User login
Large pelvic mass in a 46-year-old woman
A 46-year-old woman sought care in our emergency department (ED) for intermittent abdominal pain that she’d had for 3 weeks. The patient had no unusual family history, did not smoke or drink, and had not traveled recently. Over the previous 3 months, she’d experienced dysmenorrhea and menorrhagia during her menstrual cycle. Two days before presenting to our ED, her menstrual cycle began and she complained of persistent lower abdominal pain and hypermenorrhagia.
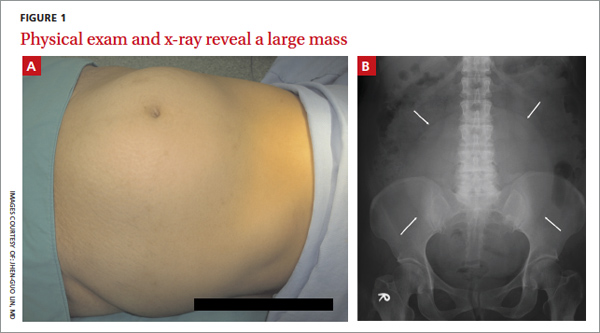
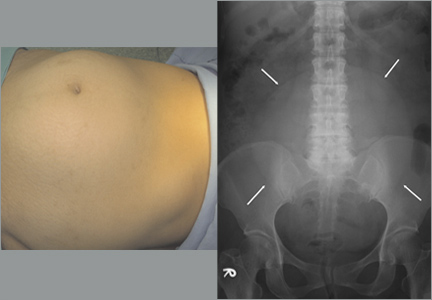
On physical examination, we noted an enlarged, palpable, fixed, firm mass in the lower abdomen (FIGURE 1A). We also noted considerably decreased bowel sounds on auscultation. A kidney, ureter, and bladder (KUB) x-ray revealed a soft tissue mass shadow in the pelvis (FIGURE 1B).
What is your diagnosis?
How would you treat this patient?
Diagnosis: Uterine fibroid
A uterine fibroid, also known as a leiomyoma, is a benign tumor that is composed of smooth muscle tissue and fibrous connective tissue. It is the most common pelvic tumor found in the female body.1 Unlike cancerous tumors, fibroids usually grow slowly and do not break away or invade other parts of the body. Patients can have a single fi- broid or multiple fibroids varying in size and location.1
Fibroids tend to affect women of a certain age. Approximately one in 3 women develops fibroids, and those between the ages of 30 and 40 are at greatest risk.1,2 Estrogen, growth hormone, and progesterone affect the growth rate of these tumors. Fibroids— especially very small ones—are usually asymptomatic, but can cause symptoms as they enlarge. Typical patient complaints in- clude lower abdominal pain, menorrhagia (with anemia), dysmenorrhea, and abnormal uterine bleeding.2,3
A growing fibroid may outpace its blood supply. The result: various forms of degeneration, including hyaline or myxoid degeneration, calcification, cystic degeneration, and red degeneration (infarction of fibroid during pregnancy).
Based on its position within the uterus, a fibroid can be submucosal, intramural, or subserosal. Uterine fibroids are usually diagnosed based on a clinical history and pelvic examination; the presence of a fibroid is confirmed by ultrasound, magnetic resonance imaging (MRI), computed tomography, saline infusion sonography, or hysterosalpingography.4
Is it a fibroid or a uterine sarcoma?
A rapidly growing uterine mass is not a reliable indicator of a uterine sarcoma in a woman of reproductive age.5 However, rapid tumor growth in a menopausal woman who is not on hormonal replacement therapy may be an indicator of uterine sarcoma.5
A diagnosis of uterine sarcoma is confirmed by histological examination fol- lowing myomectomy or hysterectomy for a presumed fibroid. However, a careful ultrasound evaluation may also identify features suggestive of sarcoma5—typically, mixed echogenic and poor echogenic areas with central necrosis.6 Color Doppler can reveal irregular vessel distribution, low imped- ance to flow, and high peak systolic velocity.6 If a sarcoma is suspected after ultrasound evaluation, an MRI can be helpful in further evaluation.7
How best to manage uterine fibroids?
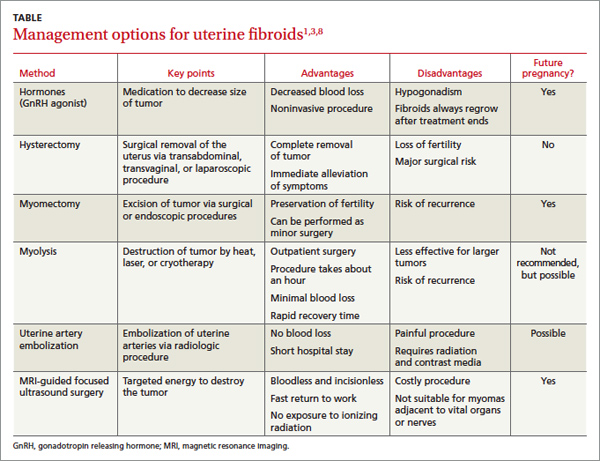
Small fibroids that are asymptomatic or cause only minor problems are not usually treated. However, if a fibroid is large or results in pain or excessive bleeding, further management may be needed. Management of fibroids may be nonsurgical or surgical (TABLE).1,3,8 Factors that affect management choices include the patient’s desire to become pregnant or preserve her uterus, symptom severity, and tumor characteristics.
A good outcome for our patient
Based on our patient’s KUB x-ray, we suspected malignancy, so we consulted a gynecologist for a sonographic examination. The ultrasound revealed a heterogeneous mass with calcification.
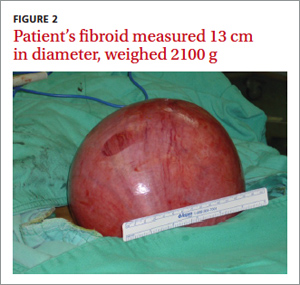
The patient underwent a hysterectomy. The solitary soft tissue mass that was removed measured 13 cm in diameter and weighed 2100 g (FIGURE 2). Histopathological analysis revealed that the fibroid was madeup of myometrium and fibrous connective tissue. After hospital discharge, the patient resumed all of her normal activities with no recurrence.
CORRESPONDENCE
Jhen-Guo Lin, MD, Department of Obstetrics and Gynecology, Taoyuan Armed Forces General Hospital, No. 168, Zhongxing Road, Longtan Township, Taoyuan County 32551, Taiwan (ROC); [email protected]
1. Levy BS. Modern management of uterine fibroids. Acta Obstet Gynecol Scand. 2008;87:812-823.
2. Jolley S. An overview of uterine fibroids. Nursing Stand. 2009; 24:44-48.
3. Evans P, Brunsell S. Uterine fibroid tumors: diagnosis and treatment. Am Fam Physician. 2007;75:1503-1508.
4. Frishman GN, Jurema MW. Myomas and myomectomy. J Minim Invasive Gynecol. 2005;12:443-456.
5. Amant F, Coosemans A, Debiec-Rychter M, et al. Clinical management of uterine sarcomas. Lancet Oncol. 2009;10:1188-1198.
6. Russell DJ. The female pelvic mass. Diagnosis and management. Med Clin North Am. 1995;79:1481-1493.
7. Rha SE, Byun JY, Jung SE, et al. CT and MRI of uterine sarcomasand their mimickers. AJR Am J Roentgenol. 2003;181:1369-1374.
8. Kim YS, Kim JH, Rhim H, et al. Volumetric MR-guided high-in- tensity focused ultrasound ablation with a one-layer strategy to treat large uterine fibroids: initial clinical outcomes. Radiology. 2012;263:600-609
A 46-year-old woman sought care in our emergency department (ED) for intermittent abdominal pain that she’d had for 3 weeks. The patient had no unusual family history, did not smoke or drink, and had not traveled recently. Over the previous 3 months, she’d experienced dysmenorrhea and menorrhagia during her menstrual cycle. Two days before presenting to our ED, her menstrual cycle began and she complained of persistent lower abdominal pain and hypermenorrhagia.
On physical examination, we noted an enlarged, palpable, fixed, firm mass in the lower abdomen (FIGURE 1A). We also noted considerably decreased bowel sounds on auscultation. A kidney, ureter, and bladder (KUB) x-ray revealed a soft tissue mass shadow in the pelvis (FIGURE 1B).
What is your diagnosis?
How would you treat this patient?
Diagnosis: Uterine fibroid
A uterine fibroid, also known as a leiomyoma, is a benign tumor that is composed of smooth muscle tissue and fibrous connective tissue. It is the most common pelvic tumor found in the female body.1 Unlike cancerous tumors, fibroids usually grow slowly and do not break away or invade other parts of the body. Patients can have a single fi- broid or multiple fibroids varying in size and location.1
Fibroids tend to affect women of a certain age. Approximately one in 3 women develops fibroids, and those between the ages of 30 and 40 are at greatest risk.1,2 Estrogen, growth hormone, and progesterone affect the growth rate of these tumors. Fibroids— especially very small ones—are usually asymptomatic, but can cause symptoms as they enlarge. Typical patient complaints in- clude lower abdominal pain, menorrhagia (with anemia), dysmenorrhea, and abnormal uterine bleeding.2,3
A growing fibroid may outpace its blood supply. The result: various forms of degeneration, including hyaline or myxoid degeneration, calcification, cystic degeneration, and red degeneration (infarction of fibroid during pregnancy).
Based on its position within the uterus, a fibroid can be submucosal, intramural, or subserosal. Uterine fibroids are usually diagnosed based on a clinical history and pelvic examination; the presence of a fibroid is confirmed by ultrasound, magnetic resonance imaging (MRI), computed tomography, saline infusion sonography, or hysterosalpingography.4
Is it a fibroid or a uterine sarcoma?
A rapidly growing uterine mass is not a reliable indicator of a uterine sarcoma in a woman of reproductive age.5 However, rapid tumor growth in a menopausal woman who is not on hormonal replacement therapy may be an indicator of uterine sarcoma.5
A diagnosis of uterine sarcoma is confirmed by histological examination fol- lowing myomectomy or hysterectomy for a presumed fibroid. However, a careful ultrasound evaluation may also identify features suggestive of sarcoma5—typically, mixed echogenic and poor echogenic areas with central necrosis.6 Color Doppler can reveal irregular vessel distribution, low imped- ance to flow, and high peak systolic velocity.6 If a sarcoma is suspected after ultrasound evaluation, an MRI can be helpful in further evaluation.7
How best to manage uterine fibroids?
Small fibroids that are asymptomatic or cause only minor problems are not usually treated. However, if a fibroid is large or results in pain or excessive bleeding, further management may be needed. Management of fibroids may be nonsurgical or surgical (TABLE).1,3,8 Factors that affect management choices include the patient’s desire to become pregnant or preserve her uterus, symptom severity, and tumor characteristics.
A good outcome for our patient
Based on our patient’s KUB x-ray, we suspected malignancy, so we consulted a gynecologist for a sonographic examination. The ultrasound revealed a heterogeneous mass with calcification.
The patient underwent a hysterectomy. The solitary soft tissue mass that was removed measured 13 cm in diameter and weighed 2100 g (FIGURE 2). Histopathological analysis revealed that the fibroid was madeup of myometrium and fibrous connective tissue. After hospital discharge, the patient resumed all of her normal activities with no recurrence.
CORRESPONDENCE
Jhen-Guo Lin, MD, Department of Obstetrics and Gynecology, Taoyuan Armed Forces General Hospital, No. 168, Zhongxing Road, Longtan Township, Taoyuan County 32551, Taiwan (ROC); [email protected]
A 46-year-old woman sought care in our emergency department (ED) for intermittent abdominal pain that she’d had for 3 weeks. The patient had no unusual family history, did not smoke or drink, and had not traveled recently. Over the previous 3 months, she’d experienced dysmenorrhea and menorrhagia during her menstrual cycle. Two days before presenting to our ED, her menstrual cycle began and she complained of persistent lower abdominal pain and hypermenorrhagia.
On physical examination, we noted an enlarged, palpable, fixed, firm mass in the lower abdomen (FIGURE 1A). We also noted considerably decreased bowel sounds on auscultation. A kidney, ureter, and bladder (KUB) x-ray revealed a soft tissue mass shadow in the pelvis (FIGURE 1B).
What is your diagnosis?
How would you treat this patient?
Diagnosis: Uterine fibroid
A uterine fibroid, also known as a leiomyoma, is a benign tumor that is composed of smooth muscle tissue and fibrous connective tissue. It is the most common pelvic tumor found in the female body.1 Unlike cancerous tumors, fibroids usually grow slowly and do not break away or invade other parts of the body. Patients can have a single fi- broid or multiple fibroids varying in size and location.1
Fibroids tend to affect women of a certain age. Approximately one in 3 women develops fibroids, and those between the ages of 30 and 40 are at greatest risk.1,2 Estrogen, growth hormone, and progesterone affect the growth rate of these tumors. Fibroids— especially very small ones—are usually asymptomatic, but can cause symptoms as they enlarge. Typical patient complaints in- clude lower abdominal pain, menorrhagia (with anemia), dysmenorrhea, and abnormal uterine bleeding.2,3
A growing fibroid may outpace its blood supply. The result: various forms of degeneration, including hyaline or myxoid degeneration, calcification, cystic degeneration, and red degeneration (infarction of fibroid during pregnancy).
Based on its position within the uterus, a fibroid can be submucosal, intramural, or subserosal. Uterine fibroids are usually diagnosed based on a clinical history and pelvic examination; the presence of a fibroid is confirmed by ultrasound, magnetic resonance imaging (MRI), computed tomography, saline infusion sonography, or hysterosalpingography.4
Is it a fibroid or a uterine sarcoma?
A rapidly growing uterine mass is not a reliable indicator of a uterine sarcoma in a woman of reproductive age.5 However, rapid tumor growth in a menopausal woman who is not on hormonal replacement therapy may be an indicator of uterine sarcoma.5
A diagnosis of uterine sarcoma is confirmed by histological examination fol- lowing myomectomy or hysterectomy for a presumed fibroid. However, a careful ultrasound evaluation may also identify features suggestive of sarcoma5—typically, mixed echogenic and poor echogenic areas with central necrosis.6 Color Doppler can reveal irregular vessel distribution, low imped- ance to flow, and high peak systolic velocity.6 If a sarcoma is suspected after ultrasound evaluation, an MRI can be helpful in further evaluation.7
How best to manage uterine fibroids?
Small fibroids that are asymptomatic or cause only minor problems are not usually treated. However, if a fibroid is large or results in pain or excessive bleeding, further management may be needed. Management of fibroids may be nonsurgical or surgical (TABLE).1,3,8 Factors that affect management choices include the patient’s desire to become pregnant or preserve her uterus, symptom severity, and tumor characteristics.
A good outcome for our patient
Based on our patient’s KUB x-ray, we suspected malignancy, so we consulted a gynecologist for a sonographic examination. The ultrasound revealed a heterogeneous mass with calcification.
The patient underwent a hysterectomy. The solitary soft tissue mass that was removed measured 13 cm in diameter and weighed 2100 g (FIGURE 2). Histopathological analysis revealed that the fibroid was madeup of myometrium and fibrous connective tissue. After hospital discharge, the patient resumed all of her normal activities with no recurrence.
CORRESPONDENCE
Jhen-Guo Lin, MD, Department of Obstetrics and Gynecology, Taoyuan Armed Forces General Hospital, No. 168, Zhongxing Road, Longtan Township, Taoyuan County 32551, Taiwan (ROC); [email protected]
1. Levy BS. Modern management of uterine fibroids. Acta Obstet Gynecol Scand. 2008;87:812-823.
2. Jolley S. An overview of uterine fibroids. Nursing Stand. 2009; 24:44-48.
3. Evans P, Brunsell S. Uterine fibroid tumors: diagnosis and treatment. Am Fam Physician. 2007;75:1503-1508.
4. Frishman GN, Jurema MW. Myomas and myomectomy. J Minim Invasive Gynecol. 2005;12:443-456.
5. Amant F, Coosemans A, Debiec-Rychter M, et al. Clinical management of uterine sarcomas. Lancet Oncol. 2009;10:1188-1198.
6. Russell DJ. The female pelvic mass. Diagnosis and management. Med Clin North Am. 1995;79:1481-1493.
7. Rha SE, Byun JY, Jung SE, et al. CT and MRI of uterine sarcomasand their mimickers. AJR Am J Roentgenol. 2003;181:1369-1374.
8. Kim YS, Kim JH, Rhim H, et al. Volumetric MR-guided high-in- tensity focused ultrasound ablation with a one-layer strategy to treat large uterine fibroids: initial clinical outcomes. Radiology. 2012;263:600-609
1. Levy BS. Modern management of uterine fibroids. Acta Obstet Gynecol Scand. 2008;87:812-823.
2. Jolley S. An overview of uterine fibroids. Nursing Stand. 2009; 24:44-48.
3. Evans P, Brunsell S. Uterine fibroid tumors: diagnosis and treatment. Am Fam Physician. 2007;75:1503-1508.
4. Frishman GN, Jurema MW. Myomas and myomectomy. J Minim Invasive Gynecol. 2005;12:443-456.
5. Amant F, Coosemans A, Debiec-Rychter M, et al. Clinical management of uterine sarcomas. Lancet Oncol. 2009;10:1188-1198.
6. Russell DJ. The female pelvic mass. Diagnosis and management. Med Clin North Am. 1995;79:1481-1493.
7. Rha SE, Byun JY, Jung SE, et al. CT and MRI of uterine sarcomasand their mimickers. AJR Am J Roentgenol. 2003;181:1369-1374.
8. Kim YS, Kim JH, Rhim H, et al. Volumetric MR-guided high-in- tensity focused ultrasound ablation with a one-layer strategy to treat large uterine fibroids: initial clinical outcomes. Radiology. 2012;263:600-609