User login
ABSTRACT
Purpose Primary care physicians are at the center of a national prescription opioid epidemic, with little training or knowledge about the management of patients on opioids for chronic noncancer pain (CNCP). We developed an electronic medical record (EMR)-based protocol and educational intervention to standardize documentation and management of patients prescribed opioids by primary care providers. Our objective was to evaluate provider adherence to this protocol, attitudes toward the management of these patients, and knowledge of opioid prescribing.
Methods We trained providers and select staff from 3 primary care practices at the Division of General Internal Medicine at the University of Pennsylvania in the use of a protocol for managing patients taking opioids for CNCP. The following served as measures of protocol adherence: 1) the provider used a standard diagnosis (chronic pain, ICD-9 code 338.29A) in the problem list, 2) the provider ordered at least one urine drug screen (UDS) for the patient in the past year, and 3) the patient came in for at least one office visit every 6 months. We assessed physician and staff attitudes and knowledge with pre- and post-intervention surveys. Adherence to the protocol was linked to a monetary incentive.
Results Provider adherence to the protocol significantly improved measured outcomes. The number of UDSs ordered increased by 145%, and the diagnosis of chronic pain on the problem list increased by 424%. There was a statistically significant improvement in providers’ role adequacy, role support, and job satisfaction/role-related self-esteem when working with patients taking opioids. In addition, provider knowledge of proper management of these patients improved significantly. Eighty-nine percent of our physicians attained the monetary incentive.
Conclusions We developed a quality improvement intervention that addressed the need for better regulation of opioid prescribing, resulted in increased adherence to best-practice guidelines, and improved provider knowledge and attitudes.
Primary care physicians often express dissatisfaction with their competency in treating patients with opioids,1 and at our institution, this includes residents and faculty, as well. Their concern, combined with apprehension about patient safety and the potential for addiction, can hinder appropriate opioid management.1 We asked: Could a protocol that structures the intervention improve physician competence and performance in prescribing opioids and reduce patient risk?
Physician concerns are well-founded. Nonmedical use of prescription opioids is second only to smoking marijuana in the illicit use of drugs in the United States.2 Since 2003, more overdose deaths have involved opioid analgesics than heroin and cocaine combined, leading the Centers for Disease Control and Prevention to declare in 2012 that the problem was a “national epidemic.”3 The Washington State Medical Quality Assurance Commission now mandates extensive patient evaluation and documentation, the use of a Controlled Medication Agreement (CMA), and specific education requirements for physicians prescribing long-acting or high-dose opioids.4
Necessary adjustments going forward. As the nation moves toward more regulated prescribing of opioids, physicians will need to develop a consistent approach to this complicated task. Primary care doctors must be at the center of this effort, as they generate most opioid prescriptions for the treatment of CNCP. Currently, providers vary widely in their management of this condition,5-7 and recommended corrective steps include increased education8 and improved adherence to national guidelines. Our contention—and the basis of our study—was that a clinical protocol for opioid prescribing could improve the care that physicians and staff were providing to CNCP patients, as well as improve the satisfaction that clinicians felt in providing this care.
Our protocol intervention. Prior to our protocol intervention, no guidelines existed for managing patients on long-term opioid therapy in the clinical practices of the University of Pennsylvania Division of General Internal Medicine. Our providers, too, varied widely in their prescribing and management. Though regular urine drug screening is known to improve detection of opioid misuse and decrease the problem in patients treated for CNCP,9,10 a study reviewing opioid prescribing practices in our clinics from 2004 to 2007 showed that physicians ordered UDSs for only 8% of patients.11 Furthermore, only half of patients (49.8%) had regular office visits—even those at high risk for opioid misuse.11
|
Based on expert opinion and national best-practice guidelines, we created a division-wide quality improvement intervention for opioid prescribing. The protocol required standardized evaluation and documentation of a patient’s pain history and treatment plan, and the use of a UDS and a CMA, which is known to decrease emergency room visits and improve physician satisfaction, respectively.9,10 We trained attending physicians and staff on the protocol, and they in turn taught residents at their practice sites. The goal of this study was to determine whether this initiative would result in adherence to the protocol and improve provider and staff knowledge and satisfaction with management of patients prescribed opioids for CNCP.
METHODS
The intervention consisted of (1) the development of an EMR-based protocol to standardize documentation and management of patients with CNCP taking opioids; (2) instruction on using the protocol and on key components of opioid management; (3) collection of data; and (4) a monetary incentive for attending physicians to adhere to the protocol. We measured the impact of this intervention by assessing physician compliance with the protocol, provider satisfaction, and knowledge.
Protocol and process
We developed a division-wide protocol for managing primary-care patients with CNCP taking opioids, based on national guidelines, expert input, best practice data, and EMR capabilities (EpicCare Ambulatory Medical Record, version Summer 2009).
Health system experts from anesthesia, pain management, and psychiatry met regularly with our monthly workgroup to review the latest literature on UDSs and CMAs, and to assess best practices researched by the Center for Evidence Based Practice at our institution. We trained providers on the following steps:
• select patients who are taking opioids for CNCP (ie, receiving >2 opioid prescriptions in the 6 months prior to the intervention for a nonlimited pain condition)
• risk stratify these patients using the Opioid Risk Tool12
• follow high-risk patients monthly; low-to-moderate-risk patients every 3 to 6 months
• use a standard diagnosis (chronic pain, ICD-9 code 338.29A) in the EMR problem list
• complete a standardized EMR “smart set” documenting evaluation and management in the overview section of the EMR’s chronic pain diagnosis module (TABLE 1)
• complete a CMA
• order a UDS at regular intervals (at least one per year; every 1-3 months in high-risk patients)
• designate one provider (in the EMR) to be responsible for opioid prescribing. Medical residents were encouraged to specify a “Continuity Attending” to maintain continuity of care when they were not in clinic.
Educational intervention
The principal investigator conducted 4 training sessions that were available to all attending physicians and staff, to review the protocol as well as information on best practices in opioid prescribing. One session was a Quality Improvement Grand Rounds for the division, and 3 sessions were open presentations within each participating practice. During all sessions, we taught the protocol, provided instruction on riskstratifying patients, reviewed the definition and prevalence of chronic pain, described the national opioid problem, detailed the components of proper documentation, and explained how to interpret and manage UDS results.
We trained categorical internal medicine interns for 1 hour during their mandatory clinical lecture series. Primary care track residents received 4 hours of training as part of their regular educational program.
Ongoing education for attending physicians occurred at 4 bimonthly opioid management case conferences, where difficult cases were presented to a rotating panel of experts from pain medicine, addiction psychiatry, and primary care. We held regular noon conferences on opioid management for residents.
Monetary incentive for physicians
Our division further aided our efforts by offering a monetary incentive ($1500) to attending physicians who achieved all 3 of the following measures of adherence with at least 80% of their chronic pain patients: at least one UDS in the past year, an office visit at least every 6 months, and a chronic pain diagnosis on the problem list in the EMR.
Data feedback
We gave providers a list of their patients receiving >2 opioid prescriptions over 6 months, and were able to exclude those patients treated for a limited pain condition. For the remainder of patients, physicians received quarterly individual reports on their adherence to the protocol.
Study population
Three internal medicine clinical practices of the University of Pennsylvania in Philadelphia took part in this initiative. We included all attending providers at these practices in the analysis assessing adherence to the protocol. Those who consented and completed a survey were included in the survey analysis. Providers were attending physicians and nurse practitioners. In Practice 1, primary care track residents are fully integrated into the practice and were included in the survey as their extended training was timed with our intervention. We did not survey residents at the other practices due to their variable schedules and inability to train as a group.
Staff included registered nurses, licensed practical nurses, medical assistants, and patient service representatives. Because nurses and medical assistants are responsible for medication refills, they received education specifically about this intervention. The remaining staff also received instruction, as they have personal interactions with patients at the provider visit, and thus their attitudes were important to measure. Participants completed surveys at the time of the educational sessions and again 9 months following implementation of the intervention. This was a one-year intervention, with 3 initial months of teaching; the study period therefore lasted 9 months. Since surveys were anonymous, we could not link results to specific individuals. However, we provided post-intervention surveys only to those who reported completing the initial survey.
Survey design and administration
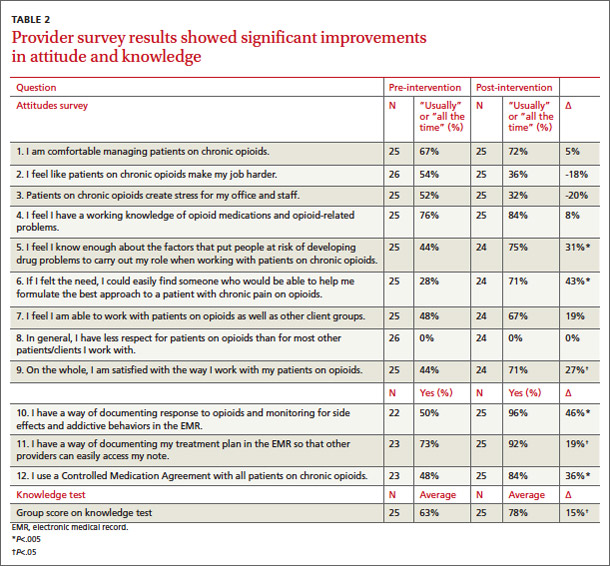
The provider survey contained an attitude component and a knowledge component (TABLE 2). The attitude component consisted of 6 items taken from the Drug Problems Perceptions Questionnaire,13 to address role adequacy, support, and self-esteem, as well as job satisfaction (the words “drug users” were replaced with “patients on [chronic] opioids”). We created an additional 3 items to further explore these domains (items 1-3). Three additional items addressed provider access to EMR specific tools (items 10-12).
The knowledge survey consisted of multiple choice questions created by the study team, and it reflected best practice guidelines for opioid management for CNCP and knowledge of protocol elements. Items included the definition of chronic pain, opioid medications not included on the UDS, interpretation of UDS results, addiction risk, intervals for office visits for patients on chronic opioid therapy, and pain medication dose escalation.
The staff survey included similar attitude components and a modified knowledge portion regarding which patients should have a CMA, where to document a CMA in the EMR, addiction risk, intervals for office visits, and how to handle early prescription refill requests.
Evaluation and statistical analysis
To assess the impact of the intervention, we chose 2 measures of physician adherence with the protocol (UDS and chronic pain diagnosis) because of our ability to access these measures within our approved protocol.
Individual attitude survey questions were compared using paired t-tests. We averaged knowledge test scores, and also used the paired t-test to compare pre- and posttest averages. We used Stata 11.2 (StataCorp LP, 2009) to analyze survey data.
This study was sponsored by the Matthew Slap Research Award and approved by the University of Pennsylvania Institutional Review Board.
RESULTS
Practice demographics
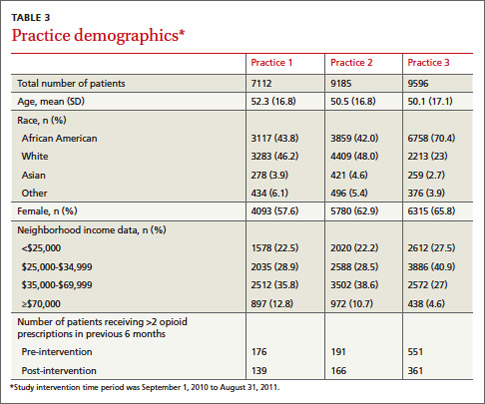
The 3 practices are located within the same zip code, a few city blocks from one another. Despite geographic proximity of the practices, their populations differ racially and ethnically as well as in neighborhood income distributions (TABLE 3). In all 3 practices, the total number of patients prescribed >2 opioid medications declined during the year-long study period. Practice 3 had the sharpest decline in the number of patients prescribed chronic opioids, likely due to provider turnover during the study period. Practices 1 and 2 had the highest adherence to guidelines. The marked variability in adoption of guidelines likely reflects a number of factors: the difference in baseline opioid prescribing (highest in Practice 3), the presence of physician champions in Practices 1 and 2, and more intensive training of the primary care residents in Practice 1.
Protocol adherence
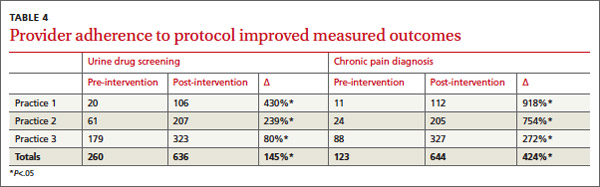
We measured provider adherence to the protocol by comparing data from the year before the intervention to the year following the start of the intervention for the number of UDSs ordered, the number of chronic pain diagnoses on patients’ EMR problem lists, and the number of office visits with CNCP patients. UDSs ordered increased by 145% across all 3 practices, with the largest improvement seen in Practice 1 (430%; P<.05). Documentation of a chronic pain diagnosis in the EMR problem list increased by 424% across practices, with the largest improvement seen again in Practice 1 (918%, P<.05) (TABLE 4). Based on this performance, 24 of 27 (89%) full time physicians qualified for the financial incentive. We chose not to include the third measure (number of office visits) for analysis, as we discovered that >90% of patients were seen at least every 6 months before the intervention.
Survey results
Before the protocol training, we surveyed 26 providers and 33 staff members. Nine months after the initiation of the protocol, 25 providers and 26 staff were again surveyed. Surveys were anonymous so we were unable to link knowledge gains to individuals.
Providers exhibited statistically significant improvement of attitude for role adequacy (item 5), role support (item 6), job satisfaction/role-related self-esteem (item 9), and access to EMR-specific tools (items 10-12) (TABLE 2). In addition, the knowledge test score increased by 15% (P<.05) in the postintervention survey.
Staff surveys showed statistically significant improvement of attitude for job satisfaction/role-related self-esteem. There was no improvement in knowledge for staff, which is likely due to variability in training.
DISCUSSION
More than 40% of opioid prescriptions in the United States are written by primary care physicians.14 Therefore, interventions that enhance provider knowledge, institute best practices, and support role-related self-esteem in opioid management are vital to our profession.
Through a straightforward protocol, we greatly increased the number of UDSs ordered (145%) and documentation of chronic pain on the problem list (424%). By increasing adherence to best practice standards, we believe this protocol will lead to improved management of patients with CNCP by providing objective urine data to guide a treatment plan, patient education with the CMA, and a documented evaluation and care plan.
In addition to fostering adherence to the protocol, our multicomponent intervention resulted in marked improvement of provider and staff attitudes toward patients taking opioids for CNCP (TABLE 2). Participants’ satisfaction in working with these patients improved significantly (27%), as did their confidence in knowing whom to ask for help with management (43%). After this intervention, physicians reported a nonstatistically significant but large reductions in the perception that patients on opioids create stress for the office (-20%), and that patients on opioids make their job harder (-18%). Knowledge about chronic opioid prescribing also improved significantly for providers (15%).
At all practices, the number of patients receiving opioids decreased, likely due to the protocol intervention.
Previous studies have shown low adoption of best practices in opioid management without a structured intervention.10 Our findings suggest that a multicomponent quality improvement intervention that combines education, financial incentive, and a structured protocol can positively impact provider and staff attitudes and adherence to best practices in caring for patients with CNCP taking opioid medications. We believe that similar interventions could be adapted by other primary care clinics with a comparable favorable impact on physician behavior, attitudes, and knowledge.
Limitations
Our findings may not apply to nonacademic practices, as we required training and the use of an EMR. Additionally, our urban patient populations may not be generalizable to rural, suburban, or other populations in the management of patients taking prescription opioids. Further, the monetary incentive, which was included in a yearly incentive package at our institution, may not be feasible at other sites.
We did not design this study to allow for practice-level comparisons or to assess patient level variables. Analysis of patient data on safety, aberrant behavior, abnormal UDS results, and the impact of the intervention on these outcomes was outside of the scope of this study. We were unable to determine whether physician turnover, particularly high in one practice, could be linked to the results.
Providers often neglected to indicate their level of training on surveys, and we were therefore unable to compare adherence and knowledge between residents and attending physicians. Additionally, we lacked approval to search individual charts to completely investigate the components of our protocol (for example, completion of a CMA or UDS). Lastly, we did not design the study to control for confounders on a provider level (such as age, gender, and years of experience). A more comprehensive review of these important variables is warranted to assess the degree to which division- or practice-level quality improvement interventions can affect provider and patient behavior change and enhance patient safety.
CORRESPONDENCE
Robin E. Canada, MD, Medical Arts Building, Suite 102, 38th and Market Sts, Philadelphia, PA 19104; [email protected]
Acknowledgement
The authors gratefully acknowledge Judy Shea, PhD and Joanna Starrels, MD, who provided valuable comments in the development of this manuscript.
1. Lin JJ, Alfandre D, Moore C. Physician attitudes toward opioid prescribing for patients with persistent noncancer pain. Clin J Pain. 2007;23:799-803.
2. Hughes A, Sathe N, Spagnola K. (2009). State estimates of substance use from the 2006-2007 National Surveys on Drug Use and Health. Rockville, MD: Office of Applied Studies, Substance Abuse and Mental Health Services Administration; 2009. NSDUH Series H-35, HHS Publication No. SMA 09-4362.
3. Centers for Disease Control and Prevention (CDC). CDC grand rounds: prescription drug overdoses - a US epidemic. MMWR Morb Mortal Wkly Rep. 2012;61:10-13.
4. Washington State Department of Health- Medical Quality Assurance Commission. Rule-Making Order CR-103. University of Washington Web site. Available at: http://depts.washington.edu/anesth/education/forms/pain/WAC-Rules-CR-103P.pdf. Accessed February 1, 2012.
5. Leverence RR, Williams RL, Potter M, et al. Chronic non-cancer pain: a siren for primary care—a report from the PRImary Care MultiEthnic Network (PRIME Net). J Am Board Fam Med. 2011;24:551-561.
6. Green CR, Wheeler JR, LaPorte F, et al. How well is chronic pain managed? Who does it well? Pain Med. 2002;3:56-65.
7. Webster BS, Cifuentes M, Verma S, et al. Geographic variation in opioid prescribing for acute, work-related, low back pain and associated factors: a multilevel analysis. Am J Ind Med. 2009;52:162-171.
8. Gunderson EW, Coffin PO, Chang N, et al. The interface between substance abuse and chronic pain management in primary care: a curriculum for medical residents. Subst Abus. 2009;30:253-260.
9. Manchikanti L, Manchukonda R, Pampati V, et al. Does random urine drug testing reduce illicit drug use in chronic pain patients receiving opioids? Pain Physician. 2006;9:123-129.
10. Starrels JL, Becker WC, Alford DP, et al. Systematic review: treatment agreements and urine drug testing to reduce opioid misuse in patients with chronic pain. Ann Intern Med. 2010;152:712-720.
11. Starrels JL, Becker WC, Weiner MG, et al. Low use of opioid risk reduction strategies in primary care even for high risk patients with chronic pain. J Gen Intern Med. 2011;26:958-964.
12. Webster LR, Webster RM. Predicting aberrant behaviors in opioid- treated patients: preliminary validation of the Opioid Risk Tool. Pain Med. 2005;6:432-442.
13. Watson H, Maclaren W, Kerr S. Staff attitudes toward working with drug users: development of the Drug Problems Perceptions Questionnaire. Addiction. 2007;102:206-215.
14. Okie S. A flood of opioids, a rising tide of deaths. N Engl J Med. 2010;363:1981-1985.
ABSTRACT
Purpose Primary care physicians are at the center of a national prescription opioid epidemic, with little training or knowledge about the management of patients on opioids for chronic noncancer pain (CNCP). We developed an electronic medical record (EMR)-based protocol and educational intervention to standardize documentation and management of patients prescribed opioids by primary care providers. Our objective was to evaluate provider adherence to this protocol, attitudes toward the management of these patients, and knowledge of opioid prescribing.
Methods We trained providers and select staff from 3 primary care practices at the Division of General Internal Medicine at the University of Pennsylvania in the use of a protocol for managing patients taking opioids for CNCP. The following served as measures of protocol adherence: 1) the provider used a standard diagnosis (chronic pain, ICD-9 code 338.29A) in the problem list, 2) the provider ordered at least one urine drug screen (UDS) for the patient in the past year, and 3) the patient came in for at least one office visit every 6 months. We assessed physician and staff attitudes and knowledge with pre- and post-intervention surveys. Adherence to the protocol was linked to a monetary incentive.
Results Provider adherence to the protocol significantly improved measured outcomes. The number of UDSs ordered increased by 145%, and the diagnosis of chronic pain on the problem list increased by 424%. There was a statistically significant improvement in providers’ role adequacy, role support, and job satisfaction/role-related self-esteem when working with patients taking opioids. In addition, provider knowledge of proper management of these patients improved significantly. Eighty-nine percent of our physicians attained the monetary incentive.
Conclusions We developed a quality improvement intervention that addressed the need for better regulation of opioid prescribing, resulted in increased adherence to best-practice guidelines, and improved provider knowledge and attitudes.
Primary care physicians often express dissatisfaction with their competency in treating patients with opioids,1 and at our institution, this includes residents and faculty, as well. Their concern, combined with apprehension about patient safety and the potential for addiction, can hinder appropriate opioid management.1 We asked: Could a protocol that structures the intervention improve physician competence and performance in prescribing opioids and reduce patient risk?
Physician concerns are well-founded. Nonmedical use of prescription opioids is second only to smoking marijuana in the illicit use of drugs in the United States.2 Since 2003, more overdose deaths have involved opioid analgesics than heroin and cocaine combined, leading the Centers for Disease Control and Prevention to declare in 2012 that the problem was a “national epidemic.”3 The Washington State Medical Quality Assurance Commission now mandates extensive patient evaluation and documentation, the use of a Controlled Medication Agreement (CMA), and specific education requirements for physicians prescribing long-acting or high-dose opioids.4
Necessary adjustments going forward. As the nation moves toward more regulated prescribing of opioids, physicians will need to develop a consistent approach to this complicated task. Primary care doctors must be at the center of this effort, as they generate most opioid prescriptions for the treatment of CNCP. Currently, providers vary widely in their management of this condition,5-7 and recommended corrective steps include increased education8 and improved adherence to national guidelines. Our contention—and the basis of our study—was that a clinical protocol for opioid prescribing could improve the care that physicians and staff were providing to CNCP patients, as well as improve the satisfaction that clinicians felt in providing this care.
Our protocol intervention. Prior to our protocol intervention, no guidelines existed for managing patients on long-term opioid therapy in the clinical practices of the University of Pennsylvania Division of General Internal Medicine. Our providers, too, varied widely in their prescribing and management. Though regular urine drug screening is known to improve detection of opioid misuse and decrease the problem in patients treated for CNCP,9,10 a study reviewing opioid prescribing practices in our clinics from 2004 to 2007 showed that physicians ordered UDSs for only 8% of patients.11 Furthermore, only half of patients (49.8%) had regular office visits—even those at high risk for opioid misuse.11
|
Based on expert opinion and national best-practice guidelines, we created a division-wide quality improvement intervention for opioid prescribing. The protocol required standardized evaluation and documentation of a patient’s pain history and treatment plan, and the use of a UDS and a CMA, which is known to decrease emergency room visits and improve physician satisfaction, respectively.9,10 We trained attending physicians and staff on the protocol, and they in turn taught residents at their practice sites. The goal of this study was to determine whether this initiative would result in adherence to the protocol and improve provider and staff knowledge and satisfaction with management of patients prescribed opioids for CNCP.
METHODS
The intervention consisted of (1) the development of an EMR-based protocol to standardize documentation and management of patients with CNCP taking opioids; (2) instruction on using the protocol and on key components of opioid management; (3) collection of data; and (4) a monetary incentive for attending physicians to adhere to the protocol. We measured the impact of this intervention by assessing physician compliance with the protocol, provider satisfaction, and knowledge.
Protocol and process
We developed a division-wide protocol for managing primary-care patients with CNCP taking opioids, based on national guidelines, expert input, best practice data, and EMR capabilities (EpicCare Ambulatory Medical Record, version Summer 2009).
Health system experts from anesthesia, pain management, and psychiatry met regularly with our monthly workgroup to review the latest literature on UDSs and CMAs, and to assess best practices researched by the Center for Evidence Based Practice at our institution. We trained providers on the following steps:
• select patients who are taking opioids for CNCP (ie, receiving >2 opioid prescriptions in the 6 months prior to the intervention for a nonlimited pain condition)
• risk stratify these patients using the Opioid Risk Tool12
• follow high-risk patients monthly; low-to-moderate-risk patients every 3 to 6 months
• use a standard diagnosis (chronic pain, ICD-9 code 338.29A) in the EMR problem list
• complete a standardized EMR “smart set” documenting evaluation and management in the overview section of the EMR’s chronic pain diagnosis module (TABLE 1)
• complete a CMA
• order a UDS at regular intervals (at least one per year; every 1-3 months in high-risk patients)
• designate one provider (in the EMR) to be responsible for opioid prescribing. Medical residents were encouraged to specify a “Continuity Attending” to maintain continuity of care when they were not in clinic.
Educational intervention
The principal investigator conducted 4 training sessions that were available to all attending physicians and staff, to review the protocol as well as information on best practices in opioid prescribing. One session was a Quality Improvement Grand Rounds for the division, and 3 sessions were open presentations within each participating practice. During all sessions, we taught the protocol, provided instruction on riskstratifying patients, reviewed the definition and prevalence of chronic pain, described the national opioid problem, detailed the components of proper documentation, and explained how to interpret and manage UDS results.
We trained categorical internal medicine interns for 1 hour during their mandatory clinical lecture series. Primary care track residents received 4 hours of training as part of their regular educational program.
Ongoing education for attending physicians occurred at 4 bimonthly opioid management case conferences, where difficult cases were presented to a rotating panel of experts from pain medicine, addiction psychiatry, and primary care. We held regular noon conferences on opioid management for residents.
Monetary incentive for physicians
Our division further aided our efforts by offering a monetary incentive ($1500) to attending physicians who achieved all 3 of the following measures of adherence with at least 80% of their chronic pain patients: at least one UDS in the past year, an office visit at least every 6 months, and a chronic pain diagnosis on the problem list in the EMR.
Data feedback
We gave providers a list of their patients receiving >2 opioid prescriptions over 6 months, and were able to exclude those patients treated for a limited pain condition. For the remainder of patients, physicians received quarterly individual reports on their adherence to the protocol.
Study population
Three internal medicine clinical practices of the University of Pennsylvania in Philadelphia took part in this initiative. We included all attending providers at these practices in the analysis assessing adherence to the protocol. Those who consented and completed a survey were included in the survey analysis. Providers were attending physicians and nurse practitioners. In Practice 1, primary care track residents are fully integrated into the practice and were included in the survey as their extended training was timed with our intervention. We did not survey residents at the other practices due to their variable schedules and inability to train as a group.
Staff included registered nurses, licensed practical nurses, medical assistants, and patient service representatives. Because nurses and medical assistants are responsible for medication refills, they received education specifically about this intervention. The remaining staff also received instruction, as they have personal interactions with patients at the provider visit, and thus their attitudes were important to measure. Participants completed surveys at the time of the educational sessions and again 9 months following implementation of the intervention. This was a one-year intervention, with 3 initial months of teaching; the study period therefore lasted 9 months. Since surveys were anonymous, we could not link results to specific individuals. However, we provided post-intervention surveys only to those who reported completing the initial survey.
Survey design and administration
The provider survey contained an attitude component and a knowledge component (TABLE 2). The attitude component consisted of 6 items taken from the Drug Problems Perceptions Questionnaire,13 to address role adequacy, support, and self-esteem, as well as job satisfaction (the words “drug users” were replaced with “patients on [chronic] opioids”). We created an additional 3 items to further explore these domains (items 1-3). Three additional items addressed provider access to EMR specific tools (items 10-12).
The knowledge survey consisted of multiple choice questions created by the study team, and it reflected best practice guidelines for opioid management for CNCP and knowledge of protocol elements. Items included the definition of chronic pain, opioid medications not included on the UDS, interpretation of UDS results, addiction risk, intervals for office visits for patients on chronic opioid therapy, and pain medication dose escalation.
The staff survey included similar attitude components and a modified knowledge portion regarding which patients should have a CMA, where to document a CMA in the EMR, addiction risk, intervals for office visits, and how to handle early prescription refill requests.
Evaluation and statistical analysis
To assess the impact of the intervention, we chose 2 measures of physician adherence with the protocol (UDS and chronic pain diagnosis) because of our ability to access these measures within our approved protocol.
Individual attitude survey questions were compared using paired t-tests. We averaged knowledge test scores, and also used the paired t-test to compare pre- and posttest averages. We used Stata 11.2 (StataCorp LP, 2009) to analyze survey data.
This study was sponsored by the Matthew Slap Research Award and approved by the University of Pennsylvania Institutional Review Board.
RESULTS
Practice demographics
The 3 practices are located within the same zip code, a few city blocks from one another. Despite geographic proximity of the practices, their populations differ racially and ethnically as well as in neighborhood income distributions (TABLE 3). In all 3 practices, the total number of patients prescribed >2 opioid medications declined during the year-long study period. Practice 3 had the sharpest decline in the number of patients prescribed chronic opioids, likely due to provider turnover during the study period. Practices 1 and 2 had the highest adherence to guidelines. The marked variability in adoption of guidelines likely reflects a number of factors: the difference in baseline opioid prescribing (highest in Practice 3), the presence of physician champions in Practices 1 and 2, and more intensive training of the primary care residents in Practice 1.
Protocol adherence
We measured provider adherence to the protocol by comparing data from the year before the intervention to the year following the start of the intervention for the number of UDSs ordered, the number of chronic pain diagnoses on patients’ EMR problem lists, and the number of office visits with CNCP patients. UDSs ordered increased by 145% across all 3 practices, with the largest improvement seen in Practice 1 (430%; P<.05). Documentation of a chronic pain diagnosis in the EMR problem list increased by 424% across practices, with the largest improvement seen again in Practice 1 (918%, P<.05) (TABLE 4). Based on this performance, 24 of 27 (89%) full time physicians qualified for the financial incentive. We chose not to include the third measure (number of office visits) for analysis, as we discovered that >90% of patients were seen at least every 6 months before the intervention.
Survey results
Before the protocol training, we surveyed 26 providers and 33 staff members. Nine months after the initiation of the protocol, 25 providers and 26 staff were again surveyed. Surveys were anonymous so we were unable to link knowledge gains to individuals.
Providers exhibited statistically significant improvement of attitude for role adequacy (item 5), role support (item 6), job satisfaction/role-related self-esteem (item 9), and access to EMR-specific tools (items 10-12) (TABLE 2). In addition, the knowledge test score increased by 15% (P<.05) in the postintervention survey.
Staff surveys showed statistically significant improvement of attitude for job satisfaction/role-related self-esteem. There was no improvement in knowledge for staff, which is likely due to variability in training.
DISCUSSION
More than 40% of opioid prescriptions in the United States are written by primary care physicians.14 Therefore, interventions that enhance provider knowledge, institute best practices, and support role-related self-esteem in opioid management are vital to our profession.
Through a straightforward protocol, we greatly increased the number of UDSs ordered (145%) and documentation of chronic pain on the problem list (424%). By increasing adherence to best practice standards, we believe this protocol will lead to improved management of patients with CNCP by providing objective urine data to guide a treatment plan, patient education with the CMA, and a documented evaluation and care plan.
In addition to fostering adherence to the protocol, our multicomponent intervention resulted in marked improvement of provider and staff attitudes toward patients taking opioids for CNCP (TABLE 2). Participants’ satisfaction in working with these patients improved significantly (27%), as did their confidence in knowing whom to ask for help with management (43%). After this intervention, physicians reported a nonstatistically significant but large reductions in the perception that patients on opioids create stress for the office (-20%), and that patients on opioids make their job harder (-18%). Knowledge about chronic opioid prescribing also improved significantly for providers (15%).
At all practices, the number of patients receiving opioids decreased, likely due to the protocol intervention.
Previous studies have shown low adoption of best practices in opioid management without a structured intervention.10 Our findings suggest that a multicomponent quality improvement intervention that combines education, financial incentive, and a structured protocol can positively impact provider and staff attitudes and adherence to best practices in caring for patients with CNCP taking opioid medications. We believe that similar interventions could be adapted by other primary care clinics with a comparable favorable impact on physician behavior, attitudes, and knowledge.
Limitations
Our findings may not apply to nonacademic practices, as we required training and the use of an EMR. Additionally, our urban patient populations may not be generalizable to rural, suburban, or other populations in the management of patients taking prescription opioids. Further, the monetary incentive, which was included in a yearly incentive package at our institution, may not be feasible at other sites.
We did not design this study to allow for practice-level comparisons or to assess patient level variables. Analysis of patient data on safety, aberrant behavior, abnormal UDS results, and the impact of the intervention on these outcomes was outside of the scope of this study. We were unable to determine whether physician turnover, particularly high in one practice, could be linked to the results.
Providers often neglected to indicate their level of training on surveys, and we were therefore unable to compare adherence and knowledge between residents and attending physicians. Additionally, we lacked approval to search individual charts to completely investigate the components of our protocol (for example, completion of a CMA or UDS). Lastly, we did not design the study to control for confounders on a provider level (such as age, gender, and years of experience). A more comprehensive review of these important variables is warranted to assess the degree to which division- or practice-level quality improvement interventions can affect provider and patient behavior change and enhance patient safety.
CORRESPONDENCE
Robin E. Canada, MD, Medical Arts Building, Suite 102, 38th and Market Sts, Philadelphia, PA 19104; [email protected]
Acknowledgement
The authors gratefully acknowledge Judy Shea, PhD and Joanna Starrels, MD, who provided valuable comments in the development of this manuscript.
ABSTRACT
Purpose Primary care physicians are at the center of a national prescription opioid epidemic, with little training or knowledge about the management of patients on opioids for chronic noncancer pain (CNCP). We developed an electronic medical record (EMR)-based protocol and educational intervention to standardize documentation and management of patients prescribed opioids by primary care providers. Our objective was to evaluate provider adherence to this protocol, attitudes toward the management of these patients, and knowledge of opioid prescribing.
Methods We trained providers and select staff from 3 primary care practices at the Division of General Internal Medicine at the University of Pennsylvania in the use of a protocol for managing patients taking opioids for CNCP. The following served as measures of protocol adherence: 1) the provider used a standard diagnosis (chronic pain, ICD-9 code 338.29A) in the problem list, 2) the provider ordered at least one urine drug screen (UDS) for the patient in the past year, and 3) the patient came in for at least one office visit every 6 months. We assessed physician and staff attitudes and knowledge with pre- and post-intervention surveys. Adherence to the protocol was linked to a monetary incentive.
Results Provider adherence to the protocol significantly improved measured outcomes. The number of UDSs ordered increased by 145%, and the diagnosis of chronic pain on the problem list increased by 424%. There was a statistically significant improvement in providers’ role adequacy, role support, and job satisfaction/role-related self-esteem when working with patients taking opioids. In addition, provider knowledge of proper management of these patients improved significantly. Eighty-nine percent of our physicians attained the monetary incentive.
Conclusions We developed a quality improvement intervention that addressed the need for better regulation of opioid prescribing, resulted in increased adherence to best-practice guidelines, and improved provider knowledge and attitudes.
Primary care physicians often express dissatisfaction with their competency in treating patients with opioids,1 and at our institution, this includes residents and faculty, as well. Their concern, combined with apprehension about patient safety and the potential for addiction, can hinder appropriate opioid management.1 We asked: Could a protocol that structures the intervention improve physician competence and performance in prescribing opioids and reduce patient risk?
Physician concerns are well-founded. Nonmedical use of prescription opioids is second only to smoking marijuana in the illicit use of drugs in the United States.2 Since 2003, more overdose deaths have involved opioid analgesics than heroin and cocaine combined, leading the Centers for Disease Control and Prevention to declare in 2012 that the problem was a “national epidemic.”3 The Washington State Medical Quality Assurance Commission now mandates extensive patient evaluation and documentation, the use of a Controlled Medication Agreement (CMA), and specific education requirements for physicians prescribing long-acting or high-dose opioids.4
Necessary adjustments going forward. As the nation moves toward more regulated prescribing of opioids, physicians will need to develop a consistent approach to this complicated task. Primary care doctors must be at the center of this effort, as they generate most opioid prescriptions for the treatment of CNCP. Currently, providers vary widely in their management of this condition,5-7 and recommended corrective steps include increased education8 and improved adherence to national guidelines. Our contention—and the basis of our study—was that a clinical protocol for opioid prescribing could improve the care that physicians and staff were providing to CNCP patients, as well as improve the satisfaction that clinicians felt in providing this care.
Our protocol intervention. Prior to our protocol intervention, no guidelines existed for managing patients on long-term opioid therapy in the clinical practices of the University of Pennsylvania Division of General Internal Medicine. Our providers, too, varied widely in their prescribing and management. Though regular urine drug screening is known to improve detection of opioid misuse and decrease the problem in patients treated for CNCP,9,10 a study reviewing opioid prescribing practices in our clinics from 2004 to 2007 showed that physicians ordered UDSs for only 8% of patients.11 Furthermore, only half of patients (49.8%) had regular office visits—even those at high risk for opioid misuse.11
|
Based on expert opinion and national best-practice guidelines, we created a division-wide quality improvement intervention for opioid prescribing. The protocol required standardized evaluation and documentation of a patient’s pain history and treatment plan, and the use of a UDS and a CMA, which is known to decrease emergency room visits and improve physician satisfaction, respectively.9,10 We trained attending physicians and staff on the protocol, and they in turn taught residents at their practice sites. The goal of this study was to determine whether this initiative would result in adherence to the protocol and improve provider and staff knowledge and satisfaction with management of patients prescribed opioids for CNCP.
METHODS
The intervention consisted of (1) the development of an EMR-based protocol to standardize documentation and management of patients with CNCP taking opioids; (2) instruction on using the protocol and on key components of opioid management; (3) collection of data; and (4) a monetary incentive for attending physicians to adhere to the protocol. We measured the impact of this intervention by assessing physician compliance with the protocol, provider satisfaction, and knowledge.
Protocol and process
We developed a division-wide protocol for managing primary-care patients with CNCP taking opioids, based on national guidelines, expert input, best practice data, and EMR capabilities (EpicCare Ambulatory Medical Record, version Summer 2009).
Health system experts from anesthesia, pain management, and psychiatry met regularly with our monthly workgroup to review the latest literature on UDSs and CMAs, and to assess best practices researched by the Center for Evidence Based Practice at our institution. We trained providers on the following steps:
• select patients who are taking opioids for CNCP (ie, receiving >2 opioid prescriptions in the 6 months prior to the intervention for a nonlimited pain condition)
• risk stratify these patients using the Opioid Risk Tool12
• follow high-risk patients monthly; low-to-moderate-risk patients every 3 to 6 months
• use a standard diagnosis (chronic pain, ICD-9 code 338.29A) in the EMR problem list
• complete a standardized EMR “smart set” documenting evaluation and management in the overview section of the EMR’s chronic pain diagnosis module (TABLE 1)
• complete a CMA
• order a UDS at regular intervals (at least one per year; every 1-3 months in high-risk patients)
• designate one provider (in the EMR) to be responsible for opioid prescribing. Medical residents were encouraged to specify a “Continuity Attending” to maintain continuity of care when they were not in clinic.
Educational intervention
The principal investigator conducted 4 training sessions that were available to all attending physicians and staff, to review the protocol as well as information on best practices in opioid prescribing. One session was a Quality Improvement Grand Rounds for the division, and 3 sessions were open presentations within each participating practice. During all sessions, we taught the protocol, provided instruction on riskstratifying patients, reviewed the definition and prevalence of chronic pain, described the national opioid problem, detailed the components of proper documentation, and explained how to interpret and manage UDS results.
We trained categorical internal medicine interns for 1 hour during their mandatory clinical lecture series. Primary care track residents received 4 hours of training as part of their regular educational program.
Ongoing education for attending physicians occurred at 4 bimonthly opioid management case conferences, where difficult cases were presented to a rotating panel of experts from pain medicine, addiction psychiatry, and primary care. We held regular noon conferences on opioid management for residents.
Monetary incentive for physicians
Our division further aided our efforts by offering a monetary incentive ($1500) to attending physicians who achieved all 3 of the following measures of adherence with at least 80% of their chronic pain patients: at least one UDS in the past year, an office visit at least every 6 months, and a chronic pain diagnosis on the problem list in the EMR.
Data feedback
We gave providers a list of their patients receiving >2 opioid prescriptions over 6 months, and were able to exclude those patients treated for a limited pain condition. For the remainder of patients, physicians received quarterly individual reports on their adherence to the protocol.
Study population
Three internal medicine clinical practices of the University of Pennsylvania in Philadelphia took part in this initiative. We included all attending providers at these practices in the analysis assessing adherence to the protocol. Those who consented and completed a survey were included in the survey analysis. Providers were attending physicians and nurse practitioners. In Practice 1, primary care track residents are fully integrated into the practice and were included in the survey as their extended training was timed with our intervention. We did not survey residents at the other practices due to their variable schedules and inability to train as a group.
Staff included registered nurses, licensed practical nurses, medical assistants, and patient service representatives. Because nurses and medical assistants are responsible for medication refills, they received education specifically about this intervention. The remaining staff also received instruction, as they have personal interactions with patients at the provider visit, and thus their attitudes were important to measure. Participants completed surveys at the time of the educational sessions and again 9 months following implementation of the intervention. This was a one-year intervention, with 3 initial months of teaching; the study period therefore lasted 9 months. Since surveys were anonymous, we could not link results to specific individuals. However, we provided post-intervention surveys only to those who reported completing the initial survey.
Survey design and administration
The provider survey contained an attitude component and a knowledge component (TABLE 2). The attitude component consisted of 6 items taken from the Drug Problems Perceptions Questionnaire,13 to address role adequacy, support, and self-esteem, as well as job satisfaction (the words “drug users” were replaced with “patients on [chronic] opioids”). We created an additional 3 items to further explore these domains (items 1-3). Three additional items addressed provider access to EMR specific tools (items 10-12).
The knowledge survey consisted of multiple choice questions created by the study team, and it reflected best practice guidelines for opioid management for CNCP and knowledge of protocol elements. Items included the definition of chronic pain, opioid medications not included on the UDS, interpretation of UDS results, addiction risk, intervals for office visits for patients on chronic opioid therapy, and pain medication dose escalation.
The staff survey included similar attitude components and a modified knowledge portion regarding which patients should have a CMA, where to document a CMA in the EMR, addiction risk, intervals for office visits, and how to handle early prescription refill requests.
Evaluation and statistical analysis
To assess the impact of the intervention, we chose 2 measures of physician adherence with the protocol (UDS and chronic pain diagnosis) because of our ability to access these measures within our approved protocol.
Individual attitude survey questions were compared using paired t-tests. We averaged knowledge test scores, and also used the paired t-test to compare pre- and posttest averages. We used Stata 11.2 (StataCorp LP, 2009) to analyze survey data.
This study was sponsored by the Matthew Slap Research Award and approved by the University of Pennsylvania Institutional Review Board.
RESULTS
Practice demographics
The 3 practices are located within the same zip code, a few city blocks from one another. Despite geographic proximity of the practices, their populations differ racially and ethnically as well as in neighborhood income distributions (TABLE 3). In all 3 practices, the total number of patients prescribed >2 opioid medications declined during the year-long study period. Practice 3 had the sharpest decline in the number of patients prescribed chronic opioids, likely due to provider turnover during the study period. Practices 1 and 2 had the highest adherence to guidelines. The marked variability in adoption of guidelines likely reflects a number of factors: the difference in baseline opioid prescribing (highest in Practice 3), the presence of physician champions in Practices 1 and 2, and more intensive training of the primary care residents in Practice 1.
Protocol adherence
We measured provider adherence to the protocol by comparing data from the year before the intervention to the year following the start of the intervention for the number of UDSs ordered, the number of chronic pain diagnoses on patients’ EMR problem lists, and the number of office visits with CNCP patients. UDSs ordered increased by 145% across all 3 practices, with the largest improvement seen in Practice 1 (430%; P<.05). Documentation of a chronic pain diagnosis in the EMR problem list increased by 424% across practices, with the largest improvement seen again in Practice 1 (918%, P<.05) (TABLE 4). Based on this performance, 24 of 27 (89%) full time physicians qualified for the financial incentive. We chose not to include the third measure (number of office visits) for analysis, as we discovered that >90% of patients were seen at least every 6 months before the intervention.
Survey results
Before the protocol training, we surveyed 26 providers and 33 staff members. Nine months after the initiation of the protocol, 25 providers and 26 staff were again surveyed. Surveys were anonymous so we were unable to link knowledge gains to individuals.
Providers exhibited statistically significant improvement of attitude for role adequacy (item 5), role support (item 6), job satisfaction/role-related self-esteem (item 9), and access to EMR-specific tools (items 10-12) (TABLE 2). In addition, the knowledge test score increased by 15% (P<.05) in the postintervention survey.
Staff surveys showed statistically significant improvement of attitude for job satisfaction/role-related self-esteem. There was no improvement in knowledge for staff, which is likely due to variability in training.
DISCUSSION
More than 40% of opioid prescriptions in the United States are written by primary care physicians.14 Therefore, interventions that enhance provider knowledge, institute best practices, and support role-related self-esteem in opioid management are vital to our profession.
Through a straightforward protocol, we greatly increased the number of UDSs ordered (145%) and documentation of chronic pain on the problem list (424%). By increasing adherence to best practice standards, we believe this protocol will lead to improved management of patients with CNCP by providing objective urine data to guide a treatment plan, patient education with the CMA, and a documented evaluation and care plan.
In addition to fostering adherence to the protocol, our multicomponent intervention resulted in marked improvement of provider and staff attitudes toward patients taking opioids for CNCP (TABLE 2). Participants’ satisfaction in working with these patients improved significantly (27%), as did their confidence in knowing whom to ask for help with management (43%). After this intervention, physicians reported a nonstatistically significant but large reductions in the perception that patients on opioids create stress for the office (-20%), and that patients on opioids make their job harder (-18%). Knowledge about chronic opioid prescribing also improved significantly for providers (15%).
At all practices, the number of patients receiving opioids decreased, likely due to the protocol intervention.
Previous studies have shown low adoption of best practices in opioid management without a structured intervention.10 Our findings suggest that a multicomponent quality improvement intervention that combines education, financial incentive, and a structured protocol can positively impact provider and staff attitudes and adherence to best practices in caring for patients with CNCP taking opioid medications. We believe that similar interventions could be adapted by other primary care clinics with a comparable favorable impact on physician behavior, attitudes, and knowledge.
Limitations
Our findings may not apply to nonacademic practices, as we required training and the use of an EMR. Additionally, our urban patient populations may not be generalizable to rural, suburban, or other populations in the management of patients taking prescription opioids. Further, the monetary incentive, which was included in a yearly incentive package at our institution, may not be feasible at other sites.
We did not design this study to allow for practice-level comparisons or to assess patient level variables. Analysis of patient data on safety, aberrant behavior, abnormal UDS results, and the impact of the intervention on these outcomes was outside of the scope of this study. We were unable to determine whether physician turnover, particularly high in one practice, could be linked to the results.
Providers often neglected to indicate their level of training on surveys, and we were therefore unable to compare adherence and knowledge between residents and attending physicians. Additionally, we lacked approval to search individual charts to completely investigate the components of our protocol (for example, completion of a CMA or UDS). Lastly, we did not design the study to control for confounders on a provider level (such as age, gender, and years of experience). A more comprehensive review of these important variables is warranted to assess the degree to which division- or practice-level quality improvement interventions can affect provider and patient behavior change and enhance patient safety.
CORRESPONDENCE
Robin E. Canada, MD, Medical Arts Building, Suite 102, 38th and Market Sts, Philadelphia, PA 19104; [email protected]
Acknowledgement
The authors gratefully acknowledge Judy Shea, PhD and Joanna Starrels, MD, who provided valuable comments in the development of this manuscript.
1. Lin JJ, Alfandre D, Moore C. Physician attitudes toward opioid prescribing for patients with persistent noncancer pain. Clin J Pain. 2007;23:799-803.
2. Hughes A, Sathe N, Spagnola K. (2009). State estimates of substance use from the 2006-2007 National Surveys on Drug Use and Health. Rockville, MD: Office of Applied Studies, Substance Abuse and Mental Health Services Administration; 2009. NSDUH Series H-35, HHS Publication No. SMA 09-4362.
3. Centers for Disease Control and Prevention (CDC). CDC grand rounds: prescription drug overdoses - a US epidemic. MMWR Morb Mortal Wkly Rep. 2012;61:10-13.
4. Washington State Department of Health- Medical Quality Assurance Commission. Rule-Making Order CR-103. University of Washington Web site. Available at: http://depts.washington.edu/anesth/education/forms/pain/WAC-Rules-CR-103P.pdf. Accessed February 1, 2012.
5. Leverence RR, Williams RL, Potter M, et al. Chronic non-cancer pain: a siren for primary care—a report from the PRImary Care MultiEthnic Network (PRIME Net). J Am Board Fam Med. 2011;24:551-561.
6. Green CR, Wheeler JR, LaPorte F, et al. How well is chronic pain managed? Who does it well? Pain Med. 2002;3:56-65.
7. Webster BS, Cifuentes M, Verma S, et al. Geographic variation in opioid prescribing for acute, work-related, low back pain and associated factors: a multilevel analysis. Am J Ind Med. 2009;52:162-171.
8. Gunderson EW, Coffin PO, Chang N, et al. The interface between substance abuse and chronic pain management in primary care: a curriculum for medical residents. Subst Abus. 2009;30:253-260.
9. Manchikanti L, Manchukonda R, Pampati V, et al. Does random urine drug testing reduce illicit drug use in chronic pain patients receiving opioids? Pain Physician. 2006;9:123-129.
10. Starrels JL, Becker WC, Alford DP, et al. Systematic review: treatment agreements and urine drug testing to reduce opioid misuse in patients with chronic pain. Ann Intern Med. 2010;152:712-720.
11. Starrels JL, Becker WC, Weiner MG, et al. Low use of opioid risk reduction strategies in primary care even for high risk patients with chronic pain. J Gen Intern Med. 2011;26:958-964.
12. Webster LR, Webster RM. Predicting aberrant behaviors in opioid- treated patients: preliminary validation of the Opioid Risk Tool. Pain Med. 2005;6:432-442.
13. Watson H, Maclaren W, Kerr S. Staff attitudes toward working with drug users: development of the Drug Problems Perceptions Questionnaire. Addiction. 2007;102:206-215.
14. Okie S. A flood of opioids, a rising tide of deaths. N Engl J Med. 2010;363:1981-1985.
1. Lin JJ, Alfandre D, Moore C. Physician attitudes toward opioid prescribing for patients with persistent noncancer pain. Clin J Pain. 2007;23:799-803.
2. Hughes A, Sathe N, Spagnola K. (2009). State estimates of substance use from the 2006-2007 National Surveys on Drug Use and Health. Rockville, MD: Office of Applied Studies, Substance Abuse and Mental Health Services Administration; 2009. NSDUH Series H-35, HHS Publication No. SMA 09-4362.
3. Centers for Disease Control and Prevention (CDC). CDC grand rounds: prescription drug overdoses - a US epidemic. MMWR Morb Mortal Wkly Rep. 2012;61:10-13.
4. Washington State Department of Health- Medical Quality Assurance Commission. Rule-Making Order CR-103. University of Washington Web site. Available at: http://depts.washington.edu/anesth/education/forms/pain/WAC-Rules-CR-103P.pdf. Accessed February 1, 2012.
5. Leverence RR, Williams RL, Potter M, et al. Chronic non-cancer pain: a siren for primary care—a report from the PRImary Care MultiEthnic Network (PRIME Net). J Am Board Fam Med. 2011;24:551-561.
6. Green CR, Wheeler JR, LaPorte F, et al. How well is chronic pain managed? Who does it well? Pain Med. 2002;3:56-65.
7. Webster BS, Cifuentes M, Verma S, et al. Geographic variation in opioid prescribing for acute, work-related, low back pain and associated factors: a multilevel analysis. Am J Ind Med. 2009;52:162-171.
8. Gunderson EW, Coffin PO, Chang N, et al. The interface between substance abuse and chronic pain management in primary care: a curriculum for medical residents. Subst Abus. 2009;30:253-260.
9. Manchikanti L, Manchukonda R, Pampati V, et al. Does random urine drug testing reduce illicit drug use in chronic pain patients receiving opioids? Pain Physician. 2006;9:123-129.
10. Starrels JL, Becker WC, Alford DP, et al. Systematic review: treatment agreements and urine drug testing to reduce opioid misuse in patients with chronic pain. Ann Intern Med. 2010;152:712-720.
11. Starrels JL, Becker WC, Weiner MG, et al. Low use of opioid risk reduction strategies in primary care even for high risk patients with chronic pain. J Gen Intern Med. 2011;26:958-964.
12. Webster LR, Webster RM. Predicting aberrant behaviors in opioid- treated patients: preliminary validation of the Opioid Risk Tool. Pain Med. 2005;6:432-442.
13. Watson H, Maclaren W, Kerr S. Staff attitudes toward working with drug users: development of the Drug Problems Perceptions Questionnaire. Addiction. 2007;102:206-215.
14. Okie S. A flood of opioids, a rising tide of deaths. N Engl J Med. 2010;363:1981-1985.
