User login
Damian McNamara is a journalist for Medscape Medical News and MDedge. He worked full-time for MDedge as the Miami Bureau covering a dozen medical specialties during 2001-2012, then as a freelancer for Medscape and MDedge, before being hired on staff by Medscape in 2018. Now the two companies are one. He uses what he learned in school – Damian has a BS in chemistry and an MS in science, health and environmental reporting/journalism. He works out of a home office in Miami, with a 100-pound chocolate lab known to snore under his desk during work hours.
Patients Prefer New Scale for Depression Remission
BOCA RATON, FLA. – "Just what we need – another scale," Dr. Mark Zimmerman said, tongue-in-cheek, as he started to explain why he and his colleagues developed the Remission From Depression Questionnaire.
Current measures define remission based on a lack of depressive symptoms alone, which is insufficient, Dr. Zimmerman said at the annual meeting of the New Clinical Drug Evaluation Unit, sponsored by the National Institute of Mental Health.

In a previous study of 514 depressed outpatients (J. Psychiatr. Res. 2008;42:797-801), "we found symptom resolution was not the most important consideration of depression remission," Dr. Zimmerman said. "Multiple factors were identified, so from a patient point of view, symptom-based definitions of remission are too narrow."
So Dr. Zimmerman and his colleagues developed the multidimensional Remission From Depression Questionnaire (RDQ), and conducted two studies to test reliability, validity, and patient preferences.
The RDQ assesses seven constructs: symptoms of depression, other symptoms, coping ability, positive mental health, functioning, life satisfaction, and general sense of well being. When the researchers compared remitters to nonremitters, significant differences were found on the RDQ total scale, depressive symptoms, and other symptoms. These findings support the RDQ as a valid measure, said Dr. Zimmerman, director of outpatient psychiatry at Rhode Island Hospital and with the department of psychiatry and human behavior at Brown University, both in Providence.
In the first study, Dr. Zimmerman and his colleagues compared responses from 102 depressed outpatients on the 41-item RDQ and the 16-item Quick Inventory of Depressive Symptomatology (QIDS). "They did not know we had developed one of these measures," he said.
There were no differences between the two measures on completion time. They were "equally burdensome and equally understandable," Dr. Zimmerman said.
Participants also reported their preference using a nine-item measure. Twice as many reported the RDQ more accurately described their overall state, 48%, vs. 24% for the QIDS. Nearly half said they preferred to complete the RDQ, 46%, compared with 22% who preferred completing the QIDS.
"Our conclusion from the first study is ... patients prefer the multifactorial RDQ scale more than a symptoms-based measure."
In a second study, the investigators asked 247 mildly depressed outpatients in ongoing treatment to complete the RDQ. The QIDS average score was 9.8, and the Hamilton Depression Rating Scale average score was 8.6. The RDQ correlated 0.62 with Hamilton scale and 0.70 with the Clinical Global Impression-Severity scale.
Dr. Zimmerman and his colleagues also split the cohort into remitters vs. nonremitters. Significant differences were found between these groups on the RDQ total score, 18 vs. 43; the depressive symptoms score, 5 vs. 12; and the other symptoms score, 2.8 vs. 5.7.
"The RDQ is a reliable and valid measure that evaluates multiple domains," Dr. Zimmerman said.
A group of 60 of the 247 patients waited and completed the RDQ measure a second time to test its reliability. The test-retest reliability and internal consistency were all greater than 0.8, Dr. Zimmerman said.
The next step is to assess the RDQ as an outcome measure in an acute treatment study of depression, Dr. Zimmerman said. An unanswered question is: Does the RDQ do a better job of predicting relapse compared to just a symptom-based scale?
Dr. Zimmerman said he had no disclosures. The studies were funded by Eli Lilly.
BOCA RATON, FLA. – "Just what we need – another scale," Dr. Mark Zimmerman said, tongue-in-cheek, as he started to explain why he and his colleagues developed the Remission From Depression Questionnaire.
Current measures define remission based on a lack of depressive symptoms alone, which is insufficient, Dr. Zimmerman said at the annual meeting of the New Clinical Drug Evaluation Unit, sponsored by the National Institute of Mental Health.
In a previous study of 514 depressed outpatients (J. Psychiatr. Res. 2008;42:797-801), "we found symptom resolution was not the most important consideration of depression remission," Dr. Zimmerman said. "Multiple factors were identified, so from a patient point of view, symptom-based definitions of remission are too narrow."
So Dr. Zimmerman and his colleagues developed the multidimensional Remission From Depression Questionnaire (RDQ), and conducted two studies to test reliability, validity, and patient preferences.
The RDQ assesses seven constructs: symptoms of depression, other symptoms, coping ability, positive mental health, functioning, life satisfaction, and general sense of well being. When the researchers compared remitters to nonremitters, significant differences were found on the RDQ total scale, depressive symptoms, and other symptoms. These findings support the RDQ as a valid measure, said Dr. Zimmerman, director of outpatient psychiatry at Rhode Island Hospital and with the department of psychiatry and human behavior at Brown University, both in Providence.
In the first study, Dr. Zimmerman and his colleagues compared responses from 102 depressed outpatients on the 41-item RDQ and the 16-item Quick Inventory of Depressive Symptomatology (QIDS). "They did not know we had developed one of these measures," he said.
There were no differences between the two measures on completion time. They were "equally burdensome and equally understandable," Dr. Zimmerman said.
Participants also reported their preference using a nine-item measure. Twice as many reported the RDQ more accurately described their overall state, 48%, vs. 24% for the QIDS. Nearly half said they preferred to complete the RDQ, 46%, compared with 22% who preferred completing the QIDS.
"Our conclusion from the first study is ... patients prefer the multifactorial RDQ scale more than a symptoms-based measure."
In a second study, the investigators asked 247 mildly depressed outpatients in ongoing treatment to complete the RDQ. The QIDS average score was 9.8, and the Hamilton Depression Rating Scale average score was 8.6. The RDQ correlated 0.62 with Hamilton scale and 0.70 with the Clinical Global Impression-Severity scale.
Dr. Zimmerman and his colleagues also split the cohort into remitters vs. nonremitters. Significant differences were found between these groups on the RDQ total score, 18 vs. 43; the depressive symptoms score, 5 vs. 12; and the other symptoms score, 2.8 vs. 5.7.
"The RDQ is a reliable and valid measure that evaluates multiple domains," Dr. Zimmerman said.
A group of 60 of the 247 patients waited and completed the RDQ measure a second time to test its reliability. The test-retest reliability and internal consistency were all greater than 0.8, Dr. Zimmerman said.
The next step is to assess the RDQ as an outcome measure in an acute treatment study of depression, Dr. Zimmerman said. An unanswered question is: Does the RDQ do a better job of predicting relapse compared to just a symptom-based scale?
Dr. Zimmerman said he had no disclosures. The studies were funded by Eli Lilly.
BOCA RATON, FLA. – "Just what we need – another scale," Dr. Mark Zimmerman said, tongue-in-cheek, as he started to explain why he and his colleagues developed the Remission From Depression Questionnaire.
Current measures define remission based on a lack of depressive symptoms alone, which is insufficient, Dr. Zimmerman said at the annual meeting of the New Clinical Drug Evaluation Unit, sponsored by the National Institute of Mental Health.
In a previous study of 514 depressed outpatients (J. Psychiatr. Res. 2008;42:797-801), "we found symptom resolution was not the most important consideration of depression remission," Dr. Zimmerman said. "Multiple factors were identified, so from a patient point of view, symptom-based definitions of remission are too narrow."
So Dr. Zimmerman and his colleagues developed the multidimensional Remission From Depression Questionnaire (RDQ), and conducted two studies to test reliability, validity, and patient preferences.
The RDQ assesses seven constructs: symptoms of depression, other symptoms, coping ability, positive mental health, functioning, life satisfaction, and general sense of well being. When the researchers compared remitters to nonremitters, significant differences were found on the RDQ total scale, depressive symptoms, and other symptoms. These findings support the RDQ as a valid measure, said Dr. Zimmerman, director of outpatient psychiatry at Rhode Island Hospital and with the department of psychiatry and human behavior at Brown University, both in Providence.
In the first study, Dr. Zimmerman and his colleagues compared responses from 102 depressed outpatients on the 41-item RDQ and the 16-item Quick Inventory of Depressive Symptomatology (QIDS). "They did not know we had developed one of these measures," he said.
There were no differences between the two measures on completion time. They were "equally burdensome and equally understandable," Dr. Zimmerman said.
Participants also reported their preference using a nine-item measure. Twice as many reported the RDQ more accurately described their overall state, 48%, vs. 24% for the QIDS. Nearly half said they preferred to complete the RDQ, 46%, compared with 22% who preferred completing the QIDS.
"Our conclusion from the first study is ... patients prefer the multifactorial RDQ scale more than a symptoms-based measure."
In a second study, the investigators asked 247 mildly depressed outpatients in ongoing treatment to complete the RDQ. The QIDS average score was 9.8, and the Hamilton Depression Rating Scale average score was 8.6. The RDQ correlated 0.62 with Hamilton scale and 0.70 with the Clinical Global Impression-Severity scale.
Dr. Zimmerman and his colleagues also split the cohort into remitters vs. nonremitters. Significant differences were found between these groups on the RDQ total score, 18 vs. 43; the depressive symptoms score, 5 vs. 12; and the other symptoms score, 2.8 vs. 5.7.
"The RDQ is a reliable and valid measure that evaluates multiple domains," Dr. Zimmerman said.
A group of 60 of the 247 patients waited and completed the RDQ measure a second time to test its reliability. The test-retest reliability and internal consistency were all greater than 0.8, Dr. Zimmerman said.
The next step is to assess the RDQ as an outcome measure in an acute treatment study of depression, Dr. Zimmerman said. An unanswered question is: Does the RDQ do a better job of predicting relapse compared to just a symptom-based scale?
Dr. Zimmerman said he had no disclosures. The studies were funded by Eli Lilly.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE NEW CLINICAL DRUG EVALUATION UNIT
Major Finding: A total 48% of patients said the Remission From Depression Questionnaire more accurately described their overall state, compared with 24% who preferred the Quick Inventory of Depressive Symptomatology.
Data Source: Survey of 102 depressed outpatients.
Disclosures: Eli Lilly sponsored the studies. Dr. Zimmerman said he had no relevant disclosures.
Botox Improves Migraine Regardless of Medication History
BERLIN – People never treated for their chronic migraines and those who failed a previous first-line medication reported similar reductions in frequency of headache days after treatment with onabotulinumtoxinA in a post hoc comparison study of the two phase III studies that Allergan used to gain approval for the new indication.
Some migraine medications work better in treatment-naïve patients, compared with those with a past marred by partial responses or one or more failures to first-line prophylactic therapies.

For this reason, Dr. Sheena K. Aurora and her associates assessed data from the two Phase 3 Research Evaluating Migraine Prophylaxis Therapy (PREEMPT) studies (Headache 2010;50:921-36) determine if onabotulinumtoxinA treatment works the same way. They compared 575 participants with a history of migraine prophylaxis use to another 809 participants who never tried such a first-line medication, as defined by the British Association for the Study of Headache (BASH). Amitriptyline and propranolol were the most common previous medications.
There was no significant difference in the reduction of frequency of headache days with onabotulinumtoxinA between previously-treated and untreated patients, Dr. Aurora said at the International Headache Congress, which was sponsored by the International Headache Society and the American Headache Society. A total 45% of patients with a history of first-line medication use versus 50% of those with no such history had a significant reduction in frequency of headache days.
"OnabotulinumtoxinA is an effective treatment of chronic migraine patients who previously failed BASH first-line migraine prophylactic meds and those naïve to BASH first-line migraine prophylactic treatment," said Dr. Aurora, a neurologist specializing in headache, migraine, and movement disorders at the Swedish Pain and Headache Center in Seattle.
Patients also experienced significant improvements in several secondary outcome measures that did not differ significantly between groups. These outcomes included frequency of migraine days, number of moderate to severe headache days, total cumulative hours of headache on headache days, and percentage of participants who reported severe migraines with a 60 or higher on the Headache Impact Test (HIT-6).
patient reports of improvements in health-related quality of life and disability did not differ significantly between groups, Dr. Aurora said.
The BASH guidelines assign medications to first-, second-, and third-line categories for prophylaxis against episodic migraines. However, many physicians use the same medicines to help chronic migraine sufferers, Dr. Aurora said, so the study answers a clinically relevant question.
Chronic migraine affects approximately 2% of the global population. Chronic migraine sufferers also report greater disability than patients with episodic migraine, according to Dr. Andrew Blumenfeld, who spoke during a separate session at the congress. "Chronic migraineurs experience a higher percentage of severe disability on more headache days than episodic migraineurs."
The burden of illness could be an additional criterion to define chronic migraine beyond the traditional cutoff of 15 or more affected days per month, said Dr. Blumenfeld, who was the lead author on a study comparing disability status and migraine frequency (Cephalalgia 2011;31:301-15). He is a neurologist in private practice in Encinitas, Calif.
The PREEMPT studies included 1,384 highly disabled migraine patients who reported 15 or more days per month with a headache lasting at least 4 hours per day. The 24-week, multicenter, double-blind study researchers randomized 688 of these men and women ages 18 to 65 years old to onabotulinumtoxinA and another 696 to placebo. A 32-week, open-label phase followed the acute treatment study. "There was a cumulative benefit over time – most patients continued to receive treatment benefit after five treatment cycles," Dr. David Dodick, one of the PREEMPT investigators, said in a separate presentation at the congress. "In clinical practice, patients should be administered at least two treatment cycles. If they have absolutely no response, do not proceed."
"You can tell patients that almost 70% of patients treated with [onabotulinumtoxinA] had 50% or more reduction in headache days at 56 weeks," said Dr. Dodick, professor of neurology at the Mayo Clinic in Phoenix, Ariz.
The mechanism of action of onabotulinumtoxinA in chronic migraine remains to be elucidated, Dr. Dodick said. "I don’t think any of us know how the prophylactic medications work in practice." In animal models, peripheral injections of the toxin reduced pain and c-fos protein expression in the spinal dorsal horn and inhibited central sensitization of spinal and medullary dorsal horn neurons, he said. "Clearly, injecting botulinum toxin peripherally has an effect on neurons centrally. Is it trans-synaptic spread or reduction in afferent drive or a combination of the two?"
A recommended injection method for chronic migraine based on the PREEMPT studies is explained, including a diagram of onabotulinumtoxinA injection sites, was published last year (Headache 2010;50:1406-18).
Allergan funded the post hoc analysis. Dr. Aurora said she is a member of the Allergan medical advisory board. Dr. Blumenfeld and Dr. Dodick have received funding from Allergan.
BERLIN – People never treated for their chronic migraines and those who failed a previous first-line medication reported similar reductions in frequency of headache days after treatment with onabotulinumtoxinA in a post hoc comparison study of the two phase III studies that Allergan used to gain approval for the new indication.
Some migraine medications work better in treatment-naïve patients, compared with those with a past marred by partial responses or one or more failures to first-line prophylactic therapies.
For this reason, Dr. Sheena K. Aurora and her associates assessed data from the two Phase 3 Research Evaluating Migraine Prophylaxis Therapy (PREEMPT) studies (Headache 2010;50:921-36) determine if onabotulinumtoxinA treatment works the same way. They compared 575 participants with a history of migraine prophylaxis use to another 809 participants who never tried such a first-line medication, as defined by the British Association for the Study of Headache (BASH). Amitriptyline and propranolol were the most common previous medications.
There was no significant difference in the reduction of frequency of headache days with onabotulinumtoxinA between previously-treated and untreated patients, Dr. Aurora said at the International Headache Congress, which was sponsored by the International Headache Society and the American Headache Society. A total 45% of patients with a history of first-line medication use versus 50% of those with no such history had a significant reduction in frequency of headache days.
"OnabotulinumtoxinA is an effective treatment of chronic migraine patients who previously failed BASH first-line migraine prophylactic meds and those naïve to BASH first-line migraine prophylactic treatment," said Dr. Aurora, a neurologist specializing in headache, migraine, and movement disorders at the Swedish Pain and Headache Center in Seattle.
Patients also experienced significant improvements in several secondary outcome measures that did not differ significantly between groups. These outcomes included frequency of migraine days, number of moderate to severe headache days, total cumulative hours of headache on headache days, and percentage of participants who reported severe migraines with a 60 or higher on the Headache Impact Test (HIT-6).
patient reports of improvements in health-related quality of life and disability did not differ significantly between groups, Dr. Aurora said.
The BASH guidelines assign medications to first-, second-, and third-line categories for prophylaxis against episodic migraines. However, many physicians use the same medicines to help chronic migraine sufferers, Dr. Aurora said, so the study answers a clinically relevant question.
Chronic migraine affects approximately 2% of the global population. Chronic migraine sufferers also report greater disability than patients with episodic migraine, according to Dr. Andrew Blumenfeld, who spoke during a separate session at the congress. "Chronic migraineurs experience a higher percentage of severe disability on more headache days than episodic migraineurs."
The burden of illness could be an additional criterion to define chronic migraine beyond the traditional cutoff of 15 or more affected days per month, said Dr. Blumenfeld, who was the lead author on a study comparing disability status and migraine frequency (Cephalalgia 2011;31:301-15). He is a neurologist in private practice in Encinitas, Calif.
The PREEMPT studies included 1,384 highly disabled migraine patients who reported 15 or more days per month with a headache lasting at least 4 hours per day. The 24-week, multicenter, double-blind study researchers randomized 688 of these men and women ages 18 to 65 years old to onabotulinumtoxinA and another 696 to placebo. A 32-week, open-label phase followed the acute treatment study. "There was a cumulative benefit over time – most patients continued to receive treatment benefit after five treatment cycles," Dr. David Dodick, one of the PREEMPT investigators, said in a separate presentation at the congress. "In clinical practice, patients should be administered at least two treatment cycles. If they have absolutely no response, do not proceed."
"You can tell patients that almost 70% of patients treated with [onabotulinumtoxinA] had 50% or more reduction in headache days at 56 weeks," said Dr. Dodick, professor of neurology at the Mayo Clinic in Phoenix, Ariz.
The mechanism of action of onabotulinumtoxinA in chronic migraine remains to be elucidated, Dr. Dodick said. "I don’t think any of us know how the prophylactic medications work in practice." In animal models, peripheral injections of the toxin reduced pain and c-fos protein expression in the spinal dorsal horn and inhibited central sensitization of spinal and medullary dorsal horn neurons, he said. "Clearly, injecting botulinum toxin peripherally has an effect on neurons centrally. Is it trans-synaptic spread or reduction in afferent drive or a combination of the two?"
A recommended injection method for chronic migraine based on the PREEMPT studies is explained, including a diagram of onabotulinumtoxinA injection sites, was published last year (Headache 2010;50:1406-18).
Allergan funded the post hoc analysis. Dr. Aurora said she is a member of the Allergan medical advisory board. Dr. Blumenfeld and Dr. Dodick have received funding from Allergan.
BERLIN – People never treated for their chronic migraines and those who failed a previous first-line medication reported similar reductions in frequency of headache days after treatment with onabotulinumtoxinA in a post hoc comparison study of the two phase III studies that Allergan used to gain approval for the new indication.
Some migraine medications work better in treatment-naïve patients, compared with those with a past marred by partial responses or one or more failures to first-line prophylactic therapies.
For this reason, Dr. Sheena K. Aurora and her associates assessed data from the two Phase 3 Research Evaluating Migraine Prophylaxis Therapy (PREEMPT) studies (Headache 2010;50:921-36) determine if onabotulinumtoxinA treatment works the same way. They compared 575 participants with a history of migraine prophylaxis use to another 809 participants who never tried such a first-line medication, as defined by the British Association for the Study of Headache (BASH). Amitriptyline and propranolol were the most common previous medications.
There was no significant difference in the reduction of frequency of headache days with onabotulinumtoxinA between previously-treated and untreated patients, Dr. Aurora said at the International Headache Congress, which was sponsored by the International Headache Society and the American Headache Society. A total 45% of patients with a history of first-line medication use versus 50% of those with no such history had a significant reduction in frequency of headache days.
"OnabotulinumtoxinA is an effective treatment of chronic migraine patients who previously failed BASH first-line migraine prophylactic meds and those naïve to BASH first-line migraine prophylactic treatment," said Dr. Aurora, a neurologist specializing in headache, migraine, and movement disorders at the Swedish Pain and Headache Center in Seattle.
Patients also experienced significant improvements in several secondary outcome measures that did not differ significantly between groups. These outcomes included frequency of migraine days, number of moderate to severe headache days, total cumulative hours of headache on headache days, and percentage of participants who reported severe migraines with a 60 or higher on the Headache Impact Test (HIT-6).
patient reports of improvements in health-related quality of life and disability did not differ significantly between groups, Dr. Aurora said.
The BASH guidelines assign medications to first-, second-, and third-line categories for prophylaxis against episodic migraines. However, many physicians use the same medicines to help chronic migraine sufferers, Dr. Aurora said, so the study answers a clinically relevant question.
Chronic migraine affects approximately 2% of the global population. Chronic migraine sufferers also report greater disability than patients with episodic migraine, according to Dr. Andrew Blumenfeld, who spoke during a separate session at the congress. "Chronic migraineurs experience a higher percentage of severe disability on more headache days than episodic migraineurs."
The burden of illness could be an additional criterion to define chronic migraine beyond the traditional cutoff of 15 or more affected days per month, said Dr. Blumenfeld, who was the lead author on a study comparing disability status and migraine frequency (Cephalalgia 2011;31:301-15). He is a neurologist in private practice in Encinitas, Calif.
The PREEMPT studies included 1,384 highly disabled migraine patients who reported 15 or more days per month with a headache lasting at least 4 hours per day. The 24-week, multicenter, double-blind study researchers randomized 688 of these men and women ages 18 to 65 years old to onabotulinumtoxinA and another 696 to placebo. A 32-week, open-label phase followed the acute treatment study. "There was a cumulative benefit over time – most patients continued to receive treatment benefit after five treatment cycles," Dr. David Dodick, one of the PREEMPT investigators, said in a separate presentation at the congress. "In clinical practice, patients should be administered at least two treatment cycles. If they have absolutely no response, do not proceed."
"You can tell patients that almost 70% of patients treated with [onabotulinumtoxinA] had 50% or more reduction in headache days at 56 weeks," said Dr. Dodick, professor of neurology at the Mayo Clinic in Phoenix, Ariz.
The mechanism of action of onabotulinumtoxinA in chronic migraine remains to be elucidated, Dr. Dodick said. "I don’t think any of us know how the prophylactic medications work in practice." In animal models, peripheral injections of the toxin reduced pain and c-fos protein expression in the spinal dorsal horn and inhibited central sensitization of spinal and medullary dorsal horn neurons, he said. "Clearly, injecting botulinum toxin peripherally has an effect on neurons centrally. Is it trans-synaptic spread or reduction in afferent drive or a combination of the two?"
A recommended injection method for chronic migraine based on the PREEMPT studies is explained, including a diagram of onabotulinumtoxinA injection sites, was published last year (Headache 2010;50:1406-18).
Allergan funded the post hoc analysis. Dr. Aurora said she is a member of the Allergan medical advisory board. Dr. Blumenfeld and Dr. Dodick have received funding from Allergan.
FROM THE INTERNATIONAL HEADACHE CONGRESS
Major Finding: A total 45% of 575 first-line treatment-naïve chronic migraine sufferers significantly responded to onabotulinumtoxinA treatment vs. 50% of 809 others with no such medication history.
Data Source: Post hoc analysis of the PREEMPT chronic migraine study.
Disclosures: The study was funded by Allergan. Dr. Aurora is on the Allergan medical advisory board. Dr. Blumenfeld and Dr. Dodick have received funding from Allergan.
Evidence Builds for Distinct Headache 'Attributed to Airplane Travel'
BERLIN – Reports from airline passengers who experience sudden onset, severe, and short duration headaches – primarily during landing – contain enough common and unique features to support a new, distinct form of headache, according to a study.
"There are some peculiar, common characteristics," Dr. Federico Mainardi said at the International Headache Congress, which was sponsored by the International Headache Society and the American Headache Society. A total of 63 people who responded to a questionnaire cited the common factors of strict unilateral presentation, absence of companion symptoms, and spontaneous resolution once they were on the ground and at the airport.
Sinus conditions sometimes cause severe headaches in migraine patients, Dr. Mainardi said, but only two participants reported concurrent sinusitis. This and other physiologic explanations were ruled out for the remainder, including a subset who underwent MRI and sinus CT scanning, said Dr. Mainardi, a neurologist at the Headache Centre at S.S. Giovanni e Paolo Hospital, Venice, Italy.
Because 60 of the 63 participants had at least one attack occur during the landing phase, Dr. Mainardi suggested that patients with a history of these attacks should take nonsteroidal anti-inflammatory drug prophylaxis either before takeoff on a short flight or during a longer flight. Some respondents reported that this strategy prevented subsequent attacks. He reminded clinicians to rule out organic pathology when a patient reports one of these in-flight headache attacks.
A majority of the participants (46) did not experience a "headache attributed to airplane travel" during their first experience flying. Many people experienced repeat attacks, including 15 patients who reported attacks on more than half their flights and 9 who suffered an attack each time they flew.
Dr. Mainardi described his first case and, together with seven other cases published in the literature, he and his colleagues devised specific criteria for these headaches (J. Headache Pain. 2007;8:196-9). The criteria include repeated attacks, occurrence during airplane travel, duration up to 20 minutes, and fronto-periorbital location.
Dr. Mainardi said that after the publication of the criteria he and his associates received e-mails from people worldwide experiencing the same kind of headache. "This is not an infrequent condition."
Of these 69 contacts, 63 returned a completed questionnaire in which they described and rated their experience. Their mean age was 37 years, and 41 (65%) of the respondents were men. Using International Classification of Headache Disorders (ICHD-II) criteria on the questionnaire, 35 (56%) had a concomitant primary headache, including 15 who reported tension type headaches, 11 who reported migraine with aura, and 3 who met criteria for probable tension type headache. Six reported more than one primary headache type. No participant suffered from cluster headache.
All patients rated their attacks as "severe" or "very severe." These headaches negatively influenced the decision to fly in the future for 44 respondents (70%). This reflects the severity of the pain, Dr. Mainardi said.
All patients denied alcohol consumption prior to the attacks and none gained relief from measures such as chewing, swallowing, or performing a Valsalva maneuver. The duration of flight was not a factor associated with the headache attacks, Dr. Mainardi said.
New cases continue to come forward, and he and his colleagues had identified 74 cases at the time of the congress. Based on more recent experience, he suggested two modifications to the criteria proposed in 2007: an increase in duration up to 30 minutes and expansion of the anatomic location of these attacks to include the parietal region.
Headache attributed to airplane travel is not included in the ICHD-II. Therefore, Dr. Mainardi said, "This should be proposed as a new entity in the forthcoming edition of the ICHD-III."
He said that he had no relevant financial disclosures.
BERLIN – Reports from airline passengers who experience sudden onset, severe, and short duration headaches – primarily during landing – contain enough common and unique features to support a new, distinct form of headache, according to a study.
"There are some peculiar, common characteristics," Dr. Federico Mainardi said at the International Headache Congress, which was sponsored by the International Headache Society and the American Headache Society. A total of 63 people who responded to a questionnaire cited the common factors of strict unilateral presentation, absence of companion symptoms, and spontaneous resolution once they were on the ground and at the airport.
Sinus conditions sometimes cause severe headaches in migraine patients, Dr. Mainardi said, but only two participants reported concurrent sinusitis. This and other physiologic explanations were ruled out for the remainder, including a subset who underwent MRI and sinus CT scanning, said Dr. Mainardi, a neurologist at the Headache Centre at S.S. Giovanni e Paolo Hospital, Venice, Italy.
Because 60 of the 63 participants had at least one attack occur during the landing phase, Dr. Mainardi suggested that patients with a history of these attacks should take nonsteroidal anti-inflammatory drug prophylaxis either before takeoff on a short flight or during a longer flight. Some respondents reported that this strategy prevented subsequent attacks. He reminded clinicians to rule out organic pathology when a patient reports one of these in-flight headache attacks.
A majority of the participants (46) did not experience a "headache attributed to airplane travel" during their first experience flying. Many people experienced repeat attacks, including 15 patients who reported attacks on more than half their flights and 9 who suffered an attack each time they flew.
Dr. Mainardi described his first case and, together with seven other cases published in the literature, he and his colleagues devised specific criteria for these headaches (J. Headache Pain. 2007;8:196-9). The criteria include repeated attacks, occurrence during airplane travel, duration up to 20 minutes, and fronto-periorbital location.
Dr. Mainardi said that after the publication of the criteria he and his associates received e-mails from people worldwide experiencing the same kind of headache. "This is not an infrequent condition."
Of these 69 contacts, 63 returned a completed questionnaire in which they described and rated their experience. Their mean age was 37 years, and 41 (65%) of the respondents were men. Using International Classification of Headache Disorders (ICHD-II) criteria on the questionnaire, 35 (56%) had a concomitant primary headache, including 15 who reported tension type headaches, 11 who reported migraine with aura, and 3 who met criteria for probable tension type headache. Six reported more than one primary headache type. No participant suffered from cluster headache.
All patients rated their attacks as "severe" or "very severe." These headaches negatively influenced the decision to fly in the future for 44 respondents (70%). This reflects the severity of the pain, Dr. Mainardi said.
All patients denied alcohol consumption prior to the attacks and none gained relief from measures such as chewing, swallowing, or performing a Valsalva maneuver. The duration of flight was not a factor associated with the headache attacks, Dr. Mainardi said.
New cases continue to come forward, and he and his colleagues had identified 74 cases at the time of the congress. Based on more recent experience, he suggested two modifications to the criteria proposed in 2007: an increase in duration up to 30 minutes and expansion of the anatomic location of these attacks to include the parietal region.
Headache attributed to airplane travel is not included in the ICHD-II. Therefore, Dr. Mainardi said, "This should be proposed as a new entity in the forthcoming edition of the ICHD-III."
He said that he had no relevant financial disclosures.
BERLIN – Reports from airline passengers who experience sudden onset, severe, and short duration headaches – primarily during landing – contain enough common and unique features to support a new, distinct form of headache, according to a study.
"There are some peculiar, common characteristics," Dr. Federico Mainardi said at the International Headache Congress, which was sponsored by the International Headache Society and the American Headache Society. A total of 63 people who responded to a questionnaire cited the common factors of strict unilateral presentation, absence of companion symptoms, and spontaneous resolution once they were on the ground and at the airport.
Sinus conditions sometimes cause severe headaches in migraine patients, Dr. Mainardi said, but only two participants reported concurrent sinusitis. This and other physiologic explanations were ruled out for the remainder, including a subset who underwent MRI and sinus CT scanning, said Dr. Mainardi, a neurologist at the Headache Centre at S.S. Giovanni e Paolo Hospital, Venice, Italy.
Because 60 of the 63 participants had at least one attack occur during the landing phase, Dr. Mainardi suggested that patients with a history of these attacks should take nonsteroidal anti-inflammatory drug prophylaxis either before takeoff on a short flight or during a longer flight. Some respondents reported that this strategy prevented subsequent attacks. He reminded clinicians to rule out organic pathology when a patient reports one of these in-flight headache attacks.
A majority of the participants (46) did not experience a "headache attributed to airplane travel" during their first experience flying. Many people experienced repeat attacks, including 15 patients who reported attacks on more than half their flights and 9 who suffered an attack each time they flew.
Dr. Mainardi described his first case and, together with seven other cases published in the literature, he and his colleagues devised specific criteria for these headaches (J. Headache Pain. 2007;8:196-9). The criteria include repeated attacks, occurrence during airplane travel, duration up to 20 minutes, and fronto-periorbital location.
Dr. Mainardi said that after the publication of the criteria he and his associates received e-mails from people worldwide experiencing the same kind of headache. "This is not an infrequent condition."
Of these 69 contacts, 63 returned a completed questionnaire in which they described and rated their experience. Their mean age was 37 years, and 41 (65%) of the respondents were men. Using International Classification of Headache Disorders (ICHD-II) criteria on the questionnaire, 35 (56%) had a concomitant primary headache, including 15 who reported tension type headaches, 11 who reported migraine with aura, and 3 who met criteria for probable tension type headache. Six reported more than one primary headache type. No participant suffered from cluster headache.
All patients rated their attacks as "severe" or "very severe." These headaches negatively influenced the decision to fly in the future for 44 respondents (70%). This reflects the severity of the pain, Dr. Mainardi said.
All patients denied alcohol consumption prior to the attacks and none gained relief from measures such as chewing, swallowing, or performing a Valsalva maneuver. The duration of flight was not a factor associated with the headache attacks, Dr. Mainardi said.
New cases continue to come forward, and he and his colleagues had identified 74 cases at the time of the congress. Based on more recent experience, he suggested two modifications to the criteria proposed in 2007: an increase in duration up to 30 minutes and expansion of the anatomic location of these attacks to include the parietal region.
Headache attributed to airplane travel is not included in the ICHD-II. Therefore, Dr. Mainardi said, "This should be proposed as a new entity in the forthcoming edition of the ICHD-III."
He said that he had no relevant financial disclosures.
FROM THE INTERNATIONAL HEADACHE CONGRESS
Major Finding: Of 63 patients who shared common characteristics for a new form of headache attributed to airplane travel, 60 reported having at least one attack occur during the landing phase.
Data Source: A questionnaire-based study of 63 people with headache attributed to airplane travel.
Disclosures: Dr. Mainardi said that he had no relevant financial disclosures.
ADHD Stimulants May Not Delay Male Puberty
DENVER – Although some studies show a delay in growth among boys taking stimulants for attention-deficit/hyperactivity disorder, the medications may not postpone pubertal onset, a new study has shown.
“Given that growth has been associated with pubertal onset, one might hypothesize that stimulant medication might affect the onset of puberty,” Jennifer M. Steffes said at the meeting. “Few data exist, however, as to the potential association.”
Ms. Steffes and her colleagues studied a multiethnic cohort of 3,868 boys who were seen at 141 clinical practices in the SSCIB (Secondary Sexual Characteristics in Boys) study. In all, 277 (7%) were taking stimulant medication. Clinicians received standardized training and evaluated genital development, pubic hair growth, and testicular volume for these boys (aged 6-16 years).
There were no significant differences between medicated and nonmedicated participants. The mean onset of genital growth (Tanner stage II) in the stimulant group was 9.84 years vs. 9.85 years in the nonstimulant group. The mean onset of pubic hair (Tanner stage II) in the stimulant group was 11.49 years vs. 11.14 years, and testicular volume of 3 mL or greater was observed in the stimulant group at a median 10.11 years, compared with 9.80 years among those who were not taking stimulant medication.
“Our results suggest that there is no difference in age of pubertal onset between boys taking stimulant medication and their nonmedicated counterparts,” Ms. Steffes said.
“For clinicians, our research should be used as reassurance to parents – should stimulant medication be recommended – that the use of these stimulants will not delay pubertal maturation,” said Ms. Steffes, an investigator for the PROS (Pediatric Research in Office Settings) research network at the American Academy of Pediatrics.
In addition, there were no significant differences in age of pubertal onset by race or ethnicity. The study included 1,979 white, 963 black, and 926 Hispanic children. Consecutive children and adolescents who were seen for well-child visits in 2005-2010 in 41 states were recruited through practices that participated in PROS, the Academic Pediatric Association's CORNET (Continuity Research Network), and the NMA PedsNet (National Medical Association's Pediatric Research Network).
Participants in the stimulant cohort took the medications regularly for 3 consecutive months within the past year. Testicular volume measurements were standardized via a modified Prader orchidometer.
Rigorous clinician training, use of the orchidometer, and inclusion of a broadly-representative geographic sample of children are among the strengths of the study, Ms. Steffes said. Limitations include its cross-sectional design. Also, stimulant use was reported from multiple sources (chart review and self- or parent report).
A meeting attendee asked about the science behind the evidence pointing to delayed growth with stimulant medications. Ms. Steffes deferred to a study coauthor in the audience.
“There [are some] data for a number of psychoactive medications possibly altering growth hormone release,” Dr. Steven A. Dowshen said. “The problem with the studies is … there really is inconsistency in terms of effects [of stimulants] on linear growth, although those [children] who show it tend to show a slowing of linear growth. The commonly accepted end point, though, is that eventually those kids catch up.
“That brings up the possibility, certainly to an endocrinologist, that the effects on growth might be mediated by delayed puberty. So in essence, the drug might be creating a constitutional growth delay,” added Dr. Dowshen, a private practice pediatric endocrinologist in Wilmington, Del. “One of the reasons we were interested in looking at the data from PROS was to [test] that hypothesis. And that wasn't the case.”
Ms. Steffes said she received a research grant from Pfizer to fund this project.
DENVER – Although some studies show a delay in growth among boys taking stimulants for attention-deficit/hyperactivity disorder, the medications may not postpone pubertal onset, a new study has shown.
“Given that growth has been associated with pubertal onset, one might hypothesize that stimulant medication might affect the onset of puberty,” Jennifer M. Steffes said at the meeting. “Few data exist, however, as to the potential association.”
Ms. Steffes and her colleagues studied a multiethnic cohort of 3,868 boys who were seen at 141 clinical practices in the SSCIB (Secondary Sexual Characteristics in Boys) study. In all, 277 (7%) were taking stimulant medication. Clinicians received standardized training and evaluated genital development, pubic hair growth, and testicular volume for these boys (aged 6-16 years).
There were no significant differences between medicated and nonmedicated participants. The mean onset of genital growth (Tanner stage II) in the stimulant group was 9.84 years vs. 9.85 years in the nonstimulant group. The mean onset of pubic hair (Tanner stage II) in the stimulant group was 11.49 years vs. 11.14 years, and testicular volume of 3 mL or greater was observed in the stimulant group at a median 10.11 years, compared with 9.80 years among those who were not taking stimulant medication.
“Our results suggest that there is no difference in age of pubertal onset between boys taking stimulant medication and their nonmedicated counterparts,” Ms. Steffes said.
“For clinicians, our research should be used as reassurance to parents – should stimulant medication be recommended – that the use of these stimulants will not delay pubertal maturation,” said Ms. Steffes, an investigator for the PROS (Pediatric Research in Office Settings) research network at the American Academy of Pediatrics.
In addition, there were no significant differences in age of pubertal onset by race or ethnicity. The study included 1,979 white, 963 black, and 926 Hispanic children. Consecutive children and adolescents who were seen for well-child visits in 2005-2010 in 41 states were recruited through practices that participated in PROS, the Academic Pediatric Association's CORNET (Continuity Research Network), and the NMA PedsNet (National Medical Association's Pediatric Research Network).
Participants in the stimulant cohort took the medications regularly for 3 consecutive months within the past year. Testicular volume measurements were standardized via a modified Prader orchidometer.
Rigorous clinician training, use of the orchidometer, and inclusion of a broadly-representative geographic sample of children are among the strengths of the study, Ms. Steffes said. Limitations include its cross-sectional design. Also, stimulant use was reported from multiple sources (chart review and self- or parent report).
A meeting attendee asked about the science behind the evidence pointing to delayed growth with stimulant medications. Ms. Steffes deferred to a study coauthor in the audience.
“There [are some] data for a number of psychoactive medications possibly altering growth hormone release,” Dr. Steven A. Dowshen said. “The problem with the studies is … there really is inconsistency in terms of effects [of stimulants] on linear growth, although those [children] who show it tend to show a slowing of linear growth. The commonly accepted end point, though, is that eventually those kids catch up.
“That brings up the possibility, certainly to an endocrinologist, that the effects on growth might be mediated by delayed puberty. So in essence, the drug might be creating a constitutional growth delay,” added Dr. Dowshen, a private practice pediatric endocrinologist in Wilmington, Del. “One of the reasons we were interested in looking at the data from PROS was to [test] that hypothesis. And that wasn't the case.”
Ms. Steffes said she received a research grant from Pfizer to fund this project.
DENVER – Although some studies show a delay in growth among boys taking stimulants for attention-deficit/hyperactivity disorder, the medications may not postpone pubertal onset, a new study has shown.
“Given that growth has been associated with pubertal onset, one might hypothesize that stimulant medication might affect the onset of puberty,” Jennifer M. Steffes said at the meeting. “Few data exist, however, as to the potential association.”
Ms. Steffes and her colleagues studied a multiethnic cohort of 3,868 boys who were seen at 141 clinical practices in the SSCIB (Secondary Sexual Characteristics in Boys) study. In all, 277 (7%) were taking stimulant medication. Clinicians received standardized training and evaluated genital development, pubic hair growth, and testicular volume for these boys (aged 6-16 years).
There were no significant differences between medicated and nonmedicated participants. The mean onset of genital growth (Tanner stage II) in the stimulant group was 9.84 years vs. 9.85 years in the nonstimulant group. The mean onset of pubic hair (Tanner stage II) in the stimulant group was 11.49 years vs. 11.14 years, and testicular volume of 3 mL or greater was observed in the stimulant group at a median 10.11 years, compared with 9.80 years among those who were not taking stimulant medication.
“Our results suggest that there is no difference in age of pubertal onset between boys taking stimulant medication and their nonmedicated counterparts,” Ms. Steffes said.
“For clinicians, our research should be used as reassurance to parents – should stimulant medication be recommended – that the use of these stimulants will not delay pubertal maturation,” said Ms. Steffes, an investigator for the PROS (Pediatric Research in Office Settings) research network at the American Academy of Pediatrics.
In addition, there were no significant differences in age of pubertal onset by race or ethnicity. The study included 1,979 white, 963 black, and 926 Hispanic children. Consecutive children and adolescents who were seen for well-child visits in 2005-2010 in 41 states were recruited through practices that participated in PROS, the Academic Pediatric Association's CORNET (Continuity Research Network), and the NMA PedsNet (National Medical Association's Pediatric Research Network).
Participants in the stimulant cohort took the medications regularly for 3 consecutive months within the past year. Testicular volume measurements were standardized via a modified Prader orchidometer.
Rigorous clinician training, use of the orchidometer, and inclusion of a broadly-representative geographic sample of children are among the strengths of the study, Ms. Steffes said. Limitations include its cross-sectional design. Also, stimulant use was reported from multiple sources (chart review and self- or parent report).
A meeting attendee asked about the science behind the evidence pointing to delayed growth with stimulant medications. Ms. Steffes deferred to a study coauthor in the audience.
“There [are some] data for a number of psychoactive medications possibly altering growth hormone release,” Dr. Steven A. Dowshen said. “The problem with the studies is … there really is inconsistency in terms of effects [of stimulants] on linear growth, although those [children] who show it tend to show a slowing of linear growth. The commonly accepted end point, though, is that eventually those kids catch up.
“That brings up the possibility, certainly to an endocrinologist, that the effects on growth might be mediated by delayed puberty. So in essence, the drug might be creating a constitutional growth delay,” added Dr. Dowshen, a private practice pediatric endocrinologist in Wilmington, Del. “One of the reasons we were interested in looking at the data from PROS was to [test] that hypothesis. And that wasn't the case.”
Ms. Steffes said she received a research grant from Pfizer to fund this project.
From the Annual Meeting of the Pediatric Academic Societies
Histrelin Implant May Work for Up to 2 Years
DENVER – A subdermal implant that was approved to treat central precocious puberty for 1 year may in fact last twice as long, according to an ongoing, prospective, observational study.
The histrelin implant suppresses early activation of the hypothalamic-pituitary-gonadal (HPG) axis in children experiencing central precocious puberty, Dr. Katherine A. Lewis said at the meeting Endo Pharmaceuticals' 50-mg Supprelin LA implant accomplishes this through the daily release of 65-mcg histrelin, a potent gonadotropin-releasing hormone analogue (GnRHa).
“If you calculate this out, theoretically it could maintain [HPG axis] suppression for 2 years,” Dr. Lewis said.
The researchers enrolled 32 children with a clinical or biochemical diagnosis of central precocious puberty. They then assessed the 7 boys and 25 girls at baseline and every 6 months for growth and pubertal stage.
So far, 29 children have completed 1 year of the study and 18 have completed the full 24 months. Bone age x-rays were taken at baseline and at 12 and 24 months.
Ultrasensitive luteinizing hormone (LH) testing was performed at 6 and 18 months. Any patient with an ultrasensitive LH value greater than 1 IU/L also underwent a GnRHa stimulation test. Otherwise, participants had GnRHa stimulation testing at 12 and 24 months.
Peak LH was 0.9 IU/L at 1 year (range, 0.2-2.2), well within the definition of HPG suppression used in the study (peak LH less than 4.0 IU/L). The researchers found that peak LH was 1.0 IU/L at 24 months. “So clearly all patients had HPG axis suppression on their stimulation tests,” said Dr. Lewis, a pediatric endocrinology fellow at Riley Hospital for Children, Indianapolis.
“The histrelin implant maintains continued HPG axis suppression when left in place for 2 years,” Dr. Lewis said. “Obviously, this has some implications for clinical care and could potentially lead to reduced cost and reduced number of procedures for patients undergoing treatment for central precocious puberty.”
Implants were removed before the end of the study in two patients who demonstrated progression of puberty, Dr. Lewis said. For example, one patient had the implant removed at 18 months because of increasing breast development and advancing bone age. The other patient had the implant removed at 22 months because of increasing breast development. However, both patients still demonstrated complete biochemical HPG axis suppression according to GnRHa stimulation testing just prior to implant removal (peak LH values of 0.04 IU/L and 0.06 IU/L, respectively).
“We are looking at [those data] for additional information that will give us any idea why” these two patients progressed despite the biochemical suppression, Dr. Lewis said. An initial theory about androgen excess was not supported. Both patients did have significant weight gain during the study, she added.
In all, 19 children were naive to treatment and 13 were previously treated with depot leuprolide, Dr. Lewis said. Mean age at implantation time was 7.2 years (range, 2.5-10.8 years). Median weight was 30 kg. Two girls had a history of menarche, but no patient achieved menarche during the study.
The bone age to chronological age ratio at 12 months was 1.25 vs. 1.22 at 24 months. “This was a mild difference and not statically significant,” Dr. Lewis said.
DENVER – A subdermal implant that was approved to treat central precocious puberty for 1 year may in fact last twice as long, according to an ongoing, prospective, observational study.
The histrelin implant suppresses early activation of the hypothalamic-pituitary-gonadal (HPG) axis in children experiencing central precocious puberty, Dr. Katherine A. Lewis said at the meeting Endo Pharmaceuticals' 50-mg Supprelin LA implant accomplishes this through the daily release of 65-mcg histrelin, a potent gonadotropin-releasing hormone analogue (GnRHa).
“If you calculate this out, theoretically it could maintain [HPG axis] suppression for 2 years,” Dr. Lewis said.
The researchers enrolled 32 children with a clinical or biochemical diagnosis of central precocious puberty. They then assessed the 7 boys and 25 girls at baseline and every 6 months for growth and pubertal stage.
So far, 29 children have completed 1 year of the study and 18 have completed the full 24 months. Bone age x-rays were taken at baseline and at 12 and 24 months.
Ultrasensitive luteinizing hormone (LH) testing was performed at 6 and 18 months. Any patient with an ultrasensitive LH value greater than 1 IU/L also underwent a GnRHa stimulation test. Otherwise, participants had GnRHa stimulation testing at 12 and 24 months.
Peak LH was 0.9 IU/L at 1 year (range, 0.2-2.2), well within the definition of HPG suppression used in the study (peak LH less than 4.0 IU/L). The researchers found that peak LH was 1.0 IU/L at 24 months. “So clearly all patients had HPG axis suppression on their stimulation tests,” said Dr. Lewis, a pediatric endocrinology fellow at Riley Hospital for Children, Indianapolis.
“The histrelin implant maintains continued HPG axis suppression when left in place for 2 years,” Dr. Lewis said. “Obviously, this has some implications for clinical care and could potentially lead to reduced cost and reduced number of procedures for patients undergoing treatment for central precocious puberty.”
Implants were removed before the end of the study in two patients who demonstrated progression of puberty, Dr. Lewis said. For example, one patient had the implant removed at 18 months because of increasing breast development and advancing bone age. The other patient had the implant removed at 22 months because of increasing breast development. However, both patients still demonstrated complete biochemical HPG axis suppression according to GnRHa stimulation testing just prior to implant removal (peak LH values of 0.04 IU/L and 0.06 IU/L, respectively).
“We are looking at [those data] for additional information that will give us any idea why” these two patients progressed despite the biochemical suppression, Dr. Lewis said. An initial theory about androgen excess was not supported. Both patients did have significant weight gain during the study, she added.
In all, 19 children were naive to treatment and 13 were previously treated with depot leuprolide, Dr. Lewis said. Mean age at implantation time was 7.2 years (range, 2.5-10.8 years). Median weight was 30 kg. Two girls had a history of menarche, but no patient achieved menarche during the study.
The bone age to chronological age ratio at 12 months was 1.25 vs. 1.22 at 24 months. “This was a mild difference and not statically significant,” Dr. Lewis said.
DENVER – A subdermal implant that was approved to treat central precocious puberty for 1 year may in fact last twice as long, according to an ongoing, prospective, observational study.
The histrelin implant suppresses early activation of the hypothalamic-pituitary-gonadal (HPG) axis in children experiencing central precocious puberty, Dr. Katherine A. Lewis said at the meeting Endo Pharmaceuticals' 50-mg Supprelin LA implant accomplishes this through the daily release of 65-mcg histrelin, a potent gonadotropin-releasing hormone analogue (GnRHa).
“If you calculate this out, theoretically it could maintain [HPG axis] suppression for 2 years,” Dr. Lewis said.
The researchers enrolled 32 children with a clinical or biochemical diagnosis of central precocious puberty. They then assessed the 7 boys and 25 girls at baseline and every 6 months for growth and pubertal stage.
So far, 29 children have completed 1 year of the study and 18 have completed the full 24 months. Bone age x-rays were taken at baseline and at 12 and 24 months.
Ultrasensitive luteinizing hormone (LH) testing was performed at 6 and 18 months. Any patient with an ultrasensitive LH value greater than 1 IU/L also underwent a GnRHa stimulation test. Otherwise, participants had GnRHa stimulation testing at 12 and 24 months.
Peak LH was 0.9 IU/L at 1 year (range, 0.2-2.2), well within the definition of HPG suppression used in the study (peak LH less than 4.0 IU/L). The researchers found that peak LH was 1.0 IU/L at 24 months. “So clearly all patients had HPG axis suppression on their stimulation tests,” said Dr. Lewis, a pediatric endocrinology fellow at Riley Hospital for Children, Indianapolis.
“The histrelin implant maintains continued HPG axis suppression when left in place for 2 years,” Dr. Lewis said. “Obviously, this has some implications for clinical care and could potentially lead to reduced cost and reduced number of procedures for patients undergoing treatment for central precocious puberty.”
Implants were removed before the end of the study in two patients who demonstrated progression of puberty, Dr. Lewis said. For example, one patient had the implant removed at 18 months because of increasing breast development and advancing bone age. The other patient had the implant removed at 22 months because of increasing breast development. However, both patients still demonstrated complete biochemical HPG axis suppression according to GnRHa stimulation testing just prior to implant removal (peak LH values of 0.04 IU/L and 0.06 IU/L, respectively).
“We are looking at [those data] for additional information that will give us any idea why” these two patients progressed despite the biochemical suppression, Dr. Lewis said. An initial theory about androgen excess was not supported. Both patients did have significant weight gain during the study, she added.
In all, 19 children were naive to treatment and 13 were previously treated with depot leuprolide, Dr. Lewis said. Mean age at implantation time was 7.2 years (range, 2.5-10.8 years). Median weight was 30 kg. Two girls had a history of menarche, but no patient achieved menarche during the study.
The bone age to chronological age ratio at 12 months was 1.25 vs. 1.22 at 24 months. “This was a mild difference and not statically significant,” Dr. Lewis said.
FROM THE ANNUAL MEETING OF THE PEDIATRIC ACADEMIC SOCIETIES
Major Finding: Peak luteinizing hormone levels were 0.9 IU/L
at 1 year and 1.0 IU/L at 2 years, indicating continued suppression of
the HPG axis.
Data Source: Ongoing, prospective, observational study of 32 children with a histrelin implant placed for central precocious puberty.
Disclosures: The study was unfunded. Dr. Lewis said that she had no relevant disclosures.
AAP: Community Health Activity Has Declined
Major Finding: Forty percent of pediatricians reported involvement in child health in their communities in 2010, compared with 45% in 2004.
Data Source: American Academy of Pediatrics periodic surveys for 2004 and 2010.
Disclosures: Dr. Minkovitz said she had no relevant financial disclosures.
Fewer pediatricians participated in community child health initiatives in 2010 than in 2004, according to a study that compared two periodic American Academy of Pediatrics surveys.
In 2010, 40% of 820 pediatricians reported caring for children in their community (other than their own patients). This figure significantly decreased from 45% of 881 who reported such involvement in 2004, Dr. Cynthia S. Minkovitz said.
“The bad news is the rate is going down. The good news is we're higher than other specialties, at least 10 percentage points higher than others,” Dr. Minkovitz said in response to a question at the annual meeting of the Pediatric Academic Societies.
Despite the decrease, perspectives regarding the importance of community pediatrics remained unchanged, Dr. Minkovitz said. “More than three-quarters feel 'moderately' or 'very responsible' for child health in both years.”
Of those who did get involved in child health outside their day-to-day practices, a greater percentage of pediatricians did so as unpaid volunteers: 86% in 2010 vs. 80% in 2004, according to this study contrasting two national, mailed surveys.
Practice constraints and changing demographics in the pediatrician workforce may play a role. Older age, not having children of their own 5 years or younger, and practicing in a rural setting were factors associated with community involvement. For example, 47% of pediatricians older than 50 years reported involvement, compared with 44% of those aged 40-50 years, 40% of those 35-39 years, and 33% of those 34 years or younger.
Women comprised a greater percentage of survey respondents in 2010, 59%, vs. 52% in 2004. The percentage of pediatricians who said general pediatrics accounts for more than half of their practice was 67% in 2010, down from 72% in 2004. Likewise, the percentage who reported a rural practice was 9% in 2010, vs. 13% in 2004.
In addition, more respondents in 2010 reported receiving formal training in community pediatrics before medical school (5% vs. 3%) and during residency (28% vs. 22%), compared with respondents in 2004, said Dr. Minkovitz, director of the women's and children's health policy center at the Johns Hopkins Bloomberg School of Public Health in Baltimore.
In a multivariate analysis, formal training (odds ratio 2.10) and older age (OR 1.38) were significant, independent predictors associated with community child health involvement.
The response rates of 58% and 60% for the two surveys are consistent with rates from other national physician surveys, and represent a strength of the study.
Major Finding: Forty percent of pediatricians reported involvement in child health in their communities in 2010, compared with 45% in 2004.
Data Source: American Academy of Pediatrics periodic surveys for 2004 and 2010.
Disclosures: Dr. Minkovitz said she had no relevant financial disclosures.
Fewer pediatricians participated in community child health initiatives in 2010 than in 2004, according to a study that compared two periodic American Academy of Pediatrics surveys.
In 2010, 40% of 820 pediatricians reported caring for children in their community (other than their own patients). This figure significantly decreased from 45% of 881 who reported such involvement in 2004, Dr. Cynthia S. Minkovitz said.
“The bad news is the rate is going down. The good news is we're higher than other specialties, at least 10 percentage points higher than others,” Dr. Minkovitz said in response to a question at the annual meeting of the Pediatric Academic Societies.
Despite the decrease, perspectives regarding the importance of community pediatrics remained unchanged, Dr. Minkovitz said. “More than three-quarters feel 'moderately' or 'very responsible' for child health in both years.”
Of those who did get involved in child health outside their day-to-day practices, a greater percentage of pediatricians did so as unpaid volunteers: 86% in 2010 vs. 80% in 2004, according to this study contrasting two national, mailed surveys.
Practice constraints and changing demographics in the pediatrician workforce may play a role. Older age, not having children of their own 5 years or younger, and practicing in a rural setting were factors associated with community involvement. For example, 47% of pediatricians older than 50 years reported involvement, compared with 44% of those aged 40-50 years, 40% of those 35-39 years, and 33% of those 34 years or younger.
Women comprised a greater percentage of survey respondents in 2010, 59%, vs. 52% in 2004. The percentage of pediatricians who said general pediatrics accounts for more than half of their practice was 67% in 2010, down from 72% in 2004. Likewise, the percentage who reported a rural practice was 9% in 2010, vs. 13% in 2004.
In addition, more respondents in 2010 reported receiving formal training in community pediatrics before medical school (5% vs. 3%) and during residency (28% vs. 22%), compared with respondents in 2004, said Dr. Minkovitz, director of the women's and children's health policy center at the Johns Hopkins Bloomberg School of Public Health in Baltimore.
In a multivariate analysis, formal training (odds ratio 2.10) and older age (OR 1.38) were significant, independent predictors associated with community child health involvement.
The response rates of 58% and 60% for the two surveys are consistent with rates from other national physician surveys, and represent a strength of the study.
Major Finding: Forty percent of pediatricians reported involvement in child health in their communities in 2010, compared with 45% in 2004.
Data Source: American Academy of Pediatrics periodic surveys for 2004 and 2010.
Disclosures: Dr. Minkovitz said she had no relevant financial disclosures.
Fewer pediatricians participated in community child health initiatives in 2010 than in 2004, according to a study that compared two periodic American Academy of Pediatrics surveys.
In 2010, 40% of 820 pediatricians reported caring for children in their community (other than their own patients). This figure significantly decreased from 45% of 881 who reported such involvement in 2004, Dr. Cynthia S. Minkovitz said.
“The bad news is the rate is going down. The good news is we're higher than other specialties, at least 10 percentage points higher than others,” Dr. Minkovitz said in response to a question at the annual meeting of the Pediatric Academic Societies.
Despite the decrease, perspectives regarding the importance of community pediatrics remained unchanged, Dr. Minkovitz said. “More than three-quarters feel 'moderately' or 'very responsible' for child health in both years.”
Of those who did get involved in child health outside their day-to-day practices, a greater percentage of pediatricians did so as unpaid volunteers: 86% in 2010 vs. 80% in 2004, according to this study contrasting two national, mailed surveys.
Practice constraints and changing demographics in the pediatrician workforce may play a role. Older age, not having children of their own 5 years or younger, and practicing in a rural setting were factors associated with community involvement. For example, 47% of pediatricians older than 50 years reported involvement, compared with 44% of those aged 40-50 years, 40% of those 35-39 years, and 33% of those 34 years or younger.
Women comprised a greater percentage of survey respondents in 2010, 59%, vs. 52% in 2004. The percentage of pediatricians who said general pediatrics accounts for more than half of their practice was 67% in 2010, down from 72% in 2004. Likewise, the percentage who reported a rural practice was 9% in 2010, vs. 13% in 2004.
In addition, more respondents in 2010 reported receiving formal training in community pediatrics before medical school (5% vs. 3%) and during residency (28% vs. 22%), compared with respondents in 2004, said Dr. Minkovitz, director of the women's and children's health policy center at the Johns Hopkins Bloomberg School of Public Health in Baltimore.
In a multivariate analysis, formal training (odds ratio 2.10) and older age (OR 1.38) were significant, independent predictors associated with community child health involvement.
The response rates of 58% and 60% for the two surveys are consistent with rates from other national physician surveys, and represent a strength of the study.
Buprenorphine Beats Tramadol as Heroin Detox
BOCA RATON, FLA. – Not all agents available to detoxify a person with a heroin addiction are created equal.
In a prospective comparison study, people who took buprenorphine experienced significantly fewer withdrawal symptoms and fewer serious adverse events over 10 days, compared with detoxification with tramadol.
Previous retrospective studies showed that buprenorphine was more effective than tramadol for acute heroin withdrawal, Dr. Jatinder M. Chawla said (Am. J. Addict. 2006;15:186-91; J. Addict. Dis. 2003;22:5-12). However, "there are some problems with buprenorphine," such as more abuse potential and a greater risk for respiratory depression, compared with tramadol, said Dr. Chawla, a psychiatry resident at SUNY Downstate Medical Center in Brooklyn, N.Y.
Also, tramadol is easier to administer in an outpatient setting because it’s an oral, nonscheduled medication compared with the sublingual, schedule III buprenorphine.
"We wanted to look at this in a prospective study," Dr. Chawla said in an interview at the annual meeting of the New Clinical Drug Evaluation Unit, sponsored by the National Institute of Mental Health.
Dr. Chawla and his associates assessed 62 men with a diagnosis of opiate dependence syndrome who had been admitted to the National Drug Dependence Treatment Centre in New Delhi, India. They were equally randomized to 10 days of buprenorphine or tramadol. Participants were aged 20-45 years. In all, 39 patients completed the 10-day study and were assessed further. Retention was not significantly different, with 21 buprenorphine and 18 tramadol patients remaining until study end.
No significant differences were found between groups in baseline Addiction Severity Index score; mean age of initiation of heroin use; duration of daily use; or average intake of heroin in the past month.
However, the researchers did find significant differences on the Subjective (SOWS) and Objective Opioid Withdrawal Scale (OOWS) scores. For example, the mean SOWS score was significantly lower in the buprenorphine group on the second, third, and ninth days of detoxification (suggesting greater efficacy). In addition, the mean OOWS score was significantly lower on days 2 and 3 in the buprenorphine group, compared with the tramadol group.
Participants also completed a visual analog scale daily to rate their satisfaction with treatment. Again, on days 2 and 3 of detoxification, people taking buprenorphine rated their satisfaction significantly higher than those taking tramadol.
Three patients in the tramadol group experienced seizures. "Tramadol has the risk of inducing seizures at higher doses," Dr. Chawla said. The seizures occurred on days 4 and 6, when drug was tapered up to a higher dose, he added.
Nausea and dizziness also were reported by people in the tramadol group. Headache, drowsiness, and dizziness were the most common adverse event reports in the buprenorphine group.
Despite these findings, Dr. Chawla said that tramadol still has advantages over buprenorphine and is not absolutely contraindicated. Additional caution is warranted for people with a history of seizures. Tramadol could be an option for patients with mild to moderate heroin dependence who are at risk of becoming addicted to buprenorphine, he said. In addition, a lower dose of tramadol could potentially minimize adverse events.
A small sample size and data from a single center are potential limitations of the study, Dr. Chawla said.
The study was unfunded. Dr. Chawla received a New Investigator Award at the NCDEU meeting for this study. He said he had no relevant financial disclosures.
BOCA RATON, FLA. – Not all agents available to detoxify a person with a heroin addiction are created equal.
In a prospective comparison study, people who took buprenorphine experienced significantly fewer withdrawal symptoms and fewer serious adverse events over 10 days, compared with detoxification with tramadol.
Previous retrospective studies showed that buprenorphine was more effective than tramadol for acute heroin withdrawal, Dr. Jatinder M. Chawla said (Am. J. Addict. 2006;15:186-91; J. Addict. Dis. 2003;22:5-12). However, "there are some problems with buprenorphine," such as more abuse potential and a greater risk for respiratory depression, compared with tramadol, said Dr. Chawla, a psychiatry resident at SUNY Downstate Medical Center in Brooklyn, N.Y.
Also, tramadol is easier to administer in an outpatient setting because it’s an oral, nonscheduled medication compared with the sublingual, schedule III buprenorphine.
"We wanted to look at this in a prospective study," Dr. Chawla said in an interview at the annual meeting of the New Clinical Drug Evaluation Unit, sponsored by the National Institute of Mental Health.
Dr. Chawla and his associates assessed 62 men with a diagnosis of opiate dependence syndrome who had been admitted to the National Drug Dependence Treatment Centre in New Delhi, India. They were equally randomized to 10 days of buprenorphine or tramadol. Participants were aged 20-45 years. In all, 39 patients completed the 10-day study and were assessed further. Retention was not significantly different, with 21 buprenorphine and 18 tramadol patients remaining until study end.
No significant differences were found between groups in baseline Addiction Severity Index score; mean age of initiation of heroin use; duration of daily use; or average intake of heroin in the past month.
However, the researchers did find significant differences on the Subjective (SOWS) and Objective Opioid Withdrawal Scale (OOWS) scores. For example, the mean SOWS score was significantly lower in the buprenorphine group on the second, third, and ninth days of detoxification (suggesting greater efficacy). In addition, the mean OOWS score was significantly lower on days 2 and 3 in the buprenorphine group, compared with the tramadol group.
Participants also completed a visual analog scale daily to rate their satisfaction with treatment. Again, on days 2 and 3 of detoxification, people taking buprenorphine rated their satisfaction significantly higher than those taking tramadol.
Three patients in the tramadol group experienced seizures. "Tramadol has the risk of inducing seizures at higher doses," Dr. Chawla said. The seizures occurred on days 4 and 6, when drug was tapered up to a higher dose, he added.
Nausea and dizziness also were reported by people in the tramadol group. Headache, drowsiness, and dizziness were the most common adverse event reports in the buprenorphine group.
Despite these findings, Dr. Chawla said that tramadol still has advantages over buprenorphine and is not absolutely contraindicated. Additional caution is warranted for people with a history of seizures. Tramadol could be an option for patients with mild to moderate heroin dependence who are at risk of becoming addicted to buprenorphine, he said. In addition, a lower dose of tramadol could potentially minimize adverse events.
A small sample size and data from a single center are potential limitations of the study, Dr. Chawla said.
The study was unfunded. Dr. Chawla received a New Investigator Award at the NCDEU meeting for this study. He said he had no relevant financial disclosures.
BOCA RATON, FLA. – Not all agents available to detoxify a person with a heroin addiction are created equal.
In a prospective comparison study, people who took buprenorphine experienced significantly fewer withdrawal symptoms and fewer serious adverse events over 10 days, compared with detoxification with tramadol.
Previous retrospective studies showed that buprenorphine was more effective than tramadol for acute heroin withdrawal, Dr. Jatinder M. Chawla said (Am. J. Addict. 2006;15:186-91; J. Addict. Dis. 2003;22:5-12). However, "there are some problems with buprenorphine," such as more abuse potential and a greater risk for respiratory depression, compared with tramadol, said Dr. Chawla, a psychiatry resident at SUNY Downstate Medical Center in Brooklyn, N.Y.
Also, tramadol is easier to administer in an outpatient setting because it’s an oral, nonscheduled medication compared with the sublingual, schedule III buprenorphine.
"We wanted to look at this in a prospective study," Dr. Chawla said in an interview at the annual meeting of the New Clinical Drug Evaluation Unit, sponsored by the National Institute of Mental Health.
Dr. Chawla and his associates assessed 62 men with a diagnosis of opiate dependence syndrome who had been admitted to the National Drug Dependence Treatment Centre in New Delhi, India. They were equally randomized to 10 days of buprenorphine or tramadol. Participants were aged 20-45 years. In all, 39 patients completed the 10-day study and were assessed further. Retention was not significantly different, with 21 buprenorphine and 18 tramadol patients remaining until study end.
No significant differences were found between groups in baseline Addiction Severity Index score; mean age of initiation of heroin use; duration of daily use; or average intake of heroin in the past month.
However, the researchers did find significant differences on the Subjective (SOWS) and Objective Opioid Withdrawal Scale (OOWS) scores. For example, the mean SOWS score was significantly lower in the buprenorphine group on the second, third, and ninth days of detoxification (suggesting greater efficacy). In addition, the mean OOWS score was significantly lower on days 2 and 3 in the buprenorphine group, compared with the tramadol group.
Participants also completed a visual analog scale daily to rate their satisfaction with treatment. Again, on days 2 and 3 of detoxification, people taking buprenorphine rated their satisfaction significantly higher than those taking tramadol.
Three patients in the tramadol group experienced seizures. "Tramadol has the risk of inducing seizures at higher doses," Dr. Chawla said. The seizures occurred on days 4 and 6, when drug was tapered up to a higher dose, he added.
Nausea and dizziness also were reported by people in the tramadol group. Headache, drowsiness, and dizziness were the most common adverse event reports in the buprenorphine group.
Despite these findings, Dr. Chawla said that tramadol still has advantages over buprenorphine and is not absolutely contraindicated. Additional caution is warranted for people with a history of seizures. Tramadol could be an option for patients with mild to moderate heroin dependence who are at risk of becoming addicted to buprenorphine, he said. In addition, a lower dose of tramadol could potentially minimize adverse events.
A small sample size and data from a single center are potential limitations of the study, Dr. Chawla said.
The study was unfunded. Dr. Chawla received a New Investigator Award at the NCDEU meeting for this study. He said he had no relevant financial disclosures.
FROM A MEETING OF THE NEW CLINICAL DRUG EVALUATION UNIT SPONSORED BY THE NATIONAL INSTITUTE OF MENTAL HEALTH
Major Finding: Mean subjective withdrawal scores during 10 days of heroin detoxification were significantly lower for buprenorphine vs. tramadol on days 2, 3, and 9.
Data Source: Single center, randomized, prospective study of 62 men with heroin dependence syndrome.
Disclosures: Dr. Chawla said he had no relevant disclosures.
Experimental Autism Spectrum Drug Improves Symptoms
BOCA RATON, FLA. – Social withdrawal and irritability significantly improved when children with autism spectrum disorder took arbaclofen, a new medication in development, according to an open label, multicenter study.
Boosted by promising results with arbaclofen in fragile X syndrome – the leading known cause of inherited autism spectrum disorder (ASD) – Dr. Jeremy M. Veenstra-VanderWeele and his associates launched a study with 32 children and adolescents.
This is the first step to determine whether the GABA-B agonist would help people with ASD who do not have fragile X syndrome, Dr. Veenstra-VanderWeele said in an interview at the annual meeting of the New Clinical Drug Evaluation Unit sponsored by the National Institute of Mental Health.
Children showed significant improvement on the Aberrant Behavior Checklist social withdrawal subscale, from a mean 18.1 at baseline to 12.6 after 8 weeks, based on an intent-to-treat analysis. In addition, the researchers rated more than half – 20 of the 32 kids – as "much improved" or "very much improved" on the Clinical Global Impression for Improvement measure.
At the same time, mean scores on the Aberrant Behavior Checklist Irritability subscale significantly improved from 24.7 to 17.3.
"We saw a lot of promising improvements in people who were taking the medicine," said Dr. Veenstra-VanderWeele, assistant professor in psychiatry at Vanderbilt University in Nashville.
"We did see some adverse events, as you would expect. None of these were terribly severe, and most of them looked similar to fluctuations in peoples’ baseline behavior," Dr. Veenstra-VanderWeele said. One severe adverse event was increased aggression during a planned taper of arbaclofen.
"The medicine was very well tolerated, especially in contrast to available medicines in autism, which, unfortunately, can have significant side effects," Dr. Veenstra-VanderWeele said.
Two participants discontinued because of increased agitation or aggression, and another five discontinued for other reasons, so 25 children and adolescents aged 6 years to 17 years completed the 8-week study. All participants met DSM-IV and Autism Diagnostic Interview (ADI-R) for autism spectrum disorder.
A double-blind, placebo-controlled study with up to 150 people is underway to confirm these results, Dr. Veenstra-VanderWeele said. When the Food and Drug Administration might approve arbaclofen for treatment of ASD is difficult to determine, he added. "The study initiating now will probably take about 6 months. Then I would anticipate there would be one more follow-up study if that study is positive."
"One really positive thing is this agent ... is closely related to a medication that has been available for decades: baclofen," Dr. Veenstra-VanderWeele said. "Because of that, the safety profile is fairly easy to predict, in contrast to a lot of investigational agents where you really have no idea going in."
Seaside Therapeutics funded the study. Dr. Veenstra-VanderWeele said he receives research funding from Seaside Therapeutics, Novartis, and Roche Pharmaceuticals.
BOCA RATON, FLA. – Social withdrawal and irritability significantly improved when children with autism spectrum disorder took arbaclofen, a new medication in development, according to an open label, multicenter study.
Boosted by promising results with arbaclofen in fragile X syndrome – the leading known cause of inherited autism spectrum disorder (ASD) – Dr. Jeremy M. Veenstra-VanderWeele and his associates launched a study with 32 children and adolescents.
This is the first step to determine whether the GABA-B agonist would help people with ASD who do not have fragile X syndrome, Dr. Veenstra-VanderWeele said in an interview at the annual meeting of the New Clinical Drug Evaluation Unit sponsored by the National Institute of Mental Health.
Children showed significant improvement on the Aberrant Behavior Checklist social withdrawal subscale, from a mean 18.1 at baseline to 12.6 after 8 weeks, based on an intent-to-treat analysis. In addition, the researchers rated more than half – 20 of the 32 kids – as "much improved" or "very much improved" on the Clinical Global Impression for Improvement measure.
At the same time, mean scores on the Aberrant Behavior Checklist Irritability subscale significantly improved from 24.7 to 17.3.
"We saw a lot of promising improvements in people who were taking the medicine," said Dr. Veenstra-VanderWeele, assistant professor in psychiatry at Vanderbilt University in Nashville.
"We did see some adverse events, as you would expect. None of these were terribly severe, and most of them looked similar to fluctuations in peoples’ baseline behavior," Dr. Veenstra-VanderWeele said. One severe adverse event was increased aggression during a planned taper of arbaclofen.
"The medicine was very well tolerated, especially in contrast to available medicines in autism, which, unfortunately, can have significant side effects," Dr. Veenstra-VanderWeele said.
Two participants discontinued because of increased agitation or aggression, and another five discontinued for other reasons, so 25 children and adolescents aged 6 years to 17 years completed the 8-week study. All participants met DSM-IV and Autism Diagnostic Interview (ADI-R) for autism spectrum disorder.
A double-blind, placebo-controlled study with up to 150 people is underway to confirm these results, Dr. Veenstra-VanderWeele said. When the Food and Drug Administration might approve arbaclofen for treatment of ASD is difficult to determine, he added. "The study initiating now will probably take about 6 months. Then I would anticipate there would be one more follow-up study if that study is positive."
"One really positive thing is this agent ... is closely related to a medication that has been available for decades: baclofen," Dr. Veenstra-VanderWeele said. "Because of that, the safety profile is fairly easy to predict, in contrast to a lot of investigational agents where you really have no idea going in."
Seaside Therapeutics funded the study. Dr. Veenstra-VanderWeele said he receives research funding from Seaside Therapeutics, Novartis, and Roche Pharmaceuticals.
BOCA RATON, FLA. – Social withdrawal and irritability significantly improved when children with autism spectrum disorder took arbaclofen, a new medication in development, according to an open label, multicenter study.
Boosted by promising results with arbaclofen in fragile X syndrome – the leading known cause of inherited autism spectrum disorder (ASD) – Dr. Jeremy M. Veenstra-VanderWeele and his associates launched a study with 32 children and adolescents.
This is the first step to determine whether the GABA-B agonist would help people with ASD who do not have fragile X syndrome, Dr. Veenstra-VanderWeele said in an interview at the annual meeting of the New Clinical Drug Evaluation Unit sponsored by the National Institute of Mental Health.
Children showed significant improvement on the Aberrant Behavior Checklist social withdrawal subscale, from a mean 18.1 at baseline to 12.6 after 8 weeks, based on an intent-to-treat analysis. In addition, the researchers rated more than half – 20 of the 32 kids – as "much improved" or "very much improved" on the Clinical Global Impression for Improvement measure.
At the same time, mean scores on the Aberrant Behavior Checklist Irritability subscale significantly improved from 24.7 to 17.3.
"We saw a lot of promising improvements in people who were taking the medicine," said Dr. Veenstra-VanderWeele, assistant professor in psychiatry at Vanderbilt University in Nashville.
"We did see some adverse events, as you would expect. None of these were terribly severe, and most of them looked similar to fluctuations in peoples’ baseline behavior," Dr. Veenstra-VanderWeele said. One severe adverse event was increased aggression during a planned taper of arbaclofen.
"The medicine was very well tolerated, especially in contrast to available medicines in autism, which, unfortunately, can have significant side effects," Dr. Veenstra-VanderWeele said.
Two participants discontinued because of increased agitation or aggression, and another five discontinued for other reasons, so 25 children and adolescents aged 6 years to 17 years completed the 8-week study. All participants met DSM-IV and Autism Diagnostic Interview (ADI-R) for autism spectrum disorder.
A double-blind, placebo-controlled study with up to 150 people is underway to confirm these results, Dr. Veenstra-VanderWeele said. When the Food and Drug Administration might approve arbaclofen for treatment of ASD is difficult to determine, he added. "The study initiating now will probably take about 6 months. Then I would anticipate there would be one more follow-up study if that study is positive."
"One really positive thing is this agent ... is closely related to a medication that has been available for decades: baclofen," Dr. Veenstra-VanderWeele said. "Because of that, the safety profile is fairly easy to predict, in contrast to a lot of investigational agents where you really have no idea going in."
Seaside Therapeutics funded the study. Dr. Veenstra-VanderWeele said he receives research funding from Seaside Therapeutics, Novartis, and Roche Pharmaceuticals.
FROM THE ANNUAL MEETING OF THE NEW CLINICAL DRUG EVALUATION UNIT
Major Finding: Children treated with arbaclofen significantly improved from a mean 18.1 to 12.6 score on the Aberrant Behavior Checklist Social Withdrawal subscale and from a mean 24.7 to 17.3 on the Irritability subscale after 8 weeks.
Data Source: An intent-to-treat analysis of 32 children in an open label, multicenter study.
Disclosures: Seaside Therapeutics funded the study. Dr. Veenstra-VanderWeele said he receives research funding from Seaside, Novartis, and Roche Pharmaceuticals.
IOM Report on Pain Ignores Rheumatologists
Rheumatologists are on the front lines of pain management, yet they were not consulted by the Institute of Medicine committee that wrote a comprehensive new report on pain.
An estimated 25 million Americans have osteoarthritis and 1.7 million have rheumatoid arthritis, according to the National Institute of Arthritis and Musculoskeletal Diseases. Arguably, these figures place rheumatologists at the eye of the nation’s pain storm.
The report "ignores the fact that there are different types of pain specialists. When they talk about a pain specialist, they are talking about an anesthesia-oriented pain specialist, not those who deal with pain as a specialty, like rheumatology or neurology," Dr. Roy Altman said in an interview. "Because this report was [written by] a predominance of anesthesiologists, a couple of pediatric people, one neurologist, plus a lot of epidemiologists, it doesn’t really approach the people on the front line who are dealing with the pain."
The author specialties are more procedure-oriented toward pain, Dr. Altman said, versus the more nonpharmacologic and pharmacologic approaches taken by internists, other primary care physicians, and rheumatologists.
A greater awareness of pain and its adverse health consequences, improved patient education and self management, and an increased emphasis on prevention are major strategies in a comprehensive new report on pain from the Institute of Medicine (IOM).
Health care providers are among those the report authors task with fostering a transition to better pain management in the United States. "Among steps to improving care, health care providers should increasingly aim at tailoring pain care to each person’s experience, and self management of pain should be promoted. Also, primary care physicians – who handle most front-line pain care – should collaborate with pain specialists in cases where pain persists," according to a brief of the report.
This collaboration is "critical," Dr. Nancy E. Lane said in an interview. "Patients with chronic pain seek out a number of different physicians, the care is not coordinated, and the patients can suffer." Dr. Lane is professor of medicine and rheumatology at the University of California, Davis and director of the UC Davis Center for Healthy Aging.
As part of the 2010 Patient Prevention and Affordable Care Act, the U.S. Department of Health and Human Services charged the IOM with assessment of the state of pain in the United States from a public health perspective. The 19 committee members also prioritized strategies for improvements in the "Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research" report, released in June.
"There is one major problem with the report, and that is the selection of people [who] wrote it. There are no primary care physicians and there are no rheumatologists involved," Dr. Altman, professor emeritus of rheumatology at the University of California, Los Angeles, said in an interview. "In other words, it excludes a lot of the people who treat pain."
The report "won’t change anything in my specialty," Dr. Altman said. "Rheumatologists, as a group, have already titled ourselves as the specialists for pain for the rheumatic diseases.
Dr. Lane was a bit more positive about the impact of the report. "It reminds me to always be vigilant about taking a thorough pain history and talking to my patients about their pain, how they are managing it, and filling in the gaps."
The committee estimated that 116 million Americans experience chronic pain. They state the cost of medical treatment and lost productivity associated with pain in the United States is an estimated $635 billion each year. To reach the vast multitude of people with various types of pain, the nation must adopt a population-level prevention and management strategy, the authors stated.
Strategies include:
• A heightened awareness of pain and its health consequences.
• An emphasis on the prevention of pain.
• Improved pain assessment and management within federal health care and financial programs.
• Patient education on management of their own pain through public health communication strategies.
• Decreasing disparities in the pain experience among subgroups of Americans.
The emphasis on patient self-management of pain also is critical, Dr. Lane said. "Education on pain and how to treat it will empower the patients, just as the arthritis self-help classes have done for years. They improve self efficacy."
"You cannot control pain if the patient does not deal with it," Dr. Altman agreed. "If a patient doesn’t have an investment and take control of their pain, they are not going to get better."
"Fibromyalgia is so prominent throughout the country," he added, "that to think about not having the patient invested in their pain control is really an exercise in futility."
Improvement of pain management and prevention efforts among underdiagnosed and/or undertreated subpopulations is another tenet of the report. Those at risk include surgery and cancer patients; people at the end of life; racial and ethnic minorities; people with lower income and education levels; women, children, and older people; and military veterans. This need is not unique to pain, Dr. Altman said. "That same disparity exists in all medical care. People who are at risk for not having pain control are the people who are at risk for not getting medical care. It’s the same population."
Strategies to reduce barriers to pain care are among the recommendations that should be implemented by the end of 2012, the report committee said. Support of greater collaboration between pain specialists and primary care clinicians also should be established by the end of next year.
In addition, an existing institute within the National Institutes of Health should become the lead institute and responsible for moving pain research forward as well by the end of 2012, the report states. The NIH Pain Consortium also should take a stronger leadership role in fostering the necessary research. Dr. Altman was somewhat pessimistic about these proposals. "They make a recommendation in here that the NIH devotes some specific groups to pain control. Good luck with that in this financial climate."
Ongoing efforts to enact the remaining recommendations in the report, the authors stated, should be finalized by the end of 2015.
Dr. Lane and Dr. Altman said that they had no relevant financial disclosures.
The report is available from the IOM website.
Rheumatologists are on the front lines of pain management, yet they were not consulted by the Institute of Medicine committee that wrote a comprehensive new report on pain.
An estimated 25 million Americans have osteoarthritis and 1.7 million have rheumatoid arthritis, according to the National Institute of Arthritis and Musculoskeletal Diseases. Arguably, these figures place rheumatologists at the eye of the nation’s pain storm.
The report "ignores the fact that there are different types of pain specialists. When they talk about a pain specialist, they are talking about an anesthesia-oriented pain specialist, not those who deal with pain as a specialty, like rheumatology or neurology," Dr. Roy Altman said in an interview. "Because this report was [written by] a predominance of anesthesiologists, a couple of pediatric people, one neurologist, plus a lot of epidemiologists, it doesn’t really approach the people on the front line who are dealing with the pain."
The author specialties are more procedure-oriented toward pain, Dr. Altman said, versus the more nonpharmacologic and pharmacologic approaches taken by internists, other primary care physicians, and rheumatologists.
A greater awareness of pain and its adverse health consequences, improved patient education and self management, and an increased emphasis on prevention are major strategies in a comprehensive new report on pain from the Institute of Medicine (IOM).
Health care providers are among those the report authors task with fostering a transition to better pain management in the United States. "Among steps to improving care, health care providers should increasingly aim at tailoring pain care to each person’s experience, and self management of pain should be promoted. Also, primary care physicians – who handle most front-line pain care – should collaborate with pain specialists in cases where pain persists," according to a brief of the report.
This collaboration is "critical," Dr. Nancy E. Lane said in an interview. "Patients with chronic pain seek out a number of different physicians, the care is not coordinated, and the patients can suffer." Dr. Lane is professor of medicine and rheumatology at the University of California, Davis and director of the UC Davis Center for Healthy Aging.
As part of the 2010 Patient Prevention and Affordable Care Act, the U.S. Department of Health and Human Services charged the IOM with assessment of the state of pain in the United States from a public health perspective. The 19 committee members also prioritized strategies for improvements in the "Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research" report, released in June.
"There is one major problem with the report, and that is the selection of people [who] wrote it. There are no primary care physicians and there are no rheumatologists involved," Dr. Altman, professor emeritus of rheumatology at the University of California, Los Angeles, said in an interview. "In other words, it excludes a lot of the people who treat pain."
The report "won’t change anything in my specialty," Dr. Altman said. "Rheumatologists, as a group, have already titled ourselves as the specialists for pain for the rheumatic diseases.
Dr. Lane was a bit more positive about the impact of the report. "It reminds me to always be vigilant about taking a thorough pain history and talking to my patients about their pain, how they are managing it, and filling in the gaps."
The committee estimated that 116 million Americans experience chronic pain. They state the cost of medical treatment and lost productivity associated with pain in the United States is an estimated $635 billion each year. To reach the vast multitude of people with various types of pain, the nation must adopt a population-level prevention and management strategy, the authors stated.
Strategies include:
• A heightened awareness of pain and its health consequences.
• An emphasis on the prevention of pain.
• Improved pain assessment and management within federal health care and financial programs.
• Patient education on management of their own pain through public health communication strategies.
• Decreasing disparities in the pain experience among subgroups of Americans.
The emphasis on patient self-management of pain also is critical, Dr. Lane said. "Education on pain and how to treat it will empower the patients, just as the arthritis self-help classes have done for years. They improve self efficacy."
"You cannot control pain if the patient does not deal with it," Dr. Altman agreed. "If a patient doesn’t have an investment and take control of their pain, they are not going to get better."
"Fibromyalgia is so prominent throughout the country," he added, "that to think about not having the patient invested in their pain control is really an exercise in futility."
Improvement of pain management and prevention efforts among underdiagnosed and/or undertreated subpopulations is another tenet of the report. Those at risk include surgery and cancer patients; people at the end of life; racial and ethnic minorities; people with lower income and education levels; women, children, and older people; and military veterans. This need is not unique to pain, Dr. Altman said. "That same disparity exists in all medical care. People who are at risk for not having pain control are the people who are at risk for not getting medical care. It’s the same population."
Strategies to reduce barriers to pain care are among the recommendations that should be implemented by the end of 2012, the report committee said. Support of greater collaboration between pain specialists and primary care clinicians also should be established by the end of next year.
In addition, an existing institute within the National Institutes of Health should become the lead institute and responsible for moving pain research forward as well by the end of 2012, the report states. The NIH Pain Consortium also should take a stronger leadership role in fostering the necessary research. Dr. Altman was somewhat pessimistic about these proposals. "They make a recommendation in here that the NIH devotes some specific groups to pain control. Good luck with that in this financial climate."
Ongoing efforts to enact the remaining recommendations in the report, the authors stated, should be finalized by the end of 2015.
Dr. Lane and Dr. Altman said that they had no relevant financial disclosures.
The report is available from the IOM website.
Rheumatologists are on the front lines of pain management, yet they were not consulted by the Institute of Medicine committee that wrote a comprehensive new report on pain.
An estimated 25 million Americans have osteoarthritis and 1.7 million have rheumatoid arthritis, according to the National Institute of Arthritis and Musculoskeletal Diseases. Arguably, these figures place rheumatologists at the eye of the nation’s pain storm.
The report "ignores the fact that there are different types of pain specialists. When they talk about a pain specialist, they are talking about an anesthesia-oriented pain specialist, not those who deal with pain as a specialty, like rheumatology or neurology," Dr. Roy Altman said in an interview. "Because this report was [written by] a predominance of anesthesiologists, a couple of pediatric people, one neurologist, plus a lot of epidemiologists, it doesn’t really approach the people on the front line who are dealing with the pain."
The author specialties are more procedure-oriented toward pain, Dr. Altman said, versus the more nonpharmacologic and pharmacologic approaches taken by internists, other primary care physicians, and rheumatologists.
A greater awareness of pain and its adverse health consequences, improved patient education and self management, and an increased emphasis on prevention are major strategies in a comprehensive new report on pain from the Institute of Medicine (IOM).
Health care providers are among those the report authors task with fostering a transition to better pain management in the United States. "Among steps to improving care, health care providers should increasingly aim at tailoring pain care to each person’s experience, and self management of pain should be promoted. Also, primary care physicians – who handle most front-line pain care – should collaborate with pain specialists in cases where pain persists," according to a brief of the report.
This collaboration is "critical," Dr. Nancy E. Lane said in an interview. "Patients with chronic pain seek out a number of different physicians, the care is not coordinated, and the patients can suffer." Dr. Lane is professor of medicine and rheumatology at the University of California, Davis and director of the UC Davis Center for Healthy Aging.
As part of the 2010 Patient Prevention and Affordable Care Act, the U.S. Department of Health and Human Services charged the IOM with assessment of the state of pain in the United States from a public health perspective. The 19 committee members also prioritized strategies for improvements in the "Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research" report, released in June.
"There is one major problem with the report, and that is the selection of people [who] wrote it. There are no primary care physicians and there are no rheumatologists involved," Dr. Altman, professor emeritus of rheumatology at the University of California, Los Angeles, said in an interview. "In other words, it excludes a lot of the people who treat pain."
The report "won’t change anything in my specialty," Dr. Altman said. "Rheumatologists, as a group, have already titled ourselves as the specialists for pain for the rheumatic diseases.
Dr. Lane was a bit more positive about the impact of the report. "It reminds me to always be vigilant about taking a thorough pain history and talking to my patients about their pain, how they are managing it, and filling in the gaps."
The committee estimated that 116 million Americans experience chronic pain. They state the cost of medical treatment and lost productivity associated with pain in the United States is an estimated $635 billion each year. To reach the vast multitude of people with various types of pain, the nation must adopt a population-level prevention and management strategy, the authors stated.
Strategies include:
• A heightened awareness of pain and its health consequences.
• An emphasis on the prevention of pain.
• Improved pain assessment and management within federal health care and financial programs.
• Patient education on management of their own pain through public health communication strategies.
• Decreasing disparities in the pain experience among subgroups of Americans.
The emphasis on patient self-management of pain also is critical, Dr. Lane said. "Education on pain and how to treat it will empower the patients, just as the arthritis self-help classes have done for years. They improve self efficacy."
"You cannot control pain if the patient does not deal with it," Dr. Altman agreed. "If a patient doesn’t have an investment and take control of their pain, they are not going to get better."
"Fibromyalgia is so prominent throughout the country," he added, "that to think about not having the patient invested in their pain control is really an exercise in futility."
Improvement of pain management and prevention efforts among underdiagnosed and/or undertreated subpopulations is another tenet of the report. Those at risk include surgery and cancer patients; people at the end of life; racial and ethnic minorities; people with lower income and education levels; women, children, and older people; and military veterans. This need is not unique to pain, Dr. Altman said. "That same disparity exists in all medical care. People who are at risk for not having pain control are the people who are at risk for not getting medical care. It’s the same population."
Strategies to reduce barriers to pain care are among the recommendations that should be implemented by the end of 2012, the report committee said. Support of greater collaboration between pain specialists and primary care clinicians also should be established by the end of next year.
In addition, an existing institute within the National Institutes of Health should become the lead institute and responsible for moving pain research forward as well by the end of 2012, the report states. The NIH Pain Consortium also should take a stronger leadership role in fostering the necessary research. Dr. Altman was somewhat pessimistic about these proposals. "They make a recommendation in here that the NIH devotes some specific groups to pain control. Good luck with that in this financial climate."
Ongoing efforts to enact the remaining recommendations in the report, the authors stated, should be finalized by the end of 2015.
Dr. Lane and Dr. Altman said that they had no relevant financial disclosures.
The report is available from the IOM website.
EXPERT ANALYSIS OF AN INSTITUTE OF MEDICINE REPORT
Study Finds Early Onset of Puberty in Girls
DENVER – A majority of girls start puberty before age 10 years, according to researchers for a longitudinal study who found young ages for onset of breast and pubic hair development.
Tanner stage II breast development ranged from 9% of 7-year-old girls to 91% of 11-year-olds in this ongoing study of 444 healthy girls. Similarly, 10% of the 7-year-olds had Tanner stage II pubic hair development, as did 86% of the 11-year-olds. A total of 75% achieved Tanner stage II or greater breast development, and 57% achieved Tanner stage II or greater pubic hair development by age 10 years.
"Observations from this longitudinal cohort study confirm that girls’ pubertal development is starting earlier," Dr. Louise C. Greenspan said at the annual meeting of the Pediatric Academic Societies, where she presented data for the first 5 years. Data from the first 2 years were previously published (Pediatrics 2010;126:e583-90).
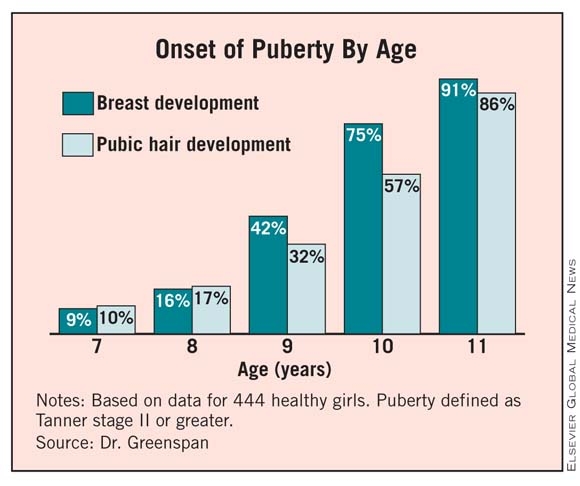
|
A higher body mass index (BMI) and black ethnicity were associated with earlier onset of puberty, said Dr. Greenspan, a pediatric endocrinologist at the Kaiser Permanente San Francisco Medical Center. Girls were aged 6-8 years in 2005 or 2006 when they were initially enrolled in the Cohort Study of Young Girls’ Nutrition, Environment, and Transitions (CYGNET). Participants are 42% white, 24% Hispanic, 22% black, and 12% Asian, "a historically understudied group in this field."
"When we break this down by ethnicity ... not surprisingly, the black girls were earlier for all stages of breast development," Dr. Greenspan said, whereas white girls were the later bloomers at all stages of breast development.
The black girls also were earlier for all stages of pubic hair development. By age 11 years, for example, almost 98% were at Tanner stage II or higher. "The difference here is that the Asian girls were the later girls, basically all the way along, for pubic hair development," Dr. Greenspan said.
Girls who were below the 85th percentile for BMI were the later bloomers at all stages of pubertal development, Dr. Greenspan said. She added that when girls had a high body-fat percentage on bioelectrical impedance analysis, examiners palpated them to try to distinguish fat from glandular tissue. In a similar fashion, the slimmer girls were the later developers of pubic hair at Tanner stage II.
Breast-development findings in the current study are similar to those reported by investigators for American Academy of Pediatrics’ Pediatric Research in Office Settings (PROS) research network.
"For breast stage, there were some variations, but it was pretty much on par," Dr. Greenspan said. However, for pubic hair, CYGNET participants had earlier rates of development versus those in the PROS cross-sectional study (Pediatrics 1997;99:505-12).
A meeting attendee asked Dr. Greenspan if she and her associates assessed BMI differences by ethnicity.
"We don’t have the power in our smaller cohort," she said. "We are looking at that in the larger 1,200 cohort."
The Relation Between Puberty and Breast Cancer
In addition to the San Francisco cohort, investigators are prospectively evaluating girls in Cincinnati and New York as part of the larger Breast Cancer and the Environment Research Program. This federally funded study is assessing the effect of early environmental exposures that could potentially trigger earlier pubertal development, and thus increase the risk of breast cancer. "We know that age of menarche is a risk for breast cancer," Dr. Greenspan said.
"There is growing evidence that timing of exposures may be important to determining breast cancer risk, and puberty may be an important window of susceptibility," Dr. Greenspan said.
The CYGNET study just entered year 6. Annual visits include a physical examination, evaluation of urine and blood samples, activity measurements, food recall, and questionnaires. One expert instructed all research staff to rate Tanner sexual maturity ratings.
Evaluation of tempo and menarche is a future goal for the CYGNET researchers. By the end of year 5, fewer than 20 girls have had menarche, Dr. Greenspan said.
"That is not enough yet to report. We are following the girls through at least year 10," so those data will be coming out, she added.
The Breast Cancer and the Environment Research Program is funded by the National Institute of Environmental Health Sciences and the National Cancer Institute. Dr. Greenspan said that she had no relevant financial disclosures.
DENVER – A majority of girls start puberty before age 10 years, according to researchers for a longitudinal study who found young ages for onset of breast and pubic hair development.
Tanner stage II breast development ranged from 9% of 7-year-old girls to 91% of 11-year-olds in this ongoing study of 444 healthy girls. Similarly, 10% of the 7-year-olds had Tanner stage II pubic hair development, as did 86% of the 11-year-olds. A total of 75% achieved Tanner stage II or greater breast development, and 57% achieved Tanner stage II or greater pubic hair development by age 10 years.
"Observations from this longitudinal cohort study confirm that girls’ pubertal development is starting earlier," Dr. Louise C. Greenspan said at the annual meeting of the Pediatric Academic Societies, where she presented data for the first 5 years. Data from the first 2 years were previously published (Pediatrics 2010;126:e583-90).
|
|
A higher body mass index (BMI) and black ethnicity were associated with earlier onset of puberty, said Dr. Greenspan, a pediatric endocrinologist at the Kaiser Permanente San Francisco Medical Center. Girls were aged 6-8 years in 2005 or 2006 when they were initially enrolled in the Cohort Study of Young Girls’ Nutrition, Environment, and Transitions (CYGNET). Participants are 42% white, 24% Hispanic, 22% black, and 12% Asian, "a historically understudied group in this field."
"When we break this down by ethnicity ... not surprisingly, the black girls were earlier for all stages of breast development," Dr. Greenspan said, whereas white girls were the later bloomers at all stages of breast development.
The black girls also were earlier for all stages of pubic hair development. By age 11 years, for example, almost 98% were at Tanner stage II or higher. "The difference here is that the Asian girls were the later girls, basically all the way along, for pubic hair development," Dr. Greenspan said.
Girls who were below the 85th percentile for BMI were the later bloomers at all stages of pubertal development, Dr. Greenspan said. She added that when girls had a high body-fat percentage on bioelectrical impedance analysis, examiners palpated them to try to distinguish fat from glandular tissue. In a similar fashion, the slimmer girls were the later developers of pubic hair at Tanner stage II.
Breast-development findings in the current study are similar to those reported by investigators for American Academy of Pediatrics’ Pediatric Research in Office Settings (PROS) research network.
"For breast stage, there were some variations, but it was pretty much on par," Dr. Greenspan said. However, for pubic hair, CYGNET participants had earlier rates of development versus those in the PROS cross-sectional study (Pediatrics 1997;99:505-12).
A meeting attendee asked Dr. Greenspan if she and her associates assessed BMI differences by ethnicity.
"We don’t have the power in our smaller cohort," she said. "We are looking at that in the larger 1,200 cohort."
The Relation Between Puberty and Breast Cancer
In addition to the San Francisco cohort, investigators are prospectively evaluating girls in Cincinnati and New York as part of the larger Breast Cancer and the Environment Research Program. This federally funded study is assessing the effect of early environmental exposures that could potentially trigger earlier pubertal development, and thus increase the risk of breast cancer. "We know that age of menarche is a risk for breast cancer," Dr. Greenspan said.
"There is growing evidence that timing of exposures may be important to determining breast cancer risk, and puberty may be an important window of susceptibility," Dr. Greenspan said.
The CYGNET study just entered year 6. Annual visits include a physical examination, evaluation of urine and blood samples, activity measurements, food recall, and questionnaires. One expert instructed all research staff to rate Tanner sexual maturity ratings.
Evaluation of tempo and menarche is a future goal for the CYGNET researchers. By the end of year 5, fewer than 20 girls have had menarche, Dr. Greenspan said.
"That is not enough yet to report. We are following the girls through at least year 10," so those data will be coming out, she added.
The Breast Cancer and the Environment Research Program is funded by the National Institute of Environmental Health Sciences and the National Cancer Institute. Dr. Greenspan said that she had no relevant financial disclosures.
DENVER – A majority of girls start puberty before age 10 years, according to researchers for a longitudinal study who found young ages for onset of breast and pubic hair development.
Tanner stage II breast development ranged from 9% of 7-year-old girls to 91% of 11-year-olds in this ongoing study of 444 healthy girls. Similarly, 10% of the 7-year-olds had Tanner stage II pubic hair development, as did 86% of the 11-year-olds. A total of 75% achieved Tanner stage II or greater breast development, and 57% achieved Tanner stage II or greater pubic hair development by age 10 years.
"Observations from this longitudinal cohort study confirm that girls’ pubertal development is starting earlier," Dr. Louise C. Greenspan said at the annual meeting of the Pediatric Academic Societies, where she presented data for the first 5 years. Data from the first 2 years were previously published (Pediatrics 2010;126:e583-90).
|
|
A higher body mass index (BMI) and black ethnicity were associated with earlier onset of puberty, said Dr. Greenspan, a pediatric endocrinologist at the Kaiser Permanente San Francisco Medical Center. Girls were aged 6-8 years in 2005 or 2006 when they were initially enrolled in the Cohort Study of Young Girls’ Nutrition, Environment, and Transitions (CYGNET). Participants are 42% white, 24% Hispanic, 22% black, and 12% Asian, "a historically understudied group in this field."
"When we break this down by ethnicity ... not surprisingly, the black girls were earlier for all stages of breast development," Dr. Greenspan said, whereas white girls were the later bloomers at all stages of breast development.
The black girls also were earlier for all stages of pubic hair development. By age 11 years, for example, almost 98% were at Tanner stage II or higher. "The difference here is that the Asian girls were the later girls, basically all the way along, for pubic hair development," Dr. Greenspan said.
Girls who were below the 85th percentile for BMI were the later bloomers at all stages of pubertal development, Dr. Greenspan said. She added that when girls had a high body-fat percentage on bioelectrical impedance analysis, examiners palpated them to try to distinguish fat from glandular tissue. In a similar fashion, the slimmer girls were the later developers of pubic hair at Tanner stage II.
Breast-development findings in the current study are similar to those reported by investigators for American Academy of Pediatrics’ Pediatric Research in Office Settings (PROS) research network.
"For breast stage, there were some variations, but it was pretty much on par," Dr. Greenspan said. However, for pubic hair, CYGNET participants had earlier rates of development versus those in the PROS cross-sectional study (Pediatrics 1997;99:505-12).
A meeting attendee asked Dr. Greenspan if she and her associates assessed BMI differences by ethnicity.
"We don’t have the power in our smaller cohort," she said. "We are looking at that in the larger 1,200 cohort."
The Relation Between Puberty and Breast Cancer
In addition to the San Francisco cohort, investigators are prospectively evaluating girls in Cincinnati and New York as part of the larger Breast Cancer and the Environment Research Program. This federally funded study is assessing the effect of early environmental exposures that could potentially trigger earlier pubertal development, and thus increase the risk of breast cancer. "We know that age of menarche is a risk for breast cancer," Dr. Greenspan said.
"There is growing evidence that timing of exposures may be important to determining breast cancer risk, and puberty may be an important window of susceptibility," Dr. Greenspan said.
The CYGNET study just entered year 6. Annual visits include a physical examination, evaluation of urine and blood samples, activity measurements, food recall, and questionnaires. One expert instructed all research staff to rate Tanner sexual maturity ratings.
Evaluation of tempo and menarche is a future goal for the CYGNET researchers. By the end of year 5, fewer than 20 girls have had menarche, Dr. Greenspan said.
"That is not enough yet to report. We are following the girls through at least year 10," so those data will be coming out, she added.
The Breast Cancer and the Environment Research Program is funded by the National Institute of Environmental Health Sciences and the National Cancer Institute. Dr. Greenspan said that she had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE PEDIATRIC ACADEMIC SOCIETIES
Major Finding: A total of 75% achieved Tanner stage II or greater breast development and 57% achieved Tanner stage II or greater pubic hair development by age 10 years.
Data Source: The 5-year data for 444 healthy girls from the ongoing, longitudinal CYGNET.
Disclosures: Dr. Greenspan said she had no relevant financial disclosures. The investigation is part of a larger study sponsored by the National Institute of Environmental Health Sciences and the National Cancer Institute.