User login
The Hospitalist only
Psychiatric Hospitalist Model Supported by New Outcomes Research from UK
Unpublished data from a British study of dedicated psychiatric hospitalists shows clear improvements in 17 of 23 measured outcomes, according to the study's lead researcher.
Julian Beezhold, MD, a consultant in emergency psychiatry at Norfolk and Suffolk NHS Foundation Trust (formerly Norfolk and Waveney Mental Health Foundation Trust) presented the data at the annual meeting of the American Psychiatric Association in May in Philadelphia.
The researchers investigated 5,000 patients over nearly eight years. By switching coverage from 13 consultant psychiatrists to dedicated-unit psychiatric hospitalists, the study showed lengths of stay on two inpatient psychiatry units cut in half (just over 11 days from nearly 22 days). Researchers also found reductions in violent episodes and self-harm. Demand for beds on the units declined steadily during the study, resulting in consolidation down to one unit.
"We found overwhelming, robust evidence showing clear benefit from a hospitalist model of care," Dr. Beezhold says. "We found that dedicated doctors are able to achieve better quality of care simply because they are there, able to respond to crises and to change treatment plans more quickly when that is needed."
Psychiatry practice differs from most specialty practice in the United Kingdom, he adds, but the recent trend has been toward a larger division between office-based and hospital-based practices.
In the U.S., models of coverage for acute psychiatric patients include specialized psychiatric hospitals, dedicated psychiatric units within general hospitals, and patients admitted to general hospital units whose psychiatric care is managed by consultation-liaison psychiatrists, says Abigail Donovan, MD, a psychiatrist at Massachusetts General Hospital in Boston.
"At Mass General, we have access to all of these approaches," she says, adding that the new data "reinforces the way we've been doing things with dedicated psychiatric hospitalists—showing the tangible results of this model."
Unpublished data from a British study of dedicated psychiatric hospitalists shows clear improvements in 17 of 23 measured outcomes, according to the study's lead researcher.
Julian Beezhold, MD, a consultant in emergency psychiatry at Norfolk and Suffolk NHS Foundation Trust (formerly Norfolk and Waveney Mental Health Foundation Trust) presented the data at the annual meeting of the American Psychiatric Association in May in Philadelphia.
The researchers investigated 5,000 patients over nearly eight years. By switching coverage from 13 consultant psychiatrists to dedicated-unit psychiatric hospitalists, the study showed lengths of stay on two inpatient psychiatry units cut in half (just over 11 days from nearly 22 days). Researchers also found reductions in violent episodes and self-harm. Demand for beds on the units declined steadily during the study, resulting in consolidation down to one unit.
"We found overwhelming, robust evidence showing clear benefit from a hospitalist model of care," Dr. Beezhold says. "We found that dedicated doctors are able to achieve better quality of care simply because they are there, able to respond to crises and to change treatment plans more quickly when that is needed."
Psychiatry practice differs from most specialty practice in the United Kingdom, he adds, but the recent trend has been toward a larger division between office-based and hospital-based practices.
In the U.S., models of coverage for acute psychiatric patients include specialized psychiatric hospitals, dedicated psychiatric units within general hospitals, and patients admitted to general hospital units whose psychiatric care is managed by consultation-liaison psychiatrists, says Abigail Donovan, MD, a psychiatrist at Massachusetts General Hospital in Boston.
"At Mass General, we have access to all of these approaches," she says, adding that the new data "reinforces the way we've been doing things with dedicated psychiatric hospitalists—showing the tangible results of this model."
Unpublished data from a British study of dedicated psychiatric hospitalists shows clear improvements in 17 of 23 measured outcomes, according to the study's lead researcher.
Julian Beezhold, MD, a consultant in emergency psychiatry at Norfolk and Suffolk NHS Foundation Trust (formerly Norfolk and Waveney Mental Health Foundation Trust) presented the data at the annual meeting of the American Psychiatric Association in May in Philadelphia.
The researchers investigated 5,000 patients over nearly eight years. By switching coverage from 13 consultant psychiatrists to dedicated-unit psychiatric hospitalists, the study showed lengths of stay on two inpatient psychiatry units cut in half (just over 11 days from nearly 22 days). Researchers also found reductions in violent episodes and self-harm. Demand for beds on the units declined steadily during the study, resulting in consolidation down to one unit.
"We found overwhelming, robust evidence showing clear benefit from a hospitalist model of care," Dr. Beezhold says. "We found that dedicated doctors are able to achieve better quality of care simply because they are there, able to respond to crises and to change treatment plans more quickly when that is needed."
Psychiatry practice differs from most specialty practice in the United Kingdom, he adds, but the recent trend has been toward a larger division between office-based and hospital-based practices.
In the U.S., models of coverage for acute psychiatric patients include specialized psychiatric hospitals, dedicated psychiatric units within general hospitals, and patients admitted to general hospital units whose psychiatric care is managed by consultation-liaison psychiatrists, says Abigail Donovan, MD, a psychiatrist at Massachusetts General Hospital in Boston.
"At Mass General, we have access to all of these approaches," she says, adding that the new data "reinforces the way we've been doing things with dedicated psychiatric hospitalists—showing the tangible results of this model."
Tech Takes Off: Videoconferences in medical settings is more acceptable and affordable, but hurdles remain
Picture this likely scenario: You’re a hospitalist in a remote setting, and a patient with stroke symptoms is rushed in by ambulance. Numbness has overcome one side of his body. Dizziness disrupts his balance, his speech becomes slurred, and his vision is blurred. Treatment must be started swiftly to halt irreversible brain damage. The nearest neurologist is located hours away, but thanks to advanced video technology, you’re able to instantly consult face to face with that specialist to help ensure optimal recovery for the patient.
Such applications of telemedicine are becoming more mainstream and affordable, facilitating discussions and decisions between healthcare providers while improving patient access to specialty care in emergencies and other situations.
Remote hospitalist services include videoconferencing for patient monitoring and assessment of various clinical services, says Jona
Advantages and Challenges
Remote patient monitoring in ICUs is on the upswing, filling gaps in the shortage of physicians specializing in critical care. Some unit administrators have established off-site command centers for these specialists to follow multiple facilities with the assistance of video technology and to intervene at urgent times.1
In a neonatal ICU, this type of live-feed technology allows for a face-to-face interaction with a pediatric pulmonologist, for example, when a premature infant is exhibiting symptoms of respiratory distress in the middle of the night, says David Cattell-Gordon, MSW, director of the Office of Telemedicine at the University of Virginia in Charlottesville.
Similarly, in rural areas where women don’t have immediate access to high-risk obstetricians, telemedicine makes it possible to consult with maternal-fetal medicine specialists from a distance, boosting the chances for pregnant mothers with complex conditions to carry healthy babies to term, says Cattell-Gordon. “Our approach has been to bring telemedicine to hospitals and clinics in communities where that resource [specialists] otherwise is unavailable,” he adds.
—Matthew Harbison, MD, medical director, Sound Physicians hospitalist services, Memorial Hermann-Texas Medical Center
Compared with telephone conversations, the advantages of video consultations are multifold: They display a patient’s facial expressions, gestures, and other body language, which might assist with the diagnosis and prescribed treatment, says Kerry Weiner, MD, chief clinical officer for IPC: The Hospitalist Company in North Hollywood, Calif., which has a presence in about 900 facilities in 25 states.
When the strength of that assessment depends on visual inspection, the technology can be particularly helpful. “The weak part of it is when you need to touch” to guide that assessment, Dr. Weiner says. That’s when the technology isn’t as useful. Still, he adds, “We use teleconferencing all over the place in a Skype-like manner, only more sophisticated. It’s more encrypted.”
Interacting within a secure network is crucial to protect privacy, says Peter Kragel, MD, clinical director of the Telemedicine Center at East Carolina University’s Brody School of Medicine in Greenville, N.C. As with any form of communication that transmits identifiable patient information, healthcare providers must comply with HIPAA guidelines when employing videoconferencing services similar to Skype.
“Because of concerns about compliance with encryption and confidentiality regulations, we do not use [videoconferencing] here,” Dr. Kragel says.
Additionally, “telemedicine isn’t always appropriate for patient care,” Linkous says. “All of this depends on the circumstances and needs of the patient. Obviously, surgery requires a direct physician-patient interaction, except for robotic surgery.” For hospitals that don’t have any neurology coverage, telemedicine robots can assist with outside consults for time-sensitive stroke care.
—Jonathan D. Linkous, CEO, American Telemedicine Association
Videoconferencing isn’t necessary for all telemedicine encounters, Linkous says. Teledermatology and retinal screening use “store and forward” communication of images, which allows for the electronic transmission of images and documents in non-emergent situations in which immediate video isn’t necessary.
“As a society, we’ve become more comfortable with the technology,” says Matthew Harbison, MD, medical director of Sound Physicians hospitalist services at Memorial Hermann-Texas Medical Center in Houston. “And as the technology continues to develop, ultimately there will be [more of] a role, but how large that will be is difficult to predict.” He adds that “the advantages are obviously in low-staffed places or staffing-challenged sites.”
Moving Ahead
As experts continue to iron out the kinks and as communities obtain greater access to broadband signals, telemedicine equipment is moving to advanced high-definition platforms. Meanwhile, the expense has come down considerably since its inception in the mid-1990s. A high-definition setup that once cost upward of $130,000 is now available for less than $10,000, Cattell-Gordon says.
The digital transmission also can assist in patient follow-up after discharge from the hospital and in monitoring various chronic diseases from home. It’s an effective tool for medical staff meetings and training purposes as well.
IPC's hospitalists have been using the technology to communicate with each other, brainstorming across regions of the country. “Because we’re a national company,” Dr. Weiner says, “this has changed the game in terms of being able to collaborate.”
Susan Kreimer is a freelance medical writer based in New York.
Reference
1. Thomas EJ, Lucke JF, Wueste L, Weavind L, Patel B. Association of telemedicine for remote monitoring of intensive care patients with mortality, complications, and length of stay. JAMA. 2009;302:2671-2678.
Picture this likely scenario: You’re a hospitalist in a remote setting, and a patient with stroke symptoms is rushed in by ambulance. Numbness has overcome one side of his body. Dizziness disrupts his balance, his speech becomes slurred, and his vision is blurred. Treatment must be started swiftly to halt irreversible brain damage. The nearest neurologist is located hours away, but thanks to advanced video technology, you’re able to instantly consult face to face with that specialist to help ensure optimal recovery for the patient.
Such applications of telemedicine are becoming more mainstream and affordable, facilitating discussions and decisions between healthcare providers while improving patient access to specialty care in emergencies and other situations.
Remote hospitalist services include videoconferencing for patient monitoring and assessment of various clinical services, says Jona
Advantages and Challenges
Remote patient monitoring in ICUs is on the upswing, filling gaps in the shortage of physicians specializing in critical care. Some unit administrators have established off-site command centers for these specialists to follow multiple facilities with the assistance of video technology and to intervene at urgent times.1
In a neonatal ICU, this type of live-feed technology allows for a face-to-face interaction with a pediatric pulmonologist, for example, when a premature infant is exhibiting symptoms of respiratory distress in the middle of the night, says David Cattell-Gordon, MSW, director of the Office of Telemedicine at the University of Virginia in Charlottesville.
Similarly, in rural areas where women don’t have immediate access to high-risk obstetricians, telemedicine makes it possible to consult with maternal-fetal medicine specialists from a distance, boosting the chances for pregnant mothers with complex conditions to carry healthy babies to term, says Cattell-Gordon. “Our approach has been to bring telemedicine to hospitals and clinics in communities where that resource [specialists] otherwise is unavailable,” he adds.
—Matthew Harbison, MD, medical director, Sound Physicians hospitalist services, Memorial Hermann-Texas Medical Center
Compared with telephone conversations, the advantages of video consultations are multifold: They display a patient’s facial expressions, gestures, and other body language, which might assist with the diagnosis and prescribed treatment, says Kerry Weiner, MD, chief clinical officer for IPC: The Hospitalist Company in North Hollywood, Calif., which has a presence in about 900 facilities in 25 states.
When the strength of that assessment depends on visual inspection, the technology can be particularly helpful. “The weak part of it is when you need to touch” to guide that assessment, Dr. Weiner says. That’s when the technology isn’t as useful. Still, he adds, “We use teleconferencing all over the place in a Skype-like manner, only more sophisticated. It’s more encrypted.”
Interacting within a secure network is crucial to protect privacy, says Peter Kragel, MD, clinical director of the Telemedicine Center at East Carolina University’s Brody School of Medicine in Greenville, N.C. As with any form of communication that transmits identifiable patient information, healthcare providers must comply with HIPAA guidelines when employing videoconferencing services similar to Skype.
“Because of concerns about compliance with encryption and confidentiality regulations, we do not use [videoconferencing] here,” Dr. Kragel says.
Additionally, “telemedicine isn’t always appropriate for patient care,” Linkous says. “All of this depends on the circumstances and needs of the patient. Obviously, surgery requires a direct physician-patient interaction, except for robotic surgery.” For hospitals that don’t have any neurology coverage, telemedicine robots can assist with outside consults for time-sensitive stroke care.
—Jonathan D. Linkous, CEO, American Telemedicine Association
Videoconferencing isn’t necessary for all telemedicine encounters, Linkous says. Teledermatology and retinal screening use “store and forward” communication of images, which allows for the electronic transmission of images and documents in non-emergent situations in which immediate video isn’t necessary.
“As a society, we’ve become more comfortable with the technology,” says Matthew Harbison, MD, medical director of Sound Physicians hospitalist services at Memorial Hermann-Texas Medical Center in Houston. “And as the technology continues to develop, ultimately there will be [more of] a role, but how large that will be is difficult to predict.” He adds that “the advantages are obviously in low-staffed places or staffing-challenged sites.”
Moving Ahead
As experts continue to iron out the kinks and as communities obtain greater access to broadband signals, telemedicine equipment is moving to advanced high-definition platforms. Meanwhile, the expense has come down considerably since its inception in the mid-1990s. A high-definition setup that once cost upward of $130,000 is now available for less than $10,000, Cattell-Gordon says.
The digital transmission also can assist in patient follow-up after discharge from the hospital and in monitoring various chronic diseases from home. It’s an effective tool for medical staff meetings and training purposes as well.
IPC's hospitalists have been using the technology to communicate with each other, brainstorming across regions of the country. “Because we’re a national company,” Dr. Weiner says, “this has changed the game in terms of being able to collaborate.”
Susan Kreimer is a freelance medical writer based in New York.
Reference
1. Thomas EJ, Lucke JF, Wueste L, Weavind L, Patel B. Association of telemedicine for remote monitoring of intensive care patients with mortality, complications, and length of stay. JAMA. 2009;302:2671-2678.
Picture this likely scenario: You’re a hospitalist in a remote setting, and a patient with stroke symptoms is rushed in by ambulance. Numbness has overcome one side of his body. Dizziness disrupts his balance, his speech becomes slurred, and his vision is blurred. Treatment must be started swiftly to halt irreversible brain damage. The nearest neurologist is located hours away, but thanks to advanced video technology, you’re able to instantly consult face to face with that specialist to help ensure optimal recovery for the patient.
Such applications of telemedicine are becoming more mainstream and affordable, facilitating discussions and decisions between healthcare providers while improving patient access to specialty care in emergencies and other situations.
Remote hospitalist services include videoconferencing for patient monitoring and assessment of various clinical services, says Jona
Advantages and Challenges
Remote patient monitoring in ICUs is on the upswing, filling gaps in the shortage of physicians specializing in critical care. Some unit administrators have established off-site command centers for these specialists to follow multiple facilities with the assistance of video technology and to intervene at urgent times.1
In a neonatal ICU, this type of live-feed technology allows for a face-to-face interaction with a pediatric pulmonologist, for example, when a premature infant is exhibiting symptoms of respiratory distress in the middle of the night, says David Cattell-Gordon, MSW, director of the Office of Telemedicine at the University of Virginia in Charlottesville.
Similarly, in rural areas where women don’t have immediate access to high-risk obstetricians, telemedicine makes it possible to consult with maternal-fetal medicine specialists from a distance, boosting the chances for pregnant mothers with complex conditions to carry healthy babies to term, says Cattell-Gordon. “Our approach has been to bring telemedicine to hospitals and clinics in communities where that resource [specialists] otherwise is unavailable,” he adds.
—Matthew Harbison, MD, medical director, Sound Physicians hospitalist services, Memorial Hermann-Texas Medical Center
Compared with telephone conversations, the advantages of video consultations are multifold: They display a patient’s facial expressions, gestures, and other body language, which might assist with the diagnosis and prescribed treatment, says Kerry Weiner, MD, chief clinical officer for IPC: The Hospitalist Company in North Hollywood, Calif., which has a presence in about 900 facilities in 25 states.
When the strength of that assessment depends on visual inspection, the technology can be particularly helpful. “The weak part of it is when you need to touch” to guide that assessment, Dr. Weiner says. That’s when the technology isn’t as useful. Still, he adds, “We use teleconferencing all over the place in a Skype-like manner, only more sophisticated. It’s more encrypted.”
Interacting within a secure network is crucial to protect privacy, says Peter Kragel, MD, clinical director of the Telemedicine Center at East Carolina University’s Brody School of Medicine in Greenville, N.C. As with any form of communication that transmits identifiable patient information, healthcare providers must comply with HIPAA guidelines when employing videoconferencing services similar to Skype.
“Because of concerns about compliance with encryption and confidentiality regulations, we do not use [videoconferencing] here,” Dr. Kragel says.
Additionally, “telemedicine isn’t always appropriate for patient care,” Linkous says. “All of this depends on the circumstances and needs of the patient. Obviously, surgery requires a direct physician-patient interaction, except for robotic surgery.” For hospitals that don’t have any neurology coverage, telemedicine robots can assist with outside consults for time-sensitive stroke care.
—Jonathan D. Linkous, CEO, American Telemedicine Association
Videoconferencing isn’t necessary for all telemedicine encounters, Linkous says. Teledermatology and retinal screening use “store and forward” communication of images, which allows for the electronic transmission of images and documents in non-emergent situations in which immediate video isn’t necessary.
“As a society, we’ve become more comfortable with the technology,” says Matthew Harbison, MD, medical director of Sound Physicians hospitalist services at Memorial Hermann-Texas Medical Center in Houston. “And as the technology continues to develop, ultimately there will be [more of] a role, but how large that will be is difficult to predict.” He adds that “the advantages are obviously in low-staffed places or staffing-challenged sites.”
Moving Ahead
As experts continue to iron out the kinks and as communities obtain greater access to broadband signals, telemedicine equipment is moving to advanced high-definition platforms. Meanwhile, the expense has come down considerably since its inception in the mid-1990s. A high-definition setup that once cost upward of $130,000 is now available for less than $10,000, Cattell-Gordon says.
The digital transmission also can assist in patient follow-up after discharge from the hospital and in monitoring various chronic diseases from home. It’s an effective tool for medical staff meetings and training purposes as well.
IPC's hospitalists have been using the technology to communicate with each other, brainstorming across regions of the country. “Because we’re a national company,” Dr. Weiner says, “this has changed the game in terms of being able to collaborate.”
Susan Kreimer is a freelance medical writer based in New York.
Reference
1. Thomas EJ, Lucke JF, Wueste L, Weavind L, Patel B. Association of telemedicine for remote monitoring of intensive care patients with mortality, complications, and length of stay. JAMA. 2009;302:2671-2678.
Physician Noncompete Clauses
A hospitalist was recently offered a lucrative position in his community and was concerned that his previous employment agreement would prohibit him from accepting the new job opportunity. His former employment contract contained a noncompetition clause that made him and his prospective employer rightfully concerned. Upon a comprehensive review of his former employment contract, the noncompetition provision was not as restrictive as he and his prospective employer had previously thought. As it turned out, in his case, and in many others, the noncompetition clause was penetrable, and the physician accepted the new employment offer knowing he was not in violation of his previous contract.
What Is a Noncompetition Clause?
A noncompetition clause, also known as a covenant not to compete or a restrictive covenant, is a provision in a contract that precludes one party from engaging in competition with another party by working 1) in a particular field, 2) within a specific geographic area, and 3) for a stated period of time. A well-written noncompetition provision will prevent a physician from practicing within a certain geographical area surrounding the employer or the employer’s hospital relationships and for a prescribed period of time after the termination of the physician’s employment.
Often, the physician will be permitted to practice within the parameters of the restricted geographical area or time period if they (or the prospective employer) “buy out” of the clause. This is an especially good option when the reasonableness of the noncompetition is not black and white, and both parties want to avoid the expense of litigating the enforceability of the noncompetition clause. Otherwise, in the event the physician breaches the noncompetition clause, the former employer will usually first seek injunctive relief that prohibits the physician’s new employment, then follow with a request for monetary damages arising from the physician’s breach.
In states where noncompetition clauses for physicians are enforceable, the provision must: 1) protect the employer’s legitimate business interest, 2) be specific in geographical scope, and 3) have a narrowly tailored durational scope. Each of these factors is described below. If the language in the clause is vague or does not clearly describe the exact terms of the restrictions on practice, the clause might be unenforceable or open to greater interpretation than either party anticipated.
Do Employers Have a Legitimate Business Interest to Protect?
In order for a noncompetition clause to be enforceable, it must protect the employer’s legitimate business interest. Some examples of a legitimate business interest in the HM context are the employer’s goodwill and the retention of the employer’s clients (hospitals and medical practices). Moreover, since noncompetition clauses are not looked upon with favor by courts because they operate as a restraint of trade, the language needs to be narrowly tailored in order to protect the employer’s legitimate interests.
Is Geographical Scope Reasonable?
Noncompetition clauses must also specify the restricted geographical area where the physician is prohibited from practicing. However, whether a geographical scope is overly broad will not only depend on state law, but also the location of the employer and the surrounding community.
Typically, contracts will provide a radius in miles surrounding the employer’s location or locations as the restricted territory. But whether a geographic limitation is “reasonable” is a relative term. A five-mile radius in an urban area like New York City might be home to millions of people, whereas a five-mile radius in a suburb of New York might only be home to a few thousand people. For hospitalists, the geographic restriction might prohibit the physician from practicing at or for the employer’s clients (e.g. hospitals).
Although the following might seem obviously overly broad to some, a review of contracts with the following geographic restrictions should be considered red flags:
- Prohibition to practice anywhere in the U.S.;
- Prohibition to practice anywhere in a specific state;
- Prohibition to practice in a territory comprised of excessive miles from the employer’s location; and
- Prohibition to practice in certain counties.
Please note that exclusion to practice in certain counties might be overly broad in some situations but might be acceptable in others. For example, a hospitalist sold his ownership stake in his practice, and part of the deal required him to agree not to practice in Los Angeles County. This particular county restriction would be difficult, if not impossible, to enforce because Los Angeles County includes more than 80 cities and covers more than 4,000 square miles.
Is Durational Scope Reasonable?
A noncompetition clause should identify the length of time in which the physician is prohibited from practicing within the restricted geographic area. Whether the durational scope is reasonable will vary from state to state. As a general rule of thumb, if the restricted time frame is two years or less after termination of the contract, the time restriction will likely be considered “reasonable.” However, state laws vary on whether time restraints in excess of two years are enforceable.
A common pitfall with time restrictions is excessiveness based on the state’s laws and the specific circumstances of the physician and the employer. In negotiating the restricted length of time in a noncompetition clause, it is more common to have a longer time restriction when a physician is selling an ownership interest in a practice than for a physician entering into an employment relationship.
Prospective Employers: What You Need to Know
Great care must be taken when hiring a physician. States recognize the legal theory of interference with a contract. If an employer is recruiting a hospitalist who is subject to an employment agreement with a noncompetition clause, the prospective employer must be very careful in the recruiting process. It is recommended that the employment agreement include a representation by the physician-employee that he or she is not subject to any other agreement that would prohibit the physician from entering into the new employment relationship.
If a prospective employer is aware of an existing employment contract that contains practice restrictions on a recruited physician, the prospective employer could be held responsible for damages if a dispute arises between the parties.
It’s All in the Words
Although it might seem like semantics, a few words can change your future. Before you put pen to paper, be sure to have any contract containing a noncompetition clause reviewed by a lawyer who is well-versed in your state’s laws. If you have already signed an agreement with a noncompetition clause and you are considering your next career move, a lawyer can shed some light on a seemingly impenetrable clause.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
A hospitalist was recently offered a lucrative position in his community and was concerned that his previous employment agreement would prohibit him from accepting the new job opportunity. His former employment contract contained a noncompetition clause that made him and his prospective employer rightfully concerned. Upon a comprehensive review of his former employment contract, the noncompetition provision was not as restrictive as he and his prospective employer had previously thought. As it turned out, in his case, and in many others, the noncompetition clause was penetrable, and the physician accepted the new employment offer knowing he was not in violation of his previous contract.
What Is a Noncompetition Clause?
A noncompetition clause, also known as a covenant not to compete or a restrictive covenant, is a provision in a contract that precludes one party from engaging in competition with another party by working 1) in a particular field, 2) within a specific geographic area, and 3) for a stated period of time. A well-written noncompetition provision will prevent a physician from practicing within a certain geographical area surrounding the employer or the employer’s hospital relationships and for a prescribed period of time after the termination of the physician’s employment.
Often, the physician will be permitted to practice within the parameters of the restricted geographical area or time period if they (or the prospective employer) “buy out” of the clause. This is an especially good option when the reasonableness of the noncompetition is not black and white, and both parties want to avoid the expense of litigating the enforceability of the noncompetition clause. Otherwise, in the event the physician breaches the noncompetition clause, the former employer will usually first seek injunctive relief that prohibits the physician’s new employment, then follow with a request for monetary damages arising from the physician’s breach.
In states where noncompetition clauses for physicians are enforceable, the provision must: 1) protect the employer’s legitimate business interest, 2) be specific in geographical scope, and 3) have a narrowly tailored durational scope. Each of these factors is described below. If the language in the clause is vague or does not clearly describe the exact terms of the restrictions on practice, the clause might be unenforceable or open to greater interpretation than either party anticipated.
Do Employers Have a Legitimate Business Interest to Protect?
In order for a noncompetition clause to be enforceable, it must protect the employer’s legitimate business interest. Some examples of a legitimate business interest in the HM context are the employer’s goodwill and the retention of the employer’s clients (hospitals and medical practices). Moreover, since noncompetition clauses are not looked upon with favor by courts because they operate as a restraint of trade, the language needs to be narrowly tailored in order to protect the employer’s legitimate interests.
Is Geographical Scope Reasonable?
Noncompetition clauses must also specify the restricted geographical area where the physician is prohibited from practicing. However, whether a geographical scope is overly broad will not only depend on state law, but also the location of the employer and the surrounding community.
Typically, contracts will provide a radius in miles surrounding the employer’s location or locations as the restricted territory. But whether a geographic limitation is “reasonable” is a relative term. A five-mile radius in an urban area like New York City might be home to millions of people, whereas a five-mile radius in a suburb of New York might only be home to a few thousand people. For hospitalists, the geographic restriction might prohibit the physician from practicing at or for the employer’s clients (e.g. hospitals).
Although the following might seem obviously overly broad to some, a review of contracts with the following geographic restrictions should be considered red flags:
- Prohibition to practice anywhere in the U.S.;
- Prohibition to practice anywhere in a specific state;
- Prohibition to practice in a territory comprised of excessive miles from the employer’s location; and
- Prohibition to practice in certain counties.
Please note that exclusion to practice in certain counties might be overly broad in some situations but might be acceptable in others. For example, a hospitalist sold his ownership stake in his practice, and part of the deal required him to agree not to practice in Los Angeles County. This particular county restriction would be difficult, if not impossible, to enforce because Los Angeles County includes more than 80 cities and covers more than 4,000 square miles.
Is Durational Scope Reasonable?
A noncompetition clause should identify the length of time in which the physician is prohibited from practicing within the restricted geographic area. Whether the durational scope is reasonable will vary from state to state. As a general rule of thumb, if the restricted time frame is two years or less after termination of the contract, the time restriction will likely be considered “reasonable.” However, state laws vary on whether time restraints in excess of two years are enforceable.
A common pitfall with time restrictions is excessiveness based on the state’s laws and the specific circumstances of the physician and the employer. In negotiating the restricted length of time in a noncompetition clause, it is more common to have a longer time restriction when a physician is selling an ownership interest in a practice than for a physician entering into an employment relationship.
Prospective Employers: What You Need to Know
Great care must be taken when hiring a physician. States recognize the legal theory of interference with a contract. If an employer is recruiting a hospitalist who is subject to an employment agreement with a noncompetition clause, the prospective employer must be very careful in the recruiting process. It is recommended that the employment agreement include a representation by the physician-employee that he or she is not subject to any other agreement that would prohibit the physician from entering into the new employment relationship.
If a prospective employer is aware of an existing employment contract that contains practice restrictions on a recruited physician, the prospective employer could be held responsible for damages if a dispute arises between the parties.
It’s All in the Words
Although it might seem like semantics, a few words can change your future. Before you put pen to paper, be sure to have any contract containing a noncompetition clause reviewed by a lawyer who is well-versed in your state’s laws. If you have already signed an agreement with a noncompetition clause and you are considering your next career move, a lawyer can shed some light on a seemingly impenetrable clause.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
A hospitalist was recently offered a lucrative position in his community and was concerned that his previous employment agreement would prohibit him from accepting the new job opportunity. His former employment contract contained a noncompetition clause that made him and his prospective employer rightfully concerned. Upon a comprehensive review of his former employment contract, the noncompetition provision was not as restrictive as he and his prospective employer had previously thought. As it turned out, in his case, and in many others, the noncompetition clause was penetrable, and the physician accepted the new employment offer knowing he was not in violation of his previous contract.
What Is a Noncompetition Clause?
A noncompetition clause, also known as a covenant not to compete or a restrictive covenant, is a provision in a contract that precludes one party from engaging in competition with another party by working 1) in a particular field, 2) within a specific geographic area, and 3) for a stated period of time. A well-written noncompetition provision will prevent a physician from practicing within a certain geographical area surrounding the employer or the employer’s hospital relationships and for a prescribed period of time after the termination of the physician’s employment.
Often, the physician will be permitted to practice within the parameters of the restricted geographical area or time period if they (or the prospective employer) “buy out” of the clause. This is an especially good option when the reasonableness of the noncompetition is not black and white, and both parties want to avoid the expense of litigating the enforceability of the noncompetition clause. Otherwise, in the event the physician breaches the noncompetition clause, the former employer will usually first seek injunctive relief that prohibits the physician’s new employment, then follow with a request for monetary damages arising from the physician’s breach.
In states where noncompetition clauses for physicians are enforceable, the provision must: 1) protect the employer’s legitimate business interest, 2) be specific in geographical scope, and 3) have a narrowly tailored durational scope. Each of these factors is described below. If the language in the clause is vague or does not clearly describe the exact terms of the restrictions on practice, the clause might be unenforceable or open to greater interpretation than either party anticipated.
Do Employers Have a Legitimate Business Interest to Protect?
In order for a noncompetition clause to be enforceable, it must protect the employer’s legitimate business interest. Some examples of a legitimate business interest in the HM context are the employer’s goodwill and the retention of the employer’s clients (hospitals and medical practices). Moreover, since noncompetition clauses are not looked upon with favor by courts because they operate as a restraint of trade, the language needs to be narrowly tailored in order to protect the employer’s legitimate interests.
Is Geographical Scope Reasonable?
Noncompetition clauses must also specify the restricted geographical area where the physician is prohibited from practicing. However, whether a geographical scope is overly broad will not only depend on state law, but also the location of the employer and the surrounding community.
Typically, contracts will provide a radius in miles surrounding the employer’s location or locations as the restricted territory. But whether a geographic limitation is “reasonable” is a relative term. A five-mile radius in an urban area like New York City might be home to millions of people, whereas a five-mile radius in a suburb of New York might only be home to a few thousand people. For hospitalists, the geographic restriction might prohibit the physician from practicing at or for the employer’s clients (e.g. hospitals).
Although the following might seem obviously overly broad to some, a review of contracts with the following geographic restrictions should be considered red flags:
- Prohibition to practice anywhere in the U.S.;
- Prohibition to practice anywhere in a specific state;
- Prohibition to practice in a territory comprised of excessive miles from the employer’s location; and
- Prohibition to practice in certain counties.
Please note that exclusion to practice in certain counties might be overly broad in some situations but might be acceptable in others. For example, a hospitalist sold his ownership stake in his practice, and part of the deal required him to agree not to practice in Los Angeles County. This particular county restriction would be difficult, if not impossible, to enforce because Los Angeles County includes more than 80 cities and covers more than 4,000 square miles.
Is Durational Scope Reasonable?
A noncompetition clause should identify the length of time in which the physician is prohibited from practicing within the restricted geographic area. Whether the durational scope is reasonable will vary from state to state. As a general rule of thumb, if the restricted time frame is two years or less after termination of the contract, the time restriction will likely be considered “reasonable.” However, state laws vary on whether time restraints in excess of two years are enforceable.
A common pitfall with time restrictions is excessiveness based on the state’s laws and the specific circumstances of the physician and the employer. In negotiating the restricted length of time in a noncompetition clause, it is more common to have a longer time restriction when a physician is selling an ownership interest in a practice than for a physician entering into an employment relationship.
Prospective Employers: What You Need to Know
Great care must be taken when hiring a physician. States recognize the legal theory of interference with a contract. If an employer is recruiting a hospitalist who is subject to an employment agreement with a noncompetition clause, the prospective employer must be very careful in the recruiting process. It is recommended that the employment agreement include a representation by the physician-employee that he or she is not subject to any other agreement that would prohibit the physician from entering into the new employment relationship.
If a prospective employer is aware of an existing employment contract that contains practice restrictions on a recruited physician, the prospective employer could be held responsible for damages if a dispute arises between the parties.
It’s All in the Words
Although it might seem like semantics, a few words can change your future. Before you put pen to paper, be sure to have any contract containing a noncompetition clause reviewed by a lawyer who is well-versed in your state’s laws. If you have already signed an agreement with a noncompetition clause and you are considering your next career move, a lawyer can shed some light on a seemingly impenetrable clause.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Unit-Based Rounding: A Holy Grail?

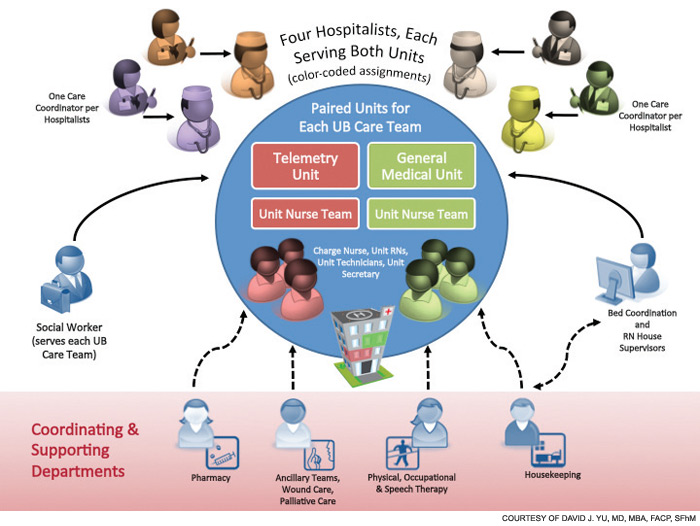
The adult inpatient medicine service at Presbyterian Medical Group (PMG) in Albuquerque, N.M, has been utilizing a unit-based care model (UBCM) with multidisciplinary rounding for the past two years. Due to the positive results, what initially started on two medicine floors telemetry and non-telemetry quickly spread to all of the medicine floors. With implementation of Unit Base 4 in April, all of the medicine beds at Presbyterian will be run using a UBCM.
Set within an inner-city hospital, the medicine service is one of the largest single-site HM programs in the country. The group has 46 FTE requirements and performed more than 15,000 admissions and consults in 2011.
Background
In early 2010, however, the HM service was in crisis. Daily starting census on a typical rounding team was 18 to 20 patients per day, and the average length of stay (LOS) for the group was close to five days. Morale among the hospitalists was low, mainly due to the patient load and multiple throughput issues. Simply stated, the program was at a tipping point.
It was at this time that a Lean Six Sigma Project was initiated to examine the throughput issues. This project expanded rapidly, with input from physicians, nurses, care coordinators, and ancillary staff, and eventually morphed into the UBCM.
The original UBCM premise was to have four geographically isolated hospitalists staff a telemetry floor, and four unit-based hospitalists staff a non-telemetry floor. The isolation guaranteed a lower starting average census for the rounding hospitalists. Each hospitalist on the UBCM would be assigned one specific care coordinator. The multidisciplinary round then occurred at the whiteboard with the hospitalists, nurses, care coordinators, and ancillary staff. The whiteboard had the floor’s census and pertinent care coordination information. The UBCM utilized several tools: visual management (white board), dedicated workspace for the hospitalist team members, standardization of work for team members, and self-regulating governance.
UBCM does not focus specifically on standardization of management of specific disease processes but on standardization of communication and interaction between various team members. For example, at multidisciplinary rounds, the charge nurses and care coordinators ask specific questions regarding estimated discharge date, level of care issues (i.e. observation vs. admission), downgrade to telemetry, and discharge issues. The new practice model had these original goals:
- Reduce average LOS, thereby increasing patient encounters through backfill;
- Improve patient satisfaction; and
- Improve financial outcomes.
The Financial Case for UBCM
The UBCM team worked closely with the finance department to create a business model with a net present value proposal for each unit-base rollout. This included the cost of hiring an additional FTE for each UBCM, but it meant each UBCM rounding team had a lower starting census.
The results have been very exciting.
The average LOS dropped to 4.6 days from 5.06 days in 2011; in 2012, the group’s LOS is at 4.40 days. By lowering average LOS with available backfill population, the group was able to increase patient discharges 15% (to 14,411 in 2011 from 12,503 in 2010).
The financial modeling for Unit Base 1 was based on the addition of PMG’s inpatient medicine service to the contribution margin by increasing patient encounters; the model for Unit Base 2 was based on savings through variable expenditures by decreasing average LOS. After 21 months, Unit Base 1 added $2.2 million to the contribution margin; after 15 months, Unit Base 2 lowered variable expenditure of $1.3 million.
The significant drop in average LOS has allowed the hospital to close a nine-bed temporary holding floor, which was created in 2009 to relieve ED congestion. This was a realized savings of $800,000 of a fixed cost.
Other Key Measures
Patient satisfaction scores have been encouraging; however, the group is realizing that the same hospitalists are scoring lower on the medicine floor with the older physical plant than on the floor with the newer physical plant. The percentage of downgrades from telemetry to non-telemetry significantly improved.
Additionally, there was initially skepticism among the hospitalists and the nursing staff. The biggest concern was that multidisciplinary rounding could not be successfully implemented on a busy medicine or telemetry floor during one of the busiest times of the day, at 9 a.m. However, team members quickly discovered that multidisciplinary rounds were an efficient way of communicating and prioritizing their time and resources. They also quickly realized the benefit to their daily workflow, and now leverage this tool to increase efficiency.
Having hospitalists geographically isolated and creating an environment that encourages communication has changed the culture of the inpatient workplace. The relationship between the hospitalists, nurses, ancillary staff, and care coordinators has improved significantly.

Try It for Yourself
Having practiced traditional internal medicine for nine years prior to becoming a hospitalist, I realize that many hospitalists are still rounding based on traditional models. But with such a system, ask yourself:
- Does a busy hospitalist always communicate the plan of care with the nurse?
- Does a hospitalist communicate with the care coordinator or physical therapist for each patient?
- Does a hospitalist leverage the fact that he or she is hospital-based to the maximum efficiency?
The answer in the vast majority of HM groups is “no.” With a UBCM approach, the efficiencies, the quality, and the communication improvements are baked into the process. We did not admonish our staff to perform “quality,” nor did we “improve communication.” We feel that we have found the holy grail of hospital medicine. The UBCM approach solves many of our problems, allows us to hire more hospitalists, and benefits our hospital’s bottom line.
Dr. Yu is medical director of the adult inpatient medicine service at Presbyterian Medical Group, Albuquerque, N.M. He is a former member of Team Hospitalist.
The adult inpatient medicine service at Presbyterian Medical Group (PMG) in Albuquerque, N.M, has been utilizing a unit-based care model (UBCM) with multidisciplinary rounding for the past two years. Due to the positive results, what initially started on two medicine floors telemetry and non-telemetry quickly spread to all of the medicine floors. With implementation of Unit Base 4 in April, all of the medicine beds at Presbyterian will be run using a UBCM.
Set within an inner-city hospital, the medicine service is one of the largest single-site HM programs in the country. The group has 46 FTE requirements and performed more than 15,000 admissions and consults in 2011.
Background
In early 2010, however, the HM service was in crisis. Daily starting census on a typical rounding team was 18 to 20 patients per day, and the average length of stay (LOS) for the group was close to five days. Morale among the hospitalists was low, mainly due to the patient load and multiple throughput issues. Simply stated, the program was at a tipping point.
It was at this time that a Lean Six Sigma Project was initiated to examine the throughput issues. This project expanded rapidly, with input from physicians, nurses, care coordinators, and ancillary staff, and eventually morphed into the UBCM.
The original UBCM premise was to have four geographically isolated hospitalists staff a telemetry floor, and four unit-based hospitalists staff a non-telemetry floor. The isolation guaranteed a lower starting average census for the rounding hospitalists. Each hospitalist on the UBCM would be assigned one specific care coordinator. The multidisciplinary round then occurred at the whiteboard with the hospitalists, nurses, care coordinators, and ancillary staff. The whiteboard had the floor’s census and pertinent care coordination information. The UBCM utilized several tools: visual management (white board), dedicated workspace for the hospitalist team members, standardization of work for team members, and self-regulating governance.
UBCM does not focus specifically on standardization of management of specific disease processes but on standardization of communication and interaction between various team members. For example, at multidisciplinary rounds, the charge nurses and care coordinators ask specific questions regarding estimated discharge date, level of care issues (i.e. observation vs. admission), downgrade to telemetry, and discharge issues. The new practice model had these original goals:
- Reduce average LOS, thereby increasing patient encounters through backfill;
- Improve patient satisfaction; and
- Improve financial outcomes.
The Financial Case for UBCM
The UBCM team worked closely with the finance department to create a business model with a net present value proposal for each unit-base rollout. This included the cost of hiring an additional FTE for each UBCM, but it meant each UBCM rounding team had a lower starting census.
The results have been very exciting.
The average LOS dropped to 4.6 days from 5.06 days in 2011; in 2012, the group’s LOS is at 4.40 days. By lowering average LOS with available backfill population, the group was able to increase patient discharges 15% (to 14,411 in 2011 from 12,503 in 2010).
The financial modeling for Unit Base 1 was based on the addition of PMG’s inpatient medicine service to the contribution margin by increasing patient encounters; the model for Unit Base 2 was based on savings through variable expenditures by decreasing average LOS. After 21 months, Unit Base 1 added $2.2 million to the contribution margin; after 15 months, Unit Base 2 lowered variable expenditure of $1.3 million.
The significant drop in average LOS has allowed the hospital to close a nine-bed temporary holding floor, which was created in 2009 to relieve ED congestion. This was a realized savings of $800,000 of a fixed cost.
Other Key Measures
Patient satisfaction scores have been encouraging; however, the group is realizing that the same hospitalists are scoring lower on the medicine floor with the older physical plant than on the floor with the newer physical plant. The percentage of downgrades from telemetry to non-telemetry significantly improved.
Additionally, there was initially skepticism among the hospitalists and the nursing staff. The biggest concern was that multidisciplinary rounding could not be successfully implemented on a busy medicine or telemetry floor during one of the busiest times of the day, at 9 a.m. However, team members quickly discovered that multidisciplinary rounds were an efficient way of communicating and prioritizing their time and resources. They also quickly realized the benefit to their daily workflow, and now leverage this tool to increase efficiency.
Having hospitalists geographically isolated and creating an environment that encourages communication has changed the culture of the inpatient workplace. The relationship between the hospitalists, nurses, ancillary staff, and care coordinators has improved significantly.
Try It for Yourself
Having practiced traditional internal medicine for nine years prior to becoming a hospitalist, I realize that many hospitalists are still rounding based on traditional models. But with such a system, ask yourself:
- Does a busy hospitalist always communicate the plan of care with the nurse?
- Does a hospitalist communicate with the care coordinator or physical therapist for each patient?
- Does a hospitalist leverage the fact that he or she is hospital-based to the maximum efficiency?
The answer in the vast majority of HM groups is “no.” With a UBCM approach, the efficiencies, the quality, and the communication improvements are baked into the process. We did not admonish our staff to perform “quality,” nor did we “improve communication.” We feel that we have found the holy grail of hospital medicine. The UBCM approach solves many of our problems, allows us to hire more hospitalists, and benefits our hospital’s bottom line.
Dr. Yu is medical director of the adult inpatient medicine service at Presbyterian Medical Group, Albuquerque, N.M. He is a former member of Team Hospitalist.
The adult inpatient medicine service at Presbyterian Medical Group (PMG) in Albuquerque, N.M, has been utilizing a unit-based care model (UBCM) with multidisciplinary rounding for the past two years. Due to the positive results, what initially started on two medicine floors telemetry and non-telemetry quickly spread to all of the medicine floors. With implementation of Unit Base 4 in April, all of the medicine beds at Presbyterian will be run using a UBCM.
Set within an inner-city hospital, the medicine service is one of the largest single-site HM programs in the country. The group has 46 FTE requirements and performed more than 15,000 admissions and consults in 2011.
Background
In early 2010, however, the HM service was in crisis. Daily starting census on a typical rounding team was 18 to 20 patients per day, and the average length of stay (LOS) for the group was close to five days. Morale among the hospitalists was low, mainly due to the patient load and multiple throughput issues. Simply stated, the program was at a tipping point.
It was at this time that a Lean Six Sigma Project was initiated to examine the throughput issues. This project expanded rapidly, with input from physicians, nurses, care coordinators, and ancillary staff, and eventually morphed into the UBCM.
The original UBCM premise was to have four geographically isolated hospitalists staff a telemetry floor, and four unit-based hospitalists staff a non-telemetry floor. The isolation guaranteed a lower starting average census for the rounding hospitalists. Each hospitalist on the UBCM would be assigned one specific care coordinator. The multidisciplinary round then occurred at the whiteboard with the hospitalists, nurses, care coordinators, and ancillary staff. The whiteboard had the floor’s census and pertinent care coordination information. The UBCM utilized several tools: visual management (white board), dedicated workspace for the hospitalist team members, standardization of work for team members, and self-regulating governance.
UBCM does not focus specifically on standardization of management of specific disease processes but on standardization of communication and interaction between various team members. For example, at multidisciplinary rounds, the charge nurses and care coordinators ask specific questions regarding estimated discharge date, level of care issues (i.e. observation vs. admission), downgrade to telemetry, and discharge issues. The new practice model had these original goals:
- Reduce average LOS, thereby increasing patient encounters through backfill;
- Improve patient satisfaction; and
- Improve financial outcomes.
The Financial Case for UBCM
The UBCM team worked closely with the finance department to create a business model with a net present value proposal for each unit-base rollout. This included the cost of hiring an additional FTE for each UBCM, but it meant each UBCM rounding team had a lower starting census.
The results have been very exciting.
The average LOS dropped to 4.6 days from 5.06 days in 2011; in 2012, the group’s LOS is at 4.40 days. By lowering average LOS with available backfill population, the group was able to increase patient discharges 15% (to 14,411 in 2011 from 12,503 in 2010).
The financial modeling for Unit Base 1 was based on the addition of PMG’s inpatient medicine service to the contribution margin by increasing patient encounters; the model for Unit Base 2 was based on savings through variable expenditures by decreasing average LOS. After 21 months, Unit Base 1 added $2.2 million to the contribution margin; after 15 months, Unit Base 2 lowered variable expenditure of $1.3 million.
The significant drop in average LOS has allowed the hospital to close a nine-bed temporary holding floor, which was created in 2009 to relieve ED congestion. This was a realized savings of $800,000 of a fixed cost.
Other Key Measures
Patient satisfaction scores have been encouraging; however, the group is realizing that the same hospitalists are scoring lower on the medicine floor with the older physical plant than on the floor with the newer physical plant. The percentage of downgrades from telemetry to non-telemetry significantly improved.
Additionally, there was initially skepticism among the hospitalists and the nursing staff. The biggest concern was that multidisciplinary rounding could not be successfully implemented on a busy medicine or telemetry floor during one of the busiest times of the day, at 9 a.m. However, team members quickly discovered that multidisciplinary rounds were an efficient way of communicating and prioritizing their time and resources. They also quickly realized the benefit to their daily workflow, and now leverage this tool to increase efficiency.
Having hospitalists geographically isolated and creating an environment that encourages communication has changed the culture of the inpatient workplace. The relationship between the hospitalists, nurses, ancillary staff, and care coordinators has improved significantly.
Try It for Yourself
Having practiced traditional internal medicine for nine years prior to becoming a hospitalist, I realize that many hospitalists are still rounding based on traditional models. But with such a system, ask yourself:
- Does a busy hospitalist always communicate the plan of care with the nurse?
- Does a hospitalist communicate with the care coordinator or physical therapist for each patient?
- Does a hospitalist leverage the fact that he or she is hospital-based to the maximum efficiency?
The answer in the vast majority of HM groups is “no.” With a UBCM approach, the efficiencies, the quality, and the communication improvements are baked into the process. We did not admonish our staff to perform “quality,” nor did we “improve communication.” We feel that we have found the holy grail of hospital medicine. The UBCM approach solves many of our problems, allows us to hire more hospitalists, and benefits our hospital’s bottom line.
Dr. Yu is medical director of the adult inpatient medicine service at Presbyterian Medical Group, Albuquerque, N.M. He is a former member of Team Hospitalist.
Whac-a-Mole Regulation

Let’s be honest. How many times in the past (insert any timeline here; month, week, day, minute) have you heard a disparaging comment about a hospital regulatory agency? They usually sound something like, “Well, I’ll be darned if I am going to let CMS tell me how to practice medicine” or “So is this another Joint Commission thing?”
I understand the frustration. The healthcare industry is incredibly regulated. So much so that I, and countless others in hospital administration offices around the country, relinquish an inordinate amount of time figuring out what it is we are supposed to be complying with, then figuring how we are actually going to do it. It often has been equated to Whac-a-Mole, a game that requires more eyeballs and arm strength than an extraterrestrial possesses. There are many reasons that underlie the frustration and lead to the disparaging comments:
- Some requirements are not perfectly evidence-based. Not all process measures actually correlate with any outcomes; just because someone checks an oxygen saturation on every pneumonia patient doesn’t mean anything else improves for the patient.
- Some requirements are poorly implemented. I think we can all agree that counseling patients to stop smoking is a laudable goal. However, “smoking cessation counseling” is often relegated to uttering a short phrase (“you know you should really quit smoking”) while holding the exit-door handle, then checking the box for documentation. This “counseling session” is probably as effective as declaring every day a Great American Smokeout.
- Some regulations result in unintended consequences when implemented into large, complicated organizations. An obvious example is the time to first antibiotic in pneumonia patients, which resulted in frequent and unnecessary antibiotic utilization in patients who did not have pneumonia.
- Some are just extremely difficult to accomplish with high reliability. An example here is time to PCI for heart attacks. It’s clearly the right thing to do, and clearly very difficult to get it completed, on time, on every single patient. And 99% compliance is just not good enough, because the 1% matters.
And as a result of these imperfections, “noncompliance” leads to lots of emails, rework, restructuring, and at times downright bickering—hence, the disparaging comments.
Regulatory Origins and Missions
But let’s back up for a minute and think about why healthcare regulations exist: Many local, state, and federal agencies have enhanced the scrutiny of healthcare over time because, quite frankly, the healthcare industry did not regulate itself very well. We insisted for decades that patients were each too unique to be “cook-booked,” that medicine was an art as much as it was a science, and that “it’s just complicated.”
It took a few (too many) high-profile deaths and a few common-sense publications to incense the public, our payors, and our regulators. Who is not familiar with the 98,000-preventable-deaths-a-year statistic? Not only is that figure sobering, but it also is quite difficult to untether from our reputation. Henceforth, over the course of decades, a multitude of moles have emerged, littering the landscape and sparing no area of the healthcare industry.
So let’s back up another minute and think about what these agencies are trying to do: Could it be that most regulatory agencies really do want to leverage large-scale improvements in patient outcomes, at the best value?
Take this vision statement, as an example: “All people always experience the safest, highest-quality, best-value healthcare across all settings.”
Sounds like the kind of healthcare I want for my kids and my mom. That is the vision statement of the Joint Commission.
How about this vision statement: “CMS is a major force and a trustworthy partner for the continual improvement of health and healthcare for all Americans.”
Not too shabby.
So why do we view regulators like moles? Why do we arm ourselves with big, black mallets ready to strike when we see them emerge from the corner of our eye?
HM-Mole Alliance
Whac-a-Mole is an unwinnable game. No player has ever whacked all the moles. If you have not been to your local arcade lately, the game starts out slow, such that most players can keep pace; it then accelerates, such that several moles are outside the holes simultaneously, and their time above ground becomes consecutively shorter. You can add mallets, even add players, but generally they end up getting in each other’s way, communication breaks down, and one mole gets whacked twice, while another exits unscathed, only to break the soil elsewhere.
Maybe a better strategy is to have a strategy—to work with our “trustworthy partners” to align our vision statements, anticipate the vermin’s approach, and fill the holes (or chasms) before anything has a chance to squeeze through. Maybe we should tell them where the moles are, because we actually already know what they look like and where they dwell. Why don’t we tell them which moles are the most dangerous, the most annoying, or are the most likely to tear up the topsoil into an irreparable state?
What about all the issues that no one is telling us we have to comply with—for example, a universal allergy list across the spectrum of care, or a perfectly reliable system to ensure that a patient with an epidural catheter cannot be anticoagulated? Such a list is endless, and no one is telling us we have to address the majority of the items on the list.
It comes down to this: What kind of healthcare do you want for yourself, your family, and the patients who trust you? I’d rather not have a reactive, frantic race to obliterate the next torrid creature that has arisen. I suggest a proactive, strategic pathway of tilling the soil.
In anticipation of a universal vote for the latter, join me in congratulating the healthcare industry in holding ourselves accountable, embracing a new era of transparency and collaboration, and routinely going beyond the expectations of our regulators. And leaving the mallet in the arcade.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Let’s be honest. How many times in the past (insert any timeline here; month, week, day, minute) have you heard a disparaging comment about a hospital regulatory agency? They usually sound something like, “Well, I’ll be darned if I am going to let CMS tell me how to practice medicine” or “So is this another Joint Commission thing?”
I understand the frustration. The healthcare industry is incredibly regulated. So much so that I, and countless others in hospital administration offices around the country, relinquish an inordinate amount of time figuring out what it is we are supposed to be complying with, then figuring how we are actually going to do it. It often has been equated to Whac-a-Mole, a game that requires more eyeballs and arm strength than an extraterrestrial possesses. There are many reasons that underlie the frustration and lead to the disparaging comments:
- Some requirements are not perfectly evidence-based. Not all process measures actually correlate with any outcomes; just because someone checks an oxygen saturation on every pneumonia patient doesn’t mean anything else improves for the patient.
- Some requirements are poorly implemented. I think we can all agree that counseling patients to stop smoking is a laudable goal. However, “smoking cessation counseling” is often relegated to uttering a short phrase (“you know you should really quit smoking”) while holding the exit-door handle, then checking the box for documentation. This “counseling session” is probably as effective as declaring every day a Great American Smokeout.
- Some regulations result in unintended consequences when implemented into large, complicated organizations. An obvious example is the time to first antibiotic in pneumonia patients, which resulted in frequent and unnecessary antibiotic utilization in patients who did not have pneumonia.
- Some are just extremely difficult to accomplish with high reliability. An example here is time to PCI for heart attacks. It’s clearly the right thing to do, and clearly very difficult to get it completed, on time, on every single patient. And 99% compliance is just not good enough, because the 1% matters.
And as a result of these imperfections, “noncompliance” leads to lots of emails, rework, restructuring, and at times downright bickering—hence, the disparaging comments.
Regulatory Origins and Missions
But let’s back up for a minute and think about why healthcare regulations exist: Many local, state, and federal agencies have enhanced the scrutiny of healthcare over time because, quite frankly, the healthcare industry did not regulate itself very well. We insisted for decades that patients were each too unique to be “cook-booked,” that medicine was an art as much as it was a science, and that “it’s just complicated.”
It took a few (too many) high-profile deaths and a few common-sense publications to incense the public, our payors, and our regulators. Who is not familiar with the 98,000-preventable-deaths-a-year statistic? Not only is that figure sobering, but it also is quite difficult to untether from our reputation. Henceforth, over the course of decades, a multitude of moles have emerged, littering the landscape and sparing no area of the healthcare industry.
So let’s back up another minute and think about what these agencies are trying to do: Could it be that most regulatory agencies really do want to leverage large-scale improvements in patient outcomes, at the best value?
Take this vision statement, as an example: “All people always experience the safest, highest-quality, best-value healthcare across all settings.”
Sounds like the kind of healthcare I want for my kids and my mom. That is the vision statement of the Joint Commission.
How about this vision statement: “CMS is a major force and a trustworthy partner for the continual improvement of health and healthcare for all Americans.”
Not too shabby.
So why do we view regulators like moles? Why do we arm ourselves with big, black mallets ready to strike when we see them emerge from the corner of our eye?
HM-Mole Alliance
Whac-a-Mole is an unwinnable game. No player has ever whacked all the moles. If you have not been to your local arcade lately, the game starts out slow, such that most players can keep pace; it then accelerates, such that several moles are outside the holes simultaneously, and their time above ground becomes consecutively shorter. You can add mallets, even add players, but generally they end up getting in each other’s way, communication breaks down, and one mole gets whacked twice, while another exits unscathed, only to break the soil elsewhere.
Maybe a better strategy is to have a strategy—to work with our “trustworthy partners” to align our vision statements, anticipate the vermin’s approach, and fill the holes (or chasms) before anything has a chance to squeeze through. Maybe we should tell them where the moles are, because we actually already know what they look like and where they dwell. Why don’t we tell them which moles are the most dangerous, the most annoying, or are the most likely to tear up the topsoil into an irreparable state?
What about all the issues that no one is telling us we have to comply with—for example, a universal allergy list across the spectrum of care, or a perfectly reliable system to ensure that a patient with an epidural catheter cannot be anticoagulated? Such a list is endless, and no one is telling us we have to address the majority of the items on the list.
It comes down to this: What kind of healthcare do you want for yourself, your family, and the patients who trust you? I’d rather not have a reactive, frantic race to obliterate the next torrid creature that has arisen. I suggest a proactive, strategic pathway of tilling the soil.
In anticipation of a universal vote for the latter, join me in congratulating the healthcare industry in holding ourselves accountable, embracing a new era of transparency and collaboration, and routinely going beyond the expectations of our regulators. And leaving the mallet in the arcade.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Let’s be honest. How many times in the past (insert any timeline here; month, week, day, minute) have you heard a disparaging comment about a hospital regulatory agency? They usually sound something like, “Well, I’ll be darned if I am going to let CMS tell me how to practice medicine” or “So is this another Joint Commission thing?”
I understand the frustration. The healthcare industry is incredibly regulated. So much so that I, and countless others in hospital administration offices around the country, relinquish an inordinate amount of time figuring out what it is we are supposed to be complying with, then figuring how we are actually going to do it. It often has been equated to Whac-a-Mole, a game that requires more eyeballs and arm strength than an extraterrestrial possesses. There are many reasons that underlie the frustration and lead to the disparaging comments:
- Some requirements are not perfectly evidence-based. Not all process measures actually correlate with any outcomes; just because someone checks an oxygen saturation on every pneumonia patient doesn’t mean anything else improves for the patient.
- Some requirements are poorly implemented. I think we can all agree that counseling patients to stop smoking is a laudable goal. However, “smoking cessation counseling” is often relegated to uttering a short phrase (“you know you should really quit smoking”) while holding the exit-door handle, then checking the box for documentation. This “counseling session” is probably as effective as declaring every day a Great American Smokeout.
- Some regulations result in unintended consequences when implemented into large, complicated organizations. An obvious example is the time to first antibiotic in pneumonia patients, which resulted in frequent and unnecessary antibiotic utilization in patients who did not have pneumonia.
- Some are just extremely difficult to accomplish with high reliability. An example here is time to PCI for heart attacks. It’s clearly the right thing to do, and clearly very difficult to get it completed, on time, on every single patient. And 99% compliance is just not good enough, because the 1% matters.
And as a result of these imperfections, “noncompliance” leads to lots of emails, rework, restructuring, and at times downright bickering—hence, the disparaging comments.
Regulatory Origins and Missions
But let’s back up for a minute and think about why healthcare regulations exist: Many local, state, and federal agencies have enhanced the scrutiny of healthcare over time because, quite frankly, the healthcare industry did not regulate itself very well. We insisted for decades that patients were each too unique to be “cook-booked,” that medicine was an art as much as it was a science, and that “it’s just complicated.”
It took a few (too many) high-profile deaths and a few common-sense publications to incense the public, our payors, and our regulators. Who is not familiar with the 98,000-preventable-deaths-a-year statistic? Not only is that figure sobering, but it also is quite difficult to untether from our reputation. Henceforth, over the course of decades, a multitude of moles have emerged, littering the landscape and sparing no area of the healthcare industry.
So let’s back up another minute and think about what these agencies are trying to do: Could it be that most regulatory agencies really do want to leverage large-scale improvements in patient outcomes, at the best value?
Take this vision statement, as an example: “All people always experience the safest, highest-quality, best-value healthcare across all settings.”
Sounds like the kind of healthcare I want for my kids and my mom. That is the vision statement of the Joint Commission.
How about this vision statement: “CMS is a major force and a trustworthy partner for the continual improvement of health and healthcare for all Americans.”
Not too shabby.
So why do we view regulators like moles? Why do we arm ourselves with big, black mallets ready to strike when we see them emerge from the corner of our eye?
HM-Mole Alliance
Whac-a-Mole is an unwinnable game. No player has ever whacked all the moles. If you have not been to your local arcade lately, the game starts out slow, such that most players can keep pace; it then accelerates, such that several moles are outside the holes simultaneously, and their time above ground becomes consecutively shorter. You can add mallets, even add players, but generally they end up getting in each other’s way, communication breaks down, and one mole gets whacked twice, while another exits unscathed, only to break the soil elsewhere.
Maybe a better strategy is to have a strategy—to work with our “trustworthy partners” to align our vision statements, anticipate the vermin’s approach, and fill the holes (or chasms) before anything has a chance to squeeze through. Maybe we should tell them where the moles are, because we actually already know what they look like and where they dwell. Why don’t we tell them which moles are the most dangerous, the most annoying, or are the most likely to tear up the topsoil into an irreparable state?
What about all the issues that no one is telling us we have to comply with—for example, a universal allergy list across the spectrum of care, or a perfectly reliable system to ensure that a patient with an epidural catheter cannot be anticoagulated? Such a list is endless, and no one is telling us we have to address the majority of the items on the list.
It comes down to this: What kind of healthcare do you want for yourself, your family, and the patients who trust you? I’d rather not have a reactive, frantic race to obliterate the next torrid creature that has arisen. I suggest a proactive, strategic pathway of tilling the soil.
In anticipation of a universal vote for the latter, join me in congratulating the healthcare industry in holding ourselves accountable, embracing a new era of transparency and collaboration, and routinely going beyond the expectations of our regulators. And leaving the mallet in the arcade.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Rural Hospitalist Practice: First Among Equals
Louis O’Boyle, DO, FACP, FHM, says hospitalists with an entrepreneurial bent can use flexibility and creativity to design HM programs that meet the unique needs of small or rural hospitals. He owns a hospitalist practice, Advanced Inpatient Medicine, which serves 98-bed Wayne Memorial Hospital in Honesdale, Pa., population 4,874.
“In 2006, the largest group of community physicians locally said they were not going to do hospital coverage or take unassigned hospitalized patients anymore,” Dr. O’Boyle says. The hospital first brought in an out-of-town consultant to provide hospitalist services, but in 2009, Dr. O’Boyle seized the opportunity to fill the need. He formed his own company, which employs five hospitalists providing 24/7 coverage (clinicians rotate between 8 a.m.-to-4 p.m. shifts and 4 p.m.-to-8 a.m. shifts). The hospitalist on duty can often go home after the ED slows down, he says, although hiring a sixth hospitalist would make it easier to provide a 24-hour presence.

“Our hospitalists see an average of 12 patients a day, so we’re not running too hard. You can take time to do a good job, and still have supper with your kids some workdays. In a rural area, you can still get away with that,” Dr. O’Boyle says. “We have a good salary, work schedule, and caseload. We have a great team, with everyone on board with what we’re trying to do.”
Members of Dr. O’Boyle’s group sit on all of the hospital’s committees. Many have a say in changes that go on at the hospital. The group is active in quality and safety projects and research on readmission rates. The program has been so successful that he is negotiating to cover several other hospitals in the region.
“Another key to the success of this program is our fiscal responsibility, demonstrating the value we bring to the hospital,” he says. “We align our goals with the hospital’s goals. We have cut length of stay by an average of three-quarters of a day. We were very involved with the IT department in setting up EHR and CPOE to our specifications. There is a whole list of things we do to justify our worth, and our subsidy payment from the hospital is particularly low.”
Dr. O’Boyle, in addition to his practice-management responsibilities, works alongside his colleagues. “It’s not like I’m the boss—more like I’m first among equals,” he says. “We meet as a team once a month.”
Louis O’Boyle, DO, FACP, FHM, says hospitalists with an entrepreneurial bent can use flexibility and creativity to design HM programs that meet the unique needs of small or rural hospitals. He owns a hospitalist practice, Advanced Inpatient Medicine, which serves 98-bed Wayne Memorial Hospital in Honesdale, Pa., population 4,874.
“In 2006, the largest group of community physicians locally said they were not going to do hospital coverage or take unassigned hospitalized patients anymore,” Dr. O’Boyle says. The hospital first brought in an out-of-town consultant to provide hospitalist services, but in 2009, Dr. O’Boyle seized the opportunity to fill the need. He formed his own company, which employs five hospitalists providing 24/7 coverage (clinicians rotate between 8 a.m.-to-4 p.m. shifts and 4 p.m.-to-8 a.m. shifts). The hospitalist on duty can often go home after the ED slows down, he says, although hiring a sixth hospitalist would make it easier to provide a 24-hour presence.
“Our hospitalists see an average of 12 patients a day, so we’re not running too hard. You can take time to do a good job, and still have supper with your kids some workdays. In a rural area, you can still get away with that,” Dr. O’Boyle says. “We have a good salary, work schedule, and caseload. We have a great team, with everyone on board with what we’re trying to do.”
Members of Dr. O’Boyle’s group sit on all of the hospital’s committees. Many have a say in changes that go on at the hospital. The group is active in quality and safety projects and research on readmission rates. The program has been so successful that he is negotiating to cover several other hospitals in the region.
“Another key to the success of this program is our fiscal responsibility, demonstrating the value we bring to the hospital,” he says. “We align our goals with the hospital’s goals. We have cut length of stay by an average of three-quarters of a day. We were very involved with the IT department in setting up EHR and CPOE to our specifications. There is a whole list of things we do to justify our worth, and our subsidy payment from the hospital is particularly low.”
Dr. O’Boyle, in addition to his practice-management responsibilities, works alongside his colleagues. “It’s not like I’m the boss—more like I’m first among equals,” he says. “We meet as a team once a month.”
Louis O’Boyle, DO, FACP, FHM, says hospitalists with an entrepreneurial bent can use flexibility and creativity to design HM programs that meet the unique needs of small or rural hospitals. He owns a hospitalist practice, Advanced Inpatient Medicine, which serves 98-bed Wayne Memorial Hospital in Honesdale, Pa., population 4,874.
“In 2006, the largest group of community physicians locally said they were not going to do hospital coverage or take unassigned hospitalized patients anymore,” Dr. O’Boyle says. The hospital first brought in an out-of-town consultant to provide hospitalist services, but in 2009, Dr. O’Boyle seized the opportunity to fill the need. He formed his own company, which employs five hospitalists providing 24/7 coverage (clinicians rotate between 8 a.m.-to-4 p.m. shifts and 4 p.m.-to-8 a.m. shifts). The hospitalist on duty can often go home after the ED slows down, he says, although hiring a sixth hospitalist would make it easier to provide a 24-hour presence.
“Our hospitalists see an average of 12 patients a day, so we’re not running too hard. You can take time to do a good job, and still have supper with your kids some workdays. In a rural area, you can still get away with that,” Dr. O’Boyle says. “We have a good salary, work schedule, and caseload. We have a great team, with everyone on board with what we’re trying to do.”
Members of Dr. O’Boyle’s group sit on all of the hospital’s committees. Many have a say in changes that go on at the hospital. The group is active in quality and safety projects and research on readmission rates. The program has been so successful that he is negotiating to cover several other hospitals in the region.
“Another key to the success of this program is our fiscal responsibility, demonstrating the value we bring to the hospital,” he says. “We align our goals with the hospital’s goals. We have cut length of stay by an average of three-quarters of a day. We were very involved with the IT department in setting up EHR and CPOE to our specifications. There is a whole list of things we do to justify our worth, and our subsidy payment from the hospital is particularly low.”
Dr. O’Boyle, in addition to his practice-management responsibilities, works alongside his colleagues. “It’s not like I’m the boss—more like I’m first among equals,” he says. “We meet as a team once a month.”
Rural Healthcare Facts
The obstacles faced by healthcare providers and patients in rural areas are vastly different than those in urban areas. Rural Americans face a unique combination of factors that create disparities in healthcare not found in urban areas:
- Only about 10% of physicians practice in rural America despite the fact that nearly one-fourth of the population lives in these areas.
- Rural residents tend to be poorer. On the average, per capita income is $7,417 lower than in urban areas, and rural Americans are more likely to live below the poverty line. The disparity in incomes is even greater for minorities living in rural areas. Nearly 24% of rural children live in poverty.
- Hypertension is higher in rural than urban areas (101.3 per 1,000 individuals in MSAs and 128.8 per 1,000 individuals in non-MSAs).
- 20% of nonmetropolitan counties lack mental health services, compared with 5% of metropolitan counties.
- Medicare payments to rural hospitals and physicians are dramatically less than those to their urban counterparts for equivalent services. And more than 470 rural hospitals have closed in the past 25 years.
- Medicare patients with acute myocardial infarction (AMI) who were treated in rural hospitals were less likely than those treated in urban hospitals to receive recommended treatments and had significantly higher adjusted 30-day post-AMI death rates from all causes than those in urban hospitals.
- Rural residents have greater transportation difficulties reaching healthcare providers, often traveling great distances to reach a doctor or hospital.
Source: www.ruralhealthweb.org
The obstacles faced by healthcare providers and patients in rural areas are vastly different than those in urban areas. Rural Americans face a unique combination of factors that create disparities in healthcare not found in urban areas:
- Only about 10% of physicians practice in rural America despite the fact that nearly one-fourth of the population lives in these areas.
- Rural residents tend to be poorer. On the average, per capita income is $7,417 lower than in urban areas, and rural Americans are more likely to live below the poverty line. The disparity in incomes is even greater for minorities living in rural areas. Nearly 24% of rural children live in poverty.
- Hypertension is higher in rural than urban areas (101.3 per 1,000 individuals in MSAs and 128.8 per 1,000 individuals in non-MSAs).
- 20% of nonmetropolitan counties lack mental health services, compared with 5% of metropolitan counties.
- Medicare payments to rural hospitals and physicians are dramatically less than those to their urban counterparts for equivalent services. And more than 470 rural hospitals have closed in the past 25 years.
- Medicare patients with acute myocardial infarction (AMI) who were treated in rural hospitals were less likely than those treated in urban hospitals to receive recommended treatments and had significantly higher adjusted 30-day post-AMI death rates from all causes than those in urban hospitals.
- Rural residents have greater transportation difficulties reaching healthcare providers, often traveling great distances to reach a doctor or hospital.
Source: www.ruralhealthweb.org
The obstacles faced by healthcare providers and patients in rural areas are vastly different than those in urban areas. Rural Americans face a unique combination of factors that create disparities in healthcare not found in urban areas:
- Only about 10% of physicians practice in rural America despite the fact that nearly one-fourth of the population lives in these areas.
- Rural residents tend to be poorer. On the average, per capita income is $7,417 lower than in urban areas, and rural Americans are more likely to live below the poverty line. The disparity in incomes is even greater for minorities living in rural areas. Nearly 24% of rural children live in poverty.
- Hypertension is higher in rural than urban areas (101.3 per 1,000 individuals in MSAs and 128.8 per 1,000 individuals in non-MSAs).
- 20% of nonmetropolitan counties lack mental health services, compared with 5% of metropolitan counties.
- Medicare payments to rural hospitals and physicians are dramatically less than those to their urban counterparts for equivalent services. And more than 470 rural hospitals have closed in the past 25 years.
- Medicare patients with acute myocardial infarction (AMI) who were treated in rural hospitals were less likely than those treated in urban hospitals to receive recommended treatments and had significantly higher adjusted 30-day post-AMI death rates from all causes than those in urban hospitals.
- Rural residents have greater transportation difficulties reaching healthcare providers, often traveling great distances to reach a doctor or hospital.
Source: www.ruralhealthweb.org
Resources for the Rural Hospitalist
SHM immediate past president Joseph Ming Wah Li, MD, SFHM, practices hospital medicine at Beth Israel Deaconess Medical Center in Boston, but Oklahoma is where he grew up, went to medical school, and performed rural rotations. Some parts of hospitalist practice are the same at big and small hospitals, urban and rural settings, he says.
“Recruitment of high-quality physicians is always a challenge,” Dr. Li says. “That’s where SHM can help.”
SHM’s Career Center, official publications, and the SHM annual meeting are excellent avenues for recruitment, Dr. Li says. SHM also offers online practice-management tools and a variety of collaborative resources—SQUINT, a searchable repository of innovative QI methods and systems, and an electronic QI toolkit known as eQUIPS—to help rural hospitalists.
Based in Kansas City, the National Rural Health Association (www.ruralhealthweb.org) provides additional resources for small, rural hospitals. The NRHA is working with the Office of the National Coordinator for Health IT and 62 Regional Extension Centers to help rural providers with EHR adoption and implementation, guiding them to meet meaningful-use standards.
“NRHA is a member organization with multiple constituencies,” says Brock Slabach, senior vice president for member services. “If anybody in hospital medicine works in a rural community and wants to connect with an organization like ours, we don’t have a lot of hospitalist members, but we would welcome them.”
SHM immediate past president Joseph Ming Wah Li, MD, SFHM, practices hospital medicine at Beth Israel Deaconess Medical Center in Boston, but Oklahoma is where he grew up, went to medical school, and performed rural rotations. Some parts of hospitalist practice are the same at big and small hospitals, urban and rural settings, he says.
“Recruitment of high-quality physicians is always a challenge,” Dr. Li says. “That’s where SHM can help.”
SHM’s Career Center, official publications, and the SHM annual meeting are excellent avenues for recruitment, Dr. Li says. SHM also offers online practice-management tools and a variety of collaborative resources—SQUINT, a searchable repository of innovative QI methods and systems, and an electronic QI toolkit known as eQUIPS—to help rural hospitalists.
Based in Kansas City, the National Rural Health Association (www.ruralhealthweb.org) provides additional resources for small, rural hospitals. The NRHA is working with the Office of the National Coordinator for Health IT and 62 Regional Extension Centers to help rural providers with EHR adoption and implementation, guiding them to meet meaningful-use standards.
“NRHA is a member organization with multiple constituencies,” says Brock Slabach, senior vice president for member services. “If anybody in hospital medicine works in a rural community and wants to connect with an organization like ours, we don’t have a lot of hospitalist members, but we would welcome them.”
SHM immediate past president Joseph Ming Wah Li, MD, SFHM, practices hospital medicine at Beth Israel Deaconess Medical Center in Boston, but Oklahoma is where he grew up, went to medical school, and performed rural rotations. Some parts of hospitalist practice are the same at big and small hospitals, urban and rural settings, he says.
“Recruitment of high-quality physicians is always a challenge,” Dr. Li says. “That’s where SHM can help.”
SHM’s Career Center, official publications, and the SHM annual meeting are excellent avenues for recruitment, Dr. Li says. SHM also offers online practice-management tools and a variety of collaborative resources—SQUINT, a searchable repository of innovative QI methods and systems, and an electronic QI toolkit known as eQUIPS—to help rural hospitalists.
Based in Kansas City, the National Rural Health Association (www.ruralhealthweb.org) provides additional resources for small, rural hospitals. The NRHA is working with the Office of the National Coordinator for Health IT and 62 Regional Extension Centers to help rural providers with EHR adoption and implementation, guiding them to meet meaningful-use standards.
“NRHA is a member organization with multiple constituencies,” says Brock Slabach, senior vice president for member services. “If anybody in hospital medicine works in a rural community and wants to connect with an organization like ours, we don’t have a lot of hospitalist members, but we would welcome them.”
Evaluating a Hospitalist: A New Way of Measurement
Medicine in the past 10-20 years has seen major changes driven by changes in payment systems, lifestyle changes, and changes in training patterns. One such change is the hospitalist model of medicine. The advent of hospitalist practice has turned work-life balance on its head, as far as medicine is concerned.
All along, professionalism required that we pay unquestionable attention to the patient, the profession, and the organization—reporting early to work, staying until the work is done, taking work home, and answering the phone on the nights when we were on call. On weekends, finishing pending dictation was normal. The 20-minute mill of outpatient practice has driven primary medicine to a breaking point.
As the pressures of the primary-care job got worse, there came an exit in the form of the hospitalist model. HM provided shift work that could be adjusted to the needs of the physician.
This new kind of job, however, has its own problems. Physicians choosing the normalcy of shift work did not realize that they would give up professional independence. Hospitalists now are governed by the laws of shift work, and at the same time remain governed by the laws of their profession. It is likely when in need they will stay behind and get the work done. And it has been seen that hospitalists do visit the doctors’ lounge, have professional interests outside of direct patient care, and sometimes leave the hospital when their admits and discharges are complete.
And so the shift-work model has, at times, resulted in friction between hospital administration and hospitalists. It could be understood that, from an employer’s perspective, hospitals are paying on an hourly basis and thus expect the hospitalist group to be on site 24/7, sticking around even if there is no work. However, the argument from the hospitalist perspective is that when needed, I stay extra. It should be OK that on low-census days we should be able to leave for a cup of coffee and still be reachable, ready to come in if need arises.
So how do hospitalist-physician professionalism and shift work co-exist? It’s a big question, one that organizations around the country will be looking to solve in the next few years. How this question is answered is going to impact quality of care, recruitment, and staff satisfaction. Each answer will impact the staff and patients.
Keeping in mind outcomes that both parties are looking for, I think a proper plan can be worked out. I suggest hospital administrators adopt the following value-based measurements to evaluate hospitalist clinicians, and establish a compensation system where a minimum amount of production must be met.
Work relative value units (wRVUs). Work RVUs provide a consistent method to measure physician productivity. If one HM clinician’s numbers are below the group average, they might need a lesson in billing, along with a report of their productivity numbers and group expectations.
Patient encounters per day. The average number of patients seen per day (patients seen divided by number of shifts worked) should be measured on a quarterly basis. This metric should provide a measure of the work done by the physician; however, it needs to be offset by your group’s turnover rate (as discussed below).
Length of stay (LOS). Most HM groups are measuring LOS. It is the reason hospitalists exist. Not much more needs to be said about this measure of work performance.
Percentage of patient turnover. A good hospitalist will have a high patient turnover figure (total discharges divided by total encounters per day). This is important to know; it’s even better if accompanied by a short LOS.
New admissions per shift. Again, if there is an outlier, that metric should be detected rather easily.
Patient satisfaction. More and more, this is becoming an important measure of physician quality and is essential for competitive marketplaces. Of course, the quality of medical care will have its own parameters. And it is best left to use the existing, longstanding parameters that are used for the rest of the doctors in your system. There is no need to create an alternative system for the hospitalist.
If all of the above measures are better than the average hospitalist in the locality, then no one should worry about the hospitalist’s other activities, be it involvement in committee work, research, or browsing a newspaper or a cup of coffee in the doctors’ lounge. After all, one of the main reasons physicians opted for HM practice was to have the ability to control their workday.
This will, in my opinion, improve workforce satisfaction and improve productivity. It only makes common sense. It may be a hard pill to swallow for the administrators, but it is the right medicine for the doctor.
Rwoof Reshi, MD, hospitalist, St. Joe’s Hospital, St. Paul, Minn.
Medicine in the past 10-20 years has seen major changes driven by changes in payment systems, lifestyle changes, and changes in training patterns. One such change is the hospitalist model of medicine. The advent of hospitalist practice has turned work-life balance on its head, as far as medicine is concerned.
All along, professionalism required that we pay unquestionable attention to the patient, the profession, and the organization—reporting early to work, staying until the work is done, taking work home, and answering the phone on the nights when we were on call. On weekends, finishing pending dictation was normal. The 20-minute mill of outpatient practice has driven primary medicine to a breaking point.
As the pressures of the primary-care job got worse, there came an exit in the form of the hospitalist model. HM provided shift work that could be adjusted to the needs of the physician.
This new kind of job, however, has its own problems. Physicians choosing the normalcy of shift work did not realize that they would give up professional independence. Hospitalists now are governed by the laws of shift work, and at the same time remain governed by the laws of their profession. It is likely when in need they will stay behind and get the work done. And it has been seen that hospitalists do visit the doctors’ lounge, have professional interests outside of direct patient care, and sometimes leave the hospital when their admits and discharges are complete.
And so the shift-work model has, at times, resulted in friction between hospital administration and hospitalists. It could be understood that, from an employer’s perspective, hospitals are paying on an hourly basis and thus expect the hospitalist group to be on site 24/7, sticking around even if there is no work. However, the argument from the hospitalist perspective is that when needed, I stay extra. It should be OK that on low-census days we should be able to leave for a cup of coffee and still be reachable, ready to come in if need arises.
So how do hospitalist-physician professionalism and shift work co-exist? It’s a big question, one that organizations around the country will be looking to solve in the next few years. How this question is answered is going to impact quality of care, recruitment, and staff satisfaction. Each answer will impact the staff and patients.
Keeping in mind outcomes that both parties are looking for, I think a proper plan can be worked out. I suggest hospital administrators adopt the following value-based measurements to evaluate hospitalist clinicians, and establish a compensation system where a minimum amount of production must be met.
Work relative value units (wRVUs). Work RVUs provide a consistent method to measure physician productivity. If one HM clinician’s numbers are below the group average, they might need a lesson in billing, along with a report of their productivity numbers and group expectations.
Patient encounters per day. The average number of patients seen per day (patients seen divided by number of shifts worked) should be measured on a quarterly basis. This metric should provide a measure of the work done by the physician; however, it needs to be offset by your group’s turnover rate (as discussed below).
Length of stay (LOS). Most HM groups are measuring LOS. It is the reason hospitalists exist. Not much more needs to be said about this measure of work performance.
Percentage of patient turnover. A good hospitalist will have a high patient turnover figure (total discharges divided by total encounters per day). This is important to know; it’s even better if accompanied by a short LOS.
New admissions per shift. Again, if there is an outlier, that metric should be detected rather easily.
Patient satisfaction. More and more, this is becoming an important measure of physician quality and is essential for competitive marketplaces. Of course, the quality of medical care will have its own parameters. And it is best left to use the existing, longstanding parameters that are used for the rest of the doctors in your system. There is no need to create an alternative system for the hospitalist.
If all of the above measures are better than the average hospitalist in the locality, then no one should worry about the hospitalist’s other activities, be it involvement in committee work, research, or browsing a newspaper or a cup of coffee in the doctors’ lounge. After all, one of the main reasons physicians opted for HM practice was to have the ability to control their workday.
This will, in my opinion, improve workforce satisfaction and improve productivity. It only makes common sense. It may be a hard pill to swallow for the administrators, but it is the right medicine for the doctor.
Rwoof Reshi, MD, hospitalist, St. Joe’s Hospital, St. Paul, Minn.
Medicine in the past 10-20 years has seen major changes driven by changes in payment systems, lifestyle changes, and changes in training patterns. One such change is the hospitalist model of medicine. The advent of hospitalist practice has turned work-life balance on its head, as far as medicine is concerned.
All along, professionalism required that we pay unquestionable attention to the patient, the profession, and the organization—reporting early to work, staying until the work is done, taking work home, and answering the phone on the nights when we were on call. On weekends, finishing pending dictation was normal. The 20-minute mill of outpatient practice has driven primary medicine to a breaking point.
As the pressures of the primary-care job got worse, there came an exit in the form of the hospitalist model. HM provided shift work that could be adjusted to the needs of the physician.
This new kind of job, however, has its own problems. Physicians choosing the normalcy of shift work did not realize that they would give up professional independence. Hospitalists now are governed by the laws of shift work, and at the same time remain governed by the laws of their profession. It is likely when in need they will stay behind and get the work done. And it has been seen that hospitalists do visit the doctors’ lounge, have professional interests outside of direct patient care, and sometimes leave the hospital when their admits and discharges are complete.
And so the shift-work model has, at times, resulted in friction between hospital administration and hospitalists. It could be understood that, from an employer’s perspective, hospitals are paying on an hourly basis and thus expect the hospitalist group to be on site 24/7, sticking around even if there is no work. However, the argument from the hospitalist perspective is that when needed, I stay extra. It should be OK that on low-census days we should be able to leave for a cup of coffee and still be reachable, ready to come in if need arises.
So how do hospitalist-physician professionalism and shift work co-exist? It’s a big question, one that organizations around the country will be looking to solve in the next few years. How this question is answered is going to impact quality of care, recruitment, and staff satisfaction. Each answer will impact the staff and patients.
Keeping in mind outcomes that both parties are looking for, I think a proper plan can be worked out. I suggest hospital administrators adopt the following value-based measurements to evaluate hospitalist clinicians, and establish a compensation system where a minimum amount of production must be met.
Work relative value units (wRVUs). Work RVUs provide a consistent method to measure physician productivity. If one HM clinician’s numbers are below the group average, they might need a lesson in billing, along with a report of their productivity numbers and group expectations.
Patient encounters per day. The average number of patients seen per day (patients seen divided by number of shifts worked) should be measured on a quarterly basis. This metric should provide a measure of the work done by the physician; however, it needs to be offset by your group’s turnover rate (as discussed below).
Length of stay (LOS). Most HM groups are measuring LOS. It is the reason hospitalists exist. Not much more needs to be said about this measure of work performance.
Percentage of patient turnover. A good hospitalist will have a high patient turnover figure (total discharges divided by total encounters per day). This is important to know; it’s even better if accompanied by a short LOS.
New admissions per shift. Again, if there is an outlier, that metric should be detected rather easily.
Patient satisfaction. More and more, this is becoming an important measure of physician quality and is essential for competitive marketplaces. Of course, the quality of medical care will have its own parameters. And it is best left to use the existing, longstanding parameters that are used for the rest of the doctors in your system. There is no need to create an alternative system for the hospitalist.
If all of the above measures are better than the average hospitalist in the locality, then no one should worry about the hospitalist’s other activities, be it involvement in committee work, research, or browsing a newspaper or a cup of coffee in the doctors’ lounge. After all, one of the main reasons physicians opted for HM practice was to have the ability to control their workday.
This will, in my opinion, improve workforce satisfaction and improve productivity. It only makes common sense. It may be a hard pill to swallow for the administrators, but it is the right medicine for the doctor.
Rwoof Reshi, MD, hospitalist, St. Joe’s Hospital, St. Paul, Minn.
ONLINE EXCLUSIVE: International Clinicians Can Bolster Rural HM Group Recruiting Efforts
Where do rural hospitals look if they are having trouble attracting hospitalists to their communities—and keeping them there? One target should be graduates of international medical schools. Brian Bossard, MD, FACP, FHM, director of Inpatient Physician Associates in Lincoln, Neb., estimates that he has recruited 40 physicians to HM practice at the three hospitals his group serves, and at least a dozen of them were international medical graduates (IMGs).
Dr. Bossard works closely with a specialized immigration attorney, Elahe Najfabadi of the Offices of Carl Shusterman in Los Angeles. “There are lots of barriers to address to negotiate positive outcomes,” Dr. Bossard says. “You need an attorney you can rely on thoroughly.”

—Brian Bossard, MD, FACP, FHM, director of Inpatient Physician Associates in Lincoln, Neb.
There are basically two categories of visas for IMGs: H-1B visas, which are capped nationally but allow doctors the flexibility to move around, and J-1 visas, which allow clinicians to remain in the U.S. while completing their medical studies. J-1 visas expire after two years, but physicians often are granted waivers and remain in the U.S.
According to Najfabadi, each state is allowed 30 physician J-1 visa waivers annually. Physicians must work in underserved areas, including rural communities, and those physicians must stay in the job for three years.
When it comes to the J-1 waiver program, timelines, deadlines, requirements for employers, and other regulations vary by state.
“In one state, we’ve had cases where the state wants verification of the doctor’s approved immigration status before issuing the medical license,” Najfabadi says.
The Immigration and Naturalization Service requires a valid license or a letter from the state that the physician is eligible in order to grant an H-1B permit. Najfabadi encourages potential rural employers of IMGs to learn the rules in their state, and to take advantage of such resources such as the IMG Task Force (http://www.imgtaskforce.org/).
“What I have found is that we get exceedingly high-quality physicians to provide care in rural communities,” Dr. Bossard says. “I love working with them.”
Larry Beresford is a freelance writer in Oakland, Calif.
Where do rural hospitals look if they are having trouble attracting hospitalists to their communities—and keeping them there? One target should be graduates of international medical schools. Brian Bossard, MD, FACP, FHM, director of Inpatient Physician Associates in Lincoln, Neb., estimates that he has recruited 40 physicians to HM practice at the three hospitals his group serves, and at least a dozen of them were international medical graduates (IMGs).
Dr. Bossard works closely with a specialized immigration attorney, Elahe Najfabadi of the Offices of Carl Shusterman in Los Angeles. “There are lots of barriers to address to negotiate positive outcomes,” Dr. Bossard says. “You need an attorney you can rely on thoroughly.”
—Brian Bossard, MD, FACP, FHM, director of Inpatient Physician Associates in Lincoln, Neb.
There are basically two categories of visas for IMGs: H-1B visas, which are capped nationally but allow doctors the flexibility to move around, and J-1 visas, which allow clinicians to remain in the U.S. while completing their medical studies. J-1 visas expire after two years, but physicians often are granted waivers and remain in the U.S.
According to Najfabadi, each state is allowed 30 physician J-1 visa waivers annually. Physicians must work in underserved areas, including rural communities, and those physicians must stay in the job for three years.
When it comes to the J-1 waiver program, timelines, deadlines, requirements for employers, and other regulations vary by state.
“In one state, we’ve had cases where the state wants verification of the doctor’s approved immigration status before issuing the medical license,” Najfabadi says.
The Immigration and Naturalization Service requires a valid license or a letter from the state that the physician is eligible in order to grant an H-1B permit. Najfabadi encourages potential rural employers of IMGs to learn the rules in their state, and to take advantage of such resources such as the IMG Task Force (http://www.imgtaskforce.org/).
“What I have found is that we get exceedingly high-quality physicians to provide care in rural communities,” Dr. Bossard says. “I love working with them.”
Larry Beresford is a freelance writer in Oakland, Calif.
Where do rural hospitals look if they are having trouble attracting hospitalists to their communities—and keeping them there? One target should be graduates of international medical schools. Brian Bossard, MD, FACP, FHM, director of Inpatient Physician Associates in Lincoln, Neb., estimates that he has recruited 40 physicians to HM practice at the three hospitals his group serves, and at least a dozen of them were international medical graduates (IMGs).
Dr. Bossard works closely with a specialized immigration attorney, Elahe Najfabadi of the Offices of Carl Shusterman in Los Angeles. “There are lots of barriers to address to negotiate positive outcomes,” Dr. Bossard says. “You need an attorney you can rely on thoroughly.”
—Brian Bossard, MD, FACP, FHM, director of Inpatient Physician Associates in Lincoln, Neb.
There are basically two categories of visas for IMGs: H-1B visas, which are capped nationally but allow doctors the flexibility to move around, and J-1 visas, which allow clinicians to remain in the U.S. while completing their medical studies. J-1 visas expire after two years, but physicians often are granted waivers and remain in the U.S.
According to Najfabadi, each state is allowed 30 physician J-1 visa waivers annually. Physicians must work in underserved areas, including rural communities, and those physicians must stay in the job for three years.
When it comes to the J-1 waiver program, timelines, deadlines, requirements for employers, and other regulations vary by state.
“In one state, we’ve had cases where the state wants verification of the doctor’s approved immigration status before issuing the medical license,” Najfabadi says.
The Immigration and Naturalization Service requires a valid license or a letter from the state that the physician is eligible in order to grant an H-1B permit. Najfabadi encourages potential rural employers of IMGs to learn the rules in their state, and to take advantage of such resources such as the IMG Task Force (http://www.imgtaskforce.org/).
“What I have found is that we get exceedingly high-quality physicians to provide care in rural communities,” Dr. Bossard says. “I love working with them.”
Larry Beresford is a freelance writer in Oakland, Calif.