User login
What is the recommended workup for a man with a first UTI?
obtain a urine culture in all men with suspected urinary tract infection (UTI), to reliably diagnose an infection (strength of recommendation [SOR]: C).
For further evaluation, ultrasonography with abdominal radiography appears at least as accurate as an intravenous pyelogram (IVP) for detecting urinary tract abnormalities such as hydronephrosis, stones, or outlet obstruction (SOR: C; single small poor-quality cohort study).
Imaging of the urinary tract is not supported by the literature, for low-risk males <45 years of age after their first UTI (SOR: C; expert opinion, very small cohort study). unfortunately, there is scant literature, mostly of poor quality, to guide decisions on work-up of men with a suspected UTI.
Imaging not likely to enlighten
Peter C. Smith, MD
University of Colorado Health Sciences Center
The vast majority of men with a first UTI in my practice have a preexisting, well-defined risk factor, such as a chronic indwelling catheter, immune compromise, or known prostatic hypertrophy. In otherwise healthy men with symptoms suggestive of UTI, the first order of business is to make the correct diagnosis: Is it cystitis? Pyelonephritis? Urethritis? Prostatitis?
Some of you may be surprised by the recommendation to forgo further evaluation in the majority of males with a simple first UTI. However, the underlying cause is readily apparent in the majority, and imaging adds little to a careful history and physical exam.
The proportion of men with UTI who actually meet the low-risk criteria (younger than 50, not prostatitis or urethritis, no symptoms suggesting outflow obstruction, no hematuria, etc) is vanishingly small. only that small minority of men over 50 without an obvious cause for their infection will need more evaluation. this review conforms well to current primary care practice.
Evidence summary
Limiting further evaluation of men with a first UTI to those at increased risk (TABLE) may reduce unnecessary radiological, endoscopic, or urodynamic investigation.
Approximately 20% of all UTIs occur in men,1-3 and the lifetime prevalence is about 14%.3 The incidence in elderly men is high, often attributable to a bladder outflow obstruction.4 (For this review, the definition of UTI is limited to bacterial infections of the kidney, ureter, or bladder, and does not include urethritis, epididymitis, prostatitis, or orchitis.)
TABLE
Conditions that increase risk of urinary tract infection in men3,7,9,10
| Immunocompromised |
| Uncircumcised |
| Engaging in anal intercourse |
| Age >65 years |
| Institutional care |
| Bladder outlet obstruction |
| Anatomic functional abnormalities of the urinary tract with incomplete bladder emptying (e.g., neurogenic bladder, vesicoureteric reflux) |
| Previous urinary tract surgery |
| Recent procedures: cystoscopy, catheterization, or transrectal prostate biopsy |
Get a urine culture
A urine culture is recommended to reliably diagnose an infection and guide treatment.5
- A cohort of 66 men (mean age, 66±13 years) presenting to a VA urology clinic for procedures, dysuria, or bacteriuria had urine samples taken while voiding, as well as directly from the bladder, either via suprapubic aspiration or urethral catheterization. Using bladder cultures as a gold standard, midstream urine culture had a specificity and sensitivity of >97% at a threshold of 1000 CFU/mL.6
The usual organisms are colonic bacteria: Escherichia coli (75%), enterococci (20%), and, less commonly, Klebsiella and Proteus.4
No need for routine imaging
Consider a workup for men who have no response to antibiotic therapy or have persistent hematuria.
There is little evidence to support routine imaging in low-risk men with a first UTI, whether with or without fever:
- A very small prospective study of 29 heterosexual, circumcised men 16 to 45 years old (those who were sexually active had a steady partner) who were hospitalized with a first febrile UTI failed to find any significant structural or functional urinary tract abnormalities.4
- Another small prospective study of 85 men, 18 to 86 years of age, with febrile UTI, concluded that routine imaging of the upper urinary tract was unnecessary, and that, if indicated, further workup should focus on the lower urinary tract.7 Abnormalities in this group were suggested by a history of voiding problems, hematuria, or recurrent infection. One limitation of this study was the incomplete urodynamic and endoscopic evaluation of the lower urinary tract.
- Another study enrolled 114 men, 18 to 85 years of age, with proven UTIs, who underwent ultrasonography and plain radiography, as well as an IVP.8 (Only 100 had complete data at enrollment.) All men had urinary flow rates measured. The combination of a plain abdominal film and ultrasonography detected more abnormalities than an IVP. (The primary role of the plain film was in detecting urinary calculi.)
Final “clinical” diagnoses were reported, but the study did not report a comparison of clinical and radiological findings. Almost half of the abnormalities were lower tract obstructions (bladder outlet obstruction, underactive detrusor, and chronic retention). There was no comment on the importance or treatment of any abnormalities found.
Recommendations from others
PRODIGY (from the British National Health Service) recommends:
- Men under 45 years with a first UTI who respond well to antibiotic treatment are not likely to have a urologic abnormality.9
- Older men who do not respond well to antibiotics or who have recurrent UTIs are likely to have abnormalities and may benefit from further investigation.9
Neither the American Academy of Urology, the US Preventive Services Task Force, nor the Agency for Healthcare Research and Quality has published guidelines for evaluation of adult men with a first UTI.
1. Foxman B. Epidemiology of urinary tract infections: Incidence, morbidity, and economic costs. Am J Med 2002;113(suppl 1A):5S-13S
2. lipsky BA. Urinary tract infections in men. epidemiology, pathophysiology, diagnosis, and treatment. Ann Intern Med 1989;110:138-150.
3. Griebling TL. Urologic diseases in America project: Trends in resource use for urinary tract infections in men. J Urol 2005;173:1288-1294.
4. Abarbanel J, Engelstein D, Lask D, Livne PM. Urinary tract infection in men younger than 45 years of age: Is there a need for urologic investigation? Urology 2003;62:27-29.
5. Hummers-Pradier E, Ohse AM, Koch M, Heizmann WR, Kochen MM. Urinary tract infection in men. Int J Clin Pharmacol Ther 2004;42:360-366.
6. Lipsky BA, Ireton RC, Fihn SD, Hackett R, Berger RE. Diagnosis of bacturia in Men: Specimen Collection and Culture interpretation. J Infect Dis 1987;155:847-853.
7. Ulleryd P, Zackrisson B, Aus G, Bergdahl S, Hugosson J, Sandberg T. Selective urological evaluation in men with febrile urinary tract infection. BJU Int 2001;88:15-20.
8. Andrews SJ, Brooks PT, Hanbury DC, King CM, Prendergast CM, Boustead GB, et al. Ultrasonography and abdominal radiography versus intravenous urography in investigation of urinary tract infection in men: Prospective incident cohort study. BMJ 2002;324:454-456.
9. PRODIGY Knowledge (2006). Urinary tract infection (lower) - men. Sowerby Centre for Health Informatics at Newcastle, Ltd (SCHIN). Available at: www.prodigy.nhs.uk/urinary_tract_infection_lower_men. Accessed on July 18, 2007.
10. Lipsky BA. Managing urinary tract infections in men. Hosp Pract (Minneap) 2000;35:53-59.
obtain a urine culture in all men with suspected urinary tract infection (UTI), to reliably diagnose an infection (strength of recommendation [SOR]: C).
For further evaluation, ultrasonography with abdominal radiography appears at least as accurate as an intravenous pyelogram (IVP) for detecting urinary tract abnormalities such as hydronephrosis, stones, or outlet obstruction (SOR: C; single small poor-quality cohort study).
Imaging of the urinary tract is not supported by the literature, for low-risk males <45 years of age after their first UTI (SOR: C; expert opinion, very small cohort study). unfortunately, there is scant literature, mostly of poor quality, to guide decisions on work-up of men with a suspected UTI.
Imaging not likely to enlighten
Peter C. Smith, MD
University of Colorado Health Sciences Center
The vast majority of men with a first UTI in my practice have a preexisting, well-defined risk factor, such as a chronic indwelling catheter, immune compromise, or known prostatic hypertrophy. In otherwise healthy men with symptoms suggestive of UTI, the first order of business is to make the correct diagnosis: Is it cystitis? Pyelonephritis? Urethritis? Prostatitis?
Some of you may be surprised by the recommendation to forgo further evaluation in the majority of males with a simple first UTI. However, the underlying cause is readily apparent in the majority, and imaging adds little to a careful history and physical exam.
The proportion of men with UTI who actually meet the low-risk criteria (younger than 50, not prostatitis or urethritis, no symptoms suggesting outflow obstruction, no hematuria, etc) is vanishingly small. only that small minority of men over 50 without an obvious cause for their infection will need more evaluation. this review conforms well to current primary care practice.
Evidence summary
Limiting further evaluation of men with a first UTI to those at increased risk (TABLE) may reduce unnecessary radiological, endoscopic, or urodynamic investigation.
Approximately 20% of all UTIs occur in men,1-3 and the lifetime prevalence is about 14%.3 The incidence in elderly men is high, often attributable to a bladder outflow obstruction.4 (For this review, the definition of UTI is limited to bacterial infections of the kidney, ureter, or bladder, and does not include urethritis, epididymitis, prostatitis, or orchitis.)
TABLE
Conditions that increase risk of urinary tract infection in men3,7,9,10
| Immunocompromised |
| Uncircumcised |
| Engaging in anal intercourse |
| Age >65 years |
| Institutional care |
| Bladder outlet obstruction |
| Anatomic functional abnormalities of the urinary tract with incomplete bladder emptying (e.g., neurogenic bladder, vesicoureteric reflux) |
| Previous urinary tract surgery |
| Recent procedures: cystoscopy, catheterization, or transrectal prostate biopsy |
Get a urine culture
A urine culture is recommended to reliably diagnose an infection and guide treatment.5
- A cohort of 66 men (mean age, 66±13 years) presenting to a VA urology clinic for procedures, dysuria, or bacteriuria had urine samples taken while voiding, as well as directly from the bladder, either via suprapubic aspiration or urethral catheterization. Using bladder cultures as a gold standard, midstream urine culture had a specificity and sensitivity of >97% at a threshold of 1000 CFU/mL.6
The usual organisms are colonic bacteria: Escherichia coli (75%), enterococci (20%), and, less commonly, Klebsiella and Proteus.4
No need for routine imaging
Consider a workup for men who have no response to antibiotic therapy or have persistent hematuria.
There is little evidence to support routine imaging in low-risk men with a first UTI, whether with or without fever:
- A very small prospective study of 29 heterosexual, circumcised men 16 to 45 years old (those who were sexually active had a steady partner) who were hospitalized with a first febrile UTI failed to find any significant structural or functional urinary tract abnormalities.4
- Another small prospective study of 85 men, 18 to 86 years of age, with febrile UTI, concluded that routine imaging of the upper urinary tract was unnecessary, and that, if indicated, further workup should focus on the lower urinary tract.7 Abnormalities in this group were suggested by a history of voiding problems, hematuria, or recurrent infection. One limitation of this study was the incomplete urodynamic and endoscopic evaluation of the lower urinary tract.
- Another study enrolled 114 men, 18 to 85 years of age, with proven UTIs, who underwent ultrasonography and plain radiography, as well as an IVP.8 (Only 100 had complete data at enrollment.) All men had urinary flow rates measured. The combination of a plain abdominal film and ultrasonography detected more abnormalities than an IVP. (The primary role of the plain film was in detecting urinary calculi.)
Final “clinical” diagnoses were reported, but the study did not report a comparison of clinical and radiological findings. Almost half of the abnormalities were lower tract obstructions (bladder outlet obstruction, underactive detrusor, and chronic retention). There was no comment on the importance or treatment of any abnormalities found.
Recommendations from others
PRODIGY (from the British National Health Service) recommends:
- Men under 45 years with a first UTI who respond well to antibiotic treatment are not likely to have a urologic abnormality.9
- Older men who do not respond well to antibiotics or who have recurrent UTIs are likely to have abnormalities and may benefit from further investigation.9
Neither the American Academy of Urology, the US Preventive Services Task Force, nor the Agency for Healthcare Research and Quality has published guidelines for evaluation of adult men with a first UTI.
obtain a urine culture in all men with suspected urinary tract infection (UTI), to reliably diagnose an infection (strength of recommendation [SOR]: C).
For further evaluation, ultrasonography with abdominal radiography appears at least as accurate as an intravenous pyelogram (IVP) for detecting urinary tract abnormalities such as hydronephrosis, stones, or outlet obstruction (SOR: C; single small poor-quality cohort study).
Imaging of the urinary tract is not supported by the literature, for low-risk males <45 years of age after their first UTI (SOR: C; expert opinion, very small cohort study). unfortunately, there is scant literature, mostly of poor quality, to guide decisions on work-up of men with a suspected UTI.
Imaging not likely to enlighten
Peter C. Smith, MD
University of Colorado Health Sciences Center
The vast majority of men with a first UTI in my practice have a preexisting, well-defined risk factor, such as a chronic indwelling catheter, immune compromise, or known prostatic hypertrophy. In otherwise healthy men with symptoms suggestive of UTI, the first order of business is to make the correct diagnosis: Is it cystitis? Pyelonephritis? Urethritis? Prostatitis?
Some of you may be surprised by the recommendation to forgo further evaluation in the majority of males with a simple first UTI. However, the underlying cause is readily apparent in the majority, and imaging adds little to a careful history and physical exam.
The proportion of men with UTI who actually meet the low-risk criteria (younger than 50, not prostatitis or urethritis, no symptoms suggesting outflow obstruction, no hematuria, etc) is vanishingly small. only that small minority of men over 50 without an obvious cause for their infection will need more evaluation. this review conforms well to current primary care practice.
Evidence summary
Limiting further evaluation of men with a first UTI to those at increased risk (TABLE) may reduce unnecessary radiological, endoscopic, or urodynamic investigation.
Approximately 20% of all UTIs occur in men,1-3 and the lifetime prevalence is about 14%.3 The incidence in elderly men is high, often attributable to a bladder outflow obstruction.4 (For this review, the definition of UTI is limited to bacterial infections of the kidney, ureter, or bladder, and does not include urethritis, epididymitis, prostatitis, or orchitis.)
TABLE
Conditions that increase risk of urinary tract infection in men3,7,9,10
| Immunocompromised |
| Uncircumcised |
| Engaging in anal intercourse |
| Age >65 years |
| Institutional care |
| Bladder outlet obstruction |
| Anatomic functional abnormalities of the urinary tract with incomplete bladder emptying (e.g., neurogenic bladder, vesicoureteric reflux) |
| Previous urinary tract surgery |
| Recent procedures: cystoscopy, catheterization, or transrectal prostate biopsy |
Get a urine culture
A urine culture is recommended to reliably diagnose an infection and guide treatment.5
- A cohort of 66 men (mean age, 66±13 years) presenting to a VA urology clinic for procedures, dysuria, or bacteriuria had urine samples taken while voiding, as well as directly from the bladder, either via suprapubic aspiration or urethral catheterization. Using bladder cultures as a gold standard, midstream urine culture had a specificity and sensitivity of >97% at a threshold of 1000 CFU/mL.6
The usual organisms are colonic bacteria: Escherichia coli (75%), enterococci (20%), and, less commonly, Klebsiella and Proteus.4
No need for routine imaging
Consider a workup for men who have no response to antibiotic therapy or have persistent hematuria.
There is little evidence to support routine imaging in low-risk men with a first UTI, whether with or without fever:
- A very small prospective study of 29 heterosexual, circumcised men 16 to 45 years old (those who were sexually active had a steady partner) who were hospitalized with a first febrile UTI failed to find any significant structural or functional urinary tract abnormalities.4
- Another small prospective study of 85 men, 18 to 86 years of age, with febrile UTI, concluded that routine imaging of the upper urinary tract was unnecessary, and that, if indicated, further workup should focus on the lower urinary tract.7 Abnormalities in this group were suggested by a history of voiding problems, hematuria, or recurrent infection. One limitation of this study was the incomplete urodynamic and endoscopic evaluation of the lower urinary tract.
- Another study enrolled 114 men, 18 to 85 years of age, with proven UTIs, who underwent ultrasonography and plain radiography, as well as an IVP.8 (Only 100 had complete data at enrollment.) All men had urinary flow rates measured. The combination of a plain abdominal film and ultrasonography detected more abnormalities than an IVP. (The primary role of the plain film was in detecting urinary calculi.)
Final “clinical” diagnoses were reported, but the study did not report a comparison of clinical and radiological findings. Almost half of the abnormalities were lower tract obstructions (bladder outlet obstruction, underactive detrusor, and chronic retention). There was no comment on the importance or treatment of any abnormalities found.
Recommendations from others
PRODIGY (from the British National Health Service) recommends:
- Men under 45 years with a first UTI who respond well to antibiotic treatment are not likely to have a urologic abnormality.9
- Older men who do not respond well to antibiotics or who have recurrent UTIs are likely to have abnormalities and may benefit from further investigation.9
Neither the American Academy of Urology, the US Preventive Services Task Force, nor the Agency for Healthcare Research and Quality has published guidelines for evaluation of adult men with a first UTI.
1. Foxman B. Epidemiology of urinary tract infections: Incidence, morbidity, and economic costs. Am J Med 2002;113(suppl 1A):5S-13S
2. lipsky BA. Urinary tract infections in men. epidemiology, pathophysiology, diagnosis, and treatment. Ann Intern Med 1989;110:138-150.
3. Griebling TL. Urologic diseases in America project: Trends in resource use for urinary tract infections in men. J Urol 2005;173:1288-1294.
4. Abarbanel J, Engelstein D, Lask D, Livne PM. Urinary tract infection in men younger than 45 years of age: Is there a need for urologic investigation? Urology 2003;62:27-29.
5. Hummers-Pradier E, Ohse AM, Koch M, Heizmann WR, Kochen MM. Urinary tract infection in men. Int J Clin Pharmacol Ther 2004;42:360-366.
6. Lipsky BA, Ireton RC, Fihn SD, Hackett R, Berger RE. Diagnosis of bacturia in Men: Specimen Collection and Culture interpretation. J Infect Dis 1987;155:847-853.
7. Ulleryd P, Zackrisson B, Aus G, Bergdahl S, Hugosson J, Sandberg T. Selective urological evaluation in men with febrile urinary tract infection. BJU Int 2001;88:15-20.
8. Andrews SJ, Brooks PT, Hanbury DC, King CM, Prendergast CM, Boustead GB, et al. Ultrasonography and abdominal radiography versus intravenous urography in investigation of urinary tract infection in men: Prospective incident cohort study. BMJ 2002;324:454-456.
9. PRODIGY Knowledge (2006). Urinary tract infection (lower) - men. Sowerby Centre for Health Informatics at Newcastle, Ltd (SCHIN). Available at: www.prodigy.nhs.uk/urinary_tract_infection_lower_men. Accessed on July 18, 2007.
10. Lipsky BA. Managing urinary tract infections in men. Hosp Pract (Minneap) 2000;35:53-59.
1. Foxman B. Epidemiology of urinary tract infections: Incidence, morbidity, and economic costs. Am J Med 2002;113(suppl 1A):5S-13S
2. lipsky BA. Urinary tract infections in men. epidemiology, pathophysiology, diagnosis, and treatment. Ann Intern Med 1989;110:138-150.
3. Griebling TL. Urologic diseases in America project: Trends in resource use for urinary tract infections in men. J Urol 2005;173:1288-1294.
4. Abarbanel J, Engelstein D, Lask D, Livne PM. Urinary tract infection in men younger than 45 years of age: Is there a need for urologic investigation? Urology 2003;62:27-29.
5. Hummers-Pradier E, Ohse AM, Koch M, Heizmann WR, Kochen MM. Urinary tract infection in men. Int J Clin Pharmacol Ther 2004;42:360-366.
6. Lipsky BA, Ireton RC, Fihn SD, Hackett R, Berger RE. Diagnosis of bacturia in Men: Specimen Collection and Culture interpretation. J Infect Dis 1987;155:847-853.
7. Ulleryd P, Zackrisson B, Aus G, Bergdahl S, Hugosson J, Sandberg T. Selective urological evaluation in men with febrile urinary tract infection. BJU Int 2001;88:15-20.
8. Andrews SJ, Brooks PT, Hanbury DC, King CM, Prendergast CM, Boustead GB, et al. Ultrasonography and abdominal radiography versus intravenous urography in investigation of urinary tract infection in men: Prospective incident cohort study. BMJ 2002;324:454-456.
9. PRODIGY Knowledge (2006). Urinary tract infection (lower) - men. Sowerby Centre for Health Informatics at Newcastle, Ltd (SCHIN). Available at: www.prodigy.nhs.uk/urinary_tract_infection_lower_men. Accessed on July 18, 2007.
10. Lipsky BA. Managing urinary tract infections in men. Hosp Pract (Minneap) 2000;35:53-59.
Evidence-based answers from the Family Physicians Inquiries Network
Stress tests: How to make a calculated choice
- Estimate pretest probability of CAD in patients with chest pain on the basis of age, sex, pain characteristics, and cardiovascular risk factors (B).
- Low pretest probability patients should undergo an exercise treadmill test alone (C).
- Intermediate pretest probability patients, including those with complete right bundle branch block or less than 1 mm ST depression at rest should have an exercise treadmill test without imaging (B). Patients with an electronically paced ventricular rhythm (C) or left bundle-branch block (B) require myocardial perfusion imaging.
- In high pretest probability patients, coronary angiography is an appropriate initial strategy for CAD diagnosis (C).
- In women, the data are insufficient to justify routine stress imaging tests as the initial test for CAD (C).
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Are you a wise “consumer” of stress tests? That is: Do you consider your patient’s CAD probability score before ordering an exercise treadmill test or pharmacologic stress myocardial imaging (PSMI)? Are you as well-versed as you’d like to be on the predictive value of things like the Duke Treadmill Score?
If your answer is No to either question, this review may help guide your use of stress tests, based on evidence.
What is the pretest probability of CAD?
The decision to order an exercise stress test or a PSMI should be based on history, physical examination, and pretest probability for CAD. You can estimate the pretest probability for CAD in a chest pain patient based on the patient’s age, sex, and pain characteristics.1
Determine whether symptoms are typical, atypical, or nonanginal, based on whether the chest pain is substernal, brought on by exertion, or relieved by rest or nitroglycerin.2
To recap:
- Typical angina requires all 3 pain characteristics
- Atypical angina, only 2
- Nonanginal chest pain, 1.2
Use this information (along with the patient’s age) to determine whether he has a high, intermediate, low, or very low likelihood of CAD (TABLE 1). From the low, to the intermediate, to the high pretest probability levels, the positive predictive value increases progressively (21%, 62%, and 92%) and the negative predictive value decreases progressively (94%, 72%, and 28%).3 (These values are based on a review of symptomatic patients who had angiography following stress testing.)
TABLE 1
How to determine pretest probability of coronary artery disease
| STEP 1 | STEP 2 | STEP 3 | ||||||
|---|---|---|---|---|---|---|---|---|
| Ask 3 questions: | Total the number of “yes” answers to identify symptom pattern: | Find the cell in the matrix (below) where age, gender, and symptom pattern converge: | ||||||
| 0 of 3=Asymptomatic | High probability | >90% | |||||
| 1 of 3=Nonanginal chest pain | Intermediate | 10%–90% | ||||||
| 2 of 3=Atypical angina | Low | <10% | ||||||
| 3 of 3=Typical angina | Very low | <5% | ||||||
| AGE (YRS) | SYMPTOMS | |||||||
| ASYMPTOMATIC | NONANGINAL CHEST PAIN | ATYPICAL ANGINA | TYPICAL ANGINA | |||||
| MEN | WOMEN | MEN | WOMEN | MEN | WOMEN | MEN | WOMEN | |
| 35–45 | Very low | Very low | Intermediate | Very low | Intermediate | Intermediate | Intermediate | Intermediate |
| 45–55 | Low | Very low | Intermediate | Low | Intermediate | Intermediate | High | Intermediate |
| 55–65 | Intermediate | Low | Intermediate | Intermediate | Intermediate | Intermediate | High | Intermediate |
| 65–75 | Intermediate | Intermediate | Intermediate | Intermediate | Intermediate | Intermediate | High | High |
| Adapted from Diamond GA.2 | ||||||||
Your patients’ score dictates whether testing is required, and if so what kind.
Very low pretest probability patients should not have an exercise test, since they have a high risk of false-positive results. Evaluate and treat them for noncardiac causes of chest pain and begin primary prevention of CAD.
Low pretest probability patients should undergo exercise treadmill testing alone since negative results carry a high negative predictive value in both men and women, but positive test results may be false and can be evaluated by more studies.3
Intermediate pretest probability patients, including those with complete right bundle branch block or less than 1 mm ST depression at rest should have an exercise treadmill test without imaging modality.3-5 However, intermediate pretest probability patients with baseline ECG abnormalities such as electronically paced ventricular rhythm or left bundle-branch block will require myocardial perfusion imaging.5
High pretest probability patients should have coronary angiography as an initial strategy for diagnosis of CAD.3
History, exam, and ECG determine test suitability
Can your patient take an exercise stress test, or will he need a pharmacologic stress test instead? (See “A guide to sensitivity, specificity, and likelihood ratios for stress tests.”) Can he pedal a bicycle, walk, or exercise for 6 minutes? On physical examination, take note of his gait, mobility, and limb strength.
What medications is the patient taking? Digoxin may cause false ST changes, beta-blockers may prevent attaining maximum heart rate, and antihypertensive agents and vasodilators may alter the blood pressure response, producing a false negative result. Nitrates attenuate angina and the associated ST depression of ischemia.6 In addition, metabolic abnormalities and cocaine or alcohol use may affect heart rate, metabolic oxygen demand and the ability to perform the exercise treadmill testing.
On examination, document murmurs, rhythm abnormalities, vascular bruits, and abnormal pulses. Limit laboratory studies to recent cardiac damage screening if indicated. Screen with a resting ECG for arrhythmias, conduction abnormalities or preexisting cardiac damage. ST-segment (≥1 mm) and T-wave changes such as inversions secondary to strain or old injury or conduction abnormalities such as bundle branch blocks and prolonged QT interval may obscure exercise treadmill testing findings. Consider spirometry for patients with asthma or chronic lung disease.
Exercise treadmill testing
Sensitivity varies from 45% to 67% and specificity 72% to 90% with operator and patient variables.6 An abnormal test in a man at a heart rate of 85% of predicted maximum for age has a sensitivity of about 65% and a specificity of 85% for CAD. In women, one meta-analysis demonstrated a sensitivity of only 61% and a specificity of only 70%.8
PSMI
Pharmacologic stress myocardial imaging is similar to exercise treadmill testing. Dipyridamole and adenosine PSMI with thallium T1 201 or technetium Tc 99m have a similar sensitivity of 90%, and specificity of 70% for detection of CAD.6
Echocardiography
Overall sensitivity for exercise echocardiography was about 85% and for dobutamine stress echocardiography 82%. Dobutamine has a higher sensitivity than vasodilator echocardiography.6
Likelihood ratios (LR) for exercise treadmill testing and PSMI
Based on a review of coronary artery disease with chest pain as the symptom and a reference standard of a coronary angiogram with >70% narrowing of one or more arteries, or >50% left main, the LR varies for sex and for each different study. The positive LR (LR+) for exercise treadmill testing is 3.00 for men and 2.00 for women. The negative LR (LR–) for exercise treadmill testing is 0.650 for men and 0.560 for women. LR+ for exercise treadmill testing with thallium imaging is 5.9 (generally), but 2.20 for women; LR–is 0.200 and is 0.340 for women. Dipyridamole PSMI, LR+ is 3.30 and LR- is 0.180.16
The decisive factors
Absolute contraindications to exercise treadmill testing include recent MI; significant aortic stenosis,7 and weight exceeding equipment capacity. Relative contraindications to exercise treadmill testing (which can be superseded if the benefits of exercise outweigh the risks) include: hypertension (systolic >200 mm Hg/diastolic >110 mm Hg),5 left main coronary stenosis and stenotic valvular disease. (For more on “Contraindications to exercise testing,” see TABLE 2.)
The role of imaging: Important, yes—routine, no
An important element of stress testing is, of course, the imaging method(s) that will be used. The options include myocardial perfusion imaging with thallium Tl 201 or technetium Tc 99m, and echocardiography.
Indications for myocardial perfusion imaging with exercise treadmill testing are a high pretest probability for CAD, an abnormal baseline ECG such as left bundle branch block, previous myocardial damage or coronary revascularization, or a previous equivocal or unexpected exercise ECG result. In women with an intermediate pretest probability for CAD, the sensitivity and specificity of an exercise treadmill testing is less than in men, which suggests that nuclear imaging would improve this test.8 There is, however, insufficient data to justify initial routine stress imaging tests in women.1
TABLE 2
Contraindications to exercise testing
| ABSOLUTE |
|---|
|
| RELATIVE CONTRAINDICATIONS (CAN BE SUPERSEDED IF THE BENEFITS OF EXERCISE OUTWEIGH THE RISKS) |
|
| Source: Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Exercise Testing). 2002. Available at: www.acc.org/qualityandscience/clinical/guidelines/exercise/exercise_clean.pdf Accessed: March 6, 2007. |
Of the 2 agents used for myocardial perfusion imaging, technetium Tc 99m has more favorable imaging characteristics.9 It has a shorter half-life (6 hours) than thallium Tl 201 (73 hours), and larger doses of technetium Tc99m may be used, permitting the assessment of ventricular function.10
Echocardiography may also be done with either exercise treadmill testing or PSMI to evaluate relative myocardial perfusion. While radionuclide technique assesses relative myocardial perfusion, echocardiography also evaluates global and regional function. Indications for echocardiography are similar to myocardial perfusion imaging but also include the need for prognostic information after MI, and to assess physiologic significance of a lesion or to determine the success of an intervention.
Time for the test: Selecting the protocol
While the Bruce exercise treadmill testing protocol is the most commonly used (82% of tests)11 in healthy adults, it may not be appropriate for women or the elderly as most protocols were developed for the evaluation of men.12 A ramp method with gradual increase in grade each minute is preferred by some clinicians when patients are unable to perform a standard Bruce protocol. Another option, the Modified Bruce protocol, which is more gradual than the standard Bruce protocol; it has two 3-minute warm-up stages.12
The 3 PSMI protocols include adenosine, dipyridamole, and dobutamine. Each has a different administration routine,9 though ECG, blood pressure and pulse are taken every minute for all 3.
- Adenosine is infused with a pump over 6 minutes and technetium Tc99m is injected 3 minutes into the infusion.
- Dipyridamole is infused over 4 minutes and technetium Tc99m is injected 2 to no more than 5 minutes after the infusion. Theophylline is injected, after dipyridamole if necessary, no earlier than 1 minute after technetium Tc99m is administered to avoid interference with the uptake.
- Dobutamine is titrated with a dose increase every 3 minutes. Tc99m is injected after the first minute at the highest concentration. (Typically dobutamine is used with echocardiography.6)
Adenosine
A potent vasodilator, this endogenous nucleoside is rapidly cleared (half-life, <10 seconds) along with its side effects of flushing, headache, and nausea.
Dipyridamole
This coronary vasodilator inhibits the uptake of adenosine. The same side effects as adenosine—flushing, headache, nausea—may last longer with dipyridamole (half-life,13 hours) but they are more common with adenosine and are relieved by administering theophylline.
All methylxanthines may interfere with either dipyridamole or adenosine and should be held for 24 to 48 hours prior to examination.
- Avoid both adenosine and dipyridamole in patients with asthma, severe COPD (FEV1<30%), second- or third-degree heart block, hypotension, or those who are on oral dipyridamole.
Dobutamine
This synthetic catecholamine increases heart rate, systolic blood pressure, and myocardial contractility, thereby provoking ischemia. Dobutamine (half-life 2 minutes) is not affected by methylxanthines.
- It is preferred in patients who are unable to use adenosine or dipyridamole.
- Caution is needed in patients with systolic BP less than 100 mm Hg, hypertension, ventricular ectopy, and glaucoma.
- Side effects can be reversed with beta-blockers.
Ideal endpoints and the realities that may creep in
The ideal endpoint in an exercise treadmill testing is 100% of the age-predicted maximum heart rate (220–age). Eighty-five percent of maximum heart rate is the minimum for an acceptable test.
Absolute contraindications
Absolute indicators for stopping an exercise treadmill test are either a 10 mm Hg systolic drop in blood pressure from standing baseline, moderate to severe angina symptoms, feelings of syncope, skin color changes suggestive of hypoxia or hypotension, ischemic ST changes, or the patient’s desire to stop.
Relative contraindications
Relative indicators to stop include fatigue, shortness of breath, leg pain, increased arrhythmias—particularly PVCs that increase with the exercise level—and blood pressure ≥250 systolic or 115 diastolic.6
Ideally, PSMI evaluations are terminated according to the prescribed length of infusions. They will also be terminated if a patient develops wheezing, severe or increasing chest pain or hypotension, neurological symptoms, ST-segment elevation abnormalities, or arrhythmias. To reverse the side effects of adenosine or dipyridamole, aminophylline IV will be administered (1–2 mg/kg slowly, up to 250 mg).
Heart of the matter: What a report should cover
Assuming you have ordered the stress test (and not done it yourself), a complete report should include
- ST changes
- symptoms during testing
- reason for ending the test
- estimation of exercise capacity
- blood pressure response
- the presence and frequency of arrhythmias or ectopy.
Abnormal. ST segment change is the most important ECG finding in a positive test; it’s defined as >1 mm horizontal or down sloping depression or elevation, at least 60 to 80 milliseconds after the end of the QRS complex and should prompt further workup to confirm CAD.5 An abnormal ECG during a PSMI test indicates an elevated risk of multivessel CAD and should prompt further evaluation regardless of normal myocardial perfusion imaging.13
Duke Treadmill Score
Duke Treadmill Score (DTS)=exercise time–(5 × ST deviation) - (4 × exercise angina), with 0=no angina during exercise, 1=nonlimiting angina, and 2=exercise-limiting angina.
The score typically ranges from –25 to +15.4
- Low risk: > +5
- Moderate risk: –10 to +4
- High risk: < –11
Elderly Alternative Treadmill Score (for patients over 65 years of age)
This score has 2 variables in common with the Duke Treadmill Score (exercise duration or the MET equivalent and millimeters of ST changes). It also has 2 different variables (drop in exercise systolic blood pressure below resting value and history of congestive heart failure [CHF] or use of digoxin [Dig]).17,18
The score is calculated as follows: 5 × (CHF/Dig [yes=1; no=0]) + exercise-induced ST depression in millimeters + change in systolic blood pressure score–METs
Systolic blood pressure score:
- 0 for an increase >40 mm Hg
- 1 for an increase of 31–40 mm Hg
- 2 for an increase of 21–30 mm Hg
- 3 for an increase of 11–20 mm Hg
- 4 for an increase of 0–10 mm Hg
- 5 for a reduction below standing systolic pre-exercise blood pressure.
A score of < –2 is low risk, –2 to 2 is moderate risk, and >2 is high risk.
Equivocal. Reports that come back as equivocal will have ECG changes nondiagnostic of ischemia such as alterations in P- or T-wave morphology and nondiagnostic changes in AV conduction, particularly if changes revert to baseline during the rest period. Unifocal PACs or PVCs (<5/min) are not specific indicators for CAD and the development of bundle branch blocks are nondiagnostic findings. Equivocal results need additional testing such as myocardial perfusion imaging or angiography to document ischemia if the pretest probability is high.
Incomplete or failure. If your patient’s test involves equipment failure or if he (or the operator) was unable to complete the test, you should get a report to that effect. Depending on the nature of the failure, you may need to repeat the test, consider PSMI, or make a cardiology referral.
Duke Treadmill Score
A helpful calculation following treadmill testing
If your patient had a positive or negative exercise treadmill test, consider calculating his Duke Treadmill Score (DTS), which is predictive of 5-year survival and significant severe CAD for patients who are younger than 75 years.4,14
DTS helps you to exclude low-risk patients from further invasive testing and ensure high-risk patients receive further evaluation and appropriate treatment. DTS appears to be more useful in women with an intermediate pretest score but not with a low pretest score.15
The DTS score typically ranges from –25 to +15.5 Patients at low risk will have a score of > +5), moderate risk will have scores ranging from –10 to +4, and those at high risk will have a score of ≤–11.4
A modified DTS is used for patients older than 65 years who may have a limited exercise capacity, controlled asymptomatic congestive heart failure, or be on digoxin, which may affect their ability to perform a maximal exercise treadmill test.5 The values for the Elderly Alternative Treadmill Score are as follows: low risk (< –2); moderate risk (–2 to 2); and high risk (>2). (See “The calculations behind the scores.”)
Bottom line
DTS scores, Elderly Alternative Treadmill Scores, and pre–stress test CAD probability scores are all extremely useful. Integrating them into your practice can ensure that patients get the prompt care they may need, while sparing them unnecessary tests along the way.
FIGURE
Template for dictating noninvasive cardiac tests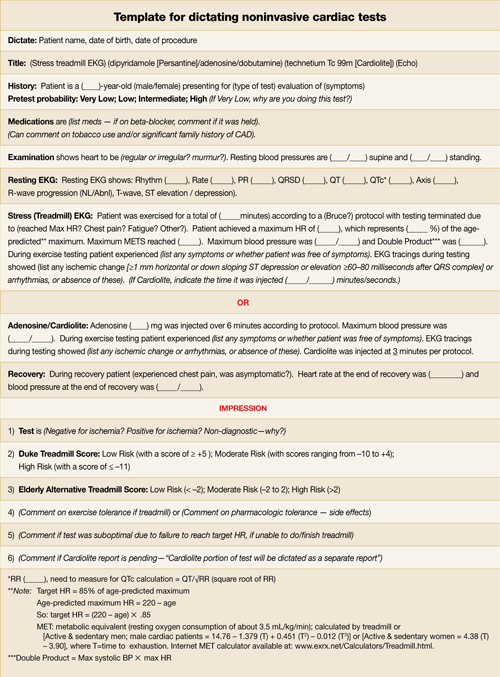
Correspondence
Dennis P. Breen, MD, Eau Claire Family Medicine Clinic, 617 Clairemont Avenue, Eau Claire, WI 54701. [email protected]
1. Snow V, Barry P, Fihn SD, et al. Evaluation of primary care patients with chronic stable angina: guidelines from the American College of Physicians. Ann Intern Med 2004;141:57-64.
2. Diamond GA. A clinically relevant classification of chest discomfort. J Am Coll Cardiol 1983;1:574-575.
3. Morise AP. Are the American College of Cardiology/American Heart Association guidelines for exercise testing for suspected coronary artery disease correct? Chest 2000;118:535-541.
4. Shaw LJ, Peterson ED, Shaw LK, et al. Use of a prognostic treadmill score in identifying diagnostic coronary disease subgroups. Circulation 1998;98:1622-1630.
5. Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Exercise Testing). 2002. Available at: www.acc.org/qualityandscience/clinical/guidelines/exercise/exercise_clean.pdf. Accessed on March 6, 2007.
6. Gibbons RJ, Chatterjee K, Daley J, et al. ACC/AHA/ACP-ASIM guidelines for the management of patients with chronic stable angina: A report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on Management of Patients with Chronic Stable Angina). J Am Coll Cardiol 1999;33:2092-2197.
7. Pellikka PA, Sarano ME, Nishimura RA, et al. Outcome of 622 adults with asymptomatic, hemodynamically significant aortic stenosis during prolonged follow-up. Circulation 2005;111:3290-3295.
8. Lewis JF, McGorray S, Lin L, et al. Exercise treadmill testing using a modified exercise protocol in women with suspected myocardial ischemia: Findings from the national heart, lung and blood institute-sponsored women’s ischemia syndrome evaluation (WISE). Am Heart J 2005;149:527-533.
9. Klocke FJ, Baird MG, Lorell BH, et al. ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging—executive summary: A report of the American College of Cardiology/American Heart Association task force on practice guidelines (ACC/AHA/ASNC committee to revise the 1995 guidelines for the clinical use of cardiac radionuclide imaging). J Am Coll Cardiol 2003;42:1318-1333.
10. Lee TH, Boucher CA. Clinical practice. noninvasive tests in patients with stable coronary artery disease. N Engl J Med 2001;344:1840-1845.
11. Myers J, Voodi L, Umann T, Froelicher VF. A survey of exercise testing: Methods, utilization, interpretation, and safety in the VAHCS. J Cardiopulm Rehabil 2000;20:251-258.
12. Ashley EA, Myers J, Froelicher V. Exercise testing in clinical medicine. Lancet 2000;356:1592-1597.
13. Cosmai EM, Heller GV. The clinical importance of electrocardiographic changes during pharmacologic stress testing with radionuclide myocardial perfusion imaging. J Nucl Cardiol 2005;12:466-472.
14. Kwok JM, Miller TD, Hodge DO, Gibbons RJ. Prognostic value of the duke treadmill score in the elderly. J Am Coll Cardiol 2002;39:1475-1481.
15. Morise AP, Olson MB, Merz NB, et al. Validation of the accuracy of pretest and exercise test scores in women with a low prevalence of coronary disease. The NHLBI-sponsored Women’s Ischemia Syndrome Evaluation (WISE) Study. Am Heart J 2004;147:1085-1092.
16. InfoRetriever [web site] Clinical Rules and Calculators (2007). InfoRetriever Search Results, Exercise Testing, Diagnostic Tests, Chest Pain. Available at: www.infopoems.com/irsearch/display_article.cfm?resource=D&article=34. Accessed on January 26, 2007.
17. Morrow K, Morris CK, Froelicher VF, et al. Prediction of cardiovascular death in men undergoing noninvasive evaluation for coronary artery disease. Ann Intern Med 1993;118:689-695.
18. Kwok JF, Christian TE. Effective use of the exercise stress test to detect and predict coronary artery disease. Emerg Med 2001;33:12-22.Available at: www.emedmag.com/html/pre/fea/features/051501.asp. Accessed on March 7, 2007.
- Estimate pretest probability of CAD in patients with chest pain on the basis of age, sex, pain characteristics, and cardiovascular risk factors (B).
- Low pretest probability patients should undergo an exercise treadmill test alone (C).
- Intermediate pretest probability patients, including those with complete right bundle branch block or less than 1 mm ST depression at rest should have an exercise treadmill test without imaging (B). Patients with an electronically paced ventricular rhythm (C) or left bundle-branch block (B) require myocardial perfusion imaging.
- In high pretest probability patients, coronary angiography is an appropriate initial strategy for CAD diagnosis (C).
- In women, the data are insufficient to justify routine stress imaging tests as the initial test for CAD (C).
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Are you a wise “consumer” of stress tests? That is: Do you consider your patient’s CAD probability score before ordering an exercise treadmill test or pharmacologic stress myocardial imaging (PSMI)? Are you as well-versed as you’d like to be on the predictive value of things like the Duke Treadmill Score?
If your answer is No to either question, this review may help guide your use of stress tests, based on evidence.
What is the pretest probability of CAD?
The decision to order an exercise stress test or a PSMI should be based on history, physical examination, and pretest probability for CAD. You can estimate the pretest probability for CAD in a chest pain patient based on the patient’s age, sex, and pain characteristics.1
Determine whether symptoms are typical, atypical, or nonanginal, based on whether the chest pain is substernal, brought on by exertion, or relieved by rest or nitroglycerin.2
To recap:
- Typical angina requires all 3 pain characteristics
- Atypical angina, only 2
- Nonanginal chest pain, 1.2
Use this information (along with the patient’s age) to determine whether he has a high, intermediate, low, or very low likelihood of CAD (TABLE 1). From the low, to the intermediate, to the high pretest probability levels, the positive predictive value increases progressively (21%, 62%, and 92%) and the negative predictive value decreases progressively (94%, 72%, and 28%).3 (These values are based on a review of symptomatic patients who had angiography following stress testing.)
TABLE 1
How to determine pretest probability of coronary artery disease
| STEP 1 | STEP 2 | STEP 3 | ||||||
|---|---|---|---|---|---|---|---|---|
| Ask 3 questions: | Total the number of “yes” answers to identify symptom pattern: | Find the cell in the matrix (below) where age, gender, and symptom pattern converge: | ||||||
| 0 of 3=Asymptomatic | High probability | >90% | |||||
| 1 of 3=Nonanginal chest pain | Intermediate | 10%–90% | ||||||
| 2 of 3=Atypical angina | Low | <10% | ||||||
| 3 of 3=Typical angina | Very low | <5% | ||||||
| AGE (YRS) | SYMPTOMS | |||||||
| ASYMPTOMATIC | NONANGINAL CHEST PAIN | ATYPICAL ANGINA | TYPICAL ANGINA | |||||
| MEN | WOMEN | MEN | WOMEN | MEN | WOMEN | MEN | WOMEN | |
| 35–45 | Very low | Very low | Intermediate | Very low | Intermediate | Intermediate | Intermediate | Intermediate |
| 45–55 | Low | Very low | Intermediate | Low | Intermediate | Intermediate | High | Intermediate |
| 55–65 | Intermediate | Low | Intermediate | Intermediate | Intermediate | Intermediate | High | Intermediate |
| 65–75 | Intermediate | Intermediate | Intermediate | Intermediate | Intermediate | Intermediate | High | High |
| Adapted from Diamond GA.2 | ||||||||
Your patients’ score dictates whether testing is required, and if so what kind.
Very low pretest probability patients should not have an exercise test, since they have a high risk of false-positive results. Evaluate and treat them for noncardiac causes of chest pain and begin primary prevention of CAD.
Low pretest probability patients should undergo exercise treadmill testing alone since negative results carry a high negative predictive value in both men and women, but positive test results may be false and can be evaluated by more studies.3
Intermediate pretest probability patients, including those with complete right bundle branch block or less than 1 mm ST depression at rest should have an exercise treadmill test without imaging modality.3-5 However, intermediate pretest probability patients with baseline ECG abnormalities such as electronically paced ventricular rhythm or left bundle-branch block will require myocardial perfusion imaging.5
High pretest probability patients should have coronary angiography as an initial strategy for diagnosis of CAD.3
History, exam, and ECG determine test suitability
Can your patient take an exercise stress test, or will he need a pharmacologic stress test instead? (See “A guide to sensitivity, specificity, and likelihood ratios for stress tests.”) Can he pedal a bicycle, walk, or exercise for 6 minutes? On physical examination, take note of his gait, mobility, and limb strength.
What medications is the patient taking? Digoxin may cause false ST changes, beta-blockers may prevent attaining maximum heart rate, and antihypertensive agents and vasodilators may alter the blood pressure response, producing a false negative result. Nitrates attenuate angina and the associated ST depression of ischemia.6 In addition, metabolic abnormalities and cocaine or alcohol use may affect heart rate, metabolic oxygen demand and the ability to perform the exercise treadmill testing.
On examination, document murmurs, rhythm abnormalities, vascular bruits, and abnormal pulses. Limit laboratory studies to recent cardiac damage screening if indicated. Screen with a resting ECG for arrhythmias, conduction abnormalities or preexisting cardiac damage. ST-segment (≥1 mm) and T-wave changes such as inversions secondary to strain or old injury or conduction abnormalities such as bundle branch blocks and prolonged QT interval may obscure exercise treadmill testing findings. Consider spirometry for patients with asthma or chronic lung disease.
Exercise treadmill testing
Sensitivity varies from 45% to 67% and specificity 72% to 90% with operator and patient variables.6 An abnormal test in a man at a heart rate of 85% of predicted maximum for age has a sensitivity of about 65% and a specificity of 85% for CAD. In women, one meta-analysis demonstrated a sensitivity of only 61% and a specificity of only 70%.8
PSMI
Pharmacologic stress myocardial imaging is similar to exercise treadmill testing. Dipyridamole and adenosine PSMI with thallium T1 201 or technetium Tc 99m have a similar sensitivity of 90%, and specificity of 70% for detection of CAD.6
Echocardiography
Overall sensitivity for exercise echocardiography was about 85% and for dobutamine stress echocardiography 82%. Dobutamine has a higher sensitivity than vasodilator echocardiography.6
Likelihood ratios (LR) for exercise treadmill testing and PSMI
Based on a review of coronary artery disease with chest pain as the symptom and a reference standard of a coronary angiogram with >70% narrowing of one or more arteries, or >50% left main, the LR varies for sex and for each different study. The positive LR (LR+) for exercise treadmill testing is 3.00 for men and 2.00 for women. The negative LR (LR–) for exercise treadmill testing is 0.650 for men and 0.560 for women. LR+ for exercise treadmill testing with thallium imaging is 5.9 (generally), but 2.20 for women; LR–is 0.200 and is 0.340 for women. Dipyridamole PSMI, LR+ is 3.30 and LR- is 0.180.16
The decisive factors
Absolute contraindications to exercise treadmill testing include recent MI; significant aortic stenosis,7 and weight exceeding equipment capacity. Relative contraindications to exercise treadmill testing (which can be superseded if the benefits of exercise outweigh the risks) include: hypertension (systolic >200 mm Hg/diastolic >110 mm Hg),5 left main coronary stenosis and stenotic valvular disease. (For more on “Contraindications to exercise testing,” see TABLE 2.)
The role of imaging: Important, yes—routine, no
An important element of stress testing is, of course, the imaging method(s) that will be used. The options include myocardial perfusion imaging with thallium Tl 201 or technetium Tc 99m, and echocardiography.
Indications for myocardial perfusion imaging with exercise treadmill testing are a high pretest probability for CAD, an abnormal baseline ECG such as left bundle branch block, previous myocardial damage or coronary revascularization, or a previous equivocal or unexpected exercise ECG result. In women with an intermediate pretest probability for CAD, the sensitivity and specificity of an exercise treadmill testing is less than in men, which suggests that nuclear imaging would improve this test.8 There is, however, insufficient data to justify initial routine stress imaging tests in women.1
TABLE 2
Contraindications to exercise testing
| ABSOLUTE |
|---|
|
| RELATIVE CONTRAINDICATIONS (CAN BE SUPERSEDED IF THE BENEFITS OF EXERCISE OUTWEIGH THE RISKS) |
|
| Source: Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Exercise Testing). 2002. Available at: www.acc.org/qualityandscience/clinical/guidelines/exercise/exercise_clean.pdf Accessed: March 6, 2007. |
Of the 2 agents used for myocardial perfusion imaging, technetium Tc 99m has more favorable imaging characteristics.9 It has a shorter half-life (6 hours) than thallium Tl 201 (73 hours), and larger doses of technetium Tc99m may be used, permitting the assessment of ventricular function.10
Echocardiography may also be done with either exercise treadmill testing or PSMI to evaluate relative myocardial perfusion. While radionuclide technique assesses relative myocardial perfusion, echocardiography also evaluates global and regional function. Indications for echocardiography are similar to myocardial perfusion imaging but also include the need for prognostic information after MI, and to assess physiologic significance of a lesion or to determine the success of an intervention.
Time for the test: Selecting the protocol
While the Bruce exercise treadmill testing protocol is the most commonly used (82% of tests)11 in healthy adults, it may not be appropriate for women or the elderly as most protocols were developed for the evaluation of men.12 A ramp method with gradual increase in grade each minute is preferred by some clinicians when patients are unable to perform a standard Bruce protocol. Another option, the Modified Bruce protocol, which is more gradual than the standard Bruce protocol; it has two 3-minute warm-up stages.12
The 3 PSMI protocols include adenosine, dipyridamole, and dobutamine. Each has a different administration routine,9 though ECG, blood pressure and pulse are taken every minute for all 3.
- Adenosine is infused with a pump over 6 minutes and technetium Tc99m is injected 3 minutes into the infusion.
- Dipyridamole is infused over 4 minutes and technetium Tc99m is injected 2 to no more than 5 minutes after the infusion. Theophylline is injected, after dipyridamole if necessary, no earlier than 1 minute after technetium Tc99m is administered to avoid interference with the uptake.
- Dobutamine is titrated with a dose increase every 3 minutes. Tc99m is injected after the first minute at the highest concentration. (Typically dobutamine is used with echocardiography.6)
Adenosine
A potent vasodilator, this endogenous nucleoside is rapidly cleared (half-life, <10 seconds) along with its side effects of flushing, headache, and nausea.
Dipyridamole
This coronary vasodilator inhibits the uptake of adenosine. The same side effects as adenosine—flushing, headache, nausea—may last longer with dipyridamole (half-life,13 hours) but they are more common with adenosine and are relieved by administering theophylline.
All methylxanthines may interfere with either dipyridamole or adenosine and should be held for 24 to 48 hours prior to examination.
- Avoid both adenosine and dipyridamole in patients with asthma, severe COPD (FEV1<30%), second- or third-degree heart block, hypotension, or those who are on oral dipyridamole.
Dobutamine
This synthetic catecholamine increases heart rate, systolic blood pressure, and myocardial contractility, thereby provoking ischemia. Dobutamine (half-life 2 minutes) is not affected by methylxanthines.
- It is preferred in patients who are unable to use adenosine or dipyridamole.
- Caution is needed in patients with systolic BP less than 100 mm Hg, hypertension, ventricular ectopy, and glaucoma.
- Side effects can be reversed with beta-blockers.
Ideal endpoints and the realities that may creep in
The ideal endpoint in an exercise treadmill testing is 100% of the age-predicted maximum heart rate (220–age). Eighty-five percent of maximum heart rate is the minimum for an acceptable test.
Absolute contraindications
Absolute indicators for stopping an exercise treadmill test are either a 10 mm Hg systolic drop in blood pressure from standing baseline, moderate to severe angina symptoms, feelings of syncope, skin color changes suggestive of hypoxia or hypotension, ischemic ST changes, or the patient’s desire to stop.
Relative contraindications
Relative indicators to stop include fatigue, shortness of breath, leg pain, increased arrhythmias—particularly PVCs that increase with the exercise level—and blood pressure ≥250 systolic or 115 diastolic.6
Ideally, PSMI evaluations are terminated according to the prescribed length of infusions. They will also be terminated if a patient develops wheezing, severe or increasing chest pain or hypotension, neurological symptoms, ST-segment elevation abnormalities, or arrhythmias. To reverse the side effects of adenosine or dipyridamole, aminophylline IV will be administered (1–2 mg/kg slowly, up to 250 mg).
Heart of the matter: What a report should cover
Assuming you have ordered the stress test (and not done it yourself), a complete report should include
- ST changes
- symptoms during testing
- reason for ending the test
- estimation of exercise capacity
- blood pressure response
- the presence and frequency of arrhythmias or ectopy.
Abnormal. ST segment change is the most important ECG finding in a positive test; it’s defined as >1 mm horizontal or down sloping depression or elevation, at least 60 to 80 milliseconds after the end of the QRS complex and should prompt further workup to confirm CAD.5 An abnormal ECG during a PSMI test indicates an elevated risk of multivessel CAD and should prompt further evaluation regardless of normal myocardial perfusion imaging.13
Duke Treadmill Score
Duke Treadmill Score (DTS)=exercise time–(5 × ST deviation) - (4 × exercise angina), with 0=no angina during exercise, 1=nonlimiting angina, and 2=exercise-limiting angina.
The score typically ranges from –25 to +15.4
- Low risk: > +5
- Moderate risk: –10 to +4
- High risk: < –11
Elderly Alternative Treadmill Score (for patients over 65 years of age)
This score has 2 variables in common with the Duke Treadmill Score (exercise duration or the MET equivalent and millimeters of ST changes). It also has 2 different variables (drop in exercise systolic blood pressure below resting value and history of congestive heart failure [CHF] or use of digoxin [Dig]).17,18
The score is calculated as follows: 5 × (CHF/Dig [yes=1; no=0]) + exercise-induced ST depression in millimeters + change in systolic blood pressure score–METs
Systolic blood pressure score:
- 0 for an increase >40 mm Hg
- 1 for an increase of 31–40 mm Hg
- 2 for an increase of 21–30 mm Hg
- 3 for an increase of 11–20 mm Hg
- 4 for an increase of 0–10 mm Hg
- 5 for a reduction below standing systolic pre-exercise blood pressure.
A score of < –2 is low risk, –2 to 2 is moderate risk, and >2 is high risk.
Equivocal. Reports that come back as equivocal will have ECG changes nondiagnostic of ischemia such as alterations in P- or T-wave morphology and nondiagnostic changes in AV conduction, particularly if changes revert to baseline during the rest period. Unifocal PACs or PVCs (<5/min) are not specific indicators for CAD and the development of bundle branch blocks are nondiagnostic findings. Equivocal results need additional testing such as myocardial perfusion imaging or angiography to document ischemia if the pretest probability is high.
Incomplete or failure. If your patient’s test involves equipment failure or if he (or the operator) was unable to complete the test, you should get a report to that effect. Depending on the nature of the failure, you may need to repeat the test, consider PSMI, or make a cardiology referral.
Duke Treadmill Score
A helpful calculation following treadmill testing
If your patient had a positive or negative exercise treadmill test, consider calculating his Duke Treadmill Score (DTS), which is predictive of 5-year survival and significant severe CAD for patients who are younger than 75 years.4,14
DTS helps you to exclude low-risk patients from further invasive testing and ensure high-risk patients receive further evaluation and appropriate treatment. DTS appears to be more useful in women with an intermediate pretest score but not with a low pretest score.15
The DTS score typically ranges from –25 to +15.5 Patients at low risk will have a score of > +5), moderate risk will have scores ranging from –10 to +4, and those at high risk will have a score of ≤–11.4
A modified DTS is used for patients older than 65 years who may have a limited exercise capacity, controlled asymptomatic congestive heart failure, or be on digoxin, which may affect their ability to perform a maximal exercise treadmill test.5 The values for the Elderly Alternative Treadmill Score are as follows: low risk (< –2); moderate risk (–2 to 2); and high risk (>2). (See “The calculations behind the scores.”)
Bottom line
DTS scores, Elderly Alternative Treadmill Scores, and pre–stress test CAD probability scores are all extremely useful. Integrating them into your practice can ensure that patients get the prompt care they may need, while sparing them unnecessary tests along the way.
FIGURE
Template for dictating noninvasive cardiac tests
Correspondence
Dennis P. Breen, MD, Eau Claire Family Medicine Clinic, 617 Clairemont Avenue, Eau Claire, WI 54701. [email protected]
- Estimate pretest probability of CAD in patients with chest pain on the basis of age, sex, pain characteristics, and cardiovascular risk factors (B).
- Low pretest probability patients should undergo an exercise treadmill test alone (C).
- Intermediate pretest probability patients, including those with complete right bundle branch block or less than 1 mm ST depression at rest should have an exercise treadmill test without imaging (B). Patients with an electronically paced ventricular rhythm (C) or left bundle-branch block (B) require myocardial perfusion imaging.
- In high pretest probability patients, coronary angiography is an appropriate initial strategy for CAD diagnosis (C).
- In women, the data are insufficient to justify routine stress imaging tests as the initial test for CAD (C).
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Are you a wise “consumer” of stress tests? That is: Do you consider your patient’s CAD probability score before ordering an exercise treadmill test or pharmacologic stress myocardial imaging (PSMI)? Are you as well-versed as you’d like to be on the predictive value of things like the Duke Treadmill Score?
If your answer is No to either question, this review may help guide your use of stress tests, based on evidence.
What is the pretest probability of CAD?
The decision to order an exercise stress test or a PSMI should be based on history, physical examination, and pretest probability for CAD. You can estimate the pretest probability for CAD in a chest pain patient based on the patient’s age, sex, and pain characteristics.1
Determine whether symptoms are typical, atypical, or nonanginal, based on whether the chest pain is substernal, brought on by exertion, or relieved by rest or nitroglycerin.2
To recap:
- Typical angina requires all 3 pain characteristics
- Atypical angina, only 2
- Nonanginal chest pain, 1.2
Use this information (along with the patient’s age) to determine whether he has a high, intermediate, low, or very low likelihood of CAD (TABLE 1). From the low, to the intermediate, to the high pretest probability levels, the positive predictive value increases progressively (21%, 62%, and 92%) and the negative predictive value decreases progressively (94%, 72%, and 28%).3 (These values are based on a review of symptomatic patients who had angiography following stress testing.)
TABLE 1
How to determine pretest probability of coronary artery disease
| STEP 1 | STEP 2 | STEP 3 | ||||||
|---|---|---|---|---|---|---|---|---|
| Ask 3 questions: | Total the number of “yes” answers to identify symptom pattern: | Find the cell in the matrix (below) where age, gender, and symptom pattern converge: | ||||||
| 0 of 3=Asymptomatic | High probability | >90% | |||||
| 1 of 3=Nonanginal chest pain | Intermediate | 10%–90% | ||||||
| 2 of 3=Atypical angina | Low | <10% | ||||||
| 3 of 3=Typical angina | Very low | <5% | ||||||
| AGE (YRS) | SYMPTOMS | |||||||
| ASYMPTOMATIC | NONANGINAL CHEST PAIN | ATYPICAL ANGINA | TYPICAL ANGINA | |||||
| MEN | WOMEN | MEN | WOMEN | MEN | WOMEN | MEN | WOMEN | |
| 35–45 | Very low | Very low | Intermediate | Very low | Intermediate | Intermediate | Intermediate | Intermediate |
| 45–55 | Low | Very low | Intermediate | Low | Intermediate | Intermediate | High | Intermediate |
| 55–65 | Intermediate | Low | Intermediate | Intermediate | Intermediate | Intermediate | High | Intermediate |
| 65–75 | Intermediate | Intermediate | Intermediate | Intermediate | Intermediate | Intermediate | High | High |
| Adapted from Diamond GA.2 | ||||||||
Your patients’ score dictates whether testing is required, and if so what kind.
Very low pretest probability patients should not have an exercise test, since they have a high risk of false-positive results. Evaluate and treat them for noncardiac causes of chest pain and begin primary prevention of CAD.
Low pretest probability patients should undergo exercise treadmill testing alone since negative results carry a high negative predictive value in both men and women, but positive test results may be false and can be evaluated by more studies.3
Intermediate pretest probability patients, including those with complete right bundle branch block or less than 1 mm ST depression at rest should have an exercise treadmill test without imaging modality.3-5 However, intermediate pretest probability patients with baseline ECG abnormalities such as electronically paced ventricular rhythm or left bundle-branch block will require myocardial perfusion imaging.5
High pretest probability patients should have coronary angiography as an initial strategy for diagnosis of CAD.3
History, exam, and ECG determine test suitability
Can your patient take an exercise stress test, or will he need a pharmacologic stress test instead? (See “A guide to sensitivity, specificity, and likelihood ratios for stress tests.”) Can he pedal a bicycle, walk, or exercise for 6 minutes? On physical examination, take note of his gait, mobility, and limb strength.
What medications is the patient taking? Digoxin may cause false ST changes, beta-blockers may prevent attaining maximum heart rate, and antihypertensive agents and vasodilators may alter the blood pressure response, producing a false negative result. Nitrates attenuate angina and the associated ST depression of ischemia.6 In addition, metabolic abnormalities and cocaine or alcohol use may affect heart rate, metabolic oxygen demand and the ability to perform the exercise treadmill testing.
On examination, document murmurs, rhythm abnormalities, vascular bruits, and abnormal pulses. Limit laboratory studies to recent cardiac damage screening if indicated. Screen with a resting ECG for arrhythmias, conduction abnormalities or preexisting cardiac damage. ST-segment (≥1 mm) and T-wave changes such as inversions secondary to strain or old injury or conduction abnormalities such as bundle branch blocks and prolonged QT interval may obscure exercise treadmill testing findings. Consider spirometry for patients with asthma or chronic lung disease.
Exercise treadmill testing
Sensitivity varies from 45% to 67% and specificity 72% to 90% with operator and patient variables.6 An abnormal test in a man at a heart rate of 85% of predicted maximum for age has a sensitivity of about 65% and a specificity of 85% for CAD. In women, one meta-analysis demonstrated a sensitivity of only 61% and a specificity of only 70%.8
PSMI
Pharmacologic stress myocardial imaging is similar to exercise treadmill testing. Dipyridamole and adenosine PSMI with thallium T1 201 or technetium Tc 99m have a similar sensitivity of 90%, and specificity of 70% for detection of CAD.6
Echocardiography
Overall sensitivity for exercise echocardiography was about 85% and for dobutamine stress echocardiography 82%. Dobutamine has a higher sensitivity than vasodilator echocardiography.6
Likelihood ratios (LR) for exercise treadmill testing and PSMI
Based on a review of coronary artery disease with chest pain as the symptom and a reference standard of a coronary angiogram with >70% narrowing of one or more arteries, or >50% left main, the LR varies for sex and for each different study. The positive LR (LR+) for exercise treadmill testing is 3.00 for men and 2.00 for women. The negative LR (LR–) for exercise treadmill testing is 0.650 for men and 0.560 for women. LR+ for exercise treadmill testing with thallium imaging is 5.9 (generally), but 2.20 for women; LR–is 0.200 and is 0.340 for women. Dipyridamole PSMI, LR+ is 3.30 and LR- is 0.180.16
The decisive factors
Absolute contraindications to exercise treadmill testing include recent MI; significant aortic stenosis,7 and weight exceeding equipment capacity. Relative contraindications to exercise treadmill testing (which can be superseded if the benefits of exercise outweigh the risks) include: hypertension (systolic >200 mm Hg/diastolic >110 mm Hg),5 left main coronary stenosis and stenotic valvular disease. (For more on “Contraindications to exercise testing,” see TABLE 2.)
The role of imaging: Important, yes—routine, no
An important element of stress testing is, of course, the imaging method(s) that will be used. The options include myocardial perfusion imaging with thallium Tl 201 or technetium Tc 99m, and echocardiography.
Indications for myocardial perfusion imaging with exercise treadmill testing are a high pretest probability for CAD, an abnormal baseline ECG such as left bundle branch block, previous myocardial damage or coronary revascularization, or a previous equivocal or unexpected exercise ECG result. In women with an intermediate pretest probability for CAD, the sensitivity and specificity of an exercise treadmill testing is less than in men, which suggests that nuclear imaging would improve this test.8 There is, however, insufficient data to justify initial routine stress imaging tests in women.1
TABLE 2
Contraindications to exercise testing
| ABSOLUTE |
|---|
|
| RELATIVE CONTRAINDICATIONS (CAN BE SUPERSEDED IF THE BENEFITS OF EXERCISE OUTWEIGH THE RISKS) |
|
| Source: Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Exercise Testing). 2002. Available at: www.acc.org/qualityandscience/clinical/guidelines/exercise/exercise_clean.pdf Accessed: March 6, 2007. |
Of the 2 agents used for myocardial perfusion imaging, technetium Tc 99m has more favorable imaging characteristics.9 It has a shorter half-life (6 hours) than thallium Tl 201 (73 hours), and larger doses of technetium Tc99m may be used, permitting the assessment of ventricular function.10
Echocardiography may also be done with either exercise treadmill testing or PSMI to evaluate relative myocardial perfusion. While radionuclide technique assesses relative myocardial perfusion, echocardiography also evaluates global and regional function. Indications for echocardiography are similar to myocardial perfusion imaging but also include the need for prognostic information after MI, and to assess physiologic significance of a lesion or to determine the success of an intervention.
Time for the test: Selecting the protocol
While the Bruce exercise treadmill testing protocol is the most commonly used (82% of tests)11 in healthy adults, it may not be appropriate for women or the elderly as most protocols were developed for the evaluation of men.12 A ramp method with gradual increase in grade each minute is preferred by some clinicians when patients are unable to perform a standard Bruce protocol. Another option, the Modified Bruce protocol, which is more gradual than the standard Bruce protocol; it has two 3-minute warm-up stages.12
The 3 PSMI protocols include adenosine, dipyridamole, and dobutamine. Each has a different administration routine,9 though ECG, blood pressure and pulse are taken every minute for all 3.
- Adenosine is infused with a pump over 6 minutes and technetium Tc99m is injected 3 minutes into the infusion.
- Dipyridamole is infused over 4 minutes and technetium Tc99m is injected 2 to no more than 5 minutes after the infusion. Theophylline is injected, after dipyridamole if necessary, no earlier than 1 minute after technetium Tc99m is administered to avoid interference with the uptake.
- Dobutamine is titrated with a dose increase every 3 minutes. Tc99m is injected after the first minute at the highest concentration. (Typically dobutamine is used with echocardiography.6)
Adenosine
A potent vasodilator, this endogenous nucleoside is rapidly cleared (half-life, <10 seconds) along with its side effects of flushing, headache, and nausea.
Dipyridamole
This coronary vasodilator inhibits the uptake of adenosine. The same side effects as adenosine—flushing, headache, nausea—may last longer with dipyridamole (half-life,13 hours) but they are more common with adenosine and are relieved by administering theophylline.
All methylxanthines may interfere with either dipyridamole or adenosine and should be held for 24 to 48 hours prior to examination.
- Avoid both adenosine and dipyridamole in patients with asthma, severe COPD (FEV1<30%), second- or third-degree heart block, hypotension, or those who are on oral dipyridamole.
Dobutamine
This synthetic catecholamine increases heart rate, systolic blood pressure, and myocardial contractility, thereby provoking ischemia. Dobutamine (half-life 2 minutes) is not affected by methylxanthines.
- It is preferred in patients who are unable to use adenosine or dipyridamole.
- Caution is needed in patients with systolic BP less than 100 mm Hg, hypertension, ventricular ectopy, and glaucoma.
- Side effects can be reversed with beta-blockers.
Ideal endpoints and the realities that may creep in
The ideal endpoint in an exercise treadmill testing is 100% of the age-predicted maximum heart rate (220–age). Eighty-five percent of maximum heart rate is the minimum for an acceptable test.
Absolute contraindications
Absolute indicators for stopping an exercise treadmill test are either a 10 mm Hg systolic drop in blood pressure from standing baseline, moderate to severe angina symptoms, feelings of syncope, skin color changes suggestive of hypoxia or hypotension, ischemic ST changes, or the patient’s desire to stop.
Relative contraindications
Relative indicators to stop include fatigue, shortness of breath, leg pain, increased arrhythmias—particularly PVCs that increase with the exercise level—and blood pressure ≥250 systolic or 115 diastolic.6
Ideally, PSMI evaluations are terminated according to the prescribed length of infusions. They will also be terminated if a patient develops wheezing, severe or increasing chest pain or hypotension, neurological symptoms, ST-segment elevation abnormalities, or arrhythmias. To reverse the side effects of adenosine or dipyridamole, aminophylline IV will be administered (1–2 mg/kg slowly, up to 250 mg).
Heart of the matter: What a report should cover
Assuming you have ordered the stress test (and not done it yourself), a complete report should include
- ST changes
- symptoms during testing
- reason for ending the test
- estimation of exercise capacity
- blood pressure response
- the presence and frequency of arrhythmias or ectopy.
Abnormal. ST segment change is the most important ECG finding in a positive test; it’s defined as >1 mm horizontal or down sloping depression or elevation, at least 60 to 80 milliseconds after the end of the QRS complex and should prompt further workup to confirm CAD.5 An abnormal ECG during a PSMI test indicates an elevated risk of multivessel CAD and should prompt further evaluation regardless of normal myocardial perfusion imaging.13
Duke Treadmill Score
Duke Treadmill Score (DTS)=exercise time–(5 × ST deviation) - (4 × exercise angina), with 0=no angina during exercise, 1=nonlimiting angina, and 2=exercise-limiting angina.
The score typically ranges from –25 to +15.4
- Low risk: > +5
- Moderate risk: –10 to +4
- High risk: < –11
Elderly Alternative Treadmill Score (for patients over 65 years of age)
This score has 2 variables in common with the Duke Treadmill Score (exercise duration or the MET equivalent and millimeters of ST changes). It also has 2 different variables (drop in exercise systolic blood pressure below resting value and history of congestive heart failure [CHF] or use of digoxin [Dig]).17,18
The score is calculated as follows: 5 × (CHF/Dig [yes=1; no=0]) + exercise-induced ST depression in millimeters + change in systolic blood pressure score–METs
Systolic blood pressure score:
- 0 for an increase >40 mm Hg
- 1 for an increase of 31–40 mm Hg
- 2 for an increase of 21–30 mm Hg
- 3 for an increase of 11–20 mm Hg
- 4 for an increase of 0–10 mm Hg
- 5 for a reduction below standing systolic pre-exercise blood pressure.
A score of < –2 is low risk, –2 to 2 is moderate risk, and >2 is high risk.
Equivocal. Reports that come back as equivocal will have ECG changes nondiagnostic of ischemia such as alterations in P- or T-wave morphology and nondiagnostic changes in AV conduction, particularly if changes revert to baseline during the rest period. Unifocal PACs or PVCs (<5/min) are not specific indicators for CAD and the development of bundle branch blocks are nondiagnostic findings. Equivocal results need additional testing such as myocardial perfusion imaging or angiography to document ischemia if the pretest probability is high.
Incomplete or failure. If your patient’s test involves equipment failure or if he (or the operator) was unable to complete the test, you should get a report to that effect. Depending on the nature of the failure, you may need to repeat the test, consider PSMI, or make a cardiology referral.
Duke Treadmill Score
A helpful calculation following treadmill testing
If your patient had a positive or negative exercise treadmill test, consider calculating his Duke Treadmill Score (DTS), which is predictive of 5-year survival and significant severe CAD for patients who are younger than 75 years.4,14
DTS helps you to exclude low-risk patients from further invasive testing and ensure high-risk patients receive further evaluation and appropriate treatment. DTS appears to be more useful in women with an intermediate pretest score but not with a low pretest score.15
The DTS score typically ranges from –25 to +15.5 Patients at low risk will have a score of > +5), moderate risk will have scores ranging from –10 to +4, and those at high risk will have a score of ≤–11.4
A modified DTS is used for patients older than 65 years who may have a limited exercise capacity, controlled asymptomatic congestive heart failure, or be on digoxin, which may affect their ability to perform a maximal exercise treadmill test.5 The values for the Elderly Alternative Treadmill Score are as follows: low risk (< –2); moderate risk (–2 to 2); and high risk (>2). (See “The calculations behind the scores.”)
Bottom line
DTS scores, Elderly Alternative Treadmill Scores, and pre–stress test CAD probability scores are all extremely useful. Integrating them into your practice can ensure that patients get the prompt care they may need, while sparing them unnecessary tests along the way.
FIGURE
Template for dictating noninvasive cardiac tests
Correspondence
Dennis P. Breen, MD, Eau Claire Family Medicine Clinic, 617 Clairemont Avenue, Eau Claire, WI 54701. [email protected]
1. Snow V, Barry P, Fihn SD, et al. Evaluation of primary care patients with chronic stable angina: guidelines from the American College of Physicians. Ann Intern Med 2004;141:57-64.
2. Diamond GA. A clinically relevant classification of chest discomfort. J Am Coll Cardiol 1983;1:574-575.
3. Morise AP. Are the American College of Cardiology/American Heart Association guidelines for exercise testing for suspected coronary artery disease correct? Chest 2000;118:535-541.
4. Shaw LJ, Peterson ED, Shaw LK, et al. Use of a prognostic treadmill score in identifying diagnostic coronary disease subgroups. Circulation 1998;98:1622-1630.
5. Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Exercise Testing). 2002. Available at: www.acc.org/qualityandscience/clinical/guidelines/exercise/exercise_clean.pdf. Accessed on March 6, 2007.
6. Gibbons RJ, Chatterjee K, Daley J, et al. ACC/AHA/ACP-ASIM guidelines for the management of patients with chronic stable angina: A report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on Management of Patients with Chronic Stable Angina). J Am Coll Cardiol 1999;33:2092-2197.
7. Pellikka PA, Sarano ME, Nishimura RA, et al. Outcome of 622 adults with asymptomatic, hemodynamically significant aortic stenosis during prolonged follow-up. Circulation 2005;111:3290-3295.
8. Lewis JF, McGorray S, Lin L, et al. Exercise treadmill testing using a modified exercise protocol in women with suspected myocardial ischemia: Findings from the national heart, lung and blood institute-sponsored women’s ischemia syndrome evaluation (WISE). Am Heart J 2005;149:527-533.
9. Klocke FJ, Baird MG, Lorell BH, et al. ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging—executive summary: A report of the American College of Cardiology/American Heart Association task force on practice guidelines (ACC/AHA/ASNC committee to revise the 1995 guidelines for the clinical use of cardiac radionuclide imaging). J Am Coll Cardiol 2003;42:1318-1333.
10. Lee TH, Boucher CA. Clinical practice. noninvasive tests in patients with stable coronary artery disease. N Engl J Med 2001;344:1840-1845.
11. Myers J, Voodi L, Umann T, Froelicher VF. A survey of exercise testing: Methods, utilization, interpretation, and safety in the VAHCS. J Cardiopulm Rehabil 2000;20:251-258.
12. Ashley EA, Myers J, Froelicher V. Exercise testing in clinical medicine. Lancet 2000;356:1592-1597.
13. Cosmai EM, Heller GV. The clinical importance of electrocardiographic changes during pharmacologic stress testing with radionuclide myocardial perfusion imaging. J Nucl Cardiol 2005;12:466-472.
14. Kwok JM, Miller TD, Hodge DO, Gibbons RJ. Prognostic value of the duke treadmill score in the elderly. J Am Coll Cardiol 2002;39:1475-1481.
15. Morise AP, Olson MB, Merz NB, et al. Validation of the accuracy of pretest and exercise test scores in women with a low prevalence of coronary disease. The NHLBI-sponsored Women’s Ischemia Syndrome Evaluation (WISE) Study. Am Heart J 2004;147:1085-1092.
16. InfoRetriever [web site] Clinical Rules and Calculators (2007). InfoRetriever Search Results, Exercise Testing, Diagnostic Tests, Chest Pain. Available at: www.infopoems.com/irsearch/display_article.cfm?resource=D&article=34. Accessed on January 26, 2007.
17. Morrow K, Morris CK, Froelicher VF, et al. Prediction of cardiovascular death in men undergoing noninvasive evaluation for coronary artery disease. Ann Intern Med 1993;118:689-695.
18. Kwok JF, Christian TE. Effective use of the exercise stress test to detect and predict coronary artery disease. Emerg Med 2001;33:12-22.Available at: www.emedmag.com/html/pre/fea/features/051501.asp. Accessed on March 7, 2007.
1. Snow V, Barry P, Fihn SD, et al. Evaluation of primary care patients with chronic stable angina: guidelines from the American College of Physicians. Ann Intern Med 2004;141:57-64.
2. Diamond GA. A clinically relevant classification of chest discomfort. J Am Coll Cardiol 1983;1:574-575.
3. Morise AP. Are the American College of Cardiology/American Heart Association guidelines for exercise testing for suspected coronary artery disease correct? Chest 2000;118:535-541.
4. Shaw LJ, Peterson ED, Shaw LK, et al. Use of a prognostic treadmill score in identifying diagnostic coronary disease subgroups. Circulation 1998;98:1622-1630.
5. Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guideline update for exercise testing: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Exercise Testing). 2002. Available at: www.acc.org/qualityandscience/clinical/guidelines/exercise/exercise_clean.pdf. Accessed on March 6, 2007.
6. Gibbons RJ, Chatterjee K, Daley J, et al. ACC/AHA/ACP-ASIM guidelines for the management of patients with chronic stable angina: A report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on Management of Patients with Chronic Stable Angina). J Am Coll Cardiol 1999;33:2092-2197.
7. Pellikka PA, Sarano ME, Nishimura RA, et al. Outcome of 622 adults with asymptomatic, hemodynamically significant aortic stenosis during prolonged follow-up. Circulation 2005;111:3290-3295.
8. Lewis JF, McGorray S, Lin L, et al. Exercise treadmill testing using a modified exercise protocol in women with suspected myocardial ischemia: Findings from the national heart, lung and blood institute-sponsored women’s ischemia syndrome evaluation (WISE). Am Heart J 2005;149:527-533.
9. Klocke FJ, Baird MG, Lorell BH, et al. ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging—executive summary: A report of the American College of Cardiology/American Heart Association task force on practice guidelines (ACC/AHA/ASNC committee to revise the 1995 guidelines for the clinical use of cardiac radionuclide imaging). J Am Coll Cardiol 2003;42:1318-1333.
10. Lee TH, Boucher CA. Clinical practice. noninvasive tests in patients with stable coronary artery disease. N Engl J Med 2001;344:1840-1845.
11. Myers J, Voodi L, Umann T, Froelicher VF. A survey of exercise testing: Methods, utilization, interpretation, and safety in the VAHCS. J Cardiopulm Rehabil 2000;20:251-258.
12. Ashley EA, Myers J, Froelicher V. Exercise testing in clinical medicine. Lancet 2000;356:1592-1597.
13. Cosmai EM, Heller GV. The clinical importance of electrocardiographic changes during pharmacologic stress testing with radionuclide myocardial perfusion imaging. J Nucl Cardiol 2005;12:466-472.
14. Kwok JM, Miller TD, Hodge DO, Gibbons RJ. Prognostic value of the duke treadmill score in the elderly. J Am Coll Cardiol 2002;39:1475-1481.
15. Morise AP, Olson MB, Merz NB, et al. Validation of the accuracy of pretest and exercise test scores in women with a low prevalence of coronary disease. The NHLBI-sponsored Women’s Ischemia Syndrome Evaluation (WISE) Study. Am Heart J 2004;147:1085-1092.
16. InfoRetriever [web site] Clinical Rules and Calculators (2007). InfoRetriever Search Results, Exercise Testing, Diagnostic Tests, Chest Pain. Available at: www.infopoems.com/irsearch/display_article.cfm?resource=D&article=34. Accessed on January 26, 2007.
17. Morrow K, Morris CK, Froelicher VF, et al. Prediction of cardiovascular death in men undergoing noninvasive evaluation for coronary artery disease. Ann Intern Med 1993;118:689-695.
18. Kwok JF, Christian TE. Effective use of the exercise stress test to detect and predict coronary artery disease. Emerg Med 2001;33:12-22.Available at: www.emedmag.com/html/pre/fea/features/051501.asp. Accessed on March 7, 2007.