User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Marijuana use dramatically increases risk of heart problems, stroke
Regularly using marijuana can significantly increase a person’s risk of heart attack, heart failure, and stroke, according to a pair of new studies that will be presented at a major upcoming medical conference.
People who use marijuana daily have a 34% increased risk of heart failure, compared with people who don’t use the drug, according to one of the new studies.
The new findings leverage health data from 157,000 people in the National Institutes of Health “All of Us” research program. Researchers analyzed whether marijuana users were more likely to experience heart failure than nonusers over the course of nearly 4 years. The results indicated that coronary artery disease was behind marijuana users’ increased risk. (Coronary artery disease is the buildup of plaque on the walls of the arteries that supply blood to the heart.)
The research was conducted by a team at Medstar Health, a large Maryland health care system that operates 10 hospitals plus hundreds of clinics. The findings will be presented at the American Heart Association’s Scientific Sessions 2023 in Philadelphia.
“Our results should encourage more researchers to study the use of marijuana to better understand its health implications, especially on cardiovascular risk,” said researcher Yakubu Bene-Alhasan, MD, MPH, a doctor at Medstar Health in Baltimore. “We want to provide the population with high-quality information on marijuana use and to help inform policy decisions at the state level, to educate patients, and to guide health care professionals.”
About one in five people in the United States use marijuana, according to the Centers for Disease Control and Prevention. The majority of U.S. states allow marijuana to be used legally for medical purposes, and more than 20 states have legalized recreational marijuana, a tracker from the National Conference of State Legislatures shows.
A second study that will be presented at the conference shows that older people with any combination of type 2 diabetes, high blood pressure, and high cholesterol who use marijuana have an increased risk for a major heart or brain event, compared with people who never used the drug.
The researchers analyzed data for more than 28,000 people age 65 and older who had health conditions that put them at risk for heart problems and whose medical records showed they were marijuana users but not tobacco users. The results showed at least a 20% increased risk of heart attack, stroke, cardiac arrest, or arrhythmia (irregular heartbeat).
The findings are significant because medical professionals have long said that research on the long-term health effects of using marijuana are limited.
“The latest research about cannabis use indicates that smoking and inhaling cannabis increases concentrations of blood carboxyhemoglobin (carbon monoxide, a poisonous gas), tar (partly burned combustible matter) similar to the effects of inhaling a tobacco cigarette, both of which have been linked to heart muscle disease, chest pain, heart rhythm disturbances, heart attacks and other serious conditions,” said Robert L. Page II, PharmD, MSPH, chair of the volunteer writing group for the 2020 American Heart Association Scientific Statement: Medical Marijuana, Recreational Cannabis, and Cardiovascular Health, in a statement. “Together with the results of these two research studies, the cardiovascular risks of cannabis use are becoming clearer and should be carefully considered and monitored by health care professionals and the public.”
A version of this article first appeared on WebMD.com.
Regularly using marijuana can significantly increase a person’s risk of heart attack, heart failure, and stroke, according to a pair of new studies that will be presented at a major upcoming medical conference.
People who use marijuana daily have a 34% increased risk of heart failure, compared with people who don’t use the drug, according to one of the new studies.
The new findings leverage health data from 157,000 people in the National Institutes of Health “All of Us” research program. Researchers analyzed whether marijuana users were more likely to experience heart failure than nonusers over the course of nearly 4 years. The results indicated that coronary artery disease was behind marijuana users’ increased risk. (Coronary artery disease is the buildup of plaque on the walls of the arteries that supply blood to the heart.)
The research was conducted by a team at Medstar Health, a large Maryland health care system that operates 10 hospitals plus hundreds of clinics. The findings will be presented at the American Heart Association’s Scientific Sessions 2023 in Philadelphia.
“Our results should encourage more researchers to study the use of marijuana to better understand its health implications, especially on cardiovascular risk,” said researcher Yakubu Bene-Alhasan, MD, MPH, a doctor at Medstar Health in Baltimore. “We want to provide the population with high-quality information on marijuana use and to help inform policy decisions at the state level, to educate patients, and to guide health care professionals.”
About one in five people in the United States use marijuana, according to the Centers for Disease Control and Prevention. The majority of U.S. states allow marijuana to be used legally for medical purposes, and more than 20 states have legalized recreational marijuana, a tracker from the National Conference of State Legislatures shows.
A second study that will be presented at the conference shows that older people with any combination of type 2 diabetes, high blood pressure, and high cholesterol who use marijuana have an increased risk for a major heart or brain event, compared with people who never used the drug.
The researchers analyzed data for more than 28,000 people age 65 and older who had health conditions that put them at risk for heart problems and whose medical records showed they were marijuana users but not tobacco users. The results showed at least a 20% increased risk of heart attack, stroke, cardiac arrest, or arrhythmia (irregular heartbeat).
The findings are significant because medical professionals have long said that research on the long-term health effects of using marijuana are limited.
“The latest research about cannabis use indicates that smoking and inhaling cannabis increases concentrations of blood carboxyhemoglobin (carbon monoxide, a poisonous gas), tar (partly burned combustible matter) similar to the effects of inhaling a tobacco cigarette, both of which have been linked to heart muscle disease, chest pain, heart rhythm disturbances, heart attacks and other serious conditions,” said Robert L. Page II, PharmD, MSPH, chair of the volunteer writing group for the 2020 American Heart Association Scientific Statement: Medical Marijuana, Recreational Cannabis, and Cardiovascular Health, in a statement. “Together with the results of these two research studies, the cardiovascular risks of cannabis use are becoming clearer and should be carefully considered and monitored by health care professionals and the public.”
A version of this article first appeared on WebMD.com.
Regularly using marijuana can significantly increase a person’s risk of heart attack, heart failure, and stroke, according to a pair of new studies that will be presented at a major upcoming medical conference.
People who use marijuana daily have a 34% increased risk of heart failure, compared with people who don’t use the drug, according to one of the new studies.
The new findings leverage health data from 157,000 people in the National Institutes of Health “All of Us” research program. Researchers analyzed whether marijuana users were more likely to experience heart failure than nonusers over the course of nearly 4 years. The results indicated that coronary artery disease was behind marijuana users’ increased risk. (Coronary artery disease is the buildup of plaque on the walls of the arteries that supply blood to the heart.)
The research was conducted by a team at Medstar Health, a large Maryland health care system that operates 10 hospitals plus hundreds of clinics. The findings will be presented at the American Heart Association’s Scientific Sessions 2023 in Philadelphia.
“Our results should encourage more researchers to study the use of marijuana to better understand its health implications, especially on cardiovascular risk,” said researcher Yakubu Bene-Alhasan, MD, MPH, a doctor at Medstar Health in Baltimore. “We want to provide the population with high-quality information on marijuana use and to help inform policy decisions at the state level, to educate patients, and to guide health care professionals.”
About one in five people in the United States use marijuana, according to the Centers for Disease Control and Prevention. The majority of U.S. states allow marijuana to be used legally for medical purposes, and more than 20 states have legalized recreational marijuana, a tracker from the National Conference of State Legislatures shows.
A second study that will be presented at the conference shows that older people with any combination of type 2 diabetes, high blood pressure, and high cholesterol who use marijuana have an increased risk for a major heart or brain event, compared with people who never used the drug.
The researchers analyzed data for more than 28,000 people age 65 and older who had health conditions that put them at risk for heart problems and whose medical records showed they were marijuana users but not tobacco users. The results showed at least a 20% increased risk of heart attack, stroke, cardiac arrest, or arrhythmia (irregular heartbeat).
The findings are significant because medical professionals have long said that research on the long-term health effects of using marijuana are limited.
“The latest research about cannabis use indicates that smoking and inhaling cannabis increases concentrations of blood carboxyhemoglobin (carbon monoxide, a poisonous gas), tar (partly burned combustible matter) similar to the effects of inhaling a tobacco cigarette, both of which have been linked to heart muscle disease, chest pain, heart rhythm disturbances, heart attacks and other serious conditions,” said Robert L. Page II, PharmD, MSPH, chair of the volunteer writing group for the 2020 American Heart Association Scientific Statement: Medical Marijuana, Recreational Cannabis, and Cardiovascular Health, in a statement. “Together with the results of these two research studies, the cardiovascular risks of cannabis use are becoming clearer and should be carefully considered and monitored by health care professionals and the public.”
A version of this article first appeared on WebMD.com.
FROM AHA 2023
Body dysmorphic disorder diagnosis guidelines completed in Europe
BERLIN – were outlined in a late-breaker presentation at the annual Congress of the European Academy of Dermatology and Venereology.
The development of guidelines for BDD, a disorder familiar to many clinical dermatologists, is intended as a practical tool, according to Maria-Angeliki Gkini, MD, who has appointments at both Bart’s Health NHS Trust in London and the 401 General Army Hospital in Athens.

“BDD is a relatively common disorder in which the patients are preoccupied with a perceived defect or defects,” Dr. Gkini explained. “This affects them so intensely that it affects their mental health and their quality of life.”
In the DSM-5, published by the American Psychiatric Association, BDD is specifically defined as a preoccupation with “one or more perceived defects or flaws in physical appearance that are not observable or appear slight to others.” But Dr. Gkini said that BDD can also develop as a comorbidity of dermatological disorders that are visible.
These patients are challenging because they are difficult to please, added Dr. Gkini, who said they commonly become involved in doctor shopping, leaving negative reviews on social media for the clinicians they have cycled through. The problem is that the defects they seek to resolve typically stem from distorted perceptions.
BDD is related to obsessive-compulsive disorder by the frequency with which patients pursue repetitive behaviors related to their preoccupation, such as intensive grooming, frequent trips to the mirror, or difficulty in focusing on topics other than their own appearance.
The process to develop the soon-to-be-published guidelines began with a literature search. Of the approximately 3,200 articles identified on BDD, only 10 involved randomized controlled trials. Moreover, even the quality of these trials was considered “low to very low” by the experts who reviewed them, Dr. Gkini said.
One explanation is that psychodermatology has only recently started to attract more research interest, and better studies are now underway, she noted.
However, because of the dearth of high quality evidence now available, the guideline development relied on a Delphi method to reach consensus based on expert opinion in discussion of the available data.
Consensus reached by 17 experts
Specifically, 17 experts, all of whom were members of the European Society for Dermatology and Psychiatry proceeded to systematically address a series of clinical questions and recommendations. Consensus was defined as at least 75% of the participants strongly agreeing or agreeing. Several rounds of discussion were often required.
Among the conclusions, the guidelines support uniform screening for BDD in all patients prior to cosmetic procedures. In identifying depression, anxiety, and distorted perceptions, simple tools, such as the Patient Health Questionnaire might be adequate for an initial evaluation, but Dr. Gkini also recommended routinely inquiring about suicidal ideation, which has been reported in up to 80% of individuals with BDD.
Other instruments for screening that can be considered include DSM-5 criteria for BDD and the Body Dysmorphic Disorder Questionnaire–Dermatology Version, which might be particularly useful and appropriate for dermatologists.
One of the reasons to screen for BDD is that these patients often convince themselves that some specific procedure is needed to resolve the source of their obsession. The goal of screening is to verify that it is the dermatologic concern, not an underlying psychiatric disorder that is driving their search for relief. The risk of dermatologic interventions is not only that expectations are not met, but the patient’s perception of a failed intervention “sometimes makes these worse,” Dr. Gkini explained.
Collaboration with psychiatrists recommended
The guidelines include suggestions for treatment of BDD. Of these, SSRIs are recommended at high relative doses, according to Dr. Gkini. Consistent with the consensus recommendation of collaborating with mental health specialists, she said that the recommendations acknowledge evidence of greater benefits when SSRIs are combined with psychotherapy.
Katharine A. Phillips, MD, professor of psychiatry at Weill Cornell Medicine, New York, has been conducting BDD research for several years and has written numerous books and articles about this topic, including a review in the journal Focus. She cautioned that, because of a normal concern for appearance, BDD is easily missed by dermatologists.
“For BDD to be diagnosed, the preoccupation with a nonexistent or slight defect in appearance must cause clinically significant distress or impairment in functioning,” she said in an interview. “This is necessary to differentiate BDD from more normal and common appearance concerns that do not qualify for the diagnosis”
She specified that patients should be considered for cognitive-behavioral therapy rather than psychotherapy, a generic term that covers many forms of treatment. She said that most other types of psychotherapy “are probably not effective” for BDD.
Dr. Phillips highly endorsed the development of BDD guidelines for dermatologists because of the frequency with which physicians in this specialty encounter BDD – and believes that more attention to this diagnosis is needed.
“I recommend that dermatologists who have a patient with BDD collaborate with a psychiatrist in delivering care with an SSRI,” she said. “High doses of these medications are often needed to effectively treat BDD.”
Dr. Gkini reported financial relationships with AbbVie, Almirall, Celgene, Eli Lilly, Janssen, LEO, Novartis, Sanofi, and Regenlab. Dr. Phillips reported no relevant financial relationships.
BERLIN – were outlined in a late-breaker presentation at the annual Congress of the European Academy of Dermatology and Venereology.
The development of guidelines for BDD, a disorder familiar to many clinical dermatologists, is intended as a practical tool, according to Maria-Angeliki Gkini, MD, who has appointments at both Bart’s Health NHS Trust in London and the 401 General Army Hospital in Athens.
“BDD is a relatively common disorder in which the patients are preoccupied with a perceived defect or defects,” Dr. Gkini explained. “This affects them so intensely that it affects their mental health and their quality of life.”
In the DSM-5, published by the American Psychiatric Association, BDD is specifically defined as a preoccupation with “one or more perceived defects or flaws in physical appearance that are not observable or appear slight to others.” But Dr. Gkini said that BDD can also develop as a comorbidity of dermatological disorders that are visible.
These patients are challenging because they are difficult to please, added Dr. Gkini, who said they commonly become involved in doctor shopping, leaving negative reviews on social media for the clinicians they have cycled through. The problem is that the defects they seek to resolve typically stem from distorted perceptions.
BDD is related to obsessive-compulsive disorder by the frequency with which patients pursue repetitive behaviors related to their preoccupation, such as intensive grooming, frequent trips to the mirror, or difficulty in focusing on topics other than their own appearance.
The process to develop the soon-to-be-published guidelines began with a literature search. Of the approximately 3,200 articles identified on BDD, only 10 involved randomized controlled trials. Moreover, even the quality of these trials was considered “low to very low” by the experts who reviewed them, Dr. Gkini said.
One explanation is that psychodermatology has only recently started to attract more research interest, and better studies are now underway, she noted.
However, because of the dearth of high quality evidence now available, the guideline development relied on a Delphi method to reach consensus based on expert opinion in discussion of the available data.
Consensus reached by 17 experts
Specifically, 17 experts, all of whom were members of the European Society for Dermatology and Psychiatry proceeded to systematically address a series of clinical questions and recommendations. Consensus was defined as at least 75% of the participants strongly agreeing or agreeing. Several rounds of discussion were often required.
Among the conclusions, the guidelines support uniform screening for BDD in all patients prior to cosmetic procedures. In identifying depression, anxiety, and distorted perceptions, simple tools, such as the Patient Health Questionnaire might be adequate for an initial evaluation, but Dr. Gkini also recommended routinely inquiring about suicidal ideation, which has been reported in up to 80% of individuals with BDD.
Other instruments for screening that can be considered include DSM-5 criteria for BDD and the Body Dysmorphic Disorder Questionnaire–Dermatology Version, which might be particularly useful and appropriate for dermatologists.
One of the reasons to screen for BDD is that these patients often convince themselves that some specific procedure is needed to resolve the source of their obsession. The goal of screening is to verify that it is the dermatologic concern, not an underlying psychiatric disorder that is driving their search for relief. The risk of dermatologic interventions is not only that expectations are not met, but the patient’s perception of a failed intervention “sometimes makes these worse,” Dr. Gkini explained.
Collaboration with psychiatrists recommended
The guidelines include suggestions for treatment of BDD. Of these, SSRIs are recommended at high relative doses, according to Dr. Gkini. Consistent with the consensus recommendation of collaborating with mental health specialists, she said that the recommendations acknowledge evidence of greater benefits when SSRIs are combined with psychotherapy.
Katharine A. Phillips, MD, professor of psychiatry at Weill Cornell Medicine, New York, has been conducting BDD research for several years and has written numerous books and articles about this topic, including a review in the journal Focus. She cautioned that, because of a normal concern for appearance, BDD is easily missed by dermatologists.
“For BDD to be diagnosed, the preoccupation with a nonexistent or slight defect in appearance must cause clinically significant distress or impairment in functioning,” she said in an interview. “This is necessary to differentiate BDD from more normal and common appearance concerns that do not qualify for the diagnosis”
She specified that patients should be considered for cognitive-behavioral therapy rather than psychotherapy, a generic term that covers many forms of treatment. She said that most other types of psychotherapy “are probably not effective” for BDD.
Dr. Phillips highly endorsed the development of BDD guidelines for dermatologists because of the frequency with which physicians in this specialty encounter BDD – and believes that more attention to this diagnosis is needed.
“I recommend that dermatologists who have a patient with BDD collaborate with a psychiatrist in delivering care with an SSRI,” she said. “High doses of these medications are often needed to effectively treat BDD.”
Dr. Gkini reported financial relationships with AbbVie, Almirall, Celgene, Eli Lilly, Janssen, LEO, Novartis, Sanofi, and Regenlab. Dr. Phillips reported no relevant financial relationships.
BERLIN – were outlined in a late-breaker presentation at the annual Congress of the European Academy of Dermatology and Venereology.
The development of guidelines for BDD, a disorder familiar to many clinical dermatologists, is intended as a practical tool, according to Maria-Angeliki Gkini, MD, who has appointments at both Bart’s Health NHS Trust in London and the 401 General Army Hospital in Athens.
“BDD is a relatively common disorder in which the patients are preoccupied with a perceived defect or defects,” Dr. Gkini explained. “This affects them so intensely that it affects their mental health and their quality of life.”
In the DSM-5, published by the American Psychiatric Association, BDD is specifically defined as a preoccupation with “one or more perceived defects or flaws in physical appearance that are not observable or appear slight to others.” But Dr. Gkini said that BDD can also develop as a comorbidity of dermatological disorders that are visible.
These patients are challenging because they are difficult to please, added Dr. Gkini, who said they commonly become involved in doctor shopping, leaving negative reviews on social media for the clinicians they have cycled through. The problem is that the defects they seek to resolve typically stem from distorted perceptions.
BDD is related to obsessive-compulsive disorder by the frequency with which patients pursue repetitive behaviors related to their preoccupation, such as intensive grooming, frequent trips to the mirror, or difficulty in focusing on topics other than their own appearance.
The process to develop the soon-to-be-published guidelines began with a literature search. Of the approximately 3,200 articles identified on BDD, only 10 involved randomized controlled trials. Moreover, even the quality of these trials was considered “low to very low” by the experts who reviewed them, Dr. Gkini said.
One explanation is that psychodermatology has only recently started to attract more research interest, and better studies are now underway, she noted.
However, because of the dearth of high quality evidence now available, the guideline development relied on a Delphi method to reach consensus based on expert opinion in discussion of the available data.
Consensus reached by 17 experts
Specifically, 17 experts, all of whom were members of the European Society for Dermatology and Psychiatry proceeded to systematically address a series of clinical questions and recommendations. Consensus was defined as at least 75% of the participants strongly agreeing or agreeing. Several rounds of discussion were often required.
Among the conclusions, the guidelines support uniform screening for BDD in all patients prior to cosmetic procedures. In identifying depression, anxiety, and distorted perceptions, simple tools, such as the Patient Health Questionnaire might be adequate for an initial evaluation, but Dr. Gkini also recommended routinely inquiring about suicidal ideation, which has been reported in up to 80% of individuals with BDD.
Other instruments for screening that can be considered include DSM-5 criteria for BDD and the Body Dysmorphic Disorder Questionnaire–Dermatology Version, which might be particularly useful and appropriate for dermatologists.
One of the reasons to screen for BDD is that these patients often convince themselves that some specific procedure is needed to resolve the source of their obsession. The goal of screening is to verify that it is the dermatologic concern, not an underlying psychiatric disorder that is driving their search for relief. The risk of dermatologic interventions is not only that expectations are not met, but the patient’s perception of a failed intervention “sometimes makes these worse,” Dr. Gkini explained.
Collaboration with psychiatrists recommended
The guidelines include suggestions for treatment of BDD. Of these, SSRIs are recommended at high relative doses, according to Dr. Gkini. Consistent with the consensus recommendation of collaborating with mental health specialists, she said that the recommendations acknowledge evidence of greater benefits when SSRIs are combined with psychotherapy.
Katharine A. Phillips, MD, professor of psychiatry at Weill Cornell Medicine, New York, has been conducting BDD research for several years and has written numerous books and articles about this topic, including a review in the journal Focus. She cautioned that, because of a normal concern for appearance, BDD is easily missed by dermatologists.
“For BDD to be diagnosed, the preoccupation with a nonexistent or slight defect in appearance must cause clinically significant distress or impairment in functioning,” she said in an interview. “This is necessary to differentiate BDD from more normal and common appearance concerns that do not qualify for the diagnosis”
She specified that patients should be considered for cognitive-behavioral therapy rather than psychotherapy, a generic term that covers many forms of treatment. She said that most other types of psychotherapy “are probably not effective” for BDD.
Dr. Phillips highly endorsed the development of BDD guidelines for dermatologists because of the frequency with which physicians in this specialty encounter BDD – and believes that more attention to this diagnosis is needed.
“I recommend that dermatologists who have a patient with BDD collaborate with a psychiatrist in delivering care with an SSRI,” she said. “High doses of these medications are often needed to effectively treat BDD.”
Dr. Gkini reported financial relationships with AbbVie, Almirall, Celgene, Eli Lilly, Janssen, LEO, Novartis, Sanofi, and Regenlab. Dr. Phillips reported no relevant financial relationships.
AT THE EADV CONGRESS
EMR prompt boosts albuminuria measurement in T2D
PHILADELPHIA – An electronic medical record alert to primary care physicians that their adult patients with type 2 diabetes were due for an albuminuria and renal-function check boosted screening for chronic kidney disease (CKD) by roughly half compared with the preintervention rate in a single U.S. academic health system.
“Screening rates for CKD more rapidly improved after implementation” of the EMR alert, said Maggy M. Spolnik, MD, at Kidney Week 2023, organized by the American Society of Nephrology.
“There was an immediate and ongoing effect over a year,” said Dr. Spolnik, a nephrologist at Indiana University in Indianapolis.

However, CKD screening rates in the primary care setting remain a challenge. In the study, the EMR alert produced a urine albumin-to-creatinine ratio (UACR) screening rate of about 26% of patient encounters, she reported. While this was significantly above the roughly 17% rate that had persisted for months before the intervention, it still fell short of the universal annual screening for adults with type 2 diabetes not previously diagnosed with CKD recommended by medical groups such as the American Diabetes Association and the Kidney Disease: Improving Global Outcomes organization. The U.S. Preventive Services Task Force’s assessment in 2012 concluded inadequate information existed at that time to make recommendations about CKD screening, but the group is now revisiting the issue.
‘Albuminuria is an earlier marker’ than eGFR
“Primary care physicians need to regularly monitor albuminuria in adults with type 2 diabetes,” commented Karen A. Griffin, MD, a nephrologist and professor at Loyola University in Maywood, Ill. “By the time you diagnose CKD based on reduced estimated glomerular filtration rate (eGFR), a patient has already lost more than half their renal function. Albuminuria is an earlier marker of a problem,” Dr. Griffin said in an interview.
Primary care physicians have been slow to adopt at least annual checks on both eGFR and the urinary albumin-to-creatinine ratio (UACR) in their adult patients with type 2 diabetes. Dr. Spolnik cited reasons such as the brief 15-minute consultation that primary care physicians have when seeing a patient, and an often confusing ordering menu that gives a UACR test various other names such as tests for microalbuminuria or macroalbuminuria.
To simplify ordering, the EMR prompt assessed in Dr. Spolnik’s study called the test “kidney screening” that automatically bundled an order for both eGFR calculation with UACR measurement. Another limitation is that UACR measurement requires a urine sample, which patients often find inconvenient to provide at the time of their examination.
The study run by Dr. Spolnik involved 10,744 adults with type 2 diabetes without an existing diagnosis of CKD seen in an outpatient, primary care visit to the UVA Health system centered in Charlottesville, Va. during April 2021–April 2022. A total of 23,419 encounters served as usual-care controls. The intervention period with active EMR alerts for kidney screening included 10,204 similar patients seen during April 2022–April 2023 in a total of 20,358 encounters. The patients averaged about 61-62 years old, and about 45% were men.
Bundling alerts into a single pop-up
The primary care clinicians who received the prompts were generally receptive to them, but they asked the researchers to bundle the UACR and eGFR measurement prompts along with any other alerts they received in the EMR into a single on-screen pop-up.
Dr. Spolnik acknowledged the need for further research and refinement to the prompt. For example, she wants to assess prompts for patients identified as having CKD that would promote best-practice management, including lifestyle and medical interventions. She also envisions expanding the prompts to also include other, related disorders such as hypertension.
But she and her colleagues were convinced enough by the results that they have not only continued the program at UVA Health but they also expanded it, starting in October 2023, to the academic primary care practice at Indiana University.
If the Indiana University trial confirms the efficacy seen in Virginia, the next step might be inclusion by Epic of the CKD screening alert as a routine option in the EMR software it distributes to its U.S. clients, Dr. Spolnik said in an interview.
Dr. Spolnik and Dr. Griffin had no disclosures.
PHILADELPHIA – An electronic medical record alert to primary care physicians that their adult patients with type 2 diabetes were due for an albuminuria and renal-function check boosted screening for chronic kidney disease (CKD) by roughly half compared with the preintervention rate in a single U.S. academic health system.
“Screening rates for CKD more rapidly improved after implementation” of the EMR alert, said Maggy M. Spolnik, MD, at Kidney Week 2023, organized by the American Society of Nephrology.
“There was an immediate and ongoing effect over a year,” said Dr. Spolnik, a nephrologist at Indiana University in Indianapolis.
However, CKD screening rates in the primary care setting remain a challenge. In the study, the EMR alert produced a urine albumin-to-creatinine ratio (UACR) screening rate of about 26% of patient encounters, she reported. While this was significantly above the roughly 17% rate that had persisted for months before the intervention, it still fell short of the universal annual screening for adults with type 2 diabetes not previously diagnosed with CKD recommended by medical groups such as the American Diabetes Association and the Kidney Disease: Improving Global Outcomes organization. The U.S. Preventive Services Task Force’s assessment in 2012 concluded inadequate information existed at that time to make recommendations about CKD screening, but the group is now revisiting the issue.
‘Albuminuria is an earlier marker’ than eGFR
“Primary care physicians need to regularly monitor albuminuria in adults with type 2 diabetes,” commented Karen A. Griffin, MD, a nephrologist and professor at Loyola University in Maywood, Ill. “By the time you diagnose CKD based on reduced estimated glomerular filtration rate (eGFR), a patient has already lost more than half their renal function. Albuminuria is an earlier marker of a problem,” Dr. Griffin said in an interview.
Primary care physicians have been slow to adopt at least annual checks on both eGFR and the urinary albumin-to-creatinine ratio (UACR) in their adult patients with type 2 diabetes. Dr. Spolnik cited reasons such as the brief 15-minute consultation that primary care physicians have when seeing a patient, and an often confusing ordering menu that gives a UACR test various other names such as tests for microalbuminuria or macroalbuminuria.
To simplify ordering, the EMR prompt assessed in Dr. Spolnik’s study called the test “kidney screening” that automatically bundled an order for both eGFR calculation with UACR measurement. Another limitation is that UACR measurement requires a urine sample, which patients often find inconvenient to provide at the time of their examination.
The study run by Dr. Spolnik involved 10,744 adults with type 2 diabetes without an existing diagnosis of CKD seen in an outpatient, primary care visit to the UVA Health system centered in Charlottesville, Va. during April 2021–April 2022. A total of 23,419 encounters served as usual-care controls. The intervention period with active EMR alerts for kidney screening included 10,204 similar patients seen during April 2022–April 2023 in a total of 20,358 encounters. The patients averaged about 61-62 years old, and about 45% were men.
Bundling alerts into a single pop-up
The primary care clinicians who received the prompts were generally receptive to them, but they asked the researchers to bundle the UACR and eGFR measurement prompts along with any other alerts they received in the EMR into a single on-screen pop-up.
Dr. Spolnik acknowledged the need for further research and refinement to the prompt. For example, she wants to assess prompts for patients identified as having CKD that would promote best-practice management, including lifestyle and medical interventions. She also envisions expanding the prompts to also include other, related disorders such as hypertension.
But she and her colleagues were convinced enough by the results that they have not only continued the program at UVA Health but they also expanded it, starting in October 2023, to the academic primary care practice at Indiana University.
If the Indiana University trial confirms the efficacy seen in Virginia, the next step might be inclusion by Epic of the CKD screening alert as a routine option in the EMR software it distributes to its U.S. clients, Dr. Spolnik said in an interview.
Dr. Spolnik and Dr. Griffin had no disclosures.
PHILADELPHIA – An electronic medical record alert to primary care physicians that their adult patients with type 2 diabetes were due for an albuminuria and renal-function check boosted screening for chronic kidney disease (CKD) by roughly half compared with the preintervention rate in a single U.S. academic health system.
“Screening rates for CKD more rapidly improved after implementation” of the EMR alert, said Maggy M. Spolnik, MD, at Kidney Week 2023, organized by the American Society of Nephrology.
“There was an immediate and ongoing effect over a year,” said Dr. Spolnik, a nephrologist at Indiana University in Indianapolis.
However, CKD screening rates in the primary care setting remain a challenge. In the study, the EMR alert produced a urine albumin-to-creatinine ratio (UACR) screening rate of about 26% of patient encounters, she reported. While this was significantly above the roughly 17% rate that had persisted for months before the intervention, it still fell short of the universal annual screening for adults with type 2 diabetes not previously diagnosed with CKD recommended by medical groups such as the American Diabetes Association and the Kidney Disease: Improving Global Outcomes organization. The U.S. Preventive Services Task Force’s assessment in 2012 concluded inadequate information existed at that time to make recommendations about CKD screening, but the group is now revisiting the issue.
‘Albuminuria is an earlier marker’ than eGFR
“Primary care physicians need to regularly monitor albuminuria in adults with type 2 diabetes,” commented Karen A. Griffin, MD, a nephrologist and professor at Loyola University in Maywood, Ill. “By the time you diagnose CKD based on reduced estimated glomerular filtration rate (eGFR), a patient has already lost more than half their renal function. Albuminuria is an earlier marker of a problem,” Dr. Griffin said in an interview.
Primary care physicians have been slow to adopt at least annual checks on both eGFR and the urinary albumin-to-creatinine ratio (UACR) in their adult patients with type 2 diabetes. Dr. Spolnik cited reasons such as the brief 15-minute consultation that primary care physicians have when seeing a patient, and an often confusing ordering menu that gives a UACR test various other names such as tests for microalbuminuria or macroalbuminuria.
To simplify ordering, the EMR prompt assessed in Dr. Spolnik’s study called the test “kidney screening” that automatically bundled an order for both eGFR calculation with UACR measurement. Another limitation is that UACR measurement requires a urine sample, which patients often find inconvenient to provide at the time of their examination.
The study run by Dr. Spolnik involved 10,744 adults with type 2 diabetes without an existing diagnosis of CKD seen in an outpatient, primary care visit to the UVA Health system centered in Charlottesville, Va. during April 2021–April 2022. A total of 23,419 encounters served as usual-care controls. The intervention period with active EMR alerts for kidney screening included 10,204 similar patients seen during April 2022–April 2023 in a total of 20,358 encounters. The patients averaged about 61-62 years old, and about 45% were men.
Bundling alerts into a single pop-up
The primary care clinicians who received the prompts were generally receptive to them, but they asked the researchers to bundle the UACR and eGFR measurement prompts along with any other alerts they received in the EMR into a single on-screen pop-up.
Dr. Spolnik acknowledged the need for further research and refinement to the prompt. For example, she wants to assess prompts for patients identified as having CKD that would promote best-practice management, including lifestyle and medical interventions. She also envisions expanding the prompts to also include other, related disorders such as hypertension.
But she and her colleagues were convinced enough by the results that they have not only continued the program at UVA Health but they also expanded it, starting in October 2023, to the academic primary care practice at Indiana University.
If the Indiana University trial confirms the efficacy seen in Virginia, the next step might be inclusion by Epic of the CKD screening alert as a routine option in the EMR software it distributes to its U.S. clients, Dr. Spolnik said in an interview.
Dr. Spolnik and Dr. Griffin had no disclosures.
REPORTING FROM KIDNEY WEEK 2023
Enhanced natural killer cell therapy shows promise in Alzheimer’s
BOSTON – .
SNK01, being developed by NKGen Biotech, is an autologous, nongenetically modified NK cell product that has enhanced cytotoxicity and activating receptor expression.
“When we give these enhanced natural killer cells intravenously, not only do they get into the brain, but we’ve shown, through CSF biomarker data, that they reduce both amyloid and tau proteins, dramatically reducing the neuroinflammation,” said Paul Song, MD, chief executive officer of NKGen Biotech.
“Remarkably,” in the first 6 months, 90% of patients with Alzheimer’s disease demonstrated improvement or maintained stable cognitive function, based on the Alzheimer’s Disease Composite Score (ADCOMS), suggesting that SNK01 may do more than simply slow disease progression, Dr. Song said.
The findings were presented at the 16th Clinical Trials on Alzheimer’s Disease (CTAD) conference.
Sound rationale
NK cells are an essential part of the innate immune system that can shape the adaptive response by eliminating activated (not resting) autologous CD4+ T cells. Weak or deficient NK cells have been found to correlate with various diseases, including autoimmune diseases, and emerging data suggest an autoimmune component to Alzheimer’s disease.
The phase 1 study evaluated the safety, tolerability, and exploratory efficacy of SNK01 given intravenously in escalating doses every 3 weeks (four treatments in total).
Participants included 10 patients with Alzheimer’s disease confirmed by imaging. Five had mild Alzheimer’s disease, three had moderate Alzheimer’s disease, and two had advanced Alzheimer’s disease, based on baseline Clinical Dementia Rating–Sum of Boxes (CDR-SB) scores. Median baseline CDR-SB score was 9 (range, 4-18).
Cognitive assessments included CDR-SB, Mini-Mental State Examination (MMSE), Alzheimer’s disease Assessment Scale-Cognitive Subscale (ADAS-Cog) and ADCOMS. CSF biomarker analyses were performed at baseline and at 1 and 12 weeks after the final dose (weeks 11 and 22, respectively).
NK cells were successfully activated and expanded in all 10 patients and no treatment-related adverse events were observed.
Based on the CSF biomarker data, SNK01 crossed the blood–brain barrier and reduced CSF amyloid-beta 42/40 and pTau181 levels and neuroinflammation, as measured by glial fibrillary acid protein (GFAP), and the effects appeared to persist 12 weeks after the final dose.
The exploratory efficacy data show that, 1 week after final dose (week 11), compared with baseline, 30% of patients showed clinical improvement on the composite ADCOMS and 60% had a stable ADCOMS score; 50%-70% of patients were stable or improved on the CDR-SB, ADAS-Cog and/or MMSE.
“One patient went from a MMSE score of 14, which is moderate dementia, to 22, which is mild cognitive impairment,” said Dr. Song.
At 12 weeks after the final dose (week 22), 44%-89% of patients remained stable or improved in all cognitive scores compared with week 11; and 50% of the patients with stable ADCOMS scores at week 11 remained stable.
Based on the positive phase 1 data, the Food and Drug Administration has approved a phase 1/2a study in patients with moderate Alzheimer’s disease. “The trial will use a much higher dose and a prolonged dosing regimen and we think we’ll see even more dramatic results with more sustained higher dosing,” Dr. Song said.
Down the road, it will be interesting to see how NK cell therapy could “complement” anti-amyloid and anti-tau therapies, he added.
Ideal treatment approach
Commenting on this research, Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, said NK cells have “natural abilities that could make them an ideal treatment approach for Alzheimer’s and similar neurodegenerative diseases.
“NK cells have properties that allow them to recognize and destroy diseased brain cells while leaving healthy cells intact, without causing excessive inflammation or autoimmune issues. It has historically been difficult to get immune cells to access the privileged immunological environment of the brain,” Dr. Lakhan explained.
“However, this line of early research shows that NK cells safely crosses the blood–brain barrier, infiltrates brain tissue, and may stave off Alzheimer’s disease as measured by biomarkers and clinical symptoms,” he noted.
“This emerging cell-based immunotherapy is highly-specific to the cells responsible for Alzheimer’s, avoids drug resistance, has long-lasting results, and has fewer side effects than drug counterparts,” Dr. Lakhan said.
The trial was sponsored by NKGen Biotech. Dr. Song and six coauthors are employees and shareholders in the company. Dr. Lakhan reports no relevant financial relationships.
A version of this article appeared on Medscape.com.
BOSTON – .
SNK01, being developed by NKGen Biotech, is an autologous, nongenetically modified NK cell product that has enhanced cytotoxicity and activating receptor expression.
“When we give these enhanced natural killer cells intravenously, not only do they get into the brain, but we’ve shown, through CSF biomarker data, that they reduce both amyloid and tau proteins, dramatically reducing the neuroinflammation,” said Paul Song, MD, chief executive officer of NKGen Biotech.
“Remarkably,” in the first 6 months, 90% of patients with Alzheimer’s disease demonstrated improvement or maintained stable cognitive function, based on the Alzheimer’s Disease Composite Score (ADCOMS), suggesting that SNK01 may do more than simply slow disease progression, Dr. Song said.
The findings were presented at the 16th Clinical Trials on Alzheimer’s Disease (CTAD) conference.
Sound rationale
NK cells are an essential part of the innate immune system that can shape the adaptive response by eliminating activated (not resting) autologous CD4+ T cells. Weak or deficient NK cells have been found to correlate with various diseases, including autoimmune diseases, and emerging data suggest an autoimmune component to Alzheimer’s disease.
The phase 1 study evaluated the safety, tolerability, and exploratory efficacy of SNK01 given intravenously in escalating doses every 3 weeks (four treatments in total).
Participants included 10 patients with Alzheimer’s disease confirmed by imaging. Five had mild Alzheimer’s disease, three had moderate Alzheimer’s disease, and two had advanced Alzheimer’s disease, based on baseline Clinical Dementia Rating–Sum of Boxes (CDR-SB) scores. Median baseline CDR-SB score was 9 (range, 4-18).
Cognitive assessments included CDR-SB, Mini-Mental State Examination (MMSE), Alzheimer’s disease Assessment Scale-Cognitive Subscale (ADAS-Cog) and ADCOMS. CSF biomarker analyses were performed at baseline and at 1 and 12 weeks after the final dose (weeks 11 and 22, respectively).
NK cells were successfully activated and expanded in all 10 patients and no treatment-related adverse events were observed.
Based on the CSF biomarker data, SNK01 crossed the blood–brain barrier and reduced CSF amyloid-beta 42/40 and pTau181 levels and neuroinflammation, as measured by glial fibrillary acid protein (GFAP), and the effects appeared to persist 12 weeks after the final dose.
The exploratory efficacy data show that, 1 week after final dose (week 11), compared with baseline, 30% of patients showed clinical improvement on the composite ADCOMS and 60% had a stable ADCOMS score; 50%-70% of patients were stable or improved on the CDR-SB, ADAS-Cog and/or MMSE.
“One patient went from a MMSE score of 14, which is moderate dementia, to 22, which is mild cognitive impairment,” said Dr. Song.
At 12 weeks after the final dose (week 22), 44%-89% of patients remained stable or improved in all cognitive scores compared with week 11; and 50% of the patients with stable ADCOMS scores at week 11 remained stable.
Based on the positive phase 1 data, the Food and Drug Administration has approved a phase 1/2a study in patients with moderate Alzheimer’s disease. “The trial will use a much higher dose and a prolonged dosing regimen and we think we’ll see even more dramatic results with more sustained higher dosing,” Dr. Song said.
Down the road, it will be interesting to see how NK cell therapy could “complement” anti-amyloid and anti-tau therapies, he added.
Ideal treatment approach
Commenting on this research, Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, said NK cells have “natural abilities that could make them an ideal treatment approach for Alzheimer’s and similar neurodegenerative diseases.
“NK cells have properties that allow them to recognize and destroy diseased brain cells while leaving healthy cells intact, without causing excessive inflammation or autoimmune issues. It has historically been difficult to get immune cells to access the privileged immunological environment of the brain,” Dr. Lakhan explained.
“However, this line of early research shows that NK cells safely crosses the blood–brain barrier, infiltrates brain tissue, and may stave off Alzheimer’s disease as measured by biomarkers and clinical symptoms,” he noted.
“This emerging cell-based immunotherapy is highly-specific to the cells responsible for Alzheimer’s, avoids drug resistance, has long-lasting results, and has fewer side effects than drug counterparts,” Dr. Lakhan said.
The trial was sponsored by NKGen Biotech. Dr. Song and six coauthors are employees and shareholders in the company. Dr. Lakhan reports no relevant financial relationships.
A version of this article appeared on Medscape.com.
BOSTON – .
SNK01, being developed by NKGen Biotech, is an autologous, nongenetically modified NK cell product that has enhanced cytotoxicity and activating receptor expression.
“When we give these enhanced natural killer cells intravenously, not only do they get into the brain, but we’ve shown, through CSF biomarker data, that they reduce both amyloid and tau proteins, dramatically reducing the neuroinflammation,” said Paul Song, MD, chief executive officer of NKGen Biotech.
“Remarkably,” in the first 6 months, 90% of patients with Alzheimer’s disease demonstrated improvement or maintained stable cognitive function, based on the Alzheimer’s Disease Composite Score (ADCOMS), suggesting that SNK01 may do more than simply slow disease progression, Dr. Song said.
The findings were presented at the 16th Clinical Trials on Alzheimer’s Disease (CTAD) conference.
Sound rationale
NK cells are an essential part of the innate immune system that can shape the adaptive response by eliminating activated (not resting) autologous CD4+ T cells. Weak or deficient NK cells have been found to correlate with various diseases, including autoimmune diseases, and emerging data suggest an autoimmune component to Alzheimer’s disease.
The phase 1 study evaluated the safety, tolerability, and exploratory efficacy of SNK01 given intravenously in escalating doses every 3 weeks (four treatments in total).
Participants included 10 patients with Alzheimer’s disease confirmed by imaging. Five had mild Alzheimer’s disease, three had moderate Alzheimer’s disease, and two had advanced Alzheimer’s disease, based on baseline Clinical Dementia Rating–Sum of Boxes (CDR-SB) scores. Median baseline CDR-SB score was 9 (range, 4-18).
Cognitive assessments included CDR-SB, Mini-Mental State Examination (MMSE), Alzheimer’s disease Assessment Scale-Cognitive Subscale (ADAS-Cog) and ADCOMS. CSF biomarker analyses were performed at baseline and at 1 and 12 weeks after the final dose (weeks 11 and 22, respectively).
NK cells were successfully activated and expanded in all 10 patients and no treatment-related adverse events were observed.
Based on the CSF biomarker data, SNK01 crossed the blood–brain barrier and reduced CSF amyloid-beta 42/40 and pTau181 levels and neuroinflammation, as measured by glial fibrillary acid protein (GFAP), and the effects appeared to persist 12 weeks after the final dose.
The exploratory efficacy data show that, 1 week after final dose (week 11), compared with baseline, 30% of patients showed clinical improvement on the composite ADCOMS and 60% had a stable ADCOMS score; 50%-70% of patients were stable or improved on the CDR-SB, ADAS-Cog and/or MMSE.
“One patient went from a MMSE score of 14, which is moderate dementia, to 22, which is mild cognitive impairment,” said Dr. Song.
At 12 weeks after the final dose (week 22), 44%-89% of patients remained stable or improved in all cognitive scores compared with week 11; and 50% of the patients with stable ADCOMS scores at week 11 remained stable.
Based on the positive phase 1 data, the Food and Drug Administration has approved a phase 1/2a study in patients with moderate Alzheimer’s disease. “The trial will use a much higher dose and a prolonged dosing regimen and we think we’ll see even more dramatic results with more sustained higher dosing,” Dr. Song said.
Down the road, it will be interesting to see how NK cell therapy could “complement” anti-amyloid and anti-tau therapies, he added.
Ideal treatment approach
Commenting on this research, Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, said NK cells have “natural abilities that could make them an ideal treatment approach for Alzheimer’s and similar neurodegenerative diseases.
“NK cells have properties that allow them to recognize and destroy diseased brain cells while leaving healthy cells intact, without causing excessive inflammation or autoimmune issues. It has historically been difficult to get immune cells to access the privileged immunological environment of the brain,” Dr. Lakhan explained.
“However, this line of early research shows that NK cells safely crosses the blood–brain barrier, infiltrates brain tissue, and may stave off Alzheimer’s disease as measured by biomarkers and clinical symptoms,” he noted.
“This emerging cell-based immunotherapy is highly-specific to the cells responsible for Alzheimer’s, avoids drug resistance, has long-lasting results, and has fewer side effects than drug counterparts,” Dr. Lakhan said.
The trial was sponsored by NKGen Biotech. Dr. Song and six coauthors are employees and shareholders in the company. Dr. Lakhan reports no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM CTAD 2023
Drug-coated balloon beats conventional angioplasty for high-risk patients with in-stent restenosis
SAN FRANCISCO – For the treatment of coronary artery in-stent restenosis, angioplasty with a drug-coated balloon (AGENT DCB; Boston Scientific) was superior to conventional balloon angioplasty in preventing target lesion failure at 1 year in a high-risk patient population.
Approximate 50% reductions in the rates of target lesion restenosis and target vessel myocardial infarction (MI) accounted for the superior findings with the AGENT DCB over conventional balloon angioplasty.
Robert Yeh, MD, of Beth Israel Deaconess Medical Center in Boston reported at the annual Transcatheter Cardiovascular Therapeutics congress. “This represented a 38% relative risk reduction as well as a 10% absolute risk reduction in the endpoint. The P value for superiority was 0.0063, highly statistically significant.”
In-stent restenosis is clinically challenging and accounts for about 10% of all percutaneous coronary interventions. “Sometimes these patients have multiple layers, and that could be a third or fourth layer of stent, something that we try to avoid,” he said.
Drug-coated balloons, which are not currently approved in the United States, can deliver drugs that inhibit blockages from reforming, “without leaving additional layers of metal behind,” he added. Such devices are already available in Europe and Japan.
AGENT IDE was a prospective, multicenter, superiority trial that randomly assigned 480 patients 2:1 to the AGENT DCB (n = 321) or to conventional balloon angioplasty (n = 159). Randomization occurred after successful pre-dilation of the target vessel.
The trial included patients with in-stent restenosis previously treated with a bare metal or a drug-eluting stent with lesion lengths < 26 mm (reference vessel diameter: > 2 mm to ≤ 4), and percent diameter stenosis of more than 70% if they were asymptomatic or of more than 50% if they were symptomatic. Patients were excluded if they had a recent ST-elevation MI, bifurcation, saphenous vein or arterial graft, or thrombus in the target vessel.
All received dual antiplatelet therapy for at least 1 month and then antiplatelet monotherapy for the duration of the trial. The primary endpoint was target lesion failure at 1 year, a composite of target lesion restenosis, target vessel-related MI, or cardiac death. More than 93% of patients in each arm were available for evaluation of the primary endpoint.
The two groups were well balanced at baseline: Approximate age was 68 years, 27% were women, and three quarters were White. Approximately 28%-32% had had a prior coronary artery bypass graft, 20%-22% had previous heart failure, and about 22% had a history of left main coronary artery disease. Half had diabetes, and about half had stable angina.
Multiple stent layers were common in 43% of each group. Stenosis diameter was about 65% at baseline for the two groups and was reduced to 22% post procedure.
Outcomes all favored AGENT DCB
In the AGENT DCB group, the technical success rate was 92.9% vs 89.3% for balloon angioplasty. Intravascular imaging was used during the procedure in 72.3% of DCB cases and in 76.7% of balloon cases.
Besides demonstrating a nearly 38% reduction in the primary endpoint of target lesion failure at 1 year for the DCB over conventional balloon angioplasty, DCB nearly halved the rate of target lesion revascularization and target vessel MI and was superior on other measures of clinical outcome.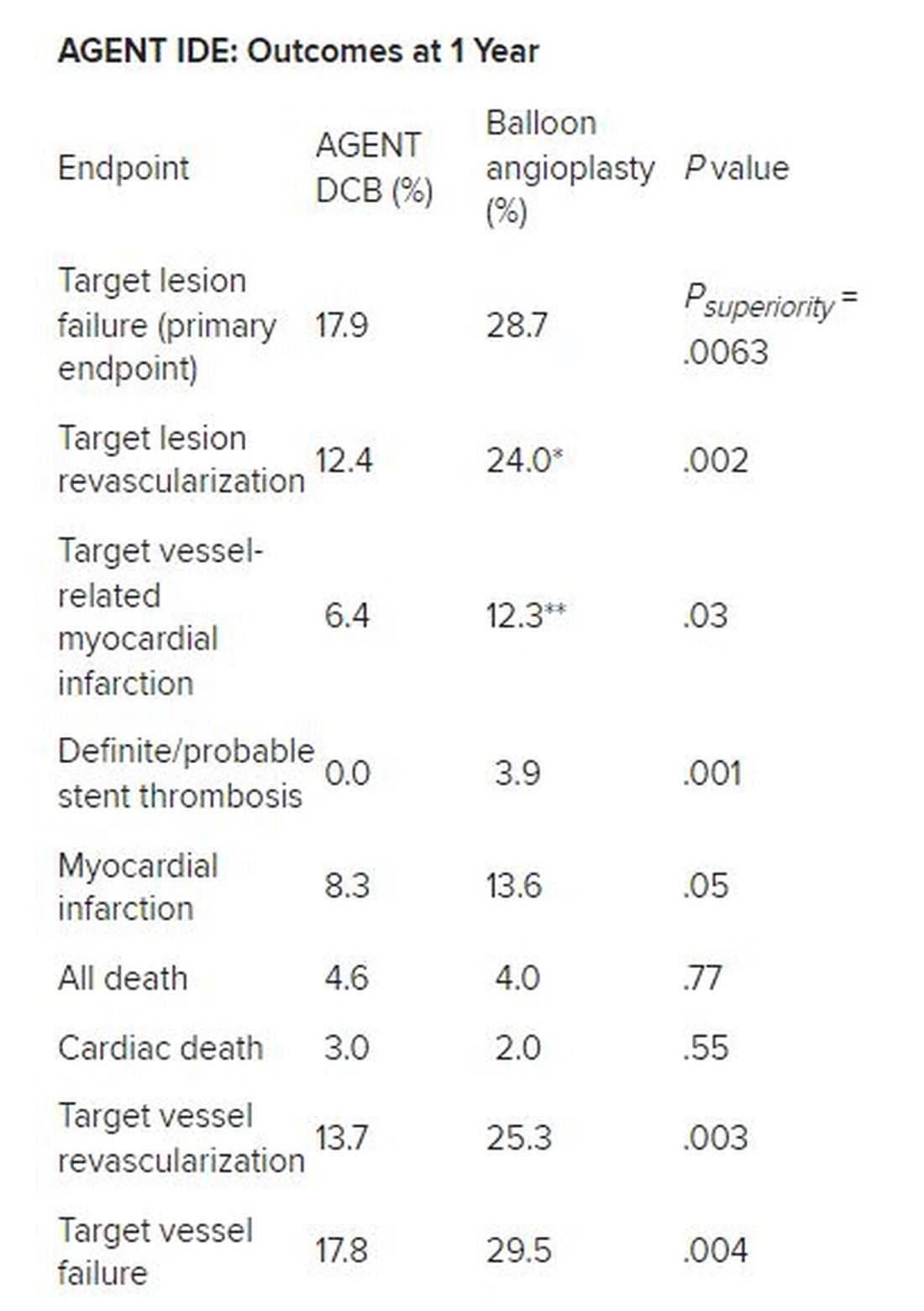
*Hazard ratio, 0.49; 95% CI, 0.31-0.79; ** HR, 0.51; 95% CI, 0.27-0.95
There was no stent rethrombosis with the DCB vs 3.9% with the conventional balloon angioplasty. Of note, there were no differences between the groups in terms of cardiac or noncardiac death.
Subgroup analyses of the primary outcome in terms of sex, age, diabetes, vessel size, or single or multiple stent layers all trended in favor of AGENT DCB but were not statistically significant for interaction.
The study is being expanded to include 600 patients. This device is a US Food and Drug Administration–designated breakthrough device, “and this pivotal trial will be the primary evidence used to support FDA approval,” Dr. Yeh said. “And given the marked superiority over conventional balloon angioplasty, I believe that the AGENT DCB is likely to become an important new treatment option for patients with coronary stenosis in the United States.”
Long overdue
Róisín Colleran, MBBCh, of the Cardiovascular Research Institute Dublin at Mater Private Hospital in Ireland, the designated discussant, first congratulated Dr. Yeh and his coinvestigators on the study’s conduct and findings.
“This study is long overdue,” she said. As Dr. Yeh noted, about 10% of PCI procedures are done for in-stent restenosis, Dr. Colleran said, but in 2023, there is still no coronary drug eluting balloon approved for this indication in the US, despite the class 1 recommendation in the 2014 European guidelines.
She pointed to the trial results, saying they are “clear...a significant reduction in target lesion failure driven by halving in rates of both target lesion revascularization and target vessel MI.”
Strengths of the study are it is the largest of its kind to date, with 480 patients, conducted at 40 US centers, using device-specific endpoints. There was a “very high” intravascular imaging rate of 75% in a cohort with a high risk for in-stent restenosis, consisting of 50% of patients with diabetes and more than 40% with multiple stents.
“The main limitation is the choice of comparator,” Dr. Colleran said. Balloon angioplasty is inferior to both stenting and drug coated balloon therapy for treatment of in-stent restenosis but is the standard of care in the United States, she noted. “I think...for regulatory reasons this was the comparator chosen,” she said.
“I think the implications are clear,” Dr. Colleran added. “This trial should provide a basis for regulatory approval of the drug coated balloon treatment of in-stent restenosis in the U.S. and finally provide this as an available treatment option for such patients.”
Dr. Yeh reported receiving grant/research support from Abbott Vascular, BD Bard, Boston Scientific, Cook Medical, Philips Medical, and Medtronic, and consulting for Abbott Vascular, Boston Scientific, CathWorks, Elixir Medical, Infraredx, Medtronic, Shockwave Medical, and Zol. Dr. Colleran had no disclosures. The trial was supported by Boston Scientific.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – For the treatment of coronary artery in-stent restenosis, angioplasty with a drug-coated balloon (AGENT DCB; Boston Scientific) was superior to conventional balloon angioplasty in preventing target lesion failure at 1 year in a high-risk patient population.
Approximate 50% reductions in the rates of target lesion restenosis and target vessel myocardial infarction (MI) accounted for the superior findings with the AGENT DCB over conventional balloon angioplasty.
Robert Yeh, MD, of Beth Israel Deaconess Medical Center in Boston reported at the annual Transcatheter Cardiovascular Therapeutics congress. “This represented a 38% relative risk reduction as well as a 10% absolute risk reduction in the endpoint. The P value for superiority was 0.0063, highly statistically significant.”
In-stent restenosis is clinically challenging and accounts for about 10% of all percutaneous coronary interventions. “Sometimes these patients have multiple layers, and that could be a third or fourth layer of stent, something that we try to avoid,” he said.
Drug-coated balloons, which are not currently approved in the United States, can deliver drugs that inhibit blockages from reforming, “without leaving additional layers of metal behind,” he added. Such devices are already available in Europe and Japan.
AGENT IDE was a prospective, multicenter, superiority trial that randomly assigned 480 patients 2:1 to the AGENT DCB (n = 321) or to conventional balloon angioplasty (n = 159). Randomization occurred after successful pre-dilation of the target vessel.
The trial included patients with in-stent restenosis previously treated with a bare metal or a drug-eluting stent with lesion lengths < 26 mm (reference vessel diameter: > 2 mm to ≤ 4), and percent diameter stenosis of more than 70% if they were asymptomatic or of more than 50% if they were symptomatic. Patients were excluded if they had a recent ST-elevation MI, bifurcation, saphenous vein or arterial graft, or thrombus in the target vessel.
All received dual antiplatelet therapy for at least 1 month and then antiplatelet monotherapy for the duration of the trial. The primary endpoint was target lesion failure at 1 year, a composite of target lesion restenosis, target vessel-related MI, or cardiac death. More than 93% of patients in each arm were available for evaluation of the primary endpoint.
The two groups were well balanced at baseline: Approximate age was 68 years, 27% were women, and three quarters were White. Approximately 28%-32% had had a prior coronary artery bypass graft, 20%-22% had previous heart failure, and about 22% had a history of left main coronary artery disease. Half had diabetes, and about half had stable angina.
Multiple stent layers were common in 43% of each group. Stenosis diameter was about 65% at baseline for the two groups and was reduced to 22% post procedure.
Outcomes all favored AGENT DCB
In the AGENT DCB group, the technical success rate was 92.9% vs 89.3% for balloon angioplasty. Intravascular imaging was used during the procedure in 72.3% of DCB cases and in 76.7% of balloon cases.
Besides demonstrating a nearly 38% reduction in the primary endpoint of target lesion failure at 1 year for the DCB over conventional balloon angioplasty, DCB nearly halved the rate of target lesion revascularization and target vessel MI and was superior on other measures of clinical outcome.
*Hazard ratio, 0.49; 95% CI, 0.31-0.79; ** HR, 0.51; 95% CI, 0.27-0.95
There was no stent rethrombosis with the DCB vs 3.9% with the conventional balloon angioplasty. Of note, there were no differences between the groups in terms of cardiac or noncardiac death.
Subgroup analyses of the primary outcome in terms of sex, age, diabetes, vessel size, or single or multiple stent layers all trended in favor of AGENT DCB but were not statistically significant for interaction.
The study is being expanded to include 600 patients. This device is a US Food and Drug Administration–designated breakthrough device, “and this pivotal trial will be the primary evidence used to support FDA approval,” Dr. Yeh said. “And given the marked superiority over conventional balloon angioplasty, I believe that the AGENT DCB is likely to become an important new treatment option for patients with coronary stenosis in the United States.”
Long overdue
Róisín Colleran, MBBCh, of the Cardiovascular Research Institute Dublin at Mater Private Hospital in Ireland, the designated discussant, first congratulated Dr. Yeh and his coinvestigators on the study’s conduct and findings.
“This study is long overdue,” she said. As Dr. Yeh noted, about 10% of PCI procedures are done for in-stent restenosis, Dr. Colleran said, but in 2023, there is still no coronary drug eluting balloon approved for this indication in the US, despite the class 1 recommendation in the 2014 European guidelines.
She pointed to the trial results, saying they are “clear...a significant reduction in target lesion failure driven by halving in rates of both target lesion revascularization and target vessel MI.”
Strengths of the study are it is the largest of its kind to date, with 480 patients, conducted at 40 US centers, using device-specific endpoints. There was a “very high” intravascular imaging rate of 75% in a cohort with a high risk for in-stent restenosis, consisting of 50% of patients with diabetes and more than 40% with multiple stents.
“The main limitation is the choice of comparator,” Dr. Colleran said. Balloon angioplasty is inferior to both stenting and drug coated balloon therapy for treatment of in-stent restenosis but is the standard of care in the United States, she noted. “I think...for regulatory reasons this was the comparator chosen,” she said.
“I think the implications are clear,” Dr. Colleran added. “This trial should provide a basis for regulatory approval of the drug coated balloon treatment of in-stent restenosis in the U.S. and finally provide this as an available treatment option for such patients.”
Dr. Yeh reported receiving grant/research support from Abbott Vascular, BD Bard, Boston Scientific, Cook Medical, Philips Medical, and Medtronic, and consulting for Abbott Vascular, Boston Scientific, CathWorks, Elixir Medical, Infraredx, Medtronic, Shockwave Medical, and Zol. Dr. Colleran had no disclosures. The trial was supported by Boston Scientific.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – For the treatment of coronary artery in-stent restenosis, angioplasty with a drug-coated balloon (AGENT DCB; Boston Scientific) was superior to conventional balloon angioplasty in preventing target lesion failure at 1 year in a high-risk patient population.
Approximate 50% reductions in the rates of target lesion restenosis and target vessel myocardial infarction (MI) accounted for the superior findings with the AGENT DCB over conventional balloon angioplasty.
Robert Yeh, MD, of Beth Israel Deaconess Medical Center in Boston reported at the annual Transcatheter Cardiovascular Therapeutics congress. “This represented a 38% relative risk reduction as well as a 10% absolute risk reduction in the endpoint. The P value for superiority was 0.0063, highly statistically significant.”
In-stent restenosis is clinically challenging and accounts for about 10% of all percutaneous coronary interventions. “Sometimes these patients have multiple layers, and that could be a third or fourth layer of stent, something that we try to avoid,” he said.
Drug-coated balloons, which are not currently approved in the United States, can deliver drugs that inhibit blockages from reforming, “without leaving additional layers of metal behind,” he added. Such devices are already available in Europe and Japan.
AGENT IDE was a prospective, multicenter, superiority trial that randomly assigned 480 patients 2:1 to the AGENT DCB (n = 321) or to conventional balloon angioplasty (n = 159). Randomization occurred after successful pre-dilation of the target vessel.
The trial included patients with in-stent restenosis previously treated with a bare metal or a drug-eluting stent with lesion lengths < 26 mm (reference vessel diameter: > 2 mm to ≤ 4), and percent diameter stenosis of more than 70% if they were asymptomatic or of more than 50% if they were symptomatic. Patients were excluded if they had a recent ST-elevation MI, bifurcation, saphenous vein or arterial graft, or thrombus in the target vessel.
All received dual antiplatelet therapy for at least 1 month and then antiplatelet monotherapy for the duration of the trial. The primary endpoint was target lesion failure at 1 year, a composite of target lesion restenosis, target vessel-related MI, or cardiac death. More than 93% of patients in each arm were available for evaluation of the primary endpoint.
The two groups were well balanced at baseline: Approximate age was 68 years, 27% were women, and three quarters were White. Approximately 28%-32% had had a prior coronary artery bypass graft, 20%-22% had previous heart failure, and about 22% had a history of left main coronary artery disease. Half had diabetes, and about half had stable angina.
Multiple stent layers were common in 43% of each group. Stenosis diameter was about 65% at baseline for the two groups and was reduced to 22% post procedure.
Outcomes all favored AGENT DCB
In the AGENT DCB group, the technical success rate was 92.9% vs 89.3% for balloon angioplasty. Intravascular imaging was used during the procedure in 72.3% of DCB cases and in 76.7% of balloon cases.
Besides demonstrating a nearly 38% reduction in the primary endpoint of target lesion failure at 1 year for the DCB over conventional balloon angioplasty, DCB nearly halved the rate of target lesion revascularization and target vessel MI and was superior on other measures of clinical outcome.
*Hazard ratio, 0.49; 95% CI, 0.31-0.79; ** HR, 0.51; 95% CI, 0.27-0.95
There was no stent rethrombosis with the DCB vs 3.9% with the conventional balloon angioplasty. Of note, there were no differences between the groups in terms of cardiac or noncardiac death.
Subgroup analyses of the primary outcome in terms of sex, age, diabetes, vessel size, or single or multiple stent layers all trended in favor of AGENT DCB but were not statistically significant for interaction.
The study is being expanded to include 600 patients. This device is a US Food and Drug Administration–designated breakthrough device, “and this pivotal trial will be the primary evidence used to support FDA approval,” Dr. Yeh said. “And given the marked superiority over conventional balloon angioplasty, I believe that the AGENT DCB is likely to become an important new treatment option for patients with coronary stenosis in the United States.”
Long overdue
Róisín Colleran, MBBCh, of the Cardiovascular Research Institute Dublin at Mater Private Hospital in Ireland, the designated discussant, first congratulated Dr. Yeh and his coinvestigators on the study’s conduct and findings.
“This study is long overdue,” she said. As Dr. Yeh noted, about 10% of PCI procedures are done for in-stent restenosis, Dr. Colleran said, but in 2023, there is still no coronary drug eluting balloon approved for this indication in the US, despite the class 1 recommendation in the 2014 European guidelines.
She pointed to the trial results, saying they are “clear...a significant reduction in target lesion failure driven by halving in rates of both target lesion revascularization and target vessel MI.”
Strengths of the study are it is the largest of its kind to date, with 480 patients, conducted at 40 US centers, using device-specific endpoints. There was a “very high” intravascular imaging rate of 75% in a cohort with a high risk for in-stent restenosis, consisting of 50% of patients with diabetes and more than 40% with multiple stents.
“The main limitation is the choice of comparator,” Dr. Colleran said. Balloon angioplasty is inferior to both stenting and drug coated balloon therapy for treatment of in-stent restenosis but is the standard of care in the United States, she noted. “I think...for regulatory reasons this was the comparator chosen,” she said.
“I think the implications are clear,” Dr. Colleran added. “This trial should provide a basis for regulatory approval of the drug coated balloon treatment of in-stent restenosis in the U.S. and finally provide this as an available treatment option for such patients.”
Dr. Yeh reported receiving grant/research support from Abbott Vascular, BD Bard, Boston Scientific, Cook Medical, Philips Medical, and Medtronic, and consulting for Abbott Vascular, Boston Scientific, CathWorks, Elixir Medical, Infraredx, Medtronic, Shockwave Medical, and Zol. Dr. Colleran had no disclosures. The trial was supported by Boston Scientific.
A version of this article first appeared on Medscape.com.
AT TCT 2023
Genetic therapies bring change to neurology clinics
PHOENIX – New therapies are on the horizon for genetic neuromuscular diseases, and this will raise both hopes for patients and challenges for neurologists. , according to Nicolas Madigan, MBBCh, PhD, who spoke at the 2023 annual meeting of the American Association for Neuromuscular and Electrodiagnostic Medicine (AANEM).
“I think we will very soon be in a position to tell these patients that they might actually have a better treatment outcome with a genetic treatment than if they had a sporadic or inflammatory disorder,” said Dr. Madigan, who is an assistant professor of clinical research at Mayo Clinic, Rochester, N.Y.
To illustrate how genetic therapies are changing neurology practice, Dr. Madigan focused his talk on CMT neuropathy, which is the most common hereditary neuropathy and, as a result, has become a prime focus of gene therapy development. “In a city of about a million people, there will be 100-800 patients with one of these disorders,” said Dr. Madigan.
Case report illustrates a change in approach
There are more than 100 known genes that can contribute to CMT, but about 90% of patients harbor alterations in one of four genes: PMP22, GJB1, MFN2, and MPZ.
The trick is determining which patients are candidates for genetic testing, according to Dr. Madigan. He presented a case report of a 39-year-old woman who had experienced sensory symptoms for years, with a sudden exacerbation along with allodynia following COVID-19 vaccination. Her cerebrospinal fluid protein was high and outside electromyography indicated mild demyelinating neuropathy, consistent with chronic inflammatory demyelinating polyradiculoneuropathy (CIDP). After her insurance denied IVIG treatment, she received solumedrol, but her symptoms worsened and she was referred to Dr. Madigan.
After 6 months of methotrexate treatment, her sensory symptoms had not improved, and she was referred for genetic testing, which revealed a truncating mutation of the MPZ gene. “What I learned from this case really was that, in a young patient with conduction slowing, you might be considering CIDP. It might actually be better to do genetic testing first as opposed to starting inflammatory neuropathy type treatments with respect to cost – the genetic tests costs $300 versus tens of thousands of dollars for IVIG – and for [patient] welfare as well,” said Dr. Madigan.
Specifically, when clinical signs point to inherited neuropathy and there is conduction slowing, “the biggest bang for your buck might to be to go straight to PMP22 deletion or duplication testing and see if you can get a diagnosis. If that is negative or the clinical features are not as you might suspect, then, if you have other supportive features such as a very young age or there’s predominance of motor or sensory symptoms, you could test more broadly with a panel. If both of these are negative, then you could consider exome sequencing if the clinical phenotype really is consistent with that,” said Dr. Madigan.
The treatment landscape
With a diagnosis in hand, it’s possible to turn to treatment options, and the CMT landscape is promising. Dr. Madigan’s group recently reviewed 286 CMT clinical trials published between 1999 and 2022, 86% of which were interventions. Most were procedures based on carpal or cubital tunnel release, extracorporeal shockwave therapy, or nerve hydrodissection.
The small-molecule drug combination PXT3003 (Pharnext) – comprising baclofen, naltrexone, and sorbitol – downregulated PMP22 mRNA expression and led to improved myelination in animal models. It is currently being studied in a phase 2 clinical trial. Other approaches include supplements, stem cells, anesthetics, and various devices.
Genetic therapy is in the preclinical stage, including gene replacement using adeno-associated virus (AAV) vectors, gene silencing using antisense oligonucleotides or RNA interference, and gene editing using CRISPR-Cas 9 approaches.
Gene replacement strategies include delivering a normal copy of the gene, a supportive gene, or a gene that delays or reduces axon degeneration. Gene silencing targets PMP22, while CRISPR-Cas9 gene editing aims for PMP22 or neurofilament light polypeptide (NEFL) gene knockout.
The most clinically advanced AAV program delivers neurotrophin-3 via the viral vector to the target muscle, which has been demonstrated to improve symptoms in a mouse model using a muscle-specific promoter. A phase 1/2a trial will test the approach in three patients.
In the antisense space, chemical advances have improved the profile of the RNA, including modifications that influence inflammatory properties, stability, and targeting of specific tissues through conjugation to specific lipids, proteins, or antibodies. A 2018 study sponsored by DTxPharma showed that the formulation could improve outcomes and histologic myelination in a mouse model. In the wake of Novartis’s acquisition of the technology, Dr. Madigan anticipates that clinical trials will likely begin in 2024.
Finally, CRISPR-Cas9 targeting of a promoter region that leads to PMP22 transcription improved remyelination and electrophysiological parameters after injection into the sciatic nerve of mice.
A need for genetic counseling
Advances in testing and therapies represent exciting developments, but they also create a need for genetic counselors, according to Dr. Madigan. His clinic has two certified genetic counselors who meet with patients and discuss testing options, including risks and benefits to family members. The counselors also provide psychological support and assist in shared decision-making. They also handle testing paperwork, which eases the burden on physicians.
If the tests are negative, the genetic counselor informs the patient and lets them know of any additional testing required. In case of a positive test, the genetic counselor informs the patient, but the physician also makes contact to discuss clinical implications of the result. “I think it’s working extremely well, and I would encourage all practices to begin to explore those options moving forward,” said Dr. Madigan.
During the Q&A session after the talk, an audience member noted that genetic counselors are not covered by insurance, which places a financial burden on providers to hire them. He noted that his facility has a large clinical genomics department that was able to fund the two counselors, though they are both part-time. “It wasn’t easy. I think there was at least a year of trying to work out how to do it in terms of finding positions and negotiating, but I think once it’s accomplished it’s incredibly cost effective in terms of getting patients what they need from that perspective, and helping with the testing,” said Dr. Madigan.
Dr. Madigan reported no relevant financial disclosures.
PHOENIX – New therapies are on the horizon for genetic neuromuscular diseases, and this will raise both hopes for patients and challenges for neurologists. , according to Nicolas Madigan, MBBCh, PhD, who spoke at the 2023 annual meeting of the American Association for Neuromuscular and Electrodiagnostic Medicine (AANEM).
“I think we will very soon be in a position to tell these patients that they might actually have a better treatment outcome with a genetic treatment than if they had a sporadic or inflammatory disorder,” said Dr. Madigan, who is an assistant professor of clinical research at Mayo Clinic, Rochester, N.Y.
To illustrate how genetic therapies are changing neurology practice, Dr. Madigan focused his talk on CMT neuropathy, which is the most common hereditary neuropathy and, as a result, has become a prime focus of gene therapy development. “In a city of about a million people, there will be 100-800 patients with one of these disorders,” said Dr. Madigan.
Case report illustrates a change in approach
There are more than 100 known genes that can contribute to CMT, but about 90% of patients harbor alterations in one of four genes: PMP22, GJB1, MFN2, and MPZ.
The trick is determining which patients are candidates for genetic testing, according to Dr. Madigan. He presented a case report of a 39-year-old woman who had experienced sensory symptoms for years, with a sudden exacerbation along with allodynia following COVID-19 vaccination. Her cerebrospinal fluid protein was high and outside electromyography indicated mild demyelinating neuropathy, consistent with chronic inflammatory demyelinating polyradiculoneuropathy (CIDP). After her insurance denied IVIG treatment, she received solumedrol, but her symptoms worsened and she was referred to Dr. Madigan.
After 6 months of methotrexate treatment, her sensory symptoms had not improved, and she was referred for genetic testing, which revealed a truncating mutation of the MPZ gene. “What I learned from this case really was that, in a young patient with conduction slowing, you might be considering CIDP. It might actually be better to do genetic testing first as opposed to starting inflammatory neuropathy type treatments with respect to cost – the genetic tests costs $300 versus tens of thousands of dollars for IVIG – and for [patient] welfare as well,” said Dr. Madigan.
Specifically, when clinical signs point to inherited neuropathy and there is conduction slowing, “the biggest bang for your buck might to be to go straight to PMP22 deletion or duplication testing and see if you can get a diagnosis. If that is negative or the clinical features are not as you might suspect, then, if you have other supportive features such as a very young age or there’s predominance of motor or sensory symptoms, you could test more broadly with a panel. If both of these are negative, then you could consider exome sequencing if the clinical phenotype really is consistent with that,” said Dr. Madigan.
The treatment landscape
With a diagnosis in hand, it’s possible to turn to treatment options, and the CMT landscape is promising. Dr. Madigan’s group recently reviewed 286 CMT clinical trials published between 1999 and 2022, 86% of which were interventions. Most were procedures based on carpal or cubital tunnel release, extracorporeal shockwave therapy, or nerve hydrodissection.
The small-molecule drug combination PXT3003 (Pharnext) – comprising baclofen, naltrexone, and sorbitol – downregulated PMP22 mRNA expression and led to improved myelination in animal models. It is currently being studied in a phase 2 clinical trial. Other approaches include supplements, stem cells, anesthetics, and various devices.
Genetic therapy is in the preclinical stage, including gene replacement using adeno-associated virus (AAV) vectors, gene silencing using antisense oligonucleotides or RNA interference, and gene editing using CRISPR-Cas 9 approaches.
Gene replacement strategies include delivering a normal copy of the gene, a supportive gene, or a gene that delays or reduces axon degeneration. Gene silencing targets PMP22, while CRISPR-Cas9 gene editing aims for PMP22 or neurofilament light polypeptide (NEFL) gene knockout.
The most clinically advanced AAV program delivers neurotrophin-3 via the viral vector to the target muscle, which has been demonstrated to improve symptoms in a mouse model using a muscle-specific promoter. A phase 1/2a trial will test the approach in three patients.
In the antisense space, chemical advances have improved the profile of the RNA, including modifications that influence inflammatory properties, stability, and targeting of specific tissues through conjugation to specific lipids, proteins, or antibodies. A 2018 study sponsored by DTxPharma showed that the formulation could improve outcomes and histologic myelination in a mouse model. In the wake of Novartis’s acquisition of the technology, Dr. Madigan anticipates that clinical trials will likely begin in 2024.
Finally, CRISPR-Cas9 targeting of a promoter region that leads to PMP22 transcription improved remyelination and electrophysiological parameters after injection into the sciatic nerve of mice.
A need for genetic counseling
Advances in testing and therapies represent exciting developments, but they also create a need for genetic counselors, according to Dr. Madigan. His clinic has two certified genetic counselors who meet with patients and discuss testing options, including risks and benefits to family members. The counselors also provide psychological support and assist in shared decision-making. They also handle testing paperwork, which eases the burden on physicians.
If the tests are negative, the genetic counselor informs the patient and lets them know of any additional testing required. In case of a positive test, the genetic counselor informs the patient, but the physician also makes contact to discuss clinical implications of the result. “I think it’s working extremely well, and I would encourage all practices to begin to explore those options moving forward,” said Dr. Madigan.
During the Q&A session after the talk, an audience member noted that genetic counselors are not covered by insurance, which places a financial burden on providers to hire them. He noted that his facility has a large clinical genomics department that was able to fund the two counselors, though they are both part-time. “It wasn’t easy. I think there was at least a year of trying to work out how to do it in terms of finding positions and negotiating, but I think once it’s accomplished it’s incredibly cost effective in terms of getting patients what they need from that perspective, and helping with the testing,” said Dr. Madigan.
Dr. Madigan reported no relevant financial disclosures.
PHOENIX – New therapies are on the horizon for genetic neuromuscular diseases, and this will raise both hopes for patients and challenges for neurologists. , according to Nicolas Madigan, MBBCh, PhD, who spoke at the 2023 annual meeting of the American Association for Neuromuscular and Electrodiagnostic Medicine (AANEM).
“I think we will very soon be in a position to tell these patients that they might actually have a better treatment outcome with a genetic treatment than if they had a sporadic or inflammatory disorder,” said Dr. Madigan, who is an assistant professor of clinical research at Mayo Clinic, Rochester, N.Y.
To illustrate how genetic therapies are changing neurology practice, Dr. Madigan focused his talk on CMT neuropathy, which is the most common hereditary neuropathy and, as a result, has become a prime focus of gene therapy development. “In a city of about a million people, there will be 100-800 patients with one of these disorders,” said Dr. Madigan.
Case report illustrates a change in approach
There are more than 100 known genes that can contribute to CMT, but about 90% of patients harbor alterations in one of four genes: PMP22, GJB1, MFN2, and MPZ.
The trick is determining which patients are candidates for genetic testing, according to Dr. Madigan. He presented a case report of a 39-year-old woman who had experienced sensory symptoms for years, with a sudden exacerbation along with allodynia following COVID-19 vaccination. Her cerebrospinal fluid protein was high and outside electromyography indicated mild demyelinating neuropathy, consistent with chronic inflammatory demyelinating polyradiculoneuropathy (CIDP). After her insurance denied IVIG treatment, she received solumedrol, but her symptoms worsened and she was referred to Dr. Madigan.
After 6 months of methotrexate treatment, her sensory symptoms had not improved, and she was referred for genetic testing, which revealed a truncating mutation of the MPZ gene. “What I learned from this case really was that, in a young patient with conduction slowing, you might be considering CIDP. It might actually be better to do genetic testing first as opposed to starting inflammatory neuropathy type treatments with respect to cost – the genetic tests costs $300 versus tens of thousands of dollars for IVIG – and for [patient] welfare as well,” said Dr. Madigan.
Specifically, when clinical signs point to inherited neuropathy and there is conduction slowing, “the biggest bang for your buck might to be to go straight to PMP22 deletion or duplication testing and see if you can get a diagnosis. If that is negative or the clinical features are not as you might suspect, then, if you have other supportive features such as a very young age or there’s predominance of motor or sensory symptoms, you could test more broadly with a panel. If both of these are negative, then you could consider exome sequencing if the clinical phenotype really is consistent with that,” said Dr. Madigan.
The treatment landscape
With a diagnosis in hand, it’s possible to turn to treatment options, and the CMT landscape is promising. Dr. Madigan’s group recently reviewed 286 CMT clinical trials published between 1999 and 2022, 86% of which were interventions. Most were procedures based on carpal or cubital tunnel release, extracorporeal shockwave therapy, or nerve hydrodissection.
The small-molecule drug combination PXT3003 (Pharnext) – comprising baclofen, naltrexone, and sorbitol – downregulated PMP22 mRNA expression and led to improved myelination in animal models. It is currently being studied in a phase 2 clinical trial. Other approaches include supplements, stem cells, anesthetics, and various devices.
Genetic therapy is in the preclinical stage, including gene replacement using adeno-associated virus (AAV) vectors, gene silencing using antisense oligonucleotides or RNA interference, and gene editing using CRISPR-Cas 9 approaches.
Gene replacement strategies include delivering a normal copy of the gene, a supportive gene, or a gene that delays or reduces axon degeneration. Gene silencing targets PMP22, while CRISPR-Cas9 gene editing aims for PMP22 or neurofilament light polypeptide (NEFL) gene knockout.
The most clinically advanced AAV program delivers neurotrophin-3 via the viral vector to the target muscle, which has been demonstrated to improve symptoms in a mouse model using a muscle-specific promoter. A phase 1/2a trial will test the approach in three patients.
In the antisense space, chemical advances have improved the profile of the RNA, including modifications that influence inflammatory properties, stability, and targeting of specific tissues through conjugation to specific lipids, proteins, or antibodies. A 2018 study sponsored by DTxPharma showed that the formulation could improve outcomes and histologic myelination in a mouse model. In the wake of Novartis’s acquisition of the technology, Dr. Madigan anticipates that clinical trials will likely begin in 2024.
Finally, CRISPR-Cas9 targeting of a promoter region that leads to PMP22 transcription improved remyelination and electrophysiological parameters after injection into the sciatic nerve of mice.
A need for genetic counseling
Advances in testing and therapies represent exciting developments, but they also create a need for genetic counselors, according to Dr. Madigan. His clinic has two certified genetic counselors who meet with patients and discuss testing options, including risks and benefits to family members. The counselors also provide psychological support and assist in shared decision-making. They also handle testing paperwork, which eases the burden on physicians.
If the tests are negative, the genetic counselor informs the patient and lets them know of any additional testing required. In case of a positive test, the genetic counselor informs the patient, but the physician also makes contact to discuss clinical implications of the result. “I think it’s working extremely well, and I would encourage all practices to begin to explore those options moving forward,” said Dr. Madigan.
During the Q&A session after the talk, an audience member noted that genetic counselors are not covered by insurance, which places a financial burden on providers to hire them. He noted that his facility has a large clinical genomics department that was able to fund the two counselors, though they are both part-time. “It wasn’t easy. I think there was at least a year of trying to work out how to do it in terms of finding positions and negotiating, but I think once it’s accomplished it’s incredibly cost effective in terms of getting patients what they need from that perspective, and helping with the testing,” said Dr. Madigan.
Dr. Madigan reported no relevant financial disclosures.
At AANEM 2023
Adverse events related to embryo transfer catheters may be underreported to the FDA
, according to a new study presented at the American Society for Reproductive Medicine’s 2023 meeting.
ETCs are medical devices used routinely in assisted reproduction. The findings highlight the need for increased vigilance in tracking and reporting adverse events associated with these devices, according to the investigators.
“With hundreds of thousands of embryo transfers being performed per year, surveillance of the safety, performance, and quality of embryo transfer catheter devices is critical and should not be taken for granted,” said Anita Madison, MD, MPH, from the division of reproductive endocrinology and infertility at Johns Hopkins School of Medicine, Baltimore, who led the study. “There are a variety of transfer catheters with different indications, with little data on the superiority and safety of the brands compared to one another.”
Although the number of reported adverse events associated with ETCs is relatively small, the problems can significantly affect patient care, the researchers said.
Dr. Madison and her colleagues used the Manufacturer and User Facility Device Experience (MAUDE) database to identify adverse events associated with ETC devices. The MAUDE database is a voluntary reporting system that holds hundreds of thousands of medical device reports of suspected device-associated deaths, injuries, and malfunctions reported to the FDA annually.
For each adverse event in the database linked to an ECT, the researchers collected information related to the brand of the device, the nature of the event, and the nature of the reporter. The researchers omitted the device and manufacturer names from the presentation of the study findings, delineating them only as “Brand 1,” “Brand 2,” “Brand 3,” “Brand 4,” or “Other.”
Problems with devices included contamination, packaging problems, malfunction, mechanical flaws, and material separation. Patient-level adverse events included retaining of foreign body, trauma, malfunction, or failed embryo transfer.
Between 2014 and 2023, Dr. Madison and her colleagues identified 101 adverse events associated with ECTs in the database. About 25% of these occurred in 2018, with 27 cases reported. Contamination was the most prevalent problem, found in 68 reports; oil was the most common contaminant.
The distribution of types of adverse events varied, depending on ETC brand. A breakdown of occurrences revealed high numbers for Brand 2, with 52 adverse events. Although Brand 3 accounted for only 16 adverse events, the majority of these were related to device separation.
“That finding stood out,” Dr. Madison said.
Nearly 1 in 4 (22%) of all reported incidents led to overt patient harm. Retention of a foreign body was the prime type of injury, occurring in 12 cases. Malfunction and injury were found in four cases each, with two failed embryo transfers reported, Dr. Madison said.
Because the majority of these adverse event reports were submitted by manufacturers (87%) and were rarely submitted by end users (for example, physicians, lab staff), the researchers said their findings likely underestimate such problems.
“I’m surprised the [number of reported adverse events] is as low as it is,” said Kimball Pomeroy, PhD, scientific director at the World Egg and Sperm Bank, Scottsdale, Ariz., who was not part of the study team. “Laboratories are required to report failed devices; they have to have a plan for that.”

“It just comes down to underreporting,” added Valerie L. Baker, MD, director in the Division of Reproductive Endocrinology and Infertility at Johns Hopkins Medicine, Lutherville, Md., who was not affiliated with the study.
“In two of these reports, they failed to transfer the embryo; they actually lost the embryo,” Dr. Pomeroy added. “That’s drastic for those patients; it’s a serious problem that needs to be addressed.”
Citing these findings, the authors underscored the need for heightened surveillance of ETC devices and recommend further studies to assess the sensitivity of these procedures for attempting pregnancy. They urge physicians and lab staff involved in these procedures to exercise continued vigilance and to improve the reporting of problems with ETC devices.
Dr. Madison, Dr. Baker, and Dr. Pomeroy report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to a new study presented at the American Society for Reproductive Medicine’s 2023 meeting.
ETCs are medical devices used routinely in assisted reproduction. The findings highlight the need for increased vigilance in tracking and reporting adverse events associated with these devices, according to the investigators.
“With hundreds of thousands of embryo transfers being performed per year, surveillance of the safety, performance, and quality of embryo transfer catheter devices is critical and should not be taken for granted,” said Anita Madison, MD, MPH, from the division of reproductive endocrinology and infertility at Johns Hopkins School of Medicine, Baltimore, who led the study. “There are a variety of transfer catheters with different indications, with little data on the superiority and safety of the brands compared to one another.”
Although the number of reported adverse events associated with ETCs is relatively small, the problems can significantly affect patient care, the researchers said.
Dr. Madison and her colleagues used the Manufacturer and User Facility Device Experience (MAUDE) database to identify adverse events associated with ETC devices. The MAUDE database is a voluntary reporting system that holds hundreds of thousands of medical device reports of suspected device-associated deaths, injuries, and malfunctions reported to the FDA annually.
For each adverse event in the database linked to an ECT, the researchers collected information related to the brand of the device, the nature of the event, and the nature of the reporter. The researchers omitted the device and manufacturer names from the presentation of the study findings, delineating them only as “Brand 1,” “Brand 2,” “Brand 3,” “Brand 4,” or “Other.”
Problems with devices included contamination, packaging problems, malfunction, mechanical flaws, and material separation. Patient-level adverse events included retaining of foreign body, trauma, malfunction, or failed embryo transfer.
Between 2014 and 2023, Dr. Madison and her colleagues identified 101 adverse events associated with ECTs in the database. About 25% of these occurred in 2018, with 27 cases reported. Contamination was the most prevalent problem, found in 68 reports; oil was the most common contaminant.
The distribution of types of adverse events varied, depending on ETC brand. A breakdown of occurrences revealed high numbers for Brand 2, with 52 adverse events. Although Brand 3 accounted for only 16 adverse events, the majority of these were related to device separation.
“That finding stood out,” Dr. Madison said.
Nearly 1 in 4 (22%) of all reported incidents led to overt patient harm. Retention of a foreign body was the prime type of injury, occurring in 12 cases. Malfunction and injury were found in four cases each, with two failed embryo transfers reported, Dr. Madison said.
Because the majority of these adverse event reports were submitted by manufacturers (87%) and were rarely submitted by end users (for example, physicians, lab staff), the researchers said their findings likely underestimate such problems.
“I’m surprised the [number of reported adverse events] is as low as it is,” said Kimball Pomeroy, PhD, scientific director at the World Egg and Sperm Bank, Scottsdale, Ariz., who was not part of the study team. “Laboratories are required to report failed devices; they have to have a plan for that.”
“It just comes down to underreporting,” added Valerie L. Baker, MD, director in the Division of Reproductive Endocrinology and Infertility at Johns Hopkins Medicine, Lutherville, Md., who was not affiliated with the study.
“In two of these reports, they failed to transfer the embryo; they actually lost the embryo,” Dr. Pomeroy added. “That’s drastic for those patients; it’s a serious problem that needs to be addressed.”
Citing these findings, the authors underscored the need for heightened surveillance of ETC devices and recommend further studies to assess the sensitivity of these procedures for attempting pregnancy. They urge physicians and lab staff involved in these procedures to exercise continued vigilance and to improve the reporting of problems with ETC devices.
Dr. Madison, Dr. Baker, and Dr. Pomeroy report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to a new study presented at the American Society for Reproductive Medicine’s 2023 meeting.
ETCs are medical devices used routinely in assisted reproduction. The findings highlight the need for increased vigilance in tracking and reporting adverse events associated with these devices, according to the investigators.
“With hundreds of thousands of embryo transfers being performed per year, surveillance of the safety, performance, and quality of embryo transfer catheter devices is critical and should not be taken for granted,” said Anita Madison, MD, MPH, from the division of reproductive endocrinology and infertility at Johns Hopkins School of Medicine, Baltimore, who led the study. “There are a variety of transfer catheters with different indications, with little data on the superiority and safety of the brands compared to one another.”
Although the number of reported adverse events associated with ETCs is relatively small, the problems can significantly affect patient care, the researchers said.
Dr. Madison and her colleagues used the Manufacturer and User Facility Device Experience (MAUDE) database to identify adverse events associated with ETC devices. The MAUDE database is a voluntary reporting system that holds hundreds of thousands of medical device reports of suspected device-associated deaths, injuries, and malfunctions reported to the FDA annually.
For each adverse event in the database linked to an ECT, the researchers collected information related to the brand of the device, the nature of the event, and the nature of the reporter. The researchers omitted the device and manufacturer names from the presentation of the study findings, delineating them only as “Brand 1,” “Brand 2,” “Brand 3,” “Brand 4,” or “Other.”
Problems with devices included contamination, packaging problems, malfunction, mechanical flaws, and material separation. Patient-level adverse events included retaining of foreign body, trauma, malfunction, or failed embryo transfer.
Between 2014 and 2023, Dr. Madison and her colleagues identified 101 adverse events associated with ECTs in the database. About 25% of these occurred in 2018, with 27 cases reported. Contamination was the most prevalent problem, found in 68 reports; oil was the most common contaminant.
The distribution of types of adverse events varied, depending on ETC brand. A breakdown of occurrences revealed high numbers for Brand 2, with 52 adverse events. Although Brand 3 accounted for only 16 adverse events, the majority of these were related to device separation.
“That finding stood out,” Dr. Madison said.
Nearly 1 in 4 (22%) of all reported incidents led to overt patient harm. Retention of a foreign body was the prime type of injury, occurring in 12 cases. Malfunction and injury were found in four cases each, with two failed embryo transfers reported, Dr. Madison said.
Because the majority of these adverse event reports were submitted by manufacturers (87%) and were rarely submitted by end users (for example, physicians, lab staff), the researchers said their findings likely underestimate such problems.
“I’m surprised the [number of reported adverse events] is as low as it is,” said Kimball Pomeroy, PhD, scientific director at the World Egg and Sperm Bank, Scottsdale, Ariz., who was not part of the study team. “Laboratories are required to report failed devices; they have to have a plan for that.”
“It just comes down to underreporting,” added Valerie L. Baker, MD, director in the Division of Reproductive Endocrinology and Infertility at Johns Hopkins Medicine, Lutherville, Md., who was not affiliated with the study.
“In two of these reports, they failed to transfer the embryo; they actually lost the embryo,” Dr. Pomeroy added. “That’s drastic for those patients; it’s a serious problem that needs to be addressed.”
Citing these findings, the authors underscored the need for heightened surveillance of ETC devices and recommend further studies to assess the sensitivity of these procedures for attempting pregnancy. They urge physicians and lab staff involved in these procedures to exercise continued vigilance and to improve the reporting of problems with ETC devices.
Dr. Madison, Dr. Baker, and Dr. Pomeroy report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ASRM 2023
Digital tool clarifies menopause symptoms
GLASGOW – An interactive digital decision tool that individualizes menopause care received praise from primary care clinicians in the United Kingdom, who said it could improve patient care and streamline office visits.
“Access to hormone replacement therapy [HRT], as well as decision-making around treatment for menopausal symptoms, is often complicated by concerns around its safety, and there is still a knowledge and a confidence gap among health care professionals causing reluctance to prescribe HRT,” said Aini Kamal, MSc, from University College London. Ms. Kamal presented results of a survey about the tool at the annual meeting of the Royal College of General Practitioners.
For the study, Ms. Kamal, Daniel Reisel, MBBS, PhD, a gynecologist at UCL, and colleagues evaluated Wellspring with doctors, nurses, and pharmacists.
“Ensuring that women receive education around symptoms, so that they are empowered, is a key part of optimizing their care and sharing decision-making,” Dr. Reisel said in an interview. He added that U.K. primary care had seen an increase in cases of women presenting with symptoms associated with the perimenopause and menopause at a time when U.K. Members of Parliament are debating whether to make it mandatory for all women to have menopause check-up in their early 40s.
The online survey was completed by 280 participants, and respondents were primarily GPs with several years of relevant prescribing practice. Of those, 93% found information from national guidelines to be accurately presented in the tool, and 97% said they would recommend this decision aid to other health care professionals, Ms. Kamal reported.
Nearly all participants said they could see themselves using the tool with patients in the clinic or as an adjunct to virtual sessions. “This [finding] was particularly important because it demonstrates the clinical potential this tool has,” she said.
One consult, too many problems
Louise Newson, MBChB, who runs the U.K.’s largest menopause clinic, said primary care appointments are often time-pressured and follow a “’one problem-one consultation’” policy. As such, women are often thinking ‘Do I go with my joint pains, or my palpitations, tinnitus, or what?’ If a patient presents with tinnitus, a doctor might focus on the potential of an inner ear problem rather than a hormone deficiency, but I do know that if the woman is perimenopausal or menopausal, we often look to replace the missing hormones, and then if the tinnitus doesn’t improve we can revisit the ear problem.”
Dr. Newson noted that 17% of women in her clinics have had more than six GP visits in the year before she sees them, but in the year following, this figure drops to 1%. Acknowledging that a menopause consultation for a GP is time-consuming, Dr. Newson pointed out that taking time initially with the patient “means it will reduce the number of future consultations quickly, but more importantly, we also know that taking HRT reduces long-term risk of serious diseases, including heart disease and osteoporosis.”
The digital tool can be used by both doctors and patients to help women work through their symptoms and equip them with knowledge so their GP visits are more productive.
“When we see women who are empowered with knowledge [about menopause symptoms], then the consultations are quicker and essentially place the patient central to the discussion,” Dr. Newson said.
Ed Russell-Smith, MBChB, a GP in Scotland who moderated the session, said the tool “lays out a nicely structured approach and provides modern treatment options and resources for patients.”
However, he added “we also need to remember there are potential harms to be done from HRT too. It’s vitally important that while patients might see HRT as a panacea, doctors need to balance this with the risks involved for each individual. As a tool, I think Wellspring can help us in this respect to apply general principles to that patient and individualize treatment.”
Dr. Reisel, Dr. Newson, Ms. Kamal, and Dr. Russell-Smith disclosed no relevant financial relationships. The Wellspring Decision Aid was supported by UCL’s Institute for Women’s Health. The Newson Health clinic is fully private, but research is done via the nonprofit arm, which is supported by the clinic. There is no pharma involvement.
A version of this article first appeared on Medscape.com.
GLASGOW – An interactive digital decision tool that individualizes menopause care received praise from primary care clinicians in the United Kingdom, who said it could improve patient care and streamline office visits.
“Access to hormone replacement therapy [HRT], as well as decision-making around treatment for menopausal symptoms, is often complicated by concerns around its safety, and there is still a knowledge and a confidence gap among health care professionals causing reluctance to prescribe HRT,” said Aini Kamal, MSc, from University College London. Ms. Kamal presented results of a survey about the tool at the annual meeting of the Royal College of General Practitioners.
For the study, Ms. Kamal, Daniel Reisel, MBBS, PhD, a gynecologist at UCL, and colleagues evaluated Wellspring with doctors, nurses, and pharmacists.
“Ensuring that women receive education around symptoms, so that they are empowered, is a key part of optimizing their care and sharing decision-making,” Dr. Reisel said in an interview. He added that U.K. primary care had seen an increase in cases of women presenting with symptoms associated with the perimenopause and menopause at a time when U.K. Members of Parliament are debating whether to make it mandatory for all women to have menopause check-up in their early 40s.
The online survey was completed by 280 participants, and respondents were primarily GPs with several years of relevant prescribing practice. Of those, 93% found information from national guidelines to be accurately presented in the tool, and 97% said they would recommend this decision aid to other health care professionals, Ms. Kamal reported.
Nearly all participants said they could see themselves using the tool with patients in the clinic or as an adjunct to virtual sessions. “This [finding] was particularly important because it demonstrates the clinical potential this tool has,” she said.
One consult, too many problems
Louise Newson, MBChB, who runs the U.K.’s largest menopause clinic, said primary care appointments are often time-pressured and follow a “’one problem-one consultation’” policy. As such, women are often thinking ‘Do I go with my joint pains, or my palpitations, tinnitus, or what?’ If a patient presents with tinnitus, a doctor might focus on the potential of an inner ear problem rather than a hormone deficiency, but I do know that if the woman is perimenopausal or menopausal, we often look to replace the missing hormones, and then if the tinnitus doesn’t improve we can revisit the ear problem.”
Dr. Newson noted that 17% of women in her clinics have had more than six GP visits in the year before she sees them, but in the year following, this figure drops to 1%. Acknowledging that a menopause consultation for a GP is time-consuming, Dr. Newson pointed out that taking time initially with the patient “means it will reduce the number of future consultations quickly, but more importantly, we also know that taking HRT reduces long-term risk of serious diseases, including heart disease and osteoporosis.”
The digital tool can be used by both doctors and patients to help women work through their symptoms and equip them with knowledge so their GP visits are more productive.
“When we see women who are empowered with knowledge [about menopause symptoms], then the consultations are quicker and essentially place the patient central to the discussion,” Dr. Newson said.
Ed Russell-Smith, MBChB, a GP in Scotland who moderated the session, said the tool “lays out a nicely structured approach and provides modern treatment options and resources for patients.”
However, he added “we also need to remember there are potential harms to be done from HRT too. It’s vitally important that while patients might see HRT as a panacea, doctors need to balance this with the risks involved for each individual. As a tool, I think Wellspring can help us in this respect to apply general principles to that patient and individualize treatment.”
Dr. Reisel, Dr. Newson, Ms. Kamal, and Dr. Russell-Smith disclosed no relevant financial relationships. The Wellspring Decision Aid was supported by UCL’s Institute for Women’s Health. The Newson Health clinic is fully private, but research is done via the nonprofit arm, which is supported by the clinic. There is no pharma involvement.
A version of this article first appeared on Medscape.com.
GLASGOW – An interactive digital decision tool that individualizes menopause care received praise from primary care clinicians in the United Kingdom, who said it could improve patient care and streamline office visits.
“Access to hormone replacement therapy [HRT], as well as decision-making around treatment for menopausal symptoms, is often complicated by concerns around its safety, and there is still a knowledge and a confidence gap among health care professionals causing reluctance to prescribe HRT,” said Aini Kamal, MSc, from University College London. Ms. Kamal presented results of a survey about the tool at the annual meeting of the Royal College of General Practitioners.
For the study, Ms. Kamal, Daniel Reisel, MBBS, PhD, a gynecologist at UCL, and colleagues evaluated Wellspring with doctors, nurses, and pharmacists.
“Ensuring that women receive education around symptoms, so that they are empowered, is a key part of optimizing their care and sharing decision-making,” Dr. Reisel said in an interview. He added that U.K. primary care had seen an increase in cases of women presenting with symptoms associated with the perimenopause and menopause at a time when U.K. Members of Parliament are debating whether to make it mandatory for all women to have menopause check-up in their early 40s.
The online survey was completed by 280 participants, and respondents were primarily GPs with several years of relevant prescribing practice. Of those, 93% found information from national guidelines to be accurately presented in the tool, and 97% said they would recommend this decision aid to other health care professionals, Ms. Kamal reported.
Nearly all participants said they could see themselves using the tool with patients in the clinic or as an adjunct to virtual sessions. “This [finding] was particularly important because it demonstrates the clinical potential this tool has,” she said.
One consult, too many problems
Louise Newson, MBChB, who runs the U.K.’s largest menopause clinic, said primary care appointments are often time-pressured and follow a “’one problem-one consultation’” policy. As such, women are often thinking ‘Do I go with my joint pains, or my palpitations, tinnitus, or what?’ If a patient presents with tinnitus, a doctor might focus on the potential of an inner ear problem rather than a hormone deficiency, but I do know that if the woman is perimenopausal or menopausal, we often look to replace the missing hormones, and then if the tinnitus doesn’t improve we can revisit the ear problem.”
Dr. Newson noted that 17% of women in her clinics have had more than six GP visits in the year before she sees them, but in the year following, this figure drops to 1%. Acknowledging that a menopause consultation for a GP is time-consuming, Dr. Newson pointed out that taking time initially with the patient “means it will reduce the number of future consultations quickly, but more importantly, we also know that taking HRT reduces long-term risk of serious diseases, including heart disease and osteoporosis.”
The digital tool can be used by both doctors and patients to help women work through their symptoms and equip them with knowledge so their GP visits are more productive.
“When we see women who are empowered with knowledge [about menopause symptoms], then the consultations are quicker and essentially place the patient central to the discussion,” Dr. Newson said.
Ed Russell-Smith, MBChB, a GP in Scotland who moderated the session, said the tool “lays out a nicely structured approach and provides modern treatment options and resources for patients.”
However, he added “we also need to remember there are potential harms to be done from HRT too. It’s vitally important that while patients might see HRT as a panacea, doctors need to balance this with the risks involved for each individual. As a tool, I think Wellspring can help us in this respect to apply general principles to that patient and individualize treatment.”
Dr. Reisel, Dr. Newson, Ms. Kamal, and Dr. Russell-Smith disclosed no relevant financial relationships. The Wellspring Decision Aid was supported by UCL’s Institute for Women’s Health. The Newson Health clinic is fully private, but research is done via the nonprofit arm, which is supported by the clinic. There is no pharma involvement.
A version of this article first appeared on Medscape.com.
AT RCGP 2023
Popular liver supplements lack data supporting efficacy, study shows
The 10 best-selling liver health supplements on Amazon bring in an estimated $2.5 million each month. But none of them contain ingredients recommended by major groups of doctors who treat liver issues in the United States or Europe.
Like many supplements, popular online liver products are unregulated, meaning they do not have to meet the same safety and effectiveness standards as prescription medications.
Sales of liver supplements are growing, particularly in the last few years, said Ahmed Eltelbany, MD, MPH, a first-year gastrointestinal fellow at the University of New Mexico. One reason could be increased alcohol use during the COVID-19 pandemic.
Some manufacturers make bold claims on Amazon, said Dr. Eltelbany, author of a study that looked into the supplements. “The most recurrent claims were that their supplements maintain normal liver function, are scientifically formulated, and – my personal favorite – are a highly effective liver detox formulation developed according to the latest scientific findings.”
Does natural mean safe?
Many supplements are marketed as “liver cleansing,” for “liver detox,” or for “liver support,” Dr. Eltelbany said as he presented the study results at the annual meeting of the American College of Gastroenterology.
“People take these supplements because they believe they’re natural and therefore they’re safe,” said Paul Y. Kwo, MD, who moderated a session on the study at the meeting, when asked to comment. “As I tell every patient in clinic, a great white shark is natural, a scorpion is natural, and so is a hurricane. So just because they’re natural doesn’t mean they’re safe.”
At the same time, “it’s not that every supplement is bad for you. Nonetheless, there’s just a dizzying array of these out there” said Dr. Kwo, a professor of medicine at Stanford Medicine in Redwood, Calif.
“We have to be very cautious,” he said. For example, some people might believe that “if a little bit of a supplement is good, a tremendous amount must be really good.” The antioxidant turmeric, for example, has a pretty good safety record, he said. But this past year, some liver toxicity concerns arose about preparations with “very, very high concentrations” of turmeric.
The top 10 sellers
Dr. Eltelbany and colleagues studied prices for 1-month supplies, monthly sales, and revenue for the top 10 liver supplements sold on Amazon on June 3, 2023:
Ranking by sales:
- 1. Liver Cleanse Detox & Repair Formula – Herbal Liver Supplement with Milk Thistle, Dandelion Root, Organic Turmeric and Artichoke Extract for Liver Health – Silymarin Milk Thistle Detox Capsules
- 2. Ancestral Supplements Grass Fed Beef Liver Capsules. Supports Energy Production, Detoxification, Digestion, Immunity and Full Body Wellness, Non-GMO, Freeze Dried Liver Health Supplement, 180 Capsules
- 3. Bronson Milk Thistle 1,000 mg Silymarin Marianum & Dandelion Root Liver Health Support, 120 Capsules
- 4. PUREHEALTH RESEARCH Liver Supplement – Herbal Liver Cleanse Detox & Repair with Milk Thistle, Artichoke Extract, Dandelion Root, Turmeric, Berberine to Healthy Liver Renew with 11 Natural Nutrients
- 5. TUDCA Bile Salts Liver Support Supplement, 500-mg Servings, Liver and Gallbladder Cleanse Supplement (60 Capsules 250 mg) Genuine Bile Acid. TUDCA Strong Bitter Taste by Double Wood
- 6. 28-in-1 Liver Cleanse Detox & Repair Fatty Liver Formula, Milk Thistle Silymarin, Artichoke Extract, Dandelion & Apple Cider Vinegar – Liver Health Supplement Support Pills – Vegan Capsules
- 7. Vita-Liver Liver Health Supplement – Support Liver Cleanse & Detox – Liquid Delivery for Absorption – Milk Thistle, Artichoke, Chanca Piedra, Dandelion & More
- 8. Liver Supplement with Milk Thistle, Liver Detox Formula, Artichoke and Turmeric. Supports Liver Health Defense & Liver Renew. Liver Cleanse Detox & Repair for Fatty Liver Support. 60 Capsules
- 9. Liver Cleanse Detox & Repair. Milk Thistle Extract with Silymarin 80%, Artichoke Extract, Dandelion Root, Chicory, 25+ Herbs – Premium Liver Health Formula, Liver Support Detox Health Formula – Liver Support Detox Cleanse Supplement
- 10. Arazo Nutrition Liver Cleanse Detox & Repair Formula – Milk Thistle Herbal Support Supplement: Silymarin, Beet, Artichoke, Dandelion, Chicory Root
The investigators found a total of 65 unique ingredients. “Most of these ingredients have historical uses linked to liver health. But our research revealed that strong scientific evidence supporting the efficacy of any of these supplements is currently lacking,” Dr. Eltelbany said. They started the study by creating a new account on Amazon to make sure the search would not be influenced by prior shopping or purchases. They next searched for supplements using the keywords “liver” and “cleanse.” To figure out sales numbers, they used the AMZScout proprietary analytics software that Amazon sellers use to track sales.
Reviewing the reviews
The researchers discovered an average 11,526 reviews for each supplement product. The average rating was 4.42 stars out of 5.
Using Fakespot.com, proprietary Amazon customer review software that analyzes the timing and language of reviews, they found that only 65% of product reviews were genuine.
“We felt it was crucial to vet the authenticity of customer feedback,” Dr. Eltelbany said.
Few other options?
Liver disease remains a persistent and significant global health burden. Despite advances in many areas of gastroenterology, there remains no curative treatment for liver cirrhosis, Dr. Eltelbany said.
The primary option for people with end-stage liver disease is a liver transplant. “However, given the scarcity of donors and the vast number of patients in need, many individuals, unfortunately, do not get a timely transplant,” he said. “This void of treatment options and the desperation to find relief often drives patients towards alternative therapies.”
Also, online shopping has made getting these supplements “as simple as a click away. But what’s more concerning is the trust placed in these products by our patients,” Dr. Eltelbany said.
“There’s a strong need for rigorous scientific investigation into the actual health benefits of any liver detox supplements,” he said. “Above all, patient education remains paramount, warning them of potential risks and unknowns of these supplements.”
A version of this article appeared on WebMD.com.
The 10 best-selling liver health supplements on Amazon bring in an estimated $2.5 million each month. But none of them contain ingredients recommended by major groups of doctors who treat liver issues in the United States or Europe.
Like many supplements, popular online liver products are unregulated, meaning they do not have to meet the same safety and effectiveness standards as prescription medications.
Sales of liver supplements are growing, particularly in the last few years, said Ahmed Eltelbany, MD, MPH, a first-year gastrointestinal fellow at the University of New Mexico. One reason could be increased alcohol use during the COVID-19 pandemic.
Some manufacturers make bold claims on Amazon, said Dr. Eltelbany, author of a study that looked into the supplements. “The most recurrent claims were that their supplements maintain normal liver function, are scientifically formulated, and – my personal favorite – are a highly effective liver detox formulation developed according to the latest scientific findings.”
Does natural mean safe?
Many supplements are marketed as “liver cleansing,” for “liver detox,” or for “liver support,” Dr. Eltelbany said as he presented the study results at the annual meeting of the American College of Gastroenterology.
“People take these supplements because they believe they’re natural and therefore they’re safe,” said Paul Y. Kwo, MD, who moderated a session on the study at the meeting, when asked to comment. “As I tell every patient in clinic, a great white shark is natural, a scorpion is natural, and so is a hurricane. So just because they’re natural doesn’t mean they’re safe.”
At the same time, “it’s not that every supplement is bad for you. Nonetheless, there’s just a dizzying array of these out there” said Dr. Kwo, a professor of medicine at Stanford Medicine in Redwood, Calif.
“We have to be very cautious,” he said. For example, some people might believe that “if a little bit of a supplement is good, a tremendous amount must be really good.” The antioxidant turmeric, for example, has a pretty good safety record, he said. But this past year, some liver toxicity concerns arose about preparations with “very, very high concentrations” of turmeric.
The top 10 sellers
Dr. Eltelbany and colleagues studied prices for 1-month supplies, monthly sales, and revenue for the top 10 liver supplements sold on Amazon on June 3, 2023:
Ranking by sales:
- 1. Liver Cleanse Detox & Repair Formula – Herbal Liver Supplement with Milk Thistle, Dandelion Root, Organic Turmeric and Artichoke Extract for Liver Health – Silymarin Milk Thistle Detox Capsules
- 2. Ancestral Supplements Grass Fed Beef Liver Capsules. Supports Energy Production, Detoxification, Digestion, Immunity and Full Body Wellness, Non-GMO, Freeze Dried Liver Health Supplement, 180 Capsules
- 3. Bronson Milk Thistle 1,000 mg Silymarin Marianum & Dandelion Root Liver Health Support, 120 Capsules
- 4. PUREHEALTH RESEARCH Liver Supplement – Herbal Liver Cleanse Detox & Repair with Milk Thistle, Artichoke Extract, Dandelion Root, Turmeric, Berberine to Healthy Liver Renew with 11 Natural Nutrients
- 5. TUDCA Bile Salts Liver Support Supplement, 500-mg Servings, Liver and Gallbladder Cleanse Supplement (60 Capsules 250 mg) Genuine Bile Acid. TUDCA Strong Bitter Taste by Double Wood
- 6. 28-in-1 Liver Cleanse Detox & Repair Fatty Liver Formula, Milk Thistle Silymarin, Artichoke Extract, Dandelion & Apple Cider Vinegar – Liver Health Supplement Support Pills – Vegan Capsules
- 7. Vita-Liver Liver Health Supplement – Support Liver Cleanse & Detox – Liquid Delivery for Absorption – Milk Thistle, Artichoke, Chanca Piedra, Dandelion & More
- 8. Liver Supplement with Milk Thistle, Liver Detox Formula, Artichoke and Turmeric. Supports Liver Health Defense & Liver Renew. Liver Cleanse Detox & Repair for Fatty Liver Support. 60 Capsules
- 9. Liver Cleanse Detox & Repair. Milk Thistle Extract with Silymarin 80%, Artichoke Extract, Dandelion Root, Chicory, 25+ Herbs – Premium Liver Health Formula, Liver Support Detox Health Formula – Liver Support Detox Cleanse Supplement
- 10. Arazo Nutrition Liver Cleanse Detox & Repair Formula – Milk Thistle Herbal Support Supplement: Silymarin, Beet, Artichoke, Dandelion, Chicory Root
The investigators found a total of 65 unique ingredients. “Most of these ingredients have historical uses linked to liver health. But our research revealed that strong scientific evidence supporting the efficacy of any of these supplements is currently lacking,” Dr. Eltelbany said. They started the study by creating a new account on Amazon to make sure the search would not be influenced by prior shopping or purchases. They next searched for supplements using the keywords “liver” and “cleanse.” To figure out sales numbers, they used the AMZScout proprietary analytics software that Amazon sellers use to track sales.
Reviewing the reviews
The researchers discovered an average 11,526 reviews for each supplement product. The average rating was 4.42 stars out of 5.
Using Fakespot.com, proprietary Amazon customer review software that analyzes the timing and language of reviews, they found that only 65% of product reviews were genuine.
“We felt it was crucial to vet the authenticity of customer feedback,” Dr. Eltelbany said.
Few other options?
Liver disease remains a persistent and significant global health burden. Despite advances in many areas of gastroenterology, there remains no curative treatment for liver cirrhosis, Dr. Eltelbany said.
The primary option for people with end-stage liver disease is a liver transplant. “However, given the scarcity of donors and the vast number of patients in need, many individuals, unfortunately, do not get a timely transplant,” he said. “This void of treatment options and the desperation to find relief often drives patients towards alternative therapies.”
Also, online shopping has made getting these supplements “as simple as a click away. But what’s more concerning is the trust placed in these products by our patients,” Dr. Eltelbany said.
“There’s a strong need for rigorous scientific investigation into the actual health benefits of any liver detox supplements,” he said. “Above all, patient education remains paramount, warning them of potential risks and unknowns of these supplements.”
A version of this article appeared on WebMD.com.
The 10 best-selling liver health supplements on Amazon bring in an estimated $2.5 million each month. But none of them contain ingredients recommended by major groups of doctors who treat liver issues in the United States or Europe.
Like many supplements, popular online liver products are unregulated, meaning they do not have to meet the same safety and effectiveness standards as prescription medications.
Sales of liver supplements are growing, particularly in the last few years, said Ahmed Eltelbany, MD, MPH, a first-year gastrointestinal fellow at the University of New Mexico. One reason could be increased alcohol use during the COVID-19 pandemic.
Some manufacturers make bold claims on Amazon, said Dr. Eltelbany, author of a study that looked into the supplements. “The most recurrent claims were that their supplements maintain normal liver function, are scientifically formulated, and – my personal favorite – are a highly effective liver detox formulation developed according to the latest scientific findings.”
Does natural mean safe?
Many supplements are marketed as “liver cleansing,” for “liver detox,” or for “liver support,” Dr. Eltelbany said as he presented the study results at the annual meeting of the American College of Gastroenterology.
“People take these supplements because they believe they’re natural and therefore they’re safe,” said Paul Y. Kwo, MD, who moderated a session on the study at the meeting, when asked to comment. “As I tell every patient in clinic, a great white shark is natural, a scorpion is natural, and so is a hurricane. So just because they’re natural doesn’t mean they’re safe.”
At the same time, “it’s not that every supplement is bad for you. Nonetheless, there’s just a dizzying array of these out there” said Dr. Kwo, a professor of medicine at Stanford Medicine in Redwood, Calif.
“We have to be very cautious,” he said. For example, some people might believe that “if a little bit of a supplement is good, a tremendous amount must be really good.” The antioxidant turmeric, for example, has a pretty good safety record, he said. But this past year, some liver toxicity concerns arose about preparations with “very, very high concentrations” of turmeric.
The top 10 sellers
Dr. Eltelbany and colleagues studied prices for 1-month supplies, monthly sales, and revenue for the top 10 liver supplements sold on Amazon on June 3, 2023:
Ranking by sales:
- 1. Liver Cleanse Detox & Repair Formula – Herbal Liver Supplement with Milk Thistle, Dandelion Root, Organic Turmeric and Artichoke Extract for Liver Health – Silymarin Milk Thistle Detox Capsules
- 2. Ancestral Supplements Grass Fed Beef Liver Capsules. Supports Energy Production, Detoxification, Digestion, Immunity and Full Body Wellness, Non-GMO, Freeze Dried Liver Health Supplement, 180 Capsules
- 3. Bronson Milk Thistle 1,000 mg Silymarin Marianum & Dandelion Root Liver Health Support, 120 Capsules
- 4. PUREHEALTH RESEARCH Liver Supplement – Herbal Liver Cleanse Detox & Repair with Milk Thistle, Artichoke Extract, Dandelion Root, Turmeric, Berberine to Healthy Liver Renew with 11 Natural Nutrients
- 5. TUDCA Bile Salts Liver Support Supplement, 500-mg Servings, Liver and Gallbladder Cleanse Supplement (60 Capsules 250 mg) Genuine Bile Acid. TUDCA Strong Bitter Taste by Double Wood
- 6. 28-in-1 Liver Cleanse Detox & Repair Fatty Liver Formula, Milk Thistle Silymarin, Artichoke Extract, Dandelion & Apple Cider Vinegar – Liver Health Supplement Support Pills – Vegan Capsules
- 7. Vita-Liver Liver Health Supplement – Support Liver Cleanse & Detox – Liquid Delivery for Absorption – Milk Thistle, Artichoke, Chanca Piedra, Dandelion & More
- 8. Liver Supplement with Milk Thistle, Liver Detox Formula, Artichoke and Turmeric. Supports Liver Health Defense & Liver Renew. Liver Cleanse Detox & Repair for Fatty Liver Support. 60 Capsules
- 9. Liver Cleanse Detox & Repair. Milk Thistle Extract with Silymarin 80%, Artichoke Extract, Dandelion Root, Chicory, 25+ Herbs – Premium Liver Health Formula, Liver Support Detox Health Formula – Liver Support Detox Cleanse Supplement
- 10. Arazo Nutrition Liver Cleanse Detox & Repair Formula – Milk Thistle Herbal Support Supplement: Silymarin, Beet, Artichoke, Dandelion, Chicory Root
The investigators found a total of 65 unique ingredients. “Most of these ingredients have historical uses linked to liver health. But our research revealed that strong scientific evidence supporting the efficacy of any of these supplements is currently lacking,” Dr. Eltelbany said. They started the study by creating a new account on Amazon to make sure the search would not be influenced by prior shopping or purchases. They next searched for supplements using the keywords “liver” and “cleanse.” To figure out sales numbers, they used the AMZScout proprietary analytics software that Amazon sellers use to track sales.
Reviewing the reviews
The researchers discovered an average 11,526 reviews for each supplement product. The average rating was 4.42 stars out of 5.
Using Fakespot.com, proprietary Amazon customer review software that analyzes the timing and language of reviews, they found that only 65% of product reviews were genuine.
“We felt it was crucial to vet the authenticity of customer feedback,” Dr. Eltelbany said.
Few other options?
Liver disease remains a persistent and significant global health burden. Despite advances in many areas of gastroenterology, there remains no curative treatment for liver cirrhosis, Dr. Eltelbany said.
The primary option for people with end-stage liver disease is a liver transplant. “However, given the scarcity of donors and the vast number of patients in need, many individuals, unfortunately, do not get a timely transplant,” he said. “This void of treatment options and the desperation to find relief often drives patients towards alternative therapies.”
Also, online shopping has made getting these supplements “as simple as a click away. But what’s more concerning is the trust placed in these products by our patients,” Dr. Eltelbany said.
“There’s a strong need for rigorous scientific investigation into the actual health benefits of any liver detox supplements,” he said. “Above all, patient education remains paramount, warning them of potential risks and unknowns of these supplements.”
A version of this article appeared on WebMD.com.
FROM ACG 2023
Five times greater suicide risk for trans, gender-diverse teens in ED
WASHINGTON – , according to a study presented at the annual meeting of the American Academy of Pediatrics.
“The take-home message here is this study emphasizes the importance of universal screening to identify gender-diverse youth at risk,” Amanda Burnside, PhD, assistant professor of psychiatry and behavioral sciences at Ann and Robert H. Lurie Children’s Hospital of Chicago and Northwestern University, told attendees. “We really need to develop robust strategies and systems to link better mental health services.”

Suicide rates in transgender and gender-diverse youth are exceptionally high among youth in the U.S., Dr. Burnside said during her presentation. For example, the 2022 LGBTQ health survey from the Trevor Project found that much higher percentages of transgender and gender nonconforming youth had considered suicide in the past year compared with cisgender youth, even within the LGBTQ umbrella. Among nearly 34,000 LGBTQ youth aged 13-24, nearly half of trans females (48%) and more than half of trans males (59%) had considered suicide, compared with 28% of cisgender males and 37% of cisgender females. The rate among nonbinary/genderqueer individuals was 53%, and it was 48% for those questioning their gender.
Current methods of identifying trans and gender-diverse (TGD) youth in the hospital, however, may not actually be capturing the entire population.
“In health care settings, research involving TGD individuals has historically been limited to specialized clinic populations or youth with gender-specific diagnostic codes documented in the electronic medical record,” an approach that “likely significantly underestimates the prevalence of TGD youth in health care settings.” While at least one study has attempted to bridge this gap by searching the EMR for keywords, that study only tried to identify trans youth and not other youth on the gender diversity spectrum, such as nonbinary youth or those questioning their gender identity. Dr. Burnside and her colleagues therefore designed a study that used keywords to identify both trans youth and other gender-diverse youth who visited the ED so they could assess the rate of positive suicide screens in this population.
Underestimating the population at risk?
The researchers conducted a retrospective cross-sectional study of EMR data for all ED visits during which the patient underwent suicide screening. For the period of November 2019 to August 2022, they collected data on the screening results and the patient’s gender identity, age, race/ethnicity, insurance status, chief complaint in the ED and child opportunity index, which assess a youth’s access to resources based on geography. The suicide screener used was the Ask Suicide–Screening Questions (ASQ) tool.
The keywords they looked for in the EMR to identify trans and gender-diverse youth included transgender, pronouns, agender, gender dysphoria, male-to-female, female-to-male, nonbinary, preferred name, and they/them (captured as a complete term, not as “they” and “them” separately).
“If a keyword was present, the surrounding text was extracted and reviewed by two members of our team,” Dr. Burnside explained in her presentation. “We categorized keywords into either indicative of gender-diverse identity or not, and if it wasn’t clear based on the text extracted, we would conduct a manual chart review,” though that only occurred in about 3% of cases, she added.
Among 15,413 ED encounters with a suicide screen, the researchers identified 1,126 of these keywords in the EMR, among which 91.2% were classified as referring to a gender-diverse patient. Nearly all of the words were at least 90% effective in identify a gender-diverse youth, Dr. Burnside said, and all of the 197 instances of “they/them” were classified as gender diverse.
The accuracy was a little lower for the two keywords that appeared most frequently: For “pronouns,” 86.3% of 306 instances were classified as gender diverse, and for “transgender,” 83.1% of 207 instances were classified as gender diverse. Since some providers ask all patients their pronouns, the presence of “pronouns” in the EMR alone did not necessarily indicate the patient was gender diverse, Dr. Burnside said. A common reason the term “transgender” occurred in the EMR of non–gender diverse patients is that the department’s list of crisis resources includes transgender hotlines.
After identifying all the keywords, the researchers determined how many of these occurred in unique ED encounters and removed those with incomplete screening. Overall, they found 565 encounters by 399 gender-diverse individuals who had a suicide screening, representing 4.6% of total visits. This percentage is slightly lower than recent population-based estimates of gender-diverse youth, the researchers noted.
This population ranged from 8 to 23 years old, and 43% were publicly insured. The chief complaint for most of the patients (77.5%) was a mental health one. They were predominantly White (43%) or Hispanic (35%), with 10% Black youth, 4% Asian youth, and 8% youth who were “other” or two or more races. About half (52%) lived in a neighborhood with a “low” or “very low” child opportunity index.
Within this population, 81% of the patients screened positive on the suicide screening, compared with 23% positive screens across all ED visits. One in ten (10%) gender-diverse youth had active suicidal ideation, compared with 3.4% of the rest of the ED patient population. The researchers calculated that gender-diverse youth had 5.35 times greater odds of screening positive than cisgender youth in the ED (95% confidence interval [CI] 8.7-15.92). Further, a quarter (25%) of the trans and gender-diverse youth who screened positive for suicide risk had come to the ED for a primary complaint unrelated to mental health.
“We had a kid who came in because he broke his arm who had active suicidal ideation,” study coauthor Jennifer A. Hoffmann, MD, assistant professor of pediatrics at the Ann & Robert H. Lurie Children’s Hospital of Chicago and Northwestern University, mentioned after the presentation. That particular patient even had a suicide plan, but was identified as actively suicidal only because of the screening. In other cases, she said, a youth may come in with self-inflicted injuries, and while those are the primary complaint, they are linked with suicidal ideation.

Among the study’s limitations are that gender identity is not necessarily being systematically assessed during visits, misspellings might have missed some youth, and their search strategy has not yet been externally validated, though they plan to seek that.
“Overall, however, this study did demonstrate that keyword searching is a promising technique to identify and prioritize gender-diverse youth in health services research,” Dr. Burnside said. In addition to showing the feasibility of using a keyword search strategy for identifying gender-diverse youth, Dr. Burnside noted that 31% of the encounters were identified by just one of the keywords they used, “highlighting the importance of using a comprehensive list of keywords to identify gender-diverse youth.”
Uncovering valuable information
Jason Rafferty, MD, MPH, EdM, clinical assistant professor of pediatrics and of psychiatry and human behavior at Brown University, Providence, R.I., who attended the presentation, noted that the study provides information on a population that’s often difficult to get through traditional EMR research methods.

“A lot of medical record systems don’t have uniform ways of capturing [gender diversity], but what we know as providers is that kids are really struggling and that it’s not a surprise that we’re seeing these disparities with suicidality,” Dr. Rafferty said.
The study also provides more discrete estimates by age than what most other current research measures, which tends to be lifetime suicidality as opposed to suicidal thoughts or attempts within the past year, Dr. Rafferty added.
”What this shows is, for adolescents, the risk of suicide is something we need to be paying attention to. Because it’s not that it’s something that only happens in adults, this really dispels a lot of the misquoting of the data that’s out there.” That kind of information is valuable for determining resource allocation, he said. “A disparity like this really underlies the importance of mental health resources in this field,” he said.
Dr. Burnside, Dr. Hoffmann, and Dr. Rafferty had no disclosures, and no external funding sources were noted.
WASHINGTON – , according to a study presented at the annual meeting of the American Academy of Pediatrics.
“The take-home message here is this study emphasizes the importance of universal screening to identify gender-diverse youth at risk,” Amanda Burnside, PhD, assistant professor of psychiatry and behavioral sciences at Ann and Robert H. Lurie Children’s Hospital of Chicago and Northwestern University, told attendees. “We really need to develop robust strategies and systems to link better mental health services.”
Suicide rates in transgender and gender-diverse youth are exceptionally high among youth in the U.S., Dr. Burnside said during her presentation. For example, the 2022 LGBTQ health survey from the Trevor Project found that much higher percentages of transgender and gender nonconforming youth had considered suicide in the past year compared with cisgender youth, even within the LGBTQ umbrella. Among nearly 34,000 LGBTQ youth aged 13-24, nearly half of trans females (48%) and more than half of trans males (59%) had considered suicide, compared with 28% of cisgender males and 37% of cisgender females. The rate among nonbinary/genderqueer individuals was 53%, and it was 48% for those questioning their gender.
Current methods of identifying trans and gender-diverse (TGD) youth in the hospital, however, may not actually be capturing the entire population.
“In health care settings, research involving TGD individuals has historically been limited to specialized clinic populations or youth with gender-specific diagnostic codes documented in the electronic medical record,” an approach that “likely significantly underestimates the prevalence of TGD youth in health care settings.” While at least one study has attempted to bridge this gap by searching the EMR for keywords, that study only tried to identify trans youth and not other youth on the gender diversity spectrum, such as nonbinary youth or those questioning their gender identity. Dr. Burnside and her colleagues therefore designed a study that used keywords to identify both trans youth and other gender-diverse youth who visited the ED so they could assess the rate of positive suicide screens in this population.
Underestimating the population at risk?
The researchers conducted a retrospective cross-sectional study of EMR data for all ED visits during which the patient underwent suicide screening. For the period of November 2019 to August 2022, they collected data on the screening results and the patient’s gender identity, age, race/ethnicity, insurance status, chief complaint in the ED and child opportunity index, which assess a youth’s access to resources based on geography. The suicide screener used was the Ask Suicide–Screening Questions (ASQ) tool.
The keywords they looked for in the EMR to identify trans and gender-diverse youth included transgender, pronouns, agender, gender dysphoria, male-to-female, female-to-male, nonbinary, preferred name, and they/them (captured as a complete term, not as “they” and “them” separately).
“If a keyword was present, the surrounding text was extracted and reviewed by two members of our team,” Dr. Burnside explained in her presentation. “We categorized keywords into either indicative of gender-diverse identity or not, and if it wasn’t clear based on the text extracted, we would conduct a manual chart review,” though that only occurred in about 3% of cases, she added.
Among 15,413 ED encounters with a suicide screen, the researchers identified 1,126 of these keywords in the EMR, among which 91.2% were classified as referring to a gender-diverse patient. Nearly all of the words were at least 90% effective in identify a gender-diverse youth, Dr. Burnside said, and all of the 197 instances of “they/them” were classified as gender diverse.
The accuracy was a little lower for the two keywords that appeared most frequently: For “pronouns,” 86.3% of 306 instances were classified as gender diverse, and for “transgender,” 83.1% of 207 instances were classified as gender diverse. Since some providers ask all patients their pronouns, the presence of “pronouns” in the EMR alone did not necessarily indicate the patient was gender diverse, Dr. Burnside said. A common reason the term “transgender” occurred in the EMR of non–gender diverse patients is that the department’s list of crisis resources includes transgender hotlines.
After identifying all the keywords, the researchers determined how many of these occurred in unique ED encounters and removed those with incomplete screening. Overall, they found 565 encounters by 399 gender-diverse individuals who had a suicide screening, representing 4.6% of total visits. This percentage is slightly lower than recent population-based estimates of gender-diverse youth, the researchers noted.
This population ranged from 8 to 23 years old, and 43% were publicly insured. The chief complaint for most of the patients (77.5%) was a mental health one. They were predominantly White (43%) or Hispanic (35%), with 10% Black youth, 4% Asian youth, and 8% youth who were “other” or two or more races. About half (52%) lived in a neighborhood with a “low” or “very low” child opportunity index.
Within this population, 81% of the patients screened positive on the suicide screening, compared with 23% positive screens across all ED visits. One in ten (10%) gender-diverse youth had active suicidal ideation, compared with 3.4% of the rest of the ED patient population. The researchers calculated that gender-diverse youth had 5.35 times greater odds of screening positive than cisgender youth in the ED (95% confidence interval [CI] 8.7-15.92). Further, a quarter (25%) of the trans and gender-diverse youth who screened positive for suicide risk had come to the ED for a primary complaint unrelated to mental health.
“We had a kid who came in because he broke his arm who had active suicidal ideation,” study coauthor Jennifer A. Hoffmann, MD, assistant professor of pediatrics at the Ann & Robert H. Lurie Children’s Hospital of Chicago and Northwestern University, mentioned after the presentation. That particular patient even had a suicide plan, but was identified as actively suicidal only because of the screening. In other cases, she said, a youth may come in with self-inflicted injuries, and while those are the primary complaint, they are linked with suicidal ideation.
Among the study’s limitations are that gender identity is not necessarily being systematically assessed during visits, misspellings might have missed some youth, and their search strategy has not yet been externally validated, though they plan to seek that.
“Overall, however, this study did demonstrate that keyword searching is a promising technique to identify and prioritize gender-diverse youth in health services research,” Dr. Burnside said. In addition to showing the feasibility of using a keyword search strategy for identifying gender-diverse youth, Dr. Burnside noted that 31% of the encounters were identified by just one of the keywords they used, “highlighting the importance of using a comprehensive list of keywords to identify gender-diverse youth.”
Uncovering valuable information
Jason Rafferty, MD, MPH, EdM, clinical assistant professor of pediatrics and of psychiatry and human behavior at Brown University, Providence, R.I., who attended the presentation, noted that the study provides information on a population that’s often difficult to get through traditional EMR research methods.
“A lot of medical record systems don’t have uniform ways of capturing [gender diversity], but what we know as providers is that kids are really struggling and that it’s not a surprise that we’re seeing these disparities with suicidality,” Dr. Rafferty said.
The study also provides more discrete estimates by age than what most other current research measures, which tends to be lifetime suicidality as opposed to suicidal thoughts or attempts within the past year, Dr. Rafferty added.
”What this shows is, for adolescents, the risk of suicide is something we need to be paying attention to. Because it’s not that it’s something that only happens in adults, this really dispels a lot of the misquoting of the data that’s out there.” That kind of information is valuable for determining resource allocation, he said. “A disparity like this really underlies the importance of mental health resources in this field,” he said.
Dr. Burnside, Dr. Hoffmann, and Dr. Rafferty had no disclosures, and no external funding sources were noted.
WASHINGTON – , according to a study presented at the annual meeting of the American Academy of Pediatrics.
“The take-home message here is this study emphasizes the importance of universal screening to identify gender-diverse youth at risk,” Amanda Burnside, PhD, assistant professor of psychiatry and behavioral sciences at Ann and Robert H. Lurie Children’s Hospital of Chicago and Northwestern University, told attendees. “We really need to develop robust strategies and systems to link better mental health services.”
Suicide rates in transgender and gender-diverse youth are exceptionally high among youth in the U.S., Dr. Burnside said during her presentation. For example, the 2022 LGBTQ health survey from the Trevor Project found that much higher percentages of transgender and gender nonconforming youth had considered suicide in the past year compared with cisgender youth, even within the LGBTQ umbrella. Among nearly 34,000 LGBTQ youth aged 13-24, nearly half of trans females (48%) and more than half of trans males (59%) had considered suicide, compared with 28% of cisgender males and 37% of cisgender females. The rate among nonbinary/genderqueer individuals was 53%, and it was 48% for those questioning their gender.
Current methods of identifying trans and gender-diverse (TGD) youth in the hospital, however, may not actually be capturing the entire population.
“In health care settings, research involving TGD individuals has historically been limited to specialized clinic populations or youth with gender-specific diagnostic codes documented in the electronic medical record,” an approach that “likely significantly underestimates the prevalence of TGD youth in health care settings.” While at least one study has attempted to bridge this gap by searching the EMR for keywords, that study only tried to identify trans youth and not other youth on the gender diversity spectrum, such as nonbinary youth or those questioning their gender identity. Dr. Burnside and her colleagues therefore designed a study that used keywords to identify both trans youth and other gender-diverse youth who visited the ED so they could assess the rate of positive suicide screens in this population.
Underestimating the population at risk?
The researchers conducted a retrospective cross-sectional study of EMR data for all ED visits during which the patient underwent suicide screening. For the period of November 2019 to August 2022, they collected data on the screening results and the patient’s gender identity, age, race/ethnicity, insurance status, chief complaint in the ED and child opportunity index, which assess a youth’s access to resources based on geography. The suicide screener used was the Ask Suicide–Screening Questions (ASQ) tool.
The keywords they looked for in the EMR to identify trans and gender-diverse youth included transgender, pronouns, agender, gender dysphoria, male-to-female, female-to-male, nonbinary, preferred name, and they/them (captured as a complete term, not as “they” and “them” separately).
“If a keyword was present, the surrounding text was extracted and reviewed by two members of our team,” Dr. Burnside explained in her presentation. “We categorized keywords into either indicative of gender-diverse identity or not, and if it wasn’t clear based on the text extracted, we would conduct a manual chart review,” though that only occurred in about 3% of cases, she added.
Among 15,413 ED encounters with a suicide screen, the researchers identified 1,126 of these keywords in the EMR, among which 91.2% were classified as referring to a gender-diverse patient. Nearly all of the words were at least 90% effective in identify a gender-diverse youth, Dr. Burnside said, and all of the 197 instances of “they/them” were classified as gender diverse.
The accuracy was a little lower for the two keywords that appeared most frequently: For “pronouns,” 86.3% of 306 instances were classified as gender diverse, and for “transgender,” 83.1% of 207 instances were classified as gender diverse. Since some providers ask all patients their pronouns, the presence of “pronouns” in the EMR alone did not necessarily indicate the patient was gender diverse, Dr. Burnside said. A common reason the term “transgender” occurred in the EMR of non–gender diverse patients is that the department’s list of crisis resources includes transgender hotlines.
After identifying all the keywords, the researchers determined how many of these occurred in unique ED encounters and removed those with incomplete screening. Overall, they found 565 encounters by 399 gender-diverse individuals who had a suicide screening, representing 4.6% of total visits. This percentage is slightly lower than recent population-based estimates of gender-diverse youth, the researchers noted.
This population ranged from 8 to 23 years old, and 43% were publicly insured. The chief complaint for most of the patients (77.5%) was a mental health one. They were predominantly White (43%) or Hispanic (35%), with 10% Black youth, 4% Asian youth, and 8% youth who were “other” or two or more races. About half (52%) lived in a neighborhood with a “low” or “very low” child opportunity index.
Within this population, 81% of the patients screened positive on the suicide screening, compared with 23% positive screens across all ED visits. One in ten (10%) gender-diverse youth had active suicidal ideation, compared with 3.4% of the rest of the ED patient population. The researchers calculated that gender-diverse youth had 5.35 times greater odds of screening positive than cisgender youth in the ED (95% confidence interval [CI] 8.7-15.92). Further, a quarter (25%) of the trans and gender-diverse youth who screened positive for suicide risk had come to the ED for a primary complaint unrelated to mental health.
“We had a kid who came in because he broke his arm who had active suicidal ideation,” study coauthor Jennifer A. Hoffmann, MD, assistant professor of pediatrics at the Ann & Robert H. Lurie Children’s Hospital of Chicago and Northwestern University, mentioned after the presentation. That particular patient even had a suicide plan, but was identified as actively suicidal only because of the screening. In other cases, she said, a youth may come in with self-inflicted injuries, and while those are the primary complaint, they are linked with suicidal ideation.
Among the study’s limitations are that gender identity is not necessarily being systematically assessed during visits, misspellings might have missed some youth, and their search strategy has not yet been externally validated, though they plan to seek that.
“Overall, however, this study did demonstrate that keyword searching is a promising technique to identify and prioritize gender-diverse youth in health services research,” Dr. Burnside said. In addition to showing the feasibility of using a keyword search strategy for identifying gender-diverse youth, Dr. Burnside noted that 31% of the encounters were identified by just one of the keywords they used, “highlighting the importance of using a comprehensive list of keywords to identify gender-diverse youth.”
Uncovering valuable information
Jason Rafferty, MD, MPH, EdM, clinical assistant professor of pediatrics and of psychiatry and human behavior at Brown University, Providence, R.I., who attended the presentation, noted that the study provides information on a population that’s often difficult to get through traditional EMR research methods.
“A lot of medical record systems don’t have uniform ways of capturing [gender diversity], but what we know as providers is that kids are really struggling and that it’s not a surprise that we’re seeing these disparities with suicidality,” Dr. Rafferty said.
The study also provides more discrete estimates by age than what most other current research measures, which tends to be lifetime suicidality as opposed to suicidal thoughts or attempts within the past year, Dr. Rafferty added.
”What this shows is, for adolescents, the risk of suicide is something we need to be paying attention to. Because it’s not that it’s something that only happens in adults, this really dispels a lot of the misquoting of the data that’s out there.” That kind of information is valuable for determining resource allocation, he said. “A disparity like this really underlies the importance of mental health resources in this field,” he said.
Dr. Burnside, Dr. Hoffmann, and Dr. Rafferty had no disclosures, and no external funding sources were noted.
AT AAP 2023