User login
In the Literature: HM-Related Research You Need to Know
In This Edition
Literature at a Glance
A guide to this month’s studies
- Early ambulation and LOS in geriatric patients
- Patient-safety movement and hospital harm rates
- Lifestyle modification and weight loss
- Outcomes of transcatheter aortic-valve implantation
- Tool for predicting mortality in advanced dementia
- Residents’ opinion of new duty-hour regulations
- Renal ultrasound predictor for acute kidney injury
- Romiplostim use in immune thrombocytopenia
Increasing Ambulation within 48 Hours of Admission Decreases LOS by Two Days
Clinical question: Is there an association between an early increase in ambulation and length of stay (LOS) in geriatric patients admitted with an acute illness?
Background: Early ambulation leading to better recovery in such illnesses as pneumonia and myocardial infarction is well known, as is early ambulation after hip fracture surgery to prevent complications. However, no specific guidelines exist in regard to ambulation in older patients.
Study design: Prospective, nonblinded study.
Setting: Acute-care geriatric unit in an academic medical center.
Synopsis: A total of 162 patients 65 or older were studied. Data were collected during a four-month period in 2009. A Step Activity Monitor (SAM) was placed on admission. Patients were instructed to walk as usual. Investigators measured the number of steps taken per day and change in steps between the first and second day.
Patients averaged 662.1 steps per day, with a mean step change of 196.5 steps. The adjusted mean difference in LOS for patients who increased their total steps by 600 or more between the first and second day was 2.13 days (95% CI, 1.05-3.97). Patients who had low or negative changes in steps had longer LOS. The 32 patients who walked more than 600 steps were more likely to be men (P=0.02), independently ambulate (P<0.01), and have admitting orders of “ambulate with assist” (P=0.03).
One limitation of this study is that patients who walked more might have been less ill or very functional on admission.
Bottom line: Increasing ambulation early in a hospitalization (first two days) is associated with a decreased LOS in an elderly population.
Citation: Fisher SR, Kuo YF, Graham JE, Ottenbacher KJ, Ostir GV. Early ambulation and length of stay in older adults hospitalized for acute illness. Arch Intern Med. 2010;170(21):1942-1943.
Despite Efforts to Improve Patient Safety in Hospitals, No Reduction in Longitudinal Rates of Harm
Clinical question: As hospitals focus more on programs to improve patient safety, has the rate of harms decreased?
Background: Since the Institute of Medicine published a groundbreaking report (To Err is Human) a little more than a decade ago, policymakers, hospitals, and healthcare organizations have focused more on efforts to improve patient safety with the goal of reducing harms. It is not clear if these efforts have reduced harms.
Study design: Retrospective chart review.
Setting: Ten hospitals in North Carolina.
Synopsis: Ten charts per quarter were randomly selected from each hospital from January 2002 through December 2007. Internal and external reviewers used the IHI Global Trigger Tool for Measuring Adverse Events to identify rates of harm. Harms were classified into categories of severity and assessed for preventability.
Kappa scores were generally higher for internal reviewers, indicating higher reliability for internal reviewers. Internal reviewers identified 588 harms for 10,415 patient days (25.1 harms per 100 patient days), which occurred in 423 unique patients (18.1%). A majority (63.1%) of harms were considered preventable. Forty-one percent of harms were temporary and required intervention; 2.4% caused or contributed to a patient’s death.
There was no significant change over time in the rate of harms (regardless of reviewer type) even after adjusting for demographics.
This study is limited because it is based only in North Carolina hospitals. It was not powered to evaluate change in individual hospitals. There might have been unmeasurable improvements that were not accounted for by the trigger tool.
Bottom line: Despite a higher focus on patient safety, investigators did not find a decrease in the rate of harms. A majority of the harms were preventable. This study should not preclude efforts to continue to improve patient safety.
Citation: Landrigan CP, Parry GJ, Bones CB, Hackbarth AD, Goldmann DA, Sharek PJ. Temporal trends in rates of patient harm resulting from medical care. N Engl J Med. 2010;363(22):2124-2134.
Intensive Lifestyle Modification Improves Weight Loss in Severely Obese Individuals
Clinical question: Does the combination of diet modification and increased physical activity lead to weight loss and improve health risks in severely obese patients?
Background: Obesity is at epidemic proportions, but there are no evidence-based treatment guidelines for severe obesity.
Study design: Randomized, single-blind trial.
Setting: Community volunteers.
Synopsis: A total of 130 individuals with a body mass index (BMI) of ≥35 were randomized to receive lifestyle interventions consisting of diet and initial physical activity for 12 months, or diet for six months and delayed physical activity for the remainder of the year.
The initial-physical-activity group demonstrated greater weight loss at six months, but the overall weight loss did not differ between the two groups. At 12 months, the initial physical activity group lost 12.1 kg and the delayed-physical-activity group lost 9.87 kg. Both groups demonstrated significantly reduced blood pressure, reduced serum liver enzymes, and improved insulin resistance.
Candidates with a history of coronary artery disease, uncontrolled blood pressure, or diabetes were excluded. Participants were provided with prepackaged meal replacements for the first six months and received financial compensation for participation in the study.
This study is limited by the fact that a majority of the participants were female (85.1%). Providing meals to the participants also limits the application of this program to the general public.
Bottom line: The results of this study reflect the importance of diet and exercise on weight loss in obese individuals. However, adherence to the goals of the study required multiple individual and group meetings throughout the year, the provision of prepackaged meals, and some financial incentive for compliance.
Citation: Goodpaster GH, Delany JP, Otto AD, et al. Effects of diet and physical activity interventions on weight loss and cardiometabolic risk factors in severely obese adults: a randomized trial. JAMA. 2010;304 (16):1795-1802.
Transcatheter Aortic-Valve Implantation Is Superior to Standard Nonoperative Therapy for Symptomatic Aortic Stenosis
Clinical question: Is there a mortality benefit to transcatheter valve implantation over standard therapy in nonsurgical candidates with severe aortic stenosis (AS)?
Background: Untreated, symptomatic AS has a high rate of death, but a significant proportion of patients with severe aortic stenosis are poor surgical candidates. Available since 2002, transcatheter aortic-valve implantation (TAVI) is a promising, nonsurgical treatment option for severe AS. However, to date, TAVI has lacked rigorous clinical data.
Study design: Prospective, multicenter, randomized, active-treatment-controlled clinical trial.
Setting: Twenty-one centers, 17 of which were in the U.S.
Synopsis: A total of 358 patients with severe AS who were considered nonsurgical candidates were randomized to either TAVI or standard therapy. A majority (83.8%) of the patients in the standard group underwent balloon aortic valvuloplasty.
Researchers found a significant reduction (HR 0.55, 95% CI 0.40 to 0.74, P<0.001) in all-cause mortality at one year in those patients undergoing TAVI (30.7%) vs. standard therapy (50.7%). Additional benefits included lower rates of the composite endpoints of death from any cause or repeat hospitalization (42.5% vs. 71.6%, P<0.001) and NYHA Functional Class III or IV symptoms (25.2% vs. 58.0%, P<0.001) at one year. However, higher incidences of major strokes (5.0% vs. 1.6%, P=0.06) and major vascular complications (16.2% vs. 1.1%, P<0.001) were seen.
While the one-year mortality benefit of TAVI over standard nonoperative therapy was clearly demonstrated by this study, hospitalists should interpret these data cautiously with respect to their inpatient populations as exclusion criteria were extensive, including bicuspid or noncalcified aortic valve, LVEF less than 20%, and severe renal insufficiency. Additionally, the entity of standard therapy was poorly delineated.
Bottom line: TAVI should be considered in patients with severe aortic stenosis who are not suitable surgical candidates.
Citation: Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-1607.
ADEPT Score Better Predicts Six-Month Mortality in Nursing Home Residents with Advanced Dementia
Clinical question: Are current Medicare hospice eligibility guidelines accurate enough to predict six-month survival in nursing home residents with dementia when compared with the Advanced Dementia Prognostic Tool (ADEPT)?
Background: Incorrectly estimating the life expectancy in almost 5 million nursing home residents with dementia prevents enrollment to palliative care and hospice for those who would benefit most. Creating and validating a mortality risk score would allow increased services to these residents.
Study design: Prospective cohort study.
Setting: Twenty-one nursing homes in Boston.
Synopsis: A total of 606 nursing home residents with advanced dementia were recruited for this study. Each resident was assessed for Medicare hospice eligibility and assigned an ADEPT score. Mortality rate was determined six months later. These two assessment tools were compared regarding their ability to predict six-month mortality.
The mean ADEPT score was 10.1 (range of 1.0-32.5), with a higher score meaning worse prognosis. Sixty-five residents (10.7%) met Medicare hospice eligibility guidelines. A total of 111 residents (18.3%) died.
The ADEPT score was more sensitive (90% vs. 20%) but less specific (28.3% vs. 89%) than Medicare guidelines. The area under the receiver operating characteristic (AUROC) curve was 0.67 (95% CI, 0.62-0.72) for ADEPT and 0.55 (95% CI, 0.51-0.59) for Medicare.
ADEPT was slightly better than hospice guidelines in predicting six-month mortality.
This study was limited in that the resident data were collected at a single random time point and might not reflect reality, as with palliative care and hospice, there usually is a decline in status that stimulates the referrals.
Bottom line: The ADEPT score might better estimate the six-month mortality in nursing home residents with dementia, which can help expand the enrollment of palliative care and hospice for these residents.
Citation: Mitchell SL, Miller SC, Teno JM, Kiely DK, Davis RB, Shaffer ML. Prediction of 6-month survival of nursing home residents with advanced dementia using ADEPT vs hospice eligibility guidelines. JAMA. 2010;304(17):1929-1935.
Residents Concerned about How New ACGME Duty-Hour Restrictions Will Impact Patient Care and Education
Clinical question: How do residents believe the forthcoming revised ACGME Rules for Supervision and Duty Hours will impact their residency?
Background: On July 1, revised ACGME duty-hour rules go into effect, limiting PGY-1 residents to 16-hour duty periods and PGY-2 and above to 28 hours. The effect these recommendations will have on patient care and resident education is unknown.
Study design: Twenty-question electronic, anonymous survey.
Setting: Twenty-three medical centers in the U.S., including residents from all disciplines and years in training.
Synopsis: Twenty-two percent of residents responded to the survey (n=2,521). Overall, 48% of residents disagreed with this statement: “Overall the changes will have a positive effect on education,” while only 26% agreed. Approximately half of those surveyed agreed that the revisions would improve their quality of life, but the same percentage also believed the revisions would increase the length of their residencies.
Residents reacted negatively to the idea that the proposed changes would improve patient safety and quality of care delivered, promote education over service obligations, and prepare them to assume senior roles. In free-text comments, residents expressed concerns about an increased number of handoffs and decreased continuity of care.
While the sample size is large and diverse, results of this survey can be affected by voluntary response bias and, therefore, could be skewed toward more extreme responses (in this case, more negative responses). The wide distribution of the responses suggests this might not be the case.
Bottom line: Residents do not believe the new requirements—though they could improve their quality of life—will positively impact patient care and education.
Citation: Drolet BC, Spalluto LB, Fischer SA. Residents’ perspectives on ACGME regulation of supervision and duty hours—a national survey. N Engl J Med. 2010;363(23):e34(1)-e34.
Decision Rule Might Help Clinicians Decide When to Order Renal Ultrasound to Evaluate Hospitalized Patients with Acute Kidney Injury
Clinical question: Can a clinical prediction rule aid clinicians in deciding when to order a renal ultrasound (RUS) in hospitalized patients with acute kidney injury?
Background: RUS routinely is obtained in patients admitted with acute kidney injury (AKI) to rule out obstruction as a cause of AKI. It is not known if this test adds any additional information in the routine evaluation of AKI and if obtaining the test is cost-effective.
Study design: Cross-sectional study.
Setting: Yale-New Haven Hospital in Connecticut.
Synopsis: This study evaluated 997 inpatients with AKI who underwent RUS. Outcome events were RUS identification of hydronephrosis (HN) or hydronephrosis requiring intervention (HNRI). The patients were divided into two samples: 200 in derivation sample and 797 in validation sample. The derivation sample was used to identify specific factors associated with HN. Seven clinical variables were identified and were used to create three risk groups: low, medium, and high.
In the validation sample, 10.6% of patients had HN and 3.3% had HNRI. The negative predictive value for HN was 96.9%, sensitivity 91.8%, and negative likelihood ratio 0.27. The number needed to screen (NNS) low-risk patients for HN was 32 and 223 for HNRI. Based on their findings, if the patient was classified low-risk, clinicians might be able to delay or avoid ordering RUS.
The major limitation of this study was that it was based at a single institution. This study only evaluated RUS obtained in patients who were hospitalized and might not be applicable to outpatients.
Bottom line: RUS was not found to change clinical management in patients with AKI and classified as low-risk for HN. Limiting RUS to patients who are high-risk for obstruction will increase the chance of finding useful clinical information that can change management decisions and limit cost of unnecessary testing.
Citation: Licurse A, Kim MC, Dziura J, et al. Renal ultrasonography in the evaluation of acute kidney injury: developing a risk stratification framework. Arch Intern Med. 2010;170(21):1900-1907.
Romiplostim Has Higher Rate of Platelet Response and Fewer Adverse Events in Patients with Immune Thrombocytopenia
Clinical question: Does the use of romiplostim lead to increased platelet counts and lower rates of splenectomy and other adverse events when compared with standard therapy in patients with immune thrombocytopenia?
Background: Romiplostim is a thrombopoetin mimetic used to increase platelet counts in immune thrombocytopenia. Initial treatments for this disease involve glucocorticoids or intravenous immune globulin. Most patients require second-line medical or surgical therapies, including splenectomy.
Study design: Randomized, open-label controlled trial.
Setting: Eighty-five medical centers in North America, Europe, and Australia.
Synopsis: A total of 234 patients were randomized in a 2:1 ratio to receive either romiplostim or the medical standard of care. Co-primary endpoints were the incidence of treatment failure and the incidence of splenectomy; secondary endpoints included time to splenectomy, platelet count, platelet response, and quality of life. Treatment failure was defined as a platelet count of 20x109 per liter or lower for four weeks, or a major bleeding event.
At the end of 52 weeks, patients receiving romiplostim had higher platelet counts, fewer bleeding events, less need for splenectomy (9% vs. 36%), and a better quality of life.
The short-term use of romiplostim in this study was not associated with an increase in adverse events when compared with standard therapy. However, maintenance of the elevated platelet count, which results from romiplostim treatment, requires continuous use of the drug; the long-term effects are unknown.
Bottom line: In patients with immune thrombocytopenia, romiplostim leads to increased platelet counts, decreased bleeding events, and decreased need for splenectomy compared to standard of care. However, the cost of the medication, when compared with current therapies, could be prohibitive.
Citation: Kuter DJ, Rummel M, Boccia R, et al. Romiplostim or standard of care in patients with immune thrombocytopenia. N Engl J Med. 2010;363(20):1889-1899. TH
Pediatric HM Literature
Parental History Portends Persistent Chronic Abdominal Pain in Children

Clinical question: What is the quality of the current evidence for potential prognostic factors of persistent chronic abdominal pain in children?
Background: Chronic abdominal pain (CAP) is a prevalent condition in childhood that might be associated with increased healthcare costs, including hospital admission. Retrospective studies have implicated psychosocial factors as being of prognostic relevance, but these are unable to offer greater insight into the relationship given the complex nature of this chronic illness.
Study design: Systematic review of literature.
Setting: MEDLINE, EMBASE, and PsycINFO.
Synopsis: The databases were searched through June 2008 for articles that focused on children 4 to 18 years of age; used criteria for CAP as defined by Apley and Naish, von Baeyer and Walker, or the Rome Committee; and demonstrated prospective determination of outcomes. Eight studies were included in the final review, and the levels of evidence were graded based on assessment of risk for bias.
Female sex and severity of baseline abdominal pain did not predict persistence of CAP, although there was conflicting evidence as to the role of psychological factors. There was moderate evidence that having a parent with functional gastrointestinal (GI) symptoms predicted persistence of CAP in children, and there was weak evidence that having parents who eschew psychological factors in favor of searching for an organic explanation predicted persistence of CAP.
Due to a limited number of studies or conflicting associations, conclusions regarding the following factors could not be drawn: age, educational level, duration of CAP, associated symptoms, socioeconomic status, and history of two or more surgical operations.
In addition, the univariate analysis used by the included studies might not be appropriate for such a multifactorially complex disease. Nevertheless, this study challenges the conventional wisdom that psychological factors predict persistence of pain and should remind clinicians to assess for parental functional GI disorders in this patient population.
Bottom line: Parental history of functional GI disorders predicts persistence of CAP in children.
Citation: Gieteling MJ, Bierma-Zeinstra SM, van Leeuwen Y, Passchier J, Berger MY. Prognostic factors for persistence of chronic abdominal pain in children. J Pediatr Gastroenterol Nutr. 2011;52(2):154-161.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Early ambulation and LOS in geriatric patients
- Patient-safety movement and hospital harm rates
- Lifestyle modification and weight loss
- Outcomes of transcatheter aortic-valve implantation
- Tool for predicting mortality in advanced dementia
- Residents’ opinion of new duty-hour regulations
- Renal ultrasound predictor for acute kidney injury
- Romiplostim use in immune thrombocytopenia
Increasing Ambulation within 48 Hours of Admission Decreases LOS by Two Days
Clinical question: Is there an association between an early increase in ambulation and length of stay (LOS) in geriatric patients admitted with an acute illness?
Background: Early ambulation leading to better recovery in such illnesses as pneumonia and myocardial infarction is well known, as is early ambulation after hip fracture surgery to prevent complications. However, no specific guidelines exist in regard to ambulation in older patients.
Study design: Prospective, nonblinded study.
Setting: Acute-care geriatric unit in an academic medical center.
Synopsis: A total of 162 patients 65 or older were studied. Data were collected during a four-month period in 2009. A Step Activity Monitor (SAM) was placed on admission. Patients were instructed to walk as usual. Investigators measured the number of steps taken per day and change in steps between the first and second day.
Patients averaged 662.1 steps per day, with a mean step change of 196.5 steps. The adjusted mean difference in LOS for patients who increased their total steps by 600 or more between the first and second day was 2.13 days (95% CI, 1.05-3.97). Patients who had low or negative changes in steps had longer LOS. The 32 patients who walked more than 600 steps were more likely to be men (P=0.02), independently ambulate (P<0.01), and have admitting orders of “ambulate with assist” (P=0.03).
One limitation of this study is that patients who walked more might have been less ill or very functional on admission.
Bottom line: Increasing ambulation early in a hospitalization (first two days) is associated with a decreased LOS in an elderly population.
Citation: Fisher SR, Kuo YF, Graham JE, Ottenbacher KJ, Ostir GV. Early ambulation and length of stay in older adults hospitalized for acute illness. Arch Intern Med. 2010;170(21):1942-1943.
Despite Efforts to Improve Patient Safety in Hospitals, No Reduction in Longitudinal Rates of Harm
Clinical question: As hospitals focus more on programs to improve patient safety, has the rate of harms decreased?
Background: Since the Institute of Medicine published a groundbreaking report (To Err is Human) a little more than a decade ago, policymakers, hospitals, and healthcare organizations have focused more on efforts to improve patient safety with the goal of reducing harms. It is not clear if these efforts have reduced harms.
Study design: Retrospective chart review.
Setting: Ten hospitals in North Carolina.
Synopsis: Ten charts per quarter were randomly selected from each hospital from January 2002 through December 2007. Internal and external reviewers used the IHI Global Trigger Tool for Measuring Adverse Events to identify rates of harm. Harms were classified into categories of severity and assessed for preventability.
Kappa scores were generally higher for internal reviewers, indicating higher reliability for internal reviewers. Internal reviewers identified 588 harms for 10,415 patient days (25.1 harms per 100 patient days), which occurred in 423 unique patients (18.1%). A majority (63.1%) of harms were considered preventable. Forty-one percent of harms were temporary and required intervention; 2.4% caused or contributed to a patient’s death.
There was no significant change over time in the rate of harms (regardless of reviewer type) even after adjusting for demographics.
This study is limited because it is based only in North Carolina hospitals. It was not powered to evaluate change in individual hospitals. There might have been unmeasurable improvements that were not accounted for by the trigger tool.
Bottom line: Despite a higher focus on patient safety, investigators did not find a decrease in the rate of harms. A majority of the harms were preventable. This study should not preclude efforts to continue to improve patient safety.
Citation: Landrigan CP, Parry GJ, Bones CB, Hackbarth AD, Goldmann DA, Sharek PJ. Temporal trends in rates of patient harm resulting from medical care. N Engl J Med. 2010;363(22):2124-2134.
Intensive Lifestyle Modification Improves Weight Loss in Severely Obese Individuals
Clinical question: Does the combination of diet modification and increased physical activity lead to weight loss and improve health risks in severely obese patients?
Background: Obesity is at epidemic proportions, but there are no evidence-based treatment guidelines for severe obesity.
Study design: Randomized, single-blind trial.
Setting: Community volunteers.
Synopsis: A total of 130 individuals with a body mass index (BMI) of ≥35 were randomized to receive lifestyle interventions consisting of diet and initial physical activity for 12 months, or diet for six months and delayed physical activity for the remainder of the year.
The initial-physical-activity group demonstrated greater weight loss at six months, but the overall weight loss did not differ between the two groups. At 12 months, the initial physical activity group lost 12.1 kg and the delayed-physical-activity group lost 9.87 kg. Both groups demonstrated significantly reduced blood pressure, reduced serum liver enzymes, and improved insulin resistance.
Candidates with a history of coronary artery disease, uncontrolled blood pressure, or diabetes were excluded. Participants were provided with prepackaged meal replacements for the first six months and received financial compensation for participation in the study.
This study is limited by the fact that a majority of the participants were female (85.1%). Providing meals to the participants also limits the application of this program to the general public.
Bottom line: The results of this study reflect the importance of diet and exercise on weight loss in obese individuals. However, adherence to the goals of the study required multiple individual and group meetings throughout the year, the provision of prepackaged meals, and some financial incentive for compliance.
Citation: Goodpaster GH, Delany JP, Otto AD, et al. Effects of diet and physical activity interventions on weight loss and cardiometabolic risk factors in severely obese adults: a randomized trial. JAMA. 2010;304 (16):1795-1802.
Transcatheter Aortic-Valve Implantation Is Superior to Standard Nonoperative Therapy for Symptomatic Aortic Stenosis
Clinical question: Is there a mortality benefit to transcatheter valve implantation over standard therapy in nonsurgical candidates with severe aortic stenosis (AS)?
Background: Untreated, symptomatic AS has a high rate of death, but a significant proportion of patients with severe aortic stenosis are poor surgical candidates. Available since 2002, transcatheter aortic-valve implantation (TAVI) is a promising, nonsurgical treatment option for severe AS. However, to date, TAVI has lacked rigorous clinical data.
Study design: Prospective, multicenter, randomized, active-treatment-controlled clinical trial.
Setting: Twenty-one centers, 17 of which were in the U.S.
Synopsis: A total of 358 patients with severe AS who were considered nonsurgical candidates were randomized to either TAVI or standard therapy. A majority (83.8%) of the patients in the standard group underwent balloon aortic valvuloplasty.
Researchers found a significant reduction (HR 0.55, 95% CI 0.40 to 0.74, P<0.001) in all-cause mortality at one year in those patients undergoing TAVI (30.7%) vs. standard therapy (50.7%). Additional benefits included lower rates of the composite endpoints of death from any cause or repeat hospitalization (42.5% vs. 71.6%, P<0.001) and NYHA Functional Class III or IV symptoms (25.2% vs. 58.0%, P<0.001) at one year. However, higher incidences of major strokes (5.0% vs. 1.6%, P=0.06) and major vascular complications (16.2% vs. 1.1%, P<0.001) were seen.
While the one-year mortality benefit of TAVI over standard nonoperative therapy was clearly demonstrated by this study, hospitalists should interpret these data cautiously with respect to their inpatient populations as exclusion criteria were extensive, including bicuspid or noncalcified aortic valve, LVEF less than 20%, and severe renal insufficiency. Additionally, the entity of standard therapy was poorly delineated.
Bottom line: TAVI should be considered in patients with severe aortic stenosis who are not suitable surgical candidates.
Citation: Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-1607.
ADEPT Score Better Predicts Six-Month Mortality in Nursing Home Residents with Advanced Dementia
Clinical question: Are current Medicare hospice eligibility guidelines accurate enough to predict six-month survival in nursing home residents with dementia when compared with the Advanced Dementia Prognostic Tool (ADEPT)?
Background: Incorrectly estimating the life expectancy in almost 5 million nursing home residents with dementia prevents enrollment to palliative care and hospice for those who would benefit most. Creating and validating a mortality risk score would allow increased services to these residents.
Study design: Prospective cohort study.
Setting: Twenty-one nursing homes in Boston.
Synopsis: A total of 606 nursing home residents with advanced dementia were recruited for this study. Each resident was assessed for Medicare hospice eligibility and assigned an ADEPT score. Mortality rate was determined six months later. These two assessment tools were compared regarding their ability to predict six-month mortality.
The mean ADEPT score was 10.1 (range of 1.0-32.5), with a higher score meaning worse prognosis. Sixty-five residents (10.7%) met Medicare hospice eligibility guidelines. A total of 111 residents (18.3%) died.
The ADEPT score was more sensitive (90% vs. 20%) but less specific (28.3% vs. 89%) than Medicare guidelines. The area under the receiver operating characteristic (AUROC) curve was 0.67 (95% CI, 0.62-0.72) for ADEPT and 0.55 (95% CI, 0.51-0.59) for Medicare.
ADEPT was slightly better than hospice guidelines in predicting six-month mortality.
This study was limited in that the resident data were collected at a single random time point and might not reflect reality, as with palliative care and hospice, there usually is a decline in status that stimulates the referrals.
Bottom line: The ADEPT score might better estimate the six-month mortality in nursing home residents with dementia, which can help expand the enrollment of palliative care and hospice for these residents.
Citation: Mitchell SL, Miller SC, Teno JM, Kiely DK, Davis RB, Shaffer ML. Prediction of 6-month survival of nursing home residents with advanced dementia using ADEPT vs hospice eligibility guidelines. JAMA. 2010;304(17):1929-1935.
Residents Concerned about How New ACGME Duty-Hour Restrictions Will Impact Patient Care and Education
Clinical question: How do residents believe the forthcoming revised ACGME Rules for Supervision and Duty Hours will impact their residency?
Background: On July 1, revised ACGME duty-hour rules go into effect, limiting PGY-1 residents to 16-hour duty periods and PGY-2 and above to 28 hours. The effect these recommendations will have on patient care and resident education is unknown.
Study design: Twenty-question electronic, anonymous survey.
Setting: Twenty-three medical centers in the U.S., including residents from all disciplines and years in training.
Synopsis: Twenty-two percent of residents responded to the survey (n=2,521). Overall, 48% of residents disagreed with this statement: “Overall the changes will have a positive effect on education,” while only 26% agreed. Approximately half of those surveyed agreed that the revisions would improve their quality of life, but the same percentage also believed the revisions would increase the length of their residencies.
Residents reacted negatively to the idea that the proposed changes would improve patient safety and quality of care delivered, promote education over service obligations, and prepare them to assume senior roles. In free-text comments, residents expressed concerns about an increased number of handoffs and decreased continuity of care.
While the sample size is large and diverse, results of this survey can be affected by voluntary response bias and, therefore, could be skewed toward more extreme responses (in this case, more negative responses). The wide distribution of the responses suggests this might not be the case.
Bottom line: Residents do not believe the new requirements—though they could improve their quality of life—will positively impact patient care and education.
Citation: Drolet BC, Spalluto LB, Fischer SA. Residents’ perspectives on ACGME regulation of supervision and duty hours—a national survey. N Engl J Med. 2010;363(23):e34(1)-e34.
Decision Rule Might Help Clinicians Decide When to Order Renal Ultrasound to Evaluate Hospitalized Patients with Acute Kidney Injury
Clinical question: Can a clinical prediction rule aid clinicians in deciding when to order a renal ultrasound (RUS) in hospitalized patients with acute kidney injury?
Background: RUS routinely is obtained in patients admitted with acute kidney injury (AKI) to rule out obstruction as a cause of AKI. It is not known if this test adds any additional information in the routine evaluation of AKI and if obtaining the test is cost-effective.
Study design: Cross-sectional study.
Setting: Yale-New Haven Hospital in Connecticut.
Synopsis: This study evaluated 997 inpatients with AKI who underwent RUS. Outcome events were RUS identification of hydronephrosis (HN) or hydronephrosis requiring intervention (HNRI). The patients were divided into two samples: 200 in derivation sample and 797 in validation sample. The derivation sample was used to identify specific factors associated with HN. Seven clinical variables were identified and were used to create three risk groups: low, medium, and high.
In the validation sample, 10.6% of patients had HN and 3.3% had HNRI. The negative predictive value for HN was 96.9%, sensitivity 91.8%, and negative likelihood ratio 0.27. The number needed to screen (NNS) low-risk patients for HN was 32 and 223 for HNRI. Based on their findings, if the patient was classified low-risk, clinicians might be able to delay or avoid ordering RUS.
The major limitation of this study was that it was based at a single institution. This study only evaluated RUS obtained in patients who were hospitalized and might not be applicable to outpatients.
Bottom line: RUS was not found to change clinical management in patients with AKI and classified as low-risk for HN. Limiting RUS to patients who are high-risk for obstruction will increase the chance of finding useful clinical information that can change management decisions and limit cost of unnecessary testing.
Citation: Licurse A, Kim MC, Dziura J, et al. Renal ultrasonography in the evaluation of acute kidney injury: developing a risk stratification framework. Arch Intern Med. 2010;170(21):1900-1907.
Romiplostim Has Higher Rate of Platelet Response and Fewer Adverse Events in Patients with Immune Thrombocytopenia
Clinical question: Does the use of romiplostim lead to increased platelet counts and lower rates of splenectomy and other adverse events when compared with standard therapy in patients with immune thrombocytopenia?
Background: Romiplostim is a thrombopoetin mimetic used to increase platelet counts in immune thrombocytopenia. Initial treatments for this disease involve glucocorticoids or intravenous immune globulin. Most patients require second-line medical or surgical therapies, including splenectomy.
Study design: Randomized, open-label controlled trial.
Setting: Eighty-five medical centers in North America, Europe, and Australia.
Synopsis: A total of 234 patients were randomized in a 2:1 ratio to receive either romiplostim or the medical standard of care. Co-primary endpoints were the incidence of treatment failure and the incidence of splenectomy; secondary endpoints included time to splenectomy, platelet count, platelet response, and quality of life. Treatment failure was defined as a platelet count of 20x109 per liter or lower for four weeks, or a major bleeding event.
At the end of 52 weeks, patients receiving romiplostim had higher platelet counts, fewer bleeding events, less need for splenectomy (9% vs. 36%), and a better quality of life.
The short-term use of romiplostim in this study was not associated with an increase in adverse events when compared with standard therapy. However, maintenance of the elevated platelet count, which results from romiplostim treatment, requires continuous use of the drug; the long-term effects are unknown.
Bottom line: In patients with immune thrombocytopenia, romiplostim leads to increased platelet counts, decreased bleeding events, and decreased need for splenectomy compared to standard of care. However, the cost of the medication, when compared with current therapies, could be prohibitive.
Citation: Kuter DJ, Rummel M, Boccia R, et al. Romiplostim or standard of care in patients with immune thrombocytopenia. N Engl J Med. 2010;363(20):1889-1899. TH
Pediatric HM Literature
Parental History Portends Persistent Chronic Abdominal Pain in Children
Clinical question: What is the quality of the current evidence for potential prognostic factors of persistent chronic abdominal pain in children?
Background: Chronic abdominal pain (CAP) is a prevalent condition in childhood that might be associated with increased healthcare costs, including hospital admission. Retrospective studies have implicated psychosocial factors as being of prognostic relevance, but these are unable to offer greater insight into the relationship given the complex nature of this chronic illness.
Study design: Systematic review of literature.
Setting: MEDLINE, EMBASE, and PsycINFO.
Synopsis: The databases were searched through June 2008 for articles that focused on children 4 to 18 years of age; used criteria for CAP as defined by Apley and Naish, von Baeyer and Walker, or the Rome Committee; and demonstrated prospective determination of outcomes. Eight studies were included in the final review, and the levels of evidence were graded based on assessment of risk for bias.
Female sex and severity of baseline abdominal pain did not predict persistence of CAP, although there was conflicting evidence as to the role of psychological factors. There was moderate evidence that having a parent with functional gastrointestinal (GI) symptoms predicted persistence of CAP in children, and there was weak evidence that having parents who eschew psychological factors in favor of searching for an organic explanation predicted persistence of CAP.
Due to a limited number of studies or conflicting associations, conclusions regarding the following factors could not be drawn: age, educational level, duration of CAP, associated symptoms, socioeconomic status, and history of two or more surgical operations.
In addition, the univariate analysis used by the included studies might not be appropriate for such a multifactorially complex disease. Nevertheless, this study challenges the conventional wisdom that psychological factors predict persistence of pain and should remind clinicians to assess for parental functional GI disorders in this patient population.
Bottom line: Parental history of functional GI disorders predicts persistence of CAP in children.
Citation: Gieteling MJ, Bierma-Zeinstra SM, van Leeuwen Y, Passchier J, Berger MY. Prognostic factors for persistence of chronic abdominal pain in children. J Pediatr Gastroenterol Nutr. 2011;52(2):154-161.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Early ambulation and LOS in geriatric patients
- Patient-safety movement and hospital harm rates
- Lifestyle modification and weight loss
- Outcomes of transcatheter aortic-valve implantation
- Tool for predicting mortality in advanced dementia
- Residents’ opinion of new duty-hour regulations
- Renal ultrasound predictor for acute kidney injury
- Romiplostim use in immune thrombocytopenia
Increasing Ambulation within 48 Hours of Admission Decreases LOS by Two Days
Clinical question: Is there an association between an early increase in ambulation and length of stay (LOS) in geriatric patients admitted with an acute illness?
Background: Early ambulation leading to better recovery in such illnesses as pneumonia and myocardial infarction is well known, as is early ambulation after hip fracture surgery to prevent complications. However, no specific guidelines exist in regard to ambulation in older patients.
Study design: Prospective, nonblinded study.
Setting: Acute-care geriatric unit in an academic medical center.
Synopsis: A total of 162 patients 65 or older were studied. Data were collected during a four-month period in 2009. A Step Activity Monitor (SAM) was placed on admission. Patients were instructed to walk as usual. Investigators measured the number of steps taken per day and change in steps between the first and second day.
Patients averaged 662.1 steps per day, with a mean step change of 196.5 steps. The adjusted mean difference in LOS for patients who increased their total steps by 600 or more between the first and second day was 2.13 days (95% CI, 1.05-3.97). Patients who had low or negative changes in steps had longer LOS. The 32 patients who walked more than 600 steps were more likely to be men (P=0.02), independently ambulate (P<0.01), and have admitting orders of “ambulate with assist” (P=0.03).
One limitation of this study is that patients who walked more might have been less ill or very functional on admission.
Bottom line: Increasing ambulation early in a hospitalization (first two days) is associated with a decreased LOS in an elderly population.
Citation: Fisher SR, Kuo YF, Graham JE, Ottenbacher KJ, Ostir GV. Early ambulation and length of stay in older adults hospitalized for acute illness. Arch Intern Med. 2010;170(21):1942-1943.
Despite Efforts to Improve Patient Safety in Hospitals, No Reduction in Longitudinal Rates of Harm
Clinical question: As hospitals focus more on programs to improve patient safety, has the rate of harms decreased?
Background: Since the Institute of Medicine published a groundbreaking report (To Err is Human) a little more than a decade ago, policymakers, hospitals, and healthcare organizations have focused more on efforts to improve patient safety with the goal of reducing harms. It is not clear if these efforts have reduced harms.
Study design: Retrospective chart review.
Setting: Ten hospitals in North Carolina.
Synopsis: Ten charts per quarter were randomly selected from each hospital from January 2002 through December 2007. Internal and external reviewers used the IHI Global Trigger Tool for Measuring Adverse Events to identify rates of harm. Harms were classified into categories of severity and assessed for preventability.
Kappa scores were generally higher for internal reviewers, indicating higher reliability for internal reviewers. Internal reviewers identified 588 harms for 10,415 patient days (25.1 harms per 100 patient days), which occurred in 423 unique patients (18.1%). A majority (63.1%) of harms were considered preventable. Forty-one percent of harms were temporary and required intervention; 2.4% caused or contributed to a patient’s death.
There was no significant change over time in the rate of harms (regardless of reviewer type) even after adjusting for demographics.
This study is limited because it is based only in North Carolina hospitals. It was not powered to evaluate change in individual hospitals. There might have been unmeasurable improvements that were not accounted for by the trigger tool.
Bottom line: Despite a higher focus on patient safety, investigators did not find a decrease in the rate of harms. A majority of the harms were preventable. This study should not preclude efforts to continue to improve patient safety.
Citation: Landrigan CP, Parry GJ, Bones CB, Hackbarth AD, Goldmann DA, Sharek PJ. Temporal trends in rates of patient harm resulting from medical care. N Engl J Med. 2010;363(22):2124-2134.
Intensive Lifestyle Modification Improves Weight Loss in Severely Obese Individuals
Clinical question: Does the combination of diet modification and increased physical activity lead to weight loss and improve health risks in severely obese patients?
Background: Obesity is at epidemic proportions, but there are no evidence-based treatment guidelines for severe obesity.
Study design: Randomized, single-blind trial.
Setting: Community volunteers.
Synopsis: A total of 130 individuals with a body mass index (BMI) of ≥35 were randomized to receive lifestyle interventions consisting of diet and initial physical activity for 12 months, or diet for six months and delayed physical activity for the remainder of the year.
The initial-physical-activity group demonstrated greater weight loss at six months, but the overall weight loss did not differ between the two groups. At 12 months, the initial physical activity group lost 12.1 kg and the delayed-physical-activity group lost 9.87 kg. Both groups demonstrated significantly reduced blood pressure, reduced serum liver enzymes, and improved insulin resistance.
Candidates with a history of coronary artery disease, uncontrolled blood pressure, or diabetes were excluded. Participants were provided with prepackaged meal replacements for the first six months and received financial compensation for participation in the study.
This study is limited by the fact that a majority of the participants were female (85.1%). Providing meals to the participants also limits the application of this program to the general public.
Bottom line: The results of this study reflect the importance of diet and exercise on weight loss in obese individuals. However, adherence to the goals of the study required multiple individual and group meetings throughout the year, the provision of prepackaged meals, and some financial incentive for compliance.
Citation: Goodpaster GH, Delany JP, Otto AD, et al. Effects of diet and physical activity interventions on weight loss and cardiometabolic risk factors in severely obese adults: a randomized trial. JAMA. 2010;304 (16):1795-1802.
Transcatheter Aortic-Valve Implantation Is Superior to Standard Nonoperative Therapy for Symptomatic Aortic Stenosis
Clinical question: Is there a mortality benefit to transcatheter valve implantation over standard therapy in nonsurgical candidates with severe aortic stenosis (AS)?
Background: Untreated, symptomatic AS has a high rate of death, but a significant proportion of patients with severe aortic stenosis are poor surgical candidates. Available since 2002, transcatheter aortic-valve implantation (TAVI) is a promising, nonsurgical treatment option for severe AS. However, to date, TAVI has lacked rigorous clinical data.
Study design: Prospective, multicenter, randomized, active-treatment-controlled clinical trial.
Setting: Twenty-one centers, 17 of which were in the U.S.
Synopsis: A total of 358 patients with severe AS who were considered nonsurgical candidates were randomized to either TAVI or standard therapy. A majority (83.8%) of the patients in the standard group underwent balloon aortic valvuloplasty.
Researchers found a significant reduction (HR 0.55, 95% CI 0.40 to 0.74, P<0.001) in all-cause mortality at one year in those patients undergoing TAVI (30.7%) vs. standard therapy (50.7%). Additional benefits included lower rates of the composite endpoints of death from any cause or repeat hospitalization (42.5% vs. 71.6%, P<0.001) and NYHA Functional Class III or IV symptoms (25.2% vs. 58.0%, P<0.001) at one year. However, higher incidences of major strokes (5.0% vs. 1.6%, P=0.06) and major vascular complications (16.2% vs. 1.1%, P<0.001) were seen.
While the one-year mortality benefit of TAVI over standard nonoperative therapy was clearly demonstrated by this study, hospitalists should interpret these data cautiously with respect to their inpatient populations as exclusion criteria were extensive, including bicuspid or noncalcified aortic valve, LVEF less than 20%, and severe renal insufficiency. Additionally, the entity of standard therapy was poorly delineated.
Bottom line: TAVI should be considered in patients with severe aortic stenosis who are not suitable surgical candidates.
Citation: Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-1607.
ADEPT Score Better Predicts Six-Month Mortality in Nursing Home Residents with Advanced Dementia
Clinical question: Are current Medicare hospice eligibility guidelines accurate enough to predict six-month survival in nursing home residents with dementia when compared with the Advanced Dementia Prognostic Tool (ADEPT)?
Background: Incorrectly estimating the life expectancy in almost 5 million nursing home residents with dementia prevents enrollment to palliative care and hospice for those who would benefit most. Creating and validating a mortality risk score would allow increased services to these residents.
Study design: Prospective cohort study.
Setting: Twenty-one nursing homes in Boston.
Synopsis: A total of 606 nursing home residents with advanced dementia were recruited for this study. Each resident was assessed for Medicare hospice eligibility and assigned an ADEPT score. Mortality rate was determined six months later. These two assessment tools were compared regarding their ability to predict six-month mortality.
The mean ADEPT score was 10.1 (range of 1.0-32.5), with a higher score meaning worse prognosis. Sixty-five residents (10.7%) met Medicare hospice eligibility guidelines. A total of 111 residents (18.3%) died.
The ADEPT score was more sensitive (90% vs. 20%) but less specific (28.3% vs. 89%) than Medicare guidelines. The area under the receiver operating characteristic (AUROC) curve was 0.67 (95% CI, 0.62-0.72) for ADEPT and 0.55 (95% CI, 0.51-0.59) for Medicare.
ADEPT was slightly better than hospice guidelines in predicting six-month mortality.
This study was limited in that the resident data were collected at a single random time point and might not reflect reality, as with palliative care and hospice, there usually is a decline in status that stimulates the referrals.
Bottom line: The ADEPT score might better estimate the six-month mortality in nursing home residents with dementia, which can help expand the enrollment of palliative care and hospice for these residents.
Citation: Mitchell SL, Miller SC, Teno JM, Kiely DK, Davis RB, Shaffer ML. Prediction of 6-month survival of nursing home residents with advanced dementia using ADEPT vs hospice eligibility guidelines. JAMA. 2010;304(17):1929-1935.
Residents Concerned about How New ACGME Duty-Hour Restrictions Will Impact Patient Care and Education
Clinical question: How do residents believe the forthcoming revised ACGME Rules for Supervision and Duty Hours will impact their residency?
Background: On July 1, revised ACGME duty-hour rules go into effect, limiting PGY-1 residents to 16-hour duty periods and PGY-2 and above to 28 hours. The effect these recommendations will have on patient care and resident education is unknown.
Study design: Twenty-question electronic, anonymous survey.
Setting: Twenty-three medical centers in the U.S., including residents from all disciplines and years in training.
Synopsis: Twenty-two percent of residents responded to the survey (n=2,521). Overall, 48% of residents disagreed with this statement: “Overall the changes will have a positive effect on education,” while only 26% agreed. Approximately half of those surveyed agreed that the revisions would improve their quality of life, but the same percentage also believed the revisions would increase the length of their residencies.
Residents reacted negatively to the idea that the proposed changes would improve patient safety and quality of care delivered, promote education over service obligations, and prepare them to assume senior roles. In free-text comments, residents expressed concerns about an increased number of handoffs and decreased continuity of care.
While the sample size is large and diverse, results of this survey can be affected by voluntary response bias and, therefore, could be skewed toward more extreme responses (in this case, more negative responses). The wide distribution of the responses suggests this might not be the case.
Bottom line: Residents do not believe the new requirements—though they could improve their quality of life—will positively impact patient care and education.
Citation: Drolet BC, Spalluto LB, Fischer SA. Residents’ perspectives on ACGME regulation of supervision and duty hours—a national survey. N Engl J Med. 2010;363(23):e34(1)-e34.
Decision Rule Might Help Clinicians Decide When to Order Renal Ultrasound to Evaluate Hospitalized Patients with Acute Kidney Injury
Clinical question: Can a clinical prediction rule aid clinicians in deciding when to order a renal ultrasound (RUS) in hospitalized patients with acute kidney injury?
Background: RUS routinely is obtained in patients admitted with acute kidney injury (AKI) to rule out obstruction as a cause of AKI. It is not known if this test adds any additional information in the routine evaluation of AKI and if obtaining the test is cost-effective.
Study design: Cross-sectional study.
Setting: Yale-New Haven Hospital in Connecticut.
Synopsis: This study evaluated 997 inpatients with AKI who underwent RUS. Outcome events were RUS identification of hydronephrosis (HN) or hydronephrosis requiring intervention (HNRI). The patients were divided into two samples: 200 in derivation sample and 797 in validation sample. The derivation sample was used to identify specific factors associated with HN. Seven clinical variables were identified and were used to create three risk groups: low, medium, and high.
In the validation sample, 10.6% of patients had HN and 3.3% had HNRI. The negative predictive value for HN was 96.9%, sensitivity 91.8%, and negative likelihood ratio 0.27. The number needed to screen (NNS) low-risk patients for HN was 32 and 223 for HNRI. Based on their findings, if the patient was classified low-risk, clinicians might be able to delay or avoid ordering RUS.
The major limitation of this study was that it was based at a single institution. This study only evaluated RUS obtained in patients who were hospitalized and might not be applicable to outpatients.
Bottom line: RUS was not found to change clinical management in patients with AKI and classified as low-risk for HN. Limiting RUS to patients who are high-risk for obstruction will increase the chance of finding useful clinical information that can change management decisions and limit cost of unnecessary testing.
Citation: Licurse A, Kim MC, Dziura J, et al. Renal ultrasonography in the evaluation of acute kidney injury: developing a risk stratification framework. Arch Intern Med. 2010;170(21):1900-1907.
Romiplostim Has Higher Rate of Platelet Response and Fewer Adverse Events in Patients with Immune Thrombocytopenia
Clinical question: Does the use of romiplostim lead to increased platelet counts and lower rates of splenectomy and other adverse events when compared with standard therapy in patients with immune thrombocytopenia?
Background: Romiplostim is a thrombopoetin mimetic used to increase platelet counts in immune thrombocytopenia. Initial treatments for this disease involve glucocorticoids or intravenous immune globulin. Most patients require second-line medical or surgical therapies, including splenectomy.
Study design: Randomized, open-label controlled trial.
Setting: Eighty-five medical centers in North America, Europe, and Australia.
Synopsis: A total of 234 patients were randomized in a 2:1 ratio to receive either romiplostim or the medical standard of care. Co-primary endpoints were the incidence of treatment failure and the incidence of splenectomy; secondary endpoints included time to splenectomy, platelet count, platelet response, and quality of life. Treatment failure was defined as a platelet count of 20x109 per liter or lower for four weeks, or a major bleeding event.
At the end of 52 weeks, patients receiving romiplostim had higher platelet counts, fewer bleeding events, less need for splenectomy (9% vs. 36%), and a better quality of life.
The short-term use of romiplostim in this study was not associated with an increase in adverse events when compared with standard therapy. However, maintenance of the elevated platelet count, which results from romiplostim treatment, requires continuous use of the drug; the long-term effects are unknown.
Bottom line: In patients with immune thrombocytopenia, romiplostim leads to increased platelet counts, decreased bleeding events, and decreased need for splenectomy compared to standard of care. However, the cost of the medication, when compared with current therapies, could be prohibitive.
Citation: Kuter DJ, Rummel M, Boccia R, et al. Romiplostim or standard of care in patients with immune thrombocytopenia. N Engl J Med. 2010;363(20):1889-1899. TH
Pediatric HM Literature
Parental History Portends Persistent Chronic Abdominal Pain in Children
Clinical question: What is the quality of the current evidence for potential prognostic factors of persistent chronic abdominal pain in children?
Background: Chronic abdominal pain (CAP) is a prevalent condition in childhood that might be associated with increased healthcare costs, including hospital admission. Retrospective studies have implicated psychosocial factors as being of prognostic relevance, but these are unable to offer greater insight into the relationship given the complex nature of this chronic illness.
Study design: Systematic review of literature.
Setting: MEDLINE, EMBASE, and PsycINFO.
Synopsis: The databases were searched through June 2008 for articles that focused on children 4 to 18 years of age; used criteria for CAP as defined by Apley and Naish, von Baeyer and Walker, or the Rome Committee; and demonstrated prospective determination of outcomes. Eight studies were included in the final review, and the levels of evidence were graded based on assessment of risk for bias.
Female sex and severity of baseline abdominal pain did not predict persistence of CAP, although there was conflicting evidence as to the role of psychological factors. There was moderate evidence that having a parent with functional gastrointestinal (GI) symptoms predicted persistence of CAP in children, and there was weak evidence that having parents who eschew psychological factors in favor of searching for an organic explanation predicted persistence of CAP.
Due to a limited number of studies or conflicting associations, conclusions regarding the following factors could not be drawn: age, educational level, duration of CAP, associated symptoms, socioeconomic status, and history of two or more surgical operations.
In addition, the univariate analysis used by the included studies might not be appropriate for such a multifactorially complex disease. Nevertheless, this study challenges the conventional wisdom that psychological factors predict persistence of pain and should remind clinicians to assess for parental functional GI disorders in this patient population.
Bottom line: Parental history of functional GI disorders predicts persistence of CAP in children.
Citation: Gieteling MJ, Bierma-Zeinstra SM, van Leeuwen Y, Passchier J, Berger MY. Prognostic factors for persistence of chronic abdominal pain in children. J Pediatr Gastroenterol Nutr. 2011;52(2):154-161.
In the Literature: HM-Related Research You Need to Know
In This Edition
Literature at a Glance
A guide to this month’s studies
- Risk of adverse events with opioid use
- Drug of choice for outpatient treatment of cellulitis
- Preventing hospital falls
- Post-hospital outcomes based on status of PCP follow-up
- LOS, mortality, and readmission based on insurance
- Antiplatelets added to warfarin for atrial fibrillation.
- Cognitive effects of severe sepsis
- Effect of preoperative furosemide use
ED Visits Are Higher among Recipients of Chronic Opioid Therapy
Clinical question: Is there an association between the use of prescription opioids and adverse outcomes?
Background: Chronic opioid therapy is a common strategy for managing chronic, noncancer pain. There has been an increase in overdose deaths and ED visits (EDV) involving the use of prescription opioids.
Study design: Retrospective study from claims records.
Setting: Population in the Health Core Integrated Research Database, containing large, commercial insurance plans in 14 states, and Arkansas Medicaid.
Synopsis: Patients 18 and older without cancer diagnoses who used prescription opioids for at least 90 continuous days within a six-month period from 2000 to 2005 were examined for risk factors for EDVs and alcohol- or drug-related encounters (ADEs) in the 12 months following 90 days or more of prescribed opioids.
Patients with diagnoses of headache, back pain, and pre-existing substance-use disorders had significantly higher EDVs and ADEs. Opioid dose at morphine-equivalent doses over 120 mg per day doubled the risk of ADEs. The use of short-acting Schedule II opioids was associated with EDVs (relative risk, 1.09-1.74). The use of long-acting Schedule II opioids was strongly associated with ADEs (relative risk, 1.64-4.00).
Bottom line: In adults with noncancer pain prescribed opioids for 90 days or more, short-acting Schedule II opioid use was associated with an increased number of EDVs, and long-acting opioid use was associated with an increased number of ADEs. Minimizing Schedule II opioid prescription in these higher-risk patients might be prudent to increase patient safety.
Citation: Braden JB, Russo J, Fan MI, et al. Emergency department visits among recipients of chronic opioid therapy. Arch Intern Med. 2010; 170(16):1425-1432.
Empiric Outpatient Therapy with Trimethoprim-Sulfamethoxazole or Clindamycin Is Preferred for Cellulitis
Clinical question: What is the best empiric outpatient oral antibiotic treatment for cellulitis in areas with a high prevalence of community-associated MRSA infections?
Background: The increasing rates of community-associated MRSA skin and soft-tissue infections have raised concerns that such beta-lactams as cephalexin and other semisynthetic penicillins are not appropriate for empiric outpatient therapy for cellulitis.
Study design: Three-year, retrospective cohort study.
Setting: A teaching clinic of a tertiary-care medical center in Hawaii.
Synopsis: More than 540 patients with cellulitis were identified from January 2005 to December 2007. Of these, 139 patients were excluded for reasons such as hospitalization, surgical intervention, etc. In the final cohort of 405 patients, the three most commonly prescribed oral antibiotics were cephalexin (44%), trimethoprim-sulfamethoxazole (38%), and clindamycin (10%). Other antibiotics accounted for the remaining 8%.
MRSA was recovered in 62% of positive culture specimens. The success rate of trimethoprim-sulfamethoxazole was 91% vs. 74% in the cephalexin group (P<0.001). Clindamycin success rates were higher than those of cephalexin in patients who had subsequently confirmed MRSA infections (P=0.01) and moderately severe cellulitis (P=0.03) and were obese (P=0.04).
Bottom line: Antibiotics with activity against community-acquired MRSA (e.g. trimethroprim-sulfamethoxazole and clinidamycin) are the preferred empiric outpatient therapy for cellulitis in areas with a high prevalence of community-acquired MRSA.
Citation: Khawcharoenporn T, Tice A. Empiric outpatient therapy with trimethoprim-sulfamethoxazole, cephalexin, or clindamycin for cellulitis. Am J Med. 2010;123(10):942-950.
Patient-Specific Screening with Health Information Technology Prevents Falls
Clinical question: Does a fall-prevention toolkit using health information technology decrease patient falls in acute-care hospitals?
Background: Inpatient falls and fall-related injuries result in substantial morbidity and additional healthcare costs. While specific fall-prevention strategies were a longstanding target for intervention, little evidence exists to link them with decreased fall rates.
Study design: Cluster-randomized study.
Setting: Four urban hospitals in Massachusetts.
Synopsis: Comparing patient fall rates in four acute-care hospitals between units providing usual care (5,104 patients) and units using a health information technology (HIT)-linked fall prevention toolkit (5,160 patients), this study demonstrated significant fall reduction in older inpatients. The intervention integrated existing workflow and validated fall risk assessment (Morse Falls Scale) into an HIT software application that tailored fall-prevention interventions to patients’ specific fall risk determinants. The toolkit produced bed posters, patient education handouts, and plans of care communicating patient-specific alerts to key stakeholders.
The primary outcome was patient falls per 1,000 patient-days during the six-month intervention period. The number of patients with falls was significantly different (P=0.02) between control (n=87) and intervention (n=67) units. The toolkit prevented one fall per 862 patient-days.
This nonblinded study was limited by the fact that it was conducted in a single health system. The toolkit was not effective in patients less than 65 years of age. Additionally, the sample size did not have sufficient power to detect effectiveness in preventing repeat falls or falls with injury.
Bottom line: Patient-specific fall prevention strategy coupled with HIT reduces falls in older inpatients.
Citation: Dykes PC, Carroll DL, Hurley A, et al. Fall prevention in acute care hospitals: a randomized trial. JAMA. 2010;304(17):1912-1918.
Lack of Timely Outpatient Follow-Up Results in Higher Readmission Rates
Clinical question: Does timely primary-care-physician (PCP) follow-up improve outcomes and prevent hospital readmissions?
Background: Active PCP involvement is key to interventions aimed at reducing readmissions and ensuring effective ongoing patient care. Some studies suggest increased overall resource utilization when PCP follow-up occurs after hospitalization. Resource utilization and clinical outcomes after hospitalization related to timely PCP follow-up have not been adequately studied.
Study design: Prospective cohort.
Setting: An urban, academic, 425-bed tertiary-care center in Colorado.
Synopsis: From a convenience sample of 121 patients admitted to general medicine services during winter months, 65 patients completed the study. Demographics, diagnosis, payor source, and PCP information were collected upon enrollment. Post-discharge phone calls and patient surveys were used to determine follow-up and readmission status. Timely PCP follow-up was defined as a visit with a PCP or specialist related to the discharge diagnosis within four weeks of hospital discharge.
Thirty-day readmission rates and hospital length of stay were compared for those with timely PCP follow-up and those without. Less than half of general-medicine inpatients received timely PCP follow-up post-discharge. Lack of timely PCP follow-up was associated with younger age, a 10-fold increase in 30-day readmission for the same condition, and a trend toward longer length of stay. However, hospital readmission for any condition did not differ with lack of timely PCP follow-up.
This small, single-center study with convenience sample enrollment might not represent all medical inpatients or diagnoses. Determination of same-condition readmission was potentially subjective.
Bottom line: Patients who lack timely post-discharge follow-up have higher readmission rates for the same medical condition.
Citation: Misky GJ, Wald HL, Coleman EA. Post-hospitalization transitions: examining the effects of timing of primary care provider follow-up. J Hosp Med. 2010;5(7):392-397.
Compared with Uninsured and Medicaid Patients, Privately Insured Patients Admitted for Acute MI, Stroke, and Pneumonia Have Better Mortality Rates
Clinical question: Do outcomes for insured and underinsured patients vary for three of the most common medical conditions for which patients are hospitalized: acute myocardial infarction (AMI), stroke, and pneumonia?
Background: The ideal healthcare system would provide quality care to all individuals regardless of insurance status. Nevertheless, disparities in outcomes for the insured and underinsured or uninsured are well-documented in the outpatient setting but not as well in the inpatient setting. More needs to be done to address these potential disparities.
Study design: Retrospective database analysis.
Setting: Database including 20% of all U.S. community hospitals, including public hospitals, academic medical centers, and specialty hospitals.
Synopsis: This study utilized a database of 8 million discharges from more than 1,000 hospitals and isolated patients 18-64 years old (154,381 patients). Privately insured, uninsured, and Medicaid patients’ data were reviewed for in-hospital mortality, length of stay (LOS), and cost per hospitalization. The analysis took into account disease severity, comorbidities, and the proportion of underinsured patients receiving care in each hospital when insurance-related disparities were examined.
Compared with the privately insured, in-hospital mortality and LOS for AMI and stroke were significantly higher for uninsured and Medicaid patients. Among pneumonia patients, Medicaid patients had significantly higher in-hospital mortality and LOS than the other two groups. Cost per hospitalization was highest for all three conditions in the Medicaid group; the uninsured group had the lowest costs for all three conditions.
Unfortunately, the three conditions analyzed only comprise 8% of annual hospital discharges, so the findings cannot be generalized. Also, deaths occurring soon after hospital discharge were not included, and uninsured and Medicaid patients are likely to have more severe diseases, which, rather than insurance status, could account for the mortality differences.
Bottom line: In-hospital mortality and resource use for three common medical conditions vary significantly between privately insured and uninsured or Medicaid patients, highlighting the need to take measures to close this gap.
Citation: Hasan O, Orav EJ, LeRoi LS. Insurance status and hospital care for myocardial infarction, stroke, and pneumonia. J Hosp Med. 2010;5(8);452-459.
Warfarin Monotherapy Best in Prevention of Thromboembolic Events for Atrial Fibrillation Patients
Clinical question: Is there a benefit to adding an antiplatelet agent to warfarin for the prevention of thromboembolic stroke in atrial fibrillation?
Background: Many physicians prescribe various combinations of aspirin, clopidogrel, and warfarin, as these treatments are endorsed in guidelines and expert statements. The use of these medications, however, has not been studied in a setting large enough to understand the safety of these therapies.
Study design: Retrospective cohort.
Setting: All Danish hospitals.
Synopsis: All hospitalized patients in Denmark from 1997 to 2006 who were identified with new onset atrial fibrillation (n=118,606) were monitored for outcomes and the use of aspirin, clopidogrel, and warfarin. These patients were followed for a mean of 3.3 years with the primary endpoint being admission to a hospital for a diagnosis of bleeding and a secondary endpoint of stroke.
Bleeding occurred in 13,573 patients (11.4%). The incidence of bleeding was highest in the first 180 days and then leveled off. Hazard ratios were computed with warfarin monotherapy as a reference. Only the hazard ratio for aspirin monotherapy (0.93) was lower (confidence interval [CI] 0.88-0.98). The highest risk of bleeding was with the triple therapy warfarin-aspirin-clopidogrel, which had a hazard ratio of 3.70 (CI 2.89-4.76).
For strokes, the hazard ratio was slightly better for warfarin-clopidogrel (0.70), although the CI was wide at 0.35-1.4 compared to warfarin monotherapy as a reference. Hazard ratios for monotherapy with clopidogrel or aspirin, dual therapy, and triple therapy all were worse, ranging from 1.27 to 1.86.
Bottom line: Warfarin as a monotherapy might have a bleeding risk comparable to that of aspirin or clopidogrel alone, and prevents more strokes than various combinations of these medications.
Citation: Hansen ML, Sørensen R, Clausen MT, et al. Risk of bleeding with single, dual, or triple therapy with warfarin, aspirin, and clopidogrel in patients with atrial fibrillation. Arch Intern Med. 2010;170 (16):1433-1441.
Cognitive and Physical Function Declines in Elderly Severe Sepsis Survivors
Clinical question: Is there a change in cognitive and physical functioning after severe sepsis?
Background: Disability is associated with increased mortality, decreased quality of life, and increased burdens by families and healthcare costs. After severe sepsis, the lasting effects of debility have not been investigated in any large studies.
Study design: Prospective cohort.
Setting: Hospitalized Medicare patients participating in the Health and Retirement Study.
Synopsis: Patients (n=1194) were followed for a minimum of one year between 1998 and 2006. The outcomes were measured by multiple personal interviews before and after a severe sepsis episode. Cognitive impairment was measured using three validated questionnaires dependent upon age or if a proxy was the respondent. For functional limitations, a questionnaire concerning instrumental and basic activities of daily living was used.
Cognitive impairment for those with moderate to severe impairment increased to 16.7% from 6.1% after a sepsis episode with an odds ratio of 3.34 (95% confidence interval 1.53-7.25). There was no significant increase in nonsevere sepsis hospitalized comparison patients (n=5574). All survivors with severe sepsis had a functional decline of 1.5 activities. The comparison group had about a 0.4 activity decline. All of these deficits endured throughout the study.
The authors provide comments that there should be a system-based approach in preventing severe sepsis, its burdens, and its costs. Suggestions include preventing delirium, initiating better standards of care, and involving therapists earlier to prevent immobility.
Bottom line: Severe sepsis is independently associated with enduring cognitive and physical functional declines, which strain families and our healthcare system.
Citation: Iwashyna TJ, Ely EW, Smith DM, Langa KM. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 2010;304(16):1787-1794.
Furosemide on Day of Elective Noncardiac Surgery Does Not Increase Risk of Intraoperative Hypotension
Clinical question: For patients chronically treated with loop diuretics, does withholding furosemide on the day of elective noncardiac surgery prevent intraoperative hypotension?
Background: Recent studies have questioned the safety of blood-pressure-lowering medications administered on the day of surgery. Beta-blockers have been associated with an increase in strokes and death perioperatively, and angiotensin receptor blockers (ARB) are frequently withheld on the day of surgery to avoid intraoperative hypotension. The effect of loop diuretics is uncertain.
Study design: Double-blind, randomized, placebo-controlled study.
Setting: Three North American university centers.
Synopsis: One hundred ninety-three patients were instructed to take furosemide or placebo on the day they underwent noncardiac surgery. The primary outcome measure was perioperative hypotension defined as a SBP <90 mmHg for more than five minutes, a 35% drop in the mean arterial blood pressure, or the need for a vasopressor agent. The number of cardiovascular complications (acute heart failure, acute coronary syndrome, arrhythmia, acute cerebrovascular event) and deaths also were analyzed.
Concerns have been raised that loop diuretics might predispose patients to a higher risk of intraoperative hypotension during noncardiac surgery. This trial showed no significant difference in the rates of intraoperative hypotension in patients who were administered furosemide versus those who were not. Although cardiovascular complications occurred more frequently in the furosemide group, the difference was not statistically significant.
Important limitations of the study were recognized. A larger population of patients could have revealed a statistically significant difference in cardiovascular outcomes in the furosemide group. Also, an anesthetic protocol was not utilized, which raises questions about the interaction of furosemide and effect on blood pressure with certain anesthetics.
Bottom line: Administering furosemide prior to surgery in chronic users does not appreciably increase the rate of intraoperative hypotension or cardiovascular events.
Citation: Khan NA, Campbell NR, Frost SD, et al. Risk of intraoperative hypotension with loop diuretics: a randomized controlled trial. Am J Med. 2010;123(11):1059e1-1059e8.
Pediatric HM Literature
Computerized Physician Order Entry Decreases Hospitalwide Mortality
Clinical question: What is the effect of computerized physician order entry (CPOE) on hospitalwide mortality?
Background: CPOE has been touted as a key method for improving the quality and safety of patient care. To date, however, studies have not demonstrated definitive benefits, with one study demonstrating an increase in mortality rates in a critical-care unit after CPOE implementation.
Study design: Retrospective cohort study.
Setting: Quaternary-care academic children’s hospital.
Synopsis: More than 97,000 nonobstetric patients admitted to Lucile Packard Children’s Hospital (LCPH) at Stanford University in Palo Alto, Calif., from January 2001 to April 2009 were included in the analysis. The patients were divided into pre- and postintervention groups. The intervention was defined as a “big bang” activation of CPOE on Nov. 4, 2007, affecting 90% of the inpatient beds at LCPH.
After the intervention, mean monthly unadjusted mortality rates decreased to 0.716 deaths from 1.008 per 100 discharges. After adjustment for severity of illness and a rapid-response team (which had previously been shown to decrease mortality rates), mortality rates postintervention continued to remain significantly lower.
This study revealed an impressive reduction in perhaps the ultimate outcome measure: hospitalwide mortality. The authors went to extensive lengths to adjust for potential confounding factors to include delayed implementation of CPOE in the ICUs. As with many complex process improvement efforts, the devil might be in the details of local context and culture. Thus, the software might have been less important than the manner in which the institution adapted to its functionality. Those seeking to replicate these results will need to be mindful of the requisite organizational changes in communication, order standardization, and data retrieval.
Bottom line: CPOE implementation has the potential to significantly reduce hospitalwide mortality rates.
Citation: Longhurst CA, Parast L, Sandborg CI, et al. Decrease in hospital-wide mortality rate after implementation of a commercially sold computerized physician order entry system. Pediatrics. 2010;126(1):e1-e8.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Risk of adverse events with opioid use
- Drug of choice for outpatient treatment of cellulitis
- Preventing hospital falls
- Post-hospital outcomes based on status of PCP follow-up
- LOS, mortality, and readmission based on insurance
- Antiplatelets added to warfarin for atrial fibrillation.
- Cognitive effects of severe sepsis
- Effect of preoperative furosemide use
ED Visits Are Higher among Recipients of Chronic Opioid Therapy
Clinical question: Is there an association between the use of prescription opioids and adverse outcomes?
Background: Chronic opioid therapy is a common strategy for managing chronic, noncancer pain. There has been an increase in overdose deaths and ED visits (EDV) involving the use of prescription opioids.
Study design: Retrospective study from claims records.
Setting: Population in the Health Core Integrated Research Database, containing large, commercial insurance plans in 14 states, and Arkansas Medicaid.
Synopsis: Patients 18 and older without cancer diagnoses who used prescription opioids for at least 90 continuous days within a six-month period from 2000 to 2005 were examined for risk factors for EDVs and alcohol- or drug-related encounters (ADEs) in the 12 months following 90 days or more of prescribed opioids.
Patients with diagnoses of headache, back pain, and pre-existing substance-use disorders had significantly higher EDVs and ADEs. Opioid dose at morphine-equivalent doses over 120 mg per day doubled the risk of ADEs. The use of short-acting Schedule II opioids was associated with EDVs (relative risk, 1.09-1.74). The use of long-acting Schedule II opioids was strongly associated with ADEs (relative risk, 1.64-4.00).
Bottom line: In adults with noncancer pain prescribed opioids for 90 days or more, short-acting Schedule II opioid use was associated with an increased number of EDVs, and long-acting opioid use was associated with an increased number of ADEs. Minimizing Schedule II opioid prescription in these higher-risk patients might be prudent to increase patient safety.
Citation: Braden JB, Russo J, Fan MI, et al. Emergency department visits among recipients of chronic opioid therapy. Arch Intern Med. 2010; 170(16):1425-1432.
Empiric Outpatient Therapy with Trimethoprim-Sulfamethoxazole or Clindamycin Is Preferred for Cellulitis
Clinical question: What is the best empiric outpatient oral antibiotic treatment for cellulitis in areas with a high prevalence of community-associated MRSA infections?
Background: The increasing rates of community-associated MRSA skin and soft-tissue infections have raised concerns that such beta-lactams as cephalexin and other semisynthetic penicillins are not appropriate for empiric outpatient therapy for cellulitis.
Study design: Three-year, retrospective cohort study.
Setting: A teaching clinic of a tertiary-care medical center in Hawaii.
Synopsis: More than 540 patients with cellulitis were identified from January 2005 to December 2007. Of these, 139 patients were excluded for reasons such as hospitalization, surgical intervention, etc. In the final cohort of 405 patients, the three most commonly prescribed oral antibiotics were cephalexin (44%), trimethoprim-sulfamethoxazole (38%), and clindamycin (10%). Other antibiotics accounted for the remaining 8%.
MRSA was recovered in 62% of positive culture specimens. The success rate of trimethoprim-sulfamethoxazole was 91% vs. 74% in the cephalexin group (P<0.001). Clindamycin success rates were higher than those of cephalexin in patients who had subsequently confirmed MRSA infections (P=0.01) and moderately severe cellulitis (P=0.03) and were obese (P=0.04).
Bottom line: Antibiotics with activity against community-acquired MRSA (e.g. trimethroprim-sulfamethoxazole and clinidamycin) are the preferred empiric outpatient therapy for cellulitis in areas with a high prevalence of community-acquired MRSA.
Citation: Khawcharoenporn T, Tice A. Empiric outpatient therapy with trimethoprim-sulfamethoxazole, cephalexin, or clindamycin for cellulitis. Am J Med. 2010;123(10):942-950.
Patient-Specific Screening with Health Information Technology Prevents Falls
Clinical question: Does a fall-prevention toolkit using health information technology decrease patient falls in acute-care hospitals?
Background: Inpatient falls and fall-related injuries result in substantial morbidity and additional healthcare costs. While specific fall-prevention strategies were a longstanding target for intervention, little evidence exists to link them with decreased fall rates.
Study design: Cluster-randomized study.
Setting: Four urban hospitals in Massachusetts.
Synopsis: Comparing patient fall rates in four acute-care hospitals between units providing usual care (5,104 patients) and units using a health information technology (HIT)-linked fall prevention toolkit (5,160 patients), this study demonstrated significant fall reduction in older inpatients. The intervention integrated existing workflow and validated fall risk assessment (Morse Falls Scale) into an HIT software application that tailored fall-prevention interventions to patients’ specific fall risk determinants. The toolkit produced bed posters, patient education handouts, and plans of care communicating patient-specific alerts to key stakeholders.
The primary outcome was patient falls per 1,000 patient-days during the six-month intervention period. The number of patients with falls was significantly different (P=0.02) between control (n=87) and intervention (n=67) units. The toolkit prevented one fall per 862 patient-days.
This nonblinded study was limited by the fact that it was conducted in a single health system. The toolkit was not effective in patients less than 65 years of age. Additionally, the sample size did not have sufficient power to detect effectiveness in preventing repeat falls or falls with injury.
Bottom line: Patient-specific fall prevention strategy coupled with HIT reduces falls in older inpatients.
Citation: Dykes PC, Carroll DL, Hurley A, et al. Fall prevention in acute care hospitals: a randomized trial. JAMA. 2010;304(17):1912-1918.
Lack of Timely Outpatient Follow-Up Results in Higher Readmission Rates
Clinical question: Does timely primary-care-physician (PCP) follow-up improve outcomes and prevent hospital readmissions?
Background: Active PCP involvement is key to interventions aimed at reducing readmissions and ensuring effective ongoing patient care. Some studies suggest increased overall resource utilization when PCP follow-up occurs after hospitalization. Resource utilization and clinical outcomes after hospitalization related to timely PCP follow-up have not been adequately studied.
Study design: Prospective cohort.
Setting: An urban, academic, 425-bed tertiary-care center in Colorado.
Synopsis: From a convenience sample of 121 patients admitted to general medicine services during winter months, 65 patients completed the study. Demographics, diagnosis, payor source, and PCP information were collected upon enrollment. Post-discharge phone calls and patient surveys were used to determine follow-up and readmission status. Timely PCP follow-up was defined as a visit with a PCP or specialist related to the discharge diagnosis within four weeks of hospital discharge.
Thirty-day readmission rates and hospital length of stay were compared for those with timely PCP follow-up and those without. Less than half of general-medicine inpatients received timely PCP follow-up post-discharge. Lack of timely PCP follow-up was associated with younger age, a 10-fold increase in 30-day readmission for the same condition, and a trend toward longer length of stay. However, hospital readmission for any condition did not differ with lack of timely PCP follow-up.
This small, single-center study with convenience sample enrollment might not represent all medical inpatients or diagnoses. Determination of same-condition readmission was potentially subjective.
Bottom line: Patients who lack timely post-discharge follow-up have higher readmission rates for the same medical condition.
Citation: Misky GJ, Wald HL, Coleman EA. Post-hospitalization transitions: examining the effects of timing of primary care provider follow-up. J Hosp Med. 2010;5(7):392-397.
Compared with Uninsured and Medicaid Patients, Privately Insured Patients Admitted for Acute MI, Stroke, and Pneumonia Have Better Mortality Rates
Clinical question: Do outcomes for insured and underinsured patients vary for three of the most common medical conditions for which patients are hospitalized: acute myocardial infarction (AMI), stroke, and pneumonia?
Background: The ideal healthcare system would provide quality care to all individuals regardless of insurance status. Nevertheless, disparities in outcomes for the insured and underinsured or uninsured are well-documented in the outpatient setting but not as well in the inpatient setting. More needs to be done to address these potential disparities.
Study design: Retrospective database analysis.
Setting: Database including 20% of all U.S. community hospitals, including public hospitals, academic medical centers, and specialty hospitals.
Synopsis: This study utilized a database of 8 million discharges from more than 1,000 hospitals and isolated patients 18-64 years old (154,381 patients). Privately insured, uninsured, and Medicaid patients’ data were reviewed for in-hospital mortality, length of stay (LOS), and cost per hospitalization. The analysis took into account disease severity, comorbidities, and the proportion of underinsured patients receiving care in each hospital when insurance-related disparities were examined.
Compared with the privately insured, in-hospital mortality and LOS for AMI and stroke were significantly higher for uninsured and Medicaid patients. Among pneumonia patients, Medicaid patients had significantly higher in-hospital mortality and LOS than the other two groups. Cost per hospitalization was highest for all three conditions in the Medicaid group; the uninsured group had the lowest costs for all three conditions.
Unfortunately, the three conditions analyzed only comprise 8% of annual hospital discharges, so the findings cannot be generalized. Also, deaths occurring soon after hospital discharge were not included, and uninsured and Medicaid patients are likely to have more severe diseases, which, rather than insurance status, could account for the mortality differences.
Bottom line: In-hospital mortality and resource use for three common medical conditions vary significantly between privately insured and uninsured or Medicaid patients, highlighting the need to take measures to close this gap.
Citation: Hasan O, Orav EJ, LeRoi LS. Insurance status and hospital care for myocardial infarction, stroke, and pneumonia. J Hosp Med. 2010;5(8);452-459.
Warfarin Monotherapy Best in Prevention of Thromboembolic Events for Atrial Fibrillation Patients
Clinical question: Is there a benefit to adding an antiplatelet agent to warfarin for the prevention of thromboembolic stroke in atrial fibrillation?
Background: Many physicians prescribe various combinations of aspirin, clopidogrel, and warfarin, as these treatments are endorsed in guidelines and expert statements. The use of these medications, however, has not been studied in a setting large enough to understand the safety of these therapies.
Study design: Retrospective cohort.
Setting: All Danish hospitals.
Synopsis: All hospitalized patients in Denmark from 1997 to 2006 who were identified with new onset atrial fibrillation (n=118,606) were monitored for outcomes and the use of aspirin, clopidogrel, and warfarin. These patients were followed for a mean of 3.3 years with the primary endpoint being admission to a hospital for a diagnosis of bleeding and a secondary endpoint of stroke.
Bleeding occurred in 13,573 patients (11.4%). The incidence of bleeding was highest in the first 180 days and then leveled off. Hazard ratios were computed with warfarin monotherapy as a reference. Only the hazard ratio for aspirin monotherapy (0.93) was lower (confidence interval [CI] 0.88-0.98). The highest risk of bleeding was with the triple therapy warfarin-aspirin-clopidogrel, which had a hazard ratio of 3.70 (CI 2.89-4.76).
For strokes, the hazard ratio was slightly better for warfarin-clopidogrel (0.70), although the CI was wide at 0.35-1.4 compared to warfarin monotherapy as a reference. Hazard ratios for monotherapy with clopidogrel or aspirin, dual therapy, and triple therapy all were worse, ranging from 1.27 to 1.86.
Bottom line: Warfarin as a monotherapy might have a bleeding risk comparable to that of aspirin or clopidogrel alone, and prevents more strokes than various combinations of these medications.
Citation: Hansen ML, Sørensen R, Clausen MT, et al. Risk of bleeding with single, dual, or triple therapy with warfarin, aspirin, and clopidogrel in patients with atrial fibrillation. Arch Intern Med. 2010;170 (16):1433-1441.
Cognitive and Physical Function Declines in Elderly Severe Sepsis Survivors
Clinical question: Is there a change in cognitive and physical functioning after severe sepsis?
Background: Disability is associated with increased mortality, decreased quality of life, and increased burdens by families and healthcare costs. After severe sepsis, the lasting effects of debility have not been investigated in any large studies.
Study design: Prospective cohort.
Setting: Hospitalized Medicare patients participating in the Health and Retirement Study.
Synopsis: Patients (n=1194) were followed for a minimum of one year between 1998 and 2006. The outcomes were measured by multiple personal interviews before and after a severe sepsis episode. Cognitive impairment was measured using three validated questionnaires dependent upon age or if a proxy was the respondent. For functional limitations, a questionnaire concerning instrumental and basic activities of daily living was used.
Cognitive impairment for those with moderate to severe impairment increased to 16.7% from 6.1% after a sepsis episode with an odds ratio of 3.34 (95% confidence interval 1.53-7.25). There was no significant increase in nonsevere sepsis hospitalized comparison patients (n=5574). All survivors with severe sepsis had a functional decline of 1.5 activities. The comparison group had about a 0.4 activity decline. All of these deficits endured throughout the study.
The authors provide comments that there should be a system-based approach in preventing severe sepsis, its burdens, and its costs. Suggestions include preventing delirium, initiating better standards of care, and involving therapists earlier to prevent immobility.
Bottom line: Severe sepsis is independently associated with enduring cognitive and physical functional declines, which strain families and our healthcare system.
Citation: Iwashyna TJ, Ely EW, Smith DM, Langa KM. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 2010;304(16):1787-1794.
Furosemide on Day of Elective Noncardiac Surgery Does Not Increase Risk of Intraoperative Hypotension
Clinical question: For patients chronically treated with loop diuretics, does withholding furosemide on the day of elective noncardiac surgery prevent intraoperative hypotension?
Background: Recent studies have questioned the safety of blood-pressure-lowering medications administered on the day of surgery. Beta-blockers have been associated with an increase in strokes and death perioperatively, and angiotensin receptor blockers (ARB) are frequently withheld on the day of surgery to avoid intraoperative hypotension. The effect of loop diuretics is uncertain.
Study design: Double-blind, randomized, placebo-controlled study.
Setting: Three North American university centers.
Synopsis: One hundred ninety-three patients were instructed to take furosemide or placebo on the day they underwent noncardiac surgery. The primary outcome measure was perioperative hypotension defined as a SBP <90 mmHg for more than five minutes, a 35% drop in the mean arterial blood pressure, or the need for a vasopressor agent. The number of cardiovascular complications (acute heart failure, acute coronary syndrome, arrhythmia, acute cerebrovascular event) and deaths also were analyzed.
Concerns have been raised that loop diuretics might predispose patients to a higher risk of intraoperative hypotension during noncardiac surgery. This trial showed no significant difference in the rates of intraoperative hypotension in patients who were administered furosemide versus those who were not. Although cardiovascular complications occurred more frequently in the furosemide group, the difference was not statistically significant.
Important limitations of the study were recognized. A larger population of patients could have revealed a statistically significant difference in cardiovascular outcomes in the furosemide group. Also, an anesthetic protocol was not utilized, which raises questions about the interaction of furosemide and effect on blood pressure with certain anesthetics.
Bottom line: Administering furosemide prior to surgery in chronic users does not appreciably increase the rate of intraoperative hypotension or cardiovascular events.
Citation: Khan NA, Campbell NR, Frost SD, et al. Risk of intraoperative hypotension with loop diuretics: a randomized controlled trial. Am J Med. 2010;123(11):1059e1-1059e8.
Pediatric HM Literature
Computerized Physician Order Entry Decreases Hospitalwide Mortality
Clinical question: What is the effect of computerized physician order entry (CPOE) on hospitalwide mortality?
Background: CPOE has been touted as a key method for improving the quality and safety of patient care. To date, however, studies have not demonstrated definitive benefits, with one study demonstrating an increase in mortality rates in a critical-care unit after CPOE implementation.
Study design: Retrospective cohort study.
Setting: Quaternary-care academic children’s hospital.
Synopsis: More than 97,000 nonobstetric patients admitted to Lucile Packard Children’s Hospital (LCPH) at Stanford University in Palo Alto, Calif., from January 2001 to April 2009 were included in the analysis. The patients were divided into pre- and postintervention groups. The intervention was defined as a “big bang” activation of CPOE on Nov. 4, 2007, affecting 90% of the inpatient beds at LCPH.
After the intervention, mean monthly unadjusted mortality rates decreased to 0.716 deaths from 1.008 per 100 discharges. After adjustment for severity of illness and a rapid-response team (which had previously been shown to decrease mortality rates), mortality rates postintervention continued to remain significantly lower.
This study revealed an impressive reduction in perhaps the ultimate outcome measure: hospitalwide mortality. The authors went to extensive lengths to adjust for potential confounding factors to include delayed implementation of CPOE in the ICUs. As with many complex process improvement efforts, the devil might be in the details of local context and culture. Thus, the software might have been less important than the manner in which the institution adapted to its functionality. Those seeking to replicate these results will need to be mindful of the requisite organizational changes in communication, order standardization, and data retrieval.
Bottom line: CPOE implementation has the potential to significantly reduce hospitalwide mortality rates.
Citation: Longhurst CA, Parast L, Sandborg CI, et al. Decrease in hospital-wide mortality rate after implementation of a commercially sold computerized physician order entry system. Pediatrics. 2010;126(1):e1-e8.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Risk of adverse events with opioid use
- Drug of choice for outpatient treatment of cellulitis
- Preventing hospital falls
- Post-hospital outcomes based on status of PCP follow-up
- LOS, mortality, and readmission based on insurance
- Antiplatelets added to warfarin for atrial fibrillation.
- Cognitive effects of severe sepsis
- Effect of preoperative furosemide use
ED Visits Are Higher among Recipients of Chronic Opioid Therapy
Clinical question: Is there an association between the use of prescription opioids and adverse outcomes?
Background: Chronic opioid therapy is a common strategy for managing chronic, noncancer pain. There has been an increase in overdose deaths and ED visits (EDV) involving the use of prescription opioids.
Study design: Retrospective study from claims records.
Setting: Population in the Health Core Integrated Research Database, containing large, commercial insurance plans in 14 states, and Arkansas Medicaid.
Synopsis: Patients 18 and older without cancer diagnoses who used prescription opioids for at least 90 continuous days within a six-month period from 2000 to 2005 were examined for risk factors for EDVs and alcohol- or drug-related encounters (ADEs) in the 12 months following 90 days or more of prescribed opioids.
Patients with diagnoses of headache, back pain, and pre-existing substance-use disorders had significantly higher EDVs and ADEs. Opioid dose at morphine-equivalent doses over 120 mg per day doubled the risk of ADEs. The use of short-acting Schedule II opioids was associated with EDVs (relative risk, 1.09-1.74). The use of long-acting Schedule II opioids was strongly associated with ADEs (relative risk, 1.64-4.00).
Bottom line: In adults with noncancer pain prescribed opioids for 90 days or more, short-acting Schedule II opioid use was associated with an increased number of EDVs, and long-acting opioid use was associated with an increased number of ADEs. Minimizing Schedule II opioid prescription in these higher-risk patients might be prudent to increase patient safety.
Citation: Braden JB, Russo J, Fan MI, et al. Emergency department visits among recipients of chronic opioid therapy. Arch Intern Med. 2010; 170(16):1425-1432.
Empiric Outpatient Therapy with Trimethoprim-Sulfamethoxazole or Clindamycin Is Preferred for Cellulitis
Clinical question: What is the best empiric outpatient oral antibiotic treatment for cellulitis in areas with a high prevalence of community-associated MRSA infections?
Background: The increasing rates of community-associated MRSA skin and soft-tissue infections have raised concerns that such beta-lactams as cephalexin and other semisynthetic penicillins are not appropriate for empiric outpatient therapy for cellulitis.
Study design: Three-year, retrospective cohort study.
Setting: A teaching clinic of a tertiary-care medical center in Hawaii.
Synopsis: More than 540 patients with cellulitis were identified from January 2005 to December 2007. Of these, 139 patients were excluded for reasons such as hospitalization, surgical intervention, etc. In the final cohort of 405 patients, the three most commonly prescribed oral antibiotics were cephalexin (44%), trimethoprim-sulfamethoxazole (38%), and clindamycin (10%). Other antibiotics accounted for the remaining 8%.
MRSA was recovered in 62% of positive culture specimens. The success rate of trimethoprim-sulfamethoxazole was 91% vs. 74% in the cephalexin group (P<0.001). Clindamycin success rates were higher than those of cephalexin in patients who had subsequently confirmed MRSA infections (P=0.01) and moderately severe cellulitis (P=0.03) and were obese (P=0.04).
Bottom line: Antibiotics with activity against community-acquired MRSA (e.g. trimethroprim-sulfamethoxazole and clinidamycin) are the preferred empiric outpatient therapy for cellulitis in areas with a high prevalence of community-acquired MRSA.
Citation: Khawcharoenporn T, Tice A. Empiric outpatient therapy with trimethoprim-sulfamethoxazole, cephalexin, or clindamycin for cellulitis. Am J Med. 2010;123(10):942-950.
Patient-Specific Screening with Health Information Technology Prevents Falls
Clinical question: Does a fall-prevention toolkit using health information technology decrease patient falls in acute-care hospitals?
Background: Inpatient falls and fall-related injuries result in substantial morbidity and additional healthcare costs. While specific fall-prevention strategies were a longstanding target for intervention, little evidence exists to link them with decreased fall rates.
Study design: Cluster-randomized study.
Setting: Four urban hospitals in Massachusetts.
Synopsis: Comparing patient fall rates in four acute-care hospitals between units providing usual care (5,104 patients) and units using a health information technology (HIT)-linked fall prevention toolkit (5,160 patients), this study demonstrated significant fall reduction in older inpatients. The intervention integrated existing workflow and validated fall risk assessment (Morse Falls Scale) into an HIT software application that tailored fall-prevention interventions to patients’ specific fall risk determinants. The toolkit produced bed posters, patient education handouts, and plans of care communicating patient-specific alerts to key stakeholders.
The primary outcome was patient falls per 1,000 patient-days during the six-month intervention period. The number of patients with falls was significantly different (P=0.02) between control (n=87) and intervention (n=67) units. The toolkit prevented one fall per 862 patient-days.
This nonblinded study was limited by the fact that it was conducted in a single health system. The toolkit was not effective in patients less than 65 years of age. Additionally, the sample size did not have sufficient power to detect effectiveness in preventing repeat falls or falls with injury.
Bottom line: Patient-specific fall prevention strategy coupled with HIT reduces falls in older inpatients.
Citation: Dykes PC, Carroll DL, Hurley A, et al. Fall prevention in acute care hospitals: a randomized trial. JAMA. 2010;304(17):1912-1918.
Lack of Timely Outpatient Follow-Up Results in Higher Readmission Rates
Clinical question: Does timely primary-care-physician (PCP) follow-up improve outcomes and prevent hospital readmissions?
Background: Active PCP involvement is key to interventions aimed at reducing readmissions and ensuring effective ongoing patient care. Some studies suggest increased overall resource utilization when PCP follow-up occurs after hospitalization. Resource utilization and clinical outcomes after hospitalization related to timely PCP follow-up have not been adequately studied.
Study design: Prospective cohort.
Setting: An urban, academic, 425-bed tertiary-care center in Colorado.
Synopsis: From a convenience sample of 121 patients admitted to general medicine services during winter months, 65 patients completed the study. Demographics, diagnosis, payor source, and PCP information were collected upon enrollment. Post-discharge phone calls and patient surveys were used to determine follow-up and readmission status. Timely PCP follow-up was defined as a visit with a PCP or specialist related to the discharge diagnosis within four weeks of hospital discharge.
Thirty-day readmission rates and hospital length of stay were compared for those with timely PCP follow-up and those without. Less than half of general-medicine inpatients received timely PCP follow-up post-discharge. Lack of timely PCP follow-up was associated with younger age, a 10-fold increase in 30-day readmission for the same condition, and a trend toward longer length of stay. However, hospital readmission for any condition did not differ with lack of timely PCP follow-up.
This small, single-center study with convenience sample enrollment might not represent all medical inpatients or diagnoses. Determination of same-condition readmission was potentially subjective.
Bottom line: Patients who lack timely post-discharge follow-up have higher readmission rates for the same medical condition.
Citation: Misky GJ, Wald HL, Coleman EA. Post-hospitalization transitions: examining the effects of timing of primary care provider follow-up. J Hosp Med. 2010;5(7):392-397.
Compared with Uninsured and Medicaid Patients, Privately Insured Patients Admitted for Acute MI, Stroke, and Pneumonia Have Better Mortality Rates
Clinical question: Do outcomes for insured and underinsured patients vary for three of the most common medical conditions for which patients are hospitalized: acute myocardial infarction (AMI), stroke, and pneumonia?
Background: The ideal healthcare system would provide quality care to all individuals regardless of insurance status. Nevertheless, disparities in outcomes for the insured and underinsured or uninsured are well-documented in the outpatient setting but not as well in the inpatient setting. More needs to be done to address these potential disparities.
Study design: Retrospective database analysis.
Setting: Database including 20% of all U.S. community hospitals, including public hospitals, academic medical centers, and specialty hospitals.
Synopsis: This study utilized a database of 8 million discharges from more than 1,000 hospitals and isolated patients 18-64 years old (154,381 patients). Privately insured, uninsured, and Medicaid patients’ data were reviewed for in-hospital mortality, length of stay (LOS), and cost per hospitalization. The analysis took into account disease severity, comorbidities, and the proportion of underinsured patients receiving care in each hospital when insurance-related disparities were examined.
Compared with the privately insured, in-hospital mortality and LOS for AMI and stroke were significantly higher for uninsured and Medicaid patients. Among pneumonia patients, Medicaid patients had significantly higher in-hospital mortality and LOS than the other two groups. Cost per hospitalization was highest for all three conditions in the Medicaid group; the uninsured group had the lowest costs for all three conditions.
Unfortunately, the three conditions analyzed only comprise 8% of annual hospital discharges, so the findings cannot be generalized. Also, deaths occurring soon after hospital discharge were not included, and uninsured and Medicaid patients are likely to have more severe diseases, which, rather than insurance status, could account for the mortality differences.
Bottom line: In-hospital mortality and resource use for three common medical conditions vary significantly between privately insured and uninsured or Medicaid patients, highlighting the need to take measures to close this gap.
Citation: Hasan O, Orav EJ, LeRoi LS. Insurance status and hospital care for myocardial infarction, stroke, and pneumonia. J Hosp Med. 2010;5(8);452-459.
Warfarin Monotherapy Best in Prevention of Thromboembolic Events for Atrial Fibrillation Patients
Clinical question: Is there a benefit to adding an antiplatelet agent to warfarin for the prevention of thromboembolic stroke in atrial fibrillation?
Background: Many physicians prescribe various combinations of aspirin, clopidogrel, and warfarin, as these treatments are endorsed in guidelines and expert statements. The use of these medications, however, has not been studied in a setting large enough to understand the safety of these therapies.
Study design: Retrospective cohort.
Setting: All Danish hospitals.
Synopsis: All hospitalized patients in Denmark from 1997 to 2006 who were identified with new onset atrial fibrillation (n=118,606) were monitored for outcomes and the use of aspirin, clopidogrel, and warfarin. These patients were followed for a mean of 3.3 years with the primary endpoint being admission to a hospital for a diagnosis of bleeding and a secondary endpoint of stroke.
Bleeding occurred in 13,573 patients (11.4%). The incidence of bleeding was highest in the first 180 days and then leveled off. Hazard ratios were computed with warfarin monotherapy as a reference. Only the hazard ratio for aspirin monotherapy (0.93) was lower (confidence interval [CI] 0.88-0.98). The highest risk of bleeding was with the triple therapy warfarin-aspirin-clopidogrel, which had a hazard ratio of 3.70 (CI 2.89-4.76).
For strokes, the hazard ratio was slightly better for warfarin-clopidogrel (0.70), although the CI was wide at 0.35-1.4 compared to warfarin monotherapy as a reference. Hazard ratios for monotherapy with clopidogrel or aspirin, dual therapy, and triple therapy all were worse, ranging from 1.27 to 1.86.
Bottom line: Warfarin as a monotherapy might have a bleeding risk comparable to that of aspirin or clopidogrel alone, and prevents more strokes than various combinations of these medications.
Citation: Hansen ML, Sørensen R, Clausen MT, et al. Risk of bleeding with single, dual, or triple therapy with warfarin, aspirin, and clopidogrel in patients with atrial fibrillation. Arch Intern Med. 2010;170 (16):1433-1441.
Cognitive and Physical Function Declines in Elderly Severe Sepsis Survivors
Clinical question: Is there a change in cognitive and physical functioning after severe sepsis?
Background: Disability is associated with increased mortality, decreased quality of life, and increased burdens by families and healthcare costs. After severe sepsis, the lasting effects of debility have not been investigated in any large studies.
Study design: Prospective cohort.
Setting: Hospitalized Medicare patients participating in the Health and Retirement Study.
Synopsis: Patients (n=1194) were followed for a minimum of one year between 1998 and 2006. The outcomes were measured by multiple personal interviews before and after a severe sepsis episode. Cognitive impairment was measured using three validated questionnaires dependent upon age or if a proxy was the respondent. For functional limitations, a questionnaire concerning instrumental and basic activities of daily living was used.
Cognitive impairment for those with moderate to severe impairment increased to 16.7% from 6.1% after a sepsis episode with an odds ratio of 3.34 (95% confidence interval 1.53-7.25). There was no significant increase in nonsevere sepsis hospitalized comparison patients (n=5574). All survivors with severe sepsis had a functional decline of 1.5 activities. The comparison group had about a 0.4 activity decline. All of these deficits endured throughout the study.
The authors provide comments that there should be a system-based approach in preventing severe sepsis, its burdens, and its costs. Suggestions include preventing delirium, initiating better standards of care, and involving therapists earlier to prevent immobility.
Bottom line: Severe sepsis is independently associated with enduring cognitive and physical functional declines, which strain families and our healthcare system.
Citation: Iwashyna TJ, Ely EW, Smith DM, Langa KM. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 2010;304(16):1787-1794.
Furosemide on Day of Elective Noncardiac Surgery Does Not Increase Risk of Intraoperative Hypotension
Clinical question: For patients chronically treated with loop diuretics, does withholding furosemide on the day of elective noncardiac surgery prevent intraoperative hypotension?
Background: Recent studies have questioned the safety of blood-pressure-lowering medications administered on the day of surgery. Beta-blockers have been associated with an increase in strokes and death perioperatively, and angiotensin receptor blockers (ARB) are frequently withheld on the day of surgery to avoid intraoperative hypotension. The effect of loop diuretics is uncertain.
Study design: Double-blind, randomized, placebo-controlled study.
Setting: Three North American university centers.
Synopsis: One hundred ninety-three patients were instructed to take furosemide or placebo on the day they underwent noncardiac surgery. The primary outcome measure was perioperative hypotension defined as a SBP <90 mmHg for more than five minutes, a 35% drop in the mean arterial blood pressure, or the need for a vasopressor agent. The number of cardiovascular complications (acute heart failure, acute coronary syndrome, arrhythmia, acute cerebrovascular event) and deaths also were analyzed.
Concerns have been raised that loop diuretics might predispose patients to a higher risk of intraoperative hypotension during noncardiac surgery. This trial showed no significant difference in the rates of intraoperative hypotension in patients who were administered furosemide versus those who were not. Although cardiovascular complications occurred more frequently in the furosemide group, the difference was not statistically significant.
Important limitations of the study were recognized. A larger population of patients could have revealed a statistically significant difference in cardiovascular outcomes in the furosemide group. Also, an anesthetic protocol was not utilized, which raises questions about the interaction of furosemide and effect on blood pressure with certain anesthetics.
Bottom line: Administering furosemide prior to surgery in chronic users does not appreciably increase the rate of intraoperative hypotension or cardiovascular events.
Citation: Khan NA, Campbell NR, Frost SD, et al. Risk of intraoperative hypotension with loop diuretics: a randomized controlled trial. Am J Med. 2010;123(11):1059e1-1059e8.
Pediatric HM Literature
Computerized Physician Order Entry Decreases Hospitalwide Mortality
Clinical question: What is the effect of computerized physician order entry (CPOE) on hospitalwide mortality?
Background: CPOE has been touted as a key method for improving the quality and safety of patient care. To date, however, studies have not demonstrated definitive benefits, with one study demonstrating an increase in mortality rates in a critical-care unit after CPOE implementation.
Study design: Retrospective cohort study.
Setting: Quaternary-care academic children’s hospital.
Synopsis: More than 97,000 nonobstetric patients admitted to Lucile Packard Children’s Hospital (LCPH) at Stanford University in Palo Alto, Calif., from January 2001 to April 2009 were included in the analysis. The patients were divided into pre- and postintervention groups. The intervention was defined as a “big bang” activation of CPOE on Nov. 4, 2007, affecting 90% of the inpatient beds at LCPH.
After the intervention, mean monthly unadjusted mortality rates decreased to 0.716 deaths from 1.008 per 100 discharges. After adjustment for severity of illness and a rapid-response team (which had previously been shown to decrease mortality rates), mortality rates postintervention continued to remain significantly lower.
This study revealed an impressive reduction in perhaps the ultimate outcome measure: hospitalwide mortality. The authors went to extensive lengths to adjust for potential confounding factors to include delayed implementation of CPOE in the ICUs. As with many complex process improvement efforts, the devil might be in the details of local context and culture. Thus, the software might have been less important than the manner in which the institution adapted to its functionality. Those seeking to replicate these results will need to be mindful of the requisite organizational changes in communication, order standardization, and data retrieval.
Bottom line: CPOE implementation has the potential to significantly reduce hospitalwide mortality rates.
Citation: Longhurst CA, Parast L, Sandborg CI, et al. Decrease in hospital-wide mortality rate after implementation of a commercially sold computerized physician order entry system. Pediatrics. 2010;126(1):e1-e8.
In the Literature: HM-Related Research You Need to Know
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effects of extended VTE prophylaxis in medical patients
- Outcomes with and without preprocedural statins
- Association of subclinical hypothyroidism and CHD
- BP treatment after intracerebral hemorrhage
- Outcomes of ICD therapy in the elderly
- Systems delays and outcomes of STEMI
- D-dimer to predict recurrent VTE
- Stocking height and risk of post-stroke DVT
Extending Anticoagulant Prophylaxis after Medical Hospitalization Decreases VTE, Increases Major Bleeding
Clinical question: For patients with acute medical illness, does extending low-molecular-weight heparin (LMWH) administration for up to 28 days after discharge reduce the incidence of venous thromboembolism (VTE)?
Background: DVT and pulmonary embolism (PE) are common hospital-acquired complications. LMWH has been shown to reduce VTE for medical and surgical patients, and extended-duration LMWH reduces VTE in high-risk surgical patients. Whether extending anticoagulant prophylaxis after discharge for acutely ill medical patients with reduced mobility improves outcomes is unknown.
Study design: Randomized, placebo-controlled trial.
Setting: Three hundred seventy hospitals in 20 countries.
Synopsis: Eligible patients were >40 years old, hospitalized with acute medical illness, and had reduced mobility for ≥3 days. Patients received enoxaparin 40 mg SC daily prophylaxis while hospitalized and were then randomized to an additional 28±4 days of enoxaparin or placebo. Patients received a screening ultrasound to assess for asymptomatic DVT. The primary outcome was a composite of asymptomatic proximal DVT, symptomatic DVT or PE, or fatal PE during the period of extended prophylaxis.
An interim analysis indicated that extended prophylaxis was ineffective; at that time, the protocol was amended to target patients with severe immobility or with moderate immobility plus an additional risk factor (e.g. cancer, prior VTE, or age >75).
The study found that extended prophylaxis decreased the composite VTE outcome (2.5% vs 4.0%, P<0.05) and symptomatic VTE (0.2% vs 1.0%, P<0.05). The incidence of major bleeding was increased in the extended prophylaxis group (0.8% vs 0.3%, P<0.05). There was no difference in mortality.
The unplanned, midstudy protocol amendment to target higher-risk patients is a concern, though the final analyses included patients pre- and post-amendment.
Bottom line: Extending LMWH beyond hospitalization for patients admitted with acute medical illness and decreased mobility decreases VTE, but increases major bleeding.
Citation: Hull RD, Schellong SM, Tapson VF, et al. Extended-duration venous thromboembolism prophylaxis in acutely ill medical patients with recently reduced mobility: a randomized trial. Ann Intern Med. 2010;153(1);8-18.
Preprocedural Statin Therapy Reduces Postprocedural Myocardial Infarction
Clinical question: Does statin therapy reduce periprocedural cardiovascular events?
Background: Myocardial infarction (MI) and death are inherent risks of invasive procedures. Reduction of these risks in certain patient populations has been shown with the use of a beta blockade. Statins have shown promise during acute coronary syndrome. Questions remain about the role of statin therapy before invasive procedures in reducing adverse cardiovascular events.
Study design: Meta-analysis of randomized controlled trials.
Setting: Twenty-one studies involving 4,805 patients, published from inception of MEDLINE, Cochrane, and Clinicaltrials to February 2010.
Synopsis: The use of statins one to seven days preprocedure significantly reduced post-procedural MI in percutaneous coronary interventions (PCI) (P<0.0001). Statins given approximately four weeks in advance of noncardiac surgical procedures also significantly reduced postprocedural MI (P=0.004). An absolute risk reduction of 5.8% for postprocedural MI was found after PCI and 4.1% in noncardiac surgical procedures.
Statins did not show a significant reduction in postprocedural MI (P=0.40) or all-cause mortality (P=0.15) in coronary artery bypass graft surgery (CABG). However, statins did reduce post-CABG atrial fibrillation (P<0.0001).
The 21 studies used a variety of drugs and doses. However, the PCI studies favored atorvastatin 40 mg; more than half the CABG studies used atorvastatin 20 mg; and 91% of the noncardiac surgical studies used fluvastatin 80 mg. Dedicated trials are needed to demonstrate optimal statin agent, dose, and timing of therapy.
Bottom line: Preprocedural statin therapy reduces postprocedural MI after both PCI and noncardiac procedures but not after CABG.
Citation: Winchester DE, Wen X, Xie L, Bavry AA. Evidence of pre-procedural statin therapy: a meta-analysis of randomized trials. J Am Coll Cardiol. 2010;56(19); 1099-1109.
Subclinical Hypothyroidism Increases the Risk of Coronary Heart Disease and Mortality
Clinical question: What are the risks of coronary heart disease (CHD) and mortality among adults with subclinical hypothyroidism?
Background: Subclinical hypo-thyroidism is defined as an elevated serum thyroid stimulating hormone (TSH) level with a normal T4 concentration. Controversy exists regarding the treatment of subclinical hypothyroidism. Because of the association with hyperlipidemia and atherosclerosis, treatment of subclinical hypothyroidism is thought to be beneficial. Previous data from large prospective cohort studies regarding this association are conflicting.
Study design: Study-level meta-analysis of prospective cohort studies.
Setting: Eleven prospective cohorts in the U.S., Europe, Australia, Brazil, and Japan from 1972 to 2007.
Synopsis: Among 55,287 adults, 3,450 (6.2%) had subclinical hypothyroidism and 51,837 were euthyroid. Using Cox proportional hazard models, the association of subclinical hypothyroidism with CHD and mortality were determined for each cohort.
The risk of CHD events and CHD mortality increased with higher TSH concentrations.
In age- and sex-adjusted analyses, the hazard ratio (HR) for CHD events were as follows: HR=1.0 (TSH=4.5-6.9 mIU/L); HR=1.17 (TSH=7-9.9 mIU/L), and HR=1.89 (TSH=10-19.9 mIU/L). Similarly, HRs for CHD mortality showed an increasing trend: 1.09, 1.42, and 1.58, respectively.
Although the association is clearly established here, randomized controlled trials are needed to address whether thyroxine replacement can prevent CHD and the TSH threshold that will provide the most clinical benefit.
Bottom line: Subclinical hypo-thyroidism is associated with an increased risk for CHD events and mortality, primarily in patients with TSH concentrations of 10 mIU/L or higher.
Citation: Rodondi N, den Elzen WP, Bauer DC, et al. Subclinical hypothyroidism and the risk of coronary heart disease and mortality. JAMA. 2010;304(12): 1365-1374.
Reduction in Hematoma Growth after Acute Intracerebral Hemorrhage Associated with Lower Blood Pressure
Clinical question: Does intensive systolic blood pressure (SBP) <140 mmHg within one hour reduce hematoma growth after acute intracerebral bleeding?
Background: Early elevation of blood pressure after an acute intracerebral bleed is strongly associated with hematoma growth and worse outcomes. The pilot phase of the Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial (INTERACT) showed that early intensive blood pressure lowering reduced hematoma growth within six hours after onset of intracerebral hemorrhage.
Study design: Randomized controlled trial in which patients received an early intensive blood-pressure-lowering treatment (goal SBP<140 mmHg within one hour) or the AHA recommended best practice guidelines (goal SBP <180 mmHg), which were published in 1999.
Setting: Network of hospitals in China, South Korea, and Australia.
Synopsis: From 2005 to 2007, the study examined 404 patients with computed-tomography (CT) evidence of intracerebral hemorrhage, elevated SBP (150 mmHg-220 mmHg), and ability to commence BP lowering treatment within six hours of onset. Hematoma volumes were measured in the intensive treatment and guideline groups based on CT scans done at baseline and after 24 hours.
No significant association was found between the baseline SBP and the absolute or proportional growth of the hematoma. However, in the intensively treated patients who achieved target SBP within the first 24 hours, a significant association was found with the absolute and proportional hematoma growth.
Maximum reduction of hematoma growth occurred in the group with a median SBP of 135 mmHg.
This single-observational study did not include patients with severe intracranial bleeding who died or required surgical evacuation within the first 24 hours.
Hematoma size reduction did not improve survival or outcomes.
Bottom line: Intensive SBP lowering from 140 mmHg to 130 mmHg within one hour reduces hematoma growth after an intracranial hemorrhage.
Citation: Arima H, Anderson CS, Wang JG, et al. Lower treatment blood pressure is associated with the greatest reduction in hematoma growth after acute intracerebral hemorrhage. Hypertension. 2010;56(5):852-858.
Implantable Cardioverter-Defibrillator (ICD) Therapy for Primary Prevention of Sudden Cardiac Death Might Not Provide Survival Benefit to Elderly
Clinical question: Does ICD therapy for primary prevention of sudden cardiac death in individuals with severe left ventricular dysfunction improve survival in elderly patients?
Background: Several clinical trials of select individuals with severe left ventricular dysfunction (EF <40%) have demonstrated that ICD therapy is associated with a reduction in overall mortality. Given the costs and risks associated with ICD placement, it is important to assess how this therapy affects survival in younger versus older individuals.
Study design: Meta-analysis of five randomized controlled trials.
Setting: Five trials (MADIT-II, DEFINITE, DINAMIT, SCDHeFT, and IRIS).
Synopsis: All included studies compared ICD therapy to standard medical care in the primary prevention of sudden cardiac death in individuals with severe left ventricular dysfunction. Elderly patients comprised 44% of the 5,783 patients included in the study; elderly patients were defined as >65 in three studies, and >60 in two studies. Pooled analysis of the three trials examining ICD use for primary prevention found a nonsignificant reduction in all-cause mortality compared with medical therapy in elderly patients (HR 0.81 [95% CI 0.62 to 1.05], P=0.11). The two remaining studies involving post-MI patients showed no statistically significant reduction in mortality in elderly patients.
In contrast, pooled data from younger patients in the five trials showed that prophylactic ICD therapy reduced all-cause mortality.
None of the selected trials demonstrated evidence of selection, performance, detection, or attrition bias. Only a small number of studies were included, and four potentially relevant trials were not included because mortality data by age group were not available.
Trials including cardiac resynchronization therapy (CRT) were excluded from this meta-analysis, and elderly patients meeting criteria for CRT comprise an important group that must be considered separately.
Bottom line: There is no definitive reduction in mortality with prophylactic ICD therapy in elderly patients with severe left ventricular dysfunction.
Citation: Santangeli P, Di Biase L, Dello Russo A, et al. Meta-analysis: age and effectiveness of prophylactic implantable cardioverter-defibrillators. Ann Intern Med. 2010;153(9):592-599.
System Delay Is Mortality Marker in STEMI Patients Treated with Primary PCI
Clinical question: What is the relationship between system delays to reperfusion therapy and mortality in patients with ST-segment-elevation myocardial infarction (STEMI)?
Background: In patients with STEMI, an early reperfusion strategy is often sought, and several studies have focused on the association between door-to-balloon delay and outcomes. Focusing more broadly on the time from first contact with the healthcare system to the initiation of reperfusion therapy (system delay) might be a more relevant approach.
Study design: Historical follow-up study.
Setting: Three high-volume PCI centers in Denmark.
Synopsis: Using population-based medical registries of 6,209 Danish patients treated for STEMI with percutaneous coronary intervention (PCI), the authors examined the association between delays in reperfusion therapy and mortality. System delay encompassed the entire time from first contact with the healthcare system to the initiation of reperfusion therapy.
Overall, shorter system delay was associated with significantly decreased mortality, as were the individual components of system delay (prehospital delay and door-to-balloon delay). The shortest delays (0-60 minutes) corresponded to a mortality rate of 15%, and the longest delays (181-360 minutes) corresponded to a mortality rate of 31%. Patients were followed for a median of 3.4 years.
This study is unique, as it is the first to look at the association between system delay and outcomes in patients with STEMI transported by EMS and treated with primary PCI. The study highlights the harmful impact of longer system delays on mortality. Limitations of this study include possible underestimation of system delay and challenges surrounding the right marker for reperfusion.
Bottom line: System delay might serve as a broad, comprehensive marker for predicting mortality in patients with STEMI treated with primary PCI.
Citation: Terkelsen CJ, Sorensen JT, Maeng M, et al. System delay and mortality among patients with STEMI treated with primary percutaneous coronary intervention. JAMA. 2010;304(7): 763-771.
D-Dimer Is Effective in Determining the Risk of VTE Recurrence after First Unprovoked Event
Clinical question: Does the timing, patient age, or cut point level affect the predictive value of a D-dimer in predicting VTE recurrence after a first unprovoked event?
Background: Anticoagulation duration after a first unprovoked VTE is at least three months, but it can be indefinite in patients with stable anticoagulation and low bleeding risk. Measuring a D-dimer level after discontinuation of anticoagulation is helpful in determining which patients might benefit from prolonged anticoagulation. However, several unanswered questions remain regarding D-dimer testing.
Study design: Patient-level meta-analysis.
Setting: Pooled patient-level data from seven prospective studies.
Synopsis: Patient-level data were obtained for all patients enrolled using post-treatment D-dimer measurement to predict recurrent VTE in patients with a first unprovoked VTE who had completed at least three months of anticoagulation therapy. The mean length of follow-up was 30 months. Patients with a positive D-dimer had recurrent VTE at a rate of 8.8 per 100 patient-years while those with a negative D-dimer had a rate of 3.7 per 100 patient-years.
Univariate analysis revealed an HR of 2.59 for patients with a positive versus a negative test result. The analysis also showed that the timing of the test, the age of the patient, and the actual cut points used for the various D-dimer tests did not affect the analysis significantly.
These studies’ strength is their large sample sizes and the use of prospective studies. The weaknesses include a mostly white patient population and incomplete data on all patients.
Bottom line: D-dimer testing is useful in predicting VTE recurrence after treatment for a first unprovoked event regardless of patient age, post-treatment timing, or the assay cut point used.
Citation: Douketis J, Tosetto A, Marcucci M, et al. Patient-level meta-analysis: effect of measurement timing, threshold, and patient age on ability of D-dimer testing to assess recurrence risk after unprovoked venous thromboembolism. Ann Intern Med. 2010;153(8): 523-531.
Thigh-High Stockings Are Better than Knee-High Stockings for Post-Stroke DVT Prophylaxis
Clinical question: Are thigh-high compression stockings better then knee-high stockings in immobilized acute-stroke patients?
Background: DVT is common in hospitalized stroke patients with immobility. Graduated compression stockings are often used for DVT prophylaxis, but the CLOTS-1 trial recently found that thigh-high stockings were ineffective after acute stroke. It is unclear if the more commonly used knee-high stockings are more effective than thigh-high stockings.
Study design: Parallel-group trial (the CLOTS-2 trial).
Setting: One hundred twelve hospitals in nine countries.
Synopsis: More than 3,100 patients with acute stroke and immobilization were recruited from January 2002 to May 2009. Patients were randomized to receive thigh-high or knee-high stockings. Patients also received usual care, including anticoagulants and a screening ultrasound for asymptomatic proximal DVT at seven to 10 days. Approximately 640 patients in each group also underwent ultrasound at 25-30 days.
Overall, 6.3% of patients in the thigh-high group had DVT, compared with 8.8% in the knee-high group (P=0.007). There were no significant differences in the secondary outcomes of pulmonary embolism or death. The thigh-high stockings had a higher number of adverse skin events. Enrollment was stopped early when the CLOTS-1 trial showed no difference in DVT rates between thigh-high stockings and no stockings.
Bottom line: Knee-high graduated compression stockings lead to worse outcomes than thigh-high stockings for DVT prophylaxis in immobilized acute-stroke patients.
Citation: CLOTS (Clots in Legs Or sTockings after Stroke) Trial Collaboration. Thigh-length versus below-knee stockings for deep venous thrombosis prophylaxis after stroke: a randomized trial. Ann Intern Med. 2010;153(9):553-562. TH
Pediatric HM Literature
Co-Infection with Pertussis in Infants Hospitalized for Bronchiolitis

Clinical question: How often are infants admitted with bronchiolitis co-infected with Bordatella pertussis?
Background: Infants admitted for bronchiolitis have previously been reported to have co-infection with B. pertussis. Given the nonspecific symptoms associated with early B. pertussis infection, as well as the epidemiology of ongoing outbreaks, it might be useful to better define the risk of co-infection in the seasonal surge of acute bronchiolitis.
Study design: Retrospective cohort study.
Setting: One university hospital in Finland.
Synopsis: A prior study had generated nasopharyngeal aspirate samples for viral antigen detection from 205 healthy, full-term infants younger than 6 months hospitalized for bronchiolitis from 2001 to 2004. Of these samples, 142 (69%) were of quality sufficient for B. pertussis PCR testing in 2009.
Twelve (8.5%) of the 142 infants admitted with bronchiolitis were found to have B. pertussis. Eleven of the 12 infants were co-infected with at least one other virus (RSV in eight of them). Infants who tested positive for pertussis were more often found to have coughing spells (41.7% vs. 14.6% in those who tested negative).
The reported rate of co-infection in this study is higher than other recent reports from the U.S., likely due to the fact that samples were collected during a time period when the incidence of pertussis was relatively high in Finland.
Nevertheless, given the magnitude of a recent pertussis outbreak in California, it might be useful to consider co-infection in young infants admitted for bronchiolitis in areas with a relatively higher incidence of pertussis.
Although the retrospective nature of this study and the lack of a reported definition of coughing spells make further conclusions difficult to draw, cough might deserve further scrutiny during bronchiolitis season.
Bottom line: Consider co-infection with pertussis in young infants admitted with bronchiolitis.
Citation: Nuolivirta K, Koponen P, He Q, et al. Bordatella pertussis infection is common in nonvaccinated infants admitted for bronchiolitis. Pediatr Infect Dis J. 2010;29(11):1013-1015.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effects of extended VTE prophylaxis in medical patients
- Outcomes with and without preprocedural statins
- Association of subclinical hypothyroidism and CHD
- BP treatment after intracerebral hemorrhage
- Outcomes of ICD therapy in the elderly
- Systems delays and outcomes of STEMI
- D-dimer to predict recurrent VTE
- Stocking height and risk of post-stroke DVT
Extending Anticoagulant Prophylaxis after Medical Hospitalization Decreases VTE, Increases Major Bleeding
Clinical question: For patients with acute medical illness, does extending low-molecular-weight heparin (LMWH) administration for up to 28 days after discharge reduce the incidence of venous thromboembolism (VTE)?
Background: DVT and pulmonary embolism (PE) are common hospital-acquired complications. LMWH has been shown to reduce VTE for medical and surgical patients, and extended-duration LMWH reduces VTE in high-risk surgical patients. Whether extending anticoagulant prophylaxis after discharge for acutely ill medical patients with reduced mobility improves outcomes is unknown.
Study design: Randomized, placebo-controlled trial.
Setting: Three hundred seventy hospitals in 20 countries.
Synopsis: Eligible patients were >40 years old, hospitalized with acute medical illness, and had reduced mobility for ≥3 days. Patients received enoxaparin 40 mg SC daily prophylaxis while hospitalized and were then randomized to an additional 28±4 days of enoxaparin or placebo. Patients received a screening ultrasound to assess for asymptomatic DVT. The primary outcome was a composite of asymptomatic proximal DVT, symptomatic DVT or PE, or fatal PE during the period of extended prophylaxis.
An interim analysis indicated that extended prophylaxis was ineffective; at that time, the protocol was amended to target patients with severe immobility or with moderate immobility plus an additional risk factor (e.g. cancer, prior VTE, or age >75).
The study found that extended prophylaxis decreased the composite VTE outcome (2.5% vs 4.0%, P<0.05) and symptomatic VTE (0.2% vs 1.0%, P<0.05). The incidence of major bleeding was increased in the extended prophylaxis group (0.8% vs 0.3%, P<0.05). There was no difference in mortality.
The unplanned, midstudy protocol amendment to target higher-risk patients is a concern, though the final analyses included patients pre- and post-amendment.
Bottom line: Extending LMWH beyond hospitalization for patients admitted with acute medical illness and decreased mobility decreases VTE, but increases major bleeding.
Citation: Hull RD, Schellong SM, Tapson VF, et al. Extended-duration venous thromboembolism prophylaxis in acutely ill medical patients with recently reduced mobility: a randomized trial. Ann Intern Med. 2010;153(1);8-18.
Preprocedural Statin Therapy Reduces Postprocedural Myocardial Infarction
Clinical question: Does statin therapy reduce periprocedural cardiovascular events?
Background: Myocardial infarction (MI) and death are inherent risks of invasive procedures. Reduction of these risks in certain patient populations has been shown with the use of a beta blockade. Statins have shown promise during acute coronary syndrome. Questions remain about the role of statin therapy before invasive procedures in reducing adverse cardiovascular events.
Study design: Meta-analysis of randomized controlled trials.
Setting: Twenty-one studies involving 4,805 patients, published from inception of MEDLINE, Cochrane, and Clinicaltrials to February 2010.
Synopsis: The use of statins one to seven days preprocedure significantly reduced post-procedural MI in percutaneous coronary interventions (PCI) (P<0.0001). Statins given approximately four weeks in advance of noncardiac surgical procedures also significantly reduced postprocedural MI (P=0.004). An absolute risk reduction of 5.8% for postprocedural MI was found after PCI and 4.1% in noncardiac surgical procedures.
Statins did not show a significant reduction in postprocedural MI (P=0.40) or all-cause mortality (P=0.15) in coronary artery bypass graft surgery (CABG). However, statins did reduce post-CABG atrial fibrillation (P<0.0001).
The 21 studies used a variety of drugs and doses. However, the PCI studies favored atorvastatin 40 mg; more than half the CABG studies used atorvastatin 20 mg; and 91% of the noncardiac surgical studies used fluvastatin 80 mg. Dedicated trials are needed to demonstrate optimal statin agent, dose, and timing of therapy.
Bottom line: Preprocedural statin therapy reduces postprocedural MI after both PCI and noncardiac procedures but not after CABG.
Citation: Winchester DE, Wen X, Xie L, Bavry AA. Evidence of pre-procedural statin therapy: a meta-analysis of randomized trials. J Am Coll Cardiol. 2010;56(19); 1099-1109.
Subclinical Hypothyroidism Increases the Risk of Coronary Heart Disease and Mortality
Clinical question: What are the risks of coronary heart disease (CHD) and mortality among adults with subclinical hypothyroidism?
Background: Subclinical hypo-thyroidism is defined as an elevated serum thyroid stimulating hormone (TSH) level with a normal T4 concentration. Controversy exists regarding the treatment of subclinical hypothyroidism. Because of the association with hyperlipidemia and atherosclerosis, treatment of subclinical hypothyroidism is thought to be beneficial. Previous data from large prospective cohort studies regarding this association are conflicting.
Study design: Study-level meta-analysis of prospective cohort studies.
Setting: Eleven prospective cohorts in the U.S., Europe, Australia, Brazil, and Japan from 1972 to 2007.
Synopsis: Among 55,287 adults, 3,450 (6.2%) had subclinical hypothyroidism and 51,837 were euthyroid. Using Cox proportional hazard models, the association of subclinical hypothyroidism with CHD and mortality were determined for each cohort.
The risk of CHD events and CHD mortality increased with higher TSH concentrations.
In age- and sex-adjusted analyses, the hazard ratio (HR) for CHD events were as follows: HR=1.0 (TSH=4.5-6.9 mIU/L); HR=1.17 (TSH=7-9.9 mIU/L), and HR=1.89 (TSH=10-19.9 mIU/L). Similarly, HRs for CHD mortality showed an increasing trend: 1.09, 1.42, and 1.58, respectively.
Although the association is clearly established here, randomized controlled trials are needed to address whether thyroxine replacement can prevent CHD and the TSH threshold that will provide the most clinical benefit.
Bottom line: Subclinical hypo-thyroidism is associated with an increased risk for CHD events and mortality, primarily in patients with TSH concentrations of 10 mIU/L or higher.
Citation: Rodondi N, den Elzen WP, Bauer DC, et al. Subclinical hypothyroidism and the risk of coronary heart disease and mortality. JAMA. 2010;304(12): 1365-1374.
Reduction in Hematoma Growth after Acute Intracerebral Hemorrhage Associated with Lower Blood Pressure
Clinical question: Does intensive systolic blood pressure (SBP) <140 mmHg within one hour reduce hematoma growth after acute intracerebral bleeding?
Background: Early elevation of blood pressure after an acute intracerebral bleed is strongly associated with hematoma growth and worse outcomes. The pilot phase of the Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial (INTERACT) showed that early intensive blood pressure lowering reduced hematoma growth within six hours after onset of intracerebral hemorrhage.
Study design: Randomized controlled trial in which patients received an early intensive blood-pressure-lowering treatment (goal SBP<140 mmHg within one hour) or the AHA recommended best practice guidelines (goal SBP <180 mmHg), which were published in 1999.
Setting: Network of hospitals in China, South Korea, and Australia.
Synopsis: From 2005 to 2007, the study examined 404 patients with computed-tomography (CT) evidence of intracerebral hemorrhage, elevated SBP (150 mmHg-220 mmHg), and ability to commence BP lowering treatment within six hours of onset. Hematoma volumes were measured in the intensive treatment and guideline groups based on CT scans done at baseline and after 24 hours.
No significant association was found between the baseline SBP and the absolute or proportional growth of the hematoma. However, in the intensively treated patients who achieved target SBP within the first 24 hours, a significant association was found with the absolute and proportional hematoma growth.
Maximum reduction of hematoma growth occurred in the group with a median SBP of 135 mmHg.
This single-observational study did not include patients with severe intracranial bleeding who died or required surgical evacuation within the first 24 hours.
Hematoma size reduction did not improve survival or outcomes.
Bottom line: Intensive SBP lowering from 140 mmHg to 130 mmHg within one hour reduces hematoma growth after an intracranial hemorrhage.
Citation: Arima H, Anderson CS, Wang JG, et al. Lower treatment blood pressure is associated with the greatest reduction in hematoma growth after acute intracerebral hemorrhage. Hypertension. 2010;56(5):852-858.
Implantable Cardioverter-Defibrillator (ICD) Therapy for Primary Prevention of Sudden Cardiac Death Might Not Provide Survival Benefit to Elderly
Clinical question: Does ICD therapy for primary prevention of sudden cardiac death in individuals with severe left ventricular dysfunction improve survival in elderly patients?
Background: Several clinical trials of select individuals with severe left ventricular dysfunction (EF <40%) have demonstrated that ICD therapy is associated with a reduction in overall mortality. Given the costs and risks associated with ICD placement, it is important to assess how this therapy affects survival in younger versus older individuals.
Study design: Meta-analysis of five randomized controlled trials.
Setting: Five trials (MADIT-II, DEFINITE, DINAMIT, SCDHeFT, and IRIS).
Synopsis: All included studies compared ICD therapy to standard medical care in the primary prevention of sudden cardiac death in individuals with severe left ventricular dysfunction. Elderly patients comprised 44% of the 5,783 patients included in the study; elderly patients were defined as >65 in three studies, and >60 in two studies. Pooled analysis of the three trials examining ICD use for primary prevention found a nonsignificant reduction in all-cause mortality compared with medical therapy in elderly patients (HR 0.81 [95% CI 0.62 to 1.05], P=0.11). The two remaining studies involving post-MI patients showed no statistically significant reduction in mortality in elderly patients.
In contrast, pooled data from younger patients in the five trials showed that prophylactic ICD therapy reduced all-cause mortality.
None of the selected trials demonstrated evidence of selection, performance, detection, or attrition bias. Only a small number of studies were included, and four potentially relevant trials were not included because mortality data by age group were not available.
Trials including cardiac resynchronization therapy (CRT) were excluded from this meta-analysis, and elderly patients meeting criteria for CRT comprise an important group that must be considered separately.
Bottom line: There is no definitive reduction in mortality with prophylactic ICD therapy in elderly patients with severe left ventricular dysfunction.
Citation: Santangeli P, Di Biase L, Dello Russo A, et al. Meta-analysis: age and effectiveness of prophylactic implantable cardioverter-defibrillators. Ann Intern Med. 2010;153(9):592-599.
System Delay Is Mortality Marker in STEMI Patients Treated with Primary PCI
Clinical question: What is the relationship between system delays to reperfusion therapy and mortality in patients with ST-segment-elevation myocardial infarction (STEMI)?
Background: In patients with STEMI, an early reperfusion strategy is often sought, and several studies have focused on the association between door-to-balloon delay and outcomes. Focusing more broadly on the time from first contact with the healthcare system to the initiation of reperfusion therapy (system delay) might be a more relevant approach.
Study design: Historical follow-up study.
Setting: Three high-volume PCI centers in Denmark.
Synopsis: Using population-based medical registries of 6,209 Danish patients treated for STEMI with percutaneous coronary intervention (PCI), the authors examined the association between delays in reperfusion therapy and mortality. System delay encompassed the entire time from first contact with the healthcare system to the initiation of reperfusion therapy.
Overall, shorter system delay was associated with significantly decreased mortality, as were the individual components of system delay (prehospital delay and door-to-balloon delay). The shortest delays (0-60 minutes) corresponded to a mortality rate of 15%, and the longest delays (181-360 minutes) corresponded to a mortality rate of 31%. Patients were followed for a median of 3.4 years.
This study is unique, as it is the first to look at the association between system delay and outcomes in patients with STEMI transported by EMS and treated with primary PCI. The study highlights the harmful impact of longer system delays on mortality. Limitations of this study include possible underestimation of system delay and challenges surrounding the right marker for reperfusion.
Bottom line: System delay might serve as a broad, comprehensive marker for predicting mortality in patients with STEMI treated with primary PCI.
Citation: Terkelsen CJ, Sorensen JT, Maeng M, et al. System delay and mortality among patients with STEMI treated with primary percutaneous coronary intervention. JAMA. 2010;304(7): 763-771.
D-Dimer Is Effective in Determining the Risk of VTE Recurrence after First Unprovoked Event
Clinical question: Does the timing, patient age, or cut point level affect the predictive value of a D-dimer in predicting VTE recurrence after a first unprovoked event?
Background: Anticoagulation duration after a first unprovoked VTE is at least three months, but it can be indefinite in patients with stable anticoagulation and low bleeding risk. Measuring a D-dimer level after discontinuation of anticoagulation is helpful in determining which patients might benefit from prolonged anticoagulation. However, several unanswered questions remain regarding D-dimer testing.
Study design: Patient-level meta-analysis.
Setting: Pooled patient-level data from seven prospective studies.
Synopsis: Patient-level data were obtained for all patients enrolled using post-treatment D-dimer measurement to predict recurrent VTE in patients with a first unprovoked VTE who had completed at least three months of anticoagulation therapy. The mean length of follow-up was 30 months. Patients with a positive D-dimer had recurrent VTE at a rate of 8.8 per 100 patient-years while those with a negative D-dimer had a rate of 3.7 per 100 patient-years.
Univariate analysis revealed an HR of 2.59 for patients with a positive versus a negative test result. The analysis also showed that the timing of the test, the age of the patient, and the actual cut points used for the various D-dimer tests did not affect the analysis significantly.
These studies’ strength is their large sample sizes and the use of prospective studies. The weaknesses include a mostly white patient population and incomplete data on all patients.
Bottom line: D-dimer testing is useful in predicting VTE recurrence after treatment for a first unprovoked event regardless of patient age, post-treatment timing, or the assay cut point used.
Citation: Douketis J, Tosetto A, Marcucci M, et al. Patient-level meta-analysis: effect of measurement timing, threshold, and patient age on ability of D-dimer testing to assess recurrence risk after unprovoked venous thromboembolism. Ann Intern Med. 2010;153(8): 523-531.
Thigh-High Stockings Are Better than Knee-High Stockings for Post-Stroke DVT Prophylaxis
Clinical question: Are thigh-high compression stockings better then knee-high stockings in immobilized acute-stroke patients?
Background: DVT is common in hospitalized stroke patients with immobility. Graduated compression stockings are often used for DVT prophylaxis, but the CLOTS-1 trial recently found that thigh-high stockings were ineffective after acute stroke. It is unclear if the more commonly used knee-high stockings are more effective than thigh-high stockings.
Study design: Parallel-group trial (the CLOTS-2 trial).
Setting: One hundred twelve hospitals in nine countries.
Synopsis: More than 3,100 patients with acute stroke and immobilization were recruited from January 2002 to May 2009. Patients were randomized to receive thigh-high or knee-high stockings. Patients also received usual care, including anticoagulants and a screening ultrasound for asymptomatic proximal DVT at seven to 10 days. Approximately 640 patients in each group also underwent ultrasound at 25-30 days.
Overall, 6.3% of patients in the thigh-high group had DVT, compared with 8.8% in the knee-high group (P=0.007). There were no significant differences in the secondary outcomes of pulmonary embolism or death. The thigh-high stockings had a higher number of adverse skin events. Enrollment was stopped early when the CLOTS-1 trial showed no difference in DVT rates between thigh-high stockings and no stockings.
Bottom line: Knee-high graduated compression stockings lead to worse outcomes than thigh-high stockings for DVT prophylaxis in immobilized acute-stroke patients.
Citation: CLOTS (Clots in Legs Or sTockings after Stroke) Trial Collaboration. Thigh-length versus below-knee stockings for deep venous thrombosis prophylaxis after stroke: a randomized trial. Ann Intern Med. 2010;153(9):553-562. TH
Pediatric HM Literature
Co-Infection with Pertussis in Infants Hospitalized for Bronchiolitis
Clinical question: How often are infants admitted with bronchiolitis co-infected with Bordatella pertussis?
Background: Infants admitted for bronchiolitis have previously been reported to have co-infection with B. pertussis. Given the nonspecific symptoms associated with early B. pertussis infection, as well as the epidemiology of ongoing outbreaks, it might be useful to better define the risk of co-infection in the seasonal surge of acute bronchiolitis.
Study design: Retrospective cohort study.
Setting: One university hospital in Finland.
Synopsis: A prior study had generated nasopharyngeal aspirate samples for viral antigen detection from 205 healthy, full-term infants younger than 6 months hospitalized for bronchiolitis from 2001 to 2004. Of these samples, 142 (69%) were of quality sufficient for B. pertussis PCR testing in 2009.
Twelve (8.5%) of the 142 infants admitted with bronchiolitis were found to have B. pertussis. Eleven of the 12 infants were co-infected with at least one other virus (RSV in eight of them). Infants who tested positive for pertussis were more often found to have coughing spells (41.7% vs. 14.6% in those who tested negative).
The reported rate of co-infection in this study is higher than other recent reports from the U.S., likely due to the fact that samples were collected during a time period when the incidence of pertussis was relatively high in Finland.
Nevertheless, given the magnitude of a recent pertussis outbreak in California, it might be useful to consider co-infection in young infants admitted for bronchiolitis in areas with a relatively higher incidence of pertussis.
Although the retrospective nature of this study and the lack of a reported definition of coughing spells make further conclusions difficult to draw, cough might deserve further scrutiny during bronchiolitis season.
Bottom line: Consider co-infection with pertussis in young infants admitted with bronchiolitis.
Citation: Nuolivirta K, Koponen P, He Q, et al. Bordatella pertussis infection is common in nonvaccinated infants admitted for bronchiolitis. Pediatr Infect Dis J. 2010;29(11):1013-1015.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effects of extended VTE prophylaxis in medical patients
- Outcomes with and without preprocedural statins
- Association of subclinical hypothyroidism and CHD
- BP treatment after intracerebral hemorrhage
- Outcomes of ICD therapy in the elderly
- Systems delays and outcomes of STEMI
- D-dimer to predict recurrent VTE
- Stocking height and risk of post-stroke DVT
Extending Anticoagulant Prophylaxis after Medical Hospitalization Decreases VTE, Increases Major Bleeding
Clinical question: For patients with acute medical illness, does extending low-molecular-weight heparin (LMWH) administration for up to 28 days after discharge reduce the incidence of venous thromboembolism (VTE)?
Background: DVT and pulmonary embolism (PE) are common hospital-acquired complications. LMWH has been shown to reduce VTE for medical and surgical patients, and extended-duration LMWH reduces VTE in high-risk surgical patients. Whether extending anticoagulant prophylaxis after discharge for acutely ill medical patients with reduced mobility improves outcomes is unknown.
Study design: Randomized, placebo-controlled trial.
Setting: Three hundred seventy hospitals in 20 countries.
Synopsis: Eligible patients were >40 years old, hospitalized with acute medical illness, and had reduced mobility for ≥3 days. Patients received enoxaparin 40 mg SC daily prophylaxis while hospitalized and were then randomized to an additional 28±4 days of enoxaparin or placebo. Patients received a screening ultrasound to assess for asymptomatic DVT. The primary outcome was a composite of asymptomatic proximal DVT, symptomatic DVT or PE, or fatal PE during the period of extended prophylaxis.
An interim analysis indicated that extended prophylaxis was ineffective; at that time, the protocol was amended to target patients with severe immobility or with moderate immobility plus an additional risk factor (e.g. cancer, prior VTE, or age >75).
The study found that extended prophylaxis decreased the composite VTE outcome (2.5% vs 4.0%, P<0.05) and symptomatic VTE (0.2% vs 1.0%, P<0.05). The incidence of major bleeding was increased in the extended prophylaxis group (0.8% vs 0.3%, P<0.05). There was no difference in mortality.
The unplanned, midstudy protocol amendment to target higher-risk patients is a concern, though the final analyses included patients pre- and post-amendment.
Bottom line: Extending LMWH beyond hospitalization for patients admitted with acute medical illness and decreased mobility decreases VTE, but increases major bleeding.
Citation: Hull RD, Schellong SM, Tapson VF, et al. Extended-duration venous thromboembolism prophylaxis in acutely ill medical patients with recently reduced mobility: a randomized trial. Ann Intern Med. 2010;153(1);8-18.
Preprocedural Statin Therapy Reduces Postprocedural Myocardial Infarction
Clinical question: Does statin therapy reduce periprocedural cardiovascular events?
Background: Myocardial infarction (MI) and death are inherent risks of invasive procedures. Reduction of these risks in certain patient populations has been shown with the use of a beta blockade. Statins have shown promise during acute coronary syndrome. Questions remain about the role of statin therapy before invasive procedures in reducing adverse cardiovascular events.
Study design: Meta-analysis of randomized controlled trials.
Setting: Twenty-one studies involving 4,805 patients, published from inception of MEDLINE, Cochrane, and Clinicaltrials to February 2010.
Synopsis: The use of statins one to seven days preprocedure significantly reduced post-procedural MI in percutaneous coronary interventions (PCI) (P<0.0001). Statins given approximately four weeks in advance of noncardiac surgical procedures also significantly reduced postprocedural MI (P=0.004). An absolute risk reduction of 5.8% for postprocedural MI was found after PCI and 4.1% in noncardiac surgical procedures.
Statins did not show a significant reduction in postprocedural MI (P=0.40) or all-cause mortality (P=0.15) in coronary artery bypass graft surgery (CABG). However, statins did reduce post-CABG atrial fibrillation (P<0.0001).
The 21 studies used a variety of drugs and doses. However, the PCI studies favored atorvastatin 40 mg; more than half the CABG studies used atorvastatin 20 mg; and 91% of the noncardiac surgical studies used fluvastatin 80 mg. Dedicated trials are needed to demonstrate optimal statin agent, dose, and timing of therapy.
Bottom line: Preprocedural statin therapy reduces postprocedural MI after both PCI and noncardiac procedures but not after CABG.
Citation: Winchester DE, Wen X, Xie L, Bavry AA. Evidence of pre-procedural statin therapy: a meta-analysis of randomized trials. J Am Coll Cardiol. 2010;56(19); 1099-1109.
Subclinical Hypothyroidism Increases the Risk of Coronary Heart Disease and Mortality
Clinical question: What are the risks of coronary heart disease (CHD) and mortality among adults with subclinical hypothyroidism?
Background: Subclinical hypo-thyroidism is defined as an elevated serum thyroid stimulating hormone (TSH) level with a normal T4 concentration. Controversy exists regarding the treatment of subclinical hypothyroidism. Because of the association with hyperlipidemia and atherosclerosis, treatment of subclinical hypothyroidism is thought to be beneficial. Previous data from large prospective cohort studies regarding this association are conflicting.
Study design: Study-level meta-analysis of prospective cohort studies.
Setting: Eleven prospective cohorts in the U.S., Europe, Australia, Brazil, and Japan from 1972 to 2007.
Synopsis: Among 55,287 adults, 3,450 (6.2%) had subclinical hypothyroidism and 51,837 were euthyroid. Using Cox proportional hazard models, the association of subclinical hypothyroidism with CHD and mortality were determined for each cohort.
The risk of CHD events and CHD mortality increased with higher TSH concentrations.
In age- and sex-adjusted analyses, the hazard ratio (HR) for CHD events were as follows: HR=1.0 (TSH=4.5-6.9 mIU/L); HR=1.17 (TSH=7-9.9 mIU/L), and HR=1.89 (TSH=10-19.9 mIU/L). Similarly, HRs for CHD mortality showed an increasing trend: 1.09, 1.42, and 1.58, respectively.
Although the association is clearly established here, randomized controlled trials are needed to address whether thyroxine replacement can prevent CHD and the TSH threshold that will provide the most clinical benefit.
Bottom line: Subclinical hypo-thyroidism is associated with an increased risk for CHD events and mortality, primarily in patients with TSH concentrations of 10 mIU/L or higher.
Citation: Rodondi N, den Elzen WP, Bauer DC, et al. Subclinical hypothyroidism and the risk of coronary heart disease and mortality. JAMA. 2010;304(12): 1365-1374.
Reduction in Hematoma Growth after Acute Intracerebral Hemorrhage Associated with Lower Blood Pressure
Clinical question: Does intensive systolic blood pressure (SBP) <140 mmHg within one hour reduce hematoma growth after acute intracerebral bleeding?
Background: Early elevation of blood pressure after an acute intracerebral bleed is strongly associated with hematoma growth and worse outcomes. The pilot phase of the Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial (INTERACT) showed that early intensive blood pressure lowering reduced hematoma growth within six hours after onset of intracerebral hemorrhage.
Study design: Randomized controlled trial in which patients received an early intensive blood-pressure-lowering treatment (goal SBP<140 mmHg within one hour) or the AHA recommended best practice guidelines (goal SBP <180 mmHg), which were published in 1999.
Setting: Network of hospitals in China, South Korea, and Australia.
Synopsis: From 2005 to 2007, the study examined 404 patients with computed-tomography (CT) evidence of intracerebral hemorrhage, elevated SBP (150 mmHg-220 mmHg), and ability to commence BP lowering treatment within six hours of onset. Hematoma volumes were measured in the intensive treatment and guideline groups based on CT scans done at baseline and after 24 hours.
No significant association was found between the baseline SBP and the absolute or proportional growth of the hematoma. However, in the intensively treated patients who achieved target SBP within the first 24 hours, a significant association was found with the absolute and proportional hematoma growth.
Maximum reduction of hematoma growth occurred in the group with a median SBP of 135 mmHg.
This single-observational study did not include patients with severe intracranial bleeding who died or required surgical evacuation within the first 24 hours.
Hematoma size reduction did not improve survival or outcomes.
Bottom line: Intensive SBP lowering from 140 mmHg to 130 mmHg within one hour reduces hematoma growth after an intracranial hemorrhage.
Citation: Arima H, Anderson CS, Wang JG, et al. Lower treatment blood pressure is associated with the greatest reduction in hematoma growth after acute intracerebral hemorrhage. Hypertension. 2010;56(5):852-858.
Implantable Cardioverter-Defibrillator (ICD) Therapy for Primary Prevention of Sudden Cardiac Death Might Not Provide Survival Benefit to Elderly
Clinical question: Does ICD therapy for primary prevention of sudden cardiac death in individuals with severe left ventricular dysfunction improve survival in elderly patients?
Background: Several clinical trials of select individuals with severe left ventricular dysfunction (EF <40%) have demonstrated that ICD therapy is associated with a reduction in overall mortality. Given the costs and risks associated with ICD placement, it is important to assess how this therapy affects survival in younger versus older individuals.
Study design: Meta-analysis of five randomized controlled trials.
Setting: Five trials (MADIT-II, DEFINITE, DINAMIT, SCDHeFT, and IRIS).
Synopsis: All included studies compared ICD therapy to standard medical care in the primary prevention of sudden cardiac death in individuals with severe left ventricular dysfunction. Elderly patients comprised 44% of the 5,783 patients included in the study; elderly patients were defined as >65 in three studies, and >60 in two studies. Pooled analysis of the three trials examining ICD use for primary prevention found a nonsignificant reduction in all-cause mortality compared with medical therapy in elderly patients (HR 0.81 [95% CI 0.62 to 1.05], P=0.11). The two remaining studies involving post-MI patients showed no statistically significant reduction in mortality in elderly patients.
In contrast, pooled data from younger patients in the five trials showed that prophylactic ICD therapy reduced all-cause mortality.
None of the selected trials demonstrated evidence of selection, performance, detection, or attrition bias. Only a small number of studies were included, and four potentially relevant trials were not included because mortality data by age group were not available.
Trials including cardiac resynchronization therapy (CRT) were excluded from this meta-analysis, and elderly patients meeting criteria for CRT comprise an important group that must be considered separately.
Bottom line: There is no definitive reduction in mortality with prophylactic ICD therapy in elderly patients with severe left ventricular dysfunction.
Citation: Santangeli P, Di Biase L, Dello Russo A, et al. Meta-analysis: age and effectiveness of prophylactic implantable cardioverter-defibrillators. Ann Intern Med. 2010;153(9):592-599.
System Delay Is Mortality Marker in STEMI Patients Treated with Primary PCI
Clinical question: What is the relationship between system delays to reperfusion therapy and mortality in patients with ST-segment-elevation myocardial infarction (STEMI)?
Background: In patients with STEMI, an early reperfusion strategy is often sought, and several studies have focused on the association between door-to-balloon delay and outcomes. Focusing more broadly on the time from first contact with the healthcare system to the initiation of reperfusion therapy (system delay) might be a more relevant approach.
Study design: Historical follow-up study.
Setting: Three high-volume PCI centers in Denmark.
Synopsis: Using population-based medical registries of 6,209 Danish patients treated for STEMI with percutaneous coronary intervention (PCI), the authors examined the association between delays in reperfusion therapy and mortality. System delay encompassed the entire time from first contact with the healthcare system to the initiation of reperfusion therapy.
Overall, shorter system delay was associated with significantly decreased mortality, as were the individual components of system delay (prehospital delay and door-to-balloon delay). The shortest delays (0-60 minutes) corresponded to a mortality rate of 15%, and the longest delays (181-360 minutes) corresponded to a mortality rate of 31%. Patients were followed for a median of 3.4 years.
This study is unique, as it is the first to look at the association between system delay and outcomes in patients with STEMI transported by EMS and treated with primary PCI. The study highlights the harmful impact of longer system delays on mortality. Limitations of this study include possible underestimation of system delay and challenges surrounding the right marker for reperfusion.
Bottom line: System delay might serve as a broad, comprehensive marker for predicting mortality in patients with STEMI treated with primary PCI.
Citation: Terkelsen CJ, Sorensen JT, Maeng M, et al. System delay and mortality among patients with STEMI treated with primary percutaneous coronary intervention. JAMA. 2010;304(7): 763-771.
D-Dimer Is Effective in Determining the Risk of VTE Recurrence after First Unprovoked Event
Clinical question: Does the timing, patient age, or cut point level affect the predictive value of a D-dimer in predicting VTE recurrence after a first unprovoked event?
Background: Anticoagulation duration after a first unprovoked VTE is at least three months, but it can be indefinite in patients with stable anticoagulation and low bleeding risk. Measuring a D-dimer level after discontinuation of anticoagulation is helpful in determining which patients might benefit from prolonged anticoagulation. However, several unanswered questions remain regarding D-dimer testing.
Study design: Patient-level meta-analysis.
Setting: Pooled patient-level data from seven prospective studies.
Synopsis: Patient-level data were obtained for all patients enrolled using post-treatment D-dimer measurement to predict recurrent VTE in patients with a first unprovoked VTE who had completed at least three months of anticoagulation therapy. The mean length of follow-up was 30 months. Patients with a positive D-dimer had recurrent VTE at a rate of 8.8 per 100 patient-years while those with a negative D-dimer had a rate of 3.7 per 100 patient-years.
Univariate analysis revealed an HR of 2.59 for patients with a positive versus a negative test result. The analysis also showed that the timing of the test, the age of the patient, and the actual cut points used for the various D-dimer tests did not affect the analysis significantly.
These studies’ strength is their large sample sizes and the use of prospective studies. The weaknesses include a mostly white patient population and incomplete data on all patients.
Bottom line: D-dimer testing is useful in predicting VTE recurrence after treatment for a first unprovoked event regardless of patient age, post-treatment timing, or the assay cut point used.
Citation: Douketis J, Tosetto A, Marcucci M, et al. Patient-level meta-analysis: effect of measurement timing, threshold, and patient age on ability of D-dimer testing to assess recurrence risk after unprovoked venous thromboembolism. Ann Intern Med. 2010;153(8): 523-531.
Thigh-High Stockings Are Better than Knee-High Stockings for Post-Stroke DVT Prophylaxis
Clinical question: Are thigh-high compression stockings better then knee-high stockings in immobilized acute-stroke patients?
Background: DVT is common in hospitalized stroke patients with immobility. Graduated compression stockings are often used for DVT prophylaxis, but the CLOTS-1 trial recently found that thigh-high stockings were ineffective after acute stroke. It is unclear if the more commonly used knee-high stockings are more effective than thigh-high stockings.
Study design: Parallel-group trial (the CLOTS-2 trial).
Setting: One hundred twelve hospitals in nine countries.
Synopsis: More than 3,100 patients with acute stroke and immobilization were recruited from January 2002 to May 2009. Patients were randomized to receive thigh-high or knee-high stockings. Patients also received usual care, including anticoagulants and a screening ultrasound for asymptomatic proximal DVT at seven to 10 days. Approximately 640 patients in each group also underwent ultrasound at 25-30 days.
Overall, 6.3% of patients in the thigh-high group had DVT, compared with 8.8% in the knee-high group (P=0.007). There were no significant differences in the secondary outcomes of pulmonary embolism or death. The thigh-high stockings had a higher number of adverse skin events. Enrollment was stopped early when the CLOTS-1 trial showed no difference in DVT rates between thigh-high stockings and no stockings.
Bottom line: Knee-high graduated compression stockings lead to worse outcomes than thigh-high stockings for DVT prophylaxis in immobilized acute-stroke patients.
Citation: CLOTS (Clots in Legs Or sTockings after Stroke) Trial Collaboration. Thigh-length versus below-knee stockings for deep venous thrombosis prophylaxis after stroke: a randomized trial. Ann Intern Med. 2010;153(9):553-562. TH
Pediatric HM Literature
Co-Infection with Pertussis in Infants Hospitalized for Bronchiolitis
Clinical question: How often are infants admitted with bronchiolitis co-infected with Bordatella pertussis?
Background: Infants admitted for bronchiolitis have previously been reported to have co-infection with B. pertussis. Given the nonspecific symptoms associated with early B. pertussis infection, as well as the epidemiology of ongoing outbreaks, it might be useful to better define the risk of co-infection in the seasonal surge of acute bronchiolitis.
Study design: Retrospective cohort study.
Setting: One university hospital in Finland.
Synopsis: A prior study had generated nasopharyngeal aspirate samples for viral antigen detection from 205 healthy, full-term infants younger than 6 months hospitalized for bronchiolitis from 2001 to 2004. Of these samples, 142 (69%) were of quality sufficient for B. pertussis PCR testing in 2009.
Twelve (8.5%) of the 142 infants admitted with bronchiolitis were found to have B. pertussis. Eleven of the 12 infants were co-infected with at least one other virus (RSV in eight of them). Infants who tested positive for pertussis were more often found to have coughing spells (41.7% vs. 14.6% in those who tested negative).
The reported rate of co-infection in this study is higher than other recent reports from the U.S., likely due to the fact that samples were collected during a time period when the incidence of pertussis was relatively high in Finland.
Nevertheless, given the magnitude of a recent pertussis outbreak in California, it might be useful to consider co-infection in young infants admitted for bronchiolitis in areas with a relatively higher incidence of pertussis.
Although the retrospective nature of this study and the lack of a reported definition of coughing spells make further conclusions difficult to draw, cough might deserve further scrutiny during bronchiolitis season.
Bottom line: Consider co-infection with pertussis in young infants admitted with bronchiolitis.
Citation: Nuolivirta K, Koponen P, He Q, et al. Bordatella pertussis infection is common in nonvaccinated infants admitted for bronchiolitis. Pediatr Infect Dis J. 2010;29(11):1013-1015.
In the Literature: HM-Related Research You Need to Know
In This Edition
Literature at a Glance
A guide to this month’s studies
- Characteristics of CA-MRSA
- Association of gurgling with morbidity and mortality
- Antibiotics for active ulcerative colitis
- TIPS for cirrhosis-induced variceal bleeding
- Steroid dose, route in COPD exacerbations
- Effect of reminders and stop orders on urinary catheter use
- Outcomes of chest-compression-only CPR
- Albumin levels and risk of surgical-site infections
Characteristics of Community-Acquired methicillin-resistant Staphylococcus aureus Pneumonia in an Academic Medical Center
Clinical question: What are the clinical features and epidemiology of community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) pneumonia?
Background: CA-MRSA is an emerging cause of pneumonia. The genetic makeup of most CA-MRSA strains is different than that of nosocomial MRSA. Typically, CA-MRSA is resistant to methicillin, beta-lactams, and erythromycin, but it retains susceptibility to trimethoprim-sulfamethoxazole (TMP/sulfa) and clindamycin.
In addition, the most common strain of CA-MRSA carries the Panton-Valentine leukocidin (PVL) toxin, which is associated with necrotizing pneumonia and high mortality rates.
Study design: Retrospective case series.
Setting: A 1,100-bed teaching hospital in Chicago.
Synopsis: Of the 5,955 discharges with a diagnosis-related group (DRG) code of pneumonia, 15 met criteria for CA-MRSA, or <1% of all inpatient community-acquired pneumonia cases. All 15 CA-MRSA strains were positive for PVL.
Seven of the 15 patients never were admitted to the ICU, while seven patients required mechanical ventilation. Seven patients were immunocompromised; one patient presented with preceding influenza; seven patients presented with hemoptysis; and eight patients demonstrated findings of lung necrosis on CT scan. Two patients died; both were immunocompromised.
Although the initial antibiotic regimen varied considerably, 14 patients ultimately received either clindamycin or linezolid.
Bottom line: CA-MRSA pneumonia is an uncommon subset of community-acquired pneumonia admissions. Approximately half the patients admitted with CA-MRSA presented with features of severe pneumonia. Nearly all were treated with antibiotics that inhibit exotoxin production, and the associated mortality rate of 13% was lower than previously reported.
Citation: Lobo JL, Reed KD, Wunderink RG. Expanded clinical presentation of community-acquired methicillin-resistant Staphylococcus aureus pneumonia. Chest. 2010;138(1):130-136.
Gurgling Breath Sounds in Hospitalized Patients Might Predict Subsequent Pneumonia Development
Clinical question: Can gurgling sounds over the glottis during speech or quiet breathing predict hospital-acquired pneumonia (HAP)?
Background: HAP is a relatively frequent complication of hospitalization. HAP usually portends an increase in morbidity and mortality. Patients in the hospital might have disease states that inhibit the reflexes that normally eliminate secretions from above or below their glottis, increasing the risk of pneumonia.
Study design: Prospective cohort.
Setting: A 350-bed community teaching hospital in Bridgeport, Conn.
Synopsis: All patients admitted to a respiratory-care unit and general medical ward from December 2008 to April 2009 underwent auscultation over their glottis by study personnel. Patients with gurgles heard during speech or quiet breathing on auscultation and patients without gurgles were entered into the study in a 1:3 fashion, until 20 patients with gurgles and 60 patients without gurgles had been enrolled. Patients were followed for the development of clinical and radiographic evidence of HAP, ICU transfer, and in-hospital death.
Both dementia and treatment with opiates were independent predictors of gurgle in multivariate analysis. HAP occurred in 55% of the patients with gurgle versus 1.7% of patients without gurgle. In addition, 50% of the patients with gurgle required transfer to the ICU, compared with only 3.3% of patients without gurgle. In-hospital mortality was 30% among patients with gurgle versus 11.7% among patients without gurgle.
Bottom line: In patients admitted to the medical service of a community teaching hospital, gurgling sounds heard over the glottis during speech or quiet inspiration are independently associated with the development of HAP, ICU transfer, and in-hospital mortality.
Citation: Vazquez R, Gheorghe C, Ramos F, Dadu R, Amoateng-Adjepong Y, Manthous CA. Gurgling breath sounds may predict hospital-acquired pneumonia. Chest. 2010;138(2):284-288.
Treatment of Active Ulcerative Colitis with Triple Antibiotic Therapy Provides Better Response than Placebo
Clinical question: Does combination antibiotic therapy induce and/or maintain remission of active ulcerative colitis (UC)?
Background: Mouse models and other experimental evidence have suggested a pathogenic role for microbes in the development and/or exacerbation of ulcerative colitis, although antibiotic human trials have produced conflicting results. Recently, Fusobacterium varium was shown to be present in the gastrointestinal (GI) tract of most UC patients, and a pilot study using targeted antibacterials demonstrated efficacy in treating active UC.
Study design: Randomized, double-blind, placebo-controlled, multicenter trial.
Setting: Eleven hospitals in Japan.
Synopsis: Patients with mild to severe chronic relapsing UC were randomly assigned to either combination antibiotic therapy or placebo. All previous UC treatment regimens were continued in study patients, with the exception of steroids, which were tapered slowly if possible. Patients in the antibiotic group received a two-week combination therapy of amoxicillin, tetracycline, and metronidazole. Patients were followed weekly or monthly and underwent periodic exams and colonoscopies to assess clinical and endoscopic improvement for 12 months.
One hundred five patients were enrolled in each group. The clinical response rate at one year in patients treated with antibiotics was 44.8% versus 22.8% in the placebo group. Remission at one year was achieved in 26.7% of patients treated with antibiotics versus 14.9% of placebo patients. Endoscopic response rates and steroid discontinuation rates were higher in the antibiotic-treated groups. Effects were most pronounced in the group of patients with active disease.
Bottom line: Triple antibiotic therapy with amoxicillin, tetracycline, and metronidazole, when compared with placebo, was associated with improvement in clinical symptoms, endoscopic findings, remission rates, and steroid withdrawal in patients with active ulcerative colitis.
Citation: Ohkusa T, Kato K, Terao S, et al. Newly developed antibiotic combination therapy for ulcerative colitis: a double-blind placebo-controlled multicenter trial. Am J Gastroenterol. 2010;105(8):1820-1829.
Early TIPS Outperformed Optimal Medical Therapy in Patients with Advanced Cirrhosis and Variceal Bleeding
Clinical question: Does early treatment with a transjugular intrahepatic portosystemic shunt (TIPS) improve outcomes in patients with advanced cirrhosis and variceal bleeding?
Background: Current management guidelines for variceal bleeding include treatment with vasoactive drugs and serial endoscopy, yet treatment failure occurs in 10% to 15% of patients. TIPS is highly effective in controlling bleeding in such patients, but it historically has been reserved for patients who repeatedly fail preventive strategies.
Study design: Randomized controlled trial.
Setting: Nine European centers.
Synopsis: Sixty-three patients with advanced cirrhosis and acute esophageal variceal bleeding treated with optimal medical therapy were randomized within 24 hours of admission to either 1) early TIPS (polytetrafluoroethylene-covered stents) within 72 hours of randomization, or 2) ongoing optimal medical therapy with vasoactive drugs, treatment with a nonselective beta-blocker, and endoscopic band ligation.
During the median 16-month follow-up, rebleeding or failure to control bleeding occurred in 45% of patients in the optimal medical therapy group versus 3% of patients in the early TIPS group. One-year actuarial survival was 61% in the optimal medical therapy group versus 86% in the early-TIPS group. Remarkably, encephalopathy was less common in the early-TIPS group, and adverse events as a whole were similar in both groups.
Bottom line: Early use of TIPS was superior to optimal medical therapy for patients with advanced cirrhosis hospitalized for acute variceal bleeding at high risk for treatment failure.
Citation: García-Pagán JC, Caca K, Bureau C, et al. Early use of TIPS in patients with cirrhosis and variceal bleeding. N Engl J Med. 2010;362(25):2370-2379.
Low-Dose Oral Corticosteroids As Effective As High-Dose Intravenous Therapy in COPD Exacerbations
Clinical question: In patients hospitalized with acute exacerbation of chronic obstructive pulmonary disease (COPD), what are the outcomes of those initially treated with low doses of steroids administered orally compared with those initially treated with higher doses intravenously?
Background: COPD affects 6% of adults in the U.S., and acute exacerbation of COPD is one of the leading causes of hospitalization nationwide. Systemic corticosteroids are beneficial for patients hospitalized with acute exacerbation of COPD; however, optimal dose and route of administration are uncertain.
Study design: Retrospective cohort.
Setting: Four hundred fourteen U.S. acute-care hospitals; most were small to midsize nonteaching facilities serving urban patient populations.
Synopsis: Almost 80,000 patients admitted to a non-ICU setting with a diagnosis of acute exacerbation of COPD from 2006 to 2007, and who received systemic corticosteroids during the first two hospital days, were included in the study. In contrast to clinical guidelines recommending the use of low-dose oral corticosteroids, 92% of study participants were treated initially with intravenous steroids, whereas 8% received oral treatment. The primary composite outcome measure—need for mechanical ventilation after the second hospital day, inpatient mortality, or readmission for COPD within 30 days—was no worse in patients treated with oral steroids. Risk of treatment failure, length of stay, and cost were significantly lower among orally treated patients.
Bottom line: High-dose intravenous steroids appear to be no more effective than low-dose oral steroids for acute exacerbation of COPD. The authors recommend a randomized controlled trial be conducted to compare these two management strategies.
Citation: Lindenauer PK, Pekow PS, Lahti MC, Lee Y, Benjamin EM, Rothberg MB. Association of corticosteroid dose and route of administration with risk of treatment failure in acute exacerbation of chronic obstructive pulmonary disease. JAMA. 2010;303(23):2359-2367.
Reminders and Stop Orders Reduce Catheter-Associated Urinary Tract Infections
Clinical question: Do interventions that remind clinicians of the presence of urinary catheters and prompt timely removal decrease the rate of catheter-associated urinary tract infections (CA-UTI)?
Background: CA-UTI is a common yet preventable hospital-acquired infection. Many catheters are placed unnecessarily, remain in use without physician awareness, and are not removed promptly when no longer needed.
Study design: Systematic review and meta-analysis of 13 preintervention and postintervention quasi-experimental trials and one randomized controlled trial.
Setting: Studies conducted in the U.S., Canada, Europe, and Asia.
Synopsis: This literature search revealed 14 articles that used a reminder or stop-order intervention to prompt removal of urinary catheters and reported pre- and postintervention outcomes for CA-UTI rates, duration of urinary catheter use, and recatheterization need. Five studies used stop orders and nine studies used reminder interventions.
Use of a stop order or reminder reduced the rate of CA-UTI (episodes per 1,000 catheter days) by 52%. Mean duration of catheterization decreased by 37%, which resulted in 2.61 fewer days of catheterization per patient in the intervention versus control groups. Recatheterization rates were similar in the control and intervention groups.
Bottom line: Urinary catheter reminders and stop orders are low-cost strategies that appear to reduce the rate of CA-UTI.
Citation: Meddings J, Rogers MA, Macy M, Saint S. Systematic review and meta-analysis: reminder systems to reduce catheter-associated urinary tract infections and urinary catheter use in hospitalized patients. Clin Infect Dis. 2010;51(5):550-560.
Chest-Compression-Only Bystander CPR Increases Survival
Clinical question: Is bystander cardiopulmonary resuscitation (CPR) with chest compressions alone or chest compressions with rescue breathing superior in out-of-hospital adult cardiac arrest?
Background: Out-of-hospital cardiac arrest claims hundreds of thousands of lives each year. Early initiation of CPR by a layperson can increase a patient’s chances of surviving and having a favorable long-term neurologic recovery. Although traditional CPR consists of chest compression with rescue breathing, chest compression alone might be more acceptable to many laypersons and has the potential advantage of fewer compression interruptions.
Study design: Multicenter randomized trial.
Setting: Two EMSs in Washington state and one in London.
Synopsis: Patients were initially eligible for this study if a dispatcher determined that the patient was unconscious and not breathing, and that bystander CPR was not yet under way. If the caller was willing to undertake CPR with the dispatcher’s assistance, a randomization envelope containing CPR instructions was opened. Patients with arrest due to trauma, drowning, or asphyxiation were excluded, as were those under 18 years of age.
No significant difference was observed between the two groups in the percentage of patients who survived to hospital discharge or who survived with a favorable neurologic outcome. However, subgroup analyses showed a trend toward a higher percentage of patients surviving to hospital discharge with chest compressions alone, as compared with chest compressions with rescue breathing for patients with a cardiac cause of arrest and for those with shockable rhythms.
Bottom line: Dispatcher CPR instruction consisting of chest compression alone was noninferior to conventional CPR with rescue breathing, and it showed a trend toward better outcomes in cardiac cause of arrest.
Citation: Rea TD, Fahrenbruch C, Culley L, et al. CPR with chest compression alone or with rescue breathing. N Engl J Med. 2010;363(5):423-433.
Low Albumin Is Associated with Postoperative Wound Infections
Clinical question: What is the relationship between preoperative serum albumin levels and postoperative surgical-site infections (SSI)?
Background: Poor nutritional status is associated with adverse surgical outcomes. Serum albumin can both reflect nutritional status and function as a negative acute phase reactant, i.e., decreases in the setting of inflammation. It is uncertain whether low preoperative albumin levels are associated with postoperative SSI risk.
Study design: Retrospective cohort with multivariate analysis.
Setting: Four centers in Ireland.
Synopsis: Patients undergoing GI surgery (n=524) were prospectively followed as part of an SSI database. Demographic data, American Society of Anesthesia class, serum albumin levels, and presence and severity of SSI data were collected on all patients. Follow-up extended to 30 days.
SSI developed in 20% of patients. Patients who developed a SSI had lower serum albumin levels (mean 3.0 g/dL versus 3.6 g/dL). A serum albumin level less than 3.0 g/dL was associated with greater risk of SSI (relative risk 5.68), deeper SSI, and prolonged length of stay.
Bottom line: After controlling for other variables, serum albumin lower than 3.0 g/dL is independently associated with SSI frequency and severity.
Citation: Hennessey DB, Burke JP, Ni-Dhonochu T, Shields C, Winter DC, Mealy K. Preoperative hypoalbuminemia is an independent risk factor for the development of surgical site infection following gastrointestinal surgery: a multi-institutional study. Ann Surg. 2010;252 (2):325-329. TH
Pediatric HM Literature
Nebulized Hypertonic Saline Alone Safe to Study in Bronchiolitis

Clinical question: Is nebulized 3% saline solution safe to use alone in infants with bronchiolitis?
Background: Nebulized 3% (hypertonic) saline is increasingly used in the treatment of infants hospitalized with bronchiolitis. Studies to date have primarily investigated its efficacy in conjunction with bronchodilators due to a theoretical risk of bronchospasm. The safety profile of hypertonic saline alone in bronchiolitis is unknown.
Study design: Retrospective cohort study.
Setting: A single children’s hospital.
Synopsis: An existing QI database was reviewed during one winter season. One hundred fifty-four records were analyzed, comprising previously healthy infants with acute bronchiolitis. Hypertonic (3%) saline delivered more than four hours before and after albuterol was considered to have been given alone. Adverse events were not defined a priori, and documentation of symptoms related to medication administration was encouraged via a new comment section of a pathway scoring system.
Sixty-eight patients received 444 doses of hypertonic saline, 377 (85%) of which were administered alone. Four adverse events (1.0%) occurred in the group without adjunctive bronchodilator therapy; one adverse event (1.1%) occurred after concomitant delivery of albuterol and 3% saline. Rates of readmission and transfer to higher level of care were similar between those that did and did not receive hypertonic saline.
The potential for under-ascertainment of adverse events is significant with the retrospective design and frequency of underreporting in most hospitals. In addition, adverse events related to medication administration might be particularly difficult to assess in such dynamic diseases as bronchiolitis. Nevertheless, this study does suggest that adverse event rates are low with hypertonic saline alone, paving the way for future studies to assess its efficacy without bronchodilators clouding the picture.
Bottom line: Nebulized 3% saline has a low rate of adverse events in infants with acute bronchiolitis.
Citation: Ralston S, Hill V, Martinez M. Nebulized hypertonic saline without adjunctive bronchodilators for children with bronchiolitis. Pediatrics. 2010;126(3):e520-e525.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Characteristics of CA-MRSA
- Association of gurgling with morbidity and mortality
- Antibiotics for active ulcerative colitis
- TIPS for cirrhosis-induced variceal bleeding
- Steroid dose, route in COPD exacerbations
- Effect of reminders and stop orders on urinary catheter use
- Outcomes of chest-compression-only CPR
- Albumin levels and risk of surgical-site infections
Characteristics of Community-Acquired methicillin-resistant Staphylococcus aureus Pneumonia in an Academic Medical Center
Clinical question: What are the clinical features and epidemiology of community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) pneumonia?
Background: CA-MRSA is an emerging cause of pneumonia. The genetic makeup of most CA-MRSA strains is different than that of nosocomial MRSA. Typically, CA-MRSA is resistant to methicillin, beta-lactams, and erythromycin, but it retains susceptibility to trimethoprim-sulfamethoxazole (TMP/sulfa) and clindamycin.
In addition, the most common strain of CA-MRSA carries the Panton-Valentine leukocidin (PVL) toxin, which is associated with necrotizing pneumonia and high mortality rates.
Study design: Retrospective case series.
Setting: A 1,100-bed teaching hospital in Chicago.
Synopsis: Of the 5,955 discharges with a diagnosis-related group (DRG) code of pneumonia, 15 met criteria for CA-MRSA, or <1% of all inpatient community-acquired pneumonia cases. All 15 CA-MRSA strains were positive for PVL.
Seven of the 15 patients never were admitted to the ICU, while seven patients required mechanical ventilation. Seven patients were immunocompromised; one patient presented with preceding influenza; seven patients presented with hemoptysis; and eight patients demonstrated findings of lung necrosis on CT scan. Two patients died; both were immunocompromised.
Although the initial antibiotic regimen varied considerably, 14 patients ultimately received either clindamycin or linezolid.
Bottom line: CA-MRSA pneumonia is an uncommon subset of community-acquired pneumonia admissions. Approximately half the patients admitted with CA-MRSA presented with features of severe pneumonia. Nearly all were treated with antibiotics that inhibit exotoxin production, and the associated mortality rate of 13% was lower than previously reported.
Citation: Lobo JL, Reed KD, Wunderink RG. Expanded clinical presentation of community-acquired methicillin-resistant Staphylococcus aureus pneumonia. Chest. 2010;138(1):130-136.
Gurgling Breath Sounds in Hospitalized Patients Might Predict Subsequent Pneumonia Development
Clinical question: Can gurgling sounds over the glottis during speech or quiet breathing predict hospital-acquired pneumonia (HAP)?
Background: HAP is a relatively frequent complication of hospitalization. HAP usually portends an increase in morbidity and mortality. Patients in the hospital might have disease states that inhibit the reflexes that normally eliminate secretions from above or below their glottis, increasing the risk of pneumonia.
Study design: Prospective cohort.
Setting: A 350-bed community teaching hospital in Bridgeport, Conn.
Synopsis: All patients admitted to a respiratory-care unit and general medical ward from December 2008 to April 2009 underwent auscultation over their glottis by study personnel. Patients with gurgles heard during speech or quiet breathing on auscultation and patients without gurgles were entered into the study in a 1:3 fashion, until 20 patients with gurgles and 60 patients without gurgles had been enrolled. Patients were followed for the development of clinical and radiographic evidence of HAP, ICU transfer, and in-hospital death.
Both dementia and treatment with opiates were independent predictors of gurgle in multivariate analysis. HAP occurred in 55% of the patients with gurgle versus 1.7% of patients without gurgle. In addition, 50% of the patients with gurgle required transfer to the ICU, compared with only 3.3% of patients without gurgle. In-hospital mortality was 30% among patients with gurgle versus 11.7% among patients without gurgle.
Bottom line: In patients admitted to the medical service of a community teaching hospital, gurgling sounds heard over the glottis during speech or quiet inspiration are independently associated with the development of HAP, ICU transfer, and in-hospital mortality.
Citation: Vazquez R, Gheorghe C, Ramos F, Dadu R, Amoateng-Adjepong Y, Manthous CA. Gurgling breath sounds may predict hospital-acquired pneumonia. Chest. 2010;138(2):284-288.
Treatment of Active Ulcerative Colitis with Triple Antibiotic Therapy Provides Better Response than Placebo
Clinical question: Does combination antibiotic therapy induce and/or maintain remission of active ulcerative colitis (UC)?
Background: Mouse models and other experimental evidence have suggested a pathogenic role for microbes in the development and/or exacerbation of ulcerative colitis, although antibiotic human trials have produced conflicting results. Recently, Fusobacterium varium was shown to be present in the gastrointestinal (GI) tract of most UC patients, and a pilot study using targeted antibacterials demonstrated efficacy in treating active UC.
Study design: Randomized, double-blind, placebo-controlled, multicenter trial.
Setting: Eleven hospitals in Japan.
Synopsis: Patients with mild to severe chronic relapsing UC were randomly assigned to either combination antibiotic therapy or placebo. All previous UC treatment regimens were continued in study patients, with the exception of steroids, which were tapered slowly if possible. Patients in the antibiotic group received a two-week combination therapy of amoxicillin, tetracycline, and metronidazole. Patients were followed weekly or monthly and underwent periodic exams and colonoscopies to assess clinical and endoscopic improvement for 12 months.
One hundred five patients were enrolled in each group. The clinical response rate at one year in patients treated with antibiotics was 44.8% versus 22.8% in the placebo group. Remission at one year was achieved in 26.7% of patients treated with antibiotics versus 14.9% of placebo patients. Endoscopic response rates and steroid discontinuation rates were higher in the antibiotic-treated groups. Effects were most pronounced in the group of patients with active disease.
Bottom line: Triple antibiotic therapy with amoxicillin, tetracycline, and metronidazole, when compared with placebo, was associated with improvement in clinical symptoms, endoscopic findings, remission rates, and steroid withdrawal in patients with active ulcerative colitis.
Citation: Ohkusa T, Kato K, Terao S, et al. Newly developed antibiotic combination therapy for ulcerative colitis: a double-blind placebo-controlled multicenter trial. Am J Gastroenterol. 2010;105(8):1820-1829.
Early TIPS Outperformed Optimal Medical Therapy in Patients with Advanced Cirrhosis and Variceal Bleeding
Clinical question: Does early treatment with a transjugular intrahepatic portosystemic shunt (TIPS) improve outcomes in patients with advanced cirrhosis and variceal bleeding?
Background: Current management guidelines for variceal bleeding include treatment with vasoactive drugs and serial endoscopy, yet treatment failure occurs in 10% to 15% of patients. TIPS is highly effective in controlling bleeding in such patients, but it historically has been reserved for patients who repeatedly fail preventive strategies.
Study design: Randomized controlled trial.
Setting: Nine European centers.
Synopsis: Sixty-three patients with advanced cirrhosis and acute esophageal variceal bleeding treated with optimal medical therapy were randomized within 24 hours of admission to either 1) early TIPS (polytetrafluoroethylene-covered stents) within 72 hours of randomization, or 2) ongoing optimal medical therapy with vasoactive drugs, treatment with a nonselective beta-blocker, and endoscopic band ligation.
During the median 16-month follow-up, rebleeding or failure to control bleeding occurred in 45% of patients in the optimal medical therapy group versus 3% of patients in the early TIPS group. One-year actuarial survival was 61% in the optimal medical therapy group versus 86% in the early-TIPS group. Remarkably, encephalopathy was less common in the early-TIPS group, and adverse events as a whole were similar in both groups.
Bottom line: Early use of TIPS was superior to optimal medical therapy for patients with advanced cirrhosis hospitalized for acute variceal bleeding at high risk for treatment failure.
Citation: García-Pagán JC, Caca K, Bureau C, et al. Early use of TIPS in patients with cirrhosis and variceal bleeding. N Engl J Med. 2010;362(25):2370-2379.
Low-Dose Oral Corticosteroids As Effective As High-Dose Intravenous Therapy in COPD Exacerbations
Clinical question: In patients hospitalized with acute exacerbation of chronic obstructive pulmonary disease (COPD), what are the outcomes of those initially treated with low doses of steroids administered orally compared with those initially treated with higher doses intravenously?
Background: COPD affects 6% of adults in the U.S., and acute exacerbation of COPD is one of the leading causes of hospitalization nationwide. Systemic corticosteroids are beneficial for patients hospitalized with acute exacerbation of COPD; however, optimal dose and route of administration are uncertain.
Study design: Retrospective cohort.
Setting: Four hundred fourteen U.S. acute-care hospitals; most were small to midsize nonteaching facilities serving urban patient populations.
Synopsis: Almost 80,000 patients admitted to a non-ICU setting with a diagnosis of acute exacerbation of COPD from 2006 to 2007, and who received systemic corticosteroids during the first two hospital days, were included in the study. In contrast to clinical guidelines recommending the use of low-dose oral corticosteroids, 92% of study participants were treated initially with intravenous steroids, whereas 8% received oral treatment. The primary composite outcome measure—need for mechanical ventilation after the second hospital day, inpatient mortality, or readmission for COPD within 30 days—was no worse in patients treated with oral steroids. Risk of treatment failure, length of stay, and cost were significantly lower among orally treated patients.
Bottom line: High-dose intravenous steroids appear to be no more effective than low-dose oral steroids for acute exacerbation of COPD. The authors recommend a randomized controlled trial be conducted to compare these two management strategies.
Citation: Lindenauer PK, Pekow PS, Lahti MC, Lee Y, Benjamin EM, Rothberg MB. Association of corticosteroid dose and route of administration with risk of treatment failure in acute exacerbation of chronic obstructive pulmonary disease. JAMA. 2010;303(23):2359-2367.
Reminders and Stop Orders Reduce Catheter-Associated Urinary Tract Infections
Clinical question: Do interventions that remind clinicians of the presence of urinary catheters and prompt timely removal decrease the rate of catheter-associated urinary tract infections (CA-UTI)?
Background: CA-UTI is a common yet preventable hospital-acquired infection. Many catheters are placed unnecessarily, remain in use without physician awareness, and are not removed promptly when no longer needed.
Study design: Systematic review and meta-analysis of 13 preintervention and postintervention quasi-experimental trials and one randomized controlled trial.
Setting: Studies conducted in the U.S., Canada, Europe, and Asia.
Synopsis: This literature search revealed 14 articles that used a reminder or stop-order intervention to prompt removal of urinary catheters and reported pre- and postintervention outcomes for CA-UTI rates, duration of urinary catheter use, and recatheterization need. Five studies used stop orders and nine studies used reminder interventions.
Use of a stop order or reminder reduced the rate of CA-UTI (episodes per 1,000 catheter days) by 52%. Mean duration of catheterization decreased by 37%, which resulted in 2.61 fewer days of catheterization per patient in the intervention versus control groups. Recatheterization rates were similar in the control and intervention groups.
Bottom line: Urinary catheter reminders and stop orders are low-cost strategies that appear to reduce the rate of CA-UTI.
Citation: Meddings J, Rogers MA, Macy M, Saint S. Systematic review and meta-analysis: reminder systems to reduce catheter-associated urinary tract infections and urinary catheter use in hospitalized patients. Clin Infect Dis. 2010;51(5):550-560.
Chest-Compression-Only Bystander CPR Increases Survival
Clinical question: Is bystander cardiopulmonary resuscitation (CPR) with chest compressions alone or chest compressions with rescue breathing superior in out-of-hospital adult cardiac arrest?
Background: Out-of-hospital cardiac arrest claims hundreds of thousands of lives each year. Early initiation of CPR by a layperson can increase a patient’s chances of surviving and having a favorable long-term neurologic recovery. Although traditional CPR consists of chest compression with rescue breathing, chest compression alone might be more acceptable to many laypersons and has the potential advantage of fewer compression interruptions.
Study design: Multicenter randomized trial.
Setting: Two EMSs in Washington state and one in London.
Synopsis: Patients were initially eligible for this study if a dispatcher determined that the patient was unconscious and not breathing, and that bystander CPR was not yet under way. If the caller was willing to undertake CPR with the dispatcher’s assistance, a randomization envelope containing CPR instructions was opened. Patients with arrest due to trauma, drowning, or asphyxiation were excluded, as were those under 18 years of age.
No significant difference was observed between the two groups in the percentage of patients who survived to hospital discharge or who survived with a favorable neurologic outcome. However, subgroup analyses showed a trend toward a higher percentage of patients surviving to hospital discharge with chest compressions alone, as compared with chest compressions with rescue breathing for patients with a cardiac cause of arrest and for those with shockable rhythms.
Bottom line: Dispatcher CPR instruction consisting of chest compression alone was noninferior to conventional CPR with rescue breathing, and it showed a trend toward better outcomes in cardiac cause of arrest.
Citation: Rea TD, Fahrenbruch C, Culley L, et al. CPR with chest compression alone or with rescue breathing. N Engl J Med. 2010;363(5):423-433.
Low Albumin Is Associated with Postoperative Wound Infections
Clinical question: What is the relationship between preoperative serum albumin levels and postoperative surgical-site infections (SSI)?
Background: Poor nutritional status is associated with adverse surgical outcomes. Serum albumin can both reflect nutritional status and function as a negative acute phase reactant, i.e., decreases in the setting of inflammation. It is uncertain whether low preoperative albumin levels are associated with postoperative SSI risk.
Study design: Retrospective cohort with multivariate analysis.
Setting: Four centers in Ireland.
Synopsis: Patients undergoing GI surgery (n=524) were prospectively followed as part of an SSI database. Demographic data, American Society of Anesthesia class, serum albumin levels, and presence and severity of SSI data were collected on all patients. Follow-up extended to 30 days.
SSI developed in 20% of patients. Patients who developed a SSI had lower serum albumin levels (mean 3.0 g/dL versus 3.6 g/dL). A serum albumin level less than 3.0 g/dL was associated with greater risk of SSI (relative risk 5.68), deeper SSI, and prolonged length of stay.
Bottom line: After controlling for other variables, serum albumin lower than 3.0 g/dL is independently associated with SSI frequency and severity.
Citation: Hennessey DB, Burke JP, Ni-Dhonochu T, Shields C, Winter DC, Mealy K. Preoperative hypoalbuminemia is an independent risk factor for the development of surgical site infection following gastrointestinal surgery: a multi-institutional study. Ann Surg. 2010;252 (2):325-329. TH
Pediatric HM Literature
Nebulized Hypertonic Saline Alone Safe to Study in Bronchiolitis
Clinical question: Is nebulized 3% saline solution safe to use alone in infants with bronchiolitis?
Background: Nebulized 3% (hypertonic) saline is increasingly used in the treatment of infants hospitalized with bronchiolitis. Studies to date have primarily investigated its efficacy in conjunction with bronchodilators due to a theoretical risk of bronchospasm. The safety profile of hypertonic saline alone in bronchiolitis is unknown.
Study design: Retrospective cohort study.
Setting: A single children’s hospital.
Synopsis: An existing QI database was reviewed during one winter season. One hundred fifty-four records were analyzed, comprising previously healthy infants with acute bronchiolitis. Hypertonic (3%) saline delivered more than four hours before and after albuterol was considered to have been given alone. Adverse events were not defined a priori, and documentation of symptoms related to medication administration was encouraged via a new comment section of a pathway scoring system.
Sixty-eight patients received 444 doses of hypertonic saline, 377 (85%) of which were administered alone. Four adverse events (1.0%) occurred in the group without adjunctive bronchodilator therapy; one adverse event (1.1%) occurred after concomitant delivery of albuterol and 3% saline. Rates of readmission and transfer to higher level of care were similar between those that did and did not receive hypertonic saline.
The potential for under-ascertainment of adverse events is significant with the retrospective design and frequency of underreporting in most hospitals. In addition, adverse events related to medication administration might be particularly difficult to assess in such dynamic diseases as bronchiolitis. Nevertheless, this study does suggest that adverse event rates are low with hypertonic saline alone, paving the way for future studies to assess its efficacy without bronchodilators clouding the picture.
Bottom line: Nebulized 3% saline has a low rate of adverse events in infants with acute bronchiolitis.
Citation: Ralston S, Hill V, Martinez M. Nebulized hypertonic saline without adjunctive bronchodilators for children with bronchiolitis. Pediatrics. 2010;126(3):e520-e525.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Characteristics of CA-MRSA
- Association of gurgling with morbidity and mortality
- Antibiotics for active ulcerative colitis
- TIPS for cirrhosis-induced variceal bleeding
- Steroid dose, route in COPD exacerbations
- Effect of reminders and stop orders on urinary catheter use
- Outcomes of chest-compression-only CPR
- Albumin levels and risk of surgical-site infections
Characteristics of Community-Acquired methicillin-resistant Staphylococcus aureus Pneumonia in an Academic Medical Center
Clinical question: What are the clinical features and epidemiology of community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) pneumonia?
Background: CA-MRSA is an emerging cause of pneumonia. The genetic makeup of most CA-MRSA strains is different than that of nosocomial MRSA. Typically, CA-MRSA is resistant to methicillin, beta-lactams, and erythromycin, but it retains susceptibility to trimethoprim-sulfamethoxazole (TMP/sulfa) and clindamycin.
In addition, the most common strain of CA-MRSA carries the Panton-Valentine leukocidin (PVL) toxin, which is associated with necrotizing pneumonia and high mortality rates.
Study design: Retrospective case series.
Setting: A 1,100-bed teaching hospital in Chicago.
Synopsis: Of the 5,955 discharges with a diagnosis-related group (DRG) code of pneumonia, 15 met criteria for CA-MRSA, or <1% of all inpatient community-acquired pneumonia cases. All 15 CA-MRSA strains were positive for PVL.
Seven of the 15 patients never were admitted to the ICU, while seven patients required mechanical ventilation. Seven patients were immunocompromised; one patient presented with preceding influenza; seven patients presented with hemoptysis; and eight patients demonstrated findings of lung necrosis on CT scan. Two patients died; both were immunocompromised.
Although the initial antibiotic regimen varied considerably, 14 patients ultimately received either clindamycin or linezolid.
Bottom line: CA-MRSA pneumonia is an uncommon subset of community-acquired pneumonia admissions. Approximately half the patients admitted with CA-MRSA presented with features of severe pneumonia. Nearly all were treated with antibiotics that inhibit exotoxin production, and the associated mortality rate of 13% was lower than previously reported.
Citation: Lobo JL, Reed KD, Wunderink RG. Expanded clinical presentation of community-acquired methicillin-resistant Staphylococcus aureus pneumonia. Chest. 2010;138(1):130-136.
Gurgling Breath Sounds in Hospitalized Patients Might Predict Subsequent Pneumonia Development
Clinical question: Can gurgling sounds over the glottis during speech or quiet breathing predict hospital-acquired pneumonia (HAP)?
Background: HAP is a relatively frequent complication of hospitalization. HAP usually portends an increase in morbidity and mortality. Patients in the hospital might have disease states that inhibit the reflexes that normally eliminate secretions from above or below their glottis, increasing the risk of pneumonia.
Study design: Prospective cohort.
Setting: A 350-bed community teaching hospital in Bridgeport, Conn.
Synopsis: All patients admitted to a respiratory-care unit and general medical ward from December 2008 to April 2009 underwent auscultation over their glottis by study personnel. Patients with gurgles heard during speech or quiet breathing on auscultation and patients without gurgles were entered into the study in a 1:3 fashion, until 20 patients with gurgles and 60 patients without gurgles had been enrolled. Patients were followed for the development of clinical and radiographic evidence of HAP, ICU transfer, and in-hospital death.
Both dementia and treatment with opiates were independent predictors of gurgle in multivariate analysis. HAP occurred in 55% of the patients with gurgle versus 1.7% of patients without gurgle. In addition, 50% of the patients with gurgle required transfer to the ICU, compared with only 3.3% of patients without gurgle. In-hospital mortality was 30% among patients with gurgle versus 11.7% among patients without gurgle.
Bottom line: In patients admitted to the medical service of a community teaching hospital, gurgling sounds heard over the glottis during speech or quiet inspiration are independently associated with the development of HAP, ICU transfer, and in-hospital mortality.
Citation: Vazquez R, Gheorghe C, Ramos F, Dadu R, Amoateng-Adjepong Y, Manthous CA. Gurgling breath sounds may predict hospital-acquired pneumonia. Chest. 2010;138(2):284-288.
Treatment of Active Ulcerative Colitis with Triple Antibiotic Therapy Provides Better Response than Placebo
Clinical question: Does combination antibiotic therapy induce and/or maintain remission of active ulcerative colitis (UC)?
Background: Mouse models and other experimental evidence have suggested a pathogenic role for microbes in the development and/or exacerbation of ulcerative colitis, although antibiotic human trials have produced conflicting results. Recently, Fusobacterium varium was shown to be present in the gastrointestinal (GI) tract of most UC patients, and a pilot study using targeted antibacterials demonstrated efficacy in treating active UC.
Study design: Randomized, double-blind, placebo-controlled, multicenter trial.
Setting: Eleven hospitals in Japan.
Synopsis: Patients with mild to severe chronic relapsing UC were randomly assigned to either combination antibiotic therapy or placebo. All previous UC treatment regimens were continued in study patients, with the exception of steroids, which were tapered slowly if possible. Patients in the antibiotic group received a two-week combination therapy of amoxicillin, tetracycline, and metronidazole. Patients were followed weekly or monthly and underwent periodic exams and colonoscopies to assess clinical and endoscopic improvement for 12 months.
One hundred five patients were enrolled in each group. The clinical response rate at one year in patients treated with antibiotics was 44.8% versus 22.8% in the placebo group. Remission at one year was achieved in 26.7% of patients treated with antibiotics versus 14.9% of placebo patients. Endoscopic response rates and steroid discontinuation rates were higher in the antibiotic-treated groups. Effects were most pronounced in the group of patients with active disease.
Bottom line: Triple antibiotic therapy with amoxicillin, tetracycline, and metronidazole, when compared with placebo, was associated with improvement in clinical symptoms, endoscopic findings, remission rates, and steroid withdrawal in patients with active ulcerative colitis.
Citation: Ohkusa T, Kato K, Terao S, et al. Newly developed antibiotic combination therapy for ulcerative colitis: a double-blind placebo-controlled multicenter trial. Am J Gastroenterol. 2010;105(8):1820-1829.
Early TIPS Outperformed Optimal Medical Therapy in Patients with Advanced Cirrhosis and Variceal Bleeding
Clinical question: Does early treatment with a transjugular intrahepatic portosystemic shunt (TIPS) improve outcomes in patients with advanced cirrhosis and variceal bleeding?
Background: Current management guidelines for variceal bleeding include treatment with vasoactive drugs and serial endoscopy, yet treatment failure occurs in 10% to 15% of patients. TIPS is highly effective in controlling bleeding in such patients, but it historically has been reserved for patients who repeatedly fail preventive strategies.
Study design: Randomized controlled trial.
Setting: Nine European centers.
Synopsis: Sixty-three patients with advanced cirrhosis and acute esophageal variceal bleeding treated with optimal medical therapy were randomized within 24 hours of admission to either 1) early TIPS (polytetrafluoroethylene-covered stents) within 72 hours of randomization, or 2) ongoing optimal medical therapy with vasoactive drugs, treatment with a nonselective beta-blocker, and endoscopic band ligation.
During the median 16-month follow-up, rebleeding or failure to control bleeding occurred in 45% of patients in the optimal medical therapy group versus 3% of patients in the early TIPS group. One-year actuarial survival was 61% in the optimal medical therapy group versus 86% in the early-TIPS group. Remarkably, encephalopathy was less common in the early-TIPS group, and adverse events as a whole were similar in both groups.
Bottom line: Early use of TIPS was superior to optimal medical therapy for patients with advanced cirrhosis hospitalized for acute variceal bleeding at high risk for treatment failure.
Citation: García-Pagán JC, Caca K, Bureau C, et al. Early use of TIPS in patients with cirrhosis and variceal bleeding. N Engl J Med. 2010;362(25):2370-2379.
Low-Dose Oral Corticosteroids As Effective As High-Dose Intravenous Therapy in COPD Exacerbations
Clinical question: In patients hospitalized with acute exacerbation of chronic obstructive pulmonary disease (COPD), what are the outcomes of those initially treated with low doses of steroids administered orally compared with those initially treated with higher doses intravenously?
Background: COPD affects 6% of adults in the U.S., and acute exacerbation of COPD is one of the leading causes of hospitalization nationwide. Systemic corticosteroids are beneficial for patients hospitalized with acute exacerbation of COPD; however, optimal dose and route of administration are uncertain.
Study design: Retrospective cohort.
Setting: Four hundred fourteen U.S. acute-care hospitals; most were small to midsize nonteaching facilities serving urban patient populations.
Synopsis: Almost 80,000 patients admitted to a non-ICU setting with a diagnosis of acute exacerbation of COPD from 2006 to 2007, and who received systemic corticosteroids during the first two hospital days, were included in the study. In contrast to clinical guidelines recommending the use of low-dose oral corticosteroids, 92% of study participants were treated initially with intravenous steroids, whereas 8% received oral treatment. The primary composite outcome measure—need for mechanical ventilation after the second hospital day, inpatient mortality, or readmission for COPD within 30 days—was no worse in patients treated with oral steroids. Risk of treatment failure, length of stay, and cost were significantly lower among orally treated patients.
Bottom line: High-dose intravenous steroids appear to be no more effective than low-dose oral steroids for acute exacerbation of COPD. The authors recommend a randomized controlled trial be conducted to compare these two management strategies.
Citation: Lindenauer PK, Pekow PS, Lahti MC, Lee Y, Benjamin EM, Rothberg MB. Association of corticosteroid dose and route of administration with risk of treatment failure in acute exacerbation of chronic obstructive pulmonary disease. JAMA. 2010;303(23):2359-2367.
Reminders and Stop Orders Reduce Catheter-Associated Urinary Tract Infections
Clinical question: Do interventions that remind clinicians of the presence of urinary catheters and prompt timely removal decrease the rate of catheter-associated urinary tract infections (CA-UTI)?
Background: CA-UTI is a common yet preventable hospital-acquired infection. Many catheters are placed unnecessarily, remain in use without physician awareness, and are not removed promptly when no longer needed.
Study design: Systematic review and meta-analysis of 13 preintervention and postintervention quasi-experimental trials and one randomized controlled trial.
Setting: Studies conducted in the U.S., Canada, Europe, and Asia.
Synopsis: This literature search revealed 14 articles that used a reminder or stop-order intervention to prompt removal of urinary catheters and reported pre- and postintervention outcomes for CA-UTI rates, duration of urinary catheter use, and recatheterization need. Five studies used stop orders and nine studies used reminder interventions.
Use of a stop order or reminder reduced the rate of CA-UTI (episodes per 1,000 catheter days) by 52%. Mean duration of catheterization decreased by 37%, which resulted in 2.61 fewer days of catheterization per patient in the intervention versus control groups. Recatheterization rates were similar in the control and intervention groups.
Bottom line: Urinary catheter reminders and stop orders are low-cost strategies that appear to reduce the rate of CA-UTI.
Citation: Meddings J, Rogers MA, Macy M, Saint S. Systematic review and meta-analysis: reminder systems to reduce catheter-associated urinary tract infections and urinary catheter use in hospitalized patients. Clin Infect Dis. 2010;51(5):550-560.
Chest-Compression-Only Bystander CPR Increases Survival
Clinical question: Is bystander cardiopulmonary resuscitation (CPR) with chest compressions alone or chest compressions with rescue breathing superior in out-of-hospital adult cardiac arrest?
Background: Out-of-hospital cardiac arrest claims hundreds of thousands of lives each year. Early initiation of CPR by a layperson can increase a patient’s chances of surviving and having a favorable long-term neurologic recovery. Although traditional CPR consists of chest compression with rescue breathing, chest compression alone might be more acceptable to many laypersons and has the potential advantage of fewer compression interruptions.
Study design: Multicenter randomized trial.
Setting: Two EMSs in Washington state and one in London.
Synopsis: Patients were initially eligible for this study if a dispatcher determined that the patient was unconscious and not breathing, and that bystander CPR was not yet under way. If the caller was willing to undertake CPR with the dispatcher’s assistance, a randomization envelope containing CPR instructions was opened. Patients with arrest due to trauma, drowning, or asphyxiation were excluded, as were those under 18 years of age.
No significant difference was observed between the two groups in the percentage of patients who survived to hospital discharge or who survived with a favorable neurologic outcome. However, subgroup analyses showed a trend toward a higher percentage of patients surviving to hospital discharge with chest compressions alone, as compared with chest compressions with rescue breathing for patients with a cardiac cause of arrest and for those with shockable rhythms.
Bottom line: Dispatcher CPR instruction consisting of chest compression alone was noninferior to conventional CPR with rescue breathing, and it showed a trend toward better outcomes in cardiac cause of arrest.
Citation: Rea TD, Fahrenbruch C, Culley L, et al. CPR with chest compression alone or with rescue breathing. N Engl J Med. 2010;363(5):423-433.
Low Albumin Is Associated with Postoperative Wound Infections
Clinical question: What is the relationship between preoperative serum albumin levels and postoperative surgical-site infections (SSI)?
Background: Poor nutritional status is associated with adverse surgical outcomes. Serum albumin can both reflect nutritional status and function as a negative acute phase reactant, i.e., decreases in the setting of inflammation. It is uncertain whether low preoperative albumin levels are associated with postoperative SSI risk.
Study design: Retrospective cohort with multivariate analysis.
Setting: Four centers in Ireland.
Synopsis: Patients undergoing GI surgery (n=524) were prospectively followed as part of an SSI database. Demographic data, American Society of Anesthesia class, serum albumin levels, and presence and severity of SSI data were collected on all patients. Follow-up extended to 30 days.
SSI developed in 20% of patients. Patients who developed a SSI had lower serum albumin levels (mean 3.0 g/dL versus 3.6 g/dL). A serum albumin level less than 3.0 g/dL was associated with greater risk of SSI (relative risk 5.68), deeper SSI, and prolonged length of stay.
Bottom line: After controlling for other variables, serum albumin lower than 3.0 g/dL is independently associated with SSI frequency and severity.
Citation: Hennessey DB, Burke JP, Ni-Dhonochu T, Shields C, Winter DC, Mealy K. Preoperative hypoalbuminemia is an independent risk factor for the development of surgical site infection following gastrointestinal surgery: a multi-institutional study. Ann Surg. 2010;252 (2):325-329. TH
Pediatric HM Literature
Nebulized Hypertonic Saline Alone Safe to Study in Bronchiolitis
Clinical question: Is nebulized 3% saline solution safe to use alone in infants with bronchiolitis?
Background: Nebulized 3% (hypertonic) saline is increasingly used in the treatment of infants hospitalized with bronchiolitis. Studies to date have primarily investigated its efficacy in conjunction with bronchodilators due to a theoretical risk of bronchospasm. The safety profile of hypertonic saline alone in bronchiolitis is unknown.
Study design: Retrospective cohort study.
Setting: A single children’s hospital.
Synopsis: An existing QI database was reviewed during one winter season. One hundred fifty-four records were analyzed, comprising previously healthy infants with acute bronchiolitis. Hypertonic (3%) saline delivered more than four hours before and after albuterol was considered to have been given alone. Adverse events were not defined a priori, and documentation of symptoms related to medication administration was encouraged via a new comment section of a pathway scoring system.
Sixty-eight patients received 444 doses of hypertonic saline, 377 (85%) of which were administered alone. Four adverse events (1.0%) occurred in the group without adjunctive bronchodilator therapy; one adverse event (1.1%) occurred after concomitant delivery of albuterol and 3% saline. Rates of readmission and transfer to higher level of care were similar between those that did and did not receive hypertonic saline.
The potential for under-ascertainment of adverse events is significant with the retrospective design and frequency of underreporting in most hospitals. In addition, adverse events related to medication administration might be particularly difficult to assess in such dynamic diseases as bronchiolitis. Nevertheless, this study does suggest that adverse event rates are low with hypertonic saline alone, paving the way for future studies to assess its efficacy without bronchodilators clouding the picture.
Bottom line: Nebulized 3% saline has a low rate of adverse events in infants with acute bronchiolitis.
Citation: Ralston S, Hill V, Martinez M. Nebulized hypertonic saline without adjunctive bronchodilators for children with bronchiolitis. Pediatrics. 2010;126(3):e520-e525.
Pediatric HM Literature Review
Clinical question: What is the relationship between duration of intravenous (IV) antibiotic therapy and treatment failure in infants <6 months of age hospitalized with urinary tract infections (UTIs)?
Background: There is an inadequate evidence base to drive decisions regarding duration of IV antibiotic therapy in young infants hospitalized with UTIs. Documented variability exists in length of stay (LOS) and resource utilization for these infants, which might be a direct result of practice variation with respect to IV therapy.
Study design: Retrospective cohort study.
Setting: Twenty-four freestanding children’s hospitals.
Synopsis: The Pediatric Health Information System (PHIS) administrative database was used to identify healthy infants <6 months of age admitted with a primary or secondary diagnosis of UTI or pyelonephritis from 1999 to 2004 to participating hospitals. Duration of IV therapy was defined as a dichotomous variable with three days (short course: three days) selected because it was the median length of therapy. Treatment failure was defined as readmission within 30 days.
More than 12,300 records were analyzed. Male gender, neonatal status, black race, Hispanic ethnicity, nonprivate insurance, severity of illness, known bacteremia, known genitourinary tract disorders, and specific hospital were independently associated with increased likelihood of long-course (four days) therapy.
Unadjusted analysis initially revealed that long-course therapy was significantly associated with a higher rate of treatment failure. After multivariate (to include propensity scores) adjustment, a significant association between treatment duration and failure was no longer identified. Treatment failure association with known genitourinary abnormalities and higher severity of illness remained.
A significant limitation of this study is the potential for multivariate analysis to fail to mitigate a bias toward sicker patients receiving longer duration of antibiotic therapy and, thus, having a higher likelihood of treatment failure. In addition, the greater question of when IV antibiotics (and hospital admission) are indicated in this population was not addressed by the study design.
Nonetheless, the data likely support a limited utility to long-course IV antibiotic therapy in this population. The study also adds to the evolving picture of considerable and widespread variation in physician practice.
Bottom line: Short-course IV therapy for infants with UTIs does not increase risk of treatment failure.
Citation: Brady PW, Conway PH, Goudie A. Length of intravenous antibiotic therapy and treatment failure in infants with urinary tract infections. Pediatrics. 2010;126(2):196-203.
Reviewed by Pediatric Editor Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Clinical question: What is the relationship between duration of intravenous (IV) antibiotic therapy and treatment failure in infants <6 months of age hospitalized with urinary tract infections (UTIs)?
Background: There is an inadequate evidence base to drive decisions regarding duration of IV antibiotic therapy in young infants hospitalized with UTIs. Documented variability exists in length of stay (LOS) and resource utilization for these infants, which might be a direct result of practice variation with respect to IV therapy.
Study design: Retrospective cohort study.
Setting: Twenty-four freestanding children’s hospitals.
Synopsis: The Pediatric Health Information System (PHIS) administrative database was used to identify healthy infants <6 months of age admitted with a primary or secondary diagnosis of UTI or pyelonephritis from 1999 to 2004 to participating hospitals. Duration of IV therapy was defined as a dichotomous variable with three days (short course: three days) selected because it was the median length of therapy. Treatment failure was defined as readmission within 30 days.
More than 12,300 records were analyzed. Male gender, neonatal status, black race, Hispanic ethnicity, nonprivate insurance, severity of illness, known bacteremia, known genitourinary tract disorders, and specific hospital were independently associated with increased likelihood of long-course (four days) therapy.
Unadjusted analysis initially revealed that long-course therapy was significantly associated with a higher rate of treatment failure. After multivariate (to include propensity scores) adjustment, a significant association between treatment duration and failure was no longer identified. Treatment failure association with known genitourinary abnormalities and higher severity of illness remained.
A significant limitation of this study is the potential for multivariate analysis to fail to mitigate a bias toward sicker patients receiving longer duration of antibiotic therapy and, thus, having a higher likelihood of treatment failure. In addition, the greater question of when IV antibiotics (and hospital admission) are indicated in this population was not addressed by the study design.
Nonetheless, the data likely support a limited utility to long-course IV antibiotic therapy in this population. The study also adds to the evolving picture of considerable and widespread variation in physician practice.
Bottom line: Short-course IV therapy for infants with UTIs does not increase risk of treatment failure.
Citation: Brady PW, Conway PH, Goudie A. Length of intravenous antibiotic therapy and treatment failure in infants with urinary tract infections. Pediatrics. 2010;126(2):196-203.
Reviewed by Pediatric Editor Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Clinical question: What is the relationship between duration of intravenous (IV) antibiotic therapy and treatment failure in infants <6 months of age hospitalized with urinary tract infections (UTIs)?
Background: There is an inadequate evidence base to drive decisions regarding duration of IV antibiotic therapy in young infants hospitalized with UTIs. Documented variability exists in length of stay (LOS) and resource utilization for these infants, which might be a direct result of practice variation with respect to IV therapy.
Study design: Retrospective cohort study.
Setting: Twenty-four freestanding children’s hospitals.
Synopsis: The Pediatric Health Information System (PHIS) administrative database was used to identify healthy infants <6 months of age admitted with a primary or secondary diagnosis of UTI or pyelonephritis from 1999 to 2004 to participating hospitals. Duration of IV therapy was defined as a dichotomous variable with three days (short course: three days) selected because it was the median length of therapy. Treatment failure was defined as readmission within 30 days.
More than 12,300 records were analyzed. Male gender, neonatal status, black race, Hispanic ethnicity, nonprivate insurance, severity of illness, known bacteremia, known genitourinary tract disorders, and specific hospital were independently associated with increased likelihood of long-course (four days) therapy.
Unadjusted analysis initially revealed that long-course therapy was significantly associated with a higher rate of treatment failure. After multivariate (to include propensity scores) adjustment, a significant association between treatment duration and failure was no longer identified. Treatment failure association with known genitourinary abnormalities and higher severity of illness remained.
A significant limitation of this study is the potential for multivariate analysis to fail to mitigate a bias toward sicker patients receiving longer duration of antibiotic therapy and, thus, having a higher likelihood of treatment failure. In addition, the greater question of when IV antibiotics (and hospital admission) are indicated in this population was not addressed by the study design.
Nonetheless, the data likely support a limited utility to long-course IV antibiotic therapy in this population. The study also adds to the evolving picture of considerable and widespread variation in physician practice.
Bottom line: Short-course IV therapy for infants with UTIs does not increase risk of treatment failure.
Citation: Brady PW, Conway PH, Goudie A. Length of intravenous antibiotic therapy and treatment failure in infants with urinary tract infections. Pediatrics. 2010;126(2):196-203.
Reviewed by Pediatric Editor Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Should HM Redefine Its Role as Provider and Adjust Expectations for Inpatient Care?

Did you happen to read a recent New York Times article (www.nytimes.com/2010/05/27/us/27hosp.html) about hospitalists? I thought the article was great, but I was surprised by some of the negative reader feedback. What did you think?
George Eppley, MD
Reed, Ga.
Dr. Hospitalist responds: I read the NYT article by Jane Gross, “New Breed of Specialist Steps in for Family Doctor,” which was published May 26. The accompanying reader comment section is available at http://newoldage.blogs.nytimes.com/2010/05/26/in-hospitals-new-fingers -on-the-pulse/?ref=us.
The article provides the statistics that all of us in HM have come to know: HM is the fastest-growing medical specialty in the U.S. and, over the past decade, the number of hospitalists in the U.S. has grown from hundreds to 30,000. Gross talks about the care a hospitalist at the Hospital of the University of Pennsylvania provides for her patient. She highlights the challenges of transitions of care and references the work being done by hospitalists and SHM to make sure patients are making safe transitions. While the article was largely supportive of HM, she does provide a shade of balance when she mentions the risks to the patient when hospitalists fail to do their job when it comes to communication.
As a practicing hospitalist, I kind of wished I had stopped reading at the end of the article. I honestly did not like most of what I read in the reader comment section. Although the article was a feel-good story, I think it is fair to say the reader comments were largely negative. I understand that readers with negative experiences with hospitalists might be more likely to post a comment; nevertheless, some of the comments are hard to ignore—mainly because I suspect some of it is true.
One reader from Raleigh, N.C., wrote, “Hospitalists proved inept at contacting the patients’ existing doctors or even talking to the patients. Then, on discharge to nursing homes for further recovery, the ball was dropped further, with very poor communication of medication dosages, etc.” Yikes! What happened to the communication and the medication reconciliation process?
A reader from Massachusetts wrote about “the hospitalist … (who) ordered five blood draws in the space of several hours to replicate tests that had already been taken by the primary-care physician before admission.” So, not only are hospitalists poor communicators and do not do a good job with transitions of care, but their care is also driving up the cost of healthcare needlessly?
The most positive comments seem to come from outpatient providers and, quite honestly, I found them lukewarm at best. A PCP from Charleston, S.C., wrote, “I no longer have to cancel the appointments of the patients at the last minute in order to attend to an emergency occurring outside my office. It is a very efficient system.” Glad to hear the hospitalist relationship is working out for you, Dr. PCP, but as a patient in the hospital, I am worried more about the competency of this doctor, whom I have never met before this hospitalization, as opposed to how this doctor is going to make you more “efficient” in your office practice.
I came away with several thoughts after reading the article and the comments.
First, we need to set the right expectations. Is this the equivalent of the star athlete who makes a brash statement followed shortly thereafter by the statement, “I was misquoted”? Well … maybe. Are we who we say we are? The headline is “New Breed of Specialist Steps in for Family Doctor.”
As a practicing hospitalist, I never describe myself as replacing the family doctor, because this is the worst position I could put myself in. A patient might have a relationship with a family doctor for three or four decades. This family doctor might not only care for this patient, but also his children and grandchildren. The patient visits the family doctor at least once a year for a checkup. But when the patient is as sick as they have ever been in their life and needs their family doctor whom they trust, I am supposed to “step in” for this family doctor? Good luck trying to meet that standard. It’s like putting me next to Justin Timberlake on stage at a teenybopper concert. Who do you think is going to look better in that sort of comparison?
We, as hospitalists, should never allow anyone to think we are replacing their family doctor. We are here to work with the family doctor to provide the best care possible. Do surgeons, medical subspecialists, or ED doctors “replace” the family doctor? No way! They are working with the family doctor. Perhaps the problem here is that we have not set the appropriate expectations for our patients.
Next, we need to be clear in saying what we say we do or doing we what we say we do. A line in this article bothers me more than any of the reader comments: “The most compelling argument in favor of hospitalists, who are now in 5,000 institutions, from academic giants like the Hospital of the University of Pennsylvania to small community hospitals to innovators like the Mayo and Cleveland Clinics—is that they are there all the time.”
Why does it bother me so much? It is troubling because it is misleading and might simply be untrue. Many hospitalists are not there “all the time.” While many of our hospitalist programs have providers in the hospital 24 hours a day, many do not. I know a number of hospitalists who make rounds at multiple hospitals throughout the day. Are they really hospitalists or are they inpatient rounders?
Hospitalists are physicians defined by their location, not unlike ED physicians. Do we have ED doctors going from hospital to hospital, leaving nurses alone to care for patients when they are at another hospital? So what do we expect from our hospitalists? Should they be in the hospital 24/7? That would seem to be more consistent with the thought that “they are there all the time.” Remember, Gross did not say hospitalists are “reachable” all the time. She did say hospitalists are “on top of everything that happens to a patient—from entry through treatment and discharge.” It is time that we, as hospitalists, uniformly meet those expectations. Patients all over the country are figuring out that not all hospitalists are doing what they are supposed to do when it comes to communications and establishing safe transitions of care. Remember the adage: It does not take many rotten apples to spoil the barrel.
Last, let us talk more about how hospitalists can provide patient-centric care, as opposed to cost savings and carrying out President Obama’s marching orders. The article describes how a study published in the Journal of the American Medical Association found that patients have a reduced length of stay in the hospital when cared for by hospitalists; how hospitalists are being viewed as leaders in healthcare reform; and how the hospitalist spends her nonclinical time “design(ing) computer programs to contain costs.” Do not get me wrong. I am supportive as anyone of the notion that hospitalists should provide cost-effective care. But the reality is that our patients’ No. 1 priority is to believe that their doctor is providing the best care possible. They do not want to feel someone is short-changing them.
Talk all you want to insurers and hospitals about cost savings, but when speaking with patients, I think it makes more sense to discuss the quality as opposed to cost of care. Ask your next patient whether they give a hoot what you do when you are not caring for them. TH
Did you happen to read a recent New York Times article (www.nytimes.com/2010/05/27/us/27hosp.html) about hospitalists? I thought the article was great, but I was surprised by some of the negative reader feedback. What did you think?
George Eppley, MD
Reed, Ga.
Dr. Hospitalist responds: I read the NYT article by Jane Gross, “New Breed of Specialist Steps in for Family Doctor,” which was published May 26. The accompanying reader comment section is available at http://newoldage.blogs.nytimes.com/2010/05/26/in-hospitals-new-fingers -on-the-pulse/?ref=us.
The article provides the statistics that all of us in HM have come to know: HM is the fastest-growing medical specialty in the U.S. and, over the past decade, the number of hospitalists in the U.S. has grown from hundreds to 30,000. Gross talks about the care a hospitalist at the Hospital of the University of Pennsylvania provides for her patient. She highlights the challenges of transitions of care and references the work being done by hospitalists and SHM to make sure patients are making safe transitions. While the article was largely supportive of HM, she does provide a shade of balance when she mentions the risks to the patient when hospitalists fail to do their job when it comes to communication.
As a practicing hospitalist, I kind of wished I had stopped reading at the end of the article. I honestly did not like most of what I read in the reader comment section. Although the article was a feel-good story, I think it is fair to say the reader comments were largely negative. I understand that readers with negative experiences with hospitalists might be more likely to post a comment; nevertheless, some of the comments are hard to ignore—mainly because I suspect some of it is true.
One reader from Raleigh, N.C., wrote, “Hospitalists proved inept at contacting the patients’ existing doctors or even talking to the patients. Then, on discharge to nursing homes for further recovery, the ball was dropped further, with very poor communication of medication dosages, etc.” Yikes! What happened to the communication and the medication reconciliation process?
A reader from Massachusetts wrote about “the hospitalist … (who) ordered five blood draws in the space of several hours to replicate tests that had already been taken by the primary-care physician before admission.” So, not only are hospitalists poor communicators and do not do a good job with transitions of care, but their care is also driving up the cost of healthcare needlessly?
The most positive comments seem to come from outpatient providers and, quite honestly, I found them lukewarm at best. A PCP from Charleston, S.C., wrote, “I no longer have to cancel the appointments of the patients at the last minute in order to attend to an emergency occurring outside my office. It is a very efficient system.” Glad to hear the hospitalist relationship is working out for you, Dr. PCP, but as a patient in the hospital, I am worried more about the competency of this doctor, whom I have never met before this hospitalization, as opposed to how this doctor is going to make you more “efficient” in your office practice.
I came away with several thoughts after reading the article and the comments.
First, we need to set the right expectations. Is this the equivalent of the star athlete who makes a brash statement followed shortly thereafter by the statement, “I was misquoted”? Well … maybe. Are we who we say we are? The headline is “New Breed of Specialist Steps in for Family Doctor.”
As a practicing hospitalist, I never describe myself as replacing the family doctor, because this is the worst position I could put myself in. A patient might have a relationship with a family doctor for three or four decades. This family doctor might not only care for this patient, but also his children and grandchildren. The patient visits the family doctor at least once a year for a checkup. But when the patient is as sick as they have ever been in their life and needs their family doctor whom they trust, I am supposed to “step in” for this family doctor? Good luck trying to meet that standard. It’s like putting me next to Justin Timberlake on stage at a teenybopper concert. Who do you think is going to look better in that sort of comparison?
We, as hospitalists, should never allow anyone to think we are replacing their family doctor. We are here to work with the family doctor to provide the best care possible. Do surgeons, medical subspecialists, or ED doctors “replace” the family doctor? No way! They are working with the family doctor. Perhaps the problem here is that we have not set the appropriate expectations for our patients.
Next, we need to be clear in saying what we say we do or doing we what we say we do. A line in this article bothers me more than any of the reader comments: “The most compelling argument in favor of hospitalists, who are now in 5,000 institutions, from academic giants like the Hospital of the University of Pennsylvania to small community hospitals to innovators like the Mayo and Cleveland Clinics—is that they are there all the time.”
Why does it bother me so much? It is troubling because it is misleading and might simply be untrue. Many hospitalists are not there “all the time.” While many of our hospitalist programs have providers in the hospital 24 hours a day, many do not. I know a number of hospitalists who make rounds at multiple hospitals throughout the day. Are they really hospitalists or are they inpatient rounders?
Hospitalists are physicians defined by their location, not unlike ED physicians. Do we have ED doctors going from hospital to hospital, leaving nurses alone to care for patients when they are at another hospital? So what do we expect from our hospitalists? Should they be in the hospital 24/7? That would seem to be more consistent with the thought that “they are there all the time.” Remember, Gross did not say hospitalists are “reachable” all the time. She did say hospitalists are “on top of everything that happens to a patient—from entry through treatment and discharge.” It is time that we, as hospitalists, uniformly meet those expectations. Patients all over the country are figuring out that not all hospitalists are doing what they are supposed to do when it comes to communications and establishing safe transitions of care. Remember the adage: It does not take many rotten apples to spoil the barrel.
Last, let us talk more about how hospitalists can provide patient-centric care, as opposed to cost savings and carrying out President Obama’s marching orders. The article describes how a study published in the Journal of the American Medical Association found that patients have a reduced length of stay in the hospital when cared for by hospitalists; how hospitalists are being viewed as leaders in healthcare reform; and how the hospitalist spends her nonclinical time “design(ing) computer programs to contain costs.” Do not get me wrong. I am supportive as anyone of the notion that hospitalists should provide cost-effective care. But the reality is that our patients’ No. 1 priority is to believe that their doctor is providing the best care possible. They do not want to feel someone is short-changing them.
Talk all you want to insurers and hospitals about cost savings, but when speaking with patients, I think it makes more sense to discuss the quality as opposed to cost of care. Ask your next patient whether they give a hoot what you do when you are not caring for them. TH
Did you happen to read a recent New York Times article (www.nytimes.com/2010/05/27/us/27hosp.html) about hospitalists? I thought the article was great, but I was surprised by some of the negative reader feedback. What did you think?
George Eppley, MD
Reed, Ga.
Dr. Hospitalist responds: I read the NYT article by Jane Gross, “New Breed of Specialist Steps in for Family Doctor,” which was published May 26. The accompanying reader comment section is available at http://newoldage.blogs.nytimes.com/2010/05/26/in-hospitals-new-fingers -on-the-pulse/?ref=us.
The article provides the statistics that all of us in HM have come to know: HM is the fastest-growing medical specialty in the U.S. and, over the past decade, the number of hospitalists in the U.S. has grown from hundreds to 30,000. Gross talks about the care a hospitalist at the Hospital of the University of Pennsylvania provides for her patient. She highlights the challenges of transitions of care and references the work being done by hospitalists and SHM to make sure patients are making safe transitions. While the article was largely supportive of HM, she does provide a shade of balance when she mentions the risks to the patient when hospitalists fail to do their job when it comes to communication.
As a practicing hospitalist, I kind of wished I had stopped reading at the end of the article. I honestly did not like most of what I read in the reader comment section. Although the article was a feel-good story, I think it is fair to say the reader comments were largely negative. I understand that readers with negative experiences with hospitalists might be more likely to post a comment; nevertheless, some of the comments are hard to ignore—mainly because I suspect some of it is true.
One reader from Raleigh, N.C., wrote, “Hospitalists proved inept at contacting the patients’ existing doctors or even talking to the patients. Then, on discharge to nursing homes for further recovery, the ball was dropped further, with very poor communication of medication dosages, etc.” Yikes! What happened to the communication and the medication reconciliation process?
A reader from Massachusetts wrote about “the hospitalist … (who) ordered five blood draws in the space of several hours to replicate tests that had already been taken by the primary-care physician before admission.” So, not only are hospitalists poor communicators and do not do a good job with transitions of care, but their care is also driving up the cost of healthcare needlessly?
The most positive comments seem to come from outpatient providers and, quite honestly, I found them lukewarm at best. A PCP from Charleston, S.C., wrote, “I no longer have to cancel the appointments of the patients at the last minute in order to attend to an emergency occurring outside my office. It is a very efficient system.” Glad to hear the hospitalist relationship is working out for you, Dr. PCP, but as a patient in the hospital, I am worried more about the competency of this doctor, whom I have never met before this hospitalization, as opposed to how this doctor is going to make you more “efficient” in your office practice.
I came away with several thoughts after reading the article and the comments.
First, we need to set the right expectations. Is this the equivalent of the star athlete who makes a brash statement followed shortly thereafter by the statement, “I was misquoted”? Well … maybe. Are we who we say we are? The headline is “New Breed of Specialist Steps in for Family Doctor.”
As a practicing hospitalist, I never describe myself as replacing the family doctor, because this is the worst position I could put myself in. A patient might have a relationship with a family doctor for three or four decades. This family doctor might not only care for this patient, but also his children and grandchildren. The patient visits the family doctor at least once a year for a checkup. But when the patient is as sick as they have ever been in their life and needs their family doctor whom they trust, I am supposed to “step in” for this family doctor? Good luck trying to meet that standard. It’s like putting me next to Justin Timberlake on stage at a teenybopper concert. Who do you think is going to look better in that sort of comparison?
We, as hospitalists, should never allow anyone to think we are replacing their family doctor. We are here to work with the family doctor to provide the best care possible. Do surgeons, medical subspecialists, or ED doctors “replace” the family doctor? No way! They are working with the family doctor. Perhaps the problem here is that we have not set the appropriate expectations for our patients.
Next, we need to be clear in saying what we say we do or doing we what we say we do. A line in this article bothers me more than any of the reader comments: “The most compelling argument in favor of hospitalists, who are now in 5,000 institutions, from academic giants like the Hospital of the University of Pennsylvania to small community hospitals to innovators like the Mayo and Cleveland Clinics—is that they are there all the time.”
Why does it bother me so much? It is troubling because it is misleading and might simply be untrue. Many hospitalists are not there “all the time.” While many of our hospitalist programs have providers in the hospital 24 hours a day, many do not. I know a number of hospitalists who make rounds at multiple hospitals throughout the day. Are they really hospitalists or are they inpatient rounders?
Hospitalists are physicians defined by their location, not unlike ED physicians. Do we have ED doctors going from hospital to hospital, leaving nurses alone to care for patients when they are at another hospital? So what do we expect from our hospitalists? Should they be in the hospital 24/7? That would seem to be more consistent with the thought that “they are there all the time.” Remember, Gross did not say hospitalists are “reachable” all the time. She did say hospitalists are “on top of everything that happens to a patient—from entry through treatment and discharge.” It is time that we, as hospitalists, uniformly meet those expectations. Patients all over the country are figuring out that not all hospitalists are doing what they are supposed to do when it comes to communications and establishing safe transitions of care. Remember the adage: It does not take many rotten apples to spoil the barrel.
Last, let us talk more about how hospitalists can provide patient-centric care, as opposed to cost savings and carrying out President Obama’s marching orders. The article describes how a study published in the Journal of the American Medical Association found that patients have a reduced length of stay in the hospital when cared for by hospitalists; how hospitalists are being viewed as leaders in healthcare reform; and how the hospitalist spends her nonclinical time “design(ing) computer programs to contain costs.” Do not get me wrong. I am supportive as anyone of the notion that hospitalists should provide cost-effective care. But the reality is that our patients’ No. 1 priority is to believe that their doctor is providing the best care possible. They do not want to feel someone is short-changing them.
Talk all you want to insurers and hospitals about cost savings, but when speaking with patients, I think it makes more sense to discuss the quality as opposed to cost of care. Ask your next patient whether they give a hoot what you do when you are not caring for them. TH
How should Parkinson’s disease be managed perioperatively?
Case
A 67-year-old female with moderately advanced Parkinson’s disease (PD) had a mechanical fall in her home, which resulted in a humeral fracture. The fall occurred in the morning before she was able to take her medications and was related to her difficulty in initiating movements.
On her current regimen, her PD symptoms are controlled. She is able to perform daily living activities independently and ambulates without assistance. She also performs more complex tasks (e.g., cooking and managing her finances). She has not exhibited any symptoms consistent with dementia. She occasionally experiences dyspnea on exertion and dysphagia, but she has not been evaluated for these complaints. She takes carbidopa/levodopa (CD/LD) 25 mg/100 mg four times a day, amantadine 100 mg twice daily, and ropinirole 3 mg three times a day.
She is scheduled for open reduction internal fixation of her fracture; the orthopedic surgeon has requested a perioperative risk assessment and recommendations concerning her medications. How should PD be managed perioperatively?
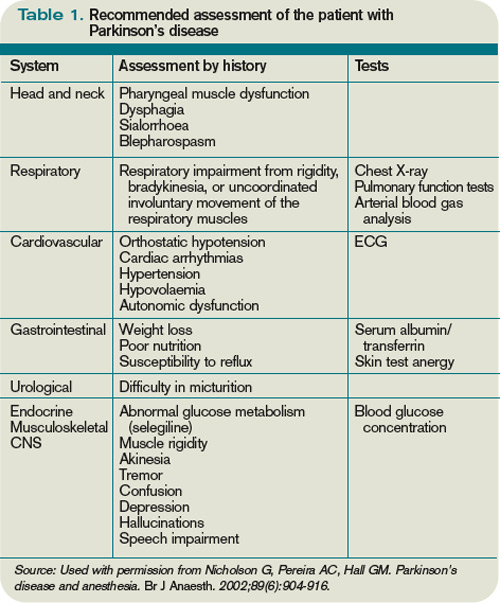
Overview
Advances in surgical and anesthetic techniques, in combination with an aging population, have contributed to an increasing number of geriatric patients undergoing surgery. As many as 50% of Americans older than 65 will undergo a surgical procedure; hospitalists will comanage many of these patients in the perioperative period.1
Although cardiopulmonary disorders receive a great deal of attention with regard to perioperative risk assessment, other comorbid conditions also contribute to perioperative risk—namely, disorders specific to the elderly population. Parkinson’s disease is one such condition that deserves attention.
PD is a progressive, neurodegenerative condition associated with loss of dopaminergic neurons and the presence of Lewy bodies within the substantia nigra and other areas of the brain and peripheral autonomic nervous system.2 Cardinal clinical features include rigidity, bradykinesia, and resting tremor. A supportive feature is a consistent response to levodopa. Postural instability, cognitive impairment, and autonomic dysfunction usually occur later in the disease.3,4
As the population ages, Parkinson’s disease is becoming more prevalent, affecting approximately 1% of individuals older than 60.5 These patients pose a specific challenge to the hospitalist, not only because the multiorgan system manifestations of PD can raise surgical risk, but also due to the direct effects of dopaminergic medications used to treat PD, lack of a parenteral route for these medications in NPO patients, and the risks associated with abrupt withdrawal of these medications.
Although surgical risk in PD patients has received intermittent attention in surgical, anesthesia, and neurology literature, there is no broad consensus statement or treatment guideline for the perioperative approach.
Literature Review
A retrospective cohort of 51 PD patients undergoing various types of surgery revealed that PD patients have a longer hospital stay than matched cohorts.6 Pepper et al studied a cohort of 234 PD patients in the Veterans Administration population who were undergoing a variety of surgeries.7 They found that patients with PD had a longer acute hospital stay and had higher in-hospital mortality.7 The multisystem manifestations of PD might account for this global increase in perioperative risk.
The following are reviews of organ-system manifestations of PD and their relevance to the perioperative period.
Motor: The motor symptoms of PD place patients at increased risk for falls and might impair their ability to participate in rehabilitation. Mueller et al demonstrated that there was a significantly increased risk of postoperative falls and a higher need for inpatient rehabilitation due to motor difficulties in the PD cohort.6
Pulmonary: PD patients have increased risk of abnormal pulmonary function secondary to rigidity and akinesia. Increased airway resistance and decreased lung elastic recoil lead to obstructive lung disease.8,9 Rigidity of voluntary chest wall and upper airway muscles leads to a restrictive lung disease pattern.8,10 Furthermore, respiratory dyskinesia is a common side effect of levodopa, which can result in restrictive and dyskinetic ventilation.11 As a consequence of disordered respiratory mechanics (especially in combination with disordered swallow mechanics), PD patients are at increased risk of lower respiratory infections. In fact, pneumonia remains the leading cause of mortality among PD patients.11
Not surprisingly, several cohorts have suggested that PD patients undergoing surgical procedures are at higher risk for atelectasis, pneumonia, and postoperative respiratory failure.7,12 Postoperative VTE rates are not statistically different between PD patients and matched cohorts.
Gastrointestinal: Abnor-malities in muscles of the mouth, pharynx, and esophagus account for the dysphagia commonly noted in PD.13 Barium swallow tests are abnormal in 80% or more of PD patients.14 Dysphagia can lead to aspiration, as well as inadequate oral intake, resulting in pneumonia and malnutrition, respectively.15 Dysfunction of the myenteric plexus (evidenced by Lewy Body deposition) accounts for gastrointestinal dysmotility manifested as gastroparesis, ileus, and slow colonic transit, which results in constipation.16
PD patients in the postoperative period are at risk for swallowing difficulties, which increases the risk of aspiration and might delay initiation of oral medications. Gastroparesis threatens appropriate delivery of oral medications for adequate absorption. In addition, postoperative ileus and constipation can pose challenges.
Cardiovascular: Such cardiac sympathetic abnormalities as orthostatic hypotension, postprandial or exercise-induced hypotension, impaired heart rate variability, and dysrhythmias are common in PD.17 Pepper et al found a trend toward increased risk of hypotension and acute myocardial infarction (MI) in PD patients undergoing surgery.7
Genitourinary: Urinary complaints (e.g., nocturia, frequency, urgency, and urge incontinence) are common in PD patients.18 These clinical complaints correspond to involuntary detrusor contractions (detrusor hyperreflexia).19 Pepper et al found an increased risk of postoperative urinary tract infection in PD patients.7

Cognitive: A recognized feature of advanced PD is cognitive impairment. Studies estimate the prevalence of dementia in cohorts of PD patients is from 28% to 44%. PD with dementia has been associated with shortened survival, impaired quality of life, and increased caregiver distress.20 Pepper et al noted a trend toward increased incidence of postoperative delirium in their cohort of 234 PD patients undergoing surgery.7
Medication: Management of anti-Parkinsonian medications in the perioperative period poses unique challenges. These medications’ prodopaminergic effects can lead to hemodynamic compromise and are potentially arrhythmogenic. At the same time, abrupt withdrawal of these medications can lead to a potentially lethal condition called Parkinsonism-hyperpyrexia syndrome (PHS), which is clinically similar to neuroleptic malignant syndrome.21 PHS is characterized by very high fever, extreme muscle rigidity, autonomic instability, altered consciousness, and multiple severe systemic complications (e.g., acute renal failure, disseminated intravascular coagulation, autonomic failure, aspiration pneumonia, and infections). PHS occurs in up to 4% of PD patients; mortality is reported to be from 4% for treated to 20% for untreated episodes.22-24
As many as 30% of patients who survive a PHS episode have worsening of their PD symptoms and never return to their pre-PHS baseline. PHS prevention in hospitalized patients by uninterrupted administration of PD medications should be the goal. Early recognition and aggressive treatment is key to successful recovery.
Furthermore, even brief interruption of medications can lead to decompensation of Parkinsonian symptoms, which not only delays recovery from surgery, but also increases the risk for multisystem complications as discussed above.25 Traditional anti-Parkinsonian medications can only be delivered orally, presenting significant challenges for NPO patients, especially those undergoing enteric surgery requiring bowel rest.
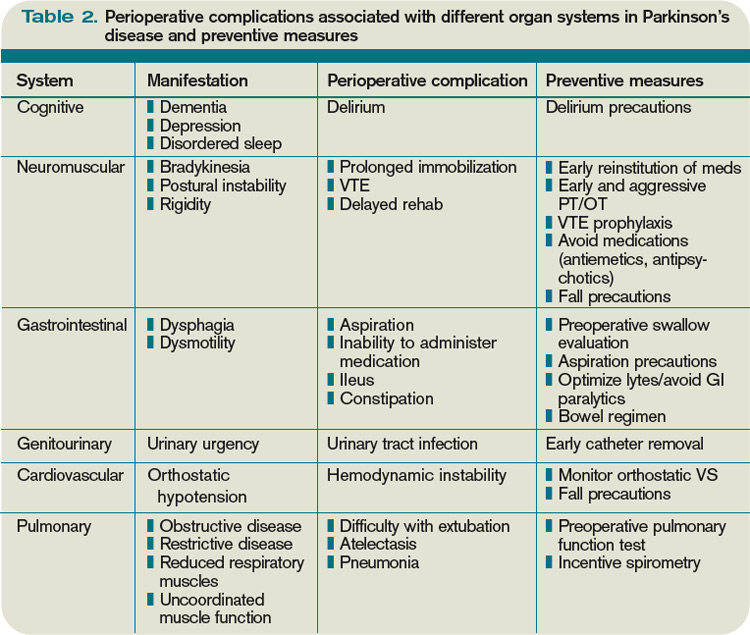
Case reports describe various approaches to medication management in the perioperative period, but no single consensus statement (or treatment guideline) exists. The most common clinical scenarios are:
- Patient undergoes short surgery and is able to take oral medication immediately after the procedure (e.g., orthopedic, eye);
- Patient undergoes more lengthy surgery and will be able to take enteric medications perioperatively (e.g., longer orthopedic surgeries, genitourinary); and
- Patient undergoes lengthy procedure in which they will be required to adhere to bowel rest (e.g., bowel resection).
Depending on the category, the approach to medication management might differ.
Furuya et al describe a 70-year-old male with PD who had previously experienced perioperative complications associated with his medication management, including postoperative rigidity, dysphagia, and difficulty maintaining respiratory secretions.26 These symptoms were reversed with intravenous levodopa. However, the patient experienced hypotension and premature ventricular contractions as side effects of this therapy. This patient was scheduled to undergo hepatic lobectomy. Given his previous complications, Furuya et al provided enteral administration of CD/LD via nasogastric tube every two hours during the surgery, with placement of a duodenostomy for postoperative administration of CD/LD. The patient maintained hemodynamic stability throughout the perioperative period and emerged from anesthesia smoothly with no muscle rigidity or postoperative complications.26
Fujii et al described three cases of PD patients undergoing gastrointestinal surgery. They suggested that the dose of medication required to control symptoms should be minimized before surgery to avoid withdrawal symptoms. They also described the use of intravenous levodopa immediately, postoperatively, while the patient was unable to tolerate enteric medications, and suggested the use of prokinetics to prevent ileus and maximize drug absorption.27
Gálvez-Jiménez et al discuss the limitations of intravenous levodopa, including hemodynamic compromise, need for escalating doses, frequent adjustments to maintain effect, and large amount of fluids required. They propose the use of subcutaneous apomorphine, which is a potent D1/D2 dopamine agonist in conjunction with rectal domeperidone, a D2 antagonist with poor blood-brain-barrier penetration, to counteract the peripheral dopaminergic side effects. The main limitation to this approach is that domeperidone is not available in the U.S.28
Intravenous antihistamines and anticholinergics are readily available. However, they show limited efficacy in halting Parkinsonian symptoms and carry multiple side effects (e.g., confusion, delay in gastrointestinal recovery, and urinary retention).28
Various anesthesiologists agree with administering anti-PD medications immediately, preoperatively, and restarting medications as soon as possible postoperatively. However, they do not provide uniform treatment guidelines regarding specific medication management.29,30
Deep-brain-stimulation (DBS) management: DBS is an effective treatment for advanced PD. There are more than 60,000 patients around the world who have DBS for various conditions, mostly for PD. Therefore, it is increasingly likely that hospitalists will encounter hospitalized patients with advanced PD who are treated both pharmacologically and with DBS. It is important to recognize that stimulation, just like PD medications, cannot be stopped suddenly. If there is any concern of the DBS system malfunctioning (i.e., fracture of the hardware during a fall), the neurologist or neurosurgeon managing the DBS should be contacted immediately. Certain diagnostic tests (MRI) and treatment procedures (diathermy) are contraindicated, and if done inappropriately, can result in permanent brain damage.31,32,33
During surgeries requiring blood-vessel cauterization, DBS should be temporarily turned off. This can be done with the patient’s handheld device or, preferably, by a trained technician usually available through 24/7 technical support services provided by the manufacturer.
Summary of recommendations: There are no clear treatment guidelines regarding the optimal perioperative management of PD patients. The following measures are based on available data and are extensions of routine perioperative management; however, there is no evidence to demonstrate their efficacy in decreasing complication rates among patients with PD:
- A thorough preoperative history and physical examination should include Parkinsonian signs and symptoms, precise medication regimen with doses and timing of intake, effects of medication withdrawal or missed doses, type of surgery planned, and comorbid conditions;
- Depending on symptoms mentioned in the history, consider further testing for dysphagia (preoperative swallow evaluation) and dyspnea (preoperative pulmonary function tests);
- The major goal of medication management in the perioperative period is to continue administration of dopamine replacement therapy as close to the outpatient regimen as possible.
- Titrate down dose of anti-Parkinsonian medications to lowest possible dose prior to surgery if prolonged NPO status is anticipated;
- Ensure medications are administered immediately prior to surgery;
- For short, nonenteric procedures, resume outpatient medication doses and timing of administration as soon as possible postoperatively. For longer, nonenteric surgeries, consider placement of nasogastric tube for medication delivery during procedure and immediately postoperatively;
- If the major limitation of oral medication intake is dysphagia, the use of orally disintegrated formulation CD/LD (parcopa) is helpful;
- For longer enteric surgeries in which patient must be on bowel rest, recommend consultation with neurologist specialized in movement disorders to guide use of intravenous or subcutaneous agents. Transdermal delivery systems of the dopamine agonist rotigotine are in the process of being approved in the U.S. market and might be helpful for this purpose;
- Initiation of tube feeding, when co-administered with levodopa, might result in sudden changes in medication absorption and potential worsening of PD symptoms; feeding should be started slowly and preferably at night when the body’s dopamine requirements are lower;
- Consider use of promotility agents;
- If apomorphine or intravenous LD are not available, consider trial of intravenous anticholinergics or antihistamines, carefully observing for potential cognitive and behavioral side effects;
- Avoid such dopamine antagonists as droperidol, haloperidol, risperidone, metaclopramide, prochlorperazine, or promethazine, as these medications can worsen Parkinsonian symptoms; and
- If patient was on MAO-B inhibitors (selegiline, rasagiline) before surgery, be aware of multiple potential interactions with various medications that are commonly used in perioperative period, including anesthesia agents and certain analgesics, specifically meperidine. These interactions include serotonin syndrome, and can be life-threatening.34
- Psychiatric considerations: delirium precautions;
- Motor considerations: early PT/OT, early referral to inpatient rehabilitation; fall precautions;
- Pulmonary considerations: institute aggressive incentive spirometry, postural drainage, management of respiratory secretions, and breathing exercises; VTE prophylaxis;
- Gastrointestinal considerations: aspiration precautions and prompt speech therapy to evaluate for aspiration and to teach appropriate swallow techniques (chin tuck); institute aggressive bowel regimen; maximize fluids, electrolytes, and avoid narcotics to prevent precipitating or exacerbating ileus;
- Cardiovascular considerations: monitor orthostatic vital signs; fall precautions to avoid syncopal falls; and
- Genitourinary considerations: early urinary catheter removal; vigilance in monitoring for urinary tract infection.
Back to the Case
The patient underwent repair of her fracture, was extubated, and recovered from general anesthesia without incident. She was evaluated in the postanesthesia care unit, at which time she had a slight tremor and mild rigidity. She was immediately given a dose of her CD/LD, and her evening doses of amantadine and ropinirole were resumed. The patient had no significant flare of her Parkinsonian symptoms and did not exhibit any evidence of PHS.
A postoperative consultation was placed for speech therapy, physical therapy, and occupational therapy. She was given low-molecular-weight heparin for VTE prophylaxis and asked to use incentive spirometry. On postoperative day one, she complained of urinary frequency. A urinalysis was consistent with possible infection. She was discharged home on her previous medication regimen, in addition to antibiotics for cystitis.
If the procedure had not been emergent, the patient might have benefited from a preoperative swallow evaluation, given her dysphagia. Consultation with a speech therapist would have ensured that the patient was educated regarding aspiration precautions. Although this patient did not have difficulty with extubation or experience postoperative respiratory failure, abnormal preoperative pulmonary function tests might have prompted the anesthesiologists to consider alternative low-risk techniques (e.g., a local nerve block).
Bottom Line
Perioperative management of patients with Parkinson’s disease requires knowledge of the multisystem disease characteristics that raise perioperative risk and the effects of the medications used to treat PD. To date, no clear treatment guidelines exist for the optimal perioperative management of PD patients.
However, vigilance in detecting possible complications and instituting attentive perioperative care can aid a hospitalist consultant in improving overall care for these patients. TH
Dr. Patel is a medical resident at the University of Colorado Denver. Dr. Stickrath is a hospitalist at the Denver VA Medical Center and instructor of medicine at the University of Colorado Denver. Dr. Anderson is a hospitalist at the Denver VA Medical Center and assistant professor of medicine at the University of Colorado Denver. Dr. Klepitskaya is a neurologist and assistant professor of neurology at the University of Colorado Denver.
References
- Ersan T. Perioperative management of the geriatric patient. Web MD website. Available at: http://emedicine.medscape.com/article/285433-overview. Accessed May 10, 2010.
- Braak H, Del Tredici K, Rüb U, de Vos RA, Jansen Steur EN, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging. 2003;24(2):197-211.
- Ward CD, Gibb WR. Research diagnostic criteria for Parkinson’s disease. Adv Neurol. 1990;53:245-249.
- Stern MB, Koller WC. Parkinsonian Syndromes. New York: Informa Healthcare Publishing; 1993.
- Nutt JG, Wooten GF. Clinical practice. Diagnosis and initial management of Parkinson’s disease. N Engl J Med. 2005;353(10):1021-1027.
- Mueller MC, Jüptner U, Wuellner U, et al. Parkinson’s disease influences the perioperative risk profile in surgery. Langenbecks Arch Surg. 2009;394(3):511-515.
- Pepper PV, Goldstein MK. Postoperative complications in Parkinson’s disease. J Am Geriatr Soc. 1999;47(8):967-972.
- Shill H, Stacy M. Respiratory function in Parkinson’s disease. Clin Neurosci. 1998;5(2):131-135.
- Neu HC, Connolly JJ Jr., Schwertley FW, Ladwig HA, Brody AW. Obstructive respiratory dysfunction in parkinsonian patients. Ann Rev Respir Dis. 1967;95(1):33-47.
- Chokroverty S. The spectrum of ventilatory disturbances in movement disorders. In: Chokroverty S, ed. Movement Disorders. Great Neck, New York: PMA Publishing Corp.; 1990:365-392.
- Shill H, Stacy M. Respiratory complications of Parkinson’s disease. Semin Respir Crit Care Med. 2002;23(3):261-265.
- Easdown LJ, Tessler KJ, Minuk J. Upper airway involvement in Parkinson’s disease resulting in postoperative respiratory failure. Can J Anaesth. 1995;42(4):344-347.
- Pfeiffer RF. Gastrointestinal dysfunction in Parkinson’s disease. Lancet Neurol. 2003;2(2):107-116.
- Castell JA, Johnston BT, Colcher A, Li Q, Gideon RM, Castell DO. Manometric abnormalities of the oesophagus in patients with Parkinson’s disease. Neurogastroenterol Motil. 2001;13(4):361-364.
- Marcason W. What are the primary nutritional issues for a patient with Parkinson’s disease? J Am Diet Assoc. 2009;109(7):1316.
- Djaldetti R, Lev N, Melamed E. Lesions outside the CNS in Parkinson’s disease. Mov Disord. 2009;24(6):793-800.
- Orimo S, Takahashi A, Uchihara T, Mori F, Kakita A, Wakabayashi K, Takahashi H. Degeneration of cardiac sympathetic nerve begins in the early disease process of Parkinson’s disease. Brain Pathol. 2007;17(1):24-30.
- Lemack GE, Dewey RB Jr., Roehrborn CG, O’Suilleabhain PE, Zimmern PE. Questionnaire-based assessment of bladder dysfunction in patients with mild to moderate Parkinson’s disease. Urology. 2000;56(2):250-254.
- Singer C. Urinary dysfunction in Parkinson’s disease. Clin Neurosci. 1998;5(2):78-86.
- Leverenz JB, Quinn JF, Zabetian C, Zhang J, Montine KS, Montine TJ. Cognitive impairment and dementia in patients with Parkinson disease. Curr Top Med Chem. 2009;9(10):903-912.
- Factor SA, Santiago A. Parkinson-hyperpyrexia syndrome in Parkinson’s disease. In: Frucht S, Fahn S, eds. Movement Disorder Emergencies: Diagnosis and Treatment. New York: Humana Press; 2005:29-40.
- Reed AP, Han DG: Intraoperative exacerbation of Parkinson’s disease. Anesth Analg. 1992;75(5):850-853.
- Harada T, Mitsuoka K, Kumagai R, et al. Clinical features of malignant syndrome in Parkinson’s disease and related neurological disorders. Parkinsonism Relat Disord. 2003;9(Suppl 1):S15-23.
- Onofrj M, Thomas A. Acute akinesia in Parkinson disease. Neurology. 2005;64(7):1162-1169.
- Serrano-Dueñas M. Neuroleptic malignant syndrome-like, or—dopaminergic malignant syndrome—due to levodopa therapy withdrawal. Clinical features in 11 patients. Parkinsonism Relat Disord. 2003;9(3):175-178.
- Furuya R, Hirai A, Andoh T, Kudoh I, Okumura F. Successful perioperative management of a patient with Parkinson’s disease by enteral levodopa administration under propofol anesthesia. Anesthesiology. 1998;89(1):261-263.
- Fujii T, Nakabayashi T, Hashimoto S, Kuwano H. Successful perioperative management of patients with Parkinson’s disease following gastrointestinal surgery: report of three cases. Surg Today. 2009;39(9):807-810.
- Gálvez-Jiménez N, Lang AE. The perioperative management of Parkinson’s disease revisited. Neurol Clin. 2004;22(2):367-377.
- Kalenka A, Schwarz A. Anasthesia and Parkinson’s disease: how to manage with new therapies? Curr Opin Anesthesiol. 2009;22(3):419-424.
- Nicholson G, Pereira AC, Hall GM. Parkinson’s disease and anesthesia. Br J Anaesthesia. 2002;89(6):904-916.
- Rezai AR, Baker KB, Tkach JA, et al. Is magnetic resonance imaging safe for patients with neurostimulation systems used for deep brain stimulation? Neurosurgery. 2005:57(5):1056-1062.
- Henderson JM, Tkach J, Phillips M, Baker K, Shellock FG, Rezai AR. Permanent neurological deficit related to magnetic resonance imaging in a patient with implanted deep brain stimulation electrodes for Parkinson’s disease: case report. Neurosurgery. 2005:57(5):E1063.
- Nutt JG, Anderson VC, Peacock JH, Hammerstad JP, Burchiel KJ. DBS and diathermy interaction induces severe CNS damage. Neurology. 2001;56 (10):1384-1386.
- Gordon PH, Frucht SJ. Neuroleptic malignant syndrome in advanced Parkinson’s disease. Mov Disord. 2001;16(5):960-962.
Case
A 67-year-old female with moderately advanced Parkinson’s disease (PD) had a mechanical fall in her home, which resulted in a humeral fracture. The fall occurred in the morning before she was able to take her medications and was related to her difficulty in initiating movements.
On her current regimen, her PD symptoms are controlled. She is able to perform daily living activities independently and ambulates without assistance. She also performs more complex tasks (e.g., cooking and managing her finances). She has not exhibited any symptoms consistent with dementia. She occasionally experiences dyspnea on exertion and dysphagia, but she has not been evaluated for these complaints. She takes carbidopa/levodopa (CD/LD) 25 mg/100 mg four times a day, amantadine 100 mg twice daily, and ropinirole 3 mg three times a day.
She is scheduled for open reduction internal fixation of her fracture; the orthopedic surgeon has requested a perioperative risk assessment and recommendations concerning her medications. How should PD be managed perioperatively?
Overview
Advances in surgical and anesthetic techniques, in combination with an aging population, have contributed to an increasing number of geriatric patients undergoing surgery. As many as 50% of Americans older than 65 will undergo a surgical procedure; hospitalists will comanage many of these patients in the perioperative period.1
Although cardiopulmonary disorders receive a great deal of attention with regard to perioperative risk assessment, other comorbid conditions also contribute to perioperative risk—namely, disorders specific to the elderly population. Parkinson’s disease is one such condition that deserves attention.
PD is a progressive, neurodegenerative condition associated with loss of dopaminergic neurons and the presence of Lewy bodies within the substantia nigra and other areas of the brain and peripheral autonomic nervous system.2 Cardinal clinical features include rigidity, bradykinesia, and resting tremor. A supportive feature is a consistent response to levodopa. Postural instability, cognitive impairment, and autonomic dysfunction usually occur later in the disease.3,4
As the population ages, Parkinson’s disease is becoming more prevalent, affecting approximately 1% of individuals older than 60.5 These patients pose a specific challenge to the hospitalist, not only because the multiorgan system manifestations of PD can raise surgical risk, but also due to the direct effects of dopaminergic medications used to treat PD, lack of a parenteral route for these medications in NPO patients, and the risks associated with abrupt withdrawal of these medications.
Although surgical risk in PD patients has received intermittent attention in surgical, anesthesia, and neurology literature, there is no broad consensus statement or treatment guideline for the perioperative approach.
Literature Review
A retrospective cohort of 51 PD patients undergoing various types of surgery revealed that PD patients have a longer hospital stay than matched cohorts.6 Pepper et al studied a cohort of 234 PD patients in the Veterans Administration population who were undergoing a variety of surgeries.7 They found that patients with PD had a longer acute hospital stay and had higher in-hospital mortality.7 The multisystem manifestations of PD might account for this global increase in perioperative risk.
The following are reviews of organ-system manifestations of PD and their relevance to the perioperative period.
Motor: The motor symptoms of PD place patients at increased risk for falls and might impair their ability to participate in rehabilitation. Mueller et al demonstrated that there was a significantly increased risk of postoperative falls and a higher need for inpatient rehabilitation due to motor difficulties in the PD cohort.6
Pulmonary: PD patients have increased risk of abnormal pulmonary function secondary to rigidity and akinesia. Increased airway resistance and decreased lung elastic recoil lead to obstructive lung disease.8,9 Rigidity of voluntary chest wall and upper airway muscles leads to a restrictive lung disease pattern.8,10 Furthermore, respiratory dyskinesia is a common side effect of levodopa, which can result in restrictive and dyskinetic ventilation.11 As a consequence of disordered respiratory mechanics (especially in combination with disordered swallow mechanics), PD patients are at increased risk of lower respiratory infections. In fact, pneumonia remains the leading cause of mortality among PD patients.11
Not surprisingly, several cohorts have suggested that PD patients undergoing surgical procedures are at higher risk for atelectasis, pneumonia, and postoperative respiratory failure.7,12 Postoperative VTE rates are not statistically different between PD patients and matched cohorts.
Gastrointestinal: Abnor-malities in muscles of the mouth, pharynx, and esophagus account for the dysphagia commonly noted in PD.13 Barium swallow tests are abnormal in 80% or more of PD patients.14 Dysphagia can lead to aspiration, as well as inadequate oral intake, resulting in pneumonia and malnutrition, respectively.15 Dysfunction of the myenteric plexus (evidenced by Lewy Body deposition) accounts for gastrointestinal dysmotility manifested as gastroparesis, ileus, and slow colonic transit, which results in constipation.16
PD patients in the postoperative period are at risk for swallowing difficulties, which increases the risk of aspiration and might delay initiation of oral medications. Gastroparesis threatens appropriate delivery of oral medications for adequate absorption. In addition, postoperative ileus and constipation can pose challenges.
Cardiovascular: Such cardiac sympathetic abnormalities as orthostatic hypotension, postprandial or exercise-induced hypotension, impaired heart rate variability, and dysrhythmias are common in PD.17 Pepper et al found a trend toward increased risk of hypotension and acute myocardial infarction (MI) in PD patients undergoing surgery.7
Genitourinary: Urinary complaints (e.g., nocturia, frequency, urgency, and urge incontinence) are common in PD patients.18 These clinical complaints correspond to involuntary detrusor contractions (detrusor hyperreflexia).19 Pepper et al found an increased risk of postoperative urinary tract infection in PD patients.7
Cognitive: A recognized feature of advanced PD is cognitive impairment. Studies estimate the prevalence of dementia in cohorts of PD patients is from 28% to 44%. PD with dementia has been associated with shortened survival, impaired quality of life, and increased caregiver distress.20 Pepper et al noted a trend toward increased incidence of postoperative delirium in their cohort of 234 PD patients undergoing surgery.7
Medication: Management of anti-Parkinsonian medications in the perioperative period poses unique challenges. These medications’ prodopaminergic effects can lead to hemodynamic compromise and are potentially arrhythmogenic. At the same time, abrupt withdrawal of these medications can lead to a potentially lethal condition called Parkinsonism-hyperpyrexia syndrome (PHS), which is clinically similar to neuroleptic malignant syndrome.21 PHS is characterized by very high fever, extreme muscle rigidity, autonomic instability, altered consciousness, and multiple severe systemic complications (e.g., acute renal failure, disseminated intravascular coagulation, autonomic failure, aspiration pneumonia, and infections). PHS occurs in up to 4% of PD patients; mortality is reported to be from 4% for treated to 20% for untreated episodes.22-24
As many as 30% of patients who survive a PHS episode have worsening of their PD symptoms and never return to their pre-PHS baseline. PHS prevention in hospitalized patients by uninterrupted administration of PD medications should be the goal. Early recognition and aggressive treatment is key to successful recovery.
Furthermore, even brief interruption of medications can lead to decompensation of Parkinsonian symptoms, which not only delays recovery from surgery, but also increases the risk for multisystem complications as discussed above.25 Traditional anti-Parkinsonian medications can only be delivered orally, presenting significant challenges for NPO patients, especially those undergoing enteric surgery requiring bowel rest.
Case reports describe various approaches to medication management in the perioperative period, but no single consensus statement (or treatment guideline) exists. The most common clinical scenarios are:
- Patient undergoes short surgery and is able to take oral medication immediately after the procedure (e.g., orthopedic, eye);
- Patient undergoes more lengthy surgery and will be able to take enteric medications perioperatively (e.g., longer orthopedic surgeries, genitourinary); and
- Patient undergoes lengthy procedure in which they will be required to adhere to bowel rest (e.g., bowel resection).
Depending on the category, the approach to medication management might differ.
Furuya et al describe a 70-year-old male with PD who had previously experienced perioperative complications associated with his medication management, including postoperative rigidity, dysphagia, and difficulty maintaining respiratory secretions.26 These symptoms were reversed with intravenous levodopa. However, the patient experienced hypotension and premature ventricular contractions as side effects of this therapy. This patient was scheduled to undergo hepatic lobectomy. Given his previous complications, Furuya et al provided enteral administration of CD/LD via nasogastric tube every two hours during the surgery, with placement of a duodenostomy for postoperative administration of CD/LD. The patient maintained hemodynamic stability throughout the perioperative period and emerged from anesthesia smoothly with no muscle rigidity or postoperative complications.26
Fujii et al described three cases of PD patients undergoing gastrointestinal surgery. They suggested that the dose of medication required to control symptoms should be minimized before surgery to avoid withdrawal symptoms. They also described the use of intravenous levodopa immediately, postoperatively, while the patient was unable to tolerate enteric medications, and suggested the use of prokinetics to prevent ileus and maximize drug absorption.27
Gálvez-Jiménez et al discuss the limitations of intravenous levodopa, including hemodynamic compromise, need for escalating doses, frequent adjustments to maintain effect, and large amount of fluids required. They propose the use of subcutaneous apomorphine, which is a potent D1/D2 dopamine agonist in conjunction with rectal domeperidone, a D2 antagonist with poor blood-brain-barrier penetration, to counteract the peripheral dopaminergic side effects. The main limitation to this approach is that domeperidone is not available in the U.S.28
Intravenous antihistamines and anticholinergics are readily available. However, they show limited efficacy in halting Parkinsonian symptoms and carry multiple side effects (e.g., confusion, delay in gastrointestinal recovery, and urinary retention).28
Various anesthesiologists agree with administering anti-PD medications immediately, preoperatively, and restarting medications as soon as possible postoperatively. However, they do not provide uniform treatment guidelines regarding specific medication management.29,30
Deep-brain-stimulation (DBS) management: DBS is an effective treatment for advanced PD. There are more than 60,000 patients around the world who have DBS for various conditions, mostly for PD. Therefore, it is increasingly likely that hospitalists will encounter hospitalized patients with advanced PD who are treated both pharmacologically and with DBS. It is important to recognize that stimulation, just like PD medications, cannot be stopped suddenly. If there is any concern of the DBS system malfunctioning (i.e., fracture of the hardware during a fall), the neurologist or neurosurgeon managing the DBS should be contacted immediately. Certain diagnostic tests (MRI) and treatment procedures (diathermy) are contraindicated, and if done inappropriately, can result in permanent brain damage.31,32,33
During surgeries requiring blood-vessel cauterization, DBS should be temporarily turned off. This can be done with the patient’s handheld device or, preferably, by a trained technician usually available through 24/7 technical support services provided by the manufacturer.
Summary of recommendations: There are no clear treatment guidelines regarding the optimal perioperative management of PD patients. The following measures are based on available data and are extensions of routine perioperative management; however, there is no evidence to demonstrate their efficacy in decreasing complication rates among patients with PD:
- A thorough preoperative history and physical examination should include Parkinsonian signs and symptoms, precise medication regimen with doses and timing of intake, effects of medication withdrawal or missed doses, type of surgery planned, and comorbid conditions;
- Depending on symptoms mentioned in the history, consider further testing for dysphagia (preoperative swallow evaluation) and dyspnea (preoperative pulmonary function tests);
- The major goal of medication management in the perioperative period is to continue administration of dopamine replacement therapy as close to the outpatient regimen as possible.
- Titrate down dose of anti-Parkinsonian medications to lowest possible dose prior to surgery if prolonged NPO status is anticipated;
- Ensure medications are administered immediately prior to surgery;
- For short, nonenteric procedures, resume outpatient medication doses and timing of administration as soon as possible postoperatively. For longer, nonenteric surgeries, consider placement of nasogastric tube for medication delivery during procedure and immediately postoperatively;
- If the major limitation of oral medication intake is dysphagia, the use of orally disintegrated formulation CD/LD (parcopa) is helpful;
- For longer enteric surgeries in which patient must be on bowel rest, recommend consultation with neurologist specialized in movement disorders to guide use of intravenous or subcutaneous agents. Transdermal delivery systems of the dopamine agonist rotigotine are in the process of being approved in the U.S. market and might be helpful for this purpose;
- Initiation of tube feeding, when co-administered with levodopa, might result in sudden changes in medication absorption and potential worsening of PD symptoms; feeding should be started slowly and preferably at night when the body’s dopamine requirements are lower;
- Consider use of promotility agents;
- If apomorphine or intravenous LD are not available, consider trial of intravenous anticholinergics or antihistamines, carefully observing for potential cognitive and behavioral side effects;
- Avoid such dopamine antagonists as droperidol, haloperidol, risperidone, metaclopramide, prochlorperazine, or promethazine, as these medications can worsen Parkinsonian symptoms; and
- If patient was on MAO-B inhibitors (selegiline, rasagiline) before surgery, be aware of multiple potential interactions with various medications that are commonly used in perioperative period, including anesthesia agents and certain analgesics, specifically meperidine. These interactions include serotonin syndrome, and can be life-threatening.34
- Psychiatric considerations: delirium precautions;
- Motor considerations: early PT/OT, early referral to inpatient rehabilitation; fall precautions;
- Pulmonary considerations: institute aggressive incentive spirometry, postural drainage, management of respiratory secretions, and breathing exercises; VTE prophylaxis;
- Gastrointestinal considerations: aspiration precautions and prompt speech therapy to evaluate for aspiration and to teach appropriate swallow techniques (chin tuck); institute aggressive bowel regimen; maximize fluids, electrolytes, and avoid narcotics to prevent precipitating or exacerbating ileus;
- Cardiovascular considerations: monitor orthostatic vital signs; fall precautions to avoid syncopal falls; and
- Genitourinary considerations: early urinary catheter removal; vigilance in monitoring for urinary tract infection.
Back to the Case
The patient underwent repair of her fracture, was extubated, and recovered from general anesthesia without incident. She was evaluated in the postanesthesia care unit, at which time she had a slight tremor and mild rigidity. She was immediately given a dose of her CD/LD, and her evening doses of amantadine and ropinirole were resumed. The patient had no significant flare of her Parkinsonian symptoms and did not exhibit any evidence of PHS.
A postoperative consultation was placed for speech therapy, physical therapy, and occupational therapy. She was given low-molecular-weight heparin for VTE prophylaxis and asked to use incentive spirometry. On postoperative day one, she complained of urinary frequency. A urinalysis was consistent with possible infection. She was discharged home on her previous medication regimen, in addition to antibiotics for cystitis.
If the procedure had not been emergent, the patient might have benefited from a preoperative swallow evaluation, given her dysphagia. Consultation with a speech therapist would have ensured that the patient was educated regarding aspiration precautions. Although this patient did not have difficulty with extubation or experience postoperative respiratory failure, abnormal preoperative pulmonary function tests might have prompted the anesthesiologists to consider alternative low-risk techniques (e.g., a local nerve block).
Bottom Line
Perioperative management of patients with Parkinson’s disease requires knowledge of the multisystem disease characteristics that raise perioperative risk and the effects of the medications used to treat PD. To date, no clear treatment guidelines exist for the optimal perioperative management of PD patients.
However, vigilance in detecting possible complications and instituting attentive perioperative care can aid a hospitalist consultant in improving overall care for these patients. TH
Dr. Patel is a medical resident at the University of Colorado Denver. Dr. Stickrath is a hospitalist at the Denver VA Medical Center and instructor of medicine at the University of Colorado Denver. Dr. Anderson is a hospitalist at the Denver VA Medical Center and assistant professor of medicine at the University of Colorado Denver. Dr. Klepitskaya is a neurologist and assistant professor of neurology at the University of Colorado Denver.
References
- Ersan T. Perioperative management of the geriatric patient. Web MD website. Available at: http://emedicine.medscape.com/article/285433-overview. Accessed May 10, 2010.
- Braak H, Del Tredici K, Rüb U, de Vos RA, Jansen Steur EN, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging. 2003;24(2):197-211.
- Ward CD, Gibb WR. Research diagnostic criteria for Parkinson’s disease. Adv Neurol. 1990;53:245-249.
- Stern MB, Koller WC. Parkinsonian Syndromes. New York: Informa Healthcare Publishing; 1993.
- Nutt JG, Wooten GF. Clinical practice. Diagnosis and initial management of Parkinson’s disease. N Engl J Med. 2005;353(10):1021-1027.
- Mueller MC, Jüptner U, Wuellner U, et al. Parkinson’s disease influences the perioperative risk profile in surgery. Langenbecks Arch Surg. 2009;394(3):511-515.
- Pepper PV, Goldstein MK. Postoperative complications in Parkinson’s disease. J Am Geriatr Soc. 1999;47(8):967-972.
- Shill H, Stacy M. Respiratory function in Parkinson’s disease. Clin Neurosci. 1998;5(2):131-135.
- Neu HC, Connolly JJ Jr., Schwertley FW, Ladwig HA, Brody AW. Obstructive respiratory dysfunction in parkinsonian patients. Ann Rev Respir Dis. 1967;95(1):33-47.
- Chokroverty S. The spectrum of ventilatory disturbances in movement disorders. In: Chokroverty S, ed. Movement Disorders. Great Neck, New York: PMA Publishing Corp.; 1990:365-392.
- Shill H, Stacy M. Respiratory complications of Parkinson’s disease. Semin Respir Crit Care Med. 2002;23(3):261-265.
- Easdown LJ, Tessler KJ, Minuk J. Upper airway involvement in Parkinson’s disease resulting in postoperative respiratory failure. Can J Anaesth. 1995;42(4):344-347.
- Pfeiffer RF. Gastrointestinal dysfunction in Parkinson’s disease. Lancet Neurol. 2003;2(2):107-116.
- Castell JA, Johnston BT, Colcher A, Li Q, Gideon RM, Castell DO. Manometric abnormalities of the oesophagus in patients with Parkinson’s disease. Neurogastroenterol Motil. 2001;13(4):361-364.
- Marcason W. What are the primary nutritional issues for a patient with Parkinson’s disease? J Am Diet Assoc. 2009;109(7):1316.
- Djaldetti R, Lev N, Melamed E. Lesions outside the CNS in Parkinson’s disease. Mov Disord. 2009;24(6):793-800.
- Orimo S, Takahashi A, Uchihara T, Mori F, Kakita A, Wakabayashi K, Takahashi H. Degeneration of cardiac sympathetic nerve begins in the early disease process of Parkinson’s disease. Brain Pathol. 2007;17(1):24-30.
- Lemack GE, Dewey RB Jr., Roehrborn CG, O’Suilleabhain PE, Zimmern PE. Questionnaire-based assessment of bladder dysfunction in patients with mild to moderate Parkinson’s disease. Urology. 2000;56(2):250-254.
- Singer C. Urinary dysfunction in Parkinson’s disease. Clin Neurosci. 1998;5(2):78-86.
- Leverenz JB, Quinn JF, Zabetian C, Zhang J, Montine KS, Montine TJ. Cognitive impairment and dementia in patients with Parkinson disease. Curr Top Med Chem. 2009;9(10):903-912.
- Factor SA, Santiago A. Parkinson-hyperpyrexia syndrome in Parkinson’s disease. In: Frucht S, Fahn S, eds. Movement Disorder Emergencies: Diagnosis and Treatment. New York: Humana Press; 2005:29-40.
- Reed AP, Han DG: Intraoperative exacerbation of Parkinson’s disease. Anesth Analg. 1992;75(5):850-853.
- Harada T, Mitsuoka K, Kumagai R, et al. Clinical features of malignant syndrome in Parkinson’s disease and related neurological disorders. Parkinsonism Relat Disord. 2003;9(Suppl 1):S15-23.
- Onofrj M, Thomas A. Acute akinesia in Parkinson disease. Neurology. 2005;64(7):1162-1169.
- Serrano-Dueñas M. Neuroleptic malignant syndrome-like, or—dopaminergic malignant syndrome—due to levodopa therapy withdrawal. Clinical features in 11 patients. Parkinsonism Relat Disord. 2003;9(3):175-178.
- Furuya R, Hirai A, Andoh T, Kudoh I, Okumura F. Successful perioperative management of a patient with Parkinson’s disease by enteral levodopa administration under propofol anesthesia. Anesthesiology. 1998;89(1):261-263.
- Fujii T, Nakabayashi T, Hashimoto S, Kuwano H. Successful perioperative management of patients with Parkinson’s disease following gastrointestinal surgery: report of three cases. Surg Today. 2009;39(9):807-810.
- Gálvez-Jiménez N, Lang AE. The perioperative management of Parkinson’s disease revisited. Neurol Clin. 2004;22(2):367-377.
- Kalenka A, Schwarz A. Anasthesia and Parkinson’s disease: how to manage with new therapies? Curr Opin Anesthesiol. 2009;22(3):419-424.
- Nicholson G, Pereira AC, Hall GM. Parkinson’s disease and anesthesia. Br J Anaesthesia. 2002;89(6):904-916.
- Rezai AR, Baker KB, Tkach JA, et al. Is magnetic resonance imaging safe for patients with neurostimulation systems used for deep brain stimulation? Neurosurgery. 2005:57(5):1056-1062.
- Henderson JM, Tkach J, Phillips M, Baker K, Shellock FG, Rezai AR. Permanent neurological deficit related to magnetic resonance imaging in a patient with implanted deep brain stimulation electrodes for Parkinson’s disease: case report. Neurosurgery. 2005:57(5):E1063.
- Nutt JG, Anderson VC, Peacock JH, Hammerstad JP, Burchiel KJ. DBS and diathermy interaction induces severe CNS damage. Neurology. 2001;56 (10):1384-1386.
- Gordon PH, Frucht SJ. Neuroleptic malignant syndrome in advanced Parkinson’s disease. Mov Disord. 2001;16(5):960-962.
Case
A 67-year-old female with moderately advanced Parkinson’s disease (PD) had a mechanical fall in her home, which resulted in a humeral fracture. The fall occurred in the morning before she was able to take her medications and was related to her difficulty in initiating movements.
On her current regimen, her PD symptoms are controlled. She is able to perform daily living activities independently and ambulates without assistance. She also performs more complex tasks (e.g., cooking and managing her finances). She has not exhibited any symptoms consistent with dementia. She occasionally experiences dyspnea on exertion and dysphagia, but she has not been evaluated for these complaints. She takes carbidopa/levodopa (CD/LD) 25 mg/100 mg four times a day, amantadine 100 mg twice daily, and ropinirole 3 mg three times a day.
She is scheduled for open reduction internal fixation of her fracture; the orthopedic surgeon has requested a perioperative risk assessment and recommendations concerning her medications. How should PD be managed perioperatively?
Overview
Advances in surgical and anesthetic techniques, in combination with an aging population, have contributed to an increasing number of geriatric patients undergoing surgery. As many as 50% of Americans older than 65 will undergo a surgical procedure; hospitalists will comanage many of these patients in the perioperative period.1
Although cardiopulmonary disorders receive a great deal of attention with regard to perioperative risk assessment, other comorbid conditions also contribute to perioperative risk—namely, disorders specific to the elderly population. Parkinson’s disease is one such condition that deserves attention.
PD is a progressive, neurodegenerative condition associated with loss of dopaminergic neurons and the presence of Lewy bodies within the substantia nigra and other areas of the brain and peripheral autonomic nervous system.2 Cardinal clinical features include rigidity, bradykinesia, and resting tremor. A supportive feature is a consistent response to levodopa. Postural instability, cognitive impairment, and autonomic dysfunction usually occur later in the disease.3,4
As the population ages, Parkinson’s disease is becoming more prevalent, affecting approximately 1% of individuals older than 60.5 These patients pose a specific challenge to the hospitalist, not only because the multiorgan system manifestations of PD can raise surgical risk, but also due to the direct effects of dopaminergic medications used to treat PD, lack of a parenteral route for these medications in NPO patients, and the risks associated with abrupt withdrawal of these medications.
Although surgical risk in PD patients has received intermittent attention in surgical, anesthesia, and neurology literature, there is no broad consensus statement or treatment guideline for the perioperative approach.
Literature Review
A retrospective cohort of 51 PD patients undergoing various types of surgery revealed that PD patients have a longer hospital stay than matched cohorts.6 Pepper et al studied a cohort of 234 PD patients in the Veterans Administration population who were undergoing a variety of surgeries.7 They found that patients with PD had a longer acute hospital stay and had higher in-hospital mortality.7 The multisystem manifestations of PD might account for this global increase in perioperative risk.
The following are reviews of organ-system manifestations of PD and their relevance to the perioperative period.
Motor: The motor symptoms of PD place patients at increased risk for falls and might impair their ability to participate in rehabilitation. Mueller et al demonstrated that there was a significantly increased risk of postoperative falls and a higher need for inpatient rehabilitation due to motor difficulties in the PD cohort.6
Pulmonary: PD patients have increased risk of abnormal pulmonary function secondary to rigidity and akinesia. Increased airway resistance and decreased lung elastic recoil lead to obstructive lung disease.8,9 Rigidity of voluntary chest wall and upper airway muscles leads to a restrictive lung disease pattern.8,10 Furthermore, respiratory dyskinesia is a common side effect of levodopa, which can result in restrictive and dyskinetic ventilation.11 As a consequence of disordered respiratory mechanics (especially in combination with disordered swallow mechanics), PD patients are at increased risk of lower respiratory infections. In fact, pneumonia remains the leading cause of mortality among PD patients.11
Not surprisingly, several cohorts have suggested that PD patients undergoing surgical procedures are at higher risk for atelectasis, pneumonia, and postoperative respiratory failure.7,12 Postoperative VTE rates are not statistically different between PD patients and matched cohorts.
Gastrointestinal: Abnor-malities in muscles of the mouth, pharynx, and esophagus account for the dysphagia commonly noted in PD.13 Barium swallow tests are abnormal in 80% or more of PD patients.14 Dysphagia can lead to aspiration, as well as inadequate oral intake, resulting in pneumonia and malnutrition, respectively.15 Dysfunction of the myenteric plexus (evidenced by Lewy Body deposition) accounts for gastrointestinal dysmotility manifested as gastroparesis, ileus, and slow colonic transit, which results in constipation.16
PD patients in the postoperative period are at risk for swallowing difficulties, which increases the risk of aspiration and might delay initiation of oral medications. Gastroparesis threatens appropriate delivery of oral medications for adequate absorption. In addition, postoperative ileus and constipation can pose challenges.
Cardiovascular: Such cardiac sympathetic abnormalities as orthostatic hypotension, postprandial or exercise-induced hypotension, impaired heart rate variability, and dysrhythmias are common in PD.17 Pepper et al found a trend toward increased risk of hypotension and acute myocardial infarction (MI) in PD patients undergoing surgery.7
Genitourinary: Urinary complaints (e.g., nocturia, frequency, urgency, and urge incontinence) are common in PD patients.18 These clinical complaints correspond to involuntary detrusor contractions (detrusor hyperreflexia).19 Pepper et al found an increased risk of postoperative urinary tract infection in PD patients.7
Cognitive: A recognized feature of advanced PD is cognitive impairment. Studies estimate the prevalence of dementia in cohorts of PD patients is from 28% to 44%. PD with dementia has been associated with shortened survival, impaired quality of life, and increased caregiver distress.20 Pepper et al noted a trend toward increased incidence of postoperative delirium in their cohort of 234 PD patients undergoing surgery.7
Medication: Management of anti-Parkinsonian medications in the perioperative period poses unique challenges. These medications’ prodopaminergic effects can lead to hemodynamic compromise and are potentially arrhythmogenic. At the same time, abrupt withdrawal of these medications can lead to a potentially lethal condition called Parkinsonism-hyperpyrexia syndrome (PHS), which is clinically similar to neuroleptic malignant syndrome.21 PHS is characterized by very high fever, extreme muscle rigidity, autonomic instability, altered consciousness, and multiple severe systemic complications (e.g., acute renal failure, disseminated intravascular coagulation, autonomic failure, aspiration pneumonia, and infections). PHS occurs in up to 4% of PD patients; mortality is reported to be from 4% for treated to 20% for untreated episodes.22-24
As many as 30% of patients who survive a PHS episode have worsening of their PD symptoms and never return to their pre-PHS baseline. PHS prevention in hospitalized patients by uninterrupted administration of PD medications should be the goal. Early recognition and aggressive treatment is key to successful recovery.
Furthermore, even brief interruption of medications can lead to decompensation of Parkinsonian symptoms, which not only delays recovery from surgery, but also increases the risk for multisystem complications as discussed above.25 Traditional anti-Parkinsonian medications can only be delivered orally, presenting significant challenges for NPO patients, especially those undergoing enteric surgery requiring bowel rest.
Case reports describe various approaches to medication management in the perioperative period, but no single consensus statement (or treatment guideline) exists. The most common clinical scenarios are:
- Patient undergoes short surgery and is able to take oral medication immediately after the procedure (e.g., orthopedic, eye);
- Patient undergoes more lengthy surgery and will be able to take enteric medications perioperatively (e.g., longer orthopedic surgeries, genitourinary); and
- Patient undergoes lengthy procedure in which they will be required to adhere to bowel rest (e.g., bowel resection).
Depending on the category, the approach to medication management might differ.
Furuya et al describe a 70-year-old male with PD who had previously experienced perioperative complications associated with his medication management, including postoperative rigidity, dysphagia, and difficulty maintaining respiratory secretions.26 These symptoms were reversed with intravenous levodopa. However, the patient experienced hypotension and premature ventricular contractions as side effects of this therapy. This patient was scheduled to undergo hepatic lobectomy. Given his previous complications, Furuya et al provided enteral administration of CD/LD via nasogastric tube every two hours during the surgery, with placement of a duodenostomy for postoperative administration of CD/LD. The patient maintained hemodynamic stability throughout the perioperative period and emerged from anesthesia smoothly with no muscle rigidity or postoperative complications.26
Fujii et al described three cases of PD patients undergoing gastrointestinal surgery. They suggested that the dose of medication required to control symptoms should be minimized before surgery to avoid withdrawal symptoms. They also described the use of intravenous levodopa immediately, postoperatively, while the patient was unable to tolerate enteric medications, and suggested the use of prokinetics to prevent ileus and maximize drug absorption.27
Gálvez-Jiménez et al discuss the limitations of intravenous levodopa, including hemodynamic compromise, need for escalating doses, frequent adjustments to maintain effect, and large amount of fluids required. They propose the use of subcutaneous apomorphine, which is a potent D1/D2 dopamine agonist in conjunction with rectal domeperidone, a D2 antagonist with poor blood-brain-barrier penetration, to counteract the peripheral dopaminergic side effects. The main limitation to this approach is that domeperidone is not available in the U.S.28
Intravenous antihistamines and anticholinergics are readily available. However, they show limited efficacy in halting Parkinsonian symptoms and carry multiple side effects (e.g., confusion, delay in gastrointestinal recovery, and urinary retention).28
Various anesthesiologists agree with administering anti-PD medications immediately, preoperatively, and restarting medications as soon as possible postoperatively. However, they do not provide uniform treatment guidelines regarding specific medication management.29,30
Deep-brain-stimulation (DBS) management: DBS is an effective treatment for advanced PD. There are more than 60,000 patients around the world who have DBS for various conditions, mostly for PD. Therefore, it is increasingly likely that hospitalists will encounter hospitalized patients with advanced PD who are treated both pharmacologically and with DBS. It is important to recognize that stimulation, just like PD medications, cannot be stopped suddenly. If there is any concern of the DBS system malfunctioning (i.e., fracture of the hardware during a fall), the neurologist or neurosurgeon managing the DBS should be contacted immediately. Certain diagnostic tests (MRI) and treatment procedures (diathermy) are contraindicated, and if done inappropriately, can result in permanent brain damage.31,32,33
During surgeries requiring blood-vessel cauterization, DBS should be temporarily turned off. This can be done with the patient’s handheld device or, preferably, by a trained technician usually available through 24/7 technical support services provided by the manufacturer.
Summary of recommendations: There are no clear treatment guidelines regarding the optimal perioperative management of PD patients. The following measures are based on available data and are extensions of routine perioperative management; however, there is no evidence to demonstrate their efficacy in decreasing complication rates among patients with PD:
- A thorough preoperative history and physical examination should include Parkinsonian signs and symptoms, precise medication regimen with doses and timing of intake, effects of medication withdrawal or missed doses, type of surgery planned, and comorbid conditions;
- Depending on symptoms mentioned in the history, consider further testing for dysphagia (preoperative swallow evaluation) and dyspnea (preoperative pulmonary function tests);
- The major goal of medication management in the perioperative period is to continue administration of dopamine replacement therapy as close to the outpatient regimen as possible.
- Titrate down dose of anti-Parkinsonian medications to lowest possible dose prior to surgery if prolonged NPO status is anticipated;
- Ensure medications are administered immediately prior to surgery;
- For short, nonenteric procedures, resume outpatient medication doses and timing of administration as soon as possible postoperatively. For longer, nonenteric surgeries, consider placement of nasogastric tube for medication delivery during procedure and immediately postoperatively;
- If the major limitation of oral medication intake is dysphagia, the use of orally disintegrated formulation CD/LD (parcopa) is helpful;
- For longer enteric surgeries in which patient must be on bowel rest, recommend consultation with neurologist specialized in movement disorders to guide use of intravenous or subcutaneous agents. Transdermal delivery systems of the dopamine agonist rotigotine are in the process of being approved in the U.S. market and might be helpful for this purpose;
- Initiation of tube feeding, when co-administered with levodopa, might result in sudden changes in medication absorption and potential worsening of PD symptoms; feeding should be started slowly and preferably at night when the body’s dopamine requirements are lower;
- Consider use of promotility agents;
- If apomorphine or intravenous LD are not available, consider trial of intravenous anticholinergics or antihistamines, carefully observing for potential cognitive and behavioral side effects;
- Avoid such dopamine antagonists as droperidol, haloperidol, risperidone, metaclopramide, prochlorperazine, or promethazine, as these medications can worsen Parkinsonian symptoms; and
- If patient was on MAO-B inhibitors (selegiline, rasagiline) before surgery, be aware of multiple potential interactions with various medications that are commonly used in perioperative period, including anesthesia agents and certain analgesics, specifically meperidine. These interactions include serotonin syndrome, and can be life-threatening.34
- Psychiatric considerations: delirium precautions;
- Motor considerations: early PT/OT, early referral to inpatient rehabilitation; fall precautions;
- Pulmonary considerations: institute aggressive incentive spirometry, postural drainage, management of respiratory secretions, and breathing exercises; VTE prophylaxis;
- Gastrointestinal considerations: aspiration precautions and prompt speech therapy to evaluate for aspiration and to teach appropriate swallow techniques (chin tuck); institute aggressive bowel regimen; maximize fluids, electrolytes, and avoid narcotics to prevent precipitating or exacerbating ileus;
- Cardiovascular considerations: monitor orthostatic vital signs; fall precautions to avoid syncopal falls; and
- Genitourinary considerations: early urinary catheter removal; vigilance in monitoring for urinary tract infection.
Back to the Case
The patient underwent repair of her fracture, was extubated, and recovered from general anesthesia without incident. She was evaluated in the postanesthesia care unit, at which time she had a slight tremor and mild rigidity. She was immediately given a dose of her CD/LD, and her evening doses of amantadine and ropinirole were resumed. The patient had no significant flare of her Parkinsonian symptoms and did not exhibit any evidence of PHS.
A postoperative consultation was placed for speech therapy, physical therapy, and occupational therapy. She was given low-molecular-weight heparin for VTE prophylaxis and asked to use incentive spirometry. On postoperative day one, she complained of urinary frequency. A urinalysis was consistent with possible infection. She was discharged home on her previous medication regimen, in addition to antibiotics for cystitis.
If the procedure had not been emergent, the patient might have benefited from a preoperative swallow evaluation, given her dysphagia. Consultation with a speech therapist would have ensured that the patient was educated regarding aspiration precautions. Although this patient did not have difficulty with extubation or experience postoperative respiratory failure, abnormal preoperative pulmonary function tests might have prompted the anesthesiologists to consider alternative low-risk techniques (e.g., a local nerve block).
Bottom Line
Perioperative management of patients with Parkinson’s disease requires knowledge of the multisystem disease characteristics that raise perioperative risk and the effects of the medications used to treat PD. To date, no clear treatment guidelines exist for the optimal perioperative management of PD patients.
However, vigilance in detecting possible complications and instituting attentive perioperative care can aid a hospitalist consultant in improving overall care for these patients. TH
Dr. Patel is a medical resident at the University of Colorado Denver. Dr. Stickrath is a hospitalist at the Denver VA Medical Center and instructor of medicine at the University of Colorado Denver. Dr. Anderson is a hospitalist at the Denver VA Medical Center and assistant professor of medicine at the University of Colorado Denver. Dr. Klepitskaya is a neurologist and assistant professor of neurology at the University of Colorado Denver.
References
- Ersan T. Perioperative management of the geriatric patient. Web MD website. Available at: http://emedicine.medscape.com/article/285433-overview. Accessed May 10, 2010.
- Braak H, Del Tredici K, Rüb U, de Vos RA, Jansen Steur EN, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging. 2003;24(2):197-211.
- Ward CD, Gibb WR. Research diagnostic criteria for Parkinson’s disease. Adv Neurol. 1990;53:245-249.
- Stern MB, Koller WC. Parkinsonian Syndromes. New York: Informa Healthcare Publishing; 1993.
- Nutt JG, Wooten GF. Clinical practice. Diagnosis and initial management of Parkinson’s disease. N Engl J Med. 2005;353(10):1021-1027.
- Mueller MC, Jüptner U, Wuellner U, et al. Parkinson’s disease influences the perioperative risk profile in surgery. Langenbecks Arch Surg. 2009;394(3):511-515.
- Pepper PV, Goldstein MK. Postoperative complications in Parkinson’s disease. J Am Geriatr Soc. 1999;47(8):967-972.
- Shill H, Stacy M. Respiratory function in Parkinson’s disease. Clin Neurosci. 1998;5(2):131-135.
- Neu HC, Connolly JJ Jr., Schwertley FW, Ladwig HA, Brody AW. Obstructive respiratory dysfunction in parkinsonian patients. Ann Rev Respir Dis. 1967;95(1):33-47.
- Chokroverty S. The spectrum of ventilatory disturbances in movement disorders. In: Chokroverty S, ed. Movement Disorders. Great Neck, New York: PMA Publishing Corp.; 1990:365-392.
- Shill H, Stacy M. Respiratory complications of Parkinson’s disease. Semin Respir Crit Care Med. 2002;23(3):261-265.
- Easdown LJ, Tessler KJ, Minuk J. Upper airway involvement in Parkinson’s disease resulting in postoperative respiratory failure. Can J Anaesth. 1995;42(4):344-347.
- Pfeiffer RF. Gastrointestinal dysfunction in Parkinson’s disease. Lancet Neurol. 2003;2(2):107-116.
- Castell JA, Johnston BT, Colcher A, Li Q, Gideon RM, Castell DO. Manometric abnormalities of the oesophagus in patients with Parkinson’s disease. Neurogastroenterol Motil. 2001;13(4):361-364.
- Marcason W. What are the primary nutritional issues for a patient with Parkinson’s disease? J Am Diet Assoc. 2009;109(7):1316.
- Djaldetti R, Lev N, Melamed E. Lesions outside the CNS in Parkinson’s disease. Mov Disord. 2009;24(6):793-800.
- Orimo S, Takahashi A, Uchihara T, Mori F, Kakita A, Wakabayashi K, Takahashi H. Degeneration of cardiac sympathetic nerve begins in the early disease process of Parkinson’s disease. Brain Pathol. 2007;17(1):24-30.
- Lemack GE, Dewey RB Jr., Roehrborn CG, O’Suilleabhain PE, Zimmern PE. Questionnaire-based assessment of bladder dysfunction in patients with mild to moderate Parkinson’s disease. Urology. 2000;56(2):250-254.
- Singer C. Urinary dysfunction in Parkinson’s disease. Clin Neurosci. 1998;5(2):78-86.
- Leverenz JB, Quinn JF, Zabetian C, Zhang J, Montine KS, Montine TJ. Cognitive impairment and dementia in patients with Parkinson disease. Curr Top Med Chem. 2009;9(10):903-912.
- Factor SA, Santiago A. Parkinson-hyperpyrexia syndrome in Parkinson’s disease. In: Frucht S, Fahn S, eds. Movement Disorder Emergencies: Diagnosis and Treatment. New York: Humana Press; 2005:29-40.
- Reed AP, Han DG: Intraoperative exacerbation of Parkinson’s disease. Anesth Analg. 1992;75(5):850-853.
- Harada T, Mitsuoka K, Kumagai R, et al. Clinical features of malignant syndrome in Parkinson’s disease and related neurological disorders. Parkinsonism Relat Disord. 2003;9(Suppl 1):S15-23.
- Onofrj M, Thomas A. Acute akinesia in Parkinson disease. Neurology. 2005;64(7):1162-1169.
- Serrano-Dueñas M. Neuroleptic malignant syndrome-like, or—dopaminergic malignant syndrome—due to levodopa therapy withdrawal. Clinical features in 11 patients. Parkinsonism Relat Disord. 2003;9(3):175-178.
- Furuya R, Hirai A, Andoh T, Kudoh I, Okumura F. Successful perioperative management of a patient with Parkinson’s disease by enteral levodopa administration under propofol anesthesia. Anesthesiology. 1998;89(1):261-263.
- Fujii T, Nakabayashi T, Hashimoto S, Kuwano H. Successful perioperative management of patients with Parkinson’s disease following gastrointestinal surgery: report of three cases. Surg Today. 2009;39(9):807-810.
- Gálvez-Jiménez N, Lang AE. The perioperative management of Parkinson’s disease revisited. Neurol Clin. 2004;22(2):367-377.
- Kalenka A, Schwarz A. Anasthesia and Parkinson’s disease: how to manage with new therapies? Curr Opin Anesthesiol. 2009;22(3):419-424.
- Nicholson G, Pereira AC, Hall GM. Parkinson’s disease and anesthesia. Br J Anaesthesia. 2002;89(6):904-916.
- Rezai AR, Baker KB, Tkach JA, et al. Is magnetic resonance imaging safe for patients with neurostimulation systems used for deep brain stimulation? Neurosurgery. 2005:57(5):1056-1062.
- Henderson JM, Tkach J, Phillips M, Baker K, Shellock FG, Rezai AR. Permanent neurological deficit related to magnetic resonance imaging in a patient with implanted deep brain stimulation electrodes for Parkinson’s disease: case report. Neurosurgery. 2005:57(5):E1063.
- Nutt JG, Anderson VC, Peacock JH, Hammerstad JP, Burchiel KJ. DBS and diathermy interaction induces severe CNS damage. Neurology. 2001;56 (10):1384-1386.
- Gordon PH, Frucht SJ. Neuroleptic malignant syndrome in advanced Parkinson’s disease. Mov Disord. 2001;16(5):960-962.
Article on Anniversary of Medical Errors Report Missed Key Points
Donald Berwick, MD, MPP, FRCP, is honest, forthright, and accurate, as always. Christine Cassel, MD, is correct: We need to change the culture in medical school. However, diagnostic errors aren’t “emerging” as a medical error—they’ve been with us all along.
I would point to Maureen Thiel as one example. She was the victim of repeated diagnostic errors in the late 1990s. Her widower, Bill Thiel, has been a patient-safety advocate ever since (www.maureensmission.org).
“Failure to rescue” is an emerging medical error. Lori Nerbonne of New Hampshire Patient Voices has a story of a failure to rescue that ultimately took her mother’s life.
Lewis Blackman, a healthy 15-year-old boy, died in 2000. He slowly bled to death over the course of several days after being admitted to the hospital for an elective procedure. I’m sure his mother, Helen Haskell, can share his story. She is the director of the Empowered Patient Coalition. You can find her and other advocates listed at www.empoweredpatientcoalition.org/patient-advocate-directory.
What’s missing from your November cover story, “Medical Mistakes, 10 Years Post-Op,” and the accompanying timeline is what really sparked the patient-safety movement. It was the 100,000 Lives Campaign in tandem with medical-error victims and their families. Unfortunately, those numbers have grown exponentially in recent years.
With the exception of Dr. Berwick and Johns Hopkins, our nation’s political and healthcare “leaders” have not taken the initiative with patient safety. And make no mistake: They have been pushed.
Dr. Berwick is leading. We are pushing.
“To Err is Human—To Delay is Deadly” is the message patient-safety advocates took to Washington on Nov. 17, 2009. We think the IOM report should be acted on before it’s commemorated. It should not be a surprise that patient-safety advocates were excluded from this article. We have been dismissed and ignored by the medical profession for years. Why is that? History should not overlook the substantial contribution made by the grassroots advocates.
Lisa Lindell,
Webster, Texas
Author, PULSE of America
Coalition state coordinator
Donald Berwick, MD, MPP, FRCP, is honest, forthright, and accurate, as always. Christine Cassel, MD, is correct: We need to change the culture in medical school. However, diagnostic errors aren’t “emerging” as a medical error—they’ve been with us all along.
I would point to Maureen Thiel as one example. She was the victim of repeated diagnostic errors in the late 1990s. Her widower, Bill Thiel, has been a patient-safety advocate ever since (www.maureensmission.org).
“Failure to rescue” is an emerging medical error. Lori Nerbonne of New Hampshire Patient Voices has a story of a failure to rescue that ultimately took her mother’s life.
Lewis Blackman, a healthy 15-year-old boy, died in 2000. He slowly bled to death over the course of several days after being admitted to the hospital for an elective procedure. I’m sure his mother, Helen Haskell, can share his story. She is the director of the Empowered Patient Coalition. You can find her and other advocates listed at www.empoweredpatientcoalition.org/patient-advocate-directory.
What’s missing from your November cover story, “Medical Mistakes, 10 Years Post-Op,” and the accompanying timeline is what really sparked the patient-safety movement. It was the 100,000 Lives Campaign in tandem with medical-error victims and their families. Unfortunately, those numbers have grown exponentially in recent years.
With the exception of Dr. Berwick and Johns Hopkins, our nation’s political and healthcare “leaders” have not taken the initiative with patient safety. And make no mistake: They have been pushed.
Dr. Berwick is leading. We are pushing.
“To Err is Human—To Delay is Deadly” is the message patient-safety advocates took to Washington on Nov. 17, 2009. We think the IOM report should be acted on before it’s commemorated. It should not be a surprise that patient-safety advocates were excluded from this article. We have been dismissed and ignored by the medical profession for years. Why is that? History should not overlook the substantial contribution made by the grassroots advocates.
Lisa Lindell,
Webster, Texas
Author, PULSE of America
Coalition state coordinator
Donald Berwick, MD, MPP, FRCP, is honest, forthright, and accurate, as always. Christine Cassel, MD, is correct: We need to change the culture in medical school. However, diagnostic errors aren’t “emerging” as a medical error—they’ve been with us all along.
I would point to Maureen Thiel as one example. She was the victim of repeated diagnostic errors in the late 1990s. Her widower, Bill Thiel, has been a patient-safety advocate ever since (www.maureensmission.org).
“Failure to rescue” is an emerging medical error. Lori Nerbonne of New Hampshire Patient Voices has a story of a failure to rescue that ultimately took her mother’s life.
Lewis Blackman, a healthy 15-year-old boy, died in 2000. He slowly bled to death over the course of several days after being admitted to the hospital for an elective procedure. I’m sure his mother, Helen Haskell, can share his story. She is the director of the Empowered Patient Coalition. You can find her and other advocates listed at www.empoweredpatientcoalition.org/patient-advocate-directory.
What’s missing from your November cover story, “Medical Mistakes, 10 Years Post-Op,” and the accompanying timeline is what really sparked the patient-safety movement. It was the 100,000 Lives Campaign in tandem with medical-error victims and their families. Unfortunately, those numbers have grown exponentially in recent years.
With the exception of Dr. Berwick and Johns Hopkins, our nation’s political and healthcare “leaders” have not taken the initiative with patient safety. And make no mistake: They have been pushed.
Dr. Berwick is leading. We are pushing.
“To Err is Human—To Delay is Deadly” is the message patient-safety advocates took to Washington on Nov. 17, 2009. We think the IOM report should be acted on before it’s commemorated. It should not be a surprise that patient-safety advocates were excluded from this article. We have been dismissed and ignored by the medical profession for years. Why is that? History should not overlook the substantial contribution made by the grassroots advocates.
Lisa Lindell,
Webster, Texas
Author, PULSE of America
Coalition state coordinator