User login
Online Diagnosis of Sexually Transmitted Infections? Ethicist Says We Are Nowhere Close
This transcript has been edited for clarity.
There has been a large amount of news lately about dating online and dating apps. Probably the most common way younger people find potential partners is to go online and see who’s there that they might want to meet.
Online dating is also notorious for being full of scammers. There are all kinds of people out there that you have to be careful of, who are trying to rip you off by saying, “Send me money, I’m in trouble,” or “Now that we have a relationship, will you support my particular entrepreneurial idea?” Certainly, dangers are there.
Another danger we don’t talk much about is meeting people who have sexually transmitted diseases. That’s been a problem before websites and before dating apps. I think the opportunity of meeting more people — strangers, people you don’t really know — who may not tell you the truth about their health, and particularly their sexual health, is really out there.
It’s always good medical advice to tell people to practice safe sex, and that often involves a man wearing a condom. It certainly is the case that we want to attend not just to the prevention of unwanted pregnancy but also to the transmission of diseases. I think it’s very important to tell women of reproductive age to get their HPV shot to try to reduce cancers in their reproductive systems, or sometimes in men — anal cancers, or even being a transmitter of disease.
Even then, certainly one wants to recommend that, in an age where some people are going to meet many partners that they don’t know well or don’t have much background with, it’s wise to try to prevent diseases using the vaccines we’ve got, using the contraceptive methods that will prevent disease transmission, and reminding people to ask about sex life.
I did come across a website that just startled me. It’s called HeHealth, and basically it says to men, if you are conscientious about your sex life, take a picture of your penis, send it to us, and we have doctors — I presume they’re US doctors but I don’t know — who will diagnose venereal diseases based on that picture. I presume women could also say, “Before we have sex, or now that we’re approaching that possibility, I want you to send a picture to this company on this website.”
Now, a couple of reminders. I think we all know this, but just because you’re not manifesting symptoms on your reproductive organs doesn’t mean you don’t have a sexual disease. It’s not a reliable measure. Yes, maybe you could have somebody say: “Oh, that looks nasty. I’m not sure you ought to have sex right now, and maybe you should go get some treatment.” This is going to miss many cases and is not a reliable indicator that your partner is safe in terms of not transmitting diseases to you.
It also isn’t clear what they do with these images. Do they keep them? Who can see them? Could they resell them? What sort of privacy protection have you got if you decide to use this?
There’s another issue here, which is, if they misdiagnose someone and you do catch a sexual disease, who’s liable? Can you go after them for using doctors who weren’t competent or transmitting images that weren’t really adequate because you didn’t know how to take that picture properly when you sent that off to them? There are many unknowns.
The bottom line is that we’re in a different world, I think, of romance. We’re in a world where some people are going to meet more partners. Some people are going to meet more strangers. One approach is to have us take pictures of ourselves, send them off to who knows where, and ask for a green light to go ahead and have sexual relations. I don’t think we’re anywhere close to being able to rely on that as a way to avoid the risks of unprotected sexual behavior.
We do know what to do in dealing with patients who are sexually active. First, we have to ask them. Then we’ve got to recommend available vaccinations to prevent the transmission of some cancers, the HPV vaccine. Then they need that reminder about safe sexual practices not only to protect against unwanted pregnancy, but still, in this day and age, to protect against syphilis, which is on the rise, plus HIV, gonorrhea, chlamydia, and other sexually transmissible diseases.
I’m not going to rely on the penis picture to make the world safe for sex. I think we have to still use the old-fashioned techniques of education and prevention to do the best we can.
Dr. Caplan is director of the Division of Medical Ethics at New York University Langone Medical Center, New York City. He reported conflicts of interest with Johnson & Johnson’s Panel for Compassionate Drug Use and Medscape.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
There has been a large amount of news lately about dating online and dating apps. Probably the most common way younger people find potential partners is to go online and see who’s there that they might want to meet.
Online dating is also notorious for being full of scammers. There are all kinds of people out there that you have to be careful of, who are trying to rip you off by saying, “Send me money, I’m in trouble,” or “Now that we have a relationship, will you support my particular entrepreneurial idea?” Certainly, dangers are there.
Another danger we don’t talk much about is meeting people who have sexually transmitted diseases. That’s been a problem before websites and before dating apps. I think the opportunity of meeting more people — strangers, people you don’t really know — who may not tell you the truth about their health, and particularly their sexual health, is really out there.
It’s always good medical advice to tell people to practice safe sex, and that often involves a man wearing a condom. It certainly is the case that we want to attend not just to the prevention of unwanted pregnancy but also to the transmission of diseases. I think it’s very important to tell women of reproductive age to get their HPV shot to try to reduce cancers in their reproductive systems, or sometimes in men — anal cancers, or even being a transmitter of disease.
Even then, certainly one wants to recommend that, in an age where some people are going to meet many partners that they don’t know well or don’t have much background with, it’s wise to try to prevent diseases using the vaccines we’ve got, using the contraceptive methods that will prevent disease transmission, and reminding people to ask about sex life.
I did come across a website that just startled me. It’s called HeHealth, and basically it says to men, if you are conscientious about your sex life, take a picture of your penis, send it to us, and we have doctors — I presume they’re US doctors but I don’t know — who will diagnose venereal diseases based on that picture. I presume women could also say, “Before we have sex, or now that we’re approaching that possibility, I want you to send a picture to this company on this website.”
Now, a couple of reminders. I think we all know this, but just because you’re not manifesting symptoms on your reproductive organs doesn’t mean you don’t have a sexual disease. It’s not a reliable measure. Yes, maybe you could have somebody say: “Oh, that looks nasty. I’m not sure you ought to have sex right now, and maybe you should go get some treatment.” This is going to miss many cases and is not a reliable indicator that your partner is safe in terms of not transmitting diseases to you.
It also isn’t clear what they do with these images. Do they keep them? Who can see them? Could they resell them? What sort of privacy protection have you got if you decide to use this?
There’s another issue here, which is, if they misdiagnose someone and you do catch a sexual disease, who’s liable? Can you go after them for using doctors who weren’t competent or transmitting images that weren’t really adequate because you didn’t know how to take that picture properly when you sent that off to them? There are many unknowns.
The bottom line is that we’re in a different world, I think, of romance. We’re in a world where some people are going to meet more partners. Some people are going to meet more strangers. One approach is to have us take pictures of ourselves, send them off to who knows where, and ask for a green light to go ahead and have sexual relations. I don’t think we’re anywhere close to being able to rely on that as a way to avoid the risks of unprotected sexual behavior.
We do know what to do in dealing with patients who are sexually active. First, we have to ask them. Then we’ve got to recommend available vaccinations to prevent the transmission of some cancers, the HPV vaccine. Then they need that reminder about safe sexual practices not only to protect against unwanted pregnancy, but still, in this day and age, to protect against syphilis, which is on the rise, plus HIV, gonorrhea, chlamydia, and other sexually transmissible diseases.
I’m not going to rely on the penis picture to make the world safe for sex. I think we have to still use the old-fashioned techniques of education and prevention to do the best we can.
Dr. Caplan is director of the Division of Medical Ethics at New York University Langone Medical Center, New York City. He reported conflicts of interest with Johnson & Johnson’s Panel for Compassionate Drug Use and Medscape.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
There has been a large amount of news lately about dating online and dating apps. Probably the most common way younger people find potential partners is to go online and see who’s there that they might want to meet.
Online dating is also notorious for being full of scammers. There are all kinds of people out there that you have to be careful of, who are trying to rip you off by saying, “Send me money, I’m in trouble,” or “Now that we have a relationship, will you support my particular entrepreneurial idea?” Certainly, dangers are there.
Another danger we don’t talk much about is meeting people who have sexually transmitted diseases. That’s been a problem before websites and before dating apps. I think the opportunity of meeting more people — strangers, people you don’t really know — who may not tell you the truth about their health, and particularly their sexual health, is really out there.
It’s always good medical advice to tell people to practice safe sex, and that often involves a man wearing a condom. It certainly is the case that we want to attend not just to the prevention of unwanted pregnancy but also to the transmission of diseases. I think it’s very important to tell women of reproductive age to get their HPV shot to try to reduce cancers in their reproductive systems, or sometimes in men — anal cancers, or even being a transmitter of disease.
Even then, certainly one wants to recommend that, in an age where some people are going to meet many partners that they don’t know well or don’t have much background with, it’s wise to try to prevent diseases using the vaccines we’ve got, using the contraceptive methods that will prevent disease transmission, and reminding people to ask about sex life.
I did come across a website that just startled me. It’s called HeHealth, and basically it says to men, if you are conscientious about your sex life, take a picture of your penis, send it to us, and we have doctors — I presume they’re US doctors but I don’t know — who will diagnose venereal diseases based on that picture. I presume women could also say, “Before we have sex, or now that we’re approaching that possibility, I want you to send a picture to this company on this website.”
Now, a couple of reminders. I think we all know this, but just because you’re not manifesting symptoms on your reproductive organs doesn’t mean you don’t have a sexual disease. It’s not a reliable measure. Yes, maybe you could have somebody say: “Oh, that looks nasty. I’m not sure you ought to have sex right now, and maybe you should go get some treatment.” This is going to miss many cases and is not a reliable indicator that your partner is safe in terms of not transmitting diseases to you.
It also isn’t clear what they do with these images. Do they keep them? Who can see them? Could they resell them? What sort of privacy protection have you got if you decide to use this?
There’s another issue here, which is, if they misdiagnose someone and you do catch a sexual disease, who’s liable? Can you go after them for using doctors who weren’t competent or transmitting images that weren’t really adequate because you didn’t know how to take that picture properly when you sent that off to them? There are many unknowns.
The bottom line is that we’re in a different world, I think, of romance. We’re in a world where some people are going to meet more partners. Some people are going to meet more strangers. One approach is to have us take pictures of ourselves, send them off to who knows where, and ask for a green light to go ahead and have sexual relations. I don’t think we’re anywhere close to being able to rely on that as a way to avoid the risks of unprotected sexual behavior.
We do know what to do in dealing with patients who are sexually active. First, we have to ask them. Then we’ve got to recommend available vaccinations to prevent the transmission of some cancers, the HPV vaccine. Then they need that reminder about safe sexual practices not only to protect against unwanted pregnancy, but still, in this day and age, to protect against syphilis, which is on the rise, plus HIV, gonorrhea, chlamydia, and other sexually transmissible diseases.
I’m not going to rely on the penis picture to make the world safe for sex. I think we have to still use the old-fashioned techniques of education and prevention to do the best we can.
Dr. Caplan is director of the Division of Medical Ethics at New York University Langone Medical Center, New York City. He reported conflicts of interest with Johnson & Johnson’s Panel for Compassionate Drug Use and Medscape.
A version of this article first appeared on Medscape.com.
Should You Offer Medical Credit Cards?
Editor’s note: This is Dr. Eastern’s last “Managing Your Practice” column for Dermatology News. After his first column was published in 1986, Dr. Eastern continued writing his column monthly until the mid-1990s, resuming in 2005. In total, he has written over 300 columns on topics relevant to medical practice, ranging from hiring employees, selling and merging practices, complying with OSHA, and avoiding embezzlement, to electronic health records, burnout, medical assistants, negative online reviews, artificial intelligence in the office, and more. In the future, he will continue to provide commentary on practice issues with an occasional guest editorial.
Medicare reimbursement cuts, increasing overhead and staff salaries, and inflation have made running a profitable private practice increasingly challenging, particularly for rural and smaller offices. Medical credit cards are an increasingly popular choice to fill this gap.

Traditionally, these cards were used to help cover procedures insurance didn’t cover — such as cosmetic procedures — but over the years, they have been expanded to cover other healthcare charges, mostly for patients who are paying out of pocket due to inadequate insurance or other reasons.
Advantages for physicians include immediate payment from the credit card company and reduced billing and collection costs. Patients are also less likely to delay or defer treatment if they can charge the payment and pay it back in installments.
The first step in offering medical credit cards is signing up with one or more third-party card companies. CareCredit is the most common provider in the medical credit card market. Other vendors include Wells Fargo, AccessOne, Alphaeon Credit, and iCare Financial. (As always, I have no financial interest in any product or service mentioned in this column.) A member of your staff signs patients up, and the credit card company checks their credit. If approved, the card company pays you your fee and assumes responsibility for collecting from the patient.
The interest charge on medical credit cards is often deferred for a period of time, typically between 6 and 24 months. If patients pay off the debt within this time, they can avoid paying interest. But, like other credit cards, if they make late payments or have an unpaid balance once the promotional period ends, they may end up with interest and fees totaling 25%-30% or more. It is important to make it very clear to your patients that payments are interest-free only if they are all made on time and within the promotional period.

According to a Consumer Financial Protection Bureau report released earlier this year, deferred interest medical credit cards or loans were used to pay nearly $23 billion in healthcare expenses from 2018 to 2020. Individuals unable to complete payment during the promotional period paid $1 billion in deferred interest payments during that period.
Despite the growing popularity of medical credit cards among physicians, it is worth noting that some consumer groups view them as predatory financial products, marketed toward people in tough financial situations. A coalition of 60 health advocacy groups has urged the Biden Administration to ban deferred interest medical credit cards. So there is that much more reason to choose candidates for medical credit cards carefully, and to make them fully aware of what obligations they are assuming.
Patients who do not think they can pay off the balance within the interest-free time frame should probably be advised to pursue an alternative payment method, such as using a conventional credit card, taking out a personal or home-equity loan, or borrowing from a retirement savings account. Some physicians are willing to negotiate a reduced fee for patients who agree to pay cash at the time of service.
Those who do choose to apply for a medical credit card should be informed of their options, which can vary considerably depending on the product and the third-party vendor. Some medical credit products can be used only for elective procedures, but some can be used more broadly for various medical expenses. Check to make sure that each patient’s financing option can be used for his or her desired medical service.
Some payment products can only be used at specific practices or groups, while others can be used at a variety of medical offices and hospitals. If a patient arrives with a medical credit card already in hand, confirm that it is one that your office accepts.
Interest rates generally vary with each card and vendor. Make patients aware of when interest rates start accruing and if the plan offers a fixed or variable APR, or if it charges compounding interest. Confirm if there is a deferred interest option, and if so, for how long.
Different medical credit products also have varying fees and payment schedules. See that each patient reads the terms of the agreement to understand when interest may start to accrue or change, as well as when certain fees may apply. Understanding when the payments are due will help them avoid additional fees, including late fees. Some medical payment plans may also have administrative or processing fees. If so, patients should be made aware of them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, New Jersey. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Editor’s note: This is Dr. Eastern’s last “Managing Your Practice” column for Dermatology News. After his first column was published in 1986, Dr. Eastern continued writing his column monthly until the mid-1990s, resuming in 2005. In total, he has written over 300 columns on topics relevant to medical practice, ranging from hiring employees, selling and merging practices, complying with OSHA, and avoiding embezzlement, to electronic health records, burnout, medical assistants, negative online reviews, artificial intelligence in the office, and more. In the future, he will continue to provide commentary on practice issues with an occasional guest editorial.
Medicare reimbursement cuts, increasing overhead and staff salaries, and inflation have made running a profitable private practice increasingly challenging, particularly for rural and smaller offices. Medical credit cards are an increasingly popular choice to fill this gap.
Traditionally, these cards were used to help cover procedures insurance didn’t cover — such as cosmetic procedures — but over the years, they have been expanded to cover other healthcare charges, mostly for patients who are paying out of pocket due to inadequate insurance or other reasons.
Advantages for physicians include immediate payment from the credit card company and reduced billing and collection costs. Patients are also less likely to delay or defer treatment if they can charge the payment and pay it back in installments.
The first step in offering medical credit cards is signing up with one or more third-party card companies. CareCredit is the most common provider in the medical credit card market. Other vendors include Wells Fargo, AccessOne, Alphaeon Credit, and iCare Financial. (As always, I have no financial interest in any product or service mentioned in this column.) A member of your staff signs patients up, and the credit card company checks their credit. If approved, the card company pays you your fee and assumes responsibility for collecting from the patient.
The interest charge on medical credit cards is often deferred for a period of time, typically between 6 and 24 months. If patients pay off the debt within this time, they can avoid paying interest. But, like other credit cards, if they make late payments or have an unpaid balance once the promotional period ends, they may end up with interest and fees totaling 25%-30% or more. It is important to make it very clear to your patients that payments are interest-free only if they are all made on time and within the promotional period.
According to a Consumer Financial Protection Bureau report released earlier this year, deferred interest medical credit cards or loans were used to pay nearly $23 billion in healthcare expenses from 2018 to 2020. Individuals unable to complete payment during the promotional period paid $1 billion in deferred interest payments during that period.
Despite the growing popularity of medical credit cards among physicians, it is worth noting that some consumer groups view them as predatory financial products, marketed toward people in tough financial situations. A coalition of 60 health advocacy groups has urged the Biden Administration to ban deferred interest medical credit cards. So there is that much more reason to choose candidates for medical credit cards carefully, and to make them fully aware of what obligations they are assuming.
Patients who do not think they can pay off the balance within the interest-free time frame should probably be advised to pursue an alternative payment method, such as using a conventional credit card, taking out a personal or home-equity loan, or borrowing from a retirement savings account. Some physicians are willing to negotiate a reduced fee for patients who agree to pay cash at the time of service.
Those who do choose to apply for a medical credit card should be informed of their options, which can vary considerably depending on the product and the third-party vendor. Some medical credit products can be used only for elective procedures, but some can be used more broadly for various medical expenses. Check to make sure that each patient’s financing option can be used for his or her desired medical service.
Some payment products can only be used at specific practices or groups, while others can be used at a variety of medical offices and hospitals. If a patient arrives with a medical credit card already in hand, confirm that it is one that your office accepts.
Interest rates generally vary with each card and vendor. Make patients aware of when interest rates start accruing and if the plan offers a fixed or variable APR, or if it charges compounding interest. Confirm if there is a deferred interest option, and if so, for how long.
Different medical credit products also have varying fees and payment schedules. See that each patient reads the terms of the agreement to understand when interest may start to accrue or change, as well as when certain fees may apply. Understanding when the payments are due will help them avoid additional fees, including late fees. Some medical payment plans may also have administrative or processing fees. If so, patients should be made aware of them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, New Jersey. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Editor’s note: This is Dr. Eastern’s last “Managing Your Practice” column for Dermatology News. After his first column was published in 1986, Dr. Eastern continued writing his column monthly until the mid-1990s, resuming in 2005. In total, he has written over 300 columns on topics relevant to medical practice, ranging from hiring employees, selling and merging practices, complying with OSHA, and avoiding embezzlement, to electronic health records, burnout, medical assistants, negative online reviews, artificial intelligence in the office, and more. In the future, he will continue to provide commentary on practice issues with an occasional guest editorial.
Medicare reimbursement cuts, increasing overhead and staff salaries, and inflation have made running a profitable private practice increasingly challenging, particularly for rural and smaller offices. Medical credit cards are an increasingly popular choice to fill this gap.
Traditionally, these cards were used to help cover procedures insurance didn’t cover — such as cosmetic procedures — but over the years, they have been expanded to cover other healthcare charges, mostly for patients who are paying out of pocket due to inadequate insurance or other reasons.
Advantages for physicians include immediate payment from the credit card company and reduced billing and collection costs. Patients are also less likely to delay or defer treatment if they can charge the payment and pay it back in installments.
The first step in offering medical credit cards is signing up with one or more third-party card companies. CareCredit is the most common provider in the medical credit card market. Other vendors include Wells Fargo, AccessOne, Alphaeon Credit, and iCare Financial. (As always, I have no financial interest in any product or service mentioned in this column.) A member of your staff signs patients up, and the credit card company checks their credit. If approved, the card company pays you your fee and assumes responsibility for collecting from the patient.
The interest charge on medical credit cards is often deferred for a period of time, typically between 6 and 24 months. If patients pay off the debt within this time, they can avoid paying interest. But, like other credit cards, if they make late payments or have an unpaid balance once the promotional period ends, they may end up with interest and fees totaling 25%-30% or more. It is important to make it very clear to your patients that payments are interest-free only if they are all made on time and within the promotional period.
According to a Consumer Financial Protection Bureau report released earlier this year, deferred interest medical credit cards or loans were used to pay nearly $23 billion in healthcare expenses from 2018 to 2020. Individuals unable to complete payment during the promotional period paid $1 billion in deferred interest payments during that period.
Despite the growing popularity of medical credit cards among physicians, it is worth noting that some consumer groups view them as predatory financial products, marketed toward people in tough financial situations. A coalition of 60 health advocacy groups has urged the Biden Administration to ban deferred interest medical credit cards. So there is that much more reason to choose candidates for medical credit cards carefully, and to make them fully aware of what obligations they are assuming.
Patients who do not think they can pay off the balance within the interest-free time frame should probably be advised to pursue an alternative payment method, such as using a conventional credit card, taking out a personal or home-equity loan, or borrowing from a retirement savings account. Some physicians are willing to negotiate a reduced fee for patients who agree to pay cash at the time of service.
Those who do choose to apply for a medical credit card should be informed of their options, which can vary considerably depending on the product and the third-party vendor. Some medical credit products can be used only for elective procedures, but some can be used more broadly for various medical expenses. Check to make sure that each patient’s financing option can be used for his or her desired medical service.
Some payment products can only be used at specific practices or groups, while others can be used at a variety of medical offices and hospitals. If a patient arrives with a medical credit card already in hand, confirm that it is one that your office accepts.
Interest rates generally vary with each card and vendor. Make patients aware of when interest rates start accruing and if the plan offers a fixed or variable APR, or if it charges compounding interest. Confirm if there is a deferred interest option, and if so, for how long.
Different medical credit products also have varying fees and payment schedules. See that each patient reads the terms of the agreement to understand when interest may start to accrue or change, as well as when certain fees may apply. Understanding when the payments are due will help them avoid additional fees, including late fees. Some medical payment plans may also have administrative or processing fees. If so, patients should be made aware of them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, New Jersey. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Pruritic, violaceous papules in a patient with renal cell carcinoma
Pembrolizumab (Keytruda) is a programmed cell death protein 1 (PD-1) blocking antibody used to treat different malignancies including melanoma, non–small cell lung cancer, and other advanced solid tumors and hematologic malignancies. and drug rash with eosinophilia and systemic symptoms (DRESS).
Lichen planus-like adverse drug reactions, as seen in this patient, are also referred to as lichenoid drug eruption or drug-induced lichen planus. This cutaneous reaction is one of the more rare side effects of pembrolizumab. It should be noted that in lichenoid reactions, keratinocytes expressing PD-L1 are particularly affected, leading to a dense CD4/CD8 positive lymphocytic infiltration in the basal layer, necrosis of keratinocytes, acanthosis, and hypergranulosis. Subsequently, the cutaneous adverse reaction is a target effect of the PD-1/PD-L1 pathway and not a general hypersensitivity reaction. Clinically, both lichen planus and lichenoid drug eruptions exhibit erythematous papules and plaques. Lichenoid drug eruptions, however, can be scaly, pruritic, and heal with more hyperpigmentation.
A skin biopsy revealed irregular epidermal hyperplasia with jagged rete ridges. Within the dermis, there was a lichenoid inflammatory cell infiltrate obscuring the dermal-epidermal junction. The inflammatory cell infiltrate contained lymphocytes, histiocytes, and eosinophils. A diagnosis of a lichen planus-like adverse drug reaction to pembrolizumab was favored.
If the reaction is mild, topical corticosteroids and oral antihistamines can help with the drug-induced lichen planus. For more severe cases, systemic steroids can be given to help ease the reaction. Physicians should be aware of potential adverse drug effects that can mimic other medical conditions.

The case and photo were submitted by Ms. Towe, Nova Southeastern University College of Osteopathic Medicine, Davie, Florida, and Dr. Berke, Three Rivers Dermatology, Coraopolis, Pennsylvania. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
Bansal A et al. Indian Dermatol Online J. 2023 Apr 4;14(3):391-4. doi: 10.4103/idoj.idoj_377_22.
Sethi A, Raj M. Cureus. 2021 Mar 8;13(3):e13768. doi: 10.7759/cureus.13768.
Pembrolizumab (Keytruda) is a programmed cell death protein 1 (PD-1) blocking antibody used to treat different malignancies including melanoma, non–small cell lung cancer, and other advanced solid tumors and hematologic malignancies. and drug rash with eosinophilia and systemic symptoms (DRESS).
Lichen planus-like adverse drug reactions, as seen in this patient, are also referred to as lichenoid drug eruption or drug-induced lichen planus. This cutaneous reaction is one of the more rare side effects of pembrolizumab. It should be noted that in lichenoid reactions, keratinocytes expressing PD-L1 are particularly affected, leading to a dense CD4/CD8 positive lymphocytic infiltration in the basal layer, necrosis of keratinocytes, acanthosis, and hypergranulosis. Subsequently, the cutaneous adverse reaction is a target effect of the PD-1/PD-L1 pathway and not a general hypersensitivity reaction. Clinically, both lichen planus and lichenoid drug eruptions exhibit erythematous papules and plaques. Lichenoid drug eruptions, however, can be scaly, pruritic, and heal with more hyperpigmentation.
A skin biopsy revealed irregular epidermal hyperplasia with jagged rete ridges. Within the dermis, there was a lichenoid inflammatory cell infiltrate obscuring the dermal-epidermal junction. The inflammatory cell infiltrate contained lymphocytes, histiocytes, and eosinophils. A diagnosis of a lichen planus-like adverse drug reaction to pembrolizumab was favored.
If the reaction is mild, topical corticosteroids and oral antihistamines can help with the drug-induced lichen planus. For more severe cases, systemic steroids can be given to help ease the reaction. Physicians should be aware of potential adverse drug effects that can mimic other medical conditions.
The case and photo were submitted by Ms. Towe, Nova Southeastern University College of Osteopathic Medicine, Davie, Florida, and Dr. Berke, Three Rivers Dermatology, Coraopolis, Pennsylvania. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
Bansal A et al. Indian Dermatol Online J. 2023 Apr 4;14(3):391-4. doi: 10.4103/idoj.idoj_377_22.
Sethi A, Raj M. Cureus. 2021 Mar 8;13(3):e13768. doi: 10.7759/cureus.13768.
Pembrolizumab (Keytruda) is a programmed cell death protein 1 (PD-1) blocking antibody used to treat different malignancies including melanoma, non–small cell lung cancer, and other advanced solid tumors and hematologic malignancies. and drug rash with eosinophilia and systemic symptoms (DRESS).
Lichen planus-like adverse drug reactions, as seen in this patient, are also referred to as lichenoid drug eruption or drug-induced lichen planus. This cutaneous reaction is one of the more rare side effects of pembrolizumab. It should be noted that in lichenoid reactions, keratinocytes expressing PD-L1 are particularly affected, leading to a dense CD4/CD8 positive lymphocytic infiltration in the basal layer, necrosis of keratinocytes, acanthosis, and hypergranulosis. Subsequently, the cutaneous adverse reaction is a target effect of the PD-1/PD-L1 pathway and not a general hypersensitivity reaction. Clinically, both lichen planus and lichenoid drug eruptions exhibit erythematous papules and plaques. Lichenoid drug eruptions, however, can be scaly, pruritic, and heal with more hyperpigmentation.
A skin biopsy revealed irregular epidermal hyperplasia with jagged rete ridges. Within the dermis, there was a lichenoid inflammatory cell infiltrate obscuring the dermal-epidermal junction. The inflammatory cell infiltrate contained lymphocytes, histiocytes, and eosinophils. A diagnosis of a lichen planus-like adverse drug reaction to pembrolizumab was favored.
If the reaction is mild, topical corticosteroids and oral antihistamines can help with the drug-induced lichen planus. For more severe cases, systemic steroids can be given to help ease the reaction. Physicians should be aware of potential adverse drug effects that can mimic other medical conditions.
The case and photo were submitted by Ms. Towe, Nova Southeastern University College of Osteopathic Medicine, Davie, Florida, and Dr. Berke, Three Rivers Dermatology, Coraopolis, Pennsylvania. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
Bansal A et al. Indian Dermatol Online J. 2023 Apr 4;14(3):391-4. doi: 10.4103/idoj.idoj_377_22.
Sethi A, Raj M. Cureus. 2021 Mar 8;13(3):e13768. doi: 10.7759/cureus.13768.

Managing Heart Failure in Women: Key Differences and Clinical Tips
This transcript has been edited for clarity.
Hi. I’m Dr Eileen Hsich. I’m the medical director for heart transplantation at the Cleveland Clinic, and my specialty is sex differences in heart failure. I’m excited to talk to you about heart failure treatment in women, addressing the differences in managing heart failure in women as well as practical tips for clinicians. You think that I’m going to be starting off by telling you about the differences in how we’re going to manage the patients, but I’m not. The reason I’m not going to do that is because our national guidelines are not sex specific.
What I’m really going to discuss with you today are the data so that you can decide for yourself what we should do and whether there really are differences. As we begin, I always think about the prevalence of the disease. Currently, there are 6.7 million Americans with heart failure, and approximately 45% of them are women. Globally, our best research shows that there are over 56 million people living with heart failure, and half of them are women.
We also know that there are different underlying causes in women and men. For women, the four risk factors are hypertension, diabetes, atrial fibrillation (AFib), and left bundle branch block. I know you knew about hypertension. Diabetes may not have been right up there in your mind. You see many women with AFib, so I know that you were thinking about it. We’re going to come back to left bundle branch block; it really is very interesting.
For men, it is the risk for heart failure development after a myocardial infarction. Men are more likely to have an ischemic cardiomyopathy. It is also important to state that when women have heart failure, it is often with more preserved ejection fraction. We know that heart failure with preserved ejection fraction (HFpEF) is more common in women and heart failure with reduced ejection fraction (HFrEF) is more common in men.
Now we’re going to talk about the four pillars in medical management, and we’re going to start out with the easy medications that show no sex differences in benefit. The mineralocorticoid receptor antagonists (MRAs) show that there are no sex differences in regard to benefit. Women benefit as much as men, based on two of the largest studies, which were the RALES study, which studied heart failure that was ischemic and nonischemic, and then the EPHESUS study, which was specific to patients who had myocardial infarction. There was a mortality benefit in the women.
The next set of drugs that we’re going to mention are the sodium-glucose cotransporter 2 (SGLT2) inhibitors. The combined endpoint for women and men was a combined endpoint of death and heart failure hospitalization. No matter what the ejection fraction was, women benefited like men for this drug.
The third class of agents that I want to discuss is the beta-blockers, which are really very interesting because they’re so powerful. The studies for these drugs were stopped prematurely. When you take into consideration that women are underenrolled in clinical trials, remember that the studies for these drugs were stopped, so there weren’t that many women. The fact that we showed a mortality benefit is really important.
The first drug that we’re going to refer to is bisoprolol because CIBIS II was the first trial for this drug to demonstrate a mortality benefit in women and men. The second drug that I want to mention is metoprolol XL, which did not demonstrate a mortality benefit in the MERIT-HF study, but did demonstrate a benefit in reduced heart failure hospitalizations, which is also very important.
The third drug is carvedilol, which had been shown to reduce a combined endpoint of mortality and heart failure hospitalizations for patients with moderate symptoms. When I talk about these studies, they have anywhere from 250 to 1000 women enrolled, so these are relatively small studies and they still did demonstrate a benefit.
When we talk about angiotensin receptor–neprilysin inhibitors (ARNI), I think that’s when it gets a little complex. The data are not very clear because ARNI is a combination pill — sacubitril combined with valsartan. When you have an ideal control for a study and you want to know what your magic ingredient is, which is the sacubitril, you really want to compare valsartan with ARNI so that you can find out what your magic little ingredient is doing.
When we had the PARAGON-HF study, which was for HFpEF patients who had an ejection fraction greater than 45%, there was a benefit in the women and not in the men, and that really was in the women with the lower ejection fractions. That’s very interesting because the control was valsartan.
When we had the PARADIGM-HF study, that was more complex. The control was an angiotensin-converting enzyme (ACE) inhibitor, which is not an ideal control for women since, even in a meta-analysis that had over 1000 women, there has not been a proven benefit. The confidence intervals remain wide. Therefore, it’s not quite a fair comparison to randomize women to ARNI versus an ACE inhibitor. Comparing ARNI to valsartan would be better in order to determine the additional benefit of sacubitril since valsartan alone has already been shown, in the Val-HeFT study, to reduce heart failure hospitalizations in women — although not mortality. There was a benefit.
When you look at the PARADIGM-HF study, which was for HFrEF patients, and you see that there is a benefit in the women, where the combined endpoint was heart failure hospitalization and mortality, you then see that there’s a figure that shows what happens when we look at mortality alone. The benefit is not driven by mortality; it’s driven by heart failure hospitalizations for the women, for which valsartan already had been shown to do this. Therefore, I don’t know if sacubitril/valsartan is more powerful because we didn’t have the right control in studies. From my standpoint, the data really are not there. We can all have our own biased opinions.
When we talk about devices, that gets really interesting because it goes back to those risk factors. We’re going to start with implantable cardioverter defibrillators (ICDs). We have shown in many ICD trials that women and men had similar survival. There were very few women in these device trials. If you think the medical trials had only a few women, just imagine what the ICD trials had.
Santangeli and colleagues hypothesized that an ICD only saves you from sudden death. It doesn›t really save you from anything else. In heart failure, women do live longer than men. Is this device really saving you? They weren’t interested in all-cause mortality; they were interested in whether the device fired appropriately for ventricular tachycardia or ventricular fibrillation. They demonstrated in that meta-analysis that it was not very clear that women had the benefit. The rationale behind that comes from the MADIT studies that showed that men were more likely than women to have ventricular arrhythmias.
This is also true based on the Seattle Heart Failure Model. The derivation cohort had very few ICDs at that time, and women were less likely than men to have ventricular arrhythmias as the cause of death. It’s not that we shouldn’t put them in — I very strongly believe that we should — but we don’t have that data.
In fact, in the Santangeli and colleagues study, women were more likely to have inappropriate firing for AFib. Remember that we talked about how one of the risk factors for heart failure was AFib. Women are more likely to have AFib and the ICD firing for AFib and not ventricular arrhythmias. This may be dependent on the type of cardiomyopathy.
Next, we’re going to talk about biventricular pacemakers. Women tend to benefit more so that there is an improvement in symptoms and survival. What is fascinating is that left bundle branch block is a risk factor for the development of heart failure in women, which makes this next statement even more fascinating.
The FDA does their own analysis when they are reviewing devices and everything else, and they published one of them in JAMA Internal Medicine, taking three studies and seeing the benefit in women and men. They found that everybody benefits when the left bundle branch block has a QRS greater than 150 milliseconds. But with a QRS between 130 and 149 milliseconds, only the women benefited. That›s fascinating because that is a risk factor — the development of the left bundle branch block causing heart failure in women. It makes you wonder whether you are correcting something that actually was responsible for their heart failure.
In advanced heart failure, we have left ventricular assist devices (LVADs) and heart transplantation. For years, we couldn’t get LVADs small enough to fit in women. When they were larger, there were complications that were more common in women, such as stroke. With the newer devices — the HeartMate 3 is small, for instance — complications for everyone are very infrequent, and women and men benefit. I’m going to encourage clinicians to use them.
For heart transplantation, as I mentioned before, women tend to get HFpEF. I didn’t mention that they get heart failure when they’re older, for the most part. There are fewer women who are transplanted than men and eligible at younger ages. What we had for decades was that women were dying while they were on the waitlist for heart transplantation at a faster rate than men but living longer after transplantation. As LVADs became more appropriately sized for women, the complication rates went down; and we did see an improvement on the waitlist mortality rate before we changed the allocation system. But it really wasn’t until after we changed the allocation system in 2018 that we saw great success. Now, women have similar survival while on the waitlist. They’re transplanted at a faster rate despite the fact that they’re less likely to receive the temporary mechanical support, and they tend to still do very well.
We have some differences in therapy response. Thank you.
Dr. Hsich disclosed ties with Natera, DEFINE steering committee (no money), and MEDCAC (Medicare/Medicaid) committee. She received research grant from the National Institutes of Health.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Dr Eileen Hsich. I’m the medical director for heart transplantation at the Cleveland Clinic, and my specialty is sex differences in heart failure. I’m excited to talk to you about heart failure treatment in women, addressing the differences in managing heart failure in women as well as practical tips for clinicians. You think that I’m going to be starting off by telling you about the differences in how we’re going to manage the patients, but I’m not. The reason I’m not going to do that is because our national guidelines are not sex specific.
What I’m really going to discuss with you today are the data so that you can decide for yourself what we should do and whether there really are differences. As we begin, I always think about the prevalence of the disease. Currently, there are 6.7 million Americans with heart failure, and approximately 45% of them are women. Globally, our best research shows that there are over 56 million people living with heart failure, and half of them are women.
We also know that there are different underlying causes in women and men. For women, the four risk factors are hypertension, diabetes, atrial fibrillation (AFib), and left bundle branch block. I know you knew about hypertension. Diabetes may not have been right up there in your mind. You see many women with AFib, so I know that you were thinking about it. We’re going to come back to left bundle branch block; it really is very interesting.
For men, it is the risk for heart failure development after a myocardial infarction. Men are more likely to have an ischemic cardiomyopathy. It is also important to state that when women have heart failure, it is often with more preserved ejection fraction. We know that heart failure with preserved ejection fraction (HFpEF) is more common in women and heart failure with reduced ejection fraction (HFrEF) is more common in men.
Now we’re going to talk about the four pillars in medical management, and we’re going to start out with the easy medications that show no sex differences in benefit. The mineralocorticoid receptor antagonists (MRAs) show that there are no sex differences in regard to benefit. Women benefit as much as men, based on two of the largest studies, which were the RALES study, which studied heart failure that was ischemic and nonischemic, and then the EPHESUS study, which was specific to patients who had myocardial infarction. There was a mortality benefit in the women.
The next set of drugs that we’re going to mention are the sodium-glucose cotransporter 2 (SGLT2) inhibitors. The combined endpoint for women and men was a combined endpoint of death and heart failure hospitalization. No matter what the ejection fraction was, women benefited like men for this drug.
The third class of agents that I want to discuss is the beta-blockers, which are really very interesting because they’re so powerful. The studies for these drugs were stopped prematurely. When you take into consideration that women are underenrolled in clinical trials, remember that the studies for these drugs were stopped, so there weren’t that many women. The fact that we showed a mortality benefit is really important.
The first drug that we’re going to refer to is bisoprolol because CIBIS II was the first trial for this drug to demonstrate a mortality benefit in women and men. The second drug that I want to mention is metoprolol XL, which did not demonstrate a mortality benefit in the MERIT-HF study, but did demonstrate a benefit in reduced heart failure hospitalizations, which is also very important.
The third drug is carvedilol, which had been shown to reduce a combined endpoint of mortality and heart failure hospitalizations for patients with moderate symptoms. When I talk about these studies, they have anywhere from 250 to 1000 women enrolled, so these are relatively small studies and they still did demonstrate a benefit.
When we talk about angiotensin receptor–neprilysin inhibitors (ARNI), I think that’s when it gets a little complex. The data are not very clear because ARNI is a combination pill — sacubitril combined with valsartan. When you have an ideal control for a study and you want to know what your magic ingredient is, which is the sacubitril, you really want to compare valsartan with ARNI so that you can find out what your magic little ingredient is doing.
When we had the PARAGON-HF study, which was for HFpEF patients who had an ejection fraction greater than 45%, there was a benefit in the women and not in the men, and that really was in the women with the lower ejection fractions. That’s very interesting because the control was valsartan.
When we had the PARADIGM-HF study, that was more complex. The control was an angiotensin-converting enzyme (ACE) inhibitor, which is not an ideal control for women since, even in a meta-analysis that had over 1000 women, there has not been a proven benefit. The confidence intervals remain wide. Therefore, it’s not quite a fair comparison to randomize women to ARNI versus an ACE inhibitor. Comparing ARNI to valsartan would be better in order to determine the additional benefit of sacubitril since valsartan alone has already been shown, in the Val-HeFT study, to reduce heart failure hospitalizations in women — although not mortality. There was a benefit.
When you look at the PARADIGM-HF study, which was for HFrEF patients, and you see that there is a benefit in the women, where the combined endpoint was heart failure hospitalization and mortality, you then see that there’s a figure that shows what happens when we look at mortality alone. The benefit is not driven by mortality; it’s driven by heart failure hospitalizations for the women, for which valsartan already had been shown to do this. Therefore, I don’t know if sacubitril/valsartan is more powerful because we didn’t have the right control in studies. From my standpoint, the data really are not there. We can all have our own biased opinions.
When we talk about devices, that gets really interesting because it goes back to those risk factors. We’re going to start with implantable cardioverter defibrillators (ICDs). We have shown in many ICD trials that women and men had similar survival. There were very few women in these device trials. If you think the medical trials had only a few women, just imagine what the ICD trials had.
Santangeli and colleagues hypothesized that an ICD only saves you from sudden death. It doesn›t really save you from anything else. In heart failure, women do live longer than men. Is this device really saving you? They weren’t interested in all-cause mortality; they were interested in whether the device fired appropriately for ventricular tachycardia or ventricular fibrillation. They demonstrated in that meta-analysis that it was not very clear that women had the benefit. The rationale behind that comes from the MADIT studies that showed that men were more likely than women to have ventricular arrhythmias.
This is also true based on the Seattle Heart Failure Model. The derivation cohort had very few ICDs at that time, and women were less likely than men to have ventricular arrhythmias as the cause of death. It’s not that we shouldn’t put them in — I very strongly believe that we should — but we don’t have that data.
In fact, in the Santangeli and colleagues study, women were more likely to have inappropriate firing for AFib. Remember that we talked about how one of the risk factors for heart failure was AFib. Women are more likely to have AFib and the ICD firing for AFib and not ventricular arrhythmias. This may be dependent on the type of cardiomyopathy.
Next, we’re going to talk about biventricular pacemakers. Women tend to benefit more so that there is an improvement in symptoms and survival. What is fascinating is that left bundle branch block is a risk factor for the development of heart failure in women, which makes this next statement even more fascinating.
The FDA does their own analysis when they are reviewing devices and everything else, and they published one of them in JAMA Internal Medicine, taking three studies and seeing the benefit in women and men. They found that everybody benefits when the left bundle branch block has a QRS greater than 150 milliseconds. But with a QRS between 130 and 149 milliseconds, only the women benefited. That›s fascinating because that is a risk factor — the development of the left bundle branch block causing heart failure in women. It makes you wonder whether you are correcting something that actually was responsible for their heart failure.
In advanced heart failure, we have left ventricular assist devices (LVADs) and heart transplantation. For years, we couldn’t get LVADs small enough to fit in women. When they were larger, there were complications that were more common in women, such as stroke. With the newer devices — the HeartMate 3 is small, for instance — complications for everyone are very infrequent, and women and men benefit. I’m going to encourage clinicians to use them.
For heart transplantation, as I mentioned before, women tend to get HFpEF. I didn’t mention that they get heart failure when they’re older, for the most part. There are fewer women who are transplanted than men and eligible at younger ages. What we had for decades was that women were dying while they were on the waitlist for heart transplantation at a faster rate than men but living longer after transplantation. As LVADs became more appropriately sized for women, the complication rates went down; and we did see an improvement on the waitlist mortality rate before we changed the allocation system. But it really wasn’t until after we changed the allocation system in 2018 that we saw great success. Now, women have similar survival while on the waitlist. They’re transplanted at a faster rate despite the fact that they’re less likely to receive the temporary mechanical support, and they tend to still do very well.
We have some differences in therapy response. Thank you.
Dr. Hsich disclosed ties with Natera, DEFINE steering committee (no money), and MEDCAC (Medicare/Medicaid) committee. She received research grant from the National Institutes of Health.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Dr Eileen Hsich. I’m the medical director for heart transplantation at the Cleveland Clinic, and my specialty is sex differences in heart failure. I’m excited to talk to you about heart failure treatment in women, addressing the differences in managing heart failure in women as well as practical tips for clinicians. You think that I’m going to be starting off by telling you about the differences in how we’re going to manage the patients, but I’m not. The reason I’m not going to do that is because our national guidelines are not sex specific.
What I’m really going to discuss with you today are the data so that you can decide for yourself what we should do and whether there really are differences. As we begin, I always think about the prevalence of the disease. Currently, there are 6.7 million Americans with heart failure, and approximately 45% of them are women. Globally, our best research shows that there are over 56 million people living with heart failure, and half of them are women.
We also know that there are different underlying causes in women and men. For women, the four risk factors are hypertension, diabetes, atrial fibrillation (AFib), and left bundle branch block. I know you knew about hypertension. Diabetes may not have been right up there in your mind. You see many women with AFib, so I know that you were thinking about it. We’re going to come back to left bundle branch block; it really is very interesting.
For men, it is the risk for heart failure development after a myocardial infarction. Men are more likely to have an ischemic cardiomyopathy. It is also important to state that when women have heart failure, it is often with more preserved ejection fraction. We know that heart failure with preserved ejection fraction (HFpEF) is more common in women and heart failure with reduced ejection fraction (HFrEF) is more common in men.
Now we’re going to talk about the four pillars in medical management, and we’re going to start out with the easy medications that show no sex differences in benefit. The mineralocorticoid receptor antagonists (MRAs) show that there are no sex differences in regard to benefit. Women benefit as much as men, based on two of the largest studies, which were the RALES study, which studied heart failure that was ischemic and nonischemic, and then the EPHESUS study, which was specific to patients who had myocardial infarction. There was a mortality benefit in the women.
The next set of drugs that we’re going to mention are the sodium-glucose cotransporter 2 (SGLT2) inhibitors. The combined endpoint for women and men was a combined endpoint of death and heart failure hospitalization. No matter what the ejection fraction was, women benefited like men for this drug.
The third class of agents that I want to discuss is the beta-blockers, which are really very interesting because they’re so powerful. The studies for these drugs were stopped prematurely. When you take into consideration that women are underenrolled in clinical trials, remember that the studies for these drugs were stopped, so there weren’t that many women. The fact that we showed a mortality benefit is really important.
The first drug that we’re going to refer to is bisoprolol because CIBIS II was the first trial for this drug to demonstrate a mortality benefit in women and men. The second drug that I want to mention is metoprolol XL, which did not demonstrate a mortality benefit in the MERIT-HF study, but did demonstrate a benefit in reduced heart failure hospitalizations, which is also very important.
The third drug is carvedilol, which had been shown to reduce a combined endpoint of mortality and heart failure hospitalizations for patients with moderate symptoms. When I talk about these studies, they have anywhere from 250 to 1000 women enrolled, so these are relatively small studies and they still did demonstrate a benefit.
When we talk about angiotensin receptor–neprilysin inhibitors (ARNI), I think that’s when it gets a little complex. The data are not very clear because ARNI is a combination pill — sacubitril combined with valsartan. When you have an ideal control for a study and you want to know what your magic ingredient is, which is the sacubitril, you really want to compare valsartan with ARNI so that you can find out what your magic little ingredient is doing.
When we had the PARAGON-HF study, which was for HFpEF patients who had an ejection fraction greater than 45%, there was a benefit in the women and not in the men, and that really was in the women with the lower ejection fractions. That’s very interesting because the control was valsartan.
When we had the PARADIGM-HF study, that was more complex. The control was an angiotensin-converting enzyme (ACE) inhibitor, which is not an ideal control for women since, even in a meta-analysis that had over 1000 women, there has not been a proven benefit. The confidence intervals remain wide. Therefore, it’s not quite a fair comparison to randomize women to ARNI versus an ACE inhibitor. Comparing ARNI to valsartan would be better in order to determine the additional benefit of sacubitril since valsartan alone has already been shown, in the Val-HeFT study, to reduce heart failure hospitalizations in women — although not mortality. There was a benefit.
When you look at the PARADIGM-HF study, which was for HFrEF patients, and you see that there is a benefit in the women, where the combined endpoint was heart failure hospitalization and mortality, you then see that there’s a figure that shows what happens when we look at mortality alone. The benefit is not driven by mortality; it’s driven by heart failure hospitalizations for the women, for which valsartan already had been shown to do this. Therefore, I don’t know if sacubitril/valsartan is more powerful because we didn’t have the right control in studies. From my standpoint, the data really are not there. We can all have our own biased opinions.
When we talk about devices, that gets really interesting because it goes back to those risk factors. We’re going to start with implantable cardioverter defibrillators (ICDs). We have shown in many ICD trials that women and men had similar survival. There were very few women in these device trials. If you think the medical trials had only a few women, just imagine what the ICD trials had.
Santangeli and colleagues hypothesized that an ICD only saves you from sudden death. It doesn›t really save you from anything else. In heart failure, women do live longer than men. Is this device really saving you? They weren’t interested in all-cause mortality; they were interested in whether the device fired appropriately for ventricular tachycardia or ventricular fibrillation. They demonstrated in that meta-analysis that it was not very clear that women had the benefit. The rationale behind that comes from the MADIT studies that showed that men were more likely than women to have ventricular arrhythmias.
This is also true based on the Seattle Heart Failure Model. The derivation cohort had very few ICDs at that time, and women were less likely than men to have ventricular arrhythmias as the cause of death. It’s not that we shouldn’t put them in — I very strongly believe that we should — but we don’t have that data.
In fact, in the Santangeli and colleagues study, women were more likely to have inappropriate firing for AFib. Remember that we talked about how one of the risk factors for heart failure was AFib. Women are more likely to have AFib and the ICD firing for AFib and not ventricular arrhythmias. This may be dependent on the type of cardiomyopathy.
Next, we’re going to talk about biventricular pacemakers. Women tend to benefit more so that there is an improvement in symptoms and survival. What is fascinating is that left bundle branch block is a risk factor for the development of heart failure in women, which makes this next statement even more fascinating.
The FDA does their own analysis when they are reviewing devices and everything else, and they published one of them in JAMA Internal Medicine, taking three studies and seeing the benefit in women and men. They found that everybody benefits when the left bundle branch block has a QRS greater than 150 milliseconds. But with a QRS between 130 and 149 milliseconds, only the women benefited. That›s fascinating because that is a risk factor — the development of the left bundle branch block causing heart failure in women. It makes you wonder whether you are correcting something that actually was responsible for their heart failure.
In advanced heart failure, we have left ventricular assist devices (LVADs) and heart transplantation. For years, we couldn’t get LVADs small enough to fit in women. When they were larger, there were complications that were more common in women, such as stroke. With the newer devices — the HeartMate 3 is small, for instance — complications for everyone are very infrequent, and women and men benefit. I’m going to encourage clinicians to use them.
For heart transplantation, as I mentioned before, women tend to get HFpEF. I didn’t mention that they get heart failure when they’re older, for the most part. There are fewer women who are transplanted than men and eligible at younger ages. What we had for decades was that women were dying while they were on the waitlist for heart transplantation at a faster rate than men but living longer after transplantation. As LVADs became more appropriately sized for women, the complication rates went down; and we did see an improvement on the waitlist mortality rate before we changed the allocation system. But it really wasn’t until after we changed the allocation system in 2018 that we saw great success. Now, women have similar survival while on the waitlist. They’re transplanted at a faster rate despite the fact that they’re less likely to receive the temporary mechanical support, and they tend to still do very well.
We have some differences in therapy response. Thank you.
Dr. Hsich disclosed ties with Natera, DEFINE steering committee (no money), and MEDCAC (Medicare/Medicaid) committee. She received research grant from the National Institutes of Health.
A version of this article appeared on Medscape.com.
‘Just Be Prepared’: MD Finds Overdose Victim in an Alley
Emergencies happen anywhere, anytime, and sometimes, medical professionals find themselves in situations where they are the only ones who can help. Is There a Doctor in the House? is a Medscape Medical News series telling these stories.
I had worked a normal 7:00 a.m. to 3:00 p.m. shift in our emergency department. It was a nice day out, so I put my headphones in and started walking home through the Capitol Hill neighborhood in Denver. I passed a couple of buildings and reached an alleyway. At that moment, I glanced over.
Two guys were standing over a third person who was down on the ground. One of the people standing was on the phone. I paused for a second and thought, that doesn’t look right.
The guy on the ground was clearly out. And the other two were looking concerned like they didn’t know what to do.
I walked up the alley and asked, “What’s going on? Can I help?” One of the guys explained that they had just found this man lying here and had already called 911. They sounded a little bit out of their element. They certainly weren’t medically trained.
I leaned down next to the man on the ground. He was probably in his mid-to-late 40s. Unconscious. I always start with, “Hello? Can you hear me?” No response.
I felt for a pulse and he had one, but he didn’t appear to be breathing. I thought, I know what this is. I said, “Sir, I’m going to open your eyes.” I opened his eyes, and his pupils were tiny. It was almost certainly an opioid overdose.
And I had naloxone in my bag.
I got it out and started to assemble it. I didn’t have Narcan, which is the easy one. I had to put this kit together, draw up the medication, and put on the little nasal atomizer.
The two other guys were standing there watching. Then the one on the phone walked down to the end of the alley to where the ambulance was probably going to arrive so he could wave them down.
I gave the man the 4 mg of naloxone, two in each nostril.
He still wasn’t breathing. I did a basic maneuver where you lift his jaw a little bit to help open up the airway.
Suddenly, he started breathing again. I couldn’t do any meaningful measurements of his oxygen saturation or anything like that. I just kind of looked at him and thought, Okay, he has a pulse. He’s breathing now. That’s good.
Luckily, the cavalry arrived soon after that. Our Denver Health paramedics pulled up into the alley, and one of them recognized me from the ER. I explained that I had already given the guy naloxone. They did their assessment, and he still wasn’t breathing well, so they gave him some breaths with a mask and a bag.
We got him onto the gurney and into the back of the ambulance. They started an IV. He seemed to be breathing okay by then, and his numbers looked okay. But he wasn’t awake yet by any means.
I handed off care to them and disposed of my sharp in the ambulance. Then they took him into the ER that I had just left moments ago.
The two other guys had already disappeared. I think they saw the ambulance and thought, our job is done. So, I didn’t end up talking to them at all.
So, just like that ... I started walking home again.
I like to think of myself as a cool, calm, collected person working in the ER. But my heart was definitely going fast at that point. I called my wife to tell her about the crazy thing that just happened, and she could hear in my voice how amped up I was.
In the ER, it’s very common to see patients who need naloxone, have opioid toxicity, or have received Narcan in the community. Luckily, this man was found right away. He had likely overdosed only a few minutes earlier. Those scenarios can go bad very quickly. If there’s no one there, people often die.
That’s why I started carrying naloxone.
Now, I encourage all my friends to have some, and I suggest all medical professionals to keep some with them. Just be prepared. Put it in your backpack, your purse, keep it in the house, in the car, wherever. The nasal autoinjectors are incredibly easy. Like, stick it up the nose, push the big red button. Done.
When we train lay people to administer Narcan, we try to keep it simple. If you see someone, and they’re not responsive, not breathing, just give it. It’s not that there’s no possible harm if you’re wrong. But the benefits so vastly outweigh the risks that we are very aggressive to say, go ahead and give it.
I think we all have a responsibility to care for our communities. Obviously, that can take a lot of different forms. I had the privilege of being in the right place at the right time with the right tool to potentially save a life. That was the form it took for me that day.
Later, I followed up with a friend who took care of the man in the ER. He went through our standard procedure, being monitored to make sure the opioids didn’t outlast the naloxone. We have a lot of resources and next steps for people that have opioid use disorder. He was made aware of those. And then he walked out. I never saw him again.
It’s not the sexy part of our job in emergency medicine, not the super high–intensity adrenaline rush–type work, but a lot of what we do is talk to people like this guy. We counsel them. We think about their longer-term health and not just the overdose. This is an incredibly high-risk population in terms of their mortality risk from the opioid use disorder. It’s astronomical.
I obviously believed in this work before, but that day changed something for me. It added a layer of urgency. Now, when I have a moment in the emergency room to connect with someone, I know the reality — this person sitting in front of me could die in an alley. Maybe not today, but next week or next month.
I have the naloxone in my bag. Just in case.
Patrick Joynt, MD, is an emergency medicine physician with Denver Health in Denver.
Are you a medical professional with a dramatic story outside the clinic? Medscape Medical News would love to consider your story for Is There a Doctor in the House? Please email your contact information and a short summary to [email protected].
A version of this article appeared on Medscape.com .
Emergencies happen anywhere, anytime, and sometimes, medical professionals find themselves in situations where they are the only ones who can help. Is There a Doctor in the House? is a Medscape Medical News series telling these stories.
I had worked a normal 7:00 a.m. to 3:00 p.m. shift in our emergency department. It was a nice day out, so I put my headphones in and started walking home through the Capitol Hill neighborhood in Denver. I passed a couple of buildings and reached an alleyway. At that moment, I glanced over.
Two guys were standing over a third person who was down on the ground. One of the people standing was on the phone. I paused for a second and thought, that doesn’t look right.
The guy on the ground was clearly out. And the other two were looking concerned like they didn’t know what to do.
I walked up the alley and asked, “What’s going on? Can I help?” One of the guys explained that they had just found this man lying here and had already called 911. They sounded a little bit out of their element. They certainly weren’t medically trained.
I leaned down next to the man on the ground. He was probably in his mid-to-late 40s. Unconscious. I always start with, “Hello? Can you hear me?” No response.
I felt for a pulse and he had one, but he didn’t appear to be breathing. I thought, I know what this is. I said, “Sir, I’m going to open your eyes.” I opened his eyes, and his pupils were tiny. It was almost certainly an opioid overdose.
And I had naloxone in my bag.
I got it out and started to assemble it. I didn’t have Narcan, which is the easy one. I had to put this kit together, draw up the medication, and put on the little nasal atomizer.
The two other guys were standing there watching. Then the one on the phone walked down to the end of the alley to where the ambulance was probably going to arrive so he could wave them down.
I gave the man the 4 mg of naloxone, two in each nostril.
He still wasn’t breathing. I did a basic maneuver where you lift his jaw a little bit to help open up the airway.
Suddenly, he started breathing again. I couldn’t do any meaningful measurements of his oxygen saturation or anything like that. I just kind of looked at him and thought, Okay, he has a pulse. He’s breathing now. That’s good.
Luckily, the cavalry arrived soon after that. Our Denver Health paramedics pulled up into the alley, and one of them recognized me from the ER. I explained that I had already given the guy naloxone. They did their assessment, and he still wasn’t breathing well, so they gave him some breaths with a mask and a bag.
We got him onto the gurney and into the back of the ambulance. They started an IV. He seemed to be breathing okay by then, and his numbers looked okay. But he wasn’t awake yet by any means.
I handed off care to them and disposed of my sharp in the ambulance. Then they took him into the ER that I had just left moments ago.
The two other guys had already disappeared. I think they saw the ambulance and thought, our job is done. So, I didn’t end up talking to them at all.
So, just like that ... I started walking home again.
I like to think of myself as a cool, calm, collected person working in the ER. But my heart was definitely going fast at that point. I called my wife to tell her about the crazy thing that just happened, and she could hear in my voice how amped up I was.
In the ER, it’s very common to see patients who need naloxone, have opioid toxicity, or have received Narcan in the community. Luckily, this man was found right away. He had likely overdosed only a few minutes earlier. Those scenarios can go bad very quickly. If there’s no one there, people often die.
That’s why I started carrying naloxone.
Now, I encourage all my friends to have some, and I suggest all medical professionals to keep some with them. Just be prepared. Put it in your backpack, your purse, keep it in the house, in the car, wherever. The nasal autoinjectors are incredibly easy. Like, stick it up the nose, push the big red button. Done.
When we train lay people to administer Narcan, we try to keep it simple. If you see someone, and they’re not responsive, not breathing, just give it. It’s not that there’s no possible harm if you’re wrong. But the benefits so vastly outweigh the risks that we are very aggressive to say, go ahead and give it.
I think we all have a responsibility to care for our communities. Obviously, that can take a lot of different forms. I had the privilege of being in the right place at the right time with the right tool to potentially save a life. That was the form it took for me that day.
Later, I followed up with a friend who took care of the man in the ER. He went through our standard procedure, being monitored to make sure the opioids didn’t outlast the naloxone. We have a lot of resources and next steps for people that have opioid use disorder. He was made aware of those. And then he walked out. I never saw him again.
It’s not the sexy part of our job in emergency medicine, not the super high–intensity adrenaline rush–type work, but a lot of what we do is talk to people like this guy. We counsel them. We think about their longer-term health and not just the overdose. This is an incredibly high-risk population in terms of their mortality risk from the opioid use disorder. It’s astronomical.
I obviously believed in this work before, but that day changed something for me. It added a layer of urgency. Now, when I have a moment in the emergency room to connect with someone, I know the reality — this person sitting in front of me could die in an alley. Maybe not today, but next week or next month.
I have the naloxone in my bag. Just in case.
Patrick Joynt, MD, is an emergency medicine physician with Denver Health in Denver.
Are you a medical professional with a dramatic story outside the clinic? Medscape Medical News would love to consider your story for Is There a Doctor in the House? Please email your contact information and a short summary to [email protected].
A version of this article appeared on Medscape.com .
Emergencies happen anywhere, anytime, and sometimes, medical professionals find themselves in situations where they are the only ones who can help. Is There a Doctor in the House? is a Medscape Medical News series telling these stories.
I had worked a normal 7:00 a.m. to 3:00 p.m. shift in our emergency department. It was a nice day out, so I put my headphones in and started walking home through the Capitol Hill neighborhood in Denver. I passed a couple of buildings and reached an alleyway. At that moment, I glanced over.
Two guys were standing over a third person who was down on the ground. One of the people standing was on the phone. I paused for a second and thought, that doesn’t look right.
The guy on the ground was clearly out. And the other two were looking concerned like they didn’t know what to do.
I walked up the alley and asked, “What’s going on? Can I help?” One of the guys explained that they had just found this man lying here and had already called 911. They sounded a little bit out of their element. They certainly weren’t medically trained.
I leaned down next to the man on the ground. He was probably in his mid-to-late 40s. Unconscious. I always start with, “Hello? Can you hear me?” No response.
I felt for a pulse and he had one, but he didn’t appear to be breathing. I thought, I know what this is. I said, “Sir, I’m going to open your eyes.” I opened his eyes, and his pupils were tiny. It was almost certainly an opioid overdose.
And I had naloxone in my bag.
I got it out and started to assemble it. I didn’t have Narcan, which is the easy one. I had to put this kit together, draw up the medication, and put on the little nasal atomizer.
The two other guys were standing there watching. Then the one on the phone walked down to the end of the alley to where the ambulance was probably going to arrive so he could wave them down.
I gave the man the 4 mg of naloxone, two in each nostril.
He still wasn’t breathing. I did a basic maneuver where you lift his jaw a little bit to help open up the airway.
Suddenly, he started breathing again. I couldn’t do any meaningful measurements of his oxygen saturation or anything like that. I just kind of looked at him and thought, Okay, he has a pulse. He’s breathing now. That’s good.
Luckily, the cavalry arrived soon after that. Our Denver Health paramedics pulled up into the alley, and one of them recognized me from the ER. I explained that I had already given the guy naloxone. They did their assessment, and he still wasn’t breathing well, so they gave him some breaths with a mask and a bag.
We got him onto the gurney and into the back of the ambulance. They started an IV. He seemed to be breathing okay by then, and his numbers looked okay. But he wasn’t awake yet by any means.
I handed off care to them and disposed of my sharp in the ambulance. Then they took him into the ER that I had just left moments ago.
The two other guys had already disappeared. I think they saw the ambulance and thought, our job is done. So, I didn’t end up talking to them at all.
So, just like that ... I started walking home again.
I like to think of myself as a cool, calm, collected person working in the ER. But my heart was definitely going fast at that point. I called my wife to tell her about the crazy thing that just happened, and she could hear in my voice how amped up I was.
In the ER, it’s very common to see patients who need naloxone, have opioid toxicity, or have received Narcan in the community. Luckily, this man was found right away. He had likely overdosed only a few minutes earlier. Those scenarios can go bad very quickly. If there’s no one there, people often die.
That’s why I started carrying naloxone.
Now, I encourage all my friends to have some, and I suggest all medical professionals to keep some with them. Just be prepared. Put it in your backpack, your purse, keep it in the house, in the car, wherever. The nasal autoinjectors are incredibly easy. Like, stick it up the nose, push the big red button. Done.
When we train lay people to administer Narcan, we try to keep it simple. If you see someone, and they’re not responsive, not breathing, just give it. It’s not that there’s no possible harm if you’re wrong. But the benefits so vastly outweigh the risks that we are very aggressive to say, go ahead and give it.
I think we all have a responsibility to care for our communities. Obviously, that can take a lot of different forms. I had the privilege of being in the right place at the right time with the right tool to potentially save a life. That was the form it took for me that day.
Later, I followed up with a friend who took care of the man in the ER. He went through our standard procedure, being monitored to make sure the opioids didn’t outlast the naloxone. We have a lot of resources and next steps for people that have opioid use disorder. He was made aware of those. And then he walked out. I never saw him again.
It’s not the sexy part of our job in emergency medicine, not the super high–intensity adrenaline rush–type work, but a lot of what we do is talk to people like this guy. We counsel them. We think about their longer-term health and not just the overdose. This is an incredibly high-risk population in terms of their mortality risk from the opioid use disorder. It’s astronomical.
I obviously believed in this work before, but that day changed something for me. It added a layer of urgency. Now, when I have a moment in the emergency room to connect with someone, I know the reality — this person sitting in front of me could die in an alley. Maybe not today, but next week or next month.
I have the naloxone in my bag. Just in case.
Patrick Joynt, MD, is an emergency medicine physician with Denver Health in Denver.
Are you a medical professional with a dramatic story outside the clinic? Medscape Medical News would love to consider your story for Is There a Doctor in the House? Please email your contact information and a short summary to [email protected].
A version of this article appeared on Medscape.com .
Long COVID Can’t Be Solved Until We Decide What It Is
This transcript has been edited for clarity.
I want to help people suffering from long COVID as much as anyone. But we have a real problem. In brief, we are being too inclusive. The first thing you learn, when you start studying the epidemiology of diseases, is that you need a good case definition. And our case definition for long COVID sucks. Just last week, the National Academies of Sciences, Engineering, and Medicine (NASEM) issued a definition of long COVID with the aim of “improving consistency, documentation, and treatment.” Good news, right? Here’s the definition: “Long COVID is an infection-associated chronic condition that occurs after SARS-CoV-2 infection and is present for at least 3 months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems.”
This is not helpful. The symptoms can be in any organ system, can be continuous or relapsing and remitting. Basically, if you’ve had COVID — and essentially all of us have by now — and you have any symptom, even one that comes and goes, 3 months after that, it’s long COVID. They don’t even specify that it has to be a new symptom.
And I have sort of a case study in this problem today, based on a paper getting a lot of press suggesting that one out of every five people has long COVID.
We are talking about this study, “Epidemiologic Features of Recovery From SARS-CoV-2 Infection,” appearing in JAMA Network Open this week. While I think the idea is important, the study really highlights why it can be so hard to study long COVID.
As part of efforts to understand long COVID, the National Institutes of Health (NIH) leveraged 14 of its ongoing cohort studies. The NIH has multiple longitudinal cohort studies that follow various groups of people over time. You may have heard of the REGARDS study, for example, which focuses on cardiovascular risks to people living in the southern United States. Or the ARIC study, which followed adults in four communities across the United States for the development of heart disease. All 14 of the cohorts in this study are long-running projects with ongoing data collection. So, it was not a huge lift to add some questions to the yearly surveys and studies the participants were already getting.
To wit: “Do you think that you have had COVID-19?” and “Would you say that you are completely recovered now?” Those who said they weren’t fully recovered were asked how long it had been since their infection, and anyone who answered with a duration > 90 days was considered to have long COVID.
So, we have self-report of infection, self-report of duration of symptoms, and self-report of recovery. This is fine, of course; individuals’ perceptions of their own health are meaningful. But the vagaries inherent in those perceptions are going to muddy the waters as we attempt to discover the true nature of the long COVID syndrome.
But let’s look at some results. Out of 4708 individuals studied, 842 (17.9%) had not recovered by 90 days.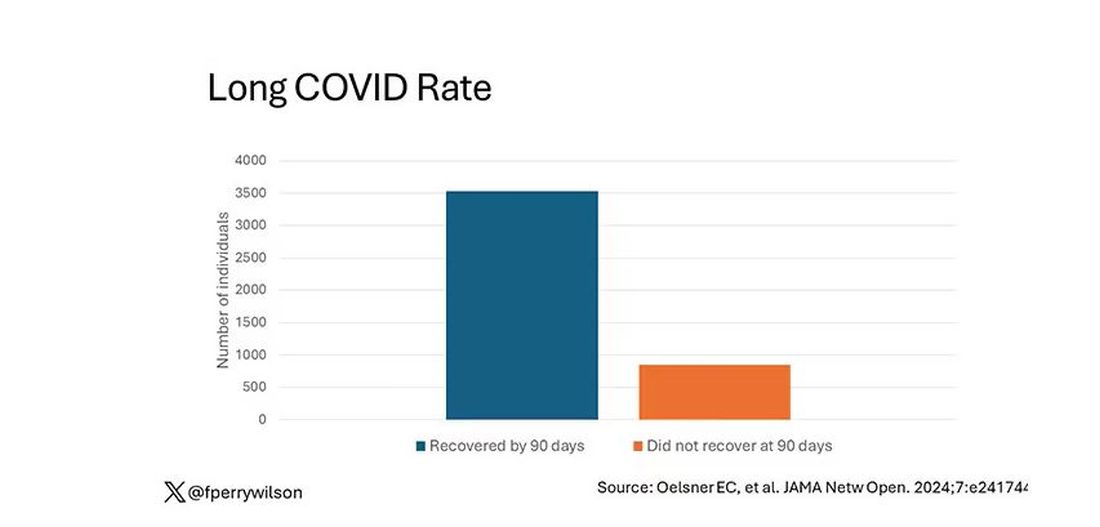
This study included not only people hospitalized with COVID, as some prior long COVID studies did, but people self-diagnosed, tested at home, etc. This estimate is as reflective of the broader US population as we can get.
And there are some interesting trends here.
Recovery time was longer in the first waves of COVID than in the Omicron wave.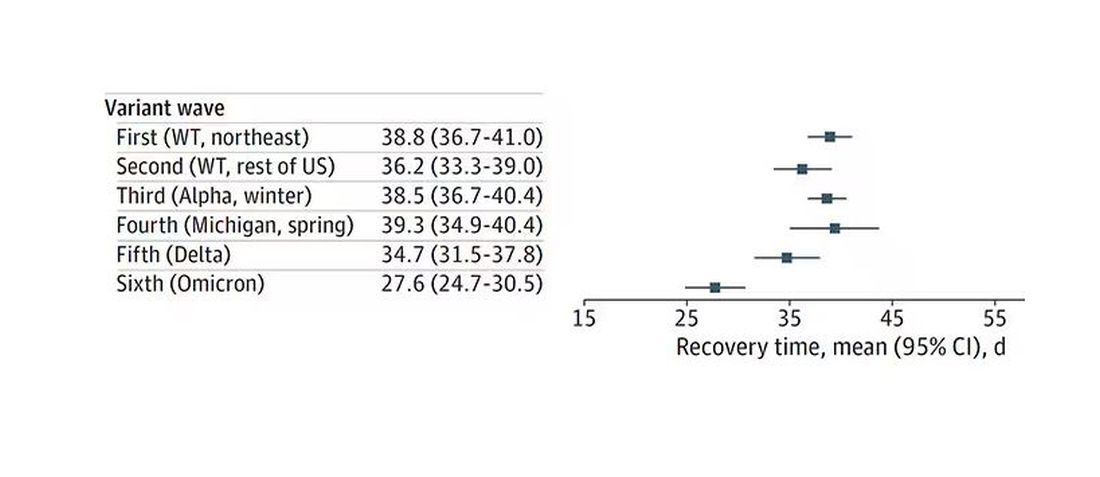
Recovery times were longer for smokers, those with diabetes, and those who were obese.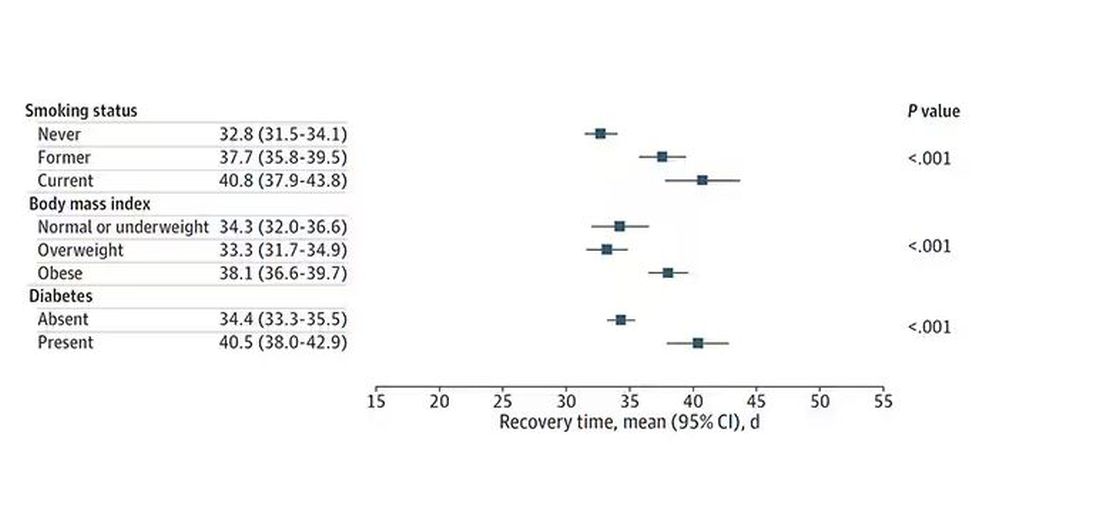
Recovery times were longer if the disease was more severe, in general. Though there is an unusual finding that women had longer recovery times despite their lower average severity of illness.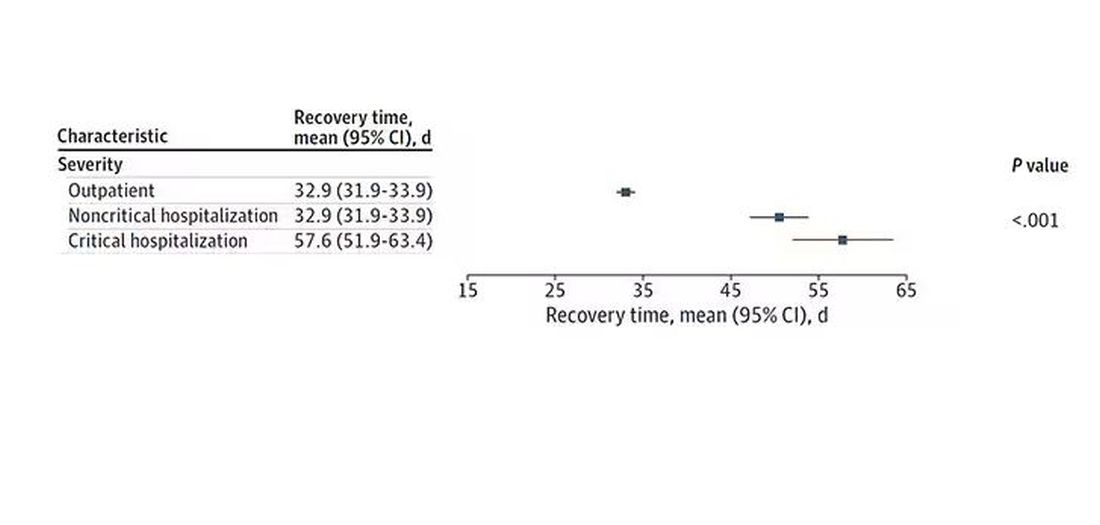
Vaccination was associated with shorter recovery times, as you can see here. 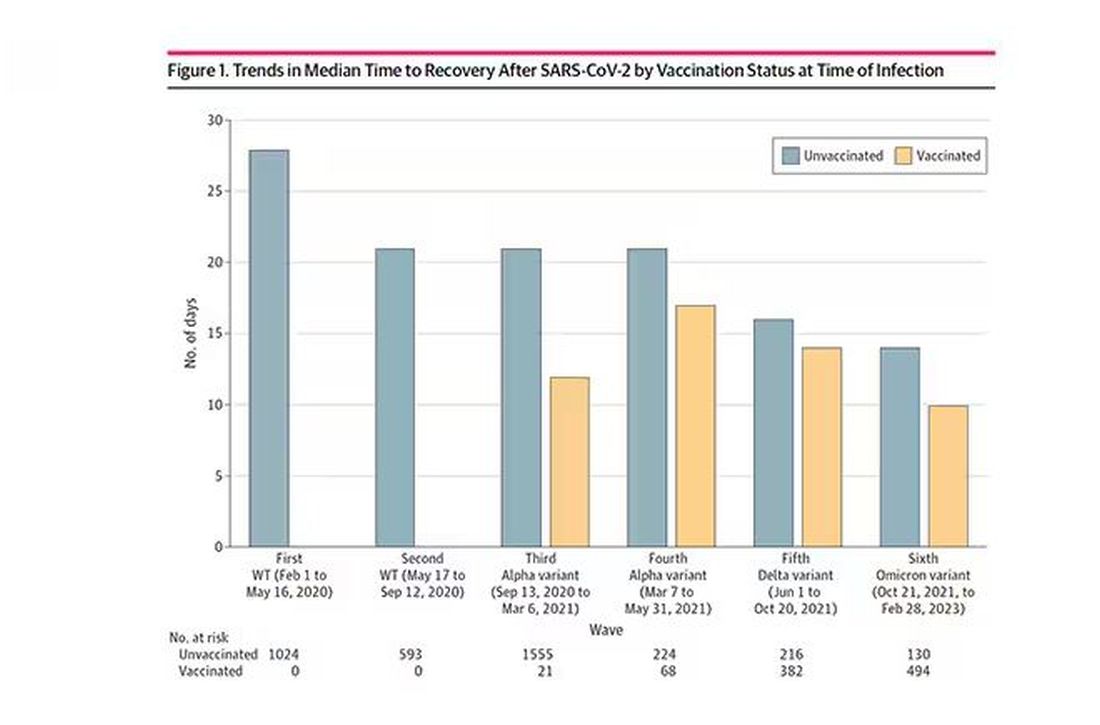
This is all quite interesting. It’s clear that people feel they are sick for a while after COVID. But we need to understand whether these symptoms are due to the lingering effects of a bad infection that knocks you down a peg, or to an ongoing syndrome — this thing we call long COVID — that has a physiologic basis and thus can be treated. And this study doesn’t help us much with that.
Not that this was the authors’ intention. This is a straight-up epidemiology study. But the problem is deeper than that. Let’s imagine that you want to really dig into this long COVID thing and get blood samples from people with it, ideally from controls with some other respiratory virus infection, and do all kinds of genetic and proteomic studies and stuff to really figure out what’s going on. Who do you enroll to be in the long COVID group? Do you enroll anyone who says they had COVID and still has some symptom more than 90 days after? You are going to find an awful lot of eligible people, and I guarantee that if there is a pathognomonic signature of long COVID, not all of them will have it.
And what about other respiratory viruses? This study in The Lancet Infectious Diseases compared long-term outcomes among hospitalized patients with COVID vs influenza. In general, the COVID outcomes are worse, but let’s not knock the concept of “long flu.” Across the board, roughly 50% of people report symptoms across any given organ system.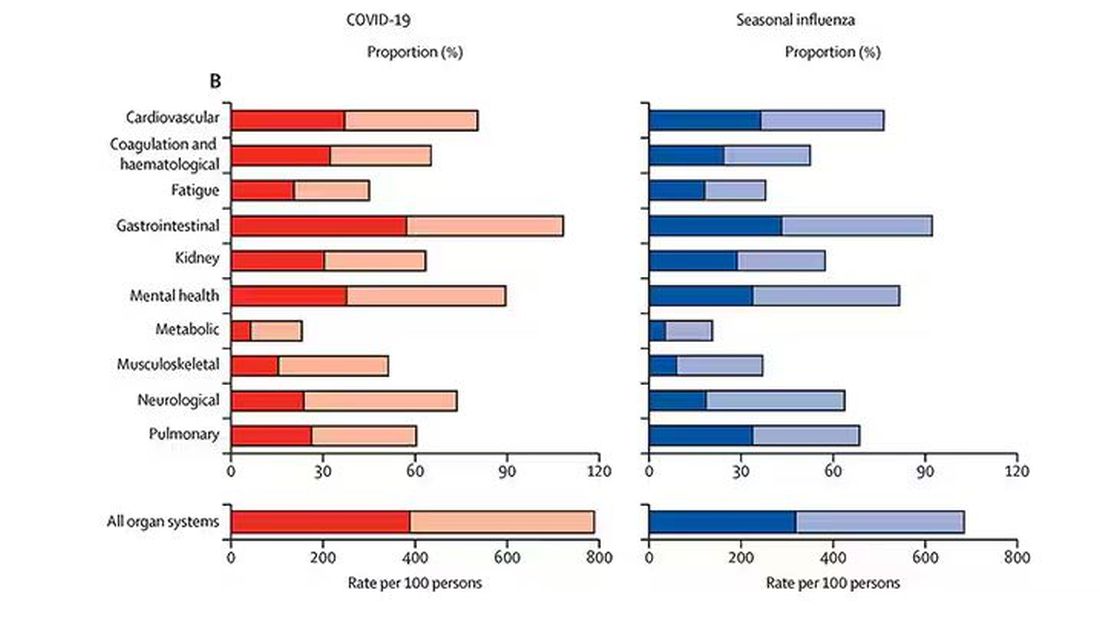
What this is all about is something called misclassification bias, a form of information bias that arises in a study where you label someone as diseased when they are not, or vice versa. If this happens at random, it’s bad; you’ve lost your ability to distinguish characteristics from the diseased and nondiseased population.
When it’s not random, it’s really bad. If we are more likely to misclassify women as having long COVID, for example, then it will appear that long COVID is more likely among women, or more likely among those with higher estrogen levels, or something. And that might simply be wrong.
I’m not saying that’s what happened here; this study does a really great job of what it set out to do, which was to describe the patterns of lingering symptoms after COVID. But we are not going to make progress toward understanding long COVID until we are less inclusive with our case definition. To paraphrase Syndrome from The Incredibles: If everyone has long COVID, then no one does.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
I want to help people suffering from long COVID as much as anyone. But we have a real problem. In brief, we are being too inclusive. The first thing you learn, when you start studying the epidemiology of diseases, is that you need a good case definition. And our case definition for long COVID sucks. Just last week, the National Academies of Sciences, Engineering, and Medicine (NASEM) issued a definition of long COVID with the aim of “improving consistency, documentation, and treatment.” Good news, right? Here’s the definition: “Long COVID is an infection-associated chronic condition that occurs after SARS-CoV-2 infection and is present for at least 3 months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems.”
This is not helpful. The symptoms can be in any organ system, can be continuous or relapsing and remitting. Basically, if you’ve had COVID — and essentially all of us have by now — and you have any symptom, even one that comes and goes, 3 months after that, it’s long COVID. They don’t even specify that it has to be a new symptom.
And I have sort of a case study in this problem today, based on a paper getting a lot of press suggesting that one out of every five people has long COVID.
We are talking about this study, “Epidemiologic Features of Recovery From SARS-CoV-2 Infection,” appearing in JAMA Network Open this week. While I think the idea is important, the study really highlights why it can be so hard to study long COVID.
As part of efforts to understand long COVID, the National Institutes of Health (NIH) leveraged 14 of its ongoing cohort studies. The NIH has multiple longitudinal cohort studies that follow various groups of people over time. You may have heard of the REGARDS study, for example, which focuses on cardiovascular risks to people living in the southern United States. Or the ARIC study, which followed adults in four communities across the United States for the development of heart disease. All 14 of the cohorts in this study are long-running projects with ongoing data collection. So, it was not a huge lift to add some questions to the yearly surveys and studies the participants were already getting.
To wit: “Do you think that you have had COVID-19?” and “Would you say that you are completely recovered now?” Those who said they weren’t fully recovered were asked how long it had been since their infection, and anyone who answered with a duration > 90 days was considered to have long COVID.
So, we have self-report of infection, self-report of duration of symptoms, and self-report of recovery. This is fine, of course; individuals’ perceptions of their own health are meaningful. But the vagaries inherent in those perceptions are going to muddy the waters as we attempt to discover the true nature of the long COVID syndrome.
But let’s look at some results. Out of 4708 individuals studied, 842 (17.9%) had not recovered by 90 days.
This study included not only people hospitalized with COVID, as some prior long COVID studies did, but people self-diagnosed, tested at home, etc. This estimate is as reflective of the broader US population as we can get.
And there are some interesting trends here.
Recovery time was longer in the first waves of COVID than in the Omicron wave.
Recovery times were longer for smokers, those with diabetes, and those who were obese.
Recovery times were longer if the disease was more severe, in general. Though there is an unusual finding that women had longer recovery times despite their lower average severity of illness.
Vaccination was associated with shorter recovery times, as you can see here.
This is all quite interesting. It’s clear that people feel they are sick for a while after COVID. But we need to understand whether these symptoms are due to the lingering effects of a bad infection that knocks you down a peg, or to an ongoing syndrome — this thing we call long COVID — that has a physiologic basis and thus can be treated. And this study doesn’t help us much with that.
Not that this was the authors’ intention. This is a straight-up epidemiology study. But the problem is deeper than that. Let’s imagine that you want to really dig into this long COVID thing and get blood samples from people with it, ideally from controls with some other respiratory virus infection, and do all kinds of genetic and proteomic studies and stuff to really figure out what’s going on. Who do you enroll to be in the long COVID group? Do you enroll anyone who says they had COVID and still has some symptom more than 90 days after? You are going to find an awful lot of eligible people, and I guarantee that if there is a pathognomonic signature of long COVID, not all of them will have it.
And what about other respiratory viruses? This study in The Lancet Infectious Diseases compared long-term outcomes among hospitalized patients with COVID vs influenza. In general, the COVID outcomes are worse, but let’s not knock the concept of “long flu.” Across the board, roughly 50% of people report symptoms across any given organ system.
What this is all about is something called misclassification bias, a form of information bias that arises in a study where you label someone as diseased when they are not, or vice versa. If this happens at random, it’s bad; you’ve lost your ability to distinguish characteristics from the diseased and nondiseased population.
When it’s not random, it’s really bad. If we are more likely to misclassify women as having long COVID, for example, then it will appear that long COVID is more likely among women, or more likely among those with higher estrogen levels, or something. And that might simply be wrong.
I’m not saying that’s what happened here; this study does a really great job of what it set out to do, which was to describe the patterns of lingering symptoms after COVID. But we are not going to make progress toward understanding long COVID until we are less inclusive with our case definition. To paraphrase Syndrome from The Incredibles: If everyone has long COVID, then no one does.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
I want to help people suffering from long COVID as much as anyone. But we have a real problem. In brief, we are being too inclusive. The first thing you learn, when you start studying the epidemiology of diseases, is that you need a good case definition. And our case definition for long COVID sucks. Just last week, the National Academies of Sciences, Engineering, and Medicine (NASEM) issued a definition of long COVID with the aim of “improving consistency, documentation, and treatment.” Good news, right? Here’s the definition: “Long COVID is an infection-associated chronic condition that occurs after SARS-CoV-2 infection and is present for at least 3 months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems.”
This is not helpful. The symptoms can be in any organ system, can be continuous or relapsing and remitting. Basically, if you’ve had COVID — and essentially all of us have by now — and you have any symptom, even one that comes and goes, 3 months after that, it’s long COVID. They don’t even specify that it has to be a new symptom.
And I have sort of a case study in this problem today, based on a paper getting a lot of press suggesting that one out of every five people has long COVID.
We are talking about this study, “Epidemiologic Features of Recovery From SARS-CoV-2 Infection,” appearing in JAMA Network Open this week. While I think the idea is important, the study really highlights why it can be so hard to study long COVID.
As part of efforts to understand long COVID, the National Institutes of Health (NIH) leveraged 14 of its ongoing cohort studies. The NIH has multiple longitudinal cohort studies that follow various groups of people over time. You may have heard of the REGARDS study, for example, which focuses on cardiovascular risks to people living in the southern United States. Or the ARIC study, which followed adults in four communities across the United States for the development of heart disease. All 14 of the cohorts in this study are long-running projects with ongoing data collection. So, it was not a huge lift to add some questions to the yearly surveys and studies the participants were already getting.
To wit: “Do you think that you have had COVID-19?” and “Would you say that you are completely recovered now?” Those who said they weren’t fully recovered were asked how long it had been since their infection, and anyone who answered with a duration > 90 days was considered to have long COVID.
So, we have self-report of infection, self-report of duration of symptoms, and self-report of recovery. This is fine, of course; individuals’ perceptions of their own health are meaningful. But the vagaries inherent in those perceptions are going to muddy the waters as we attempt to discover the true nature of the long COVID syndrome.
But let’s look at some results. Out of 4708 individuals studied, 842 (17.9%) had not recovered by 90 days.
This study included not only people hospitalized with COVID, as some prior long COVID studies did, but people self-diagnosed, tested at home, etc. This estimate is as reflective of the broader US population as we can get.
And there are some interesting trends here.
Recovery time was longer in the first waves of COVID than in the Omicron wave.
Recovery times were longer for smokers, those with diabetes, and those who were obese.
Recovery times were longer if the disease was more severe, in general. Though there is an unusual finding that women had longer recovery times despite their lower average severity of illness.
Vaccination was associated with shorter recovery times, as you can see here.
This is all quite interesting. It’s clear that people feel they are sick for a while after COVID. But we need to understand whether these symptoms are due to the lingering effects of a bad infection that knocks you down a peg, or to an ongoing syndrome — this thing we call long COVID — that has a physiologic basis and thus can be treated. And this study doesn’t help us much with that.
Not that this was the authors’ intention. This is a straight-up epidemiology study. But the problem is deeper than that. Let’s imagine that you want to really dig into this long COVID thing and get blood samples from people with it, ideally from controls with some other respiratory virus infection, and do all kinds of genetic and proteomic studies and stuff to really figure out what’s going on. Who do you enroll to be in the long COVID group? Do you enroll anyone who says they had COVID and still has some symptom more than 90 days after? You are going to find an awful lot of eligible people, and I guarantee that if there is a pathognomonic signature of long COVID, not all of them will have it.
And what about other respiratory viruses? This study in The Lancet Infectious Diseases compared long-term outcomes among hospitalized patients with COVID vs influenza. In general, the COVID outcomes are worse, but let’s not knock the concept of “long flu.” Across the board, roughly 50% of people report symptoms across any given organ system.
What this is all about is something called misclassification bias, a form of information bias that arises in a study where you label someone as diseased when they are not, or vice versa. If this happens at random, it’s bad; you’ve lost your ability to distinguish characteristics from the diseased and nondiseased population.
When it’s not random, it’s really bad. If we are more likely to misclassify women as having long COVID, for example, then it will appear that long COVID is more likely among women, or more likely among those with higher estrogen levels, or something. And that might simply be wrong.
I’m not saying that’s what happened here; this study does a really great job of what it set out to do, which was to describe the patterns of lingering symptoms after COVID. But we are not going to make progress toward understanding long COVID until we are less inclusive with our case definition. To paraphrase Syndrome from The Incredibles: If everyone has long COVID, then no one does.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Acute Sore Throat in Primary Care: When to Reach for the Antibiotics
This transcript has been edited for clarity.
There is a helpful consensus from experts on the best management of patients with acute sore throat. This is a common problem in primary care, and one for which there is a lot of evidence, opinion, and ultimately overprescribing of antibiotics. This consensus presents a pragmatic clinical approach aimed at decreasing overprescribing, yet detecting which patients are likely to benefit from treatment with antibiotics.
Let’s first go over the evidence that forms the basis for the recommendations, then the recommended approach. First, a sore throat can be caused by many different viruses, as well as group A streptococcus (GAS), the group C streptococcus S dysgalactiae, and fusobacterium. We sometimes think of throat cultures as telling us the definitive etiology of a sore throat. In fact, children commonly are colonized with GAS even when not infected — 35% of the time, when GAS is detected on throat swab in a child, GAS is not the cause of the sore throat. Very few adults are colonized with GAS.
Sore throats are usually self-limited, whether they are treated with antibiotics or not, but occasionally complications can occur. Suppurative complications include peritonsillar abscess, sinusitis and sepsis. Nonsuppurative complications are primarily glomerulonephritis and rheumatic fever, which can lead to rheumatic heart disease.
Antibiotics. Antibiotics have three potential benefits in acute sore throat: to reduce the risk of developing rheumatic heart disease, reduce the duration and severity of symptoms, and treat suppurative complications. The risk for rheumatic heart disease has almost vanished in high-income countries, but not in low-income countries. Thus, antibiotic treatment of acute sore throat due to GAS may benefit those in living in, and those who recently emigrated from, low-income countries.
Patients with suppurative complications should be identified because antibiotics are important for this group. Although antibiotics are prescribed primarily to prevent rheumatic fever in this population, they may be mildly helpful in reducing a patient’s symptoms.
Testing. The sensitivity and specificity of high-quality point-of-care tests (POCTs) are on par with those of cultures, with the advantage that the results are available within minutes. Negative tests reduce unneeded antibiotic prescriptions.
Given this evidence, the authors recommend an approach that puts a lot of emphasis on two major things: the risk for rheumatic fever, and clinical assessment. On the basis of these factors, a decision is made about the utility of POCTs and treatment with antibiotics for GAS. The risk for rheumatic fever is based on epidemiology: If the patient is in a low-income country or has recently immigrated from one, then the risk is high, and if not, the risk is low.
Complicated vs uncomplicated? This is determined by clinical assessment of the severity of the patient’s illness, including general appearance. Uncomplicated sore throat means that the patient:
- Is not getting worse after 3 days of illness
- Has a duration of illness ≤ 5 days or is getting better after day 5
- Has mild to moderate symptom severity (bilateral throat pain, the ability to open the mouth fully, and absence of a sandpaper or scarlatiniform rash or strawberry tongue)
For patients with uncomplicated sore throat and low risk for rheumatic fever, the main goals are to reduce antibiotic use and provide symptomatic relief. For these patients, an assessment such as the Centor score can be done. Those with a low Centor score (0-2) can be treated with analgesics and there is no need for a POCT.
In patients with a higher Centor score, the consensus gives two choices: They can either be tested (and treated if the testing is positive), or it is reasonable to forgo testing and use a wait-and-see strategy, with reevaluation if they are getting worse after day 3 or not improving after day 5 days of their illness. Illnesses that last longer than 5 days with sore throat and fatigue should prompt consideration of alternative diagnoses, such as infectious mononucleosis.
For patients with potentially complicated sore throat — including indicators such as worsening symptoms after 3 days or worsening after initiation of antibiotics, inability to open the mouth fully, unilateral neck pain or swelling, or rigors — should undergo a careful evaluation. The need for further testing in these patients, including labs and imaging, should be decided on a case-by-case basis. If the patient appears seriously ill, don’t rely solely on POCT for GAS, but think about other diagnoses.
Rheumatic fever. The approach is very different in patients at high risk for rheumatic fever. POCT for GAS is recommended irrespective of their clinical score, and antibiotics should be prescribed if it’s positive for GAS. If a POCT is unavailable, then the consensus recommends prescribing antibiotics for all high-risk patients who have acute sore throat.
This approach is sensible and puts a lot of emphasis on clinical evaluation, though it should be noted that this approach is considerably different from that in the 2012 Infectious Diseases Society of America guidelines.
Dr. Skolnik, professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly and Company, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
There is a helpful consensus from experts on the best management of patients with acute sore throat. This is a common problem in primary care, and one for which there is a lot of evidence, opinion, and ultimately overprescribing of antibiotics. This consensus presents a pragmatic clinical approach aimed at decreasing overprescribing, yet detecting which patients are likely to benefit from treatment with antibiotics.
Let’s first go over the evidence that forms the basis for the recommendations, then the recommended approach. First, a sore throat can be caused by many different viruses, as well as group A streptococcus (GAS), the group C streptococcus S dysgalactiae, and fusobacterium. We sometimes think of throat cultures as telling us the definitive etiology of a sore throat. In fact, children commonly are colonized with GAS even when not infected — 35% of the time, when GAS is detected on throat swab in a child, GAS is not the cause of the sore throat. Very few adults are colonized with GAS.
Sore throats are usually self-limited, whether they are treated with antibiotics or not, but occasionally complications can occur. Suppurative complications include peritonsillar abscess, sinusitis and sepsis. Nonsuppurative complications are primarily glomerulonephritis and rheumatic fever, which can lead to rheumatic heart disease.
Antibiotics. Antibiotics have three potential benefits in acute sore throat: to reduce the risk of developing rheumatic heart disease, reduce the duration and severity of symptoms, and treat suppurative complications. The risk for rheumatic heart disease has almost vanished in high-income countries, but not in low-income countries. Thus, antibiotic treatment of acute sore throat due to GAS may benefit those in living in, and those who recently emigrated from, low-income countries.
Patients with suppurative complications should be identified because antibiotics are important for this group. Although antibiotics are prescribed primarily to prevent rheumatic fever in this population, they may be mildly helpful in reducing a patient’s symptoms.
Testing. The sensitivity and specificity of high-quality point-of-care tests (POCTs) are on par with those of cultures, with the advantage that the results are available within minutes. Negative tests reduce unneeded antibiotic prescriptions.
Given this evidence, the authors recommend an approach that puts a lot of emphasis on two major things: the risk for rheumatic fever, and clinical assessment. On the basis of these factors, a decision is made about the utility of POCTs and treatment with antibiotics for GAS. The risk for rheumatic fever is based on epidemiology: If the patient is in a low-income country or has recently immigrated from one, then the risk is high, and if not, the risk is low.
Complicated vs uncomplicated? This is determined by clinical assessment of the severity of the patient’s illness, including general appearance. Uncomplicated sore throat means that the patient:
- Is not getting worse after 3 days of illness
- Has a duration of illness ≤ 5 days or is getting better after day 5
- Has mild to moderate symptom severity (bilateral throat pain, the ability to open the mouth fully, and absence of a sandpaper or scarlatiniform rash or strawberry tongue)
For patients with uncomplicated sore throat and low risk for rheumatic fever, the main goals are to reduce antibiotic use and provide symptomatic relief. For these patients, an assessment such as the Centor score can be done. Those with a low Centor score (0-2) can be treated with analgesics and there is no need for a POCT.
In patients with a higher Centor score, the consensus gives two choices: They can either be tested (and treated if the testing is positive), or it is reasonable to forgo testing and use a wait-and-see strategy, with reevaluation if they are getting worse after day 3 or not improving after day 5 days of their illness. Illnesses that last longer than 5 days with sore throat and fatigue should prompt consideration of alternative diagnoses, such as infectious mononucleosis.
For patients with potentially complicated sore throat — including indicators such as worsening symptoms after 3 days or worsening after initiation of antibiotics, inability to open the mouth fully, unilateral neck pain or swelling, or rigors — should undergo a careful evaluation. The need for further testing in these patients, including labs and imaging, should be decided on a case-by-case basis. If the patient appears seriously ill, don’t rely solely on POCT for GAS, but think about other diagnoses.
Rheumatic fever. The approach is very different in patients at high risk for rheumatic fever. POCT for GAS is recommended irrespective of their clinical score, and antibiotics should be prescribed if it’s positive for GAS. If a POCT is unavailable, then the consensus recommends prescribing antibiotics for all high-risk patients who have acute sore throat.
This approach is sensible and puts a lot of emphasis on clinical evaluation, though it should be noted that this approach is considerably different from that in the 2012 Infectious Diseases Society of America guidelines.
Dr. Skolnik, professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly and Company, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
There is a helpful consensus from experts on the best management of patients with acute sore throat. This is a common problem in primary care, and one for which there is a lot of evidence, opinion, and ultimately overprescribing of antibiotics. This consensus presents a pragmatic clinical approach aimed at decreasing overprescribing, yet detecting which patients are likely to benefit from treatment with antibiotics.
Let’s first go over the evidence that forms the basis for the recommendations, then the recommended approach. First, a sore throat can be caused by many different viruses, as well as group A streptococcus (GAS), the group C streptococcus S dysgalactiae, and fusobacterium. We sometimes think of throat cultures as telling us the definitive etiology of a sore throat. In fact, children commonly are colonized with GAS even when not infected — 35% of the time, when GAS is detected on throat swab in a child, GAS is not the cause of the sore throat. Very few adults are colonized with GAS.
Sore throats are usually self-limited, whether they are treated with antibiotics or not, but occasionally complications can occur. Suppurative complications include peritonsillar abscess, sinusitis and sepsis. Nonsuppurative complications are primarily glomerulonephritis and rheumatic fever, which can lead to rheumatic heart disease.
Antibiotics. Antibiotics have three potential benefits in acute sore throat: to reduce the risk of developing rheumatic heart disease, reduce the duration and severity of symptoms, and treat suppurative complications. The risk for rheumatic heart disease has almost vanished in high-income countries, but not in low-income countries. Thus, antibiotic treatment of acute sore throat due to GAS may benefit those in living in, and those who recently emigrated from, low-income countries.
Patients with suppurative complications should be identified because antibiotics are important for this group. Although antibiotics are prescribed primarily to prevent rheumatic fever in this population, they may be mildly helpful in reducing a patient’s symptoms.
Testing. The sensitivity and specificity of high-quality point-of-care tests (POCTs) are on par with those of cultures, with the advantage that the results are available within minutes. Negative tests reduce unneeded antibiotic prescriptions.
Given this evidence, the authors recommend an approach that puts a lot of emphasis on two major things: the risk for rheumatic fever, and clinical assessment. On the basis of these factors, a decision is made about the utility of POCTs and treatment with antibiotics for GAS. The risk for rheumatic fever is based on epidemiology: If the patient is in a low-income country or has recently immigrated from one, then the risk is high, and if not, the risk is low.
Complicated vs uncomplicated? This is determined by clinical assessment of the severity of the patient’s illness, including general appearance. Uncomplicated sore throat means that the patient:
- Is not getting worse after 3 days of illness
- Has a duration of illness ≤ 5 days or is getting better after day 5
- Has mild to moderate symptom severity (bilateral throat pain, the ability to open the mouth fully, and absence of a sandpaper or scarlatiniform rash or strawberry tongue)
For patients with uncomplicated sore throat and low risk for rheumatic fever, the main goals are to reduce antibiotic use and provide symptomatic relief. For these patients, an assessment such as the Centor score can be done. Those with a low Centor score (0-2) can be treated with analgesics and there is no need for a POCT.
In patients with a higher Centor score, the consensus gives two choices: They can either be tested (and treated if the testing is positive), or it is reasonable to forgo testing and use a wait-and-see strategy, with reevaluation if they are getting worse after day 3 or not improving after day 5 days of their illness. Illnesses that last longer than 5 days with sore throat and fatigue should prompt consideration of alternative diagnoses, such as infectious mononucleosis.
For patients with potentially complicated sore throat — including indicators such as worsening symptoms after 3 days or worsening after initiation of antibiotics, inability to open the mouth fully, unilateral neck pain or swelling, or rigors — should undergo a careful evaluation. The need for further testing in these patients, including labs and imaging, should be decided on a case-by-case basis. If the patient appears seriously ill, don’t rely solely on POCT for GAS, but think about other diagnoses.
Rheumatic fever. The approach is very different in patients at high risk for rheumatic fever. POCT for GAS is recommended irrespective of their clinical score, and antibiotics should be prescribed if it’s positive for GAS. If a POCT is unavailable, then the consensus recommends prescribing antibiotics for all high-risk patients who have acute sore throat.
This approach is sensible and puts a lot of emphasis on clinical evaluation, though it should be noted that this approach is considerably different from that in the 2012 Infectious Diseases Society of America guidelines.
Dr. Skolnik, professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly and Company, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article appeared on Medscape.com.
Gynecologic Oncology Consult: Update on Endometrial Cancer Treatment
While rates of most other cancers have declined or plateaued, the incidence and mortality rate of endometrial cancer continue to rise.1 The landscape of endometrial cancer treatment has evolved quickly over the past 2-3 years. While surgery and radiation therapy remain the mainstay of treatment for early-stage disease, the development of multiple targeted therapeutics has led to additional treatment options in advanced-stage disease and more aggressive tumor types, which are both associated with a poorer prognosis.

In this update, we highlight the recent advances in these targeted therapies in endometrial cancer. We review the landmark NRG-GY018 and RUBY trials, which demonstrated that checkpoint inhibitors improve outcomes in women with advanced endometrial cancer. We discuss an immunotherapy and antivascular endothelial growth factor (VEGF) combination useful in certain tumors lacking biomarker expression. We also highlight progress against endometrial cancers that overexpress human epidermal growth factor receptor 2 (HER2), demonstrated in the DESTINY PanTumor-02 trial.
PD-1 inhibitors
Programmed cell death protein 1 (PD-1) is an inhibitory receptor expressed on T cells that binds to programmed cell death ligand 1 (PD-L1). PD-L1 is expressed on many immune cells but can also be expressed on tumor cells. The interaction of PD-L1 expressed on the surface of endometrial cancer cells with the PD-1 receptor on T cells results in diminished T-cell function, eliminating the immune system’s ability to attack the tumor cells. Treatment with a PD-1 inhibitor prevents this ligand-receptor interaction and restores cancer-fighting function to T cells.

Pembrolizumab, an antibody against the PD-1 receptor, has been used as single-agent treatment for recurrent endometrial cancer since the KEYNOTE-158 study demonstrated clinical benefit in patients with mismatch repair deficient (dMMR) tumors.2
Additionally, in 2022, Makker et al. published results from a phase 3 trial3 evaluating immunotherapy in the treatment of recurrent endometrial cancer, specifically in patients with mismatch repair proficient (pMMR) tumors. They compared the combination of pembrolizumab and lenvatinib, an oral inhibitor of VEGF, to physician’s choice next-line chemotherapy in over 800 patients with advanced or recurrent endometrial cancer. They found that progression-free survival (PFS) was significantly improved from a median of 3.8 months with chemotherapy to a median of 6.6 months with pembrolizumab and lenvatinib in the pMMR population. Overall survival was also improved from 12 months to 17.4 months in the pMMR population.
With the clear benefit of immunotherapy in the recurrent setting established, Eskander and colleagues were the first to evaluate treatment with pembrolizumab as upfront treatment in the NRG-GY018 trial,4 comparing standard first-line chemotherapy (carboplatin and paclitaxel) with or without the addition of pembrolizumab. This randomized, international, phase 3 trial included over 800 patients with advanced or recurrent endometrial cancer of any histology except carcinosarcoma. Patients received carboplatin and paclitaxel with either pembrolizumab or placebo, followed by maintenance pembrolizumab or placebo. The results showed an improvement in PFS with the addition of immunotherapy, with a risk of disease progression or death with pembrolizumab 70% lower than with placebo in patients with dMMR tumors and 46% lower than with placebo in patients with pMMR tumors.
In the similar randomized, international, phase 3 RUBY trial,5 Mirza and colleagues compared standard chemotherapy with or without the addition of another PD-1 inhibitor, dostarlimab, in almost 500 patients with advanced or recurrent endometrial cancer of any histology. They found that the addition of dostarlimab to standard chemotherapy significantly improved PFS. Unpublished data presented at the Society of Gynecologic Oncology annual meeting in March also demonstrated an improvement in overall survival.6 As in NRG-GY018, they found a substantial benefit again in the dMMR population.
The results of these three landmark trials demonstrate the increasing role for immunotherapy in endometrial cancer, especially at the time of initial treatment, and how biomarkers can help direct treatment options.
Takeaway
Use of PD-1 inhibitors improves clinical outcomes in both the upfront and recurrent treatment settings. The magnitude of benefit of treatment with PD-1 inhibitors is greater in patients with dMMR tumors.
Anti-HER2 therapies
HER2 is a cell surface protein that can become overexpressed and promote tumorigenesis. It is used as a prognostic biomarker and a therapeutic target in breast, stomach, and colon cancer, but it has also been identified at high rates (20%-30%) in the most aggressive histologic subtypes in endometrial cancer (serous, clear cell, and carcinosarcoma). Trastuzumab is a monoclonal antibody directed against HER2, most commonly used in HER2-positive breast cancer. In 2018, a phase 2 trial demonstrated that trastuzumab combined with standard chemotherapy improved PFS in serous endometrial cancers that overexpress HER2.7 These results were important and promising given both the poor prognosis associated with the aggressive serous histology and the relative lack of effective therapies at the time of recurrence.
Recently, antibody-drug conjugates (ADCs) have come to the forefront of cancer-directed therapies. ADCs deliver chemotherapy agents directly to cancer cells via a monoclonal antibody that binds to a specific target on the cancer cells. Trastuzumab-deruxtecan (T-DXd) is an ADC consisting of an anti-HER2 monoclonal antibody, a topoisomerase I inhibitor payload, and a cleavable linker. T-DXd was evaluated in the tumor-agnostic phase 2 DESTINY-PanTumor02 trial,8 which included endometrial, ovarian, and cervical cancer cohorts, in addition to four other nongynecologic malignancies. In this study, 40 patients with advanced or recurrent malignancies overexpressing HER2 in each cohort were treated with T-DXd.
The results within the endometrial cancer cohort were particularly promising. The overall response rate in endometrial cancer was an astounding 57.5% with a median PFS of over 11 months. Even higher response rates were seen in endometrial cancer patients whose tumors demonstrated higher rates of HER2 overexpression. These results are unprecedented in a cohort in which most patients had seen at least 2 prior lines of therapy. Ocular and pulmonary toxicities are of particular interest with use of ADCs, but they were mostly low grade and manageable in this study.
Takeaway
Anti-HER2 therapies, including antibody-drug conjugates, are effective in treating patients with some of the highest-risk endometrial cancers when they overexpress this protein.
Dr. Haag is a gynecologic oncology fellow in the Department of Obstetrics and Gynecology, University of North Carolina Hospitals, Chapel Hill. Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill. They have no conflicts of interest.
References
1. Siegel R et al. CA Cancer J. 2024;74(1):12-49.
2. Marabelle A et al. J Clin Oncol. 2020;38(1):1-10.
3. Makker V et al. N Engl J Med. 2022;386(5):437-48.
4. Eskander RN et al. N Engl J Med. 2023;388(23):2159-70.
5. Mirza MR et al. N Engl J Med. 2023;388(23):2145-58.
6. Powell MA et al, editors. Society of Gynecologic Oncology Annual Meeting on Women’s Cancer, 2024; San Diego, CA.
7. Fader AN et al. J Clin Oncol. 2018;36(20):2044-51.
8. Meric-Bernstam F et al. J Clin Oncol. 2024;42(1):47-58.
While rates of most other cancers have declined or plateaued, the incidence and mortality rate of endometrial cancer continue to rise.1 The landscape of endometrial cancer treatment has evolved quickly over the past 2-3 years. While surgery and radiation therapy remain the mainstay of treatment for early-stage disease, the development of multiple targeted therapeutics has led to additional treatment options in advanced-stage disease and more aggressive tumor types, which are both associated with a poorer prognosis.
In this update, we highlight the recent advances in these targeted therapies in endometrial cancer. We review the landmark NRG-GY018 and RUBY trials, which demonstrated that checkpoint inhibitors improve outcomes in women with advanced endometrial cancer. We discuss an immunotherapy and antivascular endothelial growth factor (VEGF) combination useful in certain tumors lacking biomarker expression. We also highlight progress against endometrial cancers that overexpress human epidermal growth factor receptor 2 (HER2), demonstrated in the DESTINY PanTumor-02 trial.
PD-1 inhibitors
Programmed cell death protein 1 (PD-1) is an inhibitory receptor expressed on T cells that binds to programmed cell death ligand 1 (PD-L1). PD-L1 is expressed on many immune cells but can also be expressed on tumor cells. The interaction of PD-L1 expressed on the surface of endometrial cancer cells with the PD-1 receptor on T cells results in diminished T-cell function, eliminating the immune system’s ability to attack the tumor cells. Treatment with a PD-1 inhibitor prevents this ligand-receptor interaction and restores cancer-fighting function to T cells.
Pembrolizumab, an antibody against the PD-1 receptor, has been used as single-agent treatment for recurrent endometrial cancer since the KEYNOTE-158 study demonstrated clinical benefit in patients with mismatch repair deficient (dMMR) tumors.2
Additionally, in 2022, Makker et al. published results from a phase 3 trial3 evaluating immunotherapy in the treatment of recurrent endometrial cancer, specifically in patients with mismatch repair proficient (pMMR) tumors. They compared the combination of pembrolizumab and lenvatinib, an oral inhibitor of VEGF, to physician’s choice next-line chemotherapy in over 800 patients with advanced or recurrent endometrial cancer. They found that progression-free survival (PFS) was significantly improved from a median of 3.8 months with chemotherapy to a median of 6.6 months with pembrolizumab and lenvatinib in the pMMR population. Overall survival was also improved from 12 months to 17.4 months in the pMMR population.
With the clear benefit of immunotherapy in the recurrent setting established, Eskander and colleagues were the first to evaluate treatment with pembrolizumab as upfront treatment in the NRG-GY018 trial,4 comparing standard first-line chemotherapy (carboplatin and paclitaxel) with or without the addition of pembrolizumab. This randomized, international, phase 3 trial included over 800 patients with advanced or recurrent endometrial cancer of any histology except carcinosarcoma. Patients received carboplatin and paclitaxel with either pembrolizumab or placebo, followed by maintenance pembrolizumab or placebo. The results showed an improvement in PFS with the addition of immunotherapy, with a risk of disease progression or death with pembrolizumab 70% lower than with placebo in patients with dMMR tumors and 46% lower than with placebo in patients with pMMR tumors.
In the similar randomized, international, phase 3 RUBY trial,5 Mirza and colleagues compared standard chemotherapy with or without the addition of another PD-1 inhibitor, dostarlimab, in almost 500 patients with advanced or recurrent endometrial cancer of any histology. They found that the addition of dostarlimab to standard chemotherapy significantly improved PFS. Unpublished data presented at the Society of Gynecologic Oncology annual meeting in March also demonstrated an improvement in overall survival.6 As in NRG-GY018, they found a substantial benefit again in the dMMR population.
The results of these three landmark trials demonstrate the increasing role for immunotherapy in endometrial cancer, especially at the time of initial treatment, and how biomarkers can help direct treatment options.
Takeaway
Use of PD-1 inhibitors improves clinical outcomes in both the upfront and recurrent treatment settings. The magnitude of benefit of treatment with PD-1 inhibitors is greater in patients with dMMR tumors.
Anti-HER2 therapies
HER2 is a cell surface protein that can become overexpressed and promote tumorigenesis. It is used as a prognostic biomarker and a therapeutic target in breast, stomach, and colon cancer, but it has also been identified at high rates (20%-30%) in the most aggressive histologic subtypes in endometrial cancer (serous, clear cell, and carcinosarcoma). Trastuzumab is a monoclonal antibody directed against HER2, most commonly used in HER2-positive breast cancer. In 2018, a phase 2 trial demonstrated that trastuzumab combined with standard chemotherapy improved PFS in serous endometrial cancers that overexpress HER2.7 These results were important and promising given both the poor prognosis associated with the aggressive serous histology and the relative lack of effective therapies at the time of recurrence.
Recently, antibody-drug conjugates (ADCs) have come to the forefront of cancer-directed therapies. ADCs deliver chemotherapy agents directly to cancer cells via a monoclonal antibody that binds to a specific target on the cancer cells. Trastuzumab-deruxtecan (T-DXd) is an ADC consisting of an anti-HER2 monoclonal antibody, a topoisomerase I inhibitor payload, and a cleavable linker. T-DXd was evaluated in the tumor-agnostic phase 2 DESTINY-PanTumor02 trial,8 which included endometrial, ovarian, and cervical cancer cohorts, in addition to four other nongynecologic malignancies. In this study, 40 patients with advanced or recurrent malignancies overexpressing HER2 in each cohort were treated with T-DXd.
The results within the endometrial cancer cohort were particularly promising. The overall response rate in endometrial cancer was an astounding 57.5% with a median PFS of over 11 months. Even higher response rates were seen in endometrial cancer patients whose tumors demonstrated higher rates of HER2 overexpression. These results are unprecedented in a cohort in which most patients had seen at least 2 prior lines of therapy. Ocular and pulmonary toxicities are of particular interest with use of ADCs, but they were mostly low grade and manageable in this study.
Takeaway
Anti-HER2 therapies, including antibody-drug conjugates, are effective in treating patients with some of the highest-risk endometrial cancers when they overexpress this protein.
Dr. Haag is a gynecologic oncology fellow in the Department of Obstetrics and Gynecology, University of North Carolina Hospitals, Chapel Hill. Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill. They have no conflicts of interest.
References
1. Siegel R et al. CA Cancer J. 2024;74(1):12-49.
2. Marabelle A et al. J Clin Oncol. 2020;38(1):1-10.
3. Makker V et al. N Engl J Med. 2022;386(5):437-48.
4. Eskander RN et al. N Engl J Med. 2023;388(23):2159-70.
5. Mirza MR et al. N Engl J Med. 2023;388(23):2145-58.
6. Powell MA et al, editors. Society of Gynecologic Oncology Annual Meeting on Women’s Cancer, 2024; San Diego, CA.
7. Fader AN et al. J Clin Oncol. 2018;36(20):2044-51.
8. Meric-Bernstam F et al. J Clin Oncol. 2024;42(1):47-58.
While rates of most other cancers have declined or plateaued, the incidence and mortality rate of endometrial cancer continue to rise.1 The landscape of endometrial cancer treatment has evolved quickly over the past 2-3 years. While surgery and radiation therapy remain the mainstay of treatment for early-stage disease, the development of multiple targeted therapeutics has led to additional treatment options in advanced-stage disease and more aggressive tumor types, which are both associated with a poorer prognosis.
In this update, we highlight the recent advances in these targeted therapies in endometrial cancer. We review the landmark NRG-GY018 and RUBY trials, which demonstrated that checkpoint inhibitors improve outcomes in women with advanced endometrial cancer. We discuss an immunotherapy and antivascular endothelial growth factor (VEGF) combination useful in certain tumors lacking biomarker expression. We also highlight progress against endometrial cancers that overexpress human epidermal growth factor receptor 2 (HER2), demonstrated in the DESTINY PanTumor-02 trial.
PD-1 inhibitors
Programmed cell death protein 1 (PD-1) is an inhibitory receptor expressed on T cells that binds to programmed cell death ligand 1 (PD-L1). PD-L1 is expressed on many immune cells but can also be expressed on tumor cells. The interaction of PD-L1 expressed on the surface of endometrial cancer cells with the PD-1 receptor on T cells results in diminished T-cell function, eliminating the immune system’s ability to attack the tumor cells. Treatment with a PD-1 inhibitor prevents this ligand-receptor interaction and restores cancer-fighting function to T cells.
Pembrolizumab, an antibody against the PD-1 receptor, has been used as single-agent treatment for recurrent endometrial cancer since the KEYNOTE-158 study demonstrated clinical benefit in patients with mismatch repair deficient (dMMR) tumors.2
Additionally, in 2022, Makker et al. published results from a phase 3 trial3 evaluating immunotherapy in the treatment of recurrent endometrial cancer, specifically in patients with mismatch repair proficient (pMMR) tumors. They compared the combination of pembrolizumab and lenvatinib, an oral inhibitor of VEGF, to physician’s choice next-line chemotherapy in over 800 patients with advanced or recurrent endometrial cancer. They found that progression-free survival (PFS) was significantly improved from a median of 3.8 months with chemotherapy to a median of 6.6 months with pembrolizumab and lenvatinib in the pMMR population. Overall survival was also improved from 12 months to 17.4 months in the pMMR population.
With the clear benefit of immunotherapy in the recurrent setting established, Eskander and colleagues were the first to evaluate treatment with pembrolizumab as upfront treatment in the NRG-GY018 trial,4 comparing standard first-line chemotherapy (carboplatin and paclitaxel) with or without the addition of pembrolizumab. This randomized, international, phase 3 trial included over 800 patients with advanced or recurrent endometrial cancer of any histology except carcinosarcoma. Patients received carboplatin and paclitaxel with either pembrolizumab or placebo, followed by maintenance pembrolizumab or placebo. The results showed an improvement in PFS with the addition of immunotherapy, with a risk of disease progression or death with pembrolizumab 70% lower than with placebo in patients with dMMR tumors and 46% lower than with placebo in patients with pMMR tumors.
In the similar randomized, international, phase 3 RUBY trial,5 Mirza and colleagues compared standard chemotherapy with or without the addition of another PD-1 inhibitor, dostarlimab, in almost 500 patients with advanced or recurrent endometrial cancer of any histology. They found that the addition of dostarlimab to standard chemotherapy significantly improved PFS. Unpublished data presented at the Society of Gynecologic Oncology annual meeting in March also demonstrated an improvement in overall survival.6 As in NRG-GY018, they found a substantial benefit again in the dMMR population.
The results of these three landmark trials demonstrate the increasing role for immunotherapy in endometrial cancer, especially at the time of initial treatment, and how biomarkers can help direct treatment options.
Takeaway
Use of PD-1 inhibitors improves clinical outcomes in both the upfront and recurrent treatment settings. The magnitude of benefit of treatment with PD-1 inhibitors is greater in patients with dMMR tumors.
Anti-HER2 therapies
HER2 is a cell surface protein that can become overexpressed and promote tumorigenesis. It is used as a prognostic biomarker and a therapeutic target in breast, stomach, and colon cancer, but it has also been identified at high rates (20%-30%) in the most aggressive histologic subtypes in endometrial cancer (serous, clear cell, and carcinosarcoma). Trastuzumab is a monoclonal antibody directed against HER2, most commonly used in HER2-positive breast cancer. In 2018, a phase 2 trial demonstrated that trastuzumab combined with standard chemotherapy improved PFS in serous endometrial cancers that overexpress HER2.7 These results were important and promising given both the poor prognosis associated with the aggressive serous histology and the relative lack of effective therapies at the time of recurrence.
Recently, antibody-drug conjugates (ADCs) have come to the forefront of cancer-directed therapies. ADCs deliver chemotherapy agents directly to cancer cells via a monoclonal antibody that binds to a specific target on the cancer cells. Trastuzumab-deruxtecan (T-DXd) is an ADC consisting of an anti-HER2 monoclonal antibody, a topoisomerase I inhibitor payload, and a cleavable linker. T-DXd was evaluated in the tumor-agnostic phase 2 DESTINY-PanTumor02 trial,8 which included endometrial, ovarian, and cervical cancer cohorts, in addition to four other nongynecologic malignancies. In this study, 40 patients with advanced or recurrent malignancies overexpressing HER2 in each cohort were treated with T-DXd.
The results within the endometrial cancer cohort were particularly promising. The overall response rate in endometrial cancer was an astounding 57.5% with a median PFS of over 11 months. Even higher response rates were seen in endometrial cancer patients whose tumors demonstrated higher rates of HER2 overexpression. These results are unprecedented in a cohort in which most patients had seen at least 2 prior lines of therapy. Ocular and pulmonary toxicities are of particular interest with use of ADCs, but they were mostly low grade and manageable in this study.
Takeaway
Anti-HER2 therapies, including antibody-drug conjugates, are effective in treating patients with some of the highest-risk endometrial cancers when they overexpress this protein.
Dr. Haag is a gynecologic oncology fellow in the Department of Obstetrics and Gynecology, University of North Carolina Hospitals, Chapel Hill. Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill. They have no conflicts of interest.
References
1. Siegel R et al. CA Cancer J. 2024;74(1):12-49.
2. Marabelle A et al. J Clin Oncol. 2020;38(1):1-10.
3. Makker V et al. N Engl J Med. 2022;386(5):437-48.
4. Eskander RN et al. N Engl J Med. 2023;388(23):2159-70.
5. Mirza MR et al. N Engl J Med. 2023;388(23):2145-58.
6. Powell MA et al, editors. Society of Gynecologic Oncology Annual Meeting on Women’s Cancer, 2024; San Diego, CA.
7. Fader AN et al. J Clin Oncol. 2018;36(20):2044-51.
8. Meric-Bernstam F et al. J Clin Oncol. 2024;42(1):47-58.
The Management of Anxiety in Primary Care
This transcript has been edited for clarity.
Matthew F. Watto, MD: Welcome back to The Curbsiders. I’m Dr. Matthew Frank Watto, here with my great friend and America’s primary care physician, Dr. Paul Nelson Williams. Paul, are you ready to talk about anxiety?
Paul N. Williams, MD: Always. It’s one of my favorite topics.
Dr. Watto: We had a great guest for this podcast on anxiety — Dr. Jessi Gold, who gave us a lot of practical tips. The way she talks to her patients about anxiety is really useful. When patients say “my anxiety” or “I feel anxious,” she considers that a symptom. Anxiety can be a diagnosis or a symptom. You need to clarify what they mean when they refer to their anxiety and dig into how it affects their life.
We asked her about the Generalized Anxiety Disorder (GAD)-7 score. Like most of the experts we’ve talked to, she’s internalized that, so she doesn’t need to rely on a questionnaire. But I still rely on a questionnaire when I’m taking a history for anxiety.
We also asked her how she explains anxiety to patients. I don’t know about you, Paul, but I’ve never really thought about explaining to patients why they have anxiety.
Dr. Williams: I’ve done my best to try to normalize it, but I haven’t actually talked to patients about the evolutionary advantage of anxiety.
Dr. Watto: She frames it to patients this way: As we were evolving, it was somewhat of an advantage to be hypervigilant, to have some anxiety and a healthy amount of fear so that you weren’t killed or eaten. But now, in the modern world, anxiety isn’t playing to our advantage. Anxiety is not making them safer; it’s making their lives worse. She explains to patients that she’s trying to help them overcome that.
In terms of pharmacotherapy for anxiety, I always think about SSRIs as one of the first steps. Why not use an SNRI as first-line treatment?
Dr. Williams: I was glad we had this conversation because I feel, for whatever reason, a bit more comfortable treating depression than anxiety. In any case, Dr. Gold reaches for the SSRI first, in part because getting off an SNRI (for example, to switch to something else) can be absolutely miserable. The discontinuation effects can be severe enough to have to bridge some patients with a benzodiazepine to get them fully off the SNRI. So, an SNRI is not the first drug you should necessarily reach for.
She thinks about using an SNRI if she has tried a couple of SSRIs that have been ineffective, or if the patient has a comorbid condition that might also benefit from the SNRI in the same way that you might use a tricyclic antidepressant in the patient with both migraines and anxiety. An SNRI might be a good medication to consider in the patient with neuropathic pain and anxiety but rarely as a first-line treatment, because if it doesn’t work out, getting the patient off that medication can be a challenge.
Dr. Watto: She mentioned venlafaxine as being especially difficult to get people off of. I’ve heard that bupropion should never be used in anxiety, and if you give it, you are a terrible doctor. What did we learn about that?
Dr. Williams: It’s a drug I’ve hesitated to prescribe to patients with anxiety or even comorbid anxiety. I’m a little bit nervous for someone who has depression and anxiety to prescribe bupropion because it can be activating and make things worse. But Dr. Gold says that she has seen bupropion work for some patients so she will consider it, especially for patients who don’t want to gain weight, or for whom sexual side effects would be bothersome. So, it’s not always the wrong answer. In her expert opinion, you can try it and see how the patient responds, using shared decision-making and letting the patient know that they may not tolerate it as well as other medications.
Dr. Watto: She sees a lot of younger people — students, working professionals — who do not want to gain weight, and that’s understandable. She will tell patients, “We can try bupropion, but if you get more anxious, we might not be able to continue it. We might have to use one of the first-line agents instead.”
Dr. Williams: We talked about mirtazapine as well. She tells patients they are going to gain weight with it. You have to have that conversation with the patient to see whether that is something they are willing to tolerate. If so, mirtazapine might be worth a try, but you have to be upfront about the potential side effects and know what the medications you’re prescribing will do to patients.
Dr. Watto: We asked her about benzodiazepines. For as-needed medication for people who are experiencing panic or anxiety attacks, she prescribes propranolol 10-20 mg twice a day as needed, which is a low dose. In primary care, we use higher doses for migraine prophylaxis.
She uses propranolol because for some patients, it’s the physical symptoms of anxiety that are bothering them. She can calm down the physical symptoms with that and get by without needing to use a benzodiazepine.
But what about thoughts that make people anxious? Can we change people’s thoughts with medication?
Dr. Williams: Dr. Gold made the point that we can medicate away insomnia, for the most part. We can medicate away the physical symptoms of anxiety, which can be really bothersome. But we can’t medicate away thoughts and thought patterns. You can make patients feel better with medications, but you may not be able to get rid of the persistent bothersome thoughts. That’s where cognitive-behavioral therapy can be especially helpful. Most of these patients would benefit from therapy.
Dr. Watto: I completely agree with that. We talked about so many great things with Dr. Gold, but we can’t recap all of it here. Please click on this link to hear the full podcast episode.
Dr. Watto is Clinical Assistant Professor, Department of Medicine, Perelman School of Medicine at University of Pennsylvania; Internist, Department of Medicine, Hospital Medicine Section, Pennsylvania Hospital, Philadelphia, Pennsylvania. He has disclosed no relevant financial relationships. Dr. Williams is Associate Professor of Clinical Medicine, Department of General Internal Medicine, Lewis Katz School of Medicine; Staff Physician, Department of General Internal Medicine, Temple Internal Medicine Associates, Philadelphia, Pennsylvania. He disclosed receiving income from The Curbsiders. The Curbsiders is an internal medicine podcast, in which three board-certified internists interview experts on clinically important topics. In a collaboration with Medscape, the Curbsiders share clinical pearls and practice-changing knowledge from selected podcasts.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Matthew F. Watto, MD: Welcome back to The Curbsiders. I’m Dr. Matthew Frank Watto, here with my great friend and America’s primary care physician, Dr. Paul Nelson Williams. Paul, are you ready to talk about anxiety?
Paul N. Williams, MD: Always. It’s one of my favorite topics.
Dr. Watto: We had a great guest for this podcast on anxiety — Dr. Jessi Gold, who gave us a lot of practical tips. The way she talks to her patients about anxiety is really useful. When patients say “my anxiety” or “I feel anxious,” she considers that a symptom. Anxiety can be a diagnosis or a symptom. You need to clarify what they mean when they refer to their anxiety and dig into how it affects their life.
We asked her about the Generalized Anxiety Disorder (GAD)-7 score. Like most of the experts we’ve talked to, she’s internalized that, so she doesn’t need to rely on a questionnaire. But I still rely on a questionnaire when I’m taking a history for anxiety.
We also asked her how she explains anxiety to patients. I don’t know about you, Paul, but I’ve never really thought about explaining to patients why they have anxiety.
Dr. Williams: I’ve done my best to try to normalize it, but I haven’t actually talked to patients about the evolutionary advantage of anxiety.
Dr. Watto: She frames it to patients this way: As we were evolving, it was somewhat of an advantage to be hypervigilant, to have some anxiety and a healthy amount of fear so that you weren’t killed or eaten. But now, in the modern world, anxiety isn’t playing to our advantage. Anxiety is not making them safer; it’s making their lives worse. She explains to patients that she’s trying to help them overcome that.
In terms of pharmacotherapy for anxiety, I always think about SSRIs as one of the first steps. Why not use an SNRI as first-line treatment?
Dr. Williams: I was glad we had this conversation because I feel, for whatever reason, a bit more comfortable treating depression than anxiety. In any case, Dr. Gold reaches for the SSRI first, in part because getting off an SNRI (for example, to switch to something else) can be absolutely miserable. The discontinuation effects can be severe enough to have to bridge some patients with a benzodiazepine to get them fully off the SNRI. So, an SNRI is not the first drug you should necessarily reach for.
She thinks about using an SNRI if she has tried a couple of SSRIs that have been ineffective, or if the patient has a comorbid condition that might also benefit from the SNRI in the same way that you might use a tricyclic antidepressant in the patient with both migraines and anxiety. An SNRI might be a good medication to consider in the patient with neuropathic pain and anxiety but rarely as a first-line treatment, because if it doesn’t work out, getting the patient off that medication can be a challenge.
Dr. Watto: She mentioned venlafaxine as being especially difficult to get people off of. I’ve heard that bupropion should never be used in anxiety, and if you give it, you are a terrible doctor. What did we learn about that?
Dr. Williams: It’s a drug I’ve hesitated to prescribe to patients with anxiety or even comorbid anxiety. I’m a little bit nervous for someone who has depression and anxiety to prescribe bupropion because it can be activating and make things worse. But Dr. Gold says that she has seen bupropion work for some patients so she will consider it, especially for patients who don’t want to gain weight, or for whom sexual side effects would be bothersome. So, it’s not always the wrong answer. In her expert opinion, you can try it and see how the patient responds, using shared decision-making and letting the patient know that they may not tolerate it as well as other medications.
Dr. Watto: She sees a lot of younger people — students, working professionals — who do not want to gain weight, and that’s understandable. She will tell patients, “We can try bupropion, but if you get more anxious, we might not be able to continue it. We might have to use one of the first-line agents instead.”
Dr. Williams: We talked about mirtazapine as well. She tells patients they are going to gain weight with it. You have to have that conversation with the patient to see whether that is something they are willing to tolerate. If so, mirtazapine might be worth a try, but you have to be upfront about the potential side effects and know what the medications you’re prescribing will do to patients.
Dr. Watto: We asked her about benzodiazepines. For as-needed medication for people who are experiencing panic or anxiety attacks, she prescribes propranolol 10-20 mg twice a day as needed, which is a low dose. In primary care, we use higher doses for migraine prophylaxis.
She uses propranolol because for some patients, it’s the physical symptoms of anxiety that are bothering them. She can calm down the physical symptoms with that and get by without needing to use a benzodiazepine.
But what about thoughts that make people anxious? Can we change people’s thoughts with medication?
Dr. Williams: Dr. Gold made the point that we can medicate away insomnia, for the most part. We can medicate away the physical symptoms of anxiety, which can be really bothersome. But we can’t medicate away thoughts and thought patterns. You can make patients feel better with medications, but you may not be able to get rid of the persistent bothersome thoughts. That’s where cognitive-behavioral therapy can be especially helpful. Most of these patients would benefit from therapy.
Dr. Watto: I completely agree with that. We talked about so many great things with Dr. Gold, but we can’t recap all of it here. Please click on this link to hear the full podcast episode.
Dr. Watto is Clinical Assistant Professor, Department of Medicine, Perelman School of Medicine at University of Pennsylvania; Internist, Department of Medicine, Hospital Medicine Section, Pennsylvania Hospital, Philadelphia, Pennsylvania. He has disclosed no relevant financial relationships. Dr. Williams is Associate Professor of Clinical Medicine, Department of General Internal Medicine, Lewis Katz School of Medicine; Staff Physician, Department of General Internal Medicine, Temple Internal Medicine Associates, Philadelphia, Pennsylvania. He disclosed receiving income from The Curbsiders. The Curbsiders is an internal medicine podcast, in which three board-certified internists interview experts on clinically important topics. In a collaboration with Medscape, the Curbsiders share clinical pearls and practice-changing knowledge from selected podcasts.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Matthew F. Watto, MD: Welcome back to The Curbsiders. I’m Dr. Matthew Frank Watto, here with my great friend and America’s primary care physician, Dr. Paul Nelson Williams. Paul, are you ready to talk about anxiety?
Paul N. Williams, MD: Always. It’s one of my favorite topics.
Dr. Watto: We had a great guest for this podcast on anxiety — Dr. Jessi Gold, who gave us a lot of practical tips. The way she talks to her patients about anxiety is really useful. When patients say “my anxiety” or “I feel anxious,” she considers that a symptom. Anxiety can be a diagnosis or a symptom. You need to clarify what they mean when they refer to their anxiety and dig into how it affects their life.
We asked her about the Generalized Anxiety Disorder (GAD)-7 score. Like most of the experts we’ve talked to, she’s internalized that, so she doesn’t need to rely on a questionnaire. But I still rely on a questionnaire when I’m taking a history for anxiety.
We also asked her how she explains anxiety to patients. I don’t know about you, Paul, but I’ve never really thought about explaining to patients why they have anxiety.
Dr. Williams: I’ve done my best to try to normalize it, but I haven’t actually talked to patients about the evolutionary advantage of anxiety.
Dr. Watto: She frames it to patients this way: As we were evolving, it was somewhat of an advantage to be hypervigilant, to have some anxiety and a healthy amount of fear so that you weren’t killed or eaten. But now, in the modern world, anxiety isn’t playing to our advantage. Anxiety is not making them safer; it’s making their lives worse. She explains to patients that she’s trying to help them overcome that.
In terms of pharmacotherapy for anxiety, I always think about SSRIs as one of the first steps. Why not use an SNRI as first-line treatment?
Dr. Williams: I was glad we had this conversation because I feel, for whatever reason, a bit more comfortable treating depression than anxiety. In any case, Dr. Gold reaches for the SSRI first, in part because getting off an SNRI (for example, to switch to something else) can be absolutely miserable. The discontinuation effects can be severe enough to have to bridge some patients with a benzodiazepine to get them fully off the SNRI. So, an SNRI is not the first drug you should necessarily reach for.
She thinks about using an SNRI if she has tried a couple of SSRIs that have been ineffective, or if the patient has a comorbid condition that might also benefit from the SNRI in the same way that you might use a tricyclic antidepressant in the patient with both migraines and anxiety. An SNRI might be a good medication to consider in the patient with neuropathic pain and anxiety but rarely as a first-line treatment, because if it doesn’t work out, getting the patient off that medication can be a challenge.
Dr. Watto: She mentioned venlafaxine as being especially difficult to get people off of. I’ve heard that bupropion should never be used in anxiety, and if you give it, you are a terrible doctor. What did we learn about that?
Dr. Williams: It’s a drug I’ve hesitated to prescribe to patients with anxiety or even comorbid anxiety. I’m a little bit nervous for someone who has depression and anxiety to prescribe bupropion because it can be activating and make things worse. But Dr. Gold says that she has seen bupropion work for some patients so she will consider it, especially for patients who don’t want to gain weight, or for whom sexual side effects would be bothersome. So, it’s not always the wrong answer. In her expert opinion, you can try it and see how the patient responds, using shared decision-making and letting the patient know that they may not tolerate it as well as other medications.
Dr. Watto: She sees a lot of younger people — students, working professionals — who do not want to gain weight, and that’s understandable. She will tell patients, “We can try bupropion, but if you get more anxious, we might not be able to continue it. We might have to use one of the first-line agents instead.”
Dr. Williams: We talked about mirtazapine as well. She tells patients they are going to gain weight with it. You have to have that conversation with the patient to see whether that is something they are willing to tolerate. If so, mirtazapine might be worth a try, but you have to be upfront about the potential side effects and know what the medications you’re prescribing will do to patients.
Dr. Watto: We asked her about benzodiazepines. For as-needed medication for people who are experiencing panic or anxiety attacks, she prescribes propranolol 10-20 mg twice a day as needed, which is a low dose. In primary care, we use higher doses for migraine prophylaxis.
She uses propranolol because for some patients, it’s the physical symptoms of anxiety that are bothering them. She can calm down the physical symptoms with that and get by without needing to use a benzodiazepine.
But what about thoughts that make people anxious? Can we change people’s thoughts with medication?
Dr. Williams: Dr. Gold made the point that we can medicate away insomnia, for the most part. We can medicate away the physical symptoms of anxiety, which can be really bothersome. But we can’t medicate away thoughts and thought patterns. You can make patients feel better with medications, but you may not be able to get rid of the persistent bothersome thoughts. That’s where cognitive-behavioral therapy can be especially helpful. Most of these patients would benefit from therapy.
Dr. Watto: I completely agree with that. We talked about so many great things with Dr. Gold, but we can’t recap all of it here. Please click on this link to hear the full podcast episode.
Dr. Watto is Clinical Assistant Professor, Department of Medicine, Perelman School of Medicine at University of Pennsylvania; Internist, Department of Medicine, Hospital Medicine Section, Pennsylvania Hospital, Philadelphia, Pennsylvania. He has disclosed no relevant financial relationships. Dr. Williams is Associate Professor of Clinical Medicine, Department of General Internal Medicine, Lewis Katz School of Medicine; Staff Physician, Department of General Internal Medicine, Temple Internal Medicine Associates, Philadelphia, Pennsylvania. He disclosed receiving income from The Curbsiders. The Curbsiders is an internal medicine podcast, in which three board-certified internists interview experts on clinically important topics. In a collaboration with Medscape, the Curbsiders share clinical pearls and practice-changing knowledge from selected podcasts.
A version of this article appeared on Medscape.com.
How to Better Diagnose and Manage Rumination Syndrome
Rumination syndrome is a well-recognized functional disorder characterized by the regurgitation of food or liquid in the absence of retching or nausea.
Evidence suggests that the prevalence of rumination syndrome is increasing. In a 2022 health survey study conducted across 26 countries — the largest epidemiologic study to date on rumination syndrome — investigators reported that it had a global prevalence of 3.1% in adults. This was higher than reported in most prior country-specific studies. More recently, a systematic review and meta-analysis from 2024 reported the pooled prevalence of rumination syndrome as 3.7% in adults and 0.4% in children. Both reports noted that female gender, anxiety, and depression were independent risk factors associated with rumination syndrome.
Recognition of this disorder is crucial in order for clinicians to better diagnose and manage it in their patients.
Making the Diagnosis
The diagnosis of rumination syndrome is currently based on the Rome IV consensus criteria, which were last updated in 2016. These include three diagnostic criteria essential to remember as discriminant for rumination syndrome:
- Regurgitation is the effortless return of gastric contents (recognizable food) retrograde back into the esophagus and/or mouth.
- This is not preceded by retching and not associated with nausea.
- These symptoms must have started at least 6 months before evaluation, been evident over the past 3 months, and occurred at least two to three times per month.
Although this diagnosis will be highly suspected after taking an astute clinical history, you will still need to rule out the presence of underlying organic disease.
Nearly one quarter of patients with eating disorders — which commonly accompany gastrointestinal disorders — will not have been diagnosed by the time they visit with a gastroenterologist. Therefore, gastroenterologists should be vigilant in screening for eating disorders. Notably, severe weight loss, malnutrition, electrolyte abnormalities, and dental erosions (due to acid etching) are uncommon in rumination syndrome. If such symptoms are present, it increases the possibility of an underlying eating disorder rather than primary regurgitation.
Previously, there were no published, validated questionnaires to assess the diagnosis or symptomatic response to therapies for rumination syndrome. This has recently changed with the development of a novel eight-point questionnaire that assesses frequency, severity, type of regurgitant, timing of regurgitation in relation to the meal, weight loss, and use of and response to proton pump inhibitors.
This questionnaire was recently implemented in five patients diagnosed with rumination syndrome. Albeit an extremely small trial, it nonetheless showed clinical improvement in scores associated with therapeutic intervention. Further evaluation of this tool is needed.
The diagnosis of rumination syndrome can be confirmed using impedance manometry in persons with evidence of reflux extending to the proximal esophagus, which is associated with an intragastric pressure > 30 mmHg in adults or > 25 mmHg in children.
Gastric emptying studies are typically not required to make a diagnosis unless the clinical symptoms are atypical and an alternative motility disorder is suspected. Endoscopy is performed to rule out a mechanical disorder.
Histopathologic Evidence
New data indicate that there may be specific histologic changes associated with rumination syndrome. A 2023 meta-analysis reported that patients with rumination syndrome had duodenal histologic evidence of increased lymphocytes and eosinophils, which have been associated with epithelial barrier dysfunction, microbial changes, and systemic immune activation in eosinophilic duodenitis.
If these histologic changes are validated, they may suggest future novel diagnostic and treatment approaches, at least for a subset of people with rumination syndrome.
Best Available Treatments
The first-line therapeutic treatment for rumination syndrome is diaphragmatic breathing.
I recommended using diaphragmatic breathing for this indication in a previous commentary, in which I noted that it can essentially serve as yoga for the diaphragm and abdominal muscles and advised patients to focus on breathing “through” their belly button.
Patients are instructed to breath in through their nose for 4-6 seconds, hold their breath for 2-3 seconds, and then breath out slowly against pursed lips. They can be supine or upright but should sense their abdominal muscles expand with inhaling, not move their chest wall, and completely relax their abdominal muscles upon exhaling.
Although there is no standard frequency or duration for diaphragmatic breathing, I routinely recommend patients try it after each meal for 10-15 minutes and, if possible, more during the day and in times of stress or anxiety.
Cognitive-behavioral therapies have been shown to be effective alternatives to diaphragmatic breathing.
There is some evidence that hypnosis and biofeedback-guided control of abdominothoracic muscle activity can also be effective options in treating rumination syndrome.
Robust data on pharmacologic treatments for rumination syndrome are lacking, with the exception of a randomized crossover study of baclofen. In this study, baclofen (10 mg three times daily) was significantly more effective than placebo (P = .04) in reducing regurgitation events. Investigators theorized that baclofen counteracts transient lower esophageal sphincter (LES) relaxations by increasing basal LES pressure, thereby potentially reducing regurgitation episodes. The most notable treatment side effects were somnolence, confusion, and dizziness, which may limit its extended use.
A Potentially Reversible Habit
Rumination syndrome is considered an acquired habit and, therefore, should be reversible.
Although there is no recent evidence in the literature that rumination syndrome contributes to a reduced survival rate, older data suggested adult mortality rates of 12%-20% (mostly in patients who were institutionalized). Additionally, rumination syndrome has been shown to diminish quality of life.
The best approach to improving the clinical outcomes of patients with rumination syndrome is to enlist a collaborative interprofessional team that includes physicians, behavioral therapists, and nurses to coordinate and optimize existing treatment strategies.
David A. Johnson, MD, is professor of medicine and chief of gastroenterology at Eastern Virginia Medical School in Norfolk, Virginia, and a past president of the American College of Gastroenterology. His primary focus is the clinical practice of gastroenterology. He has published extensively in the internal medicine/gastroenterology literature, with principal research interests in esophageal and colon disease, and more recently in sleep and microbiome effects on gastrointestinal health and disease. He has disclosed the following relevant financial relationships: advisor to ISOTHRIVE and Johnson & Johnson.
A version of this article first appeared on Medscape.com.
Rumination syndrome is a well-recognized functional disorder characterized by the regurgitation of food or liquid in the absence of retching or nausea.
Evidence suggests that the prevalence of rumination syndrome is increasing. In a 2022 health survey study conducted across 26 countries — the largest epidemiologic study to date on rumination syndrome — investigators reported that it had a global prevalence of 3.1% in adults. This was higher than reported in most prior country-specific studies. More recently, a systematic review and meta-analysis from 2024 reported the pooled prevalence of rumination syndrome as 3.7% in adults and 0.4% in children. Both reports noted that female gender, anxiety, and depression were independent risk factors associated with rumination syndrome.
Recognition of this disorder is crucial in order for clinicians to better diagnose and manage it in their patients.
Making the Diagnosis
The diagnosis of rumination syndrome is currently based on the Rome IV consensus criteria, which were last updated in 2016. These include three diagnostic criteria essential to remember as discriminant for rumination syndrome:
- Regurgitation is the effortless return of gastric contents (recognizable food) retrograde back into the esophagus and/or mouth.
- This is not preceded by retching and not associated with nausea.
- These symptoms must have started at least 6 months before evaluation, been evident over the past 3 months, and occurred at least two to three times per month.
Although this diagnosis will be highly suspected after taking an astute clinical history, you will still need to rule out the presence of underlying organic disease.
Nearly one quarter of patients with eating disorders — which commonly accompany gastrointestinal disorders — will not have been diagnosed by the time they visit with a gastroenterologist. Therefore, gastroenterologists should be vigilant in screening for eating disorders. Notably, severe weight loss, malnutrition, electrolyte abnormalities, and dental erosions (due to acid etching) are uncommon in rumination syndrome. If such symptoms are present, it increases the possibility of an underlying eating disorder rather than primary regurgitation.
Previously, there were no published, validated questionnaires to assess the diagnosis or symptomatic response to therapies for rumination syndrome. This has recently changed with the development of a novel eight-point questionnaire that assesses frequency, severity, type of regurgitant, timing of regurgitation in relation to the meal, weight loss, and use of and response to proton pump inhibitors.
This questionnaire was recently implemented in five patients diagnosed with rumination syndrome. Albeit an extremely small trial, it nonetheless showed clinical improvement in scores associated with therapeutic intervention. Further evaluation of this tool is needed.
The diagnosis of rumination syndrome can be confirmed using impedance manometry in persons with evidence of reflux extending to the proximal esophagus, which is associated with an intragastric pressure > 30 mmHg in adults or > 25 mmHg in children.
Gastric emptying studies are typically not required to make a diagnosis unless the clinical symptoms are atypical and an alternative motility disorder is suspected. Endoscopy is performed to rule out a mechanical disorder.
Histopathologic Evidence
New data indicate that there may be specific histologic changes associated with rumination syndrome. A 2023 meta-analysis reported that patients with rumination syndrome had duodenal histologic evidence of increased lymphocytes and eosinophils, which have been associated with epithelial barrier dysfunction, microbial changes, and systemic immune activation in eosinophilic duodenitis.
If these histologic changes are validated, they may suggest future novel diagnostic and treatment approaches, at least for a subset of people with rumination syndrome.
Best Available Treatments
The first-line therapeutic treatment for rumination syndrome is diaphragmatic breathing.
I recommended using diaphragmatic breathing for this indication in a previous commentary, in which I noted that it can essentially serve as yoga for the diaphragm and abdominal muscles and advised patients to focus on breathing “through” their belly button.
Patients are instructed to breath in through their nose for 4-6 seconds, hold their breath for 2-3 seconds, and then breath out slowly against pursed lips. They can be supine or upright but should sense their abdominal muscles expand with inhaling, not move their chest wall, and completely relax their abdominal muscles upon exhaling.
Although there is no standard frequency or duration for diaphragmatic breathing, I routinely recommend patients try it after each meal for 10-15 minutes and, if possible, more during the day and in times of stress or anxiety.
Cognitive-behavioral therapies have been shown to be effective alternatives to diaphragmatic breathing.
There is some evidence that hypnosis and biofeedback-guided control of abdominothoracic muscle activity can also be effective options in treating rumination syndrome.
Robust data on pharmacologic treatments for rumination syndrome are lacking, with the exception of a randomized crossover study of baclofen. In this study, baclofen (10 mg three times daily) was significantly more effective than placebo (P = .04) in reducing regurgitation events. Investigators theorized that baclofen counteracts transient lower esophageal sphincter (LES) relaxations by increasing basal LES pressure, thereby potentially reducing regurgitation episodes. The most notable treatment side effects were somnolence, confusion, and dizziness, which may limit its extended use.
A Potentially Reversible Habit
Rumination syndrome is considered an acquired habit and, therefore, should be reversible.
Although there is no recent evidence in the literature that rumination syndrome contributes to a reduced survival rate, older data suggested adult mortality rates of 12%-20% (mostly in patients who were institutionalized). Additionally, rumination syndrome has been shown to diminish quality of life.
The best approach to improving the clinical outcomes of patients with rumination syndrome is to enlist a collaborative interprofessional team that includes physicians, behavioral therapists, and nurses to coordinate and optimize existing treatment strategies.
David A. Johnson, MD, is professor of medicine and chief of gastroenterology at Eastern Virginia Medical School in Norfolk, Virginia, and a past president of the American College of Gastroenterology. His primary focus is the clinical practice of gastroenterology. He has published extensively in the internal medicine/gastroenterology literature, with principal research interests in esophageal and colon disease, and more recently in sleep and microbiome effects on gastrointestinal health and disease. He has disclosed the following relevant financial relationships: advisor to ISOTHRIVE and Johnson & Johnson.
A version of this article first appeared on Medscape.com.
Rumination syndrome is a well-recognized functional disorder characterized by the regurgitation of food or liquid in the absence of retching or nausea.
Evidence suggests that the prevalence of rumination syndrome is increasing. In a 2022 health survey study conducted across 26 countries — the largest epidemiologic study to date on rumination syndrome — investigators reported that it had a global prevalence of 3.1% in adults. This was higher than reported in most prior country-specific studies. More recently, a systematic review and meta-analysis from 2024 reported the pooled prevalence of rumination syndrome as 3.7% in adults and 0.4% in children. Both reports noted that female gender, anxiety, and depression were independent risk factors associated with rumination syndrome.
Recognition of this disorder is crucial in order for clinicians to better diagnose and manage it in their patients.
Making the Diagnosis
The diagnosis of rumination syndrome is currently based on the Rome IV consensus criteria, which were last updated in 2016. These include three diagnostic criteria essential to remember as discriminant for rumination syndrome:
- Regurgitation is the effortless return of gastric contents (recognizable food) retrograde back into the esophagus and/or mouth.
- This is not preceded by retching and not associated with nausea.
- These symptoms must have started at least 6 months before evaluation, been evident over the past 3 months, and occurred at least two to three times per month.
Although this diagnosis will be highly suspected after taking an astute clinical history, you will still need to rule out the presence of underlying organic disease.
Nearly one quarter of patients with eating disorders — which commonly accompany gastrointestinal disorders — will not have been diagnosed by the time they visit with a gastroenterologist. Therefore, gastroenterologists should be vigilant in screening for eating disorders. Notably, severe weight loss, malnutrition, electrolyte abnormalities, and dental erosions (due to acid etching) are uncommon in rumination syndrome. If such symptoms are present, it increases the possibility of an underlying eating disorder rather than primary regurgitation.
Previously, there were no published, validated questionnaires to assess the diagnosis or symptomatic response to therapies for rumination syndrome. This has recently changed with the development of a novel eight-point questionnaire that assesses frequency, severity, type of regurgitant, timing of regurgitation in relation to the meal, weight loss, and use of and response to proton pump inhibitors.
This questionnaire was recently implemented in five patients diagnosed with rumination syndrome. Albeit an extremely small trial, it nonetheless showed clinical improvement in scores associated with therapeutic intervention. Further evaluation of this tool is needed.
The diagnosis of rumination syndrome can be confirmed using impedance manometry in persons with evidence of reflux extending to the proximal esophagus, which is associated with an intragastric pressure > 30 mmHg in adults or > 25 mmHg in children.
Gastric emptying studies are typically not required to make a diagnosis unless the clinical symptoms are atypical and an alternative motility disorder is suspected. Endoscopy is performed to rule out a mechanical disorder.
Histopathologic Evidence
New data indicate that there may be specific histologic changes associated with rumination syndrome. A 2023 meta-analysis reported that patients with rumination syndrome had duodenal histologic evidence of increased lymphocytes and eosinophils, which have been associated with epithelial barrier dysfunction, microbial changes, and systemic immune activation in eosinophilic duodenitis.
If these histologic changes are validated, they may suggest future novel diagnostic and treatment approaches, at least for a subset of people with rumination syndrome.
Best Available Treatments
The first-line therapeutic treatment for rumination syndrome is diaphragmatic breathing.
I recommended using diaphragmatic breathing for this indication in a previous commentary, in which I noted that it can essentially serve as yoga for the diaphragm and abdominal muscles and advised patients to focus on breathing “through” their belly button.
Patients are instructed to breath in through their nose for 4-6 seconds, hold their breath for 2-3 seconds, and then breath out slowly against pursed lips. They can be supine or upright but should sense their abdominal muscles expand with inhaling, not move their chest wall, and completely relax their abdominal muscles upon exhaling.
Although there is no standard frequency or duration for diaphragmatic breathing, I routinely recommend patients try it after each meal for 10-15 minutes and, if possible, more during the day and in times of stress or anxiety.
Cognitive-behavioral therapies have been shown to be effective alternatives to diaphragmatic breathing.
There is some evidence that hypnosis and biofeedback-guided control of abdominothoracic muscle activity can also be effective options in treating rumination syndrome.
Robust data on pharmacologic treatments for rumination syndrome are lacking, with the exception of a randomized crossover study of baclofen. In this study, baclofen (10 mg three times daily) was significantly more effective than placebo (P = .04) in reducing regurgitation events. Investigators theorized that baclofen counteracts transient lower esophageal sphincter (LES) relaxations by increasing basal LES pressure, thereby potentially reducing regurgitation episodes. The most notable treatment side effects were somnolence, confusion, and dizziness, which may limit its extended use.
A Potentially Reversible Habit
Rumination syndrome is considered an acquired habit and, therefore, should be reversible.
Although there is no recent evidence in the literature that rumination syndrome contributes to a reduced survival rate, older data suggested adult mortality rates of 12%-20% (mostly in patients who were institutionalized). Additionally, rumination syndrome has been shown to diminish quality of life.
The best approach to improving the clinical outcomes of patients with rumination syndrome is to enlist a collaborative interprofessional team that includes physicians, behavioral therapists, and nurses to coordinate and optimize existing treatment strategies.
David A. Johnson, MD, is professor of medicine and chief of gastroenterology at Eastern Virginia Medical School in Norfolk, Virginia, and a past president of the American College of Gastroenterology. His primary focus is the clinical practice of gastroenterology. He has published extensively in the internal medicine/gastroenterology literature, with principal research interests in esophageal and colon disease, and more recently in sleep and microbiome effects on gastrointestinal health and disease. He has disclosed the following relevant financial relationships: advisor to ISOTHRIVE and Johnson & Johnson.
A version of this article first appeared on Medscape.com.