User login
The Hospitalist only
Survey Shows Five-Year Decrease in Employee Benefits, Paid Time Off for Hospitalists
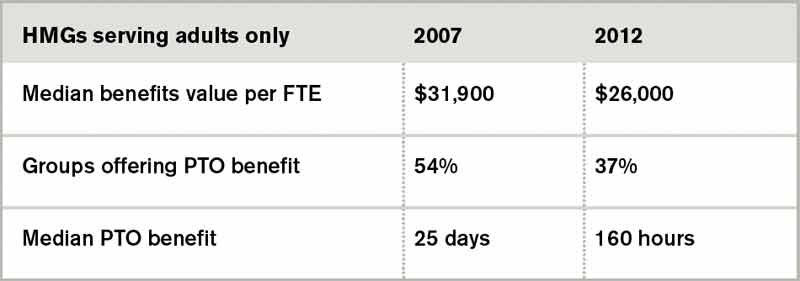
For the first time in several years, SHM included questions about employee benefits and paid time off in its 2012 State of Hospital Medicine survey. The median value of benefits per physician FTE reported by HM groups serving adults only was $26,000, according to the 2012 survey. But what a surprise it was when survey respondents in 2007 reported median benefits of $31,900.
I admit to being flummoxed by the decrease. The definition of “benefits” was identical in both surveys. The only difference is that in 2007, SHM collected actual benefit cost for each individual on the individual questionnaire; in 2012, we asked for the average benefits per FTE for the group. One possible explanation is that some respondents simply guessed about the average, because they didn’t have to report data for individual doctors. Of course, it’s also possible that groups are requiring physicians to pay a higher proportion of insurance premiums or are reducing retirement plan contributions due to the weak economy. But in the work I do with hospitalist groups around the country, I rarely see benefit costs below about $35,000.
Source: 2012 State of Hospital Medicine report
Another interesting finding from the 2012 survey is that 37% of adult medicine groups reported offering paid time off (PTO), down from 54% in 2007. Even among groups using a seven-on/seven-off schedule, the PTO rate was only 44%. Does this represent a survey design or respondent input error, differences in respondent populations, or an actual shift in the prevalence of PTO benefits? I suspect it’s the latter, because the median amount of PTO time awarded has also declined. In 2007, adult HMGs reported a median of 25 PTO days annually. In 2012, the median for those groups offering PTO was 160 hours of PTO, which represents somewhere around 13 to 20 days, depending on shift length.
Why might PTO benefits be declining? I suppose it could be belt-tightening associated with the poor economy. But I think many HM groups simply have found PTO benefits difficult to administer and fraught with unintended consequences. Many groups are so thinly staffed that for someone to take a PTO day, someone else must work extra to cover. Then, when the covering doctor takes PTO, the first doctor must work extra—effectively offsetting the value of PTO. And if a hospitalist takes PTO and also works extra shifts in the same pay period, do these two offset each other? Or does the doctor get paid for both the PTO days and the extra shift days?
For clinicians such as hospitalists, whose work is defined in highly variable, shift-based schedules that include a lot of night and weekend work, it becomes very difficult to determine which of the days not worked were PTO days versus just days the doctor wasn’t scheduled.
Personally, I don’t think it makes much sense for most hospitalists to have PTO. Don’t get me wrong—I think hospitalists should be paid well and have generous amounts of time off in exchange for long, challenging workdays and a disproportionate amount of night and weekend work. But arbitrarily assigning some of the days not worked as PTO while others are just unscheduled days seems unnecessarily complex.
Time will tell if the specialty as a whole agrees with me or not.
Leslie Flores is a principal in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
For the first time in several years, SHM included questions about employee benefits and paid time off in its 2012 State of Hospital Medicine survey. The median value of benefits per physician FTE reported by HM groups serving adults only was $26,000, according to the 2012 survey. But what a surprise it was when survey respondents in 2007 reported median benefits of $31,900.
I admit to being flummoxed by the decrease. The definition of “benefits” was identical in both surveys. The only difference is that in 2007, SHM collected actual benefit cost for each individual on the individual questionnaire; in 2012, we asked for the average benefits per FTE for the group. One possible explanation is that some respondents simply guessed about the average, because they didn’t have to report data for individual doctors. Of course, it’s also possible that groups are requiring physicians to pay a higher proportion of insurance premiums or are reducing retirement plan contributions due to the weak economy. But in the work I do with hospitalist groups around the country, I rarely see benefit costs below about $35,000.
Source: 2012 State of Hospital Medicine report
Another interesting finding from the 2012 survey is that 37% of adult medicine groups reported offering paid time off (PTO), down from 54% in 2007. Even among groups using a seven-on/seven-off schedule, the PTO rate was only 44%. Does this represent a survey design or respondent input error, differences in respondent populations, or an actual shift in the prevalence of PTO benefits? I suspect it’s the latter, because the median amount of PTO time awarded has also declined. In 2007, adult HMGs reported a median of 25 PTO days annually. In 2012, the median for those groups offering PTO was 160 hours of PTO, which represents somewhere around 13 to 20 days, depending on shift length.
Why might PTO benefits be declining? I suppose it could be belt-tightening associated with the poor economy. But I think many HM groups simply have found PTO benefits difficult to administer and fraught with unintended consequences. Many groups are so thinly staffed that for someone to take a PTO day, someone else must work extra to cover. Then, when the covering doctor takes PTO, the first doctor must work extra—effectively offsetting the value of PTO. And if a hospitalist takes PTO and also works extra shifts in the same pay period, do these two offset each other? Or does the doctor get paid for both the PTO days and the extra shift days?
For clinicians such as hospitalists, whose work is defined in highly variable, shift-based schedules that include a lot of night and weekend work, it becomes very difficult to determine which of the days not worked were PTO days versus just days the doctor wasn’t scheduled.
Personally, I don’t think it makes much sense for most hospitalists to have PTO. Don’t get me wrong—I think hospitalists should be paid well and have generous amounts of time off in exchange for long, challenging workdays and a disproportionate amount of night and weekend work. But arbitrarily assigning some of the days not worked as PTO while others are just unscheduled days seems unnecessarily complex.
Time will tell if the specialty as a whole agrees with me or not.
Leslie Flores is a principal in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
For the first time in several years, SHM included questions about employee benefits and paid time off in its 2012 State of Hospital Medicine survey. The median value of benefits per physician FTE reported by HM groups serving adults only was $26,000, according to the 2012 survey. But what a surprise it was when survey respondents in 2007 reported median benefits of $31,900.
I admit to being flummoxed by the decrease. The definition of “benefits” was identical in both surveys. The only difference is that in 2007, SHM collected actual benefit cost for each individual on the individual questionnaire; in 2012, we asked for the average benefits per FTE for the group. One possible explanation is that some respondents simply guessed about the average, because they didn’t have to report data for individual doctors. Of course, it’s also possible that groups are requiring physicians to pay a higher proportion of insurance premiums or are reducing retirement plan contributions due to the weak economy. But in the work I do with hospitalist groups around the country, I rarely see benefit costs below about $35,000.
Source: 2012 State of Hospital Medicine report
Another interesting finding from the 2012 survey is that 37% of adult medicine groups reported offering paid time off (PTO), down from 54% in 2007. Even among groups using a seven-on/seven-off schedule, the PTO rate was only 44%. Does this represent a survey design or respondent input error, differences in respondent populations, or an actual shift in the prevalence of PTO benefits? I suspect it’s the latter, because the median amount of PTO time awarded has also declined. In 2007, adult HMGs reported a median of 25 PTO days annually. In 2012, the median for those groups offering PTO was 160 hours of PTO, which represents somewhere around 13 to 20 days, depending on shift length.
Why might PTO benefits be declining? I suppose it could be belt-tightening associated with the poor economy. But I think many HM groups simply have found PTO benefits difficult to administer and fraught with unintended consequences. Many groups are so thinly staffed that for someone to take a PTO day, someone else must work extra to cover. Then, when the covering doctor takes PTO, the first doctor must work extra—effectively offsetting the value of PTO. And if a hospitalist takes PTO and also works extra shifts in the same pay period, do these two offset each other? Or does the doctor get paid for both the PTO days and the extra shift days?
For clinicians such as hospitalists, whose work is defined in highly variable, shift-based schedules that include a lot of night and weekend work, it becomes very difficult to determine which of the days not worked were PTO days versus just days the doctor wasn’t scheduled.
Personally, I don’t think it makes much sense for most hospitalists to have PTO. Don’t get me wrong—I think hospitalists should be paid well and have generous amounts of time off in exchange for long, challenging workdays and a disproportionate amount of night and weekend work. But arbitrarily assigning some of the days not worked as PTO while others are just unscheduled days seems unnecessarily complex.
Time will tell if the specialty as a whole agrees with me or not.
Leslie Flores is a principal in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
HMX Term of the Month: Achievement Points
Awarded to a hospital by comparing an individual hospital’s performance measure rates during a certain period with all hospitals’ rates during the baseline period.
Awarded to a hospital by comparing an individual hospital’s performance measure rates during a certain period with all hospitals’ rates during the baseline period.
Awarded to a hospital by comparing an individual hospital’s performance measure rates during a certain period with all hospitals’ rates during the baseline period.
Is Your Hospital Medicine Group a Good Candidate for Project BOOST?
Does your team have:
- Eagerness to improve their discharge processes and reduce unnecessary readmissions and avoidable adverse events in the post-discharge period?
- A multidisciplinary team in place capable of working collaboratively to redesign existing care processes?
- A dedicated leader to manage the process of tailoring the BOOST intervention to your site’s needs and implementing BOOST?
- Support of at least one executive sponsor who can meet with the team monthly?
- Access to data support personnel needed to collect baseline and post-implementation data?
Does your team have:
- Eagerness to improve their discharge processes and reduce unnecessary readmissions and avoidable adverse events in the post-discharge period?
- A multidisciplinary team in place capable of working collaboratively to redesign existing care processes?
- A dedicated leader to manage the process of tailoring the BOOST intervention to your site’s needs and implementing BOOST?
- Support of at least one executive sponsor who can meet with the team monthly?
- Access to data support personnel needed to collect baseline and post-implementation data?
Does your team have:
- Eagerness to improve their discharge processes and reduce unnecessary readmissions and avoidable adverse events in the post-discharge period?
- A multidisciplinary team in place capable of working collaboratively to redesign existing care processes?
- A dedicated leader to manage the process of tailoring the BOOST intervention to your site’s needs and implementing BOOST?
- Support of at least one executive sponsor who can meet with the team monthly?
- Access to data support personnel needed to collect baseline and post-implementation data?
Hospitalists Urged to Help Reduce 30-Day Readmission Rate
For hospitals across the country, 2013 is the year to address readmissions and find practical solutions. In January, the Journal of the American Medical Association dedicated
an entire issue to the vexing problem of hospital readmissions. In his audio summary of the issue, JAMA editor Howard Bauchner, MD, notes that it “came together organically,” based on increased submissions and attention to 30-day readmissions.
Among nearly a dozen articles focused on readmissions, discharge, and transitions of care, Project BOOST principal investigator Mark V. Williams, MD, FACP, MHM, makes the case for a community-based approach in an editorial titled “A Requirement to Reduce Readmissions: Take Care of the Patient, Not Just the Disease.” In the piece, he advocates for “broad patient-centered approaches that engage all members of a care team, especially front-line clinicians and use proven quality-improvement [QI] methods.” He goes on to link the concepts to the principles taught by Project BOOST.
After all, readmissions are expensive, and not just for hospitals, which is why private insurers and the Centers for Medicare & Medicaid Services (CMS) are investing resources to improve discharge processes, reduce readmissions, and reduce costs.
Many adverse events that happen after discharge are predictable using assessment tools and methods in the Project BOOST program, Dr. Williams says. Hospitalists can—and should, according to many—improve the system to protect patients.
And while systemwide change doesn’t happen overnight, it does have to start somewhere, as leaders at the 150-plus Project BOOST sites nationwide can attest Now is the time to begin planning to join the Project BOOST 2013 cohort. Applications will be accepted through this summer; training will begin in the fall. But participation is limited, and successful applicants often need time to prepare their applications, which must include letters of support from a site executive and the development of a multidisciplinary team. For more information, visit www.hospitalmedicine.org/boost.
Brendon Shank is SHM’s associate vice president of communications.
For hospitals across the country, 2013 is the year to address readmissions and find practical solutions. In January, the Journal of the American Medical Association dedicated
an entire issue to the vexing problem of hospital readmissions. In his audio summary of the issue, JAMA editor Howard Bauchner, MD, notes that it “came together organically,” based on increased submissions and attention to 30-day readmissions.
Among nearly a dozen articles focused on readmissions, discharge, and transitions of care, Project BOOST principal investigator Mark V. Williams, MD, FACP, MHM, makes the case for a community-based approach in an editorial titled “A Requirement to Reduce Readmissions: Take Care of the Patient, Not Just the Disease.” In the piece, he advocates for “broad patient-centered approaches that engage all members of a care team, especially front-line clinicians and use proven quality-improvement [QI] methods.” He goes on to link the concepts to the principles taught by Project BOOST.
After all, readmissions are expensive, and not just for hospitals, which is why private insurers and the Centers for Medicare & Medicaid Services (CMS) are investing resources to improve discharge processes, reduce readmissions, and reduce costs.
Many adverse events that happen after discharge are predictable using assessment tools and methods in the Project BOOST program, Dr. Williams says. Hospitalists can—and should, according to many—improve the system to protect patients.
And while systemwide change doesn’t happen overnight, it does have to start somewhere, as leaders at the 150-plus Project BOOST sites nationwide can attest Now is the time to begin planning to join the Project BOOST 2013 cohort. Applications will be accepted through this summer; training will begin in the fall. But participation is limited, and successful applicants often need time to prepare their applications, which must include letters of support from a site executive and the development of a multidisciplinary team. For more information, visit www.hospitalmedicine.org/boost.
Brendon Shank is SHM’s associate vice president of communications.
For hospitals across the country, 2013 is the year to address readmissions and find practical solutions. In January, the Journal of the American Medical Association dedicated
an entire issue to the vexing problem of hospital readmissions. In his audio summary of the issue, JAMA editor Howard Bauchner, MD, notes that it “came together organically,” based on increased submissions and attention to 30-day readmissions.
Among nearly a dozen articles focused on readmissions, discharge, and transitions of care, Project BOOST principal investigator Mark V. Williams, MD, FACP, MHM, makes the case for a community-based approach in an editorial titled “A Requirement to Reduce Readmissions: Take Care of the Patient, Not Just the Disease.” In the piece, he advocates for “broad patient-centered approaches that engage all members of a care team, especially front-line clinicians and use proven quality-improvement [QI] methods.” He goes on to link the concepts to the principles taught by Project BOOST.
After all, readmissions are expensive, and not just for hospitals, which is why private insurers and the Centers for Medicare & Medicaid Services (CMS) are investing resources to improve discharge processes, reduce readmissions, and reduce costs.
Many adverse events that happen after discharge are predictable using assessment tools and methods in the Project BOOST program, Dr. Williams says. Hospitalists can—and should, according to many—improve the system to protect patients.
And while systemwide change doesn’t happen overnight, it does have to start somewhere, as leaders at the 150-plus Project BOOST sites nationwide can attest Now is the time to begin planning to join the Project BOOST 2013 cohort. Applications will be accepted through this summer; training will begin in the fall. But participation is limited, and successful applicants often need time to prepare their applications, which must include letters of support from a site executive and the development of a multidisciplinary team. For more information, visit www.hospitalmedicine.org/boost.
Brendon Shank is SHM’s associate vice president of communications.
Physicians Exercise Their Entrepreneurial Skills, Creativity to Pursue Passions Beyond Clinical Medicine
After years of juggling more than one career, Kulleni Gebreyes, MD, MBA, had a tough decision to make. "I'm a little bit of a glutton for punishment," she admits with a chuckle. While overseeing quality improvement (QI) for a healthcare foundation, she had negotiated to take off every other Friday and work several ED shifts per month on weekends at two local hospitals.
Then, in January 2012, Dr. Gebreyes began a new full-time position as a director at PricewaterhouseCoopers in McLean, Va. It became too time-consuming and exhausting to treat patients and consult in healthcare industries, says the mother of two children, who are 7 and 4.
Dr. Gebreyes is among a growing number of physicians who, after a number of years, opt to give up clinical medicine for nonclinical roles in healthcare or other industries altogether. "You are ready for transition when the new choice excites and energizes you," she explains, "and not necessarily when your first choice disappoints you."
A career shift offers new opportunities for broadening one's horizons while often striking a better work-life balance. Many clinicians make the transition slowly and wisely, and some take an expected financial hit as they carve out an entrepreneurial and creative path.
"Modern medicine is very difficult. You can burn out if you're not careful," says Dan Hale, MD, FAAP, a pediatric hospitalist in the Floating Hospital for Children at Tufts Medical Center in Boston.
Stepping off the merry-go-round can help you regroup. Fortunately, he adds, hospitalists can exercise more flexibility in scheduling than physicians in different specialties. Some hospitalists prefer to work nights and weekends in order to free up weekdays for other activities. Others decrease their clinical shifts and devote more time to teaching, research, or administration.
For those who decide to leave medicine completely, "hospitalists definitely have people skills day to day in their jobs that are applicable in multiple other careers," says Dr. Hale, a Team Hospitalist member. "Becoming a physician requires so much dedication and hard work, so you will succeed in whatever career you choose."
The Society of Physician Entrepreneurs (www.sopenet.org) is expanding by about 150 to 200 new members each month. Founded in 2008 and officially launched in January 2011, the society has more than 4,700 members globally. The interdisciplinary network includes physicians and innovators in other professions—from law to information technology to product development.
Its purpose is to "bring all the stakeholders together in one virtual space to collaborate," says co-founder and president Arlen Meyers, MD, MBA, professor in the departments of otolaryngology, dentistry, and engineering at the University of Colorado Denver, where he directs the graduate program in bio-innovation and entrepreneurship.
"The opportunities for physician entrepreneurs include working with industry, consulting, creating their own company, and much more," Dr. Meyers says. "As domain experts, physicians are in a unique position to add value to the innovation chain.

–Maren Grainger-Monsen, MD, filmmaker-in-residence and director of the bioethics and film program, Stanford Center for Biomedical Ethics, Stanford, Calif.
"However, to leave practice and be successful at something nonclinical requires education, experience, and networks," he says. "Doing what you did successfully in your last career won't be a guarantee of success in your next career, so you have to be willing to pay your dues and accept the risk."
The Writer
Deborah Shlian, MD, MBA, a former family medicine physician and managed-care executive in California, has evolved into a medical management consultant and an author of both fiction and nonfiction titles. Dr. Shlian, who now lives in Boca Raton, Fla., had always wanted to write. Her father, an internist, encouraged the pursuit of medicine, so she followed in his footsteps.

"I wanted to emulate what he did," she says. Over time, she realized that "doctors have a lot of skills that are applicable to other endeavors."
She and her husband, Joel Shlian, MD, MBA, also a former family medicine physician, fully gave up clinical practice about 10 years ago after doing it part time for a decade. The Shlians met as students at the University of Maryland School of Medicine in 1970. Initially, their new business concentrated on physician executive recruitment. As clients requested other services, the Shlians helped identify nonphysician managers as well. Clients included established, as well as start-up health plans, academic institutions, utilization review, and healthcare consulting companies.
Given the accelerated changes in healthcare delivery, earning a graduate education in business is not a quick and easy avenue to another career. "An MBA should never be viewed as the means to 'get out of medical practice,'" Dr. Shlian says in her new book, "Lessons Learned: Stories from Women in Medical Management," released this month by the American College of Physician Executives.
"In fact, I would submit that if you really hate clinical medicine, medical management is not for you," she says. "It can be every bit as demanding and frustrating as clinical practice."
The Entrepreneur
Jeffrey N. Hausfeld, MD, MBA, FACS, completed an MBA program on evenings and weekends. After graduation in 2005, he gave up his 24-year practice of otolaryngology and facial plastic surgery. He continued his education by obtaining a graduate certificate in leadership coaching and organizational development. Then he became involved in the first of several business ventures, capitalizing on his clinical experience.

"Doctors don't have a trusted partner to do their debt collections," says Dr. Hausfeld, co-founder and treasurer of the Society of Physician Entrepreneurs. His own negative experiences with debt-collection agencies contributed to his "understanding the obstacles and objections to create this kind of an entity."

—Kulleni Gebreyes, MD, MBA, director of healthcare consulting, PricewaterhouseCoopers, McLean, Va.
Hence the emergence of FMS Financial Solutions, based in Greenbelt, Md. "This seemed to be a very natural fit for me," says Dr. Hausfeld, who is the managing director. By collecting money owed to physicians, hospitals, and surgical centers, he has increased the revenues of his business fourfold since 2006. The company has 24 full- and part-time workers.
Meanwhile, his son, Joshua, who joined him in the healthcare MBA program at Johns Hopkins University in Baltimore and now works for an investment banking firm that provides real estate loans for senior housing, introduced Dr. Hausfeld to a group of Midwest-based assisted-living-facility developers. Four years ago, they struck a deal to provide private equity funding and create Memory Care Communities of Illinois, with Dr. Hausfeld serving as president. The 24-hour residential facilities are home to patients with Alzheimer's disease and dementia.
To some degree, he misses practicing medicine, but Dr. Hausfeld is enthusiastic about making a difference in even more people's lives than he did as a physician and surgeon.
"I've done 10,000 ear, nose, and throat operations. If I did 1,000 more, how much would I be changing the world?" Dr. Hausfeld says. Ultimately, "you find a way to leave a bigger footprint."

His entrepreneurial spirit has led to other consulting roles. For instance, he is trying to help two startup companies—one in the medical device arena, the other in information technology—grow by leaps and bounds.
The Director
Maren Grainger-Monsen, MD, has made her mark as an award-winning physician filmmaker. She is filmmaker-in-residence and director of the bioethics and film program at the Stanford Center for Biomedical Ethics in Palo Alto, Calif. She studied at the London Film School and received her medical training at the University of Washington in Seattle and Stanford University School of Medicine.
"I have really enjoyed using all of my medical background and knowledge and applying it toward film," Dr. Grainger-Monsen says of her position at Stanford, which she has held since 1998. "It's very grounding. It gives you a purpose."
Her one-hour documentary "Rare," which features a family with a very uncommon genetic disease, aired last August on PBS. Another film, "The Revolutionary Optimists," follows a group of aspiring youngsters in the slums of Calcutta, India, who battle poverty and transform their neighborhoods from the inside out. One-hour and 80-minute versions of the film are slated to air on the PBS series "Independent Lens" as part of the Women and Girls Lead Global partnership.
–Dan Hale, MD, FAAP, a pediatric hospitalist in the Floating Hospital for Children at Tufts Medical Center in Boston
Dr. Grainger-Monsen co-produced and co-directed both films with Nicole Newnham, an independent documentary filmmaker who is in residence at Stanford's bioethics and film program.
As an undergraduate art history major, Dr. Grainger-Monsen became interested in social and ethical issues in medicine. Later, films shown in medical school struck a chord with her. She was amazed at how images could resonate with viewers and trigger animated debate. During the summer between her first and second years of medical school, she was inspired to study film at New York University.
Dr. Grainger-Monsen eventually trained in emergency medicine at Stanford and completed a fellowship in palliative care at Stanford-affiliated Palo Alto Veterans Administration Hospital. For years, she split her career between working in community ER clinics and producing films. Her films are large-scale projects that may take five years or longer to make, and she raises all the funds to bring them to fruition.
"I really do find documentary filmmaking tremendously gratifying," Dr. Grainger-Monsen says of the chance "to talk with all different kinds of people in all different situations and walk in their shoes, with them, for a time. That is what I'm trying to share with the audience."
In creating character-driven documentaries, she aims to spark discussions about important issues in contemporary medicine. "I hope my films can help increase understanding and empathy," she says, "and result in improvements to the delivery of healthcare and reduction of disparities on multiple levels."
Susan Kreimer is a freelance writer in New York.
After years of juggling more than one career, Kulleni Gebreyes, MD, MBA, had a tough decision to make. "I'm a little bit of a glutton for punishment," she admits with a chuckle. While overseeing quality improvement (QI) for a healthcare foundation, she had negotiated to take off every other Friday and work several ED shifts per month on weekends at two local hospitals.
Then, in January 2012, Dr. Gebreyes began a new full-time position as a director at PricewaterhouseCoopers in McLean, Va. It became too time-consuming and exhausting to treat patients and consult in healthcare industries, says the mother of two children, who are 7 and 4.
Dr. Gebreyes is among a growing number of physicians who, after a number of years, opt to give up clinical medicine for nonclinical roles in healthcare or other industries altogether. "You are ready for transition when the new choice excites and energizes you," she explains, "and not necessarily when your first choice disappoints you."
A career shift offers new opportunities for broadening one's horizons while often striking a better work-life balance. Many clinicians make the transition slowly and wisely, and some take an expected financial hit as they carve out an entrepreneurial and creative path.
"Modern medicine is very difficult. You can burn out if you're not careful," says Dan Hale, MD, FAAP, a pediatric hospitalist in the Floating Hospital for Children at Tufts Medical Center in Boston.
Stepping off the merry-go-round can help you regroup. Fortunately, he adds, hospitalists can exercise more flexibility in scheduling than physicians in different specialties. Some hospitalists prefer to work nights and weekends in order to free up weekdays for other activities. Others decrease their clinical shifts and devote more time to teaching, research, or administration.
For those who decide to leave medicine completely, "hospitalists definitely have people skills day to day in their jobs that are applicable in multiple other careers," says Dr. Hale, a Team Hospitalist member. "Becoming a physician requires so much dedication and hard work, so you will succeed in whatever career you choose."
The Society of Physician Entrepreneurs (www.sopenet.org) is expanding by about 150 to 200 new members each month. Founded in 2008 and officially launched in January 2011, the society has more than 4,700 members globally. The interdisciplinary network includes physicians and innovators in other professions—from law to information technology to product development.
Its purpose is to "bring all the stakeholders together in one virtual space to collaborate," says co-founder and president Arlen Meyers, MD, MBA, professor in the departments of otolaryngology, dentistry, and engineering at the University of Colorado Denver, where he directs the graduate program in bio-innovation and entrepreneurship.
"The opportunities for physician entrepreneurs include working with industry, consulting, creating their own company, and much more," Dr. Meyers says. "As domain experts, physicians are in a unique position to add value to the innovation chain.
–Maren Grainger-Monsen, MD, filmmaker-in-residence and director of the bioethics and film program, Stanford Center for Biomedical Ethics, Stanford, Calif.
"However, to leave practice and be successful at something nonclinical requires education, experience, and networks," he says. "Doing what you did successfully in your last career won't be a guarantee of success in your next career, so you have to be willing to pay your dues and accept the risk."
The Writer
Deborah Shlian, MD, MBA, a former family medicine physician and managed-care executive in California, has evolved into a medical management consultant and an author of both fiction and nonfiction titles. Dr. Shlian, who now lives in Boca Raton, Fla., had always wanted to write. Her father, an internist, encouraged the pursuit of medicine, so she followed in his footsteps.
"I wanted to emulate what he did," she says. Over time, she realized that "doctors have a lot of skills that are applicable to other endeavors."
She and her husband, Joel Shlian, MD, MBA, also a former family medicine physician, fully gave up clinical practice about 10 years ago after doing it part time for a decade. The Shlians met as students at the University of Maryland School of Medicine in 1970. Initially, their new business concentrated on physician executive recruitment. As clients requested other services, the Shlians helped identify nonphysician managers as well. Clients included established, as well as start-up health plans, academic institutions, utilization review, and healthcare consulting companies.
Given the accelerated changes in healthcare delivery, earning a graduate education in business is not a quick and easy avenue to another career. "An MBA should never be viewed as the means to 'get out of medical practice,'" Dr. Shlian says in her new book, "Lessons Learned: Stories from Women in Medical Management," released this month by the American College of Physician Executives.
"In fact, I would submit that if you really hate clinical medicine, medical management is not for you," she says. "It can be every bit as demanding and frustrating as clinical practice."
The Entrepreneur
Jeffrey N. Hausfeld, MD, MBA, FACS, completed an MBA program on evenings and weekends. After graduation in 2005, he gave up his 24-year practice of otolaryngology and facial plastic surgery. He continued his education by obtaining a graduate certificate in leadership coaching and organizational development. Then he became involved in the first of several business ventures, capitalizing on his clinical experience.
"Doctors don't have a trusted partner to do their debt collections," says Dr. Hausfeld, co-founder and treasurer of the Society of Physician Entrepreneurs. His own negative experiences with debt-collection agencies contributed to his "understanding the obstacles and objections to create this kind of an entity."
—Kulleni Gebreyes, MD, MBA, director of healthcare consulting, PricewaterhouseCoopers, McLean, Va.
Hence the emergence of FMS Financial Solutions, based in Greenbelt, Md. "This seemed to be a very natural fit for me," says Dr. Hausfeld, who is the managing director. By collecting money owed to physicians, hospitals, and surgical centers, he has increased the revenues of his business fourfold since 2006. The company has 24 full- and part-time workers.
Meanwhile, his son, Joshua, who joined him in the healthcare MBA program at Johns Hopkins University in Baltimore and now works for an investment banking firm that provides real estate loans for senior housing, introduced Dr. Hausfeld to a group of Midwest-based assisted-living-facility developers. Four years ago, they struck a deal to provide private equity funding and create Memory Care Communities of Illinois, with Dr. Hausfeld serving as president. The 24-hour residential facilities are home to patients with Alzheimer's disease and dementia.
To some degree, he misses practicing medicine, but Dr. Hausfeld is enthusiastic about making a difference in even more people's lives than he did as a physician and surgeon.
"I've done 10,000 ear, nose, and throat operations. If I did 1,000 more, how much would I be changing the world?" Dr. Hausfeld says. Ultimately, "you find a way to leave a bigger footprint."
His entrepreneurial spirit has led to other consulting roles. For instance, he is trying to help two startup companies—one in the medical device arena, the other in information technology—grow by leaps and bounds.
The Director
Maren Grainger-Monsen, MD, has made her mark as an award-winning physician filmmaker. She is filmmaker-in-residence and director of the bioethics and film program at the Stanford Center for Biomedical Ethics in Palo Alto, Calif. She studied at the London Film School and received her medical training at the University of Washington in Seattle and Stanford University School of Medicine.
"I have really enjoyed using all of my medical background and knowledge and applying it toward film," Dr. Grainger-Monsen says of her position at Stanford, which she has held since 1998. "It's very grounding. It gives you a purpose."
Her one-hour documentary "Rare," which features a family with a very uncommon genetic disease, aired last August on PBS. Another film, "The Revolutionary Optimists," follows a group of aspiring youngsters in the slums of Calcutta, India, who battle poverty and transform their neighborhoods from the inside out. One-hour and 80-minute versions of the film are slated to air on the PBS series "Independent Lens" as part of the Women and Girls Lead Global partnership.
–Dan Hale, MD, FAAP, a pediatric hospitalist in the Floating Hospital for Children at Tufts Medical Center in Boston
Dr. Grainger-Monsen co-produced and co-directed both films with Nicole Newnham, an independent documentary filmmaker who is in residence at Stanford's bioethics and film program.
As an undergraduate art history major, Dr. Grainger-Monsen became interested in social and ethical issues in medicine. Later, films shown in medical school struck a chord with her. She was amazed at how images could resonate with viewers and trigger animated debate. During the summer between her first and second years of medical school, she was inspired to study film at New York University.
Dr. Grainger-Monsen eventually trained in emergency medicine at Stanford and completed a fellowship in palliative care at Stanford-affiliated Palo Alto Veterans Administration Hospital. For years, she split her career between working in community ER clinics and producing films. Her films are large-scale projects that may take five years or longer to make, and she raises all the funds to bring them to fruition.
"I really do find documentary filmmaking tremendously gratifying," Dr. Grainger-Monsen says of the chance "to talk with all different kinds of people in all different situations and walk in their shoes, with them, for a time. That is what I'm trying to share with the audience."
In creating character-driven documentaries, she aims to spark discussions about important issues in contemporary medicine. "I hope my films can help increase understanding and empathy," she says, "and result in improvements to the delivery of healthcare and reduction of disparities on multiple levels."
Susan Kreimer is a freelance writer in New York.
After years of juggling more than one career, Kulleni Gebreyes, MD, MBA, had a tough decision to make. "I'm a little bit of a glutton for punishment," she admits with a chuckle. While overseeing quality improvement (QI) for a healthcare foundation, she had negotiated to take off every other Friday and work several ED shifts per month on weekends at two local hospitals.
Then, in January 2012, Dr. Gebreyes began a new full-time position as a director at PricewaterhouseCoopers in McLean, Va. It became too time-consuming and exhausting to treat patients and consult in healthcare industries, says the mother of two children, who are 7 and 4.
Dr. Gebreyes is among a growing number of physicians who, after a number of years, opt to give up clinical medicine for nonclinical roles in healthcare or other industries altogether. "You are ready for transition when the new choice excites and energizes you," she explains, "and not necessarily when your first choice disappoints you."
A career shift offers new opportunities for broadening one's horizons while often striking a better work-life balance. Many clinicians make the transition slowly and wisely, and some take an expected financial hit as they carve out an entrepreneurial and creative path.
"Modern medicine is very difficult. You can burn out if you're not careful," says Dan Hale, MD, FAAP, a pediatric hospitalist in the Floating Hospital for Children at Tufts Medical Center in Boston.
Stepping off the merry-go-round can help you regroup. Fortunately, he adds, hospitalists can exercise more flexibility in scheduling than physicians in different specialties. Some hospitalists prefer to work nights and weekends in order to free up weekdays for other activities. Others decrease their clinical shifts and devote more time to teaching, research, or administration.
For those who decide to leave medicine completely, "hospitalists definitely have people skills day to day in their jobs that are applicable in multiple other careers," says Dr. Hale, a Team Hospitalist member. "Becoming a physician requires so much dedication and hard work, so you will succeed in whatever career you choose."
The Society of Physician Entrepreneurs (www.sopenet.org) is expanding by about 150 to 200 new members each month. Founded in 2008 and officially launched in January 2011, the society has more than 4,700 members globally. The interdisciplinary network includes physicians and innovators in other professions—from law to information technology to product development.
Its purpose is to "bring all the stakeholders together in one virtual space to collaborate," says co-founder and president Arlen Meyers, MD, MBA, professor in the departments of otolaryngology, dentistry, and engineering at the University of Colorado Denver, where he directs the graduate program in bio-innovation and entrepreneurship.
"The opportunities for physician entrepreneurs include working with industry, consulting, creating their own company, and much more," Dr. Meyers says. "As domain experts, physicians are in a unique position to add value to the innovation chain.
–Maren Grainger-Monsen, MD, filmmaker-in-residence and director of the bioethics and film program, Stanford Center for Biomedical Ethics, Stanford, Calif.
"However, to leave practice and be successful at something nonclinical requires education, experience, and networks," he says. "Doing what you did successfully in your last career won't be a guarantee of success in your next career, so you have to be willing to pay your dues and accept the risk."
The Writer
Deborah Shlian, MD, MBA, a former family medicine physician and managed-care executive in California, has evolved into a medical management consultant and an author of both fiction and nonfiction titles. Dr. Shlian, who now lives in Boca Raton, Fla., had always wanted to write. Her father, an internist, encouraged the pursuit of medicine, so she followed in his footsteps.
"I wanted to emulate what he did," she says. Over time, she realized that "doctors have a lot of skills that are applicable to other endeavors."
She and her husband, Joel Shlian, MD, MBA, also a former family medicine physician, fully gave up clinical practice about 10 years ago after doing it part time for a decade. The Shlians met as students at the University of Maryland School of Medicine in 1970. Initially, their new business concentrated on physician executive recruitment. As clients requested other services, the Shlians helped identify nonphysician managers as well. Clients included established, as well as start-up health plans, academic institutions, utilization review, and healthcare consulting companies.
Given the accelerated changes in healthcare delivery, earning a graduate education in business is not a quick and easy avenue to another career. "An MBA should never be viewed as the means to 'get out of medical practice,'" Dr. Shlian says in her new book, "Lessons Learned: Stories from Women in Medical Management," released this month by the American College of Physician Executives.
"In fact, I would submit that if you really hate clinical medicine, medical management is not for you," she says. "It can be every bit as demanding and frustrating as clinical practice."
The Entrepreneur
Jeffrey N. Hausfeld, MD, MBA, FACS, completed an MBA program on evenings and weekends. After graduation in 2005, he gave up his 24-year practice of otolaryngology and facial plastic surgery. He continued his education by obtaining a graduate certificate in leadership coaching and organizational development. Then he became involved in the first of several business ventures, capitalizing on his clinical experience.
"Doctors don't have a trusted partner to do their debt collections," says Dr. Hausfeld, co-founder and treasurer of the Society of Physician Entrepreneurs. His own negative experiences with debt-collection agencies contributed to his "understanding the obstacles and objections to create this kind of an entity."
—Kulleni Gebreyes, MD, MBA, director of healthcare consulting, PricewaterhouseCoopers, McLean, Va.
Hence the emergence of FMS Financial Solutions, based in Greenbelt, Md. "This seemed to be a very natural fit for me," says Dr. Hausfeld, who is the managing director. By collecting money owed to physicians, hospitals, and surgical centers, he has increased the revenues of his business fourfold since 2006. The company has 24 full- and part-time workers.
Meanwhile, his son, Joshua, who joined him in the healthcare MBA program at Johns Hopkins University in Baltimore and now works for an investment banking firm that provides real estate loans for senior housing, introduced Dr. Hausfeld to a group of Midwest-based assisted-living-facility developers. Four years ago, they struck a deal to provide private equity funding and create Memory Care Communities of Illinois, with Dr. Hausfeld serving as president. The 24-hour residential facilities are home to patients with Alzheimer's disease and dementia.
To some degree, he misses practicing medicine, but Dr. Hausfeld is enthusiastic about making a difference in even more people's lives than he did as a physician and surgeon.
"I've done 10,000 ear, nose, and throat operations. If I did 1,000 more, how much would I be changing the world?" Dr. Hausfeld says. Ultimately, "you find a way to leave a bigger footprint."
His entrepreneurial spirit has led to other consulting roles. For instance, he is trying to help two startup companies—one in the medical device arena, the other in information technology—grow by leaps and bounds.
The Director
Maren Grainger-Monsen, MD, has made her mark as an award-winning physician filmmaker. She is filmmaker-in-residence and director of the bioethics and film program at the Stanford Center for Biomedical Ethics in Palo Alto, Calif. She studied at the London Film School and received her medical training at the University of Washington in Seattle and Stanford University School of Medicine.
"I have really enjoyed using all of my medical background and knowledge and applying it toward film," Dr. Grainger-Monsen says of her position at Stanford, which she has held since 1998. "It's very grounding. It gives you a purpose."
Her one-hour documentary "Rare," which features a family with a very uncommon genetic disease, aired last August on PBS. Another film, "The Revolutionary Optimists," follows a group of aspiring youngsters in the slums of Calcutta, India, who battle poverty and transform their neighborhoods from the inside out. One-hour and 80-minute versions of the film are slated to air on the PBS series "Independent Lens" as part of the Women and Girls Lead Global partnership.
–Dan Hale, MD, FAAP, a pediatric hospitalist in the Floating Hospital for Children at Tufts Medical Center in Boston
Dr. Grainger-Monsen co-produced and co-directed both films with Nicole Newnham, an independent documentary filmmaker who is in residence at Stanford's bioethics and film program.
As an undergraduate art history major, Dr. Grainger-Monsen became interested in social and ethical issues in medicine. Later, films shown in medical school struck a chord with her. She was amazed at how images could resonate with viewers and trigger animated debate. During the summer between her first and second years of medical school, she was inspired to study film at New York University.
Dr. Grainger-Monsen eventually trained in emergency medicine at Stanford and completed a fellowship in palliative care at Stanford-affiliated Palo Alto Veterans Administration Hospital. For years, she split her career between working in community ER clinics and producing films. Her films are large-scale projects that may take five years or longer to make, and she raises all the funds to bring them to fruition.
"I really do find documentary filmmaking tremendously gratifying," Dr. Grainger-Monsen says of the chance "to talk with all different kinds of people in all different situations and walk in their shoes, with them, for a time. That is what I'm trying to share with the audience."
In creating character-driven documentaries, she aims to spark discussions about important issues in contemporary medicine. "I hope my films can help increase understanding and empathy," she says, "and result in improvements to the delivery of healthcare and reduction of disparities on multiple levels."
Susan Kreimer is a freelance writer in New York.
Week On, Week Off Schedules Make Balancing Work-Life Demands Tough for Some Hospitalists

Ask supporters and detractors of the seven-on/seven-off schedule their favorite (or least favorite) aspect of the model, and they’ll say the same thing: how it impacts work-life balance.
Heads: “For me, I know that there’s that balance,” says Dr. Houser, who works in Rapid City, S.D. “I know that there are going to be some holidays, some weekends where I’m not going to go to the soccer game or go to the volleyball game or see the choir practice. But the other side of me knows that I will be able to make it up to the kids, if it was something that I missed. I’ll be able to devote that time that I really like to devote to my family when I’m off.”
Tails: “I really believe that [seven-on/seven-off] scheduling is probably more desirable to Generation Y, which tends to have a lot more life quality and life balance as part of their mentality,” says Eshbaugh, the administrator in Traverse City, Mich. “I think the older generation of physicians, especially because they came out of the outpatient world, they were used to working five days a week, every week.”
Ask supporters and detractors of the seven-on/seven-off schedule their favorite (or least favorite) aspect of the model, and they’ll say the same thing: how it impacts work-life balance.
Heads: “For me, I know that there’s that balance,” says Dr. Houser, who works in Rapid City, S.D. “I know that there are going to be some holidays, some weekends where I’m not going to go to the soccer game or go to the volleyball game or see the choir practice. But the other side of me knows that I will be able to make it up to the kids, if it was something that I missed. I’ll be able to devote that time that I really like to devote to my family when I’m off.”
Tails: “I really believe that [seven-on/seven-off] scheduling is probably more desirable to Generation Y, which tends to have a lot more life quality and life balance as part of their mentality,” says Eshbaugh, the administrator in Traverse City, Mich. “I think the older generation of physicians, especially because they came out of the outpatient world, they were used to working five days a week, every week.”
Ask supporters and detractors of the seven-on/seven-off schedule their favorite (or least favorite) aspect of the model, and they’ll say the same thing: how it impacts work-life balance.
Heads: “For me, I know that there’s that balance,” says Dr. Houser, who works in Rapid City, S.D. “I know that there are going to be some holidays, some weekends where I’m not going to go to the soccer game or go to the volleyball game or see the choir practice. But the other side of me knows that I will be able to make it up to the kids, if it was something that I missed. I’ll be able to devote that time that I really like to devote to my family when I’m off.”
Tails: “I really believe that [seven-on/seven-off] scheduling is probably more desirable to Generation Y, which tends to have a lot more life quality and life balance as part of their mentality,” says Eshbaugh, the administrator in Traverse City, Mich. “I think the older generation of physicians, especially because they came out of the outpatient world, they were used to working five days a week, every week.”
Experts Debate Pros and Cons of Seven Days On, Seven Days Off Work Schedule

—Jeff Taylor, president, chief operating officer, IPC: The Hospitalist Co., North Hollywood, Calif.
Robert Houser, MD, MBA, co-medical director of Rapid City Regional Hospital in Rapid City, S.D., left his primary-care practice a little more than 10 years ago to become a hospitalist. At the time, his new schedule—working seven days in a row, then taking off seven days in a row—struck him as odd. But the idea of being able to throw himself completely and alternately into both his job and his family appealed to him. More than a decade later, he still believes his schedule is a perfect mix of personal and professional time.
Bradley Eshbaugh, MBA, FACMPE, chief administrator of Hospitalists of Northern Michigan (HNM) in Traverse City, Mich., and a SHM Administrators’ Committee member, doesn’t see it that way. His hospitalists tell him the work-a-week, skip-a-week schedule is too inflexible for the work-life balance they crave. Even when newly hired physicians accustomed to the week-on/week-off schedule ask if they can continue it, Eshbaugh says, most quickly realize the flexible-schedule option that HNM utilizes offers them a more balanced approach to time off work.


Welcome to the world of seven-on/seven-off scheduling, where detractors and supporters often have the same reasons for their differing viewpoints. Those who favor the model say that its simple-to-implement block approach to scheduling allows physicians to know far in advance when their time off is. That allows clinicians to plan their lives way in advance, a carrot hospitalist groups have used for more than a decade to attract new hires. Those who prefer other scheduling methods say the seven-on/seven-off model’s rigidity leaves little flexibility to deal with the unscheduled inevitabilities of life (sickness, personal time, maternity leave, resignations, etc.) and is not the best construct to match staffing to the busiest admissions periods.
And while everyone agrees that the seven-on/seven-off model is among the most popular, there is as yet no clinical data that show whether its practitioners are more or less likely to provide higher-quality care. So the oft-asked question of whether the schedule is sustainable comes down not to care delivery but financial pressure. Three-quarters of HM groups (HMGs) rely on their host hospitals for financial support, and that support-per-FTE at nonacademic groups serving only adults rose to an median of $140,204 this year, according to SHM’s 2012 State of Hospital Medicine report—a 40% increase over data in the 2010 SHM/MGMA‐ACMPE survey.
“When we started in this business 15 years ago, the average hospital might have three to five hospitalists, maybe a subsidy of $300,000 to $500,000,” says Martin Buser, a partner in Hospitalist Management Resources of Del Mar, Calif. “That same program today is probably running 15 to 20 hospitalists, a subsidy of $3 million-plus. It’s really strongly on the radar screen for administrators to look at, ‘Can I keep affording this, or do I need to find less expensive ways to get the same result?’”
Viewpoints Vary
The origins of the seven-on/seven-off schedule are a bit murky. Some believe it was borrowed from the shift-work model in the ED. Others think it has roots in the nursing ranks. Still others think that in the nascent days of HM, two- and three-physician groups developed the schedule by simply splitting monthly schedules by weeks. Regardless of pedigree, the model has grown to be just about the most common schedule for HMGs serving adults only. The State of Hospital Medicine report reported that 41.9% of adult groups use the seven-on/seven-off schedule, with 41.6% reporting their schedule as “variable” and “other.”
SHM has never queried hospitalists specifically about their schedules before, so no comparative data are available for information. Interestingly, the State of Hospital Medicine report found that hospitalist management companies and private HM groups were less likely to use the seven-on/seven-off schedule than hospital-owned or academic groups.
Jeff Taylor, president and chief operating officer of IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif., says just 10% of his 1,400 providers nationwide uses the seven-on/seven-off construct. He argues the model “is economically inefficient.” For example, he says, take a hospital with a census of around 60 inpatients per day. An HM group that wants to limit daily censuses to about 15 patients would need four doctors to staff that patient load. Using the seven-on/seven-off schedule, the group would need eight dayside hospitalists (not counting nocturnists). In a more traditional staffing model of a five-day workweek and call coverage, a group likely could handle the same workload with five FTE hospitalists, Taylor says.
“We have been doing some education with hospitals over the last three or four years of just doing the math,” he adds. “How many doctors would you need to staff this census? … We often give a dual proposal. This is how much it will cost for seven-on/seven-off; this is how much it will cost with the Monday-through-Friday model. Obviously, the Monday-through-Friday model is a lower cost, but it may take a little bit longer to get it staffed.”
Staffing difficulties—particularly recruitment and retention—are a major driver of the popularity of the seven-on/seven-off schedule, says Gregory Martinek, DO, FHM, medical director of Lexington Hospitalists in Altoona, Pa. He says it’s tough to recruit hospitalists to work in a small town in central Pennsylvania, so offering a schedule those physicians want to work is helpful.

In fact, Dr. Martinek offers his hospitalists an extra week of vacation in addition to the 26 weeks they don’t work. That allows some of his foreign-born physicians to take a three-week break from work, which many use as a chance to return to their birth countries.
“We had trouble recruiting when we had a different model,” Dr. Martinek says. “This has really worked for us. It’s allowed us to recruit.”
Cost Concerns
How do HM group leaders answer C-suite questions about whether the expenses associated with the seven-on/seven-off model are worth it? The short answer is data. Know basic metrics on length of stay, cost of care, etc., before having that conversation. For example, a traditional 40-hour workweek is 2,080 hours per annum (and probably less with vacation time). And while some might think that 26 weeks off a year equates to fewer hours, 26 weeks of 12-hour shifts totals 2,184 hours.
Per Danielsson, MD, medical director of Swedish Hospital Medicine in Seattle, says his group uses a hybrid seven-on/seven-off schedule that has demonstrated that their cost-of-care delivery is consistently $1,000 to $1,500 less per case than other physicians’ cases at Swedish Medical Center—and those other physicians often take care of patients with the same diagnoses.

—Kristi Gylten, MBA, director, hospitalist services, Rapid City (S.D.) Regional Hospital, SHM Administrators’ Committee member
“When you have those kinds of numbers, and you’re doing 7,000 admissions per year, the numbers add up quickly,” Dr. Danielsson says.
Kristi Gylten, MBA, director of hospitalist services at Rapid City Regional Hospital and a member of SHM’s Administrators’ Committee, says hospitalist group leaders should urge their administrations to look at more than just financial statements when judging the value of an HM group, particularly in rural areas.
“Our program started with three physicians in 2004 and has grown to over 30 in 2012,” she says. “There has been such great value brought to our community and our medical staff and our patients, just over and above what the bottom line would show on a monthly operational statement, that we don’t have the bean-counters knocking on our door.”
IPC’s Taylor says a complicating factor in moving away from the seven-on/seven-off format is the passion physicians have for their schedules. Or, to use his words: “You make major changes to schedules at great peril.”
John Frehse, managing partner of Core Practice, a Chicago consultancy that designs and implements labor strategies for shift-work operations, says that managers and administrators looking to change schedules often shy away from the upheaval.
“This emotional and potentially disruptive environment is something that makes them say, ‘We’re getting away with it now, so let’s not change it. Why rock the boat?’” Frehse explains. “They should be saying, ‘What is the methodology to get this out of here and put in something that’s financially responsible for the organization?’”
Practice Concerns
Ten years ago, Dr. Houser found the seven-on/seven-off schedule “a little bit unusual.” Now, his workweek of seven 10-hour days in a row seems natural. Even so, he understands those who voice concerns about hospitalized patients who would not be happy to know their hospitalist was on his 60th, 70th, or 80th hour of work that week.
“The physician’s side of me stays in a mode where I know I have to be a resource to the patient and I have to be a resource to my colleagues, and so I don’t think terms of being mentally drained,” he says. “Whether I’m starting or finishing, I just want to be as fresh as I can to approach those problems and mentally stay in the game that way. If I start thinking about being fatigued or tired, I feel like I won’t be able to provide the type of care that I can for that patient.”
Some groups using the seven-on/seven-off model allow physicians to leave the hospital at slow times while requiring they be on call. That allows hospitalists to recharge a bit midweek while ensuring that there is enough staff to provide coverage. Dr. Martinek says there’s no need to “hold them in the hospital if there is no work to do.” Daytime hospitalists also split admission to lighten the workload, he says.
Taylor says another practical concern for hospitalists working the seven-on/seven-off schedule is how engaged they can be with their institutions, particularly when they aren’t there half the year for committee meetings, staff gatherings—even water cooler conversation.
“I just have difficulty understanding how if half your workforce is gone every other week, how that group of doctors can become as integrated and ingrained and as part of the fabric of that facility as people who are there every week,” he says. “There are people who disagree with me on that, obviously.”
Richard Quinn is a freelance writer in New Jersey.
—Jeff Taylor, president, chief operating officer, IPC: The Hospitalist Co., North Hollywood, Calif.
Robert Houser, MD, MBA, co-medical director of Rapid City Regional Hospital in Rapid City, S.D., left his primary-care practice a little more than 10 years ago to become a hospitalist. At the time, his new schedule—working seven days in a row, then taking off seven days in a row—struck him as odd. But the idea of being able to throw himself completely and alternately into both his job and his family appealed to him. More than a decade later, he still believes his schedule is a perfect mix of personal and professional time.
Bradley Eshbaugh, MBA, FACMPE, chief administrator of Hospitalists of Northern Michigan (HNM) in Traverse City, Mich., and a SHM Administrators’ Committee member, doesn’t see it that way. His hospitalists tell him the work-a-week, skip-a-week schedule is too inflexible for the work-life balance they crave. Even when newly hired physicians accustomed to the week-on/week-off schedule ask if they can continue it, Eshbaugh says, most quickly realize the flexible-schedule option that HNM utilizes offers them a more balanced approach to time off work.
Welcome to the world of seven-on/seven-off scheduling, where detractors and supporters often have the same reasons for their differing viewpoints. Those who favor the model say that its simple-to-implement block approach to scheduling allows physicians to know far in advance when their time off is. That allows clinicians to plan their lives way in advance, a carrot hospitalist groups have used for more than a decade to attract new hires. Those who prefer other scheduling methods say the seven-on/seven-off model’s rigidity leaves little flexibility to deal with the unscheduled inevitabilities of life (sickness, personal time, maternity leave, resignations, etc.) and is not the best construct to match staffing to the busiest admissions periods.
And while everyone agrees that the seven-on/seven-off model is among the most popular, there is as yet no clinical data that show whether its practitioners are more or less likely to provide higher-quality care. So the oft-asked question of whether the schedule is sustainable comes down not to care delivery but financial pressure. Three-quarters of HM groups (HMGs) rely on their host hospitals for financial support, and that support-per-FTE at nonacademic groups serving only adults rose to an median of $140,204 this year, according to SHM’s 2012 State of Hospital Medicine report—a 40% increase over data in the 2010 SHM/MGMA‐ACMPE survey.
“When we started in this business 15 years ago, the average hospital might have three to five hospitalists, maybe a subsidy of $300,000 to $500,000,” says Martin Buser, a partner in Hospitalist Management Resources of Del Mar, Calif. “That same program today is probably running 15 to 20 hospitalists, a subsidy of $3 million-plus. It’s really strongly on the radar screen for administrators to look at, ‘Can I keep affording this, or do I need to find less expensive ways to get the same result?’”
Viewpoints Vary
The origins of the seven-on/seven-off schedule are a bit murky. Some believe it was borrowed from the shift-work model in the ED. Others think it has roots in the nursing ranks. Still others think that in the nascent days of HM, two- and three-physician groups developed the schedule by simply splitting monthly schedules by weeks. Regardless of pedigree, the model has grown to be just about the most common schedule for HMGs serving adults only. The State of Hospital Medicine report reported that 41.9% of adult groups use the seven-on/seven-off schedule, with 41.6% reporting their schedule as “variable” and “other.”
SHM has never queried hospitalists specifically about their schedules before, so no comparative data are available for information. Interestingly, the State of Hospital Medicine report found that hospitalist management companies and private HM groups were less likely to use the seven-on/seven-off schedule than hospital-owned or academic groups.
Jeff Taylor, president and chief operating officer of IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif., says just 10% of his 1,400 providers nationwide uses the seven-on/seven-off construct. He argues the model “is economically inefficient.” For example, he says, take a hospital with a census of around 60 inpatients per day. An HM group that wants to limit daily censuses to about 15 patients would need four doctors to staff that patient load. Using the seven-on/seven-off schedule, the group would need eight dayside hospitalists (not counting nocturnists). In a more traditional staffing model of a five-day workweek and call coverage, a group likely could handle the same workload with five FTE hospitalists, Taylor says.
“We have been doing some education with hospitals over the last three or four years of just doing the math,” he adds. “How many doctors would you need to staff this census? … We often give a dual proposal. This is how much it will cost for seven-on/seven-off; this is how much it will cost with the Monday-through-Friday model. Obviously, the Monday-through-Friday model is a lower cost, but it may take a little bit longer to get it staffed.”
Staffing difficulties—particularly recruitment and retention—are a major driver of the popularity of the seven-on/seven-off schedule, says Gregory Martinek, DO, FHM, medical director of Lexington Hospitalists in Altoona, Pa. He says it’s tough to recruit hospitalists to work in a small town in central Pennsylvania, so offering a schedule those physicians want to work is helpful.
In fact, Dr. Martinek offers his hospitalists an extra week of vacation in addition to the 26 weeks they don’t work. That allows some of his foreign-born physicians to take a three-week break from work, which many use as a chance to return to their birth countries.
“We had trouble recruiting when we had a different model,” Dr. Martinek says. “This has really worked for us. It’s allowed us to recruit.”
Cost Concerns
How do HM group leaders answer C-suite questions about whether the expenses associated with the seven-on/seven-off model are worth it? The short answer is data. Know basic metrics on length of stay, cost of care, etc., before having that conversation. For example, a traditional 40-hour workweek is 2,080 hours per annum (and probably less with vacation time). And while some might think that 26 weeks off a year equates to fewer hours, 26 weeks of 12-hour shifts totals 2,184 hours.
Per Danielsson, MD, medical director of Swedish Hospital Medicine in Seattle, says his group uses a hybrid seven-on/seven-off schedule that has demonstrated that their cost-of-care delivery is consistently $1,000 to $1,500 less per case than other physicians’ cases at Swedish Medical Center—and those other physicians often take care of patients with the same diagnoses.
—Kristi Gylten, MBA, director, hospitalist services, Rapid City (S.D.) Regional Hospital, SHM Administrators’ Committee member
“When you have those kinds of numbers, and you’re doing 7,000 admissions per year, the numbers add up quickly,” Dr. Danielsson says.
Kristi Gylten, MBA, director of hospitalist services at Rapid City Regional Hospital and a member of SHM’s Administrators’ Committee, says hospitalist group leaders should urge their administrations to look at more than just financial statements when judging the value of an HM group, particularly in rural areas.
“Our program started with three physicians in 2004 and has grown to over 30 in 2012,” she says. “There has been such great value brought to our community and our medical staff and our patients, just over and above what the bottom line would show on a monthly operational statement, that we don’t have the bean-counters knocking on our door.”
IPC’s Taylor says a complicating factor in moving away from the seven-on/seven-off format is the passion physicians have for their schedules. Or, to use his words: “You make major changes to schedules at great peril.”
John Frehse, managing partner of Core Practice, a Chicago consultancy that designs and implements labor strategies for shift-work operations, says that managers and administrators looking to change schedules often shy away from the upheaval.
“This emotional and potentially disruptive environment is something that makes them say, ‘We’re getting away with it now, so let’s not change it. Why rock the boat?’” Frehse explains. “They should be saying, ‘What is the methodology to get this out of here and put in something that’s financially responsible for the organization?’”
Practice Concerns
Ten years ago, Dr. Houser found the seven-on/seven-off schedule “a little bit unusual.” Now, his workweek of seven 10-hour days in a row seems natural. Even so, he understands those who voice concerns about hospitalized patients who would not be happy to know their hospitalist was on his 60th, 70th, or 80th hour of work that week.
“The physician’s side of me stays in a mode where I know I have to be a resource to the patient and I have to be a resource to my colleagues, and so I don’t think terms of being mentally drained,” he says. “Whether I’m starting or finishing, I just want to be as fresh as I can to approach those problems and mentally stay in the game that way. If I start thinking about being fatigued or tired, I feel like I won’t be able to provide the type of care that I can for that patient.”
Some groups using the seven-on/seven-off model allow physicians to leave the hospital at slow times while requiring they be on call. That allows hospitalists to recharge a bit midweek while ensuring that there is enough staff to provide coverage. Dr. Martinek says there’s no need to “hold them in the hospital if there is no work to do.” Daytime hospitalists also split admission to lighten the workload, he says.
Taylor says another practical concern for hospitalists working the seven-on/seven-off schedule is how engaged they can be with their institutions, particularly when they aren’t there half the year for committee meetings, staff gatherings—even water cooler conversation.
“I just have difficulty understanding how if half your workforce is gone every other week, how that group of doctors can become as integrated and ingrained and as part of the fabric of that facility as people who are there every week,” he says. “There are people who disagree with me on that, obviously.”
Richard Quinn is a freelance writer in New Jersey.
—Jeff Taylor, president, chief operating officer, IPC: The Hospitalist Co., North Hollywood, Calif.
Robert Houser, MD, MBA, co-medical director of Rapid City Regional Hospital in Rapid City, S.D., left his primary-care practice a little more than 10 years ago to become a hospitalist. At the time, his new schedule—working seven days in a row, then taking off seven days in a row—struck him as odd. But the idea of being able to throw himself completely and alternately into both his job and his family appealed to him. More than a decade later, he still believes his schedule is a perfect mix of personal and professional time.
Bradley Eshbaugh, MBA, FACMPE, chief administrator of Hospitalists of Northern Michigan (HNM) in Traverse City, Mich., and a SHM Administrators’ Committee member, doesn’t see it that way. His hospitalists tell him the work-a-week, skip-a-week schedule is too inflexible for the work-life balance they crave. Even when newly hired physicians accustomed to the week-on/week-off schedule ask if they can continue it, Eshbaugh says, most quickly realize the flexible-schedule option that HNM utilizes offers them a more balanced approach to time off work.
Welcome to the world of seven-on/seven-off scheduling, where detractors and supporters often have the same reasons for their differing viewpoints. Those who favor the model say that its simple-to-implement block approach to scheduling allows physicians to know far in advance when their time off is. That allows clinicians to plan their lives way in advance, a carrot hospitalist groups have used for more than a decade to attract new hires. Those who prefer other scheduling methods say the seven-on/seven-off model’s rigidity leaves little flexibility to deal with the unscheduled inevitabilities of life (sickness, personal time, maternity leave, resignations, etc.) and is not the best construct to match staffing to the busiest admissions periods.
And while everyone agrees that the seven-on/seven-off model is among the most popular, there is as yet no clinical data that show whether its practitioners are more or less likely to provide higher-quality care. So the oft-asked question of whether the schedule is sustainable comes down not to care delivery but financial pressure. Three-quarters of HM groups (HMGs) rely on their host hospitals for financial support, and that support-per-FTE at nonacademic groups serving only adults rose to an median of $140,204 this year, according to SHM’s 2012 State of Hospital Medicine report—a 40% increase over data in the 2010 SHM/MGMA‐ACMPE survey.
“When we started in this business 15 years ago, the average hospital might have three to five hospitalists, maybe a subsidy of $300,000 to $500,000,” says Martin Buser, a partner in Hospitalist Management Resources of Del Mar, Calif. “That same program today is probably running 15 to 20 hospitalists, a subsidy of $3 million-plus. It’s really strongly on the radar screen for administrators to look at, ‘Can I keep affording this, or do I need to find less expensive ways to get the same result?’”
Viewpoints Vary
The origins of the seven-on/seven-off schedule are a bit murky. Some believe it was borrowed from the shift-work model in the ED. Others think it has roots in the nursing ranks. Still others think that in the nascent days of HM, two- and three-physician groups developed the schedule by simply splitting monthly schedules by weeks. Regardless of pedigree, the model has grown to be just about the most common schedule for HMGs serving adults only. The State of Hospital Medicine report reported that 41.9% of adult groups use the seven-on/seven-off schedule, with 41.6% reporting their schedule as “variable” and “other.”
SHM has never queried hospitalists specifically about their schedules before, so no comparative data are available for information. Interestingly, the State of Hospital Medicine report found that hospitalist management companies and private HM groups were less likely to use the seven-on/seven-off schedule than hospital-owned or academic groups.
Jeff Taylor, president and chief operating officer of IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif., says just 10% of his 1,400 providers nationwide uses the seven-on/seven-off construct. He argues the model “is economically inefficient.” For example, he says, take a hospital with a census of around 60 inpatients per day. An HM group that wants to limit daily censuses to about 15 patients would need four doctors to staff that patient load. Using the seven-on/seven-off schedule, the group would need eight dayside hospitalists (not counting nocturnists). In a more traditional staffing model of a five-day workweek and call coverage, a group likely could handle the same workload with five FTE hospitalists, Taylor says.
“We have been doing some education with hospitals over the last three or four years of just doing the math,” he adds. “How many doctors would you need to staff this census? … We often give a dual proposal. This is how much it will cost for seven-on/seven-off; this is how much it will cost with the Monday-through-Friday model. Obviously, the Monday-through-Friday model is a lower cost, but it may take a little bit longer to get it staffed.”
Staffing difficulties—particularly recruitment and retention—are a major driver of the popularity of the seven-on/seven-off schedule, says Gregory Martinek, DO, FHM, medical director of Lexington Hospitalists in Altoona, Pa. He says it’s tough to recruit hospitalists to work in a small town in central Pennsylvania, so offering a schedule those physicians want to work is helpful.
In fact, Dr. Martinek offers his hospitalists an extra week of vacation in addition to the 26 weeks they don’t work. That allows some of his foreign-born physicians to take a three-week break from work, which many use as a chance to return to their birth countries.
“We had trouble recruiting when we had a different model,” Dr. Martinek says. “This has really worked for us. It’s allowed us to recruit.”
Cost Concerns
How do HM group leaders answer C-suite questions about whether the expenses associated with the seven-on/seven-off model are worth it? The short answer is data. Know basic metrics on length of stay, cost of care, etc., before having that conversation. For example, a traditional 40-hour workweek is 2,080 hours per annum (and probably less with vacation time). And while some might think that 26 weeks off a year equates to fewer hours, 26 weeks of 12-hour shifts totals 2,184 hours.
Per Danielsson, MD, medical director of Swedish Hospital Medicine in Seattle, says his group uses a hybrid seven-on/seven-off schedule that has demonstrated that their cost-of-care delivery is consistently $1,000 to $1,500 less per case than other physicians’ cases at Swedish Medical Center—and those other physicians often take care of patients with the same diagnoses.
—Kristi Gylten, MBA, director, hospitalist services, Rapid City (S.D.) Regional Hospital, SHM Administrators’ Committee member
“When you have those kinds of numbers, and you’re doing 7,000 admissions per year, the numbers add up quickly,” Dr. Danielsson says.
Kristi Gylten, MBA, director of hospitalist services at Rapid City Regional Hospital and a member of SHM’s Administrators’ Committee, says hospitalist group leaders should urge their administrations to look at more than just financial statements when judging the value of an HM group, particularly in rural areas.
“Our program started with three physicians in 2004 and has grown to over 30 in 2012,” she says. “There has been such great value brought to our community and our medical staff and our patients, just over and above what the bottom line would show on a monthly operational statement, that we don’t have the bean-counters knocking on our door.”
IPC’s Taylor says a complicating factor in moving away from the seven-on/seven-off format is the passion physicians have for their schedules. Or, to use his words: “You make major changes to schedules at great peril.”
John Frehse, managing partner of Core Practice, a Chicago consultancy that designs and implements labor strategies for shift-work operations, says that managers and administrators looking to change schedules often shy away from the upheaval.
“This emotional and potentially disruptive environment is something that makes them say, ‘We’re getting away with it now, so let’s not change it. Why rock the boat?’” Frehse explains. “They should be saying, ‘What is the methodology to get this out of here and put in something that’s financially responsible for the organization?’”
Practice Concerns
Ten years ago, Dr. Houser found the seven-on/seven-off schedule “a little bit unusual.” Now, his workweek of seven 10-hour days in a row seems natural. Even so, he understands those who voice concerns about hospitalized patients who would not be happy to know their hospitalist was on his 60th, 70th, or 80th hour of work that week.
“The physician’s side of me stays in a mode where I know I have to be a resource to the patient and I have to be a resource to my colleagues, and so I don’t think terms of being mentally drained,” he says. “Whether I’m starting or finishing, I just want to be as fresh as I can to approach those problems and mentally stay in the game that way. If I start thinking about being fatigued or tired, I feel like I won’t be able to provide the type of care that I can for that patient.”
Some groups using the seven-on/seven-off model allow physicians to leave the hospital at slow times while requiring they be on call. That allows hospitalists to recharge a bit midweek while ensuring that there is enough staff to provide coverage. Dr. Martinek says there’s no need to “hold them in the hospital if there is no work to do.” Daytime hospitalists also split admission to lighten the workload, he says.
Taylor says another practical concern for hospitalists working the seven-on/seven-off schedule is how engaged they can be with their institutions, particularly when they aren’t there half the year for committee meetings, staff gatherings—even water cooler conversation.
“I just have difficulty understanding how if half your workforce is gone every other week, how that group of doctors can become as integrated and ingrained and as part of the fabric of that facility as people who are there every week,” he says. “There are people who disagree with me on that, obviously.”
Richard Quinn is a freelance writer in New Jersey.
Former Hospitalist Gets Satisfaction Helping Physicians Launch Nonclinical Careers

Q&A with Philippa Kennealy, MD, MPH, CPCC, PCC, founder and owner of The Entrepreneurial MD (www.entrepreneurialmd.com).
Question: What type of business do you operate?
Answer: I’m a physician development and business coach. My role is to help physicians who are struggling with launching a nonclinical career or a new business, or revamping a medical practice to become a satisfying venture. Although I am personally based in Los Angeles, The Entrepreneurial MD clients can be located anywhere in the world as long as we both have phone or Internet access. About 95% of my clients are not located in Los Angeles. I’m 57 years old. I was 41 when I left medical practice and went on to have several more careers.
Q: Why did you give up the practice of medicine?
A: I left my five-member private family practice in mid-1996, after joining my group in the middle of 1988. I realized that not only was I feeling unfulfilled and frustrated by work, but that I was even starting to dread it. I particularly dreaded the nights and weekends on call—for the latter, I started getting that “sick in the stomach” feeling on Mondays. I also realized that I had become bored with the repetition of the work and loved the idea of learning a whole lot of new stuff. I had embarked on my master’s degree in public health at UCLA around that time (mid-1995) and became completely energized by being a student again in a class of adult learners.
In short, I was deeply restless, in my early 40s, and ready for a change.
Q: How would you advise other MDs who are considering the pros/cons of not seeing patients anymore?
A: Above all else, it is important to get to really know yourself. Give yourself the gift of real reflection rather than just reaction. Upon such reflection, I knew that what truly energized me in clinical practice was my connection to people rather than being able to use a stethoscope or remove a mole. I also recognized that this “passion” was portable—unless I was locked away in a room with only a computer for company, I would thrive professionally no matter what I chose next, as long as it involved being in a helping relationship with others.
Engage in conversation with others who are like-minded—your mentors, people who have made career changes, your significant others. Do your homework and recognize that in the end, it is only you who can make the decision whether to stay or leave. Be compelled to make changes in your life because you are moving toward new opportunities rather than merely running away.
Q: Can you name some pros and cons for physicians interested in a career change?
A: The pros: interesting challenges, a chance to remake your career, re-engage your brain, feel challenged; reinvent yourself, strive for the dream(s) that you may have put on hold many years before or gave up because you did medicine to please others; acquire new skills, which may be fun.
The cons: risky if unplanned, you may have to take an income hit for a while, you may be a victim of “the grass is always greener” [mindset], you may never discover what you really want if you are simply acting from dissatisfaction and aren’t willing to do the work of change. It feels scary, and it takes a certain amount of inner courage and external support to make the move.
Q&A with Philippa Kennealy, MD, MPH, CPCC, PCC, founder and owner of The Entrepreneurial MD (www.entrepreneurialmd.com).
Question: What type of business do you operate?
Answer: I’m a physician development and business coach. My role is to help physicians who are struggling with launching a nonclinical career or a new business, or revamping a medical practice to become a satisfying venture. Although I am personally based in Los Angeles, The Entrepreneurial MD clients can be located anywhere in the world as long as we both have phone or Internet access. About 95% of my clients are not located in Los Angeles. I’m 57 years old. I was 41 when I left medical practice and went on to have several more careers.
Q: Why did you give up the practice of medicine?
A: I left my five-member private family practice in mid-1996, after joining my group in the middle of 1988. I realized that not only was I feeling unfulfilled and frustrated by work, but that I was even starting to dread it. I particularly dreaded the nights and weekends on call—for the latter, I started getting that “sick in the stomach” feeling on Mondays. I also realized that I had become bored with the repetition of the work and loved the idea of learning a whole lot of new stuff. I had embarked on my master’s degree in public health at UCLA around that time (mid-1995) and became completely energized by being a student again in a class of adult learners.
In short, I was deeply restless, in my early 40s, and ready for a change.
Q: How would you advise other MDs who are considering the pros/cons of not seeing patients anymore?
A: Above all else, it is important to get to really know yourself. Give yourself the gift of real reflection rather than just reaction. Upon such reflection, I knew that what truly energized me in clinical practice was my connection to people rather than being able to use a stethoscope or remove a mole. I also recognized that this “passion” was portable—unless I was locked away in a room with only a computer for company, I would thrive professionally no matter what I chose next, as long as it involved being in a helping relationship with others.
Engage in conversation with others who are like-minded—your mentors, people who have made career changes, your significant others. Do your homework and recognize that in the end, it is only you who can make the decision whether to stay or leave. Be compelled to make changes in your life because you are moving toward new opportunities rather than merely running away.
Q: Can you name some pros and cons for physicians interested in a career change?
A: The pros: interesting challenges, a chance to remake your career, re-engage your brain, feel challenged; reinvent yourself, strive for the dream(s) that you may have put on hold many years before or gave up because you did medicine to please others; acquire new skills, which may be fun.
The cons: risky if unplanned, you may have to take an income hit for a while, you may be a victim of “the grass is always greener” [mindset], you may never discover what you really want if you are simply acting from dissatisfaction and aren’t willing to do the work of change. It feels scary, and it takes a certain amount of inner courage and external support to make the move.
Q&A with Philippa Kennealy, MD, MPH, CPCC, PCC, founder and owner of The Entrepreneurial MD (www.entrepreneurialmd.com).
Question: What type of business do you operate?
Answer: I’m a physician development and business coach. My role is to help physicians who are struggling with launching a nonclinical career or a new business, or revamping a medical practice to become a satisfying venture. Although I am personally based in Los Angeles, The Entrepreneurial MD clients can be located anywhere in the world as long as we both have phone or Internet access. About 95% of my clients are not located in Los Angeles. I’m 57 years old. I was 41 when I left medical practice and went on to have several more careers.
Q: Why did you give up the practice of medicine?
A: I left my five-member private family practice in mid-1996, after joining my group in the middle of 1988. I realized that not only was I feeling unfulfilled and frustrated by work, but that I was even starting to dread it. I particularly dreaded the nights and weekends on call—for the latter, I started getting that “sick in the stomach” feeling on Mondays. I also realized that I had become bored with the repetition of the work and loved the idea of learning a whole lot of new stuff. I had embarked on my master’s degree in public health at UCLA around that time (mid-1995) and became completely energized by being a student again in a class of adult learners.
In short, I was deeply restless, in my early 40s, and ready for a change.
Q: How would you advise other MDs who are considering the pros/cons of not seeing patients anymore?
A: Above all else, it is important to get to really know yourself. Give yourself the gift of real reflection rather than just reaction. Upon such reflection, I knew that what truly energized me in clinical practice was my connection to people rather than being able to use a stethoscope or remove a mole. I also recognized that this “passion” was portable—unless I was locked away in a room with only a computer for company, I would thrive professionally no matter what I chose next, as long as it involved being in a helping relationship with others.
Engage in conversation with others who are like-minded—your mentors, people who have made career changes, your significant others. Do your homework and recognize that in the end, it is only you who can make the decision whether to stay or leave. Be compelled to make changes in your life because you are moving toward new opportunities rather than merely running away.
Q: Can you name some pros and cons for physicians interested in a career change?
A: The pros: interesting challenges, a chance to remake your career, re-engage your brain, feel challenged; reinvent yourself, strive for the dream(s) that you may have put on hold many years before or gave up because you did medicine to please others; acquire new skills, which may be fun.
The cons: risky if unplanned, you may have to take an income hit for a while, you may be a victim of “the grass is always greener” [mindset], you may never discover what you really want if you are simply acting from dissatisfaction and aren’t willing to do the work of change. It feels scary, and it takes a certain amount of inner courage and external support to make the move.
Medicare Billing Regulations for Nonphysician Providers Vary by State, Facility
Nurse practitioners (NPs) and physician assistants (PAs), referred to as nonphysician providers (NPPs) in billing policy, provide many different services in the hospital setting. Roles include:
- Rounding independently and following patients of varying acuity with physician supervision. The NPP may ask the physician to see the patient, as necessary, if a change in the patient’s condition arises and warrants physician evaluation.
- Providing prompt consultative
- services when the physician is not
- readily available.
- Rounding alongside the physician and expediting the work of admission services through a combined effort.
Hospitalist programs may elect one model over another, or utilize NPPs according to existing need and shifting census. Employers must be aware of state and federal regulations, facility-imposed standards of care, and billing requirements surrounding NPP services.
Medicare Enrollment and Billing Eligibility
Certified PAs and NPs may provide covered services to Medicare beneficiaries in accordance with their state scope of practice under state law and corresponding supervision/collaboration requirements. They can submit claims for these services, providing they meet enrollment qualifications.1
PAs must have:
- Graduated from a PA educational program accredited by the Accreditation Review Commission on Education for the Physician Assistant (or its predecessor agencies, the Commission on Accreditation of Allied Health Education Programs (CAAHEP) and the Committee on Allied Health Education and Accreditation (CAHEA); or
- Passed the national certification examination administered by the National Commission on Certification of Physician Assistants (NCCPA); and
- A license as a PA in the practicing state.
NPs must:
- Be a registered nurse who is authorized and licensed by the state to practice as a nurse practitioner by Dec. 31, 2000; or
- After Jan. 1, 2001, be a registered nurse who is authorized and licensed by the state to practice as an NP and be certified by a recognized national certifying body that has established standards for NPs (e.g. American Academy of Nurse Practitioners, American Nurses Credentialing Center, AACN Certification Corp., or National Board on Certification of Hospice and Palliative Nurses); and
- Possess a master’s degree in nursing.
Independent Billing
NPPs can see patients in any setting without the presence of a physician. The physician is not required to see the patient but must be available by phone or beeper in accordance with supervisory/collaborative guidelines. Physician cosignature is not required unless mandated by state law or the facility.
NPPs document and report their services according to the Centers for Medicare & Medicaid Services (CMS) Documentation Guidelines (available at www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/EMDOC.html). The NPP should be listed as the rendering provider on the claim form. Currently, insurance programs Medicare and Aetna Inc. consistently enroll and recognize NPPs as billing providers and reimburse these services at 85% of the allowable physician rate.2
Shared/Split Billing
When two providers (a physician and NPP) from the same group (direct employment or a lease arrangement contractually linking the providers) perform a service for the same patient on the same calendar day, CMS allows the combined services to be reported under a single provider’s name.
Allowable services. NPPs are only limited by the state scope of practice under state law, and the facility rules in which the NPPs practice. Services must be performed under the appropriate level of supervision or collaboration. Medicare reimburses reasonable and necessary services not otherwise excluded from coverage.
However, shared/split rules restrict the services reported under this billing model, recognizing only evaluation and management (E/M) services (and not procedures) provided in the ED, outpatient hospital clinics, or inpatient hospital (i.e. facility-based services). Shared/split rules do not involve all types of E/M services. For hospitalist programs, critical-care services (99291-99292) are excluded.3
Physician requirement. Shared/split rules require a face-to-face patient encounter by each provider on the same calendar day. There are no billing mandates requiring the NPP to see the patient before the physician does, although practice style might govern this decision.4 CMS does not specify the extent of provider involvement, but it could be established by local Medicare contractor requirements. Some contractors reference physician participation as a “substantive” service without further elaboration on specific parameters. Therefore, the physician determines the critical or key portion of his/her personal service. Minimalistic documentation can be problematic for quality or medicolegal aspects of patient care, and physicians might benefit from a more detailed notation of participation.
Documentation. Physician documentation must include an attestation that supports the physician encounter (e.g. “Patient seen and examined by me”), the individual with whom the service is shared (e.g. “Agree with note by X”), their portion of the rendered service (e.g. “Pulse oximetry 94% on room air. Audible rhonchi at bilateral lung bases. Start O2 2L nasal cannula. Obtain CXR”), the date, and a legible signature. NPP documentation should include as similar reference to the physician with whom the service is being shared for better charge capture. It alerts coders, auditors, and payor representatives to consider both notes in support of the billed service and ensures that the correct notes are sent to the payor in the event of claim denial and subsequent appeal.
Although the visit level is supported by both provider services, only one claim may be submitted for a shared/split service. The rendering provider listed on the claim can be the physician (reimbursed at 100% of the Medicare allowable physician rate) or the NPP (reimbursed at 85% of the allowable physician rate).
Non-Medicare Claims
Shared/split billing policy only applies to Medicare beneficiaries, while independent billing policy applies to Medicare and Aetna. Excessive costs prevent most other non-Medicare insurers from credentialing and enrollment NPPs. Absence of payor policy does not disqualify reimbursement for shared services, but it does require additional measures to establish recognition of NPP services and a corresponding reimbursement model.
After determining payor mix, develop a reasonable guideline for those payors who do not enroll NPPs. Delineate, in writing, a predetermined time frame for guideline implementation unless the payor can provide an alternate billing option. Some experts suggest physician groups outline the following key issues when structuring a billing option5:
- Type of NPPs involved in patient care;
- Category of services provided;
- Service location(s);
- Physician involvement;
- Mechanism for reporting services; and
- Documentation requirements.
Guidelines can be developed for any of the billing options (independent, “incident-to,” shared/split). Be sure to obtain written payor response before initiating the billing process.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
NPP Billing Reminders

Discharge day management (99238-99239) often is delegated to qualified NPPs.3 Because this service is time-based, the final code selection is based upon the total time spent with the patient, and on the patient’s unit/floor, coordinating care prior to the patient leaving the hospital on the day of discharge. If this service is solely provided by the NPP, the NPP must report the appropriate code under his/her own name on the claim form (for eligible payors). If this service is shared with the physician, report the code representing the cumulative, documented time in both notes, provided that each note identifies the face-toface service from each provider, and his/her corresponding participation.

Many questions arise about NPPs performing the admission service because NPPs might not be given “admitting” privileges by the facility in which they practice. NPPs may provide and/or participate in services according to their state scope practice and facility-imposed guidelines. Billing policy supports state law and will reimburse any “independent” service permitted by the state. Facilities may limit NPP scope of practice by disallowing independent admission service but permittin a shared service with the physician. If this service is shared with the physician, report the code representing the cumulative, documented encounter, provided that each note identifies the face-to-face service from each provider, and his/her corresponding participation

Prior to Medicare’s elimination of consultation services (99241-99245, 99251-99255), shared/split billing rules excluded consultations from this claim-reporting model.3 Since the elimination of consults, “consultations” are reported as initial hospital care services (99221-99223).3 Therefore, consultative services can be shared by NPPs and physicians, and reported as a cumulative initial hospital service through the shared/ split billing model. Other payors still accept consultation codes and do not have a specified shared/split model. This allows for the consultative service to be reported as a cumulative NPP/physician effort under the physician name, as long as a written contractual agreement exists allowing this billing option.
References
- Centers for Medicare & Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 190-200. Centers for Medicare & Medicaid website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/bp102c15.pdf. Accessed Nov. 5, 2012.
- Aetna Inc. Aetna office links updates. Reminder: Reimbursement change for mid-level practitioners. Aetna Inc. website. Available at www.aetna.com/provider/data/OLU_MA_JUN2010_final.pdf. Accessed Nov. 6, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. Centers for Medicare & Medicaid website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan 21, 2013.
- Pohlig, C. Nonphysician Providers in Your Practice. In: Coding for Chest Medicine 2011. Northbrook, Ill.: American College of Chest Physicians, 2010.
Nurse practitioners (NPs) and physician assistants (PAs), referred to as nonphysician providers (NPPs) in billing policy, provide many different services in the hospital setting. Roles include:
- Rounding independently and following patients of varying acuity with physician supervision. The NPP may ask the physician to see the patient, as necessary, if a change in the patient’s condition arises and warrants physician evaluation.
- Providing prompt consultative
- services when the physician is not
- readily available.
- Rounding alongside the physician and expediting the work of admission services through a combined effort.
Hospitalist programs may elect one model over another, or utilize NPPs according to existing need and shifting census. Employers must be aware of state and federal regulations, facility-imposed standards of care, and billing requirements surrounding NPP services.
Medicare Enrollment and Billing Eligibility
Certified PAs and NPs may provide covered services to Medicare beneficiaries in accordance with their state scope of practice under state law and corresponding supervision/collaboration requirements. They can submit claims for these services, providing they meet enrollment qualifications.1
PAs must have:
- Graduated from a PA educational program accredited by the Accreditation Review Commission on Education for the Physician Assistant (or its predecessor agencies, the Commission on Accreditation of Allied Health Education Programs (CAAHEP) and the Committee on Allied Health Education and Accreditation (CAHEA); or
- Passed the national certification examination administered by the National Commission on Certification of Physician Assistants (NCCPA); and
- A license as a PA in the practicing state.
NPs must:
- Be a registered nurse who is authorized and licensed by the state to practice as a nurse practitioner by Dec. 31, 2000; or
- After Jan. 1, 2001, be a registered nurse who is authorized and licensed by the state to practice as an NP and be certified by a recognized national certifying body that has established standards for NPs (e.g. American Academy of Nurse Practitioners, American Nurses Credentialing Center, AACN Certification Corp., or National Board on Certification of Hospice and Palliative Nurses); and
- Possess a master’s degree in nursing.
Independent Billing
NPPs can see patients in any setting without the presence of a physician. The physician is not required to see the patient but must be available by phone or beeper in accordance with supervisory/collaborative guidelines. Physician cosignature is not required unless mandated by state law or the facility.
NPPs document and report their services according to the Centers for Medicare & Medicaid Services (CMS) Documentation Guidelines (available at www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/EMDOC.html). The NPP should be listed as the rendering provider on the claim form. Currently, insurance programs Medicare and Aetna Inc. consistently enroll and recognize NPPs as billing providers and reimburse these services at 85% of the allowable physician rate.2
Shared/Split Billing
When two providers (a physician and NPP) from the same group (direct employment or a lease arrangement contractually linking the providers) perform a service for the same patient on the same calendar day, CMS allows the combined services to be reported under a single provider’s name.
Allowable services. NPPs are only limited by the state scope of practice under state law, and the facility rules in which the NPPs practice. Services must be performed under the appropriate level of supervision or collaboration. Medicare reimburses reasonable and necessary services not otherwise excluded from coverage.
However, shared/split rules restrict the services reported under this billing model, recognizing only evaluation and management (E/M) services (and not procedures) provided in the ED, outpatient hospital clinics, or inpatient hospital (i.e. facility-based services). Shared/split rules do not involve all types of E/M services. For hospitalist programs, critical-care services (99291-99292) are excluded.3
Physician requirement. Shared/split rules require a face-to-face patient encounter by each provider on the same calendar day. There are no billing mandates requiring the NPP to see the patient before the physician does, although practice style might govern this decision.4 CMS does not specify the extent of provider involvement, but it could be established by local Medicare contractor requirements. Some contractors reference physician participation as a “substantive” service without further elaboration on specific parameters. Therefore, the physician determines the critical or key portion of his/her personal service. Minimalistic documentation can be problematic for quality or medicolegal aspects of patient care, and physicians might benefit from a more detailed notation of participation.
Documentation. Physician documentation must include an attestation that supports the physician encounter (e.g. “Patient seen and examined by me”), the individual with whom the service is shared (e.g. “Agree with note by X”), their portion of the rendered service (e.g. “Pulse oximetry 94% on room air. Audible rhonchi at bilateral lung bases. Start O2 2L nasal cannula. Obtain CXR”), the date, and a legible signature. NPP documentation should include as similar reference to the physician with whom the service is being shared for better charge capture. It alerts coders, auditors, and payor representatives to consider both notes in support of the billed service and ensures that the correct notes are sent to the payor in the event of claim denial and subsequent appeal.
Although the visit level is supported by both provider services, only one claim may be submitted for a shared/split service. The rendering provider listed on the claim can be the physician (reimbursed at 100% of the Medicare allowable physician rate) or the NPP (reimbursed at 85% of the allowable physician rate).
Non-Medicare Claims
Shared/split billing policy only applies to Medicare beneficiaries, while independent billing policy applies to Medicare and Aetna. Excessive costs prevent most other non-Medicare insurers from credentialing and enrollment NPPs. Absence of payor policy does not disqualify reimbursement for shared services, but it does require additional measures to establish recognition of NPP services and a corresponding reimbursement model.
After determining payor mix, develop a reasonable guideline for those payors who do not enroll NPPs. Delineate, in writing, a predetermined time frame for guideline implementation unless the payor can provide an alternate billing option. Some experts suggest physician groups outline the following key issues when structuring a billing option5:
- Type of NPPs involved in patient care;
- Category of services provided;
- Service location(s);
- Physician involvement;
- Mechanism for reporting services; and
- Documentation requirements.
Guidelines can be developed for any of the billing options (independent, “incident-to,” shared/split). Be sure to obtain written payor response before initiating the billing process.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
NPP Billing Reminders
Discharge day management (99238-99239) often is delegated to qualified NPPs.3 Because this service is time-based, the final code selection is based upon the total time spent with the patient, and on the patient’s unit/floor, coordinating care prior to the patient leaving the hospital on the day of discharge. If this service is solely provided by the NPP, the NPP must report the appropriate code under his/her own name on the claim form (for eligible payors). If this service is shared with the physician, report the code representing the cumulative, documented time in both notes, provided that each note identifies the face-toface service from each provider, and his/her corresponding participation.
Many questions arise about NPPs performing the admission service because NPPs might not be given “admitting” privileges by the facility in which they practice. NPPs may provide and/or participate in services according to their state scope practice and facility-imposed guidelines. Billing policy supports state law and will reimburse any “independent” service permitted by the state. Facilities may limit NPP scope of practice by disallowing independent admission service but permittin a shared service with the physician. If this service is shared with the physician, report the code representing the cumulative, documented encounter, provided that each note identifies the face-to-face service from each provider, and his/her corresponding participation
Prior to Medicare’s elimination of consultation services (99241-99245, 99251-99255), shared/split billing rules excluded consultations from this claim-reporting model.3 Since the elimination of consults, “consultations” are reported as initial hospital care services (99221-99223).3 Therefore, consultative services can be shared by NPPs and physicians, and reported as a cumulative initial hospital service through the shared/ split billing model. Other payors still accept consultation codes and do not have a specified shared/split model. This allows for the consultative service to be reported as a cumulative NPP/physician effort under the physician name, as long as a written contractual agreement exists allowing this billing option.
References
- Centers for Medicare & Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 190-200. Centers for Medicare & Medicaid website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/bp102c15.pdf. Accessed Nov. 5, 2012.
- Aetna Inc. Aetna office links updates. Reminder: Reimbursement change for mid-level practitioners. Aetna Inc. website. Available at www.aetna.com/provider/data/OLU_MA_JUN2010_final.pdf. Accessed Nov. 6, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. Centers for Medicare & Medicaid website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan 21, 2013.
- Pohlig, C. Nonphysician Providers in Your Practice. In: Coding for Chest Medicine 2011. Northbrook, Ill.: American College of Chest Physicians, 2010.
Nurse practitioners (NPs) and physician assistants (PAs), referred to as nonphysician providers (NPPs) in billing policy, provide many different services in the hospital setting. Roles include:
- Rounding independently and following patients of varying acuity with physician supervision. The NPP may ask the physician to see the patient, as necessary, if a change in the patient’s condition arises and warrants physician evaluation.
- Providing prompt consultative
- services when the physician is not
- readily available.
- Rounding alongside the physician and expediting the work of admission services through a combined effort.
Hospitalist programs may elect one model over another, or utilize NPPs according to existing need and shifting census. Employers must be aware of state and federal regulations, facility-imposed standards of care, and billing requirements surrounding NPP services.
Medicare Enrollment and Billing Eligibility
Certified PAs and NPs may provide covered services to Medicare beneficiaries in accordance with their state scope of practice under state law and corresponding supervision/collaboration requirements. They can submit claims for these services, providing they meet enrollment qualifications.1
PAs must have:
- Graduated from a PA educational program accredited by the Accreditation Review Commission on Education for the Physician Assistant (or its predecessor agencies, the Commission on Accreditation of Allied Health Education Programs (CAAHEP) and the Committee on Allied Health Education and Accreditation (CAHEA); or
- Passed the national certification examination administered by the National Commission on Certification of Physician Assistants (NCCPA); and
- A license as a PA in the practicing state.
NPs must:
- Be a registered nurse who is authorized and licensed by the state to practice as a nurse practitioner by Dec. 31, 2000; or
- After Jan. 1, 2001, be a registered nurse who is authorized and licensed by the state to practice as an NP and be certified by a recognized national certifying body that has established standards for NPs (e.g. American Academy of Nurse Practitioners, American Nurses Credentialing Center, AACN Certification Corp., or National Board on Certification of Hospice and Palliative Nurses); and
- Possess a master’s degree in nursing.
Independent Billing
NPPs can see patients in any setting without the presence of a physician. The physician is not required to see the patient but must be available by phone or beeper in accordance with supervisory/collaborative guidelines. Physician cosignature is not required unless mandated by state law or the facility.
NPPs document and report their services according to the Centers for Medicare & Medicaid Services (CMS) Documentation Guidelines (available at www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/EMDOC.html). The NPP should be listed as the rendering provider on the claim form. Currently, insurance programs Medicare and Aetna Inc. consistently enroll and recognize NPPs as billing providers and reimburse these services at 85% of the allowable physician rate.2
Shared/Split Billing
When two providers (a physician and NPP) from the same group (direct employment or a lease arrangement contractually linking the providers) perform a service for the same patient on the same calendar day, CMS allows the combined services to be reported under a single provider’s name.
Allowable services. NPPs are only limited by the state scope of practice under state law, and the facility rules in which the NPPs practice. Services must be performed under the appropriate level of supervision or collaboration. Medicare reimburses reasonable and necessary services not otherwise excluded from coverage.
However, shared/split rules restrict the services reported under this billing model, recognizing only evaluation and management (E/M) services (and not procedures) provided in the ED, outpatient hospital clinics, or inpatient hospital (i.e. facility-based services). Shared/split rules do not involve all types of E/M services. For hospitalist programs, critical-care services (99291-99292) are excluded.3
Physician requirement. Shared/split rules require a face-to-face patient encounter by each provider on the same calendar day. There are no billing mandates requiring the NPP to see the patient before the physician does, although practice style might govern this decision.4 CMS does not specify the extent of provider involvement, but it could be established by local Medicare contractor requirements. Some contractors reference physician participation as a “substantive” service without further elaboration on specific parameters. Therefore, the physician determines the critical or key portion of his/her personal service. Minimalistic documentation can be problematic for quality or medicolegal aspects of patient care, and physicians might benefit from a more detailed notation of participation.
Documentation. Physician documentation must include an attestation that supports the physician encounter (e.g. “Patient seen and examined by me”), the individual with whom the service is shared (e.g. “Agree with note by X”), their portion of the rendered service (e.g. “Pulse oximetry 94% on room air. Audible rhonchi at bilateral lung bases. Start O2 2L nasal cannula. Obtain CXR”), the date, and a legible signature. NPP documentation should include as similar reference to the physician with whom the service is being shared for better charge capture. It alerts coders, auditors, and payor representatives to consider both notes in support of the billed service and ensures that the correct notes are sent to the payor in the event of claim denial and subsequent appeal.
Although the visit level is supported by both provider services, only one claim may be submitted for a shared/split service. The rendering provider listed on the claim can be the physician (reimbursed at 100% of the Medicare allowable physician rate) or the NPP (reimbursed at 85% of the allowable physician rate).
Non-Medicare Claims
Shared/split billing policy only applies to Medicare beneficiaries, while independent billing policy applies to Medicare and Aetna. Excessive costs prevent most other non-Medicare insurers from credentialing and enrollment NPPs. Absence of payor policy does not disqualify reimbursement for shared services, but it does require additional measures to establish recognition of NPP services and a corresponding reimbursement model.
After determining payor mix, develop a reasonable guideline for those payors who do not enroll NPPs. Delineate, in writing, a predetermined time frame for guideline implementation unless the payor can provide an alternate billing option. Some experts suggest physician groups outline the following key issues when structuring a billing option5:
- Type of NPPs involved in patient care;
- Category of services provided;
- Service location(s);
- Physician involvement;
- Mechanism for reporting services; and
- Documentation requirements.
Guidelines can be developed for any of the billing options (independent, “incident-to,” shared/split). Be sure to obtain written payor response before initiating the billing process.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
NPP Billing Reminders
Discharge day management (99238-99239) often is delegated to qualified NPPs.3 Because this service is time-based, the final code selection is based upon the total time spent with the patient, and on the patient’s unit/floor, coordinating care prior to the patient leaving the hospital on the day of discharge. If this service is solely provided by the NPP, the NPP must report the appropriate code under his/her own name on the claim form (for eligible payors). If this service is shared with the physician, report the code representing the cumulative, documented time in both notes, provided that each note identifies the face-toface service from each provider, and his/her corresponding participation.
Many questions arise about NPPs performing the admission service because NPPs might not be given “admitting” privileges by the facility in which they practice. NPPs may provide and/or participate in services according to their state scope practice and facility-imposed guidelines. Billing policy supports state law and will reimburse any “independent” service permitted by the state. Facilities may limit NPP scope of practice by disallowing independent admission service but permittin a shared service with the physician. If this service is shared with the physician, report the code representing the cumulative, documented encounter, provided that each note identifies the face-to-face service from each provider, and his/her corresponding participation
Prior to Medicare’s elimination of consultation services (99241-99245, 99251-99255), shared/split billing rules excluded consultations from this claim-reporting model.3 Since the elimination of consults, “consultations” are reported as initial hospital care services (99221-99223).3 Therefore, consultative services can be shared by NPPs and physicians, and reported as a cumulative initial hospital service through the shared/ split billing model. Other payors still accept consultation codes and do not have a specified shared/split model. This allows for the consultative service to be reported as a cumulative NPP/physician effort under the physician name, as long as a written contractual agreement exists allowing this billing option.
References
- Centers for Medicare & Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 190-200. Centers for Medicare & Medicaid website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/bp102c15.pdf. Accessed Nov. 5, 2012.
- Aetna Inc. Aetna office links updates. Reminder: Reimbursement change for mid-level practitioners. Aetna Inc. website. Available at www.aetna.com/provider/data/OLU_MA_JUN2010_final.pdf. Accessed Nov. 6, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. Centers for Medicare & Medicaid website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan 21, 2013.
- Pohlig, C. Nonphysician Providers in Your Practice. In: Coding for Chest Medicine 2011. Northbrook, Ill.: American College of Chest Physicians, 2010.
Affordable Care Act Provides Two-Year Increase in Medicaid Payments for Primary-Care Services
Some hospitalist groups can expect a bump in total revenue over the next two years, thanks to the Medicaid-to-Medicare parity regulation that was included in the Affordable Care Act. But whether the increase in reimbursement lasts beyond 2014 is anyone’s guess.
The regulation, which the Centers for Medicare & Medicaid Services (CMS) released in November and made effective Jan. 1, increases Medicaid payments for certain primary-care services to 100% of Medicare levels this year and next. States will receive an estimated $11 billion over the next two years to fund the program, according to the American Academy of Family Physicians (AAFP). Eligible providers include physicians, physician assistants (PAs), and nurse practitioners (NPs), who self-attest they are board-certified in family, pediatric, or general internal medicine; it also includes those doctors, PAs, or NPs who self-attest that at least 60% of all Medicaid services they bill or provide in a managed-care environment are for specific evaluation and management (E&M) and vaccine administration codes.1
The concept is to boost Medicaid participation by improving historically lagging reimbursement rates.2 To wit, CMS’ Office of the Actuary estimates the parity rule will add more than 10,000 new primary-care physicians (PCPs) to the Medicaid participation ranks.3
SHM Public Policy Committee member Brad Flansbaum, DO, MPH, SFHM, says that hospitalists who deal with Medicaid populations can expect at least some increase in their revenue over the next two years. For example, he says, take an HM group earning $100,000 a year in Medicaid revenue. Now consider Urban Institute figures that show, in 2012, Medicaid physician fees on average were 66% of Medicare physician fees (with wide state variations). The parity rule now pays that hypothetical HM group about $150,000.
“It’s simple math,” Dr. Flansbaum says. “I would emphasize that the bump in pay is going to be proportional to the percentage of Medicaid patients that you see. There are some doctors who see an awful lot of Medicaid patients in safety-net and public hospitals, and that money, when it comes back to departments and divisions, can be used for things that a lot of these places never had the means to do before. It could be salary, but it could also mean hiring more people, more resources. It makes a difference.”
Public Policy Committee chair Ron Greeno, MD, FCCP, MHM, says SHM advocated for the parity regulation, as Medicaid has historically paid for only about 70% of the healthcare delivered to patients. Although the parity issue has not gathered as much attention as other facets of the healthcare reform movement, having CMS recognize that delivery of primary care is not restricted to traditional offices is one he and SHM are particularly proud of.
“This is a correction long in coming,” Dr. Greeno says. “We’re happy hospitalists were included in the group of people that will achieve that parity.”

Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City, says few physicians are even aware of the provision, in part because of a widespread frustration with Medicaid’s historic reimbursements rates.
“It’s almost a foregone conclusion that Medicaid never pays, reimbursement always goes down, and the interactions with Medicaid are always increasingly difficult,” Dr. Flansbaum adds.
The question for physicians and policy wonks now is what happens to the parity regulation after its scheduled expiration Dec. 31, 2014. Several medical societies, including SHM and the American College of Physicians (ACP), lobbied Congress to make sure the parity regulation was not impacted by the “fiscal cliff” negotiations. The next step is to craft a permanent funding source to pay for it.
“Unless Congress acts to permanently extend and fund this provision, a sudden return to disparate and inadequate payment for primary services needed by Medicaid patients after only two years will again threaten to restrict their access to such needed services,” AAFP said in a statement after the rule was implemented. “It would once again shut out people who have come to know and depend on their primary care physicians. Only by extending Medicaid parity with Medicare can we ensure that these Americans continue to have uninterrupted medical care in the future.”

—Brad Flansbaum, DO, MPH, SFHM, Lenox Hill Hospital, New York City, SHM Public Policy Committee member
SHM recommended that CMS work with the states to facilitate timely data collection designed to determine the effects on the quality and efficiency of care being received under Medicaid as a result of the enhanced fees. CMS agreed with this recommendation and the resulting data, hopefully, will make the case for continuing the enhanced payment following 2014.
Dr. Flansbaum says SHM’s policy team will continue to work on the issue, but given the precarious state of federal budgets and political dysfunction in Washington, it’s too early to know whether a funding source will be identified to pay for parity in 2015 and beyond—especially as politicians have yet to craft long-term solutions to issues including the sustainable-growth rate formula and other specialists, including radiologists and obstetricians, lobby to be eligible for the parity pay. However, he is hopeful that physicians who see the added impact of parity pay in the next two years will lobby Congress to find a way to continue the higher reimbursement.
“I can’t tell you whether or not when you put on the scale of all the priorities whether it’s going to be a new Air Force bomber, another $50 billion into Medicare for physicians, or an educational system upgrade,” he says. “I don’t know where the government is going to assign its priorities. Will the money be there to extend both the two-year Medicaid and the reprieve? And if the answer is yes, will it be extended to other providers beyond just primary-care practitioners? It’s anyone’s guess.”
Richard Quinn is a freelance writer in New Jersey.
References
- FAQ: Medicaid/Medicare Parity Regulation. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Images/Advocacy_Image/pdf/Parity_FAQ_Final.pdf. Accessed Jan. 27, 2013.
- Centers for Medicare & Medicaid Services. Medicaid program; payments for services furnished by certain primary care physicians and charges for vaccine administration under the Vaccines for Children program. Federal Register website. Available at: http://www.gpo.gov/fdsys/pkg/FR-2012-11-06/pdf/2012-26507.pdf. Accessed Jan. 15, 2013.
- Bindman A. JAMA Forum: Warning: Dangerous physician payment cliffs ahead. Journal of the American Medical Association website. Available at: http://newsatjama.jama.com/2013/01/10/jama-forum-warning-dangerous-physician-payment-cliffs-ahead/.Accessed Jan. 15, 2013.
Some hospitalist groups can expect a bump in total revenue over the next two years, thanks to the Medicaid-to-Medicare parity regulation that was included in the Affordable Care Act. But whether the increase in reimbursement lasts beyond 2014 is anyone’s guess.
The regulation, which the Centers for Medicare & Medicaid Services (CMS) released in November and made effective Jan. 1, increases Medicaid payments for certain primary-care services to 100% of Medicare levels this year and next. States will receive an estimated $11 billion over the next two years to fund the program, according to the American Academy of Family Physicians (AAFP). Eligible providers include physicians, physician assistants (PAs), and nurse practitioners (NPs), who self-attest they are board-certified in family, pediatric, or general internal medicine; it also includes those doctors, PAs, or NPs who self-attest that at least 60% of all Medicaid services they bill or provide in a managed-care environment are for specific evaluation and management (E&M) and vaccine administration codes.1
The concept is to boost Medicaid participation by improving historically lagging reimbursement rates.2 To wit, CMS’ Office of the Actuary estimates the parity rule will add more than 10,000 new primary-care physicians (PCPs) to the Medicaid participation ranks.3
SHM Public Policy Committee member Brad Flansbaum, DO, MPH, SFHM, says that hospitalists who deal with Medicaid populations can expect at least some increase in their revenue over the next two years. For example, he says, take an HM group earning $100,000 a year in Medicaid revenue. Now consider Urban Institute figures that show, in 2012, Medicaid physician fees on average were 66% of Medicare physician fees (with wide state variations). The parity rule now pays that hypothetical HM group about $150,000.
“It’s simple math,” Dr. Flansbaum says. “I would emphasize that the bump in pay is going to be proportional to the percentage of Medicaid patients that you see. There are some doctors who see an awful lot of Medicaid patients in safety-net and public hospitals, and that money, when it comes back to departments and divisions, can be used for things that a lot of these places never had the means to do before. It could be salary, but it could also mean hiring more people, more resources. It makes a difference.”
Public Policy Committee chair Ron Greeno, MD, FCCP, MHM, says SHM advocated for the parity regulation, as Medicaid has historically paid for only about 70% of the healthcare delivered to patients. Although the parity issue has not gathered as much attention as other facets of the healthcare reform movement, having CMS recognize that delivery of primary care is not restricted to traditional offices is one he and SHM are particularly proud of.
“This is a correction long in coming,” Dr. Greeno says. “We’re happy hospitalists were included in the group of people that will achieve that parity.”
Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City, says few physicians are even aware of the provision, in part because of a widespread frustration with Medicaid’s historic reimbursements rates.
“It’s almost a foregone conclusion that Medicaid never pays, reimbursement always goes down, and the interactions with Medicaid are always increasingly difficult,” Dr. Flansbaum adds.
The question for physicians and policy wonks now is what happens to the parity regulation after its scheduled expiration Dec. 31, 2014. Several medical societies, including SHM and the American College of Physicians (ACP), lobbied Congress to make sure the parity regulation was not impacted by the “fiscal cliff” negotiations. The next step is to craft a permanent funding source to pay for it.
“Unless Congress acts to permanently extend and fund this provision, a sudden return to disparate and inadequate payment for primary services needed by Medicaid patients after only two years will again threaten to restrict their access to such needed services,” AAFP said in a statement after the rule was implemented. “It would once again shut out people who have come to know and depend on their primary care physicians. Only by extending Medicaid parity with Medicare can we ensure that these Americans continue to have uninterrupted medical care in the future.”
—Brad Flansbaum, DO, MPH, SFHM, Lenox Hill Hospital, New York City, SHM Public Policy Committee member
SHM recommended that CMS work with the states to facilitate timely data collection designed to determine the effects on the quality and efficiency of care being received under Medicaid as a result of the enhanced fees. CMS agreed with this recommendation and the resulting data, hopefully, will make the case for continuing the enhanced payment following 2014.
Dr. Flansbaum says SHM’s policy team will continue to work on the issue, but given the precarious state of federal budgets and political dysfunction in Washington, it’s too early to know whether a funding source will be identified to pay for parity in 2015 and beyond—especially as politicians have yet to craft long-term solutions to issues including the sustainable-growth rate formula and other specialists, including radiologists and obstetricians, lobby to be eligible for the parity pay. However, he is hopeful that physicians who see the added impact of parity pay in the next two years will lobby Congress to find a way to continue the higher reimbursement.
“I can’t tell you whether or not when you put on the scale of all the priorities whether it’s going to be a new Air Force bomber, another $50 billion into Medicare for physicians, or an educational system upgrade,” he says. “I don’t know where the government is going to assign its priorities. Will the money be there to extend both the two-year Medicaid and the reprieve? And if the answer is yes, will it be extended to other providers beyond just primary-care practitioners? It’s anyone’s guess.”
Richard Quinn is a freelance writer in New Jersey.
References
- FAQ: Medicaid/Medicare Parity Regulation. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Images/Advocacy_Image/pdf/Parity_FAQ_Final.pdf. Accessed Jan. 27, 2013.
- Centers for Medicare & Medicaid Services. Medicaid program; payments for services furnished by certain primary care physicians and charges for vaccine administration under the Vaccines for Children program. Federal Register website. Available at: http://www.gpo.gov/fdsys/pkg/FR-2012-11-06/pdf/2012-26507.pdf. Accessed Jan. 15, 2013.
- Bindman A. JAMA Forum: Warning: Dangerous physician payment cliffs ahead. Journal of the American Medical Association website. Available at: http://newsatjama.jama.com/2013/01/10/jama-forum-warning-dangerous-physician-payment-cliffs-ahead/.Accessed Jan. 15, 2013.
Some hospitalist groups can expect a bump in total revenue over the next two years, thanks to the Medicaid-to-Medicare parity regulation that was included in the Affordable Care Act. But whether the increase in reimbursement lasts beyond 2014 is anyone’s guess.
The regulation, which the Centers for Medicare & Medicaid Services (CMS) released in November and made effective Jan. 1, increases Medicaid payments for certain primary-care services to 100% of Medicare levels this year and next. States will receive an estimated $11 billion over the next two years to fund the program, according to the American Academy of Family Physicians (AAFP). Eligible providers include physicians, physician assistants (PAs), and nurse practitioners (NPs), who self-attest they are board-certified in family, pediatric, or general internal medicine; it also includes those doctors, PAs, or NPs who self-attest that at least 60% of all Medicaid services they bill or provide in a managed-care environment are for specific evaluation and management (E&M) and vaccine administration codes.1
The concept is to boost Medicaid participation by improving historically lagging reimbursement rates.2 To wit, CMS’ Office of the Actuary estimates the parity rule will add more than 10,000 new primary-care physicians (PCPs) to the Medicaid participation ranks.3
SHM Public Policy Committee member Brad Flansbaum, DO, MPH, SFHM, says that hospitalists who deal with Medicaid populations can expect at least some increase in their revenue over the next two years. For example, he says, take an HM group earning $100,000 a year in Medicaid revenue. Now consider Urban Institute figures that show, in 2012, Medicaid physician fees on average were 66% of Medicare physician fees (with wide state variations). The parity rule now pays that hypothetical HM group about $150,000.
“It’s simple math,” Dr. Flansbaum says. “I would emphasize that the bump in pay is going to be proportional to the percentage of Medicaid patients that you see. There are some doctors who see an awful lot of Medicaid patients in safety-net and public hospitals, and that money, when it comes back to departments and divisions, can be used for things that a lot of these places never had the means to do before. It could be salary, but it could also mean hiring more people, more resources. It makes a difference.”
Public Policy Committee chair Ron Greeno, MD, FCCP, MHM, says SHM advocated for the parity regulation, as Medicaid has historically paid for only about 70% of the healthcare delivered to patients. Although the parity issue has not gathered as much attention as other facets of the healthcare reform movement, having CMS recognize that delivery of primary care is not restricted to traditional offices is one he and SHM are particularly proud of.
“This is a correction long in coming,” Dr. Greeno says. “We’re happy hospitalists were included in the group of people that will achieve that parity.”
Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City, says few physicians are even aware of the provision, in part because of a widespread frustration with Medicaid’s historic reimbursements rates.
“It’s almost a foregone conclusion that Medicaid never pays, reimbursement always goes down, and the interactions with Medicaid are always increasingly difficult,” Dr. Flansbaum adds.
The question for physicians and policy wonks now is what happens to the parity regulation after its scheduled expiration Dec. 31, 2014. Several medical societies, including SHM and the American College of Physicians (ACP), lobbied Congress to make sure the parity regulation was not impacted by the “fiscal cliff” negotiations. The next step is to craft a permanent funding source to pay for it.
“Unless Congress acts to permanently extend and fund this provision, a sudden return to disparate and inadequate payment for primary services needed by Medicaid patients after only two years will again threaten to restrict their access to such needed services,” AAFP said in a statement after the rule was implemented. “It would once again shut out people who have come to know and depend on their primary care physicians. Only by extending Medicaid parity with Medicare can we ensure that these Americans continue to have uninterrupted medical care in the future.”
—Brad Flansbaum, DO, MPH, SFHM, Lenox Hill Hospital, New York City, SHM Public Policy Committee member
SHM recommended that CMS work with the states to facilitate timely data collection designed to determine the effects on the quality and efficiency of care being received under Medicaid as a result of the enhanced fees. CMS agreed with this recommendation and the resulting data, hopefully, will make the case for continuing the enhanced payment following 2014.
Dr. Flansbaum says SHM’s policy team will continue to work on the issue, but given the precarious state of federal budgets and political dysfunction in Washington, it’s too early to know whether a funding source will be identified to pay for parity in 2015 and beyond—especially as politicians have yet to craft long-term solutions to issues including the sustainable-growth rate formula and other specialists, including radiologists and obstetricians, lobby to be eligible for the parity pay. However, he is hopeful that physicians who see the added impact of parity pay in the next two years will lobby Congress to find a way to continue the higher reimbursement.
“I can’t tell you whether or not when you put on the scale of all the priorities whether it’s going to be a new Air Force bomber, another $50 billion into Medicare for physicians, or an educational system upgrade,” he says. “I don’t know where the government is going to assign its priorities. Will the money be there to extend both the two-year Medicaid and the reprieve? And if the answer is yes, will it be extended to other providers beyond just primary-care practitioners? It’s anyone’s guess.”
Richard Quinn is a freelance writer in New Jersey.
References
- FAQ: Medicaid/Medicare Parity Regulation. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Images/Advocacy_Image/pdf/Parity_FAQ_Final.pdf. Accessed Jan. 27, 2013.
- Centers for Medicare & Medicaid Services. Medicaid program; payments for services furnished by certain primary care physicians and charges for vaccine administration under the Vaccines for Children program. Federal Register website. Available at: http://www.gpo.gov/fdsys/pkg/FR-2012-11-06/pdf/2012-26507.pdf. Accessed Jan. 15, 2013.
- Bindman A. JAMA Forum: Warning: Dangerous physician payment cliffs ahead. Journal of the American Medical Association website. Available at: http://newsatjama.jama.com/2013/01/10/jama-forum-warning-dangerous-physician-payment-cliffs-ahead/.Accessed Jan. 15, 2013.