User login
Diabetes Hub contains news and clinical review articles for physicians seeking the most up-to-date information on the rapidly evolving options for treating and preventing Type 2 Diabetes in at-risk patients. The Diabetes Hub is powered by Frontline Medical Communications.
Weight gain after GDM linked to type 2 diabetes
Women who had gestational diabetes mellitus and gained weight after pregnancy were significantly more likely to progress to type 2 diabetes, according to a study.
Among the 1,695 women in the Diabetes & Women’s Health study with a history of gestational diabetes mellitus (GDM), researchers documented 259 incident cases of type 2 diabetes during up to 18 years of follow-up. Each 1 kg/m2 increase in baseline body mass index was associated with a 16% higher risk of type 2 diabetes (hazard ratio, 1.16).
Each 5 kg of weight gain after the development of GDM was associated with a 27% higher risk of type 2 diabetes (HR, 1.27).
“Our findings provide evidence to support the recent call from the [National Diabetes Education Program] and highlight the importance of achieving and maintaining a healthy weight in these high-risk women to prevent future development of type 2 diabetes,” the researchers wrote.
The study was supported by the National Institute of Child Health and Human Development, part of the National Institutes of Health.
Read the full study in Diabetologia (doi: 10.1007/s00125-015-3537-4).
Women who had gestational diabetes mellitus and gained weight after pregnancy were significantly more likely to progress to type 2 diabetes, according to a study.
Among the 1,695 women in the Diabetes & Women’s Health study with a history of gestational diabetes mellitus (GDM), researchers documented 259 incident cases of type 2 diabetes during up to 18 years of follow-up. Each 1 kg/m2 increase in baseline body mass index was associated with a 16% higher risk of type 2 diabetes (hazard ratio, 1.16).
Each 5 kg of weight gain after the development of GDM was associated with a 27% higher risk of type 2 diabetes (HR, 1.27).
“Our findings provide evidence to support the recent call from the [National Diabetes Education Program] and highlight the importance of achieving and maintaining a healthy weight in these high-risk women to prevent future development of type 2 diabetes,” the researchers wrote.
The study was supported by the National Institute of Child Health and Human Development, part of the National Institutes of Health.
Read the full study in Diabetologia (doi: 10.1007/s00125-015-3537-4).
Women who had gestational diabetes mellitus and gained weight after pregnancy were significantly more likely to progress to type 2 diabetes, according to a study.
Among the 1,695 women in the Diabetes & Women’s Health study with a history of gestational diabetes mellitus (GDM), researchers documented 259 incident cases of type 2 diabetes during up to 18 years of follow-up. Each 1 kg/m2 increase in baseline body mass index was associated with a 16% higher risk of type 2 diabetes (hazard ratio, 1.16).
Each 5 kg of weight gain after the development of GDM was associated with a 27% higher risk of type 2 diabetes (HR, 1.27).
“Our findings provide evidence to support the recent call from the [National Diabetes Education Program] and highlight the importance of achieving and maintaining a healthy weight in these high-risk women to prevent future development of type 2 diabetes,” the researchers wrote.
The study was supported by the National Institute of Child Health and Human Development, part of the National Institutes of Health.
Read the full study in Diabetologia (doi: 10.1007/s00125-015-3537-4).
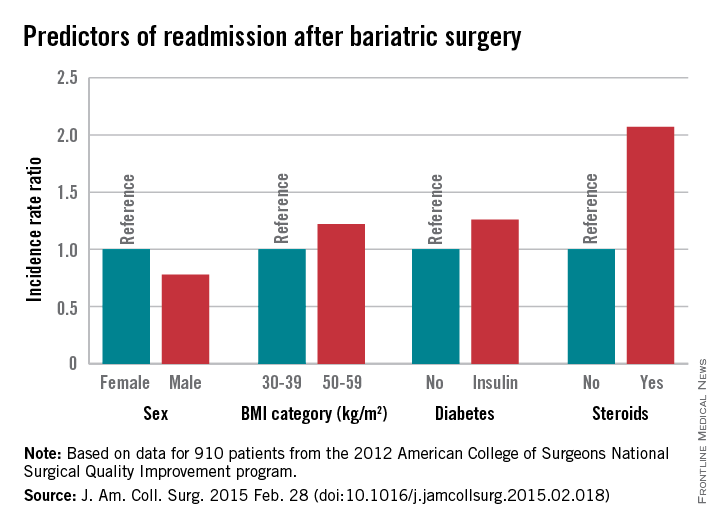
Several factors predict postbariatric surgery readmission
Bariatric surgery is generally safe and readmissions are rare, but prolonged operative time, operation complexity, and major postoperative complications are among several risk factors for readmission identified in a large retrospective cohort.
Of 18,186 patients from the 2012 American College of Surgeons National Surgical Quality Improvement program (ACS NSQIP) database who had bariatric surgery as a primary procedure, 5% were readmitted. Of 815 patients with any major complication, 31% were readmitted. Factors found on multivariate analysis to significantly predict readmission within 30 days were age, sex, body mass index, American Society of Anesthesiology (ASA) risk class, diabetes status, hypertension, and steroid use, Dr. Christa R. Abraham of Albany (N.Y.) Medical College and her colleagues reported online in the Journal of the American College of Surgeons.

Further, all major postoperative complications were significant predictors of readmission, including bleeding requiring transfusion, urinary tract infections, and superficial surgical site infection (SSI). Other significant predictors were deep SSI, organ space SSI, wound disruption, pneumonia, unplanned intubation, mechanical ventilation for more than 48 hours, pulmonary embolism, deep vein thrombosis, and sepsis, the investigators said (J. Am. Coll. Surg. 2015 [doi:10.1016/j.jamcollsurg.2015.02.018]).
Of the patients included in the study, 1,819 had a laparoscopic gastric band, 9,613 had laparoscopic Roux-en-Y gastric bypass, 6,439 had gastroplasties, and 315 had open Roux-en-Y gastric bypass. All had a BMI of at least 30 kg/m2, and had a postsurgery length of stay of 14 days or fewer. Most were ASA risk class 3 or lower, and most were functionally independent.
Complications were more common with laparoscopic and open Roux-en-y gastric bypass (5.5% and 11.8%, respectively) rather than with gastroplasty and sleeve (3.4%) and laparoscopic banding (1.4%).
The findings are of value, because while bariatric surgery is a low-risk procedure, and it is extremely common; in 2013 there were 179,000 such surgeries performed in the United States.
“Bariatric surgery is one of the fastest-growing surgical interest areas, making analysis of patient outcomes and reasons for readmission important,” the investigators explained.
The ability to identify high-risk patients could allow for targeted interventions to prevent readmission, they said.
For example, steroid use, which was identified as a risk factor in the current study, is modifiable.
“In our practice, steroids are discontinued for 6 weeks prior to bariatric surgery and patients who are steroid dependent are unlikely to undergo bariatric surgery,” they said.
Additionally, they “try to minimize readmission for patients with infections by treating with antibiotics following operation and continuing antibiotics at discharge.”
The investigators noted that the ACS NSQIP MORBPROB (estimated probability of morbidity) tool is a good tool for predicting readmission among prospective bariatric patients, although it may not fully capture the effect of preexisting conditions.
“These data led us to change our own practice by risk-stratifying patients with higher ASA and BMI to consider surgical options, and to begin early surveillance soon after discharge,” they said.
The authors reported having no disclosures.
Bariatric surgery is generally safe and readmissions are rare, but prolonged operative time, operation complexity, and major postoperative complications are among several risk factors for readmission identified in a large retrospective cohort.
Of 18,186 patients from the 2012 American College of Surgeons National Surgical Quality Improvement program (ACS NSQIP) database who had bariatric surgery as a primary procedure, 5% were readmitted. Of 815 patients with any major complication, 31% were readmitted. Factors found on multivariate analysis to significantly predict readmission within 30 days were age, sex, body mass index, American Society of Anesthesiology (ASA) risk class, diabetes status, hypertension, and steroid use, Dr. Christa R. Abraham of Albany (N.Y.) Medical College and her colleagues reported online in the Journal of the American College of Surgeons.
Further, all major postoperative complications were significant predictors of readmission, including bleeding requiring transfusion, urinary tract infections, and superficial surgical site infection (SSI). Other significant predictors were deep SSI, organ space SSI, wound disruption, pneumonia, unplanned intubation, mechanical ventilation for more than 48 hours, pulmonary embolism, deep vein thrombosis, and sepsis, the investigators said (J. Am. Coll. Surg. 2015 [doi:10.1016/j.jamcollsurg.2015.02.018]).
Of the patients included in the study, 1,819 had a laparoscopic gastric band, 9,613 had laparoscopic Roux-en-Y gastric bypass, 6,439 had gastroplasties, and 315 had open Roux-en-Y gastric bypass. All had a BMI of at least 30 kg/m2, and had a postsurgery length of stay of 14 days or fewer. Most were ASA risk class 3 or lower, and most were functionally independent.
Complications were more common with laparoscopic and open Roux-en-y gastric bypass (5.5% and 11.8%, respectively) rather than with gastroplasty and sleeve (3.4%) and laparoscopic banding (1.4%).
The findings are of value, because while bariatric surgery is a low-risk procedure, and it is extremely common; in 2013 there were 179,000 such surgeries performed in the United States.
“Bariatric surgery is one of the fastest-growing surgical interest areas, making analysis of patient outcomes and reasons for readmission important,” the investigators explained.
The ability to identify high-risk patients could allow for targeted interventions to prevent readmission, they said.
For example, steroid use, which was identified as a risk factor in the current study, is modifiable.
“In our practice, steroids are discontinued for 6 weeks prior to bariatric surgery and patients who are steroid dependent are unlikely to undergo bariatric surgery,” they said.
Additionally, they “try to minimize readmission for patients with infections by treating with antibiotics following operation and continuing antibiotics at discharge.”
The investigators noted that the ACS NSQIP MORBPROB (estimated probability of morbidity) tool is a good tool for predicting readmission among prospective bariatric patients, although it may not fully capture the effect of preexisting conditions.
“These data led us to change our own practice by risk-stratifying patients with higher ASA and BMI to consider surgical options, and to begin early surveillance soon after discharge,” they said.
The authors reported having no disclosures.
Bariatric surgery is generally safe and readmissions are rare, but prolonged operative time, operation complexity, and major postoperative complications are among several risk factors for readmission identified in a large retrospective cohort.
Of 18,186 patients from the 2012 American College of Surgeons National Surgical Quality Improvement program (ACS NSQIP) database who had bariatric surgery as a primary procedure, 5% were readmitted. Of 815 patients with any major complication, 31% were readmitted. Factors found on multivariate analysis to significantly predict readmission within 30 days were age, sex, body mass index, American Society of Anesthesiology (ASA) risk class, diabetes status, hypertension, and steroid use, Dr. Christa R. Abraham of Albany (N.Y.) Medical College and her colleagues reported online in the Journal of the American College of Surgeons.
Further, all major postoperative complications were significant predictors of readmission, including bleeding requiring transfusion, urinary tract infections, and superficial surgical site infection (SSI). Other significant predictors were deep SSI, organ space SSI, wound disruption, pneumonia, unplanned intubation, mechanical ventilation for more than 48 hours, pulmonary embolism, deep vein thrombosis, and sepsis, the investigators said (J. Am. Coll. Surg. 2015 [doi:10.1016/j.jamcollsurg.2015.02.018]).
Of the patients included in the study, 1,819 had a laparoscopic gastric band, 9,613 had laparoscopic Roux-en-Y gastric bypass, 6,439 had gastroplasties, and 315 had open Roux-en-Y gastric bypass. All had a BMI of at least 30 kg/m2, and had a postsurgery length of stay of 14 days or fewer. Most were ASA risk class 3 or lower, and most were functionally independent.
Complications were more common with laparoscopic and open Roux-en-y gastric bypass (5.5% and 11.8%, respectively) rather than with gastroplasty and sleeve (3.4%) and laparoscopic banding (1.4%).
The findings are of value, because while bariatric surgery is a low-risk procedure, and it is extremely common; in 2013 there were 179,000 such surgeries performed in the United States.
“Bariatric surgery is one of the fastest-growing surgical interest areas, making analysis of patient outcomes and reasons for readmission important,” the investigators explained.
The ability to identify high-risk patients could allow for targeted interventions to prevent readmission, they said.
For example, steroid use, which was identified as a risk factor in the current study, is modifiable.
“In our practice, steroids are discontinued for 6 weeks prior to bariatric surgery and patients who are steroid dependent are unlikely to undergo bariatric surgery,” they said.
Additionally, they “try to minimize readmission for patients with infections by treating with antibiotics following operation and continuing antibiotics at discharge.”
The investigators noted that the ACS NSQIP MORBPROB (estimated probability of morbidity) tool is a good tool for predicting readmission among prospective bariatric patients, although it may not fully capture the effect of preexisting conditions.
“These data led us to change our own practice by risk-stratifying patients with higher ASA and BMI to consider surgical options, and to begin early surveillance soon after discharge,” they said.
The authors reported having no disclosures.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF SURGEONS
Key clinical point: Knowing risk factors for readmission after bariatric surgery can allow for targeted interventions.
Major finding: Steroid use is among several risk factors for readmission following bariatric surgery (incidence rate ratio, 2.07)
Data source: A retrospective cohort study involving 18,186 patients.
Disclosures: The authors reported having no disclosures.

Midlife blood pressure patterns predict CVD, mortality risk
BALTIMORE – Distinct patterns of blood pressure changes in midlife are associated with varying degrees of risk for cardiovascular disease and death, according to a multisite study.
These patterns of change contributed to risk for both CVD and mortality, separate from the known association of absolute elevation of systolic blood pressure with CVD and death. Natalia Petruski-Ivleva of the University of North Carolina, Chapel Hill, and colleagues identified SBP patterns emerging from the biracial, multisite Atherosclerosis Risk in Communities (ARIC) study and presented the results at the American Heart Association Epidemiology and Prevention, Lifestyle and Cardiometabolic Health 2015 Scientific Sessions.

The study included 9,882 patients from the ARIC population who had recorded BPs at four study visits between 1987 and 1998, and whose outcomes were tracked over the period from 1987 to 2011. Median follow-up after the last study visit was 13.2 years. Participants were grouped by patterns of change in SBP over time using a latent class growth model; this analytic model allowed for the discovery of similar groups of cases within the data.
Results were adjusted for age and demographic characteristics, as well as for self-reported hypertension medication use. In addition to all-cause mortality, outcomes included coronary heart disease, heart failure, and stroke.
In all, six distinct patterns emerged of change in SBP over the study visit period, with three groups having SBPs consistently below the threshold of 140 mm Hg, and three other groups showing varying patterns of elevation. About 84% of participants fell into one of the three groups that showed parallel patterns of SBP change, with pressures slowly rising over time, but never exceeding 140 mm Hg. The remainder of participants were grouped into three other patterns. One showed a steep increase over time from an initial SBP just under 140 mm Hg to a final reading just over 160 mm Hg; a second showed high and sustained SBPs of more than 160 mm Hg at all study visits. Finally, some participants had initially elevated SBPs that fell to the normal range by the end of the study.
Overall, analysis showed a gradient of risk, with lower SBP associated with lower risk of CVD and death. This was true even for those participants in the first three groups, whose SBPs stayed below 140 mm Hg throughout. Notably, the pattern of steep increase of already elevated SBP, as well as that of sustained elevated blood pressures, were both associated with the highest all-cause mortality. Reducing SBP to less than 140 mm Hg was not associated with reduced risk of CHD in the final group.
The three higher-risk groups were more likely to be obese, black, on hypertension medication, and have diabetes. They were also older on average than participants with the three nonelevated patterns.
These patterns of change, said Ms. Petruski-Ivleva, “contribute varying amounts of risk of CVD and mortality in addition to the risk imparted by the absolute SBP level.” Though the clinical significance of these patterns of blood pressure change needs more examination, she said that the results underscore the cumulative impact of elevated SBP through midlife.
BALTIMORE – Distinct patterns of blood pressure changes in midlife are associated with varying degrees of risk for cardiovascular disease and death, according to a multisite study.
These patterns of change contributed to risk for both CVD and mortality, separate from the known association of absolute elevation of systolic blood pressure with CVD and death. Natalia Petruski-Ivleva of the University of North Carolina, Chapel Hill, and colleagues identified SBP patterns emerging from the biracial, multisite Atherosclerosis Risk in Communities (ARIC) study and presented the results at the American Heart Association Epidemiology and Prevention, Lifestyle and Cardiometabolic Health 2015 Scientific Sessions.
The study included 9,882 patients from the ARIC population who had recorded BPs at four study visits between 1987 and 1998, and whose outcomes were tracked over the period from 1987 to 2011. Median follow-up after the last study visit was 13.2 years. Participants were grouped by patterns of change in SBP over time using a latent class growth model; this analytic model allowed for the discovery of similar groups of cases within the data.
Results were adjusted for age and demographic characteristics, as well as for self-reported hypertension medication use. In addition to all-cause mortality, outcomes included coronary heart disease, heart failure, and stroke.
In all, six distinct patterns emerged of change in SBP over the study visit period, with three groups having SBPs consistently below the threshold of 140 mm Hg, and three other groups showing varying patterns of elevation. About 84% of participants fell into one of the three groups that showed parallel patterns of SBP change, with pressures slowly rising over time, but never exceeding 140 mm Hg. The remainder of participants were grouped into three other patterns. One showed a steep increase over time from an initial SBP just under 140 mm Hg to a final reading just over 160 mm Hg; a second showed high and sustained SBPs of more than 160 mm Hg at all study visits. Finally, some participants had initially elevated SBPs that fell to the normal range by the end of the study.
Overall, analysis showed a gradient of risk, with lower SBP associated with lower risk of CVD and death. This was true even for those participants in the first three groups, whose SBPs stayed below 140 mm Hg throughout. Notably, the pattern of steep increase of already elevated SBP, as well as that of sustained elevated blood pressures, were both associated with the highest all-cause mortality. Reducing SBP to less than 140 mm Hg was not associated with reduced risk of CHD in the final group.
The three higher-risk groups were more likely to be obese, black, on hypertension medication, and have diabetes. They were also older on average than participants with the three nonelevated patterns.
These patterns of change, said Ms. Petruski-Ivleva, “contribute varying amounts of risk of CVD and mortality in addition to the risk imparted by the absolute SBP level.” Though the clinical significance of these patterns of blood pressure change needs more examination, she said that the results underscore the cumulative impact of elevated SBP through midlife.
BALTIMORE – Distinct patterns of blood pressure changes in midlife are associated with varying degrees of risk for cardiovascular disease and death, according to a multisite study.
These patterns of change contributed to risk for both CVD and mortality, separate from the known association of absolute elevation of systolic blood pressure with CVD and death. Natalia Petruski-Ivleva of the University of North Carolina, Chapel Hill, and colleagues identified SBP patterns emerging from the biracial, multisite Atherosclerosis Risk in Communities (ARIC) study and presented the results at the American Heart Association Epidemiology and Prevention, Lifestyle and Cardiometabolic Health 2015 Scientific Sessions.
The study included 9,882 patients from the ARIC population who had recorded BPs at four study visits between 1987 and 1998, and whose outcomes were tracked over the period from 1987 to 2011. Median follow-up after the last study visit was 13.2 years. Participants were grouped by patterns of change in SBP over time using a latent class growth model; this analytic model allowed for the discovery of similar groups of cases within the data.
Results were adjusted for age and demographic characteristics, as well as for self-reported hypertension medication use. In addition to all-cause mortality, outcomes included coronary heart disease, heart failure, and stroke.
In all, six distinct patterns emerged of change in SBP over the study visit period, with three groups having SBPs consistently below the threshold of 140 mm Hg, and three other groups showing varying patterns of elevation. About 84% of participants fell into one of the three groups that showed parallel patterns of SBP change, with pressures slowly rising over time, but never exceeding 140 mm Hg. The remainder of participants were grouped into three other patterns. One showed a steep increase over time from an initial SBP just under 140 mm Hg to a final reading just over 160 mm Hg; a second showed high and sustained SBPs of more than 160 mm Hg at all study visits. Finally, some participants had initially elevated SBPs that fell to the normal range by the end of the study.
Overall, analysis showed a gradient of risk, with lower SBP associated with lower risk of CVD and death. This was true even for those participants in the first three groups, whose SBPs stayed below 140 mm Hg throughout. Notably, the pattern of steep increase of already elevated SBP, as well as that of sustained elevated blood pressures, were both associated with the highest all-cause mortality. Reducing SBP to less than 140 mm Hg was not associated with reduced risk of CHD in the final group.
The three higher-risk groups were more likely to be obese, black, on hypertension medication, and have diabetes. They were also older on average than participants with the three nonelevated patterns.
These patterns of change, said Ms. Petruski-Ivleva, “contribute varying amounts of risk of CVD and mortality in addition to the risk imparted by the absolute SBP level.” Though the clinical significance of these patterns of blood pressure change needs more examination, she said that the results underscore the cumulative impact of elevated SBP through midlife.
AT AHA EPI/LIFESTYLE 2015
Key clinical point: Systolic blood pressures at midlife fall into patterns associated with varying degrees of CVD risk.
Major finding: Lower SBP was associated with lower risk of CVD and death, and a pattern of steep increase of already elevated SBP was associated with higher all-cause mortality.
Data source: Analysis of longitudinal change in SBP of nearly 10,000 participants in the multiracial, multisite ARIC study.
Disclosures: ARIC is supported by the National Heart, Lung, and Blood Institute. No authors reported financial disclosures.

CDC, AMA launch nationwide prediabetes awareness initiative
The Centers for Disease Control and Prevention have joined the American Medical Association to create a new program aimed at reducing the number of Americans diagnosed with type 2 diabetes, one of the most common chronic medical conditions in the United States.
The initiative, entitled “Prevent Diabetes STAT: Screen, Test, Act – Today,” will focus on individuals who have prediabetes, which is characterized by having blood glucose levels that are higher than normal but not high enough to be considered diabetic. Unless they are able to lose weight through diet and exercise, 15%-30% of prediabetic individuals are diagnosed with type 2 diabetes within 5 years of becoming prediabetic.

“This isn’t just a concern: It’s a crisis,” said AMA president Robert M. Wah, during a telebriefing on Thursday. “It’s not only taking a physical and emotional toll on people living with prediabetes, but it also takes an economic toll on our country. More than $245 billion in health care spending and reduced productivity is directly linked to diabetes,” Dr. Wah said.
“The truth is, our health care system simply can not sustain the growing number of people developing diabetes,” said Ann Albright, Ph.D., director of the CDC’s Division of Diabetes Translation, during the same telebriefing. “Research shows that screening, testing, and referring people who are at risk for type 2 diabetes is critical, [and] that when people know they have prediabetes, they are more likely to take action.”
To that end, the AMA and CDC have created an online “toolkit” that allows health care providers and patients to understand the risks and signs of prediabetes. The toolkit will offer resources on how to prevent high blood glucose levels from progressing to type 2 diabetes. Additionally, both organizations have created an online screening tool that allows visitors to determine their risk for prediabetes.

Health care providers are another key component of Prevent Diabetes STAT, said Dr. Wah and Dr. Albright, who urged physicians and health care teams to actively screen patients using either the CDC’s Prediabetes Screening Test or the American Diabetes Association’s Type 2 Diabetes Risk Test, test for prediabetes using one of three recommended blood tests, and refer prediabetic patients to a CDC-recognized prevention program.
Prevent Diabetes STAT is intended to be a multiyear program. It represents an expansion of previous efforts undertaken individually by the CDC and AMA to combat the growing diabetes epidemic. In 2012, the CDC created the National Diabetes Prevention Program, using data from the National Institutes of Health, to create a framework of more than 500 programs designed to help people with diabetes institute meaningful lifestyle changes. The AMA launched a similar initiative in 2013 known as Improving Health Outcomes, which included partnering with YMCAs around the country to refer at-risk youths to diabetes prevention programs recognized by the CDC.
“We have seen significant progress, but we’ve really got to be sure that we get this [diabetes initiative] to a larger number of people,” said Dr. Albright. “We need to allow this to be scaled nationally [by] taking the successes that we’ve had and the lessons that we’ve learned, [but] in order to do that, people have to receive a diagnosis of prediabetes so that they can get connected to these services.”
According to the AMA, there are currently more than 86 million individuals in the United States living with prediabetes, yet roughly 90% of those people don’t even know they have it. The CDC estimates that the number of individuals diagnosed with diabetes in the United States more than tripled from 1980 to 2011, going from 5.6 million to nearly 21 million in just over 30 years. In 2011, 19.6 million American adults were diagnosed with diabetes; right now, according to the AMA and CDC, more than 33% of American adults are living with prediabetes.
The Centers for Disease Control and Prevention have joined the American Medical Association to create a new program aimed at reducing the number of Americans diagnosed with type 2 diabetes, one of the most common chronic medical conditions in the United States.
The initiative, entitled “Prevent Diabetes STAT: Screen, Test, Act – Today,” will focus on individuals who have prediabetes, which is characterized by having blood glucose levels that are higher than normal but not high enough to be considered diabetic. Unless they are able to lose weight through diet and exercise, 15%-30% of prediabetic individuals are diagnosed with type 2 diabetes within 5 years of becoming prediabetic.
“This isn’t just a concern: It’s a crisis,” said AMA president Robert M. Wah, during a telebriefing on Thursday. “It’s not only taking a physical and emotional toll on people living with prediabetes, but it also takes an economic toll on our country. More than $245 billion in health care spending and reduced productivity is directly linked to diabetes,” Dr. Wah said.
“The truth is, our health care system simply can not sustain the growing number of people developing diabetes,” said Ann Albright, Ph.D., director of the CDC’s Division of Diabetes Translation, during the same telebriefing. “Research shows that screening, testing, and referring people who are at risk for type 2 diabetes is critical, [and] that when people know they have prediabetes, they are more likely to take action.”
To that end, the AMA and CDC have created an online “toolkit” that allows health care providers and patients to understand the risks and signs of prediabetes. The toolkit will offer resources on how to prevent high blood glucose levels from progressing to type 2 diabetes. Additionally, both organizations have created an online screening tool that allows visitors to determine their risk for prediabetes.
Health care providers are another key component of Prevent Diabetes STAT, said Dr. Wah and Dr. Albright, who urged physicians and health care teams to actively screen patients using either the CDC’s Prediabetes Screening Test or the American Diabetes Association’s Type 2 Diabetes Risk Test, test for prediabetes using one of three recommended blood tests, and refer prediabetic patients to a CDC-recognized prevention program.
Prevent Diabetes STAT is intended to be a multiyear program. It represents an expansion of previous efforts undertaken individually by the CDC and AMA to combat the growing diabetes epidemic. In 2012, the CDC created the National Diabetes Prevention Program, using data from the National Institutes of Health, to create a framework of more than 500 programs designed to help people with diabetes institute meaningful lifestyle changes. The AMA launched a similar initiative in 2013 known as Improving Health Outcomes, which included partnering with YMCAs around the country to refer at-risk youths to diabetes prevention programs recognized by the CDC.
“We have seen significant progress, but we’ve really got to be sure that we get this [diabetes initiative] to a larger number of people,” said Dr. Albright. “We need to allow this to be scaled nationally [by] taking the successes that we’ve had and the lessons that we’ve learned, [but] in order to do that, people have to receive a diagnosis of prediabetes so that they can get connected to these services.”
According to the AMA, there are currently more than 86 million individuals in the United States living with prediabetes, yet roughly 90% of those people don’t even know they have it. The CDC estimates that the number of individuals diagnosed with diabetes in the United States more than tripled from 1980 to 2011, going from 5.6 million to nearly 21 million in just over 30 years. In 2011, 19.6 million American adults were diagnosed with diabetes; right now, according to the AMA and CDC, more than 33% of American adults are living with prediabetes.
The Centers for Disease Control and Prevention have joined the American Medical Association to create a new program aimed at reducing the number of Americans diagnosed with type 2 diabetes, one of the most common chronic medical conditions in the United States.
The initiative, entitled “Prevent Diabetes STAT: Screen, Test, Act – Today,” will focus on individuals who have prediabetes, which is characterized by having blood glucose levels that are higher than normal but not high enough to be considered diabetic. Unless they are able to lose weight through diet and exercise, 15%-30% of prediabetic individuals are diagnosed with type 2 diabetes within 5 years of becoming prediabetic.
“This isn’t just a concern: It’s a crisis,” said AMA president Robert M. Wah, during a telebriefing on Thursday. “It’s not only taking a physical and emotional toll on people living with prediabetes, but it also takes an economic toll on our country. More than $245 billion in health care spending and reduced productivity is directly linked to diabetes,” Dr. Wah said.
“The truth is, our health care system simply can not sustain the growing number of people developing diabetes,” said Ann Albright, Ph.D., director of the CDC’s Division of Diabetes Translation, during the same telebriefing. “Research shows that screening, testing, and referring people who are at risk for type 2 diabetes is critical, [and] that when people know they have prediabetes, they are more likely to take action.”
To that end, the AMA and CDC have created an online “toolkit” that allows health care providers and patients to understand the risks and signs of prediabetes. The toolkit will offer resources on how to prevent high blood glucose levels from progressing to type 2 diabetes. Additionally, both organizations have created an online screening tool that allows visitors to determine their risk for prediabetes.
Health care providers are another key component of Prevent Diabetes STAT, said Dr. Wah and Dr. Albright, who urged physicians and health care teams to actively screen patients using either the CDC’s Prediabetes Screening Test or the American Diabetes Association’s Type 2 Diabetes Risk Test, test for prediabetes using one of three recommended blood tests, and refer prediabetic patients to a CDC-recognized prevention program.
Prevent Diabetes STAT is intended to be a multiyear program. It represents an expansion of previous efforts undertaken individually by the CDC and AMA to combat the growing diabetes epidemic. In 2012, the CDC created the National Diabetes Prevention Program, using data from the National Institutes of Health, to create a framework of more than 500 programs designed to help people with diabetes institute meaningful lifestyle changes. The AMA launched a similar initiative in 2013 known as Improving Health Outcomes, which included partnering with YMCAs around the country to refer at-risk youths to diabetes prevention programs recognized by the CDC.
“We have seen significant progress, but we’ve really got to be sure that we get this [diabetes initiative] to a larger number of people,” said Dr. Albright. “We need to allow this to be scaled nationally [by] taking the successes that we’ve had and the lessons that we’ve learned, [but] in order to do that, people have to receive a diagnosis of prediabetes so that they can get connected to these services.”
According to the AMA, there are currently more than 86 million individuals in the United States living with prediabetes, yet roughly 90% of those people don’t even know they have it. The CDC estimates that the number of individuals diagnosed with diabetes in the United States more than tripled from 1980 to 2011, going from 5.6 million to nearly 21 million in just over 30 years. In 2011, 19.6 million American adults were diagnosed with diabetes; right now, according to the AMA and CDC, more than 33% of American adults are living with prediabetes.
FROM A CDC/AMA TELEBRIEFING

ACS NSQIP data: Laparoscopic sleeve gastrectomy is at least as safe as gastric bypass
Laparoscopic sleeve gastrectomy is associated with lower rates of morbidity and similar mortality when compared with laparoscopic Roux-en-Y gastric bypass, according to an analysis of 2010-2011 data from the American College of Surgeons National Surgical Quality Improvement Program database.
Of 24,117 patients included in the analysis, 79.5% underwent laparoscopic Roux-en-Y gastric bypass (LGB), and 20.5% had laparoscopic sleeve gastrectomy (LSG). Of note, the proportion of LSG cases increased from 14.6% in 2010 to 24.8% in 2011, Dr. Monica T. Young of the University of California Irvine Medical Center, Orange, Calif., and her colleagues reported.

Those who underwent LGB had a significantly higher rate of 30-day risk-adjusted morbidity (odds ratio, 1.32). The 30-day mortality rate was 0.15% with bypass and 0.10% for sleeve gastrectomy, the investigators said (J. Am. Coll. Surg. 2015 [doi:
10.1016/j.jamcollsurg.2015.01.059]).
Further, sleeve gastrectomy was associated with shorter operative time (101 vs. 133 minutes) and with lower rates of blood loss requiring transfusion (0.65% vs. 1.5%), deep wound infections (0.06% vs. 0.20%), sepsis (0.34% vs. 0.58%), overall serious morbidity (3.8% vs. 5.8%), and reoperations within 30 days (1.6% vs. 2.5%).
The rate of deep venous thrombosis, however, was significantly higher with sleeve gastrectomy (0.47% vs. 0.21%). Deep vein thrombosis was the only complication found to be higher after LSG, they noted.
Older patients, those with a higher body mass index, and those who smoked or had hypertension were at significantly greater risk of serious morbidity.
Given the increasing popularity and use of sleeve gastrectomy as seen both in this study and nationally – with a reported increase in utilization from 0.9% in 2008 to 36.3% in 2012, it is important to compare outcomes with LSG with those for the preferred Roux-en-Y bypass surgery, the investigators said, noting that few large-scale studies have compared outcomes with the two procedures.
“Over the past decade, laparoscopic sleeve gastrectomy has emerged as a common utilized bariatric procedure. LSG has several advantages over LGB including preservation of endoscopic access to the upper gastrointestinal tract, avoidance of intestinal anastomosis, and prevention of dumping syndrome by pylorus preservation,” they wrote, adding that studies increasingly demonstrate its efficacy for weight loss.
The current findings support those of other recent studies, and a comparison of the data with those from 2007 to 2010 from the ACS NSQIP database showed that while reoperation rates after gastric bypass and sleeve gastrectomy have declined dramatically over time, readmission rates remain elevated.
“Therefore, it appears that further quality improvement initiatives are necessary to reduce the rate of readmissions after bariatric surgery,” the investigators wrote, noting that a national collaborative to reduce 30-day readmissions by 20% (the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program, or MBSAQIP) is currently enrolling.
Additional randomized controlled trials are also needed to evaluate differences in long-term outcomes between the two procedures, they concluded.
The authors reported having no relevant financial disclosures.
Laparoscopic sleeve gastrectomy is associated with lower rates of morbidity and similar mortality when compared with laparoscopic Roux-en-Y gastric bypass, according to an analysis of 2010-2011 data from the American College of Surgeons National Surgical Quality Improvement Program database.
Of 24,117 patients included in the analysis, 79.5% underwent laparoscopic Roux-en-Y gastric bypass (LGB), and 20.5% had laparoscopic sleeve gastrectomy (LSG). Of note, the proportion of LSG cases increased from 14.6% in 2010 to 24.8% in 2011, Dr. Monica T. Young of the University of California Irvine Medical Center, Orange, Calif., and her colleagues reported.
Those who underwent LGB had a significantly higher rate of 30-day risk-adjusted morbidity (odds ratio, 1.32). The 30-day mortality rate was 0.15% with bypass and 0.10% for sleeve gastrectomy, the investigators said (J. Am. Coll. Surg. 2015 [doi:
10.1016/j.jamcollsurg.2015.01.059]).
Further, sleeve gastrectomy was associated with shorter operative time (101 vs. 133 minutes) and with lower rates of blood loss requiring transfusion (0.65% vs. 1.5%), deep wound infections (0.06% vs. 0.20%), sepsis (0.34% vs. 0.58%), overall serious morbidity (3.8% vs. 5.8%), and reoperations within 30 days (1.6% vs. 2.5%).
The rate of deep venous thrombosis, however, was significantly higher with sleeve gastrectomy (0.47% vs. 0.21%). Deep vein thrombosis was the only complication found to be higher after LSG, they noted.
Older patients, those with a higher body mass index, and those who smoked or had hypertension were at significantly greater risk of serious morbidity.
Given the increasing popularity and use of sleeve gastrectomy as seen both in this study and nationally – with a reported increase in utilization from 0.9% in 2008 to 36.3% in 2012, it is important to compare outcomes with LSG with those for the preferred Roux-en-Y bypass surgery, the investigators said, noting that few large-scale studies have compared outcomes with the two procedures.
“Over the past decade, laparoscopic sleeve gastrectomy has emerged as a common utilized bariatric procedure. LSG has several advantages over LGB including preservation of endoscopic access to the upper gastrointestinal tract, avoidance of intestinal anastomosis, and prevention of dumping syndrome by pylorus preservation,” they wrote, adding that studies increasingly demonstrate its efficacy for weight loss.
The current findings support those of other recent studies, and a comparison of the data with those from 2007 to 2010 from the ACS NSQIP database showed that while reoperation rates after gastric bypass and sleeve gastrectomy have declined dramatically over time, readmission rates remain elevated.
“Therefore, it appears that further quality improvement initiatives are necessary to reduce the rate of readmissions after bariatric surgery,” the investigators wrote, noting that a national collaborative to reduce 30-day readmissions by 20% (the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program, or MBSAQIP) is currently enrolling.
Additional randomized controlled trials are also needed to evaluate differences in long-term outcomes between the two procedures, they concluded.
The authors reported having no relevant financial disclosures.
Laparoscopic sleeve gastrectomy is associated with lower rates of morbidity and similar mortality when compared with laparoscopic Roux-en-Y gastric bypass, according to an analysis of 2010-2011 data from the American College of Surgeons National Surgical Quality Improvement Program database.
Of 24,117 patients included in the analysis, 79.5% underwent laparoscopic Roux-en-Y gastric bypass (LGB), and 20.5% had laparoscopic sleeve gastrectomy (LSG). Of note, the proportion of LSG cases increased from 14.6% in 2010 to 24.8% in 2011, Dr. Monica T. Young of the University of California Irvine Medical Center, Orange, Calif., and her colleagues reported.
Those who underwent LGB had a significantly higher rate of 30-day risk-adjusted morbidity (odds ratio, 1.32). The 30-day mortality rate was 0.15% with bypass and 0.10% for sleeve gastrectomy, the investigators said (J. Am. Coll. Surg. 2015 [doi:
10.1016/j.jamcollsurg.2015.01.059]).
Further, sleeve gastrectomy was associated with shorter operative time (101 vs. 133 minutes) and with lower rates of blood loss requiring transfusion (0.65% vs. 1.5%), deep wound infections (0.06% vs. 0.20%), sepsis (0.34% vs. 0.58%), overall serious morbidity (3.8% vs. 5.8%), and reoperations within 30 days (1.6% vs. 2.5%).
The rate of deep venous thrombosis, however, was significantly higher with sleeve gastrectomy (0.47% vs. 0.21%). Deep vein thrombosis was the only complication found to be higher after LSG, they noted.
Older patients, those with a higher body mass index, and those who smoked or had hypertension were at significantly greater risk of serious morbidity.
Given the increasing popularity and use of sleeve gastrectomy as seen both in this study and nationally – with a reported increase in utilization from 0.9% in 2008 to 36.3% in 2012, it is important to compare outcomes with LSG with those for the preferred Roux-en-Y bypass surgery, the investigators said, noting that few large-scale studies have compared outcomes with the two procedures.
“Over the past decade, laparoscopic sleeve gastrectomy has emerged as a common utilized bariatric procedure. LSG has several advantages over LGB including preservation of endoscopic access to the upper gastrointestinal tract, avoidance of intestinal anastomosis, and prevention of dumping syndrome by pylorus preservation,” they wrote, adding that studies increasingly demonstrate its efficacy for weight loss.
The current findings support those of other recent studies, and a comparison of the data with those from 2007 to 2010 from the ACS NSQIP database showed that while reoperation rates after gastric bypass and sleeve gastrectomy have declined dramatically over time, readmission rates remain elevated.
“Therefore, it appears that further quality improvement initiatives are necessary to reduce the rate of readmissions after bariatric surgery,” the investigators wrote, noting that a national collaborative to reduce 30-day readmissions by 20% (the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program, or MBSAQIP) is currently enrolling.
Additional randomized controlled trials are also needed to evaluate differences in long-term outcomes between the two procedures, they concluded.
The authors reported having no relevant financial disclosures.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF SURGEONS
Key clinical point: Laparoscopic sleeve gastrectomy appears to have numerous advantages over laparoscopic Roux-en-Y gastric bypass.
Major finding: Patients who underwent LGB had a significantly higher rate of 30-day risk-adjusted morbidity (odds ratio, 1.32).
Data source: An analysis of data from the ACS NSQIP database.
Disclosures: The authors reported having no relevant financial disclosures.

Long-acting basal insulins aim to reduce hypoglycemia
NEW YORK – Three new insulins hold the potential for decreasing the risk of severe hypoglycemia episodes in patients with diabetes, Dr. Elizabeth R. Seaquist said at the annual advanced postgraduate course held by the American Diabetes Association.
None of the products are yet available in the the United States, although one of the insulins was approved in February by the Food and Drug Administration and is expected to be on the market later this year. The new insulin glargine (Toujeo; Sanofi), a once-daily long-acting basal insulin, received its FDA approval on Feb. 25.
Toujeo has a flatter glycemic profile and a longer duration of action than does its predecessor insulin glargine, Lantus, said Dr. Seaquist, professor of medicine and the Pennock Family Chair in Diabetes Research at the University of Minnesota, Minneapolis.

The approval of Toujeo was based on results from the EDITION clinical trial series, which included more than 3,500 adults with type 1 or type 2 diabetes. In those studies, once-daily Toujeo was compared with once-daily insulin Lantus in open-label, randomized, active-control, parallel, treat-to-target studies of up to 26 weeks of duration with 6 months’ safety extension, according to a Sanofi press release.
Insulin degludec, a once-daily, long-acting basal insulin analogue, is available in the European Union as Tresiba (Novo Nordisk) at strengths of 100 U/mL and 200 U/mL. The FDA denied its approval in 2013, after a review committee expressed concern about a potential increased risk of major cardiovascular events. The FDA has requested that additional cardiovascular data from a dedicated cardiovascular outcomes trial be provided before considering approval.
Basal insulin peglispro (Lilly) has successfully completed all its phase III studies and is on track for FDA submission this year. The primary efficacy endpoint of noninferior HbA1c, compared with insulin glargine was met in both the IMAGINE-1 and IMAGINE-3 trials, and significantly more patients taking basal insulin peglispro achieved an HbA1c of less than 7%. Further, patients taking basal insulin peglispro experienced weight loss and patients taking insulin glargine experienced weight gain, according to Lilly press releases.
Both trials – in which patients were taking mealtime and basal insulin – also found a significantly lower rate of nocturnal hypoglycemia with basal insulin peglispro. Because of a higher rate of daytime hypoglycemic events, however, there was a statistically significant increase in the rate of total hypoglycemia for patients taking basal insulin peglispro.
In the open-label IMAGINE-1 trial, patients taking basal insulin peglispro reported a statistically significant higher rate of severe hypoglycemic events. However, in the larger, blinded IMAGINE-3 trial the rate of severe hypoglycemic events for treatment with basal insulin peglispro was numerically lower, but the difference was not statistically significant.
The fear of hypoglycemia can prompt patients to be nonadherent with their insulin regimen, Dr. Seaquist said. “And we all know that many patients don’t reach their glycemic goal, so they need additional medications that then put them at an increased risk of hypoglycemia.”
According to one review article, an intensively treated individual with type 1 diabetes can experience up to 10 episodes of symptomatic hypoglycemia per week and severe temporarily disabling hypoglycemia at least once a year. Hypoglycemia is also relatively common in type 2 diabetes, with prevalence rates of 70%-80% in clinical trials using insulin to achieve good metabolic control.
Dr. Seaquist disclosed that she is a consultant for Sanofi Aventis, the maker of Toujeo.
NEW YORK – Three new insulins hold the potential for decreasing the risk of severe hypoglycemia episodes in patients with diabetes, Dr. Elizabeth R. Seaquist said at the annual advanced postgraduate course held by the American Diabetes Association.
None of the products are yet available in the the United States, although one of the insulins was approved in February by the Food and Drug Administration and is expected to be on the market later this year. The new insulin glargine (Toujeo; Sanofi), a once-daily long-acting basal insulin, received its FDA approval on Feb. 25.
Toujeo has a flatter glycemic profile and a longer duration of action than does its predecessor insulin glargine, Lantus, said Dr. Seaquist, professor of medicine and the Pennock Family Chair in Diabetes Research at the University of Minnesota, Minneapolis.
The approval of Toujeo was based on results from the EDITION clinical trial series, which included more than 3,500 adults with type 1 or type 2 diabetes. In those studies, once-daily Toujeo was compared with once-daily insulin Lantus in open-label, randomized, active-control, parallel, treat-to-target studies of up to 26 weeks of duration with 6 months’ safety extension, according to a Sanofi press release.
Insulin degludec, a once-daily, long-acting basal insulin analogue, is available in the European Union as Tresiba (Novo Nordisk) at strengths of 100 U/mL and 200 U/mL. The FDA denied its approval in 2013, after a review committee expressed concern about a potential increased risk of major cardiovascular events. The FDA has requested that additional cardiovascular data from a dedicated cardiovascular outcomes trial be provided before considering approval.
Basal insulin peglispro (Lilly) has successfully completed all its phase III studies and is on track for FDA submission this year. The primary efficacy endpoint of noninferior HbA1c, compared with insulin glargine was met in both the IMAGINE-1 and IMAGINE-3 trials, and significantly more patients taking basal insulin peglispro achieved an HbA1c of less than 7%. Further, patients taking basal insulin peglispro experienced weight loss and patients taking insulin glargine experienced weight gain, according to Lilly press releases.
Both trials – in which patients were taking mealtime and basal insulin – also found a significantly lower rate of nocturnal hypoglycemia with basal insulin peglispro. Because of a higher rate of daytime hypoglycemic events, however, there was a statistically significant increase in the rate of total hypoglycemia for patients taking basal insulin peglispro.
In the open-label IMAGINE-1 trial, patients taking basal insulin peglispro reported a statistically significant higher rate of severe hypoglycemic events. However, in the larger, blinded IMAGINE-3 trial the rate of severe hypoglycemic events for treatment with basal insulin peglispro was numerically lower, but the difference was not statistically significant.
The fear of hypoglycemia can prompt patients to be nonadherent with their insulin regimen, Dr. Seaquist said. “And we all know that many patients don’t reach their glycemic goal, so they need additional medications that then put them at an increased risk of hypoglycemia.”
According to one review article, an intensively treated individual with type 1 diabetes can experience up to 10 episodes of symptomatic hypoglycemia per week and severe temporarily disabling hypoglycemia at least once a year. Hypoglycemia is also relatively common in type 2 diabetes, with prevalence rates of 70%-80% in clinical trials using insulin to achieve good metabolic control.
Dr. Seaquist disclosed that she is a consultant for Sanofi Aventis, the maker of Toujeo.
NEW YORK – Three new insulins hold the potential for decreasing the risk of severe hypoglycemia episodes in patients with diabetes, Dr. Elizabeth R. Seaquist said at the annual advanced postgraduate course held by the American Diabetes Association.
None of the products are yet available in the the United States, although one of the insulins was approved in February by the Food and Drug Administration and is expected to be on the market later this year. The new insulin glargine (Toujeo; Sanofi), a once-daily long-acting basal insulin, received its FDA approval on Feb. 25.
Toujeo has a flatter glycemic profile and a longer duration of action than does its predecessor insulin glargine, Lantus, said Dr. Seaquist, professor of medicine and the Pennock Family Chair in Diabetes Research at the University of Minnesota, Minneapolis.
The approval of Toujeo was based on results from the EDITION clinical trial series, which included more than 3,500 adults with type 1 or type 2 diabetes. In those studies, once-daily Toujeo was compared with once-daily insulin Lantus in open-label, randomized, active-control, parallel, treat-to-target studies of up to 26 weeks of duration with 6 months’ safety extension, according to a Sanofi press release.
Insulin degludec, a once-daily, long-acting basal insulin analogue, is available in the European Union as Tresiba (Novo Nordisk) at strengths of 100 U/mL and 200 U/mL. The FDA denied its approval in 2013, after a review committee expressed concern about a potential increased risk of major cardiovascular events. The FDA has requested that additional cardiovascular data from a dedicated cardiovascular outcomes trial be provided before considering approval.
Basal insulin peglispro (Lilly) has successfully completed all its phase III studies and is on track for FDA submission this year. The primary efficacy endpoint of noninferior HbA1c, compared with insulin glargine was met in both the IMAGINE-1 and IMAGINE-3 trials, and significantly more patients taking basal insulin peglispro achieved an HbA1c of less than 7%. Further, patients taking basal insulin peglispro experienced weight loss and patients taking insulin glargine experienced weight gain, according to Lilly press releases.
Both trials – in which patients were taking mealtime and basal insulin – also found a significantly lower rate of nocturnal hypoglycemia with basal insulin peglispro. Because of a higher rate of daytime hypoglycemic events, however, there was a statistically significant increase in the rate of total hypoglycemia for patients taking basal insulin peglispro.
In the open-label IMAGINE-1 trial, patients taking basal insulin peglispro reported a statistically significant higher rate of severe hypoglycemic events. However, in the larger, blinded IMAGINE-3 trial the rate of severe hypoglycemic events for treatment with basal insulin peglispro was numerically lower, but the difference was not statistically significant.
The fear of hypoglycemia can prompt patients to be nonadherent with their insulin regimen, Dr. Seaquist said. “And we all know that many patients don’t reach their glycemic goal, so they need additional medications that then put them at an increased risk of hypoglycemia.”
According to one review article, an intensively treated individual with type 1 diabetes can experience up to 10 episodes of symptomatic hypoglycemia per week and severe temporarily disabling hypoglycemia at least once a year. Hypoglycemia is also relatively common in type 2 diabetes, with prevalence rates of 70%-80% in clinical trials using insulin to achieve good metabolic control.
Dr. Seaquist disclosed that she is a consultant for Sanofi Aventis, the maker of Toujeo.
EXPERT ANALYSIS FROM THE ADA ADVANCED POSTGRADUATE COURSE

Diet’s link to RA risk centers on alcohol, fish, sugar consumption
SNOWMASS, COLO. – Moderate alcohol intake and fish consumption are the two dietary factors supported by the strongest epidemiologic evidence for a protective effect against development of rheumatoid arthritis, while sugar-sweetened sodas are associated with increased risk of the disease.
“Sugar-sweetened soft drinks are now the primary source of sugar in the American diet. This consumption has increased astronomically over the past 30 years,” Dr. Karen H. Costenbader observed at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.

Obesity, one consequence of America’s love affair with sugar, is a moderately potent independent risk factor for RA, according to several studies, including one carried out by Dr. Costenbader and her colleagues at Brigham and Women’s Hospital and Harvard University, Boston.
They followed nearly 220,000 women enrolled in the Nurses Health Study (NHS) and NHS II prospective cohort studies. During 4.7 million person-years of follow-up, women who were diagnosed with RA before age 55 were 45% more likely to be overweight and 65% more likely to be obese than were women without RA at that age. The association was stronger for seropositive than seronegative RA. Moreover, in an analysis that considered cumulative years of obesity as something akin to pack-years of smoking, the investigators found strong evidence of a dose effect, such that 10 cumulative years of being obese was associated with a 37% increased risk of RA by age 55 (Ann. Rheum. Dis. 2014;73:1914-22).
These findings were consistent with the results of a retrospective, population-based study of Olmsted County, Minn., residents conducted by investigators at the Mayo Clinic. They found that a history of obesity was associated with a 24% increased likelihood of developing RA. The investigators calculated that obesity could account for 52% of the sharp increase in the incidence of RA seen in the county, as elsewhere, between 1985 and 2007 (Arthritis Care Res. 2013;65:71-7).
The mechanism by which obesity may boost the development of RA is unknown. Speculation has focused on inflammation as the likely mediator. Visceral fat secretes proinflammatory cytokines, with resultant elevations in C-reactive protein, TNF-alpha, and other biomarkers of systemic inflammation, Dr. Costenbader said.
The importance of eating fish as a protector against developing RA is also supported by multiple epidemiologic studies. Investigators at the Karolinska Institute in Stockholm demonstrated in a study of 1,889 Swedish RA patients and 2,145 controls that eating oily fish on as few as 1-3 occasions per month was associated with a 20% reduction in the odds of developing RA (Epidemiology 2009;20:896-901).
The Swedish findings were confirmed in a recent, not-yet-published analysis of women enrolled in the Nurses’ Health Study and NHS II. Dr. Costenbader and coworkers showed that eating fish at least once per month was associated with a 28% reduction in RA risk, compared with never-eaters of fish.
The evidence for a preventive effect of eating fish and a contributory role of obesity in the development of RA is sufficiently strong that these two behavioral factors have been incorporated in the Personalized Risk Estimator for Rheumatoid Arthritis (PRE-RA) Family Study. This is an ongoing National Institutes of Health–funded, prospective, randomized, controlled trial being conducted by Dr. Costenbader and others at Brigham and Women’s Hospital.
The PRE-RA Family Study is designed to compare the willingness to change RA-associated behaviors among first-degree relatives of RA patients after exposure to an online personalized risk-estimation tool and education program. The four behavioral factors included in the risk estimator – and targeted for change in the online risk education program – are cigarette smoking, excess body weight, low fish intake, and poor oral health.
Dr. Costenbader said “the sweet spot” for alcohol consumption in terms of reducing RA risk was 5.0-9.9 g/day – equivalent to one-half to one drink – in an analysis of incident RA cases she and her coinvestigators performed in the NHS and NHS II cohorts (Arthritis Rheumatol. 2014;66:1998-2005).
In the sugar-sweetened soda study, she and her coworkers found that nurses who drank more than one serving per day had a 63% greater risk of developing seropositive RA compared with those who consumed less than one per month. Restricting the analysis to women with onset of RA after age 55, the association grew markedly stronger, with one or more soft drinks per day linked to a 2.64-fold increased risk (Am. J. Clin. Nutr. 2014;100:959-67).
Lots of other dietary factors, including coffee, tea, red meat, protein, vitamins and antioxidant-rich foods, and the Mediterranean diet pattern, have been looked at by various investigators. None have panned out.
Dr. Costenbader’s research is supported by the NIH and the Arthritis Foundation. She reported having no financial conflicts.
SNOWMASS, COLO. – Moderate alcohol intake and fish consumption are the two dietary factors supported by the strongest epidemiologic evidence for a protective effect against development of rheumatoid arthritis, while sugar-sweetened sodas are associated with increased risk of the disease.
“Sugar-sweetened soft drinks are now the primary source of sugar in the American diet. This consumption has increased astronomically over the past 30 years,” Dr. Karen H. Costenbader observed at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
Obesity, one consequence of America’s love affair with sugar, is a moderately potent independent risk factor for RA, according to several studies, including one carried out by Dr. Costenbader and her colleagues at Brigham and Women’s Hospital and Harvard University, Boston.
They followed nearly 220,000 women enrolled in the Nurses Health Study (NHS) and NHS II prospective cohort studies. During 4.7 million person-years of follow-up, women who were diagnosed with RA before age 55 were 45% more likely to be overweight and 65% more likely to be obese than were women without RA at that age. The association was stronger for seropositive than seronegative RA. Moreover, in an analysis that considered cumulative years of obesity as something akin to pack-years of smoking, the investigators found strong evidence of a dose effect, such that 10 cumulative years of being obese was associated with a 37% increased risk of RA by age 55 (Ann. Rheum. Dis. 2014;73:1914-22).
These findings were consistent with the results of a retrospective, population-based study of Olmsted County, Minn., residents conducted by investigators at the Mayo Clinic. They found that a history of obesity was associated with a 24% increased likelihood of developing RA. The investigators calculated that obesity could account for 52% of the sharp increase in the incidence of RA seen in the county, as elsewhere, between 1985 and 2007 (Arthritis Care Res. 2013;65:71-7).
The mechanism by which obesity may boost the development of RA is unknown. Speculation has focused on inflammation as the likely mediator. Visceral fat secretes proinflammatory cytokines, with resultant elevations in C-reactive protein, TNF-alpha, and other biomarkers of systemic inflammation, Dr. Costenbader said.
The importance of eating fish as a protector against developing RA is also supported by multiple epidemiologic studies. Investigators at the Karolinska Institute in Stockholm demonstrated in a study of 1,889 Swedish RA patients and 2,145 controls that eating oily fish on as few as 1-3 occasions per month was associated with a 20% reduction in the odds of developing RA (Epidemiology 2009;20:896-901).
The Swedish findings were confirmed in a recent, not-yet-published analysis of women enrolled in the Nurses’ Health Study and NHS II. Dr. Costenbader and coworkers showed that eating fish at least once per month was associated with a 28% reduction in RA risk, compared with never-eaters of fish.
The evidence for a preventive effect of eating fish and a contributory role of obesity in the development of RA is sufficiently strong that these two behavioral factors have been incorporated in the Personalized Risk Estimator for Rheumatoid Arthritis (PRE-RA) Family Study. This is an ongoing National Institutes of Health–funded, prospective, randomized, controlled trial being conducted by Dr. Costenbader and others at Brigham and Women’s Hospital.
The PRE-RA Family Study is designed to compare the willingness to change RA-associated behaviors among first-degree relatives of RA patients after exposure to an online personalized risk-estimation tool and education program. The four behavioral factors included in the risk estimator – and targeted for change in the online risk education program – are cigarette smoking, excess body weight, low fish intake, and poor oral health.
Dr. Costenbader said “the sweet spot” for alcohol consumption in terms of reducing RA risk was 5.0-9.9 g/day – equivalent to one-half to one drink – in an analysis of incident RA cases she and her coinvestigators performed in the NHS and NHS II cohorts (Arthritis Rheumatol. 2014;66:1998-2005).
In the sugar-sweetened soda study, she and her coworkers found that nurses who drank more than one serving per day had a 63% greater risk of developing seropositive RA compared with those who consumed less than one per month. Restricting the analysis to women with onset of RA after age 55, the association grew markedly stronger, with one or more soft drinks per day linked to a 2.64-fold increased risk (Am. J. Clin. Nutr. 2014;100:959-67).
Lots of other dietary factors, including coffee, tea, red meat, protein, vitamins and antioxidant-rich foods, and the Mediterranean diet pattern, have been looked at by various investigators. None have panned out.
Dr. Costenbader’s research is supported by the NIH and the Arthritis Foundation. She reported having no financial conflicts.
SNOWMASS, COLO. – Moderate alcohol intake and fish consumption are the two dietary factors supported by the strongest epidemiologic evidence for a protective effect against development of rheumatoid arthritis, while sugar-sweetened sodas are associated with increased risk of the disease.
“Sugar-sweetened soft drinks are now the primary source of sugar in the American diet. This consumption has increased astronomically over the past 30 years,” Dr. Karen H. Costenbader observed at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
Obesity, one consequence of America’s love affair with sugar, is a moderately potent independent risk factor for RA, according to several studies, including one carried out by Dr. Costenbader and her colleagues at Brigham and Women’s Hospital and Harvard University, Boston.
They followed nearly 220,000 women enrolled in the Nurses Health Study (NHS) and NHS II prospective cohort studies. During 4.7 million person-years of follow-up, women who were diagnosed with RA before age 55 were 45% more likely to be overweight and 65% more likely to be obese than were women without RA at that age. The association was stronger for seropositive than seronegative RA. Moreover, in an analysis that considered cumulative years of obesity as something akin to pack-years of smoking, the investigators found strong evidence of a dose effect, such that 10 cumulative years of being obese was associated with a 37% increased risk of RA by age 55 (Ann. Rheum. Dis. 2014;73:1914-22).
These findings were consistent with the results of a retrospective, population-based study of Olmsted County, Minn., residents conducted by investigators at the Mayo Clinic. They found that a history of obesity was associated with a 24% increased likelihood of developing RA. The investigators calculated that obesity could account for 52% of the sharp increase in the incidence of RA seen in the county, as elsewhere, between 1985 and 2007 (Arthritis Care Res. 2013;65:71-7).
The mechanism by which obesity may boost the development of RA is unknown. Speculation has focused on inflammation as the likely mediator. Visceral fat secretes proinflammatory cytokines, with resultant elevations in C-reactive protein, TNF-alpha, and other biomarkers of systemic inflammation, Dr. Costenbader said.
The importance of eating fish as a protector against developing RA is also supported by multiple epidemiologic studies. Investigators at the Karolinska Institute in Stockholm demonstrated in a study of 1,889 Swedish RA patients and 2,145 controls that eating oily fish on as few as 1-3 occasions per month was associated with a 20% reduction in the odds of developing RA (Epidemiology 2009;20:896-901).
The Swedish findings were confirmed in a recent, not-yet-published analysis of women enrolled in the Nurses’ Health Study and NHS II. Dr. Costenbader and coworkers showed that eating fish at least once per month was associated with a 28% reduction in RA risk, compared with never-eaters of fish.
The evidence for a preventive effect of eating fish and a contributory role of obesity in the development of RA is sufficiently strong that these two behavioral factors have been incorporated in the Personalized Risk Estimator for Rheumatoid Arthritis (PRE-RA) Family Study. This is an ongoing National Institutes of Health–funded, prospective, randomized, controlled trial being conducted by Dr. Costenbader and others at Brigham and Women’s Hospital.
The PRE-RA Family Study is designed to compare the willingness to change RA-associated behaviors among first-degree relatives of RA patients after exposure to an online personalized risk-estimation tool and education program. The four behavioral factors included in the risk estimator – and targeted for change in the online risk education program – are cigarette smoking, excess body weight, low fish intake, and poor oral health.
Dr. Costenbader said “the sweet spot” for alcohol consumption in terms of reducing RA risk was 5.0-9.9 g/day – equivalent to one-half to one drink – in an analysis of incident RA cases she and her coinvestigators performed in the NHS and NHS II cohorts (Arthritis Rheumatol. 2014;66:1998-2005).
In the sugar-sweetened soda study, she and her coworkers found that nurses who drank more than one serving per day had a 63% greater risk of developing seropositive RA compared with those who consumed less than one per month. Restricting the analysis to women with onset of RA after age 55, the association grew markedly stronger, with one or more soft drinks per day linked to a 2.64-fold increased risk (Am. J. Clin. Nutr. 2014;100:959-67).
Lots of other dietary factors, including coffee, tea, red meat, protein, vitamins and antioxidant-rich foods, and the Mediterranean diet pattern, have been looked at by various investigators. None have panned out.
Dr. Costenbader’s research is supported by the NIH and the Arthritis Foundation. She reported having no financial conflicts.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM

Statins for all eligible under new guidelines could save lives
BALTIMORE – If all Americans eligible for statins under new American College of Cardiology/American Heart Association guidelines actually took them, thousands of deaths per year from cardiovascular disease might be prevented but at a cost of increased incidence of diabetes and myopathy.
The 2013 ACC/AHA guidelines expand criteria for the use of statins for primary prevention of CVD to more Americans (Circulation 2015;131:A05). Compliance with those guidelines would save 7,930 lives per year that would have been lost to CVD, according to Quanhe Yang, Ph.D., of the Centers for Disease Control and Prevention’s Division for Heart Disease and Stroke Prevention, and colleagues from the CDC and Emory University, Atlanta. Dr. Yang presented the findings at the American Heart Association Epidemiology and Prevention, Lifestyle and Cardiometabolic Health 2015 Scientific Sessions.
Statins are now indicated for primary prevention of CVD for anyone with an LDL cholesterol level greater than or equal to 190 mg/dL, for individuals aged 40-75 years with diabetes, and for those aged 40-75 years with LDL cholesterol greater than or equal to 70 mg/dL but less than 190 mg/dL who have at least a 7.5% estimated 10-year risk of developing atherosclerotic CVD. This means that an additional 24.2 million Americans are now eligible for statins but are not taking one, according to Dr. Yang and coinvestigators. However, “no study has assessed the potential impact of statin therapy under the new guidelines,” said Dr. Yang.
In order to obtain treatment group-specific atherosclerotic CVD, investigators first estimated hazard ratios for each treatment group by sex from the National Health and Nutrition Examination Survey III (NHANES III)–linked Mortality files. These hazard ratios were then applied to data from NHANES 2005-2010, the 2010 Multiple Cause of Death file, and the 2010 U.S. census to obtain age/race/sex-specific atherosclerotic CVD for each treatment group.
Applying the per-group hazard ratios, Dr. Yang and colleagues calculated that an annual 7,930 atherosclerotic CVD deaths would be prevented with full statin compliance, a reduction of 12.6%. However, modeling predicted an additional 16,400 additional cases of diabetes caused by statin use, he cautioned. More cases of myopathy would also occur, though the estimated number depends on whether the rate is derived from randomized, controlled trials (RCTs) or from population-based reports of myopathy. If the RCT data are used, just 1,510 excess cases of myopathy would be seen, in contrast to the 36,100 cases predicted by population-based data.
The study could model deaths caused by CVD only and not the reduction in disease burden of CVD that would result if all of the additional 24.2 million Americans took a statin, Dr Yang noted. Other limitations of the study included the lack of agreement in incidence of myopathy between RCTs and population-based studies, as well as the likelihood that the risk of diabetes increases with age and higher statin dose – effects not accounted for in the study.
Questioning after the talk focused on sex-specific differences in statin takers. For example, statin-associated diabetes is more common in women than men, another effect not accounted for in the study’s modeling, noted an audience member. Additionally, given that women have been underrepresented in clinical trials in general and in those for CVD in particular, some modeling assumptions in the present study may also lack full generalizability to women at risk for CVD.
BALTIMORE – If all Americans eligible for statins under new American College of Cardiology/American Heart Association guidelines actually took them, thousands of deaths per year from cardiovascular disease might be prevented but at a cost of increased incidence of diabetes and myopathy.
The 2013 ACC/AHA guidelines expand criteria for the use of statins for primary prevention of CVD to more Americans (Circulation 2015;131:A05). Compliance with those guidelines would save 7,930 lives per year that would have been lost to CVD, according to Quanhe Yang, Ph.D., of the Centers for Disease Control and Prevention’s Division for Heart Disease and Stroke Prevention, and colleagues from the CDC and Emory University, Atlanta. Dr. Yang presented the findings at the American Heart Association Epidemiology and Prevention, Lifestyle and Cardiometabolic Health 2015 Scientific Sessions.
Statins are now indicated for primary prevention of CVD for anyone with an LDL cholesterol level greater than or equal to 190 mg/dL, for individuals aged 40-75 years with diabetes, and for those aged 40-75 years with LDL cholesterol greater than or equal to 70 mg/dL but less than 190 mg/dL who have at least a 7.5% estimated 10-year risk of developing atherosclerotic CVD. This means that an additional 24.2 million Americans are now eligible for statins but are not taking one, according to Dr. Yang and coinvestigators. However, “no study has assessed the potential impact of statin therapy under the new guidelines,” said Dr. Yang.
In order to obtain treatment group-specific atherosclerotic CVD, investigators first estimated hazard ratios for each treatment group by sex from the National Health and Nutrition Examination Survey III (NHANES III)–linked Mortality files. These hazard ratios were then applied to data from NHANES 2005-2010, the 2010 Multiple Cause of Death file, and the 2010 U.S. census to obtain age/race/sex-specific atherosclerotic CVD for each treatment group.
Applying the per-group hazard ratios, Dr. Yang and colleagues calculated that an annual 7,930 atherosclerotic CVD deaths would be prevented with full statin compliance, a reduction of 12.6%. However, modeling predicted an additional 16,400 additional cases of diabetes caused by statin use, he cautioned. More cases of myopathy would also occur, though the estimated number depends on whether the rate is derived from randomized, controlled trials (RCTs) or from population-based reports of myopathy. If the RCT data are used, just 1,510 excess cases of myopathy would be seen, in contrast to the 36,100 cases predicted by population-based data.
The study could model deaths caused by CVD only and not the reduction in disease burden of CVD that would result if all of the additional 24.2 million Americans took a statin, Dr Yang noted. Other limitations of the study included the lack of agreement in incidence of myopathy between RCTs and population-based studies, as well as the likelihood that the risk of diabetes increases with age and higher statin dose – effects not accounted for in the study.
Questioning after the talk focused on sex-specific differences in statin takers. For example, statin-associated diabetes is more common in women than men, another effect not accounted for in the study’s modeling, noted an audience member. Additionally, given that women have been underrepresented in clinical trials in general and in those for CVD in particular, some modeling assumptions in the present study may also lack full generalizability to women at risk for CVD.
BALTIMORE – If all Americans eligible for statins under new American College of Cardiology/American Heart Association guidelines actually took them, thousands of deaths per year from cardiovascular disease might be prevented but at a cost of increased incidence of diabetes and myopathy.
The 2013 ACC/AHA guidelines expand criteria for the use of statins for primary prevention of CVD to more Americans (Circulation 2015;131:A05). Compliance with those guidelines would save 7,930 lives per year that would have been lost to CVD, according to Quanhe Yang, Ph.D., of the Centers for Disease Control and Prevention’s Division for Heart Disease and Stroke Prevention, and colleagues from the CDC and Emory University, Atlanta. Dr. Yang presented the findings at the American Heart Association Epidemiology and Prevention, Lifestyle and Cardiometabolic Health 2015 Scientific Sessions.
Statins are now indicated for primary prevention of CVD for anyone with an LDL cholesterol level greater than or equal to 190 mg/dL, for individuals aged 40-75 years with diabetes, and for those aged 40-75 years with LDL cholesterol greater than or equal to 70 mg/dL but less than 190 mg/dL who have at least a 7.5% estimated 10-year risk of developing atherosclerotic CVD. This means that an additional 24.2 million Americans are now eligible for statins but are not taking one, according to Dr. Yang and coinvestigators. However, “no study has assessed the potential impact of statin therapy under the new guidelines,” said Dr. Yang.
In order to obtain treatment group-specific atherosclerotic CVD, investigators first estimated hazard ratios for each treatment group by sex from the National Health and Nutrition Examination Survey III (NHANES III)–linked Mortality files. These hazard ratios were then applied to data from NHANES 2005-2010, the 2010 Multiple Cause of Death file, and the 2010 U.S. census to obtain age/race/sex-specific atherosclerotic CVD for each treatment group.
Applying the per-group hazard ratios, Dr. Yang and colleagues calculated that an annual 7,930 atherosclerotic CVD deaths would be prevented with full statin compliance, a reduction of 12.6%. However, modeling predicted an additional 16,400 additional cases of diabetes caused by statin use, he cautioned. More cases of myopathy would also occur, though the estimated number depends on whether the rate is derived from randomized, controlled trials (RCTs) or from population-based reports of myopathy. If the RCT data are used, just 1,510 excess cases of myopathy would be seen, in contrast to the 36,100 cases predicted by population-based data.
The study could model deaths caused by CVD only and not the reduction in disease burden of CVD that would result if all of the additional 24.2 million Americans took a statin, Dr Yang noted. Other limitations of the study included the lack of agreement in incidence of myopathy between RCTs and population-based studies, as well as the likelihood that the risk of diabetes increases with age and higher statin dose – effects not accounted for in the study.
Questioning after the talk focused on sex-specific differences in statin takers. For example, statin-associated diabetes is more common in women than men, another effect not accounted for in the study’s modeling, noted an audience member. Additionally, given that women have been underrepresented in clinical trials in general and in those for CVD in particular, some modeling assumptions in the present study may also lack full generalizability to women at risk for CVD.
AT AHA EPI/LIFESTYLE 2015MEETING
Key clinical point: New statin guidelines, if followed, could save lives but increase cases of myopathy and diabetes.
Major finding: Up to 12.6% of current deaths from CVD could be prevented if all guideline-eligible Americans took statins; saving of these lives would come at the cost of excess cases of diabetes and myopathy.
Data source: Analysis of U.S. census data and data from the NHANES study, together with meta-analysis of RCTs, used to model outcomes for 100% guideline-eligible statin use.
Disclosures: No authors reported financial disclosures.
Achieving diabetes treatment goals rarely influenced by provider beliefs
Primary care providers’ beliefs about diabetic treatment and glycated hemoglobin goals have a relatively small impact on patients achieving their diabetes treatment goals, researchers said.
A study linking the survey responses from 149 primary care providers to the health records of their 18,346 patients with diabetes showed that only two survey responses bore any significant relationship to patients’ glycemic control.
The 21% of responders who agreed with the statement that “current research did not support HbA1c levels below 7%” were 13% less likely to have patients with HbA1c levels below 7%, compared with responders who were neutral about that statement (odds ratio, 0.87; 95% confidence interval, 0.78-0.97; P = .02), according to Dr. Erin S. LeBlanc of the Kaiser Permanente Center for Health Research in Portland, Ore., and her coauthors.
Similarly, the 21% of providers who disagreed with the statement that “some patients will have an HbA1c greater than 9% no matter what I do” were 16% more likely to have patients achieving an HbA1cbelow 7% (OR, 1.16; 95%CI 1.03-1.30; P= .01) than those providers who were neutral about the statement.
“To the best of our knowledge, no previous research has linked what clinicians identify as patient and care setting barriers to the documented glycemic control of their patients,” they wrote (BMJ Open Diab. Res. Care 2015 Feb. 24).
The survey highlighted psychosocial issues, resistance to lifestyle change, and noncompliance as the most common patient-related barriers to achieving optimal control.
On the question of what factors might delay pharmacologic intensification, providers singled out patients’ resistance to lifestyle change and noncompliance as two factors that came into play at least 25% of the time, while unwillingness to consider insulin and psychosocial issues also played a key role.
Side effects, cost, cultural issues, and a lack of established patient-provider relationship played relatively minor roles in influencing pharmacologic intensification.
“These data suggest that patient and system barriers play a larger role than clinician beliefs and behaviors in prolonged poor control and delayed treatment intensification,” Dr. LeBlanc and her associates wrote.
“HbA1clevels were consistent across patients despite differences in their providers’ treatment behaviors, HbA1c goals, and diabetic treatment opinions,” they said.
The survey also revealed that 80% of primary care providers gave patients who were above their glycemic goals 3-6 months to work on lifestyle changes before resorting to pharmacologic therapy, while a similar percentage agreed that older patients needed less-stringent glycemic goals.
The majority also agreed that weight loss was a key component of diabetes care, but only 40% agreed that the impact of a diabetes medication on weight influenced their therapy decisions.
“Taken together, it seems that intervention to reduce barriers to glycemic control directed at providers would not produce much benefit, and that addressing these barriers may be most fruitful at the health system level,” the authors suggested.
The authors acknowledged that the survey was limited by a lack of variation in provider attitudes – possibly the result of conducting it within a single organization – as well as being of an insured population restricted to a range of treatments that did not include newer medications.
“This could affect the relative importance of cost issues in prescribing and intensification practices, and may also constrain our ability to assess the value of more therapeutic options,” they wrote.
The study was funded by AstraZeneca and Bristol-Myers Squibb. Two authors declared additional research funding from other pharmaceutical companies, while two authors were employees of Bristol-Myers Squibb.
Primary care providers’ beliefs about diabetic treatment and glycated hemoglobin goals have a relatively small impact on patients achieving their diabetes treatment goals, researchers said.
A study linking the survey responses from 149 primary care providers to the health records of their 18,346 patients with diabetes showed that only two survey responses bore any significant relationship to patients’ glycemic control.
The 21% of responders who agreed with the statement that “current research did not support HbA1c levels below 7%” were 13% less likely to have patients with HbA1c levels below 7%, compared with responders who were neutral about that statement (odds ratio, 0.87; 95% confidence interval, 0.78-0.97; P = .02), according to Dr. Erin S. LeBlanc of the Kaiser Permanente Center for Health Research in Portland, Ore., and her coauthors.
Similarly, the 21% of providers who disagreed with the statement that “some patients will have an HbA1c greater than 9% no matter what I do” were 16% more likely to have patients achieving an HbA1cbelow 7% (OR, 1.16; 95%CI 1.03-1.30; P= .01) than those providers who were neutral about the statement.
“To the best of our knowledge, no previous research has linked what clinicians identify as patient and care setting barriers to the documented glycemic control of their patients,” they wrote (BMJ Open Diab. Res. Care 2015 Feb. 24).
The survey highlighted psychosocial issues, resistance to lifestyle change, and noncompliance as the most common patient-related barriers to achieving optimal control.
On the question of what factors might delay pharmacologic intensification, providers singled out patients’ resistance to lifestyle change and noncompliance as two factors that came into play at least 25% of the time, while unwillingness to consider insulin and psychosocial issues also played a key role.
Side effects, cost, cultural issues, and a lack of established patient-provider relationship played relatively minor roles in influencing pharmacologic intensification.
“These data suggest that patient and system barriers play a larger role than clinician beliefs and behaviors in prolonged poor control and delayed treatment intensification,” Dr. LeBlanc and her associates wrote.
“HbA1clevels were consistent across patients despite differences in their providers’ treatment behaviors, HbA1c goals, and diabetic treatment opinions,” they said.
The survey also revealed that 80% of primary care providers gave patients who were above their glycemic goals 3-6 months to work on lifestyle changes before resorting to pharmacologic therapy, while a similar percentage agreed that older patients needed less-stringent glycemic goals.
The majority also agreed that weight loss was a key component of diabetes care, but only 40% agreed that the impact of a diabetes medication on weight influenced their therapy decisions.
“Taken together, it seems that intervention to reduce barriers to glycemic control directed at providers would not produce much benefit, and that addressing these barriers may be most fruitful at the health system level,” the authors suggested.
The authors acknowledged that the survey was limited by a lack of variation in provider attitudes – possibly the result of conducting it within a single organization – as well as being of an insured population restricted to a range of treatments that did not include newer medications.
“This could affect the relative importance of cost issues in prescribing and intensification practices, and may also constrain our ability to assess the value of more therapeutic options,” they wrote.
The study was funded by AstraZeneca and Bristol-Myers Squibb. Two authors declared additional research funding from other pharmaceutical companies, while two authors were employees of Bristol-Myers Squibb.
Primary care providers’ beliefs about diabetic treatment and glycated hemoglobin goals have a relatively small impact on patients achieving their diabetes treatment goals, researchers said.
A study linking the survey responses from 149 primary care providers to the health records of their 18,346 patients with diabetes showed that only two survey responses bore any significant relationship to patients’ glycemic control.
The 21% of responders who agreed with the statement that “current research did not support HbA1c levels below 7%” were 13% less likely to have patients with HbA1c levels below 7%, compared with responders who were neutral about that statement (odds ratio, 0.87; 95% confidence interval, 0.78-0.97; P = .02), according to Dr. Erin S. LeBlanc of the Kaiser Permanente Center for Health Research in Portland, Ore., and her coauthors.
Similarly, the 21% of providers who disagreed with the statement that “some patients will have an HbA1c greater than 9% no matter what I do” were 16% more likely to have patients achieving an HbA1cbelow 7% (OR, 1.16; 95%CI 1.03-1.30; P= .01) than those providers who were neutral about the statement.
“To the best of our knowledge, no previous research has linked what clinicians identify as patient and care setting barriers to the documented glycemic control of their patients,” they wrote (BMJ Open Diab. Res. Care 2015 Feb. 24).
The survey highlighted psychosocial issues, resistance to lifestyle change, and noncompliance as the most common patient-related barriers to achieving optimal control.
On the question of what factors might delay pharmacologic intensification, providers singled out patients’ resistance to lifestyle change and noncompliance as two factors that came into play at least 25% of the time, while unwillingness to consider insulin and psychosocial issues also played a key role.
Side effects, cost, cultural issues, and a lack of established patient-provider relationship played relatively minor roles in influencing pharmacologic intensification.
“These data suggest that patient and system barriers play a larger role than clinician beliefs and behaviors in prolonged poor control and delayed treatment intensification,” Dr. LeBlanc and her associates wrote.
“HbA1clevels were consistent across patients despite differences in their providers’ treatment behaviors, HbA1c goals, and diabetic treatment opinions,” they said.
The survey also revealed that 80% of primary care providers gave patients who were above their glycemic goals 3-6 months to work on lifestyle changes before resorting to pharmacologic therapy, while a similar percentage agreed that older patients needed less-stringent glycemic goals.
The majority also agreed that weight loss was a key component of diabetes care, but only 40% agreed that the impact of a diabetes medication on weight influenced their therapy decisions.
“Taken together, it seems that intervention to reduce barriers to glycemic control directed at providers would not produce much benefit, and that addressing these barriers may be most fruitful at the health system level,” the authors suggested.
The authors acknowledged that the survey was limited by a lack of variation in provider attitudes – possibly the result of conducting it within a single organization – as well as being of an insured population restricted to a range of treatments that did not include newer medications.
“This could affect the relative importance of cost issues in prescribing and intensification practices, and may also constrain our ability to assess the value of more therapeutic options,” they wrote.
The study was funded by AstraZeneca and Bristol-Myers Squibb. Two authors declared additional research funding from other pharmaceutical companies, while two authors were employees of Bristol-Myers Squibb.
FROM BMJ OPEN DIABETES RESEARCH AND CARE
Key clinical point: Primary care providers’ beliefs about diabetes treatment have a relatively small impact on patients achieving treatment goals.
Major finding: Responders who agreed that “current research did not support HbA1c levels below 7%” were 13% less likely to have patients with HbA1c levels below 7%, compared with responders who were neutral about that statement.
Data source: Survey of 149 health care providers and their 18,346 patients with diabetes.
Disclosures: The study was funded by AstraZeneca and Bristol-Myers Squibb. Two authors declared additional research funding from other pharmaceutical companies, while two authors were employees of Bristol-Myers Squibb.
Type 2 diabetes lower in familial hypercholesterolemia
The prevalence of type 2 diabetes appears to be significantly lower in patients with familial hypercholesterolemia than in their unaffected relatives, according to a report published online March 10 in JAMA.
In an observational cross-sectional analysis of data from a nationwide Dutch registry of familial hypercholesterolemia, the prevalence of type 2 diabetes was 1.75% in 25,137 patients with the disorder, compared with 2.93% in 38,183 of their unaffected relatives. If this finding is confirmed in further research, it would support the hypothesis that cellular cholesterol metabolism plays a role in the development of type 2 diabetes, “perhaps because increased intracellular cholesterol levels are detrimental for pancreatic beta-cell function,” said Dr. Joost Besseling of the department of vascular medicine, Academic Medical Centre, Amsterdam, and his associates.
Patients with familial hypercholesterolemia require strict clinical follow-up, and it has been noticed – but, until now, not substantiated – that they are less prone to developing type 2 diabetes.
In what they described as the first study to examine this relationship, Dr. Besseling and his colleagues found that the strong inverse association (odds ratio, 0.62; 95% confidence interval, 0.55-0.69) between familial hypercholesterolemia and type 2 diabetes was consistent across every subgroup they evaluated, regardless of patient age, statin use, smoking status, and other possible confounding factors.
In addition, they found that the severity of the genetic mutation underlying the familial hypercholesterolemia also correlated, in an inverse dose-response manner, with the prevalence of type 2 diabetes (JAMA 2015;313:1029-36).
If these findings are confirmed, “they might provide support for development of new approaches to the prevention and treatment of type 2 diabetes by improving function and survival of pancreatic beta cells,” the investigators said.
The findings by Besseling et al. should allay any concerns physicians may have about using statins in patients who have familial hypercholesterolemia. The drugs are now known to promote type 2 diabetes in the general population, but these patients appear to be at low risk for that metabolic disorder.
The study results do not, and should not, alter the use of these important medications in patients at elevated cardiovascular risk, who clearly benefit from statin therapy.
Dr. David Preiss and Dr. Naveed Sattar are at the BHF Glasgow Cardiovascular Research Centre at the University of Glasgow. Dr. Preiss reported serving as a consultant for Sanofi-Aventis; Dr. Sattar reported financial relationships with Amgen, Kowa Pharmaceuticals, and Sanofi-Aventis. They made these remarks in an editorial accompanying Dr. Besseling’s report (JAMA 2015;313:1016-7).
The findings by Besseling et al. should allay any concerns physicians may have about using statins in patients who have familial hypercholesterolemia. The drugs are now known to promote type 2 diabetes in the general population, but these patients appear to be at low risk for that metabolic disorder.
The study results do not, and should not, alter the use of these important medications in patients at elevated cardiovascular risk, who clearly benefit from statin therapy.
Dr. David Preiss and Dr. Naveed Sattar are at the BHF Glasgow Cardiovascular Research Centre at the University of Glasgow. Dr. Preiss reported serving as a consultant for Sanofi-Aventis; Dr. Sattar reported financial relationships with Amgen, Kowa Pharmaceuticals, and Sanofi-Aventis. They made these remarks in an editorial accompanying Dr. Besseling’s report (JAMA 2015;313:1016-7).
The findings by Besseling et al. should allay any concerns physicians may have about using statins in patients who have familial hypercholesterolemia. The drugs are now known to promote type 2 diabetes in the general population, but these patients appear to be at low risk for that metabolic disorder.
The study results do not, and should not, alter the use of these important medications in patients at elevated cardiovascular risk, who clearly benefit from statin therapy.
Dr. David Preiss and Dr. Naveed Sattar are at the BHF Glasgow Cardiovascular Research Centre at the University of Glasgow. Dr. Preiss reported serving as a consultant for Sanofi-Aventis; Dr. Sattar reported financial relationships with Amgen, Kowa Pharmaceuticals, and Sanofi-Aventis. They made these remarks in an editorial accompanying Dr. Besseling’s report (JAMA 2015;313:1016-7).
The prevalence of type 2 diabetes appears to be significantly lower in patients with familial hypercholesterolemia than in their unaffected relatives, according to a report published online March 10 in JAMA.
In an observational cross-sectional analysis of data from a nationwide Dutch registry of familial hypercholesterolemia, the prevalence of type 2 diabetes was 1.75% in 25,137 patients with the disorder, compared with 2.93% in 38,183 of their unaffected relatives. If this finding is confirmed in further research, it would support the hypothesis that cellular cholesterol metabolism plays a role in the development of type 2 diabetes, “perhaps because increased intracellular cholesterol levels are detrimental for pancreatic beta-cell function,” said Dr. Joost Besseling of the department of vascular medicine, Academic Medical Centre, Amsterdam, and his associates.
Patients with familial hypercholesterolemia require strict clinical follow-up, and it has been noticed – but, until now, not substantiated – that they are less prone to developing type 2 diabetes.
In what they described as the first study to examine this relationship, Dr. Besseling and his colleagues found that the strong inverse association (odds ratio, 0.62; 95% confidence interval, 0.55-0.69) between familial hypercholesterolemia and type 2 diabetes was consistent across every subgroup they evaluated, regardless of patient age, statin use, smoking status, and other possible confounding factors.
In addition, they found that the severity of the genetic mutation underlying the familial hypercholesterolemia also correlated, in an inverse dose-response manner, with the prevalence of type 2 diabetes (JAMA 2015;313:1029-36).
If these findings are confirmed, “they might provide support for development of new approaches to the prevention and treatment of type 2 diabetes by improving function and survival of pancreatic beta cells,” the investigators said.
The prevalence of type 2 diabetes appears to be significantly lower in patients with familial hypercholesterolemia than in their unaffected relatives, according to a report published online March 10 in JAMA.
In an observational cross-sectional analysis of data from a nationwide Dutch registry of familial hypercholesterolemia, the prevalence of type 2 diabetes was 1.75% in 25,137 patients with the disorder, compared with 2.93% in 38,183 of their unaffected relatives. If this finding is confirmed in further research, it would support the hypothesis that cellular cholesterol metabolism plays a role in the development of type 2 diabetes, “perhaps because increased intracellular cholesterol levels are detrimental for pancreatic beta-cell function,” said Dr. Joost Besseling of the department of vascular medicine, Academic Medical Centre, Amsterdam, and his associates.
Patients with familial hypercholesterolemia require strict clinical follow-up, and it has been noticed – but, until now, not substantiated – that they are less prone to developing type 2 diabetes.
In what they described as the first study to examine this relationship, Dr. Besseling and his colleagues found that the strong inverse association (odds ratio, 0.62; 95% confidence interval, 0.55-0.69) between familial hypercholesterolemia and type 2 diabetes was consistent across every subgroup they evaluated, regardless of patient age, statin use, smoking status, and other possible confounding factors.
In addition, they found that the severity of the genetic mutation underlying the familial hypercholesterolemia also correlated, in an inverse dose-response manner, with the prevalence of type 2 diabetes (JAMA 2015;313:1029-36).
If these findings are confirmed, “they might provide support for development of new approaches to the prevention and treatment of type 2 diabetes by improving function and survival of pancreatic beta cells,” the investigators said.
FROM JAMA
Key clinical point: The prevalence of type 2 diabetes appears to be significantly lower in patients with familial hypercholesterolemia than in their unaffected relatives.
Major finding: The prevalence of type 2 diabetes was 1.75% in 25,137 patients with the familial hypercholesterolemia, compared with 2.93% in 38,183 of their unaffected relatives.
Data source: An observational cross-sectional analysis of data for 63,320 people in the Dutch national registry of familial hypercholesterolemia.
Disclosures: The study sponsor was not specified; the familial hypercholesterolemia registry is subsidized by the Dutch government. Dr. Besseling reported having no financial disclosures; his associates reported ties to Aegerion, Amgen, AstraZeneca, Boehringer Ingelheim, Cerenis, Eli Lilly, Genzyme, JSiS, MSD, Novartis, Pfizer, Regeneron, Roche, and Sanofi.