User login
Richard Quinn is an award-winning journalist with 15 years’ experience. He has worked at the Asbury Park Press in New Jersey and The Virginian-Pilot in Norfolk, Va., and currently is managing editor for a leading commercial real estate publication. His freelance work has appeared in The Jewish State, The Hospitalist, The Rheumatologist, ACEP Now, and ENT Today. He lives in New Jersey with his wife and three cats.
Teachable Moments
With World Stroke Day scheduled for Saturday, a frequent speaker for the National Stroke Association (NSA) wants to remind hospitalists to push their patients to know their risk factors.
"They have an excellent opportunity to be an educator, particularly because of that captive audience," says David Willis, MD, a primary-care physician in Ocala, Fla., who frequently holds educational events for the NSA.
Dr. Willis cites data from a 2010 survey (PDF) compiled by NSA and Boehringer Ingelheim Pharmaceuticals that shows while more than 75% of healthcare providers reported talking to patients about atrial fibrillation (AF) and stroke, nearly half don't recall the conversation. And just 40% of patients initiate the discussion.
Dr. Willis, who served on the steering committee that interpreted the survey results, says that hospitalists dealing with AF patients can "quarterback" care plans and help improve communication with post-discharge physicians, be they primary care or specialists.
"We may not be getting that thought across as well as we think we are," he says.
Improved communication and transitions will become more important as unnecessary readmissions related to AF or stroke financially impact physicians because the government may reduce reimbursements for repeated hospital visits. Dr. Willis suggests that hospitalists take the reins of integrating their patient education efforts into checklists, health information technology, or some formalized process.
"My experience is, if you create protocols, they usually work better than educating people at a provider level," he says.
With World Stroke Day scheduled for Saturday, a frequent speaker for the National Stroke Association (NSA) wants to remind hospitalists to push their patients to know their risk factors.
"They have an excellent opportunity to be an educator, particularly because of that captive audience," says David Willis, MD, a primary-care physician in Ocala, Fla., who frequently holds educational events for the NSA.
Dr. Willis cites data from a 2010 survey (PDF) compiled by NSA and Boehringer Ingelheim Pharmaceuticals that shows while more than 75% of healthcare providers reported talking to patients about atrial fibrillation (AF) and stroke, nearly half don't recall the conversation. And just 40% of patients initiate the discussion.
Dr. Willis, who served on the steering committee that interpreted the survey results, says that hospitalists dealing with AF patients can "quarterback" care plans and help improve communication with post-discharge physicians, be they primary care or specialists.
"We may not be getting that thought across as well as we think we are," he says.
Improved communication and transitions will become more important as unnecessary readmissions related to AF or stroke financially impact physicians because the government may reduce reimbursements for repeated hospital visits. Dr. Willis suggests that hospitalists take the reins of integrating their patient education efforts into checklists, health information technology, or some formalized process.
"My experience is, if you create protocols, they usually work better than educating people at a provider level," he says.
With World Stroke Day scheduled for Saturday, a frequent speaker for the National Stroke Association (NSA) wants to remind hospitalists to push their patients to know their risk factors.
"They have an excellent opportunity to be an educator, particularly because of that captive audience," says David Willis, MD, a primary-care physician in Ocala, Fla., who frequently holds educational events for the NSA.
Dr. Willis cites data from a 2010 survey (PDF) compiled by NSA and Boehringer Ingelheim Pharmaceuticals that shows while more than 75% of healthcare providers reported talking to patients about atrial fibrillation (AF) and stroke, nearly half don't recall the conversation. And just 40% of patients initiate the discussion.
Dr. Willis, who served on the steering committee that interpreted the survey results, says that hospitalists dealing with AF patients can "quarterback" care plans and help improve communication with post-discharge physicians, be they primary care or specialists.
"We may not be getting that thought across as well as we think we are," he says.
Improved communication and transitions will become more important as unnecessary readmissions related to AF or stroke financially impact physicians because the government may reduce reimbursements for repeated hospital visits. Dr. Willis suggests that hospitalists take the reins of integrating their patient education efforts into checklists, health information technology, or some formalized process.
"My experience is, if you create protocols, they usually work better than educating people at a provider level," he says.
Seal of Approval
A report in this month's Journal of Hospital Medicine suggests that hospitals accredited by the Joint Commission outperform those that aren't when it comes to treatment of acute myocardial infarction (AMI), heart failure (HF), and pneumonia.
The study, "Hospital Performance Trends on National Quality Measures and the Association with Joint Commission Accreditation," also found that over a five-year reporting period, accredited institutions improved more than their non-accredited counterparts. HM pioneer Robert Wachter, MD, MHM, chief of the Division of Hospital Medicine at the University of California at San Francisco, was a coauthor of the study.
Joint Commission staffers and fellow coauthors Jerod Loeb, PhD, executive vice president of the Division of Healthcare Quality Evaluation at the Joint Commission, and Stephen Schmaltz, MPH, PhD, associate director of the Department of Health Services Research, say that researchers were not able to compare hospitals based on accreditation and quality control until the commission and the Centers for Medicare & Medicaid Services (CMS) adopted identical measures in 2004.
"We had a strong suspicion that accredited facilities would perform better, which was demonstrable in a statistically significant manner," Dr. Loeb says. "Of course, we worried that one of the questions that reviewers or others who read this might ask is, 'Sure, this is what we might expect from the Joint Commission to say that.' This is why the data is publically available, from us and CMS. Anyone can do the same type of analyses we’ve done and clearly come up with the very same conclusion.”
The next step of the research, Drs. Loeb and Schmaltz say, is to try to delineate whether the "gold seal" of accreditation is what "actually promotes improved performance or is a marker for other characteristics associated with such performance."
"There is something to this broad rubric associated with accreditation that is actually making a difference in the context of measures that matter...to clinical outcomes," Dr. Loeb adds. "This isn't the end of the game for us by any stretch of the imagination. It's clear that more research is needed."
A report in this month's Journal of Hospital Medicine suggests that hospitals accredited by the Joint Commission outperform those that aren't when it comes to treatment of acute myocardial infarction (AMI), heart failure (HF), and pneumonia.
The study, "Hospital Performance Trends on National Quality Measures and the Association with Joint Commission Accreditation," also found that over a five-year reporting period, accredited institutions improved more than their non-accredited counterparts. HM pioneer Robert Wachter, MD, MHM, chief of the Division of Hospital Medicine at the University of California at San Francisco, was a coauthor of the study.
Joint Commission staffers and fellow coauthors Jerod Loeb, PhD, executive vice president of the Division of Healthcare Quality Evaluation at the Joint Commission, and Stephen Schmaltz, MPH, PhD, associate director of the Department of Health Services Research, say that researchers were not able to compare hospitals based on accreditation and quality control until the commission and the Centers for Medicare & Medicaid Services (CMS) adopted identical measures in 2004.
"We had a strong suspicion that accredited facilities would perform better, which was demonstrable in a statistically significant manner," Dr. Loeb says. "Of course, we worried that one of the questions that reviewers or others who read this might ask is, 'Sure, this is what we might expect from the Joint Commission to say that.' This is why the data is publically available, from us and CMS. Anyone can do the same type of analyses we’ve done and clearly come up with the very same conclusion.”
The next step of the research, Drs. Loeb and Schmaltz say, is to try to delineate whether the "gold seal" of accreditation is what "actually promotes improved performance or is a marker for other characteristics associated with such performance."
"There is something to this broad rubric associated with accreditation that is actually making a difference in the context of measures that matter...to clinical outcomes," Dr. Loeb adds. "This isn't the end of the game for us by any stretch of the imagination. It's clear that more research is needed."
A report in this month's Journal of Hospital Medicine suggests that hospitals accredited by the Joint Commission outperform those that aren't when it comes to treatment of acute myocardial infarction (AMI), heart failure (HF), and pneumonia.
The study, "Hospital Performance Trends on National Quality Measures and the Association with Joint Commission Accreditation," also found that over a five-year reporting period, accredited institutions improved more than their non-accredited counterparts. HM pioneer Robert Wachter, MD, MHM, chief of the Division of Hospital Medicine at the University of California at San Francisco, was a coauthor of the study.
Joint Commission staffers and fellow coauthors Jerod Loeb, PhD, executive vice president of the Division of Healthcare Quality Evaluation at the Joint Commission, and Stephen Schmaltz, MPH, PhD, associate director of the Department of Health Services Research, say that researchers were not able to compare hospitals based on accreditation and quality control until the commission and the Centers for Medicare & Medicaid Services (CMS) adopted identical measures in 2004.
"We had a strong suspicion that accredited facilities would perform better, which was demonstrable in a statistically significant manner," Dr. Loeb says. "Of course, we worried that one of the questions that reviewers or others who read this might ask is, 'Sure, this is what we might expect from the Joint Commission to say that.' This is why the data is publically available, from us and CMS. Anyone can do the same type of analyses we’ve done and clearly come up with the very same conclusion.”
The next step of the research, Drs. Loeb and Schmaltz say, is to try to delineate whether the "gold seal" of accreditation is what "actually promotes improved performance or is a marker for other characteristics associated with such performance."
"There is something to this broad rubric associated with accreditation that is actually making a difference in the context of measures that matter...to clinical outcomes," Dr. Loeb adds. "This isn't the end of the game for us by any stretch of the imagination. It's clear that more research is needed."
NQF Launches Interactive Quality-Measurement Tool
Quality-minded hospitalists now have a new research tool at their disposal. In the past few weeks, the National Quality Forum (NQF) unveiled a beta-test version of its Quality Positioning System (QPS), a searchable and interactive database of NQF-endorsed quality measures on a host of medical topics.
The database, which won’t have an official launch until 2012, allows users to create lists of measurements or view lists that other institutions have put together, dubbed portfolios. The idea is that as more users post public portfolios, the more physicians across the country can see what measures work where.
“This is a brand-new tool, so we’re starting to see more and more portfolios created,” said Diane Stollenwerk, MPP, NQF’s vice president of community alliances. “The more people who use the portfolio function in QPS, the more valuable the portfolios and QPS will become for end users.”
HM groups can use the site to create private portfolios that can be shared just among group members. NQF will provide automatic updates on those measures a user is interested in, giving the site an interactive feature. Stollenwerk says future added value in the site will be pushed in part by user feedback. She is hopeful that users will not only create lists of which measures they use, but also comment on their experience in using those measures in specific situations.
“A foundational role QPS can play is simply creating a shared space for people to have the conversation,” Stollenwerk adds.
Quality-minded hospitalists now have a new research tool at their disposal. In the past few weeks, the National Quality Forum (NQF) unveiled a beta-test version of its Quality Positioning System (QPS), a searchable and interactive database of NQF-endorsed quality measures on a host of medical topics.
The database, which won’t have an official launch until 2012, allows users to create lists of measurements or view lists that other institutions have put together, dubbed portfolios. The idea is that as more users post public portfolios, the more physicians across the country can see what measures work where.
“This is a brand-new tool, so we’re starting to see more and more portfolios created,” said Diane Stollenwerk, MPP, NQF’s vice president of community alliances. “The more people who use the portfolio function in QPS, the more valuable the portfolios and QPS will become for end users.”
HM groups can use the site to create private portfolios that can be shared just among group members. NQF will provide automatic updates on those measures a user is interested in, giving the site an interactive feature. Stollenwerk says future added value in the site will be pushed in part by user feedback. She is hopeful that users will not only create lists of which measures they use, but also comment on their experience in using those measures in specific situations.
“A foundational role QPS can play is simply creating a shared space for people to have the conversation,” Stollenwerk adds.
Quality-minded hospitalists now have a new research tool at their disposal. In the past few weeks, the National Quality Forum (NQF) unveiled a beta-test version of its Quality Positioning System (QPS), a searchable and interactive database of NQF-endorsed quality measures on a host of medical topics.
The database, which won’t have an official launch until 2012, allows users to create lists of measurements or view lists that other institutions have put together, dubbed portfolios. The idea is that as more users post public portfolios, the more physicians across the country can see what measures work where.
“This is a brand-new tool, so we’re starting to see more and more portfolios created,” said Diane Stollenwerk, MPP, NQF’s vice president of community alliances. “The more people who use the portfolio function in QPS, the more valuable the portfolios and QPS will become for end users.”
HM groups can use the site to create private portfolios that can be shared just among group members. NQF will provide automatic updates on those measures a user is interested in, giving the site an interactive feature. Stollenwerk says future added value in the site will be pushed in part by user feedback. She is hopeful that users will not only create lists of which measures they use, but also comment on their experience in using those measures in specific situations.
“A foundational role QPS can play is simply creating a shared space for people to have the conversation,” Stollenwerk adds.
Temporary Staffing Common in HM, Study Reports
One in 10 hospitalists has worked locum tenens in the past year, according to a study of the practice released this week.
Locum Leaders, a locum tenens staffing agency in Alpharetta, Ga., put the study together this summer to define for the first time just how prevalent the practice of temporary staffing is and what motivates physicians to do the work. The report found that of hospitalists who work as locums tenens, 82% do it in addition to their full-time jobs and 11% do it as their full-time jobs.
Robert Harrington Jr., MD, SFHM, chief medical officer for Locum Leaders and an SHM board member, says the phenomenon allows some hospitalists to learn more about an institution before signing a long-term contract. It also affords other physicians flexibility, higher earning potential, or just the chance to "try something on for size before they buy."
"On the physician side, there are opportunities out there for you to not strain yourself immensely to increase your compensation, to travel to places you may not normally get to go, and to see how different programs are structured and operate," he says. "To see a more worldly view of hospital medicine."
For hospitals, even though locum physicians can cost more in salary, they can provide an opportunity for savings, as the hospital does not have to contribute to healthcare, pensions, or other costs. To wit, locum physicians can gross 30% to 40% more per year for the same number of shifts as a typical FTE hospitalist.
"They're all independent contractors," Dr. Harrington adds. "The increase in compensation that locum tenens physicians are able to demand, for the most part, comes from the difference between having a full-time employee versus an independent contractor."
One in 10 hospitalists has worked locum tenens in the past year, according to a study of the practice released this week.
Locum Leaders, a locum tenens staffing agency in Alpharetta, Ga., put the study together this summer to define for the first time just how prevalent the practice of temporary staffing is and what motivates physicians to do the work. The report found that of hospitalists who work as locums tenens, 82% do it in addition to their full-time jobs and 11% do it as their full-time jobs.
Robert Harrington Jr., MD, SFHM, chief medical officer for Locum Leaders and an SHM board member, says the phenomenon allows some hospitalists to learn more about an institution before signing a long-term contract. It also affords other physicians flexibility, higher earning potential, or just the chance to "try something on for size before they buy."
"On the physician side, there are opportunities out there for you to not strain yourself immensely to increase your compensation, to travel to places you may not normally get to go, and to see how different programs are structured and operate," he says. "To see a more worldly view of hospital medicine."
For hospitals, even though locum physicians can cost more in salary, they can provide an opportunity for savings, as the hospital does not have to contribute to healthcare, pensions, or other costs. To wit, locum physicians can gross 30% to 40% more per year for the same number of shifts as a typical FTE hospitalist.
"They're all independent contractors," Dr. Harrington adds. "The increase in compensation that locum tenens physicians are able to demand, for the most part, comes from the difference between having a full-time employee versus an independent contractor."
One in 10 hospitalists has worked locum tenens in the past year, according to a study of the practice released this week.
Locum Leaders, a locum tenens staffing agency in Alpharetta, Ga., put the study together this summer to define for the first time just how prevalent the practice of temporary staffing is and what motivates physicians to do the work. The report found that of hospitalists who work as locums tenens, 82% do it in addition to their full-time jobs and 11% do it as their full-time jobs.
Robert Harrington Jr., MD, SFHM, chief medical officer for Locum Leaders and an SHM board member, says the phenomenon allows some hospitalists to learn more about an institution before signing a long-term contract. It also affords other physicians flexibility, higher earning potential, or just the chance to "try something on for size before they buy."
"On the physician side, there are opportunities out there for you to not strain yourself immensely to increase your compensation, to travel to places you may not normally get to go, and to see how different programs are structured and operate," he says. "To see a more worldly view of hospital medicine."
For hospitals, even though locum physicians can cost more in salary, they can provide an opportunity for savings, as the hospital does not have to contribute to healthcare, pensions, or other costs. To wit, locum physicians can gross 30% to 40% more per year for the same number of shifts as a typical FTE hospitalist.
"They're all independent contractors," Dr. Harrington adds. "The increase in compensation that locum tenens physicians are able to demand, for the most part, comes from the difference between having a full-time employee versus an independent contractor."
Transferring “Boarders” Could Save Millions
A pilot project that transferred “boarded” patients from one hospital’s ED to an inpatient bed at another nearby hospital in the same health system suggests that the concept could save hospitals millions.
“Improvement in Emergency Department Treatment Capacity: A Health System Integration Approach” was the subject of an oral presentation at HM11 in Dallas. Lead researcher Diego Martinez-Vasquez, MD, MPH, FACP, CPE, medical director for clinical resource utilization at Franklin Square Hospital Center in Baltimore, conducted the research in the University of Maryland medical system.
In the project, 265 patients who consented were transferred 1.3 miles to a sister hospital. Without “boarders”—admitted patients held in the ED—Dr. Martinez-Vasquez’s team found that the referring hospital could have regained enough capacity for an additional 2.9 patients per day. The project also showed median net revenue of $520,000 for the referring hospital and $1.9 million for the accepting hospital.
“The hospitalist group at the receiving hospital was the instrument that facilitated this program,” Dr. Martinez-Vasquez says. “But really what kept my attention was that healthcare systems sometimes don’t use resources effectively. So when I looked at the problem that this particular hospital was having regarding increased boarding time and decreased treatment capacity, I said, ‘Well, one way to resolve this issue is to develop a process that connects two system hospitals and their bed resources.’ ”
A pilot project that transferred “boarded” patients from one hospital’s ED to an inpatient bed at another nearby hospital in the same health system suggests that the concept could save hospitals millions.
“Improvement in Emergency Department Treatment Capacity: A Health System Integration Approach” was the subject of an oral presentation at HM11 in Dallas. Lead researcher Diego Martinez-Vasquez, MD, MPH, FACP, CPE, medical director for clinical resource utilization at Franklin Square Hospital Center in Baltimore, conducted the research in the University of Maryland medical system.
In the project, 265 patients who consented were transferred 1.3 miles to a sister hospital. Without “boarders”—admitted patients held in the ED—Dr. Martinez-Vasquez’s team found that the referring hospital could have regained enough capacity for an additional 2.9 patients per day. The project also showed median net revenue of $520,000 for the referring hospital and $1.9 million for the accepting hospital.
“The hospitalist group at the receiving hospital was the instrument that facilitated this program,” Dr. Martinez-Vasquez says. “But really what kept my attention was that healthcare systems sometimes don’t use resources effectively. So when I looked at the problem that this particular hospital was having regarding increased boarding time and decreased treatment capacity, I said, ‘Well, one way to resolve this issue is to develop a process that connects two system hospitals and their bed resources.’ ”
A pilot project that transferred “boarded” patients from one hospital’s ED to an inpatient bed at another nearby hospital in the same health system suggests that the concept could save hospitals millions.
“Improvement in Emergency Department Treatment Capacity: A Health System Integration Approach” was the subject of an oral presentation at HM11 in Dallas. Lead researcher Diego Martinez-Vasquez, MD, MPH, FACP, CPE, medical director for clinical resource utilization at Franklin Square Hospital Center in Baltimore, conducted the research in the University of Maryland medical system.
In the project, 265 patients who consented were transferred 1.3 miles to a sister hospital. Without “boarders”—admitted patients held in the ED—Dr. Martinez-Vasquez’s team found that the referring hospital could have regained enough capacity for an additional 2.9 patients per day. The project also showed median net revenue of $520,000 for the referring hospital and $1.9 million for the accepting hospital.
“The hospitalist group at the receiving hospital was the instrument that facilitated this program,” Dr. Martinez-Vasquez says. “But really what kept my attention was that healthcare systems sometimes don’t use resources effectively. So when I looked at the problem that this particular hospital was having regarding increased boarding time and decreased treatment capacity, I said, ‘Well, one way to resolve this issue is to develop a process that connects two system hospitals and their bed resources.’ ”
The Earlier, the Better
Every morning at 8 a.m., a multidisciplinary team at Wayne Memorial Hospital in Honesdale, Pa., a rural pocket of about 5,000 people about 30 miles northeast of Scranton, gathers to discuss discharge planning. Representatives from social services, home health, nursing, physical therapy, pharmacy, and the HM group attend the meeting. Each stakeholder weighs in, listens to others, and voices concerns when applicable.
“We go through each patient in the morning, briefly, and go through the plan so that when there’s a discharge coming, everybody is on the same page and can try to get everything organized,” says Louis O’Boyle, DO, FACP, FHM, medical director of Advanced Inpatient Medicine, the hospitalist program contracted by Wayne Memorial, which has 98 acute-care beds. “The hospital has reminded us to be cognizant of getting that early discharge, and it’s become almost so rote now that we don’t even have to worry about it. It’s just a thing we do.”
Better bed management is a new mantra for hospitalists nationwide, because fewer open beds means fewer dollars for both the physician and the hospital. Better bed management also means improved patient satisfaction scores, as most patients would rather be at home (and those scores in the coming years will factor into Medicare reimbursement). And better bed management means reduced backlogs across the hospital, particularly “boarders” in the ED.
“The pressure really is on the hospital for a number of reasons,” says Ken Simone, DO, SFHM, president of Hospitalist and Practice Solutions in Veazie, Maine, and a member of Team Hospitalist. “In terms of reimbursement, the sooner they can get a patient out of the hospital, it opens bed space for patients in the emergency department. It eases up bottlenecks because the patient in the ED may not need the bed that is being opened, but they may need an ICU bed, and the ICU patient is stable enough to be transferred to that medical bed that you’re opening up. So it’s a domino effect, and it certainly helps with creating a better flow within the hospital.”
It sounds simple, of course: Discharge inpatients early in the day and fill that bed with another patient, akin to a busy restaurant flipping tables to reduce the line stretching out the front door. The more customers, the more money made—both for the restaurant (i.e. hospital) and the servers (i.e. providers). And the less potential customers wait, the happier they are with their service.
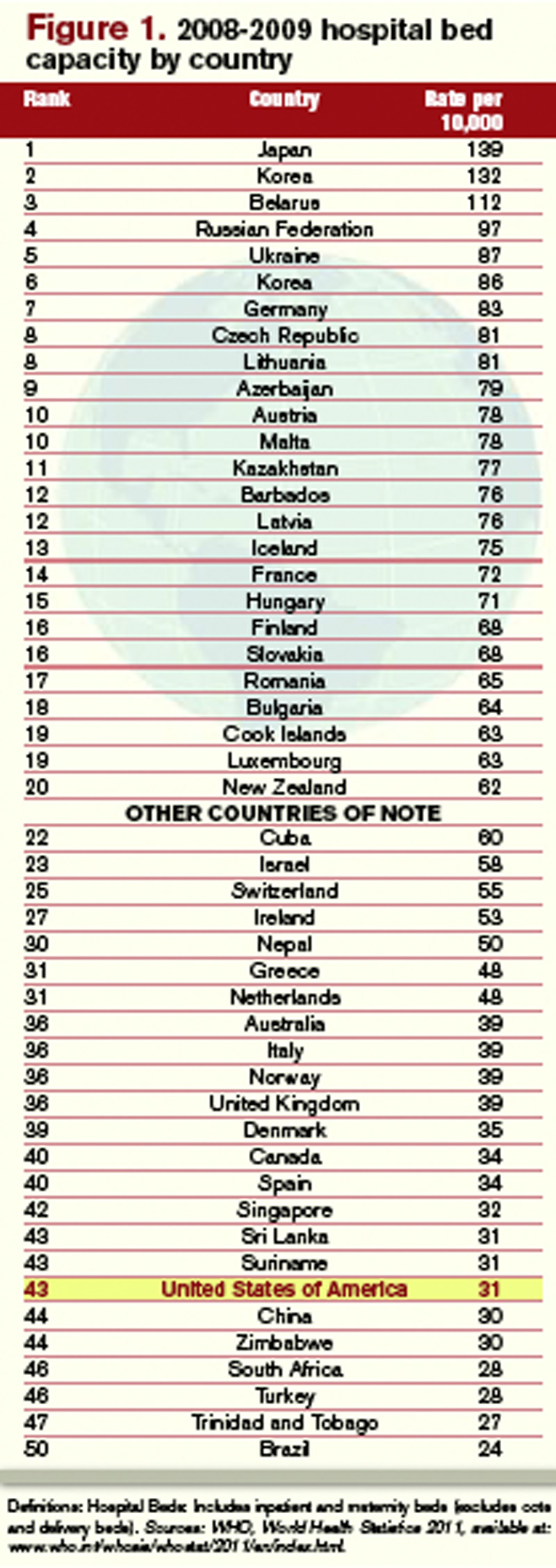
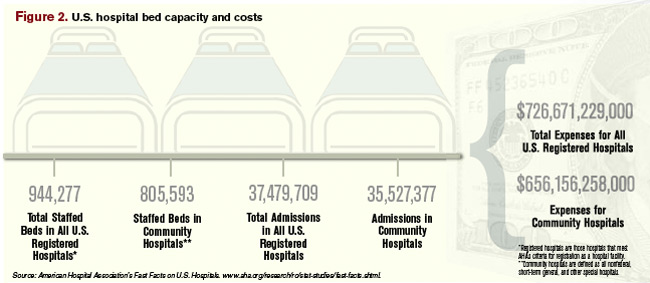
But adding new beds, at nearly $1 million per bed inclusive of the space, infrastructure, and technology, is unacceptable math for most U.S. hospitals struggling to make ends meet in a tough economy.1 By contrast, an aggressive bed-management approach creates virtual bed capacity that creates more revenue-generating opportunities without those costs. And as Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) surveys tie patient satisfaction more directly to compensation, the more attention that will be focused on the discharge, as it will be the last process the patient experiences, and the one they likely will remember the most.
So if everyone agrees that discharging inpatients earlier in the day is a good idea, what’s the holdup? Interviews with more than a half-dozen hospitalists show a handful of factors that are present in all hospitals, large and small, academic and community:
- Downstream complications. HM is only one piece of the discharge puzzle. Hospitalists might be ready to discharge, but without that last test, or the ability to reach a pharmacist, the process slows. Even when discharge is complete, the room needs to be cleared and cleaned.
- Rounding protocols. Hospital-ists intuitively round on the sickest patients first, but that time-honored tradition has the byproduct of pushing those patients most likely to be sent home to the end of the line, automatically delaying discharges.
- Shift flexibility. Many hospitalist groups have morning shifts that begin at 8 a.m. Given the time it takes to craft discharge orders and deal with inevitable wrinkles in the process, that almost guarantees discharges will be pushed to later in the day.
- Hospital infrastructure. Insti-tutional bed management begins at the top, with a commitment across departments that discharge procedures are a shared priority. Without such across-the-board buy-in, the best hospitalists can do is fight against the tide. For example, a room could be vacated at 10 a.m., but housekeeping isn’t notified (or prepared) to clean the room for two hours because there is no institutional procedure in place to govern that decision.
“It’s harder than you think,” Dr. O’Boyle admits. “There are always extraneous factors that can delay the hospitalists from getting [discharges] done.”
Continued below...

Bed Management
Early-day discharge is just one pathway to improve “patient flow” and, therefore, bed management, according to a recent editorial in Health Affairs jointly penned by executives from the Institute for Healthcare Optimization in Newton, Mass., and the Institute for Healthcare Improvement in Cambridge, Mass.1
Other techniques are:
- Reducing length of stay (LOS): Hospitalists have long focused on keeping patient stays at a minimum, although many researchers have argued that LOS can only be reduced to a point. Quality and patient safety issues in the Affordable Care Act might actually increase LOS, as hospitalists and other physicians work to reduce 30-day readmissions by ensuring everything is done right the first time.
- Expanding capacity: At an estimated cost of $1 million to add one new bed to a hospital, it is simply unlikely that institutions will be in a fiscal position to add physical beds in the next few years.
- Increasing staff: “Here again,” the authors state flatly, “pressures on hospital systems and operating margins make it unlikely that hospitals will dramatically increase their payrolls.”
No Consensus
Although a variety of techniques can help improve early day discharge, all have hurdles. Two of the most common suggestions are geographic rounding and discharge lounges. A third is the active bed-management (ABM) model that hospitalist Eric Howell, MD, SFHM, associate professor of medicine at Johns Hopkins University and director of Johns Hopkins Bayview Medical Center’s HM division, wrote about in the Annals of Internal Medicine in December 2008.2
Geographic rounding, also dubbed unit-based setups, can help improve bed management because all participants are co-located; however, the gains likely are not enough to motivate an institution to implement the model without demonstrated improvements to other systems as well, says John Nelson, MD, FACP, MHM, cofounder and past president of SHM and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants.
Discharge lounges—areas usually administered by a nurse and billed as a place for patients to gather after they’ve been formally discharged but before they have arranged a ride to physically leave the hospital—have been adopted by many hospitals. Dr. Simone and others question the liability issues associated with keeping discharged patients under the watch of hospital staff and also wonder whether the setup can have a negative impact on patient satisfaction. (For more on discharge lounges, check out “Solution of Problem,” at www.the-hospitalist.org.)

—David Bachman, MD, senior medical director for transitions of care, MaineHealth Clinical Integration, Portland, Maine
David Bachman, MD, senior medical director for transitions of care at MaineHealth Clinical Integration in Portland, Maine, and a former hospital administrator in New England, sees hospitalists as a lynchpin to the discharge process, but he also urges them to get the hospital to see them as “change agents” who need institutional support to make significant improvements.
“You’re trying to run cases through and it’s all dependent on downstream activity,” Dr. Bachman says. “If the hospitalist can push back and get this recognized as a hospital issue, that’s the only time when this problem can be solved. Hospitalists are a piece of the puzzle, but it’s not just them.”
Ideas to Chew On
Mitchell Wilson, MD, SFHM, chief medical officer for Eagle Hospital Physicians in Atlanta, agrees that reprioritizing physician rounds to encourage discharges would push patients out earlier, but he wants to see more physician assistants and nurse practitioners (PAs and NPs) blended into those rounds. The partnership would be a relatively simple and direct way for physicians to pass off nonclinical or less-intensive duties that afford them more time to focus on discharge planning. A dedicated nurse for HM service and the use of telemedicine could be folded into HM practices to help.
Each of the techniques would serve to get patients out earlier on what is arguably the most costly day of their stay. “Hospitals generally lose money on the last day of a patient’s stay,” Dr. Wilson says. “When appropriate from a patient care standpoint, discharging your patient and getting the bed ready for the next patient sooner is definitely an advantage for the hospital, and for the next patient.”
Dr. Bachman says one of the main hurdles to that process is no single provider “has clear responsibility and oversight. … It’s this diffuse responsibility.” That’s where Dr. Howell and colleagues thought ABM would work well. At Hopkins Bayview, hospitalists staffed an active bed-management program that rounded twice daily in ICUs and visited the ED regularly. The hospitalist on the 12-hour shift had no other duties, a luxury that HM pioneer Robert Wachter, MD, MHM, described at the time as “freeing him or her up to act as a full-time air traffic controller for all medical patients.”
The intervention reduced ED throughput for admitted patients by 98 minutes, to 360 minutes from 458 minutes. It also cut the amount of time the ED diverted ambulances because of overcrowding—the so-called “yellow alert”—by 6%, and the amount of time ambulances were diverted due to a lack of ICU beds—“red alert”—by 27%. Dr. Howell, an SHM board member, says the results showed how hospitalists can lead throughput change through institutions but that more work needs to be done to focus on early-day discharge.
“The hospital medicine side may be incentivized for early discharges,” he says, “but the hospital systems may not.”
Dr. Howell pushes for “2-by-10,” shorthand for identifying two patients daily who could be discharged by 10 a.m. because “the ED doesn’t necessarily need more beds for 24 hours. They need more beds early in the day.” But in keeping with the ABM model, Dr. Howell believes fiscal and personnel resources have to be dedicated to the problem to expect results. In the Hopkins Bayview intervention, Dr. Wachter, professor and associate chairman of the Department of Medicine at the University of California at San Francisco, chief of the division of hospital medicine, and chief of the medical service at UCSF Medical Center, estimated the annual costs of ABM at close to $1 million a year, given the likely need for four to six full-time equivalent hospitalists, according to a post on his Wachter’s World blog (www.wachtersworld. com) after the report was published.
One idea Dr. Howell suggests to push earlier discharges is restructuring physician workweeks, setting aside certain days for admission and certain days for follow-ups. If two shifts of follow-up days are scheduled after two days of admissions, it’s likely a hospitalist could follow a patient through their entire stay, he says. “You have to structure the doctor’s day to focus on discharges first,” he adds.
Dr. Howell also believes multidisciplinary rounds are key to earlier discharges. At Wayne Memorial Hospital and other places that have instituted such teams, discharge usually is just one byproduct of a construct ultimately aimed at quality improvement. Wayne Memorial’s Dr. O’Boyle says that since the team approach was initiated in September 2009, the hospital’s LOS has dropped by 0.75 days and patient satisfaction scores have risen about 25%. Those metrics will be key data points in the years to come as discharges and readmissions become tied to reimbursement via healthcare reform (see “Value-Based Purchasing Raises the Stakes,” May 2011).

“One of the biggest factors for readmissions are things like pharmacy errors, and lack of follow-up, and other loose ends that, if you’re in too much of a hurry to get people out and you don’t have the whole team approach and make sure all your I’s are dotted and T’s are crossed, then they have an increased chance of coming back,” Dr. O’Boyle says. “So we focus on patient satisfaction, and we focus on the discharge day and the discharge time to prevent readmissions and to maximize patient satisfaction. That’s the bottom line for the hospital…It’s interesting how the bottom line seems to follow quality.”
Continued below...
Inherent Conflicts?
Early-day discharge actually can be a bad thing in some cases, Dr. Nelson says. Think of a case in which a patient might be ready for discharge in the late evening or during an overnight. To wait until the morning to send that patient home might not be the best approach.

—Louis O’Boyle, DO, FACP, FHM, medical director, Advanced Inpatient Medicine, Honesdale, Pa.
“The place that manages length of stay most efficiently probably has plenty of late-day discharge,” he says.
Another potential conflict getting in the way of early-day discharge is what Dr. Wilson calls “admission competition.” For example, a hospitalist is working on discharge papers early in the morning but is then called away for a consult on an acute-care case in the ED or elsewhere. Each of the duties is important, but conflicting duties leave the hospitalist having to make choices.
“It’s not all straightforward,” Dr. Nelson says.
Emergency Nurses Association President AnnMarie Papa, DNP, RN, CEN, NE-BC, FAEN, says that collaboration between nurses and physicians is an answer to such competition. Calling the problem a “wrinkle across the system,” Papa says that without hospital administrators taking point and declaring the issue of discharge a priority, little wholesale improvement will be made. Even then, physicians and nurses—as the two main groups interacting with the patient—have to work together, she adds.
“Hospitalists have to partner with nurses,” Papa says, imploring physicians and nurses to work together on discharge decisions. “If the physicians and nurses collaborate on the decision and plans of care for the patients and the care they’re giving them and the discharge instructions, then it’s a win-win for everybody.”
Richard Quinn is a freelance writer based in New Jersey.
Reference
- Litvak E, Bisognano M. More patients, less payment: increasing hospital efficiency in the aftermath of health reform. Health Affairs. 2011;30(1): 76-80.
- Howell E, Bessman E, Kravet S, Kolodner K, Marshall R, Wright S. Active bed management by hospitalists and emergency department throughput. Ann Int Med. 2008;149(11):804-810.
Every morning at 8 a.m., a multidisciplinary team at Wayne Memorial Hospital in Honesdale, Pa., a rural pocket of about 5,000 people about 30 miles northeast of Scranton, gathers to discuss discharge planning. Representatives from social services, home health, nursing, physical therapy, pharmacy, and the HM group attend the meeting. Each stakeholder weighs in, listens to others, and voices concerns when applicable.
“We go through each patient in the morning, briefly, and go through the plan so that when there’s a discharge coming, everybody is on the same page and can try to get everything organized,” says Louis O’Boyle, DO, FACP, FHM, medical director of Advanced Inpatient Medicine, the hospitalist program contracted by Wayne Memorial, which has 98 acute-care beds. “The hospital has reminded us to be cognizant of getting that early discharge, and it’s become almost so rote now that we don’t even have to worry about it. It’s just a thing we do.”
Better bed management is a new mantra for hospitalists nationwide, because fewer open beds means fewer dollars for both the physician and the hospital. Better bed management also means improved patient satisfaction scores, as most patients would rather be at home (and those scores in the coming years will factor into Medicare reimbursement). And better bed management means reduced backlogs across the hospital, particularly “boarders” in the ED.
“The pressure really is on the hospital for a number of reasons,” says Ken Simone, DO, SFHM, president of Hospitalist and Practice Solutions in Veazie, Maine, and a member of Team Hospitalist. “In terms of reimbursement, the sooner they can get a patient out of the hospital, it opens bed space for patients in the emergency department. It eases up bottlenecks because the patient in the ED may not need the bed that is being opened, but they may need an ICU bed, and the ICU patient is stable enough to be transferred to that medical bed that you’re opening up. So it’s a domino effect, and it certainly helps with creating a better flow within the hospital.”
It sounds simple, of course: Discharge inpatients early in the day and fill that bed with another patient, akin to a busy restaurant flipping tables to reduce the line stretching out the front door. The more customers, the more money made—both for the restaurant (i.e. hospital) and the servers (i.e. providers). And the less potential customers wait, the happier they are with their service.
But adding new beds, at nearly $1 million per bed inclusive of the space, infrastructure, and technology, is unacceptable math for most U.S. hospitals struggling to make ends meet in a tough economy.1 By contrast, an aggressive bed-management approach creates virtual bed capacity that creates more revenue-generating opportunities without those costs. And as Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) surveys tie patient satisfaction more directly to compensation, the more attention that will be focused on the discharge, as it will be the last process the patient experiences, and the one they likely will remember the most.
So if everyone agrees that discharging inpatients earlier in the day is a good idea, what’s the holdup? Interviews with more than a half-dozen hospitalists show a handful of factors that are present in all hospitals, large and small, academic and community:
- Downstream complications. HM is only one piece of the discharge puzzle. Hospitalists might be ready to discharge, but without that last test, or the ability to reach a pharmacist, the process slows. Even when discharge is complete, the room needs to be cleared and cleaned.
- Rounding protocols. Hospital-ists intuitively round on the sickest patients first, but that time-honored tradition has the byproduct of pushing those patients most likely to be sent home to the end of the line, automatically delaying discharges.
- Shift flexibility. Many hospitalist groups have morning shifts that begin at 8 a.m. Given the time it takes to craft discharge orders and deal with inevitable wrinkles in the process, that almost guarantees discharges will be pushed to later in the day.
- Hospital infrastructure. Insti-tutional bed management begins at the top, with a commitment across departments that discharge procedures are a shared priority. Without such across-the-board buy-in, the best hospitalists can do is fight against the tide. For example, a room could be vacated at 10 a.m., but housekeeping isn’t notified (or prepared) to clean the room for two hours because there is no institutional procedure in place to govern that decision.
“It’s harder than you think,” Dr. O’Boyle admits. “There are always extraneous factors that can delay the hospitalists from getting [discharges] done.”
Continued below...
Bed Management
Early-day discharge is just one pathway to improve “patient flow” and, therefore, bed management, according to a recent editorial in Health Affairs jointly penned by executives from the Institute for Healthcare Optimization in Newton, Mass., and the Institute for Healthcare Improvement in Cambridge, Mass.1
Other techniques are:
- Reducing length of stay (LOS): Hospitalists have long focused on keeping patient stays at a minimum, although many researchers have argued that LOS can only be reduced to a point. Quality and patient safety issues in the Affordable Care Act might actually increase LOS, as hospitalists and other physicians work to reduce 30-day readmissions by ensuring everything is done right the first time.
- Expanding capacity: At an estimated cost of $1 million to add one new bed to a hospital, it is simply unlikely that institutions will be in a fiscal position to add physical beds in the next few years.
- Increasing staff: “Here again,” the authors state flatly, “pressures on hospital systems and operating margins make it unlikely that hospitals will dramatically increase their payrolls.”
No Consensus
Although a variety of techniques can help improve early day discharge, all have hurdles. Two of the most common suggestions are geographic rounding and discharge lounges. A third is the active bed-management (ABM) model that hospitalist Eric Howell, MD, SFHM, associate professor of medicine at Johns Hopkins University and director of Johns Hopkins Bayview Medical Center’s HM division, wrote about in the Annals of Internal Medicine in December 2008.2
Geographic rounding, also dubbed unit-based setups, can help improve bed management because all participants are co-located; however, the gains likely are not enough to motivate an institution to implement the model without demonstrated improvements to other systems as well, says John Nelson, MD, FACP, MHM, cofounder and past president of SHM and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants.
Discharge lounges—areas usually administered by a nurse and billed as a place for patients to gather after they’ve been formally discharged but before they have arranged a ride to physically leave the hospital—have been adopted by many hospitals. Dr. Simone and others question the liability issues associated with keeping discharged patients under the watch of hospital staff and also wonder whether the setup can have a negative impact on patient satisfaction. (For more on discharge lounges, check out “Solution of Problem,” at www.the-hospitalist.org.)
—David Bachman, MD, senior medical director for transitions of care, MaineHealth Clinical Integration, Portland, Maine
David Bachman, MD, senior medical director for transitions of care at MaineHealth Clinical Integration in Portland, Maine, and a former hospital administrator in New England, sees hospitalists as a lynchpin to the discharge process, but he also urges them to get the hospital to see them as “change agents” who need institutional support to make significant improvements.
“You’re trying to run cases through and it’s all dependent on downstream activity,” Dr. Bachman says. “If the hospitalist can push back and get this recognized as a hospital issue, that’s the only time when this problem can be solved. Hospitalists are a piece of the puzzle, but it’s not just them.”
Ideas to Chew On
Mitchell Wilson, MD, SFHM, chief medical officer for Eagle Hospital Physicians in Atlanta, agrees that reprioritizing physician rounds to encourage discharges would push patients out earlier, but he wants to see more physician assistants and nurse practitioners (PAs and NPs) blended into those rounds. The partnership would be a relatively simple and direct way for physicians to pass off nonclinical or less-intensive duties that afford them more time to focus on discharge planning. A dedicated nurse for HM service and the use of telemedicine could be folded into HM practices to help.
Each of the techniques would serve to get patients out earlier on what is arguably the most costly day of their stay. “Hospitals generally lose money on the last day of a patient’s stay,” Dr. Wilson says. “When appropriate from a patient care standpoint, discharging your patient and getting the bed ready for the next patient sooner is definitely an advantage for the hospital, and for the next patient.”
Dr. Bachman says one of the main hurdles to that process is no single provider “has clear responsibility and oversight. … It’s this diffuse responsibility.” That’s where Dr. Howell and colleagues thought ABM would work well. At Hopkins Bayview, hospitalists staffed an active bed-management program that rounded twice daily in ICUs and visited the ED regularly. The hospitalist on the 12-hour shift had no other duties, a luxury that HM pioneer Robert Wachter, MD, MHM, described at the time as “freeing him or her up to act as a full-time air traffic controller for all medical patients.”
The intervention reduced ED throughput for admitted patients by 98 minutes, to 360 minutes from 458 minutes. It also cut the amount of time the ED diverted ambulances because of overcrowding—the so-called “yellow alert”—by 6%, and the amount of time ambulances were diverted due to a lack of ICU beds—“red alert”—by 27%. Dr. Howell, an SHM board member, says the results showed how hospitalists can lead throughput change through institutions but that more work needs to be done to focus on early-day discharge.
“The hospital medicine side may be incentivized for early discharges,” he says, “but the hospital systems may not.”
Dr. Howell pushes for “2-by-10,” shorthand for identifying two patients daily who could be discharged by 10 a.m. because “the ED doesn’t necessarily need more beds for 24 hours. They need more beds early in the day.” But in keeping with the ABM model, Dr. Howell believes fiscal and personnel resources have to be dedicated to the problem to expect results. In the Hopkins Bayview intervention, Dr. Wachter, professor and associate chairman of the Department of Medicine at the University of California at San Francisco, chief of the division of hospital medicine, and chief of the medical service at UCSF Medical Center, estimated the annual costs of ABM at close to $1 million a year, given the likely need for four to six full-time equivalent hospitalists, according to a post on his Wachter’s World blog (www.wachtersworld. com) after the report was published.
One idea Dr. Howell suggests to push earlier discharges is restructuring physician workweeks, setting aside certain days for admission and certain days for follow-ups. If two shifts of follow-up days are scheduled after two days of admissions, it’s likely a hospitalist could follow a patient through their entire stay, he says. “You have to structure the doctor’s day to focus on discharges first,” he adds.
Dr. Howell also believes multidisciplinary rounds are key to earlier discharges. At Wayne Memorial Hospital and other places that have instituted such teams, discharge usually is just one byproduct of a construct ultimately aimed at quality improvement. Wayne Memorial’s Dr. O’Boyle says that since the team approach was initiated in September 2009, the hospital’s LOS has dropped by 0.75 days and patient satisfaction scores have risen about 25%. Those metrics will be key data points in the years to come as discharges and readmissions become tied to reimbursement via healthcare reform (see “Value-Based Purchasing Raises the Stakes,” May 2011).
“One of the biggest factors for readmissions are things like pharmacy errors, and lack of follow-up, and other loose ends that, if you’re in too much of a hurry to get people out and you don’t have the whole team approach and make sure all your I’s are dotted and T’s are crossed, then they have an increased chance of coming back,” Dr. O’Boyle says. “So we focus on patient satisfaction, and we focus on the discharge day and the discharge time to prevent readmissions and to maximize patient satisfaction. That’s the bottom line for the hospital…It’s interesting how the bottom line seems to follow quality.”
Continued below...
Inherent Conflicts?
Early-day discharge actually can be a bad thing in some cases, Dr. Nelson says. Think of a case in which a patient might be ready for discharge in the late evening or during an overnight. To wait until the morning to send that patient home might not be the best approach.
—Louis O’Boyle, DO, FACP, FHM, medical director, Advanced Inpatient Medicine, Honesdale, Pa.
“The place that manages length of stay most efficiently probably has plenty of late-day discharge,” he says.
Another potential conflict getting in the way of early-day discharge is what Dr. Wilson calls “admission competition.” For example, a hospitalist is working on discharge papers early in the morning but is then called away for a consult on an acute-care case in the ED or elsewhere. Each of the duties is important, but conflicting duties leave the hospitalist having to make choices.
“It’s not all straightforward,” Dr. Nelson says.
Emergency Nurses Association President AnnMarie Papa, DNP, RN, CEN, NE-BC, FAEN, says that collaboration between nurses and physicians is an answer to such competition. Calling the problem a “wrinkle across the system,” Papa says that without hospital administrators taking point and declaring the issue of discharge a priority, little wholesale improvement will be made. Even then, physicians and nurses—as the two main groups interacting with the patient—have to work together, she adds.
“Hospitalists have to partner with nurses,” Papa says, imploring physicians and nurses to work together on discharge decisions. “If the physicians and nurses collaborate on the decision and plans of care for the patients and the care they’re giving them and the discharge instructions, then it’s a win-win for everybody.”
Richard Quinn is a freelance writer based in New Jersey.
Reference
- Litvak E, Bisognano M. More patients, less payment: increasing hospital efficiency in the aftermath of health reform. Health Affairs. 2011;30(1): 76-80.
- Howell E, Bessman E, Kravet S, Kolodner K, Marshall R, Wright S. Active bed management by hospitalists and emergency department throughput. Ann Int Med. 2008;149(11):804-810.
Every morning at 8 a.m., a multidisciplinary team at Wayne Memorial Hospital in Honesdale, Pa., a rural pocket of about 5,000 people about 30 miles northeast of Scranton, gathers to discuss discharge planning. Representatives from social services, home health, nursing, physical therapy, pharmacy, and the HM group attend the meeting. Each stakeholder weighs in, listens to others, and voices concerns when applicable.
“We go through each patient in the morning, briefly, and go through the plan so that when there’s a discharge coming, everybody is on the same page and can try to get everything organized,” says Louis O’Boyle, DO, FACP, FHM, medical director of Advanced Inpatient Medicine, the hospitalist program contracted by Wayne Memorial, which has 98 acute-care beds. “The hospital has reminded us to be cognizant of getting that early discharge, and it’s become almost so rote now that we don’t even have to worry about it. It’s just a thing we do.”
Better bed management is a new mantra for hospitalists nationwide, because fewer open beds means fewer dollars for both the physician and the hospital. Better bed management also means improved patient satisfaction scores, as most patients would rather be at home (and those scores in the coming years will factor into Medicare reimbursement). And better bed management means reduced backlogs across the hospital, particularly “boarders” in the ED.
“The pressure really is on the hospital for a number of reasons,” says Ken Simone, DO, SFHM, president of Hospitalist and Practice Solutions in Veazie, Maine, and a member of Team Hospitalist. “In terms of reimbursement, the sooner they can get a patient out of the hospital, it opens bed space for patients in the emergency department. It eases up bottlenecks because the patient in the ED may not need the bed that is being opened, but they may need an ICU bed, and the ICU patient is stable enough to be transferred to that medical bed that you’re opening up. So it’s a domino effect, and it certainly helps with creating a better flow within the hospital.”
It sounds simple, of course: Discharge inpatients early in the day and fill that bed with another patient, akin to a busy restaurant flipping tables to reduce the line stretching out the front door. The more customers, the more money made—both for the restaurant (i.e. hospital) and the servers (i.e. providers). And the less potential customers wait, the happier they are with their service.
But adding new beds, at nearly $1 million per bed inclusive of the space, infrastructure, and technology, is unacceptable math for most U.S. hospitals struggling to make ends meet in a tough economy.1 By contrast, an aggressive bed-management approach creates virtual bed capacity that creates more revenue-generating opportunities without those costs. And as Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) surveys tie patient satisfaction more directly to compensation, the more attention that will be focused on the discharge, as it will be the last process the patient experiences, and the one they likely will remember the most.
So if everyone agrees that discharging inpatients earlier in the day is a good idea, what’s the holdup? Interviews with more than a half-dozen hospitalists show a handful of factors that are present in all hospitals, large and small, academic and community:
- Downstream complications. HM is only one piece of the discharge puzzle. Hospitalists might be ready to discharge, but without that last test, or the ability to reach a pharmacist, the process slows. Even when discharge is complete, the room needs to be cleared and cleaned.
- Rounding protocols. Hospital-ists intuitively round on the sickest patients first, but that time-honored tradition has the byproduct of pushing those patients most likely to be sent home to the end of the line, automatically delaying discharges.
- Shift flexibility. Many hospitalist groups have morning shifts that begin at 8 a.m. Given the time it takes to craft discharge orders and deal with inevitable wrinkles in the process, that almost guarantees discharges will be pushed to later in the day.
- Hospital infrastructure. Insti-tutional bed management begins at the top, with a commitment across departments that discharge procedures are a shared priority. Without such across-the-board buy-in, the best hospitalists can do is fight against the tide. For example, a room could be vacated at 10 a.m., but housekeeping isn’t notified (or prepared) to clean the room for two hours because there is no institutional procedure in place to govern that decision.
“It’s harder than you think,” Dr. O’Boyle admits. “There are always extraneous factors that can delay the hospitalists from getting [discharges] done.”
Continued below...
Bed Management
Early-day discharge is just one pathway to improve “patient flow” and, therefore, bed management, according to a recent editorial in Health Affairs jointly penned by executives from the Institute for Healthcare Optimization in Newton, Mass., and the Institute for Healthcare Improvement in Cambridge, Mass.1
Other techniques are:
- Reducing length of stay (LOS): Hospitalists have long focused on keeping patient stays at a minimum, although many researchers have argued that LOS can only be reduced to a point. Quality and patient safety issues in the Affordable Care Act might actually increase LOS, as hospitalists and other physicians work to reduce 30-day readmissions by ensuring everything is done right the first time.
- Expanding capacity: At an estimated cost of $1 million to add one new bed to a hospital, it is simply unlikely that institutions will be in a fiscal position to add physical beds in the next few years.
- Increasing staff: “Here again,” the authors state flatly, “pressures on hospital systems and operating margins make it unlikely that hospitals will dramatically increase their payrolls.”
No Consensus
Although a variety of techniques can help improve early day discharge, all have hurdles. Two of the most common suggestions are geographic rounding and discharge lounges. A third is the active bed-management (ABM) model that hospitalist Eric Howell, MD, SFHM, associate professor of medicine at Johns Hopkins University and director of Johns Hopkins Bayview Medical Center’s HM division, wrote about in the Annals of Internal Medicine in December 2008.2
Geographic rounding, also dubbed unit-based setups, can help improve bed management because all participants are co-located; however, the gains likely are not enough to motivate an institution to implement the model without demonstrated improvements to other systems as well, says John Nelson, MD, FACP, MHM, cofounder and past president of SHM and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants.
Discharge lounges—areas usually administered by a nurse and billed as a place for patients to gather after they’ve been formally discharged but before they have arranged a ride to physically leave the hospital—have been adopted by many hospitals. Dr. Simone and others question the liability issues associated with keeping discharged patients under the watch of hospital staff and also wonder whether the setup can have a negative impact on patient satisfaction. (For more on discharge lounges, check out “Solution of Problem,” at www.the-hospitalist.org.)
—David Bachman, MD, senior medical director for transitions of care, MaineHealth Clinical Integration, Portland, Maine
David Bachman, MD, senior medical director for transitions of care at MaineHealth Clinical Integration in Portland, Maine, and a former hospital administrator in New England, sees hospitalists as a lynchpin to the discharge process, but he also urges them to get the hospital to see them as “change agents” who need institutional support to make significant improvements.
“You’re trying to run cases through and it’s all dependent on downstream activity,” Dr. Bachman says. “If the hospitalist can push back and get this recognized as a hospital issue, that’s the only time when this problem can be solved. Hospitalists are a piece of the puzzle, but it’s not just them.”
Ideas to Chew On
Mitchell Wilson, MD, SFHM, chief medical officer for Eagle Hospital Physicians in Atlanta, agrees that reprioritizing physician rounds to encourage discharges would push patients out earlier, but he wants to see more physician assistants and nurse practitioners (PAs and NPs) blended into those rounds. The partnership would be a relatively simple and direct way for physicians to pass off nonclinical or less-intensive duties that afford them more time to focus on discharge planning. A dedicated nurse for HM service and the use of telemedicine could be folded into HM practices to help.
Each of the techniques would serve to get patients out earlier on what is arguably the most costly day of their stay. “Hospitals generally lose money on the last day of a patient’s stay,” Dr. Wilson says. “When appropriate from a patient care standpoint, discharging your patient and getting the bed ready for the next patient sooner is definitely an advantage for the hospital, and for the next patient.”
Dr. Bachman says one of the main hurdles to that process is no single provider “has clear responsibility and oversight. … It’s this diffuse responsibility.” That’s where Dr. Howell and colleagues thought ABM would work well. At Hopkins Bayview, hospitalists staffed an active bed-management program that rounded twice daily in ICUs and visited the ED regularly. The hospitalist on the 12-hour shift had no other duties, a luxury that HM pioneer Robert Wachter, MD, MHM, described at the time as “freeing him or her up to act as a full-time air traffic controller for all medical patients.”
The intervention reduced ED throughput for admitted patients by 98 minutes, to 360 minutes from 458 minutes. It also cut the amount of time the ED diverted ambulances because of overcrowding—the so-called “yellow alert”—by 6%, and the amount of time ambulances were diverted due to a lack of ICU beds—“red alert”—by 27%. Dr. Howell, an SHM board member, says the results showed how hospitalists can lead throughput change through institutions but that more work needs to be done to focus on early-day discharge.
“The hospital medicine side may be incentivized for early discharges,” he says, “but the hospital systems may not.”
Dr. Howell pushes for “2-by-10,” shorthand for identifying two patients daily who could be discharged by 10 a.m. because “the ED doesn’t necessarily need more beds for 24 hours. They need more beds early in the day.” But in keeping with the ABM model, Dr. Howell believes fiscal and personnel resources have to be dedicated to the problem to expect results. In the Hopkins Bayview intervention, Dr. Wachter, professor and associate chairman of the Department of Medicine at the University of California at San Francisco, chief of the division of hospital medicine, and chief of the medical service at UCSF Medical Center, estimated the annual costs of ABM at close to $1 million a year, given the likely need for four to six full-time equivalent hospitalists, according to a post on his Wachter’s World blog (www.wachtersworld. com) after the report was published.
One idea Dr. Howell suggests to push earlier discharges is restructuring physician workweeks, setting aside certain days for admission and certain days for follow-ups. If two shifts of follow-up days are scheduled after two days of admissions, it’s likely a hospitalist could follow a patient through their entire stay, he says. “You have to structure the doctor’s day to focus on discharges first,” he adds.
Dr. Howell also believes multidisciplinary rounds are key to earlier discharges. At Wayne Memorial Hospital and other places that have instituted such teams, discharge usually is just one byproduct of a construct ultimately aimed at quality improvement. Wayne Memorial’s Dr. O’Boyle says that since the team approach was initiated in September 2009, the hospital’s LOS has dropped by 0.75 days and patient satisfaction scores have risen about 25%. Those metrics will be key data points in the years to come as discharges and readmissions become tied to reimbursement via healthcare reform (see “Value-Based Purchasing Raises the Stakes,” May 2011).
“One of the biggest factors for readmissions are things like pharmacy errors, and lack of follow-up, and other loose ends that, if you’re in too much of a hurry to get people out and you don’t have the whole team approach and make sure all your I’s are dotted and T’s are crossed, then they have an increased chance of coming back,” Dr. O’Boyle says. “So we focus on patient satisfaction, and we focus on the discharge day and the discharge time to prevent readmissions and to maximize patient satisfaction. That’s the bottom line for the hospital…It’s interesting how the bottom line seems to follow quality.”
Continued below...
Inherent Conflicts?
Early-day discharge actually can be a bad thing in some cases, Dr. Nelson says. Think of a case in which a patient might be ready for discharge in the late evening or during an overnight. To wait until the morning to send that patient home might not be the best approach.
—Louis O’Boyle, DO, FACP, FHM, medical director, Advanced Inpatient Medicine, Honesdale, Pa.
“The place that manages length of stay most efficiently probably has plenty of late-day discharge,” he says.
Another potential conflict getting in the way of early-day discharge is what Dr. Wilson calls “admission competition.” For example, a hospitalist is working on discharge papers early in the morning but is then called away for a consult on an acute-care case in the ED or elsewhere. Each of the duties is important, but conflicting duties leave the hospitalist having to make choices.
“It’s not all straightforward,” Dr. Nelson says.
Emergency Nurses Association President AnnMarie Papa, DNP, RN, CEN, NE-BC, FAEN, says that collaboration between nurses and physicians is an answer to such competition. Calling the problem a “wrinkle across the system,” Papa says that without hospital administrators taking point and declaring the issue of discharge a priority, little wholesale improvement will be made. Even then, physicians and nurses—as the two main groups interacting with the patient—have to work together, she adds.
“Hospitalists have to partner with nurses,” Papa says, imploring physicians and nurses to work together on discharge decisions. “If the physicians and nurses collaborate on the decision and plans of care for the patients and the care they’re giving them and the discharge instructions, then it’s a win-win for everybody.”
Richard Quinn is a freelance writer based in New Jersey.
Reference
- Litvak E, Bisognano M. More patients, less payment: increasing hospital efficiency in the aftermath of health reform. Health Affairs. 2011;30(1): 76-80.
- Howell E, Bessman E, Kravet S, Kolodner K, Marshall R, Wright S. Active bed management by hospitalists and emergency department throughput. Ann Int Med. 2008;149(11):804-810.
Study: Rural Hospitals Behind IT Curve
Only a sliver of rural hospitals would meet the Center for Medicare & Medicaid Services’ (CMS) criteria to qualify for “meaningful use” of health information technology (HIT), according to a new study, but that could be a window for HM group leaders to take the reins of technology projects.
“[Hospitalists] could be very useful as a champion,” says Brock Slabach, MPH, FACHE, senior vice president for member services at the National Rural Health Association.
The new report showed that 5% of rural hospitals could demonstrate meaningful use of an electronic health record (EHR) system, as opposed to 9% of urban hospitals (J Rural Health. 2011;27(3):329-337). The number dips to 3% for critical-access hospitals. EHR usage often is used as a benchmark for HIT implementation.
CMS has allotted $20 billion for physicians and hospitals to adopt new technologies, but entities must prove they have met “meaningful use” requirements.
Slabach, who spent 20 years as an administrator at Field Memorial Community Hospital in Centreville, Miss., says the major hurdle for HIT implementation at rural hospitals is a lack of knowledge. But if hospitalists can show other physicians the value of HIT, others will follow, he adds.
“Somebody who may not have any informatics background, but is willing to grab a hold of the system, learn its applications, develop methods to spread the knowledge to the rest of the medical staff, is critical,” Slabach says. “It just takes that one or two [people] to get the momentum starting, in terms of a transition to what for a lot of middle-aged and older physicians is a completely new world.”
Only a sliver of rural hospitals would meet the Center for Medicare & Medicaid Services’ (CMS) criteria to qualify for “meaningful use” of health information technology (HIT), according to a new study, but that could be a window for HM group leaders to take the reins of technology projects.
“[Hospitalists] could be very useful as a champion,” says Brock Slabach, MPH, FACHE, senior vice president for member services at the National Rural Health Association.
The new report showed that 5% of rural hospitals could demonstrate meaningful use of an electronic health record (EHR) system, as opposed to 9% of urban hospitals (J Rural Health. 2011;27(3):329-337). The number dips to 3% for critical-access hospitals. EHR usage often is used as a benchmark for HIT implementation.
CMS has allotted $20 billion for physicians and hospitals to adopt new technologies, but entities must prove they have met “meaningful use” requirements.
Slabach, who spent 20 years as an administrator at Field Memorial Community Hospital in Centreville, Miss., says the major hurdle for HIT implementation at rural hospitals is a lack of knowledge. But if hospitalists can show other physicians the value of HIT, others will follow, he adds.
“Somebody who may not have any informatics background, but is willing to grab a hold of the system, learn its applications, develop methods to spread the knowledge to the rest of the medical staff, is critical,” Slabach says. “It just takes that one or two [people] to get the momentum starting, in terms of a transition to what for a lot of middle-aged and older physicians is a completely new world.”
Only a sliver of rural hospitals would meet the Center for Medicare & Medicaid Services’ (CMS) criteria to qualify for “meaningful use” of health information technology (HIT), according to a new study, but that could be a window for HM group leaders to take the reins of technology projects.
“[Hospitalists] could be very useful as a champion,” says Brock Slabach, MPH, FACHE, senior vice president for member services at the National Rural Health Association.
The new report showed that 5% of rural hospitals could demonstrate meaningful use of an electronic health record (EHR) system, as opposed to 9% of urban hospitals (J Rural Health. 2011;27(3):329-337). The number dips to 3% for critical-access hospitals. EHR usage often is used as a benchmark for HIT implementation.
CMS has allotted $20 billion for physicians and hospitals to adopt new technologies, but entities must prove they have met “meaningful use” requirements.
Slabach, who spent 20 years as an administrator at Field Memorial Community Hospital in Centreville, Miss., says the major hurdle for HIT implementation at rural hospitals is a lack of knowledge. But if hospitalists can show other physicians the value of HIT, others will follow, he adds.
“Somebody who may not have any informatics background, but is willing to grab a hold of the system, learn its applications, develop methods to spread the knowledge to the rest of the medical staff, is critical,” Slabach says. “It just takes that one or two [people] to get the momentum starting, in terms of a transition to what for a lot of middle-aged and older physicians is a completely new world.”
ONLINE EXCLUSIVE: A Discharge Solution—or Problem?
In a bit of counterintuition, an empty discharge lounge might be the most successful kind.
Christine Collins, executive director of patient access services at Brigham and Women’s Hospital in Boston, says that the lounge should be a service for discharged patients who have completed medical treatment, but who for some reason remain unable to leave the institution. Such cases can include waiting on a prescription from the pharmacy, or simply waiting on a relative or friend to arrive with transportation.
—Christine Collins, executive director, patient access services, Brigham and Women’s Hospital, Boston
She does not view Brigham’s discharge lounge, a room with lounge chairs and light meals that is staffed by a registered nurse, as the answer to the throughput conundrum hospitals across the country face each and every day. So when the lounge is empty, it means patients have been discharged without any hang-ups.
“It’s not a patient-care area,” Collins says. “They’re people that should be home.”
Some view discharge lounges as a potential aid in smoothing out the discharge process. In theory, patients ready to be medically discharged but unable to leave the hospital have a place to go. But keeping the patients in the building, and under the eye of a nurse, could create liability issues, says Ken Simone, DO, SFHM, president of Hospitalist and Practice Solutions in Veazie, Maine, and a member of Team Hospitalist. Dr. Simone also wonders how the lounge concept impacts patient satisfaction, as some could view it negatively if they’re told they have to sit in what could be construed as a back-end waiting room.
“People need to assess what they’re doing it for and is it really accomplishing what they want it to accomplish,” Collins says.
Discharge lounges “can’t be another nursing unit because a patient is supposed to be discharged. ... Whether you have a discharge lounge or not, you need to improve your systems so that the patients leave when they leave.”
Richard Quinn is a freelance writer based in New Jersey.
In a bit of counterintuition, an empty discharge lounge might be the most successful kind.
Christine Collins, executive director of patient access services at Brigham and Women’s Hospital in Boston, says that the lounge should be a service for discharged patients who have completed medical treatment, but who for some reason remain unable to leave the institution. Such cases can include waiting on a prescription from the pharmacy, or simply waiting on a relative or friend to arrive with transportation.
—Christine Collins, executive director, patient access services, Brigham and Women’s Hospital, Boston
She does not view Brigham’s discharge lounge, a room with lounge chairs and light meals that is staffed by a registered nurse, as the answer to the throughput conundrum hospitals across the country face each and every day. So when the lounge is empty, it means patients have been discharged without any hang-ups.
“It’s not a patient-care area,” Collins says. “They’re people that should be home.”
Some view discharge lounges as a potential aid in smoothing out the discharge process. In theory, patients ready to be medically discharged but unable to leave the hospital have a place to go. But keeping the patients in the building, and under the eye of a nurse, could create liability issues, says Ken Simone, DO, SFHM, president of Hospitalist and Practice Solutions in Veazie, Maine, and a member of Team Hospitalist. Dr. Simone also wonders how the lounge concept impacts patient satisfaction, as some could view it negatively if they’re told they have to sit in what could be construed as a back-end waiting room.
“People need to assess what they’re doing it for and is it really accomplishing what they want it to accomplish,” Collins says.
Discharge lounges “can’t be another nursing unit because a patient is supposed to be discharged. ... Whether you have a discharge lounge or not, you need to improve your systems so that the patients leave when they leave.”
Richard Quinn is a freelance writer based in New Jersey.
In a bit of counterintuition, an empty discharge lounge might be the most successful kind.
Christine Collins, executive director of patient access services at Brigham and Women’s Hospital in Boston, says that the lounge should be a service for discharged patients who have completed medical treatment, but who for some reason remain unable to leave the institution. Such cases can include waiting on a prescription from the pharmacy, or simply waiting on a relative or friend to arrive with transportation.
—Christine Collins, executive director, patient access services, Brigham and Women’s Hospital, Boston
She does not view Brigham’s discharge lounge, a room with lounge chairs and light meals that is staffed by a registered nurse, as the answer to the throughput conundrum hospitals across the country face each and every day. So when the lounge is empty, it means patients have been discharged without any hang-ups.
“It’s not a patient-care area,” Collins says. “They’re people that should be home.”
Some view discharge lounges as a potential aid in smoothing out the discharge process. In theory, patients ready to be medically discharged but unable to leave the hospital have a place to go. But keeping the patients in the building, and under the eye of a nurse, could create liability issues, says Ken Simone, DO, SFHM, president of Hospitalist and Practice Solutions in Veazie, Maine, and a member of Team Hospitalist. Dr. Simone also wonders how the lounge concept impacts patient satisfaction, as some could view it negatively if they’re told they have to sit in what could be construed as a back-end waiting room.
“People need to assess what they’re doing it for and is it really accomplishing what they want it to accomplish,” Collins says.
Discharge lounges “can’t be another nursing unit because a patient is supposed to be discharged. ... Whether you have a discharge lounge or not, you need to improve your systems so that the patients leave when they leave.”
Richard Quinn is a freelance writer based in New Jersey.
ONLINE EXCLUSIVE: Experts discuss strategies to improve early discharges
Tackling Readmissions Together
A new report in the Journal of Hospital Medicine suggests that more than 60% of 30-day readmissions are viewed as potentially preventable by hospitalists.
The study, “Hospitalists Assess the Causes of Early Hospital Readmissions,” found that of 298 cases reviewed, 15% were deemed “preventable” by a team of 17 hospitalist reviewers at Providence Health & Services in Portland, Ore. (DOI: 10.1002/jhm.909). Another 40% were tagged as “possibly preventable,” the authors reported.
When the reviewers analyzed cases to determine what interventions could have prevented readmissions, team-based approaches were the answer much of the time, says lead author and hospitalist Douglas Koekkoek, MD. Those potential answers included earlier follow-up conversations with primary-care physicians (PCPs), palliative care-consults, and more education about home-care management.
“When a physician looks at just his locus of control, they tend to be a little pessimistic,” Dr. Koekkoek says. “When they take a systems approach ... then they gain that optimism.”
The report found that in 23% of the cases, hospitalists found that extending length of stay by a day or two could have prevented a readmission. Dr. Koekkoek says that inherent conflict?balancing the cost of every hospitalized day against keeping patients long enough to prevent readmission?is “the bread and butter of hospitalist care.”
“There is going to be a natural conflict of ‘I can’t keep people in the hospital forever,’” he adds.
Given that the federal government is likely to start reducing reimbursements for unnecessary readmissions, Dr. Koekkoek says HM groups have to view their work as one front in the battle to keep patients from returning. And that has to include outpatient physicians, patient education, and other techniques.
“The take-home is we are part of a care team,” he adds. “And the team extends beyond the hospital’s walls.”
A new report in the Journal of Hospital Medicine suggests that more than 60% of 30-day readmissions are viewed as potentially preventable by hospitalists.
The study, “Hospitalists Assess the Causes of Early Hospital Readmissions,” found that of 298 cases reviewed, 15% were deemed “preventable” by a team of 17 hospitalist reviewers at Providence Health & Services in Portland, Ore. (DOI: 10.1002/jhm.909). Another 40% were tagged as “possibly preventable,” the authors reported.
When the reviewers analyzed cases to determine what interventions could have prevented readmissions, team-based approaches were the answer much of the time, says lead author and hospitalist Douglas Koekkoek, MD. Those potential answers included earlier follow-up conversations with primary-care physicians (PCPs), palliative care-consults, and more education about home-care management.
“When a physician looks at just his locus of control, they tend to be a little pessimistic,” Dr. Koekkoek says. “When they take a systems approach ... then they gain that optimism.”
The report found that in 23% of the cases, hospitalists found that extending length of stay by a day or two could have prevented a readmission. Dr. Koekkoek says that inherent conflict?balancing the cost of every hospitalized day against keeping patients long enough to prevent readmission?is “the bread and butter of hospitalist care.”
“There is going to be a natural conflict of ‘I can’t keep people in the hospital forever,’” he adds.
Given that the federal government is likely to start reducing reimbursements for unnecessary readmissions, Dr. Koekkoek says HM groups have to view their work as one front in the battle to keep patients from returning. And that has to include outpatient physicians, patient education, and other techniques.
“The take-home is we are part of a care team,” he adds. “And the team extends beyond the hospital’s walls.”
A new report in the Journal of Hospital Medicine suggests that more than 60% of 30-day readmissions are viewed as potentially preventable by hospitalists.
The study, “Hospitalists Assess the Causes of Early Hospital Readmissions,” found that of 298 cases reviewed, 15% were deemed “preventable” by a team of 17 hospitalist reviewers at Providence Health & Services in Portland, Ore. (DOI: 10.1002/jhm.909). Another 40% were tagged as “possibly preventable,” the authors reported.
When the reviewers analyzed cases to determine what interventions could have prevented readmissions, team-based approaches were the answer much of the time, says lead author and hospitalist Douglas Koekkoek, MD. Those potential answers included earlier follow-up conversations with primary-care physicians (PCPs), palliative care-consults, and more education about home-care management.
“When a physician looks at just his locus of control, they tend to be a little pessimistic,” Dr. Koekkoek says. “When they take a systems approach ... then they gain that optimism.”
The report found that in 23% of the cases, hospitalists found that extending length of stay by a day or two could have prevented a readmission. Dr. Koekkoek says that inherent conflict?balancing the cost of every hospitalized day against keeping patients long enough to prevent readmission?is “the bread and butter of hospitalist care.”
“There is going to be a natural conflict of ‘I can’t keep people in the hospital forever,’” he adds.
Given that the federal government is likely to start reducing reimbursements for unnecessary readmissions, Dr. Koekkoek says HM groups have to view their work as one front in the battle to keep patients from returning. And that has to include outpatient physicians, patient education, and other techniques.
“The take-home is we are part of a care team,” he adds. “And the team extends beyond the hospital’s walls.”