User login
Official Newspaper of the American College of Surgeons
5 ways White House can use its muscle to undercut Obamacare
President Donald Trump has vowed to “let Obamacare fail,” after legislative efforts to undo the Affordable Care Act have stalled.
He and congressional Republicans have repeatedly portrayed the Affordable Care Act insurance marketplaces, also known as exchanges, as being in a “death spiral.” But independent analyses have concluded that such spontaneous disintegration isn’t happening.
In a number of ways, the Trump administration’s policies are pushing Obamacare into the vortex.
Reports from Standard & Poor’s, the Congressional Budget Office and the Kaiser Family Foundation all suggest that the exchanges – where people can shop for coverage, often with the help of a government subsidy – are stabilizing. (Kaiser Health News is an editorially independent program of the foundation.)

“The administration has a lot of power to undermine the markets and make them dysfunctional,” said Sabrina Corlette, a research professor at Georgetown University’s Center on Health Insurance Reforms, who specializes in private insurance markets.
Here’s a look at five ways the White House is already working to weaken the health law, and what that means for consumers.
‘Cost-sharing reductions’
Under the ACA, when someone’s income falls between 100% and 250% of the federal poverty level – up to about $29,000 for an individual or around $61,000 for a family of four – marketplace carriers must offer a plan with “cost-sharing reductions” (CSRs) that reduce consumers’ out-of-pocket expenses.
Reducing cost-sharing – generally copayments and deductibles – makes plans more expensive for the insurers. The Obama administration used its rule-making power to set up direct payments to carriers to help offset this burden. The Trump White House has inherited that responsibility but also has the power to end the payment program.
The nonpartisan Congressional Budget Office estimated CSR subsidies in 2017 would total about $7 billion. Without that money, analysts say, more insurers might choose to exit, limiting options for consumers, and letting the insurers who remain charge higher prices.
Trump has been committedly noncommittal, publicly indicating he would like to halt the subsidies, but so far – on a month-to-month basis – letting them continue.
The uncertainty makes insurance companies skittish about participating, analysts noted. It’s also one reason some plans say they have had to increase their rates, noted Charles Gaba, a Michigan-based blogger who tracks ACA sign-ups. For instance: When filing plans for the 2018 marketplace, carriers on average raised premiums by about 34% – with about 20 points stemming from CSR uncertainty, Mr. Gaba said, based on an analysis of 21 states’ initial rate filings. Dropping the subsidies altogether would be even more damaging.
Weaken the mandate
The White House has already signaled it does not want to enforce the individual mandate – the health law’s requirement that all people have coverage. And administration officials have repeated that position.
Meanwhile, in January, it issued an executive order that encouraged U.S. agencies to grant exemptions and waive or defer health law provisions that could put financial strain on companies or individuals – which could also be applied to the individual mandate.
For 2016 tax returns, though, the Internal Revenue Service continued to impose a financial penalty on people who didn’t have health insurance and who didn’t qualify for an exemption.
But enforcement may be waning. This year, the IRS was supposed to reject tax returns if people didn’t indicate whether they had coverage, flagging them for a potential penalty. Instead, it continued processing them, citing Trump’s executive order.
If the IRS has already processed any tax refunds for consumers, then they “don’t have much leverage” when attempting to collect the mandate fee, said Timothy Jost, emeritus law professor at Washington and Lee University in Virginia and an expert on health reform.
Enforcement of the mandate, economists note, is crucial to ensuring that enough healthy people buy coverage to balance the costs of sicker beneficiaries.
But even with the mandate in effect, the efforts to defang it bring confusion.
“A lot of people believe the Trump administration is not enforcing it,” Mr. Jost said.
As a result, healthy people may become less likely to buy insurance, even as sick ones continue seeking it. That means higher prices, and a shakier pool.
“If they don’t think they’re going to get healthy people in the risk pool, they’re going to increase their rates further to protect themselves,” Mr. Jost said. “And as they raise their rates further to protect themselves, people … start to drop out.”
Thus, the president’s position on the mandate is leaving insurance carriers and commissioners “apprehensive,” noted Mike Kreidler, Washington state’s insurance commissioner.
A bare market
Skittishness on the part of insurers could lead them to drop out of some marketplaces, leaving consumers in some areas with few or no choices. Those “bare markets” are possible under even stable circumstances – and preventing them requires active federal involvement.
Under the Obama administration, high-level officials were “on the phone daily with insurance company executives … trying to get them to participate,” Ms. Corlette said. “It was very much an all-hands-on-deck, ‘we’re going to make it work for you guys’ kind of communication.”
And so far Trump’s Department of Health and Human Services doesn’t appear to be emphasizing this kind of essential outreach, both Ms. Corlette and Mr. Jost suggested. A few months ago, Mr. Kreidler agreed, HHS staffers appeared interested in helping states fill their bare counties – but that support has since dwindled.
“This may be sort of under the radar, but it can have real, lasting effects” for consumer choice, Ms. Corlette said.
All quiet on the enrollment front
The administration could further undermine the marketplace by dropping outreach to consumers. It’s already a shorter enrollment period this year – spanning 6 weeks instead of 3 months, from Nov. 1 to Dec. 15 – though that change was already slated to eventually take effect.
That shorter period means people may miss the memo on signing up – or at least need an extra push, Ms. Corlette said. And that’s another way the administration could undermine the marketplaces: simply choosing not to advertise them.
Last sign-up season, HHS stopped open enrollment advertising in January, pulling ads a few days before the period ended. Enrollment dropped compared with previous years, Mr. Jost and Mr. Gaba noted, with young, healthy people being more likely not to buy coverage.
The administration also just stopped funding federal contractors that supported efforts by community groups and other organizations in some of the nation’s largest cities to sign up people.
Dropping advertising, shortening open enrollment, or simply scaling back on technical maintenance for the marketplace website could all have significant impact, Ms. Corlette said. People who are sick and need insurance will likely seek it out, but those who are healthier – for whom health insurance is a less pressing priority – could miss the boat.
Again, Mr. Jost said, that affects insurer participation.
“Insurance is a product that needs to be sold,” he said. “If the insurers believe they’re not going to get any help at all in marketing their product,” he added, fewer will want to enter the marketplace.
Word of (bad) mouth
HHS has taken an active role in criticizing the health law – pushing press releases and videos that argue it has helped more than hurt. That strategy could do a lot of harm, experts said.
If consumers keep hearing the law is failing, Mr. Jost noted, some will ultimately believe it, buying coverage only if they need it and thereby skewing the insurance risk pool.
Perceived hostility also has an effect on insurers, steering them away from marketplace participation.
“When you undermine confidence in the marketplace, you don’t need a Ph.D. in economics to know it’s not good long term,” Ms. Corlette said.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
President Donald Trump has vowed to “let Obamacare fail,” after legislative efforts to undo the Affordable Care Act have stalled.
He and congressional Republicans have repeatedly portrayed the Affordable Care Act insurance marketplaces, also known as exchanges, as being in a “death spiral.” But independent analyses have concluded that such spontaneous disintegration isn’t happening.
In a number of ways, the Trump administration’s policies are pushing Obamacare into the vortex.
Reports from Standard & Poor’s, the Congressional Budget Office and the Kaiser Family Foundation all suggest that the exchanges – where people can shop for coverage, often with the help of a government subsidy – are stabilizing. (Kaiser Health News is an editorially independent program of the foundation.)
“The administration has a lot of power to undermine the markets and make them dysfunctional,” said Sabrina Corlette, a research professor at Georgetown University’s Center on Health Insurance Reforms, who specializes in private insurance markets.
Here’s a look at five ways the White House is already working to weaken the health law, and what that means for consumers.
‘Cost-sharing reductions’
Under the ACA, when someone’s income falls between 100% and 250% of the federal poverty level – up to about $29,000 for an individual or around $61,000 for a family of four – marketplace carriers must offer a plan with “cost-sharing reductions” (CSRs) that reduce consumers’ out-of-pocket expenses.
Reducing cost-sharing – generally copayments and deductibles – makes plans more expensive for the insurers. The Obama administration used its rule-making power to set up direct payments to carriers to help offset this burden. The Trump White House has inherited that responsibility but also has the power to end the payment program.
The nonpartisan Congressional Budget Office estimated CSR subsidies in 2017 would total about $7 billion. Without that money, analysts say, more insurers might choose to exit, limiting options for consumers, and letting the insurers who remain charge higher prices.
Trump has been committedly noncommittal, publicly indicating he would like to halt the subsidies, but so far – on a month-to-month basis – letting them continue.
The uncertainty makes insurance companies skittish about participating, analysts noted. It’s also one reason some plans say they have had to increase their rates, noted Charles Gaba, a Michigan-based blogger who tracks ACA sign-ups. For instance: When filing plans for the 2018 marketplace, carriers on average raised premiums by about 34% – with about 20 points stemming from CSR uncertainty, Mr. Gaba said, based on an analysis of 21 states’ initial rate filings. Dropping the subsidies altogether would be even more damaging.
Weaken the mandate
The White House has already signaled it does not want to enforce the individual mandate – the health law’s requirement that all people have coverage. And administration officials have repeated that position.
Meanwhile, in January, it issued an executive order that encouraged U.S. agencies to grant exemptions and waive or defer health law provisions that could put financial strain on companies or individuals – which could also be applied to the individual mandate.
For 2016 tax returns, though, the Internal Revenue Service continued to impose a financial penalty on people who didn’t have health insurance and who didn’t qualify for an exemption.
But enforcement may be waning. This year, the IRS was supposed to reject tax returns if people didn’t indicate whether they had coverage, flagging them for a potential penalty. Instead, it continued processing them, citing Trump’s executive order.
If the IRS has already processed any tax refunds for consumers, then they “don’t have much leverage” when attempting to collect the mandate fee, said Timothy Jost, emeritus law professor at Washington and Lee University in Virginia and an expert on health reform.
Enforcement of the mandate, economists note, is crucial to ensuring that enough healthy people buy coverage to balance the costs of sicker beneficiaries.
But even with the mandate in effect, the efforts to defang it bring confusion.
“A lot of people believe the Trump administration is not enforcing it,” Mr. Jost said.
As a result, healthy people may become less likely to buy insurance, even as sick ones continue seeking it. That means higher prices, and a shakier pool.
“If they don’t think they’re going to get healthy people in the risk pool, they’re going to increase their rates further to protect themselves,” Mr. Jost said. “And as they raise their rates further to protect themselves, people … start to drop out.”
Thus, the president’s position on the mandate is leaving insurance carriers and commissioners “apprehensive,” noted Mike Kreidler, Washington state’s insurance commissioner.
A bare market
Skittishness on the part of insurers could lead them to drop out of some marketplaces, leaving consumers in some areas with few or no choices. Those “bare markets” are possible under even stable circumstances – and preventing them requires active federal involvement.
Under the Obama administration, high-level officials were “on the phone daily with insurance company executives … trying to get them to participate,” Ms. Corlette said. “It was very much an all-hands-on-deck, ‘we’re going to make it work for you guys’ kind of communication.”
And so far Trump’s Department of Health and Human Services doesn’t appear to be emphasizing this kind of essential outreach, both Ms. Corlette and Mr. Jost suggested. A few months ago, Mr. Kreidler agreed, HHS staffers appeared interested in helping states fill their bare counties – but that support has since dwindled.
“This may be sort of under the radar, but it can have real, lasting effects” for consumer choice, Ms. Corlette said.
All quiet on the enrollment front
The administration could further undermine the marketplace by dropping outreach to consumers. It’s already a shorter enrollment period this year – spanning 6 weeks instead of 3 months, from Nov. 1 to Dec. 15 – though that change was already slated to eventually take effect.
That shorter period means people may miss the memo on signing up – or at least need an extra push, Ms. Corlette said. And that’s another way the administration could undermine the marketplaces: simply choosing not to advertise them.
Last sign-up season, HHS stopped open enrollment advertising in January, pulling ads a few days before the period ended. Enrollment dropped compared with previous years, Mr. Jost and Mr. Gaba noted, with young, healthy people being more likely not to buy coverage.
The administration also just stopped funding federal contractors that supported efforts by community groups and other organizations in some of the nation’s largest cities to sign up people.
Dropping advertising, shortening open enrollment, or simply scaling back on technical maintenance for the marketplace website could all have significant impact, Ms. Corlette said. People who are sick and need insurance will likely seek it out, but those who are healthier – for whom health insurance is a less pressing priority – could miss the boat.
Again, Mr. Jost said, that affects insurer participation.
“Insurance is a product that needs to be sold,” he said. “If the insurers believe they’re not going to get any help at all in marketing their product,” he added, fewer will want to enter the marketplace.
Word of (bad) mouth
HHS has taken an active role in criticizing the health law – pushing press releases and videos that argue it has helped more than hurt. That strategy could do a lot of harm, experts said.
If consumers keep hearing the law is failing, Mr. Jost noted, some will ultimately believe it, buying coverage only if they need it and thereby skewing the insurance risk pool.
Perceived hostility also has an effect on insurers, steering them away from marketplace participation.
“When you undermine confidence in the marketplace, you don’t need a Ph.D. in economics to know it’s not good long term,” Ms. Corlette said.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
President Donald Trump has vowed to “let Obamacare fail,” after legislative efforts to undo the Affordable Care Act have stalled.
He and congressional Republicans have repeatedly portrayed the Affordable Care Act insurance marketplaces, also known as exchanges, as being in a “death spiral.” But independent analyses have concluded that such spontaneous disintegration isn’t happening.
In a number of ways, the Trump administration’s policies are pushing Obamacare into the vortex.
Reports from Standard & Poor’s, the Congressional Budget Office and the Kaiser Family Foundation all suggest that the exchanges – where people can shop for coverage, often with the help of a government subsidy – are stabilizing. (Kaiser Health News is an editorially independent program of the foundation.)
“The administration has a lot of power to undermine the markets and make them dysfunctional,” said Sabrina Corlette, a research professor at Georgetown University’s Center on Health Insurance Reforms, who specializes in private insurance markets.
Here’s a look at five ways the White House is already working to weaken the health law, and what that means for consumers.
‘Cost-sharing reductions’
Under the ACA, when someone’s income falls between 100% and 250% of the federal poverty level – up to about $29,000 for an individual or around $61,000 for a family of four – marketplace carriers must offer a plan with “cost-sharing reductions” (CSRs) that reduce consumers’ out-of-pocket expenses.
Reducing cost-sharing – generally copayments and deductibles – makes plans more expensive for the insurers. The Obama administration used its rule-making power to set up direct payments to carriers to help offset this burden. The Trump White House has inherited that responsibility but also has the power to end the payment program.
The nonpartisan Congressional Budget Office estimated CSR subsidies in 2017 would total about $7 billion. Without that money, analysts say, more insurers might choose to exit, limiting options for consumers, and letting the insurers who remain charge higher prices.
Trump has been committedly noncommittal, publicly indicating he would like to halt the subsidies, but so far – on a month-to-month basis – letting them continue.
The uncertainty makes insurance companies skittish about participating, analysts noted. It’s also one reason some plans say they have had to increase their rates, noted Charles Gaba, a Michigan-based blogger who tracks ACA sign-ups. For instance: When filing plans for the 2018 marketplace, carriers on average raised premiums by about 34% – with about 20 points stemming from CSR uncertainty, Mr. Gaba said, based on an analysis of 21 states’ initial rate filings. Dropping the subsidies altogether would be even more damaging.
Weaken the mandate
The White House has already signaled it does not want to enforce the individual mandate – the health law’s requirement that all people have coverage. And administration officials have repeated that position.
Meanwhile, in January, it issued an executive order that encouraged U.S. agencies to grant exemptions and waive or defer health law provisions that could put financial strain on companies or individuals – which could also be applied to the individual mandate.
For 2016 tax returns, though, the Internal Revenue Service continued to impose a financial penalty on people who didn’t have health insurance and who didn’t qualify for an exemption.
But enforcement may be waning. This year, the IRS was supposed to reject tax returns if people didn’t indicate whether they had coverage, flagging them for a potential penalty. Instead, it continued processing them, citing Trump’s executive order.
If the IRS has already processed any tax refunds for consumers, then they “don’t have much leverage” when attempting to collect the mandate fee, said Timothy Jost, emeritus law professor at Washington and Lee University in Virginia and an expert on health reform.
Enforcement of the mandate, economists note, is crucial to ensuring that enough healthy people buy coverage to balance the costs of sicker beneficiaries.
But even with the mandate in effect, the efforts to defang it bring confusion.
“A lot of people believe the Trump administration is not enforcing it,” Mr. Jost said.
As a result, healthy people may become less likely to buy insurance, even as sick ones continue seeking it. That means higher prices, and a shakier pool.
“If they don’t think they’re going to get healthy people in the risk pool, they’re going to increase their rates further to protect themselves,” Mr. Jost said. “And as they raise their rates further to protect themselves, people … start to drop out.”
Thus, the president’s position on the mandate is leaving insurance carriers and commissioners “apprehensive,” noted Mike Kreidler, Washington state’s insurance commissioner.
A bare market
Skittishness on the part of insurers could lead them to drop out of some marketplaces, leaving consumers in some areas with few or no choices. Those “bare markets” are possible under even stable circumstances – and preventing them requires active federal involvement.
Under the Obama administration, high-level officials were “on the phone daily with insurance company executives … trying to get them to participate,” Ms. Corlette said. “It was very much an all-hands-on-deck, ‘we’re going to make it work for you guys’ kind of communication.”
And so far Trump’s Department of Health and Human Services doesn’t appear to be emphasizing this kind of essential outreach, both Ms. Corlette and Mr. Jost suggested. A few months ago, Mr. Kreidler agreed, HHS staffers appeared interested in helping states fill their bare counties – but that support has since dwindled.
“This may be sort of under the radar, but it can have real, lasting effects” for consumer choice, Ms. Corlette said.
All quiet on the enrollment front
The administration could further undermine the marketplace by dropping outreach to consumers. It’s already a shorter enrollment period this year – spanning 6 weeks instead of 3 months, from Nov. 1 to Dec. 15 – though that change was already slated to eventually take effect.
That shorter period means people may miss the memo on signing up – or at least need an extra push, Ms. Corlette said. And that’s another way the administration could undermine the marketplaces: simply choosing not to advertise them.
Last sign-up season, HHS stopped open enrollment advertising in January, pulling ads a few days before the period ended. Enrollment dropped compared with previous years, Mr. Jost and Mr. Gaba noted, with young, healthy people being more likely not to buy coverage.
The administration also just stopped funding federal contractors that supported efforts by community groups and other organizations in some of the nation’s largest cities to sign up people.
Dropping advertising, shortening open enrollment, or simply scaling back on technical maintenance for the marketplace website could all have significant impact, Ms. Corlette said. People who are sick and need insurance will likely seek it out, but those who are healthier – for whom health insurance is a less pressing priority – could miss the boat.
Again, Mr. Jost said, that affects insurer participation.
“Insurance is a product that needs to be sold,” he said. “If the insurers believe they’re not going to get any help at all in marketing their product,” he added, fewer will want to enter the marketplace.
Word of (bad) mouth
HHS has taken an active role in criticizing the health law – pushing press releases and videos that argue it has helped more than hurt. That strategy could do a lot of harm, experts said.
If consumers keep hearing the law is failing, Mr. Jost noted, some will ultimately believe it, buying coverage only if they need it and thereby skewing the insurance risk pool.
Perceived hostility also has an effect on insurers, steering them away from marketplace participation.
“When you undermine confidence in the marketplace, you don’t need a Ph.D. in economics to know it’s not good long term,” Ms. Corlette said.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
The right choice? Surgical ethics and the history of surgery
In the almost 30 years since I started surgical residency, the attention to ethical issues in surgery has dramatically changed. Although surgeons still faced ethical dilemmas decades ago, there was little specific attention paid to highlighting these ethical issues in the past. Today, for many reasons, specific attention to the ethical issues in the care of surgical patients is a widespread phenomenon. We see articles in surgical journals about ethical issues and it is commonplace to find sessions devoted to various surgical ethics topics at many surgical society meetings. The American College of Surgeons is even publishing a textbook of surgical ethics in the upcoming months.
This contemporary attention to ethics in surgery seems to be a recent phenomenon. One of my senior colleagues, in commenting on how much more specific attention we pay to ethical issues today, once jokingly stated that he had trained in surgery “before there was ethics.” Although we laughed at the idea that there was a time before ethics, my own experience and my discussions with many retired surgeons, including my father, have led me to believe that things are very different today than several decades ago. I thought that although there were certainly ethically challenging cases in the past that demanded surgeons to make tough choices, such cases I thought were unlikely to be called out as ethics cases.

According to the short publication, the address was given to the Meath Hospital and County Dublin Infirmary at the “opening of the session” on Monday, Oct. 8, 1894. Dr. Stokes’ words on that date seem to have been addressed primarily to medical students, but many of the topics he touched upon resonate with ongoing ethical issues in the care of patients today.
When addressing the innovative ideas of antisepsis, Dr. Stokes wrote: “…it might be that in the minds of some zealous operators, it may have had a tendency to beget an overweening confidence in the powers of our art. The result has been that the ethical principles which should always guide us in our operative work have, at times, I think, been neglected, and operations undertaken that, in the present state of our knowledge, have, I fear, overleaped the pale of legitimate surgery.” In these sentences, Dr. Stokes is addressing the worry that overconfident surgeons might recommend operations that may put their patients at significant risk. Here, he is addressing an issue that remains problematic today as surgeons must often temper their enthusiasm for an innovative operation in the context of the potential complications that the patient will be put at risk for.
Later, Dr. Stokes goes on to use the term “surgical ethics” for perhaps the first time in the surgical literature when he writes: “A consideration of surgical ethics that frequently exercises the mind of the operating surgeon is the question of the principles that should guide him in dealing with cancerous growths. The question as to what constitutes justification in dealing with them in an operative way is ever present and surrounded with difficulty, as the result of such interference must end in weal or woe, satisfaction or regret to the patient as to the operator.” Although the language is somewhat different, Dr. Stokes is challenging surgeons to address a central question in the care of every patient with cancer:
Do the risks of the operation outweigh the potential benefits to the patient?
Although this question is central to all surgical decision making, Dr. Stokes’ specific attention to this question in relation to cancer surgery is a reflection of the understanding, even in the 1890s, that cancers most frequently led to death with or without aggressive surgical intervention. Although patients commonly are willing to put themselves at significant risk for even a small chance of benefit when the alternative is death, surgeons must carefully weigh risks and benefits when deciding when to offer surgery to such vulnerable patients.
The words of Sir William Stokes seem strangely modern in their emphasis on surgeon judgment. The question of “what should we offer to our patient?” is one that apparently is not new. The overarching question of whether the risks outweigh the benefits of innovative operations or challenging cancer procedures are as relevant to surgeons today as they were to a thoughtful surgeon in 1894. The questions that Dr. Stokes raised could have been lifted directly from the M & M discussion at any number of surgical departments today. This early work in surgical ethics should remind us of the importance of carefully considering when we should offer risky surgery to vulnerable patients who often believe that surgery is their only option for cure.
Dr. Angelos is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
In the almost 30 years since I started surgical residency, the attention to ethical issues in surgery has dramatically changed. Although surgeons still faced ethical dilemmas decades ago, there was little specific attention paid to highlighting these ethical issues in the past. Today, for many reasons, specific attention to the ethical issues in the care of surgical patients is a widespread phenomenon. We see articles in surgical journals about ethical issues and it is commonplace to find sessions devoted to various surgical ethics topics at many surgical society meetings. The American College of Surgeons is even publishing a textbook of surgical ethics in the upcoming months.
This contemporary attention to ethics in surgery seems to be a recent phenomenon. One of my senior colleagues, in commenting on how much more specific attention we pay to ethical issues today, once jokingly stated that he had trained in surgery “before there was ethics.” Although we laughed at the idea that there was a time before ethics, my own experience and my discussions with many retired surgeons, including my father, have led me to believe that things are very different today than several decades ago. I thought that although there were certainly ethically challenging cases in the past that demanded surgeons to make tough choices, such cases I thought were unlikely to be called out as ethics cases.
According to the short publication, the address was given to the Meath Hospital and County Dublin Infirmary at the “opening of the session” on Monday, Oct. 8, 1894. Dr. Stokes’ words on that date seem to have been addressed primarily to medical students, but many of the topics he touched upon resonate with ongoing ethical issues in the care of patients today.
When addressing the innovative ideas of antisepsis, Dr. Stokes wrote: “…it might be that in the minds of some zealous operators, it may have had a tendency to beget an overweening confidence in the powers of our art. The result has been that the ethical principles which should always guide us in our operative work have, at times, I think, been neglected, and operations undertaken that, in the present state of our knowledge, have, I fear, overleaped the pale of legitimate surgery.” In these sentences, Dr. Stokes is addressing the worry that overconfident surgeons might recommend operations that may put their patients at significant risk. Here, he is addressing an issue that remains problematic today as surgeons must often temper their enthusiasm for an innovative operation in the context of the potential complications that the patient will be put at risk for.
Later, Dr. Stokes goes on to use the term “surgical ethics” for perhaps the first time in the surgical literature when he writes: “A consideration of surgical ethics that frequently exercises the mind of the operating surgeon is the question of the principles that should guide him in dealing with cancerous growths. The question as to what constitutes justification in dealing with them in an operative way is ever present and surrounded with difficulty, as the result of such interference must end in weal or woe, satisfaction or regret to the patient as to the operator.” Although the language is somewhat different, Dr. Stokes is challenging surgeons to address a central question in the care of every patient with cancer:
Do the risks of the operation outweigh the potential benefits to the patient?
Although this question is central to all surgical decision making, Dr. Stokes’ specific attention to this question in relation to cancer surgery is a reflection of the understanding, even in the 1890s, that cancers most frequently led to death with or without aggressive surgical intervention. Although patients commonly are willing to put themselves at significant risk for even a small chance of benefit when the alternative is death, surgeons must carefully weigh risks and benefits when deciding when to offer surgery to such vulnerable patients.
The words of Sir William Stokes seem strangely modern in their emphasis on surgeon judgment. The question of “what should we offer to our patient?” is one that apparently is not new. The overarching question of whether the risks outweigh the benefits of innovative operations or challenging cancer procedures are as relevant to surgeons today as they were to a thoughtful surgeon in 1894. The questions that Dr. Stokes raised could have been lifted directly from the M & M discussion at any number of surgical departments today. This early work in surgical ethics should remind us of the importance of carefully considering when we should offer risky surgery to vulnerable patients who often believe that surgery is their only option for cure.
Dr. Angelos is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
In the almost 30 years since I started surgical residency, the attention to ethical issues in surgery has dramatically changed. Although surgeons still faced ethical dilemmas decades ago, there was little specific attention paid to highlighting these ethical issues in the past. Today, for many reasons, specific attention to the ethical issues in the care of surgical patients is a widespread phenomenon. We see articles in surgical journals about ethical issues and it is commonplace to find sessions devoted to various surgical ethics topics at many surgical society meetings. The American College of Surgeons is even publishing a textbook of surgical ethics in the upcoming months.
This contemporary attention to ethics in surgery seems to be a recent phenomenon. One of my senior colleagues, in commenting on how much more specific attention we pay to ethical issues today, once jokingly stated that he had trained in surgery “before there was ethics.” Although we laughed at the idea that there was a time before ethics, my own experience and my discussions with many retired surgeons, including my father, have led me to believe that things are very different today than several decades ago. I thought that although there were certainly ethically challenging cases in the past that demanded surgeons to make tough choices, such cases I thought were unlikely to be called out as ethics cases.
According to the short publication, the address was given to the Meath Hospital and County Dublin Infirmary at the “opening of the session” on Monday, Oct. 8, 1894. Dr. Stokes’ words on that date seem to have been addressed primarily to medical students, but many of the topics he touched upon resonate with ongoing ethical issues in the care of patients today.
When addressing the innovative ideas of antisepsis, Dr. Stokes wrote: “…it might be that in the minds of some zealous operators, it may have had a tendency to beget an overweening confidence in the powers of our art. The result has been that the ethical principles which should always guide us in our operative work have, at times, I think, been neglected, and operations undertaken that, in the present state of our knowledge, have, I fear, overleaped the pale of legitimate surgery.” In these sentences, Dr. Stokes is addressing the worry that overconfident surgeons might recommend operations that may put their patients at significant risk. Here, he is addressing an issue that remains problematic today as surgeons must often temper their enthusiasm for an innovative operation in the context of the potential complications that the patient will be put at risk for.
Later, Dr. Stokes goes on to use the term “surgical ethics” for perhaps the first time in the surgical literature when he writes: “A consideration of surgical ethics that frequently exercises the mind of the operating surgeon is the question of the principles that should guide him in dealing with cancerous growths. The question as to what constitutes justification in dealing with them in an operative way is ever present and surrounded with difficulty, as the result of such interference must end in weal or woe, satisfaction or regret to the patient as to the operator.” Although the language is somewhat different, Dr. Stokes is challenging surgeons to address a central question in the care of every patient with cancer:
Do the risks of the operation outweigh the potential benefits to the patient?
Although this question is central to all surgical decision making, Dr. Stokes’ specific attention to this question in relation to cancer surgery is a reflection of the understanding, even in the 1890s, that cancers most frequently led to death with or without aggressive surgical intervention. Although patients commonly are willing to put themselves at significant risk for even a small chance of benefit when the alternative is death, surgeons must carefully weigh risks and benefits when deciding when to offer surgery to such vulnerable patients.
The words of Sir William Stokes seem strangely modern in their emphasis on surgeon judgment. The question of “what should we offer to our patient?” is one that apparently is not new. The overarching question of whether the risks outweigh the benefits of innovative operations or challenging cancer procedures are as relevant to surgeons today as they were to a thoughtful surgeon in 1894. The questions that Dr. Stokes raised could have been lifted directly from the M & M discussion at any number of surgical departments today. This early work in surgical ethics should remind us of the importance of carefully considering when we should offer risky surgery to vulnerable patients who often believe that surgery is their only option for cure.
Dr. Angelos is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
The surgical sky may not be falling
Unlike Dr. Elsey (“Surgery can be demanding work: Grit needed,” Letter to the Editor, May 2017, p. 6) and many others in various surgical publications, I have NOT enjoyed recent discussions about my generation’s perceived lack of readiness for independent practice following general surgery residency. Having been subjected to another round this month of “Why The Surgical Sky Is Falling,” I would like to take a moment to offer a different viewpoint.
I graduated from Tufts Medical Center’s general surgery residency in June 2014. After taking the written board exams, I started practice in a hospital-based group in Maine that same summer. My partners, both with 20+ years of experience, instituted a probationary period for observation of skill (ostensibly, and with good-natured teasing, to ensure I would not harm their patients, though I suspect such a thing is fairly universal for a new grad to receive institutional privileges), and, after convincing them I was not a reckless maniac, within a few months I was “on my own” in the operating room. I relied heavily on colleagues those first 18 months in practice, and ,if they ever grew weary of my asking advice about hemorrhoids, biliary colic, and diverticular disease, they never displayed perceptible annoyance. They were, and are, the best mentors I could have had.

Metrics and studies that rely on resident self-evaluation – and conversely, ones that rely on “objective” identification of resident strengths and weaknesses by faculty – are subject to the very bias that has dominated this argument for years. If you tell us we are not good enough or lacking in some capacity, often enough, we inevitably will start to believe it. Then, you will reinforce that same belief in your perception of us, which drives the wedge further into an increasingly irreconcilable situation.
I had a decent self-opinion of my surgical skill as a chief resident, but, on any given day, the number I would have assigned to my own “readiness” for independence would have varied greatly for any number of reasons. I did not contend with much in the way of spirited discouragement or admonishment regarding my skill progression over 5 years, but, in keeping with the “gritty” surgical personality espoused by Dr. Elsey in his letter, I’m not sure I would have let that stop me. Honestly though, it’s impossible to say how it would have affected my confidence to leave residency straight for attendinghood had I been subjected to daily thrashings over 5 years regarding my lack of attending-level skill.
It seems to me, some of the current teaching generation has displayed an inability to connect with their pupils. The majority of surgical residents in 2017 are millennials, and the “good old ways” of effective teaching through guilt, embarrassment, and punitive action will not work. Browbeaters need not apply, for you already have lost this war. For better or worse, educators must find a way to engage these residents on a positive emotional level at the same time as they engage on a higher intellectual plane.
Before the coffee spurts across your OR lounge and the surgical hats start flying fast and furious, let me clarify: In no way do I support the notion that general surgery residents should be coddled, pampered, or emotionally shielded from the gut-wrenching difficulty of practicing surgery. It was imperative in my education that I learned how to be wrong, how to admit it, and how to take ownership of my actions, whether right or wrong. Thankfully, I had a few good examples in Boston, and I’ll never forget the impact they made on my education. But, those lessons were reinforced in a way that made me WANT to weave them into the fabric of my surgical life. Never a heavy-handed dictum; without ego or audience; lacking the morose condescension associated with “those giants” of classical surgical training – what I received in my training was a whole-person engagement that fulfilled my desire to succeed and allowed me the room to grow up as an adult learner without feeling too akin to a 16-year-old, grounded and without car keys, when I had the audacity to make a mistake. Some tried this tack, but my grit won. Somewhere in Lawrenceville, Ga., I hope Dr. Elsey is smiling.
Those who taught best in my residency did so by example. They did it by letting me drive the ship, by giving credit when I did well, by educating when I did not. They did it by making me understand a patient is not a statistic, that you can be honest and kind and a giver of hope all at the same time and that a true surgeon does not need to brag and boast about her accomplishments, nor does he imperiously tear down those lower than himself on the “hierarchy.” The best of the best at Tufts Medical Center showed me what it means when a good person sits in an exam room with a hurting human being and starts the healing process with a kind smile, a gentle touch, words of reassurance, and confidence in his ability to change that patient’s life for the better.
Could it be that we need more of that – and less devotion to metrics – in surgical education? What might training become if we focus entirely on the patient and stop worrying about how the statistics make us all look? What would happen if educators traded nostalgia for engagement with their pupils? It may just be me, but all that sounds suspiciously ... old school, no?
So, before I have to choke down another article explaining how my contemporaries and I represent a kind of global warming to the long-established surgical polar ice caps, let me assure you that at least one young whippersnapper made it out of modern (read: postduty hours) surgical training and actually found a little success – and more than a bit of professional satisfaction – in the unforgiving world of independent general surgery by adhering to the same principles that guided Zollinger and DeBakey, Graham and Fisher: Do what is right for the patient, every single time, to the very best of your God-given and man-made ability. Those are some time-tested lessons I am very proud to have learned.
And, if you want the real story about my 3 years in practice, talk to my partners here in Maine. There is no critique quite like daily proximity. For what it’s worth, they have tolerated me splendidly.
Dr. Crosslin is a general surgeon practicing in Rockport, Maine, and an FACS Initiate, October 2017.
Unlike Dr. Elsey (“Surgery can be demanding work: Grit needed,” Letter to the Editor, May 2017, p. 6) and many others in various surgical publications, I have NOT enjoyed recent discussions about my generation’s perceived lack of readiness for independent practice following general surgery residency. Having been subjected to another round this month of “Why The Surgical Sky Is Falling,” I would like to take a moment to offer a different viewpoint.
I graduated from Tufts Medical Center’s general surgery residency in June 2014. After taking the written board exams, I started practice in a hospital-based group in Maine that same summer. My partners, both with 20+ years of experience, instituted a probationary period for observation of skill (ostensibly, and with good-natured teasing, to ensure I would not harm their patients, though I suspect such a thing is fairly universal for a new grad to receive institutional privileges), and, after convincing them I was not a reckless maniac, within a few months I was “on my own” in the operating room. I relied heavily on colleagues those first 18 months in practice, and ,if they ever grew weary of my asking advice about hemorrhoids, biliary colic, and diverticular disease, they never displayed perceptible annoyance. They were, and are, the best mentors I could have had.
Metrics and studies that rely on resident self-evaluation – and conversely, ones that rely on “objective” identification of resident strengths and weaknesses by faculty – are subject to the very bias that has dominated this argument for years. If you tell us we are not good enough or lacking in some capacity, often enough, we inevitably will start to believe it. Then, you will reinforce that same belief in your perception of us, which drives the wedge further into an increasingly irreconcilable situation.
I had a decent self-opinion of my surgical skill as a chief resident, but, on any given day, the number I would have assigned to my own “readiness” for independence would have varied greatly for any number of reasons. I did not contend with much in the way of spirited discouragement or admonishment regarding my skill progression over 5 years, but, in keeping with the “gritty” surgical personality espoused by Dr. Elsey in his letter, I’m not sure I would have let that stop me. Honestly though, it’s impossible to say how it would have affected my confidence to leave residency straight for attendinghood had I been subjected to daily thrashings over 5 years regarding my lack of attending-level skill.
It seems to me, some of the current teaching generation has displayed an inability to connect with their pupils. The majority of surgical residents in 2017 are millennials, and the “good old ways” of effective teaching through guilt, embarrassment, and punitive action will not work. Browbeaters need not apply, for you already have lost this war. For better or worse, educators must find a way to engage these residents on a positive emotional level at the same time as they engage on a higher intellectual plane.
Before the coffee spurts across your OR lounge and the surgical hats start flying fast and furious, let me clarify: In no way do I support the notion that general surgery residents should be coddled, pampered, or emotionally shielded from the gut-wrenching difficulty of practicing surgery. It was imperative in my education that I learned how to be wrong, how to admit it, and how to take ownership of my actions, whether right or wrong. Thankfully, I had a few good examples in Boston, and I’ll never forget the impact they made on my education. But, those lessons were reinforced in a way that made me WANT to weave them into the fabric of my surgical life. Never a heavy-handed dictum; without ego or audience; lacking the morose condescension associated with “those giants” of classical surgical training – what I received in my training was a whole-person engagement that fulfilled my desire to succeed and allowed me the room to grow up as an adult learner without feeling too akin to a 16-year-old, grounded and without car keys, when I had the audacity to make a mistake. Some tried this tack, but my grit won. Somewhere in Lawrenceville, Ga., I hope Dr. Elsey is smiling.
Those who taught best in my residency did so by example. They did it by letting me drive the ship, by giving credit when I did well, by educating when I did not. They did it by making me understand a patient is not a statistic, that you can be honest and kind and a giver of hope all at the same time and that a true surgeon does not need to brag and boast about her accomplishments, nor does he imperiously tear down those lower than himself on the “hierarchy.” The best of the best at Tufts Medical Center showed me what it means when a good person sits in an exam room with a hurting human being and starts the healing process with a kind smile, a gentle touch, words of reassurance, and confidence in his ability to change that patient’s life for the better.
Could it be that we need more of that – and less devotion to metrics – in surgical education? What might training become if we focus entirely on the patient and stop worrying about how the statistics make us all look? What would happen if educators traded nostalgia for engagement with their pupils? It may just be me, but all that sounds suspiciously ... old school, no?
So, before I have to choke down another article explaining how my contemporaries and I represent a kind of global warming to the long-established surgical polar ice caps, let me assure you that at least one young whippersnapper made it out of modern (read: postduty hours) surgical training and actually found a little success – and more than a bit of professional satisfaction – in the unforgiving world of independent general surgery by adhering to the same principles that guided Zollinger and DeBakey, Graham and Fisher: Do what is right for the patient, every single time, to the very best of your God-given and man-made ability. Those are some time-tested lessons I am very proud to have learned.
And, if you want the real story about my 3 years in practice, talk to my partners here in Maine. There is no critique quite like daily proximity. For what it’s worth, they have tolerated me splendidly.
Dr. Crosslin is a general surgeon practicing in Rockport, Maine, and an FACS Initiate, October 2017.
Unlike Dr. Elsey (“Surgery can be demanding work: Grit needed,” Letter to the Editor, May 2017, p. 6) and many others in various surgical publications, I have NOT enjoyed recent discussions about my generation’s perceived lack of readiness for independent practice following general surgery residency. Having been subjected to another round this month of “Why The Surgical Sky Is Falling,” I would like to take a moment to offer a different viewpoint.
I graduated from Tufts Medical Center’s general surgery residency in June 2014. After taking the written board exams, I started practice in a hospital-based group in Maine that same summer. My partners, both with 20+ years of experience, instituted a probationary period for observation of skill (ostensibly, and with good-natured teasing, to ensure I would not harm their patients, though I suspect such a thing is fairly universal for a new grad to receive institutional privileges), and, after convincing them I was not a reckless maniac, within a few months I was “on my own” in the operating room. I relied heavily on colleagues those first 18 months in practice, and ,if they ever grew weary of my asking advice about hemorrhoids, biliary colic, and diverticular disease, they never displayed perceptible annoyance. They were, and are, the best mentors I could have had.
Metrics and studies that rely on resident self-evaluation – and conversely, ones that rely on “objective” identification of resident strengths and weaknesses by faculty – are subject to the very bias that has dominated this argument for years. If you tell us we are not good enough or lacking in some capacity, often enough, we inevitably will start to believe it. Then, you will reinforce that same belief in your perception of us, which drives the wedge further into an increasingly irreconcilable situation.
I had a decent self-opinion of my surgical skill as a chief resident, but, on any given day, the number I would have assigned to my own “readiness” for independence would have varied greatly for any number of reasons. I did not contend with much in the way of spirited discouragement or admonishment regarding my skill progression over 5 years, but, in keeping with the “gritty” surgical personality espoused by Dr. Elsey in his letter, I’m not sure I would have let that stop me. Honestly though, it’s impossible to say how it would have affected my confidence to leave residency straight for attendinghood had I been subjected to daily thrashings over 5 years regarding my lack of attending-level skill.
It seems to me, some of the current teaching generation has displayed an inability to connect with their pupils. The majority of surgical residents in 2017 are millennials, and the “good old ways” of effective teaching through guilt, embarrassment, and punitive action will not work. Browbeaters need not apply, for you already have lost this war. For better or worse, educators must find a way to engage these residents on a positive emotional level at the same time as they engage on a higher intellectual plane.
Before the coffee spurts across your OR lounge and the surgical hats start flying fast and furious, let me clarify: In no way do I support the notion that general surgery residents should be coddled, pampered, or emotionally shielded from the gut-wrenching difficulty of practicing surgery. It was imperative in my education that I learned how to be wrong, how to admit it, and how to take ownership of my actions, whether right or wrong. Thankfully, I had a few good examples in Boston, and I’ll never forget the impact they made on my education. But, those lessons were reinforced in a way that made me WANT to weave them into the fabric of my surgical life. Never a heavy-handed dictum; without ego or audience; lacking the morose condescension associated with “those giants” of classical surgical training – what I received in my training was a whole-person engagement that fulfilled my desire to succeed and allowed me the room to grow up as an adult learner without feeling too akin to a 16-year-old, grounded and without car keys, when I had the audacity to make a mistake. Some tried this tack, but my grit won. Somewhere in Lawrenceville, Ga., I hope Dr. Elsey is smiling.
Those who taught best in my residency did so by example. They did it by letting me drive the ship, by giving credit when I did well, by educating when I did not. They did it by making me understand a patient is not a statistic, that you can be honest and kind and a giver of hope all at the same time and that a true surgeon does not need to brag and boast about her accomplishments, nor does he imperiously tear down those lower than himself on the “hierarchy.” The best of the best at Tufts Medical Center showed me what it means when a good person sits in an exam room with a hurting human being and starts the healing process with a kind smile, a gentle touch, words of reassurance, and confidence in his ability to change that patient’s life for the better.
Could it be that we need more of that – and less devotion to metrics – in surgical education? What might training become if we focus entirely on the patient and stop worrying about how the statistics make us all look? What would happen if educators traded nostalgia for engagement with their pupils? It may just be me, but all that sounds suspiciously ... old school, no?
So, before I have to choke down another article explaining how my contemporaries and I represent a kind of global warming to the long-established surgical polar ice caps, let me assure you that at least one young whippersnapper made it out of modern (read: postduty hours) surgical training and actually found a little success – and more than a bit of professional satisfaction – in the unforgiving world of independent general surgery by adhering to the same principles that guided Zollinger and DeBakey, Graham and Fisher: Do what is right for the patient, every single time, to the very best of your God-given and man-made ability. Those are some time-tested lessons I am very proud to have learned.
And, if you want the real story about my 3 years in practice, talk to my partners here in Maine. There is no critique quite like daily proximity. For what it’s worth, they have tolerated me splendidly.
Dr. Crosslin is a general surgeon practicing in Rockport, Maine, and an FACS Initiate, October 2017.

From the Editors: A crisis of confidence?
As today’s surgical residents complete their residencies and enter practice, we are compelled to ask, Is their level of confidence and independence different from that of, say, the class of 1978? Have circumstances of training changed to such a degree that graduating residents’ beliefs in their own judgment have been undermined?
The answer is yes: The conditions and circumstances of training have changed substantially. Our attendings were strong role models, but they were not as omnipresent as are today’s faculty, particularly in the operating room. We, therefore, felt a greater sense of autonomy than do today’s trainees.

It is unquestionably true that our medical and surgical world has become so much more complex that mastery of the broad range of knowledge and skills encompassing general surgery has become daunting. It is indeed too much to ask that a graduating surgeon be a master at biliary surgery, foregut surgery, head and neck surgery, trauma, critical care, and all the rest.
If we are honest with ourselves, Was our confidence really that much greater in 1978? I think that most of us were scared to death that we would make wrong decisions or encounter a problem that we would be unable to handle in those first few years of practice. That is why most of us chose to enter a practice with a senior partner or partners whose brains we could pick if need be. Of course, it wasn’t fashionable to admit it because surgeons were supposed to behave as though they always had everything under control and had the utmost confidence. Mostly we did, but it was most helpful to run a sticky, complicated patient problem by our all-wise senior partner. Even then, with all our clinical experience and independence, we weren’t as polished or confident as surgeons on graduation day from residency than we would become after 8 or 10 years of practice.
So, what’s different now? From the time that they are pups, today’s residents somehow get the impression that they can’t become good surgeons in the 80-hour work week, that they lack stamina and resolve of past generations, and that they need to do a fellowship to get respect or know enough to do a good job. Although the cause of these problems is placed at the feet of the ACGME, hospital administration, American Board of Surgery, or the residents themselves, surgical faculty should shoulder some of the responsibility. Faculty can and should make changes to their teaching and assessment techniques to better address the realities of today’s generation and today’s surgical realities.
I would maintain that it is possible to produce competent surgeons in five years of training but only if training is revised to reflect the changed circumstances of surgical practice. It must be intentional and evidence-based, much like the surgical practice we wish to promote. It should include simulation supervised by expert surgeons who can immediately correct errors, mandated practice at skills until the resident has passed a competency exam in that skill before taking it into the human operating skill, specific and honest but respectful assessment of the resident’s operative skills, and graduated responsibility with eventual autonomy as the goal. This kind of training can’t happen if the faculty feel bound more by demands of the clock and the pressure to generate more relative value units than by their responsibility to their trainees to coach them in clinical decision-making and technical skills. It is possible as an intending to be present but not make all the decisions. Instead of “Do this!” one need only ask, “What do you want to do?” and then pause for the trainee to respond.
Whenever it isn’t a dire and pressing emergency, what can follow is an honest interchange of ideas. For that to happen, the relationship requires mutual trust and respect. On the faculty’s part, there should be an understanding that there is often more than one acceptable way to proceed and that the resident is not only smart and diligent but usually just as motivated to do the best for his or her patient as is the faculty member. On the resident’s part, there should be the expectation that the faculty member will engage the resident in thoughtful discussion in response to his or her question, even if the answer was not the faculty’s favored way of handling the problem.
Having been a surgical faculty member for almost 40 years and a general surgery program director for 20, I would argue that today’s surgical residents are every bit as dedicated and conscientious as we were. Since there is more to learn and less time to learn it, we faculty need to be more efficient in our teaching and assessment, which means using every opportunity we have to help them become as competent and confident as possible by June 30 of their chief residency year.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
As today’s surgical residents complete their residencies and enter practice, we are compelled to ask, Is their level of confidence and independence different from that of, say, the class of 1978? Have circumstances of training changed to such a degree that graduating residents’ beliefs in their own judgment have been undermined?
The answer is yes: The conditions and circumstances of training have changed substantially. Our attendings were strong role models, but they were not as omnipresent as are today’s faculty, particularly in the operating room. We, therefore, felt a greater sense of autonomy than do today’s trainees.
It is unquestionably true that our medical and surgical world has become so much more complex that mastery of the broad range of knowledge and skills encompassing general surgery has become daunting. It is indeed too much to ask that a graduating surgeon be a master at biliary surgery, foregut surgery, head and neck surgery, trauma, critical care, and all the rest.
If we are honest with ourselves, Was our confidence really that much greater in 1978? I think that most of us were scared to death that we would make wrong decisions or encounter a problem that we would be unable to handle in those first few years of practice. That is why most of us chose to enter a practice with a senior partner or partners whose brains we could pick if need be. Of course, it wasn’t fashionable to admit it because surgeons were supposed to behave as though they always had everything under control and had the utmost confidence. Mostly we did, but it was most helpful to run a sticky, complicated patient problem by our all-wise senior partner. Even then, with all our clinical experience and independence, we weren’t as polished or confident as surgeons on graduation day from residency than we would become after 8 or 10 years of practice.
So, what’s different now? From the time that they are pups, today’s residents somehow get the impression that they can’t become good surgeons in the 80-hour work week, that they lack stamina and resolve of past generations, and that they need to do a fellowship to get respect or know enough to do a good job. Although the cause of these problems is placed at the feet of the ACGME, hospital administration, American Board of Surgery, or the residents themselves, surgical faculty should shoulder some of the responsibility. Faculty can and should make changes to their teaching and assessment techniques to better address the realities of today’s generation and today’s surgical realities.
I would maintain that it is possible to produce competent surgeons in five years of training but only if training is revised to reflect the changed circumstances of surgical practice. It must be intentional and evidence-based, much like the surgical practice we wish to promote. It should include simulation supervised by expert surgeons who can immediately correct errors, mandated practice at skills until the resident has passed a competency exam in that skill before taking it into the human operating skill, specific and honest but respectful assessment of the resident’s operative skills, and graduated responsibility with eventual autonomy as the goal. This kind of training can’t happen if the faculty feel bound more by demands of the clock and the pressure to generate more relative value units than by their responsibility to their trainees to coach them in clinical decision-making and technical skills. It is possible as an intending to be present but not make all the decisions. Instead of “Do this!” one need only ask, “What do you want to do?” and then pause for the trainee to respond.
Whenever it isn’t a dire and pressing emergency, what can follow is an honest interchange of ideas. For that to happen, the relationship requires mutual trust and respect. On the faculty’s part, there should be an understanding that there is often more than one acceptable way to proceed and that the resident is not only smart and diligent but usually just as motivated to do the best for his or her patient as is the faculty member. On the resident’s part, there should be the expectation that the faculty member will engage the resident in thoughtful discussion in response to his or her question, even if the answer was not the faculty’s favored way of handling the problem.
Having been a surgical faculty member for almost 40 years and a general surgery program director for 20, I would argue that today’s surgical residents are every bit as dedicated and conscientious as we were. Since there is more to learn and less time to learn it, we faculty need to be more efficient in our teaching and assessment, which means using every opportunity we have to help them become as competent and confident as possible by June 30 of their chief residency year.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
As today’s surgical residents complete their residencies and enter practice, we are compelled to ask, Is their level of confidence and independence different from that of, say, the class of 1978? Have circumstances of training changed to such a degree that graduating residents’ beliefs in their own judgment have been undermined?
The answer is yes: The conditions and circumstances of training have changed substantially. Our attendings were strong role models, but they were not as omnipresent as are today’s faculty, particularly in the operating room. We, therefore, felt a greater sense of autonomy than do today’s trainees.
It is unquestionably true that our medical and surgical world has become so much more complex that mastery of the broad range of knowledge and skills encompassing general surgery has become daunting. It is indeed too much to ask that a graduating surgeon be a master at biliary surgery, foregut surgery, head and neck surgery, trauma, critical care, and all the rest.
If we are honest with ourselves, Was our confidence really that much greater in 1978? I think that most of us were scared to death that we would make wrong decisions or encounter a problem that we would be unable to handle in those first few years of practice. That is why most of us chose to enter a practice with a senior partner or partners whose brains we could pick if need be. Of course, it wasn’t fashionable to admit it because surgeons were supposed to behave as though they always had everything under control and had the utmost confidence. Mostly we did, but it was most helpful to run a sticky, complicated patient problem by our all-wise senior partner. Even then, with all our clinical experience and independence, we weren’t as polished or confident as surgeons on graduation day from residency than we would become after 8 or 10 years of practice.
So, what’s different now? From the time that they are pups, today’s residents somehow get the impression that they can’t become good surgeons in the 80-hour work week, that they lack stamina and resolve of past generations, and that they need to do a fellowship to get respect or know enough to do a good job. Although the cause of these problems is placed at the feet of the ACGME, hospital administration, American Board of Surgery, or the residents themselves, surgical faculty should shoulder some of the responsibility. Faculty can and should make changes to their teaching and assessment techniques to better address the realities of today’s generation and today’s surgical realities.
I would maintain that it is possible to produce competent surgeons in five years of training but only if training is revised to reflect the changed circumstances of surgical practice. It must be intentional and evidence-based, much like the surgical practice we wish to promote. It should include simulation supervised by expert surgeons who can immediately correct errors, mandated practice at skills until the resident has passed a competency exam in that skill before taking it into the human operating skill, specific and honest but respectful assessment of the resident’s operative skills, and graduated responsibility with eventual autonomy as the goal. This kind of training can’t happen if the faculty feel bound more by demands of the clock and the pressure to generate more relative value units than by their responsibility to their trainees to coach them in clinical decision-making and technical skills. It is possible as an intending to be present but not make all the decisions. Instead of “Do this!” one need only ask, “What do you want to do?” and then pause for the trainee to respond.
Whenever it isn’t a dire and pressing emergency, what can follow is an honest interchange of ideas. For that to happen, the relationship requires mutual trust and respect. On the faculty’s part, there should be an understanding that there is often more than one acceptable way to proceed and that the resident is not only smart and diligent but usually just as motivated to do the best for his or her patient as is the faculty member. On the resident’s part, there should be the expectation that the faculty member will engage the resident in thoughtful discussion in response to his or her question, even if the answer was not the faculty’s favored way of handling the problem.
Having been a surgical faculty member for almost 40 years and a general surgery program director for 20, I would argue that today’s surgical residents are every bit as dedicated and conscientious as we were. Since there is more to learn and less time to learn it, we faculty need to be more efficient in our teaching and assessment, which means using every opportunity we have to help them become as competent and confident as possible by June 30 of their chief residency year.
Dr. Deveney is professor of surgery and vice chair of education in the department of surgery, Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
SSC Women’s Committee hosts leadership symposium teaser
The Society of Surgical Chairs (SSC) Women’s Committee hosted a leadership symposium for 40 women surgeons April 18–19 at the Union League of Philadelphia, PA, immediately preceding the annual meeting of the American Surgical Association. The event was sponsored by the American College of Surgeons (ACS) Foundation, Johnson & Johnson Ethicon, and the SSC Women’s Committee.
Anne C. Mosenthal, MD, FACS, Benjamin F. Rush, Jr. Endowed Chair and professor and chair of surgery at Rutgers New Jersey Medical School, Newark, and chair of the SSC’s Women’s Committee led the daylong educational program, which featured the following sessions:
• A team from Johnson & Johnson Ethicon spoke on the Changing Healthcare Landscape.
• Larry R. Kaiser, MD, FACS, Lewis Katz Dean, School of Medicine, senior executive vice-president for Health Affairs, Temple University, and president and chief executive officer (CEO), Temple University Health System, Philadelphia, spoke on the Healthcare System and Academic Medicine.
• ACS President-Elect Barbara L. Bass, MD, FACS, the John F. and Carolyn Bookout Distinguished Endowed Chair and chair, department of surgery, Houston Methodist Hospital, TX; and Past-Chair of the ACS Board of Regents Julie A. Freischlag, MD, FACS, president and CEO, Wake Forest Baptist Medical Center, Winston-Salem, NC, spoke on leadership challenges.
• Sandra Humbles, vice-president of Global Educational Solutions for One Medical Devices at Johnson & Johnson, and Vice-Chair of the ACS Board of Regents Leigh A. Neumayer, MD, MS, FACS, professor and chair, department of surgery, University of Arizona College of Medicine, Tucson, led a session on Performance, Impact, and Exposure.
• Dr. Mosenthal moderated a panel discussion on advancing women to leadership roles, which included the following panelists: Daniel V. Schidlow, MD, Drexel University, Walter H. and Leonore Annenberg Dean and senior vice-president, medical affairs, at Drexel University College of Medicine; Nancy Spector, MD, executive director, executive leadership in academic medicine, and associate dean for faculty development, Drexel University College of Medicine; Mary T. Hawn, MD, FACS, professor of surgery and chair, department of surgery, Stanford University, CA; and Jeffrey B. Matthews, MD, FACS, Dallas B. Phemister Professor of Surgery and chair, department of surgery, University of Chicago, IL.
The ACS Foundation hosted a dinner for the SSC Women’s Committee members and Shane Hollett, ACS Foundation Executive Director, spoke with them about the future of women in philanthropy.
The Society of Surgical Chairs (SSC) Women’s Committee hosted a leadership symposium for 40 women surgeons April 18–19 at the Union League of Philadelphia, PA, immediately preceding the annual meeting of the American Surgical Association. The event was sponsored by the American College of Surgeons (ACS) Foundation, Johnson & Johnson Ethicon, and the SSC Women’s Committee.
Anne C. Mosenthal, MD, FACS, Benjamin F. Rush, Jr. Endowed Chair and professor and chair of surgery at Rutgers New Jersey Medical School, Newark, and chair of the SSC’s Women’s Committee led the daylong educational program, which featured the following sessions:
• A team from Johnson & Johnson Ethicon spoke on the Changing Healthcare Landscape.
• Larry R. Kaiser, MD, FACS, Lewis Katz Dean, School of Medicine, senior executive vice-president for Health Affairs, Temple University, and president and chief executive officer (CEO), Temple University Health System, Philadelphia, spoke on the Healthcare System and Academic Medicine.
• ACS President-Elect Barbara L. Bass, MD, FACS, the John F. and Carolyn Bookout Distinguished Endowed Chair and chair, department of surgery, Houston Methodist Hospital, TX; and Past-Chair of the ACS Board of Regents Julie A. Freischlag, MD, FACS, president and CEO, Wake Forest Baptist Medical Center, Winston-Salem, NC, spoke on leadership challenges.
• Sandra Humbles, vice-president of Global Educational Solutions for One Medical Devices at Johnson & Johnson, and Vice-Chair of the ACS Board of Regents Leigh A. Neumayer, MD, MS, FACS, professor and chair, department of surgery, University of Arizona College of Medicine, Tucson, led a session on Performance, Impact, and Exposure.
• Dr. Mosenthal moderated a panel discussion on advancing women to leadership roles, which included the following panelists: Daniel V. Schidlow, MD, Drexel University, Walter H. and Leonore Annenberg Dean and senior vice-president, medical affairs, at Drexel University College of Medicine; Nancy Spector, MD, executive director, executive leadership in academic medicine, and associate dean for faculty development, Drexel University College of Medicine; Mary T. Hawn, MD, FACS, professor of surgery and chair, department of surgery, Stanford University, CA; and Jeffrey B. Matthews, MD, FACS, Dallas B. Phemister Professor of Surgery and chair, department of surgery, University of Chicago, IL.
The ACS Foundation hosted a dinner for the SSC Women’s Committee members and Shane Hollett, ACS Foundation Executive Director, spoke with them about the future of women in philanthropy.
The Society of Surgical Chairs (SSC) Women’s Committee hosted a leadership symposium for 40 women surgeons April 18–19 at the Union League of Philadelphia, PA, immediately preceding the annual meeting of the American Surgical Association. The event was sponsored by the American College of Surgeons (ACS) Foundation, Johnson & Johnson Ethicon, and the SSC Women’s Committee.
Anne C. Mosenthal, MD, FACS, Benjamin F. Rush, Jr. Endowed Chair and professor and chair of surgery at Rutgers New Jersey Medical School, Newark, and chair of the SSC’s Women’s Committee led the daylong educational program, which featured the following sessions:
• A team from Johnson & Johnson Ethicon spoke on the Changing Healthcare Landscape.
• Larry R. Kaiser, MD, FACS, Lewis Katz Dean, School of Medicine, senior executive vice-president for Health Affairs, Temple University, and president and chief executive officer (CEO), Temple University Health System, Philadelphia, spoke on the Healthcare System and Academic Medicine.
• ACS President-Elect Barbara L. Bass, MD, FACS, the John F. and Carolyn Bookout Distinguished Endowed Chair and chair, department of surgery, Houston Methodist Hospital, TX; and Past-Chair of the ACS Board of Regents Julie A. Freischlag, MD, FACS, president and CEO, Wake Forest Baptist Medical Center, Winston-Salem, NC, spoke on leadership challenges.
• Sandra Humbles, vice-president of Global Educational Solutions for One Medical Devices at Johnson & Johnson, and Vice-Chair of the ACS Board of Regents Leigh A. Neumayer, MD, MS, FACS, professor and chair, department of surgery, University of Arizona College of Medicine, Tucson, led a session on Performance, Impact, and Exposure.
• Dr. Mosenthal moderated a panel discussion on advancing women to leadership roles, which included the following panelists: Daniel V. Schidlow, MD, Drexel University, Walter H. and Leonore Annenberg Dean and senior vice-president, medical affairs, at Drexel University College of Medicine; Nancy Spector, MD, executive director, executive leadership in academic medicine, and associate dean for faculty development, Drexel University College of Medicine; Mary T. Hawn, MD, FACS, professor of surgery and chair, department of surgery, Stanford University, CA; and Jeffrey B. Matthews, MD, FACS, Dallas B. Phemister Professor of Surgery and chair, department of surgery, University of Chicago, IL.
The ACS Foundation hosted a dinner for the SSC Women’s Committee members and Shane Hollett, ACS Foundation Executive Director, spoke with them about the future of women in philanthropy.
NAPRC Now Accepting Applications from Hospitals teaser
National Accreditation Program for Rectal CancerRectal cancer programs interested in earning accreditation from the new National Accreditation Program for Rectal Cancer (NAPRC) may now apply for participation in the program. The goal of the NAPRC is to ensure that rectal cancer patients receive appropriate care using a multidisciplinary approach.
The NAPRC was developed through collaboration between the American College of Surgeons (ACS) Commission on Cancer (CoC) and the Optimizing the Surgical Treatment of Rectal Cancer (OSTRiCh) Consortium, with input from other stakeholder organizations. The NAPRC formed as a response to the success European countries have had in treating rectal cancer, while the quality of care in the U.S. has continued to vary.
Representatives from OSTRiCh presented data highlighting these differences to the CoC Accreditation Committee, which eventually led to the development of a standards manual and six pilot surveys to form the NAPRC, explained Steven D. Wexner, MD, FACS, a colorectal surgeon, ACS Regent, and member of the NAPRC Steering Committee. The standards evaluate program management, clinical services, and quality improvement efforts. The NAPRC also offers educational modules created and maintained by content experts from the American Society of Colon and Rectal Surgeons, College of American Pathologists, and American College of Radiology.
To attain accreditation from the NAPRC, cancer programs must assess and demonstrate compliance with the requirements for all standards outlined in The National Accreditation Program for Rectal Cancer Standards Manual: 2017 Edition, available at facs.org/quality-programs/cancer/naprc/standards.
For more information about the NAPRC, visit the ACS website at facs.org/quality-programs/cancer/naprc, contact [email protected], and read the ACS press release at facs.org/media/press-releases/2017/naprc062117.
National Accreditation Program for Rectal CancerRectal cancer programs interested in earning accreditation from the new National Accreditation Program for Rectal Cancer (NAPRC) may now apply for participation in the program. The goal of the NAPRC is to ensure that rectal cancer patients receive appropriate care using a multidisciplinary approach.
The NAPRC was developed through collaboration between the American College of Surgeons (ACS) Commission on Cancer (CoC) and the Optimizing the Surgical Treatment of Rectal Cancer (OSTRiCh) Consortium, with input from other stakeholder organizations. The NAPRC formed as a response to the success European countries have had in treating rectal cancer, while the quality of care in the U.S. has continued to vary.
Representatives from OSTRiCh presented data highlighting these differences to the CoC Accreditation Committee, which eventually led to the development of a standards manual and six pilot surveys to form the NAPRC, explained Steven D. Wexner, MD, FACS, a colorectal surgeon, ACS Regent, and member of the NAPRC Steering Committee. The standards evaluate program management, clinical services, and quality improvement efforts. The NAPRC also offers educational modules created and maintained by content experts from the American Society of Colon and Rectal Surgeons, College of American Pathologists, and American College of Radiology.
To attain accreditation from the NAPRC, cancer programs must assess and demonstrate compliance with the requirements for all standards outlined in The National Accreditation Program for Rectal Cancer Standards Manual: 2017 Edition, available at facs.org/quality-programs/cancer/naprc/standards.
For more information about the NAPRC, visit the ACS website at facs.org/quality-programs/cancer/naprc, contact [email protected], and read the ACS press release at facs.org/media/press-releases/2017/naprc062117.
National Accreditation Program for Rectal CancerRectal cancer programs interested in earning accreditation from the new National Accreditation Program for Rectal Cancer (NAPRC) may now apply for participation in the program. The goal of the NAPRC is to ensure that rectal cancer patients receive appropriate care using a multidisciplinary approach.
The NAPRC was developed through collaboration between the American College of Surgeons (ACS) Commission on Cancer (CoC) and the Optimizing the Surgical Treatment of Rectal Cancer (OSTRiCh) Consortium, with input from other stakeholder organizations. The NAPRC formed as a response to the success European countries have had in treating rectal cancer, while the quality of care in the U.S. has continued to vary.
Representatives from OSTRiCh presented data highlighting these differences to the CoC Accreditation Committee, which eventually led to the development of a standards manual and six pilot surveys to form the NAPRC, explained Steven D. Wexner, MD, FACS, a colorectal surgeon, ACS Regent, and member of the NAPRC Steering Committee. The standards evaluate program management, clinical services, and quality improvement efforts. The NAPRC also offers educational modules created and maintained by content experts from the American Society of Colon and Rectal Surgeons, College of American Pathologists, and American College of Radiology.
To attain accreditation from the NAPRC, cancer programs must assess and demonstrate compliance with the requirements for all standards outlined in The National Accreditation Program for Rectal Cancer Standards Manual: 2017 Edition, available at facs.org/quality-programs/cancer/naprc/standards.
For more information about the NAPRC, visit the ACS website at facs.org/quality-programs/cancer/naprc, contact [email protected], and read the ACS press release at facs.org/media/press-releases/2017/naprc062117.
ACSPA-SurgeonsPAC maintains strong presence at 2017 Advocacy Summit teaser
During the American College of Surgeons (ACS) Leadership & Advocacy Summit 2017 in Washington, DC, May 6–9, the ACS Professional Association political action committee (ACSPA-SurgeonsPAC) raised more than $61,000 from more than 175 members, staff, and other attendees. In addition to raising funds to elect and reelect congressional candidates who support a pro-surgeon, pro-surgical patient agenda, the Advocacy Summit provided an opportunity to recognize 2017 SurgeonsPAC contributors. SurgeonsPAC notably recognized Gary Timmerman, MD, FACS, as its newest Willens Society member. To become a member of the Willens Society—SurgeonsPAC’s highest giving level named in memory of Past-PAC Vice-Chair Mitchell Willens, MD, FACS—members must pledge a sum total of $25,000 over 10 years.
SurgeonsPAC events showcased ACSPA members’ broad-based commitment to the PAC, particularly at the SurgeonsPAC-sponsored reception at the Smithsonian American Art Museum and National Portrait Gallery, which more than 175 program participants attended. Guests enjoyed VIP access to special exhibitions and views of downtown Washington, DC.
Other SurgeonsPAC-sponsored events included a political luncheon featuring special guest speaker Mara Liasson, national political correspondent for National Public Radio, and presentation of the 2016 PAC awards. For the second consecutive year, South Dakota achieved the highest percent of PAC participation. California was recognized for most dollars raised, and Michael Coburn, MD, FACS, professor and chairman, Scott Department of Urology, and the Russell and Mary Hugh Scott Chair in Urology, Baylor College of Medicine, Houston, TX, received the Warshaw-PAC MVP Award (named in honor of Andrew L. Warshaw, MD, FACS, founder of the PAC) for his leadership raising funds within the ACS Committee on Trauma.
To learn more about SurgeonsPAC fundraising or disbursements, visit www.surgeonspac.org (log in: ACS username and password) or contact ACSPA-SurgeonsPAC staff at 202-672-1520 or [email protected]. For more information about the College’s legislative priorities, go to www.surgeonsvoice.org. ♦
Note
Contributions to ACSPA-SurgeonsPAC are not deductible as charitable contributions for federal income tax purposes. Contributions are voluntary, and all members of ACSPA have the right to refuse to contribute without reprisal. Federal law prohibits ACSPA-SurgeonsPAC from accepting contributions from foreign nations. By law, if your contributions are made using a personal check or credit card, ACSPA-SurgeonsPAC may only use your contribution to support candidates in federal elections. All corporate contributions to ACSPA-SurgeonsPAC will be used for educational and administrative fees of ACSPA and other activities permissible under federal law. Federal law requires ACSPA-SurgeonsPAC to use its best efforts to collect and report the name, mailing address, occupation, and the name of the employer of individuals whose contributions exceed $200 in a calendar year. ACSPA-SurgeonsPAC is a program of the ACSPA, which is exempt from federal income tax under section 501c (6) of the Internal Revenue Code.
During the American College of Surgeons (ACS) Leadership & Advocacy Summit 2017 in Washington, DC, May 6–9, the ACS Professional Association political action committee (ACSPA-SurgeonsPAC) raised more than $61,000 from more than 175 members, staff, and other attendees. In addition to raising funds to elect and reelect congressional candidates who support a pro-surgeon, pro-surgical patient agenda, the Advocacy Summit provided an opportunity to recognize 2017 SurgeonsPAC contributors. SurgeonsPAC notably recognized Gary Timmerman, MD, FACS, as its newest Willens Society member. To become a member of the Willens Society—SurgeonsPAC’s highest giving level named in memory of Past-PAC Vice-Chair Mitchell Willens, MD, FACS—members must pledge a sum total of $25,000 over 10 years.
SurgeonsPAC events showcased ACSPA members’ broad-based commitment to the PAC, particularly at the SurgeonsPAC-sponsored reception at the Smithsonian American Art Museum and National Portrait Gallery, which more than 175 program participants attended. Guests enjoyed VIP access to special exhibitions and views of downtown Washington, DC.
Other SurgeonsPAC-sponsored events included a political luncheon featuring special guest speaker Mara Liasson, national political correspondent for National Public Radio, and presentation of the 2016 PAC awards. For the second consecutive year, South Dakota achieved the highest percent of PAC participation. California was recognized for most dollars raised, and Michael Coburn, MD, FACS, professor and chairman, Scott Department of Urology, and the Russell and Mary Hugh Scott Chair in Urology, Baylor College of Medicine, Houston, TX, received the Warshaw-PAC MVP Award (named in honor of Andrew L. Warshaw, MD, FACS, founder of the PAC) for his leadership raising funds within the ACS Committee on Trauma.
To learn more about SurgeonsPAC fundraising or disbursements, visit www.surgeonspac.org (log in: ACS username and password) or contact ACSPA-SurgeonsPAC staff at 202-672-1520 or [email protected]. For more information about the College’s legislative priorities, go to www.surgeonsvoice.org. ♦
Note
Contributions to ACSPA-SurgeonsPAC are not deductible as charitable contributions for federal income tax purposes. Contributions are voluntary, and all members of ACSPA have the right to refuse to contribute without reprisal. Federal law prohibits ACSPA-SurgeonsPAC from accepting contributions from foreign nations. By law, if your contributions are made using a personal check or credit card, ACSPA-SurgeonsPAC may only use your contribution to support candidates in federal elections. All corporate contributions to ACSPA-SurgeonsPAC will be used for educational and administrative fees of ACSPA and other activities permissible under federal law. Federal law requires ACSPA-SurgeonsPAC to use its best efforts to collect and report the name, mailing address, occupation, and the name of the employer of individuals whose contributions exceed $200 in a calendar year. ACSPA-SurgeonsPAC is a program of the ACSPA, which is exempt from federal income tax under section 501c (6) of the Internal Revenue Code.
During the American College of Surgeons (ACS) Leadership & Advocacy Summit 2017 in Washington, DC, May 6–9, the ACS Professional Association political action committee (ACSPA-SurgeonsPAC) raised more than $61,000 from more than 175 members, staff, and other attendees. In addition to raising funds to elect and reelect congressional candidates who support a pro-surgeon, pro-surgical patient agenda, the Advocacy Summit provided an opportunity to recognize 2017 SurgeonsPAC contributors. SurgeonsPAC notably recognized Gary Timmerman, MD, FACS, as its newest Willens Society member. To become a member of the Willens Society—SurgeonsPAC’s highest giving level named in memory of Past-PAC Vice-Chair Mitchell Willens, MD, FACS—members must pledge a sum total of $25,000 over 10 years.
SurgeonsPAC events showcased ACSPA members’ broad-based commitment to the PAC, particularly at the SurgeonsPAC-sponsored reception at the Smithsonian American Art Museum and National Portrait Gallery, which more than 175 program participants attended. Guests enjoyed VIP access to special exhibitions and views of downtown Washington, DC.
Other SurgeonsPAC-sponsored events included a political luncheon featuring special guest speaker Mara Liasson, national political correspondent for National Public Radio, and presentation of the 2016 PAC awards. For the second consecutive year, South Dakota achieved the highest percent of PAC participation. California was recognized for most dollars raised, and Michael Coburn, MD, FACS, professor and chairman, Scott Department of Urology, and the Russell and Mary Hugh Scott Chair in Urology, Baylor College of Medicine, Houston, TX, received the Warshaw-PAC MVP Award (named in honor of Andrew L. Warshaw, MD, FACS, founder of the PAC) for his leadership raising funds within the ACS Committee on Trauma.
To learn more about SurgeonsPAC fundraising or disbursements, visit www.surgeonspac.org (log in: ACS username and password) or contact ACSPA-SurgeonsPAC staff at 202-672-1520 or [email protected]. For more information about the College’s legislative priorities, go to www.surgeonsvoice.org. ♦
Note
Contributions to ACSPA-SurgeonsPAC are not deductible as charitable contributions for federal income tax purposes. Contributions are voluntary, and all members of ACSPA have the right to refuse to contribute without reprisal. Federal law prohibits ACSPA-SurgeonsPAC from accepting contributions from foreign nations. By law, if your contributions are made using a personal check or credit card, ACSPA-SurgeonsPAC may only use your contribution to support candidates in federal elections. All corporate contributions to ACSPA-SurgeonsPAC will be used for educational and administrative fees of ACSPA and other activities permissible under federal law. Federal law requires ACSPA-SurgeonsPAC to use its best efforts to collect and report the name, mailing address, occupation, and the name of the employer of individuals whose contributions exceed $200 in a calendar year. ACSPA-SurgeonsPAC is a program of the ACSPA, which is exempt from federal income tax under section 501c (6) of the Internal Revenue Code.
Inaugural Chapter Officer Leadership Program promotes best practices for effective chapter management
The inaugural Chapter Officer Leadership Program took place May 6 in Washington, DC, prior to the kickoff of the American College of Surgeons (ACS) 2017 Leadership & Advocacy Summit. The program was designed to provide chapter officers with the tools they need to succeed as leaders and with an opportunity to network and share best practices with colleagues in similar roles.
More than 30 ACS chapter officers, primarily chapter Presidents and Presidents-Elect, attended the all-day session at the Renaissance Downtown Hotel.
“The Chapter Officer Leadership Program is an important component of the ACS strategy to support our domestic chapters,” said Patricia L. Turner, MD, FACS, Director, ACS Division of Member Services, Chicago, IL. “Chapters provide a significant benefit for our members, and this new approach to leadership education will help to ensure that our chapter officers are provided the support they need to deliver high-quality programs and services to ACS members.”
A range of leadership presentations
Program speakers represented a mix of ACS leadership, former and current chapter leaders, and ACS administrators, and addressed topics aimed at providing attendees with the skills and knowledge they need to effectively manage a chapter. Specific presentations included the following:
• Members Services Pillar Update on Efforts to Support Chapters
• Leading in Your Setting: How Effective Leaders Use Multiple Leadership Styles to Impact Change
• ACS Resources for Chapters
• Strategic Planning Strategies for ACS Chapters
• Panel Discussion: What I Wish I Knew Before Becoming a Chapter President
• Results of the 2016 Chapter Survey
• Chapter Communications & Marketing
• Volunteerism through Operation Giving Back: How Can We Help?
• Grassroots Advocacy at the State Level: Making Chapters Strong Advocates for Surgeons
• Resident and Associate Society and Young Fellows Association Engagement in Chapters
• Chapter Involvement in Stop the Bleed®
• Funding Chapter Activities through Sponsorship and Philanthropy
The day concluded with an opportunity for program attendees to discuss issues of concern with members of the Board of Governors Chapter Activities Domestic Workgroup, which serves as an advocate for ACS chapters in the U.S. and Canada. This meeting gave chapter leaders the opportunity to provide feedback on initiatives that the workgroup has been working on over the last year. One such initiative is revising the ACS Chapter Guidebook, a living document that is housed on the ACS website and that will be updated as new topics of interest arise, such as how to effectively use social media to promote chapter activities. The guidebook is available at facs.org/member-services/chapters/guidebook.
The agenda and presentations from the Chapter Officer Leadership Program are available at facs.org/member-services/chapters/acs-events/2017-leadership. For more information about chapter support services, contact Luke Moreau at [email protected] or 312-202-5737.
Mr. Moreau is Manager, Domestic Chapter Services, ACS Division of Member Services, Chicago, IL.
The inaugural Chapter Officer Leadership Program took place May 6 in Washington, DC, prior to the kickoff of the American College of Surgeons (ACS) 2017 Leadership & Advocacy Summit. The program was designed to provide chapter officers with the tools they need to succeed as leaders and with an opportunity to network and share best practices with colleagues in similar roles.
More than 30 ACS chapter officers, primarily chapter Presidents and Presidents-Elect, attended the all-day session at the Renaissance Downtown Hotel.
“The Chapter Officer Leadership Program is an important component of the ACS strategy to support our domestic chapters,” said Patricia L. Turner, MD, FACS, Director, ACS Division of Member Services, Chicago, IL. “Chapters provide a significant benefit for our members, and this new approach to leadership education will help to ensure that our chapter officers are provided the support they need to deliver high-quality programs and services to ACS members.”
A range of leadership presentations
Program speakers represented a mix of ACS leadership, former and current chapter leaders, and ACS administrators, and addressed topics aimed at providing attendees with the skills and knowledge they need to effectively manage a chapter. Specific presentations included the following:
• Members Services Pillar Update on Efforts to Support Chapters
• Leading in Your Setting: How Effective Leaders Use Multiple Leadership Styles to Impact Change
• ACS Resources for Chapters
• Strategic Planning Strategies for ACS Chapters
• Panel Discussion: What I Wish I Knew Before Becoming a Chapter President
• Results of the 2016 Chapter Survey
• Chapter Communications & Marketing
• Volunteerism through Operation Giving Back: How Can We Help?
• Grassroots Advocacy at the State Level: Making Chapters Strong Advocates for Surgeons
• Resident and Associate Society and Young Fellows Association Engagement in Chapters
• Chapter Involvement in Stop the Bleed®
• Funding Chapter Activities through Sponsorship and Philanthropy
The day concluded with an opportunity for program attendees to discuss issues of concern with members of the Board of Governors Chapter Activities Domestic Workgroup, which serves as an advocate for ACS chapters in the U.S. and Canada. This meeting gave chapter leaders the opportunity to provide feedback on initiatives that the workgroup has been working on over the last year. One such initiative is revising the ACS Chapter Guidebook, a living document that is housed on the ACS website and that will be updated as new topics of interest arise, such as how to effectively use social media to promote chapter activities. The guidebook is available at facs.org/member-services/chapters/guidebook.
The agenda and presentations from the Chapter Officer Leadership Program are available at facs.org/member-services/chapters/acs-events/2017-leadership. For more information about chapter support services, contact Luke Moreau at [email protected] or 312-202-5737.
Mr. Moreau is Manager, Domestic Chapter Services, ACS Division of Member Services, Chicago, IL.
The inaugural Chapter Officer Leadership Program took place May 6 in Washington, DC, prior to the kickoff of the American College of Surgeons (ACS) 2017 Leadership & Advocacy Summit. The program was designed to provide chapter officers with the tools they need to succeed as leaders and with an opportunity to network and share best practices with colleagues in similar roles.
More than 30 ACS chapter officers, primarily chapter Presidents and Presidents-Elect, attended the all-day session at the Renaissance Downtown Hotel.
“The Chapter Officer Leadership Program is an important component of the ACS strategy to support our domestic chapters,” said Patricia L. Turner, MD, FACS, Director, ACS Division of Member Services, Chicago, IL. “Chapters provide a significant benefit for our members, and this new approach to leadership education will help to ensure that our chapter officers are provided the support they need to deliver high-quality programs and services to ACS members.”
A range of leadership presentations
Program speakers represented a mix of ACS leadership, former and current chapter leaders, and ACS administrators, and addressed topics aimed at providing attendees with the skills and knowledge they need to effectively manage a chapter. Specific presentations included the following:
• Members Services Pillar Update on Efforts to Support Chapters
• Leading in Your Setting: How Effective Leaders Use Multiple Leadership Styles to Impact Change
• ACS Resources for Chapters
• Strategic Planning Strategies for ACS Chapters
• Panel Discussion: What I Wish I Knew Before Becoming a Chapter President
• Results of the 2016 Chapter Survey
• Chapter Communications & Marketing
• Volunteerism through Operation Giving Back: How Can We Help?
• Grassroots Advocacy at the State Level: Making Chapters Strong Advocates for Surgeons
• Resident and Associate Society and Young Fellows Association Engagement in Chapters
• Chapter Involvement in Stop the Bleed®
• Funding Chapter Activities through Sponsorship and Philanthropy
The day concluded with an opportunity for program attendees to discuss issues of concern with members of the Board of Governors Chapter Activities Domestic Workgroup, which serves as an advocate for ACS chapters in the U.S. and Canada. This meeting gave chapter leaders the opportunity to provide feedback on initiatives that the workgroup has been working on over the last year. One such initiative is revising the ACS Chapter Guidebook, a living document that is housed on the ACS website and that will be updated as new topics of interest arise, such as how to effectively use social media to promote chapter activities. The guidebook is available at facs.org/member-services/chapters/guidebook.
The agenda and presentations from the Chapter Officer Leadership Program are available at facs.org/member-services/chapters/acs-events/2017-leadership. For more information about chapter support services, contact Luke Moreau at [email protected] or 312-202-5737.
Mr. Moreau is Manager, Domestic Chapter Services, ACS Division of Member Services, Chicago, IL.
From the Washington Office: Ensuring an adequate surgical workforce in underserved areas
Increasing evidence indicates a current and growing shortage of surgeons available to serve our nation’s population. As Fellows, we clearly recognize that a shortage of general surgeons is a critical component of this crisis in our nation’s health care workforce. Accordingly, the American College of Surgeons (ACS) is urging policy makers to take appropriate action to recognize that surgeons are uniquely trained and qualified to provide certain necessary, lifesaving procedures through the designation of a formal surgical shortage area.
The ACS is pleased that the Ensuring Access to General Surgery Act of 2017 (S.1351 and H.R.2906) was recently introduced in both the Senate and the House of Representatives. The text of the bill, which is the same in both the Senate and House versions, can be found here: https://www.grassley.senate.gov/sites/default/files/constituents/surgery%20bill.pdf. The legislation has bipartisan sponsorship in both legislative bodies by Senators Charles Grassley (R-IA) and Brian Schatz (D-HI) and Representatives Larry Bucshon, MD, FACS (R-IN) and Ami Bera, MD (D-CA) in the House. This legislation directs the Secretary of the Department of Health and Human Services (HHS), through the Health Resources Services Administration (HRSA), to conduct a study on general surgery workforce shortage areas and provide a general surgery shortage area designation.

Senator Grassley’s office issued a press release on June 15, 2017, in which he, Senator Schatz, Representative Bucshon, and Representative Bera individually delineate the reasons why it is critically important to define and designate general surgery shortage areas. For those interested, that press release can be found here: https://www.grassley.senate.gov/news/news-releases/bipartisan-bill-grassley-schatz-bucshon-bera-would-help-document-areas.
Fellows who visited the offices of their representatives and senators in May as part of the ACS Leadership and Advocacy Summit were able to personally discuss this initiative with members and their staff at that time. Now that the legislation has been officially introduced in both houses of Congress, I would respectfully ask that all Fellows take the 3 minutes necessary to make their voice heard by logging on to www.surgeonsvoice.org and clicking on the Take Action tab on the right side of the landing page to send an e-mail message urging support of the Ensuring Access to General Surgery Act by their individual representatives and both senators.
Until next month …
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
Increasing evidence indicates a current and growing shortage of surgeons available to serve our nation’s population. As Fellows, we clearly recognize that a shortage of general surgeons is a critical component of this crisis in our nation’s health care workforce. Accordingly, the American College of Surgeons (ACS) is urging policy makers to take appropriate action to recognize that surgeons are uniquely trained and qualified to provide certain necessary, lifesaving procedures through the designation of a formal surgical shortage area.
The ACS is pleased that the Ensuring Access to General Surgery Act of 2017 (S.1351 and H.R.2906) was recently introduced in both the Senate and the House of Representatives. The text of the bill, which is the same in both the Senate and House versions, can be found here: https://www.grassley.senate.gov/sites/default/files/constituents/surgery%20bill.pdf. The legislation has bipartisan sponsorship in both legislative bodies by Senators Charles Grassley (R-IA) and Brian Schatz (D-HI) and Representatives Larry Bucshon, MD, FACS (R-IN) and Ami Bera, MD (D-CA) in the House. This legislation directs the Secretary of the Department of Health and Human Services (HHS), through the Health Resources Services Administration (HRSA), to conduct a study on general surgery workforce shortage areas and provide a general surgery shortage area designation.
Senator Grassley’s office issued a press release on June 15, 2017, in which he, Senator Schatz, Representative Bucshon, and Representative Bera individually delineate the reasons why it is critically important to define and designate general surgery shortage areas. For those interested, that press release can be found here: https://www.grassley.senate.gov/news/news-releases/bipartisan-bill-grassley-schatz-bucshon-bera-would-help-document-areas.
Fellows who visited the offices of their representatives and senators in May as part of the ACS Leadership and Advocacy Summit were able to personally discuss this initiative with members and their staff at that time. Now that the legislation has been officially introduced in both houses of Congress, I would respectfully ask that all Fellows take the 3 minutes necessary to make their voice heard by logging on to www.surgeonsvoice.org and clicking on the Take Action tab on the right side of the landing page to send an e-mail message urging support of the Ensuring Access to General Surgery Act by their individual representatives and both senators.
Until next month …
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
Increasing evidence indicates a current and growing shortage of surgeons available to serve our nation’s population. As Fellows, we clearly recognize that a shortage of general surgeons is a critical component of this crisis in our nation’s health care workforce. Accordingly, the American College of Surgeons (ACS) is urging policy makers to take appropriate action to recognize that surgeons are uniquely trained and qualified to provide certain necessary, lifesaving procedures through the designation of a formal surgical shortage area.
The ACS is pleased that the Ensuring Access to General Surgery Act of 2017 (S.1351 and H.R.2906) was recently introduced in both the Senate and the House of Representatives. The text of the bill, which is the same in both the Senate and House versions, can be found here: https://www.grassley.senate.gov/sites/default/files/constituents/surgery%20bill.pdf. The legislation has bipartisan sponsorship in both legislative bodies by Senators Charles Grassley (R-IA) and Brian Schatz (D-HI) and Representatives Larry Bucshon, MD, FACS (R-IN) and Ami Bera, MD (D-CA) in the House. This legislation directs the Secretary of the Department of Health and Human Services (HHS), through the Health Resources Services Administration (HRSA), to conduct a study on general surgery workforce shortage areas and provide a general surgery shortage area designation.
Senator Grassley’s office issued a press release on June 15, 2017, in which he, Senator Schatz, Representative Bucshon, and Representative Bera individually delineate the reasons why it is critically important to define and designate general surgery shortage areas. For those interested, that press release can be found here: https://www.grassley.senate.gov/news/news-releases/bipartisan-bill-grassley-schatz-bucshon-bera-would-help-document-areas.
Fellows who visited the offices of their representatives and senators in May as part of the ACS Leadership and Advocacy Summit were able to personally discuss this initiative with members and their staff at that time. Now that the legislation has been officially introduced in both houses of Congress, I would respectfully ask that all Fellows take the 3 minutes necessary to make their voice heard by logging on to www.surgeonsvoice.org and clicking on the Take Action tab on the right side of the landing page to send an e-mail message urging support of the Ensuring Access to General Surgery Act by their individual representatives and both senators.
Until next month …
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
Physician compensation growing but at a slightly slower pace
Physicians working in large multispecialty groups saw their compensation increase in 2016, albeit at a slower pace than in 2015, according to survey results reported by AMGA.
The 2017 Medical Group Compensation and Productivity Survey shows that the overall weighted average increase in physician compensation for the calendar year 2016 was 2.9%, slightly lower than the 3.1% increase seen in 2015. Doctors in more than three-quarters (77%) of specialties saw increases in 2016.
Opthalmologic surgery saw the largest compensation increase at 7.7%, followed by cardiothoracic surgery (7.0%), hematology and medical oncology (6.7%), allergy/immunology (5.9%) and pulmonary disease (5.6%). Emergency medicine saw a decrease in compensation of 2.0% in 2016 after experiencing a 9.6% increase in 2015.
Value-based payment is beginning to factor into the growth in payment by specialty. Overall, about 8% of compensation is being linked to value-based pay, and that number is expected to rise, with some medical practice groups linking 15% or more of compensation to value-based metrics.
“In almost all of the groups that I have worked with in the last few years on [compensation] design, that has been one of the drivers of decision to do the compensation redesign is to allocate to the value-based metrics,” Wayne Hartley, vice president of AMGA Consulting, said in an interview. 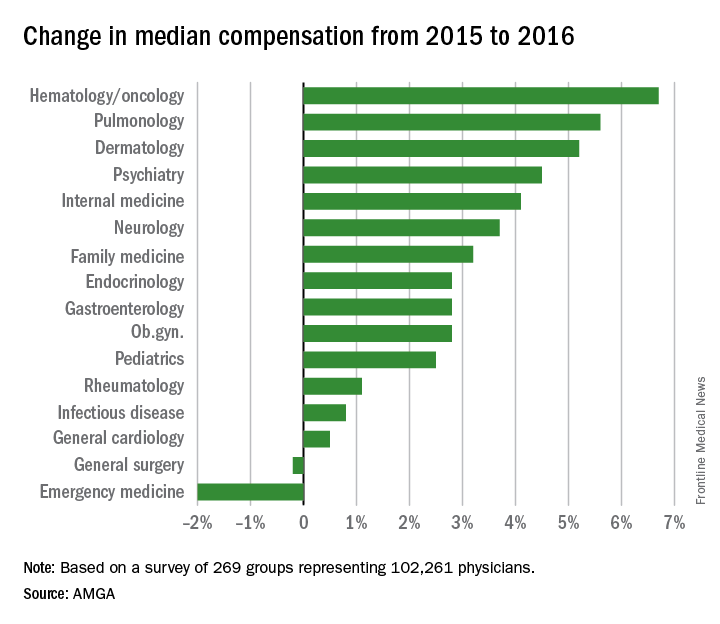
AMGA said that the data covers responses from 269 medical groups covering more than 102,000 providers and is representative of large multispecialty groups and integrated health systems that average 380 providers per group.
Physicians working in large multispecialty groups saw their compensation increase in 2016, albeit at a slower pace than in 2015, according to survey results reported by AMGA.
The 2017 Medical Group Compensation and Productivity Survey shows that the overall weighted average increase in physician compensation for the calendar year 2016 was 2.9%, slightly lower than the 3.1% increase seen in 2015. Doctors in more than three-quarters (77%) of specialties saw increases in 2016.
Opthalmologic surgery saw the largest compensation increase at 7.7%, followed by cardiothoracic surgery (7.0%), hematology and medical oncology (6.7%), allergy/immunology (5.9%) and pulmonary disease (5.6%). Emergency medicine saw a decrease in compensation of 2.0% in 2016 after experiencing a 9.6% increase in 2015.
Value-based payment is beginning to factor into the growth in payment by specialty. Overall, about 8% of compensation is being linked to value-based pay, and that number is expected to rise, with some medical practice groups linking 15% or more of compensation to value-based metrics.
“In almost all of the groups that I have worked with in the last few years on [compensation] design, that has been one of the drivers of decision to do the compensation redesign is to allocate to the value-based metrics,” Wayne Hartley, vice president of AMGA Consulting, said in an interview.
AMGA said that the data covers responses from 269 medical groups covering more than 102,000 providers and is representative of large multispecialty groups and integrated health systems that average 380 providers per group.
Physicians working in large multispecialty groups saw their compensation increase in 2016, albeit at a slower pace than in 2015, according to survey results reported by AMGA.
The 2017 Medical Group Compensation and Productivity Survey shows that the overall weighted average increase in physician compensation for the calendar year 2016 was 2.9%, slightly lower than the 3.1% increase seen in 2015. Doctors in more than three-quarters (77%) of specialties saw increases in 2016.
Opthalmologic surgery saw the largest compensation increase at 7.7%, followed by cardiothoracic surgery (7.0%), hematology and medical oncology (6.7%), allergy/immunology (5.9%) and pulmonary disease (5.6%). Emergency medicine saw a decrease in compensation of 2.0% in 2016 after experiencing a 9.6% increase in 2015.
Value-based payment is beginning to factor into the growth in payment by specialty. Overall, about 8% of compensation is being linked to value-based pay, and that number is expected to rise, with some medical practice groups linking 15% or more of compensation to value-based metrics.
“In almost all of the groups that I have worked with in the last few years on [compensation] design, that has been one of the drivers of decision to do the compensation redesign is to allocate to the value-based metrics,” Wayne Hartley, vice president of AMGA Consulting, said in an interview.
AMGA said that the data covers responses from 269 medical groups covering more than 102,000 providers and is representative of large multispecialty groups and integrated health systems that average 380 providers per group.