User login
Standardization of the Discharge Process for Inpatient Hematology and Oncology
Purpose/Rationale: To standardize the discharge process for the hematology/oncology inpatient service at Hines VA Hospital to improve the transition of care
Background: The landmark 1999 report from the Institute of Medicine, To Err is Human, identified the impact of medical error on mortality and morbidity. Medical errors tend to occur during transitions of care. At Hines VA Hospital, a multidisciplinary team delivers specialized care to veterans on the hematology/oncology service. However, resident physicians staffing the inpatient hematology/oncology service may be unfamiliar with the unique needs of the service and population. Currently there is no standardized discharge process in place. Prior studies have demonstrated improved outcomes following standardization of the discharge process for hematology patients. The authors aim to develop and implement a standardized discharge process to minimize risk for medical error.
Method/Approach: A multidisciplinary team of hematology and oncology staff was formed, including attending physicians, fellows, residents, advanced practice nurses, registered nurses, clinical pharmacists, and patient care coordinators, and several interviews were conducted. A standardized discharge process was developed in the form of guidelines and expectations. These include an explanation of unique features of the hematology/oncology service and expectations of medication reconciliation with emphasis placed on antiemetics, antimicrobial prophylaxis, and bowel regimen when appropriate, ambulatory hematology/oncology follow up within 1-2 weeks, primary care followup, communication with ambulatory hematology/oncology physician, written discharge instructions, and bedside teaching when appropriate. The standardized process will be taught to rotating resident physicians in the form of both online orientation and an in-person orientation. Outcome measures were identified including key components of medication reconciliation, time to hematology & oncology clinic visit, time to primary care visit, communication of discharge with outpatient hematology/oncology physician, and 30-day readmission rate.
Conclusions: All patients discharged during the twomonth period prior to and all patients discharged after the implementation of the standardized process will be reviewed; the above-mentioned variables will be recorded. Outcomes will be compared. Interim multidisciplinary team focus group meetings will be held every quarter to review and refine the process.
Purpose/Rationale: To standardize the discharge process for the hematology/oncology inpatient service at Hines VA Hospital to improve the transition of care
Background: The landmark 1999 report from the Institute of Medicine, To Err is Human, identified the impact of medical error on mortality and morbidity. Medical errors tend to occur during transitions of care. At Hines VA Hospital, a multidisciplinary team delivers specialized care to veterans on the hematology/oncology service. However, resident physicians staffing the inpatient hematology/oncology service may be unfamiliar with the unique needs of the service and population. Currently there is no standardized discharge process in place. Prior studies have demonstrated improved outcomes following standardization of the discharge process for hematology patients. The authors aim to develop and implement a standardized discharge process to minimize risk for medical error.
Method/Approach: A multidisciplinary team of hematology and oncology staff was formed, including attending physicians, fellows, residents, advanced practice nurses, registered nurses, clinical pharmacists, and patient care coordinators, and several interviews were conducted. A standardized discharge process was developed in the form of guidelines and expectations. These include an explanation of unique features of the hematology/oncology service and expectations of medication reconciliation with emphasis placed on antiemetics, antimicrobial prophylaxis, and bowel regimen when appropriate, ambulatory hematology/oncology follow up within 1-2 weeks, primary care followup, communication with ambulatory hematology/oncology physician, written discharge instructions, and bedside teaching when appropriate. The standardized process will be taught to rotating resident physicians in the form of both online orientation and an in-person orientation. Outcome measures were identified including key components of medication reconciliation, time to hematology & oncology clinic visit, time to primary care visit, communication of discharge with outpatient hematology/oncology physician, and 30-day readmission rate.
Conclusions: All patients discharged during the twomonth period prior to and all patients discharged after the implementation of the standardized process will be reviewed; the above-mentioned variables will be recorded. Outcomes will be compared. Interim multidisciplinary team focus group meetings will be held every quarter to review and refine the process.
Purpose/Rationale: To standardize the discharge process for the hematology/oncology inpatient service at Hines VA Hospital to improve the transition of care
Background: The landmark 1999 report from the Institute of Medicine, To Err is Human, identified the impact of medical error on mortality and morbidity. Medical errors tend to occur during transitions of care. At Hines VA Hospital, a multidisciplinary team delivers specialized care to veterans on the hematology/oncology service. However, resident physicians staffing the inpatient hematology/oncology service may be unfamiliar with the unique needs of the service and population. Currently there is no standardized discharge process in place. Prior studies have demonstrated improved outcomes following standardization of the discharge process for hematology patients. The authors aim to develop and implement a standardized discharge process to minimize risk for medical error.
Method/Approach: A multidisciplinary team of hematology and oncology staff was formed, including attending physicians, fellows, residents, advanced practice nurses, registered nurses, clinical pharmacists, and patient care coordinators, and several interviews were conducted. A standardized discharge process was developed in the form of guidelines and expectations. These include an explanation of unique features of the hematology/oncology service and expectations of medication reconciliation with emphasis placed on antiemetics, antimicrobial prophylaxis, and bowel regimen when appropriate, ambulatory hematology/oncology follow up within 1-2 weeks, primary care followup, communication with ambulatory hematology/oncology physician, written discharge instructions, and bedside teaching when appropriate. The standardized process will be taught to rotating resident physicians in the form of both online orientation and an in-person orientation. Outcome measures were identified including key components of medication reconciliation, time to hematology & oncology clinic visit, time to primary care visit, communication of discharge with outpatient hematology/oncology physician, and 30-day readmission rate.
Conclusions: All patients discharged during the twomonth period prior to and all patients discharged after the implementation of the standardized process will be reviewed; the above-mentioned variables will be recorded. Outcomes will be compared. Interim multidisciplinary team focus group meetings will be held every quarter to review and refine the process.
Genomic Medicine Service Uses Group Telehealth Appointments to Reduce Wait Times From 5 Months To ~1 Week
Purpose/Rationale: Genomic Medicine Service (GMS) fields 100+ consults weekly. Due to an increase in the number of consults received, without an equal increase in staffing, the wait time for a non-urgent appointment approached 6 months. We explored the use of Group Telehealth
appointments (GTAs) for individuals referred for a family history of breast cancer as one way to reduce these wait times.
Background: While oncology specializes in those with cancer, they are often asked to see unaffected individuals with a family history of cancer who need risk assessments, management recommendations, and/or genetic testing. Many of these are then referred to GMS.
GMS uses the VA telehealth infrastructure to provide genetic evaluation to 84 VAMCs. We typically schedule appointments for one-hour, with an inability to double book due to the limitations of multi-site telehealth. As risk assessment for unaffected individuals is not urgent, these Veterans were scheduled routinely. As GMS got busier, wait times for routine appointments approached 6 months.
Methods/Approach: As part of a Leadership Development Institute, one of the authors (RAR) conceived and implemented a process whereby we held GTAs for unaffected individuals with family histories of breast cancer for whom we would most likely recommend testing an affected
relative. Before the GTA, we mailed a Breast Cancer Risk Assessment (BCRA) form to collect personal/family history. Patients who complete the GTA and BCRA were sent letters that included risk assessments and testing and screening recommendations. 4 GTAs are held each month.
We recorded the number of patients scheduled, appointments attended, and BCRA forms returned. The presentation will review results of an initial 3-month period, during which we held 14 GTAs with 97 patients scheduled, 65 seen, and 58 who turned in BCRAs. We compared time
spent on patients, documentation, and risk assessment in GTAs with the time needed for individual visits for the same number of people. We modeled time saved under a range of assumptions.
Conclusions: Our GTAs were successful, allowing our providers to more efficiently use their time and reducing our wait times. We have expanded our GTAs to include non-breast cancers and reasons for referral.
Purpose/Rationale: Genomic Medicine Service (GMS) fields 100+ consults weekly. Due to an increase in the number of consults received, without an equal increase in staffing, the wait time for a non-urgent appointment approached 6 months. We explored the use of Group Telehealth
appointments (GTAs) for individuals referred for a family history of breast cancer as one way to reduce these wait times.
Background: While oncology specializes in those with cancer, they are often asked to see unaffected individuals with a family history of cancer who need risk assessments, management recommendations, and/or genetic testing. Many of these are then referred to GMS.
GMS uses the VA telehealth infrastructure to provide genetic evaluation to 84 VAMCs. We typically schedule appointments for one-hour, with an inability to double book due to the limitations of multi-site telehealth. As risk assessment for unaffected individuals is not urgent, these Veterans were scheduled routinely. As GMS got busier, wait times for routine appointments approached 6 months.
Methods/Approach: As part of a Leadership Development Institute, one of the authors (RAR) conceived and implemented a process whereby we held GTAs for unaffected individuals with family histories of breast cancer for whom we would most likely recommend testing an affected
relative. Before the GTA, we mailed a Breast Cancer Risk Assessment (BCRA) form to collect personal/family history. Patients who complete the GTA and BCRA were sent letters that included risk assessments and testing and screening recommendations. 4 GTAs are held each month.
We recorded the number of patients scheduled, appointments attended, and BCRA forms returned. The presentation will review results of an initial 3-month period, during which we held 14 GTAs with 97 patients scheduled, 65 seen, and 58 who turned in BCRAs. We compared time
spent on patients, documentation, and risk assessment in GTAs with the time needed for individual visits for the same number of people. We modeled time saved under a range of assumptions.
Conclusions: Our GTAs were successful, allowing our providers to more efficiently use their time and reducing our wait times. We have expanded our GTAs to include non-breast cancers and reasons for referral.
Purpose/Rationale: Genomic Medicine Service (GMS) fields 100+ consults weekly. Due to an increase in the number of consults received, without an equal increase in staffing, the wait time for a non-urgent appointment approached 6 months. We explored the use of Group Telehealth
appointments (GTAs) for individuals referred for a family history of breast cancer as one way to reduce these wait times.
Background: While oncology specializes in those with cancer, they are often asked to see unaffected individuals with a family history of cancer who need risk assessments, management recommendations, and/or genetic testing. Many of these are then referred to GMS.
GMS uses the VA telehealth infrastructure to provide genetic evaluation to 84 VAMCs. We typically schedule appointments for one-hour, with an inability to double book due to the limitations of multi-site telehealth. As risk assessment for unaffected individuals is not urgent, these Veterans were scheduled routinely. As GMS got busier, wait times for routine appointments approached 6 months.
Methods/Approach: As part of a Leadership Development Institute, one of the authors (RAR) conceived and implemented a process whereby we held GTAs for unaffected individuals with family histories of breast cancer for whom we would most likely recommend testing an affected
relative. Before the GTA, we mailed a Breast Cancer Risk Assessment (BCRA) form to collect personal/family history. Patients who complete the GTA and BCRA were sent letters that included risk assessments and testing and screening recommendations. 4 GTAs are held each month.
We recorded the number of patients scheduled, appointments attended, and BCRA forms returned. The presentation will review results of an initial 3-month period, during which we held 14 GTAs with 97 patients scheduled, 65 seen, and 58 who turned in BCRAs. We compared time
spent on patients, documentation, and risk assessment in GTAs with the time needed for individual visits for the same number of people. We modeled time saved under a range of assumptions.
Conclusions: Our GTAs were successful, allowing our providers to more efficiently use their time and reducing our wait times. We have expanded our GTAs to include non-breast cancers and reasons for referral.
Optimization of Palliative Oncology Care Within the VA Healthcare System–Assessing the Availability of Outpatient Palliative Care Within VA Oncology Clinic
Purpose: Palliative care is essential to oncology. The purpose of this project was to characterize the interface between VA oncologists and palliative care specialists in the outpatient setting and to identify barriers to outpatient palliative oncology care in the VA.
Background: The American Society of Clinical Oncology (ASCO) recommends palliative care for all patients with metastatic lung cancer and other symptomatic advanced malignancies. The VA mandates palliative care inpatient consult teams for all medical facilities. It is not clearly known how palliative care is integrated into standard VA outpatient oncology practice. The 2016 VHA Cancer Care Survey was a comprehensive assessment of 140 VA facilities regarding their cancer care infrastructure. On this survey, 23% of sites (N=32) reported that they were not able to provide adequate palliative oncology care in the outpatient setting.
Methods: We contacted clinicians at each of these 32 sites to characterize the outpatient oncology/palliative care interface and identify potential barriers.
Results: Of the 32 sites, 17 reported that they provided limited oncologic care and generally referred patients to other facilities for cancer treatment. The remaining 15 sites reported providing full oncology services. These 15 sites employed a variety of methods to engage palliative care specialists. These included referring patients to a separate outpatient palliative care clinic or a home-based provider; consulting the inpatient palliative care team to evaluate the patient while in the cancer clinic; working with an oncology social worker; or arranging a tele-consult with a remote palliative care specialist. Barriers to providing outpatient palliative care included not enough palliative care staff, not enough clinic space, and patients or oncologists declining a palliative care referral. Clinicians expressed that they would provide more outpatient palliative care if they
had more palliative care staff, more clinic space, and more palliative care training for oncologists.
Conclusions: This project identified that some sites have found creative approaches to providing outpatient palliative oncology care. In addition, clinicians emphasized the ongoing need for additional specialty palliative care staff, primary palliative care training for oncologists, and clinic space in order to provide optimal outpatient palliative oncology care for VA patients.
Purpose: Palliative care is essential to oncology. The purpose of this project was to characterize the interface between VA oncologists and palliative care specialists in the outpatient setting and to identify barriers to outpatient palliative oncology care in the VA.
Background: The American Society of Clinical Oncology (ASCO) recommends palliative care for all patients with metastatic lung cancer and other symptomatic advanced malignancies. The VA mandates palliative care inpatient consult teams for all medical facilities. It is not clearly known how palliative care is integrated into standard VA outpatient oncology practice. The 2016 VHA Cancer Care Survey was a comprehensive assessment of 140 VA facilities regarding their cancer care infrastructure. On this survey, 23% of sites (N=32) reported that they were not able to provide adequate palliative oncology care in the outpatient setting.
Methods: We contacted clinicians at each of these 32 sites to characterize the outpatient oncology/palliative care interface and identify potential barriers.
Results: Of the 32 sites, 17 reported that they provided limited oncologic care and generally referred patients to other facilities for cancer treatment. The remaining 15 sites reported providing full oncology services. These 15 sites employed a variety of methods to engage palliative care specialists. These included referring patients to a separate outpatient palliative care clinic or a home-based provider; consulting the inpatient palliative care team to evaluate the patient while in the cancer clinic; working with an oncology social worker; or arranging a tele-consult with a remote palliative care specialist. Barriers to providing outpatient palliative care included not enough palliative care staff, not enough clinic space, and patients or oncologists declining a palliative care referral. Clinicians expressed that they would provide more outpatient palliative care if they
had more palliative care staff, more clinic space, and more palliative care training for oncologists.
Conclusions: This project identified that some sites have found creative approaches to providing outpatient palliative oncology care. In addition, clinicians emphasized the ongoing need for additional specialty palliative care staff, primary palliative care training for oncologists, and clinic space in order to provide optimal outpatient palliative oncology care for VA patients.
Purpose: Palliative care is essential to oncology. The purpose of this project was to characterize the interface between VA oncologists and palliative care specialists in the outpatient setting and to identify barriers to outpatient palliative oncology care in the VA.
Background: The American Society of Clinical Oncology (ASCO) recommends palliative care for all patients with metastatic lung cancer and other symptomatic advanced malignancies. The VA mandates palliative care inpatient consult teams for all medical facilities. It is not clearly known how palliative care is integrated into standard VA outpatient oncology practice. The 2016 VHA Cancer Care Survey was a comprehensive assessment of 140 VA facilities regarding their cancer care infrastructure. On this survey, 23% of sites (N=32) reported that they were not able to provide adequate palliative oncology care in the outpatient setting.
Methods: We contacted clinicians at each of these 32 sites to characterize the outpatient oncology/palliative care interface and identify potential barriers.
Results: Of the 32 sites, 17 reported that they provided limited oncologic care and generally referred patients to other facilities for cancer treatment. The remaining 15 sites reported providing full oncology services. These 15 sites employed a variety of methods to engage palliative care specialists. These included referring patients to a separate outpatient palliative care clinic or a home-based provider; consulting the inpatient palliative care team to evaluate the patient while in the cancer clinic; working with an oncology social worker; or arranging a tele-consult with a remote palliative care specialist. Barriers to providing outpatient palliative care included not enough palliative care staff, not enough clinic space, and patients or oncologists declining a palliative care referral. Clinicians expressed that they would provide more outpatient palliative care if they
had more palliative care staff, more clinic space, and more palliative care training for oncologists.
Conclusions: This project identified that some sites have found creative approaches to providing outpatient palliative oncology care. In addition, clinicians emphasized the ongoing need for additional specialty palliative care staff, primary palliative care training for oncologists, and clinic space in order to provide optimal outpatient palliative oncology care for VA patients.
More than half of urine drug screens showed improper medication use
LAS VEGAS –

Of almost 4 million urine screens examined, 52% were discordant for the screen-ordered drugs, Jeffrey Gudin, MD, said at the annual PAINWeek. Most common was the combination of opioids and benzodiazepines, which accounted for 21% of the discordant samples – and, in 64% of these cases, at least one of the drugs was not prescribed.
“Drug testing is a standard of care in pain management, and it’s the only objective way to know what patients are really taking,” said Dr. Gudin, director of pain and palliative care at Englewood (N.J.) Hospital and Medical Center. “What this tells us is that, if we just ask our patients, half the time they won’t tell you the whole story. More than 50% of the time things don’t match up. To me this is just unbelievable.”
Quest Diagnostics compiled these data, and many more, in its “Health Trends Report: Drug Misuse in America 2018.”
The report examines 3.9 million routine drug screens ordered by primary care and pain physicians during 2011-2017. It not only looks at prescription drug use and misuse but also tracks illicit drugs in both general and substance abuse patient populations. The findings reported at PAINWeek were based on 456,675 screens from 276,953 patients conducted in 2017. These results were included in the Quest Diagnostics medMATCH reports, which indicated what tested drugs were prescribed and whether these drugs were detected in the specimen.
The following were found among the discordant screens identified in 2017:
- 45% were positive for nonprescribed or illicit drugs in addition to all the prescribed drugs.
- 34% did not show all the drugs they had been prescribed, or any other tested drug.
- 22% did not show all the drugs they had been prescribed but were positive for other illicit or nonprescribed drugs.
The tests were ordered as a part of routine care – an important point, Dr. Gudin said in an interview. “These are not ‘gotcha tests,’ ” intended to catch patients unawares. “These are regularly ordered screens that are standard of care in pain management.”
The report found that men and women were equally likely to misuse medications (52% each). There were some age-related differences, with misuse peaking in young adulthood: 60% of 18- to 24-year-olds and 56% of 25- to 45-year-olds. Misuse dropped off in those aged 55-64 years (52%) and in those 65 years and older (43%). But even children showed evidence of medication misuse, with about 41% of samples from children aged 10 years and younger being discordant.
The rates of misuse were about 50% in Medicare and private pay patients, but around 65% in Medicaid patients.
There was some good news: In the general patient population, opioid use was down by 12% from 2016 – the largest annual decrease Quest has noted since 2012. Several factors probably contributed to that decline, including shifts in clinical care and payer reimbursement, as well as regulatory and legislative restrictions.
“This shows that we’re doing better on the pain management front,” Dr. Gudin said. “But in substance use disorder settings, we saw 400% increases for both fentanyl and heroin. The addiction front it out of control.”
More than 27% of all specimens that came from substance abuse treatment centers were positive for nonprescribed fentanyl and 10% were positive for heroin. “We also saw that, in 2016, 45% of those heroin-positive samples had fentanyl in them, and in 2017, 83% did.”
Although not discussed at PAINWeek, the report also noted a rise in gabapentin misuse. The antiepileptic is now the 10th most commonly prescribed drug in the United States, the report noted, with 68 million prescriptions dispensed last year. The report found that 9.5% of tests showed nonprescription gabapentin. In the subset of samples obtained from substance abuse treatment centers, gabapentin misuse increased by 800% from 2016 – the most dramatic increase of any of the tracked drugs.
The combination of gabapentin and opioids is risky, the report noted. Opioid-related deaths are 49% more common among those taking both than those taking opioids only.
SOURCE: Gudin J et al. PAINWeek 2018, abstract 44.
LAS VEGAS –
Of almost 4 million urine screens examined, 52% were discordant for the screen-ordered drugs, Jeffrey Gudin, MD, said at the annual PAINWeek. Most common was the combination of opioids and benzodiazepines, which accounted for 21% of the discordant samples – and, in 64% of these cases, at least one of the drugs was not prescribed.
“Drug testing is a standard of care in pain management, and it’s the only objective way to know what patients are really taking,” said Dr. Gudin, director of pain and palliative care at Englewood (N.J.) Hospital and Medical Center. “What this tells us is that, if we just ask our patients, half the time they won’t tell you the whole story. More than 50% of the time things don’t match up. To me this is just unbelievable.”
Quest Diagnostics compiled these data, and many more, in its “Health Trends Report: Drug Misuse in America 2018.”
The report examines 3.9 million routine drug screens ordered by primary care and pain physicians during 2011-2017. It not only looks at prescription drug use and misuse but also tracks illicit drugs in both general and substance abuse patient populations. The findings reported at PAINWeek were based on 456,675 screens from 276,953 patients conducted in 2017. These results were included in the Quest Diagnostics medMATCH reports, which indicated what tested drugs were prescribed and whether these drugs were detected in the specimen.
The following were found among the discordant screens identified in 2017:
- 45% were positive for nonprescribed or illicit drugs in addition to all the prescribed drugs.
- 34% did not show all the drugs they had been prescribed, or any other tested drug.
- 22% did not show all the drugs they had been prescribed but were positive for other illicit or nonprescribed drugs.
The tests were ordered as a part of routine care – an important point, Dr. Gudin said in an interview. “These are not ‘gotcha tests,’ ” intended to catch patients unawares. “These are regularly ordered screens that are standard of care in pain management.”
The report found that men and women were equally likely to misuse medications (52% each). There were some age-related differences, with misuse peaking in young adulthood: 60% of 18- to 24-year-olds and 56% of 25- to 45-year-olds. Misuse dropped off in those aged 55-64 years (52%) and in those 65 years and older (43%). But even children showed evidence of medication misuse, with about 41% of samples from children aged 10 years and younger being discordant.
The rates of misuse were about 50% in Medicare and private pay patients, but around 65% in Medicaid patients.
There was some good news: In the general patient population, opioid use was down by 12% from 2016 – the largest annual decrease Quest has noted since 2012. Several factors probably contributed to that decline, including shifts in clinical care and payer reimbursement, as well as regulatory and legislative restrictions.
“This shows that we’re doing better on the pain management front,” Dr. Gudin said. “But in substance use disorder settings, we saw 400% increases for both fentanyl and heroin. The addiction front it out of control.”
More than 27% of all specimens that came from substance abuse treatment centers were positive for nonprescribed fentanyl and 10% were positive for heroin. “We also saw that, in 2016, 45% of those heroin-positive samples had fentanyl in them, and in 2017, 83% did.”
Although not discussed at PAINWeek, the report also noted a rise in gabapentin misuse. The antiepileptic is now the 10th most commonly prescribed drug in the United States, the report noted, with 68 million prescriptions dispensed last year. The report found that 9.5% of tests showed nonprescription gabapentin. In the subset of samples obtained from substance abuse treatment centers, gabapentin misuse increased by 800% from 2016 – the most dramatic increase of any of the tracked drugs.
The combination of gabapentin and opioids is risky, the report noted. Opioid-related deaths are 49% more common among those taking both than those taking opioids only.
SOURCE: Gudin J et al. PAINWeek 2018, abstract 44.
LAS VEGAS –
Of almost 4 million urine screens examined, 52% were discordant for the screen-ordered drugs, Jeffrey Gudin, MD, said at the annual PAINWeek. Most common was the combination of opioids and benzodiazepines, which accounted for 21% of the discordant samples – and, in 64% of these cases, at least one of the drugs was not prescribed.
“Drug testing is a standard of care in pain management, and it’s the only objective way to know what patients are really taking,” said Dr. Gudin, director of pain and palliative care at Englewood (N.J.) Hospital and Medical Center. “What this tells us is that, if we just ask our patients, half the time they won’t tell you the whole story. More than 50% of the time things don’t match up. To me this is just unbelievable.”
Quest Diagnostics compiled these data, and many more, in its “Health Trends Report: Drug Misuse in America 2018.”
The report examines 3.9 million routine drug screens ordered by primary care and pain physicians during 2011-2017. It not only looks at prescription drug use and misuse but also tracks illicit drugs in both general and substance abuse patient populations. The findings reported at PAINWeek were based on 456,675 screens from 276,953 patients conducted in 2017. These results were included in the Quest Diagnostics medMATCH reports, which indicated what tested drugs were prescribed and whether these drugs were detected in the specimen.
The following were found among the discordant screens identified in 2017:
- 45% were positive for nonprescribed or illicit drugs in addition to all the prescribed drugs.
- 34% did not show all the drugs they had been prescribed, or any other tested drug.
- 22% did not show all the drugs they had been prescribed but were positive for other illicit or nonprescribed drugs.
The tests were ordered as a part of routine care – an important point, Dr. Gudin said in an interview. “These are not ‘gotcha tests,’ ” intended to catch patients unawares. “These are regularly ordered screens that are standard of care in pain management.”
The report found that men and women were equally likely to misuse medications (52% each). There were some age-related differences, with misuse peaking in young adulthood: 60% of 18- to 24-year-olds and 56% of 25- to 45-year-olds. Misuse dropped off in those aged 55-64 years (52%) and in those 65 years and older (43%). But even children showed evidence of medication misuse, with about 41% of samples from children aged 10 years and younger being discordant.
The rates of misuse were about 50% in Medicare and private pay patients, but around 65% in Medicaid patients.
There was some good news: In the general patient population, opioid use was down by 12% from 2016 – the largest annual decrease Quest has noted since 2012. Several factors probably contributed to that decline, including shifts in clinical care and payer reimbursement, as well as regulatory and legislative restrictions.
“This shows that we’re doing better on the pain management front,” Dr. Gudin said. “But in substance use disorder settings, we saw 400% increases for both fentanyl and heroin. The addiction front it out of control.”
More than 27% of all specimens that came from substance abuse treatment centers were positive for nonprescribed fentanyl and 10% were positive for heroin. “We also saw that, in 2016, 45% of those heroin-positive samples had fentanyl in them, and in 2017, 83% did.”
Although not discussed at PAINWeek, the report also noted a rise in gabapentin misuse. The antiepileptic is now the 10th most commonly prescribed drug in the United States, the report noted, with 68 million prescriptions dispensed last year. The report found that 9.5% of tests showed nonprescription gabapentin. In the subset of samples obtained from substance abuse treatment centers, gabapentin misuse increased by 800% from 2016 – the most dramatic increase of any of the tracked drugs.
The combination of gabapentin and opioids is risky, the report noted. Opioid-related deaths are 49% more common among those taking both than those taking opioids only.
SOURCE: Gudin J et al. PAINWeek 2018, abstract 44.
REPORTING FROM PAINWEEK 2018
Key clinical point: More than half of patients undergoing urine drug screens were misusing medications.
Major finding: The samples were discordant for the queried drug in 52% of samples.
Study details: The study was based on 3.9 million drug screens ordered during 2011-2017.
Disclosures: The findings were included in Quest Diagnostics’ “Health Trends Report: Drug Misuse in America 2018.”
Source: Gudin J et al. PAINWeek, Abstract 44.
Improving Patient Safety, One Hematology/Oncology Order Set a Time. An Outpatient VA Oncology Clinic Experience
Purpose: A VISN initiative in 2015 led to development of hematology/oncology medication order sets to improve the translation of medication orders from CPRS provider order entry program to pharmacy verification program in VistA. Our purpose is to report the incidence of averted errors due to hematology/oncology medication order translation issues prior to order set initiative as compared to incidence post-order set initiative.
Background: Hematology/oncology medication orders at this outpatient VA oncology clinic are prescribed via provider order entry within CPRS. Safety concerns existed due to inefficient communication between CPRS order entry and pharmacy verification within VistA. A pharmacist verifying orders within VistA was required to re-enter critical medication order information such as drug dose into VistA. In order to find the dose ordered by a provider, the verification pharmacist
advanced at least one screen in VistA then returned to the original VistA verification screen to enter drug dose.
Methods: Incidence of averted errors related to hematology/oncology medication order translation issues between CPRS and VistA are reported for the 2-year time period (October 2013 through September 2015) prior to order set initiative and for the 2-year time period (October 2015 through September 2017) after beginning the order set initiative. Additional information includes facility resources, such as: treatment area, providers, staffing, oncology pharmacy, pharmacy ADPAC, and CACs; mechanisms of orders and notes entering/recording; dosing and safety checks;
and available order sets.
Results: The incidence rate of averted errors related to hematology/oncology medication order translation issues prior to order set initiative was 0.379% as compared to 0.128% rate of averted errors in the two years post order set initiative. Results showed hematology/oncology medication order sets used at this facility positively impacted the incidence of averted errors attributed to translation issues from CPRS to VistA. With fewer averted errors, patient safety increased.
Implications: Using limited VA resources, order sets were implemented for use at this VA outpatient oncology clinic. The hematology/oncology health care team worked together to provide vigilant oversight of order sets and to incorporate necessary revisions, updates, and additions. With fewer averted errors, the effectiveness of this initiative is quantified with improved patient care, safety and efficiency.
Purpose: A VISN initiative in 2015 led to development of hematology/oncology medication order sets to improve the translation of medication orders from CPRS provider order entry program to pharmacy verification program in VistA. Our purpose is to report the incidence of averted errors due to hematology/oncology medication order translation issues prior to order set initiative as compared to incidence post-order set initiative.
Background: Hematology/oncology medication orders at this outpatient VA oncology clinic are prescribed via provider order entry within CPRS. Safety concerns existed due to inefficient communication between CPRS order entry and pharmacy verification within VistA. A pharmacist verifying orders within VistA was required to re-enter critical medication order information such as drug dose into VistA. In order to find the dose ordered by a provider, the verification pharmacist
advanced at least one screen in VistA then returned to the original VistA verification screen to enter drug dose.
Methods: Incidence of averted errors related to hematology/oncology medication order translation issues between CPRS and VistA are reported for the 2-year time period (October 2013 through September 2015) prior to order set initiative and for the 2-year time period (October 2015 through September 2017) after beginning the order set initiative. Additional information includes facility resources, such as: treatment area, providers, staffing, oncology pharmacy, pharmacy ADPAC, and CACs; mechanisms of orders and notes entering/recording; dosing and safety checks;
and available order sets.
Results: The incidence rate of averted errors related to hematology/oncology medication order translation issues prior to order set initiative was 0.379% as compared to 0.128% rate of averted errors in the two years post order set initiative. Results showed hematology/oncology medication order sets used at this facility positively impacted the incidence of averted errors attributed to translation issues from CPRS to VistA. With fewer averted errors, patient safety increased.
Implications: Using limited VA resources, order sets were implemented for use at this VA outpatient oncology clinic. The hematology/oncology health care team worked together to provide vigilant oversight of order sets and to incorporate necessary revisions, updates, and additions. With fewer averted errors, the effectiveness of this initiative is quantified with improved patient care, safety and efficiency.
Purpose: A VISN initiative in 2015 led to development of hematology/oncology medication order sets to improve the translation of medication orders from CPRS provider order entry program to pharmacy verification program in VistA. Our purpose is to report the incidence of averted errors due to hematology/oncology medication order translation issues prior to order set initiative as compared to incidence post-order set initiative.
Background: Hematology/oncology medication orders at this outpatient VA oncology clinic are prescribed via provider order entry within CPRS. Safety concerns existed due to inefficient communication between CPRS order entry and pharmacy verification within VistA. A pharmacist verifying orders within VistA was required to re-enter critical medication order information such as drug dose into VistA. In order to find the dose ordered by a provider, the verification pharmacist
advanced at least one screen in VistA then returned to the original VistA verification screen to enter drug dose.
Methods: Incidence of averted errors related to hematology/oncology medication order translation issues between CPRS and VistA are reported for the 2-year time period (October 2013 through September 2015) prior to order set initiative and for the 2-year time period (October 2015 through September 2017) after beginning the order set initiative. Additional information includes facility resources, such as: treatment area, providers, staffing, oncology pharmacy, pharmacy ADPAC, and CACs; mechanisms of orders and notes entering/recording; dosing and safety checks;
and available order sets.
Results: The incidence rate of averted errors related to hematology/oncology medication order translation issues prior to order set initiative was 0.379% as compared to 0.128% rate of averted errors in the two years post order set initiative. Results showed hematology/oncology medication order sets used at this facility positively impacted the incidence of averted errors attributed to translation issues from CPRS to VistA. With fewer averted errors, patient safety increased.
Implications: Using limited VA resources, order sets were implemented for use at this VA outpatient oncology clinic. The hematology/oncology health care team worked together to provide vigilant oversight of order sets and to incorporate necessary revisions, updates, and additions. With fewer averted errors, the effectiveness of this initiative is quantified with improved patient care, safety and efficiency.
Oncology Nursing Professionalism: Advocating and Developing Oncology Certified Nurses
Introduction: The Commission on Cancer (COC), the New Mexico VA Health Care System (NMVAHCS) accrediting body for cancer care, mandates 25% of nurses maintain oncology nurse certification (OCN) to validate competency. However, the NMVAHCS remains deficient: threatening facility ability to maintain accreditation. Per the Oncology Nursing Certification Corporation, Albuquerque maintains 160 OCNs. However, 50% have retired and the remaining 50% are over 52. Leaving approximately 40 OCN nurses in a population of 500,000. This problem was not only a NMVAHCS problem, but a community problem: affecting quality of oncology care.
Problem: Not only is certification required for COC accredited facilities, it represents validation of expertise and skill set. Validation serves to build trust of Veterans, enables superior clinical judgment, and contributes to improved outcomes. With the Choice Program, many Veterans can leave the VAHCS. Certification serves to build necessary confidence required to keep Veterans within the VAHCS.
Methods: Barriers prohibiting certification were identified through survey of oncology nurses. Nurses reported fear related to failure, study material costs, exam fees, lack of mentors, and lack of internal leadership encouragement and support as barriers of certification. Funding was sought to provide a review course for 40 nurses, study guides, reimbursement of course and exam fees and held June 2017 in Albuquerque, New Mexico. A second review course, held during the 2017 AVAHO meeting, was conducted for another 24 nurses. The courses aimed to build confidence and decrease barriers. Both exceeded capacity.
Results: As a result of the Albuquerque course, VISN 22 and non-VA nurses attended from several states. Each received
a 30% reduction in exam fees and were eligible for exam reimbursement after passing: 50% of attendees are now OCNs.
The AVAHO course, to date, has resulted in an additional 2 OCNs, 2 certification renewals, and an additional 5 are registered for the exam. Those not taking the exam cite lack of leadership support and encouragement as the main
barrier.
Implications: Certification validates care provided and builds Veterans trust: necessary with Choice. Facilities that retain a strong foundation of OCNs, mentor staff, and maintain leadership support remain more apt to produce and sustain certified nurses. Therefore, leadership buy-in remains essential.
Introduction: The Commission on Cancer (COC), the New Mexico VA Health Care System (NMVAHCS) accrediting body for cancer care, mandates 25% of nurses maintain oncology nurse certification (OCN) to validate competency. However, the NMVAHCS remains deficient: threatening facility ability to maintain accreditation. Per the Oncology Nursing Certification Corporation, Albuquerque maintains 160 OCNs. However, 50% have retired and the remaining 50% are over 52. Leaving approximately 40 OCN nurses in a population of 500,000. This problem was not only a NMVAHCS problem, but a community problem: affecting quality of oncology care.
Problem: Not only is certification required for COC accredited facilities, it represents validation of expertise and skill set. Validation serves to build trust of Veterans, enables superior clinical judgment, and contributes to improved outcomes. With the Choice Program, many Veterans can leave the VAHCS. Certification serves to build necessary confidence required to keep Veterans within the VAHCS.
Methods: Barriers prohibiting certification were identified through survey of oncology nurses. Nurses reported fear related to failure, study material costs, exam fees, lack of mentors, and lack of internal leadership encouragement and support as barriers of certification. Funding was sought to provide a review course for 40 nurses, study guides, reimbursement of course and exam fees and held June 2017 in Albuquerque, New Mexico. A second review course, held during the 2017 AVAHO meeting, was conducted for another 24 nurses. The courses aimed to build confidence and decrease barriers. Both exceeded capacity.
Results: As a result of the Albuquerque course, VISN 22 and non-VA nurses attended from several states. Each received
a 30% reduction in exam fees and were eligible for exam reimbursement after passing: 50% of attendees are now OCNs.
The AVAHO course, to date, has resulted in an additional 2 OCNs, 2 certification renewals, and an additional 5 are registered for the exam. Those not taking the exam cite lack of leadership support and encouragement as the main
barrier.
Implications: Certification validates care provided and builds Veterans trust: necessary with Choice. Facilities that retain a strong foundation of OCNs, mentor staff, and maintain leadership support remain more apt to produce and sustain certified nurses. Therefore, leadership buy-in remains essential.
Introduction: The Commission on Cancer (COC), the New Mexico VA Health Care System (NMVAHCS) accrediting body for cancer care, mandates 25% of nurses maintain oncology nurse certification (OCN) to validate competency. However, the NMVAHCS remains deficient: threatening facility ability to maintain accreditation. Per the Oncology Nursing Certification Corporation, Albuquerque maintains 160 OCNs. However, 50% have retired and the remaining 50% are over 52. Leaving approximately 40 OCN nurses in a population of 500,000. This problem was not only a NMVAHCS problem, but a community problem: affecting quality of oncology care.
Problem: Not only is certification required for COC accredited facilities, it represents validation of expertise and skill set. Validation serves to build trust of Veterans, enables superior clinical judgment, and contributes to improved outcomes. With the Choice Program, many Veterans can leave the VAHCS. Certification serves to build necessary confidence required to keep Veterans within the VAHCS.
Methods: Barriers prohibiting certification were identified through survey of oncology nurses. Nurses reported fear related to failure, study material costs, exam fees, lack of mentors, and lack of internal leadership encouragement and support as barriers of certification. Funding was sought to provide a review course for 40 nurses, study guides, reimbursement of course and exam fees and held June 2017 in Albuquerque, New Mexico. A second review course, held during the 2017 AVAHO meeting, was conducted for another 24 nurses. The courses aimed to build confidence and decrease barriers. Both exceeded capacity.
Results: As a result of the Albuquerque course, VISN 22 and non-VA nurses attended from several states. Each received
a 30% reduction in exam fees and were eligible for exam reimbursement after passing: 50% of attendees are now OCNs.
The AVAHO course, to date, has resulted in an additional 2 OCNs, 2 certification renewals, and an additional 5 are registered for the exam. Those not taking the exam cite lack of leadership support and encouragement as the main
barrier.
Implications: Certification validates care provided and builds Veterans trust: necessary with Choice. Facilities that retain a strong foundation of OCNs, mentor staff, and maintain leadership support remain more apt to produce and sustain certified nurses. Therefore, leadership buy-in remains essential.
Use of Simulated Patients to Teach Goals of Care Conversations
Background: Understanding a patient’s expectations with treatment for their cancer is an important first step in caring for patients with cancer. Establishing goals of care allows providers to understand what their patients are willing to endure especially if they have a limited life expectancy. It provides a plan of care that is agreed upon by both the patient and provider. However, talking to patients about goals of care requires a skill set that many providers have not fully developed.
The use of simulated patients (SPs) has been shown to be an effective method to teach communication skills. However, many people feel intimidated when they are asked to work with SPs, especially if their conversations are viewed and critiqued by others. At the Pittsburgh VA we have developed a method that uses SPs to teach communication skills in a comfortable non-threatening environment for the learner. We tested this method with our Oncology providers.
Methods: Oncologists, nurses and social workers attended a meeting where they were asked to view a scenario where a patient and his family( SPs) were informed that the patient had progression of his cancer. In the first scenario the information was presented to SPs focusing on the cancer and treatment options. In the second scenario the same information was presented by an oncologist trained in palliative care focusing on the patient’s understanding of his disease and his goals of care. SPs were asked to contrast and comment on the different styles. The audience was then asked to provide comments and feedback.
Results: Twenty-two participants provided feedback. Twenty one of the participants agreed or strongly agreed that the simulation improved their knowledge and skill set and was done in a safe and comfortable learning environment.
Conclusions: Using SPs and allowing providers to contrast different styles of communicating the same set of information can be an effective and non-threatening teaching method of teaching communication skills. Longitudinal review of patient records will further help to determine the effectiveness of this method of training.
Background: Understanding a patient’s expectations with treatment for their cancer is an important first step in caring for patients with cancer. Establishing goals of care allows providers to understand what their patients are willing to endure especially if they have a limited life expectancy. It provides a plan of care that is agreed upon by both the patient and provider. However, talking to patients about goals of care requires a skill set that many providers have not fully developed.
The use of simulated patients (SPs) has been shown to be an effective method to teach communication skills. However, many people feel intimidated when they are asked to work with SPs, especially if their conversations are viewed and critiqued by others. At the Pittsburgh VA we have developed a method that uses SPs to teach communication skills in a comfortable non-threatening environment for the learner. We tested this method with our Oncology providers.
Methods: Oncologists, nurses and social workers attended a meeting where they were asked to view a scenario where a patient and his family( SPs) were informed that the patient had progression of his cancer. In the first scenario the information was presented to SPs focusing on the cancer and treatment options. In the second scenario the same information was presented by an oncologist trained in palliative care focusing on the patient’s understanding of his disease and his goals of care. SPs were asked to contrast and comment on the different styles. The audience was then asked to provide comments and feedback.
Results: Twenty-two participants provided feedback. Twenty one of the participants agreed or strongly agreed that the simulation improved their knowledge and skill set and was done in a safe and comfortable learning environment.
Conclusions: Using SPs and allowing providers to contrast different styles of communicating the same set of information can be an effective and non-threatening teaching method of teaching communication skills. Longitudinal review of patient records will further help to determine the effectiveness of this method of training.
Background: Understanding a patient’s expectations with treatment for their cancer is an important first step in caring for patients with cancer. Establishing goals of care allows providers to understand what their patients are willing to endure especially if they have a limited life expectancy. It provides a plan of care that is agreed upon by both the patient and provider. However, talking to patients about goals of care requires a skill set that many providers have not fully developed.
The use of simulated patients (SPs) has been shown to be an effective method to teach communication skills. However, many people feel intimidated when they are asked to work with SPs, especially if their conversations are viewed and critiqued by others. At the Pittsburgh VA we have developed a method that uses SPs to teach communication skills in a comfortable non-threatening environment for the learner. We tested this method with our Oncology providers.
Methods: Oncologists, nurses and social workers attended a meeting where they were asked to view a scenario where a patient and his family( SPs) were informed that the patient had progression of his cancer. In the first scenario the information was presented to SPs focusing on the cancer and treatment options. In the second scenario the same information was presented by an oncologist trained in palliative care focusing on the patient’s understanding of his disease and his goals of care. SPs were asked to contrast and comment on the different styles. The audience was then asked to provide comments and feedback.
Results: Twenty-two participants provided feedback. Twenty one of the participants agreed or strongly agreed that the simulation improved their knowledge and skill set and was done in a safe and comfortable learning environment.
Conclusions: Using SPs and allowing providers to contrast different styles of communicating the same set of information can be an effective and non-threatening teaching method of teaching communication skills. Longitudinal review of patient records will further help to determine the effectiveness of this method of training.
Model of Integrated Oncology- Palliative Care in an Outpatient Setting
Background: Early introduction of palliative care for oncology patients has demonstrated enhanced quality of life and satisfaction. We developed a model for integrating palliative care into outpatient oncology care.
Hypothesis: Optimal integration of oncology and palliative care requires palliative care clinician’s presence at initial, and many subsequent, patient encounters.
Objective: To implement and evaluate outpatient integrated oncology and palliative care.
Method: In January 2015, we implemented an integrated outpatient practice of oncology and palliative care with: Pre-clinic “huddle” among palliative care and oncology staff to identify patients in need of palliative care; shared palliative care-oncology appointments. Initial visit: New oncology patients are seen by an oncologist and palliative care physician together. Palliative care physician introduces palliative care and initiates advance care planning. Concurrent oncology-palliative care follow-up: High-risk patients (aggressive histology, progressing disease, etc) are followed by oncologist and palliative care physician. Palliative care physician facilitates goals of care discussions and addresses symptom management. End-of-life care: Hospice care remains a part of oncology care. Palliative care physician and oncology team co-manage all oncology patients enrolled in hospice care.
Results: Increase in palliative care consults from oncology clinics: After this intervention, there is a 10-fold increase in number of palliative care consultation requests from oncology clinics from fiscal year 2014 to 2017. Increase in percentage of inpatients deaths with prior palliative care consultation: Since the implementation of this model, there is an increase in the percentage of inpatient deaths with prior palliative care consultations; from 75% in fiscal year 2014 to 97% in fiscal year 2017.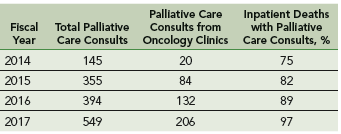
Challenges/Limitations: Single clinic setting, with one oncologist and palliative care physician, palliative care staffing, clinic space, administrative support.
Conclusions: Studies are needed to show impact of palliative care integration on acute care utilization, hospice care accession and satisfaction with care. There is a need to explore improved training and structures for both oncology and palliative care teams.
Background: Early introduction of palliative care for oncology patients has demonstrated enhanced quality of life and satisfaction. We developed a model for integrating palliative care into outpatient oncology care.
Hypothesis: Optimal integration of oncology and palliative care requires palliative care clinician’s presence at initial, and many subsequent, patient encounters.
Objective: To implement and evaluate outpatient integrated oncology and palliative care.
Method: In January 2015, we implemented an integrated outpatient practice of oncology and palliative care with: Pre-clinic “huddle” among palliative care and oncology staff to identify patients in need of palliative care; shared palliative care-oncology appointments. Initial visit: New oncology patients are seen by an oncologist and palliative care physician together. Palliative care physician introduces palliative care and initiates advance care planning. Concurrent oncology-palliative care follow-up: High-risk patients (aggressive histology, progressing disease, etc) are followed by oncologist and palliative care physician. Palliative care physician facilitates goals of care discussions and addresses symptom management. End-of-life care: Hospice care remains a part of oncology care. Palliative care physician and oncology team co-manage all oncology patients enrolled in hospice care.
Results: Increase in palliative care consults from oncology clinics: After this intervention, there is a 10-fold increase in number of palliative care consultation requests from oncology clinics from fiscal year 2014 to 2017. Increase in percentage of inpatients deaths with prior palliative care consultation: Since the implementation of this model, there is an increase in the percentage of inpatient deaths with prior palliative care consultations; from 75% in fiscal year 2014 to 97% in fiscal year 2017.
Challenges/Limitations: Single clinic setting, with one oncologist and palliative care physician, palliative care staffing, clinic space, administrative support.
Conclusions: Studies are needed to show impact of palliative care integration on acute care utilization, hospice care accession and satisfaction with care. There is a need to explore improved training and structures for both oncology and palliative care teams.
Background: Early introduction of palliative care for oncology patients has demonstrated enhanced quality of life and satisfaction. We developed a model for integrating palliative care into outpatient oncology care.
Hypothesis: Optimal integration of oncology and palliative care requires palliative care clinician’s presence at initial, and many subsequent, patient encounters.
Objective: To implement and evaluate outpatient integrated oncology and palliative care.
Method: In January 2015, we implemented an integrated outpatient practice of oncology and palliative care with: Pre-clinic “huddle” among palliative care and oncology staff to identify patients in need of palliative care; shared palliative care-oncology appointments. Initial visit: New oncology patients are seen by an oncologist and palliative care physician together. Palliative care physician introduces palliative care and initiates advance care planning. Concurrent oncology-palliative care follow-up: High-risk patients (aggressive histology, progressing disease, etc) are followed by oncologist and palliative care physician. Palliative care physician facilitates goals of care discussions and addresses symptom management. End-of-life care: Hospice care remains a part of oncology care. Palliative care physician and oncology team co-manage all oncology patients enrolled in hospice care.
Results: Increase in palliative care consults from oncology clinics: After this intervention, there is a 10-fold increase in number of palliative care consultation requests from oncology clinics from fiscal year 2014 to 2017. Increase in percentage of inpatients deaths with prior palliative care consultation: Since the implementation of this model, there is an increase in the percentage of inpatient deaths with prior palliative care consultations; from 75% in fiscal year 2014 to 97% in fiscal year 2017.
Challenges/Limitations: Single clinic setting, with one oncologist and palliative care physician, palliative care staffing, clinic space, administrative support.
Conclusions: Studies are needed to show impact of palliative care integration on acute care utilization, hospice care accession and satisfaction with care. There is a need to explore improved training and structures for both oncology and palliative care teams.
Better ICU staff communication with family may improve end-of-life choices
A nurse-led support intervention for the families of critically ill patients did little to ease families’ psychological symptoms, but it did improve their perception of staff communication and family-centered care in the intensive care unit.

The length of ICU stay was also significantly shorter and the in-unit death rate higher among patients whose families received the intervention – a finding that suggests difficult end-of-life choices may have been eased, reported Douglas B. White, MD, and his colleagues (N Engl J Med. 2018;378:2365-75).
“The intervention resulted in significant improvements in markers of the quality of decision making, including the patient- and family-centeredness of care and the quality of clinician-family communication. Taken together, these findings suggest that the intervention allowed surrogates to transition a patient’s treatment to comfort-focused care when doing so aligned with the patient’s values,” wrote Dr. White of the University of Pittsburgh. “A previous study that was conducted in the context of advanced illness suggested that treatment that accords with the patient’s preferences may lead to shorter survival among those who prioritize comfort over longevity.”
The trial randomized 1,420 patients and their family surrogates in five ICUs to usual care, or to the multicomponent family-support intervention. The primary outcome was change in the surrogates’ scores on the Hospital Anxiety Depression Scale (HADS) at 6 months. The secondary outcomes were changes in Impact of Event Scale (IES; a measure of posttraumatic stress) the Quality of Communication (QOC) scale, quality of clinician-family communication measured by the Patient Perception of Patient Centeredness (PPPC) scale and the mean length of ICU stay.
The intervention was delivered by nurses who received special training on communication and other skills needed to support the families of critically ill patients. Nurses met with families every day and arranged regular meetings with ICU clinicians. A quality improvement specialist incorporated the family support into daily work flow.
In a fully adjusted model, there was no significant between-group difference in the 6-month HADS scores (11.7 vs. 12 points). Likewise, there was no significant difference between the groups in the mean IES score at 6 months.
Family members in the active group did rate the quality of clinician-family communication as significantly better, and they also gave significantly higher ratings to the quality of patient- and family-centered care during the ICU stay.
The shorter length of stay was reflected in the time to death among patients who died during the stay (4.4 days in the intervention group vs. 6.8 days in the control group), although there was no significant difference in length of stay among patients who survived to discharge. Significantly more patients in the intervention group died in the ICU as well (36% vs. 28.5%); however, there was no significant difference in 6-month mortality (60.4% vs. 55.4%).
The study was supported by an Innovation Award from the University of Pittsburgh Medical Center Health System and by the Greenwell Foundation. Dr. White reported having no financial disclosures
Although the results by White and colleagues “cannot be interpreted as clinically directive,” the study offers a glimpse of the path forward in improving the experience of families with critically ill loved ones, Daniela Lamas, MD, wrote in an accompanying editorial (N Engl J Med. 2018; 378:2431-2).
The study didn’t meet its primary endpoint of reducing surrogates’ psychological symptoms at 6 months, but it did lead to an improved ICU experience, with better clinician communication. There was another finding that deserves a close look: In the intervention group, ICU length of stay was shorter and in-hospital mortality greater, although mortality among those who survived to discharge was similar at 6 months.
These findings suggest that the intervention did not lead to the premature death of patients who would have otherwise done well, but rather was associated with a shorter dying process for those who faced a dismal prognosis, according to Dr. Lamas.
“As we increasingly look beyond mortality as the primary outcome that matters, seeking to maximize quality of life and minimize suffering, this work represents an ‘end of the beginning’ by suggesting the next steps in moving closer to achieving these goals.”
Dr. Lamas is a pulmonary and critical care doctor at Brigham & Women’s Hospital and on the faculty at Harvard Medical School, Boston.
Although the results by White and colleagues “cannot be interpreted as clinically directive,” the study offers a glimpse of the path forward in improving the experience of families with critically ill loved ones, Daniela Lamas, MD, wrote in an accompanying editorial (N Engl J Med. 2018; 378:2431-2).
The study didn’t meet its primary endpoint of reducing surrogates’ psychological symptoms at 6 months, but it did lead to an improved ICU experience, with better clinician communication. There was another finding that deserves a close look: In the intervention group, ICU length of stay was shorter and in-hospital mortality greater, although mortality among those who survived to discharge was similar at 6 months.
These findings suggest that the intervention did not lead to the premature death of patients who would have otherwise done well, but rather was associated with a shorter dying process for those who faced a dismal prognosis, according to Dr. Lamas.
“As we increasingly look beyond mortality as the primary outcome that matters, seeking to maximize quality of life and minimize suffering, this work represents an ‘end of the beginning’ by suggesting the next steps in moving closer to achieving these goals.”
Dr. Lamas is a pulmonary and critical care doctor at Brigham & Women’s Hospital and on the faculty at Harvard Medical School, Boston.
Although the results by White and colleagues “cannot be interpreted as clinically directive,” the study offers a glimpse of the path forward in improving the experience of families with critically ill loved ones, Daniela Lamas, MD, wrote in an accompanying editorial (N Engl J Med. 2018; 378:2431-2).
The study didn’t meet its primary endpoint of reducing surrogates’ psychological symptoms at 6 months, but it did lead to an improved ICU experience, with better clinician communication. There was another finding that deserves a close look: In the intervention group, ICU length of stay was shorter and in-hospital mortality greater, although mortality among those who survived to discharge was similar at 6 months.
These findings suggest that the intervention did not lead to the premature death of patients who would have otherwise done well, but rather was associated with a shorter dying process for those who faced a dismal prognosis, according to Dr. Lamas.
“As we increasingly look beyond mortality as the primary outcome that matters, seeking to maximize quality of life and minimize suffering, this work represents an ‘end of the beginning’ by suggesting the next steps in moving closer to achieving these goals.”
Dr. Lamas is a pulmonary and critical care doctor at Brigham & Women’s Hospital and on the faculty at Harvard Medical School, Boston.
A nurse-led support intervention for the families of critically ill patients did little to ease families’ psychological symptoms, but it did improve their perception of staff communication and family-centered care in the intensive care unit.
The length of ICU stay was also significantly shorter and the in-unit death rate higher among patients whose families received the intervention – a finding that suggests difficult end-of-life choices may have been eased, reported Douglas B. White, MD, and his colleagues (N Engl J Med. 2018;378:2365-75).
“The intervention resulted in significant improvements in markers of the quality of decision making, including the patient- and family-centeredness of care and the quality of clinician-family communication. Taken together, these findings suggest that the intervention allowed surrogates to transition a patient’s treatment to comfort-focused care when doing so aligned with the patient’s values,” wrote Dr. White of the University of Pittsburgh. “A previous study that was conducted in the context of advanced illness suggested that treatment that accords with the patient’s preferences may lead to shorter survival among those who prioritize comfort over longevity.”
The trial randomized 1,420 patients and their family surrogates in five ICUs to usual care, or to the multicomponent family-support intervention. The primary outcome was change in the surrogates’ scores on the Hospital Anxiety Depression Scale (HADS) at 6 months. The secondary outcomes were changes in Impact of Event Scale (IES; a measure of posttraumatic stress) the Quality of Communication (QOC) scale, quality of clinician-family communication measured by the Patient Perception of Patient Centeredness (PPPC) scale and the mean length of ICU stay.
The intervention was delivered by nurses who received special training on communication and other skills needed to support the families of critically ill patients. Nurses met with families every day and arranged regular meetings with ICU clinicians. A quality improvement specialist incorporated the family support into daily work flow.
In a fully adjusted model, there was no significant between-group difference in the 6-month HADS scores (11.7 vs. 12 points). Likewise, there was no significant difference between the groups in the mean IES score at 6 months.
Family members in the active group did rate the quality of clinician-family communication as significantly better, and they also gave significantly higher ratings to the quality of patient- and family-centered care during the ICU stay.
The shorter length of stay was reflected in the time to death among patients who died during the stay (4.4 days in the intervention group vs. 6.8 days in the control group), although there was no significant difference in length of stay among patients who survived to discharge. Significantly more patients in the intervention group died in the ICU as well (36% vs. 28.5%); however, there was no significant difference in 6-month mortality (60.4% vs. 55.4%).
The study was supported by an Innovation Award from the University of Pittsburgh Medical Center Health System and by the Greenwell Foundation. Dr. White reported having no financial disclosures
A nurse-led support intervention for the families of critically ill patients did little to ease families’ psychological symptoms, but it did improve their perception of staff communication and family-centered care in the intensive care unit.
The length of ICU stay was also significantly shorter and the in-unit death rate higher among patients whose families received the intervention – a finding that suggests difficult end-of-life choices may have been eased, reported Douglas B. White, MD, and his colleagues (N Engl J Med. 2018;378:2365-75).
“The intervention resulted in significant improvements in markers of the quality of decision making, including the patient- and family-centeredness of care and the quality of clinician-family communication. Taken together, these findings suggest that the intervention allowed surrogates to transition a patient’s treatment to comfort-focused care when doing so aligned with the patient’s values,” wrote Dr. White of the University of Pittsburgh. “A previous study that was conducted in the context of advanced illness suggested that treatment that accords with the patient’s preferences may lead to shorter survival among those who prioritize comfort over longevity.”
The trial randomized 1,420 patients and their family surrogates in five ICUs to usual care, or to the multicomponent family-support intervention. The primary outcome was change in the surrogates’ scores on the Hospital Anxiety Depression Scale (HADS) at 6 months. The secondary outcomes were changes in Impact of Event Scale (IES; a measure of posttraumatic stress) the Quality of Communication (QOC) scale, quality of clinician-family communication measured by the Patient Perception of Patient Centeredness (PPPC) scale and the mean length of ICU stay.
The intervention was delivered by nurses who received special training on communication and other skills needed to support the families of critically ill patients. Nurses met with families every day and arranged regular meetings with ICU clinicians. A quality improvement specialist incorporated the family support into daily work flow.
In a fully adjusted model, there was no significant between-group difference in the 6-month HADS scores (11.7 vs. 12 points). Likewise, there was no significant difference between the groups in the mean IES score at 6 months.
Family members in the active group did rate the quality of clinician-family communication as significantly better, and they also gave significantly higher ratings to the quality of patient- and family-centered care during the ICU stay.
The shorter length of stay was reflected in the time to death among patients who died during the stay (4.4 days in the intervention group vs. 6.8 days in the control group), although there was no significant difference in length of stay among patients who survived to discharge. Significantly more patients in the intervention group died in the ICU as well (36% vs. 28.5%); however, there was no significant difference in 6-month mortality (60.4% vs. 55.4%).
The study was supported by an Innovation Award from the University of Pittsburgh Medical Center Health System and by the Greenwell Foundation. Dr. White reported having no financial disclosures
FROM NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: A family communication intervention didn’t improve 6-month psychological symptoms among those with loved ones in intensive care units.
Major finding: There was no significant difference on the Hospital Anxiety and Depression Scale at 6 months (11.7 vs. 12 points).
Study details: The study randomized 1,420 ICU patients and surrogates to the intervention or to usual care.
Disclosures: The study was supported by an Innovation Award from the University of Pittsburgh Medical Center Health System and by the Greenwell Foundation. Dr. White had no financial disclosures.
Source: White et al. N Engl J Med. 2018;378:2365-75.
Medicare hospital deaths decline, hospice usage increases
Since 2000, Medicare beneficiaries have become less likely to die in hospitals, and more likely to die in their homes or in community health care facilities.
A review of Medicare records also determined that there was a decline in health care transitions in the final 3 days of life for these patients, Joan M. Teno, MD, and her colleagues wrote in JAMA.
It is not possible to identify a specific reason for the shift, wrote Dr. Teno, professor of medicine at the Oregon Health & Science University, Portland. Between the study years of 2000 and 2015, there were several large efforts to improve care at the end of life.
“Since 2009, programs ranging from ensuring informed patient decision making to enhanced care coordination have had the goal of improving care at the end of life. Specific interventions have included promoting conversations about the goals of care, continued growth of hospice services and palliative care, and the debate and passage of the Affordable Care Act … It is difficult to disentangle efforts such as public education, promotion of advance directives through the Patient Self- Determination Act, increased access to hospice and palliative care services, financial incentives of payment policies, and other secular changes.”
The study mined data from the Centers for Medicare & Medicaid Services, and examined end-of-life outcomes among two Medicare groups: Medicare fee-for-service recipients (1,361,870) during 2009-2015, and Medicare Advantage recipients (871,845), comparing 2011 and 2015. The mean age of both cohorts was 82 years.
Outcomes included site of death and “potentially burdensome transitions,” during the last days of life. These were defined as three or more hospitalizations in the previous 3 months, or two or more hospitalizations for pneumonia, urinary tract infection, dehydration, or sepsis during the last 120 days of life. Prolonged mechanical ventilation also was deemed potentially burdensome.
Among fee-for-service recipients, deaths in acute care hospitals declined from 32.6% to19.8%. Deaths in nursing homes remained steady, at 27.2% and 24.9%. Many of these deaths (42.9%) were preceded by a stay in an ICU. There was a transient increase in end-of-life ICU use, around 2009, but by 2015, the percentage was down to 29%, compared with 65.2% in 2000.
Transitions between a nursing home and hospital in the last 90 days of life were 0.49/person in 2000 and 0.33/person in 2015. Hospitalizations for infection or dehydration fell from 14.6% to12.2%. Hospitalization with prolonged ventilation fell from 3.1% to 2.5%.
Dying in hospice care increased from 21.6% to 50.4%, and people were taking advantage of hospice services longer: the proportion using short-term services (3 days or less) fell from 9.8% to 7.7%.
Among Medicare Advantage recipients, the numbers were somewhat different. More than 50% of recipients entered hospice care in both 2011 and 2015; in both years, 8% had services for more than 3 days. About 27% had ICU care in the last days of life, in both years. Compared to fee-for-service recipients, fewer Medicare Advantage patients were in nursing homes at the time of death, and that number declined from 2011 to 2015 (37.7% to 33.2%).
In each year, about 10% of these patients had a hospitalization for dehydration or infection, and 3% had a stay requiring prolonged mechanical ventilation in each year. The mean number of health care transitions remained steady, at 0.23 and 0.21 per person each year.
Dr. Teno had no financial disclosures.
SOURCE: Teno JM et al. JAMA. 2018 Jun 25. doi: 10.1001/jama.2018.8981.
Since 2000, Medicare beneficiaries have become less likely to die in hospitals, and more likely to die in their homes or in community health care facilities.
A review of Medicare records also determined that there was a decline in health care transitions in the final 3 days of life for these patients, Joan M. Teno, MD, and her colleagues wrote in JAMA.
It is not possible to identify a specific reason for the shift, wrote Dr. Teno, professor of medicine at the Oregon Health & Science University, Portland. Between the study years of 2000 and 2015, there were several large efforts to improve care at the end of life.
“Since 2009, programs ranging from ensuring informed patient decision making to enhanced care coordination have had the goal of improving care at the end of life. Specific interventions have included promoting conversations about the goals of care, continued growth of hospice services and palliative care, and the debate and passage of the Affordable Care Act … It is difficult to disentangle efforts such as public education, promotion of advance directives through the Patient Self- Determination Act, increased access to hospice and palliative care services, financial incentives of payment policies, and other secular changes.”
The study mined data from the Centers for Medicare & Medicaid Services, and examined end-of-life outcomes among two Medicare groups: Medicare fee-for-service recipients (1,361,870) during 2009-2015, and Medicare Advantage recipients (871,845), comparing 2011 and 2015. The mean age of both cohorts was 82 years.
Outcomes included site of death and “potentially burdensome transitions,” during the last days of life. These were defined as three or more hospitalizations in the previous 3 months, or two or more hospitalizations for pneumonia, urinary tract infection, dehydration, or sepsis during the last 120 days of life. Prolonged mechanical ventilation also was deemed potentially burdensome.
Among fee-for-service recipients, deaths in acute care hospitals declined from 32.6% to19.8%. Deaths in nursing homes remained steady, at 27.2% and 24.9%. Many of these deaths (42.9%) were preceded by a stay in an ICU. There was a transient increase in end-of-life ICU use, around 2009, but by 2015, the percentage was down to 29%, compared with 65.2% in 2000.
Transitions between a nursing home and hospital in the last 90 days of life were 0.49/person in 2000 and 0.33/person in 2015. Hospitalizations for infection or dehydration fell from 14.6% to12.2%. Hospitalization with prolonged ventilation fell from 3.1% to 2.5%.
Dying in hospice care increased from 21.6% to 50.4%, and people were taking advantage of hospice services longer: the proportion using short-term services (3 days or less) fell from 9.8% to 7.7%.
Among Medicare Advantage recipients, the numbers were somewhat different. More than 50% of recipients entered hospice care in both 2011 and 2015; in both years, 8% had services for more than 3 days. About 27% had ICU care in the last days of life, in both years. Compared to fee-for-service recipients, fewer Medicare Advantage patients were in nursing homes at the time of death, and that number declined from 2011 to 2015 (37.7% to 33.2%).
In each year, about 10% of these patients had a hospitalization for dehydration or infection, and 3% had a stay requiring prolonged mechanical ventilation in each year. The mean number of health care transitions remained steady, at 0.23 and 0.21 per person each year.
Dr. Teno had no financial disclosures.
SOURCE: Teno JM et al. JAMA. 2018 Jun 25. doi: 10.1001/jama.2018.8981.
Since 2000, Medicare beneficiaries have become less likely to die in hospitals, and more likely to die in their homes or in community health care facilities.
A review of Medicare records also determined that there was a decline in health care transitions in the final 3 days of life for these patients, Joan M. Teno, MD, and her colleagues wrote in JAMA.
It is not possible to identify a specific reason for the shift, wrote Dr. Teno, professor of medicine at the Oregon Health & Science University, Portland. Between the study years of 2000 and 2015, there were several large efforts to improve care at the end of life.
“Since 2009, programs ranging from ensuring informed patient decision making to enhanced care coordination have had the goal of improving care at the end of life. Specific interventions have included promoting conversations about the goals of care, continued growth of hospice services and palliative care, and the debate and passage of the Affordable Care Act … It is difficult to disentangle efforts such as public education, promotion of advance directives through the Patient Self- Determination Act, increased access to hospice and palliative care services, financial incentives of payment policies, and other secular changes.”
The study mined data from the Centers for Medicare & Medicaid Services, and examined end-of-life outcomes among two Medicare groups: Medicare fee-for-service recipients (1,361,870) during 2009-2015, and Medicare Advantage recipients (871,845), comparing 2011 and 2015. The mean age of both cohorts was 82 years.
Outcomes included site of death and “potentially burdensome transitions,” during the last days of life. These were defined as three or more hospitalizations in the previous 3 months, or two or more hospitalizations for pneumonia, urinary tract infection, dehydration, or sepsis during the last 120 days of life. Prolonged mechanical ventilation also was deemed potentially burdensome.
Among fee-for-service recipients, deaths in acute care hospitals declined from 32.6% to19.8%. Deaths in nursing homes remained steady, at 27.2% and 24.9%. Many of these deaths (42.9%) were preceded by a stay in an ICU. There was a transient increase in end-of-life ICU use, around 2009, but by 2015, the percentage was down to 29%, compared with 65.2% in 2000.
Transitions between a nursing home and hospital in the last 90 days of life were 0.49/person in 2000 and 0.33/person in 2015. Hospitalizations for infection or dehydration fell from 14.6% to12.2%. Hospitalization with prolonged ventilation fell from 3.1% to 2.5%.
Dying in hospice care increased from 21.6% to 50.4%, and people were taking advantage of hospice services longer: the proportion using short-term services (3 days or less) fell from 9.8% to 7.7%.
Among Medicare Advantage recipients, the numbers were somewhat different. More than 50% of recipients entered hospice care in both 2011 and 2015; in both years, 8% had services for more than 3 days. About 27% had ICU care in the last days of life, in both years. Compared to fee-for-service recipients, fewer Medicare Advantage patients were in nursing homes at the time of death, and that number declined from 2011 to 2015 (37.7% to 33.2%).
In each year, about 10% of these patients had a hospitalization for dehydration or infection, and 3% had a stay requiring prolonged mechanical ventilation in each year. The mean number of health care transitions remained steady, at 0.23 and 0.21 per person each year.
Dr. Teno had no financial disclosures.
SOURCE: Teno JM et al. JAMA. 2018 Jun 25. doi: 10.1001/jama.2018.8981.
FROM JAMA
Key clinical point: During 2000-2015, Medicare recipients became less likely to die in hospitals.
Major finding:
Study details: The retrospective study comprised more than 2.3 million Medicare recipients.
Disclosures: Dr. Teno had no financial disclosures.
Source: Teno JM et al. JAMA. 2018 Jun 25. doi: 10.1001/jama.2018.8981.