User login
Study provides new insights regarding HSCs, FA
with Fanconi anemia
Image by Michael Milsom
Environmental stress is a major factor driving DNA damage in hematopoietic stem cells (HSCs), according to research published in Nature.
Investigators found that repeated exposure to such stress induces accelerated tissue aging and may cause cancer.
In examining HSCs’ response to stress, the team also gained new insight regarding Fanconi anemia.
The investigators noted that, under normal conditions, HSCs exist in a state of dormancy. They rarely divide and have very low energy demands.
“Our theory was that this state of dormancy protected hematopoietic stem cells from DNA damage and therefore protects them from premature aging,” said study author Michael Milsom, PhD, of The Heidelberg Institute for Stem Cell Technology and Experimental Medicine in Germany.
However, under conditions of stress, such as during chronic blood loss or infection, HSCs are driven into a state of rapid cell division in order to produce new blood cells and repair the damaged tissue.
“The stem cells go from a state of rest to very high activity within a short space of time, requiring them to rapidly increase their metabolic rate, synthesize new DNA, and coordinate cell division,” Dr Milsom explained. “Suddenly having to simultaneously execute these complicated functions dramatically increases the likelihood that something will go wrong.”
Indeed, the investigators’ experiments showed that the increased energy demands during stress results in elevated production of reactive metabolites that can directly damage DNA. If this happens at the same time a cell is trying to replicate its DNA, this can cause cell death or the acquisition of mutations that may cause cancer.
Normal stem cells can repair the majority of this stress-induced DNA damage, the investigators noted. However, the more HSCs are exposed to stress, the more likely they are to inefficiently repair the damage and then die or mutate.
“We believe that this model perfectly explains the gradual accumulation of DNA damage in stem cells with age and the associated reduction in the ability of a tissue to maintain and repair itself as you get older,” Dr Milsom said.
He and his colleagues also examined how this stress response impacts a mouse model of Fanconi anemia. These mice have the same DNA repair defect found in humans with the disease, but the mice never spontaneously develop the bone marrow failure observed in nearly all patients.
“We felt that stress-induced DNA damage was the missing ingredient that was required to cause hematopoietic stem cell depletion in these mice,” Dr Milsom said.
When mice with Fanconi anemia were exposed to stimulation mimicking a prolonged viral infection, they were unable to efficiently repair the resulting DNA damage, and their stem cells failed.
In the same space of time that normal mice showed a gradual decline in HSC numbers, the stem cells in Fanconi anemia mice were almost completely depleted, resulting in bone marrow failure and an inadequate production of blood cells to sustain life.
“This perfectly recapitulates what happens to Fanconi anemia patients and now gives us an opportunity to understand how this disease works and how we might better treat it,” Dr Milsom said. ![]()
with Fanconi anemia
Image by Michael Milsom
Environmental stress is a major factor driving DNA damage in hematopoietic stem cells (HSCs), according to research published in Nature.
Investigators found that repeated exposure to such stress induces accelerated tissue aging and may cause cancer.
In examining HSCs’ response to stress, the team also gained new insight regarding Fanconi anemia.
The investigators noted that, under normal conditions, HSCs exist in a state of dormancy. They rarely divide and have very low energy demands.
“Our theory was that this state of dormancy protected hematopoietic stem cells from DNA damage and therefore protects them from premature aging,” said study author Michael Milsom, PhD, of The Heidelberg Institute for Stem Cell Technology and Experimental Medicine in Germany.
However, under conditions of stress, such as during chronic blood loss or infection, HSCs are driven into a state of rapid cell division in order to produce new blood cells and repair the damaged tissue.
“The stem cells go from a state of rest to very high activity within a short space of time, requiring them to rapidly increase their metabolic rate, synthesize new DNA, and coordinate cell division,” Dr Milsom explained. “Suddenly having to simultaneously execute these complicated functions dramatically increases the likelihood that something will go wrong.”
Indeed, the investigators’ experiments showed that the increased energy demands during stress results in elevated production of reactive metabolites that can directly damage DNA. If this happens at the same time a cell is trying to replicate its DNA, this can cause cell death or the acquisition of mutations that may cause cancer.
Normal stem cells can repair the majority of this stress-induced DNA damage, the investigators noted. However, the more HSCs are exposed to stress, the more likely they are to inefficiently repair the damage and then die or mutate.
“We believe that this model perfectly explains the gradual accumulation of DNA damage in stem cells with age and the associated reduction in the ability of a tissue to maintain and repair itself as you get older,” Dr Milsom said.
He and his colleagues also examined how this stress response impacts a mouse model of Fanconi anemia. These mice have the same DNA repair defect found in humans with the disease, but the mice never spontaneously develop the bone marrow failure observed in nearly all patients.
“We felt that stress-induced DNA damage was the missing ingredient that was required to cause hematopoietic stem cell depletion in these mice,” Dr Milsom said.
When mice with Fanconi anemia were exposed to stimulation mimicking a prolonged viral infection, they were unable to efficiently repair the resulting DNA damage, and their stem cells failed.
In the same space of time that normal mice showed a gradual decline in HSC numbers, the stem cells in Fanconi anemia mice were almost completely depleted, resulting in bone marrow failure and an inadequate production of blood cells to sustain life.
“This perfectly recapitulates what happens to Fanconi anemia patients and now gives us an opportunity to understand how this disease works and how we might better treat it,” Dr Milsom said. ![]()
with Fanconi anemia
Image by Michael Milsom
Environmental stress is a major factor driving DNA damage in hematopoietic stem cells (HSCs), according to research published in Nature.
Investigators found that repeated exposure to such stress induces accelerated tissue aging and may cause cancer.
In examining HSCs’ response to stress, the team also gained new insight regarding Fanconi anemia.
The investigators noted that, under normal conditions, HSCs exist in a state of dormancy. They rarely divide and have very low energy demands.
“Our theory was that this state of dormancy protected hematopoietic stem cells from DNA damage and therefore protects them from premature aging,” said study author Michael Milsom, PhD, of The Heidelberg Institute for Stem Cell Technology and Experimental Medicine in Germany.
However, under conditions of stress, such as during chronic blood loss or infection, HSCs are driven into a state of rapid cell division in order to produce new blood cells and repair the damaged tissue.
“The stem cells go from a state of rest to very high activity within a short space of time, requiring them to rapidly increase their metabolic rate, synthesize new DNA, and coordinate cell division,” Dr Milsom explained. “Suddenly having to simultaneously execute these complicated functions dramatically increases the likelihood that something will go wrong.”
Indeed, the investigators’ experiments showed that the increased energy demands during stress results in elevated production of reactive metabolites that can directly damage DNA. If this happens at the same time a cell is trying to replicate its DNA, this can cause cell death or the acquisition of mutations that may cause cancer.
Normal stem cells can repair the majority of this stress-induced DNA damage, the investigators noted. However, the more HSCs are exposed to stress, the more likely they are to inefficiently repair the damage and then die or mutate.
“We believe that this model perfectly explains the gradual accumulation of DNA damage in stem cells with age and the associated reduction in the ability of a tissue to maintain and repair itself as you get older,” Dr Milsom said.
He and his colleagues also examined how this stress response impacts a mouse model of Fanconi anemia. These mice have the same DNA repair defect found in humans with the disease, but the mice never spontaneously develop the bone marrow failure observed in nearly all patients.
“We felt that stress-induced DNA damage was the missing ingredient that was required to cause hematopoietic stem cell depletion in these mice,” Dr Milsom said.
When mice with Fanconi anemia were exposed to stimulation mimicking a prolonged viral infection, they were unable to efficiently repair the resulting DNA damage, and their stem cells failed.
In the same space of time that normal mice showed a gradual decline in HSC numbers, the stem cells in Fanconi anemia mice were almost completely depleted, resulting in bone marrow failure and an inadequate production of blood cells to sustain life.
“This perfectly recapitulates what happens to Fanconi anemia patients and now gives us an opportunity to understand how this disease works and how we might better treat it,” Dr Milsom said. ![]()
How cancer patients make treatment decisions

patient and her father
Photo by Rhoda Baer
A survey of more than 5000 cancer patients suggests there are a number of factors that might make a patient more likely to involve family members in treatment decisions.
A patient’s gender, age, marital status, native language, insurance status, and even past military service all appeared to impact family involvement in care decisions.
Gabriela Hobbs, MD, of Harvard Medical School in Boston, Massachusetts, and her colleagues conducted this research and reported the results in Cancer.
The researchers surveyed 5284 patients with a new diagnosis of lung or colon cancer, asking patients how they involved their families in treatment decisions.
Only 1.5% of patients reported complete family control over decisions. Nearly half of patients (49.4%) said they and family members shared decision-making responsibilities equally, 22.1% of patients reported some family input, and 28.5% reported little or no input from their families.
Asian and Hispanic patients who did not speak English were more likely than their peers to report equally shared decisions with their families. Likewise, patients who were married, female, older, and insured were more likely to share decision-making equally with their families.
Veterans were the least likely to share decision-making with their families, even when the researchers adjusted for marital status and social support.
“Understanding how patients vary in their inclusion of family members in decisions—by ethnicity, language spoken, marital status, sex, age, insurance status, and veteran status—may help physicians to better assess their patients’ preferences for engaging family members in decisions,” Dr Hobbs said.
“As we move to more patient-centered models of care, such assessments may help doctors personalize the care they offer their patients.”
Dr Hobbs noted that as therapies for cancer patients improve, they are also becoming increasingly complex, making it challenging for patients and providers to determine the optimal therapy for each patient. Therefore, knowing how patients make decisions and understanding the role families play in decision-making is crucial for optimizing patient participation in treatment decisions.
“Our study suggests that not all patients wish to include family in the same way,” Dr Hobbs said. “By raising awareness of these preferences, we hope that physicians will be aware of these variations and elicit their patient’s preference on how they wish to include, or not to include, families in decision-making.” ![]()
patient and her father
Photo by Rhoda Baer
A survey of more than 5000 cancer patients suggests there are a number of factors that might make a patient more likely to involve family members in treatment decisions.
A patient’s gender, age, marital status, native language, insurance status, and even past military service all appeared to impact family involvement in care decisions.
Gabriela Hobbs, MD, of Harvard Medical School in Boston, Massachusetts, and her colleagues conducted this research and reported the results in Cancer.
The researchers surveyed 5284 patients with a new diagnosis of lung or colon cancer, asking patients how they involved their families in treatment decisions.
Only 1.5% of patients reported complete family control over decisions. Nearly half of patients (49.4%) said they and family members shared decision-making responsibilities equally, 22.1% of patients reported some family input, and 28.5% reported little or no input from their families.
Asian and Hispanic patients who did not speak English were more likely than their peers to report equally shared decisions with their families. Likewise, patients who were married, female, older, and insured were more likely to share decision-making equally with their families.
Veterans were the least likely to share decision-making with their families, even when the researchers adjusted for marital status and social support.
“Understanding how patients vary in their inclusion of family members in decisions—by ethnicity, language spoken, marital status, sex, age, insurance status, and veteran status—may help physicians to better assess their patients’ preferences for engaging family members in decisions,” Dr Hobbs said.
“As we move to more patient-centered models of care, such assessments may help doctors personalize the care they offer their patients.”
Dr Hobbs noted that as therapies for cancer patients improve, they are also becoming increasingly complex, making it challenging for patients and providers to determine the optimal therapy for each patient. Therefore, knowing how patients make decisions and understanding the role families play in decision-making is crucial for optimizing patient participation in treatment decisions.
“Our study suggests that not all patients wish to include family in the same way,” Dr Hobbs said. “By raising awareness of these preferences, we hope that physicians will be aware of these variations and elicit their patient’s preference on how they wish to include, or not to include, families in decision-making.” ![]()
patient and her father
Photo by Rhoda Baer
A survey of more than 5000 cancer patients suggests there are a number of factors that might make a patient more likely to involve family members in treatment decisions.
A patient’s gender, age, marital status, native language, insurance status, and even past military service all appeared to impact family involvement in care decisions.
Gabriela Hobbs, MD, of Harvard Medical School in Boston, Massachusetts, and her colleagues conducted this research and reported the results in Cancer.
The researchers surveyed 5284 patients with a new diagnosis of lung or colon cancer, asking patients how they involved their families in treatment decisions.
Only 1.5% of patients reported complete family control over decisions. Nearly half of patients (49.4%) said they and family members shared decision-making responsibilities equally, 22.1% of patients reported some family input, and 28.5% reported little or no input from their families.
Asian and Hispanic patients who did not speak English were more likely than their peers to report equally shared decisions with their families. Likewise, patients who were married, female, older, and insured were more likely to share decision-making equally with their families.
Veterans were the least likely to share decision-making with their families, even when the researchers adjusted for marital status and social support.
“Understanding how patients vary in their inclusion of family members in decisions—by ethnicity, language spoken, marital status, sex, age, insurance status, and veteran status—may help physicians to better assess their patients’ preferences for engaging family members in decisions,” Dr Hobbs said.
“As we move to more patient-centered models of care, such assessments may help doctors personalize the care they offer their patients.”
Dr Hobbs noted that as therapies for cancer patients improve, they are also becoming increasingly complex, making it challenging for patients and providers to determine the optimal therapy for each patient. Therefore, knowing how patients make decisions and understanding the role families play in decision-making is crucial for optimizing patient participation in treatment decisions.
“Our study suggests that not all patients wish to include family in the same way,” Dr Hobbs said. “By raising awareness of these preferences, we hope that physicians will be aware of these variations and elicit their patient’s preference on how they wish to include, or not to include, families in decision-making.” ![]()
Artemisinin-resistant malaria found across Myanmar

Photo by James Gathany
Resistance to the antimalarial drug artemisinin is present in Myanmar and has reached within 25 km of the Indian border, according to research published in The Lancet Infectious Diseases.
Researchers believe the spread of artemisinin-resistant malaria parasites into neighboring India would pose a serious threat to the global control and eradication of malaria.
And if drug resistance continues to spread, millions of lives could be at risk.
Kyaw Myo Tun, MD, of the Myanmar Oxford Clinical Research Unit in Yangon, Myanmar, and colleagues uncovered artemisinin resistance by analyzing parasite samples collected at 55 malaria treatment centers across Myanmar.
The group set out to determine if the samples carried mutations in specific regions of the parasite’s kelch gene (K13)—a known genetic marker of artemisinin resistance. And they confirmed the existance of resistant parasites in Homalin, in the Sagaing Region, which is located only 25 km from the Indian border.
“Myanmar is considered the frontline in the battle against artemisinin resistance, as it forms a gateway for resistance to spread to the rest of the world,” said Charles Woodrow, MD, of the University of Oxford in the UK.
“With artemisinins, we are in the unusual position of having molecular markers for resistance before resistance has spread globally. The more we understand about the current situation in the border regions, the better prepared we are to adapt and implement strategies to overcome the spread of further drug resistance.”
The researchers obtained the DNA sequences of 940 samples of Plasmodium falciparum malaria parasites from across Myanmar and neighboring border regions in Thailand and Bangladesh between 2013 and 2014. Of those 940 samples, 371 (39%) carried a resistance-conferring K13 mutation.
“We were able to gather patient samples rapidly across Myanmar, sometimes using discarded malaria blood diagnostic tests, and then test these immediately for the K13 marker, and so generate real-time information on the spread of resistance” said Mallika Imwong, PhD, of Mahidol University in Bangkok, Thailand.
Using this information, the researchers developed maps to display the predicted extent of artemisinin resistance determined by the prevalence of K13 mutations. The maps suggested the overall prevalence of K13 mutations was greater than 10% in large areas of the east and north of Myanmar, including areas close to the border with India.
“The identification of the K13 markers of resistance has transformed our ability to monitor the spread and emergence of artemisinin resistance,” said Philippe Guerin, MD, of the Worldwide Antimalarial Resistance Network in Oxford, UK.
“However, this study highlights that the pace at which artemisinin resistance is spreading or emerging is alarming. We need a more vigorous international effort to address this issue in border regions.” ![]()
Photo by James Gathany
Resistance to the antimalarial drug artemisinin is present in Myanmar and has reached within 25 km of the Indian border, according to research published in The Lancet Infectious Diseases.
Researchers believe the spread of artemisinin-resistant malaria parasites into neighboring India would pose a serious threat to the global control and eradication of malaria.
And if drug resistance continues to spread, millions of lives could be at risk.
Kyaw Myo Tun, MD, of the Myanmar Oxford Clinical Research Unit in Yangon, Myanmar, and colleagues uncovered artemisinin resistance by analyzing parasite samples collected at 55 malaria treatment centers across Myanmar.
The group set out to determine if the samples carried mutations in specific regions of the parasite’s kelch gene (K13)—a known genetic marker of artemisinin resistance. And they confirmed the existance of resistant parasites in Homalin, in the Sagaing Region, which is located only 25 km from the Indian border.
“Myanmar is considered the frontline in the battle against artemisinin resistance, as it forms a gateway for resistance to spread to the rest of the world,” said Charles Woodrow, MD, of the University of Oxford in the UK.
“With artemisinins, we are in the unusual position of having molecular markers for resistance before resistance has spread globally. The more we understand about the current situation in the border regions, the better prepared we are to adapt and implement strategies to overcome the spread of further drug resistance.”
The researchers obtained the DNA sequences of 940 samples of Plasmodium falciparum malaria parasites from across Myanmar and neighboring border regions in Thailand and Bangladesh between 2013 and 2014. Of those 940 samples, 371 (39%) carried a resistance-conferring K13 mutation.
“We were able to gather patient samples rapidly across Myanmar, sometimes using discarded malaria blood diagnostic tests, and then test these immediately for the K13 marker, and so generate real-time information on the spread of resistance” said Mallika Imwong, PhD, of Mahidol University in Bangkok, Thailand.
Using this information, the researchers developed maps to display the predicted extent of artemisinin resistance determined by the prevalence of K13 mutations. The maps suggested the overall prevalence of K13 mutations was greater than 10% in large areas of the east and north of Myanmar, including areas close to the border with India.
“The identification of the K13 markers of resistance has transformed our ability to monitor the spread and emergence of artemisinin resistance,” said Philippe Guerin, MD, of the Worldwide Antimalarial Resistance Network in Oxford, UK.
“However, this study highlights that the pace at which artemisinin resistance is spreading or emerging is alarming. We need a more vigorous international effort to address this issue in border regions.” ![]()
Photo by James Gathany
Resistance to the antimalarial drug artemisinin is present in Myanmar and has reached within 25 km of the Indian border, according to research published in The Lancet Infectious Diseases.
Researchers believe the spread of artemisinin-resistant malaria parasites into neighboring India would pose a serious threat to the global control and eradication of malaria.
And if drug resistance continues to spread, millions of lives could be at risk.
Kyaw Myo Tun, MD, of the Myanmar Oxford Clinical Research Unit in Yangon, Myanmar, and colleagues uncovered artemisinin resistance by analyzing parasite samples collected at 55 malaria treatment centers across Myanmar.
The group set out to determine if the samples carried mutations in specific regions of the parasite’s kelch gene (K13)—a known genetic marker of artemisinin resistance. And they confirmed the existance of resistant parasites in Homalin, in the Sagaing Region, which is located only 25 km from the Indian border.
“Myanmar is considered the frontline in the battle against artemisinin resistance, as it forms a gateway for resistance to spread to the rest of the world,” said Charles Woodrow, MD, of the University of Oxford in the UK.
“With artemisinins, we are in the unusual position of having molecular markers for resistance before resistance has spread globally. The more we understand about the current situation in the border regions, the better prepared we are to adapt and implement strategies to overcome the spread of further drug resistance.”
The researchers obtained the DNA sequences of 940 samples of Plasmodium falciparum malaria parasites from across Myanmar and neighboring border regions in Thailand and Bangladesh between 2013 and 2014. Of those 940 samples, 371 (39%) carried a resistance-conferring K13 mutation.
“We were able to gather patient samples rapidly across Myanmar, sometimes using discarded malaria blood diagnostic tests, and then test these immediately for the K13 marker, and so generate real-time information on the spread of resistance” said Mallika Imwong, PhD, of Mahidol University in Bangkok, Thailand.
Using this information, the researchers developed maps to display the predicted extent of artemisinin resistance determined by the prevalence of K13 mutations. The maps suggested the overall prevalence of K13 mutations was greater than 10% in large areas of the east and north of Myanmar, including areas close to the border with India.
“The identification of the K13 markers of resistance has transformed our ability to monitor the spread and emergence of artemisinin resistance,” said Philippe Guerin, MD, of the Worldwide Antimalarial Resistance Network in Oxford, UK.
“However, this study highlights that the pace at which artemisinin resistance is spreading or emerging is alarming. We need a more vigorous international effort to address this issue in border regions.” ![]()
EC expands indication for lenalidomide in MM

Photo courtesy of Celgene
The European Commission (EC) has expanded the marketing authorization for lenalidomide (Revlimid), just 2 days after the US Food and Drug Administration did the same.
Lenalidomide is now approved in the European Union (EU) to treat adults with previously untreated multiple myeloma (MM) who are not eligible for hematopoietic stem cell transplant. These patients can receive the drug continuously until
disease progression.
Lenalidomide was already approved in the EU for use in combination with dexamethasone to treat adults with MM who have received at least 1 prior therapy.
Lenalidomide is also approved in the EU to treat patients with transfusion-dependent anemia due to low- or intermediate-1-risk myelodysplastic syndromes associated with 5q deletion when other therapeutic options are insufficient or inadequate.
“Having a new treatment option now available for patients newly diagnosed with multiple myeloma is a real step forward,” said Thierry Facon, MD, of CHRU Lille in France.
“Treating patients continuously until disease progression is supported by several clinical studies and will have an important impact on how we manage the disease over the long-term.”
The EC’s decision to extend the approved use of lenalidomide was based on the results of 2 studies: MM-015 and MM-020, also known as FIRST.
The FIRST trial
In the phase 3 FIRST trial, researchers enrolled 1623 patients who were newly diagnosed with MM and not eligible for transplant.
Patients were randomized to receive lenalidomide and dexamethasone (Rd) in 28-day cycles until disease progression (n=535), 18 cycles of lenalidomide and dexamethasone (Rd18) for 72 weeks (n=541), or melphalan, prednisone, and thalidomide (MPT) for 72 weeks (n=547).
Response rates were significantly better with continuous Rd (75%) and Rd18 (73%) than with MPT (62%, P<0.001 for both comparisons). Complete response rates were 15%, 14%, and 9%, respectively.
The median progression-free survival was 25.5 months with continuous Rd, 20.7 months with Rd18, and 21.2 months with MPT.
This resulted in a 28% reduction in the risk of progression or death for patients treated with continuous Rd compared with those treated with MPT (hazard ratio[HR]=0.72, P<0.001) and a 30% reduction compared with Rd18 (HR=0.70, P<0.001).
The pre-planned interim analysis of overall survival showed a 22% reduction in the risk of death for continuous Rd vs MPT (HR=0.78, P=0.02), but the difference did not cross the pre-specified superiority boundary (P<0.0096).
Adverse events reported in 20% or more of patients in the continuous Rd, Rd18, or MPT arms included diarrhea (45.5%, 38.5%, 16.5%), anemia (43.8%, 35.7%, 42.3%), neutropenia (35.0%, 33.0%, 60.6%), fatigue (32.5%, 32.8%, 28.5%), back pain (32.0%, 26.9%, 21.4%), insomnia (27.6%, 23.5%, 9.8%), asthenia (28.2%, 22.8%, 22.9%), rash (26.1%, 28.0%, 19.4%), decreased appetite (23.1%, 21.3%, 13.3%), cough (22.7%, 17.4%, 12.6%), pyrexia (21.4%, 18.9%, 14.0%), muscle spasms (20.5%, 18.9%, 11.3%), and abdominal pain (20.5%, 14.4%, 11.1%).
The incidence of invasive second primary malignancies was 3% in patients taking continuous Rd, 6% in patients taking Rd18, and 5% in those taking MPT. The overall incidence of solid tumors was identical in the continuous Rd and MPT arms (3%) and 5% in the Rd18 arm.
The MM-015 trial
In the phase 3 MM-015 study, researchers enrolled 459 patients who were 65 or older and newly diagnosed with MM.
The team compared melphalan-prednisone-lenalidomide induction followed by lenalidomide maintenance (MPR-R) with melphalan-prednisone-lenalidomide (MPR) or melphalan-prednisone (MP) followed by placebo maintenance.
Patients who received MPR-R or MPR had significantly better response rates than patients who received MP, at 77%, 68%, and 50%, respectively (P<0.001 and P=0.002, respectively, for the comparison with MP).
And the median progression-free survival was significantly longer with MPR-R (31 months) than with MPR (14 months, HR=0.49, P<0.001) or MP (13 months, HR=0.40, P<0.001).
During induction, the most frequent adverse events were hematologic. Grade 4 neutropenia occurred in 35% of patients in the MPR-R arm, 32% in the MPR arm, and 8% in the MP arm. The 3-year rate of second primary malignancies was 7%, 7%, and 3%, respectively. ![]()
Photo courtesy of Celgene
The European Commission (EC) has expanded the marketing authorization for lenalidomide (Revlimid), just 2 days after the US Food and Drug Administration did the same.
Lenalidomide is now approved in the European Union (EU) to treat adults with previously untreated multiple myeloma (MM) who are not eligible for hematopoietic stem cell transplant. These patients can receive the drug continuously until
disease progression.
Lenalidomide was already approved in the EU for use in combination with dexamethasone to treat adults with MM who have received at least 1 prior therapy.
Lenalidomide is also approved in the EU to treat patients with transfusion-dependent anemia due to low- or intermediate-1-risk myelodysplastic syndromes associated with 5q deletion when other therapeutic options are insufficient or inadequate.
“Having a new treatment option now available for patients newly diagnosed with multiple myeloma is a real step forward,” said Thierry Facon, MD, of CHRU Lille in France.
“Treating patients continuously until disease progression is supported by several clinical studies and will have an important impact on how we manage the disease over the long-term.”
The EC’s decision to extend the approved use of lenalidomide was based on the results of 2 studies: MM-015 and MM-020, also known as FIRST.
The FIRST trial
In the phase 3 FIRST trial, researchers enrolled 1623 patients who were newly diagnosed with MM and not eligible for transplant.
Patients were randomized to receive lenalidomide and dexamethasone (Rd) in 28-day cycles until disease progression (n=535), 18 cycles of lenalidomide and dexamethasone (Rd18) for 72 weeks (n=541), or melphalan, prednisone, and thalidomide (MPT) for 72 weeks (n=547).
Response rates were significantly better with continuous Rd (75%) and Rd18 (73%) than with MPT (62%, P<0.001 for both comparisons). Complete response rates were 15%, 14%, and 9%, respectively.
The median progression-free survival was 25.5 months with continuous Rd, 20.7 months with Rd18, and 21.2 months with MPT.
This resulted in a 28% reduction in the risk of progression or death for patients treated with continuous Rd compared with those treated with MPT (hazard ratio[HR]=0.72, P<0.001) and a 30% reduction compared with Rd18 (HR=0.70, P<0.001).
The pre-planned interim analysis of overall survival showed a 22% reduction in the risk of death for continuous Rd vs MPT (HR=0.78, P=0.02), but the difference did not cross the pre-specified superiority boundary (P<0.0096).
Adverse events reported in 20% or more of patients in the continuous Rd, Rd18, or MPT arms included diarrhea (45.5%, 38.5%, 16.5%), anemia (43.8%, 35.7%, 42.3%), neutropenia (35.0%, 33.0%, 60.6%), fatigue (32.5%, 32.8%, 28.5%), back pain (32.0%, 26.9%, 21.4%), insomnia (27.6%, 23.5%, 9.8%), asthenia (28.2%, 22.8%, 22.9%), rash (26.1%, 28.0%, 19.4%), decreased appetite (23.1%, 21.3%, 13.3%), cough (22.7%, 17.4%, 12.6%), pyrexia (21.4%, 18.9%, 14.0%), muscle spasms (20.5%, 18.9%, 11.3%), and abdominal pain (20.5%, 14.4%, 11.1%).
The incidence of invasive second primary malignancies was 3% in patients taking continuous Rd, 6% in patients taking Rd18, and 5% in those taking MPT. The overall incidence of solid tumors was identical in the continuous Rd and MPT arms (3%) and 5% in the Rd18 arm.
The MM-015 trial
In the phase 3 MM-015 study, researchers enrolled 459 patients who were 65 or older and newly diagnosed with MM.
The team compared melphalan-prednisone-lenalidomide induction followed by lenalidomide maintenance (MPR-R) with melphalan-prednisone-lenalidomide (MPR) or melphalan-prednisone (MP) followed by placebo maintenance.
Patients who received MPR-R or MPR had significantly better response rates than patients who received MP, at 77%, 68%, and 50%, respectively (P<0.001 and P=0.002, respectively, for the comparison with MP).
And the median progression-free survival was significantly longer with MPR-R (31 months) than with MPR (14 months, HR=0.49, P<0.001) or MP (13 months, HR=0.40, P<0.001).
During induction, the most frequent adverse events were hematologic. Grade 4 neutropenia occurred in 35% of patients in the MPR-R arm, 32% in the MPR arm, and 8% in the MP arm. The 3-year rate of second primary malignancies was 7%, 7%, and 3%, respectively. ![]()
Photo courtesy of Celgene
The European Commission (EC) has expanded the marketing authorization for lenalidomide (Revlimid), just 2 days after the US Food and Drug Administration did the same.
Lenalidomide is now approved in the European Union (EU) to treat adults with previously untreated multiple myeloma (MM) who are not eligible for hematopoietic stem cell transplant. These patients can receive the drug continuously until
disease progression.
Lenalidomide was already approved in the EU for use in combination with dexamethasone to treat adults with MM who have received at least 1 prior therapy.
Lenalidomide is also approved in the EU to treat patients with transfusion-dependent anemia due to low- or intermediate-1-risk myelodysplastic syndromes associated with 5q deletion when other therapeutic options are insufficient or inadequate.
“Having a new treatment option now available for patients newly diagnosed with multiple myeloma is a real step forward,” said Thierry Facon, MD, of CHRU Lille in France.
“Treating patients continuously until disease progression is supported by several clinical studies and will have an important impact on how we manage the disease over the long-term.”
The EC’s decision to extend the approved use of lenalidomide was based on the results of 2 studies: MM-015 and MM-020, also known as FIRST.
The FIRST trial
In the phase 3 FIRST trial, researchers enrolled 1623 patients who were newly diagnosed with MM and not eligible for transplant.
Patients were randomized to receive lenalidomide and dexamethasone (Rd) in 28-day cycles until disease progression (n=535), 18 cycles of lenalidomide and dexamethasone (Rd18) for 72 weeks (n=541), or melphalan, prednisone, and thalidomide (MPT) for 72 weeks (n=547).
Response rates were significantly better with continuous Rd (75%) and Rd18 (73%) than with MPT (62%, P<0.001 for both comparisons). Complete response rates were 15%, 14%, and 9%, respectively.
The median progression-free survival was 25.5 months with continuous Rd, 20.7 months with Rd18, and 21.2 months with MPT.
This resulted in a 28% reduction in the risk of progression or death for patients treated with continuous Rd compared with those treated with MPT (hazard ratio[HR]=0.72, P<0.001) and a 30% reduction compared with Rd18 (HR=0.70, P<0.001).
The pre-planned interim analysis of overall survival showed a 22% reduction in the risk of death for continuous Rd vs MPT (HR=0.78, P=0.02), but the difference did not cross the pre-specified superiority boundary (P<0.0096).
Adverse events reported in 20% or more of patients in the continuous Rd, Rd18, or MPT arms included diarrhea (45.5%, 38.5%, 16.5%), anemia (43.8%, 35.7%, 42.3%), neutropenia (35.0%, 33.0%, 60.6%), fatigue (32.5%, 32.8%, 28.5%), back pain (32.0%, 26.9%, 21.4%), insomnia (27.6%, 23.5%, 9.8%), asthenia (28.2%, 22.8%, 22.9%), rash (26.1%, 28.0%, 19.4%), decreased appetite (23.1%, 21.3%, 13.3%), cough (22.7%, 17.4%, 12.6%), pyrexia (21.4%, 18.9%, 14.0%), muscle spasms (20.5%, 18.9%, 11.3%), and abdominal pain (20.5%, 14.4%, 11.1%).
The incidence of invasive second primary malignancies was 3% in patients taking continuous Rd, 6% in patients taking Rd18, and 5% in those taking MPT. The overall incidence of solid tumors was identical in the continuous Rd and MPT arms (3%) and 5% in the Rd18 arm.
The MM-015 trial
In the phase 3 MM-015 study, researchers enrolled 459 patients who were 65 or older and newly diagnosed with MM.
The team compared melphalan-prednisone-lenalidomide induction followed by lenalidomide maintenance (MPR-R) with melphalan-prednisone-lenalidomide (MPR) or melphalan-prednisone (MP) followed by placebo maintenance.
Patients who received MPR-R or MPR had significantly better response rates than patients who received MP, at 77%, 68%, and 50%, respectively (P<0.001 and P=0.002, respectively, for the comparison with MP).
And the median progression-free survival was significantly longer with MPR-R (31 months) than with MPR (14 months, HR=0.49, P<0.001) or MP (13 months, HR=0.40, P<0.001).
During induction, the most frequent adverse events were hematologic. Grade 4 neutropenia occurred in 35% of patients in the MPR-R arm, 32% in the MPR arm, and 8% in the MP arm. The 3-year rate of second primary malignancies was 7%, 7%, and 3%, respectively. ![]()
Evolutionary findings may aid cancer drug development

Photo by Darren Baker
By tracking the evolution of Abl and Src, investigators have made discoveries that may aid the design of highly specific cancer drugs.
Abl and Src are 2 nearly identical protein kinases with a predilection to cause cancer in humans, mainly chronic myeloid leukemia and colon cancer.
The proteins are separated by 146 amino acids and one big difference: Abl is susceptible to treatment with the tyrosine kinase inhibitor imatinib (Gleevec), but Src is not.
Dorothee Kern, PhD, of Brandeis University in Waltham, Massachusetts, and her colleagues traced the journey of these 2 proteins over 1 billion years of evolution, pinpointing the exact evolutionary shifts that caused imatinib to bind well with one protein and poorly with the other.
This new approach to researching enzymes and their binding sites may have a major impact on the development of cancer drugs, the investigators said.
They published their findings in Science.
To determine why imatinib binds with Abl but not Src, Dr Kern and her colleagues turned back the evolutionary clock 1 billion years.
This revealed Abl and Src’s common ancestor, a primitive protein in yeast the team dubbed “ANC-AS.” They mapped out the family tree, searching for changes in amino acids and molecular mechanisms.
“Src and Abl differ by 146 amino acids, and we were looking for the handful that dictate Gleevec specificity,” Dr Kern said. “It was like finding a needle in a haystack and could only be done by our evolutionary approach.”
As ANC-AS evolved in more complex organisms, it began to specialize and branch into proteins with different regulation, roles, and catalysis processes—creating Abl and Src.
By following this progression, while testing the proteins’ affinity to imatinib along the way, the investigators were able to whittle down the 146 different amino acids to 15 that are responsible for imatinib specificity.
These 15 amino acids play a role in Abl’s conformational equilibrium—a process in which the protein transitions between 2 structures. The main difference between Abl and Src, when it comes to binding with imatinib, is the relative times the proteins spend in each configuration, resulting in a major difference in their binding energies.
By understanding how and why imatinib works on Abl—and doesn’t work on Src—scientists have a jumping off point to design other drugs with a high affinity and specificity, and a strong binding on cancerous proteins.
“Understanding the molecular basis for Gleevec specificity has opened the door wider to designing good drugs,” Dr Kern said. “Our results pave the way for a different approach to rational drug design.” ![]()
Photo by Darren Baker
By tracking the evolution of Abl and Src, investigators have made discoveries that may aid the design of highly specific cancer drugs.
Abl and Src are 2 nearly identical protein kinases with a predilection to cause cancer in humans, mainly chronic myeloid leukemia and colon cancer.
The proteins are separated by 146 amino acids and one big difference: Abl is susceptible to treatment with the tyrosine kinase inhibitor imatinib (Gleevec), but Src is not.
Dorothee Kern, PhD, of Brandeis University in Waltham, Massachusetts, and her colleagues traced the journey of these 2 proteins over 1 billion years of evolution, pinpointing the exact evolutionary shifts that caused imatinib to bind well with one protein and poorly with the other.
This new approach to researching enzymes and their binding sites may have a major impact on the development of cancer drugs, the investigators said.
They published their findings in Science.
To determine why imatinib binds with Abl but not Src, Dr Kern and her colleagues turned back the evolutionary clock 1 billion years.
This revealed Abl and Src’s common ancestor, a primitive protein in yeast the team dubbed “ANC-AS.” They mapped out the family tree, searching for changes in amino acids and molecular mechanisms.
“Src and Abl differ by 146 amino acids, and we were looking for the handful that dictate Gleevec specificity,” Dr Kern said. “It was like finding a needle in a haystack and could only be done by our evolutionary approach.”
As ANC-AS evolved in more complex organisms, it began to specialize and branch into proteins with different regulation, roles, and catalysis processes—creating Abl and Src.
By following this progression, while testing the proteins’ affinity to imatinib along the way, the investigators were able to whittle down the 146 different amino acids to 15 that are responsible for imatinib specificity.
These 15 amino acids play a role in Abl’s conformational equilibrium—a process in which the protein transitions between 2 structures. The main difference between Abl and Src, when it comes to binding with imatinib, is the relative times the proteins spend in each configuration, resulting in a major difference in their binding energies.
By understanding how and why imatinib works on Abl—and doesn’t work on Src—scientists have a jumping off point to design other drugs with a high affinity and specificity, and a strong binding on cancerous proteins.
“Understanding the molecular basis for Gleevec specificity has opened the door wider to designing good drugs,” Dr Kern said. “Our results pave the way for a different approach to rational drug design.” ![]()
Photo by Darren Baker
By tracking the evolution of Abl and Src, investigators have made discoveries that may aid the design of highly specific cancer drugs.
Abl and Src are 2 nearly identical protein kinases with a predilection to cause cancer in humans, mainly chronic myeloid leukemia and colon cancer.
The proteins are separated by 146 amino acids and one big difference: Abl is susceptible to treatment with the tyrosine kinase inhibitor imatinib (Gleevec), but Src is not.
Dorothee Kern, PhD, of Brandeis University in Waltham, Massachusetts, and her colleagues traced the journey of these 2 proteins over 1 billion years of evolution, pinpointing the exact evolutionary shifts that caused imatinib to bind well with one protein and poorly with the other.
This new approach to researching enzymes and their binding sites may have a major impact on the development of cancer drugs, the investigators said.
They published their findings in Science.
To determine why imatinib binds with Abl but not Src, Dr Kern and her colleagues turned back the evolutionary clock 1 billion years.
This revealed Abl and Src’s common ancestor, a primitive protein in yeast the team dubbed “ANC-AS.” They mapped out the family tree, searching for changes in amino acids and molecular mechanisms.
“Src and Abl differ by 146 amino acids, and we were looking for the handful that dictate Gleevec specificity,” Dr Kern said. “It was like finding a needle in a haystack and could only be done by our evolutionary approach.”
As ANC-AS evolved in more complex organisms, it began to specialize and branch into proteins with different regulation, roles, and catalysis processes—creating Abl and Src.
By following this progression, while testing the proteins’ affinity to imatinib along the way, the investigators were able to whittle down the 146 different amino acids to 15 that are responsible for imatinib specificity.
These 15 amino acids play a role in Abl’s conformational equilibrium—a process in which the protein transitions between 2 structures. The main difference between Abl and Src, when it comes to binding with imatinib, is the relative times the proteins spend in each configuration, resulting in a major difference in their binding energies.
By understanding how and why imatinib works on Abl—and doesn’t work on Src—scientists have a jumping off point to design other drugs with a high affinity and specificity, and a strong binding on cancerous proteins.
“Understanding the molecular basis for Gleevec specificity has opened the door wider to designing good drugs,” Dr Kern said. “Our results pave the way for a different approach to rational drug design.” ![]()
Generic enoxaparin launched in US

Image by Kevin MacKenzie
Teva Pharmaceutical Industries Ltd. has launched the generic equivalent of the low-molecular-weight heparin Lovenox (enoxaparin sodium injection) in 7 dosage strengths in the US.
Enoxaparin can be used to prevent deep vein thrombosis (DVT) in patients undergoing abdominal surgery, those receiving a hip or knee replacement, and patients at risk of thromboembolic complications due to severely restricted mobility during acute illness.
When administered with warfarin, enoxaparin can be used for inpatient treatment of acute DVT, with or without pulmonary embolism (PE). Enoxaparin given in conjunction with warfarin may also be used for outpatient treatment of acute DVT without PE.
When given concurrently with aspirin, enoxaparin can be used to prevent ischemic complications of unstable angina and non-Q-wave myocardial infarction. Enoxaparin may also be used to treat acute ST-segment elevation myocardial infarction that is managed medically or with subsequent percutaneous coronary intervention.
Teva’s Enoxaparin Sodium Injection USP is available in the following doses:
- 30 mg/0.3 mL syringe, 10 x 0.3 mL
- 40 mg/0.4 mL syringe, 10 x 0.4 mL
- 60 mg/0.6 mL syringe, 10 x 0.6 mL
- 80 mg/0.8 mL syringe, 10 x 0.8 mL
- 100 mg/mL syringe, 10 x 1 mL
- 120 mg/0.8 mL syringe, 10 x 0.8 mL
- 150 mg/mL syringe, 10 x 1 mL.
Safety information
Enoxaparin’s label contains a boxed warning detailing the risk of epidural or spinal hematomas that can occur in patients who are anticoagulated with low-molecular-weight heparins or heparinoids and are receiving neuraxial anesthesia or undergoing spinal puncture. The hematomas may result in long-term or permanent paralysis.
Enoxaparin is contraindicated in patients with active major bleeding, thrombocytopenia with a positive in vitro test for antiplatelet antibody in the presence of enoxaparin, or known hypersensitivity to enoxaparin, heparin, or pork products.
Serious adverse reactions reported with enoxaparin include increased risk of hemorrhage and thrombocytopenia.
Enoxaparin should be used with extreme caution in patients who have conditions with an increased risk of hemorrhage or in patients treated concomitantly with platelet inhibitors. Major hemorrhages, including retroperitoneal and intracranial bleeding, have been reported with enoxaparin. Some of these cases have been fatal.
Bleeding can occur at any site during enoxaparin treatment. The drug should be used with care in patients with a bleeding diathesis, uncontrolled arterial hypertension, or a history of recent gastrointestinal ulceration, diabetic retinopathy, renal dysfunction, and hemorrhage.
In clinical trials, the most common adverse reactions associated with enoxaparin (occurring in more than 1% of patients) were bleeding, anemia, thrombocytopenia, elevation of serum aminotransferase, diarrhea, and nausea. Mild local irritation, pain, hematoma, ecchymosis, and erythema may follow subcutaneous injection.
For additional information on enoxaparin, see the full prescribing information. ![]()
Image by Kevin MacKenzie
Teva Pharmaceutical Industries Ltd. has launched the generic equivalent of the low-molecular-weight heparin Lovenox (enoxaparin sodium injection) in 7 dosage strengths in the US.
Enoxaparin can be used to prevent deep vein thrombosis (DVT) in patients undergoing abdominal surgery, those receiving a hip or knee replacement, and patients at risk of thromboembolic complications due to severely restricted mobility during acute illness.
When administered with warfarin, enoxaparin can be used for inpatient treatment of acute DVT, with or without pulmonary embolism (PE). Enoxaparin given in conjunction with warfarin may also be used for outpatient treatment of acute DVT without PE.
When given concurrently with aspirin, enoxaparin can be used to prevent ischemic complications of unstable angina and non-Q-wave myocardial infarction. Enoxaparin may also be used to treat acute ST-segment elevation myocardial infarction that is managed medically or with subsequent percutaneous coronary intervention.
Teva’s Enoxaparin Sodium Injection USP is available in the following doses:
- 30 mg/0.3 mL syringe, 10 x 0.3 mL
- 40 mg/0.4 mL syringe, 10 x 0.4 mL
- 60 mg/0.6 mL syringe, 10 x 0.6 mL
- 80 mg/0.8 mL syringe, 10 x 0.8 mL
- 100 mg/mL syringe, 10 x 1 mL
- 120 mg/0.8 mL syringe, 10 x 0.8 mL
- 150 mg/mL syringe, 10 x 1 mL.
Safety information
Enoxaparin’s label contains a boxed warning detailing the risk of epidural or spinal hematomas that can occur in patients who are anticoagulated with low-molecular-weight heparins or heparinoids and are receiving neuraxial anesthesia or undergoing spinal puncture. The hematomas may result in long-term or permanent paralysis.
Enoxaparin is contraindicated in patients with active major bleeding, thrombocytopenia with a positive in vitro test for antiplatelet antibody in the presence of enoxaparin, or known hypersensitivity to enoxaparin, heparin, or pork products.
Serious adverse reactions reported with enoxaparin include increased risk of hemorrhage and thrombocytopenia.
Enoxaparin should be used with extreme caution in patients who have conditions with an increased risk of hemorrhage or in patients treated concomitantly with platelet inhibitors. Major hemorrhages, including retroperitoneal and intracranial bleeding, have been reported with enoxaparin. Some of these cases have been fatal.
Bleeding can occur at any site during enoxaparin treatment. The drug should be used with care in patients with a bleeding diathesis, uncontrolled arterial hypertension, or a history of recent gastrointestinal ulceration, diabetic retinopathy, renal dysfunction, and hemorrhage.
In clinical trials, the most common adverse reactions associated with enoxaparin (occurring in more than 1% of patients) were bleeding, anemia, thrombocytopenia, elevation of serum aminotransferase, diarrhea, and nausea. Mild local irritation, pain, hematoma, ecchymosis, and erythema may follow subcutaneous injection.
For additional information on enoxaparin, see the full prescribing information. ![]()
Image by Kevin MacKenzie
Teva Pharmaceutical Industries Ltd. has launched the generic equivalent of the low-molecular-weight heparin Lovenox (enoxaparin sodium injection) in 7 dosage strengths in the US.
Enoxaparin can be used to prevent deep vein thrombosis (DVT) in patients undergoing abdominal surgery, those receiving a hip or knee replacement, and patients at risk of thromboembolic complications due to severely restricted mobility during acute illness.
When administered with warfarin, enoxaparin can be used for inpatient treatment of acute DVT, with or without pulmonary embolism (PE). Enoxaparin given in conjunction with warfarin may also be used for outpatient treatment of acute DVT without PE.
When given concurrently with aspirin, enoxaparin can be used to prevent ischemic complications of unstable angina and non-Q-wave myocardial infarction. Enoxaparin may also be used to treat acute ST-segment elevation myocardial infarction that is managed medically or with subsequent percutaneous coronary intervention.
Teva’s Enoxaparin Sodium Injection USP is available in the following doses:
- 30 mg/0.3 mL syringe, 10 x 0.3 mL
- 40 mg/0.4 mL syringe, 10 x 0.4 mL
- 60 mg/0.6 mL syringe, 10 x 0.6 mL
- 80 mg/0.8 mL syringe, 10 x 0.8 mL
- 100 mg/mL syringe, 10 x 1 mL
- 120 mg/0.8 mL syringe, 10 x 0.8 mL
- 150 mg/mL syringe, 10 x 1 mL.
Safety information
Enoxaparin’s label contains a boxed warning detailing the risk of epidural or spinal hematomas that can occur in patients who are anticoagulated with low-molecular-weight heparins or heparinoids and are receiving neuraxial anesthesia or undergoing spinal puncture. The hematomas may result in long-term or permanent paralysis.
Enoxaparin is contraindicated in patients with active major bleeding, thrombocytopenia with a positive in vitro test for antiplatelet antibody in the presence of enoxaparin, or known hypersensitivity to enoxaparin, heparin, or pork products.
Serious adverse reactions reported with enoxaparin include increased risk of hemorrhage and thrombocytopenia.
Enoxaparin should be used with extreme caution in patients who have conditions with an increased risk of hemorrhage or in patients treated concomitantly with platelet inhibitors. Major hemorrhages, including retroperitoneal and intracranial bleeding, have been reported with enoxaparin. Some of these cases have been fatal.
Bleeding can occur at any site during enoxaparin treatment. The drug should be used with care in patients with a bleeding diathesis, uncontrolled arterial hypertension, or a history of recent gastrointestinal ulceration, diabetic retinopathy, renal dysfunction, and hemorrhage.
In clinical trials, the most common adverse reactions associated with enoxaparin (occurring in more than 1% of patients) were bleeding, anemia, thrombocytopenia, elevation of serum aminotransferase, diarrhea, and nausea. Mild local irritation, pain, hematoma, ecchymosis, and erythema may follow subcutaneous injection.
For additional information on enoxaparin, see the full prescribing information. ![]()
Group produces malaria vaccine candidate from algae
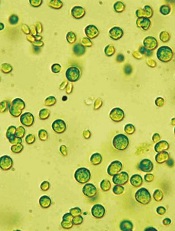
Image from Bielefeld University
A vaccine candidate generated using algae may be able to prevent the transmission of malaria from infected hosts to mosquitoes, preclinical research suggests.
Researchers used Chlamydomonas reinhardtii microalgae to produce recombinant Pfs25 protein.
When paired with human-compatible adjuvants—glucopyranosal lipid A (GLA) plus squalene oil-in-water emulsion—the protein generated antibodies that nearly eliminated malaria infection in mosquitoes.
The researchers reported these results in Infection and Immunity.
“Most malaria vaccine approaches are aimed at preventing humans from becoming infected when bitten by mosquitoes that carry the parasite,” said study author Joseph Vinetz, MD, of the University of California, San Diego.
“Our approach is to prevent transmission of the malaria parasite from infected humans to mosquitoes. This approach is similar to that of the current measles vaccine, which is such a hot topic of discussion these days, because the goal is to generate herd immunity in a population. We think that this approach is key to global malaria elimination too.”
Dr Vinetz and his colleagues wanted to produce a large quantity of properly folded Pfs25, a protein found on the surface of the malaria parasite’s reproductive cells, which are only present within the mosquito’s gut after it feeds on a malaria-infected blood meal.
Since antibodies against Pfs25 can halt the parasite’s lifecycle in the mosquito, they might also block transmission of the parasite to the next host. However, properly folded Pfs25 that induces transmission-blocking antibodies has been difficult to produce in the lab.
To overcome this problem, the researchers turned to Chlamydomonas reinhardtii. They introduced the Pfs25 gene into the algae by shooting the DNA into the plant cell’s nucleus.
After they let the algae do the work of replicating, building, and folding the protein, the team was able to purify enough functional Pfs25 for testing.
They also tested different adjuvants, which help stimulate the immune system’s response to Pfs25. They tested alum alone, GLA plus alum, squalene oil-in-water emulsion, and GLA plus squalene oil-in-water emulsion.
The best Pfs25/adjuvant combination—GLA plus squalene oil-in-water emulsion—elicited a uniquely robust antibody response in mice with high affinity and avidity—antibodies that specifically and strongly reacted with the malaria parasite’s reproductive cells.
The researchers then fed mosquitoes malaria parasites in the presence of control serum or immune serum collected from mice vaccinated with algae-produced Pfs25 in the presence of the adjuvants.
Eight days later, the team examined the mosquitoes’ guts for the presence of the malaria parasite. And they found that 4.2% (1/24) of mosquitoes that consumed the Pfs25/adjuvant-treated mouse serum were positive for the malaria parasite, compared to 70% (28/40) of control mosquitoes.
“We are really excited to see that Pfs25 produced by algae can effectively prevent malaria parasites from developing within the mosquito,” said study author Stephen Mayfield, PhD, of the University of California, San Diego.
“With the low cost of algal production, this may be the only system that can make an economic malaria vaccine. Now, we’re looking forward to comparing algae-produced Pfs25 and adjuvant head-to-head against other approaches to malaria vaccine production and administration.” ![]()
Image from Bielefeld University
A vaccine candidate generated using algae may be able to prevent the transmission of malaria from infected hosts to mosquitoes, preclinical research suggests.
Researchers used Chlamydomonas reinhardtii microalgae to produce recombinant Pfs25 protein.
When paired with human-compatible adjuvants—glucopyranosal lipid A (GLA) plus squalene oil-in-water emulsion—the protein generated antibodies that nearly eliminated malaria infection in mosquitoes.
The researchers reported these results in Infection and Immunity.
“Most malaria vaccine approaches are aimed at preventing humans from becoming infected when bitten by mosquitoes that carry the parasite,” said study author Joseph Vinetz, MD, of the University of California, San Diego.
“Our approach is to prevent transmission of the malaria parasite from infected humans to mosquitoes. This approach is similar to that of the current measles vaccine, which is such a hot topic of discussion these days, because the goal is to generate herd immunity in a population. We think that this approach is key to global malaria elimination too.”
Dr Vinetz and his colleagues wanted to produce a large quantity of properly folded Pfs25, a protein found on the surface of the malaria parasite’s reproductive cells, which are only present within the mosquito’s gut after it feeds on a malaria-infected blood meal.
Since antibodies against Pfs25 can halt the parasite’s lifecycle in the mosquito, they might also block transmission of the parasite to the next host. However, properly folded Pfs25 that induces transmission-blocking antibodies has been difficult to produce in the lab.
To overcome this problem, the researchers turned to Chlamydomonas reinhardtii. They introduced the Pfs25 gene into the algae by shooting the DNA into the plant cell’s nucleus.
After they let the algae do the work of replicating, building, and folding the protein, the team was able to purify enough functional Pfs25 for testing.
They also tested different adjuvants, which help stimulate the immune system’s response to Pfs25. They tested alum alone, GLA plus alum, squalene oil-in-water emulsion, and GLA plus squalene oil-in-water emulsion.
The best Pfs25/adjuvant combination—GLA plus squalene oil-in-water emulsion—elicited a uniquely robust antibody response in mice with high affinity and avidity—antibodies that specifically and strongly reacted with the malaria parasite’s reproductive cells.
The researchers then fed mosquitoes malaria parasites in the presence of control serum or immune serum collected from mice vaccinated with algae-produced Pfs25 in the presence of the adjuvants.
Eight days later, the team examined the mosquitoes’ guts for the presence of the malaria parasite. And they found that 4.2% (1/24) of mosquitoes that consumed the Pfs25/adjuvant-treated mouse serum were positive for the malaria parasite, compared to 70% (28/40) of control mosquitoes.
“We are really excited to see that Pfs25 produced by algae can effectively prevent malaria parasites from developing within the mosquito,” said study author Stephen Mayfield, PhD, of the University of California, San Diego.
“With the low cost of algal production, this may be the only system that can make an economic malaria vaccine. Now, we’re looking forward to comparing algae-produced Pfs25 and adjuvant head-to-head against other approaches to malaria vaccine production and administration.” ![]()
Image from Bielefeld University
A vaccine candidate generated using algae may be able to prevent the transmission of malaria from infected hosts to mosquitoes, preclinical research suggests.
Researchers used Chlamydomonas reinhardtii microalgae to produce recombinant Pfs25 protein.
When paired with human-compatible adjuvants—glucopyranosal lipid A (GLA) plus squalene oil-in-water emulsion—the protein generated antibodies that nearly eliminated malaria infection in mosquitoes.
The researchers reported these results in Infection and Immunity.
“Most malaria vaccine approaches are aimed at preventing humans from becoming infected when bitten by mosquitoes that carry the parasite,” said study author Joseph Vinetz, MD, of the University of California, San Diego.
“Our approach is to prevent transmission of the malaria parasite from infected humans to mosquitoes. This approach is similar to that of the current measles vaccine, which is such a hot topic of discussion these days, because the goal is to generate herd immunity in a population. We think that this approach is key to global malaria elimination too.”
Dr Vinetz and his colleagues wanted to produce a large quantity of properly folded Pfs25, a protein found on the surface of the malaria parasite’s reproductive cells, which are only present within the mosquito’s gut after it feeds on a malaria-infected blood meal.
Since antibodies against Pfs25 can halt the parasite’s lifecycle in the mosquito, they might also block transmission of the parasite to the next host. However, properly folded Pfs25 that induces transmission-blocking antibodies has been difficult to produce in the lab.
To overcome this problem, the researchers turned to Chlamydomonas reinhardtii. They introduced the Pfs25 gene into the algae by shooting the DNA into the plant cell’s nucleus.
After they let the algae do the work of replicating, building, and folding the protein, the team was able to purify enough functional Pfs25 for testing.
They also tested different adjuvants, which help stimulate the immune system’s response to Pfs25. They tested alum alone, GLA plus alum, squalene oil-in-water emulsion, and GLA plus squalene oil-in-water emulsion.
The best Pfs25/adjuvant combination—GLA plus squalene oil-in-water emulsion—elicited a uniquely robust antibody response in mice with high affinity and avidity—antibodies that specifically and strongly reacted with the malaria parasite’s reproductive cells.
The researchers then fed mosquitoes malaria parasites in the presence of control serum or immune serum collected from mice vaccinated with algae-produced Pfs25 in the presence of the adjuvants.
Eight days later, the team examined the mosquitoes’ guts for the presence of the malaria parasite. And they found that 4.2% (1/24) of mosquitoes that consumed the Pfs25/adjuvant-treated mouse serum were positive for the malaria parasite, compared to 70% (28/40) of control mosquitoes.
“We are really excited to see that Pfs25 produced by algae can effectively prevent malaria parasites from developing within the mosquito,” said study author Stephen Mayfield, PhD, of the University of California, San Diego.
“With the low cost of algal production, this may be the only system that can make an economic malaria vaccine. Now, we’re looking forward to comparing algae-produced Pfs25 and adjuvant head-to-head against other approaches to malaria vaccine production and administration.”
Silk-based bone marrow system produces functional platelets

proplatelets (green) that will
become mature platelets
Image from Tufts University
Researchers say they’ve developed a 3-dimensional system that reproduces the structure and physiology of human bone marrow.
Using this silk-based bone marrow niche tissue system, the team was able to manufacture functional human platelets.
The system might also prove useful for studying platelet-related diseases and predicting the efficacy of new drugs, according to the researchers, who said the new system could be a more precise and cheaper alternative to animal models.
“There are many diseases where platelet production or function is impaired,” said Alessandra Balduini, MD, of Tufts University in Medford, Massachusetts.
“New insight into the formation of platelets would have a major impact on patients and healthcare. In this tissue system, we can culture patient-derived megakaryocytes—the bone marrow cells that make platelets—and also endothelial cells, which are found in bone marrow and promote platelet production, to design patient-specific drug administration regimens.”
Dr Balduini and her colleagues described the system in Blood.
The system combined microtubes spun of silk, collagen, and fibronectin surrounded by a porous silk sponge. Megakaryocytes—some derived from patients—were seeded into the engineered microvasculature.
The researchers were able to increase platelet production in the bioreactor by embedding the silk with active endothelial cells and endothelial-related molecular proteins that support platelet formation.
The special properties of silk protein were essential to successfully mimicking the bone marrow microenvironment, said study author David Kaplan, PhD, of Tufts University.
“Silk protein possesses a unique molecular structure that enables it to be modeled in a wide variety of forms and stiffnesses, characteristics that have been shown to affect platelet formation and release,” Dr Kaplan said.
“Furthermore, silk is biocompatible and has the ability to stabilize bioactive agents at normal temperatures. Therefore, we can ‘functionalize’ it by adding such agents.”
In addition, the silk is nonactivating to platelets, which allowed the researchers to collect functional platelets from the bioreactor. Tests showed the platelets were able to aggregate and clot.
Although the number of platelets produced per megakaryocyte was lower than normally made in the body, the researchers said the system represents a significant advance over previous models. The scalable nature of the bioreactor system provides engineering options to increase the yield of platelets in ongoing studies.
In addition to providing a platform for studying the processes that regulate platelet production and related diseases, the researchers hope the platelets produced can be used as a source of growth factors for wound healing in regenerative medicine.
“The need for platelet production systems to treat patients with related diseases is significant,” Dr Kaplan said. “This patient-specific system could provide new insight and options for clinical treatments.”
“Further, the platelets can be generated on demand, avoiding the complications of storage problems, and in greater quantities and with better quality and control in terms of morphology and function.”
proplatelets (green) that will
become mature platelets
Image from Tufts University
Researchers say they’ve developed a 3-dimensional system that reproduces the structure and physiology of human bone marrow.
Using this silk-based bone marrow niche tissue system, the team was able to manufacture functional human platelets.
The system might also prove useful for studying platelet-related diseases and predicting the efficacy of new drugs, according to the researchers, who said the new system could be a more precise and cheaper alternative to animal models.
“There are many diseases where platelet production or function is impaired,” said Alessandra Balduini, MD, of Tufts University in Medford, Massachusetts.
“New insight into the formation of platelets would have a major impact on patients and healthcare. In this tissue system, we can culture patient-derived megakaryocytes—the bone marrow cells that make platelets—and also endothelial cells, which are found in bone marrow and promote platelet production, to design patient-specific drug administration regimens.”
Dr Balduini and her colleagues described the system in Blood.
The system combined microtubes spun of silk, collagen, and fibronectin surrounded by a porous silk sponge. Megakaryocytes—some derived from patients—were seeded into the engineered microvasculature.
The researchers were able to increase platelet production in the bioreactor by embedding the silk with active endothelial cells and endothelial-related molecular proteins that support platelet formation.
The special properties of silk protein were essential to successfully mimicking the bone marrow microenvironment, said study author David Kaplan, PhD, of Tufts University.
“Silk protein possesses a unique molecular structure that enables it to be modeled in a wide variety of forms and stiffnesses, characteristics that have been shown to affect platelet formation and release,” Dr Kaplan said.
“Furthermore, silk is biocompatible and has the ability to stabilize bioactive agents at normal temperatures. Therefore, we can ‘functionalize’ it by adding such agents.”
In addition, the silk is nonactivating to platelets, which allowed the researchers to collect functional platelets from the bioreactor. Tests showed the platelets were able to aggregate and clot.
Although the number of platelets produced per megakaryocyte was lower than normally made in the body, the researchers said the system represents a significant advance over previous models. The scalable nature of the bioreactor system provides engineering options to increase the yield of platelets in ongoing studies.
In addition to providing a platform for studying the processes that regulate platelet production and related diseases, the researchers hope the platelets produced can be used as a source of growth factors for wound healing in regenerative medicine.
“The need for platelet production systems to treat patients with related diseases is significant,” Dr Kaplan said. “This patient-specific system could provide new insight and options for clinical treatments.”
“Further, the platelets can be generated on demand, avoiding the complications of storage problems, and in greater quantities and with better quality and control in terms of morphology and function.”
proplatelets (green) that will
become mature platelets
Image from Tufts University
Researchers say they’ve developed a 3-dimensional system that reproduces the structure and physiology of human bone marrow.
Using this silk-based bone marrow niche tissue system, the team was able to manufacture functional human platelets.
The system might also prove useful for studying platelet-related diseases and predicting the efficacy of new drugs, according to the researchers, who said the new system could be a more precise and cheaper alternative to animal models.
“There are many diseases where platelet production or function is impaired,” said Alessandra Balduini, MD, of Tufts University in Medford, Massachusetts.
“New insight into the formation of platelets would have a major impact on patients and healthcare. In this tissue system, we can culture patient-derived megakaryocytes—the bone marrow cells that make platelets—and also endothelial cells, which are found in bone marrow and promote platelet production, to design patient-specific drug administration regimens.”
Dr Balduini and her colleagues described the system in Blood.
The system combined microtubes spun of silk, collagen, and fibronectin surrounded by a porous silk sponge. Megakaryocytes—some derived from patients—were seeded into the engineered microvasculature.
The researchers were able to increase platelet production in the bioreactor by embedding the silk with active endothelial cells and endothelial-related molecular proteins that support platelet formation.
The special properties of silk protein were essential to successfully mimicking the bone marrow microenvironment, said study author David Kaplan, PhD, of Tufts University.
“Silk protein possesses a unique molecular structure that enables it to be modeled in a wide variety of forms and stiffnesses, characteristics that have been shown to affect platelet formation and release,” Dr Kaplan said.
“Furthermore, silk is biocompatible and has the ability to stabilize bioactive agents at normal temperatures. Therefore, we can ‘functionalize’ it by adding such agents.”
In addition, the silk is nonactivating to platelets, which allowed the researchers to collect functional platelets from the bioreactor. Tests showed the platelets were able to aggregate and clot.
Although the number of platelets produced per megakaryocyte was lower than normally made in the body, the researchers said the system represents a significant advance over previous models. The scalable nature of the bioreactor system provides engineering options to increase the yield of platelets in ongoing studies.
In addition to providing a platform for studying the processes that regulate platelet production and related diseases, the researchers hope the platelets produced can be used as a source of growth factors for wound healing in regenerative medicine.
“The need for platelet production systems to treat patients with related diseases is significant,” Dr Kaplan said. “This patient-specific system could provide new insight and options for clinical treatments.”
“Further, the platelets can be generated on demand, avoiding the complications of storage problems, and in greater quantities and with better quality and control in terms of morphology and function.”
FDA approves drug for newly diagnosed MM

The US Food and Drug Administration (FDA) has expanded the existing indication for lenalidomide (Revlimid)—in combination with dexamethasone—to include patients with newly diagnosed multiple myeloma (MM).
The FDA previously approved lenalidomide in combination with dexamethasone to treat MM patients who had received at least 1 prior therapy.
Lenalidomide is also FDA-approved to treat mantle cell lymphoma patients who have failed 2 prior therapies, including bortezomib.
And the drug is approved to treat patients with transfusion-dependent anemia due to low- or intermediate-1-risk myelodysplastic syndromes associated with 5q deletion, with or without additional cytogenetic abnormalities.
“The approval of Revlimid as an option for use in all patients with multiple myeloma represents a new paradigm in the management of this disease,” said Kenneth Anderson, MD, of Dana-Farber/Brigham and Women’s Cancer Center in Boston, Massachusetts.
“We now have clinical evidence demonstrating that starting and keeping newly diagnosed multiple myeloma patients on Revlimid significantly improves progression-free survival.”
The FDA’s latest approval of lenalidomide was based on safety and efficacy results from phase 3 studies, particularly the FIRST trial.
The FIRST trial
In this phase 3 trial, researchers enrolled 1623 patients who were newly diagnosed with MM and not eligible for stem cell transplant.
Patients were randomized to receive lenalidomide and dexamethasone (Rd) in 28-day cycles until disease progression (n=535), 18 cycles of lenalidomide and dexamethasone (Rd18) for 72 weeks (n=541), or melphalan, prednisone, and thalidomide (MPT) for 72 weeks (n=547).
Response rates were significantly better with continuous Rd (75%) and Rd18 (73%) than with MPT (62%, P<0.001 for both comparisons). Complete response rates were 15%, 14%, and 9%, respectively.
The median progression-free survival was 25.5 months with continuous Rd, 20.7 months with Rd18, and 21.2 months with MPT.
This resulted in a 28% reduction in the risk of progression or death for patients treated with continuous Rd compared with those treated with MPT (hazard ratio[HR]=0.72, P<0.001) and a 30% reduction compared with Rd18 (HR=0.70, P<0.001).
The pre-planned interim analysis of overall survival showed a 22% reduction in the risk of death for continuous Rd vs MPT (HR=0.78, P=0.02), but the difference did not cross the pre-specified superiority boundary (P<0.0096).
Adverse events reported in 20% or more of patients in the continuous Rd, Rd18, or MPT arms included diarrhea (45.5%, 38.5%, 16.5%), anemia (43.8%, 35.7%, 42.3%), neutropenia (35.0%, 33.0%, 60.6%), fatigue (32.5%, 32.8%, 28.5%), back pain (32.0%, 26.9%, 21.4%), insomnia (27.6%, 23.5%, 9.8%), asthenia (28.2%, 22.8%, 22.9%), rash (26.1%, 28.0%, 19.4%), decreased appetite (23.1%, 21.3%, 13.3%), cough (22.7%, 17.4%, 12.6%), pyrexia (21.4%, 18.9%, 14.0%), muscle spasms (20.5%, 18.9%, 11.3%) and abdominal pain (20.5%, 14.4%, 11.1%).
The most frequently reported grade 3/4 events in the continuous Rd arm (until disease progression) were neutropenia (27.8%), anemia (18.2%), thrombocytopenia (8.3%), pneumonia (11.3%), asthenia (7.7%), fatigue (7.3%), back pain (7%), hypokalemia (6.6%), rash (7.3%), cataract (5.8%), dyspnea (5.6%), deep vein thrombosis (5.6%), and hyperglycemia (5.3%).
The incidence of invasive second primary malignancies was 3% in the continuous Rd arm, 6% in the Rd18 arm, and 5% in the MPT arm. The overall incidence of solid tumors was identical in the continuous Rd and MPT arms (3%) and 5% in the Rd18 arm.
The US Food and Drug Administration (FDA) has expanded the existing indication for lenalidomide (Revlimid)—in combination with dexamethasone—to include patients with newly diagnosed multiple myeloma (MM).
The FDA previously approved lenalidomide in combination with dexamethasone to treat MM patients who had received at least 1 prior therapy.
Lenalidomide is also FDA-approved to treat mantle cell lymphoma patients who have failed 2 prior therapies, including bortezomib.
And the drug is approved to treat patients with transfusion-dependent anemia due to low- or intermediate-1-risk myelodysplastic syndromes associated with 5q deletion, with or without additional cytogenetic abnormalities.
“The approval of Revlimid as an option for use in all patients with multiple myeloma represents a new paradigm in the management of this disease,” said Kenneth Anderson, MD, of Dana-Farber/Brigham and Women’s Cancer Center in Boston, Massachusetts.
“We now have clinical evidence demonstrating that starting and keeping newly diagnosed multiple myeloma patients on Revlimid significantly improves progression-free survival.”
The FDA’s latest approval of lenalidomide was based on safety and efficacy results from phase 3 studies, particularly the FIRST trial.
The FIRST trial
In this phase 3 trial, researchers enrolled 1623 patients who were newly diagnosed with MM and not eligible for stem cell transplant.
Patients were randomized to receive lenalidomide and dexamethasone (Rd) in 28-day cycles until disease progression (n=535), 18 cycles of lenalidomide and dexamethasone (Rd18) for 72 weeks (n=541), or melphalan, prednisone, and thalidomide (MPT) for 72 weeks (n=547).
Response rates were significantly better with continuous Rd (75%) and Rd18 (73%) than with MPT (62%, P<0.001 for both comparisons). Complete response rates were 15%, 14%, and 9%, respectively.
The median progression-free survival was 25.5 months with continuous Rd, 20.7 months with Rd18, and 21.2 months with MPT.
This resulted in a 28% reduction in the risk of progression or death for patients treated with continuous Rd compared with those treated with MPT (hazard ratio[HR]=0.72, P<0.001) and a 30% reduction compared with Rd18 (HR=0.70, P<0.001).
The pre-planned interim analysis of overall survival showed a 22% reduction in the risk of death for continuous Rd vs MPT (HR=0.78, P=0.02), but the difference did not cross the pre-specified superiority boundary (P<0.0096).
Adverse events reported in 20% or more of patients in the continuous Rd, Rd18, or MPT arms included diarrhea (45.5%, 38.5%, 16.5%), anemia (43.8%, 35.7%, 42.3%), neutropenia (35.0%, 33.0%, 60.6%), fatigue (32.5%, 32.8%, 28.5%), back pain (32.0%, 26.9%, 21.4%), insomnia (27.6%, 23.5%, 9.8%), asthenia (28.2%, 22.8%, 22.9%), rash (26.1%, 28.0%, 19.4%), decreased appetite (23.1%, 21.3%, 13.3%), cough (22.7%, 17.4%, 12.6%), pyrexia (21.4%, 18.9%, 14.0%), muscle spasms (20.5%, 18.9%, 11.3%) and abdominal pain (20.5%, 14.4%, 11.1%).
The most frequently reported grade 3/4 events in the continuous Rd arm (until disease progression) were neutropenia (27.8%), anemia (18.2%), thrombocytopenia (8.3%), pneumonia (11.3%), asthenia (7.7%), fatigue (7.3%), back pain (7%), hypokalemia (6.6%), rash (7.3%), cataract (5.8%), dyspnea (5.6%), deep vein thrombosis (5.6%), and hyperglycemia (5.3%).
The incidence of invasive second primary malignancies was 3% in the continuous Rd arm, 6% in the Rd18 arm, and 5% in the MPT arm. The overall incidence of solid tumors was identical in the continuous Rd and MPT arms (3%) and 5% in the Rd18 arm.
The US Food and Drug Administration (FDA) has expanded the existing indication for lenalidomide (Revlimid)—in combination with dexamethasone—to include patients with newly diagnosed multiple myeloma (MM).
The FDA previously approved lenalidomide in combination with dexamethasone to treat MM patients who had received at least 1 prior therapy.
Lenalidomide is also FDA-approved to treat mantle cell lymphoma patients who have failed 2 prior therapies, including bortezomib.
And the drug is approved to treat patients with transfusion-dependent anemia due to low- or intermediate-1-risk myelodysplastic syndromes associated with 5q deletion, with or without additional cytogenetic abnormalities.
“The approval of Revlimid as an option for use in all patients with multiple myeloma represents a new paradigm in the management of this disease,” said Kenneth Anderson, MD, of Dana-Farber/Brigham and Women’s Cancer Center in Boston, Massachusetts.
“We now have clinical evidence demonstrating that starting and keeping newly diagnosed multiple myeloma patients on Revlimid significantly improves progression-free survival.”
The FDA’s latest approval of lenalidomide was based on safety and efficacy results from phase 3 studies, particularly the FIRST trial.
The FIRST trial
In this phase 3 trial, researchers enrolled 1623 patients who were newly diagnosed with MM and not eligible for stem cell transplant.
Patients were randomized to receive lenalidomide and dexamethasone (Rd) in 28-day cycles until disease progression (n=535), 18 cycles of lenalidomide and dexamethasone (Rd18) for 72 weeks (n=541), or melphalan, prednisone, and thalidomide (MPT) for 72 weeks (n=547).
Response rates were significantly better with continuous Rd (75%) and Rd18 (73%) than with MPT (62%, P<0.001 for both comparisons). Complete response rates were 15%, 14%, and 9%, respectively.
The median progression-free survival was 25.5 months with continuous Rd, 20.7 months with Rd18, and 21.2 months with MPT.
This resulted in a 28% reduction in the risk of progression or death for patients treated with continuous Rd compared with those treated with MPT (hazard ratio[HR]=0.72, P<0.001) and a 30% reduction compared with Rd18 (HR=0.70, P<0.001).
The pre-planned interim analysis of overall survival showed a 22% reduction in the risk of death for continuous Rd vs MPT (HR=0.78, P=0.02), but the difference did not cross the pre-specified superiority boundary (P<0.0096).
Adverse events reported in 20% or more of patients in the continuous Rd, Rd18, or MPT arms included diarrhea (45.5%, 38.5%, 16.5%), anemia (43.8%, 35.7%, 42.3%), neutropenia (35.0%, 33.0%, 60.6%), fatigue (32.5%, 32.8%, 28.5%), back pain (32.0%, 26.9%, 21.4%), insomnia (27.6%, 23.5%, 9.8%), asthenia (28.2%, 22.8%, 22.9%), rash (26.1%, 28.0%, 19.4%), decreased appetite (23.1%, 21.3%, 13.3%), cough (22.7%, 17.4%, 12.6%), pyrexia (21.4%, 18.9%, 14.0%), muscle spasms (20.5%, 18.9%, 11.3%) and abdominal pain (20.5%, 14.4%, 11.1%).
The most frequently reported grade 3/4 events in the continuous Rd arm (until disease progression) were neutropenia (27.8%), anemia (18.2%), thrombocytopenia (8.3%), pneumonia (11.3%), asthenia (7.7%), fatigue (7.3%), back pain (7%), hypokalemia (6.6%), rash (7.3%), cataract (5.8%), dyspnea (5.6%), deep vein thrombosis (5.6%), and hyperglycemia (5.3%).
The incidence of invasive second primary malignancies was 3% in the continuous Rd arm, 6% in the Rd18 arm, and 5% in the MPT arm. The overall incidence of solid tumors was identical in the continuous Rd and MPT arms (3%) and 5% in the Rd18 arm.
Researchers map the human epigenome

to the Epigenome Roadmap
Image by Nik Spencer/Nature
Scientists have created new maps of the human epigenome that may help unravel the complex links between DNA and disease.
Researchers supported by the Common Fund’s Epigenomics Program have mapped the epigenomes of more than 100 types of cells and tissues, providing new insight into which parts of the genome are used to make a particular type of cell.
The group published an article describing the epigenome maps in the journal Nature.
Twenty-three additional papers in Nature Publishing Group journals show how these maps can be used to study human biology.
The papers are available on Nature’s Epigenome Roadmap site.
For the Roadmap Epigenomics Project, scientists compared epigenomic signatures and established their differences across a variety of cell types. The resulting information may help us understand how changes to the genome and epigenome can lead to cancers and other conditions.
“These 111 reference epigenome maps are essentially a vocabulary book that helps us decipher each DNA segment in distinct cell and tissue types,” said Bing Ren, PhD, of the University of California, San Diego.
For cancer research, the new data will hasten a merging of genomic and epigenomic perspectives that was already underway, according to Joseph F. Costello, PhD, of the University of California, San Francisco.
“You’ve had cancer researchers studying the genome—the role of mutations, deletions, and so on—and others studying epigenomes,” Dr Costello said. “They’ve almost been working on parallel tracks, and they didn’t talk to each other all that much.”
“Over the past 5 or 6 years, there’s been a reframing of the discussion, because the most recurrent mutations in cancer affect epigenomic regulators. So the way mutations in the genome play out is through epigenomic mechanisms, and major pharmaceutical companies now view epigenomes as an important target.”
to the Epigenome Roadmap
Image by Nik Spencer/Nature
Scientists have created new maps of the human epigenome that may help unravel the complex links between DNA and disease.
Researchers supported by the Common Fund’s Epigenomics Program have mapped the epigenomes of more than 100 types of cells and tissues, providing new insight into which parts of the genome are used to make a particular type of cell.
The group published an article describing the epigenome maps in the journal Nature.
Twenty-three additional papers in Nature Publishing Group journals show how these maps can be used to study human biology.
The papers are available on Nature’s Epigenome Roadmap site.
For the Roadmap Epigenomics Project, scientists compared epigenomic signatures and established their differences across a variety of cell types. The resulting information may help us understand how changes to the genome and epigenome can lead to cancers and other conditions.
“These 111 reference epigenome maps are essentially a vocabulary book that helps us decipher each DNA segment in distinct cell and tissue types,” said Bing Ren, PhD, of the University of California, San Diego.
For cancer research, the new data will hasten a merging of genomic and epigenomic perspectives that was already underway, according to Joseph F. Costello, PhD, of the University of California, San Francisco.
“You’ve had cancer researchers studying the genome—the role of mutations, deletions, and so on—and others studying epigenomes,” Dr Costello said. “They’ve almost been working on parallel tracks, and they didn’t talk to each other all that much.”
“Over the past 5 or 6 years, there’s been a reframing of the discussion, because the most recurrent mutations in cancer affect epigenomic regulators. So the way mutations in the genome play out is through epigenomic mechanisms, and major pharmaceutical companies now view epigenomes as an important target.”
to the Epigenome Roadmap
Image by Nik Spencer/Nature
Scientists have created new maps of the human epigenome that may help unravel the complex links between DNA and disease.
Researchers supported by the Common Fund’s Epigenomics Program have mapped the epigenomes of more than 100 types of cells and tissues, providing new insight into which parts of the genome are used to make a particular type of cell.
The group published an article describing the epigenome maps in the journal Nature.
Twenty-three additional papers in Nature Publishing Group journals show how these maps can be used to study human biology.
The papers are available on Nature’s Epigenome Roadmap site.
For the Roadmap Epigenomics Project, scientists compared epigenomic signatures and established their differences across a variety of cell types. The resulting information may help us understand how changes to the genome and epigenome can lead to cancers and other conditions.
“These 111 reference epigenome maps are essentially a vocabulary book that helps us decipher each DNA segment in distinct cell and tissue types,” said Bing Ren, PhD, of the University of California, San Diego.
For cancer research, the new data will hasten a merging of genomic and epigenomic perspectives that was already underway, according to Joseph F. Costello, PhD, of the University of California, San Francisco.
“You’ve had cancer researchers studying the genome—the role of mutations, deletions, and so on—and others studying epigenomes,” Dr Costello said. “They’ve almost been working on parallel tracks, and they didn’t talk to each other all that much.”
“Over the past 5 or 6 years, there’s been a reframing of the discussion, because the most recurrent mutations in cancer affect epigenomic regulators. So the way mutations in the genome play out is through epigenomic mechanisms, and major pharmaceutical companies now view epigenomes as an important target.”