User login
Official Newspaper of the American College of Surgeons
ACL repair: ‘We have to do better’
SNOWMASS, COLO. – A novel approach to repairing anterior cruciate ligament injuries – and perhaps thereby avoiding a downstream tidal wave of knee osteoarthritis – is creating major buzz in sports medicine circles.
“You’ll probably hear much more about this bioenhanced repair, with the expectation of achieving strength equal to that of ACL reconstruction and perhaps preventing the development of osteoarthritis 15 years down the road,” Dr. M. Timothy Hresko predicted at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.

He cited research led by his colleague Dr. Martha M. Murray of Boston Children’s Hospital, which has resulted in development of a surgical technique combining a tissue-engineered composite scaffold with a suture repair of the torn ACL in what Dr. Murray has termed a bioenhanced repair.
Her work, to date preclinical, has garnered major awards from both the American Orthopaedic Society for Sports Medicine and the American Academy of Orthopaedic Surgeons. The Food and Drug Administration recently granted approval for the first clinical safety studies, to begin this year.
There is a major unmet need for better methods of repairing ACL injuries. They’re common, with an estimated 550,000 cases per year. The peak incidence occurs in 15- to 19-year-old female athletes. And the current gold standard therapy consisting of ACL reconstruction using an allograft or hamstring graft has a disturbingly high failure rate, both early and late. The graft failure rate is up to 20% in the first 2 years, climbing to 50% at 10 years.
“We just have to do better,” conceded Dr. Hresko, an orthopedic surgeon at Harvard Medical School, Boston, and Boston Children’s Hospital.
“One of the interesting and unfortunate facts,” he continued, “is that roughly 80% of people who have an ACL injury, with or without reconstruction, are still going to have osteoarthritis 14 years after the injury. So, if this is your 15-year-old daughter who plays basketball, she’ll only be 30 and will already have degenerative arthritis of the knee at what should still be a very active period of life.”
The bioenhanced repair now under study uses an extracellular matrix-based scaffold, which is loaded with a few milliliters of the patient’s own platelet-enriched plasma. The scaffold is applied between the torn ligament ends in order to stimulate collagen production and promote ligament healing. The suture repair of the ligament entails much less trauma than does standard reconstructive surgery.
In large-animal studies, the bioenhanced repair resulted in the same yield load, stiffness, and other desirable biomechanical properties at 1 year as with major reconstructive surgery. However, while premature posttraumatic osteoarthritis occurred in 80% of the knees treated with standard ACL reconstruction, there was no evidence of such damage 1 year following bioenhanced repair. Nor have adverse reactions to the scaffold been noted in the porcine model.
Dr. Hresko reported serving as a consultant to Depuy Spine.
SNOWMASS, COLO. – A novel approach to repairing anterior cruciate ligament injuries – and perhaps thereby avoiding a downstream tidal wave of knee osteoarthritis – is creating major buzz in sports medicine circles.
“You’ll probably hear much more about this bioenhanced repair, with the expectation of achieving strength equal to that of ACL reconstruction and perhaps preventing the development of osteoarthritis 15 years down the road,” Dr. M. Timothy Hresko predicted at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
He cited research led by his colleague Dr. Martha M. Murray of Boston Children’s Hospital, which has resulted in development of a surgical technique combining a tissue-engineered composite scaffold with a suture repair of the torn ACL in what Dr. Murray has termed a bioenhanced repair.
Her work, to date preclinical, has garnered major awards from both the American Orthopaedic Society for Sports Medicine and the American Academy of Orthopaedic Surgeons. The Food and Drug Administration recently granted approval for the first clinical safety studies, to begin this year.
There is a major unmet need for better methods of repairing ACL injuries. They’re common, with an estimated 550,000 cases per year. The peak incidence occurs in 15- to 19-year-old female athletes. And the current gold standard therapy consisting of ACL reconstruction using an allograft or hamstring graft has a disturbingly high failure rate, both early and late. The graft failure rate is up to 20% in the first 2 years, climbing to 50% at 10 years.
“We just have to do better,” conceded Dr. Hresko, an orthopedic surgeon at Harvard Medical School, Boston, and Boston Children’s Hospital.
“One of the interesting and unfortunate facts,” he continued, “is that roughly 80% of people who have an ACL injury, with or without reconstruction, are still going to have osteoarthritis 14 years after the injury. So, if this is your 15-year-old daughter who plays basketball, she’ll only be 30 and will already have degenerative arthritis of the knee at what should still be a very active period of life.”
The bioenhanced repair now under study uses an extracellular matrix-based scaffold, which is loaded with a few milliliters of the patient’s own platelet-enriched plasma. The scaffold is applied between the torn ligament ends in order to stimulate collagen production and promote ligament healing. The suture repair of the ligament entails much less trauma than does standard reconstructive surgery.
In large-animal studies, the bioenhanced repair resulted in the same yield load, stiffness, and other desirable biomechanical properties at 1 year as with major reconstructive surgery. However, while premature posttraumatic osteoarthritis occurred in 80% of the knees treated with standard ACL reconstruction, there was no evidence of such damage 1 year following bioenhanced repair. Nor have adverse reactions to the scaffold been noted in the porcine model.
Dr. Hresko reported serving as a consultant to Depuy Spine.
SNOWMASS, COLO. – A novel approach to repairing anterior cruciate ligament injuries – and perhaps thereby avoiding a downstream tidal wave of knee osteoarthritis – is creating major buzz in sports medicine circles.
“You’ll probably hear much more about this bioenhanced repair, with the expectation of achieving strength equal to that of ACL reconstruction and perhaps preventing the development of osteoarthritis 15 years down the road,” Dr. M. Timothy Hresko predicted at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
He cited research led by his colleague Dr. Martha M. Murray of Boston Children’s Hospital, which has resulted in development of a surgical technique combining a tissue-engineered composite scaffold with a suture repair of the torn ACL in what Dr. Murray has termed a bioenhanced repair.
Her work, to date preclinical, has garnered major awards from both the American Orthopaedic Society for Sports Medicine and the American Academy of Orthopaedic Surgeons. The Food and Drug Administration recently granted approval for the first clinical safety studies, to begin this year.
There is a major unmet need for better methods of repairing ACL injuries. They’re common, with an estimated 550,000 cases per year. The peak incidence occurs in 15- to 19-year-old female athletes. And the current gold standard therapy consisting of ACL reconstruction using an allograft or hamstring graft has a disturbingly high failure rate, both early and late. The graft failure rate is up to 20% in the first 2 years, climbing to 50% at 10 years.
“We just have to do better,” conceded Dr. Hresko, an orthopedic surgeon at Harvard Medical School, Boston, and Boston Children’s Hospital.
“One of the interesting and unfortunate facts,” he continued, “is that roughly 80% of people who have an ACL injury, with or without reconstruction, are still going to have osteoarthritis 14 years after the injury. So, if this is your 15-year-old daughter who plays basketball, she’ll only be 30 and will already have degenerative arthritis of the knee at what should still be a very active period of life.”
The bioenhanced repair now under study uses an extracellular matrix-based scaffold, which is loaded with a few milliliters of the patient’s own platelet-enriched plasma. The scaffold is applied between the torn ligament ends in order to stimulate collagen production and promote ligament healing. The suture repair of the ligament entails much less trauma than does standard reconstructive surgery.
In large-animal studies, the bioenhanced repair resulted in the same yield load, stiffness, and other desirable biomechanical properties at 1 year as with major reconstructive surgery. However, while premature posttraumatic osteoarthritis occurred in 80% of the knees treated with standard ACL reconstruction, there was no evidence of such damage 1 year following bioenhanced repair. Nor have adverse reactions to the scaffold been noted in the porcine model.
Dr. Hresko reported serving as a consultant to Depuy Spine.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM
VIDEO: Many stroke patients may miss out on clot-retrieval options
NASHVILLE, TENN. – A 1 million–patient analysis of the Get With the Guidelines database found striking improvements in outcomes after ischemic stroke.
Despite the proven benefits of new-generation clot-retrieval devices, however, only about 2% of such stroke patients undergo endovascular therapy.
In a video interview at the International Stroke Conference, Dr. Bijoy Menon of the department of clinical neurosciences at the University of Calgary (Alta.), who presented the findings at the conference, discussed this apparent clinical paradox.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Menon’s study echoes findings of the landmark Endovascular Treatment for Small Core and Proximal Occlusion Ischemic Stroke (ESCAPE) trial, which found dramatically improved stroke outcomes after endovascular therapy.
But the benefits of such treatment should never outweigh the need for thoroughly screening patients and carefully considering their recovery prospects, Dr. Michael Hill, professor of neurology at the University of Calgary and primary investigator on the ESCAPE study, cautioned in another video interview at the meeting.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
NASHVILLE, TENN. – A 1 million–patient analysis of the Get With the Guidelines database found striking improvements in outcomes after ischemic stroke.
Despite the proven benefits of new-generation clot-retrieval devices, however, only about 2% of such stroke patients undergo endovascular therapy.
In a video interview at the International Stroke Conference, Dr. Bijoy Menon of the department of clinical neurosciences at the University of Calgary (Alta.), who presented the findings at the conference, discussed this apparent clinical paradox.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Menon’s study echoes findings of the landmark Endovascular Treatment for Small Core and Proximal Occlusion Ischemic Stroke (ESCAPE) trial, which found dramatically improved stroke outcomes after endovascular therapy.
But the benefits of such treatment should never outweigh the need for thoroughly screening patients and carefully considering their recovery prospects, Dr. Michael Hill, professor of neurology at the University of Calgary and primary investigator on the ESCAPE study, cautioned in another video interview at the meeting.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
NASHVILLE, TENN. – A 1 million–patient analysis of the Get With the Guidelines database found striking improvements in outcomes after ischemic stroke.
Despite the proven benefits of new-generation clot-retrieval devices, however, only about 2% of such stroke patients undergo endovascular therapy.
In a video interview at the International Stroke Conference, Dr. Bijoy Menon of the department of clinical neurosciences at the University of Calgary (Alta.), who presented the findings at the conference, discussed this apparent clinical paradox.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Menon’s study echoes findings of the landmark Endovascular Treatment for Small Core and Proximal Occlusion Ischemic Stroke (ESCAPE) trial, which found dramatically improved stroke outcomes after endovascular therapy.
But the benefits of such treatment should never outweigh the need for thoroughly screening patients and carefully considering their recovery prospects, Dr. Michael Hill, professor of neurology at the University of Calgary and primary investigator on the ESCAPE study, cautioned in another video interview at the meeting.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
AT THE INTERNATIONAL STROKE CONFERENCE

VTE risk climbs in patients on contact isolation
LAKE BUENA VISTA, FLA. – Trauma patients on contact isolation were nearly six times more likely to develop venous thromboembolism (VTE) as those who were not isolated, based on an analysis of 4,317 patients.
VTE occurred in 17.5% (44/251) of patients on contact isolation and 3.5% (141/4,066) of patients who were not isolated (P < .0001). Injury Severity Score (ISS), age, male gender, and obesity also were significantly associated with the risk of VTE.
The relationship between VTE risk and contact isolation remained significant after adjusting for gender, age, ISS, and comorbidities (odds ratio, 3.28; P < .0001), Dr. Robert Ferguson reported at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Odds ratios also were significantly elevated for obesity (OR, 2.35; P < .006), male gender (OR, 2.1; P < .0001), ISS (OR, 1.08; P < .0001), and age (OR, 1.02; P < .0001). The presence of diabetes, dementia/Alzheimer’s, history of cerebrovascular accident, psychiatric disease, cirrhosis, cancer, or alcohol abuse was not statistically significant.
The increased risk for VTE in trauma patients on contact isolation “is likely multifactorial in nature and is related but not limited to decreased ambulation, noncompliance with prophylaxis, and restricted access by staff,” said Dr. Ferguson, a third-year resident at the Virginia Tech, Roanoke.
The risk:benefit ratio of contact isolation in the trauma population needs to be reevaluated, the researchers concluded. “We encourage hospital committees to alter protocols and supplement strategies such as staff education, dedicated ambulation areas and/or isolation wards, and eliminate contact isolation following routine methicillin-resistant Staphylococcus aureus surveillance screening.”
Dr. Ferguson and his coauthors reported having no financial disclosures.
LAKE BUENA VISTA, FLA. – Trauma patients on contact isolation were nearly six times more likely to develop venous thromboembolism (VTE) as those who were not isolated, based on an analysis of 4,317 patients.
VTE occurred in 17.5% (44/251) of patients on contact isolation and 3.5% (141/4,066) of patients who were not isolated (P < .0001). Injury Severity Score (ISS), age, male gender, and obesity also were significantly associated with the risk of VTE.
The relationship between VTE risk and contact isolation remained significant after adjusting for gender, age, ISS, and comorbidities (odds ratio, 3.28; P < .0001), Dr. Robert Ferguson reported at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Odds ratios also were significantly elevated for obesity (OR, 2.35; P < .006), male gender (OR, 2.1; P < .0001), ISS (OR, 1.08; P < .0001), and age (OR, 1.02; P < .0001). The presence of diabetes, dementia/Alzheimer’s, history of cerebrovascular accident, psychiatric disease, cirrhosis, cancer, or alcohol abuse was not statistically significant.
The increased risk for VTE in trauma patients on contact isolation “is likely multifactorial in nature and is related but not limited to decreased ambulation, noncompliance with prophylaxis, and restricted access by staff,” said Dr. Ferguson, a third-year resident at the Virginia Tech, Roanoke.
The risk:benefit ratio of contact isolation in the trauma population needs to be reevaluated, the researchers concluded. “We encourage hospital committees to alter protocols and supplement strategies such as staff education, dedicated ambulation areas and/or isolation wards, and eliminate contact isolation following routine methicillin-resistant Staphylococcus aureus surveillance screening.”
Dr. Ferguson and his coauthors reported having no financial disclosures.
LAKE BUENA VISTA, FLA. – Trauma patients on contact isolation were nearly six times more likely to develop venous thromboembolism (VTE) as those who were not isolated, based on an analysis of 4,317 patients.
VTE occurred in 17.5% (44/251) of patients on contact isolation and 3.5% (141/4,066) of patients who were not isolated (P < .0001). Injury Severity Score (ISS), age, male gender, and obesity also were significantly associated with the risk of VTE.
The relationship between VTE risk and contact isolation remained significant after adjusting for gender, age, ISS, and comorbidities (odds ratio, 3.28; P < .0001), Dr. Robert Ferguson reported at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Odds ratios also were significantly elevated for obesity (OR, 2.35; P < .006), male gender (OR, 2.1; P < .0001), ISS (OR, 1.08; P < .0001), and age (OR, 1.02; P < .0001). The presence of diabetes, dementia/Alzheimer’s, history of cerebrovascular accident, psychiatric disease, cirrhosis, cancer, or alcohol abuse was not statistically significant.
The increased risk for VTE in trauma patients on contact isolation “is likely multifactorial in nature and is related but not limited to decreased ambulation, noncompliance with prophylaxis, and restricted access by staff,” said Dr. Ferguson, a third-year resident at the Virginia Tech, Roanoke.
The risk:benefit ratio of contact isolation in the trauma population needs to be reevaluated, the researchers concluded. “We encourage hospital committees to alter protocols and supplement strategies such as staff education, dedicated ambulation areas and/or isolation wards, and eliminate contact isolation following routine methicillin-resistant Staphylococcus aureus surveillance screening.”
Dr. Ferguson and his coauthors reported having no financial disclosures.
AT THE EAST SCIENTIFIC ASSEMBLY
Key clinical point: Trauma patients on contact isolation are significantly predisposed to develop VTE.
Major finding: VTE occurred in 17.5% of patients on contact isolation and 3.5% not isolated (P < .0001).
Data source: Retrospective analysis of 4,317 trauma patients.
Disclosures: Dr. Ferguson and his coauthors reported having no financial disclosures.
Certified ACS trauma centers move the dial on patient outcomes
LAKE BUENA VISTA, FLA. – Patients undergoing emergency general surgery appear to fare better if managed at a certified acute care surgery trauma center, a nationwide analysis suggests.
“Patients managed at acute care surgery trauma centers had lower complication rates, shorter hospital length of stay, and lower hospital costs,” lead study author Dr. Mazhar Khalil said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Several single-institution studies have reported improved patient outcomes and system efficiencies following the 2008 creation of the American Association for the Surgery of Trauma (AAST) Acute Care Surgery fellowship. The ACS model has been endorsed by several professional organizations including EAST and the American College of Surgeons, but national outcomes have never been studied.

Dr. Khalil and his colleagues conducted a 1-year retrospective analysis of 131,410 patients who underwent emergency general surgery in 2011 in the National Inpatient Sample (NIS) database. The NIS is the largest all-payer, in-patient database in the United States and represents a stratified sample of 20% of all hospital discharges including 4,121 hospitals across 44 states.
ICD-9 codes were used to identify emergency general surgery procedures, defined as appendectomy, cholecystectomy, hernia repair, and small and large bowel resections. A total of 75,930 patients (58%) were managed at non–trauma centers (NTC), 47,753 (36%) at trauma centers (TC), and 7,727 (6%) at acute care surgery trauma centers (ACS-TC). Weekend admission rates were constant across all three groups at about 24%, as were the types of procedures performed.
In-hospital complications occurred in 18.1% of patients managed at AAST-certified acute care surgery trauma centers versus 18.7% among those at non–trauma centers and 19.4% at trauma centers (P = .04), Dr. Khalil, an international trauma fellow at the University of Arizona in Tucson, reported.
Between-group differences reached statistical significance for urinary tract infections (6.5% vs. 6.8% vs. 7.2%; P = .02), but not for the other complications of pneumonia, surgical site infection, sepsis, or reoperation.
AAST-certified ACS-TC patients had significantly shorter hospital stays than NTC or TC patients (7.2 days vs. 7.9 days vs. 8.5 days; P = .04) and lower average hospital costs ($60,000 vs. $70,000 vs. $67,000; P = .03), he said.
There was no difference in mortality across the three groups (2.1% vs. 2.4% vs. 2.2%; P = .12).
In multivariable analysis adjusted for age, gender, race, Charlson comorbidity index, type of procedure, complications, and weekend admission, patients at AAST-certified ACS-TC centers had lower odds than those at trauma centers for in-hospital complications (Odds ratio, 0.95 vs. 1.1) and hospital length of stay (OR, 0.91 vs. 1.2). Again, mortality was similar (OR, 0.98 vs. 1.07), Dr. Khalil said.
“The AAST-verified acute care surgery model should be a potential component of trauma programs practicing emergency general surgery,” he concluded.
During a discussion of the paper, concerns were raised that the results would be viewed as an overarching judgment of acute care surgery and whether the investigators could be certain the trauma centers were appropriately classified and the surgeries performed by an ACS fellow. Without correct classification, the entire premise of the paper could be undermined, it was argued.
Trauma center status was determined using the location of the center as provided in the NIS and cross-referenced with the American College of Surgeons Trauma registry, Dr. Khalil said. It was not possible to identify the centers that practice the ACS model, but are not certified by AAST.
He went on to say, “All these studies do is set up a foundation for future prospective studies. They are not definitive, authoritative answers to say that this is better than that.”
Dr. Khalil and his coauthors reported having no financial disclosures.
LAKE BUENA VISTA, FLA. – Patients undergoing emergency general surgery appear to fare better if managed at a certified acute care surgery trauma center, a nationwide analysis suggests.
“Patients managed at acute care surgery trauma centers had lower complication rates, shorter hospital length of stay, and lower hospital costs,” lead study author Dr. Mazhar Khalil said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Several single-institution studies have reported improved patient outcomes and system efficiencies following the 2008 creation of the American Association for the Surgery of Trauma (AAST) Acute Care Surgery fellowship. The ACS model has been endorsed by several professional organizations including EAST and the American College of Surgeons, but national outcomes have never been studied.
Dr. Khalil and his colleagues conducted a 1-year retrospective analysis of 131,410 patients who underwent emergency general surgery in 2011 in the National Inpatient Sample (NIS) database. The NIS is the largest all-payer, in-patient database in the United States and represents a stratified sample of 20% of all hospital discharges including 4,121 hospitals across 44 states.
ICD-9 codes were used to identify emergency general surgery procedures, defined as appendectomy, cholecystectomy, hernia repair, and small and large bowel resections. A total of 75,930 patients (58%) were managed at non–trauma centers (NTC), 47,753 (36%) at trauma centers (TC), and 7,727 (6%) at acute care surgery trauma centers (ACS-TC). Weekend admission rates were constant across all three groups at about 24%, as were the types of procedures performed.
In-hospital complications occurred in 18.1% of patients managed at AAST-certified acute care surgery trauma centers versus 18.7% among those at non–trauma centers and 19.4% at trauma centers (P = .04), Dr. Khalil, an international trauma fellow at the University of Arizona in Tucson, reported.
Between-group differences reached statistical significance for urinary tract infections (6.5% vs. 6.8% vs. 7.2%; P = .02), but not for the other complications of pneumonia, surgical site infection, sepsis, or reoperation.
AAST-certified ACS-TC patients had significantly shorter hospital stays than NTC or TC patients (7.2 days vs. 7.9 days vs. 8.5 days; P = .04) and lower average hospital costs ($60,000 vs. $70,000 vs. $67,000; P = .03), he said.
There was no difference in mortality across the three groups (2.1% vs. 2.4% vs. 2.2%; P = .12).
In multivariable analysis adjusted for age, gender, race, Charlson comorbidity index, type of procedure, complications, and weekend admission, patients at AAST-certified ACS-TC centers had lower odds than those at trauma centers for in-hospital complications (Odds ratio, 0.95 vs. 1.1) and hospital length of stay (OR, 0.91 vs. 1.2). Again, mortality was similar (OR, 0.98 vs. 1.07), Dr. Khalil said.
“The AAST-verified acute care surgery model should be a potential component of trauma programs practicing emergency general surgery,” he concluded.
During a discussion of the paper, concerns were raised that the results would be viewed as an overarching judgment of acute care surgery and whether the investigators could be certain the trauma centers were appropriately classified and the surgeries performed by an ACS fellow. Without correct classification, the entire premise of the paper could be undermined, it was argued.
Trauma center status was determined using the location of the center as provided in the NIS and cross-referenced with the American College of Surgeons Trauma registry, Dr. Khalil said. It was not possible to identify the centers that practice the ACS model, but are not certified by AAST.
He went on to say, “All these studies do is set up a foundation for future prospective studies. They are not definitive, authoritative answers to say that this is better than that.”
Dr. Khalil and his coauthors reported having no financial disclosures.
LAKE BUENA VISTA, FLA. – Patients undergoing emergency general surgery appear to fare better if managed at a certified acute care surgery trauma center, a nationwide analysis suggests.
“Patients managed at acute care surgery trauma centers had lower complication rates, shorter hospital length of stay, and lower hospital costs,” lead study author Dr. Mazhar Khalil said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Several single-institution studies have reported improved patient outcomes and system efficiencies following the 2008 creation of the American Association for the Surgery of Trauma (AAST) Acute Care Surgery fellowship. The ACS model has been endorsed by several professional organizations including EAST and the American College of Surgeons, but national outcomes have never been studied.
Dr. Khalil and his colleagues conducted a 1-year retrospective analysis of 131,410 patients who underwent emergency general surgery in 2011 in the National Inpatient Sample (NIS) database. The NIS is the largest all-payer, in-patient database in the United States and represents a stratified sample of 20% of all hospital discharges including 4,121 hospitals across 44 states.
ICD-9 codes were used to identify emergency general surgery procedures, defined as appendectomy, cholecystectomy, hernia repair, and small and large bowel resections. A total of 75,930 patients (58%) were managed at non–trauma centers (NTC), 47,753 (36%) at trauma centers (TC), and 7,727 (6%) at acute care surgery trauma centers (ACS-TC). Weekend admission rates were constant across all three groups at about 24%, as were the types of procedures performed.
In-hospital complications occurred in 18.1% of patients managed at AAST-certified acute care surgery trauma centers versus 18.7% among those at non–trauma centers and 19.4% at trauma centers (P = .04), Dr. Khalil, an international trauma fellow at the University of Arizona in Tucson, reported.
Between-group differences reached statistical significance for urinary tract infections (6.5% vs. 6.8% vs. 7.2%; P = .02), but not for the other complications of pneumonia, surgical site infection, sepsis, or reoperation.
AAST-certified ACS-TC patients had significantly shorter hospital stays than NTC or TC patients (7.2 days vs. 7.9 days vs. 8.5 days; P = .04) and lower average hospital costs ($60,000 vs. $70,000 vs. $67,000; P = .03), he said.
There was no difference in mortality across the three groups (2.1% vs. 2.4% vs. 2.2%; P = .12).
In multivariable analysis adjusted for age, gender, race, Charlson comorbidity index, type of procedure, complications, and weekend admission, patients at AAST-certified ACS-TC centers had lower odds than those at trauma centers for in-hospital complications (Odds ratio, 0.95 vs. 1.1) and hospital length of stay (OR, 0.91 vs. 1.2). Again, mortality was similar (OR, 0.98 vs. 1.07), Dr. Khalil said.
“The AAST-verified acute care surgery model should be a potential component of trauma programs practicing emergency general surgery,” he concluded.
During a discussion of the paper, concerns were raised that the results would be viewed as an overarching judgment of acute care surgery and whether the investigators could be certain the trauma centers were appropriately classified and the surgeries performed by an ACS fellow. Without correct classification, the entire premise of the paper could be undermined, it was argued.
Trauma center status was determined using the location of the center as provided in the NIS and cross-referenced with the American College of Surgeons Trauma registry, Dr. Khalil said. It was not possible to identify the centers that practice the ACS model, but are not certified by AAST.
He went on to say, “All these studies do is set up a foundation for future prospective studies. They are not definitive, authoritative answers to say that this is better than that.”
Dr. Khalil and his coauthors reported having no financial disclosures.
AT THE EAST SCIENTIFIC ASSEMBLY
Key clinical point: Patients managed at certified acute care surgery trauma centers had fewer complications, shorter hospital stays, and lower hospital costs.
Major finding: In-hospital complications rates were lower in patients at ACS trauma centers than at non–trauma centers and trauma centers (18.1% vs. 18.7% vs. 19.4%; P =.04).
Data source: Retrospective analysis of 131,410 emergency general surgery patients.
Disclosures: Dr. Khalil and his coauthors reported having no financial disclosures.

Accurate ID of nonsalvageable trauma patients improves trauma center performance metrics
LAKE BUENA VISTA, FL – When does no sign of life mean a patient is unsalvageable?
A study has found that up to 33% of patients who local providers determined had no signs of life went on to live, and 10% of patients whose heart stopped before reaching the hospital actually survived.
Historically, there’s been significant variation across trauma centers and registries of how unsalvageable patients are identified. This presents a problem when measuring trauma center performance, particularly when you consider that 25% of deaths occur within 15 minutes of arrival at high-volume trauma centers, Dr. James P. Byrne, with the University of Toronto, explained.
“Variation within inclusion and exclusion criteria can lead to big differences in risk-adjusted trauma center mortality. Therefore, there’s a need for the adoption of a single-best definition for unsalvageable patients,” he said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
To that end, three case definitions of the unsalvageable patient were proposed based on data from the 2012-2013 American College of Surgeons Trauma Quality Improvement Program (ACS TQIP) database. They were no signs of life as determined by local providers (NSOL), prehospital cardiac arrest (PHCA) as entered into local trauma registries, and a PROXY for death established by the ACS TQIP and defined as an emergency department heart rate of 0 and an ED systolic blood pressure of 0 and a Glasgow Coma Scale motor component of 1.
Over the study period, 223,643 patients from 192 trauma centers met the inclusion criteria of at least 16 years of age, blunt or penetrating mechanism of injury, and known hospital discharge status. In-hospital mortality was 7.2%.
NSOL and PHCA, had positive predictive values low enough (66.58% and 89.71%) such that 33% and 10% of patients meeting these criteria went on to survive.
The PROXY had excellent predictive utility for death (PPV 99.09%), with just 0.9% of PROXY patients going on to survive (22/2,424), he said.
To test its validity, the investigators looked more closely at the 2,424 patients who met PROXY criteria (15% of all deaths). PROXY patients mostly fell into two distinct groups: severe multisystem blunt injury caused by motor vehicle collision (MVC) and penetrating trauma to the head or chest caused by firearm, Dr. Byrne said. The median time to death was 8 minutes, with 87% dying in the ED.
Among the 22 unexpected PROXY survivors, 77% had penetrating trauma. Most had isolated injuries to the heart, lung, or large blood vessels and underwent thoracotomy (71%) or open cardiac massage (35%).
“We feel these patients are adequately explained for the most part, even though they come in without vital signs, as patients that have some chance for survival with prompt hemorrhage control surgery or cardiac repair,” Dr. Byrne said.
PROXY patients with penetrating injury rather than blunt injury were more likely to be male (90% vs. 73%), younger (34 years vs. 44 years), and fall victim to firearms or stabbing than an MVC (88% & 12% vs. 59%).
Overall, patients with penetrating injury were 10 times more likely to meet PROXY criteria than those with blunt injury (5.7% vs. 0.6%; P < .001).
“The characteristics of the PROXY patients, as well as the significant association with penetrating trauma, is something that we know to be true for patients who die early from trauma,” Dr. Byrne said.
In contrast, the 13,659 patients who died without meeting PROXY criteria were older (mean age, 60 years), 72% had severe head injury from falls or MVC, and their median time to death was 52 hours.
“We feel these patients represent alternative trajectories to death that are not predicted by presenting characteristics,” he said. “This actually lends construct validity to the PROXY definition since it was able to isolate patients who died early, while excluding those patients who died later and might have a chance for a modifiable outcome.”
Finally, a hierarchical linear model that calculated risk-adjusted mortality was used to look at the influence of including nonsalvageable patients on trauma center performance. Based on the model, 36 trauma centers (19%) were below-average performers and 29 (15%) were above-average performers.
After excluding PROXY patients, 64% of trauma centers changed rank, 17% by three or more positions, but only two centers changed outlier status. The latter suggests that inclusion of unsalvageable PROXY patients would have a minor impact on risk-adjusted mortality used for peer-to-peer benchmarking. However, their inclusion could have a big impact on benchmarking at centers that receive unsalvageable patients more frequently and therefore, PROXY should be used to exclude them from registries, Dr. Byrne said.
Poster discussion comoderator Christopher J. Dente from Emory University in Atlanta, said the reason the PROXY model performs so well is that it is something that could easily translate from the bedside into a registry and from a registry to a national database, whereas measures like “no signs of life” have to translate from the field to the bedside to the registry and then TQIP.
“The same is true for prehospital cardiac arrest, which you’d think would be a little more tangible, but isn’t necessarily,” Dr. Dente said. “This is incredibly important work.”
Dr. Byrne and his coauthors reported having no financial disclosures.
Byrne et al.’s study evaluating three criteria for identifying unsalvageable trauma patients demonstrates the critical role that high-quality data can play in quality improvement efforts. Using data from the American College of Surgeons Trauma Quality Improvement Program (ACS TQIP), they developed a proxy measure that resulted in less than 1% of patients being incorrectly classified as unsalvageable.
Having an accurate, easy-to-calculate model for predicting survival is essential in applying these findings at the point of care, as the decision of whether or not to perform a resuscitative thoracotomy must be made expediently. An accurate model also allows resources to be concentrated on those who might derive the most benefit and minimizes the known harms, particularly to health care providers, and costs associated with resuscitative thoracotomies. Finally, an accurate model is necessary to ensure that benchmarking accurately reflects quality of care rather than case mix, and that efforts are appropriately directed toward those centers whose adjusted mortality is above expected, whether or not they are outliers.
Future efforts should be directed toward evaluating whether implementation of this proxy measure into clinical practice improves not just survival but survival with good functional status at a longer term end point.
Dr. Lillian S. Kao is an ACS Fellow and associate professor of surgery at the University of Texas Health Science Center at Houston.
Byrne et al.’s study evaluating three criteria for identifying unsalvageable trauma patients demonstrates the critical role that high-quality data can play in quality improvement efforts. Using data from the American College of Surgeons Trauma Quality Improvement Program (ACS TQIP), they developed a proxy measure that resulted in less than 1% of patients being incorrectly classified as unsalvageable.
Having an accurate, easy-to-calculate model for predicting survival is essential in applying these findings at the point of care, as the decision of whether or not to perform a resuscitative thoracotomy must be made expediently. An accurate model also allows resources to be concentrated on those who might derive the most benefit and minimizes the known harms, particularly to health care providers, and costs associated with resuscitative thoracotomies. Finally, an accurate model is necessary to ensure that benchmarking accurately reflects quality of care rather than case mix, and that efforts are appropriately directed toward those centers whose adjusted mortality is above expected, whether or not they are outliers.
Future efforts should be directed toward evaluating whether implementation of this proxy measure into clinical practice improves not just survival but survival with good functional status at a longer term end point.
Dr. Lillian S. Kao is an ACS Fellow and associate professor of surgery at the University of Texas Health Science Center at Houston.
Byrne et al.’s study evaluating three criteria for identifying unsalvageable trauma patients demonstrates the critical role that high-quality data can play in quality improvement efforts. Using data from the American College of Surgeons Trauma Quality Improvement Program (ACS TQIP), they developed a proxy measure that resulted in less than 1% of patients being incorrectly classified as unsalvageable.
Having an accurate, easy-to-calculate model for predicting survival is essential in applying these findings at the point of care, as the decision of whether or not to perform a resuscitative thoracotomy must be made expediently. An accurate model also allows resources to be concentrated on those who might derive the most benefit and minimizes the known harms, particularly to health care providers, and costs associated with resuscitative thoracotomies. Finally, an accurate model is necessary to ensure that benchmarking accurately reflects quality of care rather than case mix, and that efforts are appropriately directed toward those centers whose adjusted mortality is above expected, whether or not they are outliers.
Future efforts should be directed toward evaluating whether implementation of this proxy measure into clinical practice improves not just survival but survival with good functional status at a longer term end point.
Dr. Lillian S. Kao is an ACS Fellow and associate professor of surgery at the University of Texas Health Science Center at Houston.
LAKE BUENA VISTA, FL – When does no sign of life mean a patient is unsalvageable?
A study has found that up to 33% of patients who local providers determined had no signs of life went on to live, and 10% of patients whose heart stopped before reaching the hospital actually survived.
Historically, there’s been significant variation across trauma centers and registries of how unsalvageable patients are identified. This presents a problem when measuring trauma center performance, particularly when you consider that 25% of deaths occur within 15 minutes of arrival at high-volume trauma centers, Dr. James P. Byrne, with the University of Toronto, explained.
“Variation within inclusion and exclusion criteria can lead to big differences in risk-adjusted trauma center mortality. Therefore, there’s a need for the adoption of a single-best definition for unsalvageable patients,” he said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
To that end, three case definitions of the unsalvageable patient were proposed based on data from the 2012-2013 American College of Surgeons Trauma Quality Improvement Program (ACS TQIP) database. They were no signs of life as determined by local providers (NSOL), prehospital cardiac arrest (PHCA) as entered into local trauma registries, and a PROXY for death established by the ACS TQIP and defined as an emergency department heart rate of 0 and an ED systolic blood pressure of 0 and a Glasgow Coma Scale motor component of 1.
Over the study period, 223,643 patients from 192 trauma centers met the inclusion criteria of at least 16 years of age, blunt or penetrating mechanism of injury, and known hospital discharge status. In-hospital mortality was 7.2%.
NSOL and PHCA, had positive predictive values low enough (66.58% and 89.71%) such that 33% and 10% of patients meeting these criteria went on to survive.
The PROXY had excellent predictive utility for death (PPV 99.09%), with just 0.9% of PROXY patients going on to survive (22/2,424), he said.
To test its validity, the investigators looked more closely at the 2,424 patients who met PROXY criteria (15% of all deaths). PROXY patients mostly fell into two distinct groups: severe multisystem blunt injury caused by motor vehicle collision (MVC) and penetrating trauma to the head or chest caused by firearm, Dr. Byrne said. The median time to death was 8 minutes, with 87% dying in the ED.
Among the 22 unexpected PROXY survivors, 77% had penetrating trauma. Most had isolated injuries to the heart, lung, or large blood vessels and underwent thoracotomy (71%) or open cardiac massage (35%).
“We feel these patients are adequately explained for the most part, even though they come in without vital signs, as patients that have some chance for survival with prompt hemorrhage control surgery or cardiac repair,” Dr. Byrne said.
PROXY patients with penetrating injury rather than blunt injury were more likely to be male (90% vs. 73%), younger (34 years vs. 44 years), and fall victim to firearms or stabbing than an MVC (88% & 12% vs. 59%).
Overall, patients with penetrating injury were 10 times more likely to meet PROXY criteria than those with blunt injury (5.7% vs. 0.6%; P < .001).
“The characteristics of the PROXY patients, as well as the significant association with penetrating trauma, is something that we know to be true for patients who die early from trauma,” Dr. Byrne said.
In contrast, the 13,659 patients who died without meeting PROXY criteria were older (mean age, 60 years), 72% had severe head injury from falls or MVC, and their median time to death was 52 hours.
“We feel these patients represent alternative trajectories to death that are not predicted by presenting characteristics,” he said. “This actually lends construct validity to the PROXY definition since it was able to isolate patients who died early, while excluding those patients who died later and might have a chance for a modifiable outcome.”
Finally, a hierarchical linear model that calculated risk-adjusted mortality was used to look at the influence of including nonsalvageable patients on trauma center performance. Based on the model, 36 trauma centers (19%) were below-average performers and 29 (15%) were above-average performers.
After excluding PROXY patients, 64% of trauma centers changed rank, 17% by three or more positions, but only two centers changed outlier status. The latter suggests that inclusion of unsalvageable PROXY patients would have a minor impact on risk-adjusted mortality used for peer-to-peer benchmarking. However, their inclusion could have a big impact on benchmarking at centers that receive unsalvageable patients more frequently and therefore, PROXY should be used to exclude them from registries, Dr. Byrne said.
Poster discussion comoderator Christopher J. Dente from Emory University in Atlanta, said the reason the PROXY model performs so well is that it is something that could easily translate from the bedside into a registry and from a registry to a national database, whereas measures like “no signs of life” have to translate from the field to the bedside to the registry and then TQIP.
“The same is true for prehospital cardiac arrest, which you’d think would be a little more tangible, but isn’t necessarily,” Dr. Dente said. “This is incredibly important work.”
Dr. Byrne and his coauthors reported having no financial disclosures.
LAKE BUENA VISTA, FL – When does no sign of life mean a patient is unsalvageable?
A study has found that up to 33% of patients who local providers determined had no signs of life went on to live, and 10% of patients whose heart stopped before reaching the hospital actually survived.
Historically, there’s been significant variation across trauma centers and registries of how unsalvageable patients are identified. This presents a problem when measuring trauma center performance, particularly when you consider that 25% of deaths occur within 15 minutes of arrival at high-volume trauma centers, Dr. James P. Byrne, with the University of Toronto, explained.
“Variation within inclusion and exclusion criteria can lead to big differences in risk-adjusted trauma center mortality. Therefore, there’s a need for the adoption of a single-best definition for unsalvageable patients,” he said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
To that end, three case definitions of the unsalvageable patient were proposed based on data from the 2012-2013 American College of Surgeons Trauma Quality Improvement Program (ACS TQIP) database. They were no signs of life as determined by local providers (NSOL), prehospital cardiac arrest (PHCA) as entered into local trauma registries, and a PROXY for death established by the ACS TQIP and defined as an emergency department heart rate of 0 and an ED systolic blood pressure of 0 and a Glasgow Coma Scale motor component of 1.
Over the study period, 223,643 patients from 192 trauma centers met the inclusion criteria of at least 16 years of age, blunt or penetrating mechanism of injury, and known hospital discharge status. In-hospital mortality was 7.2%.
NSOL and PHCA, had positive predictive values low enough (66.58% and 89.71%) such that 33% and 10% of patients meeting these criteria went on to survive.
The PROXY had excellent predictive utility for death (PPV 99.09%), with just 0.9% of PROXY patients going on to survive (22/2,424), he said.
To test its validity, the investigators looked more closely at the 2,424 patients who met PROXY criteria (15% of all deaths). PROXY patients mostly fell into two distinct groups: severe multisystem blunt injury caused by motor vehicle collision (MVC) and penetrating trauma to the head or chest caused by firearm, Dr. Byrne said. The median time to death was 8 minutes, with 87% dying in the ED.
Among the 22 unexpected PROXY survivors, 77% had penetrating trauma. Most had isolated injuries to the heart, lung, or large blood vessels and underwent thoracotomy (71%) or open cardiac massage (35%).
“We feel these patients are adequately explained for the most part, even though they come in without vital signs, as patients that have some chance for survival with prompt hemorrhage control surgery or cardiac repair,” Dr. Byrne said.
PROXY patients with penetrating injury rather than blunt injury were more likely to be male (90% vs. 73%), younger (34 years vs. 44 years), and fall victim to firearms or stabbing than an MVC (88% & 12% vs. 59%).
Overall, patients with penetrating injury were 10 times more likely to meet PROXY criteria than those with blunt injury (5.7% vs. 0.6%; P < .001).
“The characteristics of the PROXY patients, as well as the significant association with penetrating trauma, is something that we know to be true for patients who die early from trauma,” Dr. Byrne said.
In contrast, the 13,659 patients who died without meeting PROXY criteria were older (mean age, 60 years), 72% had severe head injury from falls or MVC, and their median time to death was 52 hours.
“We feel these patients represent alternative trajectories to death that are not predicted by presenting characteristics,” he said. “This actually lends construct validity to the PROXY definition since it was able to isolate patients who died early, while excluding those patients who died later and might have a chance for a modifiable outcome.”
Finally, a hierarchical linear model that calculated risk-adjusted mortality was used to look at the influence of including nonsalvageable patients on trauma center performance. Based on the model, 36 trauma centers (19%) were below-average performers and 29 (15%) were above-average performers.
After excluding PROXY patients, 64% of trauma centers changed rank, 17% by three or more positions, but only two centers changed outlier status. The latter suggests that inclusion of unsalvageable PROXY patients would have a minor impact on risk-adjusted mortality used for peer-to-peer benchmarking. However, their inclusion could have a big impact on benchmarking at centers that receive unsalvageable patients more frequently and therefore, PROXY should be used to exclude them from registries, Dr. Byrne said.
Poster discussion comoderator Christopher J. Dente from Emory University in Atlanta, said the reason the PROXY model performs so well is that it is something that could easily translate from the bedside into a registry and from a registry to a national database, whereas measures like “no signs of life” have to translate from the field to the bedside to the registry and then TQIP.
“The same is true for prehospital cardiac arrest, which you’d think would be a little more tangible, but isn’t necessarily,” Dr. Dente said. “This is incredibly important work.”
Dr. Byrne and his coauthors reported having no financial disclosures.
AT THE EAST SCIENTIFIC ASSEMBLY 2015
Key clinical point: The ACS TQIP proxy definition of DOA should be used to exclude unsalvageable patients from peer-to-peer benchmarking and performance improvement efforts.
Major finding: Just 0.9% of patients identified as being unsalvageable by the PROXY criteria went on to survive.
Data source: Retrospective analysis of 223,643 trauma patients in the ACS TQIP database.
Disclosures: Dr. Byrne and his coauthors reported having no financial disclosures.
Feds: ACA enrollment extended for some
The federal government has extended the deadline to sign up for health insurance coverage through the federal marketplace for those last-minute enrollees who encountered difficulties.
According to a notice posted Feb. 16 at www.HealthCare.gov, the Health and Human Services Department has made an exception for people who have one of the following scenarios: They tried to meet the Feb. 15 deadline but did not complete enrollment because of higher-than-normal wait times at the Marketplace Call Center during Feb. 13-15, or they encountered technical issues with the marketplace website.
During the Valentine’s Day weekend – the last weekend for enrollment – technical issues prevented some users from having their income verified and any potential subsidies calculated.
For affected individuals, the deadline for enrollment is now Feb. 22.
At least 28 states have at least one plan accepting enrollees past the Feb. 15 deadline, some as far as Feb. 28.
The federal government has extended the deadline to sign up for health insurance coverage through the federal marketplace for those last-minute enrollees who encountered difficulties.
According to a notice posted Feb. 16 at www.HealthCare.gov, the Health and Human Services Department has made an exception for people who have one of the following scenarios: They tried to meet the Feb. 15 deadline but did not complete enrollment because of higher-than-normal wait times at the Marketplace Call Center during Feb. 13-15, or they encountered technical issues with the marketplace website.
During the Valentine’s Day weekend – the last weekend for enrollment – technical issues prevented some users from having their income verified and any potential subsidies calculated.
For affected individuals, the deadline for enrollment is now Feb. 22.
At least 28 states have at least one plan accepting enrollees past the Feb. 15 deadline, some as far as Feb. 28.
The federal government has extended the deadline to sign up for health insurance coverage through the federal marketplace for those last-minute enrollees who encountered difficulties.
According to a notice posted Feb. 16 at www.HealthCare.gov, the Health and Human Services Department has made an exception for people who have one of the following scenarios: They tried to meet the Feb. 15 deadline but did not complete enrollment because of higher-than-normal wait times at the Marketplace Call Center during Feb. 13-15, or they encountered technical issues with the marketplace website.
During the Valentine’s Day weekend – the last weekend for enrollment – technical issues prevented some users from having their income verified and any potential subsidies calculated.
For affected individuals, the deadline for enrollment is now Feb. 22.
At least 28 states have at least one plan accepting enrollees past the Feb. 15 deadline, some as far as Feb. 28.
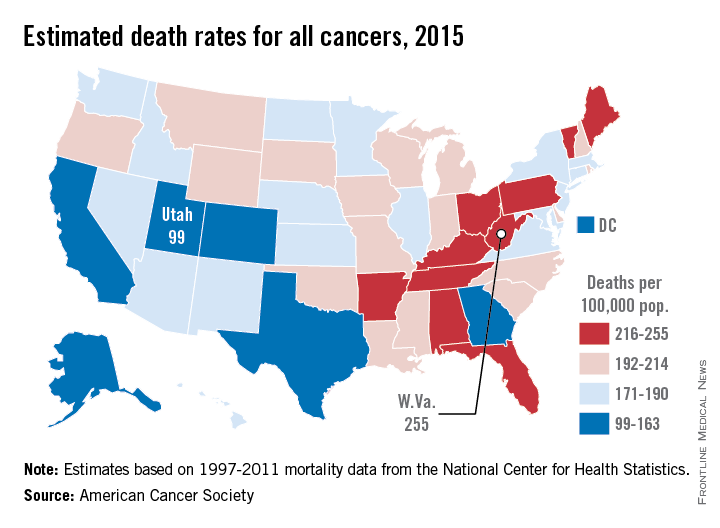
Cancer mortality lowest in western United States
Utah will have the lowest cancer mortality rate in the United States in 2015, according to a report from the American Cancer Society.
While 11 states are predicted to have fewer cancer-related deaths in 2015 than 2014, the mortality rate will be lowest in Utah, with just 99 deaths per 100,000 people. Alaska and Colorado will have the next lowest mortality rates at 141 and 142 per 100,000 people, respectively. West Virginia is estimated to have the highest cancer mortality rate at 255 per 100,000 people, followed by Kentucky and Arkansas at 231 and 228, respectively. The national cancer mortality rate will be 185 per 100,000.
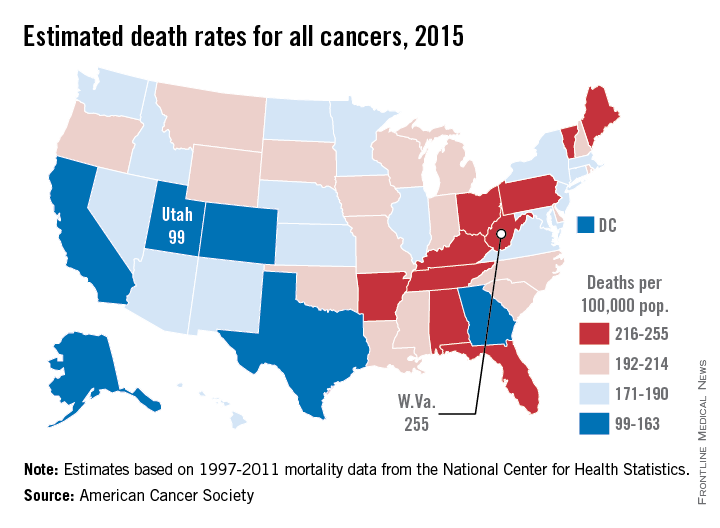
There will be about 1.66 million new cases of cancer in 2015 and about 590,000 deaths. Female breast cancer will probably be the most common with 231,000 new cases, but with an estimated 221,000 new cases each, lung/bronchus and prostate cancer also will rank high. Lung and bronchus cancer will be the most common cause of death, with 158,000 deaths predicted in 2015, more than a quarter of overall cancer deaths, according to the ACS.
Socioeconomic status makes a big difference in both cancer incidence and mortality. Cancer can stem from a higher likelihood to engage in risky behavior such as smoking, an unhealthy diet, or a sedentary lifestyle. Demographics matter more than ethnicity for cancer mortality, as “cancer mortality rates among both black and non-Hispanic white men with 12 or fewer years of education are almost 3 times higher than those of college graduates for all cancers combined and 4-5 times higher for lung cancer,” the ACS said.
Estimated data were based on 1995-2011 cancer incidence rates collected by the National Center for Health Statistics and the ACS.
Utah will have the lowest cancer mortality rate in the United States in 2015, according to a report from the American Cancer Society.
While 11 states are predicted to have fewer cancer-related deaths in 2015 than 2014, the mortality rate will be lowest in Utah, with just 99 deaths per 100,000 people. Alaska and Colorado will have the next lowest mortality rates at 141 and 142 per 100,000 people, respectively. West Virginia is estimated to have the highest cancer mortality rate at 255 per 100,000 people, followed by Kentucky and Arkansas at 231 and 228, respectively. The national cancer mortality rate will be 185 per 100,000.
There will be about 1.66 million new cases of cancer in 2015 and about 590,000 deaths. Female breast cancer will probably be the most common with 231,000 new cases, but with an estimated 221,000 new cases each, lung/bronchus and prostate cancer also will rank high. Lung and bronchus cancer will be the most common cause of death, with 158,000 deaths predicted in 2015, more than a quarter of overall cancer deaths, according to the ACS.
Socioeconomic status makes a big difference in both cancer incidence and mortality. Cancer can stem from a higher likelihood to engage in risky behavior such as smoking, an unhealthy diet, or a sedentary lifestyle. Demographics matter more than ethnicity for cancer mortality, as “cancer mortality rates among both black and non-Hispanic white men with 12 or fewer years of education are almost 3 times higher than those of college graduates for all cancers combined and 4-5 times higher for lung cancer,” the ACS said.
Estimated data were based on 1995-2011 cancer incidence rates collected by the National Center for Health Statistics and the ACS.
Utah will have the lowest cancer mortality rate in the United States in 2015, according to a report from the American Cancer Society.
While 11 states are predicted to have fewer cancer-related deaths in 2015 than 2014, the mortality rate will be lowest in Utah, with just 99 deaths per 100,000 people. Alaska and Colorado will have the next lowest mortality rates at 141 and 142 per 100,000 people, respectively. West Virginia is estimated to have the highest cancer mortality rate at 255 per 100,000 people, followed by Kentucky and Arkansas at 231 and 228, respectively. The national cancer mortality rate will be 185 per 100,000.
There will be about 1.66 million new cases of cancer in 2015 and about 590,000 deaths. Female breast cancer will probably be the most common with 231,000 new cases, but with an estimated 221,000 new cases each, lung/bronchus and prostate cancer also will rank high. Lung and bronchus cancer will be the most common cause of death, with 158,000 deaths predicted in 2015, more than a quarter of overall cancer deaths, according to the ACS.
Socioeconomic status makes a big difference in both cancer incidence and mortality. Cancer can stem from a higher likelihood to engage in risky behavior such as smoking, an unhealthy diet, or a sedentary lifestyle. Demographics matter more than ethnicity for cancer mortality, as “cancer mortality rates among both black and non-Hispanic white men with 12 or fewer years of education are almost 3 times higher than those of college graduates for all cancers combined and 4-5 times higher for lung cancer,” the ACS said.
Estimated data were based on 1995-2011 cancer incidence rates collected by the National Center for Health Statistics and the ACS.
New scoring system for small bowel–obstruction severity
LAKE BUENA VISTA, FLA. – A novel three-item scoring system reliably categorizes severity of small bowel obstruction and is more strongly associated with in-hospital mortality than the American Association for the Surgery of Trauma anatomic score alone.
The AAST developed a scoring system to standardize the severity of small-bowel obstruction (SBO) based on anatomic criteria. Its authors have subsequently recommended, however, that other parametersare needed that would take into consideration the entirety of the patient’s clinical situation (J. Trauma Acute Care Surg. 2014;77:705-8 and J. Trauma Acute Care Surg. 2014;76:884-7).

To that end, investigators at the Mayo Clinic in Rochester, Minn., created the Acute General Emergency Surgical Severity-Small Bowel Obstruction (AGESS-SBO) system that incorporates presenting physiology and pre-existing comorbidities with anatomic criteria.
“It’s evident that the complications and patient outcomes clearly depend on the extent of the involvement of the diseased organ, but also depend on the hosting environment, which means the patient’s physiology and pre-existing conditions,” Dr. Yaser Baghdadi explained at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
He reported a cohort study involving 377 patients who were treated for SBO at the Mayo Clinic between 2009 and 2012 and evaluated using anatomic criteria and the AGESS-SBO, which uses a 5-point scoring system for each of its three scales.
Most patients (57%) received a score of 1 on the AGESS-SBO anatomic involvement scale for a partial SBO without need of operation, while only 1% had a score of 5, indicating strangulation and perforation with diffuse peritoneal contamination.
On the physiology scale, 58.6% had no physiologic derangement or a score of 0, 36% had a score of 1 because of systemic inflammatory response syndrome, and only 1.1% had a score of 5 for multiple organ dysfunction syndrome.
A Charlson comorbid score of 1 or 2 earned 32% of patients 1 point on the comorbidity scale, while 4% had a score of 5 because of a Charlson score of 9 or more.
In all, 215 patients (57%) had nonoperative treatment and 162 patients (43%) underwent surgical exploration. The median overall AGESS-SBO score was 6 points (interquartile range [IQR], 3-13 points).
The median length of stay (LOS) was 5 days (IQR, 3-9.5 days), with 94 patients (25%) having a stay exceeding 9.5 days, Dr. Baghdadi said in the poster presentation. In-hospital complications occurred in 82 patients (22%) and eight patients (2%) died during their hospital stay.
Comparison of the areas under receiver operative characteristic curves revealed a statistically significant greater association between the AGESS-SBO score and in-hospital mortality than the AAST anatomic score (AUC, 0.79 vs. 0.55, P value = .015), reported Dr. Baghdadi, a research fellow in the Mayo Clinic’s trauma division.
The two scoring systems had comparable ability to predict in-hospital complications (AUC, 0.72 vs. 0.69; P = .42) and extended LOS (AUC, 0.72 vs. 0.74; P = .47). The lack of statistical significance favoring the AGESS-SBO may be because these outcomes would be more likely in patients requiring surgery and the analysis combined patients who did and did not require operative care, he said in an interview.
“The AGESS-SBO system is a useful tool to classify the disease severity among SBO patients compared to the AAST anatomic score alone. We are planning to run a prospective study to validate what we have found,” he added.
Dr. Baghdadi and his coauthors reported having no financial disclosures.
LAKE BUENA VISTA, FLA. – A novel three-item scoring system reliably categorizes severity of small bowel obstruction and is more strongly associated with in-hospital mortality than the American Association for the Surgery of Trauma anatomic score alone.
The AAST developed a scoring system to standardize the severity of small-bowel obstruction (SBO) based on anatomic criteria. Its authors have subsequently recommended, however, that other parametersare needed that would take into consideration the entirety of the patient’s clinical situation (J. Trauma Acute Care Surg. 2014;77:705-8 and J. Trauma Acute Care Surg. 2014;76:884-7).
To that end, investigators at the Mayo Clinic in Rochester, Minn., created the Acute General Emergency Surgical Severity-Small Bowel Obstruction (AGESS-SBO) system that incorporates presenting physiology and pre-existing comorbidities with anatomic criteria.
“It’s evident that the complications and patient outcomes clearly depend on the extent of the involvement of the diseased organ, but also depend on the hosting environment, which means the patient’s physiology and pre-existing conditions,” Dr. Yaser Baghdadi explained at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
He reported a cohort study involving 377 patients who were treated for SBO at the Mayo Clinic between 2009 and 2012 and evaluated using anatomic criteria and the AGESS-SBO, which uses a 5-point scoring system for each of its three scales.
Most patients (57%) received a score of 1 on the AGESS-SBO anatomic involvement scale for a partial SBO without need of operation, while only 1% had a score of 5, indicating strangulation and perforation with diffuse peritoneal contamination.
On the physiology scale, 58.6% had no physiologic derangement or a score of 0, 36% had a score of 1 because of systemic inflammatory response syndrome, and only 1.1% had a score of 5 for multiple organ dysfunction syndrome.
A Charlson comorbid score of 1 or 2 earned 32% of patients 1 point on the comorbidity scale, while 4% had a score of 5 because of a Charlson score of 9 or more.
In all, 215 patients (57%) had nonoperative treatment and 162 patients (43%) underwent surgical exploration. The median overall AGESS-SBO score was 6 points (interquartile range [IQR], 3-13 points).
The median length of stay (LOS) was 5 days (IQR, 3-9.5 days), with 94 patients (25%) having a stay exceeding 9.5 days, Dr. Baghdadi said in the poster presentation. In-hospital complications occurred in 82 patients (22%) and eight patients (2%) died during their hospital stay.
Comparison of the areas under receiver operative characteristic curves revealed a statistically significant greater association between the AGESS-SBO score and in-hospital mortality than the AAST anatomic score (AUC, 0.79 vs. 0.55, P value = .015), reported Dr. Baghdadi, a research fellow in the Mayo Clinic’s trauma division.
The two scoring systems had comparable ability to predict in-hospital complications (AUC, 0.72 vs. 0.69; P = .42) and extended LOS (AUC, 0.72 vs. 0.74; P = .47). The lack of statistical significance favoring the AGESS-SBO may be because these outcomes would be more likely in patients requiring surgery and the analysis combined patients who did and did not require operative care, he said in an interview.
“The AGESS-SBO system is a useful tool to classify the disease severity among SBO patients compared to the AAST anatomic score alone. We are planning to run a prospective study to validate what we have found,” he added.
Dr. Baghdadi and his coauthors reported having no financial disclosures.
LAKE BUENA VISTA, FLA. – A novel three-item scoring system reliably categorizes severity of small bowel obstruction and is more strongly associated with in-hospital mortality than the American Association for the Surgery of Trauma anatomic score alone.
The AAST developed a scoring system to standardize the severity of small-bowel obstruction (SBO) based on anatomic criteria. Its authors have subsequently recommended, however, that other parametersare needed that would take into consideration the entirety of the patient’s clinical situation (J. Trauma Acute Care Surg. 2014;77:705-8 and J. Trauma Acute Care Surg. 2014;76:884-7).
To that end, investigators at the Mayo Clinic in Rochester, Minn., created the Acute General Emergency Surgical Severity-Small Bowel Obstruction (AGESS-SBO) system that incorporates presenting physiology and pre-existing comorbidities with anatomic criteria.
“It’s evident that the complications and patient outcomes clearly depend on the extent of the involvement of the diseased organ, but also depend on the hosting environment, which means the patient’s physiology and pre-existing conditions,” Dr. Yaser Baghdadi explained at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
He reported a cohort study involving 377 patients who were treated for SBO at the Mayo Clinic between 2009 and 2012 and evaluated using anatomic criteria and the AGESS-SBO, which uses a 5-point scoring system for each of its three scales.
Most patients (57%) received a score of 1 on the AGESS-SBO anatomic involvement scale for a partial SBO without need of operation, while only 1% had a score of 5, indicating strangulation and perforation with diffuse peritoneal contamination.
On the physiology scale, 58.6% had no physiologic derangement or a score of 0, 36% had a score of 1 because of systemic inflammatory response syndrome, and only 1.1% had a score of 5 for multiple organ dysfunction syndrome.
A Charlson comorbid score of 1 or 2 earned 32% of patients 1 point on the comorbidity scale, while 4% had a score of 5 because of a Charlson score of 9 or more.
In all, 215 patients (57%) had nonoperative treatment and 162 patients (43%) underwent surgical exploration. The median overall AGESS-SBO score was 6 points (interquartile range [IQR], 3-13 points).
The median length of stay (LOS) was 5 days (IQR, 3-9.5 days), with 94 patients (25%) having a stay exceeding 9.5 days, Dr. Baghdadi said in the poster presentation. In-hospital complications occurred in 82 patients (22%) and eight patients (2%) died during their hospital stay.
Comparison of the areas under receiver operative characteristic curves revealed a statistically significant greater association between the AGESS-SBO score and in-hospital mortality than the AAST anatomic score (AUC, 0.79 vs. 0.55, P value = .015), reported Dr. Baghdadi, a research fellow in the Mayo Clinic’s trauma division.
The two scoring systems had comparable ability to predict in-hospital complications (AUC, 0.72 vs. 0.69; P = .42) and extended LOS (AUC, 0.72 vs. 0.74; P = .47). The lack of statistical significance favoring the AGESS-SBO may be because these outcomes would be more likely in patients requiring surgery and the analysis combined patients who did and did not require operative care, he said in an interview.
“The AGESS-SBO system is a useful tool to classify the disease severity among SBO patients compared to the AAST anatomic score alone. We are planning to run a prospective study to validate what we have found,” he added.
Dr. Baghdadi and his coauthors reported having no financial disclosures.
AT THE EAST SCIENTIFIC ASSEMBLY
Key clinical point: Adding presenting physiology and comorbidities to anatomic criteria provides a reliable tool to categorize severity of small-bowel obstruction.
Major finding: The AGESS-SBO score was significantly associated with in-hospital mortality, versus the AAST anatomic score (area under ROC curves: 0.79 vs. 0.55; P = .015).
Data source: A cohort study of 377 patients treated for small-bowel obstruction.
Disclosures: Dr. Baghdadi and his coauthors reported having no financial disclosures.
Base deficit and lactate vary with resuscitation fluid type
LAKE BUENA VISTA, FLA. – Base deficit and lactate after resuscitation were measurably different based on the type of crystalloid solution used in a class I hemorrhage model.
Further, an award-winning prospective study found that, compared with lactated Ringer’s or no intravenous fluid, normal saline results in significantly higher postresuscitation sodium and chloride levels and significantly lower ionized calcium and bicarbonate.
Taken together, these derangements are important because blood gases are one of the first objective measurements performed in acute trauma patients, Dr. Samuel Wade Ross said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).

“We might actually be overestimating the amount of shock due specifically to the iatrogenic cause of crystalloid solutions,” he said. “Additionally, this goes beyond just trauma because all medicine – surgery, anesthesia, and critical care – use crystalloid. And it should be in the back of our minds when using normal saline that this contributes to acidosis and that lactated Ringer’s can falsely elevate lactate levels.”
The analysis involved 157 voluntary blood donors, who donated 0.5 L and were then randomly assigned to normal saline, lactated Ringer’s (LR), or no IV fluid. The percentage of total blood volume lost was about 11%, which is consistent with a class I hemorrhage model, said Dr. Ross of the Carolinas Medical Center in Charlotte, N.C.
Base deficit, which is used to guide the volume of fluid needed for trauma patients’ resuscitation, was similar before administration of normal saline, lactated Ringer’s, or no IV fluid (–0.24 vs. 0.33 vs. 0.04).
After fluid administration, however, the normal saline group had almost five times the base deficit of the no IV fluid group (–3.06 vs. –0.65) and almost 10 times the base deficit of the LR group (–3.06 vs. –0.34). The differences were statistically significant, even using a conservative statistical correction with a P value cutoff of 0.0167, he said.
Preresuscitation lactate levels also were similar in the LR, normal saline, and no IV groups (1.05 mmol/L vs. 1.12 mmol/L vs. 1.10 mmol/L).
Postresuscitation, however, lactate increased by roughly 50% in the LR group vs. the normal saline group (1.54 mmol/L vs. 1.0 mmol/L) and was elevated compared with no IV fluid (1.54 mmol/L vs. 1.36 mmol/L). Both findings were statistically significant (P < .0167).
This is the first time these differences have been quantified and runs contrary to the dogma that serum lactate does not increase with the use of LR because of enzymatic clearance of the molecule in the liver, said Dr. Ross, the EAST 2015 Raymond Alexander Residents Paper Competition winner.
“With ongoing shock, lactate rises and clinicians use that as a guide for further fluid resuscitation. Thus, lactate levels could be falsely elevated with LR use, and drive further decisions for unnecessary and potentially harmful additional resuscitation and procedures,” he said in an interview.
As noted above, use of normal saline rather than LR or no IV fluid resulted in significantly higher postresuscitation sodium (141.7 mmol/L vs. 139.8 mmol/L vs. 139.8 mmol/L) and chloride (107.3 mmol/L vs. 102.3 mmol/L vs. 102.9 mmol/L), and significantly lower ionized calcium (1.15 vs. 1.22 vs. 1.24), pH (7.32 vs. 7.34 vs. 7.36), and bicarbonate (23 mmol/L vs. 25.3 mmol/L vs. 24.6 mmol/L; all P values < .001).
“The two recommended isotonic crystalloid fluids used for hemorrhagic and other forms of shock – normal saline and lactated Ringer’s – have been in use since the 19th century and early 20th century,” senior author Dr. Ronald F. Sing said in an interview. “Despite the tremendous advances in shock and resuscitation, we have identified, and actually confirmed, potentially confounding factors related to both LR and [normal saline] for resuscitation. Our next goal is to examine other crystalloid solutions and their impacts not only on shock markers, but inflammatory markers,” he added.
Future studies also will use animal models to look at class II-IV hemorrhage and increased follow-up time.
The study was supported by the Carolinas Trauma Network. Dr. Ross and his coauthors reported having no financial disclosures.
LAKE BUENA VISTA, FLA. – Base deficit and lactate after resuscitation were measurably different based on the type of crystalloid solution used in a class I hemorrhage model.
Further, an award-winning prospective study found that, compared with lactated Ringer’s or no intravenous fluid, normal saline results in significantly higher postresuscitation sodium and chloride levels and significantly lower ionized calcium and bicarbonate.
Taken together, these derangements are important because blood gases are one of the first objective measurements performed in acute trauma patients, Dr. Samuel Wade Ross said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
“We might actually be overestimating the amount of shock due specifically to the iatrogenic cause of crystalloid solutions,” he said. “Additionally, this goes beyond just trauma because all medicine – surgery, anesthesia, and critical care – use crystalloid. And it should be in the back of our minds when using normal saline that this contributes to acidosis and that lactated Ringer’s can falsely elevate lactate levels.”
The analysis involved 157 voluntary blood donors, who donated 0.5 L and were then randomly assigned to normal saline, lactated Ringer’s (LR), or no IV fluid. The percentage of total blood volume lost was about 11%, which is consistent with a class I hemorrhage model, said Dr. Ross of the Carolinas Medical Center in Charlotte, N.C.
Base deficit, which is used to guide the volume of fluid needed for trauma patients’ resuscitation, was similar before administration of normal saline, lactated Ringer’s, or no IV fluid (–0.24 vs. 0.33 vs. 0.04).
After fluid administration, however, the normal saline group had almost five times the base deficit of the no IV fluid group (–3.06 vs. –0.65) and almost 10 times the base deficit of the LR group (–3.06 vs. –0.34). The differences were statistically significant, even using a conservative statistical correction with a P value cutoff of 0.0167, he said.
Preresuscitation lactate levels also were similar in the LR, normal saline, and no IV groups (1.05 mmol/L vs. 1.12 mmol/L vs. 1.10 mmol/L).
Postresuscitation, however, lactate increased by roughly 50% in the LR group vs. the normal saline group (1.54 mmol/L vs. 1.0 mmol/L) and was elevated compared with no IV fluid (1.54 mmol/L vs. 1.36 mmol/L). Both findings were statistically significant (P < .0167).
This is the first time these differences have been quantified and runs contrary to the dogma that serum lactate does not increase with the use of LR because of enzymatic clearance of the molecule in the liver, said Dr. Ross, the EAST 2015 Raymond Alexander Residents Paper Competition winner.
“With ongoing shock, lactate rises and clinicians use that as a guide for further fluid resuscitation. Thus, lactate levels could be falsely elevated with LR use, and drive further decisions for unnecessary and potentially harmful additional resuscitation and procedures,” he said in an interview.
As noted above, use of normal saline rather than LR or no IV fluid resulted in significantly higher postresuscitation sodium (141.7 mmol/L vs. 139.8 mmol/L vs. 139.8 mmol/L) and chloride (107.3 mmol/L vs. 102.3 mmol/L vs. 102.9 mmol/L), and significantly lower ionized calcium (1.15 vs. 1.22 vs. 1.24), pH (7.32 vs. 7.34 vs. 7.36), and bicarbonate (23 mmol/L vs. 25.3 mmol/L vs. 24.6 mmol/L; all P values < .001).
“The two recommended isotonic crystalloid fluids used for hemorrhagic and other forms of shock – normal saline and lactated Ringer’s – have been in use since the 19th century and early 20th century,” senior author Dr. Ronald F. Sing said in an interview. “Despite the tremendous advances in shock and resuscitation, we have identified, and actually confirmed, potentially confounding factors related to both LR and [normal saline] for resuscitation. Our next goal is to examine other crystalloid solutions and their impacts not only on shock markers, but inflammatory markers,” he added.
Future studies also will use animal models to look at class II-IV hemorrhage and increased follow-up time.
The study was supported by the Carolinas Trauma Network. Dr. Ross and his coauthors reported having no financial disclosures.
LAKE BUENA VISTA, FLA. – Base deficit and lactate after resuscitation were measurably different based on the type of crystalloid solution used in a class I hemorrhage model.
Further, an award-winning prospective study found that, compared with lactated Ringer’s or no intravenous fluid, normal saline results in significantly higher postresuscitation sodium and chloride levels and significantly lower ionized calcium and bicarbonate.
Taken together, these derangements are important because blood gases are one of the first objective measurements performed in acute trauma patients, Dr. Samuel Wade Ross said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
“We might actually be overestimating the amount of shock due specifically to the iatrogenic cause of crystalloid solutions,” he said. “Additionally, this goes beyond just trauma because all medicine – surgery, anesthesia, and critical care – use crystalloid. And it should be in the back of our minds when using normal saline that this contributes to acidosis and that lactated Ringer’s can falsely elevate lactate levels.”
The analysis involved 157 voluntary blood donors, who donated 0.5 L and were then randomly assigned to normal saline, lactated Ringer’s (LR), or no IV fluid. The percentage of total blood volume lost was about 11%, which is consistent with a class I hemorrhage model, said Dr. Ross of the Carolinas Medical Center in Charlotte, N.C.
Base deficit, which is used to guide the volume of fluid needed for trauma patients’ resuscitation, was similar before administration of normal saline, lactated Ringer’s, or no IV fluid (–0.24 vs. 0.33 vs. 0.04).
After fluid administration, however, the normal saline group had almost five times the base deficit of the no IV fluid group (–3.06 vs. –0.65) and almost 10 times the base deficit of the LR group (–3.06 vs. –0.34). The differences were statistically significant, even using a conservative statistical correction with a P value cutoff of 0.0167, he said.
Preresuscitation lactate levels also were similar in the LR, normal saline, and no IV groups (1.05 mmol/L vs. 1.12 mmol/L vs. 1.10 mmol/L).
Postresuscitation, however, lactate increased by roughly 50% in the LR group vs. the normal saline group (1.54 mmol/L vs. 1.0 mmol/L) and was elevated compared with no IV fluid (1.54 mmol/L vs. 1.36 mmol/L). Both findings were statistically significant (P < .0167).
This is the first time these differences have been quantified and runs contrary to the dogma that serum lactate does not increase with the use of LR because of enzymatic clearance of the molecule in the liver, said Dr. Ross, the EAST 2015 Raymond Alexander Residents Paper Competition winner.
“With ongoing shock, lactate rises and clinicians use that as a guide for further fluid resuscitation. Thus, lactate levels could be falsely elevated with LR use, and drive further decisions for unnecessary and potentially harmful additional resuscitation and procedures,” he said in an interview.
As noted above, use of normal saline rather than LR or no IV fluid resulted in significantly higher postresuscitation sodium (141.7 mmol/L vs. 139.8 mmol/L vs. 139.8 mmol/L) and chloride (107.3 mmol/L vs. 102.3 mmol/L vs. 102.9 mmol/L), and significantly lower ionized calcium (1.15 vs. 1.22 vs. 1.24), pH (7.32 vs. 7.34 vs. 7.36), and bicarbonate (23 mmol/L vs. 25.3 mmol/L vs. 24.6 mmol/L; all P values < .001).
“The two recommended isotonic crystalloid fluids used for hemorrhagic and other forms of shock – normal saline and lactated Ringer’s – have been in use since the 19th century and early 20th century,” senior author Dr. Ronald F. Sing said in an interview. “Despite the tremendous advances in shock and resuscitation, we have identified, and actually confirmed, potentially confounding factors related to both LR and [normal saline] for resuscitation. Our next goal is to examine other crystalloid solutions and their impacts not only on shock markers, but inflammatory markers,” he added.
Future studies also will use animal models to look at class II-IV hemorrhage and increased follow-up time.
The study was supported by the Carolinas Trauma Network. Dr. Ross and his coauthors reported having no financial disclosures.
AT THE EAST SCIENTIFIC ASSEMBLY
Key clinical point: Quantifiable differences exist in base deficit and lactate based on the type of resuscitation fluid used in a class I hemorrhage model.
Major finding: Base deficit was dramatically lower after normal saline vs. no intravenous fluid or lactated Ringer’s (–3.06 vs. –0.65 vs. –0.34; P <.001).
Data source: Prospective study in 157 blood donors.
Disclosures: The study was supported by the Carolinas Trauma Network. Dr. Ross and his coauthors reported having no financial disclosures.

VIDEO: Cast a wider net for intimate partner and sexual violence
LAKE BUENA VISTA, FLA. – Screening for intimate partner and sexual violence occurs sporadically in trauma centers, typically among women and when there is a suspicious mechanism of injury.
In hopes of reaching a broader population, investigators at the Ryder Trauma Center at the University of Miami conducted a prospective pilot study to determine the feasibility of universal screening for intimate partner and sexual violence in all patients presenting at the level I trauma center.
In all, 399 consecutive patients were eligible, with 40% screened using a four-item questionnaire that asks patients how often their partner physically hurt, insulted, threatened with harm, and screamed at them (HITS) and the SAVE (screen, ask, validate, evaluate) method developed in Florida to screen for sexual violence. Both instruments were available in English, Spanish, and Haitian French.
Over a 4-month period, 14% of patients scored positive for physical and psychological abuse – and even more surprising, 8% scored positive for sexual violence, lead study author Dr. Tanya Zakrison reported at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
“Interestingly, there was no significant difference between men and women. They were all scoring at an equal rate,” Dr. Zakrison said. Patients who scored positive on HITS or SAVE were also found across all ethnicities and all age groups.
“The last thing that was quite surprising for us to find was that only 14% of patients who were HITS positive were actually admitted as a result of intimate partner or interpersonal violence, and none of the patients who scored positive for SAVE were admitted to trauma because of this,” she added. “Again, they’re coming in for the motor vehicle collisions, falls from standing, or other mechanisms of injury.”
To learn more about the intervention and its impact at Ryder Trauma, watch our video interview.
Dr. Zakrison and her coauthors reported no relevant financial conflicts.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LAKE BUENA VISTA, FLA. – Screening for intimate partner and sexual violence occurs sporadically in trauma centers, typically among women and when there is a suspicious mechanism of injury.
In hopes of reaching a broader population, investigators at the Ryder Trauma Center at the University of Miami conducted a prospective pilot study to determine the feasibility of universal screening for intimate partner and sexual violence in all patients presenting at the level I trauma center.
In all, 399 consecutive patients were eligible, with 40% screened using a four-item questionnaire that asks patients how often their partner physically hurt, insulted, threatened with harm, and screamed at them (HITS) and the SAVE (screen, ask, validate, evaluate) method developed in Florida to screen for sexual violence. Both instruments were available in English, Spanish, and Haitian French.
Over a 4-month period, 14% of patients scored positive for physical and psychological abuse – and even more surprising, 8% scored positive for sexual violence, lead study author Dr. Tanya Zakrison reported at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
“Interestingly, there was no significant difference between men and women. They were all scoring at an equal rate,” Dr. Zakrison said. Patients who scored positive on HITS or SAVE were also found across all ethnicities and all age groups.
“The last thing that was quite surprising for us to find was that only 14% of patients who were HITS positive were actually admitted as a result of intimate partner or interpersonal violence, and none of the patients who scored positive for SAVE were admitted to trauma because of this,” she added. “Again, they’re coming in for the motor vehicle collisions, falls from standing, or other mechanisms of injury.”
To learn more about the intervention and its impact at Ryder Trauma, watch our video interview.
Dr. Zakrison and her coauthors reported no relevant financial conflicts.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LAKE BUENA VISTA, FLA. – Screening for intimate partner and sexual violence occurs sporadically in trauma centers, typically among women and when there is a suspicious mechanism of injury.
In hopes of reaching a broader population, investigators at the Ryder Trauma Center at the University of Miami conducted a prospective pilot study to determine the feasibility of universal screening for intimate partner and sexual violence in all patients presenting at the level I trauma center.
In all, 399 consecutive patients were eligible, with 40% screened using a four-item questionnaire that asks patients how often their partner physically hurt, insulted, threatened with harm, and screamed at them (HITS) and the SAVE (screen, ask, validate, evaluate) method developed in Florida to screen for sexual violence. Both instruments were available in English, Spanish, and Haitian French.
Over a 4-month period, 14% of patients scored positive for physical and psychological abuse – and even more surprising, 8% scored positive for sexual violence, lead study author Dr. Tanya Zakrison reported at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
“Interestingly, there was no significant difference between men and women. They were all scoring at an equal rate,” Dr. Zakrison said. Patients who scored positive on HITS or SAVE were also found across all ethnicities and all age groups.
“The last thing that was quite surprising for us to find was that only 14% of patients who were HITS positive were actually admitted as a result of intimate partner or interpersonal violence, and none of the patients who scored positive for SAVE were admitted to trauma because of this,” she added. “Again, they’re coming in for the motor vehicle collisions, falls from standing, or other mechanisms of injury.”
To learn more about the intervention and its impact at Ryder Trauma, watch our video interview.
Dr. Zakrison and her coauthors reported no relevant financial conflicts.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE EAST SCIENTIFIC ASSEMBLY
