User login
Official Newspaper of the American College of Surgeons
VIDEO: Outpatient hysterectomies offer advantages for surgeons, patients
NATIONAL HARBOR, MD. – Moving hysterectomy and advanced gynecologic procedures to the ambulatory surgical environment is better for patients, surgeons, and the health care system, Richard B. Rosenfield, MD, who is in private practice in Portland, Ore., said at the AAGL Global Congress.
“We’ve been basically proving this model over the last decade by performing advanced laparoscopic surgery in the outpatient environment, and we do this for a number of reasons,” Dr. Rosenfield said in an interview. “The patients get to go home the same day, which they typically enjoy, we avoid the hospital-acquired infections, which is great, and in addition to that, the physicians tend to really appreciate the efficiency of an outpatient center.”
But with the focus on value-based payment under federal health programs, there should also be a greater focus on getting more high-volume surgeons to perform their procedures, he said. The idea is to lower the hospital readmissions, complications, and infections that could arise during procedures by less experienced surgeons and redirect the cost savings toward payments for surgeons with better outcomes, Dr. Rosenfield said. But this should be coupled with training and mentoring for lower-volume surgeons, he said.
Dr. Rosenfield reported having no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
NATIONAL HARBOR, MD. – Moving hysterectomy and advanced gynecologic procedures to the ambulatory surgical environment is better for patients, surgeons, and the health care system, Richard B. Rosenfield, MD, who is in private practice in Portland, Ore., said at the AAGL Global Congress.
“We’ve been basically proving this model over the last decade by performing advanced laparoscopic surgery in the outpatient environment, and we do this for a number of reasons,” Dr. Rosenfield said in an interview. “The patients get to go home the same day, which they typically enjoy, we avoid the hospital-acquired infections, which is great, and in addition to that, the physicians tend to really appreciate the efficiency of an outpatient center.”
But with the focus on value-based payment under federal health programs, there should also be a greater focus on getting more high-volume surgeons to perform their procedures, he said. The idea is to lower the hospital readmissions, complications, and infections that could arise during procedures by less experienced surgeons and redirect the cost savings toward payments for surgeons with better outcomes, Dr. Rosenfield said. But this should be coupled with training and mentoring for lower-volume surgeons, he said.
Dr. Rosenfield reported having no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
NATIONAL HARBOR, MD. – Moving hysterectomy and advanced gynecologic procedures to the ambulatory surgical environment is better for patients, surgeons, and the health care system, Richard B. Rosenfield, MD, who is in private practice in Portland, Ore., said at the AAGL Global Congress.
“We’ve been basically proving this model over the last decade by performing advanced laparoscopic surgery in the outpatient environment, and we do this for a number of reasons,” Dr. Rosenfield said in an interview. “The patients get to go home the same day, which they typically enjoy, we avoid the hospital-acquired infections, which is great, and in addition to that, the physicians tend to really appreciate the efficiency of an outpatient center.”
But with the focus on value-based payment under federal health programs, there should also be a greater focus on getting more high-volume surgeons to perform their procedures, he said. The idea is to lower the hospital readmissions, complications, and infections that could arise during procedures by less experienced surgeons and redirect the cost savings toward payments for surgeons with better outcomes, Dr. Rosenfield said. But this should be coupled with training and mentoring for lower-volume surgeons, he said.
Dr. Rosenfield reported having no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
AT AAGL 2017

After warning, codeine use after tonsillectomy drops, doesn’t stop
– and there has been inappropriate substitution of other opioids rather than nonopioid pain relievers such as ibuprofen, said Kao-Ping Chua, MD, PhD, of the University of Chicago, and his associates.
Codeine has been one of the most commonly prescribed analgesics for children after tonsillectomies and adenoidectomies because it was considered safe.
The FDA issued a boxed warning Feb. 20, 2013, recommending against codeine use in all children undergoing tonsillectomy and/or adenoidectomy. Also, children with obstructive sleep apnea are at risk of opioid-related respiratory depression.
A retrospective study of 362,992 children aged 0-18 years who underwent tonsillectomy and/or adenoidectomy was undertaken in 2010-2015, prior to and after the FDA issued the boxed warning against codeine use. In January 2010, codeine products were prescribed in 47% of cases, compared with 48% for hydrocodone, 4% for oxycodone, and less than 1% for other opioid products. In December 2015, codeine was prescribed in 9% of cases, compared with 73% for hydrocodone, 17% for oxycodone, and less than 1% for other opioid products.
“The unadjusted proportion of children receiving alternative opioids rose substantially during the study period, presumably because of factors other than the investigation itself,” said Dr. Chua and his associates. “This increase deserves further examination, given the abuse liability associated with higher-potency opioids, as well as the growing evidence of genetic variability in the metabolism of many alternative opioids, including oxycodone and tramadol.
“Future quality-improvement efforts should focus on eliminating this residual inappropriate codeine prescribing, and on encouraging the use of effective nonopioid medications such as ibuprofen,” the investigators said.
Read more in Pediatrics (2017 Nov 16. doi: 10.1542/ peds.2017-1765).
– and there has been inappropriate substitution of other opioids rather than nonopioid pain relievers such as ibuprofen, said Kao-Ping Chua, MD, PhD, of the University of Chicago, and his associates.
Codeine has been one of the most commonly prescribed analgesics for children after tonsillectomies and adenoidectomies because it was considered safe.
The FDA issued a boxed warning Feb. 20, 2013, recommending against codeine use in all children undergoing tonsillectomy and/or adenoidectomy. Also, children with obstructive sleep apnea are at risk of opioid-related respiratory depression.
A retrospective study of 362,992 children aged 0-18 years who underwent tonsillectomy and/or adenoidectomy was undertaken in 2010-2015, prior to and after the FDA issued the boxed warning against codeine use. In January 2010, codeine products were prescribed in 47% of cases, compared with 48% for hydrocodone, 4% for oxycodone, and less than 1% for other opioid products. In December 2015, codeine was prescribed in 9% of cases, compared with 73% for hydrocodone, 17% for oxycodone, and less than 1% for other opioid products.
“The unadjusted proportion of children receiving alternative opioids rose substantially during the study period, presumably because of factors other than the investigation itself,” said Dr. Chua and his associates. “This increase deserves further examination, given the abuse liability associated with higher-potency opioids, as well as the growing evidence of genetic variability in the metabolism of many alternative opioids, including oxycodone and tramadol.
“Future quality-improvement efforts should focus on eliminating this residual inappropriate codeine prescribing, and on encouraging the use of effective nonopioid medications such as ibuprofen,” the investigators said.
Read more in Pediatrics (2017 Nov 16. doi: 10.1542/ peds.2017-1765).
– and there has been inappropriate substitution of other opioids rather than nonopioid pain relievers such as ibuprofen, said Kao-Ping Chua, MD, PhD, of the University of Chicago, and his associates.
Codeine has been one of the most commonly prescribed analgesics for children after tonsillectomies and adenoidectomies because it was considered safe.
The FDA issued a boxed warning Feb. 20, 2013, recommending against codeine use in all children undergoing tonsillectomy and/or adenoidectomy. Also, children with obstructive sleep apnea are at risk of opioid-related respiratory depression.
A retrospective study of 362,992 children aged 0-18 years who underwent tonsillectomy and/or adenoidectomy was undertaken in 2010-2015, prior to and after the FDA issued the boxed warning against codeine use. In January 2010, codeine products were prescribed in 47% of cases, compared with 48% for hydrocodone, 4% for oxycodone, and less than 1% for other opioid products. In December 2015, codeine was prescribed in 9% of cases, compared with 73% for hydrocodone, 17% for oxycodone, and less than 1% for other opioid products.
“The unadjusted proportion of children receiving alternative opioids rose substantially during the study period, presumably because of factors other than the investigation itself,” said Dr. Chua and his associates. “This increase deserves further examination, given the abuse liability associated with higher-potency opioids, as well as the growing evidence of genetic variability in the metabolism of many alternative opioids, including oxycodone and tramadol.
“Future quality-improvement efforts should focus on eliminating this residual inappropriate codeine prescribing, and on encouraging the use of effective nonopioid medications such as ibuprofen,” the investigators said.
Read more in Pediatrics (2017 Nov 16. doi: 10.1542/ peds.2017-1765).
FROM PEDIATRICS
VIDEO: Bariatric experts discuss recent experience with gastric balloon devices
Two experts on bariatric surgery spoke at the Minimally Invasive Surgery Symposium, held in Las Vegas. Jaime Ponce, MD, FACS, and John Morton, MD, FACS, discussed several different types of gastric balloon devices and the factors guiding their use for patients. Dr. Morton suggested that the balloon devices could serve as an intermediate treatment between medications and surgery.

Two experts on bariatric surgery spoke at the Minimally Invasive Surgery Symposium, held in Las Vegas. Jaime Ponce, MD, FACS, and John Morton, MD, FACS, discussed several different types of gastric balloon devices and the factors guiding their use for patients. Dr. Morton suggested that the balloon devices could serve as an intermediate treatment between medications and surgery.
Two experts on bariatric surgery spoke at the Minimally Invasive Surgery Symposium, held in Las Vegas. Jaime Ponce, MD, FACS, and John Morton, MD, FACS, discussed several different types of gastric balloon devices and the factors guiding their use for patients. Dr. Morton suggested that the balloon devices could serve as an intermediate treatment between medications and surgery.
Higher BMI linked to lower risk of hysterectomy reoperation
NATIONAL HARBOR, MD. – Women with a greater body mass index (BMI) were less likely to need reoperation after hysterectomy, according to findings presented at the AAGL Global Congress.
“What’s unusual is women who are considered overweight or obese are generally thought to be at higher risk of any complication, including reoperation,” Janelle Moulder, MD, of the department of ob.gyn. at the University of Tennessee, Knoxville, said in an interview prior to the meeting. “We don’t have enough data to say what exactly might be protective. And to see that women who are at normal or below normal BMI were at increased risk makes you pause as to what could potentially put them at risk.”
Dr. Moulder and her colleagues analyzed data on 28,487 women who underwent an abdominal, vaginal, or laparoscopic hysterectomy from 2014 to 2015. The data came from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database.
Patients were excluded if they had cancer, their surgery was not performed by a gynecologist, or their BMI data was missing.
A majority of patients (13,000) had a BMI of 30 kg/m2 or greater.
Compared with patients with a normal BMI of 24 kg/m2, patients with a BMI of 39 kg/m2 had the lowest odds of reoperation (adjusted odds ratio, 0.73; P = .02). Patients with BMIs of 29 kg/m2 and 34 kg/m2 were also at lower odds of reoperation, with adjusted odds ratios of 0.83 (P = .003) and 0.75 (P = .005), respectively.
Patients with a low normal BMI of 18.5 kg/m2 were at a higher risk of reoperation (aOR = 1.33; P = .001).
Researchers were unable to comment on women with a BMI of 45 kg/m2 or greater, due to the limited number of women in this group.
Researchers did not have access to the reason for reoperation, which may have limited the scope of the study.
“The next thing to be evaluated is what is the protective effect of the increasing BMI on reoperation and also look at variables that may put low normal BMI women at risk for reoperation,” Dr. Moulder said.
The researchers reported having no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
NATIONAL HARBOR, MD. – Women with a greater body mass index (BMI) were less likely to need reoperation after hysterectomy, according to findings presented at the AAGL Global Congress.
“What’s unusual is women who are considered overweight or obese are generally thought to be at higher risk of any complication, including reoperation,” Janelle Moulder, MD, of the department of ob.gyn. at the University of Tennessee, Knoxville, said in an interview prior to the meeting. “We don’t have enough data to say what exactly might be protective. And to see that women who are at normal or below normal BMI were at increased risk makes you pause as to what could potentially put them at risk.”
Dr. Moulder and her colleagues analyzed data on 28,487 women who underwent an abdominal, vaginal, or laparoscopic hysterectomy from 2014 to 2015. The data came from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database.
Patients were excluded if they had cancer, their surgery was not performed by a gynecologist, or their BMI data was missing.
A majority of patients (13,000) had a BMI of 30 kg/m2 or greater.
Compared with patients with a normal BMI of 24 kg/m2, patients with a BMI of 39 kg/m2 had the lowest odds of reoperation (adjusted odds ratio, 0.73; P = .02). Patients with BMIs of 29 kg/m2 and 34 kg/m2 were also at lower odds of reoperation, with adjusted odds ratios of 0.83 (P = .003) and 0.75 (P = .005), respectively.
Patients with a low normal BMI of 18.5 kg/m2 were at a higher risk of reoperation (aOR = 1.33; P = .001).
Researchers were unable to comment on women with a BMI of 45 kg/m2 or greater, due to the limited number of women in this group.
Researchers did not have access to the reason for reoperation, which may have limited the scope of the study.
“The next thing to be evaluated is what is the protective effect of the increasing BMI on reoperation and also look at variables that may put low normal BMI women at risk for reoperation,” Dr. Moulder said.
The researchers reported having no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
NATIONAL HARBOR, MD. – Women with a greater body mass index (BMI) were less likely to need reoperation after hysterectomy, according to findings presented at the AAGL Global Congress.
“What’s unusual is women who are considered overweight or obese are generally thought to be at higher risk of any complication, including reoperation,” Janelle Moulder, MD, of the department of ob.gyn. at the University of Tennessee, Knoxville, said in an interview prior to the meeting. “We don’t have enough data to say what exactly might be protective. And to see that women who are at normal or below normal BMI were at increased risk makes you pause as to what could potentially put them at risk.”
Dr. Moulder and her colleagues analyzed data on 28,487 women who underwent an abdominal, vaginal, or laparoscopic hysterectomy from 2014 to 2015. The data came from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database.
Patients were excluded if they had cancer, their surgery was not performed by a gynecologist, or their BMI data was missing.
A majority of patients (13,000) had a BMI of 30 kg/m2 or greater.
Compared with patients with a normal BMI of 24 kg/m2, patients with a BMI of 39 kg/m2 had the lowest odds of reoperation (adjusted odds ratio, 0.73; P = .02). Patients with BMIs of 29 kg/m2 and 34 kg/m2 were also at lower odds of reoperation, with adjusted odds ratios of 0.83 (P = .003) and 0.75 (P = .005), respectively.
Patients with a low normal BMI of 18.5 kg/m2 were at a higher risk of reoperation (aOR = 1.33; P = .001).
Researchers were unable to comment on women with a BMI of 45 kg/m2 or greater, due to the limited number of women in this group.
Researchers did not have access to the reason for reoperation, which may have limited the scope of the study.
“The next thing to be evaluated is what is the protective effect of the increasing BMI on reoperation and also look at variables that may put low normal BMI women at risk for reoperation,” Dr. Moulder said.
The researchers reported having no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
AT AAGL 2017
Key clinical point:
Major finding: Patients with a BMI of 39 kg/m2 less likely to need a reoperation after hysterectomy (aOR, .73; P = .02).
Data source: Retrospective study of 28,487 women who underwent a hysterectomy from 2014 to 2015 from the American College of Surgeons National Surgical Quality Improvement Program database.
Disclosures: The researchers reported having no relevant financial disclosures.
Heart transplantation: Preop LVAD erases adverse impact of pulmonary hypertension
COLORADO SPRINGS – Reconsideration of the role of pulmonary hypertension in heart transplant outcomes is appropriate in the emerging era of the use of left ventricular assist devices (LVADs) as bridge to transplant, according to Ann C. Gaffey, MD, of the University of Pennsylvania, Philadelphia.
“Pulmonary hypertension secondary to congestive heart failure more than likely can be reversed to the values acceptable for heart transplant by the use of an LVAD. For bridge-to-transplant patients, pretransplant pulmonary hypertension does not affect recipient outcomes post transplantation,” she said at the annual meeting of the Western Thoracic Surgical Association.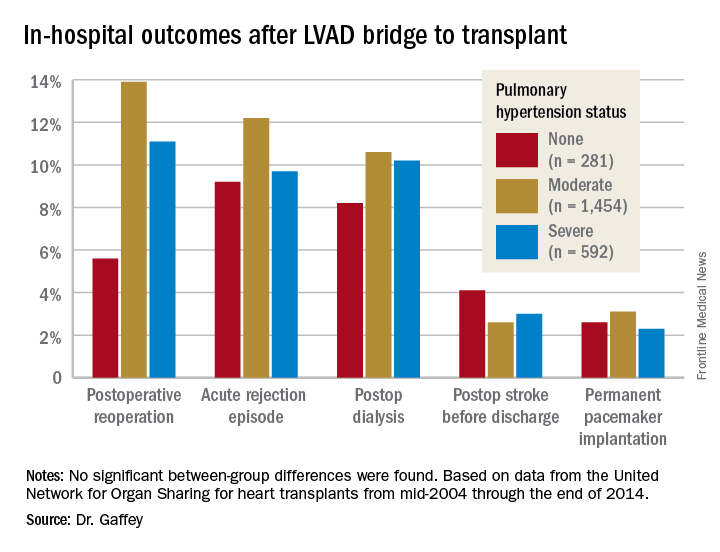
Vasodilators are prescribed in an effort to reduce PH; however, 40% of patients with PH are unresponsive to the medications and have therefore been excluded from consideration as potential candidates for a donor heart.
But the growing use of LVADs as a bridge to transplant has changed all that, Dr. Gaffey said. As supporting evidence, she presented a retrospective analysis of the United Network for Organ Sharing database on adult heart transplants from mid-2004 through the end of 2014.
The review turned up 3,951 heart transplant recipients who had been bridged to transplant with an LVAD. Dr. Gaffey and her coinvestigators divided them into three groups: 281 patients without pretransplant PH; 1,454 with moderate PH as defined by 1-3 Wood units; and 592 with severe PH and more than 3 Wood units.
The three groups didn’t differ in terms of age, sex, wait-list time, or the prevalence of diabetes or renal, liver, or cerebrovascular disease. Nor did their donors differ in age, sex, left ventricular function, or allograft ischemic time.
Key in-hospital outcomes were similar between the groups with no, mild, and severe PH.
Moreover, there was no between-group difference in the rate of rejection at 1 year. Five-year survival rates were closely similar in the three groups, in the mid-70s.
Audience member Nahush A. Mokadam, MD, rose to praise Dr. Gaffey’s report.
“This is a great and important study. I think as a group we have been too conservative with pulmonary hypertension, so thank you for shining a good light on it,” said Dr. Mokadam of the University of Washington, Seattle.
Dr. Gaffey reported having no financial conflicts regarding the study, which was conducted free of commercial support.
COLORADO SPRINGS – Reconsideration of the role of pulmonary hypertension in heart transplant outcomes is appropriate in the emerging era of the use of left ventricular assist devices (LVADs) as bridge to transplant, according to Ann C. Gaffey, MD, of the University of Pennsylvania, Philadelphia.
“Pulmonary hypertension secondary to congestive heart failure more than likely can be reversed to the values acceptable for heart transplant by the use of an LVAD. For bridge-to-transplant patients, pretransplant pulmonary hypertension does not affect recipient outcomes post transplantation,” she said at the annual meeting of the Western Thoracic Surgical Association.
Vasodilators are prescribed in an effort to reduce PH; however, 40% of patients with PH are unresponsive to the medications and have therefore been excluded from consideration as potential candidates for a donor heart.
But the growing use of LVADs as a bridge to transplant has changed all that, Dr. Gaffey said. As supporting evidence, she presented a retrospective analysis of the United Network for Organ Sharing database on adult heart transplants from mid-2004 through the end of 2014.
The review turned up 3,951 heart transplant recipients who had been bridged to transplant with an LVAD. Dr. Gaffey and her coinvestigators divided them into three groups: 281 patients without pretransplant PH; 1,454 with moderate PH as defined by 1-3 Wood units; and 592 with severe PH and more than 3 Wood units.
The three groups didn’t differ in terms of age, sex, wait-list time, or the prevalence of diabetes or renal, liver, or cerebrovascular disease. Nor did their donors differ in age, sex, left ventricular function, or allograft ischemic time.
Key in-hospital outcomes were similar between the groups with no, mild, and severe PH.
Moreover, there was no between-group difference in the rate of rejection at 1 year. Five-year survival rates were closely similar in the three groups, in the mid-70s.
Audience member Nahush A. Mokadam, MD, rose to praise Dr. Gaffey’s report.
“This is a great and important study. I think as a group we have been too conservative with pulmonary hypertension, so thank you for shining a good light on it,” said Dr. Mokadam of the University of Washington, Seattle.
Dr. Gaffey reported having no financial conflicts regarding the study, which was conducted free of commercial support.
COLORADO SPRINGS – Reconsideration of the role of pulmonary hypertension in heart transplant outcomes is appropriate in the emerging era of the use of left ventricular assist devices (LVADs) as bridge to transplant, according to Ann C. Gaffey, MD, of the University of Pennsylvania, Philadelphia.
“Pulmonary hypertension secondary to congestive heart failure more than likely can be reversed to the values acceptable for heart transplant by the use of an LVAD. For bridge-to-transplant patients, pretransplant pulmonary hypertension does not affect recipient outcomes post transplantation,” she said at the annual meeting of the Western Thoracic Surgical Association.
Vasodilators are prescribed in an effort to reduce PH; however, 40% of patients with PH are unresponsive to the medications and have therefore been excluded from consideration as potential candidates for a donor heart.
But the growing use of LVADs as a bridge to transplant has changed all that, Dr. Gaffey said. As supporting evidence, she presented a retrospective analysis of the United Network for Organ Sharing database on adult heart transplants from mid-2004 through the end of 2014.
The review turned up 3,951 heart transplant recipients who had been bridged to transplant with an LVAD. Dr. Gaffey and her coinvestigators divided them into three groups: 281 patients without pretransplant PH; 1,454 with moderate PH as defined by 1-3 Wood units; and 592 with severe PH and more than 3 Wood units.
The three groups didn’t differ in terms of age, sex, wait-list time, or the prevalence of diabetes or renal, liver, or cerebrovascular disease. Nor did their donors differ in age, sex, left ventricular function, or allograft ischemic time.
Key in-hospital outcomes were similar between the groups with no, mild, and severe PH.
Moreover, there was no between-group difference in the rate of rejection at 1 year. Five-year survival rates were closely similar in the three groups, in the mid-70s.
Audience member Nahush A. Mokadam, MD, rose to praise Dr. Gaffey’s report.
“This is a great and important study. I think as a group we have been too conservative with pulmonary hypertension, so thank you for shining a good light on it,” said Dr. Mokadam of the University of Washington, Seattle.
Dr. Gaffey reported having no financial conflicts regarding the study, which was conducted free of commercial support.
AT THE WTSA ANNUAL MEETING
Key clinical point:
Major finding: It’s time to reconsider the practice of excluding patients with pulmonary hypertension from consideration for a donor heart.
Data source: A retrospective analysis of the United Network for Organ Sharing database including outcomes out to 5 years on 3,951 heart transplant recipients who had been bridged to transplant with an LVAD, most of whom had moderate or severe pulmonary hypertension before transplant.
Disclosures: This study was conducted free of commercial support. The presenter reported having no relevant financial conflicts of interest.
Keep PCI patients on aspirin for noncardiac surgery
ANAHEIM, CALIF. – For every 1,000 patients with a history of percutaneous coronary intervention undergoing noncardiac surgery, perioperative aspirin would prevent 59 myocardial infarctions but cause 8 major/life-threatening bleeds, according to a substudy of the POISE-2 trial presented at the American Heart Association scientific sessions.
For patients with previous PCI undergoing noncardiac surgery, “I think aspirin will be more likely to benefit them than harm them,” so long as they are not having an operation where bleeding would be devastating.” These include “delicate neurosurgery in which, if you bleed into your spine, you end up paralyzed,” said lead investigator Michelle Graham, MD, an interventional cardiologist and professor of cardiology at the University of Alberta, Edmonton.

The original multisite POISE-2 trial (Perioperative Ischemic Evaluation 2) evaluated the effect of perioperative aspirin for noncardiac surgery. Patients were randomized to receive 200 mg aspirin or placebo within 4 hours of surgery and then 100 mg aspirin or placebo in the early postoperative period. There was no significant effect on the composite rate of death or myocardial infarction, but an increased risk of serious bleeding (N Engl J Med. 2014 Apr 17;370[16]:1494-503).
The new substudy focused on the 470 patients with previous PCIs, because such patients are known to have a higher risk for postop complications. More than half received bare-metal stents and a quarter got drug-eluting stents; in most of the rest, the stent type was not known. The median duration from PCI to noncardiac surgery was 64 months, ranging from 34 to 113 months. Patients with bare-metal stents placed within 6 weeks or drug-eluting stents within a year, were excluded.
Overall, 234 patients were randomized to the aspirin group, and 236 to placebo. Among those who came in on chronic, daily aspirin therapy – as almost all of the PCI subjects did – those who were randomized to perioperative aspirin stayed on daily 100 mg aspirin for a week postop, and then flipped back to whatever dose they were on at home. Likewise, placebo patients resumed their home aspirin after 1 week.
The results were very different from the main trial. At 30 days’ follow-up, just 6% of patients in the aspirin arm reached the primary endpoint of death or MI, versus 11.5% in the placebo group, a statistically significant 50% reduction.
This difference was driven almost entirely by a reduction in MIs. Whereas 5.1% of patients in the aspirin arm had MIs, 11% of the placebo group did, a significant 64% reduction. Meanwhile, the risk of major or life-threatening bleeding was not only similar between groups, but also to the overall trial, noted in 5.6% of aspirin and 4.2% of placebo subjects.
Over 75% of the participants were men, almost 60% were undergoing a major surgery, 30% had diabetes, and many had hypertension. Very few were on direct oral anticoagulants. The two arms were well matched, with a median age of about 68 years.
Simultaneously with Dr. Graham’s presentation, the results were published online (Ann Intern Med. 2017 Nov 14; doi: 10.7326/M17-2341)
The work was funded mostly by the Canadian Institutes of Health Research. Bayer supplied the aspirin. Dr. Graham has no industry disclosures.
ANAHEIM, CALIF. – For every 1,000 patients with a history of percutaneous coronary intervention undergoing noncardiac surgery, perioperative aspirin would prevent 59 myocardial infarctions but cause 8 major/life-threatening bleeds, according to a substudy of the POISE-2 trial presented at the American Heart Association scientific sessions.
For patients with previous PCI undergoing noncardiac surgery, “I think aspirin will be more likely to benefit them than harm them,” so long as they are not having an operation where bleeding would be devastating.” These include “delicate neurosurgery in which, if you bleed into your spine, you end up paralyzed,” said lead investigator Michelle Graham, MD, an interventional cardiologist and professor of cardiology at the University of Alberta, Edmonton.
The original multisite POISE-2 trial (Perioperative Ischemic Evaluation 2) evaluated the effect of perioperative aspirin for noncardiac surgery. Patients were randomized to receive 200 mg aspirin or placebo within 4 hours of surgery and then 100 mg aspirin or placebo in the early postoperative period. There was no significant effect on the composite rate of death or myocardial infarction, but an increased risk of serious bleeding (N Engl J Med. 2014 Apr 17;370[16]:1494-503).
The new substudy focused on the 470 patients with previous PCIs, because such patients are known to have a higher risk for postop complications. More than half received bare-metal stents and a quarter got drug-eluting stents; in most of the rest, the stent type was not known. The median duration from PCI to noncardiac surgery was 64 months, ranging from 34 to 113 months. Patients with bare-metal stents placed within 6 weeks or drug-eluting stents within a year, were excluded.
Overall, 234 patients were randomized to the aspirin group, and 236 to placebo. Among those who came in on chronic, daily aspirin therapy – as almost all of the PCI subjects did – those who were randomized to perioperative aspirin stayed on daily 100 mg aspirin for a week postop, and then flipped back to whatever dose they were on at home. Likewise, placebo patients resumed their home aspirin after 1 week.
The results were very different from the main trial. At 30 days’ follow-up, just 6% of patients in the aspirin arm reached the primary endpoint of death or MI, versus 11.5% in the placebo group, a statistically significant 50% reduction.
This difference was driven almost entirely by a reduction in MIs. Whereas 5.1% of patients in the aspirin arm had MIs, 11% of the placebo group did, a significant 64% reduction. Meanwhile, the risk of major or life-threatening bleeding was not only similar between groups, but also to the overall trial, noted in 5.6% of aspirin and 4.2% of placebo subjects.
Over 75% of the participants were men, almost 60% were undergoing a major surgery, 30% had diabetes, and many had hypertension. Very few were on direct oral anticoagulants. The two arms were well matched, with a median age of about 68 years.
Simultaneously with Dr. Graham’s presentation, the results were published online (Ann Intern Med. 2017 Nov 14; doi: 10.7326/M17-2341)
The work was funded mostly by the Canadian Institutes of Health Research. Bayer supplied the aspirin. Dr. Graham has no industry disclosures.
ANAHEIM, CALIF. – For every 1,000 patients with a history of percutaneous coronary intervention undergoing noncardiac surgery, perioperative aspirin would prevent 59 myocardial infarctions but cause 8 major/life-threatening bleeds, according to a substudy of the POISE-2 trial presented at the American Heart Association scientific sessions.
For patients with previous PCI undergoing noncardiac surgery, “I think aspirin will be more likely to benefit them than harm them,” so long as they are not having an operation where bleeding would be devastating.” These include “delicate neurosurgery in which, if you bleed into your spine, you end up paralyzed,” said lead investigator Michelle Graham, MD, an interventional cardiologist and professor of cardiology at the University of Alberta, Edmonton.
The original multisite POISE-2 trial (Perioperative Ischemic Evaluation 2) evaluated the effect of perioperative aspirin for noncardiac surgery. Patients were randomized to receive 200 mg aspirin or placebo within 4 hours of surgery and then 100 mg aspirin or placebo in the early postoperative period. There was no significant effect on the composite rate of death or myocardial infarction, but an increased risk of serious bleeding (N Engl J Med. 2014 Apr 17;370[16]:1494-503).
The new substudy focused on the 470 patients with previous PCIs, because such patients are known to have a higher risk for postop complications. More than half received bare-metal stents and a quarter got drug-eluting stents; in most of the rest, the stent type was not known. The median duration from PCI to noncardiac surgery was 64 months, ranging from 34 to 113 months. Patients with bare-metal stents placed within 6 weeks or drug-eluting stents within a year, were excluded.
Overall, 234 patients were randomized to the aspirin group, and 236 to placebo. Among those who came in on chronic, daily aspirin therapy – as almost all of the PCI subjects did – those who were randomized to perioperative aspirin stayed on daily 100 mg aspirin for a week postop, and then flipped back to whatever dose they were on at home. Likewise, placebo patients resumed their home aspirin after 1 week.
The results were very different from the main trial. At 30 days’ follow-up, just 6% of patients in the aspirin arm reached the primary endpoint of death or MI, versus 11.5% in the placebo group, a statistically significant 50% reduction.
This difference was driven almost entirely by a reduction in MIs. Whereas 5.1% of patients in the aspirin arm had MIs, 11% of the placebo group did, a significant 64% reduction. Meanwhile, the risk of major or life-threatening bleeding was not only similar between groups, but also to the overall trial, noted in 5.6% of aspirin and 4.2% of placebo subjects.
Over 75% of the participants were men, almost 60% were undergoing a major surgery, 30% had diabetes, and many had hypertension. Very few were on direct oral anticoagulants. The two arms were well matched, with a median age of about 68 years.
Simultaneously with Dr. Graham’s presentation, the results were published online (Ann Intern Med. 2017 Nov 14; doi: 10.7326/M17-2341)
The work was funded mostly by the Canadian Institutes of Health Research. Bayer supplied the aspirin. Dr. Graham has no industry disclosures.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: For every 1,000 patients with a history of percutaneous coronary intervention undergoing noncardiac surgery, perioperative aspirin would prevent 59 myocardial infarctions but cause 8 major/life-threatening bleeds.
Data source: POISE-2, a randomized trial of 470 PCI patients.
Disclosures: The work was funded mostly by the Canadian Institutes of Health Research. Bayer supplied the aspirin. The lead investigator has no industry disclosures.
VIDEO: Innovative technology is opening doors for vaginal hysterectomy
NATIONAL HARBOR, MD. – Innovative tools for vaginal hysterectomy were in the spotlight during a surgical demonstration at the AAGL Global Congress.
“I think it’s really compelling that we use the technologies that the AAGL is known for investigating and teaching each other,” said Charles Rardin, MD, director of the robotic surgery program at Women & Infants Hospital, Providence, R.I. “It’s nice to see a renewed interest in some newer technologies and applying them to vaginal hysterectomy.”
The presentation of new tools comes as the number of vaginal hysterectomies have decreased and laparoscopic procedures are on the rise. The rate of vaginal hysterectomy in the United States has fallen from 24.8% in 1998 to 16.7% in 2010, according to the Nationwide Inpatient Sample from the Agency for Healthcare Research and Quality.
Surgeons demonstrated new tools with the intent of showing physicians that the benefits some associate with laparoscopic procedures, such as having easier access or a better sense of the uterus, can be associated with vaginal hysterectomy as well.
Advanced tools, such as a self-retaining retractor and 3-D camera systems, could make it easier to teach students by allowing more mobility and easier visual access, Dr. Rardin said in a video interview.
The tutorial ended with a demonstration of the natural orifice transluminal endoscopic surgery tool that allows laparoscopic tools to be introduced through the vaginal pathway.
All the tools exhibited at AAGL are currently available.
Dr. Rardin reported having no relevant financial disclosures.
On Twitter @eaztweets
NATIONAL HARBOR, MD. – Innovative tools for vaginal hysterectomy were in the spotlight during a surgical demonstration at the AAGL Global Congress.
“I think it’s really compelling that we use the technologies that the AAGL is known for investigating and teaching each other,” said Charles Rardin, MD, director of the robotic surgery program at Women & Infants Hospital, Providence, R.I. “It’s nice to see a renewed interest in some newer technologies and applying them to vaginal hysterectomy.”
The presentation of new tools comes as the number of vaginal hysterectomies have decreased and laparoscopic procedures are on the rise. The rate of vaginal hysterectomy in the United States has fallen from 24.8% in 1998 to 16.7% in 2010, according to the Nationwide Inpatient Sample from the Agency for Healthcare Research and Quality.
Surgeons demonstrated new tools with the intent of showing physicians that the benefits some associate with laparoscopic procedures, such as having easier access or a better sense of the uterus, can be associated with vaginal hysterectomy as well.
Advanced tools, such as a self-retaining retractor and 3-D camera systems, could make it easier to teach students by allowing more mobility and easier visual access, Dr. Rardin said in a video interview.
The tutorial ended with a demonstration of the natural orifice transluminal endoscopic surgery tool that allows laparoscopic tools to be introduced through the vaginal pathway.
All the tools exhibited at AAGL are currently available.
Dr. Rardin reported having no relevant financial disclosures.
On Twitter @eaztweets
NATIONAL HARBOR, MD. – Innovative tools for vaginal hysterectomy were in the spotlight during a surgical demonstration at the AAGL Global Congress.
“I think it’s really compelling that we use the technologies that the AAGL is known for investigating and teaching each other,” said Charles Rardin, MD, director of the robotic surgery program at Women & Infants Hospital, Providence, R.I. “It’s nice to see a renewed interest in some newer technologies and applying them to vaginal hysterectomy.”
The presentation of new tools comes as the number of vaginal hysterectomies have decreased and laparoscopic procedures are on the rise. The rate of vaginal hysterectomy in the United States has fallen from 24.8% in 1998 to 16.7% in 2010, according to the Nationwide Inpatient Sample from the Agency for Healthcare Research and Quality.
Surgeons demonstrated new tools with the intent of showing physicians that the benefits some associate with laparoscopic procedures, such as having easier access or a better sense of the uterus, can be associated with vaginal hysterectomy as well.
Advanced tools, such as a self-retaining retractor and 3-D camera systems, could make it easier to teach students by allowing more mobility and easier visual access, Dr. Rardin said in a video interview.
The tutorial ended with a demonstration of the natural orifice transluminal endoscopic surgery tool that allows laparoscopic tools to be introduced through the vaginal pathway.
All the tools exhibited at AAGL are currently available.
Dr. Rardin reported having no relevant financial disclosures.
On Twitter @eaztweets
AT AAGL 2017

VIDEO: MISS 2017– Hot topics, innovations, debates
Philip R. Schauer, MD, FACS, discusses innovations, hot topics, and controversies covered in the sessions of this year’s Minimally Invasive Surgery Symposium, held in Las Vegas. In addition to highlighting what’s new this year, Dr. Schauer also spoke about plans for next year’s meeting and what makes the MISS unique and valuable to attendees.

Philip R. Schauer, MD, FACS, discusses innovations, hot topics, and controversies covered in the sessions of this year’s Minimally Invasive Surgery Symposium, held in Las Vegas. In addition to highlighting what’s new this year, Dr. Schauer also spoke about plans for next year’s meeting and what makes the MISS unique and valuable to attendees.
Philip R. Schauer, MD, FACS, discusses innovations, hot topics, and controversies covered in the sessions of this year’s Minimally Invasive Surgery Symposium, held in Las Vegas. In addition to highlighting what’s new this year, Dr. Schauer also spoke about plans for next year’s meeting and what makes the MISS unique and valuable to attendees.
Large database analysis suggests safety of bariatric surgery in seniors
NATIONAL HARBOR, MD. – despite a slight increase in unadjusted mortality rates, according to an analysis of data from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP).
Based on data that was collected in 2015 and submitted to MBSAQIP, “bariatric surgery is safe in the elderly, even in those 70 years old and older,” reported Tallal Zeni, MD, director of the Michigan Bariatric Institute in Livonia.

There were 16,568 patients older than age 60 years entered into the MBSAQIP database in 2015. When those were compared with the 117,443 younger patients, the unadjusted rates of morbidity (6.5% vs. 6.0%) and mortality (0.3% vs. 0.1%) were higher for the older patients, but “they are close,” according to Dr. Zeni. Both rates reached significance by the conventional definition (P < .05), but he suggested that they are lower in this study than those in prior studies of MBSAQIP datasets and that they are acceptable relative to the anticipated health benefits.
Above the age of 60 years, no correlation could be made between increasing age and increasing risk of morbidity, mortality, or rate of reoperations, according to Dr. Zeni.
Why should bariatric surgery be considered in older patients? He cited data from a study that showed the life expectancy in a 70-year-old without functional limitations is 13 years. As a result, he added, “it behooves us to provide them with the best quality of life we can.”
Relative to prior MBSAQIP evaluations of bariatric surgery in the elderly, the proportion of patients undergoing sleeve gastrectomy relative to gastric bypass has been increasing, Dr. Zeni reported. In the analysis, approximately two-thirds of the bariatric procedures were performed with sleeve gastrectomy, which is higher relative to what previous MBSAQIP analyses have shown.
Based on rates of morbidity for those two surgical approaches in the analysis, that trend makes sense. While the higher 30-day mortality for gastric bypass, compared with sleeve gastrectomy, was not significant (0.38% vs. 0.26%; P = .221), all-cause morbidity was almost two times greater for those undergoing gastric bypass than it was for those undergoing sleeve gastrectomy (10.61% vs. 5.81%; P < .001), Dr. Zeni reported.
However, some of that difference may be explained by baseline disparities between the two groups. In the gastric bypass group, there were higher rates of preoperative diabetes (54% vs. 40%; P < .001), sleep apnea (57% vs. 50%; P < .001) and hyperlipidemia (59% vs. 54%; P < .001). Also, gastric bypass patients were more likely to have a history of a previous bariatric procedure (11% vs. 8.5%; P < .001) and to be in the American Society of Anesthesiologists Physical Status score of 3 (84% vs. 80%; P < .001), according to Dr. Zeni.
The specific complications more common in the gastric bypass group than the sleeve gastrectomy group included anastomotic leak (0.56% vs. 0.3%; P = .017), surgical site infection (1.74% vs. 0.61%; P < .001), pneumonia (0.87% vs. 0.32%; P < .001), and bleeding (1.14% vs. 0.5%; P = .024). Although the average operating time was 40 minutes longer in the bypass group, there were no significant differences in thromboembolic complications.
Overall, despite a modest increase in the risk of complications for bariatric surgery in elderly patients, that risk can be considered acceptable in relation to the potential health benefits, according to Dr. Zeni. He suggested that the data might encourage further growth in the rates of bariatric procedures among patients older than 60 years.
Dr. Zeni reports no relevant financial relationships.
NATIONAL HARBOR, MD. – despite a slight increase in unadjusted mortality rates, according to an analysis of data from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP).
Based on data that was collected in 2015 and submitted to MBSAQIP, “bariatric surgery is safe in the elderly, even in those 70 years old and older,” reported Tallal Zeni, MD, director of the Michigan Bariatric Institute in Livonia.
There were 16,568 patients older than age 60 years entered into the MBSAQIP database in 2015. When those were compared with the 117,443 younger patients, the unadjusted rates of morbidity (6.5% vs. 6.0%) and mortality (0.3% vs. 0.1%) were higher for the older patients, but “they are close,” according to Dr. Zeni. Both rates reached significance by the conventional definition (P < .05), but he suggested that they are lower in this study than those in prior studies of MBSAQIP datasets and that they are acceptable relative to the anticipated health benefits.
Above the age of 60 years, no correlation could be made between increasing age and increasing risk of morbidity, mortality, or rate of reoperations, according to Dr. Zeni.
Why should bariatric surgery be considered in older patients? He cited data from a study that showed the life expectancy in a 70-year-old without functional limitations is 13 years. As a result, he added, “it behooves us to provide them with the best quality of life we can.”
Relative to prior MBSAQIP evaluations of bariatric surgery in the elderly, the proportion of patients undergoing sleeve gastrectomy relative to gastric bypass has been increasing, Dr. Zeni reported. In the analysis, approximately two-thirds of the bariatric procedures were performed with sleeve gastrectomy, which is higher relative to what previous MBSAQIP analyses have shown.
Based on rates of morbidity for those two surgical approaches in the analysis, that trend makes sense. While the higher 30-day mortality for gastric bypass, compared with sleeve gastrectomy, was not significant (0.38% vs. 0.26%; P = .221), all-cause morbidity was almost two times greater for those undergoing gastric bypass than it was for those undergoing sleeve gastrectomy (10.61% vs. 5.81%; P < .001), Dr. Zeni reported.
However, some of that difference may be explained by baseline disparities between the two groups. In the gastric bypass group, there were higher rates of preoperative diabetes (54% vs. 40%; P < .001), sleep apnea (57% vs. 50%; P < .001) and hyperlipidemia (59% vs. 54%; P < .001). Also, gastric bypass patients were more likely to have a history of a previous bariatric procedure (11% vs. 8.5%; P < .001) and to be in the American Society of Anesthesiologists Physical Status score of 3 (84% vs. 80%; P < .001), according to Dr. Zeni.
The specific complications more common in the gastric bypass group than the sleeve gastrectomy group included anastomotic leak (0.56% vs. 0.3%; P = .017), surgical site infection (1.74% vs. 0.61%; P < .001), pneumonia (0.87% vs. 0.32%; P < .001), and bleeding (1.14% vs. 0.5%; P = .024). Although the average operating time was 40 minutes longer in the bypass group, there were no significant differences in thromboembolic complications.
Overall, despite a modest increase in the risk of complications for bariatric surgery in elderly patients, that risk can be considered acceptable in relation to the potential health benefits, according to Dr. Zeni. He suggested that the data might encourage further growth in the rates of bariatric procedures among patients older than 60 years.
Dr. Zeni reports no relevant financial relationships.
NATIONAL HARBOR, MD. – despite a slight increase in unadjusted mortality rates, according to an analysis of data from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP).
Based on data that was collected in 2015 and submitted to MBSAQIP, “bariatric surgery is safe in the elderly, even in those 70 years old and older,” reported Tallal Zeni, MD, director of the Michigan Bariatric Institute in Livonia.
There were 16,568 patients older than age 60 years entered into the MBSAQIP database in 2015. When those were compared with the 117,443 younger patients, the unadjusted rates of morbidity (6.5% vs. 6.0%) and mortality (0.3% vs. 0.1%) were higher for the older patients, but “they are close,” according to Dr. Zeni. Both rates reached significance by the conventional definition (P < .05), but he suggested that they are lower in this study than those in prior studies of MBSAQIP datasets and that they are acceptable relative to the anticipated health benefits.
Above the age of 60 years, no correlation could be made between increasing age and increasing risk of morbidity, mortality, or rate of reoperations, according to Dr. Zeni.
Why should bariatric surgery be considered in older patients? He cited data from a study that showed the life expectancy in a 70-year-old without functional limitations is 13 years. As a result, he added, “it behooves us to provide them with the best quality of life we can.”
Relative to prior MBSAQIP evaluations of bariatric surgery in the elderly, the proportion of patients undergoing sleeve gastrectomy relative to gastric bypass has been increasing, Dr. Zeni reported. In the analysis, approximately two-thirds of the bariatric procedures were performed with sleeve gastrectomy, which is higher relative to what previous MBSAQIP analyses have shown.
Based on rates of morbidity for those two surgical approaches in the analysis, that trend makes sense. While the higher 30-day mortality for gastric bypass, compared with sleeve gastrectomy, was not significant (0.38% vs. 0.26%; P = .221), all-cause morbidity was almost two times greater for those undergoing gastric bypass than it was for those undergoing sleeve gastrectomy (10.61% vs. 5.81%; P < .001), Dr. Zeni reported.
However, some of that difference may be explained by baseline disparities between the two groups. In the gastric bypass group, there were higher rates of preoperative diabetes (54% vs. 40%; P < .001), sleep apnea (57% vs. 50%; P < .001) and hyperlipidemia (59% vs. 54%; P < .001). Also, gastric bypass patients were more likely to have a history of a previous bariatric procedure (11% vs. 8.5%; P < .001) and to be in the American Society of Anesthesiologists Physical Status score of 3 (84% vs. 80%; P < .001), according to Dr. Zeni.
The specific complications more common in the gastric bypass group than the sleeve gastrectomy group included anastomotic leak (0.56% vs. 0.3%; P = .017), surgical site infection (1.74% vs. 0.61%; P < .001), pneumonia (0.87% vs. 0.32%; P < .001), and bleeding (1.14% vs. 0.5%; P = .024). Although the average operating time was 40 minutes longer in the bypass group, there were no significant differences in thromboembolic complications.
Overall, despite a modest increase in the risk of complications for bariatric surgery in elderly patients, that risk can be considered acceptable in relation to the potential health benefits, according to Dr. Zeni. He suggested that the data might encourage further growth in the rates of bariatric procedures among patients older than 60 years.
Dr. Zeni reports no relevant financial relationships.
AT OBESITY WEEK 2017
Key clinical point: Based on mortality and morbidity rates, bariatric surgery is acceptably safe in patients older than 60 years of age.
Major finding: Compared with patients younger than 60 years, older patients had only modestly increased rates of morbidity (6.5% vs. 6.0%) and mortality (0.3% vs. 0.1%).
Data source: A retrospective database analysis.
Disclosures: Dr. Zeni reports no relevant financial relationships.
Fibroids associated with lower chance of unsuspected malignancy
NATIONAL HARBOR, MD. – Women undergoing hysterectomy or myomectomy for benign indications, who also had fibroids, were less likely to have a malignant diagnosis, according to a study presented at the AAGL Global Congress.
These findings could change the conversation when it comes to counseling patients about the risks associated with morcellation, a procedure that was strongly discouraged by the FDA in 2014 due to the concern that it might have the potential to spread malignancy.
“There’s a lot of things going on in the media about morcellation and risk of malignancy at the time of benign fibroid surgery, but this research actually makes apparent the higher risk of malignancy when fibroids are not present,” Farah Alvi, MD, a second-year fellow at Northwestern University, Chicago, said in an interview. Despite the concerns regarding morcellation and malignancy, this research suggests that patients who have fibroids at time of surgery may have a lower chance of malignancy, compared with patients who have other indications for surgery, she explained.
Dr. Alvi and her colleagues studied 2,987 hysterectomy or myomectomy patients with benign indications between January 2005 and December 2014.
Among patients studied, researchers found 33 confirmed malignant or borderline tumors, 16 of 1,790 (0.89%) in the leiomyoma group and 17 of 1,197 (1.42%) in the group with other indications (P = 0.04). The malignancies/borderline tumors included three leiomyosarcomas, two endometrial sarcomas, two endometrioid adenocarcinomas, one granulose cell tumor, three smooth muscle tumors of uncertain malignant potential, three atypical leiomyoma, and one serous papillary borderline ovarian tumor.
Of those with leiomyomata, 1 in 600 patients were diagnosed with leiomyosarcoma, compared with a risk of 1 in 350 for unanticipated malignancy in general.
Patients with surgical indications of symptomatic leiomyoma had an odds ratio of 0.63 (P = .18) for diagnosis of an unanticipated malignancy, compared with those without leiomyoma, according to Dr. Alvi. The odds of malignancy were also reduced in patients with uterine sizes of 15-20 weeks (OR, 0.65; P = .43) and those with specimen sizes of 250-500 grams (OR, 0.68; P = .64).
These findings will have implications for how physicians counsel women undergoing minimally invasive hysterectomy or myomectomy, Dr. Alvi said.
“In counseling patients about morcellation, we often have quoted them an estimated risk of 1 in 458 for leiomyosarcoma, based on the FDA morcellation warnings, and one thing we can learn is that risk is actually much lower than we think it is,” Dr. Alvi said.
The findings also suggest a shift in focus toward identifying the factors that put women at higher risk for malignancy. For example, older age is one of the most significant risk factors identified in the study, she added.
Dr. Alvi reported having no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
NATIONAL HARBOR, MD. – Women undergoing hysterectomy or myomectomy for benign indications, who also had fibroids, were less likely to have a malignant diagnosis, according to a study presented at the AAGL Global Congress.
These findings could change the conversation when it comes to counseling patients about the risks associated with morcellation, a procedure that was strongly discouraged by the FDA in 2014 due to the concern that it might have the potential to spread malignancy.
“There’s a lot of things going on in the media about morcellation and risk of malignancy at the time of benign fibroid surgery, but this research actually makes apparent the higher risk of malignancy when fibroids are not present,” Farah Alvi, MD, a second-year fellow at Northwestern University, Chicago, said in an interview. Despite the concerns regarding morcellation and malignancy, this research suggests that patients who have fibroids at time of surgery may have a lower chance of malignancy, compared with patients who have other indications for surgery, she explained.
Dr. Alvi and her colleagues studied 2,987 hysterectomy or myomectomy patients with benign indications between January 2005 and December 2014.
Among patients studied, researchers found 33 confirmed malignant or borderline tumors, 16 of 1,790 (0.89%) in the leiomyoma group and 17 of 1,197 (1.42%) in the group with other indications (P = 0.04). The malignancies/borderline tumors included three leiomyosarcomas, two endometrial sarcomas, two endometrioid adenocarcinomas, one granulose cell tumor, three smooth muscle tumors of uncertain malignant potential, three atypical leiomyoma, and one serous papillary borderline ovarian tumor.
Of those with leiomyomata, 1 in 600 patients were diagnosed with leiomyosarcoma, compared with a risk of 1 in 350 for unanticipated malignancy in general.
Patients with surgical indications of symptomatic leiomyoma had an odds ratio of 0.63 (P = .18) for diagnosis of an unanticipated malignancy, compared with those without leiomyoma, according to Dr. Alvi. The odds of malignancy were also reduced in patients with uterine sizes of 15-20 weeks (OR, 0.65; P = .43) and those with specimen sizes of 250-500 grams (OR, 0.68; P = .64).
These findings will have implications for how physicians counsel women undergoing minimally invasive hysterectomy or myomectomy, Dr. Alvi said.
“In counseling patients about morcellation, we often have quoted them an estimated risk of 1 in 458 for leiomyosarcoma, based on the FDA morcellation warnings, and one thing we can learn is that risk is actually much lower than we think it is,” Dr. Alvi said.
The findings also suggest a shift in focus toward identifying the factors that put women at higher risk for malignancy. For example, older age is one of the most significant risk factors identified in the study, she added.
Dr. Alvi reported having no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
NATIONAL HARBOR, MD. – Women undergoing hysterectomy or myomectomy for benign indications, who also had fibroids, were less likely to have a malignant diagnosis, according to a study presented at the AAGL Global Congress.
These findings could change the conversation when it comes to counseling patients about the risks associated with morcellation, a procedure that was strongly discouraged by the FDA in 2014 due to the concern that it might have the potential to spread malignancy.
“There’s a lot of things going on in the media about morcellation and risk of malignancy at the time of benign fibroid surgery, but this research actually makes apparent the higher risk of malignancy when fibroids are not present,” Farah Alvi, MD, a second-year fellow at Northwestern University, Chicago, said in an interview. Despite the concerns regarding morcellation and malignancy, this research suggests that patients who have fibroids at time of surgery may have a lower chance of malignancy, compared with patients who have other indications for surgery, she explained.
Dr. Alvi and her colleagues studied 2,987 hysterectomy or myomectomy patients with benign indications between January 2005 and December 2014.
Among patients studied, researchers found 33 confirmed malignant or borderline tumors, 16 of 1,790 (0.89%) in the leiomyoma group and 17 of 1,197 (1.42%) in the group with other indications (P = 0.04). The malignancies/borderline tumors included three leiomyosarcomas, two endometrial sarcomas, two endometrioid adenocarcinomas, one granulose cell tumor, three smooth muscle tumors of uncertain malignant potential, three atypical leiomyoma, and one serous papillary borderline ovarian tumor.
Of those with leiomyomata, 1 in 600 patients were diagnosed with leiomyosarcoma, compared with a risk of 1 in 350 for unanticipated malignancy in general.
Patients with surgical indications of symptomatic leiomyoma had an odds ratio of 0.63 (P = .18) for diagnosis of an unanticipated malignancy, compared with those without leiomyoma, according to Dr. Alvi. The odds of malignancy were also reduced in patients with uterine sizes of 15-20 weeks (OR, 0.65; P = .43) and those with specimen sizes of 250-500 grams (OR, 0.68; P = .64).
These findings will have implications for how physicians counsel women undergoing minimally invasive hysterectomy or myomectomy, Dr. Alvi said.
“In counseling patients about morcellation, we often have quoted them an estimated risk of 1 in 458 for leiomyosarcoma, based on the FDA morcellation warnings, and one thing we can learn is that risk is actually much lower than we think it is,” Dr. Alvi said.
The findings also suggest a shift in focus toward identifying the factors that put women at higher risk for malignancy. For example, older age is one of the most significant risk factors identified in the study, she added.
Dr. Alvi reported having no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
AT AAGL 2017
Key clinical point:
Major finding: Patients with preoperative indication of symptomatic leiomyoma had an odds ratio of 0.63 (P = .18) of having a diagnosis of malignancy.
Data source: Retrospective study of 2,987 hysterectomies or myomectomies between January 2005 and December 2014.
Disclosures: Dr. Alvi reported having no relevant financial disclosures.