User login
Mental health apps: What to tell patients
Have your patients asked you about smartphone apps? If they haven’t yet, they may soon, as interest in apps for mental health continues to expand. There are now >10,000 mental health–related smartphone apps.1 The rapid rise of these apps is partly due to their potential to transform a patient’s smartphone into a monitoring and therapeutic platform, capable of capturing mental health symptoms in real time and delivering on-the-go therapy. Setting aside questions about the potential of mobile health, 2 urgent questions remain for the busy psychiatrist in clinical practice: What is the current evidence base for mental health apps, and what should you tell your patients about them?
For most apps, evidence of efficacy is limited
While the evidence base for mental health smartphone apps continues to expand, for many of these apps, there is no evidence of effectiveness. The growing consensus is that most commercially available apps are not evidence-based and some are even dangerous. For example, researchers who examined >700 mindfulness apps on the iTunes and Google Play stores found that only 4% provided acceptable mindfulness training and education.2 Another study of 58 apps that claimed to offer sobriety assessments found that none had ever been formally evaluated.3 Evidence-based reviews of suicide prevention apps have identified potentially harmful apps,4 and studies evaluating apps for bipolar disorder5 and depression6 have yielded similar results—few have any evidence supporting their use, and some offer dangerous and harmful advice. For example, researchers found that one app for bipolar disorder advised patients who are experiencing a manic episode to drink alcohol.5 Currently, the vast majority of commercially available apps are not appropriate for clinical care. This finding is not unique to mental health; similar findings have been reported for apps for cancer.7 The bottom line is that the apps that your patients are finding, and perhaps already using, may not be useful or effective.
However, early studies have demonstrated efficacy of some apps for several conditions, including schizophrenia,8 depression,9 anxiety disorders,10 and suicidal ideation.11 Although many of the apps evaluated in these studies are not available to the public, or still require large-scale assessment before they are ready for mainstream clinical care, this research demonstrates that mental health apps can help improve treatment outcomes. As this research develops, a wave of evidence-based and effective mental health apps may be available in the near future.
Although it is unknown how many patients are presently using mental health apps, there is strong anecdotal evidence that an increasing number of patients who use these apps and other forms of digital technology are finding some benefits. In many cases, patients may actually be ahead of the research. For example, one study that conducted an online survey of patients with schizophrenia noted that some patients are using their smartphones to play music to help block auditory hallucinations.12
Why online reviews are of limited use
As this evidence continues to mature, and with an ever-growing number of mental health apps available on commercial marketplaces, busy psychiatrists need to navigate this complex space. Even psychiatrists who decide to not use apps as part of care still need to be knowledgeable about them, because patients are likely to ask about the benefits of using apps, and they will expect an informed response. How would you reply if your patient asked you about a new mood-tracking app he or she recently heard about? On what would you base your recommendation and opinion?
Reading online app reviews for guidance is not a good solution. A recent study found little relationship between the star ratings of health apps and the quality of those apps,13 which suggests that a 5-star rating on the app store is of limited use.
Unlike medications whose ingredients do not change over time, or manualized psychotherapies that use specific protocols, mental health apps are dynamic and constantly changing.14 Think of how often the apps on your smartphone update. Thus, the version of a mental health app that your patient downloads today may be very different from the version that received a favorable user review last month. And just as there is no single medication or therapy that is ideal for every patient, neither is there a single “best” app for all patients with the same disorder. Picking an app is a personal decision that cannot be made based on a single score or numeric rating. Furthermore, the validity of app rating systems is unclear. One study found a wide variation in the interrater reliability of measures used to evaluate apps from sources that included PsyberGuide, the Anxiety and Depression Association of America, and the research literature. Quality measures such as effectiveness, ease of use, and performance had relatively poor interrater reliability.15 This means that, for example, an app that one patient finds “easy to use” may be difficult to use for another. Thus, providing patients with suggestions based on an app’s ratings may result in providing information that sounds useful, but often is misleading.
A model for evaluating apps
One possible solution is a risk-based and personalized assessment approach to evaluating mental health apps. Although it does not offer scoring or recommendations of specific apps, the American Psychiatric Association (APA) App Evaluation Model (Figure) provides a framework to guide discussion and informed decision-making about apps. (The authors of this article helped create this model, but receive no compensation for that volunteer work.) The pyramid shape reflects the hierarchical nature of the model. To begin the process, start at the base of the pyramid and work upward.
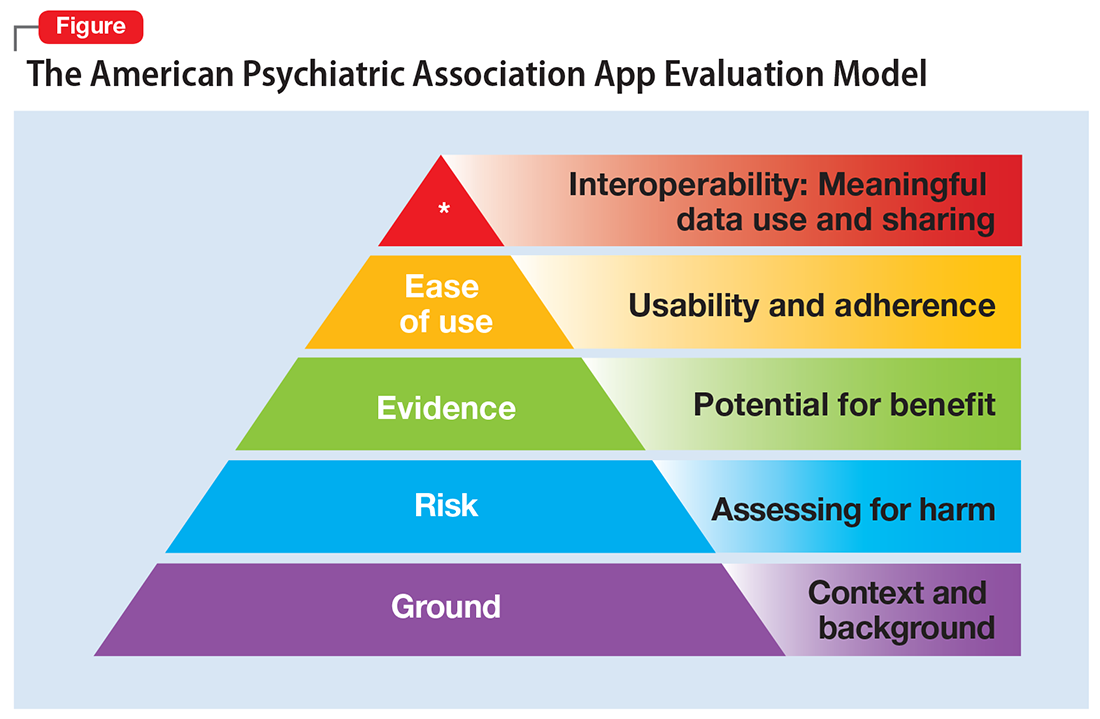
Ground. First, consider the context of the app by determining basic facts, such as who made it, how much it costs, and its technology requirements. This ground layer establishes the credibility of the app’s creator by questioning his or her reputation, ability to update the app, and funding sources. Understanding the app’s business model also will help you determine whether the app will stand the test of time: Will it continue to exist next month or next year, or will a lack of reliable funding lead the vendor to abandon it?
Risk. The next layer assesses the risk, privacy, and security features of the app. Many mental health apps actively aim to avoid falling under the jurisdiction of U.S. federal health care privacy rules, such as the Health Insurance Portability and Accountability Act of 1996, so there is no guarantee that sensitive data supplied to an app will be protected. The true cost of a “free” app often is your patient’s personal mental health information, which the app’s developer may accumulate and sell for profit. Thus, it is wise to check the privacy policy to learn where your patient’s data goes. Furthermore, patients and psychiatrists must be vigilant that malware-infected apps can be uploaded to the app store, which can further compromise privacy.16 You may be surprised to learn that many apps lack a privacy policy, which means there are no protections for personal information or safeguards against the misuse of mental health data.17 Checking that an app at least promises to digitally protect mental health data through encryption and secure storage also is a good step.
The goal of considering these factors is not to create a score, but rather to be aware of them and consider them in the context of the specific app, patient, and clinical situation. Doing so helps determine whether the app meets the appropriate risk, privacy, and security standards for your patient.
Evidence. The next layer of the evaluation framework is evidence. The goal is to seek an app with clinical evidence of effectiveness. Simply put, if a patient is going to use an app, he should use one that works. An app without formal evidence may be effective, but it is important to make sure the patient is aware that these claims have not been verified. Many apps claim that they offer cognitive-behavioral therapy or mindfulness therapy, but few deliver on such claims.18 It is wise to try an app before recommending it to a patient to ensure that it does what it claims it does, and does not offer dangerous or harmful recommendations.
Ease of use. Across all health apps, there is growing recognition that most downloaded apps are never used. Patient engagement with mental health apps appears to rapidly decline over the first week of use.19 There also is emerging evidence that many apps are not user-friendly. A recent study of several common mood-tracking apps found that patients with depression had difficulty entering and accessing their data.20 Because many psychiatric disorders are chronic or last at least several months, it is especially important to consider how engaging and usable the app will be for your patient. Usability varies from patient to patient, so it is best to check directly with your patient regarding his comfort with apps and mobile technology. Offering check-ins and support to help patients keep on track with apps may be critical for successful outcomes.
Interoperability. The final layer of the model is data sharing and interoperability. It is important to determine if the data collected or generated by the app are available to you, the patient, the treatment team, and others involved in the patient’s care. As mental health treatment moves toward integrated care, apps that fragment care (by not sharing information) impede care. Check if the app can share data with an electronic medical record, or if there is a plan to review and act on data from the app as part of your patient’s treatment plan.
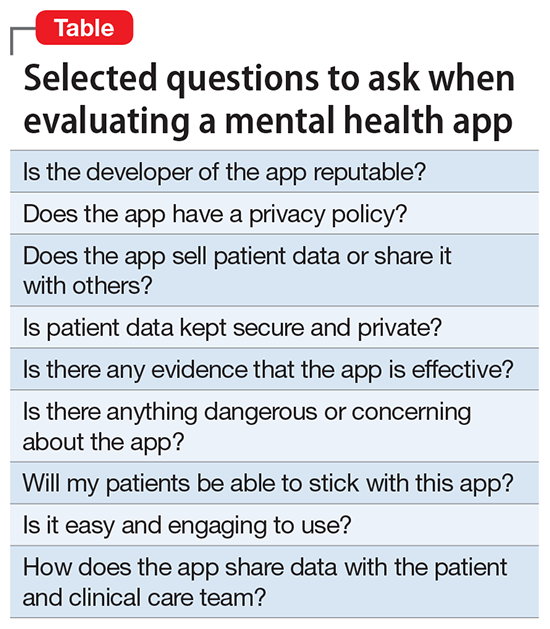
More information about the APA App Evaluation Model, including additional factors to consider within each layer, is available from the APA for free at https://www.psychiatry.org/psychiatrists/practice/mental-health-apps/app-evaluation-model. For a sample of factors to consider when evaluating a mental health app, see the Table.
A reasonable strategy
Although the APA App Evaluation Model does not endorse any particular app, it can help guide more informed decision-making. As the evidence on mental health apps continues to evolve, it will become easier to make definitive statements on what constitutes a useful app. For now, the best strategy when discussing mental health apps with patients is to combine the use of this model with your clinical judgment.
1. Torous J, Roberts LW. Needed innovation in digital health and smartphone applications for mental health: transparency and trust. JAMA Psychiatry. 2017;74(5):437-438.
2. Mani M, Kavanagh DJ, Hides L, et al. Review and evaluation of mindfulness-based iPhone apps. JMIR Mhealth Uhealth. 2015;3(3):e82. doi: 10.2196/mhealth.4328.
3. Wilson H, Stoyanov SR, Gandabhai S, et al. The quality and accuracy of mobile apps to prevent driving after drinking alcohol. JMIR Mhealth Uhealth. 2016;4(3):e98. doi: 10.2196/mhealth.5961.
4. Larsen ME, Nicholas J, Christensen H. A systematic assessment of smartphone tools for suicide prevention. PLoS One. 2016;11(4):e0152285. doi: 10.1371/journal.pone.0152285.
5. Nicholas J, Larsen ME, Proudfoot J, et al. Mobile apps for bipolar disorder: a systematic review of features and content quality. J Med Internet Res. 2015;17(8):e198. doi: 10.2196/jmir.4581.
6. Shen N, Levitan MJ, Johnson A, et al. Finding a depression app: a review and content analysis of the depression app marketplace. JMIR Mhealth Uhealth. 2015;3(1):e16. doi: 10.2196/mhealth.3713.
7. Davis SW, Oakley-Girvan I. Achieving value in mobile health applications for cancer survivors. J Cancer Surviv. 2017;11(4):498-504.
8. Ben-Zeev D, Brenner CJ, Begale M, et al. Feasibility, acceptability, and preliminary efficacy of a smartphone intervention for schizophrenia. Schizophr Bull. 2014;40(6):1244-1253.
9. Mohr DC, Tomasino KN, Lattie EG, et al. IntelliCare: an eclectic, skills-based app suite for the treatment of depression and anxiety. J Med Internet Res. 2017;19(1):e10. doi: 10.2196/jmir.6645.
10. Tighe J, Shand F, Ridani R, et al. Ibobbly mobile health intervention for suicide prevention in Australian Indigenous youth: a pilot randomised controlled trial. BMJ Open. 2017;7(1):e013518. doi: 10.1136/bmjopen-2016-013518.
11. Firth J, Torous J, Nicholas J, et al. Can smartphone mental health interventions reduce symptoms of anxiety? A meta-analysis of randomized controlled trials. J Affect Disord. 2017;218:15-22.
12. Gay K, Torous J, Joseph A, et al. Digital technology use among individuals with schizophrenia: results of an online survey. JMIR Mental Health. 2016;3(2):e15. doi: 10.2196/mental.5379.
13. Singh K, Drouin K, Newmark LP, et al. Many mobile health apps target high-need, high-cost populations, but gaps remain. Health Aff (Millwood). 2016;35(12):2310-2318.
14. Larsen ME, Nicholas J, Christensen H. Quantifying app store dynamics: longitudinal tracking of mental health apps. JMIR Mhealth Uhealth. 2016;4(3):e96. doi: 10.2196/mhealth.6020.
15. Powell AC, Torous J, Chan S, et al. Interrater reliability of mHealth app rating measures: analysis of top depression and smoking cessation apps. JMIR Mhealth Uhealth. 2016;4(1):e15. doi: 10.2196/mhealth.5176.
16. Ducklin P. Apple’s XcodeGhost malware still in the machine…. https://nakedsecurity.sophos.com/2015/11/09/apples-xcodeghost-malware-still-in-the-machine. Published November 9, 2015. Accessed May 11, 2017.
17. Rosenfeld L, Torous J, Vahia IV. Data security and privacy in apps for dementia: an analysis of existing privacy policies. Am J Geriatr Psychiatry. 2017;25(8):873-877.
18. Torous J, Levin ME, Ahern DK, et al. Cognitive behavioral mobile applications: clinical studies, marketplace overview, and research agenda. Cogn Behav Pract. 2017;24(2):215-225.
19. Owen JE, Jaworski BK, Kuhn E, et al. mHealth in the wild: using novel data to examine the reach, use, and impact of PTSD coach. JMIR Ment Health. 2015;2(1):e7. doi: 10.2196/mental.3935.
20. Sarkar U, Gourley GI, Lyles CR, et al. Usability of commercially available mobile applications for diverse patients. J Gen Intern Med. 2016;31(12):1417-1426.
Have your patients asked you about smartphone apps? If they haven’t yet, they may soon, as interest in apps for mental health continues to expand. There are now >10,000 mental health–related smartphone apps.1 The rapid rise of these apps is partly due to their potential to transform a patient’s smartphone into a monitoring and therapeutic platform, capable of capturing mental health symptoms in real time and delivering on-the-go therapy. Setting aside questions about the potential of mobile health, 2 urgent questions remain for the busy psychiatrist in clinical practice: What is the current evidence base for mental health apps, and what should you tell your patients about them?
For most apps, evidence of efficacy is limited
While the evidence base for mental health smartphone apps continues to expand, for many of these apps, there is no evidence of effectiveness. The growing consensus is that most commercially available apps are not evidence-based and some are even dangerous. For example, researchers who examined >700 mindfulness apps on the iTunes and Google Play stores found that only 4% provided acceptable mindfulness training and education.2 Another study of 58 apps that claimed to offer sobriety assessments found that none had ever been formally evaluated.3 Evidence-based reviews of suicide prevention apps have identified potentially harmful apps,4 and studies evaluating apps for bipolar disorder5 and depression6 have yielded similar results—few have any evidence supporting their use, and some offer dangerous and harmful advice. For example, researchers found that one app for bipolar disorder advised patients who are experiencing a manic episode to drink alcohol.5 Currently, the vast majority of commercially available apps are not appropriate for clinical care. This finding is not unique to mental health; similar findings have been reported for apps for cancer.7 The bottom line is that the apps that your patients are finding, and perhaps already using, may not be useful or effective.
However, early studies have demonstrated efficacy of some apps for several conditions, including schizophrenia,8 depression,9 anxiety disorders,10 and suicidal ideation.11 Although many of the apps evaluated in these studies are not available to the public, or still require large-scale assessment before they are ready for mainstream clinical care, this research demonstrates that mental health apps can help improve treatment outcomes. As this research develops, a wave of evidence-based and effective mental health apps may be available in the near future.
Although it is unknown how many patients are presently using mental health apps, there is strong anecdotal evidence that an increasing number of patients who use these apps and other forms of digital technology are finding some benefits. In many cases, patients may actually be ahead of the research. For example, one study that conducted an online survey of patients with schizophrenia noted that some patients are using their smartphones to play music to help block auditory hallucinations.12
Why online reviews are of limited use
As this evidence continues to mature, and with an ever-growing number of mental health apps available on commercial marketplaces, busy psychiatrists need to navigate this complex space. Even psychiatrists who decide to not use apps as part of care still need to be knowledgeable about them, because patients are likely to ask about the benefits of using apps, and they will expect an informed response. How would you reply if your patient asked you about a new mood-tracking app he or she recently heard about? On what would you base your recommendation and opinion?
Reading online app reviews for guidance is not a good solution. A recent study found little relationship between the star ratings of health apps and the quality of those apps,13 which suggests that a 5-star rating on the app store is of limited use.
Unlike medications whose ingredients do not change over time, or manualized psychotherapies that use specific protocols, mental health apps are dynamic and constantly changing.14 Think of how often the apps on your smartphone update. Thus, the version of a mental health app that your patient downloads today may be very different from the version that received a favorable user review last month. And just as there is no single medication or therapy that is ideal for every patient, neither is there a single “best” app for all patients with the same disorder. Picking an app is a personal decision that cannot be made based on a single score or numeric rating. Furthermore, the validity of app rating systems is unclear. One study found a wide variation in the interrater reliability of measures used to evaluate apps from sources that included PsyberGuide, the Anxiety and Depression Association of America, and the research literature. Quality measures such as effectiveness, ease of use, and performance had relatively poor interrater reliability.15 This means that, for example, an app that one patient finds “easy to use” may be difficult to use for another. Thus, providing patients with suggestions based on an app’s ratings may result in providing information that sounds useful, but often is misleading.
A model for evaluating apps
One possible solution is a risk-based and personalized assessment approach to evaluating mental health apps. Although it does not offer scoring or recommendations of specific apps, the American Psychiatric Association (APA) App Evaluation Model (Figure) provides a framework to guide discussion and informed decision-making about apps. (The authors of this article helped create this model, but receive no compensation for that volunteer work.) The pyramid shape reflects the hierarchical nature of the model. To begin the process, start at the base of the pyramid and work upward.
Ground. First, consider the context of the app by determining basic facts, such as who made it, how much it costs, and its technology requirements. This ground layer establishes the credibility of the app’s creator by questioning his or her reputation, ability to update the app, and funding sources. Understanding the app’s business model also will help you determine whether the app will stand the test of time: Will it continue to exist next month or next year, or will a lack of reliable funding lead the vendor to abandon it?
Risk. The next layer assesses the risk, privacy, and security features of the app. Many mental health apps actively aim to avoid falling under the jurisdiction of U.S. federal health care privacy rules, such as the Health Insurance Portability and Accountability Act of 1996, so there is no guarantee that sensitive data supplied to an app will be protected. The true cost of a “free” app often is your patient’s personal mental health information, which the app’s developer may accumulate and sell for profit. Thus, it is wise to check the privacy policy to learn where your patient’s data goes. Furthermore, patients and psychiatrists must be vigilant that malware-infected apps can be uploaded to the app store, which can further compromise privacy.16 You may be surprised to learn that many apps lack a privacy policy, which means there are no protections for personal information or safeguards against the misuse of mental health data.17 Checking that an app at least promises to digitally protect mental health data through encryption and secure storage also is a good step.
The goal of considering these factors is not to create a score, but rather to be aware of them and consider them in the context of the specific app, patient, and clinical situation. Doing so helps determine whether the app meets the appropriate risk, privacy, and security standards for your patient.
Evidence. The next layer of the evaluation framework is evidence. The goal is to seek an app with clinical evidence of effectiveness. Simply put, if a patient is going to use an app, he should use one that works. An app without formal evidence may be effective, but it is important to make sure the patient is aware that these claims have not been verified. Many apps claim that they offer cognitive-behavioral therapy or mindfulness therapy, but few deliver on such claims.18 It is wise to try an app before recommending it to a patient to ensure that it does what it claims it does, and does not offer dangerous or harmful recommendations.
Ease of use. Across all health apps, there is growing recognition that most downloaded apps are never used. Patient engagement with mental health apps appears to rapidly decline over the first week of use.19 There also is emerging evidence that many apps are not user-friendly. A recent study of several common mood-tracking apps found that patients with depression had difficulty entering and accessing their data.20 Because many psychiatric disorders are chronic or last at least several months, it is especially important to consider how engaging and usable the app will be for your patient. Usability varies from patient to patient, so it is best to check directly with your patient regarding his comfort with apps and mobile technology. Offering check-ins and support to help patients keep on track with apps may be critical for successful outcomes.
Interoperability. The final layer of the model is data sharing and interoperability. It is important to determine if the data collected or generated by the app are available to you, the patient, the treatment team, and others involved in the patient’s care. As mental health treatment moves toward integrated care, apps that fragment care (by not sharing information) impede care. Check if the app can share data with an electronic medical record, or if there is a plan to review and act on data from the app as part of your patient’s treatment plan.
More information about the APA App Evaluation Model, including additional factors to consider within each layer, is available from the APA for free at https://www.psychiatry.org/psychiatrists/practice/mental-health-apps/app-evaluation-model. For a sample of factors to consider when evaluating a mental health app, see the Table.
A reasonable strategy
Although the APA App Evaluation Model does not endorse any particular app, it can help guide more informed decision-making. As the evidence on mental health apps continues to evolve, it will become easier to make definitive statements on what constitutes a useful app. For now, the best strategy when discussing mental health apps with patients is to combine the use of this model with your clinical judgment.
Have your patients asked you about smartphone apps? If they haven’t yet, they may soon, as interest in apps for mental health continues to expand. There are now >10,000 mental health–related smartphone apps.1 The rapid rise of these apps is partly due to their potential to transform a patient’s smartphone into a monitoring and therapeutic platform, capable of capturing mental health symptoms in real time and delivering on-the-go therapy. Setting aside questions about the potential of mobile health, 2 urgent questions remain for the busy psychiatrist in clinical practice: What is the current evidence base for mental health apps, and what should you tell your patients about them?
For most apps, evidence of efficacy is limited
While the evidence base for mental health smartphone apps continues to expand, for many of these apps, there is no evidence of effectiveness. The growing consensus is that most commercially available apps are not evidence-based and some are even dangerous. For example, researchers who examined >700 mindfulness apps on the iTunes and Google Play stores found that only 4% provided acceptable mindfulness training and education.2 Another study of 58 apps that claimed to offer sobriety assessments found that none had ever been formally evaluated.3 Evidence-based reviews of suicide prevention apps have identified potentially harmful apps,4 and studies evaluating apps for bipolar disorder5 and depression6 have yielded similar results—few have any evidence supporting their use, and some offer dangerous and harmful advice. For example, researchers found that one app for bipolar disorder advised patients who are experiencing a manic episode to drink alcohol.5 Currently, the vast majority of commercially available apps are not appropriate for clinical care. This finding is not unique to mental health; similar findings have been reported for apps for cancer.7 The bottom line is that the apps that your patients are finding, and perhaps already using, may not be useful or effective.
However, early studies have demonstrated efficacy of some apps for several conditions, including schizophrenia,8 depression,9 anxiety disorders,10 and suicidal ideation.11 Although many of the apps evaluated in these studies are not available to the public, or still require large-scale assessment before they are ready for mainstream clinical care, this research demonstrates that mental health apps can help improve treatment outcomes. As this research develops, a wave of evidence-based and effective mental health apps may be available in the near future.
Although it is unknown how many patients are presently using mental health apps, there is strong anecdotal evidence that an increasing number of patients who use these apps and other forms of digital technology are finding some benefits. In many cases, patients may actually be ahead of the research. For example, one study that conducted an online survey of patients with schizophrenia noted that some patients are using their smartphones to play music to help block auditory hallucinations.12
Why online reviews are of limited use
As this evidence continues to mature, and with an ever-growing number of mental health apps available on commercial marketplaces, busy psychiatrists need to navigate this complex space. Even psychiatrists who decide to not use apps as part of care still need to be knowledgeable about them, because patients are likely to ask about the benefits of using apps, and they will expect an informed response. How would you reply if your patient asked you about a new mood-tracking app he or she recently heard about? On what would you base your recommendation and opinion?
Reading online app reviews for guidance is not a good solution. A recent study found little relationship between the star ratings of health apps and the quality of those apps,13 which suggests that a 5-star rating on the app store is of limited use.
Unlike medications whose ingredients do not change over time, or manualized psychotherapies that use specific protocols, mental health apps are dynamic and constantly changing.14 Think of how often the apps on your smartphone update. Thus, the version of a mental health app that your patient downloads today may be very different from the version that received a favorable user review last month. And just as there is no single medication or therapy that is ideal for every patient, neither is there a single “best” app for all patients with the same disorder. Picking an app is a personal decision that cannot be made based on a single score or numeric rating. Furthermore, the validity of app rating systems is unclear. One study found a wide variation in the interrater reliability of measures used to evaluate apps from sources that included PsyberGuide, the Anxiety and Depression Association of America, and the research literature. Quality measures such as effectiveness, ease of use, and performance had relatively poor interrater reliability.15 This means that, for example, an app that one patient finds “easy to use” may be difficult to use for another. Thus, providing patients with suggestions based on an app’s ratings may result in providing information that sounds useful, but often is misleading.
A model for evaluating apps
One possible solution is a risk-based and personalized assessment approach to evaluating mental health apps. Although it does not offer scoring or recommendations of specific apps, the American Psychiatric Association (APA) App Evaluation Model (Figure) provides a framework to guide discussion and informed decision-making about apps. (The authors of this article helped create this model, but receive no compensation for that volunteer work.) The pyramid shape reflects the hierarchical nature of the model. To begin the process, start at the base of the pyramid and work upward.
Ground. First, consider the context of the app by determining basic facts, such as who made it, how much it costs, and its technology requirements. This ground layer establishes the credibility of the app’s creator by questioning his or her reputation, ability to update the app, and funding sources. Understanding the app’s business model also will help you determine whether the app will stand the test of time: Will it continue to exist next month or next year, or will a lack of reliable funding lead the vendor to abandon it?
Risk. The next layer assesses the risk, privacy, and security features of the app. Many mental health apps actively aim to avoid falling under the jurisdiction of U.S. federal health care privacy rules, such as the Health Insurance Portability and Accountability Act of 1996, so there is no guarantee that sensitive data supplied to an app will be protected. The true cost of a “free” app often is your patient’s personal mental health information, which the app’s developer may accumulate and sell for profit. Thus, it is wise to check the privacy policy to learn where your patient’s data goes. Furthermore, patients and psychiatrists must be vigilant that malware-infected apps can be uploaded to the app store, which can further compromise privacy.16 You may be surprised to learn that many apps lack a privacy policy, which means there are no protections for personal information or safeguards against the misuse of mental health data.17 Checking that an app at least promises to digitally protect mental health data through encryption and secure storage also is a good step.
The goal of considering these factors is not to create a score, but rather to be aware of them and consider them in the context of the specific app, patient, and clinical situation. Doing so helps determine whether the app meets the appropriate risk, privacy, and security standards for your patient.
Evidence. The next layer of the evaluation framework is evidence. The goal is to seek an app with clinical evidence of effectiveness. Simply put, if a patient is going to use an app, he should use one that works. An app without formal evidence may be effective, but it is important to make sure the patient is aware that these claims have not been verified. Many apps claim that they offer cognitive-behavioral therapy or mindfulness therapy, but few deliver on such claims.18 It is wise to try an app before recommending it to a patient to ensure that it does what it claims it does, and does not offer dangerous or harmful recommendations.
Ease of use. Across all health apps, there is growing recognition that most downloaded apps are never used. Patient engagement with mental health apps appears to rapidly decline over the first week of use.19 There also is emerging evidence that many apps are not user-friendly. A recent study of several common mood-tracking apps found that patients with depression had difficulty entering and accessing their data.20 Because many psychiatric disorders are chronic or last at least several months, it is especially important to consider how engaging and usable the app will be for your patient. Usability varies from patient to patient, so it is best to check directly with your patient regarding his comfort with apps and mobile technology. Offering check-ins and support to help patients keep on track with apps may be critical for successful outcomes.
Interoperability. The final layer of the model is data sharing and interoperability. It is important to determine if the data collected or generated by the app are available to you, the patient, the treatment team, and others involved in the patient’s care. As mental health treatment moves toward integrated care, apps that fragment care (by not sharing information) impede care. Check if the app can share data with an electronic medical record, or if there is a plan to review and act on data from the app as part of your patient’s treatment plan.
More information about the APA App Evaluation Model, including additional factors to consider within each layer, is available from the APA for free at https://www.psychiatry.org/psychiatrists/practice/mental-health-apps/app-evaluation-model. For a sample of factors to consider when evaluating a mental health app, see the Table.
A reasonable strategy
Although the APA App Evaluation Model does not endorse any particular app, it can help guide more informed decision-making. As the evidence on mental health apps continues to evolve, it will become easier to make definitive statements on what constitutes a useful app. For now, the best strategy when discussing mental health apps with patients is to combine the use of this model with your clinical judgment.
1. Torous J, Roberts LW. Needed innovation in digital health and smartphone applications for mental health: transparency and trust. JAMA Psychiatry. 2017;74(5):437-438.
2. Mani M, Kavanagh DJ, Hides L, et al. Review and evaluation of mindfulness-based iPhone apps. JMIR Mhealth Uhealth. 2015;3(3):e82. doi: 10.2196/mhealth.4328.
3. Wilson H, Stoyanov SR, Gandabhai S, et al. The quality and accuracy of mobile apps to prevent driving after drinking alcohol. JMIR Mhealth Uhealth. 2016;4(3):e98. doi: 10.2196/mhealth.5961.
4. Larsen ME, Nicholas J, Christensen H. A systematic assessment of smartphone tools for suicide prevention. PLoS One. 2016;11(4):e0152285. doi: 10.1371/journal.pone.0152285.
5. Nicholas J, Larsen ME, Proudfoot J, et al. Mobile apps for bipolar disorder: a systematic review of features and content quality. J Med Internet Res. 2015;17(8):e198. doi: 10.2196/jmir.4581.
6. Shen N, Levitan MJ, Johnson A, et al. Finding a depression app: a review and content analysis of the depression app marketplace. JMIR Mhealth Uhealth. 2015;3(1):e16. doi: 10.2196/mhealth.3713.
7. Davis SW, Oakley-Girvan I. Achieving value in mobile health applications for cancer survivors. J Cancer Surviv. 2017;11(4):498-504.
8. Ben-Zeev D, Brenner CJ, Begale M, et al. Feasibility, acceptability, and preliminary efficacy of a smartphone intervention for schizophrenia. Schizophr Bull. 2014;40(6):1244-1253.
9. Mohr DC, Tomasino KN, Lattie EG, et al. IntelliCare: an eclectic, skills-based app suite for the treatment of depression and anxiety. J Med Internet Res. 2017;19(1):e10. doi: 10.2196/jmir.6645.
10. Tighe J, Shand F, Ridani R, et al. Ibobbly mobile health intervention for suicide prevention in Australian Indigenous youth: a pilot randomised controlled trial. BMJ Open. 2017;7(1):e013518. doi: 10.1136/bmjopen-2016-013518.
11. Firth J, Torous J, Nicholas J, et al. Can smartphone mental health interventions reduce symptoms of anxiety? A meta-analysis of randomized controlled trials. J Affect Disord. 2017;218:15-22.
12. Gay K, Torous J, Joseph A, et al. Digital technology use among individuals with schizophrenia: results of an online survey. JMIR Mental Health. 2016;3(2):e15. doi: 10.2196/mental.5379.
13. Singh K, Drouin K, Newmark LP, et al. Many mobile health apps target high-need, high-cost populations, but gaps remain. Health Aff (Millwood). 2016;35(12):2310-2318.
14. Larsen ME, Nicholas J, Christensen H. Quantifying app store dynamics: longitudinal tracking of mental health apps. JMIR Mhealth Uhealth. 2016;4(3):e96. doi: 10.2196/mhealth.6020.
15. Powell AC, Torous J, Chan S, et al. Interrater reliability of mHealth app rating measures: analysis of top depression and smoking cessation apps. JMIR Mhealth Uhealth. 2016;4(1):e15. doi: 10.2196/mhealth.5176.
16. Ducklin P. Apple’s XcodeGhost malware still in the machine…. https://nakedsecurity.sophos.com/2015/11/09/apples-xcodeghost-malware-still-in-the-machine. Published November 9, 2015. Accessed May 11, 2017.
17. Rosenfeld L, Torous J, Vahia IV. Data security and privacy in apps for dementia: an analysis of existing privacy policies. Am J Geriatr Psychiatry. 2017;25(8):873-877.
18. Torous J, Levin ME, Ahern DK, et al. Cognitive behavioral mobile applications: clinical studies, marketplace overview, and research agenda. Cogn Behav Pract. 2017;24(2):215-225.
19. Owen JE, Jaworski BK, Kuhn E, et al. mHealth in the wild: using novel data to examine the reach, use, and impact of PTSD coach. JMIR Ment Health. 2015;2(1):e7. doi: 10.2196/mental.3935.
20. Sarkar U, Gourley GI, Lyles CR, et al. Usability of commercially available mobile applications for diverse patients. J Gen Intern Med. 2016;31(12):1417-1426.
1. Torous J, Roberts LW. Needed innovation in digital health and smartphone applications for mental health: transparency and trust. JAMA Psychiatry. 2017;74(5):437-438.
2. Mani M, Kavanagh DJ, Hides L, et al. Review and evaluation of mindfulness-based iPhone apps. JMIR Mhealth Uhealth. 2015;3(3):e82. doi: 10.2196/mhealth.4328.
3. Wilson H, Stoyanov SR, Gandabhai S, et al. The quality and accuracy of mobile apps to prevent driving after drinking alcohol. JMIR Mhealth Uhealth. 2016;4(3):e98. doi: 10.2196/mhealth.5961.
4. Larsen ME, Nicholas J, Christensen H. A systematic assessment of smartphone tools for suicide prevention. PLoS One. 2016;11(4):e0152285. doi: 10.1371/journal.pone.0152285.
5. Nicholas J, Larsen ME, Proudfoot J, et al. Mobile apps for bipolar disorder: a systematic review of features and content quality. J Med Internet Res. 2015;17(8):e198. doi: 10.2196/jmir.4581.
6. Shen N, Levitan MJ, Johnson A, et al. Finding a depression app: a review and content analysis of the depression app marketplace. JMIR Mhealth Uhealth. 2015;3(1):e16. doi: 10.2196/mhealth.3713.
7. Davis SW, Oakley-Girvan I. Achieving value in mobile health applications for cancer survivors. J Cancer Surviv. 2017;11(4):498-504.
8. Ben-Zeev D, Brenner CJ, Begale M, et al. Feasibility, acceptability, and preliminary efficacy of a smartphone intervention for schizophrenia. Schizophr Bull. 2014;40(6):1244-1253.
9. Mohr DC, Tomasino KN, Lattie EG, et al. IntelliCare: an eclectic, skills-based app suite for the treatment of depression and anxiety. J Med Internet Res. 2017;19(1):e10. doi: 10.2196/jmir.6645.
10. Tighe J, Shand F, Ridani R, et al. Ibobbly mobile health intervention for suicide prevention in Australian Indigenous youth: a pilot randomised controlled trial. BMJ Open. 2017;7(1):e013518. doi: 10.1136/bmjopen-2016-013518.
11. Firth J, Torous J, Nicholas J, et al. Can smartphone mental health interventions reduce symptoms of anxiety? A meta-analysis of randomized controlled trials. J Affect Disord. 2017;218:15-22.
12. Gay K, Torous J, Joseph A, et al. Digital technology use among individuals with schizophrenia: results of an online survey. JMIR Mental Health. 2016;3(2):e15. doi: 10.2196/mental.5379.
13. Singh K, Drouin K, Newmark LP, et al. Many mobile health apps target high-need, high-cost populations, but gaps remain. Health Aff (Millwood). 2016;35(12):2310-2318.
14. Larsen ME, Nicholas J, Christensen H. Quantifying app store dynamics: longitudinal tracking of mental health apps. JMIR Mhealth Uhealth. 2016;4(3):e96. doi: 10.2196/mhealth.6020.
15. Powell AC, Torous J, Chan S, et al. Interrater reliability of mHealth app rating measures: analysis of top depression and smoking cessation apps. JMIR Mhealth Uhealth. 2016;4(1):e15. doi: 10.2196/mhealth.5176.
16. Ducklin P. Apple’s XcodeGhost malware still in the machine…. https://nakedsecurity.sophos.com/2015/11/09/apples-xcodeghost-malware-still-in-the-machine. Published November 9, 2015. Accessed May 11, 2017.
17. Rosenfeld L, Torous J, Vahia IV. Data security and privacy in apps for dementia: an analysis of existing privacy policies. Am J Geriatr Psychiatry. 2017;25(8):873-877.
18. Torous J, Levin ME, Ahern DK, et al. Cognitive behavioral mobile applications: clinical studies, marketplace overview, and research agenda. Cogn Behav Pract. 2017;24(2):215-225.
19. Owen JE, Jaworski BK, Kuhn E, et al. mHealth in the wild: using novel data to examine the reach, use, and impact of PTSD coach. JMIR Ment Health. 2015;2(1):e7. doi: 10.2196/mental.3935.
20. Sarkar U, Gourley GI, Lyles CR, et al. Usability of commercially available mobile applications for diverse patients. J Gen Intern Med. 2016;31(12):1417-1426.

A prescription to improve drug regimens?
Technology companies are offering two new computerized tools to reduce the “trial and error” of prescribing. Thanks to quantitative EEG (QEEG) testing and pharmacogenetic testing, you may one day be able to consistently choose medications that offer optimal benefit and minimal adverse events—without subjecting patients to unsuccessful trials.
How quantitative eeg works
QEEG adds modern computer and statistical analyses to traditional EEG recordings. The computer creates a graphic display on a schematic map of the head. The procedure is often called brain electrical activity mapping (BEAM) or simply “mapping.”1
QEEG is nearly identical to EEG, but approximately 50% more electrodes are applied to the scalp. The additional electrodes provide better definition and about twice the data compared with traditional EEG.
The UCLA Quantitative EEG Laboratory developed cordance,2 a QEEG measure, to study regional brain activity. Cordance is calculated with reference to absolute and relative power measures from the various electrodes on the brain. It is more closely correlated than traditional EEG with regional cerebral perfusion, which may offer clues to brain activity under different conditions such as depression and medication treatment.
What the data show
Several studies suggest that QEEG can trace response to medication.
Cook et al3 used QEEG in a double-blind study comparing response to fluoxetine, 20 mg/d, and placebo across 8 weeks in 24 adults with unipolar major depression. Subjects were classified as concordant or discordant depending on how many electrodes showed discordance.
Concordant patients showed a more-robust response to fluoxetine than did the discordant group, as evidenced by lower Beck Depression Inventory and Hamilton Rating Scale for Depression (HRSD) scores. The findings suggest that cordance may identify patients who will or will not respond to an antidepressant.
Cook et al4 also used cordance to measure response to fluoxetine, 20 mg/d, venlafaxine, 150 mg/d, or placebo in 51 adults with unipolar depression. Responders to antidepressants (defined as HRSD score ≤10) showed decreased prefrontal cordance after 48 hours and 1 week, suggesting that the prefrontal region may mediate antidepressant response.
A recent study in Korea5 investigated the effects of methylphenidate, 0.7 mg/kg/d (range 15 to 35 mg/d) on QEEG patterns in 20 boys ages 6 to 12 while at work or rest. Numerous changes in band waves were seen during continuous performance tests, but none were reported while the subjects were at rest. This suggests that methylphenidate exerts greater electrophysiologic influence during attention-related tasks.
Clinical applicability
QEEG has just begun to enter mainstream practice, with vendors offering analysis services. As patients increasingly demand improved diagnostic reliability and medication effectiveness, QEEG use could become a standard of practice within 5 years.
Lexicor offers a QEEG analysis to diagnose attention-deficit/hyperactivity disorder based on theta/beta band wave ratio. Lexicor says its analysis offers 86% to 90% sensitivity and 94% to 98% specificity, both far greater than traditional methods such as the Child Behavior Checklist, Behavior Assessment System for Children, and Devereaux Scales of Mental Disorder.
Major health plans offer limited coverage of quantitative EEG testing, however, so many patients would pay $200 or more for tests out of pocket. Also, the American Academy of Neurology and American Clinical Neurophysiology Society endorse QEEG for use in screening for and assessing epilepsy, but not in mental disorders,6 making insurers less likely to cover these tests for psychiatric purposes.
Pharmacogenetic testing
With the sequencing of the human genome and improved speed of genetic analysis, pharmacogenetic testing could supplement quantitative EEG in identifying an appropriate medication.
Companies such as Genelex (www.healthanddna.com/professional/pharmacogenetics.html) and Signature Genetics (www.signaturegenetics.com) have begun offering tests to detect variants of the cytochrome-P(CYP) 2C9, 2C19, 2D6, and 1A2 genes. The findings indicate if the patient will metabolize a medication too slowly or rapidly through these pathways. Psychiatrists can then adjust the dosage accordingly or try another medication. Physicians can order any combination of gene tests, which cost about $150 to $200 each, or all available tests for a discounted price of approximately $600.
Genelex and Signature Genetics can create individualized CYP-450 function reports to facilitate prescribing and customized reports that take into account the patient’s medication and diet regimen. Genelex also offers an Internet-based software tool, GeneMedRx, which allows doctors to customize medication regimens based on potential drug-drug interactions and genomic information.
Signature Genetics offers a prospective assessment of drugs based on genetic test results. This assessment provides a comprehensive report of which medications are affected by the test results.
Genetic profiling can help psychiatrists improve the likelihood of treatment success and minimize potential drug-drug interactions and adverse reactions. Patients will be more satisfied, knowing that their medications fit their individual needs. Also, as more is learned about genetic analysis, genetic testing could one day reveal susceptibility to Alzheimer’s disease, heart attack risk, or other medical problems.
As with QEEG, however, few insurance companies cover genetic testing. Also, insurance companies might charge higher premiums to patients found to have a higher likelihood of developing certain diseases.
Related resources
- Indiana University School of Medicine. Drug interactions table. http://medicine.iupui.edu/flockhart/clinlist.htm.
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
1. Children’s Hospital Boston. Child Health A to Z. What is qEEG? Available at: http://www.childrenshospital.org/az/Site1509/printerfriendlypageS1509P0.html. Accessed March 16, 2006.
2. UCLA Quantitative EEG Laboratory. QEEG Cordance. Available at: http://www.qeeg.npi.ucla.edu/cordance. Accessed March 16, 2006.
3. Cook IA, Leuchter AF, Witte E, et al. Neurophysiologic predictors of treatment response to fluoxetine in major depression. Psychiatry Res 1999;85:263-73.
4. Cook IA, Leuchter AF, Morgan M, et al. Early changes in prefrontal activity characterize clinical responders to antidepressants. Neuropsychopharmacology 2002;27:120-31.
5. Song DH, Shin DW, Jon DI, Ha EH. Effects of methylphenidate on quantitative EEG of boys with attention-deficit hyperactivity disorder in continuous performance test. Yonsei Med J 2005;46:34-41.
6. Nuwer M. Assessment of digital EEG, quantitative EEG, and EEG brain mapping: report of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology 1997;49:277-92.
Technology companies are offering two new computerized tools to reduce the “trial and error” of prescribing. Thanks to quantitative EEG (QEEG) testing and pharmacogenetic testing, you may one day be able to consistently choose medications that offer optimal benefit and minimal adverse events—without subjecting patients to unsuccessful trials.
How quantitative eeg works
QEEG adds modern computer and statistical analyses to traditional EEG recordings. The computer creates a graphic display on a schematic map of the head. The procedure is often called brain electrical activity mapping (BEAM) or simply “mapping.”1
QEEG is nearly identical to EEG, but approximately 50% more electrodes are applied to the scalp. The additional electrodes provide better definition and about twice the data compared with traditional EEG.
The UCLA Quantitative EEG Laboratory developed cordance,2 a QEEG measure, to study regional brain activity. Cordance is calculated with reference to absolute and relative power measures from the various electrodes on the brain. It is more closely correlated than traditional EEG with regional cerebral perfusion, which may offer clues to brain activity under different conditions such as depression and medication treatment.
What the data show
Several studies suggest that QEEG can trace response to medication.
Cook et al3 used QEEG in a double-blind study comparing response to fluoxetine, 20 mg/d, and placebo across 8 weeks in 24 adults with unipolar major depression. Subjects were classified as concordant or discordant depending on how many electrodes showed discordance.
Concordant patients showed a more-robust response to fluoxetine than did the discordant group, as evidenced by lower Beck Depression Inventory and Hamilton Rating Scale for Depression (HRSD) scores. The findings suggest that cordance may identify patients who will or will not respond to an antidepressant.
Cook et al4 also used cordance to measure response to fluoxetine, 20 mg/d, venlafaxine, 150 mg/d, or placebo in 51 adults with unipolar depression. Responders to antidepressants (defined as HRSD score ≤10) showed decreased prefrontal cordance after 48 hours and 1 week, suggesting that the prefrontal region may mediate antidepressant response.
A recent study in Korea5 investigated the effects of methylphenidate, 0.7 mg/kg/d (range 15 to 35 mg/d) on QEEG patterns in 20 boys ages 6 to 12 while at work or rest. Numerous changes in band waves were seen during continuous performance tests, but none were reported while the subjects were at rest. This suggests that methylphenidate exerts greater electrophysiologic influence during attention-related tasks.
Clinical applicability
QEEG has just begun to enter mainstream practice, with vendors offering analysis services. As patients increasingly demand improved diagnostic reliability and medication effectiveness, QEEG use could become a standard of practice within 5 years.
Lexicor offers a QEEG analysis to diagnose attention-deficit/hyperactivity disorder based on theta/beta band wave ratio. Lexicor says its analysis offers 86% to 90% sensitivity and 94% to 98% specificity, both far greater than traditional methods such as the Child Behavior Checklist, Behavior Assessment System for Children, and Devereaux Scales of Mental Disorder.
Major health plans offer limited coverage of quantitative EEG testing, however, so many patients would pay $200 or more for tests out of pocket. Also, the American Academy of Neurology and American Clinical Neurophysiology Society endorse QEEG for use in screening for and assessing epilepsy, but not in mental disorders,6 making insurers less likely to cover these tests for psychiatric purposes.
Pharmacogenetic testing
With the sequencing of the human genome and improved speed of genetic analysis, pharmacogenetic testing could supplement quantitative EEG in identifying an appropriate medication.
Companies such as Genelex (www.healthanddna.com/professional/pharmacogenetics.html) and Signature Genetics (www.signaturegenetics.com) have begun offering tests to detect variants of the cytochrome-P(CYP) 2C9, 2C19, 2D6, and 1A2 genes. The findings indicate if the patient will metabolize a medication too slowly or rapidly through these pathways. Psychiatrists can then adjust the dosage accordingly or try another medication. Physicians can order any combination of gene tests, which cost about $150 to $200 each, or all available tests for a discounted price of approximately $600.
Genelex and Signature Genetics can create individualized CYP-450 function reports to facilitate prescribing and customized reports that take into account the patient’s medication and diet regimen. Genelex also offers an Internet-based software tool, GeneMedRx, which allows doctors to customize medication regimens based on potential drug-drug interactions and genomic information.
Signature Genetics offers a prospective assessment of drugs based on genetic test results. This assessment provides a comprehensive report of which medications are affected by the test results.
Genetic profiling can help psychiatrists improve the likelihood of treatment success and minimize potential drug-drug interactions and adverse reactions. Patients will be more satisfied, knowing that their medications fit their individual needs. Also, as more is learned about genetic analysis, genetic testing could one day reveal susceptibility to Alzheimer’s disease, heart attack risk, or other medical problems.
As with QEEG, however, few insurance companies cover genetic testing. Also, insurance companies might charge higher premiums to patients found to have a higher likelihood of developing certain diseases.
Related resources
- Indiana University School of Medicine. Drug interactions table. http://medicine.iupui.edu/flockhart/clinlist.htm.
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
Technology companies are offering two new computerized tools to reduce the “trial and error” of prescribing. Thanks to quantitative EEG (QEEG) testing and pharmacogenetic testing, you may one day be able to consistently choose medications that offer optimal benefit and minimal adverse events—without subjecting patients to unsuccessful trials.
How quantitative eeg works
QEEG adds modern computer and statistical analyses to traditional EEG recordings. The computer creates a graphic display on a schematic map of the head. The procedure is often called brain electrical activity mapping (BEAM) or simply “mapping.”1
QEEG is nearly identical to EEG, but approximately 50% more electrodes are applied to the scalp. The additional electrodes provide better definition and about twice the data compared with traditional EEG.
The UCLA Quantitative EEG Laboratory developed cordance,2 a QEEG measure, to study regional brain activity. Cordance is calculated with reference to absolute and relative power measures from the various electrodes on the brain. It is more closely correlated than traditional EEG with regional cerebral perfusion, which may offer clues to brain activity under different conditions such as depression and medication treatment.
What the data show
Several studies suggest that QEEG can trace response to medication.
Cook et al3 used QEEG in a double-blind study comparing response to fluoxetine, 20 mg/d, and placebo across 8 weeks in 24 adults with unipolar major depression. Subjects were classified as concordant or discordant depending on how many electrodes showed discordance.
Concordant patients showed a more-robust response to fluoxetine than did the discordant group, as evidenced by lower Beck Depression Inventory and Hamilton Rating Scale for Depression (HRSD) scores. The findings suggest that cordance may identify patients who will or will not respond to an antidepressant.
Cook et al4 also used cordance to measure response to fluoxetine, 20 mg/d, venlafaxine, 150 mg/d, or placebo in 51 adults with unipolar depression. Responders to antidepressants (defined as HRSD score ≤10) showed decreased prefrontal cordance after 48 hours and 1 week, suggesting that the prefrontal region may mediate antidepressant response.
A recent study in Korea5 investigated the effects of methylphenidate, 0.7 mg/kg/d (range 15 to 35 mg/d) on QEEG patterns in 20 boys ages 6 to 12 while at work or rest. Numerous changes in band waves were seen during continuous performance tests, but none were reported while the subjects were at rest. This suggests that methylphenidate exerts greater electrophysiologic influence during attention-related tasks.
Clinical applicability
QEEG has just begun to enter mainstream practice, with vendors offering analysis services. As patients increasingly demand improved diagnostic reliability and medication effectiveness, QEEG use could become a standard of practice within 5 years.
Lexicor offers a QEEG analysis to diagnose attention-deficit/hyperactivity disorder based on theta/beta band wave ratio. Lexicor says its analysis offers 86% to 90% sensitivity and 94% to 98% specificity, both far greater than traditional methods such as the Child Behavior Checklist, Behavior Assessment System for Children, and Devereaux Scales of Mental Disorder.
Major health plans offer limited coverage of quantitative EEG testing, however, so many patients would pay $200 or more for tests out of pocket. Also, the American Academy of Neurology and American Clinical Neurophysiology Society endorse QEEG for use in screening for and assessing epilepsy, but not in mental disorders,6 making insurers less likely to cover these tests for psychiatric purposes.
Pharmacogenetic testing
With the sequencing of the human genome and improved speed of genetic analysis, pharmacogenetic testing could supplement quantitative EEG in identifying an appropriate medication.
Companies such as Genelex (www.healthanddna.com/professional/pharmacogenetics.html) and Signature Genetics (www.signaturegenetics.com) have begun offering tests to detect variants of the cytochrome-P(CYP) 2C9, 2C19, 2D6, and 1A2 genes. The findings indicate if the patient will metabolize a medication too slowly or rapidly through these pathways. Psychiatrists can then adjust the dosage accordingly or try another medication. Physicians can order any combination of gene tests, which cost about $150 to $200 each, or all available tests for a discounted price of approximately $600.
Genelex and Signature Genetics can create individualized CYP-450 function reports to facilitate prescribing and customized reports that take into account the patient’s medication and diet regimen. Genelex also offers an Internet-based software tool, GeneMedRx, which allows doctors to customize medication regimens based on potential drug-drug interactions and genomic information.
Signature Genetics offers a prospective assessment of drugs based on genetic test results. This assessment provides a comprehensive report of which medications are affected by the test results.
Genetic profiling can help psychiatrists improve the likelihood of treatment success and minimize potential drug-drug interactions and adverse reactions. Patients will be more satisfied, knowing that their medications fit their individual needs. Also, as more is learned about genetic analysis, genetic testing could one day reveal susceptibility to Alzheimer’s disease, heart attack risk, or other medical problems.
As with QEEG, however, few insurance companies cover genetic testing. Also, insurance companies might charge higher premiums to patients found to have a higher likelihood of developing certain diseases.
Related resources
- Indiana University School of Medicine. Drug interactions table. http://medicine.iupui.edu/flockhart/clinlist.htm.
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
1. Children’s Hospital Boston. Child Health A to Z. What is qEEG? Available at: http://www.childrenshospital.org/az/Site1509/printerfriendlypageS1509P0.html. Accessed March 16, 2006.
2. UCLA Quantitative EEG Laboratory. QEEG Cordance. Available at: http://www.qeeg.npi.ucla.edu/cordance. Accessed March 16, 2006.
3. Cook IA, Leuchter AF, Witte E, et al. Neurophysiologic predictors of treatment response to fluoxetine in major depression. Psychiatry Res 1999;85:263-73.
4. Cook IA, Leuchter AF, Morgan M, et al. Early changes in prefrontal activity characterize clinical responders to antidepressants. Neuropsychopharmacology 2002;27:120-31.
5. Song DH, Shin DW, Jon DI, Ha EH. Effects of methylphenidate on quantitative EEG of boys with attention-deficit hyperactivity disorder in continuous performance test. Yonsei Med J 2005;46:34-41.
6. Nuwer M. Assessment of digital EEG, quantitative EEG, and EEG brain mapping: report of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology 1997;49:277-92.
1. Children’s Hospital Boston. Child Health A to Z. What is qEEG? Available at: http://www.childrenshospital.org/az/Site1509/printerfriendlypageS1509P0.html. Accessed March 16, 2006.
2. UCLA Quantitative EEG Laboratory. QEEG Cordance. Available at: http://www.qeeg.npi.ucla.edu/cordance. Accessed March 16, 2006.
3. Cook IA, Leuchter AF, Witte E, et al. Neurophysiologic predictors of treatment response to fluoxetine in major depression. Psychiatry Res 1999;85:263-73.
4. Cook IA, Leuchter AF, Morgan M, et al. Early changes in prefrontal activity characterize clinical responders to antidepressants. Neuropsychopharmacology 2002;27:120-31.
5. Song DH, Shin DW, Jon DI, Ha EH. Effects of methylphenidate on quantitative EEG of boys with attention-deficit hyperactivity disorder in continuous performance test. Yonsei Med J 2005;46:34-41.
6. Nuwer M. Assessment of digital EEG, quantitative EEG, and EEG brain mapping: report of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology 1997;49:277-92.
Blogs: Personal and professional
Text:
Once reserved for personal diaries, the Web log or “blog” has become a powerful cybertool for self-expression, news, and debate. Physicians are increasingly using blogs to communicate and stay abreast, and advances in search engine technology make blogs easy to find and easier to start.
This article reviews numerous uses for blogs, plus information on starting your own.
The birth of the blog
Blogs started as public online diaries that provided a forum for self-expression and support. Blogs are similar to personal home pages and newsletters, except that authors update the content more frequently—daily in many cases—and readers can post comments for public viewing. Blogs combine elements of individual and group psychotherapy with a public journal.
Patients and families, for example, use schizophrenia.com to list their favorite blogs or create their own. Moodswing.org lists blogs for persons with bipolar disorder and their families.
Medical professionals also have discovered the therapeutic benefits of blog writing. Crazy Tracy features a psychiatric nurse’s musings about her work and personal life. Physicians post their experiences with patients and their thoughts about health care on blogs such as Intueri.org and Shrinkette.
Although blogs are public, many if not most authors keep identifying information out of their author profiles. Posting your e-mail address on a blog, for example, may open the door to viruses, spamming, or identity theft.
Also, recounting a specific case on a blog could breach patient confidentiality. Instead, post abstract case information to protect the patient’s anonymity.
Blog evolution
Blogs are also becoming well entrenched in business. Most corporate Web sites include blogs for employees to make announcements about products and services. Compared with discussion forums such as Invision Power Board, a blog helps create a sense of community without the constraints of defined topic headings seen in a bulletin board.
Google’s 2003 purchase of Pyra Labs—which developed Blogger, the easy-to-use blog creation site—helped push blogs into the mainstream. Even the CIA is using enterprise-based blog software to collect, organize, and publish information on its Intranet. (See “Psyber Psychiatry. Web logs: Blogging into the future,” January 2003.)
Medical blogs. A growing number of blogs, such as PsychNotes, AATP Interactive, and CodeBlueBlog, disseminate medical news. Authors cull information from clinical journals and Web sites to discuss their opinions and draw attention to new findings. Many medical blogs link to others, using pieces of code from blogLinker or Blogroller, so finding medical blogs is easy.
Some search engines and directories allow users to search exclusively for blogs. Technorati, a well-known blog search engine, searches based on links to sites and keyword tags. The blog sites’ authors choose the keywords, such as “schizophrenia” or “psychiatry.” Keyword tags can be linked to Web sites offering other services, such as photo sharing and listing favorite Web sites.
Social tagging
Even search engines cannot keep up with the growing number of sites proliferating on the Web. Enter social tagging, through which users can share common interests by storing links to Web sites. Blog users can use social tagging to consolidate links to other blogs.
Social tagging sites such as del.icio.us, Furl, and Shadows allow users to store URLs of sites they want to save and share. After creating an account, the user adds URLs with keyword tags into a database. Users can search the database for sites of interest. Using the keyword “psychiatry” on del.icio.us, for example, I found the Virtual Hospital Emergency Services Handbook and other mental health references. Each site found under the keyword also lists the number of users who have added that site to their “favorites” list.
Flickr and Buzznet offer a similar service to help users find photos related to keywords; these photos can be linked to blogs.
Rollyo and Wink are similar to social tagging sites, but with a twist. After establishing an account, users create a specialized search using a keyword tag but specify which Web sites to search. This type of keyword search could be more productive than conventional Web searches if the user knows which sites may produce useful results.
Although the Internet continues to grow almost exponentially, social tagging helps create a sense of community and a shared knowledge base. At SuprGlu, users gather content from other social tagging sites where they have an account. Ning expands upon this process, providing a free online service for building social blogs and connecting blog users based on common interests. These sites and services help make the Internet a much smaller and more useful place.
Starting your own blog
Not long ago, bloggers needed special software to post links to other blogs and comments from readers. Also, archiving previous posts required some skill, as this process was not automated.
Today, blog creation sites take the technical difficulty out of creating and hosting blogs, allowing authors to use the Web browser to edit and then publish the blog. These services, however, may have limited ‘skins’ or templates to customize your site’s look, and your URL will be based on the host name, such as boredhousewife.blogspot.com. You can circumvent this problem by registering your own URL and purchasing blog creation software such as Movable Type.
Send questions about blogs or this column to Dr. Luo or e-mail to [email protected].
Disclosure:
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions he expresses in this column are his own and do not necessarily reflect those of Current Psychiatry.
Text:
Once reserved for personal diaries, the Web log or “blog” has become a powerful cybertool for self-expression, news, and debate. Physicians are increasingly using blogs to communicate and stay abreast, and advances in search engine technology make blogs easy to find and easier to start.
This article reviews numerous uses for blogs, plus information on starting your own.
The birth of the blog
Blogs started as public online diaries that provided a forum for self-expression and support. Blogs are similar to personal home pages and newsletters, except that authors update the content more frequently—daily in many cases—and readers can post comments for public viewing. Blogs combine elements of individual and group psychotherapy with a public journal.
Patients and families, for example, use schizophrenia.com to list their favorite blogs or create their own. Moodswing.org lists blogs for persons with bipolar disorder and their families.
Medical professionals also have discovered the therapeutic benefits of blog writing. Crazy Tracy features a psychiatric nurse’s musings about her work and personal life. Physicians post their experiences with patients and their thoughts about health care on blogs such as Intueri.org and Shrinkette.
Although blogs are public, many if not most authors keep identifying information out of their author profiles. Posting your e-mail address on a blog, for example, may open the door to viruses, spamming, or identity theft.
Also, recounting a specific case on a blog could breach patient confidentiality. Instead, post abstract case information to protect the patient’s anonymity.
Blog evolution
Blogs are also becoming well entrenched in business. Most corporate Web sites include blogs for employees to make announcements about products and services. Compared with discussion forums such as Invision Power Board, a blog helps create a sense of community without the constraints of defined topic headings seen in a bulletin board.
Google’s 2003 purchase of Pyra Labs—which developed Blogger, the easy-to-use blog creation site—helped push blogs into the mainstream. Even the CIA is using enterprise-based blog software to collect, organize, and publish information on its Intranet. (See “Psyber Psychiatry. Web logs: Blogging into the future,” January 2003.)
Medical blogs. A growing number of blogs, such as PsychNotes, AATP Interactive, and CodeBlueBlog, disseminate medical news. Authors cull information from clinical journals and Web sites to discuss their opinions and draw attention to new findings. Many medical blogs link to others, using pieces of code from blogLinker or Blogroller, so finding medical blogs is easy.
Some search engines and directories allow users to search exclusively for blogs. Technorati, a well-known blog search engine, searches based on links to sites and keyword tags. The blog sites’ authors choose the keywords, such as “schizophrenia” or “psychiatry.” Keyword tags can be linked to Web sites offering other services, such as photo sharing and listing favorite Web sites.
Social tagging
Even search engines cannot keep up with the growing number of sites proliferating on the Web. Enter social tagging, through which users can share common interests by storing links to Web sites. Blog users can use social tagging to consolidate links to other blogs.
Social tagging sites such as del.icio.us, Furl, and Shadows allow users to store URLs of sites they want to save and share. After creating an account, the user adds URLs with keyword tags into a database. Users can search the database for sites of interest. Using the keyword “psychiatry” on del.icio.us, for example, I found the Virtual Hospital Emergency Services Handbook and other mental health references. Each site found under the keyword also lists the number of users who have added that site to their “favorites” list.
Flickr and Buzznet offer a similar service to help users find photos related to keywords; these photos can be linked to blogs.
Rollyo and Wink are similar to social tagging sites, but with a twist. After establishing an account, users create a specialized search using a keyword tag but specify which Web sites to search. This type of keyword search could be more productive than conventional Web searches if the user knows which sites may produce useful results.
Although the Internet continues to grow almost exponentially, social tagging helps create a sense of community and a shared knowledge base. At SuprGlu, users gather content from other social tagging sites where they have an account. Ning expands upon this process, providing a free online service for building social blogs and connecting blog users based on common interests. These sites and services help make the Internet a much smaller and more useful place.
Starting your own blog
Not long ago, bloggers needed special software to post links to other blogs and comments from readers. Also, archiving previous posts required some skill, as this process was not automated.
Today, blog creation sites take the technical difficulty out of creating and hosting blogs, allowing authors to use the Web browser to edit and then publish the blog. These services, however, may have limited ‘skins’ or templates to customize your site’s look, and your URL will be based on the host name, such as boredhousewife.blogspot.com. You can circumvent this problem by registering your own URL and purchasing blog creation software such as Movable Type.
Send questions about blogs or this column to Dr. Luo or e-mail to [email protected].
Disclosure:
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions he expresses in this column are his own and do not necessarily reflect those of Current Psychiatry.
Text:
Once reserved for personal diaries, the Web log or “blog” has become a powerful cybertool for self-expression, news, and debate. Physicians are increasingly using blogs to communicate and stay abreast, and advances in search engine technology make blogs easy to find and easier to start.
This article reviews numerous uses for blogs, plus information on starting your own.
The birth of the blog
Blogs started as public online diaries that provided a forum for self-expression and support. Blogs are similar to personal home pages and newsletters, except that authors update the content more frequently—daily in many cases—and readers can post comments for public viewing. Blogs combine elements of individual and group psychotherapy with a public journal.
Patients and families, for example, use schizophrenia.com to list their favorite blogs or create their own. Moodswing.org lists blogs for persons with bipolar disorder and their families.
Medical professionals also have discovered the therapeutic benefits of blog writing. Crazy Tracy features a psychiatric nurse’s musings about her work and personal life. Physicians post their experiences with patients and their thoughts about health care on blogs such as Intueri.org and Shrinkette.
Although blogs are public, many if not most authors keep identifying information out of their author profiles. Posting your e-mail address on a blog, for example, may open the door to viruses, spamming, or identity theft.
Also, recounting a specific case on a blog could breach patient confidentiality. Instead, post abstract case information to protect the patient’s anonymity.
Blog evolution
Blogs are also becoming well entrenched in business. Most corporate Web sites include blogs for employees to make announcements about products and services. Compared with discussion forums such as Invision Power Board, a blog helps create a sense of community without the constraints of defined topic headings seen in a bulletin board.
Google’s 2003 purchase of Pyra Labs—which developed Blogger, the easy-to-use blog creation site—helped push blogs into the mainstream. Even the CIA is using enterprise-based blog software to collect, organize, and publish information on its Intranet. (See “Psyber Psychiatry. Web logs: Blogging into the future,” January 2003.)
Medical blogs. A growing number of blogs, such as PsychNotes, AATP Interactive, and CodeBlueBlog, disseminate medical news. Authors cull information from clinical journals and Web sites to discuss their opinions and draw attention to new findings. Many medical blogs link to others, using pieces of code from blogLinker or Blogroller, so finding medical blogs is easy.
Some search engines and directories allow users to search exclusively for blogs. Technorati, a well-known blog search engine, searches based on links to sites and keyword tags. The blog sites’ authors choose the keywords, such as “schizophrenia” or “psychiatry.” Keyword tags can be linked to Web sites offering other services, such as photo sharing and listing favorite Web sites.
Social tagging
Even search engines cannot keep up with the growing number of sites proliferating on the Web. Enter social tagging, through which users can share common interests by storing links to Web sites. Blog users can use social tagging to consolidate links to other blogs.
Social tagging sites such as del.icio.us, Furl, and Shadows allow users to store URLs of sites they want to save and share. After creating an account, the user adds URLs with keyword tags into a database. Users can search the database for sites of interest. Using the keyword “psychiatry” on del.icio.us, for example, I found the Virtual Hospital Emergency Services Handbook and other mental health references. Each site found under the keyword also lists the number of users who have added that site to their “favorites” list.
Flickr and Buzznet offer a similar service to help users find photos related to keywords; these photos can be linked to blogs.
Rollyo and Wink are similar to social tagging sites, but with a twist. After establishing an account, users create a specialized search using a keyword tag but specify which Web sites to search. This type of keyword search could be more productive than conventional Web searches if the user knows which sites may produce useful results.
Although the Internet continues to grow almost exponentially, social tagging helps create a sense of community and a shared knowledge base. At SuprGlu, users gather content from other social tagging sites where they have an account. Ning expands upon this process, providing a free online service for building social blogs and connecting blog users based on common interests. These sites and services help make the Internet a much smaller and more useful place.
Starting your own blog
Not long ago, bloggers needed special software to post links to other blogs and comments from readers. Also, archiving previous posts required some skill, as this process was not automated.
Today, blog creation sites take the technical difficulty out of creating and hosting blogs, allowing authors to use the Web browser to edit and then publish the blog. These services, however, may have limited ‘skins’ or templates to customize your site’s look, and your URL will be based on the host name, such as boredhousewife.blogspot.com. You can circumvent this problem by registering your own URL and purchasing blog creation software such as Movable Type.
Send questions about blogs or this column to Dr. Luo or e-mail to [email protected].
Disclosure:
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions he expresses in this column are his own and do not necessarily reflect those of Current Psychiatry.
VoIP: The right call for your practice?
Voice-over Internet protocol (VoIP), once a cutting-edge telecommunications innovation, has quickly reached the information age mainstream (See Fast facts). Homes and businesses are increasingly using broadband Internet connections to make inexpensive long-distance telephone calls.
Can VoIP help you communicate efficiently and cost-effectively with patients, staff, and colleagues? Read on.
How VoIP works
VoIP lets you make telephone calls using your Internet connection or other computer network. Calls from one PC to another are free, while calls from a PC to a landline or mobile phone are not.
In the most basic VoIP, a user at a computer with a microphone headset calls a similarly equipped user by entering an e-mail address or user name on a network, such as Skype’s “SkypeOut” program. Software transmits the audio signal over the Internet. The technology is similar to that of a mobile phone, which requires cellular towers to send packets of your audio signal.
eBay recently purchased Skype for $1.3 billion in cash and $1.3 billion in eBay stock. VoIP use will likely become more widespread after the eBay takeover, industry observers predict. For more information, see http://news.bbc.co.uk/1/hi/technology/4238258.stm.
For as little as 17 cents per minute, you can call from your computer to a regular telephone number anywhere in the world. Skype, SunRocket, and Vonage are among the more popular and inexpensive VoIP providers (Table). In addition to “SkypeOut,” Google, Yahoo, and MSN also offer free PC-to-PC calling with voice conferencing.
Another Skype service, “SkypeIn,” offers portable local numbers that allow callers—using a computer or a regular phone—to reach you wherever you go. You can be traveling in Paris and receive a phone call at a local Internet café with your notebook computer, yet the caller pays only the regular rate to call your number.
Only Skype offers software that allows telecommunication via Pocket PC. Blackberry is not supported for VoIP communication and SunRocket and Vonage do not offer PDA support.
Table
VoIP Providers
| Provider | Service within USA and Canada | Service to India–New Delhi |
|---|---|---|
| Skype | $0.021/minute | $0.154/minute |
| SunRocket | $24.95/month unlimited | $0.12/minute |
| Vonage | $24.95/month unlimited | $0.17/minute |
VoIP advantages
The ability to make free or low-cost calls to any location worldwide is an obvious advantage. For clinical use, VoIP can help psychiatrists reach patients who travel frequently and have Internet access.
For the psychiatrist who shuttles between offices, a portable number offers flexibility. Psychiatrists attending national meetings or CME courses can use VoIP to contact colleagues or communicate with patients or staff back home.
Online phone communication is also secure, because VoIP data packets are encrypted as they are sent over the Internet.
VoIP users may be able to eliminate their local telephone service and pay only for broadband Internet access. For emergencies when the Internet is not working, a mobile phone may be sufficient backup.
If you prefer a traditional phone to a microphone headset, you can use a phone equipped with a universal serial bus (USB) connector to make online calls. Skype offers phones with built-in USB connectors, while Vonage and SunRocket offer adapters that connect to regular phones and specialized phone adapters that connect to a phone, computer, or fax machine.
Skype, SunRocket, and Vonage offer call waiting and voice mail functions. Many VoIP software clients also offer text messaging and conference calling, allowing you to use your computer to type notes or send files while making a VoIP call. Some VoIP providers, such as Yahoo! Messenger, offer a video signal as well.
Skype offers a Pocket PC software client that lets you make telephone calls while connected to the Internet with a Pocket PC personal digital assistant (PDA). Having a Pocket PC with unlimited monthly wireless Internet data service and using SkypeOut to make mobile telephone calls for 2.4 cents per minute within the continental United States can help control combined PDA/phone charges. Skype will release a Palm OS version of this software sometime this month.1
Drawbacks
When your Internet access is down, you cannot make or receive VoIP calls. Also, as with mobile phones, the connection at times may be dropped or sound somewhat muffled. Overall, VoIP sound quality is on par with mobile phones, but not as good as conventional landline phones.
If traffic over your Internet connection is heavy—with downloads and other applications competing for bandwidth—connection quality can suffer. One solution is to use a router that gives priority to the VoIP application and its data. A router, similar to a “traffic cop” on a shared Internet connection, knows which data to send to and from the different computers/devices and the Internet connection.2 The D-Link Broadband Phone Service VoIP Router, for example, enables VoIP calls and Internet sharing.
VoIP inboxes theoretically are vulnerable to spam attacks because of e-mail addresses associated with accounts. Qovia is seeking a patent for technology designed to guard against VoIP spam, but VoIP spam attacks have not yet been reported because VoIP has only recently become popular.2
As mentioned, VoIP could eliminate the need for a regular telephone line, but if you use a digital subscriber line (DSL) for Internet access, you will need to keep at least a local telephone service.
Telecommunication: the future
The development of faster Internet access with Internet2 could lead to consolidation in the communications industry, allowing voice, data, video and other media to be managed via one connection. Internet2 is a consortium of universities working with industry and government to develop and deploy advanced network applications and technologies for the creation of tomorrow’s Internet.
Related resources
- 1. Federal Communications Commission. Voice-over Internet protocol: frequently asked questions. http://www.fcc.gov/voip/
- 2. Internet2. http://www.internet2.edu/
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
(accessed Oct. 3, 2005)
1. Rojas P. Skype coming to Palm next month? Engadget Sept. 14, 2005. Available at: http://www.engadget.com/entry/1016803924623324/.
2. Qovia files patents for voice spam blocking technology. Available at: http://www.qovia.com/company/news/06.28.2004_voip_spam_patent_app_final.htm.
Voice-over Internet protocol (VoIP), once a cutting-edge telecommunications innovation, has quickly reached the information age mainstream (See Fast facts). Homes and businesses are increasingly using broadband Internet connections to make inexpensive long-distance telephone calls.
Can VoIP help you communicate efficiently and cost-effectively with patients, staff, and colleagues? Read on.
How VoIP works
VoIP lets you make telephone calls using your Internet connection or other computer network. Calls from one PC to another are free, while calls from a PC to a landline or mobile phone are not.
In the most basic VoIP, a user at a computer with a microphone headset calls a similarly equipped user by entering an e-mail address or user name on a network, such as Skype’s “SkypeOut” program. Software transmits the audio signal over the Internet. The technology is similar to that of a mobile phone, which requires cellular towers to send packets of your audio signal.
eBay recently purchased Skype for $1.3 billion in cash and $1.3 billion in eBay stock. VoIP use will likely become more widespread after the eBay takeover, industry observers predict. For more information, see http://news.bbc.co.uk/1/hi/technology/4238258.stm.
For as little as 17 cents per minute, you can call from your computer to a regular telephone number anywhere in the world. Skype, SunRocket, and Vonage are among the more popular and inexpensive VoIP providers (Table). In addition to “SkypeOut,” Google, Yahoo, and MSN also offer free PC-to-PC calling with voice conferencing.
Another Skype service, “SkypeIn,” offers portable local numbers that allow callers—using a computer or a regular phone—to reach you wherever you go. You can be traveling in Paris and receive a phone call at a local Internet café with your notebook computer, yet the caller pays only the regular rate to call your number.
Only Skype offers software that allows telecommunication via Pocket PC. Blackberry is not supported for VoIP communication and SunRocket and Vonage do not offer PDA support.
Table
VoIP Providers
| Provider | Service within USA and Canada | Service to India–New Delhi |
|---|---|---|
| Skype | $0.021/minute | $0.154/minute |
| SunRocket | $24.95/month unlimited | $0.12/minute |
| Vonage | $24.95/month unlimited | $0.17/minute |
VoIP advantages
The ability to make free or low-cost calls to any location worldwide is an obvious advantage. For clinical use, VoIP can help psychiatrists reach patients who travel frequently and have Internet access.
For the psychiatrist who shuttles between offices, a portable number offers flexibility. Psychiatrists attending national meetings or CME courses can use VoIP to contact colleagues or communicate with patients or staff back home.
Online phone communication is also secure, because VoIP data packets are encrypted as they are sent over the Internet.
VoIP users may be able to eliminate their local telephone service and pay only for broadband Internet access. For emergencies when the Internet is not working, a mobile phone may be sufficient backup.
If you prefer a traditional phone to a microphone headset, you can use a phone equipped with a universal serial bus (USB) connector to make online calls. Skype offers phones with built-in USB connectors, while Vonage and SunRocket offer adapters that connect to regular phones and specialized phone adapters that connect to a phone, computer, or fax machine.
Skype, SunRocket, and Vonage offer call waiting and voice mail functions. Many VoIP software clients also offer text messaging and conference calling, allowing you to use your computer to type notes or send files while making a VoIP call. Some VoIP providers, such as Yahoo! Messenger, offer a video signal as well.
Skype offers a Pocket PC software client that lets you make telephone calls while connected to the Internet with a Pocket PC personal digital assistant (PDA). Having a Pocket PC with unlimited monthly wireless Internet data service and using SkypeOut to make mobile telephone calls for 2.4 cents per minute within the continental United States can help control combined PDA/phone charges. Skype will release a Palm OS version of this software sometime this month.1
Drawbacks
When your Internet access is down, you cannot make or receive VoIP calls. Also, as with mobile phones, the connection at times may be dropped or sound somewhat muffled. Overall, VoIP sound quality is on par with mobile phones, but not as good as conventional landline phones.
If traffic over your Internet connection is heavy—with downloads and other applications competing for bandwidth—connection quality can suffer. One solution is to use a router that gives priority to the VoIP application and its data. A router, similar to a “traffic cop” on a shared Internet connection, knows which data to send to and from the different computers/devices and the Internet connection.2 The D-Link Broadband Phone Service VoIP Router, for example, enables VoIP calls and Internet sharing.
VoIP inboxes theoretically are vulnerable to spam attacks because of e-mail addresses associated with accounts. Qovia is seeking a patent for technology designed to guard against VoIP spam, but VoIP spam attacks have not yet been reported because VoIP has only recently become popular.2
As mentioned, VoIP could eliminate the need for a regular telephone line, but if you use a digital subscriber line (DSL) for Internet access, you will need to keep at least a local telephone service.
Telecommunication: the future
The development of faster Internet access with Internet2 could lead to consolidation in the communications industry, allowing voice, data, video and other media to be managed via one connection. Internet2 is a consortium of universities working with industry and government to develop and deploy advanced network applications and technologies for the creation of tomorrow’s Internet.
Related resources
- 1. Federal Communications Commission. Voice-over Internet protocol: frequently asked questions. http://www.fcc.gov/voip/
- 2. Internet2. http://www.internet2.edu/
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
Voice-over Internet protocol (VoIP), once a cutting-edge telecommunications innovation, has quickly reached the information age mainstream (See Fast facts). Homes and businesses are increasingly using broadband Internet connections to make inexpensive long-distance telephone calls.
Can VoIP help you communicate efficiently and cost-effectively with patients, staff, and colleagues? Read on.
How VoIP works
VoIP lets you make telephone calls using your Internet connection or other computer network. Calls from one PC to another are free, while calls from a PC to a landline or mobile phone are not.
In the most basic VoIP, a user at a computer with a microphone headset calls a similarly equipped user by entering an e-mail address or user name on a network, such as Skype’s “SkypeOut” program. Software transmits the audio signal over the Internet. The technology is similar to that of a mobile phone, which requires cellular towers to send packets of your audio signal.
eBay recently purchased Skype for $1.3 billion in cash and $1.3 billion in eBay stock. VoIP use will likely become more widespread after the eBay takeover, industry observers predict. For more information, see http://news.bbc.co.uk/1/hi/technology/4238258.stm.
For as little as 17 cents per minute, you can call from your computer to a regular telephone number anywhere in the world. Skype, SunRocket, and Vonage are among the more popular and inexpensive VoIP providers (Table). In addition to “SkypeOut,” Google, Yahoo, and MSN also offer free PC-to-PC calling with voice conferencing.
Another Skype service, “SkypeIn,” offers portable local numbers that allow callers—using a computer or a regular phone—to reach you wherever you go. You can be traveling in Paris and receive a phone call at a local Internet café with your notebook computer, yet the caller pays only the regular rate to call your number.
Only Skype offers software that allows telecommunication via Pocket PC. Blackberry is not supported for VoIP communication and SunRocket and Vonage do not offer PDA support.
Table
VoIP Providers
| Provider | Service within USA and Canada | Service to India–New Delhi |
|---|---|---|
| Skype | $0.021/minute | $0.154/minute |
| SunRocket | $24.95/month unlimited | $0.12/minute |
| Vonage | $24.95/month unlimited | $0.17/minute |
VoIP advantages
The ability to make free or low-cost calls to any location worldwide is an obvious advantage. For clinical use, VoIP can help psychiatrists reach patients who travel frequently and have Internet access.
For the psychiatrist who shuttles between offices, a portable number offers flexibility. Psychiatrists attending national meetings or CME courses can use VoIP to contact colleagues or communicate with patients or staff back home.
Online phone communication is also secure, because VoIP data packets are encrypted as they are sent over the Internet.
VoIP users may be able to eliminate their local telephone service and pay only for broadband Internet access. For emergencies when the Internet is not working, a mobile phone may be sufficient backup.
If you prefer a traditional phone to a microphone headset, you can use a phone equipped with a universal serial bus (USB) connector to make online calls. Skype offers phones with built-in USB connectors, while Vonage and SunRocket offer adapters that connect to regular phones and specialized phone adapters that connect to a phone, computer, or fax machine.
Skype, SunRocket, and Vonage offer call waiting and voice mail functions. Many VoIP software clients also offer text messaging and conference calling, allowing you to use your computer to type notes or send files while making a VoIP call. Some VoIP providers, such as Yahoo! Messenger, offer a video signal as well.
Skype offers a Pocket PC software client that lets you make telephone calls while connected to the Internet with a Pocket PC personal digital assistant (PDA). Having a Pocket PC with unlimited monthly wireless Internet data service and using SkypeOut to make mobile telephone calls for 2.4 cents per minute within the continental United States can help control combined PDA/phone charges. Skype will release a Palm OS version of this software sometime this month.1
Drawbacks
When your Internet access is down, you cannot make or receive VoIP calls. Also, as with mobile phones, the connection at times may be dropped or sound somewhat muffled. Overall, VoIP sound quality is on par with mobile phones, but not as good as conventional landline phones.
If traffic over your Internet connection is heavy—with downloads and other applications competing for bandwidth—connection quality can suffer. One solution is to use a router that gives priority to the VoIP application and its data. A router, similar to a “traffic cop” on a shared Internet connection, knows which data to send to and from the different computers/devices and the Internet connection.2 The D-Link Broadband Phone Service VoIP Router, for example, enables VoIP calls and Internet sharing.
VoIP inboxes theoretically are vulnerable to spam attacks because of e-mail addresses associated with accounts. Qovia is seeking a patent for technology designed to guard against VoIP spam, but VoIP spam attacks have not yet been reported because VoIP has only recently become popular.2
As mentioned, VoIP could eliminate the need for a regular telephone line, but if you use a digital subscriber line (DSL) for Internet access, you will need to keep at least a local telephone service.
Telecommunication: the future
The development of faster Internet access with Internet2 could lead to consolidation in the communications industry, allowing voice, data, video and other media to be managed via one connection. Internet2 is a consortium of universities working with industry and government to develop and deploy advanced network applications and technologies for the creation of tomorrow’s Internet.
Related resources
- 1. Federal Communications Commission. Voice-over Internet protocol: frequently asked questions. http://www.fcc.gov/voip/
- 2. Internet2. http://www.internet2.edu/
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
(accessed Oct. 3, 2005)
1. Rojas P. Skype coming to Palm next month? Engadget Sept. 14, 2005. Available at: http://www.engadget.com/entry/1016803924623324/.
2. Qovia files patents for voice spam blocking technology. Available at: http://www.qovia.com/company/news/06.28.2004_voip_spam_patent_app_final.htm.
(accessed Oct. 3, 2005)
1. Rojas P. Skype coming to Palm next month? Engadget Sept. 14, 2005. Available at: http://www.engadget.com/entry/1016803924623324/.
2. Qovia files patents for voice spam blocking technology. Available at: http://www.qovia.com/company/news/06.28.2004_voip_spam_patent_app_final.htm.
A prescription to improve drug regimens?
One day we may be able to consistently choose medications that offer optimal benefit and minimal adverse events—without subjecting our patients to unsuccessful trials. Thanks to quantitative EEG (OEEG) testing and pharmacogenetic testing, that day may be coming closer.
How quantitative eeg works
QEEG adds modern computer and statistical analyses to traditional EEG recordings. The computer creates a graphic display on a schematic map of the head. The procedure is often called brain electrical activity mapping (BEAM) or simply “mapping.” New tool: Genotyping makes prescribing safer, more effective, Current Psychiatry, September 2004.) Physicians can order any combination of gene tests, which cost about $150 to $200 each, or all available tests for a discounted price of approximately $600.
Genelex and Signature Genetics can create individualized CYP-450 function reports to facilitate prescribing and customized reports that take into account the patient’s medication and diet regimen. Genelex also offers an Internet-based software tool, GeneMedRx, which allows doctors to customize medication regimens based on both potential drug-drug interactions and genomic information.
Signature Genetics offers a prospective assessment of drugs based on genetic test results. This assessment provides a comprehensive report of which medications are affected by the test results.
Genetic profiling can help psychiatrists improve the likelihood of treatment success and minimize potential drug-drug interactions and adverse reactions. Patients will be more satisfied, knowing that their medications fit their individual needs. Also, as more is learned about genetic analysis, genetic testing could one day reveal susceptibility to Alzheimer’s disease, heart attack risk, or other medical problems.
As with quantitative EEG, however, few insurance companies cover genetic testing. Also, patients found to have a higher likelihood of developing certain diseases could potentially be charged higher health insurance premiums.
Related resources
Indiana University School of Medicine. Drug interactions table. http://medicine.iupui.edu/flockhart/clinlist.htm
Luo J. Psyber Psychiatry. Prescribing Information: scroll with the changes (online, handheld resources on drug-drug interaction, medications’ effect on CYP-450 system. Current Psychiatry 2003;2(8 online edition). http://www.currentpsychiatry.com/article_pages.asp?AID=666&UID=8877
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
(accessed July 27, 2005)
1. Children’s Hospital Boston. Child Health A to Z. What is qEEG? Available at: http://www.childrenshospital.org/cfapps/A2ZtopicDisplay.cfm?Topic=Quan titative%20EEG
2. UCLA Quantitative EEG Laboratory. QEEG Cordance. Available at: http://www.qeeg.npi.ucla.edu/cordance/
3. Cook IA, Leuchter AF, Witte E, et al. Neurophysiologic predictors of treatment response to fluoxetine in major depression. Psychiatry Res 1999;85:263-73.
4. Cook IA, Leuchter AF, Morgan M, et al. Early changes in prefrontal activity characterize clinical responders to antidepressants. Neuropsychopharmacology 2002;27:120-31.
5. Song DH, Shin DW, Jon DI, Ha EH. Effects of methylphenidate on quantitative EEG of boys with attention-deficit hyperactivity disorder in continuous performance test. Yonsei Med J 2005;46:34-41.
6. Nuwer M. Assessment of digital EEG, quantitative EEG, and EEG brain mapping: report of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology 1997;49:277-92.
One day we may be able to consistently choose medications that offer optimal benefit and minimal adverse events—without subjecting our patients to unsuccessful trials. Thanks to quantitative EEG (OEEG) testing and pharmacogenetic testing, that day may be coming closer.
How quantitative eeg works
QEEG adds modern computer and statistical analyses to traditional EEG recordings. The computer creates a graphic display on a schematic map of the head. The procedure is often called brain electrical activity mapping (BEAM) or simply “mapping.” New tool: Genotyping makes prescribing safer, more effective, Current Psychiatry, September 2004.) Physicians can order any combination of gene tests, which cost about $150 to $200 each, or all available tests for a discounted price of approximately $600.
Genelex and Signature Genetics can create individualized CYP-450 function reports to facilitate prescribing and customized reports that take into account the patient’s medication and diet regimen. Genelex also offers an Internet-based software tool, GeneMedRx, which allows doctors to customize medication regimens based on both potential drug-drug interactions and genomic information.
Signature Genetics offers a prospective assessment of drugs based on genetic test results. This assessment provides a comprehensive report of which medications are affected by the test results.
Genetic profiling can help psychiatrists improve the likelihood of treatment success and minimize potential drug-drug interactions and adverse reactions. Patients will be more satisfied, knowing that their medications fit their individual needs. Also, as more is learned about genetic analysis, genetic testing could one day reveal susceptibility to Alzheimer’s disease, heart attack risk, or other medical problems.
As with quantitative EEG, however, few insurance companies cover genetic testing. Also, patients found to have a higher likelihood of developing certain diseases could potentially be charged higher health insurance premiums.
Related resources
Indiana University School of Medicine. Drug interactions table. http://medicine.iupui.edu/flockhart/clinlist.htm
Luo J. Psyber Psychiatry. Prescribing Information: scroll with the changes (online, handheld resources on drug-drug interaction, medications’ effect on CYP-450 system. Current Psychiatry 2003;2(8 online edition). http://www.currentpsychiatry.com/article_pages.asp?AID=666&UID=8877
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
One day we may be able to consistently choose medications that offer optimal benefit and minimal adverse events—without subjecting our patients to unsuccessful trials. Thanks to quantitative EEG (OEEG) testing and pharmacogenetic testing, that day may be coming closer.
How quantitative eeg works
QEEG adds modern computer and statistical analyses to traditional EEG recordings. The computer creates a graphic display on a schematic map of the head. The procedure is often called brain electrical activity mapping (BEAM) or simply “mapping.” New tool: Genotyping makes prescribing safer, more effective, Current Psychiatry, September 2004.) Physicians can order any combination of gene tests, which cost about $150 to $200 each, or all available tests for a discounted price of approximately $600.
Genelex and Signature Genetics can create individualized CYP-450 function reports to facilitate prescribing and customized reports that take into account the patient’s medication and diet regimen. Genelex also offers an Internet-based software tool, GeneMedRx, which allows doctors to customize medication regimens based on both potential drug-drug interactions and genomic information.
Signature Genetics offers a prospective assessment of drugs based on genetic test results. This assessment provides a comprehensive report of which medications are affected by the test results.
Genetic profiling can help psychiatrists improve the likelihood of treatment success and minimize potential drug-drug interactions and adverse reactions. Patients will be more satisfied, knowing that their medications fit their individual needs. Also, as more is learned about genetic analysis, genetic testing could one day reveal susceptibility to Alzheimer’s disease, heart attack risk, or other medical problems.
As with quantitative EEG, however, few insurance companies cover genetic testing. Also, patients found to have a higher likelihood of developing certain diseases could potentially be charged higher health insurance premiums.
Related resources
Indiana University School of Medicine. Drug interactions table. http://medicine.iupui.edu/flockhart/clinlist.htm
Luo J. Psyber Psychiatry. Prescribing Information: scroll with the changes (online, handheld resources on drug-drug interaction, medications’ effect on CYP-450 system. Current Psychiatry 2003;2(8 online edition). http://www.currentpsychiatry.com/article_pages.asp?AID=666&UID=8877
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
(accessed July 27, 2005)
1. Children’s Hospital Boston. Child Health A to Z. What is qEEG? Available at: http://www.childrenshospital.org/cfapps/A2ZtopicDisplay.cfm?Topic=Quan titative%20EEG
2. UCLA Quantitative EEG Laboratory. QEEG Cordance. Available at: http://www.qeeg.npi.ucla.edu/cordance/
3. Cook IA, Leuchter AF, Witte E, et al. Neurophysiologic predictors of treatment response to fluoxetine in major depression. Psychiatry Res 1999;85:263-73.
4. Cook IA, Leuchter AF, Morgan M, et al. Early changes in prefrontal activity characterize clinical responders to antidepressants. Neuropsychopharmacology 2002;27:120-31.
5. Song DH, Shin DW, Jon DI, Ha EH. Effects of methylphenidate on quantitative EEG of boys with attention-deficit hyperactivity disorder in continuous performance test. Yonsei Med J 2005;46:34-41.
6. Nuwer M. Assessment of digital EEG, quantitative EEG, and EEG brain mapping: report of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology 1997;49:277-92.
(accessed July 27, 2005)
1. Children’s Hospital Boston. Child Health A to Z. What is qEEG? Available at: http://www.childrenshospital.org/cfapps/A2ZtopicDisplay.cfm?Topic=Quan titative%20EEG
2. UCLA Quantitative EEG Laboratory. QEEG Cordance. Available at: http://www.qeeg.npi.ucla.edu/cordance/
3. Cook IA, Leuchter AF, Witte E, et al. Neurophysiologic predictors of treatment response to fluoxetine in major depression. Psychiatry Res 1999;85:263-73.
4. Cook IA, Leuchter AF, Morgan M, et al. Early changes in prefrontal activity characterize clinical responders to antidepressants. Neuropsychopharmacology 2002;27:120-31.
5. Song DH, Shin DW, Jon DI, Ha EH. Effects of methylphenidate on quantitative EEG of boys with attention-deficit hyperactivity disorder in continuous performance test. Yonsei Med J 2005;46:34-41.
6. Nuwer M. Assessment of digital EEG, quantitative EEG, and EEG brain mapping: report of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology 1997;49:277-92.
Data backup: Don’t wait for the next crash
We know backing up data is important yet few of us do it consistently, either because we don’t think of it or cannot spare the time. Also, because today’s computers are less expensive and more reliable than before, many doctors think a system crash “can’t happen to me.”
Don’t wait for a power surge or hard drive failure to obliterate your crucial files or documents. This article describes numerous ways to back up and store data, each with different features. Your needs will determine which method is best for you.
HARD DRIVE FAILURE
Hard drives, which store information on platters via electrical charges, are vulnerable. They are rated with a mean time between failure (MTBF),1 which indicates how long on average a hard drive will work before it fails. Although the average MTBF is 50 years, electrical discharges such as power surges or lightning storms can force failure much sooner.
Viruses—if programmed to do so—can also corrupt hard drives. Most viruses propagate to another computer, using your computer as a host.
Companies such as Dataleach can recover information from your hard drive, but recovery may take days.
BASIC BACKUP TOOLS
CD-ROM-burning programs such as Nero Burning ROM are one way to back up data. Most computers purchased within the last 2 years have a built-in CD-ROM burner—a device that reads and creates CD-ROMs—along with CD-burning software.
Keep in mind the size of the disk you are using. CD-ROMs have a maximum capacity of 700 megabytes, but file location information consumes about 10 megabytes. A DVD-ROM can hold 4.7 gigabytes, almost 7 times the capacity of a CD-ROM.
Also consider expense. Recordable CDs on average cost 25 cents per disk. Recordable DVDs are more expensive (between 50 cents and $1 per disk depending on quantity purchased) but could save you money if you’re storing several gigabytes of data. The average cost per 100 megabytes of backup is 3.6 cents with CDs and 1.5 cents with DVDs.
Avoid rewriteable CD and DVDs—disks that can be erased and used again. Although such a disk may minimize backup costs, another computer may be unable to read it.
Alternate storage devices offer varying speeds and capacities. For example, a portable USB flash drive may be useful for storing less than 2 gigabytes. If you need more capacity, external USB hard drives can store up to 80 gigabytes. You can download or store a file within seconds with either device if it has a USB 2.0 transfer speed rating.
Zip drives, which can hold 750 megabytes, were once popular but have become less useful because they lack speed. Tape backup systems are extremely fast and can hold 130 gigabytes, but these devices are expensive and used more for large-scale business server backup.
‘WHICH FILES SHOULD I BACK UP?’
Obviously, you should back up electronic medical and billing records as well as documents created in your Microsoft Office suite.
Don’t ignore other critical information sources, such as Web browser bookmarks and e-mails, but remember that your mail, address book, and account information may be stored in different places depending on your e-mail program.
If you use a recordable CD or DVD, you must determine one by one which directories and files to archive. Nero has an easy-to-use “wizard” that guides you through this process. Nero also lets you automate backup: You would no loner have to remember to do it. Backing up e-mail and browser-bookmarked sites will be difficult, however, unless you know where they are kept.
Products such as Genie Backup Home Manager and NovaBACKUP have built-in search/inventory capability and back up to CDs or DVDs. Also, once the first backup is created, these programs can determine if the files have changed. Thus, subsequent backups will duplicate only files or modifications created since the previous backup. Specialized back-up programs also encrypt information and compress data to conserve space.
SCHEDULING DATA BACKUP
If you don’t create a schedule for backup, chances are it will never get done.
Ideally, you should back up data daily at a set time, such as at noon or closing.
Many psychiatrists, however, probably need a longer interval depending on how long backup takes (anywhere from 5 to 20 minutes depending on volume of data) and whether the information is critical. Also, a file cannot be duplicated while in use, as two computer programs cannot share a file in order to protect the data.
STORING BACKUP
After creating your backup:
- keep the backup and the software used to create it at another location in case of fire or theft
- test with your staff the process of restoring the information to the original hard drive, so that you will learn how to do it and how long it takes to get your computers running.
ALTERNATIVE BACKUP METHODS
If you have broadband Internet access via DSL or cable modem, consider using online backup services offered by Connected or Xdrive. Your data will be safe once you’ve downloaded and installed their software, designated files, and determined backup frequency. These online services also store the data at a remote site in case of fire or theft. Some physicians, however, may feel uncomfortable keeping data on another server for security reasons.
The Mirra Personal Server, an alternative to off-site backup, can be connected to one computer or a network and can back up one or all computers. This server can also synchronize files between computers and allow access to them over the Internet.
For real-time backup, a RAID array2 (redundant array of inexpensive drives) is your only choice. With RAID level 1, two hard drives record simultaneously. When one drive fails, another continues to work and has the information. A RAID array requires a specialized drive controller card, which costs around $150, or specialized software.3 Controller cards are widely available on the Internet (use search terms “Mac Raid controller” or “PC raid controller”), and raid arrays are available for any platform.
THE FUTURE
As multimedia become integrated into medical records and software programs create more information, physicians will need more storage space. New storage technologies such as the HD-DVD and Blu-Ray4 offer up to 25 to 30 gigabytes per disc. Similar to the VHS-Betamax wars of the 1980s, manufacturers are vying to make these high-density storage devices the future storage standard. Also, perpendicular recording technology is increasing hard drive storage capacity.5
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
(accessed April 22, 2005 )
1. Webopedia: What is MTBF? Available at: http://www.webopedia.com/TERM/M/MTBF.html.
2. ACITS open VMS services: Introduction to RAID technology. Available at: http://www.utexas.edu/cc/vms/about/raid.html.
3. The PC Guide: RAID. Available at: http://www.pcguide.com/ref/hdd/perf/raid/index.htm.
4. Wikipedia: HD-DVD. Available at: http://en.wikipedia.org/wiki/HD-DVD.
5. Dahl E. PC drive reaches 500 GB. PC World ‘News & Trends,’ May 2005. Available at: http://www.pcworld.com/news/article/0,aid,120102,00.asp.
We know backing up data is important yet few of us do it consistently, either because we don’t think of it or cannot spare the time. Also, because today’s computers are less expensive and more reliable than before, many doctors think a system crash “can’t happen to me.”
Don’t wait for a power surge or hard drive failure to obliterate your crucial files or documents. This article describes numerous ways to back up and store data, each with different features. Your needs will determine which method is best for you.
HARD DRIVE FAILURE
Hard drives, which store information on platters via electrical charges, are vulnerable. They are rated with a mean time between failure (MTBF),1 which indicates how long on average a hard drive will work before it fails. Although the average MTBF is 50 years, electrical discharges such as power surges or lightning storms can force failure much sooner.
Viruses—if programmed to do so—can also corrupt hard drives. Most viruses propagate to another computer, using your computer as a host.
Companies such as Dataleach can recover information from your hard drive, but recovery may take days.
BASIC BACKUP TOOLS
CD-ROM-burning programs such as Nero Burning ROM are one way to back up data. Most computers purchased within the last 2 years have a built-in CD-ROM burner—a device that reads and creates CD-ROMs—along with CD-burning software.
Keep in mind the size of the disk you are using. CD-ROMs have a maximum capacity of 700 megabytes, but file location information consumes about 10 megabytes. A DVD-ROM can hold 4.7 gigabytes, almost 7 times the capacity of a CD-ROM.
Also consider expense. Recordable CDs on average cost 25 cents per disk. Recordable DVDs are more expensive (between 50 cents and $1 per disk depending on quantity purchased) but could save you money if you’re storing several gigabytes of data. The average cost per 100 megabytes of backup is 3.6 cents with CDs and 1.5 cents with DVDs.
Avoid rewriteable CD and DVDs—disks that can be erased and used again. Although such a disk may minimize backup costs, another computer may be unable to read it.
Alternate storage devices offer varying speeds and capacities. For example, a portable USB flash drive may be useful for storing less than 2 gigabytes. If you need more capacity, external USB hard drives can store up to 80 gigabytes. You can download or store a file within seconds with either device if it has a USB 2.0 transfer speed rating.
Zip drives, which can hold 750 megabytes, were once popular but have become less useful because they lack speed. Tape backup systems are extremely fast and can hold 130 gigabytes, but these devices are expensive and used more for large-scale business server backup.
‘WHICH FILES SHOULD I BACK UP?’
Obviously, you should back up electronic medical and billing records as well as documents created in your Microsoft Office suite.
Don’t ignore other critical information sources, such as Web browser bookmarks and e-mails, but remember that your mail, address book, and account information may be stored in different places depending on your e-mail program.
If you use a recordable CD or DVD, you must determine one by one which directories and files to archive. Nero has an easy-to-use “wizard” that guides you through this process. Nero also lets you automate backup: You would no loner have to remember to do it. Backing up e-mail and browser-bookmarked sites will be difficult, however, unless you know where they are kept.
Products such as Genie Backup Home Manager and NovaBACKUP have built-in search/inventory capability and back up to CDs or DVDs. Also, once the first backup is created, these programs can determine if the files have changed. Thus, subsequent backups will duplicate only files or modifications created since the previous backup. Specialized back-up programs also encrypt information and compress data to conserve space.
SCHEDULING DATA BACKUP
If you don’t create a schedule for backup, chances are it will never get done.
Ideally, you should back up data daily at a set time, such as at noon or closing.
Many psychiatrists, however, probably need a longer interval depending on how long backup takes (anywhere from 5 to 20 minutes depending on volume of data) and whether the information is critical. Also, a file cannot be duplicated while in use, as two computer programs cannot share a file in order to protect the data.
STORING BACKUP
After creating your backup:
- keep the backup and the software used to create it at another location in case of fire or theft
- test with your staff the process of restoring the information to the original hard drive, so that you will learn how to do it and how long it takes to get your computers running.
ALTERNATIVE BACKUP METHODS
If you have broadband Internet access via DSL or cable modem, consider using online backup services offered by Connected or Xdrive. Your data will be safe once you’ve downloaded and installed their software, designated files, and determined backup frequency. These online services also store the data at a remote site in case of fire or theft. Some physicians, however, may feel uncomfortable keeping data on another server for security reasons.
The Mirra Personal Server, an alternative to off-site backup, can be connected to one computer or a network and can back up one or all computers. This server can also synchronize files between computers and allow access to them over the Internet.
For real-time backup, a RAID array2 (redundant array of inexpensive drives) is your only choice. With RAID level 1, two hard drives record simultaneously. When one drive fails, another continues to work and has the information. A RAID array requires a specialized drive controller card, which costs around $150, or specialized software.3 Controller cards are widely available on the Internet (use search terms “Mac Raid controller” or “PC raid controller”), and raid arrays are available for any platform.
THE FUTURE
As multimedia become integrated into medical records and software programs create more information, physicians will need more storage space. New storage technologies such as the HD-DVD and Blu-Ray4 offer up to 25 to 30 gigabytes per disc. Similar to the VHS-Betamax wars of the 1980s, manufacturers are vying to make these high-density storage devices the future storage standard. Also, perpendicular recording technology is increasing hard drive storage capacity.5
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
We know backing up data is important yet few of us do it consistently, either because we don’t think of it or cannot spare the time. Also, because today’s computers are less expensive and more reliable than before, many doctors think a system crash “can’t happen to me.”
Don’t wait for a power surge or hard drive failure to obliterate your crucial files or documents. This article describes numerous ways to back up and store data, each with different features. Your needs will determine which method is best for you.
HARD DRIVE FAILURE
Hard drives, which store information on platters via electrical charges, are vulnerable. They are rated with a mean time between failure (MTBF),1 which indicates how long on average a hard drive will work before it fails. Although the average MTBF is 50 years, electrical discharges such as power surges or lightning storms can force failure much sooner.
Viruses—if programmed to do so—can also corrupt hard drives. Most viruses propagate to another computer, using your computer as a host.
Companies such as Dataleach can recover information from your hard drive, but recovery may take days.
BASIC BACKUP TOOLS
CD-ROM-burning programs such as Nero Burning ROM are one way to back up data. Most computers purchased within the last 2 years have a built-in CD-ROM burner—a device that reads and creates CD-ROMs—along with CD-burning software.
Keep in mind the size of the disk you are using. CD-ROMs have a maximum capacity of 700 megabytes, but file location information consumes about 10 megabytes. A DVD-ROM can hold 4.7 gigabytes, almost 7 times the capacity of a CD-ROM.
Also consider expense. Recordable CDs on average cost 25 cents per disk. Recordable DVDs are more expensive (between 50 cents and $1 per disk depending on quantity purchased) but could save you money if you’re storing several gigabytes of data. The average cost per 100 megabytes of backup is 3.6 cents with CDs and 1.5 cents with DVDs.
Avoid rewriteable CD and DVDs—disks that can be erased and used again. Although such a disk may minimize backup costs, another computer may be unable to read it.
Alternate storage devices offer varying speeds and capacities. For example, a portable USB flash drive may be useful for storing less than 2 gigabytes. If you need more capacity, external USB hard drives can store up to 80 gigabytes. You can download or store a file within seconds with either device if it has a USB 2.0 transfer speed rating.
Zip drives, which can hold 750 megabytes, were once popular but have become less useful because they lack speed. Tape backup systems are extremely fast and can hold 130 gigabytes, but these devices are expensive and used more for large-scale business server backup.
‘WHICH FILES SHOULD I BACK UP?’
Obviously, you should back up electronic medical and billing records as well as documents created in your Microsoft Office suite.
Don’t ignore other critical information sources, such as Web browser bookmarks and e-mails, but remember that your mail, address book, and account information may be stored in different places depending on your e-mail program.
If you use a recordable CD or DVD, you must determine one by one which directories and files to archive. Nero has an easy-to-use “wizard” that guides you through this process. Nero also lets you automate backup: You would no loner have to remember to do it. Backing up e-mail and browser-bookmarked sites will be difficult, however, unless you know where they are kept.
Products such as Genie Backup Home Manager and NovaBACKUP have built-in search/inventory capability and back up to CDs or DVDs. Also, once the first backup is created, these programs can determine if the files have changed. Thus, subsequent backups will duplicate only files or modifications created since the previous backup. Specialized back-up programs also encrypt information and compress data to conserve space.
SCHEDULING DATA BACKUP
If you don’t create a schedule for backup, chances are it will never get done.
Ideally, you should back up data daily at a set time, such as at noon or closing.
Many psychiatrists, however, probably need a longer interval depending on how long backup takes (anywhere from 5 to 20 minutes depending on volume of data) and whether the information is critical. Also, a file cannot be duplicated while in use, as two computer programs cannot share a file in order to protect the data.
STORING BACKUP
After creating your backup:
- keep the backup and the software used to create it at another location in case of fire or theft
- test with your staff the process of restoring the information to the original hard drive, so that you will learn how to do it and how long it takes to get your computers running.
ALTERNATIVE BACKUP METHODS
If you have broadband Internet access via DSL or cable modem, consider using online backup services offered by Connected or Xdrive. Your data will be safe once you’ve downloaded and installed their software, designated files, and determined backup frequency. These online services also store the data at a remote site in case of fire or theft. Some physicians, however, may feel uncomfortable keeping data on another server for security reasons.
The Mirra Personal Server, an alternative to off-site backup, can be connected to one computer or a network and can back up one or all computers. This server can also synchronize files between computers and allow access to them over the Internet.
For real-time backup, a RAID array2 (redundant array of inexpensive drives) is your only choice. With RAID level 1, two hard drives record simultaneously. When one drive fails, another continues to work and has the information. A RAID array requires a specialized drive controller card, which costs around $150, or specialized software.3 Controller cards are widely available on the Internet (use search terms “Mac Raid controller” or “PC raid controller”), and raid arrays are available for any platform.
THE FUTURE
As multimedia become integrated into medical records and software programs create more information, physicians will need more storage space. New storage technologies such as the HD-DVD and Blu-Ray4 offer up to 25 to 30 gigabytes per disc. Similar to the VHS-Betamax wars of the 1980s, manufacturers are vying to make these high-density storage devices the future storage standard. Also, perpendicular recording technology is increasing hard drive storage capacity.5
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
(accessed April 22, 2005 )
1. Webopedia: What is MTBF? Available at: http://www.webopedia.com/TERM/M/MTBF.html.
2. ACITS open VMS services: Introduction to RAID technology. Available at: http://www.utexas.edu/cc/vms/about/raid.html.
3. The PC Guide: RAID. Available at: http://www.pcguide.com/ref/hdd/perf/raid/index.htm.
4. Wikipedia: HD-DVD. Available at: http://en.wikipedia.org/wiki/HD-DVD.
5. Dahl E. PC drive reaches 500 GB. PC World ‘News & Trends,’ May 2005. Available at: http://www.pcworld.com/news/article/0,aid,120102,00.asp.
(accessed April 22, 2005 )
1. Webopedia: What is MTBF? Available at: http://www.webopedia.com/TERM/M/MTBF.html.
2. ACITS open VMS services: Introduction to RAID technology. Available at: http://www.utexas.edu/cc/vms/about/raid.html.
3. The PC Guide: RAID. Available at: http://www.pcguide.com/ref/hdd/perf/raid/index.htm.
4. Wikipedia: HD-DVD. Available at: http://en.wikipedia.org/wiki/HD-DVD.
5. Dahl E. PC drive reaches 500 GB. PC World ‘News & Trends,’ May 2005. Available at: http://www.pcworld.com/news/article/0,aid,120102,00.asp.
Printing on the go
You need a printout now, but you’re at a meeting, in a hotel, or at the hospital. What do you do?
Printers have become more compact and versatile, and numerous remote printing solutions exist with more on the way. This article reviews the options to help you print anytime, anywhere.
Portable printers
HP and Canon make inkjet printers that weigh approximately 4 lbs but are portable and compatible with most systems. These printers can be connected to your notebook via a USB or parallel port cable, or wirelessly with Bluetooth or infrared. Built with high-resolution inkjet nozzles, portable printers provide sharp printouts and can even print photos (although this can quickly drain their small ink cartridges).
By contrast, the Psyber Psychiatry, December 2003). WiFi makes printing from your hotel room relatively easy.
Psyber Psychiatry, December 2004).
First, make sure the program you used to create the document is compatible with the business center’s computers. Because most business centers use the free Adobe document reader, your best bet is to convert the file to Adobe PDF, which maintains its format. Use PDFCreator or PrimoPDF to convert the file; both are free and work on Windows computers. Mac users can download the Mac-Net Freeware PDF file creator.
The future
Imagine a pocket-size device that prints onto a blank page as you move it across.
PrintDreams is developing such a device using its random-movement printing technology (RMPT). PrintDreams reports that the scanning device can print any document with 100% accuracy, though it seems best suited to text. The device is still a year or two from reaching the mainstream; PrintDreams is licensing its technology to other printer manufacturers.
Also, don’t be surprised if cellular phones one day have the capability to print e-mail attachments using Bluetooth or general packet radio service (GPRS), a very fast data transfer protocol on a GSM network.
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
You need a printout now, but you’re at a meeting, in a hotel, or at the hospital. What do you do?
Printers have become more compact and versatile, and numerous remote printing solutions exist with more on the way. This article reviews the options to help you print anytime, anywhere.
Portable printers
HP and Canon make inkjet printers that weigh approximately 4 lbs but are portable and compatible with most systems. These printers can be connected to your notebook via a USB or parallel port cable, or wirelessly with Bluetooth or infrared. Built with high-resolution inkjet nozzles, portable printers provide sharp printouts and can even print photos (although this can quickly drain their small ink cartridges).
By contrast, the Psyber Psychiatry, December 2003). WiFi makes printing from your hotel room relatively easy.
Psyber Psychiatry, December 2004).
First, make sure the program you used to create the document is compatible with the business center’s computers. Because most business centers use the free Adobe document reader, your best bet is to convert the file to Adobe PDF, which maintains its format. Use PDFCreator or PrimoPDF to convert the file; both are free and work on Windows computers. Mac users can download the Mac-Net Freeware PDF file creator.
The future
Imagine a pocket-size device that prints onto a blank page as you move it across.
PrintDreams is developing such a device using its random-movement printing technology (RMPT). PrintDreams reports that the scanning device can print any document with 100% accuracy, though it seems best suited to text. The device is still a year or two from reaching the mainstream; PrintDreams is licensing its technology to other printer manufacturers.
Also, don’t be surprised if cellular phones one day have the capability to print e-mail attachments using Bluetooth or general packet radio service (GPRS), a very fast data transfer protocol on a GSM network.
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
You need a printout now, but you’re at a meeting, in a hotel, or at the hospital. What do you do?
Printers have become more compact and versatile, and numerous remote printing solutions exist with more on the way. This article reviews the options to help you print anytime, anywhere.
Portable printers
HP and Canon make inkjet printers that weigh approximately 4 lbs but are portable and compatible with most systems. These printers can be connected to your notebook via a USB or parallel port cable, or wirelessly with Bluetooth or infrared. Built with high-resolution inkjet nozzles, portable printers provide sharp printouts and can even print photos (although this can quickly drain their small ink cartridges).
By contrast, the Psyber Psychiatry, December 2003). WiFi makes printing from your hotel room relatively easy.
Psyber Psychiatry, December 2004).
First, make sure the program you used to create the document is compatible with the business center’s computers. Because most business centers use the free Adobe document reader, your best bet is to convert the file to Adobe PDF, which maintains its format. Use PDFCreator or PrimoPDF to convert the file; both are free and work on Windows computers. Mac users can download the Mac-Net Freeware PDF file creator.
The future
Imagine a pocket-size device that prints onto a blank page as you move it across.
PrintDreams is developing such a device using its random-movement printing technology (RMPT). PrintDreams reports that the scanning device can print any document with 100% accuracy, though it seems best suited to text. The device is still a year or two from reaching the mainstream; PrintDreams is licensing its technology to other printer manufacturers.
Also, don’t be surprised if cellular phones one day have the capability to print e-mail attachments using Bluetooth or general packet radio service (GPRS), a very fast data transfer protocol on a GSM network.
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
Printing on the go
You need a printout now, but you’re at a meeting, in a hotel, or at the hospital. What do you do?
Printers have become more compact and versatile, and numerous remote printing solutions exist with more on the way. This article reviews the options to help you print anytime, anywhere.
Portable printers
HP and Canon make inkjet printers that weigh approximately 4 lbs but are portable and compatible with most systems. These printers can be connected to your notebook via a USB or parallel port cable, or wirelessly with Bluetooth or infrared. Built with high-resolution inkjet nozzles, portable printers provide sharp printouts and can even print photos (although this can quickly drain their small ink cartridges).
By contrast, the Psyber Psychiatry, December 2003). WiFi makes printing from your hotel room relatively easy.
Psyber Psychiatry, December 2004).
First, make sure the program you used to create the document is compatible with the business center’s computers. Because most business centers use the free Adobe document reader, your best bet is to convert the file to Adobe PDF, which maintains its format. Use PDFCreator or PrimoPDF to convert the file; both are free and work on Windows computers. Mac users can download the Mac-Net Freeware PDF file creator.
The future
Imagine a pocket-size device that prints onto a blank page as you move it across.
PrintDreams is developing such a device using its random-movement printing technology (RMPT). PrintDreams reports that the scanning device can print any document with 100% accuracy, though it seems best suited to text. The device is still a year or two from reaching the mainstream; PrintDreams is licensing its technology to other printer manufacturers.
Also, don’t be surprised if cellular phones one day have the capability to print e-mail attachments using Bluetooth or general packet radio service (GPRS), a very fast data transfer protocol on a GSM network.
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
You need a printout now, but you’re at a meeting, in a hotel, or at the hospital. What do you do?
Printers have become more compact and versatile, and numerous remote printing solutions exist with more on the way. This article reviews the options to help you print anytime, anywhere.
Portable printers
HP and Canon make inkjet printers that weigh approximately 4 lbs but are portable and compatible with most systems. These printers can be connected to your notebook via a USB or parallel port cable, or wirelessly with Bluetooth or infrared. Built with high-resolution inkjet nozzles, portable printers provide sharp printouts and can even print photos (although this can quickly drain their small ink cartridges).
By contrast, the Psyber Psychiatry, December 2003). WiFi makes printing from your hotel room relatively easy.
Psyber Psychiatry, December 2004).
First, make sure the program you used to create the document is compatible with the business center’s computers. Because most business centers use the free Adobe document reader, your best bet is to convert the file to Adobe PDF, which maintains its format. Use PDFCreator or PrimoPDF to convert the file; both are free and work on Windows computers. Mac users can download the Mac-Net Freeware PDF file creator.
The future
Imagine a pocket-size device that prints onto a blank page as you move it across.
PrintDreams is developing such a device using its random-movement printing technology (RMPT). PrintDreams reports that the scanning device can print any document with 100% accuracy, though it seems best suited to text. The device is still a year or two from reaching the mainstream; PrintDreams is licensing its technology to other printer manufacturers.
Also, don’t be surprised if cellular phones one day have the capability to print e-mail attachments using Bluetooth or general packet radio service (GPRS), a very fast data transfer protocol on a GSM network.
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
You need a printout now, but you’re at a meeting, in a hotel, or at the hospital. What do you do?
Printers have become more compact and versatile, and numerous remote printing solutions exist with more on the way. This article reviews the options to help you print anytime, anywhere.
Portable printers
HP and Canon make inkjet printers that weigh approximately 4 lbs but are portable and compatible with most systems. These printers can be connected to your notebook via a USB or parallel port cable, or wirelessly with Bluetooth or infrared. Built with high-resolution inkjet nozzles, portable printers provide sharp printouts and can even print photos (although this can quickly drain their small ink cartridges).
By contrast, the Psyber Psychiatry, December 2003). WiFi makes printing from your hotel room relatively easy.
Psyber Psychiatry, December 2004).
First, make sure the program you used to create the document is compatible with the business center’s computers. Because most business centers use the free Adobe document reader, your best bet is to convert the file to Adobe PDF, which maintains its format. Use PDFCreator or PrimoPDF to convert the file; both are free and work on Windows computers. Mac users can download the Mac-Net Freeware PDF file creator.
The future
Imagine a pocket-size device that prints onto a blank page as you move it across.
PrintDreams is developing such a device using its random-movement printing technology (RMPT). PrintDreams reports that the scanning device can print any document with 100% accuracy, though it seems best suited to text. The device is still a year or two from reaching the mainstream; PrintDreams is licensing its technology to other printer manufacturers.
Also, don’t be surprised if cellular phones one day have the capability to print e-mail attachments using Bluetooth or general packet radio service (GPRS), a very fast data transfer protocol on a GSM network.
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
E-mailing on the run
Many physicians communicate with patients or colleagues via e-mail but lose this connectivity when they travel. If you find traditional home and office e-mail accounts are no longer enough, several e-mail access options can help you stay connected anytime.
How e-mail works
Typical home e-mail accounts-known as post office protocol (POP) accounts-use a client-server access method. The client-such as Outlook Express, Eudora, or Netscape Mail-checks the server for mail, which is then downloaded onto the home computer. Once downloaded, the message is gone from the server.
By contrast, an Internet message access protocol (IMAP) account offers more capabilities, such as allowing users to store e-mail on the server and organize mail into folders.December 2003). Also, some public locations such as New York’s Bryant Park offer free wireless Internet as a public service.2 Personal digital assistants or notebook computers with wireless capability, such as the Tungsten TC or the Toshiba e800, are best suited to this type of access.
Dial-up Internet service is possible over your cell phone. Most mobile phone carriers charge extra for data transmission, and you will need a specific cable to connect your phone to your computer. Bluetooth wireless technology can eliminate the need for cables but beware: Data transfer is much slower with Bluetooth than with other methods.
Third-generation networks (3G)-higher-speed protocols that allow faster data transmission for multimedia-have been touted as the next best service from mobile phone providers. Wireless devices such as the Palm Treo or the Research in Motion BlackBerry are specifically designed for this type of access. Monthly data service costs approximately $30 for unlimited downloads or less when bundled with a voice plan. Access is limited to the cellular coverage area, however.
Wireless access protocol, an alternative to 3G, lets you access e-mail via your mobile phone. This service, available from mobile service providers for an additional monthly fee (about $10), lets you read mail on the phone screen, but there are several drawbacks:
- Some people may find the text too small to read.
- Text entry via the telephone keypad can be difficult. You either tap a key multiple times to select letters or use word prediction based on letters entered.
- Not all phones available for each carrier can perform this function.
Wireless access protocol is well suited to reading e-mails. To compose an e-mail, however, you need to choose letters by clicking on numbers, which can be very difficult.
Many physicians communicate with patients or colleagues via e-mail but lose this connectivity when they travel. If you find traditional home and office e-mail accounts are no longer enough, several e-mail access options can help you stay connected anytime.
How e-mail works
Typical home e-mail accounts-known as post office protocol (POP) accounts-use a client-server access method. The client-such as Outlook Express, Eudora, or Netscape Mail-checks the server for mail, which is then downloaded onto the home computer. Once downloaded, the message is gone from the server.
By contrast, an Internet message access protocol (IMAP) account offers more capabilities, such as allowing users to store e-mail on the server and organize mail into folders.December 2003). Also, some public locations such as New York’s Bryant Park offer free wireless Internet as a public service.2 Personal digital assistants or notebook computers with wireless capability, such as the Tungsten TC or the Toshiba e800, are best suited to this type of access.
Dial-up Internet service is possible over your cell phone. Most mobile phone carriers charge extra for data transmission, and you will need a specific cable to connect your phone to your computer. Bluetooth wireless technology can eliminate the need for cables but beware: Data transfer is much slower with Bluetooth than with other methods.
Third-generation networks (3G)-higher-speed protocols that allow faster data transmission for multimedia-have been touted as the next best service from mobile phone providers. Wireless devices such as the Palm Treo or the Research in Motion BlackBerry are specifically designed for this type of access. Monthly data service costs approximately $30 for unlimited downloads or less when bundled with a voice plan. Access is limited to the cellular coverage area, however.
Wireless access protocol, an alternative to 3G, lets you access e-mail via your mobile phone. This service, available from mobile service providers for an additional monthly fee (about $10), lets you read mail on the phone screen, but there are several drawbacks:
- Some people may find the text too small to read.
- Text entry via the telephone keypad can be difficult. You either tap a key multiple times to select letters or use word prediction based on letters entered.
- Not all phones available for each carrier can perform this function.
Wireless access protocol is well suited to reading e-mails. To compose an e-mail, however, you need to choose letters by clicking on numbers, which can be very difficult.
Many physicians communicate with patients or colleagues via e-mail but lose this connectivity when they travel. If you find traditional home and office e-mail accounts are no longer enough, several e-mail access options can help you stay connected anytime.
How e-mail works
Typical home e-mail accounts-known as post office protocol (POP) accounts-use a client-server access method. The client-such as Outlook Express, Eudora, or Netscape Mail-checks the server for mail, which is then downloaded onto the home computer. Once downloaded, the message is gone from the server.
By contrast, an Internet message access protocol (IMAP) account offers more capabilities, such as allowing users to store e-mail on the server and organize mail into folders.December 2003). Also, some public locations such as New York’s Bryant Park offer free wireless Internet as a public service.2 Personal digital assistants or notebook computers with wireless capability, such as the Tungsten TC or the Toshiba e800, are best suited to this type of access.
Dial-up Internet service is possible over your cell phone. Most mobile phone carriers charge extra for data transmission, and you will need a specific cable to connect your phone to your computer. Bluetooth wireless technology can eliminate the need for cables but beware: Data transfer is much slower with Bluetooth than with other methods.
Third-generation networks (3G)-higher-speed protocols that allow faster data transmission for multimedia-have been touted as the next best service from mobile phone providers. Wireless devices such as the Palm Treo or the Research in Motion BlackBerry are specifically designed for this type of access. Monthly data service costs approximately $30 for unlimited downloads or less when bundled with a voice plan. Access is limited to the cellular coverage area, however.
Wireless access protocol, an alternative to 3G, lets you access e-mail via your mobile phone. This service, available from mobile service providers for an additional monthly fee (about $10), lets you read mail on the phone screen, but there are several drawbacks:
- Some people may find the text too small to read.
- Text entry via the telephone keypad can be difficult. You either tap a key multiple times to select letters or use word prediction based on letters entered.
- Not all phones available for each carrier can perform this function.
Wireless access protocol is well suited to reading e-mails. To compose an e-mail, however, you need to choose letters by clicking on numbers, which can be very difficult.
A holiday wish: More security and accessibility
It’s the holiday season. You’ve got better things to think about than your computers’ security and data accessibility.
Many “tech toys” can help secure your computers and let you August 2004.)
Still, notebook computers are easy to steal, and desktop computers can be stolen or infiltrated. To secure your data, you need encryption to supplement password-restricted access. Also, you should regularly save and copy data in an alternate location.
Solutions. The Authenex HDLock is a universal serial bus (USB) key that encrypts your hard drive’s contents. The device uses “two-factor authentication,” a security method that blocks access until you provide something you have (the key) and something you know (the password). Without both the key and password, encrypted data cannot be accessed. If you lose the key or forget the password, an online support section provides a one-time password.
If more than one person needs access, the Silex Technology FUS-200N USB fingerprint reader is more appropriate. This device and its accompanying software:
- provide secured access for multiple users
- encrypt files and folders
- and force users to show their fingerprints before allowing access to selected programs, such as your medical records program.
The FUS-200N is more accurate than other fingerprint recognition devices because it uses electricity rather than light patterns to record fingerprints.
Another option, the DiskOnKey Classic 2.0 USB flash drive, includes a small built-in microprocessor that lets you run your electronic medical records program or other applications from the key. CapMed uses this key to allow consumers to store their medical information on the Personal HealthKey device.
See Table 1 for more information on these security enhancement programs.
Problem. When shuttling between home and office, it makes sense to carry files on a USB flash drive. These devices are great for transporting documents because the computer sees a flash drive as just another disk drive.
Flash drives, however, are easily lost—and no psychiatrist wants to be sued for losing sensitive information.
Solutions. Some USB flash drives, such as the Sony Micro Vault, offer password protection for files and folders. Another option, the Trek Thumbdrive Touch, has a built-in fingerprint reader to guard your data (Table 2).
If you already have a favorite USB flash drive, add quick- and easy-to-use encryption software to your home and office computers. AxCrypt, a free Windows-compatible program, lets you encrypt and decrypt files with a simple right-mouse click. A similar program, Fairly Good Privacy, is Mac OS-compatible (Table 1).
Problem. You need to access critical files in both your office and home computer from either location.
Solutions. Internet-based synchronization services can simultaneously update files on both computers (Table 3). fusionOne Plus, for example, keeps files, contacts, e-mail, and calendars in sync. Contacts and calendars can also be accessed and synchronized via some mobile phones. What’s more, FusionOne Plus provides an online backup copy of your files.
LogMeIn provides free secured remote access to your office files from any computer. After your install a server program on the host computer, you can run programs and open files via a Web browser. The LogMeIn Pro version, which costs $12.95 per month, adds the ability to synchronize computers, transfer files, and distribute them over the Internet.
GoToMyPC allows you to access files and programs on a host computer and also allows Pocket PC PDA viewing as well as remote printing, but it does not provide file synchronization.
For direct computer-to-computer connection, pcAnywhere and RealVNC allow you to access files and programs on the host computer. Unlike GoToMyPC and LogMeIn, however, these programs do not offer additional password protection by verifying the user’s account.
The $200 PC Anywhere program will encrypt data between computers, whereas the free RealVNC program only provides password security. PC Anywhere synchronizes file, whereas RealVNC only helps you run the remote computer. RealVNC has enterprise versions and is developing a personal version with additional features.
Online storage can help you avoid synchronization issues. Xdrive has desktop software that creates a virtual drive for storage. When starting your computer, the software will automatically connect via the Internet to your Xdrive account. You can also change the settings of your electronic medical records program or document editing software to save data only to this Internet drive. This way, your data will always be backed up to a safe location even if your home or office computer is stolen.
Table 1
Programs, services that enhance data security
| Product | URL | Cost | Requirements |
|---|---|---|---|
| AxCrypt | http://axcrypt.sourceforge.net/ | Free | Windows 95/98/ME/NT/2K/XP |
| DiskOnKey Classic 2.0 | http://www.diskonkey.com/prod_dok2.asp | $99.50 (256 MB), $159.90 (512MB), $329.90 (1GB) | Windows 98 SE, NT 4.0, 2000, ME, XP Mac OS: 9.x, 10.0.x, 10.1.x, 10.2.x, Linux 2.4.x |
| Fairly Good Privacy | http://www.securemac.com/fgp.php | Free | Mac OS System 7 and later |
| FUS-200N | http://www.silexamerica.com/us/products/fingerprint/fus200n.html | $149 | Windows XP, 2000 |
| HDLock | http://www.authenex.com/products_hdlock.cfm | $79.95 | Windows XP, 2000 |
Table 2
Secure flash drives
| Product | URL | Cost | Requirements |
|---|---|---|---|
| Micro Vault | http://www.sonystyle.com | $45.99 (256 MB) | Windows 98, 2000, ME, XP and MAC OS 9.0 and higher |
| Thumbdrive Touch | http://www.thumbdrive.com/touch.htm | $69 (16 MB), $299 (256 MB) | Mac OS 8.6 and above, Windows 98, 2000 and ME |
Table 3
Programs, services that facilitate remote data access
| Product | URL | Cost | Requirements |
|---|---|---|---|
| fusionOne Plus | http://store.yahoo.com/fusionone/ | $69.96/yr | Microsoft Windows 95/98/NT/2000/ME/XP |
| GoToMyPC | https://www.gotomypc.com/ | $19.95/month or $179.40/yr | Microsoft Windows 95/98/NT/2000/ME/XP |
| LogMeIn | https://secure.logmein.com/go.asp?page=home | Free | Windows 2000, XP, or Server 2003 |
| LogMeIn Pro | https://secure.logmein.com/go.asp?page=home | $12.95/month | Windows 2000, XP, and Server 2003 |
| pcAnywhere | http://www.symantec.com | $199.95 | Windows® XP Home/XP Pro/ 2000/NT 4/Me/98 |
| RealVNC free edition | http://www.realvnc.com | Free | Windows 9x/2000/ NT/XP, Linux, Mac OSX |
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
poll here
It’s the holiday season. You’ve got better things to think about than your computers’ security and data accessibility.
Many “tech toys” can help secure your computers and let you August 2004.)
Still, notebook computers are easy to steal, and desktop computers can be stolen or infiltrated. To secure your data, you need encryption to supplement password-restricted access. Also, you should regularly save and copy data in an alternate location.
Solutions. The Authenex HDLock is a universal serial bus (USB) key that encrypts your hard drive’s contents. The device uses “two-factor authentication,” a security method that blocks access until you provide something you have (the key) and something you know (the password). Without both the key and password, encrypted data cannot be accessed. If you lose the key or forget the password, an online support section provides a one-time password.
If more than one person needs access, the Silex Technology FUS-200N USB fingerprint reader is more appropriate. This device and its accompanying software:
- provide secured access for multiple users
- encrypt files and folders
- and force users to show their fingerprints before allowing access to selected programs, such as your medical records program.
The FUS-200N is more accurate than other fingerprint recognition devices because it uses electricity rather than light patterns to record fingerprints.
Another option, the DiskOnKey Classic 2.0 USB flash drive, includes a small built-in microprocessor that lets you run your electronic medical records program or other applications from the key. CapMed uses this key to allow consumers to store their medical information on the Personal HealthKey device.
See Table 1 for more information on these security enhancement programs.
Problem. When shuttling between home and office, it makes sense to carry files on a USB flash drive. These devices are great for transporting documents because the computer sees a flash drive as just another disk drive.
Flash drives, however, are easily lost—and no psychiatrist wants to be sued for losing sensitive information.
Solutions. Some USB flash drives, such as the Sony Micro Vault, offer password protection for files and folders. Another option, the Trek Thumbdrive Touch, has a built-in fingerprint reader to guard your data (Table 2).
If you already have a favorite USB flash drive, add quick- and easy-to-use encryption software to your home and office computers. AxCrypt, a free Windows-compatible program, lets you encrypt and decrypt files with a simple right-mouse click. A similar program, Fairly Good Privacy, is Mac OS-compatible (Table 1).
Problem. You need to access critical files in both your office and home computer from either location.
Solutions. Internet-based synchronization services can simultaneously update files on both computers (Table 3). fusionOne Plus, for example, keeps files, contacts, e-mail, and calendars in sync. Contacts and calendars can also be accessed and synchronized via some mobile phones. What’s more, FusionOne Plus provides an online backup copy of your files.
LogMeIn provides free secured remote access to your office files from any computer. After your install a server program on the host computer, you can run programs and open files via a Web browser. The LogMeIn Pro version, which costs $12.95 per month, adds the ability to synchronize computers, transfer files, and distribute them over the Internet.
GoToMyPC allows you to access files and programs on a host computer and also allows Pocket PC PDA viewing as well as remote printing, but it does not provide file synchronization.
For direct computer-to-computer connection, pcAnywhere and RealVNC allow you to access files and programs on the host computer. Unlike GoToMyPC and LogMeIn, however, these programs do not offer additional password protection by verifying the user’s account.
The $200 PC Anywhere program will encrypt data between computers, whereas the free RealVNC program only provides password security. PC Anywhere synchronizes file, whereas RealVNC only helps you run the remote computer. RealVNC has enterprise versions and is developing a personal version with additional features.
Online storage can help you avoid synchronization issues. Xdrive has desktop software that creates a virtual drive for storage. When starting your computer, the software will automatically connect via the Internet to your Xdrive account. You can also change the settings of your electronic medical records program or document editing software to save data only to this Internet drive. This way, your data will always be backed up to a safe location even if your home or office computer is stolen.
Table 1
Programs, services that enhance data security
| Product | URL | Cost | Requirements |
|---|---|---|---|
| AxCrypt | http://axcrypt.sourceforge.net/ | Free | Windows 95/98/ME/NT/2K/XP |
| DiskOnKey Classic 2.0 | http://www.diskonkey.com/prod_dok2.asp | $99.50 (256 MB), $159.90 (512MB), $329.90 (1GB) | Windows 98 SE, NT 4.0, 2000, ME, XP Mac OS: 9.x, 10.0.x, 10.1.x, 10.2.x, Linux 2.4.x |
| Fairly Good Privacy | http://www.securemac.com/fgp.php | Free | Mac OS System 7 and later |
| FUS-200N | http://www.silexamerica.com/us/products/fingerprint/fus200n.html | $149 | Windows XP, 2000 |
| HDLock | http://www.authenex.com/products_hdlock.cfm | $79.95 | Windows XP, 2000 |
Table 2
Secure flash drives
| Product | URL | Cost | Requirements |
|---|---|---|---|
| Micro Vault | http://www.sonystyle.com | $45.99 (256 MB) | Windows 98, 2000, ME, XP and MAC OS 9.0 and higher |
| Thumbdrive Touch | http://www.thumbdrive.com/touch.htm | $69 (16 MB), $299 (256 MB) | Mac OS 8.6 and above, Windows 98, 2000 and ME |
Table 3
Programs, services that facilitate remote data access
| Product | URL | Cost | Requirements |
|---|---|---|---|
| fusionOne Plus | http://store.yahoo.com/fusionone/ | $69.96/yr | Microsoft Windows 95/98/NT/2000/ME/XP |
| GoToMyPC | https://www.gotomypc.com/ | $19.95/month or $179.40/yr | Microsoft Windows 95/98/NT/2000/ME/XP |
| LogMeIn | https://secure.logmein.com/go.asp?page=home | Free | Windows 2000, XP, or Server 2003 |
| LogMeIn Pro | https://secure.logmein.com/go.asp?page=home | $12.95/month | Windows 2000, XP, and Server 2003 |
| pcAnywhere | http://www.symantec.com | $199.95 | Windows® XP Home/XP Pro/ 2000/NT 4/Me/98 |
| RealVNC free edition | http://www.realvnc.com | Free | Windows 9x/2000/ NT/XP, Linux, Mac OSX |
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
poll here
It’s the holiday season. You’ve got better things to think about than your computers’ security and data accessibility.
Many “tech toys” can help secure your computers and let you August 2004.)
Still, notebook computers are easy to steal, and desktop computers can be stolen or infiltrated. To secure your data, you need encryption to supplement password-restricted access. Also, you should regularly save and copy data in an alternate location.
Solutions. The Authenex HDLock is a universal serial bus (USB) key that encrypts your hard drive’s contents. The device uses “two-factor authentication,” a security method that blocks access until you provide something you have (the key) and something you know (the password). Without both the key and password, encrypted data cannot be accessed. If you lose the key or forget the password, an online support section provides a one-time password.
If more than one person needs access, the Silex Technology FUS-200N USB fingerprint reader is more appropriate. This device and its accompanying software:
- provide secured access for multiple users
- encrypt files and folders
- and force users to show their fingerprints before allowing access to selected programs, such as your medical records program.
The FUS-200N is more accurate than other fingerprint recognition devices because it uses electricity rather than light patterns to record fingerprints.
Another option, the DiskOnKey Classic 2.0 USB flash drive, includes a small built-in microprocessor that lets you run your electronic medical records program or other applications from the key. CapMed uses this key to allow consumers to store their medical information on the Personal HealthKey device.
See Table 1 for more information on these security enhancement programs.
Problem. When shuttling between home and office, it makes sense to carry files on a USB flash drive. These devices are great for transporting documents because the computer sees a flash drive as just another disk drive.
Flash drives, however, are easily lost—and no psychiatrist wants to be sued for losing sensitive information.
Solutions. Some USB flash drives, such as the Sony Micro Vault, offer password protection for files and folders. Another option, the Trek Thumbdrive Touch, has a built-in fingerprint reader to guard your data (Table 2).
If you already have a favorite USB flash drive, add quick- and easy-to-use encryption software to your home and office computers. AxCrypt, a free Windows-compatible program, lets you encrypt and decrypt files with a simple right-mouse click. A similar program, Fairly Good Privacy, is Mac OS-compatible (Table 1).
Problem. You need to access critical files in both your office and home computer from either location.
Solutions. Internet-based synchronization services can simultaneously update files on both computers (Table 3). fusionOne Plus, for example, keeps files, contacts, e-mail, and calendars in sync. Contacts and calendars can also be accessed and synchronized via some mobile phones. What’s more, FusionOne Plus provides an online backup copy of your files.
LogMeIn provides free secured remote access to your office files from any computer. After your install a server program on the host computer, you can run programs and open files via a Web browser. The LogMeIn Pro version, which costs $12.95 per month, adds the ability to synchronize computers, transfer files, and distribute them over the Internet.
GoToMyPC allows you to access files and programs on a host computer and also allows Pocket PC PDA viewing as well as remote printing, but it does not provide file synchronization.
For direct computer-to-computer connection, pcAnywhere and RealVNC allow you to access files and programs on the host computer. Unlike GoToMyPC and LogMeIn, however, these programs do not offer additional password protection by verifying the user’s account.
The $200 PC Anywhere program will encrypt data between computers, whereas the free RealVNC program only provides password security. PC Anywhere synchronizes file, whereas RealVNC only helps you run the remote computer. RealVNC has enterprise versions and is developing a personal version with additional features.
Online storage can help you avoid synchronization issues. Xdrive has desktop software that creates a virtual drive for storage. When starting your computer, the software will automatically connect via the Internet to your Xdrive account. You can also change the settings of your electronic medical records program or document editing software to save data only to this Internet drive. This way, your data will always be backed up to a safe location even if your home or office computer is stolen.
Table 1
Programs, services that enhance data security
| Product | URL | Cost | Requirements |
|---|---|---|---|
| AxCrypt | http://axcrypt.sourceforge.net/ | Free | Windows 95/98/ME/NT/2K/XP |
| DiskOnKey Classic 2.0 | http://www.diskonkey.com/prod_dok2.asp | $99.50 (256 MB), $159.90 (512MB), $329.90 (1GB) | Windows 98 SE, NT 4.0, 2000, ME, XP Mac OS: 9.x, 10.0.x, 10.1.x, 10.2.x, Linux 2.4.x |
| Fairly Good Privacy | http://www.securemac.com/fgp.php | Free | Mac OS System 7 and later |
| FUS-200N | http://www.silexamerica.com/us/products/fingerprint/fus200n.html | $149 | Windows XP, 2000 |
| HDLock | http://www.authenex.com/products_hdlock.cfm | $79.95 | Windows XP, 2000 |
Table 2
Secure flash drives
| Product | URL | Cost | Requirements |
|---|---|---|---|
| Micro Vault | http://www.sonystyle.com | $45.99 (256 MB) | Windows 98, 2000, ME, XP and MAC OS 9.0 and higher |
| Thumbdrive Touch | http://www.thumbdrive.com/touch.htm | $69 (16 MB), $299 (256 MB) | Mac OS 8.6 and above, Windows 98, 2000 and ME |
Table 3
Programs, services that facilitate remote data access
| Product | URL | Cost | Requirements |
|---|---|---|---|
| fusionOne Plus | http://store.yahoo.com/fusionone/ | $69.96/yr | Microsoft Windows 95/98/NT/2000/ME/XP |
| GoToMyPC | https://www.gotomypc.com/ | $19.95/month or $179.40/yr | Microsoft Windows 95/98/NT/2000/ME/XP |
| LogMeIn | https://secure.logmein.com/go.asp?page=home | Free | Windows 2000, XP, or Server 2003 |
| LogMeIn Pro | https://secure.logmein.com/go.asp?page=home | $12.95/month | Windows 2000, XP, and Server 2003 |
| pcAnywhere | http://www.symantec.com | $199.95 | Windows® XP Home/XP Pro/ 2000/NT 4/Me/98 |
| RealVNC free edition | http://www.realvnc.com | Free | Windows 9x/2000/ NT/XP, Linux, Mac OSX |
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
poll here