User login
The Front Line of Change

We are in the midst of a true evolution of how hospitals will approach creating a culture of quality. The drivers for process improvement and management of resources have traditionally been more concerned with full occupancy and risk management, but now many external forces are raising quality improvement as a potential core competency for our nation’s hospitals.
With the push of the Institute for Healthcare Improvement (IHI), Leapfrog, and even Medicare, hospitals now must grapple with a culture change—one in which measurement and reporting of outcomes and processes will become, if not truly job one, at least in the top five. The fact that a hospital’s revenue stream through pay-for-performance (P4P) bonuses and its reputation by public reporting are at stake only serve to create a real immediacy in the coming years.
A recent SHM survey of the leaders of hospital medicine groups (HMGs) has shown that, once again, hospitalists find themselves right smack in the middle of quality improvement.
Survey Says
More than 41% of hospitalist leaders report that their HMG has a quality incentive program. This is even more prevalent at hospitals participating in P4P programs, where 60% of HMGs have quality incentives to align priorities. It is a hallmark of hospitalist groups to place a particular emphasis on the process and system improvement necessary for true measurable quality improvement. Many times, this improvement takes time away from direct and billable patient care.
Pointing to the relatively early stage in the adoption of P4P, this same survey reported that only 29% of HMGs were working in hospitals that participated in P4P programs, while 56% report their hospital did not have any P4P programs in place.
As we enter 2007, it is clear that while a small percentage of hospitals have embraced P4P the majority of hospitals are—at best—on the sidelines or still in planning mode. But those who are active in P4P have engaged their hospitalists to help them meet their goals. And everything that is coming out in the literature commonly read by the hospital C-suite promotes the promise of more reimbursement from the insurance industry and Medicare, leading to the conclusion that P4P and rewarding performance will increase in the near term.
What Can SHM Do for You?
Positioning hospitalists to play a key role in quality improvement, SHM has launched a number of initiatives and partnerships to provide hospitalists with the tools they need to help their hospitals to succeed.
As a framework of tools, SHM has now built six Web-based Quality Improvement Resource Rooms in VTE, Heart Failure, Stroke, Glycemic Control, Care Transitions in the Elderly, and Antibiotic Resistance. These practical tools and references are now available on the SHM Web site (www.hospitalmedicine.org) as are, in many cases, a comprehensive workbook that helps hospitalists to be the leaders of quality improvement change at their hospitals.
SHM realizes that, while this approach may work for the savvy, experienced quality improvement (QI) implementer, most young hospitalist leaders need a more personal, hands-on approach. With this in mind, SHM has launched its Mentored QI Implementation project. Centered around VTE prevention and supported by funding from Sanofi-Aventis, two senior hospitalist mentors will each work with 15 HMG leaders to take them step by step through the process of implementing a quality improvement process in 2007 and 2008.
To take this hands-on, supportive approach to the next level SHM (with support from a Kettering Foundation grant) will add the capability for on-site consultation—sort of a QI SWAT team that can show up at your hospital and work shoulder to shoulder with hospitalists and other members of the healthcare team to develop and implement processes that will improve patient care.
To further educate and energize hospitalist leaders who have been charged with leading this change, SHM developed the Leadership Academy. To date more than 400 hospitalist leaders have been trained in sold-out small-group sessions during the past two years. The most recent academy was held last month in Orlando, Fla.
SHM provides additional training for those who will implement quality improvement at the Quality Training precourse at the SHM Annual Meeting. In the precourse up to 100 change leaders get hands-on direction, tools, and tricks of the trade to allow them to succeed in their local efforts. The next Quality Training Precourse will be held in small group sessions on May 23, 2007, in Dallas.
The SHM Annual Meeting has consistently been a venue that allows hospitalists to hear from national thought leaders in the quality revolution. In 2006, hospitalists heard from Carolyn Clancy, MD, CEO of the Agency for Healthcare Research and Quality, and Jack Rowe, MD, CEO of Aetna Insurance Company.
At this year’s meeting Jonathan Perlin, MD, PhD, who led the cutting edge QI efforts at Veterans Affairs and who is now bringing innovation to HCA (Nashville, Tenn.), the nation’s largest hospital company, will share his ideas with us. In addition, hospitalists will hear from David Brailer, MD, PhD, President George W. Bush’s first appointee to head up national efforts for health information technology. In addition, SHM’s Bob Wachter, MD, a nationally recognized leader in QI and patient safety, will share his perspectives on hospital medicine. With Drs. Perlin, Brailer, and Wachter, SHM continues its tradition of placing innovations that are changing healthcare for the better front and center at our annual meeting.
As for the future, SHM has submitted a multi-year grant application to the Hartford Foundation (Conn.) to expand our efforts—specifically in developing implementation strategies to improve the care processes and outcomes for the senior population.
One of the key areas that emerged from SHM’s work with the Hartford Foundation is the importance of improving the transitions of care and better coordinating healthcare from the patient’s point of view. This has led SHM to partner with several national organizations to make sense of what has been a squishy subject. SHM is working closely with the American Board of Internal Medicine (ABIM) Foundation on its Stepping Up to the Plate consortium, a group of specialty physicians focusing on best practice strategies in patient-centered transitions, hand-offs, and information transfer.
In addition, SHM is working with the American College of Physicians, the AHRQ, the ABIM, the American Geriatrics Society (AGS), and the Society of General Internal Medicine to hold a National Consensus Conference in 2007 to establish policy on transitions of care. The conference will involve a broad range of stakeholders and may very well lead to the establishment of performance standards that can be applied directly to patient care.
Also SHM has been working with the Case Management Society of America to bring together the broader healthcare team on its National Transitions of Care Coalition (NTOCC) project. NTOCC includes pharmacists (American Society of Health-System Pharmacists), the C-suite (American College of Healthcare Executives), social workers (National Association of Social Workers), geriatricians (the AGS), the Joint Commission on Accreditation of Healthcare Organizations, and others. NTOCC plans to develop clear tools, guidelines, and pathways for consistent communication among patients, providers, and payers throughout the care continuum, and to look at aligning incentives for use of these tools and resources.
SHM has also worked with recognized leaders in action-oriented campaigns in QI, including the IHI—first on its “100,000 Lives Campaign,” and more recently on its “5 Million Lives Campaign.” In fact, leadership from only one medical professional society—SHM—was on the stage with Don Berwick for IHI’s national announcement at the December 2006 IHI national meeting in Orlando.
Hospitalists Lead the Charge
It is clear that our nation’s hospitals will be incentivized and mandated to create processes and produce outcomes based on national performance standards and data. This will require a re-engineering of the hospitals and their medical staffs. Hospitalists will be charged (as part of their job description) to be physician leaders in making this happen. Unfortunately, their training in medical school or residency has not provided them with all the skills in QI measurement or implementation that they will need. That is where SHM comes in.
Whether developing tools and workbooks or developing educational and implementation strategies, SHM will be innovative and on the cutting edge. Just as importantly, SHM will be on the lookout for like-minded organizations to partner with to raise the visibility and necessity of QI. We will not shy away from helping to set performance standards just because they may create initial discomfort with some of our members. We will not back off from developing creative strategies to push QI down to more than 4,000 acute care hospitals just because it is difficult and at times daunting.
Hospitalists are on the front line of change. Our patients, our institutions, our fellow physicians, and the other members of the healthcare team want and need a better system. There is no standing still. There is no turning back. The time is now. It is our turn, and hospitalists, with SHM’s help, are ready to step up and make it happen. TH
Dr. Wellikson has been CEO of SHM since 2000.
We are in the midst of a true evolution of how hospitals will approach creating a culture of quality. The drivers for process improvement and management of resources have traditionally been more concerned with full occupancy and risk management, but now many external forces are raising quality improvement as a potential core competency for our nation’s hospitals.
With the push of the Institute for Healthcare Improvement (IHI), Leapfrog, and even Medicare, hospitals now must grapple with a culture change—one in which measurement and reporting of outcomes and processes will become, if not truly job one, at least in the top five. The fact that a hospital’s revenue stream through pay-for-performance (P4P) bonuses and its reputation by public reporting are at stake only serve to create a real immediacy in the coming years.
A recent SHM survey of the leaders of hospital medicine groups (HMGs) has shown that, once again, hospitalists find themselves right smack in the middle of quality improvement.
Survey Says
More than 41% of hospitalist leaders report that their HMG has a quality incentive program. This is even more prevalent at hospitals participating in P4P programs, where 60% of HMGs have quality incentives to align priorities. It is a hallmark of hospitalist groups to place a particular emphasis on the process and system improvement necessary for true measurable quality improvement. Many times, this improvement takes time away from direct and billable patient care.
Pointing to the relatively early stage in the adoption of P4P, this same survey reported that only 29% of HMGs were working in hospitals that participated in P4P programs, while 56% report their hospital did not have any P4P programs in place.
As we enter 2007, it is clear that while a small percentage of hospitals have embraced P4P the majority of hospitals are—at best—on the sidelines or still in planning mode. But those who are active in P4P have engaged their hospitalists to help them meet their goals. And everything that is coming out in the literature commonly read by the hospital C-suite promotes the promise of more reimbursement from the insurance industry and Medicare, leading to the conclusion that P4P and rewarding performance will increase in the near term.
What Can SHM Do for You?
Positioning hospitalists to play a key role in quality improvement, SHM has launched a number of initiatives and partnerships to provide hospitalists with the tools they need to help their hospitals to succeed.
As a framework of tools, SHM has now built six Web-based Quality Improvement Resource Rooms in VTE, Heart Failure, Stroke, Glycemic Control, Care Transitions in the Elderly, and Antibiotic Resistance. These practical tools and references are now available on the SHM Web site (www.hospitalmedicine.org) as are, in many cases, a comprehensive workbook that helps hospitalists to be the leaders of quality improvement change at their hospitals.
SHM realizes that, while this approach may work for the savvy, experienced quality improvement (QI) implementer, most young hospitalist leaders need a more personal, hands-on approach. With this in mind, SHM has launched its Mentored QI Implementation project. Centered around VTE prevention and supported by funding from Sanofi-Aventis, two senior hospitalist mentors will each work with 15 HMG leaders to take them step by step through the process of implementing a quality improvement process in 2007 and 2008.
To take this hands-on, supportive approach to the next level SHM (with support from a Kettering Foundation grant) will add the capability for on-site consultation—sort of a QI SWAT team that can show up at your hospital and work shoulder to shoulder with hospitalists and other members of the healthcare team to develop and implement processes that will improve patient care.
To further educate and energize hospitalist leaders who have been charged with leading this change, SHM developed the Leadership Academy. To date more than 400 hospitalist leaders have been trained in sold-out small-group sessions during the past two years. The most recent academy was held last month in Orlando, Fla.
SHM provides additional training for those who will implement quality improvement at the Quality Training precourse at the SHM Annual Meeting. In the precourse up to 100 change leaders get hands-on direction, tools, and tricks of the trade to allow them to succeed in their local efforts. The next Quality Training Precourse will be held in small group sessions on May 23, 2007, in Dallas.
The SHM Annual Meeting has consistently been a venue that allows hospitalists to hear from national thought leaders in the quality revolution. In 2006, hospitalists heard from Carolyn Clancy, MD, CEO of the Agency for Healthcare Research and Quality, and Jack Rowe, MD, CEO of Aetna Insurance Company.
At this year’s meeting Jonathan Perlin, MD, PhD, who led the cutting edge QI efforts at Veterans Affairs and who is now bringing innovation to HCA (Nashville, Tenn.), the nation’s largest hospital company, will share his ideas with us. In addition, hospitalists will hear from David Brailer, MD, PhD, President George W. Bush’s first appointee to head up national efforts for health information technology. In addition, SHM’s Bob Wachter, MD, a nationally recognized leader in QI and patient safety, will share his perspectives on hospital medicine. With Drs. Perlin, Brailer, and Wachter, SHM continues its tradition of placing innovations that are changing healthcare for the better front and center at our annual meeting.
As for the future, SHM has submitted a multi-year grant application to the Hartford Foundation (Conn.) to expand our efforts—specifically in developing implementation strategies to improve the care processes and outcomes for the senior population.
One of the key areas that emerged from SHM’s work with the Hartford Foundation is the importance of improving the transitions of care and better coordinating healthcare from the patient’s point of view. This has led SHM to partner with several national organizations to make sense of what has been a squishy subject. SHM is working closely with the American Board of Internal Medicine (ABIM) Foundation on its Stepping Up to the Plate consortium, a group of specialty physicians focusing on best practice strategies in patient-centered transitions, hand-offs, and information transfer.
In addition, SHM is working with the American College of Physicians, the AHRQ, the ABIM, the American Geriatrics Society (AGS), and the Society of General Internal Medicine to hold a National Consensus Conference in 2007 to establish policy on transitions of care. The conference will involve a broad range of stakeholders and may very well lead to the establishment of performance standards that can be applied directly to patient care.
Also SHM has been working with the Case Management Society of America to bring together the broader healthcare team on its National Transitions of Care Coalition (NTOCC) project. NTOCC includes pharmacists (American Society of Health-System Pharmacists), the C-suite (American College of Healthcare Executives), social workers (National Association of Social Workers), geriatricians (the AGS), the Joint Commission on Accreditation of Healthcare Organizations, and others. NTOCC plans to develop clear tools, guidelines, and pathways for consistent communication among patients, providers, and payers throughout the care continuum, and to look at aligning incentives for use of these tools and resources.
SHM has also worked with recognized leaders in action-oriented campaigns in QI, including the IHI—first on its “100,000 Lives Campaign,” and more recently on its “5 Million Lives Campaign.” In fact, leadership from only one medical professional society—SHM—was on the stage with Don Berwick for IHI’s national announcement at the December 2006 IHI national meeting in Orlando.
Hospitalists Lead the Charge
It is clear that our nation’s hospitals will be incentivized and mandated to create processes and produce outcomes based on national performance standards and data. This will require a re-engineering of the hospitals and their medical staffs. Hospitalists will be charged (as part of their job description) to be physician leaders in making this happen. Unfortunately, their training in medical school or residency has not provided them with all the skills in QI measurement or implementation that they will need. That is where SHM comes in.
Whether developing tools and workbooks or developing educational and implementation strategies, SHM will be innovative and on the cutting edge. Just as importantly, SHM will be on the lookout for like-minded organizations to partner with to raise the visibility and necessity of QI. We will not shy away from helping to set performance standards just because they may create initial discomfort with some of our members. We will not back off from developing creative strategies to push QI down to more than 4,000 acute care hospitals just because it is difficult and at times daunting.
Hospitalists are on the front line of change. Our patients, our institutions, our fellow physicians, and the other members of the healthcare team want and need a better system. There is no standing still. There is no turning back. The time is now. It is our turn, and hospitalists, with SHM’s help, are ready to step up and make it happen. TH
Dr. Wellikson has been CEO of SHM since 2000.
We are in the midst of a true evolution of how hospitals will approach creating a culture of quality. The drivers for process improvement and management of resources have traditionally been more concerned with full occupancy and risk management, but now many external forces are raising quality improvement as a potential core competency for our nation’s hospitals.
With the push of the Institute for Healthcare Improvement (IHI), Leapfrog, and even Medicare, hospitals now must grapple with a culture change—one in which measurement and reporting of outcomes and processes will become, if not truly job one, at least in the top five. The fact that a hospital’s revenue stream through pay-for-performance (P4P) bonuses and its reputation by public reporting are at stake only serve to create a real immediacy in the coming years.
A recent SHM survey of the leaders of hospital medicine groups (HMGs) has shown that, once again, hospitalists find themselves right smack in the middle of quality improvement.
Survey Says
More than 41% of hospitalist leaders report that their HMG has a quality incentive program. This is even more prevalent at hospitals participating in P4P programs, where 60% of HMGs have quality incentives to align priorities. It is a hallmark of hospitalist groups to place a particular emphasis on the process and system improvement necessary for true measurable quality improvement. Many times, this improvement takes time away from direct and billable patient care.
Pointing to the relatively early stage in the adoption of P4P, this same survey reported that only 29% of HMGs were working in hospitals that participated in P4P programs, while 56% report their hospital did not have any P4P programs in place.
As we enter 2007, it is clear that while a small percentage of hospitals have embraced P4P the majority of hospitals are—at best—on the sidelines or still in planning mode. But those who are active in P4P have engaged their hospitalists to help them meet their goals. And everything that is coming out in the literature commonly read by the hospital C-suite promotes the promise of more reimbursement from the insurance industry and Medicare, leading to the conclusion that P4P and rewarding performance will increase in the near term.
What Can SHM Do for You?
Positioning hospitalists to play a key role in quality improvement, SHM has launched a number of initiatives and partnerships to provide hospitalists with the tools they need to help their hospitals to succeed.
As a framework of tools, SHM has now built six Web-based Quality Improvement Resource Rooms in VTE, Heart Failure, Stroke, Glycemic Control, Care Transitions in the Elderly, and Antibiotic Resistance. These practical tools and references are now available on the SHM Web site (www.hospitalmedicine.org) as are, in many cases, a comprehensive workbook that helps hospitalists to be the leaders of quality improvement change at their hospitals.
SHM realizes that, while this approach may work for the savvy, experienced quality improvement (QI) implementer, most young hospitalist leaders need a more personal, hands-on approach. With this in mind, SHM has launched its Mentored QI Implementation project. Centered around VTE prevention and supported by funding from Sanofi-Aventis, two senior hospitalist mentors will each work with 15 HMG leaders to take them step by step through the process of implementing a quality improvement process in 2007 and 2008.
To take this hands-on, supportive approach to the next level SHM (with support from a Kettering Foundation grant) will add the capability for on-site consultation—sort of a QI SWAT team that can show up at your hospital and work shoulder to shoulder with hospitalists and other members of the healthcare team to develop and implement processes that will improve patient care.
To further educate and energize hospitalist leaders who have been charged with leading this change, SHM developed the Leadership Academy. To date more than 400 hospitalist leaders have been trained in sold-out small-group sessions during the past two years. The most recent academy was held last month in Orlando, Fla.
SHM provides additional training for those who will implement quality improvement at the Quality Training precourse at the SHM Annual Meeting. In the precourse up to 100 change leaders get hands-on direction, tools, and tricks of the trade to allow them to succeed in their local efforts. The next Quality Training Precourse will be held in small group sessions on May 23, 2007, in Dallas.
The SHM Annual Meeting has consistently been a venue that allows hospitalists to hear from national thought leaders in the quality revolution. In 2006, hospitalists heard from Carolyn Clancy, MD, CEO of the Agency for Healthcare Research and Quality, and Jack Rowe, MD, CEO of Aetna Insurance Company.
At this year’s meeting Jonathan Perlin, MD, PhD, who led the cutting edge QI efforts at Veterans Affairs and who is now bringing innovation to HCA (Nashville, Tenn.), the nation’s largest hospital company, will share his ideas with us. In addition, hospitalists will hear from David Brailer, MD, PhD, President George W. Bush’s first appointee to head up national efforts for health information technology. In addition, SHM’s Bob Wachter, MD, a nationally recognized leader in QI and patient safety, will share his perspectives on hospital medicine. With Drs. Perlin, Brailer, and Wachter, SHM continues its tradition of placing innovations that are changing healthcare for the better front and center at our annual meeting.
As for the future, SHM has submitted a multi-year grant application to the Hartford Foundation (Conn.) to expand our efforts—specifically in developing implementation strategies to improve the care processes and outcomes for the senior population.
One of the key areas that emerged from SHM’s work with the Hartford Foundation is the importance of improving the transitions of care and better coordinating healthcare from the patient’s point of view. This has led SHM to partner with several national organizations to make sense of what has been a squishy subject. SHM is working closely with the American Board of Internal Medicine (ABIM) Foundation on its Stepping Up to the Plate consortium, a group of specialty physicians focusing on best practice strategies in patient-centered transitions, hand-offs, and information transfer.
In addition, SHM is working with the American College of Physicians, the AHRQ, the ABIM, the American Geriatrics Society (AGS), and the Society of General Internal Medicine to hold a National Consensus Conference in 2007 to establish policy on transitions of care. The conference will involve a broad range of stakeholders and may very well lead to the establishment of performance standards that can be applied directly to patient care.
Also SHM has been working with the Case Management Society of America to bring together the broader healthcare team on its National Transitions of Care Coalition (NTOCC) project. NTOCC includes pharmacists (American Society of Health-System Pharmacists), the C-suite (American College of Healthcare Executives), social workers (National Association of Social Workers), geriatricians (the AGS), the Joint Commission on Accreditation of Healthcare Organizations, and others. NTOCC plans to develop clear tools, guidelines, and pathways for consistent communication among patients, providers, and payers throughout the care continuum, and to look at aligning incentives for use of these tools and resources.
SHM has also worked with recognized leaders in action-oriented campaigns in QI, including the IHI—first on its “100,000 Lives Campaign,” and more recently on its “5 Million Lives Campaign.” In fact, leadership from only one medical professional society—SHM—was on the stage with Don Berwick for IHI’s national announcement at the December 2006 IHI national meeting in Orlando.
Hospitalists Lead the Charge
It is clear that our nation’s hospitals will be incentivized and mandated to create processes and produce outcomes based on national performance standards and data. This will require a re-engineering of the hospitals and their medical staffs. Hospitalists will be charged (as part of their job description) to be physician leaders in making this happen. Unfortunately, their training in medical school or residency has not provided them with all the skills in QI measurement or implementation that they will need. That is where SHM comes in.
Whether developing tools and workbooks or developing educational and implementation strategies, SHM will be innovative and on the cutting edge. Just as importantly, SHM will be on the lookout for like-minded organizations to partner with to raise the visibility and necessity of QI. We will not shy away from helping to set performance standards just because they may create initial discomfort with some of our members. We will not back off from developing creative strategies to push QI down to more than 4,000 acute care hospitals just because it is difficult and at times daunting.
Hospitalists are on the front line of change. Our patients, our institutions, our fellow physicians, and the other members of the healthcare team want and need a better system. There is no standing still. There is no turning back. The time is now. It is our turn, and hospitalists, with SHM’s help, are ready to step up and make it happen. TH
Dr. Wellikson has been CEO of SHM since 2000.
A Fine Formation
In the football-loving state of Michigan, legendary athletes take their cues from a coach and map their strategies for one big group effort. But Michigan is also home to what may be the first-ever homegrown regional consortium for patient safety and quality improvement—and in this case—after a huddle each team member gets to call his own plays.
The Hospitalists as Emerging Leaders in Patient Safety (HELPS) Consortium of Southeastern Michigan (funded by a grant from the Blue Cross Blue Shield of Michigan Foundation) includes representatives from nine regional hospitalist programs representing 11 hospitals and approximately 75,000 patients.1
The participants in this program identify proven patient safety practices and facilitate widespread dissemination of those practices among hospitalists.
The member institutions include academic medical centers, large private teaching and non-teaching hospitals, federal facilities, and urban and rural hospitals.
Each institution is represented by a hospitalist—usually the director of the hospitalist program or the individual most interested in and familiar with quality improvement—and a representative from quality improvement or patient safety. The issues they have addressed, which emerged from a variety of sources, such as the Agency of Healthcare Research and Quality, the National Quality Forum, and the Joint Commission on Accreditation of Healthcare Organizations, are those that are commonly encountered in hospitalist practice. These physicians “are bridging the gap between that which they know to be effective and that which is actually practiced.”1
HELPS builds on the experience of medical professionals who have united geographically dispersed physicians from the same specialty to boost quality. The HELPS consortium also aids participating institutions in evaluating outcomes after implementing a targeted patient safety practice, thereby allowing rapid cycle improvement while identifying factors associated with success.
“We have gotten the work that is being done by these different organizations out there, brought it up a notch in certain situations—we like to think—and have gotten it effectively disseminated to a larger group of hospitalists,” says Scott Flanders, MD, an associate professor of medicine at the University of Michigan (Ann Arbor), director of the hospital medicine program there, and an SHM board member.
Where They Are
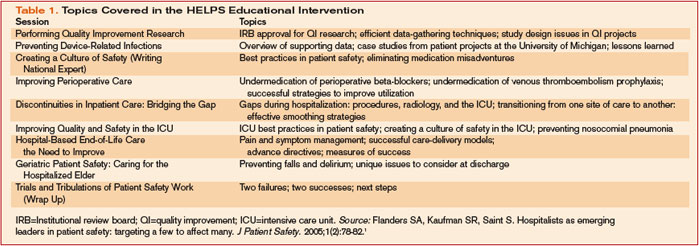
The consortium is about three-quarters of the way through its overall estimated project period, says Dr. Flanders. It originally planned to have nine gatherings over two years. (See Table 1, p. 35.) To date the consortium has held seven of those sessions and have met roughly every two to three months. End-of-life care and the final wrap-up are the only sessions still to be completed.
The individual sites took on projects that included reducing errors with heparin use in hospitalized patients, reducing falls in hospitalized patients, improving care transitions (a collaborative multidisciplinary approach), reducing unnecessary ICU admission and preventing in-hospital cardiac arrests, reducing urinary catheter infections, improving rates of appropriate deep vein thrombosis prophylaxis, and implementing best practices for reducing central line infections. A national expert conducted a session on implementing a program to reduce perioperative cardiovascular events while ensuring the appropriate use of perioperative beta-blockers.
Challenges and Lessons Learned
From the outset, the HELPS group knew that its primary challenge would be to fulfill the intention to meet as a complete group four or five times per year. “There aren’t a lot of hospitalists who have big parts of their jobs carved out for dedicated time to work on quality improvement research or patient safety,” says Dr. Flanders. “It’s part of what we do in our day, but in terms of taking on a big project, designing it, implementing it, and measuring its effect, it is hard to do in the day-to-day job of most hospitalist groups.”
He suspects that hospitalists frequently help steering committees address certain issues, “but it may not be the individual hospitalist group that is managing or driving the quality issue for an entire hospital or health system.” The HELPS physicians knew that if they could surmount the scheduling challenge, however, they would have a terrific opportunity to learn from each other and move their individual institutional patient safety initiatives forward.
They also knew that the majority of hospitalized patients receive care in community hospitals and that the culture of a community hospital differed dramatically from a tertiary-care academic medical center. Interventions would need to be tried at varied settings, and HELPS would allow that to happen. In addition, few clinically active hospitalists have developed the research expertise to evaluate an intervention rigorously at their own institution, yet decision makers often require such an evaluation when they are considering adopting a new intervention. Using the resources of an academic center such as the University of Michigan, where evaluative and methodologic expertise is available, allowed them to facilitate a resolution for that problem. “As physicians, we are helping [smaller hospitals] by facilitating data collection and data analysis for their ongoing projects,” says Dr. Flanders.
Another challenge the hospitalists faced pertained to the relative instability of hospital medicine compared with other specialties. For instance, it is probably far easier for the members of the consortium of cardiology groups working on best practices for managing acute myocardial infarction to find time to work together. In contrast, because hospital medicine is a relatively new specialty, “we are seeing a certain amount of instability,” explains Dr. Flanders. “Of our nine involved health systems, at least two had dramatic organizational and structural changes within their hospital medicine group over the last year and a half.” One hospital medicine director left, with repercussions in several areas, and, in another group, the practice was sold to a large physician management company, which meant that the HELPS data that had been collected was no longer owned by the [original] group, making their activities more complex.
What They’ve Done So Far
Dr. Flanders is not aware of any other groups of physicians from another state who have undertaken such a project. The Institute for Healthcare Improvement’s “100,000 Lives Campaign” may be similar in some ways, focusing on a few key topic areas. The Michigan Keystone Project, which concentrated on various ICU patient safety topics, is another example of a regional consortium. “But the difference is that they basically drive the agenda,” he says. “They say, ‘This is what we want you all to do, and let’s figure out how we can all do it.’ In our case, we focused on some key areas, but we did not dictate what the project was.”
The following brief recaps represent some of the projects undertaken by consortium member sites.
Falls
The University of Michigan-affiliated Ann Arbor Veterans Affairs (VA) Hospital, where Sanjay Saint, MD, MPH, is a hospitalist, has many elderly and cognitively impaired patients, so preventing falls is a big issue. “My responsibility isn’t to prevent falls but to share these best practices with others in my organization,” he says. “In fact, each project team points out where to look with a certain problem but not necessarily what to do.”
Dr. Saint brought up the issue of mattresses with lipped/raised edges to prevent patients from rolling out of bed. Following that, at least one other consortium hospital suggested to its fall prevention group that they explore the use of these lipped mattresses.
Bed alarms were another problem. Participants shared a common problem: Often, nurses wouldn’t hear a patient’s alarm go off. Other providers might reset them, but if they neglected to let the assigned nurse know the patient was calling, the patient might get tired of waiting, attempt to get out of bed, and sustain a fall. Consequently, providers in most institutions thought the alarms were not useful. But one institution identified a novel way to use bed alarms: attaching them to the nurse’s pager. Now, when the alarm goes off, it alerts the appropriate nurse directly, and because that nurse is responsible for resetting the alarm, she knows that the patient has called and needs help.
Changing Names: CARE Assistants
To avoid the use of physical or chemical restraints, many institutions have resorted to hiring “sitters” who stay at the bedside of confused or delirious patients to calm them; if patients try to get out of bed, sitters are there to coax them back in. A number of HELPS institutions shared the idea that using the term “sitter” might have been inadvertently encouraging inactivity: Too many sitters were doing just that, sitting all day, often watching television.
One of the collaborative sites now calls these employees CARE assistants, an acronym for Caring Alternative to a Restraint-free Environment. The group has predicted that calling them something different will inspire these people to “do more caring and less sitting,” says Dr. Saint. After a HELPS session, Dr. Saint submitted this idea to the key decision makers at the VA. “I could have tried by myself to resolve this dilemma for years and not come up with that idea,” he says. “Why not just take what they’ve done and modify it to suit your own environment?”
Weighty Problem: Heparin Dosing
One hospital in the consortium conducted a project on medication safety that focused on appropriate use of heparin in hospitalized patients. When the site’s hospitalists began studying the problems they were having, they realized that the weights they were using for dosing decisions were being generated in the emergency department (ED). Studying it further, they saw that, most of the time, those patients weren’t actually being weighed; nurses were simply estimating their weights. Having traced the problem to the ED, they were then able to intervene, fix the problem, and show that by doing so their rates of bleeding complications from inappropriate dosing of anticoagulants improved.
At his own institution, Dr. Flanders was participating in a group committee meeting discussing this problem. Consequently, “I was able to ask, ‘Have we looked at weights [being assessed] in the emergency department?’ Everyone involved with that project said, ‘No, why?’ And, sure enough, a similar problem existed.”
Care Transitions and Multidisciplinary Rounding
One member-team of the consortium was able to come up with a multidisciplinary team that met and rounded on patients each day and focused on the care transitions. They were able to dramatically improve staff communication, the overall discharge process, and patient satisfaction. As a result of what he learned of their successes, Dr. Flanders’ institution plans to use a similar strategy to enhance communication among healthcare providers involved in the discharge process on their hospitalist unit.
Rapid Response Teams and Input from Residents
“It’s very helpful to hear, from another site, the challenges and benefits of having hospitalists involved with the rapid response teams,” says Dr. Saint. “How did they operationalize it? What were the remaining challenges? What outcome measures did they use? How do you assess whether it’s worth the cost? What do residents think about this?
This last point turned out to be a valuable question to ask. The group included some residents at the site where this project was piloted and had a fruitful discussion. Adding the perspective of residents along with faculty, says Dr. Saint, as well as a couple of nurses and quality care managers, allows a synergy and combination of ideas that led to effective solutions. “Those are exactly the individuals who need to be around a table to overcome some of the challenges.” They have also considered inviting nursing students. “Before they get inculcated in thinking a certain way,” he says, “why not hear what they have to say?”
Dr. Saint believes, however, that this is not a step to be taken lightly. If you are going to include people, “then you have to act on their suggestions or at least hear them out and say why you’re not going to take their suggestions because a good way to get people to become jaded is to listen to their feedback and then just ignore it.”
Calling in Outside Experts
To focus on the issue of preventing hospital-acquired urinary tract infections (UTIs), the consortium invited Russell Olmstead, MPH, an infection control expert and epidemiologist at one of the HELPS sites and past president of the Michigan Society of Infection Control.
“We’d like to do a Keystone[-type] UTI project,” says Dr. Saint, referring to the federally funded statewide three-year initiative, conducted in collaboration with the Michigan Hospital Association and Johns Hopkins Research and Safety Group, that focused on applying evidence-based medicine and quality improvement efforts to prevent ventilator-associated pneumonia and central line-related infections. “We’ve called it the Bladder Bundle; that is, you bundle a group of practices together, and you give the hospitalists who want to participate a toolkit in order to roll this out.”
Although the details still need to be finalized, the project would include ensuring that patients have appropriate indication for an indwelling catheter, that the indwelling catheter is inserted in an aseptic manner, that there was some type of assessment of discontinuation after a certain amount of time, and that alternatives to an indwelling catheter are considered.
Another expert consulting with the consortium was Peter Lindenauer, MD, MSc, with the Division of Healthcare Quality, Baystate Medical Center, Springfield, Mass., and the Department of Medicine, Tufts University School of Medicine, Boston. Dr. Lindenauer came to discuss lessons he and his colleagues have learned from efforts to improve appropriate perioperative beta blocker use.
The final HELPS wrap-up session for the group will include another nationally renowned expert in patient safety.
SHARP: Research Translated into Practice
Another project initiated by the Michigan hospitalists will generate and disseminate new knowledge in the realm of clinical research. The Specialist-Hospitalist Allied Research Program (SHARP), directed by Dr. Flanders and Brahmajee Nallamothu, MD, MPH, an interventional cardiologist, is the first specialist-hospitalist clinical research program in the United States. This hospitalist delivery model alters the way clinical problems are approached and creates opportunities and challenges in implementing best practices, including those surrounding drugs and devices. A successful clinical and translational research program will combine specialists and hospitalists working collaboratively to better understand the best ways to care for inpatients.
This project is similar to what cardiology and oncology specialties have done over the last several decades, says Dr. Saint. In the future, he foresees that the NIH will increasingly focus on translating research into practice in diverse settings. Both specialists and hospitalists who work in a particular area together—such as prevention of lower extremity clots or of nosocomial infections—can use the health consortium to roll out protocols and studies in order to tackle some of the important inpatient topics.
SHARP was awarded funding through the University of Michigan Department of Medicine and was scheduled to take off in February. “Our hope is that we will be able to take advantage of and build upon the health collaborative that we have and bring in our subspecialty expertise to help inform clinical investigations,” says Dr. Saint.
Where They’re Going
Both Dr. Flanders and Dr. Saint are pleased about the HELPS consortium’s progress so far. They believe that they have found a group of people who are interested in patient safety and are willing to learn from one another and that they have done an excellent job of disseminating the best practices they have been exploring.
Ultimately, their goal is to grow this into a “more robust clinical research consortium,” says Dr. Flanders. Instead of disseminating best practices and focusing on just a few targeted patient safety quality improvement areas, they will begin to take on studies that could center around patient safety and quality improvement but will also move toward multi-center projects that might address issues related to management of common clinical problems that hospitalists are now managing and focusing on.
“We’re really excited about what we have been able to accomplish,” he says. “We’ve learned a lot about the challenges of doing this, and of course it’s never perfect. We wish we could always do more, but we’ve learned why we can’t. That will be helpful in future projects and helpful for others who are trying to tackle this same problem.” TH
Reference
- Flanders SA, Kaufman SR, Saint S. Hospitalists as emerging leaders in patient safety: targeting a few to affect many. J Patient Safety. 2005;1(2):78-82.
In the football-loving state of Michigan, legendary athletes take their cues from a coach and map their strategies for one big group effort. But Michigan is also home to what may be the first-ever homegrown regional consortium for patient safety and quality improvement—and in this case—after a huddle each team member gets to call his own plays.
The Hospitalists as Emerging Leaders in Patient Safety (HELPS) Consortium of Southeastern Michigan (funded by a grant from the Blue Cross Blue Shield of Michigan Foundation) includes representatives from nine regional hospitalist programs representing 11 hospitals and approximately 75,000 patients.1
The participants in this program identify proven patient safety practices and facilitate widespread dissemination of those practices among hospitalists.
The member institutions include academic medical centers, large private teaching and non-teaching hospitals, federal facilities, and urban and rural hospitals.
Each institution is represented by a hospitalist—usually the director of the hospitalist program or the individual most interested in and familiar with quality improvement—and a representative from quality improvement or patient safety. The issues they have addressed, which emerged from a variety of sources, such as the Agency of Healthcare Research and Quality, the National Quality Forum, and the Joint Commission on Accreditation of Healthcare Organizations, are those that are commonly encountered in hospitalist practice. These physicians “are bridging the gap between that which they know to be effective and that which is actually practiced.”1
HELPS builds on the experience of medical professionals who have united geographically dispersed physicians from the same specialty to boost quality. The HELPS consortium also aids participating institutions in evaluating outcomes after implementing a targeted patient safety practice, thereby allowing rapid cycle improvement while identifying factors associated with success.
“We have gotten the work that is being done by these different organizations out there, brought it up a notch in certain situations—we like to think—and have gotten it effectively disseminated to a larger group of hospitalists,” says Scott Flanders, MD, an associate professor of medicine at the University of Michigan (Ann Arbor), director of the hospital medicine program there, and an SHM board member.
Where They Are
The consortium is about three-quarters of the way through its overall estimated project period, says Dr. Flanders. It originally planned to have nine gatherings over two years. (See Table 1, p. 35.) To date the consortium has held seven of those sessions and have met roughly every two to three months. End-of-life care and the final wrap-up are the only sessions still to be completed.
The individual sites took on projects that included reducing errors with heparin use in hospitalized patients, reducing falls in hospitalized patients, improving care transitions (a collaborative multidisciplinary approach), reducing unnecessary ICU admission and preventing in-hospital cardiac arrests, reducing urinary catheter infections, improving rates of appropriate deep vein thrombosis prophylaxis, and implementing best practices for reducing central line infections. A national expert conducted a session on implementing a program to reduce perioperative cardiovascular events while ensuring the appropriate use of perioperative beta-blockers.
Challenges and Lessons Learned
From the outset, the HELPS group knew that its primary challenge would be to fulfill the intention to meet as a complete group four or five times per year. “There aren’t a lot of hospitalists who have big parts of their jobs carved out for dedicated time to work on quality improvement research or patient safety,” says Dr. Flanders. “It’s part of what we do in our day, but in terms of taking on a big project, designing it, implementing it, and measuring its effect, it is hard to do in the day-to-day job of most hospitalist groups.”
He suspects that hospitalists frequently help steering committees address certain issues, “but it may not be the individual hospitalist group that is managing or driving the quality issue for an entire hospital or health system.” The HELPS physicians knew that if they could surmount the scheduling challenge, however, they would have a terrific opportunity to learn from each other and move their individual institutional patient safety initiatives forward.
They also knew that the majority of hospitalized patients receive care in community hospitals and that the culture of a community hospital differed dramatically from a tertiary-care academic medical center. Interventions would need to be tried at varied settings, and HELPS would allow that to happen. In addition, few clinically active hospitalists have developed the research expertise to evaluate an intervention rigorously at their own institution, yet decision makers often require such an evaluation when they are considering adopting a new intervention. Using the resources of an academic center such as the University of Michigan, where evaluative and methodologic expertise is available, allowed them to facilitate a resolution for that problem. “As physicians, we are helping [smaller hospitals] by facilitating data collection and data analysis for their ongoing projects,” says Dr. Flanders.
Another challenge the hospitalists faced pertained to the relative instability of hospital medicine compared with other specialties. For instance, it is probably far easier for the members of the consortium of cardiology groups working on best practices for managing acute myocardial infarction to find time to work together. In contrast, because hospital medicine is a relatively new specialty, “we are seeing a certain amount of instability,” explains Dr. Flanders. “Of our nine involved health systems, at least two had dramatic organizational and structural changes within their hospital medicine group over the last year and a half.” One hospital medicine director left, with repercussions in several areas, and, in another group, the practice was sold to a large physician management company, which meant that the HELPS data that had been collected was no longer owned by the [original] group, making their activities more complex.
What They’ve Done So Far
Dr. Flanders is not aware of any other groups of physicians from another state who have undertaken such a project. The Institute for Healthcare Improvement’s “100,000 Lives Campaign” may be similar in some ways, focusing on a few key topic areas. The Michigan Keystone Project, which concentrated on various ICU patient safety topics, is another example of a regional consortium. “But the difference is that they basically drive the agenda,” he says. “They say, ‘This is what we want you all to do, and let’s figure out how we can all do it.’ In our case, we focused on some key areas, but we did not dictate what the project was.”
The following brief recaps represent some of the projects undertaken by consortium member sites.
Falls
The University of Michigan-affiliated Ann Arbor Veterans Affairs (VA) Hospital, where Sanjay Saint, MD, MPH, is a hospitalist, has many elderly and cognitively impaired patients, so preventing falls is a big issue. “My responsibility isn’t to prevent falls but to share these best practices with others in my organization,” he says. “In fact, each project team points out where to look with a certain problem but not necessarily what to do.”
Dr. Saint brought up the issue of mattresses with lipped/raised edges to prevent patients from rolling out of bed. Following that, at least one other consortium hospital suggested to its fall prevention group that they explore the use of these lipped mattresses.
Bed alarms were another problem. Participants shared a common problem: Often, nurses wouldn’t hear a patient’s alarm go off. Other providers might reset them, but if they neglected to let the assigned nurse know the patient was calling, the patient might get tired of waiting, attempt to get out of bed, and sustain a fall. Consequently, providers in most institutions thought the alarms were not useful. But one institution identified a novel way to use bed alarms: attaching them to the nurse’s pager. Now, when the alarm goes off, it alerts the appropriate nurse directly, and because that nurse is responsible for resetting the alarm, she knows that the patient has called and needs help.
Changing Names: CARE Assistants
To avoid the use of physical or chemical restraints, many institutions have resorted to hiring “sitters” who stay at the bedside of confused or delirious patients to calm them; if patients try to get out of bed, sitters are there to coax them back in. A number of HELPS institutions shared the idea that using the term “sitter” might have been inadvertently encouraging inactivity: Too many sitters were doing just that, sitting all day, often watching television.
One of the collaborative sites now calls these employees CARE assistants, an acronym for Caring Alternative to a Restraint-free Environment. The group has predicted that calling them something different will inspire these people to “do more caring and less sitting,” says Dr. Saint. After a HELPS session, Dr. Saint submitted this idea to the key decision makers at the VA. “I could have tried by myself to resolve this dilemma for years and not come up with that idea,” he says. “Why not just take what they’ve done and modify it to suit your own environment?”
Weighty Problem: Heparin Dosing
One hospital in the consortium conducted a project on medication safety that focused on appropriate use of heparin in hospitalized patients. When the site’s hospitalists began studying the problems they were having, they realized that the weights they were using for dosing decisions were being generated in the emergency department (ED). Studying it further, they saw that, most of the time, those patients weren’t actually being weighed; nurses were simply estimating their weights. Having traced the problem to the ED, they were then able to intervene, fix the problem, and show that by doing so their rates of bleeding complications from inappropriate dosing of anticoagulants improved.
At his own institution, Dr. Flanders was participating in a group committee meeting discussing this problem. Consequently, “I was able to ask, ‘Have we looked at weights [being assessed] in the emergency department?’ Everyone involved with that project said, ‘No, why?’ And, sure enough, a similar problem existed.”
Care Transitions and Multidisciplinary Rounding
One member-team of the consortium was able to come up with a multidisciplinary team that met and rounded on patients each day and focused on the care transitions. They were able to dramatically improve staff communication, the overall discharge process, and patient satisfaction. As a result of what he learned of their successes, Dr. Flanders’ institution plans to use a similar strategy to enhance communication among healthcare providers involved in the discharge process on their hospitalist unit.
Rapid Response Teams and Input from Residents
“It’s very helpful to hear, from another site, the challenges and benefits of having hospitalists involved with the rapid response teams,” says Dr. Saint. “How did they operationalize it? What were the remaining challenges? What outcome measures did they use? How do you assess whether it’s worth the cost? What do residents think about this?
This last point turned out to be a valuable question to ask. The group included some residents at the site where this project was piloted and had a fruitful discussion. Adding the perspective of residents along with faculty, says Dr. Saint, as well as a couple of nurses and quality care managers, allows a synergy and combination of ideas that led to effective solutions. “Those are exactly the individuals who need to be around a table to overcome some of the challenges.” They have also considered inviting nursing students. “Before they get inculcated in thinking a certain way,” he says, “why not hear what they have to say?”
Dr. Saint believes, however, that this is not a step to be taken lightly. If you are going to include people, “then you have to act on their suggestions or at least hear them out and say why you’re not going to take their suggestions because a good way to get people to become jaded is to listen to their feedback and then just ignore it.”
Calling in Outside Experts
To focus on the issue of preventing hospital-acquired urinary tract infections (UTIs), the consortium invited Russell Olmstead, MPH, an infection control expert and epidemiologist at one of the HELPS sites and past president of the Michigan Society of Infection Control.
“We’d like to do a Keystone[-type] UTI project,” says Dr. Saint, referring to the federally funded statewide three-year initiative, conducted in collaboration with the Michigan Hospital Association and Johns Hopkins Research and Safety Group, that focused on applying evidence-based medicine and quality improvement efforts to prevent ventilator-associated pneumonia and central line-related infections. “We’ve called it the Bladder Bundle; that is, you bundle a group of practices together, and you give the hospitalists who want to participate a toolkit in order to roll this out.”
Although the details still need to be finalized, the project would include ensuring that patients have appropriate indication for an indwelling catheter, that the indwelling catheter is inserted in an aseptic manner, that there was some type of assessment of discontinuation after a certain amount of time, and that alternatives to an indwelling catheter are considered.
Another expert consulting with the consortium was Peter Lindenauer, MD, MSc, with the Division of Healthcare Quality, Baystate Medical Center, Springfield, Mass., and the Department of Medicine, Tufts University School of Medicine, Boston. Dr. Lindenauer came to discuss lessons he and his colleagues have learned from efforts to improve appropriate perioperative beta blocker use.
The final HELPS wrap-up session for the group will include another nationally renowned expert in patient safety.
SHARP: Research Translated into Practice
Another project initiated by the Michigan hospitalists will generate and disseminate new knowledge in the realm of clinical research. The Specialist-Hospitalist Allied Research Program (SHARP), directed by Dr. Flanders and Brahmajee Nallamothu, MD, MPH, an interventional cardiologist, is the first specialist-hospitalist clinical research program in the United States. This hospitalist delivery model alters the way clinical problems are approached and creates opportunities and challenges in implementing best practices, including those surrounding drugs and devices. A successful clinical and translational research program will combine specialists and hospitalists working collaboratively to better understand the best ways to care for inpatients.
This project is similar to what cardiology and oncology specialties have done over the last several decades, says Dr. Saint. In the future, he foresees that the NIH will increasingly focus on translating research into practice in diverse settings. Both specialists and hospitalists who work in a particular area together—such as prevention of lower extremity clots or of nosocomial infections—can use the health consortium to roll out protocols and studies in order to tackle some of the important inpatient topics.
SHARP was awarded funding through the University of Michigan Department of Medicine and was scheduled to take off in February. “Our hope is that we will be able to take advantage of and build upon the health collaborative that we have and bring in our subspecialty expertise to help inform clinical investigations,” says Dr. Saint.
Where They’re Going
Both Dr. Flanders and Dr. Saint are pleased about the HELPS consortium’s progress so far. They believe that they have found a group of people who are interested in patient safety and are willing to learn from one another and that they have done an excellent job of disseminating the best practices they have been exploring.
Ultimately, their goal is to grow this into a “more robust clinical research consortium,” says Dr. Flanders. Instead of disseminating best practices and focusing on just a few targeted patient safety quality improvement areas, they will begin to take on studies that could center around patient safety and quality improvement but will also move toward multi-center projects that might address issues related to management of common clinical problems that hospitalists are now managing and focusing on.
“We’re really excited about what we have been able to accomplish,” he says. “We’ve learned a lot about the challenges of doing this, and of course it’s never perfect. We wish we could always do more, but we’ve learned why we can’t. That will be helpful in future projects and helpful for others who are trying to tackle this same problem.” TH
Reference
- Flanders SA, Kaufman SR, Saint S. Hospitalists as emerging leaders in patient safety: targeting a few to affect many. J Patient Safety. 2005;1(2):78-82.
In the football-loving state of Michigan, legendary athletes take their cues from a coach and map their strategies for one big group effort. But Michigan is also home to what may be the first-ever homegrown regional consortium for patient safety and quality improvement—and in this case—after a huddle each team member gets to call his own plays.
The Hospitalists as Emerging Leaders in Patient Safety (HELPS) Consortium of Southeastern Michigan (funded by a grant from the Blue Cross Blue Shield of Michigan Foundation) includes representatives from nine regional hospitalist programs representing 11 hospitals and approximately 75,000 patients.1
The participants in this program identify proven patient safety practices and facilitate widespread dissemination of those practices among hospitalists.
The member institutions include academic medical centers, large private teaching and non-teaching hospitals, federal facilities, and urban and rural hospitals.
Each institution is represented by a hospitalist—usually the director of the hospitalist program or the individual most interested in and familiar with quality improvement—and a representative from quality improvement or patient safety. The issues they have addressed, which emerged from a variety of sources, such as the Agency of Healthcare Research and Quality, the National Quality Forum, and the Joint Commission on Accreditation of Healthcare Organizations, are those that are commonly encountered in hospitalist practice. These physicians “are bridging the gap between that which they know to be effective and that which is actually practiced.”1
HELPS builds on the experience of medical professionals who have united geographically dispersed physicians from the same specialty to boost quality. The HELPS consortium also aids participating institutions in evaluating outcomes after implementing a targeted patient safety practice, thereby allowing rapid cycle improvement while identifying factors associated with success.
“We have gotten the work that is being done by these different organizations out there, brought it up a notch in certain situations—we like to think—and have gotten it effectively disseminated to a larger group of hospitalists,” says Scott Flanders, MD, an associate professor of medicine at the University of Michigan (Ann Arbor), director of the hospital medicine program there, and an SHM board member.
Where They Are
The consortium is about three-quarters of the way through its overall estimated project period, says Dr. Flanders. It originally planned to have nine gatherings over two years. (See Table 1, p. 35.) To date the consortium has held seven of those sessions and have met roughly every two to three months. End-of-life care and the final wrap-up are the only sessions still to be completed.
The individual sites took on projects that included reducing errors with heparin use in hospitalized patients, reducing falls in hospitalized patients, improving care transitions (a collaborative multidisciplinary approach), reducing unnecessary ICU admission and preventing in-hospital cardiac arrests, reducing urinary catheter infections, improving rates of appropriate deep vein thrombosis prophylaxis, and implementing best practices for reducing central line infections. A national expert conducted a session on implementing a program to reduce perioperative cardiovascular events while ensuring the appropriate use of perioperative beta-blockers.
Challenges and Lessons Learned
From the outset, the HELPS group knew that its primary challenge would be to fulfill the intention to meet as a complete group four or five times per year. “There aren’t a lot of hospitalists who have big parts of their jobs carved out for dedicated time to work on quality improvement research or patient safety,” says Dr. Flanders. “It’s part of what we do in our day, but in terms of taking on a big project, designing it, implementing it, and measuring its effect, it is hard to do in the day-to-day job of most hospitalist groups.”
He suspects that hospitalists frequently help steering committees address certain issues, “but it may not be the individual hospitalist group that is managing or driving the quality issue for an entire hospital or health system.” The HELPS physicians knew that if they could surmount the scheduling challenge, however, they would have a terrific opportunity to learn from each other and move their individual institutional patient safety initiatives forward.
They also knew that the majority of hospitalized patients receive care in community hospitals and that the culture of a community hospital differed dramatically from a tertiary-care academic medical center. Interventions would need to be tried at varied settings, and HELPS would allow that to happen. In addition, few clinically active hospitalists have developed the research expertise to evaluate an intervention rigorously at their own institution, yet decision makers often require such an evaluation when they are considering adopting a new intervention. Using the resources of an academic center such as the University of Michigan, where evaluative and methodologic expertise is available, allowed them to facilitate a resolution for that problem. “As physicians, we are helping [smaller hospitals] by facilitating data collection and data analysis for their ongoing projects,” says Dr. Flanders.
Another challenge the hospitalists faced pertained to the relative instability of hospital medicine compared with other specialties. For instance, it is probably far easier for the members of the consortium of cardiology groups working on best practices for managing acute myocardial infarction to find time to work together. In contrast, because hospital medicine is a relatively new specialty, “we are seeing a certain amount of instability,” explains Dr. Flanders. “Of our nine involved health systems, at least two had dramatic organizational and structural changes within their hospital medicine group over the last year and a half.” One hospital medicine director left, with repercussions in several areas, and, in another group, the practice was sold to a large physician management company, which meant that the HELPS data that had been collected was no longer owned by the [original] group, making their activities more complex.
What They’ve Done So Far
Dr. Flanders is not aware of any other groups of physicians from another state who have undertaken such a project. The Institute for Healthcare Improvement’s “100,000 Lives Campaign” may be similar in some ways, focusing on a few key topic areas. The Michigan Keystone Project, which concentrated on various ICU patient safety topics, is another example of a regional consortium. “But the difference is that they basically drive the agenda,” he says. “They say, ‘This is what we want you all to do, and let’s figure out how we can all do it.’ In our case, we focused on some key areas, but we did not dictate what the project was.”
The following brief recaps represent some of the projects undertaken by consortium member sites.
Falls
The University of Michigan-affiliated Ann Arbor Veterans Affairs (VA) Hospital, where Sanjay Saint, MD, MPH, is a hospitalist, has many elderly and cognitively impaired patients, so preventing falls is a big issue. “My responsibility isn’t to prevent falls but to share these best practices with others in my organization,” he says. “In fact, each project team points out where to look with a certain problem but not necessarily what to do.”
Dr. Saint brought up the issue of mattresses with lipped/raised edges to prevent patients from rolling out of bed. Following that, at least one other consortium hospital suggested to its fall prevention group that they explore the use of these lipped mattresses.
Bed alarms were another problem. Participants shared a common problem: Often, nurses wouldn’t hear a patient’s alarm go off. Other providers might reset them, but if they neglected to let the assigned nurse know the patient was calling, the patient might get tired of waiting, attempt to get out of bed, and sustain a fall. Consequently, providers in most institutions thought the alarms were not useful. But one institution identified a novel way to use bed alarms: attaching them to the nurse’s pager. Now, when the alarm goes off, it alerts the appropriate nurse directly, and because that nurse is responsible for resetting the alarm, she knows that the patient has called and needs help.
Changing Names: CARE Assistants
To avoid the use of physical or chemical restraints, many institutions have resorted to hiring “sitters” who stay at the bedside of confused or delirious patients to calm them; if patients try to get out of bed, sitters are there to coax them back in. A number of HELPS institutions shared the idea that using the term “sitter” might have been inadvertently encouraging inactivity: Too many sitters were doing just that, sitting all day, often watching television.
One of the collaborative sites now calls these employees CARE assistants, an acronym for Caring Alternative to a Restraint-free Environment. The group has predicted that calling them something different will inspire these people to “do more caring and less sitting,” says Dr. Saint. After a HELPS session, Dr. Saint submitted this idea to the key decision makers at the VA. “I could have tried by myself to resolve this dilemma for years and not come up with that idea,” he says. “Why not just take what they’ve done and modify it to suit your own environment?”
Weighty Problem: Heparin Dosing
One hospital in the consortium conducted a project on medication safety that focused on appropriate use of heparin in hospitalized patients. When the site’s hospitalists began studying the problems they were having, they realized that the weights they were using for dosing decisions were being generated in the emergency department (ED). Studying it further, they saw that, most of the time, those patients weren’t actually being weighed; nurses were simply estimating their weights. Having traced the problem to the ED, they were then able to intervene, fix the problem, and show that by doing so their rates of bleeding complications from inappropriate dosing of anticoagulants improved.
At his own institution, Dr. Flanders was participating in a group committee meeting discussing this problem. Consequently, “I was able to ask, ‘Have we looked at weights [being assessed] in the emergency department?’ Everyone involved with that project said, ‘No, why?’ And, sure enough, a similar problem existed.”
Care Transitions and Multidisciplinary Rounding
One member-team of the consortium was able to come up with a multidisciplinary team that met and rounded on patients each day and focused on the care transitions. They were able to dramatically improve staff communication, the overall discharge process, and patient satisfaction. As a result of what he learned of their successes, Dr. Flanders’ institution plans to use a similar strategy to enhance communication among healthcare providers involved in the discharge process on their hospitalist unit.
Rapid Response Teams and Input from Residents
“It’s very helpful to hear, from another site, the challenges and benefits of having hospitalists involved with the rapid response teams,” says Dr. Saint. “How did they operationalize it? What were the remaining challenges? What outcome measures did they use? How do you assess whether it’s worth the cost? What do residents think about this?
This last point turned out to be a valuable question to ask. The group included some residents at the site where this project was piloted and had a fruitful discussion. Adding the perspective of residents along with faculty, says Dr. Saint, as well as a couple of nurses and quality care managers, allows a synergy and combination of ideas that led to effective solutions. “Those are exactly the individuals who need to be around a table to overcome some of the challenges.” They have also considered inviting nursing students. “Before they get inculcated in thinking a certain way,” he says, “why not hear what they have to say?”
Dr. Saint believes, however, that this is not a step to be taken lightly. If you are going to include people, “then you have to act on their suggestions or at least hear them out and say why you’re not going to take their suggestions because a good way to get people to become jaded is to listen to their feedback and then just ignore it.”
Calling in Outside Experts
To focus on the issue of preventing hospital-acquired urinary tract infections (UTIs), the consortium invited Russell Olmstead, MPH, an infection control expert and epidemiologist at one of the HELPS sites and past president of the Michigan Society of Infection Control.
“We’d like to do a Keystone[-type] UTI project,” says Dr. Saint, referring to the federally funded statewide three-year initiative, conducted in collaboration with the Michigan Hospital Association and Johns Hopkins Research and Safety Group, that focused on applying evidence-based medicine and quality improvement efforts to prevent ventilator-associated pneumonia and central line-related infections. “We’ve called it the Bladder Bundle; that is, you bundle a group of practices together, and you give the hospitalists who want to participate a toolkit in order to roll this out.”
Although the details still need to be finalized, the project would include ensuring that patients have appropriate indication for an indwelling catheter, that the indwelling catheter is inserted in an aseptic manner, that there was some type of assessment of discontinuation after a certain amount of time, and that alternatives to an indwelling catheter are considered.
Another expert consulting with the consortium was Peter Lindenauer, MD, MSc, with the Division of Healthcare Quality, Baystate Medical Center, Springfield, Mass., and the Department of Medicine, Tufts University School of Medicine, Boston. Dr. Lindenauer came to discuss lessons he and his colleagues have learned from efforts to improve appropriate perioperative beta blocker use.
The final HELPS wrap-up session for the group will include another nationally renowned expert in patient safety.
SHARP: Research Translated into Practice
Another project initiated by the Michigan hospitalists will generate and disseminate new knowledge in the realm of clinical research. The Specialist-Hospitalist Allied Research Program (SHARP), directed by Dr. Flanders and Brahmajee Nallamothu, MD, MPH, an interventional cardiologist, is the first specialist-hospitalist clinical research program in the United States. This hospitalist delivery model alters the way clinical problems are approached and creates opportunities and challenges in implementing best practices, including those surrounding drugs and devices. A successful clinical and translational research program will combine specialists and hospitalists working collaboratively to better understand the best ways to care for inpatients.
This project is similar to what cardiology and oncology specialties have done over the last several decades, says Dr. Saint. In the future, he foresees that the NIH will increasingly focus on translating research into practice in diverse settings. Both specialists and hospitalists who work in a particular area together—such as prevention of lower extremity clots or of nosocomial infections—can use the health consortium to roll out protocols and studies in order to tackle some of the important inpatient topics.
SHARP was awarded funding through the University of Michigan Department of Medicine and was scheduled to take off in February. “Our hope is that we will be able to take advantage of and build upon the health collaborative that we have and bring in our subspecialty expertise to help inform clinical investigations,” says Dr. Saint.
Where They’re Going
Both Dr. Flanders and Dr. Saint are pleased about the HELPS consortium’s progress so far. They believe that they have found a group of people who are interested in patient safety and are willing to learn from one another and that they have done an excellent job of disseminating the best practices they have been exploring.
Ultimately, their goal is to grow this into a “more robust clinical research consortium,” says Dr. Flanders. Instead of disseminating best practices and focusing on just a few targeted patient safety quality improvement areas, they will begin to take on studies that could center around patient safety and quality improvement but will also move toward multi-center projects that might address issues related to management of common clinical problems that hospitalists are now managing and focusing on.
“We’re really excited about what we have been able to accomplish,” he says. “We’ve learned a lot about the challenges of doing this, and of course it’s never perfect. We wish we could always do more, but we’ve learned why we can’t. That will be helpful in future projects and helpful for others who are trying to tackle this same problem.” TH
Reference
- Flanders SA, Kaufman SR, Saint S. Hospitalists as emerging leaders in patient safety: targeting a few to affect many. J Patient Safety. 2005;1(2):78-82.
Research, innovation, and safety: Doing the right thing
Medical devices and conflict of interest: Unique issues and an industry code to address them
Guiding principles: Where are we headed?
Applications in the real world: Case studies in defining boundaries and managing innovation
Conflicts, compliance, and enforcement: Government priorities and initiatives
Proceedings of A National Dialogue on Biomedical Conflicts of Interest and Innovation Management

Supplement Editor:
Guy M. Chisolm III, PhD
Contents
From the editor
The rapidly changing landscape of biomedical conflicts of interest
Guy M. Chisolm III, PhD, Vice Chairman, Lerner Research Institute, and Professor, Department of Cell Biology, Cleveland Clinic
Opening comments
The mandate of innovation management
Delos M. Cosgrove, MD, CEO and President, Cleveland Clinic
Research, Innovation, and Safety: Doing the Right Thing
Prologue: A case study in biomedical conflicts
Nina Totenberg, Legal Affairs Correspondent, National Public Radio
Fostering innovation without compromising integrity
Philip A. Pizzo, MD, Dean and Professor of Pediatrics and of Microbiology and Immunology, Stanford University School of Medicine
Innovation and industry-academia interactions:Where conflicts arise and measures to avoid them
P. Roy Vagelos, MD, Chairman, Regeneron Pharmaceuticals, Inc.; Chairman, Theravance, Inc.; Former CEO, Merck & Co., Inc.
Overregulation of conflicts hinders medical progress
Thomas P. Stossel, MD, Professor of Medicine, Harvard Medical School
Panel discussion: Research, innovation, and safety: Doing the right thing
Moderated by Nina Totenberg, Legal Affairs Correspondent, National Public Radio
Panelists: Philip A. Pizzo, MD; Thomas P. Stossel, MD; and P. Roy Vagelos, MD
Guiding Principles:Where Are We Headed?
Conflict-of-interest management: Efforts and insights from the Association of American Medical Colleges
Darrell G. Kirch, MD, President and CEO, Association of American Medical Colleges
Medical devices and conflict of interest: Unique issues and an industry code to address them
Paul A. LaViolette, MBA, Chief Operating Officer, Boston Scientific Corporation; Member, Board of Directors, and Chairman, Special Committee on Codes of Ethics, AdvaMed
The challenge for NIH ethics policies: Preserving public trust and biomedical progress
Norka Ruiz Bravo, PhD, Deputy Director for Extramural Research, National Institutes of Health
Panel discussion: Guiding principles:Where are we headed?
Moderated by Nina Totenberg, Legal Affairs Correspondent, National Public Radio
Panelists: Darrell G. Kirch, MD; Paul A. LaViolette, MBA; and Norka Ruiz Bravo, PhD
Keynote Address
Building and retaining trust in the biomedical community
Dick Thornburgh, Counsel, K & L Gates; Former Governor of Pennsylvania; Former Attorney General of the United States
Applications in the Real World: Defining Boundaries and Managing Innovation
Interactions of the public and private sectors in drug development: Boundaries to protect scientific values while preserving innovation
Gail H. Cassell, PhD, DSc (hon), Vice President, Scientific Affairs, and Distinguished Lilly Research Scholar for Infectious Diseases, Eli Lilly and Company
Beyond disclosure: The necessity of trust in biomedical research
Jeffrey P. Kahn, PhD, MPH, Maas Family Chair in Bioethics and Director, Center for Bioethics, University of Minnesota
Panel discussion: Applications in the real world: Case studies in defining boundaries and managing innovation
Moderated by Claudia R. Adkison, JD, PhD, Executive Associate Dean, Administration and Faculty Affairs, Emory University School of Medicine
Case studies submitted by Michael J. Meehan, Esq., Senior Counsel and Corporate Assistant Secretary, Cleveland Clinic, and Claudia R. Adkison, JD, PhD
Panelists: Gail H. Cassell, PhD, DSc (hon); Jeffrey P. Kahn, PhD, MPH; Philip A. Pizzo, MD; and Thomas P. Stossel, MD
Conflicts, Compliance, and Enforcement: Government Priorities and Initiatives
Protecting subjects without hampering research progress: Guidance from the Office for Human Research Protections
Bernard A. Schwetz, DVM, PhD, Director, Office for Human Research Protections, US Department of Health and Human Services
Fraud, conflict of interest, and other enforcement issues in clinical research
James G. Sheehan, Associate US Attorney, US Attorney’s Office, US Department of Justice
Panel discussion: Conflicts, compliance, and enforcement: Government priorities and initiatives
Moderated by Jeffrey P. Kahn, PhD, MPH, Maas Family Chair in Bioethics and Director, Center for Bioethics, University of Minnesota
Panelists: Bernard A. Schwetz, DVM, PhD, and James G. Sheehan
Guidelines and Performance: Creating a Culture of Ethics
Creating an institutional conflict-of-interest policy at Johns Hopkins: Progress and lessons learned
Edward D. Miller, MD, Dean of the Medical Faculty, Johns Hopkins School of Medicine; CEO, Johns Hopkins Medicine
Managing ethical performance in organizations: Insights from the corporate world
Edward Soule, CPA, PhD, Associate Professor, McDonough School of Business, Georgetown University
Panel discussion: Guidelines and performance: Creating a culture of ethics
Moderated by Susan H. Ehringhaus, JD, Associate General Counsel for Regulatory Affairs, Association of American Medical Colleges
Panelists: Edward D. Miller, MD, and Edward Soule, CPA, PhD
Articles in these proceedings were developed by the Cleveland Clinic Journal of Medicine staff from transcripts of audiotaped presentations at the “National Dialogue on Biomedical Conflicts of Interest and Innovation Management” and then reviewed and revised by the respective speakers.
Supplement Editor:
Guy M. Chisolm III, PhD
Contents
From the editor
The rapidly changing landscape of biomedical conflicts of interest
Guy M. Chisolm III, PhD, Vice Chairman, Lerner Research Institute, and Professor, Department of Cell Biology, Cleveland Clinic
Opening comments
The mandate of innovation management
Delos M. Cosgrove, MD, CEO and President, Cleveland Clinic
Research, Innovation, and Safety: Doing the Right Thing
Prologue: A case study in biomedical conflicts
Nina Totenberg, Legal Affairs Correspondent, National Public Radio
Fostering innovation without compromising integrity
Philip A. Pizzo, MD, Dean and Professor of Pediatrics and of Microbiology and Immunology, Stanford University School of Medicine
Innovation and industry-academia interactions:Where conflicts arise and measures to avoid them
P. Roy Vagelos, MD, Chairman, Regeneron Pharmaceuticals, Inc.; Chairman, Theravance, Inc.; Former CEO, Merck & Co., Inc.
Overregulation of conflicts hinders medical progress
Thomas P. Stossel, MD, Professor of Medicine, Harvard Medical School
Panel discussion: Research, innovation, and safety: Doing the right thing
Moderated by Nina Totenberg, Legal Affairs Correspondent, National Public Radio
Panelists: Philip A. Pizzo, MD; Thomas P. Stossel, MD; and P. Roy Vagelos, MD
Guiding Principles:Where Are We Headed?
Conflict-of-interest management: Efforts and insights from the Association of American Medical Colleges
Darrell G. Kirch, MD, President and CEO, Association of American Medical Colleges
Medical devices and conflict of interest: Unique issues and an industry code to address them
Paul A. LaViolette, MBA, Chief Operating Officer, Boston Scientific Corporation; Member, Board of Directors, and Chairman, Special Committee on Codes of Ethics, AdvaMed
The challenge for NIH ethics policies: Preserving public trust and biomedical progress
Norka Ruiz Bravo, PhD, Deputy Director for Extramural Research, National Institutes of Health
Panel discussion: Guiding principles:Where are we headed?
Moderated by Nina Totenberg, Legal Affairs Correspondent, National Public Radio
Panelists: Darrell G. Kirch, MD; Paul A. LaViolette, MBA; and Norka Ruiz Bravo, PhD
Keynote Address
Building and retaining trust in the biomedical community
Dick Thornburgh, Counsel, K & L Gates; Former Governor of Pennsylvania; Former Attorney General of the United States
Applications in the Real World: Defining Boundaries and Managing Innovation
Interactions of the public and private sectors in drug development: Boundaries to protect scientific values while preserving innovation
Gail H. Cassell, PhD, DSc (hon), Vice President, Scientific Affairs, and Distinguished Lilly Research Scholar for Infectious Diseases, Eli Lilly and Company
Beyond disclosure: The necessity of trust in biomedical research
Jeffrey P. Kahn, PhD, MPH, Maas Family Chair in Bioethics and Director, Center for Bioethics, University of Minnesota
Panel discussion: Applications in the real world: Case studies in defining boundaries and managing innovation
Moderated by Claudia R. Adkison, JD, PhD, Executive Associate Dean, Administration and Faculty Affairs, Emory University School of Medicine
Case studies submitted by Michael J. Meehan, Esq., Senior Counsel and Corporate Assistant Secretary, Cleveland Clinic, and Claudia R. Adkison, JD, PhD
Panelists: Gail H. Cassell, PhD, DSc (hon); Jeffrey P. Kahn, PhD, MPH; Philip A. Pizzo, MD; and Thomas P. Stossel, MD
Conflicts, Compliance, and Enforcement: Government Priorities and Initiatives
Protecting subjects without hampering research progress: Guidance from the Office for Human Research Protections
Bernard A. Schwetz, DVM, PhD, Director, Office for Human Research Protections, US Department of Health and Human Services
Fraud, conflict of interest, and other enforcement issues in clinical research
James G. Sheehan, Associate US Attorney, US Attorney’s Office, US Department of Justice
Panel discussion: Conflicts, compliance, and enforcement: Government priorities and initiatives
Moderated by Jeffrey P. Kahn, PhD, MPH, Maas Family Chair in Bioethics and Director, Center for Bioethics, University of Minnesota
Panelists: Bernard A. Schwetz, DVM, PhD, and James G. Sheehan
Guidelines and Performance: Creating a Culture of Ethics
Creating an institutional conflict-of-interest policy at Johns Hopkins: Progress and lessons learned
Edward D. Miller, MD, Dean of the Medical Faculty, Johns Hopkins School of Medicine; CEO, Johns Hopkins Medicine
Managing ethical performance in organizations: Insights from the corporate world
Edward Soule, CPA, PhD, Associate Professor, McDonough School of Business, Georgetown University
Panel discussion: Guidelines and performance: Creating a culture of ethics
Moderated by Susan H. Ehringhaus, JD, Associate General Counsel for Regulatory Affairs, Association of American Medical Colleges
Panelists: Edward D. Miller, MD, and Edward Soule, CPA, PhD
Articles in these proceedings were developed by the Cleveland Clinic Journal of Medicine staff from transcripts of audiotaped presentations at the “National Dialogue on Biomedical Conflicts of Interest and Innovation Management” and then reviewed and revised by the respective speakers.
Supplement Editor:
Guy M. Chisolm III, PhD
Contents
From the editor
The rapidly changing landscape of biomedical conflicts of interest
Guy M. Chisolm III, PhD, Vice Chairman, Lerner Research Institute, and Professor, Department of Cell Biology, Cleveland Clinic
Opening comments
The mandate of innovation management
Delos M. Cosgrove, MD, CEO and President, Cleveland Clinic
Research, Innovation, and Safety: Doing the Right Thing
Prologue: A case study in biomedical conflicts
Nina Totenberg, Legal Affairs Correspondent, National Public Radio
Fostering innovation without compromising integrity
Philip A. Pizzo, MD, Dean and Professor of Pediatrics and of Microbiology and Immunology, Stanford University School of Medicine
Innovation and industry-academia interactions:Where conflicts arise and measures to avoid them
P. Roy Vagelos, MD, Chairman, Regeneron Pharmaceuticals, Inc.; Chairman, Theravance, Inc.; Former CEO, Merck & Co., Inc.
Overregulation of conflicts hinders medical progress
Thomas P. Stossel, MD, Professor of Medicine, Harvard Medical School
Panel discussion: Research, innovation, and safety: Doing the right thing
Moderated by Nina Totenberg, Legal Affairs Correspondent, National Public Radio
Panelists: Philip A. Pizzo, MD; Thomas P. Stossel, MD; and P. Roy Vagelos, MD
Guiding Principles:Where Are We Headed?
Conflict-of-interest management: Efforts and insights from the Association of American Medical Colleges
Darrell G. Kirch, MD, President and CEO, Association of American Medical Colleges
Medical devices and conflict of interest: Unique issues and an industry code to address them
Paul A. LaViolette, MBA, Chief Operating Officer, Boston Scientific Corporation; Member, Board of Directors, and Chairman, Special Committee on Codes of Ethics, AdvaMed
The challenge for NIH ethics policies: Preserving public trust and biomedical progress
Norka Ruiz Bravo, PhD, Deputy Director for Extramural Research, National Institutes of Health
Panel discussion: Guiding principles:Where are we headed?
Moderated by Nina Totenberg, Legal Affairs Correspondent, National Public Radio
Panelists: Darrell G. Kirch, MD; Paul A. LaViolette, MBA; and Norka Ruiz Bravo, PhD
Keynote Address
Building and retaining trust in the biomedical community
Dick Thornburgh, Counsel, K & L Gates; Former Governor of Pennsylvania; Former Attorney General of the United States
Applications in the Real World: Defining Boundaries and Managing Innovation
Interactions of the public and private sectors in drug development: Boundaries to protect scientific values while preserving innovation
Gail H. Cassell, PhD, DSc (hon), Vice President, Scientific Affairs, and Distinguished Lilly Research Scholar for Infectious Diseases, Eli Lilly and Company
Beyond disclosure: The necessity of trust in biomedical research
Jeffrey P. Kahn, PhD, MPH, Maas Family Chair in Bioethics and Director, Center for Bioethics, University of Minnesota
Panel discussion: Applications in the real world: Case studies in defining boundaries and managing innovation
Moderated by Claudia R. Adkison, JD, PhD, Executive Associate Dean, Administration and Faculty Affairs, Emory University School of Medicine
Case studies submitted by Michael J. Meehan, Esq., Senior Counsel and Corporate Assistant Secretary, Cleveland Clinic, and Claudia R. Adkison, JD, PhD
Panelists: Gail H. Cassell, PhD, DSc (hon); Jeffrey P. Kahn, PhD, MPH; Philip A. Pizzo, MD; and Thomas P. Stossel, MD
Conflicts, Compliance, and Enforcement: Government Priorities and Initiatives
Protecting subjects without hampering research progress: Guidance from the Office for Human Research Protections
Bernard A. Schwetz, DVM, PhD, Director, Office for Human Research Protections, US Department of Health and Human Services
Fraud, conflict of interest, and other enforcement issues in clinical research
James G. Sheehan, Associate US Attorney, US Attorney’s Office, US Department of Justice
Panel discussion: Conflicts, compliance, and enforcement: Government priorities and initiatives
Moderated by Jeffrey P. Kahn, PhD, MPH, Maas Family Chair in Bioethics and Director, Center for Bioethics, University of Minnesota
Panelists: Bernard A. Schwetz, DVM, PhD, and James G. Sheehan
Guidelines and Performance: Creating a Culture of Ethics
Creating an institutional conflict-of-interest policy at Johns Hopkins: Progress and lessons learned
Edward D. Miller, MD, Dean of the Medical Faculty, Johns Hopkins School of Medicine; CEO, Johns Hopkins Medicine
Managing ethical performance in organizations: Insights from the corporate world
Edward Soule, CPA, PhD, Associate Professor, McDonough School of Business, Georgetown University
Panel discussion: Guidelines and performance: Creating a culture of ethics
Moderated by Susan H. Ehringhaus, JD, Associate General Counsel for Regulatory Affairs, Association of American Medical Colleges
Panelists: Edward D. Miller, MD, and Edward Soule, CPA, PhD
Articles in these proceedings were developed by the Cleveland Clinic Journal of Medicine staff from transcripts of audiotaped presentations at the “National Dialogue on Biomedical Conflicts of Interest and Innovation Management” and then reviewed and revised by the respective speakers.
Guidelines and performance: Creating a culture of ethics
Raising hemoglobin levels to normal range for chronic kidney failure patients may be too risky
Hemoglobin concentrations in the high normal range in patients with anemia due to chronic kidney disease result in an excess risk of major adverse events, reported Arintaya Phrommintikul, MD, and colleagues from Monash University, Melbourne, Australia.
Adverse events include death, arteriovenous access thrombosis, and poorly controlled hypertension.
The investigators conducted a meta-analysis of 9 randomized controlled studies that enrolled 5143 patients treated with recombinant human erythropoietin.
Patients in the group targeted for a higher hemoglobin level (120-160 g/L) had a higher risk for all-cause mortality than patients in the lower hemoglobin target group (< 120 g/L) (risk ratio 1.17, P = 0.031).
There was also a higher risk for arteriovenous access thrombosis (risk ratio 1.34, P=0.0001) as well as a significantly higher risk of poorly controlled blood pressure (risk ratio 1.27, P=0.004) in the higher hemoglobin target group. The incidence of myocardial infarction was similar in the two groups.
Current guidelines recommend the maintenance of hemoglobin concentrations at 110 g/L or higher, based mainly on evidence of benefit in quality-of-life measures.
Current guidelines do not include an upper limit for the target hemoglobin concentration. The authors suggest that an upper limit should be added in future revisions of guideline recommendations.
The study was published in the 3 February 2007 issue of Lancet. ![]()
Hemoglobin concentrations in the high normal range in patients with anemia due to chronic kidney disease result in an excess risk of major adverse events, reported Arintaya Phrommintikul, MD, and colleagues from Monash University, Melbourne, Australia.
Adverse events include death, arteriovenous access thrombosis, and poorly controlled hypertension.
The investigators conducted a meta-analysis of 9 randomized controlled studies that enrolled 5143 patients treated with recombinant human erythropoietin.
Patients in the group targeted for a higher hemoglobin level (120-160 g/L) had a higher risk for all-cause mortality than patients in the lower hemoglobin target group (< 120 g/L) (risk ratio 1.17, P = 0.031).
There was also a higher risk for arteriovenous access thrombosis (risk ratio 1.34, P=0.0001) as well as a significantly higher risk of poorly controlled blood pressure (risk ratio 1.27, P=0.004) in the higher hemoglobin target group. The incidence of myocardial infarction was similar in the two groups.
Current guidelines recommend the maintenance of hemoglobin concentrations at 110 g/L or higher, based mainly on evidence of benefit in quality-of-life measures.
Current guidelines do not include an upper limit for the target hemoglobin concentration. The authors suggest that an upper limit should be added in future revisions of guideline recommendations.
The study was published in the 3 February 2007 issue of Lancet. ![]()
Hemoglobin concentrations in the high normal range in patients with anemia due to chronic kidney disease result in an excess risk of major adverse events, reported Arintaya Phrommintikul, MD, and colleagues from Monash University, Melbourne, Australia.
Adverse events include death, arteriovenous access thrombosis, and poorly controlled hypertension.
The investigators conducted a meta-analysis of 9 randomized controlled studies that enrolled 5143 patients treated with recombinant human erythropoietin.
Patients in the group targeted for a higher hemoglobin level (120-160 g/L) had a higher risk for all-cause mortality than patients in the lower hemoglobin target group (< 120 g/L) (risk ratio 1.17, P = 0.031).
There was also a higher risk for arteriovenous access thrombosis (risk ratio 1.34, P=0.0001) as well as a significantly higher risk of poorly controlled blood pressure (risk ratio 1.27, P=0.004) in the higher hemoglobin target group. The incidence of myocardial infarction was similar in the two groups.
Current guidelines recommend the maintenance of hemoglobin concentrations at 110 g/L or higher, based mainly on evidence of benefit in quality-of-life measures.
Current guidelines do not include an upper limit for the target hemoglobin concentration. The authors suggest that an upper limit should be added in future revisions of guideline recommendations.
The study was published in the 3 February 2007 issue of Lancet. ![]()