User login
Urinary Tract Infections Do Not Play a Significant Role in Chronic Kidney Disease

Clinical question: What is the association between childhood urinary tract infections (UTIs) and chronic kidney disease (CKD)?
Background: A traditional paradigm in pediatrics is that CKD might be caused by renal scarring as a result of recurrent UTIs, particularly in the presence of vesicoureteral reflux (VUR). Increasingly, this has been called into question as nonintervention for low-grade VUR has not impacted clinical outcomes.
Study design: Retrospective cohort and systematic literature review.
Setting: Tertiary-care hospital in Finland and PubMed database.
Synopsis: A search of the PubMed database for articles published from 1966 to 2009 relating to a potential association between CKD and UTIs yielded 10 studies reporting on 1,576 patients with UTIs and long-term evaluation for CKD. Only three of the 1,576 patients had childhood UTIs without structural kidney abnormalities as a potential cause of the CKD. VUR was not considered a structural abnormality. The authors note that no data on kidney morphology prior to UTI recurrence were available in these cases.
At the same time, the study authors reviewed the records of 366 patients with CKD at a tertiary-care hospital in Finland. They excluded 308 patients with defined noninfectious causes of CKD. Of the 58 remaining patients, three potentially had recurrent UTIs as a contributing cause to eventual CKD. All three patients had structurally abnormal kidneys on first radiologic examination, possibly suggesting pre-existing renal anomalies. The potential association between recurrent childhood UTIs without structural abnormalities and CKD appears to be less than 1%.
Limitations of this study include its retrospective design and incomplete characterization systematic review. Nevertheless, the study appears to support recent work that childhood UTIs without underlying kidney abnormalities are unlikely to result in permanent renal damage.
Bottom line: Childhood UTIs, without structural kidney abnormality, are not a significant cause of chronic kidney disease in adults.
Citation: Salo J, Ilkäheimo R, Tapiainen T, Uhari M. Childhood urinary tract infections as a cause of chronic kidney disease. Pediatrics. 2011;128:840-847.
Reviewed by Pediatric Editor Mark Shen, MD, FHM, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Clinical question: What is the association between childhood urinary tract infections (UTIs) and chronic kidney disease (CKD)?
Background: A traditional paradigm in pediatrics is that CKD might be caused by renal scarring as a result of recurrent UTIs, particularly in the presence of vesicoureteral reflux (VUR). Increasingly, this has been called into question as nonintervention for low-grade VUR has not impacted clinical outcomes.
Study design: Retrospective cohort and systematic literature review.
Setting: Tertiary-care hospital in Finland and PubMed database.
Synopsis: A search of the PubMed database for articles published from 1966 to 2009 relating to a potential association between CKD and UTIs yielded 10 studies reporting on 1,576 patients with UTIs and long-term evaluation for CKD. Only three of the 1,576 patients had childhood UTIs without structural kidney abnormalities as a potential cause of the CKD. VUR was not considered a structural abnormality. The authors note that no data on kidney morphology prior to UTI recurrence were available in these cases.
At the same time, the study authors reviewed the records of 366 patients with CKD at a tertiary-care hospital in Finland. They excluded 308 patients with defined noninfectious causes of CKD. Of the 58 remaining patients, three potentially had recurrent UTIs as a contributing cause to eventual CKD. All three patients had structurally abnormal kidneys on first radiologic examination, possibly suggesting pre-existing renal anomalies. The potential association between recurrent childhood UTIs without structural abnormalities and CKD appears to be less than 1%.
Limitations of this study include its retrospective design and incomplete characterization systematic review. Nevertheless, the study appears to support recent work that childhood UTIs without underlying kidney abnormalities are unlikely to result in permanent renal damage.
Bottom line: Childhood UTIs, without structural kidney abnormality, are not a significant cause of chronic kidney disease in adults.
Citation: Salo J, Ilkäheimo R, Tapiainen T, Uhari M. Childhood urinary tract infections as a cause of chronic kidney disease. Pediatrics. 2011;128:840-847.
Reviewed by Pediatric Editor Mark Shen, MD, FHM, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Clinical question: What is the association between childhood urinary tract infections (UTIs) and chronic kidney disease (CKD)?
Background: A traditional paradigm in pediatrics is that CKD might be caused by renal scarring as a result of recurrent UTIs, particularly in the presence of vesicoureteral reflux (VUR). Increasingly, this has been called into question as nonintervention for low-grade VUR has not impacted clinical outcomes.
Study design: Retrospective cohort and systematic literature review.
Setting: Tertiary-care hospital in Finland and PubMed database.
Synopsis: A search of the PubMed database for articles published from 1966 to 2009 relating to a potential association between CKD and UTIs yielded 10 studies reporting on 1,576 patients with UTIs and long-term evaluation for CKD. Only three of the 1,576 patients had childhood UTIs without structural kidney abnormalities as a potential cause of the CKD. VUR was not considered a structural abnormality. The authors note that no data on kidney morphology prior to UTI recurrence were available in these cases.
At the same time, the study authors reviewed the records of 366 patients with CKD at a tertiary-care hospital in Finland. They excluded 308 patients with defined noninfectious causes of CKD. Of the 58 remaining patients, three potentially had recurrent UTIs as a contributing cause to eventual CKD. All three patients had structurally abnormal kidneys on first radiologic examination, possibly suggesting pre-existing renal anomalies. The potential association between recurrent childhood UTIs without structural abnormalities and CKD appears to be less than 1%.
Limitations of this study include its retrospective design and incomplete characterization systematic review. Nevertheless, the study appears to support recent work that childhood UTIs without underlying kidney abnormalities are unlikely to result in permanent renal damage.
Bottom line: Childhood UTIs, without structural kidney abnormality, are not a significant cause of chronic kidney disease in adults.
Citation: Salo J, Ilkäheimo R, Tapiainen T, Uhari M. Childhood urinary tract infections as a cause of chronic kidney disease. Pediatrics. 2011;128:840-847.
Reviewed by Pediatric Editor Mark Shen, MD, FHM, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Guidelines for Treatment of Uncomplicated Cystitis and Pyelonephritis in Healthy, Community-Dwelling Women

Background
Uncomplicated cystitis is one of the most common indications for prescribing antimicrobial therapy to otherwise healthy women, but wide variation in prescribing practices has been described.1-2 This has prompted the need for guidelines to help providers in their selection of empiric antimicrobial regimens. Antibiotic selection should take into consideration the efficacy of individual agents, as well as their propensity for inducing resistance, altering gut flora, and increasing the risk of colonization or infection with multi-drug resistant organisms.
Guideline Update
In March 2010, the Infectious Diseases Society of America (IDSA) and the European Society for Microbiology and Infectious Diseases (ESCMID) published new guidelines for the treatment of uncomplicated cystitis and pyelonephritis in healthy, community-dwelling women.3
First-line recommended agents for empiric treatment of uncomplicated cystitis are:
- nitrofurantoin for five days;
- trimethoprim-sulfamethoxazole for three days;
- fosfomycin in a single dose; or
- pivmecillinam (where available) for three to seven days.
Although highly efficacious, fluoroquinolones are not recommended as first-line treatment for acute cystitis because of their propensity for causing “collateral damage,” especially alteration of gut flora and increased risk of multi-drug resistant infection or colonization, including methicillin-resistant Staphylococcus aureus. Oral beta-lactams (other than pivmecillinam) have generally demonstrated inferior efficacy and more adverse effects when compared with the above agents, and should be used only if none of the preferred agents can be used. Specifically, amoxicillin and ampicillin are not recommended as empiric therapy due to their low efficacy in unselected patients, though may be appropriate when culture data is available to guide therapy. Narrow spectrum cephalosporins are also a potential agent for use in certain clinical situations, although the guidelines do not make any recommendation for or against their use, given a lack of studies.
For the treatment of acute pyelonephritis, the guidelines emphasize that all patients should have urine culture and susceptibility testing in order to tailor empiric therapy to the specific uropathogen. A 5-7 day course of an oral fluoroquinolone is appropriate when the prevalence of resistance in community uropathogens is ≤10%. Where resistance is more common, an initial intravenous dose of ceftriaxone or an aminoglycoside can be administered prior to starting oral therapy. Other alternatives include a 14-day course of trimethoprim-sulfamethoxazole or an oral beta-lactam.
Women requiring hospitalization for pyelonephritis should initially be treated with an intravenous antimicrobial regimen, the choice of which should be based on local resistance patterns. Recommended intravenous agents include fluoroquinolones, aminoglycosides (with or without ampicillin), extended-spectrum cephalosporins / penicillins, or carbapenems.
Analysis
Previous guidelines for the treatment of uncomplicated cystitis and pyelonephritis were published by the IDSA in 1999.4 The guidelines were updated based on the following factors:
- continued variability in prescribing practices;1-2
- increase in antimicrobial resistance among uropathogens;
- awareness of the unintended consequences of antimicrobial therapy, such as selection of drug-resistant organisms and colonization or infection with multi-drug resistant organisms; and
- study of newer agents and different durations of therapy.
Two important differences exist between the 1999 and 2010 guidelines:
- Nitrofurantoin has taken on more prominence in the 2010 guidelines for uncomplicated cystitis. The 1999 guidelines recommended trimethoprim-sulfamethoxazole as a first-line agent and mentioned nitrofurantoin and fosfomycin as potential alternative agents, but had few studies available to inform comparative efficacy or duration of therapy.
- For the outpatient treatment of mildly-ill patients with acute pyelonephritis, the 1999 guidelines recommended 14 days of therapy regardless of the agent used; in contrast, the 2010 guidelines recommend a five- to seven-day course for oral fluoroquinolones.
The American Congress of Obstetricians and Gynecologists, American Urological Association, Association of Medical Microbiology and Infectious Diseases-Canada, and the Society for Academic Emergency Medicine have endorsed the 2010 IDSA-ESCMID guidelines. The IDSA and ESCMID plan to evaluate the need for revisions to the 2010 guidelines based on an annual review of the current literature.
HM Takeaways
The 2010 IDSA-ESCMID guidelines are a resource available to hospitalists treating acute uncomplicated cystitis and pyelonephritis. As important differences exist between the target population and the hospitalist’s patient population, there are some key points to consider for clinicians treating cystitis or pyelonephritis in hospitalized patients.
Importantly, while nitrofurantoin is favored as a first-line antimicrobial agent for cystitis in the 2010 IDSA-ESCMID guidelines, it might be problematic in hospitalized patients for several reasons:
- it is not approved or recommended for the treatment of pyelonephritis;
- it is contraindicated in patients with creatinine clearance <60 ml/min; and
- it is generally not recommended for use in patients >65 years old because of the risk of renal impairment (Beers Criteria).5
Additionally, the treatment of acute cystitis in men requires special consideration. Notably, nitrofurantoin is not recommended in men because of poor prostatic tissue penetration, and although studies are limited, some sources recommend a longer treatment duration of at least 7 days.6 Finally, hospitalized patients commonly have other conditions, such as urological abnormalities, indwelling Foley catheters, recent urinary tract instrumentation, recent use of antibiotics, risk for multi-drug resistant organisms, potential interactions with other medications, and immunosuppression. The presence of any of these factors will influence the choice of empiric therapy and may warrant treatment for complicated cystitis or pyelonephritis, which are not addressed by these guidelines.
Drs. Tarvin and Sponsler are academic hospitalists at Vanderbilt University School of Medicine in Nashville, Tenn.
References
- Huang ES, Stafford RS. National patterns in the treatment of urinary tract infections in women by ambulatory care physicians. Arch Intern Med. 2006;166:635-639.
- Kahan NR, Chinitz DP, Kahan E. Longer than recommended empiric antibiotic treatment of urinary tract infection in women: an avoidable waste of money. J Clin Pharm Therap. 2004;29:59-63.
- Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Inf Dis. 2011;52(5):e103-20.
- Warren JW, Abrutyn E, Hebel JR, Schaeffer AJ, Stamm WE. Guidelines for antimicrobial treatment of acute bacterial cystitis and acute pyelonephritis in women. Infectious Diseases Society of America. Clin Inf Dis. 1999;29(4):745-58.
- Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH. Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a U.S. consensus panel of experts. Arch Intern Med. 2003;163(22):2716-2724.
- Mehnert-Kay SA. Diagnosis and management of uncomplicated urinary tract infections. A Fam Phys. 2005;72(3):451-456.
Background
Uncomplicated cystitis is one of the most common indications for prescribing antimicrobial therapy to otherwise healthy women, but wide variation in prescribing practices has been described.1-2 This has prompted the need for guidelines to help providers in their selection of empiric antimicrobial regimens. Antibiotic selection should take into consideration the efficacy of individual agents, as well as their propensity for inducing resistance, altering gut flora, and increasing the risk of colonization or infection with multi-drug resistant organisms.
Guideline Update
In March 2010, the Infectious Diseases Society of America (IDSA) and the European Society for Microbiology and Infectious Diseases (ESCMID) published new guidelines for the treatment of uncomplicated cystitis and pyelonephritis in healthy, community-dwelling women.3
First-line recommended agents for empiric treatment of uncomplicated cystitis are:
- nitrofurantoin for five days;
- trimethoprim-sulfamethoxazole for three days;
- fosfomycin in a single dose; or
- pivmecillinam (where available) for three to seven days.
Although highly efficacious, fluoroquinolones are not recommended as first-line treatment for acute cystitis because of their propensity for causing “collateral damage,” especially alteration of gut flora and increased risk of multi-drug resistant infection or colonization, including methicillin-resistant Staphylococcus aureus. Oral beta-lactams (other than pivmecillinam) have generally demonstrated inferior efficacy and more adverse effects when compared with the above agents, and should be used only if none of the preferred agents can be used. Specifically, amoxicillin and ampicillin are not recommended as empiric therapy due to their low efficacy in unselected patients, though may be appropriate when culture data is available to guide therapy. Narrow spectrum cephalosporins are also a potential agent for use in certain clinical situations, although the guidelines do not make any recommendation for or against their use, given a lack of studies.
For the treatment of acute pyelonephritis, the guidelines emphasize that all patients should have urine culture and susceptibility testing in order to tailor empiric therapy to the specific uropathogen. A 5-7 day course of an oral fluoroquinolone is appropriate when the prevalence of resistance in community uropathogens is ≤10%. Where resistance is more common, an initial intravenous dose of ceftriaxone or an aminoglycoside can be administered prior to starting oral therapy. Other alternatives include a 14-day course of trimethoprim-sulfamethoxazole or an oral beta-lactam.
Women requiring hospitalization for pyelonephritis should initially be treated with an intravenous antimicrobial regimen, the choice of which should be based on local resistance patterns. Recommended intravenous agents include fluoroquinolones, aminoglycosides (with or without ampicillin), extended-spectrum cephalosporins / penicillins, or carbapenems.
Analysis
Previous guidelines for the treatment of uncomplicated cystitis and pyelonephritis were published by the IDSA in 1999.4 The guidelines were updated based on the following factors:
- continued variability in prescribing practices;1-2
- increase in antimicrobial resistance among uropathogens;
- awareness of the unintended consequences of antimicrobial therapy, such as selection of drug-resistant organisms and colonization or infection with multi-drug resistant organisms; and
- study of newer agents and different durations of therapy.
Two important differences exist between the 1999 and 2010 guidelines:
- Nitrofurantoin has taken on more prominence in the 2010 guidelines for uncomplicated cystitis. The 1999 guidelines recommended trimethoprim-sulfamethoxazole as a first-line agent and mentioned nitrofurantoin and fosfomycin as potential alternative agents, but had few studies available to inform comparative efficacy or duration of therapy.
- For the outpatient treatment of mildly-ill patients with acute pyelonephritis, the 1999 guidelines recommended 14 days of therapy regardless of the agent used; in contrast, the 2010 guidelines recommend a five- to seven-day course for oral fluoroquinolones.
The American Congress of Obstetricians and Gynecologists, American Urological Association, Association of Medical Microbiology and Infectious Diseases-Canada, and the Society for Academic Emergency Medicine have endorsed the 2010 IDSA-ESCMID guidelines. The IDSA and ESCMID plan to evaluate the need for revisions to the 2010 guidelines based on an annual review of the current literature.
HM Takeaways
The 2010 IDSA-ESCMID guidelines are a resource available to hospitalists treating acute uncomplicated cystitis and pyelonephritis. As important differences exist between the target population and the hospitalist’s patient population, there are some key points to consider for clinicians treating cystitis or pyelonephritis in hospitalized patients.
Importantly, while nitrofurantoin is favored as a first-line antimicrobial agent for cystitis in the 2010 IDSA-ESCMID guidelines, it might be problematic in hospitalized patients for several reasons:
- it is not approved or recommended for the treatment of pyelonephritis;
- it is contraindicated in patients with creatinine clearance <60 ml/min; and
- it is generally not recommended for use in patients >65 years old because of the risk of renal impairment (Beers Criteria).5
Additionally, the treatment of acute cystitis in men requires special consideration. Notably, nitrofurantoin is not recommended in men because of poor prostatic tissue penetration, and although studies are limited, some sources recommend a longer treatment duration of at least 7 days.6 Finally, hospitalized patients commonly have other conditions, such as urological abnormalities, indwelling Foley catheters, recent urinary tract instrumentation, recent use of antibiotics, risk for multi-drug resistant organisms, potential interactions with other medications, and immunosuppression. The presence of any of these factors will influence the choice of empiric therapy and may warrant treatment for complicated cystitis or pyelonephritis, which are not addressed by these guidelines.
Drs. Tarvin and Sponsler are academic hospitalists at Vanderbilt University School of Medicine in Nashville, Tenn.
References
- Huang ES, Stafford RS. National patterns in the treatment of urinary tract infections in women by ambulatory care physicians. Arch Intern Med. 2006;166:635-639.
- Kahan NR, Chinitz DP, Kahan E. Longer than recommended empiric antibiotic treatment of urinary tract infection in women: an avoidable waste of money. J Clin Pharm Therap. 2004;29:59-63.
- Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Inf Dis. 2011;52(5):e103-20.
- Warren JW, Abrutyn E, Hebel JR, Schaeffer AJ, Stamm WE. Guidelines for antimicrobial treatment of acute bacterial cystitis and acute pyelonephritis in women. Infectious Diseases Society of America. Clin Inf Dis. 1999;29(4):745-58.
- Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH. Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a U.S. consensus panel of experts. Arch Intern Med. 2003;163(22):2716-2724.
- Mehnert-Kay SA. Diagnosis and management of uncomplicated urinary tract infections. A Fam Phys. 2005;72(3):451-456.
Background
Uncomplicated cystitis is one of the most common indications for prescribing antimicrobial therapy to otherwise healthy women, but wide variation in prescribing practices has been described.1-2 This has prompted the need for guidelines to help providers in their selection of empiric antimicrobial regimens. Antibiotic selection should take into consideration the efficacy of individual agents, as well as their propensity for inducing resistance, altering gut flora, and increasing the risk of colonization or infection with multi-drug resistant organisms.
Guideline Update
In March 2010, the Infectious Diseases Society of America (IDSA) and the European Society for Microbiology and Infectious Diseases (ESCMID) published new guidelines for the treatment of uncomplicated cystitis and pyelonephritis in healthy, community-dwelling women.3
First-line recommended agents for empiric treatment of uncomplicated cystitis are:
- nitrofurantoin for five days;
- trimethoprim-sulfamethoxazole for three days;
- fosfomycin in a single dose; or
- pivmecillinam (where available) for three to seven days.
Although highly efficacious, fluoroquinolones are not recommended as first-line treatment for acute cystitis because of their propensity for causing “collateral damage,” especially alteration of gut flora and increased risk of multi-drug resistant infection or colonization, including methicillin-resistant Staphylococcus aureus. Oral beta-lactams (other than pivmecillinam) have generally demonstrated inferior efficacy and more adverse effects when compared with the above agents, and should be used only if none of the preferred agents can be used. Specifically, amoxicillin and ampicillin are not recommended as empiric therapy due to their low efficacy in unselected patients, though may be appropriate when culture data is available to guide therapy. Narrow spectrum cephalosporins are also a potential agent for use in certain clinical situations, although the guidelines do not make any recommendation for or against their use, given a lack of studies.
For the treatment of acute pyelonephritis, the guidelines emphasize that all patients should have urine culture and susceptibility testing in order to tailor empiric therapy to the specific uropathogen. A 5-7 day course of an oral fluoroquinolone is appropriate when the prevalence of resistance in community uropathogens is ≤10%. Where resistance is more common, an initial intravenous dose of ceftriaxone or an aminoglycoside can be administered prior to starting oral therapy. Other alternatives include a 14-day course of trimethoprim-sulfamethoxazole or an oral beta-lactam.
Women requiring hospitalization for pyelonephritis should initially be treated with an intravenous antimicrobial regimen, the choice of which should be based on local resistance patterns. Recommended intravenous agents include fluoroquinolones, aminoglycosides (with or without ampicillin), extended-spectrum cephalosporins / penicillins, or carbapenems.
Analysis
Previous guidelines for the treatment of uncomplicated cystitis and pyelonephritis were published by the IDSA in 1999.4 The guidelines were updated based on the following factors:
- continued variability in prescribing practices;1-2
- increase in antimicrobial resistance among uropathogens;
- awareness of the unintended consequences of antimicrobial therapy, such as selection of drug-resistant organisms and colonization or infection with multi-drug resistant organisms; and
- study of newer agents and different durations of therapy.
Two important differences exist between the 1999 and 2010 guidelines:
- Nitrofurantoin has taken on more prominence in the 2010 guidelines for uncomplicated cystitis. The 1999 guidelines recommended trimethoprim-sulfamethoxazole as a first-line agent and mentioned nitrofurantoin and fosfomycin as potential alternative agents, but had few studies available to inform comparative efficacy or duration of therapy.
- For the outpatient treatment of mildly-ill patients with acute pyelonephritis, the 1999 guidelines recommended 14 days of therapy regardless of the agent used; in contrast, the 2010 guidelines recommend a five- to seven-day course for oral fluoroquinolones.
The American Congress of Obstetricians and Gynecologists, American Urological Association, Association of Medical Microbiology and Infectious Diseases-Canada, and the Society for Academic Emergency Medicine have endorsed the 2010 IDSA-ESCMID guidelines. The IDSA and ESCMID plan to evaluate the need for revisions to the 2010 guidelines based on an annual review of the current literature.
HM Takeaways
The 2010 IDSA-ESCMID guidelines are a resource available to hospitalists treating acute uncomplicated cystitis and pyelonephritis. As important differences exist between the target population and the hospitalist’s patient population, there are some key points to consider for clinicians treating cystitis or pyelonephritis in hospitalized patients.
Importantly, while nitrofurantoin is favored as a first-line antimicrobial agent for cystitis in the 2010 IDSA-ESCMID guidelines, it might be problematic in hospitalized patients for several reasons:
- it is not approved or recommended for the treatment of pyelonephritis;
- it is contraindicated in patients with creatinine clearance <60 ml/min; and
- it is generally not recommended for use in patients >65 years old because of the risk of renal impairment (Beers Criteria).5
Additionally, the treatment of acute cystitis in men requires special consideration. Notably, nitrofurantoin is not recommended in men because of poor prostatic tissue penetration, and although studies are limited, some sources recommend a longer treatment duration of at least 7 days.6 Finally, hospitalized patients commonly have other conditions, such as urological abnormalities, indwelling Foley catheters, recent urinary tract instrumentation, recent use of antibiotics, risk for multi-drug resistant organisms, potential interactions with other medications, and immunosuppression. The presence of any of these factors will influence the choice of empiric therapy and may warrant treatment for complicated cystitis or pyelonephritis, which are not addressed by these guidelines.
Drs. Tarvin and Sponsler are academic hospitalists at Vanderbilt University School of Medicine in Nashville, Tenn.
References
- Huang ES, Stafford RS. National patterns in the treatment of urinary tract infections in women by ambulatory care physicians. Arch Intern Med. 2006;166:635-639.
- Kahan NR, Chinitz DP, Kahan E. Longer than recommended empiric antibiotic treatment of urinary tract infection in women: an avoidable waste of money. J Clin Pharm Therap. 2004;29:59-63.
- Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Inf Dis. 2011;52(5):e103-20.
- Warren JW, Abrutyn E, Hebel JR, Schaeffer AJ, Stamm WE. Guidelines for antimicrobial treatment of acute bacterial cystitis and acute pyelonephritis in women. Infectious Diseases Society of America. Clin Inf Dis. 1999;29(4):745-58.
- Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH. Updating the Beers criteria for potentially inappropriate medication use in older adults: results of a U.S. consensus panel of experts. Arch Intern Med. 2003;163(22):2716-2724.
- Mehnert-Kay SA. Diagnosis and management of uncomplicated urinary tract infections. A Fam Phys. 2005;72(3):451-456.
Team Hospitalist Seats 4 Members




Four hospitalists have joined Team Hospitalist, the only readerinvolvement group of its kind in HM. Each of the new members has experience in the practice of HM; many offer specialized backgrounds in pediatrics, academics, and group administration. The new members will serve two-year terms and act as special editorial consultants to the magazine.
Rajan Gurunathan, MD
Chief, section of hospital medicine, Division of General Medicine, associate attending, Department of Medicine, St. Luke’s-Roosevelt Hospital Center, New York, N.Y.
Nick Fitterman, MD, FACp, SFHM
Chief of staff and director of hospitalist services, Huntington Hospital, Huntington, N.Y., assistant professor of medicine, Hofstra University School of Medicine
Chithra R. Perumalswami, MD
Assistant professor of medicine, division of hospital medicine, section of palliative care, Northwestern University Feinberg School of Medicine, Chicago
Edward Ma, MD
Principal, The Hospitalist Consulting Group, LLC, Glen Mills, Pa., hospitalist, Chester County Hospital, West Chester, Pa.
Four hospitalists have joined Team Hospitalist, the only readerinvolvement group of its kind in HM. Each of the new members has experience in the practice of HM; many offer specialized backgrounds in pediatrics, academics, and group administration. The new members will serve two-year terms and act as special editorial consultants to the magazine.
Rajan Gurunathan, MD
Chief, section of hospital medicine, Division of General Medicine, associate attending, Department of Medicine, St. Luke’s-Roosevelt Hospital Center, New York, N.Y.
Nick Fitterman, MD, FACp, SFHM
Chief of staff and director of hospitalist services, Huntington Hospital, Huntington, N.Y., assistant professor of medicine, Hofstra University School of Medicine
Chithra R. Perumalswami, MD
Assistant professor of medicine, division of hospital medicine, section of palliative care, Northwestern University Feinberg School of Medicine, Chicago
Edward Ma, MD
Principal, The Hospitalist Consulting Group, LLC, Glen Mills, Pa., hospitalist, Chester County Hospital, West Chester, Pa.
Four hospitalists have joined Team Hospitalist, the only readerinvolvement group of its kind in HM. Each of the new members has experience in the practice of HM; many offer specialized backgrounds in pediatrics, academics, and group administration. The new members will serve two-year terms and act as special editorial consultants to the magazine.
Rajan Gurunathan, MD
Chief, section of hospital medicine, Division of General Medicine, associate attending, Department of Medicine, St. Luke’s-Roosevelt Hospital Center, New York, N.Y.
Nick Fitterman, MD, FACp, SFHM
Chief of staff and director of hospitalist services, Huntington Hospital, Huntington, N.Y., assistant professor of medicine, Hofstra University School of Medicine
Chithra R. Perumalswami, MD
Assistant professor of medicine, division of hospital medicine, section of palliative care, Northwestern University Feinberg School of Medicine, Chicago
Edward Ma, MD
Principal, The Hospitalist Consulting Group, LLC, Glen Mills, Pa., hospitalist, Chester County Hospital, West Chester, Pa.
SHM Offers Multitude of Educational, Professional Development Opportunities
In addition to the annual meeting, SHM and its partners bring hospitalists the very best in education, professional development, and networking in the form of in-person meetings.
July: Pediatric Hospital Medicine
Every year, hundreds of pediatric hospitalists come together to share their passion for caring for hospitalized children. This year, Pediatric Hospital Medicine 2012 will convene July 19-22 at the Northern Kentucky Convention Center, just outside Cincinnati. The meeting is co-sponsored by the Academic Pediatric Association, SHM, and the American Academy of Pediatrics.
For details and to register, visit www.hospitalmedicine.org/events.
October: Leadership Academy
SHM’s Leadership Academy continues to create the next generation of hospitalist leaders and sharpen the skills of existing leaders.
SHM will present its next industry-leading Leadership Academy Oct. 1-4 in Scottsdale, Ariz. The program will feature the popular “Foundations of Effective Leadership” course and the second-level “Advanced Leadership: Strategies and Tools for Personal Leadership Excellence” course.
Both courses build leadership skills for hospitalists, or, as more than one hospitalist has called the curriculum, “everything they don’t teach you in medical school.”
In the highly interactive, four-day “Foundations of Effective Leadership” course, hospitalists learn how to evaluate personal leadership strengths and weaknesses, create and execute a communication strategy for key team members, understand key hospital drivers, and examine how hospital metrics are derived.
The “Advanced Leadership: Strategies and Tools for Personal Leadership Excellence” program provides skills building for hospitalists who want to drive culture change through specific leadership behaviors and actions. It also delves deep into financial storytelling, effective professional negotiation activities with proven techniques, and more.
“Advanced Leadership” is a second-level course and is open only to hospitalists who have completed the “Foundations of Effective Leadership” course, or who have earned an advanced management degree, such as an MBA.
Both courses are required for the new Leadership Certification program, which gives hospitalists the ability to demonstrate their leadership skills through certification.
Hospitalists planning to take any Leadership Academy course should note that, starting in 2013, Leadership Academy courses will be offered only in the fall.
For details and registration, visit www.hospitalmedicine.org/leadership.
Anytime: Online Education
Hospitalists working to demonstrate their expertise and commitment to HM through the Focused Practice in Hospital Medicine designation can earn Maintenance of Certification (MOC) self-evaluation points and CME credit online at www.hospitalmedicine.org/mkm.
SHM’s Medical Knowledge Modules are online learning and self-evaluation tools that provide the user with industry-leading instruction on quality-improvement (QI) theory; project design; system processes; measurement; chance science; tools for implementation; epidemiology of patient safety; and error types, disclosure, prevention strategies, and theory.
Three Medical Knowledge Modules are available: Hospital QI and Patient Safety, Hospital QI and Patient Safety II, and Pediatric Hospital QI and Patient Safety. Each online module consists of 25 multiple-choice questions. If the correct answer is chosen, the module provides a rationale explaining why that answer was correct. When an incorrect answer is selected, users are encouraged to try again.
Each module will earn hospitalists 10 self-evaluation points for diplomates enrolled in ABIM’s MOC program and three AMA PRA Category 1 CME Credits.
SHM will continue to roll out other topics throughout 2012.
Brendon Shank is SHM associate vice president of communications.
In addition to the annual meeting, SHM and its partners bring hospitalists the very best in education, professional development, and networking in the form of in-person meetings.
July: Pediatric Hospital Medicine
Every year, hundreds of pediatric hospitalists come together to share their passion for caring for hospitalized children. This year, Pediatric Hospital Medicine 2012 will convene July 19-22 at the Northern Kentucky Convention Center, just outside Cincinnati. The meeting is co-sponsored by the Academic Pediatric Association, SHM, and the American Academy of Pediatrics.
For details and to register, visit www.hospitalmedicine.org/events.
October: Leadership Academy
SHM’s Leadership Academy continues to create the next generation of hospitalist leaders and sharpen the skills of existing leaders.
SHM will present its next industry-leading Leadership Academy Oct. 1-4 in Scottsdale, Ariz. The program will feature the popular “Foundations of Effective Leadership” course and the second-level “Advanced Leadership: Strategies and Tools for Personal Leadership Excellence” course.
Both courses build leadership skills for hospitalists, or, as more than one hospitalist has called the curriculum, “everything they don’t teach you in medical school.”
In the highly interactive, four-day “Foundations of Effective Leadership” course, hospitalists learn how to evaluate personal leadership strengths and weaknesses, create and execute a communication strategy for key team members, understand key hospital drivers, and examine how hospital metrics are derived.
The “Advanced Leadership: Strategies and Tools for Personal Leadership Excellence” program provides skills building for hospitalists who want to drive culture change through specific leadership behaviors and actions. It also delves deep into financial storytelling, effective professional negotiation activities with proven techniques, and more.
“Advanced Leadership” is a second-level course and is open only to hospitalists who have completed the “Foundations of Effective Leadership” course, or who have earned an advanced management degree, such as an MBA.
Both courses are required for the new Leadership Certification program, which gives hospitalists the ability to demonstrate their leadership skills through certification.
Hospitalists planning to take any Leadership Academy course should note that, starting in 2013, Leadership Academy courses will be offered only in the fall.
For details and registration, visit www.hospitalmedicine.org/leadership.
Anytime: Online Education
Hospitalists working to demonstrate their expertise and commitment to HM through the Focused Practice in Hospital Medicine designation can earn Maintenance of Certification (MOC) self-evaluation points and CME credit online at www.hospitalmedicine.org/mkm.
SHM’s Medical Knowledge Modules are online learning and self-evaluation tools that provide the user with industry-leading instruction on quality-improvement (QI) theory; project design; system processes; measurement; chance science; tools for implementation; epidemiology of patient safety; and error types, disclosure, prevention strategies, and theory.
Three Medical Knowledge Modules are available: Hospital QI and Patient Safety, Hospital QI and Patient Safety II, and Pediatric Hospital QI and Patient Safety. Each online module consists of 25 multiple-choice questions. If the correct answer is chosen, the module provides a rationale explaining why that answer was correct. When an incorrect answer is selected, users are encouraged to try again.
Each module will earn hospitalists 10 self-evaluation points for diplomates enrolled in ABIM’s MOC program and three AMA PRA Category 1 CME Credits.
SHM will continue to roll out other topics throughout 2012.
Brendon Shank is SHM associate vice president of communications.
In addition to the annual meeting, SHM and its partners bring hospitalists the very best in education, professional development, and networking in the form of in-person meetings.
July: Pediatric Hospital Medicine
Every year, hundreds of pediatric hospitalists come together to share their passion for caring for hospitalized children. This year, Pediatric Hospital Medicine 2012 will convene July 19-22 at the Northern Kentucky Convention Center, just outside Cincinnati. The meeting is co-sponsored by the Academic Pediatric Association, SHM, and the American Academy of Pediatrics.
For details and to register, visit www.hospitalmedicine.org/events.
October: Leadership Academy
SHM’s Leadership Academy continues to create the next generation of hospitalist leaders and sharpen the skills of existing leaders.
SHM will present its next industry-leading Leadership Academy Oct. 1-4 in Scottsdale, Ariz. The program will feature the popular “Foundations of Effective Leadership” course and the second-level “Advanced Leadership: Strategies and Tools for Personal Leadership Excellence” course.
Both courses build leadership skills for hospitalists, or, as more than one hospitalist has called the curriculum, “everything they don’t teach you in medical school.”
In the highly interactive, four-day “Foundations of Effective Leadership” course, hospitalists learn how to evaluate personal leadership strengths and weaknesses, create and execute a communication strategy for key team members, understand key hospital drivers, and examine how hospital metrics are derived.
The “Advanced Leadership: Strategies and Tools for Personal Leadership Excellence” program provides skills building for hospitalists who want to drive culture change through specific leadership behaviors and actions. It also delves deep into financial storytelling, effective professional negotiation activities with proven techniques, and more.
“Advanced Leadership” is a second-level course and is open only to hospitalists who have completed the “Foundations of Effective Leadership” course, or who have earned an advanced management degree, such as an MBA.
Both courses are required for the new Leadership Certification program, which gives hospitalists the ability to demonstrate their leadership skills through certification.
Hospitalists planning to take any Leadership Academy course should note that, starting in 2013, Leadership Academy courses will be offered only in the fall.
For details and registration, visit www.hospitalmedicine.org/leadership.
Anytime: Online Education
Hospitalists working to demonstrate their expertise and commitment to HM through the Focused Practice in Hospital Medicine designation can earn Maintenance of Certification (MOC) self-evaluation points and CME credit online at www.hospitalmedicine.org/mkm.
SHM’s Medical Knowledge Modules are online learning and self-evaluation tools that provide the user with industry-leading instruction on quality-improvement (QI) theory; project design; system processes; measurement; chance science; tools for implementation; epidemiology of patient safety; and error types, disclosure, prevention strategies, and theory.
Three Medical Knowledge Modules are available: Hospital QI and Patient Safety, Hospital QI and Patient Safety II, and Pediatric Hospital QI and Patient Safety. Each online module consists of 25 multiple-choice questions. If the correct answer is chosen, the module provides a rationale explaining why that answer was correct. When an incorrect answer is selected, users are encouraged to try again.
Each module will earn hospitalists 10 self-evaluation points for diplomates enrolled in ABIM’s MOC program and three AMA PRA Category 1 CME Credits.
SHM will continue to roll out other topics throughout 2012.
Brendon Shank is SHM associate vice president of communications.
Survey Insights: The Unique Connection between Compensation and Productivity
Perhaps one of the most interesting concepts in the 2011 SHM/MGMA State of Hospital Medicine report is illustrated by the potentially confusing graph, at right, which is reproduced from the report. By taking a few minutes to fully understand what the graph portrays, users can gain valuable insights into the relationship between productivity and compensation.
Let’s say I’m a hospitalist and my annual work RVU (wRVU) productivity is in the bottom 25% (first quartile) of all of the hospitalists who responded to the survey. My total compensation is likely to be relatively low—a median of $188,800—but my compensation per unit of work is likely to be relatively high—a median of $73.85 per wRVU.
On the other hand, if I’m a hospitalist with productivity in the top 25% of all hospitalists (fourth quartile), my overall compensation will probably be much higher—a median of $260,283—but my average compensation per unit of work has probably gone down quite a bit (note the median of $40.82 per wRVU).
Why is it that my compensation has gone up, but not at the same rate as my productivity?
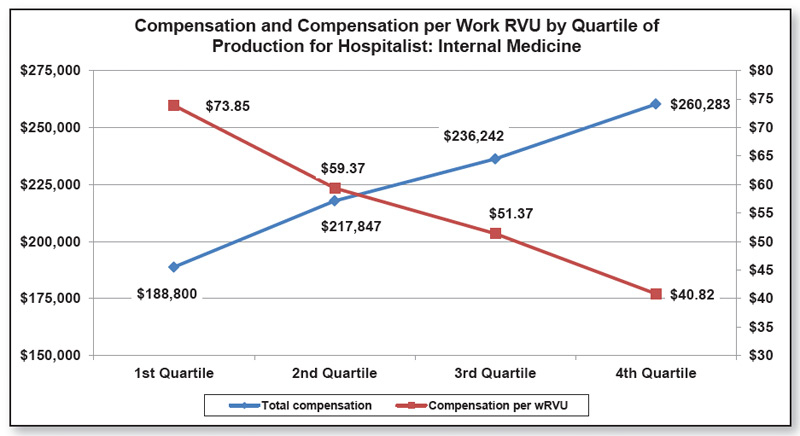
Well, despite the increasing popularity of productivity incentives among HM groups in recent years, the majority of hospitalists still receive most of their pay in the form of a fixed salary. In fact, the survey, at right, found that the average hospitalist compensation package consists of about 80% fixed-base compensation, 16% productivity incentive, and 4% quality/performance incentive. Such compensation models give clear advantages to hospitalists with low productivity, and disadvantages to those with very high productivity.
Yes, many hospitalists can earn at least a bit more if they increase their productivity, but it’s often pennies on the dollar because neither their base salary nor their quality bonus components increase as their productivity goes up. Some of you might argue that compensation should rise in a straight line along with productivity, as it does in a practice with a 100% productivity-based compensation plan (some know this as the “eat what you treat” plan).
But what rises in a straight line can also fall in a straight line, and few hospitalists are comfortable with the risk of significant drops in income if their volume decreases for some reason.
Others might argue that it’s a good thing for compensation increases to taper off at high productivity levels, since this provides at least some reward for working harder but is less likely to incentivize people to work at unreasonable levels. And a few might argue that compensation per unit of work should actually increase at high productivity levels because once a hospitalist has covered their base salary and contribution to practice overhead, any additional revenue they bring into the practice is pure profit.
I have my opinions about these things, and I’m sure you do, too. But one of the things I like best about HM is the wide variety of practices out there. With so many hospitalist practices and so much variety, there’s a compensation model out there somewhere to suit everyone.
Perhaps one of the most interesting concepts in the 2011 SHM/MGMA State of Hospital Medicine report is illustrated by the potentially confusing graph, at right, which is reproduced from the report. By taking a few minutes to fully understand what the graph portrays, users can gain valuable insights into the relationship between productivity and compensation.
Let’s say I’m a hospitalist and my annual work RVU (wRVU) productivity is in the bottom 25% (first quartile) of all of the hospitalists who responded to the survey. My total compensation is likely to be relatively low—a median of $188,800—but my compensation per unit of work is likely to be relatively high—a median of $73.85 per wRVU.
On the other hand, if I’m a hospitalist with productivity in the top 25% of all hospitalists (fourth quartile), my overall compensation will probably be much higher—a median of $260,283—but my average compensation per unit of work has probably gone down quite a bit (note the median of $40.82 per wRVU).
Why is it that my compensation has gone up, but not at the same rate as my productivity?
Well, despite the increasing popularity of productivity incentives among HM groups in recent years, the majority of hospitalists still receive most of their pay in the form of a fixed salary. In fact, the survey, at right, found that the average hospitalist compensation package consists of about 80% fixed-base compensation, 16% productivity incentive, and 4% quality/performance incentive. Such compensation models give clear advantages to hospitalists with low productivity, and disadvantages to those with very high productivity.
Yes, many hospitalists can earn at least a bit more if they increase their productivity, but it’s often pennies on the dollar because neither their base salary nor their quality bonus components increase as their productivity goes up. Some of you might argue that compensation should rise in a straight line along with productivity, as it does in a practice with a 100% productivity-based compensation plan (some know this as the “eat what you treat” plan).
But what rises in a straight line can also fall in a straight line, and few hospitalists are comfortable with the risk of significant drops in income if their volume decreases for some reason.
Others might argue that it’s a good thing for compensation increases to taper off at high productivity levels, since this provides at least some reward for working harder but is less likely to incentivize people to work at unreasonable levels. And a few might argue that compensation per unit of work should actually increase at high productivity levels because once a hospitalist has covered their base salary and contribution to practice overhead, any additional revenue they bring into the practice is pure profit.
I have my opinions about these things, and I’m sure you do, too. But one of the things I like best about HM is the wide variety of practices out there. With so many hospitalist practices and so much variety, there’s a compensation model out there somewhere to suit everyone.
Perhaps one of the most interesting concepts in the 2011 SHM/MGMA State of Hospital Medicine report is illustrated by the potentially confusing graph, at right, which is reproduced from the report. By taking a few minutes to fully understand what the graph portrays, users can gain valuable insights into the relationship between productivity and compensation.
Let’s say I’m a hospitalist and my annual work RVU (wRVU) productivity is in the bottom 25% (first quartile) of all of the hospitalists who responded to the survey. My total compensation is likely to be relatively low—a median of $188,800—but my compensation per unit of work is likely to be relatively high—a median of $73.85 per wRVU.
On the other hand, if I’m a hospitalist with productivity in the top 25% of all hospitalists (fourth quartile), my overall compensation will probably be much higher—a median of $260,283—but my average compensation per unit of work has probably gone down quite a bit (note the median of $40.82 per wRVU).
Why is it that my compensation has gone up, but not at the same rate as my productivity?
Well, despite the increasing popularity of productivity incentives among HM groups in recent years, the majority of hospitalists still receive most of their pay in the form of a fixed salary. In fact, the survey, at right, found that the average hospitalist compensation package consists of about 80% fixed-base compensation, 16% productivity incentive, and 4% quality/performance incentive. Such compensation models give clear advantages to hospitalists with low productivity, and disadvantages to those with very high productivity.
Yes, many hospitalists can earn at least a bit more if they increase their productivity, but it’s often pennies on the dollar because neither their base salary nor their quality bonus components increase as their productivity goes up. Some of you might argue that compensation should rise in a straight line along with productivity, as it does in a practice with a 100% productivity-based compensation plan (some know this as the “eat what you treat” plan).
But what rises in a straight line can also fall in a straight line, and few hospitalists are comfortable with the risk of significant drops in income if their volume decreases for some reason.
Others might argue that it’s a good thing for compensation increases to taper off at high productivity levels, since this provides at least some reward for working harder but is less likely to incentivize people to work at unreasonable levels. And a few might argue that compensation per unit of work should actually increase at high productivity levels because once a hospitalist has covered their base salary and contribution to practice overhead, any additional revenue they bring into the practice is pure profit.
I have my opinions about these things, and I’m sure you do, too. But one of the things I like best about HM is the wide variety of practices out there. With so many hospitalist practices and so much variety, there’s a compensation model out there somewhere to suit everyone.
HM On the Move


Meadowview Regional Medical Center in Maysville, Ky., recently added a hospitalist program as part of its renovation campaign. Jeff Dickerson, MD, Ignacio Calvo, MD, and nurse practitioner Abe Keating are heading up the new hospitalist team.
Eric McFarling, MD, a hospitalist at St. Cloud Hospital in St. Cloud, Minn., received the Physician of Excellence Award from employees and peers. The award recognizes commitment to patient satisfaction and teamwork.
Emily Hebert, MD, an internal-medicine hospitalist at Baylor University Medical Center in Waco, Texas, was awarded the 2011 Texas Medical Association’s Anson Jones, MD, Award in the Physician Excellence in Reporting category for her work as medical expert for the local ABC affiliate. She recently joined the staff at The Cooper Clinic in Dallas as a preventive- medicine physician, specializing in internal medicine and pediatrics.
Business Moves
IPC: the Hospitalist Co. has signed agreements to acquire Inpatient Clinical Solutions Inc. (ICS), an acute-care practice headquartered in Coral Springs, Fla., and the hospitalist practice of Lionel J. Gatien, DO, PA, based in Jacksonville, Fla. IPC expects to add approximately 116,000 patient visits on an annual basis from these acquisitions.
Glendale, Calif.-based Apollo Medical Holdings Inc., a hospitalist-, critical-care and multi-disciplinary care-management service, has appointed Edward “Ted” Schreck chairman of the board. Schreck is a senior healthcare executive with 37 years of experience in both the private and public healthcare sectors.
Carlisle (Pa.) Regional Medical Center has added a 12-member hospitalist team to its list of medical departments. The team will be known as Hospitalists of Central Pennsylvania. Michael Hilden, MD, will serve as group director.
—Alexandra Schultz
Meadowview Regional Medical Center in Maysville, Ky., recently added a hospitalist program as part of its renovation campaign. Jeff Dickerson, MD, Ignacio Calvo, MD, and nurse practitioner Abe Keating are heading up the new hospitalist team.
Eric McFarling, MD, a hospitalist at St. Cloud Hospital in St. Cloud, Minn., received the Physician of Excellence Award from employees and peers. The award recognizes commitment to patient satisfaction and teamwork.
Emily Hebert, MD, an internal-medicine hospitalist at Baylor University Medical Center in Waco, Texas, was awarded the 2011 Texas Medical Association’s Anson Jones, MD, Award in the Physician Excellence in Reporting category for her work as medical expert for the local ABC affiliate. She recently joined the staff at The Cooper Clinic in Dallas as a preventive- medicine physician, specializing in internal medicine and pediatrics.
Business Moves
IPC: the Hospitalist Co. has signed agreements to acquire Inpatient Clinical Solutions Inc. (ICS), an acute-care practice headquartered in Coral Springs, Fla., and the hospitalist practice of Lionel J. Gatien, DO, PA, based in Jacksonville, Fla. IPC expects to add approximately 116,000 patient visits on an annual basis from these acquisitions.
Glendale, Calif.-based Apollo Medical Holdings Inc., a hospitalist-, critical-care and multi-disciplinary care-management service, has appointed Edward “Ted” Schreck chairman of the board. Schreck is a senior healthcare executive with 37 years of experience in both the private and public healthcare sectors.
Carlisle (Pa.) Regional Medical Center has added a 12-member hospitalist team to its list of medical departments. The team will be known as Hospitalists of Central Pennsylvania. Michael Hilden, MD, will serve as group director.
—Alexandra Schultz
Meadowview Regional Medical Center in Maysville, Ky., recently added a hospitalist program as part of its renovation campaign. Jeff Dickerson, MD, Ignacio Calvo, MD, and nurse practitioner Abe Keating are heading up the new hospitalist team.
Eric McFarling, MD, a hospitalist at St. Cloud Hospital in St. Cloud, Minn., received the Physician of Excellence Award from employees and peers. The award recognizes commitment to patient satisfaction and teamwork.
Emily Hebert, MD, an internal-medicine hospitalist at Baylor University Medical Center in Waco, Texas, was awarded the 2011 Texas Medical Association’s Anson Jones, MD, Award in the Physician Excellence in Reporting category for her work as medical expert for the local ABC affiliate. She recently joined the staff at The Cooper Clinic in Dallas as a preventive- medicine physician, specializing in internal medicine and pediatrics.
Business Moves
IPC: the Hospitalist Co. has signed agreements to acquire Inpatient Clinical Solutions Inc. (ICS), an acute-care practice headquartered in Coral Springs, Fla., and the hospitalist practice of Lionel J. Gatien, DO, PA, based in Jacksonville, Fla. IPC expects to add approximately 116,000 patient visits on an annual basis from these acquisitions.
Glendale, Calif.-based Apollo Medical Holdings Inc., a hospitalist-, critical-care and multi-disciplinary care-management service, has appointed Edward “Ted” Schreck chairman of the board. Schreck is a senior healthcare executive with 37 years of experience in both the private and public healthcare sectors.
Carlisle (Pa.) Regional Medical Center has added a 12-member hospitalist team to its list of medical departments. The team will be known as Hospitalists of Central Pennsylvania. Michael Hilden, MD, will serve as group director.
—Alexandra Schultz
Meaninful Use of HIT: Are Hospitalists Eligible?
On March 7, the Centers for Medicare & Medicaid Services (CMS) released a proposed rule: Medicare and Medicaid Programs; Electronic Health Record Incentive Program—Stage 2. This rule is more commonly known as “Stage 2 of meaningful use.” At more than 130 pages, the rule builds upon Stage 1 of the program mainly by increasing measurement thresholds and requiring higher levels of system functionality.
Although there are no major surprises within the proposed rule, there is always one very basic yet very important question that surfaces when meaningful use makes headlines: Are hospitalists eligible for health information technology (HIT) incentives and thus subject to the meaningful use requirements?
“No” is the short answer to this question. Although physicians, including hospitalists, are considered eligible professionals (EPs) under the HIT incentive program, a subset of EPs are defined as hospital-based EPs and, therefore, are not subject to the program’s requirements. CMS defines a hospital-based eligible professional as an EP who furnishes 90% or more of their covered professional services in either the inpatient division or ED of a hospital.
While some may call this an exemption for hospitalists, it is not that definitive. Hospitalists are still “eligible,” and the determination is not made by specialty, but by pattern of practice. This means that hospitalists could find themselves on the hook for future penalties if their practice patterns expand beyond CMS’ 90% threshold.
An example of this would be a hospitalist who spends time doing rounds at a nursing home. Today, this might constitute only a small percentage of a hospitalist’s practice, but with an increasingly aging population, it is not inconceivable that this small percentage could exceed 10% within five or 10 years.
With this in mind, and a similar scenario also present in the Electronic Prescribing Incentive Program (eRx), SHM has consistently pointed out the issue to CMS and is working to find an acceptable solution.
Although hospitalists are not currently subject to physician meaningful-use requirements, the program has another category of eligibility that will certainly affect hospitalists: the eligible hospital, or EH. Many hospitalists are directly involved with HIT implementation efforts at their institutions or are indirectly working with these systems as they are implemented and expanded in hospitals across the country.
Given the 90% eligibility threshold and the role of HIT in hospitals, it is important for hospitalists to stay current and informed on meaningful use and HIT policy. Involvement with one of SHM’s HIT related committees is a clear way to stay informed in this ever-evolving area, and SHM’s efforts can be reviewed on the Advocacy page of SHM’s website: www.hospitalmedicine.org/advocacy.
For the most up-to-date information on what is being done at the federal level, the Office of the National Coordinator (ONC) has a wealth of information available at www.healthit.gov/.
SHM will continue to monitor and analyze developments and changes to EHR policy, but it also looks to you, its members, for experience and insight.
On March 7, the Centers for Medicare & Medicaid Services (CMS) released a proposed rule: Medicare and Medicaid Programs; Electronic Health Record Incentive Program—Stage 2. This rule is more commonly known as “Stage 2 of meaningful use.” At more than 130 pages, the rule builds upon Stage 1 of the program mainly by increasing measurement thresholds and requiring higher levels of system functionality.
Although there are no major surprises within the proposed rule, there is always one very basic yet very important question that surfaces when meaningful use makes headlines: Are hospitalists eligible for health information technology (HIT) incentives and thus subject to the meaningful use requirements?
“No” is the short answer to this question. Although physicians, including hospitalists, are considered eligible professionals (EPs) under the HIT incentive program, a subset of EPs are defined as hospital-based EPs and, therefore, are not subject to the program’s requirements. CMS defines a hospital-based eligible professional as an EP who furnishes 90% or more of their covered professional services in either the inpatient division or ED of a hospital.
While some may call this an exemption for hospitalists, it is not that definitive. Hospitalists are still “eligible,” and the determination is not made by specialty, but by pattern of practice. This means that hospitalists could find themselves on the hook for future penalties if their practice patterns expand beyond CMS’ 90% threshold.
An example of this would be a hospitalist who spends time doing rounds at a nursing home. Today, this might constitute only a small percentage of a hospitalist’s practice, but with an increasingly aging population, it is not inconceivable that this small percentage could exceed 10% within five or 10 years.
With this in mind, and a similar scenario also present in the Electronic Prescribing Incentive Program (eRx), SHM has consistently pointed out the issue to CMS and is working to find an acceptable solution.
Although hospitalists are not currently subject to physician meaningful-use requirements, the program has another category of eligibility that will certainly affect hospitalists: the eligible hospital, or EH. Many hospitalists are directly involved with HIT implementation efforts at their institutions or are indirectly working with these systems as they are implemented and expanded in hospitals across the country.
Given the 90% eligibility threshold and the role of HIT in hospitals, it is important for hospitalists to stay current and informed on meaningful use and HIT policy. Involvement with one of SHM’s HIT related committees is a clear way to stay informed in this ever-evolving area, and SHM’s efforts can be reviewed on the Advocacy page of SHM’s website: www.hospitalmedicine.org/advocacy.
For the most up-to-date information on what is being done at the federal level, the Office of the National Coordinator (ONC) has a wealth of information available at www.healthit.gov/.
SHM will continue to monitor and analyze developments and changes to EHR policy, but it also looks to you, its members, for experience and insight.
On March 7, the Centers for Medicare & Medicaid Services (CMS) released a proposed rule: Medicare and Medicaid Programs; Electronic Health Record Incentive Program—Stage 2. This rule is more commonly known as “Stage 2 of meaningful use.” At more than 130 pages, the rule builds upon Stage 1 of the program mainly by increasing measurement thresholds and requiring higher levels of system functionality.
Although there are no major surprises within the proposed rule, there is always one very basic yet very important question that surfaces when meaningful use makes headlines: Are hospitalists eligible for health information technology (HIT) incentives and thus subject to the meaningful use requirements?
“No” is the short answer to this question. Although physicians, including hospitalists, are considered eligible professionals (EPs) under the HIT incentive program, a subset of EPs are defined as hospital-based EPs and, therefore, are not subject to the program’s requirements. CMS defines a hospital-based eligible professional as an EP who furnishes 90% or more of their covered professional services in either the inpatient division or ED of a hospital.
While some may call this an exemption for hospitalists, it is not that definitive. Hospitalists are still “eligible,” and the determination is not made by specialty, but by pattern of practice. This means that hospitalists could find themselves on the hook for future penalties if their practice patterns expand beyond CMS’ 90% threshold.
An example of this would be a hospitalist who spends time doing rounds at a nursing home. Today, this might constitute only a small percentage of a hospitalist’s practice, but with an increasingly aging population, it is not inconceivable that this small percentage could exceed 10% within five or 10 years.
With this in mind, and a similar scenario also present in the Electronic Prescribing Incentive Program (eRx), SHM has consistently pointed out the issue to CMS and is working to find an acceptable solution.
Although hospitalists are not currently subject to physician meaningful-use requirements, the program has another category of eligibility that will certainly affect hospitalists: the eligible hospital, or EH. Many hospitalists are directly involved with HIT implementation efforts at their institutions or are indirectly working with these systems as they are implemented and expanded in hospitals across the country.
Given the 90% eligibility threshold and the role of HIT in hospitals, it is important for hospitalists to stay current and informed on meaningful use and HIT policy. Involvement with one of SHM’s HIT related committees is a clear way to stay informed in this ever-evolving area, and SHM’s efforts can be reviewed on the Advocacy page of SHM’s website: www.hospitalmedicine.org/advocacy.
For the most up-to-date information on what is being done at the federal level, the Office of the National Coordinator (ONC) has a wealth of information available at www.healthit.gov/.
SHM will continue to monitor and analyze developments and changes to EHR policy, but it also looks to you, its members, for experience and insight.
Beware Hospital Compare? New Measures Highlight Questions Surrounding Healthcare Quality Report Cards

—Anne-Marie J. Audet, MD, MSc, SM, vice president, Health System Quality and Efficiency, Commonwealth Fund
The Centers for Medicare & Medicaid Services (CMS) has been publicly reporting performance measures on its Hospital Compare website (www.hospitalcompare.hhs.gov) since 2005, focusing on processes of care, patient outcomes, patient satisfaction, patient safety, and other measures. A recent addition of patient-safety metrics has rekindled skeptical questions about the validity, purpose, and effectiveness of public healthcare quality report cards, while highlighting the need for hospitalists and their institutions to remain vigilant in the struggle to ensure that they are compared and rewarded fairly and appropriately.
Provocative Measures
Last fall, CMS began posting “Serious Complications and Deaths” measures, developed by the Agency for Healthcare Research and Quality (AHRQ). The measures score individual hospitals according to the rates at which their patients suffer from:
- Pneumothorax due to medical treatment;
- Post-operative VTE;
- Post-operative abdominal or pelvic dehiscence; and
- Accidental lacerations from medical treatment.
Four other serious complication measures (pressure ulcers, catheter and bloodstream infections, and hip fractures from falling after surgery) are folded into a separate composite score for each hospital, while another composite score for “Deaths for Certain Conditions” is based on a hospital’s post-admission mortality rate for hip fractures, acute MI, heart failure, stroke, GI bleed, and pneumonia.
National and local media reports have thrust these dramatic metrics into the public eye, putting many hospitals on the spot to explain their putative breaches of patient safety. A closer inspection of the metrics, however, reveals plausible criticisms of their shortcomings.
Methodological Weakness
The new metrics are derived from Medicare claims data instead of medical chart abstractions, which experts say weakens their validity significantly and makes their use for provider profiling questionable. Moreover, claims data are based on records that were never designed to capture the sort of clinical nuances needed for valid and equitable risk adjustment (see “Methodological Challenges to Quality Metrics,” below). “Serious Complications and Deaths” rates based on these data, critics maintain, lack validity for meaningful hospital comparisons because they can exaggerate problems at hospitals that treat a high volume of complicated patients and use more invasive procedures to do so, such as teaching hospitals in academic medical centers.1
The ante gets upped when CMS eventually begins adding patient-safety measures to the Hospital Value-Based Purchasing (HVBP) program, which rewards or punishes hospitals financially, depending on their performance on the metrics. CMS is considering adding the Serious Complications and Deaths measures to the HVPB program in the near future.
As the science of documenting and reporting patient harm struggles to find its footing, physicians and hospitals have to be more vigilant than ever to adopt a unified, organized approach to advocate the most appropriate processes and outcomes for which they will be held accountable, and avoid being cast in a reactive mode when metrics are imposed on them, says Patrick J. Torcson, MD, MMM, FACP, SFHM, chair of SHM’s Performance Measurement and Reporting Committee, and director of hospital medicine at St. Tammany Parish Hospital in Shreveport, La.
Last year, SHM sent comments to then-CMS administrator Don Berwick, expressing concern that the patient-safety measures CMS proposes to include in the HVBP program in fiscal-year 2014 are not endorsed by the National Quality Forum (NQF), that they are derived from billing and payment data that are not intended to be used primarily for clinical purposes, that the outcome measures are not entirely preventable even with the best of care, and that they are not adequately risk-adjusted.
“While it’s easy to agree with the experts that Hospital Compare’s patient-safety measures are not ready for prime time, it’s no longer acceptable simply to say, ‘These metrics are irrelevant,’” Dr. Torcson cautions. “We also must be aware of the evolution and inexorable movement of the nation’s healthcare quality and safety agenda. SHM embraces the triple aim of providing better care to our patients, promoting better health of patient populations, and doing so at a lower cost.”
The Power of “Why?”
Despite its imperfections, Hospital Compare’s greatest value is the power of its transparency, which fosters healthy discussion among providers, patients, and payors, according to Anne-Marie J. Audet, MD, MSc, SM, vice president for Health System Quality and Efficiency for the Commonwealth Fund. “That transparency gets providers’ attention and leads them to make changes that can translate into better performance,” she says, noting how hospital care for patients with heart attack, heart failure, and pneumonia has steadily improved in recent years, with the worst performers in 2009 doing as well or better than the best performers in 2004.
“There are also examples of hospitals that have gone from a median of four central line-associated bloodstream infections (CLABSI) per 1,000 line-days to zero because they decided not to take the status quo as acceptable,” says Stephen C. Schoenbaum, MD, MPH, special advisor to the president of the Josiah Macy Jr. Foundation. Dr. Schoenbaum played a significant role in the development of the Healthcare Effectiveness Data and Information Set, or HEDIS.
“There is no such thing as a perfect measure in which some adjustment or better collection method would not affect the numbers,” he notes. “Ideally, you want any publicly reported measure to get the poorer performers to come up with a way to explain their result. Or, even better, to improve their result.”
Methodological criticisms of CMS’ new “Serious Complications and Deaths” measures may be justified, Dr. Audet concedes, but she also notes that rigorous validation and reliability testing of quality measures is an expensive process. “To get where we want to go in American healthcare, we need a more thoroughly supported measure development infrastructure,” she says.
“In the meantime, providers will be probing the implications of their numbers, asking why they got the numbers they did, and what can be done about it. This attention can only lead to improvement, both in the measures themselves and in the care delivered.”
Indeed, one of the hospitals that was listed as having a high rate of accidental cuts and lacerations in the new measures found most of those cuts had been intended by the surgeon but erroneously billed to Medicare under the code for an accidental cut. Even with its methodological flaws, the Hospital Compare data led to root-cause analysis and improvement in coding.
Hospitalists’ Role
Hospitalists, according to Dr. Torcson, will be critical to the successful performance of hospitals under the HVPB program, as experts in quality and quality-measurement adherence. Hospitalists care for more hospitalized patients than any other physician group, and many believe they are uniquely positioned to lead the system-level changes and quality-improvement (QI) efforts that will be required.
“Hospitalists and their hospitals, practicing in alignment, become champions for their patients,” Dr. Torcson says. “SHM supported the HVBP program, and we foresee that the alignment of performance and payment within the program will inevitably result in better clinical outcomes for our patients.”
Chris Guadagnino is a freelance writer in Philadelphia.
References
- Experts question Medicare’s effort to rate hospitals’ patient safety records. Kaiser Health News website. Available at: http://www.kaiserhealthnews.org/Stories/2012/February/13/medicare-hospital-patient-safety-records.aspx. Accessed March 12, 2012.
- Shahian DM, Iezzoni LI, Meyer GS, Kirle L, Normand ST. Hospital-wide mortality as a quality metric: conceptual and methodological challenges. Am J Med Qual. 2012;27:112.
—Anne-Marie J. Audet, MD, MSc, SM, vice president, Health System Quality and Efficiency, Commonwealth Fund
The Centers for Medicare & Medicaid Services (CMS) has been publicly reporting performance measures on its Hospital Compare website (www.hospitalcompare.hhs.gov) since 2005, focusing on processes of care, patient outcomes, patient satisfaction, patient safety, and other measures. A recent addition of patient-safety metrics has rekindled skeptical questions about the validity, purpose, and effectiveness of public healthcare quality report cards, while highlighting the need for hospitalists and their institutions to remain vigilant in the struggle to ensure that they are compared and rewarded fairly and appropriately.
Provocative Measures
Last fall, CMS began posting “Serious Complications and Deaths” measures, developed by the Agency for Healthcare Research and Quality (AHRQ). The measures score individual hospitals according to the rates at which their patients suffer from:
- Pneumothorax due to medical treatment;
- Post-operative VTE;
- Post-operative abdominal or pelvic dehiscence; and
- Accidental lacerations from medical treatment.
Four other serious complication measures (pressure ulcers, catheter and bloodstream infections, and hip fractures from falling after surgery) are folded into a separate composite score for each hospital, while another composite score for “Deaths for Certain Conditions” is based on a hospital’s post-admission mortality rate for hip fractures, acute MI, heart failure, stroke, GI bleed, and pneumonia.
National and local media reports have thrust these dramatic metrics into the public eye, putting many hospitals on the spot to explain their putative breaches of patient safety. A closer inspection of the metrics, however, reveals plausible criticisms of their shortcomings.
Methodological Weakness
The new metrics are derived from Medicare claims data instead of medical chart abstractions, which experts say weakens their validity significantly and makes their use for provider profiling questionable. Moreover, claims data are based on records that were never designed to capture the sort of clinical nuances needed for valid and equitable risk adjustment (see “Methodological Challenges to Quality Metrics,” below). “Serious Complications and Deaths” rates based on these data, critics maintain, lack validity for meaningful hospital comparisons because they can exaggerate problems at hospitals that treat a high volume of complicated patients and use more invasive procedures to do so, such as teaching hospitals in academic medical centers.1
The ante gets upped when CMS eventually begins adding patient-safety measures to the Hospital Value-Based Purchasing (HVBP) program, which rewards or punishes hospitals financially, depending on their performance on the metrics. CMS is considering adding the Serious Complications and Deaths measures to the HVPB program in the near future.
As the science of documenting and reporting patient harm struggles to find its footing, physicians and hospitals have to be more vigilant than ever to adopt a unified, organized approach to advocate the most appropriate processes and outcomes for which they will be held accountable, and avoid being cast in a reactive mode when metrics are imposed on them, says Patrick J. Torcson, MD, MMM, FACP, SFHM, chair of SHM’s Performance Measurement and Reporting Committee, and director of hospital medicine at St. Tammany Parish Hospital in Shreveport, La.
Last year, SHM sent comments to then-CMS administrator Don Berwick, expressing concern that the patient-safety measures CMS proposes to include in the HVBP program in fiscal-year 2014 are not endorsed by the National Quality Forum (NQF), that they are derived from billing and payment data that are not intended to be used primarily for clinical purposes, that the outcome measures are not entirely preventable even with the best of care, and that they are not adequately risk-adjusted.
“While it’s easy to agree with the experts that Hospital Compare’s patient-safety measures are not ready for prime time, it’s no longer acceptable simply to say, ‘These metrics are irrelevant,’” Dr. Torcson cautions. “We also must be aware of the evolution and inexorable movement of the nation’s healthcare quality and safety agenda. SHM embraces the triple aim of providing better care to our patients, promoting better health of patient populations, and doing so at a lower cost.”
The Power of “Why?”
Despite its imperfections, Hospital Compare’s greatest value is the power of its transparency, which fosters healthy discussion among providers, patients, and payors, according to Anne-Marie J. Audet, MD, MSc, SM, vice president for Health System Quality and Efficiency for the Commonwealth Fund. “That transparency gets providers’ attention and leads them to make changes that can translate into better performance,” she says, noting how hospital care for patients with heart attack, heart failure, and pneumonia has steadily improved in recent years, with the worst performers in 2009 doing as well or better than the best performers in 2004.
“There are also examples of hospitals that have gone from a median of four central line-associated bloodstream infections (CLABSI) per 1,000 line-days to zero because they decided not to take the status quo as acceptable,” says Stephen C. Schoenbaum, MD, MPH, special advisor to the president of the Josiah Macy Jr. Foundation. Dr. Schoenbaum played a significant role in the development of the Healthcare Effectiveness Data and Information Set, or HEDIS.
“There is no such thing as a perfect measure in which some adjustment or better collection method would not affect the numbers,” he notes. “Ideally, you want any publicly reported measure to get the poorer performers to come up with a way to explain their result. Or, even better, to improve their result.”
Methodological criticisms of CMS’ new “Serious Complications and Deaths” measures may be justified, Dr. Audet concedes, but she also notes that rigorous validation and reliability testing of quality measures is an expensive process. “To get where we want to go in American healthcare, we need a more thoroughly supported measure development infrastructure,” she says.
“In the meantime, providers will be probing the implications of their numbers, asking why they got the numbers they did, and what can be done about it. This attention can only lead to improvement, both in the measures themselves and in the care delivered.”
Indeed, one of the hospitals that was listed as having a high rate of accidental cuts and lacerations in the new measures found most of those cuts had been intended by the surgeon but erroneously billed to Medicare under the code for an accidental cut. Even with its methodological flaws, the Hospital Compare data led to root-cause analysis and improvement in coding.
Hospitalists’ Role
Hospitalists, according to Dr. Torcson, will be critical to the successful performance of hospitals under the HVPB program, as experts in quality and quality-measurement adherence. Hospitalists care for more hospitalized patients than any other physician group, and many believe they are uniquely positioned to lead the system-level changes and quality-improvement (QI) efforts that will be required.
“Hospitalists and their hospitals, practicing in alignment, become champions for their patients,” Dr. Torcson says. “SHM supported the HVBP program, and we foresee that the alignment of performance and payment within the program will inevitably result in better clinical outcomes for our patients.”
Chris Guadagnino is a freelance writer in Philadelphia.
References
- Experts question Medicare’s effort to rate hospitals’ patient safety records. Kaiser Health News website. Available at: http://www.kaiserhealthnews.org/Stories/2012/February/13/medicare-hospital-patient-safety-records.aspx. Accessed March 12, 2012.
- Shahian DM, Iezzoni LI, Meyer GS, Kirle L, Normand ST. Hospital-wide mortality as a quality metric: conceptual and methodological challenges. Am J Med Qual. 2012;27:112.
—Anne-Marie J. Audet, MD, MSc, SM, vice president, Health System Quality and Efficiency, Commonwealth Fund
The Centers for Medicare & Medicaid Services (CMS) has been publicly reporting performance measures on its Hospital Compare website (www.hospitalcompare.hhs.gov) since 2005, focusing on processes of care, patient outcomes, patient satisfaction, patient safety, and other measures. A recent addition of patient-safety metrics has rekindled skeptical questions about the validity, purpose, and effectiveness of public healthcare quality report cards, while highlighting the need for hospitalists and their institutions to remain vigilant in the struggle to ensure that they are compared and rewarded fairly and appropriately.
Provocative Measures
Last fall, CMS began posting “Serious Complications and Deaths” measures, developed by the Agency for Healthcare Research and Quality (AHRQ). The measures score individual hospitals according to the rates at which their patients suffer from:
- Pneumothorax due to medical treatment;
- Post-operative VTE;
- Post-operative abdominal or pelvic dehiscence; and
- Accidental lacerations from medical treatment.
Four other serious complication measures (pressure ulcers, catheter and bloodstream infections, and hip fractures from falling after surgery) are folded into a separate composite score for each hospital, while another composite score for “Deaths for Certain Conditions” is based on a hospital’s post-admission mortality rate for hip fractures, acute MI, heart failure, stroke, GI bleed, and pneumonia.
National and local media reports have thrust these dramatic metrics into the public eye, putting many hospitals on the spot to explain their putative breaches of patient safety. A closer inspection of the metrics, however, reveals plausible criticisms of their shortcomings.
Methodological Weakness
The new metrics are derived from Medicare claims data instead of medical chart abstractions, which experts say weakens their validity significantly and makes their use for provider profiling questionable. Moreover, claims data are based on records that were never designed to capture the sort of clinical nuances needed for valid and equitable risk adjustment (see “Methodological Challenges to Quality Metrics,” below). “Serious Complications and Deaths” rates based on these data, critics maintain, lack validity for meaningful hospital comparisons because they can exaggerate problems at hospitals that treat a high volume of complicated patients and use more invasive procedures to do so, such as teaching hospitals in academic medical centers.1
The ante gets upped when CMS eventually begins adding patient-safety measures to the Hospital Value-Based Purchasing (HVBP) program, which rewards or punishes hospitals financially, depending on their performance on the metrics. CMS is considering adding the Serious Complications and Deaths measures to the HVPB program in the near future.
As the science of documenting and reporting patient harm struggles to find its footing, physicians and hospitals have to be more vigilant than ever to adopt a unified, organized approach to advocate the most appropriate processes and outcomes for which they will be held accountable, and avoid being cast in a reactive mode when metrics are imposed on them, says Patrick J. Torcson, MD, MMM, FACP, SFHM, chair of SHM’s Performance Measurement and Reporting Committee, and director of hospital medicine at St. Tammany Parish Hospital in Shreveport, La.
Last year, SHM sent comments to then-CMS administrator Don Berwick, expressing concern that the patient-safety measures CMS proposes to include in the HVBP program in fiscal-year 2014 are not endorsed by the National Quality Forum (NQF), that they are derived from billing and payment data that are not intended to be used primarily for clinical purposes, that the outcome measures are not entirely preventable even with the best of care, and that they are not adequately risk-adjusted.
“While it’s easy to agree with the experts that Hospital Compare’s patient-safety measures are not ready for prime time, it’s no longer acceptable simply to say, ‘These metrics are irrelevant,’” Dr. Torcson cautions. “We also must be aware of the evolution and inexorable movement of the nation’s healthcare quality and safety agenda. SHM embraces the triple aim of providing better care to our patients, promoting better health of patient populations, and doing so at a lower cost.”
The Power of “Why?”
Despite its imperfections, Hospital Compare’s greatest value is the power of its transparency, which fosters healthy discussion among providers, patients, and payors, according to Anne-Marie J. Audet, MD, MSc, SM, vice president for Health System Quality and Efficiency for the Commonwealth Fund. “That transparency gets providers’ attention and leads them to make changes that can translate into better performance,” she says, noting how hospital care for patients with heart attack, heart failure, and pneumonia has steadily improved in recent years, with the worst performers in 2009 doing as well or better than the best performers in 2004.
“There are also examples of hospitals that have gone from a median of four central line-associated bloodstream infections (CLABSI) per 1,000 line-days to zero because they decided not to take the status quo as acceptable,” says Stephen C. Schoenbaum, MD, MPH, special advisor to the president of the Josiah Macy Jr. Foundation. Dr. Schoenbaum played a significant role in the development of the Healthcare Effectiveness Data and Information Set, or HEDIS.
“There is no such thing as a perfect measure in which some adjustment or better collection method would not affect the numbers,” he notes. “Ideally, you want any publicly reported measure to get the poorer performers to come up with a way to explain their result. Or, even better, to improve their result.”
Methodological criticisms of CMS’ new “Serious Complications and Deaths” measures may be justified, Dr. Audet concedes, but she also notes that rigorous validation and reliability testing of quality measures is an expensive process. “To get where we want to go in American healthcare, we need a more thoroughly supported measure development infrastructure,” she says.
“In the meantime, providers will be probing the implications of their numbers, asking why they got the numbers they did, and what can be done about it. This attention can only lead to improvement, both in the measures themselves and in the care delivered.”
Indeed, one of the hospitals that was listed as having a high rate of accidental cuts and lacerations in the new measures found most of those cuts had been intended by the surgeon but erroneously billed to Medicare under the code for an accidental cut. Even with its methodological flaws, the Hospital Compare data led to root-cause analysis and improvement in coding.
Hospitalists’ Role
Hospitalists, according to Dr. Torcson, will be critical to the successful performance of hospitals under the HVPB program, as experts in quality and quality-measurement adherence. Hospitalists care for more hospitalized patients than any other physician group, and many believe they are uniquely positioned to lead the system-level changes and quality-improvement (QI) efforts that will be required.
“Hospitalists and their hospitals, practicing in alignment, become champions for their patients,” Dr. Torcson says. “SHM supported the HVBP program, and we foresee that the alignment of performance and payment within the program will inevitably result in better clinical outcomes for our patients.”
Chris Guadagnino is a freelance writer in Philadelphia.
References
- Experts question Medicare’s effort to rate hospitals’ patient safety records. Kaiser Health News website. Available at: http://www.kaiserhealthnews.org/Stories/2012/February/13/medicare-hospital-patient-safety-records.aspx. Accessed March 12, 2012.
- Shahian DM, Iezzoni LI, Meyer GS, Kirle L, Normand ST. Hospital-wide mortality as a quality metric: conceptual and methodological challenges. Am J Med Qual. 2012;27:112.
Cleveland Clinic Builds Urgency around Patient Experiences
Efforts to create a greater sense of urgency over patient satisfaction within the hospitalist service at the Cleveland Clinic using an eight-step model for changing organizational culture were outlined in an abstract presented at HM11.
“Attention to the doctor-patient experience should be our guiding principle,” explains lead author and hospitalist Vicente Velez, MD. “No matter how complex the science of medicine gets, the art is equally important.” Physicians can be taught skills in effective communication with their patients and families, Dr. Velez adds.
The initiative began four years ago after the department identified low patient satisfaction scores as a “credibility crisis.” Leadership sprung into action, promoting a vision that HM should be known for its ability to communicate. “Regardless of individual communication style, a proper self-introduction, eliciting the patient’s perspective, and an explanation of the daily plan of care were things we all had to develop as habits,” he says.
Individual projects to advance the agenda included:
- Communication training offered to all physicians at the Cleveland Clinic;
- New business cards with the hospitalists’ pictures on them;
- A pre-discharge “fly-by” visit from the hospitalist;
- Post-discharge callbacks to patients; and
- Joint physician-nurse rounding.
The service now shares its Hospital Consumer Assessment of Healthcare Providers and Systems Survey (HCAHPS) satisfaction scores for individual physicians in small groups or one-on-one meetings. The department recognizes high performers. Overall satisfaction scores rose to between 76% and 86%, up from 69% at the start of the project, Dr. Velez says.
Reference
Efforts to create a greater sense of urgency over patient satisfaction within the hospitalist service at the Cleveland Clinic using an eight-step model for changing organizational culture were outlined in an abstract presented at HM11.
“Attention to the doctor-patient experience should be our guiding principle,” explains lead author and hospitalist Vicente Velez, MD. “No matter how complex the science of medicine gets, the art is equally important.” Physicians can be taught skills in effective communication with their patients and families, Dr. Velez adds.
The initiative began four years ago after the department identified low patient satisfaction scores as a “credibility crisis.” Leadership sprung into action, promoting a vision that HM should be known for its ability to communicate. “Regardless of individual communication style, a proper self-introduction, eliciting the patient’s perspective, and an explanation of the daily plan of care were things we all had to develop as habits,” he says.
Individual projects to advance the agenda included:
- Communication training offered to all physicians at the Cleveland Clinic;
- New business cards with the hospitalists’ pictures on them;
- A pre-discharge “fly-by” visit from the hospitalist;
- Post-discharge callbacks to patients; and
- Joint physician-nurse rounding.
The service now shares its Hospital Consumer Assessment of Healthcare Providers and Systems Survey (HCAHPS) satisfaction scores for individual physicians in small groups or one-on-one meetings. The department recognizes high performers. Overall satisfaction scores rose to between 76% and 86%, up from 69% at the start of the project, Dr. Velez says.
Reference
Efforts to create a greater sense of urgency over patient satisfaction within the hospitalist service at the Cleveland Clinic using an eight-step model for changing organizational culture were outlined in an abstract presented at HM11.
“Attention to the doctor-patient experience should be our guiding principle,” explains lead author and hospitalist Vicente Velez, MD. “No matter how complex the science of medicine gets, the art is equally important.” Physicians can be taught skills in effective communication with their patients and families, Dr. Velez adds.
The initiative began four years ago after the department identified low patient satisfaction scores as a “credibility crisis.” Leadership sprung into action, promoting a vision that HM should be known for its ability to communicate. “Regardless of individual communication style, a proper self-introduction, eliciting the patient’s perspective, and an explanation of the daily plan of care were things we all had to develop as habits,” he says.
Individual projects to advance the agenda included:
- Communication training offered to all physicians at the Cleveland Clinic;
- New business cards with the hospitalists’ pictures on them;
- A pre-discharge “fly-by” visit from the hospitalist;
- Post-discharge callbacks to patients; and
- Joint physician-nurse rounding.
The service now shares its Hospital Consumer Assessment of Healthcare Providers and Systems Survey (HCAHPS) satisfaction scores for individual physicians in small groups or one-on-one meetings. The department recognizes high performers. Overall satisfaction scores rose to between 76% and 86%, up from 69% at the start of the project, Dr. Velez says.
Reference
By the Numbers: 3,000
Approximate number of million-dollar hospitalization bills in Northern California hospitals in 2010, up from 430 a decade earlier, according to statistics from the Office of Statewide Health Planning and Development.1 More than 20% of the giant bills—typically for complicated, life-saving procedures and lengthy hospital stays following critical illness or trauma—went to the parents of newborn babies with catastrophic illnesses. Organ transplants were also associated with extended hospital stays and million-dollar price tags.
Medical bills are a major factor in two-thirds of personal bankruptcy cases, although most of the largest bills will be lowered significantly, as much as 80%, after negotiations between hospitals and insurers.
Reference
Approximate number of million-dollar hospitalization bills in Northern California hospitals in 2010, up from 430 a decade earlier, according to statistics from the Office of Statewide Health Planning and Development.1 More than 20% of the giant bills—typically for complicated, life-saving procedures and lengthy hospital stays following critical illness or trauma—went to the parents of newborn babies with catastrophic illnesses. Organ transplants were also associated with extended hospital stays and million-dollar price tags.
Medical bills are a major factor in two-thirds of personal bankruptcy cases, although most of the largest bills will be lowered significantly, as much as 80%, after negotiations between hospitals and insurers.
Reference
Approximate number of million-dollar hospitalization bills in Northern California hospitals in 2010, up from 430 a decade earlier, according to statistics from the Office of Statewide Health Planning and Development.1 More than 20% of the giant bills—typically for complicated, life-saving procedures and lengthy hospital stays following critical illness or trauma—went to the parents of newborn babies with catastrophic illnesses. Organ transplants were also associated with extended hospital stays and million-dollar price tags.
Medical bills are a major factor in two-thirds of personal bankruptcy cases, although most of the largest bills will be lowered significantly, as much as 80%, after negotiations between hospitals and insurers.