User login
The Hospitalist only
Converse Like a Leader
Communication is an integral part of a hospitalist’s job: from admission interviews to conveying orders to nursing staff, communicating clearly and precisely is part of numerous best practices. When a hospitalist assumes a leadership role, however, the types and styles of communication change. A committee chair or department head must be aware of the messages they send—both literally and in the most general sense of the term. This transition to leadership can be tough.
“Physician communication is focused on clinical outcome. That’s easy for someone trained in medicine. But in leadership communication, there may not be a defined outcome,” says Timothy J. Keogh, PhD, assistant professor at The Citadel School of Business Administration in Charleston, S.C. “That’s a difficult switch from clinician to leader; maybe half of the problems a leader faces can’t be solved.”
Dr. Keogh and William F. Martin, PsyD, MPH, summarized their research data in “Managing Medical Groups: 21st Century Challenges and the Impact of Physician Leadership Styles,” published in the September-October 2004 issue of Journal of Medical Practice Management.
The Basics
The most basic communication skill a hospitalist leader should practice, according to Dr. Keogh, is “being less direct than [he or she] would like to be.” Dr. Keogh, who teaches communication skills as part of SHM’s Leadership Academy, says, “Data shows that physicians prefer to be more precise and cover topics quickly. In a leadership role, the initial part of the communication or conversation needs to be chattier. Some physicians believe that this uses up too much time, but, in fact, it doesn’t take that long and it’s a necessary step.” Acknowledge others’ need for connection by making eye contact, pausing, and exchanging quick pleasantries. “Leaders need to be able to say things in passing, greet people, et cetera,” Dr. Keogh stresses.
But what about in-depth communication?
Management Topics
If you supervise hospitalists, you can condense discussions of your expectations—at least compared with managers in business fields. “Physicians are skilled, well-trained individuals, so you don’t have to do so much of this,” Dr. Keogh says. “They have an internal sense of quality and you don’t really need to motivate them. It’s a matter of adjusting the edges.”
A hospitalist supervisor might need to address a situation in which a physician on the team has been disruptive or needs a disciplinary talk. In these instances, Dr. Keogh says, “The leader has to somehow collect data on what the hospitalist has displayed that doesn’t fit in with teamwork. The hard part is that the data is likely to be hearsay—what was said by whom, when. That’s management.”
For example, you might receive complaints from nursing staff of abrupt or rude behavior from a hospitalist. “Physicians may not think of this as data, but it is. What someone said or did, or gestured,” Dr. Keogh points out. “You have to be able to say, ‘Here’s what we know happened on this date. Help me understand what happened, because we have to change this. This behavior is not acceptable.’”
The key to all official management communication is to carefully consider how to frame the conversation and keep it flowing for both parties: Speak with hospitalists, not to them. Here is an example: “In a performance appraisal, one suggestion we make is to have a conversation about data,” Dr. Keogh explains. “Look at some numbers on quality assurance, patient load, or whatever you’re discussing. Do your homework and allow the other person to have a look at the data before you sit down with them. That’s a sign of respect.”
Styles of Communication
Dr. Keogh’s training for physician executives—including what he teaches at the Leadership Academy—is based on the personality profile system developed by Carlson Learning Company (now Inscape Publishing).1 The DiSC model outlines behavior or characteristic leadership preferences in four dimensions:
- Dominance (D): People who score high in this category have behavioral characteristics that include being motivated by control over tasks and work environment, directing others, and achieving specific stretch goals. In general, physician managers who score high on dominance tend to be results-focused, fast-paced, and value autonomy.
- Influence (I): People who score high in this category are motivated by interacting with others, giving and receiving immediate feedback, and acknowledging emotions as well as facts.
- Steadiness (S): People who score high in this category are motivated by job security, predictability, and clearly defined expectations.
- Conscientiousness (C): People who score high in this category are motivated by needing to be right, working alone, and preferring to work on tasks rather than dealing with people.
“This model provides groundwork for seeing that other people have different ways, different preferences of communicating,” Dr. Keogh says. In his own research, he says, he has found “nearly half of all physicians are some combination of time-sensitive and perfectionist,” meaning they fit the dominance style.
The trick to effective communication is learning to modify your style when necessary. Task-focused individuals must practice taking a minute for a greeting or a pleasantry, even if it initially goes against their routine. “Someone who is extremely outgoing and open can have trouble, too,” Dr. Keogh points out. “You can’t start a conversation with a lot of chit-chat, if you’re addressing someone who is direct. … That won’t work, either.”
The solution is to practice stepping outside of your normal communication style. “You can learn how to adjust your style, how to flex to others’ styles,” Dr. Keogh says. “Depending on whom you’re communicating with, you can mirror the style of the other person.” This helps to ensure that what you’re saying is received and understood.
Practicing new ways to communicate means making a fundamental shift in your behavior. It sounds difficult, but Dr. Keogh promises it’s not.
“The transition is not as hard as you think, because hospitalists have been trained to do patient interviews,” he says. “They’re skilled at observation and listening. In the transition to leadership, they sometimes forget that they have these skills and can use these to be a great leader.”” TH
Jane Jerrard is a medical writer based in Chicago. She also writes “Public Policy” for The Hospitalist.
Reference
1. Straw J. The 4-Dimensional Manager: DiSC Strategies for Managing Different People in the Best Ways. San Francisco: Berrett-Koehler Publishers, Inc.; 2002.
Communication is an integral part of a hospitalist’s job: from admission interviews to conveying orders to nursing staff, communicating clearly and precisely is part of numerous best practices. When a hospitalist assumes a leadership role, however, the types and styles of communication change. A committee chair or department head must be aware of the messages they send—both literally and in the most general sense of the term. This transition to leadership can be tough.
“Physician communication is focused on clinical outcome. That’s easy for someone trained in medicine. But in leadership communication, there may not be a defined outcome,” says Timothy J. Keogh, PhD, assistant professor at The Citadel School of Business Administration in Charleston, S.C. “That’s a difficult switch from clinician to leader; maybe half of the problems a leader faces can’t be solved.”
Dr. Keogh and William F. Martin, PsyD, MPH, summarized their research data in “Managing Medical Groups: 21st Century Challenges and the Impact of Physician Leadership Styles,” published in the September-October 2004 issue of Journal of Medical Practice Management.
The Basics
The most basic communication skill a hospitalist leader should practice, according to Dr. Keogh, is “being less direct than [he or she] would like to be.” Dr. Keogh, who teaches communication skills as part of SHM’s Leadership Academy, says, “Data shows that physicians prefer to be more precise and cover topics quickly. In a leadership role, the initial part of the communication or conversation needs to be chattier. Some physicians believe that this uses up too much time, but, in fact, it doesn’t take that long and it’s a necessary step.” Acknowledge others’ need for connection by making eye contact, pausing, and exchanging quick pleasantries. “Leaders need to be able to say things in passing, greet people, et cetera,” Dr. Keogh stresses.
But what about in-depth communication?
Management Topics
If you supervise hospitalists, you can condense discussions of your expectations—at least compared with managers in business fields. “Physicians are skilled, well-trained individuals, so you don’t have to do so much of this,” Dr. Keogh says. “They have an internal sense of quality and you don’t really need to motivate them. It’s a matter of adjusting the edges.”
A hospitalist supervisor might need to address a situation in which a physician on the team has been disruptive or needs a disciplinary talk. In these instances, Dr. Keogh says, “The leader has to somehow collect data on what the hospitalist has displayed that doesn’t fit in with teamwork. The hard part is that the data is likely to be hearsay—what was said by whom, when. That’s management.”
For example, you might receive complaints from nursing staff of abrupt or rude behavior from a hospitalist. “Physicians may not think of this as data, but it is. What someone said or did, or gestured,” Dr. Keogh points out. “You have to be able to say, ‘Here’s what we know happened on this date. Help me understand what happened, because we have to change this. This behavior is not acceptable.’”
The key to all official management communication is to carefully consider how to frame the conversation and keep it flowing for both parties: Speak with hospitalists, not to them. Here is an example: “In a performance appraisal, one suggestion we make is to have a conversation about data,” Dr. Keogh explains. “Look at some numbers on quality assurance, patient load, or whatever you’re discussing. Do your homework and allow the other person to have a look at the data before you sit down with them. That’s a sign of respect.”
Styles of Communication
Dr. Keogh’s training for physician executives—including what he teaches at the Leadership Academy—is based on the personality profile system developed by Carlson Learning Company (now Inscape Publishing).1 The DiSC model outlines behavior or characteristic leadership preferences in four dimensions:
- Dominance (D): People who score high in this category have behavioral characteristics that include being motivated by control over tasks and work environment, directing others, and achieving specific stretch goals. In general, physician managers who score high on dominance tend to be results-focused, fast-paced, and value autonomy.
- Influence (I): People who score high in this category are motivated by interacting with others, giving and receiving immediate feedback, and acknowledging emotions as well as facts.
- Steadiness (S): People who score high in this category are motivated by job security, predictability, and clearly defined expectations.
- Conscientiousness (C): People who score high in this category are motivated by needing to be right, working alone, and preferring to work on tasks rather than dealing with people.
“This model provides groundwork for seeing that other people have different ways, different preferences of communicating,” Dr. Keogh says. In his own research, he says, he has found “nearly half of all physicians are some combination of time-sensitive and perfectionist,” meaning they fit the dominance style.
The trick to effective communication is learning to modify your style when necessary. Task-focused individuals must practice taking a minute for a greeting or a pleasantry, even if it initially goes against their routine. “Someone who is extremely outgoing and open can have trouble, too,” Dr. Keogh points out. “You can’t start a conversation with a lot of chit-chat, if you’re addressing someone who is direct. … That won’t work, either.”
The solution is to practice stepping outside of your normal communication style. “You can learn how to adjust your style, how to flex to others’ styles,” Dr. Keogh says. “Depending on whom you’re communicating with, you can mirror the style of the other person.” This helps to ensure that what you’re saying is received and understood.
Practicing new ways to communicate means making a fundamental shift in your behavior. It sounds difficult, but Dr. Keogh promises it’s not.
“The transition is not as hard as you think, because hospitalists have been trained to do patient interviews,” he says. “They’re skilled at observation and listening. In the transition to leadership, they sometimes forget that they have these skills and can use these to be a great leader.”” TH
Jane Jerrard is a medical writer based in Chicago. She also writes “Public Policy” for The Hospitalist.
Reference
1. Straw J. The 4-Dimensional Manager: DiSC Strategies for Managing Different People in the Best Ways. San Francisco: Berrett-Koehler Publishers, Inc.; 2002.
Communication is an integral part of a hospitalist’s job: from admission interviews to conveying orders to nursing staff, communicating clearly and precisely is part of numerous best practices. When a hospitalist assumes a leadership role, however, the types and styles of communication change. A committee chair or department head must be aware of the messages they send—both literally and in the most general sense of the term. This transition to leadership can be tough.
“Physician communication is focused on clinical outcome. That’s easy for someone trained in medicine. But in leadership communication, there may not be a defined outcome,” says Timothy J. Keogh, PhD, assistant professor at The Citadel School of Business Administration in Charleston, S.C. “That’s a difficult switch from clinician to leader; maybe half of the problems a leader faces can’t be solved.”
Dr. Keogh and William F. Martin, PsyD, MPH, summarized their research data in “Managing Medical Groups: 21st Century Challenges and the Impact of Physician Leadership Styles,” published in the September-October 2004 issue of Journal of Medical Practice Management.
The Basics
The most basic communication skill a hospitalist leader should practice, according to Dr. Keogh, is “being less direct than [he or she] would like to be.” Dr. Keogh, who teaches communication skills as part of SHM’s Leadership Academy, says, “Data shows that physicians prefer to be more precise and cover topics quickly. In a leadership role, the initial part of the communication or conversation needs to be chattier. Some physicians believe that this uses up too much time, but, in fact, it doesn’t take that long and it’s a necessary step.” Acknowledge others’ need for connection by making eye contact, pausing, and exchanging quick pleasantries. “Leaders need to be able to say things in passing, greet people, et cetera,” Dr. Keogh stresses.
But what about in-depth communication?
Management Topics
If you supervise hospitalists, you can condense discussions of your expectations—at least compared with managers in business fields. “Physicians are skilled, well-trained individuals, so you don’t have to do so much of this,” Dr. Keogh says. “They have an internal sense of quality and you don’t really need to motivate them. It’s a matter of adjusting the edges.”
A hospitalist supervisor might need to address a situation in which a physician on the team has been disruptive or needs a disciplinary talk. In these instances, Dr. Keogh says, “The leader has to somehow collect data on what the hospitalist has displayed that doesn’t fit in with teamwork. The hard part is that the data is likely to be hearsay—what was said by whom, when. That’s management.”
For example, you might receive complaints from nursing staff of abrupt or rude behavior from a hospitalist. “Physicians may not think of this as data, but it is. What someone said or did, or gestured,” Dr. Keogh points out. “You have to be able to say, ‘Here’s what we know happened on this date. Help me understand what happened, because we have to change this. This behavior is not acceptable.’”
The key to all official management communication is to carefully consider how to frame the conversation and keep it flowing for both parties: Speak with hospitalists, not to them. Here is an example: “In a performance appraisal, one suggestion we make is to have a conversation about data,” Dr. Keogh explains. “Look at some numbers on quality assurance, patient load, or whatever you’re discussing. Do your homework and allow the other person to have a look at the data before you sit down with them. That’s a sign of respect.”
Styles of Communication
Dr. Keogh’s training for physician executives—including what he teaches at the Leadership Academy—is based on the personality profile system developed by Carlson Learning Company (now Inscape Publishing).1 The DiSC model outlines behavior or characteristic leadership preferences in four dimensions:
- Dominance (D): People who score high in this category have behavioral characteristics that include being motivated by control over tasks and work environment, directing others, and achieving specific stretch goals. In general, physician managers who score high on dominance tend to be results-focused, fast-paced, and value autonomy.
- Influence (I): People who score high in this category are motivated by interacting with others, giving and receiving immediate feedback, and acknowledging emotions as well as facts.
- Steadiness (S): People who score high in this category are motivated by job security, predictability, and clearly defined expectations.
- Conscientiousness (C): People who score high in this category are motivated by needing to be right, working alone, and preferring to work on tasks rather than dealing with people.
“This model provides groundwork for seeing that other people have different ways, different preferences of communicating,” Dr. Keogh says. In his own research, he says, he has found “nearly half of all physicians are some combination of time-sensitive and perfectionist,” meaning they fit the dominance style.
The trick to effective communication is learning to modify your style when necessary. Task-focused individuals must practice taking a minute for a greeting or a pleasantry, even if it initially goes against their routine. “Someone who is extremely outgoing and open can have trouble, too,” Dr. Keogh points out. “You can’t start a conversation with a lot of chit-chat, if you’re addressing someone who is direct. … That won’t work, either.”
The solution is to practice stepping outside of your normal communication style. “You can learn how to adjust your style, how to flex to others’ styles,” Dr. Keogh says. “Depending on whom you’re communicating with, you can mirror the style of the other person.” This helps to ensure that what you’re saying is received and understood.
Practicing new ways to communicate means making a fundamental shift in your behavior. It sounds difficult, but Dr. Keogh promises it’s not.
“The transition is not as hard as you think, because hospitalists have been trained to do patient interviews,” he says. “They’re skilled at observation and listening. In the transition to leadership, they sometimes forget that they have these skills and can use these to be a great leader.”” TH
Jane Jerrard is a medical writer based in Chicago. She also writes “Public Policy” for The Hospitalist.
Reference
1. Straw J. The 4-Dimensional Manager: DiSC Strategies for Managing Different People in the Best Ways. San Francisco: Berrett-Koehler Publishers, Inc.; 2002.
Never-Event Implications
The Center for Medicare and Medicaid Services (CMS) recently announced federal payor programs no longer reimburses for medical services rendered to treat certain complications of care. Although CMS chose the majority of these complications because they are “reasonably preventable by following evidence-based guidelines,” the national media and patient advocacy groups have adopted the term “never events” to describe them.
Aside from the payment implications, CMS’ new policy affects the liability risk of any person providing inpatient care, regardless of whether a federal payor is involved.
In its press release announcing the new payment policy, CMS stated, “when you enter the hospital for treatment of one medical problem, you don’t expect to leave with additional injuries, infections, or serious conditions that occur during the course of your stay.” Recognizing “some of these complications may not be avoidable,” CMS found “too often patients suffer from injuries or illnesses that could have been prevented if the hospital had taken proper precautions.”
Consequently, “as part of its commitment to improve the quality of care [patients] receive during a hospital stay,” CMS policy is targeted at reducing “hospital-acquired conditions like certain infections, advanced bed sores, or fractures;” and “preventable medical errors, like performing surgery on the wrong side of the body, that should never happen.”
The list of “never events” covered under the CMS payment policy can be organized into three categories: surgical events, medical products and devices, and case management. The following breaks down each category:
Case Management
- Stage III and Stage IV pressure ulcers;
- Air embolism;
- Manifestations of poor control of blood sugar levels; and
- Fracture, burns, joint dislocations, and other injuries occurring from falls or other trauma suffered while an inpatient.
Surgical Events
- Surgery on wrong body part;
- Surgery on the wrong patient;
- Wrong surgery on a patient;
- Retention of a foreign object, such as a sponge or needle, inadvertently left in a patient after surgery;
- Surgical site infection following a coronary artery bypass graft;
- Surgical site infection following bariatric surgery;
- Surgical site infection following certain orthopedic procedures; and
- Deep vein thrombosis or pulmonary embolism following certain orthopedic procedures.
Medical Products and Devices
- Transfusion of wrong blood type;
- Catheter associated urinary tract infection; and
- Vascular catheter associated infections.
It’s easy to see why some of the complications made the list. Wrong-side surgery or surgery on the wrong patient are the quintessential cases where liability is generally uncontested. There is not much one can do to satisfactorily explain to a patient, or a jury, why a surgeon and surgical team operated on the wrong body part.
In other cases, however, such as fatal pulmonary embolus, death can occur even when a patient has been appropriately managed. In fact, medical literature demonstrates a small percentage of patients will develop deep vein thrombosis or pulmonary embolus even after having received therapeutic doses of heparin.
Reasonable Expectations
In any case involving a “never event,” we expect plaintiffs’ attorneys to argue CMS’ reimbursement determination is tantamount to a finding of substandard care. In other words, plaintiffs’ attorneys will argue a physician acted negligently simply because the patient incurred one of the proscribed complications. It’s a compelling argument because the federal government has essentially concluded these complications do not occur if physicians and hospitals pay attention while providing care.
You may have heard the Latin phrase res ipsa loquitur; it translates to “the thing speaks for itself.” Legally, res ipsa loquitur states a rule of law where a jury must presume a defendant was negligent when a certain type of injury occurs. The burden then shifts to the defendant to prove the injury occurred in the absence of negligence. The res ipsa rule originated in 1863 when a plaintiff was struck by a barrel of flour falling from a second-story window. The barrel caused the judge hearing the case to remark, “It is the duty of persons who keep barrels in a warehouse to take care that they do not roll out, and I think that such a case would, beyond all doubt, afford prima facie evidence of negligence. A barrel could not roll out of a warehouse without some negligence. … [I]f there are any facts inconsistent with negligence, it is for the defendant to prove them.” Thus, res ipsa is grounded in the notion everyone knows barrels aren’t supposed to fall from second-floor windows.
Traditionally, res ipsa applied only in a small class of medical malpractice cases, such as retained objects following surgery. In such cases, jurors are just as capable as medical professionals in understanding someone was negligent. For example, it does not take expert testimony to establish there has been negligence when a surgical instrument is left in a patient. There’s simply no compelling medical reason for a surgeon to leave an instrument in a patient’s abdomen.
In contrast, res ipsa generally has not applied in cases involving pulmonary embolus because the process of thromboembolic disease is beyond the average juror’s understanding and death by pulmonary embolus would not give rise to a presumption of negligence.
Where res ipsa applies, it’s a powerful concept. If res ipsa were found to apply to pulmonary embolus cases, the jury would be instructed it is the duty of a physician caring for a post-surgical patient to take care that the patient does not develop pulmonary embolus. Thus, a jury would begin with the presumption a patient would not develop pulmonary embolus absent negligence. The physician would then be left with the burden to prove otherwise. Given such a charge, it is foreseeable a jury could return a verdict against a physician, even if the physician managed the patient’s care appropriately and ordered appropriate prophylaxis.
Take Extra Precaution
To prevent CMS' reimbursement decisions from becoming the functional equivalent of a res ipsa instruction, physicians need to raise the level of precaution they employ against “never event” complications. At the heart of CMS' decision is its statement “never event” complications are “reasonably preventable by following evidence-based guidelines.” When a condition is only “reasonably preventable,” instead of “absolutely preventable,” a defense lawyer retains the ability to argue some patients will develop the condition even when the care was entirely appropriate.
We believe most jurors understand the inherent difficulties of caring for sick patients, and the risks that exist every time a patient undergoes a surgical procedure. The defense lawyer’s challenge is convincing a jury the patient received appropriate care, notwithstanding the complication.
Because CMS refers to “evidence-based guidelines,” physicians must know and follow the guidelines. The first step is becoming familiar with the complications CMS will deny reimbursement, and then regularly review the available guidelines to identify practices to reduce or eliminate the complication. Re-evaluate and update your practice whenever new information becomes available.
A consistent cycle of evaluating and responding to complications will afford the defense lawyer the ability to argue the physician and hospital complied with “evidence-based guidelines” and the patient’s case represents one of the unfortunate incidents where a patient suffers a complication despite receiving the highest-level of care.
In our experience, many providers initially create good systems, but run into trouble in the follow up. Make sure you respond to new or additional information or methods of practice. Without this follow up, CMS’ reimbursement decisions have the potential to create malpractice liabilities for all inpatient providers. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, University of Colorado Denver.
The Center for Medicare and Medicaid Services (CMS) recently announced federal payor programs no longer reimburses for medical services rendered to treat certain complications of care. Although CMS chose the majority of these complications because they are “reasonably preventable by following evidence-based guidelines,” the national media and patient advocacy groups have adopted the term “never events” to describe them.
Aside from the payment implications, CMS’ new policy affects the liability risk of any person providing inpatient care, regardless of whether a federal payor is involved.
In its press release announcing the new payment policy, CMS stated, “when you enter the hospital for treatment of one medical problem, you don’t expect to leave with additional injuries, infections, or serious conditions that occur during the course of your stay.” Recognizing “some of these complications may not be avoidable,” CMS found “too often patients suffer from injuries or illnesses that could have been prevented if the hospital had taken proper precautions.”
Consequently, “as part of its commitment to improve the quality of care [patients] receive during a hospital stay,” CMS policy is targeted at reducing “hospital-acquired conditions like certain infections, advanced bed sores, or fractures;” and “preventable medical errors, like performing surgery on the wrong side of the body, that should never happen.”
The list of “never events” covered under the CMS payment policy can be organized into three categories: surgical events, medical products and devices, and case management. The following breaks down each category:
Case Management
- Stage III and Stage IV pressure ulcers;
- Air embolism;
- Manifestations of poor control of blood sugar levels; and
- Fracture, burns, joint dislocations, and other injuries occurring from falls or other trauma suffered while an inpatient.
Surgical Events
- Surgery on wrong body part;
- Surgery on the wrong patient;
- Wrong surgery on a patient;
- Retention of a foreign object, such as a sponge or needle, inadvertently left in a patient after surgery;
- Surgical site infection following a coronary artery bypass graft;
- Surgical site infection following bariatric surgery;
- Surgical site infection following certain orthopedic procedures; and
- Deep vein thrombosis or pulmonary embolism following certain orthopedic procedures.
Medical Products and Devices
- Transfusion of wrong blood type;
- Catheter associated urinary tract infection; and
- Vascular catheter associated infections.
It’s easy to see why some of the complications made the list. Wrong-side surgery or surgery on the wrong patient are the quintessential cases where liability is generally uncontested. There is not much one can do to satisfactorily explain to a patient, or a jury, why a surgeon and surgical team operated on the wrong body part.
In other cases, however, such as fatal pulmonary embolus, death can occur even when a patient has been appropriately managed. In fact, medical literature demonstrates a small percentage of patients will develop deep vein thrombosis or pulmonary embolus even after having received therapeutic doses of heparin.
Reasonable Expectations
In any case involving a “never event,” we expect plaintiffs’ attorneys to argue CMS’ reimbursement determination is tantamount to a finding of substandard care. In other words, plaintiffs’ attorneys will argue a physician acted negligently simply because the patient incurred one of the proscribed complications. It’s a compelling argument because the federal government has essentially concluded these complications do not occur if physicians and hospitals pay attention while providing care.
You may have heard the Latin phrase res ipsa loquitur; it translates to “the thing speaks for itself.” Legally, res ipsa loquitur states a rule of law where a jury must presume a defendant was negligent when a certain type of injury occurs. The burden then shifts to the defendant to prove the injury occurred in the absence of negligence. The res ipsa rule originated in 1863 when a plaintiff was struck by a barrel of flour falling from a second-story window. The barrel caused the judge hearing the case to remark, “It is the duty of persons who keep barrels in a warehouse to take care that they do not roll out, and I think that such a case would, beyond all doubt, afford prima facie evidence of negligence. A barrel could not roll out of a warehouse without some negligence. … [I]f there are any facts inconsistent with negligence, it is for the defendant to prove them.” Thus, res ipsa is grounded in the notion everyone knows barrels aren’t supposed to fall from second-floor windows.
Traditionally, res ipsa applied only in a small class of medical malpractice cases, such as retained objects following surgery. In such cases, jurors are just as capable as medical professionals in understanding someone was negligent. For example, it does not take expert testimony to establish there has been negligence when a surgical instrument is left in a patient. There’s simply no compelling medical reason for a surgeon to leave an instrument in a patient’s abdomen.
In contrast, res ipsa generally has not applied in cases involving pulmonary embolus because the process of thromboembolic disease is beyond the average juror’s understanding and death by pulmonary embolus would not give rise to a presumption of negligence.
Where res ipsa applies, it’s a powerful concept. If res ipsa were found to apply to pulmonary embolus cases, the jury would be instructed it is the duty of a physician caring for a post-surgical patient to take care that the patient does not develop pulmonary embolus. Thus, a jury would begin with the presumption a patient would not develop pulmonary embolus absent negligence. The physician would then be left with the burden to prove otherwise. Given such a charge, it is foreseeable a jury could return a verdict against a physician, even if the physician managed the patient’s care appropriately and ordered appropriate prophylaxis.
Take Extra Precaution
To prevent CMS' reimbursement decisions from becoming the functional equivalent of a res ipsa instruction, physicians need to raise the level of precaution they employ against “never event” complications. At the heart of CMS' decision is its statement “never event” complications are “reasonably preventable by following evidence-based guidelines.” When a condition is only “reasonably preventable,” instead of “absolutely preventable,” a defense lawyer retains the ability to argue some patients will develop the condition even when the care was entirely appropriate.
We believe most jurors understand the inherent difficulties of caring for sick patients, and the risks that exist every time a patient undergoes a surgical procedure. The defense lawyer’s challenge is convincing a jury the patient received appropriate care, notwithstanding the complication.
Because CMS refers to “evidence-based guidelines,” physicians must know and follow the guidelines. The first step is becoming familiar with the complications CMS will deny reimbursement, and then regularly review the available guidelines to identify practices to reduce or eliminate the complication. Re-evaluate and update your practice whenever new information becomes available.
A consistent cycle of evaluating and responding to complications will afford the defense lawyer the ability to argue the physician and hospital complied with “evidence-based guidelines” and the patient’s case represents one of the unfortunate incidents where a patient suffers a complication despite receiving the highest-level of care.
In our experience, many providers initially create good systems, but run into trouble in the follow up. Make sure you respond to new or additional information or methods of practice. Without this follow up, CMS’ reimbursement decisions have the potential to create malpractice liabilities for all inpatient providers. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, University of Colorado Denver.
The Center for Medicare and Medicaid Services (CMS) recently announced federal payor programs no longer reimburses for medical services rendered to treat certain complications of care. Although CMS chose the majority of these complications because they are “reasonably preventable by following evidence-based guidelines,” the national media and patient advocacy groups have adopted the term “never events” to describe them.
Aside from the payment implications, CMS’ new policy affects the liability risk of any person providing inpatient care, regardless of whether a federal payor is involved.
In its press release announcing the new payment policy, CMS stated, “when you enter the hospital for treatment of one medical problem, you don’t expect to leave with additional injuries, infections, or serious conditions that occur during the course of your stay.” Recognizing “some of these complications may not be avoidable,” CMS found “too often patients suffer from injuries or illnesses that could have been prevented if the hospital had taken proper precautions.”
Consequently, “as part of its commitment to improve the quality of care [patients] receive during a hospital stay,” CMS policy is targeted at reducing “hospital-acquired conditions like certain infections, advanced bed sores, or fractures;” and “preventable medical errors, like performing surgery on the wrong side of the body, that should never happen.”
The list of “never events” covered under the CMS payment policy can be organized into three categories: surgical events, medical products and devices, and case management. The following breaks down each category:
Case Management
- Stage III and Stage IV pressure ulcers;
- Air embolism;
- Manifestations of poor control of blood sugar levels; and
- Fracture, burns, joint dislocations, and other injuries occurring from falls or other trauma suffered while an inpatient.
Surgical Events
- Surgery on wrong body part;
- Surgery on the wrong patient;
- Wrong surgery on a patient;
- Retention of a foreign object, such as a sponge or needle, inadvertently left in a patient after surgery;
- Surgical site infection following a coronary artery bypass graft;
- Surgical site infection following bariatric surgery;
- Surgical site infection following certain orthopedic procedures; and
- Deep vein thrombosis or pulmonary embolism following certain orthopedic procedures.
Medical Products and Devices
- Transfusion of wrong blood type;
- Catheter associated urinary tract infection; and
- Vascular catheter associated infections.
It’s easy to see why some of the complications made the list. Wrong-side surgery or surgery on the wrong patient are the quintessential cases where liability is generally uncontested. There is not much one can do to satisfactorily explain to a patient, or a jury, why a surgeon and surgical team operated on the wrong body part.
In other cases, however, such as fatal pulmonary embolus, death can occur even when a patient has been appropriately managed. In fact, medical literature demonstrates a small percentage of patients will develop deep vein thrombosis or pulmonary embolus even after having received therapeutic doses of heparin.
Reasonable Expectations
In any case involving a “never event,” we expect plaintiffs’ attorneys to argue CMS’ reimbursement determination is tantamount to a finding of substandard care. In other words, plaintiffs’ attorneys will argue a physician acted negligently simply because the patient incurred one of the proscribed complications. It’s a compelling argument because the federal government has essentially concluded these complications do not occur if physicians and hospitals pay attention while providing care.
You may have heard the Latin phrase res ipsa loquitur; it translates to “the thing speaks for itself.” Legally, res ipsa loquitur states a rule of law where a jury must presume a defendant was negligent when a certain type of injury occurs. The burden then shifts to the defendant to prove the injury occurred in the absence of negligence. The res ipsa rule originated in 1863 when a plaintiff was struck by a barrel of flour falling from a second-story window. The barrel caused the judge hearing the case to remark, “It is the duty of persons who keep barrels in a warehouse to take care that they do not roll out, and I think that such a case would, beyond all doubt, afford prima facie evidence of negligence. A barrel could not roll out of a warehouse without some negligence. … [I]f there are any facts inconsistent with negligence, it is for the defendant to prove them.” Thus, res ipsa is grounded in the notion everyone knows barrels aren’t supposed to fall from second-floor windows.
Traditionally, res ipsa applied only in a small class of medical malpractice cases, such as retained objects following surgery. In such cases, jurors are just as capable as medical professionals in understanding someone was negligent. For example, it does not take expert testimony to establish there has been negligence when a surgical instrument is left in a patient. There’s simply no compelling medical reason for a surgeon to leave an instrument in a patient’s abdomen.
In contrast, res ipsa generally has not applied in cases involving pulmonary embolus because the process of thromboembolic disease is beyond the average juror’s understanding and death by pulmonary embolus would not give rise to a presumption of negligence.
Where res ipsa applies, it’s a powerful concept. If res ipsa were found to apply to pulmonary embolus cases, the jury would be instructed it is the duty of a physician caring for a post-surgical patient to take care that the patient does not develop pulmonary embolus. Thus, a jury would begin with the presumption a patient would not develop pulmonary embolus absent negligence. The physician would then be left with the burden to prove otherwise. Given such a charge, it is foreseeable a jury could return a verdict against a physician, even if the physician managed the patient’s care appropriately and ordered appropriate prophylaxis.
Take Extra Precaution
To prevent CMS' reimbursement decisions from becoming the functional equivalent of a res ipsa instruction, physicians need to raise the level of precaution they employ against “never event” complications. At the heart of CMS' decision is its statement “never event” complications are “reasonably preventable by following evidence-based guidelines.” When a condition is only “reasonably preventable,” instead of “absolutely preventable,” a defense lawyer retains the ability to argue some patients will develop the condition even when the care was entirely appropriate.
We believe most jurors understand the inherent difficulties of caring for sick patients, and the risks that exist every time a patient undergoes a surgical procedure. The defense lawyer’s challenge is convincing a jury the patient received appropriate care, notwithstanding the complication.
Because CMS refers to “evidence-based guidelines,” physicians must know and follow the guidelines. The first step is becoming familiar with the complications CMS will deny reimbursement, and then regularly review the available guidelines to identify practices to reduce or eliminate the complication. Re-evaluate and update your practice whenever new information becomes available.
A consistent cycle of evaluating and responding to complications will afford the defense lawyer the ability to argue the physician and hospital complied with “evidence-based guidelines” and the patient’s case represents one of the unfortunate incidents where a patient suffers a complication despite receiving the highest-level of care.
In our experience, many providers initially create good systems, but run into trouble in the follow up. Make sure you respond to new or additional information or methods of practice. Without this follow up, CMS’ reimbursement decisions have the potential to create malpractice liabilities for all inpatient providers. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, University of Colorado Denver.
Focused on Patient Care
Julia S. Wright, MD, spent 10 years in traditional practice before joining the University of Wisconsin School of Medicine and Public Health in Madison. Now a clinical associate professor and section head of hospital medicine, the title has changed and the professional demands have intensified. The mission, however, remains the same.
Every decision she’s made in her career—whether it be medical, managerial, financial, or even her seemingly curious choice of college majors—has been guided by one basic question: What will this mean for the quality of patient care? “It may sound cliché, but that’s always the bottom line,” Dr. Wright says. “It’s why I do what I do.”
You spent 10 years in traditional practice before becoming a hospitalist. How did that prepare you for what you’re doing now?
Answer: That experience is a tremendous asset. I made the switch to inpatient medicine because that was the arena I enjoyed the most. But having had experience in the outpatient setting gives me a better understanding of the continuum of care, and my clinical skills have been honed by that experience. I also have an understanding of the strengths of the primary care physicians (PCP), as well as the breadth of the problems they are able to take on.
How does that help you?
A: It really helps in the patient transition, especially on the return side, when patients go back to their PCP after hospitalization. Having an understanding of what resources are available to PCPs helps to determine an appropriate time to discharge a patient. Someone without that experience may have a tendency to think every loose end has to be tied up, or they may make changes that wind up making things more difficult for PCP. But if you have an understanding of a PCP’s capabilities, maybe the patient can be discharged a little earlier.
The University of Wisconsin’s hospitalist program started in 2005. You were named director in 2006. How exciting is it to guide a new program and help it develop?
A: It’s been a tremendous experience. When I joined, we had six hospitalists. Now we have 19. But it was strategic growth; it wasn’t haphazard.
What do you mean by strategic growth?
A: We didn’t simply say, ‘We need more people.’ Every time we brought somebody on, we really made sure it was going to be someone who would add value to the program and be beneficial to the hospital. We were worried, as we got bigger, that it’d be hard to keep the same cohesiveness and that same espirit de corps. During the interviews and the search process, we’re not just asking, ‘Are they qualified?’ We’re asking, ‘Are they a really good fit?’ And everybody has different areas of interest within the group. Some are more research-inclined; one developed a curriculum; some are more clinically oriented. That allows each hospitalist to have an identity in the group. That translated into a good expansion, and it’s been a win-win for us.
What makes someone a good fit for your program?
A: It sounds cliché, but I think the key to a strong developing program is to have a strong sense of what the group values. For us, we value the academic experience. For people going into academic medicine, the struggle is to be able to provide value to the hospital and yet stay academic. Our hospitalists are very clear—that’s our vision. With the support of the hospital and the department, we were able to do both at the same time.
Can you pinpoint one experience that you’ve had that made you realize you’re doing what you’re meant to do?
A: The biggest reward is always patient care. I enjoy the direct patient experience as much as I always have, and that’s what keeps me in the game.
What have you enjoyed most about your transition to a leadership role?
A: I really enjoy the position, not because of the hierarchy, but because of the opportunities afforded by it. I get to interact with hospital medicine staff and the department of medicine chair, and the vice chairs. I’ve been able to interact with others in hospital medicine across the country, and that has been a great experience.
Some hospitalists enjoy what they do because they don’t have to handle the business side of operations or deal with the administrative hassles that private physicians face. In your role, though, you do have to face those challenges. Is that a drawback?
A: I do have to pay attention to the numbers. That’s the bottom line. But it’s something I actually really enjoy. When it comes to awareness of the balance sheet, there’s a division between the leadership level and the clinician level. It’s hard to bridge that chasm of, ‘I’m here for patient care and I don’t necessarily focus on the numbers.’
How do you bridge the chasm?
A: It’s something we should be emphasizing more in hospital medicine. Some people may think it’s distasteful to think about, but it’s something hospitals do need to care about. There’s not enough of that trickling down. This is a huge area for potential growth. It’s important to have an understanding of the importance of the bottom line without feeling too much like it’s threatening the quality of the practice or getting in the way of what we want to be doing.
What other changes are in store for hospital medicine?
A: If you look at the traditional role of a hospitalist, you do a few things on the side of quality, but basically you’re seeing patients. The theory is there could be market saturation, because there are only a certain number of patients you can see in a hospital. But now hospitalists are seen as a physician resource that didn’t exist before. You have a group of doctors that understand patient care very well and are available to make changes and implement initiatives within a hospital. That’s going to lead to more roles besides direct patient care role. Hospitalists are going to be in charge of a number of administrative duties or assume administrative positions within hospitals. Because we’re branching out into other areas of hospital-based care, we’ll see more growth and still see high demand.
One of your primary medical interests is healthcare for Spanish-speaking families. Why is that so important to you?
A: My interest in working with the Latino population comes from my own background. I was a Spanish literature major at Northwestern University, and I’ve had a lot of opportunities to travel. When I started practicing, a large number of the patients were Latino. It became clear how important it is for us to understand what’s happening in our communities. We need to know what patients are coming in, what their demographics are, what their experiences have been, and what their needs are. Everything we do in a hospital translates to what’s happening outside the hospital.
Hospital medicine is quite a switch from Spanish literature. How’d that come about?
A: Actually, it was planned. I always knew I was going to medical school, but I really enjoy linguistics and language. I kept that balance. I didn’t want to be too science-oriented. It was one of those left brain-right brain things.
What is the biggest challenge facing hospital medicine?
A: The challenge is going to be retaining hospitalists and trying to avoid burnout.
How do you address the retention issue?
A: A big part of retention is making people feel happy in their field. It’s about allowing them to feel like they’re contributing in their particular area of physician interest, making them feel like their contributions are valued, making them feel like they can effect change, and making them feel like they’re really part of a team. We’ve been able to keep those as priorities.
How about the risk of burnout?
A: We have to find ways to balance our professions with our personal lives. Everybody’s looking for that balance. I have a husband and three children, so I want it, too. We really have to be reasonable. An important part of being good doctors is being good human beings.
What’s next for you personally?
A: Expanding research and developing a fellowship are two of the primary areas of focus. We also want to focus on triage and flow, and improving the throughput. Beyond that, it’s going to be program expansion, just like it’s been. That’s going to keep me busy. TH
Mark Leiser is a freelance writer in New Jersey.
Julia S. Wright, MD, spent 10 years in traditional practice before joining the University of Wisconsin School of Medicine and Public Health in Madison. Now a clinical associate professor and section head of hospital medicine, the title has changed and the professional demands have intensified. The mission, however, remains the same.
Every decision she’s made in her career—whether it be medical, managerial, financial, or even her seemingly curious choice of college majors—has been guided by one basic question: What will this mean for the quality of patient care? “It may sound cliché, but that’s always the bottom line,” Dr. Wright says. “It’s why I do what I do.”
You spent 10 years in traditional practice before becoming a hospitalist. How did that prepare you for what you’re doing now?
Answer: That experience is a tremendous asset. I made the switch to inpatient medicine because that was the arena I enjoyed the most. But having had experience in the outpatient setting gives me a better understanding of the continuum of care, and my clinical skills have been honed by that experience. I also have an understanding of the strengths of the primary care physicians (PCP), as well as the breadth of the problems they are able to take on.
How does that help you?
A: It really helps in the patient transition, especially on the return side, when patients go back to their PCP after hospitalization. Having an understanding of what resources are available to PCPs helps to determine an appropriate time to discharge a patient. Someone without that experience may have a tendency to think every loose end has to be tied up, or they may make changes that wind up making things more difficult for PCP. But if you have an understanding of a PCP’s capabilities, maybe the patient can be discharged a little earlier.
The University of Wisconsin’s hospitalist program started in 2005. You were named director in 2006. How exciting is it to guide a new program and help it develop?
A: It’s been a tremendous experience. When I joined, we had six hospitalists. Now we have 19. But it was strategic growth; it wasn’t haphazard.
What do you mean by strategic growth?
A: We didn’t simply say, ‘We need more people.’ Every time we brought somebody on, we really made sure it was going to be someone who would add value to the program and be beneficial to the hospital. We were worried, as we got bigger, that it’d be hard to keep the same cohesiveness and that same espirit de corps. During the interviews and the search process, we’re not just asking, ‘Are they qualified?’ We’re asking, ‘Are they a really good fit?’ And everybody has different areas of interest within the group. Some are more research-inclined; one developed a curriculum; some are more clinically oriented. That allows each hospitalist to have an identity in the group. That translated into a good expansion, and it’s been a win-win for us.
What makes someone a good fit for your program?
A: It sounds cliché, but I think the key to a strong developing program is to have a strong sense of what the group values. For us, we value the academic experience. For people going into academic medicine, the struggle is to be able to provide value to the hospital and yet stay academic. Our hospitalists are very clear—that’s our vision. With the support of the hospital and the department, we were able to do both at the same time.
Can you pinpoint one experience that you’ve had that made you realize you’re doing what you’re meant to do?
A: The biggest reward is always patient care. I enjoy the direct patient experience as much as I always have, and that’s what keeps me in the game.
What have you enjoyed most about your transition to a leadership role?
A: I really enjoy the position, not because of the hierarchy, but because of the opportunities afforded by it. I get to interact with hospital medicine staff and the department of medicine chair, and the vice chairs. I’ve been able to interact with others in hospital medicine across the country, and that has been a great experience.
Some hospitalists enjoy what they do because they don’t have to handle the business side of operations or deal with the administrative hassles that private physicians face. In your role, though, you do have to face those challenges. Is that a drawback?
A: I do have to pay attention to the numbers. That’s the bottom line. But it’s something I actually really enjoy. When it comes to awareness of the balance sheet, there’s a division between the leadership level and the clinician level. It’s hard to bridge that chasm of, ‘I’m here for patient care and I don’t necessarily focus on the numbers.’
How do you bridge the chasm?
A: It’s something we should be emphasizing more in hospital medicine. Some people may think it’s distasteful to think about, but it’s something hospitals do need to care about. There’s not enough of that trickling down. This is a huge area for potential growth. It’s important to have an understanding of the importance of the bottom line without feeling too much like it’s threatening the quality of the practice or getting in the way of what we want to be doing.
What other changes are in store for hospital medicine?
A: If you look at the traditional role of a hospitalist, you do a few things on the side of quality, but basically you’re seeing patients. The theory is there could be market saturation, because there are only a certain number of patients you can see in a hospital. But now hospitalists are seen as a physician resource that didn’t exist before. You have a group of doctors that understand patient care very well and are available to make changes and implement initiatives within a hospital. That’s going to lead to more roles besides direct patient care role. Hospitalists are going to be in charge of a number of administrative duties or assume administrative positions within hospitals. Because we’re branching out into other areas of hospital-based care, we’ll see more growth and still see high demand.
One of your primary medical interests is healthcare for Spanish-speaking families. Why is that so important to you?
A: My interest in working with the Latino population comes from my own background. I was a Spanish literature major at Northwestern University, and I’ve had a lot of opportunities to travel. When I started practicing, a large number of the patients were Latino. It became clear how important it is for us to understand what’s happening in our communities. We need to know what patients are coming in, what their demographics are, what their experiences have been, and what their needs are. Everything we do in a hospital translates to what’s happening outside the hospital.
Hospital medicine is quite a switch from Spanish literature. How’d that come about?
A: Actually, it was planned. I always knew I was going to medical school, but I really enjoy linguistics and language. I kept that balance. I didn’t want to be too science-oriented. It was one of those left brain-right brain things.
What is the biggest challenge facing hospital medicine?
A: The challenge is going to be retaining hospitalists and trying to avoid burnout.
How do you address the retention issue?
A: A big part of retention is making people feel happy in their field. It’s about allowing them to feel like they’re contributing in their particular area of physician interest, making them feel like their contributions are valued, making them feel like they can effect change, and making them feel like they’re really part of a team. We’ve been able to keep those as priorities.
How about the risk of burnout?
A: We have to find ways to balance our professions with our personal lives. Everybody’s looking for that balance. I have a husband and three children, so I want it, too. We really have to be reasonable. An important part of being good doctors is being good human beings.
What’s next for you personally?
A: Expanding research and developing a fellowship are two of the primary areas of focus. We also want to focus on triage and flow, and improving the throughput. Beyond that, it’s going to be program expansion, just like it’s been. That’s going to keep me busy. TH
Mark Leiser is a freelance writer in New Jersey.
Julia S. Wright, MD, spent 10 years in traditional practice before joining the University of Wisconsin School of Medicine and Public Health in Madison. Now a clinical associate professor and section head of hospital medicine, the title has changed and the professional demands have intensified. The mission, however, remains the same.
Every decision she’s made in her career—whether it be medical, managerial, financial, or even her seemingly curious choice of college majors—has been guided by one basic question: What will this mean for the quality of patient care? “It may sound cliché, but that’s always the bottom line,” Dr. Wright says. “It’s why I do what I do.”
You spent 10 years in traditional practice before becoming a hospitalist. How did that prepare you for what you’re doing now?
Answer: That experience is a tremendous asset. I made the switch to inpatient medicine because that was the arena I enjoyed the most. But having had experience in the outpatient setting gives me a better understanding of the continuum of care, and my clinical skills have been honed by that experience. I also have an understanding of the strengths of the primary care physicians (PCP), as well as the breadth of the problems they are able to take on.
How does that help you?
A: It really helps in the patient transition, especially on the return side, when patients go back to their PCP after hospitalization. Having an understanding of what resources are available to PCPs helps to determine an appropriate time to discharge a patient. Someone without that experience may have a tendency to think every loose end has to be tied up, or they may make changes that wind up making things more difficult for PCP. But if you have an understanding of a PCP’s capabilities, maybe the patient can be discharged a little earlier.
The University of Wisconsin’s hospitalist program started in 2005. You were named director in 2006. How exciting is it to guide a new program and help it develop?
A: It’s been a tremendous experience. When I joined, we had six hospitalists. Now we have 19. But it was strategic growth; it wasn’t haphazard.
What do you mean by strategic growth?
A: We didn’t simply say, ‘We need more people.’ Every time we brought somebody on, we really made sure it was going to be someone who would add value to the program and be beneficial to the hospital. We were worried, as we got bigger, that it’d be hard to keep the same cohesiveness and that same espirit de corps. During the interviews and the search process, we’re not just asking, ‘Are they qualified?’ We’re asking, ‘Are they a really good fit?’ And everybody has different areas of interest within the group. Some are more research-inclined; one developed a curriculum; some are more clinically oriented. That allows each hospitalist to have an identity in the group. That translated into a good expansion, and it’s been a win-win for us.
What makes someone a good fit for your program?
A: It sounds cliché, but I think the key to a strong developing program is to have a strong sense of what the group values. For us, we value the academic experience. For people going into academic medicine, the struggle is to be able to provide value to the hospital and yet stay academic. Our hospitalists are very clear—that’s our vision. With the support of the hospital and the department, we were able to do both at the same time.
Can you pinpoint one experience that you’ve had that made you realize you’re doing what you’re meant to do?
A: The biggest reward is always patient care. I enjoy the direct patient experience as much as I always have, and that’s what keeps me in the game.
What have you enjoyed most about your transition to a leadership role?
A: I really enjoy the position, not because of the hierarchy, but because of the opportunities afforded by it. I get to interact with hospital medicine staff and the department of medicine chair, and the vice chairs. I’ve been able to interact with others in hospital medicine across the country, and that has been a great experience.
Some hospitalists enjoy what they do because they don’t have to handle the business side of operations or deal with the administrative hassles that private physicians face. In your role, though, you do have to face those challenges. Is that a drawback?
A: I do have to pay attention to the numbers. That’s the bottom line. But it’s something I actually really enjoy. When it comes to awareness of the balance sheet, there’s a division between the leadership level and the clinician level. It’s hard to bridge that chasm of, ‘I’m here for patient care and I don’t necessarily focus on the numbers.’
How do you bridge the chasm?
A: It’s something we should be emphasizing more in hospital medicine. Some people may think it’s distasteful to think about, but it’s something hospitals do need to care about. There’s not enough of that trickling down. This is a huge area for potential growth. It’s important to have an understanding of the importance of the bottom line without feeling too much like it’s threatening the quality of the practice or getting in the way of what we want to be doing.
What other changes are in store for hospital medicine?
A: If you look at the traditional role of a hospitalist, you do a few things on the side of quality, but basically you’re seeing patients. The theory is there could be market saturation, because there are only a certain number of patients you can see in a hospital. But now hospitalists are seen as a physician resource that didn’t exist before. You have a group of doctors that understand patient care very well and are available to make changes and implement initiatives within a hospital. That’s going to lead to more roles besides direct patient care role. Hospitalists are going to be in charge of a number of administrative duties or assume administrative positions within hospitals. Because we’re branching out into other areas of hospital-based care, we’ll see more growth and still see high demand.
One of your primary medical interests is healthcare for Spanish-speaking families. Why is that so important to you?
A: My interest in working with the Latino population comes from my own background. I was a Spanish literature major at Northwestern University, and I’ve had a lot of opportunities to travel. When I started practicing, a large number of the patients were Latino. It became clear how important it is for us to understand what’s happening in our communities. We need to know what patients are coming in, what their demographics are, what their experiences have been, and what their needs are. Everything we do in a hospital translates to what’s happening outside the hospital.
Hospital medicine is quite a switch from Spanish literature. How’d that come about?
A: Actually, it was planned. I always knew I was going to medical school, but I really enjoy linguistics and language. I kept that balance. I didn’t want to be too science-oriented. It was one of those left brain-right brain things.
What is the biggest challenge facing hospital medicine?
A: The challenge is going to be retaining hospitalists and trying to avoid burnout.
How do you address the retention issue?
A: A big part of retention is making people feel happy in their field. It’s about allowing them to feel like they’re contributing in their particular area of physician interest, making them feel like their contributions are valued, making them feel like they can effect change, and making them feel like they’re really part of a team. We’ve been able to keep those as priorities.
How about the risk of burnout?
A: We have to find ways to balance our professions with our personal lives. Everybody’s looking for that balance. I have a husband and three children, so I want it, too. We really have to be reasonable. An important part of being good doctors is being good human beings.
What’s next for you personally?
A: Expanding research and developing a fellowship are two of the primary areas of focus. We also want to focus on triage and flow, and improving the throughput. Beyond that, it’s going to be program expansion, just like it’s been. That’s going to keep me busy. TH
Mark Leiser is a freelance writer in New Jersey.
“Caregiver Culture” and End-of-Life Discussions
When it comes to discussing a patient’s wishes for code status care, practices at the institution play a more important role than almost any other factor, according to a new study, “Factors Associated with Discussion of Care Plans and Code Status at the Time of Hospital Admission: Results from the Multicenter Hospitalist Study,” in the Journal of Hospital Medicine.
“What was most surprising to me was how variable the discussion rate was,” lead author Andrew Auerbach, MD, tells The Hospitalist. “It had little or nothing to do with how sick the patient was, or with the type of institution in which the discussion took place.”
Hospitalists are no more or less likely to document such discussions than doctors in any other specialty, says Dr. Auerbach, a hospitalist and associate professor of medicine at the University of California San Francisco. He and his colleagues analyzed data from patients admitted to the general medicine services at six academic medical centers as part of the Multicenter Hospitalist Study. Each site complied with requirements established by the Patient Self-Determination Act (PSDA), which says patients must be informed of their right to create an advance directive.
None of the hospitals in the study had established guidelines or formal policies regarding physician-patient discussions about code status or end-of-life care. Patients were interviewed immediately after informed consent was obtained, usually within 24 hours of admission. In each case, the authors determined whether or not the patient had had a care discussion, defined as a documented discussion “between patients (or family) and at least one physician … during the first 24 hours of hospitalization,” the authors write. “Care discussions needed to specify that the person who wrote the note had actually spoken with the patient or their family for the purposes of determining preferences for care, and that this discussion resulted in a specific care plan.”
A notation, such as “the patient continues to want full efforts,” qualified as a care discussion. Less-specific comments, such as “DNR/DNI” or “spoke with family, questions answered,” did not qualify. “These were all really, really sick people, and it was important to assess their wishes for care,” Dr. Auerbach says. Individually, PSDA or durable power of attorney may not adequately convey a patient’s true wishes, because often times the measures involve nothing more than having the patient or family complete a form. “The true marker is a conversation,” he says.
—Andrew Auerbach, MD, University of California San Francisco
By the Numbers
Of 17,097 patients interviewed, only 1,776 (10.4%) had a documented care discussion within 24 hours of hospital admission. The frequency of discussions varied from a low of 2.8% at one institution, to a high of 24.9% at another.
On unadjusted analysis, patients with documented care discussions were more likely to have living wills, durable powers of attorney, or the names of surrogate decision-makers in their charts (P<0.0001 for all categories). These patients were older, more likely to be white, and more likely to be on Medicare, compared to patients without documented care discussions.
The unadjusted analysis also showed patients with care discussions were more likely to be married, but less likely to be living in their own home or apartment, and, not surprisingly, more likely to have been hospitalized at least once within the previous 12 months. Overall, the general health of patients with care discussions was poorer than those without. Patients with documented discussions were more likely to report needing help within the past month with chores or bathing or dressing themselves, than were patients who did not have care discussions. Cancer, depression, and a history of stroke were common among patients with care discussions. Compared to patients without documented discussions, those who did have the discussion appear to want more of a say in their care: they were less likely to agree with the study statements, “I prefer my doctor give me choices regarding my care,” and “I prefer to leave care decisions to my physician.”
The authors found multivariate analysis showed many of these factors turn out to have only a moderate association with a documented care discussion, with adjusted odds ratios of less than 2.0. The strongest predictors were the existence of informal notations describing pre-hospital care wishes, with odds ratios ranging from 3.22 to 11.32, compared to people with no such documentation, and site of enrollment, with odds ratios of 1.74 to 5.14.
The Caregiver Culture
These findings suggest the “caregiver culture” at any given institution is a stronger determinant of a patient participating in a documented care discussion than other, more intuitive factors, such as medical condition or socioeconomic characteristics, or even whether or not the patient has a pre-existing advance directive or durable power of attorney, Dr. Auerbach explains. “It may just be a part of what some hospitals do. It’s driven by what your peers are doing and by local practices.”
Based on the results of the study, Dr. Auerbach and his co-authors suggest simply establishing mandates to document code status on admission probably will not encourage more conversations of this nature, “unless sites also develop an approach to using this newly documented information as a prompt for subsequent discussions.” The Patient Self-Determination Act went into effect in 1991, but its effect on improving communication around end-of-life care remains uncertain, the authors note. It might be why California passed a new law, effective as of January 2009, requiring physicians and health care organizations in the state to provide terminally ill patients who ask about their end-of-life care options with comprehensive information and counseling. Such discussions must cover advance directives, hospice care, and the right to receive palliative care. The new law is the first of its kind in the nation, but proponents of the legislation hope it will serve as a model for other states to adopt.1
“Documentation has an impact on quality of care. Lots of errors are driven by code status,” Dr. Auerbach points out. “If a patient is admitted in the middle of the night, when the doctor checks in on him the next day, he can look at the chart and see that his partner documented the care discussion the night before. That is incredibly helpful.” TH
Norra MacReady is a medical writer based in California.
Reference
1. O’Reilly KB. California law mandates discussing end-of-life options. Am Med News Web site. Available at amaassn.org/amednews/2008/11/10/prsc1110.htm. Last accessed November 6, 2008.
When it comes to discussing a patient’s wishes for code status care, practices at the institution play a more important role than almost any other factor, according to a new study, “Factors Associated with Discussion of Care Plans and Code Status at the Time of Hospital Admission: Results from the Multicenter Hospitalist Study,” in the Journal of Hospital Medicine.
“What was most surprising to me was how variable the discussion rate was,” lead author Andrew Auerbach, MD, tells The Hospitalist. “It had little or nothing to do with how sick the patient was, or with the type of institution in which the discussion took place.”
Hospitalists are no more or less likely to document such discussions than doctors in any other specialty, says Dr. Auerbach, a hospitalist and associate professor of medicine at the University of California San Francisco. He and his colleagues analyzed data from patients admitted to the general medicine services at six academic medical centers as part of the Multicenter Hospitalist Study. Each site complied with requirements established by the Patient Self-Determination Act (PSDA), which says patients must be informed of their right to create an advance directive.
None of the hospitals in the study had established guidelines or formal policies regarding physician-patient discussions about code status or end-of-life care. Patients were interviewed immediately after informed consent was obtained, usually within 24 hours of admission. In each case, the authors determined whether or not the patient had had a care discussion, defined as a documented discussion “between patients (or family) and at least one physician … during the first 24 hours of hospitalization,” the authors write. “Care discussions needed to specify that the person who wrote the note had actually spoken with the patient or their family for the purposes of determining preferences for care, and that this discussion resulted in a specific care plan.”
A notation, such as “the patient continues to want full efforts,” qualified as a care discussion. Less-specific comments, such as “DNR/DNI” or “spoke with family, questions answered,” did not qualify. “These were all really, really sick people, and it was important to assess their wishes for care,” Dr. Auerbach says. Individually, PSDA or durable power of attorney may not adequately convey a patient’s true wishes, because often times the measures involve nothing more than having the patient or family complete a form. “The true marker is a conversation,” he says.
—Andrew Auerbach, MD, University of California San Francisco
By the Numbers
Of 17,097 patients interviewed, only 1,776 (10.4%) had a documented care discussion within 24 hours of hospital admission. The frequency of discussions varied from a low of 2.8% at one institution, to a high of 24.9% at another.
On unadjusted analysis, patients with documented care discussions were more likely to have living wills, durable powers of attorney, or the names of surrogate decision-makers in their charts (P<0.0001 for all categories). These patients were older, more likely to be white, and more likely to be on Medicare, compared to patients without documented care discussions.
The unadjusted analysis also showed patients with care discussions were more likely to be married, but less likely to be living in their own home or apartment, and, not surprisingly, more likely to have been hospitalized at least once within the previous 12 months. Overall, the general health of patients with care discussions was poorer than those without. Patients with documented discussions were more likely to report needing help within the past month with chores or bathing or dressing themselves, than were patients who did not have care discussions. Cancer, depression, and a history of stroke were common among patients with care discussions. Compared to patients without documented discussions, those who did have the discussion appear to want more of a say in their care: they were less likely to agree with the study statements, “I prefer my doctor give me choices regarding my care,” and “I prefer to leave care decisions to my physician.”
The authors found multivariate analysis showed many of these factors turn out to have only a moderate association with a documented care discussion, with adjusted odds ratios of less than 2.0. The strongest predictors were the existence of informal notations describing pre-hospital care wishes, with odds ratios ranging from 3.22 to 11.32, compared to people with no such documentation, and site of enrollment, with odds ratios of 1.74 to 5.14.
The Caregiver Culture
These findings suggest the “caregiver culture” at any given institution is a stronger determinant of a patient participating in a documented care discussion than other, more intuitive factors, such as medical condition or socioeconomic characteristics, or even whether or not the patient has a pre-existing advance directive or durable power of attorney, Dr. Auerbach explains. “It may just be a part of what some hospitals do. It’s driven by what your peers are doing and by local practices.”
Based on the results of the study, Dr. Auerbach and his co-authors suggest simply establishing mandates to document code status on admission probably will not encourage more conversations of this nature, “unless sites also develop an approach to using this newly documented information as a prompt for subsequent discussions.” The Patient Self-Determination Act went into effect in 1991, but its effect on improving communication around end-of-life care remains uncertain, the authors note. It might be why California passed a new law, effective as of January 2009, requiring physicians and health care organizations in the state to provide terminally ill patients who ask about their end-of-life care options with comprehensive information and counseling. Such discussions must cover advance directives, hospice care, and the right to receive palliative care. The new law is the first of its kind in the nation, but proponents of the legislation hope it will serve as a model for other states to adopt.1
“Documentation has an impact on quality of care. Lots of errors are driven by code status,” Dr. Auerbach points out. “If a patient is admitted in the middle of the night, when the doctor checks in on him the next day, he can look at the chart and see that his partner documented the care discussion the night before. That is incredibly helpful.” TH
Norra MacReady is a medical writer based in California.
Reference
1. O’Reilly KB. California law mandates discussing end-of-life options. Am Med News Web site. Available at amaassn.org/amednews/2008/11/10/prsc1110.htm. Last accessed November 6, 2008.
When it comes to discussing a patient’s wishes for code status care, practices at the institution play a more important role than almost any other factor, according to a new study, “Factors Associated with Discussion of Care Plans and Code Status at the Time of Hospital Admission: Results from the Multicenter Hospitalist Study,” in the Journal of Hospital Medicine.
“What was most surprising to me was how variable the discussion rate was,” lead author Andrew Auerbach, MD, tells The Hospitalist. “It had little or nothing to do with how sick the patient was, or with the type of institution in which the discussion took place.”
Hospitalists are no more or less likely to document such discussions than doctors in any other specialty, says Dr. Auerbach, a hospitalist and associate professor of medicine at the University of California San Francisco. He and his colleagues analyzed data from patients admitted to the general medicine services at six academic medical centers as part of the Multicenter Hospitalist Study. Each site complied with requirements established by the Patient Self-Determination Act (PSDA), which says patients must be informed of their right to create an advance directive.
None of the hospitals in the study had established guidelines or formal policies regarding physician-patient discussions about code status or end-of-life care. Patients were interviewed immediately after informed consent was obtained, usually within 24 hours of admission. In each case, the authors determined whether or not the patient had had a care discussion, defined as a documented discussion “between patients (or family) and at least one physician … during the first 24 hours of hospitalization,” the authors write. “Care discussions needed to specify that the person who wrote the note had actually spoken with the patient or their family for the purposes of determining preferences for care, and that this discussion resulted in a specific care plan.”
A notation, such as “the patient continues to want full efforts,” qualified as a care discussion. Less-specific comments, such as “DNR/DNI” or “spoke with family, questions answered,” did not qualify. “These were all really, really sick people, and it was important to assess their wishes for care,” Dr. Auerbach says. Individually, PSDA or durable power of attorney may not adequately convey a patient’s true wishes, because often times the measures involve nothing more than having the patient or family complete a form. “The true marker is a conversation,” he says.
—Andrew Auerbach, MD, University of California San Francisco
By the Numbers
Of 17,097 patients interviewed, only 1,776 (10.4%) had a documented care discussion within 24 hours of hospital admission. The frequency of discussions varied from a low of 2.8% at one institution, to a high of 24.9% at another.
On unadjusted analysis, patients with documented care discussions were more likely to have living wills, durable powers of attorney, or the names of surrogate decision-makers in their charts (P<0.0001 for all categories). These patients were older, more likely to be white, and more likely to be on Medicare, compared to patients without documented care discussions.
The unadjusted analysis also showed patients with care discussions were more likely to be married, but less likely to be living in their own home or apartment, and, not surprisingly, more likely to have been hospitalized at least once within the previous 12 months. Overall, the general health of patients with care discussions was poorer than those without. Patients with documented discussions were more likely to report needing help within the past month with chores or bathing or dressing themselves, than were patients who did not have care discussions. Cancer, depression, and a history of stroke were common among patients with care discussions. Compared to patients without documented discussions, those who did have the discussion appear to want more of a say in their care: they were less likely to agree with the study statements, “I prefer my doctor give me choices regarding my care,” and “I prefer to leave care decisions to my physician.”
The authors found multivariate analysis showed many of these factors turn out to have only a moderate association with a documented care discussion, with adjusted odds ratios of less than 2.0. The strongest predictors were the existence of informal notations describing pre-hospital care wishes, with odds ratios ranging from 3.22 to 11.32, compared to people with no such documentation, and site of enrollment, with odds ratios of 1.74 to 5.14.
The Caregiver Culture
These findings suggest the “caregiver culture” at any given institution is a stronger determinant of a patient participating in a documented care discussion than other, more intuitive factors, such as medical condition or socioeconomic characteristics, or even whether or not the patient has a pre-existing advance directive or durable power of attorney, Dr. Auerbach explains. “It may just be a part of what some hospitals do. It’s driven by what your peers are doing and by local practices.”
Based on the results of the study, Dr. Auerbach and his co-authors suggest simply establishing mandates to document code status on admission probably will not encourage more conversations of this nature, “unless sites also develop an approach to using this newly documented information as a prompt for subsequent discussions.” The Patient Self-Determination Act went into effect in 1991, but its effect on improving communication around end-of-life care remains uncertain, the authors note. It might be why California passed a new law, effective as of January 2009, requiring physicians and health care organizations in the state to provide terminally ill patients who ask about their end-of-life care options with comprehensive information and counseling. Such discussions must cover advance directives, hospice care, and the right to receive palliative care. The new law is the first of its kind in the nation, but proponents of the legislation hope it will serve as a model for other states to adopt.1
“Documentation has an impact on quality of care. Lots of errors are driven by code status,” Dr. Auerbach points out. “If a patient is admitted in the middle of the night, when the doctor checks in on him the next day, he can look at the chart and see that his partner documented the care discussion the night before. That is incredibly helpful.” TH
Norra MacReady is a medical writer based in California.
Reference
1. O’Reilly KB. California law mandates discussing end-of-life options. Am Med News Web site. Available at amaassn.org/amednews/2008/11/10/prsc1110.htm. Last accessed November 6, 2008.
QTc Interval Prolongation
Terfenadine, cisapride, astemizole … do you remember these drugs? They all were removed from the U.S. market subsequent to adverse outcomes related to QTc interval prolongation, including ventricular arrhythmias.1-3 Many drugs prolong the QTc interval, particularly if a drug is combined with others that affect its metabolism.
QTc interval prolongation can lead to torsades de pointes (TdP). Certain individuals are particularly predisposed to developing TdP, including: women, people with hypokalemia or hypomagnesemia, and those with a history of congenital or idiopathic QTc syndrome, cardiac arrest, syncope, congestive heart failure, bradycardia, baseline QT prolongation, renal failure, or cardiac failure.4 Some agents can prolong the QTc interval by five to 10 milliseconds and cause TdP, while others require a 50-millisecond increase or more.
Drugs that confer a risk of ventricular arrhythmias include: disopyramide, dofetilide, ibutilide, procainamide, quinidine, sotalol, and amiodarone (antiarrhythmic agents); clarithromycin, erythromycin, levofloxacin, gatifloxacin, gemifloxacin, moxifloxacin, telithromycin (anti-infectives); domperidone and droperidol antiemetics; chlorpromazine, haloperidol, mesoridazine, thioridazine, and pimozide (antipsychotics); amitriptyline, desipramine, doxepin, fluoxetine, imipramine, sertraline, and venlafaxine (antidepressants); fluconazole, itraconazole, and ketoconazole (antifungals); naratriptan, sumatriptan, and zolmitriptan; and methadone.4-8 Other related agents, such as voriconazole and ondansetron, have been reported to cause QTc prolongation.
Drugs of special concern are those that frequently inhibit the metabolism of other agents, including erythromycin, clarithromycin, ketoconazole, itraconazole, amiodarone, and quinidine, and many antidepressants and antiretroviral agents. Of the deaths associated with drug-induced QTc prolongation related to the prokinetic agent cisapride, many were due to drug interactions with an imidazole or macrolide antibiotic. In these cases, increased serum concentrations of cisapride occurred due to inhibition of the cytochrome P450 CYP3A4 isoenzyme.9
If treatment with a drug that has the potential for causing QTc prolongation is begun, tell your patient to report any “potential cardiac” symptoms, such as palpitations, syncope, or near-syncope with or without palpitations, to a member of the healthcare team. Always be on the lookout for any concomitant conditions or treatments that can cause hypokalemia (e.g., diuretic use, gastroenteritis, diarrhea, excessive vomiting), or other agents that inhibit drug metabolism.
Obtaining a complete medication history, including the use of herbal products and over-the-counter medications, can help identify and prevent QTc prolongation from a drug interaction. A routine, 12-lead electrocardiogram (EKG) should be utilized during treatment to detect asymptomatic QTc prolongation or abnormal postectopic QTc intervals. Additionally, any patient predisposed to QTc prolongation should have an EKG performed before commencing treatment as well as after treatment is complete. If a drug prolongs the QTc interval beyond normal limits, the benefit of continuing the drug should be weighed against the risk of serious adverse cardiac events.10 TH
Michele B Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
1. Kupec IF. Seldane and generic terfenadine withdrawn from market. Food and Drug Administration Web site. Available at: www.fda.gov/bbs/topics/answers/ ans00853.html. Accessed Nov. 7, 2008.
2. Zalewski JM. Cisapride withdrawal requires alternate therapy. Cleveland Clinic Web site. Available at: www.clevelandclinicmeded.com/medicalpubs/pharmacy/mayjune2000/cisapride.htm. Accessed Nov. 7, 2008.
3. Drugs removed from or restricted in the U.S. market because of drug interactions. Food and Drug Administration Web site. Available at: www.fda.gov/cder/drug/drugReactions/CERT%20Educational%20Module%201/sld013.htm. Updated Dec. 22, 2008. Accessed Nov. 7, 2008.
4. Roden DM. Drug-induced prolongation of the QT interval. N Engl J Med. 2004;350:1013-1022.
5. Pham CP, de Feiter PW, van der Kuy PHM, van Mook WN. Long QTc interval and torsades de pointes caused by fluconazole. Ann Pharmacother. 2006;40:1456-1461.
6. Nykamp DL, Blackmon CL, Schmidt PE, Roberson AG. QTc prolongation associated with combination therapy of levofloxacin, imipramine, and fluoxetine. Ann Pharmacother. 1005;39:543-546.
7. Philips JA, Marty FM, Stone RM et al. Torsades de pointes associated with voriconazole use. Transpl Infect Dis. 2007;9:33-36.
8. Charbit B, Alvarez JC, Dasque E, Abe E, Démolis JL, Funck-Brentano C. Droperidol and ondansetron-induced QT interval prolongation. Anesthesiol. 2008;109:206-212.
9. Yap YG, Camm AJ. Drug induced qt prolongation and torsades de pointes. Heart. 2003;89:1363-1372.
10. Jayasinghe R, Registrar S, Kovoor P. Drugs and the QTc interval. Aust Prescr. 2002;25:63-65.
11. Atacand HCT 32/25 mg gives patients and physicians more treatment flexibility. Available at: www.pharmacitelink.com/news/2008/08/14_az.pdf. Accessed Nov. 4, 2008.
12. FDA approves astellas’ vaprisol (conivaptan hydrochloride injection) premixed in 5% dextrose for the treatment of hyponatremia. Sandoz Web site. Available at: sandoz.yellowbrix.com/pages/sandoz/Story.nsp?story_id=122559939. Accessed Nov. 4, 2008.
13. U.S. FDA drug shortages. Available at: www.fda.gov/cder/drug/shortages/default.htm#Foscavir. Accessed Nov. 3, 2008.
14. FDA Drug Shortages. Food and Drug Administration Web site. Available at: www.fda.gov/cder/drug/ shortages/discontinuation.pdf. Accessed Nov. 6, 2008.
15. Waknine Y. FDA safety changes: mirena, zyvox, orencia. Medscape Web site. Available at: www.medscape.com/viewarticle/580101. Accessed Nov. 3, 2008.
16. MannKind and Pfizer announce collaboration for certain exubera patients to transition to Mannkind’s inhaled insulin therapy. Drugs.com Web site. Available at: www.drugs.com/news/mannkind-pfizer-announce-collaboration-certain-exubera-patients-transition-mannkind-s-inhaled-13677.html. Accessed Nov. 3, 2008.
17. MannKind reports positive data from a phase 3 clinical study of technosphere insulin in Type 1 diabetics. Drugs.com Web site. Available at: www.drugs.com/ clinical_trials/mannkind-reports-positive-data-phase-3-clinical-study-technosphere-insulin-type-1-diabetes-5554.html. Accessed Nov. 3, 2008.
18. Bratulic A. Sanofi-aventis to halt all Acomplia trials. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=34DAB2DC3D7A48939A1D24AB97204CB4&logRowId=263560. Accessed Nov. 6, 2008.
Terfenadine, cisapride, astemizole … do you remember these drugs? They all were removed from the U.S. market subsequent to adverse outcomes related to QTc interval prolongation, including ventricular arrhythmias.1-3 Many drugs prolong the QTc interval, particularly if a drug is combined with others that affect its metabolism.
QTc interval prolongation can lead to torsades de pointes (TdP). Certain individuals are particularly predisposed to developing TdP, including: women, people with hypokalemia or hypomagnesemia, and those with a history of congenital or idiopathic QTc syndrome, cardiac arrest, syncope, congestive heart failure, bradycardia, baseline QT prolongation, renal failure, or cardiac failure.4 Some agents can prolong the QTc interval by five to 10 milliseconds and cause TdP, while others require a 50-millisecond increase or more.
Drugs that confer a risk of ventricular arrhythmias include: disopyramide, dofetilide, ibutilide, procainamide, quinidine, sotalol, and amiodarone (antiarrhythmic agents); clarithromycin, erythromycin, levofloxacin, gatifloxacin, gemifloxacin, moxifloxacin, telithromycin (anti-infectives); domperidone and droperidol antiemetics; chlorpromazine, haloperidol, mesoridazine, thioridazine, and pimozide (antipsychotics); amitriptyline, desipramine, doxepin, fluoxetine, imipramine, sertraline, and venlafaxine (antidepressants); fluconazole, itraconazole, and ketoconazole (antifungals); naratriptan, sumatriptan, and zolmitriptan; and methadone.4-8 Other related agents, such as voriconazole and ondansetron, have been reported to cause QTc prolongation.
Drugs of special concern are those that frequently inhibit the metabolism of other agents, including erythromycin, clarithromycin, ketoconazole, itraconazole, amiodarone, and quinidine, and many antidepressants and antiretroviral agents. Of the deaths associated with drug-induced QTc prolongation related to the prokinetic agent cisapride, many were due to drug interactions with an imidazole or macrolide antibiotic. In these cases, increased serum concentrations of cisapride occurred due to inhibition of the cytochrome P450 CYP3A4 isoenzyme.9
If treatment with a drug that has the potential for causing QTc prolongation is begun, tell your patient to report any “potential cardiac” symptoms, such as palpitations, syncope, or near-syncope with or without palpitations, to a member of the healthcare team. Always be on the lookout for any concomitant conditions or treatments that can cause hypokalemia (e.g., diuretic use, gastroenteritis, diarrhea, excessive vomiting), or other agents that inhibit drug metabolism.
Obtaining a complete medication history, including the use of herbal products and over-the-counter medications, can help identify and prevent QTc prolongation from a drug interaction. A routine, 12-lead electrocardiogram (EKG) should be utilized during treatment to detect asymptomatic QTc prolongation or abnormal postectopic QTc intervals. Additionally, any patient predisposed to QTc prolongation should have an EKG performed before commencing treatment as well as after treatment is complete. If a drug prolongs the QTc interval beyond normal limits, the benefit of continuing the drug should be weighed against the risk of serious adverse cardiac events.10 TH
Michele B Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
1. Kupec IF. Seldane and generic terfenadine withdrawn from market. Food and Drug Administration Web site. Available at: www.fda.gov/bbs/topics/answers/ ans00853.html. Accessed Nov. 7, 2008.
2. Zalewski JM. Cisapride withdrawal requires alternate therapy. Cleveland Clinic Web site. Available at: www.clevelandclinicmeded.com/medicalpubs/pharmacy/mayjune2000/cisapride.htm. Accessed Nov. 7, 2008.
3. Drugs removed from or restricted in the U.S. market because of drug interactions. Food and Drug Administration Web site. Available at: www.fda.gov/cder/drug/drugReactions/CERT%20Educational%20Module%201/sld013.htm. Updated Dec. 22, 2008. Accessed Nov. 7, 2008.
4. Roden DM. Drug-induced prolongation of the QT interval. N Engl J Med. 2004;350:1013-1022.
5. Pham CP, de Feiter PW, van der Kuy PHM, van Mook WN. Long QTc interval and torsades de pointes caused by fluconazole. Ann Pharmacother. 2006;40:1456-1461.
6. Nykamp DL, Blackmon CL, Schmidt PE, Roberson AG. QTc prolongation associated with combination therapy of levofloxacin, imipramine, and fluoxetine. Ann Pharmacother. 1005;39:543-546.
7. Philips JA, Marty FM, Stone RM et al. Torsades de pointes associated with voriconazole use. Transpl Infect Dis. 2007;9:33-36.
8. Charbit B, Alvarez JC, Dasque E, Abe E, Démolis JL, Funck-Brentano C. Droperidol and ondansetron-induced QT interval prolongation. Anesthesiol. 2008;109:206-212.
9. Yap YG, Camm AJ. Drug induced qt prolongation and torsades de pointes. Heart. 2003;89:1363-1372.
10. Jayasinghe R, Registrar S, Kovoor P. Drugs and the QTc interval. Aust Prescr. 2002;25:63-65.
11. Atacand HCT 32/25 mg gives patients and physicians more treatment flexibility. Available at: www.pharmacitelink.com/news/2008/08/14_az.pdf. Accessed Nov. 4, 2008.
12. FDA approves astellas’ vaprisol (conivaptan hydrochloride injection) premixed in 5% dextrose for the treatment of hyponatremia. Sandoz Web site. Available at: sandoz.yellowbrix.com/pages/sandoz/Story.nsp?story_id=122559939. Accessed Nov. 4, 2008.
13. U.S. FDA drug shortages. Available at: www.fda.gov/cder/drug/shortages/default.htm#Foscavir. Accessed Nov. 3, 2008.
14. FDA Drug Shortages. Food and Drug Administration Web site. Available at: www.fda.gov/cder/drug/ shortages/discontinuation.pdf. Accessed Nov. 6, 2008.
15. Waknine Y. FDA safety changes: mirena, zyvox, orencia. Medscape Web site. Available at: www.medscape.com/viewarticle/580101. Accessed Nov. 3, 2008.
16. MannKind and Pfizer announce collaboration for certain exubera patients to transition to Mannkind’s inhaled insulin therapy. Drugs.com Web site. Available at: www.drugs.com/news/mannkind-pfizer-announce-collaboration-certain-exubera-patients-transition-mannkind-s-inhaled-13677.html. Accessed Nov. 3, 2008.
17. MannKind reports positive data from a phase 3 clinical study of technosphere insulin in Type 1 diabetics. Drugs.com Web site. Available at: www.drugs.com/ clinical_trials/mannkind-reports-positive-data-phase-3-clinical-study-technosphere-insulin-type-1-diabetes-5554.html. Accessed Nov. 3, 2008.
18. Bratulic A. Sanofi-aventis to halt all Acomplia trials. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=34DAB2DC3D7A48939A1D24AB97204CB4&logRowId=263560. Accessed Nov. 6, 2008.
Terfenadine, cisapride, astemizole … do you remember these drugs? They all were removed from the U.S. market subsequent to adverse outcomes related to QTc interval prolongation, including ventricular arrhythmias.1-3 Many drugs prolong the QTc interval, particularly if a drug is combined with others that affect its metabolism.
QTc interval prolongation can lead to torsades de pointes (TdP). Certain individuals are particularly predisposed to developing TdP, including: women, people with hypokalemia or hypomagnesemia, and those with a history of congenital or idiopathic QTc syndrome, cardiac arrest, syncope, congestive heart failure, bradycardia, baseline QT prolongation, renal failure, or cardiac failure.4 Some agents can prolong the QTc interval by five to 10 milliseconds and cause TdP, while others require a 50-millisecond increase or more.
Drugs that confer a risk of ventricular arrhythmias include: disopyramide, dofetilide, ibutilide, procainamide, quinidine, sotalol, and amiodarone (antiarrhythmic agents); clarithromycin, erythromycin, levofloxacin, gatifloxacin, gemifloxacin, moxifloxacin, telithromycin (anti-infectives); domperidone and droperidol antiemetics; chlorpromazine, haloperidol, mesoridazine, thioridazine, and pimozide (antipsychotics); amitriptyline, desipramine, doxepin, fluoxetine, imipramine, sertraline, and venlafaxine (antidepressants); fluconazole, itraconazole, and ketoconazole (antifungals); naratriptan, sumatriptan, and zolmitriptan; and methadone.4-8 Other related agents, such as voriconazole and ondansetron, have been reported to cause QTc prolongation.
Drugs of special concern are those that frequently inhibit the metabolism of other agents, including erythromycin, clarithromycin, ketoconazole, itraconazole, amiodarone, and quinidine, and many antidepressants and antiretroviral agents. Of the deaths associated with drug-induced QTc prolongation related to the prokinetic agent cisapride, many were due to drug interactions with an imidazole or macrolide antibiotic. In these cases, increased serum concentrations of cisapride occurred due to inhibition of the cytochrome P450 CYP3A4 isoenzyme.9
If treatment with a drug that has the potential for causing QTc prolongation is begun, tell your patient to report any “potential cardiac” symptoms, such as palpitations, syncope, or near-syncope with or without palpitations, to a member of the healthcare team. Always be on the lookout for any concomitant conditions or treatments that can cause hypokalemia (e.g., diuretic use, gastroenteritis, diarrhea, excessive vomiting), or other agents that inhibit drug metabolism.
Obtaining a complete medication history, including the use of herbal products and over-the-counter medications, can help identify and prevent QTc prolongation from a drug interaction. A routine, 12-lead electrocardiogram (EKG) should be utilized during treatment to detect asymptomatic QTc prolongation or abnormal postectopic QTc intervals. Additionally, any patient predisposed to QTc prolongation should have an EKG performed before commencing treatment as well as after treatment is complete. If a drug prolongs the QTc interval beyond normal limits, the benefit of continuing the drug should be weighed against the risk of serious adverse cardiac events.10 TH
Michele B Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
1. Kupec IF. Seldane and generic terfenadine withdrawn from market. Food and Drug Administration Web site. Available at: www.fda.gov/bbs/topics/answers/ ans00853.html. Accessed Nov. 7, 2008.
2. Zalewski JM. Cisapride withdrawal requires alternate therapy. Cleveland Clinic Web site. Available at: www.clevelandclinicmeded.com/medicalpubs/pharmacy/mayjune2000/cisapride.htm. Accessed Nov. 7, 2008.
3. Drugs removed from or restricted in the U.S. market because of drug interactions. Food and Drug Administration Web site. Available at: www.fda.gov/cder/drug/drugReactions/CERT%20Educational%20Module%201/sld013.htm. Updated Dec. 22, 2008. Accessed Nov. 7, 2008.
4. Roden DM. Drug-induced prolongation of the QT interval. N Engl J Med. 2004;350:1013-1022.
5. Pham CP, de Feiter PW, van der Kuy PHM, van Mook WN. Long QTc interval and torsades de pointes caused by fluconazole. Ann Pharmacother. 2006;40:1456-1461.
6. Nykamp DL, Blackmon CL, Schmidt PE, Roberson AG. QTc prolongation associated with combination therapy of levofloxacin, imipramine, and fluoxetine. Ann Pharmacother. 1005;39:543-546.
7. Philips JA, Marty FM, Stone RM et al. Torsades de pointes associated with voriconazole use. Transpl Infect Dis. 2007;9:33-36.
8. Charbit B, Alvarez JC, Dasque E, Abe E, Démolis JL, Funck-Brentano C. Droperidol and ondansetron-induced QT interval prolongation. Anesthesiol. 2008;109:206-212.
9. Yap YG, Camm AJ. Drug induced qt prolongation and torsades de pointes. Heart. 2003;89:1363-1372.
10. Jayasinghe R, Registrar S, Kovoor P. Drugs and the QTc interval. Aust Prescr. 2002;25:63-65.
11. Atacand HCT 32/25 mg gives patients and physicians more treatment flexibility. Available at: www.pharmacitelink.com/news/2008/08/14_az.pdf. Accessed Nov. 4, 2008.
12. FDA approves astellas’ vaprisol (conivaptan hydrochloride injection) premixed in 5% dextrose for the treatment of hyponatremia. Sandoz Web site. Available at: sandoz.yellowbrix.com/pages/sandoz/Story.nsp?story_id=122559939. Accessed Nov. 4, 2008.
13. U.S. FDA drug shortages. Available at: www.fda.gov/cder/drug/shortages/default.htm#Foscavir. Accessed Nov. 3, 2008.
14. FDA Drug Shortages. Food and Drug Administration Web site. Available at: www.fda.gov/cder/drug/ shortages/discontinuation.pdf. Accessed Nov. 6, 2008.
15. Waknine Y. FDA safety changes: mirena, zyvox, orencia. Medscape Web site. Available at: www.medscape.com/viewarticle/580101. Accessed Nov. 3, 2008.
16. MannKind and Pfizer announce collaboration for certain exubera patients to transition to Mannkind’s inhaled insulin therapy. Drugs.com Web site. Available at: www.drugs.com/news/mannkind-pfizer-announce-collaboration-certain-exubera-patients-transition-mannkind-s-inhaled-13677.html. Accessed Nov. 3, 2008.
17. MannKind reports positive data from a phase 3 clinical study of technosphere insulin in Type 1 diabetics. Drugs.com Web site. Available at: www.drugs.com/ clinical_trials/mannkind-reports-positive-data-phase-3-clinical-study-technosphere-insulin-type-1-diabetes-5554.html. Accessed Nov. 3, 2008.
18. Bratulic A. Sanofi-aventis to halt all Acomplia trials. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=34DAB2DC3D7A48939A1D24AB97204CB4&logRowId=263560. Accessed Nov. 6, 2008.
At Work in Washington

SHM’s 20-member Public Policy Committee, headed by Eric Siegal, MD, had a busy 2008 addressing the many legislative and regulatory issues affecting hospitalists. As a result of our efforts, SHM’s visibility with key lawmakers, the Medicare Payment Advisory Commission (MedPAC), and the Centers for Medicare and Medicaid Services (CMS) has increased significantly, and policymakers now routinely turn to us for advice and expertise. Here is an update on how the committee represents hospital medicine—and your interests—in our nation’s capital.
Medicare Payment Cuts Prevented
Earlier this year, SHM’s Public Policy Committee (PPC) worked tirelessly to secure passage of H.R. 6331, the Medicare Improvements for Patients and Providers Act (MIPPA). It blocked the 10.6% physician payment cut, which was scheduled to go into effect July 1, 2008, and extended current payment rates through Dec. 31, 2009 Thanks in part to concerted advocacy by SHM and its members, Congress voted overwhelmingly July 15 to override President Bush’s veto of this measure. The new law (P.L. 110-275) includes 18 months of relief from scheduled cuts in Part B Medicare payments, other increases in reimbursement for inpatient evaluation and management services, and several SHM-supported quality improvement initiatives.
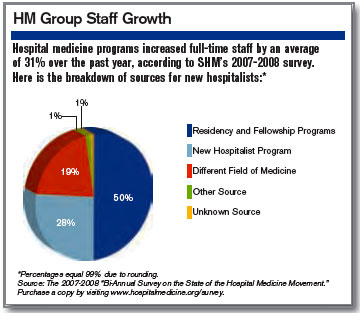
Beginning Jan. 1, hospitalists will see a 1.1% increase in Part B payments, instead of a projected 5.4% cut. SHM strongly supported provisions of the bill, which requires CMS to apply budget-neutral adjustments for 2007 and 2008 to the conversion factor. This change will result in an estimated average gain of another 3% in total Medicare payments for hospitalists.
SHM also supported continued funding of the Physician Quality Reporting Initiative (PQRI) and other quality provisions contained in MIPPA. Under the new Medicare act, hospitalists who successfully report quality measures are eligible for a bonus payment in 2009 and 2010 of 2% (up from 1.5%) of their total Medicare allowed charges. The new law also requires the U.S. Secretary of Health and Human Services (HHS) to develop a plan to transition to a value-based purchasing program for physician services.
SHM took multiple steps to influence MIPPA’s successful passage. Here are a few of those steps:
- When Sen. Max Baucus (D-Montana), chair of the Senate Finance Committee, announced he was working on legislation to reverse the pending cuts in Medicare payments, the PPC immediately commended his efforts and offered our assistance with the bill, specifically focusing on quality improvement provisions.
- Sen. Baucus introduced S. 3101, which formed the basis of the final Medicare bill, H.R. 6331, in June. On June 9, the PPC sent a letter to Sen. Baucus, formally supporting his efforts to address the pending payment reductions and praising other provisions in the bill promoting quality reporting, including continuation of the PQRI program; a requirement that measures be endorsed by a consensus-based, standard-setting entity such as the National Quality Forum, which CMS posts on its Web site the list of providers who participate in the PQRI; and that HHS provide confidential feedback to providers regarding their resource use.
- In a July 10 letter, we urged President Bush to immediately sign H.R. 6331 into law, stating, “This legislation, passed by bipartisan margins in both the House and Senate, contains many positive elements for hospitalists and their patients, and deserves your support.”
- As part of our advocacy efforts, the PPC launched a comprehensive, grassroots campaign to pass MIPPA, sending an unprecedented number of communications to inform and mobilize SHM members. In the month leading up to final passage of H.R. 6331, we sent 12 legislative e-mail updates to SHM members, urging each member to contact his or her lawmakers via our legislation action center. As a result of this outreach, hospitalists generated a total of 1,269 messages to members of Congress, urging policy makers to stop the Medicare cuts to physician payments. We thank all of you who visited the action center and contacted your lawmakers. Your efforts were vital to the success of SHM’s campaign to stop the cuts and passage of H.R. 6331.
Payment Advisory Commission Interaction
The PPC has made SHM’s engagement with the influential Medicare Payment Advisory Commission a top priority. An independent Congressional agency established by the Balanced Budget Act of 1997, MedPAC advises Congress on issues affecting the Medicare program. Our efforts to educate the commission and staff about hospital medicine are paying off. Through attendance at MedPAC meetings, as well as conference calls and face-to-face meetings with staff, SHM has educated the commission about the positive contributions hospitalists are making throughout the country.
PPC members attended MedPAC’s March 5, 2008, meeting and addressed the commission during the public comment period. The PPC offered to further educate the commission regarding the role hospital medicine can play in Medicare reform. In June, key SHM leaders met with MedPAC staff, including executive director Mark Miller, in Washington to discuss hospital medicine and SHM’s quality improvement initiatives, including Project BOOST. At MedPAC’s request, the PPC has worked to develop a “starter set” of metrics to define high-performing hospitalist programs. It might form a basis for future value-based purchasing initiatives.
Also in June, MedPAC released its report to Congress on “Reforming the Delivery System,” which contained extensive information and feedback from SHM.
The PPC continues to monitor MedPAC’s work, particularly its recommendations for changes in Medicare payment for care provided around a hospitalization to encourage care coordination and efficiency. To reduce hospital readmissions, the commission’s June report to Congress recommended, among other things, that CMS conduct a voluntary pilot program to test bundled payment for all services around a hospitalization for select conditions.
Value-Based Purchasing
Together with SHM’s Performance and Standards Committee, the PPC continues to monitor and comment on CMS’s value-based purchasing (VBP) initiatives, as well as educate SHM members on what the initiatives mean for hospitalists. On June 11, SHM hosted a teleconference on VBP. It featured Thomas Valuck, MD, JD, medical officer and senior adviser, Center for Medicare Management, CMS. In his presentation, Dr. Valuck acknowledged the unique role hospitalists play in VBP programs, and he commended SHM for its proactive stance and constructive engagement with CMS.
On Aug. 29, the PPC submitted comments on CMS’s proposed FY 2009 physician payment rule. This rule proposed additional improvements to the PQRI; discussed CMS’s interest in developing a “Physician Compare” Web site to report quality of care and value for services provided by physicians; solicited comments on CMS’s proposed preventable hospital-acquired conditions; and proposed a new, targeted exception to the physician self-referral statute for programs using economic incentives to foster high quality, cost-effective care. Visit http://www.hospital medicine.org/Content/Navigation Menu/AdvocacyPolicy/LegislativeRegulatoryUpdates/Legislative_Regulato.htm for a summary of the final rule.
Increased AHRQ Appropriations
Through its participation in the Friends of Agency for Healthcare Research and Quality (AHRQ) coalition, visits to Congressional offices by members and staff, and grassroots advocacy via our legislative action center, SHM continues to advocate for increased funding for this important agency. Last fall, President Bush signed a continuing resolution, P.L. 110-329, which funds government agencies, including AHRQ, at current levels through March 6. The resolution was necessary because none of the 12 individual FY 2009 appropriations bills, including the Labor Department-Health and Human Services-Education Department measure, which contains funding for AHRQ and the National Institutes of Health, had been enacted into law. Early this year lawmakers are expected to attempt to pass the remaining appropriations bills and forward them to President-elect Obama.
What’s Ahead?
This year promises to be busy on the healthcare policy front. SHM is poised to make major contributions to the debate, given its advocacy on key issues over the past year and the goodwill it has generated among policymakers. The PPC will devote considerable time to crafting hospital medicine-specific recommendations on health reform, including bundling and its implications for hospitalists; and providing input to CMS’s value-based purchasing initiatives, including the agency’s report to Congress, which is due May 2010. We also will continue to pursue a separate CMS specialty billing code for hospitalists.
The PPC strives to keep SHM members informed about legislative and regulatory activities through monthly updates posted to the advocacy section of the SHM Web site, articles in The Hospitalist, and items in the new SHM e-Wire. Letters to Congress and CMS are located on the Web site, as well.
When an important issue arises, you likely will receive an e-mail urging you to visit our legislative action center (www.hospitalmedicine.org/beheard) and contact your members of Congress. We depend on your involvement in the legislative process in order to be effective in Washington. TH
Laura Allendorf is senior advisor for advocacy and government affairs for the Society of Hospital Medicine. Contact her at [email protected].
SHM’s 20-member Public Policy Committee, headed by Eric Siegal, MD, had a busy 2008 addressing the many legislative and regulatory issues affecting hospitalists. As a result of our efforts, SHM’s visibility with key lawmakers, the Medicare Payment Advisory Commission (MedPAC), and the Centers for Medicare and Medicaid Services (CMS) has increased significantly, and policymakers now routinely turn to us for advice and expertise. Here is an update on how the committee represents hospital medicine—and your interests—in our nation’s capital.
Medicare Payment Cuts Prevented
Earlier this year, SHM’s Public Policy Committee (PPC) worked tirelessly to secure passage of H.R. 6331, the Medicare Improvements for Patients and Providers Act (MIPPA). It blocked the 10.6% physician payment cut, which was scheduled to go into effect July 1, 2008, and extended current payment rates through Dec. 31, 2009 Thanks in part to concerted advocacy by SHM and its members, Congress voted overwhelmingly July 15 to override President Bush’s veto of this measure. The new law (P.L. 110-275) includes 18 months of relief from scheduled cuts in Part B Medicare payments, other increases in reimbursement for inpatient evaluation and management services, and several SHM-supported quality improvement initiatives.
Beginning Jan. 1, hospitalists will see a 1.1% increase in Part B payments, instead of a projected 5.4% cut. SHM strongly supported provisions of the bill, which requires CMS to apply budget-neutral adjustments for 2007 and 2008 to the conversion factor. This change will result in an estimated average gain of another 3% in total Medicare payments for hospitalists.
SHM also supported continued funding of the Physician Quality Reporting Initiative (PQRI) and other quality provisions contained in MIPPA. Under the new Medicare act, hospitalists who successfully report quality measures are eligible for a bonus payment in 2009 and 2010 of 2% (up from 1.5%) of their total Medicare allowed charges. The new law also requires the U.S. Secretary of Health and Human Services (HHS) to develop a plan to transition to a value-based purchasing program for physician services.
SHM took multiple steps to influence MIPPA’s successful passage. Here are a few of those steps:
- When Sen. Max Baucus (D-Montana), chair of the Senate Finance Committee, announced he was working on legislation to reverse the pending cuts in Medicare payments, the PPC immediately commended his efforts and offered our assistance with the bill, specifically focusing on quality improvement provisions.
- Sen. Baucus introduced S. 3101, which formed the basis of the final Medicare bill, H.R. 6331, in June. On June 9, the PPC sent a letter to Sen. Baucus, formally supporting his efforts to address the pending payment reductions and praising other provisions in the bill promoting quality reporting, including continuation of the PQRI program; a requirement that measures be endorsed by a consensus-based, standard-setting entity such as the National Quality Forum, which CMS posts on its Web site the list of providers who participate in the PQRI; and that HHS provide confidential feedback to providers regarding their resource use.
- In a July 10 letter, we urged President Bush to immediately sign H.R. 6331 into law, stating, “This legislation, passed by bipartisan margins in both the House and Senate, contains many positive elements for hospitalists and their patients, and deserves your support.”
- As part of our advocacy efforts, the PPC launched a comprehensive, grassroots campaign to pass MIPPA, sending an unprecedented number of communications to inform and mobilize SHM members. In the month leading up to final passage of H.R. 6331, we sent 12 legislative e-mail updates to SHM members, urging each member to contact his or her lawmakers via our legislation action center. As a result of this outreach, hospitalists generated a total of 1,269 messages to members of Congress, urging policy makers to stop the Medicare cuts to physician payments. We thank all of you who visited the action center and contacted your lawmakers. Your efforts were vital to the success of SHM’s campaign to stop the cuts and passage of H.R. 6331.
Payment Advisory Commission Interaction
The PPC has made SHM’s engagement with the influential Medicare Payment Advisory Commission a top priority. An independent Congressional agency established by the Balanced Budget Act of 1997, MedPAC advises Congress on issues affecting the Medicare program. Our efforts to educate the commission and staff about hospital medicine are paying off. Through attendance at MedPAC meetings, as well as conference calls and face-to-face meetings with staff, SHM has educated the commission about the positive contributions hospitalists are making throughout the country.
PPC members attended MedPAC’s March 5, 2008, meeting and addressed the commission during the public comment period. The PPC offered to further educate the commission regarding the role hospital medicine can play in Medicare reform. In June, key SHM leaders met with MedPAC staff, including executive director Mark Miller, in Washington to discuss hospital medicine and SHM’s quality improvement initiatives, including Project BOOST. At MedPAC’s request, the PPC has worked to develop a “starter set” of metrics to define high-performing hospitalist programs. It might form a basis for future value-based purchasing initiatives.
Also in June, MedPAC released its report to Congress on “Reforming the Delivery System,” which contained extensive information and feedback from SHM.
The PPC continues to monitor MedPAC’s work, particularly its recommendations for changes in Medicare payment for care provided around a hospitalization to encourage care coordination and efficiency. To reduce hospital readmissions, the commission’s June report to Congress recommended, among other things, that CMS conduct a voluntary pilot program to test bundled payment for all services around a hospitalization for select conditions.
Value-Based Purchasing
Together with SHM’s Performance and Standards Committee, the PPC continues to monitor and comment on CMS’s value-based purchasing (VBP) initiatives, as well as educate SHM members on what the initiatives mean for hospitalists. On June 11, SHM hosted a teleconference on VBP. It featured Thomas Valuck, MD, JD, medical officer and senior adviser, Center for Medicare Management, CMS. In his presentation, Dr. Valuck acknowledged the unique role hospitalists play in VBP programs, and he commended SHM for its proactive stance and constructive engagement with CMS.
On Aug. 29, the PPC submitted comments on CMS’s proposed FY 2009 physician payment rule. This rule proposed additional improvements to the PQRI; discussed CMS’s interest in developing a “Physician Compare” Web site to report quality of care and value for services provided by physicians; solicited comments on CMS’s proposed preventable hospital-acquired conditions; and proposed a new, targeted exception to the physician self-referral statute for programs using economic incentives to foster high quality, cost-effective care. Visit http://www.hospital medicine.org/Content/Navigation Menu/AdvocacyPolicy/LegislativeRegulatoryUpdates/Legislative_Regulato.htm for a summary of the final rule.
Increased AHRQ Appropriations
Through its participation in the Friends of Agency for Healthcare Research and Quality (AHRQ) coalition, visits to Congressional offices by members and staff, and grassroots advocacy via our legislative action center, SHM continues to advocate for increased funding for this important agency. Last fall, President Bush signed a continuing resolution, P.L. 110-329, which funds government agencies, including AHRQ, at current levels through March 6. The resolution was necessary because none of the 12 individual FY 2009 appropriations bills, including the Labor Department-Health and Human Services-Education Department measure, which contains funding for AHRQ and the National Institutes of Health, had been enacted into law. Early this year lawmakers are expected to attempt to pass the remaining appropriations bills and forward them to President-elect Obama.
What’s Ahead?
This year promises to be busy on the healthcare policy front. SHM is poised to make major contributions to the debate, given its advocacy on key issues over the past year and the goodwill it has generated among policymakers. The PPC will devote considerable time to crafting hospital medicine-specific recommendations on health reform, including bundling and its implications for hospitalists; and providing input to CMS’s value-based purchasing initiatives, including the agency’s report to Congress, which is due May 2010. We also will continue to pursue a separate CMS specialty billing code for hospitalists.
The PPC strives to keep SHM members informed about legislative and regulatory activities through monthly updates posted to the advocacy section of the SHM Web site, articles in The Hospitalist, and items in the new SHM e-Wire. Letters to Congress and CMS are located on the Web site, as well.
When an important issue arises, you likely will receive an e-mail urging you to visit our legislative action center (www.hospitalmedicine.org/beheard) and contact your members of Congress. We depend on your involvement in the legislative process in order to be effective in Washington. TH
Laura Allendorf is senior advisor for advocacy and government affairs for the Society of Hospital Medicine. Contact her at [email protected].
SHM’s 20-member Public Policy Committee, headed by Eric Siegal, MD, had a busy 2008 addressing the many legislative and regulatory issues affecting hospitalists. As a result of our efforts, SHM’s visibility with key lawmakers, the Medicare Payment Advisory Commission (MedPAC), and the Centers for Medicare and Medicaid Services (CMS) has increased significantly, and policymakers now routinely turn to us for advice and expertise. Here is an update on how the committee represents hospital medicine—and your interests—in our nation’s capital.
Medicare Payment Cuts Prevented
Earlier this year, SHM’s Public Policy Committee (PPC) worked tirelessly to secure passage of H.R. 6331, the Medicare Improvements for Patients and Providers Act (MIPPA). It blocked the 10.6% physician payment cut, which was scheduled to go into effect July 1, 2008, and extended current payment rates through Dec. 31, 2009 Thanks in part to concerted advocacy by SHM and its members, Congress voted overwhelmingly July 15 to override President Bush’s veto of this measure. The new law (P.L. 110-275) includes 18 months of relief from scheduled cuts in Part B Medicare payments, other increases in reimbursement for inpatient evaluation and management services, and several SHM-supported quality improvement initiatives.
Beginning Jan. 1, hospitalists will see a 1.1% increase in Part B payments, instead of a projected 5.4% cut. SHM strongly supported provisions of the bill, which requires CMS to apply budget-neutral adjustments for 2007 and 2008 to the conversion factor. This change will result in an estimated average gain of another 3% in total Medicare payments for hospitalists.
SHM also supported continued funding of the Physician Quality Reporting Initiative (PQRI) and other quality provisions contained in MIPPA. Under the new Medicare act, hospitalists who successfully report quality measures are eligible for a bonus payment in 2009 and 2010 of 2% (up from 1.5%) of their total Medicare allowed charges. The new law also requires the U.S. Secretary of Health and Human Services (HHS) to develop a plan to transition to a value-based purchasing program for physician services.
SHM took multiple steps to influence MIPPA’s successful passage. Here are a few of those steps:
- When Sen. Max Baucus (D-Montana), chair of the Senate Finance Committee, announced he was working on legislation to reverse the pending cuts in Medicare payments, the PPC immediately commended his efforts and offered our assistance with the bill, specifically focusing on quality improvement provisions.
- Sen. Baucus introduced S. 3101, which formed the basis of the final Medicare bill, H.R. 6331, in June. On June 9, the PPC sent a letter to Sen. Baucus, formally supporting his efforts to address the pending payment reductions and praising other provisions in the bill promoting quality reporting, including continuation of the PQRI program; a requirement that measures be endorsed by a consensus-based, standard-setting entity such as the National Quality Forum, which CMS posts on its Web site the list of providers who participate in the PQRI; and that HHS provide confidential feedback to providers regarding their resource use.
- In a July 10 letter, we urged President Bush to immediately sign H.R. 6331 into law, stating, “This legislation, passed by bipartisan margins in both the House and Senate, contains many positive elements for hospitalists and their patients, and deserves your support.”
- As part of our advocacy efforts, the PPC launched a comprehensive, grassroots campaign to pass MIPPA, sending an unprecedented number of communications to inform and mobilize SHM members. In the month leading up to final passage of H.R. 6331, we sent 12 legislative e-mail updates to SHM members, urging each member to contact his or her lawmakers via our legislation action center. As a result of this outreach, hospitalists generated a total of 1,269 messages to members of Congress, urging policy makers to stop the Medicare cuts to physician payments. We thank all of you who visited the action center and contacted your lawmakers. Your efforts were vital to the success of SHM’s campaign to stop the cuts and passage of H.R. 6331.
Payment Advisory Commission Interaction
The PPC has made SHM’s engagement with the influential Medicare Payment Advisory Commission a top priority. An independent Congressional agency established by the Balanced Budget Act of 1997, MedPAC advises Congress on issues affecting the Medicare program. Our efforts to educate the commission and staff about hospital medicine are paying off. Through attendance at MedPAC meetings, as well as conference calls and face-to-face meetings with staff, SHM has educated the commission about the positive contributions hospitalists are making throughout the country.
PPC members attended MedPAC’s March 5, 2008, meeting and addressed the commission during the public comment period. The PPC offered to further educate the commission regarding the role hospital medicine can play in Medicare reform. In June, key SHM leaders met with MedPAC staff, including executive director Mark Miller, in Washington to discuss hospital medicine and SHM’s quality improvement initiatives, including Project BOOST. At MedPAC’s request, the PPC has worked to develop a “starter set” of metrics to define high-performing hospitalist programs. It might form a basis for future value-based purchasing initiatives.
Also in June, MedPAC released its report to Congress on “Reforming the Delivery System,” which contained extensive information and feedback from SHM.
The PPC continues to monitor MedPAC’s work, particularly its recommendations for changes in Medicare payment for care provided around a hospitalization to encourage care coordination and efficiency. To reduce hospital readmissions, the commission’s June report to Congress recommended, among other things, that CMS conduct a voluntary pilot program to test bundled payment for all services around a hospitalization for select conditions.
Value-Based Purchasing
Together with SHM’s Performance and Standards Committee, the PPC continues to monitor and comment on CMS’s value-based purchasing (VBP) initiatives, as well as educate SHM members on what the initiatives mean for hospitalists. On June 11, SHM hosted a teleconference on VBP. It featured Thomas Valuck, MD, JD, medical officer and senior adviser, Center for Medicare Management, CMS. In his presentation, Dr. Valuck acknowledged the unique role hospitalists play in VBP programs, and he commended SHM for its proactive stance and constructive engagement with CMS.
On Aug. 29, the PPC submitted comments on CMS’s proposed FY 2009 physician payment rule. This rule proposed additional improvements to the PQRI; discussed CMS’s interest in developing a “Physician Compare” Web site to report quality of care and value for services provided by physicians; solicited comments on CMS’s proposed preventable hospital-acquired conditions; and proposed a new, targeted exception to the physician self-referral statute for programs using economic incentives to foster high quality, cost-effective care. Visit http://www.hospital medicine.org/Content/Navigation Menu/AdvocacyPolicy/LegislativeRegulatoryUpdates/Legislative_Regulato.htm for a summary of the final rule.
Increased AHRQ Appropriations
Through its participation in the Friends of Agency for Healthcare Research and Quality (AHRQ) coalition, visits to Congressional offices by members and staff, and grassroots advocacy via our legislative action center, SHM continues to advocate for increased funding for this important agency. Last fall, President Bush signed a continuing resolution, P.L. 110-329, which funds government agencies, including AHRQ, at current levels through March 6. The resolution was necessary because none of the 12 individual FY 2009 appropriations bills, including the Labor Department-Health and Human Services-Education Department measure, which contains funding for AHRQ and the National Institutes of Health, had been enacted into law. Early this year lawmakers are expected to attempt to pass the remaining appropriations bills and forward them to President-elect Obama.
What’s Ahead?
This year promises to be busy on the healthcare policy front. SHM is poised to make major contributions to the debate, given its advocacy on key issues over the past year and the goodwill it has generated among policymakers. The PPC will devote considerable time to crafting hospital medicine-specific recommendations on health reform, including bundling and its implications for hospitalists; and providing input to CMS’s value-based purchasing initiatives, including the agency’s report to Congress, which is due May 2010. We also will continue to pursue a separate CMS specialty billing code for hospitalists.
The PPC strives to keep SHM members informed about legislative and regulatory activities through monthly updates posted to the advocacy section of the SHM Web site, articles in The Hospitalist, and items in the new SHM e-Wire. Letters to Congress and CMS are located on the Web site, as well.
When an important issue arises, you likely will receive an e-mail urging you to visit our legislative action center (www.hospitalmedicine.org/beheard) and contact your members of Congress. We depend on your involvement in the legislative process in order to be effective in Washington. TH
Laura Allendorf is senior advisor for advocacy and government affairs for the Society of Hospital Medicine. Contact her at [email protected].
Non-Physician Providers Critical to Hospital Medicine Practices
Non-Physician Providers Critical to Hospital Medicine Practices
In “Maximizing NPPs in Hospitalist Practices” (Practice Management, October 2008, p. 69), John Nelson, MD, implies a financial advantage to hiring nurse practitioners (NPs) rather than physician assistants (PAs):
“A PA’s work will nearly always require a physician being physically present during some portion of the patient visit and co-signing chart notes and orders. Nurse practitioners, on the other hand, may be able to perform certain patient-care activities independently. Medicare and other payers typically reimburse at 85% of the rate customarily paid to MDs for the same service.”
Dr. Nelson: Do you mean to imply NPs providing hospitalist coverage should function independently, without any physician supervision, oversight, or input? I do not know of any hospitals that allow NPs to admit and manage patients independently, despite their independent practice status. In my opinion, it would be detrimental to patient care to allow non-physician providers to provide completely independent, unsupervised hospital care.
In addition, I know of no hospital practice setting that requires a physician to be physically present during a PA’s exam. In all hospital practice settings that I am aware of, a supervising or attending physician (not necessarily the one on the PA’s license), must see the patient at some time each day, not necessarily at the same time as the PA.
In that scenario, the physician pays a brief visit to the patient to corroborate the PA’s exam and plan. The physician then writes a brief, seen-and-agreed note, and can bill 100% of the Medicare reimbursement, not the 85% for a NP visit. How this compares economically depends, of course, on relative salaries. But it provides physician oversight of the NPP, which assumedly will improve quality of care (though I have no studies to cite to that effect).
Do you have some other reason for your anti-PA, pro-NP bias? Is your personal experience colored by working with more competent NPs, in your opinion, and less competent PAs? Perhaps that would make for a more interesting, better-defined column.
Richard Buckberg, PA-C, Maine Medical Center, Portland, Maine
SHM’s Non-Physician Provider (NPP) Committee was delighted to see the recent article by Dr. Nelson, MD, regarding the use of NPPs in hospital medicine. These columns spotlighted HM’s increasing utilization of NPPs, a role that only is expected to increase in number and breadth, based on the increasing need for competent, comprehensive care of the acutely ill.
Dr. Nelson made many excellent points that may benefit from some clarification or expansion. Dr. Nelson states a PA “will nearly always require a physician being physically present during some portion of the patient visit and co-signing chart notes and orders.” This is incorrect, and seems to imply PAs are more difficult to assimilate into practice than NPs. Depending upon variability in legal limitations and hospital bylaws, both PAs and NPs may see a patient without a physician present. In order to bill for a shared visit and receive 100% reimbursement, the attending physician needs to have a face-to-face encounter with that patient at some point in the day and document a portion of the evaluation and management (e.g., history, physical exam, or medical decision-making).
Alternatively, in most states, both NPs and PAs can see patients independently and bill for their services at 85% of the physician’s Medicare rate. Obtaining 100% reimbursement for NPP services when using the shared billing model is efficient and simple. Though variability exists, more specifically in hospital culture, utilization of these roles can positively impact the bottom line of reimbursement. Therefore, it is essential to understand all of the regulations before developing a business model incorporating NPPs.
Dr. Nelson also points out that using NPPs in a clerical fashion, such as discharge planning, is not optimizing the NPPs capabilities. This point is well taken. If clerical assistance is needed, hire the appropriate discipline.
He also says in order to integrate and maximize the benefit of the NPP to a particular practice, a careful analysis of the needs of the practice should be performed prior to hiring. This will allow both physicians and the NPP to have clear expectations. An emphasis should be placed on the importance of recognizing the level of experience will likely impact the role. For example, utilizing a new graduate in a short-stay observation unit with limited diagnoses and treatments may make sense, but utilizing an NPP as a nocturnist, cross-covering and independently admitting patients, would require an NPP with years of experience. It is crucial to hire the right NPP with the right qualifications and experience for the job.
Dr. Nelson states patient satisfaction may decline by adding NPPs to the practice. Rather than focusing on possible dilution of a patient experience with the addition of another healthcare provider, one should instead consider the potential of adding another perspective to the team. Two providers with unique educational backgrounds and insight may indeed be better than one. Utilization of NPPs can increase face time with patients, subsequently increasing patient satisfaction. Additionally, research in outpatient settings shows no difference in patient satisfaction between physicians and NPPs; more research in inpatient settings needs to be performed.
We encourage HMG directors to refer to our expanded section on SHM’s Web site, “Practice Resources,” which has a wealth of information regarding NPP utilization. The NPP committee will be hosting two courses at the annual meeting, “The Basics: Can NPs/PAs Meet Our Needs,” and “Advanced Concepts: Three Different Practice Models.”
Jina Saltzman, PA-C, University of Chicago Medical Center
Dear readers: My main goal in writing the column was to indicate that NPs and PAs could be valuable contributors to many hospitalist practices. Yet, many practices fail to create the optimal role for them, one that contributes to patient outcomes, efficiency and economic health, and provides a rewarding role for the NPP.
I do not have an anti-PA, pro-NP bias. My intention was not to take sides regarding whether PAs or NPs are more skilled or better for patients. I think that is a function of the individual, much more than their training certificate (same with MDs). I did not intend to imply “nurse practitioners providing hospitalist coverage should function independently, without any physician supervision, oversight, or input.”
Lastly, I did make a factual error regarding the differences in physician supervision required for NPs and PAs. Saltzman’s letter above addresses the error. TH
Non-Physician Providers Critical to Hospital Medicine Practices
In “Maximizing NPPs in Hospitalist Practices” (Practice Management, October 2008, p. 69), John Nelson, MD, implies a financial advantage to hiring nurse practitioners (NPs) rather than physician assistants (PAs):
“A PA’s work will nearly always require a physician being physically present during some portion of the patient visit and co-signing chart notes and orders. Nurse practitioners, on the other hand, may be able to perform certain patient-care activities independently. Medicare and other payers typically reimburse at 85% of the rate customarily paid to MDs for the same service.”
Dr. Nelson: Do you mean to imply NPs providing hospitalist coverage should function independently, without any physician supervision, oversight, or input? I do not know of any hospitals that allow NPs to admit and manage patients independently, despite their independent practice status. In my opinion, it would be detrimental to patient care to allow non-physician providers to provide completely independent, unsupervised hospital care.
In addition, I know of no hospital practice setting that requires a physician to be physically present during a PA’s exam. In all hospital practice settings that I am aware of, a supervising or attending physician (not necessarily the one on the PA’s license), must see the patient at some time each day, not necessarily at the same time as the PA.
In that scenario, the physician pays a brief visit to the patient to corroborate the PA’s exam and plan. The physician then writes a brief, seen-and-agreed note, and can bill 100% of the Medicare reimbursement, not the 85% for a NP visit. How this compares economically depends, of course, on relative salaries. But it provides physician oversight of the NPP, which assumedly will improve quality of care (though I have no studies to cite to that effect).
Do you have some other reason for your anti-PA, pro-NP bias? Is your personal experience colored by working with more competent NPs, in your opinion, and less competent PAs? Perhaps that would make for a more interesting, better-defined column.
Richard Buckberg, PA-C, Maine Medical Center, Portland, Maine
SHM’s Non-Physician Provider (NPP) Committee was delighted to see the recent article by Dr. Nelson, MD, regarding the use of NPPs in hospital medicine. These columns spotlighted HM’s increasing utilization of NPPs, a role that only is expected to increase in number and breadth, based on the increasing need for competent, comprehensive care of the acutely ill.
Dr. Nelson made many excellent points that may benefit from some clarification or expansion. Dr. Nelson states a PA “will nearly always require a physician being physically present during some portion of the patient visit and co-signing chart notes and orders.” This is incorrect, and seems to imply PAs are more difficult to assimilate into practice than NPs. Depending upon variability in legal limitations and hospital bylaws, both PAs and NPs may see a patient without a physician present. In order to bill for a shared visit and receive 100% reimbursement, the attending physician needs to have a face-to-face encounter with that patient at some point in the day and document a portion of the evaluation and management (e.g., history, physical exam, or medical decision-making).
Alternatively, in most states, both NPs and PAs can see patients independently and bill for their services at 85% of the physician’s Medicare rate. Obtaining 100% reimbursement for NPP services when using the shared billing model is efficient and simple. Though variability exists, more specifically in hospital culture, utilization of these roles can positively impact the bottom line of reimbursement. Therefore, it is essential to understand all of the regulations before developing a business model incorporating NPPs.
Dr. Nelson also points out that using NPPs in a clerical fashion, such as discharge planning, is not optimizing the NPPs capabilities. This point is well taken. If clerical assistance is needed, hire the appropriate discipline.
He also says in order to integrate and maximize the benefit of the NPP to a particular practice, a careful analysis of the needs of the practice should be performed prior to hiring. This will allow both physicians and the NPP to have clear expectations. An emphasis should be placed on the importance of recognizing the level of experience will likely impact the role. For example, utilizing a new graduate in a short-stay observation unit with limited diagnoses and treatments may make sense, but utilizing an NPP as a nocturnist, cross-covering and independently admitting patients, would require an NPP with years of experience. It is crucial to hire the right NPP with the right qualifications and experience for the job.
Dr. Nelson states patient satisfaction may decline by adding NPPs to the practice. Rather than focusing on possible dilution of a patient experience with the addition of another healthcare provider, one should instead consider the potential of adding another perspective to the team. Two providers with unique educational backgrounds and insight may indeed be better than one. Utilization of NPPs can increase face time with patients, subsequently increasing patient satisfaction. Additionally, research in outpatient settings shows no difference in patient satisfaction between physicians and NPPs; more research in inpatient settings needs to be performed.
We encourage HMG directors to refer to our expanded section on SHM’s Web site, “Practice Resources,” which has a wealth of information regarding NPP utilization. The NPP committee will be hosting two courses at the annual meeting, “The Basics: Can NPs/PAs Meet Our Needs,” and “Advanced Concepts: Three Different Practice Models.”
Jina Saltzman, PA-C, University of Chicago Medical Center
Dear readers: My main goal in writing the column was to indicate that NPs and PAs could be valuable contributors to many hospitalist practices. Yet, many practices fail to create the optimal role for them, one that contributes to patient outcomes, efficiency and economic health, and provides a rewarding role for the NPP.
I do not have an anti-PA, pro-NP bias. My intention was not to take sides regarding whether PAs or NPs are more skilled or better for patients. I think that is a function of the individual, much more than their training certificate (same with MDs). I did not intend to imply “nurse practitioners providing hospitalist coverage should function independently, without any physician supervision, oversight, or input.”
Lastly, I did make a factual error regarding the differences in physician supervision required for NPs and PAs. Saltzman’s letter above addresses the error. TH
Non-Physician Providers Critical to Hospital Medicine Practices
In “Maximizing NPPs in Hospitalist Practices” (Practice Management, October 2008, p. 69), John Nelson, MD, implies a financial advantage to hiring nurse practitioners (NPs) rather than physician assistants (PAs):
“A PA’s work will nearly always require a physician being physically present during some portion of the patient visit and co-signing chart notes and orders. Nurse practitioners, on the other hand, may be able to perform certain patient-care activities independently. Medicare and other payers typically reimburse at 85% of the rate customarily paid to MDs for the same service.”
Dr. Nelson: Do you mean to imply NPs providing hospitalist coverage should function independently, without any physician supervision, oversight, or input? I do not know of any hospitals that allow NPs to admit and manage patients independently, despite their independent practice status. In my opinion, it would be detrimental to patient care to allow non-physician providers to provide completely independent, unsupervised hospital care.
In addition, I know of no hospital practice setting that requires a physician to be physically present during a PA’s exam. In all hospital practice settings that I am aware of, a supervising or attending physician (not necessarily the one on the PA’s license), must see the patient at some time each day, not necessarily at the same time as the PA.
In that scenario, the physician pays a brief visit to the patient to corroborate the PA’s exam and plan. The physician then writes a brief, seen-and-agreed note, and can bill 100% of the Medicare reimbursement, not the 85% for a NP visit. How this compares economically depends, of course, on relative salaries. But it provides physician oversight of the NPP, which assumedly will improve quality of care (though I have no studies to cite to that effect).
Do you have some other reason for your anti-PA, pro-NP bias? Is your personal experience colored by working with more competent NPs, in your opinion, and less competent PAs? Perhaps that would make for a more interesting, better-defined column.
Richard Buckberg, PA-C, Maine Medical Center, Portland, Maine
SHM’s Non-Physician Provider (NPP) Committee was delighted to see the recent article by Dr. Nelson, MD, regarding the use of NPPs in hospital medicine. These columns spotlighted HM’s increasing utilization of NPPs, a role that only is expected to increase in number and breadth, based on the increasing need for competent, comprehensive care of the acutely ill.
Dr. Nelson made many excellent points that may benefit from some clarification or expansion. Dr. Nelson states a PA “will nearly always require a physician being physically present during some portion of the patient visit and co-signing chart notes and orders.” This is incorrect, and seems to imply PAs are more difficult to assimilate into practice than NPs. Depending upon variability in legal limitations and hospital bylaws, both PAs and NPs may see a patient without a physician present. In order to bill for a shared visit and receive 100% reimbursement, the attending physician needs to have a face-to-face encounter with that patient at some point in the day and document a portion of the evaluation and management (e.g., history, physical exam, or medical decision-making).
Alternatively, in most states, both NPs and PAs can see patients independently and bill for their services at 85% of the physician’s Medicare rate. Obtaining 100% reimbursement for NPP services when using the shared billing model is efficient and simple. Though variability exists, more specifically in hospital culture, utilization of these roles can positively impact the bottom line of reimbursement. Therefore, it is essential to understand all of the regulations before developing a business model incorporating NPPs.
Dr. Nelson also points out that using NPPs in a clerical fashion, such as discharge planning, is not optimizing the NPPs capabilities. This point is well taken. If clerical assistance is needed, hire the appropriate discipline.
He also says in order to integrate and maximize the benefit of the NPP to a particular practice, a careful analysis of the needs of the practice should be performed prior to hiring. This will allow both physicians and the NPP to have clear expectations. An emphasis should be placed on the importance of recognizing the level of experience will likely impact the role. For example, utilizing a new graduate in a short-stay observation unit with limited diagnoses and treatments may make sense, but utilizing an NPP as a nocturnist, cross-covering and independently admitting patients, would require an NPP with years of experience. It is crucial to hire the right NPP with the right qualifications and experience for the job.
Dr. Nelson states patient satisfaction may decline by adding NPPs to the practice. Rather than focusing on possible dilution of a patient experience with the addition of another healthcare provider, one should instead consider the potential of adding another perspective to the team. Two providers with unique educational backgrounds and insight may indeed be better than one. Utilization of NPPs can increase face time with patients, subsequently increasing patient satisfaction. Additionally, research in outpatient settings shows no difference in patient satisfaction between physicians and NPPs; more research in inpatient settings needs to be performed.
We encourage HMG directors to refer to our expanded section on SHM’s Web site, “Practice Resources,” which has a wealth of information regarding NPP utilization. The NPP committee will be hosting two courses at the annual meeting, “The Basics: Can NPs/PAs Meet Our Needs,” and “Advanced Concepts: Three Different Practice Models.”
Jina Saltzman, PA-C, University of Chicago Medical Center
Dear readers: My main goal in writing the column was to indicate that NPs and PAs could be valuable contributors to many hospitalist practices. Yet, many practices fail to create the optimal role for them, one that contributes to patient outcomes, efficiency and economic health, and provides a rewarding role for the NPP.
I do not have an anti-PA, pro-NP bias. My intention was not to take sides regarding whether PAs or NPs are more skilled or better for patients. I think that is a function of the individual, much more than their training certificate (same with MDs). I did not intend to imply “nurse practitioners providing hospitalist coverage should function independently, without any physician supervision, oversight, or input.”
Lastly, I did make a factual error regarding the differences in physician supervision required for NPs and PAs. Saltzman’s letter above addresses the error. TH
Staffing Strategies

One of the most difficult challenges in staffing a hospitalist practice is handling the unpredictable daily fluctuations in patient volume. It isn’t difficult to decide how many hospitalists will work each day to handle the average number of daily visits (aka encounters), but the actual number of visits on any given day is almost always significantly different than the average. I think many groups could more effectively handle day-to-day variations in workload by eliminating predetermined lengths of the shifts that the doctors work. It isn’t a perfect strategy, but it is worth some consideration by nearly any practice. Let me explain.

First, think about how the workload for a typical day might be represented. For many or most practices it often looks something like the wavy line in Figure 1. (See Figure 1, p. 52.)
Of course, the line representing a day’s work will be different every day, but I’ve tried to draw it in a way that represents a typical day.
In Figure 2 (see p. 52), I’ve added horizontal bars to represent a common way that groups might schedule four daytime doctors who each work 7 a.m. to 7 p.m., and one night doctor working 7 p.m. to 7 a.m. The four horizontal bars represent the four day doctors, and the one horizontal bar at the bottom right represents the one night doctor. Ideally, the manpower (horizontal bars) should match the workload (wavy line) every hour of the day.
This graph shows that—at least for this particular day—there are many hours in the afternoon when there is excess manpower. The doctors may be sitting around waiting for their shift to end or waiting to see if it will suddenly get busy again. We all know that happens unpredictably. And from about 7 p.m. to about 11:30 p.m., the single night doctor has more work than he/she can reasonably handle.
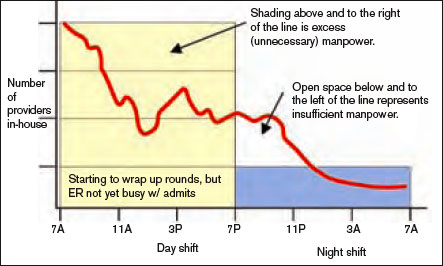
In fact, there probably isn’t ever a day when the work that needs to be done is just the right amount for all four doctors from 7 a.m. to 7 p.m. with a sudden drop at 7 p.m. that is just right for one doctor for the next 12 hours. Because the doctors have scheduled themselves to work 12-hour shifts, they know in advance that their manpower will quite regularly fail to match the workload for that day.
Groups have devised a number of strategies to try to get manpower to more closely match the unpredictable workload for a given day. These include having a member of the group available on standby (often called “jeopardy”) for that day; this physician comes in only if it is unusually busy. Some groups have a patient volume cap to prevent the practice from becoming too busy. I think a cap is a poor strategy that should be used only as a last resort, and I will discuss this in detail in a future column. Other groups have a swing shift from late in the afternoon until around 11 p.m. or so to help with evening admits and cross cover. And an often overlooked but potentially valuable strategy is to eliminate clearly specified start and stop times for the shifts that the doctors work. For an idea of what that might look like, see Figure 3 (p. 52).
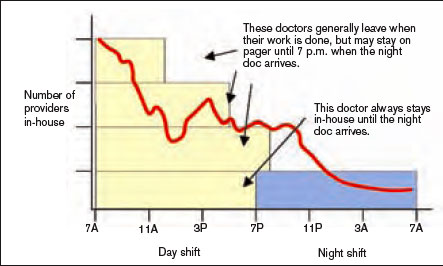
Notice that the right-hand side of each yellow bar in Figures 2 and 3 is indistinct. That is meant to show that the precise time that the doctor leaves varies, depending on the day’s workload. That way the manpower can be adjusted from one day to the next to more closely match the workload than if the doctors work fixed shifts of a specified duration. On some days, all of the doctors may stay 12 hours or more, but on many days at least some of the doctors will end up leaving in less than 12 hours. If all day doctors work a 12-hour shift, they have provided 48 hours—four doctors at 12 hours each—of physician manpower, but if there is some flexibility about when the doctors leave, the same four day doctors could provide between about 34 and 52 hours of manpower, depending on the day’s workload.
If your practice is contracted to keep a doctor in the hospital around the clock, you will probably need the night doctor and at least one day doctor to stay around—even if it is a slow day. But the other doctors might be able to leave when their work is done. And it is also reasonable for some groups to eliminate precise times that the doctors start working in the morning each day, though they might be required to be available by pager by a specified time in the morning.
One common concern about such a system is how to handle issues that arise with the patients cared for by a doctor who has left. I think it is best for the doctor to stay available by pager and handle simple issues by phone. For more complicated issues (e.g., a patient who needs attention at the bedside) the doctor could either come back to the hospital or phone another member of the practice (e.g., the doctor required to stay at least 12 hours that day) and see if he or she can handle the emergency.
All of the specifics of a system that allows doctors to leave when their work is done rather than according to shifts of a predetermined number of hours would be too long for this column. But they aren’t complicated, and given the variability that exists in the number of daily patient visits to any hospitalist practice, the application of this kind of approach is well worth considering. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
One of the most difficult challenges in staffing a hospitalist practice is handling the unpredictable daily fluctuations in patient volume. It isn’t difficult to decide how many hospitalists will work each day to handle the average number of daily visits (aka encounters), but the actual number of visits on any given day is almost always significantly different than the average. I think many groups could more effectively handle day-to-day variations in workload by eliminating predetermined lengths of the shifts that the doctors work. It isn’t a perfect strategy, but it is worth some consideration by nearly any practice. Let me explain.
First, think about how the workload for a typical day might be represented. For many or most practices it often looks something like the wavy line in Figure 1. (See Figure 1, p. 52.)
Of course, the line representing a day’s work will be different every day, but I’ve tried to draw it in a way that represents a typical day.
In Figure 2 (see p. 52), I’ve added horizontal bars to represent a common way that groups might schedule four daytime doctors who each work 7 a.m. to 7 p.m., and one night doctor working 7 p.m. to 7 a.m. The four horizontal bars represent the four day doctors, and the one horizontal bar at the bottom right represents the one night doctor. Ideally, the manpower (horizontal bars) should match the workload (wavy line) every hour of the day.
This graph shows that—at least for this particular day—there are many hours in the afternoon when there is excess manpower. The doctors may be sitting around waiting for their shift to end or waiting to see if it will suddenly get busy again. We all know that happens unpredictably. And from about 7 p.m. to about 11:30 p.m., the single night doctor has more work than he/she can reasonably handle.
In fact, there probably isn’t ever a day when the work that needs to be done is just the right amount for all four doctors from 7 a.m. to 7 p.m. with a sudden drop at 7 p.m. that is just right for one doctor for the next 12 hours. Because the doctors have scheduled themselves to work 12-hour shifts, they know in advance that their manpower will quite regularly fail to match the workload for that day.
Groups have devised a number of strategies to try to get manpower to more closely match the unpredictable workload for a given day. These include having a member of the group available on standby (often called “jeopardy”) for that day; this physician comes in only if it is unusually busy. Some groups have a patient volume cap to prevent the practice from becoming too busy. I think a cap is a poor strategy that should be used only as a last resort, and I will discuss this in detail in a future column. Other groups have a swing shift from late in the afternoon until around 11 p.m. or so to help with evening admits and cross cover. And an often overlooked but potentially valuable strategy is to eliminate clearly specified start and stop times for the shifts that the doctors work. For an idea of what that might look like, see Figure 3 (p. 52).
Notice that the right-hand side of each yellow bar in Figures 2 and 3 is indistinct. That is meant to show that the precise time that the doctor leaves varies, depending on the day’s workload. That way the manpower can be adjusted from one day to the next to more closely match the workload than if the doctors work fixed shifts of a specified duration. On some days, all of the doctors may stay 12 hours or more, but on many days at least some of the doctors will end up leaving in less than 12 hours. If all day doctors work a 12-hour shift, they have provided 48 hours—four doctors at 12 hours each—of physician manpower, but if there is some flexibility about when the doctors leave, the same four day doctors could provide between about 34 and 52 hours of manpower, depending on the day’s workload.
If your practice is contracted to keep a doctor in the hospital around the clock, you will probably need the night doctor and at least one day doctor to stay around—even if it is a slow day. But the other doctors might be able to leave when their work is done. And it is also reasonable for some groups to eliminate precise times that the doctors start working in the morning each day, though they might be required to be available by pager by a specified time in the morning.
One common concern about such a system is how to handle issues that arise with the patients cared for by a doctor who has left. I think it is best for the doctor to stay available by pager and handle simple issues by phone. For more complicated issues (e.g., a patient who needs attention at the bedside) the doctor could either come back to the hospital or phone another member of the practice (e.g., the doctor required to stay at least 12 hours that day) and see if he or she can handle the emergency.
All of the specifics of a system that allows doctors to leave when their work is done rather than according to shifts of a predetermined number of hours would be too long for this column. But they aren’t complicated, and given the variability that exists in the number of daily patient visits to any hospitalist practice, the application of this kind of approach is well worth considering. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
One of the most difficult challenges in staffing a hospitalist practice is handling the unpredictable daily fluctuations in patient volume. It isn’t difficult to decide how many hospitalists will work each day to handle the average number of daily visits (aka encounters), but the actual number of visits on any given day is almost always significantly different than the average. I think many groups could more effectively handle day-to-day variations in workload by eliminating predetermined lengths of the shifts that the doctors work. It isn’t a perfect strategy, but it is worth some consideration by nearly any practice. Let me explain.
First, think about how the workload for a typical day might be represented. For many or most practices it often looks something like the wavy line in Figure 1. (See Figure 1, p. 52.)
Of course, the line representing a day’s work will be different every day, but I’ve tried to draw it in a way that represents a typical day.
In Figure 2 (see p. 52), I’ve added horizontal bars to represent a common way that groups might schedule four daytime doctors who each work 7 a.m. to 7 p.m., and one night doctor working 7 p.m. to 7 a.m. The four horizontal bars represent the four day doctors, and the one horizontal bar at the bottom right represents the one night doctor. Ideally, the manpower (horizontal bars) should match the workload (wavy line) every hour of the day.
This graph shows that—at least for this particular day—there are many hours in the afternoon when there is excess manpower. The doctors may be sitting around waiting for their shift to end or waiting to see if it will suddenly get busy again. We all know that happens unpredictably. And from about 7 p.m. to about 11:30 p.m., the single night doctor has more work than he/she can reasonably handle.
In fact, there probably isn’t ever a day when the work that needs to be done is just the right amount for all four doctors from 7 a.m. to 7 p.m. with a sudden drop at 7 p.m. that is just right for one doctor for the next 12 hours. Because the doctors have scheduled themselves to work 12-hour shifts, they know in advance that their manpower will quite regularly fail to match the workload for that day.
Groups have devised a number of strategies to try to get manpower to more closely match the unpredictable workload for a given day. These include having a member of the group available on standby (often called “jeopardy”) for that day; this physician comes in only if it is unusually busy. Some groups have a patient volume cap to prevent the practice from becoming too busy. I think a cap is a poor strategy that should be used only as a last resort, and I will discuss this in detail in a future column. Other groups have a swing shift from late in the afternoon until around 11 p.m. or so to help with evening admits and cross cover. And an often overlooked but potentially valuable strategy is to eliminate clearly specified start and stop times for the shifts that the doctors work. For an idea of what that might look like, see Figure 3 (p. 52).
Notice that the right-hand side of each yellow bar in Figures 2 and 3 is indistinct. That is meant to show that the precise time that the doctor leaves varies, depending on the day’s workload. That way the manpower can be adjusted from one day to the next to more closely match the workload than if the doctors work fixed shifts of a specified duration. On some days, all of the doctors may stay 12 hours or more, but on many days at least some of the doctors will end up leaving in less than 12 hours. If all day doctors work a 12-hour shift, they have provided 48 hours—four doctors at 12 hours each—of physician manpower, but if there is some flexibility about when the doctors leave, the same four day doctors could provide between about 34 and 52 hours of manpower, depending on the day’s workload.
If your practice is contracted to keep a doctor in the hospital around the clock, you will probably need the night doctor and at least one day doctor to stay around—even if it is a slow day. But the other doctors might be able to leave when their work is done. And it is also reasonable for some groups to eliminate precise times that the doctors start working in the morning each day, though they might be required to be available by pager by a specified time in the morning.
One common concern about such a system is how to handle issues that arise with the patients cared for by a doctor who has left. I think it is best for the doctor to stay available by pager and handle simple issues by phone. For more complicated issues (e.g., a patient who needs attention at the bedside) the doctor could either come back to the hospital or phone another member of the practice (e.g., the doctor required to stay at least 12 hours that day) and see if he or she can handle the emergency.
All of the specifics of a system that allows doctors to leave when their work is done rather than according to shifts of a predetermined number of hours would be too long for this column. But they aren’t complicated, and given the variability that exists in the number of daily patient visits to any hospitalist practice, the application of this kind of approach is well worth considering. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
It’s Good to Be Country

Think a big hospital is where it’s at? Not according to Randy Ferrance, DC, MD, a hospitalist at Riverside Tappahanock Hospital, a 67-bed facility in rural Tappahannock, Va. The community is home to 2,172 residents and located about an hour east of Richmond, just up river from the Chesapeake Bay. Dr. Ferrance, a former chiropractor who has been practicing as a hospitalist at Riverside since 2002, recently spoke with The Hospitalist about why he enjoys the rural setting.
How is Riverside Tappahanock different from other hospitalist groups you’ve worked at?
Answer: The thing I like about it is I get to wear a lot of different hats. We don’t have intensivists; we manage our own ventilators and do our own critical care. And we’re also limited by the number of specialists we have, so of course, anything that is too difficult for us to do we transfer out. I don’t manage consultants, which seems like what hospitalists at a lot of big hospitals do. I’m often wondering what those hospitalists are left doing. Here we have cardiologists available to us, and as far as other specialists go, we have one gastroenterologist and a part-time nephrologist. I like the fact that I’m actually treating and not just stepping back and watching others treat. I especially like the ICU. This way I get to do critical care, and I think do it fairly well.
What are the challenges at a rural hospital?
A: A number of people just assume that, since we are just a small hospital, we can’t be giving good care. They come through the doors and they immediately want us to transfer them to a bigger hospital.
Is there a need for more rural hospitalists?
A: There have been times in the past when we’ve had trouble getting people [recruits] to look at us just because of the location, although I think we’re in a great location. We’re not far from Richmond, not far from good things to do.
Is there a solution to the recruitment problem?
A: The bottom line is we need more primary care physicians. We’re pretty selective and we’ve managed to do well despite that.
How many patients, on average, do you see?
A: We average about five admissions a day. We tend to follow about eight patients at a time. We don’t really do shifts. We take call a quarter of the time, doing admissions for a 24-hour stretch, averaging seven or eight calls in a month. Then we round on our post call days, as well, and the days in between. On average, we take every third day call, with a week off each month. We work 90 hours a week—pretty awful hours. So this is clearly a drawback. There are only four of us here, so if one of us were taken ill, we’d either have to get a [temporary doctor] or pick up the slack.
What are the other drawbacks to a rural hospital?
A: Our denominators are so small that, if we miss aspirin on arrival for one patient, it can pull us from first to the fourth in quality ratings. Everything has to be perfect. We can’t make any omissions. I think it certainly adds to perception. People in small towns talk a lot, and what people talk about are things that did not go well. They don’t talk about things that did go well.
What advice do you have for those considering a position at a rural hospital?
A: You have to be willing to work more than you would at a larger hospital, but I think you get to do more, which is more rewarding from my point of view.
What can rural hospitalists teach other hospitalists?
A: We probably can teach workload management a bit better. I think we can also talk about quality referral patterns. The things we need to do to make sure our quality numbers are good are probably a lot more stringent because our capture needs to be better. TH
Think a big hospital is where it’s at? Not according to Randy Ferrance, DC, MD, a hospitalist at Riverside Tappahanock Hospital, a 67-bed facility in rural Tappahannock, Va. The community is home to 2,172 residents and located about an hour east of Richmond, just up river from the Chesapeake Bay. Dr. Ferrance, a former chiropractor who has been practicing as a hospitalist at Riverside since 2002, recently spoke with The Hospitalist about why he enjoys the rural setting.
How is Riverside Tappahanock different from other hospitalist groups you’ve worked at?
Answer: The thing I like about it is I get to wear a lot of different hats. We don’t have intensivists; we manage our own ventilators and do our own critical care. And we’re also limited by the number of specialists we have, so of course, anything that is too difficult for us to do we transfer out. I don’t manage consultants, which seems like what hospitalists at a lot of big hospitals do. I’m often wondering what those hospitalists are left doing. Here we have cardiologists available to us, and as far as other specialists go, we have one gastroenterologist and a part-time nephrologist. I like the fact that I’m actually treating and not just stepping back and watching others treat. I especially like the ICU. This way I get to do critical care, and I think do it fairly well.
What are the challenges at a rural hospital?
A: A number of people just assume that, since we are just a small hospital, we can’t be giving good care. They come through the doors and they immediately want us to transfer them to a bigger hospital.
Is there a need for more rural hospitalists?
A: There have been times in the past when we’ve had trouble getting people [recruits] to look at us just because of the location, although I think we’re in a great location. We’re not far from Richmond, not far from good things to do.
Is there a solution to the recruitment problem?
A: The bottom line is we need more primary care physicians. We’re pretty selective and we’ve managed to do well despite that.
How many patients, on average, do you see?
A: We average about five admissions a day. We tend to follow about eight patients at a time. We don’t really do shifts. We take call a quarter of the time, doing admissions for a 24-hour stretch, averaging seven or eight calls in a month. Then we round on our post call days, as well, and the days in between. On average, we take every third day call, with a week off each month. We work 90 hours a week—pretty awful hours. So this is clearly a drawback. There are only four of us here, so if one of us were taken ill, we’d either have to get a [temporary doctor] or pick up the slack.
What are the other drawbacks to a rural hospital?
A: Our denominators are so small that, if we miss aspirin on arrival for one patient, it can pull us from first to the fourth in quality ratings. Everything has to be perfect. We can’t make any omissions. I think it certainly adds to perception. People in small towns talk a lot, and what people talk about are things that did not go well. They don’t talk about things that did go well.
What advice do you have for those considering a position at a rural hospital?
A: You have to be willing to work more than you would at a larger hospital, but I think you get to do more, which is more rewarding from my point of view.
What can rural hospitalists teach other hospitalists?
A: We probably can teach workload management a bit better. I think we can also talk about quality referral patterns. The things we need to do to make sure our quality numbers are good are probably a lot more stringent because our capture needs to be better. TH
Think a big hospital is where it’s at? Not according to Randy Ferrance, DC, MD, a hospitalist at Riverside Tappahanock Hospital, a 67-bed facility in rural Tappahannock, Va. The community is home to 2,172 residents and located about an hour east of Richmond, just up river from the Chesapeake Bay. Dr. Ferrance, a former chiropractor who has been practicing as a hospitalist at Riverside since 2002, recently spoke with The Hospitalist about why he enjoys the rural setting.
How is Riverside Tappahanock different from other hospitalist groups you’ve worked at?
Answer: The thing I like about it is I get to wear a lot of different hats. We don’t have intensivists; we manage our own ventilators and do our own critical care. And we’re also limited by the number of specialists we have, so of course, anything that is too difficult for us to do we transfer out. I don’t manage consultants, which seems like what hospitalists at a lot of big hospitals do. I’m often wondering what those hospitalists are left doing. Here we have cardiologists available to us, and as far as other specialists go, we have one gastroenterologist and a part-time nephrologist. I like the fact that I’m actually treating and not just stepping back and watching others treat. I especially like the ICU. This way I get to do critical care, and I think do it fairly well.
What are the challenges at a rural hospital?
A: A number of people just assume that, since we are just a small hospital, we can’t be giving good care. They come through the doors and they immediately want us to transfer them to a bigger hospital.
Is there a need for more rural hospitalists?
A: There have been times in the past when we’ve had trouble getting people [recruits] to look at us just because of the location, although I think we’re in a great location. We’re not far from Richmond, not far from good things to do.
Is there a solution to the recruitment problem?
A: The bottom line is we need more primary care physicians. We’re pretty selective and we’ve managed to do well despite that.
How many patients, on average, do you see?
A: We average about five admissions a day. We tend to follow about eight patients at a time. We don’t really do shifts. We take call a quarter of the time, doing admissions for a 24-hour stretch, averaging seven or eight calls in a month. Then we round on our post call days, as well, and the days in between. On average, we take every third day call, with a week off each month. We work 90 hours a week—pretty awful hours. So this is clearly a drawback. There are only four of us here, so if one of us were taken ill, we’d either have to get a [temporary doctor] or pick up the slack.
What are the other drawbacks to a rural hospital?
A: Our denominators are so small that, if we miss aspirin on arrival for one patient, it can pull us from first to the fourth in quality ratings. Everything has to be perfect. We can’t make any omissions. I think it certainly adds to perception. People in small towns talk a lot, and what people talk about are things that did not go well. They don’t talk about things that did go well.
What advice do you have for those considering a position at a rural hospital?
A: You have to be willing to work more than you would at a larger hospital, but I think you get to do more, which is more rewarding from my point of view.
What can rural hospitalists teach other hospitalists?
A: We probably can teach workload management a bit better. I think we can also talk about quality referral patterns. The things we need to do to make sure our quality numbers are good are probably a lot more stringent because our capture needs to be better. TH
When should a hospitalized patient be transfused?
Case
A 65-year-old male nursing home resident is sent to the emergency room with a productive cough, fever, and low blood pressure, and is diagnosed with community-acquired pneumonia. He has a history of tobacco abuse, hypertension, and a right middle cerebral artery stroke. His admission labs show a hemoglobin level of 9.0 g/dL. The day after admission his hypotension has resolved and he reports feeling much better after two liters of intravenous fluids and antibiotics. However, his hemoglobin level is 7.9 g/dL. There is no evidence of bleeding. Should this hospitalized patient be transfused?
Overview
When to give a red blood cell transfusion is a clinical question commonly encountered by hospitalists. Individuals with acute blood loss, chronic blood loss, anemia of chronic disease, and hemolytic anemia often are given transfusions. Hospitalists serving as consultants may be asked when to transfuse patients perioperatively.
It is estimated up to 25% of the red blood cells transfused in the U.S. are inappropriate.1-4 Many physicians transfuse based on a number, rather than on objective findings. Overuse is common because of the wide availability of red blood cells, the belief complications are infrequent, and an unfounded fear of adverse outcomes if a patient is not transfused.
Tachycardia, low blood pressure, and declining oxygen saturations are signs clinicians can use when making the decision to transfuse. Electrocardiographic changes associated with tissue hypoxia can occur at a hemoglobin level <5 g/dL in healthy adults. Studies show mortality and morbidity increase rapidly at levels <5.0 to 6.0 g/dL.5 Currently, no diagnostic serological test exists for tissue hypoxia, which is the physiologic reason to give red blood cells.
Red blood cell transfusion can be a life-saving therapy; however, it is not a benign intervention. It is estimated 10% of transfusion reactions will have some adverse event.6 Red blood cell use exposes patients to hemolytic transfusion reactions, infections, and transfusion related acute lung injury.7,8 Additionally, unnecessary economic expenses are incurred and a scarce resource is diverted from other patients.
Hospitalists should be able to describe the indications for red blood cell transfusion and understand the evidence for and against its use. Physicians who appreciate the risks and benefits of red blood cell use tend to transfuse less blood that those who less informed. 9, 10
Review of the Data
General outcomes: Despite the long history of red blood cell transfusion, which dates back to 1818, when James Blundell successfully saved a woman exsanguinating from a postpartum hemorrhage, little evidence has been accumulated for its appropriate use. In the 1980s, the discovery of the human immunodeficiency virus sparked blood product safety concerns. This stimulated research and a debate over red blood cell transfusion practices, with a growing body of literature unsupportive of transfusion for an arbitrary trigger, for example the “10/30 rule,” which referred to 10 g/dL hemoglobin or hematocrit of 30%.9
Observational studies have raised concerns by linking morbidity and mortality to red blood cell use. Among 1,958 surgical patients who refused blood transfusion on religious grounds, there was an increase in mortality when hemoglobin levels were <6.0 g/dL. Hemoglobin levels higher than 7.0 g/dL showed no increased mortality.11 A recent comprehensive review included 272,596 surgical, trauma, and ICU patients in 45 observational studies. The review included studies with end points, including mortality, infections, multiorgan dysfunction syndrome, and acute respiratory distress syndrome, and concluded transfusions are associated with a higher risk of morbidity and mortality.12 (see Figure 1, p. 20)
Higher rates of infection associated with transfusions occurred in patients with post-operative trauma, acute injuries, gastrointestinal cancer undergoing surgery, coronary bypass surgery, hip surgery, burns, critical illness, and patients requiring ventilation. (see Figure 2, p. 21)12 The increased infection risk likely is due to the transient depression of the immune system induced by red blood cell transfusion. Prolonged hospital stays in postoperative colorectal surgery patients and ICU patients have been associated with transfusions.13
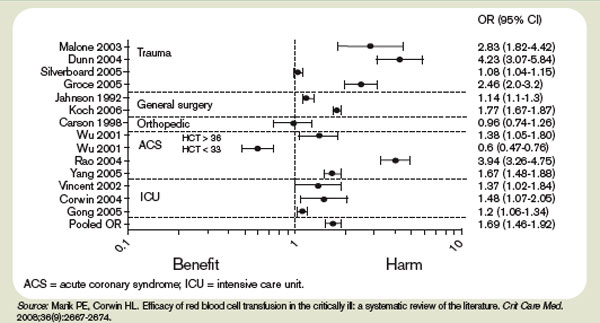
A meta-analysis of the few randomized controlled trials favors the restrictive use of red blood cells. The preponderance of the evidence comes from the Transfusion Requirements in Critical Care (TRICC) trial.14 This randomized control trial in critically ill medical and surgical patients demonstrated a restrictive strategy (transfusion trigger of <7.0 g/dL) and was as effective as a liberal transfusion strategy (transfusion trigger <10.0 g/dL). (see Figure 3, p. 22) Indeed, patients in the restrictive arm of the trial, who were less ill and under age 55 had a lower mortality rate than those who were transfused liberally.15 To date, there are no hospital-based randomized control trials that evaluate outcomes of anemic non-ICU medical patients.
This evidence has created a growing consensus that a restrictive use of blood results in improved patient outcomes. In patients without cardiovascular disease the evidence suggests most patients tolerate a hemoglobin level of 7.0 g/dL.5
Cardiac Patients
Experimental and clinical evidence suggests patients with cardiovascular disease are less tolerant of anemia. Patients with coronary disease are more likely to have adverse outcomes than those without coronary disease, if they do not have a red blood cell transfusion.11,16
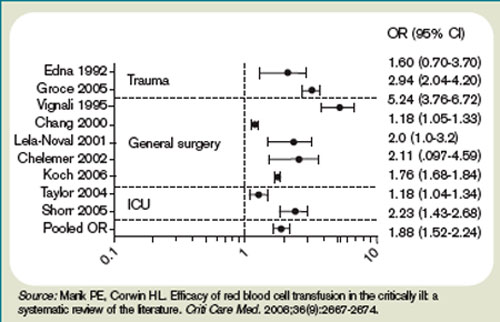
The myocardium has a higher oxygen extraction ratio compared to the tissue oxygen extraction ratio, making it more sensitive to anemia.17,18 The presence of cardiac disease may require a higher threshold to transfuse blood; however, the precise recommended threshold remains controversial. A restrictive red blood cell transfusion strategy (maintaining the hemoglobin between 7.0 g/dL and 9.0 g/dL) appeared to be safe in most critically ill patients with cardiovascular disease.14
The data is more conflicting for patients with an acute coronary syndrome (ACS). Some studies have found increased mortality and another concluded ACS decreased with red blood cell use.19-21 Further research is needed to determine when red blood cells should be given to patients with coronary disease.
Gastrointestinal Bleeding
The decision to transfuse for gastrointestinal (GI) bleeding takes into account the site and etiology of the bleeding, availability of treatments, and risk of continued bleeding. Once the blood loss is controlled, a decision must be made on how to treat the anemia. Currently, no studies have looked at outcomes for patients who did and did not receive blood for an acute or chronic GI bleed.
Additionally, no studies have been conducted to delineate when to transfuse patients with chronic GI blood loss. Studies of patients with an acute GI bleed and cardiovascular disease have shown an increase in mortality, but it is unknown if the use of specific transfusion triggers affects outcomes in this group.

In patients with GI bleeding, experts feel the use of red blood cells should be guided by available evidence. For patients without cardiac disease, red blood cell transfusion is rarely required following definitive treatment and cessation of blood loss unless the hemoglobin is <7.0 g/dL.22
Back to the Case
The patient described in our case should not be transfused unless he has clinical signs or symptoms of tissue hypoxemia. An appropriate workup for his anemia should be initiated and, if an etiology identified, definitive treatment or intervention applied.
Bottom Line
Unless there are clinical signs of tissue hypoxia, symptomatic anemia, or a hemoglobin of <7.0 g/dL, red blood cell transfusion is not recommended, unless the patient has active ACS or significant underlying coronary disease. TH
Dr. Dressler is associate program director, assistant professor of medicine, Division of General Internal Medicine, Emory University Hospital, Atlanta. Dr. VanderEnde is assistant professor of medicine, Division of General Internal Medicine, Emory University Hospital, Atlanta.
References
1. Welch HG, Meehan KR, Goodnough LT. Prudent strategies for elective red blood cell transfusion. Ann Intern Med. 1992;116(5):393-402.
2. Tartter PI, Barron DM. Unnecessary blood transfusions in elective colorectal cancer surgery. Transfusion. 1985;25(2):113-115.
3. Saxena S, Weiner JM, Rabinowitz A, Fridey J, Shulman IA, Carmel R. Transfusion practice in medical patients. Arch Int Med. 1993;153(22):2575-80.
4. Palermo G, Bove J, Katz AJ. Patterns of blood use in Connecticut. Transfusion. 1980;20(6):704-710.
5. Carson JL, Reynolds RC. In search of the transfusion threshold. Hematology. 2005;10(Suppl 1):86-88.
6. Walker RH. Special report: transfusion risks. Am J Clin Pathol. 1987;88(3):374-378.
7. Blajchman MA, Vamvakas EC. The continuing risk of transfusion-transmitted infections. N Engl J Med. 2006;355(13):1303-1305.
8. Spiess BD. Risks of transfusion: outcome focus. Transfusion. 2004;44(Suppl 12):4S-14S.
9. Salem-Schatz SR, Avorn J, Soumerai SB. Influence of clinical knowledge, organizational context, and practice style on transfusion decision-making. JAMA. 1990;264(4):476-483.
10. Wilson K, MacDougall L, Fergusson D, Graham I, Tinmouth A, Hebert PC. The effectiveness of interventions to reduce physician’s levels of inappropriate transfusion: what can be learned from a systematic review of the literature. Transfusion. 2002;42(9):1224-1229.
11. Carson JL, Duff A, Poses RM, et al. Effect of anemia and cardiovascular disease on surgical mortality and morbidity. Lancet. 1996;348(9034):1055-1060.
12. Marik PE, Corwin HL. Efficacy of red blood cell transfusion in the critically ill: a systematic review of the literature. Crit Care Med. 2008;36(9):2667-2674.
13. Raghavan M, Marik PE. Anemia, allogenic blood transfusion, and immunomodulation in the critically ill. Chest. 2005;127(1):295-307.
14. Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion requirements in critical care investigators, Canadian critical care trials group. N Engl J Med. 1999;340(6):409-417.
15. Carson JL, Hill S, Carless P, Hebert P, Henry D. Transfusion triggers: a systematic review of the literature. Transfus Med Rev. 2002;16(3):187-199.
16. Sabatine MS, Morrow DA, Giugliano RP, et al. Association of hemoglobin levels with clinical outcomes in acute coronary syndromes. Circulation. 2005; 111(16):2042-2049.
17. Jan KM, Chien S. Effect of hematocrit variations on coronary hemodynamics and oxygen utilization. Am J Physiol. 1977;233(1):H106-H113.
18. Wilderson DK RASL, Gould SA, Sehgal HL, Moss GS. Limits of cardiac compensation in anemic baboons. Surgery. 1988;103(6):665-670.
19. Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA. 2004; 292(13):1555-1562.
20. Wu WC, Rathore SS, Wang Y, Radford MJ, Krumholz HM. Blood transfusion in elderly patients with acute myocardial infarction. N Engl J Med. 2001; 345(17):1230-1236.
21. Hebert PC, Fergusson DA. Do transfusions get to the heart of the matter? JAMA. 2004;292(13):1610-1612.
22. Hearnshaw S, Travis S, Murphy M. The role of blood transfusion in the management of upper and lower intestinal tract bleeding. Best Pract Res Clin Gastroenterology. 2008;22(2):355-371.
Case
A 65-year-old male nursing home resident is sent to the emergency room with a productive cough, fever, and low blood pressure, and is diagnosed with community-acquired pneumonia. He has a history of tobacco abuse, hypertension, and a right middle cerebral artery stroke. His admission labs show a hemoglobin level of 9.0 g/dL. The day after admission his hypotension has resolved and he reports feeling much better after two liters of intravenous fluids and antibiotics. However, his hemoglobin level is 7.9 g/dL. There is no evidence of bleeding. Should this hospitalized patient be transfused?
Overview
When to give a red blood cell transfusion is a clinical question commonly encountered by hospitalists. Individuals with acute blood loss, chronic blood loss, anemia of chronic disease, and hemolytic anemia often are given transfusions. Hospitalists serving as consultants may be asked when to transfuse patients perioperatively.
It is estimated up to 25% of the red blood cells transfused in the U.S. are inappropriate.1-4 Many physicians transfuse based on a number, rather than on objective findings. Overuse is common because of the wide availability of red blood cells, the belief complications are infrequent, and an unfounded fear of adverse outcomes if a patient is not transfused.
Tachycardia, low blood pressure, and declining oxygen saturations are signs clinicians can use when making the decision to transfuse. Electrocardiographic changes associated with tissue hypoxia can occur at a hemoglobin level <5 g/dL in healthy adults. Studies show mortality and morbidity increase rapidly at levels <5.0 to 6.0 g/dL.5 Currently, no diagnostic serological test exists for tissue hypoxia, which is the physiologic reason to give red blood cells.
Red blood cell transfusion can be a life-saving therapy; however, it is not a benign intervention. It is estimated 10% of transfusion reactions will have some adverse event.6 Red blood cell use exposes patients to hemolytic transfusion reactions, infections, and transfusion related acute lung injury.7,8 Additionally, unnecessary economic expenses are incurred and a scarce resource is diverted from other patients.
Hospitalists should be able to describe the indications for red blood cell transfusion and understand the evidence for and against its use. Physicians who appreciate the risks and benefits of red blood cell use tend to transfuse less blood that those who less informed. 9, 10
Review of the Data
General outcomes: Despite the long history of red blood cell transfusion, which dates back to 1818, when James Blundell successfully saved a woman exsanguinating from a postpartum hemorrhage, little evidence has been accumulated for its appropriate use. In the 1980s, the discovery of the human immunodeficiency virus sparked blood product safety concerns. This stimulated research and a debate over red blood cell transfusion practices, with a growing body of literature unsupportive of transfusion for an arbitrary trigger, for example the “10/30 rule,” which referred to 10 g/dL hemoglobin or hematocrit of 30%.9
Observational studies have raised concerns by linking morbidity and mortality to red blood cell use. Among 1,958 surgical patients who refused blood transfusion on religious grounds, there was an increase in mortality when hemoglobin levels were <6.0 g/dL. Hemoglobin levels higher than 7.0 g/dL showed no increased mortality.11 A recent comprehensive review included 272,596 surgical, trauma, and ICU patients in 45 observational studies. The review included studies with end points, including mortality, infections, multiorgan dysfunction syndrome, and acute respiratory distress syndrome, and concluded transfusions are associated with a higher risk of morbidity and mortality.12 (see Figure 1, p. 20)
Higher rates of infection associated with transfusions occurred in patients with post-operative trauma, acute injuries, gastrointestinal cancer undergoing surgery, coronary bypass surgery, hip surgery, burns, critical illness, and patients requiring ventilation. (see Figure 2, p. 21)12 The increased infection risk likely is due to the transient depression of the immune system induced by red blood cell transfusion. Prolonged hospital stays in postoperative colorectal surgery patients and ICU patients have been associated with transfusions.13
A meta-analysis of the few randomized controlled trials favors the restrictive use of red blood cells. The preponderance of the evidence comes from the Transfusion Requirements in Critical Care (TRICC) trial.14 This randomized control trial in critically ill medical and surgical patients demonstrated a restrictive strategy (transfusion trigger of <7.0 g/dL) and was as effective as a liberal transfusion strategy (transfusion trigger <10.0 g/dL). (see Figure 3, p. 22) Indeed, patients in the restrictive arm of the trial, who were less ill and under age 55 had a lower mortality rate than those who were transfused liberally.15 To date, there are no hospital-based randomized control trials that evaluate outcomes of anemic non-ICU medical patients.
This evidence has created a growing consensus that a restrictive use of blood results in improved patient outcomes. In patients without cardiovascular disease the evidence suggests most patients tolerate a hemoglobin level of 7.0 g/dL.5
Cardiac Patients
Experimental and clinical evidence suggests patients with cardiovascular disease are less tolerant of anemia. Patients with coronary disease are more likely to have adverse outcomes than those without coronary disease, if they do not have a red blood cell transfusion.11,16
The myocardium has a higher oxygen extraction ratio compared to the tissue oxygen extraction ratio, making it more sensitive to anemia.17,18 The presence of cardiac disease may require a higher threshold to transfuse blood; however, the precise recommended threshold remains controversial. A restrictive red blood cell transfusion strategy (maintaining the hemoglobin between 7.0 g/dL and 9.0 g/dL) appeared to be safe in most critically ill patients with cardiovascular disease.14
The data is more conflicting for patients with an acute coronary syndrome (ACS). Some studies have found increased mortality and another concluded ACS decreased with red blood cell use.19-21 Further research is needed to determine when red blood cells should be given to patients with coronary disease.
Gastrointestinal Bleeding
The decision to transfuse for gastrointestinal (GI) bleeding takes into account the site and etiology of the bleeding, availability of treatments, and risk of continued bleeding. Once the blood loss is controlled, a decision must be made on how to treat the anemia. Currently, no studies have looked at outcomes for patients who did and did not receive blood for an acute or chronic GI bleed.
Additionally, no studies have been conducted to delineate when to transfuse patients with chronic GI blood loss. Studies of patients with an acute GI bleed and cardiovascular disease have shown an increase in mortality, but it is unknown if the use of specific transfusion triggers affects outcomes in this group.
In patients with GI bleeding, experts feel the use of red blood cells should be guided by available evidence. For patients without cardiac disease, red blood cell transfusion is rarely required following definitive treatment and cessation of blood loss unless the hemoglobin is <7.0 g/dL.22
Back to the Case
The patient described in our case should not be transfused unless he has clinical signs or symptoms of tissue hypoxemia. An appropriate workup for his anemia should be initiated and, if an etiology identified, definitive treatment or intervention applied.
Bottom Line
Unless there are clinical signs of tissue hypoxia, symptomatic anemia, or a hemoglobin of <7.0 g/dL, red blood cell transfusion is not recommended, unless the patient has active ACS or significant underlying coronary disease. TH
Dr. Dressler is associate program director, assistant professor of medicine, Division of General Internal Medicine, Emory University Hospital, Atlanta. Dr. VanderEnde is assistant professor of medicine, Division of General Internal Medicine, Emory University Hospital, Atlanta.
References
1. Welch HG, Meehan KR, Goodnough LT. Prudent strategies for elective red blood cell transfusion. Ann Intern Med. 1992;116(5):393-402.
2. Tartter PI, Barron DM. Unnecessary blood transfusions in elective colorectal cancer surgery. Transfusion. 1985;25(2):113-115.
3. Saxena S, Weiner JM, Rabinowitz A, Fridey J, Shulman IA, Carmel R. Transfusion practice in medical patients. Arch Int Med. 1993;153(22):2575-80.
4. Palermo G, Bove J, Katz AJ. Patterns of blood use in Connecticut. Transfusion. 1980;20(6):704-710.
5. Carson JL, Reynolds RC. In search of the transfusion threshold. Hematology. 2005;10(Suppl 1):86-88.
6. Walker RH. Special report: transfusion risks. Am J Clin Pathol. 1987;88(3):374-378.
7. Blajchman MA, Vamvakas EC. The continuing risk of transfusion-transmitted infections. N Engl J Med. 2006;355(13):1303-1305.
8. Spiess BD. Risks of transfusion: outcome focus. Transfusion. 2004;44(Suppl 12):4S-14S.
9. Salem-Schatz SR, Avorn J, Soumerai SB. Influence of clinical knowledge, organizational context, and practice style on transfusion decision-making. JAMA. 1990;264(4):476-483.
10. Wilson K, MacDougall L, Fergusson D, Graham I, Tinmouth A, Hebert PC. The effectiveness of interventions to reduce physician’s levels of inappropriate transfusion: what can be learned from a systematic review of the literature. Transfusion. 2002;42(9):1224-1229.
11. Carson JL, Duff A, Poses RM, et al. Effect of anemia and cardiovascular disease on surgical mortality and morbidity. Lancet. 1996;348(9034):1055-1060.
12. Marik PE, Corwin HL. Efficacy of red blood cell transfusion in the critically ill: a systematic review of the literature. Crit Care Med. 2008;36(9):2667-2674.
13. Raghavan M, Marik PE. Anemia, allogenic blood transfusion, and immunomodulation in the critically ill. Chest. 2005;127(1):295-307.
14. Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion requirements in critical care investigators, Canadian critical care trials group. N Engl J Med. 1999;340(6):409-417.
15. Carson JL, Hill S, Carless P, Hebert P, Henry D. Transfusion triggers: a systematic review of the literature. Transfus Med Rev. 2002;16(3):187-199.
16. Sabatine MS, Morrow DA, Giugliano RP, et al. Association of hemoglobin levels with clinical outcomes in acute coronary syndromes. Circulation. 2005; 111(16):2042-2049.
17. Jan KM, Chien S. Effect of hematocrit variations on coronary hemodynamics and oxygen utilization. Am J Physiol. 1977;233(1):H106-H113.
18. Wilderson DK RASL, Gould SA, Sehgal HL, Moss GS. Limits of cardiac compensation in anemic baboons. Surgery. 1988;103(6):665-670.
19. Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA. 2004; 292(13):1555-1562.
20. Wu WC, Rathore SS, Wang Y, Radford MJ, Krumholz HM. Blood transfusion in elderly patients with acute myocardial infarction. N Engl J Med. 2001; 345(17):1230-1236.
21. Hebert PC, Fergusson DA. Do transfusions get to the heart of the matter? JAMA. 2004;292(13):1610-1612.
22. Hearnshaw S, Travis S, Murphy M. The role of blood transfusion in the management of upper and lower intestinal tract bleeding. Best Pract Res Clin Gastroenterology. 2008;22(2):355-371.
Case
A 65-year-old male nursing home resident is sent to the emergency room with a productive cough, fever, and low blood pressure, and is diagnosed with community-acquired pneumonia. He has a history of tobacco abuse, hypertension, and a right middle cerebral artery stroke. His admission labs show a hemoglobin level of 9.0 g/dL. The day after admission his hypotension has resolved and he reports feeling much better after two liters of intravenous fluids and antibiotics. However, his hemoglobin level is 7.9 g/dL. There is no evidence of bleeding. Should this hospitalized patient be transfused?
Overview
When to give a red blood cell transfusion is a clinical question commonly encountered by hospitalists. Individuals with acute blood loss, chronic blood loss, anemia of chronic disease, and hemolytic anemia often are given transfusions. Hospitalists serving as consultants may be asked when to transfuse patients perioperatively.
It is estimated up to 25% of the red blood cells transfused in the U.S. are inappropriate.1-4 Many physicians transfuse based on a number, rather than on objective findings. Overuse is common because of the wide availability of red blood cells, the belief complications are infrequent, and an unfounded fear of adverse outcomes if a patient is not transfused.
Tachycardia, low blood pressure, and declining oxygen saturations are signs clinicians can use when making the decision to transfuse. Electrocardiographic changes associated with tissue hypoxia can occur at a hemoglobin level <5 g/dL in healthy adults. Studies show mortality and morbidity increase rapidly at levels <5.0 to 6.0 g/dL.5 Currently, no diagnostic serological test exists for tissue hypoxia, which is the physiologic reason to give red blood cells.
Red blood cell transfusion can be a life-saving therapy; however, it is not a benign intervention. It is estimated 10% of transfusion reactions will have some adverse event.6 Red blood cell use exposes patients to hemolytic transfusion reactions, infections, and transfusion related acute lung injury.7,8 Additionally, unnecessary economic expenses are incurred and a scarce resource is diverted from other patients.
Hospitalists should be able to describe the indications for red blood cell transfusion and understand the evidence for and against its use. Physicians who appreciate the risks and benefits of red blood cell use tend to transfuse less blood that those who less informed. 9, 10
Review of the Data
General outcomes: Despite the long history of red blood cell transfusion, which dates back to 1818, when James Blundell successfully saved a woman exsanguinating from a postpartum hemorrhage, little evidence has been accumulated for its appropriate use. In the 1980s, the discovery of the human immunodeficiency virus sparked blood product safety concerns. This stimulated research and a debate over red blood cell transfusion practices, with a growing body of literature unsupportive of transfusion for an arbitrary trigger, for example the “10/30 rule,” which referred to 10 g/dL hemoglobin or hematocrit of 30%.9
Observational studies have raised concerns by linking morbidity and mortality to red blood cell use. Among 1,958 surgical patients who refused blood transfusion on religious grounds, there was an increase in mortality when hemoglobin levels were <6.0 g/dL. Hemoglobin levels higher than 7.0 g/dL showed no increased mortality.11 A recent comprehensive review included 272,596 surgical, trauma, and ICU patients in 45 observational studies. The review included studies with end points, including mortality, infections, multiorgan dysfunction syndrome, and acute respiratory distress syndrome, and concluded transfusions are associated with a higher risk of morbidity and mortality.12 (see Figure 1, p. 20)
Higher rates of infection associated with transfusions occurred in patients with post-operative trauma, acute injuries, gastrointestinal cancer undergoing surgery, coronary bypass surgery, hip surgery, burns, critical illness, and patients requiring ventilation. (see Figure 2, p. 21)12 The increased infection risk likely is due to the transient depression of the immune system induced by red blood cell transfusion. Prolonged hospital stays in postoperative colorectal surgery patients and ICU patients have been associated with transfusions.13
A meta-analysis of the few randomized controlled trials favors the restrictive use of red blood cells. The preponderance of the evidence comes from the Transfusion Requirements in Critical Care (TRICC) trial.14 This randomized control trial in critically ill medical and surgical patients demonstrated a restrictive strategy (transfusion trigger of <7.0 g/dL) and was as effective as a liberal transfusion strategy (transfusion trigger <10.0 g/dL). (see Figure 3, p. 22) Indeed, patients in the restrictive arm of the trial, who were less ill and under age 55 had a lower mortality rate than those who were transfused liberally.15 To date, there are no hospital-based randomized control trials that evaluate outcomes of anemic non-ICU medical patients.
This evidence has created a growing consensus that a restrictive use of blood results in improved patient outcomes. In patients without cardiovascular disease the evidence suggests most patients tolerate a hemoglobin level of 7.0 g/dL.5
Cardiac Patients
Experimental and clinical evidence suggests patients with cardiovascular disease are less tolerant of anemia. Patients with coronary disease are more likely to have adverse outcomes than those without coronary disease, if they do not have a red blood cell transfusion.11,16
The myocardium has a higher oxygen extraction ratio compared to the tissue oxygen extraction ratio, making it more sensitive to anemia.17,18 The presence of cardiac disease may require a higher threshold to transfuse blood; however, the precise recommended threshold remains controversial. A restrictive red blood cell transfusion strategy (maintaining the hemoglobin between 7.0 g/dL and 9.0 g/dL) appeared to be safe in most critically ill patients with cardiovascular disease.14
The data is more conflicting for patients with an acute coronary syndrome (ACS). Some studies have found increased mortality and another concluded ACS decreased with red blood cell use.19-21 Further research is needed to determine when red blood cells should be given to patients with coronary disease.
Gastrointestinal Bleeding
The decision to transfuse for gastrointestinal (GI) bleeding takes into account the site and etiology of the bleeding, availability of treatments, and risk of continued bleeding. Once the blood loss is controlled, a decision must be made on how to treat the anemia. Currently, no studies have looked at outcomes for patients who did and did not receive blood for an acute or chronic GI bleed.
Additionally, no studies have been conducted to delineate when to transfuse patients with chronic GI blood loss. Studies of patients with an acute GI bleed and cardiovascular disease have shown an increase in mortality, but it is unknown if the use of specific transfusion triggers affects outcomes in this group.
In patients with GI bleeding, experts feel the use of red blood cells should be guided by available evidence. For patients without cardiac disease, red blood cell transfusion is rarely required following definitive treatment and cessation of blood loss unless the hemoglobin is <7.0 g/dL.22
Back to the Case
The patient described in our case should not be transfused unless he has clinical signs or symptoms of tissue hypoxemia. An appropriate workup for his anemia should be initiated and, if an etiology identified, definitive treatment or intervention applied.
Bottom Line
Unless there are clinical signs of tissue hypoxia, symptomatic anemia, or a hemoglobin of <7.0 g/dL, red blood cell transfusion is not recommended, unless the patient has active ACS or significant underlying coronary disease. TH
Dr. Dressler is associate program director, assistant professor of medicine, Division of General Internal Medicine, Emory University Hospital, Atlanta. Dr. VanderEnde is assistant professor of medicine, Division of General Internal Medicine, Emory University Hospital, Atlanta.
References
1. Welch HG, Meehan KR, Goodnough LT. Prudent strategies for elective red blood cell transfusion. Ann Intern Med. 1992;116(5):393-402.
2. Tartter PI, Barron DM. Unnecessary blood transfusions in elective colorectal cancer surgery. Transfusion. 1985;25(2):113-115.
3. Saxena S, Weiner JM, Rabinowitz A, Fridey J, Shulman IA, Carmel R. Transfusion practice in medical patients. Arch Int Med. 1993;153(22):2575-80.
4. Palermo G, Bove J, Katz AJ. Patterns of blood use in Connecticut. Transfusion. 1980;20(6):704-710.
5. Carson JL, Reynolds RC. In search of the transfusion threshold. Hematology. 2005;10(Suppl 1):86-88.
6. Walker RH. Special report: transfusion risks. Am J Clin Pathol. 1987;88(3):374-378.
7. Blajchman MA, Vamvakas EC. The continuing risk of transfusion-transmitted infections. N Engl J Med. 2006;355(13):1303-1305.
8. Spiess BD. Risks of transfusion: outcome focus. Transfusion. 2004;44(Suppl 12):4S-14S.
9. Salem-Schatz SR, Avorn J, Soumerai SB. Influence of clinical knowledge, organizational context, and practice style on transfusion decision-making. JAMA. 1990;264(4):476-483.
10. Wilson K, MacDougall L, Fergusson D, Graham I, Tinmouth A, Hebert PC. The effectiveness of interventions to reduce physician’s levels of inappropriate transfusion: what can be learned from a systematic review of the literature. Transfusion. 2002;42(9):1224-1229.
11. Carson JL, Duff A, Poses RM, et al. Effect of anemia and cardiovascular disease on surgical mortality and morbidity. Lancet. 1996;348(9034):1055-1060.
12. Marik PE, Corwin HL. Efficacy of red blood cell transfusion in the critically ill: a systematic review of the literature. Crit Care Med. 2008;36(9):2667-2674.
13. Raghavan M, Marik PE. Anemia, allogenic blood transfusion, and immunomodulation in the critically ill. Chest. 2005;127(1):295-307.
14. Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion requirements in critical care investigators, Canadian critical care trials group. N Engl J Med. 1999;340(6):409-417.
15. Carson JL, Hill S, Carless P, Hebert P, Henry D. Transfusion triggers: a systematic review of the literature. Transfus Med Rev. 2002;16(3):187-199.
16. Sabatine MS, Morrow DA, Giugliano RP, et al. Association of hemoglobin levels with clinical outcomes in acute coronary syndromes. Circulation. 2005; 111(16):2042-2049.
17. Jan KM, Chien S. Effect of hematocrit variations on coronary hemodynamics and oxygen utilization. Am J Physiol. 1977;233(1):H106-H113.
18. Wilderson DK RASL, Gould SA, Sehgal HL, Moss GS. Limits of cardiac compensation in anemic baboons. Surgery. 1988;103(6):665-670.
19. Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA. 2004; 292(13):1555-1562.
20. Wu WC, Rathore SS, Wang Y, Radford MJ, Krumholz HM. Blood transfusion in elderly patients with acute myocardial infarction. N Engl J Med. 2001; 345(17):1230-1236.
21. Hebert PC, Fergusson DA. Do transfusions get to the heart of the matter? JAMA. 2004;292(13):1610-1612.
22. Hearnshaw S, Travis S, Murphy M. The role of blood transfusion in the management of upper and lower intestinal tract bleeding. Best Pract Res Clin Gastroenterology. 2008;22(2):355-371.