User login
CASE Should you remove a 6-cm cyst?
Mrs. M, 34, complains of sudden-onset, left lower quadrant pain that woke her from sleep. She has no nausea, vomiting, fever, or abnormal bleeding. Vital signs and temperature are normal. She has a tender left lower quadrant with normal bowel sounds. The pelvic exam reveals a 6-cm tender, but mobile, left adnexal mass, and transvaginal pelvic sonography shows a 6.3-cm cystic mass with a thick septation and some internal echoes. Is surgery necessary?
Few cysts present with sudden pain unless they are undergoing torsion, are hemorrhagic, or are in the process of rupturing. Therefore, in the case of Mrs. M, these benign conditions should be considered first. Cancer is very unlikely to be the cause of sudden pain.
A common phenomenon, and usually benign
How widespread are ovarian cysts? About 8% of asymptomatic women between the ages of 25 and 40 have ovarian cysts larger than 2.5 cm.1 A study of women 50 or older found unilocular cysts smaller than 10 cm in 18% of cases.2 Although many cysts resolve spontaneously, some women may be subjected to unnecessary surgery because of concerns about ovarian cancer. In actuality, various studies have shown that cysts found prior to menopause are benign in 87% to 93% of women, and cysts found after menopause are benign in 55% to 92% of cases.3 The gynecologist’s dilemma is to differentiate between cysts that require surgery and those that do not.
This article details the careful assessment that should guide this important decision.
Detorsion of the twisted ovary restores function
In addition, when torsion is present, rather than resort to removal of the adnexa, simply untwist it, even if the tissue does not appear to be viable. Studies have shown that this maneuver leads to a return of ovarian function, as evidenced by follicle formation on subsequent sonograms. In addition, no case of thromboembolism has ever been reported following detorsion of an adnexa.4
Physical clues to the type of cyst
The pelvic examination can yield important clues. For example, a mass that is compressible, smooth, and freely mobile is likely to be benign.
As already noted, tenderness is more common with a hemorrhagic cyst or with torsion, and is rarely associated with cancer. A solid, fixed, irregular mass, however, should raise the suspicion of cancer.
If ascites or an abdominal mass is found, assume the patient has cancer until proven otherwise.
Sonographic appearance
If you do not perform the sonogram yourself, it is a good idea to view the actual images. The reason: Many radiologists use the term “complex” to describe all cysts other than totally clear, simple cysts (FIGURE 1). However, many benign entities are complex, such as dermoid cysts, endometriomas, hemorrhagic cysts (FIGURE 2), and cystadenomas. Careful scrutiny of the images and, at times, other imaging studies, can help determine the most likely diagnosis.
Dermoid cysts can often be confirmed by limited computed tomography scan when fat (sebaceous material), teeth, or bone are seen within the ovary.
Torsion may be suspected when Doppler imaging shows decreased or absent blood flow to the ovary.
A small amount of free fluid in the pelvis is an indication of possible cyst rupture.
If a hemorrhagic cyst is present, a follow-up sonogram about 2 weeks later may show either a smaller cyst or changes in the internal echoes consistent with an organizing clot (FIGURE 2).
False-positive CA 125 rate in young women: 70%
Markers such as CA 125 are rarely helpful in determining how to manage a cyst in a young woman and should be avoided in the premenopausal population. Abnormally high CA-125 values can occur with endometriosis, functional cysts, fibroids or adenomyosis, pelvic infection, pregnancy, and cyclic elevations associated with the menses.
In a premenopausal woman, the chance of a false-positive CA-125 reading is about 70%,5 whereas 50% of women with stage I ovarian cancer have a negative test.6
2 useful markers
Very young women are at risk for developing germ-cell tumors, which may produce β human chorionic gonadotropin or alpha fetoprotein. Thus, these tumor markers are sometimes helpful in this patient population.
FIGURE 1 Hallmarks of a benign cyst
Cysts with smooth borders and without septations, excrescences, or solid parts are likely to be benign.
Management options for premenopausal patients
CASE What is the next step?
In Mrs. M’s case, the first option should be observation and a repeat sonogram in about 2 weeks. Analgesics and rest can be helpful to control pain. Reassure her that the pain should diminish in a few days, although it sometimes takes longer.
Skip the birth control pills
Even with unilocular cysts presumed to be follicular, oral contraceptives do not speed resolution. When 80 premenopausal women with 3- to 6-cm unilocular cysts were randomized to no therapy, low-dose oral contraceptives, or high-dose oral contraceptives and followed with sonography, resolution rates were the same in all 3 groups after 10 weeks.7 Almost 90% of the cysts had resolved after 5 weeks, even in women not taking oral contraceptives.
Pain may warrant surgery
In rare cases, a woman may have such severe pain that rest and analgesics are ineffective, and surgery is warranted for pain alone. In other cases, a cyst that appears functional or hemorrhagic on sonography but persists more than 8 weeks may justify removal to rule out neoplasia.
Intraoperative considerations
After the laparoscope and any accessory cannulas are inserted, wash the pelvis and upper abdomen with saline and collect a sample for cytologic analysis. Carefully assess the pelvis and upper abdomen; any peritoneal excrescences or thick adhesions to the mass should be noted, biopsied, and sent for frozen section.
Make every effort to save the ovary
In a premenopausal woman with a presumptively benign ovarian cyst who requires surgery for pain or because the cyst fails to resolve, surgery should aim to conserve the ovary, if at all possible. Even with a large cyst (6 cm or larger), ovarian conservation is possible. Laparoscopic surgery, which involves a short hospital stay and faster postoperative recovery, should be considered unless neoplasia is suspected.
Keep the cyst intact if possible
After placing the cannulas and assessing the pelvis and abdomen, grasp the utero-ovarian ligament with an atraumatic grasper to bring the ovary into view. Inspect the ovary and desiccate (with monopolar cautery) a 1-cm area of thick ovarian capsule, preferably on the less vascular, antimesenteric portion of the ovary.
Using the laparoscopic scissors, incise the capsule superficially along the long axis of the ovary, exposing the cyst wall below. Grasp the edge of the ovarian capsule with a 5-mm grasping forceps. Insert an irrigating instrument between the cyst wall and the ovarian capsule. Use a high-pressure stream of fluid and the blunt edge of the instrument to dissect the cyst away from the ovary.
Keep the cyst intact as long as possible to facilitate dissection. Once the cyst is as free as possible, incise and empty it using the suction irrigator. Grasp the cyst wall with the 5-mm ovarian biopsy forceps and the ovary itself with an atraumatic grasper. Using traction and countertraction, tease the cyst away from the ovarian capsule.
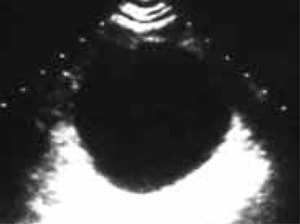
FIGURE 2 Hemorrhagic cyst at detection

Hemorrhagic cysts may have internal echoes, a sign of blood clots within the cyst.
...and 2 weeks later

Two weeks later the cyst is smaller and the clots are in the process of reabsorption.A cyst usually can be removed intact from the abdominal cavity through a 5- or 11-mm canula. If it is too large, bisect it prior to removal.
After removal, inspect the cyst for papillations, septa, or thickening of the wall. If malignancy is suspected, send the cyst for frozen section. If malignancy is confirmed, be prepared to proceed with staging laparotomy immediately.
Postmenopausal women
CASE Is a 4-cm cyst likely to be cancer?
Mrs. J, 67, visits her internist complaining of dull, achy abdominal pain associated with some bloating. A pelvic sonogram reveals a 4.1-cm cyst of the right ovary with well-defined borders; no septations, excrescences, or solid parts; and no free fluid in the pelvis. The left ovary is 3 cm and appears normal. The internist refers Mrs. J to you for further evaluation and management.
By the time you see her, Mrs. J is experiencing very little pain and bloating. However, she is concerned about the cyst and worries that she may have ovarian cancer. She has not experienced any increased abdominal girth, change in appetite or weight, or vaginal bleeding.
When you examine her, you find a normal abdomen with no ascites or abdominal mass. The pelvic exam is normal, too, except for a nontender, slightly enlarged right adnexa, which is difficult to palpate fully.
Mrs. J wants to know if you plan to remove the cyst. What do you tell her?
In this case, the cyst is probably incidental to the abdominal pain Mrs. J experienced at presentation. Because most cysts are benign, observation and repeat sonograms are justified unless the patient’s CA-125 level is found to be elevated or the size or complexity of the cyst increases. Mrs. J has a CA-125 level of 12, and her sonographic findings have not changed since the initial exam, so she can be managed with repeat imaging and blood tests in 2 months.
Data point to safety of surveillance
A sonographic study of asymptomatic postmenopausal women found that about 6% had cysts smaller than 5 cm at initial screening.8 Of the 256 women noted to have these simple cysts, 125 resolved spontaneously within 6 weeks. Among the 131 women with persistent unilocular cysts, 45 requested surgery, and no cancers were found. Among the 86 women who elected to be followed with repeat sonograms and CA-125 levels, no cancers were found after a mean follow-up of 18 months.
A more recent study involved 15,106 women age 50 or older who were screened with transvaginal sonography.2 Of these, 2,763 (18%) had unilocular cysts less than 10 cm in size. Seventy percent of the women had resolution of the cysts within 6 weeks, and none of the 220 women with persistent unilocular cysts developed ovarian cancer after a mean follow-up of 6.8 years.
In properly selected patients, risk of cancer was close to nil
An early study9 focused on 61 postmenopausal women with unilateral, cystic adnexal masses, benign-appearing sonograms, and normal CA-125 levels. These women were managed with laparoscopic oophorectomy. All had benign masses.
Another prospective study involved 228 postmenopausal women with a pelvic mass, 53 of whom had pelvic and sonographic exams suggestive of a benign mass and a CA-125 level below 35 U/mL. All 53 had a benign mass.10
Enlarging, complex cysts and elevated CA 125
In a study of 250 women with complex cystic ovarian tumors smaller than 10 cm (89% were <5 cm in size), more than half the cysts resolved spontaneously.8 However, 7 ovarian carcinomas were found. Thus, observation is not recommended for women with these findings. As might be expected, 6 of the 7 women found to have ovarian cancer had progression of cyst size and/or complexity by the 2-month follow-up sonogram.
Another study11 found that, among 226 postmenopausal women followed with sonograms and CA-125 levels after an initial finding of a unilocular ovarian cyst smaller than 5 cm, cyst size increased in only 54 women, all of whom were operated upon. Two malignancies were found, both in women with elevated CA-125 levels. None of the women whose cyst size remained the same had ovarian cancer.
CASE What is the next step?
When you suggest that Mrs. J be followed with another sonogram and CA-125 level in 2 months, she agrees. At that follow-up, no change in the size or internal architecture of the cyst is noted, and the CA 125 is normal. You ask her to return in 6 and 12 months for repeat sonograms and blood tests, all of which are normal.
At this point, surveillance can shift to yearly pelvic exams. Because women are understandably worried about ovarian cancer, they should be counseled about the importance of careful follow-up. Subjecting them to unnecessary surgery is not advised because of the very real risks of complications from anesthesia and surgery in postmenopausal women.
When surgery is warranted for postmenopausal women
Some women may be symptomatic from larger cysts, or they may not be comfortable with, or available for, close follow-up. In these cases, surgery may be warranted. Women with cysts that are increasing in size, or noted to have a change in internal architecture at the time of sonographic assessment, should also have surgery.
Remove the entire ovary
The entire ovary should be removed in postmenopausal women for complete pathologic analysis.
Technique. Grasp the utero-ovarian ligament and pull it medially to expose the infundibulopelvic ligament. I use a 5-mm bipolar cutting forceps to desiccate and divide the ligament, taking care to identify the ureter and make sure it is well away from the area to be desiccated. Then desiccate and divide the mesosalpinx and follow it to the corneal portion of the fallopian tube. Place the ovary in a laparoscopic sac. Many versions of these sacs exist, but for large cysts I prefer the Cook LapSac (Cook Urological, Spencer, Ind), which has sizes as large as 20×28 cm. These sacs are strong and almost impermeable and hence less likely to tear and allow spillage of the cyst contents into the peritoneal cavity. To keep the neck of the sac open, fill it with irrigating fluid. Once the adnexa is placed in the sac, suction the irrigating fluid and bring the neck of the bag out through an 11-mm port. The cyst can then be aspirated and decompressed to allow removal.
Frozen section is a must. After removal, inspect the cyst wall and obtain frozen sections. If malignancy is found, perform immediate staging laparotomy using a midline incision.
The author reports no financial relationships relevant to this article.
1. Borgfeldt C, Andolf E. Transvaginal sonographic ovarian findings in a random sample of women 25-40 years old. Ultrasound Obstet Gynecol. 1999;13:345-350.
2. Modesitt SC, Pavlik EJ, Ueland FR, DePriest PD, Kryscio RJ, van Nagell JR, Jr. Risk of malignancy in unilocular cystic tumors less than 10 centimeters in diameter. Obstet Gynecol. 2003;102:594-599.
3. Koonings P, Campbell K, Mishell D. Relative frequency of primary ovarian neoplasms. A 10-year review. Obstet Gynecol. 1989;79:921-926.
4. Cohen SB, Oelsner G, Seidman DS, Admon D, Mashiach S, Goldenberg M. Laparoscopic detorsion allows sparing of the twisted ischemic adnexa. J Am Assoc Gynecol Laparosc. 1999;6:139-143.
5. Vasilev SA, Schlaerth JB, Campeau J, Morrow CP. Serum CA 125 levels in preoperative evaluation of pelvic masses. Obstet Gynecol. 1988;71:751-756.
6. Jacobs I, Bast RC, Jr. The CA 125 tumour-associated antigen: a review of the literature. Hum Reprod. 1989;4:1-12.
7. Parker WH, Berek JS. Laparoscopic management of the adnexal mass. Obstet Gynecol Clin North Am. 1994;21:79-92.
8. Bailey CL, Ueland FR, Land GL, et al. The malignant potential of small cystic ovarian tumors in women over 50 years of age. Gynecol Oncol. 1998;69:3-7.
9. Parker WH, Levine RL, Howard FM, Sansone B, Berek JS. A multicenter study of laparoscopic management of selected cystic adnexal masses in postmenopausal women. J Am Coll Surg. 1994;179:733-737.
10. Schutter EM, Kenemans P, Sohn C, et al. Diagnostic value of pelvic examination, ultrasound, and serum CA 125 in postmenopausal women with a pelvic mass. An international multicenter study. Cancer. 1994;74:1398-1406.
11. Nardo LG, Kroon ND, Reginald PW. Persistent unilocular ovarian cysts in a general population of postmenopausal women: is there a place for expectant management? Obstet Gynecol. 2003;102:589-593.
CASE Should you remove a 6-cm cyst?
Mrs. M, 34, complains of sudden-onset, left lower quadrant pain that woke her from sleep. She has no nausea, vomiting, fever, or abnormal bleeding. Vital signs and temperature are normal. She has a tender left lower quadrant with normal bowel sounds. The pelvic exam reveals a 6-cm tender, but mobile, left adnexal mass, and transvaginal pelvic sonography shows a 6.3-cm cystic mass with a thick septation and some internal echoes. Is surgery necessary?
Few cysts present with sudden pain unless they are undergoing torsion, are hemorrhagic, or are in the process of rupturing. Therefore, in the case of Mrs. M, these benign conditions should be considered first. Cancer is very unlikely to be the cause of sudden pain.
A common phenomenon, and usually benign
How widespread are ovarian cysts? About 8% of asymptomatic women between the ages of 25 and 40 have ovarian cysts larger than 2.5 cm.1 A study of women 50 or older found unilocular cysts smaller than 10 cm in 18% of cases.2 Although many cysts resolve spontaneously, some women may be subjected to unnecessary surgery because of concerns about ovarian cancer. In actuality, various studies have shown that cysts found prior to menopause are benign in 87% to 93% of women, and cysts found after menopause are benign in 55% to 92% of cases.3 The gynecologist’s dilemma is to differentiate between cysts that require surgery and those that do not.
This article details the careful assessment that should guide this important decision.
Detorsion of the twisted ovary restores function
In addition, when torsion is present, rather than resort to removal of the adnexa, simply untwist it, even if the tissue does not appear to be viable. Studies have shown that this maneuver leads to a return of ovarian function, as evidenced by follicle formation on subsequent sonograms. In addition, no case of thromboembolism has ever been reported following detorsion of an adnexa.4
Physical clues to the type of cyst
The pelvic examination can yield important clues. For example, a mass that is compressible, smooth, and freely mobile is likely to be benign.
As already noted, tenderness is more common with a hemorrhagic cyst or with torsion, and is rarely associated with cancer. A solid, fixed, irregular mass, however, should raise the suspicion of cancer.
If ascites or an abdominal mass is found, assume the patient has cancer until proven otherwise.
Sonographic appearance
If you do not perform the sonogram yourself, it is a good idea to view the actual images. The reason: Many radiologists use the term “complex” to describe all cysts other than totally clear, simple cysts (FIGURE 1). However, many benign entities are complex, such as dermoid cysts, endometriomas, hemorrhagic cysts (FIGURE 2), and cystadenomas. Careful scrutiny of the images and, at times, other imaging studies, can help determine the most likely diagnosis.
Dermoid cysts can often be confirmed by limited computed tomography scan when fat (sebaceous material), teeth, or bone are seen within the ovary.
Torsion may be suspected when Doppler imaging shows decreased or absent blood flow to the ovary.
A small amount of free fluid in the pelvis is an indication of possible cyst rupture.
If a hemorrhagic cyst is present, a follow-up sonogram about 2 weeks later may show either a smaller cyst or changes in the internal echoes consistent with an organizing clot (FIGURE 2).
False-positive CA 125 rate in young women: 70%
Markers such as CA 125 are rarely helpful in determining how to manage a cyst in a young woman and should be avoided in the premenopausal population. Abnormally high CA-125 values can occur with endometriosis, functional cysts, fibroids or adenomyosis, pelvic infection, pregnancy, and cyclic elevations associated with the menses.
In a premenopausal woman, the chance of a false-positive CA-125 reading is about 70%,5 whereas 50% of women with stage I ovarian cancer have a negative test.6
2 useful markers
Very young women are at risk for developing germ-cell tumors, which may produce β human chorionic gonadotropin or alpha fetoprotein. Thus, these tumor markers are sometimes helpful in this patient population.
FIGURE 1 Hallmarks of a benign cyst
Cysts with smooth borders and without septations, excrescences, or solid parts are likely to be benign.
Management options for premenopausal patients
CASE What is the next step?
In Mrs. M’s case, the first option should be observation and a repeat sonogram in about 2 weeks. Analgesics and rest can be helpful to control pain. Reassure her that the pain should diminish in a few days, although it sometimes takes longer.
Skip the birth control pills
Even with unilocular cysts presumed to be follicular, oral contraceptives do not speed resolution. When 80 premenopausal women with 3- to 6-cm unilocular cysts were randomized to no therapy, low-dose oral contraceptives, or high-dose oral contraceptives and followed with sonography, resolution rates were the same in all 3 groups after 10 weeks.7 Almost 90% of the cysts had resolved after 5 weeks, even in women not taking oral contraceptives.
Pain may warrant surgery
In rare cases, a woman may have such severe pain that rest and analgesics are ineffective, and surgery is warranted for pain alone. In other cases, a cyst that appears functional or hemorrhagic on sonography but persists more than 8 weeks may justify removal to rule out neoplasia.
Intraoperative considerations
After the laparoscope and any accessory cannulas are inserted, wash the pelvis and upper abdomen with saline and collect a sample for cytologic analysis. Carefully assess the pelvis and upper abdomen; any peritoneal excrescences or thick adhesions to the mass should be noted, biopsied, and sent for frozen section.
Make every effort to save the ovary
In a premenopausal woman with a presumptively benign ovarian cyst who requires surgery for pain or because the cyst fails to resolve, surgery should aim to conserve the ovary, if at all possible. Even with a large cyst (6 cm or larger), ovarian conservation is possible. Laparoscopic surgery, which involves a short hospital stay and faster postoperative recovery, should be considered unless neoplasia is suspected.
Keep the cyst intact if possible
After placing the cannulas and assessing the pelvis and abdomen, grasp the utero-ovarian ligament with an atraumatic grasper to bring the ovary into view. Inspect the ovary and desiccate (with monopolar cautery) a 1-cm area of thick ovarian capsule, preferably on the less vascular, antimesenteric portion of the ovary.
Using the laparoscopic scissors, incise the capsule superficially along the long axis of the ovary, exposing the cyst wall below. Grasp the edge of the ovarian capsule with a 5-mm grasping forceps. Insert an irrigating instrument between the cyst wall and the ovarian capsule. Use a high-pressure stream of fluid and the blunt edge of the instrument to dissect the cyst away from the ovary.
Keep the cyst intact as long as possible to facilitate dissection. Once the cyst is as free as possible, incise and empty it using the suction irrigator. Grasp the cyst wall with the 5-mm ovarian biopsy forceps and the ovary itself with an atraumatic grasper. Using traction and countertraction, tease the cyst away from the ovarian capsule.
FIGURE 2 Hemorrhagic cyst at detection
Hemorrhagic cysts may have internal echoes, a sign of blood clots within the cyst.
...and 2 weeks later
Two weeks later the cyst is smaller and the clots are in the process of reabsorption.A cyst usually can be removed intact from the abdominal cavity through a 5- or 11-mm canula. If it is too large, bisect it prior to removal.
After removal, inspect the cyst for papillations, septa, or thickening of the wall. If malignancy is suspected, send the cyst for frozen section. If malignancy is confirmed, be prepared to proceed with staging laparotomy immediately.
Postmenopausal women
CASE Is a 4-cm cyst likely to be cancer?
Mrs. J, 67, visits her internist complaining of dull, achy abdominal pain associated with some bloating. A pelvic sonogram reveals a 4.1-cm cyst of the right ovary with well-defined borders; no septations, excrescences, or solid parts; and no free fluid in the pelvis. The left ovary is 3 cm and appears normal. The internist refers Mrs. J to you for further evaluation and management.
By the time you see her, Mrs. J is experiencing very little pain and bloating. However, she is concerned about the cyst and worries that she may have ovarian cancer. She has not experienced any increased abdominal girth, change in appetite or weight, or vaginal bleeding.
When you examine her, you find a normal abdomen with no ascites or abdominal mass. The pelvic exam is normal, too, except for a nontender, slightly enlarged right adnexa, which is difficult to palpate fully.
Mrs. J wants to know if you plan to remove the cyst. What do you tell her?
In this case, the cyst is probably incidental to the abdominal pain Mrs. J experienced at presentation. Because most cysts are benign, observation and repeat sonograms are justified unless the patient’s CA-125 level is found to be elevated or the size or complexity of the cyst increases. Mrs. J has a CA-125 level of 12, and her sonographic findings have not changed since the initial exam, so she can be managed with repeat imaging and blood tests in 2 months.
Data point to safety of surveillance
A sonographic study of asymptomatic postmenopausal women found that about 6% had cysts smaller than 5 cm at initial screening.8 Of the 256 women noted to have these simple cysts, 125 resolved spontaneously within 6 weeks. Among the 131 women with persistent unilocular cysts, 45 requested surgery, and no cancers were found. Among the 86 women who elected to be followed with repeat sonograms and CA-125 levels, no cancers were found after a mean follow-up of 18 months.
A more recent study involved 15,106 women age 50 or older who were screened with transvaginal sonography.2 Of these, 2,763 (18%) had unilocular cysts less than 10 cm in size. Seventy percent of the women had resolution of the cysts within 6 weeks, and none of the 220 women with persistent unilocular cysts developed ovarian cancer after a mean follow-up of 6.8 years.
In properly selected patients, risk of cancer was close to nil
An early study9 focused on 61 postmenopausal women with unilateral, cystic adnexal masses, benign-appearing sonograms, and normal CA-125 levels. These women were managed with laparoscopic oophorectomy. All had benign masses.
Another prospective study involved 228 postmenopausal women with a pelvic mass, 53 of whom had pelvic and sonographic exams suggestive of a benign mass and a CA-125 level below 35 U/mL. All 53 had a benign mass.10
Enlarging, complex cysts and elevated CA 125
In a study of 250 women with complex cystic ovarian tumors smaller than 10 cm (89% were <5 cm in size), more than half the cysts resolved spontaneously.8 However, 7 ovarian carcinomas were found. Thus, observation is not recommended for women with these findings. As might be expected, 6 of the 7 women found to have ovarian cancer had progression of cyst size and/or complexity by the 2-month follow-up sonogram.
Another study11 found that, among 226 postmenopausal women followed with sonograms and CA-125 levels after an initial finding of a unilocular ovarian cyst smaller than 5 cm, cyst size increased in only 54 women, all of whom were operated upon. Two malignancies were found, both in women with elevated CA-125 levels. None of the women whose cyst size remained the same had ovarian cancer.
CASE What is the next step?
When you suggest that Mrs. J be followed with another sonogram and CA-125 level in 2 months, she agrees. At that follow-up, no change in the size or internal architecture of the cyst is noted, and the CA 125 is normal. You ask her to return in 6 and 12 months for repeat sonograms and blood tests, all of which are normal.
At this point, surveillance can shift to yearly pelvic exams. Because women are understandably worried about ovarian cancer, they should be counseled about the importance of careful follow-up. Subjecting them to unnecessary surgery is not advised because of the very real risks of complications from anesthesia and surgery in postmenopausal women.
When surgery is warranted for postmenopausal women
Some women may be symptomatic from larger cysts, or they may not be comfortable with, or available for, close follow-up. In these cases, surgery may be warranted. Women with cysts that are increasing in size, or noted to have a change in internal architecture at the time of sonographic assessment, should also have surgery.
Remove the entire ovary
The entire ovary should be removed in postmenopausal women for complete pathologic analysis.
Technique. Grasp the utero-ovarian ligament and pull it medially to expose the infundibulopelvic ligament. I use a 5-mm bipolar cutting forceps to desiccate and divide the ligament, taking care to identify the ureter and make sure it is well away from the area to be desiccated. Then desiccate and divide the mesosalpinx and follow it to the corneal portion of the fallopian tube. Place the ovary in a laparoscopic sac. Many versions of these sacs exist, but for large cysts I prefer the Cook LapSac (Cook Urological, Spencer, Ind), which has sizes as large as 20×28 cm. These sacs are strong and almost impermeable and hence less likely to tear and allow spillage of the cyst contents into the peritoneal cavity. To keep the neck of the sac open, fill it with irrigating fluid. Once the adnexa is placed in the sac, suction the irrigating fluid and bring the neck of the bag out through an 11-mm port. The cyst can then be aspirated and decompressed to allow removal.
Frozen section is a must. After removal, inspect the cyst wall and obtain frozen sections. If malignancy is found, perform immediate staging laparotomy using a midline incision.
The author reports no financial relationships relevant to this article.
CASE Should you remove a 6-cm cyst?
Mrs. M, 34, complains of sudden-onset, left lower quadrant pain that woke her from sleep. She has no nausea, vomiting, fever, or abnormal bleeding. Vital signs and temperature are normal. She has a tender left lower quadrant with normal bowel sounds. The pelvic exam reveals a 6-cm tender, but mobile, left adnexal mass, and transvaginal pelvic sonography shows a 6.3-cm cystic mass with a thick septation and some internal echoes. Is surgery necessary?
Few cysts present with sudden pain unless they are undergoing torsion, are hemorrhagic, or are in the process of rupturing. Therefore, in the case of Mrs. M, these benign conditions should be considered first. Cancer is very unlikely to be the cause of sudden pain.
A common phenomenon, and usually benign
How widespread are ovarian cysts? About 8% of asymptomatic women between the ages of 25 and 40 have ovarian cysts larger than 2.5 cm.1 A study of women 50 or older found unilocular cysts smaller than 10 cm in 18% of cases.2 Although many cysts resolve spontaneously, some women may be subjected to unnecessary surgery because of concerns about ovarian cancer. In actuality, various studies have shown that cysts found prior to menopause are benign in 87% to 93% of women, and cysts found after menopause are benign in 55% to 92% of cases.3 The gynecologist’s dilemma is to differentiate between cysts that require surgery and those that do not.
This article details the careful assessment that should guide this important decision.
Detorsion of the twisted ovary restores function
In addition, when torsion is present, rather than resort to removal of the adnexa, simply untwist it, even if the tissue does not appear to be viable. Studies have shown that this maneuver leads to a return of ovarian function, as evidenced by follicle formation on subsequent sonograms. In addition, no case of thromboembolism has ever been reported following detorsion of an adnexa.4
Physical clues to the type of cyst
The pelvic examination can yield important clues. For example, a mass that is compressible, smooth, and freely mobile is likely to be benign.
As already noted, tenderness is more common with a hemorrhagic cyst or with torsion, and is rarely associated with cancer. A solid, fixed, irregular mass, however, should raise the suspicion of cancer.
If ascites or an abdominal mass is found, assume the patient has cancer until proven otherwise.
Sonographic appearance
If you do not perform the sonogram yourself, it is a good idea to view the actual images. The reason: Many radiologists use the term “complex” to describe all cysts other than totally clear, simple cysts (FIGURE 1). However, many benign entities are complex, such as dermoid cysts, endometriomas, hemorrhagic cysts (FIGURE 2), and cystadenomas. Careful scrutiny of the images and, at times, other imaging studies, can help determine the most likely diagnosis.
Dermoid cysts can often be confirmed by limited computed tomography scan when fat (sebaceous material), teeth, or bone are seen within the ovary.
Torsion may be suspected when Doppler imaging shows decreased or absent blood flow to the ovary.
A small amount of free fluid in the pelvis is an indication of possible cyst rupture.
If a hemorrhagic cyst is present, a follow-up sonogram about 2 weeks later may show either a smaller cyst or changes in the internal echoes consistent with an organizing clot (FIGURE 2).
False-positive CA 125 rate in young women: 70%
Markers such as CA 125 are rarely helpful in determining how to manage a cyst in a young woman and should be avoided in the premenopausal population. Abnormally high CA-125 values can occur with endometriosis, functional cysts, fibroids or adenomyosis, pelvic infection, pregnancy, and cyclic elevations associated with the menses.
In a premenopausal woman, the chance of a false-positive CA-125 reading is about 70%,5 whereas 50% of women with stage I ovarian cancer have a negative test.6
2 useful markers
Very young women are at risk for developing germ-cell tumors, which may produce β human chorionic gonadotropin or alpha fetoprotein. Thus, these tumor markers are sometimes helpful in this patient population.
FIGURE 1 Hallmarks of a benign cyst
Cysts with smooth borders and without septations, excrescences, or solid parts are likely to be benign.
Management options for premenopausal patients
CASE What is the next step?
In Mrs. M’s case, the first option should be observation and a repeat sonogram in about 2 weeks. Analgesics and rest can be helpful to control pain. Reassure her that the pain should diminish in a few days, although it sometimes takes longer.
Skip the birth control pills
Even with unilocular cysts presumed to be follicular, oral contraceptives do not speed resolution. When 80 premenopausal women with 3- to 6-cm unilocular cysts were randomized to no therapy, low-dose oral contraceptives, or high-dose oral contraceptives and followed with sonography, resolution rates were the same in all 3 groups after 10 weeks.7 Almost 90% of the cysts had resolved after 5 weeks, even in women not taking oral contraceptives.
Pain may warrant surgery
In rare cases, a woman may have such severe pain that rest and analgesics are ineffective, and surgery is warranted for pain alone. In other cases, a cyst that appears functional or hemorrhagic on sonography but persists more than 8 weeks may justify removal to rule out neoplasia.
Intraoperative considerations
After the laparoscope and any accessory cannulas are inserted, wash the pelvis and upper abdomen with saline and collect a sample for cytologic analysis. Carefully assess the pelvis and upper abdomen; any peritoneal excrescences or thick adhesions to the mass should be noted, biopsied, and sent for frozen section.
Make every effort to save the ovary
In a premenopausal woman with a presumptively benign ovarian cyst who requires surgery for pain or because the cyst fails to resolve, surgery should aim to conserve the ovary, if at all possible. Even with a large cyst (6 cm or larger), ovarian conservation is possible. Laparoscopic surgery, which involves a short hospital stay and faster postoperative recovery, should be considered unless neoplasia is suspected.
Keep the cyst intact if possible
After placing the cannulas and assessing the pelvis and abdomen, grasp the utero-ovarian ligament with an atraumatic grasper to bring the ovary into view. Inspect the ovary and desiccate (with monopolar cautery) a 1-cm area of thick ovarian capsule, preferably on the less vascular, antimesenteric portion of the ovary.
Using the laparoscopic scissors, incise the capsule superficially along the long axis of the ovary, exposing the cyst wall below. Grasp the edge of the ovarian capsule with a 5-mm grasping forceps. Insert an irrigating instrument between the cyst wall and the ovarian capsule. Use a high-pressure stream of fluid and the blunt edge of the instrument to dissect the cyst away from the ovary.
Keep the cyst intact as long as possible to facilitate dissection. Once the cyst is as free as possible, incise and empty it using the suction irrigator. Grasp the cyst wall with the 5-mm ovarian biopsy forceps and the ovary itself with an atraumatic grasper. Using traction and countertraction, tease the cyst away from the ovarian capsule.
FIGURE 2 Hemorrhagic cyst at detection
Hemorrhagic cysts may have internal echoes, a sign of blood clots within the cyst.
...and 2 weeks later
Two weeks later the cyst is smaller and the clots are in the process of reabsorption.A cyst usually can be removed intact from the abdominal cavity through a 5- or 11-mm canula. If it is too large, bisect it prior to removal.
After removal, inspect the cyst for papillations, septa, or thickening of the wall. If malignancy is suspected, send the cyst for frozen section. If malignancy is confirmed, be prepared to proceed with staging laparotomy immediately.
Postmenopausal women
CASE Is a 4-cm cyst likely to be cancer?
Mrs. J, 67, visits her internist complaining of dull, achy abdominal pain associated with some bloating. A pelvic sonogram reveals a 4.1-cm cyst of the right ovary with well-defined borders; no septations, excrescences, or solid parts; and no free fluid in the pelvis. The left ovary is 3 cm and appears normal. The internist refers Mrs. J to you for further evaluation and management.
By the time you see her, Mrs. J is experiencing very little pain and bloating. However, she is concerned about the cyst and worries that she may have ovarian cancer. She has not experienced any increased abdominal girth, change in appetite or weight, or vaginal bleeding.
When you examine her, you find a normal abdomen with no ascites or abdominal mass. The pelvic exam is normal, too, except for a nontender, slightly enlarged right adnexa, which is difficult to palpate fully.
Mrs. J wants to know if you plan to remove the cyst. What do you tell her?
In this case, the cyst is probably incidental to the abdominal pain Mrs. J experienced at presentation. Because most cysts are benign, observation and repeat sonograms are justified unless the patient’s CA-125 level is found to be elevated or the size or complexity of the cyst increases. Mrs. J has a CA-125 level of 12, and her sonographic findings have not changed since the initial exam, so she can be managed with repeat imaging and blood tests in 2 months.
Data point to safety of surveillance
A sonographic study of asymptomatic postmenopausal women found that about 6% had cysts smaller than 5 cm at initial screening.8 Of the 256 women noted to have these simple cysts, 125 resolved spontaneously within 6 weeks. Among the 131 women with persistent unilocular cysts, 45 requested surgery, and no cancers were found. Among the 86 women who elected to be followed with repeat sonograms and CA-125 levels, no cancers were found after a mean follow-up of 18 months.
A more recent study involved 15,106 women age 50 or older who were screened with transvaginal sonography.2 Of these, 2,763 (18%) had unilocular cysts less than 10 cm in size. Seventy percent of the women had resolution of the cysts within 6 weeks, and none of the 220 women with persistent unilocular cysts developed ovarian cancer after a mean follow-up of 6.8 years.
In properly selected patients, risk of cancer was close to nil
An early study9 focused on 61 postmenopausal women with unilateral, cystic adnexal masses, benign-appearing sonograms, and normal CA-125 levels. These women were managed with laparoscopic oophorectomy. All had benign masses.
Another prospective study involved 228 postmenopausal women with a pelvic mass, 53 of whom had pelvic and sonographic exams suggestive of a benign mass and a CA-125 level below 35 U/mL. All 53 had a benign mass.10
Enlarging, complex cysts and elevated CA 125
In a study of 250 women with complex cystic ovarian tumors smaller than 10 cm (89% were <5 cm in size), more than half the cysts resolved spontaneously.8 However, 7 ovarian carcinomas were found. Thus, observation is not recommended for women with these findings. As might be expected, 6 of the 7 women found to have ovarian cancer had progression of cyst size and/or complexity by the 2-month follow-up sonogram.
Another study11 found that, among 226 postmenopausal women followed with sonograms and CA-125 levels after an initial finding of a unilocular ovarian cyst smaller than 5 cm, cyst size increased in only 54 women, all of whom were operated upon. Two malignancies were found, both in women with elevated CA-125 levels. None of the women whose cyst size remained the same had ovarian cancer.
CASE What is the next step?
When you suggest that Mrs. J be followed with another sonogram and CA-125 level in 2 months, she agrees. At that follow-up, no change in the size or internal architecture of the cyst is noted, and the CA 125 is normal. You ask her to return in 6 and 12 months for repeat sonograms and blood tests, all of which are normal.
At this point, surveillance can shift to yearly pelvic exams. Because women are understandably worried about ovarian cancer, they should be counseled about the importance of careful follow-up. Subjecting them to unnecessary surgery is not advised because of the very real risks of complications from anesthesia and surgery in postmenopausal women.
When surgery is warranted for postmenopausal women
Some women may be symptomatic from larger cysts, or they may not be comfortable with, or available for, close follow-up. In these cases, surgery may be warranted. Women with cysts that are increasing in size, or noted to have a change in internal architecture at the time of sonographic assessment, should also have surgery.
Remove the entire ovary
The entire ovary should be removed in postmenopausal women for complete pathologic analysis.
Technique. Grasp the utero-ovarian ligament and pull it medially to expose the infundibulopelvic ligament. I use a 5-mm bipolar cutting forceps to desiccate and divide the ligament, taking care to identify the ureter and make sure it is well away from the area to be desiccated. Then desiccate and divide the mesosalpinx and follow it to the corneal portion of the fallopian tube. Place the ovary in a laparoscopic sac. Many versions of these sacs exist, but for large cysts I prefer the Cook LapSac (Cook Urological, Spencer, Ind), which has sizes as large as 20×28 cm. These sacs are strong and almost impermeable and hence less likely to tear and allow spillage of the cyst contents into the peritoneal cavity. To keep the neck of the sac open, fill it with irrigating fluid. Once the adnexa is placed in the sac, suction the irrigating fluid and bring the neck of the bag out through an 11-mm port. The cyst can then be aspirated and decompressed to allow removal.
Frozen section is a must. After removal, inspect the cyst wall and obtain frozen sections. If malignancy is found, perform immediate staging laparotomy using a midline incision.
The author reports no financial relationships relevant to this article.
1. Borgfeldt C, Andolf E. Transvaginal sonographic ovarian findings in a random sample of women 25-40 years old. Ultrasound Obstet Gynecol. 1999;13:345-350.
2. Modesitt SC, Pavlik EJ, Ueland FR, DePriest PD, Kryscio RJ, van Nagell JR, Jr. Risk of malignancy in unilocular cystic tumors less than 10 centimeters in diameter. Obstet Gynecol. 2003;102:594-599.
3. Koonings P, Campbell K, Mishell D. Relative frequency of primary ovarian neoplasms. A 10-year review. Obstet Gynecol. 1989;79:921-926.
4. Cohen SB, Oelsner G, Seidman DS, Admon D, Mashiach S, Goldenberg M. Laparoscopic detorsion allows sparing of the twisted ischemic adnexa. J Am Assoc Gynecol Laparosc. 1999;6:139-143.
5. Vasilev SA, Schlaerth JB, Campeau J, Morrow CP. Serum CA 125 levels in preoperative evaluation of pelvic masses. Obstet Gynecol. 1988;71:751-756.
6. Jacobs I, Bast RC, Jr. The CA 125 tumour-associated antigen: a review of the literature. Hum Reprod. 1989;4:1-12.
7. Parker WH, Berek JS. Laparoscopic management of the adnexal mass. Obstet Gynecol Clin North Am. 1994;21:79-92.
8. Bailey CL, Ueland FR, Land GL, et al. The malignant potential of small cystic ovarian tumors in women over 50 years of age. Gynecol Oncol. 1998;69:3-7.
9. Parker WH, Levine RL, Howard FM, Sansone B, Berek JS. A multicenter study of laparoscopic management of selected cystic adnexal masses in postmenopausal women. J Am Coll Surg. 1994;179:733-737.
10. Schutter EM, Kenemans P, Sohn C, et al. Diagnostic value of pelvic examination, ultrasound, and serum CA 125 in postmenopausal women with a pelvic mass. An international multicenter study. Cancer. 1994;74:1398-1406.
11. Nardo LG, Kroon ND, Reginald PW. Persistent unilocular ovarian cysts in a general population of postmenopausal women: is there a place for expectant management? Obstet Gynecol. 2003;102:589-593.
1. Borgfeldt C, Andolf E. Transvaginal sonographic ovarian findings in a random sample of women 25-40 years old. Ultrasound Obstet Gynecol. 1999;13:345-350.
2. Modesitt SC, Pavlik EJ, Ueland FR, DePriest PD, Kryscio RJ, van Nagell JR, Jr. Risk of malignancy in unilocular cystic tumors less than 10 centimeters in diameter. Obstet Gynecol. 2003;102:594-599.
3. Koonings P, Campbell K, Mishell D. Relative frequency of primary ovarian neoplasms. A 10-year review. Obstet Gynecol. 1989;79:921-926.
4. Cohen SB, Oelsner G, Seidman DS, Admon D, Mashiach S, Goldenberg M. Laparoscopic detorsion allows sparing of the twisted ischemic adnexa. J Am Assoc Gynecol Laparosc. 1999;6:139-143.
5. Vasilev SA, Schlaerth JB, Campeau J, Morrow CP. Serum CA 125 levels in preoperative evaluation of pelvic masses. Obstet Gynecol. 1988;71:751-756.
6. Jacobs I, Bast RC, Jr. The CA 125 tumour-associated antigen: a review of the literature. Hum Reprod. 1989;4:1-12.
7. Parker WH, Berek JS. Laparoscopic management of the adnexal mass. Obstet Gynecol Clin North Am. 1994;21:79-92.
8. Bailey CL, Ueland FR, Land GL, et al. The malignant potential of small cystic ovarian tumors in women over 50 years of age. Gynecol Oncol. 1998;69:3-7.
9. Parker WH, Levine RL, Howard FM, Sansone B, Berek JS. A multicenter study of laparoscopic management of selected cystic adnexal masses in postmenopausal women. J Am Coll Surg. 1994;179:733-737.
10. Schutter EM, Kenemans P, Sohn C, et al. Diagnostic value of pelvic examination, ultrasound, and serum CA 125 in postmenopausal women with a pelvic mass. An international multicenter study. Cancer. 1994;74:1398-1406.
11. Nardo LG, Kroon ND, Reginald PW. Persistent unilocular ovarian cysts in a general population of postmenopausal women: is there a place for expectant management? Obstet Gynecol. 2003;102:589-593.