User login
Topical Hypochlorous Acid for Acne Vulgaris: Mechanisms, Clinical Evidence, and Therapeutic Potential
Topical Hypochlorous Acid for Acne Vulgaris: Mechanisms, Clinical Evidence, and Therapeutic Potential
Acne vulgaris, a chronic inflammatory disease of the pilosebaceous unit, is among the most prevalent dermatologic conditions worldwide. Though symptoms range in severity, patients can experience painful irritation and scarring that can lead to substantial psychological distress and impact quality of life. Cutibacterium acnes plays a central role in acne development through biofilm formation, lipase activity, and activation of innate immune pathways, which together contribute to a cycle of inflammation and comedogenesis.1
First-line treatments for acne vulgaris include topical benzoyl peroxide, topical retinoids, and topical antibiotics, while oral spironolactone and tetracyclines can be used alongside topical therapies for more extensive disease. Additionally, isotretinoin is generally reserved for severe or refractory cases. While these therapies are effective, each has notable limitations and adverse effects that in some cases limit adherence and efficacy. The most common adverse effects seen with topical acne therapies include irritation and dryness. Systemic therapies such as spironolactone can cause fatigue, dizziness, and birth defects, while prolonged antibiotic use can promote the risk for antimicrobial resistance.2
Hypochlorous acid (HOCl) is a naturally occurring weak acid produced by neutrophils and currently is approved by the US Food and Drug Administration for wound cleansing, burn management, and dermal lesion irrigation. Although it is not approved for the treatment of acne, stabilized HOCl formulations have been used off label in dermatology for this purpose. Interest in HOCl stems from its broad-spectrum antimicrobial activity against C acnes, anti-inflammatory properties, and favorable safety profile. This literature review examines the mechanism of action, clinical evidence, and potential role of HOCl in acne management, contextualizing its use relative to current standard therapies.
Methods
A narrative literature review was conducted to identify and synthesize peer-reviewed evidence on the use of HOCl in dermatology, with emphasis on its potential role in acne management. Searches were performed using PubMed and Scopus databases. Search terms included combinations of hypochlorous acid, acne, acne vulgaris, dermatology, antimicrobial, anti-inflammatory, biofilm, and skin barrier. Eligible publications included original research articles, randomized controlled trials, retrospective studies, preclinical in vitro and in vivo studies, and systematic reviews published in English between January 2000 and December 2024. Titles and abstracts were screened for relevance, and the final selection included 16 peer-reviewed articles that met the inclusion criteria.
Results
Hypochlorous acid exhibits rapid, broad-spectrum antimicrobial activity against gram-positive and gram-negative bacteria and fungi. In vitro time-kill assays demonstrated that stabilized HOCl was bactericidal against a variety of pathogens, including methicillin-resistant Staphylococcus aureus, methicillin-sensitive S aureus, Staphylococcus epidermidis, Corynebacterium species, Streptococcus pyogenes, Pseudomonas aeruginosa, Candida albicans, and C acnes. Specifically, HOCl achieved 99.99% or greater kill within 2 minutes.3 Moreover, HOCl’s antimicrobial efficacy against this panel of organisms was found to be comparable to or greater than that of commonly used antiseptics, including povidone-iodine, chlorhexidine gluconate, and isopropyl alcohol.3 An additional study using HOCl stabilized in 0.9% saline (pH, 3.5-4.0) confirmed its rapid activity across gram-positive, gram-negative, and fungal species, again demonstrating 99.99 % or greater reduction within 1 to 2 minutes of exposure.4
Hypochlorous acid also has demonstrated substantial biofilm-disruptive properties. In vitro studies demonstrated that HOCl can penetrate and disrupt early-stage biofilms by oxidizing extracellular polymeric substances and damaging bacterial membranes; however, while HOCl was effective at destroying immature biofilms and preventing biofilm formation, its efficacy against mature, fully established biofilms was more limited.5 Thus, topical HOCl may be most effective during the early colonization phase of acne, helping to prevent biofilm maturation and subsequent inflammatory lesion formation. Unlike traditional topical and oral antibiotics, HOCl’s nonspecific oxidative mechanism of action is less likely to contribute to microbial resistance. These findings highlight HOCl as a rapid, broad-spectrum antimicrobial with additional biofilm-disruptive activity, supporting its potential role as an early-intervention therapeutic in acne treatment.
In addition to its antimicrobial effects, HOCl is a potent anti-inflammatory molecule that exerts its anti-inflammatory effects through several mechanisms. HOCl acts as a mast cell membrane stabilizer, inhibiting degranulation. Hypochlorous acid also has been demonstrated to reduce levels of leukotriene B4 and interleukin (IL) 2, which supports that HOCl has both antipruritic and anti-inflammatory properties.6 In keratinocytes and immune cells, HOCl has been shown to suppress the transcription of multiple proinflammatory cytokines by oxidizing IκB kinase β, which then prevents the activation of the nuclear factor kappa B (NF-κB) signaling pathway.7 Additionally, in a murine model of atopic dermatitis, treatment with HOCl resulted in a downregulation of key proinflammatory and Th2-associated cytokines, including IL-1β, IL-4, IL-6, IL-13, tumor necrosis factor α, thymus and activation-regulated chemokine, thymic stromal lymphopoietin, and IL-31. Parallel in vitro assays revealed that HOCl inhibited phosphorylation of mitogen-activated protein kinase (MAPK) and inhibitor of κB, which inhibits the downstream proinflammatory pathways, thereby elucidating a mechanistic basis for its anti-inflammatory effects.8 C acnes has been shown to activate the toll-like receptor 2 pathway on keratinocytes and macrophages, triggering NF-κB–dependent release of IL-1β and tumor necrosis factor α.9
By inhibiting these same signaling pathways, HOCl may attenuate the inflammatory response associated with acne lesions while simultaneously reducing microbial load. These combined anti-inflammatory and antimicrobial effects also may contribute to improved healing outcomes. Emerging clinical evidence supports HOCl’s benefit in minimizing scarring and postinflammatory sequelae. A comparative study evaluating a silicone-based scar gel containing HOCl vs silicone gel alone found that the HOCl-containing formulation produced greater improvement in hypertrophic and keloid scar appearance and overall scar texture.10 These findings suggest that HOCl may have beneficial effects on wound healing and scar remodeling.
In murine models of acute radiation dermatitis, topical HOCl reduced NF-κB–dependent gene expression, decreased epidermal ulceration, and promoted re-epithelialization to near-normal histologic appearance.7 A double-blind, randomized controlled trial evaluating topical sodium hypochlorite 0.005%, which is a compound in equilibrium with HOCl under physiologic pH, demonstrated a statistically significant reduction in papules among patients with mild to moderate acne after 1 month of treatment (P<.0001). Female participants exhibited greater lesion improvement, suggesting possible hormonal or immunologic modulation of response.11 Although limited in scale, this literature review provides preliminary clinical support for the therapeutic potential of HOCl in the treatment of acne. Collectively, these findings highlight the potential of HOCl as an emerging treatment in acne and other dermatologic conditions.
Comment
Traditional acne therapies include topical agents such as benzoyl peroxide, topical retinoids (eg, tretinoin, adapalene), and salicylic acid, as well as systemic agents such as oral antibiotics, spironolactone, and isotretinoin. While these treatments are effective, their use may be limited by irritation, antibiotic resistance, and systemic adverse effects.
Hypochlorous acid is a potential adjunctive option that acts locally with minimal irritation and without hormonal or systemic activity.12 Its antimicrobial and anti-inflammatory mechanisms target key pathogenic pathways in acne while maintaining excellent cutaneous tolerability. In a randomized, double-blind, placebo-controlled trial of 89 patients comparing topical HOCl solution with benzoyl peroxide for mild to moderate acne, HOCl demonstrated comparable improvement in lesion counts.13 Importantly, no local adverse effects were reported in either group and no dose adjustments were needed during the 12-week treatment period. Although both agents were effective, the absence of irritation with HOCl contrasts with the dryness and erythema frequently associated with benzoyl peroxide.
Additionally, a clinical trial comparing HOCl 0.01% with standard antiseptics, including isopropyl alcohol, povidone-iodine, and chlorhexidine gluconate, showed that HOCl achieved comparable antibacterial reductions while remaining well tolerated and free of facial adverse effects.14 Similarly, studies evaluating HOCl’s antimicrobial efficacy have confirmed that it is nontoxic to periocular and facial tissues, further supporting its safety for use on delicate skin regions.3 Importantly, in an experimental model evaluating both healthy skin and skin with experimentally induced irritant contact dermatitis, repeated application of an HOCl-based formulation did not impair skin barrier function, underscoring its excellent cutaneous compatibility even under inflammatory conditions.15 Ultimately, these findings suggest that HOCl offers efficacy comparable to benzoyl peroxide and retinoids while eliminating the irritation and barrier disruption that can limit the use of these first-line agents.
Topical antibiotics such as clindamycin and erythromycin are used widely for their antimicrobial and anti-inflammatory properties but increasingly are undermined by antibiotic resistance. In contrast, HOCl has been shown to reduce bacterial load without altering microbial diversity, supporting its role as a resistance-neutral antimicrobial option for acne management.16 These characteristics position HOCl as a well-tolerated, resistance-neutral adjunctive treatment that warrants further investigation through larger, controlled trials.
Topical HOCl formulations, particularly those available as sprays or misting solutions, have gained attention on social media for their ease of use and versatility. Although formal studies evaluating adherence or outcomes in this context are currently limited, this emerging consumer trend underscores the perceived convenience of HOCl compared with traditional acne therapies. These formulations can be applied throughout the day, including between exercise and work, supporting adherence among patients with active lifestyles. In contrast to many conventional topical agents that require specific application timing, cleansing routines, or avoidance of cosmetic products, HOCl sprays offer flexible use without disrupting daily activities. These characteristics highlight HOCl’s potential as a user-friendly option that may support consistent application and optimize therapeutic outcomes.
Conclusion
The addition of HOCl to acne treatment regimens offers several potential benefits. Its antimicrobial and anti-inflammatory properties may help prevent new papules and pustules, while its favorable tolerability profile minimizes irritation and systemic adverse effects. Preliminary data also suggest efficacy in androgen-mediated acne, though additional studies are needed to confirm these findings.¹¹ Current evidence remains limited by small sample sizes, short follow-up durations, and a lack of comparative studies among available formulations. Accordingly, HOCl should be considered an adjunctive rather than replacement therapy pending larger studies with longer follow-up.
- Vasam M, Korutla S, Bohara RA. Acne vulgaris: a review of the pathophysiology, treatment, and recent nanotechnology based advances. Biochem Biophys Rep. 2023;36:101578.
- Reynolds RV, Yeung H, Cheng CE, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024;90:1006.E1-1006.E30.
- Anagnostopoulos AG, Rong A, Miller D, et al. 0.01% hypochlorous acid as an alternative skin antiseptic: an in vitro comparison. Dermatol Surg. 2018;44:1489-1493.
- Wang L, Bassiri M, Najafi R, et al. Hypochlorous acid as a potential wound care agent: part I. stabilized hypochlorous acid: a component of the inorganic armamentarium of innate immunity. J Burns Wounds. 2007;6:E5.
- Ortega-Peña S, Hidalgo-González C, Robson MC, et al. In vitro microbicidal, anti-biofilm and cytotoxic effects of different commercial antiseptics. Int Wound J. 2017;14:470-479.
- Gold MH, Andriessen A, Bhatia AC, et al. Topical stabilized hypochlorous acid: the future gold standard for wound care and scar management in dermatologic and plastic surgery procedures. J Cosmet Dermatol. 2020;19:270-277.
- Leung TH, Zhang LF, Wang J, et al. Topical hypochlorite ameliorates NF-κB–mediated skin diseases in mice. J Clin Invest. 2013;123:5361-5370.
- Fukuyama T, Martel BC, Linder KE, et al. Hypochlorous acid is antipruritic and anti‐inflammatory in a mouse model of atopic dermatitis. Clin Exp Allergy. 2018;48:78-88.
- Lheure C, Grange PA, Ollagnier G, et al. TLR-2 recognizes Propionibacterium acnes CAMP factor 1 from highly inflammatory strains. PLoS ONE. 2016;11:E0167237.
- Gold MH, Andriessen A, Dayan SH, et al. Hypochlorous acid gel technology—its impact on postprocedure treatment and scar prevention. J Cosmet Dermatol. 2017;16:162-167.
- Dorostkar A, Ghahartars M, Namazi MR, et al. Sodium hypochlorite 0.005% versus placebo in the treatment of mild to moderate acne: a double-blind randomized controlled trial. Dermatol Pract Concept. Published online May 20, 2021.
- del Rosso JQ, Bhatia N. Status report on topical hypochlorous acid: clinical relevance of specific formulations, potential modes of action, and study outcomes. J Clin Aesthet Dermatol. 2018;11:36-39.
- Tirado-Sánchez A, Ponce-Olivera RM. Efficacy and tolerance of superoxidized solution in the treatment of mild to moderate inflammatory acne. a double-blinded, placebo- controlled, parallel-group, randomized, clinical trial. J Dermatolog Treat. 2009;20:289-292.
- Tran AQ, Topilow N, Rong A, et al. Comparison of skin antiseptic agents and the role of 0.01% hypochlorous acid. Aesthet Surg J. 2021;41:1170-1175.
- Yüksel YT, Sonne M, Nørreslet LB, et al. Skin barrier response to active chlorine hand disinfectant—an experimental study comparing skin barrier response to active chlorine hand disinfectant and alcohol-based hand rub on healthy skin and eczematous skin. Skin Res Technol. 2022;28:89-97.
- Stroman D, Mintun K, Epstein A, et al. Reduction in bacterial load using hypochlorous acid hygiene solution on ocular skin. OPTH. 2017;11:707-714.
Acne vulgaris, a chronic inflammatory disease of the pilosebaceous unit, is among the most prevalent dermatologic conditions worldwide. Though symptoms range in severity, patients can experience painful irritation and scarring that can lead to substantial psychological distress and impact quality of life. Cutibacterium acnes plays a central role in acne development through biofilm formation, lipase activity, and activation of innate immune pathways, which together contribute to a cycle of inflammation and comedogenesis.1
First-line treatments for acne vulgaris include topical benzoyl peroxide, topical retinoids, and topical antibiotics, while oral spironolactone and tetracyclines can be used alongside topical therapies for more extensive disease. Additionally, isotretinoin is generally reserved for severe or refractory cases. While these therapies are effective, each has notable limitations and adverse effects that in some cases limit adherence and efficacy. The most common adverse effects seen with topical acne therapies include irritation and dryness. Systemic therapies such as spironolactone can cause fatigue, dizziness, and birth defects, while prolonged antibiotic use can promote the risk for antimicrobial resistance.2
Hypochlorous acid (HOCl) is a naturally occurring weak acid produced by neutrophils and currently is approved by the US Food and Drug Administration for wound cleansing, burn management, and dermal lesion irrigation. Although it is not approved for the treatment of acne, stabilized HOCl formulations have been used off label in dermatology for this purpose. Interest in HOCl stems from its broad-spectrum antimicrobial activity against C acnes, anti-inflammatory properties, and favorable safety profile. This literature review examines the mechanism of action, clinical evidence, and potential role of HOCl in acne management, contextualizing its use relative to current standard therapies.
Methods
A narrative literature review was conducted to identify and synthesize peer-reviewed evidence on the use of HOCl in dermatology, with emphasis on its potential role in acne management. Searches were performed using PubMed and Scopus databases. Search terms included combinations of hypochlorous acid, acne, acne vulgaris, dermatology, antimicrobial, anti-inflammatory, biofilm, and skin barrier. Eligible publications included original research articles, randomized controlled trials, retrospective studies, preclinical in vitro and in vivo studies, and systematic reviews published in English between January 2000 and December 2024. Titles and abstracts were screened for relevance, and the final selection included 16 peer-reviewed articles that met the inclusion criteria.
Results
Hypochlorous acid exhibits rapid, broad-spectrum antimicrobial activity against gram-positive and gram-negative bacteria and fungi. In vitro time-kill assays demonstrated that stabilized HOCl was bactericidal against a variety of pathogens, including methicillin-resistant Staphylococcus aureus, methicillin-sensitive S aureus, Staphylococcus epidermidis, Corynebacterium species, Streptococcus pyogenes, Pseudomonas aeruginosa, Candida albicans, and C acnes. Specifically, HOCl achieved 99.99% or greater kill within 2 minutes.3 Moreover, HOCl’s antimicrobial efficacy against this panel of organisms was found to be comparable to or greater than that of commonly used antiseptics, including povidone-iodine, chlorhexidine gluconate, and isopropyl alcohol.3 An additional study using HOCl stabilized in 0.9% saline (pH, 3.5-4.0) confirmed its rapid activity across gram-positive, gram-negative, and fungal species, again demonstrating 99.99 % or greater reduction within 1 to 2 minutes of exposure.4
Hypochlorous acid also has demonstrated substantial biofilm-disruptive properties. In vitro studies demonstrated that HOCl can penetrate and disrupt early-stage biofilms by oxidizing extracellular polymeric substances and damaging bacterial membranes; however, while HOCl was effective at destroying immature biofilms and preventing biofilm formation, its efficacy against mature, fully established biofilms was more limited.5 Thus, topical HOCl may be most effective during the early colonization phase of acne, helping to prevent biofilm maturation and subsequent inflammatory lesion formation. Unlike traditional topical and oral antibiotics, HOCl’s nonspecific oxidative mechanism of action is less likely to contribute to microbial resistance. These findings highlight HOCl as a rapid, broad-spectrum antimicrobial with additional biofilm-disruptive activity, supporting its potential role as an early-intervention therapeutic in acne treatment.
In addition to its antimicrobial effects, HOCl is a potent anti-inflammatory molecule that exerts its anti-inflammatory effects through several mechanisms. HOCl acts as a mast cell membrane stabilizer, inhibiting degranulation. Hypochlorous acid also has been demonstrated to reduce levels of leukotriene B4 and interleukin (IL) 2, which supports that HOCl has both antipruritic and anti-inflammatory properties.6 In keratinocytes and immune cells, HOCl has been shown to suppress the transcription of multiple proinflammatory cytokines by oxidizing IκB kinase β, which then prevents the activation of the nuclear factor kappa B (NF-κB) signaling pathway.7 Additionally, in a murine model of atopic dermatitis, treatment with HOCl resulted in a downregulation of key proinflammatory and Th2-associated cytokines, including IL-1β, IL-4, IL-6, IL-13, tumor necrosis factor α, thymus and activation-regulated chemokine, thymic stromal lymphopoietin, and IL-31. Parallel in vitro assays revealed that HOCl inhibited phosphorylation of mitogen-activated protein kinase (MAPK) and inhibitor of κB, which inhibits the downstream proinflammatory pathways, thereby elucidating a mechanistic basis for its anti-inflammatory effects.8 C acnes has been shown to activate the toll-like receptor 2 pathway on keratinocytes and macrophages, triggering NF-κB–dependent release of IL-1β and tumor necrosis factor α.9
By inhibiting these same signaling pathways, HOCl may attenuate the inflammatory response associated with acne lesions while simultaneously reducing microbial load. These combined anti-inflammatory and antimicrobial effects also may contribute to improved healing outcomes. Emerging clinical evidence supports HOCl’s benefit in minimizing scarring and postinflammatory sequelae. A comparative study evaluating a silicone-based scar gel containing HOCl vs silicone gel alone found that the HOCl-containing formulation produced greater improvement in hypertrophic and keloid scar appearance and overall scar texture.10 These findings suggest that HOCl may have beneficial effects on wound healing and scar remodeling.
In murine models of acute radiation dermatitis, topical HOCl reduced NF-κB–dependent gene expression, decreased epidermal ulceration, and promoted re-epithelialization to near-normal histologic appearance.7 A double-blind, randomized controlled trial evaluating topical sodium hypochlorite 0.005%, which is a compound in equilibrium with HOCl under physiologic pH, demonstrated a statistically significant reduction in papules among patients with mild to moderate acne after 1 month of treatment (P<.0001). Female participants exhibited greater lesion improvement, suggesting possible hormonal or immunologic modulation of response.11 Although limited in scale, this literature review provides preliminary clinical support for the therapeutic potential of HOCl in the treatment of acne. Collectively, these findings highlight the potential of HOCl as an emerging treatment in acne and other dermatologic conditions.
Comment
Traditional acne therapies include topical agents such as benzoyl peroxide, topical retinoids (eg, tretinoin, adapalene), and salicylic acid, as well as systemic agents such as oral antibiotics, spironolactone, and isotretinoin. While these treatments are effective, their use may be limited by irritation, antibiotic resistance, and systemic adverse effects.
Hypochlorous acid is a potential adjunctive option that acts locally with minimal irritation and without hormonal or systemic activity.12 Its antimicrobial and anti-inflammatory mechanisms target key pathogenic pathways in acne while maintaining excellent cutaneous tolerability. In a randomized, double-blind, placebo-controlled trial of 89 patients comparing topical HOCl solution with benzoyl peroxide for mild to moderate acne, HOCl demonstrated comparable improvement in lesion counts.13 Importantly, no local adverse effects were reported in either group and no dose adjustments were needed during the 12-week treatment period. Although both agents were effective, the absence of irritation with HOCl contrasts with the dryness and erythema frequently associated with benzoyl peroxide.
Additionally, a clinical trial comparing HOCl 0.01% with standard antiseptics, including isopropyl alcohol, povidone-iodine, and chlorhexidine gluconate, showed that HOCl achieved comparable antibacterial reductions while remaining well tolerated and free of facial adverse effects.14 Similarly, studies evaluating HOCl’s antimicrobial efficacy have confirmed that it is nontoxic to periocular and facial tissues, further supporting its safety for use on delicate skin regions.3 Importantly, in an experimental model evaluating both healthy skin and skin with experimentally induced irritant contact dermatitis, repeated application of an HOCl-based formulation did not impair skin barrier function, underscoring its excellent cutaneous compatibility even under inflammatory conditions.15 Ultimately, these findings suggest that HOCl offers efficacy comparable to benzoyl peroxide and retinoids while eliminating the irritation and barrier disruption that can limit the use of these first-line agents.
Topical antibiotics such as clindamycin and erythromycin are used widely for their antimicrobial and anti-inflammatory properties but increasingly are undermined by antibiotic resistance. In contrast, HOCl has been shown to reduce bacterial load without altering microbial diversity, supporting its role as a resistance-neutral antimicrobial option for acne management.16 These characteristics position HOCl as a well-tolerated, resistance-neutral adjunctive treatment that warrants further investigation through larger, controlled trials.
Topical HOCl formulations, particularly those available as sprays or misting solutions, have gained attention on social media for their ease of use and versatility. Although formal studies evaluating adherence or outcomes in this context are currently limited, this emerging consumer trend underscores the perceived convenience of HOCl compared with traditional acne therapies. These formulations can be applied throughout the day, including between exercise and work, supporting adherence among patients with active lifestyles. In contrast to many conventional topical agents that require specific application timing, cleansing routines, or avoidance of cosmetic products, HOCl sprays offer flexible use without disrupting daily activities. These characteristics highlight HOCl’s potential as a user-friendly option that may support consistent application and optimize therapeutic outcomes.
Conclusion
The addition of HOCl to acne treatment regimens offers several potential benefits. Its antimicrobial and anti-inflammatory properties may help prevent new papules and pustules, while its favorable tolerability profile minimizes irritation and systemic adverse effects. Preliminary data also suggest efficacy in androgen-mediated acne, though additional studies are needed to confirm these findings.¹¹ Current evidence remains limited by small sample sizes, short follow-up durations, and a lack of comparative studies among available formulations. Accordingly, HOCl should be considered an adjunctive rather than replacement therapy pending larger studies with longer follow-up.
Acne vulgaris, a chronic inflammatory disease of the pilosebaceous unit, is among the most prevalent dermatologic conditions worldwide. Though symptoms range in severity, patients can experience painful irritation and scarring that can lead to substantial psychological distress and impact quality of life. Cutibacterium acnes plays a central role in acne development through biofilm formation, lipase activity, and activation of innate immune pathways, which together contribute to a cycle of inflammation and comedogenesis.1
First-line treatments for acne vulgaris include topical benzoyl peroxide, topical retinoids, and topical antibiotics, while oral spironolactone and tetracyclines can be used alongside topical therapies for more extensive disease. Additionally, isotretinoin is generally reserved for severe or refractory cases. While these therapies are effective, each has notable limitations and adverse effects that in some cases limit adherence and efficacy. The most common adverse effects seen with topical acne therapies include irritation and dryness. Systemic therapies such as spironolactone can cause fatigue, dizziness, and birth defects, while prolonged antibiotic use can promote the risk for antimicrobial resistance.2
Hypochlorous acid (HOCl) is a naturally occurring weak acid produced by neutrophils and currently is approved by the US Food and Drug Administration for wound cleansing, burn management, and dermal lesion irrigation. Although it is not approved for the treatment of acne, stabilized HOCl formulations have been used off label in dermatology for this purpose. Interest in HOCl stems from its broad-spectrum antimicrobial activity against C acnes, anti-inflammatory properties, and favorable safety profile. This literature review examines the mechanism of action, clinical evidence, and potential role of HOCl in acne management, contextualizing its use relative to current standard therapies.
Methods
A narrative literature review was conducted to identify and synthesize peer-reviewed evidence on the use of HOCl in dermatology, with emphasis on its potential role in acne management. Searches were performed using PubMed and Scopus databases. Search terms included combinations of hypochlorous acid, acne, acne vulgaris, dermatology, antimicrobial, anti-inflammatory, biofilm, and skin barrier. Eligible publications included original research articles, randomized controlled trials, retrospective studies, preclinical in vitro and in vivo studies, and systematic reviews published in English between January 2000 and December 2024. Titles and abstracts were screened for relevance, and the final selection included 16 peer-reviewed articles that met the inclusion criteria.
Results
Hypochlorous acid exhibits rapid, broad-spectrum antimicrobial activity against gram-positive and gram-negative bacteria and fungi. In vitro time-kill assays demonstrated that stabilized HOCl was bactericidal against a variety of pathogens, including methicillin-resistant Staphylococcus aureus, methicillin-sensitive S aureus, Staphylococcus epidermidis, Corynebacterium species, Streptococcus pyogenes, Pseudomonas aeruginosa, Candida albicans, and C acnes. Specifically, HOCl achieved 99.99% or greater kill within 2 minutes.3 Moreover, HOCl’s antimicrobial efficacy against this panel of organisms was found to be comparable to or greater than that of commonly used antiseptics, including povidone-iodine, chlorhexidine gluconate, and isopropyl alcohol.3 An additional study using HOCl stabilized in 0.9% saline (pH, 3.5-4.0) confirmed its rapid activity across gram-positive, gram-negative, and fungal species, again demonstrating 99.99 % or greater reduction within 1 to 2 minutes of exposure.4
Hypochlorous acid also has demonstrated substantial biofilm-disruptive properties. In vitro studies demonstrated that HOCl can penetrate and disrupt early-stage biofilms by oxidizing extracellular polymeric substances and damaging bacterial membranes; however, while HOCl was effective at destroying immature biofilms and preventing biofilm formation, its efficacy against mature, fully established biofilms was more limited.5 Thus, topical HOCl may be most effective during the early colonization phase of acne, helping to prevent biofilm maturation and subsequent inflammatory lesion formation. Unlike traditional topical and oral antibiotics, HOCl’s nonspecific oxidative mechanism of action is less likely to contribute to microbial resistance. These findings highlight HOCl as a rapid, broad-spectrum antimicrobial with additional biofilm-disruptive activity, supporting its potential role as an early-intervention therapeutic in acne treatment.
In addition to its antimicrobial effects, HOCl is a potent anti-inflammatory molecule that exerts its anti-inflammatory effects through several mechanisms. HOCl acts as a mast cell membrane stabilizer, inhibiting degranulation. Hypochlorous acid also has been demonstrated to reduce levels of leukotriene B4 and interleukin (IL) 2, which supports that HOCl has both antipruritic and anti-inflammatory properties.6 In keratinocytes and immune cells, HOCl has been shown to suppress the transcription of multiple proinflammatory cytokines by oxidizing IκB kinase β, which then prevents the activation of the nuclear factor kappa B (NF-κB) signaling pathway.7 Additionally, in a murine model of atopic dermatitis, treatment with HOCl resulted in a downregulation of key proinflammatory and Th2-associated cytokines, including IL-1β, IL-4, IL-6, IL-13, tumor necrosis factor α, thymus and activation-regulated chemokine, thymic stromal lymphopoietin, and IL-31. Parallel in vitro assays revealed that HOCl inhibited phosphorylation of mitogen-activated protein kinase (MAPK) and inhibitor of κB, which inhibits the downstream proinflammatory pathways, thereby elucidating a mechanistic basis for its anti-inflammatory effects.8 C acnes has been shown to activate the toll-like receptor 2 pathway on keratinocytes and macrophages, triggering NF-κB–dependent release of IL-1β and tumor necrosis factor α.9
By inhibiting these same signaling pathways, HOCl may attenuate the inflammatory response associated with acne lesions while simultaneously reducing microbial load. These combined anti-inflammatory and antimicrobial effects also may contribute to improved healing outcomes. Emerging clinical evidence supports HOCl’s benefit in minimizing scarring and postinflammatory sequelae. A comparative study evaluating a silicone-based scar gel containing HOCl vs silicone gel alone found that the HOCl-containing formulation produced greater improvement in hypertrophic and keloid scar appearance and overall scar texture.10 These findings suggest that HOCl may have beneficial effects on wound healing and scar remodeling.
In murine models of acute radiation dermatitis, topical HOCl reduced NF-κB–dependent gene expression, decreased epidermal ulceration, and promoted re-epithelialization to near-normal histologic appearance.7 A double-blind, randomized controlled trial evaluating topical sodium hypochlorite 0.005%, which is a compound in equilibrium with HOCl under physiologic pH, demonstrated a statistically significant reduction in papules among patients with mild to moderate acne after 1 month of treatment (P<.0001). Female participants exhibited greater lesion improvement, suggesting possible hormonal or immunologic modulation of response.11 Although limited in scale, this literature review provides preliminary clinical support for the therapeutic potential of HOCl in the treatment of acne. Collectively, these findings highlight the potential of HOCl as an emerging treatment in acne and other dermatologic conditions.
Comment
Traditional acne therapies include topical agents such as benzoyl peroxide, topical retinoids (eg, tretinoin, adapalene), and salicylic acid, as well as systemic agents such as oral antibiotics, spironolactone, and isotretinoin. While these treatments are effective, their use may be limited by irritation, antibiotic resistance, and systemic adverse effects.
Hypochlorous acid is a potential adjunctive option that acts locally with minimal irritation and without hormonal or systemic activity.12 Its antimicrobial and anti-inflammatory mechanisms target key pathogenic pathways in acne while maintaining excellent cutaneous tolerability. In a randomized, double-blind, placebo-controlled trial of 89 patients comparing topical HOCl solution with benzoyl peroxide for mild to moderate acne, HOCl demonstrated comparable improvement in lesion counts.13 Importantly, no local adverse effects were reported in either group and no dose adjustments were needed during the 12-week treatment period. Although both agents were effective, the absence of irritation with HOCl contrasts with the dryness and erythema frequently associated with benzoyl peroxide.
Additionally, a clinical trial comparing HOCl 0.01% with standard antiseptics, including isopropyl alcohol, povidone-iodine, and chlorhexidine gluconate, showed that HOCl achieved comparable antibacterial reductions while remaining well tolerated and free of facial adverse effects.14 Similarly, studies evaluating HOCl’s antimicrobial efficacy have confirmed that it is nontoxic to periocular and facial tissues, further supporting its safety for use on delicate skin regions.3 Importantly, in an experimental model evaluating both healthy skin and skin with experimentally induced irritant contact dermatitis, repeated application of an HOCl-based formulation did not impair skin barrier function, underscoring its excellent cutaneous compatibility even under inflammatory conditions.15 Ultimately, these findings suggest that HOCl offers efficacy comparable to benzoyl peroxide and retinoids while eliminating the irritation and barrier disruption that can limit the use of these first-line agents.
Topical antibiotics such as clindamycin and erythromycin are used widely for their antimicrobial and anti-inflammatory properties but increasingly are undermined by antibiotic resistance. In contrast, HOCl has been shown to reduce bacterial load without altering microbial diversity, supporting its role as a resistance-neutral antimicrobial option for acne management.16 These characteristics position HOCl as a well-tolerated, resistance-neutral adjunctive treatment that warrants further investigation through larger, controlled trials.
Topical HOCl formulations, particularly those available as sprays or misting solutions, have gained attention on social media for their ease of use and versatility. Although formal studies evaluating adherence or outcomes in this context are currently limited, this emerging consumer trend underscores the perceived convenience of HOCl compared with traditional acne therapies. These formulations can be applied throughout the day, including between exercise and work, supporting adherence among patients with active lifestyles. In contrast to many conventional topical agents that require specific application timing, cleansing routines, or avoidance of cosmetic products, HOCl sprays offer flexible use without disrupting daily activities. These characteristics highlight HOCl’s potential as a user-friendly option that may support consistent application and optimize therapeutic outcomes.
Conclusion
The addition of HOCl to acne treatment regimens offers several potential benefits. Its antimicrobial and anti-inflammatory properties may help prevent new papules and pustules, while its favorable tolerability profile minimizes irritation and systemic adverse effects. Preliminary data also suggest efficacy in androgen-mediated acne, though additional studies are needed to confirm these findings.¹¹ Current evidence remains limited by small sample sizes, short follow-up durations, and a lack of comparative studies among available formulations. Accordingly, HOCl should be considered an adjunctive rather than replacement therapy pending larger studies with longer follow-up.
- Vasam M, Korutla S, Bohara RA. Acne vulgaris: a review of the pathophysiology, treatment, and recent nanotechnology based advances. Biochem Biophys Rep. 2023;36:101578.
- Reynolds RV, Yeung H, Cheng CE, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024;90:1006.E1-1006.E30.
- Anagnostopoulos AG, Rong A, Miller D, et al. 0.01% hypochlorous acid as an alternative skin antiseptic: an in vitro comparison. Dermatol Surg. 2018;44:1489-1493.
- Wang L, Bassiri M, Najafi R, et al. Hypochlorous acid as a potential wound care agent: part I. stabilized hypochlorous acid: a component of the inorganic armamentarium of innate immunity. J Burns Wounds. 2007;6:E5.
- Ortega-Peña S, Hidalgo-González C, Robson MC, et al. In vitro microbicidal, anti-biofilm and cytotoxic effects of different commercial antiseptics. Int Wound J. 2017;14:470-479.
- Gold MH, Andriessen A, Bhatia AC, et al. Topical stabilized hypochlorous acid: the future gold standard for wound care and scar management in dermatologic and plastic surgery procedures. J Cosmet Dermatol. 2020;19:270-277.
- Leung TH, Zhang LF, Wang J, et al. Topical hypochlorite ameliorates NF-κB–mediated skin diseases in mice. J Clin Invest. 2013;123:5361-5370.
- Fukuyama T, Martel BC, Linder KE, et al. Hypochlorous acid is antipruritic and anti‐inflammatory in a mouse model of atopic dermatitis. Clin Exp Allergy. 2018;48:78-88.
- Lheure C, Grange PA, Ollagnier G, et al. TLR-2 recognizes Propionibacterium acnes CAMP factor 1 from highly inflammatory strains. PLoS ONE. 2016;11:E0167237.
- Gold MH, Andriessen A, Dayan SH, et al. Hypochlorous acid gel technology—its impact on postprocedure treatment and scar prevention. J Cosmet Dermatol. 2017;16:162-167.
- Dorostkar A, Ghahartars M, Namazi MR, et al. Sodium hypochlorite 0.005% versus placebo in the treatment of mild to moderate acne: a double-blind randomized controlled trial. Dermatol Pract Concept. Published online May 20, 2021.
- del Rosso JQ, Bhatia N. Status report on topical hypochlorous acid: clinical relevance of specific formulations, potential modes of action, and study outcomes. J Clin Aesthet Dermatol. 2018;11:36-39.
- Tirado-Sánchez A, Ponce-Olivera RM. Efficacy and tolerance of superoxidized solution in the treatment of mild to moderate inflammatory acne. a double-blinded, placebo- controlled, parallel-group, randomized, clinical trial. J Dermatolog Treat. 2009;20:289-292.
- Tran AQ, Topilow N, Rong A, et al. Comparison of skin antiseptic agents and the role of 0.01% hypochlorous acid. Aesthet Surg J. 2021;41:1170-1175.
- Yüksel YT, Sonne M, Nørreslet LB, et al. Skin barrier response to active chlorine hand disinfectant—an experimental study comparing skin barrier response to active chlorine hand disinfectant and alcohol-based hand rub on healthy skin and eczematous skin. Skin Res Technol. 2022;28:89-97.
- Stroman D, Mintun K, Epstein A, et al. Reduction in bacterial load using hypochlorous acid hygiene solution on ocular skin. OPTH. 2017;11:707-714.
- Vasam M, Korutla S, Bohara RA. Acne vulgaris: a review of the pathophysiology, treatment, and recent nanotechnology based advances. Biochem Biophys Rep. 2023;36:101578.
- Reynolds RV, Yeung H, Cheng CE, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024;90:1006.E1-1006.E30.
- Anagnostopoulos AG, Rong A, Miller D, et al. 0.01% hypochlorous acid as an alternative skin antiseptic: an in vitro comparison. Dermatol Surg. 2018;44:1489-1493.
- Wang L, Bassiri M, Najafi R, et al. Hypochlorous acid as a potential wound care agent: part I. stabilized hypochlorous acid: a component of the inorganic armamentarium of innate immunity. J Burns Wounds. 2007;6:E5.
- Ortega-Peña S, Hidalgo-González C, Robson MC, et al. In vitro microbicidal, anti-biofilm and cytotoxic effects of different commercial antiseptics. Int Wound J. 2017;14:470-479.
- Gold MH, Andriessen A, Bhatia AC, et al. Topical stabilized hypochlorous acid: the future gold standard for wound care and scar management in dermatologic and plastic surgery procedures. J Cosmet Dermatol. 2020;19:270-277.
- Leung TH, Zhang LF, Wang J, et al. Topical hypochlorite ameliorates NF-κB–mediated skin diseases in mice. J Clin Invest. 2013;123:5361-5370.
- Fukuyama T, Martel BC, Linder KE, et al. Hypochlorous acid is antipruritic and anti‐inflammatory in a mouse model of atopic dermatitis. Clin Exp Allergy. 2018;48:78-88.
- Lheure C, Grange PA, Ollagnier G, et al. TLR-2 recognizes Propionibacterium acnes CAMP factor 1 from highly inflammatory strains. PLoS ONE. 2016;11:E0167237.
- Gold MH, Andriessen A, Dayan SH, et al. Hypochlorous acid gel technology—its impact on postprocedure treatment and scar prevention. J Cosmet Dermatol. 2017;16:162-167.
- Dorostkar A, Ghahartars M, Namazi MR, et al. Sodium hypochlorite 0.005% versus placebo in the treatment of mild to moderate acne: a double-blind randomized controlled trial. Dermatol Pract Concept. Published online May 20, 2021.
- del Rosso JQ, Bhatia N. Status report on topical hypochlorous acid: clinical relevance of specific formulations, potential modes of action, and study outcomes. J Clin Aesthet Dermatol. 2018;11:36-39.
- Tirado-Sánchez A, Ponce-Olivera RM. Efficacy and tolerance of superoxidized solution in the treatment of mild to moderate inflammatory acne. a double-blinded, placebo- controlled, parallel-group, randomized, clinical trial. J Dermatolog Treat. 2009;20:289-292.
- Tran AQ, Topilow N, Rong A, et al. Comparison of skin antiseptic agents and the role of 0.01% hypochlorous acid. Aesthet Surg J. 2021;41:1170-1175.
- Yüksel YT, Sonne M, Nørreslet LB, et al. Skin barrier response to active chlorine hand disinfectant—an experimental study comparing skin barrier response to active chlorine hand disinfectant and alcohol-based hand rub on healthy skin and eczematous skin. Skin Res Technol. 2022;28:89-97.
- Stroman D, Mintun K, Epstein A, et al. Reduction in bacterial load using hypochlorous acid hygiene solution on ocular skin. OPTH. 2017;11:707-714.
Topical Hypochlorous Acid for Acne Vulgaris: Mechanisms, Clinical Evidence, and Therapeutic Potential
Topical Hypochlorous Acid for Acne Vulgaris: Mechanisms, Clinical Evidence, and Therapeutic Potential
Practice Points
- First-line treatments for acne vulgaris are effective but often limited by local irritation, systemic adverse effects, and antibiotic resistance.
- Hypochlorous acid (HOCl) shows rapid, broad-spectrum antimicrobial and biofilm-disruptive activity against Cutibacterium acnes and other pathogens, with a low propensity for resistance.
- Emerging clinical data indicate HOCl formulations deliver efficacy comparable to standard topical treatments with superior tolerability and no barrier disruption, supporting its use as a well-tolerated adjunct in acne management.

Rare Case of Necrobiotic Xanthogranuloma on the Scalp
Rare Case of Necrobiotic Xanthogranuloma on the Scalp
To the Editor:
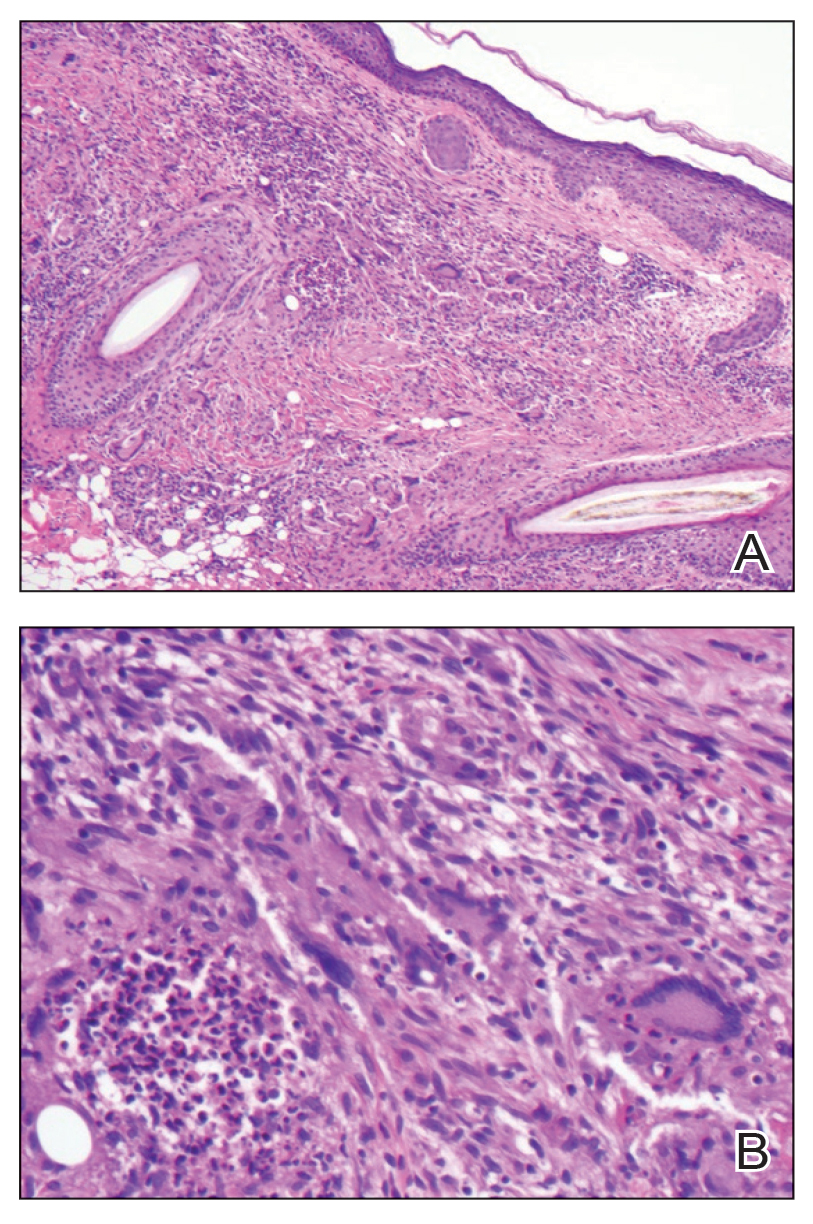
Necrobiotic xanthogranuloma (NXG) is classified as a cutaneous non–Langerhans cell histiocytosis, often seen with monoclonal gammopathy of undetermined significance or multiple myeloma.1 Clinically, it appears as a red or yellow plaque with occasional ulceration and telangiectasias, most commonly seen periorbitally and on the trunk. On pathology, NXG appears as necrobiosis, giant cells, and various inflammatory cells extending into the subcutaneous tissue.2 In this article, we describe a rare presentation of NXG in location and skin type.
A 52-year-old woman with a history of systemic lupus erythematosus (SLE) presented with alopecia and a tender lesion on the scalp of 5 years’ duration (Figure 1). The patient had no history of a similar lesion, and no other lesions were present. A biopsy performed at an outside clinic a few weeks to months prior to the initial presentation to our clinic showed NXG (Figure 2). Evaluation at our clinic revealed a 4x4-cm orange-brown annular plaque on the left parietal scalp. Serum and urine protein electrophoresis studies were negative. The patient reported she was up to date with recommended screenings such as mammography and colonoscopy.
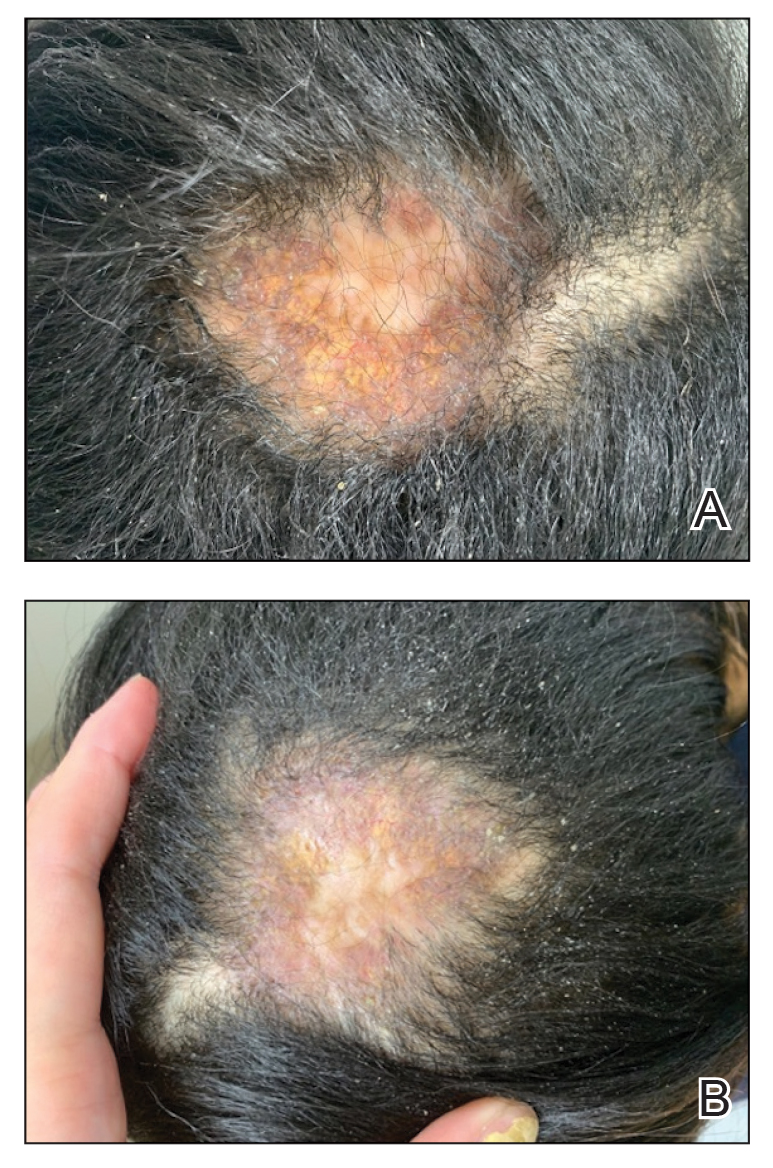
We started the patient on topical triamcinolone and topical ruxolitinib and administered intralesional triamcinolone. She was already taking hydroxychloroquine and leflunomide for SLE. Three weeks later, she returned with improved symptoms and appearance (Figure 1). She remained on intralesional triamcinolone and ruxolitinib and continues to experience improvement.
Necrobiotic xanthogranuloma is rare and typically is associated with monoclonal gammopathy.2 In one study, 83 of 100 of patients with NXG presented with or were found to have a monoclonal gammopathy.2 In another study, paraproteinemia was detected in 82.1% of patients.3 The majority of case reports and systematic reviews detail periorbital or thoracic lesions.4 The location on the scalp and lack of association with paraproteinemia make this a rare presentation of NXG. Studies may be warranted to explore any association of SLE with NXG if more cases present.
In a multicenter cross-sectional study and systematic review of 235 patients with NXG, 87% were White, 12% were Asian, and only 1% were Black or African American.3 The limited representation of skin of color raises concern for the possibility of missed diagnoses and delays in care.
Treatment of NXG often is multimodal with use of intravenous immunoglobulin, oral steroids, chlorambucil, melphalan, and other alkylating agents, and response is variable.3-6 Recent studies show treatment effectiveness with Janus kinase inhibitors in granulomatous dermatitides.7-9 As our patient was not responding to prior treatments, we decided to try ruxolitinib, and she has continued to improve with it.10,11 Interestingly, the patient experienced continued improvement with intralesional triamcinolone, which is not often reported in the literature.2-6 Overall, NXG is an extremely rare condition that requires special care in workup to rule out paraproteinemia and a thoughtful approach to treatment modalities.
- Emile JF, Abla O, Fraitag S, et al. Revised classification of histiocytoses and neoplasms of the macrophage-dendritic cell lineages. Blood. 2016;127:2672-2681.
- Spicknall KE, Mehregan DA. Necrobiotic xanthogranuloma. Int J Dermatol. 2009;48:1-10.
- Nelson CA, Zhong CS, Hashemi DA, et al. A multicenter cross-sectional study and systematic review of necrobiotic xanthogranuloma with proposed diagnostic criteria. JAMA Dermatol. 2020;156:270-279.
- Huynh KN, Nguyen BD. Histiocytosis and neoplasms of macrophagedendritic cell lineages: multimodality imaging with emphasis on PET/CT. Radiographics. 2021;41:576-594. doi: 10.1148/rg.2021200096
- Hilal T, DiCaudo DJ, Connolly SM, et al. Necrobiotic xanthogranuloma: a 30-year single-center experience. Ann Hematol. 2018;97:1471-1479.
- Oumeish OY, Oumeish I, Tarawneh M, et al. Necrobiotic xanthogranuloma associated with paraproteinemia and non- Hodgkin’s lymphoma developing into chronic lymphocytic leukemia: the first case reported in the literature and review of the literature. Int J Dermatol. 2006;45:306-310.
- Damsky W, Thakral D, McGeary MK, et al. Janus kinase inhibition induces disease remission in cutaneous sarcoidosis and granuloma annulare. J Am Acad Dermatol. 2020;82:612-621. doi:10.1016 /j.jaad.2019.05.098
- Wang A, Rahman NT, McGeary MK, et al. Treatment of granuloma annulare and suppression of proinflammatory cytokine activity with tofacitinib. J Allergy Clin Immunol. 2021;147:1795-1809. doi:10.1016 /j.jaci.2020.10.012
- Stratman S, Amara S, Tan KJ, et al. Systemic Janus kinase inhibitors in the management of granuloma annulare. Arch Dermatol Res. 2025;317:743. doi:10.1007/s00403-025-04248-1
- McPhie ML, Swales WC, Gooderham MJ. Improvement of granulomatous skin conditions with tofacitinib in three patients: a case report. SAGE Open Med Case Rep. 2021;9:2050313X211039477. doi: 10.1177/2050313X211039477
- Sood S, Heung M, Georgakopoulos JR, et al. Use of Janus kinase inhibitors for granulomatous dermatoses: a systematic review. J Am Acad Dermatol. 2023;89:357-359. doi: 10.1016/j.jaad.2023.03.024
To the Editor:
Necrobiotic xanthogranuloma (NXG) is classified as a cutaneous non–Langerhans cell histiocytosis, often seen with monoclonal gammopathy of undetermined significance or multiple myeloma.1 Clinically, it appears as a red or yellow plaque with occasional ulceration and telangiectasias, most commonly seen periorbitally and on the trunk. On pathology, NXG appears as necrobiosis, giant cells, and various inflammatory cells extending into the subcutaneous tissue.2 In this article, we describe a rare presentation of NXG in location and skin type.
A 52-year-old woman with a history of systemic lupus erythematosus (SLE) presented with alopecia and a tender lesion on the scalp of 5 years’ duration (Figure 1). The patient had no history of a similar lesion, and no other lesions were present. A biopsy performed at an outside clinic a few weeks to months prior to the initial presentation to our clinic showed NXG (Figure 2). Evaluation at our clinic revealed a 4x4-cm orange-brown annular plaque on the left parietal scalp. Serum and urine protein electrophoresis studies were negative. The patient reported she was up to date with recommended screenings such as mammography and colonoscopy.
We started the patient on topical triamcinolone and topical ruxolitinib and administered intralesional triamcinolone. She was already taking hydroxychloroquine and leflunomide for SLE. Three weeks later, she returned with improved symptoms and appearance (Figure 1). She remained on intralesional triamcinolone and ruxolitinib and continues to experience improvement.
Necrobiotic xanthogranuloma is rare and typically is associated with monoclonal gammopathy.2 In one study, 83 of 100 of patients with NXG presented with or were found to have a monoclonal gammopathy.2 In another study, paraproteinemia was detected in 82.1% of patients.3 The majority of case reports and systematic reviews detail periorbital or thoracic lesions.4 The location on the scalp and lack of association with paraproteinemia make this a rare presentation of NXG. Studies may be warranted to explore any association of SLE with NXG if more cases present.
In a multicenter cross-sectional study and systematic review of 235 patients with NXG, 87% were White, 12% were Asian, and only 1% were Black or African American.3 The limited representation of skin of color raises concern for the possibility of missed diagnoses and delays in care.
Treatment of NXG often is multimodal with use of intravenous immunoglobulin, oral steroids, chlorambucil, melphalan, and other alkylating agents, and response is variable.3-6 Recent studies show treatment effectiveness with Janus kinase inhibitors in granulomatous dermatitides.7-9 As our patient was not responding to prior treatments, we decided to try ruxolitinib, and she has continued to improve with it.10,11 Interestingly, the patient experienced continued improvement with intralesional triamcinolone, which is not often reported in the literature.2-6 Overall, NXG is an extremely rare condition that requires special care in workup to rule out paraproteinemia and a thoughtful approach to treatment modalities.
To the Editor:
Necrobiotic xanthogranuloma (NXG) is classified as a cutaneous non–Langerhans cell histiocytosis, often seen with monoclonal gammopathy of undetermined significance or multiple myeloma.1 Clinically, it appears as a red or yellow plaque with occasional ulceration and telangiectasias, most commonly seen periorbitally and on the trunk. On pathology, NXG appears as necrobiosis, giant cells, and various inflammatory cells extending into the subcutaneous tissue.2 In this article, we describe a rare presentation of NXG in location and skin type.
A 52-year-old woman with a history of systemic lupus erythematosus (SLE) presented with alopecia and a tender lesion on the scalp of 5 years’ duration (Figure 1). The patient had no history of a similar lesion, and no other lesions were present. A biopsy performed at an outside clinic a few weeks to months prior to the initial presentation to our clinic showed NXG (Figure 2). Evaluation at our clinic revealed a 4x4-cm orange-brown annular plaque on the left parietal scalp. Serum and urine protein electrophoresis studies were negative. The patient reported she was up to date with recommended screenings such as mammography and colonoscopy.
We started the patient on topical triamcinolone and topical ruxolitinib and administered intralesional triamcinolone. She was already taking hydroxychloroquine and leflunomide for SLE. Three weeks later, she returned with improved symptoms and appearance (Figure 1). She remained on intralesional triamcinolone and ruxolitinib and continues to experience improvement.
Necrobiotic xanthogranuloma is rare and typically is associated with monoclonal gammopathy.2 In one study, 83 of 100 of patients with NXG presented with or were found to have a monoclonal gammopathy.2 In another study, paraproteinemia was detected in 82.1% of patients.3 The majority of case reports and systematic reviews detail periorbital or thoracic lesions.4 The location on the scalp and lack of association with paraproteinemia make this a rare presentation of NXG. Studies may be warranted to explore any association of SLE with NXG if more cases present.
In a multicenter cross-sectional study and systematic review of 235 patients with NXG, 87% were White, 12% were Asian, and only 1% were Black or African American.3 The limited representation of skin of color raises concern for the possibility of missed diagnoses and delays in care.
Treatment of NXG often is multimodal with use of intravenous immunoglobulin, oral steroids, chlorambucil, melphalan, and other alkylating agents, and response is variable.3-6 Recent studies show treatment effectiveness with Janus kinase inhibitors in granulomatous dermatitides.7-9 As our patient was not responding to prior treatments, we decided to try ruxolitinib, and she has continued to improve with it.10,11 Interestingly, the patient experienced continued improvement with intralesional triamcinolone, which is not often reported in the literature.2-6 Overall, NXG is an extremely rare condition that requires special care in workup to rule out paraproteinemia and a thoughtful approach to treatment modalities.
- Emile JF, Abla O, Fraitag S, et al. Revised classification of histiocytoses and neoplasms of the macrophage-dendritic cell lineages. Blood. 2016;127:2672-2681.
- Spicknall KE, Mehregan DA. Necrobiotic xanthogranuloma. Int J Dermatol. 2009;48:1-10.
- Nelson CA, Zhong CS, Hashemi DA, et al. A multicenter cross-sectional study and systematic review of necrobiotic xanthogranuloma with proposed diagnostic criteria. JAMA Dermatol. 2020;156:270-279.
- Huynh KN, Nguyen BD. Histiocytosis and neoplasms of macrophagedendritic cell lineages: multimodality imaging with emphasis on PET/CT. Radiographics. 2021;41:576-594. doi: 10.1148/rg.2021200096
- Hilal T, DiCaudo DJ, Connolly SM, et al. Necrobiotic xanthogranuloma: a 30-year single-center experience. Ann Hematol. 2018;97:1471-1479.
- Oumeish OY, Oumeish I, Tarawneh M, et al. Necrobiotic xanthogranuloma associated with paraproteinemia and non- Hodgkin’s lymphoma developing into chronic lymphocytic leukemia: the first case reported in the literature and review of the literature. Int J Dermatol. 2006;45:306-310.
- Damsky W, Thakral D, McGeary MK, et al. Janus kinase inhibition induces disease remission in cutaneous sarcoidosis and granuloma annulare. J Am Acad Dermatol. 2020;82:612-621. doi:10.1016 /j.jaad.2019.05.098
- Wang A, Rahman NT, McGeary MK, et al. Treatment of granuloma annulare and suppression of proinflammatory cytokine activity with tofacitinib. J Allergy Clin Immunol. 2021;147:1795-1809. doi:10.1016 /j.jaci.2020.10.012
- Stratman S, Amara S, Tan KJ, et al. Systemic Janus kinase inhibitors in the management of granuloma annulare. Arch Dermatol Res. 2025;317:743. doi:10.1007/s00403-025-04248-1
- McPhie ML, Swales WC, Gooderham MJ. Improvement of granulomatous skin conditions with tofacitinib in three patients: a case report. SAGE Open Med Case Rep. 2021;9:2050313X211039477. doi: 10.1177/2050313X211039477
- Sood S, Heung M, Georgakopoulos JR, et al. Use of Janus kinase inhibitors for granulomatous dermatoses: a systematic review. J Am Acad Dermatol. 2023;89:357-359. doi: 10.1016/j.jaad.2023.03.024
- Emile JF, Abla O, Fraitag S, et al. Revised classification of histiocytoses and neoplasms of the macrophage-dendritic cell lineages. Blood. 2016;127:2672-2681.
- Spicknall KE, Mehregan DA. Necrobiotic xanthogranuloma. Int J Dermatol. 2009;48:1-10.
- Nelson CA, Zhong CS, Hashemi DA, et al. A multicenter cross-sectional study and systematic review of necrobiotic xanthogranuloma with proposed diagnostic criteria. JAMA Dermatol. 2020;156:270-279.
- Huynh KN, Nguyen BD. Histiocytosis and neoplasms of macrophagedendritic cell lineages: multimodality imaging with emphasis on PET/CT. Radiographics. 2021;41:576-594. doi: 10.1148/rg.2021200096
- Hilal T, DiCaudo DJ, Connolly SM, et al. Necrobiotic xanthogranuloma: a 30-year single-center experience. Ann Hematol. 2018;97:1471-1479.
- Oumeish OY, Oumeish I, Tarawneh M, et al. Necrobiotic xanthogranuloma associated with paraproteinemia and non- Hodgkin’s lymphoma developing into chronic lymphocytic leukemia: the first case reported in the literature and review of the literature. Int J Dermatol. 2006;45:306-310.
- Damsky W, Thakral D, McGeary MK, et al. Janus kinase inhibition induces disease remission in cutaneous sarcoidosis and granuloma annulare. J Am Acad Dermatol. 2020;82:612-621. doi:10.1016 /j.jaad.2019.05.098
- Wang A, Rahman NT, McGeary MK, et al. Treatment of granuloma annulare and suppression of proinflammatory cytokine activity with tofacitinib. J Allergy Clin Immunol. 2021;147:1795-1809. doi:10.1016 /j.jaci.2020.10.012
- Stratman S, Amara S, Tan KJ, et al. Systemic Janus kinase inhibitors in the management of granuloma annulare. Arch Dermatol Res. 2025;317:743. doi:10.1007/s00403-025-04248-1
- McPhie ML, Swales WC, Gooderham MJ. Improvement of granulomatous skin conditions with tofacitinib in three patients: a case report. SAGE Open Med Case Rep. 2021;9:2050313X211039477. doi: 10.1177/2050313X211039477
- Sood S, Heung M, Georgakopoulos JR, et al. Use of Janus kinase inhibitors for granulomatous dermatoses: a systematic review. J Am Acad Dermatol. 2023;89:357-359. doi: 10.1016/j.jaad.2023.03.024
Rare Case of Necrobiotic Xanthogranuloma on the Scalp
Rare Case of Necrobiotic Xanthogranuloma on the Scalp
PRACTICE POINTS
- In skin of color, necrobiotic xanthogranuloma can appear orange or brown compared to its yellow appearance in lighter skin types.
- When necrobiotic xanthogranuloma is suspected, a thorough malignancy workup should be conducted.

How Increasing Research Demands Threaten Equity in Dermatology Residency Selection and Strategies for Reform
How Increasing Research Demands Threaten Equity in Dermatology Residency Selection and Strategies for Reform
As one of the most competitive specialties in medicine, dermatology presents unique challenges for residency applicants, especially following the shift in United States Medical Licensing Examination (USMLE) Step 1 scoring to a pass/fail format.1,2 Historically, USMLE Step 1 served as a major screening metric for residency programs, with 90% of program directors in 2020 using USMLE Step 1 scores as a primary factor when deciding whether to invite applicants for interviews.1 However, the recent transition to pass/fail has made it much harder for program directors to objectively compare applicants, particularly in dermatology. In a 2020 survey, Patrinely Jr et al2 found that 77.2% of dermatology program directors agreed that this change would make it more difficult to assess candidates objectively. Consequently, research productivity has taken on greater importance as programs seek new ways to distinguish top applicants.1,2
In response to this increased emphasis on research, dermatology applicants have substantially boosted their scholarly output over the past several years. The 2022 and 2024 results from the National Residency Matching Program’s Charting Outcomes survey demonstrated a steady rise in research metrics among applicants across various specialties, with dermatology showing one of the largest increases.3,4 For instance, the average number of abstracts, presentations, and publications for matched allopathic dermatology applicants was 5.7 in 2007.5 This average increased to 20.9 in 20223 and to 27.7 in 2024,4 marking an astonishing 485% increase in 17 years. Interestingly, unmatched dermatology applicants had an average of 19.0 research products in 2024, which was similar to the average of successfully matched applicants just 2 years earlier.3,4
Engaging in research offers benefits beyond building a strong residency application. Specifically, it enhances critical thinking skills and provides hands-on experience in scientific inquiry.6 It allows students to explore dermatology topics of interest and address existing knowledge gaps within the specialty.6 Additionally, it creates opportunities to build meaningful relationships with experienced dermatologists who can guide and support students throughout their careers.7 Despite these benefits, the pursuit of research may be landscaped with obstacles, and the fervent race to obtain high research outputs may overshadow developmental advantages.8 These challenges and demands also could contribute to inequities in the residency selection process, particularly if barriers are influenced by socioeconomic and demographic disparities. As dermatology already ranks as the second least diverse specialty in medicine,9 research requirements that disproportionately disadvantage certain demographic groups risk further widening these concerning representation gaps rather than creating opportunities to address them.
Given these trends in research requirements and their potential impact on applicant success, understanding specific barriers to research engagement is essential for creating equitable opportunities in dermatology. In this study, we aimed to identify barriers to research engagement among dermatology applicants, analyze their relationship with demographic factors, assess their impact on specialty choice and research productivity, and provide actionable solutions to address these obstacles.
Methods
A cross-sectional survey was conducted targeting medical students applying to dermatology residency programs in the United States in the 2025 or 2026 match cycles as well as residents who applied to dermatology residency in the 2021 to 2024 match cycles. The 23-item survey was developed by adapting questions from several validated studies examining research barriers and experiences in medical education.6,7,10,11 Specifically, the survey included questions on demographics and background; research productivity; general research barriers; conference participation accessibility; mentorship access; and quality, career impact, and support needs. Socioeconomic background was measured via a single self-reported item asking participants to select the income class that best reflected their background growing up (low-income, lower-middle, upper-middle, or high-income); no income ranges were provided.
The survey was distributed electronically via Qualtrics between November 11, 2024, and December 30, 2024, through listserves of the Dermatology Interest Group Association (sent directly to medical students) and the Association of Professors of Dermatology (forwarded to residents by program directors). There was no way to determine the number of dermatology applicants and residents reached through either listserve. The surveys were reviewed and approved by the University of Alabama at Birmingham institutional review board (IRB-300013671).
Statistical analyses were conducted using RStudio (Posit, PBC; version 2024.12.0+467). Descriptive statistics characterized participant demographics and quantified barrier scores using frequencies and proportions. We performed regression analyses to examine relationships between demographic factors and barriers using linear regression; the relationship between barriers and research productivity correlation; and the prediction of specialty change consideration using logistic regression. For all analyses, barrier scores were rated on a scale of 0 to 3 (0=not a barrier, 1=minor barrier, 2=moderate barrier, 3=major barrier); R² values were reported to indicate strength of associations, and statistical significance was set at P<.05.
Results
Participant Demographics—A total of 136 participants completed the survey. Among the respondents, 12% identified as from a background of low-income class, 28% lower-middle class, 49% upper-middle class, and 11% high-income class. Additionally, 27% of respondents identified as underrepresented in medicine (URiM). Regarding debt levels (or expected debt levels) upon graduation from medical school, 32% reported no debt, 9% reported $1000 to $49,000 in debt, 5% reported $50,000 to $99,000 in debt, 15% reported $100,000 to $199,000 in debt, 22% reported $200,000 to $299,000 in debt, and 17% reported $300,000 in debt or higher. The majority of respondents (95%) were MD candidates, and the remaining 5% were DO candidates; additionally, 5% were participants in an MD/PhD program (eTable 1).
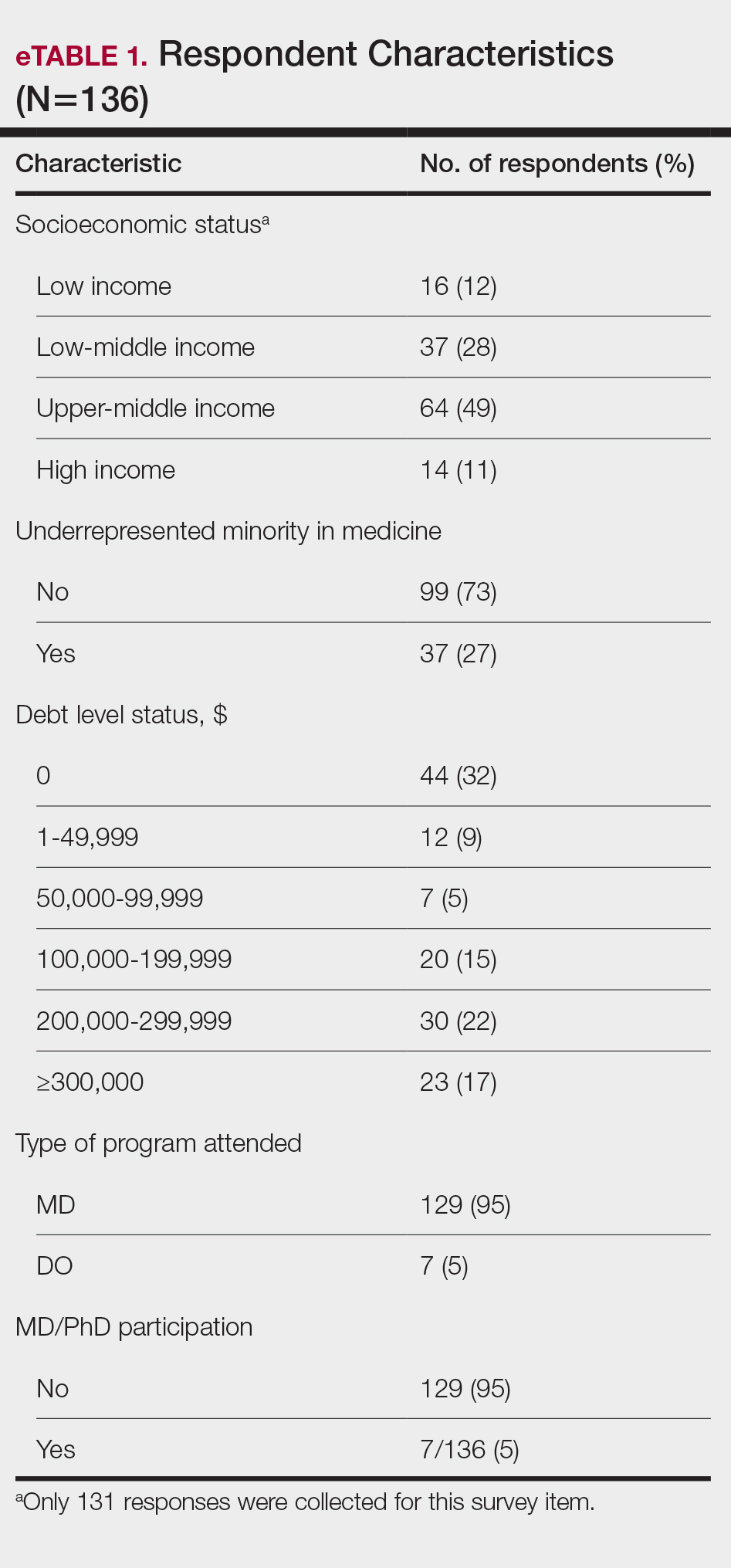
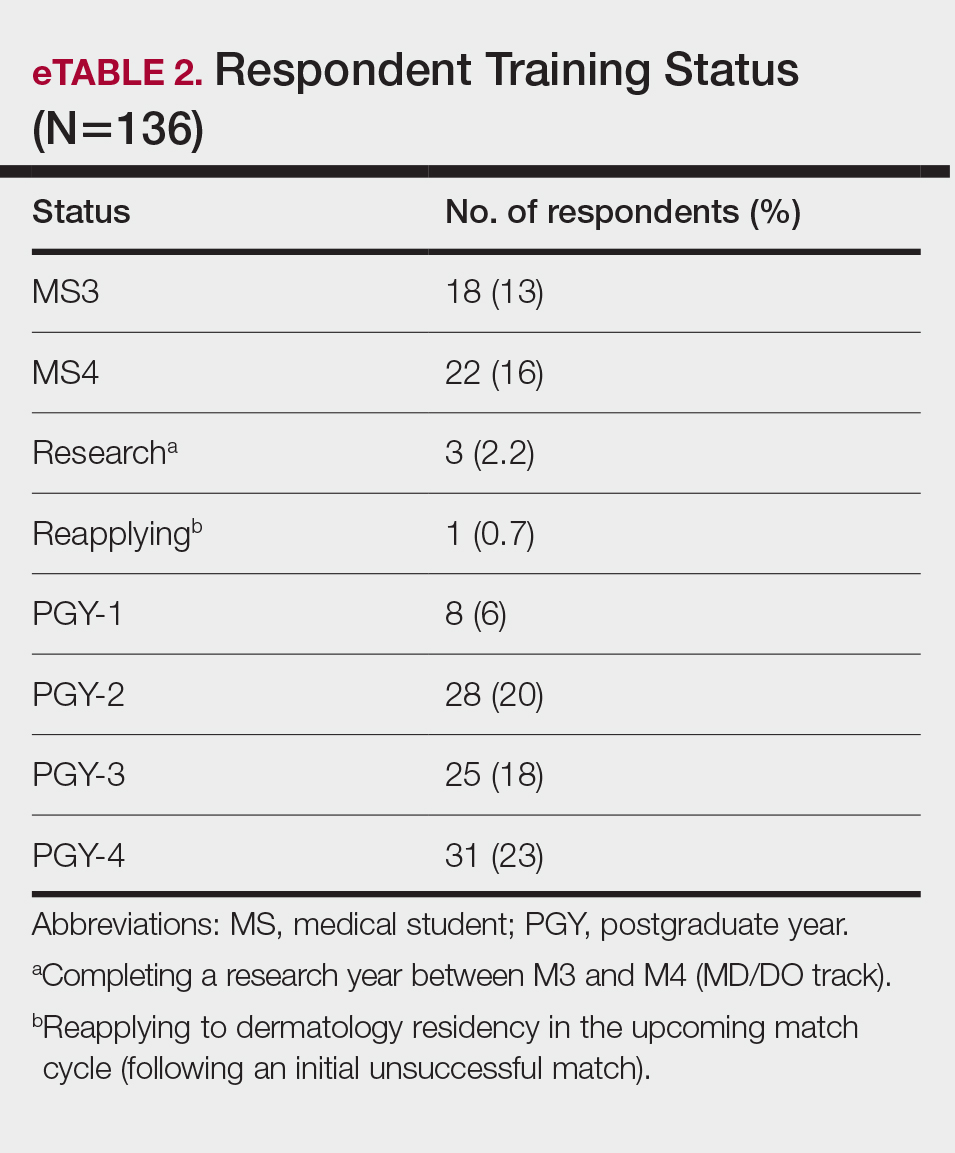
Respondents represented various stages of training: 13.2% and 16.2% were third- and fourth-year medical students, respectively, while 6.0%, 20.1%, 18.4%, and 22.8% were postgraduate year (PGY) 1, PGY-2, PGY-3, and PGY-4, respectively. A few respondents (2.9%) were participating in a research year or reapplying to dermatology residency (eTable 2).
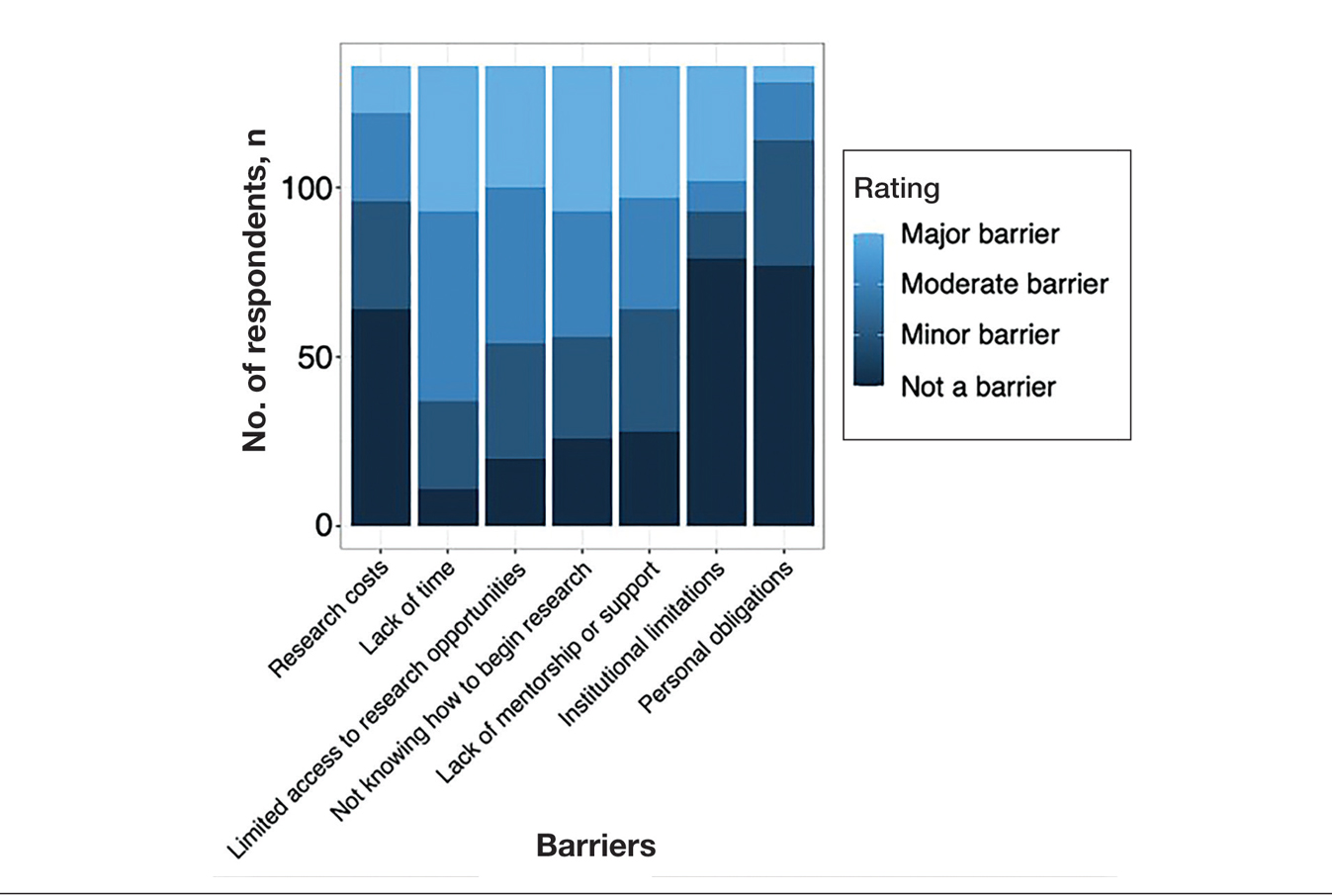
Research Barriers and Productivity—Respondents were presented with a list of potential barriers and asked to rate each as not a barrier, a minor barrier, a moderate barrier, or a major barrier. The most common barriers (ie, those with >50% of respondents rating them as a moderate or major) included lack of time, limited access to research opportunities, not knowing how to begin research, and lack of mentorship or support. Lack of time and not knowing where to begin research were reported most frequently as major barriers, with 32% of participants identifying them as such. In contrast, barriers such as financial costs and personal obligations were less frequently rated as major barriers (10% and 4%, respectively), although they still were identified as obstacles by many respondents. Interestingly, most respondents (58%) indicated that institutional limitations were not a barrier, but a separate and sizeable proportion (25%) of respondents considered it to be a major barrier (eFigure 1).
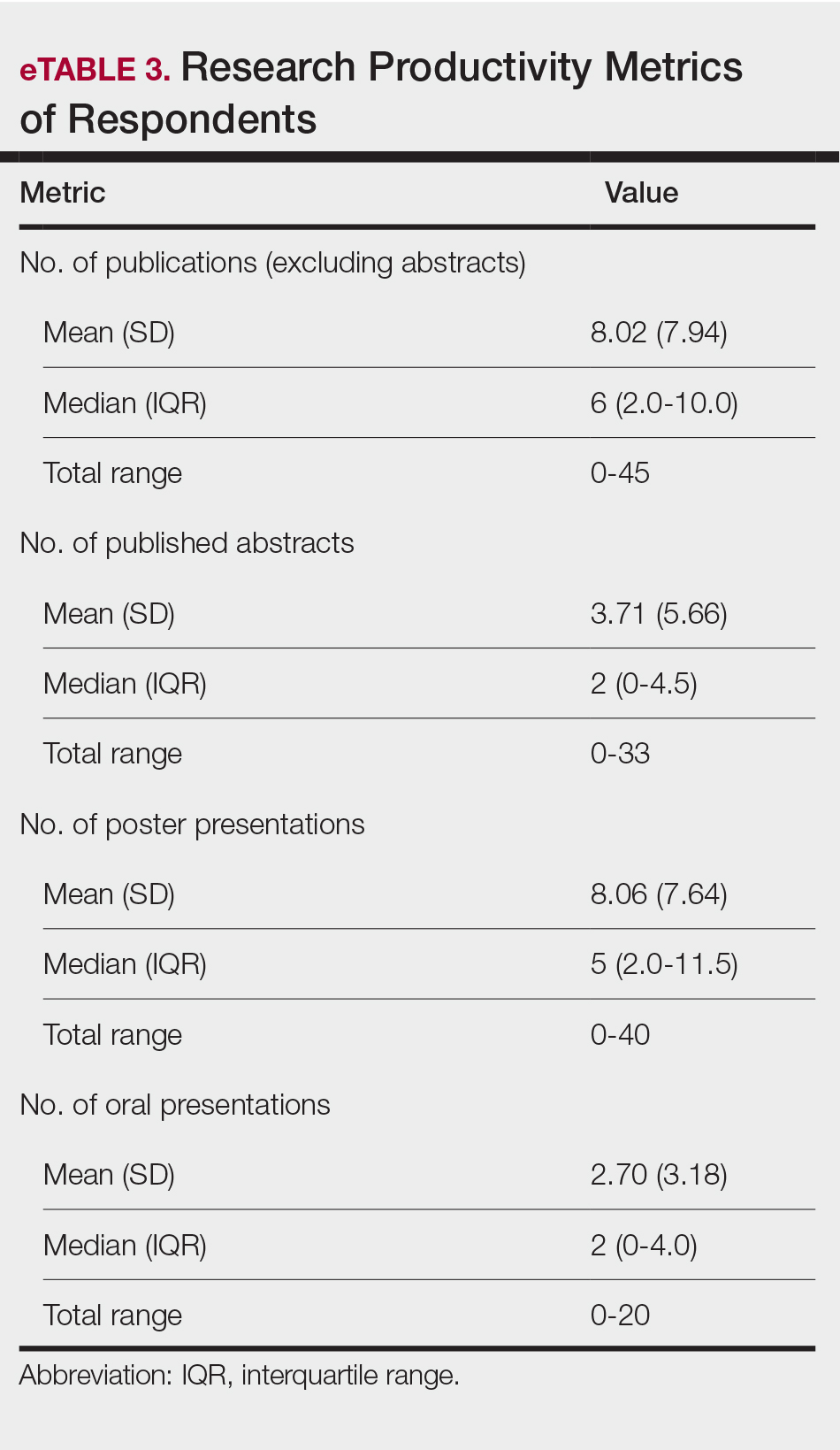
The distributions for all research metrics were right-skewed. The total range was 0 to 45 (median, 6) for number of publications (excluding abstracts), 0 to 33 (median, 2) for published abstracts, 0 to 40 (median, 5) for poster publications, and 0 to 20 (median, 2) for oral presentations (eTable 3).
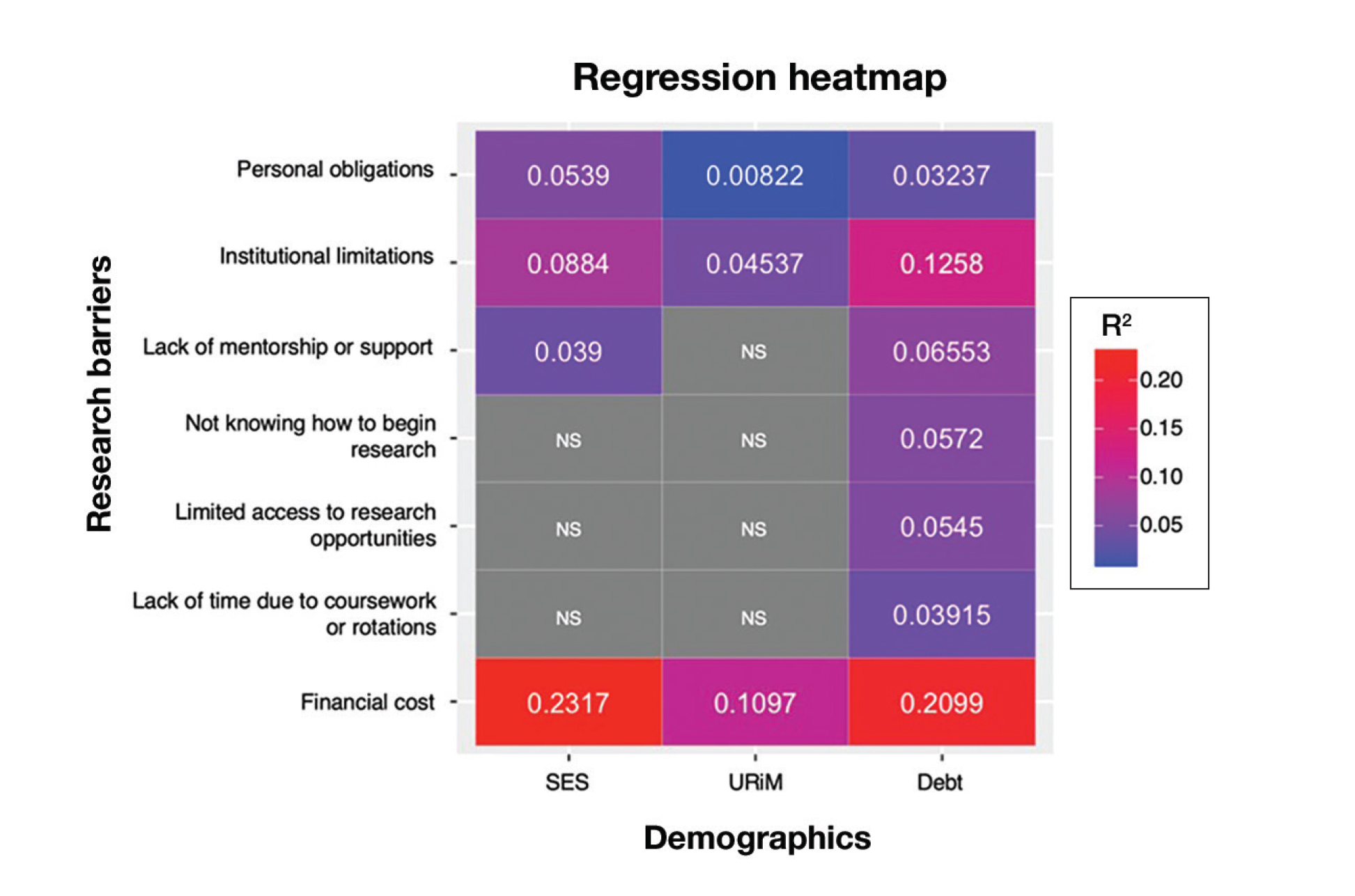
Regression Analysis—Linear regression analysis identified significant relationships between demographic variables (socioeconomic status [SES], URiM status, and debt level) and individual research barriers. The heatmap in eFigure 2 illustrates the strength of these relationships. Higher SES was predictive of lower reported financial barriers (R²=.2317; P<.0001) and lower reported institutional limitations (R²=.0884; P=.0006). A URiM status predicted higher reported financial barriers (R²=.1097; P<.0001) and institutional limitations (R²=.04537; P=.013). Also, higher debt level predicted increased financial barriers (R²=.2099; P<.0001), institutional limitations (R2=.1258; P<.0001), and lack of mentorship (R²=.06553; P=.003).
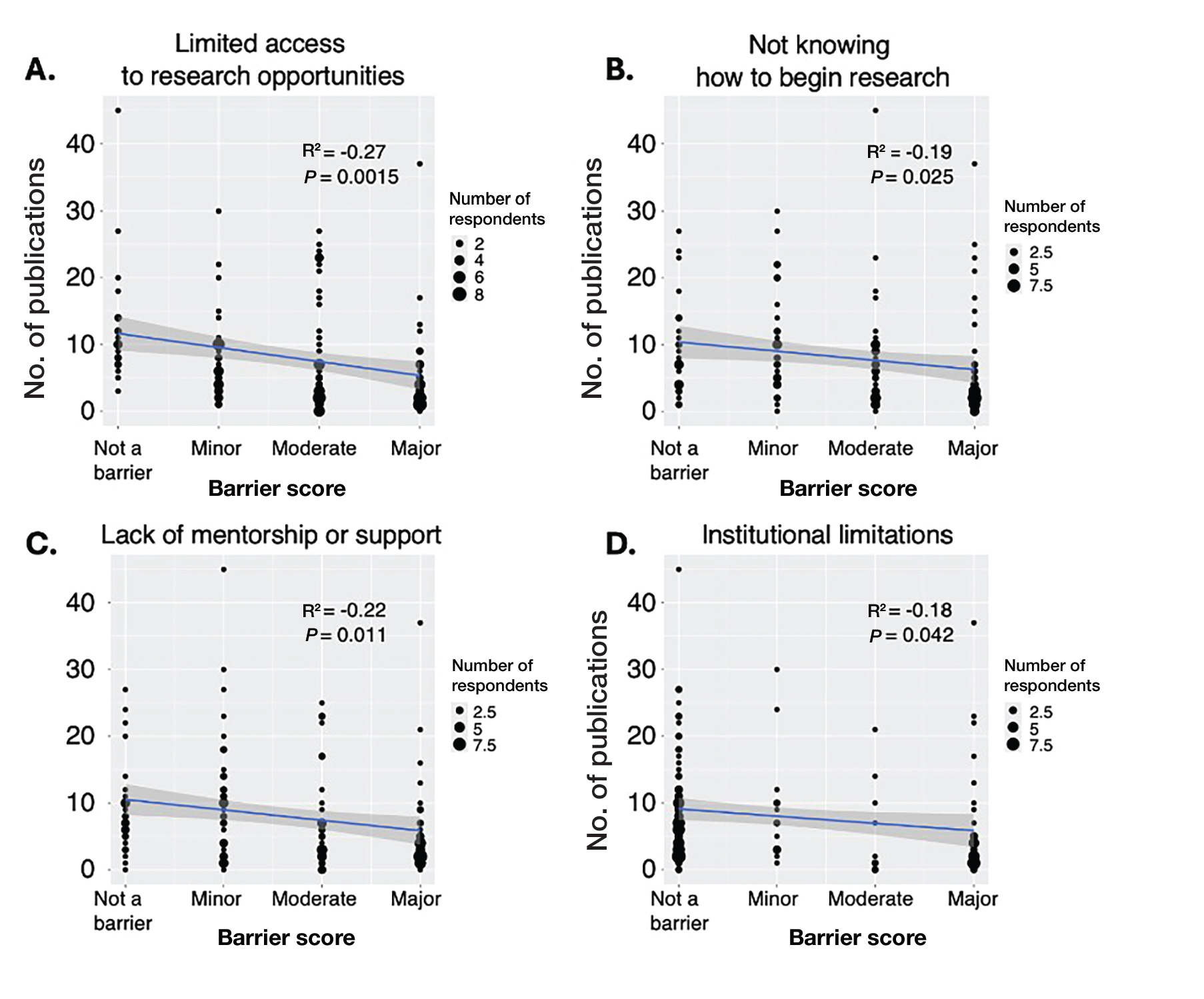
Next, the data were evaluated for correlative relationships between individual research barriers and research productivity metrics including number of publications, published abstracts and presentations (oral and poster) and total research output. While correlations were weak or nonsignificant between barriers and most research productivity metrics (published abstracts, oral and poster presentations, and total research output), the number of publications was significantly correlated with several research barriers, including limited access to research opportunities (P=.002), not knowing how to begin research (P=.025), lack of mentorship or support (P=.011), and institutional limitations (P=.042). Higher ratings for limited access to research opportunities, not knowing where to begin research, lack of mentorship or support, and institutional limitations all were negatively correlated with total number of publications (R2=−.27, –.19, −.22, and –.18, respectively)(eFigure 3).
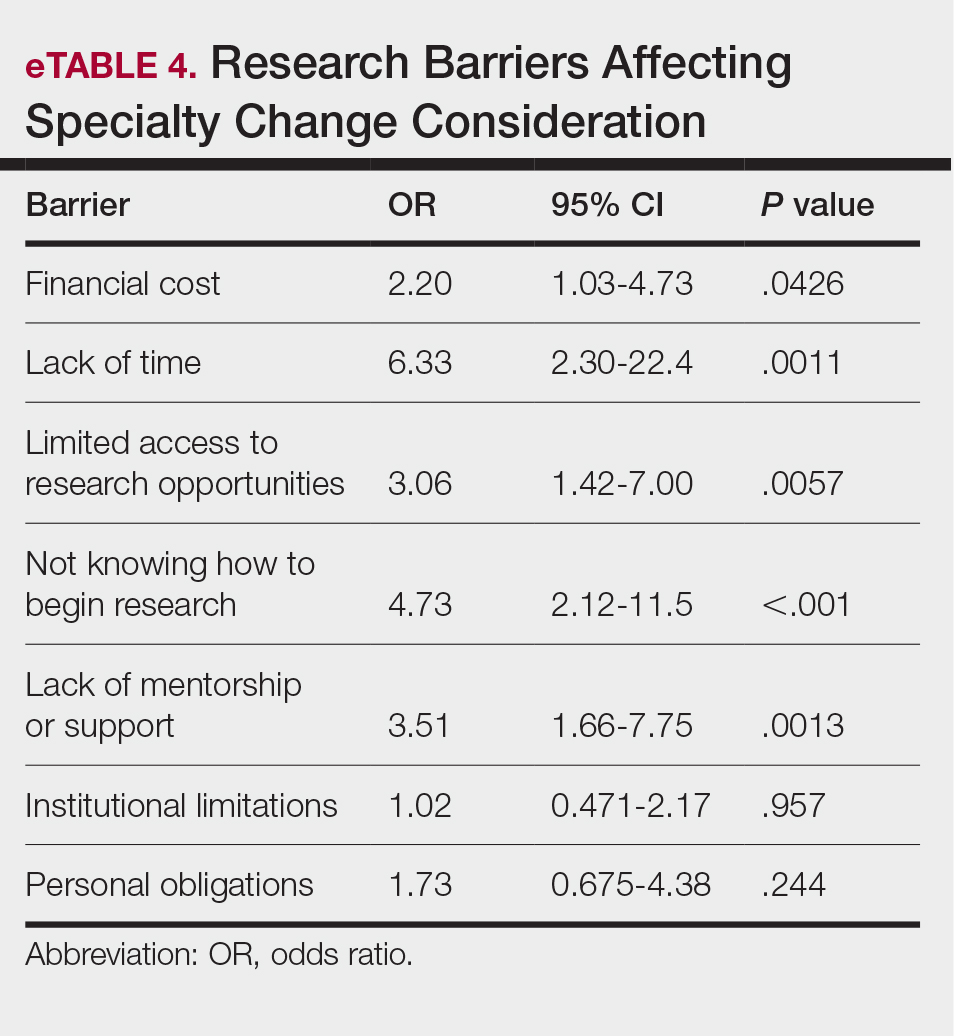
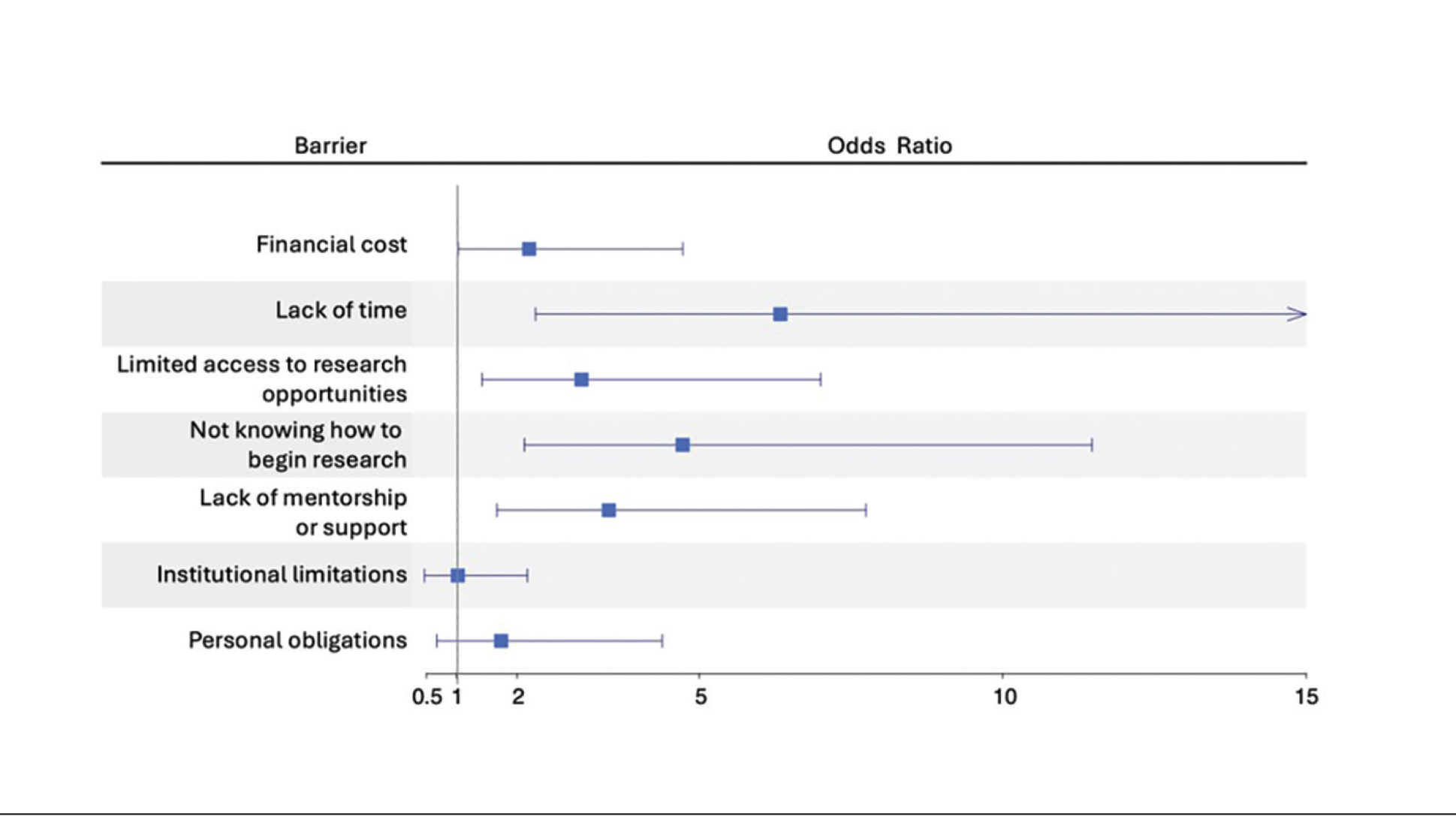
Logistic regression analysis examined the impact of research barriers on the likelihood of specialty change consideration. The results, presented in a forest plot, include odds ratios (ORs) and their corresponding 95% CIs and P values. Lack of time (P=.001) and not knowing where to begin research (P<.001) were the strongest predictors of specialty change consideration (OR, 6.3 and 4.7, respectively). Financial cost (P=.043), limited access to research opportunities (P=.006), and lack of mentorship or support (P=.001) also were significant predictors of specialty change consideration (OR, 2.2, 3.1, and 3.5, respectively). Institutional limitations and personal obligations did not predict specialty change consideration (eTable 4 and eFigure 4).
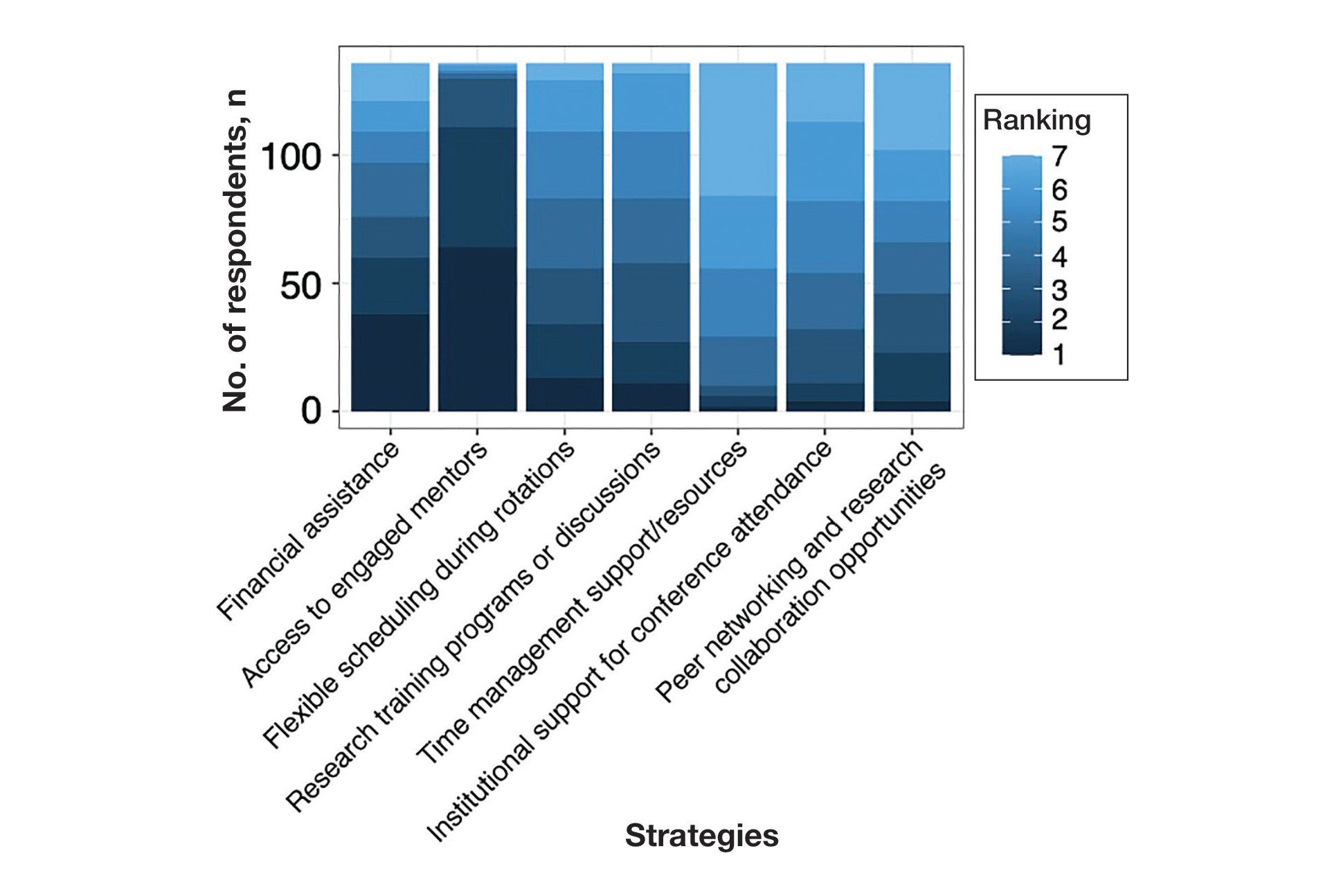
Mitigation Strategies—Mitigation strategies were ranked by respondents based on their perceived importance on a scale of 1 to 7 (1=most important, 7=least important)(eFigure 5). Respondents considered access to engaged mentors to be the most important mitigation strategy by far, with 95% ranking it in the top 3 (47% of respondents ranked it as the top most important mitigation strategy). Financial assistance was the mitigation strategy with the second highest number of respondents (28%) ranking it as the top strategy. Flexible scheduling during rotations, research training programs or discussions, and peer networking and research collaboration opportunities also were considered by respondents to be important mitigation strategies. Time management support/resources frequently was viewed as the least important mitigation strategy, with 38% of respondents ranking it last.
Comment
Our study revealed notable disparities in research barriers among dermatology applicants, with several demonstrating consistent patterns of association with SES, URiM status, and debt burden. Furthermore, the strong relationship between these barriers and decreased research productivity and specialty change consideration suggests that capable candidates may be deterred from pursuing dermatology due to surmountable obstacles rather than lack of interest or ability.
Impact of Demographic Factors on Research Barriers—All 7 general research barriers surveyed were correlated with distinct demographic predictors. Regression analyses indicated that the barrier of financial cost was significantly predicted by lower SES (R²=.2317; P<.001), URiM status (R²=.1097; P<.001), and higher debt levels (R²=.2099; P<.001)(eFigure 2). These findings are particularly concerning given the trend of dermatology applicants pursuing 1-year research fellowships, many of which are unpaid.12 In fact, Jacobson et al11 found that 71.7% (43/60) of dermatology applicants who pursued a year-long research fellowship experienced financial strain during their fellowship, with many requiring additional loans or drawing from personal savings despite already carrying substantial medical school debt of $200,000 or more. Our findings showcase how financial barriers to research disproportionately affect students from lower socioeconomic backgrounds, those who identify as URiM, and those with higher debt, creating systemic inequities in research access at a time when research productivity is increasingly vital for matching into dermatology. To address these financial barriers, institutions may consider establishing more funded research fellowships or expanding grant programs targeting students from economically disadvantaged and/or underrepresented backgrounds.
Institutional limitations (eg, the absence of a dermatology department) also was a notable barrier that was significantly predicted by lower SES (R²=.0884; P<.001) and URiM status (R²=.04537; P=.013)(eFigure 2). Students at institutions lacking dermatology programs face restricted access to mentorship and research opportunities,13 with our results demonstrating that these barriers disproportionately affect students from underresourced and minority groups. These limitations compound disparities in building competitive residency applications.14 The Women’s Dermatologic Society (WDS) has developed a model for addressing these institutional barriers through its summer research fellowship program for medical students who identify as URiM. By pairing students with WDS mentors who guide them through summer research projects, this initiative addresses access and mentorship gaps for students lacking dermatology departments at their home institution.15 The WDS program serves as a model for other organizations to adopt and expand, with particular attention to including students who identify as URiM as well as those from lower socioeconomic backgrounds.
Our results identified time constraints and lack of experience as notable research barriers. Higher debt levels significantly predicted both lack of time (R²=.03915; P=.021) and not knowing how to begin research (R²=.0572; P=.005)(eFigure 2). These statistical relationships may be explained by students with higher debt levels needing to prioritize paid work over unpaid research opportunities, limiting their engagement in research due to the scarcity of funded positions.12 The data further revealed that personal obligations, particularly family care responsibilities, were significantly predicted by both lower SES (R²=.0539; P=.008) and higher debt level (R²=.03237; P=.036)(eFigure 2). These findings demonstrate how students managing academic demands alongside financial and familial responsibilities may face compounded barriers to research engagement. To address these disparities, medical schools may consider implementing protected research time within their curricula; for example, the Emory University School of Medicine (Atlanta, Georgia) has implemented a Discovery Phase program that provides students with 5 months of protected faculty-mentored research time away from academic demands between their third and fourth years of medical school.16 Integrating similarly structured research periods across medical school curricula could help ensure equitable research opportunities for all students pursuing competitive specialties such as dermatology.8
Access to mentorship is a critical determinant of research engagement and productivity, as mentors provide valuable guidance on navigating research processes and professional development.17 Our analysis revealed that lack of mentorship was predicted by both lower SES (R²=.039; P=.023) and higher debt level (R²=.06553; P=.003)(eFigure 2). Several organizations have developed programs to address these mentorship gaps. The Skin of Color Society pairs medical students with skin of color experts while advancing its mission of increasing diversity in dermatology.18 Similarly, the American Academy of Dermatology founded a diversity mentorship program that connects students who identify as URiM with dermatologist mentors for summer research experiences.19 Notably, the Skin of Color Society’s program allows residents to serve as mentors for medical students. Involving residents and community dermatologists as potential dermatology mentors for medical students not only distributes mentorship demands more sustainably but also increases overall access to dermatology mentors. Our findings indicate that similar programs could be expanded to include more residents and community dermatologists as mentors and to target students from disadvantaged backgrounds, those facing financial constraints, and students who identify as URiM.
Impact of Research Barriers on Career Trajectories—Among survey participants, 35% reported considering changing their specialty choice due to research-related barriers. This substantial percentage likely stems from the escalating pressure to achieve increasingly high research output amidst a lack of sufficient support, time, or tools, as our results suggest. The specific barriers that most notably predicted specialty change consideration were lack of time and not knowing how to begin research (P=.001 and P<.001, respectively). Remarkably, our findings revealed that respondents who rated these as moderate or major barriers were 6.3 and 4.7 times more likely to consider changing their specialty choice, respectively. Respondents reporting financial cost (P=.043), limited access to research opportunities (P=.006), and lack of mentorship or support (P=.001) as at least moderate barriers also were 2.2 to 3.5 times more likely to consider a specialty change (eTable 4 and eFigure 4). Additionally, barriers such as limited access to research opportunities (R²=−.27; P=.002), lack of mentorship (R2=−.22; P=.011), not knowing how to begin research (R2=−.19; P=.025), and institutional limitations (R2=−.18; P=.042) all were associated with lower publication output according to our data (eFigure 3). These findings are especially concerning given current match statistics, where the trajectory of research productivity required for a successful dermatology match continues to rise sharply.3,4
Alarmingly, many of the barriers we identified—linked to both reduced research output and specialty change consideration—are associated with several demographic factors. Higher debt levels predicted greater likelihood of experiencing lack of time, insufficient mentorship, and uncertainty about initiating research, while lower SES was associated with lack of mentorship. These relationships suggest that structural barriers, rather than lack of interest or ability, may create cumulative disadvantages that deter capable candidates from pursuing dermatology or impact their success in the application process.
One potential solution to address the disproportionate emphasis on research quantity would be implementing caps on reportable research products in residency applications (eg, limiting applications to a certain number of publications, abstracts, and presentations). This change could shift applicant focus toward substantive scientific contributions rather than rapid output accumulation.8 The need for such caps was evident in our dataset, which revealed a stark contrast: some respondents reported 30 to 40 publications, while MD/PhD respondents—who dedicate 3 to 5 years to performing quality research—averaged only 7.4 publications. Implementing a research output ceiling could help alleviate barriers for applicants facing institutional and demographic disadvantages while simultaneously boosting the scientific rigor of dermatology research.8
Mitigation Strategies From Applicant Feedback—Our findings emphasize the multifaceted relationship between structural barriers and demographics in dermatology research engagement. While our statistical interpretations have outlined several potential interventions, the applicants’ perspectives on mitigation strategies offer qualitative insight. Although participants did not consistently mark financial cost and lack of mentorship as major barriers (eFigure 1), financial assistance and access to engaged mentors were among the highest-ranked mitigation strategies (eFigure 5), suggesting these resources may be fundamental to overcoming multiple structural challenges. To address these needs comprehensively, we propose a multilevel approach: at the institutional level, dermatology interest groups could establish centralized databases of research opportunities, mentorship programs, and funding sources. At the national level, dermatology organizations could consider expanding grant programs, developing virtual mentorship networks, and creating opportunities for external students through remote research projects or short-term research rotations. These interventions, informed by both our statistical analyses and applicant feedback, could help create more equitable access to research opportunities in dermatology.
Limitations
A major limitation of this study was that potential dermatology candidates who were deterred by barriers and later decided on a different specialty would not be captured in our data. As these candidates may have faced substantial barriers that caused them to choose a different path, their absence from the current data may indicate that the reported results underpredict the effect size of the true population. Another limitation is the absence of a control group, such as applicants to less competitive specialties, which would provide valuable context for whether the barriers identified are unique to dermatology.
Conclusion
Our study provides compelling evidence that research barriers in dermatology residency applications intersect with demographic factors to influence research engagement and career trajectories. Our findings suggest that without targeted intervention, increasing emphasis on research productivity may exacerbate existing disparities in dermatology. Moving forward, a coordinated effort among institutions, dermatology associations, and dermatology residency programs will be fundamental to ensure that research requirements enhance rather than impede the development of a diverse, qualified dermatology workforce.
- Ozair A, Bhat V, Detchou DKE. The US residency selection process after the United States Medical Licensing Examination Step 1 pass/fail change: overview for applicants and educators. JMIR Med Educ. 2023;9:E37069. doi:10.2196/37069
- Patrinely JR Jr, Zakria D, Drolet BC. USMLE Step 1 changes: dermatology program director perspectives and implications. Cutis. 2021;107:293-294. doi:10.12788/cutis.0277
- National Resident Matching Program. Charting outcomes in the match: US MD seniors, 2022. July 2022. Accessed February 14, 2024. https://www.nrmp.org/wp-content/uploads/2022/07/Charting-Outcomes-MD-Seniors-2022_Final.pdf
- National Resident Matching Program. Charting outcomes in the match: US MD seniors, 2024. August 2024. Accessed February 14, 2024. https://www.nrmp.org/match-data/2024/08/charting-outcomes-characteristics-of-u-s-md-seniors-who-matched-to-their-preferred-specialty-2024-main-residency-match/
- National Resident Matching Program. Charting outcomes in the match: characteristics of applicants who matched to their preferred specialty in the 2007 main residency match. July 2021. Accessed February 14, 2024. https://www.nrmp.org/wp-content/uploads/2021/07/chartingoutcomes2007.pdf
- Sanabria-de la Torre R, Quiñones-Vico MI, Ubago-Rodríguez A, et al. Medical students’ interest in research: changing trends during university training. Front Med. 2023;10. doi:10.3389/fmed.2023.1257574
- Alikhan A, Sivamani RK, Mutizwa MM, et al. Advice for medical students interested in dermatology: perspectives from fourth year students who matched. Dermatol Online J. 2009;15:7. doi:10.5070/D398p8q1m5
- Elliott B, Carmody JB. Publish or perish: the research arms race in residency selection. J Grad Med Educ. 2023;15:524-527. doi:10.4300/JGME-D-23-00262.1
- Akhiyat S, Cardwell L, Sokumbi O. Why dermatology is the second least diverse specialty in medicine: how did we get here? Clin Dermatol. 2020;38:310-315. doi:10.1016/j.clindermatol.2020.02.005
- Orebi HA, Shahin MR, Awad Allah MT, et al. Medical students’ perceptions, experiences, and barriers towards research implementation at the faculty of medicine, Tanta University. BMC Med Educ. 2023;23:902. doi:10.1186/s12909-023-04884-z
- Jacobsen A, Kabbur G, Freese RL, et al. Socioeconomic factors and financial burdens of research “gap years” for dermatology residency applicants. Int J Womens Dermatol. 2023;9:e099. doi:10.1097/JW9.0000000000000099
- Jung J, Stoff BK, Orenstein LAV. Unpaid research fellowships among dermatology residency applicants. J Am Acad Dermatol. 2022;87:1230-1231. doi:10.1016/j.jaad.2021.12.027
- Rehman R, Shareef SJ, Mohammad TF, et al. Applying to dermatology residency without a home program: advice to medical students in the COVID-19 pandemic and beyond. Clin Dermatol. 2022;40:513-515. doi:10.1016/j.clindermatol.2022.01.003
- Villa NM, Shi VY, Hsiao JL. An underrecognized barrier to the dermatology residency match: lack of a home program. Int J Womens Dermatol. 2021;7:512-513. doi:10.1016/j.ijwd.2021.02.011
- Sekyere NAN, Grimes PE, Roberts WE, et al. Turning the tide: how the Women’s Dermatologic Society leads in diversifying dermatology. Int J Womens Dermatol. 2020;7:135-136. doi:10.1016/j.ijwd.2020.12.012
- Emory School of Medicine. Four phases in four years. Accessed January 17, 2025. https://med.emory.edu/education/programs/md/curriculum/4phases/index.html
- Bhatnagar V, Diaz S, Bucur PA. The need for more mentorship in medical school. Cureus. 2020;12:E7984. doi:10.7759/cureus.7984
- Skin of Color Society. Mentorship. Accessed January 17, 2025. https://skinofcolorsociety.org/what-we-do/mentorship
- American Academy of Dermatology. Diversity Mentorship Program: information for medical students. Accessed January 17, 2025. https://www.aad.org/member/career/awards/diversity
As one of the most competitive specialties in medicine, dermatology presents unique challenges for residency applicants, especially following the shift in United States Medical Licensing Examination (USMLE) Step 1 scoring to a pass/fail format.1,2 Historically, USMLE Step 1 served as a major screening metric for residency programs, with 90% of program directors in 2020 using USMLE Step 1 scores as a primary factor when deciding whether to invite applicants for interviews.1 However, the recent transition to pass/fail has made it much harder for program directors to objectively compare applicants, particularly in dermatology. In a 2020 survey, Patrinely Jr et al2 found that 77.2% of dermatology program directors agreed that this change would make it more difficult to assess candidates objectively. Consequently, research productivity has taken on greater importance as programs seek new ways to distinguish top applicants.1,2
In response to this increased emphasis on research, dermatology applicants have substantially boosted their scholarly output over the past several years. The 2022 and 2024 results from the National Residency Matching Program’s Charting Outcomes survey demonstrated a steady rise in research metrics among applicants across various specialties, with dermatology showing one of the largest increases.3,4 For instance, the average number of abstracts, presentations, and publications for matched allopathic dermatology applicants was 5.7 in 2007.5 This average increased to 20.9 in 20223 and to 27.7 in 2024,4 marking an astonishing 485% increase in 17 years. Interestingly, unmatched dermatology applicants had an average of 19.0 research products in 2024, which was similar to the average of successfully matched applicants just 2 years earlier.3,4
Engaging in research offers benefits beyond building a strong residency application. Specifically, it enhances critical thinking skills and provides hands-on experience in scientific inquiry.6 It allows students to explore dermatology topics of interest and address existing knowledge gaps within the specialty.6 Additionally, it creates opportunities to build meaningful relationships with experienced dermatologists who can guide and support students throughout their careers.7 Despite these benefits, the pursuit of research may be landscaped with obstacles, and the fervent race to obtain high research outputs may overshadow developmental advantages.8 These challenges and demands also could contribute to inequities in the residency selection process, particularly if barriers are influenced by socioeconomic and demographic disparities. As dermatology already ranks as the second least diverse specialty in medicine,9 research requirements that disproportionately disadvantage certain demographic groups risk further widening these concerning representation gaps rather than creating opportunities to address them.
Given these trends in research requirements and their potential impact on applicant success, understanding specific barriers to research engagement is essential for creating equitable opportunities in dermatology. In this study, we aimed to identify barriers to research engagement among dermatology applicants, analyze their relationship with demographic factors, assess their impact on specialty choice and research productivity, and provide actionable solutions to address these obstacles.
Methods
A cross-sectional survey was conducted targeting medical students applying to dermatology residency programs in the United States in the 2025 or 2026 match cycles as well as residents who applied to dermatology residency in the 2021 to 2024 match cycles. The 23-item survey was developed by adapting questions from several validated studies examining research barriers and experiences in medical education.6,7,10,11 Specifically, the survey included questions on demographics and background; research productivity; general research barriers; conference participation accessibility; mentorship access; and quality, career impact, and support needs. Socioeconomic background was measured via a single self-reported item asking participants to select the income class that best reflected their background growing up (low-income, lower-middle, upper-middle, or high-income); no income ranges were provided.
The survey was distributed electronically via Qualtrics between November 11, 2024, and December 30, 2024, through listserves of the Dermatology Interest Group Association (sent directly to medical students) and the Association of Professors of Dermatology (forwarded to residents by program directors). There was no way to determine the number of dermatology applicants and residents reached through either listserve. The surveys were reviewed and approved by the University of Alabama at Birmingham institutional review board (IRB-300013671).
Statistical analyses were conducted using RStudio (Posit, PBC; version 2024.12.0+467). Descriptive statistics characterized participant demographics and quantified barrier scores using frequencies and proportions. We performed regression analyses to examine relationships between demographic factors and barriers using linear regression; the relationship between barriers and research productivity correlation; and the prediction of specialty change consideration using logistic regression. For all analyses, barrier scores were rated on a scale of 0 to 3 (0=not a barrier, 1=minor barrier, 2=moderate barrier, 3=major barrier); R² values were reported to indicate strength of associations, and statistical significance was set at P<.05.
Results
Participant Demographics—A total of 136 participants completed the survey. Among the respondents, 12% identified as from a background of low-income class, 28% lower-middle class, 49% upper-middle class, and 11% high-income class. Additionally, 27% of respondents identified as underrepresented in medicine (URiM). Regarding debt levels (or expected debt levels) upon graduation from medical school, 32% reported no debt, 9% reported $1000 to $49,000 in debt, 5% reported $50,000 to $99,000 in debt, 15% reported $100,000 to $199,000 in debt, 22% reported $200,000 to $299,000 in debt, and 17% reported $300,000 in debt or higher. The majority of respondents (95%) were MD candidates, and the remaining 5% were DO candidates; additionally, 5% were participants in an MD/PhD program (eTable 1).
Respondents represented various stages of training: 13.2% and 16.2% were third- and fourth-year medical students, respectively, while 6.0%, 20.1%, 18.4%, and 22.8% were postgraduate year (PGY) 1, PGY-2, PGY-3, and PGY-4, respectively. A few respondents (2.9%) were participating in a research year or reapplying to dermatology residency (eTable 2).
Research Barriers and Productivity—Respondents were presented with a list of potential barriers and asked to rate each as not a barrier, a minor barrier, a moderate barrier, or a major barrier. The most common barriers (ie, those with >50% of respondents rating them as a moderate or major) included lack of time, limited access to research opportunities, not knowing how to begin research, and lack of mentorship or support. Lack of time and not knowing where to begin research were reported most frequently as major barriers, with 32% of participants identifying them as such. In contrast, barriers such as financial costs and personal obligations were less frequently rated as major barriers (10% and 4%, respectively), although they still were identified as obstacles by many respondents. Interestingly, most respondents (58%) indicated that institutional limitations were not a barrier, but a separate and sizeable proportion (25%) of respondents considered it to be a major barrier (eFigure 1).
The distributions for all research metrics were right-skewed. The total range was 0 to 45 (median, 6) for number of publications (excluding abstracts), 0 to 33 (median, 2) for published abstracts, 0 to 40 (median, 5) for poster publications, and 0 to 20 (median, 2) for oral presentations (eTable 3).
Regression Analysis—Linear regression analysis identified significant relationships between demographic variables (socioeconomic status [SES], URiM status, and debt level) and individual research barriers. The heatmap in eFigure 2 illustrates the strength of these relationships. Higher SES was predictive of lower reported financial barriers (R²=.2317; P<.0001) and lower reported institutional limitations (R²=.0884; P=.0006). A URiM status predicted higher reported financial barriers (R²=.1097; P<.0001) and institutional limitations (R²=.04537; P=.013). Also, higher debt level predicted increased financial barriers (R²=.2099; P<.0001), institutional limitations (R2=.1258; P<.0001), and lack of mentorship (R²=.06553; P=.003).
Next, the data were evaluated for correlative relationships between individual research barriers and research productivity metrics including number of publications, published abstracts and presentations (oral and poster) and total research output. While correlations were weak or nonsignificant between barriers and most research productivity metrics (published abstracts, oral and poster presentations, and total research output), the number of publications was significantly correlated with several research barriers, including limited access to research opportunities (P=.002), not knowing how to begin research (P=.025), lack of mentorship or support (P=.011), and institutional limitations (P=.042). Higher ratings for limited access to research opportunities, not knowing where to begin research, lack of mentorship or support, and institutional limitations all were negatively correlated with total number of publications (R2=−.27, –.19, −.22, and –.18, respectively)(eFigure 3).
Logistic regression analysis examined the impact of research barriers on the likelihood of specialty change consideration. The results, presented in a forest plot, include odds ratios (ORs) and their corresponding 95% CIs and P values. Lack of time (P=.001) and not knowing where to begin research (P<.001) were the strongest predictors of specialty change consideration (OR, 6.3 and 4.7, respectively). Financial cost (P=.043), limited access to research opportunities (P=.006), and lack of mentorship or support (P=.001) also were significant predictors of specialty change consideration (OR, 2.2, 3.1, and 3.5, respectively). Institutional limitations and personal obligations did not predict specialty change consideration (eTable 4 and eFigure 4).
Mitigation Strategies—Mitigation strategies were ranked by respondents based on their perceived importance on a scale of 1 to 7 (1=most important, 7=least important)(eFigure 5). Respondents considered access to engaged mentors to be the most important mitigation strategy by far, with 95% ranking it in the top 3 (47% of respondents ranked it as the top most important mitigation strategy). Financial assistance was the mitigation strategy with the second highest number of respondents (28%) ranking it as the top strategy. Flexible scheduling during rotations, research training programs or discussions, and peer networking and research collaboration opportunities also were considered by respondents to be important mitigation strategies. Time management support/resources frequently was viewed as the least important mitigation strategy, with 38% of respondents ranking it last.
Comment
Our study revealed notable disparities in research barriers among dermatology applicants, with several demonstrating consistent patterns of association with SES, URiM status, and debt burden. Furthermore, the strong relationship between these barriers and decreased research productivity and specialty change consideration suggests that capable candidates may be deterred from pursuing dermatology due to surmountable obstacles rather than lack of interest or ability.
Impact of Demographic Factors on Research Barriers—All 7 general research barriers surveyed were correlated with distinct demographic predictors. Regression analyses indicated that the barrier of financial cost was significantly predicted by lower SES (R²=.2317; P<.001), URiM status (R²=.1097; P<.001), and higher debt levels (R²=.2099; P<.001)(eFigure 2). These findings are particularly concerning given the trend of dermatology applicants pursuing 1-year research fellowships, many of which are unpaid.12 In fact, Jacobson et al11 found that 71.7% (43/60) of dermatology applicants who pursued a year-long research fellowship experienced financial strain during their fellowship, with many requiring additional loans or drawing from personal savings despite already carrying substantial medical school debt of $200,000 or more. Our findings showcase how financial barriers to research disproportionately affect students from lower socioeconomic backgrounds, those who identify as URiM, and those with higher debt, creating systemic inequities in research access at a time when research productivity is increasingly vital for matching into dermatology. To address these financial barriers, institutions may consider establishing more funded research fellowships or expanding grant programs targeting students from economically disadvantaged and/or underrepresented backgrounds.
Institutional limitations (eg, the absence of a dermatology department) also was a notable barrier that was significantly predicted by lower SES (R²=.0884; P<.001) and URiM status (R²=.04537; P=.013)(eFigure 2). Students at institutions lacking dermatology programs face restricted access to mentorship and research opportunities,13 with our results demonstrating that these barriers disproportionately affect students from underresourced and minority groups. These limitations compound disparities in building competitive residency applications.14 The Women’s Dermatologic Society (WDS) has developed a model for addressing these institutional barriers through its summer research fellowship program for medical students who identify as URiM. By pairing students with WDS mentors who guide them through summer research projects, this initiative addresses access and mentorship gaps for students lacking dermatology departments at their home institution.15 The WDS program serves as a model for other organizations to adopt and expand, with particular attention to including students who identify as URiM as well as those from lower socioeconomic backgrounds.
Our results identified time constraints and lack of experience as notable research barriers. Higher debt levels significantly predicted both lack of time (R²=.03915; P=.021) and not knowing how to begin research (R²=.0572; P=.005)(eFigure 2). These statistical relationships may be explained by students with higher debt levels needing to prioritize paid work over unpaid research opportunities, limiting their engagement in research due to the scarcity of funded positions.12 The data further revealed that personal obligations, particularly family care responsibilities, were significantly predicted by both lower SES (R²=.0539; P=.008) and higher debt level (R²=.03237; P=.036)(eFigure 2). These findings demonstrate how students managing academic demands alongside financial and familial responsibilities may face compounded barriers to research engagement. To address these disparities, medical schools may consider implementing protected research time within their curricula; for example, the Emory University School of Medicine (Atlanta, Georgia) has implemented a Discovery Phase program that provides students with 5 months of protected faculty-mentored research time away from academic demands between their third and fourth years of medical school.16 Integrating similarly structured research periods across medical school curricula could help ensure equitable research opportunities for all students pursuing competitive specialties such as dermatology.8
Access to mentorship is a critical determinant of research engagement and productivity, as mentors provide valuable guidance on navigating research processes and professional development.17 Our analysis revealed that lack of mentorship was predicted by both lower SES (R²=.039; P=.023) and higher debt level (R²=.06553; P=.003)(eFigure 2). Several organizations have developed programs to address these mentorship gaps. The Skin of Color Society pairs medical students with skin of color experts while advancing its mission of increasing diversity in dermatology.18 Similarly, the American Academy of Dermatology founded a diversity mentorship program that connects students who identify as URiM with dermatologist mentors for summer research experiences.19 Notably, the Skin of Color Society’s program allows residents to serve as mentors for medical students. Involving residents and community dermatologists as potential dermatology mentors for medical students not only distributes mentorship demands more sustainably but also increases overall access to dermatology mentors. Our findings indicate that similar programs could be expanded to include more residents and community dermatologists as mentors and to target students from disadvantaged backgrounds, those facing financial constraints, and students who identify as URiM.
Impact of Research Barriers on Career Trajectories—Among survey participants, 35% reported considering changing their specialty choice due to research-related barriers. This substantial percentage likely stems from the escalating pressure to achieve increasingly high research output amidst a lack of sufficient support, time, or tools, as our results suggest. The specific barriers that most notably predicted specialty change consideration were lack of time and not knowing how to begin research (P=.001 and P<.001, respectively). Remarkably, our findings revealed that respondents who rated these as moderate or major barriers were 6.3 and 4.7 times more likely to consider changing their specialty choice, respectively. Respondents reporting financial cost (P=.043), limited access to research opportunities (P=.006), and lack of mentorship or support (P=.001) as at least moderate barriers also were 2.2 to 3.5 times more likely to consider a specialty change (eTable 4 and eFigure 4). Additionally, barriers such as limited access to research opportunities (R²=−.27; P=.002), lack of mentorship (R2=−.22; P=.011), not knowing how to begin research (R2=−.19; P=.025), and institutional limitations (R2=−.18; P=.042) all were associated with lower publication output according to our data (eFigure 3). These findings are especially concerning given current match statistics, where the trajectory of research productivity required for a successful dermatology match continues to rise sharply.3,4
Alarmingly, many of the barriers we identified—linked to both reduced research output and specialty change consideration—are associated with several demographic factors. Higher debt levels predicted greater likelihood of experiencing lack of time, insufficient mentorship, and uncertainty about initiating research, while lower SES was associated with lack of mentorship. These relationships suggest that structural barriers, rather than lack of interest or ability, may create cumulative disadvantages that deter capable candidates from pursuing dermatology or impact their success in the application process.
One potential solution to address the disproportionate emphasis on research quantity would be implementing caps on reportable research products in residency applications (eg, limiting applications to a certain number of publications, abstracts, and presentations). This change could shift applicant focus toward substantive scientific contributions rather than rapid output accumulation.8 The need for such caps was evident in our dataset, which revealed a stark contrast: some respondents reported 30 to 40 publications, while MD/PhD respondents—who dedicate 3 to 5 years to performing quality research—averaged only 7.4 publications. Implementing a research output ceiling could help alleviate barriers for applicants facing institutional and demographic disadvantages while simultaneously boosting the scientific rigor of dermatology research.8
Mitigation Strategies From Applicant Feedback—Our findings emphasize the multifaceted relationship between structural barriers and demographics in dermatology research engagement. While our statistical interpretations have outlined several potential interventions, the applicants’ perspectives on mitigation strategies offer qualitative insight. Although participants did not consistently mark financial cost and lack of mentorship as major barriers (eFigure 1), financial assistance and access to engaged mentors were among the highest-ranked mitigation strategies (eFigure 5), suggesting these resources may be fundamental to overcoming multiple structural challenges. To address these needs comprehensively, we propose a multilevel approach: at the institutional level, dermatology interest groups could establish centralized databases of research opportunities, mentorship programs, and funding sources. At the national level, dermatology organizations could consider expanding grant programs, developing virtual mentorship networks, and creating opportunities for external students through remote research projects or short-term research rotations. These interventions, informed by both our statistical analyses and applicant feedback, could help create more equitable access to research opportunities in dermatology.
Limitations
A major limitation of this study was that potential dermatology candidates who were deterred by barriers and later decided on a different specialty would not be captured in our data. As these candidates may have faced substantial barriers that caused them to choose a different path, their absence from the current data may indicate that the reported results underpredict the effect size of the true population. Another limitation is the absence of a control group, such as applicants to less competitive specialties, which would provide valuable context for whether the barriers identified are unique to dermatology.
Conclusion
Our study provides compelling evidence that research barriers in dermatology residency applications intersect with demographic factors to influence research engagement and career trajectories. Our findings suggest that without targeted intervention, increasing emphasis on research productivity may exacerbate existing disparities in dermatology. Moving forward, a coordinated effort among institutions, dermatology associations, and dermatology residency programs will be fundamental to ensure that research requirements enhance rather than impede the development of a diverse, qualified dermatology workforce.
As one of the most competitive specialties in medicine, dermatology presents unique challenges for residency applicants, especially following the shift in United States Medical Licensing Examination (USMLE) Step 1 scoring to a pass/fail format.1,2 Historically, USMLE Step 1 served as a major screening metric for residency programs, with 90% of program directors in 2020 using USMLE Step 1 scores as a primary factor when deciding whether to invite applicants for interviews.1 However, the recent transition to pass/fail has made it much harder for program directors to objectively compare applicants, particularly in dermatology. In a 2020 survey, Patrinely Jr et al2 found that 77.2% of dermatology program directors agreed that this change would make it more difficult to assess candidates objectively. Consequently, research productivity has taken on greater importance as programs seek new ways to distinguish top applicants.1,2
In response to this increased emphasis on research, dermatology applicants have substantially boosted their scholarly output over the past several years. The 2022 and 2024 results from the National Residency Matching Program’s Charting Outcomes survey demonstrated a steady rise in research metrics among applicants across various specialties, with dermatology showing one of the largest increases.3,4 For instance, the average number of abstracts, presentations, and publications for matched allopathic dermatology applicants was 5.7 in 2007.5 This average increased to 20.9 in 20223 and to 27.7 in 2024,4 marking an astonishing 485% increase in 17 years. Interestingly, unmatched dermatology applicants had an average of 19.0 research products in 2024, which was similar to the average of successfully matched applicants just 2 years earlier.3,4
Engaging in research offers benefits beyond building a strong residency application. Specifically, it enhances critical thinking skills and provides hands-on experience in scientific inquiry.6 It allows students to explore dermatology topics of interest and address existing knowledge gaps within the specialty.6 Additionally, it creates opportunities to build meaningful relationships with experienced dermatologists who can guide and support students throughout their careers.7 Despite these benefits, the pursuit of research may be landscaped with obstacles, and the fervent race to obtain high research outputs may overshadow developmental advantages.8 These challenges and demands also could contribute to inequities in the residency selection process, particularly if barriers are influenced by socioeconomic and demographic disparities. As dermatology already ranks as the second least diverse specialty in medicine,9 research requirements that disproportionately disadvantage certain demographic groups risk further widening these concerning representation gaps rather than creating opportunities to address them.
Given these trends in research requirements and their potential impact on applicant success, understanding specific barriers to research engagement is essential for creating equitable opportunities in dermatology. In this study, we aimed to identify barriers to research engagement among dermatology applicants, analyze their relationship with demographic factors, assess their impact on specialty choice and research productivity, and provide actionable solutions to address these obstacles.
Methods
A cross-sectional survey was conducted targeting medical students applying to dermatology residency programs in the United States in the 2025 or 2026 match cycles as well as residents who applied to dermatology residency in the 2021 to 2024 match cycles. The 23-item survey was developed by adapting questions from several validated studies examining research barriers and experiences in medical education.6,7,10,11 Specifically, the survey included questions on demographics and background; research productivity; general research barriers; conference participation accessibility; mentorship access; and quality, career impact, and support needs. Socioeconomic background was measured via a single self-reported item asking participants to select the income class that best reflected their background growing up (low-income, lower-middle, upper-middle, or high-income); no income ranges were provided.
The survey was distributed electronically via Qualtrics between November 11, 2024, and December 30, 2024, through listserves of the Dermatology Interest Group Association (sent directly to medical students) and the Association of Professors of Dermatology (forwarded to residents by program directors). There was no way to determine the number of dermatology applicants and residents reached through either listserve. The surveys were reviewed and approved by the University of Alabama at Birmingham institutional review board (IRB-300013671).
Statistical analyses were conducted using RStudio (Posit, PBC; version 2024.12.0+467). Descriptive statistics characterized participant demographics and quantified barrier scores using frequencies and proportions. We performed regression analyses to examine relationships between demographic factors and barriers using linear regression; the relationship between barriers and research productivity correlation; and the prediction of specialty change consideration using logistic regression. For all analyses, barrier scores were rated on a scale of 0 to 3 (0=not a barrier, 1=minor barrier, 2=moderate barrier, 3=major barrier); R² values were reported to indicate strength of associations, and statistical significance was set at P<.05.
Results
Participant Demographics—A total of 136 participants completed the survey. Among the respondents, 12% identified as from a background of low-income class, 28% lower-middle class, 49% upper-middle class, and 11% high-income class. Additionally, 27% of respondents identified as underrepresented in medicine (URiM). Regarding debt levels (or expected debt levels) upon graduation from medical school, 32% reported no debt, 9% reported $1000 to $49,000 in debt, 5% reported $50,000 to $99,000 in debt, 15% reported $100,000 to $199,000 in debt, 22% reported $200,000 to $299,000 in debt, and 17% reported $300,000 in debt or higher. The majority of respondents (95%) were MD candidates, and the remaining 5% were DO candidates; additionally, 5% were participants in an MD/PhD program (eTable 1).
Respondents represented various stages of training: 13.2% and 16.2% were third- and fourth-year medical students, respectively, while 6.0%, 20.1%, 18.4%, and 22.8% were postgraduate year (PGY) 1, PGY-2, PGY-3, and PGY-4, respectively. A few respondents (2.9%) were participating in a research year or reapplying to dermatology residency (eTable 2).
Research Barriers and Productivity—Respondents were presented with a list of potential barriers and asked to rate each as not a barrier, a minor barrier, a moderate barrier, or a major barrier. The most common barriers (ie, those with >50% of respondents rating them as a moderate or major) included lack of time, limited access to research opportunities, not knowing how to begin research, and lack of mentorship or support. Lack of time and not knowing where to begin research were reported most frequently as major barriers, with 32% of participants identifying them as such. In contrast, barriers such as financial costs and personal obligations were less frequently rated as major barriers (10% and 4%, respectively), although they still were identified as obstacles by many respondents. Interestingly, most respondents (58%) indicated that institutional limitations were not a barrier, but a separate and sizeable proportion (25%) of respondents considered it to be a major barrier (eFigure 1).
The distributions for all research metrics were right-skewed. The total range was 0 to 45 (median, 6) for number of publications (excluding abstracts), 0 to 33 (median, 2) for published abstracts, 0 to 40 (median, 5) for poster publications, and 0 to 20 (median, 2) for oral presentations (eTable 3).
Regression Analysis—Linear regression analysis identified significant relationships between demographic variables (socioeconomic status [SES], URiM status, and debt level) and individual research barriers. The heatmap in eFigure 2 illustrates the strength of these relationships. Higher SES was predictive of lower reported financial barriers (R²=.2317; P<.0001) and lower reported institutional limitations (R²=.0884; P=.0006). A URiM status predicted higher reported financial barriers (R²=.1097; P<.0001) and institutional limitations (R²=.04537; P=.013). Also, higher debt level predicted increased financial barriers (R²=.2099; P<.0001), institutional limitations (R2=.1258; P<.0001), and lack of mentorship (R²=.06553; P=.003).
Next, the data were evaluated for correlative relationships between individual research barriers and research productivity metrics including number of publications, published abstracts and presentations (oral and poster) and total research output. While correlations were weak or nonsignificant between barriers and most research productivity metrics (published abstracts, oral and poster presentations, and total research output), the number of publications was significantly correlated with several research barriers, including limited access to research opportunities (P=.002), not knowing how to begin research (P=.025), lack of mentorship or support (P=.011), and institutional limitations (P=.042). Higher ratings for limited access to research opportunities, not knowing where to begin research, lack of mentorship or support, and institutional limitations all were negatively correlated with total number of publications (R2=−.27, –.19, −.22, and –.18, respectively)(eFigure 3).
Logistic regression analysis examined the impact of research barriers on the likelihood of specialty change consideration. The results, presented in a forest plot, include odds ratios (ORs) and their corresponding 95% CIs and P values. Lack of time (P=.001) and not knowing where to begin research (P<.001) were the strongest predictors of specialty change consideration (OR, 6.3 and 4.7, respectively). Financial cost (P=.043), limited access to research opportunities (P=.006), and lack of mentorship or support (P=.001) also were significant predictors of specialty change consideration (OR, 2.2, 3.1, and 3.5, respectively). Institutional limitations and personal obligations did not predict specialty change consideration (eTable 4 and eFigure 4).
Mitigation Strategies—Mitigation strategies were ranked by respondents based on their perceived importance on a scale of 1 to 7 (1=most important, 7=least important)(eFigure 5). Respondents considered access to engaged mentors to be the most important mitigation strategy by far, with 95% ranking it in the top 3 (47% of respondents ranked it as the top most important mitigation strategy). Financial assistance was the mitigation strategy with the second highest number of respondents (28%) ranking it as the top strategy. Flexible scheduling during rotations, research training programs or discussions, and peer networking and research collaboration opportunities also were considered by respondents to be important mitigation strategies. Time management support/resources frequently was viewed as the least important mitigation strategy, with 38% of respondents ranking it last.
Comment
Our study revealed notable disparities in research barriers among dermatology applicants, with several demonstrating consistent patterns of association with SES, URiM status, and debt burden. Furthermore, the strong relationship between these barriers and decreased research productivity and specialty change consideration suggests that capable candidates may be deterred from pursuing dermatology due to surmountable obstacles rather than lack of interest or ability.
Impact of Demographic Factors on Research Barriers—All 7 general research barriers surveyed were correlated with distinct demographic predictors. Regression analyses indicated that the barrier of financial cost was significantly predicted by lower SES (R²=.2317; P<.001), URiM status (R²=.1097; P<.001), and higher debt levels (R²=.2099; P<.001)(eFigure 2). These findings are particularly concerning given the trend of dermatology applicants pursuing 1-year research fellowships, many of which are unpaid.12 In fact, Jacobson et al11 found that 71.7% (43/60) of dermatology applicants who pursued a year-long research fellowship experienced financial strain during their fellowship, with many requiring additional loans or drawing from personal savings despite already carrying substantial medical school debt of $200,000 or more. Our findings showcase how financial barriers to research disproportionately affect students from lower socioeconomic backgrounds, those who identify as URiM, and those with higher debt, creating systemic inequities in research access at a time when research productivity is increasingly vital for matching into dermatology. To address these financial barriers, institutions may consider establishing more funded research fellowships or expanding grant programs targeting students from economically disadvantaged and/or underrepresented backgrounds.
Institutional limitations (eg, the absence of a dermatology department) also was a notable barrier that was significantly predicted by lower SES (R²=.0884; P<.001) and URiM status (R²=.04537; P=.013)(eFigure 2). Students at institutions lacking dermatology programs face restricted access to mentorship and research opportunities,13 with our results demonstrating that these barriers disproportionately affect students from underresourced and minority groups. These limitations compound disparities in building competitive residency applications.14 The Women’s Dermatologic Society (WDS) has developed a model for addressing these institutional barriers through its summer research fellowship program for medical students who identify as URiM. By pairing students with WDS mentors who guide them through summer research projects, this initiative addresses access and mentorship gaps for students lacking dermatology departments at their home institution.15 The WDS program serves as a model for other organizations to adopt and expand, with particular attention to including students who identify as URiM as well as those from lower socioeconomic backgrounds.
Our results identified time constraints and lack of experience as notable research barriers. Higher debt levels significantly predicted both lack of time (R²=.03915; P=.021) and not knowing how to begin research (R²=.0572; P=.005)(eFigure 2). These statistical relationships may be explained by students with higher debt levels needing to prioritize paid work over unpaid research opportunities, limiting their engagement in research due to the scarcity of funded positions.12 The data further revealed that personal obligations, particularly family care responsibilities, were significantly predicted by both lower SES (R²=.0539; P=.008) and higher debt level (R²=.03237; P=.036)(eFigure 2). These findings demonstrate how students managing academic demands alongside financial and familial responsibilities may face compounded barriers to research engagement. To address these disparities, medical schools may consider implementing protected research time within their curricula; for example, the Emory University School of Medicine (Atlanta, Georgia) has implemented a Discovery Phase program that provides students with 5 months of protected faculty-mentored research time away from academic demands between their third and fourth years of medical school.16 Integrating similarly structured research periods across medical school curricula could help ensure equitable research opportunities for all students pursuing competitive specialties such as dermatology.8
Access to mentorship is a critical determinant of research engagement and productivity, as mentors provide valuable guidance on navigating research processes and professional development.17 Our analysis revealed that lack of mentorship was predicted by both lower SES (R²=.039; P=.023) and higher debt level (R²=.06553; P=.003)(eFigure 2). Several organizations have developed programs to address these mentorship gaps. The Skin of Color Society pairs medical students with skin of color experts while advancing its mission of increasing diversity in dermatology.18 Similarly, the American Academy of Dermatology founded a diversity mentorship program that connects students who identify as URiM with dermatologist mentors for summer research experiences.19 Notably, the Skin of Color Society’s program allows residents to serve as mentors for medical students. Involving residents and community dermatologists as potential dermatology mentors for medical students not only distributes mentorship demands more sustainably but also increases overall access to dermatology mentors. Our findings indicate that similar programs could be expanded to include more residents and community dermatologists as mentors and to target students from disadvantaged backgrounds, those facing financial constraints, and students who identify as URiM.
Impact of Research Barriers on Career Trajectories—Among survey participants, 35% reported considering changing their specialty choice due to research-related barriers. This substantial percentage likely stems from the escalating pressure to achieve increasingly high research output amidst a lack of sufficient support, time, or tools, as our results suggest. The specific barriers that most notably predicted specialty change consideration were lack of time and not knowing how to begin research (P=.001 and P<.001, respectively). Remarkably, our findings revealed that respondents who rated these as moderate or major barriers were 6.3 and 4.7 times more likely to consider changing their specialty choice, respectively. Respondents reporting financial cost (P=.043), limited access to research opportunities (P=.006), and lack of mentorship or support (P=.001) as at least moderate barriers also were 2.2 to 3.5 times more likely to consider a specialty change (eTable 4 and eFigure 4). Additionally, barriers such as limited access to research opportunities (R²=−.27; P=.002), lack of mentorship (R2=−.22; P=.011), not knowing how to begin research (R2=−.19; P=.025), and institutional limitations (R2=−.18; P=.042) all were associated with lower publication output according to our data (eFigure 3). These findings are especially concerning given current match statistics, where the trajectory of research productivity required for a successful dermatology match continues to rise sharply.3,4
Alarmingly, many of the barriers we identified—linked to both reduced research output and specialty change consideration—are associated with several demographic factors. Higher debt levels predicted greater likelihood of experiencing lack of time, insufficient mentorship, and uncertainty about initiating research, while lower SES was associated with lack of mentorship. These relationships suggest that structural barriers, rather than lack of interest or ability, may create cumulative disadvantages that deter capable candidates from pursuing dermatology or impact their success in the application process.
One potential solution to address the disproportionate emphasis on research quantity would be implementing caps on reportable research products in residency applications (eg, limiting applications to a certain number of publications, abstracts, and presentations). This change could shift applicant focus toward substantive scientific contributions rather than rapid output accumulation.8 The need for such caps was evident in our dataset, which revealed a stark contrast: some respondents reported 30 to 40 publications, while MD/PhD respondents—who dedicate 3 to 5 years to performing quality research—averaged only 7.4 publications. Implementing a research output ceiling could help alleviate barriers for applicants facing institutional and demographic disadvantages while simultaneously boosting the scientific rigor of dermatology research.8
Mitigation Strategies From Applicant Feedback—Our findings emphasize the multifaceted relationship between structural barriers and demographics in dermatology research engagement. While our statistical interpretations have outlined several potential interventions, the applicants’ perspectives on mitigation strategies offer qualitative insight. Although participants did not consistently mark financial cost and lack of mentorship as major barriers (eFigure 1), financial assistance and access to engaged mentors were among the highest-ranked mitigation strategies (eFigure 5), suggesting these resources may be fundamental to overcoming multiple structural challenges. To address these needs comprehensively, we propose a multilevel approach: at the institutional level, dermatology interest groups could establish centralized databases of research opportunities, mentorship programs, and funding sources. At the national level, dermatology organizations could consider expanding grant programs, developing virtual mentorship networks, and creating opportunities for external students through remote research projects or short-term research rotations. These interventions, informed by both our statistical analyses and applicant feedback, could help create more equitable access to research opportunities in dermatology.
Limitations
A major limitation of this study was that potential dermatology candidates who were deterred by barriers and later decided on a different specialty would not be captured in our data. As these candidates may have faced substantial barriers that caused them to choose a different path, their absence from the current data may indicate that the reported results underpredict the effect size of the true population. Another limitation is the absence of a control group, such as applicants to less competitive specialties, which would provide valuable context for whether the barriers identified are unique to dermatology.
Conclusion
Our study provides compelling evidence that research barriers in dermatology residency applications intersect with demographic factors to influence research engagement and career trajectories. Our findings suggest that without targeted intervention, increasing emphasis on research productivity may exacerbate existing disparities in dermatology. Moving forward, a coordinated effort among institutions, dermatology associations, and dermatology residency programs will be fundamental to ensure that research requirements enhance rather than impede the development of a diverse, qualified dermatology workforce.
- Ozair A, Bhat V, Detchou DKE. The US residency selection process after the United States Medical Licensing Examination Step 1 pass/fail change: overview for applicants and educators. JMIR Med Educ. 2023;9:E37069. doi:10.2196/37069
- Patrinely JR Jr, Zakria D, Drolet BC. USMLE Step 1 changes: dermatology program director perspectives and implications. Cutis. 2021;107:293-294. doi:10.12788/cutis.0277
- National Resident Matching Program. Charting outcomes in the match: US MD seniors, 2022. July 2022. Accessed February 14, 2024. https://www.nrmp.org/wp-content/uploads/2022/07/Charting-Outcomes-MD-Seniors-2022_Final.pdf
- National Resident Matching Program. Charting outcomes in the match: US MD seniors, 2024. August 2024. Accessed February 14, 2024. https://www.nrmp.org/match-data/2024/08/charting-outcomes-characteristics-of-u-s-md-seniors-who-matched-to-their-preferred-specialty-2024-main-residency-match/
- National Resident Matching Program. Charting outcomes in the match: characteristics of applicants who matched to their preferred specialty in the 2007 main residency match. July 2021. Accessed February 14, 2024. https://www.nrmp.org/wp-content/uploads/2021/07/chartingoutcomes2007.pdf
- Sanabria-de la Torre R, Quiñones-Vico MI, Ubago-Rodríguez A, et al. Medical students’ interest in research: changing trends during university training. Front Med. 2023;10. doi:10.3389/fmed.2023.1257574
- Alikhan A, Sivamani RK, Mutizwa MM, et al. Advice for medical students interested in dermatology: perspectives from fourth year students who matched. Dermatol Online J. 2009;15:7. doi:10.5070/D398p8q1m5
- Elliott B, Carmody JB. Publish or perish: the research arms race in residency selection. J Grad Med Educ. 2023;15:524-527. doi:10.4300/JGME-D-23-00262.1
- Akhiyat S, Cardwell L, Sokumbi O. Why dermatology is the second least diverse specialty in medicine: how did we get here? Clin Dermatol. 2020;38:310-315. doi:10.1016/j.clindermatol.2020.02.005
- Orebi HA, Shahin MR, Awad Allah MT, et al. Medical students’ perceptions, experiences, and barriers towards research implementation at the faculty of medicine, Tanta University. BMC Med Educ. 2023;23:902. doi:10.1186/s12909-023-04884-z
- Jacobsen A, Kabbur G, Freese RL, et al. Socioeconomic factors and financial burdens of research “gap years” for dermatology residency applicants. Int J Womens Dermatol. 2023;9:e099. doi:10.1097/JW9.0000000000000099
- Jung J, Stoff BK, Orenstein LAV. Unpaid research fellowships among dermatology residency applicants. J Am Acad Dermatol. 2022;87:1230-1231. doi:10.1016/j.jaad.2021.12.027
- Rehman R, Shareef SJ, Mohammad TF, et al. Applying to dermatology residency without a home program: advice to medical students in the COVID-19 pandemic and beyond. Clin Dermatol. 2022;40:513-515. doi:10.1016/j.clindermatol.2022.01.003
- Villa NM, Shi VY, Hsiao JL. An underrecognized barrier to the dermatology residency match: lack of a home program. Int J Womens Dermatol. 2021;7:512-513. doi:10.1016/j.ijwd.2021.02.011
- Sekyere NAN, Grimes PE, Roberts WE, et al. Turning the tide: how the Women’s Dermatologic Society leads in diversifying dermatology. Int J Womens Dermatol. 2020;7:135-136. doi:10.1016/j.ijwd.2020.12.012
- Emory School of Medicine. Four phases in four years. Accessed January 17, 2025. https://med.emory.edu/education/programs/md/curriculum/4phases/index.html
- Bhatnagar V, Diaz S, Bucur PA. The need for more mentorship in medical school. Cureus. 2020;12:E7984. doi:10.7759/cureus.7984
- Skin of Color Society. Mentorship. Accessed January 17, 2025. https://skinofcolorsociety.org/what-we-do/mentorship
- American Academy of Dermatology. Diversity Mentorship Program: information for medical students. Accessed January 17, 2025. https://www.aad.org/member/career/awards/diversity
- Ozair A, Bhat V, Detchou DKE. The US residency selection process after the United States Medical Licensing Examination Step 1 pass/fail change: overview for applicants and educators. JMIR Med Educ. 2023;9:E37069. doi:10.2196/37069
- Patrinely JR Jr, Zakria D, Drolet BC. USMLE Step 1 changes: dermatology program director perspectives and implications. Cutis. 2021;107:293-294. doi:10.12788/cutis.0277
- National Resident Matching Program. Charting outcomes in the match: US MD seniors, 2022. July 2022. Accessed February 14, 2024. https://www.nrmp.org/wp-content/uploads/2022/07/Charting-Outcomes-MD-Seniors-2022_Final.pdf
- National Resident Matching Program. Charting outcomes in the match: US MD seniors, 2024. August 2024. Accessed February 14, 2024. https://www.nrmp.org/match-data/2024/08/charting-outcomes-characteristics-of-u-s-md-seniors-who-matched-to-their-preferred-specialty-2024-main-residency-match/
- National Resident Matching Program. Charting outcomes in the match: characteristics of applicants who matched to their preferred specialty in the 2007 main residency match. July 2021. Accessed February 14, 2024. https://www.nrmp.org/wp-content/uploads/2021/07/chartingoutcomes2007.pdf
- Sanabria-de la Torre R, Quiñones-Vico MI, Ubago-Rodríguez A, et al. Medical students’ interest in research: changing trends during university training. Front Med. 2023;10. doi:10.3389/fmed.2023.1257574
- Alikhan A, Sivamani RK, Mutizwa MM, et al. Advice for medical students interested in dermatology: perspectives from fourth year students who matched. Dermatol Online J. 2009;15:7. doi:10.5070/D398p8q1m5
- Elliott B, Carmody JB. Publish or perish: the research arms race in residency selection. J Grad Med Educ. 2023;15:524-527. doi:10.4300/JGME-D-23-00262.1
- Akhiyat S, Cardwell L, Sokumbi O. Why dermatology is the second least diverse specialty in medicine: how did we get here? Clin Dermatol. 2020;38:310-315. doi:10.1016/j.clindermatol.2020.02.005
- Orebi HA, Shahin MR, Awad Allah MT, et al. Medical students’ perceptions, experiences, and barriers towards research implementation at the faculty of medicine, Tanta University. BMC Med Educ. 2023;23:902. doi:10.1186/s12909-023-04884-z
- Jacobsen A, Kabbur G, Freese RL, et al. Socioeconomic factors and financial burdens of research “gap years” for dermatology residency applicants. Int J Womens Dermatol. 2023;9:e099. doi:10.1097/JW9.0000000000000099
- Jung J, Stoff BK, Orenstein LAV. Unpaid research fellowships among dermatology residency applicants. J Am Acad Dermatol. 2022;87:1230-1231. doi:10.1016/j.jaad.2021.12.027
- Rehman R, Shareef SJ, Mohammad TF, et al. Applying to dermatology residency without a home program: advice to medical students in the COVID-19 pandemic and beyond. Clin Dermatol. 2022;40:513-515. doi:10.1016/j.clindermatol.2022.01.003
- Villa NM, Shi VY, Hsiao JL. An underrecognized barrier to the dermatology residency match: lack of a home program. Int J Womens Dermatol. 2021;7:512-513. doi:10.1016/j.ijwd.2021.02.011
- Sekyere NAN, Grimes PE, Roberts WE, et al. Turning the tide: how the Women’s Dermatologic Society leads in diversifying dermatology. Int J Womens Dermatol. 2020;7:135-136. doi:10.1016/j.ijwd.2020.12.012
- Emory School of Medicine. Four phases in four years. Accessed January 17, 2025. https://med.emory.edu/education/programs/md/curriculum/4phases/index.html
- Bhatnagar V, Diaz S, Bucur PA. The need for more mentorship in medical school. Cureus. 2020;12:E7984. doi:10.7759/cureus.7984
- Skin of Color Society. Mentorship. Accessed January 17, 2025. https://skinofcolorsociety.org/what-we-do/mentorship
- American Academy of Dermatology. Diversity Mentorship Program: information for medical students. Accessed January 17, 2025. https://www.aad.org/member/career/awards/diversity
How Increasing Research Demands Threaten Equity in Dermatology Residency Selection and Strategies for Reform
How Increasing Research Demands Threaten Equity in Dermatology Residency Selection and Strategies for Reform
Practice Points
- Dermatology programs should establish sustainable mentorship networks incorporating faculty, residents, and community dermatologists, as most applicants ranked access to engaged mentors as a top priority for overcoming research barriers.
- Protected research time and funding support for projects are critical, particularly since applicants reporting lack of time and financial barriers were more likely to consider changing their specialty choice.
- Programs should consider implementing caps on reportable research products in residency applications to shift emphasis from quantity to quality while helping address demographic disparities in research access.
