User login
Official Newspaper of the American College of Surgeons
The right choice? Surgeons, confidence, and humility
It started as an offhand comment. The patient had been on the medicine service for over a week before developing acute appendicitis with an abscess and requiring an emergency open appendectomy. He was a 68-year-old man who had longstanding medical issues that had given him many opportunities to interact with physicians in the prior few years.
On the second morning after surgery, a new team of surgical residents was rounding on him. The chief resident led the group of residents and students into the patient’s room and introduced himself as being part of the surgical team. The patient smiled and stated that he knew this was a group of surgeons. When asked why, the patient reported that he could always tell when surgeons enter the room. “You enter with an air of bravado and arrogance that the medical doctors do not exude.” The surgical residents commented on this fact to me later when I rounded on the patient, and it prompted discussion of the potential positives and negatives of confidence in surgical practice.

There is no doubt in my mind that in order to be willing to put a patient through an operation, surgeons must be confident in their skills. Surgery never achieves its benefit for patients without first causing the patient some harm. Any operation requires that the surgeon impose a violent act on the patient that, in any other context, would be illegal. In order to do such things to patients, surgeons must have a high degree of confidence.
Patients also appreciate a confident surgeon. Over the years, I have known many technically excellent surgeons who have never been as busy as they might have been because they were unable to express confidence to their patients. The opposite, however, is also true. There are surgeons who become so overconfident in their abilities that they become reckless in recommending high-risk operations to patients.
Given that patients expect their surgeons to have confidence and surgeons actually need to be confident in order to be successful, it might be surprising that the important attribute of self-confidence does not more frequently spill over into overbearing arrogance. Perhaps the most important temporizing of surgeon overconfidence is the unfortunate inevitable consequence of surgery that complications happen to even the best surgeons. We all know that the central question of the M & M conference is, “What could you have done differently?” Whether this question is answered publicly or only in the mind of the surgeon, the contemplation of the decisions made, and their consequences, is essential for each surgeon to consider in the face of every complication.
Much as the public should want surgeons to be confident, but not too confident, they should also want their surgeons to take complications seriously, but not too seriously. It is helpful for a surgeon to think about making a different choice in the future. But it would not be helpful if, in the face of a bad outcome, a surgeon decides that he or she can no longer perform surgery.
This balance between lack of confidence and overconfidence, and between thoughtful introspection and paralyzing fear of future complications, is challenging to teach to surgical residents and fellows. Part of the challenge is that often surgical faculty do not verbalize the challenges that we face in this realm. The perfect combination of confidence and humility is something that few of us have identified in our own lives, let alone are prepared to teach it authoritatively to others. Nevertheless, teaching the next generation of surgeons to recognize the tension between confidence and humility is worthwhile. And like their elders, they may well discover that achieving the right balance is a lifelong pursuit.
Dr. Angelos is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
It started as an offhand comment. The patient had been on the medicine service for over a week before developing acute appendicitis with an abscess and requiring an emergency open appendectomy. He was a 68-year-old man who had longstanding medical issues that had given him many opportunities to interact with physicians in the prior few years.
On the second morning after surgery, a new team of surgical residents was rounding on him. The chief resident led the group of residents and students into the patient’s room and introduced himself as being part of the surgical team. The patient smiled and stated that he knew this was a group of surgeons. When asked why, the patient reported that he could always tell when surgeons enter the room. “You enter with an air of bravado and arrogance that the medical doctors do not exude.” The surgical residents commented on this fact to me later when I rounded on the patient, and it prompted discussion of the potential positives and negatives of confidence in surgical practice.
There is no doubt in my mind that in order to be willing to put a patient through an operation, surgeons must be confident in their skills. Surgery never achieves its benefit for patients without first causing the patient some harm. Any operation requires that the surgeon impose a violent act on the patient that, in any other context, would be illegal. In order to do such things to patients, surgeons must have a high degree of confidence.
Patients also appreciate a confident surgeon. Over the years, I have known many technically excellent surgeons who have never been as busy as they might have been because they were unable to express confidence to their patients. The opposite, however, is also true. There are surgeons who become so overconfident in their abilities that they become reckless in recommending high-risk operations to patients.
Given that patients expect their surgeons to have confidence and surgeons actually need to be confident in order to be successful, it might be surprising that the important attribute of self-confidence does not more frequently spill over into overbearing arrogance. Perhaps the most important temporizing of surgeon overconfidence is the unfortunate inevitable consequence of surgery that complications happen to even the best surgeons. We all know that the central question of the M & M conference is, “What could you have done differently?” Whether this question is answered publicly or only in the mind of the surgeon, the contemplation of the decisions made, and their consequences, is essential for each surgeon to consider in the face of every complication.
Much as the public should want surgeons to be confident, but not too confident, they should also want their surgeons to take complications seriously, but not too seriously. It is helpful for a surgeon to think about making a different choice in the future. But it would not be helpful if, in the face of a bad outcome, a surgeon decides that he or she can no longer perform surgery.
This balance between lack of confidence and overconfidence, and between thoughtful introspection and paralyzing fear of future complications, is challenging to teach to surgical residents and fellows. Part of the challenge is that often surgical faculty do not verbalize the challenges that we face in this realm. The perfect combination of confidence and humility is something that few of us have identified in our own lives, let alone are prepared to teach it authoritatively to others. Nevertheless, teaching the next generation of surgeons to recognize the tension between confidence and humility is worthwhile. And like their elders, they may well discover that achieving the right balance is a lifelong pursuit.
Dr. Angelos is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
It started as an offhand comment. The patient had been on the medicine service for over a week before developing acute appendicitis with an abscess and requiring an emergency open appendectomy. He was a 68-year-old man who had longstanding medical issues that had given him many opportunities to interact with physicians in the prior few years.
On the second morning after surgery, a new team of surgical residents was rounding on him. The chief resident led the group of residents and students into the patient’s room and introduced himself as being part of the surgical team. The patient smiled and stated that he knew this was a group of surgeons. When asked why, the patient reported that he could always tell when surgeons enter the room. “You enter with an air of bravado and arrogance that the medical doctors do not exude.” The surgical residents commented on this fact to me later when I rounded on the patient, and it prompted discussion of the potential positives and negatives of confidence in surgical practice.
There is no doubt in my mind that in order to be willing to put a patient through an operation, surgeons must be confident in their skills. Surgery never achieves its benefit for patients without first causing the patient some harm. Any operation requires that the surgeon impose a violent act on the patient that, in any other context, would be illegal. In order to do such things to patients, surgeons must have a high degree of confidence.
Patients also appreciate a confident surgeon. Over the years, I have known many technically excellent surgeons who have never been as busy as they might have been because they were unable to express confidence to their patients. The opposite, however, is also true. There are surgeons who become so overconfident in their abilities that they become reckless in recommending high-risk operations to patients.
Given that patients expect their surgeons to have confidence and surgeons actually need to be confident in order to be successful, it might be surprising that the important attribute of self-confidence does not more frequently spill over into overbearing arrogance. Perhaps the most important temporizing of surgeon overconfidence is the unfortunate inevitable consequence of surgery that complications happen to even the best surgeons. We all know that the central question of the M & M conference is, “What could you have done differently?” Whether this question is answered publicly or only in the mind of the surgeon, the contemplation of the decisions made, and their consequences, is essential for each surgeon to consider in the face of every complication.
Much as the public should want surgeons to be confident, but not too confident, they should also want their surgeons to take complications seriously, but not too seriously. It is helpful for a surgeon to think about making a different choice in the future. But it would not be helpful if, in the face of a bad outcome, a surgeon decides that he or she can no longer perform surgery.
This balance between lack of confidence and overconfidence, and between thoughtful introspection and paralyzing fear of future complications, is challenging to teach to surgical residents and fellows. Part of the challenge is that often surgical faculty do not verbalize the challenges that we face in this realm. The perfect combination of confidence and humility is something that few of us have identified in our own lives, let alone are prepared to teach it authoritatively to others. Nevertheless, teaching the next generation of surgeons to recognize the tension between confidence and humility is worthwhile. And like their elders, they may well discover that achieving the right balance is a lifelong pursuit.
Dr. Angelos is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
Register now to participate in ACS Leadership & Advocacy Summit 2017
The American College of Surgeons (ACS) will host its sixth annual Leadership & Advocacy Summit, May 6-9 at the Renaissance Washington, DC, Downtown Hotel. The summit is a dual meeting that offers comprehensive and specialized sessions that provide volunteer leaders and advocates with the skills and tools they need to be effective in those roles. Registration for the event is now open at facs.org/summit.
Leadership Summit
The Leadership Summit provides a venue for members to connect with ACS leaders, and to participate in discussions about innovative ways to face challenges and enhance leadership skills. It begins Saturday, May 6, with an initial reception open to all registrants, followed by a full day of programming on Sunday, May 7.
More than 400 ACS leaders, members, residents, and medical students participate in the Leadership portion of the summit. Topics will focus on honing the communication and strategic thinking skills necessary for effective leadership in and out of the operating room. Speakers will address topics such as leadership strategies, ethics in leadership, common mistakes in leadership, team building, managing critical situations, and domestic volunteerism. In addition, a portion of the meeting will be dedicated to sharing ACS chapter success stories and working to identify strategies to enhance and strengthen chapters.
Advocacy Summit
The Advocacy Summit provides the best opportunity to attain the skills and knowledge needed to become a seasoned surgeon advocate. With a new presidential administration and Congress, it is vital that surgeons make the trip to Washington to observe and participate in the evolving political environment.
Since last year’s summit, many details about physician payment under the Medicare Access and CHIP (Children’s Health Insurance Program) Reauthorization Act (MACRA) of 2015 have been set. At the Advocacy Summit, surgeons will be briefed on the steps they must now take to start complying with MACRA, and ACS staff will help members navigate the many additional legislative changes that are likely to occur.
The Advocacy Summit will begin Sunday, May 7, with a dinner and keynote address. Past speakers have included political commentator Chris Matthews, U.S. Army Gen. (Retired) Stanley A. McChrystal, author Thomas Goetz, and journalists Bob Woodward and George Will.
Sessions planned for the following day will focus on the political climate in Washington, and speakers will provide updates on important health care issues, including Medicare physician payment, graduate medical education, and ensuring patient access to the highest quality surgical care. Tuesday morning, attendees will apply what they have learned at the summit in face-to-face meetings with their senators and representatives and/or congressional staffs. This portion of the program provides an opportunity to rally surgery’s collective grassroots on issues such as physician payment, professional liability, and physician workforce.
Fellows attending the Advocacy Summit will have the opportunity to make an early impression on a new Congress. During this three-day conference, participants can expect to receive comprehensive advocacy training and learn how to use these skills throughout the year, not just when in Washington. The Advocacy Summit is the place to confer with other surgeon advocates to share ideas and meet face-to-face with key health care policymakers and legislators. Perhaps more importantly, the Advocacy Summit gives surgeons an opportunity to become the constituent their legislators know and trust to offer advice on surgical issues.
The ACS Professional Association political action committee (ACSPA-SurgeonsPAC) will host various events for members and SurgeonsPAC contributors. These events provide contributors with unique networking opportunities, advanced educational sessions aimed at helping College members become more effective surgeon-advocates, and an insider’s perspective on how to remain engaged in the political process.
In addition to raising funds to elect and/or re-elect congressional candidates who support a pro-surgeon, pro-patient agenda, SurgeonsPAC will host a reception at which PAC contributors will be recognized for their commitment to surgery and the surgical patient. Other SurgeonsPAC-sponsored events include the annual raffle, a political luncheon featuring a special guest speaker, and presentation of the 2016 PAC awards. Resident engagement opportunities will be provided as well. In addition, the SurgeonsPAC booth provides attendees with a venue to interact with ACS Division of Advocacy and Health Policy staff to learn more about the PAC and ACS advocacy efforts.
For more information about the Leadership Summit, e-mail [email protected]. For more information about the Advocacy Summit and ACSPA-SurgeonsPAC activities, e-mail [email protected] or call 202-672-1520.
The American College of Surgeons (ACS) will host its sixth annual Leadership & Advocacy Summit, May 6-9 at the Renaissance Washington, DC, Downtown Hotel. The summit is a dual meeting that offers comprehensive and specialized sessions that provide volunteer leaders and advocates with the skills and tools they need to be effective in those roles. Registration for the event is now open at facs.org/summit.
Leadership Summit
The Leadership Summit provides a venue for members to connect with ACS leaders, and to participate in discussions about innovative ways to face challenges and enhance leadership skills. It begins Saturday, May 6, with an initial reception open to all registrants, followed by a full day of programming on Sunday, May 7.
More than 400 ACS leaders, members, residents, and medical students participate in the Leadership portion of the summit. Topics will focus on honing the communication and strategic thinking skills necessary for effective leadership in and out of the operating room. Speakers will address topics such as leadership strategies, ethics in leadership, common mistakes in leadership, team building, managing critical situations, and domestic volunteerism. In addition, a portion of the meeting will be dedicated to sharing ACS chapter success stories and working to identify strategies to enhance and strengthen chapters.
Advocacy Summit
The Advocacy Summit provides the best opportunity to attain the skills and knowledge needed to become a seasoned surgeon advocate. With a new presidential administration and Congress, it is vital that surgeons make the trip to Washington to observe and participate in the evolving political environment.
Since last year’s summit, many details about physician payment under the Medicare Access and CHIP (Children’s Health Insurance Program) Reauthorization Act (MACRA) of 2015 have been set. At the Advocacy Summit, surgeons will be briefed on the steps they must now take to start complying with MACRA, and ACS staff will help members navigate the many additional legislative changes that are likely to occur.
The Advocacy Summit will begin Sunday, May 7, with a dinner and keynote address. Past speakers have included political commentator Chris Matthews, U.S. Army Gen. (Retired) Stanley A. McChrystal, author Thomas Goetz, and journalists Bob Woodward and George Will.
Sessions planned for the following day will focus on the political climate in Washington, and speakers will provide updates on important health care issues, including Medicare physician payment, graduate medical education, and ensuring patient access to the highest quality surgical care. Tuesday morning, attendees will apply what they have learned at the summit in face-to-face meetings with their senators and representatives and/or congressional staffs. This portion of the program provides an opportunity to rally surgery’s collective grassroots on issues such as physician payment, professional liability, and physician workforce.
Fellows attending the Advocacy Summit will have the opportunity to make an early impression on a new Congress. During this three-day conference, participants can expect to receive comprehensive advocacy training and learn how to use these skills throughout the year, not just when in Washington. The Advocacy Summit is the place to confer with other surgeon advocates to share ideas and meet face-to-face with key health care policymakers and legislators. Perhaps more importantly, the Advocacy Summit gives surgeons an opportunity to become the constituent their legislators know and trust to offer advice on surgical issues.
The ACS Professional Association political action committee (ACSPA-SurgeonsPAC) will host various events for members and SurgeonsPAC contributors. These events provide contributors with unique networking opportunities, advanced educational sessions aimed at helping College members become more effective surgeon-advocates, and an insider’s perspective on how to remain engaged in the political process.
In addition to raising funds to elect and/or re-elect congressional candidates who support a pro-surgeon, pro-patient agenda, SurgeonsPAC will host a reception at which PAC contributors will be recognized for their commitment to surgery and the surgical patient. Other SurgeonsPAC-sponsored events include the annual raffle, a political luncheon featuring a special guest speaker, and presentation of the 2016 PAC awards. Resident engagement opportunities will be provided as well. In addition, the SurgeonsPAC booth provides attendees with a venue to interact with ACS Division of Advocacy and Health Policy staff to learn more about the PAC and ACS advocacy efforts.
For more information about the Leadership Summit, e-mail [email protected]. For more information about the Advocacy Summit and ACSPA-SurgeonsPAC activities, e-mail [email protected] or call 202-672-1520.
The American College of Surgeons (ACS) will host its sixth annual Leadership & Advocacy Summit, May 6-9 at the Renaissance Washington, DC, Downtown Hotel. The summit is a dual meeting that offers comprehensive and specialized sessions that provide volunteer leaders and advocates with the skills and tools they need to be effective in those roles. Registration for the event is now open at facs.org/summit.
Leadership Summit
The Leadership Summit provides a venue for members to connect with ACS leaders, and to participate in discussions about innovative ways to face challenges and enhance leadership skills. It begins Saturday, May 6, with an initial reception open to all registrants, followed by a full day of programming on Sunday, May 7.
More than 400 ACS leaders, members, residents, and medical students participate in the Leadership portion of the summit. Topics will focus on honing the communication and strategic thinking skills necessary for effective leadership in and out of the operating room. Speakers will address topics such as leadership strategies, ethics in leadership, common mistakes in leadership, team building, managing critical situations, and domestic volunteerism. In addition, a portion of the meeting will be dedicated to sharing ACS chapter success stories and working to identify strategies to enhance and strengthen chapters.
Advocacy Summit
The Advocacy Summit provides the best opportunity to attain the skills and knowledge needed to become a seasoned surgeon advocate. With a new presidential administration and Congress, it is vital that surgeons make the trip to Washington to observe and participate in the evolving political environment.
Since last year’s summit, many details about physician payment under the Medicare Access and CHIP (Children’s Health Insurance Program) Reauthorization Act (MACRA) of 2015 have been set. At the Advocacy Summit, surgeons will be briefed on the steps they must now take to start complying with MACRA, and ACS staff will help members navigate the many additional legislative changes that are likely to occur.
The Advocacy Summit will begin Sunday, May 7, with a dinner and keynote address. Past speakers have included political commentator Chris Matthews, U.S. Army Gen. (Retired) Stanley A. McChrystal, author Thomas Goetz, and journalists Bob Woodward and George Will.
Sessions planned for the following day will focus on the political climate in Washington, and speakers will provide updates on important health care issues, including Medicare physician payment, graduate medical education, and ensuring patient access to the highest quality surgical care. Tuesday morning, attendees will apply what they have learned at the summit in face-to-face meetings with their senators and representatives and/or congressional staffs. This portion of the program provides an opportunity to rally surgery’s collective grassroots on issues such as physician payment, professional liability, and physician workforce.
Fellows attending the Advocacy Summit will have the opportunity to make an early impression on a new Congress. During this three-day conference, participants can expect to receive comprehensive advocacy training and learn how to use these skills throughout the year, not just when in Washington. The Advocacy Summit is the place to confer with other surgeon advocates to share ideas and meet face-to-face with key health care policymakers and legislators. Perhaps more importantly, the Advocacy Summit gives surgeons an opportunity to become the constituent their legislators know and trust to offer advice on surgical issues.
The ACS Professional Association political action committee (ACSPA-SurgeonsPAC) will host various events for members and SurgeonsPAC contributors. These events provide contributors with unique networking opportunities, advanced educational sessions aimed at helping College members become more effective surgeon-advocates, and an insider’s perspective on how to remain engaged in the political process.
In addition to raising funds to elect and/or re-elect congressional candidates who support a pro-surgeon, pro-patient agenda, SurgeonsPAC will host a reception at which PAC contributors will be recognized for their commitment to surgery and the surgical patient. Other SurgeonsPAC-sponsored events include the annual raffle, a political luncheon featuring a special guest speaker, and presentation of the 2016 PAC awards. Resident engagement opportunities will be provided as well. In addition, the SurgeonsPAC booth provides attendees with a venue to interact with ACS Division of Advocacy and Health Policy staff to learn more about the PAC and ACS advocacy efforts.
For more information about the Leadership Summit, e-mail [email protected]. For more information about the Advocacy Summit and ACSPA-SurgeonsPAC activities, e-mail [email protected] or call 202-672-1520.
Dr. Frank Lewis, ABS executive director, announces retirement
Frank R. Lewis, MD, FACS, executive director of the American Board of Surgery (ABS), announced that he will retire from the organization at the end of 2017. The ABS will conduct a national recruitment process to identify his successor, with the goal of having that individual in place in late June.
Dr. Lewis, who joined the ABS as executive director in 2002, guided the society through many significant initiatives and changes, including the creation of the Surgical Council on Resident Education (SCORE), development of a primary certificate in vascular surgery, establishment of flexible rotations in residency training, and the subsequent design and implementation of the Flexibility In duty hour Requirements for Surgical Trainees (FIRST) Trial, among others.
In addition, Dr. Lewis is past chair of the ABS and the Residency Review Committee for Surgery of the Accreditation Council for Graduate Medical Education. Dr. Lewis also served as 1995-1996 First Vice-President of the American College of Surgeons (ACS) and as the 1991-1993 Chair of the ACS Board of Governors. Read more about Dr. Lewis’ retirement and accomplishments on the ABS website at www.absurgery.org/default.jsp?news_lewis0117.
Frank R. Lewis, MD, FACS, executive director of the American Board of Surgery (ABS), announced that he will retire from the organization at the end of 2017. The ABS will conduct a national recruitment process to identify his successor, with the goal of having that individual in place in late June.
Dr. Lewis, who joined the ABS as executive director in 2002, guided the society through many significant initiatives and changes, including the creation of the Surgical Council on Resident Education (SCORE), development of a primary certificate in vascular surgery, establishment of flexible rotations in residency training, and the subsequent design and implementation of the Flexibility In duty hour Requirements for Surgical Trainees (FIRST) Trial, among others.
In addition, Dr. Lewis is past chair of the ABS and the Residency Review Committee for Surgery of the Accreditation Council for Graduate Medical Education. Dr. Lewis also served as 1995-1996 First Vice-President of the American College of Surgeons (ACS) and as the 1991-1993 Chair of the ACS Board of Governors. Read more about Dr. Lewis’ retirement and accomplishments on the ABS website at www.absurgery.org/default.jsp?news_lewis0117.
Frank R. Lewis, MD, FACS, executive director of the American Board of Surgery (ABS), announced that he will retire from the organization at the end of 2017. The ABS will conduct a national recruitment process to identify his successor, with the goal of having that individual in place in late June.
Dr. Lewis, who joined the ABS as executive director in 2002, guided the society through many significant initiatives and changes, including the creation of the Surgical Council on Resident Education (SCORE), development of a primary certificate in vascular surgery, establishment of flexible rotations in residency training, and the subsequent design and implementation of the Flexibility In duty hour Requirements for Surgical Trainees (FIRST) Trial, among others.
In addition, Dr. Lewis is past chair of the ABS and the Residency Review Committee for Surgery of the Accreditation Council for Graduate Medical Education. Dr. Lewis also served as 1995-1996 First Vice-President of the American College of Surgeons (ACS) and as the 1991-1993 Chair of the ACS Board of Governors. Read more about Dr. Lewis’ retirement and accomplishments on the ABS website at www.absurgery.org/default.jsp?news_lewis0117.
Children’s Surgery Verification Program now accepting pre-applications
The Children’s Surgical Verification (CSV) Program has announced that pre-application is now available and open online, which can be accessed at facs.org/quality-programs/childrens-surgery/childrens-surgery-verification/apply. All interested sites are welcome to complete the pre-application, but note that to be approved for site verification centers must meet all of the program standards and intend to actively pursue verification for the level sought before submitting a pre-application. Pre-review questionnaires are posted for each level of certification.
The American College of Surgeons, in collaboration with the Task Force for Children’s Surgical Care, developed the CSV standards to improve surgical care for pediatric surgical patients. These standards are the nation’s first and only multispecialty benchmarks for verifying an institution’s ability to provide appropriate levels of children’s surgical care. The program evaluates three levels of care, aligned to the standards and expected scope of practice at the pediatric hospital. The CSV Program verifies that participating centers have met these standards.
Visit the Children’s Surgery Verification Program at facs.org/quality-programs/childrens-surgery/childrens-surgery-verification for more information, or contact the program team at [email protected] with any questions.
The Children’s Surgical Verification (CSV) Program has announced that pre-application is now available and open online, which can be accessed at facs.org/quality-programs/childrens-surgery/childrens-surgery-verification/apply. All interested sites are welcome to complete the pre-application, but note that to be approved for site verification centers must meet all of the program standards and intend to actively pursue verification for the level sought before submitting a pre-application. Pre-review questionnaires are posted for each level of certification.
The American College of Surgeons, in collaboration with the Task Force for Children’s Surgical Care, developed the CSV standards to improve surgical care for pediatric surgical patients. These standards are the nation’s first and only multispecialty benchmarks for verifying an institution’s ability to provide appropriate levels of children’s surgical care. The program evaluates three levels of care, aligned to the standards and expected scope of practice at the pediatric hospital. The CSV Program verifies that participating centers have met these standards.
Visit the Children’s Surgery Verification Program at facs.org/quality-programs/childrens-surgery/childrens-surgery-verification for more information, or contact the program team at [email protected] with any questions.
The Children’s Surgical Verification (CSV) Program has announced that pre-application is now available and open online, which can be accessed at facs.org/quality-programs/childrens-surgery/childrens-surgery-verification/apply. All interested sites are welcome to complete the pre-application, but note that to be approved for site verification centers must meet all of the program standards and intend to actively pursue verification for the level sought before submitting a pre-application. Pre-review questionnaires are posted for each level of certification.
The American College of Surgeons, in collaboration with the Task Force for Children’s Surgical Care, developed the CSV standards to improve surgical care for pediatric surgical patients. These standards are the nation’s first and only multispecialty benchmarks for verifying an institution’s ability to provide appropriate levels of children’s surgical care. The program evaluates three levels of care, aligned to the standards and expected scope of practice at the pediatric hospital. The CSV Program verifies that participating centers have met these standards.
Visit the Children’s Surgery Verification Program at facs.org/quality-programs/childrens-surgery/childrens-surgery-verification for more information, or contact the program team at [email protected] with any questions.
2018-2020 ACS Clinical Scholars in Residence Program Applications Now Open
The American College of Surgeons (ACS) is accepting applications for the 2018-2020 Clinical Scholars in Residence Program, a two-year fellowship in surgical outcomes research, health services research, and health care policy performed on-site at the ACS headquarters, Chicago, IL. Applications are due April 3, 2017, and the scholar begins work July 1, 2018. Applicants must have completed two years of clinical training, be U.S. citizens, and obtain two years of program funding from their home institution or other granting agency. Applicants also must be members in good standing of the College.
The Clinical Scholar will have the opportunity to work in multiple areas within the ACS Division of Research and Optimal Patient Care to advance the College’s quality improvement initiatives and to perform research relevant to ongoing projects within the organization. Participants also will earn a master’s degree in public health in their two years with the program. The Clinical Scholar will receive strong mentorship in clinical, statistical, and health services research. Previous ACS Clinical Scholars in Residence have reported excellent, productive experiences that have allowed them to launch successful careers in this field.
Important dates for this position are as follows:
• Application deadline: April 3, 2017
• Interview notification: May 1, 2017
• Interview process: May 1-31, 2017
• Notification of appointment: June 9, 2017
• Starting date: July 1, 2018
For more information about the program and the application requirements, go to the program web page at facs.org/quality-programs/about/clinical-scholars-program/details. If you have additional questions, contact the ACS Clinical Scholars in Residence Program at [email protected].
The American College of Surgeons (ACS) is accepting applications for the 2018-2020 Clinical Scholars in Residence Program, a two-year fellowship in surgical outcomes research, health services research, and health care policy performed on-site at the ACS headquarters, Chicago, IL. Applications are due April 3, 2017, and the scholar begins work July 1, 2018. Applicants must have completed two years of clinical training, be U.S. citizens, and obtain two years of program funding from their home institution or other granting agency. Applicants also must be members in good standing of the College.
The Clinical Scholar will have the opportunity to work in multiple areas within the ACS Division of Research and Optimal Patient Care to advance the College’s quality improvement initiatives and to perform research relevant to ongoing projects within the organization. Participants also will earn a master’s degree in public health in their two years with the program. The Clinical Scholar will receive strong mentorship in clinical, statistical, and health services research. Previous ACS Clinical Scholars in Residence have reported excellent, productive experiences that have allowed them to launch successful careers in this field.
Important dates for this position are as follows:
• Application deadline: April 3, 2017
• Interview notification: May 1, 2017
• Interview process: May 1-31, 2017
• Notification of appointment: June 9, 2017
• Starting date: July 1, 2018
For more information about the program and the application requirements, go to the program web page at facs.org/quality-programs/about/clinical-scholars-program/details. If you have additional questions, contact the ACS Clinical Scholars in Residence Program at [email protected].
The American College of Surgeons (ACS) is accepting applications for the 2018-2020 Clinical Scholars in Residence Program, a two-year fellowship in surgical outcomes research, health services research, and health care policy performed on-site at the ACS headquarters, Chicago, IL. Applications are due April 3, 2017, and the scholar begins work July 1, 2018. Applicants must have completed two years of clinical training, be U.S. citizens, and obtain two years of program funding from their home institution or other granting agency. Applicants also must be members in good standing of the College.
The Clinical Scholar will have the opportunity to work in multiple areas within the ACS Division of Research and Optimal Patient Care to advance the College’s quality improvement initiatives and to perform research relevant to ongoing projects within the organization. Participants also will earn a master’s degree in public health in their two years with the program. The Clinical Scholar will receive strong mentorship in clinical, statistical, and health services research. Previous ACS Clinical Scholars in Residence have reported excellent, productive experiences that have allowed them to launch successful careers in this field.
Important dates for this position are as follows:
• Application deadline: April 3, 2017
• Interview notification: May 1, 2017
• Interview process: May 1-31, 2017
• Notification of appointment: June 9, 2017
• Starting date: July 1, 2018
For more information about the program and the application requirements, go to the program web page at facs.org/quality-programs/about/clinical-scholars-program/details. If you have additional questions, contact the ACS Clinical Scholars in Residence Program at [email protected].
The Right Choice? Surgeons, confidence, and humility
It started as an offhand comment. The patient had been on the medicine service for over a week before developing acute appendicitis with an abscess requiring an emergency open appendectomy. He was a 68-year-old man who had longstanding medical issues that had given him many opportunities to interact with physicians in the prior few years.
On the second morning after surgery, a new team of surgical residents was rounding on him. The chief resident led the group of residents and students into the patient’s room and introduced himself as being part of the surgical team. The patient smiled and stated that he knew this was a group of surgeons. When asked why, the patient reported that he could always tell when surgeons enter the room. “You enter with an air of bravado and arrogance that the medical doctors do not exude.” The surgical residents commented on this fact to me later when I rounded on the patient, and it prompted discussion of the potential positives and negatives of confidence in surgical practice.
Most successful surgeons express a level of confidence in their abilities which often exceeds that of many other physicians. Such observations have led to the joke that “surgeons are often wrong, but never in doubt.” The question is whether the expression of confidence in one’s abilities as a surgeon is a requirement of a surgeon or simply a common characteristic for many people who choose to go into the field of surgery.
There is no doubt in my mind that in order to be willing to put a patient through an operation, surgeons must be confident in their skills. Surgery never achieves its benefit for patients without first causing the patient some harm. Any operation requires that the surgeon impose a violent act on the patient that, in any other context, would be illegal. To do such things to patients, surgeons must have a high degree of confidence.
Patients also appreciate a confident surgeon. Over the years, I have known many technically excellent surgeons who have never been as busy as they might have because of their inability to express confidence to their patients. The opposite, however, is also true. There are surgeons who become so overconfident in their abilities that they become reckless in recommending high-risk operations to patients.
Given that patients expect their surgeons to be confident and surgeons actually need to be confident to be successful, it might be surprising that the important attribute of self-confidence does not more frequently spill over into overbearing arrogance. Perhaps the most important temporizing of surgeon overconfidence is the unfortunate inevitable consequence of surgery that complications happen to even the best surgeons. We all know that the central question of the M & M conference is, “What could you have done differently?” Whether this question is answered publicly or only in the mind of the surgeon, the contemplation of the decisions made, and their consequences, is essential for each surgeon to consider in the face of every complication.
Much as the public should want surgeons to be confident, but not too confident, they should also want their surgeons to take complications seriously, but not too seriously. It is helpful for a surgeon to think about making a different choice in the future. But it would not be helpful if, in the face of a bad outcome, a surgeon decides that he or she can no longer perform surgery.
This balance between lack of confidence and overconfidence, and between thoughtful introspection and paralyzing fear of future complications, is challenging to teach to surgical residents and fellows. Part of the challenge is that often surgical faculty do not verbalize the challenges that we face in this realm. The perfect combination of confidence and humility is something that few of us have identified in our own lives, let alone are prepared to teach authoritatively to others. Nevertheless, teaching the next generation of surgeons to recognize the tension between confidence and humility is worthwhile. And like their elders, they may well discover that achieving the right balance is a lifelong pursuit.
Dr. Angelos is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
It started as an offhand comment. The patient had been on the medicine service for over a week before developing acute appendicitis with an abscess requiring an emergency open appendectomy. He was a 68-year-old man who had longstanding medical issues that had given him many opportunities to interact with physicians in the prior few years.
On the second morning after surgery, a new team of surgical residents was rounding on him. The chief resident led the group of residents and students into the patient’s room and introduced himself as being part of the surgical team. The patient smiled and stated that he knew this was a group of surgeons. When asked why, the patient reported that he could always tell when surgeons enter the room. “You enter with an air of bravado and arrogance that the medical doctors do not exude.” The surgical residents commented on this fact to me later when I rounded on the patient, and it prompted discussion of the potential positives and negatives of confidence in surgical practice.
Most successful surgeons express a level of confidence in their abilities which often exceeds that of many other physicians. Such observations have led to the joke that “surgeons are often wrong, but never in doubt.” The question is whether the expression of confidence in one’s abilities as a surgeon is a requirement of a surgeon or simply a common characteristic for many people who choose to go into the field of surgery.
There is no doubt in my mind that in order to be willing to put a patient through an operation, surgeons must be confident in their skills. Surgery never achieves its benefit for patients without first causing the patient some harm. Any operation requires that the surgeon impose a violent act on the patient that, in any other context, would be illegal. To do such things to patients, surgeons must have a high degree of confidence.
Patients also appreciate a confident surgeon. Over the years, I have known many technically excellent surgeons who have never been as busy as they might have because of their inability to express confidence to their patients. The opposite, however, is also true. There are surgeons who become so overconfident in their abilities that they become reckless in recommending high-risk operations to patients.
Given that patients expect their surgeons to be confident and surgeons actually need to be confident to be successful, it might be surprising that the important attribute of self-confidence does not more frequently spill over into overbearing arrogance. Perhaps the most important temporizing of surgeon overconfidence is the unfortunate inevitable consequence of surgery that complications happen to even the best surgeons. We all know that the central question of the M & M conference is, “What could you have done differently?” Whether this question is answered publicly or only in the mind of the surgeon, the contemplation of the decisions made, and their consequences, is essential for each surgeon to consider in the face of every complication.
Much as the public should want surgeons to be confident, but not too confident, they should also want their surgeons to take complications seriously, but not too seriously. It is helpful for a surgeon to think about making a different choice in the future. But it would not be helpful if, in the face of a bad outcome, a surgeon decides that he or she can no longer perform surgery.
This balance between lack of confidence and overconfidence, and between thoughtful introspection and paralyzing fear of future complications, is challenging to teach to surgical residents and fellows. Part of the challenge is that often surgical faculty do not verbalize the challenges that we face in this realm. The perfect combination of confidence and humility is something that few of us have identified in our own lives, let alone are prepared to teach authoritatively to others. Nevertheless, teaching the next generation of surgeons to recognize the tension between confidence and humility is worthwhile. And like their elders, they may well discover that achieving the right balance is a lifelong pursuit.
Dr. Angelos is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
It started as an offhand comment. The patient had been on the medicine service for over a week before developing acute appendicitis with an abscess requiring an emergency open appendectomy. He was a 68-year-old man who had longstanding medical issues that had given him many opportunities to interact with physicians in the prior few years.
On the second morning after surgery, a new team of surgical residents was rounding on him. The chief resident led the group of residents and students into the patient’s room and introduced himself as being part of the surgical team. The patient smiled and stated that he knew this was a group of surgeons. When asked why, the patient reported that he could always tell when surgeons enter the room. “You enter with an air of bravado and arrogance that the medical doctors do not exude.” The surgical residents commented on this fact to me later when I rounded on the patient, and it prompted discussion of the potential positives and negatives of confidence in surgical practice.
Most successful surgeons express a level of confidence in their abilities which often exceeds that of many other physicians. Such observations have led to the joke that “surgeons are often wrong, but never in doubt.” The question is whether the expression of confidence in one’s abilities as a surgeon is a requirement of a surgeon or simply a common characteristic for many people who choose to go into the field of surgery.
There is no doubt in my mind that in order to be willing to put a patient through an operation, surgeons must be confident in their skills. Surgery never achieves its benefit for patients without first causing the patient some harm. Any operation requires that the surgeon impose a violent act on the patient that, in any other context, would be illegal. To do such things to patients, surgeons must have a high degree of confidence.
Patients also appreciate a confident surgeon. Over the years, I have known many technically excellent surgeons who have never been as busy as they might have because of their inability to express confidence to their patients. The opposite, however, is also true. There are surgeons who become so overconfident in their abilities that they become reckless in recommending high-risk operations to patients.
Given that patients expect their surgeons to be confident and surgeons actually need to be confident to be successful, it might be surprising that the important attribute of self-confidence does not more frequently spill over into overbearing arrogance. Perhaps the most important temporizing of surgeon overconfidence is the unfortunate inevitable consequence of surgery that complications happen to even the best surgeons. We all know that the central question of the M & M conference is, “What could you have done differently?” Whether this question is answered publicly or only in the mind of the surgeon, the contemplation of the decisions made, and their consequences, is essential for each surgeon to consider in the face of every complication.
Much as the public should want surgeons to be confident, but not too confident, they should also want their surgeons to take complications seriously, but not too seriously. It is helpful for a surgeon to think about making a different choice in the future. But it would not be helpful if, in the face of a bad outcome, a surgeon decides that he or she can no longer perform surgery.
This balance between lack of confidence and overconfidence, and between thoughtful introspection and paralyzing fear of future complications, is challenging to teach to surgical residents and fellows. Part of the challenge is that often surgical faculty do not verbalize the challenges that we face in this realm. The perfect combination of confidence and humility is something that few of us have identified in our own lives, let alone are prepared to teach authoritatively to others. Nevertheless, teaching the next generation of surgeons to recognize the tension between confidence and humility is worthwhile. And like their elders, they may well discover that achieving the right balance is a lifelong pursuit.
Dr. Angelos is the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
A Message from the President: The ACS: Dedicated to Doing What’s Right for the Patient
Do what’s right for the patient. That statement is the bedrock on which the American College of Surgeons (ACS) stands.
Throughout its nearly 104-year history, the ACS has promoted surgical education and quality improvement. The College’s dedication to education and quality can be traced to the guiding principles of its founder, Franklin H. Martin, MD, FACS. In Dr. Martin’s era, the early 20th century, medical education was in a deplorable state, as documented in the well-known Flexner report of 1910.
To help improve surgical education and training, Dr. Martin first established Surgery, Gynecology & Obstetrics (SG&O, now the Journal of the American College of Surgeons) as a practical journal for practicing surgeons, edited by active surgeons. He published an editorial in the journal inviting surgeons to “learn by watching” and encouraged “every physician in the U.S. and Canada who was interested in surgery to observe the clinics in one of the large medical centers.” Approximately 1,300 physicians responded to Dr. Martin’s charge, resulting in the first Clinical Congress of Surgeons of North America (CCSNA), November 7-9, 1910, in Chicago, IL. After the third CCSNA meeting in 1912, Dr. Martin concluded that further change was necessary, which eventually led to the formation of the ACS in November 1913.
Standards

The importance of establishing standards for hospitals and surgical training cannot be emphasized enough. These programs fundamentally changed surgical practice and training. If the College had ceased to exist after that achievement, it would have more than fulfilled the expectations of Dr. Martin and other ACS leaders. But this did not happen. Instead, the College continued to inspire quality and to maintain the highest standards for better outcomes through establishment of programs aimed at improving care for cancer and trauma patients.
Committees
The ACS Committee on Cancer published a Standardized Method for Reporting Cancer End Results in 1953. In 1965, other organizations partnered with the College to transform this committee into the Commission on Cancer (CoC), which today uses strict criteria and a rigorous on-site evaluation process to accredit more than 1,530 U.S. cancer centers. This accreditation process is used not only for initial verification of achievement of program standards, but also for periodic review for compliance to maintain accreditation.
Early in its history, the College also established a Committee on the Treatment of Fractures, which evolved into what we now know as the Committee on Trauma (COT). The COT’s guidelines for hospitals to attain or maintain verification as trauma centers—Resources for Optimal Care of the Injured Patient—was first issued in 1976 and now is in its sixth edition.
Another seminal event in trauma took place in 1976—an airplane crash involving James K. Styner, MD, FACS, and his family, in rural Nebraska. His wife died on impact, and his children were severely injured. Angered by the delays his family experienced in receiving appropriate care, Dr. Styner called for the development of adequate facilities and standardized approaches to care for severely injured patients. He combined forces with Paul E. “Skip” Collicott, MD, FACS, and other Nebraska surgeons, to develop the Advanced Trauma Life Support® program, which introduces physicians and other health care professionals around the world to best practices for initial evaluation and management of trauma patients.
ACS Regent Lenworth M. Jacobs, Jr., MD, MPH, FACS, has led more recent COT initiatives, including development of the Advanced Trauma Operative Management® course and the Hartford ConsensusTM. This panel—composed of trauma care professionals and government officials—developed the Stop the Bleed program—an initiative aimed at enhancing survival from mass casualty and active shooter events.
Another important committee that the College established to ensure surgeons are prepared to do what’s right for the patient is the Committee on Emerging Surgical Technology and Education (CESTE). Launched in 1992 with the late C. James Carrico, MD, FACS, as the inaugural Chair, CESTE was charged with developing processes to evaluate emerging surgical technology for safety and effectiveness, creating standardized education programs, and measuring outcomes. Two of the College’s most important education and quality programs sprang from CESTE—the Accredited Education Institutes, under the leadership of Ajit K. Sachdeva, MD, FACS, Director, ACS Division of Education, and the Division of Research and Optimal Patient Care, first led by R. Scott Jones, MD, FACS, and now under the purview of Clifford Y. Ko, MD, MS, FACS.
The future is in your hands
Unquestionably, the ACS and its leaders have a rich history of doing what’s right for the patient. The future, however, belongs to you. I want to encourage you to participate in all the activities of your College at the local, state, and national levels. Establish personal relationships with leaders. Be an advocate for our education and quality programs. I am confident that there are those among you who will become the leaders who will continue the evolution of the College and inspire quality, maintain the highest standards, and ensure better outcomes.
Dr. Townsend is the Robertson-Poth Distinguished Chair in General Surgery, department of surgery, University of Texas Medical Branch (UTMB), Galveston; professor of surgery, department of surgery, professor of physician assistant studies, School of Allied Health Sciences; and graduate faculty in the cell biology program, UTMB. He is the 97th President of the ACS.
Do what’s right for the patient. That statement is the bedrock on which the American College of Surgeons (ACS) stands.
Throughout its nearly 104-year history, the ACS has promoted surgical education and quality improvement. The College’s dedication to education and quality can be traced to the guiding principles of its founder, Franklin H. Martin, MD, FACS. In Dr. Martin’s era, the early 20th century, medical education was in a deplorable state, as documented in the well-known Flexner report of 1910.
To help improve surgical education and training, Dr. Martin first established Surgery, Gynecology & Obstetrics (SG&O, now the Journal of the American College of Surgeons) as a practical journal for practicing surgeons, edited by active surgeons. He published an editorial in the journal inviting surgeons to “learn by watching” and encouraged “every physician in the U.S. and Canada who was interested in surgery to observe the clinics in one of the large medical centers.” Approximately 1,300 physicians responded to Dr. Martin’s charge, resulting in the first Clinical Congress of Surgeons of North America (CCSNA), November 7-9, 1910, in Chicago, IL. After the third CCSNA meeting in 1912, Dr. Martin concluded that further change was necessary, which eventually led to the formation of the ACS in November 1913.
Standards
The importance of establishing standards for hospitals and surgical training cannot be emphasized enough. These programs fundamentally changed surgical practice and training. If the College had ceased to exist after that achievement, it would have more than fulfilled the expectations of Dr. Martin and other ACS leaders. But this did not happen. Instead, the College continued to inspire quality and to maintain the highest standards for better outcomes through establishment of programs aimed at improving care for cancer and trauma patients.
Committees
The ACS Committee on Cancer published a Standardized Method for Reporting Cancer End Results in 1953. In 1965, other organizations partnered with the College to transform this committee into the Commission on Cancer (CoC), which today uses strict criteria and a rigorous on-site evaluation process to accredit more than 1,530 U.S. cancer centers. This accreditation process is used not only for initial verification of achievement of program standards, but also for periodic review for compliance to maintain accreditation.
Early in its history, the College also established a Committee on the Treatment of Fractures, which evolved into what we now know as the Committee on Trauma (COT). The COT’s guidelines for hospitals to attain or maintain verification as trauma centers—Resources for Optimal Care of the Injured Patient—was first issued in 1976 and now is in its sixth edition.
Another seminal event in trauma took place in 1976—an airplane crash involving James K. Styner, MD, FACS, and his family, in rural Nebraska. His wife died on impact, and his children were severely injured. Angered by the delays his family experienced in receiving appropriate care, Dr. Styner called for the development of adequate facilities and standardized approaches to care for severely injured patients. He combined forces with Paul E. “Skip” Collicott, MD, FACS, and other Nebraska surgeons, to develop the Advanced Trauma Life Support® program, which introduces physicians and other health care professionals around the world to best practices for initial evaluation and management of trauma patients.
ACS Regent Lenworth M. Jacobs, Jr., MD, MPH, FACS, has led more recent COT initiatives, including development of the Advanced Trauma Operative Management® course and the Hartford ConsensusTM. This panel—composed of trauma care professionals and government officials—developed the Stop the Bleed program—an initiative aimed at enhancing survival from mass casualty and active shooter events.
Another important committee that the College established to ensure surgeons are prepared to do what’s right for the patient is the Committee on Emerging Surgical Technology and Education (CESTE). Launched in 1992 with the late C. James Carrico, MD, FACS, as the inaugural Chair, CESTE was charged with developing processes to evaluate emerging surgical technology for safety and effectiveness, creating standardized education programs, and measuring outcomes. Two of the College’s most important education and quality programs sprang from CESTE—the Accredited Education Institutes, under the leadership of Ajit K. Sachdeva, MD, FACS, Director, ACS Division of Education, and the Division of Research and Optimal Patient Care, first led by R. Scott Jones, MD, FACS, and now under the purview of Clifford Y. Ko, MD, MS, FACS.
The future is in your hands
Unquestionably, the ACS and its leaders have a rich history of doing what’s right for the patient. The future, however, belongs to you. I want to encourage you to participate in all the activities of your College at the local, state, and national levels. Establish personal relationships with leaders. Be an advocate for our education and quality programs. I am confident that there are those among you who will become the leaders who will continue the evolution of the College and inspire quality, maintain the highest standards, and ensure better outcomes.
Dr. Townsend is the Robertson-Poth Distinguished Chair in General Surgery, department of surgery, University of Texas Medical Branch (UTMB), Galveston; professor of surgery, department of surgery, professor of physician assistant studies, School of Allied Health Sciences; and graduate faculty in the cell biology program, UTMB. He is the 97th President of the ACS.
Do what’s right for the patient. That statement is the bedrock on which the American College of Surgeons (ACS) stands.
Throughout its nearly 104-year history, the ACS has promoted surgical education and quality improvement. The College’s dedication to education and quality can be traced to the guiding principles of its founder, Franklin H. Martin, MD, FACS. In Dr. Martin’s era, the early 20th century, medical education was in a deplorable state, as documented in the well-known Flexner report of 1910.
To help improve surgical education and training, Dr. Martin first established Surgery, Gynecology & Obstetrics (SG&O, now the Journal of the American College of Surgeons) as a practical journal for practicing surgeons, edited by active surgeons. He published an editorial in the journal inviting surgeons to “learn by watching” and encouraged “every physician in the U.S. and Canada who was interested in surgery to observe the clinics in one of the large medical centers.” Approximately 1,300 physicians responded to Dr. Martin’s charge, resulting in the first Clinical Congress of Surgeons of North America (CCSNA), November 7-9, 1910, in Chicago, IL. After the third CCSNA meeting in 1912, Dr. Martin concluded that further change was necessary, which eventually led to the formation of the ACS in November 1913.
Standards
The importance of establishing standards for hospitals and surgical training cannot be emphasized enough. These programs fundamentally changed surgical practice and training. If the College had ceased to exist after that achievement, it would have more than fulfilled the expectations of Dr. Martin and other ACS leaders. But this did not happen. Instead, the College continued to inspire quality and to maintain the highest standards for better outcomes through establishment of programs aimed at improving care for cancer and trauma patients.
Committees
The ACS Committee on Cancer published a Standardized Method for Reporting Cancer End Results in 1953. In 1965, other organizations partnered with the College to transform this committee into the Commission on Cancer (CoC), which today uses strict criteria and a rigorous on-site evaluation process to accredit more than 1,530 U.S. cancer centers. This accreditation process is used not only for initial verification of achievement of program standards, but also for periodic review for compliance to maintain accreditation.
Early in its history, the College also established a Committee on the Treatment of Fractures, which evolved into what we now know as the Committee on Trauma (COT). The COT’s guidelines for hospitals to attain or maintain verification as trauma centers—Resources for Optimal Care of the Injured Patient—was first issued in 1976 and now is in its sixth edition.
Another seminal event in trauma took place in 1976—an airplane crash involving James K. Styner, MD, FACS, and his family, in rural Nebraska. His wife died on impact, and his children were severely injured. Angered by the delays his family experienced in receiving appropriate care, Dr. Styner called for the development of adequate facilities and standardized approaches to care for severely injured patients. He combined forces with Paul E. “Skip” Collicott, MD, FACS, and other Nebraska surgeons, to develop the Advanced Trauma Life Support® program, which introduces physicians and other health care professionals around the world to best practices for initial evaluation and management of trauma patients.
ACS Regent Lenworth M. Jacobs, Jr., MD, MPH, FACS, has led more recent COT initiatives, including development of the Advanced Trauma Operative Management® course and the Hartford ConsensusTM. This panel—composed of trauma care professionals and government officials—developed the Stop the Bleed program—an initiative aimed at enhancing survival from mass casualty and active shooter events.
Another important committee that the College established to ensure surgeons are prepared to do what’s right for the patient is the Committee on Emerging Surgical Technology and Education (CESTE). Launched in 1992 with the late C. James Carrico, MD, FACS, as the inaugural Chair, CESTE was charged with developing processes to evaluate emerging surgical technology for safety and effectiveness, creating standardized education programs, and measuring outcomes. Two of the College’s most important education and quality programs sprang from CESTE—the Accredited Education Institutes, under the leadership of Ajit K. Sachdeva, MD, FACS, Director, ACS Division of Education, and the Division of Research and Optimal Patient Care, first led by R. Scott Jones, MD, FACS, and now under the purview of Clifford Y. Ko, MD, MS, FACS.
The future is in your hands
Unquestionably, the ACS and its leaders have a rich history of doing what’s right for the patient. The future, however, belongs to you. I want to encourage you to participate in all the activities of your College at the local, state, and national levels. Establish personal relationships with leaders. Be an advocate for our education and quality programs. I am confident that there are those among you who will become the leaders who will continue the evolution of the College and inspire quality, maintain the highest standards, and ensure better outcomes.
Dr. Townsend is the Robertson-Poth Distinguished Chair in General Surgery, department of surgery, University of Texas Medical Branch (UTMB), Galveston; professor of surgery, department of surgery, professor of physician assistant studies, School of Allied Health Sciences; and graduate faculty in the cell biology program, UTMB. He is the 97th President of the ACS.
Seema Verma dodges questions on how to improve CMS
If confirmed as Centers for Medicare & Medicaid Services administrator, Seema Verma vowed to modernize CMS programs, improve Medicaid access, and leverage technology to drive better care, but she stopped short of explaining how she would do so during her confirmation hearing Feb. 16 before the Senate Finance Committee.
Legislators grilled Ms. Verma on Medicare improvements, the fate of the Affordable Care Act (ACA), Medicaid reform, and the execution of value-based care. At every turn. Ms. Verma pledged to review current processes and work toward enhancing programs, but she declined to support or oppose specific changes. Instead, she promised to help make health care more affordable and to allow patients more flexibility in making health insurance decisions.

Much of the committee’s questioning centered on Ms. Verma’s work on the Healthy Indiana Plan (HIP), Indiana’s Medicaid expansion under the ACA. The conservative plan requires patients to pay a small amount to receive health coverage and includes a lockout period if payments are missed. Legislators repeatedly asked if Ms. Verma planned to use HIP as a model to alter the Medicaid program.
Ms. Verma countered that each state has different needs and should be allowed to develop individualized Medicaid programs that provide flexibility.
“This is about putting states in a leadership role so that they can manage their programs better,” she said. “States are closer to the people that they serve and have a better understanding of what can work in their state than the federal government. I think states should have that flexibility.”
Legislators raised concerns about Ms. Verma’s past consulting agreements with states while working for Hewlett Packard (HP), a company that had financial interests in the health programs she designed. Ms. Verma’s company, SVC, advises clients on Medicaid waivers and state plan amendment development.

Ms. Verma argued that she never negotiated on behalf of Hewlett Packard, and that the work she conducted for the states did not overlap with work she completed for HP. Her company sought an ethics opinion to ensure the arrangement was not problematic, she said.
“I hold honesty and integrity and adherence to a high ethical standard as part of my personal philosophy. That’s for me, I demand that from my employees, and I set that example for my own children,” she said. “We were never in a position where we were negotiating on behalf of HP or any other contractor with the state that we had a relationship with. If there was the potential [for a conflict], we would recuse ourselves.”
Ms. Verma dodged many specific questions, including whether she supported block grants for Medicaid, how she might improve the problem of prescription drug prices, and whether she supported Medicare as a voucher program. When asked by Sen. Sherrod Campbell Brown (D-Ohio) whether she supported an extension of the current Children’s Health Insurance Program (CHIP) for another 8 years, Ms. Verma said she supported “the reauthorization of CHIP for as long as possible.”
When asked about the value-based reforms included in MACRA (the Medicare Access & CHIP Reauthorization Act of 2015), Ms. Verma said she applauded passage of the law, but she would not go into detail about potential changes to the statute.
“I think it’s an important step forward, not only to providing more stability for providers, but also moving us to better outcomes,” she said.
Sen. Wyden grew visibly frustrated with Ms. Verma’s vague answers, saying he was disappointed that, after many questions, the stances she took in many areas were still unclear.
“You’ve been asked a lot of questions and they were not ‘gotcha’ questions,” Sen. Wyden said during the hearing. “These were questions that were appropriate given the fact that if you’re confirmed, you’re going to head an agency that’s involved with a trillion [dollars] of spending in the health care of 100 million people. We’re not really getting much of a sense of how you’d approach [these issues]. I think this committee needs answers and I think the public needs answers.”
“It is critical that we get a strong, skilled leader as CMS administrator,” he said. “Here you are, somebody who has proven to be a tremendous leader in health care, not only to Indiana but as an example to the rest of the states. All I can say is you will be a strong, skilled leader as CMS administrator.”
A relative unknown before her nomination, Ms. Verma spent 20 years designing policy projects involving Medicaid, including HIP, the nation’s first consumer-directed Medicaid program under Indiana Governor Mitch Daniels and then-Gov. Mike Pence’s HIP 2.0 waiver proposal.
Prior to consulting, Ms. Verma served as vice president of planning for the Health and Hospital Corporation of Marion County (Ind.) and as a director with the Association of State and Territorial Health Officials in Washington.
Senators have asked that Ms. Verma submit written answers to their questions, which they will review before voting on her nomination.
[email protected]
On Twitter @legal_med
If confirmed as Centers for Medicare & Medicaid Services administrator, Seema Verma vowed to modernize CMS programs, improve Medicaid access, and leverage technology to drive better care, but she stopped short of explaining how she would do so during her confirmation hearing Feb. 16 before the Senate Finance Committee.
Legislators grilled Ms. Verma on Medicare improvements, the fate of the Affordable Care Act (ACA), Medicaid reform, and the execution of value-based care. At every turn. Ms. Verma pledged to review current processes and work toward enhancing programs, but she declined to support or oppose specific changes. Instead, she promised to help make health care more affordable and to allow patients more flexibility in making health insurance decisions.
Much of the committee’s questioning centered on Ms. Verma’s work on the Healthy Indiana Plan (HIP), Indiana’s Medicaid expansion under the ACA. The conservative plan requires patients to pay a small amount to receive health coverage and includes a lockout period if payments are missed. Legislators repeatedly asked if Ms. Verma planned to use HIP as a model to alter the Medicaid program.
Ms. Verma countered that each state has different needs and should be allowed to develop individualized Medicaid programs that provide flexibility.
“This is about putting states in a leadership role so that they can manage their programs better,” she said. “States are closer to the people that they serve and have a better understanding of what can work in their state than the federal government. I think states should have that flexibility.”
Legislators raised concerns about Ms. Verma’s past consulting agreements with states while working for Hewlett Packard (HP), a company that had financial interests in the health programs she designed. Ms. Verma’s company, SVC, advises clients on Medicaid waivers and state plan amendment development.
Ms. Verma argued that she never negotiated on behalf of Hewlett Packard, and that the work she conducted for the states did not overlap with work she completed for HP. Her company sought an ethics opinion to ensure the arrangement was not problematic, she said.
“I hold honesty and integrity and adherence to a high ethical standard as part of my personal philosophy. That’s for me, I demand that from my employees, and I set that example for my own children,” she said. “We were never in a position where we were negotiating on behalf of HP or any other contractor with the state that we had a relationship with. If there was the potential [for a conflict], we would recuse ourselves.”
Ms. Verma dodged many specific questions, including whether she supported block grants for Medicaid, how she might improve the problem of prescription drug prices, and whether she supported Medicare as a voucher program. When asked by Sen. Sherrod Campbell Brown (D-Ohio) whether she supported an extension of the current Children’s Health Insurance Program (CHIP) for another 8 years, Ms. Verma said she supported “the reauthorization of CHIP for as long as possible.”
When asked about the value-based reforms included in MACRA (the Medicare Access & CHIP Reauthorization Act of 2015), Ms. Verma said she applauded passage of the law, but she would not go into detail about potential changes to the statute.
“I think it’s an important step forward, not only to providing more stability for providers, but also moving us to better outcomes,” she said.
Sen. Wyden grew visibly frustrated with Ms. Verma’s vague answers, saying he was disappointed that, after many questions, the stances she took in many areas were still unclear.
“You’ve been asked a lot of questions and they were not ‘gotcha’ questions,” Sen. Wyden said during the hearing. “These were questions that were appropriate given the fact that if you’re confirmed, you’re going to head an agency that’s involved with a trillion [dollars] of spending in the health care of 100 million people. We’re not really getting much of a sense of how you’d approach [these issues]. I think this committee needs answers and I think the public needs answers.”
“It is critical that we get a strong, skilled leader as CMS administrator,” he said. “Here you are, somebody who has proven to be a tremendous leader in health care, not only to Indiana but as an example to the rest of the states. All I can say is you will be a strong, skilled leader as CMS administrator.”
A relative unknown before her nomination, Ms. Verma spent 20 years designing policy projects involving Medicaid, including HIP, the nation’s first consumer-directed Medicaid program under Indiana Governor Mitch Daniels and then-Gov. Mike Pence’s HIP 2.0 waiver proposal.
Prior to consulting, Ms. Verma served as vice president of planning for the Health and Hospital Corporation of Marion County (Ind.) and as a director with the Association of State and Territorial Health Officials in Washington.
Senators have asked that Ms. Verma submit written answers to their questions, which they will review before voting on her nomination.
[email protected]
On Twitter @legal_med
If confirmed as Centers for Medicare & Medicaid Services administrator, Seema Verma vowed to modernize CMS programs, improve Medicaid access, and leverage technology to drive better care, but she stopped short of explaining how she would do so during her confirmation hearing Feb. 16 before the Senate Finance Committee.
Legislators grilled Ms. Verma on Medicare improvements, the fate of the Affordable Care Act (ACA), Medicaid reform, and the execution of value-based care. At every turn. Ms. Verma pledged to review current processes and work toward enhancing programs, but she declined to support or oppose specific changes. Instead, she promised to help make health care more affordable and to allow patients more flexibility in making health insurance decisions.
Much of the committee’s questioning centered on Ms. Verma’s work on the Healthy Indiana Plan (HIP), Indiana’s Medicaid expansion under the ACA. The conservative plan requires patients to pay a small amount to receive health coverage and includes a lockout period if payments are missed. Legislators repeatedly asked if Ms. Verma planned to use HIP as a model to alter the Medicaid program.
Ms. Verma countered that each state has different needs and should be allowed to develop individualized Medicaid programs that provide flexibility.
“This is about putting states in a leadership role so that they can manage their programs better,” she said. “States are closer to the people that they serve and have a better understanding of what can work in their state than the federal government. I think states should have that flexibility.”
Legislators raised concerns about Ms. Verma’s past consulting agreements with states while working for Hewlett Packard (HP), a company that had financial interests in the health programs she designed. Ms. Verma’s company, SVC, advises clients on Medicaid waivers and state plan amendment development.
Ms. Verma argued that she never negotiated on behalf of Hewlett Packard, and that the work she conducted for the states did not overlap with work she completed for HP. Her company sought an ethics opinion to ensure the arrangement was not problematic, she said.
“I hold honesty and integrity and adherence to a high ethical standard as part of my personal philosophy. That’s for me, I demand that from my employees, and I set that example for my own children,” she said. “We were never in a position where we were negotiating on behalf of HP or any other contractor with the state that we had a relationship with. If there was the potential [for a conflict], we would recuse ourselves.”
Ms. Verma dodged many specific questions, including whether she supported block grants for Medicaid, how she might improve the problem of prescription drug prices, and whether she supported Medicare as a voucher program. When asked by Sen. Sherrod Campbell Brown (D-Ohio) whether she supported an extension of the current Children’s Health Insurance Program (CHIP) for another 8 years, Ms. Verma said she supported “the reauthorization of CHIP for as long as possible.”
When asked about the value-based reforms included in MACRA (the Medicare Access & CHIP Reauthorization Act of 2015), Ms. Verma said she applauded passage of the law, but she would not go into detail about potential changes to the statute.
“I think it’s an important step forward, not only to providing more stability for providers, but also moving us to better outcomes,” she said.
Sen. Wyden grew visibly frustrated with Ms. Verma’s vague answers, saying he was disappointed that, after many questions, the stances she took in many areas were still unclear.
“You’ve been asked a lot of questions and they were not ‘gotcha’ questions,” Sen. Wyden said during the hearing. “These were questions that were appropriate given the fact that if you’re confirmed, you’re going to head an agency that’s involved with a trillion [dollars] of spending in the health care of 100 million people. We’re not really getting much of a sense of how you’d approach [these issues]. I think this committee needs answers and I think the public needs answers.”
“It is critical that we get a strong, skilled leader as CMS administrator,” he said. “Here you are, somebody who has proven to be a tremendous leader in health care, not only to Indiana but as an example to the rest of the states. All I can say is you will be a strong, skilled leader as CMS administrator.”
A relative unknown before her nomination, Ms. Verma spent 20 years designing policy projects involving Medicaid, including HIP, the nation’s first consumer-directed Medicaid program under Indiana Governor Mitch Daniels and then-Gov. Mike Pence’s HIP 2.0 waiver proposal.
Prior to consulting, Ms. Verma served as vice president of planning for the Health and Hospital Corporation of Marion County (Ind.) and as a director with the Association of State and Territorial Health Officials in Washington.
Senators have asked that Ms. Verma submit written answers to their questions, which they will review before voting on her nomination.
[email protected]
On Twitter @legal_med
CMS proposal seeks to stabilize individual insurance market
Proposed regulations from the Centers for Medicare & Medicaid Services aim to provide short-term stabilization to the individual and small group insurance markets under the Affordable Care Act.
The proposal issued Feb. 15 would make changes to special enrollment periods, open enrollment, guaranteed availability, network adequacy rules, essential community providers, and actuarial value requirements. It also changes the timeline for when insurers would need to get their qualified health plan certification. It represents a first step toward fulfilling President Trump’s Inauguration Day executive order to “minimize the unwarranted economic and regulatory burdens of the [ACA], and prepare to afford the states more flexibility and control to create a more free and open health care market.”
However, the proposed rule, if finalized as is, may not have any dramatic effect on the decision by insurers to serve the individual and small group markets.
“A plan that was going to stay is probably going to stay and be a little bit happier about these regs and a plan that was going to decide to leave, like Humana, would have left anyway,” Caroline Pearson, senior vice president at Avalere Health said in an interview. “I don’t know if it is going to materially change plan participation.”
The proposed rule would shorten open enrollment for plans purchased in the ACA marketplace. Currently, plans can be purchased from Nov. 1 to Jan. 31; the proposal would move the deadline up to Dec. 15.
“We anticipate this change could improve the risk pool because it would reduce opportunities for adverse selection by those who learn they will need services in late December and January; and will encourage healthier individuals who might have previously enrolled in partial year coverage after Dec. 15th to instead enroll in coverage for the full year,” according to the proposed rule.
CMS also proposes to tighten special enrollment by requiring preverification of special enrollment period status for all people applicants. Currently, only 50% of those seeking coverage through special enrollment are verified. The agency also is proposing to limit the plan choices available to individuals who are enrolling via a special enrollment period as a way of minimizing adverse selection.
Another proposal aimed at keeping people covered is one that allows insurers to collect unpaid premiums in the prior coverage year before enrolling a patient in the next year’s plan with the same insurer.
CMS noted in the rule that a recent survey “concluded that approximately 21% of consumers stopped premium payments in 2015. Approximately 87% of those individuals repurchased plans in 2016, while 49% of these consumers purchased the same plan they had previously stopped payment on.”
On the network adequacy front, CMS is shifting the conduct of network adequacy reviews to states, or to an accrediting entity recognized by the Department of Health & Human Services in the case of states that do not have sufficient resources to conduct adequacy reviews. Further, the proposal reduces the minimum percentage of essential community providers (those who serve predominantly low-income and medically underserved populations) in a network to 20% from the 30% instituted in 2015.
CMS said in the proposal that if these rules are finalized, it will issue separate guidance on changes to the timeline for plans to submit their bids for 2018.
Avalere’s Ms. Pearson said that she sees these proposed changes merely as a stopgap measure.
“This reg is intended to stand up the exchange markets and keep them functional while the ACA replacement plan is approved and implemented,” she said. “This is meant to prevent there from being a total loss of coverage before the ACA replacement can be put into effect.”
She added that while insurers will welcome the changes, consumers and patient advocates could push back on the proposal, particularly the actuarial flexibility that could result in smaller networks and shrinking benefits.
Indeed, America’s Health Insurance Plans offered its support of the regulation. “We commend the Administration for proposing these regulatory actions as Congress considers other critical actions necessary to help stabilize and improve the individual market for 2018,” AHIP President and CEO Marilyn Tavenner said in a statement.
The proposed changes were released online Feb. 15 and are scheduled for publication in the Federal Register on Feb. 17. Comments on the proposed changes are due to CMS by March 7.
Proposed regulations from the Centers for Medicare & Medicaid Services aim to provide short-term stabilization to the individual and small group insurance markets under the Affordable Care Act.
The proposal issued Feb. 15 would make changes to special enrollment periods, open enrollment, guaranteed availability, network adequacy rules, essential community providers, and actuarial value requirements. It also changes the timeline for when insurers would need to get their qualified health plan certification. It represents a first step toward fulfilling President Trump’s Inauguration Day executive order to “minimize the unwarranted economic and regulatory burdens of the [ACA], and prepare to afford the states more flexibility and control to create a more free and open health care market.”
However, the proposed rule, if finalized as is, may not have any dramatic effect on the decision by insurers to serve the individual and small group markets.
“A plan that was going to stay is probably going to stay and be a little bit happier about these regs and a plan that was going to decide to leave, like Humana, would have left anyway,” Caroline Pearson, senior vice president at Avalere Health said in an interview. “I don’t know if it is going to materially change plan participation.”
The proposed rule would shorten open enrollment for plans purchased in the ACA marketplace. Currently, plans can be purchased from Nov. 1 to Jan. 31; the proposal would move the deadline up to Dec. 15.
“We anticipate this change could improve the risk pool because it would reduce opportunities for adverse selection by those who learn they will need services in late December and January; and will encourage healthier individuals who might have previously enrolled in partial year coverage after Dec. 15th to instead enroll in coverage for the full year,” according to the proposed rule.
CMS also proposes to tighten special enrollment by requiring preverification of special enrollment period status for all people applicants. Currently, only 50% of those seeking coverage through special enrollment are verified. The agency also is proposing to limit the plan choices available to individuals who are enrolling via a special enrollment period as a way of minimizing adverse selection.
Another proposal aimed at keeping people covered is one that allows insurers to collect unpaid premiums in the prior coverage year before enrolling a patient in the next year’s plan with the same insurer.
CMS noted in the rule that a recent survey “concluded that approximately 21% of consumers stopped premium payments in 2015. Approximately 87% of those individuals repurchased plans in 2016, while 49% of these consumers purchased the same plan they had previously stopped payment on.”
On the network adequacy front, CMS is shifting the conduct of network adequacy reviews to states, or to an accrediting entity recognized by the Department of Health & Human Services in the case of states that do not have sufficient resources to conduct adequacy reviews. Further, the proposal reduces the minimum percentage of essential community providers (those who serve predominantly low-income and medically underserved populations) in a network to 20% from the 30% instituted in 2015.
CMS said in the proposal that if these rules are finalized, it will issue separate guidance on changes to the timeline for plans to submit their bids for 2018.
Avalere’s Ms. Pearson said that she sees these proposed changes merely as a stopgap measure.
“This reg is intended to stand up the exchange markets and keep them functional while the ACA replacement plan is approved and implemented,” she said. “This is meant to prevent there from being a total loss of coverage before the ACA replacement can be put into effect.”
She added that while insurers will welcome the changes, consumers and patient advocates could push back on the proposal, particularly the actuarial flexibility that could result in smaller networks and shrinking benefits.
Indeed, America’s Health Insurance Plans offered its support of the regulation. “We commend the Administration for proposing these regulatory actions as Congress considers other critical actions necessary to help stabilize and improve the individual market for 2018,” AHIP President and CEO Marilyn Tavenner said in a statement.
The proposed changes were released online Feb. 15 and are scheduled for publication in the Federal Register on Feb. 17. Comments on the proposed changes are due to CMS by March 7.
Proposed regulations from the Centers for Medicare & Medicaid Services aim to provide short-term stabilization to the individual and small group insurance markets under the Affordable Care Act.
The proposal issued Feb. 15 would make changes to special enrollment periods, open enrollment, guaranteed availability, network adequacy rules, essential community providers, and actuarial value requirements. It also changes the timeline for when insurers would need to get their qualified health plan certification. It represents a first step toward fulfilling President Trump’s Inauguration Day executive order to “minimize the unwarranted economic and regulatory burdens of the [ACA], and prepare to afford the states more flexibility and control to create a more free and open health care market.”
However, the proposed rule, if finalized as is, may not have any dramatic effect on the decision by insurers to serve the individual and small group markets.
“A plan that was going to stay is probably going to stay and be a little bit happier about these regs and a plan that was going to decide to leave, like Humana, would have left anyway,” Caroline Pearson, senior vice president at Avalere Health said in an interview. “I don’t know if it is going to materially change plan participation.”
The proposed rule would shorten open enrollment for plans purchased in the ACA marketplace. Currently, plans can be purchased from Nov. 1 to Jan. 31; the proposal would move the deadline up to Dec. 15.
“We anticipate this change could improve the risk pool because it would reduce opportunities for adverse selection by those who learn they will need services in late December and January; and will encourage healthier individuals who might have previously enrolled in partial year coverage after Dec. 15th to instead enroll in coverage for the full year,” according to the proposed rule.
CMS also proposes to tighten special enrollment by requiring preverification of special enrollment period status for all people applicants. Currently, only 50% of those seeking coverage through special enrollment are verified. The agency also is proposing to limit the plan choices available to individuals who are enrolling via a special enrollment period as a way of minimizing adverse selection.
Another proposal aimed at keeping people covered is one that allows insurers to collect unpaid premiums in the prior coverage year before enrolling a patient in the next year’s plan with the same insurer.
CMS noted in the rule that a recent survey “concluded that approximately 21% of consumers stopped premium payments in 2015. Approximately 87% of those individuals repurchased plans in 2016, while 49% of these consumers purchased the same plan they had previously stopped payment on.”
On the network adequacy front, CMS is shifting the conduct of network adequacy reviews to states, or to an accrediting entity recognized by the Department of Health & Human Services in the case of states that do not have sufficient resources to conduct adequacy reviews. Further, the proposal reduces the minimum percentage of essential community providers (those who serve predominantly low-income and medically underserved populations) in a network to 20% from the 30% instituted in 2015.
CMS said in the proposal that if these rules are finalized, it will issue separate guidance on changes to the timeline for plans to submit their bids for 2018.
Avalere’s Ms. Pearson said that she sees these proposed changes merely as a stopgap measure.
“This reg is intended to stand up the exchange markets and keep them functional while the ACA replacement plan is approved and implemented,” she said. “This is meant to prevent there from being a total loss of coverage before the ACA replacement can be put into effect.”
She added that while insurers will welcome the changes, consumers and patient advocates could push back on the proposal, particularly the actuarial flexibility that could result in smaller networks and shrinking benefits.
Indeed, America’s Health Insurance Plans offered its support of the regulation. “We commend the Administration for proposing these regulatory actions as Congress considers other critical actions necessary to help stabilize and improve the individual market for 2018,” AHIP President and CEO Marilyn Tavenner said in a statement.
The proposed changes were released online Feb. 15 and are scheduled for publication in the Federal Register on Feb. 17. Comments on the proposed changes are due to CMS by March 7.
Malpractice 2017: Do we need reform?
Malpractice reforms long espoused by Thomas E. Price, MD, Health & Human Services secretary, are fostering debate on whether national fixes are necessary in an improving liability landscape. Claims against health providers have decreased twofold and doctors nationwide have seen their premiums decrease steadily for a decade. But the numbers tell just part of the story, liability experts say.
“Most health policy and medical malpractice scholars would not describe the environment we’re in right now as a state of crisis, at least not compared to what we observed a decade ago,” said Anupam B. Jena, MD, PhD, health care policy professor at Harvard University, Boston, and a medical liability researcher.“But I would argue that malpractice is still a salient fact for most physicians. What’s much more important than focusing on changes over time is taking a static perspective and understanding the risk that a physician faces when it comes to malpractice.”

During just over 12 years in Congress, Dr. Price (R-Ga.) has consistently advocated for tort reform, proposing legislation that would restructure the lawsuit process. He supports damage caps and has recommended the creation of health care tribunals that would hear cases only after medical review. He has also proposed the development of national practice guidelines for doctors, which if followed could be used defensively.
“From exorbitant malpractice insurance premiums to the remarkably expensive practice of defensive medicine, it is my experience that the current culture of litigation costs patients hundreds of billions of dollars,” Dr. Price wrote in a 2009 commentary about his Empowering Patients First Act. “These costs do nothing to provide better care, but rather serve only as a defense against unyielding personal injury lawyers ...When malpractice suits are brought through specialized courts and viewed through the perspective of medically appropriate care, rather than a lottery mentality, we will see a decline in frivolous lawsuits.”
Data show lawsuits down
Claims data however, show that lawsuits against doctors are on the decline – and have been for more than 10 years. The rate of paid claims against physicians dropped from 18.6 to 9.9 paid claims per 1,000 physicians between 2002 and 2013, according to 2014 study by Michelle Mello of Stanford (Calif.) University and colleagues (JAMA. 2014;312(20):2146-2155. doi:10.1001/jama.2014.10705). Another analysis found that claims decreased from 12 claims per 100 doctors in 2003 to 6 per 100 doctors in 2016, according to a study of claims from The Doctors Company database.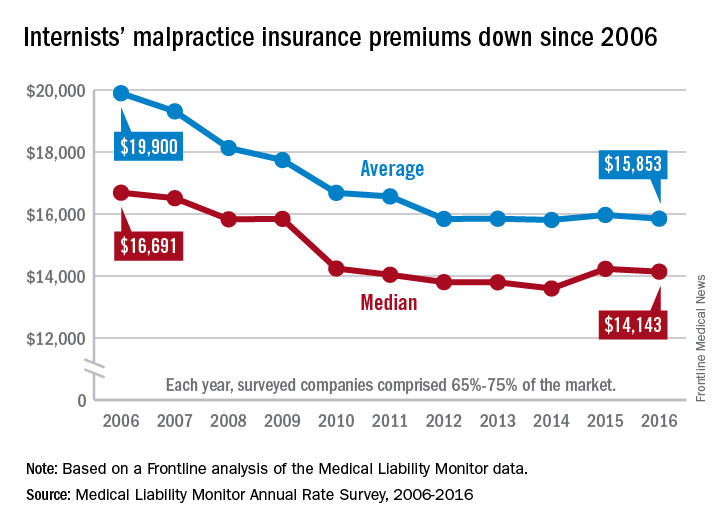
The sharp decline in claims is directly affecting premiums, which have remained nearly unchanged for years, said Michael Matray, editor of the Medical Liability Monitor (MLM), which tracks premium rates. In 2003, rate increases of 49% were commonplace, he noted, with some states reporting rises of 100%. But premiums started to fall in 2006, he said.
“We are in the midst of a 10-year soft market, the longest we’ve ever had,” Mr. Matray said in an interview. “In 2006, we started to soften. We have been soft or flat with no change since. It’s definitely unprecedented.”

In 2016, U.S. internists paid an average premium of $15,853, compared to an average premium payment of $19,900 in 2006 without inflation adjustment, according to this news organization’s analysis of MLM data. General surgeons meanwhile, paid an average of $52,905 in premiums in 2016, compared to a 2006 average of $68,186. Ob.gyns. paid an average premium of $72,999 in 2016, a drop from $93,230 in 2006.
“Generally speaking, it’s great for doctors,” Mr. Matray said. “Even if you remove the inflationary factor, there are some states where they are paying less now than they were 10 years ago.”
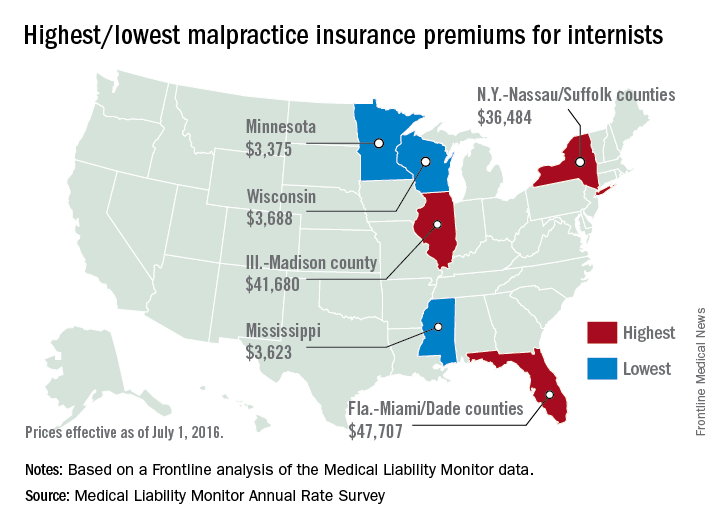
But stable premiums do not mean inexpensive insurance, noted Mike Stinson, vice president of government relations and public policy for the PIAA, a national trade association for medical liability insurers.
“They’ve certainly come down over the last few years,” Mr. Stinson said in an interview. “But they certainly are not low.”

South Florida doctors for example, are paying among the highest premiums in the nation despite an overall drop in the last 10 years. Internists in Dade County, Fla., paid $47,707 for insurance in 2016, $27,000 less than in 2006, according to MLM data. Coverage is still is not affordable, said Jason M. Goldman, MD, an internist in private practice in Coral Springs, Fla., and governor for the American College of Physicians Florida chapter.
The premiums are ridiculous,” he said in an interview. “That’s one of the reasons I went bare. Having medical insurance makes you a target, because lawyers think, ‘We can sue the insurance company and the insurance company is going to pay.’ ”
State reforms driving lawsuit decline
A combination of state reforms and patient safety initiatives are fueling the lawsuit down slide, said Paul A. Greve Jr. senior vice president/senior consultant for Willis Towers Watson Health Care Practice and coauthor of the 2016 MLM Survey report.

More than 25 states now have laws that enforce caps on noneconomic damages in medical liability cases, and in the last 15 years, a large majority have upheld such limits, Mr. Greve said. In addition, a number of states require a certificate of merit before suits can move forward, which mandate that a qualified physician verify that a defendant’s actions were likely negligent.
Patient safety programs such as internal patient safety committees, enhanced provider education, safety protocols, and communication and resolution programs, are also making an impact.
“There have been many efforts toward thinking innovatively about how we should be compensating patients more fairly and more quickly,” said Harvard’s Dr. Jena, who practices at Massachusetts General Hospital. “There are early disclosure programs that many hospitals have adopted as a movement toward that goal. The system is evolving.”
The high expense of filing a medical malpractice lawsuit is another factor detouring lawsuits, Mr. Greve added.

“It’s very expensive for [plaintiffs’ attorneys] to pursue these cases,” he said. “They have to invest a large amount of money into them and they can’t afford to take cases that have questionable liability, or they’re going to end up shelling out a lot of money and not getting anything in return.”
Malpractice system remains broken
While lawsuit and premium data paint a positive picture, the medical malpractice system remains dysfunctional for doctors and patients, said PIAA’s Mr. Stinson.
A majority of medical malpractice claims against physicians are determined to be nonmeritorious yet an average lawsuit takes roughly 4 years to resolve, he noted. Suits against doctors are dismissed by the court 54% of the time across all specialties, and among cases that go to trial, 80% end in the physician’s favor, according to a 2012 study by Dr. Jena and colleagues (JAMA Intern Med. 2012 Jun. 11 doi: 10.1001/jamainternmed.2012.1416)
“We think that’s a huge amount of resources both in time and money and human capital to get poured into cases where no payment is ever deemed appropriate,” Mr. Stinson said. “We would like to see [malpractice] reforms in part because we think you can weed out some of these claims in advance, so more of the resources can be used to determine whether or not there was negligence and if so, making that patient whole as fast as possible.”
Regardless of declining claims, most physicians will still be sued in their lifetime, Dr. Jena said. By age 65, 75% of physicians in low-risk specialties have faced a malpractice claim, and 99% of doctors in high-risk specialties have been sued, according to a 2011 study by Dr. Jena and colleagues (N Engl J Med. 2011 Aug. 18. doi: 10.1056/NEJMsa1012370)
“What really matters for physicians is not only whether they win or lose a malpractice suit, but whether they are sued in the first place,” Dr. Jena said. “Lawsuits happen quite often and over the course of a physician’s career they are quite common. So whether or not we’re in a state of malpractice crisis or not, the lifetime risk for physicians is quite real.”
The cost of defending claims continues to rise, noted Richard E. Anderson, MD, chair and CEO of The Doctors Company. At the same time, multi-million dollar malpractice verdicts have become more common.
“There’s still way too much malpractice litigation,” Dr. Anderson said. “The majority of it is fruitless, and the total cost burden borne by physicians has not decreased as much as the frequency because of the ongoing increase in severity.”
“The bottom line is defensive medicine is a huge and growing cost to all Americans,” he said. “We’re all on the hook for America’s rising health care bills. And as my increasingly infirm Baby Boomer generation gets older and weaker and sicker, those bills are going to rise that much faster. So the notion advanced by some so-called experts that we can nonetheless afford to spend a half trillion dollars a year or more on largely unnecessary testing driven in significant part by fear of litigation and giant outlier verdicts seems rather inane, and it suggests perhaps that those experts aren’t so expert.”
What would Dr. Price do?
Opinions are mixed about whether Dr. Price’s proposed reforms are the right changes for the medical liability system.
Expert panels to review claims for validity are a promising suggestion, Dr. Jena said. “Administrative courts to help identify malpractice cases that are truly malpractice early on is a good idea,” he said. “We want to have a system that prevents less meritorious cases from soaking up resources.”
But the idea may be easier said than done, said Dr. Anderson of The Doctors Company. “The devil is always in the details There is a lot of merit in [health courts] and they make a lot of sense. However, the notion of going from where we are today to an untested system, which would have to be a compromise between adversaries, would be a very challenging one.”
National clinical standards for physicians to follow and use as a safeguard could backfire, Mr. Stinson said. Bureaucracy could slow the guidelines from being promptly updated, and the standards could fail to keep up with the latest medical developments. As doctors know, medicine is not a one-size-fits-all approach, he added.
“[Guidelines] could encourage doctors to practice cookbook medicine, where they’re just going to follow the standard along without being given the opportunity to use their training and clinical experience to see whether that’s actually in the patient’s best interest,” Mr. Stinson said. “We certainly wouldn’t want to see a situation where a doctor feels diverting from a guidelines is in a patient’s best interest, but they don’t dare do it because it could subject them to a lawsuit.”
When enacting malpractice reforms, it will be critical to evaluate the intervention first to ensure the right objections are met, Dr. Jena added.
“At the end of the day, if the [legal] environment is such that it’s uncomfortable to practice medicine, that’s going to have implications for who goes into medicine and implications for ordering tests and procedures,” he said. “Any reform that attempts to make the process more efficient is a good idea because it lowers cost to the system and makes the experience better for patients and physicians.”
This article was updated 2/15/17.
[email protected]
On Twitter @legal_med
Malpractice reforms long espoused by Thomas E. Price, MD, Health & Human Services secretary, are fostering debate on whether national fixes are necessary in an improving liability landscape. Claims against health providers have decreased twofold and doctors nationwide have seen their premiums decrease steadily for a decade. But the numbers tell just part of the story, liability experts say.
“Most health policy and medical malpractice scholars would not describe the environment we’re in right now as a state of crisis, at least not compared to what we observed a decade ago,” said Anupam B. Jena, MD, PhD, health care policy professor at Harvard University, Boston, and a medical liability researcher.“But I would argue that malpractice is still a salient fact for most physicians. What’s much more important than focusing on changes over time is taking a static perspective and understanding the risk that a physician faces when it comes to malpractice.”
During just over 12 years in Congress, Dr. Price (R-Ga.) has consistently advocated for tort reform, proposing legislation that would restructure the lawsuit process. He supports damage caps and has recommended the creation of health care tribunals that would hear cases only after medical review. He has also proposed the development of national practice guidelines for doctors, which if followed could be used defensively.
“From exorbitant malpractice insurance premiums to the remarkably expensive practice of defensive medicine, it is my experience that the current culture of litigation costs patients hundreds of billions of dollars,” Dr. Price wrote in a 2009 commentary about his Empowering Patients First Act. “These costs do nothing to provide better care, but rather serve only as a defense against unyielding personal injury lawyers ...When malpractice suits are brought through specialized courts and viewed through the perspective of medically appropriate care, rather than a lottery mentality, we will see a decline in frivolous lawsuits.”
Data show lawsuits down
Claims data however, show that lawsuits against doctors are on the decline – and have been for more than 10 years. The rate of paid claims against physicians dropped from 18.6 to 9.9 paid claims per 1,000 physicians between 2002 and 2013, according to 2014 study by Michelle Mello of Stanford (Calif.) University and colleagues (JAMA. 2014;312(20):2146-2155. doi:10.1001/jama.2014.10705). Another analysis found that claims decreased from 12 claims per 100 doctors in 2003 to 6 per 100 doctors in 2016, according to a study of claims from The Doctors Company database.
The sharp decline in claims is directly affecting premiums, which have remained nearly unchanged for years, said Michael Matray, editor of the Medical Liability Monitor (MLM), which tracks premium rates. In 2003, rate increases of 49% were commonplace, he noted, with some states reporting rises of 100%. But premiums started to fall in 2006, he said.
“We are in the midst of a 10-year soft market, the longest we’ve ever had,” Mr. Matray said in an interview. “In 2006, we started to soften. We have been soft or flat with no change since. It’s definitely unprecedented.”
In 2016, U.S. internists paid an average premium of $15,853, compared to an average premium payment of $19,900 in 2006 without inflation adjustment, according to this news organization’s analysis of MLM data. General surgeons meanwhile, paid an average of $52,905 in premiums in 2016, compared to a 2006 average of $68,186. Ob.gyns. paid an average premium of $72,999 in 2016, a drop from $93,230 in 2006.
“Generally speaking, it’s great for doctors,” Mr. Matray said. “Even if you remove the inflationary factor, there are some states where they are paying less now than they were 10 years ago.”
But stable premiums do not mean inexpensive insurance, noted Mike Stinson, vice president of government relations and public policy for the PIAA, a national trade association for medical liability insurers.
“They’ve certainly come down over the last few years,” Mr. Stinson said in an interview. “But they certainly are not low.”
South Florida doctors for example, are paying among the highest premiums in the nation despite an overall drop in the last 10 years. Internists in Dade County, Fla., paid $47,707 for insurance in 2016, $27,000 less than in 2006, according to MLM data. Coverage is still is not affordable, said Jason M. Goldman, MD, an internist in private practice in Coral Springs, Fla., and governor for the American College of Physicians Florida chapter.
The premiums are ridiculous,” he said in an interview. “That’s one of the reasons I went bare. Having medical insurance makes you a target, because lawyers think, ‘We can sue the insurance company and the insurance company is going to pay.’ ”
State reforms driving lawsuit decline
A combination of state reforms and patient safety initiatives are fueling the lawsuit down slide, said Paul A. Greve Jr. senior vice president/senior consultant for Willis Towers Watson Health Care Practice and coauthor of the 2016 MLM Survey report.
More than 25 states now have laws that enforce caps on noneconomic damages in medical liability cases, and in the last 15 years, a large majority have upheld such limits, Mr. Greve said. In addition, a number of states require a certificate of merit before suits can move forward, which mandate that a qualified physician verify that a defendant’s actions were likely negligent.
Patient safety programs such as internal patient safety committees, enhanced provider education, safety protocols, and communication and resolution programs, are also making an impact.
“There have been many efforts toward thinking innovatively about how we should be compensating patients more fairly and more quickly,” said Harvard’s Dr. Jena, who practices at Massachusetts General Hospital. “There are early disclosure programs that many hospitals have adopted as a movement toward that goal. The system is evolving.”
The high expense of filing a medical malpractice lawsuit is another factor detouring lawsuits, Mr. Greve added.
“It’s very expensive for [plaintiffs’ attorneys] to pursue these cases,” he said. “They have to invest a large amount of money into them and they can’t afford to take cases that have questionable liability, or they’re going to end up shelling out a lot of money and not getting anything in return.”
Malpractice system remains broken
While lawsuit and premium data paint a positive picture, the medical malpractice system remains dysfunctional for doctors and patients, said PIAA’s Mr. Stinson.
A majority of medical malpractice claims against physicians are determined to be nonmeritorious yet an average lawsuit takes roughly 4 years to resolve, he noted. Suits against doctors are dismissed by the court 54% of the time across all specialties, and among cases that go to trial, 80% end in the physician’s favor, according to a 2012 study by Dr. Jena and colleagues (JAMA Intern Med. 2012 Jun. 11 doi: 10.1001/jamainternmed.2012.1416)
“We think that’s a huge amount of resources both in time and money and human capital to get poured into cases where no payment is ever deemed appropriate,” Mr. Stinson said. “We would like to see [malpractice] reforms in part because we think you can weed out some of these claims in advance, so more of the resources can be used to determine whether or not there was negligence and if so, making that patient whole as fast as possible.”
Regardless of declining claims, most physicians will still be sued in their lifetime, Dr. Jena said. By age 65, 75% of physicians in low-risk specialties have faced a malpractice claim, and 99% of doctors in high-risk specialties have been sued, according to a 2011 study by Dr. Jena and colleagues (N Engl J Med. 2011 Aug. 18. doi: 10.1056/NEJMsa1012370)
“What really matters for physicians is not only whether they win or lose a malpractice suit, but whether they are sued in the first place,” Dr. Jena said. “Lawsuits happen quite often and over the course of a physician’s career they are quite common. So whether or not we’re in a state of malpractice crisis or not, the lifetime risk for physicians is quite real.”
The cost of defending claims continues to rise, noted Richard E. Anderson, MD, chair and CEO of The Doctors Company. At the same time, multi-million dollar malpractice verdicts have become more common.
“There’s still way too much malpractice litigation,” Dr. Anderson said. “The majority of it is fruitless, and the total cost burden borne by physicians has not decreased as much as the frequency because of the ongoing increase in severity.”
“The bottom line is defensive medicine is a huge and growing cost to all Americans,” he said. “We’re all on the hook for America’s rising health care bills. And as my increasingly infirm Baby Boomer generation gets older and weaker and sicker, those bills are going to rise that much faster. So the notion advanced by some so-called experts that we can nonetheless afford to spend a half trillion dollars a year or more on largely unnecessary testing driven in significant part by fear of litigation and giant outlier verdicts seems rather inane, and it suggests perhaps that those experts aren’t so expert.”
What would Dr. Price do?
Opinions are mixed about whether Dr. Price’s proposed reforms are the right changes for the medical liability system.
Expert panels to review claims for validity are a promising suggestion, Dr. Jena said. “Administrative courts to help identify malpractice cases that are truly malpractice early on is a good idea,” he said. “We want to have a system that prevents less meritorious cases from soaking up resources.”
But the idea may be easier said than done, said Dr. Anderson of The Doctors Company. “The devil is always in the details There is a lot of merit in [health courts] and they make a lot of sense. However, the notion of going from where we are today to an untested system, which would have to be a compromise between adversaries, would be a very challenging one.”
National clinical standards for physicians to follow and use as a safeguard could backfire, Mr. Stinson said. Bureaucracy could slow the guidelines from being promptly updated, and the standards could fail to keep up with the latest medical developments. As doctors know, medicine is not a one-size-fits-all approach, he added.
“[Guidelines] could encourage doctors to practice cookbook medicine, where they’re just going to follow the standard along without being given the opportunity to use their training and clinical experience to see whether that’s actually in the patient’s best interest,” Mr. Stinson said. “We certainly wouldn’t want to see a situation where a doctor feels diverting from a guidelines is in a patient’s best interest, but they don’t dare do it because it could subject them to a lawsuit.”
When enacting malpractice reforms, it will be critical to evaluate the intervention first to ensure the right objections are met, Dr. Jena added.
“At the end of the day, if the [legal] environment is such that it’s uncomfortable to practice medicine, that’s going to have implications for who goes into medicine and implications for ordering tests and procedures,” he said. “Any reform that attempts to make the process more efficient is a good idea because it lowers cost to the system and makes the experience better for patients and physicians.”
This article was updated 2/15/17.
[email protected]
On Twitter @legal_med
Malpractice reforms long espoused by Thomas E. Price, MD, Health & Human Services secretary, are fostering debate on whether national fixes are necessary in an improving liability landscape. Claims against health providers have decreased twofold and doctors nationwide have seen their premiums decrease steadily for a decade. But the numbers tell just part of the story, liability experts say.
“Most health policy and medical malpractice scholars would not describe the environment we’re in right now as a state of crisis, at least not compared to what we observed a decade ago,” said Anupam B. Jena, MD, PhD, health care policy professor at Harvard University, Boston, and a medical liability researcher.“But I would argue that malpractice is still a salient fact for most physicians. What’s much more important than focusing on changes over time is taking a static perspective and understanding the risk that a physician faces when it comes to malpractice.”
During just over 12 years in Congress, Dr. Price (R-Ga.) has consistently advocated for tort reform, proposing legislation that would restructure the lawsuit process. He supports damage caps and has recommended the creation of health care tribunals that would hear cases only after medical review. He has also proposed the development of national practice guidelines for doctors, which if followed could be used defensively.
“From exorbitant malpractice insurance premiums to the remarkably expensive practice of defensive medicine, it is my experience that the current culture of litigation costs patients hundreds of billions of dollars,” Dr. Price wrote in a 2009 commentary about his Empowering Patients First Act. “These costs do nothing to provide better care, but rather serve only as a defense against unyielding personal injury lawyers ...When malpractice suits are brought through specialized courts and viewed through the perspective of medically appropriate care, rather than a lottery mentality, we will see a decline in frivolous lawsuits.”
Data show lawsuits down
Claims data however, show that lawsuits against doctors are on the decline – and have been for more than 10 years. The rate of paid claims against physicians dropped from 18.6 to 9.9 paid claims per 1,000 physicians between 2002 and 2013, according to 2014 study by Michelle Mello of Stanford (Calif.) University and colleagues (JAMA. 2014;312(20):2146-2155. doi:10.1001/jama.2014.10705). Another analysis found that claims decreased from 12 claims per 100 doctors in 2003 to 6 per 100 doctors in 2016, according to a study of claims from The Doctors Company database.
The sharp decline in claims is directly affecting premiums, which have remained nearly unchanged for years, said Michael Matray, editor of the Medical Liability Monitor (MLM), which tracks premium rates. In 2003, rate increases of 49% were commonplace, he noted, with some states reporting rises of 100%. But premiums started to fall in 2006, he said.
“We are in the midst of a 10-year soft market, the longest we’ve ever had,” Mr. Matray said in an interview. “In 2006, we started to soften. We have been soft or flat with no change since. It’s definitely unprecedented.”
In 2016, U.S. internists paid an average premium of $15,853, compared to an average premium payment of $19,900 in 2006 without inflation adjustment, according to this news organization’s analysis of MLM data. General surgeons meanwhile, paid an average of $52,905 in premiums in 2016, compared to a 2006 average of $68,186. Ob.gyns. paid an average premium of $72,999 in 2016, a drop from $93,230 in 2006.
“Generally speaking, it’s great for doctors,” Mr. Matray said. “Even if you remove the inflationary factor, there are some states where they are paying less now than they were 10 years ago.”
But stable premiums do not mean inexpensive insurance, noted Mike Stinson, vice president of government relations and public policy for the PIAA, a national trade association for medical liability insurers.
“They’ve certainly come down over the last few years,” Mr. Stinson said in an interview. “But they certainly are not low.”
South Florida doctors for example, are paying among the highest premiums in the nation despite an overall drop in the last 10 years. Internists in Dade County, Fla., paid $47,707 for insurance in 2016, $27,000 less than in 2006, according to MLM data. Coverage is still is not affordable, said Jason M. Goldman, MD, an internist in private practice in Coral Springs, Fla., and governor for the American College of Physicians Florida chapter.
The premiums are ridiculous,” he said in an interview. “That’s one of the reasons I went bare. Having medical insurance makes you a target, because lawyers think, ‘We can sue the insurance company and the insurance company is going to pay.’ ”
State reforms driving lawsuit decline
A combination of state reforms and patient safety initiatives are fueling the lawsuit down slide, said Paul A. Greve Jr. senior vice president/senior consultant for Willis Towers Watson Health Care Practice and coauthor of the 2016 MLM Survey report.
More than 25 states now have laws that enforce caps on noneconomic damages in medical liability cases, and in the last 15 years, a large majority have upheld such limits, Mr. Greve said. In addition, a number of states require a certificate of merit before suits can move forward, which mandate that a qualified physician verify that a defendant’s actions were likely negligent.
Patient safety programs such as internal patient safety committees, enhanced provider education, safety protocols, and communication and resolution programs, are also making an impact.
“There have been many efforts toward thinking innovatively about how we should be compensating patients more fairly and more quickly,” said Harvard’s Dr. Jena, who practices at Massachusetts General Hospital. “There are early disclosure programs that many hospitals have adopted as a movement toward that goal. The system is evolving.”
The high expense of filing a medical malpractice lawsuit is another factor detouring lawsuits, Mr. Greve added.
“It’s very expensive for [plaintiffs’ attorneys] to pursue these cases,” he said. “They have to invest a large amount of money into them and they can’t afford to take cases that have questionable liability, or they’re going to end up shelling out a lot of money and not getting anything in return.”
Malpractice system remains broken
While lawsuit and premium data paint a positive picture, the medical malpractice system remains dysfunctional for doctors and patients, said PIAA’s Mr. Stinson.
A majority of medical malpractice claims against physicians are determined to be nonmeritorious yet an average lawsuit takes roughly 4 years to resolve, he noted. Suits against doctors are dismissed by the court 54% of the time across all specialties, and among cases that go to trial, 80% end in the physician’s favor, according to a 2012 study by Dr. Jena and colleagues (JAMA Intern Med. 2012 Jun. 11 doi: 10.1001/jamainternmed.2012.1416)
“We think that’s a huge amount of resources both in time and money and human capital to get poured into cases where no payment is ever deemed appropriate,” Mr. Stinson said. “We would like to see [malpractice] reforms in part because we think you can weed out some of these claims in advance, so more of the resources can be used to determine whether or not there was negligence and if so, making that patient whole as fast as possible.”
Regardless of declining claims, most physicians will still be sued in their lifetime, Dr. Jena said. By age 65, 75% of physicians in low-risk specialties have faced a malpractice claim, and 99% of doctors in high-risk specialties have been sued, according to a 2011 study by Dr. Jena and colleagues (N Engl J Med. 2011 Aug. 18. doi: 10.1056/NEJMsa1012370)
“What really matters for physicians is not only whether they win or lose a malpractice suit, but whether they are sued in the first place,” Dr. Jena said. “Lawsuits happen quite often and over the course of a physician’s career they are quite common. So whether or not we’re in a state of malpractice crisis or not, the lifetime risk for physicians is quite real.”
The cost of defending claims continues to rise, noted Richard E. Anderson, MD, chair and CEO of The Doctors Company. At the same time, multi-million dollar malpractice verdicts have become more common.
“There’s still way too much malpractice litigation,” Dr. Anderson said. “The majority of it is fruitless, and the total cost burden borne by physicians has not decreased as much as the frequency because of the ongoing increase in severity.”
“The bottom line is defensive medicine is a huge and growing cost to all Americans,” he said. “We’re all on the hook for America’s rising health care bills. And as my increasingly infirm Baby Boomer generation gets older and weaker and sicker, those bills are going to rise that much faster. So the notion advanced by some so-called experts that we can nonetheless afford to spend a half trillion dollars a year or more on largely unnecessary testing driven in significant part by fear of litigation and giant outlier verdicts seems rather inane, and it suggests perhaps that those experts aren’t so expert.”
What would Dr. Price do?
Opinions are mixed about whether Dr. Price’s proposed reforms are the right changes for the medical liability system.
Expert panels to review claims for validity are a promising suggestion, Dr. Jena said. “Administrative courts to help identify malpractice cases that are truly malpractice early on is a good idea,” he said. “We want to have a system that prevents less meritorious cases from soaking up resources.”
But the idea may be easier said than done, said Dr. Anderson of The Doctors Company. “The devil is always in the details There is a lot of merit in [health courts] and they make a lot of sense. However, the notion of going from where we are today to an untested system, which would have to be a compromise between adversaries, would be a very challenging one.”
National clinical standards for physicians to follow and use as a safeguard could backfire, Mr. Stinson said. Bureaucracy could slow the guidelines from being promptly updated, and the standards could fail to keep up with the latest medical developments. As doctors know, medicine is not a one-size-fits-all approach, he added.
“[Guidelines] could encourage doctors to practice cookbook medicine, where they’re just going to follow the standard along without being given the opportunity to use their training and clinical experience to see whether that’s actually in the patient’s best interest,” Mr. Stinson said. “We certainly wouldn’t want to see a situation where a doctor feels diverting from a guidelines is in a patient’s best interest, but they don’t dare do it because it could subject them to a lawsuit.”
When enacting malpractice reforms, it will be critical to evaluate the intervention first to ensure the right objections are met, Dr. Jena added.
“At the end of the day, if the [legal] environment is such that it’s uncomfortable to practice medicine, that’s going to have implications for who goes into medicine and implications for ordering tests and procedures,” he said. “Any reform that attempts to make the process more efficient is a good idea because it lowers cost to the system and makes the experience better for patients and physicians.”
This article was updated 2/15/17.
[email protected]
On Twitter @legal_med