User login
The New Gastroenterologist goes digital
Beginning in February 2018, The New Gastroenterologist (TNG) – a supplement to GI & Hepatology News that addresses issues pertinent to trainees and early-career GIs – will switch to a primarily digital format. We are excited about this change and confident that it will allow for a more effective and widespread dissemination of content that is valuable to both AGA members and our readership more broadly.
![]()
If you have any questions about these changes, or if there are any topics you’d be interested in writing or reading about in The New Gastroenterologist, please contact Editor in Chief Bryson Katona, MD, PhD ([email protected]) or Managing Editor Ryan Farrell ([email protected]).
Beginning in February 2018, The New Gastroenterologist (TNG) – a supplement to GI & Hepatology News that addresses issues pertinent to trainees and early-career GIs – will switch to a primarily digital format. We are excited about this change and confident that it will allow for a more effective and widespread dissemination of content that is valuable to both AGA members and our readership more broadly.
![]()
If you have any questions about these changes, or if there are any topics you’d be interested in writing or reading about in The New Gastroenterologist, please contact Editor in Chief Bryson Katona, MD, PhD ([email protected]) or Managing Editor Ryan Farrell ([email protected]).
Beginning in February 2018, The New Gastroenterologist (TNG) – a supplement to GI & Hepatology News that addresses issues pertinent to trainees and early-career GIs – will switch to a primarily digital format. We are excited about this change and confident that it will allow for a more effective and widespread dissemination of content that is valuable to both AGA members and our readership more broadly.
![]()
If you have any questions about these changes, or if there are any topics you’d be interested in writing or reading about in The New Gastroenterologist, please contact Editor in Chief Bryson Katona, MD, PhD ([email protected]) or Managing Editor Ryan Farrell ([email protected]).
Submit Research to VAM
Research done? Submit it as an abstract for the 2018 Vascular Annual Meeting, set for June 20-23, 2018, in Boston. Plenaries are June 21-23 and exhibits are June 21-22.
The submission site opened Monday. The deadline for submitting abstracts is Wednesday, Jan. 17, 2018.
Abstracts may be submitted in the following categories:
- Plenary
- Vascular and Endovascular Surgical Society
- International Forum
- International Fast Talk
- Poster Competition
- Interactive Poster
Guidelines, submission policies and general information on VAM are available online.
Research done? Submit it as an abstract for the 2018 Vascular Annual Meeting, set for June 20-23, 2018, in Boston. Plenaries are June 21-23 and exhibits are June 21-22.
The submission site opened Monday. The deadline for submitting abstracts is Wednesday, Jan. 17, 2018.
Abstracts may be submitted in the following categories:
- Plenary
- Vascular and Endovascular Surgical Society
- International Forum
- International Fast Talk
- Poster Competition
- Interactive Poster
Guidelines, submission policies and general information on VAM are available online.
Research done? Submit it as an abstract for the 2018 Vascular Annual Meeting, set for June 20-23, 2018, in Boston. Plenaries are June 21-23 and exhibits are June 21-22.
The submission site opened Monday. The deadline for submitting abstracts is Wednesday, Jan. 17, 2018.
Abstracts may be submitted in the following categories:
- Plenary
- Vascular and Endovascular Surgical Society
- International Forum
- International Fast Talk
- Poster Competition
- Interactive Poster
Guidelines, submission policies and general information on VAM are available online.
This month in CHEST Editor’s picks
Original Research
Pharmacotherapy for Non-Cystic Fibrosis Bronchiectasis: Results From an NTM Info and Research Patient Survey and the Bronchiectasis and NTM Research Registry.
By Dr. E. Henkle, et al.
By Dr. A. Lautenbach, et al.
Commentary
Crotalaria (Monocrotaline) Pulmonary Hypertension: The Fiftieth Anniversary.
By Dr. J. Kay.
Original Research
Pharmacotherapy for Non-Cystic Fibrosis Bronchiectasis: Results From an NTM Info and Research Patient Survey and the Bronchiectasis and NTM Research Registry.
By Dr. E. Henkle, et al.
By Dr. A. Lautenbach, et al.
Commentary
Crotalaria (Monocrotaline) Pulmonary Hypertension: The Fiftieth Anniversary.
By Dr. J. Kay.
Original Research
Pharmacotherapy for Non-Cystic Fibrosis Bronchiectasis: Results From an NTM Info and Research Patient Survey and the Bronchiectasis and NTM Research Registry.
By Dr. E. Henkle, et al.
By Dr. A. Lautenbach, et al.
Commentary
Crotalaria (Monocrotaline) Pulmonary Hypertension: The Fiftieth Anniversary.
By Dr. J. Kay.
NAMDRC Report
In mid-September, NAMDRC, along with the American Thoracic Society, the American Association for Respiratory Care, the COPD Foundation, the American Lung Association, and others met to discuss the components of a legislative agenda for the coming years. The primary purpose behind the meeting was the premise that IF the current Republican majority would shift in either the House or Senate after the 2018 election, the community should be prepared to move an already agreed upon legislative agenda. CHEST was involved in the preliminary discussions, as well as follow-up, but was not in attendance at the meeting due to a scheduling conflict. There was also tacit agreement that as these policies are fleshed out and crafted into specific legislative language, the community would re-evaluate the current political climate to determine the value of pushing an agreed upon agenda prior to the 2018 elections.
Various patient groups were also invited to participate, but scheduling conflicts precluded some societies from participating but signaled their desire to work with the broad pulmonary medicine community to pursue common goals.

Each society brought its legislative priorities to the table, and there was active discussion on issues ranging from funding for NIH/NHLBI, to CDC and its COPD Action Plan, to a range of Medicare-related issues.
NAMDRC brought three specific Medicare coverage and payment issues to the discussion: home mechanical ventilation, payment for high flow oxygen therapy, and site of service/Section 603 issues.
Home mechanical ventilation is admittedly a complex issue, but it is moving forward in at least two political directions. First, Senator Bill Cassidy (R-LA) and a physician by training, has signaled his desire to move this issue forward, either legislatively or giving CMS one last chance to move forward through the regulatory structure. He agrees that a payment system that inhibits access to appropriate bi-level mechanical ventilators and encourages access to more complex life-sustaining ventilators, regardless of documented medical need, is appropriate. While CMS does have the authority to act, it has chosen to ignore repeated requests for action over the past 4 years.
Ironically, the House Energy and Commerce Committee, which shares jurisdiction on the House of Representatives with the Ways and Means Committee on Medicare issues, has sent a request to the Congressional Budget Office to provide a cost estimate (a “score” in Washington vernacular) of likely savings from a legislative solution to this matter. In the current political climate, a legislative proposal that actually saves $$$ is politically attractive, and we are working both the regulatory and legislative pathway to seek a workable solution.
On the oxygen therapy issue, there is growing evidence that, for a small group of Medicare beneficiaries who need high flow oxygen therapy as their disease progresses (pulmonary fibrosis, end-stage COPD, etc), there are no oxygen systems readily available to meet that need outside the home. At home, numerous concentrators can meet that need, but outside the home, the ideal solution, liquid systems, is not readily available because of the payment system tied to competitive bidding. CMS payment data indicate that a very low percentage of oxygen users need more than 4 liters per minute, and current law would make a payment adjustment unique to certain patients a very difficult hurdle, particularly in the era of competitive bidding, a legislative change is the best solution facing the community. The challenge is to craft legislative language that addresses the need but would preclude abuse by suppliers who might jump at the chance for higher payment for liquid, well above current payment levels. And because liquid systems fit into a “delivery model” business plan, contrary to portable oxygen concentrators and transfill systems, the solution is not as easy as a payment bump to make provision of liquid systems more attractive.
Site of service regulations are hitting pulmonary rehabilitation particularly hard, and CMS concedes that the only solution is a legislative one. Under current policy, a pulmonary rehab program that is located off campus but needs to expand or move from its current location (losing a lease, for example), if the expanded program is NOT within 250 yards of the main hospital campus, the program is then reimbursed at the physician fee schedule rate, a rate cut of approximately 50%. Needless to say, hospitals are not pursuing that approach. Likewise, a hospital that chooses to open a NEW program is also constrained, needing to locate within 250 yards of the main campus or face the dramatic cut in payment.
As these issues evolve and the political climate perhaps opens unique opportunities, we can expect the broad pulmonary community to pursue these and other issues.
In mid-September, NAMDRC, along with the American Thoracic Society, the American Association for Respiratory Care, the COPD Foundation, the American Lung Association, and others met to discuss the components of a legislative agenda for the coming years. The primary purpose behind the meeting was the premise that IF the current Republican majority would shift in either the House or Senate after the 2018 election, the community should be prepared to move an already agreed upon legislative agenda. CHEST was involved in the preliminary discussions, as well as follow-up, but was not in attendance at the meeting due to a scheduling conflict. There was also tacit agreement that as these policies are fleshed out and crafted into specific legislative language, the community would re-evaluate the current political climate to determine the value of pushing an agreed upon agenda prior to the 2018 elections.
Various patient groups were also invited to participate, but scheduling conflicts precluded some societies from participating but signaled their desire to work with the broad pulmonary medicine community to pursue common goals.
Each society brought its legislative priorities to the table, and there was active discussion on issues ranging from funding for NIH/NHLBI, to CDC and its COPD Action Plan, to a range of Medicare-related issues.
NAMDRC brought three specific Medicare coverage and payment issues to the discussion: home mechanical ventilation, payment for high flow oxygen therapy, and site of service/Section 603 issues.
Home mechanical ventilation is admittedly a complex issue, but it is moving forward in at least two political directions. First, Senator Bill Cassidy (R-LA) and a physician by training, has signaled his desire to move this issue forward, either legislatively or giving CMS one last chance to move forward through the regulatory structure. He agrees that a payment system that inhibits access to appropriate bi-level mechanical ventilators and encourages access to more complex life-sustaining ventilators, regardless of documented medical need, is appropriate. While CMS does have the authority to act, it has chosen to ignore repeated requests for action over the past 4 years.
Ironically, the House Energy and Commerce Committee, which shares jurisdiction on the House of Representatives with the Ways and Means Committee on Medicare issues, has sent a request to the Congressional Budget Office to provide a cost estimate (a “score” in Washington vernacular) of likely savings from a legislative solution to this matter. In the current political climate, a legislative proposal that actually saves $$$ is politically attractive, and we are working both the regulatory and legislative pathway to seek a workable solution.
On the oxygen therapy issue, there is growing evidence that, for a small group of Medicare beneficiaries who need high flow oxygen therapy as their disease progresses (pulmonary fibrosis, end-stage COPD, etc), there are no oxygen systems readily available to meet that need outside the home. At home, numerous concentrators can meet that need, but outside the home, the ideal solution, liquid systems, is not readily available because of the payment system tied to competitive bidding. CMS payment data indicate that a very low percentage of oxygen users need more than 4 liters per minute, and current law would make a payment adjustment unique to certain patients a very difficult hurdle, particularly in the era of competitive bidding, a legislative change is the best solution facing the community. The challenge is to craft legislative language that addresses the need but would preclude abuse by suppliers who might jump at the chance for higher payment for liquid, well above current payment levels. And because liquid systems fit into a “delivery model” business plan, contrary to portable oxygen concentrators and transfill systems, the solution is not as easy as a payment bump to make provision of liquid systems more attractive.
Site of service regulations are hitting pulmonary rehabilitation particularly hard, and CMS concedes that the only solution is a legislative one. Under current policy, a pulmonary rehab program that is located off campus but needs to expand or move from its current location (losing a lease, for example), if the expanded program is NOT within 250 yards of the main hospital campus, the program is then reimbursed at the physician fee schedule rate, a rate cut of approximately 50%. Needless to say, hospitals are not pursuing that approach. Likewise, a hospital that chooses to open a NEW program is also constrained, needing to locate within 250 yards of the main campus or face the dramatic cut in payment.
As these issues evolve and the political climate perhaps opens unique opportunities, we can expect the broad pulmonary community to pursue these and other issues.
In mid-September, NAMDRC, along with the American Thoracic Society, the American Association for Respiratory Care, the COPD Foundation, the American Lung Association, and others met to discuss the components of a legislative agenda for the coming years. The primary purpose behind the meeting was the premise that IF the current Republican majority would shift in either the House or Senate after the 2018 election, the community should be prepared to move an already agreed upon legislative agenda. CHEST was involved in the preliminary discussions, as well as follow-up, but was not in attendance at the meeting due to a scheduling conflict. There was also tacit agreement that as these policies are fleshed out and crafted into specific legislative language, the community would re-evaluate the current political climate to determine the value of pushing an agreed upon agenda prior to the 2018 elections.
Various patient groups were also invited to participate, but scheduling conflicts precluded some societies from participating but signaled their desire to work with the broad pulmonary medicine community to pursue common goals.
Each society brought its legislative priorities to the table, and there was active discussion on issues ranging from funding for NIH/NHLBI, to CDC and its COPD Action Plan, to a range of Medicare-related issues.
NAMDRC brought three specific Medicare coverage and payment issues to the discussion: home mechanical ventilation, payment for high flow oxygen therapy, and site of service/Section 603 issues.
Home mechanical ventilation is admittedly a complex issue, but it is moving forward in at least two political directions. First, Senator Bill Cassidy (R-LA) and a physician by training, has signaled his desire to move this issue forward, either legislatively or giving CMS one last chance to move forward through the regulatory structure. He agrees that a payment system that inhibits access to appropriate bi-level mechanical ventilators and encourages access to more complex life-sustaining ventilators, regardless of documented medical need, is appropriate. While CMS does have the authority to act, it has chosen to ignore repeated requests for action over the past 4 years.
Ironically, the House Energy and Commerce Committee, which shares jurisdiction on the House of Representatives with the Ways and Means Committee on Medicare issues, has sent a request to the Congressional Budget Office to provide a cost estimate (a “score” in Washington vernacular) of likely savings from a legislative solution to this matter. In the current political climate, a legislative proposal that actually saves $$$ is politically attractive, and we are working both the regulatory and legislative pathway to seek a workable solution.
On the oxygen therapy issue, there is growing evidence that, for a small group of Medicare beneficiaries who need high flow oxygen therapy as their disease progresses (pulmonary fibrosis, end-stage COPD, etc), there are no oxygen systems readily available to meet that need outside the home. At home, numerous concentrators can meet that need, but outside the home, the ideal solution, liquid systems, is not readily available because of the payment system tied to competitive bidding. CMS payment data indicate that a very low percentage of oxygen users need more than 4 liters per minute, and current law would make a payment adjustment unique to certain patients a very difficult hurdle, particularly in the era of competitive bidding, a legislative change is the best solution facing the community. The challenge is to craft legislative language that addresses the need but would preclude abuse by suppliers who might jump at the chance for higher payment for liquid, well above current payment levels. And because liquid systems fit into a “delivery model” business plan, contrary to portable oxygen concentrators and transfill systems, the solution is not as easy as a payment bump to make provision of liquid systems more attractive.
Site of service regulations are hitting pulmonary rehabilitation particularly hard, and CMS concedes that the only solution is a legislative one. Under current policy, a pulmonary rehab program that is located off campus but needs to expand or move from its current location (losing a lease, for example), if the expanded program is NOT within 250 yards of the main hospital campus, the program is then reimbursed at the physician fee schedule rate, a rate cut of approximately 50%. Needless to say, hospitals are not pursuing that approach. Likewise, a hospital that chooses to open a NEW program is also constrained, needing to locate within 250 yards of the main campus or face the dramatic cut in payment.
As these issues evolve and the political climate perhaps opens unique opportunities, we can expect the broad pulmonary community to pursue these and other issues.
CHEST Foundation Champions
Champion…. You ARE A CHAMPION for your patients, and as a CHEST Foundation supporter, you are a Champion for Lung Health! These words are now staples in our foundation mission. To champion lung health through clinical research and community service grants, patient education, and community service, the impact your support can have is quite profound. You are a part of an elite group to be called “champions,” and you should be celebrated for all the ways that you have championed lung health in 2017.
- YOU funded more than a half-million dollars in community service grants awarded to the next generation of CHEST leaders.
- YOU educated MILLIONS by supporting nationwide disease awareness campaigns for COPD, asthma, sarcoidosis, and lung cancer.
- YOU brought the Lung Health Experience to communities where over 1,000 people received COPD and asthma education, as well as spirometry screening.
- YOU created awareness in rare disease spaces and raised crucial support by partnering with family foundations, such as the Irv Family Foundation.
- The reach of these activities in 2017 has been astounding, and YOU, as a champion for lung health, have generated a great impact on the chest medicine community and the patients we serve.
- Now, the CHEST Foundation asks YOU to join us and support our efforts for 2018 by giving to the CHEST Foundation Annual Fund today. We ask you to help:
- Meet our fundraising goal of $700,000 for new clinical research and community service grants.
- Support NEW lung health disease awareness campaigns.
- Expand family foundation partnerships to create NEW patient resources.
- Provide NEW e-learning modules to aide patients and caregivers in managing health.
Your support today makes possible tomorrow’s advances in lung health and chest medicine. YOU believe in patient outcomes and, for that commitment, we graciously thank you. YOU save lives by supporting clinical research, patient education, and community service.
Be THE Champion for Lung Health that patients and families count on, and make an impact today. YOU can be a champion and DONATE today through a new gift to the CHEST Foundation. We cannot meet our goals for the health professionals, patients, families, and caregivers we serve without you.
Thank you for your essential continued support!

Champion…. You ARE A CHAMPION for your patients, and as a CHEST Foundation supporter, you are a Champion for Lung Health! These words are now staples in our foundation mission. To champion lung health through clinical research and community service grants, patient education, and community service, the impact your support can have is quite profound. You are a part of an elite group to be called “champions,” and you should be celebrated for all the ways that you have championed lung health in 2017.
- YOU funded more than a half-million dollars in community service grants awarded to the next generation of CHEST leaders.
- YOU educated MILLIONS by supporting nationwide disease awareness campaigns for COPD, asthma, sarcoidosis, and lung cancer.
- YOU brought the Lung Health Experience to communities where over 1,000 people received COPD and asthma education, as well as spirometry screening.
- YOU created awareness in rare disease spaces and raised crucial support by partnering with family foundations, such as the Irv Family Foundation.
- The reach of these activities in 2017 has been astounding, and YOU, as a champion for lung health, have generated a great impact on the chest medicine community and the patients we serve.
- Now, the CHEST Foundation asks YOU to join us and support our efforts for 2018 by giving to the CHEST Foundation Annual Fund today. We ask you to help:
- Meet our fundraising goal of $700,000 for new clinical research and community service grants.
- Support NEW lung health disease awareness campaigns.
- Expand family foundation partnerships to create NEW patient resources.
- Provide NEW e-learning modules to aide patients and caregivers in managing health.
Your support today makes possible tomorrow’s advances in lung health and chest medicine. YOU believe in patient outcomes and, for that commitment, we graciously thank you. YOU save lives by supporting clinical research, patient education, and community service.
Be THE Champion for Lung Health that patients and families count on, and make an impact today. YOU can be a champion and DONATE today through a new gift to the CHEST Foundation. We cannot meet our goals for the health professionals, patients, families, and caregivers we serve without you.
Thank you for your essential continued support!
Champion…. You ARE A CHAMPION for your patients, and as a CHEST Foundation supporter, you are a Champion for Lung Health! These words are now staples in our foundation mission. To champion lung health through clinical research and community service grants, patient education, and community service, the impact your support can have is quite profound. You are a part of an elite group to be called “champions,” and you should be celebrated for all the ways that you have championed lung health in 2017.
- YOU funded more than a half-million dollars in community service grants awarded to the next generation of CHEST leaders.
- YOU educated MILLIONS by supporting nationwide disease awareness campaigns for COPD, asthma, sarcoidosis, and lung cancer.
- YOU brought the Lung Health Experience to communities where over 1,000 people received COPD and asthma education, as well as spirometry screening.
- YOU created awareness in rare disease spaces and raised crucial support by partnering with family foundations, such as the Irv Family Foundation.
- The reach of these activities in 2017 has been astounding, and YOU, as a champion for lung health, have generated a great impact on the chest medicine community and the patients we serve.
- Now, the CHEST Foundation asks YOU to join us and support our efforts for 2018 by giving to the CHEST Foundation Annual Fund today. We ask you to help:
- Meet our fundraising goal of $700,000 for new clinical research and community service grants.
- Support NEW lung health disease awareness campaigns.
- Expand family foundation partnerships to create NEW patient resources.
- Provide NEW e-learning modules to aide patients and caregivers in managing health.
Your support today makes possible tomorrow’s advances in lung health and chest medicine. YOU believe in patient outcomes and, for that commitment, we graciously thank you. YOU save lives by supporting clinical research, patient education, and community service.
Be THE Champion for Lung Health that patients and families count on, and make an impact today. YOU can be a champion and DONATE today through a new gift to the CHEST Foundation. We cannot meet our goals for the health professionals, patients, families, and caregivers we serve without you.
Thank you for your essential continued support!
Urge PAs to Join New SVS Section
SVS members, please remember to urge your physician assistants -- and other PAs you know who work in a vascular setting -- to apply to become charter members of the new SVS section created for them. The first step is becoming an affiliate member of the SVS. For our new charter PA members, SVS is waiving the application fee. For more information, email [email protected] or call the SVS Membership Department at 312-334-2313.
We welcome nurses and nurse practitioners as well. Please consider becoming a part of the Society for Vascular Nursing, which makes its management home at SVS.
SVS members, please remember to urge your physician assistants -- and other PAs you know who work in a vascular setting -- to apply to become charter members of the new SVS section created for them. The first step is becoming an affiliate member of the SVS. For our new charter PA members, SVS is waiving the application fee. For more information, email [email protected] or call the SVS Membership Department at 312-334-2313.
We welcome nurses and nurse practitioners as well. Please consider becoming a part of the Society for Vascular Nursing, which makes its management home at SVS.
SVS members, please remember to urge your physician assistants -- and other PAs you know who work in a vascular setting -- to apply to become charter members of the new SVS section created for them. The first step is becoming an affiliate member of the SVS. For our new charter PA members, SVS is waiving the application fee. For more information, email [email protected] or call the SVS Membership Department at 312-334-2313.
We welcome nurses and nurse practitioners as well. Please consider becoming a part of the Society for Vascular Nursing, which makes its management home at SVS.
Apply for Wylie Scholarship
Applications are due March 2, 2018, for the Wylie Scholar Award, co-sponsored by Vascular Cures and the SVS Foundation. The three-year, $150,000 grant is awarded to a promising vascular surgeon-scientist in North America and is designed to support outstanding surgeon-scientists conducting innovative academic research in the early stages of their careers.
This year's recipient, Dr. Sean English, is conducting research on AAA. Dr. Mohamed Zayed, MD, PhD, the 2015 recipient, is investigating why diabetics develop a unique lipid profile leading to PAD. For each $150,000 award, Wylie Scholars have received $3.3 million in subsequent national research funding, for a return on investment of nearly 22 to1.
Applications are due March 2, 2018, for the Wylie Scholar Award, co-sponsored by Vascular Cures and the SVS Foundation. The three-year, $150,000 grant is awarded to a promising vascular surgeon-scientist in North America and is designed to support outstanding surgeon-scientists conducting innovative academic research in the early stages of their careers.
This year's recipient, Dr. Sean English, is conducting research on AAA. Dr. Mohamed Zayed, MD, PhD, the 2015 recipient, is investigating why diabetics develop a unique lipid profile leading to PAD. For each $150,000 award, Wylie Scholars have received $3.3 million in subsequent national research funding, for a return on investment of nearly 22 to1.
Applications are due March 2, 2018, for the Wylie Scholar Award, co-sponsored by Vascular Cures and the SVS Foundation. The three-year, $150,000 grant is awarded to a promising vascular surgeon-scientist in North America and is designed to support outstanding surgeon-scientists conducting innovative academic research in the early stages of their careers.
This year's recipient, Dr. Sean English, is conducting research on AAA. Dr. Mohamed Zayed, MD, PhD, the 2015 recipient, is investigating why diabetics develop a unique lipid profile leading to PAD. For each $150,000 award, Wylie Scholars have received $3.3 million in subsequent national research funding, for a return on investment of nearly 22 to1.
VRIC Abstracts Now Being Accepted
Abstracts for the 2018 Vascular Research Initiatives Conference are being accepted now, through Jan. 10, 2018. VRIC will be held May 9, 2018, in San Francisco, the day before the American Heart Association’s Arteriosclerosis, Thrombosis and Vascular Biology Scientific Sessions. Learn more about VRIC here.
Vascular trainees may apply for a VRIC scholarship until Jan. 10, 2018. The scholarship provides complimentary registration and a $1,000 travel stipend.
Abstracts for the 2018 Vascular Research Initiatives Conference are being accepted now, through Jan. 10, 2018. VRIC will be held May 9, 2018, in San Francisco, the day before the American Heart Association’s Arteriosclerosis, Thrombosis and Vascular Biology Scientific Sessions. Learn more about VRIC here.
Vascular trainees may apply for a VRIC scholarship until Jan. 10, 2018. The scholarship provides complimentary registration and a $1,000 travel stipend.
Abstracts for the 2018 Vascular Research Initiatives Conference are being accepted now, through Jan. 10, 2018. VRIC will be held May 9, 2018, in San Francisco, the day before the American Heart Association’s Arteriosclerosis, Thrombosis and Vascular Biology Scientific Sessions. Learn more about VRIC here.
Vascular trainees may apply for a VRIC scholarship until Jan. 10, 2018. The scholarship provides complimentary registration and a $1,000 travel stipend.
Letter from the Editor
This month we learned of the passing of Dr. Marv Sleisenger. There are few physicians who have had a greater impact on our field than Dr. Sleisenger. He was a consummate gentleman, enthusiastic teacher, great mentor, authored hundreds of research papers, and edited the most famous textbook of gastroenterology. Our thoughts and hearts are with his family and friends.

I would like to highlight our liver coverage. AASLD had their annual meeting in Washington in November. My colleague at University of Michigan (Anna Lok, MD) is the current president and helped spearhead a meeting that was packed with research and clinical information. We will be covering AASLD in greater depth in the months to come.
And while initial efforts to repeal the ACA have stalled, several key parts of the ACA continue to be modified or repealed either by Executive Orders or as part of the current tax reform efforts. We continue to view these efforts through the lens of our patients’ access to care.
John I. Allen, MD, MBA, AGAF
Editor in Chief
This month we learned of the passing of Dr. Marv Sleisenger. There are few physicians who have had a greater impact on our field than Dr. Sleisenger. He was a consummate gentleman, enthusiastic teacher, great mentor, authored hundreds of research papers, and edited the most famous textbook of gastroenterology. Our thoughts and hearts are with his family and friends.
I would like to highlight our liver coverage. AASLD had their annual meeting in Washington in November. My colleague at University of Michigan (Anna Lok, MD) is the current president and helped spearhead a meeting that was packed with research and clinical information. We will be covering AASLD in greater depth in the months to come.
And while initial efforts to repeal the ACA have stalled, several key parts of the ACA continue to be modified or repealed either by Executive Orders or as part of the current tax reform efforts. We continue to view these efforts through the lens of our patients’ access to care.
John I. Allen, MD, MBA, AGAF
Editor in Chief
This month we learned of the passing of Dr. Marv Sleisenger. There are few physicians who have had a greater impact on our field than Dr. Sleisenger. He was a consummate gentleman, enthusiastic teacher, great mentor, authored hundreds of research papers, and edited the most famous textbook of gastroenterology. Our thoughts and hearts are with his family and friends.
I would like to highlight our liver coverage. AASLD had their annual meeting in Washington in November. My colleague at University of Michigan (Anna Lok, MD) is the current president and helped spearhead a meeting that was packed with research and clinical information. We will be covering AASLD in greater depth in the months to come.
And while initial efforts to repeal the ACA have stalled, several key parts of the ACA continue to be modified or repealed either by Executive Orders or as part of the current tax reform efforts. We continue to view these efforts through the lens of our patients’ access to care.
John I. Allen, MD, MBA, AGAF
Editor in Chief

AGA’s investment in the future of GI
What will the practice of gastroenterology look like in 20 years? It is our hope that physicians will have an abundance of new tools and treatments to care for their patients suffering from digestive disorders.
How will we get there? New treatments and devices are the result of years of research.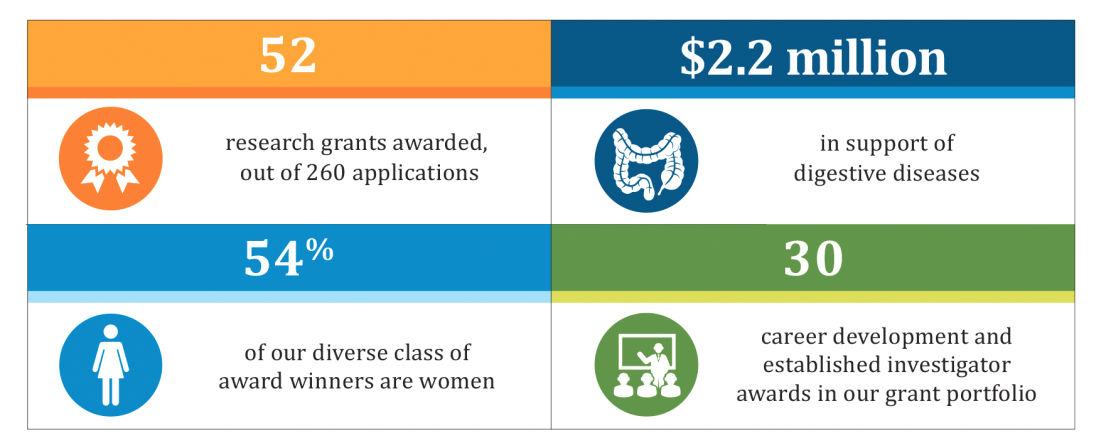
A snapshot of the foundation’s impact this year is highlighted in the chart below. The AGA Research Foundation sincerely thanks all of its donors – without your gifts, this work wouldn’t be possible. Please join us in advancing GI research with a tax-deductible gift to the AGA Research Foundation at www.gastro.org/about/aga-research-foundation.
What will the practice of gastroenterology look like in 20 years? It is our hope that physicians will have an abundance of new tools and treatments to care for their patients suffering from digestive disorders.
How will we get there? New treatments and devices are the result of years of research.
A snapshot of the foundation’s impact this year is highlighted in the chart below. The AGA Research Foundation sincerely thanks all of its donors – without your gifts, this work wouldn’t be possible. Please join us in advancing GI research with a tax-deductible gift to the AGA Research Foundation at www.gastro.org/about/aga-research-foundation.
What will the practice of gastroenterology look like in 20 years? It is our hope that physicians will have an abundance of new tools and treatments to care for their patients suffering from digestive disorders.
How will we get there? New treatments and devices are the result of years of research.
A snapshot of the foundation’s impact this year is highlighted in the chart below. The AGA Research Foundation sincerely thanks all of its donors – without your gifts, this work wouldn’t be possible. Please join us in advancing GI research with a tax-deductible gift to the AGA Research Foundation at www.gastro.org/about/aga-research-foundation.