User login
Asymptomatic Enlarging Lobulated Mass on the Lower Leg
THE DIAGNOSIS: Dermatofibroma
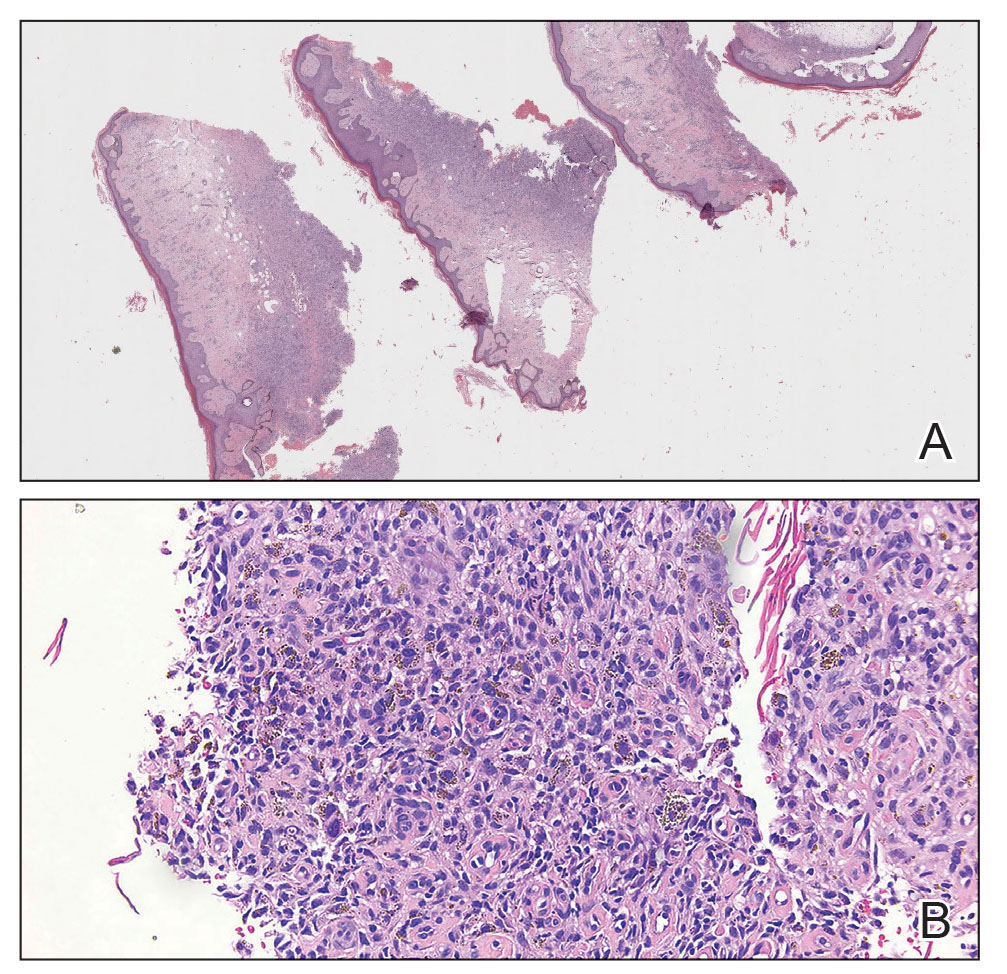
Histopathologic examination of the shave biopsy revealed fascicles of plump fibroblasts and histiocytes interposed between thick collagen bundles within the dermis, consistent with a diagnosis of dermatofibroma (DF). Dermatofibroma is a common benign skin tumor that classically manifests as brownish or reddish-brown firm papules or nodules that dimple when compressed. While the exact etiology of DF remains uncertain, it is believed to arise from a combined neoplastic and reactive fibroblastic proliferation process in response to stimuli, such as minor trauma or insect bites (as in our patient).1
On histopathology, the most common findings associated with DF are dermal proliferation of spindle-shaped fibroblasts arranged in a storiform or whorled pattern.2 In this patient, fascicles of plump fibroblasts and histiocytes were observed interspersed among thick collagen bundles within the dermis (Figure). Other histologic variants of DF include cellular, histiocytic, lipidized, angiomatous, aneurysmal, clear cell, monster cell, myxoid, keloidal, palisading, osteoclastic, and epithelioid.
On dermatoscopic examination, a pigment network is the most common feature, followed by a white scarlike patch, brown dots and globules, and vascular structures.2 Atypical DF variants can manifest with diverse clinical morphologies; one example is giant DF, which exceeds 5 cm and may exhibit an ulcerated or pedunculated appearance, as seen in our case.3 In such cases, a thorough clinical examination coupled with histopathologic analysis becomes paramount for accurate diagnosis.
Most cases of DF do not require intervention unless there are cosmetic concerns or the lesions are symptomatic. Surgical excision is a common and effective treatment method but results in scarring. Intralesional steroid injection and cryotherapy are less aggressive treatment options but have limited efficacy. Lasers, including carbon dioxide and pulsed dye lasers, are infrequently used; however, recurrence is possible with any treatment modality.4 Local recurrence is common, occurring in 26% to 50% of cases, particularly in atypical dermatofibroma variants after treatment.5 Recurrence is more likely with primary lesions larger than 1 cm.5
Several conditions share clinical features with DF, necessitating a thorough differential diagnosis. Dermatofibrosarcoma protuberans (DFSP) is a rare, locally aggressive, malignant tumor with a propensity for recurrence. It manifests as a slow-growing, red-brown, indurated plaque with irregular nodularity. Immunohistochemical staining can be used to differentiate DF from DFSP, with DF typically expressing factor XIIIa and lacking CD34, whereas DFSP exhibits CD34 positivity and lacks factor XIIIa expression.6 Another diagnosis in the differential is fibrosarcoma, a malignant tumor of fibroblasts that manifests as a painless, enlarging, poorly defined mass on the lower extremities. Histopathologic features include atypical fibroblasts and collagen with proliferation of atypical spindle-shaped cells.
Other benign lesions to consider include neurofibroma, which may manifest as a firm nodule but is derived from nerve tissue. Clinically, neurofibromas can be differentiated by their association with neurofibromatosis and softer texture. Cutaneous squamous cell carcinoma also should be considered, as it is a malignant proliferation of cutaneous epithelium that clinically manifests as a hyperkeratotic papule or plaque.5
- Hui P, J. Glusac E, Sinard JH, et al. Clonal analysis of cutaneous fibrous histiocytoma (dermatofibroma). J Cutan Pathol. 2002;29:385-389.
- Şenel E, Yuyucu Karabulut Y, Doğruer Şenel S. Clinical, histopathological, dermatoscopic and digital microscopic features of dermatofibroma: a retrospective analysis of 200 lesions. J Eur Acad Derm Venereol. 2015;29:1958-1966.
- Requena L, Fariña MC, Fuente C, et al. Giant dermatofibroma: a little-known clinical variant of dermatofibroma. J Am Acad Dermatol. 1994;30:714-718.
- Alonso-Castro L, Boixeda P, Segura-Palacios JM, et al. Dermatofibromas treated with pulsed dye laser: clinical and dermoscopic outcomes. J Cosmet Laser Ther. 2012;14:98-101.
- Gaufin M, Michaelis T, Duffy K. Cellular dermatofibroma: clinicopathologic review of 218 cases of cellular dermatofibroma to determine the clinical recurrence rate. Dermatol Surg. 2019;45:1359-1364.
- West KL, Cardona DM, Su Z, et al. Immunohistochemical markers in fibrohistiocytic lesions: factor XIIIa, CD34, S-100 and p75. Am J Dermatopathol. 2014;36:414-419.
THE DIAGNOSIS: Dermatofibroma
Histopathologic examination of the shave biopsy revealed fascicles of plump fibroblasts and histiocytes interposed between thick collagen bundles within the dermis, consistent with a diagnosis of dermatofibroma (DF). Dermatofibroma is a common benign skin tumor that classically manifests as brownish or reddish-brown firm papules or nodules that dimple when compressed. While the exact etiology of DF remains uncertain, it is believed to arise from a combined neoplastic and reactive fibroblastic proliferation process in response to stimuli, such as minor trauma or insect bites (as in our patient).1
On histopathology, the most common findings associated with DF are dermal proliferation of spindle-shaped fibroblasts arranged in a storiform or whorled pattern.2 In this patient, fascicles of plump fibroblasts and histiocytes were observed interspersed among thick collagen bundles within the dermis (Figure). Other histologic variants of DF include cellular, histiocytic, lipidized, angiomatous, aneurysmal, clear cell, monster cell, myxoid, keloidal, palisading, osteoclastic, and epithelioid.
On dermatoscopic examination, a pigment network is the most common feature, followed by a white scarlike patch, brown dots and globules, and vascular structures.2 Atypical DF variants can manifest with diverse clinical morphologies; one example is giant DF, which exceeds 5 cm and may exhibit an ulcerated or pedunculated appearance, as seen in our case.3 In such cases, a thorough clinical examination coupled with histopathologic analysis becomes paramount for accurate diagnosis.
Most cases of DF do not require intervention unless there are cosmetic concerns or the lesions are symptomatic. Surgical excision is a common and effective treatment method but results in scarring. Intralesional steroid injection and cryotherapy are less aggressive treatment options but have limited efficacy. Lasers, including carbon dioxide and pulsed dye lasers, are infrequently used; however, recurrence is possible with any treatment modality.4 Local recurrence is common, occurring in 26% to 50% of cases, particularly in atypical dermatofibroma variants after treatment.5 Recurrence is more likely with primary lesions larger than 1 cm.5
Several conditions share clinical features with DF, necessitating a thorough differential diagnosis. Dermatofibrosarcoma protuberans (DFSP) is a rare, locally aggressive, malignant tumor with a propensity for recurrence. It manifests as a slow-growing, red-brown, indurated plaque with irregular nodularity. Immunohistochemical staining can be used to differentiate DF from DFSP, with DF typically expressing factor XIIIa and lacking CD34, whereas DFSP exhibits CD34 positivity and lacks factor XIIIa expression.6 Another diagnosis in the differential is fibrosarcoma, a malignant tumor of fibroblasts that manifests as a painless, enlarging, poorly defined mass on the lower extremities. Histopathologic features include atypical fibroblasts and collagen with proliferation of atypical spindle-shaped cells.
Other benign lesions to consider include neurofibroma, which may manifest as a firm nodule but is derived from nerve tissue. Clinically, neurofibromas can be differentiated by their association with neurofibromatosis and softer texture. Cutaneous squamous cell carcinoma also should be considered, as it is a malignant proliferation of cutaneous epithelium that clinically manifests as a hyperkeratotic papule or plaque.5
THE DIAGNOSIS: Dermatofibroma
Histopathologic examination of the shave biopsy revealed fascicles of plump fibroblasts and histiocytes interposed between thick collagen bundles within the dermis, consistent with a diagnosis of dermatofibroma (DF). Dermatofibroma is a common benign skin tumor that classically manifests as brownish or reddish-brown firm papules or nodules that dimple when compressed. While the exact etiology of DF remains uncertain, it is believed to arise from a combined neoplastic and reactive fibroblastic proliferation process in response to stimuli, such as minor trauma or insect bites (as in our patient).1
On histopathology, the most common findings associated with DF are dermal proliferation of spindle-shaped fibroblasts arranged in a storiform or whorled pattern.2 In this patient, fascicles of plump fibroblasts and histiocytes were observed interspersed among thick collagen bundles within the dermis (Figure). Other histologic variants of DF include cellular, histiocytic, lipidized, angiomatous, aneurysmal, clear cell, monster cell, myxoid, keloidal, palisading, osteoclastic, and epithelioid.
On dermatoscopic examination, a pigment network is the most common feature, followed by a white scarlike patch, brown dots and globules, and vascular structures.2 Atypical DF variants can manifest with diverse clinical morphologies; one example is giant DF, which exceeds 5 cm and may exhibit an ulcerated or pedunculated appearance, as seen in our case.3 In such cases, a thorough clinical examination coupled with histopathologic analysis becomes paramount for accurate diagnosis.
Most cases of DF do not require intervention unless there are cosmetic concerns or the lesions are symptomatic. Surgical excision is a common and effective treatment method but results in scarring. Intralesional steroid injection and cryotherapy are less aggressive treatment options but have limited efficacy. Lasers, including carbon dioxide and pulsed dye lasers, are infrequently used; however, recurrence is possible with any treatment modality.4 Local recurrence is common, occurring in 26% to 50% of cases, particularly in atypical dermatofibroma variants after treatment.5 Recurrence is more likely with primary lesions larger than 1 cm.5
Several conditions share clinical features with DF, necessitating a thorough differential diagnosis. Dermatofibrosarcoma protuberans (DFSP) is a rare, locally aggressive, malignant tumor with a propensity for recurrence. It manifests as a slow-growing, red-brown, indurated plaque with irregular nodularity. Immunohistochemical staining can be used to differentiate DF from DFSP, with DF typically expressing factor XIIIa and lacking CD34, whereas DFSP exhibits CD34 positivity and lacks factor XIIIa expression.6 Another diagnosis in the differential is fibrosarcoma, a malignant tumor of fibroblasts that manifests as a painless, enlarging, poorly defined mass on the lower extremities. Histopathologic features include atypical fibroblasts and collagen with proliferation of atypical spindle-shaped cells.
Other benign lesions to consider include neurofibroma, which may manifest as a firm nodule but is derived from nerve tissue. Clinically, neurofibromas can be differentiated by their association with neurofibromatosis and softer texture. Cutaneous squamous cell carcinoma also should be considered, as it is a malignant proliferation of cutaneous epithelium that clinically manifests as a hyperkeratotic papule or plaque.5
- Hui P, J. Glusac E, Sinard JH, et al. Clonal analysis of cutaneous fibrous histiocytoma (dermatofibroma). J Cutan Pathol. 2002;29:385-389.
- Şenel E, Yuyucu Karabulut Y, Doğruer Şenel S. Clinical, histopathological, dermatoscopic and digital microscopic features of dermatofibroma: a retrospective analysis of 200 lesions. J Eur Acad Derm Venereol. 2015;29:1958-1966.
- Requena L, Fariña MC, Fuente C, et al. Giant dermatofibroma: a little-known clinical variant of dermatofibroma. J Am Acad Dermatol. 1994;30:714-718.
- Alonso-Castro L, Boixeda P, Segura-Palacios JM, et al. Dermatofibromas treated with pulsed dye laser: clinical and dermoscopic outcomes. J Cosmet Laser Ther. 2012;14:98-101.
- Gaufin M, Michaelis T, Duffy K. Cellular dermatofibroma: clinicopathologic review of 218 cases of cellular dermatofibroma to determine the clinical recurrence rate. Dermatol Surg. 2019;45:1359-1364.
- West KL, Cardona DM, Su Z, et al. Immunohistochemical markers in fibrohistiocytic lesions: factor XIIIa, CD34, S-100 and p75. Am J Dermatopathol. 2014;36:414-419.
- Hui P, J. Glusac E, Sinard JH, et al. Clonal analysis of cutaneous fibrous histiocytoma (dermatofibroma). J Cutan Pathol. 2002;29:385-389.
- Şenel E, Yuyucu Karabulut Y, Doğruer Şenel S. Clinical, histopathological, dermatoscopic and digital microscopic features of dermatofibroma: a retrospective analysis of 200 lesions. J Eur Acad Derm Venereol. 2015;29:1958-1966.
- Requena L, Fariña MC, Fuente C, et al. Giant dermatofibroma: a little-known clinical variant of dermatofibroma. J Am Acad Dermatol. 1994;30:714-718.
- Alonso-Castro L, Boixeda P, Segura-Palacios JM, et al. Dermatofibromas treated with pulsed dye laser: clinical and dermoscopic outcomes. J Cosmet Laser Ther. 2012;14:98-101.
- Gaufin M, Michaelis T, Duffy K. Cellular dermatofibroma: clinicopathologic review of 218 cases of cellular dermatofibroma to determine the clinical recurrence rate. Dermatol Surg. 2019;45:1359-1364.
- West KL, Cardona DM, Su Z, et al. Immunohistochemical markers in fibrohistiocytic lesions: factor XIIIa, CD34, S-100 and p75. Am J Dermatopathol. 2014;36:414-419.
Asymptomatic Enlarging Lobulated Mass on the Lower Leg
Asymptomatic Enlarging Lobulated Mass on the Lower Leg
A 69-year-old woman presented to the dermatology clinic with enlarging nodules on the bilateral lower legs of several years’ duration. Cutaneous examination of the legs revealed a brown, pedunculated, lobulated nodule on the lateral right lower leg measuring 5.0×1.9 cm. The patient reported that the lesion first appeared after a mosquito bite and then slowly grew over several years. A shave biopsy of the lesion was performed.

