User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Cell-Free DNA Blood Test Has High Accuracy for Detecting Colorectal Cancer
, according to a new study.
The cfDNA blood test had 83% sensitivity for CRC, 90% specificity for advanced neoplasia, and 13% sensitivity for advanced precancerous lesions. Other noninvasive screening methods have sensitivity from 67% to 94% for CRC and 22% to 43% for advanced precancerous lesions.
“The results of the study are a promising step toward developing more convenient tools to detect colorectal cancer early while it is more easily treated,” said senior author William M. Grady, MD, AGAF, medical director of the Gastrointestinal Cancer Prevention Program at the Fred Hutchinson Cancer Center in Seattle.
“The test, which has an accuracy rate for colon cancer detection similar to stool tests used for early detection of cancer, could offer an alternative for patients who may otherwise decline current screening options,” he said.
The study was published online on March 14 in The New England Journal of Medicine.
Analyzing the Blood Test’s Accuracy
Dr. Grady and colleagues conducted a multisite clinical trial called ECLIPSE, which compared the sensitivity and specificity of a cfDNA blood test (Shield, Guardant Health) against that obtained with colonoscopy, the gold standard for CRC screening. Guardant led and funded the study.
Guardant’s Shield test is designed to detect CRC through genomic alterations, aberrant methylation status, and fragmentomic patterns, which show up as an “abnormal signal detected” result. Similar blood tests are being developed as “liquid biopsy” tests for other emerging cancer screenings as well.
The study included 7861 people with average CRC risk who underwent routine screening with colonoscopy at 265 sites in the United States, including primary care and endoscopy centers in academic and community-based institutions. Eligible people were aged 45-84 years (average age, 60 years), and 53.7% were women. The race and ethnicity characteristics of the participants closely mirrored the demographic distribution in the 2020 US Census.
Overall, 54 of 65 (83.1%) participants with colonoscopy-detected CRC had a positive cfDNA blood test. However, 11 participants (16.9%) with CRC had a negative test.
The cfDNA blood test identified 42 of 48 stage I, II, or III CRCs, indicating a sensitivity of 87.5%, including 65% for stage I cancers, 100% for stage II cancers, and 100% for stage III cancers. The test also identified all 10 of the stage IV CRC cases. There were no substantial differences in sensitivity for CRC based on primary tumor location, tumor histologic grade, or demographic characteristics.
Among participants without advanced colorectal neoplasia on colonoscopy, 89.6% had a negative cfDNA blood test, and 10.4% had a positive test.
Among those with a negative colonoscopy — with no CRC, advanced precancerous lesions, or nonadvanced precancerous lesions — specificity was 89.9%.
Among 1116 participants with advanced precancerous lesions identified as the most advanced lesion on colonoscopy, the cfDNA blood test was positive for 147, indicating a sensitivity for advanced precancerous lesions of 13.2%.
Although the blood test has sensitivity similar to stool-based tests for CRC, the accuracy is lower than it is with colonoscopy, which remains the current gold standard for CRC screening, Dr. Grady said.
“Colorectal cancer is common and very preventable with screening, but only about 50% to 60% of people who are eligible for screening actually take those tests,” he said. “Getting people to be screened for cancer works best when we offer them screening options and then let them choose what works best for them.”
Future Research
Colorectal cancer is the second leading cause of cancer-related death among US adults and is now the third most diagnosed cancer for people younger than 50 years, Dr. Grady said. Although overall CRC death rates have declined in recent years, the rates among those younger than 55 years have increased since the mid-2000s.
“When colorectal cancer is found earlier and the cancer has not yet spread throughout the body, patient outcomes are much better, as reflected in 5-year survival being much better. It makes sense that an effective blood-based test could have a potential role, in particular for those not getting screened yet,” said Joshua Melson, MD, AGAF, clinical professor of medicine and director of the High-Risk Clinic for Gastrointestinal Cancers at the University of Arizona Cancer Center in Tucson.
Dr. Melson, who wasn’t involved with this study, noted that blood-based testing shows promise for cancer detection but needs additional support for real-world implementation. For instance, the Shield blood test has difficulty detecting precancerous lesions, and it remains unclear what the optimal intervals for repeat testing would be after a negative test, he said. In addition, screening programs will need to ensure they have capacity to effectively deal with a positive test result.
“For a screening program to actually work, when a noninvasive test (whether blood-based or stool-based) is read as positive, those patients need to have a follow-up colonoscopy,” he said.
Proper communication with patients will be important as well, said Gloria Coronado, PhD, associate director of Population Sciences at the University of Arizona Cancer Center, Tucson. Dr. Coronado, who wasn’t involved with this study, has developed CRC screening messages for specific patient populations and studied patient reactions to CRC blood tests.
In a study by Dr. Coronado and colleagues, among more than 2000 patients who passively declined fecal testing and had an upcoming clinic visit, CRC screening proportions were 17.5 percentage points higher in the group offered the blood test vs those offered usual care. In qualitative interviews, one patient said of the blood-based testing option, “I was screaming hallelujah!”
“Patients believed that a blood test would be more accurate than a stool-based test. However, for the detection of advanced adenomas, the reverse is true,” she said. “It will be important to balance the high acceptance and enthusiasm for the blood test with the lower performance of the blood test compared to other tests already on the market.”
In a statement accompanying the study’s publication, the American Gastroenterological Association welcomed these results as an exciting development, but cautioned that a blood-based test was not interchangeable with colonoscopy.
“The Centers for Medicare and Medicaid Services (CMS) has determined it will cover a blood test for colorectal cancer screening every three years if the test achieves 74% sensitivity for CRC, 90% specificity, and FDA approval,” the statement reads. “However, a blood test that meets only the CMS criteria will be inferior to current recommended tests and should not be recommended to replace current tests. Such a test could be recommended for patients who decline all other recommended tests, since any screening is better than no screening at all.”
Dr. Grady is a paid member of Guardant’s scientific advisory board and advised on the design and procedure of the clinical trial and data analysis. Dr. Melson previously served as consultant for Guardant. Dr. Coronado reported no relevant disclosures.
A version of this article appeared on Medscape.com .
, according to a new study.
The cfDNA blood test had 83% sensitivity for CRC, 90% specificity for advanced neoplasia, and 13% sensitivity for advanced precancerous lesions. Other noninvasive screening methods have sensitivity from 67% to 94% for CRC and 22% to 43% for advanced precancerous lesions.
“The results of the study are a promising step toward developing more convenient tools to detect colorectal cancer early while it is more easily treated,” said senior author William M. Grady, MD, AGAF, medical director of the Gastrointestinal Cancer Prevention Program at the Fred Hutchinson Cancer Center in Seattle.
“The test, which has an accuracy rate for colon cancer detection similar to stool tests used for early detection of cancer, could offer an alternative for patients who may otherwise decline current screening options,” he said.
The study was published online on March 14 in The New England Journal of Medicine.
Analyzing the Blood Test’s Accuracy
Dr. Grady and colleagues conducted a multisite clinical trial called ECLIPSE, which compared the sensitivity and specificity of a cfDNA blood test (Shield, Guardant Health) against that obtained with colonoscopy, the gold standard for CRC screening. Guardant led and funded the study.
Guardant’s Shield test is designed to detect CRC through genomic alterations, aberrant methylation status, and fragmentomic patterns, which show up as an “abnormal signal detected” result. Similar blood tests are being developed as “liquid biopsy” tests for other emerging cancer screenings as well.
The study included 7861 people with average CRC risk who underwent routine screening with colonoscopy at 265 sites in the United States, including primary care and endoscopy centers in academic and community-based institutions. Eligible people were aged 45-84 years (average age, 60 years), and 53.7% were women. The race and ethnicity characteristics of the participants closely mirrored the demographic distribution in the 2020 US Census.
Overall, 54 of 65 (83.1%) participants with colonoscopy-detected CRC had a positive cfDNA blood test. However, 11 participants (16.9%) with CRC had a negative test.
The cfDNA blood test identified 42 of 48 stage I, II, or III CRCs, indicating a sensitivity of 87.5%, including 65% for stage I cancers, 100% for stage II cancers, and 100% for stage III cancers. The test also identified all 10 of the stage IV CRC cases. There were no substantial differences in sensitivity for CRC based on primary tumor location, tumor histologic grade, or demographic characteristics.
Among participants without advanced colorectal neoplasia on colonoscopy, 89.6% had a negative cfDNA blood test, and 10.4% had a positive test.
Among those with a negative colonoscopy — with no CRC, advanced precancerous lesions, or nonadvanced precancerous lesions — specificity was 89.9%.
Among 1116 participants with advanced precancerous lesions identified as the most advanced lesion on colonoscopy, the cfDNA blood test was positive for 147, indicating a sensitivity for advanced precancerous lesions of 13.2%.
Although the blood test has sensitivity similar to stool-based tests for CRC, the accuracy is lower than it is with colonoscopy, which remains the current gold standard for CRC screening, Dr. Grady said.
“Colorectal cancer is common and very preventable with screening, but only about 50% to 60% of people who are eligible for screening actually take those tests,” he said. “Getting people to be screened for cancer works best when we offer them screening options and then let them choose what works best for them.”
Future Research
Colorectal cancer is the second leading cause of cancer-related death among US adults and is now the third most diagnosed cancer for people younger than 50 years, Dr. Grady said. Although overall CRC death rates have declined in recent years, the rates among those younger than 55 years have increased since the mid-2000s.
“When colorectal cancer is found earlier and the cancer has not yet spread throughout the body, patient outcomes are much better, as reflected in 5-year survival being much better. It makes sense that an effective blood-based test could have a potential role, in particular for those not getting screened yet,” said Joshua Melson, MD, AGAF, clinical professor of medicine and director of the High-Risk Clinic for Gastrointestinal Cancers at the University of Arizona Cancer Center in Tucson.
Dr. Melson, who wasn’t involved with this study, noted that blood-based testing shows promise for cancer detection but needs additional support for real-world implementation. For instance, the Shield blood test has difficulty detecting precancerous lesions, and it remains unclear what the optimal intervals for repeat testing would be after a negative test, he said. In addition, screening programs will need to ensure they have capacity to effectively deal with a positive test result.
“For a screening program to actually work, when a noninvasive test (whether blood-based or stool-based) is read as positive, those patients need to have a follow-up colonoscopy,” he said.
Proper communication with patients will be important as well, said Gloria Coronado, PhD, associate director of Population Sciences at the University of Arizona Cancer Center, Tucson. Dr. Coronado, who wasn’t involved with this study, has developed CRC screening messages for specific patient populations and studied patient reactions to CRC blood tests.
In a study by Dr. Coronado and colleagues, among more than 2000 patients who passively declined fecal testing and had an upcoming clinic visit, CRC screening proportions were 17.5 percentage points higher in the group offered the blood test vs those offered usual care. In qualitative interviews, one patient said of the blood-based testing option, “I was screaming hallelujah!”
“Patients believed that a blood test would be more accurate than a stool-based test. However, for the detection of advanced adenomas, the reverse is true,” she said. “It will be important to balance the high acceptance and enthusiasm for the blood test with the lower performance of the blood test compared to other tests already on the market.”
In a statement accompanying the study’s publication, the American Gastroenterological Association welcomed these results as an exciting development, but cautioned that a blood-based test was not interchangeable with colonoscopy.
“The Centers for Medicare and Medicaid Services (CMS) has determined it will cover a blood test for colorectal cancer screening every three years if the test achieves 74% sensitivity for CRC, 90% specificity, and FDA approval,” the statement reads. “However, a blood test that meets only the CMS criteria will be inferior to current recommended tests and should not be recommended to replace current tests. Such a test could be recommended for patients who decline all other recommended tests, since any screening is better than no screening at all.”
Dr. Grady is a paid member of Guardant’s scientific advisory board and advised on the design and procedure of the clinical trial and data analysis. Dr. Melson previously served as consultant for Guardant. Dr. Coronado reported no relevant disclosures.
A version of this article appeared on Medscape.com .
, according to a new study.
The cfDNA blood test had 83% sensitivity for CRC, 90% specificity for advanced neoplasia, and 13% sensitivity for advanced precancerous lesions. Other noninvasive screening methods have sensitivity from 67% to 94% for CRC and 22% to 43% for advanced precancerous lesions.
“The results of the study are a promising step toward developing more convenient tools to detect colorectal cancer early while it is more easily treated,” said senior author William M. Grady, MD, AGAF, medical director of the Gastrointestinal Cancer Prevention Program at the Fred Hutchinson Cancer Center in Seattle.
“The test, which has an accuracy rate for colon cancer detection similar to stool tests used for early detection of cancer, could offer an alternative for patients who may otherwise decline current screening options,” he said.
The study was published online on March 14 in The New England Journal of Medicine.
Analyzing the Blood Test’s Accuracy
Dr. Grady and colleagues conducted a multisite clinical trial called ECLIPSE, which compared the sensitivity and specificity of a cfDNA blood test (Shield, Guardant Health) against that obtained with colonoscopy, the gold standard for CRC screening. Guardant led and funded the study.
Guardant’s Shield test is designed to detect CRC through genomic alterations, aberrant methylation status, and fragmentomic patterns, which show up as an “abnormal signal detected” result. Similar blood tests are being developed as “liquid biopsy” tests for other emerging cancer screenings as well.
The study included 7861 people with average CRC risk who underwent routine screening with colonoscopy at 265 sites in the United States, including primary care and endoscopy centers in academic and community-based institutions. Eligible people were aged 45-84 years (average age, 60 years), and 53.7% were women. The race and ethnicity characteristics of the participants closely mirrored the demographic distribution in the 2020 US Census.
Overall, 54 of 65 (83.1%) participants with colonoscopy-detected CRC had a positive cfDNA blood test. However, 11 participants (16.9%) with CRC had a negative test.
The cfDNA blood test identified 42 of 48 stage I, II, or III CRCs, indicating a sensitivity of 87.5%, including 65% for stage I cancers, 100% for stage II cancers, and 100% for stage III cancers. The test also identified all 10 of the stage IV CRC cases. There were no substantial differences in sensitivity for CRC based on primary tumor location, tumor histologic grade, or demographic characteristics.
Among participants without advanced colorectal neoplasia on colonoscopy, 89.6% had a negative cfDNA blood test, and 10.4% had a positive test.
Among those with a negative colonoscopy — with no CRC, advanced precancerous lesions, or nonadvanced precancerous lesions — specificity was 89.9%.
Among 1116 participants with advanced precancerous lesions identified as the most advanced lesion on colonoscopy, the cfDNA blood test was positive for 147, indicating a sensitivity for advanced precancerous lesions of 13.2%.
Although the blood test has sensitivity similar to stool-based tests for CRC, the accuracy is lower than it is with colonoscopy, which remains the current gold standard for CRC screening, Dr. Grady said.
“Colorectal cancer is common and very preventable with screening, but only about 50% to 60% of people who are eligible for screening actually take those tests,” he said. “Getting people to be screened for cancer works best when we offer them screening options and then let them choose what works best for them.”
Future Research
Colorectal cancer is the second leading cause of cancer-related death among US adults and is now the third most diagnosed cancer for people younger than 50 years, Dr. Grady said. Although overall CRC death rates have declined in recent years, the rates among those younger than 55 years have increased since the mid-2000s.
“When colorectal cancer is found earlier and the cancer has not yet spread throughout the body, patient outcomes are much better, as reflected in 5-year survival being much better. It makes sense that an effective blood-based test could have a potential role, in particular for those not getting screened yet,” said Joshua Melson, MD, AGAF, clinical professor of medicine and director of the High-Risk Clinic for Gastrointestinal Cancers at the University of Arizona Cancer Center in Tucson.
Dr. Melson, who wasn’t involved with this study, noted that blood-based testing shows promise for cancer detection but needs additional support for real-world implementation. For instance, the Shield blood test has difficulty detecting precancerous lesions, and it remains unclear what the optimal intervals for repeat testing would be after a negative test, he said. In addition, screening programs will need to ensure they have capacity to effectively deal with a positive test result.
“For a screening program to actually work, when a noninvasive test (whether blood-based or stool-based) is read as positive, those patients need to have a follow-up colonoscopy,” he said.
Proper communication with patients will be important as well, said Gloria Coronado, PhD, associate director of Population Sciences at the University of Arizona Cancer Center, Tucson. Dr. Coronado, who wasn’t involved with this study, has developed CRC screening messages for specific patient populations and studied patient reactions to CRC blood tests.
In a study by Dr. Coronado and colleagues, among more than 2000 patients who passively declined fecal testing and had an upcoming clinic visit, CRC screening proportions were 17.5 percentage points higher in the group offered the blood test vs those offered usual care. In qualitative interviews, one patient said of the blood-based testing option, “I was screaming hallelujah!”
“Patients believed that a blood test would be more accurate than a stool-based test. However, for the detection of advanced adenomas, the reverse is true,” she said. “It will be important to balance the high acceptance and enthusiasm for the blood test with the lower performance of the blood test compared to other tests already on the market.”
In a statement accompanying the study’s publication, the American Gastroenterological Association welcomed these results as an exciting development, but cautioned that a blood-based test was not interchangeable with colonoscopy.
“The Centers for Medicare and Medicaid Services (CMS) has determined it will cover a blood test for colorectal cancer screening every three years if the test achieves 74% sensitivity for CRC, 90% specificity, and FDA approval,” the statement reads. “However, a blood test that meets only the CMS criteria will be inferior to current recommended tests and should not be recommended to replace current tests. Such a test could be recommended for patients who decline all other recommended tests, since any screening is better than no screening at all.”
Dr. Grady is a paid member of Guardant’s scientific advisory board and advised on the design and procedure of the clinical trial and data analysis. Dr. Melson previously served as consultant for Guardant. Dr. Coronado reported no relevant disclosures.
A version of this article appeared on Medscape.com .
FROM NEJM
Combining Targeted Drugs and Radiation in Breast Cancer: What’s Safe?
One reason is studies of new drugs typically exclude concurrent radiotherapy, said Kathy Miller, MD, a contributor to this news organization and professor of oncology and medicine at the Indiana University School of Medicine, Indianapolis, Indiana.
If trials evaluating new targeted therapies included concurrent radiotherapy, it would be challenging to identify whether toxicities came from the drug itself, the radiation, or the combination, Dr. Miller explained.
Given the limited evidence, “we tend to be cautious and conservative” and not combine therapies that “we don’t know are safe or appropriate for patients,” said Chirag Shah, MD, director of breast radiology at the Cleveland Clinic, Cleveland, Ohio.
Below is a guide to what we do and don’t know about combining radiotherapy and systemic treatments in breast cancer.
1. Immunotherapy plus radiotherapy likely safe but evidence is limited
Safety data on combining immune checkpoint inhibitors and radiotherapy in breast cancer are limited because concurrent radiotherapy has typically been excluded in pivotal trials.
The 2020 KEYNOTE-522 trial did provide a rare look at concurrent radiotherapy and immunotherapy in early triple-negative breast cancer. The analysis found “no safety concerns” with concurrent radiotherapy and pembrolizumab, lead investigator Peter Schmid, MD, of Queen Mary University of London, England, told this news organization.
Research on other solid tumor types also suggests that radiotherapy “can be considered safe” alongside immunotherapy, the authors of a recent ESTRO consensus said.
Despite evidence indicating radiotherapy alongside immunotherapy can be safe in patients with breast cancer, “certain aspects, such as patient selection, total dose, and dose per fraction, remain open for debate to achieve the best therapeutic outcomes,” the ESTRO experts cautioned.
2. CDK4/6 inhibitors may be offered with radiotherapy in some settings, not others
CDK4/6 inhibitors are now standard of care for first- or second-line treatment in patients with advanced or metastatic hormone receptor–positive, human epidermal growth factor receptor 2 (HER2)–negative breast cancer.
“Unfortunately, we found no information regarding concurrent radiotherapy in the adjuvant setting” in pivotal trials for palbociclib, abemaciclib, and ribociclib, the ESTRO authors said. In the pivotal trials for palbociclib and abemaciclib, patients had to discontinue immunotherapy before initiating radiotherapy, and in the trial for ribociclib, palliative radiotherapy was allowed for relieving bone pain only.
However, in 2023, a team of experts from 12 countries attempted to piece together the available evidence, publishing a meta-analysis of 11 retrospective studies on the safety of CDK4/6 inhibitors given concurrently with radiotherapy in patients with metastatic disease.
Although most of these studies had small patient populations, the analysis revealed that CDK4/6 inhibitors given concurrently with radiotherapy in patients with metastatic breast cancer led to a similar side-effect profile to that observed in trials of the inhibitors given sequentially with adjuvant radiotherapy.
“These findings suggest that the simultaneous administration of CDK4/6 inhibitors and radiotherapy is generally well tolerated,” the ESTRO authors concluded but added that CDK4/6 inhibitors and concomitant radiotherapy should be investigated more in the adjuvant locoregional, whole brain, and intracranial stereotactic radiotherapy settings.
The expert panel did note, however, that CDK4/6 inhibitors and concomitant radiotherapy “could be offered” during palliative and ablative extracranial radiotherapy.
3. Only offer poly (ADP-ribose) polymerase (PARP) inhibitors plus radiotherapy in clinical trial setting
PARP inhibitors olaparib (Lynparza) and talazoprib (Talzenna) are standard of care in patients with metastatic breast cancer who have BRCA1/2 gene mutations. Olaparib is also indicated for high-risk early breast cancer following neoadjuvant or adjuvant chemotherapy.
But data on combining PARP inhibitors with radiotherapy in breast cancer also remain limited.
One ongoing phase 2 trial, comparing olaparib plus radiotherapy to radiotherapy alone in 300 people with inflammatory breast cancer, is aiming to tease out the safety of the combination and whether it improves local control in patients with aggressive disease.
“The desire is to explore the exciting possibility that low doses of PARP inhibition may radiosensitize tumor cells more than normal tissues,” Reshma Jagsi, MD, chair of the Department of Radiation Oncology at Emory University School of Medicine in Atlanta, Georgia, who is leading the study.
Because of potential good or bad interactions between new systemic therapies and radiotherapy, “intentional trial design” is important, Dr. Jagsi said, so we “know the best way to combine treatments in practice to optimize outcomes.”
But given the evidence to date, the ESTRO experts advised waiting until “further research provides more comprehensive safety and efficacy data” in the primary, adjuvant, and metastatic settings. The experts also advised not offering PARP inhibitors and concomitant radiotherapy to treat advanced breast cancer outside of clinical trials.
4. Phosphoinositide 3-kinase inhibitors (PI3K) inhibitors, mammalian target of rapamycin (mTOR) inhibitors, and newer targeted agents should not be offered concurrently with radiotherapy
Clinical trial data on the safety of combining PI3K and mTOR inhibitors with radiation are thin, especially in advanced breast cancer. Typically, radiotherapy within 4 weeks before randomization, or 2 weeks for palliative radiation, was excluded in pivotal trials.
For this reason, the ESTRO team recommended that concurrent radiation with either PI3K inhibitors or mTOR inhibitors “should not be offered.”
ESTRO also cautioned against providing radiation concurrently with newer anti-HER2 tyrosine-kinase drugs, such as neratinib or tucatinib, or newer antibody-drug conjugates such as trastuzumab deruxtecan, until more data emerge on the safety of these combinations.
5. Combining older HER2-targeted drugs and radiotherapy generally safe
The ESTRO authors agreed that older anti-HER2 drugs trastuzumab (Herceptin), pertuzumab (Perjeta), and lapatinib (Tykerb) can be safely used concurrently with locoregional radiotherapy as well.
One of the biggest concerns in the field is how to combine radiation with systemic therapies in the setting of brain metastases, and the data on these older anti-HER2 drugs are relatively clear that it’s safe, Dr. Miller said.
For instance, in a 2019 study of 84 patients with 487 brain metastases, stereotactic radiosurgery given alongside lapatinib led to significantly higher rates of complete responses than stereotactic radiosurgery alone (35% vs 11%) with no increased risk for radiation necrosis.
The ESTRO team agreed, noting that the latest evidence supports the use of trastuzumab, pertuzumab, or lapatinib alongside radiotherapy for whole brain and ablative intracranial stereotactic radiotherapy.
As for older antibody-drug conjugates, trastuzumab emtansine (T-DM1) plus radiotherapy “might be considered” during adjuvant locoregional radiotherapy for breast cancer but should not be offered for whole brain and ablative intracranial stereotactic radiotherapy, the ESTRO team said.
Dr. Jagsi declared the following conflicts in a recent 2024 publication: Stock options for advisory board role in Equity Quotient; grants or contracts from Genentech; and expert witness for Kleinbard, LLC, and Hawks Quindel Law. In the Keynote-522 trial publication Dr. Schmid declared relationships with AstraZeneca, Bayer, Boehringer Ingelheim, Celgene, Eisai, Hoffmann-La Roche, Genetech, Merck, Novartis, and Pfizer. Dr. Shah reported consulting for Impedimed, Videra Surgical, and PreludeDX.
A version of this article appeared on Medscape.com.
One reason is studies of new drugs typically exclude concurrent radiotherapy, said Kathy Miller, MD, a contributor to this news organization and professor of oncology and medicine at the Indiana University School of Medicine, Indianapolis, Indiana.
If trials evaluating new targeted therapies included concurrent radiotherapy, it would be challenging to identify whether toxicities came from the drug itself, the radiation, or the combination, Dr. Miller explained.
Given the limited evidence, “we tend to be cautious and conservative” and not combine therapies that “we don’t know are safe or appropriate for patients,” said Chirag Shah, MD, director of breast radiology at the Cleveland Clinic, Cleveland, Ohio.
Below is a guide to what we do and don’t know about combining radiotherapy and systemic treatments in breast cancer.
1. Immunotherapy plus radiotherapy likely safe but evidence is limited
Safety data on combining immune checkpoint inhibitors and radiotherapy in breast cancer are limited because concurrent radiotherapy has typically been excluded in pivotal trials.
The 2020 KEYNOTE-522 trial did provide a rare look at concurrent radiotherapy and immunotherapy in early triple-negative breast cancer. The analysis found “no safety concerns” with concurrent radiotherapy and pembrolizumab, lead investigator Peter Schmid, MD, of Queen Mary University of London, England, told this news organization.
Research on other solid tumor types also suggests that radiotherapy “can be considered safe” alongside immunotherapy, the authors of a recent ESTRO consensus said.
Despite evidence indicating radiotherapy alongside immunotherapy can be safe in patients with breast cancer, “certain aspects, such as patient selection, total dose, and dose per fraction, remain open for debate to achieve the best therapeutic outcomes,” the ESTRO experts cautioned.
2. CDK4/6 inhibitors may be offered with radiotherapy in some settings, not others
CDK4/6 inhibitors are now standard of care for first- or second-line treatment in patients with advanced or metastatic hormone receptor–positive, human epidermal growth factor receptor 2 (HER2)–negative breast cancer.
“Unfortunately, we found no information regarding concurrent radiotherapy in the adjuvant setting” in pivotal trials for palbociclib, abemaciclib, and ribociclib, the ESTRO authors said. In the pivotal trials for palbociclib and abemaciclib, patients had to discontinue immunotherapy before initiating radiotherapy, and in the trial for ribociclib, palliative radiotherapy was allowed for relieving bone pain only.
However, in 2023, a team of experts from 12 countries attempted to piece together the available evidence, publishing a meta-analysis of 11 retrospective studies on the safety of CDK4/6 inhibitors given concurrently with radiotherapy in patients with metastatic disease.
Although most of these studies had small patient populations, the analysis revealed that CDK4/6 inhibitors given concurrently with radiotherapy in patients with metastatic breast cancer led to a similar side-effect profile to that observed in trials of the inhibitors given sequentially with adjuvant radiotherapy.
“These findings suggest that the simultaneous administration of CDK4/6 inhibitors and radiotherapy is generally well tolerated,” the ESTRO authors concluded but added that CDK4/6 inhibitors and concomitant radiotherapy should be investigated more in the adjuvant locoregional, whole brain, and intracranial stereotactic radiotherapy settings.
The expert panel did note, however, that CDK4/6 inhibitors and concomitant radiotherapy “could be offered” during palliative and ablative extracranial radiotherapy.
3. Only offer poly (ADP-ribose) polymerase (PARP) inhibitors plus radiotherapy in clinical trial setting
PARP inhibitors olaparib (Lynparza) and talazoprib (Talzenna) are standard of care in patients with metastatic breast cancer who have BRCA1/2 gene mutations. Olaparib is also indicated for high-risk early breast cancer following neoadjuvant or adjuvant chemotherapy.
But data on combining PARP inhibitors with radiotherapy in breast cancer also remain limited.
One ongoing phase 2 trial, comparing olaparib plus radiotherapy to radiotherapy alone in 300 people with inflammatory breast cancer, is aiming to tease out the safety of the combination and whether it improves local control in patients with aggressive disease.
“The desire is to explore the exciting possibility that low doses of PARP inhibition may radiosensitize tumor cells more than normal tissues,” Reshma Jagsi, MD, chair of the Department of Radiation Oncology at Emory University School of Medicine in Atlanta, Georgia, who is leading the study.
Because of potential good or bad interactions between new systemic therapies and radiotherapy, “intentional trial design” is important, Dr. Jagsi said, so we “know the best way to combine treatments in practice to optimize outcomes.”
But given the evidence to date, the ESTRO experts advised waiting until “further research provides more comprehensive safety and efficacy data” in the primary, adjuvant, and metastatic settings. The experts also advised not offering PARP inhibitors and concomitant radiotherapy to treat advanced breast cancer outside of clinical trials.
4. Phosphoinositide 3-kinase inhibitors (PI3K) inhibitors, mammalian target of rapamycin (mTOR) inhibitors, and newer targeted agents should not be offered concurrently with radiotherapy
Clinical trial data on the safety of combining PI3K and mTOR inhibitors with radiation are thin, especially in advanced breast cancer. Typically, radiotherapy within 4 weeks before randomization, or 2 weeks for palliative radiation, was excluded in pivotal trials.
For this reason, the ESTRO team recommended that concurrent radiation with either PI3K inhibitors or mTOR inhibitors “should not be offered.”
ESTRO also cautioned against providing radiation concurrently with newer anti-HER2 tyrosine-kinase drugs, such as neratinib or tucatinib, or newer antibody-drug conjugates such as trastuzumab deruxtecan, until more data emerge on the safety of these combinations.
5. Combining older HER2-targeted drugs and radiotherapy generally safe
The ESTRO authors agreed that older anti-HER2 drugs trastuzumab (Herceptin), pertuzumab (Perjeta), and lapatinib (Tykerb) can be safely used concurrently with locoregional radiotherapy as well.
One of the biggest concerns in the field is how to combine radiation with systemic therapies in the setting of brain metastases, and the data on these older anti-HER2 drugs are relatively clear that it’s safe, Dr. Miller said.
For instance, in a 2019 study of 84 patients with 487 brain metastases, stereotactic radiosurgery given alongside lapatinib led to significantly higher rates of complete responses than stereotactic radiosurgery alone (35% vs 11%) with no increased risk for radiation necrosis.
The ESTRO team agreed, noting that the latest evidence supports the use of trastuzumab, pertuzumab, or lapatinib alongside radiotherapy for whole brain and ablative intracranial stereotactic radiotherapy.
As for older antibody-drug conjugates, trastuzumab emtansine (T-DM1) plus radiotherapy “might be considered” during adjuvant locoregional radiotherapy for breast cancer but should not be offered for whole brain and ablative intracranial stereotactic radiotherapy, the ESTRO team said.
Dr. Jagsi declared the following conflicts in a recent 2024 publication: Stock options for advisory board role in Equity Quotient; grants or contracts from Genentech; and expert witness for Kleinbard, LLC, and Hawks Quindel Law. In the Keynote-522 trial publication Dr. Schmid declared relationships with AstraZeneca, Bayer, Boehringer Ingelheim, Celgene, Eisai, Hoffmann-La Roche, Genetech, Merck, Novartis, and Pfizer. Dr. Shah reported consulting for Impedimed, Videra Surgical, and PreludeDX.
A version of this article appeared on Medscape.com.
One reason is studies of new drugs typically exclude concurrent radiotherapy, said Kathy Miller, MD, a contributor to this news organization and professor of oncology and medicine at the Indiana University School of Medicine, Indianapolis, Indiana.
If trials evaluating new targeted therapies included concurrent radiotherapy, it would be challenging to identify whether toxicities came from the drug itself, the radiation, or the combination, Dr. Miller explained.
Given the limited evidence, “we tend to be cautious and conservative” and not combine therapies that “we don’t know are safe or appropriate for patients,” said Chirag Shah, MD, director of breast radiology at the Cleveland Clinic, Cleveland, Ohio.
Below is a guide to what we do and don’t know about combining radiotherapy and systemic treatments in breast cancer.
1. Immunotherapy plus radiotherapy likely safe but evidence is limited
Safety data on combining immune checkpoint inhibitors and radiotherapy in breast cancer are limited because concurrent radiotherapy has typically been excluded in pivotal trials.
The 2020 KEYNOTE-522 trial did provide a rare look at concurrent radiotherapy and immunotherapy in early triple-negative breast cancer. The analysis found “no safety concerns” with concurrent radiotherapy and pembrolizumab, lead investigator Peter Schmid, MD, of Queen Mary University of London, England, told this news organization.
Research on other solid tumor types also suggests that radiotherapy “can be considered safe” alongside immunotherapy, the authors of a recent ESTRO consensus said.
Despite evidence indicating radiotherapy alongside immunotherapy can be safe in patients with breast cancer, “certain aspects, such as patient selection, total dose, and dose per fraction, remain open for debate to achieve the best therapeutic outcomes,” the ESTRO experts cautioned.
2. CDK4/6 inhibitors may be offered with radiotherapy in some settings, not others
CDK4/6 inhibitors are now standard of care for first- or second-line treatment in patients with advanced or metastatic hormone receptor–positive, human epidermal growth factor receptor 2 (HER2)–negative breast cancer.
“Unfortunately, we found no information regarding concurrent radiotherapy in the adjuvant setting” in pivotal trials for palbociclib, abemaciclib, and ribociclib, the ESTRO authors said. In the pivotal trials for palbociclib and abemaciclib, patients had to discontinue immunotherapy before initiating radiotherapy, and in the trial for ribociclib, palliative radiotherapy was allowed for relieving bone pain only.
However, in 2023, a team of experts from 12 countries attempted to piece together the available evidence, publishing a meta-analysis of 11 retrospective studies on the safety of CDK4/6 inhibitors given concurrently with radiotherapy in patients with metastatic disease.
Although most of these studies had small patient populations, the analysis revealed that CDK4/6 inhibitors given concurrently with radiotherapy in patients with metastatic breast cancer led to a similar side-effect profile to that observed in trials of the inhibitors given sequentially with adjuvant radiotherapy.
“These findings suggest that the simultaneous administration of CDK4/6 inhibitors and radiotherapy is generally well tolerated,” the ESTRO authors concluded but added that CDK4/6 inhibitors and concomitant radiotherapy should be investigated more in the adjuvant locoregional, whole brain, and intracranial stereotactic radiotherapy settings.
The expert panel did note, however, that CDK4/6 inhibitors and concomitant radiotherapy “could be offered” during palliative and ablative extracranial radiotherapy.
3. Only offer poly (ADP-ribose) polymerase (PARP) inhibitors plus radiotherapy in clinical trial setting
PARP inhibitors olaparib (Lynparza) and talazoprib (Talzenna) are standard of care in patients with metastatic breast cancer who have BRCA1/2 gene mutations. Olaparib is also indicated for high-risk early breast cancer following neoadjuvant or adjuvant chemotherapy.
But data on combining PARP inhibitors with radiotherapy in breast cancer also remain limited.
One ongoing phase 2 trial, comparing olaparib plus radiotherapy to radiotherapy alone in 300 people with inflammatory breast cancer, is aiming to tease out the safety of the combination and whether it improves local control in patients with aggressive disease.
“The desire is to explore the exciting possibility that low doses of PARP inhibition may radiosensitize tumor cells more than normal tissues,” Reshma Jagsi, MD, chair of the Department of Radiation Oncology at Emory University School of Medicine in Atlanta, Georgia, who is leading the study.
Because of potential good or bad interactions between new systemic therapies and radiotherapy, “intentional trial design” is important, Dr. Jagsi said, so we “know the best way to combine treatments in practice to optimize outcomes.”
But given the evidence to date, the ESTRO experts advised waiting until “further research provides more comprehensive safety and efficacy data” in the primary, adjuvant, and metastatic settings. The experts also advised not offering PARP inhibitors and concomitant radiotherapy to treat advanced breast cancer outside of clinical trials.
4. Phosphoinositide 3-kinase inhibitors (PI3K) inhibitors, mammalian target of rapamycin (mTOR) inhibitors, and newer targeted agents should not be offered concurrently with radiotherapy
Clinical trial data on the safety of combining PI3K and mTOR inhibitors with radiation are thin, especially in advanced breast cancer. Typically, radiotherapy within 4 weeks before randomization, or 2 weeks for palliative radiation, was excluded in pivotal trials.
For this reason, the ESTRO team recommended that concurrent radiation with either PI3K inhibitors or mTOR inhibitors “should not be offered.”
ESTRO also cautioned against providing radiation concurrently with newer anti-HER2 tyrosine-kinase drugs, such as neratinib or tucatinib, or newer antibody-drug conjugates such as trastuzumab deruxtecan, until more data emerge on the safety of these combinations.
5. Combining older HER2-targeted drugs and radiotherapy generally safe
The ESTRO authors agreed that older anti-HER2 drugs trastuzumab (Herceptin), pertuzumab (Perjeta), and lapatinib (Tykerb) can be safely used concurrently with locoregional radiotherapy as well.
One of the biggest concerns in the field is how to combine radiation with systemic therapies in the setting of brain metastases, and the data on these older anti-HER2 drugs are relatively clear that it’s safe, Dr. Miller said.
For instance, in a 2019 study of 84 patients with 487 brain metastases, stereotactic radiosurgery given alongside lapatinib led to significantly higher rates of complete responses than stereotactic radiosurgery alone (35% vs 11%) with no increased risk for radiation necrosis.
The ESTRO team agreed, noting that the latest evidence supports the use of trastuzumab, pertuzumab, or lapatinib alongside radiotherapy for whole brain and ablative intracranial stereotactic radiotherapy.
As for older antibody-drug conjugates, trastuzumab emtansine (T-DM1) plus radiotherapy “might be considered” during adjuvant locoregional radiotherapy for breast cancer but should not be offered for whole brain and ablative intracranial stereotactic radiotherapy, the ESTRO team said.
Dr. Jagsi declared the following conflicts in a recent 2024 publication: Stock options for advisory board role in Equity Quotient; grants or contracts from Genentech; and expert witness for Kleinbard, LLC, and Hawks Quindel Law. In the Keynote-522 trial publication Dr. Schmid declared relationships with AstraZeneca, Bayer, Boehringer Ingelheim, Celgene, Eisai, Hoffmann-La Roche, Genetech, Merck, Novartis, and Pfizer. Dr. Shah reported consulting for Impedimed, Videra Surgical, and PreludeDX.
A version of this article appeared on Medscape.com.
FDA Approves New Esophageal Cancer Drug
The US Food and Drug Administration (FDA) has approved tislelizumab-jsgr (Tevimbra, BeiGene Ltd.) as second-line monotherapy for certain adult patients with unresectable or metastatic esophageal squamous cell carcinoma (ESCC).
Specifically, the novel checkpoint inhibitor is approved for patients with ESCC after prior systemic chemotherapy that did not include a programmed death–ligand 1 (PD-L1) inhibitor.
Approval was based on findings from the open-label, phase 3 RATIONALE 302 trial showing a statistically significant and clinically meaningful overall survival benefit with tislelizumab vs investigator’s choice of chemotherapy.
Study participants included 512 adults enrolled at 123 research sites in 11 countries in Europe, Asia, and North America. Patients were randomly assigned to receive intravenous tislelizumab, a humanized immunoglobulin G4 anti-programmed cell death protein 1 monoclonal antibody, at a dose of 200 mg every 3 weeks or investigator’s choice of standard chemotherapy with paclitaxel, docetaxel, or irinotecan until disease progression, unacceptable toxicity, or study withdrawal.
Median overall survival in the intention-to-treat population, the primary study endpoint, was 8.6 months vs 6.3 months in the chemotherapy arms (hazard ratio [HR], 0.70). The survival benefit was observed across predefined subgroups, including baseline PD-L1 status and region. The new agent was also associated with improved overall response rate (20.4% vs 9.8%) and more durable response (median duration of response of 7.1 vs 4.0 months; HR, 0.42) compared with chemotherapy.
The most common adverse reactions for tislelizumab, each occurring in at least 20% of treated patients, included increased glucose and decreased hemoglobin, lymphocytes, sodium, and albumin as well as increased alkaline phosphatase, anemia, fatigue, increased aspartate aminotransferase, musculoskeletal pain, decreased weight, increased alanine aminotransferase, and cough.
Fewer patients in the tislelizumab arm experienced grade 3 or greater treatment-emergent adverse events compared with the chemotherapy arm (46% vs 68%, respectively), and fewer patients discontinued tislelizumab vs chemotherapy due to such an event (7% vs 14%).
“Patients diagnosed with advanced or metastasized ESCC, the most common histologic subtype of esophageal cancer, often progress following initial therapy and are in need of new options,” Syma Iqbal, MD, of the Norris Comprehensive Cancer Center, Keck School of Medicine, University of Southern California, stated in the BeiGene release. “The RATIONALE 302 trial showed that patients with previously treated ESCC who received Tevimbra saw a clinically meaningful survival benefit, highlighting its potential as an important treatment option for these patients.”
The approval, which was deferred in 2022 due to COVID-19-related restrictions, marks the first for the agent in the United States. Tislelizumab should be available in the United States in the second half of 2024, BeiGene noted.
The FDA is also reviewing a Biologics License Application for the agent as a first-line treatment for patients with unresectable, locally advanced, or metastatic ESCC and for those with locally advanced unresectable or metastatic gastric or gastroesophageal junction adenocarcinoma, BeiGene announced in a press release.
A version of this article appeared on Medscape.com.
The US Food and Drug Administration (FDA) has approved tislelizumab-jsgr (Tevimbra, BeiGene Ltd.) as second-line monotherapy for certain adult patients with unresectable or metastatic esophageal squamous cell carcinoma (ESCC).
Specifically, the novel checkpoint inhibitor is approved for patients with ESCC after prior systemic chemotherapy that did not include a programmed death–ligand 1 (PD-L1) inhibitor.
Approval was based on findings from the open-label, phase 3 RATIONALE 302 trial showing a statistically significant and clinically meaningful overall survival benefit with tislelizumab vs investigator’s choice of chemotherapy.
Study participants included 512 adults enrolled at 123 research sites in 11 countries in Europe, Asia, and North America. Patients were randomly assigned to receive intravenous tislelizumab, a humanized immunoglobulin G4 anti-programmed cell death protein 1 monoclonal antibody, at a dose of 200 mg every 3 weeks or investigator’s choice of standard chemotherapy with paclitaxel, docetaxel, or irinotecan until disease progression, unacceptable toxicity, or study withdrawal.
Median overall survival in the intention-to-treat population, the primary study endpoint, was 8.6 months vs 6.3 months in the chemotherapy arms (hazard ratio [HR], 0.70). The survival benefit was observed across predefined subgroups, including baseline PD-L1 status and region. The new agent was also associated with improved overall response rate (20.4% vs 9.8%) and more durable response (median duration of response of 7.1 vs 4.0 months; HR, 0.42) compared with chemotherapy.
The most common adverse reactions for tislelizumab, each occurring in at least 20% of treated patients, included increased glucose and decreased hemoglobin, lymphocytes, sodium, and albumin as well as increased alkaline phosphatase, anemia, fatigue, increased aspartate aminotransferase, musculoskeletal pain, decreased weight, increased alanine aminotransferase, and cough.
Fewer patients in the tislelizumab arm experienced grade 3 or greater treatment-emergent adverse events compared with the chemotherapy arm (46% vs 68%, respectively), and fewer patients discontinued tislelizumab vs chemotherapy due to such an event (7% vs 14%).
“Patients diagnosed with advanced or metastasized ESCC, the most common histologic subtype of esophageal cancer, often progress following initial therapy and are in need of new options,” Syma Iqbal, MD, of the Norris Comprehensive Cancer Center, Keck School of Medicine, University of Southern California, stated in the BeiGene release. “The RATIONALE 302 trial showed that patients with previously treated ESCC who received Tevimbra saw a clinically meaningful survival benefit, highlighting its potential as an important treatment option for these patients.”
The approval, which was deferred in 2022 due to COVID-19-related restrictions, marks the first for the agent in the United States. Tislelizumab should be available in the United States in the second half of 2024, BeiGene noted.
The FDA is also reviewing a Biologics License Application for the agent as a first-line treatment for patients with unresectable, locally advanced, or metastatic ESCC and for those with locally advanced unresectable or metastatic gastric or gastroesophageal junction adenocarcinoma, BeiGene announced in a press release.
A version of this article appeared on Medscape.com.
The US Food and Drug Administration (FDA) has approved tislelizumab-jsgr (Tevimbra, BeiGene Ltd.) as second-line monotherapy for certain adult patients with unresectable or metastatic esophageal squamous cell carcinoma (ESCC).
Specifically, the novel checkpoint inhibitor is approved for patients with ESCC after prior systemic chemotherapy that did not include a programmed death–ligand 1 (PD-L1) inhibitor.
Approval was based on findings from the open-label, phase 3 RATIONALE 302 trial showing a statistically significant and clinically meaningful overall survival benefit with tislelizumab vs investigator’s choice of chemotherapy.
Study participants included 512 adults enrolled at 123 research sites in 11 countries in Europe, Asia, and North America. Patients were randomly assigned to receive intravenous tislelizumab, a humanized immunoglobulin G4 anti-programmed cell death protein 1 monoclonal antibody, at a dose of 200 mg every 3 weeks or investigator’s choice of standard chemotherapy with paclitaxel, docetaxel, or irinotecan until disease progression, unacceptable toxicity, or study withdrawal.
Median overall survival in the intention-to-treat population, the primary study endpoint, was 8.6 months vs 6.3 months in the chemotherapy arms (hazard ratio [HR], 0.70). The survival benefit was observed across predefined subgroups, including baseline PD-L1 status and region. The new agent was also associated with improved overall response rate (20.4% vs 9.8%) and more durable response (median duration of response of 7.1 vs 4.0 months; HR, 0.42) compared with chemotherapy.
The most common adverse reactions for tislelizumab, each occurring in at least 20% of treated patients, included increased glucose and decreased hemoglobin, lymphocytes, sodium, and albumin as well as increased alkaline phosphatase, anemia, fatigue, increased aspartate aminotransferase, musculoskeletal pain, decreased weight, increased alanine aminotransferase, and cough.
Fewer patients in the tislelizumab arm experienced grade 3 or greater treatment-emergent adverse events compared with the chemotherapy arm (46% vs 68%, respectively), and fewer patients discontinued tislelizumab vs chemotherapy due to such an event (7% vs 14%).
“Patients diagnosed with advanced or metastasized ESCC, the most common histologic subtype of esophageal cancer, often progress following initial therapy and are in need of new options,” Syma Iqbal, MD, of the Norris Comprehensive Cancer Center, Keck School of Medicine, University of Southern California, stated in the BeiGene release. “The RATIONALE 302 trial showed that patients with previously treated ESCC who received Tevimbra saw a clinically meaningful survival benefit, highlighting its potential as an important treatment option for these patients.”
The approval, which was deferred in 2022 due to COVID-19-related restrictions, marks the first for the agent in the United States. Tislelizumab should be available in the United States in the second half of 2024, BeiGene noted.
The FDA is also reviewing a Biologics License Application for the agent as a first-line treatment for patients with unresectable, locally advanced, or metastatic ESCC and for those with locally advanced unresectable or metastatic gastric or gastroesophageal junction adenocarcinoma, BeiGene announced in a press release.
A version of this article appeared on Medscape.com.
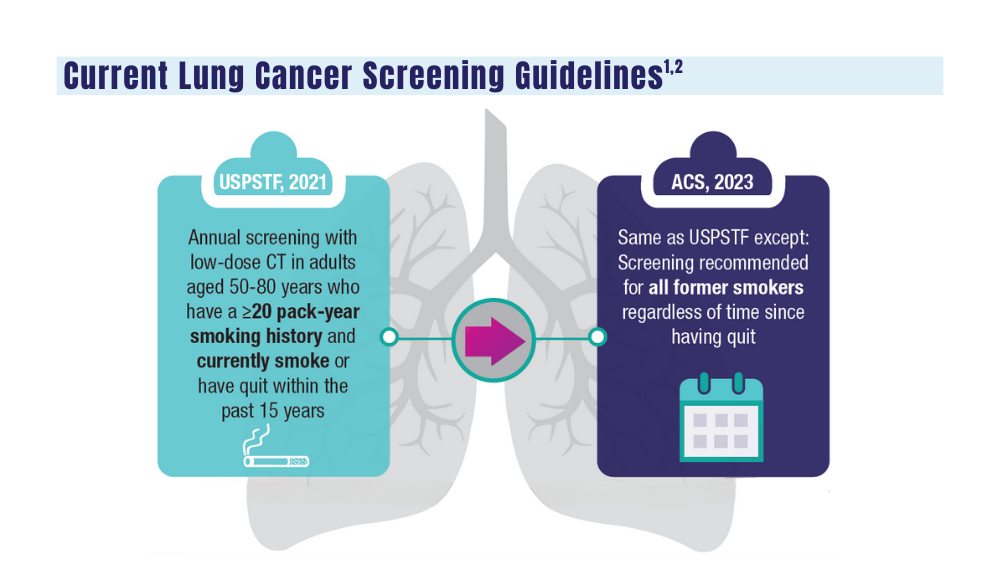
Cancer Data Trends 2024: Lung Cancer
1. Wolf AMD, Oeffinger KC, Shih TYC, et al. Screening for lung cancer: 2023 guideline update from the American Cancer Society. CA Cancer J Clin. 2023;10.3322/caac.21811. doi:10.3322/caac.21811
2. US Department of Veterans Affairs. VA promotes high-quality, patient-centered lung cancer screening for veterans. Published June 15, 2023. Accessed December 18, 2023. http://www.hsrd.research.va.gov/impacts/lcs.cfm
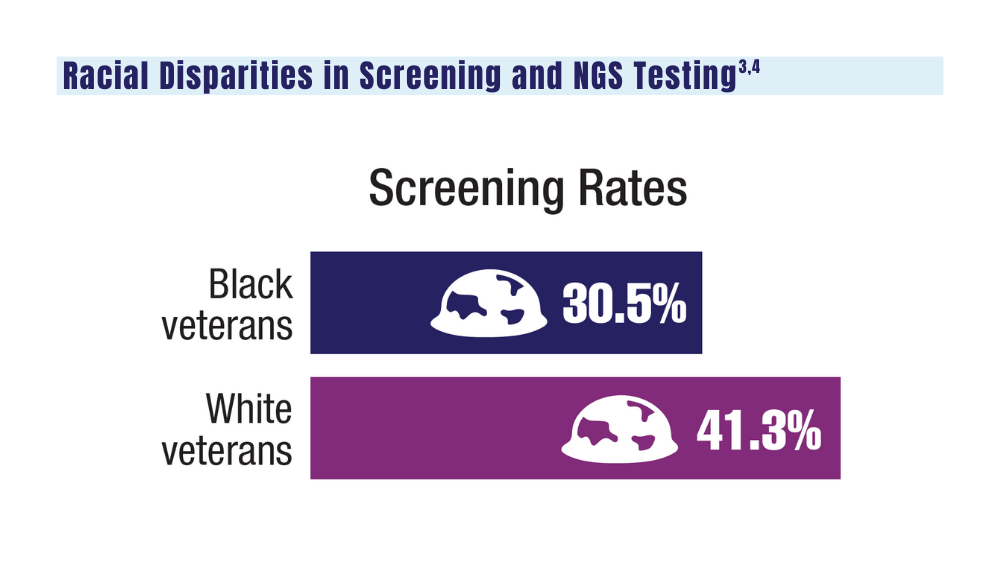
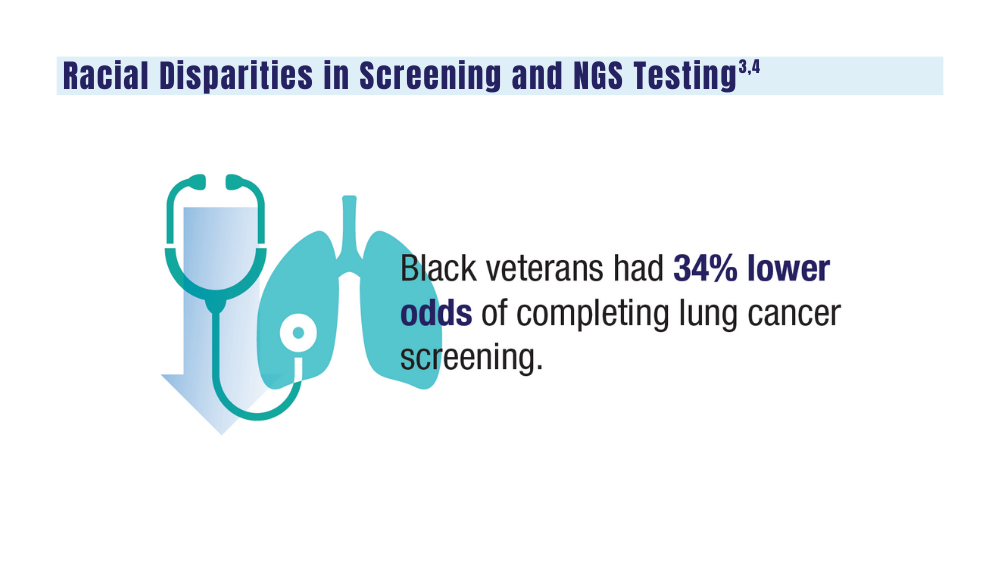
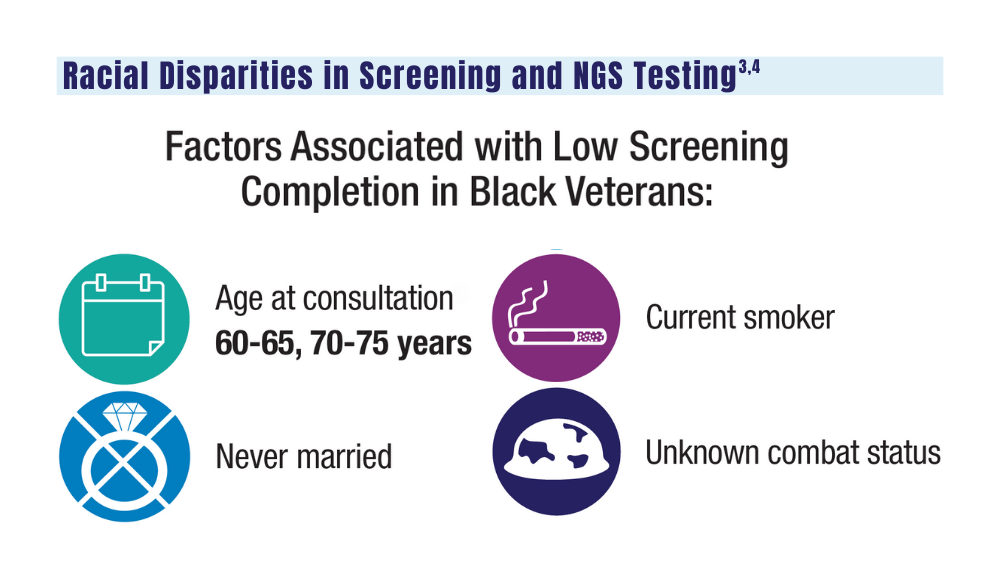
3. Navuluri N, Morrison S, Green CL, et al. Racial disparities in lung cancer screening among veterans, 2013 to 2021. JAMA Netw Open. 2023;6(6):e2318795. doi:10.1001/jamanetworkopen.2023.18795
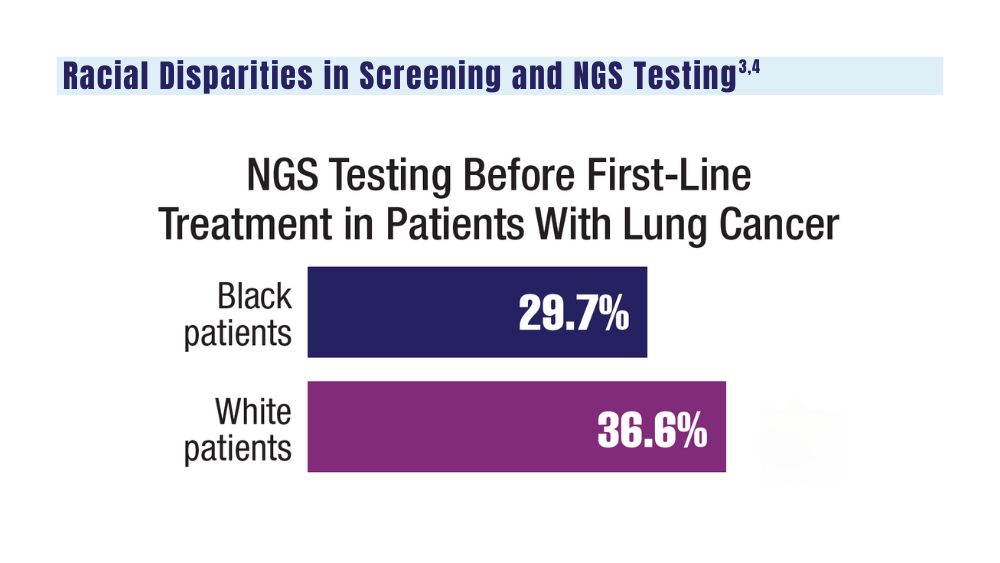
4. Bruno DS, Hess LM, Li X, Su EW, Patel M. Disparities in biomarker testing and clinical trial enrollment among patients with lung, breast, or colorectal cancers in the United States. JCO Precis Oncol. 2022;6:e2100427. doi:10.1200/PO.21.00427
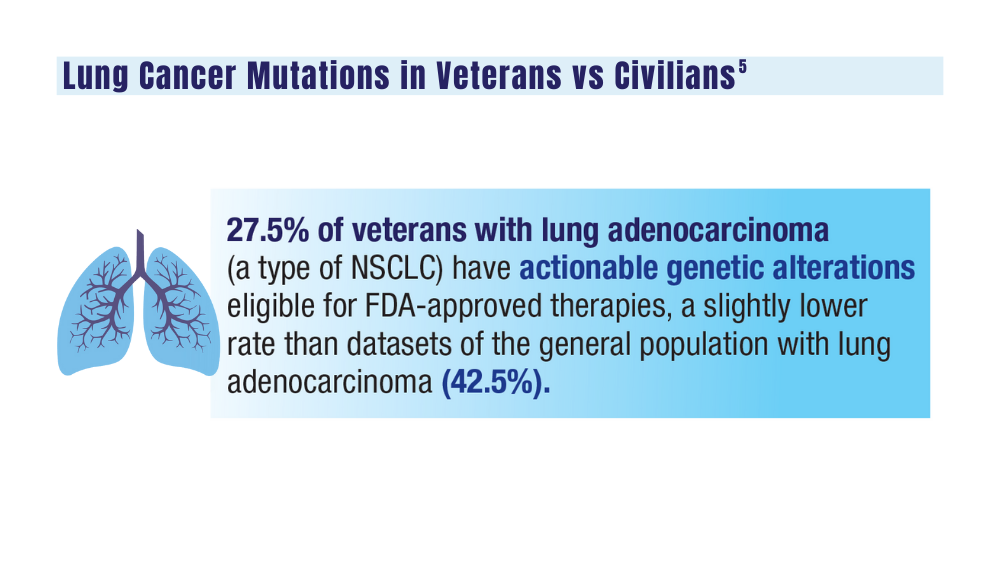
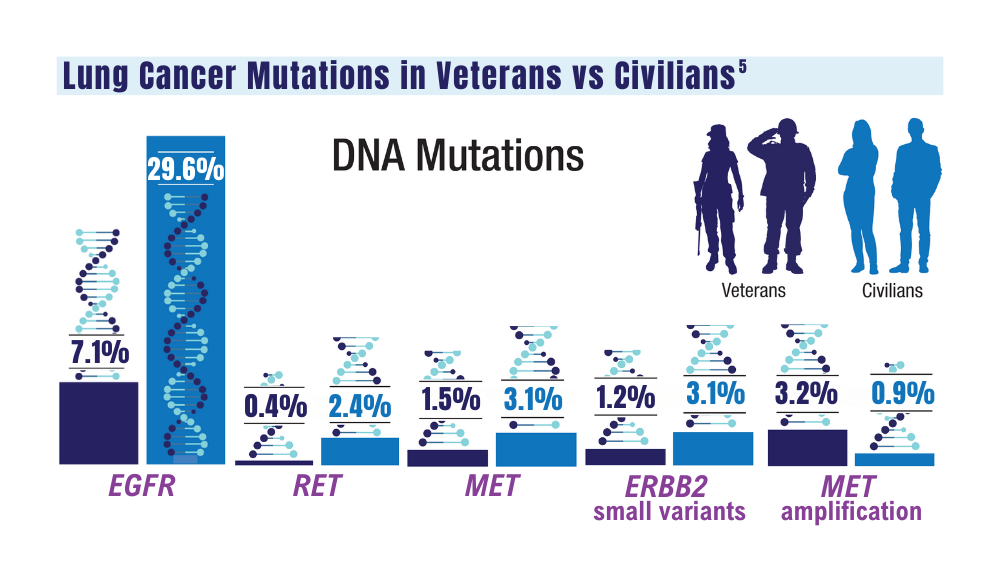
5. Jalal SI, Guo A, Ahmed S, Kelley MJ. Analysis of actionable genetic alterations in lung carcinoma from the VA National Precision Oncology Program. Semin Oncol. 2022;S0093-7754(22)00054-9. doi:10.1053/j.seminoncol.2022.06.014
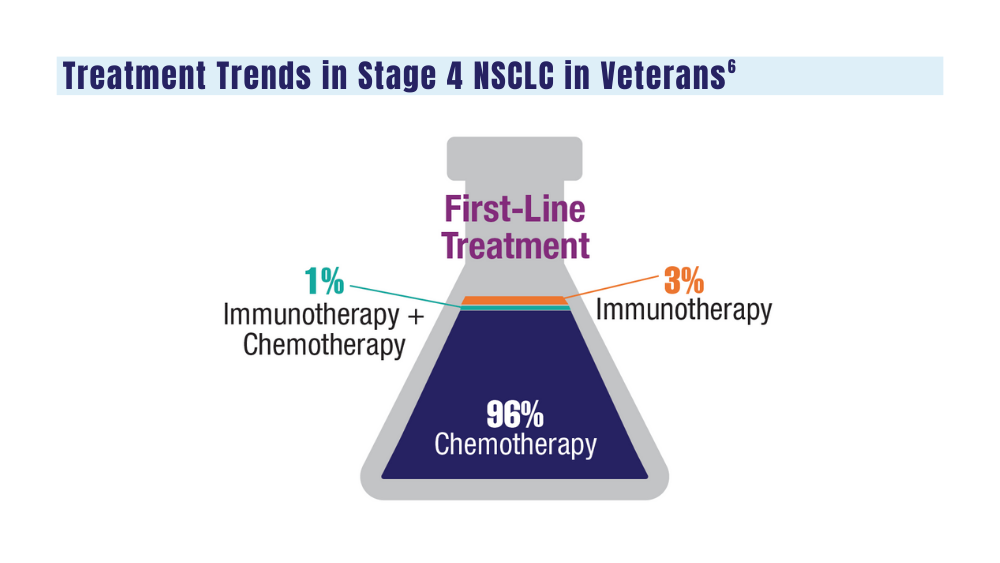
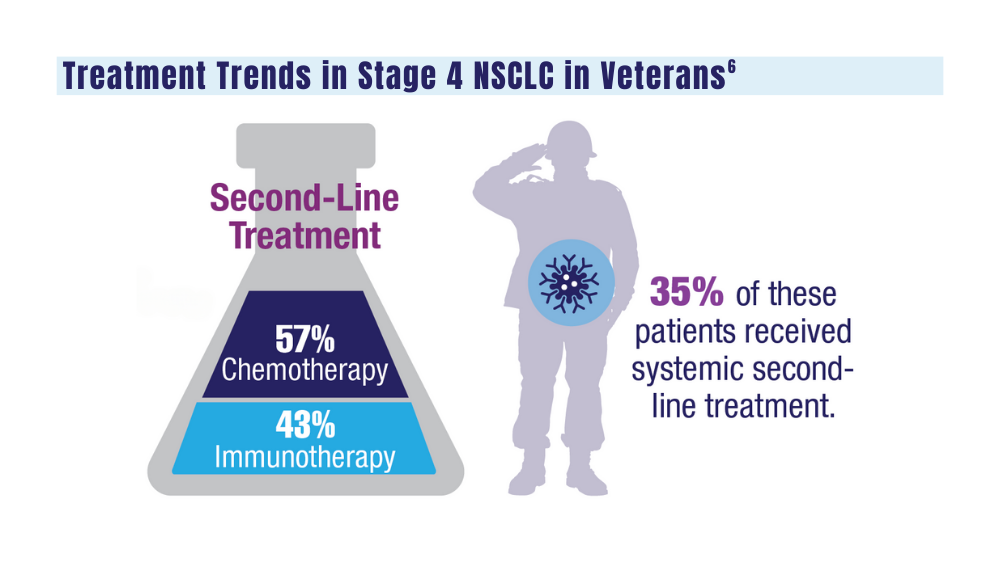
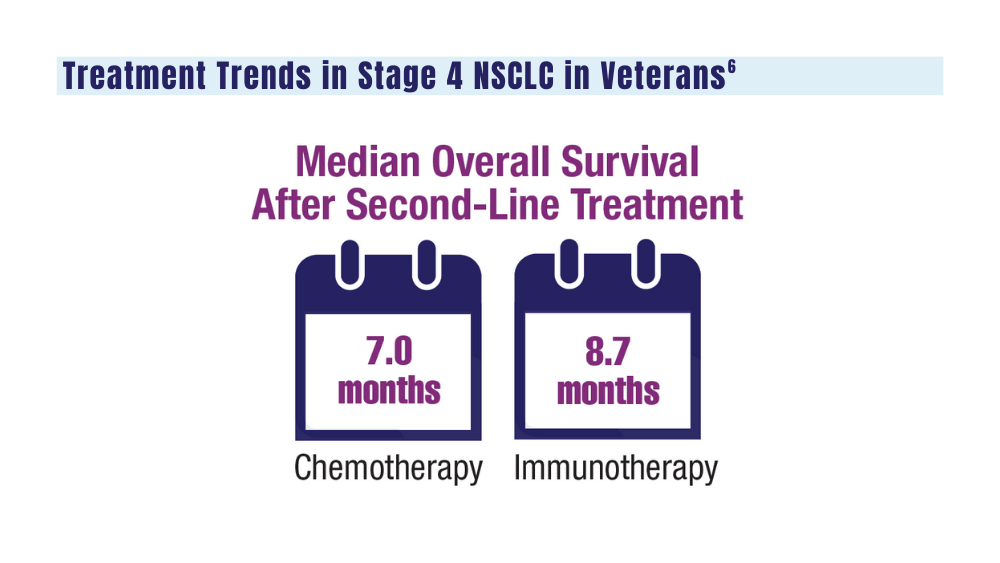
6. Williams CD, Allo MA, Gu L, Vashistha V, Press A, Kelley M. Health outcomes and healthcare resource utilization among veterans with stage IV non-small cell lung cancer treated with second-line chemotherapy versus immunotherapy. PLoS One. 2023;18(2):e0282020. doi:10.1371/journal.pone.0282020
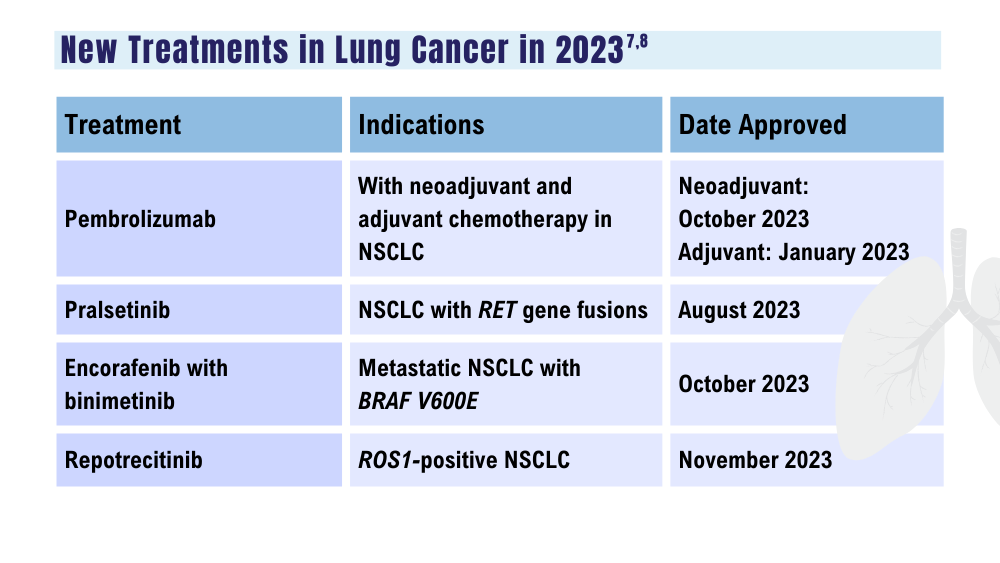
7. US Food and Drug Administration. Oncology (cancer)/hematologic malignancies approval notifications. Updated December 15, 2023. Accessed December 18, 2023. https://www.fda.gov/drugs/resources-information-approved-drugs/oncology-cancer-hematologic-malignancies-approval-notifications
8. Paz-Ares L, Chen Y, Reinmuth N, et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer: 3-year overall survival update from CASPIAN. ESMO Open. 2022;7(2):100408. doi:10.1016/j.esmoop.2022.100408
1. Wolf AMD, Oeffinger KC, Shih TYC, et al. Screening for lung cancer: 2023 guideline update from the American Cancer Society. CA Cancer J Clin. 2023;10.3322/caac.21811. doi:10.3322/caac.21811
2. US Department of Veterans Affairs. VA promotes high-quality, patient-centered lung cancer screening for veterans. Published June 15, 2023. Accessed December 18, 2023. http://www.hsrd.research.va.gov/impacts/lcs.cfm
3. Navuluri N, Morrison S, Green CL, et al. Racial disparities in lung cancer screening among veterans, 2013 to 2021. JAMA Netw Open. 2023;6(6):e2318795. doi:10.1001/jamanetworkopen.2023.18795
4. Bruno DS, Hess LM, Li X, Su EW, Patel M. Disparities in biomarker testing and clinical trial enrollment among patients with lung, breast, or colorectal cancers in the United States. JCO Precis Oncol. 2022;6:e2100427. doi:10.1200/PO.21.00427
5. Jalal SI, Guo A, Ahmed S, Kelley MJ. Analysis of actionable genetic alterations in lung carcinoma from the VA National Precision Oncology Program. Semin Oncol. 2022;S0093-7754(22)00054-9. doi:10.1053/j.seminoncol.2022.06.014
6. Williams CD, Allo MA, Gu L, Vashistha V, Press A, Kelley M. Health outcomes and healthcare resource utilization among veterans with stage IV non-small cell lung cancer treated with second-line chemotherapy versus immunotherapy. PLoS One. 2023;18(2):e0282020. doi:10.1371/journal.pone.0282020
7. US Food and Drug Administration. Oncology (cancer)/hematologic malignancies approval notifications. Updated December 15, 2023. Accessed December 18, 2023. https://www.fda.gov/drugs/resources-information-approved-drugs/oncology-cancer-hematologic-malignancies-approval-notifications
8. Paz-Ares L, Chen Y, Reinmuth N, et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer: 3-year overall survival update from CASPIAN. ESMO Open. 2022;7(2):100408. doi:10.1016/j.esmoop.2022.100408
1. Wolf AMD, Oeffinger KC, Shih TYC, et al. Screening for lung cancer: 2023 guideline update from the American Cancer Society. CA Cancer J Clin. 2023;10.3322/caac.21811. doi:10.3322/caac.21811
2. US Department of Veterans Affairs. VA promotes high-quality, patient-centered lung cancer screening for veterans. Published June 15, 2023. Accessed December 18, 2023. http://www.hsrd.research.va.gov/impacts/lcs.cfm
3. Navuluri N, Morrison S, Green CL, et al. Racial disparities in lung cancer screening among veterans, 2013 to 2021. JAMA Netw Open. 2023;6(6):e2318795. doi:10.1001/jamanetworkopen.2023.18795
4. Bruno DS, Hess LM, Li X, Su EW, Patel M. Disparities in biomarker testing and clinical trial enrollment among patients with lung, breast, or colorectal cancers in the United States. JCO Precis Oncol. 2022;6:e2100427. doi:10.1200/PO.21.00427
5. Jalal SI, Guo A, Ahmed S, Kelley MJ. Analysis of actionable genetic alterations in lung carcinoma from the VA National Precision Oncology Program. Semin Oncol. 2022;S0093-7754(22)00054-9. doi:10.1053/j.seminoncol.2022.06.014
6. Williams CD, Allo MA, Gu L, Vashistha V, Press A, Kelley M. Health outcomes and healthcare resource utilization among veterans with stage IV non-small cell lung cancer treated with second-line chemotherapy versus immunotherapy. PLoS One. 2023;18(2):e0282020. doi:10.1371/journal.pone.0282020
7. US Food and Drug Administration. Oncology (cancer)/hematologic malignancies approval notifications. Updated December 15, 2023. Accessed December 18, 2023. https://www.fda.gov/drugs/resources-information-approved-drugs/oncology-cancer-hematologic-malignancies-approval-notifications
8. Paz-Ares L, Chen Y, Reinmuth N, et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer: 3-year overall survival update from CASPIAN. ESMO Open. 2022;7(2):100408. doi:10.1016/j.esmoop.2022.100408
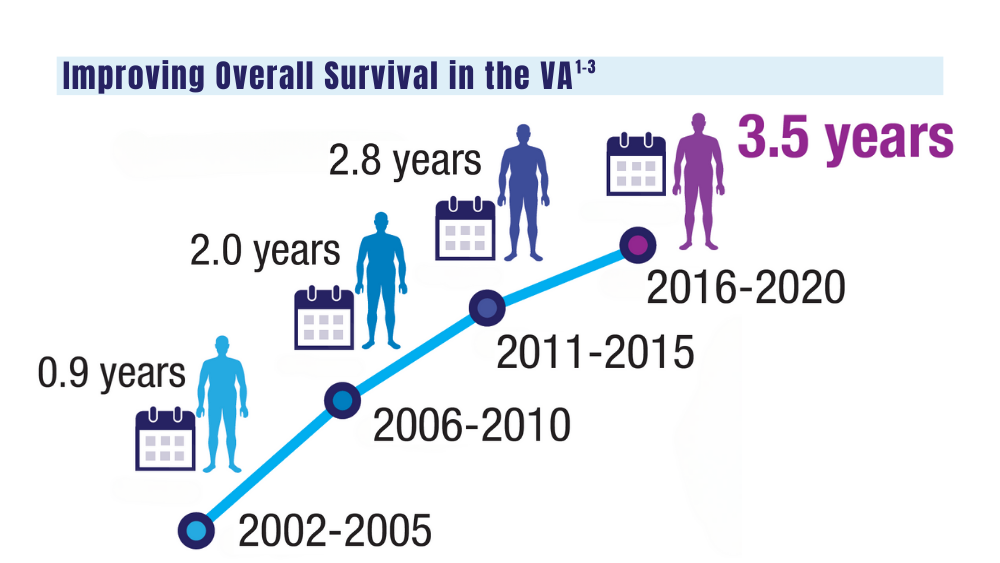
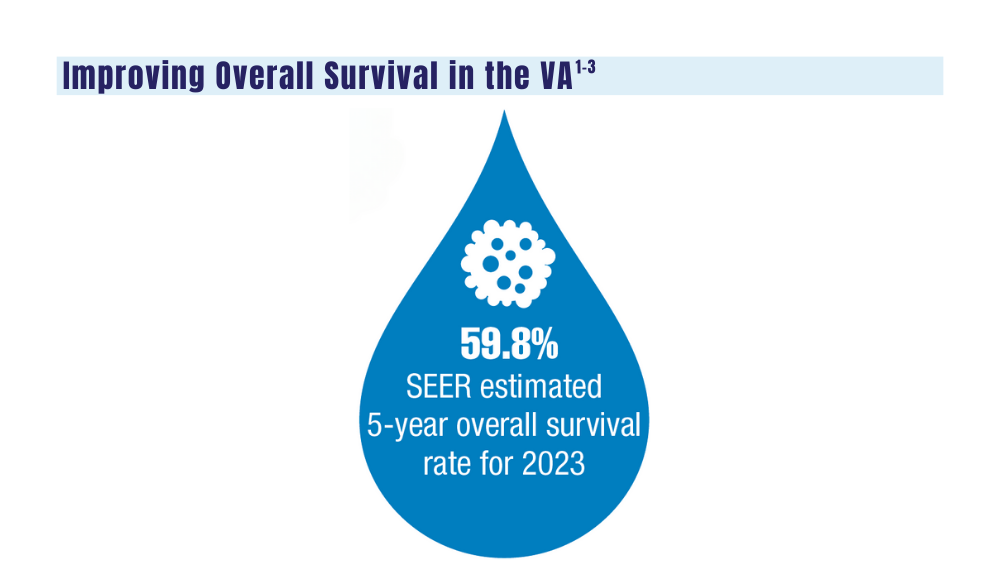
Cancer Data Trends 2024: Multiple Myeloma
1. Mahmood S, Gupta P, Ma H. Impact of time period of diagnosis, race, and military exposures on the survival of US military veterans with multiple myeloma and/or plasmacytoma. J Clin Oncol. 2023;41(16 suppl). Abstract e20061. https://doi.org/10.1200/jco.2023.41.16_suppl.e20061
2. National Cancer Institute. Cancer stat facts: myeloma. Accessed January 2, 2024. https://seer.cancer.gov/statfacts/html/mulmy.html
3. Dimopoulos MA, Moreau P, Terpos E, et al. Multiple myeloma: EHA-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up [published correction appears in Ann Oncol. 2022;33(1):117]. Ann Oncol. 2021;32(3):309-322. doi: 10.1016/j.annonc.2020.11.014
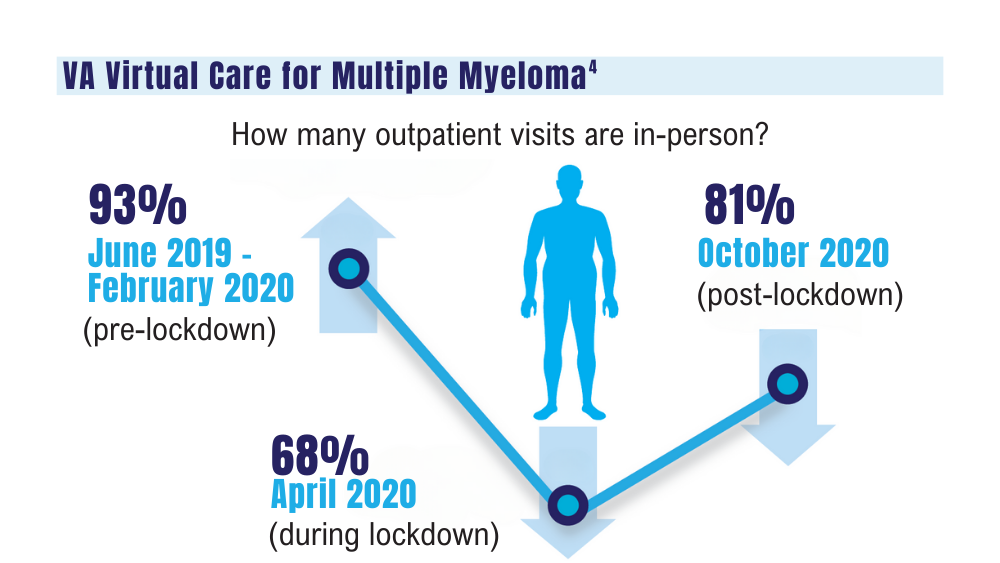
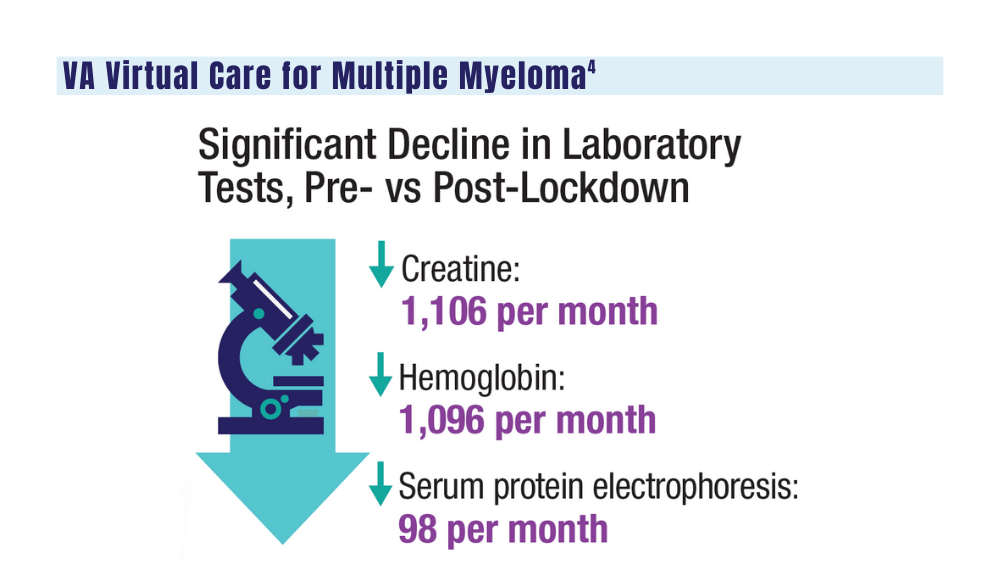
4. Su CT, Chen JC, Sussman JB. Virtual care for multiple myeloma in the COVID-19 era: interrupted time series analysis of Veterans Health Administration data. Leuk Lymphoma. 2023;64(5):1035-1039. doi: 10.1080/10428194.2023.2189989
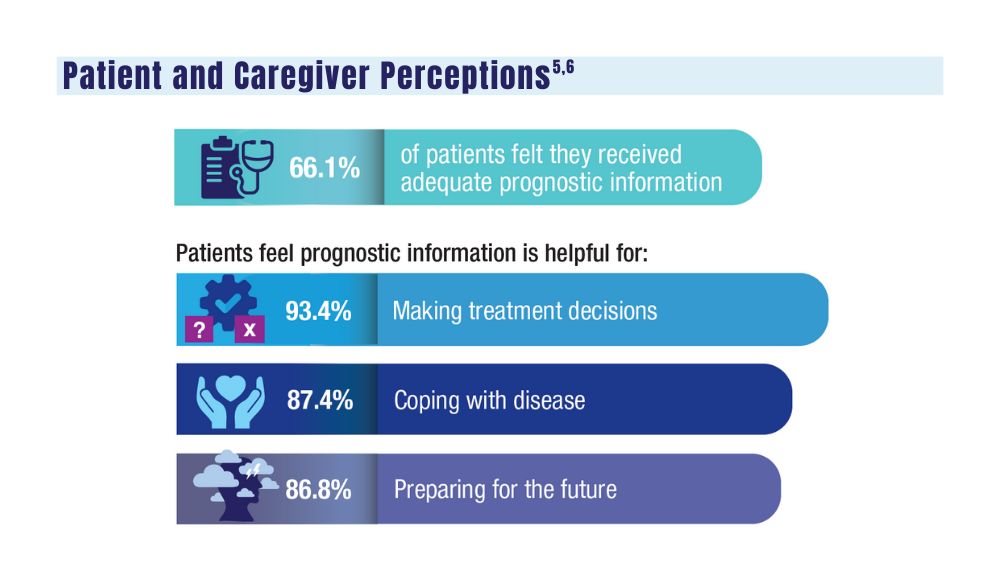
5. O’Donnell EK, Shapiro YN, Yee AJ, et al. Quality of life, psychological distress, and prognostic perceptions in patients with multiple myeloma. Cancer. 2022;128(10):1996-2004. doi: 10.1002/cncr.34134
6. O’Donnell EK, Shapiro YN, Yee AJ, et al. Quality of life, psychological distress, and prognostic perceptions in caregivers of patients with multiple myeloma. Blood Adv. 2022;6(17):4967-4974. doi: 10.1182/bloodadvances.2022007127
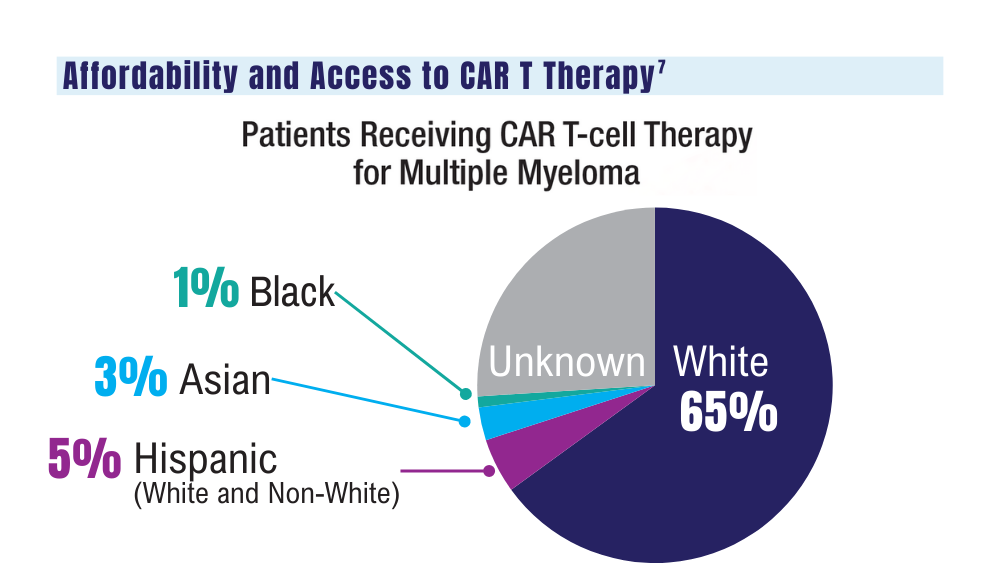
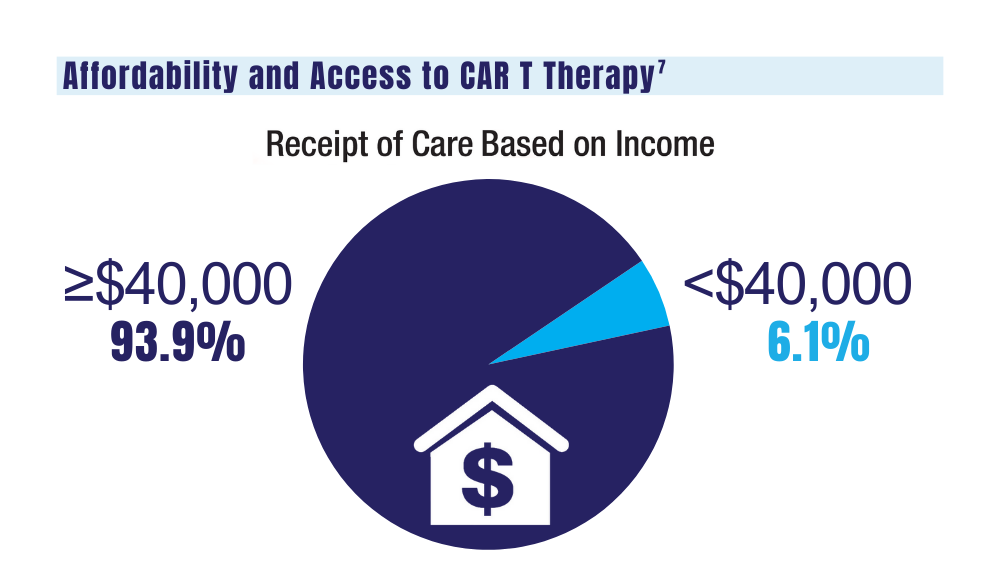
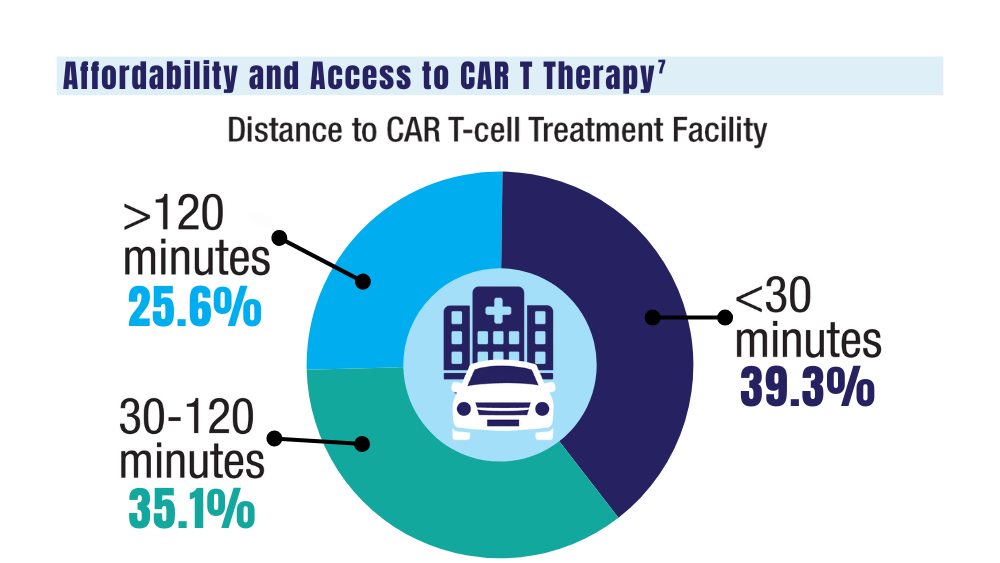
7. Ahmed N, Shahzad M, Shippey E, et al. Socioeconomic and racial disparity in chimeric antigen receptor T cell therapy access. Transplant Cell Ther. 2022;28(7):358-364. doi: 10.1016/j.jtct.2022.04.008
1. Mahmood S, Gupta P, Ma H. Impact of time period of diagnosis, race, and military exposures on the survival of US military veterans with multiple myeloma and/or plasmacytoma. J Clin Oncol. 2023;41(16 suppl). Abstract e20061. https://doi.org/10.1200/jco.2023.41.16_suppl.e20061
2. National Cancer Institute. Cancer stat facts: myeloma. Accessed January 2, 2024. https://seer.cancer.gov/statfacts/html/mulmy.html
3. Dimopoulos MA, Moreau P, Terpos E, et al. Multiple myeloma: EHA-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up [published correction appears in Ann Oncol. 2022;33(1):117]. Ann Oncol. 2021;32(3):309-322. doi: 10.1016/j.annonc.2020.11.014
4. Su CT, Chen JC, Sussman JB. Virtual care for multiple myeloma in the COVID-19 era: interrupted time series analysis of Veterans Health Administration data. Leuk Lymphoma. 2023;64(5):1035-1039. doi: 10.1080/10428194.2023.2189989
5. O’Donnell EK, Shapiro YN, Yee AJ, et al. Quality of life, psychological distress, and prognostic perceptions in patients with multiple myeloma. Cancer. 2022;128(10):1996-2004. doi: 10.1002/cncr.34134
6. O’Donnell EK, Shapiro YN, Yee AJ, et al. Quality of life, psychological distress, and prognostic perceptions in caregivers of patients with multiple myeloma. Blood Adv. 2022;6(17):4967-4974. doi: 10.1182/bloodadvances.2022007127
7. Ahmed N, Shahzad M, Shippey E, et al. Socioeconomic and racial disparity in chimeric antigen receptor T cell therapy access. Transplant Cell Ther. 2022;28(7):358-364. doi: 10.1016/j.jtct.2022.04.008
1. Mahmood S, Gupta P, Ma H. Impact of time period of diagnosis, race, and military exposures on the survival of US military veterans with multiple myeloma and/or plasmacytoma. J Clin Oncol. 2023;41(16 suppl). Abstract e20061. https://doi.org/10.1200/jco.2023.41.16_suppl.e20061
2. National Cancer Institute. Cancer stat facts: myeloma. Accessed January 2, 2024. https://seer.cancer.gov/statfacts/html/mulmy.html
3. Dimopoulos MA, Moreau P, Terpos E, et al. Multiple myeloma: EHA-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up [published correction appears in Ann Oncol. 2022;33(1):117]. Ann Oncol. 2021;32(3):309-322. doi: 10.1016/j.annonc.2020.11.014
4. Su CT, Chen JC, Sussman JB. Virtual care for multiple myeloma in the COVID-19 era: interrupted time series analysis of Veterans Health Administration data. Leuk Lymphoma. 2023;64(5):1035-1039. doi: 10.1080/10428194.2023.2189989
5. O’Donnell EK, Shapiro YN, Yee AJ, et al. Quality of life, psychological distress, and prognostic perceptions in patients with multiple myeloma. Cancer. 2022;128(10):1996-2004. doi: 10.1002/cncr.34134
6. O’Donnell EK, Shapiro YN, Yee AJ, et al. Quality of life, psychological distress, and prognostic perceptions in caregivers of patients with multiple myeloma. Blood Adv. 2022;6(17):4967-4974. doi: 10.1182/bloodadvances.2022007127
7. Ahmed N, Shahzad M, Shippey E, et al. Socioeconomic and racial disparity in chimeric antigen receptor T cell therapy access. Transplant Cell Ther. 2022;28(7):358-364. doi: 10.1016/j.jtct.2022.04.008
Survival Advantage of Adjuvant IO ‘Big News’ in Renal Cancer
This transcript has been edited for clarity.
Hi. I’m Brian Rini. I’m an Ingram Professor of Medicine at Vanderbilt-Ingram Cancer Center in Nashville, Tennessee. I think there’s three main areas: adjuvant therapy in kidney cancer, frontline therapy in advanced disease, and the refractory space.
To open with adjuvant therapy, the biggest news in kidney cancer, and probably all of GU cancer at ASCO GU this year, was the adjuvant pembrolizumab overall survival data. This KEYNOTE study had previously shown disease-free survival advantages over placebo in a population with high-risk resected kidney cancer. There was a trend toward overall survival, but it was not significant in those early analyses.
Now with nearly 5 years of follow-up, we see an overall survival advantage, with a hazard ratio in the 0.6 range — so, about a 40% reduction in the risk for death among these patients receiving adjuvant pembrolizumab (pembro). This was really important for the field. It’s been difficult to show a survival advantage, even in diseases like melanoma, which is considered at least as much, if not more immune responsive, and I think puts into perspective whether to offer this drug to high-risk resected patients. And it certainly needs to be considered for this population.
I think the balance on that — and this came out in some of the questions after the session — was around how many of the placebo recipients got salvage immune therapy, which would be a standard of care. But in the countries where this was done, it’s not really clear how many actually got therapy. We know most patients got some salvage therapy, be it local or systemic, and about half the patients got immune therapy. But some more granular detail would be necessary.
The other thing I would mention is that this was paired with the previous presentation, which was adjuvant nivolumab. It was a very similar study, a similar drug in a similar setting, but it did not show any advantages of either disease-free or overall survival. This comes on the heels of other negative studies and a negative ipilimumab/nivolumab (ipi/nivo) study in this setting, part of the same study.
The reasons for these discrepancies are not entirely clear. There’s differences in populations and duration of therapy and mechanism, and all sorts of things. I don’t think anybody’s really been able to come up with one reason why we have some negative immune trials in kidney cancer and one shiningly positive one. But be that as it may, I think the take-home was that adjuvant pembro is certainly a standard of care in high-risk disease, and a benefit/risk discussion needs to be had with each individual patient. And I think pembro will be the building block for future studies, some of which are ongoing.
The second major area of update was in frontline kidney cancer. There weren’t a lot of new data, but there were updates to the existing trials. As you may know, frontline immune-based doublet is a standard of care in this disease: either ipi/nivo or one of the immuno-oncology/tyrosine kinase inhibitor (IO/TKI) regimens. We had two updates. One was an 8-year update on ipi/nivo. It’s a really long follow-up for these patients now, and what was observed was that these results remain remarkably consistent.
The hazard ratios for benefit in terms of survival and durability of response are really consistent over the past several years — again, a hallmark of immune therapy. Over half the responders are still responding now, many years later. I think that only strengthens the position of ipi/nivo as a choice for advanced clear cell kidney cancer patients. Again, there are good long-term toxicity data, and some patients can remain off treatment in what’s called treatment-free survival. So, an important update. We look forward to future, probably 10-year, data.
The CheckMate 9ER cabozantinib/nivolumab (cabo/nivo) study was updated now with many years of follow-up, as some of the other IO/TKI regimens have as well. And I think there is a similar theme, although a few years behind in maturity from the ipi/nivo data. It shows persistence of benefit. With IO/TKI regimens, a lot of the benefit is up front. It’s high response rates. It’s progression-free survival (PFS). But we’re starting to see some of that durability.
Where it’ll land, if there will be a tail of the curve and where it will be, is unclear, but these updates are important in terms of counseling patients. Patients want to know not just what’s going to happen at their first scan but also years from now. And they’re planning to be around years from now. So, I think these data are important.
The last thing I’ll mention is a health-related quality-of-life update from what was called the 005 trial of belzutifan, an oral HIF inhibitor, compared with everolimus. We heard data at the European Society for Medical Oncology (ESMO) Congress 2023 on a PFS and response-rate advantage. The drug was approved by the US Food and Drug Administration (FDA) in late December, and now we see some quality-of-life data.
Quality-of-life questionnaires and scales have a lot of imperfections. I don’t think they necessarily capture everything we want. But in this case, it was fairly clean in that belzutifan is known to be a well-tolerated agent. The toxicity profile is clean. It’s been used for years in patients with Von Hippel-Lindau syndrome, certainly in the trials for years, and has shown good tolerance over time. So, I view these data as complementary to what we already knew about the drug, but they’re nice to see.
It’s nice to see datasets come together and show the same thing: Not only is the drug active in a refractory renal cell carcinoma (RCC) setting, but also it’s really well tolerated and does not adversely impact patients› quality of life. I use this drug a lot in refractory kidney cancer, and because it’s so well tolerated. That means it’s also combinable. And there are some very large studies in the front-end second-line space combining it, in a space where people believe that it has more activity. But there are some complementary data as we wait for the overall survival signal, hopefully, from this regimen.
So, there have been some exciting updates, mostly in the adjuvant space but also in some other spaces in kidney cancer and building upon some of the clinical advances that we had seen from previous meetings. I’m Brian Rini, and I appreciate you attending.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Brian Rini. I’m an Ingram Professor of Medicine at Vanderbilt-Ingram Cancer Center in Nashville, Tennessee. I think there’s three main areas: adjuvant therapy in kidney cancer, frontline therapy in advanced disease, and the refractory space.
To open with adjuvant therapy, the biggest news in kidney cancer, and probably all of GU cancer at ASCO GU this year, was the adjuvant pembrolizumab overall survival data. This KEYNOTE study had previously shown disease-free survival advantages over placebo in a population with high-risk resected kidney cancer. There was a trend toward overall survival, but it was not significant in those early analyses.
Now with nearly 5 years of follow-up, we see an overall survival advantage, with a hazard ratio in the 0.6 range — so, about a 40% reduction in the risk for death among these patients receiving adjuvant pembrolizumab (pembro). This was really important for the field. It’s been difficult to show a survival advantage, even in diseases like melanoma, which is considered at least as much, if not more immune responsive, and I think puts into perspective whether to offer this drug to high-risk resected patients. And it certainly needs to be considered for this population.
I think the balance on that — and this came out in some of the questions after the session — was around how many of the placebo recipients got salvage immune therapy, which would be a standard of care. But in the countries where this was done, it’s not really clear how many actually got therapy. We know most patients got some salvage therapy, be it local or systemic, and about half the patients got immune therapy. But some more granular detail would be necessary.
The other thing I would mention is that this was paired with the previous presentation, which was adjuvant nivolumab. It was a very similar study, a similar drug in a similar setting, but it did not show any advantages of either disease-free or overall survival. This comes on the heels of other negative studies and a negative ipilimumab/nivolumab (ipi/nivo) study in this setting, part of the same study.
The reasons for these discrepancies are not entirely clear. There’s differences in populations and duration of therapy and mechanism, and all sorts of things. I don’t think anybody’s really been able to come up with one reason why we have some negative immune trials in kidney cancer and one shiningly positive one. But be that as it may, I think the take-home was that adjuvant pembro is certainly a standard of care in high-risk disease, and a benefit/risk discussion needs to be had with each individual patient. And I think pembro will be the building block for future studies, some of which are ongoing.
The second major area of update was in frontline kidney cancer. There weren’t a lot of new data, but there were updates to the existing trials. As you may know, frontline immune-based doublet is a standard of care in this disease: either ipi/nivo or one of the immuno-oncology/tyrosine kinase inhibitor (IO/TKI) regimens. We had two updates. One was an 8-year update on ipi/nivo. It’s a really long follow-up for these patients now, and what was observed was that these results remain remarkably consistent.
The hazard ratios for benefit in terms of survival and durability of response are really consistent over the past several years — again, a hallmark of immune therapy. Over half the responders are still responding now, many years later. I think that only strengthens the position of ipi/nivo as a choice for advanced clear cell kidney cancer patients. Again, there are good long-term toxicity data, and some patients can remain off treatment in what’s called treatment-free survival. So, an important update. We look forward to future, probably 10-year, data.
The CheckMate 9ER cabozantinib/nivolumab (cabo/nivo) study was updated now with many years of follow-up, as some of the other IO/TKI regimens have as well. And I think there is a similar theme, although a few years behind in maturity from the ipi/nivo data. It shows persistence of benefit. With IO/TKI regimens, a lot of the benefit is up front. It’s high response rates. It’s progression-free survival (PFS). But we’re starting to see some of that durability.
Where it’ll land, if there will be a tail of the curve and where it will be, is unclear, but these updates are important in terms of counseling patients. Patients want to know not just what’s going to happen at their first scan but also years from now. And they’re planning to be around years from now. So, I think these data are important.
The last thing I’ll mention is a health-related quality-of-life update from what was called the 005 trial of belzutifan, an oral HIF inhibitor, compared with everolimus. We heard data at the European Society for Medical Oncology (ESMO) Congress 2023 on a PFS and response-rate advantage. The drug was approved by the US Food and Drug Administration (FDA) in late December, and now we see some quality-of-life data.
Quality-of-life questionnaires and scales have a lot of imperfections. I don’t think they necessarily capture everything we want. But in this case, it was fairly clean in that belzutifan is known to be a well-tolerated agent. The toxicity profile is clean. It’s been used for years in patients with Von Hippel-Lindau syndrome, certainly in the trials for years, and has shown good tolerance over time. So, I view these data as complementary to what we already knew about the drug, but they’re nice to see.
It’s nice to see datasets come together and show the same thing: Not only is the drug active in a refractory renal cell carcinoma (RCC) setting, but also it’s really well tolerated and does not adversely impact patients› quality of life. I use this drug a lot in refractory kidney cancer, and because it’s so well tolerated. That means it’s also combinable. And there are some very large studies in the front-end second-line space combining it, in a space where people believe that it has more activity. But there are some complementary data as we wait for the overall survival signal, hopefully, from this regimen.
So, there have been some exciting updates, mostly in the adjuvant space but also in some other spaces in kidney cancer and building upon some of the clinical advances that we had seen from previous meetings. I’m Brian Rini, and I appreciate you attending.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Brian Rini. I’m an Ingram Professor of Medicine at Vanderbilt-Ingram Cancer Center in Nashville, Tennessee. I think there’s three main areas: adjuvant therapy in kidney cancer, frontline therapy in advanced disease, and the refractory space.
To open with adjuvant therapy, the biggest news in kidney cancer, and probably all of GU cancer at ASCO GU this year, was the adjuvant pembrolizumab overall survival data. This KEYNOTE study had previously shown disease-free survival advantages over placebo in a population with high-risk resected kidney cancer. There was a trend toward overall survival, but it was not significant in those early analyses.
Now with nearly 5 years of follow-up, we see an overall survival advantage, with a hazard ratio in the 0.6 range — so, about a 40% reduction in the risk for death among these patients receiving adjuvant pembrolizumab (pembro). This was really important for the field. It’s been difficult to show a survival advantage, even in diseases like melanoma, which is considered at least as much, if not more immune responsive, and I think puts into perspective whether to offer this drug to high-risk resected patients. And it certainly needs to be considered for this population.
I think the balance on that — and this came out in some of the questions after the session — was around how many of the placebo recipients got salvage immune therapy, which would be a standard of care. But in the countries where this was done, it’s not really clear how many actually got therapy. We know most patients got some salvage therapy, be it local or systemic, and about half the patients got immune therapy. But some more granular detail would be necessary.
The other thing I would mention is that this was paired with the previous presentation, which was adjuvant nivolumab. It was a very similar study, a similar drug in a similar setting, but it did not show any advantages of either disease-free or overall survival. This comes on the heels of other negative studies and a negative ipilimumab/nivolumab (ipi/nivo) study in this setting, part of the same study.
The reasons for these discrepancies are not entirely clear. There’s differences in populations and duration of therapy and mechanism, and all sorts of things. I don’t think anybody’s really been able to come up with one reason why we have some negative immune trials in kidney cancer and one shiningly positive one. But be that as it may, I think the take-home was that adjuvant pembro is certainly a standard of care in high-risk disease, and a benefit/risk discussion needs to be had with each individual patient. And I think pembro will be the building block for future studies, some of which are ongoing.
The second major area of update was in frontline kidney cancer. There weren’t a lot of new data, but there were updates to the existing trials. As you may know, frontline immune-based doublet is a standard of care in this disease: either ipi/nivo or one of the immuno-oncology/tyrosine kinase inhibitor (IO/TKI) regimens. We had two updates. One was an 8-year update on ipi/nivo. It’s a really long follow-up for these patients now, and what was observed was that these results remain remarkably consistent.
The hazard ratios for benefit in terms of survival and durability of response are really consistent over the past several years — again, a hallmark of immune therapy. Over half the responders are still responding now, many years later. I think that only strengthens the position of ipi/nivo as a choice for advanced clear cell kidney cancer patients. Again, there are good long-term toxicity data, and some patients can remain off treatment in what’s called treatment-free survival. So, an important update. We look forward to future, probably 10-year, data.
The CheckMate 9ER cabozantinib/nivolumab (cabo/nivo) study was updated now with many years of follow-up, as some of the other IO/TKI regimens have as well. And I think there is a similar theme, although a few years behind in maturity from the ipi/nivo data. It shows persistence of benefit. With IO/TKI regimens, a lot of the benefit is up front. It’s high response rates. It’s progression-free survival (PFS). But we’re starting to see some of that durability.
Where it’ll land, if there will be a tail of the curve and where it will be, is unclear, but these updates are important in terms of counseling patients. Patients want to know not just what’s going to happen at their first scan but also years from now. And they’re planning to be around years from now. So, I think these data are important.
The last thing I’ll mention is a health-related quality-of-life update from what was called the 005 trial of belzutifan, an oral HIF inhibitor, compared with everolimus. We heard data at the European Society for Medical Oncology (ESMO) Congress 2023 on a PFS and response-rate advantage. The drug was approved by the US Food and Drug Administration (FDA) in late December, and now we see some quality-of-life data.
Quality-of-life questionnaires and scales have a lot of imperfections. I don’t think they necessarily capture everything we want. But in this case, it was fairly clean in that belzutifan is known to be a well-tolerated agent. The toxicity profile is clean. It’s been used for years in patients with Von Hippel-Lindau syndrome, certainly in the trials for years, and has shown good tolerance over time. So, I view these data as complementary to what we already knew about the drug, but they’re nice to see.
It’s nice to see datasets come together and show the same thing: Not only is the drug active in a refractory renal cell carcinoma (RCC) setting, but also it’s really well tolerated and does not adversely impact patients› quality of life. I use this drug a lot in refractory kidney cancer, and because it’s so well tolerated. That means it’s also combinable. And there are some very large studies in the front-end second-line space combining it, in a space where people believe that it has more activity. But there are some complementary data as we wait for the overall survival signal, hopefully, from this regimen.
So, there have been some exciting updates, mostly in the adjuvant space but also in some other spaces in kidney cancer and building upon some of the clinical advances that we had seen from previous meetings. I’m Brian Rini, and I appreciate you attending.
A version of this article first appeared on Medscape.com.
After SABR, 100% Local Control at 1 Year in Kidney Cancer
TOPLINE:
METHODOLOGY:
- SABR is a promising treatment strategy for patients with inoperable kidney cancer because it is a noninvasive procedure that does not require general anesthesia and can be used to treat stages TIa and TIb, as well as larger tumors.
- The nonrandomized, phase 2, FASTRACK II trial, conducted in Australia and the Netherlands, investigated the efficacy of SABR in 70 patients with primary RCC who had a single lesion and were considered medically inoperable, were at a high risk for surgical complications, or had declined surgery. Patients also had an Eastern Cooperative Oncology Group performance status of ≤ 2 and an estimated glomerular filtration rate above 30 mL/min.
- The median age of participants was 77 years, median body mass index was 32, and the median Charlson comorbidity index was 7; 30% of the patients were women.
- Patients with tumors ≤ 4 cm (n = 23) received a single fraction of 26 Gy SABR, while those with tumors of 4-10 cm in maximum diameter (n = 47) received 42 Gy SABR in three fractions. The median tumor size was 4.6 cm.
- The primary endpoint was local control, defined as no progression of the primary RCC.
TAKEAWAY:
- At 1 year, no patients experienced local progression of their cancer, for a 100% local control rate.
- Cancer-specific survival was also 100% at 12 months from the start of SABR treatment, while the overall survival rate was 99% at 1 year and 82% at 3 years.
- Treatment-related grade 3 adverse events, such as nausea and vomiting, colonic obstruction, and diarrhea were reported by 10% of patients, with no incidences of grade 4 treatment-related adverse events or treatment-related or cancer-related deaths.
IN PRACTICE:
“Despite a larger average tumor size (4.6 cm) than in many preexisting prospective trials of surgery or SABR in primary renal cell cancer, there were no local treatment failures observed and no patients died from cancer during the study period,” the authors noted. This trial and others “support SABR as a therapeutic option for patients with inoperable or high-risk primary renal cell cancer.”
SOURCE:
This study was led by Shankar Siva, PhD, Department of Radiation Oncology, Peter MacCallum Cancer Centre, Melbourne, Australia, and published online in The Lancet Oncology.
LIMITATIONS:
The study was limited by a small sample size and less mature data at follow-up. The absence of a control group made it impossible to assess if SABR had superior, inferior, or similar efficacy to other treatment options. The definitions of operability or technically high risk might vary between different multidisciplinary teams.
DISCLOSURES:
This study was funded by a grant from the Cancer Australia Priority-driven Collaborative Cancer Research Scheme. The study authors declared receiving grants, contracts, payments, honoraria, and research funding and having other ties with several sources.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- SABR is a promising treatment strategy for patients with inoperable kidney cancer because it is a noninvasive procedure that does not require general anesthesia and can be used to treat stages TIa and TIb, as well as larger tumors.
- The nonrandomized, phase 2, FASTRACK II trial, conducted in Australia and the Netherlands, investigated the efficacy of SABR in 70 patients with primary RCC who had a single lesion and were considered medically inoperable, were at a high risk for surgical complications, or had declined surgery. Patients also had an Eastern Cooperative Oncology Group performance status of ≤ 2 and an estimated glomerular filtration rate above 30 mL/min.
- The median age of participants was 77 years, median body mass index was 32, and the median Charlson comorbidity index was 7; 30% of the patients were women.
- Patients with tumors ≤ 4 cm (n = 23) received a single fraction of 26 Gy SABR, while those with tumors of 4-10 cm in maximum diameter (n = 47) received 42 Gy SABR in three fractions. The median tumor size was 4.6 cm.
- The primary endpoint was local control, defined as no progression of the primary RCC.
TAKEAWAY:
- At 1 year, no patients experienced local progression of their cancer, for a 100% local control rate.
- Cancer-specific survival was also 100% at 12 months from the start of SABR treatment, while the overall survival rate was 99% at 1 year and 82% at 3 years.
- Treatment-related grade 3 adverse events, such as nausea and vomiting, colonic obstruction, and diarrhea were reported by 10% of patients, with no incidences of grade 4 treatment-related adverse events or treatment-related or cancer-related deaths.
IN PRACTICE:
“Despite a larger average tumor size (4.6 cm) than in many preexisting prospective trials of surgery or SABR in primary renal cell cancer, there were no local treatment failures observed and no patients died from cancer during the study period,” the authors noted. This trial and others “support SABR as a therapeutic option for patients with inoperable or high-risk primary renal cell cancer.”
SOURCE:
This study was led by Shankar Siva, PhD, Department of Radiation Oncology, Peter MacCallum Cancer Centre, Melbourne, Australia, and published online in The Lancet Oncology.
LIMITATIONS:
The study was limited by a small sample size and less mature data at follow-up. The absence of a control group made it impossible to assess if SABR had superior, inferior, or similar efficacy to other treatment options. The definitions of operability or technically high risk might vary between different multidisciplinary teams.
DISCLOSURES:
This study was funded by a grant from the Cancer Australia Priority-driven Collaborative Cancer Research Scheme. The study authors declared receiving grants, contracts, payments, honoraria, and research funding and having other ties with several sources.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- SABR is a promising treatment strategy for patients with inoperable kidney cancer because it is a noninvasive procedure that does not require general anesthesia and can be used to treat stages TIa and TIb, as well as larger tumors.
- The nonrandomized, phase 2, FASTRACK II trial, conducted in Australia and the Netherlands, investigated the efficacy of SABR in 70 patients with primary RCC who had a single lesion and were considered medically inoperable, were at a high risk for surgical complications, or had declined surgery. Patients also had an Eastern Cooperative Oncology Group performance status of ≤ 2 and an estimated glomerular filtration rate above 30 mL/min.
- The median age of participants was 77 years, median body mass index was 32, and the median Charlson comorbidity index was 7; 30% of the patients were women.
- Patients with tumors ≤ 4 cm (n = 23) received a single fraction of 26 Gy SABR, while those with tumors of 4-10 cm in maximum diameter (n = 47) received 42 Gy SABR in three fractions. The median tumor size was 4.6 cm.
- The primary endpoint was local control, defined as no progression of the primary RCC.
TAKEAWAY:
- At 1 year, no patients experienced local progression of their cancer, for a 100% local control rate.
- Cancer-specific survival was also 100% at 12 months from the start of SABR treatment, while the overall survival rate was 99% at 1 year and 82% at 3 years.
- Treatment-related grade 3 adverse events, such as nausea and vomiting, colonic obstruction, and diarrhea were reported by 10% of patients, with no incidences of grade 4 treatment-related adverse events or treatment-related or cancer-related deaths.
IN PRACTICE:
“Despite a larger average tumor size (4.6 cm) than in many preexisting prospective trials of surgery or SABR in primary renal cell cancer, there were no local treatment failures observed and no patients died from cancer during the study period,” the authors noted. This trial and others “support SABR as a therapeutic option for patients with inoperable or high-risk primary renal cell cancer.”
SOURCE:
This study was led by Shankar Siva, PhD, Department of Radiation Oncology, Peter MacCallum Cancer Centre, Melbourne, Australia, and published online in The Lancet Oncology.
LIMITATIONS:
The study was limited by a small sample size and less mature data at follow-up. The absence of a control group made it impossible to assess if SABR had superior, inferior, or similar efficacy to other treatment options. The definitions of operability or technically high risk might vary between different multidisciplinary teams.
DISCLOSURES:
This study was funded by a grant from the Cancer Australia Priority-driven Collaborative Cancer Research Scheme. The study authors declared receiving grants, contracts, payments, honoraria, and research funding and having other ties with several sources.
A version of this article first appeared on Medscape.com.
High Marks for New CAR T Toxicity Grading Tool
“Hematotoxicity after CAR T is common and clinically relevant, but it also remains poorly understood [with] a high degree of heterogeneity in terms of grading its clinical management,” said first author Kai Rejeski, MD, in presenting on the findings at the 6th European CAR T-cell Meeting, held in Spain and jointly sponsored by the European Society for Blood and Marrow Transplantation (EBMT) and the European Hematology Association (EHA).
“We hope that this novel grading system helps with this by enabling harmonized reporting using the same nomenclature and allowing the comparison of the expected incidence rates of grade 3 or higher [hematological toxicities] across several disease entities and CAR T products,” said Dr. Rejeski, of the Adult BMT (Blood Marrow Transplant) and Cellular Therapy Service, Memorial Sloan Kettering Cancer Center, New York City.
ICAHT Grading System
In a recent meta-analysis, Dr. Rejeski and his team found that infections are the cause of as many as 49% of non–relapse related deaths after CAR T-cell therapy, representing the most common cause of death and numbering significantly more than the more prominent causes of cytokine release syndrome (CRS) or immune effector cell–associated neurotoxicity (ICANS), which paradoxically have been the focus of significantly more research. In addition, the authors have reported substantial inconsistency among CAR T centers in the grading and management of the post–CAR T cytopenias that can cause those infections, underscoring the need for better guidelines.
“The narrative around CAR T toxicity has long centered on CRS and ICANS as novel and prototypical side effects with distinct management protocols,” Dr. Rejeski said in an interview. “However, it is cytopenias and the associated infections that drive nonrelapse mortality after CAR T.”
To address the need, the EHA and EBMT established the grading system for Immune Effector Cell–Associated HematoToxicity (ICAHT) that is applicable across disease types, indications, and treatment settings.
The details of the grading system were published in September 2023 in the journal Blood. The new system, which specifically focuses on neutrophil count and timing, importantly addresses the biphasic nature of ICAHT by distinguishing “early” ICAHT, occurring within 30 days of the CAR T administration, and “late” ICAHT, occurring more that 30 days following the treatment.
By contrast, conventional grading scales for CAR T–related cytopenias, such as the Common Terminology Criteria for Adverse Events (CTCAE) scale, “neither reflect the unique quality of post–CAR T neutrophil recovery, nor do they reflect the inherent risk of infections due to protracted neutropenia,” the authors report in the study.
Real-World Evaluation
To assess the ICAHT grading system’s relevance in a real-world clinical setting of CAR T-cell therapy recipients, Dr. Rejeski and colleagues conducted a multicenter observational study, published in January 2024 in Blood Advances.
The study involved 549 patients at 12 international CAR T centers treated with BCMA- or CD19- directed CAR T therapy for relapsed/refractory B-cell malignancies.
Of the patients, 112 were treated for multiple myeloma (MM), 334 for large B cell lymphoma (LBCL), and 103 for mantle cell lymphoma (MCL).
Using the grading system, grade 3 (severe) or 4 (life-threatening) ICAHT (n = 125), was found to be strongly associated with key factors including a cumulative duration of severe neutropenia (P < .0001), the presence of multilineage cytopenias, such as severe thrombocytopenia (90%, compared with 46% in nonsevere ICAHT) and severe anemia (92% vs 49%; both P < .001), as well as the use of platelet and red blood cell transfusions.
Grade 3 or higher ICAHT was more common in patients with MCL (28%), compared with LBCL (23%) and MM (15%).
Key factors at baseline that were independently associated with severe ICAHT after multivariate adjustment included the presence of bone marrow infiltration, increased serum LDH levels, elevated CAR-HEMATOTOX scores (all P < .001), and receipt of CD28z costimulatory domain products, including axi-cel or brexu-cel (P = .01).
Those with grade 3 or higher ICAHT scores had a significantly higher rate of severe infections, compared with lower ICAHT scores (49% vs 13%; P < .0001), as well as increased nonrelapse mortality (14% vs 4.5%; P < .0001), primarily attributable to fatal infections.
Survival outcomes were also worse with grade 3 or higher ICAHT, including significantly lower rates of 1-year progression-free survival (35% vs 51%) and 1-year overall survival (52% vs 73%; both P < .0001).
Grade 3 or higher ICAHT was also significantly associated with prolonged hospital stays (median 21 vs 16 days; P < .0001).
However, contrary to findings from some previous studies, the current study showed no association between ICAHT severity and the prior administration of autologous stem cell transplant.
The number of prior treatment lines was not associated with grade 3 or higher ICAHT. However, grade 3 or higher CRS was more common as a cotoxicity (15% vs 5% without severe ICAHT), as was severe ICANS (26% vs 13%; both P < .001).
Notably, ICAHT grading showed superiority in the prediction of severe infections, compared with CTCAE grading (c-index 0.73 vs 0.55, P < .0001 vs nonsignificant).
While mild to moderate toxicity after CAR T-cell therapy has been associated with more favorable outcomes, the poor survival rates associated with severe ICAHT “underscore that high-grade toxicity and inferior treatment outcomes often go hand-in-hand,” the authors write.
Conversely, “the patients with grade 1 or 2 ICAHT exhibited excellent treatment outcomes in our study,” they point out.
Recommendations in Clinical Practice
For clinical guidance, the ICAHT grading system provides best practice recommendations based on severity for diagnostic work-up and management, such as measures including use of granulocyte-colony stimulating factor (G-CSF), anti-infective prophylaxis and stem cell boosts.
The authors add that preinfusion scoring systems, including the CAR-HEMATOTOX prognostic score, may be optimized by ICAHT grading in terms of modeling for severe or life-threatening ICAHT as an important endpoint.
“We have had an absence of the standardized severity-based guidelines that we know very well for CRS and ICANS, both in terms of the diagnostic work-up and the grading but also the management,” Dr. Rejeski said at the meeting.
“We hope that the new ICAHT grading focuses future research efforts to not only understand this important side effect better, but also develop specific management strategies that mitigate the risk of infections in high-risk patients,” Dr. Rejeski added.
“The multiply validated CAR-HEMATOTOX score, assessed at time of lymphodepletion, may be helpful in this regard,” he added.
An accompanying editorial published with the guidelines underscored that “this is the first such guideline by a major organization and is a much-needed development for the management of this important CAR T-cell–associated toxicity.”
The improved standardized reporting of ICAHT “could also inform hematotoxicity management protocols,” said the editorial authors, David Qualls, MD, of the Memorial Sloan Kettering Cancer Center in New York City and Caron Jacobson, MD, of the Dana-Farber Cancer Institute, in Boston, Massachusetts.
“While providing comprehensive recommendations for ICAHT, the EHA/EBMT guidelines also highlight important gaps in our current knowledge of ICAHT, which are significant,” the editorial authors add.
Further commenting, Ulrich Jaeger, MD, a professor of hematology at the Medical University of Vienna, Vienna, Austria, agreed that the research fills an important need in post–CAR T-cell therapy management.
“Dr. Rejeski´s work is really seminal in the field and confirmed by validation cohorts in other centers,” he said in an interview. “I think the story is absolutely clear. It will be of increasing importance, with more patients surviving. [The system] will have to be adapted to novel indications as well.”
Dr. Rejeski disclosed ties with Kite/Gilead, Novartis, GMS/Celgene, and Pierre-Fabre. Jaeger reports relationships with Novartis, Gilead Sciences, Celgene/BMS, Janssen, Roche, Miltenyi Biotec, and Innovative Medicines Initiative.
“Hematotoxicity after CAR T is common and clinically relevant, but it also remains poorly understood [with] a high degree of heterogeneity in terms of grading its clinical management,” said first author Kai Rejeski, MD, in presenting on the findings at the 6th European CAR T-cell Meeting, held in Spain and jointly sponsored by the European Society for Blood and Marrow Transplantation (EBMT) and the European Hematology Association (EHA).
“We hope that this novel grading system helps with this by enabling harmonized reporting using the same nomenclature and allowing the comparison of the expected incidence rates of grade 3 or higher [hematological toxicities] across several disease entities and CAR T products,” said Dr. Rejeski, of the Adult BMT (Blood Marrow Transplant) and Cellular Therapy Service, Memorial Sloan Kettering Cancer Center, New York City.
ICAHT Grading System
In a recent meta-analysis, Dr. Rejeski and his team found that infections are the cause of as many as 49% of non–relapse related deaths after CAR T-cell therapy, representing the most common cause of death and numbering significantly more than the more prominent causes of cytokine release syndrome (CRS) or immune effector cell–associated neurotoxicity (ICANS), which paradoxically have been the focus of significantly more research. In addition, the authors have reported substantial inconsistency among CAR T centers in the grading and management of the post–CAR T cytopenias that can cause those infections, underscoring the need for better guidelines.
“The narrative around CAR T toxicity has long centered on CRS and ICANS as novel and prototypical side effects with distinct management protocols,” Dr. Rejeski said in an interview. “However, it is cytopenias and the associated infections that drive nonrelapse mortality after CAR T.”
To address the need, the EHA and EBMT established the grading system for Immune Effector Cell–Associated HematoToxicity (ICAHT) that is applicable across disease types, indications, and treatment settings.
The details of the grading system were published in September 2023 in the journal Blood. The new system, which specifically focuses on neutrophil count and timing, importantly addresses the biphasic nature of ICAHT by distinguishing “early” ICAHT, occurring within 30 days of the CAR T administration, and “late” ICAHT, occurring more that 30 days following the treatment.
By contrast, conventional grading scales for CAR T–related cytopenias, such as the Common Terminology Criteria for Adverse Events (CTCAE) scale, “neither reflect the unique quality of post–CAR T neutrophil recovery, nor do they reflect the inherent risk of infections due to protracted neutropenia,” the authors report in the study.
Real-World Evaluation
To assess the ICAHT grading system’s relevance in a real-world clinical setting of CAR T-cell therapy recipients, Dr. Rejeski and colleagues conducted a multicenter observational study, published in January 2024 in Blood Advances.
The study involved 549 patients at 12 international CAR T centers treated with BCMA- or CD19- directed CAR T therapy for relapsed/refractory B-cell malignancies.
Of the patients, 112 were treated for multiple myeloma (MM), 334 for large B cell lymphoma (LBCL), and 103 for mantle cell lymphoma (MCL).
Using the grading system, grade 3 (severe) or 4 (life-threatening) ICAHT (n = 125), was found to be strongly associated with key factors including a cumulative duration of severe neutropenia (P < .0001), the presence of multilineage cytopenias, such as severe thrombocytopenia (90%, compared with 46% in nonsevere ICAHT) and severe anemia (92% vs 49%; both P < .001), as well as the use of platelet and red blood cell transfusions.
Grade 3 or higher ICAHT was more common in patients with MCL (28%), compared with LBCL (23%) and MM (15%).
Key factors at baseline that were independently associated with severe ICAHT after multivariate adjustment included the presence of bone marrow infiltration, increased serum LDH levels, elevated CAR-HEMATOTOX scores (all P < .001), and receipt of CD28z costimulatory domain products, including axi-cel or brexu-cel (P = .01).
Those with grade 3 or higher ICAHT scores had a significantly higher rate of severe infections, compared with lower ICAHT scores (49% vs 13%; P < .0001), as well as increased nonrelapse mortality (14% vs 4.5%; P < .0001), primarily attributable to fatal infections.
Survival outcomes were also worse with grade 3 or higher ICAHT, including significantly lower rates of 1-year progression-free survival (35% vs 51%) and 1-year overall survival (52% vs 73%; both P < .0001).
Grade 3 or higher ICAHT was also significantly associated with prolonged hospital stays (median 21 vs 16 days; P < .0001).
However, contrary to findings from some previous studies, the current study showed no association between ICAHT severity and the prior administration of autologous stem cell transplant.
The number of prior treatment lines was not associated with grade 3 or higher ICAHT. However, grade 3 or higher CRS was more common as a cotoxicity (15% vs 5% without severe ICAHT), as was severe ICANS (26% vs 13%; both P < .001).
Notably, ICAHT grading showed superiority in the prediction of severe infections, compared with CTCAE grading (c-index 0.73 vs 0.55, P < .0001 vs nonsignificant).
While mild to moderate toxicity after CAR T-cell therapy has been associated with more favorable outcomes, the poor survival rates associated with severe ICAHT “underscore that high-grade toxicity and inferior treatment outcomes often go hand-in-hand,” the authors write.
Conversely, “the patients with grade 1 or 2 ICAHT exhibited excellent treatment outcomes in our study,” they point out.
Recommendations in Clinical Practice
For clinical guidance, the ICAHT grading system provides best practice recommendations based on severity for diagnostic work-up and management, such as measures including use of granulocyte-colony stimulating factor (G-CSF), anti-infective prophylaxis and stem cell boosts.
The authors add that preinfusion scoring systems, including the CAR-HEMATOTOX prognostic score, may be optimized by ICAHT grading in terms of modeling for severe or life-threatening ICAHT as an important endpoint.
“We have had an absence of the standardized severity-based guidelines that we know very well for CRS and ICANS, both in terms of the diagnostic work-up and the grading but also the management,” Dr. Rejeski said at the meeting.
“We hope that the new ICAHT grading focuses future research efforts to not only understand this important side effect better, but also develop specific management strategies that mitigate the risk of infections in high-risk patients,” Dr. Rejeski added.
“The multiply validated CAR-HEMATOTOX score, assessed at time of lymphodepletion, may be helpful in this regard,” he added.
An accompanying editorial published with the guidelines underscored that “this is the first such guideline by a major organization and is a much-needed development for the management of this important CAR T-cell–associated toxicity.”
The improved standardized reporting of ICAHT “could also inform hematotoxicity management protocols,” said the editorial authors, David Qualls, MD, of the Memorial Sloan Kettering Cancer Center in New York City and Caron Jacobson, MD, of the Dana-Farber Cancer Institute, in Boston, Massachusetts.
“While providing comprehensive recommendations for ICAHT, the EHA/EBMT guidelines also highlight important gaps in our current knowledge of ICAHT, which are significant,” the editorial authors add.
Further commenting, Ulrich Jaeger, MD, a professor of hematology at the Medical University of Vienna, Vienna, Austria, agreed that the research fills an important need in post–CAR T-cell therapy management.
“Dr. Rejeski´s work is really seminal in the field and confirmed by validation cohorts in other centers,” he said in an interview. “I think the story is absolutely clear. It will be of increasing importance, with more patients surviving. [The system] will have to be adapted to novel indications as well.”
Dr. Rejeski disclosed ties with Kite/Gilead, Novartis, GMS/Celgene, and Pierre-Fabre. Jaeger reports relationships with Novartis, Gilead Sciences, Celgene/BMS, Janssen, Roche, Miltenyi Biotec, and Innovative Medicines Initiative.
“Hematotoxicity after CAR T is common and clinically relevant, but it also remains poorly understood [with] a high degree of heterogeneity in terms of grading its clinical management,” said first author Kai Rejeski, MD, in presenting on the findings at the 6th European CAR T-cell Meeting, held in Spain and jointly sponsored by the European Society for Blood and Marrow Transplantation (EBMT) and the European Hematology Association (EHA).
“We hope that this novel grading system helps with this by enabling harmonized reporting using the same nomenclature and allowing the comparison of the expected incidence rates of grade 3 or higher [hematological toxicities] across several disease entities and CAR T products,” said Dr. Rejeski, of the Adult BMT (Blood Marrow Transplant) and Cellular Therapy Service, Memorial Sloan Kettering Cancer Center, New York City.
ICAHT Grading System
In a recent meta-analysis, Dr. Rejeski and his team found that infections are the cause of as many as 49% of non–relapse related deaths after CAR T-cell therapy, representing the most common cause of death and numbering significantly more than the more prominent causes of cytokine release syndrome (CRS) or immune effector cell–associated neurotoxicity (ICANS), which paradoxically have been the focus of significantly more research. In addition, the authors have reported substantial inconsistency among CAR T centers in the grading and management of the post–CAR T cytopenias that can cause those infections, underscoring the need for better guidelines.
“The narrative around CAR T toxicity has long centered on CRS and ICANS as novel and prototypical side effects with distinct management protocols,” Dr. Rejeski said in an interview. “However, it is cytopenias and the associated infections that drive nonrelapse mortality after CAR T.”
To address the need, the EHA and EBMT established the grading system for Immune Effector Cell–Associated HematoToxicity (ICAHT) that is applicable across disease types, indications, and treatment settings.
The details of the grading system were published in September 2023 in the journal Blood. The new system, which specifically focuses on neutrophil count and timing, importantly addresses the biphasic nature of ICAHT by distinguishing “early” ICAHT, occurring within 30 days of the CAR T administration, and “late” ICAHT, occurring more that 30 days following the treatment.
By contrast, conventional grading scales for CAR T–related cytopenias, such as the Common Terminology Criteria for Adverse Events (CTCAE) scale, “neither reflect the unique quality of post–CAR T neutrophil recovery, nor do they reflect the inherent risk of infections due to protracted neutropenia,” the authors report in the study.
Real-World Evaluation
To assess the ICAHT grading system’s relevance in a real-world clinical setting of CAR T-cell therapy recipients, Dr. Rejeski and colleagues conducted a multicenter observational study, published in January 2024 in Blood Advances.
The study involved 549 patients at 12 international CAR T centers treated with BCMA- or CD19- directed CAR T therapy for relapsed/refractory B-cell malignancies.
Of the patients, 112 were treated for multiple myeloma (MM), 334 for large B cell lymphoma (LBCL), and 103 for mantle cell lymphoma (MCL).
Using the grading system, grade 3 (severe) or 4 (life-threatening) ICAHT (n = 125), was found to be strongly associated with key factors including a cumulative duration of severe neutropenia (P < .0001), the presence of multilineage cytopenias, such as severe thrombocytopenia (90%, compared with 46% in nonsevere ICAHT) and severe anemia (92% vs 49%; both P < .001), as well as the use of platelet and red blood cell transfusions.
Grade 3 or higher ICAHT was more common in patients with MCL (28%), compared with LBCL (23%) and MM (15%).
Key factors at baseline that were independently associated with severe ICAHT after multivariate adjustment included the presence of bone marrow infiltration, increased serum LDH levels, elevated CAR-HEMATOTOX scores (all P < .001), and receipt of CD28z costimulatory domain products, including axi-cel or brexu-cel (P = .01).
Those with grade 3 or higher ICAHT scores had a significantly higher rate of severe infections, compared with lower ICAHT scores (49% vs 13%; P < .0001), as well as increased nonrelapse mortality (14% vs 4.5%; P < .0001), primarily attributable to fatal infections.
Survival outcomes were also worse with grade 3 or higher ICAHT, including significantly lower rates of 1-year progression-free survival (35% vs 51%) and 1-year overall survival (52% vs 73%; both P < .0001).
Grade 3 or higher ICAHT was also significantly associated with prolonged hospital stays (median 21 vs 16 days; P < .0001).
However, contrary to findings from some previous studies, the current study showed no association between ICAHT severity and the prior administration of autologous stem cell transplant.
The number of prior treatment lines was not associated with grade 3 or higher ICAHT. However, grade 3 or higher CRS was more common as a cotoxicity (15% vs 5% without severe ICAHT), as was severe ICANS (26% vs 13%; both P < .001).
Notably, ICAHT grading showed superiority in the prediction of severe infections, compared with CTCAE grading (c-index 0.73 vs 0.55, P < .0001 vs nonsignificant).
While mild to moderate toxicity after CAR T-cell therapy has been associated with more favorable outcomes, the poor survival rates associated with severe ICAHT “underscore that high-grade toxicity and inferior treatment outcomes often go hand-in-hand,” the authors write.
Conversely, “the patients with grade 1 or 2 ICAHT exhibited excellent treatment outcomes in our study,” they point out.
Recommendations in Clinical Practice
For clinical guidance, the ICAHT grading system provides best practice recommendations based on severity for diagnostic work-up and management, such as measures including use of granulocyte-colony stimulating factor (G-CSF), anti-infective prophylaxis and stem cell boosts.
The authors add that preinfusion scoring systems, including the CAR-HEMATOTOX prognostic score, may be optimized by ICAHT grading in terms of modeling for severe or life-threatening ICAHT as an important endpoint.
“We have had an absence of the standardized severity-based guidelines that we know very well for CRS and ICANS, both in terms of the diagnostic work-up and the grading but also the management,” Dr. Rejeski said at the meeting.
“We hope that the new ICAHT grading focuses future research efforts to not only understand this important side effect better, but also develop specific management strategies that mitigate the risk of infections in high-risk patients,” Dr. Rejeski added.
“The multiply validated CAR-HEMATOTOX score, assessed at time of lymphodepletion, may be helpful in this regard,” he added.
An accompanying editorial published with the guidelines underscored that “this is the first such guideline by a major organization and is a much-needed development for the management of this important CAR T-cell–associated toxicity.”
The improved standardized reporting of ICAHT “could also inform hematotoxicity management protocols,” said the editorial authors, David Qualls, MD, of the Memorial Sloan Kettering Cancer Center in New York City and Caron Jacobson, MD, of the Dana-Farber Cancer Institute, in Boston, Massachusetts.
“While providing comprehensive recommendations for ICAHT, the EHA/EBMT guidelines also highlight important gaps in our current knowledge of ICAHT, which are significant,” the editorial authors add.
Further commenting, Ulrich Jaeger, MD, a professor of hematology at the Medical University of Vienna, Vienna, Austria, agreed that the research fills an important need in post–CAR T-cell therapy management.
“Dr. Rejeski´s work is really seminal in the field and confirmed by validation cohorts in other centers,” he said in an interview. “I think the story is absolutely clear. It will be of increasing importance, with more patients surviving. [The system] will have to be adapted to novel indications as well.”
Dr. Rejeski disclosed ties with Kite/Gilead, Novartis, GMS/Celgene, and Pierre-Fabre. Jaeger reports relationships with Novartis, Gilead Sciences, Celgene/BMS, Janssen, Roche, Miltenyi Biotec, and Innovative Medicines Initiative.
FROM THE 6TH EUROPEAN CAR T-CELL MEETING
Does worsening metabolic syndrome increase the risk of developing cancer?
The conditions that comprise metabolic syndrome (high blood pressure, high blood sugar, increased abdominal adiposity, and high cholesterol and triglycerides) have been associated with an increased risk of diseases, including heart disease, stroke, and type 2 diabetes, wrote Li Deng, PhD, of Capital Medical University, Beijing, China, and colleagues.
A systematic review and meta-analysis published in Diabetes Care in 2012 showed an association between the presence of metabolic syndrome and an increased risk of various cancers including liver, bladder, pancreatic, breast, and colorectal.
More recently, a 2019 study published in Diabetes showed evidence of increased risk for certain cancers (pancreatic, kidney, uterine, cervical) but no increased risk for cancer overall.
However, the reasons for this association between metabolic syndrome and cancer remain unclear, and the effect of the fluctuating nature of metabolic syndrome over time on long-term cancer risk has not been explored, the researchers wrote.
What Does New Study Add to Other Research on Metabolic Syndrome and Cancer Risk?
In the new study, published in Cancer on March 11 (doi: 10.1002/cncr.35235), 44,115 adults in China were separated into four trajectories based on metabolic syndrome scores for the period from 2006 to 2010. The scores were based on clinical evidence of metabolic syndrome, defined using the International Diabetes Federation criteria of central obesity and the presence of at least two other factors including increased triglycerides, decreased HDL cholesterol, high blood pressure (or treatment for previously diagnosed hypertension), and increased fasting plasma glucose (or previous diagnosis of type 2 diabetes).
The average age of the participants was 49 years. The four trajectories of metabolic syndrome were low-stable (10.56% of participants), moderate-low (40.84%), moderate-high (41.46%), and elevated-increasing (7.14%), based on trends from the individuals’ initial physical exams on entering the study.
Over a median follow-up period of 9.4 years (from 2010 to 2021), 2,271 cancer diagnoses were reported in the study population. Those with an elevated-increasing metabolic syndrome trajectory had 1.3 times the risk of any cancer compared with those in the low-stable group. Risk for breast cancer, endometrial cancer, kidney cancer, colorectal cancer, and liver cancer in the highest trajectory group were 2.1, 3.3, 4.5, 2.5, and 1.6 times higher, respectively, compared to the lowest group. The increased risk in the elevated-trajectory group for all cancer types persisted when the low-stable, moderate-low, and moderate-high trajectory pattern groups were combined.
The researchers also examined the impact of chronic inflammation and found that individuals with persistently high metabolic syndrome scores and concurrent chronic inflammation had the highest risks of breast, endometrial, colon, and liver cancer. However, individuals with persistently high metabolic syndrome scores and no concurrent chronic inflammation had the highest risk of kidney cancer.
What Are the Limitations of This Research?
The researchers of the current study acknowledged the lack of information on other causes of cancer, including dietary habits, hepatitis C infection, and Helicobacter pylori infection. Other limitations include the focus only on individuals from a single community of mainly middle-aged men in China that may not generalize to other populations.
Also, the metabolic syndrome trajectories did not change much over time, which may be related to the short 4-year study period.
What Is the Takeaway Message for Clinical Practice?
The results suggest that monitoring and managing metabolic syndrome could help reduce cancer risk, the researchers concluded.
“This research suggests that proactive and continuous management of metabolic syndrome may serve as an essential strategy in preventing cancer,” senior author Han-Ping Shi, MD, PhD, of Capital Medical University in Beijing, said in a press release accompanying the study.
More research is needed to assess the impact of these interventions on cancer risk, he noted. However, the data from the current study can guide future research that may lead to more targeted treatments and more effective preventive strategies, he said in a statement.
The study was supported by the National Key Research and Development Program of China. The researchers had no financial conflicts to disclose.
The conditions that comprise metabolic syndrome (high blood pressure, high blood sugar, increased abdominal adiposity, and high cholesterol and triglycerides) have been associated with an increased risk of diseases, including heart disease, stroke, and type 2 diabetes, wrote Li Deng, PhD, of Capital Medical University, Beijing, China, and colleagues.
A systematic review and meta-analysis published in Diabetes Care in 2012 showed an association between the presence of metabolic syndrome and an increased risk of various cancers including liver, bladder, pancreatic, breast, and colorectal.
More recently, a 2019 study published in Diabetes showed evidence of increased risk for certain cancers (pancreatic, kidney, uterine, cervical) but no increased risk for cancer overall.
However, the reasons for this association between metabolic syndrome and cancer remain unclear, and the effect of the fluctuating nature of metabolic syndrome over time on long-term cancer risk has not been explored, the researchers wrote.
What Does New Study Add to Other Research on Metabolic Syndrome and Cancer Risk?
In the new study, published in Cancer on March 11 (doi: 10.1002/cncr.35235), 44,115 adults in China were separated into four trajectories based on metabolic syndrome scores for the period from 2006 to 2010. The scores were based on clinical evidence of metabolic syndrome, defined using the International Diabetes Federation criteria of central obesity and the presence of at least two other factors including increased triglycerides, decreased HDL cholesterol, high blood pressure (or treatment for previously diagnosed hypertension), and increased fasting plasma glucose (or previous diagnosis of type 2 diabetes).
The average age of the participants was 49 years. The four trajectories of metabolic syndrome were low-stable (10.56% of participants), moderate-low (40.84%), moderate-high (41.46%), and elevated-increasing (7.14%), based on trends from the individuals’ initial physical exams on entering the study.
Over a median follow-up period of 9.4 years (from 2010 to 2021), 2,271 cancer diagnoses were reported in the study population. Those with an elevated-increasing metabolic syndrome trajectory had 1.3 times the risk of any cancer compared with those in the low-stable group. Risk for breast cancer, endometrial cancer, kidney cancer, colorectal cancer, and liver cancer in the highest trajectory group were 2.1, 3.3, 4.5, 2.5, and 1.6 times higher, respectively, compared to the lowest group. The increased risk in the elevated-trajectory group for all cancer types persisted when the low-stable, moderate-low, and moderate-high trajectory pattern groups were combined.
The researchers also examined the impact of chronic inflammation and found that individuals with persistently high metabolic syndrome scores and concurrent chronic inflammation had the highest risks of breast, endometrial, colon, and liver cancer. However, individuals with persistently high metabolic syndrome scores and no concurrent chronic inflammation had the highest risk of kidney cancer.
What Are the Limitations of This Research?
The researchers of the current study acknowledged the lack of information on other causes of cancer, including dietary habits, hepatitis C infection, and Helicobacter pylori infection. Other limitations include the focus only on individuals from a single community of mainly middle-aged men in China that may not generalize to other populations.
Also, the metabolic syndrome trajectories did not change much over time, which may be related to the short 4-year study period.
What Is the Takeaway Message for Clinical Practice?
The results suggest that monitoring and managing metabolic syndrome could help reduce cancer risk, the researchers concluded.
“This research suggests that proactive and continuous management of metabolic syndrome may serve as an essential strategy in preventing cancer,” senior author Han-Ping Shi, MD, PhD, of Capital Medical University in Beijing, said in a press release accompanying the study.
More research is needed to assess the impact of these interventions on cancer risk, he noted. However, the data from the current study can guide future research that may lead to more targeted treatments and more effective preventive strategies, he said in a statement.
The study was supported by the National Key Research and Development Program of China. The researchers had no financial conflicts to disclose.
The conditions that comprise metabolic syndrome (high blood pressure, high blood sugar, increased abdominal adiposity, and high cholesterol and triglycerides) have been associated with an increased risk of diseases, including heart disease, stroke, and type 2 diabetes, wrote Li Deng, PhD, of Capital Medical University, Beijing, China, and colleagues.
A systematic review and meta-analysis published in Diabetes Care in 2012 showed an association between the presence of metabolic syndrome and an increased risk of various cancers including liver, bladder, pancreatic, breast, and colorectal.
More recently, a 2019 study published in Diabetes showed evidence of increased risk for certain cancers (pancreatic, kidney, uterine, cervical) but no increased risk for cancer overall.
However, the reasons for this association between metabolic syndrome and cancer remain unclear, and the effect of the fluctuating nature of metabolic syndrome over time on long-term cancer risk has not been explored, the researchers wrote.
What Does New Study Add to Other Research on Metabolic Syndrome and Cancer Risk?
In the new study, published in Cancer on March 11 (doi: 10.1002/cncr.35235), 44,115 adults in China were separated into four trajectories based on metabolic syndrome scores for the period from 2006 to 2010. The scores were based on clinical evidence of metabolic syndrome, defined using the International Diabetes Federation criteria of central obesity and the presence of at least two other factors including increased triglycerides, decreased HDL cholesterol, high blood pressure (or treatment for previously diagnosed hypertension), and increased fasting plasma glucose (or previous diagnosis of type 2 diabetes).
The average age of the participants was 49 years. The four trajectories of metabolic syndrome were low-stable (10.56% of participants), moderate-low (40.84%), moderate-high (41.46%), and elevated-increasing (7.14%), based on trends from the individuals’ initial physical exams on entering the study.
Over a median follow-up period of 9.4 years (from 2010 to 2021), 2,271 cancer diagnoses were reported in the study population. Those with an elevated-increasing metabolic syndrome trajectory had 1.3 times the risk of any cancer compared with those in the low-stable group. Risk for breast cancer, endometrial cancer, kidney cancer, colorectal cancer, and liver cancer in the highest trajectory group were 2.1, 3.3, 4.5, 2.5, and 1.6 times higher, respectively, compared to the lowest group. The increased risk in the elevated-trajectory group for all cancer types persisted when the low-stable, moderate-low, and moderate-high trajectory pattern groups were combined.
The researchers also examined the impact of chronic inflammation and found that individuals with persistently high metabolic syndrome scores and concurrent chronic inflammation had the highest risks of breast, endometrial, colon, and liver cancer. However, individuals with persistently high metabolic syndrome scores and no concurrent chronic inflammation had the highest risk of kidney cancer.
What Are the Limitations of This Research?
The researchers of the current study acknowledged the lack of information on other causes of cancer, including dietary habits, hepatitis C infection, and Helicobacter pylori infection. Other limitations include the focus only on individuals from a single community of mainly middle-aged men in China that may not generalize to other populations.
Also, the metabolic syndrome trajectories did not change much over time, which may be related to the short 4-year study period.
What Is the Takeaway Message for Clinical Practice?
The results suggest that monitoring and managing metabolic syndrome could help reduce cancer risk, the researchers concluded.
“This research suggests that proactive and continuous management of metabolic syndrome may serve as an essential strategy in preventing cancer,” senior author Han-Ping Shi, MD, PhD, of Capital Medical University in Beijing, said in a press release accompanying the study.
More research is needed to assess the impact of these interventions on cancer risk, he noted. However, the data from the current study can guide future research that may lead to more targeted treatments and more effective preventive strategies, he said in a statement.
The study was supported by the National Key Research and Development Program of China. The researchers had no financial conflicts to disclose.
FROM CANCER
Higher Prostate Cancer Rates Seen in Black Men, but Advanced Cases Similar to White Men
There was a substantial difference in prostate cancer diagnosis across ethnic groups: 25% of Black men with a raised PSA were diagnosed with prostate cancer within 1 year of being tested, compared with 20% of White men and 13% of Asian men, in the analysis of a large primary care cohort in the United Kingdom.
Incidence of advanced prostate cancer for Asian men with a raised PSA result was 4.5%, compared with 7.5% for White men and 7.0% for Black men.
Men included in the study were aged 40 and older and had no prior cancer diagnosis. Their ethnicity and PSA test result were logged in a national dataset between 2010 and 2017.
The study of more than 730,000 men, published in BMC Medicine, didn’t explore reasons for the differences, but experts offer their thoughts on what led to the findings and what these results imply.
Why the Higher Diagnosis Rates but Not More Advanced Disease in Black Men?
Lead author Liz Down, a graduate research assistant at the University of Exeter, Exeter, England, suggests the higher diagnosis rates but not more advanced disease in Black men may be linked to genetic variations.
Her team’s studies have shown that Black men in the United Kingdom and United States have higher levels of PSA. The PSA value is used to identify patients who might benefit from specialist investigation, and current guidelines in the UK and US don’t distinguish between ethnic groups.
As most men have slow-growing prostate cancer, this may lead to a disproportionately higher number of Black men being diagnosed with prostate cancer, she said.
“One possible interpretation,” Ms. Down notes, “is that prostate cancer follows a similar trajectory in Black and White men. What is different, however, is that Black men have higher PSA levels.”
As to why the advanced-cancer incidence is similar in Black and White patients in the study, Daniel George, MD, director of genitourinary oncology at Duke Cancer Institute in Durham, North Carolina, says it’s important to understand that the Black men in this study “are not necessarily representative of the Black population at large.”
In this study, “they’re a little bit more healthcare inclined,” Dr. George notes. The study population is actively seeking the PSA test. Their socioeconomic profile might be closer to their White counterparts’, and that may make results more similar, he said.
“It’s possible that because this is a screening and not just men coming in for symptoms or cause, that we’re not seeing as much advanced disease,” he continued.
Amar Kishan, MD, chief of the genitourinary oncology service at University of California Los Angeles (UCLA) Health, says the genomic factors and environmental stressors that lead to elevated PSA counts don’t necessarily translate into aggressiveness of disease.
Why do Different Races have Different Prostate Cancer Risk?
Dr. George points out that the study also highlights that Asian men were significantly less likely to be diagnosed with prostate cancer within 1 year of the test.
The reasons for differences in prostate risk by race are complex, he notes. There are some clues that biologic factors may be at work. For instance, early puberty has a link to prostate cancer as it does to breast cancer, and height is also associated with a greater risk of prostate cancer, Dr. George said.
It’s not necessarily a racial association but there are some biological factors associated with prostate cancer later in life, he explained. “These may be enriched in certain populations, including northern Europeans and patients with African ancestries.”
The study also notes that Black men are more likely to die from prostate cancer than are White men, and Asian men are less likely than White or Black men to die from it.
Ms. Down said the difference in prostate cancer mortality between Black vs White men, in particular, may be related to a number of factors, and age, and lifetime risk of prostate cancer may play a major role, at least in the UK.
Should There Be Different ‘Normal’ PSA Levels for Different Races?
Dr. George says there is likely a need to change the system because a PSA level in one race may not signal the same risk it does in another. So medicine probably needs to standardize what a “normal” PSA is by race, he says, adding that he is a coauthor of an upcoming paper regarding that issue.
The lowest instances of prostate cancer were in Asian patients so this isn’t just a Black and White issue, Dr. George notes. “Being able to establish benchmarks by race and ethnicity is something that is probably needed in the field,” he says.
Dr. Kishan, on the other hand, says data from this study are not enough to support differentiating PSA levels based on race. He noted a limitation of the study is that it was not able to calculate the false-negative rate of PSA tests.
What are the Implications for Treating and Screening for Prostate Cancer
Dr. Kishan says there may be a role for increased intensity of screening, whether at an earlier age or with different intervals, but prostate cancer treatment should not differ by race.
“Our prior study, as well as others,” he says, “have shown that when you balance Black and White patients for every factor that might impact prognosis other than race — such as age, disease aggressiveness, etc. — Black men actually tend to have better outcomes than White men. Thus, it would mean potentially overtreating (i.e., causing unnecessary side effects) to increase treatment intensity purely based on race with the available data.”
According to the paper, prostate cancer incidence in men with higher PSA levels increases with increasing age, even when using age-adjusted thresholds.
Dr. George says we know from this study and other studies as well that Black men are more likely to be diagnosed with prostate at a younger age. “Therefore, we probably need to be thinking about screening Black men starting at a younger age. These are the men who are most likely to benefit from an intervention — patients who have life expectancies of 20 years or more.”
What are the Downsides to Overdiagnosing Prostate Cancer in Men?
“It’s one of the biggest concerns that men have in proactively seeking healthcare,” Dr. George says. “They’re more likely to undergo treatment for this disease if they’re getting screened because (clinicians are) more likely to find it.”
Some of those men, he says, are going to undergo treatment for disease that won’t ultimately kill them, but may cause complications the men shouldn’t have had at all or otherwise may have had later.
“Overtreatment is a real concern. That’s why active surveillance is so important to minimize overtreatment of patients by finding out which cancers are low risk for progression and which are becoming more aggressive,” Dr. George says.
Authors of the study write that “the potential for overdiagnosis and the subsequent psychological and physical impact of diagnosis and treatment is an important consideration.”
All authors of the new paper received financial support from Cancer Research UK, the National Institute for Health and Care Research (NIHR), and the Higgins family for the submitted work.
Dr. George reports no relevant financial relationships.
Dr. Kishan reports consulting fees and speaking honoraria from Varian Medical Systems, Janssen, and Boston Scientific; research funding from PointBioPharma, Lantheus, and Janssen; and serving on advisory boards for Lantheus, Janssen and Boston Scientific.
There was a substantial difference in prostate cancer diagnosis across ethnic groups: 25% of Black men with a raised PSA were diagnosed with prostate cancer within 1 year of being tested, compared with 20% of White men and 13% of Asian men, in the analysis of a large primary care cohort in the United Kingdom.
Incidence of advanced prostate cancer for Asian men with a raised PSA result was 4.5%, compared with 7.5% for White men and 7.0% for Black men.
Men included in the study were aged 40 and older and had no prior cancer diagnosis. Their ethnicity and PSA test result were logged in a national dataset between 2010 and 2017.
The study of more than 730,000 men, published in BMC Medicine, didn’t explore reasons for the differences, but experts offer their thoughts on what led to the findings and what these results imply.
Why the Higher Diagnosis Rates but Not More Advanced Disease in Black Men?
Lead author Liz Down, a graduate research assistant at the University of Exeter, Exeter, England, suggests the higher diagnosis rates but not more advanced disease in Black men may be linked to genetic variations.
Her team’s studies have shown that Black men in the United Kingdom and United States have higher levels of PSA. The PSA value is used to identify patients who might benefit from specialist investigation, and current guidelines in the UK and US don’t distinguish between ethnic groups.
As most men have slow-growing prostate cancer, this may lead to a disproportionately higher number of Black men being diagnosed with prostate cancer, she said.
“One possible interpretation,” Ms. Down notes, “is that prostate cancer follows a similar trajectory in Black and White men. What is different, however, is that Black men have higher PSA levels.”
As to why the advanced-cancer incidence is similar in Black and White patients in the study, Daniel George, MD, director of genitourinary oncology at Duke Cancer Institute in Durham, North Carolina, says it’s important to understand that the Black men in this study “are not necessarily representative of the Black population at large.”
In this study, “they’re a little bit more healthcare inclined,” Dr. George notes. The study population is actively seeking the PSA test. Their socioeconomic profile might be closer to their White counterparts’, and that may make results more similar, he said.
“It’s possible that because this is a screening and not just men coming in for symptoms or cause, that we’re not seeing as much advanced disease,” he continued.
Amar Kishan, MD, chief of the genitourinary oncology service at University of California Los Angeles (UCLA) Health, says the genomic factors and environmental stressors that lead to elevated PSA counts don’t necessarily translate into aggressiveness of disease.
Why do Different Races have Different Prostate Cancer Risk?
Dr. George points out that the study also highlights that Asian men were significantly less likely to be diagnosed with prostate cancer within 1 year of the test.
The reasons for differences in prostate risk by race are complex, he notes. There are some clues that biologic factors may be at work. For instance, early puberty has a link to prostate cancer as it does to breast cancer, and height is also associated with a greater risk of prostate cancer, Dr. George said.
It’s not necessarily a racial association but there are some biological factors associated with prostate cancer later in life, he explained. “These may be enriched in certain populations, including northern Europeans and patients with African ancestries.”
The study also notes that Black men are more likely to die from prostate cancer than are White men, and Asian men are less likely than White or Black men to die from it.
Ms. Down said the difference in prostate cancer mortality between Black vs White men, in particular, may be related to a number of factors, and age, and lifetime risk of prostate cancer may play a major role, at least in the UK.
Should There Be Different ‘Normal’ PSA Levels for Different Races?
Dr. George says there is likely a need to change the system because a PSA level in one race may not signal the same risk it does in another. So medicine probably needs to standardize what a “normal” PSA is by race, he says, adding that he is a coauthor of an upcoming paper regarding that issue.
The lowest instances of prostate cancer were in Asian patients so this isn’t just a Black and White issue, Dr. George notes. “Being able to establish benchmarks by race and ethnicity is something that is probably needed in the field,” he says.
Dr. Kishan, on the other hand, says data from this study are not enough to support differentiating PSA levels based on race. He noted a limitation of the study is that it was not able to calculate the false-negative rate of PSA tests.
What are the Implications for Treating and Screening for Prostate Cancer
Dr. Kishan says there may be a role for increased intensity of screening, whether at an earlier age or with different intervals, but prostate cancer treatment should not differ by race.
“Our prior study, as well as others,” he says, “have shown that when you balance Black and White patients for every factor that might impact prognosis other than race — such as age, disease aggressiveness, etc. — Black men actually tend to have better outcomes than White men. Thus, it would mean potentially overtreating (i.e., causing unnecessary side effects) to increase treatment intensity purely based on race with the available data.”
According to the paper, prostate cancer incidence in men with higher PSA levels increases with increasing age, even when using age-adjusted thresholds.
Dr. George says we know from this study and other studies as well that Black men are more likely to be diagnosed with prostate at a younger age. “Therefore, we probably need to be thinking about screening Black men starting at a younger age. These are the men who are most likely to benefit from an intervention — patients who have life expectancies of 20 years or more.”
What are the Downsides to Overdiagnosing Prostate Cancer in Men?
“It’s one of the biggest concerns that men have in proactively seeking healthcare,” Dr. George says. “They’re more likely to undergo treatment for this disease if they’re getting screened because (clinicians are) more likely to find it.”
Some of those men, he says, are going to undergo treatment for disease that won’t ultimately kill them, but may cause complications the men shouldn’t have had at all or otherwise may have had later.
“Overtreatment is a real concern. That’s why active surveillance is so important to minimize overtreatment of patients by finding out which cancers are low risk for progression and which are becoming more aggressive,” Dr. George says.
Authors of the study write that “the potential for overdiagnosis and the subsequent psychological and physical impact of diagnosis and treatment is an important consideration.”
All authors of the new paper received financial support from Cancer Research UK, the National Institute for Health and Care Research (NIHR), and the Higgins family for the submitted work.
Dr. George reports no relevant financial relationships.
Dr. Kishan reports consulting fees and speaking honoraria from Varian Medical Systems, Janssen, and Boston Scientific; research funding from PointBioPharma, Lantheus, and Janssen; and serving on advisory boards for Lantheus, Janssen and Boston Scientific.
There was a substantial difference in prostate cancer diagnosis across ethnic groups: 25% of Black men with a raised PSA were diagnosed with prostate cancer within 1 year of being tested, compared with 20% of White men and 13% of Asian men, in the analysis of a large primary care cohort in the United Kingdom.
Incidence of advanced prostate cancer for Asian men with a raised PSA result was 4.5%, compared with 7.5% for White men and 7.0% for Black men.
Men included in the study were aged 40 and older and had no prior cancer diagnosis. Their ethnicity and PSA test result were logged in a national dataset between 2010 and 2017.
The study of more than 730,000 men, published in BMC Medicine, didn’t explore reasons for the differences, but experts offer their thoughts on what led to the findings and what these results imply.
Why the Higher Diagnosis Rates but Not More Advanced Disease in Black Men?
Lead author Liz Down, a graduate research assistant at the University of Exeter, Exeter, England, suggests the higher diagnosis rates but not more advanced disease in Black men may be linked to genetic variations.
Her team’s studies have shown that Black men in the United Kingdom and United States have higher levels of PSA. The PSA value is used to identify patients who might benefit from specialist investigation, and current guidelines in the UK and US don’t distinguish between ethnic groups.
As most men have slow-growing prostate cancer, this may lead to a disproportionately higher number of Black men being diagnosed with prostate cancer, she said.
“One possible interpretation,” Ms. Down notes, “is that prostate cancer follows a similar trajectory in Black and White men. What is different, however, is that Black men have higher PSA levels.”
As to why the advanced-cancer incidence is similar in Black and White patients in the study, Daniel George, MD, director of genitourinary oncology at Duke Cancer Institute in Durham, North Carolina, says it’s important to understand that the Black men in this study “are not necessarily representative of the Black population at large.”
In this study, “they’re a little bit more healthcare inclined,” Dr. George notes. The study population is actively seeking the PSA test. Their socioeconomic profile might be closer to their White counterparts’, and that may make results more similar, he said.
“It’s possible that because this is a screening and not just men coming in for symptoms or cause, that we’re not seeing as much advanced disease,” he continued.
Amar Kishan, MD, chief of the genitourinary oncology service at University of California Los Angeles (UCLA) Health, says the genomic factors and environmental stressors that lead to elevated PSA counts don’t necessarily translate into aggressiveness of disease.
Why do Different Races have Different Prostate Cancer Risk?
Dr. George points out that the study also highlights that Asian men were significantly less likely to be diagnosed with prostate cancer within 1 year of the test.
The reasons for differences in prostate risk by race are complex, he notes. There are some clues that biologic factors may be at work. For instance, early puberty has a link to prostate cancer as it does to breast cancer, and height is also associated with a greater risk of prostate cancer, Dr. George said.
It’s not necessarily a racial association but there are some biological factors associated with prostate cancer later in life, he explained. “These may be enriched in certain populations, including northern Europeans and patients with African ancestries.”
The study also notes that Black men are more likely to die from prostate cancer than are White men, and Asian men are less likely than White or Black men to die from it.
Ms. Down said the difference in prostate cancer mortality between Black vs White men, in particular, may be related to a number of factors, and age, and lifetime risk of prostate cancer may play a major role, at least in the UK.
Should There Be Different ‘Normal’ PSA Levels for Different Races?
Dr. George says there is likely a need to change the system because a PSA level in one race may not signal the same risk it does in another. So medicine probably needs to standardize what a “normal” PSA is by race, he says, adding that he is a coauthor of an upcoming paper regarding that issue.
The lowest instances of prostate cancer were in Asian patients so this isn’t just a Black and White issue, Dr. George notes. “Being able to establish benchmarks by race and ethnicity is something that is probably needed in the field,” he says.
Dr. Kishan, on the other hand, says data from this study are not enough to support differentiating PSA levels based on race. He noted a limitation of the study is that it was not able to calculate the false-negative rate of PSA tests.
What are the Implications for Treating and Screening for Prostate Cancer
Dr. Kishan says there may be a role for increased intensity of screening, whether at an earlier age or with different intervals, but prostate cancer treatment should not differ by race.
“Our prior study, as well as others,” he says, “have shown that when you balance Black and White patients for every factor that might impact prognosis other than race — such as age, disease aggressiveness, etc. — Black men actually tend to have better outcomes than White men. Thus, it would mean potentially overtreating (i.e., causing unnecessary side effects) to increase treatment intensity purely based on race with the available data.”
According to the paper, prostate cancer incidence in men with higher PSA levels increases with increasing age, even when using age-adjusted thresholds.
Dr. George says we know from this study and other studies as well that Black men are more likely to be diagnosed with prostate at a younger age. “Therefore, we probably need to be thinking about screening Black men starting at a younger age. These are the men who are most likely to benefit from an intervention — patients who have life expectancies of 20 years or more.”
What are the Downsides to Overdiagnosing Prostate Cancer in Men?
“It’s one of the biggest concerns that men have in proactively seeking healthcare,” Dr. George says. “They’re more likely to undergo treatment for this disease if they’re getting screened because (clinicians are) more likely to find it.”
Some of those men, he says, are going to undergo treatment for disease that won’t ultimately kill them, but may cause complications the men shouldn’t have had at all or otherwise may have had later.
“Overtreatment is a real concern. That’s why active surveillance is so important to minimize overtreatment of patients by finding out which cancers are low risk for progression and which are becoming more aggressive,” Dr. George says.
Authors of the study write that “the potential for overdiagnosis and the subsequent psychological and physical impact of diagnosis and treatment is an important consideration.”
All authors of the new paper received financial support from Cancer Research UK, the National Institute for Health and Care Research (NIHR), and the Higgins family for the submitted work.
Dr. George reports no relevant financial relationships.
Dr. Kishan reports consulting fees and speaking honoraria from Varian Medical Systems, Janssen, and Boston Scientific; research funding from PointBioPharma, Lantheus, and Janssen; and serving on advisory boards for Lantheus, Janssen and Boston Scientific.
FROM BMC MEDICINE