Veterans speak of losing their innocence and longing to regain it. They ask: “Why can’t I just go back to the way I was?”
Jonathan Shay, Achilles in Vietnam1
On July 17, 2023, several media outlets covering military and federal news carried a story about the US Department of Veterans Affairs (VA) plan to conduct a major survey of moral injury in veterans.2 This is not the first such survey: There have been numerous previous studies conducted by both VA and non-VA investigators.3 Moral injury has been increasingly recognized as the signature wound of service members, especially those who fought in Operation Enduring Freedom and Operation Iraqi Freedom.4 This new VA survey can provide crucial information because we know so little about moral injury or how to help those with the condition.
At the time of this writing, there has been no official VA public statement about the study. At face value, this seemed to be strange, given that the groundbreaking research could improve the diagnosis and therapy of moral injury. According to a June 2023 VA Office of Research and Development internal announcement, the primary goal of the study is to determine the prevalence of moral injury among US veterans. The secondary goals of the study are to (1) compare those who develop moral injury and those who do not after exposure to similar traumas; and (2) conduct interviews about thoughts and experiences from 20 veterans who identify as having moral injury and 20 who do not but who have similar exposure to morally injurious events.
Data for the study will be collected through an extensive online survey from a nationally representative sample of 3000 post-9/11 war veterans. The sample will include at least 950 who served in a war zone and at least 400 who are aged 18 to 54 years. The respondents will be paid $20 for the 30 to 45 minutes survey. The collection and analysis of data are expected to take 3 or more years.
The modern version of moral injury is often associated with Jonathan Shay, MD, a VA psychiatrist.5 Shay wrote about the origin of moral injury found in Homer’s TheIliad and The Odyssey and how the poems offer ancient echoes of his therapy with modern-day combat veterans.1
There is no universal agreement on the definition of moral injury. A working definition of moral injury used in the VA suggests that it describes the difficulties that people face after doing high-stakes actions that violate a sense of what is right and just or after being forced to experience others’ immoral actions.6
Two conditions are necessary for moral injury to occur. First, an individual acts or witnesses an action that contravenes their core ethical principles. Secondly, that occurrence is experienced as a breach of the person’s moral barrier. Military personnel killing civilians to protect their lives and those of their fellow troops is a tragic example of moral injury. The translation of this for health care professionals may be the inability to save severely wounded service members in the combat theater due to the exigencies of war.7
Experts in moral injury emphasize the importance of distinguishing the phenomenon from posttraumatic stress disorder (PTSD). Unlike many psychiatric disorders, both moral injury and PTSD have known etiologies: traumatic events. An individual may have 1 or both conditions, and each can manifest anger, guilt, shame, and loss of trust in others. One way that moral injury can be distinguished from PTSD is that it goes beyond the psychological to compromise the moral and often spiritual beliefs and values of the individual. One of the characteristics that makes us human is that we have a conscience to guide us in navigating the moral field of human life, but moral injury scrambles the internal compass that discerns right and wrong, good and bad. When an individual commits an action or witnesses the perpetration of an action that crosses their personal moral boundary, their integrity is shattered, and they may lose faith in their intrinsic worth. These beliefs prevent many service members from disclosing their distress, leading some commentators to refer to moral injury as a silent or invisible wound.8
The timing of the VA’s launching of a study of moral injury of this size and scope may reflect 3 recent developments: Not unexpected in VA matters, one is political, another is benefits, and the last pertains to health care.
First, August marks the second anniversary of the withdrawal of American troops from Afghanistan. Many Afghans who assisted US forces during the war were not evacuated. For some of the troops who served in the country, these events as well as the chaotic end to the long war were experienced as a contravening of an ethical code, resulting in moral injury.9
Second, many of those service members are now calling on the federal government to recognize and respond to the detrimental impact of the withdrawal, including the high prevalence of moral injury in troops who served in Afghanistan.10 Moral injury at this time is not considered a psychiatric diagnosis; hence, not eligible for VA benefits. However, many of the psychological manifestations of moral injury, such as depression and anxiety, are established service-connected disorders.
Third, several VA studies have demonstrated that moral injury either alone or combined with PTSD substantially elevates the risk of suicide.11 Since preventing suicide is a major strategic priority for the VA, the importance of learning more about the epidemiology of moral injury is the necessary first step to developing therapeutic approaches. At a time when organized medicine is becoming increasingly technological and fragmented, launching this unprecedented survey demonstrates the VA’s commitment to delivering holistic and humanistic care of the service member: body, mind, and spirit.
This project also sends a strong message to those who lobby for shifting funding from the VA to community care or call for privatization. Veterans are different: They experience unique disorders borne of the battles they fought for our freedom. The VA has the specialized knowledge and skills in research and health care to develop the knowledge to ground innovative treatments for conditions like moral injury, PTSD, and traumatic brain injuries. VA chaplains and mental health professionals have pioneered assessment instruments and promising therapies for moral injury. Their distinctive expertise unrivaled in the civilian sector benefits not only veterans but also the wider community where there is a growing awareness of the devastating impact of moral injury, particularly on health care professionals.12 And there may have been no other time in history when this broken, violent world was more in need of moral healing and peace.
References
1. Shay J. Achilles in Vietnam: Combat Trauma and the Trials of Homecoming. Simon & Schuster; 1994.
2. Seck HH. VA lays groundwork for first major survey of moral injury in Veterans. Military Times. Accessed July 24, 2023. https://www.militarytimes.com/veterans/2023/07/17/va-lays-groundwork-for-first-major-survey-of-moral-injury-in-veterans
3. US Department of Veterans Affairs, MIRECC/CoE.Moral injury bibliography. Updated July 28, 2022. Accessed July 26, 2023. https://www.mirecc.va.gov/visn17/moralinjury/bibliography.asp
4. National Public Radio. Moral injury is the ‘signature wound’ of today’s veterans. https://www.npr.org/2014/11/11/363288341/moral-injury-is-the-signature-wound-of-today-s-veterans
5. Shay J. Moral injury. Psychoanalytic Psychol. 2014;31(2):182-191. doi.10.1037/a0036090
6. US Department of Veterans Affairs. Moral injury. Accessed July 24, 2023. https://www.mirecc.va.gov/visn17/moralinjury.asp
7. Norman SB, Maguen S. Moral injury. Accessed July 24, 2023. https://www.ptsd.va.gov/professional/treat/cooccurring/moral_injury.asp
8. Svoboda E. Moral injury is an invisible epidemic that affects millions of Americans. Scientific American. Accessed July 24, 2023. https://www.scientificamerican.com/article/moral-injury-is-an-invisible-epidemic-that-affects-millions
9. Lawrence JP. Diagnoses of moral injury are a growing part of Afghanistan legacy for U.S. personnel. Stars and Stripes. Accessed July 24, 2023. https://www.stripes.com/theaters/middle_east/2022-08-12/moral-injury-afghanistan-6862738.html
10. Kheel R. Vet group asks Biden to recognize moral injuries caused by Afghan’s war. Accessed July 24, 2023. https://www.military.com/daily-news/2022/08/30/vets-group-asks-biden-recognize-moral-injuries-caused-afghan-wars-end.html 11. Nichter B, Norman SB, Maguen S, Piertrzak RH. Moral injury and suicidal behavior among U.S. combat veterans: results from the 2019-2020 National Health and Resilience in Veterans study. Depress Anxiety. 2021;38(6):606-614. doi:10.1002/da.23145
12. Dean W, Talbot S, Dean A. Reframing clinician distress: moral injury not burnout. Fed Pract. 2019;36(9):400-402.
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies.
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies.
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies.
Veterans speak of losing their innocence and longing to regain it. They ask: “Why can’t I just go back to the way I was?”
Jonathan Shay, Achilles in Vietnam1
On July 17, 2023, several media outlets covering military and federal news carried a story about the US Department of Veterans Affairs (VA) plan to conduct a major survey of moral injury in veterans.2 This is not the first such survey: There have been numerous previous studies conducted by both VA and non-VA investigators.3 Moral injury has been increasingly recognized as the signature wound of service members, especially those who fought in Operation Enduring Freedom and Operation Iraqi Freedom.4 This new VA survey can provide crucial information because we know so little about moral injury or how to help those with the condition.
At the time of this writing, there has been no official VA public statement about the study. At face value, this seemed to be strange, given that the groundbreaking research could improve the diagnosis and therapy of moral injury. According to a June 2023 VA Office of Research and Development internal announcement, the primary goal of the study is to determine the prevalence of moral injury among US veterans. The secondary goals of the study are to (1) compare those who develop moral injury and those who do not after exposure to similar traumas; and (2) conduct interviews about thoughts and experiences from 20 veterans who identify as having moral injury and 20 who do not but who have similar exposure to morally injurious events.
Data for the study will be collected through an extensive online survey from a nationally representative sample of 3000 post-9/11 war veterans. The sample will include at least 950 who served in a war zone and at least 400 who are aged 18 to 54 years. The respondents will be paid $20 for the 30 to 45 minutes survey. The collection and analysis of data are expected to take 3 or more years.
The modern version of moral injury is often associated with Jonathan Shay, MD, a VA psychiatrist.5 Shay wrote about the origin of moral injury found in Homer’s TheIliad and The Odyssey and how the poems offer ancient echoes of his therapy with modern-day combat veterans.1
There is no universal agreement on the definition of moral injury. A working definition of moral injury used in the VA suggests that it describes the difficulties that people face after doing high-stakes actions that violate a sense of what is right and just or after being forced to experience others’ immoral actions.6
Two conditions are necessary for moral injury to occur. First, an individual acts or witnesses an action that contravenes their core ethical principles. Secondly, that occurrence is experienced as a breach of the person’s moral barrier. Military personnel killing civilians to protect their lives and those of their fellow troops is a tragic example of moral injury. The translation of this for health care professionals may be the inability to save severely wounded service members in the combat theater due to the exigencies of war.7
Experts in moral injury emphasize the importance of distinguishing the phenomenon from posttraumatic stress disorder (PTSD). Unlike many psychiatric disorders, both moral injury and PTSD have known etiologies: traumatic events. An individual may have 1 or both conditions, and each can manifest anger, guilt, shame, and loss of trust in others. One way that moral injury can be distinguished from PTSD is that it goes beyond the psychological to compromise the moral and often spiritual beliefs and values of the individual. One of the characteristics that makes us human is that we have a conscience to guide us in navigating the moral field of human life, but moral injury scrambles the internal compass that discerns right and wrong, good and bad. When an individual commits an action or witnesses the perpetration of an action that crosses their personal moral boundary, their integrity is shattered, and they may lose faith in their intrinsic worth. These beliefs prevent many service members from disclosing their distress, leading some commentators to refer to moral injury as a silent or invisible wound.8
The timing of the VA’s launching of a study of moral injury of this size and scope may reflect 3 recent developments: Not unexpected in VA matters, one is political, another is benefits, and the last pertains to health care.
First, August marks the second anniversary of the withdrawal of American troops from Afghanistan. Many Afghans who assisted US forces during the war were not evacuated. For some of the troops who served in the country, these events as well as the chaotic end to the long war were experienced as a contravening of an ethical code, resulting in moral injury.9
Second, many of those service members are now calling on the federal government to recognize and respond to the detrimental impact of the withdrawal, including the high prevalence of moral injury in troops who served in Afghanistan.10 Moral injury at this time is not considered a psychiatric diagnosis; hence, not eligible for VA benefits. However, many of the psychological manifestations of moral injury, such as depression and anxiety, are established service-connected disorders.
Third, several VA studies have demonstrated that moral injury either alone or combined with PTSD substantially elevates the risk of suicide.11 Since preventing suicide is a major strategic priority for the VA, the importance of learning more about the epidemiology of moral injury is the necessary first step to developing therapeutic approaches. At a time when organized medicine is becoming increasingly technological and fragmented, launching this unprecedented survey demonstrates the VA’s commitment to delivering holistic and humanistic care of the service member: body, mind, and spirit.
This project also sends a strong message to those who lobby for shifting funding from the VA to community care or call for privatization. Veterans are different: They experience unique disorders borne of the battles they fought for our freedom. The VA has the specialized knowledge and skills in research and health care to develop the knowledge to ground innovative treatments for conditions like moral injury, PTSD, and traumatic brain injuries. VA chaplains and mental health professionals have pioneered assessment instruments and promising therapies for moral injury. Their distinctive expertise unrivaled in the civilian sector benefits not only veterans but also the wider community where there is a growing awareness of the devastating impact of moral injury, particularly on health care professionals.12 And there may have been no other time in history when this broken, violent world was more in need of moral healing and peace.
Veterans speak of losing their innocence and longing to regain it. They ask: “Why can’t I just go back to the way I was?”
Jonathan Shay, Achilles in Vietnam1
On July 17, 2023, several media outlets covering military and federal news carried a story about the US Department of Veterans Affairs (VA) plan to conduct a major survey of moral injury in veterans.2 This is not the first such survey: There have been numerous previous studies conducted by both VA and non-VA investigators.3 Moral injury has been increasingly recognized as the signature wound of service members, especially those who fought in Operation Enduring Freedom and Operation Iraqi Freedom.4 This new VA survey can provide crucial information because we know so little about moral injury or how to help those with the condition.
At the time of this writing, there has been no official VA public statement about the study. At face value, this seemed to be strange, given that the groundbreaking research could improve the diagnosis and therapy of moral injury. According to a June 2023 VA Office of Research and Development internal announcement, the primary goal of the study is to determine the prevalence of moral injury among US veterans. The secondary goals of the study are to (1) compare those who develop moral injury and those who do not after exposure to similar traumas; and (2) conduct interviews about thoughts and experiences from 20 veterans who identify as having moral injury and 20 who do not but who have similar exposure to morally injurious events.
Data for the study will be collected through an extensive online survey from a nationally representative sample of 3000 post-9/11 war veterans. The sample will include at least 950 who served in a war zone and at least 400 who are aged 18 to 54 years. The respondents will be paid $20 for the 30 to 45 minutes survey. The collection and analysis of data are expected to take 3 or more years.
The modern version of moral injury is often associated with Jonathan Shay, MD, a VA psychiatrist.5 Shay wrote about the origin of moral injury found in Homer’s TheIliad and The Odyssey and how the poems offer ancient echoes of his therapy with modern-day combat veterans.1
There is no universal agreement on the definition of moral injury. A working definition of moral injury used in the VA suggests that it describes the difficulties that people face after doing high-stakes actions that violate a sense of what is right and just or after being forced to experience others’ immoral actions.6
Two conditions are necessary for moral injury to occur. First, an individual acts or witnesses an action that contravenes their core ethical principles. Secondly, that occurrence is experienced as a breach of the person’s moral barrier. Military personnel killing civilians to protect their lives and those of their fellow troops is a tragic example of moral injury. The translation of this for health care professionals may be the inability to save severely wounded service members in the combat theater due to the exigencies of war.7
Experts in moral injury emphasize the importance of distinguishing the phenomenon from posttraumatic stress disorder (PTSD). Unlike many psychiatric disorders, both moral injury and PTSD have known etiologies: traumatic events. An individual may have 1 or both conditions, and each can manifest anger, guilt, shame, and loss of trust in others. One way that moral injury can be distinguished from PTSD is that it goes beyond the psychological to compromise the moral and often spiritual beliefs and values of the individual. One of the characteristics that makes us human is that we have a conscience to guide us in navigating the moral field of human life, but moral injury scrambles the internal compass that discerns right and wrong, good and bad. When an individual commits an action or witnesses the perpetration of an action that crosses their personal moral boundary, their integrity is shattered, and they may lose faith in their intrinsic worth. These beliefs prevent many service members from disclosing their distress, leading some commentators to refer to moral injury as a silent or invisible wound.8
The timing of the VA’s launching of a study of moral injury of this size and scope may reflect 3 recent developments: Not unexpected in VA matters, one is political, another is benefits, and the last pertains to health care.
First, August marks the second anniversary of the withdrawal of American troops from Afghanistan. Many Afghans who assisted US forces during the war were not evacuated. For some of the troops who served in the country, these events as well as the chaotic end to the long war were experienced as a contravening of an ethical code, resulting in moral injury.9
Second, many of those service members are now calling on the federal government to recognize and respond to the detrimental impact of the withdrawal, including the high prevalence of moral injury in troops who served in Afghanistan.10 Moral injury at this time is not considered a psychiatric diagnosis; hence, not eligible for VA benefits. However, many of the psychological manifestations of moral injury, such as depression and anxiety, are established service-connected disorders.
Third, several VA studies have demonstrated that moral injury either alone or combined with PTSD substantially elevates the risk of suicide.11 Since preventing suicide is a major strategic priority for the VA, the importance of learning more about the epidemiology of moral injury is the necessary first step to developing therapeutic approaches. At a time when organized medicine is becoming increasingly technological and fragmented, launching this unprecedented survey demonstrates the VA’s commitment to delivering holistic and humanistic care of the service member: body, mind, and spirit.
This project also sends a strong message to those who lobby for shifting funding from the VA to community care or call for privatization. Veterans are different: They experience unique disorders borne of the battles they fought for our freedom. The VA has the specialized knowledge and skills in research and health care to develop the knowledge to ground innovative treatments for conditions like moral injury, PTSD, and traumatic brain injuries. VA chaplains and mental health professionals have pioneered assessment instruments and promising therapies for moral injury. Their distinctive expertise unrivaled in the civilian sector benefits not only veterans but also the wider community where there is a growing awareness of the devastating impact of moral injury, particularly on health care professionals.12 And there may have been no other time in history when this broken, violent world was more in need of moral healing and peace.
References
1. Shay J. Achilles in Vietnam: Combat Trauma and the Trials of Homecoming. Simon & Schuster; 1994.
2. Seck HH. VA lays groundwork for first major survey of moral injury in Veterans. Military Times. Accessed July 24, 2023. https://www.militarytimes.com/veterans/2023/07/17/va-lays-groundwork-for-first-major-survey-of-moral-injury-in-veterans
3. US Department of Veterans Affairs, MIRECC/CoE.Moral injury bibliography. Updated July 28, 2022. Accessed July 26, 2023. https://www.mirecc.va.gov/visn17/moralinjury/bibliography.asp
4. National Public Radio. Moral injury is the ‘signature wound’ of today’s veterans. https://www.npr.org/2014/11/11/363288341/moral-injury-is-the-signature-wound-of-today-s-veterans
5. Shay J. Moral injury. Psychoanalytic Psychol. 2014;31(2):182-191. doi.10.1037/a0036090
6. US Department of Veterans Affairs. Moral injury. Accessed July 24, 2023. https://www.mirecc.va.gov/visn17/moralinjury.asp
7. Norman SB, Maguen S. Moral injury. Accessed July 24, 2023. https://www.ptsd.va.gov/professional/treat/cooccurring/moral_injury.asp
8. Svoboda E. Moral injury is an invisible epidemic that affects millions of Americans. Scientific American. Accessed July 24, 2023. https://www.scientificamerican.com/article/moral-injury-is-an-invisible-epidemic-that-affects-millions
9. Lawrence JP. Diagnoses of moral injury are a growing part of Afghanistan legacy for U.S. personnel. Stars and Stripes. Accessed July 24, 2023. https://www.stripes.com/theaters/middle_east/2022-08-12/moral-injury-afghanistan-6862738.html
10. Kheel R. Vet group asks Biden to recognize moral injuries caused by Afghan’s war. Accessed July 24, 2023. https://www.military.com/daily-news/2022/08/30/vets-group-asks-biden-recognize-moral-injuries-caused-afghan-wars-end.html 11. Nichter B, Norman SB, Maguen S, Piertrzak RH. Moral injury and suicidal behavior among U.S. combat veterans: results from the 2019-2020 National Health and Resilience in Veterans study. Depress Anxiety. 2021;38(6):606-614. doi:10.1002/da.23145
12. Dean W, Talbot S, Dean A. Reframing clinician distress: moral injury not burnout. Fed Pract. 2019;36(9):400-402.
References
1. Shay J. Achilles in Vietnam: Combat Trauma and the Trials of Homecoming. Simon & Schuster; 1994.
2. Seck HH. VA lays groundwork for first major survey of moral injury in Veterans. Military Times. Accessed July 24, 2023. https://www.militarytimes.com/veterans/2023/07/17/va-lays-groundwork-for-first-major-survey-of-moral-injury-in-veterans
3. US Department of Veterans Affairs, MIRECC/CoE.Moral injury bibliography. Updated July 28, 2022. Accessed July 26, 2023. https://www.mirecc.va.gov/visn17/moralinjury/bibliography.asp
4. National Public Radio. Moral injury is the ‘signature wound’ of today’s veterans. https://www.npr.org/2014/11/11/363288341/moral-injury-is-the-signature-wound-of-today-s-veterans
5. Shay J. Moral injury. Psychoanalytic Psychol. 2014;31(2):182-191. doi.10.1037/a0036090
6. US Department of Veterans Affairs. Moral injury. Accessed July 24, 2023. https://www.mirecc.va.gov/visn17/moralinjury.asp
7. Norman SB, Maguen S. Moral injury. Accessed July 24, 2023. https://www.ptsd.va.gov/professional/treat/cooccurring/moral_injury.asp
8. Svoboda E. Moral injury is an invisible epidemic that affects millions of Americans. Scientific American. Accessed July 24, 2023. https://www.scientificamerican.com/article/moral-injury-is-an-invisible-epidemic-that-affects-millions
9. Lawrence JP. Diagnoses of moral injury are a growing part of Afghanistan legacy for U.S. personnel. Stars and Stripes. Accessed July 24, 2023. https://www.stripes.com/theaters/middle_east/2022-08-12/moral-injury-afghanistan-6862738.html
10. Kheel R. Vet group asks Biden to recognize moral injuries caused by Afghan’s war. Accessed July 24, 2023. https://www.military.com/daily-news/2022/08/30/vets-group-asks-biden-recognize-moral-injuries-caused-afghan-wars-end.html 11. Nichter B, Norman SB, Maguen S, Piertrzak RH. Moral injury and suicidal behavior among U.S. combat veterans: results from the 2019-2020 National Health and Resilience in Veterans study. Depress Anxiety. 2021;38(6):606-614. doi:10.1002/da.23145
12. Dean W, Talbot S, Dean A. Reframing clinician distress: moral injury not burnout. Fed Pract. 2019;36(9):400-402.
A 28-year-old woman (G1P0) is seen for a routine prenatal visit at 32 3/7 weeks’ gestation. She reports having generalized intense itching, including on her palms and soles, that is most intense at night and has been present for approximately 1 week. Her pregnancy is otherwise uncomplicated to date. Physical exam is within normal limits, with no evidence of a skin rash. Cholestasis of pregnancy is suspected, and laboratory tests are ordered, including bile acids and liver transaminases. Test results show that her aspartate transaminase (AST) and alanine transaminase (ALT) levels are mildly elevated at 55 IU/L and 41 IU/L, respectively, and several days later her bile acid level result is 21 µmol/L.
How should this patient be managed?
Intrahepatic cholestasis of pregnancy (ICP) affects 0.5% to 0.7% of pregnant individuals and results in maternal pruritus and elevated serum bile acid levels.1-3 Pruritus in ICP typically is generalized, including occurrence on the palms of the hands and soles of the feet, and it often is reported to be worse at night.4 Up to 25% of pregnant women will develop pruritus during pregnancy but the majority will not have ICP.2,5 Patients with ICP have no associated rash, but clinicians may note excoriations on exam. ICP typically presents in the third trimester of pregnancy but has been reported to occur earlier in gestation.6
Making a diagnosis of ICP
The presence of maternal pruritus in the absence of a skin condition along with elevated levels of serum bile acids are required for the diagnosis of ICP.7 Thus, a thorough history and physical exam is recommended to rule out another skin condition that could potentially explain the patient’s pruritus.
Some controversy exists regarding the bile acid level cutoff that should be used to make a diagnosis of ICP.8 It has been noted that nonfasting serum bile acid levels in pregnancy are considerably higher than those in in the nonpregnant state, and an upper limit of 18 µmol/L has been proposed as a cutoff in pregnancy.9 However, nonfasting total serum bile acids also have been shown to vary considerably by race, with levels 25.8% higher in Black women compared with those in White women and 24.3% higher in Black women compared with those in south Asian women.9 This raises the question of whether we should be using race-specific bile acid values to make a diagnosis of ICP.
Bile acid levels also vary based on whether a patient is in a fasting or postprandial state.10 Despite this variation, most guidelines do not recommend testing fasting bile acid levels as the postprandial state effect overall is small.7,9,11 The Society for Maternal-Fetal Medicine (SMFM) recommends that if a pregnancy-specific bile acid range is available from the laboratory, then the upper limit of normal for pregnancy should be used when making a diagnosis of ICP.7 The SMFM guidelines also acknowledge, however, that pregnancy-specific values rarely are available, and in this case, levels above the upper limit of normal—often 10 µmol/L should be considered diagnostic for ICP until further evidence regarding optimal bile acid cutoff levels in pregnancy becomes available.7
For patients with suspected ICP, liver transaminase levels should be measured in addition to nonfasting serum bile acid levels.7 A thorough history should include assessment for additional symptoms of liver disease, such as changes in weight, appetite, jaundice, excessive fatigue, malaise, and abdominal pain.7 Elevated transaminases levels may be associated with ICP, but they are not necessary for diagnosis. In the absence of additional clinical symptoms that suggest underlying liver disease or severe early onset ICP, additional evaluation beyond nonfasting serum bile acids and liver transaminase levels, such as liver ultrasonography or evaluation for viral or autoimmune hepatitis, is not recommended.7 Obstetric care clinicians should be aware that there is an increased incidence of preeclampsia among patients with ICP, although no specific guidance regarding further recommendations for screening is provided.7
PHOTO: CHAJAMP/SHUTTERSTOCK
Continue to: Risks associated with ICP...
Risks associated with ICP
For both patients and clinicians, the greatest concern among patients with ICP is the increased risk of stillbirth. Stillbirth risk in ICP appears to be related to serum bile acid levels and has been reported to be highest in patients with bile acid levels greater than 100 µmol/L. A systematic review and meta-analysis of ICP studies demonstrated no increased risk of stillbirth among patients with bile acid levels less than 100 µmol/L.12 These results, however, must be interpreted with extreme caution as the majority of studies included patients with ICP who were actively managed with attempts to mitigate the risk of stillbirth.7
In the absence of additional pregnancy risk factors, the risk of stillbirth among patients with ICP and serum bile acid levels between 19 and 39 µmol/L does not appear to be elevated above their baseline risk.11 The same is true for pregnant individuals with ICP and no additional pregnancy risk factors with serum bile acid levels between 40 and 99 µmol/L until approximately 38 weeks’ gestation, when the risk of stillbirth is elevated.11 The risk of stillbirth is elevated in ICP with peak bile acid levels greater than 100 µmol/L, with an absolute risk of 3.44%.11
Management of patients with ICP
Laboratory evaluation
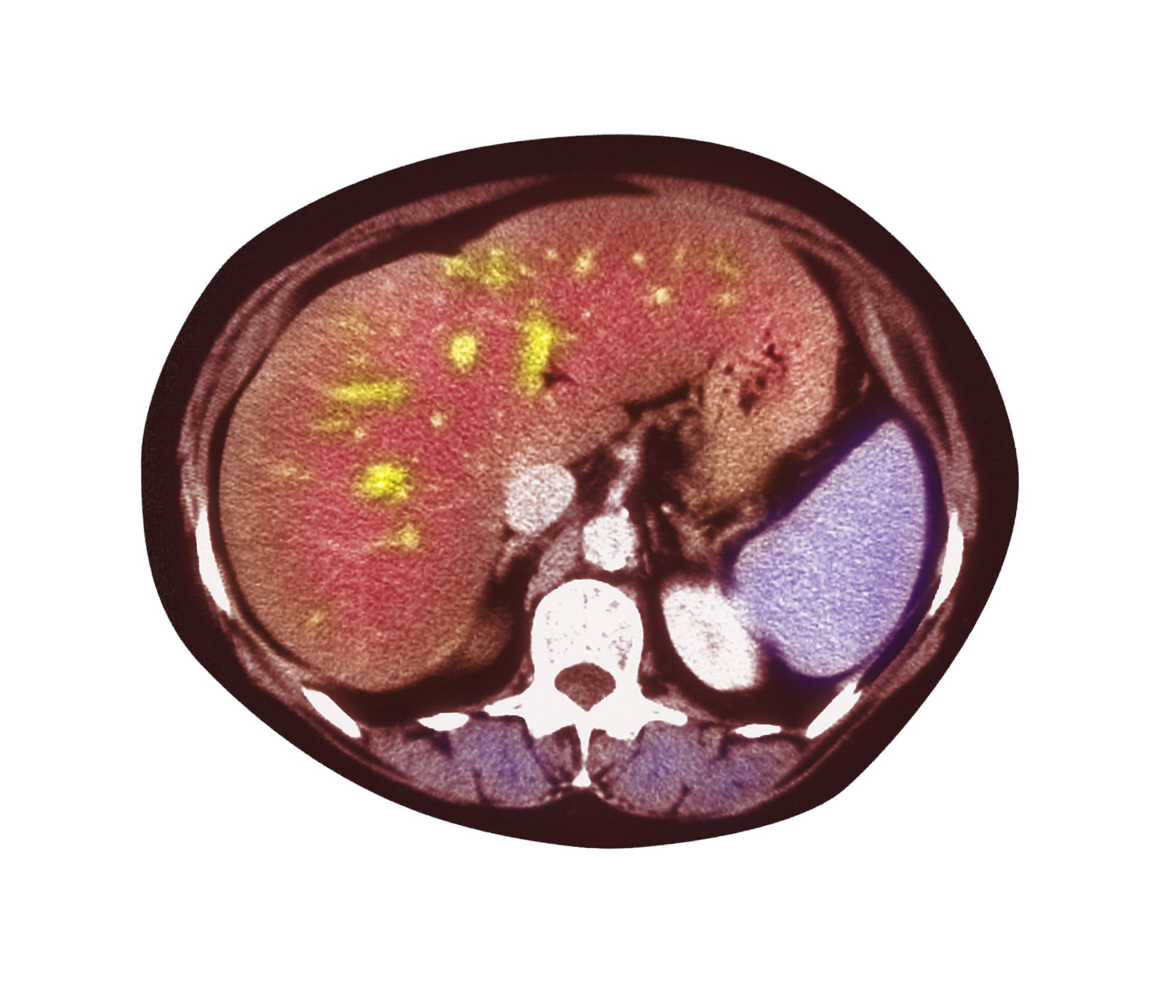
There is no consensus on the need for repeat testing of bile acid levels in patients with ICP. SMFM advises that follow-up testing of bile acid levels may help to guide delivery timing, especially in cases of severe ICP, but the society recommends against serial testing.7 By contrast, the Royal College of Obstetricians and Gynaecologists (RCOG) provides a detailed algorithm regarding time intervals between serum bile acid level testing to guide delivery timing.11 The TABLE lists the strategy for reassessment of serum bile acid levels in ICP as recommended by the RCOG.11
In the United States, bile acid testing traditionally takes several days as the testing is commonly performed at reference laboratories. We therefore suggest that clinicians consider repeating bile acid level testing in situations in which the timing of delivery may be altered if further elevations of bile acid levels were noted. This is particularly relevant for patients diagnosed with ICP early in the third trimester when repeat bile acid levels would still allow for an adjustment in delivery timing.
Antepartum fetal surveillance
Unfortunately, antepartum fetal testing for pregnant patients with ICP does not appear to reliably predict or prevent stillbirth as several studies have reported stillbirths within days of normal fetal testing.13-16 It is therefore important to counsel pregnant patients regarding monitoring of fetal movements and advise them to present for evaluation if concerns arise.
Currently, SMFM recommends that patients with ICP should begin antenatal fetal surveillance at a gestational age when abnormal fetal testing would result in delivery.7 Patients should be counseled, however, regarding the unpredictability of stillbirth with ICP in the setting of a low absolute risk of such.
Medications
While SMFM recommends a starting dose of ursodeoxycholic acid 10 to 15 mg/kg per day divided into 2 or 3 daily doses as first-line therapy for the treatment of maternal symptoms of ICP, it is important to acknowledge that the goal of treatment is to alleviate maternal symptoms as there is no evidence that ursodeoxycholic acid improves either maternal serum bile acid levels or perinatal outcomes.7,17,18 Since publication of the guidelines, ursodeoxycholic acid’s lack of benefit has been further confirmed in a meta-analysis, and thus discontinuation is not unreasonable in the absence of any improvement in maternal symptoms.18
Timing of delivery
The optimal management of ICP remains unknown. SMFM recommends delivery based on peak serum bile acid levels. Delivery is recommended at 36 weeks’ gestation with ICP and total bile acid levels greater than 100 µmol/L as these patients have the greatest risk of stillbirth.7 For patients with ICP and bile acid levels less than 100 µmol/L, delivery is recommended between 36 0/7 and 39 0/7 weeks’ gestation.7 This is a wide gestational age window for clinicians to consider timing of delivery, and certainly the risks of stillbirth should be carefully balanced with the morbidity associated with a preterm or early term delivery.
For patients with ICP who have bile acid levels greater than 40 µmol/L, it is reasonable to consider delivery earlier in the gestational age window, given an evidence of increased risk of stillbirth after 38 weeks.7,12 For patients with ICP who have bile acid levels less than 40 µmol/L, delivery closer to 39 weeks’ gestation is recommended, as the risk of stillbirth does not appear to be increased above the baseline risk.7,12 Clinicians should be aware that the presence of concomitant morbidities, such as preeclampsia and gestational diabetes, are associated with an increased risk of stillbirth and should be considered for delivery planning.19
Postpartum follow-up
Routine laboratory evaluation following delivery is not recommended.7 However, in the presence of persistent pruritus or other signs and symptoms of hepatobiliary disease, liver function tests should be repeated with referral to hepatology if results are persistently abnormal 4 to 6 weeks postpartum.7
CASE Patient follow-up and outcomes
The patient was counseled regarding the diagnosis of ICP. Following shared decision making, the patient opted to undergo twice weekly nonstress tests but was aware to carefully monitor fetal movements due to the unpredictability of stillbirth in ICP. The patient also opted to trial ursodeoxycholic acid for relief of maternal symptoms. Two weeks after her initial diagnosis, repeat total bile acid levels were stable at 22 µmol/L. Therefore, following extensive counseling, the patient opted to undergo induction of labor at 38 weeks’ gestation, with a normal outcome for mother and neonate. ●
References
Abedin P, Weaver JB, Egginton E. Intrahepatic cholestasis of pregnancy: prevalence and ethnic distribution. Ethn Health. 1999;4:35-37.
Kenyon AP, Tribe RM, Nelson-Piercy C, et al. Pruritus in pregnancy: a study of anatomical distribution and prevalence in relation to the development of obstetric cholestasis. Obstet Med. 2010;3:25-29.
Wikstrom Shemer E, Marschall HU, Ludvigsson JF, et al. Intrahepatic cholestasis of pregnancy and associated adverse pregnancy and fetal outcomes: a 12-year population-based cohort study. BJOG. 2013;120:717-723.
Ambros-Rudolph CM, Glatz M, Trauner M, et al. The importance of serum bile acid level analysis and treatment with ursodeoxycholic acid in intrahepatic cholestasis of pregnancy: a case series from central Europe. Arch Dermatol. 2007;143:757-762.
Szczech J, Wiatrowski A, Hirnle L, et al. Prevalence and relevance of pruritus in pregnancy. Biomed Res Int. 2017;2017:4238139.
Geenes V, Williamson C. Intrahepatic cholestasis of pregnancy. World J Gastroenterol. 2009;15:2049-2066.
Society for Maternal-Fetal Medicine; Lee RH, Greenberg M, Metz TD, et al. Society for Maternal-Fetal Medicine Consult Series #53: intrahepatic cholestasis of pregnancy: replaces Consult #13, April 2011. Am J Obstet Gynecol. 2021;224:B2-B9.
Horgan R, Bitas C, Abuhamad A. Intrahepatic cholestasis of pregnancy: a comparison of Society for Maternal-Fetal Medicine and the Royal College of Obstetricians and Gynaecologists’ guidelines. Am J Obstet Gynecol MFM. 2023;5:100838.
Mitchell AL, Ovadia C, Syngelaki A, et al. Re-evaluating diagnostic thresholds for intrahepatic cholestasis of pregnancy: case-control and cohort study. BJOG. 2021;128:1635-1644.
Adams A, Jacobs K, Vogel RI, et al. Bile acid determination after standardized glucose load in pregnant women. AJP Rep. 2015;5:e168-e171.
Girling J, Knight CL, Chappell L; Royal College of Obstetricians and Gynaecologists. Intrahepatic cholestasis of pregnancy: Green-top guideline no. 43, June 2022. BJOG. 2022;129:e95-e114.
Ovadia C, Seed PT, Sklavounos A, et al. Association of adverse perinatal outcomes of intrahepatic cholestasis of pregnancy with biochemical markers: results of aggregate and individual patient data meta-analyses. Lancet. 2019;393:899-909.
Alsulyman OM, Ouzounian JG, Ames-Castro M, et al. Intrahepatic cholestasis of pregnancy: perinatal outcome associated with expectant management. Am J Obstet Gynecol. 1996;175:957-960.
Herrera CA, Manuck TA, Stoddard GJ, et al. Perinatal outcomes associated with intrahepatic cholestasis of pregnancy. J Matern Fetal Neonatal Med. 2018;31:1913-1920.
Lee RH, Incerpi MH, Miller DA, et al. Sudden fetal death in intrahepatic cholestasis of pregnancy. Obstet Gynecol. 2009;113:528-531.
Sentilhes L, Verspyck E, Pia P, et al. Fetal death in a patient with intrahepatic cholestasis of pregnancy. Obstet Gynecol. 2006;107:458-460.
Chappell LC, Bell JL, Smith A, et al; PITCHES Study Group. Ursodeoxycholic acid versus placebo in women with intrahepatic cholestasis of pregnancy (PITCHES): a randomised controlled trial. Lancet. 2019;394:849-860.
Ovadia C, Sajous J, Seed PT, et al. Ursodeoxycholic acid in intrahepatic cholestasis of pregnancy: a systematic review and individual participant data meta-analysis. Lancet Gastroenterol Hepatol. 2021;6:547-558.
Geenes V, Chappell LC, Seed PT, et al. Association of severe intrahepatic cholestasis of pregnancy with adverse pregnancy outcomes: a prospective population-based case-control study. Hepatology. 2014;59:1482-1491.
A 28-year-old woman (G1P0) is seen for a routine prenatal visit at 32 3/7 weeks’ gestation. She reports having generalized intense itching, including on her palms and soles, that is most intense at night and has been present for approximately 1 week. Her pregnancy is otherwise uncomplicated to date. Physical exam is within normal limits, with no evidence of a skin rash. Cholestasis of pregnancy is suspected, and laboratory tests are ordered, including bile acids and liver transaminases. Test results show that her aspartate transaminase (AST) and alanine transaminase (ALT) levels are mildly elevated at 55 IU/L and 41 IU/L, respectively, and several days later her bile acid level result is 21 µmol/L.
How should this patient be managed?
Intrahepatic cholestasis of pregnancy (ICP) affects 0.5% to 0.7% of pregnant individuals and results in maternal pruritus and elevated serum bile acid levels.1-3 Pruritus in ICP typically is generalized, including occurrence on the palms of the hands and soles of the feet, and it often is reported to be worse at night.4 Up to 25% of pregnant women will develop pruritus during pregnancy but the majority will not have ICP.2,5 Patients with ICP have no associated rash, but clinicians may note excoriations on exam. ICP typically presents in the third trimester of pregnancy but has been reported to occur earlier in gestation.6
Making a diagnosis of ICP
The presence of maternal pruritus in the absence of a skin condition along with elevated levels of serum bile acids are required for the diagnosis of ICP.7 Thus, a thorough history and physical exam is recommended to rule out another skin condition that could potentially explain the patient’s pruritus.
Some controversy exists regarding the bile acid level cutoff that should be used to make a diagnosis of ICP.8 It has been noted that nonfasting serum bile acid levels in pregnancy are considerably higher than those in in the nonpregnant state, and an upper limit of 18 µmol/L has been proposed as a cutoff in pregnancy.9 However, nonfasting total serum bile acids also have been shown to vary considerably by race, with levels 25.8% higher in Black women compared with those in White women and 24.3% higher in Black women compared with those in south Asian women.9 This raises the question of whether we should be using race-specific bile acid values to make a diagnosis of ICP.
Bile acid levels also vary based on whether a patient is in a fasting or postprandial state.10 Despite this variation, most guidelines do not recommend testing fasting bile acid levels as the postprandial state effect overall is small.7,9,11 The Society for Maternal-Fetal Medicine (SMFM) recommends that if a pregnancy-specific bile acid range is available from the laboratory, then the upper limit of normal for pregnancy should be used when making a diagnosis of ICP.7 The SMFM guidelines also acknowledge, however, that pregnancy-specific values rarely are available, and in this case, levels above the upper limit of normal—often 10 µmol/L should be considered diagnostic for ICP until further evidence regarding optimal bile acid cutoff levels in pregnancy becomes available.7
For patients with suspected ICP, liver transaminase levels should be measured in addition to nonfasting serum bile acid levels.7 A thorough history should include assessment for additional symptoms of liver disease, such as changes in weight, appetite, jaundice, excessive fatigue, malaise, and abdominal pain.7 Elevated transaminases levels may be associated with ICP, but they are not necessary for diagnosis. In the absence of additional clinical symptoms that suggest underlying liver disease or severe early onset ICP, additional evaluation beyond nonfasting serum bile acids and liver transaminase levels, such as liver ultrasonography or evaluation for viral or autoimmune hepatitis, is not recommended.7 Obstetric care clinicians should be aware that there is an increased incidence of preeclampsia among patients with ICP, although no specific guidance regarding further recommendations for screening is provided.7
PHOTO: CHAJAMP/SHUTTERSTOCK
Continue to: Risks associated with ICP...
Risks associated with ICP
For both patients and clinicians, the greatest concern among patients with ICP is the increased risk of stillbirth. Stillbirth risk in ICP appears to be related to serum bile acid levels and has been reported to be highest in patients with bile acid levels greater than 100 µmol/L. A systematic review and meta-analysis of ICP studies demonstrated no increased risk of stillbirth among patients with bile acid levels less than 100 µmol/L.12 These results, however, must be interpreted with extreme caution as the majority of studies included patients with ICP who were actively managed with attempts to mitigate the risk of stillbirth.7
In the absence of additional pregnancy risk factors, the risk of stillbirth among patients with ICP and serum bile acid levels between 19 and 39 µmol/L does not appear to be elevated above their baseline risk.11 The same is true for pregnant individuals with ICP and no additional pregnancy risk factors with serum bile acid levels between 40 and 99 µmol/L until approximately 38 weeks’ gestation, when the risk of stillbirth is elevated.11 The risk of stillbirth is elevated in ICP with peak bile acid levels greater than 100 µmol/L, with an absolute risk of 3.44%.11
Management of patients with ICP
Laboratory evaluation
There is no consensus on the need for repeat testing of bile acid levels in patients with ICP. SMFM advises that follow-up testing of bile acid levels may help to guide delivery timing, especially in cases of severe ICP, but the society recommends against serial testing.7 By contrast, the Royal College of Obstetricians and Gynaecologists (RCOG) provides a detailed algorithm regarding time intervals between serum bile acid level testing to guide delivery timing.11 The TABLE lists the strategy for reassessment of serum bile acid levels in ICP as recommended by the RCOG.11
In the United States, bile acid testing traditionally takes several days as the testing is commonly performed at reference laboratories. We therefore suggest that clinicians consider repeating bile acid level testing in situations in which the timing of delivery may be altered if further elevations of bile acid levels were noted. This is particularly relevant for patients diagnosed with ICP early in the third trimester when repeat bile acid levels would still allow for an adjustment in delivery timing.
Antepartum fetal surveillance
Unfortunately, antepartum fetal testing for pregnant patients with ICP does not appear to reliably predict or prevent stillbirth as several studies have reported stillbirths within days of normal fetal testing.13-16 It is therefore important to counsel pregnant patients regarding monitoring of fetal movements and advise them to present for evaluation if concerns arise.
Currently, SMFM recommends that patients with ICP should begin antenatal fetal surveillance at a gestational age when abnormal fetal testing would result in delivery.7 Patients should be counseled, however, regarding the unpredictability of stillbirth with ICP in the setting of a low absolute risk of such.
Medications
While SMFM recommends a starting dose of ursodeoxycholic acid 10 to 15 mg/kg per day divided into 2 or 3 daily doses as first-line therapy for the treatment of maternal symptoms of ICP, it is important to acknowledge that the goal of treatment is to alleviate maternal symptoms as there is no evidence that ursodeoxycholic acid improves either maternal serum bile acid levels or perinatal outcomes.7,17,18 Since publication of the guidelines, ursodeoxycholic acid’s lack of benefit has been further confirmed in a meta-analysis, and thus discontinuation is not unreasonable in the absence of any improvement in maternal symptoms.18
Timing of delivery
The optimal management of ICP remains unknown. SMFM recommends delivery based on peak serum bile acid levels. Delivery is recommended at 36 weeks’ gestation with ICP and total bile acid levels greater than 100 µmol/L as these patients have the greatest risk of stillbirth.7 For patients with ICP and bile acid levels less than 100 µmol/L, delivery is recommended between 36 0/7 and 39 0/7 weeks’ gestation.7 This is a wide gestational age window for clinicians to consider timing of delivery, and certainly the risks of stillbirth should be carefully balanced with the morbidity associated with a preterm or early term delivery.
For patients with ICP who have bile acid levels greater than 40 µmol/L, it is reasonable to consider delivery earlier in the gestational age window, given an evidence of increased risk of stillbirth after 38 weeks.7,12 For patients with ICP who have bile acid levels less than 40 µmol/L, delivery closer to 39 weeks’ gestation is recommended, as the risk of stillbirth does not appear to be increased above the baseline risk.7,12 Clinicians should be aware that the presence of concomitant morbidities, such as preeclampsia and gestational diabetes, are associated with an increased risk of stillbirth and should be considered for delivery planning.19
Postpartum follow-up
Routine laboratory evaluation following delivery is not recommended.7 However, in the presence of persistent pruritus or other signs and symptoms of hepatobiliary disease, liver function tests should be repeated with referral to hepatology if results are persistently abnormal 4 to 6 weeks postpartum.7
CASE Patient follow-up and outcomes
The patient was counseled regarding the diagnosis of ICP. Following shared decision making, the patient opted to undergo twice weekly nonstress tests but was aware to carefully monitor fetal movements due to the unpredictability of stillbirth in ICP. The patient also opted to trial ursodeoxycholic acid for relief of maternal symptoms. Two weeks after her initial diagnosis, repeat total bile acid levels were stable at 22 µmol/L. Therefore, following extensive counseling, the patient opted to undergo induction of labor at 38 weeks’ gestation, with a normal outcome for mother and neonate. ●
CASE Pregnant woman with intense itching
A 28-year-old woman (G1P0) is seen for a routine prenatal visit at 32 3/7 weeks’ gestation. She reports having generalized intense itching, including on her palms and soles, that is most intense at night and has been present for approximately 1 week. Her pregnancy is otherwise uncomplicated to date. Physical exam is within normal limits, with no evidence of a skin rash. Cholestasis of pregnancy is suspected, and laboratory tests are ordered, including bile acids and liver transaminases. Test results show that her aspartate transaminase (AST) and alanine transaminase (ALT) levels are mildly elevated at 55 IU/L and 41 IU/L, respectively, and several days later her bile acid level result is 21 µmol/L.
How should this patient be managed?
Intrahepatic cholestasis of pregnancy (ICP) affects 0.5% to 0.7% of pregnant individuals and results in maternal pruritus and elevated serum bile acid levels.1-3 Pruritus in ICP typically is generalized, including occurrence on the palms of the hands and soles of the feet, and it often is reported to be worse at night.4 Up to 25% of pregnant women will develop pruritus during pregnancy but the majority will not have ICP.2,5 Patients with ICP have no associated rash, but clinicians may note excoriations on exam. ICP typically presents in the third trimester of pregnancy but has been reported to occur earlier in gestation.6
Making a diagnosis of ICP
The presence of maternal pruritus in the absence of a skin condition along with elevated levels of serum bile acids are required for the diagnosis of ICP.7 Thus, a thorough history and physical exam is recommended to rule out another skin condition that could potentially explain the patient’s pruritus.
Some controversy exists regarding the bile acid level cutoff that should be used to make a diagnosis of ICP.8 It has been noted that nonfasting serum bile acid levels in pregnancy are considerably higher than those in in the nonpregnant state, and an upper limit of 18 µmol/L has been proposed as a cutoff in pregnancy.9 However, nonfasting total serum bile acids also have been shown to vary considerably by race, with levels 25.8% higher in Black women compared with those in White women and 24.3% higher in Black women compared with those in south Asian women.9 This raises the question of whether we should be using race-specific bile acid values to make a diagnosis of ICP.
Bile acid levels also vary based on whether a patient is in a fasting or postprandial state.10 Despite this variation, most guidelines do not recommend testing fasting bile acid levels as the postprandial state effect overall is small.7,9,11 The Society for Maternal-Fetal Medicine (SMFM) recommends that if a pregnancy-specific bile acid range is available from the laboratory, then the upper limit of normal for pregnancy should be used when making a diagnosis of ICP.7 The SMFM guidelines also acknowledge, however, that pregnancy-specific values rarely are available, and in this case, levels above the upper limit of normal—often 10 µmol/L should be considered diagnostic for ICP until further evidence regarding optimal bile acid cutoff levels in pregnancy becomes available.7
For patients with suspected ICP, liver transaminase levels should be measured in addition to nonfasting serum bile acid levels.7 A thorough history should include assessment for additional symptoms of liver disease, such as changes in weight, appetite, jaundice, excessive fatigue, malaise, and abdominal pain.7 Elevated transaminases levels may be associated with ICP, but they are not necessary for diagnosis. In the absence of additional clinical symptoms that suggest underlying liver disease or severe early onset ICP, additional evaluation beyond nonfasting serum bile acids and liver transaminase levels, such as liver ultrasonography or evaluation for viral or autoimmune hepatitis, is not recommended.7 Obstetric care clinicians should be aware that there is an increased incidence of preeclampsia among patients with ICP, although no specific guidance regarding further recommendations for screening is provided.7
PHOTO: CHAJAMP/SHUTTERSTOCK
Continue to: Risks associated with ICP...
Risks associated with ICP
For both patients and clinicians, the greatest concern among patients with ICP is the increased risk of stillbirth. Stillbirth risk in ICP appears to be related to serum bile acid levels and has been reported to be highest in patients with bile acid levels greater than 100 µmol/L. A systematic review and meta-analysis of ICP studies demonstrated no increased risk of stillbirth among patients with bile acid levels less than 100 µmol/L.12 These results, however, must be interpreted with extreme caution as the majority of studies included patients with ICP who were actively managed with attempts to mitigate the risk of stillbirth.7
In the absence of additional pregnancy risk factors, the risk of stillbirth among patients with ICP and serum bile acid levels between 19 and 39 µmol/L does not appear to be elevated above their baseline risk.11 The same is true for pregnant individuals with ICP and no additional pregnancy risk factors with serum bile acid levels between 40 and 99 µmol/L until approximately 38 weeks’ gestation, when the risk of stillbirth is elevated.11 The risk of stillbirth is elevated in ICP with peak bile acid levels greater than 100 µmol/L, with an absolute risk of 3.44%.11
Management of patients with ICP
Laboratory evaluation
There is no consensus on the need for repeat testing of bile acid levels in patients with ICP. SMFM advises that follow-up testing of bile acid levels may help to guide delivery timing, especially in cases of severe ICP, but the society recommends against serial testing.7 By contrast, the Royal College of Obstetricians and Gynaecologists (RCOG) provides a detailed algorithm regarding time intervals between serum bile acid level testing to guide delivery timing.11 The TABLE lists the strategy for reassessment of serum bile acid levels in ICP as recommended by the RCOG.11
In the United States, bile acid testing traditionally takes several days as the testing is commonly performed at reference laboratories. We therefore suggest that clinicians consider repeating bile acid level testing in situations in which the timing of delivery may be altered if further elevations of bile acid levels were noted. This is particularly relevant for patients diagnosed with ICP early in the third trimester when repeat bile acid levels would still allow for an adjustment in delivery timing.
Antepartum fetal surveillance
Unfortunately, antepartum fetal testing for pregnant patients with ICP does not appear to reliably predict or prevent stillbirth as several studies have reported stillbirths within days of normal fetal testing.13-16 It is therefore important to counsel pregnant patients regarding monitoring of fetal movements and advise them to present for evaluation if concerns arise.
Currently, SMFM recommends that patients with ICP should begin antenatal fetal surveillance at a gestational age when abnormal fetal testing would result in delivery.7 Patients should be counseled, however, regarding the unpredictability of stillbirth with ICP in the setting of a low absolute risk of such.
Medications
While SMFM recommends a starting dose of ursodeoxycholic acid 10 to 15 mg/kg per day divided into 2 or 3 daily doses as first-line therapy for the treatment of maternal symptoms of ICP, it is important to acknowledge that the goal of treatment is to alleviate maternal symptoms as there is no evidence that ursodeoxycholic acid improves either maternal serum bile acid levels or perinatal outcomes.7,17,18 Since publication of the guidelines, ursodeoxycholic acid’s lack of benefit has been further confirmed in a meta-analysis, and thus discontinuation is not unreasonable in the absence of any improvement in maternal symptoms.18
Timing of delivery
The optimal management of ICP remains unknown. SMFM recommends delivery based on peak serum bile acid levels. Delivery is recommended at 36 weeks’ gestation with ICP and total bile acid levels greater than 100 µmol/L as these patients have the greatest risk of stillbirth.7 For patients with ICP and bile acid levels less than 100 µmol/L, delivery is recommended between 36 0/7 and 39 0/7 weeks’ gestation.7 This is a wide gestational age window for clinicians to consider timing of delivery, and certainly the risks of stillbirth should be carefully balanced with the morbidity associated with a preterm or early term delivery.
For patients with ICP who have bile acid levels greater than 40 µmol/L, it is reasonable to consider delivery earlier in the gestational age window, given an evidence of increased risk of stillbirth after 38 weeks.7,12 For patients with ICP who have bile acid levels less than 40 µmol/L, delivery closer to 39 weeks’ gestation is recommended, as the risk of stillbirth does not appear to be increased above the baseline risk.7,12 Clinicians should be aware that the presence of concomitant morbidities, such as preeclampsia and gestational diabetes, are associated with an increased risk of stillbirth and should be considered for delivery planning.19
Postpartum follow-up
Routine laboratory evaluation following delivery is not recommended.7 However, in the presence of persistent pruritus or other signs and symptoms of hepatobiliary disease, liver function tests should be repeated with referral to hepatology if results are persistently abnormal 4 to 6 weeks postpartum.7
CASE Patient follow-up and outcomes
The patient was counseled regarding the diagnosis of ICP. Following shared decision making, the patient opted to undergo twice weekly nonstress tests but was aware to carefully monitor fetal movements due to the unpredictability of stillbirth in ICP. The patient also opted to trial ursodeoxycholic acid for relief of maternal symptoms. Two weeks after her initial diagnosis, repeat total bile acid levels were stable at 22 µmol/L. Therefore, following extensive counseling, the patient opted to undergo induction of labor at 38 weeks’ gestation, with a normal outcome for mother and neonate. ●
References
Abedin P, Weaver JB, Egginton E. Intrahepatic cholestasis of pregnancy: prevalence and ethnic distribution. Ethn Health. 1999;4:35-37.
Kenyon AP, Tribe RM, Nelson-Piercy C, et al. Pruritus in pregnancy: a study of anatomical distribution and prevalence in relation to the development of obstetric cholestasis. Obstet Med. 2010;3:25-29.
Wikstrom Shemer E, Marschall HU, Ludvigsson JF, et al. Intrahepatic cholestasis of pregnancy and associated adverse pregnancy and fetal outcomes: a 12-year population-based cohort study. BJOG. 2013;120:717-723.
Ambros-Rudolph CM, Glatz M, Trauner M, et al. The importance of serum bile acid level analysis and treatment with ursodeoxycholic acid in intrahepatic cholestasis of pregnancy: a case series from central Europe. Arch Dermatol. 2007;143:757-762.
Szczech J, Wiatrowski A, Hirnle L, et al. Prevalence and relevance of pruritus in pregnancy. Biomed Res Int. 2017;2017:4238139.
Geenes V, Williamson C. Intrahepatic cholestasis of pregnancy. World J Gastroenterol. 2009;15:2049-2066.
Society for Maternal-Fetal Medicine; Lee RH, Greenberg M, Metz TD, et al. Society for Maternal-Fetal Medicine Consult Series #53: intrahepatic cholestasis of pregnancy: replaces Consult #13, April 2011. Am J Obstet Gynecol. 2021;224:B2-B9.
Horgan R, Bitas C, Abuhamad A. Intrahepatic cholestasis of pregnancy: a comparison of Society for Maternal-Fetal Medicine and the Royal College of Obstetricians and Gynaecologists’ guidelines. Am J Obstet Gynecol MFM. 2023;5:100838.
Mitchell AL, Ovadia C, Syngelaki A, et al. Re-evaluating diagnostic thresholds for intrahepatic cholestasis of pregnancy: case-control and cohort study. BJOG. 2021;128:1635-1644.
Adams A, Jacobs K, Vogel RI, et al. Bile acid determination after standardized glucose load in pregnant women. AJP Rep. 2015;5:e168-e171.
Girling J, Knight CL, Chappell L; Royal College of Obstetricians and Gynaecologists. Intrahepatic cholestasis of pregnancy: Green-top guideline no. 43, June 2022. BJOG. 2022;129:e95-e114.
Ovadia C, Seed PT, Sklavounos A, et al. Association of adverse perinatal outcomes of intrahepatic cholestasis of pregnancy with biochemical markers: results of aggregate and individual patient data meta-analyses. Lancet. 2019;393:899-909.
Alsulyman OM, Ouzounian JG, Ames-Castro M, et al. Intrahepatic cholestasis of pregnancy: perinatal outcome associated with expectant management. Am J Obstet Gynecol. 1996;175:957-960.
Herrera CA, Manuck TA, Stoddard GJ, et al. Perinatal outcomes associated with intrahepatic cholestasis of pregnancy. J Matern Fetal Neonatal Med. 2018;31:1913-1920.
Lee RH, Incerpi MH, Miller DA, et al. Sudden fetal death in intrahepatic cholestasis of pregnancy. Obstet Gynecol. 2009;113:528-531.
Sentilhes L, Verspyck E, Pia P, et al. Fetal death in a patient with intrahepatic cholestasis of pregnancy. Obstet Gynecol. 2006;107:458-460.
Chappell LC, Bell JL, Smith A, et al; PITCHES Study Group. Ursodeoxycholic acid versus placebo in women with intrahepatic cholestasis of pregnancy (PITCHES): a randomised controlled trial. Lancet. 2019;394:849-860.
Ovadia C, Sajous J, Seed PT, et al. Ursodeoxycholic acid in intrahepatic cholestasis of pregnancy: a systematic review and individual participant data meta-analysis. Lancet Gastroenterol Hepatol. 2021;6:547-558.
Geenes V, Chappell LC, Seed PT, et al. Association of severe intrahepatic cholestasis of pregnancy with adverse pregnancy outcomes: a prospective population-based case-control study. Hepatology. 2014;59:1482-1491.
References
Abedin P, Weaver JB, Egginton E. Intrahepatic cholestasis of pregnancy: prevalence and ethnic distribution. Ethn Health. 1999;4:35-37.
Kenyon AP, Tribe RM, Nelson-Piercy C, et al. Pruritus in pregnancy: a study of anatomical distribution and prevalence in relation to the development of obstetric cholestasis. Obstet Med. 2010;3:25-29.
Wikstrom Shemer E, Marschall HU, Ludvigsson JF, et al. Intrahepatic cholestasis of pregnancy and associated adverse pregnancy and fetal outcomes: a 12-year population-based cohort study. BJOG. 2013;120:717-723.
Ambros-Rudolph CM, Glatz M, Trauner M, et al. The importance of serum bile acid level analysis and treatment with ursodeoxycholic acid in intrahepatic cholestasis of pregnancy: a case series from central Europe. Arch Dermatol. 2007;143:757-762.
Szczech J, Wiatrowski A, Hirnle L, et al. Prevalence and relevance of pruritus in pregnancy. Biomed Res Int. 2017;2017:4238139.
Geenes V, Williamson C. Intrahepatic cholestasis of pregnancy. World J Gastroenterol. 2009;15:2049-2066.
Society for Maternal-Fetal Medicine; Lee RH, Greenberg M, Metz TD, et al. Society for Maternal-Fetal Medicine Consult Series #53: intrahepatic cholestasis of pregnancy: replaces Consult #13, April 2011. Am J Obstet Gynecol. 2021;224:B2-B9.
Horgan R, Bitas C, Abuhamad A. Intrahepatic cholestasis of pregnancy: a comparison of Society for Maternal-Fetal Medicine and the Royal College of Obstetricians and Gynaecologists’ guidelines. Am J Obstet Gynecol MFM. 2023;5:100838.
Mitchell AL, Ovadia C, Syngelaki A, et al. Re-evaluating diagnostic thresholds for intrahepatic cholestasis of pregnancy: case-control and cohort study. BJOG. 2021;128:1635-1644.
Adams A, Jacobs K, Vogel RI, et al. Bile acid determination after standardized glucose load in pregnant women. AJP Rep. 2015;5:e168-e171.
Girling J, Knight CL, Chappell L; Royal College of Obstetricians and Gynaecologists. Intrahepatic cholestasis of pregnancy: Green-top guideline no. 43, June 2022. BJOG. 2022;129:e95-e114.
Ovadia C, Seed PT, Sklavounos A, et al. Association of adverse perinatal outcomes of intrahepatic cholestasis of pregnancy with biochemical markers: results of aggregate and individual patient data meta-analyses. Lancet. 2019;393:899-909.
Alsulyman OM, Ouzounian JG, Ames-Castro M, et al. Intrahepatic cholestasis of pregnancy: perinatal outcome associated with expectant management. Am J Obstet Gynecol. 1996;175:957-960.
Herrera CA, Manuck TA, Stoddard GJ, et al. Perinatal outcomes associated with intrahepatic cholestasis of pregnancy. J Matern Fetal Neonatal Med. 2018;31:1913-1920.
Lee RH, Incerpi MH, Miller DA, et al. Sudden fetal death in intrahepatic cholestasis of pregnancy. Obstet Gynecol. 2009;113:528-531.
Sentilhes L, Verspyck E, Pia P, et al. Fetal death in a patient with intrahepatic cholestasis of pregnancy. Obstet Gynecol. 2006;107:458-460.
Chappell LC, Bell JL, Smith A, et al; PITCHES Study Group. Ursodeoxycholic acid versus placebo in women with intrahepatic cholestasis of pregnancy (PITCHES): a randomised controlled trial. Lancet. 2019;394:849-860.
Ovadia C, Sajous J, Seed PT, et al. Ursodeoxycholic acid in intrahepatic cholestasis of pregnancy: a systematic review and individual participant data meta-analysis. Lancet Gastroenterol Hepatol. 2021;6:547-558.
Geenes V, Chappell LC, Seed PT, et al. Association of severe intrahepatic cholestasis of pregnancy with adverse pregnancy outcomes: a prospective population-based case-control study. Hepatology. 2014;59:1482-1491.
The patient's history of psoriasis, along with his current skin and scalp plaque flares, symmetrical joint symptomatology, laboratory studies, and x-rays, suggest a diagnosis of symmetrical psoriatic arthritis (PsA). The rheumatologist considers ordering additional imaging to assess for subclinical enthesitis and dactylitis, and discusses treatment next steps with the patient, given inadequate control with a TNF inhibitor.
Symmetrical polyarthritis is one of the most common types of PsA and involves five or more joints in the hands, wrists, ankles, and/or feet. Among patients with PsA, 60% to 80% experience plaque psoriasis before joint-symptom onset; time to joint-symptom onset in these patients typically occurs within 10 years of a plaque psoriasis diagnosis. Involvement of DIP joints differentiates PsA from rheumatoid arthritis, as does the absence of subcutaneous nodules and a negative result for rheumatoid factor. About 30% of all people with plaque psoriasis will develop PsA, which affects an estimated 1 million people in the United States annually. Symptoms typically appear between the ages of 35 and 55 years; women are more likely than men to develop symmetrical PsA.
There are no specific diagnostic tests for PsA. Rheumatologists generally use the assessment known as the Classification Criteria for Psoriatic Arthritis, (CASPAR), which can help reveal established inflammatory articular disease through a point system based on the presence/absence of various factors. On laboratory studies, the most common characteristic abnormalities of PsA are elevated ESR and CRP levels and negative rheumatoid factor in most patients. Other abnormalities that may be present in patients with PsA include elevated serum uric acid concentration and serum immunoglobulin A, and reduced levels of circulating immune complexes. Physicians also use imaging studies, such as radiography, ultrasonography, and MRI, to help differentiate PsA from other articular diseases.
While the pathogenesis of PsA remains unclear, research has shown that disease development is associated with a complex interplay of immune-mediated inflammatory responses; genetic and environmental factors may also be involved. In addition, patients with PsA are more likely to have a high risk for comorbidities, including obesity, type 2 diabetes, hypertension, hyperlipidemia, and cardiovascular events, compared with the general population.
When patients with PsA experience both skin and joint symptoms, a multidisciplinary approach to care is advised. Multidisciplinary teams play a key role in educating patients about their treatment plans and managing their PsA symptoms. The teams also help patients determine the best approaches to exercise to help maintain current joint function, as well as helpful adjustments in daily activities that will make it easier to accommodate their disease.
Nonsteroidal anti-inflammatory drugs, whether self-prescribed or prescribed by a physician, are a common initial treatment to manage joint symptoms of PsA. Current American College of Rheumatology treatment guidelines, however, encourage early treatment with disease-modifying antirheumatic drugs (DMARDs) because approximately 40% of patients with PsA develop erosive and deforming arthritis. Several DMARDs are available, including older drugs like methotrexate, as well as newer biologic agents, such as TNF inhibitors, interleukin (IL)-17 inhibitors, IL-12/23 inhibitors, and Janus kinase inhibitors. In addition, guidelines recommend early and customized physical therapy and rehabilitation approaches for patients with PsA.
Herbert S. Diamond, MD, Professor of Medicine (retired), Temple University School of Medicine, University of Pittsburgh; Chairman, Department of Medicine Emeritus, Western Pennsylvania Hospital, Pittsburgh, PA.
Herbert S. Diamond, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The patient's history of psoriasis, along with his current skin and scalp plaque flares, symmetrical joint symptomatology, laboratory studies, and x-rays, suggest a diagnosis of symmetrical psoriatic arthritis (PsA). The rheumatologist considers ordering additional imaging to assess for subclinical enthesitis and dactylitis, and discusses treatment next steps with the patient, given inadequate control with a TNF inhibitor.
Symmetrical polyarthritis is one of the most common types of PsA and involves five or more joints in the hands, wrists, ankles, and/or feet. Among patients with PsA, 60% to 80% experience plaque psoriasis before joint-symptom onset; time to joint-symptom onset in these patients typically occurs within 10 years of a plaque psoriasis diagnosis. Involvement of DIP joints differentiates PsA from rheumatoid arthritis, as does the absence of subcutaneous nodules and a negative result for rheumatoid factor. About 30% of all people with plaque psoriasis will develop PsA, which affects an estimated 1 million people in the United States annually. Symptoms typically appear between the ages of 35 and 55 years; women are more likely than men to develop symmetrical PsA.
There are no specific diagnostic tests for PsA. Rheumatologists generally use the assessment known as the Classification Criteria for Psoriatic Arthritis, (CASPAR), which can help reveal established inflammatory articular disease through a point system based on the presence/absence of various factors. On laboratory studies, the most common characteristic abnormalities of PsA are elevated ESR and CRP levels and negative rheumatoid factor in most patients. Other abnormalities that may be present in patients with PsA include elevated serum uric acid concentration and serum immunoglobulin A, and reduced levels of circulating immune complexes. Physicians also use imaging studies, such as radiography, ultrasonography, and MRI, to help differentiate PsA from other articular diseases.
While the pathogenesis of PsA remains unclear, research has shown that disease development is associated with a complex interplay of immune-mediated inflammatory responses; genetic and environmental factors may also be involved. In addition, patients with PsA are more likely to have a high risk for comorbidities, including obesity, type 2 diabetes, hypertension, hyperlipidemia, and cardiovascular events, compared with the general population.
When patients with PsA experience both skin and joint symptoms, a multidisciplinary approach to care is advised. Multidisciplinary teams play a key role in educating patients about their treatment plans and managing their PsA symptoms. The teams also help patients determine the best approaches to exercise to help maintain current joint function, as well as helpful adjustments in daily activities that will make it easier to accommodate their disease.
Nonsteroidal anti-inflammatory drugs, whether self-prescribed or prescribed by a physician, are a common initial treatment to manage joint symptoms of PsA. Current American College of Rheumatology treatment guidelines, however, encourage early treatment with disease-modifying antirheumatic drugs (DMARDs) because approximately 40% of patients with PsA develop erosive and deforming arthritis. Several DMARDs are available, including older drugs like methotrexate, as well as newer biologic agents, such as TNF inhibitors, interleukin (IL)-17 inhibitors, IL-12/23 inhibitors, and Janus kinase inhibitors. In addition, guidelines recommend early and customized physical therapy and rehabilitation approaches for patients with PsA.
Herbert S. Diamond, MD, Professor of Medicine (retired), Temple University School of Medicine, University of Pittsburgh; Chairman, Department of Medicine Emeritus, Western Pennsylvania Hospital, Pittsburgh, PA.
Herbert S. Diamond, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The patient's history of psoriasis, along with his current skin and scalp plaque flares, symmetrical joint symptomatology, laboratory studies, and x-rays, suggest a diagnosis of symmetrical psoriatic arthritis (PsA). The rheumatologist considers ordering additional imaging to assess for subclinical enthesitis and dactylitis, and discusses treatment next steps with the patient, given inadequate control with a TNF inhibitor.
Symmetrical polyarthritis is one of the most common types of PsA and involves five or more joints in the hands, wrists, ankles, and/or feet. Among patients with PsA, 60% to 80% experience plaque psoriasis before joint-symptom onset; time to joint-symptom onset in these patients typically occurs within 10 years of a plaque psoriasis diagnosis. Involvement of DIP joints differentiates PsA from rheumatoid arthritis, as does the absence of subcutaneous nodules and a negative result for rheumatoid factor. About 30% of all people with plaque psoriasis will develop PsA, which affects an estimated 1 million people in the United States annually. Symptoms typically appear between the ages of 35 and 55 years; women are more likely than men to develop symmetrical PsA.
There are no specific diagnostic tests for PsA. Rheumatologists generally use the assessment known as the Classification Criteria for Psoriatic Arthritis, (CASPAR), which can help reveal established inflammatory articular disease through a point system based on the presence/absence of various factors. On laboratory studies, the most common characteristic abnormalities of PsA are elevated ESR and CRP levels and negative rheumatoid factor in most patients. Other abnormalities that may be present in patients with PsA include elevated serum uric acid concentration and serum immunoglobulin A, and reduced levels of circulating immune complexes. Physicians also use imaging studies, such as radiography, ultrasonography, and MRI, to help differentiate PsA from other articular diseases.
While the pathogenesis of PsA remains unclear, research has shown that disease development is associated with a complex interplay of immune-mediated inflammatory responses; genetic and environmental factors may also be involved. In addition, patients with PsA are more likely to have a high risk for comorbidities, including obesity, type 2 diabetes, hypertension, hyperlipidemia, and cardiovascular events, compared with the general population.
When patients with PsA experience both skin and joint symptoms, a multidisciplinary approach to care is advised. Multidisciplinary teams play a key role in educating patients about their treatment plans and managing their PsA symptoms. The teams also help patients determine the best approaches to exercise to help maintain current joint function, as well as helpful adjustments in daily activities that will make it easier to accommodate their disease.
Nonsteroidal anti-inflammatory drugs, whether self-prescribed or prescribed by a physician, are a common initial treatment to manage joint symptoms of PsA. Current American College of Rheumatology treatment guidelines, however, encourage early treatment with disease-modifying antirheumatic drugs (DMARDs) because approximately 40% of patients with PsA develop erosive and deforming arthritis. Several DMARDs are available, including older drugs like methotrexate, as well as newer biologic agents, such as TNF inhibitors, interleukin (IL)-17 inhibitors, IL-12/23 inhibitors, and Janus kinase inhibitors. In addition, guidelines recommend early and customized physical therapy and rehabilitation approaches for patients with PsA.
Herbert S. Diamond, MD, Professor of Medicine (retired), Temple University School of Medicine, University of Pittsburgh; Chairman, Department of Medicine Emeritus, Western Pennsylvania Hospital, Pittsburgh, PA.
Herbert S. Diamond, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
A 43-year-old White man with a 5-year history of plaque psoriasis presents to a rheumatologist on referral from his dermatologist. He had been taking a tumor necrosis factor (TNF) inhibitor, which had controlled his skin and scalp plaques since diagnosis. Lately, however, some of the plaques have begun to flare up, and the patient reports new tenderness and swelling in three of the same joints on his left and right hands and extensive fatigue. Additional medical history includes type 2 diabetes, which was diagnosed 3 years ago; soon thereafter, he started taking metformin with consistent disease control. The rheumatologist conducts a physical exam and orders laboratory studies and x-rays. Results of the laboratory studies reveal elevated levels of C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). Radiographs reveal joint-space narrowing in several distal interphalangeal (DIP) joints in both hands, with mild erosive disease.
Disallow All Ads
Content Gating
No Gating (article Unlocked/Free)
Alternative CME
Disqus Comments
Default
Gate On Date
Un-Gate On Date
Consolidated Pubs: Do Not Show Source Publication Logo
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273-282. doi:10.1016/j.ajcnut.2023.05.011.
EXPERT COMMENTARY
Preservation of function, both physical and cognitive, is key to long-term health and well-being. Age-related loss of function drives millions of people to spend an enormous amount of money each year on unregulated therapies—vitamins, supplements, infusions, hormones, and “natural” products—all toward the promise of improvement or preservation of physical strength, sexual function, and maintenance of lean body mass and cognitive abilities. Yeung and colleagues set out to determine whether the daily use of a multivitamin/mineral supplement (Centrum Silver) would impact memory in older adults.1
PHOTO: KLAVDIYAV/SHUTTERSTOCK
Details of the study
The COSMOS-Web study was designed to test the authors’ primary hypothesis that daily dietary flavanols would improve memory over 1 year.1 This study was embedded within the larger COSMOS (COcoa Supplement and Multivitamin Outcomes Study) trial, in which 21,442 people were recruited to assess the impact of flavanols and multivitamin supplements on cardiovascular and cancer outcomes.
Results of another ancillary study, the COSMOS-Mind trial (n = 2,262, average age 73, 60% female), reported no improvement with flavanols compared with placebo on a battery of tests of cognitive function administered by phone. In COSMOS-Mind, however, it was concluded that a daily multivitamin/mineral supplement improved the composite score of cognitive tests compared with placebo, particularly in participants with a history of cardiovascular disease.2
The COSMOS-Web trial recruited an additional cohort within the larger COSMOS trial from 2016–2017 (n = 3,562, average age 71, 67% female) to participate in this study specifically geared to assess memory, using the web-based ModRey test (a test of memory validated for use in a nonimpaired population). To qualify for enrollment, participants had to have access to an internet-connected computer. They were randomly assigned in a 2 x 2 study design to receive a daily multivitamin supplement or placebo; each of these cohorts was further divided into a flavanol supplementation or a placebo group. Analysis of the data showed no association between flavanol use and performance on any of the measures of memory or cognitive function.3
The COSMOS-Web trial assessed episodic recall, a function of hippocampus-mediated cognition that is particularly vulnerable to the effects of aging as demonstrated previously by neuroimaging and neuropsychological studies. The authors deployed a battery of 3 tests via a web platform for patients to complete online and independently.
The prespecified primary outcome was performance on episodic recall as measured by the ModRey test after 1 year of supplementation with multivitamins versus placebo. The ModRey test presents a series of 20 words at 3-second intervals to participants. At the conclusion of the last word, participants were asked to recall as many words as they could; after completing the 2 additional tasks, participants were asked again to recall the words. A secondary outcome of this test is the ratio of delayed to immediate recall.
Two additional tests were administered to assess cognitive performance related to different brain regions, the ModBent test (assessing novel object recognition) and the Flanker task (a measure of executive function). There was a placebo run-in phase during which participants’ adherence to daily supplement intake was ascertained. Participants were excluded if they demonstrated less than 75% adherence to study pills during the run-in placebo phase. The cognitive tasks were presented at study initiation and at yearly intervals for 3 years. The authors chose to use the results at 1 year as their primary outcome to assess the impact of supplementation during the period when adherence would be highest.
Results.At baseline, the placebo cohort recalled 7.2 words of 20 compared with 7.1 in the supplement group. In both groups there was a practice effect, with improvement in scores in the placebo group to 7.65 words and in the multivitamin group to 7.81 words. The improvement from baseline was statistically significantly better (0.71 words) in the multivitamin cohort than in the placebo group (0.45 words). There was no improvement in either group in the ModRey memory retention test (ability to recall the words after 15 minutes) or in the ModBent or Flanker tests. At 3 years of treatment, the placebo group improved by 0.92 words (SD, 3.22) whereas the multivitamin group improved by 1.13 words (SD, 3.39). These changes remained statistically significant.
The group with cardiovascular disease had lower baseline performance on the ModRey test. With supplementation, however, the improvement in this cohort was significantly greater than in those without cardiovascular disease at 1 year. The authors acknowledged that the changes were small and may not have been noticeable to the individuals, but they argued that even small changes as demonstrated in this study can have large health benefits at a population level.
The results of the COSMOS-Web trial corroborate the findings of the COSMOS-Mind study with respect to the benefits of multivitamin/mineral supplementation on cognitive test performance, particularly in a population with preexisting cardiovascular disease. The tests used across the 2 studies were different, which lends greater reliability to the findings.
Study strengths and limitations
A major strength of this study is its careful, rigorous design as a double-blind, placebo-controlled trial in a large patient population. Great care was devoted to ensuring study medication adherence. Another strength is that the cognitive tests chosen for the COSMOS-Web trial have been validated in cognitively normal populations, not those already impaired.
A limitation, however, is in the demographics of the study. The patient population was overwhelmingly White (93%), 67% were female, and they were well educated (94.8% having completed some college or beyond). Their baseline health was good; only 4.7% had a history of cardiovascular disease. Although generalizability of the study results from this population may be concerning,relative benefits of supplementation in this healthy, generally well-nourished and educated group may be lower than might be expected in a more nutritionally and educationally challenged population.
Finally, the difference between the placebo and active supplementation groups was small. Whether this less-than-1-word difference in immediate memory recall is noticeable by a patient is questionable. Both groups improved in their test performance over time—a consequence of serial cognitive tests of any kind. Although the authors calculated that the difference in recall translates to a 3-year reduction in age-related memory decline, it is hard to reconcile that with the fact that both groups actually improved over the 3 years of the study. ●
Acknowledgement
The author would like to thank JoAnn Manson, MD, DrPH, NCMP, for her assistance in evaluating the study.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
In this well-designed, randomized controlled trial by Yeung and colleagues, multivitamin/mineral supplementation improved performance on a test of immediate episodic memory at 1, 2, and 3 years compared with placebo. Given the simplicity and safety of this intervention, even with a small effect size, it makes sense to advise older patients that daily multivitamin use provides micronutrients and vitamins that may be absent in the diet or poorly absorbed by older adults. Whether this highly specific improvement in a test of hippocampal function translates into overall cognitive performance with aging remains a question.
BARBARA LEVY, MD
References
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273282. doi:10.1016/j.ajcnut.2023.05.011.
Baker LD, Manson JE, Rapp SR, et al. Effects of cocoa extract and a multivitamin on cognitive function: a randomized clinical trial. Alzheimers Dement. 2023;19:1308-1319. doi:10.1002/alz.12767.
Brickman AM, Yeung LK, Alshuler DM, et al. Dietary flavanols restore hippocampal-dependent memory in older adults with lower diet quality and lower habitual flavanol consumption. Proc Natl Acad Sci USA. 2023:120:e2216932120. doi:10.1073/ pnas.2216932120.
Barbara Levy, MD, is Clinical Professor of Obstetrics and Gynecology, George Washington University School of Medicine and Health Sciences, Washington, DC, and Voluntary Clinical Professor of Obstetrics, Gynecology and Reproductive Sciences, UC San Diego School of Medicine. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Barbara Levy, MD, is Clinical Professor of Obstetrics and Gynecology, George Washington University School of Medicine and Health Sciences, Washington, DC, and Voluntary Clinical Professor of Obstetrics, Gynecology and Reproductive Sciences, UC San Diego School of Medicine. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Author and Disclosure Information
Barbara Levy, MD, is Clinical Professor of Obstetrics and Gynecology, George Washington University School of Medicine and Health Sciences, Washington, DC, and Voluntary Clinical Professor of Obstetrics, Gynecology and Reproductive Sciences, UC San Diego School of Medicine. She serves on the OBG Management Board of Editors.
The author reports no financial relationships relevant to this article.
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273-282. doi:10.1016/j.ajcnut.2023.05.011.
EXPERT COMMENTARY
Preservation of function, both physical and cognitive, is key to long-term health and well-being. Age-related loss of function drives millions of people to spend an enormous amount of money each year on unregulated therapies—vitamins, supplements, infusions, hormones, and “natural” products—all toward the promise of improvement or preservation of physical strength, sexual function, and maintenance of lean body mass and cognitive abilities. Yeung and colleagues set out to determine whether the daily use of a multivitamin/mineral supplement (Centrum Silver) would impact memory in older adults.1
PHOTO: KLAVDIYAV/SHUTTERSTOCK
Details of the study
The COSMOS-Web study was designed to test the authors’ primary hypothesis that daily dietary flavanols would improve memory over 1 year.1 This study was embedded within the larger COSMOS (COcoa Supplement and Multivitamin Outcomes Study) trial, in which 21,442 people were recruited to assess the impact of flavanols and multivitamin supplements on cardiovascular and cancer outcomes.
Results of another ancillary study, the COSMOS-Mind trial (n = 2,262, average age 73, 60% female), reported no improvement with flavanols compared with placebo on a battery of tests of cognitive function administered by phone. In COSMOS-Mind, however, it was concluded that a daily multivitamin/mineral supplement improved the composite score of cognitive tests compared with placebo, particularly in participants with a history of cardiovascular disease.2
The COSMOS-Web trial recruited an additional cohort within the larger COSMOS trial from 2016–2017 (n = 3,562, average age 71, 67% female) to participate in this study specifically geared to assess memory, using the web-based ModRey test (a test of memory validated for use in a nonimpaired population). To qualify for enrollment, participants had to have access to an internet-connected computer. They were randomly assigned in a 2 x 2 study design to receive a daily multivitamin supplement or placebo; each of these cohorts was further divided into a flavanol supplementation or a placebo group. Analysis of the data showed no association between flavanol use and performance on any of the measures of memory or cognitive function.3
The COSMOS-Web trial assessed episodic recall, a function of hippocampus-mediated cognition that is particularly vulnerable to the effects of aging as demonstrated previously by neuroimaging and neuropsychological studies. The authors deployed a battery of 3 tests via a web platform for patients to complete online and independently.
The prespecified primary outcome was performance on episodic recall as measured by the ModRey test after 1 year of supplementation with multivitamins versus placebo. The ModRey test presents a series of 20 words at 3-second intervals to participants. At the conclusion of the last word, participants were asked to recall as many words as they could; after completing the 2 additional tasks, participants were asked again to recall the words. A secondary outcome of this test is the ratio of delayed to immediate recall.
Two additional tests were administered to assess cognitive performance related to different brain regions, the ModBent test (assessing novel object recognition) and the Flanker task (a measure of executive function). There was a placebo run-in phase during which participants’ adherence to daily supplement intake was ascertained. Participants were excluded if they demonstrated less than 75% adherence to study pills during the run-in placebo phase. The cognitive tasks were presented at study initiation and at yearly intervals for 3 years. The authors chose to use the results at 1 year as their primary outcome to assess the impact of supplementation during the period when adherence would be highest.
Results.At baseline, the placebo cohort recalled 7.2 words of 20 compared with 7.1 in the supplement group. In both groups there was a practice effect, with improvement in scores in the placebo group to 7.65 words and in the multivitamin group to 7.81 words. The improvement from baseline was statistically significantly better (0.71 words) in the multivitamin cohort than in the placebo group (0.45 words). There was no improvement in either group in the ModRey memory retention test (ability to recall the words after 15 minutes) or in the ModBent or Flanker tests. At 3 years of treatment, the placebo group improved by 0.92 words (SD, 3.22) whereas the multivitamin group improved by 1.13 words (SD, 3.39). These changes remained statistically significant.
The group with cardiovascular disease had lower baseline performance on the ModRey test. With supplementation, however, the improvement in this cohort was significantly greater than in those without cardiovascular disease at 1 year. The authors acknowledged that the changes were small and may not have been noticeable to the individuals, but they argued that even small changes as demonstrated in this study can have large health benefits at a population level.
The results of the COSMOS-Web trial corroborate the findings of the COSMOS-Mind study with respect to the benefits of multivitamin/mineral supplementation on cognitive test performance, particularly in a population with preexisting cardiovascular disease. The tests used across the 2 studies were different, which lends greater reliability to the findings.
Study strengths and limitations
A major strength of this study is its careful, rigorous design as a double-blind, placebo-controlled trial in a large patient population. Great care was devoted to ensuring study medication adherence. Another strength is that the cognitive tests chosen for the COSMOS-Web trial have been validated in cognitively normal populations, not those already impaired.
A limitation, however, is in the demographics of the study. The patient population was overwhelmingly White (93%), 67% were female, and they were well educated (94.8% having completed some college or beyond). Their baseline health was good; only 4.7% had a history of cardiovascular disease. Although generalizability of the study results from this population may be concerning,relative benefits of supplementation in this healthy, generally well-nourished and educated group may be lower than might be expected in a more nutritionally and educationally challenged population.
Finally, the difference between the placebo and active supplementation groups was small. Whether this less-than-1-word difference in immediate memory recall is noticeable by a patient is questionable. Both groups improved in their test performance over time—a consequence of serial cognitive tests of any kind. Although the authors calculated that the difference in recall translates to a 3-year reduction in age-related memory decline, it is hard to reconcile that with the fact that both groups actually improved over the 3 years of the study. ●
Acknowledgement
The author would like to thank JoAnn Manson, MD, DrPH, NCMP, for her assistance in evaluating the study.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
In this well-designed, randomized controlled trial by Yeung and colleagues, multivitamin/mineral supplementation improved performance on a test of immediate episodic memory at 1, 2, and 3 years compared with placebo. Given the simplicity and safety of this intervention, even with a small effect size, it makes sense to advise older patients that daily multivitamin use provides micronutrients and vitamins that may be absent in the diet or poorly absorbed by older adults. Whether this highly specific improvement in a test of hippocampal function translates into overall cognitive performance with aging remains a question.
BARBARA LEVY, MD
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273-282. doi:10.1016/j.ajcnut.2023.05.011.
EXPERT COMMENTARY
Preservation of function, both physical and cognitive, is key to long-term health and well-being. Age-related loss of function drives millions of people to spend an enormous amount of money each year on unregulated therapies—vitamins, supplements, infusions, hormones, and “natural” products—all toward the promise of improvement or preservation of physical strength, sexual function, and maintenance of lean body mass and cognitive abilities. Yeung and colleagues set out to determine whether the daily use of a multivitamin/mineral supplement (Centrum Silver) would impact memory in older adults.1
PHOTO: KLAVDIYAV/SHUTTERSTOCK
Details of the study
The COSMOS-Web study was designed to test the authors’ primary hypothesis that daily dietary flavanols would improve memory over 1 year.1 This study was embedded within the larger COSMOS (COcoa Supplement and Multivitamin Outcomes Study) trial, in which 21,442 people were recruited to assess the impact of flavanols and multivitamin supplements on cardiovascular and cancer outcomes.
Results of another ancillary study, the COSMOS-Mind trial (n = 2,262, average age 73, 60% female), reported no improvement with flavanols compared with placebo on a battery of tests of cognitive function administered by phone. In COSMOS-Mind, however, it was concluded that a daily multivitamin/mineral supplement improved the composite score of cognitive tests compared with placebo, particularly in participants with a history of cardiovascular disease.2
The COSMOS-Web trial recruited an additional cohort within the larger COSMOS trial from 2016–2017 (n = 3,562, average age 71, 67% female) to participate in this study specifically geared to assess memory, using the web-based ModRey test (a test of memory validated for use in a nonimpaired population). To qualify for enrollment, participants had to have access to an internet-connected computer. They were randomly assigned in a 2 x 2 study design to receive a daily multivitamin supplement or placebo; each of these cohorts was further divided into a flavanol supplementation or a placebo group. Analysis of the data showed no association between flavanol use and performance on any of the measures of memory or cognitive function.3
The COSMOS-Web trial assessed episodic recall, a function of hippocampus-mediated cognition that is particularly vulnerable to the effects of aging as demonstrated previously by neuroimaging and neuropsychological studies. The authors deployed a battery of 3 tests via a web platform for patients to complete online and independently.
The prespecified primary outcome was performance on episodic recall as measured by the ModRey test after 1 year of supplementation with multivitamins versus placebo. The ModRey test presents a series of 20 words at 3-second intervals to participants. At the conclusion of the last word, participants were asked to recall as many words as they could; after completing the 2 additional tasks, participants were asked again to recall the words. A secondary outcome of this test is the ratio of delayed to immediate recall.
Two additional tests were administered to assess cognitive performance related to different brain regions, the ModBent test (assessing novel object recognition) and the Flanker task (a measure of executive function). There was a placebo run-in phase during which participants’ adherence to daily supplement intake was ascertained. Participants were excluded if they demonstrated less than 75% adherence to study pills during the run-in placebo phase. The cognitive tasks were presented at study initiation and at yearly intervals for 3 years. The authors chose to use the results at 1 year as their primary outcome to assess the impact of supplementation during the period when adherence would be highest.
Results.At baseline, the placebo cohort recalled 7.2 words of 20 compared with 7.1 in the supplement group. In both groups there was a practice effect, with improvement in scores in the placebo group to 7.65 words and in the multivitamin group to 7.81 words. The improvement from baseline was statistically significantly better (0.71 words) in the multivitamin cohort than in the placebo group (0.45 words). There was no improvement in either group in the ModRey memory retention test (ability to recall the words after 15 minutes) or in the ModBent or Flanker tests. At 3 years of treatment, the placebo group improved by 0.92 words (SD, 3.22) whereas the multivitamin group improved by 1.13 words (SD, 3.39). These changes remained statistically significant.
The group with cardiovascular disease had lower baseline performance on the ModRey test. With supplementation, however, the improvement in this cohort was significantly greater than in those without cardiovascular disease at 1 year. The authors acknowledged that the changes were small and may not have been noticeable to the individuals, but they argued that even small changes as demonstrated in this study can have large health benefits at a population level.
The results of the COSMOS-Web trial corroborate the findings of the COSMOS-Mind study with respect to the benefits of multivitamin/mineral supplementation on cognitive test performance, particularly in a population with preexisting cardiovascular disease. The tests used across the 2 studies were different, which lends greater reliability to the findings.
Study strengths and limitations
A major strength of this study is its careful, rigorous design as a double-blind, placebo-controlled trial in a large patient population. Great care was devoted to ensuring study medication adherence. Another strength is that the cognitive tests chosen for the COSMOS-Web trial have been validated in cognitively normal populations, not those already impaired.
A limitation, however, is in the demographics of the study. The patient population was overwhelmingly White (93%), 67% were female, and they were well educated (94.8% having completed some college or beyond). Their baseline health was good; only 4.7% had a history of cardiovascular disease. Although generalizability of the study results from this population may be concerning,relative benefits of supplementation in this healthy, generally well-nourished and educated group may be lower than might be expected in a more nutritionally and educationally challenged population.
Finally, the difference between the placebo and active supplementation groups was small. Whether this less-than-1-word difference in immediate memory recall is noticeable by a patient is questionable. Both groups improved in their test performance over time—a consequence of serial cognitive tests of any kind. Although the authors calculated that the difference in recall translates to a 3-year reduction in age-related memory decline, it is hard to reconcile that with the fact that both groups actually improved over the 3 years of the study. ●
Acknowledgement
The author would like to thank JoAnn Manson, MD, DrPH, NCMP, for her assistance in evaluating the study.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
In this well-designed, randomized controlled trial by Yeung and colleagues, multivitamin/mineral supplementation improved performance on a test of immediate episodic memory at 1, 2, and 3 years compared with placebo. Given the simplicity and safety of this intervention, even with a small effect size, it makes sense to advise older patients that daily multivitamin use provides micronutrients and vitamins that may be absent in the diet or poorly absorbed by older adults. Whether this highly specific improvement in a test of hippocampal function translates into overall cognitive performance with aging remains a question.
BARBARA LEVY, MD
References
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273282. doi:10.1016/j.ajcnut.2023.05.011.
Baker LD, Manson JE, Rapp SR, et al. Effects of cocoa extract and a multivitamin on cognitive function: a randomized clinical trial. Alzheimers Dement. 2023;19:1308-1319. doi:10.1002/alz.12767.
Brickman AM, Yeung LK, Alshuler DM, et al. Dietary flavanols restore hippocampal-dependent memory in older adults with lower diet quality and lower habitual flavanol consumption. Proc Natl Acad Sci USA. 2023:120:e2216932120. doi:10.1073/ pnas.2216932120.
References
Yeung LK, Alschuler DM, Wall M, et al. Multivitamin supplementation improves memory in older adults: a randomized clinical trial. Am J Clin Nutrition. 2023;118:273282. doi:10.1016/j.ajcnut.2023.05.011.
Baker LD, Manson JE, Rapp SR, et al. Effects of cocoa extract and a multivitamin on cognitive function: a randomized clinical trial. Alzheimers Dement. 2023;19:1308-1319. doi:10.1002/alz.12767.
Brickman AM, Yeung LK, Alshuler DM, et al. Dietary flavanols restore hippocampal-dependent memory in older adults with lower diet quality and lower habitual flavanol consumption. Proc Natl Acad Sci USA. 2023:120:e2216932120. doi:10.1073/ pnas.2216932120.
Given the patient's diagnosis of stage IV MCL, the presentation of diffuse skin lesions, and the histopathologic and immunophenotyping results of those lesions, this patient is diagnosed with secondary cutaneous MCL. The hematologist-oncologist discusses the findings with the patient and presents potential next steps and treatment options.
MCL is a type of B-cell neoplasm that, with advancements in the understanding of non-Hodgkin lymphoma (NHL) in the past 30 years, has been defined as its own clinicopathologic entity by the Revised European-American Lymphoma and World Health Organization classifications. Up to 10% of all NHLs are MCL. Clinical presentation includes advanced disease with B symptoms (eg, night sweats, fever, weight loss), generalized lymphadenopathy, abdominal distention associated with hepatosplenomegaly, and fatigue. Skin manifestations are not as common as other extranodal manifestations. Primary cutaneous MCL occurs in up to 6% of patients with MCL; secondary cutaneous involvement is slightly more common, occurring in 17% of patients with MCL. Secondary cutaneous MCL usually presents in late-stage disease. Men are more likely to present with MCL than are women by a ratio of 3:1. Median age at presentation is 67 years.
Diagnosing MCL is a multipronged approach. Physical examination may reveal lymphadenopathy and hepatosplenomegaly. Lymph node biopsy and aspiration with immunophenotyping in MCL reveals monoclonal B cells expressing surface immunoglobulin (Ig), IgM, or IgD, that are characteristically CD5+ and pan B-cell antigen–positive (eg, CD19, CD20, CD22) but lack expression of CD10 and CD23 and overexpress cyclin D1. Bone marrow aspirate/biopsy are used more for staging than for diagnosis. Blood studies, including anemia and cytopenias secondary to bone marrow infiltration (with up to 40% of cases showing lymphocytosis > 4000/μL), abnormal liver function tests, and a negative Coombs test also help diagnose MCL. Secondary cutaneous MCL is diagnosed on the basis of an MCL diagnosis along with diffuse infiltration of the skin, with multiple erythematous papules and nodules coalescing to form plaques; skin biopsy and immunohistopathology showing monotonous proliferation of small- to medium-sized lymphoid cells with scant cytoplasm; irregular cleaved nuclei with coarse chromatin; and inconspicuous nucleoli as well as a spared papillary dermis.
Pathogenesis of MCL involves disordered lymphoproliferation in a subset of naive pregerminal center cells in primary follicles or in the mantle region of secondary follicles. Most cases are linked with translocation of chromosome 14 and 11, which induces overexpression of protein cyclin D1. Viral infection (Epstein-Barr virus, HIV, human T-lymphotropic virus type 1, human herpes virus 6), environmental factors, and primary and secondary immunodeficiency are also associated with the development of NHL.
Patient education should include detailed information about clinical trials, available treatment options, and associated adverse events as well as psychosocial and nutrition counseling.
Chemoimmunotherapy is standard initial treatment for MCL, but relapse is expected. Chemotherapy-free regimens with biologic targets, which were once used in second-line treatment, have increasingly become an important first-line treatment given their efficacy in the relapsed/refractory setting. Chimeric antigen receptor T-cell therapy is also a second-line treatment option. In patients with MCL and a TP53 mutation, clinical trial participation is encouraged because of poor prognosis.
Timothy J. Voorhees, MD, MSCR, Assistant Professor of Internal Medicine - Clinical, Division of Hematology, The Ohio State University James Comprehensive Cancer Center, Columbus, OH.
Timothy J. Voorhees, MD, MSCR, has disclosed the following relevant financial relationships: Received research grants from: AstraZeneca; Morphosys; Incyte; Recordati.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
Given the patient's diagnosis of stage IV MCL, the presentation of diffuse skin lesions, and the histopathologic and immunophenotyping results of those lesions, this patient is diagnosed with secondary cutaneous MCL. The hematologist-oncologist discusses the findings with the patient and presents potential next steps and treatment options.
MCL is a type of B-cell neoplasm that, with advancements in the understanding of non-Hodgkin lymphoma (NHL) in the past 30 years, has been defined as its own clinicopathologic entity by the Revised European-American Lymphoma and World Health Organization classifications. Up to 10% of all NHLs are MCL. Clinical presentation includes advanced disease with B symptoms (eg, night sweats, fever, weight loss), generalized lymphadenopathy, abdominal distention associated with hepatosplenomegaly, and fatigue. Skin manifestations are not as common as other extranodal manifestations. Primary cutaneous MCL occurs in up to 6% of patients with MCL; secondary cutaneous involvement is slightly more common, occurring in 17% of patients with MCL. Secondary cutaneous MCL usually presents in late-stage disease. Men are more likely to present with MCL than are women by a ratio of 3:1. Median age at presentation is 67 years.
Diagnosing MCL is a multipronged approach. Physical examination may reveal lymphadenopathy and hepatosplenomegaly. Lymph node biopsy and aspiration with immunophenotyping in MCL reveals monoclonal B cells expressing surface immunoglobulin (Ig), IgM, or IgD, that are characteristically CD5+ and pan B-cell antigen–positive (eg, CD19, CD20, CD22) but lack expression of CD10 and CD23 and overexpress cyclin D1. Bone marrow aspirate/biopsy are used more for staging than for diagnosis. Blood studies, including anemia and cytopenias secondary to bone marrow infiltration (with up to 40% of cases showing lymphocytosis > 4000/μL), abnormal liver function tests, and a negative Coombs test also help diagnose MCL. Secondary cutaneous MCL is diagnosed on the basis of an MCL diagnosis along with diffuse infiltration of the skin, with multiple erythematous papules and nodules coalescing to form plaques; skin biopsy and immunohistopathology showing monotonous proliferation of small- to medium-sized lymphoid cells with scant cytoplasm; irregular cleaved nuclei with coarse chromatin; and inconspicuous nucleoli as well as a spared papillary dermis.
Pathogenesis of MCL involves disordered lymphoproliferation in a subset of naive pregerminal center cells in primary follicles or in the mantle region of secondary follicles. Most cases are linked with translocation of chromosome 14 and 11, which induces overexpression of protein cyclin D1. Viral infection (Epstein-Barr virus, HIV, human T-lymphotropic virus type 1, human herpes virus 6), environmental factors, and primary and secondary immunodeficiency are also associated with the development of NHL.
Patient education should include detailed information about clinical trials, available treatment options, and associated adverse events as well as psychosocial and nutrition counseling.
Chemoimmunotherapy is standard initial treatment for MCL, but relapse is expected. Chemotherapy-free regimens with biologic targets, which were once used in second-line treatment, have increasingly become an important first-line treatment given their efficacy in the relapsed/refractory setting. Chimeric antigen receptor T-cell therapy is also a second-line treatment option. In patients with MCL and a TP53 mutation, clinical trial participation is encouraged because of poor prognosis.
Timothy J. Voorhees, MD, MSCR, Assistant Professor of Internal Medicine - Clinical, Division of Hematology, The Ohio State University James Comprehensive Cancer Center, Columbus, OH.
Timothy J. Voorhees, MD, MSCR, has disclosed the following relevant financial relationships: Received research grants from: AstraZeneca; Morphosys; Incyte; Recordati.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
Given the patient's diagnosis of stage IV MCL, the presentation of diffuse skin lesions, and the histopathologic and immunophenotyping results of those lesions, this patient is diagnosed with secondary cutaneous MCL. The hematologist-oncologist discusses the findings with the patient and presents potential next steps and treatment options.
MCL is a type of B-cell neoplasm that, with advancements in the understanding of non-Hodgkin lymphoma (NHL) in the past 30 years, has been defined as its own clinicopathologic entity by the Revised European-American Lymphoma and World Health Organization classifications. Up to 10% of all NHLs are MCL. Clinical presentation includes advanced disease with B symptoms (eg, night sweats, fever, weight loss), generalized lymphadenopathy, abdominal distention associated with hepatosplenomegaly, and fatigue. Skin manifestations are not as common as other extranodal manifestations. Primary cutaneous MCL occurs in up to 6% of patients with MCL; secondary cutaneous involvement is slightly more common, occurring in 17% of patients with MCL. Secondary cutaneous MCL usually presents in late-stage disease. Men are more likely to present with MCL than are women by a ratio of 3:1. Median age at presentation is 67 years.
Diagnosing MCL is a multipronged approach. Physical examination may reveal lymphadenopathy and hepatosplenomegaly. Lymph node biopsy and aspiration with immunophenotyping in MCL reveals monoclonal B cells expressing surface immunoglobulin (Ig), IgM, or IgD, that are characteristically CD5+ and pan B-cell antigen–positive (eg, CD19, CD20, CD22) but lack expression of CD10 and CD23 and overexpress cyclin D1. Bone marrow aspirate/biopsy are used more for staging than for diagnosis. Blood studies, including anemia and cytopenias secondary to bone marrow infiltration (with up to 40% of cases showing lymphocytosis > 4000/μL), abnormal liver function tests, and a negative Coombs test also help diagnose MCL. Secondary cutaneous MCL is diagnosed on the basis of an MCL diagnosis along with diffuse infiltration of the skin, with multiple erythematous papules and nodules coalescing to form plaques; skin biopsy and immunohistopathology showing monotonous proliferation of small- to medium-sized lymphoid cells with scant cytoplasm; irregular cleaved nuclei with coarse chromatin; and inconspicuous nucleoli as well as a spared papillary dermis.
Pathogenesis of MCL involves disordered lymphoproliferation in a subset of naive pregerminal center cells in primary follicles or in the mantle region of secondary follicles. Most cases are linked with translocation of chromosome 14 and 11, which induces overexpression of protein cyclin D1. Viral infection (Epstein-Barr virus, HIV, human T-lymphotropic virus type 1, human herpes virus 6), environmental factors, and primary and secondary immunodeficiency are also associated with the development of NHL.
Patient education should include detailed information about clinical trials, available treatment options, and associated adverse events as well as psychosocial and nutrition counseling.
Chemoimmunotherapy is standard initial treatment for MCL, but relapse is expected. Chemotherapy-free regimens with biologic targets, which were once used in second-line treatment, have increasingly become an important first-line treatment given their efficacy in the relapsed/refractory setting. Chimeric antigen receptor T-cell therapy is also a second-line treatment option. In patients with MCL and a TP53 mutation, clinical trial participation is encouraged because of poor prognosis.
Timothy J. Voorhees, MD, MSCR, Assistant Professor of Internal Medicine - Clinical, Division of Hematology, The Ohio State University James Comprehensive Cancer Center, Columbus, OH.
Timothy J. Voorhees, MD, MSCR, has disclosed the following relevant financial relationships: Received research grants from: AstraZeneca; Morphosys; Incyte; Recordati.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
A 72-year-old man presents to his hematologist-oncologist with red ulcerative nodules on both legs. Six months before, the patient was diagnosed with stage IV mantle cell lymphoma (MCL) and began chemotherapy with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP). Initial patient reports at diagnosis were abdominal distention, generalized lymphadenopathy, night sweats, and fatigue; he received a referral to hematology-oncology after his complete blood count with differential revealed anemia and cytopenias. Additional blood studies showed lymphocytosis > 4000/μL, elevated lactate dehydrogenase levels, abnormal liver function tests, and a negative result on the Coombs test. Ultrasound of the abdomen revealed hepatosplenomegaly and abdominal lymphadenopathy. The hematologist-oncologist ordered a lymph node biopsy and aspiration. Immunophenotyping showed CD5 and CD20 expression but a lack of CD23 and CD10 expression; cyclin D1 was overexpressed. Bone marrow biopsy revealed hypercellular marrow spaces showing infiltration by sheets of atypical lymphoid cells.
Because the patient presents with red ulcerative nodules on both legs, the hematologist-oncologist orders a skin biopsy of the lesions. Histopathologic evaluation shows monotonous proliferation of small- to medium-sized lymphoid cells with scant cytoplasm, irregular cleaved nuclei with coarse chromatin, and inconspicuous nucleoli as well as a spared papillary dermis. Immunophenotyping shows CD5 and CD20 expression but a lack of CD23 and CD10 expression; cyclin D1 is overexpressed.
Disallow All Ads
Content Gating
No Gating (article Unlocked/Free)
Alternative CME
Disqus Comments
Default
Gate On Date
Un-Gate On Date
Consolidated Pubs: Do Not Show Source Publication Logo
The patient's history, symptomatology, and assessments suggest a diagnosis of nonalcoholic fatty liver disease (NAFLD). The primary care physician recommends referral to a hepatologist for evaluation and possible liver biopsy.
NAFLD involves an accumulation of triglycerides and other fats in the liver (unrelated to alcohol consumption and other liver disease), with the presence of hepatic steatosis in more than 5% of hepatocytes. NAFLD affects 25% to 35% of the general population, making it the most common cause of chronic liver disease. The rate increases among patients with obesity, 80% of whom are affected by NAFLD.
NAFLD should be considered in patients with unexplained elevations in serum aminotransferases (without positive viral markers or autoantibodies and no history of alcohol use) and a high risk for steatohepatitis, including obesity. The standard NAFLD assessment for biopsy specimens is the Brunt system, and disease stage is determined using the NAFLD activity score and the amount of fibrosis present.
A study of the natural history of NAFLD in patients who were followed for 3 years showed that without pharmacologic intervention, one third experienced disease progression, one third remained stable, and one third improved. An independent risk factor for progression of nonalcoholic steatohepatitis was abnormal glucose tolerance testing. In another natural history study, a 10% higher rate of mortality over 10 years was demonstrated among those with NAFLD vs controls, with the top three causes of death being cancer, heart disease, and liver-related disease. Prevalence of chronic liver disease and cirrhosis has been shown to be elevated in Latino and Japanese American populations.
Patients with NAFLD should be seen regularly to assess for disease progression and receive guidance on weight management interventions and exercise. A weight loss of more than 5% has been shown to reduce liver fat and provide cardiometabolic benefits; a weight reduction of more than 10% can help reverse steatohepatitis or liver fibrosis. In addition to weight loss management strategies, physicians should discuss the importance of controlling hyperlipidemia, insulin resistance, and T2D with their patients and share the importance of avoiding alcohol and other hepatotoxic substances.
According to the American Association of Clinical Endocrinology Clinical Practice Guideline: "There are no U.S. Food and Drug Administration-approved medications for the treatment of NAFLD; however, some diabetes and anti-obesity medications can be beneficial. Bariatric surgery is also effective for weight loss and reducing liver fat in persons with severe obesity."
Courtney Whittle, MD, MSW, Diplomate of ABOM, Pediatric Lead, Obesity Champion, TSPMG, Weight A Minute Clinic, Atlanta, Georgia.
Courtney Whittle, MD, MSW, Diplomate of ABOM, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
Author and Disclosure Information
Reviewed by Courtney Whittle, MD, MSW, Diplomate of ABOM
Reviewed by Courtney Whittle, MD, MSW, Diplomate of ABOM
Author and Disclosure Information
Reviewed by Courtney Whittle, MD, MSW, Diplomate of ABOM
The patient's history, symptomatology, and assessments suggest a diagnosis of nonalcoholic fatty liver disease (NAFLD). The primary care physician recommends referral to a hepatologist for evaluation and possible liver biopsy.
NAFLD involves an accumulation of triglycerides and other fats in the liver (unrelated to alcohol consumption and other liver disease), with the presence of hepatic steatosis in more than 5% of hepatocytes. NAFLD affects 25% to 35% of the general population, making it the most common cause of chronic liver disease. The rate increases among patients with obesity, 80% of whom are affected by NAFLD.
NAFLD should be considered in patients with unexplained elevations in serum aminotransferases (without positive viral markers or autoantibodies and no history of alcohol use) and a high risk for steatohepatitis, including obesity. The standard NAFLD assessment for biopsy specimens is the Brunt system, and disease stage is determined using the NAFLD activity score and the amount of fibrosis present.
A study of the natural history of NAFLD in patients who were followed for 3 years showed that without pharmacologic intervention, one third experienced disease progression, one third remained stable, and one third improved. An independent risk factor for progression of nonalcoholic steatohepatitis was abnormal glucose tolerance testing. In another natural history study, a 10% higher rate of mortality over 10 years was demonstrated among those with NAFLD vs controls, with the top three causes of death being cancer, heart disease, and liver-related disease. Prevalence of chronic liver disease and cirrhosis has been shown to be elevated in Latino and Japanese American populations.
Patients with NAFLD should be seen regularly to assess for disease progression and receive guidance on weight management interventions and exercise. A weight loss of more than 5% has been shown to reduce liver fat and provide cardiometabolic benefits; a weight reduction of more than 10% can help reverse steatohepatitis or liver fibrosis. In addition to weight loss management strategies, physicians should discuss the importance of controlling hyperlipidemia, insulin resistance, and T2D with their patients and share the importance of avoiding alcohol and other hepatotoxic substances.
According to the American Association of Clinical Endocrinology Clinical Practice Guideline: "There are no U.S. Food and Drug Administration-approved medications for the treatment of NAFLD; however, some diabetes and anti-obesity medications can be beneficial. Bariatric surgery is also effective for weight loss and reducing liver fat in persons with severe obesity."
Courtney Whittle, MD, MSW, Diplomate of ABOM, Pediatric Lead, Obesity Champion, TSPMG, Weight A Minute Clinic, Atlanta, Georgia.
Courtney Whittle, MD, MSW, Diplomate of ABOM, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The patient's history, symptomatology, and assessments suggest a diagnosis of nonalcoholic fatty liver disease (NAFLD). The primary care physician recommends referral to a hepatologist for evaluation and possible liver biopsy.
NAFLD involves an accumulation of triglycerides and other fats in the liver (unrelated to alcohol consumption and other liver disease), with the presence of hepatic steatosis in more than 5% of hepatocytes. NAFLD affects 25% to 35% of the general population, making it the most common cause of chronic liver disease. The rate increases among patients with obesity, 80% of whom are affected by NAFLD.
NAFLD should be considered in patients with unexplained elevations in serum aminotransferases (without positive viral markers or autoantibodies and no history of alcohol use) and a high risk for steatohepatitis, including obesity. The standard NAFLD assessment for biopsy specimens is the Brunt system, and disease stage is determined using the NAFLD activity score and the amount of fibrosis present.
A study of the natural history of NAFLD in patients who were followed for 3 years showed that without pharmacologic intervention, one third experienced disease progression, one third remained stable, and one third improved. An independent risk factor for progression of nonalcoholic steatohepatitis was abnormal glucose tolerance testing. In another natural history study, a 10% higher rate of mortality over 10 years was demonstrated among those with NAFLD vs controls, with the top three causes of death being cancer, heart disease, and liver-related disease. Prevalence of chronic liver disease and cirrhosis has been shown to be elevated in Latino and Japanese American populations.
Patients with NAFLD should be seen regularly to assess for disease progression and receive guidance on weight management interventions and exercise. A weight loss of more than 5% has been shown to reduce liver fat and provide cardiometabolic benefits; a weight reduction of more than 10% can help reverse steatohepatitis or liver fibrosis. In addition to weight loss management strategies, physicians should discuss the importance of controlling hyperlipidemia, insulin resistance, and T2D with their patients and share the importance of avoiding alcohol and other hepatotoxic substances.
According to the American Association of Clinical Endocrinology Clinical Practice Guideline: "There are no U.S. Food and Drug Administration-approved medications for the treatment of NAFLD; however, some diabetes and anti-obesity medications can be beneficial. Bariatric surgery is also effective for weight loss and reducing liver fat in persons with severe obesity."
Courtney Whittle, MD, MSW, Diplomate of ABOM, Pediatric Lead, Obesity Champion, TSPMG, Weight A Minute Clinic, Atlanta, Georgia.
Courtney Whittle, MD, MSW, Diplomate of ABOM, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
Simon Fraser/Freeman Hospital, Newcastle upon Tyne / Science Source
A 51-year-old Hispanic man presents to his primary care physician with fatigue and pain in the upper right abdomen. Physical exam reveals ascites and splenomegaly. His height is 5 ft 8 in and weight is 274 lb; his BMI is 41.7. For the past 5 years, the patient has seen his physician for routine annual exams, during which time he has consistently met the criteria for World Health Organization Class 3 overweight (BMI ≥ 40) and has taken metformin, with varying degrees of adherence, for type 2 diabetes (T2D). Now, given the patient's symptoms and the potential for uncontrolled diabetes, the physician orders laboratory studies and viral serologies for hepatitis. Results of these assessments exclude viral infection but demonstrate abnormal levels of fasting insulin and glucose, hypertriglyceridemia, and elevated transaminase levels that are sixfold above normal levels, with an aspartate aminotransferase-to-alanine transaminase ratio < 1:1.
Disallow All Ads
Content Gating
No Gating (article Unlocked/Free)
Alternative CME
Disqus Comments
Default
Gate On Date
Un-Gate On Date
Consolidated Pubs: Do Not Show Source Publication Logo
After catching COVID-19 for the second time in July 2022, Daniel Lewis suffered persistent headaches, chest pain, and a dangerously high heart rate. He recalls that he was also so exhausted packing for a family wedding that he had to take a break to rest each time he put something into his suitcase.
Instead of attending the wedding, the 30-year-old Washington data analyst visited his doctor, who diagnosed “some postviral thing” and prescribed rest. Mr. Lewis found a new doctor, went to a long COVID clinic, and saw multiple specialists, but a year later, he’s still sick – and disabled. He meets the federal criteria for long COVID (symptoms that last more than 4 weeks).
He now uses an electric wheelchair whenever he leaves his apartment, a far cry from his pre-COVID life, when he was training for a half marathon.
“Some doctors have genuinely tried to help,” he said. “Most don’t really know what long COVID is, and ... since there’s no official guidance on what to do with long COVID patients, they just throw up their hands and say there’s nothing to do.”
That could be changing – at least the part about official guidance. New findings published in JAMA indicate we’re getting closer to unraveling what long COVID is all about and may help refine how it is defined and diagnosed. The study identified the 37 most common symptoms of long COVID, an important step toward better understanding and treatment of the condition, which affects an estimated 65 million peopleworldwide.
Although the study provides a way to systematically identify the condition, the authors were clear that this is significant but that it is only a first step. Naming symptoms is very different from understanding what causes them, and understanding them is critical for developing effective treatments, said pulmonologist Bruce Levy, MD, a study coauthor who is interim chair of medicine at Brigham and Women’s Hospital and a professor of medicine at Harvard Medical School, both in Boston.
Researchers relied on self-reported symptoms from the 9,764 participants, all adults who are part of the ongoing Researching COVID to Enhance Recovery (RECOVER) Initiative, a longitudinal study run by the National Institutes of Health. Some patients had long COVID when they signed up for the study, some developed it afterward, and some had never had it, or if they had, they were unaware.
Other studies, most of them involving smaller groups of patients, have examined long COVID biomarkers, risk factors, and specific symptoms. Dr. Levy said it’s important to have a symptom-based definition of long COVID that draws from a large cohort of patients who reported on their experiences with symptoms during the aftermath of infection. However, he pointed out that because participants volunteered for the study and were not chosen on the basis of specific criteria, they may not be representative of the more general population of patients with long COVID.
“We need this kind of evidence – it’s important to have self-reported symptoms, because clearly, the patients know what they’re feeling,” Dr. Levy said. “But it’s only part of the picture.”
Dr. Levy said the definition of long COVID needs to be further refined by ongoing research, including objective assessments of clinical findings, laboratory testing, imaging, and biomarkers.
One of the notable findings in the JAMA study is that certain symptoms tend to occur in clusters. The biostatisticians and analysts who processed the data identified four subgroups of very common symptoms that appeared together in more than 80% of the long COVID patients: loss of or change in smell and taste; postexertional malaise and fatigue; brain fog, postexertional malaise, and fatigue; and fatigue, postexertional malaise, dizziness, brain fog, gastrointestinal issues, and palpitations.
Many of those symptoms are also associated with underlying conditions not related to long COVID, which makes an accurate diagnosis a challenge.
“Just the fact that they would cluster into four groups suggests that underlying all this is not just one unifying pathobiology,” Dr. Levy said. He stressed that clinicians need to understand what’s causing the symptoms before they can properly treat patients.
He pointed out that two of the possible disease-driving mechanisms are persistence of the virus and prolonged inflammation that is slow to resolve. For patients experiencing inflammation after the virus is gone, an anti-inflammatory therapy would be most appropriate.
But if they have persistent virus, “you would want to treat with an antiviral antibiotic and not quiet down the body’s antiviral inflammatory response,” he said. “How you treat the two potential underlying causes of long COVID could thus be almost diametrically opposed, so that’s part of the importance of figuring out what is the underlying cause of those symptoms, not just identifying the symptoms themselves.”
More studies are needed to determine whether long COVID is a syndrome or is related to a singular pathobiology, experts said.
That’s consistent with the impression of long COVID researcher Harlan Krumholz, MD, the Harold H. Hines Jr. professor of medicine (cardiology) at Yale University, New Haven, Conn.
Dr. Krumholz worries that some clinicians might use the JAMA findings to dismiss patients whose symptoms meet the criteria in the scoring system developed for the study.
“It’s important for people who read this paper to know that this is preliminary,” said Dr. Krumholz, a principal investigator of another patient-focused studydesigned to understand long COVID – the Yale Listen to Immune, Symptom, and Treatment Experiences Now (LISTEN) Study. “It’s a condition we don’t understand yet.”
Dr. Krumholz said he has lost track of the number of patients he knows who, like Daniel Lewis, are ill and are unable to get answers. “There is an intense sense of inadequacy on the clinical side and the research side,” he said. “Every day people ask me, ‘Are there any evidence-based strategies?’ And so far I have to say, every day, ‘No.’ I hate to say it, but it’s kind of like every patient is on their own. They’re trying different things because they can’t wait. There is an imperative to help them.”
At the end of July, the National Institutes of Health launched phase 2 clinical trials to evaluate at least four new treatments for long COVID, all part of the RECOVER initiative. By then, Mr. Lewis, who believes his myalgic encephalomyelitis/chronic fatigue syndrome was triggered by the virus, had made plans to try an alternative, experimental therapy.
“My hope is that it will fix me,” he said. “I’m excited about those kinds of hard-hitting infusion, immunological treatment.”
As for the JAMA study, he didn’t allow himself to get excited when it was released, a function of his experience as a data analyst and long COVID patient.
“I don’t think it moves the needle much yet,” he said. “It’s the first study, and we shouldn’t expect much from the first pieces of data to come out of that. If they keep following that cohort and go deeper and deeper, they’re going to find some interesting stuff that will lead to treatments.”
A version of this article first appeared on Medscape.com.
After catching COVID-19 for the second time in July 2022, Daniel Lewis suffered persistent headaches, chest pain, and a dangerously high heart rate. He recalls that he was also so exhausted packing for a family wedding that he had to take a break to rest each time he put something into his suitcase.
Instead of attending the wedding, the 30-year-old Washington data analyst visited his doctor, who diagnosed “some postviral thing” and prescribed rest. Mr. Lewis found a new doctor, went to a long COVID clinic, and saw multiple specialists, but a year later, he’s still sick – and disabled. He meets the federal criteria for long COVID (symptoms that last more than 4 weeks).
He now uses an electric wheelchair whenever he leaves his apartment, a far cry from his pre-COVID life, when he was training for a half marathon.
“Some doctors have genuinely tried to help,” he said. “Most don’t really know what long COVID is, and ... since there’s no official guidance on what to do with long COVID patients, they just throw up their hands and say there’s nothing to do.”
That could be changing – at least the part about official guidance. New findings published in JAMA indicate we’re getting closer to unraveling what long COVID is all about and may help refine how it is defined and diagnosed. The study identified the 37 most common symptoms of long COVID, an important step toward better understanding and treatment of the condition, which affects an estimated 65 million peopleworldwide.
Although the study provides a way to systematically identify the condition, the authors were clear that this is significant but that it is only a first step. Naming symptoms is very different from understanding what causes them, and understanding them is critical for developing effective treatments, said pulmonologist Bruce Levy, MD, a study coauthor who is interim chair of medicine at Brigham and Women’s Hospital and a professor of medicine at Harvard Medical School, both in Boston.
Researchers relied on self-reported symptoms from the 9,764 participants, all adults who are part of the ongoing Researching COVID to Enhance Recovery (RECOVER) Initiative, a longitudinal study run by the National Institutes of Health. Some patients had long COVID when they signed up for the study, some developed it afterward, and some had never had it, or if they had, they were unaware.
Other studies, most of them involving smaller groups of patients, have examined long COVID biomarkers, risk factors, and specific symptoms. Dr. Levy said it’s important to have a symptom-based definition of long COVID that draws from a large cohort of patients who reported on their experiences with symptoms during the aftermath of infection. However, he pointed out that because participants volunteered for the study and were not chosen on the basis of specific criteria, they may not be representative of the more general population of patients with long COVID.
“We need this kind of evidence – it’s important to have self-reported symptoms, because clearly, the patients know what they’re feeling,” Dr. Levy said. “But it’s only part of the picture.”
Dr. Levy said the definition of long COVID needs to be further refined by ongoing research, including objective assessments of clinical findings, laboratory testing, imaging, and biomarkers.
One of the notable findings in the JAMA study is that certain symptoms tend to occur in clusters. The biostatisticians and analysts who processed the data identified four subgroups of very common symptoms that appeared together in more than 80% of the long COVID patients: loss of or change in smell and taste; postexertional malaise and fatigue; brain fog, postexertional malaise, and fatigue; and fatigue, postexertional malaise, dizziness, brain fog, gastrointestinal issues, and palpitations.
Many of those symptoms are also associated with underlying conditions not related to long COVID, which makes an accurate diagnosis a challenge.
“Just the fact that they would cluster into four groups suggests that underlying all this is not just one unifying pathobiology,” Dr. Levy said. He stressed that clinicians need to understand what’s causing the symptoms before they can properly treat patients.
He pointed out that two of the possible disease-driving mechanisms are persistence of the virus and prolonged inflammation that is slow to resolve. For patients experiencing inflammation after the virus is gone, an anti-inflammatory therapy would be most appropriate.
But if they have persistent virus, “you would want to treat with an antiviral antibiotic and not quiet down the body’s antiviral inflammatory response,” he said. “How you treat the two potential underlying causes of long COVID could thus be almost diametrically opposed, so that’s part of the importance of figuring out what is the underlying cause of those symptoms, not just identifying the symptoms themselves.”
More studies are needed to determine whether long COVID is a syndrome or is related to a singular pathobiology, experts said.
That’s consistent with the impression of long COVID researcher Harlan Krumholz, MD, the Harold H. Hines Jr. professor of medicine (cardiology) at Yale University, New Haven, Conn.
Dr. Krumholz worries that some clinicians might use the JAMA findings to dismiss patients whose symptoms meet the criteria in the scoring system developed for the study.
“It’s important for people who read this paper to know that this is preliminary,” said Dr. Krumholz, a principal investigator of another patient-focused studydesigned to understand long COVID – the Yale Listen to Immune, Symptom, and Treatment Experiences Now (LISTEN) Study. “It’s a condition we don’t understand yet.”
Dr. Krumholz said he has lost track of the number of patients he knows who, like Daniel Lewis, are ill and are unable to get answers. “There is an intense sense of inadequacy on the clinical side and the research side,” he said. “Every day people ask me, ‘Are there any evidence-based strategies?’ And so far I have to say, every day, ‘No.’ I hate to say it, but it’s kind of like every patient is on their own. They’re trying different things because they can’t wait. There is an imperative to help them.”
At the end of July, the National Institutes of Health launched phase 2 clinical trials to evaluate at least four new treatments for long COVID, all part of the RECOVER initiative. By then, Mr. Lewis, who believes his myalgic encephalomyelitis/chronic fatigue syndrome was triggered by the virus, had made plans to try an alternative, experimental therapy.
“My hope is that it will fix me,” he said. “I’m excited about those kinds of hard-hitting infusion, immunological treatment.”
As for the JAMA study, he didn’t allow himself to get excited when it was released, a function of his experience as a data analyst and long COVID patient.
“I don’t think it moves the needle much yet,” he said. “It’s the first study, and we shouldn’t expect much from the first pieces of data to come out of that. If they keep following that cohort and go deeper and deeper, they’re going to find some interesting stuff that will lead to treatments.”
A version of this article first appeared on Medscape.com.
After catching COVID-19 for the second time in July 2022, Daniel Lewis suffered persistent headaches, chest pain, and a dangerously high heart rate. He recalls that he was also so exhausted packing for a family wedding that he had to take a break to rest each time he put something into his suitcase.
Instead of attending the wedding, the 30-year-old Washington data analyst visited his doctor, who diagnosed “some postviral thing” and prescribed rest. Mr. Lewis found a new doctor, went to a long COVID clinic, and saw multiple specialists, but a year later, he’s still sick – and disabled. He meets the federal criteria for long COVID (symptoms that last more than 4 weeks).
He now uses an electric wheelchair whenever he leaves his apartment, a far cry from his pre-COVID life, when he was training for a half marathon.
“Some doctors have genuinely tried to help,” he said. “Most don’t really know what long COVID is, and ... since there’s no official guidance on what to do with long COVID patients, they just throw up their hands and say there’s nothing to do.”
That could be changing – at least the part about official guidance. New findings published in JAMA indicate we’re getting closer to unraveling what long COVID is all about and may help refine how it is defined and diagnosed. The study identified the 37 most common symptoms of long COVID, an important step toward better understanding and treatment of the condition, which affects an estimated 65 million peopleworldwide.
Although the study provides a way to systematically identify the condition, the authors were clear that this is significant but that it is only a first step. Naming symptoms is very different from understanding what causes them, and understanding them is critical for developing effective treatments, said pulmonologist Bruce Levy, MD, a study coauthor who is interim chair of medicine at Brigham and Women’s Hospital and a professor of medicine at Harvard Medical School, both in Boston.
Researchers relied on self-reported symptoms from the 9,764 participants, all adults who are part of the ongoing Researching COVID to Enhance Recovery (RECOVER) Initiative, a longitudinal study run by the National Institutes of Health. Some patients had long COVID when they signed up for the study, some developed it afterward, and some had never had it, or if they had, they were unaware.
Other studies, most of them involving smaller groups of patients, have examined long COVID biomarkers, risk factors, and specific symptoms. Dr. Levy said it’s important to have a symptom-based definition of long COVID that draws from a large cohort of patients who reported on their experiences with symptoms during the aftermath of infection. However, he pointed out that because participants volunteered for the study and were not chosen on the basis of specific criteria, they may not be representative of the more general population of patients with long COVID.
“We need this kind of evidence – it’s important to have self-reported symptoms, because clearly, the patients know what they’re feeling,” Dr. Levy said. “But it’s only part of the picture.”
Dr. Levy said the definition of long COVID needs to be further refined by ongoing research, including objective assessments of clinical findings, laboratory testing, imaging, and biomarkers.
One of the notable findings in the JAMA study is that certain symptoms tend to occur in clusters. The biostatisticians and analysts who processed the data identified four subgroups of very common symptoms that appeared together in more than 80% of the long COVID patients: loss of or change in smell and taste; postexertional malaise and fatigue; brain fog, postexertional malaise, and fatigue; and fatigue, postexertional malaise, dizziness, brain fog, gastrointestinal issues, and palpitations.
Many of those symptoms are also associated with underlying conditions not related to long COVID, which makes an accurate diagnosis a challenge.
“Just the fact that they would cluster into four groups suggests that underlying all this is not just one unifying pathobiology,” Dr. Levy said. He stressed that clinicians need to understand what’s causing the symptoms before they can properly treat patients.
He pointed out that two of the possible disease-driving mechanisms are persistence of the virus and prolonged inflammation that is slow to resolve. For patients experiencing inflammation after the virus is gone, an anti-inflammatory therapy would be most appropriate.
But if they have persistent virus, “you would want to treat with an antiviral antibiotic and not quiet down the body’s antiviral inflammatory response,” he said. “How you treat the two potential underlying causes of long COVID could thus be almost diametrically opposed, so that’s part of the importance of figuring out what is the underlying cause of those symptoms, not just identifying the symptoms themselves.”
More studies are needed to determine whether long COVID is a syndrome or is related to a singular pathobiology, experts said.
That’s consistent with the impression of long COVID researcher Harlan Krumholz, MD, the Harold H. Hines Jr. professor of medicine (cardiology) at Yale University, New Haven, Conn.
Dr. Krumholz worries that some clinicians might use the JAMA findings to dismiss patients whose symptoms meet the criteria in the scoring system developed for the study.
“It’s important for people who read this paper to know that this is preliminary,” said Dr. Krumholz, a principal investigator of another patient-focused studydesigned to understand long COVID – the Yale Listen to Immune, Symptom, and Treatment Experiences Now (LISTEN) Study. “It’s a condition we don’t understand yet.”
Dr. Krumholz said he has lost track of the number of patients he knows who, like Daniel Lewis, are ill and are unable to get answers. “There is an intense sense of inadequacy on the clinical side and the research side,” he said. “Every day people ask me, ‘Are there any evidence-based strategies?’ And so far I have to say, every day, ‘No.’ I hate to say it, but it’s kind of like every patient is on their own. They’re trying different things because they can’t wait. There is an imperative to help them.”
At the end of July, the National Institutes of Health launched phase 2 clinical trials to evaluate at least four new treatments for long COVID, all part of the RECOVER initiative. By then, Mr. Lewis, who believes his myalgic encephalomyelitis/chronic fatigue syndrome was triggered by the virus, had made plans to try an alternative, experimental therapy.
“My hope is that it will fix me,” he said. “I’m excited about those kinds of hard-hitting infusion, immunological treatment.”
As for the JAMA study, he didn’t allow himself to get excited when it was released, a function of his experience as a data analyst and long COVID patient.
“I don’t think it moves the needle much yet,” he said. “It’s the first study, and we shouldn’t expect much from the first pieces of data to come out of that. If they keep following that cohort and go deeper and deeper, they’re going to find some interesting stuff that will lead to treatments.”
A version of this article first appeared on Medscape.com.
Migraine is well known as a vascular phenomenon, but research over time has shown that vasodilation is a secondary feature of headache rather than the cause of headache pain. Calcitonin gene-related peptide (CGRP) and other vasoactive inflammatory proteins transmit nociceptive signals through the trigeminal system, and although vasodilation occurs, it is not essential for migraine attacks to occur. White matter changes on MRI are a common finding in people with migraine, and the burden of migraine often correlates with the amount of white matter changes seen. This connection highlights the indirect connection between migraine and vascular risks factors, and this study attempts to better quantify this, specifically with respect to stroke and myocardial infarction (MI).
The study by Fuglsang and colleagues was a registry-based nationwide population-based cohort study that included over 200,000 individuals with migraine, using data collected from 1996 to 2018. Participants were differentiated as having or not having migraine on the basis of prescriptions of preventive or acute migraine medications. Male and female participants were further subdivided, and these groups were compared to healthy controls. The primary endpoints were hazard ratio and absolute risk differences for developing hemorrhagic or ischemic stroke or MI among all groups.
The researchers found an increased risk for ischemic stroke that was equal among male and female participants. Hemorrhagic stroke and MI were seen to be increased in migraine, but primarily among women with migraine. This study specifically investigated what the researchers termed "premature" stroke and MI, and there remains a likelihood that estrogen could be the differentiating factor between the difference in risk between male and female participants with migraine. I have recently highlighted a number of studies investigating vascular risk factors associated with migraine; this study will help clinicians appropriately educate their patients with migraine regarding vascular risk.
The first medications reported as helpful preventively for migraine were antihypertensives, specifically beta-blockers (BB). A number of other medications in other antihypertensive subclasses have also subsequently been shown to be helpful for migraine prevention. These include angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARB), calcium channel blockers (CCB), and alpha-blockers (AB). Carcel and colleagues conducted a meta-analysis that investigated a wide variety of antihypertensive medications in multiple classes and compared the reduction in headache frequency as defined as headache days per month.
This analysis reviewed 50 studies involving over 4000 participants. The majority of the studies (35 out 50 [70%]) had a cross-over design. The medications evaluated included clonidine (an alpha agonist), candesartan (an ARB), telmisartan (an ARB), propranolol (a BB), timolol (a BB), pindolol (a BB), metoprolol (a BB), bisoprolol (a BB), atenolol (a BB), alprenolol (a BB), nimodipine (a CCB), nifedipine (a CCB), verapamil (a CCB), nicardipine (a CCB), enalapril (an ACE inhibitor), and lisinopril (an ACE inhibitor). For each class of antihypertensive, there was a lower number of monthly headache days with treatment compared with placebo; the greatest reduction was for the CCB with a mean difference of about 2 days per month. BB on average decreased headache days per month by 0.7 days. For BB, there was no clear trend to increased efficacywith increased dose. Only six trials reported the difference in blood pressure: On average, there was a 9.3 mm Hg drop in systolic and 3.0 mm Hg drop in diastolic pressure.
The authors showed that there is statistical significance for the use of antihypertensive medications for decreasing migraine days per month, and this was statistically significant separately for numerous specific drugs within the classes: clonidine, candesartan, atenolol, bisoprolol, propranolol, timolol, nicardipine, and verapamil. Antihypertensive medications remain some of the most popular first-line preventive options for migraine, and although the benefit of this class as a whole is mild (slightly more than 1 day per month), it can be an excellent option for many patients
The relationship between migraine and caffeine is necessarily controversial. Caffeine is included as a component of many over-the-counter migraine treatments, and the beneficial effect of caffeine as an acute treatment for migraine has been documented for decades. Reduction in caffeine, however, has also been established as a helpful lifestyle modification for prevention of migraine attacks. Zhang and colleagues used data from the National Health and Nutrition Examination Survey database, a program conducted by the Centers for Disease Control and Prevention to assess the health and nutritional status of adults and children in the United States.
This study sought to quantify the relationship between dietary caffeine and "severe headache." For this study, "severe headache" was defined as answering yes to the question: During the past 3 months, did you have severe headaches or migraines? Dietary caffeine intake was collected through two 24-hour dietary recall interviews, one in person and one 3-10 days later via telephone. The amount of caffeine consumed was estimated in mg/day from all caffeine-containing foods and beverages, including coffee, tea, soda, and chocolate, using the US Department of Agriculture's Food and Nutrient Database. Each participant's mean caffeine intake was defined as the difference between the first and second dietary recalls.
A large number of covariates were assessed as well, including age, race/ethnicity, body mass index, poverty-income ratio, educational level, marital status, hypertension, cancer, energy intake, protein intake, calcium intake, magnesium intake, iron intake, sodium intake, alcohol status, smoking status, and triglyceride level. A total of 8993 participants were included. Caffeine intake was divided into four groups: ≥ 0 to <40 mg/day, ≥ 40 to<200 mg/day, ≥ 200 to<400 mg/day, and ≥ 400 mg/day. After adjusting for confounders, a significant association between dietary caffeine intake and severe headaches or migraines was detected.
Curiously, in this study, only male participants were included. The authors found a clear correlation between the amount of caffeine consumed over a 24-hour period and severe migraine attacks. Further evaluation should investigate the frequency of attacks rather than just individual experience over a 3-month period. Although caffeine is helpful acutely, higher dose consumption is a risk factor for worsening migraine.
Author and Disclosure Information
Thomas Berk, MD
Neura Health and Thomas Jefferson University, Woodbury, NJ
Neura Health and Thomas Jefferson University, Woodbury, NJ
Author and Disclosure Information
Thomas Berk, MD
Neura Health and Thomas Jefferson University, Woodbury, NJ
Dr Berk scans the journal, so you don't have to!
Dr Berk scans the journal, so you don't have to!
Migraine is well known as a vascular phenomenon, but research over time has shown that vasodilation is a secondary feature of headache rather than the cause of headache pain. Calcitonin gene-related peptide (CGRP) and other vasoactive inflammatory proteins transmit nociceptive signals through the trigeminal system, and although vasodilation occurs, it is not essential for migraine attacks to occur. White matter changes on MRI are a common finding in people with migraine, and the burden of migraine often correlates with the amount of white matter changes seen. This connection highlights the indirect connection between migraine and vascular risks factors, and this study attempts to better quantify this, specifically with respect to stroke and myocardial infarction (MI).
The study by Fuglsang and colleagues was a registry-based nationwide population-based cohort study that included over 200,000 individuals with migraine, using data collected from 1996 to 2018. Participants were differentiated as having or not having migraine on the basis of prescriptions of preventive or acute migraine medications. Male and female participants were further subdivided, and these groups were compared to healthy controls. The primary endpoints were hazard ratio and absolute risk differences for developing hemorrhagic or ischemic stroke or MI among all groups.
The researchers found an increased risk for ischemic stroke that was equal among male and female participants. Hemorrhagic stroke and MI were seen to be increased in migraine, but primarily among women with migraine. This study specifically investigated what the researchers termed "premature" stroke and MI, and there remains a likelihood that estrogen could be the differentiating factor between the difference in risk between male and female participants with migraine. I have recently highlighted a number of studies investigating vascular risk factors associated with migraine; this study will help clinicians appropriately educate their patients with migraine regarding vascular risk.
The first medications reported as helpful preventively for migraine were antihypertensives, specifically beta-blockers (BB). A number of other medications in other antihypertensive subclasses have also subsequently been shown to be helpful for migraine prevention. These include angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARB), calcium channel blockers (CCB), and alpha-blockers (AB). Carcel and colleagues conducted a meta-analysis that investigated a wide variety of antihypertensive medications in multiple classes and compared the reduction in headache frequency as defined as headache days per month.
This analysis reviewed 50 studies involving over 4000 participants. The majority of the studies (35 out 50 [70%]) had a cross-over design. The medications evaluated included clonidine (an alpha agonist), candesartan (an ARB), telmisartan (an ARB), propranolol (a BB), timolol (a BB), pindolol (a BB), metoprolol (a BB), bisoprolol (a BB), atenolol (a BB), alprenolol (a BB), nimodipine (a CCB), nifedipine (a CCB), verapamil (a CCB), nicardipine (a CCB), enalapril (an ACE inhibitor), and lisinopril (an ACE inhibitor). For each class of antihypertensive, there was a lower number of monthly headache days with treatment compared with placebo; the greatest reduction was for the CCB with a mean difference of about 2 days per month. BB on average decreased headache days per month by 0.7 days. For BB, there was no clear trend to increased efficacywith increased dose. Only six trials reported the difference in blood pressure: On average, there was a 9.3 mm Hg drop in systolic and 3.0 mm Hg drop in diastolic pressure.
The authors showed that there is statistical significance for the use of antihypertensive medications for decreasing migraine days per month, and this was statistically significant separately for numerous specific drugs within the classes: clonidine, candesartan, atenolol, bisoprolol, propranolol, timolol, nicardipine, and verapamil. Antihypertensive medications remain some of the most popular first-line preventive options for migraine, and although the benefit of this class as a whole is mild (slightly more than 1 day per month), it can be an excellent option for many patients
The relationship between migraine and caffeine is necessarily controversial. Caffeine is included as a component of many over-the-counter migraine treatments, and the beneficial effect of caffeine as an acute treatment for migraine has been documented for decades. Reduction in caffeine, however, has also been established as a helpful lifestyle modification for prevention of migraine attacks. Zhang and colleagues used data from the National Health and Nutrition Examination Survey database, a program conducted by the Centers for Disease Control and Prevention to assess the health and nutritional status of adults and children in the United States.
This study sought to quantify the relationship between dietary caffeine and "severe headache." For this study, "severe headache" was defined as answering yes to the question: During the past 3 months, did you have severe headaches or migraines? Dietary caffeine intake was collected through two 24-hour dietary recall interviews, one in person and one 3-10 days later via telephone. The amount of caffeine consumed was estimated in mg/day from all caffeine-containing foods and beverages, including coffee, tea, soda, and chocolate, using the US Department of Agriculture's Food and Nutrient Database. Each participant's mean caffeine intake was defined as the difference between the first and second dietary recalls.
A large number of covariates were assessed as well, including age, race/ethnicity, body mass index, poverty-income ratio, educational level, marital status, hypertension, cancer, energy intake, protein intake, calcium intake, magnesium intake, iron intake, sodium intake, alcohol status, smoking status, and triglyceride level. A total of 8993 participants were included. Caffeine intake was divided into four groups: ≥ 0 to <40 mg/day, ≥ 40 to<200 mg/day, ≥ 200 to<400 mg/day, and ≥ 400 mg/day. After adjusting for confounders, a significant association between dietary caffeine intake and severe headaches or migraines was detected.
Curiously, in this study, only male participants were included. The authors found a clear correlation between the amount of caffeine consumed over a 24-hour period and severe migraine attacks. Further evaluation should investigate the frequency of attacks rather than just individual experience over a 3-month period. Although caffeine is helpful acutely, higher dose consumption is a risk factor for worsening migraine.
Migraine is well known as a vascular phenomenon, but research over time has shown that vasodilation is a secondary feature of headache rather than the cause of headache pain. Calcitonin gene-related peptide (CGRP) and other vasoactive inflammatory proteins transmit nociceptive signals through the trigeminal system, and although vasodilation occurs, it is not essential for migraine attacks to occur. White matter changes on MRI are a common finding in people with migraine, and the burden of migraine often correlates with the amount of white matter changes seen. This connection highlights the indirect connection between migraine and vascular risks factors, and this study attempts to better quantify this, specifically with respect to stroke and myocardial infarction (MI).
The study by Fuglsang and colleagues was a registry-based nationwide population-based cohort study that included over 200,000 individuals with migraine, using data collected from 1996 to 2018. Participants were differentiated as having or not having migraine on the basis of prescriptions of preventive or acute migraine medications. Male and female participants were further subdivided, and these groups were compared to healthy controls. The primary endpoints were hazard ratio and absolute risk differences for developing hemorrhagic or ischemic stroke or MI among all groups.
The researchers found an increased risk for ischemic stroke that was equal among male and female participants. Hemorrhagic stroke and MI were seen to be increased in migraine, but primarily among women with migraine. This study specifically investigated what the researchers termed "premature" stroke and MI, and there remains a likelihood that estrogen could be the differentiating factor between the difference in risk between male and female participants with migraine. I have recently highlighted a number of studies investigating vascular risk factors associated with migraine; this study will help clinicians appropriately educate their patients with migraine regarding vascular risk.
The first medications reported as helpful preventively for migraine were antihypertensives, specifically beta-blockers (BB). A number of other medications in other antihypertensive subclasses have also subsequently been shown to be helpful for migraine prevention. These include angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARB), calcium channel blockers (CCB), and alpha-blockers (AB). Carcel and colleagues conducted a meta-analysis that investigated a wide variety of antihypertensive medications in multiple classes and compared the reduction in headache frequency as defined as headache days per month.
This analysis reviewed 50 studies involving over 4000 participants. The majority of the studies (35 out 50 [70%]) had a cross-over design. The medications evaluated included clonidine (an alpha agonist), candesartan (an ARB), telmisartan (an ARB), propranolol (a BB), timolol (a BB), pindolol (a BB), metoprolol (a BB), bisoprolol (a BB), atenolol (a BB), alprenolol (a BB), nimodipine (a CCB), nifedipine (a CCB), verapamil (a CCB), nicardipine (a CCB), enalapril (an ACE inhibitor), and lisinopril (an ACE inhibitor). For each class of antihypertensive, there was a lower number of monthly headache days with treatment compared with placebo; the greatest reduction was for the CCB with a mean difference of about 2 days per month. BB on average decreased headache days per month by 0.7 days. For BB, there was no clear trend to increased efficacywith increased dose. Only six trials reported the difference in blood pressure: On average, there was a 9.3 mm Hg drop in systolic and 3.0 mm Hg drop in diastolic pressure.
The authors showed that there is statistical significance for the use of antihypertensive medications for decreasing migraine days per month, and this was statistically significant separately for numerous specific drugs within the classes: clonidine, candesartan, atenolol, bisoprolol, propranolol, timolol, nicardipine, and verapamil. Antihypertensive medications remain some of the most popular first-line preventive options for migraine, and although the benefit of this class as a whole is mild (slightly more than 1 day per month), it can be an excellent option for many patients
The relationship between migraine and caffeine is necessarily controversial. Caffeine is included as a component of many over-the-counter migraine treatments, and the beneficial effect of caffeine as an acute treatment for migraine has been documented for decades. Reduction in caffeine, however, has also been established as a helpful lifestyle modification for prevention of migraine attacks. Zhang and colleagues used data from the National Health and Nutrition Examination Survey database, a program conducted by the Centers for Disease Control and Prevention to assess the health and nutritional status of adults and children in the United States.
This study sought to quantify the relationship between dietary caffeine and "severe headache." For this study, "severe headache" was defined as answering yes to the question: During the past 3 months, did you have severe headaches or migraines? Dietary caffeine intake was collected through two 24-hour dietary recall interviews, one in person and one 3-10 days later via telephone. The amount of caffeine consumed was estimated in mg/day from all caffeine-containing foods and beverages, including coffee, tea, soda, and chocolate, using the US Department of Agriculture's Food and Nutrient Database. Each participant's mean caffeine intake was defined as the difference between the first and second dietary recalls.
A large number of covariates were assessed as well, including age, race/ethnicity, body mass index, poverty-income ratio, educational level, marital status, hypertension, cancer, energy intake, protein intake, calcium intake, magnesium intake, iron intake, sodium intake, alcohol status, smoking status, and triglyceride level. A total of 8993 participants were included. Caffeine intake was divided into four groups: ≥ 0 to <40 mg/day, ≥ 40 to<200 mg/day, ≥ 200 to<400 mg/day, and ≥ 400 mg/day. After adjusting for confounders, a significant association between dietary caffeine intake and severe headaches or migraines was detected.
Curiously, in this study, only male participants were included. The authors found a clear correlation between the amount of caffeine consumed over a 24-hour period and severe migraine attacks. Further evaluation should investigate the frequency of attacks rather than just individual experience over a 3-month period. Although caffeine is helpful acutely, higher dose consumption is a risk factor for worsening migraine.
Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951.
EXPERT COMMENTARY
Tamoxifen is a selective estrogen receptor modulator (SERM) approved by the US Food and Drug Administration (FDA) for both adjuvant treatment of invasive or metastatic breast cancer with hormone receptor (HR)–positive tumors (duration, 5 to 10 years) and for reduction of future breast cancers in certain high-risk individuals (duration, 5 years). It is also occasionally used for non-FDA approved indications, such as cyclic mastodynia.
Because breast cancer is among the most frequently diagnosed cancers in the United States (297,790 new cases expected in 2023) and approximately 80% are HR-positive tumors that will require hormonal adjuvant therapy,1 physicians and other gynecologic clinicians should have a working understanding of tamoxifen, including the risks and benefits associated with its use. Among the recognized serious adverse effects of tamoxifen is the increased risk of endometrial cancer in menopausal patients. This adverse effect creates a potential conundrum for clinicians who may be managing patients with tamoxifen to treat or prevent breast cancer, while also increasing the risk of another cancer. Prior prospective studies of tamoxifen have demonstrated a statistically and clinically significant increased risk of endometrial cancer in menopausal patients but not in premenopausal patients.
A recent study challenged those previous findings, suggesting that the risk of endometrial cancer is similar in both premenopausal and postmenopausal patients taking tamoxifen for treatment of breast cancer.2
Details of the study
The study by Ryu and colleagues used data from the Korean National Health Insurance Service, which covers 97% of the Korean population.2 The authors selected patients being treated for invasive breast cancer from January 1, 2003, through December 31, 2018, who were between the ages of 20 and 50 years when the breast cancer diagnosis was first made. Patients with a diagnostic code entered into their electronic health record that was consistent with menopausal status were excluded, along with any patients with a current or prior history of aromatase inhibitor use (for which one must be naturally, medically, or surgically menopausal to use). Based on these exclusions, the study cohort was then assumed to be premenopausal.
The study group included patients diagnosed with invasive breast cancer who were treated with adjuvant hormonal therapy with tamoxifen (n = 34,637), and the control group included patients with invasive breast cancer who were not treated with adjuvant hormonal therapy (n = 43,683). The primary study end point was the finding of endometrial or uterine pathology, including endometrial polyps, endometrial hyperplasia, endometrial cancer, and other uterine malignant neoplasms not originating in the endometrium (for example, uterine sarcomas).
Because this was a retrospective cohort study that included all eligible patients, the 2 groups were not matched. The treatment group was statistically older, had a higher body mass index (BMI) and a larger waist circumference, were more likely to be hypertensive, and included more patients with diabetes than the control group—all known risk factors for endometrial cancer. However, after adjusting for these 4 factors, an increased risk of endometrial cancer remained in the tamoxifen group compared with the control group (hazard ratio [HR], 3.77; 95% confidence interval [CI], 3.04–4.66). In addition, tamoxifen use was independently associated with an increased risk of endometrial polyps (HR, 3.90; 95% CI, 3.65–4.16), endometrial hyperplasia (HR, 5.56; 95% CI, 5.06–6.12), and other uterine cancers (HR, 2.27; 95% CI, 1.54–3.33). In a subgroup analysis, the risk for endometrial cancer was not higher in patients treated for more than 5 years of tamoxifen compared with those treated for 5 years or less.
Study strengths and limitations
A major strength of this study was the large number of study participants (n = 34,637 tamoxifen; n = 43,683 control), the long duration of follow-up (up to 15 years), and use of a single source of data with coverage of nearly the entire population of Korea. While the 2 study populations (tamoxifen vs no tamoxifen) were initially unbalanced in terms of endometrial cancer risk (age, BMI, concurrent diagnoses of hypertension and diabetes), the authors corrected for this with a multivariate analysis.
Furthermore, while the likely homogeneity of the study population may not make the results generalizable, the authors noted that Korean patients have a higher tendency toward early-onset breast cancer. This observation could make this cohort better suited for a study on premenopausal effects of tamoxifen.
Limitations. These data are provocative as they conflict with level 1 evidence based on multiple well-designed, double-blind, placebo-controlled randomized trials in which tamoxifen use for 5 years did not demonstrate a statistically increased risk of endometrial cancer in patients younger than age 50.3-5 Because of the importance of the question and the implications for many premenopausal women being treated with tamoxifen, we carefully evaluated the study methodology to better understand this discrepancy.
Continue to: Methodological concerns...
Methodological concerns
In the study by Ryu and colleagues, we found the definition of premenopausal to be problematic. Ultimately, if patients did not have a diagnosis of menopause in the problem summary list, they were assumed to be premenopausal if they were between the ages of 20 and 50 and not taking an aromatase inhibitor. However, important considerations in this population include the cancer stage and treatment regimens that can and do directly impact menopausal status.
Data demonstrate that early-onset breast cancer tends to be associated with more biologically aggressive characteristics that frequently require adjuvant or neoadjuvant chemotherapy.6,7 This chemotherapy regimen is comprised most commonly of Adriamycin (doxorubicin), paclitaxel, and cyclophosphamide. Cyclophosphamide is an alkylating agent that is a known gonadotoxin, and it often renders patients either temporarily or permanently menopausal due to chemotherapy-induced ovarian failure. Prior studies have demonstrated that for patients in their 40s, approximately 90% of those treated with cyclophosphamide-containing chemo-therapy for breast cancer will experience chemotherapy-induced amenorrhea (CIA).8 Although some patients in their 40s with CIA will resume ovarian function, the majority will not.8,9
Due to the lack of reliability in diagnosing CIA, blood levels of estradiol and follicle stimulating hormone are often necessary for confirmation and, even so, may be only temporary. One prospective analysis of 4 randomized neoadjuvant/adjuvant breast cancer trials used this approach and demonstrated that 85.1% of the study cohort experienced chemotherapy-induced ovarian failure at the end of their treatment, with some fluctuating back to premenopausal hormonal levels at 6 and 12 months.10
Furthermore, in the study by Ryu and colleagues, there is no description or confirmation of menstrual patterns in the study group to support the diagnosis of ongoing premenopausal status. Data on CIA and loss of ovarian function, therefore, are critical to the accurate categorization of patients as premenopausal or menopausal in this study. The study also relied on consistent and accurate recording of appropriate medical codes to capture a patient’s menopausal status, which is unclear for this particular population and health system.
In evaluating prior research, multiple studies demonstrated no increased risk of endometrial cancer in premenopausal women taking tamoxifen for breast cancer prevention (TABLE).3,5 These breast cancer prevention trials have several major advantages in assessing tamoxifen-associated endometrial cancer risk for premenopausal patients compared with the current study:
Both studies were prospective double-blind, placebo-controlled randomized clinical breast cancer prevention trials with carefully designed and measured outcomes.
Since these were breast cancer prevention trials, administration of gonadotoxic chemotherapy was not a concern. As a result, miscategorizing patients with chemotherapy-induced menopause as premenopausal would not be expected, and premature menopause would not be expected at a higher rate than the general population.
Careful histories were required prior to study entry and throughout the study, including data on menopausal status and menstrual and uterine bleeding histories.11
In these prevention trials, the effect of tamoxifen on uterine pathology demonstratedrepeatable evidence that there was a statistically significant increased risk of endometrial cancer in postmenopausal women, but there was no similar increased risk of endometrial cancer in premenopausal women (TABLE).3,5 Interestingly, the magnitude of the endometrial cancer risk found in the premenopausal patients in the study by Ryu and colleagues (RR, 3.77) is comparable to that of the menopausal group in the prevention trials, raising concern that many or most of the patients in the treatment group assumed to be premenopausal may have indeed been “menopausal” for some or all the time they were taking tamoxifen due to the possible aforementioned reasons. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
While the data from the study by Ryu and colleagues are provocative, the findings that premenopausal women are at an increased risk of endometrial cancer do not agree with those of well-designed previous trials. Our concerns about categorization bias (that is, women in the treatment group may have been menopausal for some or all the time they were taking tamoxifen but were not formally diagnosed) make the conclusion that endometrial cancer risk is increased in truly premenopausal women somewhat specious. In a Committee Opinion (last endorsed in 2020), the American College of Obstetricians and Gynecologists (ACOG) stated the following: “Postmenopausal women taking tamoxifen should be closely monitored for symptoms of endometrial hyperplasia or cancer. Premenopausal women treated with tamoxifen have no known increased risk of uterine cancer and as such require no additional monitoring beyond routine gynecologic care.”12 Based on multiple previously published studies with solid level 1 evidence and the challenges with the current study design, we continue to agree with this ACOG statement.
VERSHA PLEASANT, MD, MPH; MARK D. PEARLMAN, MD
References
Siegel RL, Miller KD, Wagle NS, et al. Cancer statistics, 2023. CA Cancer J Clin. 2023;73:17-48.
Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951-e.
Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90:1371-1388.
Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for the prevention of breast cancer: current status of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 2005;97:1652-1662.
Iqbal J, Ginsburg OM, Wijeratne TD, et al. Endometrial cancer and venous thromboembolism in women under age 50 who take tamoxifen for prevention of breast cancer: a systematic review. Cancer Treat Rev. 2012;38:318-328.
Kumar R, Abreu C, Toi M, et al. Oncobiology and treatment of breast cancer in young women. Cancer Metastasis Rev. 2022;41:749-770.
Tesch ME, Partidge AH. Treatment of breast cancer in young adults. Am Soc Clin Oncol Educ Book. 2022;42:1-12.
Han HS, Ro J, Lee KS, et al. Analysis of chemotherapy-induced amenorrhea rates by three different anthracycline and taxane containing regimens for early breast cancer. Breast Cancer Res Treat. 2009;115:335-342.
Henry NL, Xia R, Banerjee M, et al. Predictors of recovery of ovarian function during aromatase inhibitor therapy. Ann Oncol. 2013;24:2011-2016.
Furlanetto J, Marme F, Seiler S, et al. Chemotherapy-induced ovarian failure in young women with early breast cancer: prospective analysis of four randomised neoadjuvant/ adjuvant breast cancer trials. Eur J Cancer. 2021;152: 193-203.
Runowicz CD, Costantino JP, Wickerham DL, et al. Gynecologic conditions in participants in the NSABP breast cancer prevention study of tamoxifen and raloxifene (STAR). Am J Obstet Gynecol. 2011;205:535.e1-535.e5.
American College of Obstetricians and Gynecologists. Committee opinion no. 601: tamoxifen and uterine cancer. Obstet Gynecol. 2014;123:1394-1397.
Versha Pleasant, MD, MPH, is Assistant Professor and Director, Center for Cancer Genetics and Breast Health, University of Michigan Health System, Ann Arbor.
Mark D. Pearlman, MD, is Professor Emeritus and Founder, Center for Cancer Genetics and Breast Health, University of Michigan Health System, Ann Arbor.
The authors report no financial relationships relevant to this article.
Versha Pleasant, MD, MPH, is Assistant Professor and Director, Center for Cancer Genetics and Breast Health, University of Michigan Health System, Ann Arbor.
Mark D. Pearlman, MD, is Professor Emeritus and Founder, Center for Cancer Genetics and Breast Health, University of Michigan Health System, Ann Arbor.
The authors report no financial relationships relevant to this article.
Author and Disclosure Information
Versha Pleasant, MD, MPH, is Assistant Professor and Director, Center for Cancer Genetics and Breast Health, University of Michigan Health System, Ann Arbor.
Mark D. Pearlman, MD, is Professor Emeritus and Founder, Center for Cancer Genetics and Breast Health, University of Michigan Health System, Ann Arbor.
The authors report no financial relationships relevant to this article.
Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951.
EXPERT COMMENTARY
Tamoxifen is a selective estrogen receptor modulator (SERM) approved by the US Food and Drug Administration (FDA) for both adjuvant treatment of invasive or metastatic breast cancer with hormone receptor (HR)–positive tumors (duration, 5 to 10 years) and for reduction of future breast cancers in certain high-risk individuals (duration, 5 years). It is also occasionally used for non-FDA approved indications, such as cyclic mastodynia.
Because breast cancer is among the most frequently diagnosed cancers in the United States (297,790 new cases expected in 2023) and approximately 80% are HR-positive tumors that will require hormonal adjuvant therapy,1 physicians and other gynecologic clinicians should have a working understanding of tamoxifen, including the risks and benefits associated with its use. Among the recognized serious adverse effects of tamoxifen is the increased risk of endometrial cancer in menopausal patients. This adverse effect creates a potential conundrum for clinicians who may be managing patients with tamoxifen to treat or prevent breast cancer, while also increasing the risk of another cancer. Prior prospective studies of tamoxifen have demonstrated a statistically and clinically significant increased risk of endometrial cancer in menopausal patients but not in premenopausal patients.
A recent study challenged those previous findings, suggesting that the risk of endometrial cancer is similar in both premenopausal and postmenopausal patients taking tamoxifen for treatment of breast cancer.2
Details of the study
The study by Ryu and colleagues used data from the Korean National Health Insurance Service, which covers 97% of the Korean population.2 The authors selected patients being treated for invasive breast cancer from January 1, 2003, through December 31, 2018, who were between the ages of 20 and 50 years when the breast cancer diagnosis was first made. Patients with a diagnostic code entered into their electronic health record that was consistent with menopausal status were excluded, along with any patients with a current or prior history of aromatase inhibitor use (for which one must be naturally, medically, or surgically menopausal to use). Based on these exclusions, the study cohort was then assumed to be premenopausal.
The study group included patients diagnosed with invasive breast cancer who were treated with adjuvant hormonal therapy with tamoxifen (n = 34,637), and the control group included patients with invasive breast cancer who were not treated with adjuvant hormonal therapy (n = 43,683). The primary study end point was the finding of endometrial or uterine pathology, including endometrial polyps, endometrial hyperplasia, endometrial cancer, and other uterine malignant neoplasms not originating in the endometrium (for example, uterine sarcomas).
Because this was a retrospective cohort study that included all eligible patients, the 2 groups were not matched. The treatment group was statistically older, had a higher body mass index (BMI) and a larger waist circumference, were more likely to be hypertensive, and included more patients with diabetes than the control group—all known risk factors for endometrial cancer. However, after adjusting for these 4 factors, an increased risk of endometrial cancer remained in the tamoxifen group compared with the control group (hazard ratio [HR], 3.77; 95% confidence interval [CI], 3.04–4.66). In addition, tamoxifen use was independently associated with an increased risk of endometrial polyps (HR, 3.90; 95% CI, 3.65–4.16), endometrial hyperplasia (HR, 5.56; 95% CI, 5.06–6.12), and other uterine cancers (HR, 2.27; 95% CI, 1.54–3.33). In a subgroup analysis, the risk for endometrial cancer was not higher in patients treated for more than 5 years of tamoxifen compared with those treated for 5 years or less.
Study strengths and limitations
A major strength of this study was the large number of study participants (n = 34,637 tamoxifen; n = 43,683 control), the long duration of follow-up (up to 15 years), and use of a single source of data with coverage of nearly the entire population of Korea. While the 2 study populations (tamoxifen vs no tamoxifen) were initially unbalanced in terms of endometrial cancer risk (age, BMI, concurrent diagnoses of hypertension and diabetes), the authors corrected for this with a multivariate analysis.
Furthermore, while the likely homogeneity of the study population may not make the results generalizable, the authors noted that Korean patients have a higher tendency toward early-onset breast cancer. This observation could make this cohort better suited for a study on premenopausal effects of tamoxifen.
Limitations. These data are provocative as they conflict with level 1 evidence based on multiple well-designed, double-blind, placebo-controlled randomized trials in which tamoxifen use for 5 years did not demonstrate a statistically increased risk of endometrial cancer in patients younger than age 50.3-5 Because of the importance of the question and the implications for many premenopausal women being treated with tamoxifen, we carefully evaluated the study methodology to better understand this discrepancy.
Continue to: Methodological concerns...
Methodological concerns
In the study by Ryu and colleagues, we found the definition of premenopausal to be problematic. Ultimately, if patients did not have a diagnosis of menopause in the problem summary list, they were assumed to be premenopausal if they were between the ages of 20 and 50 and not taking an aromatase inhibitor. However, important considerations in this population include the cancer stage and treatment regimens that can and do directly impact menopausal status.
Data demonstrate that early-onset breast cancer tends to be associated with more biologically aggressive characteristics that frequently require adjuvant or neoadjuvant chemotherapy.6,7 This chemotherapy regimen is comprised most commonly of Adriamycin (doxorubicin), paclitaxel, and cyclophosphamide. Cyclophosphamide is an alkylating agent that is a known gonadotoxin, and it often renders patients either temporarily or permanently menopausal due to chemotherapy-induced ovarian failure. Prior studies have demonstrated that for patients in their 40s, approximately 90% of those treated with cyclophosphamide-containing chemo-therapy for breast cancer will experience chemotherapy-induced amenorrhea (CIA).8 Although some patients in their 40s with CIA will resume ovarian function, the majority will not.8,9
Due to the lack of reliability in diagnosing CIA, blood levels of estradiol and follicle stimulating hormone are often necessary for confirmation and, even so, may be only temporary. One prospective analysis of 4 randomized neoadjuvant/adjuvant breast cancer trials used this approach and demonstrated that 85.1% of the study cohort experienced chemotherapy-induced ovarian failure at the end of their treatment, with some fluctuating back to premenopausal hormonal levels at 6 and 12 months.10
Furthermore, in the study by Ryu and colleagues, there is no description or confirmation of menstrual patterns in the study group to support the diagnosis of ongoing premenopausal status. Data on CIA and loss of ovarian function, therefore, are critical to the accurate categorization of patients as premenopausal or menopausal in this study. The study also relied on consistent and accurate recording of appropriate medical codes to capture a patient’s menopausal status, which is unclear for this particular population and health system.
In evaluating prior research, multiple studies demonstrated no increased risk of endometrial cancer in premenopausal women taking tamoxifen for breast cancer prevention (TABLE).3,5 These breast cancer prevention trials have several major advantages in assessing tamoxifen-associated endometrial cancer risk for premenopausal patients compared with the current study:
Both studies were prospective double-blind, placebo-controlled randomized clinical breast cancer prevention trials with carefully designed and measured outcomes.
Since these were breast cancer prevention trials, administration of gonadotoxic chemotherapy was not a concern. As a result, miscategorizing patients with chemotherapy-induced menopause as premenopausal would not be expected, and premature menopause would not be expected at a higher rate than the general population.
Careful histories were required prior to study entry and throughout the study, including data on menopausal status and menstrual and uterine bleeding histories.11
In these prevention trials, the effect of tamoxifen on uterine pathology demonstratedrepeatable evidence that there was a statistically significant increased risk of endometrial cancer in postmenopausal women, but there was no similar increased risk of endometrial cancer in premenopausal women (TABLE).3,5 Interestingly, the magnitude of the endometrial cancer risk found in the premenopausal patients in the study by Ryu and colleagues (RR, 3.77) is comparable to that of the menopausal group in the prevention trials, raising concern that many or most of the patients in the treatment group assumed to be premenopausal may have indeed been “menopausal” for some or all the time they were taking tamoxifen due to the possible aforementioned reasons. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
While the data from the study by Ryu and colleagues are provocative, the findings that premenopausal women are at an increased risk of endometrial cancer do not agree with those of well-designed previous trials. Our concerns about categorization bias (that is, women in the treatment group may have been menopausal for some or all the time they were taking tamoxifen but were not formally diagnosed) make the conclusion that endometrial cancer risk is increased in truly premenopausal women somewhat specious. In a Committee Opinion (last endorsed in 2020), the American College of Obstetricians and Gynecologists (ACOG) stated the following: “Postmenopausal women taking tamoxifen should be closely monitored for symptoms of endometrial hyperplasia or cancer. Premenopausal women treated with tamoxifen have no known increased risk of uterine cancer and as such require no additional monitoring beyond routine gynecologic care.”12 Based on multiple previously published studies with solid level 1 evidence and the challenges with the current study design, we continue to agree with this ACOG statement.
VERSHA PLEASANT, MD, MPH; MARK D. PEARLMAN, MD
Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951.
EXPERT COMMENTARY
Tamoxifen is a selective estrogen receptor modulator (SERM) approved by the US Food and Drug Administration (FDA) for both adjuvant treatment of invasive or metastatic breast cancer with hormone receptor (HR)–positive tumors (duration, 5 to 10 years) and for reduction of future breast cancers in certain high-risk individuals (duration, 5 years). It is also occasionally used for non-FDA approved indications, such as cyclic mastodynia.
Because breast cancer is among the most frequently diagnosed cancers in the United States (297,790 new cases expected in 2023) and approximately 80% are HR-positive tumors that will require hormonal adjuvant therapy,1 physicians and other gynecologic clinicians should have a working understanding of tamoxifen, including the risks and benefits associated with its use. Among the recognized serious adverse effects of tamoxifen is the increased risk of endometrial cancer in menopausal patients. This adverse effect creates a potential conundrum for clinicians who may be managing patients with tamoxifen to treat or prevent breast cancer, while also increasing the risk of another cancer. Prior prospective studies of tamoxifen have demonstrated a statistically and clinically significant increased risk of endometrial cancer in menopausal patients but not in premenopausal patients.
A recent study challenged those previous findings, suggesting that the risk of endometrial cancer is similar in both premenopausal and postmenopausal patients taking tamoxifen for treatment of breast cancer.2
Details of the study
The study by Ryu and colleagues used data from the Korean National Health Insurance Service, which covers 97% of the Korean population.2 The authors selected patients being treated for invasive breast cancer from January 1, 2003, through December 31, 2018, who were between the ages of 20 and 50 years when the breast cancer diagnosis was first made. Patients with a diagnostic code entered into their electronic health record that was consistent with menopausal status were excluded, along with any patients with a current or prior history of aromatase inhibitor use (for which one must be naturally, medically, or surgically menopausal to use). Based on these exclusions, the study cohort was then assumed to be premenopausal.
The study group included patients diagnosed with invasive breast cancer who were treated with adjuvant hormonal therapy with tamoxifen (n = 34,637), and the control group included patients with invasive breast cancer who were not treated with adjuvant hormonal therapy (n = 43,683). The primary study end point was the finding of endometrial or uterine pathology, including endometrial polyps, endometrial hyperplasia, endometrial cancer, and other uterine malignant neoplasms not originating in the endometrium (for example, uterine sarcomas).
Because this was a retrospective cohort study that included all eligible patients, the 2 groups were not matched. The treatment group was statistically older, had a higher body mass index (BMI) and a larger waist circumference, were more likely to be hypertensive, and included more patients with diabetes than the control group—all known risk factors for endometrial cancer. However, after adjusting for these 4 factors, an increased risk of endometrial cancer remained in the tamoxifen group compared with the control group (hazard ratio [HR], 3.77; 95% confidence interval [CI], 3.04–4.66). In addition, tamoxifen use was independently associated with an increased risk of endometrial polyps (HR, 3.90; 95% CI, 3.65–4.16), endometrial hyperplasia (HR, 5.56; 95% CI, 5.06–6.12), and other uterine cancers (HR, 2.27; 95% CI, 1.54–3.33). In a subgroup analysis, the risk for endometrial cancer was not higher in patients treated for more than 5 years of tamoxifen compared with those treated for 5 years or less.
Study strengths and limitations
A major strength of this study was the large number of study participants (n = 34,637 tamoxifen; n = 43,683 control), the long duration of follow-up (up to 15 years), and use of a single source of data with coverage of nearly the entire population of Korea. While the 2 study populations (tamoxifen vs no tamoxifen) were initially unbalanced in terms of endometrial cancer risk (age, BMI, concurrent diagnoses of hypertension and diabetes), the authors corrected for this with a multivariate analysis.
Furthermore, while the likely homogeneity of the study population may not make the results generalizable, the authors noted that Korean patients have a higher tendency toward early-onset breast cancer. This observation could make this cohort better suited for a study on premenopausal effects of tamoxifen.
Limitations. These data are provocative as they conflict with level 1 evidence based on multiple well-designed, double-blind, placebo-controlled randomized trials in which tamoxifen use for 5 years did not demonstrate a statistically increased risk of endometrial cancer in patients younger than age 50.3-5 Because of the importance of the question and the implications for many premenopausal women being treated with tamoxifen, we carefully evaluated the study methodology to better understand this discrepancy.
Continue to: Methodological concerns...
Methodological concerns
In the study by Ryu and colleagues, we found the definition of premenopausal to be problematic. Ultimately, if patients did not have a diagnosis of menopause in the problem summary list, they were assumed to be premenopausal if they were between the ages of 20 and 50 and not taking an aromatase inhibitor. However, important considerations in this population include the cancer stage and treatment regimens that can and do directly impact menopausal status.
Data demonstrate that early-onset breast cancer tends to be associated with more biologically aggressive characteristics that frequently require adjuvant or neoadjuvant chemotherapy.6,7 This chemotherapy regimen is comprised most commonly of Adriamycin (doxorubicin), paclitaxel, and cyclophosphamide. Cyclophosphamide is an alkylating agent that is a known gonadotoxin, and it often renders patients either temporarily or permanently menopausal due to chemotherapy-induced ovarian failure. Prior studies have demonstrated that for patients in their 40s, approximately 90% of those treated with cyclophosphamide-containing chemo-therapy for breast cancer will experience chemotherapy-induced amenorrhea (CIA).8 Although some patients in their 40s with CIA will resume ovarian function, the majority will not.8,9
Due to the lack of reliability in diagnosing CIA, blood levels of estradiol and follicle stimulating hormone are often necessary for confirmation and, even so, may be only temporary. One prospective analysis of 4 randomized neoadjuvant/adjuvant breast cancer trials used this approach and demonstrated that 85.1% of the study cohort experienced chemotherapy-induced ovarian failure at the end of their treatment, with some fluctuating back to premenopausal hormonal levels at 6 and 12 months.10
Furthermore, in the study by Ryu and colleagues, there is no description or confirmation of menstrual patterns in the study group to support the diagnosis of ongoing premenopausal status. Data on CIA and loss of ovarian function, therefore, are critical to the accurate categorization of patients as premenopausal or menopausal in this study. The study also relied on consistent and accurate recording of appropriate medical codes to capture a patient’s menopausal status, which is unclear for this particular population and health system.
In evaluating prior research, multiple studies demonstrated no increased risk of endometrial cancer in premenopausal women taking tamoxifen for breast cancer prevention (TABLE).3,5 These breast cancer prevention trials have several major advantages in assessing tamoxifen-associated endometrial cancer risk for premenopausal patients compared with the current study:
Both studies were prospective double-blind, placebo-controlled randomized clinical breast cancer prevention trials with carefully designed and measured outcomes.
Since these were breast cancer prevention trials, administration of gonadotoxic chemotherapy was not a concern. As a result, miscategorizing patients with chemotherapy-induced menopause as premenopausal would not be expected, and premature menopause would not be expected at a higher rate than the general population.
Careful histories were required prior to study entry and throughout the study, including data on menopausal status and menstrual and uterine bleeding histories.11
In these prevention trials, the effect of tamoxifen on uterine pathology demonstratedrepeatable evidence that there was a statistically significant increased risk of endometrial cancer in postmenopausal women, but there was no similar increased risk of endometrial cancer in premenopausal women (TABLE).3,5 Interestingly, the magnitude of the endometrial cancer risk found in the premenopausal patients in the study by Ryu and colleagues (RR, 3.77) is comparable to that of the menopausal group in the prevention trials, raising concern that many or most of the patients in the treatment group assumed to be premenopausal may have indeed been “menopausal” for some or all the time they were taking tamoxifen due to the possible aforementioned reasons. ●
WHAT THIS EVIDENCE MEANS FOR PRACTICE
While the data from the study by Ryu and colleagues are provocative, the findings that premenopausal women are at an increased risk of endometrial cancer do not agree with those of well-designed previous trials. Our concerns about categorization bias (that is, women in the treatment group may have been menopausal for some or all the time they were taking tamoxifen but were not formally diagnosed) make the conclusion that endometrial cancer risk is increased in truly premenopausal women somewhat specious. In a Committee Opinion (last endorsed in 2020), the American College of Obstetricians and Gynecologists (ACOG) stated the following: “Postmenopausal women taking tamoxifen should be closely monitored for symptoms of endometrial hyperplasia or cancer. Premenopausal women treated with tamoxifen have no known increased risk of uterine cancer and as such require no additional monitoring beyond routine gynecologic care.”12 Based on multiple previously published studies with solid level 1 evidence and the challenges with the current study design, we continue to agree with this ACOG statement.
VERSHA PLEASANT, MD, MPH; MARK D. PEARLMAN, MD
References
Siegel RL, Miller KD, Wagle NS, et al. Cancer statistics, 2023. CA Cancer J Clin. 2023;73:17-48.
Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951-e.
Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90:1371-1388.
Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for the prevention of breast cancer: current status of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 2005;97:1652-1662.
Iqbal J, Ginsburg OM, Wijeratne TD, et al. Endometrial cancer and venous thromboembolism in women under age 50 who take tamoxifen for prevention of breast cancer: a systematic review. Cancer Treat Rev. 2012;38:318-328.
Kumar R, Abreu C, Toi M, et al. Oncobiology and treatment of breast cancer in young women. Cancer Metastasis Rev. 2022;41:749-770.
Tesch ME, Partidge AH. Treatment of breast cancer in young adults. Am Soc Clin Oncol Educ Book. 2022;42:1-12.
Han HS, Ro J, Lee KS, et al. Analysis of chemotherapy-induced amenorrhea rates by three different anthracycline and taxane containing regimens for early breast cancer. Breast Cancer Res Treat. 2009;115:335-342.
Henry NL, Xia R, Banerjee M, et al. Predictors of recovery of ovarian function during aromatase inhibitor therapy. Ann Oncol. 2013;24:2011-2016.
Furlanetto J, Marme F, Seiler S, et al. Chemotherapy-induced ovarian failure in young women with early breast cancer: prospective analysis of four randomised neoadjuvant/ adjuvant breast cancer trials. Eur J Cancer. 2021;152: 193-203.
Runowicz CD, Costantino JP, Wickerham DL, et al. Gynecologic conditions in participants in the NSABP breast cancer prevention study of tamoxifen and raloxifene (STAR). Am J Obstet Gynecol. 2011;205:535.e1-535.e5.
American College of Obstetricians and Gynecologists. Committee opinion no. 601: tamoxifen and uterine cancer. Obstet Gynecol. 2014;123:1394-1397.
References
Siegel RL, Miller KD, Wagle NS, et al. Cancer statistics, 2023. CA Cancer J Clin. 2023;73:17-48.
Ryu KJ, Kim MS, Lee JY, et al. Risk of endometrial polyps, hyperplasia, carcinoma, and uterine cancer after tamoxifen treatment in premenopausal women with breast cancer. JAMA Netw Open. 2022;5:e2243951-e.
Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90:1371-1388.
Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for the prevention of breast cancer: current status of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 2005;97:1652-1662.
Iqbal J, Ginsburg OM, Wijeratne TD, et al. Endometrial cancer and venous thromboembolism in women under age 50 who take tamoxifen for prevention of breast cancer: a systematic review. Cancer Treat Rev. 2012;38:318-328.
Kumar R, Abreu C, Toi M, et al. Oncobiology and treatment of breast cancer in young women. Cancer Metastasis Rev. 2022;41:749-770.
Tesch ME, Partidge AH. Treatment of breast cancer in young adults. Am Soc Clin Oncol Educ Book. 2022;42:1-12.
Han HS, Ro J, Lee KS, et al. Analysis of chemotherapy-induced amenorrhea rates by three different anthracycline and taxane containing regimens for early breast cancer. Breast Cancer Res Treat. 2009;115:335-342.
Henry NL, Xia R, Banerjee M, et al. Predictors of recovery of ovarian function during aromatase inhibitor therapy. Ann Oncol. 2013;24:2011-2016.
Furlanetto J, Marme F, Seiler S, et al. Chemotherapy-induced ovarian failure in young women with early breast cancer: prospective analysis of four randomised neoadjuvant/ adjuvant breast cancer trials. Eur J Cancer. 2021;152: 193-203.
Runowicz CD, Costantino JP, Wickerham DL, et al. Gynecologic conditions in participants in the NSABP breast cancer prevention study of tamoxifen and raloxifene (STAR). Am J Obstet Gynecol. 2011;205:535.e1-535.e5.
American College of Obstetricians and Gynecologists. Committee opinion no. 601: tamoxifen and uterine cancer. Obstet Gynecol. 2014;123:1394-1397.