User login
In the Literature

Semi-Recumbent Position to Prevent Ventilator-Associated Pneumonia: Is It Possible?
By Joseph Ming Wah Li, MD
Van Nieuwenhoven CA, Vandenbroucke-Grauls C, van Tiel FH, et al. Feasibility and effects of the semirecumbent position to prevent ventilator-associated pneumonia: a randomized study. Crit Care Med. 2006 Feb;34(2):396-402.
Ventilator-associated pneumonia (VAP) is a cause of significant morbidity and mortality among mechanically ventilated patients. Studies with radioactive-labeled enteral feeds have demonstrated an increased frequency of endotracheal aspiration of gastric contents in supine patients. The CDC guidelines for prevention of nosocomial pneumonia advise placement of mechanically ventilated patients in a semi-recumbent position as a VAP prevention measure.
Only one previous study, by Drakulovic and colleagues, has assessed this strategy to prevent VAP.1 That study demonstrated a 75% decrease in the incidence of VAP. But van Nieuwenhoven and colleagues raised two important questions about the findings from the previous study: First, the Drakulovic study placed control patients in a horizontal (zero degrees) position, which is not the standard of care in most ICUs. Most patients are placed at 10 degrees, and this position is elevated as patients are weaned. Second, the Drakulovic study measured patients only once daily but did not monitor their body positions in between the daily measurements.
Dr. van Nieuwenhoven and colleagues set out to determine whether it is feasible to keep mechanically ventilated patients in a semi-recumbent position on a continual basis and whether this measure would prevent VAP. This was a prospective multi-centered trial in which mechanically ventilated patients were randomly assigned to the semi-recumbent position with a target backrest elevation of 45 degrees or standard of care (supine position) with a backrest elevation of 10 degrees. They used a transducer with a pendulum, which was placed on the bed frame to measure the backrest elevation every 60 seconds for up to seven days. They calculated a mean degree of elevation for each patient daily. Nurses always respected the patient’s request for positioning, but a dedicated research nurse restored backrest position to the randomized position whenever possible.
Baseline characteristics for both groups were similar. For the supine (control) group, average elevations were 9.8 degrees on day one and 16.1 degrees on day seven. For the semi-recumbent group, average elevations were 28.1 degrees on day one and 22.6 degrees on day seven. There were no significant differences in numbers of patients who developed VAP in either group.
This study suggests that, despite the use of dedicated research nurses to maintain positioning, it may not be possible to keep patients’ backrests elevated to 45 degrees. Keeping patients’ backrests at an elevation of nearly 30 degrees does not appear to prevent VAP more than keeping patients’ backrests at 10 degrees, the present standard of care.
Reference
- Drakulovic MB, Torres A, Bauer TT, et al. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial. Lancet. 1999;354(9193):1851-1858.
Bar Codes in Medicine: An Opportunity for Quality Improvement
By Alex Carbo, MD
Poon EG, Cina JL, Churchill W, et al. Medication dispensing errors and potential adverse drug events before and after implementing bar code technology in the pharmacy. Ann Intern Med. 2006;145:426-434.
Medication errors and adverse drug events (ADEs) have received much attention in the literature; the use of health information technology to mitigate these errors and ADEs has now been proposed in many areas of healthcare. In an effort to decrease medication-dispensing errors, the U.S. Food and Drug Administration (FDA) mandated bar code use for all medications in hospitals, beginning in April 2006. While this technology has been extensively studied in other industries, there is little data describing its effects in the healthcare system.
Poon and colleagues set out to evaluate whether implementation of bar code technology reduced dispensing errors and the ADEs that might be caused by these miscalculations. In a before-and-after evaluation, they studied more than 350,000 dispensed medication doses in an academic medical center between February 2003 and September 2004.
During the bar code conversion process, the hospital pharmacy built a dedicated repackaging center, which was responsible for affixing a bar code to every dose of medication. These medications were then dispensed in three different configurations: two configurations required staff to verify all doses at least once using bar code scanning, and the third configuration—for commonly dispensed medications that could not be accommodated in a standard carousel machine because of their size or need for refrigeration—required scanning only one dose from each batch.
The authors found a 93% to 96% relative reduction in the incidence of target dispensing errors (P<0.001) and an 86% to 97% relative reduction in the incidence of potential ADEs (P<0.001) in the two configurations that required staff to verify all doses by scanning. The greatest reductions were seen in wrong medication errors (56%), wrong strength/dose errors (71%), wrong formulation errors (90%), and expired medication errors (100%).
In the configuration that did not require scanning of every dose, however, there was a 60% relative reduction in the incidence of target dispensing errors (P<0.001), but a 2.4-fold increase in the incidence of target potential ADEs. This included new errors attributable to wrong strength and wrong medication dispensing.
In light of the FDA’s mandate regarding bar codes, it seems that every hospital has the opportunity to improve patient safety and decrease medication error rates with the use of bar code technology. This study suggests that in order to achieve this benefit these systems should be designed to ensure that every medication dose is verified by scanning during the dispensing process.
Evaluation of a Guideline to Guide Resuscitation
By Cindy Lien, MD
Morrison LJ, Visentin LM, Kiss A, et al. Validation of a rule for termination of resuscitation in out-of-hospital cardiac arrest. N Engl J Med. 2006 Aug 3;355(5):478-487.
The survival rate of patients with out-of-hospital cardiac arrest is very low. Thus, guidelines have been developed for termination of resuscitation for those patients who have had no response to advanced cardiac life support provided by emergency medical service (EMS) personnel. Similar guidelines have not yet been developed, however, for situations in which patients receive basic life support from emergency workers trained in the use of an automated external cardiac defibrillator. Patients with little potential for survival are routinely transported to emergency departments, at significant cost to the healthcare system.
Morrison and colleagues present results from the Termination of Resuscitation (TOR) study, a prospective evaluation of a clinical prediction rule for the termination of basic life support by emergency medical personnel trained in the use of automated external defibrillators. The clinical prediction rule, previously developed in a retrospective review of case records from a large urban EMS system, recommends termination of resuscitation if there is no return of spontaneous circulation, no shock administered, and no witness of the arrest by EMS personnel.
In the current study, the authors obtained follow-up data for 1,240 adult patients in Ontario, Canada, who had suffered an arrest of presumed cardiac cause and were subsequently transported to the emergency department after resuscitative efforts. Twenty-four EMS systems participated in the study. The study found that only 0.5% of the patients for whom the clinical prediction rule recommended termination survived (four out of 776 patients). Of the 1,240 total study patients, 41 (3%) survived. The clinical prediction rule recommended continuation of resuscitative efforts for 37 of these 41 patients, resulting in a specificity of 90.2%. The positive predictive value for death was calculated to be 99.5% when termination was recommended.
The TOR trial also determined whether the addition of other criteria to the original prediction rule could further refine the specificity and positive predictive value. They found that the addition to the criteria of a response time greater than eight minutes increased the positive predictive value and specificity to 99.7% and 97.6%, respectively. When the variable “not witnessed by bystander” was added to the clinical prediction rule, both the positive predictive value and specificity increased to 100%. In other words, no patients survived if they had had a completely unwitnessed arrest, no return of spontaneous circulation, and no shocks delivered.
This study identifies a subpopulation of patients with presumed cardiac arrest for whom termination of resuscitative efforts in the field appears reasonable. The authors note that a survival rate of 1% or less has been suggested in past literature as reflective of medical futility. The TOR investigators acknowledge that their study took place before the 2005 AHA Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care were released and that their study protocols were consistent with the 2000 resuscitation guidelines. In light of this information, continued validity testing of the clinical prediction rule under the 2005 AHA protocols is needed.
Nonetheless, it is quite impressive that use of their clinical prediction rule would have resulted in transportation of only 37% of patients (464 of 1,240), rather than 100% of patients, as is currently the practice. If the guidelines described in this article are to be implemented, further studies are necessary to address the training of EMS personnel, who would carry responsibility for terminating resuscitation and notifying families of patients’ deaths.
Prevention of Ventilator-Associated Pneumonia
By Diane Sliwka, MD
Koeman M, van der Ven AJ, Hak E, et al. Oral decontamination with chlorhexidine reduces the incidence of ventilator-associated pneumonia. Am J Respir Crit Care Med. 2006 Jun;173(12):1348-1355. Epub 2006 Apr 7.
Ventilator-associated pneumonia (VAP) is an important nosocomial source of morbidity and mortality. The use of prophylactic antimicrobials to decrease VAP raises concern for antimicrobial resistance. This study evaluates the topical antiseptic chlorhexidine (CHX) as an alternative prophylactic intervention for VAP. CHX has previously been shown to decrease VAP in cardiac surgical patients, but has not been studied in higher risk, long-term-ventilated patients. Because CHX works better for gram-positive organisms, the combination of colistin and CHX (COL + CHX) was also studied for improved gram-negative coverage.
This multi-center, randomized, double-blind, placebo-controlled trial enrolled 385 adult patients. Patients who were expected to be intubated for longer than 48 hours were randomized to 3 arms: CHX alone, CHX + COL, and placebo. Exclusion criteria included known preadmission immunocompromised state, pregnancy, and physical limitation to oral application. Pneumonia was defined by clinical decision-making, which was later confirmed by three blinded intensivists’ reviews of the case records and supported by daily clinical pulmonary infection scores.
The primary endpoint of VAP was diagnosed in 52 of 385 patients: 18% placebo, 13% CHX, and 10% CHX + COL. Rate of VAP in the two treatment groups was lower than placebo and reached statistical significance when compared to placebo. The daily hazard ratio for CHX versus placebo was .352 (95% CI .160, .791); for CHX + COL versus placebo, it was .454 (95% CI .224, .925), showing a 65% and 55% reduction in the rate of pneumonia development. Multivariate analysis of variables such as gender, pulmonary admission diagnosis, colonization at time of admission, and antimicrobial use on admission did not affect the data.
The secondary endpoint of endotracheal colonization was evaluated by a twice-weekly endotracheal culture. There was no statistically significant difference in colonization among the three groups in the first (days 1-4) or third (days 9-12) time frames. During the second time frame (days 5-8), there was a statistically significant decrease in colonization for the CHX + COL treatment group when compared to both placebo (16% versus 40% p<.007) and to CHX (16% versus 38%, p<.011); this decrease is thought to be due to gram-negative coverage by COL.
The secondary endpoint of oropharyngeal colonization was evaluated for 87% of all patient days. CHX and CHX + COL were similarly effective for gram-positive bacteria when compared to placebo, with 30% and 27% reduction in rates of colonization, respectively: HR 0.695 for CHX (95% CI, 0.606, 0.796; p < 0.001) and 0.732 (95% CI, 0.640, 0.838; p < 0.001) for CHX + COL. The CHX + COL combination was more effective for gram-negative bacteria: daily HR .534 (95% CI, 0.455, 0.626; p <0.001) alone with a 47% reduction in gram-negative colonization compared to CHX.
No difference was seen in ICU mortality, duration of mechanical ventilation, or duration of ICU stay. One adverse event (tongue swelling) occurred in the CHX + COL group.
Limitations of the study include the following:
- Daily assessments on all patients were not performed;
- The placebo group had more males and more infections on admission than the other two groups, raising the question of randomization error;
- Clinical versus quantitative diagnosis of pneumonia may overestimate VAP in this study;
- It is not known how many patients were not enrolled in the study due to short anticipated ventilator times, but who later had prolonged ventilations; and
- The lack of effect on ventilator time, ICU length of stay, and mortality raises the question of the significance of these findings.
Despite these limitations, the low cost of these treatments, minimal adverse events, low risk of promoting significant antimicrobial resistance, and the finding of decreased VAP and bacterial colonization risk shown in this study support the potential benefit of topical decontamination with CHX and COL in conjunction with other measures of VAP prevention. TH
Reference
- De Riso AJ II, Ladowski JS, Dillon TA, et al. Chlorhexidine gluconate 0.12% oral rinse reduces the incidence of total nosocomial respiratory infection and nonprophylactic systemic antibiotic use in patients undergoing heart surgery. Chest. 1996;109:1556-1561.
Semi-Recumbent Position to Prevent Ventilator-Associated Pneumonia: Is It Possible?
By Joseph Ming Wah Li, MD
Van Nieuwenhoven CA, Vandenbroucke-Grauls C, van Tiel FH, et al. Feasibility and effects of the semirecumbent position to prevent ventilator-associated pneumonia: a randomized study. Crit Care Med. 2006 Feb;34(2):396-402.
Ventilator-associated pneumonia (VAP) is a cause of significant morbidity and mortality among mechanically ventilated patients. Studies with radioactive-labeled enteral feeds have demonstrated an increased frequency of endotracheal aspiration of gastric contents in supine patients. The CDC guidelines for prevention of nosocomial pneumonia advise placement of mechanically ventilated patients in a semi-recumbent position as a VAP prevention measure.
Only one previous study, by Drakulovic and colleagues, has assessed this strategy to prevent VAP.1 That study demonstrated a 75% decrease in the incidence of VAP. But van Nieuwenhoven and colleagues raised two important questions about the findings from the previous study: First, the Drakulovic study placed control patients in a horizontal (zero degrees) position, which is not the standard of care in most ICUs. Most patients are placed at 10 degrees, and this position is elevated as patients are weaned. Second, the Drakulovic study measured patients only once daily but did not monitor their body positions in between the daily measurements.
Dr. van Nieuwenhoven and colleagues set out to determine whether it is feasible to keep mechanically ventilated patients in a semi-recumbent position on a continual basis and whether this measure would prevent VAP. This was a prospective multi-centered trial in which mechanically ventilated patients were randomly assigned to the semi-recumbent position with a target backrest elevation of 45 degrees or standard of care (supine position) with a backrest elevation of 10 degrees. They used a transducer with a pendulum, which was placed on the bed frame to measure the backrest elevation every 60 seconds for up to seven days. They calculated a mean degree of elevation for each patient daily. Nurses always respected the patient’s request for positioning, but a dedicated research nurse restored backrest position to the randomized position whenever possible.
Baseline characteristics for both groups were similar. For the supine (control) group, average elevations were 9.8 degrees on day one and 16.1 degrees on day seven. For the semi-recumbent group, average elevations were 28.1 degrees on day one and 22.6 degrees on day seven. There were no significant differences in numbers of patients who developed VAP in either group.
This study suggests that, despite the use of dedicated research nurses to maintain positioning, it may not be possible to keep patients’ backrests elevated to 45 degrees. Keeping patients’ backrests at an elevation of nearly 30 degrees does not appear to prevent VAP more than keeping patients’ backrests at 10 degrees, the present standard of care.
Reference
- Drakulovic MB, Torres A, Bauer TT, et al. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial. Lancet. 1999;354(9193):1851-1858.
Bar Codes in Medicine: An Opportunity for Quality Improvement
By Alex Carbo, MD
Poon EG, Cina JL, Churchill W, et al. Medication dispensing errors and potential adverse drug events before and after implementing bar code technology in the pharmacy. Ann Intern Med. 2006;145:426-434.
Medication errors and adverse drug events (ADEs) have received much attention in the literature; the use of health information technology to mitigate these errors and ADEs has now been proposed in many areas of healthcare. In an effort to decrease medication-dispensing errors, the U.S. Food and Drug Administration (FDA) mandated bar code use for all medications in hospitals, beginning in April 2006. While this technology has been extensively studied in other industries, there is little data describing its effects in the healthcare system.
Poon and colleagues set out to evaluate whether implementation of bar code technology reduced dispensing errors and the ADEs that might be caused by these miscalculations. In a before-and-after evaluation, they studied more than 350,000 dispensed medication doses in an academic medical center between February 2003 and September 2004.
During the bar code conversion process, the hospital pharmacy built a dedicated repackaging center, which was responsible for affixing a bar code to every dose of medication. These medications were then dispensed in three different configurations: two configurations required staff to verify all doses at least once using bar code scanning, and the third configuration—for commonly dispensed medications that could not be accommodated in a standard carousel machine because of their size or need for refrigeration—required scanning only one dose from each batch.
The authors found a 93% to 96% relative reduction in the incidence of target dispensing errors (P<0.001) and an 86% to 97% relative reduction in the incidence of potential ADEs (P<0.001) in the two configurations that required staff to verify all doses by scanning. The greatest reductions were seen in wrong medication errors (56%), wrong strength/dose errors (71%), wrong formulation errors (90%), and expired medication errors (100%).
In the configuration that did not require scanning of every dose, however, there was a 60% relative reduction in the incidence of target dispensing errors (P<0.001), but a 2.4-fold increase in the incidence of target potential ADEs. This included new errors attributable to wrong strength and wrong medication dispensing.
In light of the FDA’s mandate regarding bar codes, it seems that every hospital has the opportunity to improve patient safety and decrease medication error rates with the use of bar code technology. This study suggests that in order to achieve this benefit these systems should be designed to ensure that every medication dose is verified by scanning during the dispensing process.
Evaluation of a Guideline to Guide Resuscitation
By Cindy Lien, MD
Morrison LJ, Visentin LM, Kiss A, et al. Validation of a rule for termination of resuscitation in out-of-hospital cardiac arrest. N Engl J Med. 2006 Aug 3;355(5):478-487.
The survival rate of patients with out-of-hospital cardiac arrest is very low. Thus, guidelines have been developed for termination of resuscitation for those patients who have had no response to advanced cardiac life support provided by emergency medical service (EMS) personnel. Similar guidelines have not yet been developed, however, for situations in which patients receive basic life support from emergency workers trained in the use of an automated external cardiac defibrillator. Patients with little potential for survival are routinely transported to emergency departments, at significant cost to the healthcare system.
Morrison and colleagues present results from the Termination of Resuscitation (TOR) study, a prospective evaluation of a clinical prediction rule for the termination of basic life support by emergency medical personnel trained in the use of automated external defibrillators. The clinical prediction rule, previously developed in a retrospective review of case records from a large urban EMS system, recommends termination of resuscitation if there is no return of spontaneous circulation, no shock administered, and no witness of the arrest by EMS personnel.
In the current study, the authors obtained follow-up data for 1,240 adult patients in Ontario, Canada, who had suffered an arrest of presumed cardiac cause and were subsequently transported to the emergency department after resuscitative efforts. Twenty-four EMS systems participated in the study. The study found that only 0.5% of the patients for whom the clinical prediction rule recommended termination survived (four out of 776 patients). Of the 1,240 total study patients, 41 (3%) survived. The clinical prediction rule recommended continuation of resuscitative efforts for 37 of these 41 patients, resulting in a specificity of 90.2%. The positive predictive value for death was calculated to be 99.5% when termination was recommended.
The TOR trial also determined whether the addition of other criteria to the original prediction rule could further refine the specificity and positive predictive value. They found that the addition to the criteria of a response time greater than eight minutes increased the positive predictive value and specificity to 99.7% and 97.6%, respectively. When the variable “not witnessed by bystander” was added to the clinical prediction rule, both the positive predictive value and specificity increased to 100%. In other words, no patients survived if they had had a completely unwitnessed arrest, no return of spontaneous circulation, and no shocks delivered.
This study identifies a subpopulation of patients with presumed cardiac arrest for whom termination of resuscitative efforts in the field appears reasonable. The authors note that a survival rate of 1% or less has been suggested in past literature as reflective of medical futility. The TOR investigators acknowledge that their study took place before the 2005 AHA Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care were released and that their study protocols were consistent with the 2000 resuscitation guidelines. In light of this information, continued validity testing of the clinical prediction rule under the 2005 AHA protocols is needed.
Nonetheless, it is quite impressive that use of their clinical prediction rule would have resulted in transportation of only 37% of patients (464 of 1,240), rather than 100% of patients, as is currently the practice. If the guidelines described in this article are to be implemented, further studies are necessary to address the training of EMS personnel, who would carry responsibility for terminating resuscitation and notifying families of patients’ deaths.
Prevention of Ventilator-Associated Pneumonia
By Diane Sliwka, MD
Koeman M, van der Ven AJ, Hak E, et al. Oral decontamination with chlorhexidine reduces the incidence of ventilator-associated pneumonia. Am J Respir Crit Care Med. 2006 Jun;173(12):1348-1355. Epub 2006 Apr 7.
Ventilator-associated pneumonia (VAP) is an important nosocomial source of morbidity and mortality. The use of prophylactic antimicrobials to decrease VAP raises concern for antimicrobial resistance. This study evaluates the topical antiseptic chlorhexidine (CHX) as an alternative prophylactic intervention for VAP. CHX has previously been shown to decrease VAP in cardiac surgical patients, but has not been studied in higher risk, long-term-ventilated patients. Because CHX works better for gram-positive organisms, the combination of colistin and CHX (COL + CHX) was also studied for improved gram-negative coverage.
This multi-center, randomized, double-blind, placebo-controlled trial enrolled 385 adult patients. Patients who were expected to be intubated for longer than 48 hours were randomized to 3 arms: CHX alone, CHX + COL, and placebo. Exclusion criteria included known preadmission immunocompromised state, pregnancy, and physical limitation to oral application. Pneumonia was defined by clinical decision-making, which was later confirmed by three blinded intensivists’ reviews of the case records and supported by daily clinical pulmonary infection scores.
The primary endpoint of VAP was diagnosed in 52 of 385 patients: 18% placebo, 13% CHX, and 10% CHX + COL. Rate of VAP in the two treatment groups was lower than placebo and reached statistical significance when compared to placebo. The daily hazard ratio for CHX versus placebo was .352 (95% CI .160, .791); for CHX + COL versus placebo, it was .454 (95% CI .224, .925), showing a 65% and 55% reduction in the rate of pneumonia development. Multivariate analysis of variables such as gender, pulmonary admission diagnosis, colonization at time of admission, and antimicrobial use on admission did not affect the data.
The secondary endpoint of endotracheal colonization was evaluated by a twice-weekly endotracheal culture. There was no statistically significant difference in colonization among the three groups in the first (days 1-4) or third (days 9-12) time frames. During the second time frame (days 5-8), there was a statistically significant decrease in colonization for the CHX + COL treatment group when compared to both placebo (16% versus 40% p<.007) and to CHX (16% versus 38%, p<.011); this decrease is thought to be due to gram-negative coverage by COL.
The secondary endpoint of oropharyngeal colonization was evaluated for 87% of all patient days. CHX and CHX + COL were similarly effective for gram-positive bacteria when compared to placebo, with 30% and 27% reduction in rates of colonization, respectively: HR 0.695 for CHX (95% CI, 0.606, 0.796; p < 0.001) and 0.732 (95% CI, 0.640, 0.838; p < 0.001) for CHX + COL. The CHX + COL combination was more effective for gram-negative bacteria: daily HR .534 (95% CI, 0.455, 0.626; p <0.001) alone with a 47% reduction in gram-negative colonization compared to CHX.
No difference was seen in ICU mortality, duration of mechanical ventilation, or duration of ICU stay. One adverse event (tongue swelling) occurred in the CHX + COL group.
Limitations of the study include the following:
- Daily assessments on all patients were not performed;
- The placebo group had more males and more infections on admission than the other two groups, raising the question of randomization error;
- Clinical versus quantitative diagnosis of pneumonia may overestimate VAP in this study;
- It is not known how many patients were not enrolled in the study due to short anticipated ventilator times, but who later had prolonged ventilations; and
- The lack of effect on ventilator time, ICU length of stay, and mortality raises the question of the significance of these findings.
Despite these limitations, the low cost of these treatments, minimal adverse events, low risk of promoting significant antimicrobial resistance, and the finding of decreased VAP and bacterial colonization risk shown in this study support the potential benefit of topical decontamination with CHX and COL in conjunction with other measures of VAP prevention. TH
Reference
- De Riso AJ II, Ladowski JS, Dillon TA, et al. Chlorhexidine gluconate 0.12% oral rinse reduces the incidence of total nosocomial respiratory infection and nonprophylactic systemic antibiotic use in patients undergoing heart surgery. Chest. 1996;109:1556-1561.
Semi-Recumbent Position to Prevent Ventilator-Associated Pneumonia: Is It Possible?
By Joseph Ming Wah Li, MD
Van Nieuwenhoven CA, Vandenbroucke-Grauls C, van Tiel FH, et al. Feasibility and effects of the semirecumbent position to prevent ventilator-associated pneumonia: a randomized study. Crit Care Med. 2006 Feb;34(2):396-402.
Ventilator-associated pneumonia (VAP) is a cause of significant morbidity and mortality among mechanically ventilated patients. Studies with radioactive-labeled enteral feeds have demonstrated an increased frequency of endotracheal aspiration of gastric contents in supine patients. The CDC guidelines for prevention of nosocomial pneumonia advise placement of mechanically ventilated patients in a semi-recumbent position as a VAP prevention measure.
Only one previous study, by Drakulovic and colleagues, has assessed this strategy to prevent VAP.1 That study demonstrated a 75% decrease in the incidence of VAP. But van Nieuwenhoven and colleagues raised two important questions about the findings from the previous study: First, the Drakulovic study placed control patients in a horizontal (zero degrees) position, which is not the standard of care in most ICUs. Most patients are placed at 10 degrees, and this position is elevated as patients are weaned. Second, the Drakulovic study measured patients only once daily but did not monitor their body positions in between the daily measurements.
Dr. van Nieuwenhoven and colleagues set out to determine whether it is feasible to keep mechanically ventilated patients in a semi-recumbent position on a continual basis and whether this measure would prevent VAP. This was a prospective multi-centered trial in which mechanically ventilated patients were randomly assigned to the semi-recumbent position with a target backrest elevation of 45 degrees or standard of care (supine position) with a backrest elevation of 10 degrees. They used a transducer with a pendulum, which was placed on the bed frame to measure the backrest elevation every 60 seconds for up to seven days. They calculated a mean degree of elevation for each patient daily. Nurses always respected the patient’s request for positioning, but a dedicated research nurse restored backrest position to the randomized position whenever possible.
Baseline characteristics for both groups were similar. For the supine (control) group, average elevations were 9.8 degrees on day one and 16.1 degrees on day seven. For the semi-recumbent group, average elevations were 28.1 degrees on day one and 22.6 degrees on day seven. There were no significant differences in numbers of patients who developed VAP in either group.
This study suggests that, despite the use of dedicated research nurses to maintain positioning, it may not be possible to keep patients’ backrests elevated to 45 degrees. Keeping patients’ backrests at an elevation of nearly 30 degrees does not appear to prevent VAP more than keeping patients’ backrests at 10 degrees, the present standard of care.
Reference
- Drakulovic MB, Torres A, Bauer TT, et al. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial. Lancet. 1999;354(9193):1851-1858.
Bar Codes in Medicine: An Opportunity for Quality Improvement
By Alex Carbo, MD
Poon EG, Cina JL, Churchill W, et al. Medication dispensing errors and potential adverse drug events before and after implementing bar code technology in the pharmacy. Ann Intern Med. 2006;145:426-434.
Medication errors and adverse drug events (ADEs) have received much attention in the literature; the use of health information technology to mitigate these errors and ADEs has now been proposed in many areas of healthcare. In an effort to decrease medication-dispensing errors, the U.S. Food and Drug Administration (FDA) mandated bar code use for all medications in hospitals, beginning in April 2006. While this technology has been extensively studied in other industries, there is little data describing its effects in the healthcare system.
Poon and colleagues set out to evaluate whether implementation of bar code technology reduced dispensing errors and the ADEs that might be caused by these miscalculations. In a before-and-after evaluation, they studied more than 350,000 dispensed medication doses in an academic medical center between February 2003 and September 2004.
During the bar code conversion process, the hospital pharmacy built a dedicated repackaging center, which was responsible for affixing a bar code to every dose of medication. These medications were then dispensed in three different configurations: two configurations required staff to verify all doses at least once using bar code scanning, and the third configuration—for commonly dispensed medications that could not be accommodated in a standard carousel machine because of their size or need for refrigeration—required scanning only one dose from each batch.
The authors found a 93% to 96% relative reduction in the incidence of target dispensing errors (P<0.001) and an 86% to 97% relative reduction in the incidence of potential ADEs (P<0.001) in the two configurations that required staff to verify all doses by scanning. The greatest reductions were seen in wrong medication errors (56%), wrong strength/dose errors (71%), wrong formulation errors (90%), and expired medication errors (100%).
In the configuration that did not require scanning of every dose, however, there was a 60% relative reduction in the incidence of target dispensing errors (P<0.001), but a 2.4-fold increase in the incidence of target potential ADEs. This included new errors attributable to wrong strength and wrong medication dispensing.
In light of the FDA’s mandate regarding bar codes, it seems that every hospital has the opportunity to improve patient safety and decrease medication error rates with the use of bar code technology. This study suggests that in order to achieve this benefit these systems should be designed to ensure that every medication dose is verified by scanning during the dispensing process.
Evaluation of a Guideline to Guide Resuscitation
By Cindy Lien, MD
Morrison LJ, Visentin LM, Kiss A, et al. Validation of a rule for termination of resuscitation in out-of-hospital cardiac arrest. N Engl J Med. 2006 Aug 3;355(5):478-487.
The survival rate of patients with out-of-hospital cardiac arrest is very low. Thus, guidelines have been developed for termination of resuscitation for those patients who have had no response to advanced cardiac life support provided by emergency medical service (EMS) personnel. Similar guidelines have not yet been developed, however, for situations in which patients receive basic life support from emergency workers trained in the use of an automated external cardiac defibrillator. Patients with little potential for survival are routinely transported to emergency departments, at significant cost to the healthcare system.
Morrison and colleagues present results from the Termination of Resuscitation (TOR) study, a prospective evaluation of a clinical prediction rule for the termination of basic life support by emergency medical personnel trained in the use of automated external defibrillators. The clinical prediction rule, previously developed in a retrospective review of case records from a large urban EMS system, recommends termination of resuscitation if there is no return of spontaneous circulation, no shock administered, and no witness of the arrest by EMS personnel.
In the current study, the authors obtained follow-up data for 1,240 adult patients in Ontario, Canada, who had suffered an arrest of presumed cardiac cause and were subsequently transported to the emergency department after resuscitative efforts. Twenty-four EMS systems participated in the study. The study found that only 0.5% of the patients for whom the clinical prediction rule recommended termination survived (four out of 776 patients). Of the 1,240 total study patients, 41 (3%) survived. The clinical prediction rule recommended continuation of resuscitative efforts for 37 of these 41 patients, resulting in a specificity of 90.2%. The positive predictive value for death was calculated to be 99.5% when termination was recommended.
The TOR trial also determined whether the addition of other criteria to the original prediction rule could further refine the specificity and positive predictive value. They found that the addition to the criteria of a response time greater than eight minutes increased the positive predictive value and specificity to 99.7% and 97.6%, respectively. When the variable “not witnessed by bystander” was added to the clinical prediction rule, both the positive predictive value and specificity increased to 100%. In other words, no patients survived if they had had a completely unwitnessed arrest, no return of spontaneous circulation, and no shocks delivered.
This study identifies a subpopulation of patients with presumed cardiac arrest for whom termination of resuscitative efforts in the field appears reasonable. The authors note that a survival rate of 1% or less has been suggested in past literature as reflective of medical futility. The TOR investigators acknowledge that their study took place before the 2005 AHA Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care were released and that their study protocols were consistent with the 2000 resuscitation guidelines. In light of this information, continued validity testing of the clinical prediction rule under the 2005 AHA protocols is needed.
Nonetheless, it is quite impressive that use of their clinical prediction rule would have resulted in transportation of only 37% of patients (464 of 1,240), rather than 100% of patients, as is currently the practice. If the guidelines described in this article are to be implemented, further studies are necessary to address the training of EMS personnel, who would carry responsibility for terminating resuscitation and notifying families of patients’ deaths.
Prevention of Ventilator-Associated Pneumonia
By Diane Sliwka, MD
Koeman M, van der Ven AJ, Hak E, et al. Oral decontamination with chlorhexidine reduces the incidence of ventilator-associated pneumonia. Am J Respir Crit Care Med. 2006 Jun;173(12):1348-1355. Epub 2006 Apr 7.
Ventilator-associated pneumonia (VAP) is an important nosocomial source of morbidity and mortality. The use of prophylactic antimicrobials to decrease VAP raises concern for antimicrobial resistance. This study evaluates the topical antiseptic chlorhexidine (CHX) as an alternative prophylactic intervention for VAP. CHX has previously been shown to decrease VAP in cardiac surgical patients, but has not been studied in higher risk, long-term-ventilated patients. Because CHX works better for gram-positive organisms, the combination of colistin and CHX (COL + CHX) was also studied for improved gram-negative coverage.
This multi-center, randomized, double-blind, placebo-controlled trial enrolled 385 adult patients. Patients who were expected to be intubated for longer than 48 hours were randomized to 3 arms: CHX alone, CHX + COL, and placebo. Exclusion criteria included known preadmission immunocompromised state, pregnancy, and physical limitation to oral application. Pneumonia was defined by clinical decision-making, which was later confirmed by three blinded intensivists’ reviews of the case records and supported by daily clinical pulmonary infection scores.
The primary endpoint of VAP was diagnosed in 52 of 385 patients: 18% placebo, 13% CHX, and 10% CHX + COL. Rate of VAP in the two treatment groups was lower than placebo and reached statistical significance when compared to placebo. The daily hazard ratio for CHX versus placebo was .352 (95% CI .160, .791); for CHX + COL versus placebo, it was .454 (95% CI .224, .925), showing a 65% and 55% reduction in the rate of pneumonia development. Multivariate analysis of variables such as gender, pulmonary admission diagnosis, colonization at time of admission, and antimicrobial use on admission did not affect the data.
The secondary endpoint of endotracheal colonization was evaluated by a twice-weekly endotracheal culture. There was no statistically significant difference in colonization among the three groups in the first (days 1-4) or third (days 9-12) time frames. During the second time frame (days 5-8), there was a statistically significant decrease in colonization for the CHX + COL treatment group when compared to both placebo (16% versus 40% p<.007) and to CHX (16% versus 38%, p<.011); this decrease is thought to be due to gram-negative coverage by COL.
The secondary endpoint of oropharyngeal colonization was evaluated for 87% of all patient days. CHX and CHX + COL were similarly effective for gram-positive bacteria when compared to placebo, with 30% and 27% reduction in rates of colonization, respectively: HR 0.695 for CHX (95% CI, 0.606, 0.796; p < 0.001) and 0.732 (95% CI, 0.640, 0.838; p < 0.001) for CHX + COL. The CHX + COL combination was more effective for gram-negative bacteria: daily HR .534 (95% CI, 0.455, 0.626; p <0.001) alone with a 47% reduction in gram-negative colonization compared to CHX.
No difference was seen in ICU mortality, duration of mechanical ventilation, or duration of ICU stay. One adverse event (tongue swelling) occurred in the CHX + COL group.
Limitations of the study include the following:
- Daily assessments on all patients were not performed;
- The placebo group had more males and more infections on admission than the other two groups, raising the question of randomization error;
- Clinical versus quantitative diagnosis of pneumonia may overestimate VAP in this study;
- It is not known how many patients were not enrolled in the study due to short anticipated ventilator times, but who later had prolonged ventilations; and
- The lack of effect on ventilator time, ICU length of stay, and mortality raises the question of the significance of these findings.
Despite these limitations, the low cost of these treatments, minimal adverse events, low risk of promoting significant antimicrobial resistance, and the finding of decreased VAP and bacterial colonization risk shown in this study support the potential benefit of topical decontamination with CHX and COL in conjunction with other measures of VAP prevention. TH
Reference
- De Riso AJ II, Ladowski JS, Dillon TA, et al. Chlorhexidine gluconate 0.12% oral rinse reduces the incidence of total nosocomial respiratory infection and nonprophylactic systemic antibiotic use in patients undergoing heart surgery. Chest. 1996;109:1556-1561.
An Intense Rash

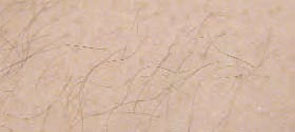
A32-year-old white male with Down syndrome was initially admitted with fever, cough, and productive sputum. He was started on appropriate antibiotics, but soon became hypoxic and developed respiratory failure requiring mechanical ventilation. The patient developed acute respiratory distress syndrome (ARDS) and eventually had a tracheostomy. On day 10, while in the intensive care unit, the patient developed multiple 1-2 mL clear vesicular eruptions with no surrounding erythema or edema. These were primarily distributed on the chest; the patient’s face was clear. TH
In dealing with this new eruption, the physician should have:
- Lowered the ambient room temperature and otherwise continued the current management.
- Performed a Tzanck smear, isolated the patient, and started acyclovir IV for presumed disseminated herpes zoster.
- Discontinued current antibiotics due to the drug reaction.
- Performed a skin biopsy for hematoxylin and eosin (H&E) stain as well as immunofluorescence for suspected primary early bullous disease (i.e., bullous pemphigoid).
- Started amphotericin.
Discussion
The correct answer is A: The physician should have lowered the ambient room temperature and continued the current management.
This patient had developed miliaria crystallina, a transient disorder of occluded sweat glands that usually results from excessive exposure to heat and humidity. Miliaria, also known as sweat rash, defines a group of disorders exhibiting eccrine gland obstruction with leakage and retention of sweat at different levels in the skin. The clinical presentation of miliaria is related to the depth of this obstruction and occurs in three main forms: miliaria crystallina, miliaria rubra, and miliaria profunda.1
Of the three variants, eccrine obstruction in miliaria crystallina occurs most superficially, at either the distal duct or pore, and drives sweat vesiculation into the stratum corneum of the epidermis.1 It is characterized by diffuse eruptions of non-inflamed, translucent vesicles of one to two millimeters, typically forming in crops on the trunk of the body. The tiny blisters have been likened to beads of sweat and are extremely fragile, rupturing spontaneously or with light friction.
Clinically, miliaria crystallina is an asymptomatic and self-limited disorder. It often occurs during the summer months and in tropical climates after prolonged exposure to heat and humidity. It is thought that overhydration of corneocytes from excessive sweating predisposes the eccrine duct to obstruction. This may be compounded by any form of occlusion, like clothing or bedding, that traps moisture and impedes the evaporation of sweat.2 Other risk factors include persistent fevers, neonate age less than two weeks, secondary to eccrine duct immaturity, and drugs such as isotretinoin and bethanechol.3,4,5
In the case of this 32-year-old male with respiratory failure, the characteristic eruption of miliaria crystallina developed on day 10 of intensive care. After lowering the ambient temperature of the patient’s room and adding the benefit of a circulatory fan, the vesicles resolved within two to three days. As this example demonstrates, the treatment of miliaria crystallina is straightforward and consists of drying the skin and preventing sweating for several days by keeping the patient in a cool, air-conditioned environment. Eventually, the keratinous plug will be shed, and normal sweating will resume.
In the literature, there is only one published report documenting two distinct cases of miliaria crystallina in the intensive care setting. At the time of onset, these two patients had been in the ICU for slightly over two weeks, and both were receiving treatment with multiple neuroautonomic agents, including—but not limited to—clonidine, a beta blocker, and opiates for pain. The innervation of eccrine glands is under sympathetic control mostly through the postsynaptic release of acetylcholine but also via adrenergic stimulation of contractile myoepithelia. While temperature and humidity are carefully regulated in most intensive care facilities, significant sweating may result from eccrine stimulation by neuroautonomic medications with intrinsic sympathomimetic activity.6 Combined with prolonged immobility, this sweating may create the perfect environment for eccrine duct obstruction and the development of miliaria crystallina.
Incidence in the intensive care setting has not been studied, but miliaria crystallina probably occurs much more frequently than it is reported. The ability to recognize the characteristic eruptions may prevent the hospitalist who encounters it from ordering unnecessary consults or diagnostics, and knowledge of its risk factors will aid both in treatment and in prevention. TH
References
- Wenzel FG, Horn TD. Nonneoplastic disorders of the eccrine glands. J Am Acad Dermatol. 1998 Jan;38(1):1–20.
- Sperling L. Chapter 3: Skin Diseases Associated with Excessive Heat, Humidity, and Sunlight. In: Textbook of Military Dermatology. Washington, D.C.: Office of The Surgeon General at TMM Publications; 1994:39-54. Available at: www.bordeninstitute.army.mil/derm/default_index.htm. Last accessed: September 8, 2006.
- Haas N, Henz BM, Weigel H. Congenital miliaria crystallina. J Am Acad Dermatol. 2002 Nov;47(5 Suppl):S270–272.
- Gupta AK, Ellis CN, Madison KC, et al. Miliaria crystallina occurring in a patient treated with isotretinoin. Cutis. 1986 Oct;38(4):275–276.
- Rochmis PG, Koplon BS. Iatrogenic miliaria crystallina due to bethanechol. Arch Dermatol. 1967 May;95(9):499–500.
- Haas N, Martens F, Henz BM. Miliaria crystallina in an intensive care setting. Clin Exp Dermatol. 2004 Jan;29 (1):32-34.
A32-year-old white male with Down syndrome was initially admitted with fever, cough, and productive sputum. He was started on appropriate antibiotics, but soon became hypoxic and developed respiratory failure requiring mechanical ventilation. The patient developed acute respiratory distress syndrome (ARDS) and eventually had a tracheostomy. On day 10, while in the intensive care unit, the patient developed multiple 1-2 mL clear vesicular eruptions with no surrounding erythema or edema. These were primarily distributed on the chest; the patient’s face was clear. TH
In dealing with this new eruption, the physician should have:
- Lowered the ambient room temperature and otherwise continued the current management.
- Performed a Tzanck smear, isolated the patient, and started acyclovir IV for presumed disseminated herpes zoster.
- Discontinued current antibiotics due to the drug reaction.
- Performed a skin biopsy for hematoxylin and eosin (H&E) stain as well as immunofluorescence for suspected primary early bullous disease (i.e., bullous pemphigoid).
- Started amphotericin.
Discussion
The correct answer is A: The physician should have lowered the ambient room temperature and continued the current management.
This patient had developed miliaria crystallina, a transient disorder of occluded sweat glands that usually results from excessive exposure to heat and humidity. Miliaria, also known as sweat rash, defines a group of disorders exhibiting eccrine gland obstruction with leakage and retention of sweat at different levels in the skin. The clinical presentation of miliaria is related to the depth of this obstruction and occurs in three main forms: miliaria crystallina, miliaria rubra, and miliaria profunda.1
Of the three variants, eccrine obstruction in miliaria crystallina occurs most superficially, at either the distal duct or pore, and drives sweat vesiculation into the stratum corneum of the epidermis.1 It is characterized by diffuse eruptions of non-inflamed, translucent vesicles of one to two millimeters, typically forming in crops on the trunk of the body. The tiny blisters have been likened to beads of sweat and are extremely fragile, rupturing spontaneously or with light friction.
Clinically, miliaria crystallina is an asymptomatic and self-limited disorder. It often occurs during the summer months and in tropical climates after prolonged exposure to heat and humidity. It is thought that overhydration of corneocytes from excessive sweating predisposes the eccrine duct to obstruction. This may be compounded by any form of occlusion, like clothing or bedding, that traps moisture and impedes the evaporation of sweat.2 Other risk factors include persistent fevers, neonate age less than two weeks, secondary to eccrine duct immaturity, and drugs such as isotretinoin and bethanechol.3,4,5
In the case of this 32-year-old male with respiratory failure, the characteristic eruption of miliaria crystallina developed on day 10 of intensive care. After lowering the ambient temperature of the patient’s room and adding the benefit of a circulatory fan, the vesicles resolved within two to three days. As this example demonstrates, the treatment of miliaria crystallina is straightforward and consists of drying the skin and preventing sweating for several days by keeping the patient in a cool, air-conditioned environment. Eventually, the keratinous plug will be shed, and normal sweating will resume.
In the literature, there is only one published report documenting two distinct cases of miliaria crystallina in the intensive care setting. At the time of onset, these two patients had been in the ICU for slightly over two weeks, and both were receiving treatment with multiple neuroautonomic agents, including—but not limited to—clonidine, a beta blocker, and opiates for pain. The innervation of eccrine glands is under sympathetic control mostly through the postsynaptic release of acetylcholine but also via adrenergic stimulation of contractile myoepithelia. While temperature and humidity are carefully regulated in most intensive care facilities, significant sweating may result from eccrine stimulation by neuroautonomic medications with intrinsic sympathomimetic activity.6 Combined with prolonged immobility, this sweating may create the perfect environment for eccrine duct obstruction and the development of miliaria crystallina.
Incidence in the intensive care setting has not been studied, but miliaria crystallina probably occurs much more frequently than it is reported. The ability to recognize the characteristic eruptions may prevent the hospitalist who encounters it from ordering unnecessary consults or diagnostics, and knowledge of its risk factors will aid both in treatment and in prevention. TH
References
- Wenzel FG, Horn TD. Nonneoplastic disorders of the eccrine glands. J Am Acad Dermatol. 1998 Jan;38(1):1–20.
- Sperling L. Chapter 3: Skin Diseases Associated with Excessive Heat, Humidity, and Sunlight. In: Textbook of Military Dermatology. Washington, D.C.: Office of The Surgeon General at TMM Publications; 1994:39-54. Available at: www.bordeninstitute.army.mil/derm/default_index.htm. Last accessed: September 8, 2006.
- Haas N, Henz BM, Weigel H. Congenital miliaria crystallina. J Am Acad Dermatol. 2002 Nov;47(5 Suppl):S270–272.
- Gupta AK, Ellis CN, Madison KC, et al. Miliaria crystallina occurring in a patient treated with isotretinoin. Cutis. 1986 Oct;38(4):275–276.
- Rochmis PG, Koplon BS. Iatrogenic miliaria crystallina due to bethanechol. Arch Dermatol. 1967 May;95(9):499–500.
- Haas N, Martens F, Henz BM. Miliaria crystallina in an intensive care setting. Clin Exp Dermatol. 2004 Jan;29 (1):32-34.
A32-year-old white male with Down syndrome was initially admitted with fever, cough, and productive sputum. He was started on appropriate antibiotics, but soon became hypoxic and developed respiratory failure requiring mechanical ventilation. The patient developed acute respiratory distress syndrome (ARDS) and eventually had a tracheostomy. On day 10, while in the intensive care unit, the patient developed multiple 1-2 mL clear vesicular eruptions with no surrounding erythema or edema. These were primarily distributed on the chest; the patient’s face was clear. TH
In dealing with this new eruption, the physician should have:
- Lowered the ambient room temperature and otherwise continued the current management.
- Performed a Tzanck smear, isolated the patient, and started acyclovir IV for presumed disseminated herpes zoster.
- Discontinued current antibiotics due to the drug reaction.
- Performed a skin biopsy for hematoxylin and eosin (H&E) stain as well as immunofluorescence for suspected primary early bullous disease (i.e., bullous pemphigoid).
- Started amphotericin.
Discussion
The correct answer is A: The physician should have lowered the ambient room temperature and continued the current management.
This patient had developed miliaria crystallina, a transient disorder of occluded sweat glands that usually results from excessive exposure to heat and humidity. Miliaria, also known as sweat rash, defines a group of disorders exhibiting eccrine gland obstruction with leakage and retention of sweat at different levels in the skin. The clinical presentation of miliaria is related to the depth of this obstruction and occurs in three main forms: miliaria crystallina, miliaria rubra, and miliaria profunda.1
Of the three variants, eccrine obstruction in miliaria crystallina occurs most superficially, at either the distal duct or pore, and drives sweat vesiculation into the stratum corneum of the epidermis.1 It is characterized by diffuse eruptions of non-inflamed, translucent vesicles of one to two millimeters, typically forming in crops on the trunk of the body. The tiny blisters have been likened to beads of sweat and are extremely fragile, rupturing spontaneously or with light friction.
Clinically, miliaria crystallina is an asymptomatic and self-limited disorder. It often occurs during the summer months and in tropical climates after prolonged exposure to heat and humidity. It is thought that overhydration of corneocytes from excessive sweating predisposes the eccrine duct to obstruction. This may be compounded by any form of occlusion, like clothing or bedding, that traps moisture and impedes the evaporation of sweat.2 Other risk factors include persistent fevers, neonate age less than two weeks, secondary to eccrine duct immaturity, and drugs such as isotretinoin and bethanechol.3,4,5
In the case of this 32-year-old male with respiratory failure, the characteristic eruption of miliaria crystallina developed on day 10 of intensive care. After lowering the ambient temperature of the patient’s room and adding the benefit of a circulatory fan, the vesicles resolved within two to three days. As this example demonstrates, the treatment of miliaria crystallina is straightforward and consists of drying the skin and preventing sweating for several days by keeping the patient in a cool, air-conditioned environment. Eventually, the keratinous plug will be shed, and normal sweating will resume.
In the literature, there is only one published report documenting two distinct cases of miliaria crystallina in the intensive care setting. At the time of onset, these two patients had been in the ICU for slightly over two weeks, and both were receiving treatment with multiple neuroautonomic agents, including—but not limited to—clonidine, a beta blocker, and opiates for pain. The innervation of eccrine glands is under sympathetic control mostly through the postsynaptic release of acetylcholine but also via adrenergic stimulation of contractile myoepithelia. While temperature and humidity are carefully regulated in most intensive care facilities, significant sweating may result from eccrine stimulation by neuroautonomic medications with intrinsic sympathomimetic activity.6 Combined with prolonged immobility, this sweating may create the perfect environment for eccrine duct obstruction and the development of miliaria crystallina.
Incidence in the intensive care setting has not been studied, but miliaria crystallina probably occurs much more frequently than it is reported. The ability to recognize the characteristic eruptions may prevent the hospitalist who encounters it from ordering unnecessary consults or diagnostics, and knowledge of its risk factors will aid both in treatment and in prevention. TH
References
- Wenzel FG, Horn TD. Nonneoplastic disorders of the eccrine glands. J Am Acad Dermatol. 1998 Jan;38(1):1–20.
- Sperling L. Chapter 3: Skin Diseases Associated with Excessive Heat, Humidity, and Sunlight. In: Textbook of Military Dermatology. Washington, D.C.: Office of The Surgeon General at TMM Publications; 1994:39-54. Available at: www.bordeninstitute.army.mil/derm/default_index.htm. Last accessed: September 8, 2006.
- Haas N, Henz BM, Weigel H. Congenital miliaria crystallina. J Am Acad Dermatol. 2002 Nov;47(5 Suppl):S270–272.
- Gupta AK, Ellis CN, Madison KC, et al. Miliaria crystallina occurring in a patient treated with isotretinoin. Cutis. 1986 Oct;38(4):275–276.
- Rochmis PG, Koplon BS. Iatrogenic miliaria crystallina due to bethanechol. Arch Dermatol. 1967 May;95(9):499–500.
- Haas N, Martens F, Henz BM. Miliaria crystallina in an intensive care setting. Clin Exp Dermatol. 2004 Jan;29 (1):32-34.
PSTF Monitors Quality

In spring 2006 SHM leadership agreed that there was a need to develop a coordinated approach to working with external organizations in the performance and standards quality arena, while collaborating with public policy and educational efforts in this area. To this end, I was hired as the SHM Senior Advisor for Quality Standards and Compliance. At around the same time, leaders from the Public Policy Committee (PPC) and Health Quality Patient Safety (HQPS) Committee joined to form a Performance and Standards Task Force (PSTF).
Purpose of the Task Force
Chaired by Patrick Torcson, MD, the PSTF works with staff to monitor the performance and quality landscape at national organizations charged with the measure development and consensus-building processes, as well as to outreach and develop liaison relationships with other professional medical societies and organizations. Ultimately, the task force wants to create a performance framework unique to and reflective of hospitalists.
Since its inception in the late spring, the PSTF has had several meetings to discuss which organizations SHM should engage with and at what level. In several cases, task force members agreed that an official member liaison should be appointed to serve as SHM’s representative to a particular organization. This serves the purpose of having a clinical expert resource available to staff with regard to the particular activities of each organization, as well as to create a consistent and reliable “SHM face” for a particular organization.
Performance Measures
SHM joined the AMA Physician Consortium for Performance Improvement (PCPI), which works with medical specialty organizations to develop physician-level performance measures. As a new member of the PCPI, SHM submitted feedback during the public comment period on perioperative care measures, the development of which was led by the American College of Surgeons, along with input from other medical specialties. SHM also participated in two expert workgroups this past summer, one on emergency medicine, focusing on treating MI and pneumonia, and another on geriatrics, which focused on falls, urinary incontinence, advanced-care planning as part of end-of-life care, and medication reconciliation as part of care coordination. Both the geriatrics and the emergency medicine measures have been released for public comment. At least through 2006, the PCPI is focusing on measures that fall under the Centers for Medicare and Medicaid Services (CMS) contract and will be included in the Physician Voluntary Reporting Program (PVRP).
The PSTF is actively recruiting leaders to participate in expert workgroups that were convened in November for both outpatient parenteral antimicrobial therapy and anesthesiology topics: perioperative normothermia and critical care. The task force will continue to evaluate the PCPI workgroups to determine which ones it should appoint members to participate in, depending on the topic area.
SHM has also become an organizational member of the National Quality Forum (NQF), a nonprofit organization that Congress, in early July, charged with endorsing consensus-based national standards for measurement and public reporting of healthcare performance data. At around the same time, NQF was seeking nominations for members of the steering committee and technical advisory panels that will oversee the work on the development of new consensus standards for hospital care. This project, sponsored by the Agency for Healthcare Research and Quality (AHRQ), will address patient safety, pediatrics, and inpatient care. The Society hopes to be fully engaged in this initiative.
In mid-October, NQF will hold its 7th Annual Meeting, a National Policy Conference on Quality, at the Grand Hyatt in Washington, D.C. This meeting will feature plenary sessions that focus on issues at the forefront of policy discussions, including incentivizing healthcare quality improvement, the role of policymakers, ways to lead professional and trade associations in improving healthcare quality, and efforts presently underway in the federal government to foster healthcare improvements. Mark Williams, MD, editor in chief of the Journal of Hospital Medicine and SHM member, will attend the policy conference as the SHM representative.
Quality Care Liaisons
In addition to fostering liaisons with organizations like PCPI and NQF, the PSTF has discussed the importance of exploring relationships with other groups, including CMS, the American College of Physicians (ACP), the Ambulatory Quality Care Alliance (AQA), and others engaged in the quality care arena.
In late spring 2006 several SHM members and staff met with CMS to discuss its PVRP in relation to hospitalists. While SHM has endorsed the PVRP, recommending that hospitalists register their intent to report and begin reporting on relevant performance measures to the extent practicable, it is clear that the 16 measures used in the PVRP have limited relevance for hospitalists because most measures used for internal medicine deal with services provided in the ambulatory setting.
Specifically, only two of the 16 measures apply to services billed by hospitalists and those only on a limited basis: aspirin on arrival for myocardial infarction and beta-blocker on arrival for MI have G-codes that can be used with the evaluation and management codes appropriate for hospitalists. In its follow-up letter to CMS staff thanking them for their time, SHM leadership also included recommendations that would expand the current number of PVRP measures that hospitalists could report on from two measures to seven.
SHM has also shared the above quality and performance improvement agenda with the staff of the ACP as well as their quality subcommittee, who have found it to be “well-reasoned and straightforward.” We anticipate having more in-depth discussions with the ACP as our quality agenda evolves.
In August, the Ambulatory Care Quality Alliance (AQA) and the Hospital Quality Alliance (HQA) joined forces to form a Quality Steering Committee in order to better coordinate the promotion of quality measurement, transparency, and improvement in care across hospital and ambulatory care settings. The PSTF is currently pursuing participation in one of the new AQA/HQA workgroups created by the steering committee, which would focus on harmonization of measures across settings.
SHM staff have also reached out to the Society of Critical Care Medicine, the Joint Commission on Accreditation of Healthcare Organizations, and the American Hospital Association to ascertain what these groups are doing in terms of quality and measure development, as well as to see how to align our efforts more closely.
In its work with all of these groups, the task force endeavors to ensure the development of performance measures that more accurately reflect services provided by hospitalists.
2007 Goals
The HQPS has developed a mechanism whereby they review measures proposed by a variety of organizations in order to evaluate which measures are relevant to individual clinicians as compared with institutional measures. It is PSTF’s goal (in conjunction with the HQPS, the PPC, and others) to recommend to the SHM board of directors which physician-level disease-specific measures are relevant to individual hospitalists and to identify where the gaps are. It hopes then to influence the scope of development of care coordination and other hospital-level measures that are in the pipeline, whether working through groups like the PCPI by taking the lead on an expert workgroup, by using the NQF consensus-building process, or by forming other key partnerships with groups like those noted above. It is likely that this work will be accomplished by some combination of these strategies.
Stay tuned for next month’s “SHM Behind the Scenes” by SHM Senior Vice President Joe Miller.
Epstein is the senior advisor for Standards and Compliance at SHM.
2005-2006 Survey Factoid
Use of PAs and NPs in hospital medicine groups
- Thirty percent of all hospital medicine groups (HMGs) employ nurse practitioners (NPs) and physician assistants (PAs).
- Those groups, on average, have 11.2 physicians and 2.8 NPs/PAs. The 70% of groups without NPs/PAs average 7.9 physicians per group.
- The following types of groups are more likely to employ NPs/PAs: academic programs, groups in the eastern U.S., and groups more than 5 years old.
- The frequency with which NPs/PAs perform certain functions in HMGs is summarized in this table:
NP/PA Function - % of HMGs
- Round daily on hospitalized patients - 83%
- Write prescriptions for patients - 82%
- Perform H & Ps upon admission - 77%
- Act as initial responder (consults, admits) - 66%
- Participate in discharge planning - 66%
- Order specialty consultations - 53%
- Assist in teaching students - 33%
- Night or weekend call - 30%
- Post discharge follow-up calls - 20%
- Emergency response; Code Blue - 14%
- Perform invasive procedures - 11%
Source: SHM’s 2005-2006 “Biannual State of the Hospital Medicine Movement” survey.
In spring 2006 SHM leadership agreed that there was a need to develop a coordinated approach to working with external organizations in the performance and standards quality arena, while collaborating with public policy and educational efforts in this area. To this end, I was hired as the SHM Senior Advisor for Quality Standards and Compliance. At around the same time, leaders from the Public Policy Committee (PPC) and Health Quality Patient Safety (HQPS) Committee joined to form a Performance and Standards Task Force (PSTF).
Purpose of the Task Force
Chaired by Patrick Torcson, MD, the PSTF works with staff to monitor the performance and quality landscape at national organizations charged with the measure development and consensus-building processes, as well as to outreach and develop liaison relationships with other professional medical societies and organizations. Ultimately, the task force wants to create a performance framework unique to and reflective of hospitalists.
Since its inception in the late spring, the PSTF has had several meetings to discuss which organizations SHM should engage with and at what level. In several cases, task force members agreed that an official member liaison should be appointed to serve as SHM’s representative to a particular organization. This serves the purpose of having a clinical expert resource available to staff with regard to the particular activities of each organization, as well as to create a consistent and reliable “SHM face” for a particular organization.
Performance Measures
SHM joined the AMA Physician Consortium for Performance Improvement (PCPI), which works with medical specialty organizations to develop physician-level performance measures. As a new member of the PCPI, SHM submitted feedback during the public comment period on perioperative care measures, the development of which was led by the American College of Surgeons, along with input from other medical specialties. SHM also participated in two expert workgroups this past summer, one on emergency medicine, focusing on treating MI and pneumonia, and another on geriatrics, which focused on falls, urinary incontinence, advanced-care planning as part of end-of-life care, and medication reconciliation as part of care coordination. Both the geriatrics and the emergency medicine measures have been released for public comment. At least through 2006, the PCPI is focusing on measures that fall under the Centers for Medicare and Medicaid Services (CMS) contract and will be included in the Physician Voluntary Reporting Program (PVRP).
The PSTF is actively recruiting leaders to participate in expert workgroups that were convened in November for both outpatient parenteral antimicrobial therapy and anesthesiology topics: perioperative normothermia and critical care. The task force will continue to evaluate the PCPI workgroups to determine which ones it should appoint members to participate in, depending on the topic area.
SHM has also become an organizational member of the National Quality Forum (NQF), a nonprofit organization that Congress, in early July, charged with endorsing consensus-based national standards for measurement and public reporting of healthcare performance data. At around the same time, NQF was seeking nominations for members of the steering committee and technical advisory panels that will oversee the work on the development of new consensus standards for hospital care. This project, sponsored by the Agency for Healthcare Research and Quality (AHRQ), will address patient safety, pediatrics, and inpatient care. The Society hopes to be fully engaged in this initiative.
In mid-October, NQF will hold its 7th Annual Meeting, a National Policy Conference on Quality, at the Grand Hyatt in Washington, D.C. This meeting will feature plenary sessions that focus on issues at the forefront of policy discussions, including incentivizing healthcare quality improvement, the role of policymakers, ways to lead professional and trade associations in improving healthcare quality, and efforts presently underway in the federal government to foster healthcare improvements. Mark Williams, MD, editor in chief of the Journal of Hospital Medicine and SHM member, will attend the policy conference as the SHM representative.
Quality Care Liaisons
In addition to fostering liaisons with organizations like PCPI and NQF, the PSTF has discussed the importance of exploring relationships with other groups, including CMS, the American College of Physicians (ACP), the Ambulatory Quality Care Alliance (AQA), and others engaged in the quality care arena.
In late spring 2006 several SHM members and staff met with CMS to discuss its PVRP in relation to hospitalists. While SHM has endorsed the PVRP, recommending that hospitalists register their intent to report and begin reporting on relevant performance measures to the extent practicable, it is clear that the 16 measures used in the PVRP have limited relevance for hospitalists because most measures used for internal medicine deal with services provided in the ambulatory setting.
Specifically, only two of the 16 measures apply to services billed by hospitalists and those only on a limited basis: aspirin on arrival for myocardial infarction and beta-blocker on arrival for MI have G-codes that can be used with the evaluation and management codes appropriate for hospitalists. In its follow-up letter to CMS staff thanking them for their time, SHM leadership also included recommendations that would expand the current number of PVRP measures that hospitalists could report on from two measures to seven.
SHM has also shared the above quality and performance improvement agenda with the staff of the ACP as well as their quality subcommittee, who have found it to be “well-reasoned and straightforward.” We anticipate having more in-depth discussions with the ACP as our quality agenda evolves.
In August, the Ambulatory Care Quality Alliance (AQA) and the Hospital Quality Alliance (HQA) joined forces to form a Quality Steering Committee in order to better coordinate the promotion of quality measurement, transparency, and improvement in care across hospital and ambulatory care settings. The PSTF is currently pursuing participation in one of the new AQA/HQA workgroups created by the steering committee, which would focus on harmonization of measures across settings.
SHM staff have also reached out to the Society of Critical Care Medicine, the Joint Commission on Accreditation of Healthcare Organizations, and the American Hospital Association to ascertain what these groups are doing in terms of quality and measure development, as well as to see how to align our efforts more closely.
In its work with all of these groups, the task force endeavors to ensure the development of performance measures that more accurately reflect services provided by hospitalists.
2007 Goals
The HQPS has developed a mechanism whereby they review measures proposed by a variety of organizations in order to evaluate which measures are relevant to individual clinicians as compared with institutional measures. It is PSTF’s goal (in conjunction with the HQPS, the PPC, and others) to recommend to the SHM board of directors which physician-level disease-specific measures are relevant to individual hospitalists and to identify where the gaps are. It hopes then to influence the scope of development of care coordination and other hospital-level measures that are in the pipeline, whether working through groups like the PCPI by taking the lead on an expert workgroup, by using the NQF consensus-building process, or by forming other key partnerships with groups like those noted above. It is likely that this work will be accomplished by some combination of these strategies.
Stay tuned for next month’s “SHM Behind the Scenes” by SHM Senior Vice President Joe Miller.
Epstein is the senior advisor for Standards and Compliance at SHM.
2005-2006 Survey Factoid
Use of PAs and NPs in hospital medicine groups
- Thirty percent of all hospital medicine groups (HMGs) employ nurse practitioners (NPs) and physician assistants (PAs).
- Those groups, on average, have 11.2 physicians and 2.8 NPs/PAs. The 70% of groups without NPs/PAs average 7.9 physicians per group.
- The following types of groups are more likely to employ NPs/PAs: academic programs, groups in the eastern U.S., and groups more than 5 years old.
- The frequency with which NPs/PAs perform certain functions in HMGs is summarized in this table:
NP/PA Function - % of HMGs
- Round daily on hospitalized patients - 83%
- Write prescriptions for patients - 82%
- Perform H & Ps upon admission - 77%
- Act as initial responder (consults, admits) - 66%
- Participate in discharge planning - 66%
- Order specialty consultations - 53%
- Assist in teaching students - 33%
- Night or weekend call - 30%
- Post discharge follow-up calls - 20%
- Emergency response; Code Blue - 14%
- Perform invasive procedures - 11%
Source: SHM’s 2005-2006 “Biannual State of the Hospital Medicine Movement” survey.
In spring 2006 SHM leadership agreed that there was a need to develop a coordinated approach to working with external organizations in the performance and standards quality arena, while collaborating with public policy and educational efforts in this area. To this end, I was hired as the SHM Senior Advisor for Quality Standards and Compliance. At around the same time, leaders from the Public Policy Committee (PPC) and Health Quality Patient Safety (HQPS) Committee joined to form a Performance and Standards Task Force (PSTF).
Purpose of the Task Force
Chaired by Patrick Torcson, MD, the PSTF works with staff to monitor the performance and quality landscape at national organizations charged with the measure development and consensus-building processes, as well as to outreach and develop liaison relationships with other professional medical societies and organizations. Ultimately, the task force wants to create a performance framework unique to and reflective of hospitalists.
Since its inception in the late spring, the PSTF has had several meetings to discuss which organizations SHM should engage with and at what level. In several cases, task force members agreed that an official member liaison should be appointed to serve as SHM’s representative to a particular organization. This serves the purpose of having a clinical expert resource available to staff with regard to the particular activities of each organization, as well as to create a consistent and reliable “SHM face” for a particular organization.
Performance Measures
SHM joined the AMA Physician Consortium for Performance Improvement (PCPI), which works with medical specialty organizations to develop physician-level performance measures. As a new member of the PCPI, SHM submitted feedback during the public comment period on perioperative care measures, the development of which was led by the American College of Surgeons, along with input from other medical specialties. SHM also participated in two expert workgroups this past summer, one on emergency medicine, focusing on treating MI and pneumonia, and another on geriatrics, which focused on falls, urinary incontinence, advanced-care planning as part of end-of-life care, and medication reconciliation as part of care coordination. Both the geriatrics and the emergency medicine measures have been released for public comment. At least through 2006, the PCPI is focusing on measures that fall under the Centers for Medicare and Medicaid Services (CMS) contract and will be included in the Physician Voluntary Reporting Program (PVRP).
The PSTF is actively recruiting leaders to participate in expert workgroups that were convened in November for both outpatient parenteral antimicrobial therapy and anesthesiology topics: perioperative normothermia and critical care. The task force will continue to evaluate the PCPI workgroups to determine which ones it should appoint members to participate in, depending on the topic area.
SHM has also become an organizational member of the National Quality Forum (NQF), a nonprofit organization that Congress, in early July, charged with endorsing consensus-based national standards for measurement and public reporting of healthcare performance data. At around the same time, NQF was seeking nominations for members of the steering committee and technical advisory panels that will oversee the work on the development of new consensus standards for hospital care. This project, sponsored by the Agency for Healthcare Research and Quality (AHRQ), will address patient safety, pediatrics, and inpatient care. The Society hopes to be fully engaged in this initiative.
In mid-October, NQF will hold its 7th Annual Meeting, a National Policy Conference on Quality, at the Grand Hyatt in Washington, D.C. This meeting will feature plenary sessions that focus on issues at the forefront of policy discussions, including incentivizing healthcare quality improvement, the role of policymakers, ways to lead professional and trade associations in improving healthcare quality, and efforts presently underway in the federal government to foster healthcare improvements. Mark Williams, MD, editor in chief of the Journal of Hospital Medicine and SHM member, will attend the policy conference as the SHM representative.
Quality Care Liaisons
In addition to fostering liaisons with organizations like PCPI and NQF, the PSTF has discussed the importance of exploring relationships with other groups, including CMS, the American College of Physicians (ACP), the Ambulatory Quality Care Alliance (AQA), and others engaged in the quality care arena.
In late spring 2006 several SHM members and staff met with CMS to discuss its PVRP in relation to hospitalists. While SHM has endorsed the PVRP, recommending that hospitalists register their intent to report and begin reporting on relevant performance measures to the extent practicable, it is clear that the 16 measures used in the PVRP have limited relevance for hospitalists because most measures used for internal medicine deal with services provided in the ambulatory setting.
Specifically, only two of the 16 measures apply to services billed by hospitalists and those only on a limited basis: aspirin on arrival for myocardial infarction and beta-blocker on arrival for MI have G-codes that can be used with the evaluation and management codes appropriate for hospitalists. In its follow-up letter to CMS staff thanking them for their time, SHM leadership also included recommendations that would expand the current number of PVRP measures that hospitalists could report on from two measures to seven.
SHM has also shared the above quality and performance improvement agenda with the staff of the ACP as well as their quality subcommittee, who have found it to be “well-reasoned and straightforward.” We anticipate having more in-depth discussions with the ACP as our quality agenda evolves.
In August, the Ambulatory Care Quality Alliance (AQA) and the Hospital Quality Alliance (HQA) joined forces to form a Quality Steering Committee in order to better coordinate the promotion of quality measurement, transparency, and improvement in care across hospital and ambulatory care settings. The PSTF is currently pursuing participation in one of the new AQA/HQA workgroups created by the steering committee, which would focus on harmonization of measures across settings.
SHM staff have also reached out to the Society of Critical Care Medicine, the Joint Commission on Accreditation of Healthcare Organizations, and the American Hospital Association to ascertain what these groups are doing in terms of quality and measure development, as well as to see how to align our efforts more closely.
In its work with all of these groups, the task force endeavors to ensure the development of performance measures that more accurately reflect services provided by hospitalists.
2007 Goals
The HQPS has developed a mechanism whereby they review measures proposed by a variety of organizations in order to evaluate which measures are relevant to individual clinicians as compared with institutional measures. It is PSTF’s goal (in conjunction with the HQPS, the PPC, and others) to recommend to the SHM board of directors which physician-level disease-specific measures are relevant to individual hospitalists and to identify where the gaps are. It hopes then to influence the scope of development of care coordination and other hospital-level measures that are in the pipeline, whether working through groups like the PCPI by taking the lead on an expert workgroup, by using the NQF consensus-building process, or by forming other key partnerships with groups like those noted above. It is likely that this work will be accomplished by some combination of these strategies.
Stay tuned for next month’s “SHM Behind the Scenes” by SHM Senior Vice President Joe Miller.
Epstein is the senior advisor for Standards and Compliance at SHM.
2005-2006 Survey Factoid
Use of PAs and NPs in hospital medicine groups
- Thirty percent of all hospital medicine groups (HMGs) employ nurse practitioners (NPs) and physician assistants (PAs).
- Those groups, on average, have 11.2 physicians and 2.8 NPs/PAs. The 70% of groups without NPs/PAs average 7.9 physicians per group.
- The following types of groups are more likely to employ NPs/PAs: academic programs, groups in the eastern U.S., and groups more than 5 years old.
- The frequency with which NPs/PAs perform certain functions in HMGs is summarized in this table:
NP/PA Function - % of HMGs
- Round daily on hospitalized patients - 83%
- Write prescriptions for patients - 82%
- Perform H & Ps upon admission - 77%
- Act as initial responder (consults, admits) - 66%
- Participate in discharge planning - 66%
- Order specialty consultations - 53%
- Assist in teaching students - 33%
- Night or weekend call - 30%
- Post discharge follow-up calls - 20%
- Emergency response; Code Blue - 14%
- Perform invasive procedures - 11%
Source: SHM’s 2005-2006 “Biannual State of the Hospital Medicine Movement” survey.
Pay Dirt

It’ s easy to find figures on what hospitalists earn these days, but if your own income doesn’t match up, does that mean you’re underpaid? Not necessarily.
The SHM Survey
There are several sources that provide figures on hospitalist income, but SHM offers an accurate, detailed—and the largest representative—picture of what hospitalists earn now. In spring 2006, SHM released its latest comprehensive survey of membership, “The 2005-2006 SHM Survey: The Authoritative Source on the State of the Hospitalist Movement.” The report is based on responses of 396 hospital medicine groups representing more than 2,500 hospitalists. However, Joseph A. Miller, senior vice president of SHM, warns that the survey’s salary figures may skew toward one or more specific demographics.
“In our survey, we have a number of respondents in each cell—academic, pediatric, etc.—as well as a range of geographic areas and other differences,” he says. “Anyone who looks at the metric needs to understand the factors behind it.”
John Nelson, MD, director, hospital practice, Overlake Hospital, Bellevue, Wash., and author of “Practice Management” for The Hospitalist, who has participated in developing and analyzing SHM surveys for years, agrees that the figures in the survey should be used as general guidelines only. “It’s easy to take individual metrics in a vacuum without considering the variables,” he warns.
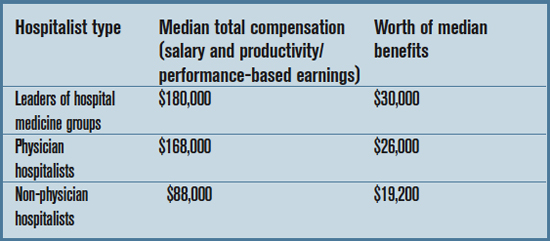
With these caveats in mind, the basic information on hospitalist compensation from the survey breaks down as follows: (table right)
To put these numbers in perspective, the median number of patient encounters per hospitalist was 2,328 per year, and the median number of work RVUs was 3,213.
Both leader- and physician-hospitalists have enjoyed an 8% increase in compensation, as well as an 8% increase in benefits, compared with the 2003-2004 survey. Non-physician hospitalists have seen a whopping increase in median income of 26% since 2003-2004. (Their benefits increased 7%.)
Perhaps the main reason for steadily increasing hospitalist incomes is that demand for hospitalists continues to exceed supply. “I’ve been trying to recruit hospitalists to my group for years,” says Dr. Nelson. “I thought that by 2002 or 2003, the number of available physicians would exceed the demand—but that hasn’t happened. It’s true that the number of doctors interested in hospital medicine has gone up pretty dramatically, but the demand went up even faster.”
By some estimates, says Dr. Nelson, there are two or three open positions for every hospitalist jobseeker.
—John Nelson, MD
Forms of Payment
To break these figures down further, income varies with type of compensation. In other words, how you are paid can influence how much you’re paid. Physician hospitalists who are paid 100% salary had a median income of $150,000. Those who are 100% productivity/performance-based make more money—a median income of $165,000; and those with a mixed-compensation model make the most of all, with a median income of $170,000.
Currently, according to the SHM survey, only 28% of respondents are 100% salary-based and 5% are 100% productivity/performance-based. The remaining majority (67%) is compensated with a combination of the two. Compared to the 2003-2004 SHM survey, the mixed compensation model increased from 47%.
“The portion of hospitalists paid via straight salary or based solely on production has been declining in the last few years,” says Dr. Nelson. “I think [a] low base and high productivity component is ideal, but [a] lower base does impede recruiting even if the total income is very attractive.”
IPC—The Hospitalist Company, one of the largest employers of hospitalists, uses the same combination of base salary and incentives for all physicians, regardless of their level of experience.
“We might change the salary figures slightly for different geographic areas, says Tim Lary, vice president of physician staffing for IPC, “but within our company, the average physician earns a little bit north of $200,000. A large portion earn over $300,000 because of our incentive plan.” That figure includes a base salary of approximately $150,000; the rest is comprised of incentives based on “typical counters” that hospitalists see, according to Lary, including productivity, quality indicators, and compliance.
Lary postulates that compensation is higher at a large organization like IPC because those employers have an infrastructure in place that ensures cost-effectiveness. “We have a 99.9% collection rate because we have a good central business office,” he says. “Small groups don’t have resources like that. We also do a great deal of training in proper coding techniques so that we can bill appropriately.”
A Grain of Salt
Before you barge in to your director’s office and ask for a raise, you should understand that the salaries summarized here have severe limitations and should be seen only as rough guidelines. There are major factors that can boost annual compensation, including:
- A heavy load of on-call, night, or weekend work;
- Employment in a geographic region with a shortage of physicians;
- Employment in a geographic region with higher physician incomes (such as the southeast);
- The type of practice you work for; and
- New practices recruiting hospitalists.
Also keep in mind that compensation totals include all bonuses and incentives received during the year.
Find Your Figure
Hospitalist income—particularly productivity-based income—is also directly affected by workload. Dr. Nelson suggests using the information in the SHM survey to find a rough guideline for productivity and compensation.
“Take the compensation figure from the survey for your region, production type, etc. and take the average production numbers from that same subgroup,” he says. “Then do the math to find the number of dollars per encounter or per RVU, and gauge your own numbers. If you have 25% more encounters, your income should be 25% higher than the average.”
The best rule of thumb for estimating what you should make, says Dr. Nelson, is to aim for five to 15% more than physicians working in traditional practice in your market. Unfortunately, information on what other doctors earn may not be readily available. Some sources (including a few listed in the sidebar to this article) provide information on all physician incomes, but is broken down by region at best. “You have to ask around,” says Dr. Nelson. “And if you’re interviewing, ask what they’re offering—then go and interview at a private practice and ask what they’re offering.”
In other words, there’s no easy way to tell if what you make is exactly on the mark for other hospitalists in your area—unless you ask those other hospitalists. But the SHM survey information should provide enough information to give you an idea. You can view an executive summary of the survey or purchase a complete copy at www.hospitalmedicine.org. TH
Jane Jerrard is the monthly writer for “Career Development.”
It’ s easy to find figures on what hospitalists earn these days, but if your own income doesn’t match up, does that mean you’re underpaid? Not necessarily.
The SHM Survey
There are several sources that provide figures on hospitalist income, but SHM offers an accurate, detailed—and the largest representative—picture of what hospitalists earn now. In spring 2006, SHM released its latest comprehensive survey of membership, “The 2005-2006 SHM Survey: The Authoritative Source on the State of the Hospitalist Movement.” The report is based on responses of 396 hospital medicine groups representing more than 2,500 hospitalists. However, Joseph A. Miller, senior vice president of SHM, warns that the survey’s salary figures may skew toward one or more specific demographics.
“In our survey, we have a number of respondents in each cell—academic, pediatric, etc.—as well as a range of geographic areas and other differences,” he says. “Anyone who looks at the metric needs to understand the factors behind it.”
John Nelson, MD, director, hospital practice, Overlake Hospital, Bellevue, Wash., and author of “Practice Management” for The Hospitalist, who has participated in developing and analyzing SHM surveys for years, agrees that the figures in the survey should be used as general guidelines only. “It’s easy to take individual metrics in a vacuum without considering the variables,” he warns.
With these caveats in mind, the basic information on hospitalist compensation from the survey breaks down as follows: (table right)
To put these numbers in perspective, the median number of patient encounters per hospitalist was 2,328 per year, and the median number of work RVUs was 3,213.
Both leader- and physician-hospitalists have enjoyed an 8% increase in compensation, as well as an 8% increase in benefits, compared with the 2003-2004 survey. Non-physician hospitalists have seen a whopping increase in median income of 26% since 2003-2004. (Their benefits increased 7%.)
Perhaps the main reason for steadily increasing hospitalist incomes is that demand for hospitalists continues to exceed supply. “I’ve been trying to recruit hospitalists to my group for years,” says Dr. Nelson. “I thought that by 2002 or 2003, the number of available physicians would exceed the demand—but that hasn’t happened. It’s true that the number of doctors interested in hospital medicine has gone up pretty dramatically, but the demand went up even faster.”
By some estimates, says Dr. Nelson, there are two or three open positions for every hospitalist jobseeker.
—John Nelson, MD
Forms of Payment
To break these figures down further, income varies with type of compensation. In other words, how you are paid can influence how much you’re paid. Physician hospitalists who are paid 100% salary had a median income of $150,000. Those who are 100% productivity/performance-based make more money—a median income of $165,000; and those with a mixed-compensation model make the most of all, with a median income of $170,000.
Currently, according to the SHM survey, only 28% of respondents are 100% salary-based and 5% are 100% productivity/performance-based. The remaining majority (67%) is compensated with a combination of the two. Compared to the 2003-2004 SHM survey, the mixed compensation model increased from 47%.
“The portion of hospitalists paid via straight salary or based solely on production has been declining in the last few years,” says Dr. Nelson. “I think [a] low base and high productivity component is ideal, but [a] lower base does impede recruiting even if the total income is very attractive.”
IPC—The Hospitalist Company, one of the largest employers of hospitalists, uses the same combination of base salary and incentives for all physicians, regardless of their level of experience.
“We might change the salary figures slightly for different geographic areas, says Tim Lary, vice president of physician staffing for IPC, “but within our company, the average physician earns a little bit north of $200,000. A large portion earn over $300,000 because of our incentive plan.” That figure includes a base salary of approximately $150,000; the rest is comprised of incentives based on “typical counters” that hospitalists see, according to Lary, including productivity, quality indicators, and compliance.
Lary postulates that compensation is higher at a large organization like IPC because those employers have an infrastructure in place that ensures cost-effectiveness. “We have a 99.9% collection rate because we have a good central business office,” he says. “Small groups don’t have resources like that. We also do a great deal of training in proper coding techniques so that we can bill appropriately.”
A Grain of Salt
Before you barge in to your director’s office and ask for a raise, you should understand that the salaries summarized here have severe limitations and should be seen only as rough guidelines. There are major factors that can boost annual compensation, including:
- A heavy load of on-call, night, or weekend work;
- Employment in a geographic region with a shortage of physicians;
- Employment in a geographic region with higher physician incomes (such as the southeast);
- The type of practice you work for; and
- New practices recruiting hospitalists.
Also keep in mind that compensation totals include all bonuses and incentives received during the year.
Find Your Figure
Hospitalist income—particularly productivity-based income—is also directly affected by workload. Dr. Nelson suggests using the information in the SHM survey to find a rough guideline for productivity and compensation.
“Take the compensation figure from the survey for your region, production type, etc. and take the average production numbers from that same subgroup,” he says. “Then do the math to find the number of dollars per encounter or per RVU, and gauge your own numbers. If you have 25% more encounters, your income should be 25% higher than the average.”
The best rule of thumb for estimating what you should make, says Dr. Nelson, is to aim for five to 15% more than physicians working in traditional practice in your market. Unfortunately, information on what other doctors earn may not be readily available. Some sources (including a few listed in the sidebar to this article) provide information on all physician incomes, but is broken down by region at best. “You have to ask around,” says Dr. Nelson. “And if you’re interviewing, ask what they’re offering—then go and interview at a private practice and ask what they’re offering.”
In other words, there’s no easy way to tell if what you make is exactly on the mark for other hospitalists in your area—unless you ask those other hospitalists. But the SHM survey information should provide enough information to give you an idea. You can view an executive summary of the survey or purchase a complete copy at www.hospitalmedicine.org. TH
Jane Jerrard is the monthly writer for “Career Development.”
It’ s easy to find figures on what hospitalists earn these days, but if your own income doesn’t match up, does that mean you’re underpaid? Not necessarily.
The SHM Survey
There are several sources that provide figures on hospitalist income, but SHM offers an accurate, detailed—and the largest representative—picture of what hospitalists earn now. In spring 2006, SHM released its latest comprehensive survey of membership, “The 2005-2006 SHM Survey: The Authoritative Source on the State of the Hospitalist Movement.” The report is based on responses of 396 hospital medicine groups representing more than 2,500 hospitalists. However, Joseph A. Miller, senior vice president of SHM, warns that the survey’s salary figures may skew toward one or more specific demographics.
“In our survey, we have a number of respondents in each cell—academic, pediatric, etc.—as well as a range of geographic areas and other differences,” he says. “Anyone who looks at the metric needs to understand the factors behind it.”
John Nelson, MD, director, hospital practice, Overlake Hospital, Bellevue, Wash., and author of “Practice Management” for The Hospitalist, who has participated in developing and analyzing SHM surveys for years, agrees that the figures in the survey should be used as general guidelines only. “It’s easy to take individual metrics in a vacuum without considering the variables,” he warns.
With these caveats in mind, the basic information on hospitalist compensation from the survey breaks down as follows: (table right)
To put these numbers in perspective, the median number of patient encounters per hospitalist was 2,328 per year, and the median number of work RVUs was 3,213.
Both leader- and physician-hospitalists have enjoyed an 8% increase in compensation, as well as an 8% increase in benefits, compared with the 2003-2004 survey. Non-physician hospitalists have seen a whopping increase in median income of 26% since 2003-2004. (Their benefits increased 7%.)
Perhaps the main reason for steadily increasing hospitalist incomes is that demand for hospitalists continues to exceed supply. “I’ve been trying to recruit hospitalists to my group for years,” says Dr. Nelson. “I thought that by 2002 or 2003, the number of available physicians would exceed the demand—but that hasn’t happened. It’s true that the number of doctors interested in hospital medicine has gone up pretty dramatically, but the demand went up even faster.”
By some estimates, says Dr. Nelson, there are two or three open positions for every hospitalist jobseeker.
—John Nelson, MD
Forms of Payment
To break these figures down further, income varies with type of compensation. In other words, how you are paid can influence how much you’re paid. Physician hospitalists who are paid 100% salary had a median income of $150,000. Those who are 100% productivity/performance-based make more money—a median income of $165,000; and those with a mixed-compensation model make the most of all, with a median income of $170,000.
Currently, according to the SHM survey, only 28% of respondents are 100% salary-based and 5% are 100% productivity/performance-based. The remaining majority (67%) is compensated with a combination of the two. Compared to the 2003-2004 SHM survey, the mixed compensation model increased from 47%.
“The portion of hospitalists paid via straight salary or based solely on production has been declining in the last few years,” says Dr. Nelson. “I think [a] low base and high productivity component is ideal, but [a] lower base does impede recruiting even if the total income is very attractive.”
IPC—The Hospitalist Company, one of the largest employers of hospitalists, uses the same combination of base salary and incentives for all physicians, regardless of their level of experience.
“We might change the salary figures slightly for different geographic areas, says Tim Lary, vice president of physician staffing for IPC, “but within our company, the average physician earns a little bit north of $200,000. A large portion earn over $300,000 because of our incentive plan.” That figure includes a base salary of approximately $150,000; the rest is comprised of incentives based on “typical counters” that hospitalists see, according to Lary, including productivity, quality indicators, and compliance.
Lary postulates that compensation is higher at a large organization like IPC because those employers have an infrastructure in place that ensures cost-effectiveness. “We have a 99.9% collection rate because we have a good central business office,” he says. “Small groups don’t have resources like that. We also do a great deal of training in proper coding techniques so that we can bill appropriately.”
A Grain of Salt
Before you barge in to your director’s office and ask for a raise, you should understand that the salaries summarized here have severe limitations and should be seen only as rough guidelines. There are major factors that can boost annual compensation, including:
- A heavy load of on-call, night, or weekend work;
- Employment in a geographic region with a shortage of physicians;
- Employment in a geographic region with higher physician incomes (such as the southeast);
- The type of practice you work for; and
- New practices recruiting hospitalists.
Also keep in mind that compensation totals include all bonuses and incentives received during the year.
Find Your Figure
Hospitalist income—particularly productivity-based income—is also directly affected by workload. Dr. Nelson suggests using the information in the SHM survey to find a rough guideline for productivity and compensation.
“Take the compensation figure from the survey for your region, production type, etc. and take the average production numbers from that same subgroup,” he says. “Then do the math to find the number of dollars per encounter or per RVU, and gauge your own numbers. If you have 25% more encounters, your income should be 25% higher than the average.”
The best rule of thumb for estimating what you should make, says Dr. Nelson, is to aim for five to 15% more than physicians working in traditional practice in your market. Unfortunately, information on what other doctors earn may not be readily available. Some sources (including a few listed in the sidebar to this article) provide information on all physician incomes, but is broken down by region at best. “You have to ask around,” says Dr. Nelson. “And if you’re interviewing, ask what they’re offering—then go and interview at a private practice and ask what they’re offering.”
In other words, there’s no easy way to tell if what you make is exactly on the mark for other hospitalists in your area—unless you ask those other hospitalists. But the SHM survey information should provide enough information to give you an idea. You can view an executive summary of the survey or purchase a complete copy at www.hospitalmedicine.org. TH
Jane Jerrard is the monthly writer for “Career Development.”
Medicare, Money, and Quality Measures

The federal government—particularly the Centers for Medicare and Medicaid Services (CMS)—is moving faster than anyone thought possible to implement “value-based purchasing,” which ties payment to quality of care and other outcomes. CMS has a congressional mandate to make value-based purchasing a reality by fiscal year 2009.
“As Congress looks at cutting physician payments, they’re very open to alternative payment methods like pay-for-performance,” says Patrick Torcson, MD, MMM, FACP, chair of SHM’s Performance and Standards Task Force, medical director, hospital medicine, St. Tammany Parish Hospital, Covington, La. “There’s tremendous political will behind this.”
Here is an overview of three CMS demonstration programs in various stages that will determine which new payment models may shape your hospital budget—and your salary—in the future.
CMS Gainsharing Demo: An Update
As reported in the October issue of The Hospitalist, CMS has been charged with establishing six three-year gainsharing pilot programs, including two in rural settings, by January 1, 2007.
CMS invited applications for the programs in mid-September, and applications were due by November 17. The six participating hospitals will provide gainsharing payments to physicians who help to save costs. The gainsharing payments will be based on net savings. Each hospital will propose multiple approaches that will both save costs and improve quality and efficiency of care.
“Gainsharing could be a better quality incentive payment model for hospitalists, [but] maybe not for other specialties,” says Dr. Torcson.
New “Gainsharing Plus” Demo—Participation Encouraged!
During Legislative Advocacy Day at the SHM Annual Meeting in Washington, D.C., in May, SHM members personally urged policymakers to broaden the concept of gainsharing and initiate demonstration projects like this that promote physician and hospital collaboration in improving care.
Four months later (in early September) CMS surprised the healthcare community with the announcement of an additional three-year demonstration program that goes beyond the traditional concept of gainsharing—one that will examine whether allowing hospitals to provide financial incentives for physicians to support better care can improve patient outcomes without increasing costs.
“SHM was pleased to hear that CMS was offering this program because we support the development of these payment models,” says Dr. Torcson.
Under the program, known as the Physician-Hospital Collaboration Demonstration (PHCD), hospitals would be paid their usual inpatient rate for the patients’ care but would be allowed to pay physicians a portion of the savings resulting from quality improvement and efficiency initiatives.
In the CMS release announcing this demonstration, former CMS Administrator Mark B. McClellan, MD, PhD, was quoted as saying, “The most costly and intensive physician services are provided in hospitals, yet our payment systems do not support steps by hospitals and doctors to work together to improve care. This demonstration program will support efforts to track and improve the overall episode of patient care, including follow-up and longer-term outcomes.”
The program will begin in 2007, and applications are due by end of business on January 9, 2007. SHM encourages members to explore the possibility of applying for one of the demonstrations with their group and their hospital administrators. Details on the PHCD are available at www.cms.hhs.gov (go to the “Medicare” page and then click the “Demonstration Projects & Evaluation Reports” page. Then click “Medicare Demonstrations).”
Of particular interest is the fact that CMS will allow participating hospitals to set the indicators to be measured. “What they’re asking for are proposals from the hospitals as to what they’ll explore—basing the program on whatever quality indicators the hospital can [use to] measure and demonstrate cost savings,” says Dr. Torcson. “CMS is providing no details regarding specific performance measures.”
Organizations eligible for the PHCD include physician groups, integrated delivery systems (IDSs), and regional coalitions of physician groups. A hospital may be included if it has an affiliation agreement with an eligible physician group. CMS has stated that preference will be given to projects developed and implemented by a consortium of physician groups and their affiliated hospitals. No more than 72 hospitals across all projects will be included in the demonstration.
“This raises the bar that any physician group has to be pretty far along already in measuring quality indicators and performance reporting,” says Dr. Torcson. “It will take a lot of infrastructure to report, measure, [and so on]. I’ll be very impressed with any group that is that far along with performance measurement and reporting. I hope a hospitalist group can be among those that step up and apply.”
Dr. Torcson believes that, while CMS did not specify hospitalists, a hospital medicine group would be uniquely positioned to participate. “Hospitalists are perfect for this,” he emphasizes.
Premier Hospital Demo: Mission Accomplished!
CMS’ first pay-for-performance demonstration program is complete. The Premier Hospital Quality Incentive Demonstration officially ended in September. CMS partnered with Premier, Inc., a nationwide alliance of not-for-profit hospitals, for the three-year demo. At the end of each of the three years, CMS rewarded the top-performing hospitals with cash bonuses. Performance was based on 33 evidence-based quality measures for inpatients with heart attack, heart failure, pneumonia, coronary artery bypass graft, and hip and knee replacements. (The individual measures were compiled into an overall quality score for each clinical condition.)
“I wish all our projects went this well,” said Mark Wynn, director of the Division of Payment Policy Demonstrations, CMS. “We’re absolutely delighted. This program shows the efficacy [of] using pay-for-performance in hospitals.”
According to analysis from Premier, Inc., if every patient in the country with pneumonia, heart bypass, acute myocardial infarction, and hip and knee replacement in 2004 had received most or all (76% to 100%) of a set of widely accepted care processes, it could have resulted in nearly 5,700 fewer deaths, 8,100 fewer complications, 10,000 fewer readmissions, and 750,000 fewer days in the hospital. In addition, hospital costs could have been as much as $1.35 billion lower.
What’s next? Wynn says that CMS is “actively looking at lessons we can use” as the agency prepares a report to be presented to Congress in 2007. “We’ll make a specific recommendation regarding pay-for-performance.”
The Future Is Coming
“Value-based purchasing is here to stay,” says Dr. Torcson. “For the significant amount of money spent on healthcare, you have to see a certain level of quality in return. This hasn’t been so obvious in healthcare. Healthcare is just starting to look like the free market in this regard. There’s a place for both pay-for-performance and gainsharing. The CMS budget is big enough for both.”
SHM is involved in pushing for these changes and wants to prepare members for any new measurement criteria that develop. “We would like for the work of the SHM Performance and Standards Task Force to result in an SHM performance agenda,” says Dr. Torcson. “We want to be able to tell members what to expect when all of these demos become a reality and be able to provide relevant information on designing their programs so that they’re ready.” TH
Jane Jerrard regularly writes “Public Policy.”
The federal government—particularly the Centers for Medicare and Medicaid Services (CMS)—is moving faster than anyone thought possible to implement “value-based purchasing,” which ties payment to quality of care and other outcomes. CMS has a congressional mandate to make value-based purchasing a reality by fiscal year 2009.
“As Congress looks at cutting physician payments, they’re very open to alternative payment methods like pay-for-performance,” says Patrick Torcson, MD, MMM, FACP, chair of SHM’s Performance and Standards Task Force, medical director, hospital medicine, St. Tammany Parish Hospital, Covington, La. “There’s tremendous political will behind this.”
Here is an overview of three CMS demonstration programs in various stages that will determine which new payment models may shape your hospital budget—and your salary—in the future.
CMS Gainsharing Demo: An Update
As reported in the October issue of The Hospitalist, CMS has been charged with establishing six three-year gainsharing pilot programs, including two in rural settings, by January 1, 2007.
CMS invited applications for the programs in mid-September, and applications were due by November 17. The six participating hospitals will provide gainsharing payments to physicians who help to save costs. The gainsharing payments will be based on net savings. Each hospital will propose multiple approaches that will both save costs and improve quality and efficiency of care.
“Gainsharing could be a better quality incentive payment model for hospitalists, [but] maybe not for other specialties,” says Dr. Torcson.
New “Gainsharing Plus” Demo—Participation Encouraged!
During Legislative Advocacy Day at the SHM Annual Meeting in Washington, D.C., in May, SHM members personally urged policymakers to broaden the concept of gainsharing and initiate demonstration projects like this that promote physician and hospital collaboration in improving care.
Four months later (in early September) CMS surprised the healthcare community with the announcement of an additional three-year demonstration program that goes beyond the traditional concept of gainsharing—one that will examine whether allowing hospitals to provide financial incentives for physicians to support better care can improve patient outcomes without increasing costs.
“SHM was pleased to hear that CMS was offering this program because we support the development of these payment models,” says Dr. Torcson.
Under the program, known as the Physician-Hospital Collaboration Demonstration (PHCD), hospitals would be paid their usual inpatient rate for the patients’ care but would be allowed to pay physicians a portion of the savings resulting from quality improvement and efficiency initiatives.
In the CMS release announcing this demonstration, former CMS Administrator Mark B. McClellan, MD, PhD, was quoted as saying, “The most costly and intensive physician services are provided in hospitals, yet our payment systems do not support steps by hospitals and doctors to work together to improve care. This demonstration program will support efforts to track and improve the overall episode of patient care, including follow-up and longer-term outcomes.”
The program will begin in 2007, and applications are due by end of business on January 9, 2007. SHM encourages members to explore the possibility of applying for one of the demonstrations with their group and their hospital administrators. Details on the PHCD are available at www.cms.hhs.gov (go to the “Medicare” page and then click the “Demonstration Projects & Evaluation Reports” page. Then click “Medicare Demonstrations).”
Of particular interest is the fact that CMS will allow participating hospitals to set the indicators to be measured. “What they’re asking for are proposals from the hospitals as to what they’ll explore—basing the program on whatever quality indicators the hospital can [use to] measure and demonstrate cost savings,” says Dr. Torcson. “CMS is providing no details regarding specific performance measures.”
Organizations eligible for the PHCD include physician groups, integrated delivery systems (IDSs), and regional coalitions of physician groups. A hospital may be included if it has an affiliation agreement with an eligible physician group. CMS has stated that preference will be given to projects developed and implemented by a consortium of physician groups and their affiliated hospitals. No more than 72 hospitals across all projects will be included in the demonstration.
“This raises the bar that any physician group has to be pretty far along already in measuring quality indicators and performance reporting,” says Dr. Torcson. “It will take a lot of infrastructure to report, measure, [and so on]. I’ll be very impressed with any group that is that far along with performance measurement and reporting. I hope a hospitalist group can be among those that step up and apply.”
Dr. Torcson believes that, while CMS did not specify hospitalists, a hospital medicine group would be uniquely positioned to participate. “Hospitalists are perfect for this,” he emphasizes.
Premier Hospital Demo: Mission Accomplished!
CMS’ first pay-for-performance demonstration program is complete. The Premier Hospital Quality Incentive Demonstration officially ended in September. CMS partnered with Premier, Inc., a nationwide alliance of not-for-profit hospitals, for the three-year demo. At the end of each of the three years, CMS rewarded the top-performing hospitals with cash bonuses. Performance was based on 33 evidence-based quality measures for inpatients with heart attack, heart failure, pneumonia, coronary artery bypass graft, and hip and knee replacements. (The individual measures were compiled into an overall quality score for each clinical condition.)
“I wish all our projects went this well,” said Mark Wynn, director of the Division of Payment Policy Demonstrations, CMS. “We’re absolutely delighted. This program shows the efficacy [of] using pay-for-performance in hospitals.”
According to analysis from Premier, Inc., if every patient in the country with pneumonia, heart bypass, acute myocardial infarction, and hip and knee replacement in 2004 had received most or all (76% to 100%) of a set of widely accepted care processes, it could have resulted in nearly 5,700 fewer deaths, 8,100 fewer complications, 10,000 fewer readmissions, and 750,000 fewer days in the hospital. In addition, hospital costs could have been as much as $1.35 billion lower.
What’s next? Wynn says that CMS is “actively looking at lessons we can use” as the agency prepares a report to be presented to Congress in 2007. “We’ll make a specific recommendation regarding pay-for-performance.”
The Future Is Coming
“Value-based purchasing is here to stay,” says Dr. Torcson. “For the significant amount of money spent on healthcare, you have to see a certain level of quality in return. This hasn’t been so obvious in healthcare. Healthcare is just starting to look like the free market in this regard. There’s a place for both pay-for-performance and gainsharing. The CMS budget is big enough for both.”
SHM is involved in pushing for these changes and wants to prepare members for any new measurement criteria that develop. “We would like for the work of the SHM Performance and Standards Task Force to result in an SHM performance agenda,” says Dr. Torcson. “We want to be able to tell members what to expect when all of these demos become a reality and be able to provide relevant information on designing their programs so that they’re ready.” TH
Jane Jerrard regularly writes “Public Policy.”
The federal government—particularly the Centers for Medicare and Medicaid Services (CMS)—is moving faster than anyone thought possible to implement “value-based purchasing,” which ties payment to quality of care and other outcomes. CMS has a congressional mandate to make value-based purchasing a reality by fiscal year 2009.
“As Congress looks at cutting physician payments, they’re very open to alternative payment methods like pay-for-performance,” says Patrick Torcson, MD, MMM, FACP, chair of SHM’s Performance and Standards Task Force, medical director, hospital medicine, St. Tammany Parish Hospital, Covington, La. “There’s tremendous political will behind this.”
Here is an overview of three CMS demonstration programs in various stages that will determine which new payment models may shape your hospital budget—and your salary—in the future.
CMS Gainsharing Demo: An Update
As reported in the October issue of The Hospitalist, CMS has been charged with establishing six three-year gainsharing pilot programs, including two in rural settings, by January 1, 2007.
CMS invited applications for the programs in mid-September, and applications were due by November 17. The six participating hospitals will provide gainsharing payments to physicians who help to save costs. The gainsharing payments will be based on net savings. Each hospital will propose multiple approaches that will both save costs and improve quality and efficiency of care.
“Gainsharing could be a better quality incentive payment model for hospitalists, [but] maybe not for other specialties,” says Dr. Torcson.
New “Gainsharing Plus” Demo—Participation Encouraged!
During Legislative Advocacy Day at the SHM Annual Meeting in Washington, D.C., in May, SHM members personally urged policymakers to broaden the concept of gainsharing and initiate demonstration projects like this that promote physician and hospital collaboration in improving care.
Four months later (in early September) CMS surprised the healthcare community with the announcement of an additional three-year demonstration program that goes beyond the traditional concept of gainsharing—one that will examine whether allowing hospitals to provide financial incentives for physicians to support better care can improve patient outcomes without increasing costs.
“SHM was pleased to hear that CMS was offering this program because we support the development of these payment models,” says Dr. Torcson.
Under the program, known as the Physician-Hospital Collaboration Demonstration (PHCD), hospitals would be paid their usual inpatient rate for the patients’ care but would be allowed to pay physicians a portion of the savings resulting from quality improvement and efficiency initiatives.
In the CMS release announcing this demonstration, former CMS Administrator Mark B. McClellan, MD, PhD, was quoted as saying, “The most costly and intensive physician services are provided in hospitals, yet our payment systems do not support steps by hospitals and doctors to work together to improve care. This demonstration program will support efforts to track and improve the overall episode of patient care, including follow-up and longer-term outcomes.”
The program will begin in 2007, and applications are due by end of business on January 9, 2007. SHM encourages members to explore the possibility of applying for one of the demonstrations with their group and their hospital administrators. Details on the PHCD are available at www.cms.hhs.gov (go to the “Medicare” page and then click the “Demonstration Projects & Evaluation Reports” page. Then click “Medicare Demonstrations).”
Of particular interest is the fact that CMS will allow participating hospitals to set the indicators to be measured. “What they’re asking for are proposals from the hospitals as to what they’ll explore—basing the program on whatever quality indicators the hospital can [use to] measure and demonstrate cost savings,” says Dr. Torcson. “CMS is providing no details regarding specific performance measures.”
Organizations eligible for the PHCD include physician groups, integrated delivery systems (IDSs), and regional coalitions of physician groups. A hospital may be included if it has an affiliation agreement with an eligible physician group. CMS has stated that preference will be given to projects developed and implemented by a consortium of physician groups and their affiliated hospitals. No more than 72 hospitals across all projects will be included in the demonstration.
“This raises the bar that any physician group has to be pretty far along already in measuring quality indicators and performance reporting,” says Dr. Torcson. “It will take a lot of infrastructure to report, measure, [and so on]. I’ll be very impressed with any group that is that far along with performance measurement and reporting. I hope a hospitalist group can be among those that step up and apply.”
Dr. Torcson believes that, while CMS did not specify hospitalists, a hospital medicine group would be uniquely positioned to participate. “Hospitalists are perfect for this,” he emphasizes.
Premier Hospital Demo: Mission Accomplished!
CMS’ first pay-for-performance demonstration program is complete. The Premier Hospital Quality Incentive Demonstration officially ended in September. CMS partnered with Premier, Inc., a nationwide alliance of not-for-profit hospitals, for the three-year demo. At the end of each of the three years, CMS rewarded the top-performing hospitals with cash bonuses. Performance was based on 33 evidence-based quality measures for inpatients with heart attack, heart failure, pneumonia, coronary artery bypass graft, and hip and knee replacements. (The individual measures were compiled into an overall quality score for each clinical condition.)
“I wish all our projects went this well,” said Mark Wynn, director of the Division of Payment Policy Demonstrations, CMS. “We’re absolutely delighted. This program shows the efficacy [of] using pay-for-performance in hospitals.”
According to analysis from Premier, Inc., if every patient in the country with pneumonia, heart bypass, acute myocardial infarction, and hip and knee replacement in 2004 had received most or all (76% to 100%) of a set of widely accepted care processes, it could have resulted in nearly 5,700 fewer deaths, 8,100 fewer complications, 10,000 fewer readmissions, and 750,000 fewer days in the hospital. In addition, hospital costs could have been as much as $1.35 billion lower.
What’s next? Wynn says that CMS is “actively looking at lessons we can use” as the agency prepares a report to be presented to Congress in 2007. “We’ll make a specific recommendation regarding pay-for-performance.”
The Future Is Coming
“Value-based purchasing is here to stay,” says Dr. Torcson. “For the significant amount of money spent on healthcare, you have to see a certain level of quality in return. This hasn’t been so obvious in healthcare. Healthcare is just starting to look like the free market in this regard. There’s a place for both pay-for-performance and gainsharing. The CMS budget is big enough for both.”
SHM is involved in pushing for these changes and wants to prepare members for any new measurement criteria that develop. “We would like for the work of the SHM Performance and Standards Task Force to result in an SHM performance agenda,” says Dr. Torcson. “We want to be able to tell members what to expect when all of these demos become a reality and be able to provide relevant information on designing their programs so that they’re ready.” TH
Jane Jerrard regularly writes “Public Policy.”
Are You Satisfied?

“(I can’t get no) satisfaction.”—The Rolling Stones
Do you know people who have good health, loving families, a healthy income, and a great house but who are still not satisfied? You may also know some people who seemingly have little to be thankful for, and yet they are very satisfied. There has been a great deal of research on this topic, specifically as it relates to job or career satisfaction. Some assume that the main component of job satisfaction is how much a person is paid. In study after study, however, compensation is never first and is often fourth or lower on the list of items that people identify as the key factors related to their satisfaction. So what are the other factors?
What Stimulates You?
The nature of the work is important. People must find their work stimulating. Everyone finds stimulation at different levels—for some it may involve being technically successful, whether they are reviewing contract language or hanging crown molding. Others find performing a procedure such as a cardiac catheterization or a lumbar puncture highly energizing. Or stimulation—for the master chess player, for example—may be found strictly on a mental level. Whatever the sweet spot, it is important to identify what you find motivating and challenging.
Overstimulating situations, on the other hand, are uncomfortable and dissatisfying. Some individuals thrive in a highly stressful environment, such as air traffic control, that others would find overwhelming.
One of the unique features of being a hospitalist is the need to work collaboratively across many disciplines to achieve results for our patients. The collegiality involved in the team approach can be invigorating and satisfying to many people. For others, it is simply frustrating.
Do You Feel Appreciated?
Recognition for a job well done is something everyone needs. We see this in our co-workers and in children when they try something and are praised for it. We all need recognition for doing a good job day after day. This seemed counterintuitive to me when I first learned about it. Gee whiz, I thought, why do I have to say, “Good job,” when people are just doing what they are supposed to do? It turns out that we all need to be recognized regularly in order to feel that we are valued and needed. It keeps us interested and motivated.
This reminds me of the old joke in which the wife says to her husband of 25 years, “Do you love me?” He replies, “Well, I told you so 15 years ago. Don’t you remember?”
This does not mean we need a financial reward every other day or a big bonus every month. It means that we desire recognition that is meaningful and timely. Studies have shown that unless the recognition is personalized, it can have a negative effect. For instance, if I don’t care for sports, rewarding me with tickets to a baseball game will seem depersonalized and will give me the feeling that no one took the time to know what is important to me.
By the same token, if praise in a public setting makes me uncomfortable, don’t create a reward banquet with great public fanfare. People prize small things like handwritten thank you notes, gift cards for places they like (Starbucks!), or opportunities for educational or other activities. A simple “thank you,” said with enthusiasm, does wonders. Respect is closely tied to recognition. If the hospitalist feels like a glorified resident, the sense of disrespect is pervasive—more on this below.
Are You in Control?
Autonomy and control over your work and work life remain key factors in career satisfaction. This includes having input not only when it comes to the schedule but also, and more importantly, with regard to the processes. Can you participate in design for your group or at the hospital? If you find that all your suggestions fall on deaf ears, then either the work environment needs some adjusting or you are always wrong! Small things can be important here. Just having the flexibility to participate in quality processes or to give input on a protocol creates a feeling of control over your work. Hospitalists who have decisions imposed on them experience a great deal of tension and may, ultimately, resign.
Is there an opportunity for promotion or further learning? An individual who feels boxed in and unable to make career improvements is often dissatisfied. This ties in to the need for challenge and the importance of the nature of the work.
We all have personal challenges that we would like the flexibility to address. You may have childcare or elder care issues. Perhaps you want to train for the next Ironman race. If you are unable to address these personal aspirations and goals, you may feel that you have no control over your life, much less your work life.
Are You Happy at Work?
Work environment—who knew how important this could be? Let’s say you are employed at a large organization, perhaps General Electric. GE controls the environment for all of its employees. The company makes sure that the lighting is adequate. It tries to protect its employees from hostility based on gender, race, or disability. GE controls work assignments, and there is a chain of command for any issue that needs to be addressed.
The hospitalist, as a member of the medical staff, may be in a much different setting. Often, hospitalists work in someone else’s environment. The nurses and physicians with whom they work are generally hired by others. The atmosphere in which they work can be hostile, devoid of respect. There is often no clear chain of command set up to resolve work environment issues. Some facilities are frustrating and challenging to work in, with insufficient translators or inadequate lab or X-ray support. Fellow medical staff members or administrators may not understand how hospitalists differ from other specialists, making the job of the hospitalist more difficult
An individual’s inability to affect the work environment due to the structure of the facility can be detrimental to morale. Are the committees structured so that hospitalists can participate in them and influence the decisions they make? Even seemingly small issues can have a big impact on a hospitalist’s feelings of control and autonomy.
What Do You Earn?
Finally, compensation. Everyone wants a fair wage for a reasonable work effort. It seems simple, but obviously there are tensions here. All things being equal, a person’s income should be competitive and fair. The definition of “fair” is often determined by the marketplace. In the field of hospitalist medicine, there is a great deal of competition for labor, so there are many opportunities to evaluate. But finding the work that is most satisfying involves attaining a combination of the abovementioned characteristics as well as evaluating location.
SHM’s Task Force Examines the Issue
So, what to do? As an organization, SHM has appointed a Career Satisfaction Task Force to study work satisfaction and to design processes that will address this issue specifically for the hospitalist workforce. As I mentioned above, this topic has been studied extensively in various employee environments for many years. Retention of valuable employees is a key component of an organization’s success. This applies to nonmedical as well as to medical fields. The emergency medicine field, for example, has done some work on the challenges specific to their physicians and has some interesting insights. We expect to share the work product of our own task force in the future.
Short-Term Help
But what to do now? If you are a hospitalist leader, ask your group for feedback. Are they finding satisfaction in the areas described above? Find ways to develop control and autonomy for your group. Encourage them to participate in shaping their own careers and futures. Recognize, recognize, recognize. You can’t say “Thank you” or “Good job” too often. Learn how your group members prefer to be recognized and try to personalize what you do for them. Remember this line from The One Minute Manager, by Kenneth Blanchard, PhD, and Spencer Johnson, MD: “Catch them doing something right.” It happens around us all day, but we take performance for granted and fail to praise and recognize.
If you are a hospitalist, help shape your own destiny. Participate, ask questions, and devise solutions. And recognize the nurses, the social worker, and your group leader.
Together we can create career satisfaction and lifelong, fulfilling work. Unlike Mick Jagger, we will then get some satisfaction! TH
Dr. Gorman is the president of SHM.
“(I can’t get no) satisfaction.”—The Rolling Stones
Do you know people who have good health, loving families, a healthy income, and a great house but who are still not satisfied? You may also know some people who seemingly have little to be thankful for, and yet they are very satisfied. There has been a great deal of research on this topic, specifically as it relates to job or career satisfaction. Some assume that the main component of job satisfaction is how much a person is paid. In study after study, however, compensation is never first and is often fourth or lower on the list of items that people identify as the key factors related to their satisfaction. So what are the other factors?
What Stimulates You?
The nature of the work is important. People must find their work stimulating. Everyone finds stimulation at different levels—for some it may involve being technically successful, whether they are reviewing contract language or hanging crown molding. Others find performing a procedure such as a cardiac catheterization or a lumbar puncture highly energizing. Or stimulation—for the master chess player, for example—may be found strictly on a mental level. Whatever the sweet spot, it is important to identify what you find motivating and challenging.
Overstimulating situations, on the other hand, are uncomfortable and dissatisfying. Some individuals thrive in a highly stressful environment, such as air traffic control, that others would find overwhelming.
One of the unique features of being a hospitalist is the need to work collaboratively across many disciplines to achieve results for our patients. The collegiality involved in the team approach can be invigorating and satisfying to many people. For others, it is simply frustrating.
Do You Feel Appreciated?
Recognition for a job well done is something everyone needs. We see this in our co-workers and in children when they try something and are praised for it. We all need recognition for doing a good job day after day. This seemed counterintuitive to me when I first learned about it. Gee whiz, I thought, why do I have to say, “Good job,” when people are just doing what they are supposed to do? It turns out that we all need to be recognized regularly in order to feel that we are valued and needed. It keeps us interested and motivated.
This reminds me of the old joke in which the wife says to her husband of 25 years, “Do you love me?” He replies, “Well, I told you so 15 years ago. Don’t you remember?”
This does not mean we need a financial reward every other day or a big bonus every month. It means that we desire recognition that is meaningful and timely. Studies have shown that unless the recognition is personalized, it can have a negative effect. For instance, if I don’t care for sports, rewarding me with tickets to a baseball game will seem depersonalized and will give me the feeling that no one took the time to know what is important to me.
By the same token, if praise in a public setting makes me uncomfortable, don’t create a reward banquet with great public fanfare. People prize small things like handwritten thank you notes, gift cards for places they like (Starbucks!), or opportunities for educational or other activities. A simple “thank you,” said with enthusiasm, does wonders. Respect is closely tied to recognition. If the hospitalist feels like a glorified resident, the sense of disrespect is pervasive—more on this below.
Are You in Control?
Autonomy and control over your work and work life remain key factors in career satisfaction. This includes having input not only when it comes to the schedule but also, and more importantly, with regard to the processes. Can you participate in design for your group or at the hospital? If you find that all your suggestions fall on deaf ears, then either the work environment needs some adjusting or you are always wrong! Small things can be important here. Just having the flexibility to participate in quality processes or to give input on a protocol creates a feeling of control over your work. Hospitalists who have decisions imposed on them experience a great deal of tension and may, ultimately, resign.
Is there an opportunity for promotion or further learning? An individual who feels boxed in and unable to make career improvements is often dissatisfied. This ties in to the need for challenge and the importance of the nature of the work.
We all have personal challenges that we would like the flexibility to address. You may have childcare or elder care issues. Perhaps you want to train for the next Ironman race. If you are unable to address these personal aspirations and goals, you may feel that you have no control over your life, much less your work life.
Are You Happy at Work?
Work environment—who knew how important this could be? Let’s say you are employed at a large organization, perhaps General Electric. GE controls the environment for all of its employees. The company makes sure that the lighting is adequate. It tries to protect its employees from hostility based on gender, race, or disability. GE controls work assignments, and there is a chain of command for any issue that needs to be addressed.
The hospitalist, as a member of the medical staff, may be in a much different setting. Often, hospitalists work in someone else’s environment. The nurses and physicians with whom they work are generally hired by others. The atmosphere in which they work can be hostile, devoid of respect. There is often no clear chain of command set up to resolve work environment issues. Some facilities are frustrating and challenging to work in, with insufficient translators or inadequate lab or X-ray support. Fellow medical staff members or administrators may not understand how hospitalists differ from other specialists, making the job of the hospitalist more difficult
An individual’s inability to affect the work environment due to the structure of the facility can be detrimental to morale. Are the committees structured so that hospitalists can participate in them and influence the decisions they make? Even seemingly small issues can have a big impact on a hospitalist’s feelings of control and autonomy.
What Do You Earn?
Finally, compensation. Everyone wants a fair wage for a reasonable work effort. It seems simple, but obviously there are tensions here. All things being equal, a person’s income should be competitive and fair. The definition of “fair” is often determined by the marketplace. In the field of hospitalist medicine, there is a great deal of competition for labor, so there are many opportunities to evaluate. But finding the work that is most satisfying involves attaining a combination of the abovementioned characteristics as well as evaluating location.
SHM’s Task Force Examines the Issue
So, what to do? As an organization, SHM has appointed a Career Satisfaction Task Force to study work satisfaction and to design processes that will address this issue specifically for the hospitalist workforce. As I mentioned above, this topic has been studied extensively in various employee environments for many years. Retention of valuable employees is a key component of an organization’s success. This applies to nonmedical as well as to medical fields. The emergency medicine field, for example, has done some work on the challenges specific to their physicians and has some interesting insights. We expect to share the work product of our own task force in the future.
Short-Term Help
But what to do now? If you are a hospitalist leader, ask your group for feedback. Are they finding satisfaction in the areas described above? Find ways to develop control and autonomy for your group. Encourage them to participate in shaping their own careers and futures. Recognize, recognize, recognize. You can’t say “Thank you” or “Good job” too often. Learn how your group members prefer to be recognized and try to personalize what you do for them. Remember this line from The One Minute Manager, by Kenneth Blanchard, PhD, and Spencer Johnson, MD: “Catch them doing something right.” It happens around us all day, but we take performance for granted and fail to praise and recognize.
If you are a hospitalist, help shape your own destiny. Participate, ask questions, and devise solutions. And recognize the nurses, the social worker, and your group leader.
Together we can create career satisfaction and lifelong, fulfilling work. Unlike Mick Jagger, we will then get some satisfaction! TH
Dr. Gorman is the president of SHM.
“(I can’t get no) satisfaction.”—The Rolling Stones
Do you know people who have good health, loving families, a healthy income, and a great house but who are still not satisfied? You may also know some people who seemingly have little to be thankful for, and yet they are very satisfied. There has been a great deal of research on this topic, specifically as it relates to job or career satisfaction. Some assume that the main component of job satisfaction is how much a person is paid. In study after study, however, compensation is never first and is often fourth or lower on the list of items that people identify as the key factors related to their satisfaction. So what are the other factors?
What Stimulates You?
The nature of the work is important. People must find their work stimulating. Everyone finds stimulation at different levels—for some it may involve being technically successful, whether they are reviewing contract language or hanging crown molding. Others find performing a procedure such as a cardiac catheterization or a lumbar puncture highly energizing. Or stimulation—for the master chess player, for example—may be found strictly on a mental level. Whatever the sweet spot, it is important to identify what you find motivating and challenging.
Overstimulating situations, on the other hand, are uncomfortable and dissatisfying. Some individuals thrive in a highly stressful environment, such as air traffic control, that others would find overwhelming.
One of the unique features of being a hospitalist is the need to work collaboratively across many disciplines to achieve results for our patients. The collegiality involved in the team approach can be invigorating and satisfying to many people. For others, it is simply frustrating.
Do You Feel Appreciated?
Recognition for a job well done is something everyone needs. We see this in our co-workers and in children when they try something and are praised for it. We all need recognition for doing a good job day after day. This seemed counterintuitive to me when I first learned about it. Gee whiz, I thought, why do I have to say, “Good job,” when people are just doing what they are supposed to do? It turns out that we all need to be recognized regularly in order to feel that we are valued and needed. It keeps us interested and motivated.
This reminds me of the old joke in which the wife says to her husband of 25 years, “Do you love me?” He replies, “Well, I told you so 15 years ago. Don’t you remember?”
This does not mean we need a financial reward every other day or a big bonus every month. It means that we desire recognition that is meaningful and timely. Studies have shown that unless the recognition is personalized, it can have a negative effect. For instance, if I don’t care for sports, rewarding me with tickets to a baseball game will seem depersonalized and will give me the feeling that no one took the time to know what is important to me.
By the same token, if praise in a public setting makes me uncomfortable, don’t create a reward banquet with great public fanfare. People prize small things like handwritten thank you notes, gift cards for places they like (Starbucks!), or opportunities for educational or other activities. A simple “thank you,” said with enthusiasm, does wonders. Respect is closely tied to recognition. If the hospitalist feels like a glorified resident, the sense of disrespect is pervasive—more on this below.
Are You in Control?
Autonomy and control over your work and work life remain key factors in career satisfaction. This includes having input not only when it comes to the schedule but also, and more importantly, with regard to the processes. Can you participate in design for your group or at the hospital? If you find that all your suggestions fall on deaf ears, then either the work environment needs some adjusting or you are always wrong! Small things can be important here. Just having the flexibility to participate in quality processes or to give input on a protocol creates a feeling of control over your work. Hospitalists who have decisions imposed on them experience a great deal of tension and may, ultimately, resign.
Is there an opportunity for promotion or further learning? An individual who feels boxed in and unable to make career improvements is often dissatisfied. This ties in to the need for challenge and the importance of the nature of the work.
We all have personal challenges that we would like the flexibility to address. You may have childcare or elder care issues. Perhaps you want to train for the next Ironman race. If you are unable to address these personal aspirations and goals, you may feel that you have no control over your life, much less your work life.
Are You Happy at Work?
Work environment—who knew how important this could be? Let’s say you are employed at a large organization, perhaps General Electric. GE controls the environment for all of its employees. The company makes sure that the lighting is adequate. It tries to protect its employees from hostility based on gender, race, or disability. GE controls work assignments, and there is a chain of command for any issue that needs to be addressed.
The hospitalist, as a member of the medical staff, may be in a much different setting. Often, hospitalists work in someone else’s environment. The nurses and physicians with whom they work are generally hired by others. The atmosphere in which they work can be hostile, devoid of respect. There is often no clear chain of command set up to resolve work environment issues. Some facilities are frustrating and challenging to work in, with insufficient translators or inadequate lab or X-ray support. Fellow medical staff members or administrators may not understand how hospitalists differ from other specialists, making the job of the hospitalist more difficult
An individual’s inability to affect the work environment due to the structure of the facility can be detrimental to morale. Are the committees structured so that hospitalists can participate in them and influence the decisions they make? Even seemingly small issues can have a big impact on a hospitalist’s feelings of control and autonomy.
What Do You Earn?
Finally, compensation. Everyone wants a fair wage for a reasonable work effort. It seems simple, but obviously there are tensions here. All things being equal, a person’s income should be competitive and fair. The definition of “fair” is often determined by the marketplace. In the field of hospitalist medicine, there is a great deal of competition for labor, so there are many opportunities to evaluate. But finding the work that is most satisfying involves attaining a combination of the abovementioned characteristics as well as evaluating location.
SHM’s Task Force Examines the Issue
So, what to do? As an organization, SHM has appointed a Career Satisfaction Task Force to study work satisfaction and to design processes that will address this issue specifically for the hospitalist workforce. As I mentioned above, this topic has been studied extensively in various employee environments for many years. Retention of valuable employees is a key component of an organization’s success. This applies to nonmedical as well as to medical fields. The emergency medicine field, for example, has done some work on the challenges specific to their physicians and has some interesting insights. We expect to share the work product of our own task force in the future.
Short-Term Help
But what to do now? If you are a hospitalist leader, ask your group for feedback. Are they finding satisfaction in the areas described above? Find ways to develop control and autonomy for your group. Encourage them to participate in shaping their own careers and futures. Recognize, recognize, recognize. You can’t say “Thank you” or “Good job” too often. Learn how your group members prefer to be recognized and try to personalize what you do for them. Remember this line from The One Minute Manager, by Kenneth Blanchard, PhD, and Spencer Johnson, MD: “Catch them doing something right.” It happens around us all day, but we take performance for granted and fail to praise and recognize.
If you are a hospitalist, help shape your own destiny. Participate, ask questions, and devise solutions. And recognize the nurses, the social worker, and your group leader.
Together we can create career satisfaction and lifelong, fulfilling work. Unlike Mick Jagger, we will then get some satisfaction! TH
Dr. Gorman is the president of SHM.
To protect and serve: Psychiatrists’ duty to patients
Patient discharged from group therapy kills psychiatrist, patient, and himself
Oakland County (MI) Circuit Court
The plaintiff, age 57, attended regular group therapy with a psychiatrist. Another patient, Mr. B, was dismissed from group therapy by the psychiatrist, but returned to the office with a gun during one of the regular sessions. Mr. B shot and killed the psychiatrist then entered the group meeting room and discharged his gun, fatally injuring another patient and wounding the plaintiff. Mr. B then turned the gun on himself and committed suicide. The plaintiff suffered gunshot wounds to the lower leg, foot, and hand and was away from work for 6 weeks.
The plaintiff alleged that the psychiatrist, his associates, and his daughter—who is also a psychiatrist at the office—knew Mr. B was dangerous and should not have been included in group therapy. The plaintiff claimed that Mr. B had a history of questionable psychotic behavior and other patients should not have been exposed to him. The psychiatrist’s associates contended that they had no way to anticipate this event and had used due care and caution in their practice.
- A $2 million verdict was returned
Dr. Grant’s observations
Warn and protect
In this case, several unavailable facts may have supported the successful negligence claim. For example, why was Mr. B dismissed from the group? Did he threaten someone in the group? Did he tell the group or the group leader about thoughts of violence or homicide? If so, perhaps a violent event was foreseeable.
Was Mr. B dismissed because of delusional or paranoid thoughts? What was done to help him, and were appropriate referrals in place? Instituting the right interventions requires clinicians to walk a fine line between preserving doctor-patient confidentiality and protecting other patients and the general public.
Doctor-patient confidentiality is deeply rooted in medical ethics and protected by law—in various forms—in all jurisdictions. Directives requiring a physician to reveal information without a patient’s consent are either legislated—and tend to be clear—or are based on court precedent, which is more open to interpretation. These mandated exceptions are purpose-specific and intended to preserve overall doctor-patient confidentiality.“Is this patient dangerous?” by John Battaglia, MD, and “Protect yourself from patient assault”, an interview between Dr. Battaglia and Lois E. Krahn, MD.
1. Kleinman I. Confidentiality and the duty to warn. Can Med Assoc J 1993;149:1783-5.
2. Chaimowitx G, Glancy G. The duty to protect. Can J Psychiatry 2002;47:1-4.
3. Tarasoff v. Regents of the University of California, 118 Cal. Rptr. 129 (Cal. 1974) (Tarasoff I), modified by Tarasoff v. Regents of the Univ. of Cal., 551 P.2d 334 (Cal. 1976) (Tarasoff II).
4. Naidu v. Laird, 539 A.2d 1064 (Del. 1988).
5. Davis v. Lhim, 335 N.W.2d 481 (Mich. App. 1983).
6. Beck J, Baxter P. The violent patient. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:153-65.
7. Buckner F, Firestone M. Where the public peril begins: 25 years after Tarasoff. J Legal Med 2000;21:187-222.
8. Corey G, Williams GT, Moline ME. Ethical and legal issues in group counseling. Ethics & Behavior 1995;5:161-83.
9. American Counseling Association code of ethics and standards of practice 2005. Available at: http://www.counseling.org/Resources/CodeOfEthics/TP/Home/CT2.aspx. Accessed October 23, 2006.
Patient discharged from group therapy kills psychiatrist, patient, and himself
Oakland County (MI) Circuit Court
The plaintiff, age 57, attended regular group therapy with a psychiatrist. Another patient, Mr. B, was dismissed from group therapy by the psychiatrist, but returned to the office with a gun during one of the regular sessions. Mr. B shot and killed the psychiatrist then entered the group meeting room and discharged his gun, fatally injuring another patient and wounding the plaintiff. Mr. B then turned the gun on himself and committed suicide. The plaintiff suffered gunshot wounds to the lower leg, foot, and hand and was away from work for 6 weeks.
The plaintiff alleged that the psychiatrist, his associates, and his daughter—who is also a psychiatrist at the office—knew Mr. B was dangerous and should not have been included in group therapy. The plaintiff claimed that Mr. B had a history of questionable psychotic behavior and other patients should not have been exposed to him. The psychiatrist’s associates contended that they had no way to anticipate this event and had used due care and caution in their practice.
- A $2 million verdict was returned
Dr. Grant’s observations
Warn and protect
In this case, several unavailable facts may have supported the successful negligence claim. For example, why was Mr. B dismissed from the group? Did he threaten someone in the group? Did he tell the group or the group leader about thoughts of violence or homicide? If so, perhaps a violent event was foreseeable.
Was Mr. B dismissed because of delusional or paranoid thoughts? What was done to help him, and were appropriate referrals in place? Instituting the right interventions requires clinicians to walk a fine line between preserving doctor-patient confidentiality and protecting other patients and the general public.
Doctor-patient confidentiality is deeply rooted in medical ethics and protected by law—in various forms—in all jurisdictions. Directives requiring a physician to reveal information without a patient’s consent are either legislated—and tend to be clear—or are based on court precedent, which is more open to interpretation. These mandated exceptions are purpose-specific and intended to preserve overall doctor-patient confidentiality.“Is this patient dangerous?” by John Battaglia, MD, and “Protect yourself from patient assault”, an interview between Dr. Battaglia and Lois E. Krahn, MD.
Patient discharged from group therapy kills psychiatrist, patient, and himself
Oakland County (MI) Circuit Court
The plaintiff, age 57, attended regular group therapy with a psychiatrist. Another patient, Mr. B, was dismissed from group therapy by the psychiatrist, but returned to the office with a gun during one of the regular sessions. Mr. B shot and killed the psychiatrist then entered the group meeting room and discharged his gun, fatally injuring another patient and wounding the plaintiff. Mr. B then turned the gun on himself and committed suicide. The plaintiff suffered gunshot wounds to the lower leg, foot, and hand and was away from work for 6 weeks.
The plaintiff alleged that the psychiatrist, his associates, and his daughter—who is also a psychiatrist at the office—knew Mr. B was dangerous and should not have been included in group therapy. The plaintiff claimed that Mr. B had a history of questionable psychotic behavior and other patients should not have been exposed to him. The psychiatrist’s associates contended that they had no way to anticipate this event and had used due care and caution in their practice.
- A $2 million verdict was returned
Dr. Grant’s observations
Warn and protect
In this case, several unavailable facts may have supported the successful negligence claim. For example, why was Mr. B dismissed from the group? Did he threaten someone in the group? Did he tell the group or the group leader about thoughts of violence or homicide? If so, perhaps a violent event was foreseeable.
Was Mr. B dismissed because of delusional or paranoid thoughts? What was done to help him, and were appropriate referrals in place? Instituting the right interventions requires clinicians to walk a fine line between preserving doctor-patient confidentiality and protecting other patients and the general public.
Doctor-patient confidentiality is deeply rooted in medical ethics and protected by law—in various forms—in all jurisdictions. Directives requiring a physician to reveal information without a patient’s consent are either legislated—and tend to be clear—or are based on court precedent, which is more open to interpretation. These mandated exceptions are purpose-specific and intended to preserve overall doctor-patient confidentiality.“Is this patient dangerous?” by John Battaglia, MD, and “Protect yourself from patient assault”, an interview between Dr. Battaglia and Lois E. Krahn, MD.
1. Kleinman I. Confidentiality and the duty to warn. Can Med Assoc J 1993;149:1783-5.
2. Chaimowitx G, Glancy G. The duty to protect. Can J Psychiatry 2002;47:1-4.
3. Tarasoff v. Regents of the University of California, 118 Cal. Rptr. 129 (Cal. 1974) (Tarasoff I), modified by Tarasoff v. Regents of the Univ. of Cal., 551 P.2d 334 (Cal. 1976) (Tarasoff II).
4. Naidu v. Laird, 539 A.2d 1064 (Del. 1988).
5. Davis v. Lhim, 335 N.W.2d 481 (Mich. App. 1983).
6. Beck J, Baxter P. The violent patient. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:153-65.
7. Buckner F, Firestone M. Where the public peril begins: 25 years after Tarasoff. J Legal Med 2000;21:187-222.
8. Corey G, Williams GT, Moline ME. Ethical and legal issues in group counseling. Ethics & Behavior 1995;5:161-83.
9. American Counseling Association code of ethics and standards of practice 2005. Available at: http://www.counseling.org/Resources/CodeOfEthics/TP/Home/CT2.aspx. Accessed October 23, 2006.
1. Kleinman I. Confidentiality and the duty to warn. Can Med Assoc J 1993;149:1783-5.
2. Chaimowitx G, Glancy G. The duty to protect. Can J Psychiatry 2002;47:1-4.
3. Tarasoff v. Regents of the University of California, 118 Cal. Rptr. 129 (Cal. 1974) (Tarasoff I), modified by Tarasoff v. Regents of the Univ. of Cal., 551 P.2d 334 (Cal. 1976) (Tarasoff II).
4. Naidu v. Laird, 539 A.2d 1064 (Del. 1988).
5. Davis v. Lhim, 335 N.W.2d 481 (Mich. App. 1983).
6. Beck J, Baxter P. The violent patient. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:153-65.
7. Buckner F, Firestone M. Where the public peril begins: 25 years after Tarasoff. J Legal Med 2000;21:187-222.
8. Corey G, Williams GT, Moline ME. Ethical and legal issues in group counseling. Ethics & Behavior 1995;5:161-83.
9. American Counseling Association code of ethics and standards of practice 2005. Available at: http://www.counseling.org/Resources/CodeOfEthics/TP/Home/CT2.aspx. Accessed October 23, 2006.
In the Literature
Statins for Stroke Prevention
By Paul J. Grant, MD
Amarenco P, Bogousslavsky J, Callahan A III, et al. Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006 Aug 22;355:549-559.
Despite recent advances, the physician’s armamentarium for secondary stroke prevention is limited. The literature regarding optimal blood pressure management for stroke prevention is sparse, and the data addressing the best antiplatelet regimen remain controversial. This is troubling, given the fact that cerebrovascular disease remains the third leading cause of death in the United States.
Although extensive data exists for the benefits of using 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors (statins) for the prevention and treatment of cardiovascular disease, little is known about their role in decreasing the risk of stroke. The highly anticipated Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) trial sought to determine if statin therapy would decrease the risk of recurrent stroke in patients with no known coronary heart disease.
This prospective, randomized, double-blind, placebo-controlled trial included 4,731 men and women with no history of coronary heart disease. Eligible patients had a history of stroke (ischemic or hemorrhagic) or a transient ischemic attack (TIA) within a one- to six-month period before randomization as diagnosed by a neurologist. All patients required a low-density lipoprotein (LDL) cholesterol level between 100 and 190 mg/dL, while exclusion criteria included atrial fibrillation. Patients were randomized either to a dosage of 80 mg of atorvastatin daily or to a placebo and were followed for a median duration of 4.9 years. The primary endpoint was fatal or nonfatal stroke.
The average patient age in this trial was 63; approximately 60% of the patients were male. A total of 265 patients reached the primary endpoint in the atorvastatin group, versus 311 patients in the placebo group. This translates to an adjusted relative risk reduction of 16% in the primary endpoint for patients receiving atorvastatin (hazard ratio 0.84; 95% confidence interval 0.71 to 0.99; p=0.03). Although there was no difference in overall mortality between the two groups, the incidence of cardiovascular events was significantly lower in those receiving atorvastatin. Interestingly, more hemorrhagic strokes were noted in the atorvastatin group. With respect to safety, no significant differences in serious adverse events were noted. The atorvastatin group did, however, encounter significantly more cases of persistently elevated aspartate aminotransferase (AST) or alanine aminotransferase (ALT), at 2.2% versus 0.5% in the placebo group.
The findings by the SPARCL investigators provide strong evidence that atorvastatin reduces the incidence of stroke recurrence. The mechanism for risk reduction with statin exposure is most likely due to the dramatic lowering of LDL cholesterol. This effect has been shown in numerous trials resulting in the reduction of cardiovascular events. The present trial observed a 53% decrease in LDL cholesterol in the atorvastatin group compared with no change in the placebo arm. In addition to their powerful lipid-lowering role, statins also appear to prevent plaque rupture, optimize endothelial function, and provide anti-inflammatory effects. These are the so-called “pleiotropic effects” of statins and may be another factor contributing to the benefits observed.
Although some physicians are already prescribing statins for stroke patients, the literature supporting this practice has been sparse. The latest guidelines for prevention of stroke in patients with ischemic stroke or TIA were published in February 2006 by the American Heart Association/American Stroke Association Council on Stroke. These guidelines state that patients with a history of ischemic stroke or TIA are “reasonable candidates” for statin therapy. One could argue that these guidelines should now be revised to include a strong recommendation for statin therapy in secondary stroke prevention.
MRSA in the Community
By Matthew T. Harbison, MD
Moran GJ, Krishnadasan A, Gorwitz RJ, et al. EMERGEncy ID Net Study Group. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med. 2006 Aug 17;355(7):666-674.
Methicillin-resistant Staphylococcus aureus (MRSA) emerged as an issue in the healthcare community not long after the introduction of methicillin in 1959. MRSA has traditionally been thought of as an issue for those individuals who have contact with the healthcare system; however, there is growing evidence that MRSA has become an entity in the greater community at large, affecting individuals who have not spent significant time in healthcare facilities. Descriptions of several community-based outbreaks have led to the understanding that community-associated MRSA has different characteristics than MRSA infections contracted in the hospital setting. The community-associated isolates are resistant to fewer antibiotics, produce different toxins, and have differing genetic complexes responsible for antibiotic resistance. The majority of the community-acquired infections are skin and soft tissue infections, although more serious infections have been reported.
Moran and colleagues conducted a prospective prevalence study in adult patients presenting to emergency departments with skin and soft tissue infections in 11 metropolitan areas in geographically diverse regions of the United States. Eligible patients 18 and older with purulent skin or soft tissue infections of less than one week’s duration had demographic and historical data collected; a wound culture was also taken. If Staphylococcus aureus was isolated, it was further evaluated by the Centers for Disease Control and Prevention (CDC) to characterize antibiotic resistance patterns, toxin production, and the type of staphylococcal cassette chromosome present.
A total of 422 patients were enrolled, with S. aureus isolated in 320 patients (76%). Of those with isolated S. aureus, 78% had MRSA (59% of the total patients enrolled). The individual site prevalence of MRSA ranged from 15 to 74% and was the predominant etiology of skin and soft tissue infections in 10 of 11 emergency departments. MRSA susceptibilities in this study were 100% to trimethoprim-sulfamethoxazole and rifampin, 95% to clindamycin, 92% to tetracycline, 60% to fluoroquinolones, and 6% to erythromycin. The authors point out that clindamycin resistance in one center was 60%; thus, individual site resistance patterns may differ significantly. Treatment data was available for 406 of the 422 patients, with the majority of those treated with incision, drainage, and antibiotics. In 100 of the 175 MRSA patients treated with antibiotics, the choice of agent was discordant with susceptibility patterns. The authors were able to contact 248 patients between two and three weeks after their visits and, of those contacted, 96% reported resolution or improvement of the wound.
Using multivariate logistic-regression analyses, the authors identified several potential risk factors for MRSA infection. These included use of any antibiotic in the past month, underlying illness, history of MRSA infection, close contact with someone with similar infection, and reported spider bite. Interestingly, being a healthcare worker, living in a long-term care facility, and being hospitalized in the past year were not shown to be significant risk factors in this study.
The results of this study highlight the emerging difficulty, which continues to evolve, with antibiotic resistance patterns. The healthcare community must be vigilant to new entities that challenge the traditional views of antibiotic resistance patterns. The high rate of community-acquired MRSA skin and soft tissue infection demonstrated in this study, in addition to the large percentage of patients prescribed antibiotics that were resistant for the strain involved, emphasizes the need to reconsider the empiric antibiotic choices for this patient population. The variability in regional resistance patterns further complicates the issue. Given the high prevalence of MRSA skin and soft tissue infections reported in this study, use of routine wound cultures appears prudent, as does the need for effective follow-up strategies for alteration of antibiotic choice if necessary. At an institutional level, development of surveillance and isolation strategies for community-acquired MRSA should be considered.
More Options for Venous Thromboembolism Treatment
By Kirsten N. Kangelaris, MD
Kearon C, Ginsberg JS, Julian JA, et al. Fixed-Dose Heparin (FIDO) Investigators. Comparison of fixed-dose weight-adjusted unfractionated heparin and low-molecular-weight heparin for acute treatment of venous thromboembolism. JAMA. 2006 Aug 23;296(8):935-942.
The standard approach to using unfractionated heparin (UFH) in the treatment of acute venous thromboembolism as a bridge to warfarin therapy requires continuous intravenous infusion with frequent dose adjustments in response to measurements of activated partial thromboplastin time (aPTT). This therapy inevitably requires inpatient management. Subcutaneous administration of weight-based low molecular weight heparin (LMWH) has been the modality of choice for outpatient treatment of venous thromboembolism because it does not require laboratory monitoring. Its use has been limited by the high cost of treatment, however. A preliminary study, released in 2000 by the FIDO group (Fixed-Dose Heparin Investigators, Kearon and colleagues), suggested that subcutaneously administered UFH could be optimally dosed based on weight rather than monitoring aPTT levels.
This follow-up, randomized, open-label, adjudicator-blinded, multi-centered, non-inferiority trial enrolled 708 patients and compared fixed-dose, subcutaneously administered UFH to LMWH in acute deep venous thrombosis and pulmonary embolism. Administration in both groups was twice daily, subcutaneous, and weight-based. UFH was given as a first dose of 333 U/kg, followed by 250 U/kg every 12 hours. LMWH was administered at a dose of 100 IU/kg every 12 hours. Both treatments overlapped with three months of warfarin therapy, and both could be administered out of hospital.
Exclusion criteria were age <18, contraindication to subcutaneous therapy, active bleeding, life expectancy under three months, long-term anticoagulation therapy, pregnancy, and creatinine level >2.3 mg/dL.
The primary endpoints were efficacy as determined by recurrent venous thromboembolism within three months and safety as determined by major bleeding within 10 days of randomization. A secondary endpoint was relationship of efficacy and safety outcomes to aPTT levels measured on day two to three of therapy for the UFH group.
Results revealed that UFH was statistically non-inferior to LMWH by all endpoints, including treatment duration, efficacy, and safety. At three months, there was no significant difference between the groups in frequency of recurrent venous thromboembolism (3.8% UFH versus 3.4% LMWH), bleeding (1.1% UFH versus 1.4% LMWH), or death. There was no association between aPTT levels and recurrent venous thromboembolism or bleeding.
Limitations of the study included reduced enrollment from the initial study design, though power was adequate due to a lower than expected incidence of recurrent venous thromboembolism in both arms (~3.6% versus the expected 6%); possible biases related to open-label design; and more post-randomization exclusions in the UFH group versus the LMWH group.
In summary, fixed-dose, unmonitored, subcutaneous UFH appears to be an effective, safe alternative to LMWH as a bridge to warfarin therapy for venous thromboembolism. Clinically, this is relevant, because UFH is approximately 15 to 20 times less expensive than LMWH. The authors appropriately call attention to two developments in clinical practice that occurred during the course of the present study and that could potentially limit the use of UFH. These are 1) the dosing option for once-daily LMWH, which improves convenience, and 2) the preference for long-term LMWH therapy over warfarin for treating cancer patients with venous thromboembolism. Despite these exceptions, UFH may prove to be a viable and economic option for venous thromboembolism treatment.
In-Hospital MI Versus MI at Presentation
By Erin M. Galbraith, MD
Maynard C, Lowy E, Rumsfeld J, et al. The prevalence and outcomes of in-hospital acute myocardial infarction in the Department of Veterans Affairs Health System. Arch Intern Med. 2006 Jul 10;166(13):1410-1416.
Much is known about the prevalence, treatment, and prognosis of acute myocardial infarction (AMI) when it occurs in the community and is the presenting diagnosis. Few studies, however, have addressed the epidemiology of in-hospital AMIs. This study by Maynard and colleagues attempts to elucidate the basic epidemiologic characteristics, treatments, and outcomes of patients who suffer in-hospital AMIs.
This retrospective cohort consisted of 7,054 patients who had been discharged with a diagnosis of AMI from 127 Veterans Health Administration (VHA) medical centers between July and August 2003. Patients who had suffered a postoperative MI or were transferred in from another hospital were excluded. Data was obtained from both the electronic and paper medical records. Of the 7,054 patients in the study, 792 (11.2%) had experienced an AMI while hospitalized for other medical problems. These 792 patients were older by approximately 4.5 years and more frequently suffered from heart failure, diabetes, chronic renal insufficiency, COPD, cerebrovascular disease, dementia, and cancer. These patients were less likely, however, to have had a previous MI, to be current smokers, or to have undergone previous angioplasty. They were also less likely to have known lipid disorders or to be taking aspirin or lipid-lowering agents.
Regarding their presentations and management, the patients who suffered in-hospital AMIs had faster heart rates and lower blood pressures. They were also up to 75% less likely to report typical symptoms of cardiac ischemia, including chest pain/pressure, shoulder pain, nausea, and diaphoresis. They were less often seen by an attending cardiologist and had more contraindications to AMI therapy; thus, these patients underwent reperfusion therapy at much lower rates, both initially and at 30 days. Their troponin levels were more frequently elevated, but they were only half as likely to have ST segment elevations at the time of diagnosis. Hospitalizations were longer for the in-hospital group, and there were higher rates of in-hospital cardiogenic shock, cardiac arrest, and death (27.3% versus 8.6%). The 30-day mortality rate was also higher (33% versus 11.9%). Multivariate logistic regression revealed an adjusted odds ratio of 2.0 (95% confidence interval 1.7 to 2.4; p<0.001) for 30-day mortality in those who experienced an in-hospital AMI versus those who presented with an AMI.
Potential reasons for the increased severity of outcomes include, but are not limited to, their many chronic comorbidities, their other acute diagnoses, the failure of the medical team to recognize cardiac ischemia in a timely manner (i.e., higher initial troponins), the inability to treat MIs appropriately secondary to contraindications to acute intervention, and the lack of an attending cardiologist presiding over their medical care. Clearly, further studies are needed to elucidate the causes of death in the 33% of patients who died, because it is unclear whether the patients died of complications from their MIs or as a result of their multiple other medical problems. Knowledge of the extent to which these patients could be managed, both medically and via interventional procedures (and why these therapies were not pursued), would also be of value.
This study emphasizes the importance of recognizing atypical presentations of AMIs and exercising vigilance in pursuing the most aggressive therapy possible, as dictated by a patient’s ability to tolerate medical and procedural interventions.
Hyperglycemia in Heart Failure
By David H. Wesorick, MD
Barsheshet A, Garty M, Grossman E, et al. Admission blood glucose level and mortality among hospitalized nondiabetic patients with heart failure. Arch Intern Med. 2006 Aug 14-28;166(15):1613-1619.
The medical literature strongly suggests that inpatient hyperglycemia is associated with a variety of poor outcomes. Little is known, however, about the relationship between hyperglycemia and heart failure. These investigators examined the association of admission blood glucose and mortality in patients who were admitted to the hospital with acute heart failure.
In this study, 1,122 patients admitted to the hospital with acute heart failure and without diabetes were divided into tertiles depending on their admission blood glucose levels. Diabetes was defined as an admission blood glucose greater than or equal to 200 mg/dl, a known diagnosis of diabetes recorded in the chart, or the presence of anti-diabetic medications on the patient’s medication list. Tertile #1 had an average admission blood glucose of 92 mg/dl (with a range of 54-102); tertile #2 had an average admission blood glucose of 113 mg/dl (with a range of 103-127); and tertile #3 had an average admission blood glucose of 147 mg/dl (with a range of 128-199). Mortality was evaluated according to tertile.
In this study, patients in tertile #3 had significantly higher inpatient mortality (7.2%) than patients in tertile #1 or #2 (3% and 4%, respectively). There was a significant association between hyperglycemia and mortality, even at 60 days follow-up, although not at six and 12 months follow-up. The association remained significant, even when patients with acute MI were excluded. Besides hyperglycemia, the authors noted that increasing age, increasing creatinine, a New York Heart Association (NYHA) functional class of III or IV, and a systolic blood pressure of lower than 115 were also significant, independent predictors of in-hospital mortality in this patient population.
For a hospitalist, the intriguing question is this: Is hyperglycemia just a marker of worse disease, or might it contribute to poorer outcomes? Clearly, hyperglycemia is associated with poorer outcomes in other types of patients, including post-surgical patients, critically ill patients, MI patients, and general medical patients.1 But is hyperglycemia just a marker of more severe illness? In heart failure, perhaps more severe decompensation results in a more profound activation of the sympathetic nervous system and a more vigorous release of stress hormones, such as cortisol and catecholamines. In that case, one might expect a sicker patient to have a higher blood glucose.
More recent studies, however, show that better control of hyperglycemia in some acutely ill patients actually results in improved outcomes, suggesting that the hyperglycemia itself might be contributing to the poorer outcomes in some cases.2-5 Hyperglycemia is known to alter human physiology in a variety of adverse ways.1 For example, hyperglycemia is known to inhibit nitric oxide production and to alter endothelial dysfunction. In a patient with acute heart failure, these alterations might be expected to have a significant effect on outcomes.
This study does not intend to answer these questions, but it does add to our understanding of the association of hyperglycemia and poor outcomes in acutely ill patients. More research is needed to examine whether or not heart failure patients, specifically, will benefit from better glycemic control in the acute setting. TH
References
- Clement S, Braithwaite SS, Magee MF, et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004 Feb;27(2):553-591.
- Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001 Nov 8;345(19):1359-1367.
- Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006 Feb 2;354(5):449-461.
- Furnary AP, Zerr KJ, Grunkemeier GL, et al. Continuous intravenous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical procedures. Ann Thorac Surg. 1999 Feb;67(2):352-362.
- Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2003 May;125(5):1007-1021.
Statins for Stroke Prevention
By Paul J. Grant, MD
Amarenco P, Bogousslavsky J, Callahan A III, et al. Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006 Aug 22;355:549-559.
Despite recent advances, the physician’s armamentarium for secondary stroke prevention is limited. The literature regarding optimal blood pressure management for stroke prevention is sparse, and the data addressing the best antiplatelet regimen remain controversial. This is troubling, given the fact that cerebrovascular disease remains the third leading cause of death in the United States.
Although extensive data exists for the benefits of using 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors (statins) for the prevention and treatment of cardiovascular disease, little is known about their role in decreasing the risk of stroke. The highly anticipated Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) trial sought to determine if statin therapy would decrease the risk of recurrent stroke in patients with no known coronary heart disease.
This prospective, randomized, double-blind, placebo-controlled trial included 4,731 men and women with no history of coronary heart disease. Eligible patients had a history of stroke (ischemic or hemorrhagic) or a transient ischemic attack (TIA) within a one- to six-month period before randomization as diagnosed by a neurologist. All patients required a low-density lipoprotein (LDL) cholesterol level between 100 and 190 mg/dL, while exclusion criteria included atrial fibrillation. Patients were randomized either to a dosage of 80 mg of atorvastatin daily or to a placebo and were followed for a median duration of 4.9 years. The primary endpoint was fatal or nonfatal stroke.
The average patient age in this trial was 63; approximately 60% of the patients were male. A total of 265 patients reached the primary endpoint in the atorvastatin group, versus 311 patients in the placebo group. This translates to an adjusted relative risk reduction of 16% in the primary endpoint for patients receiving atorvastatin (hazard ratio 0.84; 95% confidence interval 0.71 to 0.99; p=0.03). Although there was no difference in overall mortality between the two groups, the incidence of cardiovascular events was significantly lower in those receiving atorvastatin. Interestingly, more hemorrhagic strokes were noted in the atorvastatin group. With respect to safety, no significant differences in serious adverse events were noted. The atorvastatin group did, however, encounter significantly more cases of persistently elevated aspartate aminotransferase (AST) or alanine aminotransferase (ALT), at 2.2% versus 0.5% in the placebo group.
The findings by the SPARCL investigators provide strong evidence that atorvastatin reduces the incidence of stroke recurrence. The mechanism for risk reduction with statin exposure is most likely due to the dramatic lowering of LDL cholesterol. This effect has been shown in numerous trials resulting in the reduction of cardiovascular events. The present trial observed a 53% decrease in LDL cholesterol in the atorvastatin group compared with no change in the placebo arm. In addition to their powerful lipid-lowering role, statins also appear to prevent plaque rupture, optimize endothelial function, and provide anti-inflammatory effects. These are the so-called “pleiotropic effects” of statins and may be another factor contributing to the benefits observed.
Although some physicians are already prescribing statins for stroke patients, the literature supporting this practice has been sparse. The latest guidelines for prevention of stroke in patients with ischemic stroke or TIA were published in February 2006 by the American Heart Association/American Stroke Association Council on Stroke. These guidelines state that patients with a history of ischemic stroke or TIA are “reasonable candidates” for statin therapy. One could argue that these guidelines should now be revised to include a strong recommendation for statin therapy in secondary stroke prevention.
MRSA in the Community
By Matthew T. Harbison, MD
Moran GJ, Krishnadasan A, Gorwitz RJ, et al. EMERGEncy ID Net Study Group. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med. 2006 Aug 17;355(7):666-674.
Methicillin-resistant Staphylococcus aureus (MRSA) emerged as an issue in the healthcare community not long after the introduction of methicillin in 1959. MRSA has traditionally been thought of as an issue for those individuals who have contact with the healthcare system; however, there is growing evidence that MRSA has become an entity in the greater community at large, affecting individuals who have not spent significant time in healthcare facilities. Descriptions of several community-based outbreaks have led to the understanding that community-associated MRSA has different characteristics than MRSA infections contracted in the hospital setting. The community-associated isolates are resistant to fewer antibiotics, produce different toxins, and have differing genetic complexes responsible for antibiotic resistance. The majority of the community-acquired infections are skin and soft tissue infections, although more serious infections have been reported.
Moran and colleagues conducted a prospective prevalence study in adult patients presenting to emergency departments with skin and soft tissue infections in 11 metropolitan areas in geographically diverse regions of the United States. Eligible patients 18 and older with purulent skin or soft tissue infections of less than one week’s duration had demographic and historical data collected; a wound culture was also taken. If Staphylococcus aureus was isolated, it was further evaluated by the Centers for Disease Control and Prevention (CDC) to characterize antibiotic resistance patterns, toxin production, and the type of staphylococcal cassette chromosome present.
A total of 422 patients were enrolled, with S. aureus isolated in 320 patients (76%). Of those with isolated S. aureus, 78% had MRSA (59% of the total patients enrolled). The individual site prevalence of MRSA ranged from 15 to 74% and was the predominant etiology of skin and soft tissue infections in 10 of 11 emergency departments. MRSA susceptibilities in this study were 100% to trimethoprim-sulfamethoxazole and rifampin, 95% to clindamycin, 92% to tetracycline, 60% to fluoroquinolones, and 6% to erythromycin. The authors point out that clindamycin resistance in one center was 60%; thus, individual site resistance patterns may differ significantly. Treatment data was available for 406 of the 422 patients, with the majority of those treated with incision, drainage, and antibiotics. In 100 of the 175 MRSA patients treated with antibiotics, the choice of agent was discordant with susceptibility patterns. The authors were able to contact 248 patients between two and three weeks after their visits and, of those contacted, 96% reported resolution or improvement of the wound.
Using multivariate logistic-regression analyses, the authors identified several potential risk factors for MRSA infection. These included use of any antibiotic in the past month, underlying illness, history of MRSA infection, close contact with someone with similar infection, and reported spider bite. Interestingly, being a healthcare worker, living in a long-term care facility, and being hospitalized in the past year were not shown to be significant risk factors in this study.
The results of this study highlight the emerging difficulty, which continues to evolve, with antibiotic resistance patterns. The healthcare community must be vigilant to new entities that challenge the traditional views of antibiotic resistance patterns. The high rate of community-acquired MRSA skin and soft tissue infection demonstrated in this study, in addition to the large percentage of patients prescribed antibiotics that were resistant for the strain involved, emphasizes the need to reconsider the empiric antibiotic choices for this patient population. The variability in regional resistance patterns further complicates the issue. Given the high prevalence of MRSA skin and soft tissue infections reported in this study, use of routine wound cultures appears prudent, as does the need for effective follow-up strategies for alteration of antibiotic choice if necessary. At an institutional level, development of surveillance and isolation strategies for community-acquired MRSA should be considered.
More Options for Venous Thromboembolism Treatment
By Kirsten N. Kangelaris, MD
Kearon C, Ginsberg JS, Julian JA, et al. Fixed-Dose Heparin (FIDO) Investigators. Comparison of fixed-dose weight-adjusted unfractionated heparin and low-molecular-weight heparin for acute treatment of venous thromboembolism. JAMA. 2006 Aug 23;296(8):935-942.
The standard approach to using unfractionated heparin (UFH) in the treatment of acute venous thromboembolism as a bridge to warfarin therapy requires continuous intravenous infusion with frequent dose adjustments in response to measurements of activated partial thromboplastin time (aPTT). This therapy inevitably requires inpatient management. Subcutaneous administration of weight-based low molecular weight heparin (LMWH) has been the modality of choice for outpatient treatment of venous thromboembolism because it does not require laboratory monitoring. Its use has been limited by the high cost of treatment, however. A preliminary study, released in 2000 by the FIDO group (Fixed-Dose Heparin Investigators, Kearon and colleagues), suggested that subcutaneously administered UFH could be optimally dosed based on weight rather than monitoring aPTT levels.
This follow-up, randomized, open-label, adjudicator-blinded, multi-centered, non-inferiority trial enrolled 708 patients and compared fixed-dose, subcutaneously administered UFH to LMWH in acute deep venous thrombosis and pulmonary embolism. Administration in both groups was twice daily, subcutaneous, and weight-based. UFH was given as a first dose of 333 U/kg, followed by 250 U/kg every 12 hours. LMWH was administered at a dose of 100 IU/kg every 12 hours. Both treatments overlapped with three months of warfarin therapy, and both could be administered out of hospital.
Exclusion criteria were age <18, contraindication to subcutaneous therapy, active bleeding, life expectancy under three months, long-term anticoagulation therapy, pregnancy, and creatinine level >2.3 mg/dL.
The primary endpoints were efficacy as determined by recurrent venous thromboembolism within three months and safety as determined by major bleeding within 10 days of randomization. A secondary endpoint was relationship of efficacy and safety outcomes to aPTT levels measured on day two to three of therapy for the UFH group.
Results revealed that UFH was statistically non-inferior to LMWH by all endpoints, including treatment duration, efficacy, and safety. At three months, there was no significant difference between the groups in frequency of recurrent venous thromboembolism (3.8% UFH versus 3.4% LMWH), bleeding (1.1% UFH versus 1.4% LMWH), or death. There was no association between aPTT levels and recurrent venous thromboembolism or bleeding.
Limitations of the study included reduced enrollment from the initial study design, though power was adequate due to a lower than expected incidence of recurrent venous thromboembolism in both arms (~3.6% versus the expected 6%); possible biases related to open-label design; and more post-randomization exclusions in the UFH group versus the LMWH group.
In summary, fixed-dose, unmonitored, subcutaneous UFH appears to be an effective, safe alternative to LMWH as a bridge to warfarin therapy for venous thromboembolism. Clinically, this is relevant, because UFH is approximately 15 to 20 times less expensive than LMWH. The authors appropriately call attention to two developments in clinical practice that occurred during the course of the present study and that could potentially limit the use of UFH. These are 1) the dosing option for once-daily LMWH, which improves convenience, and 2) the preference for long-term LMWH therapy over warfarin for treating cancer patients with venous thromboembolism. Despite these exceptions, UFH may prove to be a viable and economic option for venous thromboembolism treatment.
In-Hospital MI Versus MI at Presentation
By Erin M. Galbraith, MD
Maynard C, Lowy E, Rumsfeld J, et al. The prevalence and outcomes of in-hospital acute myocardial infarction in the Department of Veterans Affairs Health System. Arch Intern Med. 2006 Jul 10;166(13):1410-1416.
Much is known about the prevalence, treatment, and prognosis of acute myocardial infarction (AMI) when it occurs in the community and is the presenting diagnosis. Few studies, however, have addressed the epidemiology of in-hospital AMIs. This study by Maynard and colleagues attempts to elucidate the basic epidemiologic characteristics, treatments, and outcomes of patients who suffer in-hospital AMIs.
This retrospective cohort consisted of 7,054 patients who had been discharged with a diagnosis of AMI from 127 Veterans Health Administration (VHA) medical centers between July and August 2003. Patients who had suffered a postoperative MI or were transferred in from another hospital were excluded. Data was obtained from both the electronic and paper medical records. Of the 7,054 patients in the study, 792 (11.2%) had experienced an AMI while hospitalized for other medical problems. These 792 patients were older by approximately 4.5 years and more frequently suffered from heart failure, diabetes, chronic renal insufficiency, COPD, cerebrovascular disease, dementia, and cancer. These patients were less likely, however, to have had a previous MI, to be current smokers, or to have undergone previous angioplasty. They were also less likely to have known lipid disorders or to be taking aspirin or lipid-lowering agents.
Regarding their presentations and management, the patients who suffered in-hospital AMIs had faster heart rates and lower blood pressures. They were also up to 75% less likely to report typical symptoms of cardiac ischemia, including chest pain/pressure, shoulder pain, nausea, and diaphoresis. They were less often seen by an attending cardiologist and had more contraindications to AMI therapy; thus, these patients underwent reperfusion therapy at much lower rates, both initially and at 30 days. Their troponin levels were more frequently elevated, but they were only half as likely to have ST segment elevations at the time of diagnosis. Hospitalizations were longer for the in-hospital group, and there were higher rates of in-hospital cardiogenic shock, cardiac arrest, and death (27.3% versus 8.6%). The 30-day mortality rate was also higher (33% versus 11.9%). Multivariate logistic regression revealed an adjusted odds ratio of 2.0 (95% confidence interval 1.7 to 2.4; p<0.001) for 30-day mortality in those who experienced an in-hospital AMI versus those who presented with an AMI.
Potential reasons for the increased severity of outcomes include, but are not limited to, their many chronic comorbidities, their other acute diagnoses, the failure of the medical team to recognize cardiac ischemia in a timely manner (i.e., higher initial troponins), the inability to treat MIs appropriately secondary to contraindications to acute intervention, and the lack of an attending cardiologist presiding over their medical care. Clearly, further studies are needed to elucidate the causes of death in the 33% of patients who died, because it is unclear whether the patients died of complications from their MIs or as a result of their multiple other medical problems. Knowledge of the extent to which these patients could be managed, both medically and via interventional procedures (and why these therapies were not pursued), would also be of value.
This study emphasizes the importance of recognizing atypical presentations of AMIs and exercising vigilance in pursuing the most aggressive therapy possible, as dictated by a patient’s ability to tolerate medical and procedural interventions.
Hyperglycemia in Heart Failure
By David H. Wesorick, MD
Barsheshet A, Garty M, Grossman E, et al. Admission blood glucose level and mortality among hospitalized nondiabetic patients with heart failure. Arch Intern Med. 2006 Aug 14-28;166(15):1613-1619.
The medical literature strongly suggests that inpatient hyperglycemia is associated with a variety of poor outcomes. Little is known, however, about the relationship between hyperglycemia and heart failure. These investigators examined the association of admission blood glucose and mortality in patients who were admitted to the hospital with acute heart failure.
In this study, 1,122 patients admitted to the hospital with acute heart failure and without diabetes were divided into tertiles depending on their admission blood glucose levels. Diabetes was defined as an admission blood glucose greater than or equal to 200 mg/dl, a known diagnosis of diabetes recorded in the chart, or the presence of anti-diabetic medications on the patient’s medication list. Tertile #1 had an average admission blood glucose of 92 mg/dl (with a range of 54-102); tertile #2 had an average admission blood glucose of 113 mg/dl (with a range of 103-127); and tertile #3 had an average admission blood glucose of 147 mg/dl (with a range of 128-199). Mortality was evaluated according to tertile.
In this study, patients in tertile #3 had significantly higher inpatient mortality (7.2%) than patients in tertile #1 or #2 (3% and 4%, respectively). There was a significant association between hyperglycemia and mortality, even at 60 days follow-up, although not at six and 12 months follow-up. The association remained significant, even when patients with acute MI were excluded. Besides hyperglycemia, the authors noted that increasing age, increasing creatinine, a New York Heart Association (NYHA) functional class of III or IV, and a systolic blood pressure of lower than 115 were also significant, independent predictors of in-hospital mortality in this patient population.
For a hospitalist, the intriguing question is this: Is hyperglycemia just a marker of worse disease, or might it contribute to poorer outcomes? Clearly, hyperglycemia is associated with poorer outcomes in other types of patients, including post-surgical patients, critically ill patients, MI patients, and general medical patients.1 But is hyperglycemia just a marker of more severe illness? In heart failure, perhaps more severe decompensation results in a more profound activation of the sympathetic nervous system and a more vigorous release of stress hormones, such as cortisol and catecholamines. In that case, one might expect a sicker patient to have a higher blood glucose.
More recent studies, however, show that better control of hyperglycemia in some acutely ill patients actually results in improved outcomes, suggesting that the hyperglycemia itself might be contributing to the poorer outcomes in some cases.2-5 Hyperglycemia is known to alter human physiology in a variety of adverse ways.1 For example, hyperglycemia is known to inhibit nitric oxide production and to alter endothelial dysfunction. In a patient with acute heart failure, these alterations might be expected to have a significant effect on outcomes.
This study does not intend to answer these questions, but it does add to our understanding of the association of hyperglycemia and poor outcomes in acutely ill patients. More research is needed to examine whether or not heart failure patients, specifically, will benefit from better glycemic control in the acute setting. TH
References
- Clement S, Braithwaite SS, Magee MF, et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004 Feb;27(2):553-591.
- Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001 Nov 8;345(19):1359-1367.
- Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006 Feb 2;354(5):449-461.
- Furnary AP, Zerr KJ, Grunkemeier GL, et al. Continuous intravenous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical procedures. Ann Thorac Surg. 1999 Feb;67(2):352-362.
- Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2003 May;125(5):1007-1021.
Statins for Stroke Prevention
By Paul J. Grant, MD
Amarenco P, Bogousslavsky J, Callahan A III, et al. Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006 Aug 22;355:549-559.
Despite recent advances, the physician’s armamentarium for secondary stroke prevention is limited. The literature regarding optimal blood pressure management for stroke prevention is sparse, and the data addressing the best antiplatelet regimen remain controversial. This is troubling, given the fact that cerebrovascular disease remains the third leading cause of death in the United States.
Although extensive data exists for the benefits of using 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors (statins) for the prevention and treatment of cardiovascular disease, little is known about their role in decreasing the risk of stroke. The highly anticipated Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) trial sought to determine if statin therapy would decrease the risk of recurrent stroke in patients with no known coronary heart disease.
This prospective, randomized, double-blind, placebo-controlled trial included 4,731 men and women with no history of coronary heart disease. Eligible patients had a history of stroke (ischemic or hemorrhagic) or a transient ischemic attack (TIA) within a one- to six-month period before randomization as diagnosed by a neurologist. All patients required a low-density lipoprotein (LDL) cholesterol level between 100 and 190 mg/dL, while exclusion criteria included atrial fibrillation. Patients were randomized either to a dosage of 80 mg of atorvastatin daily or to a placebo and were followed for a median duration of 4.9 years. The primary endpoint was fatal or nonfatal stroke.
The average patient age in this trial was 63; approximately 60% of the patients were male. A total of 265 patients reached the primary endpoint in the atorvastatin group, versus 311 patients in the placebo group. This translates to an adjusted relative risk reduction of 16% in the primary endpoint for patients receiving atorvastatin (hazard ratio 0.84; 95% confidence interval 0.71 to 0.99; p=0.03). Although there was no difference in overall mortality between the two groups, the incidence of cardiovascular events was significantly lower in those receiving atorvastatin. Interestingly, more hemorrhagic strokes were noted in the atorvastatin group. With respect to safety, no significant differences in serious adverse events were noted. The atorvastatin group did, however, encounter significantly more cases of persistently elevated aspartate aminotransferase (AST) or alanine aminotransferase (ALT), at 2.2% versus 0.5% in the placebo group.
The findings by the SPARCL investigators provide strong evidence that atorvastatin reduces the incidence of stroke recurrence. The mechanism for risk reduction with statin exposure is most likely due to the dramatic lowering of LDL cholesterol. This effect has been shown in numerous trials resulting in the reduction of cardiovascular events. The present trial observed a 53% decrease in LDL cholesterol in the atorvastatin group compared with no change in the placebo arm. In addition to their powerful lipid-lowering role, statins also appear to prevent plaque rupture, optimize endothelial function, and provide anti-inflammatory effects. These are the so-called “pleiotropic effects” of statins and may be another factor contributing to the benefits observed.
Although some physicians are already prescribing statins for stroke patients, the literature supporting this practice has been sparse. The latest guidelines for prevention of stroke in patients with ischemic stroke or TIA were published in February 2006 by the American Heart Association/American Stroke Association Council on Stroke. These guidelines state that patients with a history of ischemic stroke or TIA are “reasonable candidates” for statin therapy. One could argue that these guidelines should now be revised to include a strong recommendation for statin therapy in secondary stroke prevention.
MRSA in the Community
By Matthew T. Harbison, MD
Moran GJ, Krishnadasan A, Gorwitz RJ, et al. EMERGEncy ID Net Study Group. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med. 2006 Aug 17;355(7):666-674.
Methicillin-resistant Staphylococcus aureus (MRSA) emerged as an issue in the healthcare community not long after the introduction of methicillin in 1959. MRSA has traditionally been thought of as an issue for those individuals who have contact with the healthcare system; however, there is growing evidence that MRSA has become an entity in the greater community at large, affecting individuals who have not spent significant time in healthcare facilities. Descriptions of several community-based outbreaks have led to the understanding that community-associated MRSA has different characteristics than MRSA infections contracted in the hospital setting. The community-associated isolates are resistant to fewer antibiotics, produce different toxins, and have differing genetic complexes responsible for antibiotic resistance. The majority of the community-acquired infections are skin and soft tissue infections, although more serious infections have been reported.
Moran and colleagues conducted a prospective prevalence study in adult patients presenting to emergency departments with skin and soft tissue infections in 11 metropolitan areas in geographically diverse regions of the United States. Eligible patients 18 and older with purulent skin or soft tissue infections of less than one week’s duration had demographic and historical data collected; a wound culture was also taken. If Staphylococcus aureus was isolated, it was further evaluated by the Centers for Disease Control and Prevention (CDC) to characterize antibiotic resistance patterns, toxin production, and the type of staphylococcal cassette chromosome present.
A total of 422 patients were enrolled, with S. aureus isolated in 320 patients (76%). Of those with isolated S. aureus, 78% had MRSA (59% of the total patients enrolled). The individual site prevalence of MRSA ranged from 15 to 74% and was the predominant etiology of skin and soft tissue infections in 10 of 11 emergency departments. MRSA susceptibilities in this study were 100% to trimethoprim-sulfamethoxazole and rifampin, 95% to clindamycin, 92% to tetracycline, 60% to fluoroquinolones, and 6% to erythromycin. The authors point out that clindamycin resistance in one center was 60%; thus, individual site resistance patterns may differ significantly. Treatment data was available for 406 of the 422 patients, with the majority of those treated with incision, drainage, and antibiotics. In 100 of the 175 MRSA patients treated with antibiotics, the choice of agent was discordant with susceptibility patterns. The authors were able to contact 248 patients between two and three weeks after their visits and, of those contacted, 96% reported resolution or improvement of the wound.
Using multivariate logistic-regression analyses, the authors identified several potential risk factors for MRSA infection. These included use of any antibiotic in the past month, underlying illness, history of MRSA infection, close contact with someone with similar infection, and reported spider bite. Interestingly, being a healthcare worker, living in a long-term care facility, and being hospitalized in the past year were not shown to be significant risk factors in this study.
The results of this study highlight the emerging difficulty, which continues to evolve, with antibiotic resistance patterns. The healthcare community must be vigilant to new entities that challenge the traditional views of antibiotic resistance patterns. The high rate of community-acquired MRSA skin and soft tissue infection demonstrated in this study, in addition to the large percentage of patients prescribed antibiotics that were resistant for the strain involved, emphasizes the need to reconsider the empiric antibiotic choices for this patient population. The variability in regional resistance patterns further complicates the issue. Given the high prevalence of MRSA skin and soft tissue infections reported in this study, use of routine wound cultures appears prudent, as does the need for effective follow-up strategies for alteration of antibiotic choice if necessary. At an institutional level, development of surveillance and isolation strategies for community-acquired MRSA should be considered.
More Options for Venous Thromboembolism Treatment
By Kirsten N. Kangelaris, MD
Kearon C, Ginsberg JS, Julian JA, et al. Fixed-Dose Heparin (FIDO) Investigators. Comparison of fixed-dose weight-adjusted unfractionated heparin and low-molecular-weight heparin for acute treatment of venous thromboembolism. JAMA. 2006 Aug 23;296(8):935-942.
The standard approach to using unfractionated heparin (UFH) in the treatment of acute venous thromboembolism as a bridge to warfarin therapy requires continuous intravenous infusion with frequent dose adjustments in response to measurements of activated partial thromboplastin time (aPTT). This therapy inevitably requires inpatient management. Subcutaneous administration of weight-based low molecular weight heparin (LMWH) has been the modality of choice for outpatient treatment of venous thromboembolism because it does not require laboratory monitoring. Its use has been limited by the high cost of treatment, however. A preliminary study, released in 2000 by the FIDO group (Fixed-Dose Heparin Investigators, Kearon and colleagues), suggested that subcutaneously administered UFH could be optimally dosed based on weight rather than monitoring aPTT levels.
This follow-up, randomized, open-label, adjudicator-blinded, multi-centered, non-inferiority trial enrolled 708 patients and compared fixed-dose, subcutaneously administered UFH to LMWH in acute deep venous thrombosis and pulmonary embolism. Administration in both groups was twice daily, subcutaneous, and weight-based. UFH was given as a first dose of 333 U/kg, followed by 250 U/kg every 12 hours. LMWH was administered at a dose of 100 IU/kg every 12 hours. Both treatments overlapped with three months of warfarin therapy, and both could be administered out of hospital.
Exclusion criteria were age <18, contraindication to subcutaneous therapy, active bleeding, life expectancy under three months, long-term anticoagulation therapy, pregnancy, and creatinine level >2.3 mg/dL.
The primary endpoints were efficacy as determined by recurrent venous thromboembolism within three months and safety as determined by major bleeding within 10 days of randomization. A secondary endpoint was relationship of efficacy and safety outcomes to aPTT levels measured on day two to three of therapy for the UFH group.
Results revealed that UFH was statistically non-inferior to LMWH by all endpoints, including treatment duration, efficacy, and safety. At three months, there was no significant difference between the groups in frequency of recurrent venous thromboembolism (3.8% UFH versus 3.4% LMWH), bleeding (1.1% UFH versus 1.4% LMWH), or death. There was no association between aPTT levels and recurrent venous thromboembolism or bleeding.
Limitations of the study included reduced enrollment from the initial study design, though power was adequate due to a lower than expected incidence of recurrent venous thromboembolism in both arms (~3.6% versus the expected 6%); possible biases related to open-label design; and more post-randomization exclusions in the UFH group versus the LMWH group.
In summary, fixed-dose, unmonitored, subcutaneous UFH appears to be an effective, safe alternative to LMWH as a bridge to warfarin therapy for venous thromboembolism. Clinically, this is relevant, because UFH is approximately 15 to 20 times less expensive than LMWH. The authors appropriately call attention to two developments in clinical practice that occurred during the course of the present study and that could potentially limit the use of UFH. These are 1) the dosing option for once-daily LMWH, which improves convenience, and 2) the preference for long-term LMWH therapy over warfarin for treating cancer patients with venous thromboembolism. Despite these exceptions, UFH may prove to be a viable and economic option for venous thromboembolism treatment.
In-Hospital MI Versus MI at Presentation
By Erin M. Galbraith, MD
Maynard C, Lowy E, Rumsfeld J, et al. The prevalence and outcomes of in-hospital acute myocardial infarction in the Department of Veterans Affairs Health System. Arch Intern Med. 2006 Jul 10;166(13):1410-1416.
Much is known about the prevalence, treatment, and prognosis of acute myocardial infarction (AMI) when it occurs in the community and is the presenting diagnosis. Few studies, however, have addressed the epidemiology of in-hospital AMIs. This study by Maynard and colleagues attempts to elucidate the basic epidemiologic characteristics, treatments, and outcomes of patients who suffer in-hospital AMIs.
This retrospective cohort consisted of 7,054 patients who had been discharged with a diagnosis of AMI from 127 Veterans Health Administration (VHA) medical centers between July and August 2003. Patients who had suffered a postoperative MI or were transferred in from another hospital were excluded. Data was obtained from both the electronic and paper medical records. Of the 7,054 patients in the study, 792 (11.2%) had experienced an AMI while hospitalized for other medical problems. These 792 patients were older by approximately 4.5 years and more frequently suffered from heart failure, diabetes, chronic renal insufficiency, COPD, cerebrovascular disease, dementia, and cancer. These patients were less likely, however, to have had a previous MI, to be current smokers, or to have undergone previous angioplasty. They were also less likely to have known lipid disorders or to be taking aspirin or lipid-lowering agents.
Regarding their presentations and management, the patients who suffered in-hospital AMIs had faster heart rates and lower blood pressures. They were also up to 75% less likely to report typical symptoms of cardiac ischemia, including chest pain/pressure, shoulder pain, nausea, and diaphoresis. They were less often seen by an attending cardiologist and had more contraindications to AMI therapy; thus, these patients underwent reperfusion therapy at much lower rates, both initially and at 30 days. Their troponin levels were more frequently elevated, but they were only half as likely to have ST segment elevations at the time of diagnosis. Hospitalizations were longer for the in-hospital group, and there were higher rates of in-hospital cardiogenic shock, cardiac arrest, and death (27.3% versus 8.6%). The 30-day mortality rate was also higher (33% versus 11.9%). Multivariate logistic regression revealed an adjusted odds ratio of 2.0 (95% confidence interval 1.7 to 2.4; p<0.001) for 30-day mortality in those who experienced an in-hospital AMI versus those who presented with an AMI.
Potential reasons for the increased severity of outcomes include, but are not limited to, their many chronic comorbidities, their other acute diagnoses, the failure of the medical team to recognize cardiac ischemia in a timely manner (i.e., higher initial troponins), the inability to treat MIs appropriately secondary to contraindications to acute intervention, and the lack of an attending cardiologist presiding over their medical care. Clearly, further studies are needed to elucidate the causes of death in the 33% of patients who died, because it is unclear whether the patients died of complications from their MIs or as a result of their multiple other medical problems. Knowledge of the extent to which these patients could be managed, both medically and via interventional procedures (and why these therapies were not pursued), would also be of value.
This study emphasizes the importance of recognizing atypical presentations of AMIs and exercising vigilance in pursuing the most aggressive therapy possible, as dictated by a patient’s ability to tolerate medical and procedural interventions.
Hyperglycemia in Heart Failure
By David H. Wesorick, MD
Barsheshet A, Garty M, Grossman E, et al. Admission blood glucose level and mortality among hospitalized nondiabetic patients with heart failure. Arch Intern Med. 2006 Aug 14-28;166(15):1613-1619.
The medical literature strongly suggests that inpatient hyperglycemia is associated with a variety of poor outcomes. Little is known, however, about the relationship between hyperglycemia and heart failure. These investigators examined the association of admission blood glucose and mortality in patients who were admitted to the hospital with acute heart failure.
In this study, 1,122 patients admitted to the hospital with acute heart failure and without diabetes were divided into tertiles depending on their admission blood glucose levels. Diabetes was defined as an admission blood glucose greater than or equal to 200 mg/dl, a known diagnosis of diabetes recorded in the chart, or the presence of anti-diabetic medications on the patient’s medication list. Tertile #1 had an average admission blood glucose of 92 mg/dl (with a range of 54-102); tertile #2 had an average admission blood glucose of 113 mg/dl (with a range of 103-127); and tertile #3 had an average admission blood glucose of 147 mg/dl (with a range of 128-199). Mortality was evaluated according to tertile.
In this study, patients in tertile #3 had significantly higher inpatient mortality (7.2%) than patients in tertile #1 or #2 (3% and 4%, respectively). There was a significant association between hyperglycemia and mortality, even at 60 days follow-up, although not at six and 12 months follow-up. The association remained significant, even when patients with acute MI were excluded. Besides hyperglycemia, the authors noted that increasing age, increasing creatinine, a New York Heart Association (NYHA) functional class of III or IV, and a systolic blood pressure of lower than 115 were also significant, independent predictors of in-hospital mortality in this patient population.
For a hospitalist, the intriguing question is this: Is hyperglycemia just a marker of worse disease, or might it contribute to poorer outcomes? Clearly, hyperglycemia is associated with poorer outcomes in other types of patients, including post-surgical patients, critically ill patients, MI patients, and general medical patients.1 But is hyperglycemia just a marker of more severe illness? In heart failure, perhaps more severe decompensation results in a more profound activation of the sympathetic nervous system and a more vigorous release of stress hormones, such as cortisol and catecholamines. In that case, one might expect a sicker patient to have a higher blood glucose.
More recent studies, however, show that better control of hyperglycemia in some acutely ill patients actually results in improved outcomes, suggesting that the hyperglycemia itself might be contributing to the poorer outcomes in some cases.2-5 Hyperglycemia is known to alter human physiology in a variety of adverse ways.1 For example, hyperglycemia is known to inhibit nitric oxide production and to alter endothelial dysfunction. In a patient with acute heart failure, these alterations might be expected to have a significant effect on outcomes.
This study does not intend to answer these questions, but it does add to our understanding of the association of hyperglycemia and poor outcomes in acutely ill patients. More research is needed to examine whether or not heart failure patients, specifically, will benefit from better glycemic control in the acute setting. TH
References
- Clement S, Braithwaite SS, Magee MF, et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004 Feb;27(2):553-591.
- Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001 Nov 8;345(19):1359-1367.
- Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006 Feb 2;354(5):449-461.
- Furnary AP, Zerr KJ, Grunkemeier GL, et al. Continuous intravenous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical procedures. Ann Thorac Surg. 1999 Feb;67(2):352-362.
- Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2003 May;125(5):1007-1021.
Injection Pearls
A 29-year-old male warehouse worker noticed pain in his right lower quadrant. The pain was intense and poorly localized (arrow) and increased with lifting or resisted hip flexion. Appendicitis was diagnosed, but pain persisted post-operatively. Necrotizing fasciitis was suspected, but repeated debridements failed to relieve the pain.

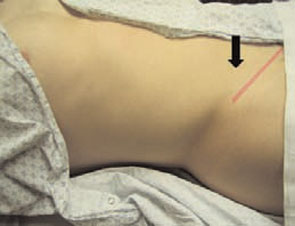
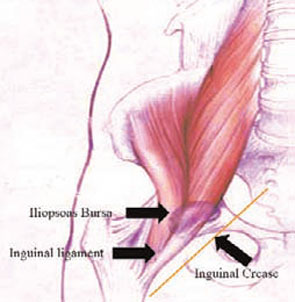
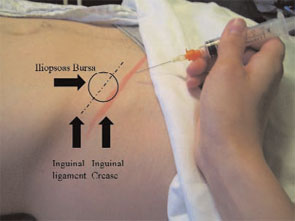

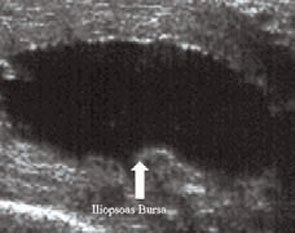
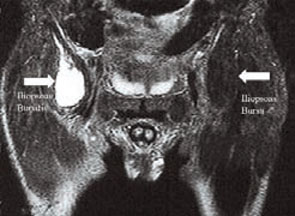
Physical Exam
The inguinal ligament runs parallel to the inguinal crease (pink pencil line—see right). About midway in its length, the ligament became difficult to identify due to an exquisitely tender doughy area (arrow). Palpation of this area reproduced the patent’s symptoms, along with poorly localized lower abdominal pain. An attempted sit-up caused similar symptoms.
Anatomy
The iliopsoas bursa is located where the inguinal ligament, the iliopsoas tendon, and the transversus tendon intersect. An inflamed iliopsoas bursa is palpable as a doughy mass below the midpoint of the length of the inguinal ligament, lateral to the femoral artery. Most often the opposite, unaffected side demonstrates a normal, pencil-thin, easily defined, non-tender inguinal ligament.
Iliopsoas Bursitis/Tendonitis
The iliopsoas bursa is the largest bursa in the body and communicates with the hip joint in 15% of patients. Bursitis/tendonitis is caused by overuse and friction as the tendon rides over the iliopectineal eminence of the pubis. The condition is associated with lifting, unloading trucks, and participating in sports requiring extensive use of the hip flexors (e.g., soccer, ballet, uphill running, hurdling, jumping). Iliopsoas bursitis/tendonitis is characterized by deep groin pain, sometimes radiating to the anterior hip or thigh, and is often accompanied by a snapping sensation. The patient may limp.
The pain is difficult for patients to localize and challenging for clinicians to reproduce. In fact, the average time from the onset of symptoms to diagnosis is 31 to 42 months. It is common for many other diagnoses to be entertained and treated with no improvement. Physical examination will reveal pain on deep palpation over the femoral triangle, where the musculotendinous junction of the iliopsoas can be palpated as a doughy diffuse area of tenderness at the midpoint of the inguinal ligament.
Pain may also be produced when the affected hip is extended or when the supine patient raises his or her heels off the table at about 15 degrees. In the latter position, the only active hip flexor is the iliopsoas.
Imaging
Although these procedures are not necessary for diagnosis, iliopsoas bursitis is best visualized using ultrasound or MRI—either of which will reveal a collection of fluid adjacent to the muscle. Treatment is conservative and consists of rest followed by stretching of the hip flexors and rotators, then strengthening and gradual return to work or sport. As in any overuse injury, biomechanical abnormalities must be sought and corrected. While most patients resolve spontaneously, corticosteroid injections are helpful in about one-third of patients. Rarely, surgical management of recalcitrant cases is warranted.
Iliopsoas Bursitis/Tendonitis Injection
The following procedure should be followed when administering a corticosteroid injection. With the fingers of one hand, identify and isolate the inguinal ligament in the area of doughy discomfort. With the other hand, insert a 1.5-inch needle to its hub, parallel to the ligament, and inject a steroid and lidocaine mixture slowly while withdrawing the needle to avoid inadvertently injecting the ligament or any tendons.
A medium-acting depot steroid gives good, long-lasting relief. A mixture of lidocaine or bupivacaine and the steroid allows for immediate relief, as well as confirmation that the steroid reached its target. TH
Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, and Dr. Ficalora is an associate professor in internal medicine at the Mayo Clinic College of Medicine.
A 29-year-old male warehouse worker noticed pain in his right lower quadrant. The pain was intense and poorly localized (arrow) and increased with lifting or resisted hip flexion. Appendicitis was diagnosed, but pain persisted post-operatively. Necrotizing fasciitis was suspected, but repeated debridements failed to relieve the pain.
Physical Exam
The inguinal ligament runs parallel to the inguinal crease (pink pencil line—see right). About midway in its length, the ligament became difficult to identify due to an exquisitely tender doughy area (arrow). Palpation of this area reproduced the patent’s symptoms, along with poorly localized lower abdominal pain. An attempted sit-up caused similar symptoms.
Anatomy
The iliopsoas bursa is located where the inguinal ligament, the iliopsoas tendon, and the transversus tendon intersect. An inflamed iliopsoas bursa is palpable as a doughy mass below the midpoint of the length of the inguinal ligament, lateral to the femoral artery. Most often the opposite, unaffected side demonstrates a normal, pencil-thin, easily defined, non-tender inguinal ligament.
Iliopsoas Bursitis/Tendonitis
The iliopsoas bursa is the largest bursa in the body and communicates with the hip joint in 15% of patients. Bursitis/tendonitis is caused by overuse and friction as the tendon rides over the iliopectineal eminence of the pubis. The condition is associated with lifting, unloading trucks, and participating in sports requiring extensive use of the hip flexors (e.g., soccer, ballet, uphill running, hurdling, jumping). Iliopsoas bursitis/tendonitis is characterized by deep groin pain, sometimes radiating to the anterior hip or thigh, and is often accompanied by a snapping sensation. The patient may limp.
The pain is difficult for patients to localize and challenging for clinicians to reproduce. In fact, the average time from the onset of symptoms to diagnosis is 31 to 42 months. It is common for many other diagnoses to be entertained and treated with no improvement. Physical examination will reveal pain on deep palpation over the femoral triangle, where the musculotendinous junction of the iliopsoas can be palpated as a doughy diffuse area of tenderness at the midpoint of the inguinal ligament.
Pain may also be produced when the affected hip is extended or when the supine patient raises his or her heels off the table at about 15 degrees. In the latter position, the only active hip flexor is the iliopsoas.
Imaging
Although these procedures are not necessary for diagnosis, iliopsoas bursitis is best visualized using ultrasound or MRI—either of which will reveal a collection of fluid adjacent to the muscle. Treatment is conservative and consists of rest followed by stretching of the hip flexors and rotators, then strengthening and gradual return to work or sport. As in any overuse injury, biomechanical abnormalities must be sought and corrected. While most patients resolve spontaneously, corticosteroid injections are helpful in about one-third of patients. Rarely, surgical management of recalcitrant cases is warranted.
Iliopsoas Bursitis/Tendonitis Injection
The following procedure should be followed when administering a corticosteroid injection. With the fingers of one hand, identify and isolate the inguinal ligament in the area of doughy discomfort. With the other hand, insert a 1.5-inch needle to its hub, parallel to the ligament, and inject a steroid and lidocaine mixture slowly while withdrawing the needle to avoid inadvertently injecting the ligament or any tendons.
A medium-acting depot steroid gives good, long-lasting relief. A mixture of lidocaine or bupivacaine and the steroid allows for immediate relief, as well as confirmation that the steroid reached its target. TH
Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, and Dr. Ficalora is an associate professor in internal medicine at the Mayo Clinic College of Medicine.
A 29-year-old male warehouse worker noticed pain in his right lower quadrant. The pain was intense and poorly localized (arrow) and increased with lifting or resisted hip flexion. Appendicitis was diagnosed, but pain persisted post-operatively. Necrotizing fasciitis was suspected, but repeated debridements failed to relieve the pain.
Physical Exam
The inguinal ligament runs parallel to the inguinal crease (pink pencil line—see right). About midway in its length, the ligament became difficult to identify due to an exquisitely tender doughy area (arrow). Palpation of this area reproduced the patent’s symptoms, along with poorly localized lower abdominal pain. An attempted sit-up caused similar symptoms.
Anatomy
The iliopsoas bursa is located where the inguinal ligament, the iliopsoas tendon, and the transversus tendon intersect. An inflamed iliopsoas bursa is palpable as a doughy mass below the midpoint of the length of the inguinal ligament, lateral to the femoral artery. Most often the opposite, unaffected side demonstrates a normal, pencil-thin, easily defined, non-tender inguinal ligament.
Iliopsoas Bursitis/Tendonitis
The iliopsoas bursa is the largest bursa in the body and communicates with the hip joint in 15% of patients. Bursitis/tendonitis is caused by overuse and friction as the tendon rides over the iliopectineal eminence of the pubis. The condition is associated with lifting, unloading trucks, and participating in sports requiring extensive use of the hip flexors (e.g., soccer, ballet, uphill running, hurdling, jumping). Iliopsoas bursitis/tendonitis is characterized by deep groin pain, sometimes radiating to the anterior hip or thigh, and is often accompanied by a snapping sensation. The patient may limp.
The pain is difficult for patients to localize and challenging for clinicians to reproduce. In fact, the average time from the onset of symptoms to diagnosis is 31 to 42 months. It is common for many other diagnoses to be entertained and treated with no improvement. Physical examination will reveal pain on deep palpation over the femoral triangle, where the musculotendinous junction of the iliopsoas can be palpated as a doughy diffuse area of tenderness at the midpoint of the inguinal ligament.
Pain may also be produced when the affected hip is extended or when the supine patient raises his or her heels off the table at about 15 degrees. In the latter position, the only active hip flexor is the iliopsoas.
Imaging
Although these procedures are not necessary for diagnosis, iliopsoas bursitis is best visualized using ultrasound or MRI—either of which will reveal a collection of fluid adjacent to the muscle. Treatment is conservative and consists of rest followed by stretching of the hip flexors and rotators, then strengthening and gradual return to work or sport. As in any overuse injury, biomechanical abnormalities must be sought and corrected. While most patients resolve spontaneously, corticosteroid injections are helpful in about one-third of patients. Rarely, surgical management of recalcitrant cases is warranted.
Iliopsoas Bursitis/Tendonitis Injection
The following procedure should be followed when administering a corticosteroid injection. With the fingers of one hand, identify and isolate the inguinal ligament in the area of doughy discomfort. With the other hand, insert a 1.5-inch needle to its hub, parallel to the ligament, and inject a steroid and lidocaine mixture slowly while withdrawing the needle to avoid inadvertently injecting the ligament or any tendons.
A medium-acting depot steroid gives good, long-lasting relief. A mixture of lidocaine or bupivacaine and the steroid allows for immediate relief, as well as confirmation that the steroid reached its target. TH
Gerhart is a third-year medical student at the Mayo Clinic College of Medicine, and Dr. Ficalora is an associate professor in internal medicine at the Mayo Clinic College of Medicine.
History of a Vitamin

What do the Japanese military, a Dutch microbiologist, sick chickens, and rice polishers have in common?
In the 1800s, Europeans colonizing Asia brought with them steam-powered machines that completely polished rice. This rice, which was thought to be superior to unpolished rice, became very popular. As Far Eastern society’s main source of thiamine was polished to oblivion, beriberi became more prevalent and problematic.
At that time, micronutrient deficiency states were still a mystery to physicians. Kanehiro Takaki (October 30, 1849–April 13, 1920), surgeon general of the Japanese Imperial Navy, noticed a connection between sailors’ diets and their development of beriberi. White rice was replaced with barley, vegetables, fish, and meat. The incidence of beriberi dropped swiftly and was eliminated in the Japanese Navy, within six years.

Meanwhile, in the Dutch Indies, beriberi was endemic and crippling. Christiaan Eijkman, a Dutch microbiologist (August 11, 1858–November 5, 1930) who had studied with bacteriologist Robert Koch (December 11, 1843-May 27, 1910) in Berlin, was sent to research the disease in Java. Eijkman was unaware of Takaki’s findings and was convinced that beriberi was an infection.
Eijkman tried to infect chickens with a microorganism isolated from the corpses of two beriberi-related deaths. While he was striving to find the causative pathogen, Eijkman noticed that all chickens, even those having no contact with either the microorganism or other chickens, developed “a disease, in many respects strikingly similar to beriberi in man.” In fact, they had developed polyneuritis. Then, miraculously, they recovered spontaneously.

Eijkman was bewildered by this sequence of events and set out to solve the poultry mystery. He discovered that the chickens, during the time that they had been ill, had been eating leftover cooked, polished white rice from the hospital kitchen. When the cook left, however, his replacement refused to relinquish leftover rice, and they were thereafter given raw, unpolished rice. After this dietary change, the chickens recovered. Eijkman concluded that a substance in unpolished rice protected chickens against infection—he was still searching for the elusive microscopic culprit—and he called this protective substance the “anti-beriberi factor.” He thought unpolished rice contained an antidote to a bacterial toxin.
In 1906, Frederick Hopkins (1861–1947) demonstrated “accessory factors” in food, those nutrients necessary to maintain good health in addition to the carbohydrates, fats, proteins, and minerals that had previously been acknowledged as vital. In 1912, a Polish biochemist, Casimir Funk (1884–1967), thought he had isolated the anti-beriberi factor and named his discovery vitamine, from “vital amine.” Although he hadn’t isolated anti-beriberi factor—it is believed that he isolated nicotinic acid—the name vitamine remained. Eventually, in 1926, researchers were able to isolate the anti-beriberi factor in rice bran extracts. In 1929, Hopkins and Eijkman were awarded the Nobel Prize in Physiology or Medicine for the discovery of vitamins.

Clinicians are now well aware of alcohol abuse and the development of Wernicke’s encephalopathy or Korsakoff amnestic syndrome. Phrases like wet (high output heart failure) and dry (peripheral neuropathy) beriberi were once commonly found on board exams. The clinical presentation of thiamine deficiency isn’t limited to alcoholics. For example, there is evidence that patients with end-stage renal disease on hemodialysis are at risk of becoming thiamine deficient and of developing “unexplained” encephalopathies.1 Patients who suffer congestive heart failure while on long-term diuretics are also at increased risk for thiamine deficiency.2
This account is a classic example of the fascinating way in which the discovery of these essential nutrients has evolved and serves as a wake-up call that emphasizes the current epidemic of malnutrition in hospitalized patients.
Protein energy malnutrition in hospitalized patients is very common. Many studies have demonstrated that the prevalence runs between 30% and 60%, depending on the patient population studied and the assessment tools used. Hospital malnutrition, independent of disease activity, has been linked to increased length of stay and heightened morbidity and mortality. It is disturbing to think that many patients are actually worse off at time of dismissal than they were at admission. Malnutrition often goes unrecognized and even when the problem is acknowledged adequate nutrition is often not provided. Patients are commonly permitted to subsist on very low nutrient intakes.3 The problem of malnutrition is likely grossly underestimated because most studies have not considered micronutrients such as trace elements and vitamins. In addition, the presence of subclinical, yet clinically important, deficiency is expected to be highly prevalent.
Early screening improves the recognition of malnourished patients and provides the opportunity to start treatment at an early stage of hospitalization. Nutritional therapy as part of a comprehensive treatment modality may result in improvement of healthcare quality. In some countries it is also a criterion for assessing the performance of hospitals. In the U.S., for example, nutritional screening in hospitals is required for accreditation by the Joint Commission on Accreditation of Healthcare Organizations and is part of the Minimal Data Set documentation in long-term care facilities.
In most institutions, nutritional screening refers to a rapid and general test that is undertaken by nursing, medical, and other staff, often at first contact with patients. This is in contrast to the detailed nutritional evaluation that is undertaken by nutrition specialists (e.g., dietitians, specialist nutrition nurses, or physicians with an interest in nutrition), often for complex problems and often following nutritional screening. The introduction of a nutrition screening program and documentation of nutritional status may also increase diagnosis-related group (DRG)-based reimbursement.
Unfortunately, a lack of standardized sensitive and specific methodologies to assess for macro- or micronutrient deficiencies makes it difficult to determine how best to screen patients. Recent literature suggests, however, that the use of a short nutrition questionnaire and an undemanding treatment plan improved nutritional care during a hospital stay.4 The use of this strategy reduced the duration of the hospital stay in a subgroup of frail malnourished patients, offering potential improvements in morbidity as well as financial benefits for the hospital.
The lessons of past discoveries should not be lost on modern medicine. Malnutrition can be made a condition of the past through the use of simple screening procedures and uncomplicated treatments. The results will benefit both patients and hospitals. TH
Michelle Schneider is a medical student at the Royal College of Surgeons in Dublin, Ireland. Dr. Egger is a senior associate consultant at the Mayo Clinic College of Medicine.
References
- Hung SC, Hung SH, Tarng DC, et al. Thiamine deficiency and unexplained encephalopathy in hemodialysis and peritoneal dialysis patients. Am J Kidney Dis. 2001;38:941-947.
- Hanninen SA, Darling PB, Sole MJ, et al. The prevalence of thiamin deficiency in hospitalized patients with congestive heart failure. J Am Coll Cardiol. 2006 Jan 17;47(2):354-361.
- Sullivan DH, Sun S, Walls RC. Protein-energy undernutrition among elderly hospitalized patients: a prospective study. JAMA. 1999 Jun;281(21):2013-2019.
- Kruizenga HM, Van Tulder MW, Seidell JC, et al. Effectiveness and cost-effectiveness of early screening and treatment of malnourished patients. Am J Clin Nutr. 2005;82(5):1082-1089.
What do the Japanese military, a Dutch microbiologist, sick chickens, and rice polishers have in common?
In the 1800s, Europeans colonizing Asia brought with them steam-powered machines that completely polished rice. This rice, which was thought to be superior to unpolished rice, became very popular. As Far Eastern society’s main source of thiamine was polished to oblivion, beriberi became more prevalent and problematic.
At that time, micronutrient deficiency states were still a mystery to physicians. Kanehiro Takaki (October 30, 1849–April 13, 1920), surgeon general of the Japanese Imperial Navy, noticed a connection between sailors’ diets and their development of beriberi. White rice was replaced with barley, vegetables, fish, and meat. The incidence of beriberi dropped swiftly and was eliminated in the Japanese Navy, within six years.
Meanwhile, in the Dutch Indies, beriberi was endemic and crippling. Christiaan Eijkman, a Dutch microbiologist (August 11, 1858–November 5, 1930) who had studied with bacteriologist Robert Koch (December 11, 1843-May 27, 1910) in Berlin, was sent to research the disease in Java. Eijkman was unaware of Takaki’s findings and was convinced that beriberi was an infection.
Eijkman tried to infect chickens with a microorganism isolated from the corpses of two beriberi-related deaths. While he was striving to find the causative pathogen, Eijkman noticed that all chickens, even those having no contact with either the microorganism or other chickens, developed “a disease, in many respects strikingly similar to beriberi in man.” In fact, they had developed polyneuritis. Then, miraculously, they recovered spontaneously.
Eijkman was bewildered by this sequence of events and set out to solve the poultry mystery. He discovered that the chickens, during the time that they had been ill, had been eating leftover cooked, polished white rice from the hospital kitchen. When the cook left, however, his replacement refused to relinquish leftover rice, and they were thereafter given raw, unpolished rice. After this dietary change, the chickens recovered. Eijkman concluded that a substance in unpolished rice protected chickens against infection—he was still searching for the elusive microscopic culprit—and he called this protective substance the “anti-beriberi factor.” He thought unpolished rice contained an antidote to a bacterial toxin.
In 1906, Frederick Hopkins (1861–1947) demonstrated “accessory factors” in food, those nutrients necessary to maintain good health in addition to the carbohydrates, fats, proteins, and minerals that had previously been acknowledged as vital. In 1912, a Polish biochemist, Casimir Funk (1884–1967), thought he had isolated the anti-beriberi factor and named his discovery vitamine, from “vital amine.” Although he hadn’t isolated anti-beriberi factor—it is believed that he isolated nicotinic acid—the name vitamine remained. Eventually, in 1926, researchers were able to isolate the anti-beriberi factor in rice bran extracts. In 1929, Hopkins and Eijkman were awarded the Nobel Prize in Physiology or Medicine for the discovery of vitamins.
Clinicians are now well aware of alcohol abuse and the development of Wernicke’s encephalopathy or Korsakoff amnestic syndrome. Phrases like wet (high output heart failure) and dry (peripheral neuropathy) beriberi were once commonly found on board exams. The clinical presentation of thiamine deficiency isn’t limited to alcoholics. For example, there is evidence that patients with end-stage renal disease on hemodialysis are at risk of becoming thiamine deficient and of developing “unexplained” encephalopathies.1 Patients who suffer congestive heart failure while on long-term diuretics are also at increased risk for thiamine deficiency.2
This account is a classic example of the fascinating way in which the discovery of these essential nutrients has evolved and serves as a wake-up call that emphasizes the current epidemic of malnutrition in hospitalized patients.
Protein energy malnutrition in hospitalized patients is very common. Many studies have demonstrated that the prevalence runs between 30% and 60%, depending on the patient population studied and the assessment tools used. Hospital malnutrition, independent of disease activity, has been linked to increased length of stay and heightened morbidity and mortality. It is disturbing to think that many patients are actually worse off at time of dismissal than they were at admission. Malnutrition often goes unrecognized and even when the problem is acknowledged adequate nutrition is often not provided. Patients are commonly permitted to subsist on very low nutrient intakes.3 The problem of malnutrition is likely grossly underestimated because most studies have not considered micronutrients such as trace elements and vitamins. In addition, the presence of subclinical, yet clinically important, deficiency is expected to be highly prevalent.
Early screening improves the recognition of malnourished patients and provides the opportunity to start treatment at an early stage of hospitalization. Nutritional therapy as part of a comprehensive treatment modality may result in improvement of healthcare quality. In some countries it is also a criterion for assessing the performance of hospitals. In the U.S., for example, nutritional screening in hospitals is required for accreditation by the Joint Commission on Accreditation of Healthcare Organizations and is part of the Minimal Data Set documentation in long-term care facilities.
In most institutions, nutritional screening refers to a rapid and general test that is undertaken by nursing, medical, and other staff, often at first contact with patients. This is in contrast to the detailed nutritional evaluation that is undertaken by nutrition specialists (e.g., dietitians, specialist nutrition nurses, or physicians with an interest in nutrition), often for complex problems and often following nutritional screening. The introduction of a nutrition screening program and documentation of nutritional status may also increase diagnosis-related group (DRG)-based reimbursement.
Unfortunately, a lack of standardized sensitive and specific methodologies to assess for macro- or micronutrient deficiencies makes it difficult to determine how best to screen patients. Recent literature suggests, however, that the use of a short nutrition questionnaire and an undemanding treatment plan improved nutritional care during a hospital stay.4 The use of this strategy reduced the duration of the hospital stay in a subgroup of frail malnourished patients, offering potential improvements in morbidity as well as financial benefits for the hospital.
The lessons of past discoveries should not be lost on modern medicine. Malnutrition can be made a condition of the past through the use of simple screening procedures and uncomplicated treatments. The results will benefit both patients and hospitals. TH
Michelle Schneider is a medical student at the Royal College of Surgeons in Dublin, Ireland. Dr. Egger is a senior associate consultant at the Mayo Clinic College of Medicine.
References
- Hung SC, Hung SH, Tarng DC, et al. Thiamine deficiency and unexplained encephalopathy in hemodialysis and peritoneal dialysis patients. Am J Kidney Dis. 2001;38:941-947.
- Hanninen SA, Darling PB, Sole MJ, et al. The prevalence of thiamin deficiency in hospitalized patients with congestive heart failure. J Am Coll Cardiol. 2006 Jan 17;47(2):354-361.
- Sullivan DH, Sun S, Walls RC. Protein-energy undernutrition among elderly hospitalized patients: a prospective study. JAMA. 1999 Jun;281(21):2013-2019.
- Kruizenga HM, Van Tulder MW, Seidell JC, et al. Effectiveness and cost-effectiveness of early screening and treatment of malnourished patients. Am J Clin Nutr. 2005;82(5):1082-1089.
What do the Japanese military, a Dutch microbiologist, sick chickens, and rice polishers have in common?
In the 1800s, Europeans colonizing Asia brought with them steam-powered machines that completely polished rice. This rice, which was thought to be superior to unpolished rice, became very popular. As Far Eastern society’s main source of thiamine was polished to oblivion, beriberi became more prevalent and problematic.
At that time, micronutrient deficiency states were still a mystery to physicians. Kanehiro Takaki (October 30, 1849–April 13, 1920), surgeon general of the Japanese Imperial Navy, noticed a connection between sailors’ diets and their development of beriberi. White rice was replaced with barley, vegetables, fish, and meat. The incidence of beriberi dropped swiftly and was eliminated in the Japanese Navy, within six years.
Meanwhile, in the Dutch Indies, beriberi was endemic and crippling. Christiaan Eijkman, a Dutch microbiologist (August 11, 1858–November 5, 1930) who had studied with bacteriologist Robert Koch (December 11, 1843-May 27, 1910) in Berlin, was sent to research the disease in Java. Eijkman was unaware of Takaki’s findings and was convinced that beriberi was an infection.
Eijkman tried to infect chickens with a microorganism isolated from the corpses of two beriberi-related deaths. While he was striving to find the causative pathogen, Eijkman noticed that all chickens, even those having no contact with either the microorganism or other chickens, developed “a disease, in many respects strikingly similar to beriberi in man.” In fact, they had developed polyneuritis. Then, miraculously, they recovered spontaneously.
Eijkman was bewildered by this sequence of events and set out to solve the poultry mystery. He discovered that the chickens, during the time that they had been ill, had been eating leftover cooked, polished white rice from the hospital kitchen. When the cook left, however, his replacement refused to relinquish leftover rice, and they were thereafter given raw, unpolished rice. After this dietary change, the chickens recovered. Eijkman concluded that a substance in unpolished rice protected chickens against infection—he was still searching for the elusive microscopic culprit—and he called this protective substance the “anti-beriberi factor.” He thought unpolished rice contained an antidote to a bacterial toxin.
In 1906, Frederick Hopkins (1861–1947) demonstrated “accessory factors” in food, those nutrients necessary to maintain good health in addition to the carbohydrates, fats, proteins, and minerals that had previously been acknowledged as vital. In 1912, a Polish biochemist, Casimir Funk (1884–1967), thought he had isolated the anti-beriberi factor and named his discovery vitamine, from “vital amine.” Although he hadn’t isolated anti-beriberi factor—it is believed that he isolated nicotinic acid—the name vitamine remained. Eventually, in 1926, researchers were able to isolate the anti-beriberi factor in rice bran extracts. In 1929, Hopkins and Eijkman were awarded the Nobel Prize in Physiology or Medicine for the discovery of vitamins.
Clinicians are now well aware of alcohol abuse and the development of Wernicke’s encephalopathy or Korsakoff amnestic syndrome. Phrases like wet (high output heart failure) and dry (peripheral neuropathy) beriberi were once commonly found on board exams. The clinical presentation of thiamine deficiency isn’t limited to alcoholics. For example, there is evidence that patients with end-stage renal disease on hemodialysis are at risk of becoming thiamine deficient and of developing “unexplained” encephalopathies.1 Patients who suffer congestive heart failure while on long-term diuretics are also at increased risk for thiamine deficiency.2
This account is a classic example of the fascinating way in which the discovery of these essential nutrients has evolved and serves as a wake-up call that emphasizes the current epidemic of malnutrition in hospitalized patients.
Protein energy malnutrition in hospitalized patients is very common. Many studies have demonstrated that the prevalence runs between 30% and 60%, depending on the patient population studied and the assessment tools used. Hospital malnutrition, independent of disease activity, has been linked to increased length of stay and heightened morbidity and mortality. It is disturbing to think that many patients are actually worse off at time of dismissal than they were at admission. Malnutrition often goes unrecognized and even when the problem is acknowledged adequate nutrition is often not provided. Patients are commonly permitted to subsist on very low nutrient intakes.3 The problem of malnutrition is likely grossly underestimated because most studies have not considered micronutrients such as trace elements and vitamins. In addition, the presence of subclinical, yet clinically important, deficiency is expected to be highly prevalent.
Early screening improves the recognition of malnourished patients and provides the opportunity to start treatment at an early stage of hospitalization. Nutritional therapy as part of a comprehensive treatment modality may result in improvement of healthcare quality. In some countries it is also a criterion for assessing the performance of hospitals. In the U.S., for example, nutritional screening in hospitals is required for accreditation by the Joint Commission on Accreditation of Healthcare Organizations and is part of the Minimal Data Set documentation in long-term care facilities.
In most institutions, nutritional screening refers to a rapid and general test that is undertaken by nursing, medical, and other staff, often at first contact with patients. This is in contrast to the detailed nutritional evaluation that is undertaken by nutrition specialists (e.g., dietitians, specialist nutrition nurses, or physicians with an interest in nutrition), often for complex problems and often following nutritional screening. The introduction of a nutrition screening program and documentation of nutritional status may also increase diagnosis-related group (DRG)-based reimbursement.
Unfortunately, a lack of standardized sensitive and specific methodologies to assess for macro- or micronutrient deficiencies makes it difficult to determine how best to screen patients. Recent literature suggests, however, that the use of a short nutrition questionnaire and an undemanding treatment plan improved nutritional care during a hospital stay.4 The use of this strategy reduced the duration of the hospital stay in a subgroup of frail malnourished patients, offering potential improvements in morbidity as well as financial benefits for the hospital.
The lessons of past discoveries should not be lost on modern medicine. Malnutrition can be made a condition of the past through the use of simple screening procedures and uncomplicated treatments. The results will benefit both patients and hospitals. TH
Michelle Schneider is a medical student at the Royal College of Surgeons in Dublin, Ireland. Dr. Egger is a senior associate consultant at the Mayo Clinic College of Medicine.
References
- Hung SC, Hung SH, Tarng DC, et al. Thiamine deficiency and unexplained encephalopathy in hemodialysis and peritoneal dialysis patients. Am J Kidney Dis. 2001;38:941-947.
- Hanninen SA, Darling PB, Sole MJ, et al. The prevalence of thiamin deficiency in hospitalized patients with congestive heart failure. J Am Coll Cardiol. 2006 Jan 17;47(2):354-361.
- Sullivan DH, Sun S, Walls RC. Protein-energy undernutrition among elderly hospitalized patients: a prospective study. JAMA. 1999 Jun;281(21):2013-2019.
- Kruizenga HM, Van Tulder MW, Seidell JC, et al. Effectiveness and cost-effectiveness of early screening and treatment of malnourished patients. Am J Clin Nutr. 2005;82(5):1082-1089.