User login
Evaluation of Health Professions Trainee Experiences Transitioning to New VHA Electronic Health Record
The Veterans Health Administration (VHA) is transitioning from its native electronic health record (EHR) Vista/Computerized Patient Record System to the commercial Cerner/Oracle Health EHR. Though this process was temporarily discontinued in April 2023 due to patient safety, usability, and reliability concerns, it resumed in April 2026. It was originally projected to cost $50 billion to implement. 1-3 As of March 9, 2024, 6 sites had transitioned to the new EHR.2 The transition is the largest of its kind in the US, offering an unparalleled opportunity to examine the effects of EHR transitions on an often overlooked part of the workforce: health professions trainees (HPTs).
HPTs serve a central role in VHA. About one-third of patients receive care directly from HPTs who make up about one-third of the VHA workforce. VHA trains > 60 clinical disciplines, comprising > 122,000 trainees annually.4,5 A paucity of literature exists exploring the experiences of HPTs during EHR transitions, and many studies are often limited to single-site or small populations. HPTs face distinct challenges and needs during EHR transitions and are particularly vulnerable to their negative impacts on retention, clinical training, and efficiency and confidence in EHR use.6-10 HPTs at VHA sites that have already transitioned to the Cerner/Oracle Health EHR identified many challenges, including significant delays in gaining EHR access, pervasive perceptions of poor training, concerns that EHR functionality issues limited patient care, and decreased ability to track clinical skill acquisition.6 These challenges may impact some HPTs more than others (eg, students on short rotations are affected more acutely by delayed EHR access and usage).
This quality improvement project evaluated HPT EHR transition experiences at the Captain James A. Lovell Federal Health Care Center (FHCC). This article contributes to the limited literature on HPT transition experiences, identifies opportunities to support HPTs, and informs broader efforts in teaching HPTs new technologies.
Methods
FHCC is jointly operated by the US Department of Defense and US Department of Veterans Affairs (VA). It treats 80,000 inpatient and outpatients annually. FHCC was the sixth VA facility to transition to the new EHR, which went live on March 9, 2024.2,11 About 700 HPTs rotate through FHCC annually. HPTs were eligible for inclusion if they were present during the March 9 transition according to a VA Office of Academic Affiliations database. A total of 216 HPTs were identified for inclusion.
Preparations for the transition included scaling down operations (ie, blocking clinician schedules, not scheduling future appointments that may conflict with the transition, making decisions on new facility- and service-line workflows, required EHR training, and speaking with support staff, including VHA National EHR Modernization Supplemental Staffing Unit [NESSU]). This evaluation was designated nonresearch/quality improvement by the VA Bedford Healthcare System Institutional Review Board.
Surveys
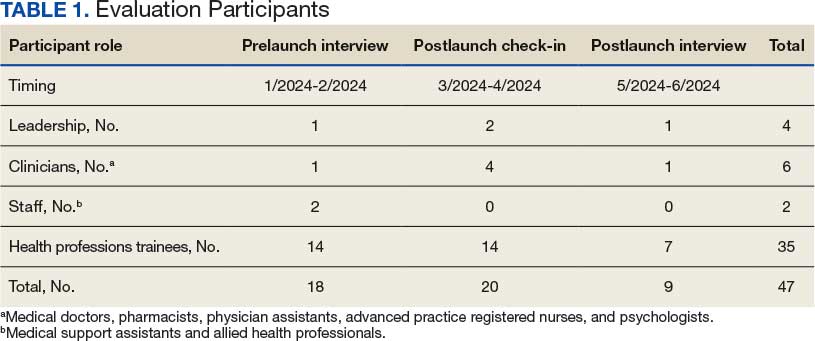
Forty-seven interviews were conducted with HPTs, site leaders, and supervisors from January 2024 to June 2024 (Table 1). Participants were identified by service leads and recruited via email; snowball sampling identified additional participants.
The evaluation team developed semistructured interview guides using grounded probes based on a pilot evaluation and existing research on EHR transitions.12 Questions focused on participant experiences preparing for the EHR transition, learning and using the site’s EHR, and the impact the transition had on clinical training experiences. Interviews were conducted at different times to capture the range of user experiences: 1 month prelaunch, 2 to 6 weeks postlaunch, and 2 months postlaunch. Interviewees were informed of participant rights and provided verbal consent.
HPTs present at FHCC at each survey’s release were emailed invitations and 2 reminders. The anonymous surveys took about 10 minutes to complete. Survey items queried HPTs about their experiences preparing to use the new EHR, perceptions of the current EHR (adapted from the System Usability Scale), satisfaction with VHA training, impact on clinical training, ability to work with preceptors and patients, and experiences with the VHA clinical learning environment (adapted from the VHA Learners Preceptor Survey).13-15 Survey questions used a 5-point Likert response scale.
Analysis
Interviewers completed postinterview summaries for team debriefing and consensus building. Interviews were coded using a priori (from piloting evaluations and relevant literature) and emergent (refined and developed from data) codes. Deductive and inductive content analyses were conducted. 16 Deductive analysis used a priori categories (eg, care coordination, EHR training). Inductive content analysis consisted of open and unstructured coding, capturing data outside a priori categories. Emergent codes captured unidentified categories. Qualitative researchers met weekly to discuss data and reach consensus on interpretation.
Descriptive analysis was conducted using top-2 box scoring (proportion responding within the 2 most favorable responses [agree/ strongly agree]). Survey data were analyzed in SAS.17 The analysis used a merging approach on simultaneously collected qualitative and quantitative data to reach findings consensus.18
Researcher and research team decisions may shape the data collected due to prior assumptions and experience.19 This analysis attempted to integrate reflexivity practices to enhance awareness of the researchers’ assumptions and positionality, including by integrating intent collaborative conversing and memorandum writing into the processes.20,21
Results
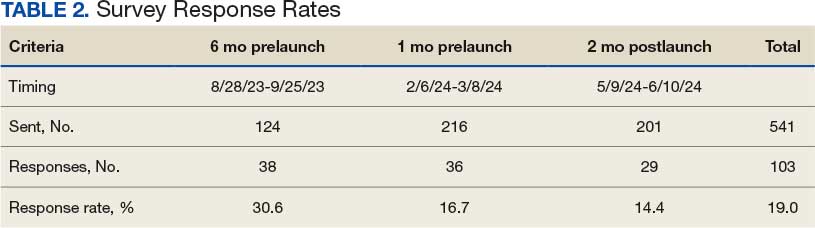
This analysis created a survey and fielded responses from HPTs present at FHCC across 3 time points (6 months prelaunch, 1 month prelaunch, and 2 months postlaunch), resulting in a total of 103 responses and an average response rate of 19.0% (Table 2). Six key findings were identified in analysis of responses: (1) critiques of transition management; (2) concerns with training; (3) hope about the EHR; (4) at-the-elbow support was essential; (5) HPTs adjusted to, and later preferred, the new EHR; and (6) transition impacted clinical training, but not overall career plans for HPTs. Findings are presented in this section, with illustrative quantitative data and qualitative data quotes available in the eAppendix.
Critiques of the Transition’s Management
While participants were aware of the transition to the new EHR, most felt they did not have enough information or time to prepare for it, indicating it was “too little, too late.” HPTs felt necessary workflow processes for Cerner/Oracle Health were not determined with enough time to learn them prior to transition. Supervisors shared that important workflow and onboarding decisions remained undecided mere weeks before the transition. Some service lines did not decrease patient loads until right before the transition, making it difficult to manage their schedules and resulting in insufficient time to learn the new EHR.
EHR Training Concerns
Overall, HPTs expressed low satisfaction with computer-based Training Management System (TMS) EHR training, believing it did not prepare them for the new EHR. The percentage of HPTs satisfied or very satisfied with the quality of TMS training was lower than that of instructor-based training pre- and posttransition, with 50% of 36 prelaunch respondents, and 43% of 29 postlaunch respondents expressing satisfaction with computer-based trainings (Figure 1). HPTs were dissatisfied with the training content. They felt it was too general and failed to teach basic tasks in the workflow for their service areas and roles, such as writing a note or order. Furthermore, poor content was exacerbated by poor and unengaging instruction, and HPTs were dissatisfied with the practice EHR used in training, which glitched frequently.
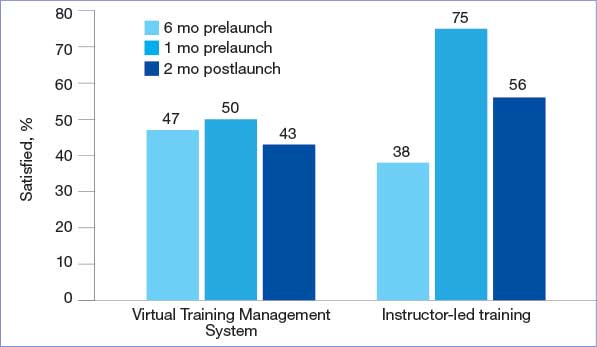
quality of electronic health record training.
EHR Transition Optimism
Even though the transition was stressful, most HPTs hoped it would be a temporary disruption and that they would quickly adjust to the new EHR. Many participants expected that once they switched to the new EHR, they would pick it up quickly. In addition, many anticipated Cerner/Oracle Health would be better and easier to use in the long run.
At-The-Elbow Support Essential
VHA peer support with NESSU was highly valued among HPTs. NESSU staff were highly knowledgeable and could provide both broad and service-line-specific support. NESSU provided prompt answers to EHR questions. This was particularly critical as other forms of in-person support were often inaccessible or absent during the transition.
HPTs found facility support helpful: 85% of 36 respondents reported being satisfied/ very satisfied with support from supervisors and preceptors, and 84% of 36 respondents were satisfied/very satisfied with technical support from facility informatics staff pretransition (n = 36) (Figure 2). NESSU and supervisor support with daily workflows were particularly helpful, as pretransition training only provided a general introduction to the EHR.
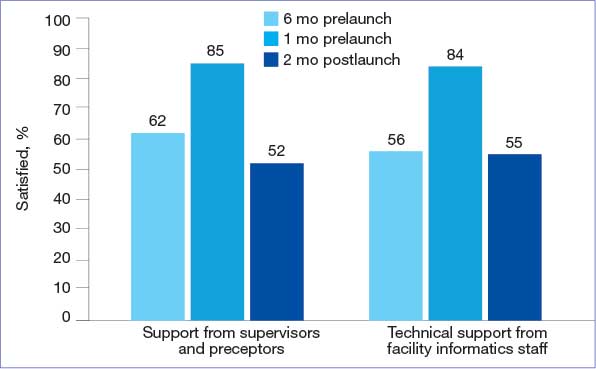
health record training.
HPTs Adjusted to and Later Preferred the New EHR
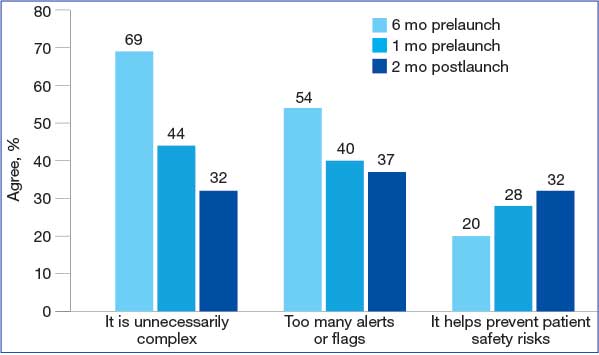
The EHR learning experience was intense but short, with many HPTs feeling able to use it only 2 to 4 weeks posttransition. Confidence grew as HPTs came to view Cerner/Oracle Health as a more integrated and intuitive system than the previous EHR. Most participants preferred the new EHR, even if they criticized some features (eg, no group documentation capabilities). Survey participants frequently rated Cerner/Oracle Health usability higher than the original. A total of 32% of 29 posttransition respondents agreed or strongly agreed that Cerner/Oracle Health helps prevent situations that can lead to patient safety risks—higher than pretransition rates. Additionally, fewer respondents found the new EHR unnecessarily complex or thought it contained too many alerts and flags compared to the original EHR (Figure 3).
health record usability.
Impact on Clinical Training, Not Career Plans
The extensive time and energy the transition demanded of HPTs caused stress and affected their clinical training. Many believed they would have learned more if their training had happened outside the transition.
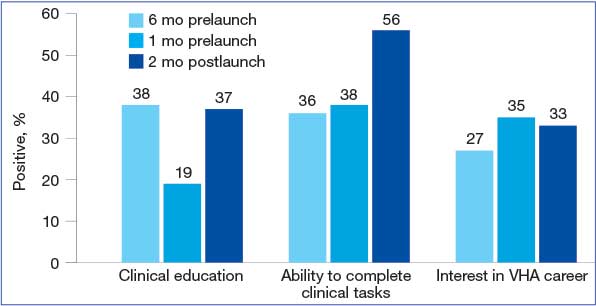
Concerns that the transition affected learning were most acutely felt pretransition. HPTs reporting that EHR implementation positively affected their clinical education fell from 38% of 36 respondents 6 months pretransition to 19% of 29 respondents 1 month pretransition, but returned to 37% posttransition (Figure 4). However, some HPTs believed there was a silver lining: it provided a learning experience they otherwise would not have had.
new Veterans Health Administration (VHA) electronic health record.
HPTs who believed the transition positively impacted their likelihood of pursuing future career opportunities within the VHA rose to 33% of 29 respondents posttransition. Overall, Cerner/Oracle Health was characterized as a tool: something used in training, but not something that precluded wanting VHA careers or having meaningful experiences, such as caring for patients.
Discussion
This evaluation addressed an underexplored aspect of EHR transitions: their impact on HPTs. It identified HPT challenges, including dissatisfaction with poor transition preparation and EHR training experiences. Promising findings include positive experiences with transition support, EHR uptake, and overall positive educational experiences despite the transition’s disruption.
When EHR users, including HPTs, are dissatisfied with transition preparations, consequent stress can lead to undesired effects, including increased burnout, inappropriate EHR use, and low work satisfaction.22-24 Negative EHR transition experiences shape HPTs’ subsequent EHR adoption, user satisfaction, as well as confidence and career intent.3,25,26 Health systems have strong incentives to implement effective transition change management.
HPTs at previous VHA EHR transition sites reported significantly more disruption to their clinical training compared with HPTs at FHCC. Academic programs were shut down at the first transition site, and HPTs expressed decreased interest in VHA careers at another, even a year posttransition.6,27 These findings are consistent with the limited literature on the adverse impacts that EHR transitions have on HPTs.7,28
HPT retention is critical. VA is mandated to prepare the next generation of HPTs for its needs, and those of the nation. The VA relies heavily on HPT retention to recruit clinicians: > 65% of VHA physicians nationwide participated in VHA training programs prior to recruitment into staff positions.5,29
VHA should invest in transition change management with demonstrated, positive impacts on HPTs, such as in-house support from clinicians. Previous research found that lack of support was a major source of stress and negative outcomes.6,27 Consequently, supporting HPTs through EHR transitions directly contributes to the VHA’s ability to attract high-quality staff from its HPTs. The challenges and promising practices described in this analysis underscore the necessity of understanding how all EHR users are affected by transitions. What happens to them has direct implications for the VA mission to provide safe, efficient care, and its mandate to provide quality clinical training to HPTs.
These findings hold hopeful implications for supporting HPT EHR use, both during and outside EHR transitions. HPTs expressing that an EHR is only 1 part of their clinical training experience suggests that change management can improve EHR transitions. HPT learning can enhance known factors that are important for HPTs in clinical training, including the health care organization’s mission, caring for patients, and personal development.
Further investigations may engage HPTs at future VHA sites making the transition to the new EHR. One focus would involve applying a learning health systems framework to examine the nature of change management efforts—and their effects on HPT transition experiences—iteratively across transition sites to evaluate the effect of the efforts. Another focus may be longitudinal engagement with HPTs at health care systems and sites transitioning to new EHRs. Research has found that disruptions to EHR usability, satisfaction, and care provision can persist for 2 years and beyond following an EHR transition.30 Evaluating the long-term effects of transitions on HPTs is of interest, given their distinct characteristics and differences from employees.
Limitations
Study data came from voluntary participants at 1 highly engaged site, raising the possibility of self-selection bias. HPT experiences at other VA and non-VA sites may differ. Employees and HPTs were engaged during a high-stress event; snowballing recruitment reach was limited by high workloads and limited time for engagement. Statistical data were descriptive and should not be interpreted as causal. Results may reflect, in part, temporal effects, and respondents include HPTs at different stages of training and with different levels of VA experience. Survey sample sizes may limit generalizability; however, merging data streams strengthened the reliability of findings.
Conclusions
The results of this analysis of FHCC HPTs were notably more positive than those of HPTs at previous VHA EHR transition sites. VHA is one of many health care systems that provide clinical training for HPTs and relies on this population to provide patient care. By highlighting challenges and positive experiences of HPTs during an EHR transition, this evaluation produces actionable insights that can inform the actions of health care systems seeking to support HPTs during disruptive EHR transitions.
- US Department of Veterans Affairs Office of the Inspector General. VA needs to strengthen controls to address electronic health record system major performance incidents. September 23, 2024. Accessed February 3, 2026. https://www.vaoig.gov/sites/default/files /reports/2024-09/vaoig-22-03591-231.pdf
- EHR deployment schedule. VA EHR Modernization. Updated February 2, 2026. Accessed February 3, 2026. https://digital.va.gov/ehr-modernization/ehr-deployment -schedule/
- Heckman J. VA in 2026 looks to get EHR rollout back on track, embark on health care reorganization. Federal News Network. December 24, 2025. Accessed February 3, 2026. https://federalnewsnetwork.com/veterans-affairs/2025/12 /va-in-2026-looks-to-get-ehr-rollout-back-on-track -embark-on-health-care-reorganization/
- US Department of Veterans Affairs Office of Academic Affiliations. Medical and dental education. Updated September 12, 2025. Accessed February 3, 2026. https://department.va.gov/academic-affiliations /medical-and-dental/
- Functions of Veterans Health Administration: health-care personnel education and training programs. 38 U.S.C. § 7302 (2026). Accessed February 3, 2026. https://uscode.house.gov/view.xhtml ?req=(title:38%20section:7302%20edition:prelim)
- Ahlness EA, Molloy-Paolillo BK, Brunner J, et al. Impacts of an electronic health record transition on Veterans Health Administration health professions trainee experience. J Gen Intern Med. 2023;38:1031-1039. doi:10.1007/s11606-023-08283-4
- Roberts DL, Mishark KJ, Alessandro STD, et al. Impact of electronic medical record transitions on the educational experiences of medical students. J Health Care Finance. 2014;41:1-5.
- Varpio L, Day K, Elliot‐Miller P, et al. The impact of adopting EHRs: how losing connectivity affects clinical reasoning. Med Educ. 2015;49:476-486. doi:10.1111/medu.12665
- Gali HE, Baxter SL, Lander L, et al. Impact of electronic health record implementation on ophthalmology trainee time expenditures. J Acad Ophthalmol (2017). 2019;11:e65-e72. doi:10.1055/s-0039-3401986
- Humphrey‐Murto S, Makus D, Moore S, et al. Training physicians and residents for the use of electronic health records— a comparative case study between two hospitals. Med Educ. 2023;57:337-348. doi:10.1111/medu.14944
- US Department of Defense. Captain James A. Lovell Federal Health Care Center: readying warriors & caring for heroes. Presentation August 10, 2022.
- Sayre G, Young J. Beyond openended questions: purposeful interview guide development to elicit rich, trustworthy data. Patient Aligned Care Teams (PACT) Demonstration Labs cyber seminar. March 21, 2018. Accessed February 3, 2026. https://www.hsrd.research.va.gov/for _researchers/cyber_seminars/catalog/transcripts/2439.doc
- Jordan PW, Thomas B, McClelland IL, Weerdmeester B, eds. Usability Evaluation In Industry. CRC Press; 1996.
- Keitz SA, Holland GJ, Melander EH, et al. The Veterans Affairs Learners’ Perceptions Survey: the foundation for educational quality improvement. Acad Med. 2003;78:910- 917. doi:10.1097/00001888-200309000-00016
- Byrne JM, Chang BK, Gilman SC, et al. The learners’ perceptions survey—primary care: assessing resident perceptions of internal medicine continuity clinics and patient- centered care. J Grad Med Educ. 2013;5:587-593. doi:10.4300/JGME-D-12-00233.1
- Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107-115. doi:10.1111/j.1365-2648.2007.04569.x
- Siller AB, Tompkins L. The big four: analyzing complex sample survey data using SAS, SPSS, STATA, and SUDAAN. Poster presented at: 31st Annual SAS Users Group International Conference; March 27, 2006; San Francisco, CA. Accessed February 3, 2026. https://support.sas.com /resources/papers/proceedings/proceedings/sugi31/172 -31.pdf
- Tashakkori A, Johnson RB, Teddlie C. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioral Sciences. 2nd ed. SAGE Publications, Inc.; 2020.
- Olmos-Vega FM, Stalmeijer RE, Varpio L, et al. A practical guide to reflexivity in qualitative research: AMEE Guide No. 149. Med Teach. 2023;45:241-251. doi:10.1080/0142159X.2022.2057287
- Mezirow J. Fostering Critical Reflection in Adulthood: A Guide to Transformative and Emancipatory Learning. JosseyBass; 1991.
- Probst B, Berenson L. The double arrow: how qualitative social work researchers use reflexivity. Qual Soc Work. 2014;13:813-827. doi:10.1177/1473325013506248
- Huang C, Koppel R, McGreevey JD 3rd, et al. Transitions from one electronic health record to another: challenges, pitfalls, and recommendations. Appl Clin Infor. 2020;11:742-754. doi:10.1055/s-0040-1718535
- Zheng K, Abraham J, Novak LL, et al. A survey of the literature on unintended consequences associated with health information technology: 2014–2015. Yearb Med Inform. 2016;25:13-29. doi:10.15265/IY-2016-036
- Campbell EM, Sittig DF, Ash JS, et al. Types of unintended consequences related to computerized provider order entry. J Am Med Inform Assoc. 2006;13:547-556. doi:10.1197/jamia.M2042
- Sittig DF, Lakhani P, Singh H. Applying requisite imagination to safeguard electronic health record transitions. JAMA. 2022;29:1014-1018. doi:10.1093/jamia/ocab291
- Ko HH, Lee TK, Leung Y, et al. Factors influencing career choices made by medical students, residents, and practising physicians. B C Med J. 2007;49:482-489.
- Brunner J, Ahlness EA, Anderson E, et al. VA’s EHR transition and health professions trainee programs: findings and impacts of a multistakeholder learning community. Learn Health Sys. 2024;9:e10460. doi:10.1002/lrh2.10460
- Rosdahl JA, Rudd M, Benjamin R, et al. Effect of the adoption of a comprehensive electronic health record on graduate medical education: perceptions of faculty and trainees. South Med J. 2018;111:476-483. doi:10.14423/SMJ.0000000000000847
- Hill C. U.S. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed February 3, 2026. https://news.va.gov/93370/medical-education-at-va -its-all-about-the-veterans
- Hanauer DA, Branford GL, Greenberg G, et al. Twoyear longitudinal assessment of physicians’ perceptions after replacement of a longstanding homegrown electronic health record: does a J-curve of satisfaction really exist? J Am Med Inform Assoc. 2017;24:e157-e165. doi:10.1093/jamia/ocw077
The Veterans Health Administration (VHA) is transitioning from its native electronic health record (EHR) Vista/Computerized Patient Record System to the commercial Cerner/Oracle Health EHR. Though this process was temporarily discontinued in April 2023 due to patient safety, usability, and reliability concerns, it resumed in April 2026. It was originally projected to cost $50 billion to implement. 1-3 As of March 9, 2024, 6 sites had transitioned to the new EHR.2 The transition is the largest of its kind in the US, offering an unparalleled opportunity to examine the effects of EHR transitions on an often overlooked part of the workforce: health professions trainees (HPTs).
HPTs serve a central role in VHA. About one-third of patients receive care directly from HPTs who make up about one-third of the VHA workforce. VHA trains > 60 clinical disciplines, comprising > 122,000 trainees annually.4,5 A paucity of literature exists exploring the experiences of HPTs during EHR transitions, and many studies are often limited to single-site or small populations. HPTs face distinct challenges and needs during EHR transitions and are particularly vulnerable to their negative impacts on retention, clinical training, and efficiency and confidence in EHR use.6-10 HPTs at VHA sites that have already transitioned to the Cerner/Oracle Health EHR identified many challenges, including significant delays in gaining EHR access, pervasive perceptions of poor training, concerns that EHR functionality issues limited patient care, and decreased ability to track clinical skill acquisition.6 These challenges may impact some HPTs more than others (eg, students on short rotations are affected more acutely by delayed EHR access and usage).
This quality improvement project evaluated HPT EHR transition experiences at the Captain James A. Lovell Federal Health Care Center (FHCC). This article contributes to the limited literature on HPT transition experiences, identifies opportunities to support HPTs, and informs broader efforts in teaching HPTs new technologies.
Methods
FHCC is jointly operated by the US Department of Defense and US Department of Veterans Affairs (VA). It treats 80,000 inpatient and outpatients annually. FHCC was the sixth VA facility to transition to the new EHR, which went live on March 9, 2024.2,11 About 700 HPTs rotate through FHCC annually. HPTs were eligible for inclusion if they were present during the March 9 transition according to a VA Office of Academic Affiliations database. A total of 216 HPTs were identified for inclusion.
Preparations for the transition included scaling down operations (ie, blocking clinician schedules, not scheduling future appointments that may conflict with the transition, making decisions on new facility- and service-line workflows, required EHR training, and speaking with support staff, including VHA National EHR Modernization Supplemental Staffing Unit [NESSU]). This evaluation was designated nonresearch/quality improvement by the VA Bedford Healthcare System Institutional Review Board.
Surveys
Forty-seven interviews were conducted with HPTs, site leaders, and supervisors from January 2024 to June 2024 (Table 1). Participants were identified by service leads and recruited via email; snowball sampling identified additional participants.
The evaluation team developed semistructured interview guides using grounded probes based on a pilot evaluation and existing research on EHR transitions.12 Questions focused on participant experiences preparing for the EHR transition, learning and using the site’s EHR, and the impact the transition had on clinical training experiences. Interviews were conducted at different times to capture the range of user experiences: 1 month prelaunch, 2 to 6 weeks postlaunch, and 2 months postlaunch. Interviewees were informed of participant rights and provided verbal consent.
HPTs present at FHCC at each survey’s release were emailed invitations and 2 reminders. The anonymous surveys took about 10 minutes to complete. Survey items queried HPTs about their experiences preparing to use the new EHR, perceptions of the current EHR (adapted from the System Usability Scale), satisfaction with VHA training, impact on clinical training, ability to work with preceptors and patients, and experiences with the VHA clinical learning environment (adapted from the VHA Learners Preceptor Survey).13-15 Survey questions used a 5-point Likert response scale.
Analysis
Interviewers completed postinterview summaries for team debriefing and consensus building. Interviews were coded using a priori (from piloting evaluations and relevant literature) and emergent (refined and developed from data) codes. Deductive and inductive content analyses were conducted. 16 Deductive analysis used a priori categories (eg, care coordination, EHR training). Inductive content analysis consisted of open and unstructured coding, capturing data outside a priori categories. Emergent codes captured unidentified categories. Qualitative researchers met weekly to discuss data and reach consensus on interpretation.
Descriptive analysis was conducted using top-2 box scoring (proportion responding within the 2 most favorable responses [agree/ strongly agree]). Survey data were analyzed in SAS.17 The analysis used a merging approach on simultaneously collected qualitative and quantitative data to reach findings consensus.18
Researcher and research team decisions may shape the data collected due to prior assumptions and experience.19 This analysis attempted to integrate reflexivity practices to enhance awareness of the researchers’ assumptions and positionality, including by integrating intent collaborative conversing and memorandum writing into the processes.20,21
Results
This analysis created a survey and fielded responses from HPTs present at FHCC across 3 time points (6 months prelaunch, 1 month prelaunch, and 2 months postlaunch), resulting in a total of 103 responses and an average response rate of 19.0% (Table 2). Six key findings were identified in analysis of responses: (1) critiques of transition management; (2) concerns with training; (3) hope about the EHR; (4) at-the-elbow support was essential; (5) HPTs adjusted to, and later preferred, the new EHR; and (6) transition impacted clinical training, but not overall career plans for HPTs. Findings are presented in this section, with illustrative quantitative data and qualitative data quotes available in the eAppendix.
Critiques of the Transition’s Management
While participants were aware of the transition to the new EHR, most felt they did not have enough information or time to prepare for it, indicating it was “too little, too late.” HPTs felt necessary workflow processes for Cerner/Oracle Health were not determined with enough time to learn them prior to transition. Supervisors shared that important workflow and onboarding decisions remained undecided mere weeks before the transition. Some service lines did not decrease patient loads until right before the transition, making it difficult to manage their schedules and resulting in insufficient time to learn the new EHR.
EHR Training Concerns
Overall, HPTs expressed low satisfaction with computer-based Training Management System (TMS) EHR training, believing it did not prepare them for the new EHR. The percentage of HPTs satisfied or very satisfied with the quality of TMS training was lower than that of instructor-based training pre- and posttransition, with 50% of 36 prelaunch respondents, and 43% of 29 postlaunch respondents expressing satisfaction with computer-based trainings (Figure 1). HPTs were dissatisfied with the training content. They felt it was too general and failed to teach basic tasks in the workflow for their service areas and roles, such as writing a note or order. Furthermore, poor content was exacerbated by poor and unengaging instruction, and HPTs were dissatisfied with the practice EHR used in training, which glitched frequently.
quality of electronic health record training.
EHR Transition Optimism
Even though the transition was stressful, most HPTs hoped it would be a temporary disruption and that they would quickly adjust to the new EHR. Many participants expected that once they switched to the new EHR, they would pick it up quickly. In addition, many anticipated Cerner/Oracle Health would be better and easier to use in the long run.
At-The-Elbow Support Essential
VHA peer support with NESSU was highly valued among HPTs. NESSU staff were highly knowledgeable and could provide both broad and service-line-specific support. NESSU provided prompt answers to EHR questions. This was particularly critical as other forms of in-person support were often inaccessible or absent during the transition.
HPTs found facility support helpful: 85% of 36 respondents reported being satisfied/ very satisfied with support from supervisors and preceptors, and 84% of 36 respondents were satisfied/very satisfied with technical support from facility informatics staff pretransition (n = 36) (Figure 2). NESSU and supervisor support with daily workflows were particularly helpful, as pretransition training only provided a general introduction to the EHR.
health record training.
HPTs Adjusted to and Later Preferred the New EHR
The EHR learning experience was intense but short, with many HPTs feeling able to use it only 2 to 4 weeks posttransition. Confidence grew as HPTs came to view Cerner/Oracle Health as a more integrated and intuitive system than the previous EHR. Most participants preferred the new EHR, even if they criticized some features (eg, no group documentation capabilities). Survey participants frequently rated Cerner/Oracle Health usability higher than the original. A total of 32% of 29 posttransition respondents agreed or strongly agreed that Cerner/Oracle Health helps prevent situations that can lead to patient safety risks—higher than pretransition rates. Additionally, fewer respondents found the new EHR unnecessarily complex or thought it contained too many alerts and flags compared to the original EHR (Figure 3).
health record usability.
Impact on Clinical Training, Not Career Plans
The extensive time and energy the transition demanded of HPTs caused stress and affected their clinical training. Many believed they would have learned more if their training had happened outside the transition.
Concerns that the transition affected learning were most acutely felt pretransition. HPTs reporting that EHR implementation positively affected their clinical education fell from 38% of 36 respondents 6 months pretransition to 19% of 29 respondents 1 month pretransition, but returned to 37% posttransition (Figure 4). However, some HPTs believed there was a silver lining: it provided a learning experience they otherwise would not have had.
new Veterans Health Administration (VHA) electronic health record.
HPTs who believed the transition positively impacted their likelihood of pursuing future career opportunities within the VHA rose to 33% of 29 respondents posttransition. Overall, Cerner/Oracle Health was characterized as a tool: something used in training, but not something that precluded wanting VHA careers or having meaningful experiences, such as caring for patients.
Discussion
This evaluation addressed an underexplored aspect of EHR transitions: their impact on HPTs. It identified HPT challenges, including dissatisfaction with poor transition preparation and EHR training experiences. Promising findings include positive experiences with transition support, EHR uptake, and overall positive educational experiences despite the transition’s disruption.
When EHR users, including HPTs, are dissatisfied with transition preparations, consequent stress can lead to undesired effects, including increased burnout, inappropriate EHR use, and low work satisfaction.22-24 Negative EHR transition experiences shape HPTs’ subsequent EHR adoption, user satisfaction, as well as confidence and career intent.3,25,26 Health systems have strong incentives to implement effective transition change management.
HPTs at previous VHA EHR transition sites reported significantly more disruption to their clinical training compared with HPTs at FHCC. Academic programs were shut down at the first transition site, and HPTs expressed decreased interest in VHA careers at another, even a year posttransition.6,27 These findings are consistent with the limited literature on the adverse impacts that EHR transitions have on HPTs.7,28
HPT retention is critical. VA is mandated to prepare the next generation of HPTs for its needs, and those of the nation. The VA relies heavily on HPT retention to recruit clinicians: > 65% of VHA physicians nationwide participated in VHA training programs prior to recruitment into staff positions.5,29
VHA should invest in transition change management with demonstrated, positive impacts on HPTs, such as in-house support from clinicians. Previous research found that lack of support was a major source of stress and negative outcomes.6,27 Consequently, supporting HPTs through EHR transitions directly contributes to the VHA’s ability to attract high-quality staff from its HPTs. The challenges and promising practices described in this analysis underscore the necessity of understanding how all EHR users are affected by transitions. What happens to them has direct implications for the VA mission to provide safe, efficient care, and its mandate to provide quality clinical training to HPTs.
These findings hold hopeful implications for supporting HPT EHR use, both during and outside EHR transitions. HPTs expressing that an EHR is only 1 part of their clinical training experience suggests that change management can improve EHR transitions. HPT learning can enhance known factors that are important for HPTs in clinical training, including the health care organization’s mission, caring for patients, and personal development.
Further investigations may engage HPTs at future VHA sites making the transition to the new EHR. One focus would involve applying a learning health systems framework to examine the nature of change management efforts—and their effects on HPT transition experiences—iteratively across transition sites to evaluate the effect of the efforts. Another focus may be longitudinal engagement with HPTs at health care systems and sites transitioning to new EHRs. Research has found that disruptions to EHR usability, satisfaction, and care provision can persist for 2 years and beyond following an EHR transition.30 Evaluating the long-term effects of transitions on HPTs is of interest, given their distinct characteristics and differences from employees.
Limitations
Study data came from voluntary participants at 1 highly engaged site, raising the possibility of self-selection bias. HPT experiences at other VA and non-VA sites may differ. Employees and HPTs were engaged during a high-stress event; snowballing recruitment reach was limited by high workloads and limited time for engagement. Statistical data were descriptive and should not be interpreted as causal. Results may reflect, in part, temporal effects, and respondents include HPTs at different stages of training and with different levels of VA experience. Survey sample sizes may limit generalizability; however, merging data streams strengthened the reliability of findings.
Conclusions
The results of this analysis of FHCC HPTs were notably more positive than those of HPTs at previous VHA EHR transition sites. VHA is one of many health care systems that provide clinical training for HPTs and relies on this population to provide patient care. By highlighting challenges and positive experiences of HPTs during an EHR transition, this evaluation produces actionable insights that can inform the actions of health care systems seeking to support HPTs during disruptive EHR transitions.
The Veterans Health Administration (VHA) is transitioning from its native electronic health record (EHR) Vista/Computerized Patient Record System to the commercial Cerner/Oracle Health EHR. Though this process was temporarily discontinued in April 2023 due to patient safety, usability, and reliability concerns, it resumed in April 2026. It was originally projected to cost $50 billion to implement. 1-3 As of March 9, 2024, 6 sites had transitioned to the new EHR.2 The transition is the largest of its kind in the US, offering an unparalleled opportunity to examine the effects of EHR transitions on an often overlooked part of the workforce: health professions trainees (HPTs).
HPTs serve a central role in VHA. About one-third of patients receive care directly from HPTs who make up about one-third of the VHA workforce. VHA trains > 60 clinical disciplines, comprising > 122,000 trainees annually.4,5 A paucity of literature exists exploring the experiences of HPTs during EHR transitions, and many studies are often limited to single-site or small populations. HPTs face distinct challenges and needs during EHR transitions and are particularly vulnerable to their negative impacts on retention, clinical training, and efficiency and confidence in EHR use.6-10 HPTs at VHA sites that have already transitioned to the Cerner/Oracle Health EHR identified many challenges, including significant delays in gaining EHR access, pervasive perceptions of poor training, concerns that EHR functionality issues limited patient care, and decreased ability to track clinical skill acquisition.6 These challenges may impact some HPTs more than others (eg, students on short rotations are affected more acutely by delayed EHR access and usage).
This quality improvement project evaluated HPT EHR transition experiences at the Captain James A. Lovell Federal Health Care Center (FHCC). This article contributes to the limited literature on HPT transition experiences, identifies opportunities to support HPTs, and informs broader efforts in teaching HPTs new technologies.
Methods
FHCC is jointly operated by the US Department of Defense and US Department of Veterans Affairs (VA). It treats 80,000 inpatient and outpatients annually. FHCC was the sixth VA facility to transition to the new EHR, which went live on March 9, 2024.2,11 About 700 HPTs rotate through FHCC annually. HPTs were eligible for inclusion if they were present during the March 9 transition according to a VA Office of Academic Affiliations database. A total of 216 HPTs were identified for inclusion.
Preparations for the transition included scaling down operations (ie, blocking clinician schedules, not scheduling future appointments that may conflict with the transition, making decisions on new facility- and service-line workflows, required EHR training, and speaking with support staff, including VHA National EHR Modernization Supplemental Staffing Unit [NESSU]). This evaluation was designated nonresearch/quality improvement by the VA Bedford Healthcare System Institutional Review Board.
Surveys
Forty-seven interviews were conducted with HPTs, site leaders, and supervisors from January 2024 to June 2024 (Table 1). Participants were identified by service leads and recruited via email; snowball sampling identified additional participants.
The evaluation team developed semistructured interview guides using grounded probes based on a pilot evaluation and existing research on EHR transitions.12 Questions focused on participant experiences preparing for the EHR transition, learning and using the site’s EHR, and the impact the transition had on clinical training experiences. Interviews were conducted at different times to capture the range of user experiences: 1 month prelaunch, 2 to 6 weeks postlaunch, and 2 months postlaunch. Interviewees were informed of participant rights and provided verbal consent.
HPTs present at FHCC at each survey’s release were emailed invitations and 2 reminders. The anonymous surveys took about 10 minutes to complete. Survey items queried HPTs about their experiences preparing to use the new EHR, perceptions of the current EHR (adapted from the System Usability Scale), satisfaction with VHA training, impact on clinical training, ability to work with preceptors and patients, and experiences with the VHA clinical learning environment (adapted from the VHA Learners Preceptor Survey).13-15 Survey questions used a 5-point Likert response scale.
Analysis
Interviewers completed postinterview summaries for team debriefing and consensus building. Interviews were coded using a priori (from piloting evaluations and relevant literature) and emergent (refined and developed from data) codes. Deductive and inductive content analyses were conducted. 16 Deductive analysis used a priori categories (eg, care coordination, EHR training). Inductive content analysis consisted of open and unstructured coding, capturing data outside a priori categories. Emergent codes captured unidentified categories. Qualitative researchers met weekly to discuss data and reach consensus on interpretation.
Descriptive analysis was conducted using top-2 box scoring (proportion responding within the 2 most favorable responses [agree/ strongly agree]). Survey data were analyzed in SAS.17 The analysis used a merging approach on simultaneously collected qualitative and quantitative data to reach findings consensus.18
Researcher and research team decisions may shape the data collected due to prior assumptions and experience.19 This analysis attempted to integrate reflexivity practices to enhance awareness of the researchers’ assumptions and positionality, including by integrating intent collaborative conversing and memorandum writing into the processes.20,21
Results
This analysis created a survey and fielded responses from HPTs present at FHCC across 3 time points (6 months prelaunch, 1 month prelaunch, and 2 months postlaunch), resulting in a total of 103 responses and an average response rate of 19.0% (Table 2). Six key findings were identified in analysis of responses: (1) critiques of transition management; (2) concerns with training; (3) hope about the EHR; (4) at-the-elbow support was essential; (5) HPTs adjusted to, and later preferred, the new EHR; and (6) transition impacted clinical training, but not overall career plans for HPTs. Findings are presented in this section, with illustrative quantitative data and qualitative data quotes available in the eAppendix.
Critiques of the Transition’s Management
While participants were aware of the transition to the new EHR, most felt they did not have enough information or time to prepare for it, indicating it was “too little, too late.” HPTs felt necessary workflow processes for Cerner/Oracle Health were not determined with enough time to learn them prior to transition. Supervisors shared that important workflow and onboarding decisions remained undecided mere weeks before the transition. Some service lines did not decrease patient loads until right before the transition, making it difficult to manage their schedules and resulting in insufficient time to learn the new EHR.
EHR Training Concerns
Overall, HPTs expressed low satisfaction with computer-based Training Management System (TMS) EHR training, believing it did not prepare them for the new EHR. The percentage of HPTs satisfied or very satisfied with the quality of TMS training was lower than that of instructor-based training pre- and posttransition, with 50% of 36 prelaunch respondents, and 43% of 29 postlaunch respondents expressing satisfaction with computer-based trainings (Figure 1). HPTs were dissatisfied with the training content. They felt it was too general and failed to teach basic tasks in the workflow for their service areas and roles, such as writing a note or order. Furthermore, poor content was exacerbated by poor and unengaging instruction, and HPTs were dissatisfied with the practice EHR used in training, which glitched frequently.
quality of electronic health record training.
EHR Transition Optimism
Even though the transition was stressful, most HPTs hoped it would be a temporary disruption and that they would quickly adjust to the new EHR. Many participants expected that once they switched to the new EHR, they would pick it up quickly. In addition, many anticipated Cerner/Oracle Health would be better and easier to use in the long run.
At-The-Elbow Support Essential
VHA peer support with NESSU was highly valued among HPTs. NESSU staff were highly knowledgeable and could provide both broad and service-line-specific support. NESSU provided prompt answers to EHR questions. This was particularly critical as other forms of in-person support were often inaccessible or absent during the transition.
HPTs found facility support helpful: 85% of 36 respondents reported being satisfied/ very satisfied with support from supervisors and preceptors, and 84% of 36 respondents were satisfied/very satisfied with technical support from facility informatics staff pretransition (n = 36) (Figure 2). NESSU and supervisor support with daily workflows were particularly helpful, as pretransition training only provided a general introduction to the EHR.
health record training.
HPTs Adjusted to and Later Preferred the New EHR
The EHR learning experience was intense but short, with many HPTs feeling able to use it only 2 to 4 weeks posttransition. Confidence grew as HPTs came to view Cerner/Oracle Health as a more integrated and intuitive system than the previous EHR. Most participants preferred the new EHR, even if they criticized some features (eg, no group documentation capabilities). Survey participants frequently rated Cerner/Oracle Health usability higher than the original. A total of 32% of 29 posttransition respondents agreed or strongly agreed that Cerner/Oracle Health helps prevent situations that can lead to patient safety risks—higher than pretransition rates. Additionally, fewer respondents found the new EHR unnecessarily complex or thought it contained too many alerts and flags compared to the original EHR (Figure 3).
health record usability.
Impact on Clinical Training, Not Career Plans
The extensive time and energy the transition demanded of HPTs caused stress and affected their clinical training. Many believed they would have learned more if their training had happened outside the transition.
Concerns that the transition affected learning were most acutely felt pretransition. HPTs reporting that EHR implementation positively affected their clinical education fell from 38% of 36 respondents 6 months pretransition to 19% of 29 respondents 1 month pretransition, but returned to 37% posttransition (Figure 4). However, some HPTs believed there was a silver lining: it provided a learning experience they otherwise would not have had.
new Veterans Health Administration (VHA) electronic health record.
HPTs who believed the transition positively impacted their likelihood of pursuing future career opportunities within the VHA rose to 33% of 29 respondents posttransition. Overall, Cerner/Oracle Health was characterized as a tool: something used in training, but not something that precluded wanting VHA careers or having meaningful experiences, such as caring for patients.
Discussion
This evaluation addressed an underexplored aspect of EHR transitions: their impact on HPTs. It identified HPT challenges, including dissatisfaction with poor transition preparation and EHR training experiences. Promising findings include positive experiences with transition support, EHR uptake, and overall positive educational experiences despite the transition’s disruption.
When EHR users, including HPTs, are dissatisfied with transition preparations, consequent stress can lead to undesired effects, including increased burnout, inappropriate EHR use, and low work satisfaction.22-24 Negative EHR transition experiences shape HPTs’ subsequent EHR adoption, user satisfaction, as well as confidence and career intent.3,25,26 Health systems have strong incentives to implement effective transition change management.
HPTs at previous VHA EHR transition sites reported significantly more disruption to their clinical training compared with HPTs at FHCC. Academic programs were shut down at the first transition site, and HPTs expressed decreased interest in VHA careers at another, even a year posttransition.6,27 These findings are consistent with the limited literature on the adverse impacts that EHR transitions have on HPTs.7,28
HPT retention is critical. VA is mandated to prepare the next generation of HPTs for its needs, and those of the nation. The VA relies heavily on HPT retention to recruit clinicians: > 65% of VHA physicians nationwide participated in VHA training programs prior to recruitment into staff positions.5,29
VHA should invest in transition change management with demonstrated, positive impacts on HPTs, such as in-house support from clinicians. Previous research found that lack of support was a major source of stress and negative outcomes.6,27 Consequently, supporting HPTs through EHR transitions directly contributes to the VHA’s ability to attract high-quality staff from its HPTs. The challenges and promising practices described in this analysis underscore the necessity of understanding how all EHR users are affected by transitions. What happens to them has direct implications for the VA mission to provide safe, efficient care, and its mandate to provide quality clinical training to HPTs.
These findings hold hopeful implications for supporting HPT EHR use, both during and outside EHR transitions. HPTs expressing that an EHR is only 1 part of their clinical training experience suggests that change management can improve EHR transitions. HPT learning can enhance known factors that are important for HPTs in clinical training, including the health care organization’s mission, caring for patients, and personal development.
Further investigations may engage HPTs at future VHA sites making the transition to the new EHR. One focus would involve applying a learning health systems framework to examine the nature of change management efforts—and their effects on HPT transition experiences—iteratively across transition sites to evaluate the effect of the efforts. Another focus may be longitudinal engagement with HPTs at health care systems and sites transitioning to new EHRs. Research has found that disruptions to EHR usability, satisfaction, and care provision can persist for 2 years and beyond following an EHR transition.30 Evaluating the long-term effects of transitions on HPTs is of interest, given their distinct characteristics and differences from employees.
Limitations
Study data came from voluntary participants at 1 highly engaged site, raising the possibility of self-selection bias. HPT experiences at other VA and non-VA sites may differ. Employees and HPTs were engaged during a high-stress event; snowballing recruitment reach was limited by high workloads and limited time for engagement. Statistical data were descriptive and should not be interpreted as causal. Results may reflect, in part, temporal effects, and respondents include HPTs at different stages of training and with different levels of VA experience. Survey sample sizes may limit generalizability; however, merging data streams strengthened the reliability of findings.
Conclusions
The results of this analysis of FHCC HPTs were notably more positive than those of HPTs at previous VHA EHR transition sites. VHA is one of many health care systems that provide clinical training for HPTs and relies on this population to provide patient care. By highlighting challenges and positive experiences of HPTs during an EHR transition, this evaluation produces actionable insights that can inform the actions of health care systems seeking to support HPTs during disruptive EHR transitions.
- US Department of Veterans Affairs Office of the Inspector General. VA needs to strengthen controls to address electronic health record system major performance incidents. September 23, 2024. Accessed February 3, 2026. https://www.vaoig.gov/sites/default/files /reports/2024-09/vaoig-22-03591-231.pdf
- EHR deployment schedule. VA EHR Modernization. Updated February 2, 2026. Accessed February 3, 2026. https://digital.va.gov/ehr-modernization/ehr-deployment -schedule/
- Heckman J. VA in 2026 looks to get EHR rollout back on track, embark on health care reorganization. Federal News Network. December 24, 2025. Accessed February 3, 2026. https://federalnewsnetwork.com/veterans-affairs/2025/12 /va-in-2026-looks-to-get-ehr-rollout-back-on-track -embark-on-health-care-reorganization/
- US Department of Veterans Affairs Office of Academic Affiliations. Medical and dental education. Updated September 12, 2025. Accessed February 3, 2026. https://department.va.gov/academic-affiliations /medical-and-dental/
- Functions of Veterans Health Administration: health-care personnel education and training programs. 38 U.S.C. § 7302 (2026). Accessed February 3, 2026. https://uscode.house.gov/view.xhtml ?req=(title:38%20section:7302%20edition:prelim)
- Ahlness EA, Molloy-Paolillo BK, Brunner J, et al. Impacts of an electronic health record transition on Veterans Health Administration health professions trainee experience. J Gen Intern Med. 2023;38:1031-1039. doi:10.1007/s11606-023-08283-4
- Roberts DL, Mishark KJ, Alessandro STD, et al. Impact of electronic medical record transitions on the educational experiences of medical students. J Health Care Finance. 2014;41:1-5.
- Varpio L, Day K, Elliot‐Miller P, et al. The impact of adopting EHRs: how losing connectivity affects clinical reasoning. Med Educ. 2015;49:476-486. doi:10.1111/medu.12665
- Gali HE, Baxter SL, Lander L, et al. Impact of electronic health record implementation on ophthalmology trainee time expenditures. J Acad Ophthalmol (2017). 2019;11:e65-e72. doi:10.1055/s-0039-3401986
- Humphrey‐Murto S, Makus D, Moore S, et al. Training physicians and residents for the use of electronic health records— a comparative case study between two hospitals. Med Educ. 2023;57:337-348. doi:10.1111/medu.14944
- US Department of Defense. Captain James A. Lovell Federal Health Care Center: readying warriors & caring for heroes. Presentation August 10, 2022.
- Sayre G, Young J. Beyond openended questions: purposeful interview guide development to elicit rich, trustworthy data. Patient Aligned Care Teams (PACT) Demonstration Labs cyber seminar. March 21, 2018. Accessed February 3, 2026. https://www.hsrd.research.va.gov/for _researchers/cyber_seminars/catalog/transcripts/2439.doc
- Jordan PW, Thomas B, McClelland IL, Weerdmeester B, eds. Usability Evaluation In Industry. CRC Press; 1996.
- Keitz SA, Holland GJ, Melander EH, et al. The Veterans Affairs Learners’ Perceptions Survey: the foundation for educational quality improvement. Acad Med. 2003;78:910- 917. doi:10.1097/00001888-200309000-00016
- Byrne JM, Chang BK, Gilman SC, et al. The learners’ perceptions survey—primary care: assessing resident perceptions of internal medicine continuity clinics and patient- centered care. J Grad Med Educ. 2013;5:587-593. doi:10.4300/JGME-D-12-00233.1
- Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107-115. doi:10.1111/j.1365-2648.2007.04569.x
- Siller AB, Tompkins L. The big four: analyzing complex sample survey data using SAS, SPSS, STATA, and SUDAAN. Poster presented at: 31st Annual SAS Users Group International Conference; March 27, 2006; San Francisco, CA. Accessed February 3, 2026. https://support.sas.com /resources/papers/proceedings/proceedings/sugi31/172 -31.pdf
- Tashakkori A, Johnson RB, Teddlie C. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioral Sciences. 2nd ed. SAGE Publications, Inc.; 2020.
- Olmos-Vega FM, Stalmeijer RE, Varpio L, et al. A practical guide to reflexivity in qualitative research: AMEE Guide No. 149. Med Teach. 2023;45:241-251. doi:10.1080/0142159X.2022.2057287
- Mezirow J. Fostering Critical Reflection in Adulthood: A Guide to Transformative and Emancipatory Learning. JosseyBass; 1991.
- Probst B, Berenson L. The double arrow: how qualitative social work researchers use reflexivity. Qual Soc Work. 2014;13:813-827. doi:10.1177/1473325013506248
- Huang C, Koppel R, McGreevey JD 3rd, et al. Transitions from one electronic health record to another: challenges, pitfalls, and recommendations. Appl Clin Infor. 2020;11:742-754. doi:10.1055/s-0040-1718535
- Zheng K, Abraham J, Novak LL, et al. A survey of the literature on unintended consequences associated with health information technology: 2014–2015. Yearb Med Inform. 2016;25:13-29. doi:10.15265/IY-2016-036
- Campbell EM, Sittig DF, Ash JS, et al. Types of unintended consequences related to computerized provider order entry. J Am Med Inform Assoc. 2006;13:547-556. doi:10.1197/jamia.M2042
- Sittig DF, Lakhani P, Singh H. Applying requisite imagination to safeguard electronic health record transitions. JAMA. 2022;29:1014-1018. doi:10.1093/jamia/ocab291
- Ko HH, Lee TK, Leung Y, et al. Factors influencing career choices made by medical students, residents, and practising physicians. B C Med J. 2007;49:482-489.
- Brunner J, Ahlness EA, Anderson E, et al. VA’s EHR transition and health professions trainee programs: findings and impacts of a multistakeholder learning community. Learn Health Sys. 2024;9:e10460. doi:10.1002/lrh2.10460
- Rosdahl JA, Rudd M, Benjamin R, et al. Effect of the adoption of a comprehensive electronic health record on graduate medical education: perceptions of faculty and trainees. South Med J. 2018;111:476-483. doi:10.14423/SMJ.0000000000000847
- Hill C. U.S. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed February 3, 2026. https://news.va.gov/93370/medical-education-at-va -its-all-about-the-veterans
- Hanauer DA, Branford GL, Greenberg G, et al. Twoyear longitudinal assessment of physicians’ perceptions after replacement of a longstanding homegrown electronic health record: does a J-curve of satisfaction really exist? J Am Med Inform Assoc. 2017;24:e157-e165. doi:10.1093/jamia/ocw077
- US Department of Veterans Affairs Office of the Inspector General. VA needs to strengthen controls to address electronic health record system major performance incidents. September 23, 2024. Accessed February 3, 2026. https://www.vaoig.gov/sites/default/files /reports/2024-09/vaoig-22-03591-231.pdf
- EHR deployment schedule. VA EHR Modernization. Updated February 2, 2026. Accessed February 3, 2026. https://digital.va.gov/ehr-modernization/ehr-deployment -schedule/
- Heckman J. VA in 2026 looks to get EHR rollout back on track, embark on health care reorganization. Federal News Network. December 24, 2025. Accessed February 3, 2026. https://federalnewsnetwork.com/veterans-affairs/2025/12 /va-in-2026-looks-to-get-ehr-rollout-back-on-track -embark-on-health-care-reorganization/
- US Department of Veterans Affairs Office of Academic Affiliations. Medical and dental education. Updated September 12, 2025. Accessed February 3, 2026. https://department.va.gov/academic-affiliations /medical-and-dental/
- Functions of Veterans Health Administration: health-care personnel education and training programs. 38 U.S.C. § 7302 (2026). Accessed February 3, 2026. https://uscode.house.gov/view.xhtml ?req=(title:38%20section:7302%20edition:prelim)
- Ahlness EA, Molloy-Paolillo BK, Brunner J, et al. Impacts of an electronic health record transition on Veterans Health Administration health professions trainee experience. J Gen Intern Med. 2023;38:1031-1039. doi:10.1007/s11606-023-08283-4
- Roberts DL, Mishark KJ, Alessandro STD, et al. Impact of electronic medical record transitions on the educational experiences of medical students. J Health Care Finance. 2014;41:1-5.
- Varpio L, Day K, Elliot‐Miller P, et al. The impact of adopting EHRs: how losing connectivity affects clinical reasoning. Med Educ. 2015;49:476-486. doi:10.1111/medu.12665
- Gali HE, Baxter SL, Lander L, et al. Impact of electronic health record implementation on ophthalmology trainee time expenditures. J Acad Ophthalmol (2017). 2019;11:e65-e72. doi:10.1055/s-0039-3401986
- Humphrey‐Murto S, Makus D, Moore S, et al. Training physicians and residents for the use of electronic health records— a comparative case study between two hospitals. Med Educ. 2023;57:337-348. doi:10.1111/medu.14944
- US Department of Defense. Captain James A. Lovell Federal Health Care Center: readying warriors & caring for heroes. Presentation August 10, 2022.
- Sayre G, Young J. Beyond openended questions: purposeful interview guide development to elicit rich, trustworthy data. Patient Aligned Care Teams (PACT) Demonstration Labs cyber seminar. March 21, 2018. Accessed February 3, 2026. https://www.hsrd.research.va.gov/for _researchers/cyber_seminars/catalog/transcripts/2439.doc
- Jordan PW, Thomas B, McClelland IL, Weerdmeester B, eds. Usability Evaluation In Industry. CRC Press; 1996.
- Keitz SA, Holland GJ, Melander EH, et al. The Veterans Affairs Learners’ Perceptions Survey: the foundation for educational quality improvement. Acad Med. 2003;78:910- 917. doi:10.1097/00001888-200309000-00016
- Byrne JM, Chang BK, Gilman SC, et al. The learners’ perceptions survey—primary care: assessing resident perceptions of internal medicine continuity clinics and patient- centered care. J Grad Med Educ. 2013;5:587-593. doi:10.4300/JGME-D-12-00233.1
- Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107-115. doi:10.1111/j.1365-2648.2007.04569.x
- Siller AB, Tompkins L. The big four: analyzing complex sample survey data using SAS, SPSS, STATA, and SUDAAN. Poster presented at: 31st Annual SAS Users Group International Conference; March 27, 2006; San Francisco, CA. Accessed February 3, 2026. https://support.sas.com /resources/papers/proceedings/proceedings/sugi31/172 -31.pdf
- Tashakkori A, Johnson RB, Teddlie C. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioral Sciences. 2nd ed. SAGE Publications, Inc.; 2020.
- Olmos-Vega FM, Stalmeijer RE, Varpio L, et al. A practical guide to reflexivity in qualitative research: AMEE Guide No. 149. Med Teach. 2023;45:241-251. doi:10.1080/0142159X.2022.2057287
- Mezirow J. Fostering Critical Reflection in Adulthood: A Guide to Transformative and Emancipatory Learning. JosseyBass; 1991.
- Probst B, Berenson L. The double arrow: how qualitative social work researchers use reflexivity. Qual Soc Work. 2014;13:813-827. doi:10.1177/1473325013506248
- Huang C, Koppel R, McGreevey JD 3rd, et al. Transitions from one electronic health record to another: challenges, pitfalls, and recommendations. Appl Clin Infor. 2020;11:742-754. doi:10.1055/s-0040-1718535
- Zheng K, Abraham J, Novak LL, et al. A survey of the literature on unintended consequences associated with health information technology: 2014–2015. Yearb Med Inform. 2016;25:13-29. doi:10.15265/IY-2016-036
- Campbell EM, Sittig DF, Ash JS, et al. Types of unintended consequences related to computerized provider order entry. J Am Med Inform Assoc. 2006;13:547-556. doi:10.1197/jamia.M2042
- Sittig DF, Lakhani P, Singh H. Applying requisite imagination to safeguard electronic health record transitions. JAMA. 2022;29:1014-1018. doi:10.1093/jamia/ocab291
- Ko HH, Lee TK, Leung Y, et al. Factors influencing career choices made by medical students, residents, and practising physicians. B C Med J. 2007;49:482-489.
- Brunner J, Ahlness EA, Anderson E, et al. VA’s EHR transition and health professions trainee programs: findings and impacts of a multistakeholder learning community. Learn Health Sys. 2024;9:e10460. doi:10.1002/lrh2.10460
- Rosdahl JA, Rudd M, Benjamin R, et al. Effect of the adoption of a comprehensive electronic health record on graduate medical education: perceptions of faculty and trainees. South Med J. 2018;111:476-483. doi:10.14423/SMJ.0000000000000847
- Hill C. U.S. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed February 3, 2026. https://news.va.gov/93370/medical-education-at-va -its-all-about-the-veterans
- Hanauer DA, Branford GL, Greenberg G, et al. Twoyear longitudinal assessment of physicians’ perceptions after replacement of a longstanding homegrown electronic health record: does a J-curve of satisfaction really exist? J Am Med Inform Assoc. 2017;24:e157-e165. doi:10.1093/jamia/ocw077
Evaluation of Health Professions Trainee Experiences Transitioning to New VHA Electronic Health Record
Evaluation of Health Professions Trainee Experiences Transitioning to New VHA Electronic Health Record
