User login
Emergency hernia surgery risk predicted by access, age, and race
JACKSONVILLE, FLA. – Age and access to medical care may be key drivers of emergency surgery for ventral hernia repair, a large retrospective study has found.
Patients who do not have health insurance, are advanced in age, are black or Hispanic, or have unrelated health problems are at significantly higher risk than other patients with hernias of having emergency surgery for ventral hernia repair, facing a higher risk of death, a higher cost, and a longer hospital stay, Dr. Lindsey Wolf said at the Association for Academic Surgery/Society of University Surgeons Academic Surgical Congress. “This study demonstrates persistent disparities in access to elective surgery care that must be understood and mitigated,” she said. “The strongest predictor was being uninsured. The self-pay group had an odds ratio of 3.5 for undergoing emergency surgery, compared with those who were primarily insured.”

The goal of the study was to identify patient and hospital factors associated with emergency ventral hernia surgery in the U.S. population, said Dr. Wolf of Brigham and Women’s Hospital in Boston. “Prior studies that have been done on predictors of emergency repair are from universally insured populations,” she said. One was a national cohort study in Denmark, and another involved the Veterans Affairs population, she said. “Both of these identified several demographic and clinical risk factors for emergency hernia repair,” she said.
The current Brigham and Women’s study involved a retrospective cross-sectional data analysis of approximately 453,000 elective and emergency ventral hernia repairs performed from 2003 to 2011 in the Nationwide Inpatient Sample. Any cases that involved a trauma diagnosis were excluded. Forty percent of the cases in the sample were emergency admissions.
When considering the effect of age, the investigators found that the aged 65-75 group had the lowest risk of emergency hernia surgery of all age groups with an odds ratio of 0.77, compared with those under 45 years. Those aged 85 and older, however, had the highest risk of all age groups with an odds ratio of 2.23. “The proportion of the cohort undergoing emergency surgery really increases drastically with age after 75 years,” Dr. Wolf said.
Other factors that had an impact on emergency hernia repair were Medicaid coverage (OR, 1.29, compared with private insurance), black race (OR, 1.64, compared with white race), Hispanic ethnicity (OR, 1.44, compared with non-Hispanic white race/ethnicity), and comorbidities, ranging from 1.13 for one comorbidity to 1.68 for three or more, compared with none.
The study also elucidated a few consequences of emergency ventral hernia repair: 2.58 times higher odds of death, a 15% greater cost per hospital stay, and 26% longer hospital stays.
“Looking forward there are both patient and provider areas to target,” Dr. Wolf said. “For patients, interventions must be designed to populations that may have poor access to elective surgical services.” She acknowledged that race was a strong predictor, “but race is a social construct that may be a proxy to many barriers to access and care.”
The study findings may also help inform surgeons on when to operate on ventral hernias. “In the absence of any clinical guidelines for when a hernia should be repaired, our results with regard to age and multiple comorbidities may assist surgeons in risk stratifying patients when considering [whether] to perform an elective repair,” she said.
Dr. Wolf and her coauthors had no relevant financial conflicts to disclose.
JACKSONVILLE, FLA. – Age and access to medical care may be key drivers of emergency surgery for ventral hernia repair, a large retrospective study has found.
Patients who do not have health insurance, are advanced in age, are black or Hispanic, or have unrelated health problems are at significantly higher risk than other patients with hernias of having emergency surgery for ventral hernia repair, facing a higher risk of death, a higher cost, and a longer hospital stay, Dr. Lindsey Wolf said at the Association for Academic Surgery/Society of University Surgeons Academic Surgical Congress. “This study demonstrates persistent disparities in access to elective surgery care that must be understood and mitigated,” she said. “The strongest predictor was being uninsured. The self-pay group had an odds ratio of 3.5 for undergoing emergency surgery, compared with those who were primarily insured.”
The goal of the study was to identify patient and hospital factors associated with emergency ventral hernia surgery in the U.S. population, said Dr. Wolf of Brigham and Women’s Hospital in Boston. “Prior studies that have been done on predictors of emergency repair are from universally insured populations,” she said. One was a national cohort study in Denmark, and another involved the Veterans Affairs population, she said. “Both of these identified several demographic and clinical risk factors for emergency hernia repair,” she said.
The current Brigham and Women’s study involved a retrospective cross-sectional data analysis of approximately 453,000 elective and emergency ventral hernia repairs performed from 2003 to 2011 in the Nationwide Inpatient Sample. Any cases that involved a trauma diagnosis were excluded. Forty percent of the cases in the sample were emergency admissions.
When considering the effect of age, the investigators found that the aged 65-75 group had the lowest risk of emergency hernia surgery of all age groups with an odds ratio of 0.77, compared with those under 45 years. Those aged 85 and older, however, had the highest risk of all age groups with an odds ratio of 2.23. “The proportion of the cohort undergoing emergency surgery really increases drastically with age after 75 years,” Dr. Wolf said.
Other factors that had an impact on emergency hernia repair were Medicaid coverage (OR, 1.29, compared with private insurance), black race (OR, 1.64, compared with white race), Hispanic ethnicity (OR, 1.44, compared with non-Hispanic white race/ethnicity), and comorbidities, ranging from 1.13 for one comorbidity to 1.68 for three or more, compared with none.
The study also elucidated a few consequences of emergency ventral hernia repair: 2.58 times higher odds of death, a 15% greater cost per hospital stay, and 26% longer hospital stays.
“Looking forward there are both patient and provider areas to target,” Dr. Wolf said. “For patients, interventions must be designed to populations that may have poor access to elective surgical services.” She acknowledged that race was a strong predictor, “but race is a social construct that may be a proxy to many barriers to access and care.”
The study findings may also help inform surgeons on when to operate on ventral hernias. “In the absence of any clinical guidelines for when a hernia should be repaired, our results with regard to age and multiple comorbidities may assist surgeons in risk stratifying patients when considering [whether] to perform an elective repair,” she said.
Dr. Wolf and her coauthors had no relevant financial conflicts to disclose.
JACKSONVILLE, FLA. – Age and access to medical care may be key drivers of emergency surgery for ventral hernia repair, a large retrospective study has found.
Patients who do not have health insurance, are advanced in age, are black or Hispanic, or have unrelated health problems are at significantly higher risk than other patients with hernias of having emergency surgery for ventral hernia repair, facing a higher risk of death, a higher cost, and a longer hospital stay, Dr. Lindsey Wolf said at the Association for Academic Surgery/Society of University Surgeons Academic Surgical Congress. “This study demonstrates persistent disparities in access to elective surgery care that must be understood and mitigated,” she said. “The strongest predictor was being uninsured. The self-pay group had an odds ratio of 3.5 for undergoing emergency surgery, compared with those who were primarily insured.”
The goal of the study was to identify patient and hospital factors associated with emergency ventral hernia surgery in the U.S. population, said Dr. Wolf of Brigham and Women’s Hospital in Boston. “Prior studies that have been done on predictors of emergency repair are from universally insured populations,” she said. One was a national cohort study in Denmark, and another involved the Veterans Affairs population, she said. “Both of these identified several demographic and clinical risk factors for emergency hernia repair,” she said.
The current Brigham and Women’s study involved a retrospective cross-sectional data analysis of approximately 453,000 elective and emergency ventral hernia repairs performed from 2003 to 2011 in the Nationwide Inpatient Sample. Any cases that involved a trauma diagnosis were excluded. Forty percent of the cases in the sample were emergency admissions.
When considering the effect of age, the investigators found that the aged 65-75 group had the lowest risk of emergency hernia surgery of all age groups with an odds ratio of 0.77, compared with those under 45 years. Those aged 85 and older, however, had the highest risk of all age groups with an odds ratio of 2.23. “The proportion of the cohort undergoing emergency surgery really increases drastically with age after 75 years,” Dr. Wolf said.
Other factors that had an impact on emergency hernia repair were Medicaid coverage (OR, 1.29, compared with private insurance), black race (OR, 1.64, compared with white race), Hispanic ethnicity (OR, 1.44, compared with non-Hispanic white race/ethnicity), and comorbidities, ranging from 1.13 for one comorbidity to 1.68 for three or more, compared with none.
The study also elucidated a few consequences of emergency ventral hernia repair: 2.58 times higher odds of death, a 15% greater cost per hospital stay, and 26% longer hospital stays.
“Looking forward there are both patient and provider areas to target,” Dr. Wolf said. “For patients, interventions must be designed to populations that may have poor access to elective surgical services.” She acknowledged that race was a strong predictor, “but race is a social construct that may be a proxy to many barriers to access and care.”
The study findings may also help inform surgeons on when to operate on ventral hernias. “In the absence of any clinical guidelines for when a hernia should be repaired, our results with regard to age and multiple comorbidities may assist surgeons in risk stratifying patients when considering [whether] to perform an elective repair,” she said.
Dr. Wolf and her coauthors had no relevant financial conflicts to disclose.
AT THE ACADEMIC SURGICAL CONGRESS
Key clinical point: Disparities among patients more likely to get emergency rather than elective ventral hernia repair include race, insurance status, and advanced age.
Major finding: Among demographic groups with a significantly higher likelihood of undergoing emergency ventral hernia repair were blacks (odds ratio, 1.64), Hispanics (OR, 1.44), and people over age 85 (OR, 2.23).
Data source: Nationwide Inpatient Sample of 453,000 adults who had inpatient ventral hernia repair from 2003 to 2011.
Disclosures: The study authors reported having no relevant financial disclosures.

Study validates cholecystectomy safe in obese
JACKSONVILLE, FLA. – Obesity has not been found to be an independent risk factor for death or serious morbidity following cholecystectomy.
Recent, single-center studies have found that cholecystectomy for acute cholecystitis is equally safe in obese and normal weight patients, a finding that a retrospective analysis of 20,979 patients drawn from the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database has confirmed.

In presenting the study at the Association for Academic Surgery/Society of University Surgeons Academic Surgical Congress, Christopher Neylan, the Harrison Surgical Scholar at the Hospital of the University of Pennsylvania, Philadelphia, reported that approximately 900,000 cholecystectomies are performed each year in the United States, about 75% of them on individuals with a body mass index of 25 kg/m2 or greater. “But limited studies into the association of BMI and outcomes following cholecystectomy are available,” Mr. Neylan said. The data from the single-center and institutional reports “may not be applicable across a national sample,” he said.
The primary study endpoint was death/serious morbidity following surgery, with secondary outcomes being system-based complications, such as cardiac and respiratory problems. “When we control for certain factors, there is no independent association between BMI class and death or serious morbidity,” he said. “Elevated BMI class does not independently increase the risk of death or serious morbidity following cholecystectomy for acute cholecystitis,” he said.
The study also found that a patient’s BMI status has no association with secondary outcomes, which included pulmonary and cardiac complications, Neylan said.
The retrospective analysis sampled patients in the ACS NSQIP database who had cholecystectomy for acute cholecystitis from 2008 to 2013. In the dataset, 46% were considered obese with a BMI of 30 or greater; the remainder with BMI less than 30 were considered normal. A total of 87% of the sample had intended laparoscopic cholecystectomy and the conversion rate to open surgery was 4%.
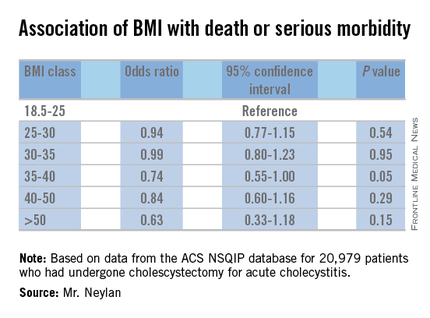
The rates of death/serious morbidity by BMI class were as follows: BMI 18.5-25, 8%; BMI 25-30, 7%; BMI 30-35, 7%; BMI 35-40, 6%; BMI 40-50, 7%; and BMI 50 or greater, 9%.
The investigators developed a multivariable model to assess the independent relationship between BMI class and the primary outcome of death or serious morbidity. The model controlled for the procedure type (open vs. laparoscopic), an interaction term between procedure type and BMI class, and patient-level characteristics such as age, smoking status and the presence of diabetes or hypertension, among other factors. Using BMI 18.5-25 as the reference group, the odds ratios for each subsequent BMI class were each less than 1, and none of the associated P values reached the level of statistical significance (P less than .01).
Mr. Neylan and his coauthors had no financial relationships to disclose.
JACKSONVILLE, FLA. – Obesity has not been found to be an independent risk factor for death or serious morbidity following cholecystectomy.
Recent, single-center studies have found that cholecystectomy for acute cholecystitis is equally safe in obese and normal weight patients, a finding that a retrospective analysis of 20,979 patients drawn from the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database has confirmed.
In presenting the study at the Association for Academic Surgery/Society of University Surgeons Academic Surgical Congress, Christopher Neylan, the Harrison Surgical Scholar at the Hospital of the University of Pennsylvania, Philadelphia, reported that approximately 900,000 cholecystectomies are performed each year in the United States, about 75% of them on individuals with a body mass index of 25 kg/m2 or greater. “But limited studies into the association of BMI and outcomes following cholecystectomy are available,” Mr. Neylan said. The data from the single-center and institutional reports “may not be applicable across a national sample,” he said.
The primary study endpoint was death/serious morbidity following surgery, with secondary outcomes being system-based complications, such as cardiac and respiratory problems. “When we control for certain factors, there is no independent association between BMI class and death or serious morbidity,” he said. “Elevated BMI class does not independently increase the risk of death or serious morbidity following cholecystectomy for acute cholecystitis,” he said.
The study also found that a patient’s BMI status has no association with secondary outcomes, which included pulmonary and cardiac complications, Neylan said.
The retrospective analysis sampled patients in the ACS NSQIP database who had cholecystectomy for acute cholecystitis from 2008 to 2013. In the dataset, 46% were considered obese with a BMI of 30 or greater; the remainder with BMI less than 30 were considered normal. A total of 87% of the sample had intended laparoscopic cholecystectomy and the conversion rate to open surgery was 4%.
The rates of death/serious morbidity by BMI class were as follows: BMI 18.5-25, 8%; BMI 25-30, 7%; BMI 30-35, 7%; BMI 35-40, 6%; BMI 40-50, 7%; and BMI 50 or greater, 9%.
The investigators developed a multivariable model to assess the independent relationship between BMI class and the primary outcome of death or serious morbidity. The model controlled for the procedure type (open vs. laparoscopic), an interaction term between procedure type and BMI class, and patient-level characteristics such as age, smoking status and the presence of diabetes or hypertension, among other factors. Using BMI 18.5-25 as the reference group, the odds ratios for each subsequent BMI class were each less than 1, and none of the associated P values reached the level of statistical significance (P less than .01).
Mr. Neylan and his coauthors had no financial relationships to disclose.
JACKSONVILLE, FLA. – Obesity has not been found to be an independent risk factor for death or serious morbidity following cholecystectomy.
Recent, single-center studies have found that cholecystectomy for acute cholecystitis is equally safe in obese and normal weight patients, a finding that a retrospective analysis of 20,979 patients drawn from the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database has confirmed.
In presenting the study at the Association for Academic Surgery/Society of University Surgeons Academic Surgical Congress, Christopher Neylan, the Harrison Surgical Scholar at the Hospital of the University of Pennsylvania, Philadelphia, reported that approximately 900,000 cholecystectomies are performed each year in the United States, about 75% of them on individuals with a body mass index of 25 kg/m2 or greater. “But limited studies into the association of BMI and outcomes following cholecystectomy are available,” Mr. Neylan said. The data from the single-center and institutional reports “may not be applicable across a national sample,” he said.
The primary study endpoint was death/serious morbidity following surgery, with secondary outcomes being system-based complications, such as cardiac and respiratory problems. “When we control for certain factors, there is no independent association between BMI class and death or serious morbidity,” he said. “Elevated BMI class does not independently increase the risk of death or serious morbidity following cholecystectomy for acute cholecystitis,” he said.
The study also found that a patient’s BMI status has no association with secondary outcomes, which included pulmonary and cardiac complications, Neylan said.
The retrospective analysis sampled patients in the ACS NSQIP database who had cholecystectomy for acute cholecystitis from 2008 to 2013. In the dataset, 46% were considered obese with a BMI of 30 or greater; the remainder with BMI less than 30 were considered normal. A total of 87% of the sample had intended laparoscopic cholecystectomy and the conversion rate to open surgery was 4%.
The rates of death/serious morbidity by BMI class were as follows: BMI 18.5-25, 8%; BMI 25-30, 7%; BMI 30-35, 7%; BMI 35-40, 6%; BMI 40-50, 7%; and BMI 50 or greater, 9%.
The investigators developed a multivariable model to assess the independent relationship between BMI class and the primary outcome of death or serious morbidity. The model controlled for the procedure type (open vs. laparoscopic), an interaction term between procedure type and BMI class, and patient-level characteristics such as age, smoking status and the presence of diabetes or hypertension, among other factors. Using BMI 18.5-25 as the reference group, the odds ratios for each subsequent BMI class were each less than 1, and none of the associated P values reached the level of statistical significance (P less than .01).
Mr. Neylan and his coauthors had no financial relationships to disclose.
AT THE ACADEMIC SURGICAL CONGRESS
Key clinical point: Cholecystectomy for acute cholecystitis has been found to have a similar safety profile in obese and normal-weight patients.
Major finding: Rates of death/serious morbidity ranged from 6% to 9% across six different weight classes ranging from normal weight to morbidly obese.
Data source: Retrospective analysis of 20,979 patients who had cholecystectomy for cholecystitis from 2008 to 2015 drawn from the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database.
Disclosures: The study authors reported having no financial disclosures.

ERAS eliminated racial disparities in postop hospital stay
JACKSONVILLE, FLA. – An enhanced recovery protocol after colorectal surgery nearly eliminated differences in hospital stays between black and white patients, according to a study based on data from the University of Alabama at Birmingham.
Dr. Tyler S. Wahl, a resident at UAB reported on the institution’s experience with the Enhanced Recovery After Surgery (ERAS) pathway at the Association of Academic Surgery/Society of University Surgeons Academic Surgical Congress. “ERAS has been shown to reduce length of stay, cost, and perioperative complications without compromising readmission or mortality rates,” Dr. Wahl said. Dr. Daniel Chu was senior author.

Surgical literature has increasingly demonstrated disparities among black patients undergoing major surgery: longer lengths of stay, more readmissions, increased postoperative mortality and lower survival rates after colorectal cancer resections, Dr. Wahl said. The UAB investigators set out to determine whether the ERAS pathway would reduce disparities in length of stay among black and white patients when compared to the traditional pathway.
Before UAB started using ERAS for colorectal patients, the average length of stay for patients undergoing colorectal surgery was 6.7 days with significant differences between black and white patients: 8 days vs. 6.1 days, respectively. However, after implementation of the ERAS pathway in January 2015, average length of stay declined to 4.7 days overall. Black patients had dramatic reductions in length of stay, compared with white patients, with stays of 3.9 days vs. 5 days, respectively.
“Not only were patients leaving much earlier, but their length of stay was also shorter than predicted using the American College of Surgeons Risk Calculator,” Dr. Wahl said.
The UAB study was a retrospective, matched cohort analysis of 258 patients – 129 patients from pre-ERAS years were compared with 129 ERAS patients from January to October 2015.
Study subjects were similar in many patient- and procedure-specific factors; however, differences in operative approach, indication, ostomy formation, and operative time did not change the predicted length of stay among races, Dr. Wahl said.
Dr. Wahl said the racial makeup of the study differs from most ERAS literature in colorectal patients. “The overall percentage of the African American population was 30% within our study, as most ERAS literature has 10% or less,” he added.
“Further work needs to be pursued to find what’s driving these dramatic results among the black population,” he said.
Dr. Wahl and coauthors had no disclosures.
JACKSONVILLE, FLA. – An enhanced recovery protocol after colorectal surgery nearly eliminated differences in hospital stays between black and white patients, according to a study based on data from the University of Alabama at Birmingham.
Dr. Tyler S. Wahl, a resident at UAB reported on the institution’s experience with the Enhanced Recovery After Surgery (ERAS) pathway at the Association of Academic Surgery/Society of University Surgeons Academic Surgical Congress. “ERAS has been shown to reduce length of stay, cost, and perioperative complications without compromising readmission or mortality rates,” Dr. Wahl said. Dr. Daniel Chu was senior author.
Surgical literature has increasingly demonstrated disparities among black patients undergoing major surgery: longer lengths of stay, more readmissions, increased postoperative mortality and lower survival rates after colorectal cancer resections, Dr. Wahl said. The UAB investigators set out to determine whether the ERAS pathway would reduce disparities in length of stay among black and white patients when compared to the traditional pathway.
Before UAB started using ERAS for colorectal patients, the average length of stay for patients undergoing colorectal surgery was 6.7 days with significant differences between black and white patients: 8 days vs. 6.1 days, respectively. However, after implementation of the ERAS pathway in January 2015, average length of stay declined to 4.7 days overall. Black patients had dramatic reductions in length of stay, compared with white patients, with stays of 3.9 days vs. 5 days, respectively.
“Not only were patients leaving much earlier, but their length of stay was also shorter than predicted using the American College of Surgeons Risk Calculator,” Dr. Wahl said.
The UAB study was a retrospective, matched cohort analysis of 258 patients – 129 patients from pre-ERAS years were compared with 129 ERAS patients from January to October 2015.
Study subjects were similar in many patient- and procedure-specific factors; however, differences in operative approach, indication, ostomy formation, and operative time did not change the predicted length of stay among races, Dr. Wahl said.
Dr. Wahl said the racial makeup of the study differs from most ERAS literature in colorectal patients. “The overall percentage of the African American population was 30% within our study, as most ERAS literature has 10% or less,” he added.
“Further work needs to be pursued to find what’s driving these dramatic results among the black population,” he said.
Dr. Wahl and coauthors had no disclosures.
JACKSONVILLE, FLA. – An enhanced recovery protocol after colorectal surgery nearly eliminated differences in hospital stays between black and white patients, according to a study based on data from the University of Alabama at Birmingham.
Dr. Tyler S. Wahl, a resident at UAB reported on the institution’s experience with the Enhanced Recovery After Surgery (ERAS) pathway at the Association of Academic Surgery/Society of University Surgeons Academic Surgical Congress. “ERAS has been shown to reduce length of stay, cost, and perioperative complications without compromising readmission or mortality rates,” Dr. Wahl said. Dr. Daniel Chu was senior author.
Surgical literature has increasingly demonstrated disparities among black patients undergoing major surgery: longer lengths of stay, more readmissions, increased postoperative mortality and lower survival rates after colorectal cancer resections, Dr. Wahl said. The UAB investigators set out to determine whether the ERAS pathway would reduce disparities in length of stay among black and white patients when compared to the traditional pathway.
Before UAB started using ERAS for colorectal patients, the average length of stay for patients undergoing colorectal surgery was 6.7 days with significant differences between black and white patients: 8 days vs. 6.1 days, respectively. However, after implementation of the ERAS pathway in January 2015, average length of stay declined to 4.7 days overall. Black patients had dramatic reductions in length of stay, compared with white patients, with stays of 3.9 days vs. 5 days, respectively.
“Not only were patients leaving much earlier, but their length of stay was also shorter than predicted using the American College of Surgeons Risk Calculator,” Dr. Wahl said.
The UAB study was a retrospective, matched cohort analysis of 258 patients – 129 patients from pre-ERAS years were compared with 129 ERAS patients from January to October 2015.
Study subjects were similar in many patient- and procedure-specific factors; however, differences in operative approach, indication, ostomy formation, and operative time did not change the predicted length of stay among races, Dr. Wahl said.
Dr. Wahl said the racial makeup of the study differs from most ERAS literature in colorectal patients. “The overall percentage of the African American population was 30% within our study, as most ERAS literature has 10% or less,” he added.
“Further work needs to be pursued to find what’s driving these dramatic results among the black population,” he said.
Dr. Wahl and coauthors had no disclosures.
FROM THE ACADEMIC SURGICAL CONGRESS
Key clinical point: Use of the ERAS pathway reduced hospital stays for all patients after colorectal surgery, with results most dramatic in black patients.
Major finding: Hospital stays declined from 6.7 days before ERAS to 4.7 days afterward, with stays for blacks declining from 8 days before ERAS to 3.9 days afterward.
Data source: Retrospective, matched cohort analysis of 258 patients – 129 patients from pre-ERAS years were compared to 129 ERAS patients from January to October 2015.
Disclosures: The study authors reported having no financial disclosures.

Finding more transplant hearts but not more donors
Heart transplant volumes in the United States have remained static since the start of the century because of improved trauma prevention and treatment, but that has challenged cardiologists to find enough donor hearts for the growing ranks of advanced heart failure patients. So a multidisciplinary team at the University of Washington in Seattle initiated a quality improvement program that doubled transplant volume without any change in transplant-related deaths by accepting hearts they would have otherwise discarded.
The study came about after the researchers determined that a large number of donor hearts from their own organ procurement program were being sent to other transplant centers. So they gathered a multidisciplinary team of transplant surgeons, cardiologists, and members of the organ procurement program to study ways to improve its center-specific organ utilization rate. The endeavor resulted in an increase in utilization rates from 28% to 49% in a year, a rate that has been sustained through a second year, according to study findings published in the January issue of the Journal of Thoracic and Cardiovascular Surgery (2016;151:238-43).
“The simple process of systematically reviewing donor turn down events as a group tended to reduce variability [and] increase confidence in expanded criteria donors and resulted in improved donor organ utilization and transplant volumes,” lead author Dr. Jason Smith and colleagues said.
The 30-day and 1-year death rates were similar before and after the quality improvement program started, but the death rates of those on the heart wait list declined from 17.2% to 12%, “which was not statistically significant,” Dr. Smith and coauthors said, “but does show that increasing use of organs that may be outside of the usual pattern has a trend toward improved wait list survival and needs to be considered when assessing donor hearts.”
Because of excellent results of heart transplants in patients with advanced heart failure, a number of investigators have proposed expanding the population of heart donors to include older people, those with higher risk of infectious disease, or with heart disease such as coronary artery disease and left ventricular hypertrophy, Dr. Smith and coauthors said. Their own review found a higher-than-expected rate of donor hearts sent to other centers from the University of Washington organ procurement program.
The multidisciplinary team analyzed the organs the University of Washington surgeons refused and sent to other institutions from July 2012 to June 2013.
For a year after that, the multidisciplinary group did real-time analysis of organ refusal along with quarterly reviews “in a non-confrontational, proactive” setting, as Dr. Smith and his colleagues described it. The group held open discussions on refused organs that were ultimately transplanted elsewhere. “The review process was facilitated to provide a constructive environment to encourage development of best practices and consistency,” the researchers noted. The quality improvement program led to an increase in the unit’s transplant volume despite fewer donor offers.
The researchers acknowledged that donor assessment has been the focus of much controversy. They pointed out that average donor age has increased over the last 20 years from 29 years to 33 years and has since retreated to 31 years, and some programs utilize donors up to their mid-60s. Also, previous studies have advocated for the use of donors who meet the criteria of the Centers for Disease Control and Prevention high risk behavior of infection as well as some drug abusers because of the low-risk of transmission and emerging evidence affirming the safety of hearts of drug users.
“The individual decision to utilize or discard a donor organ is one of the most challenging aspects of transplant medicine,” Dr. Smith and colleagues said. “It requires balancing donor risks against the exigencies of the recipient.”
Today, the multidisciplinary team evaluates each heart offered for donation and is exploring ways to accept even more donor hearts, even discarded hearts. “This represents a large, untapped pool of potential donor hearts that might add to the net number of transplants performed nationally and not merely redistribute organ usage,” Dr. Smith and colleagues said.
Dr. Smith is a consultant for Thoratec and is a primary site investigator for the EXPAND Trial sponsored by TransMedics. Dr. Todd Dardas is supported by the American College of Cardiology/Daiichi Sankyo Career Development Award. Dr. Jay Pal receives grant support from Tenax. Dr. Wayne Levy is a consultant for HeartWare, Novartis, GE Healthcare, Pharmin, and Biotronik. Dr. Claudius Mahr is a consultant for Thoratec, HeartWare and Abiomed. Dr. Nahush Mokadam is a consultant for Thoratec, HeartWare, Syncardia and St. Jude Medical, and has research grants from Thoratec, HeartWare and Syncardia. The other coauthors had no relationships to disclose.
How the University of Washington researchers brought about such a dramatic increase in donor heart utilization raises a number of questions, Dr. Nicholas Smedira of Cleveland Clinic said in his invited commentary (J Thorac Cardiovasc Surg 2016;151:243-4).
“They refer euphemistically to ‘behavioral adaptation’ and ‘frank discussions’ regarding ‘individual and group bias’ as explanations, but understanding exactly how this is accomplished is not easy,” Dr. Smedira said.
Noteworthy is that the researchers used more donors who meet Center for Disease Control and Prevention high risk criteria for infectious disease. However, cardiologists tend to weigh their decision for accepting donor hearts “by the last memorable or distressful experience,” Dr. Smedira said. Hence, many of these donor hearts go unused. At the same time, assessing risk without complete information is challenging, he said.
Besides their thought processes, other factors that influence cardiologists’ decisions on accepting donor hearts include fatigue, scheduling conflicts, reimbursement issues, and outcome metrics. He credited the University of Washington for its “courage” to examine their decision-making process, including exploring biases as well as working “collectively and blamelessly” to support their decisions. “I would encourage more transplant centers to follow a program similar to the University of Washington’s and maybe we will be hearing more yeses and fewer nos,” Dr. Smedira said.
He had no relationships to disclose.
How the University of Washington researchers brought about such a dramatic increase in donor heart utilization raises a number of questions, Dr. Nicholas Smedira of Cleveland Clinic said in his invited commentary (J Thorac Cardiovasc Surg 2016;151:243-4).
“They refer euphemistically to ‘behavioral adaptation’ and ‘frank discussions’ regarding ‘individual and group bias’ as explanations, but understanding exactly how this is accomplished is not easy,” Dr. Smedira said.
Noteworthy is that the researchers used more donors who meet Center for Disease Control and Prevention high risk criteria for infectious disease. However, cardiologists tend to weigh their decision for accepting donor hearts “by the last memorable or distressful experience,” Dr. Smedira said. Hence, many of these donor hearts go unused. At the same time, assessing risk without complete information is challenging, he said.
Besides their thought processes, other factors that influence cardiologists’ decisions on accepting donor hearts include fatigue, scheduling conflicts, reimbursement issues, and outcome metrics. He credited the University of Washington for its “courage” to examine their decision-making process, including exploring biases as well as working “collectively and blamelessly” to support their decisions. “I would encourage more transplant centers to follow a program similar to the University of Washington’s and maybe we will be hearing more yeses and fewer nos,” Dr. Smedira said.
He had no relationships to disclose.
How the University of Washington researchers brought about such a dramatic increase in donor heart utilization raises a number of questions, Dr. Nicholas Smedira of Cleveland Clinic said in his invited commentary (J Thorac Cardiovasc Surg 2016;151:243-4).
“They refer euphemistically to ‘behavioral adaptation’ and ‘frank discussions’ regarding ‘individual and group bias’ as explanations, but understanding exactly how this is accomplished is not easy,” Dr. Smedira said.
Noteworthy is that the researchers used more donors who meet Center for Disease Control and Prevention high risk criteria for infectious disease. However, cardiologists tend to weigh their decision for accepting donor hearts “by the last memorable or distressful experience,” Dr. Smedira said. Hence, many of these donor hearts go unused. At the same time, assessing risk without complete information is challenging, he said.
Besides their thought processes, other factors that influence cardiologists’ decisions on accepting donor hearts include fatigue, scheduling conflicts, reimbursement issues, and outcome metrics. He credited the University of Washington for its “courage” to examine their decision-making process, including exploring biases as well as working “collectively and blamelessly” to support their decisions. “I would encourage more transplant centers to follow a program similar to the University of Washington’s and maybe we will be hearing more yeses and fewer nos,” Dr. Smedira said.
He had no relationships to disclose.
Heart transplant volumes in the United States have remained static since the start of the century because of improved trauma prevention and treatment, but that has challenged cardiologists to find enough donor hearts for the growing ranks of advanced heart failure patients. So a multidisciplinary team at the University of Washington in Seattle initiated a quality improvement program that doubled transplant volume without any change in transplant-related deaths by accepting hearts they would have otherwise discarded.
The study came about after the researchers determined that a large number of donor hearts from their own organ procurement program were being sent to other transplant centers. So they gathered a multidisciplinary team of transplant surgeons, cardiologists, and members of the organ procurement program to study ways to improve its center-specific organ utilization rate. The endeavor resulted in an increase in utilization rates from 28% to 49% in a year, a rate that has been sustained through a second year, according to study findings published in the January issue of the Journal of Thoracic and Cardiovascular Surgery (2016;151:238-43).
“The simple process of systematically reviewing donor turn down events as a group tended to reduce variability [and] increase confidence in expanded criteria donors and resulted in improved donor organ utilization and transplant volumes,” lead author Dr. Jason Smith and colleagues said.
The 30-day and 1-year death rates were similar before and after the quality improvement program started, but the death rates of those on the heart wait list declined from 17.2% to 12%, “which was not statistically significant,” Dr. Smith and coauthors said, “but does show that increasing use of organs that may be outside of the usual pattern has a trend toward improved wait list survival and needs to be considered when assessing donor hearts.”
Because of excellent results of heart transplants in patients with advanced heart failure, a number of investigators have proposed expanding the population of heart donors to include older people, those with higher risk of infectious disease, or with heart disease such as coronary artery disease and left ventricular hypertrophy, Dr. Smith and coauthors said. Their own review found a higher-than-expected rate of donor hearts sent to other centers from the University of Washington organ procurement program.
The multidisciplinary team analyzed the organs the University of Washington surgeons refused and sent to other institutions from July 2012 to June 2013.
For a year after that, the multidisciplinary group did real-time analysis of organ refusal along with quarterly reviews “in a non-confrontational, proactive” setting, as Dr. Smith and his colleagues described it. The group held open discussions on refused organs that were ultimately transplanted elsewhere. “The review process was facilitated to provide a constructive environment to encourage development of best practices and consistency,” the researchers noted. The quality improvement program led to an increase in the unit’s transplant volume despite fewer donor offers.
The researchers acknowledged that donor assessment has been the focus of much controversy. They pointed out that average donor age has increased over the last 20 years from 29 years to 33 years and has since retreated to 31 years, and some programs utilize donors up to their mid-60s. Also, previous studies have advocated for the use of donors who meet the criteria of the Centers for Disease Control and Prevention high risk behavior of infection as well as some drug abusers because of the low-risk of transmission and emerging evidence affirming the safety of hearts of drug users.
“The individual decision to utilize or discard a donor organ is one of the most challenging aspects of transplant medicine,” Dr. Smith and colleagues said. “It requires balancing donor risks against the exigencies of the recipient.”
Today, the multidisciplinary team evaluates each heart offered for donation and is exploring ways to accept even more donor hearts, even discarded hearts. “This represents a large, untapped pool of potential donor hearts that might add to the net number of transplants performed nationally and not merely redistribute organ usage,” Dr. Smith and colleagues said.
Dr. Smith is a consultant for Thoratec and is a primary site investigator for the EXPAND Trial sponsored by TransMedics. Dr. Todd Dardas is supported by the American College of Cardiology/Daiichi Sankyo Career Development Award. Dr. Jay Pal receives grant support from Tenax. Dr. Wayne Levy is a consultant for HeartWare, Novartis, GE Healthcare, Pharmin, and Biotronik. Dr. Claudius Mahr is a consultant for Thoratec, HeartWare and Abiomed. Dr. Nahush Mokadam is a consultant for Thoratec, HeartWare, Syncardia and St. Jude Medical, and has research grants from Thoratec, HeartWare and Syncardia. The other coauthors had no relationships to disclose.
Heart transplant volumes in the United States have remained static since the start of the century because of improved trauma prevention and treatment, but that has challenged cardiologists to find enough donor hearts for the growing ranks of advanced heart failure patients. So a multidisciplinary team at the University of Washington in Seattle initiated a quality improvement program that doubled transplant volume without any change in transplant-related deaths by accepting hearts they would have otherwise discarded.
The study came about after the researchers determined that a large number of donor hearts from their own organ procurement program were being sent to other transplant centers. So they gathered a multidisciplinary team of transplant surgeons, cardiologists, and members of the organ procurement program to study ways to improve its center-specific organ utilization rate. The endeavor resulted in an increase in utilization rates from 28% to 49% in a year, a rate that has been sustained through a second year, according to study findings published in the January issue of the Journal of Thoracic and Cardiovascular Surgery (2016;151:238-43).
“The simple process of systematically reviewing donor turn down events as a group tended to reduce variability [and] increase confidence in expanded criteria donors and resulted in improved donor organ utilization and transplant volumes,” lead author Dr. Jason Smith and colleagues said.
The 30-day and 1-year death rates were similar before and after the quality improvement program started, but the death rates of those on the heart wait list declined from 17.2% to 12%, “which was not statistically significant,” Dr. Smith and coauthors said, “but does show that increasing use of organs that may be outside of the usual pattern has a trend toward improved wait list survival and needs to be considered when assessing donor hearts.”
Because of excellent results of heart transplants in patients with advanced heart failure, a number of investigators have proposed expanding the population of heart donors to include older people, those with higher risk of infectious disease, or with heart disease such as coronary artery disease and left ventricular hypertrophy, Dr. Smith and coauthors said. Their own review found a higher-than-expected rate of donor hearts sent to other centers from the University of Washington organ procurement program.
The multidisciplinary team analyzed the organs the University of Washington surgeons refused and sent to other institutions from July 2012 to June 2013.
For a year after that, the multidisciplinary group did real-time analysis of organ refusal along with quarterly reviews “in a non-confrontational, proactive” setting, as Dr. Smith and his colleagues described it. The group held open discussions on refused organs that were ultimately transplanted elsewhere. “The review process was facilitated to provide a constructive environment to encourage development of best practices and consistency,” the researchers noted. The quality improvement program led to an increase in the unit’s transplant volume despite fewer donor offers.
The researchers acknowledged that donor assessment has been the focus of much controversy. They pointed out that average donor age has increased over the last 20 years from 29 years to 33 years and has since retreated to 31 years, and some programs utilize donors up to their mid-60s. Also, previous studies have advocated for the use of donors who meet the criteria of the Centers for Disease Control and Prevention high risk behavior of infection as well as some drug abusers because of the low-risk of transmission and emerging evidence affirming the safety of hearts of drug users.
“The individual decision to utilize or discard a donor organ is one of the most challenging aspects of transplant medicine,” Dr. Smith and colleagues said. “It requires balancing donor risks against the exigencies of the recipient.”
Today, the multidisciplinary team evaluates each heart offered for donation and is exploring ways to accept even more donor hearts, even discarded hearts. “This represents a large, untapped pool of potential donor hearts that might add to the net number of transplants performed nationally and not merely redistribute organ usage,” Dr. Smith and colleagues said.
Dr. Smith is a consultant for Thoratec and is a primary site investigator for the EXPAND Trial sponsored by TransMedics. Dr. Todd Dardas is supported by the American College of Cardiology/Daiichi Sankyo Career Development Award. Dr. Jay Pal receives grant support from Tenax. Dr. Wayne Levy is a consultant for HeartWare, Novartis, GE Healthcare, Pharmin, and Biotronik. Dr. Claudius Mahr is a consultant for Thoratec, HeartWare and Abiomed. Dr. Nahush Mokadam is a consultant for Thoratec, HeartWare, Syncardia and St. Jude Medical, and has research grants from Thoratec, HeartWare and Syncardia. The other coauthors had no relationships to disclose.
Key clinical point: A group approach to systematically review rejected donor organs has led to expanded donor criteria and resulted in improved donor organ utilization and transplant volume.
Major finding: Transplant utilization rate increased from 28% to 49% with no significant change in 30-day survival after implementation of a donor review protocol.
Data source: Retrospective review of 293 total donor heart offers at a single center from July 2012 to June 2013 compared with review of 279 heart offers from July 2013 to June 2014.
Disclosures: Lead author Dr. Jason Smith is a consultant for Thoratec and is a primary site investigator for the EXPAND Trial sponsored by TransMedics. Dr. Todd Dardas is supported by the American College of Cardiology/Daiichi Sankyo Career Development Award. Dr. Jay Pal receives grant support from Tenax. Dr. Wayne Levy is a consultant for HeartWare, Novartis, GE Healthcare, Pharmin, and Biotronik. Dr. Claudius Mahr is a consultant for Thoratec, HeartWare and Abiomed. Dr. Nahush Mokadam is a consultant for Thoratec, HeartWare, Syncardia, and St. Jude Medical, and has research grants from Thoratec, HeartWare and Syncardia. The other coauthors had no relationships to disclose.
Presurgery radiation shows benefit in lung cancer
The popularity of extrapleural pneumonectomy to treat asbestos-related thoracic mesothelioma has yielded to extended pleurectomy/decortication in recent years, but a recent study suggests that the extrapleural pneumonectomy procedure can achieve good results in a new protocol that involves administering radiation therapy before surgery as opposed the more conventional approach of radiation after surgery.
Researchers at the University of Toronto reported on their protocol that uses accelerated intensity modulated radiation therapy (IMRT) for malignant pleural mesothelioma (MPM) (J Thorac Cardiovasc Surg. doi: 10.1016/j.jtcvs.2015.09.129). They call the protocol SMART, for Surgery for Mesothelioma After Radiation Therapy.
“The rationale to develop this protocol was to optimize the delivery of radiation to the whole tumor bed, sterilize the edges of the tumor to limit the risk of spillage at the time of surgery, develop a shorter treatment plan and potentiate the activation of the immune system by using a hypofractionated regimen,” wrote Dr. Marc de Perrot and colleagues.
The protocol involves delivering 25 Gy of radiation in five daily fractions over a week to the entire side of the thorax with 5 Gy boosts based on imaging, followed by extrapleural pneumonectomy (EPP) 4-6 days later. Patients with three or more positive lymph notes (ypN2 disease) also are offered adjuvant chemotherapy.
The researchers performed the protocol on 62 patients from November 2008 to October 2014, which represents 24% of all patients with MPM seen at the institution in that period. Fifty-two patients were men and ages ranged from 41 to 75 years. Clinical stage of cancer ranged from T1N0 in 10 patients, to T2N0 in 35 and T3N0 in 13 (two had T4N0 and two had T3N2). Forty-five had right-side cancers. Six patients received an extended protocol for various reasons, including tumor extending to the chest wall.
All 62 patients completed IMRT and EPP. All but one had resection and reconstruction of the diaphragm, and all but four had resection and reconstruction of the pericardium.
Overall death rate was 4.8% (three patients). Results were better in patients with epithelioid tumors, with a median survival of 51 months and disease-free survival of 47 months. Those with biphasic subtypes had median survival of 10 months and disease-free survival of 8 months. Eight patients had ipsilateral chest recurrence. “This analysis demonstrates that the SMART approach is particularly encouraging for patients with epithelial subtype,” Dr. de Perrot and coauthors said. They no longer perform the SMART protocol on patients with biphasic subtype.
The protocol was not without complications. Twenty-four patients, about 38%, had serious complications that required intervention or worse. Twelve had atrial fibrillation, but none advanced to life-threatening disease. Among other complications, four had empyema – one resulting in death – and three had pulmonary emboli. One other patient in the complications group died from pneumonia, and another died from a heart attack at home.
This is the Toronto researchers’ second attempt at studying the three-modality approach. In their first attempt, only half the patients who started with preoperative chemotherapy went onto complete the radiation after surgery because of difficulties administering it (J Thorac Cardiovasc Surg. 2007;133:111-6; J Clin Oncol. 2009;27:1413-8). Also, about 25% of patients had disease progression during induction chemotherapy and could not go onto surgery.
They designed the most recent trial to deliver radiation before surgery because of the excellent local control of cancer along with evidence that MPM tumors were radio-sensitive. “Considering the risk of disease progression on induction chemotherapy, we felt that switching the order of therapy was potentially a better option for patients with surgically resectable disease,” Dr. de Perrott and colleagues said.
The researchers cited the study’s single-center nature with a single treatment arm, and the lack of longer-term follow-up, as limitations. “However, in our own experience, this approach has been very encouraging and has become our primary option for patients with surgically resectable MPM,” they noted.
The study authors had no conflicts to disclose.
Implementing the treatment regimen for malignant pleural mesothelioma (MPM) that the Toronto researchers studied poses “several high stakes challenges,” Dr. Valerie Rusch and coauthors at Memorial Sloan-Kettering Cancer Center, New York, said in their invited commentary (J Thorac Cardiovasc Surg. doi: 10.1016/j.jtcvs.2015.10.038).

|
Dr. Valerie W. Rusch |
But they noted challenges involved with conventional multi-modality treatment for MPM, namely the 6 months of intensive treatment. However, the experience of the Toronto researchers will be difficult to replicate, they said. “Such outstanding results reflect the expertise of Dr. de Perrot and colleagues in the surgical care of MPM and the excellence of their multidisciplinary program,” Dr. Rusch and coauthors said.
The study results are among the best reported for MPM to date, they added, but they asked why. “Are they solely related to patient selection or do they reflect the true impact of a novel approach to treatment?”
Patients selected for the treatment need to be able to undergo the extrapleural pneumonectomy (EPP) and the surgeon has to be able to predict the resectability of the tumor. But limitations in existing staging methods for MPM make it difficult to predict tumor resectability. “To avoid bronchial stump leaks and other serious complications after EPP requires experience along with meticulous surgical technique and postoperative care,” Dr. Rusch and colleagues said. “Only high-volume centers of excellence could potentially reproduce these results.”
Despite the waning in popularity of EPP, the study results underscore its effectiveness in carefully selected patients – “those with epithelioid tumor histology and no tumor metastases.” To corroborate the findings, reports on other centers’ experience along with human and animal studies rather than a randomized clinical trial are needed. “Dr. de Perrot and colleagues may have been not only bold but SMART,” Dr. Rusch and colleagues said.
Implementing the treatment regimen for malignant pleural mesothelioma (MPM) that the Toronto researchers studied poses “several high stakes challenges,” Dr. Valerie Rusch and coauthors at Memorial Sloan-Kettering Cancer Center, New York, said in their invited commentary (J Thorac Cardiovasc Surg. doi: 10.1016/j.jtcvs.2015.10.038).
|
|
Dr. Valerie W. Rusch |
But they noted challenges involved with conventional multi-modality treatment for MPM, namely the 6 months of intensive treatment. However, the experience of the Toronto researchers will be difficult to replicate, they said. “Such outstanding results reflect the expertise of Dr. de Perrot and colleagues in the surgical care of MPM and the excellence of their multidisciplinary program,” Dr. Rusch and coauthors said.
The study results are among the best reported for MPM to date, they added, but they asked why. “Are they solely related to patient selection or do they reflect the true impact of a novel approach to treatment?”
Patients selected for the treatment need to be able to undergo the extrapleural pneumonectomy (EPP) and the surgeon has to be able to predict the resectability of the tumor. But limitations in existing staging methods for MPM make it difficult to predict tumor resectability. “To avoid bronchial stump leaks and other serious complications after EPP requires experience along with meticulous surgical technique and postoperative care,” Dr. Rusch and colleagues said. “Only high-volume centers of excellence could potentially reproduce these results.”
Despite the waning in popularity of EPP, the study results underscore its effectiveness in carefully selected patients – “those with epithelioid tumor histology and no tumor metastases.” To corroborate the findings, reports on other centers’ experience along with human and animal studies rather than a randomized clinical trial are needed. “Dr. de Perrot and colleagues may have been not only bold but SMART,” Dr. Rusch and colleagues said.
Implementing the treatment regimen for malignant pleural mesothelioma (MPM) that the Toronto researchers studied poses “several high stakes challenges,” Dr. Valerie Rusch and coauthors at Memorial Sloan-Kettering Cancer Center, New York, said in their invited commentary (J Thorac Cardiovasc Surg. doi: 10.1016/j.jtcvs.2015.10.038).
|
|
Dr. Valerie W. Rusch |
But they noted challenges involved with conventional multi-modality treatment for MPM, namely the 6 months of intensive treatment. However, the experience of the Toronto researchers will be difficult to replicate, they said. “Such outstanding results reflect the expertise of Dr. de Perrot and colleagues in the surgical care of MPM and the excellence of their multidisciplinary program,” Dr. Rusch and coauthors said.
The study results are among the best reported for MPM to date, they added, but they asked why. “Are they solely related to patient selection or do they reflect the true impact of a novel approach to treatment?”
Patients selected for the treatment need to be able to undergo the extrapleural pneumonectomy (EPP) and the surgeon has to be able to predict the resectability of the tumor. But limitations in existing staging methods for MPM make it difficult to predict tumor resectability. “To avoid bronchial stump leaks and other serious complications after EPP requires experience along with meticulous surgical technique and postoperative care,” Dr. Rusch and colleagues said. “Only high-volume centers of excellence could potentially reproduce these results.”
Despite the waning in popularity of EPP, the study results underscore its effectiveness in carefully selected patients – “those with epithelioid tumor histology and no tumor metastases.” To corroborate the findings, reports on other centers’ experience along with human and animal studies rather than a randomized clinical trial are needed. “Dr. de Perrot and colleagues may have been not only bold but SMART,” Dr. Rusch and colleagues said.
The popularity of extrapleural pneumonectomy to treat asbestos-related thoracic mesothelioma has yielded to extended pleurectomy/decortication in recent years, but a recent study suggests that the extrapleural pneumonectomy procedure can achieve good results in a new protocol that involves administering radiation therapy before surgery as opposed the more conventional approach of radiation after surgery.
Researchers at the University of Toronto reported on their protocol that uses accelerated intensity modulated radiation therapy (IMRT) for malignant pleural mesothelioma (MPM) (J Thorac Cardiovasc Surg. doi: 10.1016/j.jtcvs.2015.09.129). They call the protocol SMART, for Surgery for Mesothelioma After Radiation Therapy.
“The rationale to develop this protocol was to optimize the delivery of radiation to the whole tumor bed, sterilize the edges of the tumor to limit the risk of spillage at the time of surgery, develop a shorter treatment plan and potentiate the activation of the immune system by using a hypofractionated regimen,” wrote Dr. Marc de Perrot and colleagues.
The protocol involves delivering 25 Gy of radiation in five daily fractions over a week to the entire side of the thorax with 5 Gy boosts based on imaging, followed by extrapleural pneumonectomy (EPP) 4-6 days later. Patients with three or more positive lymph notes (ypN2 disease) also are offered adjuvant chemotherapy.
The researchers performed the protocol on 62 patients from November 2008 to October 2014, which represents 24% of all patients with MPM seen at the institution in that period. Fifty-two patients were men and ages ranged from 41 to 75 years. Clinical stage of cancer ranged from T1N0 in 10 patients, to T2N0 in 35 and T3N0 in 13 (two had T4N0 and two had T3N2). Forty-five had right-side cancers. Six patients received an extended protocol for various reasons, including tumor extending to the chest wall.
All 62 patients completed IMRT and EPP. All but one had resection and reconstruction of the diaphragm, and all but four had resection and reconstruction of the pericardium.
Overall death rate was 4.8% (three patients). Results were better in patients with epithelioid tumors, with a median survival of 51 months and disease-free survival of 47 months. Those with biphasic subtypes had median survival of 10 months and disease-free survival of 8 months. Eight patients had ipsilateral chest recurrence. “This analysis demonstrates that the SMART approach is particularly encouraging for patients with epithelial subtype,” Dr. de Perrot and coauthors said. They no longer perform the SMART protocol on patients with biphasic subtype.
The protocol was not without complications. Twenty-four patients, about 38%, had serious complications that required intervention or worse. Twelve had atrial fibrillation, but none advanced to life-threatening disease. Among other complications, four had empyema – one resulting in death – and three had pulmonary emboli. One other patient in the complications group died from pneumonia, and another died from a heart attack at home.
This is the Toronto researchers’ second attempt at studying the three-modality approach. In their first attempt, only half the patients who started with preoperative chemotherapy went onto complete the radiation after surgery because of difficulties administering it (J Thorac Cardiovasc Surg. 2007;133:111-6; J Clin Oncol. 2009;27:1413-8). Also, about 25% of patients had disease progression during induction chemotherapy and could not go onto surgery.
They designed the most recent trial to deliver radiation before surgery because of the excellent local control of cancer along with evidence that MPM tumors were radio-sensitive. “Considering the risk of disease progression on induction chemotherapy, we felt that switching the order of therapy was potentially a better option for patients with surgically resectable disease,” Dr. de Perrott and colleagues said.
The researchers cited the study’s single-center nature with a single treatment arm, and the lack of longer-term follow-up, as limitations. “However, in our own experience, this approach has been very encouraging and has become our primary option for patients with surgically resectable MPM,” they noted.
The study authors had no conflicts to disclose.
The popularity of extrapleural pneumonectomy to treat asbestos-related thoracic mesothelioma has yielded to extended pleurectomy/decortication in recent years, but a recent study suggests that the extrapleural pneumonectomy procedure can achieve good results in a new protocol that involves administering radiation therapy before surgery as opposed the more conventional approach of radiation after surgery.
Researchers at the University of Toronto reported on their protocol that uses accelerated intensity modulated radiation therapy (IMRT) for malignant pleural mesothelioma (MPM) (J Thorac Cardiovasc Surg. doi: 10.1016/j.jtcvs.2015.09.129). They call the protocol SMART, for Surgery for Mesothelioma After Radiation Therapy.
“The rationale to develop this protocol was to optimize the delivery of radiation to the whole tumor bed, sterilize the edges of the tumor to limit the risk of spillage at the time of surgery, develop a shorter treatment plan and potentiate the activation of the immune system by using a hypofractionated regimen,” wrote Dr. Marc de Perrot and colleagues.
The protocol involves delivering 25 Gy of radiation in five daily fractions over a week to the entire side of the thorax with 5 Gy boosts based on imaging, followed by extrapleural pneumonectomy (EPP) 4-6 days later. Patients with three or more positive lymph notes (ypN2 disease) also are offered adjuvant chemotherapy.
The researchers performed the protocol on 62 patients from November 2008 to October 2014, which represents 24% of all patients with MPM seen at the institution in that period. Fifty-two patients were men and ages ranged from 41 to 75 years. Clinical stage of cancer ranged from T1N0 in 10 patients, to T2N0 in 35 and T3N0 in 13 (two had T4N0 and two had T3N2). Forty-five had right-side cancers. Six patients received an extended protocol for various reasons, including tumor extending to the chest wall.
All 62 patients completed IMRT and EPP. All but one had resection and reconstruction of the diaphragm, and all but four had resection and reconstruction of the pericardium.
Overall death rate was 4.8% (three patients). Results were better in patients with epithelioid tumors, with a median survival of 51 months and disease-free survival of 47 months. Those with biphasic subtypes had median survival of 10 months and disease-free survival of 8 months. Eight patients had ipsilateral chest recurrence. “This analysis demonstrates that the SMART approach is particularly encouraging for patients with epithelial subtype,” Dr. de Perrot and coauthors said. They no longer perform the SMART protocol on patients with biphasic subtype.
The protocol was not without complications. Twenty-four patients, about 38%, had serious complications that required intervention or worse. Twelve had atrial fibrillation, but none advanced to life-threatening disease. Among other complications, four had empyema – one resulting in death – and three had pulmonary emboli. One other patient in the complications group died from pneumonia, and another died from a heart attack at home.
This is the Toronto researchers’ second attempt at studying the three-modality approach. In their first attempt, only half the patients who started with preoperative chemotherapy went onto complete the radiation after surgery because of difficulties administering it (J Thorac Cardiovasc Surg. 2007;133:111-6; J Clin Oncol. 2009;27:1413-8). Also, about 25% of patients had disease progression during induction chemotherapy and could not go onto surgery.
They designed the most recent trial to deliver radiation before surgery because of the excellent local control of cancer along with evidence that MPM tumors were radio-sensitive. “Considering the risk of disease progression on induction chemotherapy, we felt that switching the order of therapy was potentially a better option for patients with surgically resectable disease,” Dr. de Perrott and colleagues said.
The researchers cited the study’s single-center nature with a single treatment arm, and the lack of longer-term follow-up, as limitations. “However, in our own experience, this approach has been very encouraging and has become our primary option for patients with surgically resectable MPM,” they noted.
The study authors had no conflicts to disclose.
Key clinical point: A new protocol that involves accelerated hemithoracic intensity modulated radiation before surgery for lung mesothelioma delivered encouraging results in patients with epithelioid tumors.
Major finding: Disease-free survival was 47 months in epithelial subtypes compared with 8 months in biphasic subtypes.
Data source: A single-center population of 62 patients with malignant pleural mesothelioma treated between November 2008 and October 2014.
Disclosures: The study authors had no relationships to disclose.

Off-pump bypass may confer stroke benefit
Claims that off-pump coronary artery bypass (OPCAB) carries a lower risk of short-term stroke than conventional on-pump coronary artery bypass grafting (CABG) have been the subject of contradicting evidence, mostly because of the small size of the studies that showed a benefit, but European investigators published a meta-analysis involving more than 19,000 cases that showed what they called a “significant reduction” in the odds of a stroke.
“OPCAB was associated with a significant (28%) reduction in the odds of stroke compared with CABG,” said lead author Dr. Mariusz Kowalewski of Copernicus University in Bydgoszcz, Poland, and coauthors. The meta-analysis appeared in the January issue of the Journal of Thoracic and Cardiovascular Surgery (2016;151:60-77).
The coauthors represent 10 different centers throughout Europe. Dr. Kowalewski and three other coauthors are also with the Systemic Investigation and Research on Interventions and Outcomes MEDICINE Research Network based in Düsseldorf, Germany.
Dr. Kowalewski and colleagues said this is the largest meta-analysis of randomized clinical trials comparing short-term outcomes of the two approaches to coronary bypass. “By its unique design, this analysis is the first report to investigate the causal relationship between underlying patient risk profile and the benefits of off-pump coronary revascularization,” they noted.
The meta-analysis looked at results of three primary outcomes: death within 30 days of the operation (2.25% overall, 2% in the OPCAB group and 2.04% in the CABG group); MI 30 days after surgery (4.49% overall, 4.3% for OPCAB and 4.67% for CABG); and 30-day occurrence of stroke (1.67% overall, 1.34% for OPCAB group and 2% for CABG).
In the meta-analysis, the researchers evaluated 100 studies for potential bias and conducted three separate analyses: one of all studies; and then separate analyses of studies of more than 50 and 100 subjects, respectively. Their goal was to check if small studies were driving the results.
Dr. Kowalewski and the study team acknowledged the conflicting science surrounding the benefits of the off-pump vs. conventional bypass. They pointed out that a host of randomized studies failed to show significant differences in stroke rates between the two approaches, and that conflicting European and American guidelines on the role of off-pump surgery to provide a better neurologic outcome do not help to clarify the relative risk.
“This apparent contradiction with the available registries’ data reporting a significantly decreased incidence of stroke with OPCAB may be explained by the fact that cerebral stroke represents a relatively rare entity after CABG, and thus even the largest randomized studies are underpowered to prove a possible advantage of one technique over the other,” Dr. Kowalewski and colleagues said.
They cited the CORONARY trial (N Engl J Med. 2012;366:1489-97), the largest trial to date, with 4,752 patients, which found no difference in the rate of stroke between the two groups. Three previous meta-analyses demonstrated 30%-50% reductions in stroke, but a systemic review called those results into question (Cochrane Database Syst. Rev. 2012;3:CD007224).
The “most important” finding of their study may be the confirmation of what large registries have reported: that OPCAB is safer and more effective than conventional bypass surgery in older and sicker patients. But they acknowledged that why this is the case “remains a subject of ongoing debate.”
Dr. Kowalewski and coresearchers acknowledged a number of limitations of their meta-analysis, namely that sensitivity analysis may have missed clinically important differences in patient results and broad patient inclusion criteria. However, the random-effects model they used accounted for study variations. “The findings on significant risk profile meta-regression are further corroborated in the analysis of MI and stroke,” they said.
Coauthor Dr. Eliano Pio Navarese disclosed honoraria from Eli Lilly. The other coauthors had no relationships to disclose.
That off-pump coronary artery bypass (OPCAB) grafting provides no benefit or, at best, a negligible benefit over conventional on-pump surgery in terms of 30-day death rates and risk of myocardial infarction is a question that can be laid “safely to bed,” Dr. Fraser Rubens of the University of Ottawa Heart Institute said in his invited commentary (J Thorac Cardiovasc Surg. 2016;151:78-9).
However, less clear cut is the meta-analysis researchers’ assertion that off-pump CABG can significantly reduce the risk of future stroke, and that requires a close examination of the structural shortcomings of any meta-analysis, Dr. Rubens said. He cited a report that stated meta-analyses may inaccurately predict the outcomes of subsequent large randomized clinical trials in about one-third of all cases (N Engl J Med 1997;337:536-42).
Smaller trials like those used in a meta-analysis are more likely to be flawed because of a lax peer review or compromised methodology, Dr. Rubens said. The largest randomized trial the authors used in the meta-analysis showed “certainly no difference in stroke,” and when all trials with 200 or fewer patients were excluded, the stroke rates were 1.4% in the off-pump group vs. 1.6% in the on-pump population, he said.
To validate that difference would require a number needed to treat of 500 patients to prevent one stroke, Dr. Rubens said, “and the sample size required to prove this difference would exceed 58,000 patients per group” – whereas the large-trial cohort in this meta-analysis population was about a tenth of that.
“One must therefore assimilate this information with the worrisome evidence that off-pump surgery is associated with an increased incidence of incomplete revascularization, which is likely related to the subsequent increased need for repeat revascularization,” Dr. Rubens said.
Dr. Rubens had no disclosures.
That off-pump coronary artery bypass (OPCAB) grafting provides no benefit or, at best, a negligible benefit over conventional on-pump surgery in terms of 30-day death rates and risk of myocardial infarction is a question that can be laid “safely to bed,” Dr. Fraser Rubens of the University of Ottawa Heart Institute said in his invited commentary (J Thorac Cardiovasc Surg. 2016;151:78-9).
However, less clear cut is the meta-analysis researchers’ assertion that off-pump CABG can significantly reduce the risk of future stroke, and that requires a close examination of the structural shortcomings of any meta-analysis, Dr. Rubens said. He cited a report that stated meta-analyses may inaccurately predict the outcomes of subsequent large randomized clinical trials in about one-third of all cases (N Engl J Med 1997;337:536-42).
Smaller trials like those used in a meta-analysis are more likely to be flawed because of a lax peer review or compromised methodology, Dr. Rubens said. The largest randomized trial the authors used in the meta-analysis showed “certainly no difference in stroke,” and when all trials with 200 or fewer patients were excluded, the stroke rates were 1.4% in the off-pump group vs. 1.6% in the on-pump population, he said.
To validate that difference would require a number needed to treat of 500 patients to prevent one stroke, Dr. Rubens said, “and the sample size required to prove this difference would exceed 58,000 patients per group” – whereas the large-trial cohort in this meta-analysis population was about a tenth of that.
“One must therefore assimilate this information with the worrisome evidence that off-pump surgery is associated with an increased incidence of incomplete revascularization, which is likely related to the subsequent increased need for repeat revascularization,” Dr. Rubens said.
Dr. Rubens had no disclosures.
That off-pump coronary artery bypass (OPCAB) grafting provides no benefit or, at best, a negligible benefit over conventional on-pump surgery in terms of 30-day death rates and risk of myocardial infarction is a question that can be laid “safely to bed,” Dr. Fraser Rubens of the University of Ottawa Heart Institute said in his invited commentary (J Thorac Cardiovasc Surg. 2016;151:78-9).
However, less clear cut is the meta-analysis researchers’ assertion that off-pump CABG can significantly reduce the risk of future stroke, and that requires a close examination of the structural shortcomings of any meta-analysis, Dr. Rubens said. He cited a report that stated meta-analyses may inaccurately predict the outcomes of subsequent large randomized clinical trials in about one-third of all cases (N Engl J Med 1997;337:536-42).
Smaller trials like those used in a meta-analysis are more likely to be flawed because of a lax peer review or compromised methodology, Dr. Rubens said. The largest randomized trial the authors used in the meta-analysis showed “certainly no difference in stroke,” and when all trials with 200 or fewer patients were excluded, the stroke rates were 1.4% in the off-pump group vs. 1.6% in the on-pump population, he said.
To validate that difference would require a number needed to treat of 500 patients to prevent one stroke, Dr. Rubens said, “and the sample size required to prove this difference would exceed 58,000 patients per group” – whereas the large-trial cohort in this meta-analysis population was about a tenth of that.
“One must therefore assimilate this information with the worrisome evidence that off-pump surgery is associated with an increased incidence of incomplete revascularization, which is likely related to the subsequent increased need for repeat revascularization,” Dr. Rubens said.
Dr. Rubens had no disclosures.
Claims that off-pump coronary artery bypass (OPCAB) carries a lower risk of short-term stroke than conventional on-pump coronary artery bypass grafting (CABG) have been the subject of contradicting evidence, mostly because of the small size of the studies that showed a benefit, but European investigators published a meta-analysis involving more than 19,000 cases that showed what they called a “significant reduction” in the odds of a stroke.
“OPCAB was associated with a significant (28%) reduction in the odds of stroke compared with CABG,” said lead author Dr. Mariusz Kowalewski of Copernicus University in Bydgoszcz, Poland, and coauthors. The meta-analysis appeared in the January issue of the Journal of Thoracic and Cardiovascular Surgery (2016;151:60-77).
The coauthors represent 10 different centers throughout Europe. Dr. Kowalewski and three other coauthors are also with the Systemic Investigation and Research on Interventions and Outcomes MEDICINE Research Network based in Düsseldorf, Germany.
Dr. Kowalewski and colleagues said this is the largest meta-analysis of randomized clinical trials comparing short-term outcomes of the two approaches to coronary bypass. “By its unique design, this analysis is the first report to investigate the causal relationship between underlying patient risk profile and the benefits of off-pump coronary revascularization,” they noted.
The meta-analysis looked at results of three primary outcomes: death within 30 days of the operation (2.25% overall, 2% in the OPCAB group and 2.04% in the CABG group); MI 30 days after surgery (4.49% overall, 4.3% for OPCAB and 4.67% for CABG); and 30-day occurrence of stroke (1.67% overall, 1.34% for OPCAB group and 2% for CABG).
In the meta-analysis, the researchers evaluated 100 studies for potential bias and conducted three separate analyses: one of all studies; and then separate analyses of studies of more than 50 and 100 subjects, respectively. Their goal was to check if small studies were driving the results.
Dr. Kowalewski and the study team acknowledged the conflicting science surrounding the benefits of the off-pump vs. conventional bypass. They pointed out that a host of randomized studies failed to show significant differences in stroke rates between the two approaches, and that conflicting European and American guidelines on the role of off-pump surgery to provide a better neurologic outcome do not help to clarify the relative risk.
“This apparent contradiction with the available registries’ data reporting a significantly decreased incidence of stroke with OPCAB may be explained by the fact that cerebral stroke represents a relatively rare entity after CABG, and thus even the largest randomized studies are underpowered to prove a possible advantage of one technique over the other,” Dr. Kowalewski and colleagues said.
They cited the CORONARY trial (N Engl J Med. 2012;366:1489-97), the largest trial to date, with 4,752 patients, which found no difference in the rate of stroke between the two groups. Three previous meta-analyses demonstrated 30%-50% reductions in stroke, but a systemic review called those results into question (Cochrane Database Syst. Rev. 2012;3:CD007224).
The “most important” finding of their study may be the confirmation of what large registries have reported: that OPCAB is safer and more effective than conventional bypass surgery in older and sicker patients. But they acknowledged that why this is the case “remains a subject of ongoing debate.”
Dr. Kowalewski and coresearchers acknowledged a number of limitations of their meta-analysis, namely that sensitivity analysis may have missed clinically important differences in patient results and broad patient inclusion criteria. However, the random-effects model they used accounted for study variations. “The findings on significant risk profile meta-regression are further corroborated in the analysis of MI and stroke,” they said.
Coauthor Dr. Eliano Pio Navarese disclosed honoraria from Eli Lilly. The other coauthors had no relationships to disclose.
Claims that off-pump coronary artery bypass (OPCAB) carries a lower risk of short-term stroke than conventional on-pump coronary artery bypass grafting (CABG) have been the subject of contradicting evidence, mostly because of the small size of the studies that showed a benefit, but European investigators published a meta-analysis involving more than 19,000 cases that showed what they called a “significant reduction” in the odds of a stroke.
“OPCAB was associated with a significant (28%) reduction in the odds of stroke compared with CABG,” said lead author Dr. Mariusz Kowalewski of Copernicus University in Bydgoszcz, Poland, and coauthors. The meta-analysis appeared in the January issue of the Journal of Thoracic and Cardiovascular Surgery (2016;151:60-77).
The coauthors represent 10 different centers throughout Europe. Dr. Kowalewski and three other coauthors are also with the Systemic Investigation and Research on Interventions and Outcomes MEDICINE Research Network based in Düsseldorf, Germany.
Dr. Kowalewski and colleagues said this is the largest meta-analysis of randomized clinical trials comparing short-term outcomes of the two approaches to coronary bypass. “By its unique design, this analysis is the first report to investigate the causal relationship between underlying patient risk profile and the benefits of off-pump coronary revascularization,” they noted.
The meta-analysis looked at results of three primary outcomes: death within 30 days of the operation (2.25% overall, 2% in the OPCAB group and 2.04% in the CABG group); MI 30 days after surgery (4.49% overall, 4.3% for OPCAB and 4.67% for CABG); and 30-day occurrence of stroke (1.67% overall, 1.34% for OPCAB group and 2% for CABG).
In the meta-analysis, the researchers evaluated 100 studies for potential bias and conducted three separate analyses: one of all studies; and then separate analyses of studies of more than 50 and 100 subjects, respectively. Their goal was to check if small studies were driving the results.
Dr. Kowalewski and the study team acknowledged the conflicting science surrounding the benefits of the off-pump vs. conventional bypass. They pointed out that a host of randomized studies failed to show significant differences in stroke rates between the two approaches, and that conflicting European and American guidelines on the role of off-pump surgery to provide a better neurologic outcome do not help to clarify the relative risk.
“This apparent contradiction with the available registries’ data reporting a significantly decreased incidence of stroke with OPCAB may be explained by the fact that cerebral stroke represents a relatively rare entity after CABG, and thus even the largest randomized studies are underpowered to prove a possible advantage of one technique over the other,” Dr. Kowalewski and colleagues said.
They cited the CORONARY trial (N Engl J Med. 2012;366:1489-97), the largest trial to date, with 4,752 patients, which found no difference in the rate of stroke between the two groups. Three previous meta-analyses demonstrated 30%-50% reductions in stroke, but a systemic review called those results into question (Cochrane Database Syst. Rev. 2012;3:CD007224).
The “most important” finding of their study may be the confirmation of what large registries have reported: that OPCAB is safer and more effective than conventional bypass surgery in older and sicker patients. But they acknowledged that why this is the case “remains a subject of ongoing debate.”
Dr. Kowalewski and coresearchers acknowledged a number of limitations of their meta-analysis, namely that sensitivity analysis may have missed clinically important differences in patient results and broad patient inclusion criteria. However, the random-effects model they used accounted for study variations. “The findings on significant risk profile meta-regression are further corroborated in the analysis of MI and stroke,” they said.
Coauthor Dr. Eliano Pio Navarese disclosed honoraria from Eli Lilly. The other coauthors had no relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Off-pump coronary artery bypass is associated with a significant reduction in the odds of stroke compared with conventional coronary artery bypass grafting and should be considered in high-risk patients.
Major finding: Off-pump coronary artery bypass was associated with a 28% reduction in the odds of patients having a cerebral stroke when compared with the conventional on-pump procedure.
Data source: Meta-analysis of 100 studies with a total of 19,192 patients.
Disclosures: Coauthor Dr. Eliano Pio Navarese disclosed honoraria from Eli Lilly. The other authors had no relationships to disclose.
Post-repair MR may be worse than thought
In patients who undergo transcatheter mitral valve repair for mitral valve regurgitation (MR), residual mild (+2) regurgitation has been considered procedural success, but a team of Italian investigators has provided evidence that such a result may actually foretell far worse long-term outcomes than residual trace (≤1) MR.
The investigators from San Raffaele Scientific Institute in Milan reported their findings in the January issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg 2016;151:88-96). They compared follow-up outcomes of 223 consecutive patients with residual MR 2+ and MR ≤1 after implantation of the MitraClip system (Abbott Vascular). The procedures were performed between October 2008 and December 2014.
“In this study we found a clear unfavorable impact on follow-up outcomes of acute residual 2+ MR after MitraClip repair when compared to residual ≤1+ MR,” lead author Dr. Nicola Buzzatti and colleagues said.
The study cited a scarcity of data on the long-term impact of residual mild MR. “This topic is therefore particularly of interest, especially when assessing the convenience to expand transcatheter mitral repair procedures to intermediate or low-risk patients,” Dr. Buzzatti and coauthors said.
The study group all had moderate or greater (≥3+) MR when they underwent mitral valve repair (MVR). The post-MVR study cohort excluded patients who had residual MR of 3 or greater, which was considered a procedural failure. Four patients died within 30 days, each from a different cause: multi-organ failure, lung rupture, pneumonia with heart failure, and sudden death. The overall 30-day death rate was 1.8%.
Among the remainder of patients, the average follow-up was 20.5 months, with some follow-up extending to 75 months. The overall survival was 74.4% at 24 months and 63% at 48 months.
The study calculated the cumulative incidence function, or the probability of failure, of cardiac death in patients with residual MR ≤1 at 7.1% at 24 months and 10.9% at 48 months, compared with 26.9% at 24 months and 35.3% at 48 months in those with MR 2+. The probability of failure of recurrence of moderate or severe MR with residual MR ≤1 was 5.6% at 24 months and 13.3% at 48 months, compared with 45.2% at both 24 and 48 months with residual MR 2+. “The difference between MR ≤1 and MR=2 was significant,” Dr. Buzzatti and colleagues said.
The researchers separately evaluated outcomes among those who had functional MR (FMR) and degenerative MR (DMR). In FMR, patients with MR 2+ had a higher risk profile at baseline because of a slightly higher rate of advanced heart disease; they typically had larger ventricles with larger mitral valves and greater pulmonary pressure than the ≤1 MR patients. “Notably, these features could have impaired the surgeon’s ability to achieve acute optimal MR reduction during the MitraClip procedure,” Dr. Buzzatti and coauthors said. “For sure, advanced left ventricle remodeling was a strong independent predictor of increased cardiac death.” The study authors could not draw a similar conclusion with DMR because only three patients in the group died of cardiac causes.
MR recurrence was “remarkably higher” in MR 2+ patients, compared with the MR ≤1 group with FMR and DMR, and MR 2+ developed in 21.4% of the FMR group within 30 days of the procedure. “This poor efficacy results in a population of patients who were supposed to have had a ‘procedural success’ is striking,” Dr. Buzzatti and coauthors noted.
Dr. Buzzatti and coauthor Dr. Paolo Denti disclosed receiving consultant fees from Abbott Vascular. Coauthor Dr. Fabio Barili disclosed receiving consultant fees from St. Jude Medical. The other coauthors had no relationships to disclose.
In interpreting the findings of the Italian study and applying them in the clinic, one must consider the etiology of mitral valve regurgitation (MR) because that can determine the outcome of transcatheter mitral valve repair, Dr. Vincent Chan and Dr. Marc Ruel of the University of Ottawa Heart Institute said in their invited commentary (J Thorac Cardiovasc Surg 2016;151:97-8).
“In patients with coronary artery disease, it is well known that the presence of moderate chronic ischemic MR is associated with worse survival and more congestive heart failure compared to patients without MR,” Dr. Chan and Dr. Ruel said.
In a series his group studied, they noted that recurrent moderate MR was more common after MV repair than replacement; the survival rates between the two groups were similar (Ann Thorac Surg. 2011;92:1358-1365). That may be because late left ventricle (LV) function was similar between patients who had recurrent moderate MR and those that did not, but the Italian study did not clarify difference in late LV function between functional MR patients. “Perhaps differences in clinical outcome between patients with MR 2+ and MR ≤1+ relate to differences in ventricular function that portend mortality?” they asked.
They also called the researchers’ assertion that moderate MR impacts outcomes after repair “interesting.” They cited studies that linked effective worse outcomes to effective regurgitant orifice area (EROA) of 20-39 mm2, but that the complexity of echocardiographic measurement raises challenges in calculating EROA (Circulation. 2001;103:1759-64; N Engl J Med. 2005;352:875-83). “Also residual prolapse following MitraClip, as with any prolapse, may be brief and therefore instantaneous measures or regurgitation with pulse wave Doppler may be limited,” they said.
While percutaneous approaches to treat MR have “revolutionized” the care of these patients, the technology has its limitations, Dr. Chan and Dr. Ruel said. “Although many patients benefit from this therapy, the understanding of incomplete MR reduction with this technology continues to evolve.”
They had no disclosures.
In interpreting the findings of the Italian study and applying them in the clinic, one must consider the etiology of mitral valve regurgitation (MR) because that can determine the outcome of transcatheter mitral valve repair, Dr. Vincent Chan and Dr. Marc Ruel of the University of Ottawa Heart Institute said in their invited commentary (J Thorac Cardiovasc Surg 2016;151:97-8).
“In patients with coronary artery disease, it is well known that the presence of moderate chronic ischemic MR is associated with worse survival and more congestive heart failure compared to patients without MR,” Dr. Chan and Dr. Ruel said.
In a series his group studied, they noted that recurrent moderate MR was more common after MV repair than replacement; the survival rates between the two groups were similar (Ann Thorac Surg. 2011;92:1358-1365). That may be because late left ventricle (LV) function was similar between patients who had recurrent moderate MR and those that did not, but the Italian study did not clarify difference in late LV function between functional MR patients. “Perhaps differences in clinical outcome between patients with MR 2+ and MR ≤1+ relate to differences in ventricular function that portend mortality?” they asked.
They also called the researchers’ assertion that moderate MR impacts outcomes after repair “interesting.” They cited studies that linked effective worse outcomes to effective regurgitant orifice area (EROA) of 20-39 mm2, but that the complexity of echocardiographic measurement raises challenges in calculating EROA (Circulation. 2001;103:1759-64; N Engl J Med. 2005;352:875-83). “Also residual prolapse following MitraClip, as with any prolapse, may be brief and therefore instantaneous measures or regurgitation with pulse wave Doppler may be limited,” they said.
While percutaneous approaches to treat MR have “revolutionized” the care of these patients, the technology has its limitations, Dr. Chan and Dr. Ruel said. “Although many patients benefit from this therapy, the understanding of incomplete MR reduction with this technology continues to evolve.”
They had no disclosures.
In interpreting the findings of the Italian study and applying them in the clinic, one must consider the etiology of mitral valve regurgitation (MR) because that can determine the outcome of transcatheter mitral valve repair, Dr. Vincent Chan and Dr. Marc Ruel of the University of Ottawa Heart Institute said in their invited commentary (J Thorac Cardiovasc Surg 2016;151:97-8).
“In patients with coronary artery disease, it is well known that the presence of moderate chronic ischemic MR is associated with worse survival and more congestive heart failure compared to patients without MR,” Dr. Chan and Dr. Ruel said.
In a series his group studied, they noted that recurrent moderate MR was more common after MV repair than replacement; the survival rates between the two groups were similar (Ann Thorac Surg. 2011;92:1358-1365). That may be because late left ventricle (LV) function was similar between patients who had recurrent moderate MR and those that did not, but the Italian study did not clarify difference in late LV function between functional MR patients. “Perhaps differences in clinical outcome between patients with MR 2+ and MR ≤1+ relate to differences in ventricular function that portend mortality?” they asked.
They also called the researchers’ assertion that moderate MR impacts outcomes after repair “interesting.” They cited studies that linked effective worse outcomes to effective regurgitant orifice area (EROA) of 20-39 mm2, but that the complexity of echocardiographic measurement raises challenges in calculating EROA (Circulation. 2001;103:1759-64; N Engl J Med. 2005;352:875-83). “Also residual prolapse following MitraClip, as with any prolapse, may be brief and therefore instantaneous measures or regurgitation with pulse wave Doppler may be limited,” they said.
While percutaneous approaches to treat MR have “revolutionized” the care of these patients, the technology has its limitations, Dr. Chan and Dr. Ruel said. “Although many patients benefit from this therapy, the understanding of incomplete MR reduction with this technology continues to evolve.”
They had no disclosures.
In patients who undergo transcatheter mitral valve repair for mitral valve regurgitation (MR), residual mild (+2) regurgitation has been considered procedural success, but a team of Italian investigators has provided evidence that such a result may actually foretell far worse long-term outcomes than residual trace (≤1) MR.
The investigators from San Raffaele Scientific Institute in Milan reported their findings in the January issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg 2016;151:88-96). They compared follow-up outcomes of 223 consecutive patients with residual MR 2+ and MR ≤1 after implantation of the MitraClip system (Abbott Vascular). The procedures were performed between October 2008 and December 2014.
“In this study we found a clear unfavorable impact on follow-up outcomes of acute residual 2+ MR after MitraClip repair when compared to residual ≤1+ MR,” lead author Dr. Nicola Buzzatti and colleagues said.
The study cited a scarcity of data on the long-term impact of residual mild MR. “This topic is therefore particularly of interest, especially when assessing the convenience to expand transcatheter mitral repair procedures to intermediate or low-risk patients,” Dr. Buzzatti and coauthors said.
The study group all had moderate or greater (≥3+) MR when they underwent mitral valve repair (MVR). The post-MVR study cohort excluded patients who had residual MR of 3 or greater, which was considered a procedural failure. Four patients died within 30 days, each from a different cause: multi-organ failure, lung rupture, pneumonia with heart failure, and sudden death. The overall 30-day death rate was 1.8%.
Among the remainder of patients, the average follow-up was 20.5 months, with some follow-up extending to 75 months. The overall survival was 74.4% at 24 months and 63% at 48 months.
The study calculated the cumulative incidence function, or the probability of failure, of cardiac death in patients with residual MR ≤1 at 7.1% at 24 months and 10.9% at 48 months, compared with 26.9% at 24 months and 35.3% at 48 months in those with MR 2+. The probability of failure of recurrence of moderate or severe MR with residual MR ≤1 was 5.6% at 24 months and 13.3% at 48 months, compared with 45.2% at both 24 and 48 months with residual MR 2+. “The difference between MR ≤1 and MR=2 was significant,” Dr. Buzzatti and colleagues said.
The researchers separately evaluated outcomes among those who had functional MR (FMR) and degenerative MR (DMR). In FMR, patients with MR 2+ had a higher risk profile at baseline because of a slightly higher rate of advanced heart disease; they typically had larger ventricles with larger mitral valves and greater pulmonary pressure than the ≤1 MR patients. “Notably, these features could have impaired the surgeon’s ability to achieve acute optimal MR reduction during the MitraClip procedure,” Dr. Buzzatti and coauthors said. “For sure, advanced left ventricle remodeling was a strong independent predictor of increased cardiac death.” The study authors could not draw a similar conclusion with DMR because only three patients in the group died of cardiac causes.
MR recurrence was “remarkably higher” in MR 2+ patients, compared with the MR ≤1 group with FMR and DMR, and MR 2+ developed in 21.4% of the FMR group within 30 days of the procedure. “This poor efficacy results in a population of patients who were supposed to have had a ‘procedural success’ is striking,” Dr. Buzzatti and coauthors noted.
Dr. Buzzatti and coauthor Dr. Paolo Denti disclosed receiving consultant fees from Abbott Vascular. Coauthor Dr. Fabio Barili disclosed receiving consultant fees from St. Jude Medical. The other coauthors had no relationships to disclose.
In patients who undergo transcatheter mitral valve repair for mitral valve regurgitation (MR), residual mild (+2) regurgitation has been considered procedural success, but a team of Italian investigators has provided evidence that such a result may actually foretell far worse long-term outcomes than residual trace (≤1) MR.
The investigators from San Raffaele Scientific Institute in Milan reported their findings in the January issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg 2016;151:88-96). They compared follow-up outcomes of 223 consecutive patients with residual MR 2+ and MR ≤1 after implantation of the MitraClip system (Abbott Vascular). The procedures were performed between October 2008 and December 2014.
“In this study we found a clear unfavorable impact on follow-up outcomes of acute residual 2+ MR after MitraClip repair when compared to residual ≤1+ MR,” lead author Dr. Nicola Buzzatti and colleagues said.
The study cited a scarcity of data on the long-term impact of residual mild MR. “This topic is therefore particularly of interest, especially when assessing the convenience to expand transcatheter mitral repair procedures to intermediate or low-risk patients,” Dr. Buzzatti and coauthors said.
The study group all had moderate or greater (≥3+) MR when they underwent mitral valve repair (MVR). The post-MVR study cohort excluded patients who had residual MR of 3 or greater, which was considered a procedural failure. Four patients died within 30 days, each from a different cause: multi-organ failure, lung rupture, pneumonia with heart failure, and sudden death. The overall 30-day death rate was 1.8%.
Among the remainder of patients, the average follow-up was 20.5 months, with some follow-up extending to 75 months. The overall survival was 74.4% at 24 months and 63% at 48 months.
The study calculated the cumulative incidence function, or the probability of failure, of cardiac death in patients with residual MR ≤1 at 7.1% at 24 months and 10.9% at 48 months, compared with 26.9% at 24 months and 35.3% at 48 months in those with MR 2+. The probability of failure of recurrence of moderate or severe MR with residual MR ≤1 was 5.6% at 24 months and 13.3% at 48 months, compared with 45.2% at both 24 and 48 months with residual MR 2+. “The difference between MR ≤1 and MR=2 was significant,” Dr. Buzzatti and colleagues said.
The researchers separately evaluated outcomes among those who had functional MR (FMR) and degenerative MR (DMR). In FMR, patients with MR 2+ had a higher risk profile at baseline because of a slightly higher rate of advanced heart disease; they typically had larger ventricles with larger mitral valves and greater pulmonary pressure than the ≤1 MR patients. “Notably, these features could have impaired the surgeon’s ability to achieve acute optimal MR reduction during the MitraClip procedure,” Dr. Buzzatti and coauthors said. “For sure, advanced left ventricle remodeling was a strong independent predictor of increased cardiac death.” The study authors could not draw a similar conclusion with DMR because only three patients in the group died of cardiac causes.
MR recurrence was “remarkably higher” in MR 2+ patients, compared with the MR ≤1 group with FMR and DMR, and MR 2+ developed in 21.4% of the FMR group within 30 days of the procedure. “This poor efficacy results in a population of patients who were supposed to have had a ‘procedural success’ is striking,” Dr. Buzzatti and coauthors noted.
Dr. Buzzatti and coauthor Dr. Paolo Denti disclosed receiving consultant fees from Abbott Vascular. Coauthor Dr. Fabio Barili disclosed receiving consultant fees from St. Jude Medical. The other coauthors had no relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Residual mild mitral valve regurgitation (MR) after implantation of the MitraClip device (Abbott Vascular) was associated with worse survival, symptom relief, and risk of moderate or severe MR than residual trace MR after implantation.
Major finding: Patients with residual mild MR after MitraClip implantation had a 45% probability of recurrence of moderate or severe MR within 4 years, more than three times that of those who had residual trace MR.
Data source: Population of 223 consecutive patients with acute residual trace or mild MR after MitraClip implantation between 2008 and 2014 at a single institution.
Disclosures: Dr. Nicola Buzzatti and Dr. Paolo Denti disclosed receiving consultant fees from Abbott Vascular. Dr. Fabio Barili disclosed receiving consultant fees from St. Jude Medical. The other authors had no relationships to disclose.
Six-year Norwood-RVPA results in matched patients outperformed BT-shunt
Concerns with delayed right ventricle dysfunction have offset the early survival advantages after Norwood procedure with right ventricle to pulmonary artery conduit (NW-RVPA) over the Norwood with Blalock-Taussig shunt (NW-BT) in newborns with left ventricular outflow tract obstruction, but a recent report provides evidence that RV function between the two procedures is comparable for up to six years.
Reporting in the January issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015 Dec;150:1440–52), investigators for the Congenital Heart Surgeons’ Society (CHSS) trial found that NW-RVPA has better overall six-year survival and superior right ventricle function in the short term after surgery than NW-BT. The study involved 454 newborns with critical left ventricular outflow tract obstruction (LVOTO) in the CHSS database who had Norwood stage-1 from 2005 to 2014. Propensity matching paired 169 NW-RVPA patients with the same number of NW-BT patients for comparison. CHSS along with the Hospital for Sick Children in Toronto provided funding for the study.

“For neonates with critical LVOTO and similar baseline characteristics undergoing a Norwood stage-1 operation, the six-year overall survival and transplant-free survival were significantly better after NW-RVPA vs. NW-BT,” said Dr. Travis J. Wilder and his colleagues from the Hospital for Sick Children in Toronto.
Key questions the study sought to answer involved the clinical implications of the small variations in RV function between the two procedures, as well as the association between Norwood procedures and tricuspid valve regurgitation (TR) and overall survival.
Overall six-year survival was 70% for the NW-RVPA group vs. 55% for the NW-BT group. Right ventricle dysfunction rates three months after the procedure were lower for the NW-RVPA group, 6% vs. 16%, but rates of late RV dysfunction were less than 5% for both groups. Likewise, rates of moderate or greater TR at two years were lower in the NW-RVPA group: 11% vs. 16%.
Rates of Fontan operation after six years were higher among the NW-RVPA group (54% vs. 49%), as were transplantation rates (6% vs. 2%). Overall, 2% converted to a biventricular repair, but only after NW-RVPA; and seven patients who had NW-RVPA underwent a tricuspid valve repair, compared with four in the NW-BT group.
“For all survivors not undergoing transplantation or biventricular repair, the prevalence of late moderate or greater RV dysfunction and TR were similar between NW-BT and NW-RVPA at six years, without evidence of increased RV dysfunction for patients who underwent NW-RVPA,” Dr. Wilder and his colleagues said.
Consistent with previous studies, the CHSS study showed an early risk of death after a Norwood stage-1 operation, which may be due to a greater prevalence of significant RV dysfunction as the operation transitions from stage 1 to stage 2, Dr. Wilder and his coauthors said. “Although causation between these two time-related events cannot directly be made, it suggests that poor RV function contributes to early hazard for death,” they said.
The authors acknowledge a number of limitations with their study: the variation in the quality of echocardiogram reports from the multiple institutions involved, the inability of propensity matching to account for unmeasured factors and the influence of center and surgeon volume among participating sites. They also said that the ventriculotomy the NW-RVPA involves can lead to late aneurysm, arrhythmias, and ventricular failure. The adverse effects of ventriculotomy on long-term RV function “may not become apparent for years,” Dr. Wilder and his coauthors said.
Dr. Wilder presented a report of the original results at the 2015 American Association for Thoracic Surgery Annual meeting.
The authors had no relationships to disclose.
“It is time to have the courage to confess that we need a more overarching quality improvement strategy,” Dr. James S. Tweddell of the Children’s Hospital of Wisconsin said of the results of the Congenital Heart Surgeons’ Society (CHSS) study in his invited commentary (J Thorac Cardiovasc Surg. 2015 Dec;150:1453–4).
Dr. Tweddell said the findings of the CHSS study and the earlier Single Ventricle Reconstruction (SVR) trial (N Engl J Med. 2010;362:1980-1992) are similar in terms of transplant-free survival in newborns. And while the dates of the studies’ enrollments overlap – 2005-2008 for SVR and 2005-2014 for CHSS – the more recent findings of the CHSS study would imply an advantage in terms of survival and right ventricle function. Nonetheless, the survival rates are similar, he said. “Only about 60% of patients remain alive.”

|
Dr. James S. Tweddell |
Dr. Tweddell pointed out the CHSS study is not a randomized, controlled trial, “and the shortcomings of the prospective observational study are well known.”
In calling for a “more overarching” quality improvement measure, Dr. Tweddell said that many programs use Norwood performance as a benchmark for outcomes. He proposed collaboration among high and low performing centers, imitating the adult cardiology model. He also suggested consolidation of programs performing the Norwood procedure to eliminate low-volume centers and develop centers of excellence. “The outcome of the Norwood procedure is dependent on both program and surgeon volume,” Dr. Tweddell said.
The CHSS study “is important and identifies a potentially durable benefit to the NW-RVPA,” Dr. Tweddell said, “but perhaps now is the time to focus on strategies between programs rather than solely within programs.”
“It is time to have the courage to confess that we need a more overarching quality improvement strategy,” Dr. James S. Tweddell of the Children’s Hospital of Wisconsin said of the results of the Congenital Heart Surgeons’ Society (CHSS) study in his invited commentary (J Thorac Cardiovasc Surg. 2015 Dec;150:1453–4).
Dr. Tweddell said the findings of the CHSS study and the earlier Single Ventricle Reconstruction (SVR) trial (N Engl J Med. 2010;362:1980-1992) are similar in terms of transplant-free survival in newborns. And while the dates of the studies’ enrollments overlap – 2005-2008 for SVR and 2005-2014 for CHSS – the more recent findings of the CHSS study would imply an advantage in terms of survival and right ventricle function. Nonetheless, the survival rates are similar, he said. “Only about 60% of patients remain alive.”
|
|
Dr. James S. Tweddell |
Dr. Tweddell pointed out the CHSS study is not a randomized, controlled trial, “and the shortcomings of the prospective observational study are well known.”
In calling for a “more overarching” quality improvement measure, Dr. Tweddell said that many programs use Norwood performance as a benchmark for outcomes. He proposed collaboration among high and low performing centers, imitating the adult cardiology model. He also suggested consolidation of programs performing the Norwood procedure to eliminate low-volume centers and develop centers of excellence. “The outcome of the Norwood procedure is dependent on both program and surgeon volume,” Dr. Tweddell said.
The CHSS study “is important and identifies a potentially durable benefit to the NW-RVPA,” Dr. Tweddell said, “but perhaps now is the time to focus on strategies between programs rather than solely within programs.”
“It is time to have the courage to confess that we need a more overarching quality improvement strategy,” Dr. James S. Tweddell of the Children’s Hospital of Wisconsin said of the results of the Congenital Heart Surgeons’ Society (CHSS) study in his invited commentary (J Thorac Cardiovasc Surg. 2015 Dec;150:1453–4).
Dr. Tweddell said the findings of the CHSS study and the earlier Single Ventricle Reconstruction (SVR) trial (N Engl J Med. 2010;362:1980-1992) are similar in terms of transplant-free survival in newborns. And while the dates of the studies’ enrollments overlap – 2005-2008 for SVR and 2005-2014 for CHSS – the more recent findings of the CHSS study would imply an advantage in terms of survival and right ventricle function. Nonetheless, the survival rates are similar, he said. “Only about 60% of patients remain alive.”
|
|
Dr. James S. Tweddell |
Dr. Tweddell pointed out the CHSS study is not a randomized, controlled trial, “and the shortcomings of the prospective observational study are well known.”
In calling for a “more overarching” quality improvement measure, Dr. Tweddell said that many programs use Norwood performance as a benchmark for outcomes. He proposed collaboration among high and low performing centers, imitating the adult cardiology model. He also suggested consolidation of programs performing the Norwood procedure to eliminate low-volume centers and develop centers of excellence. “The outcome of the Norwood procedure is dependent on both program and surgeon volume,” Dr. Tweddell said.
The CHSS study “is important and identifies a potentially durable benefit to the NW-RVPA,” Dr. Tweddell said, “but perhaps now is the time to focus on strategies between programs rather than solely within programs.”
Concerns with delayed right ventricle dysfunction have offset the early survival advantages after Norwood procedure with right ventricle to pulmonary artery conduit (NW-RVPA) over the Norwood with Blalock-Taussig shunt (NW-BT) in newborns with left ventricular outflow tract obstruction, but a recent report provides evidence that RV function between the two procedures is comparable for up to six years.
Reporting in the January issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015 Dec;150:1440–52), investigators for the Congenital Heart Surgeons’ Society (CHSS) trial found that NW-RVPA has better overall six-year survival and superior right ventricle function in the short term after surgery than NW-BT. The study involved 454 newborns with critical left ventricular outflow tract obstruction (LVOTO) in the CHSS database who had Norwood stage-1 from 2005 to 2014. Propensity matching paired 169 NW-RVPA patients with the same number of NW-BT patients for comparison. CHSS along with the Hospital for Sick Children in Toronto provided funding for the study.
“For neonates with critical LVOTO and similar baseline characteristics undergoing a Norwood stage-1 operation, the six-year overall survival and transplant-free survival were significantly better after NW-RVPA vs. NW-BT,” said Dr. Travis J. Wilder and his colleagues from the Hospital for Sick Children in Toronto.
Key questions the study sought to answer involved the clinical implications of the small variations in RV function between the two procedures, as well as the association between Norwood procedures and tricuspid valve regurgitation (TR) and overall survival.
Overall six-year survival was 70% for the NW-RVPA group vs. 55% for the NW-BT group. Right ventricle dysfunction rates three months after the procedure were lower for the NW-RVPA group, 6% vs. 16%, but rates of late RV dysfunction were less than 5% for both groups. Likewise, rates of moderate or greater TR at two years were lower in the NW-RVPA group: 11% vs. 16%.
Rates of Fontan operation after six years were higher among the NW-RVPA group (54% vs. 49%), as were transplantation rates (6% vs. 2%). Overall, 2% converted to a biventricular repair, but only after NW-RVPA; and seven patients who had NW-RVPA underwent a tricuspid valve repair, compared with four in the NW-BT group.
“For all survivors not undergoing transplantation or biventricular repair, the prevalence of late moderate or greater RV dysfunction and TR were similar between NW-BT and NW-RVPA at six years, without evidence of increased RV dysfunction for patients who underwent NW-RVPA,” Dr. Wilder and his colleagues said.
Consistent with previous studies, the CHSS study showed an early risk of death after a Norwood stage-1 operation, which may be due to a greater prevalence of significant RV dysfunction as the operation transitions from stage 1 to stage 2, Dr. Wilder and his coauthors said. “Although causation between these two time-related events cannot directly be made, it suggests that poor RV function contributes to early hazard for death,” they said.
The authors acknowledge a number of limitations with their study: the variation in the quality of echocardiogram reports from the multiple institutions involved, the inability of propensity matching to account for unmeasured factors and the influence of center and surgeon volume among participating sites. They also said that the ventriculotomy the NW-RVPA involves can lead to late aneurysm, arrhythmias, and ventricular failure. The adverse effects of ventriculotomy on long-term RV function “may not become apparent for years,” Dr. Wilder and his coauthors said.
Dr. Wilder presented a report of the original results at the 2015 American Association for Thoracic Surgery Annual meeting.
The authors had no relationships to disclose.
Concerns with delayed right ventricle dysfunction have offset the early survival advantages after Norwood procedure with right ventricle to pulmonary artery conduit (NW-RVPA) over the Norwood with Blalock-Taussig shunt (NW-BT) in newborns with left ventricular outflow tract obstruction, but a recent report provides evidence that RV function between the two procedures is comparable for up to six years.
Reporting in the January issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015 Dec;150:1440–52), investigators for the Congenital Heart Surgeons’ Society (CHSS) trial found that NW-RVPA has better overall six-year survival and superior right ventricle function in the short term after surgery than NW-BT. The study involved 454 newborns with critical left ventricular outflow tract obstruction (LVOTO) in the CHSS database who had Norwood stage-1 from 2005 to 2014. Propensity matching paired 169 NW-RVPA patients with the same number of NW-BT patients for comparison. CHSS along with the Hospital for Sick Children in Toronto provided funding for the study.
“For neonates with critical LVOTO and similar baseline characteristics undergoing a Norwood stage-1 operation, the six-year overall survival and transplant-free survival were significantly better after NW-RVPA vs. NW-BT,” said Dr. Travis J. Wilder and his colleagues from the Hospital for Sick Children in Toronto.
Key questions the study sought to answer involved the clinical implications of the small variations in RV function between the two procedures, as well as the association between Norwood procedures and tricuspid valve regurgitation (TR) and overall survival.
Overall six-year survival was 70% for the NW-RVPA group vs. 55% for the NW-BT group. Right ventricle dysfunction rates three months after the procedure were lower for the NW-RVPA group, 6% vs. 16%, but rates of late RV dysfunction were less than 5% for both groups. Likewise, rates of moderate or greater TR at two years were lower in the NW-RVPA group: 11% vs. 16%.
Rates of Fontan operation after six years were higher among the NW-RVPA group (54% vs. 49%), as were transplantation rates (6% vs. 2%). Overall, 2% converted to a biventricular repair, but only after NW-RVPA; and seven patients who had NW-RVPA underwent a tricuspid valve repair, compared with four in the NW-BT group.
“For all survivors not undergoing transplantation or biventricular repair, the prevalence of late moderate or greater RV dysfunction and TR were similar between NW-BT and NW-RVPA at six years, without evidence of increased RV dysfunction for patients who underwent NW-RVPA,” Dr. Wilder and his colleagues said.
Consistent with previous studies, the CHSS study showed an early risk of death after a Norwood stage-1 operation, which may be due to a greater prevalence of significant RV dysfunction as the operation transitions from stage 1 to stage 2, Dr. Wilder and his coauthors said. “Although causation between these two time-related events cannot directly be made, it suggests that poor RV function contributes to early hazard for death,” they said.
The authors acknowledge a number of limitations with their study: the variation in the quality of echocardiogram reports from the multiple institutions involved, the inability of propensity matching to account for unmeasured factors and the influence of center and surgeon volume among participating sites. They also said that the ventriculotomy the NW-RVPA involves can lead to late aneurysm, arrhythmias, and ventricular failure. The adverse effects of ventriculotomy on long-term RV function “may not become apparent for years,” Dr. Wilder and his coauthors said.
Dr. Wilder presented a report of the original results at the 2015 American Association for Thoracic Surgery Annual meeting.
The authors had no relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOTHORACIC SURGERY
Key clinical point: For newborns with critical left ventricular outflow tract obstruction (LVOTO) undergoing Norwood stage-1 procedures, Norwood with right ventricle to pulmonary artery conduit (NW-RVPA) resulted in better survival and less short-term right-ventricle dysfunction than matched patients who had the Norwood procedure with Blalock-Taussig shunt (NW-BT).
Major finding: Overall six-year survival was 70% for the NW-RVPA group vs. 55% for the NW-BT group, and RV dysfunction rates three months after the procedure were 6% for NW-RVPA vs. 16% for NW-BT.
Data source: Prospective group of 454 newborns with LVOTO in the Congenital Heart Surgeons’ Society database.
Disclosures: The Congenital Heart Surgeons’ Society and Hospital for Sick Children, Toronto, provided funding for the study. The authors had no relationships to disclose.

Should annular dilation be a marker for concomitant tricuspid valve repair?
The idea of performing a tricuspid valve repair during a mitral valve procedure has fueled considerable debate among cardiovascular surgeons largely because the grading of tricuspid regurgitation (TR) has been an unreliable marker, so now may be the time to use a new parameter, Dr. Robert Dion of Genk, Belgium, argues in an expert opinion in the Journal of Thoracic and Cardiovascular Surgery (2015 Nov 20;150:1040-3).
“Therefore, we need a parameter hardly depending on preload,” Dr. Dion said. He noted that many authors have validated the use of annual dilatation of 40 mm or 21mm/m2.
Further, preoperative functional New York Heart Association (NYHA) class plays a major role, Dr. Dion said. TR is progressive in nature and the existence of concomitant mitral valve disease can aggravate annular dilation. The earlier surgeons operate on the mitral valve, the less frequently patients will require tricuspid valve repair at the same time, he said.

The controversy was aired in a report at the 2015 American Association for Thoracic Surgery meeting when Dr. Joanna Chikwe of Mount Sinai Hospital in New York discussed an approach that led to tricuspid valve repair at the time of mitral valve surgery in almost two-thirds of patients. Dr. Chikwe and her coauthors opted for concomitant surgery when patients had moderate TR or tricuspid annular dilatation of 40 mm or greater – a strategy that Dr. Dion said was validated because they reported comparable outcomes in terms of death, morbidity, or pacemaker need. The concomitant repair cured TR and prevented progression at seven years of follow-up; and it induced right ventricle recovery and reduced pulmonary hypertension.
In this opinion piece, Dr. Dion took issue with comments made by Dr. Tirone E. David of the University of Toronto during Dr. Chikwe’s AATS presentation. Dr. David, for whom the David reimplantation technique for aortic root replacement is named, called the technique “overkill,” according to Dr. Dion.
Specifically, Dr. Dion questioned Dr. David’s assertions that the use of rigid rings in mitral valve repair causes TR and that no evidence validates the 40-mm diameter minimum in patients with degenerative mitral valve disease. On the first point, Dr. Dion said no evidence has linked the rigidity of the mitral valve ring and progression of tricuspid regurgitation. On the second, Dr. Dion cited eight studies of progressive tricuspid annular dilation with mitral regurgitation, most of which proposed the 40-mm threshold for concomitant tricuspid valve repair. Since then, the 40-mm threshold has been adopted for both European and American guidelines and validated by five reports from 2011 to 2014.
Dr. Dion said the rationale for using annular dilation rather than TR grade rests on “three poles”: annular dilation does not depend on preload whereas the right ventricle does; documented discrepancies between clinical and hemodynamic data (J Cardiol Surg. 1994 Mar;9(2 suppl):237-41; J Am Coll Cardiol. 2004 Feb. 4;43:405-9); and the idea that TR is “bad” for the patient. He also cited disparities in the number of concomitant repairs performed at leading centers: 7%-10% at the Mayo Clinic and Dr. David’s Toronto center, 25% in Leipzig, 40%-45% in his own clinic and two others, and 65% in Dr. Chikwe’s facility.
But early intervention for mitral valve dysfunction is a key indicator of the need for concomitant tricuspid valve repair, Dr. Dion said. “The earlier we operate on the MV, the less frequently patients will require tricuspid valve repair,” he said. In his own approach, Dr. Dion uses a transseptal approach of the mitral valve. For TR greater than grade 2, he performs tricuspid repair using a semirigid ring sized on the area of the anterior leaflet tissue; and if the tenting distance is 8 mm or greater, he includes anterior leaflet augmentation. When TR grade is 2 or less, he also performs concomitant tricuspid repair when the tricuspid annulus is 40 mm or greater or when the tricuspid annulus is 3.5-4 mm in the setting of a host of other cardiac problems, from atrial fibrillation to left valve dysfunction. “Otherwise: abstention,” he said.
“The major issue here is to do everything possible to avoid the risk and outcomes of reoperative tricuspid valve surgery,” Dr. Dion said, citing in-hospital death rates of 13.2% that Dr. David reported (Ann Thorac Surg. 2013 Jan;95:119-24.) and 14.6% the Leipzig group reported (J Thorac Cardiovasc Surg. 2013 Oct; 146:841-7).While he acknowledged calls for a prospective, randomized clinical trial, Dr. Dion said the contraindications for concomitant tricuspid valve repair with mitral valve repair have already been well documented.
Dr. Dion reports consulting fees from Sorin, Edwards, Johnson & Johnson, and St. Jude Medical.
In their invited commentary, Dr. Tirone E. David of the University of Toronto and his colleagues said that performing a tricuspid valve annuloplasty (TVA) in the setting of tricuspid regurgitation (TR) or a tricuspid annulus diameter greater than 40 mm does not completely prevent the onset of new TR (J Thorac Cardiovasc Surg. 2015 Nov;150:1043-4). “Other factors play a role in its development,” they said. “Longstanding atrial fibrillation is one of them.”
“Are patients who have mitral valve (MV) repair for degenerative disease of the MV likely to develop functional TR if there is only trivial or mild TR before surgery?” Dr. David and his coauthors asked. “We are certain that some patients do, but it does not appear to be as common as patients who had MV replacement for rheumatic disease. Is it solely because the incidence of atrial fibrillation is higher in rheumatic patients?”
In a second invited commentary, Dr. Richard J. Shemin of the University of California, Los Angeles, said the discrepancies between the rates of concomitant tricuspid repair among the various centers that Dr. Robert A. Dion cited beg for resolution (J Thorac Cardiovasc Surg. 2015 Nov;150:1045-6). “The wide discrepancy can perhaps be partially resolved with a re-review of the Toronto experience and follow-up,” Dr. Shemin said. “The subset of patients with TVA greater than 40 who were not repaired and the late follow-up would be very helpful.”
The cardiothoracic surgeon faces conflicting principles when considering concomitant tricuspid valve repair, Dr. Shemin said: avoiding an unnecessary surgery when functional TR exists, or leaving a residual lesion that could lead to a risky reoperation. Hence, accurate measurements of the tricuspid valve annulus and TR are essential, Dr. Shemin said.
“The tricuspid valve has been rediscovered and further investigation will resolve the questions,” Dr. Shemin said. Likewise, Dr. David and his colleagues said the “time has come” for a multicentered clinical trial to put the issue to rest for both mitral valve replacement and repair.
In their invited commentary, Dr. Tirone E. David of the University of Toronto and his colleagues said that performing a tricuspid valve annuloplasty (TVA) in the setting of tricuspid regurgitation (TR) or a tricuspid annulus diameter greater than 40 mm does not completely prevent the onset of new TR (J Thorac Cardiovasc Surg. 2015 Nov;150:1043-4). “Other factors play a role in its development,” they said. “Longstanding atrial fibrillation is one of them.”
“Are patients who have mitral valve (MV) repair for degenerative disease of the MV likely to develop functional TR if there is only trivial or mild TR before surgery?” Dr. David and his coauthors asked. “We are certain that some patients do, but it does not appear to be as common as patients who had MV replacement for rheumatic disease. Is it solely because the incidence of atrial fibrillation is higher in rheumatic patients?”
In a second invited commentary, Dr. Richard J. Shemin of the University of California, Los Angeles, said the discrepancies between the rates of concomitant tricuspid repair among the various centers that Dr. Robert A. Dion cited beg for resolution (J Thorac Cardiovasc Surg. 2015 Nov;150:1045-6). “The wide discrepancy can perhaps be partially resolved with a re-review of the Toronto experience and follow-up,” Dr. Shemin said. “The subset of patients with TVA greater than 40 who were not repaired and the late follow-up would be very helpful.”
The cardiothoracic surgeon faces conflicting principles when considering concomitant tricuspid valve repair, Dr. Shemin said: avoiding an unnecessary surgery when functional TR exists, or leaving a residual lesion that could lead to a risky reoperation. Hence, accurate measurements of the tricuspid valve annulus and TR are essential, Dr. Shemin said.
“The tricuspid valve has been rediscovered and further investigation will resolve the questions,” Dr. Shemin said. Likewise, Dr. David and his colleagues said the “time has come” for a multicentered clinical trial to put the issue to rest for both mitral valve replacement and repair.
In their invited commentary, Dr. Tirone E. David of the University of Toronto and his colleagues said that performing a tricuspid valve annuloplasty (TVA) in the setting of tricuspid regurgitation (TR) or a tricuspid annulus diameter greater than 40 mm does not completely prevent the onset of new TR (J Thorac Cardiovasc Surg. 2015 Nov;150:1043-4). “Other factors play a role in its development,” they said. “Longstanding atrial fibrillation is one of them.”
“Are patients who have mitral valve (MV) repair for degenerative disease of the MV likely to develop functional TR if there is only trivial or mild TR before surgery?” Dr. David and his coauthors asked. “We are certain that some patients do, but it does not appear to be as common as patients who had MV replacement for rheumatic disease. Is it solely because the incidence of atrial fibrillation is higher in rheumatic patients?”
In a second invited commentary, Dr. Richard J. Shemin of the University of California, Los Angeles, said the discrepancies between the rates of concomitant tricuspid repair among the various centers that Dr. Robert A. Dion cited beg for resolution (J Thorac Cardiovasc Surg. 2015 Nov;150:1045-6). “The wide discrepancy can perhaps be partially resolved with a re-review of the Toronto experience and follow-up,” Dr. Shemin said. “The subset of patients with TVA greater than 40 who were not repaired and the late follow-up would be very helpful.”
The cardiothoracic surgeon faces conflicting principles when considering concomitant tricuspid valve repair, Dr. Shemin said: avoiding an unnecessary surgery when functional TR exists, or leaving a residual lesion that could lead to a risky reoperation. Hence, accurate measurements of the tricuspid valve annulus and TR are essential, Dr. Shemin said.
“The tricuspid valve has been rediscovered and further investigation will resolve the questions,” Dr. Shemin said. Likewise, Dr. David and his colleagues said the “time has come” for a multicentered clinical trial to put the issue to rest for both mitral valve replacement and repair.
The idea of performing a tricuspid valve repair during a mitral valve procedure has fueled considerable debate among cardiovascular surgeons largely because the grading of tricuspid regurgitation (TR) has been an unreliable marker, so now may be the time to use a new parameter, Dr. Robert Dion of Genk, Belgium, argues in an expert opinion in the Journal of Thoracic and Cardiovascular Surgery (2015 Nov 20;150:1040-3).
“Therefore, we need a parameter hardly depending on preload,” Dr. Dion said. He noted that many authors have validated the use of annual dilatation of 40 mm or 21mm/m2.
Further, preoperative functional New York Heart Association (NYHA) class plays a major role, Dr. Dion said. TR is progressive in nature and the existence of concomitant mitral valve disease can aggravate annular dilation. The earlier surgeons operate on the mitral valve, the less frequently patients will require tricuspid valve repair at the same time, he said.
The controversy was aired in a report at the 2015 American Association for Thoracic Surgery meeting when Dr. Joanna Chikwe of Mount Sinai Hospital in New York discussed an approach that led to tricuspid valve repair at the time of mitral valve surgery in almost two-thirds of patients. Dr. Chikwe and her coauthors opted for concomitant surgery when patients had moderate TR or tricuspid annular dilatation of 40 mm or greater – a strategy that Dr. Dion said was validated because they reported comparable outcomes in terms of death, morbidity, or pacemaker need. The concomitant repair cured TR and prevented progression at seven years of follow-up; and it induced right ventricle recovery and reduced pulmonary hypertension.
In this opinion piece, Dr. Dion took issue with comments made by Dr. Tirone E. David of the University of Toronto during Dr. Chikwe’s AATS presentation. Dr. David, for whom the David reimplantation technique for aortic root replacement is named, called the technique “overkill,” according to Dr. Dion.
Specifically, Dr. Dion questioned Dr. David’s assertions that the use of rigid rings in mitral valve repair causes TR and that no evidence validates the 40-mm diameter minimum in patients with degenerative mitral valve disease. On the first point, Dr. Dion said no evidence has linked the rigidity of the mitral valve ring and progression of tricuspid regurgitation. On the second, Dr. Dion cited eight studies of progressive tricuspid annular dilation with mitral regurgitation, most of which proposed the 40-mm threshold for concomitant tricuspid valve repair. Since then, the 40-mm threshold has been adopted for both European and American guidelines and validated by five reports from 2011 to 2014.
Dr. Dion said the rationale for using annular dilation rather than TR grade rests on “three poles”: annular dilation does not depend on preload whereas the right ventricle does; documented discrepancies between clinical and hemodynamic data (J Cardiol Surg. 1994 Mar;9(2 suppl):237-41; J Am Coll Cardiol. 2004 Feb. 4;43:405-9); and the idea that TR is “bad” for the patient. He also cited disparities in the number of concomitant repairs performed at leading centers: 7%-10% at the Mayo Clinic and Dr. David’s Toronto center, 25% in Leipzig, 40%-45% in his own clinic and two others, and 65% in Dr. Chikwe’s facility.
But early intervention for mitral valve dysfunction is a key indicator of the need for concomitant tricuspid valve repair, Dr. Dion said. “The earlier we operate on the MV, the less frequently patients will require tricuspid valve repair,” he said. In his own approach, Dr. Dion uses a transseptal approach of the mitral valve. For TR greater than grade 2, he performs tricuspid repair using a semirigid ring sized on the area of the anterior leaflet tissue; and if the tenting distance is 8 mm or greater, he includes anterior leaflet augmentation. When TR grade is 2 or less, he also performs concomitant tricuspid repair when the tricuspid annulus is 40 mm or greater or when the tricuspid annulus is 3.5-4 mm in the setting of a host of other cardiac problems, from atrial fibrillation to left valve dysfunction. “Otherwise: abstention,” he said.
“The major issue here is to do everything possible to avoid the risk and outcomes of reoperative tricuspid valve surgery,” Dr. Dion said, citing in-hospital death rates of 13.2% that Dr. David reported (Ann Thorac Surg. 2013 Jan;95:119-24.) and 14.6% the Leipzig group reported (J Thorac Cardiovasc Surg. 2013 Oct; 146:841-7).While he acknowledged calls for a prospective, randomized clinical trial, Dr. Dion said the contraindications for concomitant tricuspid valve repair with mitral valve repair have already been well documented.
Dr. Dion reports consulting fees from Sorin, Edwards, Johnson & Johnson, and St. Jude Medical.
The idea of performing a tricuspid valve repair during a mitral valve procedure has fueled considerable debate among cardiovascular surgeons largely because the grading of tricuspid regurgitation (TR) has been an unreliable marker, so now may be the time to use a new parameter, Dr. Robert Dion of Genk, Belgium, argues in an expert opinion in the Journal of Thoracic and Cardiovascular Surgery (2015 Nov 20;150:1040-3).
“Therefore, we need a parameter hardly depending on preload,” Dr. Dion said. He noted that many authors have validated the use of annual dilatation of 40 mm or 21mm/m2.
Further, preoperative functional New York Heart Association (NYHA) class plays a major role, Dr. Dion said. TR is progressive in nature and the existence of concomitant mitral valve disease can aggravate annular dilation. The earlier surgeons operate on the mitral valve, the less frequently patients will require tricuspid valve repair at the same time, he said.
The controversy was aired in a report at the 2015 American Association for Thoracic Surgery meeting when Dr. Joanna Chikwe of Mount Sinai Hospital in New York discussed an approach that led to tricuspid valve repair at the time of mitral valve surgery in almost two-thirds of patients. Dr. Chikwe and her coauthors opted for concomitant surgery when patients had moderate TR or tricuspid annular dilatation of 40 mm or greater – a strategy that Dr. Dion said was validated because they reported comparable outcomes in terms of death, morbidity, or pacemaker need. The concomitant repair cured TR and prevented progression at seven years of follow-up; and it induced right ventricle recovery and reduced pulmonary hypertension.
In this opinion piece, Dr. Dion took issue with comments made by Dr. Tirone E. David of the University of Toronto during Dr. Chikwe’s AATS presentation. Dr. David, for whom the David reimplantation technique for aortic root replacement is named, called the technique “overkill,” according to Dr. Dion.
Specifically, Dr. Dion questioned Dr. David’s assertions that the use of rigid rings in mitral valve repair causes TR and that no evidence validates the 40-mm diameter minimum in patients with degenerative mitral valve disease. On the first point, Dr. Dion said no evidence has linked the rigidity of the mitral valve ring and progression of tricuspid regurgitation. On the second, Dr. Dion cited eight studies of progressive tricuspid annular dilation with mitral regurgitation, most of which proposed the 40-mm threshold for concomitant tricuspid valve repair. Since then, the 40-mm threshold has been adopted for both European and American guidelines and validated by five reports from 2011 to 2014.
Dr. Dion said the rationale for using annular dilation rather than TR grade rests on “three poles”: annular dilation does not depend on preload whereas the right ventricle does; documented discrepancies between clinical and hemodynamic data (J Cardiol Surg. 1994 Mar;9(2 suppl):237-41; J Am Coll Cardiol. 2004 Feb. 4;43:405-9); and the idea that TR is “bad” for the patient. He also cited disparities in the number of concomitant repairs performed at leading centers: 7%-10% at the Mayo Clinic and Dr. David’s Toronto center, 25% in Leipzig, 40%-45% in his own clinic and two others, and 65% in Dr. Chikwe’s facility.
But early intervention for mitral valve dysfunction is a key indicator of the need for concomitant tricuspid valve repair, Dr. Dion said. “The earlier we operate on the MV, the less frequently patients will require tricuspid valve repair,” he said. In his own approach, Dr. Dion uses a transseptal approach of the mitral valve. For TR greater than grade 2, he performs tricuspid repair using a semirigid ring sized on the area of the anterior leaflet tissue; and if the tenting distance is 8 mm or greater, he includes anterior leaflet augmentation. When TR grade is 2 or less, he also performs concomitant tricuspid repair when the tricuspid annulus is 40 mm or greater or when the tricuspid annulus is 3.5-4 mm in the setting of a host of other cardiac problems, from atrial fibrillation to left valve dysfunction. “Otherwise: abstention,” he said.
“The major issue here is to do everything possible to avoid the risk and outcomes of reoperative tricuspid valve surgery,” Dr. Dion said, citing in-hospital death rates of 13.2% that Dr. David reported (Ann Thorac Surg. 2013 Jan;95:119-24.) and 14.6% the Leipzig group reported (J Thorac Cardiovasc Surg. 2013 Oct; 146:841-7).While he acknowledged calls for a prospective, randomized clinical trial, Dr. Dion said the contraindications for concomitant tricuspid valve repair with mitral valve repair have already been well documented.
Dr. Dion reports consulting fees from Sorin, Edwards, Johnson & Johnson, and St. Jude Medical.
Key clinical point: Controversy surrounds the need for concomitant tricuspid valve repair with a mitral valve procedure and what parameters the decision should be based on.
Major finding: Increasing reports have supported the use of annular dilation of 40 mm or greater as a threshold for performing concomitant tricuspid valve repair rather than grading of tricuspid regurgitation.
Data source: This Expert Opinion piece cites studies along with American and European clinical guidelines that support the 40-mm threshold.
Disclosures: Dr. Dion reports consulting fees from Sorin, Edwards, Johnson & Johnson, and St. Jude Medical.

Setting a new standard for aortic root repair?
Over the past 3 decades surgery for aortic root replacement has seen a dramatic decline in rates of death and complications, but there have been few studies comparing which technique would be best for specific patients, and those that have been done have been limited by selection bias or small patient numbers.
But a team of investigators from Weill Cornell Medical College in New York have analyzed results of three different aortic root replacement (ARR) procedures over a 17-year period and found that the rates of death during surgery and complications were less than 1% regardless of the technique. They published their results in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1120-9).

“In the current era, aortic root replacement can be performed with very low perioperative risk in high-volume aortic centers,” said Dr. Mario Gaudino and coauthors. “The type of operation performed does not affect early or late survival.”
They compared results of three different approaches to ARR performed in 890 consecutive patients in their institution from May 1997 to January 2014: mechanical composite valved graft (mCVG) in 289 patients; biologic composite valved graft (bCVG) in 421; and valve-sparing reconstruction (VSR) in 180. Then the researchers applied propensity matching to neutralize the differences in the baseline characteristics between the different procedures.
The overall rate of death from the operation was 0.2%, but the two patients who died did so in the first 5 years of the study. There were no deaths in the VSR group, and the incidence of complications after surgery was less than 0.5%. Three-year survival was 94.8% and 5-year survival was 89.4%, and reintervention rates at 5 years were 0% for the mCVG group, 2.4% for the bCVG group, and 7.3% for those who had VSR. “Although mCVG remains the gold standard for durability, bCVG and VSR are excellent options for those who either cannot take or wish to avoid long-term anticoagulation,” Dr. Gaudino and colleagues said.
At the time of surgery, 332 patients (37.3%) had at least one associated cardiac procedure, led by arch replacement (149 patients) and coronary artery bypass (81 patients). Eighty-four patients (9.4%) had two or more associated procedures. The bCVG and mCVG groups had the highest rates of associated cardiac procedures.
Before propensity matching, bCVG patients were older and had more comorbidities and worse functional class, while the mCVG group had higher rates of redo procedures and urgent or emergent operations. Connective tissue disorders were most common in the VSR group.
The results paralleled data from the Society of Thoracic Surgery’s Adult Cardiac Surgery Database, Dr. Gaudino and colleagues said, including a fivefold increase in the number of root replacements performed annually during the study period and a shift away from the traditional mCVG operation to widespread adoption of the bCVG and VSR procedures in the later years of the study.
“Surgeons with extensive experience in aortic surgery can tailor their choice of ARR to the procedure that best suits the individual patient based on their baseline characteristics,” Dr. Gaudino and coauthors said.
Dr. Gaudino and his coauthors had no disclosures.
The results of elective aortic root surgery that Dr. Mario Gaudino and his colleagues reported are “the most impressive … ever published and probably difficult, if not impossible, to reproduce,” Dr. Tirone David of the University of Toronto said in his invited commentary in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1130-1).
Dr. David cited the study’s low rates of deaths and complications. “They had only two deaths early on in their experience and no deaths among the most recent 804 patients operated on since 2002,” he said. “And there is more,” he said: only four strokes, one heart attack, one sternal infection, and only 11.2% of patients receiving blood transfusion. “And to make us ordinary surgeons even more envious, more than one-third of their patients had combined procedures,” Dr. David said.
|
Dr. Tirone David |
He said Dr. Gaudino and his colleagues have set a new standard for early outcomes of elective aortic root surgery. “These outcomes are difficult to emulate but we have to try,” Dr. David said. “To be an obsessive-compulsive surgeon who pays enormous attention to technical details is not enough because even patients who have perfectly executed operations may suffer serious and occasionally fatal postoperative complications.”
The results of elective aortic root surgery that Dr. Mario Gaudino and his colleagues reported are “the most impressive … ever published and probably difficult, if not impossible, to reproduce,” Dr. Tirone David of the University of Toronto said in his invited commentary in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1130-1).
Dr. David cited the study’s low rates of deaths and complications. “They had only two deaths early on in their experience and no deaths among the most recent 804 patients operated on since 2002,” he said. “And there is more,” he said: only four strokes, one heart attack, one sternal infection, and only 11.2% of patients receiving blood transfusion. “And to make us ordinary surgeons even more envious, more than one-third of their patients had combined procedures,” Dr. David said.
|
|
Dr. Tirone David |
He said Dr. Gaudino and his colleagues have set a new standard for early outcomes of elective aortic root surgery. “These outcomes are difficult to emulate but we have to try,” Dr. David said. “To be an obsessive-compulsive surgeon who pays enormous attention to technical details is not enough because even patients who have perfectly executed operations may suffer serious and occasionally fatal postoperative complications.”
The results of elective aortic root surgery that Dr. Mario Gaudino and his colleagues reported are “the most impressive … ever published and probably difficult, if not impossible, to reproduce,” Dr. Tirone David of the University of Toronto said in his invited commentary in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1130-1).
Dr. David cited the study’s low rates of deaths and complications. “They had only two deaths early on in their experience and no deaths among the most recent 804 patients operated on since 2002,” he said. “And there is more,” he said: only four strokes, one heart attack, one sternal infection, and only 11.2% of patients receiving blood transfusion. “And to make us ordinary surgeons even more envious, more than one-third of their patients had combined procedures,” Dr. David said.
|
|
Dr. Tirone David |
He said Dr. Gaudino and his colleagues have set a new standard for early outcomes of elective aortic root surgery. “These outcomes are difficult to emulate but we have to try,” Dr. David said. “To be an obsessive-compulsive surgeon who pays enormous attention to technical details is not enough because even patients who have perfectly executed operations may suffer serious and occasionally fatal postoperative complications.”
Over the past 3 decades surgery for aortic root replacement has seen a dramatic decline in rates of death and complications, but there have been few studies comparing which technique would be best for specific patients, and those that have been done have been limited by selection bias or small patient numbers.
But a team of investigators from Weill Cornell Medical College in New York have analyzed results of three different aortic root replacement (ARR) procedures over a 17-year period and found that the rates of death during surgery and complications were less than 1% regardless of the technique. They published their results in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1120-9).
“In the current era, aortic root replacement can be performed with very low perioperative risk in high-volume aortic centers,” said Dr. Mario Gaudino and coauthors. “The type of operation performed does not affect early or late survival.”
They compared results of three different approaches to ARR performed in 890 consecutive patients in their institution from May 1997 to January 2014: mechanical composite valved graft (mCVG) in 289 patients; biologic composite valved graft (bCVG) in 421; and valve-sparing reconstruction (VSR) in 180. Then the researchers applied propensity matching to neutralize the differences in the baseline characteristics between the different procedures.
The overall rate of death from the operation was 0.2%, but the two patients who died did so in the first 5 years of the study. There were no deaths in the VSR group, and the incidence of complications after surgery was less than 0.5%. Three-year survival was 94.8% and 5-year survival was 89.4%, and reintervention rates at 5 years were 0% for the mCVG group, 2.4% for the bCVG group, and 7.3% for those who had VSR. “Although mCVG remains the gold standard for durability, bCVG and VSR are excellent options for those who either cannot take or wish to avoid long-term anticoagulation,” Dr. Gaudino and colleagues said.
At the time of surgery, 332 patients (37.3%) had at least one associated cardiac procedure, led by arch replacement (149 patients) and coronary artery bypass (81 patients). Eighty-four patients (9.4%) had two or more associated procedures. The bCVG and mCVG groups had the highest rates of associated cardiac procedures.
Before propensity matching, bCVG patients were older and had more comorbidities and worse functional class, while the mCVG group had higher rates of redo procedures and urgent or emergent operations. Connective tissue disorders were most common in the VSR group.
The results paralleled data from the Society of Thoracic Surgery’s Adult Cardiac Surgery Database, Dr. Gaudino and colleagues said, including a fivefold increase in the number of root replacements performed annually during the study period and a shift away from the traditional mCVG operation to widespread adoption of the bCVG and VSR procedures in the later years of the study.
“Surgeons with extensive experience in aortic surgery can tailor their choice of ARR to the procedure that best suits the individual patient based on their baseline characteristics,” Dr. Gaudino and coauthors said.
Dr. Gaudino and his coauthors had no disclosures.
Over the past 3 decades surgery for aortic root replacement has seen a dramatic decline in rates of death and complications, but there have been few studies comparing which technique would be best for specific patients, and those that have been done have been limited by selection bias or small patient numbers.
But a team of investigators from Weill Cornell Medical College in New York have analyzed results of three different aortic root replacement (ARR) procedures over a 17-year period and found that the rates of death during surgery and complications were less than 1% regardless of the technique. They published their results in the Journal of Thoracic and Cardiovascular Surgery (2015;150:1120-9).
“In the current era, aortic root replacement can be performed with very low perioperative risk in high-volume aortic centers,” said Dr. Mario Gaudino and coauthors. “The type of operation performed does not affect early or late survival.”
They compared results of three different approaches to ARR performed in 890 consecutive patients in their institution from May 1997 to January 2014: mechanical composite valved graft (mCVG) in 289 patients; biologic composite valved graft (bCVG) in 421; and valve-sparing reconstruction (VSR) in 180. Then the researchers applied propensity matching to neutralize the differences in the baseline characteristics between the different procedures.
The overall rate of death from the operation was 0.2%, but the two patients who died did so in the first 5 years of the study. There were no deaths in the VSR group, and the incidence of complications after surgery was less than 0.5%. Three-year survival was 94.8% and 5-year survival was 89.4%, and reintervention rates at 5 years were 0% for the mCVG group, 2.4% for the bCVG group, and 7.3% for those who had VSR. “Although mCVG remains the gold standard for durability, bCVG and VSR are excellent options for those who either cannot take or wish to avoid long-term anticoagulation,” Dr. Gaudino and colleagues said.
At the time of surgery, 332 patients (37.3%) had at least one associated cardiac procedure, led by arch replacement (149 patients) and coronary artery bypass (81 patients). Eighty-four patients (9.4%) had two or more associated procedures. The bCVG and mCVG groups had the highest rates of associated cardiac procedures.
Before propensity matching, bCVG patients were older and had more comorbidities and worse functional class, while the mCVG group had higher rates of redo procedures and urgent or emergent operations. Connective tissue disorders were most common in the VSR group.
The results paralleled data from the Society of Thoracic Surgery’s Adult Cardiac Surgery Database, Dr. Gaudino and colleagues said, including a fivefold increase in the number of root replacements performed annually during the study period and a shift away from the traditional mCVG operation to widespread adoption of the bCVG and VSR procedures in the later years of the study.
“Surgeons with extensive experience in aortic surgery can tailor their choice of ARR to the procedure that best suits the individual patient based on their baseline characteristics,” Dr. Gaudino and coauthors said.
Dr. Gaudino and his coauthors had no disclosures.
Key clinical point: Aortic root replacement surgery can be performed with minimal risk of death and complications regardless of the approach taken.
Major finding: Overall rate of death was 0.2%, with none since 2002, and the overall rate of complications was below 0.5% in the study cohort.
Data source: Review of prospective data on 890 aortic root replacement operations performed over a 17-year period at a single center.
Disclosures: The study authors had no relationships to disclose.
