User login
NEW ORLEANS – Do you know which of your patients is likely to misuse or abuse opioid medications?
They can be stratified according to risk, but many physicians don’t know how or don’t take the time to do so, according to Dr. Lynn R. Webster, medical director of Lifetree Clinical Research in Salt Lake City and director at large for the American Academy of Pain Medicine.
It is important to try to prevent misuse or abuse, given that overdoses and deaths from prescription drugs are on the rise, said Dr. Webster at the American Medical Association House of Delegates Interim meeting.
According to the National Institute on Drug Abuse, emergency department visits involving nonmedical use of pharmaceuticals (either alone or in combination with another drug) increased 98% between 2004 and 2009, from 627,291 visits to 1.2 million visits. There was an 83% rise in emergency department visits involving adverse reactions to pharmaceuticals between 2005 and 2009, from 1.3 million to 2.3 million visits.
Opioids were the most frequently cited in those ED visits, accounting for about 50% of nonmedical use. Psychotherapeutic agents accounted for a third of the nonmedical use. According to the National Institute on Drug Abuse, the three most frequently cited drugs in those visits were hydrocodone (alone or in combination), accounting for 104,490 visits; oxycodone (alone or in combination), for 175,949 visits; and methadone, for 70,637 visits.
To properly assess and treat patients, physicians should understand and agree upon terminology, said Dr. Webster. Patients may "misuse" prescriptions if they are not taking them as directed. They aren’t seeking a high, they may just have undertreated pain, he said.
Abuse is the willful self-administration of a drug to get high. Addiction is a medical condition with complex genetic, psychosocial, and environmental factors that influence its development and manifestations. Addicts may have impaired control over drug use, compulsive use, or continued use despite harm.
"You don’t just put someone on an opioid and think you’ve done your job."
Pseudoaddiction results from undertreatment of pain, and may resolve with proper therapy. Patients in this state may manifest behavior that is misidentified as drug-seeking, according to Dr. Webster.
Even with chronic pain, "people prescribed opioids over a long period of time are going to have aberrant behavior," said Dr. Webster, noting that "it’s not a small problem." In research he conducted, up to 40% of patients in his chronic pain practice had aberrant behavior within a year of starting treatment.
But, he said, "only a small percent have the disease of addiction."
To prevent misuse and abuse, it’s important to understand patients’ motives, he said. Nonmedical users may have been prescribed pain medications, but they move on to recreational use and then, often, abuse.
Medical users generally are pain patients who are seeking more pain relief and end up misusing the drugs. They also may become abusers. In all, 40%-60% have other chronic conditions for which opioids provide relief, such as anxiety, said Dr. Webster. That use is obviously not appropriate, but it can only be prevented if physicians fully assess pain patients.
There is a constellation of risk factors that help determine potential for misuse and abuse, according to Dr. Webster.
The potency of a pharmacologic substance and how fast it works are important, as those factors help determine how much dopamine is released, and thus, the amount of reward the patient feels, said Dr. Webster. If the drug is readily available, that also determines its attractiveness.
One-fifth of the overall population is at risk for addiction. There is no on/off switch, but a continuum of risk, he explained. Biological, psychiatric, and social factors all play a role in where patients fall on that continuum. Age, gender, family history, cigarette smoking, pain severity and duration, and sleep disorders are all risk factors. Patients with a history of a psychiatric disorder, being sexual abused, or substance use disorder also are at higher risk. "We must assess mental health," said Dr. Webster, noting that patients with anxiety, depression, traumatic brain injury, and attention-deficit/hyperactivity disorder are at risk for self-medicating and overdose.
A history of legal problems and motor vehicle accidents, or poor family support and unemployment also are predictors, Dr. Webster said.
Aberrant behaviors are directly related to the duration and the intensity of pain. Patients who cannot completely eliminate their pain may resort to taking more medication, which they will see as less of a wrong than the pain itself, he said.
Physicians generally have not done a good job at evaluating these risks, and selecting and managing patients according to these factors. But how patients are managed can help determine whether they end up in the emergency room, "or going to a substance abuse treatment center or the morgue," he said.
There are tools that can be used to screen patients for risk. Among those are the Screener and Opioid Assessment for Patients With Pain (SOAPP); the Opioid Risk Tool (ORT); the Diagnosis, Intractability, Risk Efficacy (DIRE) test; and the Current Opioid Misuse Measure (COMM), which is used for patients already taking opioids.
These tests all are simple and take only 1 to 10 minutes to administer. They can be given by any physician, including primary care physicians, he said.
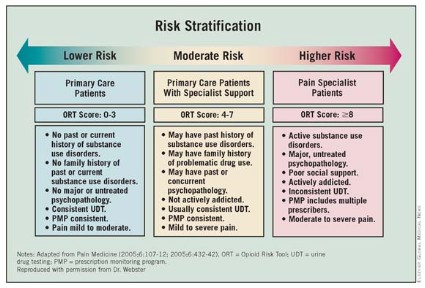
Once all the factors are taken into account, patients can be stratified according to risk. Lower-risk patients – those with moderate pain and no personal or family history of substance use disorders – can be managed by primary care physicians. Those at moderate risk may need the addition of a pain specialist. The higher-risk patients will need consultations with mental health professionals and pain physicians.
Monitoring higher-risk patients may require urine drug testing and prescription monitoring programs. Pharmacists should be kept in the loop to see whether patients are shopping around. Family and friends can be invaluable sources to help identify risky behaviors.
Physicians need to do a better job of titrating opioids and determining proper dosing. Many patients have died at initiation of opioid therapy, or from rotating from one drug to another, he said. Patients should not be allowed to determine how much of a long-acting medication they can take.
So how do doctors mitigate risk? The first order of business is to treat the pain. "Uncontrolled pain, untreated pain, I believe is the number one reason for aberrant behavior," said Dr. Webster. Physicians cannot eliminate all pain, however, so education also is crucial.
Physicians also have a duty to monitor pain patients. "You don’t just put someone on an opioid and think you’ve done your job," said Dr. Webster. A doctor would not stop managing a diabetic; pain patients need long-term management, he said.
Dr. Webster reported having no relevant conflicts of interest.
NEW ORLEANS – Do you know which of your patients is likely to misuse or abuse opioid medications?
They can be stratified according to risk, but many physicians don’t know how or don’t take the time to do so, according to Dr. Lynn R. Webster, medical director of Lifetree Clinical Research in Salt Lake City and director at large for the American Academy of Pain Medicine.
It is important to try to prevent misuse or abuse, given that overdoses and deaths from prescription drugs are on the rise, said Dr. Webster at the American Medical Association House of Delegates Interim meeting.
According to the National Institute on Drug Abuse, emergency department visits involving nonmedical use of pharmaceuticals (either alone or in combination with another drug) increased 98% between 2004 and 2009, from 627,291 visits to 1.2 million visits. There was an 83% rise in emergency department visits involving adverse reactions to pharmaceuticals between 2005 and 2009, from 1.3 million to 2.3 million visits.
Opioids were the most frequently cited in those ED visits, accounting for about 50% of nonmedical use. Psychotherapeutic agents accounted for a third of the nonmedical use. According to the National Institute on Drug Abuse, the three most frequently cited drugs in those visits were hydrocodone (alone or in combination), accounting for 104,490 visits; oxycodone (alone or in combination), for 175,949 visits; and methadone, for 70,637 visits.
To properly assess and treat patients, physicians should understand and agree upon terminology, said Dr. Webster. Patients may "misuse" prescriptions if they are not taking them as directed. They aren’t seeking a high, they may just have undertreated pain, he said.
Abuse is the willful self-administration of a drug to get high. Addiction is a medical condition with complex genetic, psychosocial, and environmental factors that influence its development and manifestations. Addicts may have impaired control over drug use, compulsive use, or continued use despite harm.
"You don’t just put someone on an opioid and think you’ve done your job."
Pseudoaddiction results from undertreatment of pain, and may resolve with proper therapy. Patients in this state may manifest behavior that is misidentified as drug-seeking, according to Dr. Webster.
Even with chronic pain, "people prescribed opioids over a long period of time are going to have aberrant behavior," said Dr. Webster, noting that "it’s not a small problem." In research he conducted, up to 40% of patients in his chronic pain practice had aberrant behavior within a year of starting treatment.
But, he said, "only a small percent have the disease of addiction."
To prevent misuse and abuse, it’s important to understand patients’ motives, he said. Nonmedical users may have been prescribed pain medications, but they move on to recreational use and then, often, abuse.
Medical users generally are pain patients who are seeking more pain relief and end up misusing the drugs. They also may become abusers. In all, 40%-60% have other chronic conditions for which opioids provide relief, such as anxiety, said Dr. Webster. That use is obviously not appropriate, but it can only be prevented if physicians fully assess pain patients.
There is a constellation of risk factors that help determine potential for misuse and abuse, according to Dr. Webster.
The potency of a pharmacologic substance and how fast it works are important, as those factors help determine how much dopamine is released, and thus, the amount of reward the patient feels, said Dr. Webster. If the drug is readily available, that also determines its attractiveness.
One-fifth of the overall population is at risk for addiction. There is no on/off switch, but a continuum of risk, he explained. Biological, psychiatric, and social factors all play a role in where patients fall on that continuum. Age, gender, family history, cigarette smoking, pain severity and duration, and sleep disorders are all risk factors. Patients with a history of a psychiatric disorder, being sexual abused, or substance use disorder also are at higher risk. "We must assess mental health," said Dr. Webster, noting that patients with anxiety, depression, traumatic brain injury, and attention-deficit/hyperactivity disorder are at risk for self-medicating and overdose.
A history of legal problems and motor vehicle accidents, or poor family support and unemployment also are predictors, Dr. Webster said.
Aberrant behaviors are directly related to the duration and the intensity of pain. Patients who cannot completely eliminate their pain may resort to taking more medication, which they will see as less of a wrong than the pain itself, he said.
Physicians generally have not done a good job at evaluating these risks, and selecting and managing patients according to these factors. But how patients are managed can help determine whether they end up in the emergency room, "or going to a substance abuse treatment center or the morgue," he said.
There are tools that can be used to screen patients for risk. Among those are the Screener and Opioid Assessment for Patients With Pain (SOAPP); the Opioid Risk Tool (ORT); the Diagnosis, Intractability, Risk Efficacy (DIRE) test; and the Current Opioid Misuse Measure (COMM), which is used for patients already taking opioids.
These tests all are simple and take only 1 to 10 minutes to administer. They can be given by any physician, including primary care physicians, he said.
Once all the factors are taken into account, patients can be stratified according to risk. Lower-risk patients – those with moderate pain and no personal or family history of substance use disorders – can be managed by primary care physicians. Those at moderate risk may need the addition of a pain specialist. The higher-risk patients will need consultations with mental health professionals and pain physicians.
Monitoring higher-risk patients may require urine drug testing and prescription monitoring programs. Pharmacists should be kept in the loop to see whether patients are shopping around. Family and friends can be invaluable sources to help identify risky behaviors.
Physicians need to do a better job of titrating opioids and determining proper dosing. Many patients have died at initiation of opioid therapy, or from rotating from one drug to another, he said. Patients should not be allowed to determine how much of a long-acting medication they can take.
So how do doctors mitigate risk? The first order of business is to treat the pain. "Uncontrolled pain, untreated pain, I believe is the number one reason for aberrant behavior," said Dr. Webster. Physicians cannot eliminate all pain, however, so education also is crucial.
Physicians also have a duty to monitor pain patients. "You don’t just put someone on an opioid and think you’ve done your job," said Dr. Webster. A doctor would not stop managing a diabetic; pain patients need long-term management, he said.
Dr. Webster reported having no relevant conflicts of interest.
NEW ORLEANS – Do you know which of your patients is likely to misuse or abuse opioid medications?
They can be stratified according to risk, but many physicians don’t know how or don’t take the time to do so, according to Dr. Lynn R. Webster, medical director of Lifetree Clinical Research in Salt Lake City and director at large for the American Academy of Pain Medicine.
It is important to try to prevent misuse or abuse, given that overdoses and deaths from prescription drugs are on the rise, said Dr. Webster at the American Medical Association House of Delegates Interim meeting.
According to the National Institute on Drug Abuse, emergency department visits involving nonmedical use of pharmaceuticals (either alone or in combination with another drug) increased 98% between 2004 and 2009, from 627,291 visits to 1.2 million visits. There was an 83% rise in emergency department visits involving adverse reactions to pharmaceuticals between 2005 and 2009, from 1.3 million to 2.3 million visits.
Opioids were the most frequently cited in those ED visits, accounting for about 50% of nonmedical use. Psychotherapeutic agents accounted for a third of the nonmedical use. According to the National Institute on Drug Abuse, the three most frequently cited drugs in those visits were hydrocodone (alone or in combination), accounting for 104,490 visits; oxycodone (alone or in combination), for 175,949 visits; and methadone, for 70,637 visits.
To properly assess and treat patients, physicians should understand and agree upon terminology, said Dr. Webster. Patients may "misuse" prescriptions if they are not taking them as directed. They aren’t seeking a high, they may just have undertreated pain, he said.
Abuse is the willful self-administration of a drug to get high. Addiction is a medical condition with complex genetic, psychosocial, and environmental factors that influence its development and manifestations. Addicts may have impaired control over drug use, compulsive use, or continued use despite harm.
"You don’t just put someone on an opioid and think you’ve done your job."
Pseudoaddiction results from undertreatment of pain, and may resolve with proper therapy. Patients in this state may manifest behavior that is misidentified as drug-seeking, according to Dr. Webster.
Even with chronic pain, "people prescribed opioids over a long period of time are going to have aberrant behavior," said Dr. Webster, noting that "it’s not a small problem." In research he conducted, up to 40% of patients in his chronic pain practice had aberrant behavior within a year of starting treatment.
But, he said, "only a small percent have the disease of addiction."
To prevent misuse and abuse, it’s important to understand patients’ motives, he said. Nonmedical users may have been prescribed pain medications, but they move on to recreational use and then, often, abuse.
Medical users generally are pain patients who are seeking more pain relief and end up misusing the drugs. They also may become abusers. In all, 40%-60% have other chronic conditions for which opioids provide relief, such as anxiety, said Dr. Webster. That use is obviously not appropriate, but it can only be prevented if physicians fully assess pain patients.
There is a constellation of risk factors that help determine potential for misuse and abuse, according to Dr. Webster.
The potency of a pharmacologic substance and how fast it works are important, as those factors help determine how much dopamine is released, and thus, the amount of reward the patient feels, said Dr. Webster. If the drug is readily available, that also determines its attractiveness.
One-fifth of the overall population is at risk for addiction. There is no on/off switch, but a continuum of risk, he explained. Biological, psychiatric, and social factors all play a role in where patients fall on that continuum. Age, gender, family history, cigarette smoking, pain severity and duration, and sleep disorders are all risk factors. Patients with a history of a psychiatric disorder, being sexual abused, or substance use disorder also are at higher risk. "We must assess mental health," said Dr. Webster, noting that patients with anxiety, depression, traumatic brain injury, and attention-deficit/hyperactivity disorder are at risk for self-medicating and overdose.
A history of legal problems and motor vehicle accidents, or poor family support and unemployment also are predictors, Dr. Webster said.
Aberrant behaviors are directly related to the duration and the intensity of pain. Patients who cannot completely eliminate their pain may resort to taking more medication, which they will see as less of a wrong than the pain itself, he said.
Physicians generally have not done a good job at evaluating these risks, and selecting and managing patients according to these factors. But how patients are managed can help determine whether they end up in the emergency room, "or going to a substance abuse treatment center or the morgue," he said.
There are tools that can be used to screen patients for risk. Among those are the Screener and Opioid Assessment for Patients With Pain (SOAPP); the Opioid Risk Tool (ORT); the Diagnosis, Intractability, Risk Efficacy (DIRE) test; and the Current Opioid Misuse Measure (COMM), which is used for patients already taking opioids.
These tests all are simple and take only 1 to 10 minutes to administer. They can be given by any physician, including primary care physicians, he said.
Once all the factors are taken into account, patients can be stratified according to risk. Lower-risk patients – those with moderate pain and no personal or family history of substance use disorders – can be managed by primary care physicians. Those at moderate risk may need the addition of a pain specialist. The higher-risk patients will need consultations with mental health professionals and pain physicians.
Monitoring higher-risk patients may require urine drug testing and prescription monitoring programs. Pharmacists should be kept in the loop to see whether patients are shopping around. Family and friends can be invaluable sources to help identify risky behaviors.
Physicians need to do a better job of titrating opioids and determining proper dosing. Many patients have died at initiation of opioid therapy, or from rotating from one drug to another, he said. Patients should not be allowed to determine how much of a long-acting medication they can take.
So how do doctors mitigate risk? The first order of business is to treat the pain. "Uncontrolled pain, untreated pain, I believe is the number one reason for aberrant behavior," said Dr. Webster. Physicians cannot eliminate all pain, however, so education also is crucial.
Physicians also have a duty to monitor pain patients. "You don’t just put someone on an opioid and think you’ve done your job," said Dr. Webster. A doctor would not stop managing a diabetic; pain patients need long-term management, he said.
Dr. Webster reported having no relevant conflicts of interest.
FROM THE AMERICAN MEDICAL ASSOCIATION HOUSE OF DELEGATES INTERIM MEETING