User login
John Nelson, MD: A New Hospitalist

Ben was just accepted to med school!!! Hopefully, more acceptances will be forthcoming. We are very proud of Ben for all his hard work. Another doctor in the family.
I was delighted to find the above message from an old friend in my inbox. It got me thinking: Will Ben become a hospitalist? Will he join his dad’s hospitalist group? Will his dad encourage him to pursue a hospitalist career or something else?
Early Hospitalist Practice
The author of that email was Ben’s dad, Chuck Wilson. Chuck is the reason I’m a hospitalist. He was a year ahead of me in residency, and while still a resident, he somehow connected with a really busy family physician in town who was looking for someone to manage his hospital patients. Not one to be bound by convention, Chuck agreed to what was at the time a nearly unheard-of arrangement. He finished residency, joined the staff of the community hospital across town from our residency, and began caring for the family physician’s hospital patients. Within days, he was fielding calls from other doctors asking him to do the same for them. Within weeks of arriving, he had begun accepting essentially all unassigned medical admissions from the ED. This was in the 1980s; Chuck was among the nation’s first real hospitalists.
I don’t think Chuck spent any time worrying about how his practice was so different from the traditional internists and family physicians in the community. He was confident he was providing a valuable service to his patients and the medical community. The rapid growth in his patient census was an indicator he was on to something, and soon he and I began talking. He was looking for a partner.
In November of my third year of residency, I decided I would put off my endocrinology fellowship for a year or two and join Chuck in his new practice. From our conversations, I anticipated that I would care for exactly the kinds of patients that filled nearly all of my time as a resident. I wouldn’t need to learn the new skills in ambulatory medicine, and wouldn’t need to make the long-term commitment expected to join a traditional primary-care practice. And I would earn a competitive compensation and have a flexible lifestyle. I soon realized that hospitalist practice provided me with all of these advantages, so more than two decades later, I still haven’t gotten around to completing the application for an endocrine fellowship.
A Loose Arrangement
For the first few years, Chuck and I didn’t bother to have any sort of legal agreement with each other. We shook hands and agreed to a “reap what you till” form of compensation, which meant we didn’t have to work exactly the same amount, and never had disagreements about how practice revenue was divided between us.
Because of Chuck’s influence, we had miniscule overhead expenses, most likely less than 10% of revenue. We each bought our own malpractice insurance, paid our biller a percent of collections, and rented a pager. That was about it for overhead.
We had no rigid scheduling algorithm, the only requirement being that at least one of us needed to be working every day. Both of us worked most weekdays, but we took time off whenever it suited us. Our scheduling meetings were usually held when we bumped into one another while rounding and went something like this:
“You OK if I take five days off starting tomorrow?”
“Sure. That’s fine.”
Meeting adjourned.
For years, we had no official name for our practice. This became a bigger issue when our group had grown to four doctors, so we defaulted to referring to the group by the first letter of the last name of each doctor, in order of tenure: The WNKL Group. A more formal name was to follow a few years later when the group was even larger, but I’ve taken delight in hearing that WNKL has persisted in some places and documents around the hospital years later, even though N, K, and L left the group long ago.
In the first few years, we never thought about developing clinical protocols or measuring our efficiency or clinical effectiveness. Chuck was confident that compared to the traditional primary-care model, we were providing higher-quality care at a lower cost. But I wasn’t so sure. After a few years, we began seeing hospital data showing that our cost per case tended to be lower, and what little data we could get regarding our quality of care suggested that it was about the same, and in some cases might be better.
A principal reason the practice has survived more than 25 years is that other than a small “tax” during their first 18 months (mainly to cover the cost of recruiting them), new doctors were regarded as equals in the business. Chuck and subsequent doctors never tried to gain an advantage over newer doctors by trying to claim a greater share of the practice’s revenue or decision-making authority.
Chuck is still in the same group he founded. In 2000, I was lured away by the chance to start a new group and live in a place that both my wife and I love. He and I have enjoyed watching our field grow up, and we take satisfaction in our roles in its evolution.
Lessons Learned
The hospitalist model of practice didn’t have a single inventor or place of origin, and anyone involved in starting a practice in the 1980s or before should be proud to have invented their practice when no blueprint existed. Creative thinking and openness to a new way of doing things were critical in developing the first hospitalist practices. They also are useful traits in trying to improve modern hospitalist practices or other segments of our healthcare system.
Like many new developments in medicine, the economic effects of our practice—lower hospital cost per case—became apparent, especially to Chuck, before data regarding quality surfaced. I wish we had gotten more serious early on about capturing whatever quality data might have been available—clearly less than what is available today—and those in new healthcare endeavors today should try to measure quality at the outset. Unlike the 1980s, the current marketplace will help ensure that happens.
Coda
There is one other really cool thing about Chuck’s email at the beginning of this column: those three exclamation points! Chuck is typically laconic and understated, and not given to such displays of emotion, but there are few things that generate more enthusiasm than a parent sharing news of a child’s success.
So, Ben, as you start med school next year, I wish you the best. You can be sure I’ll be asking for updates about your progress. The most important thing is that you find a life and career that engages you to do good work for others and provides satisfaction. And whatever you choose to do after med school, I know you’ll continue to make your parents proud.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Ben was just accepted to med school!!! Hopefully, more acceptances will be forthcoming. We are very proud of Ben for all his hard work. Another doctor in the family.
I was delighted to find the above message from an old friend in my inbox. It got me thinking: Will Ben become a hospitalist? Will he join his dad’s hospitalist group? Will his dad encourage him to pursue a hospitalist career or something else?
Early Hospitalist Practice
The author of that email was Ben’s dad, Chuck Wilson. Chuck is the reason I’m a hospitalist. He was a year ahead of me in residency, and while still a resident, he somehow connected with a really busy family physician in town who was looking for someone to manage his hospital patients. Not one to be bound by convention, Chuck agreed to what was at the time a nearly unheard-of arrangement. He finished residency, joined the staff of the community hospital across town from our residency, and began caring for the family physician’s hospital patients. Within days, he was fielding calls from other doctors asking him to do the same for them. Within weeks of arriving, he had begun accepting essentially all unassigned medical admissions from the ED. This was in the 1980s; Chuck was among the nation’s first real hospitalists.
I don’t think Chuck spent any time worrying about how his practice was so different from the traditional internists and family physicians in the community. He was confident he was providing a valuable service to his patients and the medical community. The rapid growth in his patient census was an indicator he was on to something, and soon he and I began talking. He was looking for a partner.
In November of my third year of residency, I decided I would put off my endocrinology fellowship for a year or two and join Chuck in his new practice. From our conversations, I anticipated that I would care for exactly the kinds of patients that filled nearly all of my time as a resident. I wouldn’t need to learn the new skills in ambulatory medicine, and wouldn’t need to make the long-term commitment expected to join a traditional primary-care practice. And I would earn a competitive compensation and have a flexible lifestyle. I soon realized that hospitalist practice provided me with all of these advantages, so more than two decades later, I still haven’t gotten around to completing the application for an endocrine fellowship.
A Loose Arrangement
For the first few years, Chuck and I didn’t bother to have any sort of legal agreement with each other. We shook hands and agreed to a “reap what you till” form of compensation, which meant we didn’t have to work exactly the same amount, and never had disagreements about how practice revenue was divided between us.
Because of Chuck’s influence, we had miniscule overhead expenses, most likely less than 10% of revenue. We each bought our own malpractice insurance, paid our biller a percent of collections, and rented a pager. That was about it for overhead.
We had no rigid scheduling algorithm, the only requirement being that at least one of us needed to be working every day. Both of us worked most weekdays, but we took time off whenever it suited us. Our scheduling meetings were usually held when we bumped into one another while rounding and went something like this:
“You OK if I take five days off starting tomorrow?”
“Sure. That’s fine.”
Meeting adjourned.
For years, we had no official name for our practice. This became a bigger issue when our group had grown to four doctors, so we defaulted to referring to the group by the first letter of the last name of each doctor, in order of tenure: The WNKL Group. A more formal name was to follow a few years later when the group was even larger, but I’ve taken delight in hearing that WNKL has persisted in some places and documents around the hospital years later, even though N, K, and L left the group long ago.
In the first few years, we never thought about developing clinical protocols or measuring our efficiency or clinical effectiveness. Chuck was confident that compared to the traditional primary-care model, we were providing higher-quality care at a lower cost. But I wasn’t so sure. After a few years, we began seeing hospital data showing that our cost per case tended to be lower, and what little data we could get regarding our quality of care suggested that it was about the same, and in some cases might be better.
A principal reason the practice has survived more than 25 years is that other than a small “tax” during their first 18 months (mainly to cover the cost of recruiting them), new doctors were regarded as equals in the business. Chuck and subsequent doctors never tried to gain an advantage over newer doctors by trying to claim a greater share of the practice’s revenue or decision-making authority.
Chuck is still in the same group he founded. In 2000, I was lured away by the chance to start a new group and live in a place that both my wife and I love. He and I have enjoyed watching our field grow up, and we take satisfaction in our roles in its evolution.
Lessons Learned
The hospitalist model of practice didn’t have a single inventor or place of origin, and anyone involved in starting a practice in the 1980s or before should be proud to have invented their practice when no blueprint existed. Creative thinking and openness to a new way of doing things were critical in developing the first hospitalist practices. They also are useful traits in trying to improve modern hospitalist practices or other segments of our healthcare system.
Like many new developments in medicine, the economic effects of our practice—lower hospital cost per case—became apparent, especially to Chuck, before data regarding quality surfaced. I wish we had gotten more serious early on about capturing whatever quality data might have been available—clearly less than what is available today—and those in new healthcare endeavors today should try to measure quality at the outset. Unlike the 1980s, the current marketplace will help ensure that happens.
Coda
There is one other really cool thing about Chuck’s email at the beginning of this column: those three exclamation points! Chuck is typically laconic and understated, and not given to such displays of emotion, but there are few things that generate more enthusiasm than a parent sharing news of a child’s success.
So, Ben, as you start med school next year, I wish you the best. You can be sure I’ll be asking for updates about your progress. The most important thing is that you find a life and career that engages you to do good work for others and provides satisfaction. And whatever you choose to do after med school, I know you’ll continue to make your parents proud.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Ben was just accepted to med school!!! Hopefully, more acceptances will be forthcoming. We are very proud of Ben for all his hard work. Another doctor in the family.
I was delighted to find the above message from an old friend in my inbox. It got me thinking: Will Ben become a hospitalist? Will he join his dad’s hospitalist group? Will his dad encourage him to pursue a hospitalist career or something else?
Early Hospitalist Practice
The author of that email was Ben’s dad, Chuck Wilson. Chuck is the reason I’m a hospitalist. He was a year ahead of me in residency, and while still a resident, he somehow connected with a really busy family physician in town who was looking for someone to manage his hospital patients. Not one to be bound by convention, Chuck agreed to what was at the time a nearly unheard-of arrangement. He finished residency, joined the staff of the community hospital across town from our residency, and began caring for the family physician’s hospital patients. Within days, he was fielding calls from other doctors asking him to do the same for them. Within weeks of arriving, he had begun accepting essentially all unassigned medical admissions from the ED. This was in the 1980s; Chuck was among the nation’s first real hospitalists.
I don’t think Chuck spent any time worrying about how his practice was so different from the traditional internists and family physicians in the community. He was confident he was providing a valuable service to his patients and the medical community. The rapid growth in his patient census was an indicator he was on to something, and soon he and I began talking. He was looking for a partner.
In November of my third year of residency, I decided I would put off my endocrinology fellowship for a year or two and join Chuck in his new practice. From our conversations, I anticipated that I would care for exactly the kinds of patients that filled nearly all of my time as a resident. I wouldn’t need to learn the new skills in ambulatory medicine, and wouldn’t need to make the long-term commitment expected to join a traditional primary-care practice. And I would earn a competitive compensation and have a flexible lifestyle. I soon realized that hospitalist practice provided me with all of these advantages, so more than two decades later, I still haven’t gotten around to completing the application for an endocrine fellowship.
A Loose Arrangement
For the first few years, Chuck and I didn’t bother to have any sort of legal agreement with each other. We shook hands and agreed to a “reap what you till” form of compensation, which meant we didn’t have to work exactly the same amount, and never had disagreements about how practice revenue was divided between us.
Because of Chuck’s influence, we had miniscule overhead expenses, most likely less than 10% of revenue. We each bought our own malpractice insurance, paid our biller a percent of collections, and rented a pager. That was about it for overhead.
We had no rigid scheduling algorithm, the only requirement being that at least one of us needed to be working every day. Both of us worked most weekdays, but we took time off whenever it suited us. Our scheduling meetings were usually held when we bumped into one another while rounding and went something like this:
“You OK if I take five days off starting tomorrow?”
“Sure. That’s fine.”
Meeting adjourned.
For years, we had no official name for our practice. This became a bigger issue when our group had grown to four doctors, so we defaulted to referring to the group by the first letter of the last name of each doctor, in order of tenure: The WNKL Group. A more formal name was to follow a few years later when the group was even larger, but I’ve taken delight in hearing that WNKL has persisted in some places and documents around the hospital years later, even though N, K, and L left the group long ago.
In the first few years, we never thought about developing clinical protocols or measuring our efficiency or clinical effectiveness. Chuck was confident that compared to the traditional primary-care model, we were providing higher-quality care at a lower cost. But I wasn’t so sure. After a few years, we began seeing hospital data showing that our cost per case tended to be lower, and what little data we could get regarding our quality of care suggested that it was about the same, and in some cases might be better.
A principal reason the practice has survived more than 25 years is that other than a small “tax” during their first 18 months (mainly to cover the cost of recruiting them), new doctors were regarded as equals in the business. Chuck and subsequent doctors never tried to gain an advantage over newer doctors by trying to claim a greater share of the practice’s revenue or decision-making authority.
Chuck is still in the same group he founded. In 2000, I was lured away by the chance to start a new group and live in a place that both my wife and I love. He and I have enjoyed watching our field grow up, and we take satisfaction in our roles in its evolution.
Lessons Learned
The hospitalist model of practice didn’t have a single inventor or place of origin, and anyone involved in starting a practice in the 1980s or before should be proud to have invented their practice when no blueprint existed. Creative thinking and openness to a new way of doing things were critical in developing the first hospitalist practices. They also are useful traits in trying to improve modern hospitalist practices or other segments of our healthcare system.
Like many new developments in medicine, the economic effects of our practice—lower hospital cost per case—became apparent, especially to Chuck, before data regarding quality surfaced. I wish we had gotten more serious early on about capturing whatever quality data might have been available—clearly less than what is available today—and those in new healthcare endeavors today should try to measure quality at the outset. Unlike the 1980s, the current marketplace will help ensure that happens.
Coda
There is one other really cool thing about Chuck’s email at the beginning of this column: those three exclamation points! Chuck is typically laconic and understated, and not given to such displays of emotion, but there are few things that generate more enthusiasm than a parent sharing news of a child’s success.
So, Ben, as you start med school next year, I wish you the best. You can be sure I’ll be asking for updates about your progress. The most important thing is that you find a life and career that engages you to do good work for others and provides satisfaction. And whatever you choose to do after med school, I know you’ll continue to make your parents proud.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Host of Factors Play Into Hospitalist Billing for Patient Transfers
Patient Transfers
Hospitalist billing depends on several factors. Know your role and avoid common mistakes Patient transfers can occur for many reasons: advanced technological services required, health insurance coverage, or a change in the level of care, to name a few. Patient care that is provided in the acute-care setting does not always terminate with discharge to home. Frequently, hospitalists are involved in patient transfers to another location to receive additional services: intrafacility (a different unit or related facility within the same physical plant) or interfacility (geographically separate facilities). The hospitalist must identify his or her role in the transfer and the patient’s new environment.
Physician billing in the transferred setting depends upon several factors:1
- Shared or merged medical record;
- The attending of record in each setting;
- The requirements for care rendered by the hospitalist in each setting; and
- Service dates.
Intrafacility Initial Service
Let’s examine a common example: A hospitalist serves as the “attending of record” in an inpatient hospital where acute care is required for an 83-year-old female with hypertension and diabetes who sustained a left hip fracture. The hospitalist plans to discharge the patient to the rehabilitation unit. After transfer, the rehabilitation physician becomes the attending of record, and the hospitalist might be asked to provide ongoing care for the patient’s hypertension and diabetes.
What should the hospitalist report for the initial post-transfer service? The typical options to consider are:2
- Inpatient consultation (99251-99255);
- Initial hospital care (99221-99223); and
- Subsequent hospital care (99231-99233).
Report a consultation only if the rehab attending requests an opinion or advice for an unrelated, new condition instead of previously treated conditions, and the requesting physician’s intent is for opinion or advice on management options rather than the a priori intent for the hospitalist to assume the patient’s medical care. If these requirements are met, the hospitalist may report an inpatient consultation code (99251-99255). Alternatively, if the intent or need represents a continuity of medical care provided during the acute episode of care, report the most appropriate subsequent hospital care code (99231-99233) for the hospitalist’s initial rehab visit and all follow-up services.
Initial hospital care (99221-99223) codes can only be reported for Medicare beneficiaries in place of consultation codes (99251-99255), as Medicare ceased to reimburse consultation codes.3 Most other payors who do not recognize consultation services only allow one initial hospital care code per hospitalization, reserved for the attending of record.
Interfacility Initial Service
Hospitalist groups provide patient care and coverage in many different types of facilities. Confusion often arises when the “attending of record” during acute care and the “subacute” setting (e.g. long-term acute-care hospital) are two different hospitalists from the same group practice. The hospitalist receiving the patient in the transfer facility may decide to report subsequent hospital care (99231-99233), because the group has been providing ongoing care to this patient. In this scenario, the hospitalist group could be losing revenue if an admission service (99221-99223) was not reported.
An initial hospital care service (99221-99223) is permitted when the transfer is between:
- Different hospitals;
- Different facilities under common ownership which do not have merged records; or
- Between the acute-care hospital and a PPS (prospective payment system)-exempt unit within the same hospital when there are no merged records (e.g. Medicare Part A-covered inpatient care in psychiatric, rehabilitation, critical access, and long-term care hospitals).4
In all other transfer circumstances not meeting the elements noted above, the physician should bill only the appropriate level of subsequent hospital care (99231-99233) for the date of transfer.1 Do not equate “merged records” to commonly accessible charts via an electronic medical record system or an electronic storage system. If the medical record for the patient’s acute stay is “closed” and the patient is given a separate medical record and registration for the stay in the transferred facility, consider the transfer stay as a separate admission.
Billing Two Services on Day of Transfer
Whether the transfer is classified as intrafacility or interfacility, an individual hospitalist or two separate hospitalists from the same group practice may provide the acute-care discharge and the transfer admission. A hospital discharge day management service (99238-99239) and an initial hospital care service (99221-99223) can only be reported if they do not occur on the same day.1 Physicians in the same group practice who are in the same specialty must bill and be paid as though they were a single physician; if more than one evaluation and management (face to face) service is provided on the same day to the same patient by the same physician or more than one physician in the same specialty in the same group, only one evaluation and management service may be reported.5
The Exception
CMS will allow a single hospitalist or two hospitalists from the same group practice to report a discharge day management service on the same day as an admission service. When they are billed by the same physician or group with the same date of service, contractors are instructed to pay the hospital discharge day management code (99238-99239) in addition to a nursing facility admission code (99304-99306).6
Conversely, if the patient is admitted to a hospital (99221-99223) following a nursing facility discharge (99315-99316) on the same date by the same physician/group, insurers will only reimburse the initial hospital care code. Payment for the initial hospital care service includes all work performed by the physician/group in all sites of service on that date.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is faculty for SHM’s inpatient coding course.
References available online at the-hospitalist.org
ICD-10 Update

On Sept. 5, 2012, the Centers for Medicare & Medicaid Services (CMS) published the final rule for Administration Simplification, which included a compliance date change for the International Classification of Diseases, 10th Edition (ICD-10-CM and ICD-10-PCS), Medical Data Code Sets:7
“According to a recent survey conducted by the CMS, up to one-quarter of healthcare providers believe they will not be ready for an October 1, 2013, compliance date. While the survey found no significant differences among practice settings regarding the likelihood of achieving compliance before the deadline, based on recent industry feedback we believe that larger healthcare plans and providers generally are more prepared than smaller entities. The uncertainty about provider readiness is confirmed in another recent readiness survey in which nearly 50 percent of the 2,140 provider respondents did not know when they would complete their impact assessment of the ICD-10 transition. By delaying the compliance date of ICD-10 from October 1, 2013, to October 1, 2014, we are allowing more time for covered entities to prepare for the transition to ICD-10 and to conduct thorough testing. By allowing more time to prepare, covered entities may be able to avoid costly obstacles that would otherwise emerge while in production.”7
Although providers have gained a year to adopt ICD-10, this should not deter progress toward the 2014 goal, with hopefulness that additional rulings will be made to further stall full implementation.
Patient Transfers
Hospitalist billing depends on several factors. Know your role and avoid common mistakes Patient transfers can occur for many reasons: advanced technological services required, health insurance coverage, or a change in the level of care, to name a few. Patient care that is provided in the acute-care setting does not always terminate with discharge to home. Frequently, hospitalists are involved in patient transfers to another location to receive additional services: intrafacility (a different unit or related facility within the same physical plant) or interfacility (geographically separate facilities). The hospitalist must identify his or her role in the transfer and the patient’s new environment.
Physician billing in the transferred setting depends upon several factors:1
- Shared or merged medical record;
- The attending of record in each setting;
- The requirements for care rendered by the hospitalist in each setting; and
- Service dates.
Intrafacility Initial Service
Let’s examine a common example: A hospitalist serves as the “attending of record” in an inpatient hospital where acute care is required for an 83-year-old female with hypertension and diabetes who sustained a left hip fracture. The hospitalist plans to discharge the patient to the rehabilitation unit. After transfer, the rehabilitation physician becomes the attending of record, and the hospitalist might be asked to provide ongoing care for the patient’s hypertension and diabetes.
What should the hospitalist report for the initial post-transfer service? The typical options to consider are:2
- Inpatient consultation (99251-99255);
- Initial hospital care (99221-99223); and
- Subsequent hospital care (99231-99233).
Report a consultation only if the rehab attending requests an opinion or advice for an unrelated, new condition instead of previously treated conditions, and the requesting physician’s intent is for opinion or advice on management options rather than the a priori intent for the hospitalist to assume the patient’s medical care. If these requirements are met, the hospitalist may report an inpatient consultation code (99251-99255). Alternatively, if the intent or need represents a continuity of medical care provided during the acute episode of care, report the most appropriate subsequent hospital care code (99231-99233) for the hospitalist’s initial rehab visit and all follow-up services.
Initial hospital care (99221-99223) codes can only be reported for Medicare beneficiaries in place of consultation codes (99251-99255), as Medicare ceased to reimburse consultation codes.3 Most other payors who do not recognize consultation services only allow one initial hospital care code per hospitalization, reserved for the attending of record.
Interfacility Initial Service
Hospitalist groups provide patient care and coverage in many different types of facilities. Confusion often arises when the “attending of record” during acute care and the “subacute” setting (e.g. long-term acute-care hospital) are two different hospitalists from the same group practice. The hospitalist receiving the patient in the transfer facility may decide to report subsequent hospital care (99231-99233), because the group has been providing ongoing care to this patient. In this scenario, the hospitalist group could be losing revenue if an admission service (99221-99223) was not reported.
An initial hospital care service (99221-99223) is permitted when the transfer is between:
- Different hospitals;
- Different facilities under common ownership which do not have merged records; or
- Between the acute-care hospital and a PPS (prospective payment system)-exempt unit within the same hospital when there are no merged records (e.g. Medicare Part A-covered inpatient care in psychiatric, rehabilitation, critical access, and long-term care hospitals).4
In all other transfer circumstances not meeting the elements noted above, the physician should bill only the appropriate level of subsequent hospital care (99231-99233) for the date of transfer.1 Do not equate “merged records” to commonly accessible charts via an electronic medical record system or an electronic storage system. If the medical record for the patient’s acute stay is “closed” and the patient is given a separate medical record and registration for the stay in the transferred facility, consider the transfer stay as a separate admission.
Billing Two Services on Day of Transfer
Whether the transfer is classified as intrafacility or interfacility, an individual hospitalist or two separate hospitalists from the same group practice may provide the acute-care discharge and the transfer admission. A hospital discharge day management service (99238-99239) and an initial hospital care service (99221-99223) can only be reported if they do not occur on the same day.1 Physicians in the same group practice who are in the same specialty must bill and be paid as though they were a single physician; if more than one evaluation and management (face to face) service is provided on the same day to the same patient by the same physician or more than one physician in the same specialty in the same group, only one evaluation and management service may be reported.5
The Exception
CMS will allow a single hospitalist or two hospitalists from the same group practice to report a discharge day management service on the same day as an admission service. When they are billed by the same physician or group with the same date of service, contractors are instructed to pay the hospital discharge day management code (99238-99239) in addition to a nursing facility admission code (99304-99306).6
Conversely, if the patient is admitted to a hospital (99221-99223) following a nursing facility discharge (99315-99316) on the same date by the same physician/group, insurers will only reimburse the initial hospital care code. Payment for the initial hospital care service includes all work performed by the physician/group in all sites of service on that date.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is faculty for SHM’s inpatient coding course.
References available online at the-hospitalist.org
ICD-10 Update
On Sept. 5, 2012, the Centers for Medicare & Medicaid Services (CMS) published the final rule for Administration Simplification, which included a compliance date change for the International Classification of Diseases, 10th Edition (ICD-10-CM and ICD-10-PCS), Medical Data Code Sets:7
“According to a recent survey conducted by the CMS, up to one-quarter of healthcare providers believe they will not be ready for an October 1, 2013, compliance date. While the survey found no significant differences among practice settings regarding the likelihood of achieving compliance before the deadline, based on recent industry feedback we believe that larger healthcare plans and providers generally are more prepared than smaller entities. The uncertainty about provider readiness is confirmed in another recent readiness survey in which nearly 50 percent of the 2,140 provider respondents did not know when they would complete their impact assessment of the ICD-10 transition. By delaying the compliance date of ICD-10 from October 1, 2013, to October 1, 2014, we are allowing more time for covered entities to prepare for the transition to ICD-10 and to conduct thorough testing. By allowing more time to prepare, covered entities may be able to avoid costly obstacles that would otherwise emerge while in production.”7
Although providers have gained a year to adopt ICD-10, this should not deter progress toward the 2014 goal, with hopefulness that additional rulings will be made to further stall full implementation.
Patient Transfers
Hospitalist billing depends on several factors. Know your role and avoid common mistakes Patient transfers can occur for many reasons: advanced technological services required, health insurance coverage, or a change in the level of care, to name a few. Patient care that is provided in the acute-care setting does not always terminate with discharge to home. Frequently, hospitalists are involved in patient transfers to another location to receive additional services: intrafacility (a different unit or related facility within the same physical plant) or interfacility (geographically separate facilities). The hospitalist must identify his or her role in the transfer and the patient’s new environment.
Physician billing in the transferred setting depends upon several factors:1
- Shared or merged medical record;
- The attending of record in each setting;
- The requirements for care rendered by the hospitalist in each setting; and
- Service dates.
Intrafacility Initial Service
Let’s examine a common example: A hospitalist serves as the “attending of record” in an inpatient hospital where acute care is required for an 83-year-old female with hypertension and diabetes who sustained a left hip fracture. The hospitalist plans to discharge the patient to the rehabilitation unit. After transfer, the rehabilitation physician becomes the attending of record, and the hospitalist might be asked to provide ongoing care for the patient’s hypertension and diabetes.
What should the hospitalist report for the initial post-transfer service? The typical options to consider are:2
- Inpatient consultation (99251-99255);
- Initial hospital care (99221-99223); and
- Subsequent hospital care (99231-99233).
Report a consultation only if the rehab attending requests an opinion or advice for an unrelated, new condition instead of previously treated conditions, and the requesting physician’s intent is for opinion or advice on management options rather than the a priori intent for the hospitalist to assume the patient’s medical care. If these requirements are met, the hospitalist may report an inpatient consultation code (99251-99255). Alternatively, if the intent or need represents a continuity of medical care provided during the acute episode of care, report the most appropriate subsequent hospital care code (99231-99233) for the hospitalist’s initial rehab visit and all follow-up services.
Initial hospital care (99221-99223) codes can only be reported for Medicare beneficiaries in place of consultation codes (99251-99255), as Medicare ceased to reimburse consultation codes.3 Most other payors who do not recognize consultation services only allow one initial hospital care code per hospitalization, reserved for the attending of record.
Interfacility Initial Service
Hospitalist groups provide patient care and coverage in many different types of facilities. Confusion often arises when the “attending of record” during acute care and the “subacute” setting (e.g. long-term acute-care hospital) are two different hospitalists from the same group practice. The hospitalist receiving the patient in the transfer facility may decide to report subsequent hospital care (99231-99233), because the group has been providing ongoing care to this patient. In this scenario, the hospitalist group could be losing revenue if an admission service (99221-99223) was not reported.
An initial hospital care service (99221-99223) is permitted when the transfer is between:
- Different hospitals;
- Different facilities under common ownership which do not have merged records; or
- Between the acute-care hospital and a PPS (prospective payment system)-exempt unit within the same hospital when there are no merged records (e.g. Medicare Part A-covered inpatient care in psychiatric, rehabilitation, critical access, and long-term care hospitals).4
In all other transfer circumstances not meeting the elements noted above, the physician should bill only the appropriate level of subsequent hospital care (99231-99233) for the date of transfer.1 Do not equate “merged records” to commonly accessible charts via an electronic medical record system or an electronic storage system. If the medical record for the patient’s acute stay is “closed” and the patient is given a separate medical record and registration for the stay in the transferred facility, consider the transfer stay as a separate admission.
Billing Two Services on Day of Transfer
Whether the transfer is classified as intrafacility or interfacility, an individual hospitalist or two separate hospitalists from the same group practice may provide the acute-care discharge and the transfer admission. A hospital discharge day management service (99238-99239) and an initial hospital care service (99221-99223) can only be reported if they do not occur on the same day.1 Physicians in the same group practice who are in the same specialty must bill and be paid as though they were a single physician; if more than one evaluation and management (face to face) service is provided on the same day to the same patient by the same physician or more than one physician in the same specialty in the same group, only one evaluation and management service may be reported.5
The Exception
CMS will allow a single hospitalist or two hospitalists from the same group practice to report a discharge day management service on the same day as an admission service. When they are billed by the same physician or group with the same date of service, contractors are instructed to pay the hospital discharge day management code (99238-99239) in addition to a nursing facility admission code (99304-99306).6
Conversely, if the patient is admitted to a hospital (99221-99223) following a nursing facility discharge (99315-99316) on the same date by the same physician/group, insurers will only reimburse the initial hospital care code. Payment for the initial hospital care service includes all work performed by the physician/group in all sites of service on that date.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is faculty for SHM’s inpatient coding course.
References available online at the-hospitalist.org
ICD-10 Update
On Sept. 5, 2012, the Centers for Medicare & Medicaid Services (CMS) published the final rule for Administration Simplification, which included a compliance date change for the International Classification of Diseases, 10th Edition (ICD-10-CM and ICD-10-PCS), Medical Data Code Sets:7
“According to a recent survey conducted by the CMS, up to one-quarter of healthcare providers believe they will not be ready for an October 1, 2013, compliance date. While the survey found no significant differences among practice settings regarding the likelihood of achieving compliance before the deadline, based on recent industry feedback we believe that larger healthcare plans and providers generally are more prepared than smaller entities. The uncertainty about provider readiness is confirmed in another recent readiness survey in which nearly 50 percent of the 2,140 provider respondents did not know when they would complete their impact assessment of the ICD-10 transition. By delaying the compliance date of ICD-10 from October 1, 2013, to October 1, 2014, we are allowing more time for covered entities to prepare for the transition to ICD-10 and to conduct thorough testing. By allowing more time to prepare, covered entities may be able to avoid costly obstacles that would otherwise emerge while in production.”7
Although providers have gained a year to adopt ICD-10, this should not deter progress toward the 2014 goal, with hopefulness that additional rulings will be made to further stall full implementation.
Position Paper on Critical-Care Debate Did Not Address Family Practice Physicians in ICU

Position Paper Did Not Address Family Practice Physicians in ICU
I just finished reading “The Critical-Care Debate” article in The Hospitalist’s October issue. I was quite interested in getting further follow-up and comments regarding family practice physicians’ role in critical care. Now that some hospitalist programs are utilized as “intensivists,” what are SHM and the Society of Critical Care Medicine’s (SCCM) opinions of family practitioners who are hospitalists acting in this manner? The TH article says that internal-medicine programs are insufficient for preparing internists; what are SHM and SCCM’s positions and opinions of family practice physicians being utilized as intensivists?
—Ray Nowaczyk, DO
Dr. Hospitalist responds:
Boy, and we thought this issue was politically charged before you asked that question. From my reading of the position paper (J Hosp Med. 2012;7:359-364) cited in the article, the role of family practice physicians is only alluded to, and not addressed except by its absence. The main thrust of the paper focuses specifically on physicians trained in internal medicine (IM) and how they could become “qualified” to provide ICU care. A few items stand out:
- The baseline assumption is that these would be IM-trained physicians, not family practice physicians.
- The requirements to entry wouldinclude: a) completion of IM residency; b) three years’ clinical practice as a hospitalist; and c) enrollment in the ABIM Focused Practice in Hospital Medicine Maintenance of Certification process, which, by definition, requires board certification in internal medicine.
Judging by the vocal backlash from the American College of Chest Physicians (ACCP), I imagine that even getting consensus on the points above required some fairly heavy lifting. Addressing the issue of family practitioners in HM likely was not a topic they felt could gain traction
You are absolutely correct, though, in that plenty of family practitioners practice full time as adult hospitalists (and are doing a fine job). As the paper notes, it is estimated that 6% to 8% of all hospitalists are familypractice- trained. Unfortunately, there is very little objective documentation that will allow them to demonstrate their clinical quality other than direct clinical practice or observation. There is no formal “bridge” to cross for a family practice physician wanting to receive certification in hospital medicine; this currently can only happen through ABIM.
At the same time, I do not believe that the absence of formal certification disqualifies any family practitioner from practicing quality medicine in the hospital. In fact, in my market, there are some fantastic family practice hospitalists who have been in practice in a busy, urban, Level I hospital for more than 10 years. They clearly have the clinical experience and skills that would vastly outweigh those of almost any new graduate of an internal-medicine program. Can they prove it? Not today.
I think it’s a similar discussion with IM-trained hospitalists providing ICU care. I have colleagues who actively seek to accept and care for ICU patients when it comes time for admissions, and these physicians spend much more time in direct patient care in the ICU than even some of our intensivists. Can they prove their skills? Not today. However, as noted in the Leapfrog data, at this point, only 4% of ICUs have 24/7 dedicated intensivists, so who are we kidding? We need hospitalists to provide competent ICU care. Whether we provide a pathway for objective recognition or not, it is still going to happen. It sure would be nice if it happened in a sensible way with input from the stakeholders—just as was suggested in the position paper.
Here’s a little anecdote: Many years ago, there was an ortho PA (we’ll call him Jimmy John) in our hospital, but when you called his pager number, which he also gave out routinely to patients, the message said, “You’ve reached the pager of Doctor John.” He was no doctor. Well, one of us finally asked him about it, and he replied, with a straight face: “Oh, I used to be a vet.” OK.
The point is, we all need to recognize our own skills and limitations and be able to communicate those same skills and limitations to others, especially to patients, honestly. Since honesty has its limits, then independent objective measurement is a useful adjunct. Just look at your office walls.
Position Paper Did Not Address Family Practice Physicians in ICU
I just finished reading “The Critical-Care Debate” article in The Hospitalist’s October issue. I was quite interested in getting further follow-up and comments regarding family practice physicians’ role in critical care. Now that some hospitalist programs are utilized as “intensivists,” what are SHM and the Society of Critical Care Medicine’s (SCCM) opinions of family practitioners who are hospitalists acting in this manner? The TH article says that internal-medicine programs are insufficient for preparing internists; what are SHM and SCCM’s positions and opinions of family practice physicians being utilized as intensivists?
—Ray Nowaczyk, DO
Dr. Hospitalist responds:
Boy, and we thought this issue was politically charged before you asked that question. From my reading of the position paper (J Hosp Med. 2012;7:359-364) cited in the article, the role of family practice physicians is only alluded to, and not addressed except by its absence. The main thrust of the paper focuses specifically on physicians trained in internal medicine (IM) and how they could become “qualified” to provide ICU care. A few items stand out:
- The baseline assumption is that these would be IM-trained physicians, not family practice physicians.
- The requirements to entry wouldinclude: a) completion of IM residency; b) three years’ clinical practice as a hospitalist; and c) enrollment in the ABIM Focused Practice in Hospital Medicine Maintenance of Certification process, which, by definition, requires board certification in internal medicine.
Judging by the vocal backlash from the American College of Chest Physicians (ACCP), I imagine that even getting consensus on the points above required some fairly heavy lifting. Addressing the issue of family practitioners in HM likely was not a topic they felt could gain traction
You are absolutely correct, though, in that plenty of family practitioners practice full time as adult hospitalists (and are doing a fine job). As the paper notes, it is estimated that 6% to 8% of all hospitalists are familypractice- trained. Unfortunately, there is very little objective documentation that will allow them to demonstrate their clinical quality other than direct clinical practice or observation. There is no formal “bridge” to cross for a family practice physician wanting to receive certification in hospital medicine; this currently can only happen through ABIM.
At the same time, I do not believe that the absence of formal certification disqualifies any family practitioner from practicing quality medicine in the hospital. In fact, in my market, there are some fantastic family practice hospitalists who have been in practice in a busy, urban, Level I hospital for more than 10 years. They clearly have the clinical experience and skills that would vastly outweigh those of almost any new graduate of an internal-medicine program. Can they prove it? Not today.
I think it’s a similar discussion with IM-trained hospitalists providing ICU care. I have colleagues who actively seek to accept and care for ICU patients when it comes time for admissions, and these physicians spend much more time in direct patient care in the ICU than even some of our intensivists. Can they prove their skills? Not today. However, as noted in the Leapfrog data, at this point, only 4% of ICUs have 24/7 dedicated intensivists, so who are we kidding? We need hospitalists to provide competent ICU care. Whether we provide a pathway for objective recognition or not, it is still going to happen. It sure would be nice if it happened in a sensible way with input from the stakeholders—just as was suggested in the position paper.
Here’s a little anecdote: Many years ago, there was an ortho PA (we’ll call him Jimmy John) in our hospital, but when you called his pager number, which he also gave out routinely to patients, the message said, “You’ve reached the pager of Doctor John.” He was no doctor. Well, one of us finally asked him about it, and he replied, with a straight face: “Oh, I used to be a vet.” OK.
The point is, we all need to recognize our own skills and limitations and be able to communicate those same skills and limitations to others, especially to patients, honestly. Since honesty has its limits, then independent objective measurement is a useful adjunct. Just look at your office walls.
Position Paper Did Not Address Family Practice Physicians in ICU
I just finished reading “The Critical-Care Debate” article in The Hospitalist’s October issue. I was quite interested in getting further follow-up and comments regarding family practice physicians’ role in critical care. Now that some hospitalist programs are utilized as “intensivists,” what are SHM and the Society of Critical Care Medicine’s (SCCM) opinions of family practitioners who are hospitalists acting in this manner? The TH article says that internal-medicine programs are insufficient for preparing internists; what are SHM and SCCM’s positions and opinions of family practice physicians being utilized as intensivists?
—Ray Nowaczyk, DO
Dr. Hospitalist responds:
Boy, and we thought this issue was politically charged before you asked that question. From my reading of the position paper (J Hosp Med. 2012;7:359-364) cited in the article, the role of family practice physicians is only alluded to, and not addressed except by its absence. The main thrust of the paper focuses specifically on physicians trained in internal medicine (IM) and how they could become “qualified” to provide ICU care. A few items stand out:
- The baseline assumption is that these would be IM-trained physicians, not family practice physicians.
- The requirements to entry wouldinclude: a) completion of IM residency; b) three years’ clinical practice as a hospitalist; and c) enrollment in the ABIM Focused Practice in Hospital Medicine Maintenance of Certification process, which, by definition, requires board certification in internal medicine.
Judging by the vocal backlash from the American College of Chest Physicians (ACCP), I imagine that even getting consensus on the points above required some fairly heavy lifting. Addressing the issue of family practitioners in HM likely was not a topic they felt could gain traction
You are absolutely correct, though, in that plenty of family practitioners practice full time as adult hospitalists (and are doing a fine job). As the paper notes, it is estimated that 6% to 8% of all hospitalists are familypractice- trained. Unfortunately, there is very little objective documentation that will allow them to demonstrate their clinical quality other than direct clinical practice or observation. There is no formal “bridge” to cross for a family practice physician wanting to receive certification in hospital medicine; this currently can only happen through ABIM.
At the same time, I do not believe that the absence of formal certification disqualifies any family practitioner from practicing quality medicine in the hospital. In fact, in my market, there are some fantastic family practice hospitalists who have been in practice in a busy, urban, Level I hospital for more than 10 years. They clearly have the clinical experience and skills that would vastly outweigh those of almost any new graduate of an internal-medicine program. Can they prove it? Not today.
I think it’s a similar discussion with IM-trained hospitalists providing ICU care. I have colleagues who actively seek to accept and care for ICU patients when it comes time for admissions, and these physicians spend much more time in direct patient care in the ICU than even some of our intensivists. Can they prove their skills? Not today. However, as noted in the Leapfrog data, at this point, only 4% of ICUs have 24/7 dedicated intensivists, so who are we kidding? We need hospitalists to provide competent ICU care. Whether we provide a pathway for objective recognition or not, it is still going to happen. It sure would be nice if it happened in a sensible way with input from the stakeholders—just as was suggested in the position paper.
Here’s a little anecdote: Many years ago, there was an ortho PA (we’ll call him Jimmy John) in our hospital, but when you called his pager number, which he also gave out routinely to patients, the message said, “You’ve reached the pager of Doctor John.” He was no doctor. Well, one of us finally asked him about it, and he replied, with a straight face: “Oh, I used to be a vet.” OK.
The point is, we all need to recognize our own skills and limitations and be able to communicate those same skills and limitations to others, especially to patients, honestly. Since honesty has its limits, then independent objective measurement is a useful adjunct. Just look at your office walls.
More Hospitalists Opt for Part-Time Work Schedules
An increasing number of hospitalists are pursuing part-time schedules to cater to lifestyle demands and personal desires. According to a 2010 survey conducted by the American Medical Group Management Association and Cejka Search, 21% of physicians in the U.S. are working part time, compared with only 13% in 2005.
Among those part-time physicians, the fastest-growing segments are men approaching retirement and women in the early to middle stages of their careers. Senior physicians who are tired of the commitment that comes with full-time employment increasingly are opting for part-time employment as a transition into retirement. Physicians with young children are seeking part-time employment to be more active in child-rearing.
The medical community generally has welcomed the opportunity to incorporate part-time physicians into hospital settings as a way to maintain female physicians, senior physicians, and physicians in specialties experiencing shortages. Physicians who are retained on a part-time basis should be cognizant of the following areas of the physician’s employment or independent contractor agreement:
- Independent contractor or employee status;
- Compensation;
- Benefits;
- Professional liability (malpractice) insurance; and
- Restrictive covenants.
Independent Contractor vs. Employee
Oftentimes, physicians assume that just because he or she is working part time, he or she is an independent contractor. That is an inaccurate assumption. The amount of time a physician works is not the determining factor as to whether someone is an employee or an independent contractor of the practice or hospital. Whether a physician is an employee or an independent contractor is a distinction with real consequences for tax purposes and protections under federal and state labor and employment laws.
Generally, labor and employment laws provide protections for employees, but these protections do not extend to independent contractors. With regard to taxes, if a hospitalist is an employee, the employer is required to withhold income, Social Security, and Medicare taxes, and pay unemployment tax on wages paid to the hospitalist. Conversely, if a hospitalist is an independent contractor, the practice or hospital will not withhold or pay taxes on payments to the hospitalist; rather, the individual hospitalist will be responsible for making those payments to the IRS and state tax authorities. It is imperative that the contract clearly indicates whether the hospitalist is an employee or an independent contractor, as well as the corresponding responsibilities of the parties.
Compensation and Benefits
Partial compensation for part-time work is logical, but determining a fair and competitive compensation package is not always as straightforward when it comes to part-timers. There are two general models that practices and hospitals use to determine compensation for hospitalists working part time. First, the physician may be paid a percentage of a full-time physician’s salary, based on the number of hours worked. Second, the physician may receive a per diem rate or an hourly rate. As with full-time physicians, there are various ways to formulate a part-time physician’s compensation, and the method used should be explicitly outlined in the physician’s employment or independent contractor agreement.
Benefit plans and arrangements (such as health, dental, vision, retirement plan, pension plan, disability coverage, life insurance, etc.) frequently are provided to employees and infrequently provided to independent contractors. Whether a physician who is working part time will receive benefits will vary from employer to employer. A threshold issue, however, is whether a part-time worker is even eligible to receive certain benefits. Many health, dental, and vision plans require employees to work a minimum of 30 hours a week on a regular basis, thus excluding part-time employees who work fewer hours. For retirement and pension plans, employees typically must work a minimum of 1,000 hours per year to be eligible to participate. Even if a hospitalist’s employment agreement provides that the hospitalist may receive benefits from the employer, the agreement may also provide that such a provision is subject to the terms and conditions of the particular benefit plans or arrangements.
Professional Liability (Malpractice) Insurance
While some practices or hospitals pay for a part-time physician’s malpractice insurance premiums, many shift some or all of these costs to the physician. Many insurance providers offer malpractice plans for physicians practicing part time, with reduced premiums and reduced coverage.
When negotiating a compensation package, payment for malpractice insurance should be considered. A physician also must be aware of what is excluded from coverage. For example, if a physician works part time with Hospital A and part time with Hospital B, and Hospital A provides malpractice coverage for the physician, it cannot be assumed that such coverage will cover the physician’s work with Hospital B. In this case, the physician may need a separate policy for work performed through Hospital B.
Restrictive Covenants
Although a physician might only be employed on a part-time basis, the employer might nevertheless want to protect itself by including restrictive covenants (i.e. noncompetition and nonsolicitation clauses) in the physician’s employment agreement. A part-time physician must be careful that the restrictive covenants do not jeopardize their other career objectives. For example, in the example described above with the physician working part time for both Hospital A and Hospital B, a noncompetition clause in the physician’s employment agreement with Hospital A could prohibit the physician from working at another hospital, including Hospital B.
Retaining part-time hospitalists is an increasingly attractive option for physician practices and hospitals, and part-time work is an increasingly attractive option for physicians. The items described above are just a few of the provisions that are unique to the part-time physician relationship that should be reflected in the physician’s employment or independent contractor agreement.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
An increasing number of hospitalists are pursuing part-time schedules to cater to lifestyle demands and personal desires. According to a 2010 survey conducted by the American Medical Group Management Association and Cejka Search, 21% of physicians in the U.S. are working part time, compared with only 13% in 2005.
Among those part-time physicians, the fastest-growing segments are men approaching retirement and women in the early to middle stages of their careers. Senior physicians who are tired of the commitment that comes with full-time employment increasingly are opting for part-time employment as a transition into retirement. Physicians with young children are seeking part-time employment to be more active in child-rearing.
The medical community generally has welcomed the opportunity to incorporate part-time physicians into hospital settings as a way to maintain female physicians, senior physicians, and physicians in specialties experiencing shortages. Physicians who are retained on a part-time basis should be cognizant of the following areas of the physician’s employment or independent contractor agreement:
- Independent contractor or employee status;
- Compensation;
- Benefits;
- Professional liability (malpractice) insurance; and
- Restrictive covenants.
Independent Contractor vs. Employee
Oftentimes, physicians assume that just because he or she is working part time, he or she is an independent contractor. That is an inaccurate assumption. The amount of time a physician works is not the determining factor as to whether someone is an employee or an independent contractor of the practice or hospital. Whether a physician is an employee or an independent contractor is a distinction with real consequences for tax purposes and protections under federal and state labor and employment laws.
Generally, labor and employment laws provide protections for employees, but these protections do not extend to independent contractors. With regard to taxes, if a hospitalist is an employee, the employer is required to withhold income, Social Security, and Medicare taxes, and pay unemployment tax on wages paid to the hospitalist. Conversely, if a hospitalist is an independent contractor, the practice or hospital will not withhold or pay taxes on payments to the hospitalist; rather, the individual hospitalist will be responsible for making those payments to the IRS and state tax authorities. It is imperative that the contract clearly indicates whether the hospitalist is an employee or an independent contractor, as well as the corresponding responsibilities of the parties.
Compensation and Benefits
Partial compensation for part-time work is logical, but determining a fair and competitive compensation package is not always as straightforward when it comes to part-timers. There are two general models that practices and hospitals use to determine compensation for hospitalists working part time. First, the physician may be paid a percentage of a full-time physician’s salary, based on the number of hours worked. Second, the physician may receive a per diem rate or an hourly rate. As with full-time physicians, there are various ways to formulate a part-time physician’s compensation, and the method used should be explicitly outlined in the physician’s employment or independent contractor agreement.
Benefit plans and arrangements (such as health, dental, vision, retirement plan, pension plan, disability coverage, life insurance, etc.) frequently are provided to employees and infrequently provided to independent contractors. Whether a physician who is working part time will receive benefits will vary from employer to employer. A threshold issue, however, is whether a part-time worker is even eligible to receive certain benefits. Many health, dental, and vision plans require employees to work a minimum of 30 hours a week on a regular basis, thus excluding part-time employees who work fewer hours. For retirement and pension plans, employees typically must work a minimum of 1,000 hours per year to be eligible to participate. Even if a hospitalist’s employment agreement provides that the hospitalist may receive benefits from the employer, the agreement may also provide that such a provision is subject to the terms and conditions of the particular benefit plans or arrangements.
Professional Liability (Malpractice) Insurance
While some practices or hospitals pay for a part-time physician’s malpractice insurance premiums, many shift some or all of these costs to the physician. Many insurance providers offer malpractice plans for physicians practicing part time, with reduced premiums and reduced coverage.
When negotiating a compensation package, payment for malpractice insurance should be considered. A physician also must be aware of what is excluded from coverage. For example, if a physician works part time with Hospital A and part time with Hospital B, and Hospital A provides malpractice coverage for the physician, it cannot be assumed that such coverage will cover the physician’s work with Hospital B. In this case, the physician may need a separate policy for work performed through Hospital B.
Restrictive Covenants
Although a physician might only be employed on a part-time basis, the employer might nevertheless want to protect itself by including restrictive covenants (i.e. noncompetition and nonsolicitation clauses) in the physician’s employment agreement. A part-time physician must be careful that the restrictive covenants do not jeopardize their other career objectives. For example, in the example described above with the physician working part time for both Hospital A and Hospital B, a noncompetition clause in the physician’s employment agreement with Hospital A could prohibit the physician from working at another hospital, including Hospital B.
Retaining part-time hospitalists is an increasingly attractive option for physician practices and hospitals, and part-time work is an increasingly attractive option for physicians. The items described above are just a few of the provisions that are unique to the part-time physician relationship that should be reflected in the physician’s employment or independent contractor agreement.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
An increasing number of hospitalists are pursuing part-time schedules to cater to lifestyle demands and personal desires. According to a 2010 survey conducted by the American Medical Group Management Association and Cejka Search, 21% of physicians in the U.S. are working part time, compared with only 13% in 2005.
Among those part-time physicians, the fastest-growing segments are men approaching retirement and women in the early to middle stages of their careers. Senior physicians who are tired of the commitment that comes with full-time employment increasingly are opting for part-time employment as a transition into retirement. Physicians with young children are seeking part-time employment to be more active in child-rearing.
The medical community generally has welcomed the opportunity to incorporate part-time physicians into hospital settings as a way to maintain female physicians, senior physicians, and physicians in specialties experiencing shortages. Physicians who are retained on a part-time basis should be cognizant of the following areas of the physician’s employment or independent contractor agreement:
- Independent contractor or employee status;
- Compensation;
- Benefits;
- Professional liability (malpractice) insurance; and
- Restrictive covenants.
Independent Contractor vs. Employee
Oftentimes, physicians assume that just because he or she is working part time, he or she is an independent contractor. That is an inaccurate assumption. The amount of time a physician works is not the determining factor as to whether someone is an employee or an independent contractor of the practice or hospital. Whether a physician is an employee or an independent contractor is a distinction with real consequences for tax purposes and protections under federal and state labor and employment laws.
Generally, labor and employment laws provide protections for employees, but these protections do not extend to independent contractors. With regard to taxes, if a hospitalist is an employee, the employer is required to withhold income, Social Security, and Medicare taxes, and pay unemployment tax on wages paid to the hospitalist. Conversely, if a hospitalist is an independent contractor, the practice or hospital will not withhold or pay taxes on payments to the hospitalist; rather, the individual hospitalist will be responsible for making those payments to the IRS and state tax authorities. It is imperative that the contract clearly indicates whether the hospitalist is an employee or an independent contractor, as well as the corresponding responsibilities of the parties.
Compensation and Benefits
Partial compensation for part-time work is logical, but determining a fair and competitive compensation package is not always as straightforward when it comes to part-timers. There are two general models that practices and hospitals use to determine compensation for hospitalists working part time. First, the physician may be paid a percentage of a full-time physician’s salary, based on the number of hours worked. Second, the physician may receive a per diem rate or an hourly rate. As with full-time physicians, there are various ways to formulate a part-time physician’s compensation, and the method used should be explicitly outlined in the physician’s employment or independent contractor agreement.
Benefit plans and arrangements (such as health, dental, vision, retirement plan, pension plan, disability coverage, life insurance, etc.) frequently are provided to employees and infrequently provided to independent contractors. Whether a physician who is working part time will receive benefits will vary from employer to employer. A threshold issue, however, is whether a part-time worker is even eligible to receive certain benefits. Many health, dental, and vision plans require employees to work a minimum of 30 hours a week on a regular basis, thus excluding part-time employees who work fewer hours. For retirement and pension plans, employees typically must work a minimum of 1,000 hours per year to be eligible to participate. Even if a hospitalist’s employment agreement provides that the hospitalist may receive benefits from the employer, the agreement may also provide that such a provision is subject to the terms and conditions of the particular benefit plans or arrangements.
Professional Liability (Malpractice) Insurance
While some practices or hospitals pay for a part-time physician’s malpractice insurance premiums, many shift some or all of these costs to the physician. Many insurance providers offer malpractice plans for physicians practicing part time, with reduced premiums and reduced coverage.
When negotiating a compensation package, payment for malpractice insurance should be considered. A physician also must be aware of what is excluded from coverage. For example, if a physician works part time with Hospital A and part time with Hospital B, and Hospital A provides malpractice coverage for the physician, it cannot be assumed that such coverage will cover the physician’s work with Hospital B. In this case, the physician may need a separate policy for work performed through Hospital B.
Restrictive Covenants
Although a physician might only be employed on a part-time basis, the employer might nevertheless want to protect itself by including restrictive covenants (i.e. noncompetition and nonsolicitation clauses) in the physician’s employment agreement. A part-time physician must be careful that the restrictive covenants do not jeopardize their other career objectives. For example, in the example described above with the physician working part time for both Hospital A and Hospital B, a noncompetition clause in the physician’s employment agreement with Hospital A could prohibit the physician from working at another hospital, including Hospital B.
Retaining part-time hospitalists is an increasingly attractive option for physician practices and hospitals, and part-time work is an increasingly attractive option for physicians. The items described above are just a few of the provisions that are unique to the part-time physician relationship that should be reflected in the physician’s employment or independent contractor agreement.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Hospitalist Edward Ma, MD, Embraces the Entrepreneurial Spirit

Edward Ma, MD, wasn’t sure what he wanted to be when he grew up. As a biology student at the University of Pennsylvania in Philadelphia, he says friends “peer-pressured” him to choose a career in medicine. Once the decision was made and he began his training, he found out he was pretty good at the doctor thing.
“I realized that I like this,” he says. “I told myself, ‘I’m going to go for it.’”
Dr. Ma also realized he had a liking for business, and where better to study business than at Penn’s Wharton School of Business? He hasn’t completed an MBA, but he’s taken post-grad courses focused on healthcare management. And now he’s combining that knowledge with his experiences as a hospitalist and medical director to develop a consulting business.
“That sort of evolved because I sort of have a big mouth. When I see something wrong, or something that could be done better, I tend to vocalize it,” says Dr. Ma, medical director of hospitalist services at 168-bed Brandywine Hospital in Coatesville, Pa. “The biggest opportunity is to really help a hospitalist group realize its potential and its value.”
Dr. Ma joined Team Hospitalist in April 2012. Although his side business is evolving via “word of mouth,” he still spends the majority of his time in the hospital directing a six-member HM group and caring for hospitalized patients.
Question: What do you like most about caring for patients?
Answer: I like the acuity of the care. The acuity of the illness is pretty high for our patients, and you can see very quickly the impact hospitalists can have. A lot of outpatient medicine is preventive care, so usually you don’t have an immediate problem that needs to be fixed, whereas in HM, the patients are acutely ill and there’s an ability to get these patients better—and see a change in their medical condition in a day or two. There’s more immediate gratification in terms of the effort that we put in caring for a patient.
Q: What do you like least?
A: The paperwork. At my hospital, a lot of it is computerized. But there are tons of checklists, tons of quality measures that need to be addressed, which is good. Still, it ends up bogging down our ability to take care of the patient. For example, a patient comes in for pneumonia and you have to make sure that some of their chronic issues (e.g. diabetes) are addressed. Have they had their hemoglobin A1C checked in the last 60 days? Does it really matter right now when we’re taking care of the patient’s pneumonia that we have to address this? Smoking cessation, yes, it’s very important, and we need to address this, but is it really necessary that we do this at this point when a patient is really ill? I think there’s a lot of these government regulations that they want us to take care of sometimes in the acute setting, which sometimes feels awkward or not necessarily time-appropriate.
Q: You say your training as an internist prepared you for a seamless transition to a hospitalist job, but you also think IM training is “doing a disservice to medicine.” How so?
A: Don’t get me wrong, I love hospital medicine. But I think what we really need is more primary-care doctors. This is not just my commentary on hospital medicine, but all subspecialties. I know specifically speaking that we need more outpatient internists, outpatient family physicians. If there are many internists, they’re not going to have as much need for cardiology or GI, or a lot of other subspecialties. There’s enough of a population of internists that would satisfy the need for internists and obviously the need for subspecialties.
Q: What’s the biggest change in HM you’ve witnessed since you started 10 years ago?
A: Our acceptance as a field by the medical community. Other physicians have now come to be very accepting of our role as the primary caretakers of their hospitalized patients.
Q: Do you consider yourself to have an entrepreneurial spirit or are you more of a solutions-oriented physician?
A: I have more of the entrepreneurial spirit. I’ve been talking to a lot of hospitalists, and what I encourage them to do is completely counter to the current healthcare environment. I’ve been encouraging them to say, “Let’s get a bunch of us together and set up our own hospitalist practice and do it in a way that we can have a certain level of autonomy, but also do it in a way that we can collaborate with the hospital, work intimately with them, and get certain guarantees from them. And do it privately, so that we can maintain our autonomy.” I think that’s important because I see the difference between the private practices and the practices that are owned by a health system. People just care so much more when it’s their own practice.
Q: What are the biggest challenges you face as medical director?
A: Getting everyone to work as a team. Everyone has a different schedule, differing values, and priorities. It’s very important that we work as a team because when one person does something, it impacts what somebody else does.
Q: What’s the most important thing to know when starting an HM group or fixing a broken group?
A: For fixing a group, you have to look at the values of the group of doctors. What are the values? What are the objectives? What are the professional goals? What I’ve encountered in HM is a lot of people are just coming in to get a paycheck. They come in, they do their job, and they like to take care of patients. Don’t get me wrong about that, but they like the freedom and the high competition that’s provided by hospital medicine. Oftentimes they come in, they do their jobs very well, they take care of their patients, and then they’re out the door. They don’t really have an interest in building up that practice or building up something for the hospital. We as doctors are all part of a medical community, we’re part of a medical staff, and it’s very important for us to get involved.
Q: Last year, you became president of SHM’s Philadelphia Tri-State Region chapter. What are your goals?
A: I’ve always been involved with the chapter, but I saw it as a good opportunity to network and talk with more hospitalists. I wanted to get their viewpoints on things and bounce ideas. I’m a very vocal person, so when I hear a good idea, I like to spread it amongst other people. And if I see something that someone said was bad and I hear it from enough people, I like to bring it up and discuss with everybody.
Q: What’s the best part of being an SHM member?
A: Getting to interact with a lot of my colleagues. To see what struggles they’re going through, to see that their struggles are very similar to the struggles that my group is going through, that we’re all in the same boat, and that we need to collaborate a little more to make things work. Instead of each practice trying to reinvent the wheel, we can try to work together and build off each other.
Richard Quinn is a freelance writer in New Jersey.
Edward Ma, MD, wasn’t sure what he wanted to be when he grew up. As a biology student at the University of Pennsylvania in Philadelphia, he says friends “peer-pressured” him to choose a career in medicine. Once the decision was made and he began his training, he found out he was pretty good at the doctor thing.
“I realized that I like this,” he says. “I told myself, ‘I’m going to go for it.’”
Dr. Ma also realized he had a liking for business, and where better to study business than at Penn’s Wharton School of Business? He hasn’t completed an MBA, but he’s taken post-grad courses focused on healthcare management. And now he’s combining that knowledge with his experiences as a hospitalist and medical director to develop a consulting business.
“That sort of evolved because I sort of have a big mouth. When I see something wrong, or something that could be done better, I tend to vocalize it,” says Dr. Ma, medical director of hospitalist services at 168-bed Brandywine Hospital in Coatesville, Pa. “The biggest opportunity is to really help a hospitalist group realize its potential and its value.”
Dr. Ma joined Team Hospitalist in April 2012. Although his side business is evolving via “word of mouth,” he still spends the majority of his time in the hospital directing a six-member HM group and caring for hospitalized patients.
Question: What do you like most about caring for patients?
Answer: I like the acuity of the care. The acuity of the illness is pretty high for our patients, and you can see very quickly the impact hospitalists can have. A lot of outpatient medicine is preventive care, so usually you don’t have an immediate problem that needs to be fixed, whereas in HM, the patients are acutely ill and there’s an ability to get these patients better—and see a change in their medical condition in a day or two. There’s more immediate gratification in terms of the effort that we put in caring for a patient.
Q: What do you like least?
A: The paperwork. At my hospital, a lot of it is computerized. But there are tons of checklists, tons of quality measures that need to be addressed, which is good. Still, it ends up bogging down our ability to take care of the patient. For example, a patient comes in for pneumonia and you have to make sure that some of their chronic issues (e.g. diabetes) are addressed. Have they had their hemoglobin A1C checked in the last 60 days? Does it really matter right now when we’re taking care of the patient’s pneumonia that we have to address this? Smoking cessation, yes, it’s very important, and we need to address this, but is it really necessary that we do this at this point when a patient is really ill? I think there’s a lot of these government regulations that they want us to take care of sometimes in the acute setting, which sometimes feels awkward or not necessarily time-appropriate.
Q: You say your training as an internist prepared you for a seamless transition to a hospitalist job, but you also think IM training is “doing a disservice to medicine.” How so?
A: Don’t get me wrong, I love hospital medicine. But I think what we really need is more primary-care doctors. This is not just my commentary on hospital medicine, but all subspecialties. I know specifically speaking that we need more outpatient internists, outpatient family physicians. If there are many internists, they’re not going to have as much need for cardiology or GI, or a lot of other subspecialties. There’s enough of a population of internists that would satisfy the need for internists and obviously the need for subspecialties.
Q: What’s the biggest change in HM you’ve witnessed since you started 10 years ago?
A: Our acceptance as a field by the medical community. Other physicians have now come to be very accepting of our role as the primary caretakers of their hospitalized patients.
Q: Do you consider yourself to have an entrepreneurial spirit or are you more of a solutions-oriented physician?
A: I have more of the entrepreneurial spirit. I’ve been talking to a lot of hospitalists, and what I encourage them to do is completely counter to the current healthcare environment. I’ve been encouraging them to say, “Let’s get a bunch of us together and set up our own hospitalist practice and do it in a way that we can have a certain level of autonomy, but also do it in a way that we can collaborate with the hospital, work intimately with them, and get certain guarantees from them. And do it privately, so that we can maintain our autonomy.” I think that’s important because I see the difference between the private practices and the practices that are owned by a health system. People just care so much more when it’s their own practice.
Q: What are the biggest challenges you face as medical director?
A: Getting everyone to work as a team. Everyone has a different schedule, differing values, and priorities. It’s very important that we work as a team because when one person does something, it impacts what somebody else does.
Q: What’s the most important thing to know when starting an HM group or fixing a broken group?
A: For fixing a group, you have to look at the values of the group of doctors. What are the values? What are the objectives? What are the professional goals? What I’ve encountered in HM is a lot of people are just coming in to get a paycheck. They come in, they do their job, and they like to take care of patients. Don’t get me wrong about that, but they like the freedom and the high competition that’s provided by hospital medicine. Oftentimes they come in, they do their jobs very well, they take care of their patients, and then they’re out the door. They don’t really have an interest in building up that practice or building up something for the hospital. We as doctors are all part of a medical community, we’re part of a medical staff, and it’s very important for us to get involved.
Q: Last year, you became president of SHM’s Philadelphia Tri-State Region chapter. What are your goals?
A: I’ve always been involved with the chapter, but I saw it as a good opportunity to network and talk with more hospitalists. I wanted to get their viewpoints on things and bounce ideas. I’m a very vocal person, so when I hear a good idea, I like to spread it amongst other people. And if I see something that someone said was bad and I hear it from enough people, I like to bring it up and discuss with everybody.
Q: What’s the best part of being an SHM member?
A: Getting to interact with a lot of my colleagues. To see what struggles they’re going through, to see that their struggles are very similar to the struggles that my group is going through, that we’re all in the same boat, and that we need to collaborate a little more to make things work. Instead of each practice trying to reinvent the wheel, we can try to work together and build off each other.
Richard Quinn is a freelance writer in New Jersey.
Edward Ma, MD, wasn’t sure what he wanted to be when he grew up. As a biology student at the University of Pennsylvania in Philadelphia, he says friends “peer-pressured” him to choose a career in medicine. Once the decision was made and he began his training, he found out he was pretty good at the doctor thing.
“I realized that I like this,” he says. “I told myself, ‘I’m going to go for it.’”
Dr. Ma also realized he had a liking for business, and where better to study business than at Penn’s Wharton School of Business? He hasn’t completed an MBA, but he’s taken post-grad courses focused on healthcare management. And now he’s combining that knowledge with his experiences as a hospitalist and medical director to develop a consulting business.
“That sort of evolved because I sort of have a big mouth. When I see something wrong, or something that could be done better, I tend to vocalize it,” says Dr. Ma, medical director of hospitalist services at 168-bed Brandywine Hospital in Coatesville, Pa. “The biggest opportunity is to really help a hospitalist group realize its potential and its value.”
Dr. Ma joined Team Hospitalist in April 2012. Although his side business is evolving via “word of mouth,” he still spends the majority of his time in the hospital directing a six-member HM group and caring for hospitalized patients.
Question: What do you like most about caring for patients?
Answer: I like the acuity of the care. The acuity of the illness is pretty high for our patients, and you can see very quickly the impact hospitalists can have. A lot of outpatient medicine is preventive care, so usually you don’t have an immediate problem that needs to be fixed, whereas in HM, the patients are acutely ill and there’s an ability to get these patients better—and see a change in their medical condition in a day or two. There’s more immediate gratification in terms of the effort that we put in caring for a patient.
Q: What do you like least?
A: The paperwork. At my hospital, a lot of it is computerized. But there are tons of checklists, tons of quality measures that need to be addressed, which is good. Still, it ends up bogging down our ability to take care of the patient. For example, a patient comes in for pneumonia and you have to make sure that some of their chronic issues (e.g. diabetes) are addressed. Have they had their hemoglobin A1C checked in the last 60 days? Does it really matter right now when we’re taking care of the patient’s pneumonia that we have to address this? Smoking cessation, yes, it’s very important, and we need to address this, but is it really necessary that we do this at this point when a patient is really ill? I think there’s a lot of these government regulations that they want us to take care of sometimes in the acute setting, which sometimes feels awkward or not necessarily time-appropriate.
Q: You say your training as an internist prepared you for a seamless transition to a hospitalist job, but you also think IM training is “doing a disservice to medicine.” How so?
A: Don’t get me wrong, I love hospital medicine. But I think what we really need is more primary-care doctors. This is not just my commentary on hospital medicine, but all subspecialties. I know specifically speaking that we need more outpatient internists, outpatient family physicians. If there are many internists, they’re not going to have as much need for cardiology or GI, or a lot of other subspecialties. There’s enough of a population of internists that would satisfy the need for internists and obviously the need for subspecialties.
Q: What’s the biggest change in HM you’ve witnessed since you started 10 years ago?
A: Our acceptance as a field by the medical community. Other physicians have now come to be very accepting of our role as the primary caretakers of their hospitalized patients.
Q: Do you consider yourself to have an entrepreneurial spirit or are you more of a solutions-oriented physician?
A: I have more of the entrepreneurial spirit. I’ve been talking to a lot of hospitalists, and what I encourage them to do is completely counter to the current healthcare environment. I’ve been encouraging them to say, “Let’s get a bunch of us together and set up our own hospitalist practice and do it in a way that we can have a certain level of autonomy, but also do it in a way that we can collaborate with the hospital, work intimately with them, and get certain guarantees from them. And do it privately, so that we can maintain our autonomy.” I think that’s important because I see the difference between the private practices and the practices that are owned by a health system. People just care so much more when it’s their own practice.
Q: What are the biggest challenges you face as medical director?
A: Getting everyone to work as a team. Everyone has a different schedule, differing values, and priorities. It’s very important that we work as a team because when one person does something, it impacts what somebody else does.
Q: What’s the most important thing to know when starting an HM group or fixing a broken group?
A: For fixing a group, you have to look at the values of the group of doctors. What are the values? What are the objectives? What are the professional goals? What I’ve encountered in HM is a lot of people are just coming in to get a paycheck. They come in, they do their job, and they like to take care of patients. Don’t get me wrong about that, but they like the freedom and the high competition that’s provided by hospital medicine. Oftentimes they come in, they do their jobs very well, they take care of their patients, and then they’re out the door. They don’t really have an interest in building up that practice or building up something for the hospital. We as doctors are all part of a medical community, we’re part of a medical staff, and it’s very important for us to get involved.
Q: Last year, you became president of SHM’s Philadelphia Tri-State Region chapter. What are your goals?
A: I’ve always been involved with the chapter, but I saw it as a good opportunity to network and talk with more hospitalists. I wanted to get their viewpoints on things and bounce ideas. I’m a very vocal person, so when I hear a good idea, I like to spread it amongst other people. And if I see something that someone said was bad and I hear it from enough people, I like to bring it up and discuss with everybody.
Q: What’s the best part of being an SHM member?
A: Getting to interact with a lot of my colleagues. To see what struggles they’re going through, to see that their struggles are very similar to the struggles that my group is going through, that we’re all in the same boat, and that we need to collaborate a little more to make things work. Instead of each practice trying to reinvent the wheel, we can try to work together and build off each other.
Richard Quinn is a freelance writer in New Jersey.
Variation by age in neutropenic complications among patients with cancer receiving chemotherapy
Background Age is among the most important risk factors for neutropenia-related hospitalization, but evidence is limited regarding the relative contributions of age and other risk factors.
Objective To explore the associations among patient age, other risk factors, and neutropenic complications in patients with cancer receiving myelosuppressive chemotherapy.
Methods This retrospective cohort study, which used a US commercial insurance claims database, included patients aged 40 years or older with non-Hodgkin lymphoma (NHL), breast cancer, or lung cancer who initiated chemotherapy between January 1, 2006 and March 31, 2010. The primary endpoint was the risk of neutropenia-related hospitalization during the first chemotherapy course. We used cubic spline modeling to estimate the association between neutropenia-related hospitalization and age, adjusting for patient and treatment characteristics. Logistic regression analyses examined the effects of other risk factors.
Results A total of 15,638 patients were included (NHL, n = 2,506; breast cancer, n = 9,110; lung cancer, n = 4,022), mean age 56-66 years. Neutropenia-related hospitalization occurred in 8.7% of NHL patients, 4.2% of breast cancer patients, and 3.9% of lung cancer patients. The association between age and the risk of neutropenia-related hospitalization was stronger in NHL than in lung or breast cancer. Patient comorbidities and chemotherapy characteristics had considerable effects on risk of neutropenia-related hospitalization.
Limitations Disease stage and other clinical factors could not be identified from the claims data.
Conclusion In addition to age, oncologists should evaluate individual patient risk factors including patient comorbidities and type of chemotherapy regimen.
*To read the full article, click on the PDF icon at the top of this introduction.
Background Age is among the most important risk factors for neutropenia-related hospitalization, but evidence is limited regarding the relative contributions of age and other risk factors.
Objective To explore the associations among patient age, other risk factors, and neutropenic complications in patients with cancer receiving myelosuppressive chemotherapy.
Methods This retrospective cohort study, which used a US commercial insurance claims database, included patients aged 40 years or older with non-Hodgkin lymphoma (NHL), breast cancer, or lung cancer who initiated chemotherapy between January 1, 2006 and March 31, 2010. The primary endpoint was the risk of neutropenia-related hospitalization during the first chemotherapy course. We used cubic spline modeling to estimate the association between neutropenia-related hospitalization and age, adjusting for patient and treatment characteristics. Logistic regression analyses examined the effects of other risk factors.
Results A total of 15,638 patients were included (NHL, n = 2,506; breast cancer, n = 9,110; lung cancer, n = 4,022), mean age 56-66 years. Neutropenia-related hospitalization occurred in 8.7% of NHL patients, 4.2% of breast cancer patients, and 3.9% of lung cancer patients. The association between age and the risk of neutropenia-related hospitalization was stronger in NHL than in lung or breast cancer. Patient comorbidities and chemotherapy characteristics had considerable effects on risk of neutropenia-related hospitalization.
Limitations Disease stage and other clinical factors could not be identified from the claims data.
Conclusion In addition to age, oncologists should evaluate individual patient risk factors including patient comorbidities and type of chemotherapy regimen.
*To read the full article, click on the PDF icon at the top of this introduction.
Background Age is among the most important risk factors for neutropenia-related hospitalization, but evidence is limited regarding the relative contributions of age and other risk factors.
Objective To explore the associations among patient age, other risk factors, and neutropenic complications in patients with cancer receiving myelosuppressive chemotherapy.
Methods This retrospective cohort study, which used a US commercial insurance claims database, included patients aged 40 years or older with non-Hodgkin lymphoma (NHL), breast cancer, or lung cancer who initiated chemotherapy between January 1, 2006 and March 31, 2010. The primary endpoint was the risk of neutropenia-related hospitalization during the first chemotherapy course. We used cubic spline modeling to estimate the association between neutropenia-related hospitalization and age, adjusting for patient and treatment characteristics. Logistic regression analyses examined the effects of other risk factors.
Results A total of 15,638 patients were included (NHL, n = 2,506; breast cancer, n = 9,110; lung cancer, n = 4,022), mean age 56-66 years. Neutropenia-related hospitalization occurred in 8.7% of NHL patients, 4.2% of breast cancer patients, and 3.9% of lung cancer patients. The association between age and the risk of neutropenia-related hospitalization was stronger in NHL than in lung or breast cancer. Patient comorbidities and chemotherapy characteristics had considerable effects on risk of neutropenia-related hospitalization.
Limitations Disease stage and other clinical factors could not be identified from the claims data.
Conclusion In addition to age, oncologists should evaluate individual patient risk factors including patient comorbidities and type of chemotherapy regimen.
*To read the full article, click on the PDF icon at the top of this introduction.
Working with other disciplines
Optimizing Home Health Care: Enhanced Value and Improved Outcomes
Supplement Editor:
William Zafirau, MD
Supplement Co-Editors:
Steven H. Landers, MD, MPH, and Cindy Vunovich, RN, BSN, MSM
Contents
Introduction—Medicine’s future: Helping patients stay healthy at home
Steven H. Landers, MD, MPH
Care transitions and advanced home care models
Improving patient outcomes with better care transitions: The role for home health
Michael O. Fleming, MD, and Tara Trahan Haney
Improving outcomes and lowering costs by applying advanced models of in-home care
Peter A. Boling, MD; Rashmi V. Chandekar, MD; Beth Hungate, MS, ANP-BC; Martha Purvis, MSN; Rachel Selby-Penczak, MD; and Linda J. Abbey, MD
Home care for knee replacement and heart failure
In-home care following total knee replacement
Mark I. Froimson, MD, MBA
Home-based care for heart failure: Cleveland Clinic's "Heart Care at Home" transitional care program
Eiran Z. Gorodeski, MD, MPH; Sandra Chlad, NP; and Seth Vilensky, MBA
Technology innovations and palliative care
The case for "connected health" at home
Steven H. Landers, MD, MPH
Innovative models of home-based palliative care
Margherita C. Labson, RN, MSHSA, CPHQ, CCM; Michele M. Sacco, MS; David E. Weissman, MD; Betsy Gornet, FACHE; and Brad Stuart, MD
Cleveland Clinic Journal of Medicine interview
Accountable care and patient-centered medical homes: Implications for office-based practice
An interview with David L. Longworth, MD
Supplement Editor:
William Zafirau, MD
Supplement Co-Editors:
Steven H. Landers, MD, MPH, and Cindy Vunovich, RN, BSN, MSM
Contents
Introduction—Medicine’s future: Helping patients stay healthy at home
Steven H. Landers, MD, MPH
Care transitions and advanced home care models
Improving patient outcomes with better care transitions: The role for home health
Michael O. Fleming, MD, and Tara Trahan Haney
Improving outcomes and lowering costs by applying advanced models of in-home care
Peter A. Boling, MD; Rashmi V. Chandekar, MD; Beth Hungate, MS, ANP-BC; Martha Purvis, MSN; Rachel Selby-Penczak, MD; and Linda J. Abbey, MD
Home care for knee replacement and heart failure
In-home care following total knee replacement
Mark I. Froimson, MD, MBA
Home-based care for heart failure: Cleveland Clinic's "Heart Care at Home" transitional care program
Eiran Z. Gorodeski, MD, MPH; Sandra Chlad, NP; and Seth Vilensky, MBA
Technology innovations and palliative care
The case for "connected health" at home
Steven H. Landers, MD, MPH
Innovative models of home-based palliative care
Margherita C. Labson, RN, MSHSA, CPHQ, CCM; Michele M. Sacco, MS; David E. Weissman, MD; Betsy Gornet, FACHE; and Brad Stuart, MD
Cleveland Clinic Journal of Medicine interview
Accountable care and patient-centered medical homes: Implications for office-based practice
An interview with David L. Longworth, MD
Supplement Editor:
William Zafirau, MD
Supplement Co-Editors:
Steven H. Landers, MD, MPH, and Cindy Vunovich, RN, BSN, MSM
Contents
Introduction—Medicine’s future: Helping patients stay healthy at home
Steven H. Landers, MD, MPH
Care transitions and advanced home care models
Improving patient outcomes with better care transitions: The role for home health
Michael O. Fleming, MD, and Tara Trahan Haney
Improving outcomes and lowering costs by applying advanced models of in-home care
Peter A. Boling, MD; Rashmi V. Chandekar, MD; Beth Hungate, MS, ANP-BC; Martha Purvis, MSN; Rachel Selby-Penczak, MD; and Linda J. Abbey, MD
Home care for knee replacement and heart failure
In-home care following total knee replacement
Mark I. Froimson, MD, MBA
Home-based care for heart failure: Cleveland Clinic's "Heart Care at Home" transitional care program
Eiran Z. Gorodeski, MD, MPH; Sandra Chlad, NP; and Seth Vilensky, MBA
Technology innovations and palliative care
The case for "connected health" at home
Steven H. Landers, MD, MPH
Innovative models of home-based palliative care
Margherita C. Labson, RN, MSHSA, CPHQ, CCM; Michele M. Sacco, MS; David E. Weissman, MD; Betsy Gornet, FACHE; and Brad Stuart, MD
Cleveland Clinic Journal of Medicine interview
Accountable care and patient-centered medical homes: Implications for office-based practice
An interview with David L. Longworth, MD
Introduction—Medicine’s future: Helping patients stay healthy at home
Home-based care will undoubtedly play an increasingly important role in the health care system as the United States seeks ways to provide cost-effective and compassionate care to a growing population of older adults with chronic illness. “Home health care,” a term that refers more specifically to visiting nurses, therapists, and related services, is currently the prominent home care model in this country.
Home health services were developed around the start of the 20th century to address the unmet health and social needs of vulnerable populations living in the shadows. Today, there are more than 10,000 home health agencies and visiting nurse organizations across the country that care for millions of homebound patients each year. With the onset of health reform and the increasing focus on value and “accountability,” there are many opportunities and challenges for home health providers and the physicians, hospitals, and facilities they work with to try to find the best ways to keep patients healthy at home and drive value for society.
There is a paucity of medical and health services literature to guide providers and policymakers’ decisions about the right types and approaches to care at home. Maybe this is because academic centers and American medicine became so focused on acute institutional care in the past half century that the home has been overlooked. However, that pendulum is likely swinging back as almost every sober analysis of our current health care environment suggests a need for better care for the chronically ill at home and in the community. It is important that research and academic enterprises emphasize scholarly efforts to understand and improve home and community care so that the anticipated shift in care to home is informed by the best possible evidence, ultimately ensuring that patients get the best possible care.
The articles in this online, CME-certified Cleveland Clinic Journal of Medicine supplement address contemporary topics in home health and other home-based care concepts. The authors have diverse backgrounds and discuss issues related to technology, palliative care, care transitions, heart failure, knee replacement, primary care, and health reform. Several articles share concepts and outcomes from innovative approaches being developed throughout the country to help patients succeed at home, especially when returning home from a hospitalization.
The articles should improve readers’ understanding of a wide range of initiatives and ideas for how home health and home care might look in the future delivery system. The authors also raise numerous yet-unanswered questions and opportunities for future study. The needs for further home care research from clinical, public health, and policy perspectives are evident. Health care is going home, and this transformation will be enhanced and possibly accelerated by thoughtful research and synthesis.
I am incredibly thankful to my fellow authors, and hope that we have produced a useful supplement that will help readers in their efforts to assist the most vulnerable patients and families in their efforts to remain independent at home.
Home-based care will undoubtedly play an increasingly important role in the health care system as the United States seeks ways to provide cost-effective and compassionate care to a growing population of older adults with chronic illness. “Home health care,” a term that refers more specifically to visiting nurses, therapists, and related services, is currently the prominent home care model in this country.
Home health services were developed around the start of the 20th century to address the unmet health and social needs of vulnerable populations living in the shadows. Today, there are more than 10,000 home health agencies and visiting nurse organizations across the country that care for millions of homebound patients each year. With the onset of health reform and the increasing focus on value and “accountability,” there are many opportunities and challenges for home health providers and the physicians, hospitals, and facilities they work with to try to find the best ways to keep patients healthy at home and drive value for society.
There is a paucity of medical and health services literature to guide providers and policymakers’ decisions about the right types and approaches to care at home. Maybe this is because academic centers and American medicine became so focused on acute institutional care in the past half century that the home has been overlooked. However, that pendulum is likely swinging back as almost every sober analysis of our current health care environment suggests a need for better care for the chronically ill at home and in the community. It is important that research and academic enterprises emphasize scholarly efforts to understand and improve home and community care so that the anticipated shift in care to home is informed by the best possible evidence, ultimately ensuring that patients get the best possible care.
The articles in this online, CME-certified Cleveland Clinic Journal of Medicine supplement address contemporary topics in home health and other home-based care concepts. The authors have diverse backgrounds and discuss issues related to technology, palliative care, care transitions, heart failure, knee replacement, primary care, and health reform. Several articles share concepts and outcomes from innovative approaches being developed throughout the country to help patients succeed at home, especially when returning home from a hospitalization.
The articles should improve readers’ understanding of a wide range of initiatives and ideas for how home health and home care might look in the future delivery system. The authors also raise numerous yet-unanswered questions and opportunities for future study. The needs for further home care research from clinical, public health, and policy perspectives are evident. Health care is going home, and this transformation will be enhanced and possibly accelerated by thoughtful research and synthesis.
I am incredibly thankful to my fellow authors, and hope that we have produced a useful supplement that will help readers in their efforts to assist the most vulnerable patients and families in their efforts to remain independent at home.
Home-based care will undoubtedly play an increasingly important role in the health care system as the United States seeks ways to provide cost-effective and compassionate care to a growing population of older adults with chronic illness. “Home health care,” a term that refers more specifically to visiting nurses, therapists, and related services, is currently the prominent home care model in this country.
Home health services were developed around the start of the 20th century to address the unmet health and social needs of vulnerable populations living in the shadows. Today, there are more than 10,000 home health agencies and visiting nurse organizations across the country that care for millions of homebound patients each year. With the onset of health reform and the increasing focus on value and “accountability,” there are many opportunities and challenges for home health providers and the physicians, hospitals, and facilities they work with to try to find the best ways to keep patients healthy at home and drive value for society.
There is a paucity of medical and health services literature to guide providers and policymakers’ decisions about the right types and approaches to care at home. Maybe this is because academic centers and American medicine became so focused on acute institutional care in the past half century that the home has been overlooked. However, that pendulum is likely swinging back as almost every sober analysis of our current health care environment suggests a need for better care for the chronically ill at home and in the community. It is important that research and academic enterprises emphasize scholarly efforts to understand and improve home and community care so that the anticipated shift in care to home is informed by the best possible evidence, ultimately ensuring that patients get the best possible care.
The articles in this online, CME-certified Cleveland Clinic Journal of Medicine supplement address contemporary topics in home health and other home-based care concepts. The authors have diverse backgrounds and discuss issues related to technology, palliative care, care transitions, heart failure, knee replacement, primary care, and health reform. Several articles share concepts and outcomes from innovative approaches being developed throughout the country to help patients succeed at home, especially when returning home from a hospitalization.
The articles should improve readers’ understanding of a wide range of initiatives and ideas for how home health and home care might look in the future delivery system. The authors also raise numerous yet-unanswered questions and opportunities for future study. The needs for further home care research from clinical, public health, and policy perspectives are evident. Health care is going home, and this transformation will be enhanced and possibly accelerated by thoughtful research and synthesis.
I am incredibly thankful to my fellow authors, and hope that we have produced a useful supplement that will help readers in their efforts to assist the most vulnerable patients and families in their efforts to remain independent at home.
Improving patient outcomes with better care transitions: The role for home health
The US health care system faces many challenges. Quality, cost, access, fragmentation, and misalignment of incentives are only a few. The most pressing dilemma is how this challenged system will handle the demographic wave of aging Americans. Our 21st-century population is living longer with a greater chronic disease burden than its predecessors, and has reasonable expectations of quality care. No setting portrays this challenge more clearly than that of transition: the transfer of a patient and his or her care from the hospital or facility setting to the home. Addressing this challenge requires that we adopt a set of proven effective interventions that can improve quality of care, meet the needs of the patients and families we serve, and lower the staggering economic and social burden of preventable hospital readmissions.
The Medicare system, designed in 1965, has not kept pace with the needs and challenges of the rapidly aging US population. Further, the system is not aligned with today’s—and tomorrow’s—needs. In 1965, average life expectancy for Americans was 70 years; by 2020, that average is predicted to be nearly 80 years.1 In 2000, one in eight Americans, or 12% of the US population, was aged 65 years or older.2 It is expected that by 2030, this group will represent 19% of the population. This means that in 2030, some 72 million Americans will be aged 65 or older—more than twice the number in this age group in 2000.2
The 1965 health care system focused on treating acute disease, but the health care system of the 21st century must effectively manage chronic disease. The burden of chronic disease is especially significant for aging patients, who are likely to be under the care of multiple providers and require multiple medications and ever-higher levels of professional care. The management and sequelae of chronic diseases frequently lead to impaired quality of life as well as significant expense for Medicare.
The discrepancy between our health care system and unmet needs is acutely obvious at the time of hospital discharge. In fact, the Medicare Payment Advisory Commission (MedPAC) has stated that this burden of unmet needs at hospital discharge is primarily driven by hospital admissions and readmissions.3 Thirty-day readmission rates among older Medicare beneficiaries range from 15% to 25%.4–6 Disagreement persists regarding what percentage of hospital readmissions within 30 days might be preventable. A systematic review of 34 studies has reported that, on average, 27% of readmissions were preventable.7
To address the challenge of avoidable readmissions, our home health and hospice care organization, Amedisys, Inc., developed a care transitions initiative designed to improve quality of life, improve patient outcomes, and prevent unnecessary hospital readmissions. This article, which includes an illustrative case study, describes the initiative and the outcomes observed during its first 12 months of testing.
CASE STUDY
Mrs. Smith is 84 years old and lives alone in her home. She suffers from mild to moderate dementia and heart failure (HF). Mrs. Smith’s daughter is her main caregiver, talking to Mrs. Smith multiple times a day and stopping by Mrs. Smith’s house at least two to three times a week.
Mrs. Smith was admitted to the hospital after her daughter brought her to the emergency department over the weekend because of shortness of breath. This was her third visit to the emergency department within the past year, with each visit resulting in a hospitalization. Because of questions regarding her homebound status, home health was not considered part of the care plan during either of Mrs. Smith’s previous discharges.
Hospitalists made rounds over the weekend and notified Mrs. Smith that she would be released on Tuesday morning; because of her weakness and disorientation, the hospitalist issued an order for home health and a prescription for a new HF medication. Upon hearing the news on Monday of the planned discharge, Mrs. Smith and her daughter selected the home health provider they wished to use and, within the next few hours, a care transitions coordinator (CTC) visited them in the hospital.
The CTC, a registered nurse, talked with Mrs. Smith about her illness, educating her on the impact of diet on her condition and the medications she takes, including the new medication prescribed by the hospitalist. Most importantly, the CTC talked to Mrs. Smith about her personal goals during her recovery. For example, Mrs. Smith loves to visit her granddaughter, where she spends hours at a time watching her great-grandchildren play. Mrs. Smith wants to control her HF so that she can continue these visits that bring her such joy.
Mrs. Smith’s daughter asked the CTC if she would make Mrs. Smith’s primary care physician aware of the change in medication and schedule an appointment within the next week. The CTC did so before Mrs. Smith left the hospital. She also completed a primary care discharge notification, which documented Mrs. Smith’s discharge diagnoses, discharge medications, important test results, and the date of the appointment, and e-faxed it to Mrs. Smith’s primary care physician. The CTC also communicated with the home health nurse who would care for Mrs. Smith following discharge, reviewing her clinical needs as well as her personal goals.
Mrs. Smith’s daughter was present when the home health nurse conducted the admission and in-home assessment. The home health nurse educated both Mrs. Smith and her daughter about foods that might exacerbate HF, reinforcing the education started in the hospital by the CTC. In the course of this conversation, Mrs. Smith’s daughter realized that her mother had been eating popcorn late at night when she could not sleep. The CTC helped both mother and daughter to understand that the salt in her popcorn could have an impact on Mrs. Smith’s illness that would likely result in rehospitalization and an increase in medication dosage; this educational process enhanced the patient’s understanding of her disease and likely reduced the chances of her emergency department–rehospitalization cycle continuing.
INTERVENTION
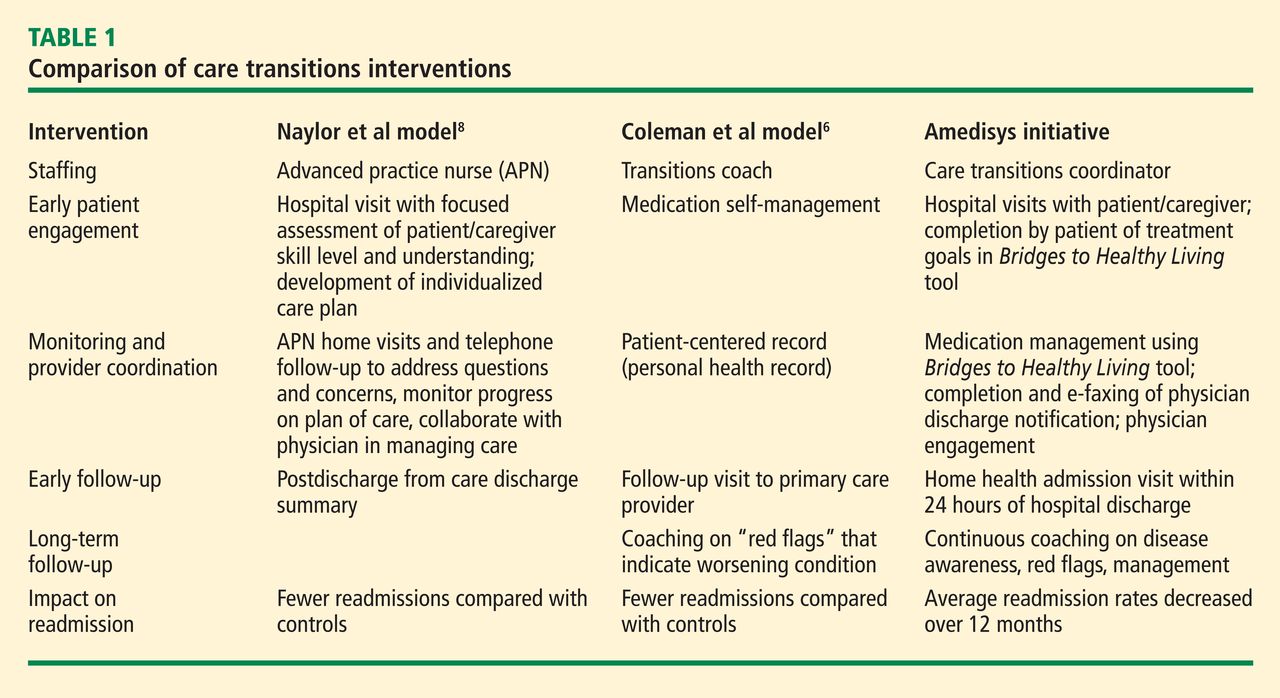
The design of the Amedisys care transitions initiative is based on work by Naylor et al8 and Coleman et al,6 who are recognized in the home health industry for their models of intervention at the time of hospital discharge. The Amedisys initiative’s objective is to prevent avoidable readmissions through patient and caregiver health coaching and care coordination, starting in the hospital and continuing through completion of the patient’s home health plan of care. Table 1 compares the essential interventions of the Naylor and Coleman models with those of the Amedisys initiative.
The Amedisys initiative includes these specific interventions:
- use of a CTC;
- early engagement of the patient, caregiver, and family with condition-specific coaching;
- careful medication management; and
- physician engagement with scheduling and reminders of physician visits early in the transition process.
Using a care transitions coordinator
Amedisys has placed CTCs in the acute care facilities that it serves. The CTC’s responsibility is to ensure that patients transition safely home from the acute care setting. With fragmentation of care, patients are most vulnerable during the initial few days postdischarge; this is particularly true for the frail elderly. Consequently, the CTC meets with the patient and caregiver as soon as possible upon his or her referral to Amedisys to plan the transition home from the facility and determine the resources needed once home. The CTC becomes the patient’s “touchpoint” for any questions or problems that arise between the time of discharge and the time when an Amedisys nurse visits the patient’s home.
Early engagement and coaching
The CTC uses a proprietary tool, Bridge to Healt0hy Living, to begin the process of early engagement, education, and coaching. This bound notebook is personalized for each patient with the CTC’s name and 24-hour phone contact information. The CTC records the patient’s diagnoses as well as social and economic barriers that may affect the patient’s outcomes. The diagnoses are written in the notebook along with a list of the patient’s medications that describes what each drug is for, its exact dosage, and instructions for taking it.
Coaching focuses on the patient’s diagnoses and capabilities, with discussion of diet and lifestyle needs and identification of “red flags” about each condition. The CTC asks the patient to describe his or her treatment goals and care plan. Ideally, the patient or a family member puts the goals and care plan in writing in the notebook in the patient’s own words; this strategy makes the goals and plan more meaningful and relevant to the patient. The CTC revisits this information at each encounter with the patient and caregiver.
Patient/family and caregiver engagement are crucial to the success of the initiative with frail, older patients.8,9 One 1998 study indicated that patient and caregiver satisfaction with home health services correlated with receiving information from the home health staff regarding medications, equipment and supplies, and self-care; further, the degree of caregiver burden was inversely related to receipt of information from the home health staff.10 The engagement required for the patient and caregiver to record the necessary information in the care transitions tool improves the likelihood of their understanding and adhering to lifestyle, behavioral, and medication recommendations.
At the time of hospital discharge, the CTC arranges the patient’s appointment with the primary care physician and records this in the patient’s notebook. The date and time for the patient’s first home nursing visit is also arranged and recorded so that the patient and caregiver know exactly when to expect that visit.
Medication management
The first home nursing visit typically occurs within 24 hours of hospital discharge. During this visit, the home health nurse reviews the Bridge to Healthy Living tool and uses it to guide care in partnership with the patient, enhancing adherence to the care plan. The nurse reviews the patient’s medications, checks them against the hospital discharge list, and then asks about other medications that might be in a cabinet or the refrigerator that the patient might be taking. At each subsequent visit, the nurse reviews the medication list and adjusts it as indicated if the patient’s physicians have changed any medication. If there has been a medication change, this is communicated by the home health nurse to all physicians caring for the patient.
The initial home nursing visit includes an environmental assessment with observation for hazards that could increase the risk for falls or other injury. The nurse also reinforces coaching on medications, red flags, and dietary or lifestyle issues that was begun by the CTC in the hospital.
Physician engagement
Physician engagement in the transition process is critical to reducing avoidable rehospitalizations. Coleman’s work has emphasized the need for the patient to follow up with his or her primary care physician within 1 week of discharge; but too frequently, the primary care physician is unaware that the patient was admitted to the hospital, and discharge summaries may take weeks to arrive. The care transitions initiative is a relationship-based, physician-led care delivery model in which the CTC serves as the funnel for information-sharing among all providers engaged with the patient. Although the CTC functions as the information manager, a successful transition requires an unprecedented level of cooperation among physicians and other health care providers. Health care is changing; outcomes must improve and costs must decrease. Therefore, this level of cooperation is no longer optional, but has become mandatory.
OUTCOMES
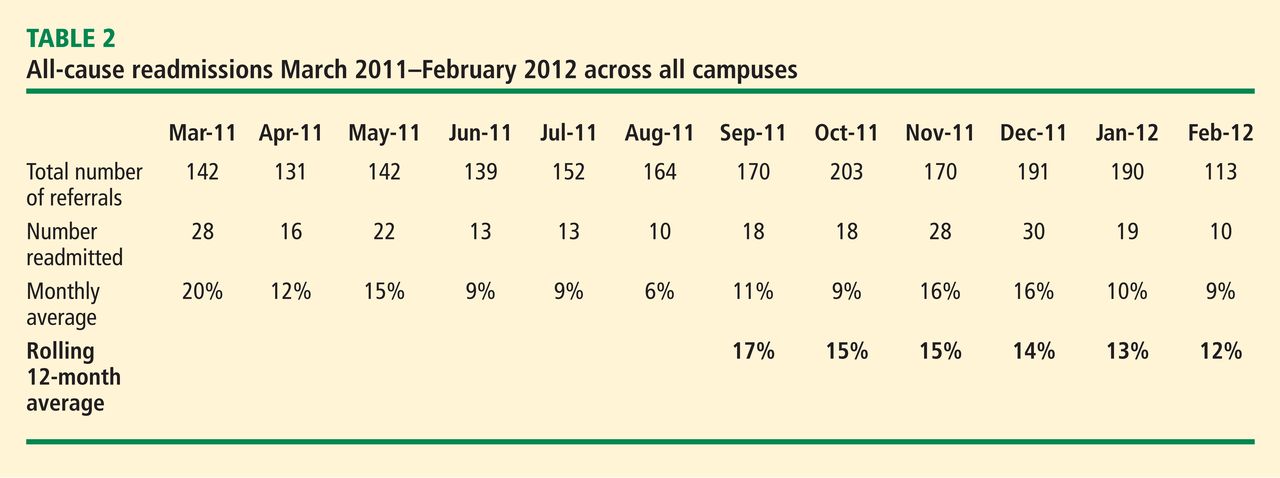
The primary outcome measure in the care transitions initiative was the rate of nonelective rehospitalization related to any cause, recurrence, or exacerbation of the index hospitalization diagnosis-related group, comorbid conditions, or new health problems. The Amedisys care transitions initiative was tested in three large, academic institutions in the northeast and southeast United States for 12 months. The 12-month average readmission rate (as calculated month by month) in the last 6 months of the study decreased from 17% to 12% (Table 2). During this period both patient and physician satisfaction were enhanced, according to internal survey data.
CALL TO ACTION
Americans want to live in their own homes as long as possible. In fact, when elderly Americans are admitted to a hospital, what is actually occurring is that they are being “discharged from their communities.”11 A health care delivery system that provides a true patient-centered approach to care recognizes that this situation often compounds issues of health care costs and quality. Adequate transitional care can provide simpler and more cost-effective options. If a CTC and follow-up care at home had been provided to Mrs. Smith and her daughter upon the first emergency room visit earlier in the year (see “Case study,” page e-S2), Mrs. Smith might have avoided multiple costly readmissions. Each member of the home health industry and its partners should be required to provide a basic set of evidence-based care transition elements to the patients they serve. By coordinating care at the time of discharge, some of the fragmentation that has become embedded in our system might be overcome.
- Life expectancy—United States. Data360 Web site. http://www.data360.org/dsg.aspx?Data_Set_Group_Id=195. Accessed August 15, 2012.
- Aging statistics. Administration on Aging Web site. http://www.aoa.gov/aoaroot/aging_statistics/index.aspx. Updated September 1, 2011. Accessed August 15, 2012.
- Report to the Congress. Medicare Payment Policy. Medicare Payment Advisory Commission Web site. http://medpac.gov/documents/Mar08_EntireReport.pdf. Published March 2008. Accessed August 15, 2012.
- Coleman EA, Min S, Chomiak A, Kramer AM. Post-hospital care transitions: patterns, complications, and risk identification. Health Serv Res 2004; 39:1449–1465.
- Quality initiatives—general information. Centers for Medicare & Medicaid Services Web site. http://www.cms.hhs.gov/QualityInitiativesGenInfo/15_MQMS.asp. Updated April 4, 2012. Accessed August 15, 2012.
- Coleman EA, Parry C, Chalmers S, Min SJ. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med 2006; 166:1822–1828.
- van Walraven C, Bennett C, Jennings A, Austin PC, Forster AJ. Proportion of hospital readmissions deemed avoidable: a systematic review [published online ahead of print]. CMAJ 2011; 183:E391–E402. 10.1503/cmaj.101860
- Naylor MD, Brooten D, Campbell R, et al. Comprehensive discharge planning and home follow-up of hospitalized elders: a randomized clinical trial. JAMA 1999; 281:613–620.
- Coleman EA, Smith JD, Frank JC, Min S, Parry C, Kramer AM. Preparing patients and caregivers to participate in care delivered across settings: the Care Transitions Intervention. J Am Geriatr Soc 2004; 52:1817–1825.
- Weaver FM, Perloff L, Waters T. Patients’ and caregivers’ transition from hospital to home: needs and recommendations. Home Health Care Serv Q 1998; 17:27–48.
- Fleming MO. The value of healthcare at home. Presented at: American Osteopathic Visiting Professorship, Louisiana State University Health System; April 12, 2012; New Orleans, LA.
The US health care system faces many challenges. Quality, cost, access, fragmentation, and misalignment of incentives are only a few. The most pressing dilemma is how this challenged system will handle the demographic wave of aging Americans. Our 21st-century population is living longer with a greater chronic disease burden than its predecessors, and has reasonable expectations of quality care. No setting portrays this challenge more clearly than that of transition: the transfer of a patient and his or her care from the hospital or facility setting to the home. Addressing this challenge requires that we adopt a set of proven effective interventions that can improve quality of care, meet the needs of the patients and families we serve, and lower the staggering economic and social burden of preventable hospital readmissions.
The Medicare system, designed in 1965, has not kept pace with the needs and challenges of the rapidly aging US population. Further, the system is not aligned with today’s—and tomorrow’s—needs. In 1965, average life expectancy for Americans was 70 years; by 2020, that average is predicted to be nearly 80 years.1 In 2000, one in eight Americans, or 12% of the US population, was aged 65 years or older.2 It is expected that by 2030, this group will represent 19% of the population. This means that in 2030, some 72 million Americans will be aged 65 or older—more than twice the number in this age group in 2000.2
The 1965 health care system focused on treating acute disease, but the health care system of the 21st century must effectively manage chronic disease. The burden of chronic disease is especially significant for aging patients, who are likely to be under the care of multiple providers and require multiple medications and ever-higher levels of professional care. The management and sequelae of chronic diseases frequently lead to impaired quality of life as well as significant expense for Medicare.
The discrepancy between our health care system and unmet needs is acutely obvious at the time of hospital discharge. In fact, the Medicare Payment Advisory Commission (MedPAC) has stated that this burden of unmet needs at hospital discharge is primarily driven by hospital admissions and readmissions.3 Thirty-day readmission rates among older Medicare beneficiaries range from 15% to 25%.4–6 Disagreement persists regarding what percentage of hospital readmissions within 30 days might be preventable. A systematic review of 34 studies has reported that, on average, 27% of readmissions were preventable.7
To address the challenge of avoidable readmissions, our home health and hospice care organization, Amedisys, Inc., developed a care transitions initiative designed to improve quality of life, improve patient outcomes, and prevent unnecessary hospital readmissions. This article, which includes an illustrative case study, describes the initiative and the outcomes observed during its first 12 months of testing.
CASE STUDY
Mrs. Smith is 84 years old and lives alone in her home. She suffers from mild to moderate dementia and heart failure (HF). Mrs. Smith’s daughter is her main caregiver, talking to Mrs. Smith multiple times a day and stopping by Mrs. Smith’s house at least two to three times a week.
Mrs. Smith was admitted to the hospital after her daughter brought her to the emergency department over the weekend because of shortness of breath. This was her third visit to the emergency department within the past year, with each visit resulting in a hospitalization. Because of questions regarding her homebound status, home health was not considered part of the care plan during either of Mrs. Smith’s previous discharges.
Hospitalists made rounds over the weekend and notified Mrs. Smith that she would be released on Tuesday morning; because of her weakness and disorientation, the hospitalist issued an order for home health and a prescription for a new HF medication. Upon hearing the news on Monday of the planned discharge, Mrs. Smith and her daughter selected the home health provider they wished to use and, within the next few hours, a care transitions coordinator (CTC) visited them in the hospital.
The CTC, a registered nurse, talked with Mrs. Smith about her illness, educating her on the impact of diet on her condition and the medications she takes, including the new medication prescribed by the hospitalist. Most importantly, the CTC talked to Mrs. Smith about her personal goals during her recovery. For example, Mrs. Smith loves to visit her granddaughter, where she spends hours at a time watching her great-grandchildren play. Mrs. Smith wants to control her HF so that she can continue these visits that bring her such joy.
Mrs. Smith’s daughter asked the CTC if she would make Mrs. Smith’s primary care physician aware of the change in medication and schedule an appointment within the next week. The CTC did so before Mrs. Smith left the hospital. She also completed a primary care discharge notification, which documented Mrs. Smith’s discharge diagnoses, discharge medications, important test results, and the date of the appointment, and e-faxed it to Mrs. Smith’s primary care physician. The CTC also communicated with the home health nurse who would care for Mrs. Smith following discharge, reviewing her clinical needs as well as her personal goals.
Mrs. Smith’s daughter was present when the home health nurse conducted the admission and in-home assessment. The home health nurse educated both Mrs. Smith and her daughter about foods that might exacerbate HF, reinforcing the education started in the hospital by the CTC. In the course of this conversation, Mrs. Smith’s daughter realized that her mother had been eating popcorn late at night when she could not sleep. The CTC helped both mother and daughter to understand that the salt in her popcorn could have an impact on Mrs. Smith’s illness that would likely result in rehospitalization and an increase in medication dosage; this educational process enhanced the patient’s understanding of her disease and likely reduced the chances of her emergency department–rehospitalization cycle continuing.
INTERVENTION
The design of the Amedisys care transitions initiative is based on work by Naylor et al8 and Coleman et al,6 who are recognized in the home health industry for their models of intervention at the time of hospital discharge. The Amedisys initiative’s objective is to prevent avoidable readmissions through patient and caregiver health coaching and care coordination, starting in the hospital and continuing through completion of the patient’s home health plan of care. Table 1 compares the essential interventions of the Naylor and Coleman models with those of the Amedisys initiative.
The Amedisys initiative includes these specific interventions:
- use of a CTC;
- early engagement of the patient, caregiver, and family with condition-specific coaching;
- careful medication management; and
- physician engagement with scheduling and reminders of physician visits early in the transition process.
Using a care transitions coordinator
Amedisys has placed CTCs in the acute care facilities that it serves. The CTC’s responsibility is to ensure that patients transition safely home from the acute care setting. With fragmentation of care, patients are most vulnerable during the initial few days postdischarge; this is particularly true for the frail elderly. Consequently, the CTC meets with the patient and caregiver as soon as possible upon his or her referral to Amedisys to plan the transition home from the facility and determine the resources needed once home. The CTC becomes the patient’s “touchpoint” for any questions or problems that arise between the time of discharge and the time when an Amedisys nurse visits the patient’s home.
Early engagement and coaching
The CTC uses a proprietary tool, Bridge to Healt0hy Living, to begin the process of early engagement, education, and coaching. This bound notebook is personalized for each patient with the CTC’s name and 24-hour phone contact information. The CTC records the patient’s diagnoses as well as social and economic barriers that may affect the patient’s outcomes. The diagnoses are written in the notebook along with a list of the patient’s medications that describes what each drug is for, its exact dosage, and instructions for taking it.
Coaching focuses on the patient’s diagnoses and capabilities, with discussion of diet and lifestyle needs and identification of “red flags” about each condition. The CTC asks the patient to describe his or her treatment goals and care plan. Ideally, the patient or a family member puts the goals and care plan in writing in the notebook in the patient’s own words; this strategy makes the goals and plan more meaningful and relevant to the patient. The CTC revisits this information at each encounter with the patient and caregiver.
Patient/family and caregiver engagement are crucial to the success of the initiative with frail, older patients.8,9 One 1998 study indicated that patient and caregiver satisfaction with home health services correlated with receiving information from the home health staff regarding medications, equipment and supplies, and self-care; further, the degree of caregiver burden was inversely related to receipt of information from the home health staff.10 The engagement required for the patient and caregiver to record the necessary information in the care transitions tool improves the likelihood of their understanding and adhering to lifestyle, behavioral, and medication recommendations.
At the time of hospital discharge, the CTC arranges the patient’s appointment with the primary care physician and records this in the patient’s notebook. The date and time for the patient’s first home nursing visit is also arranged and recorded so that the patient and caregiver know exactly when to expect that visit.
Medication management
The first home nursing visit typically occurs within 24 hours of hospital discharge. During this visit, the home health nurse reviews the Bridge to Healthy Living tool and uses it to guide care in partnership with the patient, enhancing adherence to the care plan. The nurse reviews the patient’s medications, checks them against the hospital discharge list, and then asks about other medications that might be in a cabinet or the refrigerator that the patient might be taking. At each subsequent visit, the nurse reviews the medication list and adjusts it as indicated if the patient’s physicians have changed any medication. If there has been a medication change, this is communicated by the home health nurse to all physicians caring for the patient.
The initial home nursing visit includes an environmental assessment with observation for hazards that could increase the risk for falls or other injury. The nurse also reinforces coaching on medications, red flags, and dietary or lifestyle issues that was begun by the CTC in the hospital.
Physician engagement
Physician engagement in the transition process is critical to reducing avoidable rehospitalizations. Coleman’s work has emphasized the need for the patient to follow up with his or her primary care physician within 1 week of discharge; but too frequently, the primary care physician is unaware that the patient was admitted to the hospital, and discharge summaries may take weeks to arrive. The care transitions initiative is a relationship-based, physician-led care delivery model in which the CTC serves as the funnel for information-sharing among all providers engaged with the patient. Although the CTC functions as the information manager, a successful transition requires an unprecedented level of cooperation among physicians and other health care providers. Health care is changing; outcomes must improve and costs must decrease. Therefore, this level of cooperation is no longer optional, but has become mandatory.
OUTCOMES
The primary outcome measure in the care transitions initiative was the rate of nonelective rehospitalization related to any cause, recurrence, or exacerbation of the index hospitalization diagnosis-related group, comorbid conditions, or new health problems. The Amedisys care transitions initiative was tested in three large, academic institutions in the northeast and southeast United States for 12 months. The 12-month average readmission rate (as calculated month by month) in the last 6 months of the study decreased from 17% to 12% (Table 2). During this period both patient and physician satisfaction were enhanced, according to internal survey data.
CALL TO ACTION
Americans want to live in their own homes as long as possible. In fact, when elderly Americans are admitted to a hospital, what is actually occurring is that they are being “discharged from their communities.”11 A health care delivery system that provides a true patient-centered approach to care recognizes that this situation often compounds issues of health care costs and quality. Adequate transitional care can provide simpler and more cost-effective options. If a CTC and follow-up care at home had been provided to Mrs. Smith and her daughter upon the first emergency room visit earlier in the year (see “Case study,” page e-S2), Mrs. Smith might have avoided multiple costly readmissions. Each member of the home health industry and its partners should be required to provide a basic set of evidence-based care transition elements to the patients they serve. By coordinating care at the time of discharge, some of the fragmentation that has become embedded in our system might be overcome.
The US health care system faces many challenges. Quality, cost, access, fragmentation, and misalignment of incentives are only a few. The most pressing dilemma is how this challenged system will handle the demographic wave of aging Americans. Our 21st-century population is living longer with a greater chronic disease burden than its predecessors, and has reasonable expectations of quality care. No setting portrays this challenge more clearly than that of transition: the transfer of a patient and his or her care from the hospital or facility setting to the home. Addressing this challenge requires that we adopt a set of proven effective interventions that can improve quality of care, meet the needs of the patients and families we serve, and lower the staggering economic and social burden of preventable hospital readmissions.
The Medicare system, designed in 1965, has not kept pace with the needs and challenges of the rapidly aging US population. Further, the system is not aligned with today’s—and tomorrow’s—needs. In 1965, average life expectancy for Americans was 70 years; by 2020, that average is predicted to be nearly 80 years.1 In 2000, one in eight Americans, or 12% of the US population, was aged 65 years or older.2 It is expected that by 2030, this group will represent 19% of the population. This means that in 2030, some 72 million Americans will be aged 65 or older—more than twice the number in this age group in 2000.2
The 1965 health care system focused on treating acute disease, but the health care system of the 21st century must effectively manage chronic disease. The burden of chronic disease is especially significant for aging patients, who are likely to be under the care of multiple providers and require multiple medications and ever-higher levels of professional care. The management and sequelae of chronic diseases frequently lead to impaired quality of life as well as significant expense for Medicare.
The discrepancy between our health care system and unmet needs is acutely obvious at the time of hospital discharge. In fact, the Medicare Payment Advisory Commission (MedPAC) has stated that this burden of unmet needs at hospital discharge is primarily driven by hospital admissions and readmissions.3 Thirty-day readmission rates among older Medicare beneficiaries range from 15% to 25%.4–6 Disagreement persists regarding what percentage of hospital readmissions within 30 days might be preventable. A systematic review of 34 studies has reported that, on average, 27% of readmissions were preventable.7
To address the challenge of avoidable readmissions, our home health and hospice care organization, Amedisys, Inc., developed a care transitions initiative designed to improve quality of life, improve patient outcomes, and prevent unnecessary hospital readmissions. This article, which includes an illustrative case study, describes the initiative and the outcomes observed during its first 12 months of testing.
CASE STUDY
Mrs. Smith is 84 years old and lives alone in her home. She suffers from mild to moderate dementia and heart failure (HF). Mrs. Smith’s daughter is her main caregiver, talking to Mrs. Smith multiple times a day and stopping by Mrs. Smith’s house at least two to three times a week.
Mrs. Smith was admitted to the hospital after her daughter brought her to the emergency department over the weekend because of shortness of breath. This was her third visit to the emergency department within the past year, with each visit resulting in a hospitalization. Because of questions regarding her homebound status, home health was not considered part of the care plan during either of Mrs. Smith’s previous discharges.
Hospitalists made rounds over the weekend and notified Mrs. Smith that she would be released on Tuesday morning; because of her weakness and disorientation, the hospitalist issued an order for home health and a prescription for a new HF medication. Upon hearing the news on Monday of the planned discharge, Mrs. Smith and her daughter selected the home health provider they wished to use and, within the next few hours, a care transitions coordinator (CTC) visited them in the hospital.
The CTC, a registered nurse, talked with Mrs. Smith about her illness, educating her on the impact of diet on her condition and the medications she takes, including the new medication prescribed by the hospitalist. Most importantly, the CTC talked to Mrs. Smith about her personal goals during her recovery. For example, Mrs. Smith loves to visit her granddaughter, where she spends hours at a time watching her great-grandchildren play. Mrs. Smith wants to control her HF so that she can continue these visits that bring her such joy.
Mrs. Smith’s daughter asked the CTC if she would make Mrs. Smith’s primary care physician aware of the change in medication and schedule an appointment within the next week. The CTC did so before Mrs. Smith left the hospital. She also completed a primary care discharge notification, which documented Mrs. Smith’s discharge diagnoses, discharge medications, important test results, and the date of the appointment, and e-faxed it to Mrs. Smith’s primary care physician. The CTC also communicated with the home health nurse who would care for Mrs. Smith following discharge, reviewing her clinical needs as well as her personal goals.
Mrs. Smith’s daughter was present when the home health nurse conducted the admission and in-home assessment. The home health nurse educated both Mrs. Smith and her daughter about foods that might exacerbate HF, reinforcing the education started in the hospital by the CTC. In the course of this conversation, Mrs. Smith’s daughter realized that her mother had been eating popcorn late at night when she could not sleep. The CTC helped both mother and daughter to understand that the salt in her popcorn could have an impact on Mrs. Smith’s illness that would likely result in rehospitalization and an increase in medication dosage; this educational process enhanced the patient’s understanding of her disease and likely reduced the chances of her emergency department–rehospitalization cycle continuing.
INTERVENTION
The design of the Amedisys care transitions initiative is based on work by Naylor et al8 and Coleman et al,6 who are recognized in the home health industry for their models of intervention at the time of hospital discharge. The Amedisys initiative’s objective is to prevent avoidable readmissions through patient and caregiver health coaching and care coordination, starting in the hospital and continuing through completion of the patient’s home health plan of care. Table 1 compares the essential interventions of the Naylor and Coleman models with those of the Amedisys initiative.
The Amedisys initiative includes these specific interventions:
- use of a CTC;
- early engagement of the patient, caregiver, and family with condition-specific coaching;
- careful medication management; and
- physician engagement with scheduling and reminders of physician visits early in the transition process.
Using a care transitions coordinator
Amedisys has placed CTCs in the acute care facilities that it serves. The CTC’s responsibility is to ensure that patients transition safely home from the acute care setting. With fragmentation of care, patients are most vulnerable during the initial few days postdischarge; this is particularly true for the frail elderly. Consequently, the CTC meets with the patient and caregiver as soon as possible upon his or her referral to Amedisys to plan the transition home from the facility and determine the resources needed once home. The CTC becomes the patient’s “touchpoint” for any questions or problems that arise between the time of discharge and the time when an Amedisys nurse visits the patient’s home.
Early engagement and coaching
The CTC uses a proprietary tool, Bridge to Healt0hy Living, to begin the process of early engagement, education, and coaching. This bound notebook is personalized for each patient with the CTC’s name and 24-hour phone contact information. The CTC records the patient’s diagnoses as well as social and economic barriers that may affect the patient’s outcomes. The diagnoses are written in the notebook along with a list of the patient’s medications that describes what each drug is for, its exact dosage, and instructions for taking it.
Coaching focuses on the patient’s diagnoses and capabilities, with discussion of diet and lifestyle needs and identification of “red flags” about each condition. The CTC asks the patient to describe his or her treatment goals and care plan. Ideally, the patient or a family member puts the goals and care plan in writing in the notebook in the patient’s own words; this strategy makes the goals and plan more meaningful and relevant to the patient. The CTC revisits this information at each encounter with the patient and caregiver.
Patient/family and caregiver engagement are crucial to the success of the initiative with frail, older patients.8,9 One 1998 study indicated that patient and caregiver satisfaction with home health services correlated with receiving information from the home health staff regarding medications, equipment and supplies, and self-care; further, the degree of caregiver burden was inversely related to receipt of information from the home health staff.10 The engagement required for the patient and caregiver to record the necessary information in the care transitions tool improves the likelihood of their understanding and adhering to lifestyle, behavioral, and medication recommendations.
At the time of hospital discharge, the CTC arranges the patient’s appointment with the primary care physician and records this in the patient’s notebook. The date and time for the patient’s first home nursing visit is also arranged and recorded so that the patient and caregiver know exactly when to expect that visit.
Medication management
The first home nursing visit typically occurs within 24 hours of hospital discharge. During this visit, the home health nurse reviews the Bridge to Healthy Living tool and uses it to guide care in partnership with the patient, enhancing adherence to the care plan. The nurse reviews the patient’s medications, checks them against the hospital discharge list, and then asks about other medications that might be in a cabinet or the refrigerator that the patient might be taking. At each subsequent visit, the nurse reviews the medication list and adjusts it as indicated if the patient’s physicians have changed any medication. If there has been a medication change, this is communicated by the home health nurse to all physicians caring for the patient.
The initial home nursing visit includes an environmental assessment with observation for hazards that could increase the risk for falls or other injury. The nurse also reinforces coaching on medications, red flags, and dietary or lifestyle issues that was begun by the CTC in the hospital.
Physician engagement
Physician engagement in the transition process is critical to reducing avoidable rehospitalizations. Coleman’s work has emphasized the need for the patient to follow up with his or her primary care physician within 1 week of discharge; but too frequently, the primary care physician is unaware that the patient was admitted to the hospital, and discharge summaries may take weeks to arrive. The care transitions initiative is a relationship-based, physician-led care delivery model in which the CTC serves as the funnel for information-sharing among all providers engaged with the patient. Although the CTC functions as the information manager, a successful transition requires an unprecedented level of cooperation among physicians and other health care providers. Health care is changing; outcomes must improve and costs must decrease. Therefore, this level of cooperation is no longer optional, but has become mandatory.
OUTCOMES
The primary outcome measure in the care transitions initiative was the rate of nonelective rehospitalization related to any cause, recurrence, or exacerbation of the index hospitalization diagnosis-related group, comorbid conditions, or new health problems. The Amedisys care transitions initiative was tested in three large, academic institutions in the northeast and southeast United States for 12 months. The 12-month average readmission rate (as calculated month by month) in the last 6 months of the study decreased from 17% to 12% (Table 2). During this period both patient and physician satisfaction were enhanced, according to internal survey data.
CALL TO ACTION
Americans want to live in their own homes as long as possible. In fact, when elderly Americans are admitted to a hospital, what is actually occurring is that they are being “discharged from their communities.”11 A health care delivery system that provides a true patient-centered approach to care recognizes that this situation often compounds issues of health care costs and quality. Adequate transitional care can provide simpler and more cost-effective options. If a CTC and follow-up care at home had been provided to Mrs. Smith and her daughter upon the first emergency room visit earlier in the year (see “Case study,” page e-S2), Mrs. Smith might have avoided multiple costly readmissions. Each member of the home health industry and its partners should be required to provide a basic set of evidence-based care transition elements to the patients they serve. By coordinating care at the time of discharge, some of the fragmentation that has become embedded in our system might be overcome.
- Life expectancy—United States. Data360 Web site. http://www.data360.org/dsg.aspx?Data_Set_Group_Id=195. Accessed August 15, 2012.
- Aging statistics. Administration on Aging Web site. http://www.aoa.gov/aoaroot/aging_statistics/index.aspx. Updated September 1, 2011. Accessed August 15, 2012.
- Report to the Congress. Medicare Payment Policy. Medicare Payment Advisory Commission Web site. http://medpac.gov/documents/Mar08_EntireReport.pdf. Published March 2008. Accessed August 15, 2012.
- Coleman EA, Min S, Chomiak A, Kramer AM. Post-hospital care transitions: patterns, complications, and risk identification. Health Serv Res 2004; 39:1449–1465.
- Quality initiatives—general information. Centers for Medicare & Medicaid Services Web site. http://www.cms.hhs.gov/QualityInitiativesGenInfo/15_MQMS.asp. Updated April 4, 2012. Accessed August 15, 2012.
- Coleman EA, Parry C, Chalmers S, Min SJ. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med 2006; 166:1822–1828.
- van Walraven C, Bennett C, Jennings A, Austin PC, Forster AJ. Proportion of hospital readmissions deemed avoidable: a systematic review [published online ahead of print]. CMAJ 2011; 183:E391–E402. 10.1503/cmaj.101860
- Naylor MD, Brooten D, Campbell R, et al. Comprehensive discharge planning and home follow-up of hospitalized elders: a randomized clinical trial. JAMA 1999; 281:613–620.
- Coleman EA, Smith JD, Frank JC, Min S, Parry C, Kramer AM. Preparing patients and caregivers to participate in care delivered across settings: the Care Transitions Intervention. J Am Geriatr Soc 2004; 52:1817–1825.
- Weaver FM, Perloff L, Waters T. Patients’ and caregivers’ transition from hospital to home: needs and recommendations. Home Health Care Serv Q 1998; 17:27–48.
- Fleming MO. The value of healthcare at home. Presented at: American Osteopathic Visiting Professorship, Louisiana State University Health System; April 12, 2012; New Orleans, LA.
- Life expectancy—United States. Data360 Web site. http://www.data360.org/dsg.aspx?Data_Set_Group_Id=195. Accessed August 15, 2012.
- Aging statistics. Administration on Aging Web site. http://www.aoa.gov/aoaroot/aging_statistics/index.aspx. Updated September 1, 2011. Accessed August 15, 2012.
- Report to the Congress. Medicare Payment Policy. Medicare Payment Advisory Commission Web site. http://medpac.gov/documents/Mar08_EntireReport.pdf. Published March 2008. Accessed August 15, 2012.
- Coleman EA, Min S, Chomiak A, Kramer AM. Post-hospital care transitions: patterns, complications, and risk identification. Health Serv Res 2004; 39:1449–1465.
- Quality initiatives—general information. Centers for Medicare & Medicaid Services Web site. http://www.cms.hhs.gov/QualityInitiativesGenInfo/15_MQMS.asp. Updated April 4, 2012. Accessed August 15, 2012.
- Coleman EA, Parry C, Chalmers S, Min SJ. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med 2006; 166:1822–1828.
- van Walraven C, Bennett C, Jennings A, Austin PC, Forster AJ. Proportion of hospital readmissions deemed avoidable: a systematic review [published online ahead of print]. CMAJ 2011; 183:E391–E402. 10.1503/cmaj.101860
- Naylor MD, Brooten D, Campbell R, et al. Comprehensive discharge planning and home follow-up of hospitalized elders: a randomized clinical trial. JAMA 1999; 281:613–620.
- Coleman EA, Smith JD, Frank JC, Min S, Parry C, Kramer AM. Preparing patients and caregivers to participate in care delivered across settings: the Care Transitions Intervention. J Am Geriatr Soc 2004; 52:1817–1825.
- Weaver FM, Perloff L, Waters T. Patients’ and caregivers’ transition from hospital to home: needs and recommendations. Home Health Care Serv Q 1998; 17:27–48.
- Fleming MO. The value of healthcare at home. Presented at: American Osteopathic Visiting Professorship, Louisiana State University Health System; April 12, 2012; New Orleans, LA.