User login
Richard Quinn is an award-winning journalist with 15 years’ experience. He has worked at the Asbury Park Press in New Jersey and The Virginian-Pilot in Norfolk, Va., and currently is managing editor for a leading commercial real estate publication. His freelance work has appeared in The Jewish State, The Hospitalist, The Rheumatologist, ACEP Now, and ENT Today. He lives in New Jersey with his wife and three cats.
ONLINE EXCLUSIVE: Team Hospitalist Veteran Says Compensation Will Continue Growth Pattern
Click here to listen to Dr. Simone
Click here to listen to Dr. Simone
Click here to listen to Dr. Simone
Study: Burnout Risk High for Hospitalists, Other “Front-Line” Physicians
An author of new research that shows physicians are more likely to be burned out by work than other professions says the findings underscore the need for hospitalists to find a balance between their professional and personal lives.
The Archives of Internal Medicine report, "Burnout and Satisfaction With Work-Life Balance Among US Physicians Relative to the General U.S. Population," found that physicians were more likely than "working U.S. adults" to exhibit at least one symptom of burnout (37.9% vs. 27.8%, P<0.01). Physicians also were more likely to be dissatisfied with their work-life balance (40.2% vs. 23.2%, P<0.01), according to the data.
"It's a balancing act," says Colin West, MD, PhD, FACP, of the Departments of Internal Medicine and Health Sciences Research at Mayo Clinic in Rochester, Minn. "Every physician is a little bit different. Every person is a little bit different. If everyone is able to exert some control … and do what's meaningful to them, that gives them the best shot to balance."
Of specific importance for hospitalists, the research found that "front-line specialties" (including internal medicine, general medicine, and emergency medicine) exhibited the highest risk factor for burnout. Dr. West says more research would be required to determine how at risk hospitalists are, but given their position in the healthcare spectrum, he suspects they are among those at highest risk. He believes that the healthcare system as a whole needs to address the burnout issue, as repercussions can include problematic alcohol use, broken relationships, and suicidal ideation.
"The best group is that which strikes a balance," Dr. West says. "It's probably because [those physicians are not] feeling like they're dropping a ball. If you pick work over home, or home over work, then, basically, one is left behind."
An author of new research that shows physicians are more likely to be burned out by work than other professions says the findings underscore the need for hospitalists to find a balance between their professional and personal lives.
The Archives of Internal Medicine report, "Burnout and Satisfaction With Work-Life Balance Among US Physicians Relative to the General U.S. Population," found that physicians were more likely than "working U.S. adults" to exhibit at least one symptom of burnout (37.9% vs. 27.8%, P<0.01). Physicians also were more likely to be dissatisfied with their work-life balance (40.2% vs. 23.2%, P<0.01), according to the data.
"It's a balancing act," says Colin West, MD, PhD, FACP, of the Departments of Internal Medicine and Health Sciences Research at Mayo Clinic in Rochester, Minn. "Every physician is a little bit different. Every person is a little bit different. If everyone is able to exert some control … and do what's meaningful to them, that gives them the best shot to balance."
Of specific importance for hospitalists, the research found that "front-line specialties" (including internal medicine, general medicine, and emergency medicine) exhibited the highest risk factor for burnout. Dr. West says more research would be required to determine how at risk hospitalists are, but given their position in the healthcare spectrum, he suspects they are among those at highest risk. He believes that the healthcare system as a whole needs to address the burnout issue, as repercussions can include problematic alcohol use, broken relationships, and suicidal ideation.
"The best group is that which strikes a balance," Dr. West says. "It's probably because [those physicians are not] feeling like they're dropping a ball. If you pick work over home, or home over work, then, basically, one is left behind."
An author of new research that shows physicians are more likely to be burned out by work than other professions says the findings underscore the need for hospitalists to find a balance between their professional and personal lives.
The Archives of Internal Medicine report, "Burnout and Satisfaction With Work-Life Balance Among US Physicians Relative to the General U.S. Population," found that physicians were more likely than "working U.S. adults" to exhibit at least one symptom of burnout (37.9% vs. 27.8%, P<0.01). Physicians also were more likely to be dissatisfied with their work-life balance (40.2% vs. 23.2%, P<0.01), according to the data.
"It's a balancing act," says Colin West, MD, PhD, FACP, of the Departments of Internal Medicine and Health Sciences Research at Mayo Clinic in Rochester, Minn. "Every physician is a little bit different. Every person is a little bit different. If everyone is able to exert some control … and do what's meaningful to them, that gives them the best shot to balance."
Of specific importance for hospitalists, the research found that "front-line specialties" (including internal medicine, general medicine, and emergency medicine) exhibited the highest risk factor for burnout. Dr. West says more research would be required to determine how at risk hospitalists are, but given their position in the healthcare spectrum, he suspects they are among those at highest risk. He believes that the healthcare system as a whole needs to address the burnout issue, as repercussions can include problematic alcohol use, broken relationships, and suicidal ideation.
"The best group is that which strikes a balance," Dr. West says. "It's probably because [those physicians are not] feeling like they're dropping a ball. If you pick work over home, or home over work, then, basically, one is left behind."
As Hospitalists Cement their Worth, Compensation Continues Upward Climb
Tom Smith, MD, vice president of clinical quality and hospitalist medical director at North Fulton Regional Medical Center in Alpharetta, Ga., is emotionally torn every time practice-based compensation and productivity data are published— data he will both use and defend against in negotiations with staffers and would-be staffers.
If nocturnist salaries are increasing nationally, will he have to pay his night-shift staff more?
If work relative-value units (wRVUs) are rising in his region, will he need to review how hard he is working his staff—or not hard enough?
If group leaders are receiving compensation premiums, should his top docs be paid above rank-and-file colleagues?
“There are upsides and downsides,” Dr. Smith says. “No. 1, if your compensation is good or appropriate, they sort of validate your pay and, I guess, your self-worth to some degree. But I think if you’re on the lower side, it definitely starts bringing to mind the ‘grass-is-greener scenarios.’”
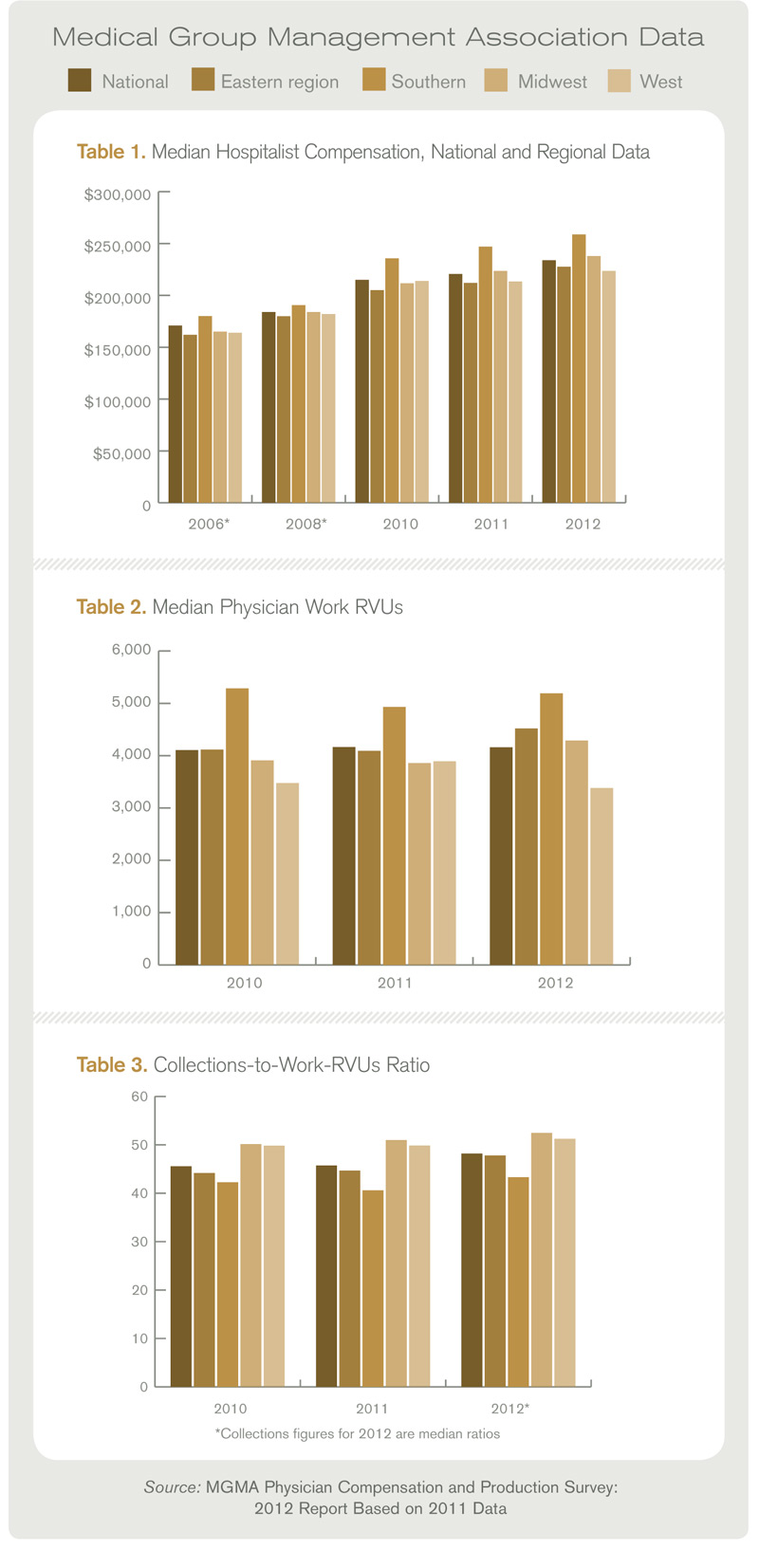
For hospitalists, the grass is green in most cases. Median compensation for adult hospitalists rose 6% to $233,855 in 2011, while productivity remained nearly static, according to the Medical Group Management Association’s (MGMA) Physician Compensation and Production Survey: 2012 Report Based on 2011 Data. The report is based on data compiled from 3,402 hospitalists nationwide; slightly more than 56% of respondents work in practices owned by hospitals/integrated delivery systems (IDS); 26% work in physician-owned groups.
The data, which excludes academic hospitalists, shows hospitalist pay has jumped more than 27% since 2008, when unadjusted figures pegged median hospitalist compensation at $183,900 nationwide. The climb comes despite little movement in the number of wRVUs hospitalists are producing. In 2011, the median physician wRVU rate was 4,159 per year, a 0.17% drop from the year prior.
The MGMA survey data will be incorporated into SHM’s annual State of Hospital Medicine report (SOHM), which features information on individual physicians and HM groups. The SOHM report received submission from 396 groups that serve adults only (for more about the survey instruments, see “Apples to Apples?”). Some 40% were employed by hospitals/IDS; a third were employed by management companies; and the rest were academic or other models. The report includes group-level data valuable to hospitalist groups, including financial data (i.e. hospital support payments and CPT code distribution), and information on staffing and scheduling.
Combined, the MGMA and SHM reports show a specialty where compensation continues to be pushed by demand outstripping supply, particularly in southern states (see Table 1). More subtly, leading hospitalists say, the data shows that much of the work that physicians now do—QI initiatives, committee leadership and leading digitalization efforts—is not completely captured by the wRVU metric, long the gold standard for measuring productivity.
“I really believe this is critical, critical information for people to have,” says William “Tex” Landis, MD, FHM, chairman of SHM’s Practice Analysis Committee. “Administrators need to have information to make sure that they’re being appropriate in the compensation that they’re paying the physicians. So everybody that’s involved in hospitalist programs is interested, or should be interested in this data, because it allows them to right resource their programs.”
Dollars and Sense
First and foremost in the MGMA data is the continued trend of rising compensation. In a seemingly endless uptick, hospitalists in the South continue to earn the most (median compensation $258,793, up from $247,000 in 2011 data). Southern hospitalists, though, only saw a 4.8% increase in compensation. The largest percentage jump (7.4%) was for hospitalists in the East (median compensation $227,656, up from $212,000 the year prior). Doctors in the East typically have the lowest compensation of the country’s four geographic regions, but this year’s data showed hospitalists in the West with the lowest figure (median compensation $223,574, up from $213,405).

Dan Fuller, president of IN Compass Health of Alpharetta, Ga., and a member of SHM’s Practice Analysis Committee, says the rising compensation makes perfect sense.
“In fact, I think it’s something we’re probably going to have to deal with for the near future,” he says, noting some in the specialty believed median compensation was ready to plateau. “And, certainly, as hospitalists are asked to do more and more, and they a play a bigger and bigger role in the facility, there should be a higher expectation that they continue to make more and more, and make a bigger impact.”
The question group leaders are asking now: how high can the compensation figures climb? Todd Evenson, MGMA director of data solutions, says there is no answer, yet. Evenson says he sees no immediate obstacles to the continued growth, as hospitalists have established themselves as major players in most hospitals.
What could determine the upper limit is “the payment mechanisms that we start to see fall out of the legislation that occurs,” he says. “As that evolves, I can’t say I know the ceiling.”
A year or two ago, Dr. Landis would have told anyone who asked that the compensation limit was in sight. Now, he believes that as long as competition makes recruitment and retention difficult, it’s hard to predict an end to the compensation growth.
“I don’t think there is a hospitalist group, whether it’s hospitalist-owned, national company, or a private group part of a large, multi-specialty clinic, there’s not a group in the country that’s not struggling with recruitment and retention,” Dr. Fuller adds.
The Value of wRVUs
One data point that has stymied the expectations of some hospitalists is the relative stability of wRVUs. The national figure has ticked up 1.26% since 2010 to 4,159 per year. But the stability is geographically deceiving. In the East and Midwest regions, hospitalist wRVUs jumped 9.8% and 9.7%, respectively. In the South and West, wRVUs fell 1.8% and 2.7%, respectively.
In whole numbers, the South continues to show the highest productivity per physician. Hospitalists in the south produced 671 more wRVUs than the next-highest regional cohort, (5,192 South vs. 4,521 East). Hospitalists in the South region also produced nearly 35% more wRVUs than their Western counterparts (5,192 vs. 3,383).
Survey experts have no explanation for why regional productivity varies so much. Regardless, the trouble with wRVUs is that they are intended to serve as a proxy of billable productivity, hospitalists say.

As HM groups and physicians become more engaged in moving from a fee-for-service payment model to one that rewards quality and value, the metric becomes less precise, says Ken Simone, DO, SFHM, founder and president of Hospitalist and Practice Solutions in Veazie, Maine, an HM consulting firm.
“Productivity in some ways is difficult to measure with hospitalists because they are also providing services [while they are] working on committees, doing IT work, or doing some research,” says Dr. Simone, a member of Team Hospitalist. “I’m very careful in how I look at a hospitalist’s productivity.”

Although some are hesitant to suggest that wRVUs have leveled, Dr. Smith, who oversees a six-hospitalist group at his 208-bed institution about 25 miles north of Atlanta, believes hospitalists “are about at capacity.”
“Particularly considering the new pressures that are on patient satisfaction, time to go in the ER, length of stay, discharge, reducing readmissions,” he says. “I think it’s going to be hard to push that number up.”

Dr. Landis, medical director of Wellspan Hospitalists in York, Pa., believes it is counter-productive to push wRVUs too high. He believes a hospitalist’s role is to provide patient care, lead process improvement, and coordinate multi-disciplinary teams. Too much of a focus on any one role takes away from physician efficacy.
“The value of a hospitalist goes well beyond the wRVU number,” he explains. “That being said, we are still in the business of seeing patients. I don’t think having a hospitalist that’s generating 1,500 RVUs and paying them at the 75th percentile is going to be very effective. You’re going to need to balance those out.”
continued below...
Apples to Apples?

Any researcher worth his academic salt will say that results are only as good as their N. And so hospitalists eager to glean data points from the MGMA’s Physician Compensation and Production Survey: 2012 Report Based on 2011 Data and SHM’s State of Hospital Medicine report need to remember that the numbers aren’t coming from the same source.
MGMA compiled compensation data on 3,402 full-time hospitalists nationwide. Slightly more than 56% of the respondents worked in hospital-owned practices, while 26% are in physician-owned groups. The rest reported “other” practice models.
SHM received submissions from 396 groups that serve adults only. Some 49% were hospital/IDS employed, 33% management companies, and the rest were academic or other models.
And while the MGMA survey data will be incorporated into SHM’s report, the information was culled from different universes. SHM encouraged its members to participate in the MGMA survey, but did not get involved beyond that. This is a change to the 2011 report, when the two groups jointly gathered data. And it is a change again from previous years, when SHM did its work separately, with little teamwork with MGMA.
While the changing methodologies can make year-to-year comparisons less precise or more difficult to craft, Dr. Landis says surveys need to evolve to ensure they’re asking the best questions and the questions users want answer to. Even then, though, he cautions ever reading too much into survey data.
“We’ve used the best tools to give good statistics, but in the end it’s not a scientific, placebo-controlled, double-blinded trial,” Dr. Landis says. “It’s a survey, and you need to keep in mind that’s what it is.”
—Richard Quinn
How Much Turnover Is Too Much Turnover?
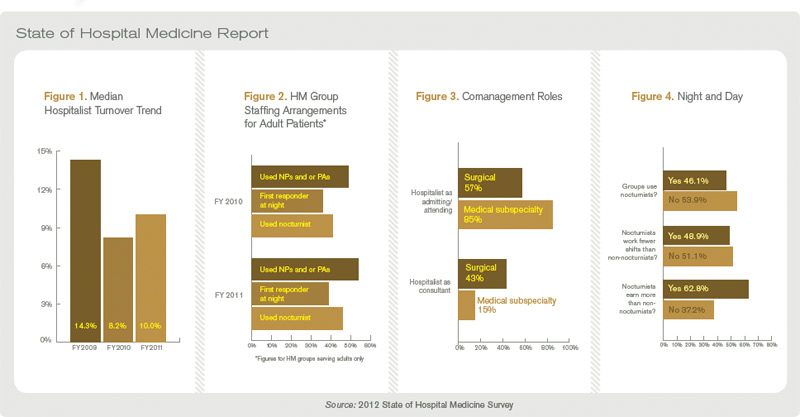
Some HM leaders were pleased last year when hospitalist turnover dropped to 8% from a 14% turnover rate the year prior. This year’s State of Hospital Medicine report pegs the turnover figure at 10%. Although just a slight increase this year, Fuller views the uptick in turnover as a burgeoning cycle. While the supply-demand curve continues to push compensation up, increased turnover will continue to impact both sides of the equation.
“I’m sure there are many fully staffed programs, but they’re dealing with turnover,” he says. “They’re dealing with attrition, physicians leaving to go to fellowships, physicians relocating...physicians wanting to retire. I think it’s a crisis, a tremendous crisis that we need to be prepared to deal with for the near future.”
Aside from turnover data, the SOHM report this year looked to break new ground by trying out new questions. The report for the first time surveyed how hospitalists perform comanagement duties. In surgical comanagement cases, the hospitalist served as the admitting or attending physician 57% of the time. The rest of the time they served as a consultant. In medical comanagement, hospitalists were the admitting/attending physician 85% of the time (see “Comanagement Roles,”).
As hospitalists find specialties even within the field, the report also looked to put data to the cohort of nocturnists. Roughly half of those covering night shifts work fewer shifts than their daytime colleagues. Moreover, 63% of nocturnists earned a differential for that work (see Figure 4).
The value of data points on emerging and existing trends is that it gives HM groups and group administrators thresholds to benchmark themselves against, Dr. Simone says.
“It also allows the HM leader to compare within a practice,” he adds. “If hospital medicine groups are performing at or above median, or are highly functional groups, it gives great feedback that they’re doing things correctly. But it also gives the leader an opportunity to make a sound business plan when he’s going to talk to the hospital [administration] for subsidy, or when he’s going to negotiate compensation for his providers for the next year. I think that’s a powerful tool.”
Interactive regional survey breakdowns
Richard Quinn is a freelance writer based in New Jersey.
How Long Can The Stool of Staffing Success Stand?

William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and chair of SHM’s Practice Analysis Committee, likes to say that hospitalists are a fundamentally necessary service in hospitals. But keeping a full complement of hospitalists is hard work—and money is a big draw.
“We have to make some way for it to be a more desirable position, and my feeling is that there are three legs that stool stands on, and that’s salary, schedule, and scope,” he says. “Those are the three things that you have to play with and if the scope of the service is going to stay the same and the schedule is going to be similar, then the third thing that’s easiest to adjust is the salary.”
Dr. Landis has no answer to when he expects compensation to stop increasing. But Leslie Flores, MHA, SHM senior advisor for practice management and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants, believes it’s dangerous to climb too high in compensation without something else changing dramatically.
“At some point,” she says, “there is a breaking point in terms of what hospitals can afford to spend to support hospitalist programs, and that is going to either cause significant salary pressure, or it’s going to cause significant pressure for hospitalists to increase their productivity and become a lot more efficient in their clinical work, or both.”
—Richard Quinn
Tom Smith, MD, vice president of clinical quality and hospitalist medical director at North Fulton Regional Medical Center in Alpharetta, Ga., is emotionally torn every time practice-based compensation and productivity data are published— data he will both use and defend against in negotiations with staffers and would-be staffers.
If nocturnist salaries are increasing nationally, will he have to pay his night-shift staff more?
If work relative-value units (wRVUs) are rising in his region, will he need to review how hard he is working his staff—or not hard enough?
If group leaders are receiving compensation premiums, should his top docs be paid above rank-and-file colleagues?
“There are upsides and downsides,” Dr. Smith says. “No. 1, if your compensation is good or appropriate, they sort of validate your pay and, I guess, your self-worth to some degree. But I think if you’re on the lower side, it definitely starts bringing to mind the ‘grass-is-greener scenarios.’”
For hospitalists, the grass is green in most cases. Median compensation for adult hospitalists rose 6% to $233,855 in 2011, while productivity remained nearly static, according to the Medical Group Management Association’s (MGMA) Physician Compensation and Production Survey: 2012 Report Based on 2011 Data. The report is based on data compiled from 3,402 hospitalists nationwide; slightly more than 56% of respondents work in practices owned by hospitals/integrated delivery systems (IDS); 26% work in physician-owned groups.
The data, which excludes academic hospitalists, shows hospitalist pay has jumped more than 27% since 2008, when unadjusted figures pegged median hospitalist compensation at $183,900 nationwide. The climb comes despite little movement in the number of wRVUs hospitalists are producing. In 2011, the median physician wRVU rate was 4,159 per year, a 0.17% drop from the year prior.
The MGMA survey data will be incorporated into SHM’s annual State of Hospital Medicine report (SOHM), which features information on individual physicians and HM groups. The SOHM report received submission from 396 groups that serve adults only (for more about the survey instruments, see “Apples to Apples?”). Some 40% were employed by hospitals/IDS; a third were employed by management companies; and the rest were academic or other models. The report includes group-level data valuable to hospitalist groups, including financial data (i.e. hospital support payments and CPT code distribution), and information on staffing and scheduling.
Combined, the MGMA and SHM reports show a specialty where compensation continues to be pushed by demand outstripping supply, particularly in southern states (see Table 1). More subtly, leading hospitalists say, the data shows that much of the work that physicians now do—QI initiatives, committee leadership and leading digitalization efforts—is not completely captured by the wRVU metric, long the gold standard for measuring productivity.
“I really believe this is critical, critical information for people to have,” says William “Tex” Landis, MD, FHM, chairman of SHM’s Practice Analysis Committee. “Administrators need to have information to make sure that they’re being appropriate in the compensation that they’re paying the physicians. So everybody that’s involved in hospitalist programs is interested, or should be interested in this data, because it allows them to right resource their programs.”
Dollars and Sense
First and foremost in the MGMA data is the continued trend of rising compensation. In a seemingly endless uptick, hospitalists in the South continue to earn the most (median compensation $258,793, up from $247,000 in 2011 data). Southern hospitalists, though, only saw a 4.8% increase in compensation. The largest percentage jump (7.4%) was for hospitalists in the East (median compensation $227,656, up from $212,000 the year prior). Doctors in the East typically have the lowest compensation of the country’s four geographic regions, but this year’s data showed hospitalists in the West with the lowest figure (median compensation $223,574, up from $213,405).
Dan Fuller, president of IN Compass Health of Alpharetta, Ga., and a member of SHM’s Practice Analysis Committee, says the rising compensation makes perfect sense.
“In fact, I think it’s something we’re probably going to have to deal with for the near future,” he says, noting some in the specialty believed median compensation was ready to plateau. “And, certainly, as hospitalists are asked to do more and more, and they a play a bigger and bigger role in the facility, there should be a higher expectation that they continue to make more and more, and make a bigger impact.”
The question group leaders are asking now: how high can the compensation figures climb? Todd Evenson, MGMA director of data solutions, says there is no answer, yet. Evenson says he sees no immediate obstacles to the continued growth, as hospitalists have established themselves as major players in most hospitals.
What could determine the upper limit is “the payment mechanisms that we start to see fall out of the legislation that occurs,” he says. “As that evolves, I can’t say I know the ceiling.”
A year or two ago, Dr. Landis would have told anyone who asked that the compensation limit was in sight. Now, he believes that as long as competition makes recruitment and retention difficult, it’s hard to predict an end to the compensation growth.
“I don’t think there is a hospitalist group, whether it’s hospitalist-owned, national company, or a private group part of a large, multi-specialty clinic, there’s not a group in the country that’s not struggling with recruitment and retention,” Dr. Fuller adds.
The Value of wRVUs
One data point that has stymied the expectations of some hospitalists is the relative stability of wRVUs. The national figure has ticked up 1.26% since 2010 to 4,159 per year. But the stability is geographically deceiving. In the East and Midwest regions, hospitalist wRVUs jumped 9.8% and 9.7%, respectively. In the South and West, wRVUs fell 1.8% and 2.7%, respectively.
In whole numbers, the South continues to show the highest productivity per physician. Hospitalists in the south produced 671 more wRVUs than the next-highest regional cohort, (5,192 South vs. 4,521 East). Hospitalists in the South region also produced nearly 35% more wRVUs than their Western counterparts (5,192 vs. 3,383).
Survey experts have no explanation for why regional productivity varies so much. Regardless, the trouble with wRVUs is that they are intended to serve as a proxy of billable productivity, hospitalists say.
As HM groups and physicians become more engaged in moving from a fee-for-service payment model to one that rewards quality and value, the metric becomes less precise, says Ken Simone, DO, SFHM, founder and president of Hospitalist and Practice Solutions in Veazie, Maine, an HM consulting firm.
“Productivity in some ways is difficult to measure with hospitalists because they are also providing services [while they are] working on committees, doing IT work, or doing some research,” says Dr. Simone, a member of Team Hospitalist. “I’m very careful in how I look at a hospitalist’s productivity.”
Although some are hesitant to suggest that wRVUs have leveled, Dr. Smith, who oversees a six-hospitalist group at his 208-bed institution about 25 miles north of Atlanta, believes hospitalists “are about at capacity.”
“Particularly considering the new pressures that are on patient satisfaction, time to go in the ER, length of stay, discharge, reducing readmissions,” he says. “I think it’s going to be hard to push that number up.”
Dr. Landis, medical director of Wellspan Hospitalists in York, Pa., believes it is counter-productive to push wRVUs too high. He believes a hospitalist’s role is to provide patient care, lead process improvement, and coordinate multi-disciplinary teams. Too much of a focus on any one role takes away from physician efficacy.
“The value of a hospitalist goes well beyond the wRVU number,” he explains. “That being said, we are still in the business of seeing patients. I don’t think having a hospitalist that’s generating 1,500 RVUs and paying them at the 75th percentile is going to be very effective. You’re going to need to balance those out.”
continued below...
Apples to Apples?
Any researcher worth his academic salt will say that results are only as good as their N. And so hospitalists eager to glean data points from the MGMA’s Physician Compensation and Production Survey: 2012 Report Based on 2011 Data and SHM’s State of Hospital Medicine report need to remember that the numbers aren’t coming from the same source.
MGMA compiled compensation data on 3,402 full-time hospitalists nationwide. Slightly more than 56% of the respondents worked in hospital-owned practices, while 26% are in physician-owned groups. The rest reported “other” practice models.
SHM received submissions from 396 groups that serve adults only. Some 49% were hospital/IDS employed, 33% management companies, and the rest were academic or other models.
And while the MGMA survey data will be incorporated into SHM’s report, the information was culled from different universes. SHM encouraged its members to participate in the MGMA survey, but did not get involved beyond that. This is a change to the 2011 report, when the two groups jointly gathered data. And it is a change again from previous years, when SHM did its work separately, with little teamwork with MGMA.
While the changing methodologies can make year-to-year comparisons less precise or more difficult to craft, Dr. Landis says surveys need to evolve to ensure they’re asking the best questions and the questions users want answer to. Even then, though, he cautions ever reading too much into survey data.
“We’ve used the best tools to give good statistics, but in the end it’s not a scientific, placebo-controlled, double-blinded trial,” Dr. Landis says. “It’s a survey, and you need to keep in mind that’s what it is.”
—Richard Quinn
How Much Turnover Is Too Much Turnover?
Some HM leaders were pleased last year when hospitalist turnover dropped to 8% from a 14% turnover rate the year prior. This year’s State of Hospital Medicine report pegs the turnover figure at 10%. Although just a slight increase this year, Fuller views the uptick in turnover as a burgeoning cycle. While the supply-demand curve continues to push compensation up, increased turnover will continue to impact both sides of the equation.
“I’m sure there are many fully staffed programs, but they’re dealing with turnover,” he says. “They’re dealing with attrition, physicians leaving to go to fellowships, physicians relocating...physicians wanting to retire. I think it’s a crisis, a tremendous crisis that we need to be prepared to deal with for the near future.”
Aside from turnover data, the SOHM report this year looked to break new ground by trying out new questions. The report for the first time surveyed how hospitalists perform comanagement duties. In surgical comanagement cases, the hospitalist served as the admitting or attending physician 57% of the time. The rest of the time they served as a consultant. In medical comanagement, hospitalists were the admitting/attending physician 85% of the time (see “Comanagement Roles,”).
As hospitalists find specialties even within the field, the report also looked to put data to the cohort of nocturnists. Roughly half of those covering night shifts work fewer shifts than their daytime colleagues. Moreover, 63% of nocturnists earned a differential for that work (see Figure 4).
The value of data points on emerging and existing trends is that it gives HM groups and group administrators thresholds to benchmark themselves against, Dr. Simone says.
“It also allows the HM leader to compare within a practice,” he adds. “If hospital medicine groups are performing at or above median, or are highly functional groups, it gives great feedback that they’re doing things correctly. But it also gives the leader an opportunity to make a sound business plan when he’s going to talk to the hospital [administration] for subsidy, or when he’s going to negotiate compensation for his providers for the next year. I think that’s a powerful tool.”
Interactive regional survey breakdowns
Richard Quinn is a freelance writer based in New Jersey.
How Long Can The Stool of Staffing Success Stand?
William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and chair of SHM’s Practice Analysis Committee, likes to say that hospitalists are a fundamentally necessary service in hospitals. But keeping a full complement of hospitalists is hard work—and money is a big draw.
“We have to make some way for it to be a more desirable position, and my feeling is that there are three legs that stool stands on, and that’s salary, schedule, and scope,” he says. “Those are the three things that you have to play with and if the scope of the service is going to stay the same and the schedule is going to be similar, then the third thing that’s easiest to adjust is the salary.”
Dr. Landis has no answer to when he expects compensation to stop increasing. But Leslie Flores, MHA, SHM senior advisor for practice management and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants, believes it’s dangerous to climb too high in compensation without something else changing dramatically.
“At some point,” she says, “there is a breaking point in terms of what hospitals can afford to spend to support hospitalist programs, and that is going to either cause significant salary pressure, or it’s going to cause significant pressure for hospitalists to increase their productivity and become a lot more efficient in their clinical work, or both.”
—Richard Quinn
Tom Smith, MD, vice president of clinical quality and hospitalist medical director at North Fulton Regional Medical Center in Alpharetta, Ga., is emotionally torn every time practice-based compensation and productivity data are published— data he will both use and defend against in negotiations with staffers and would-be staffers.
If nocturnist salaries are increasing nationally, will he have to pay his night-shift staff more?
If work relative-value units (wRVUs) are rising in his region, will he need to review how hard he is working his staff—or not hard enough?
If group leaders are receiving compensation premiums, should his top docs be paid above rank-and-file colleagues?
“There are upsides and downsides,” Dr. Smith says. “No. 1, if your compensation is good or appropriate, they sort of validate your pay and, I guess, your self-worth to some degree. But I think if you’re on the lower side, it definitely starts bringing to mind the ‘grass-is-greener scenarios.’”
For hospitalists, the grass is green in most cases. Median compensation for adult hospitalists rose 6% to $233,855 in 2011, while productivity remained nearly static, according to the Medical Group Management Association’s (MGMA) Physician Compensation and Production Survey: 2012 Report Based on 2011 Data. The report is based on data compiled from 3,402 hospitalists nationwide; slightly more than 56% of respondents work in practices owned by hospitals/integrated delivery systems (IDS); 26% work in physician-owned groups.
The data, which excludes academic hospitalists, shows hospitalist pay has jumped more than 27% since 2008, when unadjusted figures pegged median hospitalist compensation at $183,900 nationwide. The climb comes despite little movement in the number of wRVUs hospitalists are producing. In 2011, the median physician wRVU rate was 4,159 per year, a 0.17% drop from the year prior.
The MGMA survey data will be incorporated into SHM’s annual State of Hospital Medicine report (SOHM), which features information on individual physicians and HM groups. The SOHM report received submission from 396 groups that serve adults only (for more about the survey instruments, see “Apples to Apples?”). Some 40% were employed by hospitals/IDS; a third were employed by management companies; and the rest were academic or other models. The report includes group-level data valuable to hospitalist groups, including financial data (i.e. hospital support payments and CPT code distribution), and information on staffing and scheduling.
Combined, the MGMA and SHM reports show a specialty where compensation continues to be pushed by demand outstripping supply, particularly in southern states (see Table 1). More subtly, leading hospitalists say, the data shows that much of the work that physicians now do—QI initiatives, committee leadership and leading digitalization efforts—is not completely captured by the wRVU metric, long the gold standard for measuring productivity.
“I really believe this is critical, critical information for people to have,” says William “Tex” Landis, MD, FHM, chairman of SHM’s Practice Analysis Committee. “Administrators need to have information to make sure that they’re being appropriate in the compensation that they’re paying the physicians. So everybody that’s involved in hospitalist programs is interested, or should be interested in this data, because it allows them to right resource their programs.”
Dollars and Sense
First and foremost in the MGMA data is the continued trend of rising compensation. In a seemingly endless uptick, hospitalists in the South continue to earn the most (median compensation $258,793, up from $247,000 in 2011 data). Southern hospitalists, though, only saw a 4.8% increase in compensation. The largest percentage jump (7.4%) was for hospitalists in the East (median compensation $227,656, up from $212,000 the year prior). Doctors in the East typically have the lowest compensation of the country’s four geographic regions, but this year’s data showed hospitalists in the West with the lowest figure (median compensation $223,574, up from $213,405).
Dan Fuller, president of IN Compass Health of Alpharetta, Ga., and a member of SHM’s Practice Analysis Committee, says the rising compensation makes perfect sense.
“In fact, I think it’s something we’re probably going to have to deal with for the near future,” he says, noting some in the specialty believed median compensation was ready to plateau. “And, certainly, as hospitalists are asked to do more and more, and they a play a bigger and bigger role in the facility, there should be a higher expectation that they continue to make more and more, and make a bigger impact.”
The question group leaders are asking now: how high can the compensation figures climb? Todd Evenson, MGMA director of data solutions, says there is no answer, yet. Evenson says he sees no immediate obstacles to the continued growth, as hospitalists have established themselves as major players in most hospitals.
What could determine the upper limit is “the payment mechanisms that we start to see fall out of the legislation that occurs,” he says. “As that evolves, I can’t say I know the ceiling.”
A year or two ago, Dr. Landis would have told anyone who asked that the compensation limit was in sight. Now, he believes that as long as competition makes recruitment and retention difficult, it’s hard to predict an end to the compensation growth.
“I don’t think there is a hospitalist group, whether it’s hospitalist-owned, national company, or a private group part of a large, multi-specialty clinic, there’s not a group in the country that’s not struggling with recruitment and retention,” Dr. Fuller adds.
The Value of wRVUs
One data point that has stymied the expectations of some hospitalists is the relative stability of wRVUs. The national figure has ticked up 1.26% since 2010 to 4,159 per year. But the stability is geographically deceiving. In the East and Midwest regions, hospitalist wRVUs jumped 9.8% and 9.7%, respectively. In the South and West, wRVUs fell 1.8% and 2.7%, respectively.
In whole numbers, the South continues to show the highest productivity per physician. Hospitalists in the south produced 671 more wRVUs than the next-highest regional cohort, (5,192 South vs. 4,521 East). Hospitalists in the South region also produced nearly 35% more wRVUs than their Western counterparts (5,192 vs. 3,383).
Survey experts have no explanation for why regional productivity varies so much. Regardless, the trouble with wRVUs is that they are intended to serve as a proxy of billable productivity, hospitalists say.
As HM groups and physicians become more engaged in moving from a fee-for-service payment model to one that rewards quality and value, the metric becomes less precise, says Ken Simone, DO, SFHM, founder and president of Hospitalist and Practice Solutions in Veazie, Maine, an HM consulting firm.
“Productivity in some ways is difficult to measure with hospitalists because they are also providing services [while they are] working on committees, doing IT work, or doing some research,” says Dr. Simone, a member of Team Hospitalist. “I’m very careful in how I look at a hospitalist’s productivity.”
Although some are hesitant to suggest that wRVUs have leveled, Dr. Smith, who oversees a six-hospitalist group at his 208-bed institution about 25 miles north of Atlanta, believes hospitalists “are about at capacity.”
“Particularly considering the new pressures that are on patient satisfaction, time to go in the ER, length of stay, discharge, reducing readmissions,” he says. “I think it’s going to be hard to push that number up.”
Dr. Landis, medical director of Wellspan Hospitalists in York, Pa., believes it is counter-productive to push wRVUs too high. He believes a hospitalist’s role is to provide patient care, lead process improvement, and coordinate multi-disciplinary teams. Too much of a focus on any one role takes away from physician efficacy.
“The value of a hospitalist goes well beyond the wRVU number,” he explains. “That being said, we are still in the business of seeing patients. I don’t think having a hospitalist that’s generating 1,500 RVUs and paying them at the 75th percentile is going to be very effective. You’re going to need to balance those out.”
continued below...
Apples to Apples?
Any researcher worth his academic salt will say that results are only as good as their N. And so hospitalists eager to glean data points from the MGMA’s Physician Compensation and Production Survey: 2012 Report Based on 2011 Data and SHM’s State of Hospital Medicine report need to remember that the numbers aren’t coming from the same source.
MGMA compiled compensation data on 3,402 full-time hospitalists nationwide. Slightly more than 56% of the respondents worked in hospital-owned practices, while 26% are in physician-owned groups. The rest reported “other” practice models.
SHM received submissions from 396 groups that serve adults only. Some 49% were hospital/IDS employed, 33% management companies, and the rest were academic or other models.
And while the MGMA survey data will be incorporated into SHM’s report, the information was culled from different universes. SHM encouraged its members to participate in the MGMA survey, but did not get involved beyond that. This is a change to the 2011 report, when the two groups jointly gathered data. And it is a change again from previous years, when SHM did its work separately, with little teamwork with MGMA.
While the changing methodologies can make year-to-year comparisons less precise or more difficult to craft, Dr. Landis says surveys need to evolve to ensure they’re asking the best questions and the questions users want answer to. Even then, though, he cautions ever reading too much into survey data.
“We’ve used the best tools to give good statistics, but in the end it’s not a scientific, placebo-controlled, double-blinded trial,” Dr. Landis says. “It’s a survey, and you need to keep in mind that’s what it is.”
—Richard Quinn
How Much Turnover Is Too Much Turnover?
Some HM leaders were pleased last year when hospitalist turnover dropped to 8% from a 14% turnover rate the year prior. This year’s State of Hospital Medicine report pegs the turnover figure at 10%. Although just a slight increase this year, Fuller views the uptick in turnover as a burgeoning cycle. While the supply-demand curve continues to push compensation up, increased turnover will continue to impact both sides of the equation.
“I’m sure there are many fully staffed programs, but they’re dealing with turnover,” he says. “They’re dealing with attrition, physicians leaving to go to fellowships, physicians relocating...physicians wanting to retire. I think it’s a crisis, a tremendous crisis that we need to be prepared to deal with for the near future.”
Aside from turnover data, the SOHM report this year looked to break new ground by trying out new questions. The report for the first time surveyed how hospitalists perform comanagement duties. In surgical comanagement cases, the hospitalist served as the admitting or attending physician 57% of the time. The rest of the time they served as a consultant. In medical comanagement, hospitalists were the admitting/attending physician 85% of the time (see “Comanagement Roles,”).
As hospitalists find specialties even within the field, the report also looked to put data to the cohort of nocturnists. Roughly half of those covering night shifts work fewer shifts than their daytime colleagues. Moreover, 63% of nocturnists earned a differential for that work (see Figure 4).
The value of data points on emerging and existing trends is that it gives HM groups and group administrators thresholds to benchmark themselves against, Dr. Simone says.
“It also allows the HM leader to compare within a practice,” he adds. “If hospital medicine groups are performing at or above median, or are highly functional groups, it gives great feedback that they’re doing things correctly. But it also gives the leader an opportunity to make a sound business plan when he’s going to talk to the hospital [administration] for subsidy, or when he’s going to negotiate compensation for his providers for the next year. I think that’s a powerful tool.”
Interactive regional survey breakdowns
Richard Quinn is a freelance writer based in New Jersey.
How Long Can The Stool of Staffing Success Stand?
William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and chair of SHM’s Practice Analysis Committee, likes to say that hospitalists are a fundamentally necessary service in hospitals. But keeping a full complement of hospitalists is hard work—and money is a big draw.
“We have to make some way for it to be a more desirable position, and my feeling is that there are three legs that stool stands on, and that’s salary, schedule, and scope,” he says. “Those are the three things that you have to play with and if the scope of the service is going to stay the same and the schedule is going to be similar, then the third thing that’s easiest to adjust is the salary.”
Dr. Landis has no answer to when he expects compensation to stop increasing. But Leslie Flores, MHA, SHM senior advisor for practice management and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants, believes it’s dangerous to climb too high in compensation without something else changing dramatically.
“At some point,” she says, “there is a breaking point in terms of what hospitals can afford to spend to support hospitalist programs, and that is going to either cause significant salary pressure, or it’s going to cause significant pressure for hospitalists to increase their productivity and become a lot more efficient in their clinical work, or both.”
—Richard Quinn
Palliative-Care-Focused Hospitalist Appreciates Training the Next Generation

Chithra Perumalswami, MD, knew early on what she wanted to do with her life. As a teenager, she volunteered in an ED and with a hospice group, volunteerism that continued throughout her education. When she graduated from high school, she was tapped for Brown University’s Program in Liberal Medical Education, which calls itself the only baccalaureate-MD program in the Ivy League. And though she eventually turned down the offer, she pursued dual majors in cellular and molecular biology and English at the University of Michigan, where she earned her medical degree in 2004 and completed her residency.
In 2009, she participated in the Palliative Care Education and Practice Program at Harvard Medical School in Boston, a two-week post-graduate course aimed at professional development for physicians dedicated to careers in palliative-care education. “I really found that there were just so many aspects to caring for a patient as a palliative-care specialist and as a hospitalist that really strike at the heart of what being a doctor is,” says Dr. Perumalswami, assistant professor of medicine in the Division of Hospital Medicine at Northwestern Memorial Hospital in Chicago and one of four new members of Team Hospitalist. “I think it’s been an interest I’ve always had. During my residency training, I definitely experienced quite a few patient cases where I felt that we really needed to help patients and their families, and I didn’t necessarily have the best skill set to do that until I had more experience and more training.”
Dr. Perumalswami now wants to get better at her craft.
“As an academic hospitalist, it’s not just about doing research and writing papers and seeing papers,” she says, “but it’s also developing those leadership skills and helping that become an integral part of the educational experience.”
Question: What drew you to a career in HM?
Answer: I chose a career in academic hospital medicine primarily because I enjoy taking care of acutely ill, hospitalized, adult patients. I also really enjoy teaching medical students, residents, and fellows, and I enjoy doing that in the hospital setting. I think that there’s great satisfaction from taking care of a patient from admission to discharge.… I enjoyed every aspect of internal medicine, and when I graduated, I thought I could choose a subspecialty, but I felt that my skills and my expertise was really in taking care of the hospitalized patient.
Q: You have sought out extra training in palliative care and pain management. How has that impacted your career?
A: It’s not something that I necessarily started out thinking that I would specialize in, but the more I took care of hospitalized patients, the more I realized that we actually take care of a fair number of patients who have really complex symptom needs, and also really have a lot of needs with regard to recognizing when their prognosis is poor and understanding what their options are, if they’re even amenable to a palliative approach. I really felt that that was a skill that I needed to fine-tune. So I ended up gaining enough clinical experience and participating with hospice patients to the point where that’s really supplemented my hospitalist career, because what I found is that it’s made me a better hospitalist, and being a hospitalist has made me a better palliative-care doc.
Q: Working in academia, there’s no way to escape talk of the duty-hour rules recently put in place. What’s your view on the issue?
A: My view is that the work hours are here to stay. I think that there are some definite benefits that we’ve gained from having work hours. I’d say first and foremost of those gains is public trust. I think most physicians will tell you that they don’t want a physician who’s in the 36th hour of their day taking care of them when we know that studies actually can demonstrate that when you’ve been awake that long, that your cognitive abilities decline.
Q: But?
A: I think we have a lot of challenges, though, because a lot of things require creative solutions. And I think the first on that list is education, because that’s the first thing that I think has the potential to drop to the bottom of the list.
Q: In terms of HM’s growth, as you see residents coming through your program, how popular do you think the model is going to be with them moving forward?
A: I do, actually, because as an academic hospitalist, I’ve had several medical students and residents tell me, “Watching you, I think that I want to go into this field.” Or they’ll say, “What do you think about doing this for a year or two?” Or, “What do you think about subspecializing, and then being a hospitalist?” And my answer to all of them is it’s a dynamic specialty, and if you’re up for creating change and being a leader, it’s a good field, because we need people in a lot of different buckets, so to speak. We need people who have done other things in their career to contribute to our field.
Q: How do you prepare trainees for all the challenges coming down the pike?
A: A lot of the people who are doing work in medical education are starting to look to other fields to see if there are other models that we can adapt, or that we can somehow absorb into our practice. I think that there are some parts of our education which are not really formalized early on, but I think we have a lot to learn from organizational behavior circles, and systems that actually look at teams and leadership.
Q: What do the next five to 10 years hold for you?
A: All physician leaders have to stay somewhat in the clinical world. I think if you lose sight of that, you can’t be a very effective leader, or a very effective agent for change. Because part of my work is with palliative care, and I really feel that it’s affected my work as a hospitalist in a positive way, I don’t think I ever see myself leaving the clinical world completely. But I do see myself becoming, ideally, more involved with leadership and more involved with helping to train the next set of leaders.
Q: What do you see as SHM’s role specific to academic HM?
A: HM is changing the way healthcare is delivered in the U.S., and I think having an organization to represent us is vital to our success in other arenas of change—including healthcare policy and innovative care models. I see SHM as a large umbrella group, of which academic HM is one part. Academic hospitalists are increasingly involved in the education of future generations of physicians, and are uniquely poised for facilitating cascading leadership. The traditional, hierarchical model of attending-fellow-resident-medical student is shifting, and academic hospitalists are well-suited to study and explore this leadership structure and how it affects patient care, feedback, and mentoring.
Richard Quinn is a freelance writer based in New Jersey.
Chithra Perumalswami, MD, knew early on what she wanted to do with her life. As a teenager, she volunteered in an ED and with a hospice group, volunteerism that continued throughout her education. When she graduated from high school, she was tapped for Brown University’s Program in Liberal Medical Education, which calls itself the only baccalaureate-MD program in the Ivy League. And though she eventually turned down the offer, she pursued dual majors in cellular and molecular biology and English at the University of Michigan, where she earned her medical degree in 2004 and completed her residency.
In 2009, she participated in the Palliative Care Education and Practice Program at Harvard Medical School in Boston, a two-week post-graduate course aimed at professional development for physicians dedicated to careers in palliative-care education. “I really found that there were just so many aspects to caring for a patient as a palliative-care specialist and as a hospitalist that really strike at the heart of what being a doctor is,” says Dr. Perumalswami, assistant professor of medicine in the Division of Hospital Medicine at Northwestern Memorial Hospital in Chicago and one of four new members of Team Hospitalist. “I think it’s been an interest I’ve always had. During my residency training, I definitely experienced quite a few patient cases where I felt that we really needed to help patients and their families, and I didn’t necessarily have the best skill set to do that until I had more experience and more training.”
Dr. Perumalswami now wants to get better at her craft.
“As an academic hospitalist, it’s not just about doing research and writing papers and seeing papers,” she says, “but it’s also developing those leadership skills and helping that become an integral part of the educational experience.”
Question: What drew you to a career in HM?
Answer: I chose a career in academic hospital medicine primarily because I enjoy taking care of acutely ill, hospitalized, adult patients. I also really enjoy teaching medical students, residents, and fellows, and I enjoy doing that in the hospital setting. I think that there’s great satisfaction from taking care of a patient from admission to discharge.… I enjoyed every aspect of internal medicine, and when I graduated, I thought I could choose a subspecialty, but I felt that my skills and my expertise was really in taking care of the hospitalized patient.
Q: You have sought out extra training in palliative care and pain management. How has that impacted your career?
A: It’s not something that I necessarily started out thinking that I would specialize in, but the more I took care of hospitalized patients, the more I realized that we actually take care of a fair number of patients who have really complex symptom needs, and also really have a lot of needs with regard to recognizing when their prognosis is poor and understanding what their options are, if they’re even amenable to a palliative approach. I really felt that that was a skill that I needed to fine-tune. So I ended up gaining enough clinical experience and participating with hospice patients to the point where that’s really supplemented my hospitalist career, because what I found is that it’s made me a better hospitalist, and being a hospitalist has made me a better palliative-care doc.
Q: Working in academia, there’s no way to escape talk of the duty-hour rules recently put in place. What’s your view on the issue?
A: My view is that the work hours are here to stay. I think that there are some definite benefits that we’ve gained from having work hours. I’d say first and foremost of those gains is public trust. I think most physicians will tell you that they don’t want a physician who’s in the 36th hour of their day taking care of them when we know that studies actually can demonstrate that when you’ve been awake that long, that your cognitive abilities decline.
Q: But?
A: I think we have a lot of challenges, though, because a lot of things require creative solutions. And I think the first on that list is education, because that’s the first thing that I think has the potential to drop to the bottom of the list.
Q: In terms of HM’s growth, as you see residents coming through your program, how popular do you think the model is going to be with them moving forward?
A: I do, actually, because as an academic hospitalist, I’ve had several medical students and residents tell me, “Watching you, I think that I want to go into this field.” Or they’ll say, “What do you think about doing this for a year or two?” Or, “What do you think about subspecializing, and then being a hospitalist?” And my answer to all of them is it’s a dynamic specialty, and if you’re up for creating change and being a leader, it’s a good field, because we need people in a lot of different buckets, so to speak. We need people who have done other things in their career to contribute to our field.
Q: How do you prepare trainees for all the challenges coming down the pike?
A: A lot of the people who are doing work in medical education are starting to look to other fields to see if there are other models that we can adapt, or that we can somehow absorb into our practice. I think that there are some parts of our education which are not really formalized early on, but I think we have a lot to learn from organizational behavior circles, and systems that actually look at teams and leadership.
Q: What do the next five to 10 years hold for you?
A: All physician leaders have to stay somewhat in the clinical world. I think if you lose sight of that, you can’t be a very effective leader, or a very effective agent for change. Because part of my work is with palliative care, and I really feel that it’s affected my work as a hospitalist in a positive way, I don’t think I ever see myself leaving the clinical world completely. But I do see myself becoming, ideally, more involved with leadership and more involved with helping to train the next set of leaders.
Q: What do you see as SHM’s role specific to academic HM?
A: HM is changing the way healthcare is delivered in the U.S., and I think having an organization to represent us is vital to our success in other arenas of change—including healthcare policy and innovative care models. I see SHM as a large umbrella group, of which academic HM is one part. Academic hospitalists are increasingly involved in the education of future generations of physicians, and are uniquely poised for facilitating cascading leadership. The traditional, hierarchical model of attending-fellow-resident-medical student is shifting, and academic hospitalists are well-suited to study and explore this leadership structure and how it affects patient care, feedback, and mentoring.
Richard Quinn is a freelance writer based in New Jersey.
Chithra Perumalswami, MD, knew early on what she wanted to do with her life. As a teenager, she volunteered in an ED and with a hospice group, volunteerism that continued throughout her education. When she graduated from high school, she was tapped for Brown University’s Program in Liberal Medical Education, which calls itself the only baccalaureate-MD program in the Ivy League. And though she eventually turned down the offer, she pursued dual majors in cellular and molecular biology and English at the University of Michigan, where she earned her medical degree in 2004 and completed her residency.
In 2009, she participated in the Palliative Care Education and Practice Program at Harvard Medical School in Boston, a two-week post-graduate course aimed at professional development for physicians dedicated to careers in palliative-care education. “I really found that there were just so many aspects to caring for a patient as a palliative-care specialist and as a hospitalist that really strike at the heart of what being a doctor is,” says Dr. Perumalswami, assistant professor of medicine in the Division of Hospital Medicine at Northwestern Memorial Hospital in Chicago and one of four new members of Team Hospitalist. “I think it’s been an interest I’ve always had. During my residency training, I definitely experienced quite a few patient cases where I felt that we really needed to help patients and their families, and I didn’t necessarily have the best skill set to do that until I had more experience and more training.”
Dr. Perumalswami now wants to get better at her craft.
“As an academic hospitalist, it’s not just about doing research and writing papers and seeing papers,” she says, “but it’s also developing those leadership skills and helping that become an integral part of the educational experience.”
Question: What drew you to a career in HM?
Answer: I chose a career in academic hospital medicine primarily because I enjoy taking care of acutely ill, hospitalized, adult patients. I also really enjoy teaching medical students, residents, and fellows, and I enjoy doing that in the hospital setting. I think that there’s great satisfaction from taking care of a patient from admission to discharge.… I enjoyed every aspect of internal medicine, and when I graduated, I thought I could choose a subspecialty, but I felt that my skills and my expertise was really in taking care of the hospitalized patient.
Q: You have sought out extra training in palliative care and pain management. How has that impacted your career?
A: It’s not something that I necessarily started out thinking that I would specialize in, but the more I took care of hospitalized patients, the more I realized that we actually take care of a fair number of patients who have really complex symptom needs, and also really have a lot of needs with regard to recognizing when their prognosis is poor and understanding what their options are, if they’re even amenable to a palliative approach. I really felt that that was a skill that I needed to fine-tune. So I ended up gaining enough clinical experience and participating with hospice patients to the point where that’s really supplemented my hospitalist career, because what I found is that it’s made me a better hospitalist, and being a hospitalist has made me a better palliative-care doc.
Q: Working in academia, there’s no way to escape talk of the duty-hour rules recently put in place. What’s your view on the issue?
A: My view is that the work hours are here to stay. I think that there are some definite benefits that we’ve gained from having work hours. I’d say first and foremost of those gains is public trust. I think most physicians will tell you that they don’t want a physician who’s in the 36th hour of their day taking care of them when we know that studies actually can demonstrate that when you’ve been awake that long, that your cognitive abilities decline.
Q: But?
A: I think we have a lot of challenges, though, because a lot of things require creative solutions. And I think the first on that list is education, because that’s the first thing that I think has the potential to drop to the bottom of the list.
Q: In terms of HM’s growth, as you see residents coming through your program, how popular do you think the model is going to be with them moving forward?
A: I do, actually, because as an academic hospitalist, I’ve had several medical students and residents tell me, “Watching you, I think that I want to go into this field.” Or they’ll say, “What do you think about doing this for a year or two?” Or, “What do you think about subspecializing, and then being a hospitalist?” And my answer to all of them is it’s a dynamic specialty, and if you’re up for creating change and being a leader, it’s a good field, because we need people in a lot of different buckets, so to speak. We need people who have done other things in their career to contribute to our field.
Q: How do you prepare trainees for all the challenges coming down the pike?
A: A lot of the people who are doing work in medical education are starting to look to other fields to see if there are other models that we can adapt, or that we can somehow absorb into our practice. I think that there are some parts of our education which are not really formalized early on, but I think we have a lot to learn from organizational behavior circles, and systems that actually look at teams and leadership.
Q: What do the next five to 10 years hold for you?
A: All physician leaders have to stay somewhat in the clinical world. I think if you lose sight of that, you can’t be a very effective leader, or a very effective agent for change. Because part of my work is with palliative care, and I really feel that it’s affected my work as a hospitalist in a positive way, I don’t think I ever see myself leaving the clinical world completely. But I do see myself becoming, ideally, more involved with leadership and more involved with helping to train the next set of leaders.
Q: What do you see as SHM’s role specific to academic HM?
A: HM is changing the way healthcare is delivered in the U.S., and I think having an organization to represent us is vital to our success in other arenas of change—including healthcare policy and innovative care models. I see SHM as a large umbrella group, of which academic HM is one part. Academic hospitalists are increasingly involved in the education of future generations of physicians, and are uniquely poised for facilitating cascading leadership. The traditional, hierarchical model of attending-fellow-resident-medical student is shifting, and academic hospitalists are well-suited to study and explore this leadership structure and how it affects patient care, feedback, and mentoring.
Richard Quinn is a freelance writer based in New Jersey.
Still No Implementation Date Set for ICD-10
A new implementation date for the 10th revision of the International Statistical Classification of Diseases coding system (ICD-10) isn't expected to be known until after the November election, says a coding specialist. But hospitalists and others should not take that as a sign to just sit around and wait for a date.
"We're probably not going to hear anything until after the election is finished," says Brenda Edwards, CPC, CPMA, a coding and compliance specialist with Kansas Medical Mutual Insurance Co. and a trainer with AAPC. "The thing that's worrisome, though, is people think this delay we have encountered is a time to sit back and do nothing, but really we’re almost burning money by not doing anything."
An outcry from many physicians led the U.S. Department of Health and Human Services to delay the planned October 2013 implementation date. No new date has been announced.
Edwards urges physicians, billing specialists, and group leaders to use the delay as an opportunity to better prepare for the implementation. She suggests checking with vendors and preparing training programs to help adjust to the new coding initiative, which will quadruple the number of billing codes to 68,000.
"Everyone at this point should still be moving forward," she says.
At the same time, the Centers for Medicare & Medicaid Services (CMS) is seeking public comment on a new version of its ICD-10 readiness assessment. Those interested in weighing in can learn more here.
A new implementation date for the 10th revision of the International Statistical Classification of Diseases coding system (ICD-10) isn't expected to be known until after the November election, says a coding specialist. But hospitalists and others should not take that as a sign to just sit around and wait for a date.
"We're probably not going to hear anything until after the election is finished," says Brenda Edwards, CPC, CPMA, a coding and compliance specialist with Kansas Medical Mutual Insurance Co. and a trainer with AAPC. "The thing that's worrisome, though, is people think this delay we have encountered is a time to sit back and do nothing, but really we’re almost burning money by not doing anything."
An outcry from many physicians led the U.S. Department of Health and Human Services to delay the planned October 2013 implementation date. No new date has been announced.
Edwards urges physicians, billing specialists, and group leaders to use the delay as an opportunity to better prepare for the implementation. She suggests checking with vendors and preparing training programs to help adjust to the new coding initiative, which will quadruple the number of billing codes to 68,000.
"Everyone at this point should still be moving forward," she says.
At the same time, the Centers for Medicare & Medicaid Services (CMS) is seeking public comment on a new version of its ICD-10 readiness assessment. Those interested in weighing in can learn more here.
A new implementation date for the 10th revision of the International Statistical Classification of Diseases coding system (ICD-10) isn't expected to be known until after the November election, says a coding specialist. But hospitalists and others should not take that as a sign to just sit around and wait for a date.
"We're probably not going to hear anything until after the election is finished," says Brenda Edwards, CPC, CPMA, a coding and compliance specialist with Kansas Medical Mutual Insurance Co. and a trainer with AAPC. "The thing that's worrisome, though, is people think this delay we have encountered is a time to sit back and do nothing, but really we’re almost burning money by not doing anything."
An outcry from many physicians led the U.S. Department of Health and Human Services to delay the planned October 2013 implementation date. No new date has been announced.
Edwards urges physicians, billing specialists, and group leaders to use the delay as an opportunity to better prepare for the implementation. She suggests checking with vendors and preparing training programs to help adjust to the new coding initiative, which will quadruple the number of billing codes to 68,000.
"Everyone at this point should still be moving forward," she says.
At the same time, the Centers for Medicare & Medicaid Services (CMS) is seeking public comment on a new version of its ICD-10 readiness assessment. Those interested in weighing in can learn more here.
Discordant Antibiotic Use in Pediatric UTIs Associated with Higher LOS
Discordant antibiotic therapy for urinary tract infections (UTIs) is common and associated with higher length of stay (LOS) in hospitalized children, according to a study published online last month in the Journal of Hospital Medicine. But lead author Karen Jerardi, MD, division of hospital medicine at Cincinnati Children's Hospital Medical Center says the reason might be related to physicians, not their patients.
"First, use our knowledge of local resistance patterns and patient factors to select an antibiotic likely to be concordant," she says. "The second thing is [that] we probably need to analyze our practice a little bit more and try to figure out if we are just keeping patients in the hospital because we want to see them be on the concordant antibiotic for X number of hours before we send them home. Does that benefit the patient more, or are we keeping them in the hospital longer for our own peace of mind?"
The report, "Discordant Antibiotic Therapy and Length of Stay in Children Hospitalized for Urinary Tract Infection," found that discordant therapy occurred in 10% of cases in which patients had laboratory-confirmed UTIs and, in adjusted analyses, was associated with a 1.8-day increase in LOS.
Dr. Jerardi says that future studies are needed to determine whether pediatric hospitalists are extending LOS by keeping patients longer than absolutely necessary. She cautions, though, that how long a child is kept in the hospital should be determined by case-specific circumstances.
"Hopefully, this will make people analyze how they do things," she adds, "and think to themselves, 'Would I keep that patient an extra day longer because I had to switch their antibiotic—even if their fever went away, they were drinking great, and Mom and Dad were ready to go home—just for my peace of mind?'"
Discordant antibiotic therapy for urinary tract infections (UTIs) is common and associated with higher length of stay (LOS) in hospitalized children, according to a study published online last month in the Journal of Hospital Medicine. But lead author Karen Jerardi, MD, division of hospital medicine at Cincinnati Children's Hospital Medical Center says the reason might be related to physicians, not their patients.
"First, use our knowledge of local resistance patterns and patient factors to select an antibiotic likely to be concordant," she says. "The second thing is [that] we probably need to analyze our practice a little bit more and try to figure out if we are just keeping patients in the hospital because we want to see them be on the concordant antibiotic for X number of hours before we send them home. Does that benefit the patient more, or are we keeping them in the hospital longer for our own peace of mind?"
The report, "Discordant Antibiotic Therapy and Length of Stay in Children Hospitalized for Urinary Tract Infection," found that discordant therapy occurred in 10% of cases in which patients had laboratory-confirmed UTIs and, in adjusted analyses, was associated with a 1.8-day increase in LOS.
Dr. Jerardi says that future studies are needed to determine whether pediatric hospitalists are extending LOS by keeping patients longer than absolutely necessary. She cautions, though, that how long a child is kept in the hospital should be determined by case-specific circumstances.
"Hopefully, this will make people analyze how they do things," she adds, "and think to themselves, 'Would I keep that patient an extra day longer because I had to switch their antibiotic—even if their fever went away, they were drinking great, and Mom and Dad were ready to go home—just for my peace of mind?'"
Discordant antibiotic therapy for urinary tract infections (UTIs) is common and associated with higher length of stay (LOS) in hospitalized children, according to a study published online last month in the Journal of Hospital Medicine. But lead author Karen Jerardi, MD, division of hospital medicine at Cincinnati Children's Hospital Medical Center says the reason might be related to physicians, not their patients.
"First, use our knowledge of local resistance patterns and patient factors to select an antibiotic likely to be concordant," she says. "The second thing is [that] we probably need to analyze our practice a little bit more and try to figure out if we are just keeping patients in the hospital because we want to see them be on the concordant antibiotic for X number of hours before we send them home. Does that benefit the patient more, or are we keeping them in the hospital longer for our own peace of mind?"
The report, "Discordant Antibiotic Therapy and Length of Stay in Children Hospitalized for Urinary Tract Infection," found that discordant therapy occurred in 10% of cases in which patients had laboratory-confirmed UTIs and, in adjusted analyses, was associated with a 1.8-day increase in LOS.
Dr. Jerardi says that future studies are needed to determine whether pediatric hospitalists are extending LOS by keeping patients longer than absolutely necessary. She cautions, though, that how long a child is kept in the hospital should be determined by case-specific circumstances.
"Hopefully, this will make people analyze how they do things," she adds, "and think to themselves, 'Would I keep that patient an extra day longer because I had to switch their antibiotic—even if their fever went away, they were drinking great, and Mom and Dad were ready to go home—just for my peace of mind?'"
Study: Collaborative Approach to Med Rec Effective, Cost-Efficient
A paper published in the May/June issue of the Journal of Hospital Medicine shows that a collaborative approach to medication reconciliation ("med rec") appears to both prevent adverse drug events and pay for itself.
The paper, "Nurse-Pharmacist Collaboration on Medication Reconciliation Prevents Potential Harm," found that 225 of 500 surveyed patients had at least one unintended discrepancy in their house medication list (HML) on admission or discharge. And 162 of those patients had a discrepancy ranked on the upper end of the study's risk scale.
However, having nurses and pharmacists work together "allowed many discrepancies to be reconciled before causing harm," the study concluded.
"It absolutely supports the idea that we need to approach medicine as a team game," says hospitalist and lead author Lenny Feldman, MD, FACP, FAAP, SFHM, of John Hopkins School of Medicine in Baltimore. "We can't do this alone, and patients don't do better when we do this alone."
The study noted that it cost $113.64 to find one potentially harmful medication discrepancy. To offset those costs, an institution would have to prevent one discrepancy for every 290 patient encounters. The Johns Hopkins team averted 81 such events, but Dr. Feldman notes that without a control group, it’s difficult to say how many of those potential issues would have been caught at some other point in a patient's stay.
Still, he says, part of the value of a multidisciplinary approach to med rec is that it can help hospitalists improve patient care. By having nurses, physicians, and pharmacists working together, more potential adverse drug events could be prevented, Dr. Feldman says.
"That data-gathering is difficult and time-consuming, and it is not something hospitalists need do on their own," he adds.
A paper published in the May/June issue of the Journal of Hospital Medicine shows that a collaborative approach to medication reconciliation ("med rec") appears to both prevent adverse drug events and pay for itself.
The paper, "Nurse-Pharmacist Collaboration on Medication Reconciliation Prevents Potential Harm," found that 225 of 500 surveyed patients had at least one unintended discrepancy in their house medication list (HML) on admission or discharge. And 162 of those patients had a discrepancy ranked on the upper end of the study's risk scale.
However, having nurses and pharmacists work together "allowed many discrepancies to be reconciled before causing harm," the study concluded.
"It absolutely supports the idea that we need to approach medicine as a team game," says hospitalist and lead author Lenny Feldman, MD, FACP, FAAP, SFHM, of John Hopkins School of Medicine in Baltimore. "We can't do this alone, and patients don't do better when we do this alone."
The study noted that it cost $113.64 to find one potentially harmful medication discrepancy. To offset those costs, an institution would have to prevent one discrepancy for every 290 patient encounters. The Johns Hopkins team averted 81 such events, but Dr. Feldman notes that without a control group, it’s difficult to say how many of those potential issues would have been caught at some other point in a patient's stay.
Still, he says, part of the value of a multidisciplinary approach to med rec is that it can help hospitalists improve patient care. By having nurses, physicians, and pharmacists working together, more potential adverse drug events could be prevented, Dr. Feldman says.
"That data-gathering is difficult and time-consuming, and it is not something hospitalists need do on their own," he adds.
A paper published in the May/June issue of the Journal of Hospital Medicine shows that a collaborative approach to medication reconciliation ("med rec") appears to both prevent adverse drug events and pay for itself.
The paper, "Nurse-Pharmacist Collaboration on Medication Reconciliation Prevents Potential Harm," found that 225 of 500 surveyed patients had at least one unintended discrepancy in their house medication list (HML) on admission or discharge. And 162 of those patients had a discrepancy ranked on the upper end of the study's risk scale.
However, having nurses and pharmacists work together "allowed many discrepancies to be reconciled before causing harm," the study concluded.
"It absolutely supports the idea that we need to approach medicine as a team game," says hospitalist and lead author Lenny Feldman, MD, FACP, FAAP, SFHM, of John Hopkins School of Medicine in Baltimore. "We can't do this alone, and patients don't do better when we do this alone."
The study noted that it cost $113.64 to find one potentially harmful medication discrepancy. To offset those costs, an institution would have to prevent one discrepancy for every 290 patient encounters. The Johns Hopkins team averted 81 such events, but Dr. Feldman notes that without a control group, it’s difficult to say how many of those potential issues would have been caught at some other point in a patient's stay.
Still, he says, part of the value of a multidisciplinary approach to med rec is that it can help hospitalists improve patient care. By having nurses, physicians, and pharmacists working together, more potential adverse drug events could be prevented, Dr. Feldman says.
"That data-gathering is difficult and time-consuming, and it is not something hospitalists need do on their own," he adds.
Report: Pharmacist-Led Interventions Don’t Reduce Medication Errors Post-Discharge
At first blush, some hospitalists might see it as bad news that a recent report found a pharmacist-assisted medication reconciliation ("med rec") intervention did not significantly reduce clinically important medication errors after discharge. But a deeper reading of the study tells a different story, says a hospitalist who worked on the report.
"This is the latest in our growing understanding of the roles of certain interventions on transitions of care," says Jeffrey Schnipper, MD, MPH, FHM, director of clinical research and an associate physician in the general medicine division at Brigham and Women's Hospitalist Service in Boston, and co-author of the study "Effect of a Pharmacist Intervention on Clinically Important Medication Errors after Hospital Discharge." "What I don't want to have happen is for people to read this article ... and say, 'Oh, pharmacists don't make a difference.' They absolutely make a difference. This is a more nuanced issue of who do they have the biggest impact with, and 'On top of what other interventions are you doing this?'"
The researchers set out to determine whether a pharmacist-delivered intervention on patients with low health literacy (including a post-discharge telephone call) would lower adverse drug events and other clinically important medication errors. They concluded that it did not (unadjusted incidence rate ratio, 0.92 [95% CI, 0.77 to 1.10]).
Dr. Schnipper says the impact was likely muted because the patients studied had higher health-literacy levels than researchers expected. Also, because most follow-up phone calls occurred within a few days of discharge, the intervention failed to capture any events that happened in the 30 days after discharge.
He also notes that the institutions that participated in the study have already implemented multiple med-rec interventions over the past few years. Hospitals that have not focused intently on the issue could find much larger gains from implementing pharmacist-led programs.
"If you're a hospital that has not been fixated on improving medication safety and transitions of care, I think pharmacists are huge," Dr. Schnipper says. "The key, then, is to focus them on the highest-risk patients."
At first blush, some hospitalists might see it as bad news that a recent report found a pharmacist-assisted medication reconciliation ("med rec") intervention did not significantly reduce clinically important medication errors after discharge. But a deeper reading of the study tells a different story, says a hospitalist who worked on the report.
"This is the latest in our growing understanding of the roles of certain interventions on transitions of care," says Jeffrey Schnipper, MD, MPH, FHM, director of clinical research and an associate physician in the general medicine division at Brigham and Women's Hospitalist Service in Boston, and co-author of the study "Effect of a Pharmacist Intervention on Clinically Important Medication Errors after Hospital Discharge." "What I don't want to have happen is for people to read this article ... and say, 'Oh, pharmacists don't make a difference.' They absolutely make a difference. This is a more nuanced issue of who do they have the biggest impact with, and 'On top of what other interventions are you doing this?'"
The researchers set out to determine whether a pharmacist-delivered intervention on patients with low health literacy (including a post-discharge telephone call) would lower adverse drug events and other clinically important medication errors. They concluded that it did not (unadjusted incidence rate ratio, 0.92 [95% CI, 0.77 to 1.10]).
Dr. Schnipper says the impact was likely muted because the patients studied had higher health-literacy levels than researchers expected. Also, because most follow-up phone calls occurred within a few days of discharge, the intervention failed to capture any events that happened in the 30 days after discharge.
He also notes that the institutions that participated in the study have already implemented multiple med-rec interventions over the past few years. Hospitals that have not focused intently on the issue could find much larger gains from implementing pharmacist-led programs.
"If you're a hospital that has not been fixated on improving medication safety and transitions of care, I think pharmacists are huge," Dr. Schnipper says. "The key, then, is to focus them on the highest-risk patients."
At first blush, some hospitalists might see it as bad news that a recent report found a pharmacist-assisted medication reconciliation ("med rec") intervention did not significantly reduce clinically important medication errors after discharge. But a deeper reading of the study tells a different story, says a hospitalist who worked on the report.
"This is the latest in our growing understanding of the roles of certain interventions on transitions of care," says Jeffrey Schnipper, MD, MPH, FHM, director of clinical research and an associate physician in the general medicine division at Brigham and Women's Hospitalist Service in Boston, and co-author of the study "Effect of a Pharmacist Intervention on Clinically Important Medication Errors after Hospital Discharge." "What I don't want to have happen is for people to read this article ... and say, 'Oh, pharmacists don't make a difference.' They absolutely make a difference. This is a more nuanced issue of who do they have the biggest impact with, and 'On top of what other interventions are you doing this?'"
The researchers set out to determine whether a pharmacist-delivered intervention on patients with low health literacy (including a post-discharge telephone call) would lower adverse drug events and other clinically important medication errors. They concluded that it did not (unadjusted incidence rate ratio, 0.92 [95% CI, 0.77 to 1.10]).
Dr. Schnipper says the impact was likely muted because the patients studied had higher health-literacy levels than researchers expected. Also, because most follow-up phone calls occurred within a few days of discharge, the intervention failed to capture any events that happened in the 30 days after discharge.
He also notes that the institutions that participated in the study have already implemented multiple med-rec interventions over the past few years. Hospitals that have not focused intently on the issue could find much larger gains from implementing pharmacist-led programs.
"If you're a hospital that has not been fixated on improving medication safety and transitions of care, I think pharmacists are huge," Dr. Schnipper says. "The key, then, is to focus them on the highest-risk patients."
Report: Wrong-Patient Orders Occur Frequently with CPOE Systems
Hospitalist Jason Adelman, MD, MS, believes computerized physician order-entry (CPOE) systems improve workflow and help prevent many mistakes, but the automation also causes mistakes as physicians toggle back and forth between screens in the system interface.
Dr. Adelman, patient safety officer at Montefiore Medical Center in the Bronx, N.Y., and colleagues developed an automated method for measuring wrong-patient electronic orders. They found that systems that compel physicians to re-enter certain information reduced errors.
CPOE systems have "certainly prevented errors," he says, "but they've unintentionally caused errors, and the name of the game is to keep working on ways to prevent more and more errors and minimize those errors unintentionally caused by these systems."
The researchers hypothesized that some wrong-patient orders are recognized by the orderer shortly after entry, promptly retracted, then re-entered on the correct patient. Their study results, published in the Journal of the American Medical Informatics Association, used a "retract and reorder" measurement tool that flagged any orders placed on a patient that were quickly retracted and replaced with a new order set.
Using the tool, Dr. Adleman and his research team estimated that 5,246 orders were placed on the wrong patients in 2009 at Montefiore.
The study also showed that interventions helped lower the odds of wrong-patient errors. One method made physicians click on a link to verify a patient’s identity, while another required the physician to manually input information to confirm the patient’s identity. Potential other interventions included using photo identification to ensure that physicians entered orders correctly.
"I think the goal is to try to get perfection," Dr. Adelman says. "I don't know if you could ever get totally there ... but you try."
Hospitalist Jason Adelman, MD, MS, believes computerized physician order-entry (CPOE) systems improve workflow and help prevent many mistakes, but the automation also causes mistakes as physicians toggle back and forth between screens in the system interface.
Dr. Adelman, patient safety officer at Montefiore Medical Center in the Bronx, N.Y., and colleagues developed an automated method for measuring wrong-patient electronic orders. They found that systems that compel physicians to re-enter certain information reduced errors.
CPOE systems have "certainly prevented errors," he says, "but they've unintentionally caused errors, and the name of the game is to keep working on ways to prevent more and more errors and minimize those errors unintentionally caused by these systems."
The researchers hypothesized that some wrong-patient orders are recognized by the orderer shortly after entry, promptly retracted, then re-entered on the correct patient. Their study results, published in the Journal of the American Medical Informatics Association, used a "retract and reorder" measurement tool that flagged any orders placed on a patient that were quickly retracted and replaced with a new order set.
Using the tool, Dr. Adleman and his research team estimated that 5,246 orders were placed on the wrong patients in 2009 at Montefiore.
The study also showed that interventions helped lower the odds of wrong-patient errors. One method made physicians click on a link to verify a patient’s identity, while another required the physician to manually input information to confirm the patient’s identity. Potential other interventions included using photo identification to ensure that physicians entered orders correctly.
"I think the goal is to try to get perfection," Dr. Adelman says. "I don't know if you could ever get totally there ... but you try."
Hospitalist Jason Adelman, MD, MS, believes computerized physician order-entry (CPOE) systems improve workflow and help prevent many mistakes, but the automation also causes mistakes as physicians toggle back and forth between screens in the system interface.
Dr. Adelman, patient safety officer at Montefiore Medical Center in the Bronx, N.Y., and colleagues developed an automated method for measuring wrong-patient electronic orders. They found that systems that compel physicians to re-enter certain information reduced errors.
CPOE systems have "certainly prevented errors," he says, "but they've unintentionally caused errors, and the name of the game is to keep working on ways to prevent more and more errors and minimize those errors unintentionally caused by these systems."
The researchers hypothesized that some wrong-patient orders are recognized by the orderer shortly after entry, promptly retracted, then re-entered on the correct patient. Their study results, published in the Journal of the American Medical Informatics Association, used a "retract and reorder" measurement tool that flagged any orders placed on a patient that were quickly retracted and replaced with a new order set.
Using the tool, Dr. Adleman and his research team estimated that 5,246 orders were placed on the wrong patients in 2009 at Montefiore.
The study also showed that interventions helped lower the odds of wrong-patient errors. One method made physicians click on a link to verify a patient’s identity, while another required the physician to manually input information to confirm the patient’s identity. Potential other interventions included using photo identification to ensure that physicians entered orders correctly.
"I think the goal is to try to get perfection," Dr. Adelman says. "I don't know if you could ever get totally there ... but you try."
International Concern: Hospitalists around the globe face similar issues, seek answers in U.S.
They hailed from such places as Germany, Bermuda, and Brazil, yet they were searching for the same answers as their American counterparts. How do I improve our better discharge process? How can we work better with administrators or primary-care physicians (PCPs)? How can we recruit better clinicians or see more patients in a day?
Nearly 20 international hospitalists gathered to discuss ideas, exchange business cards, and report on the growth of the hospitalist model in their countries at a Special Interest Forum at HM12 in April in San Diego.
“I’m here to get together with hospitalists, colleagues in the same field. We have a new program, and I thought I could learn from meeting people already in the field,” said David McGowan, MD, a hospitalist at the only HM group in Bermuda.
Dr. McGowan, attending his first SHM annual meeting, focused his attention on practice management, leadership and quality-initiative (QI) topics. His four-doctor HM group is relatively new, and he planned to “take some stuff back to my group.”
—Rafaela Komorowski Dal Molin, hospitalist, Hospital Mae de Deus, Porto Alegre, Brazil, scientific director, Brazilian Society of Hospital Medicine
Bermuda has one hospital, in the capital city of Hamilton, for the entire island of nearly 65,000 residents. Administration has been very supportive of the HM model, according to Dr. McGowan, although the group has faced challenges in the community.
“The system is new and people are used to their primary-care physicians being in the hospital,” he said. “We have been working on that through public relations, providing good care, and ramping up our communication with the primary-care physicians in the community.
“We set the standard for the island, and I think we are making progress. The quality of care is better. … I think the potential is there for things to be better, and outcomes are going to [get] better.”
Euro Development
Not so new to the HM model of care was Stefan Reinecke, MBA, chief of the division of general internal medicine at St. Mary’s Hospital in Stuttgart, Germany. HM12 marked the third time he’d traveled to the U.S. for an HM-focused meeting, and, as before, his areas of focus were on practice management and quality.
“I think there is a need for well-trained physicians in internal medicine, with a high knowledge of quality, methods of quality measurement, and outcome measurement,” said Dr. Reinecke, whose division has 35 inpatient physicians and 20 residents.
As in the U.S., a hospitalist model requires upfront costs to the German healthcare system, and Dr. Reinecke said he and other group leaders are feeling “strong financial pressures” from administration. He said he hoped to build new quality- and systems-improvement structures into his division, and “to do it daily,” he said.
South America
One way to validate a hospitalist service is to demonstrate improvements in quality and cost of care. That’s exactly what Rafaela Komorowski Dal Molin’s group at Hospital Mae de Deus in Porto Alegre, Brazil, has done─and her chief medical officer noticed.
“Our HM service reduced length of stay,” she said, noting hospitals and payors in her country are “thinking more and more about costs of care.”
She also said administrators are learning why the HM model of care is important. “HM in USA proved we can reduce the costs, and proved we influence the length of stay,” she said. “That’s interesting to medical directors.”
Dr. Dal Molin’s six-hospitalist group began in 2009 and includes an intensivist and pulmonologist. Starting this summer, the group will begin training four residents in an HM-focused program.
Dr. Dal Molin admitted Brazil’s healthcare system is just learning about the HM model, and groups face myriad clinical, financial, and professional issues. “HM in Brazil is not recognized as a specialty yet,” she said. “We’re working on it. I’m thinking maybe in the next two years it will be recognized.”
As scientific director of the Brazilian Society of Hospital Medicine, Dr. Dal Molin was one of a small contingency of hospitalists from the Southern Hemisphere at HM12. The group is planning its second Brazilian Congress of HM Nov. 15-16 in Sao Paulo.
Richard Quinn is a freelance writer based in New Jersey.
They hailed from such places as Germany, Bermuda, and Brazil, yet they were searching for the same answers as their American counterparts. How do I improve our better discharge process? How can we work better with administrators or primary-care physicians (PCPs)? How can we recruit better clinicians or see more patients in a day?
Nearly 20 international hospitalists gathered to discuss ideas, exchange business cards, and report on the growth of the hospitalist model in their countries at a Special Interest Forum at HM12 in April in San Diego.
“I’m here to get together with hospitalists, colleagues in the same field. We have a new program, and I thought I could learn from meeting people already in the field,” said David McGowan, MD, a hospitalist at the only HM group in Bermuda.
Dr. McGowan, attending his first SHM annual meeting, focused his attention on practice management, leadership and quality-initiative (QI) topics. His four-doctor HM group is relatively new, and he planned to “take some stuff back to my group.”
—Rafaela Komorowski Dal Molin, hospitalist, Hospital Mae de Deus, Porto Alegre, Brazil, scientific director, Brazilian Society of Hospital Medicine
Bermuda has one hospital, in the capital city of Hamilton, for the entire island of nearly 65,000 residents. Administration has been very supportive of the HM model, according to Dr. McGowan, although the group has faced challenges in the community.
“The system is new and people are used to their primary-care physicians being in the hospital,” he said. “We have been working on that through public relations, providing good care, and ramping up our communication with the primary-care physicians in the community.
“We set the standard for the island, and I think we are making progress. The quality of care is better. … I think the potential is there for things to be better, and outcomes are going to [get] better.”
Euro Development
Not so new to the HM model of care was Stefan Reinecke, MBA, chief of the division of general internal medicine at St. Mary’s Hospital in Stuttgart, Germany. HM12 marked the third time he’d traveled to the U.S. for an HM-focused meeting, and, as before, his areas of focus were on practice management and quality.
“I think there is a need for well-trained physicians in internal medicine, with a high knowledge of quality, methods of quality measurement, and outcome measurement,” said Dr. Reinecke, whose division has 35 inpatient physicians and 20 residents.
As in the U.S., a hospitalist model requires upfront costs to the German healthcare system, and Dr. Reinecke said he and other group leaders are feeling “strong financial pressures” from administration. He said he hoped to build new quality- and systems-improvement structures into his division, and “to do it daily,” he said.
South America
One way to validate a hospitalist service is to demonstrate improvements in quality and cost of care. That’s exactly what Rafaela Komorowski Dal Molin’s group at Hospital Mae de Deus in Porto Alegre, Brazil, has done─and her chief medical officer noticed.
“Our HM service reduced length of stay,” she said, noting hospitals and payors in her country are “thinking more and more about costs of care.”
She also said administrators are learning why the HM model of care is important. “HM in USA proved we can reduce the costs, and proved we influence the length of stay,” she said. “That’s interesting to medical directors.”
Dr. Dal Molin’s six-hospitalist group began in 2009 and includes an intensivist and pulmonologist. Starting this summer, the group will begin training four residents in an HM-focused program.
Dr. Dal Molin admitted Brazil’s healthcare system is just learning about the HM model, and groups face myriad clinical, financial, and professional issues. “HM in Brazil is not recognized as a specialty yet,” she said. “We’re working on it. I’m thinking maybe in the next two years it will be recognized.”
As scientific director of the Brazilian Society of Hospital Medicine, Dr. Dal Molin was one of a small contingency of hospitalists from the Southern Hemisphere at HM12. The group is planning its second Brazilian Congress of HM Nov. 15-16 in Sao Paulo.
Richard Quinn is a freelance writer based in New Jersey.
They hailed from such places as Germany, Bermuda, and Brazil, yet they were searching for the same answers as their American counterparts. How do I improve our better discharge process? How can we work better with administrators or primary-care physicians (PCPs)? How can we recruit better clinicians or see more patients in a day?
Nearly 20 international hospitalists gathered to discuss ideas, exchange business cards, and report on the growth of the hospitalist model in their countries at a Special Interest Forum at HM12 in April in San Diego.
“I’m here to get together with hospitalists, colleagues in the same field. We have a new program, and I thought I could learn from meeting people already in the field,” said David McGowan, MD, a hospitalist at the only HM group in Bermuda.
Dr. McGowan, attending his first SHM annual meeting, focused his attention on practice management, leadership and quality-initiative (QI) topics. His four-doctor HM group is relatively new, and he planned to “take some stuff back to my group.”
—Rafaela Komorowski Dal Molin, hospitalist, Hospital Mae de Deus, Porto Alegre, Brazil, scientific director, Brazilian Society of Hospital Medicine
Bermuda has one hospital, in the capital city of Hamilton, for the entire island of nearly 65,000 residents. Administration has been very supportive of the HM model, according to Dr. McGowan, although the group has faced challenges in the community.
“The system is new and people are used to their primary-care physicians being in the hospital,” he said. “We have been working on that through public relations, providing good care, and ramping up our communication with the primary-care physicians in the community.
“We set the standard for the island, and I think we are making progress. The quality of care is better. … I think the potential is there for things to be better, and outcomes are going to [get] better.”
Euro Development
Not so new to the HM model of care was Stefan Reinecke, MBA, chief of the division of general internal medicine at St. Mary’s Hospital in Stuttgart, Germany. HM12 marked the third time he’d traveled to the U.S. for an HM-focused meeting, and, as before, his areas of focus were on practice management and quality.
“I think there is a need for well-trained physicians in internal medicine, with a high knowledge of quality, methods of quality measurement, and outcome measurement,” said Dr. Reinecke, whose division has 35 inpatient physicians and 20 residents.
As in the U.S., a hospitalist model requires upfront costs to the German healthcare system, and Dr. Reinecke said he and other group leaders are feeling “strong financial pressures” from administration. He said he hoped to build new quality- and systems-improvement structures into his division, and “to do it daily,” he said.
South America
One way to validate a hospitalist service is to demonstrate improvements in quality and cost of care. That’s exactly what Rafaela Komorowski Dal Molin’s group at Hospital Mae de Deus in Porto Alegre, Brazil, has done─and her chief medical officer noticed.
“Our HM service reduced length of stay,” she said, noting hospitals and payors in her country are “thinking more and more about costs of care.”
She also said administrators are learning why the HM model of care is important. “HM in USA proved we can reduce the costs, and proved we influence the length of stay,” she said. “That’s interesting to medical directors.”
Dr. Dal Molin’s six-hospitalist group began in 2009 and includes an intensivist and pulmonologist. Starting this summer, the group will begin training four residents in an HM-focused program.
Dr. Dal Molin admitted Brazil’s healthcare system is just learning about the HM model, and groups face myriad clinical, financial, and professional issues. “HM in Brazil is not recognized as a specialty yet,” she said. “We’re working on it. I’m thinking maybe in the next two years it will be recognized.”
As scientific director of the Brazilian Society of Hospital Medicine, Dr. Dal Molin was one of a small contingency of hospitalists from the Southern Hemisphere at HM12. The group is planning its second Brazilian Congress of HM Nov. 15-16 in Sao Paulo.
Richard Quinn is a freelance writer based in New Jersey.