User login
The Hospitalist only
Job Hunter’s Checklist
Apart from the part-time job that provided pocket money while you were in high school or during your undergraduate years, physicians generally have little experience in the job-hunting arena. A physician’s career path requires much skill at applying for such educational endeavors as medical school and residency training, but applying for a “real” job can be a strange concept for most.
Not lost in the equation is the fact that the application process doesn’t begin until most physicians are in their late 20s. While many of our non-physician friends are on their second or third jobs, graduating residents looking to launch their careers often struggle with the transition to the world of HM. In order to help navigate these waters, we have put together a yearlong guide to help make the transition from third-year resident to hospitalist a little smoother.

July-September
The first step in landing a job is to find a mentor who can assist you through the entire process. Choose your mentor wisely; an experienced hospitalist can provide valuable feedback during your job search. If your goal is employment with a private hospitalist group, find a hospitalist with private-practice experience.
Choose your senior-year electives carefully. Consider focusing on areas of weakness or areas that are pertinent to HM (e.g., infectious disease, cardiology, neurology, critical-care medicine). Think about an outside elective in HM.
If you haven’t done so already, now is the time to create a curriculum vitae, also known as a CV, and a cover letter. The CV is a vital document. It might be the key element in determining whether you are worthy of an interview. Work on this document early, as you will need time for edits, updates, and mentor review. The cover letter should clearly describe the type of position you want and confidently state why you would be an asset to a particular hospitalist program. Edit your words carefully; spelling errors or typos in documents can be costly.
Once the Labor Day holiday has passed, you should start requesting letters of recommendation. Think hard about who you want before asking for a letter of recommendation, as these typically carry a lot of weight in the interview selection process. Although program directors, chiefs of medicine, and hospitalists can be good choices, it is important to choose people who know you well, as they tend to generate a more personal and powerful letter. Because letter-writers often are busy people, it is appropriate to give a deadline for when you need the letter.
October-December
Actively start the job search and apply for desired positions. This is the time of year when HM jobs are heavily advertised and programs are looking to fill positions. Hospitalists are in high demand throughout the country. Some great places to find job openings are:
- SHM’s Career Center (www.hospitalmedicine.org/careers);
- Classified ad sections in the Journal of Hospital Medicine, general medicine journals, and HM news magazines like The Hospitalist (see “SHM Career Center,” p. 35); and
- Hospitals and HM groups of interest, even if they are not advertising; contact them personally.
Begin the interview process by researching the hospital and HM group in advance. Prepare appropriate interview questions. When you interview, try to meet with as many people as possible to get a feel for what the job entails. Talk to the everyday hospitalists and try to gauge how satisfied they are in their jobs.
Bring extra copies of your updated CV and look sharp. Shine your shoes. Is it time to replace the suit you used to apply for residency?
Send a thank-you note or e-mail to the person(s) you interviewed with. If possible, do this within three days of your visit. It’s an important step in the process, yet this simple task often is overlooked. Remain in contact with the HM programs you are most interested in. Think about a follow-up visit or phone call to address any unanswered questions.
January-March
Hopefully you will have one or more offers by now. This is the time to negotiate a contract and accept an offer. Review the contract carefully and don’t hesitate to ask for clarification of unclear points. Some applicants prefer to have a lawyer review the contract prior to signing (see “The Art of Negotiation,” December 2008, p. 20).
Register for your board examination. Most specialties, including internal medicine, family medicine, and pediatrics, as well as board exams for osteopathic medicine, have registration deadlines in February. Given the significant cost of applying for these exams, it pays not to be tardy, as late fees can set you back hundreds of dollars.
Apply for state medical licensure. This process varies by state, but it can take several months to complete, especially if you are applying in a state other than where you trained. For example, California recommends starting the application process six to nine months in advance. International medical graduates who require a work visa need to ensure their paperwork is processed in a timely manner.
Each hospital is different, but applications for hospital credentialing generally means filling out a mountain of paperwork. Most hospitals will perform a thorough background check, so don’t be surprised if fingerprinting is required. The hospital or hospitalist group usually helps new hires navigate through this process, which can take several weeks or even months.
April-June
Moving to a different city or state can be exciting—and stressful. Start talking to hospitalists at the facility where you will be working to get a feel for the city and recommendations for places to live. Revisit the location to become more familiar with the surroundings. Some hospitals are very helpful; some provide new hires with a real estate agent. Moving expenses often are covered as a condition of employment, but it depends on your contract.
Consider taking a vacation to either further explore relocation options or to simply relax. If you have followed the recommendations outlined in the previous months, you should have time to unwind as your residency comes to an end. Some future hospitalists like to use this time to intensify board review; others cringe at the thought.
Transitioning from resident to hospitalist is no easy task, and it shouldn’t be taken lightly. It’s not a one-month process, either, so planning is essential. Although it might seem to be a daunting journey, it’s very rewarding in the long run. TH
Dr. Grant is a hospitalist at the University of Michigan Health System in Ann Arbor. Dr. Warren-Marzola is a hospitalist at St. Luke’s Hospital in Toledo, Ohio. Both are members of SHM’s Young Physicians Committee.
Apart from the part-time job that provided pocket money while you were in high school or during your undergraduate years, physicians generally have little experience in the job-hunting arena. A physician’s career path requires much skill at applying for such educational endeavors as medical school and residency training, but applying for a “real” job can be a strange concept for most.
Not lost in the equation is the fact that the application process doesn’t begin until most physicians are in their late 20s. While many of our non-physician friends are on their second or third jobs, graduating residents looking to launch their careers often struggle with the transition to the world of HM. In order to help navigate these waters, we have put together a yearlong guide to help make the transition from third-year resident to hospitalist a little smoother.
July-September
The first step in landing a job is to find a mentor who can assist you through the entire process. Choose your mentor wisely; an experienced hospitalist can provide valuable feedback during your job search. If your goal is employment with a private hospitalist group, find a hospitalist with private-practice experience.
Choose your senior-year electives carefully. Consider focusing on areas of weakness or areas that are pertinent to HM (e.g., infectious disease, cardiology, neurology, critical-care medicine). Think about an outside elective in HM.
If you haven’t done so already, now is the time to create a curriculum vitae, also known as a CV, and a cover letter. The CV is a vital document. It might be the key element in determining whether you are worthy of an interview. Work on this document early, as you will need time for edits, updates, and mentor review. The cover letter should clearly describe the type of position you want and confidently state why you would be an asset to a particular hospitalist program. Edit your words carefully; spelling errors or typos in documents can be costly.
Once the Labor Day holiday has passed, you should start requesting letters of recommendation. Think hard about who you want before asking for a letter of recommendation, as these typically carry a lot of weight in the interview selection process. Although program directors, chiefs of medicine, and hospitalists can be good choices, it is important to choose people who know you well, as they tend to generate a more personal and powerful letter. Because letter-writers often are busy people, it is appropriate to give a deadline for when you need the letter.
October-December
Actively start the job search and apply for desired positions. This is the time of year when HM jobs are heavily advertised and programs are looking to fill positions. Hospitalists are in high demand throughout the country. Some great places to find job openings are:
- SHM’s Career Center (www.hospitalmedicine.org/careers);
- Classified ad sections in the Journal of Hospital Medicine, general medicine journals, and HM news magazines like The Hospitalist (see “SHM Career Center,” p. 35); and
- Hospitals and HM groups of interest, even if they are not advertising; contact them personally.
Begin the interview process by researching the hospital and HM group in advance. Prepare appropriate interview questions. When you interview, try to meet with as many people as possible to get a feel for what the job entails. Talk to the everyday hospitalists and try to gauge how satisfied they are in their jobs.
Bring extra copies of your updated CV and look sharp. Shine your shoes. Is it time to replace the suit you used to apply for residency?
Send a thank-you note or e-mail to the person(s) you interviewed with. If possible, do this within three days of your visit. It’s an important step in the process, yet this simple task often is overlooked. Remain in contact with the HM programs you are most interested in. Think about a follow-up visit or phone call to address any unanswered questions.
January-March
Hopefully you will have one or more offers by now. This is the time to negotiate a contract and accept an offer. Review the contract carefully and don’t hesitate to ask for clarification of unclear points. Some applicants prefer to have a lawyer review the contract prior to signing (see “The Art of Negotiation,” December 2008, p. 20).
Register for your board examination. Most specialties, including internal medicine, family medicine, and pediatrics, as well as board exams for osteopathic medicine, have registration deadlines in February. Given the significant cost of applying for these exams, it pays not to be tardy, as late fees can set you back hundreds of dollars.
Apply for state medical licensure. This process varies by state, but it can take several months to complete, especially if you are applying in a state other than where you trained. For example, California recommends starting the application process six to nine months in advance. International medical graduates who require a work visa need to ensure their paperwork is processed in a timely manner.
Each hospital is different, but applications for hospital credentialing generally means filling out a mountain of paperwork. Most hospitals will perform a thorough background check, so don’t be surprised if fingerprinting is required. The hospital or hospitalist group usually helps new hires navigate through this process, which can take several weeks or even months.
April-June
Moving to a different city or state can be exciting—and stressful. Start talking to hospitalists at the facility where you will be working to get a feel for the city and recommendations for places to live. Revisit the location to become more familiar with the surroundings. Some hospitals are very helpful; some provide new hires with a real estate agent. Moving expenses often are covered as a condition of employment, but it depends on your contract.
Consider taking a vacation to either further explore relocation options or to simply relax. If you have followed the recommendations outlined in the previous months, you should have time to unwind as your residency comes to an end. Some future hospitalists like to use this time to intensify board review; others cringe at the thought.
Transitioning from resident to hospitalist is no easy task, and it shouldn’t be taken lightly. It’s not a one-month process, either, so planning is essential. Although it might seem to be a daunting journey, it’s very rewarding in the long run. TH
Dr. Grant is a hospitalist at the University of Michigan Health System in Ann Arbor. Dr. Warren-Marzola is a hospitalist at St. Luke’s Hospital in Toledo, Ohio. Both are members of SHM’s Young Physicians Committee.
Apart from the part-time job that provided pocket money while you were in high school or during your undergraduate years, physicians generally have little experience in the job-hunting arena. A physician’s career path requires much skill at applying for such educational endeavors as medical school and residency training, but applying for a “real” job can be a strange concept for most.
Not lost in the equation is the fact that the application process doesn’t begin until most physicians are in their late 20s. While many of our non-physician friends are on their second or third jobs, graduating residents looking to launch their careers often struggle with the transition to the world of HM. In order to help navigate these waters, we have put together a yearlong guide to help make the transition from third-year resident to hospitalist a little smoother.
July-September
The first step in landing a job is to find a mentor who can assist you through the entire process. Choose your mentor wisely; an experienced hospitalist can provide valuable feedback during your job search. If your goal is employment with a private hospitalist group, find a hospitalist with private-practice experience.
Choose your senior-year electives carefully. Consider focusing on areas of weakness or areas that are pertinent to HM (e.g., infectious disease, cardiology, neurology, critical-care medicine). Think about an outside elective in HM.
If you haven’t done so already, now is the time to create a curriculum vitae, also known as a CV, and a cover letter. The CV is a vital document. It might be the key element in determining whether you are worthy of an interview. Work on this document early, as you will need time for edits, updates, and mentor review. The cover letter should clearly describe the type of position you want and confidently state why you would be an asset to a particular hospitalist program. Edit your words carefully; spelling errors or typos in documents can be costly.
Once the Labor Day holiday has passed, you should start requesting letters of recommendation. Think hard about who you want before asking for a letter of recommendation, as these typically carry a lot of weight in the interview selection process. Although program directors, chiefs of medicine, and hospitalists can be good choices, it is important to choose people who know you well, as they tend to generate a more personal and powerful letter. Because letter-writers often are busy people, it is appropriate to give a deadline for when you need the letter.
October-December
Actively start the job search and apply for desired positions. This is the time of year when HM jobs are heavily advertised and programs are looking to fill positions. Hospitalists are in high demand throughout the country. Some great places to find job openings are:
- SHM’s Career Center (www.hospitalmedicine.org/careers);
- Classified ad sections in the Journal of Hospital Medicine, general medicine journals, and HM news magazines like The Hospitalist (see “SHM Career Center,” p. 35); and
- Hospitals and HM groups of interest, even if they are not advertising; contact them personally.
Begin the interview process by researching the hospital and HM group in advance. Prepare appropriate interview questions. When you interview, try to meet with as many people as possible to get a feel for what the job entails. Talk to the everyday hospitalists and try to gauge how satisfied they are in their jobs.
Bring extra copies of your updated CV and look sharp. Shine your shoes. Is it time to replace the suit you used to apply for residency?
Send a thank-you note or e-mail to the person(s) you interviewed with. If possible, do this within three days of your visit. It’s an important step in the process, yet this simple task often is overlooked. Remain in contact with the HM programs you are most interested in. Think about a follow-up visit or phone call to address any unanswered questions.
January-March
Hopefully you will have one or more offers by now. This is the time to negotiate a contract and accept an offer. Review the contract carefully and don’t hesitate to ask for clarification of unclear points. Some applicants prefer to have a lawyer review the contract prior to signing (see “The Art of Negotiation,” December 2008, p. 20).
Register for your board examination. Most specialties, including internal medicine, family medicine, and pediatrics, as well as board exams for osteopathic medicine, have registration deadlines in February. Given the significant cost of applying for these exams, it pays not to be tardy, as late fees can set you back hundreds of dollars.
Apply for state medical licensure. This process varies by state, but it can take several months to complete, especially if you are applying in a state other than where you trained. For example, California recommends starting the application process six to nine months in advance. International medical graduates who require a work visa need to ensure their paperwork is processed in a timely manner.
Each hospital is different, but applications for hospital credentialing generally means filling out a mountain of paperwork. Most hospitals will perform a thorough background check, so don’t be surprised if fingerprinting is required. The hospital or hospitalist group usually helps new hires navigate through this process, which can take several weeks or even months.
April-June
Moving to a different city or state can be exciting—and stressful. Start talking to hospitalists at the facility where you will be working to get a feel for the city and recommendations for places to live. Revisit the location to become more familiar with the surroundings. Some hospitals are very helpful; some provide new hires with a real estate agent. Moving expenses often are covered as a condition of employment, but it depends on your contract.
Consider taking a vacation to either further explore relocation options or to simply relax. If you have followed the recommendations outlined in the previous months, you should have time to unwind as your residency comes to an end. Some future hospitalists like to use this time to intensify board review; others cringe at the thought.
Transitioning from resident to hospitalist is no easy task, and it shouldn’t be taken lightly. It’s not a one-month process, either, so planning is essential. Although it might seem to be a daunting journey, it’s very rewarding in the long run. TH
Dr. Grant is a hospitalist at the University of Michigan Health System in Ann Arbor. Dr. Warren-Marzola is a hospitalist at St. Luke’s Hospital in Toledo, Ohio. Both are members of SHM’s Young Physicians Committee.
Facility Transfers
Patient care provided in the acute setting might not always end with discharge to the patient’s home. Frequently, a hospitalist will transfer the patient to a different unit in the hospital or an off-site facility to receive additional services before returning to their home. When the patient’s condition requires a transfer to a physical medicine and rehabilitation (PM&R) unit, a psychiatric unit, a long-term acute-care facility, or a skilled nursing facility, it is important for the hospitalist to identify their role, if any, in the new area of care. Physician billing will depend on several factors:
- A shared medical record;
- The attending of record in each setting; and
- The care rendered by the hospitalist in each setting.
Intrafacility
A hospitalist serves as the “attending of record” in an inpatient hospital where acute care is required for a 68-year-old male with hypertension and diabetes who sustained a hip fracture. The care plan includes post-discharge therapy and rehabilitation. When the hospitalist transfers care to a PM&R unit within the same facility for which the hospitalist is no longer the attending of record, they might be asked to provide ongoing care for the patient’s medical conditions (e.g., diabetes and hypertension). The hospitalist’s knee-jerk reaction is to bill for an inpatient consultation for the initial service provided in the transferred setting. This would only be appropriate if the request for opinion or advice involved an unrelated, new condition, and the requesting physician’s intent is for opinion or advice on how to manage the patient and not the a priori intent for the hospitalist to assume the patient’s medical care.
If consultation requirements are met (see “Consulataion Reminder,” p. 20), the hospitalist can report an inpatient consultation code (99251-99255). However, when circumstances do not fully represent the intent or need for consultative services but rather a continuity of the medical care provided during the acute phase of the hospitalization, report the most appropriate subsequent hospital care code (99231-99233) for the initial rehab visit and all follow-up services.
On occasion, the hospitalist will be asked to perform and provide the history and physical (H&P) for the patient’s “sub-acute” phase of care, even though the hospitalist is not the attending of record. This usually happens when the attending of record cannot complete the medical requirements of the H&P, either at all or as comprehensively as the hospitalist. When this occurs, the hospitalist should not report an initial hospital care code (99221-99223) because they are not the attending of record—the physician who admits the patient and is responsible for the patient’s stay in the transferred location.
Additionally, a consultation service (99251-99255) should not be reported, because the request involves the completion of a facility-mandated form and not an opinion or advice on caring for the patient. If medical issues require the hospitalist’s evaluation and management, there is medical necessity for capturing the hospitalist’s participation as subsequent hospital care (99231-99233). If no medical conditions present for the hospitalist to manage, the service will not be considered “medically necessary” by the payor.
Interfacility
Hospitalist groups provide patient care and coverage in a variety of facilities. Confusion often arises when the attending of record during acute care and the sub-acute setting are different hospitalists from the same HM group. The hospitalist who receives the patient in the transfer facility may err on the side of caution and report subsequent hospital care (99231-99233) because the group has provided ongoing patient care. In this scenario, the hospitalist group might lose revenue if an admission service (99221-99223) was not reported.
Day of Transfer Billing
A single hospitalist or two hospitalists from the same group might bill both the hospital discharge management code (99238-99239) and an initial hospital care code (99221-99223) when the discharge and admission do not occur on the same day if the transfer is between:
- Different hospitals;
- Different facilities under common ownership that do not have merged records;* or
- Between the acute-care hospital and a prospective payment system (PPS)-exempt unit within the same hospital when there are no merged records.
In all other transfer circumstances that do not meet the elements noted above, the physician should bill only the appropriate level of subsequent hospital care (99231-99233) for the date of transfer.1 Of note, Medicare Part A covers inpatient care in psychiatric, rehabilitation, critical access, and long-term-care hospitals. Each of these specialty hospitals is exempt from the PPS established for acute-care hospitals in 1983.2 TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty of SHM’s inpatient coding course.
*Editor’s note: “Merged record” is not equivalent to commonly accessible charts via an electronic health record system. If the medical record for the patient’s acute stay is “closed” and the patient is given a separate medical record and registration for the stay in the transferred facility, consider the transfer stay as a separate admission.
References
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1E. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed June 1, 2009.
- Department of Health and Human Services. Office of Inspector General: Oversight of Medicare PPS-Exempt Hospital Services. HHS Web site. Available at: www.oig.hhs.gov/oei/reports/oei-12-02-00170.pdf. Accessed June 1, 2009.
- CMS. Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1H. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed June 1, 2009.
Patient care provided in the acute setting might not always end with discharge to the patient’s home. Frequently, a hospitalist will transfer the patient to a different unit in the hospital or an off-site facility to receive additional services before returning to their home. When the patient’s condition requires a transfer to a physical medicine and rehabilitation (PM&R) unit, a psychiatric unit, a long-term acute-care facility, or a skilled nursing facility, it is important for the hospitalist to identify their role, if any, in the new area of care. Physician billing will depend on several factors:
- A shared medical record;
- The attending of record in each setting; and
- The care rendered by the hospitalist in each setting.
Intrafacility
A hospitalist serves as the “attending of record” in an inpatient hospital where acute care is required for a 68-year-old male with hypertension and diabetes who sustained a hip fracture. The care plan includes post-discharge therapy and rehabilitation. When the hospitalist transfers care to a PM&R unit within the same facility for which the hospitalist is no longer the attending of record, they might be asked to provide ongoing care for the patient’s medical conditions (e.g., diabetes and hypertension). The hospitalist’s knee-jerk reaction is to bill for an inpatient consultation for the initial service provided in the transferred setting. This would only be appropriate if the request for opinion or advice involved an unrelated, new condition, and the requesting physician’s intent is for opinion or advice on how to manage the patient and not the a priori intent for the hospitalist to assume the patient’s medical care.
If consultation requirements are met (see “Consulataion Reminder,” p. 20), the hospitalist can report an inpatient consultation code (99251-99255). However, when circumstances do not fully represent the intent or need for consultative services but rather a continuity of the medical care provided during the acute phase of the hospitalization, report the most appropriate subsequent hospital care code (99231-99233) for the initial rehab visit and all follow-up services.
On occasion, the hospitalist will be asked to perform and provide the history and physical (H&P) for the patient’s “sub-acute” phase of care, even though the hospitalist is not the attending of record. This usually happens when the attending of record cannot complete the medical requirements of the H&P, either at all or as comprehensively as the hospitalist. When this occurs, the hospitalist should not report an initial hospital care code (99221-99223) because they are not the attending of record—the physician who admits the patient and is responsible for the patient’s stay in the transferred location.
Additionally, a consultation service (99251-99255) should not be reported, because the request involves the completion of a facility-mandated form and not an opinion or advice on caring for the patient. If medical issues require the hospitalist’s evaluation and management, there is medical necessity for capturing the hospitalist’s participation as subsequent hospital care (99231-99233). If no medical conditions present for the hospitalist to manage, the service will not be considered “medically necessary” by the payor.
Interfacility
Hospitalist groups provide patient care and coverage in a variety of facilities. Confusion often arises when the attending of record during acute care and the sub-acute setting are different hospitalists from the same HM group. The hospitalist who receives the patient in the transfer facility may err on the side of caution and report subsequent hospital care (99231-99233) because the group has provided ongoing patient care. In this scenario, the hospitalist group might lose revenue if an admission service (99221-99223) was not reported.
Day of Transfer Billing
A single hospitalist or two hospitalists from the same group might bill both the hospital discharge management code (99238-99239) and an initial hospital care code (99221-99223) when the discharge and admission do not occur on the same day if the transfer is between:
- Different hospitals;
- Different facilities under common ownership that do not have merged records;* or
- Between the acute-care hospital and a prospective payment system (PPS)-exempt unit within the same hospital when there are no merged records.
In all other transfer circumstances that do not meet the elements noted above, the physician should bill only the appropriate level of subsequent hospital care (99231-99233) for the date of transfer.1 Of note, Medicare Part A covers inpatient care in psychiatric, rehabilitation, critical access, and long-term-care hospitals. Each of these specialty hospitals is exempt from the PPS established for acute-care hospitals in 1983.2 TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty of SHM’s inpatient coding course.
*Editor’s note: “Merged record” is not equivalent to commonly accessible charts via an electronic health record system. If the medical record for the patient’s acute stay is “closed” and the patient is given a separate medical record and registration for the stay in the transferred facility, consider the transfer stay as a separate admission.
References
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1E. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed June 1, 2009.
- Department of Health and Human Services. Office of Inspector General: Oversight of Medicare PPS-Exempt Hospital Services. HHS Web site. Available at: www.oig.hhs.gov/oei/reports/oei-12-02-00170.pdf. Accessed June 1, 2009.
- CMS. Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1H. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed June 1, 2009.
Patient care provided in the acute setting might not always end with discharge to the patient’s home. Frequently, a hospitalist will transfer the patient to a different unit in the hospital or an off-site facility to receive additional services before returning to their home. When the patient’s condition requires a transfer to a physical medicine and rehabilitation (PM&R) unit, a psychiatric unit, a long-term acute-care facility, or a skilled nursing facility, it is important for the hospitalist to identify their role, if any, in the new area of care. Physician billing will depend on several factors:
- A shared medical record;
- The attending of record in each setting; and
- The care rendered by the hospitalist in each setting.
Intrafacility
A hospitalist serves as the “attending of record” in an inpatient hospital where acute care is required for a 68-year-old male with hypertension and diabetes who sustained a hip fracture. The care plan includes post-discharge therapy and rehabilitation. When the hospitalist transfers care to a PM&R unit within the same facility for which the hospitalist is no longer the attending of record, they might be asked to provide ongoing care for the patient’s medical conditions (e.g., diabetes and hypertension). The hospitalist’s knee-jerk reaction is to bill for an inpatient consultation for the initial service provided in the transferred setting. This would only be appropriate if the request for opinion or advice involved an unrelated, new condition, and the requesting physician’s intent is for opinion or advice on how to manage the patient and not the a priori intent for the hospitalist to assume the patient’s medical care.
If consultation requirements are met (see “Consulataion Reminder,” p. 20), the hospitalist can report an inpatient consultation code (99251-99255). However, when circumstances do not fully represent the intent or need for consultative services but rather a continuity of the medical care provided during the acute phase of the hospitalization, report the most appropriate subsequent hospital care code (99231-99233) for the initial rehab visit and all follow-up services.
On occasion, the hospitalist will be asked to perform and provide the history and physical (H&P) for the patient’s “sub-acute” phase of care, even though the hospitalist is not the attending of record. This usually happens when the attending of record cannot complete the medical requirements of the H&P, either at all or as comprehensively as the hospitalist. When this occurs, the hospitalist should not report an initial hospital care code (99221-99223) because they are not the attending of record—the physician who admits the patient and is responsible for the patient’s stay in the transferred location.
Additionally, a consultation service (99251-99255) should not be reported, because the request involves the completion of a facility-mandated form and not an opinion or advice on caring for the patient. If medical issues require the hospitalist’s evaluation and management, there is medical necessity for capturing the hospitalist’s participation as subsequent hospital care (99231-99233). If no medical conditions present for the hospitalist to manage, the service will not be considered “medically necessary” by the payor.
Interfacility
Hospitalist groups provide patient care and coverage in a variety of facilities. Confusion often arises when the attending of record during acute care and the sub-acute setting are different hospitalists from the same HM group. The hospitalist who receives the patient in the transfer facility may err on the side of caution and report subsequent hospital care (99231-99233) because the group has provided ongoing patient care. In this scenario, the hospitalist group might lose revenue if an admission service (99221-99223) was not reported.
Day of Transfer Billing
A single hospitalist or two hospitalists from the same group might bill both the hospital discharge management code (99238-99239) and an initial hospital care code (99221-99223) when the discharge and admission do not occur on the same day if the transfer is between:
- Different hospitals;
- Different facilities under common ownership that do not have merged records;* or
- Between the acute-care hospital and a prospective payment system (PPS)-exempt unit within the same hospital when there are no merged records.
In all other transfer circumstances that do not meet the elements noted above, the physician should bill only the appropriate level of subsequent hospital care (99231-99233) for the date of transfer.1 Of note, Medicare Part A covers inpatient care in psychiatric, rehabilitation, critical access, and long-term-care hospitals. Each of these specialty hospitals is exempt from the PPS established for acute-care hospitals in 1983.2 TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty of SHM’s inpatient coding course.
*Editor’s note: “Merged record” is not equivalent to commonly accessible charts via an electronic health record system. If the medical record for the patient’s acute stay is “closed” and the patient is given a separate medical record and registration for the stay in the transferred facility, consider the transfer stay as a separate admission.
References
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1E. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed June 1, 2009.
- Department of Health and Human Services. Office of Inspector General: Oversight of Medicare PPS-Exempt Hospital Services. HHS Web site. Available at: www.oig.hhs.gov/oei/reports/oei-12-02-00170.pdf. Accessed June 1, 2009.
- CMS. Medicare Claims Processing Manual: Chapter 12, Section 30.6.9.1H. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed June 1, 2009.
Billion-Dollar Questions
On June 30, a new government agency within the Department of Health and Human Services (HHS) called the Federal Coordinating Council for Comparative Effectiveness Research released its first report to President Obama and Congress. Authorized by the American Recovery and Reinvestment Act of 2009, the council is tasked with prioritizing and coordinating how multiple government agencies will spend the stimulus package’s $1.1 billion windfall for comparative effectiveness research (CER), which is aimed at improving healthcare outcomes in the U.S.
Of the funds, $400 million has been directed to the National Institutes of Health (NIH), $300 million to the Agency for Healthcare Research and Quality, and the remaining $400 million to the Office of the Secretary of Health and Human Services.
Patrick Conway, MD, MSc, the federal coordinating council’s executive director, is well versed in the potential impact of comparative effectiveness research on hospitalists. Just as Dr. Conway was joining the Center for Health Care Quality at Cincinnati Children’s Hospital after a fellowship at Children’s Hospital of Philadelphia, the pediatric hospitalist was named a 2007-2008 White House Fellow at HHS—the first hospitalist accepted into the program.

—Patrick Conway, MD, MSc, executive director, HHS’ Federal Coordinating Council for Comparative Effectiveness Research
In August 2008, he was tapped for the post of chief medical officer in the department’s Office of the Assistant Secretary for Planning and Evaluation.
Meanwhile, Dr. Conway still sees patients on weekends at Children’s National Medical Center in Washington, D.C. He recently talked with The Hospitalist about the challenges of coordinating research funding across multiple government agencies, how the Office of the Secretary’s $400 million allocation could be best spent, and what it all means for patient care.
Question: What are the biggest recommendations in the federal coordinating council’s report?
Answer: We approached this as “What unique role can the Office of the Secretary research funds address?” We identified data infrastructure as a potential primary investment. That includes things such as patient registries, distributed data networks, and claims databases.
Traditionally, the federal government has not invested in infrastructure because we have funded independent investigators on a one-question-by-one-question basis. The way I see this infusion of funds is it allows you to invest in data infrastructure that can then be used to answer literally hundreds of questions over time.
Secondly, we identified dissemination and translation, so how do we think about innovative ways to actually communicate directly to patients and physicians at the point of care? We also identified priority populations, including racial and ethnic minorities, persons with multiple chronic conditions, children, and the elderly. And lastly, we identified priority interventions, such as behavioral change, delivery systems, and prevention. So how do we decrease obesity, how do we decrease smoking rates?
Q: How will you address the challenge of coordinating research funding across multiple federal agencies?
A: I think the first step is doing the inventory [of CER], which is going to be an ongoing and iterative process. By doing that, then the council and the HHS have to attempt to avoid duplicating efforts and actually coordinate efforts across the federal government.
Honestly, I think the biggest challenge is these are extremely large, complex government programs. These are hundreds of millions of dollars going out to a huge variety of researchers, academic institutions, etc. One of the systems we’re trying to put in place is a better way to track what’s going on now, so we can actually coordinate going forward. It’s something as simple as we now have a common definition. We tag all money (e.g., CER), so we know exactly what we’re spending money on. That sounds really simple, but it’s actually never been done before. This is a relatively new area of emphasis for the federal government and for healthcare.
Q: What main point should hospitalists take away from this report?
A: This research will address primary questions about which medicine is best for which patient but also address larger issues, such as care coordination and how care is organized within the hospital and outside the hospital, so that we focus on the gamut of questions that have the potential to improve patient outcomes.
Q: What were some common themes you heard in the public listening sessions and online comments you solicited during the report’s preparation?
A: One of them was the importance of engaging stakeholders throughout the process, getting input from patients, physicians, policymakers. … We also heard themes about the need for infrastructure development, also the need for data infrastructure. We also heard a theme about the need for more work on research methodology and training of researchers. And then we heard a strong theme around “This needs to actually be disseminated and translated into care delivery.” So producing knowledge is helpful, but translating that knowledge into better outcomes is the ultimate goal.
Q: The report repeatedly mentions “real world” healthcare settings. Is this meant as a criticism of the idealized outcomes of efficacy research as it is typically conducted?
A: I don’t know that I would frame it as a criticism. I will say that as hospitalists, we are faced with patients every day where there’s unclear evidence about how best to manage that patient. And therefore, we need more evidence on the real questions that patients and physicians encounter in practice. I think we’ve had a long history of strong, well-funded randomized trials in this country, and I think we need to complement that with other methods of research as well, including databases, quality improvement, and measuring interventions.
Q: What are the limitations in translating all of this knowledge to interventions for the patients who need it?
A: I think the research paradigm traditionally has been: We fund an investigator. They go off for years and do their research. And then they publish it in the New England Journal [of Medicine] or JAMA, and we call that a success.
I would argue that we’re at a time where we need to think about a new paradigm, where just publishing it is some middle step. And we need to think about how you actually link the research enterprise to the care delivery enterprise, so research is rapidly implemented and you’re measuring outcomes and ensuring that research actually reaches the patients and clinicians.
Q: Are there any real-world examples of how to do this?
A: Say we had a national patient library and we thought about things that we have not traditionally thought about in healthcare—social networking, Twitter, Facebook, media channels that reach people now. How do you insert health content into those channels to actually change people’s behavior, or at least inform them? The medical establishment thinks we publish it in the New England Journal [of Medicine] and the world changes. That’s just fundamentally not true.
On the provider side, how do we think about the lay media? How do we think about channels that providers use, like UpToDate and Medscape? How do we get comparative effectiveness content into those channels that are used by providers and physicians?
Q: How should CER address the needs of patient groups that are under-represented in traditional medical studies?
A: I think that’s a huge area. Efficacy trials generally will show something works for the average patient. But the issue is, and I’ll give you a concrete example, if you are an elderly, African-American female with a couple of conditions (diabetes and heart disease), how will that treatment work for you? So I think the power of comparative effectiveness is that we, especially with the data sources we just talked about, can look at patient subgroups and get as close as possible to the individual level to really present information. Instead of [saying], this works on average patients, which includes lots of patients that don’t look at all like you, [we can] say we’ve looked and it actually works well for racial and ethnic minorities, or persons with disabilities, or the very elderly.
Q: What do you hope ultimately will come from this report?
A: On the care delivery side, this is an opportunity for hospitalists to test different interventions to improve care in the hospitals. For what I hope to achieve, I think as we invest in all these individual programs, we are building in evaluation components to assess how this impacts patient outcomes.
I think the ultimate goal is to improve patient outcomes in this country, which I know is an unbelievably grand goal, but I think you build up to that by each investment. You track what it produces and ultimately how it affects outcomes, and so you at least start to build a sense of what this program means for the nation’s health. TH
Bryn Nelson is a freelance writer based in Seattle.
On June 30, a new government agency within the Department of Health and Human Services (HHS) called the Federal Coordinating Council for Comparative Effectiveness Research released its first report to President Obama and Congress. Authorized by the American Recovery and Reinvestment Act of 2009, the council is tasked with prioritizing and coordinating how multiple government agencies will spend the stimulus package’s $1.1 billion windfall for comparative effectiveness research (CER), which is aimed at improving healthcare outcomes in the U.S.
Of the funds, $400 million has been directed to the National Institutes of Health (NIH), $300 million to the Agency for Healthcare Research and Quality, and the remaining $400 million to the Office of the Secretary of Health and Human Services.
Patrick Conway, MD, MSc, the federal coordinating council’s executive director, is well versed in the potential impact of comparative effectiveness research on hospitalists. Just as Dr. Conway was joining the Center for Health Care Quality at Cincinnati Children’s Hospital after a fellowship at Children’s Hospital of Philadelphia, the pediatric hospitalist was named a 2007-2008 White House Fellow at HHS—the first hospitalist accepted into the program.
—Patrick Conway, MD, MSc, executive director, HHS’ Federal Coordinating Council for Comparative Effectiveness Research
In August 2008, he was tapped for the post of chief medical officer in the department’s Office of the Assistant Secretary for Planning and Evaluation.
Meanwhile, Dr. Conway still sees patients on weekends at Children’s National Medical Center in Washington, D.C. He recently talked with The Hospitalist about the challenges of coordinating research funding across multiple government agencies, how the Office of the Secretary’s $400 million allocation could be best spent, and what it all means for patient care.
Question: What are the biggest recommendations in the federal coordinating council’s report?
Answer: We approached this as “What unique role can the Office of the Secretary research funds address?” We identified data infrastructure as a potential primary investment. That includes things such as patient registries, distributed data networks, and claims databases.
Traditionally, the federal government has not invested in infrastructure because we have funded independent investigators on a one-question-by-one-question basis. The way I see this infusion of funds is it allows you to invest in data infrastructure that can then be used to answer literally hundreds of questions over time.
Secondly, we identified dissemination and translation, so how do we think about innovative ways to actually communicate directly to patients and physicians at the point of care? We also identified priority populations, including racial and ethnic minorities, persons with multiple chronic conditions, children, and the elderly. And lastly, we identified priority interventions, such as behavioral change, delivery systems, and prevention. So how do we decrease obesity, how do we decrease smoking rates?
Q: How will you address the challenge of coordinating research funding across multiple federal agencies?
A: I think the first step is doing the inventory [of CER], which is going to be an ongoing and iterative process. By doing that, then the council and the HHS have to attempt to avoid duplicating efforts and actually coordinate efforts across the federal government.
Honestly, I think the biggest challenge is these are extremely large, complex government programs. These are hundreds of millions of dollars going out to a huge variety of researchers, academic institutions, etc. One of the systems we’re trying to put in place is a better way to track what’s going on now, so we can actually coordinate going forward. It’s something as simple as we now have a common definition. We tag all money (e.g., CER), so we know exactly what we’re spending money on. That sounds really simple, but it’s actually never been done before. This is a relatively new area of emphasis for the federal government and for healthcare.
Q: What main point should hospitalists take away from this report?
A: This research will address primary questions about which medicine is best for which patient but also address larger issues, such as care coordination and how care is organized within the hospital and outside the hospital, so that we focus on the gamut of questions that have the potential to improve patient outcomes.
Q: What were some common themes you heard in the public listening sessions and online comments you solicited during the report’s preparation?
A: One of them was the importance of engaging stakeholders throughout the process, getting input from patients, physicians, policymakers. … We also heard themes about the need for infrastructure development, also the need for data infrastructure. We also heard a theme about the need for more work on research methodology and training of researchers. And then we heard a strong theme around “This needs to actually be disseminated and translated into care delivery.” So producing knowledge is helpful, but translating that knowledge into better outcomes is the ultimate goal.
Q: The report repeatedly mentions “real world” healthcare settings. Is this meant as a criticism of the idealized outcomes of efficacy research as it is typically conducted?
A: I don’t know that I would frame it as a criticism. I will say that as hospitalists, we are faced with patients every day where there’s unclear evidence about how best to manage that patient. And therefore, we need more evidence on the real questions that patients and physicians encounter in practice. I think we’ve had a long history of strong, well-funded randomized trials in this country, and I think we need to complement that with other methods of research as well, including databases, quality improvement, and measuring interventions.
Q: What are the limitations in translating all of this knowledge to interventions for the patients who need it?
A: I think the research paradigm traditionally has been: We fund an investigator. They go off for years and do their research. And then they publish it in the New England Journal [of Medicine] or JAMA, and we call that a success.
I would argue that we’re at a time where we need to think about a new paradigm, where just publishing it is some middle step. And we need to think about how you actually link the research enterprise to the care delivery enterprise, so research is rapidly implemented and you’re measuring outcomes and ensuring that research actually reaches the patients and clinicians.
Q: Are there any real-world examples of how to do this?
A: Say we had a national patient library and we thought about things that we have not traditionally thought about in healthcare—social networking, Twitter, Facebook, media channels that reach people now. How do you insert health content into those channels to actually change people’s behavior, or at least inform them? The medical establishment thinks we publish it in the New England Journal [of Medicine] and the world changes. That’s just fundamentally not true.
On the provider side, how do we think about the lay media? How do we think about channels that providers use, like UpToDate and Medscape? How do we get comparative effectiveness content into those channels that are used by providers and physicians?
Q: How should CER address the needs of patient groups that are under-represented in traditional medical studies?
A: I think that’s a huge area. Efficacy trials generally will show something works for the average patient. But the issue is, and I’ll give you a concrete example, if you are an elderly, African-American female with a couple of conditions (diabetes and heart disease), how will that treatment work for you? So I think the power of comparative effectiveness is that we, especially with the data sources we just talked about, can look at patient subgroups and get as close as possible to the individual level to really present information. Instead of [saying], this works on average patients, which includes lots of patients that don’t look at all like you, [we can] say we’ve looked and it actually works well for racial and ethnic minorities, or persons with disabilities, or the very elderly.
Q: What do you hope ultimately will come from this report?
A: On the care delivery side, this is an opportunity for hospitalists to test different interventions to improve care in the hospitals. For what I hope to achieve, I think as we invest in all these individual programs, we are building in evaluation components to assess how this impacts patient outcomes.
I think the ultimate goal is to improve patient outcomes in this country, which I know is an unbelievably grand goal, but I think you build up to that by each investment. You track what it produces and ultimately how it affects outcomes, and so you at least start to build a sense of what this program means for the nation’s health. TH
Bryn Nelson is a freelance writer based in Seattle.
On June 30, a new government agency within the Department of Health and Human Services (HHS) called the Federal Coordinating Council for Comparative Effectiveness Research released its first report to President Obama and Congress. Authorized by the American Recovery and Reinvestment Act of 2009, the council is tasked with prioritizing and coordinating how multiple government agencies will spend the stimulus package’s $1.1 billion windfall for comparative effectiveness research (CER), which is aimed at improving healthcare outcomes in the U.S.
Of the funds, $400 million has been directed to the National Institutes of Health (NIH), $300 million to the Agency for Healthcare Research and Quality, and the remaining $400 million to the Office of the Secretary of Health and Human Services.
Patrick Conway, MD, MSc, the federal coordinating council’s executive director, is well versed in the potential impact of comparative effectiveness research on hospitalists. Just as Dr. Conway was joining the Center for Health Care Quality at Cincinnati Children’s Hospital after a fellowship at Children’s Hospital of Philadelphia, the pediatric hospitalist was named a 2007-2008 White House Fellow at HHS—the first hospitalist accepted into the program.
—Patrick Conway, MD, MSc, executive director, HHS’ Federal Coordinating Council for Comparative Effectiveness Research
In August 2008, he was tapped for the post of chief medical officer in the department’s Office of the Assistant Secretary for Planning and Evaluation.
Meanwhile, Dr. Conway still sees patients on weekends at Children’s National Medical Center in Washington, D.C. He recently talked with The Hospitalist about the challenges of coordinating research funding across multiple government agencies, how the Office of the Secretary’s $400 million allocation could be best spent, and what it all means for patient care.
Question: What are the biggest recommendations in the federal coordinating council’s report?
Answer: We approached this as “What unique role can the Office of the Secretary research funds address?” We identified data infrastructure as a potential primary investment. That includes things such as patient registries, distributed data networks, and claims databases.
Traditionally, the federal government has not invested in infrastructure because we have funded independent investigators on a one-question-by-one-question basis. The way I see this infusion of funds is it allows you to invest in data infrastructure that can then be used to answer literally hundreds of questions over time.
Secondly, we identified dissemination and translation, so how do we think about innovative ways to actually communicate directly to patients and physicians at the point of care? We also identified priority populations, including racial and ethnic minorities, persons with multiple chronic conditions, children, and the elderly. And lastly, we identified priority interventions, such as behavioral change, delivery systems, and prevention. So how do we decrease obesity, how do we decrease smoking rates?
Q: How will you address the challenge of coordinating research funding across multiple federal agencies?
A: I think the first step is doing the inventory [of CER], which is going to be an ongoing and iterative process. By doing that, then the council and the HHS have to attempt to avoid duplicating efforts and actually coordinate efforts across the federal government.
Honestly, I think the biggest challenge is these are extremely large, complex government programs. These are hundreds of millions of dollars going out to a huge variety of researchers, academic institutions, etc. One of the systems we’re trying to put in place is a better way to track what’s going on now, so we can actually coordinate going forward. It’s something as simple as we now have a common definition. We tag all money (e.g., CER), so we know exactly what we’re spending money on. That sounds really simple, but it’s actually never been done before. This is a relatively new area of emphasis for the federal government and for healthcare.
Q: What main point should hospitalists take away from this report?
A: This research will address primary questions about which medicine is best for which patient but also address larger issues, such as care coordination and how care is organized within the hospital and outside the hospital, so that we focus on the gamut of questions that have the potential to improve patient outcomes.
Q: What were some common themes you heard in the public listening sessions and online comments you solicited during the report’s preparation?
A: One of them was the importance of engaging stakeholders throughout the process, getting input from patients, physicians, policymakers. … We also heard themes about the need for infrastructure development, also the need for data infrastructure. We also heard a theme about the need for more work on research methodology and training of researchers. And then we heard a strong theme around “This needs to actually be disseminated and translated into care delivery.” So producing knowledge is helpful, but translating that knowledge into better outcomes is the ultimate goal.
Q: The report repeatedly mentions “real world” healthcare settings. Is this meant as a criticism of the idealized outcomes of efficacy research as it is typically conducted?
A: I don’t know that I would frame it as a criticism. I will say that as hospitalists, we are faced with patients every day where there’s unclear evidence about how best to manage that patient. And therefore, we need more evidence on the real questions that patients and physicians encounter in practice. I think we’ve had a long history of strong, well-funded randomized trials in this country, and I think we need to complement that with other methods of research as well, including databases, quality improvement, and measuring interventions.
Q: What are the limitations in translating all of this knowledge to interventions for the patients who need it?
A: I think the research paradigm traditionally has been: We fund an investigator. They go off for years and do their research. And then they publish it in the New England Journal [of Medicine] or JAMA, and we call that a success.
I would argue that we’re at a time where we need to think about a new paradigm, where just publishing it is some middle step. And we need to think about how you actually link the research enterprise to the care delivery enterprise, so research is rapidly implemented and you’re measuring outcomes and ensuring that research actually reaches the patients and clinicians.
Q: Are there any real-world examples of how to do this?
A: Say we had a national patient library and we thought about things that we have not traditionally thought about in healthcare—social networking, Twitter, Facebook, media channels that reach people now. How do you insert health content into those channels to actually change people’s behavior, or at least inform them? The medical establishment thinks we publish it in the New England Journal [of Medicine] and the world changes. That’s just fundamentally not true.
On the provider side, how do we think about the lay media? How do we think about channels that providers use, like UpToDate and Medscape? How do we get comparative effectiveness content into those channels that are used by providers and physicians?
Q: How should CER address the needs of patient groups that are under-represented in traditional medical studies?
A: I think that’s a huge area. Efficacy trials generally will show something works for the average patient. But the issue is, and I’ll give you a concrete example, if you are an elderly, African-American female with a couple of conditions (diabetes and heart disease), how will that treatment work for you? So I think the power of comparative effectiveness is that we, especially with the data sources we just talked about, can look at patient subgroups and get as close as possible to the individual level to really present information. Instead of [saying], this works on average patients, which includes lots of patients that don’t look at all like you, [we can] say we’ve looked and it actually works well for racial and ethnic minorities, or persons with disabilities, or the very elderly.
Q: What do you hope ultimately will come from this report?
A: On the care delivery side, this is an opportunity for hospitalists to test different interventions to improve care in the hospitals. For what I hope to achieve, I think as we invest in all these individual programs, we are building in evaluation components to assess how this impacts patient outcomes.
I think the ultimate goal is to improve patient outcomes in this country, which I know is an unbelievably grand goal, but I think you build up to that by each investment. You track what it produces and ultimately how it affects outcomes, and so you at least start to build a sense of what this program means for the nation’s health. TH
Bryn Nelson is a freelance writer based in Seattle.
The Downtime Dilemma
How do you spend your time off? Do you neglect your to-do list in favor of rest and relaxation, or do you race around trying to get everything done? How you use your free time affects your energy level and on-the-job enthusiasm. Hospitalists who learn to make the most of their time off reduce their stress and master the elusive work-life balance, and are more likely to avoid burnout. It’s especially true of physicians who work long hours followed by multiple days of downtime.
“I tell hospitalists … that they have to know what a sense of ‘work-life balance’ means to them,” says Iris Grimm, creator of the Balanced Physician program and founder of Marietta, Ga.-based Master Performance Inc. (www.balanced physician.com). Understanding what you need to lead a healthy, balanced life is crucial to your happiness and well-being on and off the job.
Hospitalists who work long shifts also face extended stretches of time off that are vital to recharging one’s batteries. “One of the challenges they have is to find a routine,” Grimm says. “As human beings, we prefer to have a daily routine, which is a benefit from a health standpoint. These people have different sleep patterns when they’re off, which can throw off their bodies, which in turn has an effect on health and well-being.”
—Chad Whelan, MD, FHM, assistant professor of medicine, University of Chicago
Plan to Cope
The allure of regular, extended time off—namely, the seven-day-on, seven-day-off schedule model—can factor heavily into a physician’s decision to choose an HM career. A full week off is ideal for some, but not so ideal for others.
Many think the seven-on, seven-off schedule increases the likelihood of physician burnout. Others think the exact opposite. No matter what, the “intense shift” model is not going away anytime soon, says Chad Whelan, MD, FHM, associate professor of medicine and director of the division of hospital medicine at Loyola University Chicago Stritch School of Medicine.
The first step in maximizing your personal time is to accept your schedule. “Whatever schedule you’re working, you’re going to be working when others are not,” Dr. Whelan says. “You have to recognize that, and you have to own it.”
Once you accept the fact that you’ll miss out on some activities—from dinner parties to your child’s Little League baseball games—that fall on your workdays, you can move on to a key component of maximizing your days off: the art of planning.
Planning your days off helps ensure that you don’t end up wasting them. “Your plan could include exercise, visiting with friends, and keeping up with CME,” Grimm says. Dr. Whelan agrees: “You have to do some active planning to schedule things that need to get done.” He knows from personal experience that “the mundane details are easy to drop; instead of grocery shopping, you end up ordering in. I find that if I schedule these things—even at a funky time like late at night—I’ll get them done.”
Planning works both ways. “Part of balance is using time in your off days to prepare for when you’ll be working,” Grimm says. For example, make sure you have food in your refrigerator so that you can have a healthy breakfast and occasionally prepare dinners in advance that you can quickly heat up after your shift.
Focusing your organizational skills and planning on personal “to-dos” will lighten the load of a long workday. “Automate as much as possible—such as paying bills,” Grimm advises, “and delegate what you can. The less you have to keep track of, the less stress you’ll feel and the more energy you’ll find to do what you’re paid to do.”
Time for Self
Physicians, especially those with families, need to remember to make time for themselves “so that you won’t build resentment toward others,” Grimm says. “Doing something for yourself refills your energy tank.” Whether it’s exercising, going fishing, volunteering at the community center, downloading photos from your digital camera, or reading a book, “it’s different for everyone,” Grimm points out. “You have to know what you need.”
Dr. Whelan—who is a runner—focuses on physical activity to relieve stress and re-energize his mind and body. “It’s hard, because people who are serious about exercise, however you define ‘serious,’ are told to exercise on a consistent schedule. Well, we don’t have consistent schedules,” he says. “The key is to recognize that this is a challenge and find a creative way to schedule it, just like we make other decisions creatively. You have to make an upfront commitment.”
Whatever you do to “refill your tank,” there’s a good reason to devote time to it. “The more we do for ourselves, the more we can do for others,” Grimm says. “It’s not an hour-to-hour ratio; you might just need a five-minute meditation at the end of the day. … I always challenge my clients to be aware of what gives them energy and what takes energy away from them. This is essential for work, and essential for life.”
Leave Work Behind
One of the hardest things to learn—a lesson left out of medical school texts—is how to leave the stress and responsibility of the job at the office. “These are intense jobs; they’re high-stress,” Dr. Whelan explains. “The good thing about being a hospitalist is that when you’re off, you’re off. But it’s important to be able to compartmentalize.”
Dr. Whelan learned a couple of simple strategies to help with this concept. “At the end of every work day, after you’ve signed off, dedicate some time to transition. It can be just 10 or 15 minutes. Don’t answer the phone or e-mail; just dedicate that time to transition,” he says. “Run through your day and process each part—whether that’s each patient or each administrative task—emotionally and intellectually. For each one, make a plan for what you’ll do tomorrow. Once you’ve worked through your day this way, you can allow yourself to let it go.”
He also advises hospitalists to use on-the-job time when it’s available, rather than overlapping work and personal time. “There are parts of your business that can be done when you’re not seeing patients, such as reading journals,” Dr. Whelan says. “Try to schedule those things into your [work day], so you don’t end up catching up on them at home.”
Find Your Balance
Make it a point to make the most of your time off. Plan it in advance to ensure you do what you need to do and what you want to do. Think creatively and include all types of activities. And be sure to include time for yourself.
“There are very few of us who can sustain a life made up entirely of work and still be happy,” Dr. Whelan says. “Eventually, you’ll start to resent the work, and that’s the stuff that leads to burnout. You’re also probably not doing as good a job.”
One final piece of advice: Be prepared to change.
“You need to be self-aware, and you need to realize that your definition of balance will shift with age, responsibility, and goals,” Grimm says. TH
Jane Jerrard is a freelance writer based in Chicago.
How do you spend your time off? Do you neglect your to-do list in favor of rest and relaxation, or do you race around trying to get everything done? How you use your free time affects your energy level and on-the-job enthusiasm. Hospitalists who learn to make the most of their time off reduce their stress and master the elusive work-life balance, and are more likely to avoid burnout. It’s especially true of physicians who work long hours followed by multiple days of downtime.
“I tell hospitalists … that they have to know what a sense of ‘work-life balance’ means to them,” says Iris Grimm, creator of the Balanced Physician program and founder of Marietta, Ga.-based Master Performance Inc. (www.balanced physician.com). Understanding what you need to lead a healthy, balanced life is crucial to your happiness and well-being on and off the job.
Hospitalists who work long shifts also face extended stretches of time off that are vital to recharging one’s batteries. “One of the challenges they have is to find a routine,” Grimm says. “As human beings, we prefer to have a daily routine, which is a benefit from a health standpoint. These people have different sleep patterns when they’re off, which can throw off their bodies, which in turn has an effect on health and well-being.”
—Chad Whelan, MD, FHM, assistant professor of medicine, University of Chicago
Plan to Cope
The allure of regular, extended time off—namely, the seven-day-on, seven-day-off schedule model—can factor heavily into a physician’s decision to choose an HM career. A full week off is ideal for some, but not so ideal for others.
Many think the seven-on, seven-off schedule increases the likelihood of physician burnout. Others think the exact opposite. No matter what, the “intense shift” model is not going away anytime soon, says Chad Whelan, MD, FHM, associate professor of medicine and director of the division of hospital medicine at Loyola University Chicago Stritch School of Medicine.
The first step in maximizing your personal time is to accept your schedule. “Whatever schedule you’re working, you’re going to be working when others are not,” Dr. Whelan says. “You have to recognize that, and you have to own it.”
Once you accept the fact that you’ll miss out on some activities—from dinner parties to your child’s Little League baseball games—that fall on your workdays, you can move on to a key component of maximizing your days off: the art of planning.
Planning your days off helps ensure that you don’t end up wasting them. “Your plan could include exercise, visiting with friends, and keeping up with CME,” Grimm says. Dr. Whelan agrees: “You have to do some active planning to schedule things that need to get done.” He knows from personal experience that “the mundane details are easy to drop; instead of grocery shopping, you end up ordering in. I find that if I schedule these things—even at a funky time like late at night—I’ll get them done.”
Planning works both ways. “Part of balance is using time in your off days to prepare for when you’ll be working,” Grimm says. For example, make sure you have food in your refrigerator so that you can have a healthy breakfast and occasionally prepare dinners in advance that you can quickly heat up after your shift.
Focusing your organizational skills and planning on personal “to-dos” will lighten the load of a long workday. “Automate as much as possible—such as paying bills,” Grimm advises, “and delegate what you can. The less you have to keep track of, the less stress you’ll feel and the more energy you’ll find to do what you’re paid to do.”
Time for Self
Physicians, especially those with families, need to remember to make time for themselves “so that you won’t build resentment toward others,” Grimm says. “Doing something for yourself refills your energy tank.” Whether it’s exercising, going fishing, volunteering at the community center, downloading photos from your digital camera, or reading a book, “it’s different for everyone,” Grimm points out. “You have to know what you need.”
Dr. Whelan—who is a runner—focuses on physical activity to relieve stress and re-energize his mind and body. “It’s hard, because people who are serious about exercise, however you define ‘serious,’ are told to exercise on a consistent schedule. Well, we don’t have consistent schedules,” he says. “The key is to recognize that this is a challenge and find a creative way to schedule it, just like we make other decisions creatively. You have to make an upfront commitment.”
Whatever you do to “refill your tank,” there’s a good reason to devote time to it. “The more we do for ourselves, the more we can do for others,” Grimm says. “It’s not an hour-to-hour ratio; you might just need a five-minute meditation at the end of the day. … I always challenge my clients to be aware of what gives them energy and what takes energy away from them. This is essential for work, and essential for life.”
Leave Work Behind
One of the hardest things to learn—a lesson left out of medical school texts—is how to leave the stress and responsibility of the job at the office. “These are intense jobs; they’re high-stress,” Dr. Whelan explains. “The good thing about being a hospitalist is that when you’re off, you’re off. But it’s important to be able to compartmentalize.”
Dr. Whelan learned a couple of simple strategies to help with this concept. “At the end of every work day, after you’ve signed off, dedicate some time to transition. It can be just 10 or 15 minutes. Don’t answer the phone or e-mail; just dedicate that time to transition,” he says. “Run through your day and process each part—whether that’s each patient or each administrative task—emotionally and intellectually. For each one, make a plan for what you’ll do tomorrow. Once you’ve worked through your day this way, you can allow yourself to let it go.”
He also advises hospitalists to use on-the-job time when it’s available, rather than overlapping work and personal time. “There are parts of your business that can be done when you’re not seeing patients, such as reading journals,” Dr. Whelan says. “Try to schedule those things into your [work day], so you don’t end up catching up on them at home.”
Find Your Balance
Make it a point to make the most of your time off. Plan it in advance to ensure you do what you need to do and what you want to do. Think creatively and include all types of activities. And be sure to include time for yourself.
“There are very few of us who can sustain a life made up entirely of work and still be happy,” Dr. Whelan says. “Eventually, you’ll start to resent the work, and that’s the stuff that leads to burnout. You’re also probably not doing as good a job.”
One final piece of advice: Be prepared to change.
“You need to be self-aware, and you need to realize that your definition of balance will shift with age, responsibility, and goals,” Grimm says. TH
Jane Jerrard is a freelance writer based in Chicago.
How do you spend your time off? Do you neglect your to-do list in favor of rest and relaxation, or do you race around trying to get everything done? How you use your free time affects your energy level and on-the-job enthusiasm. Hospitalists who learn to make the most of their time off reduce their stress and master the elusive work-life balance, and are more likely to avoid burnout. It’s especially true of physicians who work long hours followed by multiple days of downtime.
“I tell hospitalists … that they have to know what a sense of ‘work-life balance’ means to them,” says Iris Grimm, creator of the Balanced Physician program and founder of Marietta, Ga.-based Master Performance Inc. (www.balanced physician.com). Understanding what you need to lead a healthy, balanced life is crucial to your happiness and well-being on and off the job.
Hospitalists who work long shifts also face extended stretches of time off that are vital to recharging one’s batteries. “One of the challenges they have is to find a routine,” Grimm says. “As human beings, we prefer to have a daily routine, which is a benefit from a health standpoint. These people have different sleep patterns when they’re off, which can throw off their bodies, which in turn has an effect on health and well-being.”
—Chad Whelan, MD, FHM, assistant professor of medicine, University of Chicago
Plan to Cope
The allure of regular, extended time off—namely, the seven-day-on, seven-day-off schedule model—can factor heavily into a physician’s decision to choose an HM career. A full week off is ideal for some, but not so ideal for others.
Many think the seven-on, seven-off schedule increases the likelihood of physician burnout. Others think the exact opposite. No matter what, the “intense shift” model is not going away anytime soon, says Chad Whelan, MD, FHM, associate professor of medicine and director of the division of hospital medicine at Loyola University Chicago Stritch School of Medicine.
The first step in maximizing your personal time is to accept your schedule. “Whatever schedule you’re working, you’re going to be working when others are not,” Dr. Whelan says. “You have to recognize that, and you have to own it.”
Once you accept the fact that you’ll miss out on some activities—from dinner parties to your child’s Little League baseball games—that fall on your workdays, you can move on to a key component of maximizing your days off: the art of planning.
Planning your days off helps ensure that you don’t end up wasting them. “Your plan could include exercise, visiting with friends, and keeping up with CME,” Grimm says. Dr. Whelan agrees: “You have to do some active planning to schedule things that need to get done.” He knows from personal experience that “the mundane details are easy to drop; instead of grocery shopping, you end up ordering in. I find that if I schedule these things—even at a funky time like late at night—I’ll get them done.”
Planning works both ways. “Part of balance is using time in your off days to prepare for when you’ll be working,” Grimm says. For example, make sure you have food in your refrigerator so that you can have a healthy breakfast and occasionally prepare dinners in advance that you can quickly heat up after your shift.
Focusing your organizational skills and planning on personal “to-dos” will lighten the load of a long workday. “Automate as much as possible—such as paying bills,” Grimm advises, “and delegate what you can. The less you have to keep track of, the less stress you’ll feel and the more energy you’ll find to do what you’re paid to do.”
Time for Self
Physicians, especially those with families, need to remember to make time for themselves “so that you won’t build resentment toward others,” Grimm says. “Doing something for yourself refills your energy tank.” Whether it’s exercising, going fishing, volunteering at the community center, downloading photos from your digital camera, or reading a book, “it’s different for everyone,” Grimm points out. “You have to know what you need.”
Dr. Whelan—who is a runner—focuses on physical activity to relieve stress and re-energize his mind and body. “It’s hard, because people who are serious about exercise, however you define ‘serious,’ are told to exercise on a consistent schedule. Well, we don’t have consistent schedules,” he says. “The key is to recognize that this is a challenge and find a creative way to schedule it, just like we make other decisions creatively. You have to make an upfront commitment.”
Whatever you do to “refill your tank,” there’s a good reason to devote time to it. “The more we do for ourselves, the more we can do for others,” Grimm says. “It’s not an hour-to-hour ratio; you might just need a five-minute meditation at the end of the day. … I always challenge my clients to be aware of what gives them energy and what takes energy away from them. This is essential for work, and essential for life.”
Leave Work Behind
One of the hardest things to learn—a lesson left out of medical school texts—is how to leave the stress and responsibility of the job at the office. “These are intense jobs; they’re high-stress,” Dr. Whelan explains. “The good thing about being a hospitalist is that when you’re off, you’re off. But it’s important to be able to compartmentalize.”
Dr. Whelan learned a couple of simple strategies to help with this concept. “At the end of every work day, after you’ve signed off, dedicate some time to transition. It can be just 10 or 15 minutes. Don’t answer the phone or e-mail; just dedicate that time to transition,” he says. “Run through your day and process each part—whether that’s each patient or each administrative task—emotionally and intellectually. For each one, make a plan for what you’ll do tomorrow. Once you’ve worked through your day this way, you can allow yourself to let it go.”
He also advises hospitalists to use on-the-job time when it’s available, rather than overlapping work and personal time. “There are parts of your business that can be done when you’re not seeing patients, such as reading journals,” Dr. Whelan says. “Try to schedule those things into your [work day], so you don’t end up catching up on them at home.”
Find Your Balance
Make it a point to make the most of your time off. Plan it in advance to ensure you do what you need to do and what you want to do. Think creatively and include all types of activities. And be sure to include time for yourself.
“There are very few of us who can sustain a life made up entirely of work and still be happy,” Dr. Whelan says. “Eventually, you’ll start to resent the work, and that’s the stuff that leads to burnout. You’re also probably not doing as good a job.”
One final piece of advice: Be prepared to change.
“You need to be self-aware, and you need to realize that your definition of balance will shift with age, responsibility, and goals,” Grimm says. TH
Jane Jerrard is a freelance writer based in Chicago.
In the Literature
In This Edition
- Pharmacists and readmission rates.
- Geriatric discharge bundles and readmission rates.
- Medication reconciliation and risk of adverse drug events.
- End-of-life discussions and care outcomes.
- Effect of case management and housing for homeless adults.
- IV esomeprazole in bleeding ulcers.
- Causes of discharge delays.
- Methods to reduce ICU medication errors.
Addition of Pharmacists to Inpatient Teams Reduces Drug-Related Readmissions, Morbidity, and Costs for Elderly Patients
Clinical question: Would a ward-based pharmacist reduce morbidity, subsequent ED visits, and readmissions for elderly patients?
Background: Adverse drug events can cause significant drug-related morbidity and mortality, and lead to unnecessary healthcare costs. Elderly patients are more vulnerable to these effects given the polypharmacy often associated with their care. The effectiveness of a ward-based pharmacist intervention for elderly patients has not yet been studied.
Study design: Randomized controlled trial.
Setting: Two acute-care, internal-medicine wards at the University Hospital of Uppsala in Uppsala, Sweden.
Synopsis: Three hundred sixty-eight hospitalized patients ages 80 or older were randomized to control or intervention groups. The latter received enhanced services from a pharmacist who was integrated into the inpatient team. This individual performed medication reconciliation, reviewed the medication list, and advised the treating physician. The pharmacist educated and monitored patients during the hospitalization, counseled them at discharge, communicated pertinent medication information to the primary-care physicians (PCPs), and called the patients two months after discharge.
The primary outcome measure was the frequency of all hospital visits (ED visits plus hospital readmissions) during 12-month follow-up. The secondary outcome measure was the cost of hospital care.
The intervention group had a 16% reduction in all hospital visits and a 47% reduction in ED visits. There were five times as many drug-related readmissions in the control group compared with the intervention group, but the study did not have enough power to show a reduction in the total number of readmissions alone. The cost of hospital care minus the cost of the intervention resulted in a net savings of $230 per patient.
Bottom line: For elderly patients, adding a pharmacist to the inpatient team could lead to significant reductions in morbidity and, on a population basis, healthcare costs.
Citation: Gillespie U, Alassaad A, Henrohn D, et al. A comprehensive pharmacist intervention to reduce morbidity in patients 80 years or older: a randomized controlled trial. Arch Intern Med. 2009;169(9):894-900.
Geriatric Care Coordination at Discharge Reduces Readmission Rates at 30 Days
Clinical question: Does a discharge planning service package affect readmission rates and ED visits?
Background: Elderly patients are at high risk for readmission after a hospitalization. Coordinated care packages, although effective in congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD) management, have yielded inconsistent results in terms of decreasing readmission rates for patients with a broader range of medical issues.
Study design: Randomized controlled pilot study.
Setting: A single large academic medical center in Texas.
Synopsis: Forty-one elderly patients at high risk for readmission—because of their age and comorbidities—were enrolled within 72 hours of admission. Patients randomized to the care bundle arm received daily education about medication reconciliation, health conditions, and self-care provided by study pharmacists and nurses. The intervention required approximately 40 minutes per day: 20 to 25 minutes for the care coordinators and 20 minutes for the pharmacists. A post-discharge phone call to review medication and confirm follow-up instructions was included.
Eight patients in the control group and two patients in the intervention arm were readmitted or seen in the ED within 30 days after discharge (38% vs. 10%, P=0.004). At 60 days, the difference between the two groups was no longer significant. The intervention group had a longer time interval before its first readmission (36.2 days vs. 15.7 days). The sample was too small to determine the effect on length of hospitalization.
Limitations of the study include its small sample size and unclear costs of the intervention.
Bottom line: Geriatric discharge bundles might decrease readmission and ED visits after discharge, but larger studies are needed to confirm this finding.
Citation: Koehler BE, Richter KM, Youngblood L, et al. Reduction of 30-day post-discharge hospital readmission or emergency department (ED) visit rates in high-risk elderly medical patients through delivery of a targeted care bundle. J Hosp Med. 2009;4(4):211-218.
Computer-Assisted Medication Reconciliation Might Reduce Unintentional Drug Discrepancies with Potential for Harm
Clinical question: Does a computerized medication reconciliation intervention reduce unintentional medication discrepancies?
Background: Given the high prevalence of unintentional medication discrepancies in hospitalized patients and the potential for harm, medication reconciliation is a national patient safety goal. Little data exist on the efficacy of medication reconciliation interventions for reducing medication discrepancies.
Study design: Cluster-randomized controlled trial.
Setting: Two large academic hospitals in Boston.
Synopsis: Using 14 medical teams, the study enrolled and randomized 322 patients to a floor with intervention or to a floor with traditional care. The intervention teams utilized a computerized order entry application designed to facilitate medication reconciliation, as well as a process redesign for physicians, nurses, and pharmacists.
The primary outcome was the number of unintentional medication discrepancies with the potential for causing harm (PADEs) per patient.
Patients randomized to the intervention group had a 28% reduction in relative risk compared with the control group (1.05 PADEs vs. 1.44 PADEs; absolute relative risk 0.72 (0.52-0.99)). The absolute relative risk reduction between the two arms was 0.39 PADE per patient (NNT=2.6). The intervention was associated with a significant reduction in PADEs at discharge but not at admission. The effects of the intervention were greater in patients with a higher PADE score.
Bottom line: This computerized medication reconciliation program with process redesign was associated with reduced risk of unintentional medication discrepancies with potential for causing harms (PADEs).
Citation: Schnipper JL, Hamann C, Ndumele CD, et al. Effect of an electronic medication reconciliation application and process redesign on potential adverse drug events: a cluster-randomized trial. Arch Intern Med. 2009;169(8):771-780.
End-of-Life Discussions Associated with Lower Healthcare Costs
Clinical question: What is the impact of patient-physician discussions of end-of-life care on healthcare costs in the final week of a patient’s life?
Background: Life-sustaining medical care of patients with advanced cancer is costly, with disproportionate spending at the end of a patient’s life. The link between discussions of end-of-life care preferences and healthcare expenditure has not been studied thoroughly.
Study design: Prospective observational study.
Setting: Seven sites in Connecticut, Texas, New Hampshire, and Massachusetts.
Synopsis: More than 600 patients with advanced cancer were recruited from September 2002 through December 2007 as part of the Coping With Cancer study. The 188 patients (31%) who reported end-of-life discussions with their physicians at baseline were less likely to undergo mechanical ventilator use or resuscitation, or to be admitted or die in an intensive-care unit in the final week of life. They were more likely to receive outpatient hospice care and had less physical distress in the last week than those who did not.
The mean aggregate cost of care in this group was $1,876, which was 36% lower than in the group that did not discuss end-of-life care ($2,917), P=0.002. In addition, higher medical costs were associated with worse quality of death, as reported by caregivers.
This study is limited by its observational design.
Bottom line: Physician communication with patients regarding end-of-life care preferences is associated with lower costs in the final week of life.
Citation: Zhang B, Wright AA, Huskamp HA, et al. Health care costs in the last week of life: associations with end-of-life conversations. Arch Intern Med. 2009;169(5):480-488.
Reduction of ED Visits and Hospitalizations for Chronically Ill and Homeless Adults
Clinical question: Can a case management and housing program reduce the utilization of ED and hospital medical services among chronically ill homeless adults?
Background: Homeless adults have high rates of chronic illness, have poor access to uninterrupted primary healthcare, and frequently use costly medical services, including those provided by EDs and inpatient hospitalizations. Studies to determine the efficacy of housing and case management services in reducing hospital and ED utilization in this population are lacking.
Study design: Randomized controlled trial.
Setting: A public teaching hospital and a private nonprofit hospital in Chicago.
Synopsis: Four hundred seven chronically ill and homeless adults were randomized to receive a case management and housing intervention or traditional care following an index hospitalization. The intervention group received assistance with stable housing on discharge and biweekly case management services throughout the study period. Traditional care consisted of routine inpatient discharge planning and transportation to a shelter.
Patients were followed for 18 months for the primary outcomes: number of hospitalizations, total hospital days, and number of ED visits.
After adjusting for differences in baseline variables, the intervention group was found to have significantly lower rates of hospitalization (relative reduction 29%), total hospital days (29%), and ED visits (24%). The authors did not find a difference in mortality or quality of life between the two groups.
Limitations of this study include a small sample size, limited geographic distribution of subjects, and the lack of a cost-benefit analysis of the intervention.
Bottom line: Case management and housing interventions can decrease hospitalizations and ED visits among chronically ill homeless adults.
Citation: Sadowski LS, Kee RA, VanderWeele TJ, Buchanan D. Effect of a housing and case management program on emergency department visits and hospitalizations among chronically ill homeless adults: a randomized trial. JAMA. 2009;301(17):1771-1778.
Intravenous Esomeprazole Reduces Recurrent Bleeding from Peptic Ulcers
Clinical question: Does intravenous esomeprazole prevent recurrent peptic ulcer bleeding, compared with placebo?
Background: U.S. hospitals admit more than 300,000 patients per year for peptic ulcer bleeding. Asian studies of proton pump inhibitors have demonstrated improved outcomes in patients with bleeding caused by peptic ulcers, but these results have not been consistently replicated in studies in Western Europe or North America.
Study design: Randomized, placebo-controlled, double-blind trial.
Setting: Ninety-one hospital EDs in 16 countries.
Synopsis: The study team randomized 764 adult patients with a single bleeding gastric or duodenal ulcer after successful endoscopic hemostasis. The study group received esomeprazole (80 mg bolus, given intravenously over 30 minutes, followed by an 8 mg/hour infusion for 71.5 hours). The second group received placebo. Each group subsequently received 40 mg/day of oral esomeprazole for 27 days.
Recurrent bleeding within 72 hours was reduced by nearly half in the intravenous esomeprazole arm compared with placebo (5.9% vs. 10.3%, P=0.026). This remained significant at seven and 30 days. Intravenous esomeprazole also reduced endoscopic retreatment (6.4% vs. 11.6%; P=0.012) and demonstrated a trend toward reduction in surgery (2.7% vs. 5.4%) and all-cause mortality (0.8% vs. 2.1%).
Study limitations included a lack of standardization of endoscopic therapy across institutions.
Bottom line: Given after endoscopic hemostatis, intravenous esomeprazole followed by oral esomeprazole reduced recurrent bleeding in patients with a single duodenal or gastric ulcer.
Citation: Sung JJ, Barkun A, Kuipers EJ, et al. Intravenous esomeprazole for prevention of recurrent peptic ulcer bleeding: a randomized trial. Ann Intern Med. 2009;150(7):455-464.
Discharge Time and Duration Affected by Several Factors During Hospitalization
Clinical question: What are the factors affecting late and long discharges in a general medical unit?
Background: The mismatch between admission and discharge times is a problem for many hospitals; admissions occur early in the day whereas, discharges occur later in the day. The reasons behind delays in discharge and prolongation of discharges are not fully understood.
Study design: Prospective cohort study.
Setting: A general medical unit without house staff coverage at an academic medical center in Baltimore.
Synopsis: Care providers completed surveys on 201 consecutive discharges from January to April 2005. Outcome variables included time of discharge and discharge duration.
Mean discharge time was 3:09 p.m. Delay in discharge was associated with a need for ambulance transportation (1.5 hours), need for prescriptions to be filled at the hospital (1.4 hours), and for patients whose final test was a procedure (1.2 hours) or consult (1.1 hours).
Median discharge time was 7.6 hours. Longer discharge duration was associated with discharge to a location other than home (28.9 hours), need for consultation (14.8 hours), or need for a procedure (13.4 hours) before discharge.
African-American race, gender, age, and comorbid psychiatric and substance abuse disorders were not associated with either late or prolonged discharges.
Bottom line: Final-day tests, procedures, and consults, as well as complex discharge arrangements, prolong and delay discharges more than the characteristics of patients themselves.
Citation: Chen LM, Freitag MH, Franco M, Sullivan CD, Dickson C, Brancati FL. Natural history of late discharges from a general medical ward. J Hosp Med. 2009;4(4):226-233.
Administration of Parenteral Medication a Common Point at Which Errors Occur in ICUs
Clinical question: To what extent are medication administration errors a problem across ICUs, and what are some ways to prevent them?
Background: High-acuity and complex systems increase the likelihood of medical errors in ICUs. The first multinational Sentinel Events Evaluation study reported an ICU medication error rate of 10.5 per 100 patient days at the prescription and administration stages of medication delivery.
Study design: Multinational observational, prospective, cross-sectional study.
Setting: One hundred thirteen ICUs in 27 countries on five continents.
Synopsis: This study addressed five types of medication error at the administration stage in the ICU in a 24-hour timeframe: wrong drug, wrong dose, wrong route, wrong time, and missed medication. The main outcome measures were the number and impact of administration errors, the distribution of error characteristics, and the distribution of contributing and preventive factors.
In the 1,328 critically ill patients included in the study, 861 medication errors were reported by structured questionnaire; 441 patients were affected by the errors. The prevalence was 74.5 errors per 100 patient days, and 12 patients (0.9%) suffered permanent harm or death. Most medication administration errors occurred during routine care, not during extraordinary situations. Most were omission errors.
This study is limited by its observational design and by the fact that self-reporting also carries the risk of under-reporting.
This study points out several ways to reduce medication errors. An independent predictor of decreased risk of medication errors of all types is an established incident reporting system. Routine checking of infusion pumps at every nursing shift change also reduced this risk.
Bottom line: This study confirmed that the administration of parenteral medications is a vulnerable point across many ICUs, and incident reporting systems and routine checks of infusion pumps are effective ways to reduce the risk of this type of error.
Citation: Valentin A, Capuzzo M, Guidet B, et al. Errors in administration of parenteral drugs in intensive care units: multinational prospective study. BMJ. 2009;338:b814. TH
PEDIATRIC HM LITERATURE
The Value of Pediatric Hospitalist Programs
By Mark Shen, MD

Clinical question: What is the value of pediatric hospitalist programs to hospital leaders?
Background: The growth of the HM field has resulted in an increase in both the absolute number of hospitalists and hospitalist programs in the U.S. Although the clinical impact of this model generally has been favorable, most programs still require significant financial subsidies, typically from hospitals. The perspective of hospital leaders on the reasons for giving these subsidies to pediatric hospitalist programs has not been examined.
Study design: Mailed survey to hospital leaders.
Setting: Hospitals with a pediatric hospitalist program.
Synopsis: A random sample of 213 (out of 761) American Hospital Association hospitals with an HM program and pediatric beds were selected for study. One hundred twelve pediatric hospitalist programs were confirmed at these institutions, and hospital leaders (CEOs, presidents, CFOs, CMOs, or others) were surveyed from each facility. The response rate was 69%. Almost all of the pediatric hospitalist programs (78%) were subsidized, and the vast majority of hospital leaders thought the programs increased patient satisfaction (94%) and referring physician satisfaction (90%), while decreasing length of stay (81%) and adverse events (81%). The hospital leaders also identified those four factors as the primary reasons for subsidization of the HM programs.
Although virtually all hospital leaders responding to the survey thought that pediatric hospitalist programs improved patient and referring physician satisfaction, they only reported measuring this impact 80% and 66% of the time, respectively. Thus, this survey was unable to link actual outcomes, such as increased satisfaction or decreased length of stay, to increased quantity or likelihood of funding. The literature on pediatric hospitalist programs’ impact on satisfaction, quality, and safety remains sparse; however, now there is valuable information with respect to why hospital leaders subsidize these groups.
Bottom line: Hospital leaders subsidize pediatric HM programs based on the belief that the hospitalists positively impact patient and referring physician satisfaction.
Citation: Freed GL, Dunham KM, Switalski KE, et al. Assessing the value of pediatric hospitalist programs: the perspective of hospital leaders. Acad Pediatr. 2009;9(3):192-196.
In This Edition
- Pharmacists and readmission rates.
- Geriatric discharge bundles and readmission rates.
- Medication reconciliation and risk of adverse drug events.
- End-of-life discussions and care outcomes.
- Effect of case management and housing for homeless adults.
- IV esomeprazole in bleeding ulcers.
- Causes of discharge delays.
- Methods to reduce ICU medication errors.
Addition of Pharmacists to Inpatient Teams Reduces Drug-Related Readmissions, Morbidity, and Costs for Elderly Patients
Clinical question: Would a ward-based pharmacist reduce morbidity, subsequent ED visits, and readmissions for elderly patients?
Background: Adverse drug events can cause significant drug-related morbidity and mortality, and lead to unnecessary healthcare costs. Elderly patients are more vulnerable to these effects given the polypharmacy often associated with their care. The effectiveness of a ward-based pharmacist intervention for elderly patients has not yet been studied.
Study design: Randomized controlled trial.
Setting: Two acute-care, internal-medicine wards at the University Hospital of Uppsala in Uppsala, Sweden.
Synopsis: Three hundred sixty-eight hospitalized patients ages 80 or older were randomized to control or intervention groups. The latter received enhanced services from a pharmacist who was integrated into the inpatient team. This individual performed medication reconciliation, reviewed the medication list, and advised the treating physician. The pharmacist educated and monitored patients during the hospitalization, counseled them at discharge, communicated pertinent medication information to the primary-care physicians (PCPs), and called the patients two months after discharge.
The primary outcome measure was the frequency of all hospital visits (ED visits plus hospital readmissions) during 12-month follow-up. The secondary outcome measure was the cost of hospital care.
The intervention group had a 16% reduction in all hospital visits and a 47% reduction in ED visits. There were five times as many drug-related readmissions in the control group compared with the intervention group, but the study did not have enough power to show a reduction in the total number of readmissions alone. The cost of hospital care minus the cost of the intervention resulted in a net savings of $230 per patient.
Bottom line: For elderly patients, adding a pharmacist to the inpatient team could lead to significant reductions in morbidity and, on a population basis, healthcare costs.
Citation: Gillespie U, Alassaad A, Henrohn D, et al. A comprehensive pharmacist intervention to reduce morbidity in patients 80 years or older: a randomized controlled trial. Arch Intern Med. 2009;169(9):894-900.
Geriatric Care Coordination at Discharge Reduces Readmission Rates at 30 Days
Clinical question: Does a discharge planning service package affect readmission rates and ED visits?
Background: Elderly patients are at high risk for readmission after a hospitalization. Coordinated care packages, although effective in congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD) management, have yielded inconsistent results in terms of decreasing readmission rates for patients with a broader range of medical issues.
Study design: Randomized controlled pilot study.
Setting: A single large academic medical center in Texas.
Synopsis: Forty-one elderly patients at high risk for readmission—because of their age and comorbidities—were enrolled within 72 hours of admission. Patients randomized to the care bundle arm received daily education about medication reconciliation, health conditions, and self-care provided by study pharmacists and nurses. The intervention required approximately 40 minutes per day: 20 to 25 minutes for the care coordinators and 20 minutes for the pharmacists. A post-discharge phone call to review medication and confirm follow-up instructions was included.
Eight patients in the control group and two patients in the intervention arm were readmitted or seen in the ED within 30 days after discharge (38% vs. 10%, P=0.004). At 60 days, the difference between the two groups was no longer significant. The intervention group had a longer time interval before its first readmission (36.2 days vs. 15.7 days). The sample was too small to determine the effect on length of hospitalization.
Limitations of the study include its small sample size and unclear costs of the intervention.
Bottom line: Geriatric discharge bundles might decrease readmission and ED visits after discharge, but larger studies are needed to confirm this finding.
Citation: Koehler BE, Richter KM, Youngblood L, et al. Reduction of 30-day post-discharge hospital readmission or emergency department (ED) visit rates in high-risk elderly medical patients through delivery of a targeted care bundle. J Hosp Med. 2009;4(4):211-218.
Computer-Assisted Medication Reconciliation Might Reduce Unintentional Drug Discrepancies with Potential for Harm
Clinical question: Does a computerized medication reconciliation intervention reduce unintentional medication discrepancies?
Background: Given the high prevalence of unintentional medication discrepancies in hospitalized patients and the potential for harm, medication reconciliation is a national patient safety goal. Little data exist on the efficacy of medication reconciliation interventions for reducing medication discrepancies.
Study design: Cluster-randomized controlled trial.
Setting: Two large academic hospitals in Boston.
Synopsis: Using 14 medical teams, the study enrolled and randomized 322 patients to a floor with intervention or to a floor with traditional care. The intervention teams utilized a computerized order entry application designed to facilitate medication reconciliation, as well as a process redesign for physicians, nurses, and pharmacists.
The primary outcome was the number of unintentional medication discrepancies with the potential for causing harm (PADEs) per patient.
Patients randomized to the intervention group had a 28% reduction in relative risk compared with the control group (1.05 PADEs vs. 1.44 PADEs; absolute relative risk 0.72 (0.52-0.99)). The absolute relative risk reduction between the two arms was 0.39 PADE per patient (NNT=2.6). The intervention was associated with a significant reduction in PADEs at discharge but not at admission. The effects of the intervention were greater in patients with a higher PADE score.
Bottom line: This computerized medication reconciliation program with process redesign was associated with reduced risk of unintentional medication discrepancies with potential for causing harms (PADEs).
Citation: Schnipper JL, Hamann C, Ndumele CD, et al. Effect of an electronic medication reconciliation application and process redesign on potential adverse drug events: a cluster-randomized trial. Arch Intern Med. 2009;169(8):771-780.
End-of-Life Discussions Associated with Lower Healthcare Costs
Clinical question: What is the impact of patient-physician discussions of end-of-life care on healthcare costs in the final week of a patient’s life?
Background: Life-sustaining medical care of patients with advanced cancer is costly, with disproportionate spending at the end of a patient’s life. The link between discussions of end-of-life care preferences and healthcare expenditure has not been studied thoroughly.
Study design: Prospective observational study.
Setting: Seven sites in Connecticut, Texas, New Hampshire, and Massachusetts.
Synopsis: More than 600 patients with advanced cancer were recruited from September 2002 through December 2007 as part of the Coping With Cancer study. The 188 patients (31%) who reported end-of-life discussions with their physicians at baseline were less likely to undergo mechanical ventilator use or resuscitation, or to be admitted or die in an intensive-care unit in the final week of life. They were more likely to receive outpatient hospice care and had less physical distress in the last week than those who did not.
The mean aggregate cost of care in this group was $1,876, which was 36% lower than in the group that did not discuss end-of-life care ($2,917), P=0.002. In addition, higher medical costs were associated with worse quality of death, as reported by caregivers.
This study is limited by its observational design.
Bottom line: Physician communication with patients regarding end-of-life care preferences is associated with lower costs in the final week of life.
Citation: Zhang B, Wright AA, Huskamp HA, et al. Health care costs in the last week of life: associations with end-of-life conversations. Arch Intern Med. 2009;169(5):480-488.
Reduction of ED Visits and Hospitalizations for Chronically Ill and Homeless Adults
Clinical question: Can a case management and housing program reduce the utilization of ED and hospital medical services among chronically ill homeless adults?
Background: Homeless adults have high rates of chronic illness, have poor access to uninterrupted primary healthcare, and frequently use costly medical services, including those provided by EDs and inpatient hospitalizations. Studies to determine the efficacy of housing and case management services in reducing hospital and ED utilization in this population are lacking.
Study design: Randomized controlled trial.
Setting: A public teaching hospital and a private nonprofit hospital in Chicago.
Synopsis: Four hundred seven chronically ill and homeless adults were randomized to receive a case management and housing intervention or traditional care following an index hospitalization. The intervention group received assistance with stable housing on discharge and biweekly case management services throughout the study period. Traditional care consisted of routine inpatient discharge planning and transportation to a shelter.
Patients were followed for 18 months for the primary outcomes: number of hospitalizations, total hospital days, and number of ED visits.
After adjusting for differences in baseline variables, the intervention group was found to have significantly lower rates of hospitalization (relative reduction 29%), total hospital days (29%), and ED visits (24%). The authors did not find a difference in mortality or quality of life between the two groups.
Limitations of this study include a small sample size, limited geographic distribution of subjects, and the lack of a cost-benefit analysis of the intervention.
Bottom line: Case management and housing interventions can decrease hospitalizations and ED visits among chronically ill homeless adults.
Citation: Sadowski LS, Kee RA, VanderWeele TJ, Buchanan D. Effect of a housing and case management program on emergency department visits and hospitalizations among chronically ill homeless adults: a randomized trial. JAMA. 2009;301(17):1771-1778.
Intravenous Esomeprazole Reduces Recurrent Bleeding from Peptic Ulcers
Clinical question: Does intravenous esomeprazole prevent recurrent peptic ulcer bleeding, compared with placebo?
Background: U.S. hospitals admit more than 300,000 patients per year for peptic ulcer bleeding. Asian studies of proton pump inhibitors have demonstrated improved outcomes in patients with bleeding caused by peptic ulcers, but these results have not been consistently replicated in studies in Western Europe or North America.
Study design: Randomized, placebo-controlled, double-blind trial.
Setting: Ninety-one hospital EDs in 16 countries.
Synopsis: The study team randomized 764 adult patients with a single bleeding gastric or duodenal ulcer after successful endoscopic hemostasis. The study group received esomeprazole (80 mg bolus, given intravenously over 30 minutes, followed by an 8 mg/hour infusion for 71.5 hours). The second group received placebo. Each group subsequently received 40 mg/day of oral esomeprazole for 27 days.
Recurrent bleeding within 72 hours was reduced by nearly half in the intravenous esomeprazole arm compared with placebo (5.9% vs. 10.3%, P=0.026). This remained significant at seven and 30 days. Intravenous esomeprazole also reduced endoscopic retreatment (6.4% vs. 11.6%; P=0.012) and demonstrated a trend toward reduction in surgery (2.7% vs. 5.4%) and all-cause mortality (0.8% vs. 2.1%).
Study limitations included a lack of standardization of endoscopic therapy across institutions.
Bottom line: Given after endoscopic hemostatis, intravenous esomeprazole followed by oral esomeprazole reduced recurrent bleeding in patients with a single duodenal or gastric ulcer.
Citation: Sung JJ, Barkun A, Kuipers EJ, et al. Intravenous esomeprazole for prevention of recurrent peptic ulcer bleeding: a randomized trial. Ann Intern Med. 2009;150(7):455-464.
Discharge Time and Duration Affected by Several Factors During Hospitalization
Clinical question: What are the factors affecting late and long discharges in a general medical unit?
Background: The mismatch between admission and discharge times is a problem for many hospitals; admissions occur early in the day whereas, discharges occur later in the day. The reasons behind delays in discharge and prolongation of discharges are not fully understood.
Study design: Prospective cohort study.
Setting: A general medical unit without house staff coverage at an academic medical center in Baltimore.
Synopsis: Care providers completed surveys on 201 consecutive discharges from January to April 2005. Outcome variables included time of discharge and discharge duration.
Mean discharge time was 3:09 p.m. Delay in discharge was associated with a need for ambulance transportation (1.5 hours), need for prescriptions to be filled at the hospital (1.4 hours), and for patients whose final test was a procedure (1.2 hours) or consult (1.1 hours).
Median discharge time was 7.6 hours. Longer discharge duration was associated with discharge to a location other than home (28.9 hours), need for consultation (14.8 hours), or need for a procedure (13.4 hours) before discharge.
African-American race, gender, age, and comorbid psychiatric and substance abuse disorders were not associated with either late or prolonged discharges.
Bottom line: Final-day tests, procedures, and consults, as well as complex discharge arrangements, prolong and delay discharges more than the characteristics of patients themselves.
Citation: Chen LM, Freitag MH, Franco M, Sullivan CD, Dickson C, Brancati FL. Natural history of late discharges from a general medical ward. J Hosp Med. 2009;4(4):226-233.
Administration of Parenteral Medication a Common Point at Which Errors Occur in ICUs
Clinical question: To what extent are medication administration errors a problem across ICUs, and what are some ways to prevent them?
Background: High-acuity and complex systems increase the likelihood of medical errors in ICUs. The first multinational Sentinel Events Evaluation study reported an ICU medication error rate of 10.5 per 100 patient days at the prescription and administration stages of medication delivery.
Study design: Multinational observational, prospective, cross-sectional study.
Setting: One hundred thirteen ICUs in 27 countries on five continents.
Synopsis: This study addressed five types of medication error at the administration stage in the ICU in a 24-hour timeframe: wrong drug, wrong dose, wrong route, wrong time, and missed medication. The main outcome measures were the number and impact of administration errors, the distribution of error characteristics, and the distribution of contributing and preventive factors.
In the 1,328 critically ill patients included in the study, 861 medication errors were reported by structured questionnaire; 441 patients were affected by the errors. The prevalence was 74.5 errors per 100 patient days, and 12 patients (0.9%) suffered permanent harm or death. Most medication administration errors occurred during routine care, not during extraordinary situations. Most were omission errors.
This study is limited by its observational design and by the fact that self-reporting also carries the risk of under-reporting.
This study points out several ways to reduce medication errors. An independent predictor of decreased risk of medication errors of all types is an established incident reporting system. Routine checking of infusion pumps at every nursing shift change also reduced this risk.
Bottom line: This study confirmed that the administration of parenteral medications is a vulnerable point across many ICUs, and incident reporting systems and routine checks of infusion pumps are effective ways to reduce the risk of this type of error.
Citation: Valentin A, Capuzzo M, Guidet B, et al. Errors in administration of parenteral drugs in intensive care units: multinational prospective study. BMJ. 2009;338:b814. TH
PEDIATRIC HM LITERATURE
The Value of Pediatric Hospitalist Programs
By Mark Shen, MD
Clinical question: What is the value of pediatric hospitalist programs to hospital leaders?
Background: The growth of the HM field has resulted in an increase in both the absolute number of hospitalists and hospitalist programs in the U.S. Although the clinical impact of this model generally has been favorable, most programs still require significant financial subsidies, typically from hospitals. The perspective of hospital leaders on the reasons for giving these subsidies to pediatric hospitalist programs has not been examined.
Study design: Mailed survey to hospital leaders.
Setting: Hospitals with a pediatric hospitalist program.
Synopsis: A random sample of 213 (out of 761) American Hospital Association hospitals with an HM program and pediatric beds were selected for study. One hundred twelve pediatric hospitalist programs were confirmed at these institutions, and hospital leaders (CEOs, presidents, CFOs, CMOs, or others) were surveyed from each facility. The response rate was 69%. Almost all of the pediatric hospitalist programs (78%) were subsidized, and the vast majority of hospital leaders thought the programs increased patient satisfaction (94%) and referring physician satisfaction (90%), while decreasing length of stay (81%) and adverse events (81%). The hospital leaders also identified those four factors as the primary reasons for subsidization of the HM programs.
Although virtually all hospital leaders responding to the survey thought that pediatric hospitalist programs improved patient and referring physician satisfaction, they only reported measuring this impact 80% and 66% of the time, respectively. Thus, this survey was unable to link actual outcomes, such as increased satisfaction or decreased length of stay, to increased quantity or likelihood of funding. The literature on pediatric hospitalist programs’ impact on satisfaction, quality, and safety remains sparse; however, now there is valuable information with respect to why hospital leaders subsidize these groups.
Bottom line: Hospital leaders subsidize pediatric HM programs based on the belief that the hospitalists positively impact patient and referring physician satisfaction.
Citation: Freed GL, Dunham KM, Switalski KE, et al. Assessing the value of pediatric hospitalist programs: the perspective of hospital leaders. Acad Pediatr. 2009;9(3):192-196.
In This Edition
- Pharmacists and readmission rates.
- Geriatric discharge bundles and readmission rates.
- Medication reconciliation and risk of adverse drug events.
- End-of-life discussions and care outcomes.
- Effect of case management and housing for homeless adults.
- IV esomeprazole in bleeding ulcers.
- Causes of discharge delays.
- Methods to reduce ICU medication errors.
Addition of Pharmacists to Inpatient Teams Reduces Drug-Related Readmissions, Morbidity, and Costs for Elderly Patients
Clinical question: Would a ward-based pharmacist reduce morbidity, subsequent ED visits, and readmissions for elderly patients?
Background: Adverse drug events can cause significant drug-related morbidity and mortality, and lead to unnecessary healthcare costs. Elderly patients are more vulnerable to these effects given the polypharmacy often associated with their care. The effectiveness of a ward-based pharmacist intervention for elderly patients has not yet been studied.
Study design: Randomized controlled trial.
Setting: Two acute-care, internal-medicine wards at the University Hospital of Uppsala in Uppsala, Sweden.
Synopsis: Three hundred sixty-eight hospitalized patients ages 80 or older were randomized to control or intervention groups. The latter received enhanced services from a pharmacist who was integrated into the inpatient team. This individual performed medication reconciliation, reviewed the medication list, and advised the treating physician. The pharmacist educated and monitored patients during the hospitalization, counseled them at discharge, communicated pertinent medication information to the primary-care physicians (PCPs), and called the patients two months after discharge.
The primary outcome measure was the frequency of all hospital visits (ED visits plus hospital readmissions) during 12-month follow-up. The secondary outcome measure was the cost of hospital care.
The intervention group had a 16% reduction in all hospital visits and a 47% reduction in ED visits. There were five times as many drug-related readmissions in the control group compared with the intervention group, but the study did not have enough power to show a reduction in the total number of readmissions alone. The cost of hospital care minus the cost of the intervention resulted in a net savings of $230 per patient.
Bottom line: For elderly patients, adding a pharmacist to the inpatient team could lead to significant reductions in morbidity and, on a population basis, healthcare costs.
Citation: Gillespie U, Alassaad A, Henrohn D, et al. A comprehensive pharmacist intervention to reduce morbidity in patients 80 years or older: a randomized controlled trial. Arch Intern Med. 2009;169(9):894-900.
Geriatric Care Coordination at Discharge Reduces Readmission Rates at 30 Days
Clinical question: Does a discharge planning service package affect readmission rates and ED visits?
Background: Elderly patients are at high risk for readmission after a hospitalization. Coordinated care packages, although effective in congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD) management, have yielded inconsistent results in terms of decreasing readmission rates for patients with a broader range of medical issues.
Study design: Randomized controlled pilot study.
Setting: A single large academic medical center in Texas.
Synopsis: Forty-one elderly patients at high risk for readmission—because of their age and comorbidities—were enrolled within 72 hours of admission. Patients randomized to the care bundle arm received daily education about medication reconciliation, health conditions, and self-care provided by study pharmacists and nurses. The intervention required approximately 40 minutes per day: 20 to 25 minutes for the care coordinators and 20 minutes for the pharmacists. A post-discharge phone call to review medication and confirm follow-up instructions was included.
Eight patients in the control group and two patients in the intervention arm were readmitted or seen in the ED within 30 days after discharge (38% vs. 10%, P=0.004). At 60 days, the difference between the two groups was no longer significant. The intervention group had a longer time interval before its first readmission (36.2 days vs. 15.7 days). The sample was too small to determine the effect on length of hospitalization.
Limitations of the study include its small sample size and unclear costs of the intervention.
Bottom line: Geriatric discharge bundles might decrease readmission and ED visits after discharge, but larger studies are needed to confirm this finding.
Citation: Koehler BE, Richter KM, Youngblood L, et al. Reduction of 30-day post-discharge hospital readmission or emergency department (ED) visit rates in high-risk elderly medical patients through delivery of a targeted care bundle. J Hosp Med. 2009;4(4):211-218.
Computer-Assisted Medication Reconciliation Might Reduce Unintentional Drug Discrepancies with Potential for Harm
Clinical question: Does a computerized medication reconciliation intervention reduce unintentional medication discrepancies?
Background: Given the high prevalence of unintentional medication discrepancies in hospitalized patients and the potential for harm, medication reconciliation is a national patient safety goal. Little data exist on the efficacy of medication reconciliation interventions for reducing medication discrepancies.
Study design: Cluster-randomized controlled trial.
Setting: Two large academic hospitals in Boston.
Synopsis: Using 14 medical teams, the study enrolled and randomized 322 patients to a floor with intervention or to a floor with traditional care. The intervention teams utilized a computerized order entry application designed to facilitate medication reconciliation, as well as a process redesign for physicians, nurses, and pharmacists.
The primary outcome was the number of unintentional medication discrepancies with the potential for causing harm (PADEs) per patient.
Patients randomized to the intervention group had a 28% reduction in relative risk compared with the control group (1.05 PADEs vs. 1.44 PADEs; absolute relative risk 0.72 (0.52-0.99)). The absolute relative risk reduction between the two arms was 0.39 PADE per patient (NNT=2.6). The intervention was associated with a significant reduction in PADEs at discharge but not at admission. The effects of the intervention were greater in patients with a higher PADE score.
Bottom line: This computerized medication reconciliation program with process redesign was associated with reduced risk of unintentional medication discrepancies with potential for causing harms (PADEs).
Citation: Schnipper JL, Hamann C, Ndumele CD, et al. Effect of an electronic medication reconciliation application and process redesign on potential adverse drug events: a cluster-randomized trial. Arch Intern Med. 2009;169(8):771-780.
End-of-Life Discussions Associated with Lower Healthcare Costs
Clinical question: What is the impact of patient-physician discussions of end-of-life care on healthcare costs in the final week of a patient’s life?
Background: Life-sustaining medical care of patients with advanced cancer is costly, with disproportionate spending at the end of a patient’s life. The link between discussions of end-of-life care preferences and healthcare expenditure has not been studied thoroughly.
Study design: Prospective observational study.
Setting: Seven sites in Connecticut, Texas, New Hampshire, and Massachusetts.
Synopsis: More than 600 patients with advanced cancer were recruited from September 2002 through December 2007 as part of the Coping With Cancer study. The 188 patients (31%) who reported end-of-life discussions with their physicians at baseline were less likely to undergo mechanical ventilator use or resuscitation, or to be admitted or die in an intensive-care unit in the final week of life. They were more likely to receive outpatient hospice care and had less physical distress in the last week than those who did not.
The mean aggregate cost of care in this group was $1,876, which was 36% lower than in the group that did not discuss end-of-life care ($2,917), P=0.002. In addition, higher medical costs were associated with worse quality of death, as reported by caregivers.
This study is limited by its observational design.
Bottom line: Physician communication with patients regarding end-of-life care preferences is associated with lower costs in the final week of life.
Citation: Zhang B, Wright AA, Huskamp HA, et al. Health care costs in the last week of life: associations with end-of-life conversations. Arch Intern Med. 2009;169(5):480-488.
Reduction of ED Visits and Hospitalizations for Chronically Ill and Homeless Adults
Clinical question: Can a case management and housing program reduce the utilization of ED and hospital medical services among chronically ill homeless adults?
Background: Homeless adults have high rates of chronic illness, have poor access to uninterrupted primary healthcare, and frequently use costly medical services, including those provided by EDs and inpatient hospitalizations. Studies to determine the efficacy of housing and case management services in reducing hospital and ED utilization in this population are lacking.
Study design: Randomized controlled trial.
Setting: A public teaching hospital and a private nonprofit hospital in Chicago.
Synopsis: Four hundred seven chronically ill and homeless adults were randomized to receive a case management and housing intervention or traditional care following an index hospitalization. The intervention group received assistance with stable housing on discharge and biweekly case management services throughout the study period. Traditional care consisted of routine inpatient discharge planning and transportation to a shelter.
Patients were followed for 18 months for the primary outcomes: number of hospitalizations, total hospital days, and number of ED visits.
After adjusting for differences in baseline variables, the intervention group was found to have significantly lower rates of hospitalization (relative reduction 29%), total hospital days (29%), and ED visits (24%). The authors did not find a difference in mortality or quality of life between the two groups.
Limitations of this study include a small sample size, limited geographic distribution of subjects, and the lack of a cost-benefit analysis of the intervention.
Bottom line: Case management and housing interventions can decrease hospitalizations and ED visits among chronically ill homeless adults.
Citation: Sadowski LS, Kee RA, VanderWeele TJ, Buchanan D. Effect of a housing and case management program on emergency department visits and hospitalizations among chronically ill homeless adults: a randomized trial. JAMA. 2009;301(17):1771-1778.
Intravenous Esomeprazole Reduces Recurrent Bleeding from Peptic Ulcers
Clinical question: Does intravenous esomeprazole prevent recurrent peptic ulcer bleeding, compared with placebo?
Background: U.S. hospitals admit more than 300,000 patients per year for peptic ulcer bleeding. Asian studies of proton pump inhibitors have demonstrated improved outcomes in patients with bleeding caused by peptic ulcers, but these results have not been consistently replicated in studies in Western Europe or North America.
Study design: Randomized, placebo-controlled, double-blind trial.
Setting: Ninety-one hospital EDs in 16 countries.
Synopsis: The study team randomized 764 adult patients with a single bleeding gastric or duodenal ulcer after successful endoscopic hemostasis. The study group received esomeprazole (80 mg bolus, given intravenously over 30 minutes, followed by an 8 mg/hour infusion for 71.5 hours). The second group received placebo. Each group subsequently received 40 mg/day of oral esomeprazole for 27 days.
Recurrent bleeding within 72 hours was reduced by nearly half in the intravenous esomeprazole arm compared with placebo (5.9% vs. 10.3%, P=0.026). This remained significant at seven and 30 days. Intravenous esomeprazole also reduced endoscopic retreatment (6.4% vs. 11.6%; P=0.012) and demonstrated a trend toward reduction in surgery (2.7% vs. 5.4%) and all-cause mortality (0.8% vs. 2.1%).
Study limitations included a lack of standardization of endoscopic therapy across institutions.
Bottom line: Given after endoscopic hemostatis, intravenous esomeprazole followed by oral esomeprazole reduced recurrent bleeding in patients with a single duodenal or gastric ulcer.
Citation: Sung JJ, Barkun A, Kuipers EJ, et al. Intravenous esomeprazole for prevention of recurrent peptic ulcer bleeding: a randomized trial. Ann Intern Med. 2009;150(7):455-464.
Discharge Time and Duration Affected by Several Factors During Hospitalization
Clinical question: What are the factors affecting late and long discharges in a general medical unit?
Background: The mismatch between admission and discharge times is a problem for many hospitals; admissions occur early in the day whereas, discharges occur later in the day. The reasons behind delays in discharge and prolongation of discharges are not fully understood.
Study design: Prospective cohort study.
Setting: A general medical unit without house staff coverage at an academic medical center in Baltimore.
Synopsis: Care providers completed surveys on 201 consecutive discharges from January to April 2005. Outcome variables included time of discharge and discharge duration.
Mean discharge time was 3:09 p.m. Delay in discharge was associated with a need for ambulance transportation (1.5 hours), need for prescriptions to be filled at the hospital (1.4 hours), and for patients whose final test was a procedure (1.2 hours) or consult (1.1 hours).
Median discharge time was 7.6 hours. Longer discharge duration was associated with discharge to a location other than home (28.9 hours), need for consultation (14.8 hours), or need for a procedure (13.4 hours) before discharge.
African-American race, gender, age, and comorbid psychiatric and substance abuse disorders were not associated with either late or prolonged discharges.
Bottom line: Final-day tests, procedures, and consults, as well as complex discharge arrangements, prolong and delay discharges more than the characteristics of patients themselves.
Citation: Chen LM, Freitag MH, Franco M, Sullivan CD, Dickson C, Brancati FL. Natural history of late discharges from a general medical ward. J Hosp Med. 2009;4(4):226-233.
Administration of Parenteral Medication a Common Point at Which Errors Occur in ICUs
Clinical question: To what extent are medication administration errors a problem across ICUs, and what are some ways to prevent them?
Background: High-acuity and complex systems increase the likelihood of medical errors in ICUs. The first multinational Sentinel Events Evaluation study reported an ICU medication error rate of 10.5 per 100 patient days at the prescription and administration stages of medication delivery.
Study design: Multinational observational, prospective, cross-sectional study.
Setting: One hundred thirteen ICUs in 27 countries on five continents.
Synopsis: This study addressed five types of medication error at the administration stage in the ICU in a 24-hour timeframe: wrong drug, wrong dose, wrong route, wrong time, and missed medication. The main outcome measures were the number and impact of administration errors, the distribution of error characteristics, and the distribution of contributing and preventive factors.
In the 1,328 critically ill patients included in the study, 861 medication errors were reported by structured questionnaire; 441 patients were affected by the errors. The prevalence was 74.5 errors per 100 patient days, and 12 patients (0.9%) suffered permanent harm or death. Most medication administration errors occurred during routine care, not during extraordinary situations. Most were omission errors.
This study is limited by its observational design and by the fact that self-reporting also carries the risk of under-reporting.
This study points out several ways to reduce medication errors. An independent predictor of decreased risk of medication errors of all types is an established incident reporting system. Routine checking of infusion pumps at every nursing shift change also reduced this risk.
Bottom line: This study confirmed that the administration of parenteral medications is a vulnerable point across many ICUs, and incident reporting systems and routine checks of infusion pumps are effective ways to reduce the risk of this type of error.
Citation: Valentin A, Capuzzo M, Guidet B, et al. Errors in administration of parenteral drugs in intensive care units: multinational prospective study. BMJ. 2009;338:b814. TH
PEDIATRIC HM LITERATURE
The Value of Pediatric Hospitalist Programs
By Mark Shen, MD
Clinical question: What is the value of pediatric hospitalist programs to hospital leaders?
Background: The growth of the HM field has resulted in an increase in both the absolute number of hospitalists and hospitalist programs in the U.S. Although the clinical impact of this model generally has been favorable, most programs still require significant financial subsidies, typically from hospitals. The perspective of hospital leaders on the reasons for giving these subsidies to pediatric hospitalist programs has not been examined.
Study design: Mailed survey to hospital leaders.
Setting: Hospitals with a pediatric hospitalist program.
Synopsis: A random sample of 213 (out of 761) American Hospital Association hospitals with an HM program and pediatric beds were selected for study. One hundred twelve pediatric hospitalist programs were confirmed at these institutions, and hospital leaders (CEOs, presidents, CFOs, CMOs, or others) were surveyed from each facility. The response rate was 69%. Almost all of the pediatric hospitalist programs (78%) were subsidized, and the vast majority of hospital leaders thought the programs increased patient satisfaction (94%) and referring physician satisfaction (90%), while decreasing length of stay (81%) and adverse events (81%). The hospital leaders also identified those four factors as the primary reasons for subsidization of the HM programs.
Although virtually all hospital leaders responding to the survey thought that pediatric hospitalist programs improved patient and referring physician satisfaction, they only reported measuring this impact 80% and 66% of the time, respectively. Thus, this survey was unable to link actual outcomes, such as increased satisfaction or decreased length of stay, to increased quantity or likelihood of funding. The literature on pediatric hospitalist programs’ impact on satisfaction, quality, and safety remains sparse; however, now there is valuable information with respect to why hospital leaders subsidize these groups.
Bottom line: Hospital leaders subsidize pediatric HM programs based on the belief that the hospitalists positively impact patient and referring physician satisfaction.
Citation: Freed GL, Dunham KM, Switalski KE, et al. Assessing the value of pediatric hospitalist programs: the perspective of hospital leaders. Acad Pediatr. 2009;9(3):192-196.
Planned Partnerships
A day in the life of a hospitalist is not spent in a vacuum. Every day in hospitals across the country, hospitalists coordinate patient care with a host of other physicians, caregivers, and administrators. One minute, a hospitalist could be managing a patient’s treatment with a physician assistant; the next minute, the hospitalist could be reviewing a diagnosis from a cardiologist. The same hospitalist might finish the shift by reporting valuable quality-improvement (QI) data to the hospital’s management staff.
It’s that kind of collaboration that is the hallmark of HM, so it makes sense that the same level of collaboration take place between SHM and a bevy of other healthcare-related organizations.
“The delivery of hospital-based care is a team sport,” says Joe Miller, SHM’s executive advisor to the CEO. “It requires coordination across disciplines, from clinical to managerial. Hospital medicine is in the middle of a complex system, and we can’t do it ourselves. If we’re going to be successful, we need to forge partnerships.”
Chapter Updates
Indiana Chapter

The chapter met June 2 at the Tomato Pie Bistro in Indianapolis. The meeting kicked off with a welcome from chapter President Angela Corea, MD, assistant medical director at Saint Vincent Healthcare in Indianapolis, and nominations for the chapter’s 2010 officers.
Mark Bochan, MD, an infectious-disease specialist at St. Vincent’s, spoke to the group about candida and aspergillus infections. Special guest Scott Flanders, MD, FHM, president of SHM, discussed his thoughts on the growth of HM and the challenges currently facing hospitalists. He then opened up the floor for a brief question-and-answer session.
Palmetto/Eastern South Carolina Chapter
The chapter met May 28 at Victor’s Restaurant in Florence. Chapter president Beth Cardosi, DO, a hospitalist with McLeod Inpatient Services in Darlington, welcomed everyone and introduced the guest speaker, Kevin Shea, MD. Dr. Shea presented a program to the group on gram-negative infections in the hospital setting.
Milwaukee Chapter
The chapter met June 8 at Columbia Hospital. Four HM groups attended the meeting. Chapter goals for the coming months were set, including QI, advocacy, policy, and membership initiatives.
Those partnerships have been critical to SHM’s ability to create educational programs and practice management resources. It also factors into SHM’s efforts to enhance patient satisfaction and advocate for QI in healthcare. The list of SHM’s partner organizations and joint projects is an alphabet soup that includes the nation’s most influential professional societies, academies, and government entities, each of which is working to improve the delivery of care to hospitalized patients.
Small Start, Quick Growth
The relationship between SHM and the American Medical Association (AMA) began as a simple research project and has grown into a deeper collaboration. In 2007, the AMA’s Organized Medical Staff Section (OMSS), the department that advocates on behalf of physicians who are members of medical staffs and other organizations, wanted to increase understanding of how hospitalists, primary-care physicians, and other physicians work together in the hospital setting. The association collaborated with SHM to conduct a survey and obtain feedback from hospitalists.
The 2007 survey found that there was still work to be done between the organizations, namely the need for a set of guiding principles for a successful hospitalist practice. OMSS, SHM, AHA, and the Joint Commission developed the principles, which were recently endorsed by OMSS at the association’s annual conference in June.
“We feel they’re appropriate and make sense,” says Jim DeNuccio, director of AMA’s Organized Medical Staff, Group Practice, and Senior Physician Services.
The 2007 survey and the principles for a hospitalist practice have led to a new survey, conducted this year, to track how the issues and challenges within a hospital have changed. The initiatives are just the beginning of a long-term relationship between SHM and AMA.
“It’s very important for all of us to work together to continue to grow,” says DeNuccio, who cites AMA’s courses in practice management, QI, and patient safety as educational opportunities for hospitalists. “Our interest is in the patient. That’s what this is all about. The AMA and OMSS feel strongly that the profession needs to call the shots about how care is delivered in hospitals. They see that engaging the hospitalist is in the interest of the patient.”
SHM and AAPA: Educating Together
Hospitalists and physician assistants (PAs) work hand in hand to care for their patients. At the national level, SHM and the American Academy of Physician Assistants (AAPA) are coordinating educational programs to ensure PAs and hospitalists are properly informed and learning from the same page.
“It’s a very broad spectrum,” says Sharon Kulesz, AAPA director of alliance development and education. “We provide physician assistants with information about hospitalists, and we provide physicians with information about the benefit of working with physician assistants.”
Along with the American Academy of Nurse Practitioners (AANP), AAPA and SHM have coordinated educational programs at SHM’s annual meeting for hospitalists, and recently developed a stand-alone “Boot Camp” series for nurse practitioners and physician assistants to learn more about HM.
Kulesz notes, however, that not all of the education is exclusively for hospital-based workers. Some of the efforts are geared toward educating the public about hospitals’ patient-care teams. Regardless of the topic or the audience, the key is a comfortable working relationship between teams, she says.
“Our work with SHM is the model that I would like to use in all of our collaborations,” Kulesz says. “SHM gets us. They get what we can do and how a collaborative approach can be of benefit to everyone. It’s like an extended family.”
Patient-First Collaboration
The new Hospital Care Collaborative takes a team approach to hospital-based care. More than simply a partnership, the group brings together groups that represent healthcare professionals in the hospital—hospitalists, nurses, case managers, respiratory therapists, social workers—to find common approaches to QI and patient safety.
“As a group, the Hospital Care Collaborative is looking for ways to work together to improve the care of the hospitalized patient,” says Larry Wellikson, MD, FHM, CEO of SHM. “We’ve developed common principles, which have been ratified by each of our boards. At its core, the collaborative is looking for real-world ways to integrate medical professionals and help hospitals take a new approach to patient care.”
Part of the answer is in the education, development, and promotion of high-performance teams in hospital settings, Dr. Wellikson says. For instance, if a patient is admitted to the hospital with a blood clot, each team member has the opportunity to contribute his or her expertise and coordinate with others. The hospitalist might make the diagnosis, which leads to the prescription from the hospital pharmacist. With the diagnosis and list of prescriptions in hand, a nurse can then explain to the patient how the medications will affect their daily routine.
“In modern healthcare, no one professional or professional society can have all the perspectives you need,” Dr. Wellikson says. “In SHM’s approach, we’re looking at the hospital as a community, not a building. The problems we’re trying to solve are complex, and it requires an all-hands-on-deck approach. Knitting the perspectives and expertise together will be the key to treating the patient in the 21st century.” TH
Brendon Shank is a freelance writer based in Philadelphia.
A day in the life of a hospitalist is not spent in a vacuum. Every day in hospitals across the country, hospitalists coordinate patient care with a host of other physicians, caregivers, and administrators. One minute, a hospitalist could be managing a patient’s treatment with a physician assistant; the next minute, the hospitalist could be reviewing a diagnosis from a cardiologist. The same hospitalist might finish the shift by reporting valuable quality-improvement (QI) data to the hospital’s management staff.
It’s that kind of collaboration that is the hallmark of HM, so it makes sense that the same level of collaboration take place between SHM and a bevy of other healthcare-related organizations.
“The delivery of hospital-based care is a team sport,” says Joe Miller, SHM’s executive advisor to the CEO. “It requires coordination across disciplines, from clinical to managerial. Hospital medicine is in the middle of a complex system, and we can’t do it ourselves. If we’re going to be successful, we need to forge partnerships.”
Chapter Updates
Indiana Chapter
The chapter met June 2 at the Tomato Pie Bistro in Indianapolis. The meeting kicked off with a welcome from chapter President Angela Corea, MD, assistant medical director at Saint Vincent Healthcare in Indianapolis, and nominations for the chapter’s 2010 officers.
Mark Bochan, MD, an infectious-disease specialist at St. Vincent’s, spoke to the group about candida and aspergillus infections. Special guest Scott Flanders, MD, FHM, president of SHM, discussed his thoughts on the growth of HM and the challenges currently facing hospitalists. He then opened up the floor for a brief question-and-answer session.
Palmetto/Eastern South Carolina Chapter
The chapter met May 28 at Victor’s Restaurant in Florence. Chapter president Beth Cardosi, DO, a hospitalist with McLeod Inpatient Services in Darlington, welcomed everyone and introduced the guest speaker, Kevin Shea, MD. Dr. Shea presented a program to the group on gram-negative infections in the hospital setting.
Milwaukee Chapter
The chapter met June 8 at Columbia Hospital. Four HM groups attended the meeting. Chapter goals for the coming months were set, including QI, advocacy, policy, and membership initiatives.
Those partnerships have been critical to SHM’s ability to create educational programs and practice management resources. It also factors into SHM’s efforts to enhance patient satisfaction and advocate for QI in healthcare. The list of SHM’s partner organizations and joint projects is an alphabet soup that includes the nation’s most influential professional societies, academies, and government entities, each of which is working to improve the delivery of care to hospitalized patients.
Small Start, Quick Growth
The relationship between SHM and the American Medical Association (AMA) began as a simple research project and has grown into a deeper collaboration. In 2007, the AMA’s Organized Medical Staff Section (OMSS), the department that advocates on behalf of physicians who are members of medical staffs and other organizations, wanted to increase understanding of how hospitalists, primary-care physicians, and other physicians work together in the hospital setting. The association collaborated with SHM to conduct a survey and obtain feedback from hospitalists.
The 2007 survey found that there was still work to be done between the organizations, namely the need for a set of guiding principles for a successful hospitalist practice. OMSS, SHM, AHA, and the Joint Commission developed the principles, which were recently endorsed by OMSS at the association’s annual conference in June.
“We feel they’re appropriate and make sense,” says Jim DeNuccio, director of AMA’s Organized Medical Staff, Group Practice, and Senior Physician Services.
The 2007 survey and the principles for a hospitalist practice have led to a new survey, conducted this year, to track how the issues and challenges within a hospital have changed. The initiatives are just the beginning of a long-term relationship between SHM and AMA.
“It’s very important for all of us to work together to continue to grow,” says DeNuccio, who cites AMA’s courses in practice management, QI, and patient safety as educational opportunities for hospitalists. “Our interest is in the patient. That’s what this is all about. The AMA and OMSS feel strongly that the profession needs to call the shots about how care is delivered in hospitals. They see that engaging the hospitalist is in the interest of the patient.”
SHM and AAPA: Educating Together
Hospitalists and physician assistants (PAs) work hand in hand to care for their patients. At the national level, SHM and the American Academy of Physician Assistants (AAPA) are coordinating educational programs to ensure PAs and hospitalists are properly informed and learning from the same page.
“It’s a very broad spectrum,” says Sharon Kulesz, AAPA director of alliance development and education. “We provide physician assistants with information about hospitalists, and we provide physicians with information about the benefit of working with physician assistants.”
Along with the American Academy of Nurse Practitioners (AANP), AAPA and SHM have coordinated educational programs at SHM’s annual meeting for hospitalists, and recently developed a stand-alone “Boot Camp” series for nurse practitioners and physician assistants to learn more about HM.
Kulesz notes, however, that not all of the education is exclusively for hospital-based workers. Some of the efforts are geared toward educating the public about hospitals’ patient-care teams. Regardless of the topic or the audience, the key is a comfortable working relationship between teams, she says.
“Our work with SHM is the model that I would like to use in all of our collaborations,” Kulesz says. “SHM gets us. They get what we can do and how a collaborative approach can be of benefit to everyone. It’s like an extended family.”
Patient-First Collaboration
The new Hospital Care Collaborative takes a team approach to hospital-based care. More than simply a partnership, the group brings together groups that represent healthcare professionals in the hospital—hospitalists, nurses, case managers, respiratory therapists, social workers—to find common approaches to QI and patient safety.
“As a group, the Hospital Care Collaborative is looking for ways to work together to improve the care of the hospitalized patient,” says Larry Wellikson, MD, FHM, CEO of SHM. “We’ve developed common principles, which have been ratified by each of our boards. At its core, the collaborative is looking for real-world ways to integrate medical professionals and help hospitals take a new approach to patient care.”
Part of the answer is in the education, development, and promotion of high-performance teams in hospital settings, Dr. Wellikson says. For instance, if a patient is admitted to the hospital with a blood clot, each team member has the opportunity to contribute his or her expertise and coordinate with others. The hospitalist might make the diagnosis, which leads to the prescription from the hospital pharmacist. With the diagnosis and list of prescriptions in hand, a nurse can then explain to the patient how the medications will affect their daily routine.
“In modern healthcare, no one professional or professional society can have all the perspectives you need,” Dr. Wellikson says. “In SHM’s approach, we’re looking at the hospital as a community, not a building. The problems we’re trying to solve are complex, and it requires an all-hands-on-deck approach. Knitting the perspectives and expertise together will be the key to treating the patient in the 21st century.” TH
Brendon Shank is a freelance writer based in Philadelphia.
A day in the life of a hospitalist is not spent in a vacuum. Every day in hospitals across the country, hospitalists coordinate patient care with a host of other physicians, caregivers, and administrators. One minute, a hospitalist could be managing a patient’s treatment with a physician assistant; the next minute, the hospitalist could be reviewing a diagnosis from a cardiologist. The same hospitalist might finish the shift by reporting valuable quality-improvement (QI) data to the hospital’s management staff.
It’s that kind of collaboration that is the hallmark of HM, so it makes sense that the same level of collaboration take place between SHM and a bevy of other healthcare-related organizations.
“The delivery of hospital-based care is a team sport,” says Joe Miller, SHM’s executive advisor to the CEO. “It requires coordination across disciplines, from clinical to managerial. Hospital medicine is in the middle of a complex system, and we can’t do it ourselves. If we’re going to be successful, we need to forge partnerships.”
Chapter Updates
Indiana Chapter
The chapter met June 2 at the Tomato Pie Bistro in Indianapolis. The meeting kicked off with a welcome from chapter President Angela Corea, MD, assistant medical director at Saint Vincent Healthcare in Indianapolis, and nominations for the chapter’s 2010 officers.
Mark Bochan, MD, an infectious-disease specialist at St. Vincent’s, spoke to the group about candida and aspergillus infections. Special guest Scott Flanders, MD, FHM, president of SHM, discussed his thoughts on the growth of HM and the challenges currently facing hospitalists. He then opened up the floor for a brief question-and-answer session.
Palmetto/Eastern South Carolina Chapter
The chapter met May 28 at Victor’s Restaurant in Florence. Chapter president Beth Cardosi, DO, a hospitalist with McLeod Inpatient Services in Darlington, welcomed everyone and introduced the guest speaker, Kevin Shea, MD. Dr. Shea presented a program to the group on gram-negative infections in the hospital setting.
Milwaukee Chapter
The chapter met June 8 at Columbia Hospital. Four HM groups attended the meeting. Chapter goals for the coming months were set, including QI, advocacy, policy, and membership initiatives.
Those partnerships have been critical to SHM’s ability to create educational programs and practice management resources. It also factors into SHM’s efforts to enhance patient satisfaction and advocate for QI in healthcare. The list of SHM’s partner organizations and joint projects is an alphabet soup that includes the nation’s most influential professional societies, academies, and government entities, each of which is working to improve the delivery of care to hospitalized patients.
Small Start, Quick Growth
The relationship between SHM and the American Medical Association (AMA) began as a simple research project and has grown into a deeper collaboration. In 2007, the AMA’s Organized Medical Staff Section (OMSS), the department that advocates on behalf of physicians who are members of medical staffs and other organizations, wanted to increase understanding of how hospitalists, primary-care physicians, and other physicians work together in the hospital setting. The association collaborated with SHM to conduct a survey and obtain feedback from hospitalists.
The 2007 survey found that there was still work to be done between the organizations, namely the need for a set of guiding principles for a successful hospitalist practice. OMSS, SHM, AHA, and the Joint Commission developed the principles, which were recently endorsed by OMSS at the association’s annual conference in June.
“We feel they’re appropriate and make sense,” says Jim DeNuccio, director of AMA’s Organized Medical Staff, Group Practice, and Senior Physician Services.
The 2007 survey and the principles for a hospitalist practice have led to a new survey, conducted this year, to track how the issues and challenges within a hospital have changed. The initiatives are just the beginning of a long-term relationship between SHM and AMA.
“It’s very important for all of us to work together to continue to grow,” says DeNuccio, who cites AMA’s courses in practice management, QI, and patient safety as educational opportunities for hospitalists. “Our interest is in the patient. That’s what this is all about. The AMA and OMSS feel strongly that the profession needs to call the shots about how care is delivered in hospitals. They see that engaging the hospitalist is in the interest of the patient.”
SHM and AAPA: Educating Together
Hospitalists and physician assistants (PAs) work hand in hand to care for their patients. At the national level, SHM and the American Academy of Physician Assistants (AAPA) are coordinating educational programs to ensure PAs and hospitalists are properly informed and learning from the same page.
“It’s a very broad spectrum,” says Sharon Kulesz, AAPA director of alliance development and education. “We provide physician assistants with information about hospitalists, and we provide physicians with information about the benefit of working with physician assistants.”
Along with the American Academy of Nurse Practitioners (AANP), AAPA and SHM have coordinated educational programs at SHM’s annual meeting for hospitalists, and recently developed a stand-alone “Boot Camp” series for nurse practitioners and physician assistants to learn more about HM.
Kulesz notes, however, that not all of the education is exclusively for hospital-based workers. Some of the efforts are geared toward educating the public about hospitals’ patient-care teams. Regardless of the topic or the audience, the key is a comfortable working relationship between teams, she says.
“Our work with SHM is the model that I would like to use in all of our collaborations,” Kulesz says. “SHM gets us. They get what we can do and how a collaborative approach can be of benefit to everyone. It’s like an extended family.”
Patient-First Collaboration
The new Hospital Care Collaborative takes a team approach to hospital-based care. More than simply a partnership, the group brings together groups that represent healthcare professionals in the hospital—hospitalists, nurses, case managers, respiratory therapists, social workers—to find common approaches to QI and patient safety.
“As a group, the Hospital Care Collaborative is looking for ways to work together to improve the care of the hospitalized patient,” says Larry Wellikson, MD, FHM, CEO of SHM. “We’ve developed common principles, which have been ratified by each of our boards. At its core, the collaborative is looking for real-world ways to integrate medical professionals and help hospitals take a new approach to patient care.”
Part of the answer is in the education, development, and promotion of high-performance teams in hospital settings, Dr. Wellikson says. For instance, if a patient is admitted to the hospital with a blood clot, each team member has the opportunity to contribute his or her expertise and coordinate with others. The hospitalist might make the diagnosis, which leads to the prescription from the hospital pharmacist. With the diagnosis and list of prescriptions in hand, a nurse can then explain to the patient how the medications will affect their daily routine.
“In modern healthcare, no one professional or professional society can have all the perspectives you need,” Dr. Wellikson says. “In SHM’s approach, we’re looking at the hospital as a community, not a building. The problems we’re trying to solve are complex, and it requires an all-hands-on-deck approach. Knitting the perspectives and expertise together will be the key to treating the patient in the 21st century.” TH
Brendon Shank is a freelance writer based in Philadelphia.
Social Work
Editors’ note: “Alliances” is a new series written about the relationships that hospitalists have with members of the clinical care team—from the team members’ points of view. It’s our hope that each installment of “Alliances” will provide valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
Social workers are a natural fit with hospitalists and the hospitalist’s strongest allies and staunchest supporters, wrote Bradley Flansbaum, DO, MPH, in his Nov./Dec. 2003 article in The Hospitalist. What makes this collaboration such a positive one and what can members of these two professions learn from each other?
Dr. Flansbaum, a hospitalist and internist with the Division of Internal Medicine/Primary Care at Lenox Hill Hospital, Bronx, N.Y., and a former SHM board member, recently reiterated the benefits of the hospitalist-social worker relationship. In general, he believes that hospitalists provide a unique history-taking perspective that is useful to social workers in their work. Foremost, social workers bring a rich understanding of the available resources that patients need after discharge and a view of the patient’s nonmedical circumstances. Together, the two professionals’ daily interactions generate more effective discharge planning as a part of the multidisciplinary team.
ALWAYS THERE
Amy Lingg, MS, MPA, works on the general medicine unit at Greenwich Hospital (Conn). She says the role of the hospitalist is fairly new at Greenwich. In fact Sabitha Rajan, MD, MS, was the first one at Greenwich Hospital.
In Lingg’s view, nothing can replace the availability of the hospitalist to discuss patient cases, not only with the social worker but also as a team with the patient and family.
“[Attendings] are not there for the moment-by-moment events that happen on the unit, including availability when families are here,” says Lingg. “If I need to speak with a family and the physician’s input is important there, I can just page the hospitalist, she’s here. Whereas with an attending you have to make an appointment; you have to schedule around them. It can become difficult.”
Lingg, who works with hospitalist Dr. Rajan, director of hospitalist services at Greenwich Hospital, cites an example of the benefits of hospitalists’ 24/7 availability: “We had a fairly young woman in her mid-40s who was the divorced mother of a 17-year-old son. The father was not in the picture, and the woman was dying of alcoholic cirrhosis and liver failure. She was Dr. Rajan’s patient. One of the issues was the fact that there was no adult guardian for the son although he was going to be 18 in two months.
“So it involved a lot of talking with friends of the woman, who were sort of stepping in as surrogate guardians to him,” Lingg continues. “There were a lot of logistics [regarding] what would happen with him. We were trying to call the grandfather who was estranged. It was a very, very sensitive, very, very tricky case. It went on for days and days. … Dr. Rajan and I could work on this together on a dayto-day basis, [including] … the counseling, relaying medical knowledge to the family, what was going on clinically, trying to deal with that in a way where she was talking in one way to [the] adults and in a different, more appropriate [for the boy’s age] way to the 17-yearold son. And I can be there to help with that process.”
The situation was resolved to the satisfaction of the mother, the son, the friends, and the providers. “It was really pretty extraordinary,” she said. “I’ve talked about that a couple of times, including at a staff meetings when we were talking about getting new hospitalists. That is something I’ve described because, really, it was very special.”
TRUE TEAMWORK
Although everyone on a multidisciplinary team can bring something to the discussion that makes the team work better, social workers and hospitalists collaborate well in painting a more comprehensive picture of the patient’s lifestyle, living habits, and needs.
“In many hospitals … there’s a pattern that develops [whereby at] some time in the morning the hospitalist and social worker will get together and talk,” says Dr. Flansbaum “The hospitalist speaks the language of the social worker and knows what to tell them and how to direct them rather than just saying, ‘the patient’s homeless or the patient needs help at home.’”
After working regularly with social workers and recognizing what they need to know, he says, “the hospitalist is more likely to say, ‘the patient has Medicaid,’ or ‘the patient has this insurance,’ [or] ‘the patient has a home-health [caregiver] four hours a day and needs six or eight hours a day,’ or ‘the patient’s going to need a subacute nursing facility.’ … I think our insights are different from voluntary physicians and our face-time with social workers is more efficient.”
Sylvia Krafcik, MSSA, LISW, with MetroHealth Medical Center, Cleveland, says hospitalists are “great to work with because they’re very dedicated to the population they’re caring for, because this is their whole responsibility; they don’t have a private caseload.”
But in her view most hospitalists are focused on patients’ medical conditions and some of them are not as tuned in to all the other aspects of the patient, such as all the psychosocial dynamics.
“A lot of them are, but some aren’t,” Krafcik says. “Especially at MetroHealth, we’re a county hospital. So many of the patients that come here are poor. A lot of them are alcoholics or drug abusers. They’re homeless. They live on the streets. They don’t have a primary doctor. They’re usually not compliant with their medications.”
“Here at Metro we have a lot of patients who have extreme social circumstances that affect their medical issues so much,” says Sara Dunson, MSW, LSW, who also works as a social worker at Metro-Health. “I think the hospitalist has greater insight into the person’s environment and all the social structures that they have at home and that are going on in their life [than other physicians might].”
But there is always room for improvement.
“We had one patient who wasn’t able to read, and he never told anybody this,” says Dunson. “And as social workers, we have more of a way of finding that kind of stuff out from patients than the doctors might. And he kept coming in and coming in and was noncompliant with his medication. We eventually determined that this was why he was noncompliant and was causing all these medical issues. The doctors finally [understood] why this gentleman kept coming in with the same problems and he wasn’t taking care of himself. It wasn’t that he didn’t want to, it was just that he was having problems reading all the medications and all the discharge paperwork, and he was too ashamed to tell anybody. [Once the social workers questioned him and got this] out in the open, we were able to get him help with that.”
The doctors focused on what he was or wasn’t doing, but they hadn’t looked at why he wasn’t adherent, explains Dunson. If hospitalists do that more often, she thinks, they could save time and get better outcomes sooner.
COMMUNICATING WITH PATIENTS AND FAMILIES
“I think where hospitalists are coming from is a whole different mindset than a physician who has mainly an office practice,” said Lingg. “The office practice comes first [for them]. Some of our physicians have huge practices in town. And they’ll visit the hospital very early in the morning or in the evening. ... So if I need something in a case like that, if there was not a hospitalist involved, it would have been separate meetings for the family with the physician … and [with] me at another time.”
To hospitalists, a social worker can serve as an important adjunct in talking to the patient and family. “For example, if [social workers] are giving bad news, they warn the physician first,” says Dr. Rajan. “If they’re going to go in and tell the patient that they’re not going to qualify for any home services, they tell the physician as well so that [the hospitalist will not later be] meeting an angry patient.” In addition, she says, “for critically ill or long-term patients, social workers [can] help family members cope. Sometimes as physicians we don’t have the time or we don’t have the resources to do that.”
But this doesn’t let doctors off the hook in regard to addressing the whole person’s needs. Especially if someone has multiple medical problems, the social worker needs to know the availability and level of support for which the family can be counted.
“Social workers will ask questions such as: Are the families involved? or Is there any family?” says Krafcik. “Do they need to go in a nursing home or do they need 24-hour care at home? Is the family able to provide that? [E]very morning we meet to have team rounds. And the [team] go[es] over every patient on the floor, and then I will ask those questions if the doctor hasn’t given me that information.”
Social workers appreciate and would like hospitalists to do more listening to the patient and family for the aspects of the history and psychosocial status that the social worker will need to know.
TEACHING POINTS
In the course of their interactions, what do hospitalists and social workers teach each other that could lead to working a case more effectively and to the greater satisfaction of all involved?
Most of those we interviewed seem to think that the greatest service hospitalists provide is to teach the social worker the medical components that go along with what the social worker does every day.
“[Social workers] get a better understanding of [whether] someone comes in with heart failure or a fall or a stroke, just by repetition and also education; they get to understand after a while what’s needed for individual medical diagnoses,” says Dr. Flansbaum.
“When I know [better] what the medical condition is,” says Krafcik, “I have an idea of how much help [the patient] would need at home and their ability to function. And I would make sure that the patient gets physical therapy or occupational therapy referral or speech therapy.”
Again, perhaps the area where the social worker most teaches the hospitalist regards available resources to solve problems over and above the purely medical. “They know the social system and the needs of different forms and eligibility and what different patients are entitled to and what the system will provide,” says Dr. Flansbaum.
Dunson believes hospitalists are perceived as being more involved in a holistic way with the patient. “I always stress that it is so important to look at the whole person and not just the medical aspects,” she says. “It’s hard for the doctor sometimes to realize that this person might not be able to afford this medication and that’s why they’re noncompliant and all the other issues. So I think is important to open up to the other aspects of a person’s life and not just the medical aspects.”
CONCLUSION
Social workers’ knowledge of medical and nonmedical resources, both locally and nationally, offer hospitalists essential information that leads to designing more appropriate and effective post-discharge plans. Hospitalists can best team with social workers by consistently keeping in mind the patient’s overall circumstances and informing their colleagues of the medical information that can help social workers do their best work. TH
Writer Andrea Sattinger will write about the effect of poor communication skills in the November issue of The Hospitalist.
HOSPITALISTS AND SOCIAL WORKERS
Both sides of the clinical care team discuss the pros and cons of working together

In these … fractious healthcare times when resources are not plentiful and the expectations of patients might be higher, like getting 24-hour care at home, sometimes it might appear that the hospitalist or [another] physician is always the bringer of bad news. A good social worker can work well with the hospitalist in … letting the patient know the realistic expectations of what the system can provide [so that] we’re not in this alone. You know, ‘the world is a nail, the hospitalist is always the hammer’ kind of thing. Social workers can be very helpful in delivering information. … A good social worker can also add some “salve” to the wounds that the patient comes in with.
Some [patients] are borderline functioning or kind of on the precipice already. They come in with this problem and all of a sudden they can’t go back to the situation they were operating in prior. Social workers’ knowledge of the social safety net … is terrific, and they help us in directing what would be the best discharge plan for this patient, [including] knowing what the insurance status is, … what resources they have in place already, what else is available. … [I]t has a lot to do with discharge and recovery and functionality, and [to find out what’s the best place for the patient. They can help us with that.

Perhaps the greatest value social workers provide for all concerned is having the storehouse of knowledge of the available resources of the community. This is probably one of the most vital things to me; they can get a patient into services or programs that I didn’t even know exist. And the resources are very different in Connecticut than … in New York [where I practiced previously]. In New York there are many resources geared toward the Hispanic community, which I haven’t seen so far in Connecticut. But Connecticut has some other great resources; the local area clinic is a fantastic one.
Patients with end-of-life situations are dealt with differently in different states, too, and I wouldn’t have known about all this if it had not been for the social worker with whom I work. I also found out that there is a free program for alcohol rehabilitation in Connecticut; that does not exist in New York. We’ve sent a lot of our patients [to that]; you know they have to be the ones to initiate the call, but if they do, then that’s actually a resource for them. I wasn’t aware of that until I worked with the social workers here.
Editors’ note: “Alliances” is a new series written about the relationships that hospitalists have with members of the clinical care team—from the team members’ points of view. It’s our hope that each installment of “Alliances” will provide valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
Social workers are a natural fit with hospitalists and the hospitalist’s strongest allies and staunchest supporters, wrote Bradley Flansbaum, DO, MPH, in his Nov./Dec. 2003 article in The Hospitalist. What makes this collaboration such a positive one and what can members of these two professions learn from each other?
Dr. Flansbaum, a hospitalist and internist with the Division of Internal Medicine/Primary Care at Lenox Hill Hospital, Bronx, N.Y., and a former SHM board member, recently reiterated the benefits of the hospitalist-social worker relationship. In general, he believes that hospitalists provide a unique history-taking perspective that is useful to social workers in their work. Foremost, social workers bring a rich understanding of the available resources that patients need after discharge and a view of the patient’s nonmedical circumstances. Together, the two professionals’ daily interactions generate more effective discharge planning as a part of the multidisciplinary team.
ALWAYS THERE
Amy Lingg, MS, MPA, works on the general medicine unit at Greenwich Hospital (Conn). She says the role of the hospitalist is fairly new at Greenwich. In fact Sabitha Rajan, MD, MS, was the first one at Greenwich Hospital.
In Lingg’s view, nothing can replace the availability of the hospitalist to discuss patient cases, not only with the social worker but also as a team with the patient and family.
“[Attendings] are not there for the moment-by-moment events that happen on the unit, including availability when families are here,” says Lingg. “If I need to speak with a family and the physician’s input is important there, I can just page the hospitalist, she’s here. Whereas with an attending you have to make an appointment; you have to schedule around them. It can become difficult.”
Lingg, who works with hospitalist Dr. Rajan, director of hospitalist services at Greenwich Hospital, cites an example of the benefits of hospitalists’ 24/7 availability: “We had a fairly young woman in her mid-40s who was the divorced mother of a 17-year-old son. The father was not in the picture, and the woman was dying of alcoholic cirrhosis and liver failure. She was Dr. Rajan’s patient. One of the issues was the fact that there was no adult guardian for the son although he was going to be 18 in two months.
“So it involved a lot of talking with friends of the woman, who were sort of stepping in as surrogate guardians to him,” Lingg continues. “There were a lot of logistics [regarding] what would happen with him. We were trying to call the grandfather who was estranged. It was a very, very sensitive, very, very tricky case. It went on for days and days. … Dr. Rajan and I could work on this together on a dayto-day basis, [including] … the counseling, relaying medical knowledge to the family, what was going on clinically, trying to deal with that in a way where she was talking in one way to [the] adults and in a different, more appropriate [for the boy’s age] way to the 17-yearold son. And I can be there to help with that process.”
The situation was resolved to the satisfaction of the mother, the son, the friends, and the providers. “It was really pretty extraordinary,” she said. “I’ve talked about that a couple of times, including at a staff meetings when we were talking about getting new hospitalists. That is something I’ve described because, really, it was very special.”
TRUE TEAMWORK
Although everyone on a multidisciplinary team can bring something to the discussion that makes the team work better, social workers and hospitalists collaborate well in painting a more comprehensive picture of the patient’s lifestyle, living habits, and needs.
“In many hospitals … there’s a pattern that develops [whereby at] some time in the morning the hospitalist and social worker will get together and talk,” says Dr. Flansbaum “The hospitalist speaks the language of the social worker and knows what to tell them and how to direct them rather than just saying, ‘the patient’s homeless or the patient needs help at home.’”
After working regularly with social workers and recognizing what they need to know, he says, “the hospitalist is more likely to say, ‘the patient has Medicaid,’ or ‘the patient has this insurance,’ [or] ‘the patient has a home-health [caregiver] four hours a day and needs six or eight hours a day,’ or ‘the patient’s going to need a subacute nursing facility.’ … I think our insights are different from voluntary physicians and our face-time with social workers is more efficient.”
Sylvia Krafcik, MSSA, LISW, with MetroHealth Medical Center, Cleveland, says hospitalists are “great to work with because they’re very dedicated to the population they’re caring for, because this is their whole responsibility; they don’t have a private caseload.”
But in her view most hospitalists are focused on patients’ medical conditions and some of them are not as tuned in to all the other aspects of the patient, such as all the psychosocial dynamics.
“A lot of them are, but some aren’t,” Krafcik says. “Especially at MetroHealth, we’re a county hospital. So many of the patients that come here are poor. A lot of them are alcoholics or drug abusers. They’re homeless. They live on the streets. They don’t have a primary doctor. They’re usually not compliant with their medications.”
“Here at Metro we have a lot of patients who have extreme social circumstances that affect their medical issues so much,” says Sara Dunson, MSW, LSW, who also works as a social worker at Metro-Health. “I think the hospitalist has greater insight into the person’s environment and all the social structures that they have at home and that are going on in their life [than other physicians might].”
But there is always room for improvement.
“We had one patient who wasn’t able to read, and he never told anybody this,” says Dunson. “And as social workers, we have more of a way of finding that kind of stuff out from patients than the doctors might. And he kept coming in and coming in and was noncompliant with his medication. We eventually determined that this was why he was noncompliant and was causing all these medical issues. The doctors finally [understood] why this gentleman kept coming in with the same problems and he wasn’t taking care of himself. It wasn’t that he didn’t want to, it was just that he was having problems reading all the medications and all the discharge paperwork, and he was too ashamed to tell anybody. [Once the social workers questioned him and got this] out in the open, we were able to get him help with that.”
The doctors focused on what he was or wasn’t doing, but they hadn’t looked at why he wasn’t adherent, explains Dunson. If hospitalists do that more often, she thinks, they could save time and get better outcomes sooner.
COMMUNICATING WITH PATIENTS AND FAMILIES
“I think where hospitalists are coming from is a whole different mindset than a physician who has mainly an office practice,” said Lingg. “The office practice comes first [for them]. Some of our physicians have huge practices in town. And they’ll visit the hospital very early in the morning or in the evening. ... So if I need something in a case like that, if there was not a hospitalist involved, it would have been separate meetings for the family with the physician … and [with] me at another time.”
To hospitalists, a social worker can serve as an important adjunct in talking to the patient and family. “For example, if [social workers] are giving bad news, they warn the physician first,” says Dr. Rajan. “If they’re going to go in and tell the patient that they’re not going to qualify for any home services, they tell the physician as well so that [the hospitalist will not later be] meeting an angry patient.” In addition, she says, “for critically ill or long-term patients, social workers [can] help family members cope. Sometimes as physicians we don’t have the time or we don’t have the resources to do that.”
But this doesn’t let doctors off the hook in regard to addressing the whole person’s needs. Especially if someone has multiple medical problems, the social worker needs to know the availability and level of support for which the family can be counted.
“Social workers will ask questions such as: Are the families involved? or Is there any family?” says Krafcik. “Do they need to go in a nursing home or do they need 24-hour care at home? Is the family able to provide that? [E]very morning we meet to have team rounds. And the [team] go[es] over every patient on the floor, and then I will ask those questions if the doctor hasn’t given me that information.”
Social workers appreciate and would like hospitalists to do more listening to the patient and family for the aspects of the history and psychosocial status that the social worker will need to know.
TEACHING POINTS
In the course of their interactions, what do hospitalists and social workers teach each other that could lead to working a case more effectively and to the greater satisfaction of all involved?
Most of those we interviewed seem to think that the greatest service hospitalists provide is to teach the social worker the medical components that go along with what the social worker does every day.
“[Social workers] get a better understanding of [whether] someone comes in with heart failure or a fall or a stroke, just by repetition and also education; they get to understand after a while what’s needed for individual medical diagnoses,” says Dr. Flansbaum.
“When I know [better] what the medical condition is,” says Krafcik, “I have an idea of how much help [the patient] would need at home and their ability to function. And I would make sure that the patient gets physical therapy or occupational therapy referral or speech therapy.”
Again, perhaps the area where the social worker most teaches the hospitalist regards available resources to solve problems over and above the purely medical. “They know the social system and the needs of different forms and eligibility and what different patients are entitled to and what the system will provide,” says Dr. Flansbaum.
Dunson believes hospitalists are perceived as being more involved in a holistic way with the patient. “I always stress that it is so important to look at the whole person and not just the medical aspects,” she says. “It’s hard for the doctor sometimes to realize that this person might not be able to afford this medication and that’s why they’re noncompliant and all the other issues. So I think is important to open up to the other aspects of a person’s life and not just the medical aspects.”
CONCLUSION
Social workers’ knowledge of medical and nonmedical resources, both locally and nationally, offer hospitalists essential information that leads to designing more appropriate and effective post-discharge plans. Hospitalists can best team with social workers by consistently keeping in mind the patient’s overall circumstances and informing their colleagues of the medical information that can help social workers do their best work. TH
Writer Andrea Sattinger will write about the effect of poor communication skills in the November issue of The Hospitalist.
HOSPITALISTS AND SOCIAL WORKERS
Both sides of the clinical care team discuss the pros and cons of working together
In these … fractious healthcare times when resources are not plentiful and the expectations of patients might be higher, like getting 24-hour care at home, sometimes it might appear that the hospitalist or [another] physician is always the bringer of bad news. A good social worker can work well with the hospitalist in … letting the patient know the realistic expectations of what the system can provide [so that] we’re not in this alone. You know, ‘the world is a nail, the hospitalist is always the hammer’ kind of thing. Social workers can be very helpful in delivering information. … A good social worker can also add some “salve” to the wounds that the patient comes in with.
Some [patients] are borderline functioning or kind of on the precipice already. They come in with this problem and all of a sudden they can’t go back to the situation they were operating in prior. Social workers’ knowledge of the social safety net … is terrific, and they help us in directing what would be the best discharge plan for this patient, [including] knowing what the insurance status is, … what resources they have in place already, what else is available. … [I]t has a lot to do with discharge and recovery and functionality, and [to find out what’s the best place for the patient. They can help us with that.
Perhaps the greatest value social workers provide for all concerned is having the storehouse of knowledge of the available resources of the community. This is probably one of the most vital things to me; they can get a patient into services or programs that I didn’t even know exist. And the resources are very different in Connecticut than … in New York [where I practiced previously]. In New York there are many resources geared toward the Hispanic community, which I haven’t seen so far in Connecticut. But Connecticut has some other great resources; the local area clinic is a fantastic one.
Patients with end-of-life situations are dealt with differently in different states, too, and I wouldn’t have known about all this if it had not been for the social worker with whom I work. I also found out that there is a free program for alcohol rehabilitation in Connecticut; that does not exist in New York. We’ve sent a lot of our patients [to that]; you know they have to be the ones to initiate the call, but if they do, then that’s actually a resource for them. I wasn’t aware of that until I worked with the social workers here.
Editors’ note: “Alliances” is a new series written about the relationships that hospitalists have with members of the clinical care team—from the team members’ points of view. It’s our hope that each installment of “Alliances” will provide valuable, revealing feedback that hospitalists can use to continually improve their intrateam relationships and, ultimately, patient care.
Social workers are a natural fit with hospitalists and the hospitalist’s strongest allies and staunchest supporters, wrote Bradley Flansbaum, DO, MPH, in his Nov./Dec. 2003 article in The Hospitalist. What makes this collaboration such a positive one and what can members of these two professions learn from each other?
Dr. Flansbaum, a hospitalist and internist with the Division of Internal Medicine/Primary Care at Lenox Hill Hospital, Bronx, N.Y., and a former SHM board member, recently reiterated the benefits of the hospitalist-social worker relationship. In general, he believes that hospitalists provide a unique history-taking perspective that is useful to social workers in their work. Foremost, social workers bring a rich understanding of the available resources that patients need after discharge and a view of the patient’s nonmedical circumstances. Together, the two professionals’ daily interactions generate more effective discharge planning as a part of the multidisciplinary team.
ALWAYS THERE
Amy Lingg, MS, MPA, works on the general medicine unit at Greenwich Hospital (Conn). She says the role of the hospitalist is fairly new at Greenwich. In fact Sabitha Rajan, MD, MS, was the first one at Greenwich Hospital.
In Lingg’s view, nothing can replace the availability of the hospitalist to discuss patient cases, not only with the social worker but also as a team with the patient and family.
“[Attendings] are not there for the moment-by-moment events that happen on the unit, including availability when families are here,” says Lingg. “If I need to speak with a family and the physician’s input is important there, I can just page the hospitalist, she’s here. Whereas with an attending you have to make an appointment; you have to schedule around them. It can become difficult.”
Lingg, who works with hospitalist Dr. Rajan, director of hospitalist services at Greenwich Hospital, cites an example of the benefits of hospitalists’ 24/7 availability: “We had a fairly young woman in her mid-40s who was the divorced mother of a 17-year-old son. The father was not in the picture, and the woman was dying of alcoholic cirrhosis and liver failure. She was Dr. Rajan’s patient. One of the issues was the fact that there was no adult guardian for the son although he was going to be 18 in two months.
“So it involved a lot of talking with friends of the woman, who were sort of stepping in as surrogate guardians to him,” Lingg continues. “There were a lot of logistics [regarding] what would happen with him. We were trying to call the grandfather who was estranged. It was a very, very sensitive, very, very tricky case. It went on for days and days. … Dr. Rajan and I could work on this together on a dayto-day basis, [including] … the counseling, relaying medical knowledge to the family, what was going on clinically, trying to deal with that in a way where she was talking in one way to [the] adults and in a different, more appropriate [for the boy’s age] way to the 17-yearold son. And I can be there to help with that process.”
The situation was resolved to the satisfaction of the mother, the son, the friends, and the providers. “It was really pretty extraordinary,” she said. “I’ve talked about that a couple of times, including at a staff meetings when we were talking about getting new hospitalists. That is something I’ve described because, really, it was very special.”
TRUE TEAMWORK
Although everyone on a multidisciplinary team can bring something to the discussion that makes the team work better, social workers and hospitalists collaborate well in painting a more comprehensive picture of the patient’s lifestyle, living habits, and needs.
“In many hospitals … there’s a pattern that develops [whereby at] some time in the morning the hospitalist and social worker will get together and talk,” says Dr. Flansbaum “The hospitalist speaks the language of the social worker and knows what to tell them and how to direct them rather than just saying, ‘the patient’s homeless or the patient needs help at home.’”
After working regularly with social workers and recognizing what they need to know, he says, “the hospitalist is more likely to say, ‘the patient has Medicaid,’ or ‘the patient has this insurance,’ [or] ‘the patient has a home-health [caregiver] four hours a day and needs six or eight hours a day,’ or ‘the patient’s going to need a subacute nursing facility.’ … I think our insights are different from voluntary physicians and our face-time with social workers is more efficient.”
Sylvia Krafcik, MSSA, LISW, with MetroHealth Medical Center, Cleveland, says hospitalists are “great to work with because they’re very dedicated to the population they’re caring for, because this is their whole responsibility; they don’t have a private caseload.”
But in her view most hospitalists are focused on patients’ medical conditions and some of them are not as tuned in to all the other aspects of the patient, such as all the psychosocial dynamics.
“A lot of them are, but some aren’t,” Krafcik says. “Especially at MetroHealth, we’re a county hospital. So many of the patients that come here are poor. A lot of them are alcoholics or drug abusers. They’re homeless. They live on the streets. They don’t have a primary doctor. They’re usually not compliant with their medications.”
“Here at Metro we have a lot of patients who have extreme social circumstances that affect their medical issues so much,” says Sara Dunson, MSW, LSW, who also works as a social worker at Metro-Health. “I think the hospitalist has greater insight into the person’s environment and all the social structures that they have at home and that are going on in their life [than other physicians might].”
But there is always room for improvement.
“We had one patient who wasn’t able to read, and he never told anybody this,” says Dunson. “And as social workers, we have more of a way of finding that kind of stuff out from patients than the doctors might. And he kept coming in and coming in and was noncompliant with his medication. We eventually determined that this was why he was noncompliant and was causing all these medical issues. The doctors finally [understood] why this gentleman kept coming in with the same problems and he wasn’t taking care of himself. It wasn’t that he didn’t want to, it was just that he was having problems reading all the medications and all the discharge paperwork, and he was too ashamed to tell anybody. [Once the social workers questioned him and got this] out in the open, we were able to get him help with that.”
The doctors focused on what he was or wasn’t doing, but they hadn’t looked at why he wasn’t adherent, explains Dunson. If hospitalists do that more often, she thinks, they could save time and get better outcomes sooner.
COMMUNICATING WITH PATIENTS AND FAMILIES
“I think where hospitalists are coming from is a whole different mindset than a physician who has mainly an office practice,” said Lingg. “The office practice comes first [for them]. Some of our physicians have huge practices in town. And they’ll visit the hospital very early in the morning or in the evening. ... So if I need something in a case like that, if there was not a hospitalist involved, it would have been separate meetings for the family with the physician … and [with] me at another time.”
To hospitalists, a social worker can serve as an important adjunct in talking to the patient and family. “For example, if [social workers] are giving bad news, they warn the physician first,” says Dr. Rajan. “If they’re going to go in and tell the patient that they’re not going to qualify for any home services, they tell the physician as well so that [the hospitalist will not later be] meeting an angry patient.” In addition, she says, “for critically ill or long-term patients, social workers [can] help family members cope. Sometimes as physicians we don’t have the time or we don’t have the resources to do that.”
But this doesn’t let doctors off the hook in regard to addressing the whole person’s needs. Especially if someone has multiple medical problems, the social worker needs to know the availability and level of support for which the family can be counted.
“Social workers will ask questions such as: Are the families involved? or Is there any family?” says Krafcik. “Do they need to go in a nursing home or do they need 24-hour care at home? Is the family able to provide that? [E]very morning we meet to have team rounds. And the [team] go[es] over every patient on the floor, and then I will ask those questions if the doctor hasn’t given me that information.”
Social workers appreciate and would like hospitalists to do more listening to the patient and family for the aspects of the history and psychosocial status that the social worker will need to know.
TEACHING POINTS
In the course of their interactions, what do hospitalists and social workers teach each other that could lead to working a case more effectively and to the greater satisfaction of all involved?
Most of those we interviewed seem to think that the greatest service hospitalists provide is to teach the social worker the medical components that go along with what the social worker does every day.
“[Social workers] get a better understanding of [whether] someone comes in with heart failure or a fall or a stroke, just by repetition and also education; they get to understand after a while what’s needed for individual medical diagnoses,” says Dr. Flansbaum.
“When I know [better] what the medical condition is,” says Krafcik, “I have an idea of how much help [the patient] would need at home and their ability to function. And I would make sure that the patient gets physical therapy or occupational therapy referral or speech therapy.”
Again, perhaps the area where the social worker most teaches the hospitalist regards available resources to solve problems over and above the purely medical. “They know the social system and the needs of different forms and eligibility and what different patients are entitled to and what the system will provide,” says Dr. Flansbaum.
Dunson believes hospitalists are perceived as being more involved in a holistic way with the patient. “I always stress that it is so important to look at the whole person and not just the medical aspects,” she says. “It’s hard for the doctor sometimes to realize that this person might not be able to afford this medication and that’s why they’re noncompliant and all the other issues. So I think is important to open up to the other aspects of a person’s life and not just the medical aspects.”
CONCLUSION
Social workers’ knowledge of medical and nonmedical resources, both locally and nationally, offer hospitalists essential information that leads to designing more appropriate and effective post-discharge plans. Hospitalists can best team with social workers by consistently keeping in mind the patient’s overall circumstances and informing their colleagues of the medical information that can help social workers do their best work. TH
Writer Andrea Sattinger will write about the effect of poor communication skills in the November issue of The Hospitalist.
HOSPITALISTS AND SOCIAL WORKERS
Both sides of the clinical care team discuss the pros and cons of working together
In these … fractious healthcare times when resources are not plentiful and the expectations of patients might be higher, like getting 24-hour care at home, sometimes it might appear that the hospitalist or [another] physician is always the bringer of bad news. A good social worker can work well with the hospitalist in … letting the patient know the realistic expectations of what the system can provide [so that] we’re not in this alone. You know, ‘the world is a nail, the hospitalist is always the hammer’ kind of thing. Social workers can be very helpful in delivering information. … A good social worker can also add some “salve” to the wounds that the patient comes in with.
Some [patients] are borderline functioning or kind of on the precipice already. They come in with this problem and all of a sudden they can’t go back to the situation they were operating in prior. Social workers’ knowledge of the social safety net … is terrific, and they help us in directing what would be the best discharge plan for this patient, [including] knowing what the insurance status is, … what resources they have in place already, what else is available. … [I]t has a lot to do with discharge and recovery and functionality, and [to find out what’s the best place for the patient. They can help us with that.
Perhaps the greatest value social workers provide for all concerned is having the storehouse of knowledge of the available resources of the community. This is probably one of the most vital things to me; they can get a patient into services or programs that I didn’t even know exist. And the resources are very different in Connecticut than … in New York [where I practiced previously]. In New York there are many resources geared toward the Hispanic community, which I haven’t seen so far in Connecticut. But Connecticut has some other great resources; the local area clinic is a fantastic one.
Patients with end-of-life situations are dealt with differently in different states, too, and I wouldn’t have known about all this if it had not been for the social worker with whom I work. I also found out that there is a free program for alcohol rehabilitation in Connecticut; that does not exist in New York. We’ve sent a lot of our patients [to that]; you know they have to be the ones to initiate the call, but if they do, then that’s actually a resource for them. I wasn’t aware of that until I worked with the social workers here.
How should hypertension in pregnant patients be managed?
Case
You are consulted on a 29-year-old gravida 1 at nine weeks gestation with a two-year history of Type 2 diabetes and hypertension. She is admitted to the obstetric inpatient service for glycemic control. Although prescribed metformin and lisinopril, she ran out of both four months ago. Her current hemoglobin A1C is 9%. Her blood pressure is 140/90 mmHg in both arms, with an appropriately sized manual cuff while seated. She does not have retinopathy, nephropathy, or neuropathy. The obstetric team will begin weight-based insulin to achieve glycemic targets, and they ask for your input regarding blood-pressure management. How should one approach a pregnant patient with hypertension?
Overview
The most common chronic medical issue in reproductive-age women, essential hypertension (termed chronic hypertension in obstetric literature) contributes significantly to maternal and perinatal morbidity and mortality, primarily via increased risk of preeclampsia.
Chronic hypertension complicates up to 5% of pregnancies in the U.S., or as many as 120,000 pregnant women per year.1 Rates of chronic hypertension are expected to increase with later childbearing and increased rate of obesity. Prior to and during pregnancy, hypertension is defined as blood pressure 140/90 mmHg or higher. Chronic hypertension can be either hypertension diagnosed prior to pregnancy or elevated blood pressures identified prior to 20 weeks gestation.2 Normal pregnancy physiology leads to decreased systemic vascular resistance by the end of the first trimester, dropping systolic and diastolic blood pressure between 10 and 15 mmHg, with maximal effect mid-pregnancy followed by a gradual return to baseline.3 Therefore, chronic hypertension might be masked in early pregnancy. Normal changes in pregnancy include renal vasodilatation and increased glomerular filtration rate, so the average serum creatinine (SCr) is 0.5 mg/dL.4
Newly identified hypertension or accelerating hypertension after 20 weeks warrants close evaluation for preeclampsia. Preeclampsia is a multisystem, life-threatening disorder characterized by hypertension and proteinuria (greater than 300 mg/day). Severe forms of preeclampsia include HELLP (hemolysis, elevated liver enzymes and low platelets) syndrome and eclampsia (seizures with no other attributable cause). Superimposed preeclampsia occurs in 20% to 25% of women with chronic hypertension.5 Women with hypertensive target organ damage have an even greater likelihood of preeclampsia as well as maternal and fetal complications. Unfortunately, blood-pressure control during pregnancy has not been shown to minimize the likelihood of developing superimposed preeclampsia or associated maternal and fetal complications.6 The goal of antihypertensive management during pregnancy is to avoid acute maternal or fetal complications of severe hypertension.
Review of the Data
Q: How are hypertensive disorders of pregnancy classified?
The American College of Obstetrics and Gynecology and the National High Blood Pressure Education Program guideline committees have classified hypertensive disorders of pregnancy into four categories: chronic hypertension, preeclampsia, preeclampsia superimposed on chronic hypertension, and gestational hypertension.2,7
Chronic hypertension is defined as blood pressure 140/90 mmHg or greater on two occasions before pregnancy, prior to 20 weeks of gestation, or persisting 12 weeks postpartum. Severe hypertension is defined as diastolic blood pressure ≥110 mm Hg. Hypertensive women tend to have a greater decline in blood pressure during early pregnancy than normotensive women.8
Secondary hypertension is an important consideration in women of reproductive age. A brief screen for secondary causes includes bilateral arm pressures and femoral pulse assessment, renal bruit assessment, inquiry into snoring, gasping, and daytime somnolence, as well as measurement of serum thyrotropin, potassium, calcium, creatinine, and urinalysis. This kind of evaluation will assess for coarctation of the aorta, renal artery stenosis, obstructive sleep apnea, hyper- or hypothyroidism, hyperaldosteronism, hyperparathyroidism, and underlying renal disease.9,10 Patient reports of episodic headache, palpitations, and diaphoresis should prompt investigation for pheochromocytoma.
Hyperaldosteronism, pheochromocytoma, or hyperthyroidism might be quiescent during pregnancy but flare in the postpartum period.
Women with severe chronic hypertension or target organ damage have higher rates of superimposed preeclampsia. In these individuals, preeclampsia is more likely to present early (before 34 weeks gestation) or with severe disease.1
Preeclampsia is defined as hypertension and proteinuria (greater than 300 mg/day) at or beyond 20 weeks gestation in a previously normotensive woman. Preeclampsia rates vary from 5% to 10% of nulliparous women, to much higher rates in women with medical comorbidities or fetal factors (e.g., multiple gestations, molar pregnancies, hydrops, or triploidy). Preeclampsia’s pathogenesis is attributed to abnormal placental implantation with abnormal maternal immune adaptation, altered angiogenic factors with increased systemic vascular resistance and endothelial dysfunction leading to the clinically apparent maternal syndrome.11
Severe preeclampsia criteria include any of the following: eclampsia, HELLP syndrome (platelets less than 100,000/mm³, transaminases more than twice the upper limit of normal, and/or epigastric pain), SBP ≥160 mmHg, DBP ≥110 mmHg, proteinuria ≥5 grams per day, oliguria, pulmonary edema, placental abruption, or fetal manifestations such as intrauterine growth restriction (≤10th percentile of expected fetal weight based on gestational age), decreased amniotic fluid index, or fetal demise.2,5,12
Maternal symptoms might include headache, visual disturbances, epigastric or right upper quadrant (RUQ) pain, rapid weight gain, and severe edema. Some women remain asymptomatic. Preeclampsia can rapidly progress from “less severe” to severe. Maternal symptoms and abnormal lab findings are more predictive of adverse pregnancy outcomes than the degree of hypertension and/or proteinuria.1
It is always in the mother’s interest to deliver when preeclampsia is diagnosed, because preeclampsia will not resolve until after delivery, with hypertension and lab abnormalities sometimes persisting for months postpartum. Preeclampsia might be diagnosed before fetal viability (approximately 24 weeks gestation), although the vast majority of cases occur near term.
Risks of premature delivery must be balanced with the risks of progressively severe manifestations for the mother and fetus. Guidelines for expectant management of early (<34 weeks) preeclampsia are based on available evidence and expert opinion.13 Magnesium sulfate has been shown to be the most effective agent to minimize the likelihood of seizure in preeclamptic women.14 With an initial bolus of 4 g to 6 g IV followed by infusion of 1-2 g/hour, magnesium sulfate is usually continued for 24 to 48 hours after delivery.
Preeclampsia can first appear postpartum, most likely in the first days to weeks. A growing body of literature links preeclampsia, particularly early and/or recurrent, to subsequent increased risk for cardiovascular disease and end-stage renal disease.15
Preeclampsia superimposed on chronic hypertension is defined as the new onset or markedly increasing proteinuria or accelerating hypertension in the latter half of pregnancy. Maternal symptoms, transaminase elevation, thrombocytopenia, or fetal manifestations further support this diagnosis.
Gestational hypertension, previously known as pregnancy-induced hypertension, is defined as hypertension in the absence of proteinuria in the latter half of pregnancy. Symptoms and lab abnormalities of preeclampsia will be absent. At least half of women with hypertension in the latter half of pregnancy progress to preeclampsia, so gestational hypertension should be considered a provisional diagnosis. Severe gestational hypertension, even without proteinuria or other lab abnormalities, carries increased perinatal risk.
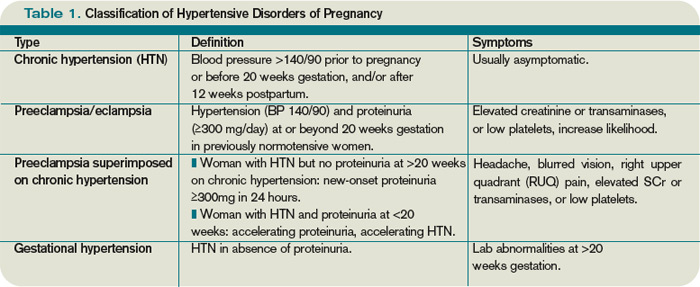
Q: What factors contribute to increased preeclampsia risk?
Maternal factors include: first pregnancy, first pregnancy with a new father, maternal age >35, particularly >40, personal or family history of preeclampsia, chronic hypertension, diabetes mellitus (Type 1, 2 or gestational), systemic lupus erythematosus, antiphospholipid antibody syndrome, renal disease, and obesity. Fetal factors include: multiple gestations, molar pregnancies, hydrops, and triploidy.5,12
Q: When should antihypertensive medications be used in pregnancy?
Most women are hesitant to expose their fetus to medication, and thus must be in therapeutic alliance with their obstetrician and consultants. The overriding principle of medication use in pregnancy is that a healthy fetus requires a healthy mother, and medication use is justified when there is definite benefit to the mother. Due to increased metabolism during pregnancy, medications otherwise dosed once per day often require two doses per day, and those dosed twice daily often require every-eight-hour dosing to maintain efficacy. Additionally, titration up every few days may be required.
Therapy goals include avoiding maternal and fetal complications from severely elevated blood pressure, as well as avoiding fetal growth restriction due to impaired uteroplacental flow. The ideal blood pressure for a hypertensive pregnant woman has not been established, but recommendations are based upon available data and expert opinion.2,5,10,12 Maternal risk of intracerebral hemorrhage increases with SBP ≥160 mmHg.16 Diastolic BP ≥110 mmHg has been associated with greater risk of placental abruption and intrauterine growth restriction.
Pharmacologic treatment generally is initiated or adjusted to achieve SBP <160 mm Hg and DBP <100 to <105 mmHg, although some societies advocate treatment initiation at 140/90 mmHg.2,5,12,17,18 If a woman has target organ damage or concomitant medical issues warranting tighter control (e.g., diabetes or pre-existing renal disease), 130/80 mmHg is preferable.19 Activity limitation and/or bed rest, although commonly recommended, have not been shown to reduce maternal or fetal morbidity or mortality, or prolong time to delivery.
An ongoing, randomized, prospective trial will compare maternal and fetal outcomes in women with mild chronic hypertension with deliberate blood-pressure stratification (goal DBP 85 mmHg vs. goal DBP 100 mmHg).20
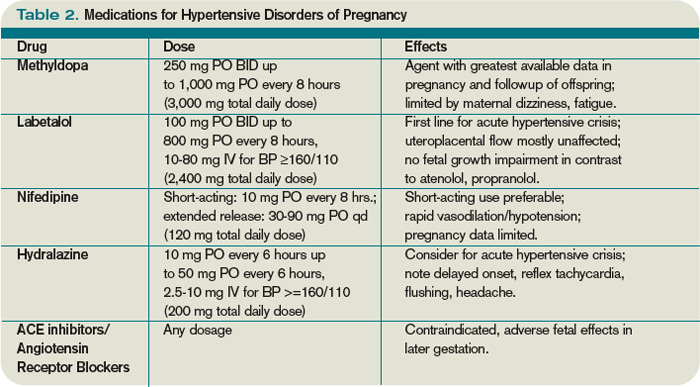
Q: What are reasonable treatment options for a woman with chronic hypertension during pregnancy?
Due to vasodilatation of pregnancy, antihypertensive agents often can be discontinued early in pregnancy with close, ongoing monitoring. The majority of women with mild chronic hypertension will have blood pressures <160/100 mmHg without medication during the first half of pregnancy.
If a woman has been using a pharmacologic agent not advisable during pregnancy, she could be switched to a preferred agent. If a woman has been using a pharmacologic agent preferred during pregnancy, she could continue this agent.
Q: What antihypertensives are favored during pregnancy?
Methyldopa and labetalol have been used extensively. Methyldopa has not been found to adversely affect cognitive development in children exposed in utero. On the maternal side, somnolence, dizziness, and dry mouth are common side effects.
Labetalol is widely used as a first- or second-line agent. It can be used intravenously or orally. Intravenous labetalol in escalating doses (10 mg, 20 mg, 40 mg, 80 mg) is the first line of acute treatment for severe hypertension/preeclampsia.
Atenolol and propranolol have been associated with fetal growth restriction, metoprolol to a lesser degree.
Metoprolol is useful in women with coronary artery disease, tachyarrhythmias, and/or requiring migraine prophylaxis during pregnancy.
Nifedipine is often used as a second-line agent, with extended-release preparation preferred. Short-acting nifedipine should be used with caution during pregnancy due to the potential for acute impairment of uteroplacental flow. However, short-acting nifedipine is used for tocolysis in pre-term labor.
Intravenous hydralazine is another option for acute treatment in the setting of severe hypertension/preeclampsia.
Angiotensin-converting enzyme (ACE) inhibitors are contraindicated during pregnancy due to association with increased rates of cardiovascular and central nervous system malformations when used in the first trimester, as well as fetal anuric renal failure when used later in pregnancy.21 Due to similar mechanisms of action, angiotensin receptor blockers (ARBs) are contraindicated.
In general, antihypertensive agents are considered compatible with lactation, with most minimally excreted into breast milk. Women requiring antihypertensive agents or almost any medication during lactation seek particular reassurance from caregivers.
It is essential to emphasize the benefit of breastfeeding for both mother and newborn, which far outweighs the risk of medication exposure to the newborn—with rare exceptions. Enalapril and captopril are considered compatible with breastfeeding by the American Academy of Pediatrics.22
Q: Can we identify and possibly prevent preeclampsia?
Escalating hypertension or maternal symptoms, especially in women with increased risk factors, warrant careful examination and laboratory assessment for preeclampsia. Physical findings may include retinal vasospasm, rales on pulmonary exam, cardiac gallop, RUQ or midepigastric tenderness from hepatic capsule stretching, nondependent edema (e.g., face, hands), or clonus on deep tendon reflex evaluation. Useful laboratory values include complete blood count, serum creatinine, hepatic transaminases, uric acid, and urinalysis.
Marked anemia or hemoconcentration, thrombocytopenia, SCr ≥0.8 mg/dL, transaminases above normal, uric acid ≥5.0 mg/dL, urine protein 1+ or greater on dipstick, are all suggestive of preeclampsia, particularly if worsened compared to prior values. Urine protein-to-creatinine ratios have not reliably correlated with 24-hour urine protein collections in preeclamptic patients, although very high or low values could be helpful.23
Women are typically admitted for fetal monitoring, 24-hour urine protein collection, and blood-pressure management during a preeclampsia evaluation.
Thus far, the only intervention shown to reduce the likelihood of preeclampsia in women at increased risk is low-dose aspirin. A recent meta-analysis noted 10% reduction of relative risk of preeclampsia and pre-term birth prior to 34 weeks in women with history of preeclampsia treated with aspirin from the second trimester onward.24 Other interventions in trials that have not displayed reduced risk include vitamin C, vitamin E, calcium, fish oil, zinc, magnesium, and antihypertensive therapy.
Back to the Case
Our patient has chronic hypertension and diabetes, so she should have a blood-pressure goal of <130/80 mmHg. She could be initiated on methyldopa or labetalol. She should have a screen for secondary hypertension via exam and serum thyrotropin, potassium, and calcium, as well as baseline “preeclampsia labs”: complete blood count, serum creatinine, transaminases, uric acid, and 24-hour urine protein assessment. Aspirin at 81 mg daily should be considered from 12 weeks gestation to delivery.
Glycemic control is critical in early gestation to avoid increased risk for congenital malformations and spontaneous abortion, and later on to minimize macrosomia. Close monitoring for maternal symptoms of preeclampsia and blood-pressure assessment is advisable. With medical comorbidities of hypertension and diabetes mellitus, the woman’s risk of preeclampsia is at least 25%. Her pregnancy dating should be confirmed by a first-trimester ultrasound.
Bottom Line
A pregnant woman with chronic hypertension should have evaluation for secondary causes of hypertension, adjustment or initiation of preferred antihypertensive agents to achieve blood pressures that minimize the risk for acute hypertensive complications and fetal growth impairment, and close monitoring for superimposed preeclampsia. TH
Dr. Hayes is an obstetric internist at Women & Infants’ Hospital and assistant professor of medicine (clinical) at the Warren Alpert Medical School of Brown University, Providence, R.I.
References
- Sibai BM. Caring for women with hypertension in pregnancy. JAMA. 2007;298(13):1566-1568.
- Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. Am J Obstet Gynecol. 2000;183:S1-S22.
- Christianson RE. Studies on blood pressure during pregnancy. I. Influence of parity and age. Am J Obstet Gynecol. 1976;125(4):509-513.
- Gibson P, Rosene-Montella K. Normal renal and vascular changes in pregnancy. In: Rosene-Montella K, Keely E, Barbour LA, Lee RV, eds. Medical Care of the Pregnant Patient. 2nd ed. Philadelphia: American College of Physicians; 2008:149-152.
- ACOG practice bulletin, No. 33, January 2002. Diagnosis and management of preeclampsia and eclampsia. Obstet Gynecol. 2002;99(1):159-167.
- Sibai BM. Chronic hypertension in pregnancy. Obstet Gynecol. 2002;100(2):369-377.
- Mulrow CD, Chiquette E, Ferrer RL, et al. Management of Chronic Hypertension During Pregnancy. Rockville: Agency for Healthcare Research and Quality; 2000.
- Pickering TG, Hall JE, Appel LJ, et al. Recommendations for blood pressure measurement in humans and experimental animals: part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Prof-essional and Public Education of the American Heart Association Council on high blood pressure Research. Circulation. 2005;111(5):697-716.
- Powrie RO. A 30-year-old woman with chronic hypertension trying to conceive. JAMA. 2007; 298(13):1548-1558.
- Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003:289(19):2560-2571.
- Widmer M, Villar J, Benigni A, Conde-Agudelo A, Karumanchi SA, Lindheimer M. Mapping the theories of preeclampsia and the role of angiogenic factors: a systematic review. Obstet Gynecol. 2007; 109(1):168-180.
- Magee LA, Helewa M, Moutquin JM, van Dadelszen P. Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy. SOGC Clinical Practice Guideline. J Obstet Gynaecol Can. 2008; 30:S1-S48.
- Sibai BM, Barton JR. Expectant management of severe preeclampsia remote from term: patient selection, treatment, and delivery indications. Am J Obstet Gynecol. 2007;196(6):514.e1-514.e1-9.
- Duley L, Gülmezoglu AM, Henderson-Smart DJ. Magnesium sulphate and other anticonvulsants for women with preeclampsia. Cochrane Database Syst Rev. 2003;(2):CD000025.
- McDonald SD, Malinowski A, Zhou Q, Yusuf S, Devereaux PJ. Cardiovascular sequelae of preeclampsia/eclampsia: a systematic review and meta-analyses. Am Heart J. 2008;156(5):918-930.
- Martin JN Jr., Thigpen BD, Moore RC, Rose CH, Cushman J, May W. Stroke and severe preeclampsia and eclampsia: a paradigm shift focusing on systolic blood pressure. Obstet Gynecol. 2005;105(2): 246-254.
- Lindheimer MD, Taler SJ, Cunningham FG. Hyper-tension in pregnancy. J Am Soc Hypertens. 2008; 2(6):484-494.
- Podymow T, August P. Update on the use of antihypertensive drugs in pregnancy. Hypertension. 2008; 51(4):960-969.
- Kitzmiller JL, Block JM, Brown FM, et al. Managing preexisting diabetes for pregnancy: summary of evidence and consensus recommendations for care. Diabetes Care. 2008;31(5):1060-1079.
- Magee LA, von Dadelszen P, Chan S, et al. The Control of Hypertension In Pregnancy Study pilot trial. BJOG. 2007;114(6):770,e13-e20.
- Cooper WO, Hernandez-Diaz S, Arbogast PG, et al. Major congenital malformations after first-trimester exposure to ACE inhibitors. N Engl J Med. 2006; 354(23):2442-2451.
- American Academy of Pediatrics Committee on Drugs. Transfer of drugs and other chemicals into human milk. Pediatrics. 2001;108(3):776-789.
- Papanna R, Mann LK, Kouides RW, Glantz JC. Protein/creatinine ratio in preeclampsia: a systematic review. Obstet Gynecol. 2008;112(1):135-144.
- Askie LM, Duley L, Henderson-Smart DJ, Stewart LA, PARIS Collaborative group. Antiplatelet agents for prevention of pre-eclampsia: a meta-analysis of individual patient data. Lancet. 2007;369(9575): 1791-1798.
Case
You are consulted on a 29-year-old gravida 1 at nine weeks gestation with a two-year history of Type 2 diabetes and hypertension. She is admitted to the obstetric inpatient service for glycemic control. Although prescribed metformin and lisinopril, she ran out of both four months ago. Her current hemoglobin A1C is 9%. Her blood pressure is 140/90 mmHg in both arms, with an appropriately sized manual cuff while seated. She does not have retinopathy, nephropathy, or neuropathy. The obstetric team will begin weight-based insulin to achieve glycemic targets, and they ask for your input regarding blood-pressure management. How should one approach a pregnant patient with hypertension?
Overview
The most common chronic medical issue in reproductive-age women, essential hypertension (termed chronic hypertension in obstetric literature) contributes significantly to maternal and perinatal morbidity and mortality, primarily via increased risk of preeclampsia.
Chronic hypertension complicates up to 5% of pregnancies in the U.S., or as many as 120,000 pregnant women per year.1 Rates of chronic hypertension are expected to increase with later childbearing and increased rate of obesity. Prior to and during pregnancy, hypertension is defined as blood pressure 140/90 mmHg or higher. Chronic hypertension can be either hypertension diagnosed prior to pregnancy or elevated blood pressures identified prior to 20 weeks gestation.2 Normal pregnancy physiology leads to decreased systemic vascular resistance by the end of the first trimester, dropping systolic and diastolic blood pressure between 10 and 15 mmHg, with maximal effect mid-pregnancy followed by a gradual return to baseline.3 Therefore, chronic hypertension might be masked in early pregnancy. Normal changes in pregnancy include renal vasodilatation and increased glomerular filtration rate, so the average serum creatinine (SCr) is 0.5 mg/dL.4
Newly identified hypertension or accelerating hypertension after 20 weeks warrants close evaluation for preeclampsia. Preeclampsia is a multisystem, life-threatening disorder characterized by hypertension and proteinuria (greater than 300 mg/day). Severe forms of preeclampsia include HELLP (hemolysis, elevated liver enzymes and low platelets) syndrome and eclampsia (seizures with no other attributable cause). Superimposed preeclampsia occurs in 20% to 25% of women with chronic hypertension.5 Women with hypertensive target organ damage have an even greater likelihood of preeclampsia as well as maternal and fetal complications. Unfortunately, blood-pressure control during pregnancy has not been shown to minimize the likelihood of developing superimposed preeclampsia or associated maternal and fetal complications.6 The goal of antihypertensive management during pregnancy is to avoid acute maternal or fetal complications of severe hypertension.
Review of the Data
Q: How are hypertensive disorders of pregnancy classified?
The American College of Obstetrics and Gynecology and the National High Blood Pressure Education Program guideline committees have classified hypertensive disorders of pregnancy into four categories: chronic hypertension, preeclampsia, preeclampsia superimposed on chronic hypertension, and gestational hypertension.2,7
Chronic hypertension is defined as blood pressure 140/90 mmHg or greater on two occasions before pregnancy, prior to 20 weeks of gestation, or persisting 12 weeks postpartum. Severe hypertension is defined as diastolic blood pressure ≥110 mm Hg. Hypertensive women tend to have a greater decline in blood pressure during early pregnancy than normotensive women.8
Secondary hypertension is an important consideration in women of reproductive age. A brief screen for secondary causes includes bilateral arm pressures and femoral pulse assessment, renal bruit assessment, inquiry into snoring, gasping, and daytime somnolence, as well as measurement of serum thyrotropin, potassium, calcium, creatinine, and urinalysis. This kind of evaluation will assess for coarctation of the aorta, renal artery stenosis, obstructive sleep apnea, hyper- or hypothyroidism, hyperaldosteronism, hyperparathyroidism, and underlying renal disease.9,10 Patient reports of episodic headache, palpitations, and diaphoresis should prompt investigation for pheochromocytoma.
Hyperaldosteronism, pheochromocytoma, or hyperthyroidism might be quiescent during pregnancy but flare in the postpartum period.
Women with severe chronic hypertension or target organ damage have higher rates of superimposed preeclampsia. In these individuals, preeclampsia is more likely to present early (before 34 weeks gestation) or with severe disease.1
Preeclampsia is defined as hypertension and proteinuria (greater than 300 mg/day) at or beyond 20 weeks gestation in a previously normotensive woman. Preeclampsia rates vary from 5% to 10% of nulliparous women, to much higher rates in women with medical comorbidities or fetal factors (e.g., multiple gestations, molar pregnancies, hydrops, or triploidy). Preeclampsia’s pathogenesis is attributed to abnormal placental implantation with abnormal maternal immune adaptation, altered angiogenic factors with increased systemic vascular resistance and endothelial dysfunction leading to the clinically apparent maternal syndrome.11
Severe preeclampsia criteria include any of the following: eclampsia, HELLP syndrome (platelets less than 100,000/mm³, transaminases more than twice the upper limit of normal, and/or epigastric pain), SBP ≥160 mmHg, DBP ≥110 mmHg, proteinuria ≥5 grams per day, oliguria, pulmonary edema, placental abruption, or fetal manifestations such as intrauterine growth restriction (≤10th percentile of expected fetal weight based on gestational age), decreased amniotic fluid index, or fetal demise.2,5,12
Maternal symptoms might include headache, visual disturbances, epigastric or right upper quadrant (RUQ) pain, rapid weight gain, and severe edema. Some women remain asymptomatic. Preeclampsia can rapidly progress from “less severe” to severe. Maternal symptoms and abnormal lab findings are more predictive of adverse pregnancy outcomes than the degree of hypertension and/or proteinuria.1
It is always in the mother’s interest to deliver when preeclampsia is diagnosed, because preeclampsia will not resolve until after delivery, with hypertension and lab abnormalities sometimes persisting for months postpartum. Preeclampsia might be diagnosed before fetal viability (approximately 24 weeks gestation), although the vast majority of cases occur near term.
Risks of premature delivery must be balanced with the risks of progressively severe manifestations for the mother and fetus. Guidelines for expectant management of early (<34 weeks) preeclampsia are based on available evidence and expert opinion.13 Magnesium sulfate has been shown to be the most effective agent to minimize the likelihood of seizure in preeclamptic women.14 With an initial bolus of 4 g to 6 g IV followed by infusion of 1-2 g/hour, magnesium sulfate is usually continued for 24 to 48 hours after delivery.
Preeclampsia can first appear postpartum, most likely in the first days to weeks. A growing body of literature links preeclampsia, particularly early and/or recurrent, to subsequent increased risk for cardiovascular disease and end-stage renal disease.15
Preeclampsia superimposed on chronic hypertension is defined as the new onset or markedly increasing proteinuria or accelerating hypertension in the latter half of pregnancy. Maternal symptoms, transaminase elevation, thrombocytopenia, or fetal manifestations further support this diagnosis.
Gestational hypertension, previously known as pregnancy-induced hypertension, is defined as hypertension in the absence of proteinuria in the latter half of pregnancy. Symptoms and lab abnormalities of preeclampsia will be absent. At least half of women with hypertension in the latter half of pregnancy progress to preeclampsia, so gestational hypertension should be considered a provisional diagnosis. Severe gestational hypertension, even without proteinuria or other lab abnormalities, carries increased perinatal risk.
Q: What factors contribute to increased preeclampsia risk?
Maternal factors include: first pregnancy, first pregnancy with a new father, maternal age >35, particularly >40, personal or family history of preeclampsia, chronic hypertension, diabetes mellitus (Type 1, 2 or gestational), systemic lupus erythematosus, antiphospholipid antibody syndrome, renal disease, and obesity. Fetal factors include: multiple gestations, molar pregnancies, hydrops, and triploidy.5,12
Q: When should antihypertensive medications be used in pregnancy?
Most women are hesitant to expose their fetus to medication, and thus must be in therapeutic alliance with their obstetrician and consultants. The overriding principle of medication use in pregnancy is that a healthy fetus requires a healthy mother, and medication use is justified when there is definite benefit to the mother. Due to increased metabolism during pregnancy, medications otherwise dosed once per day often require two doses per day, and those dosed twice daily often require every-eight-hour dosing to maintain efficacy. Additionally, titration up every few days may be required.
Therapy goals include avoiding maternal and fetal complications from severely elevated blood pressure, as well as avoiding fetal growth restriction due to impaired uteroplacental flow. The ideal blood pressure for a hypertensive pregnant woman has not been established, but recommendations are based upon available data and expert opinion.2,5,10,12 Maternal risk of intracerebral hemorrhage increases with SBP ≥160 mmHg.16 Diastolic BP ≥110 mmHg has been associated with greater risk of placental abruption and intrauterine growth restriction.
Pharmacologic treatment generally is initiated or adjusted to achieve SBP <160 mm Hg and DBP <100 to <105 mmHg, although some societies advocate treatment initiation at 140/90 mmHg.2,5,12,17,18 If a woman has target organ damage or concomitant medical issues warranting tighter control (e.g., diabetes or pre-existing renal disease), 130/80 mmHg is preferable.19 Activity limitation and/or bed rest, although commonly recommended, have not been shown to reduce maternal or fetal morbidity or mortality, or prolong time to delivery.
An ongoing, randomized, prospective trial will compare maternal and fetal outcomes in women with mild chronic hypertension with deliberate blood-pressure stratification (goal DBP 85 mmHg vs. goal DBP 100 mmHg).20
Q: What are reasonable treatment options for a woman with chronic hypertension during pregnancy?
Due to vasodilatation of pregnancy, antihypertensive agents often can be discontinued early in pregnancy with close, ongoing monitoring. The majority of women with mild chronic hypertension will have blood pressures <160/100 mmHg without medication during the first half of pregnancy.
If a woman has been using a pharmacologic agent not advisable during pregnancy, she could be switched to a preferred agent. If a woman has been using a pharmacologic agent preferred during pregnancy, she could continue this agent.
Q: What antihypertensives are favored during pregnancy?
Methyldopa and labetalol have been used extensively. Methyldopa has not been found to adversely affect cognitive development in children exposed in utero. On the maternal side, somnolence, dizziness, and dry mouth are common side effects.
Labetalol is widely used as a first- or second-line agent. It can be used intravenously or orally. Intravenous labetalol in escalating doses (10 mg, 20 mg, 40 mg, 80 mg) is the first line of acute treatment for severe hypertension/preeclampsia.
Atenolol and propranolol have been associated with fetal growth restriction, metoprolol to a lesser degree.
Metoprolol is useful in women with coronary artery disease, tachyarrhythmias, and/or requiring migraine prophylaxis during pregnancy.
Nifedipine is often used as a second-line agent, with extended-release preparation preferred. Short-acting nifedipine should be used with caution during pregnancy due to the potential for acute impairment of uteroplacental flow. However, short-acting nifedipine is used for tocolysis in pre-term labor.
Intravenous hydralazine is another option for acute treatment in the setting of severe hypertension/preeclampsia.
Angiotensin-converting enzyme (ACE) inhibitors are contraindicated during pregnancy due to association with increased rates of cardiovascular and central nervous system malformations when used in the first trimester, as well as fetal anuric renal failure when used later in pregnancy.21 Due to similar mechanisms of action, angiotensin receptor blockers (ARBs) are contraindicated.
In general, antihypertensive agents are considered compatible with lactation, with most minimally excreted into breast milk. Women requiring antihypertensive agents or almost any medication during lactation seek particular reassurance from caregivers.
It is essential to emphasize the benefit of breastfeeding for both mother and newborn, which far outweighs the risk of medication exposure to the newborn—with rare exceptions. Enalapril and captopril are considered compatible with breastfeeding by the American Academy of Pediatrics.22
Q: Can we identify and possibly prevent preeclampsia?
Escalating hypertension or maternal symptoms, especially in women with increased risk factors, warrant careful examination and laboratory assessment for preeclampsia. Physical findings may include retinal vasospasm, rales on pulmonary exam, cardiac gallop, RUQ or midepigastric tenderness from hepatic capsule stretching, nondependent edema (e.g., face, hands), or clonus on deep tendon reflex evaluation. Useful laboratory values include complete blood count, serum creatinine, hepatic transaminases, uric acid, and urinalysis.
Marked anemia or hemoconcentration, thrombocytopenia, SCr ≥0.8 mg/dL, transaminases above normal, uric acid ≥5.0 mg/dL, urine protein 1+ or greater on dipstick, are all suggestive of preeclampsia, particularly if worsened compared to prior values. Urine protein-to-creatinine ratios have not reliably correlated with 24-hour urine protein collections in preeclamptic patients, although very high or low values could be helpful.23
Women are typically admitted for fetal monitoring, 24-hour urine protein collection, and blood-pressure management during a preeclampsia evaluation.
Thus far, the only intervention shown to reduce the likelihood of preeclampsia in women at increased risk is low-dose aspirin. A recent meta-analysis noted 10% reduction of relative risk of preeclampsia and pre-term birth prior to 34 weeks in women with history of preeclampsia treated with aspirin from the second trimester onward.24 Other interventions in trials that have not displayed reduced risk include vitamin C, vitamin E, calcium, fish oil, zinc, magnesium, and antihypertensive therapy.
Back to the Case
Our patient has chronic hypertension and diabetes, so she should have a blood-pressure goal of <130/80 mmHg. She could be initiated on methyldopa or labetalol. She should have a screen for secondary hypertension via exam and serum thyrotropin, potassium, and calcium, as well as baseline “preeclampsia labs”: complete blood count, serum creatinine, transaminases, uric acid, and 24-hour urine protein assessment. Aspirin at 81 mg daily should be considered from 12 weeks gestation to delivery.
Glycemic control is critical in early gestation to avoid increased risk for congenital malformations and spontaneous abortion, and later on to minimize macrosomia. Close monitoring for maternal symptoms of preeclampsia and blood-pressure assessment is advisable. With medical comorbidities of hypertension and diabetes mellitus, the woman’s risk of preeclampsia is at least 25%. Her pregnancy dating should be confirmed by a first-trimester ultrasound.
Bottom Line
A pregnant woman with chronic hypertension should have evaluation for secondary causes of hypertension, adjustment or initiation of preferred antihypertensive agents to achieve blood pressures that minimize the risk for acute hypertensive complications and fetal growth impairment, and close monitoring for superimposed preeclampsia. TH
Dr. Hayes is an obstetric internist at Women & Infants’ Hospital and assistant professor of medicine (clinical) at the Warren Alpert Medical School of Brown University, Providence, R.I.
References
- Sibai BM. Caring for women with hypertension in pregnancy. JAMA. 2007;298(13):1566-1568.
- Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. Am J Obstet Gynecol. 2000;183:S1-S22.
- Christianson RE. Studies on blood pressure during pregnancy. I. Influence of parity and age. Am J Obstet Gynecol. 1976;125(4):509-513.
- Gibson P, Rosene-Montella K. Normal renal and vascular changes in pregnancy. In: Rosene-Montella K, Keely E, Barbour LA, Lee RV, eds. Medical Care of the Pregnant Patient. 2nd ed. Philadelphia: American College of Physicians; 2008:149-152.
- ACOG practice bulletin, No. 33, January 2002. Diagnosis and management of preeclampsia and eclampsia. Obstet Gynecol. 2002;99(1):159-167.
- Sibai BM. Chronic hypertension in pregnancy. Obstet Gynecol. 2002;100(2):369-377.
- Mulrow CD, Chiquette E, Ferrer RL, et al. Management of Chronic Hypertension During Pregnancy. Rockville: Agency for Healthcare Research and Quality; 2000.
- Pickering TG, Hall JE, Appel LJ, et al. Recommendations for blood pressure measurement in humans and experimental animals: part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Prof-essional and Public Education of the American Heart Association Council on high blood pressure Research. Circulation. 2005;111(5):697-716.
- Powrie RO. A 30-year-old woman with chronic hypertension trying to conceive. JAMA. 2007; 298(13):1548-1558.
- Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003:289(19):2560-2571.
- Widmer M, Villar J, Benigni A, Conde-Agudelo A, Karumanchi SA, Lindheimer M. Mapping the theories of preeclampsia and the role of angiogenic factors: a systematic review. Obstet Gynecol. 2007; 109(1):168-180.
- Magee LA, Helewa M, Moutquin JM, van Dadelszen P. Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy. SOGC Clinical Practice Guideline. J Obstet Gynaecol Can. 2008; 30:S1-S48.
- Sibai BM, Barton JR. Expectant management of severe preeclampsia remote from term: patient selection, treatment, and delivery indications. Am J Obstet Gynecol. 2007;196(6):514.e1-514.e1-9.
- Duley L, Gülmezoglu AM, Henderson-Smart DJ. Magnesium sulphate and other anticonvulsants for women with preeclampsia. Cochrane Database Syst Rev. 2003;(2):CD000025.
- McDonald SD, Malinowski A, Zhou Q, Yusuf S, Devereaux PJ. Cardiovascular sequelae of preeclampsia/eclampsia: a systematic review and meta-analyses. Am Heart J. 2008;156(5):918-930.
- Martin JN Jr., Thigpen BD, Moore RC, Rose CH, Cushman J, May W. Stroke and severe preeclampsia and eclampsia: a paradigm shift focusing on systolic blood pressure. Obstet Gynecol. 2005;105(2): 246-254.
- Lindheimer MD, Taler SJ, Cunningham FG. Hyper-tension in pregnancy. J Am Soc Hypertens. 2008; 2(6):484-494.
- Podymow T, August P. Update on the use of antihypertensive drugs in pregnancy. Hypertension. 2008; 51(4):960-969.
- Kitzmiller JL, Block JM, Brown FM, et al. Managing preexisting diabetes for pregnancy: summary of evidence and consensus recommendations for care. Diabetes Care. 2008;31(5):1060-1079.
- Magee LA, von Dadelszen P, Chan S, et al. The Control of Hypertension In Pregnancy Study pilot trial. BJOG. 2007;114(6):770,e13-e20.
- Cooper WO, Hernandez-Diaz S, Arbogast PG, et al. Major congenital malformations after first-trimester exposure to ACE inhibitors. N Engl J Med. 2006; 354(23):2442-2451.
- American Academy of Pediatrics Committee on Drugs. Transfer of drugs and other chemicals into human milk. Pediatrics. 2001;108(3):776-789.
- Papanna R, Mann LK, Kouides RW, Glantz JC. Protein/creatinine ratio in preeclampsia: a systematic review. Obstet Gynecol. 2008;112(1):135-144.
- Askie LM, Duley L, Henderson-Smart DJ, Stewart LA, PARIS Collaborative group. Antiplatelet agents for prevention of pre-eclampsia: a meta-analysis of individual patient data. Lancet. 2007;369(9575): 1791-1798.
Case
You are consulted on a 29-year-old gravida 1 at nine weeks gestation with a two-year history of Type 2 diabetes and hypertension. She is admitted to the obstetric inpatient service for glycemic control. Although prescribed metformin and lisinopril, she ran out of both four months ago. Her current hemoglobin A1C is 9%. Her blood pressure is 140/90 mmHg in both arms, with an appropriately sized manual cuff while seated. She does not have retinopathy, nephropathy, or neuropathy. The obstetric team will begin weight-based insulin to achieve glycemic targets, and they ask for your input regarding blood-pressure management. How should one approach a pregnant patient with hypertension?
Overview
The most common chronic medical issue in reproductive-age women, essential hypertension (termed chronic hypertension in obstetric literature) contributes significantly to maternal and perinatal morbidity and mortality, primarily via increased risk of preeclampsia.
Chronic hypertension complicates up to 5% of pregnancies in the U.S., or as many as 120,000 pregnant women per year.1 Rates of chronic hypertension are expected to increase with later childbearing and increased rate of obesity. Prior to and during pregnancy, hypertension is defined as blood pressure 140/90 mmHg or higher. Chronic hypertension can be either hypertension diagnosed prior to pregnancy or elevated blood pressures identified prior to 20 weeks gestation.2 Normal pregnancy physiology leads to decreased systemic vascular resistance by the end of the first trimester, dropping systolic and diastolic blood pressure between 10 and 15 mmHg, with maximal effect mid-pregnancy followed by a gradual return to baseline.3 Therefore, chronic hypertension might be masked in early pregnancy. Normal changes in pregnancy include renal vasodilatation and increased glomerular filtration rate, so the average serum creatinine (SCr) is 0.5 mg/dL.4
Newly identified hypertension or accelerating hypertension after 20 weeks warrants close evaluation for preeclampsia. Preeclampsia is a multisystem, life-threatening disorder characterized by hypertension and proteinuria (greater than 300 mg/day). Severe forms of preeclampsia include HELLP (hemolysis, elevated liver enzymes and low platelets) syndrome and eclampsia (seizures with no other attributable cause). Superimposed preeclampsia occurs in 20% to 25% of women with chronic hypertension.5 Women with hypertensive target organ damage have an even greater likelihood of preeclampsia as well as maternal and fetal complications. Unfortunately, blood-pressure control during pregnancy has not been shown to minimize the likelihood of developing superimposed preeclampsia or associated maternal and fetal complications.6 The goal of antihypertensive management during pregnancy is to avoid acute maternal or fetal complications of severe hypertension.
Review of the Data
Q: How are hypertensive disorders of pregnancy classified?
The American College of Obstetrics and Gynecology and the National High Blood Pressure Education Program guideline committees have classified hypertensive disorders of pregnancy into four categories: chronic hypertension, preeclampsia, preeclampsia superimposed on chronic hypertension, and gestational hypertension.2,7
Chronic hypertension is defined as blood pressure 140/90 mmHg or greater on two occasions before pregnancy, prior to 20 weeks of gestation, or persisting 12 weeks postpartum. Severe hypertension is defined as diastolic blood pressure ≥110 mm Hg. Hypertensive women tend to have a greater decline in blood pressure during early pregnancy than normotensive women.8
Secondary hypertension is an important consideration in women of reproductive age. A brief screen for secondary causes includes bilateral arm pressures and femoral pulse assessment, renal bruit assessment, inquiry into snoring, gasping, and daytime somnolence, as well as measurement of serum thyrotropin, potassium, calcium, creatinine, and urinalysis. This kind of evaluation will assess for coarctation of the aorta, renal artery stenosis, obstructive sleep apnea, hyper- or hypothyroidism, hyperaldosteronism, hyperparathyroidism, and underlying renal disease.9,10 Patient reports of episodic headache, palpitations, and diaphoresis should prompt investigation for pheochromocytoma.
Hyperaldosteronism, pheochromocytoma, or hyperthyroidism might be quiescent during pregnancy but flare in the postpartum period.
Women with severe chronic hypertension or target organ damage have higher rates of superimposed preeclampsia. In these individuals, preeclampsia is more likely to present early (before 34 weeks gestation) or with severe disease.1
Preeclampsia is defined as hypertension and proteinuria (greater than 300 mg/day) at or beyond 20 weeks gestation in a previously normotensive woman. Preeclampsia rates vary from 5% to 10% of nulliparous women, to much higher rates in women with medical comorbidities or fetal factors (e.g., multiple gestations, molar pregnancies, hydrops, or triploidy). Preeclampsia’s pathogenesis is attributed to abnormal placental implantation with abnormal maternal immune adaptation, altered angiogenic factors with increased systemic vascular resistance and endothelial dysfunction leading to the clinically apparent maternal syndrome.11
Severe preeclampsia criteria include any of the following: eclampsia, HELLP syndrome (platelets less than 100,000/mm³, transaminases more than twice the upper limit of normal, and/or epigastric pain), SBP ≥160 mmHg, DBP ≥110 mmHg, proteinuria ≥5 grams per day, oliguria, pulmonary edema, placental abruption, or fetal manifestations such as intrauterine growth restriction (≤10th percentile of expected fetal weight based on gestational age), decreased amniotic fluid index, or fetal demise.2,5,12
Maternal symptoms might include headache, visual disturbances, epigastric or right upper quadrant (RUQ) pain, rapid weight gain, and severe edema. Some women remain asymptomatic. Preeclampsia can rapidly progress from “less severe” to severe. Maternal symptoms and abnormal lab findings are more predictive of adverse pregnancy outcomes than the degree of hypertension and/or proteinuria.1
It is always in the mother’s interest to deliver when preeclampsia is diagnosed, because preeclampsia will not resolve until after delivery, with hypertension and lab abnormalities sometimes persisting for months postpartum. Preeclampsia might be diagnosed before fetal viability (approximately 24 weeks gestation), although the vast majority of cases occur near term.
Risks of premature delivery must be balanced with the risks of progressively severe manifestations for the mother and fetus. Guidelines for expectant management of early (<34 weeks) preeclampsia are based on available evidence and expert opinion.13 Magnesium sulfate has been shown to be the most effective agent to minimize the likelihood of seizure in preeclamptic women.14 With an initial bolus of 4 g to 6 g IV followed by infusion of 1-2 g/hour, magnesium sulfate is usually continued for 24 to 48 hours after delivery.
Preeclampsia can first appear postpartum, most likely in the first days to weeks. A growing body of literature links preeclampsia, particularly early and/or recurrent, to subsequent increased risk for cardiovascular disease and end-stage renal disease.15
Preeclampsia superimposed on chronic hypertension is defined as the new onset or markedly increasing proteinuria or accelerating hypertension in the latter half of pregnancy. Maternal symptoms, transaminase elevation, thrombocytopenia, or fetal manifestations further support this diagnosis.
Gestational hypertension, previously known as pregnancy-induced hypertension, is defined as hypertension in the absence of proteinuria in the latter half of pregnancy. Symptoms and lab abnormalities of preeclampsia will be absent. At least half of women with hypertension in the latter half of pregnancy progress to preeclampsia, so gestational hypertension should be considered a provisional diagnosis. Severe gestational hypertension, even without proteinuria or other lab abnormalities, carries increased perinatal risk.
Q: What factors contribute to increased preeclampsia risk?
Maternal factors include: first pregnancy, first pregnancy with a new father, maternal age >35, particularly >40, personal or family history of preeclampsia, chronic hypertension, diabetes mellitus (Type 1, 2 or gestational), systemic lupus erythematosus, antiphospholipid antibody syndrome, renal disease, and obesity. Fetal factors include: multiple gestations, molar pregnancies, hydrops, and triploidy.5,12
Q: When should antihypertensive medications be used in pregnancy?
Most women are hesitant to expose their fetus to medication, and thus must be in therapeutic alliance with their obstetrician and consultants. The overriding principle of medication use in pregnancy is that a healthy fetus requires a healthy mother, and medication use is justified when there is definite benefit to the mother. Due to increased metabolism during pregnancy, medications otherwise dosed once per day often require two doses per day, and those dosed twice daily often require every-eight-hour dosing to maintain efficacy. Additionally, titration up every few days may be required.
Therapy goals include avoiding maternal and fetal complications from severely elevated blood pressure, as well as avoiding fetal growth restriction due to impaired uteroplacental flow. The ideal blood pressure for a hypertensive pregnant woman has not been established, but recommendations are based upon available data and expert opinion.2,5,10,12 Maternal risk of intracerebral hemorrhage increases with SBP ≥160 mmHg.16 Diastolic BP ≥110 mmHg has been associated with greater risk of placental abruption and intrauterine growth restriction.
Pharmacologic treatment generally is initiated or adjusted to achieve SBP <160 mm Hg and DBP <100 to <105 mmHg, although some societies advocate treatment initiation at 140/90 mmHg.2,5,12,17,18 If a woman has target organ damage or concomitant medical issues warranting tighter control (e.g., diabetes or pre-existing renal disease), 130/80 mmHg is preferable.19 Activity limitation and/or bed rest, although commonly recommended, have not been shown to reduce maternal or fetal morbidity or mortality, or prolong time to delivery.
An ongoing, randomized, prospective trial will compare maternal and fetal outcomes in women with mild chronic hypertension with deliberate blood-pressure stratification (goal DBP 85 mmHg vs. goal DBP 100 mmHg).20
Q: What are reasonable treatment options for a woman with chronic hypertension during pregnancy?
Due to vasodilatation of pregnancy, antihypertensive agents often can be discontinued early in pregnancy with close, ongoing monitoring. The majority of women with mild chronic hypertension will have blood pressures <160/100 mmHg without medication during the first half of pregnancy.
If a woman has been using a pharmacologic agent not advisable during pregnancy, she could be switched to a preferred agent. If a woman has been using a pharmacologic agent preferred during pregnancy, she could continue this agent.
Q: What antihypertensives are favored during pregnancy?
Methyldopa and labetalol have been used extensively. Methyldopa has not been found to adversely affect cognitive development in children exposed in utero. On the maternal side, somnolence, dizziness, and dry mouth are common side effects.
Labetalol is widely used as a first- or second-line agent. It can be used intravenously or orally. Intravenous labetalol in escalating doses (10 mg, 20 mg, 40 mg, 80 mg) is the first line of acute treatment for severe hypertension/preeclampsia.
Atenolol and propranolol have been associated with fetal growth restriction, metoprolol to a lesser degree.
Metoprolol is useful in women with coronary artery disease, tachyarrhythmias, and/or requiring migraine prophylaxis during pregnancy.
Nifedipine is often used as a second-line agent, with extended-release preparation preferred. Short-acting nifedipine should be used with caution during pregnancy due to the potential for acute impairment of uteroplacental flow. However, short-acting nifedipine is used for tocolysis in pre-term labor.
Intravenous hydralazine is another option for acute treatment in the setting of severe hypertension/preeclampsia.
Angiotensin-converting enzyme (ACE) inhibitors are contraindicated during pregnancy due to association with increased rates of cardiovascular and central nervous system malformations when used in the first trimester, as well as fetal anuric renal failure when used later in pregnancy.21 Due to similar mechanisms of action, angiotensin receptor blockers (ARBs) are contraindicated.
In general, antihypertensive agents are considered compatible with lactation, with most minimally excreted into breast milk. Women requiring antihypertensive agents or almost any medication during lactation seek particular reassurance from caregivers.
It is essential to emphasize the benefit of breastfeeding for both mother and newborn, which far outweighs the risk of medication exposure to the newborn—with rare exceptions. Enalapril and captopril are considered compatible with breastfeeding by the American Academy of Pediatrics.22
Q: Can we identify and possibly prevent preeclampsia?
Escalating hypertension or maternal symptoms, especially in women with increased risk factors, warrant careful examination and laboratory assessment for preeclampsia. Physical findings may include retinal vasospasm, rales on pulmonary exam, cardiac gallop, RUQ or midepigastric tenderness from hepatic capsule stretching, nondependent edema (e.g., face, hands), or clonus on deep tendon reflex evaluation. Useful laboratory values include complete blood count, serum creatinine, hepatic transaminases, uric acid, and urinalysis.
Marked anemia or hemoconcentration, thrombocytopenia, SCr ≥0.8 mg/dL, transaminases above normal, uric acid ≥5.0 mg/dL, urine protein 1+ or greater on dipstick, are all suggestive of preeclampsia, particularly if worsened compared to prior values. Urine protein-to-creatinine ratios have not reliably correlated with 24-hour urine protein collections in preeclamptic patients, although very high or low values could be helpful.23
Women are typically admitted for fetal monitoring, 24-hour urine protein collection, and blood-pressure management during a preeclampsia evaluation.
Thus far, the only intervention shown to reduce the likelihood of preeclampsia in women at increased risk is low-dose aspirin. A recent meta-analysis noted 10% reduction of relative risk of preeclampsia and pre-term birth prior to 34 weeks in women with history of preeclampsia treated with aspirin from the second trimester onward.24 Other interventions in trials that have not displayed reduced risk include vitamin C, vitamin E, calcium, fish oil, zinc, magnesium, and antihypertensive therapy.
Back to the Case
Our patient has chronic hypertension and diabetes, so she should have a blood-pressure goal of <130/80 mmHg. She could be initiated on methyldopa or labetalol. She should have a screen for secondary hypertension via exam and serum thyrotropin, potassium, and calcium, as well as baseline “preeclampsia labs”: complete blood count, serum creatinine, transaminases, uric acid, and 24-hour urine protein assessment. Aspirin at 81 mg daily should be considered from 12 weeks gestation to delivery.
Glycemic control is critical in early gestation to avoid increased risk for congenital malformations and spontaneous abortion, and later on to minimize macrosomia. Close monitoring for maternal symptoms of preeclampsia and blood-pressure assessment is advisable. With medical comorbidities of hypertension and diabetes mellitus, the woman’s risk of preeclampsia is at least 25%. Her pregnancy dating should be confirmed by a first-trimester ultrasound.
Bottom Line
A pregnant woman with chronic hypertension should have evaluation for secondary causes of hypertension, adjustment or initiation of preferred antihypertensive agents to achieve blood pressures that minimize the risk for acute hypertensive complications and fetal growth impairment, and close monitoring for superimposed preeclampsia. TH
Dr. Hayes is an obstetric internist at Women & Infants’ Hospital and assistant professor of medicine (clinical) at the Warren Alpert Medical School of Brown University, Providence, R.I.
References
- Sibai BM. Caring for women with hypertension in pregnancy. JAMA. 2007;298(13):1566-1568.
- Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. Am J Obstet Gynecol. 2000;183:S1-S22.
- Christianson RE. Studies on blood pressure during pregnancy. I. Influence of parity and age. Am J Obstet Gynecol. 1976;125(4):509-513.
- Gibson P, Rosene-Montella K. Normal renal and vascular changes in pregnancy. In: Rosene-Montella K, Keely E, Barbour LA, Lee RV, eds. Medical Care of the Pregnant Patient. 2nd ed. Philadelphia: American College of Physicians; 2008:149-152.
- ACOG practice bulletin, No. 33, January 2002. Diagnosis and management of preeclampsia and eclampsia. Obstet Gynecol. 2002;99(1):159-167.
- Sibai BM. Chronic hypertension in pregnancy. Obstet Gynecol. 2002;100(2):369-377.
- Mulrow CD, Chiquette E, Ferrer RL, et al. Management of Chronic Hypertension During Pregnancy. Rockville: Agency for Healthcare Research and Quality; 2000.
- Pickering TG, Hall JE, Appel LJ, et al. Recommendations for blood pressure measurement in humans and experimental animals: part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Prof-essional and Public Education of the American Heart Association Council on high blood pressure Research. Circulation. 2005;111(5):697-716.
- Powrie RO. A 30-year-old woman with chronic hypertension trying to conceive. JAMA. 2007; 298(13):1548-1558.
- Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003:289(19):2560-2571.
- Widmer M, Villar J, Benigni A, Conde-Agudelo A, Karumanchi SA, Lindheimer M. Mapping the theories of preeclampsia and the role of angiogenic factors: a systematic review. Obstet Gynecol. 2007; 109(1):168-180.
- Magee LA, Helewa M, Moutquin JM, van Dadelszen P. Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy. SOGC Clinical Practice Guideline. J Obstet Gynaecol Can. 2008; 30:S1-S48.
- Sibai BM, Barton JR. Expectant management of severe preeclampsia remote from term: patient selection, treatment, and delivery indications. Am J Obstet Gynecol. 2007;196(6):514.e1-514.e1-9.
- Duley L, Gülmezoglu AM, Henderson-Smart DJ. Magnesium sulphate and other anticonvulsants for women with preeclampsia. Cochrane Database Syst Rev. 2003;(2):CD000025.
- McDonald SD, Malinowski A, Zhou Q, Yusuf S, Devereaux PJ. Cardiovascular sequelae of preeclampsia/eclampsia: a systematic review and meta-analyses. Am Heart J. 2008;156(5):918-930.
- Martin JN Jr., Thigpen BD, Moore RC, Rose CH, Cushman J, May W. Stroke and severe preeclampsia and eclampsia: a paradigm shift focusing on systolic blood pressure. Obstet Gynecol. 2005;105(2): 246-254.
- Lindheimer MD, Taler SJ, Cunningham FG. Hyper-tension in pregnancy. J Am Soc Hypertens. 2008; 2(6):484-494.
- Podymow T, August P. Update on the use of antihypertensive drugs in pregnancy. Hypertension. 2008; 51(4):960-969.
- Kitzmiller JL, Block JM, Brown FM, et al. Managing preexisting diabetes for pregnancy: summary of evidence and consensus recommendations for care. Diabetes Care. 2008;31(5):1060-1079.
- Magee LA, von Dadelszen P, Chan S, et al. The Control of Hypertension In Pregnancy Study pilot trial. BJOG. 2007;114(6):770,e13-e20.
- Cooper WO, Hernandez-Diaz S, Arbogast PG, et al. Major congenital malformations after first-trimester exposure to ACE inhibitors. N Engl J Med. 2006; 354(23):2442-2451.
- American Academy of Pediatrics Committee on Drugs. Transfer of drugs and other chemicals into human milk. Pediatrics. 2001;108(3):776-789.
- Papanna R, Mann LK, Kouides RW, Glantz JC. Protein/creatinine ratio in preeclampsia: a systematic review. Obstet Gynecol. 2008;112(1):135-144.
- Askie LM, Duley L, Henderson-Smart DJ, Stewart LA, PARIS Collaborative group. Antiplatelet agents for prevention of pre-eclampsia: a meta-analysis of individual patient data. Lancet. 2007;369(9575): 1791-1798.
Investigate Claim Denials
In order to recover the appropriate payment for services provided by hospitalists, the following must occur:
- The billing provider renders service fully, or jointly with a resident under the teaching physician guidelines or nonphysician provider under the shared/split billing rules;
- The service is completely and accurately documented in the medical record;
- The correct information is entered on the claim form that is submitted to the payor; and
- The service is determined to be a covered benefit and eligible for payment.
Claims frequently are rejected or denied. Even more frequently, the physician or billing staff does not understand the reason for the denial. The typical reaction to claim denial is twofold: “appeal with paper” and “write off.” In other words, send a copy of the physician notes to the payor and consider the claim unsuccessful and payment unable to be obtained.
Examining and understanding the payor’s initial claim determination might prompt a more successful response. Presuming the patient demographics are entered without error, the insurance information is correct, the patient is eligible for coverage, and all precertifications and authorizations were obtained, check for these other common errors.
Medical Necessity
Denials for “medical necessity” are not always what they seem. Individuals often assume that the physician reported an incorrect diagnosis code. Consider the service/procedure code when trying to formulate a response to the denial. When dealing with procedure codes, it is likely the denial is received for a mismatched diagnosis.
For example, a payor might deny a claim for cardiopulmonary resuscitation (92950) that is associated with a diagnosis code of congestive heart failure (428.0), despite this being the underlying condition that prompted the decline in the patient’s condition. The payor might only accept “cardiac arrest” (427.5) as the diagnosis for cardiopulmonary resuscitation because it was the direct reason for the procedure. After you ensure that the documentation supports the diagnosis, the claim should be resubmitted with the corrected diagnosis code.
If the “medical necessity” denial involves a covered evaluation and management (E/M) visit, it is less likely that the diagnosis code is the issue. When dealing with Medicare in particular, this type of denial likely is the result of a failure to respond to a prepayment request for documentation. Medicare issues prepayment requests for documentation for the following inpatient CPT codes: 99255, 99254, 99233, 99232, 99223, 99239, and 99292. If the documentation isn’t provided to the Medicare review department within the designated time frame, the claim is automatically denied. The reason for denial is cited as “not deemed a medical necessity.” Some providers misunderstand this remittance remark and assume that the physician assigned an incorrect diagnosis code. Although that might be true, it probably is due to a failure to respond to the prepayment documentation request. Appealing these claims requires the submission of documentation to the Medicare appeals department. Once the supporting documentation is reviewed, reimbursement is granted.
Bundling
The National Correct Coding Initiative (NCCI) identifies edits that ultimately affect claims submission and payment. The Column One/Column Two Correct Coding Edits and the Mutually Exclusive Edits list code pairs that should not be reported together on the same date by either a single physician or physicians of the same specialty within a provider group. Under some well-documented circumstances, the physician is allowed to “unbundle” the services by appending the appropriate modifier.
When services are denied as being “incidental/integral” to another reimbursed service (e.g., bundled), the claim should not automatically be resubmitted with a modifier appended to the “bundled” procedure code.
Documentation should be reviewed to determine if the denied service is separately reportable from the paid service. Only when supported by documentation can the physician append the appropriate modifier and resubmit the claim. For example, a hospitalist evaluated a patient with congestive heart failure and pleural effusions. The hospitalist determined that the patient requires placement of a central venous catheter (36556). Because the patient’s underlying condition was evaluated and resulted in the decision to place a central venous catheter, both the visit (99233) and the procedure (36556) can be reported. If submitted without modifiers, some payors may deny payment for the visit because it was not “integral” to the catheter placement. You should resubmit those claims with modifier 25.
Place of Service
Ensure that the place of service (POS) matches the service/procedure code. For example, say a hospitalist performs a consultation in the ED and determines that the patient does not need to be treated as an inpatient but provides recommendations for ED care and outpatient followup. Avoid a mismatch of the service code and the location. Consults performed in the ED should be reported with outpatient consultation codes (99241-99245) as appropriate. The correct POS should be the ED, not the inpatient hospital. Reporting outpatient codes with an inpatient POS (e.g., 21: inpatient hospital, 31: skilled nursing facility) will result in claim denial.
The same is true when trying to report inpatient consultation codes (99251-99255) in an outpatient location (e.g., 23-ED). The appropriate response for this type of denial is to resubmit the claim with the correct the POS and service/procedure code. A complete list of POS codes and corresponding definitions can be found in Chapter 26, Section 10.5 of the Medicare Claims Processing Manual, available at www.cms.hhs.gov/manuals/downloads/clm104c26.pdf.
Provider Enrollment
Provider enrollment issues occur when a physician’s national provider identifier (NPI) is not properly linked to the group practice. More often than not, the group practice receives claim rejections for enrollment issues when services involve nurse practitioners or physician assistants who have not enrolled with Medicare or cannot enroll with non-Medicare payors.
For example, a nurse practitioner independently provides a subsequent hospital-care service (e.g., 99232). The claim is submitted and Medicare reimburses the service at the correct amount as a primary insurer. The remaining balance is submitted to the secondary insurer. Because the submitted claim identifies the service provider as a nonphysician provider, who likely is not enrolled with the non-Medicare payor, the claim is rejected.
If the physician group has a contractual agreement to recognize nonphysician provider services by reporting them under the collaborating physician’s name, the claim can be resubmitted in the physician’s name. In absence of such an agreement, the claim should be written off. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty of SHM’s inpatient coding course.
Reference
- Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2008.
In order to recover the appropriate payment for services provided by hospitalists, the following must occur:
- The billing provider renders service fully, or jointly with a resident under the teaching physician guidelines or nonphysician provider under the shared/split billing rules;
- The service is completely and accurately documented in the medical record;
- The correct information is entered on the claim form that is submitted to the payor; and
- The service is determined to be a covered benefit and eligible for payment.
Claims frequently are rejected or denied. Even more frequently, the physician or billing staff does not understand the reason for the denial. The typical reaction to claim denial is twofold: “appeal with paper” and “write off.” In other words, send a copy of the physician notes to the payor and consider the claim unsuccessful and payment unable to be obtained.
Examining and understanding the payor’s initial claim determination might prompt a more successful response. Presuming the patient demographics are entered without error, the insurance information is correct, the patient is eligible for coverage, and all precertifications and authorizations were obtained, check for these other common errors.
Medical Necessity
Denials for “medical necessity” are not always what they seem. Individuals often assume that the physician reported an incorrect diagnosis code. Consider the service/procedure code when trying to formulate a response to the denial. When dealing with procedure codes, it is likely the denial is received for a mismatched diagnosis.
For example, a payor might deny a claim for cardiopulmonary resuscitation (92950) that is associated with a diagnosis code of congestive heart failure (428.0), despite this being the underlying condition that prompted the decline in the patient’s condition. The payor might only accept “cardiac arrest” (427.5) as the diagnosis for cardiopulmonary resuscitation because it was the direct reason for the procedure. After you ensure that the documentation supports the diagnosis, the claim should be resubmitted with the corrected diagnosis code.
If the “medical necessity” denial involves a covered evaluation and management (E/M) visit, it is less likely that the diagnosis code is the issue. When dealing with Medicare in particular, this type of denial likely is the result of a failure to respond to a prepayment request for documentation. Medicare issues prepayment requests for documentation for the following inpatient CPT codes: 99255, 99254, 99233, 99232, 99223, 99239, and 99292. If the documentation isn’t provided to the Medicare review department within the designated time frame, the claim is automatically denied. The reason for denial is cited as “not deemed a medical necessity.” Some providers misunderstand this remittance remark and assume that the physician assigned an incorrect diagnosis code. Although that might be true, it probably is due to a failure to respond to the prepayment documentation request. Appealing these claims requires the submission of documentation to the Medicare appeals department. Once the supporting documentation is reviewed, reimbursement is granted.
Bundling
The National Correct Coding Initiative (NCCI) identifies edits that ultimately affect claims submission and payment. The Column One/Column Two Correct Coding Edits and the Mutually Exclusive Edits list code pairs that should not be reported together on the same date by either a single physician or physicians of the same specialty within a provider group. Under some well-documented circumstances, the physician is allowed to “unbundle” the services by appending the appropriate modifier.
When services are denied as being “incidental/integral” to another reimbursed service (e.g., bundled), the claim should not automatically be resubmitted with a modifier appended to the “bundled” procedure code.
Documentation should be reviewed to determine if the denied service is separately reportable from the paid service. Only when supported by documentation can the physician append the appropriate modifier and resubmit the claim. For example, a hospitalist evaluated a patient with congestive heart failure and pleural effusions. The hospitalist determined that the patient requires placement of a central venous catheter (36556). Because the patient’s underlying condition was evaluated and resulted in the decision to place a central venous catheter, both the visit (99233) and the procedure (36556) can be reported. If submitted without modifiers, some payors may deny payment for the visit because it was not “integral” to the catheter placement. You should resubmit those claims with modifier 25.
Place of Service
Ensure that the place of service (POS) matches the service/procedure code. For example, say a hospitalist performs a consultation in the ED and determines that the patient does not need to be treated as an inpatient but provides recommendations for ED care and outpatient followup. Avoid a mismatch of the service code and the location. Consults performed in the ED should be reported with outpatient consultation codes (99241-99245) as appropriate. The correct POS should be the ED, not the inpatient hospital. Reporting outpatient codes with an inpatient POS (e.g., 21: inpatient hospital, 31: skilled nursing facility) will result in claim denial.
The same is true when trying to report inpatient consultation codes (99251-99255) in an outpatient location (e.g., 23-ED). The appropriate response for this type of denial is to resubmit the claim with the correct the POS and service/procedure code. A complete list of POS codes and corresponding definitions can be found in Chapter 26, Section 10.5 of the Medicare Claims Processing Manual, available at www.cms.hhs.gov/manuals/downloads/clm104c26.pdf.
Provider Enrollment
Provider enrollment issues occur when a physician’s national provider identifier (NPI) is not properly linked to the group practice. More often than not, the group practice receives claim rejections for enrollment issues when services involve nurse practitioners or physician assistants who have not enrolled with Medicare or cannot enroll with non-Medicare payors.
For example, a nurse practitioner independently provides a subsequent hospital-care service (e.g., 99232). The claim is submitted and Medicare reimburses the service at the correct amount as a primary insurer. The remaining balance is submitted to the secondary insurer. Because the submitted claim identifies the service provider as a nonphysician provider, who likely is not enrolled with the non-Medicare payor, the claim is rejected.
If the physician group has a contractual agreement to recognize nonphysician provider services by reporting them under the collaborating physician’s name, the claim can be resubmitted in the physician’s name. In absence of such an agreement, the claim should be written off. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty of SHM’s inpatient coding course.
Reference
- Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2008.
In order to recover the appropriate payment for services provided by hospitalists, the following must occur:
- The billing provider renders service fully, or jointly with a resident under the teaching physician guidelines or nonphysician provider under the shared/split billing rules;
- The service is completely and accurately documented in the medical record;
- The correct information is entered on the claim form that is submitted to the payor; and
- The service is determined to be a covered benefit and eligible for payment.
Claims frequently are rejected or denied. Even more frequently, the physician or billing staff does not understand the reason for the denial. The typical reaction to claim denial is twofold: “appeal with paper” and “write off.” In other words, send a copy of the physician notes to the payor and consider the claim unsuccessful and payment unable to be obtained.
Examining and understanding the payor’s initial claim determination might prompt a more successful response. Presuming the patient demographics are entered without error, the insurance information is correct, the patient is eligible for coverage, and all precertifications and authorizations were obtained, check for these other common errors.
Medical Necessity
Denials for “medical necessity” are not always what they seem. Individuals often assume that the physician reported an incorrect diagnosis code. Consider the service/procedure code when trying to formulate a response to the denial. When dealing with procedure codes, it is likely the denial is received for a mismatched diagnosis.
For example, a payor might deny a claim for cardiopulmonary resuscitation (92950) that is associated with a diagnosis code of congestive heart failure (428.0), despite this being the underlying condition that prompted the decline in the patient’s condition. The payor might only accept “cardiac arrest” (427.5) as the diagnosis for cardiopulmonary resuscitation because it was the direct reason for the procedure. After you ensure that the documentation supports the diagnosis, the claim should be resubmitted with the corrected diagnosis code.
If the “medical necessity” denial involves a covered evaluation and management (E/M) visit, it is less likely that the diagnosis code is the issue. When dealing with Medicare in particular, this type of denial likely is the result of a failure to respond to a prepayment request for documentation. Medicare issues prepayment requests for documentation for the following inpatient CPT codes: 99255, 99254, 99233, 99232, 99223, 99239, and 99292. If the documentation isn’t provided to the Medicare review department within the designated time frame, the claim is automatically denied. The reason for denial is cited as “not deemed a medical necessity.” Some providers misunderstand this remittance remark and assume that the physician assigned an incorrect diagnosis code. Although that might be true, it probably is due to a failure to respond to the prepayment documentation request. Appealing these claims requires the submission of documentation to the Medicare appeals department. Once the supporting documentation is reviewed, reimbursement is granted.
Bundling
The National Correct Coding Initiative (NCCI) identifies edits that ultimately affect claims submission and payment. The Column One/Column Two Correct Coding Edits and the Mutually Exclusive Edits list code pairs that should not be reported together on the same date by either a single physician or physicians of the same specialty within a provider group. Under some well-documented circumstances, the physician is allowed to “unbundle” the services by appending the appropriate modifier.
When services are denied as being “incidental/integral” to another reimbursed service (e.g., bundled), the claim should not automatically be resubmitted with a modifier appended to the “bundled” procedure code.
Documentation should be reviewed to determine if the denied service is separately reportable from the paid service. Only when supported by documentation can the physician append the appropriate modifier and resubmit the claim. For example, a hospitalist evaluated a patient with congestive heart failure and pleural effusions. The hospitalist determined that the patient requires placement of a central venous catheter (36556). Because the patient’s underlying condition was evaluated and resulted in the decision to place a central venous catheter, both the visit (99233) and the procedure (36556) can be reported. If submitted without modifiers, some payors may deny payment for the visit because it was not “integral” to the catheter placement. You should resubmit those claims with modifier 25.
Place of Service
Ensure that the place of service (POS) matches the service/procedure code. For example, say a hospitalist performs a consultation in the ED and determines that the patient does not need to be treated as an inpatient but provides recommendations for ED care and outpatient followup. Avoid a mismatch of the service code and the location. Consults performed in the ED should be reported with outpatient consultation codes (99241-99245) as appropriate. The correct POS should be the ED, not the inpatient hospital. Reporting outpatient codes with an inpatient POS (e.g., 21: inpatient hospital, 31: skilled nursing facility) will result in claim denial.
The same is true when trying to report inpatient consultation codes (99251-99255) in an outpatient location (e.g., 23-ED). The appropriate response for this type of denial is to resubmit the claim with the correct the POS and service/procedure code. A complete list of POS codes and corresponding definitions can be found in Chapter 26, Section 10.5 of the Medicare Claims Processing Manual, available at www.cms.hhs.gov/manuals/downloads/clm104c26.pdf.
Provider Enrollment
Provider enrollment issues occur when a physician’s national provider identifier (NPI) is not properly linked to the group practice. More often than not, the group practice receives claim rejections for enrollment issues when services involve nurse practitioners or physician assistants who have not enrolled with Medicare or cannot enroll with non-Medicare payors.
For example, a nurse practitioner independently provides a subsequent hospital-care service (e.g., 99232). The claim is submitted and Medicare reimburses the service at the correct amount as a primary insurer. The remaining balance is submitted to the secondary insurer. Because the submitted claim identifies the service provider as a nonphysician provider, who likely is not enrolled with the non-Medicare payor, the claim is rejected.
If the physician group has a contractual agreement to recognize nonphysician provider services by reporting them under the collaborating physician’s name, the claim can be resubmitted in the physician’s name. In absence of such an agreement, the claim should be written off. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty of SHM’s inpatient coding course.
Reference
- Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2008.
Pharma Pledges Price Cut
The June 22 announcement of an $80 billion deal to help reduce out-of-pocket drug costs for Medicare beneficiaries has elicited mixed reactions on what it might mean for patients, and calls for hospitalists to remain vigilant about prescription drug expenses.
Under a pledge negotiated with the White House and congressional Democrats, the pharmaceutical industry has promised a 50% discount for name-brand drugs to beneficiaries stuck in the notorious gap of the Medicare Part D prescription drug plan, commonly called the “doughnut hole” (see “Beware the Doughnut Hole,” June 2009, p. 1) In 2009, the gap in coverage kicks in after $2,700 in total drug costs and persists until $6,154 in total costs, by which point patients have spent as much as $4,350 of their own money for prescription drugs.
President Obama says the gap “has been placing a crushing burden on many older Americans who live on fixed incomes and can’t afford thousands of dollars in out-of-pocket expenses.” The AARP hails the “unique solution” as a “major step forward,” though other industry observers have taken a more circumspect stance and say they want to see tougher cost-control measures in writing.
“You don’t want to look an $80 billion gift horse in the mouth, but there’s some halitosis in this mouth,” says Bill Vaughan, a health policy analyst for Consumers Union in Washington, D.C. “It’s not as pure and altruistic as it seems at first blush, and people need to keep pushing for generics because these [brand-name drugs] are grossly overpriced.”
Under the proposal, the cost for a 30-day supply of the beta-blocker drug carvedilol (Coreg) could be halved, from $142.79 to $71.40, based on Drugstore.com’s current retail prices. Even with the savings, the drug would still cost almost four and a half times more than a generic alternative, metoprolol tartrate (Lopressor), which costs $15.99 for a 30-day supply.
The deal also includes several caveats: The pledge doesn’t address the cost of brand-name drugs before or after the coverage gap, and the doughnut-hole price reduction would go into effect only if Congress enacts healthcare reform legislation.
Battles already are looming over the fight to make generics more accessible and to eliminate the doughnut hole entirely.
“I think the sense is that … everybody is going to have to give back a little bit,” says William D. Atchley Jr., MD, FACP, FHM, chief of the division of hospital medicine for Sentara Medical Group in Norfolk, Va., and a member of SHM’s Public Policy Committee. “This is a different landscape than the early 1990s. … Stakeholders are ready to be proactive and work with people.”
News accounts suggest that the pharmaceutical industry will offer an estimated $30 billion over 10 years toward narrowing the gap, while another $50 billion in concessions still must be worked out. Even so, consumer advocates like Vaughan say the need for hospitalists to help patients avoid unnecessary drug costs remains as high as ever.
Dr. Atchley, a former member of SHM’s board of directors, says hospitalists need to know what’s available in the hospital pharmacy and maintain an open line of communication with their patients in terms of their access and ability to pay for prescriptions.
“You need to understand patients’ economic status. You need to know if they get their medication from Walmart or the [Veterans Affairs] hospital pharmacy,” he says. “Cost is an issue to our Medicare patients, and it’s important to collaborate with them to make sure they can afford the drug. If they can’t, you need to work with them to find another affordable drug that will provide the same benefit.” TH
Bryn Nelson, PhD, is a freelance writer based in Seattle.
The June 22 announcement of an $80 billion deal to help reduce out-of-pocket drug costs for Medicare beneficiaries has elicited mixed reactions on what it might mean for patients, and calls for hospitalists to remain vigilant about prescription drug expenses.
Under a pledge negotiated with the White House and congressional Democrats, the pharmaceutical industry has promised a 50% discount for name-brand drugs to beneficiaries stuck in the notorious gap of the Medicare Part D prescription drug plan, commonly called the “doughnut hole” (see “Beware the Doughnut Hole,” June 2009, p. 1) In 2009, the gap in coverage kicks in after $2,700 in total drug costs and persists until $6,154 in total costs, by which point patients have spent as much as $4,350 of their own money for prescription drugs.
President Obama says the gap “has been placing a crushing burden on many older Americans who live on fixed incomes and can’t afford thousands of dollars in out-of-pocket expenses.” The AARP hails the “unique solution” as a “major step forward,” though other industry observers have taken a more circumspect stance and say they want to see tougher cost-control measures in writing.
“You don’t want to look an $80 billion gift horse in the mouth, but there’s some halitosis in this mouth,” says Bill Vaughan, a health policy analyst for Consumers Union in Washington, D.C. “It’s not as pure and altruistic as it seems at first blush, and people need to keep pushing for generics because these [brand-name drugs] are grossly overpriced.”
Under the proposal, the cost for a 30-day supply of the beta-blocker drug carvedilol (Coreg) could be halved, from $142.79 to $71.40, based on Drugstore.com’s current retail prices. Even with the savings, the drug would still cost almost four and a half times more than a generic alternative, metoprolol tartrate (Lopressor), which costs $15.99 for a 30-day supply.
The deal also includes several caveats: The pledge doesn’t address the cost of brand-name drugs before or after the coverage gap, and the doughnut-hole price reduction would go into effect only if Congress enacts healthcare reform legislation.
Battles already are looming over the fight to make generics more accessible and to eliminate the doughnut hole entirely.
“I think the sense is that … everybody is going to have to give back a little bit,” says William D. Atchley Jr., MD, FACP, FHM, chief of the division of hospital medicine for Sentara Medical Group in Norfolk, Va., and a member of SHM’s Public Policy Committee. “This is a different landscape than the early 1990s. … Stakeholders are ready to be proactive and work with people.”
News accounts suggest that the pharmaceutical industry will offer an estimated $30 billion over 10 years toward narrowing the gap, while another $50 billion in concessions still must be worked out. Even so, consumer advocates like Vaughan say the need for hospitalists to help patients avoid unnecessary drug costs remains as high as ever.
Dr. Atchley, a former member of SHM’s board of directors, says hospitalists need to know what’s available in the hospital pharmacy and maintain an open line of communication with their patients in terms of their access and ability to pay for prescriptions.
“You need to understand patients’ economic status. You need to know if they get their medication from Walmart or the [Veterans Affairs] hospital pharmacy,” he says. “Cost is an issue to our Medicare patients, and it’s important to collaborate with them to make sure they can afford the drug. If they can’t, you need to work with them to find another affordable drug that will provide the same benefit.” TH
Bryn Nelson, PhD, is a freelance writer based in Seattle.
The June 22 announcement of an $80 billion deal to help reduce out-of-pocket drug costs for Medicare beneficiaries has elicited mixed reactions on what it might mean for patients, and calls for hospitalists to remain vigilant about prescription drug expenses.
Under a pledge negotiated with the White House and congressional Democrats, the pharmaceutical industry has promised a 50% discount for name-brand drugs to beneficiaries stuck in the notorious gap of the Medicare Part D prescription drug plan, commonly called the “doughnut hole” (see “Beware the Doughnut Hole,” June 2009, p. 1) In 2009, the gap in coverage kicks in after $2,700 in total drug costs and persists until $6,154 in total costs, by which point patients have spent as much as $4,350 of their own money for prescription drugs.
President Obama says the gap “has been placing a crushing burden on many older Americans who live on fixed incomes and can’t afford thousands of dollars in out-of-pocket expenses.” The AARP hails the “unique solution” as a “major step forward,” though other industry observers have taken a more circumspect stance and say they want to see tougher cost-control measures in writing.
“You don’t want to look an $80 billion gift horse in the mouth, but there’s some halitosis in this mouth,” says Bill Vaughan, a health policy analyst for Consumers Union in Washington, D.C. “It’s not as pure and altruistic as it seems at first blush, and people need to keep pushing for generics because these [brand-name drugs] are grossly overpriced.”
Under the proposal, the cost for a 30-day supply of the beta-blocker drug carvedilol (Coreg) could be halved, from $142.79 to $71.40, based on Drugstore.com’s current retail prices. Even with the savings, the drug would still cost almost four and a half times more than a generic alternative, metoprolol tartrate (Lopressor), which costs $15.99 for a 30-day supply.
The deal also includes several caveats: The pledge doesn’t address the cost of brand-name drugs before or after the coverage gap, and the doughnut-hole price reduction would go into effect only if Congress enacts healthcare reform legislation.
Battles already are looming over the fight to make generics more accessible and to eliminate the doughnut hole entirely.
“I think the sense is that … everybody is going to have to give back a little bit,” says William D. Atchley Jr., MD, FACP, FHM, chief of the division of hospital medicine for Sentara Medical Group in Norfolk, Va., and a member of SHM’s Public Policy Committee. “This is a different landscape than the early 1990s. … Stakeholders are ready to be proactive and work with people.”
News accounts suggest that the pharmaceutical industry will offer an estimated $30 billion over 10 years toward narrowing the gap, while another $50 billion in concessions still must be worked out. Even so, consumer advocates like Vaughan say the need for hospitalists to help patients avoid unnecessary drug costs remains as high as ever.
Dr. Atchley, a former member of SHM’s board of directors, says hospitalists need to know what’s available in the hospital pharmacy and maintain an open line of communication with their patients in terms of their access and ability to pay for prescriptions.
“You need to understand patients’ economic status. You need to know if they get their medication from Walmart or the [Veterans Affairs] hospital pharmacy,” he says. “Cost is an issue to our Medicare patients, and it’s important to collaborate with them to make sure they can afford the drug. If they can’t, you need to work with them to find another affordable drug that will provide the same benefit.” TH
Bryn Nelson, PhD, is a freelance writer based in Seattle.