User login
Safe use of SSRIs in young adults: How strong is evidence for new suicide warning?
CASE: Life is 'not worth it'
Mr. B, age 20, has taken a semester leave from college because of gradually worsening depressed mood. Over the past 2 months he has lost interest in jogging and playing piano—which he usually enjoys. He reports reduced libido, middle insomnia, loss of appetite, feeling as if his head is “full of cotton,” trouble concentrating, and waking in the morning with a sense of dread. His anxiety dissipates during the day, but he continues to feel sad and sometimes weepy, which is unusual for him.
Mr. B reports feeling hopeless at times and has had vague thoughts about life being “not worth it if I continue to feel like this” but denies specific suicide plans. Your initial impression is that Mr. B is in the midst of a major depressive episode and that a selective serotonin reuptake inhibitor (SSRI) is indicated. As you finish taking his history, you run through your mind the pros and cons of the recommendation you will make to him.
Do SSRIs raise or lower the risk for suicidal behavior in young adults such as Mr. B? The answer is complicated and goes beyond an “either/or” question, as the FDA acknowledged in May 2007 when it:
- extended the black-box warning of increased suicidality risk with antidepressants to cover adults age 18 to 24 as well as children and adolescents
- included language in the warning about the benefits of treating depression and the suicide risk associated with untreated depression, given concerns about declining antidepressant prescriptions and rising suicides among youth.1
- To help you make informed decisions when treating depression in adults, this article reviews the studies leading up to and following the FDA’s meta-analysis of antidepressant trial data in patients age 18 and older. Our goal is to provide a framework for clinical treatment of adults age 18 to 24 and those age ≥25.
The FDA meta-analysis designed to investigate a reported association between antidepressants and suicidality in children and adolescents found contradictory results:
- Pooled adverse event data from 24 pediatric antidepressant trials totaling >4,400 patients showed a higher risk of suicidal ideation or behavior (no suicides occurred) with antidepressants (4%) vs placebo (2%).
- Systematically collected suicide-related item scores from 17 of the trials showed no evidence that antidepressants worsen suicidality or cause it to emerge.
One interpretation of these findings is that antidepressants’ effect on suicidality is small and therefore subject to measurement error.
Another is ascertainment bias; any side effect associated with active medication encourages discussion with the clinician and may distort the frequency of reported adverse events.
The FDA meta-analysis also found:
- Relative risk for suicidality ranged 10-fold among agents, from 0.9 with fluoxetine to 8.8 with venlafaxine.
- Most suicide-related events occurred in subjects having the highest baseline levels of suicidality.
- Hostility and agitation emerged with SSRI use, particularly during the first month of treatment.
- Patient age, sex, or history of suicide attempt/ideation did not affect the results.
Source: Reference 7
First hints of suicidality
SSRIs revolutionized depression treatment. From 1985 to 1999, annual U.S. antidepressant prescriptions quadrupled, with SSRIs accounting for 70% of the increase (see “Antidepressants and suicide risk, 1985 to 2007”). At the same time, the age-adjusted suicide rate:
- dropped 22.5% for women (who account for twice as many antidepressant prescriptions as men)
- dropped 12.8% for men (without change in the rank order of suicide methods).2
The debate rekindled in June 2003 when the British Committee on Safety of Medicines warned against using paroxetine or venlafaxine in children. After conducting its own meta-analysis, the FDA in 2004 ordered a black-box warning about suicidality and the use of antidepressants in children and adolescents ( Box ).7
After the pediatric ‘black box.’ Antidepressant prescriptions for children and adolescents declined in the years 2003 to 2004, as did diagnosis of pediatric depression.8-10 Antidepressant prescribing also showed signs of shifting from general practitioners to psychiatrists.8 At the same time, the suicide rate among youth age 11 In patients age >60, SSRI prescriptions continued to rise and suicide rates fell,9 a pattern of change consistent with antidepressants protecting against suicide.
An independent meta-analysis by Bridge et al12 examined the pediatric trial data used in the FDA meta-analysis plus 7 additional studies. Its findings differ in 2 important ways from those of the FDA review:
- Antidepressants—including others besides fluoxetine—showed efficacy in treating anxiety disorders and depression in children and adolescents.
- The frequency of suicide-related adverse events (no trial patients committed suicide) was approximately 3% on active medication—25% lower than the FDA estimated rate—and 2% on placebo, similar to the FDA estimate.
Antidepressants and suicide risk, 1985 to 2007
| 1985 | 1990 | 1991 | 1999 | 2003 | 2004 | 2006 | 2007 |
|---|---|---|---|---|---|---|---|
| Case reports suggest link between suicide and SSRI use | FDA analysis finds no association between SSRIs and increased suicide risk | UK agency warns of suicide-related events in children treated with paroxetine and venlafaxine | FDA conducts meta-analysis, requires black-box warnings of risk of suicidality in youth taking antidepressants | FDA meta-analysis finds age-dependent effect of antidepressants on suicidality risk in adults | FDA expands warning of increased suicidality risk with antidepressants to adults age | ||
| Antidepressant prescriptions quadruple; age-adjusted suicide rate drops 22.5% for women and 12.8% for men | Pediatric depression diagnoses and antidepressant prescriptions decline; suicides increase 11% | Bridge et al meta-analysis finds 25% lower rate of suicide-related events in youth than the FDA found | |||||
What about adults?
Overall effect. A subsequent FDA meta-analysis of antidepressant clinical trial data in adults13 found 8 suicides in 372 trials totaling nearly 100,000 persons. All occurred in the 295 trials with psychiatric indications. Among these psychiatric trials, 59% had a suicidal behavior/ideation event in either the test-drug or placebo arm, and 41% had none. Eleven antidepressants were included in the meta-analysis:
- 6 SSRIs (citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, and sertraline)
- 2 SNRIs (duloxetine and venlafaxine)
- 3 others (bupropion, mirtazapine, and nefazodone).
Age-specific findings. When the FDA analysis was stratified by age, however, antidepressants’ benefit appeared greater for patients age ≥25 than for those age 18 to 24. The data suggested:
- elevated suicidality risk among adults age
- neutral or possibly protective effect for adults age 25 to 64
- protective effect in adults age ≥65 ( Table 1 ).13
FDA meta-analysis: Suicide rates by age in antidepressant trials
| Age group (yr) | Suicide rate (%)(test drug/placebo) | Suicide attempt rate (%)(test drug/placebo) |
|---|---|---|
| 18 to 24 | 0.03/0.00 | 0.55/0.27 |
| 25 to 30 | 0.00/0.03 | 0.23/0.11 |
| 31 to 64 | 0.01/0.00 | 0.13/0.15 |
| ≥65 | 0.00/0.04 | 0.03/0.25 |
| Source: Reference 13 | ||
The odds ratio for suicidal behavior (preparatory acts, attempt, or suicide) for subacts, attempt, or suicide) for subjects age 18 to 24 on test drug vs placebo was 2.31 (95% CI: 1.02, 5.64) [event rate/sample: 23/3810 vs 8/2604]. NNH was 333, which means 333 adults in this age group would need to be treated with an antidepressant for 1 to experience a suicidal behavior event that would not have happened with placebo.
1. Kuehn BM. FDA panel seeks to balance risks in warnings for antidepressants. J Am Med Assoc 2007;297:573-4.
2. Grunebaum MF, Ellis SP, Li S, et al. Antidepressants and suicide risk in the United States, 1985-1999. J Clin Psychiatry 2004;65(11):1456-62.
3. Teicher MH, Glod C, Cole JO. Emergence of intense suicidal preoccupation during fluoxetine treatment. Am J Psychiatry 1990;147:207-10.
4. King RA, Riddle MA, Chappell PB, et al. Emergence of self-destructive phenomena in children and adolescents during fluoxetine treatment. J Am Acad Child Adolesc Psychiatry 1991;30(2):179-86.
5. Rothschild AJ, Locke CA. Reexposure to fluoxetine after serious suicide attempts by three patients: the role of akathisia. J Clin Psychiatry 1991;52:491-3.
6. Beasley CM, Dornseif BE, Bosomworth JC, et al. Fluoxetine and suicide: a meta-analysis of controlled trials of treatment for depression. BMJ 1991;303:685-92.
7. Hammad TA. Review and evaluation of clinical data. Food and Drug Administration. August 16, 2004. Available at: http://www.fda.gov/ohrms/dockets/ac/04/briefing/2004-4065b1-10-TAB08-Hammads-Review.pdf. Accessed September 19, 2007.
8. Nemeroff CB, Kalali A, Keller MB, et al. Impact of publicity concerning pediatric suicidality data on physician practice patterns in the United States. Arch Gen Psychiatry 2007;64(4):466-72.
9. Gibbons RD, Brown CH, Hur K, et al. Early evidence on the effects of regulators’ suicidality warnings on SSRI prescriptions and suicide in children and adolescents. Am J Psychiatry 2007;164:1356-63.
10. Libby AM, Brent DA, Morrato EH, et al. Decline in treatment of pediatric depression after FDA advisory on risk of suicidality with SSRIs. Am J Psychiatry 2007;164(6):884-91.
11. US. Department of Health and Human Services. Centers for Disease Control and Prevention. Fatal injury reports. Web-based injury statistics query and reporting system. Available at: http://www.cdc.gov/NCIPC/wisqars. Accessed July 16, 2007.
12. Bridge JA, Iyengar S, Salary CB, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA 2007;297:1683-96.
13. Levenson M, Holland C. Statistical evaluation of suicidality in adults treated with antidepressants. In: Laughren TP. Memorandum: overview for December 13 meeting of PsychopharmacologicDrugs Advisory Committee (PDAC). Center for Drug Evaluation and Research, US Food and Drug Administration. November 16, 2006. Available at: http://www.fda.gov/ohrms/dockets/ac/06/briefing/2006-4272b1-01-FDA.pdf. Accessed October 11, 2007.
14. Bostwick JM, Pankratz VS. Affective disorders and suicide risk: a reexamination. Am J Psychiatry 2000;157(12):1925-32.
15. Lafuente-Lafuente C, Mouly S, Longas-Tejero MA, et al. Antiarrhythmic drugs for maintaining sinus rhythm after cardioversion of atrial fibrillation: a systematic review of randomized controlled trials. Arch Intern Med 2006;166(7):719-28.
16. Khan A, Khan S, Kolts R, Brown WA. Suicide rates in clinical trials of SSRIs, other antidepressants, and placebo: analysis of FDA reports. Am J Psychiatry 2003;160:790-2.
17. Jick H, Kaye JA, Jick SS. Antidepressants and the risk of suicidal behaviors. J Am Med Assoc 2004;292(3):338-43.
18. Martinez C, Rietbrock S, Wise L, et al. Antidepressant treatment and the risk of fatal and non-fatal self harm in first episode depression: nested case-control study. BMJ 2005;330(7488):389.-
19. Gunnell D, Saperia J, Ashby D. Selective serotonin reuptake inhibitors (SSRIs) and suicide in adults: meta-analysis of drug company data from placebo controlled, randomised controlled trials submitted to the MHRA’s safety review. BMJ 2005;330(7488):385-9.
20. Fergusson D, Doucette S, Glass KC, et al. Association between suicide attempts and selective serotonin reuptake inhibitors: systematic review of randomised controlled trials. BMJ 2005;330(7488):396.-
21. Juurlink DN, Mamdani MM, Kopp A, Redelmeier DA. The risk of suicide with selective serotonin reuptake inhibitors in the elderly. Am J Psychiatry 2006;163(5):813-21.
22. Isacsson G, Holmgren P, Ahlner J. Selective serotonin reuptake inhibitor antidepressants and the risk of suicide: a controlled forensic database study of 14,857 suicides. Acta Psychiatr Scand. 2005;111(4):286-90.
23. Simon GE, Savarino J, Operskalski B, Wang PS. Suicide risk during antidepressant treatment. Am J Psychiatry 2006;163(1):41-7.
24. Gibbons RD, Brown CH, Hur K, et al. Relationship between antidepressants and suicide attempts: an analysis of the Veterans Health Administration data sets. Am J Psychiatry 2007;164(7):1044-9.
25. Simon GE, Savarino J. Suicide attempts among patients starting depression treatment with medications or psychotherapy. Am J Psychiatry 2007;164(7):1029-34.
26. Mann JJ, Apter A, Bertolote J, et al. Suicide prevention strategies: a systematic review. JAMA 2005;294(16):2064-74.
27. Rich CL, Isacsson G. Suicide and antidepressants in South Alabama: evidence for improved treatment of depression. J Affect Disord 1997;45:135-42.
28. Isacsson G, Bergman U, Rich CL. Antidepressants, depression and suicide: an analysis of the San Diego study. J Affect Disord 1994;32:277-86.
29. Geddes JR, Carney SM, Davies C, et al. Relapse prevention with antidepressant drug treatment in depressive disorders: a systematic review. Lancet 2003;361(9358):653-61.
30. Gibbons RD, Hur K, Bhaumik DK, Mann JJ. The relationship between antidepressant medication use and rate of suicide. Arch Gen Psychiatry 2005;62(2):165-72.
31. Hall WD, Mant A, Mitchell PB, et al. Association between antidepressant prescribing and suicide in Australia, 1991-2000: trend analysis. BMJ 2003;326(7397):1008-11.
32. Nakagawa A, Grunebaum MF, Ellis SP, et al. Association of suicide and antidepressant prescription rates in Japan, 1999-2003. J Clin Psychiatry 2007;68(6):908-16.
33. Helgason T, Tomasson H, Zoega T. Antidepressants and public health in Iceland. Time series analysis of national data. Br J Psychiatry 2004;184:157-62.
34. March J, Silva S, Petrycki S, et al. Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for Adolescents with Depression Study (TADS) randomized controlled trial. JAMA 2004;292(7):807-20.
CASE: Life is 'not worth it'
Mr. B, age 20, has taken a semester leave from college because of gradually worsening depressed mood. Over the past 2 months he has lost interest in jogging and playing piano—which he usually enjoys. He reports reduced libido, middle insomnia, loss of appetite, feeling as if his head is “full of cotton,” trouble concentrating, and waking in the morning with a sense of dread. His anxiety dissipates during the day, but he continues to feel sad and sometimes weepy, which is unusual for him.
Mr. B reports feeling hopeless at times and has had vague thoughts about life being “not worth it if I continue to feel like this” but denies specific suicide plans. Your initial impression is that Mr. B is in the midst of a major depressive episode and that a selective serotonin reuptake inhibitor (SSRI) is indicated. As you finish taking his history, you run through your mind the pros and cons of the recommendation you will make to him.
Do SSRIs raise or lower the risk for suicidal behavior in young adults such as Mr. B? The answer is complicated and goes beyond an “either/or” question, as the FDA acknowledged in May 2007 when it:
- extended the black-box warning of increased suicidality risk with antidepressants to cover adults age 18 to 24 as well as children and adolescents
- included language in the warning about the benefits of treating depression and the suicide risk associated with untreated depression, given concerns about declining antidepressant prescriptions and rising suicides among youth.1
- To help you make informed decisions when treating depression in adults, this article reviews the studies leading up to and following the FDA’s meta-analysis of antidepressant trial data in patients age 18 and older. Our goal is to provide a framework for clinical treatment of adults age 18 to 24 and those age ≥25.
The FDA meta-analysis designed to investigate a reported association between antidepressants and suicidality in children and adolescents found contradictory results:
- Pooled adverse event data from 24 pediatric antidepressant trials totaling >4,400 patients showed a higher risk of suicidal ideation or behavior (no suicides occurred) with antidepressants (4%) vs placebo (2%).
- Systematically collected suicide-related item scores from 17 of the trials showed no evidence that antidepressants worsen suicidality or cause it to emerge.
One interpretation of these findings is that antidepressants’ effect on suicidality is small and therefore subject to measurement error.
Another is ascertainment bias; any side effect associated with active medication encourages discussion with the clinician and may distort the frequency of reported adverse events.
The FDA meta-analysis also found:
- Relative risk for suicidality ranged 10-fold among agents, from 0.9 with fluoxetine to 8.8 with venlafaxine.
- Most suicide-related events occurred in subjects having the highest baseline levels of suicidality.
- Hostility and agitation emerged with SSRI use, particularly during the first month of treatment.
- Patient age, sex, or history of suicide attempt/ideation did not affect the results.
Source: Reference 7
First hints of suicidality
SSRIs revolutionized depression treatment. From 1985 to 1999, annual U.S. antidepressant prescriptions quadrupled, with SSRIs accounting for 70% of the increase (see “Antidepressants and suicide risk, 1985 to 2007”). At the same time, the age-adjusted suicide rate:
- dropped 22.5% for women (who account for twice as many antidepressant prescriptions as men)
- dropped 12.8% for men (without change in the rank order of suicide methods).2
The debate rekindled in June 2003 when the British Committee on Safety of Medicines warned against using paroxetine or venlafaxine in children. After conducting its own meta-analysis, the FDA in 2004 ordered a black-box warning about suicidality and the use of antidepressants in children and adolescents ( Box ).7
After the pediatric ‘black box.’ Antidepressant prescriptions for children and adolescents declined in the years 2003 to 2004, as did diagnosis of pediatric depression.8-10 Antidepressant prescribing also showed signs of shifting from general practitioners to psychiatrists.8 At the same time, the suicide rate among youth age 11 In patients age >60, SSRI prescriptions continued to rise and suicide rates fell,9 a pattern of change consistent with antidepressants protecting against suicide.
An independent meta-analysis by Bridge et al12 examined the pediatric trial data used in the FDA meta-analysis plus 7 additional studies. Its findings differ in 2 important ways from those of the FDA review:
- Antidepressants—including others besides fluoxetine—showed efficacy in treating anxiety disorders and depression in children and adolescents.
- The frequency of suicide-related adverse events (no trial patients committed suicide) was approximately 3% on active medication—25% lower than the FDA estimated rate—and 2% on placebo, similar to the FDA estimate.
Antidepressants and suicide risk, 1985 to 2007
| 1985 | 1990 | 1991 | 1999 | 2003 | 2004 | 2006 | 2007 |
|---|---|---|---|---|---|---|---|
| Case reports suggest link between suicide and SSRI use | FDA analysis finds no association between SSRIs and increased suicide risk | UK agency warns of suicide-related events in children treated with paroxetine and venlafaxine | FDA conducts meta-analysis, requires black-box warnings of risk of suicidality in youth taking antidepressants | FDA meta-analysis finds age-dependent effect of antidepressants on suicidality risk in adults | FDA expands warning of increased suicidality risk with antidepressants to adults age | ||
| Antidepressant prescriptions quadruple; age-adjusted suicide rate drops 22.5% for women and 12.8% for men | Pediatric depression diagnoses and antidepressant prescriptions decline; suicides increase 11% | Bridge et al meta-analysis finds 25% lower rate of suicide-related events in youth than the FDA found | |||||
What about adults?
Overall effect. A subsequent FDA meta-analysis of antidepressant clinical trial data in adults13 found 8 suicides in 372 trials totaling nearly 100,000 persons. All occurred in the 295 trials with psychiatric indications. Among these psychiatric trials, 59% had a suicidal behavior/ideation event in either the test-drug or placebo arm, and 41% had none. Eleven antidepressants were included in the meta-analysis:
- 6 SSRIs (citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, and sertraline)
- 2 SNRIs (duloxetine and venlafaxine)
- 3 others (bupropion, mirtazapine, and nefazodone).
Age-specific findings. When the FDA analysis was stratified by age, however, antidepressants’ benefit appeared greater for patients age ≥25 than for those age 18 to 24. The data suggested:
- elevated suicidality risk among adults age
- neutral or possibly protective effect for adults age 25 to 64
- protective effect in adults age ≥65 ( Table 1 ).13
FDA meta-analysis: Suicide rates by age in antidepressant trials
| Age group (yr) | Suicide rate (%)(test drug/placebo) | Suicide attempt rate (%)(test drug/placebo) |
|---|---|---|
| 18 to 24 | 0.03/0.00 | 0.55/0.27 |
| 25 to 30 | 0.00/0.03 | 0.23/0.11 |
| 31 to 64 | 0.01/0.00 | 0.13/0.15 |
| ≥65 | 0.00/0.04 | 0.03/0.25 |
| Source: Reference 13 | ||
The odds ratio for suicidal behavior (preparatory acts, attempt, or suicide) for subacts, attempt, or suicide) for subjects age 18 to 24 on test drug vs placebo was 2.31 (95% CI: 1.02, 5.64) [event rate/sample: 23/3810 vs 8/2604]. NNH was 333, which means 333 adults in this age group would need to be treated with an antidepressant for 1 to experience a suicidal behavior event that would not have happened with placebo.
CASE: Life is 'not worth it'
Mr. B, age 20, has taken a semester leave from college because of gradually worsening depressed mood. Over the past 2 months he has lost interest in jogging and playing piano—which he usually enjoys. He reports reduced libido, middle insomnia, loss of appetite, feeling as if his head is “full of cotton,” trouble concentrating, and waking in the morning with a sense of dread. His anxiety dissipates during the day, but he continues to feel sad and sometimes weepy, which is unusual for him.
Mr. B reports feeling hopeless at times and has had vague thoughts about life being “not worth it if I continue to feel like this” but denies specific suicide plans. Your initial impression is that Mr. B is in the midst of a major depressive episode and that a selective serotonin reuptake inhibitor (SSRI) is indicated. As you finish taking his history, you run through your mind the pros and cons of the recommendation you will make to him.
Do SSRIs raise or lower the risk for suicidal behavior in young adults such as Mr. B? The answer is complicated and goes beyond an “either/or” question, as the FDA acknowledged in May 2007 when it:
- extended the black-box warning of increased suicidality risk with antidepressants to cover adults age 18 to 24 as well as children and adolescents
- included language in the warning about the benefits of treating depression and the suicide risk associated with untreated depression, given concerns about declining antidepressant prescriptions and rising suicides among youth.1
- To help you make informed decisions when treating depression in adults, this article reviews the studies leading up to and following the FDA’s meta-analysis of antidepressant trial data in patients age 18 and older. Our goal is to provide a framework for clinical treatment of adults age 18 to 24 and those age ≥25.
The FDA meta-analysis designed to investigate a reported association between antidepressants and suicidality in children and adolescents found contradictory results:
- Pooled adverse event data from 24 pediatric antidepressant trials totaling >4,400 patients showed a higher risk of suicidal ideation or behavior (no suicides occurred) with antidepressants (4%) vs placebo (2%).
- Systematically collected suicide-related item scores from 17 of the trials showed no evidence that antidepressants worsen suicidality or cause it to emerge.
One interpretation of these findings is that antidepressants’ effect on suicidality is small and therefore subject to measurement error.
Another is ascertainment bias; any side effect associated with active medication encourages discussion with the clinician and may distort the frequency of reported adverse events.
The FDA meta-analysis also found:
- Relative risk for suicidality ranged 10-fold among agents, from 0.9 with fluoxetine to 8.8 with venlafaxine.
- Most suicide-related events occurred in subjects having the highest baseline levels of suicidality.
- Hostility and agitation emerged with SSRI use, particularly during the first month of treatment.
- Patient age, sex, or history of suicide attempt/ideation did not affect the results.
Source: Reference 7
First hints of suicidality
SSRIs revolutionized depression treatment. From 1985 to 1999, annual U.S. antidepressant prescriptions quadrupled, with SSRIs accounting for 70% of the increase (see “Antidepressants and suicide risk, 1985 to 2007”). At the same time, the age-adjusted suicide rate:
- dropped 22.5% for women (who account for twice as many antidepressant prescriptions as men)
- dropped 12.8% for men (without change in the rank order of suicide methods).2
The debate rekindled in June 2003 when the British Committee on Safety of Medicines warned against using paroxetine or venlafaxine in children. After conducting its own meta-analysis, the FDA in 2004 ordered a black-box warning about suicidality and the use of antidepressants in children and adolescents ( Box ).7
After the pediatric ‘black box.’ Antidepressant prescriptions for children and adolescents declined in the years 2003 to 2004, as did diagnosis of pediatric depression.8-10 Antidepressant prescribing also showed signs of shifting from general practitioners to psychiatrists.8 At the same time, the suicide rate among youth age 11 In patients age >60, SSRI prescriptions continued to rise and suicide rates fell,9 a pattern of change consistent with antidepressants protecting against suicide.
An independent meta-analysis by Bridge et al12 examined the pediatric trial data used in the FDA meta-analysis plus 7 additional studies. Its findings differ in 2 important ways from those of the FDA review:
- Antidepressants—including others besides fluoxetine—showed efficacy in treating anxiety disorders and depression in children and adolescents.
- The frequency of suicide-related adverse events (no trial patients committed suicide) was approximately 3% on active medication—25% lower than the FDA estimated rate—and 2% on placebo, similar to the FDA estimate.
Antidepressants and suicide risk, 1985 to 2007
| 1985 | 1990 | 1991 | 1999 | 2003 | 2004 | 2006 | 2007 |
|---|---|---|---|---|---|---|---|
| Case reports suggest link between suicide and SSRI use | FDA analysis finds no association between SSRIs and increased suicide risk | UK agency warns of suicide-related events in children treated with paroxetine and venlafaxine | FDA conducts meta-analysis, requires black-box warnings of risk of suicidality in youth taking antidepressants | FDA meta-analysis finds age-dependent effect of antidepressants on suicidality risk in adults | FDA expands warning of increased suicidality risk with antidepressants to adults age | ||
| Antidepressant prescriptions quadruple; age-adjusted suicide rate drops 22.5% for women and 12.8% for men | Pediatric depression diagnoses and antidepressant prescriptions decline; suicides increase 11% | Bridge et al meta-analysis finds 25% lower rate of suicide-related events in youth than the FDA found | |||||
What about adults?
Overall effect. A subsequent FDA meta-analysis of antidepressant clinical trial data in adults13 found 8 suicides in 372 trials totaling nearly 100,000 persons. All occurred in the 295 trials with psychiatric indications. Among these psychiatric trials, 59% had a suicidal behavior/ideation event in either the test-drug or placebo arm, and 41% had none. Eleven antidepressants were included in the meta-analysis:
- 6 SSRIs (citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, and sertraline)
- 2 SNRIs (duloxetine and venlafaxine)
- 3 others (bupropion, mirtazapine, and nefazodone).
Age-specific findings. When the FDA analysis was stratified by age, however, antidepressants’ benefit appeared greater for patients age ≥25 than for those age 18 to 24. The data suggested:
- elevated suicidality risk among adults age
- neutral or possibly protective effect for adults age 25 to 64
- protective effect in adults age ≥65 ( Table 1 ).13
FDA meta-analysis: Suicide rates by age in antidepressant trials
| Age group (yr) | Suicide rate (%)(test drug/placebo) | Suicide attempt rate (%)(test drug/placebo) |
|---|---|---|
| 18 to 24 | 0.03/0.00 | 0.55/0.27 |
| 25 to 30 | 0.00/0.03 | 0.23/0.11 |
| 31 to 64 | 0.01/0.00 | 0.13/0.15 |
| ≥65 | 0.00/0.04 | 0.03/0.25 |
| Source: Reference 13 | ||
The odds ratio for suicidal behavior (preparatory acts, attempt, or suicide) for subacts, attempt, or suicide) for subjects age 18 to 24 on test drug vs placebo was 2.31 (95% CI: 1.02, 5.64) [event rate/sample: 23/3810 vs 8/2604]. NNH was 333, which means 333 adults in this age group would need to be treated with an antidepressant for 1 to experience a suicidal behavior event that would not have happened with placebo.
1. Kuehn BM. FDA panel seeks to balance risks in warnings for antidepressants. J Am Med Assoc 2007;297:573-4.
2. Grunebaum MF, Ellis SP, Li S, et al. Antidepressants and suicide risk in the United States, 1985-1999. J Clin Psychiatry 2004;65(11):1456-62.
3. Teicher MH, Glod C, Cole JO. Emergence of intense suicidal preoccupation during fluoxetine treatment. Am J Psychiatry 1990;147:207-10.
4. King RA, Riddle MA, Chappell PB, et al. Emergence of self-destructive phenomena in children and adolescents during fluoxetine treatment. J Am Acad Child Adolesc Psychiatry 1991;30(2):179-86.
5. Rothschild AJ, Locke CA. Reexposure to fluoxetine after serious suicide attempts by three patients: the role of akathisia. J Clin Psychiatry 1991;52:491-3.
6. Beasley CM, Dornseif BE, Bosomworth JC, et al. Fluoxetine and suicide: a meta-analysis of controlled trials of treatment for depression. BMJ 1991;303:685-92.
7. Hammad TA. Review and evaluation of clinical data. Food and Drug Administration. August 16, 2004. Available at: http://www.fda.gov/ohrms/dockets/ac/04/briefing/2004-4065b1-10-TAB08-Hammads-Review.pdf. Accessed September 19, 2007.
8. Nemeroff CB, Kalali A, Keller MB, et al. Impact of publicity concerning pediatric suicidality data on physician practice patterns in the United States. Arch Gen Psychiatry 2007;64(4):466-72.
9. Gibbons RD, Brown CH, Hur K, et al. Early evidence on the effects of regulators’ suicidality warnings on SSRI prescriptions and suicide in children and adolescents. Am J Psychiatry 2007;164:1356-63.
10. Libby AM, Brent DA, Morrato EH, et al. Decline in treatment of pediatric depression after FDA advisory on risk of suicidality with SSRIs. Am J Psychiatry 2007;164(6):884-91.
11. US. Department of Health and Human Services. Centers for Disease Control and Prevention. Fatal injury reports. Web-based injury statistics query and reporting system. Available at: http://www.cdc.gov/NCIPC/wisqars. Accessed July 16, 2007.
12. Bridge JA, Iyengar S, Salary CB, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA 2007;297:1683-96.
13. Levenson M, Holland C. Statistical evaluation of suicidality in adults treated with antidepressants. In: Laughren TP. Memorandum: overview for December 13 meeting of PsychopharmacologicDrugs Advisory Committee (PDAC). Center for Drug Evaluation and Research, US Food and Drug Administration. November 16, 2006. Available at: http://www.fda.gov/ohrms/dockets/ac/06/briefing/2006-4272b1-01-FDA.pdf. Accessed October 11, 2007.
14. Bostwick JM, Pankratz VS. Affective disorders and suicide risk: a reexamination. Am J Psychiatry 2000;157(12):1925-32.
15. Lafuente-Lafuente C, Mouly S, Longas-Tejero MA, et al. Antiarrhythmic drugs for maintaining sinus rhythm after cardioversion of atrial fibrillation: a systematic review of randomized controlled trials. Arch Intern Med 2006;166(7):719-28.
16. Khan A, Khan S, Kolts R, Brown WA. Suicide rates in clinical trials of SSRIs, other antidepressants, and placebo: analysis of FDA reports. Am J Psychiatry 2003;160:790-2.
17. Jick H, Kaye JA, Jick SS. Antidepressants and the risk of suicidal behaviors. J Am Med Assoc 2004;292(3):338-43.
18. Martinez C, Rietbrock S, Wise L, et al. Antidepressant treatment and the risk of fatal and non-fatal self harm in first episode depression: nested case-control study. BMJ 2005;330(7488):389.-
19. Gunnell D, Saperia J, Ashby D. Selective serotonin reuptake inhibitors (SSRIs) and suicide in adults: meta-analysis of drug company data from placebo controlled, randomised controlled trials submitted to the MHRA’s safety review. BMJ 2005;330(7488):385-9.
20. Fergusson D, Doucette S, Glass KC, et al. Association between suicide attempts and selective serotonin reuptake inhibitors: systematic review of randomised controlled trials. BMJ 2005;330(7488):396.-
21. Juurlink DN, Mamdani MM, Kopp A, Redelmeier DA. The risk of suicide with selective serotonin reuptake inhibitors in the elderly. Am J Psychiatry 2006;163(5):813-21.
22. Isacsson G, Holmgren P, Ahlner J. Selective serotonin reuptake inhibitor antidepressants and the risk of suicide: a controlled forensic database study of 14,857 suicides. Acta Psychiatr Scand. 2005;111(4):286-90.
23. Simon GE, Savarino J, Operskalski B, Wang PS. Suicide risk during antidepressant treatment. Am J Psychiatry 2006;163(1):41-7.
24. Gibbons RD, Brown CH, Hur K, et al. Relationship between antidepressants and suicide attempts: an analysis of the Veterans Health Administration data sets. Am J Psychiatry 2007;164(7):1044-9.
25. Simon GE, Savarino J. Suicide attempts among patients starting depression treatment with medications or psychotherapy. Am J Psychiatry 2007;164(7):1029-34.
26. Mann JJ, Apter A, Bertolote J, et al. Suicide prevention strategies: a systematic review. JAMA 2005;294(16):2064-74.
27. Rich CL, Isacsson G. Suicide and antidepressants in South Alabama: evidence for improved treatment of depression. J Affect Disord 1997;45:135-42.
28. Isacsson G, Bergman U, Rich CL. Antidepressants, depression and suicide: an analysis of the San Diego study. J Affect Disord 1994;32:277-86.
29. Geddes JR, Carney SM, Davies C, et al. Relapse prevention with antidepressant drug treatment in depressive disorders: a systematic review. Lancet 2003;361(9358):653-61.
30. Gibbons RD, Hur K, Bhaumik DK, Mann JJ. The relationship between antidepressant medication use and rate of suicide. Arch Gen Psychiatry 2005;62(2):165-72.
31. Hall WD, Mant A, Mitchell PB, et al. Association between antidepressant prescribing and suicide in Australia, 1991-2000: trend analysis. BMJ 2003;326(7397):1008-11.
32. Nakagawa A, Grunebaum MF, Ellis SP, et al. Association of suicide and antidepressant prescription rates in Japan, 1999-2003. J Clin Psychiatry 2007;68(6):908-16.
33. Helgason T, Tomasson H, Zoega T. Antidepressants and public health in Iceland. Time series analysis of national data. Br J Psychiatry 2004;184:157-62.
34. March J, Silva S, Petrycki S, et al. Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for Adolescents with Depression Study (TADS) randomized controlled trial. JAMA 2004;292(7):807-20.
1. Kuehn BM. FDA panel seeks to balance risks in warnings for antidepressants. J Am Med Assoc 2007;297:573-4.
2. Grunebaum MF, Ellis SP, Li S, et al. Antidepressants and suicide risk in the United States, 1985-1999. J Clin Psychiatry 2004;65(11):1456-62.
3. Teicher MH, Glod C, Cole JO. Emergence of intense suicidal preoccupation during fluoxetine treatment. Am J Psychiatry 1990;147:207-10.
4. King RA, Riddle MA, Chappell PB, et al. Emergence of self-destructive phenomena in children and adolescents during fluoxetine treatment. J Am Acad Child Adolesc Psychiatry 1991;30(2):179-86.
5. Rothschild AJ, Locke CA. Reexposure to fluoxetine after serious suicide attempts by three patients: the role of akathisia. J Clin Psychiatry 1991;52:491-3.
6. Beasley CM, Dornseif BE, Bosomworth JC, et al. Fluoxetine and suicide: a meta-analysis of controlled trials of treatment for depression. BMJ 1991;303:685-92.
7. Hammad TA. Review and evaluation of clinical data. Food and Drug Administration. August 16, 2004. Available at: http://www.fda.gov/ohrms/dockets/ac/04/briefing/2004-4065b1-10-TAB08-Hammads-Review.pdf. Accessed September 19, 2007.
8. Nemeroff CB, Kalali A, Keller MB, et al. Impact of publicity concerning pediatric suicidality data on physician practice patterns in the United States. Arch Gen Psychiatry 2007;64(4):466-72.
9. Gibbons RD, Brown CH, Hur K, et al. Early evidence on the effects of regulators’ suicidality warnings on SSRI prescriptions and suicide in children and adolescents. Am J Psychiatry 2007;164:1356-63.
10. Libby AM, Brent DA, Morrato EH, et al. Decline in treatment of pediatric depression after FDA advisory on risk of suicidality with SSRIs. Am J Psychiatry 2007;164(6):884-91.
11. US. Department of Health and Human Services. Centers for Disease Control and Prevention. Fatal injury reports. Web-based injury statistics query and reporting system. Available at: http://www.cdc.gov/NCIPC/wisqars. Accessed July 16, 2007.
12. Bridge JA, Iyengar S, Salary CB, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA 2007;297:1683-96.
13. Levenson M, Holland C. Statistical evaluation of suicidality in adults treated with antidepressants. In: Laughren TP. Memorandum: overview for December 13 meeting of PsychopharmacologicDrugs Advisory Committee (PDAC). Center for Drug Evaluation and Research, US Food and Drug Administration. November 16, 2006. Available at: http://www.fda.gov/ohrms/dockets/ac/06/briefing/2006-4272b1-01-FDA.pdf. Accessed October 11, 2007.
14. Bostwick JM, Pankratz VS. Affective disorders and suicide risk: a reexamination. Am J Psychiatry 2000;157(12):1925-32.
15. Lafuente-Lafuente C, Mouly S, Longas-Tejero MA, et al. Antiarrhythmic drugs for maintaining sinus rhythm after cardioversion of atrial fibrillation: a systematic review of randomized controlled trials. Arch Intern Med 2006;166(7):719-28.
16. Khan A, Khan S, Kolts R, Brown WA. Suicide rates in clinical trials of SSRIs, other antidepressants, and placebo: analysis of FDA reports. Am J Psychiatry 2003;160:790-2.
17. Jick H, Kaye JA, Jick SS. Antidepressants and the risk of suicidal behaviors. J Am Med Assoc 2004;292(3):338-43.
18. Martinez C, Rietbrock S, Wise L, et al. Antidepressant treatment and the risk of fatal and non-fatal self harm in first episode depression: nested case-control study. BMJ 2005;330(7488):389.-
19. Gunnell D, Saperia J, Ashby D. Selective serotonin reuptake inhibitors (SSRIs) and suicide in adults: meta-analysis of drug company data from placebo controlled, randomised controlled trials submitted to the MHRA’s safety review. BMJ 2005;330(7488):385-9.
20. Fergusson D, Doucette S, Glass KC, et al. Association between suicide attempts and selective serotonin reuptake inhibitors: systematic review of randomised controlled trials. BMJ 2005;330(7488):396.-
21. Juurlink DN, Mamdani MM, Kopp A, Redelmeier DA. The risk of suicide with selective serotonin reuptake inhibitors in the elderly. Am J Psychiatry 2006;163(5):813-21.
22. Isacsson G, Holmgren P, Ahlner J. Selective serotonin reuptake inhibitor antidepressants and the risk of suicide: a controlled forensic database study of 14,857 suicides. Acta Psychiatr Scand. 2005;111(4):286-90.
23. Simon GE, Savarino J, Operskalski B, Wang PS. Suicide risk during antidepressant treatment. Am J Psychiatry 2006;163(1):41-7.
24. Gibbons RD, Brown CH, Hur K, et al. Relationship between antidepressants and suicide attempts: an analysis of the Veterans Health Administration data sets. Am J Psychiatry 2007;164(7):1044-9.
25. Simon GE, Savarino J. Suicide attempts among patients starting depression treatment with medications or psychotherapy. Am J Psychiatry 2007;164(7):1029-34.
26. Mann JJ, Apter A, Bertolote J, et al. Suicide prevention strategies: a systematic review. JAMA 2005;294(16):2064-74.
27. Rich CL, Isacsson G. Suicide and antidepressants in South Alabama: evidence for improved treatment of depression. J Affect Disord 1997;45:135-42.
28. Isacsson G, Bergman U, Rich CL. Antidepressants, depression and suicide: an analysis of the San Diego study. J Affect Disord 1994;32:277-86.
29. Geddes JR, Carney SM, Davies C, et al. Relapse prevention with antidepressant drug treatment in depressive disorders: a systematic review. Lancet 2003;361(9358):653-61.
30. Gibbons RD, Hur K, Bhaumik DK, Mann JJ. The relationship between antidepressant medication use and rate of suicide. Arch Gen Psychiatry 2005;62(2):165-72.
31. Hall WD, Mant A, Mitchell PB, et al. Association between antidepressant prescribing and suicide in Australia, 1991-2000: trend analysis. BMJ 2003;326(7397):1008-11.
32. Nakagawa A, Grunebaum MF, Ellis SP, et al. Association of suicide and antidepressant prescription rates in Japan, 1999-2003. J Clin Psychiatry 2007;68(6):908-16.
33. Helgason T, Tomasson H, Zoega T. Antidepressants and public health in Iceland. Time series analysis of national data. Br J Psychiatry 2004;184:157-62.
34. March J, Silva S, Petrycki S, et al. Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for Adolescents with Depression Study (TADS) randomized controlled trial. JAMA 2004;292(7):807-20.
Modafinil: Not just for sleep disorders?
Ms. B, a middle-aged mother of 3, is being monitored for bipolar disorder. She has a history of stimulant abuse but has been in remission for 5 years. She complains of excessive daytime sleepiness. Most days she wakes at 7 AM, but sleeps on several occasions during the day. She also complains of fatigue and lack of motivation.
She is being treated with lithium, venlafaxine, and zolpidem and reports good adherence. Basic laboratory work and serum lithium levels are within acceptable ranges. Her symptoms do not improve when venlafaxine is titrated from 225 mg/d to 300 mg/d. She also reports previously failed trials with bupropion and fluoxetine.
We decide to try a psychostimulant as an augmenting agent. Because of her past stimulant abuse, we add modafinil, 100 mg/d and increase to 200 mg/d. Ms. B reports improvement in her daytime sleepiness and fatigue and—except for a mild headache—tolerates the medication well.
Modafinil is being investigated for potential roles in managing inattention, excess sleepiness, fatigue, and cognitive dysfunction associated with:
- mood disorders (major depression and bipolar depression)
- attention-deficit/hyperactivity disorder (ADHD)
- schizophrenia
- cocaine dependence.
This article discusses how the drug promotes wakefulness, how it might improve cognitive function, and what the evidence reveals about off-label indications.
How it works
Although modafinil’s precise mechanism of action is unknown, it is believed to promote wakefulness more selectively than conventional stimulants such as amphetamine and methylphenidate. Modafinil does not bind to norepinephrine, serotonin, dopamine, or benzodiazepine receptors.1,2 It might target specific hypothalamic regions such as the tuberomammillary nucleus and orexin neurons, which are peptide neurotransmitters that promote wakefulness.3,4
Clinical trials found that modafinil has beneficial effects on:
- working memory, recognition memory, and sustained attention in healthy humans
- prefrontal-dependent cognitive functions in schizophrenia, major depression, and adult ADHD.5
Evidence for approved indications
Modafinil is indicated to improve wakefulness in patients who have excessive sleepiness associated with narcolepsy, obstructive sleep apnea, or shift work sleep disorder. It was approved for reducing excessive sleepiness in narcoleptic patients after two 9-week placebo-controlled clinical trials. The drug significantly reduced sleepiness and improved overall disease status as measured by the Clinical Global Impression of Change (CGI-C) scale.6,7
In patients with shift work sleep disorder, a 12-week placebo-controlled clinical trial found that modafinil significantly improved sleep latency and CGI-C scores.10
Dosage and side effects. For patients with narcolepsy or obstructive sleep apnea, the recommended dose is 200 mg given in the morning.11 For patients prescribed modafinil for work-time wakefulness, the dose is 200 mg 1 hour before their work shift. Lower doses are recommended for patients who are elderly or have hepatic impairment. Those with severe hepatic impairment typically are prescribed 100 mg/d.11 Modafinil is rapidly absorbed and is metabolized primarily by the liver (Table 1). A summary of potential drug-drug interactions appears in Table 2.11
In pivotal trials, adverse events that occurred more frequently with modafinil than with placebo and in >5% of the study population included headache, nausea, nervousness, rhinitis, diarrhea, back pain, insomnia, dizziness, and dyspepsia. Headache was most commonly reported; in most patients, it resolved soon after they started taking modafinil. Post-marketing reports have included cases of psychosis, mania, and suspected serious skin reactions, including Stevens-Johnson syndrome.11 Modafinil lacks euphorigenic properties and has minimal potential for abuse.12
Table 1
Modafinil’s pharmacokinetics
| Absorbed rapidly, with peak plasma concentrations at 2 to 4 hours |
| Apparent steady states reached after 2 to 4 days of dosing |
| Half-life: 15 hours |
| Major route of elimination (~90%) is metabolism, primarily by the liver |
Selected drug-drug interactions with modafinil
| Action of modafinil | Potential drug interactions |
|---|---|
| Increases elimination of CYP 3A4 substrates | Carbamazepine, phenytoin may decrease modafinil levels Azole antifungals, protease inhibitors, and erythromycin may increase modafinil levels |
| Inhibits CYP 2C19 enzyme | Modafinil may increase levels of citalopram, diazepam, and sertraline |
| Decreases absorption of ethinyl estradiol | Modafinil can decrease effectiveness of oral contraceptives |
| CYP: cytochrome P-450 | |
| Source: Reference 11 | |
Evidence for off-label uses
Major depressive disorder (MDD). The fatigue and excessive sleepiness often seen with MDD often persist after other depressive symptoms have remitted with antidepressant treatment.13 Patients with these symptoms might benefit from modafinil’s stimulating properties. Conventional stimulants such as methylphenidate have been used to improve neurovegetative symptoms of depression, but modafinil offers several advantages:
- decreased adverse CNS effects
- fewer drug-drug interactions
- minimal risk for dependence or abuse.
A 6-week open-label study of 25 depressed patients with residual fatigue and sleepiness showed that adjunctive modafinil, 100 to 200 mg/d, significantly improved these symptoms, as well as Hamilton Rating Scale for Depression (HAM-D) score, as early as week 2. Seventy-six percent of patients responded to treatment, defined as a >50% reduction in HAM-D scores.16
Several open-label studies and case re-ports have evaluated adjunctive modafinil use in patients with:
- depression characterized by ongoing lethargy or apathy17
- depression with atypical features18
- seasonal affective disorder19
- partial response to antidepressants.20,21
Bipolar depression. A 6-week, double-blind, placebo-controlled trial randomly assigned 85 patients with bipolar depression to adjunctive modafinil, 100 to 200 mg/d, or placebo for 6 weeks (Table 3).22 The number of patients receiving an antidepressant or mood stabilizer was not significantly different between the modafinil and placebo groups.
The primary outcome measure was change in the Inventory for Depressive Symptoms (IDS) score from baseline to endpoint. Forty-four percent of patients receiving modafinil achieved a ≥50% reduction in IDS score, compared with 23% of the placebo group; this difference was statistically significant (P=0.03).
In this study, modafinil was well tolerated and did not induce mania or hypomania. Cases of modafinil-induced mania have been reported elsewhere.23,24
The mechanisms of modafinil’s antidepressant effects are unclear. The drug does not cause release of norepinephrine or dopamine. One study proposed that modafinil acts by releasing histamine and activating noradrenaline receptors.25 Activation of these receptors increases dopamine and norepinephrine in these areas, and excites histaminergic tuberomammillary neurons, increasing histamine levels. Another trial suggested that modafinil may improve mood by mechanisms similar to the antidepressant effects induced by sleep deprivation.26
Summary. Modafinil may have a role in managing residual fatigue and excessive sleepiness associated with MDD and bipolar depression. Evidence for a mood-elevating effect is minimal; additional studies are needed. Adjunctive modafinil and conventional stimulants have not been compared head-to-head in patients with mood disorders. Modafinil’s tolerability profile and lack of euphorigenic and reinforcing properties make it a potentially attractive alternative, however.
ADHD. Approximately 30% of ADHD patients do not respond to or are unable to tolerate conventional stimulant medications such as methylphenidate and dextroamphetamine.27 Several studies have evaluated modafinil as a potential treatment for ADHD based on the drug’s action on arousal and attention systems. Although modafinil’s precise mechanism of action in ADHD is unknown, proposed mechanisms include:
- hypothalamic and cerebral cortex neuronal activation
- action on histamine that results in internal vigilance.28
Can modafinil help patients with mood disorders?
| Author | Study design | Modafinil dose | Conclusion |
|---|---|---|---|
| Major depressive disorder | |||
| Fava et al, 200514 | 8-week, double-blind, placebo-controlled; 331 subjects with partial or no response to SSRI monotherapy | 200 mg/d | No significant difference between modafinil and placebo at final visit |
| DeBattista et al, 200315 | 6-week, double-blind, placebo-controlled; 136 subjects with partial response to antidepressant therapy | 100 to 400 mg/d | Significant improvement in sleepiness by week 1 and fatigue by week 2, but differences between modafinil and placebo were not statistically significant by end of study |
| Konuk et al, 200616 | 6-week, open-label; 25 subjects with residual sleepiness or fatigue after SSRI therapy | 100 to 200 mg/d | All patients showed significant improvement in sleepiness, fatigue, and HAM-D scores |
| Bipolar depression | |||
| Frye et al, 200722 | 6-week, double-blind, placebo-controlled trial; 85 subjects who did not respond to a mood stabilizer with or without concomitant antidepressant therapy | 100 to 200 mg/d (mean 177 mg/d) | 44% of modafinil patients achieved ≥50% reduction in IDS score compared with 23% in placebo group (P=0.03) |
| HAM-D: Hamilton Rating Scale for Depression; IDS: Inventory for Depressive Symptoms; SSRI: selective serotonin reuptake inhibitor | |||
CASE 2: Another Tx for ADHD
Matt, age 8, is referred to our outpatient child psychiatric clinic after his parents noted declining school performance associated with increased aggression and irritability. Our assessment strongly supports a diagnosis of ADHD without comorbid conditions. We start Matt on methylphenidate, 5 mg twice daily, which quickly improves his ADHD symptoms. However, the medication causes GI side effects and profound sleep and weight changes.
Matt’s parents request that their son be treated with a different type of agent. A trial of atomoxetine is not as effective as the initial methylphenidate dosage and produces similar side effects. We then consider modafinil because of its side effect profile. We start Matt on 100 mg once daily and titrate up to 200 mg/d 4 weeks later. Matt and his parents notice an immediate improvement in his ADHD symptoms with no side effects.
In children and adolescents. Wigal et al29 reviewed pooled data from 3 randomized, double-blind, placebo-controlled studies of modafinil in pediatric ADHD (Table 4). Modafinil was well tolerated and improved ADHD symptoms and behaviors regardless of patients’ stimulant use history.
In a recent open-label study, 220 children and young adolescents with ADHD who had completed 4 weeks of a double-blind, placebo-controlled trial were evaluated for an additional 8 weeks. Modafinil improved ADHD symptoms and overall clinical condition as determined by the parent- or clinician-completed ADHD Rating Scale-IV Home Version, the parent-completed Conners’ ADHD/DSM-IV Scale Parent Version, and the clinician-rated CGI scale.30 Insomnia, headache, and decreased appetite were the most commonly reported adverse events.
In adults. The results of 2 double-blind, placebo-controlled trials of modafinil in adults with ADHD have been positive:
- In 1 study, modafinil (mean 206.8 mg/d) was more effective than placebo and comparable to dextroamphetamine in improving ADHD symptoms.31
- In another, modafinil (a single 200-mg dose) increased cognitive performance during treatment.32
Schizophrenia. Double-blind, randomized placebo-controlled studies have evaluated modafinil for improving cognitive function and reducing negative symptoms in patients with schizophrenia. Results have been inconsistent.
One double-blind, randomized, placebo-controlled crossover study of 20 patients with chronic schizophrenia found that modafinil, 200 mg/d, significantly improved short-term verbal memory span and attentional set shifting—the ability to discriminate and selectively attend to various stimulus dimensions (Table 5).33 Two other controlled studies showed no differences between the effects of modafinil and placebo on schizophrenia’s fatigue, cognition, or positive or negative symptoms.34,35
Summary. Although open-label studies have shown modafinil has beneficial effects on cognitive symptoms, controlled data are scarce. Reports of modafinil-induced psychosis or mania11 may limit the drug’s usefulness in schizophrenia patients.
Cocaine dependence. No medications are FDA-approved for treating cocaine dependence. A placebo-controlled, double-blind trial found that modafinil blunts cocaine euphoria under controlled conditions.36 This effect is hypothesized to be secondary to modafinil’s glutamate-enhancing and gamma-aminobutyric acid inhibitory effects.37
Summary. A single study supports using modafinil to improve outcomes in cocaine-dependent patients receiving standardized psychosocial treatment. More research is needed.
Table 4
Modafinil and ADHD: What the evidence says
| Author | Study design | Modafinil dosage | Conclusion |
|---|---|---|---|
| Wigal et al, 200629 | Analysis of data from 3 double-blind, placebo-controlled trials; total 638 children/adolescents, some of whom had received prior stimulant therapy | 170 to 425 mg/d | Whether or not patients received prior stimulant treatment, modafinil significantly improved ADHD symptoms and was well tolerated |
| Boellner et al, 200630 | 8-week, open-label extension of a 4-week double-blind, placebo-controlled trial; 220 subjects ages 6-14 | 100 to 400 mg/d | Modafinil improved ADHD symptoms and overall clinical condition |
| Taylor et al, 200031 | 2-week, double-blind, placebo-controlled crossover comparing modafinil with dextroamphetamine; 22 adults | Mean 206.8 mg/d | Both modafinil and dextroamphetamine significantly improved ADHD symptoms compared with placebo |
| Turner et al, 200432 | Double-blind, placebo-controlled crossover; 20 adults | Single 200-mg dose | Modafinil improved results on cognitive tests, including short-term memory span, visual memory, spatial planning, and sustained attention |
| ADHD: attention-deficit/hyperactivity disorder | |||
Table 5
Modafinil for schizophrenia or cocaine dependence:
More research is needed
| Author | Study design | Modafinil dosage | Conclusion |
|---|---|---|---|
| Schizophrenia | |||
| Turner et al, 200433 | Double-blind, placebo-controlled crossover; 20 adults | 200 mg/d | Modafinil significantly improved attentional set shifting and short-term verbal memory span |
| Sevy et al, 200534 | 8-week, double-blind, placebo-controlled; 24 subjects | Up to 200 mg/d | No significant difference between modafinil and placebo in reducing fatigue or positive or negative symptoms or in improving cognition |
| Pierre et al, 200735 | 8-week, double-blind, placebo-controlled; 20 subjects | 100 to 200 mg/d | Modafinil did not significantly improve neurocognitive or negative symptoms |
| Cocaine dependence | |||
| Dackis et al, 200538 | 8-week, double-blind, placebo-controlled; 62 cocaine-dependent subjects | 400 mg/d | Patients receiving modafinil provided significantly more cocaine-negative urine samples and were significantly more likely to achieve =3 weeks cocaine abstinence than those receiving placebo |
Related resource
- Ballon JS, Feifel D. A systematic review of modafinil: potential clinical uses and mechanisms of action. J Clin Psychiatry 2006;67(4):554-66.
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Carbamazepine • Carbatrol, Tegretol, others
- Citalopram • Celexa
- Dextroamphetamine • Dexedrine, DextroStat
- Diazepam • Valium
- Erythromycin • Ery-Tab, Eryc, others
- Fluoxetine • Prozac
- Lithium • Eskalith, Lithobid
- Methylphenidate • Ritalin, others
- Modafinil • Provigil
- Phenytoin • Dilantin
- Sertraline • Zoloft
- Venlafaxine • Effexor
- Zolpidem • Ambien
Dr. Ramaswamy receives research support from Bristol-Myers Squibb, Shire, and Forest Pharmaceuticals and is a consultant to Dainippon Sumitomo Pharma.
Dr. Mattai reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Wilson receives research support from, is a consultant to, or is a speaker for the National Institute of Mental Health, the Substance Abuse and Mental Health Services Administration, the Veterans Administration, the State of Nebraska, the State of Ohio, Health Futures Foundation, Inc., Abbott Laboratories, Astra-Zeneca, Bristol-Myers Squibb, Elan, Eli Lilly and Company, GlaxoSmithKline, Janssen, Ortho-McNeil, Pfizer, and Wyeth.
1. Mignot E, Nishino S, Guilleminault C, et al. Modafinil binds to dopamine uptake carrier site with low affinity. Sleep 1994;17:436-7.
2. Lin J-S, Hou Y, Jouvet M. Potential brain neuronal targets for amphetamine, methylphenidate, and modafinil induced wakefulness, evidenced by c-fos immunocytochemistry in the cat. Proc Natl Acad Sci USA 1996;93:14128-33.
3. Scammell TE, Estabrooke IV, McCarthy MT, et al. Hypothalamic arousal regions are activated during modafinil-induced wakefulness. J Neurosci 2000;20(22):8620-8.
4. Stenberg D. Neuroanatomy and neurochemistry of sleep. Cell Mol Life Sci 2007;64(10):1187-204.
5. Minzenberg MJ, Carter CS. Modafinil: a review of neurochemical actions and effects on cognition. Neuropsychopharmacology In press.
6. U.S. Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil for the treatment of pathological somnolence in narcolepsy. Ann Neurol 1998;43(1):88-97.
7. U.S. Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil as a treatment for the excessive daytime somnolence of narcolepsy. Neurology 2000;54:1166-75.
8. Black JE, Hirshkowitz M. Modafinil for treatment of residual excessive sleepiness in nasal continuous positive airway pressure-treated obstructive sleep apnea/hypopnea syndrome. Sleep 2005;28(4):464-71.
9. Pack AI, Black JE, Schwartz JR, Matheson JK. Modafinil as adjunct therapy for daytime sleepiness in obstructive sleep apnea. Am J Respir Crit Care Med 2001;164(9):1675-81.
10. Czeisler CA, Walsh JK, Roth T, et al. and the U.S. Modafinil in Shift Work Sleep Disorder Study Group. Modafinil for excessive sleepiness associated with shift-work sleep disorder. N Engl J Med. 2005;353(5):476-86. Published correction appears in: N Engl J Med 2005;353(10):1078.-
11. Provigil [package insert] West Chester, PA: Cephalon Inc; 2004.
12. Myrick H, Malcolm R, Taylor B, et al. Modafinil: preclinical, clinical, and post-marketing surveillance—a review of abuse liability issues. Ann Clin Psychiatry 2004;16(2):101-9.
13. Baldwin DS, Papakostas GI. Symptoms of fatigue and sleepiness in major depressive disorder. J Clin Psychiatry 2006;67(suppl 6):9-15.
14. Fava M, Thase ME, DeBattista C. A multicenter, placebo-controlled study of modafinil augmentation in partial responders to selective serotonin reuptake inhibitors with persistent fatigue and sleepiness. J Clin Psychiatry 2005;66(1):85-93.
15. DeBattista C, Doghramji K, Menza MA, et al. and the Modafinil in Depression Study Group. Adjunct modafinil for the short-term treatment of fatigue and sleepiness in patients with major depressive disorder: a preliminary double-blind, placebo-controlled study. J Clin Psychiatry 2003;64(9):1057-64.
16. Konuk N, Atasoy N, Atik L, Akay O. Open-label study of adjunct modafinil for the treatment of patients with fatigue, sleepiness, and major depression treated with selective serotonin reuptake inhibitors. Adv Ther 2006;23(4):646-54.
17. Markovitz PJ, Wagner S. An open-label trial of modafinil augmentation in patients with partial response to antidepressant therapy. J Clin Psychopharmacol 2003;23(2):207-9.
18. Vaishnavi S, Gadde K, Alamy S, et al. Modafinil for atypical depression: effects of open-label and double-blind discontinuation treatment. J Clin Psychopharmacol 2006; 26(4): 373-8. Published correction appears in: J Clin Psychopharmacol. 2006;26(5):523.
19. Lundt L. Modafinil treatment in patients with seasonal affective disorder/winter depression: an open-label pilot study. J Affect Disord 2004;81(2):173-8.
20. DeBattista C, Lembke A, Solvason HB, et al. A prospective trial of modafinil as an adjunctive treatment of major depression. J Clin Psychopharmacol 2004;24(1):87-90.
21. Rasmussen NA, Schroder P, Olsen LR, et al. Modafinil augmentation in depressed patients with partial response to antidepressants: a pilot study on self-reported symptoms covered by the Major Depression Inventory (MDI) and the Symptom Checklist (SCL-92). Nord J Psychiatry 2005;59(3):173-8.
22. Frye MA, Grunze H, Suppes T, et al. A placebo-controlled evaluation of adjunctive modafinil in the treatment of bipolar depression. Am J Psychiatry 2007;164:1242-9.
23. Wolf J, Fiedler U, Anghelescu I, Schwertfeger N. Manic switch in a patient with treatment-resistant bipolar depression treated with modafinil. J Clin Psychiatry 2006;67(11):1817.-
24. Vorspan F, Warot D, Consoli A, et al. Mania in a boy treated with modafinil for narcolepsy. Am J Psychiatry 2005;162(4):813-4.
25. McClellan KJ, Spencer CM. Modafinil: a review of its pharmacology and clinical efficacy in the management of narcolepsy. CNS Drugs 1998;9(4):311-24.
26. Ballon JS, Feifel D. A systematic review of modafinil: potential clinical uses and mechanisms of action. J Clin Psychiatry 2006;67(4):554-66.
27. Dulcan M. Practice parameters for the assessment and treatment of children, adolescents and adults with attentiondeficit hyperactivity disorder. American Academy of Child and Adolescent Psychiatry. J Am Acad Child Adolesc Psychiatry 1997;36(suppl 10):85S-121S.
28. Lindsay SE, Gudelsky GA, Heaton PC. Use of modafinil for the treatment of attention deficit/hyperactivity disorder. Ann Pharmacother 2006;40(10):1829-33.
29. Wigal SB, Biederman J, Swanson JM, et al. Efficacy and safety of modafinil film-coated tablets in children and adolescents with or without prior stimulant treatment for attention-deficit/hyperactivity disorder: pooled analysis of 3 randomized, double-blind, placebo-controlled studies. Prim Care Companion J Clin Psychiatry 2006;8(6):352-60.
30. Boellner SW, Earl CQ, Arora S. Modafinil in children and adolescents with attention-deficit/hyperactivity disorder: a preliminary 8-week, open-label study. Curr Med Res Opin 2006;22(12):2457-65.
31. Taylor FB, Russo J. Efficacy of modafinil compared to dextroamphetamine for the treatment of attention deficit hyperactivity disorder in adults. J Child Adolesc Psychopharmacol 2000;10(4):311-20.
32. Turner DC, Clark L, Dowson J, et al. Modafinil improves cognition and response inhibition in adult attention-deficit/ hyperactivity disorder. Biol Psychiatry 2004;55(10):1031-40.
33. Turner DC, Clark L, Pomarol-Clotet E, et al. Modafinil improves cognition and attentional set shifting in patients with chronic schizophrenia. Neuropsychopharmacology 2004;29(7):1363-73.
34. Sevy S, Rosenthal MH, Alvir J, et al. Double-blind, placebo-controlled study of modafinil for fatigue and cognition in schizophrenia patients treated with psychotropic medications. J Clin Psychiatry 2005;66(7):839-43.
35. Pierre JM, Peloian JH, Wirshing DA, et al. A randomized, double-blind, placebo-controlled trial of modafinil for negative symptoms in schizophrenia. J Clin Psychiatry 2007;68(5):705-10.
36. Dackis CA, Lynch KG, Yu E, et al. Modafinil and cocaine: a double-blind, placebo-controlled drug interaction study. Drug Alcohol Depend 2003;70(1):29-37.
37. Perez de la Mora M, Aguilar-Garcia A, Ramon-Frias T, et al. Effects of the vigilance promoting drug modafinil on the synthesis of GABA and glutamate in slices of rat hypothalamus. Neurosci Lett 1999;259:181-5.
38. Dackis CA, Kampman KM, Lynch KG, et al. A double-blind, placebo-controlled trial of modafinil for cocaine dependence. Neuropsychopharmacology 2005;30(1):205-11.
Ms. B, a middle-aged mother of 3, is being monitored for bipolar disorder. She has a history of stimulant abuse but has been in remission for 5 years. She complains of excessive daytime sleepiness. Most days she wakes at 7 AM, but sleeps on several occasions during the day. She also complains of fatigue and lack of motivation.
She is being treated with lithium, venlafaxine, and zolpidem and reports good adherence. Basic laboratory work and serum lithium levels are within acceptable ranges. Her symptoms do not improve when venlafaxine is titrated from 225 mg/d to 300 mg/d. She also reports previously failed trials with bupropion and fluoxetine.
We decide to try a psychostimulant as an augmenting agent. Because of her past stimulant abuse, we add modafinil, 100 mg/d and increase to 200 mg/d. Ms. B reports improvement in her daytime sleepiness and fatigue and—except for a mild headache—tolerates the medication well.
Modafinil is being investigated for potential roles in managing inattention, excess sleepiness, fatigue, and cognitive dysfunction associated with:
- mood disorders (major depression and bipolar depression)
- attention-deficit/hyperactivity disorder (ADHD)
- schizophrenia
- cocaine dependence.
This article discusses how the drug promotes wakefulness, how it might improve cognitive function, and what the evidence reveals about off-label indications.
How it works
Although modafinil’s precise mechanism of action is unknown, it is believed to promote wakefulness more selectively than conventional stimulants such as amphetamine and methylphenidate. Modafinil does not bind to norepinephrine, serotonin, dopamine, or benzodiazepine receptors.1,2 It might target specific hypothalamic regions such as the tuberomammillary nucleus and orexin neurons, which are peptide neurotransmitters that promote wakefulness.3,4
Clinical trials found that modafinil has beneficial effects on:
- working memory, recognition memory, and sustained attention in healthy humans
- prefrontal-dependent cognitive functions in schizophrenia, major depression, and adult ADHD.5
Evidence for approved indications
Modafinil is indicated to improve wakefulness in patients who have excessive sleepiness associated with narcolepsy, obstructive sleep apnea, or shift work sleep disorder. It was approved for reducing excessive sleepiness in narcoleptic patients after two 9-week placebo-controlled clinical trials. The drug significantly reduced sleepiness and improved overall disease status as measured by the Clinical Global Impression of Change (CGI-C) scale.6,7
In patients with shift work sleep disorder, a 12-week placebo-controlled clinical trial found that modafinil significantly improved sleep latency and CGI-C scores.10
Dosage and side effects. For patients with narcolepsy or obstructive sleep apnea, the recommended dose is 200 mg given in the morning.11 For patients prescribed modafinil for work-time wakefulness, the dose is 200 mg 1 hour before their work shift. Lower doses are recommended for patients who are elderly or have hepatic impairment. Those with severe hepatic impairment typically are prescribed 100 mg/d.11 Modafinil is rapidly absorbed and is metabolized primarily by the liver (Table 1). A summary of potential drug-drug interactions appears in Table 2.11
In pivotal trials, adverse events that occurred more frequently with modafinil than with placebo and in >5% of the study population included headache, nausea, nervousness, rhinitis, diarrhea, back pain, insomnia, dizziness, and dyspepsia. Headache was most commonly reported; in most patients, it resolved soon after they started taking modafinil. Post-marketing reports have included cases of psychosis, mania, and suspected serious skin reactions, including Stevens-Johnson syndrome.11 Modafinil lacks euphorigenic properties and has minimal potential for abuse.12
Table 1
Modafinil’s pharmacokinetics
| Absorbed rapidly, with peak plasma concentrations at 2 to 4 hours |
| Apparent steady states reached after 2 to 4 days of dosing |
| Half-life: 15 hours |
| Major route of elimination (~90%) is metabolism, primarily by the liver |
Selected drug-drug interactions with modafinil
| Action of modafinil | Potential drug interactions |
|---|---|
| Increases elimination of CYP 3A4 substrates | Carbamazepine, phenytoin may decrease modafinil levels Azole antifungals, protease inhibitors, and erythromycin may increase modafinil levels |
| Inhibits CYP 2C19 enzyme | Modafinil may increase levels of citalopram, diazepam, and sertraline |
| Decreases absorption of ethinyl estradiol | Modafinil can decrease effectiveness of oral contraceptives |
| CYP: cytochrome P-450 | |
| Source: Reference 11 | |
Evidence for off-label uses
Major depressive disorder (MDD). The fatigue and excessive sleepiness often seen with MDD often persist after other depressive symptoms have remitted with antidepressant treatment.13 Patients with these symptoms might benefit from modafinil’s stimulating properties. Conventional stimulants such as methylphenidate have been used to improve neurovegetative symptoms of depression, but modafinil offers several advantages:
- decreased adverse CNS effects
- fewer drug-drug interactions
- minimal risk for dependence or abuse.
A 6-week open-label study of 25 depressed patients with residual fatigue and sleepiness showed that adjunctive modafinil, 100 to 200 mg/d, significantly improved these symptoms, as well as Hamilton Rating Scale for Depression (HAM-D) score, as early as week 2. Seventy-six percent of patients responded to treatment, defined as a >50% reduction in HAM-D scores.16
Several open-label studies and case re-ports have evaluated adjunctive modafinil use in patients with:
- depression characterized by ongoing lethargy or apathy17
- depression with atypical features18
- seasonal affective disorder19
- partial response to antidepressants.20,21
Bipolar depression. A 6-week, double-blind, placebo-controlled trial randomly assigned 85 patients with bipolar depression to adjunctive modafinil, 100 to 200 mg/d, or placebo for 6 weeks (Table 3).22 The number of patients receiving an antidepressant or mood stabilizer was not significantly different between the modafinil and placebo groups.
The primary outcome measure was change in the Inventory for Depressive Symptoms (IDS) score from baseline to endpoint. Forty-four percent of patients receiving modafinil achieved a ≥50% reduction in IDS score, compared with 23% of the placebo group; this difference was statistically significant (P=0.03).
In this study, modafinil was well tolerated and did not induce mania or hypomania. Cases of modafinil-induced mania have been reported elsewhere.23,24
The mechanisms of modafinil’s antidepressant effects are unclear. The drug does not cause release of norepinephrine or dopamine. One study proposed that modafinil acts by releasing histamine and activating noradrenaline receptors.25 Activation of these receptors increases dopamine and norepinephrine in these areas, and excites histaminergic tuberomammillary neurons, increasing histamine levels. Another trial suggested that modafinil may improve mood by mechanisms similar to the antidepressant effects induced by sleep deprivation.26
Summary. Modafinil may have a role in managing residual fatigue and excessive sleepiness associated with MDD and bipolar depression. Evidence for a mood-elevating effect is minimal; additional studies are needed. Adjunctive modafinil and conventional stimulants have not been compared head-to-head in patients with mood disorders. Modafinil’s tolerability profile and lack of euphorigenic and reinforcing properties make it a potentially attractive alternative, however.
ADHD. Approximately 30% of ADHD patients do not respond to or are unable to tolerate conventional stimulant medications such as methylphenidate and dextroamphetamine.27 Several studies have evaluated modafinil as a potential treatment for ADHD based on the drug’s action on arousal and attention systems. Although modafinil’s precise mechanism of action in ADHD is unknown, proposed mechanisms include:
- hypothalamic and cerebral cortex neuronal activation
- action on histamine that results in internal vigilance.28
Can modafinil help patients with mood disorders?
| Author | Study design | Modafinil dose | Conclusion |
|---|---|---|---|
| Major depressive disorder | |||
| Fava et al, 200514 | 8-week, double-blind, placebo-controlled; 331 subjects with partial or no response to SSRI monotherapy | 200 mg/d | No significant difference between modafinil and placebo at final visit |
| DeBattista et al, 200315 | 6-week, double-blind, placebo-controlled; 136 subjects with partial response to antidepressant therapy | 100 to 400 mg/d | Significant improvement in sleepiness by week 1 and fatigue by week 2, but differences between modafinil and placebo were not statistically significant by end of study |
| Konuk et al, 200616 | 6-week, open-label; 25 subjects with residual sleepiness or fatigue after SSRI therapy | 100 to 200 mg/d | All patients showed significant improvement in sleepiness, fatigue, and HAM-D scores |
| Bipolar depression | |||
| Frye et al, 200722 | 6-week, double-blind, placebo-controlled trial; 85 subjects who did not respond to a mood stabilizer with or without concomitant antidepressant therapy | 100 to 200 mg/d (mean 177 mg/d) | 44% of modafinil patients achieved ≥50% reduction in IDS score compared with 23% in placebo group (P=0.03) |
| HAM-D: Hamilton Rating Scale for Depression; IDS: Inventory for Depressive Symptoms; SSRI: selective serotonin reuptake inhibitor | |||
CASE 2: Another Tx for ADHD
Matt, age 8, is referred to our outpatient child psychiatric clinic after his parents noted declining school performance associated with increased aggression and irritability. Our assessment strongly supports a diagnosis of ADHD without comorbid conditions. We start Matt on methylphenidate, 5 mg twice daily, which quickly improves his ADHD symptoms. However, the medication causes GI side effects and profound sleep and weight changes.
Matt’s parents request that their son be treated with a different type of agent. A trial of atomoxetine is not as effective as the initial methylphenidate dosage and produces similar side effects. We then consider modafinil because of its side effect profile. We start Matt on 100 mg once daily and titrate up to 200 mg/d 4 weeks later. Matt and his parents notice an immediate improvement in his ADHD symptoms with no side effects.
In children and adolescents. Wigal et al29 reviewed pooled data from 3 randomized, double-blind, placebo-controlled studies of modafinil in pediatric ADHD (Table 4). Modafinil was well tolerated and improved ADHD symptoms and behaviors regardless of patients’ stimulant use history.
In a recent open-label study, 220 children and young adolescents with ADHD who had completed 4 weeks of a double-blind, placebo-controlled trial were evaluated for an additional 8 weeks. Modafinil improved ADHD symptoms and overall clinical condition as determined by the parent- or clinician-completed ADHD Rating Scale-IV Home Version, the parent-completed Conners’ ADHD/DSM-IV Scale Parent Version, and the clinician-rated CGI scale.30 Insomnia, headache, and decreased appetite were the most commonly reported adverse events.
In adults. The results of 2 double-blind, placebo-controlled trials of modafinil in adults with ADHD have been positive:
- In 1 study, modafinil (mean 206.8 mg/d) was more effective than placebo and comparable to dextroamphetamine in improving ADHD symptoms.31
- In another, modafinil (a single 200-mg dose) increased cognitive performance during treatment.32
Schizophrenia. Double-blind, randomized placebo-controlled studies have evaluated modafinil for improving cognitive function and reducing negative symptoms in patients with schizophrenia. Results have been inconsistent.
One double-blind, randomized, placebo-controlled crossover study of 20 patients with chronic schizophrenia found that modafinil, 200 mg/d, significantly improved short-term verbal memory span and attentional set shifting—the ability to discriminate and selectively attend to various stimulus dimensions (Table 5).33 Two other controlled studies showed no differences between the effects of modafinil and placebo on schizophrenia’s fatigue, cognition, or positive or negative symptoms.34,35
Summary. Although open-label studies have shown modafinil has beneficial effects on cognitive symptoms, controlled data are scarce. Reports of modafinil-induced psychosis or mania11 may limit the drug’s usefulness in schizophrenia patients.
Cocaine dependence. No medications are FDA-approved for treating cocaine dependence. A placebo-controlled, double-blind trial found that modafinil blunts cocaine euphoria under controlled conditions.36 This effect is hypothesized to be secondary to modafinil’s glutamate-enhancing and gamma-aminobutyric acid inhibitory effects.37
Summary. A single study supports using modafinil to improve outcomes in cocaine-dependent patients receiving standardized psychosocial treatment. More research is needed.
Table 4
Modafinil and ADHD: What the evidence says
| Author | Study design | Modafinil dosage | Conclusion |
|---|---|---|---|
| Wigal et al, 200629 | Analysis of data from 3 double-blind, placebo-controlled trials; total 638 children/adolescents, some of whom had received prior stimulant therapy | 170 to 425 mg/d | Whether or not patients received prior stimulant treatment, modafinil significantly improved ADHD symptoms and was well tolerated |
| Boellner et al, 200630 | 8-week, open-label extension of a 4-week double-blind, placebo-controlled trial; 220 subjects ages 6-14 | 100 to 400 mg/d | Modafinil improved ADHD symptoms and overall clinical condition |
| Taylor et al, 200031 | 2-week, double-blind, placebo-controlled crossover comparing modafinil with dextroamphetamine; 22 adults | Mean 206.8 mg/d | Both modafinil and dextroamphetamine significantly improved ADHD symptoms compared with placebo |
| Turner et al, 200432 | Double-blind, placebo-controlled crossover; 20 adults | Single 200-mg dose | Modafinil improved results on cognitive tests, including short-term memory span, visual memory, spatial planning, and sustained attention |
| ADHD: attention-deficit/hyperactivity disorder | |||
Table 5
Modafinil for schizophrenia or cocaine dependence:
More research is needed
| Author | Study design | Modafinil dosage | Conclusion |
|---|---|---|---|
| Schizophrenia | |||
| Turner et al, 200433 | Double-blind, placebo-controlled crossover; 20 adults | 200 mg/d | Modafinil significantly improved attentional set shifting and short-term verbal memory span |
| Sevy et al, 200534 | 8-week, double-blind, placebo-controlled; 24 subjects | Up to 200 mg/d | No significant difference between modafinil and placebo in reducing fatigue or positive or negative symptoms or in improving cognition |
| Pierre et al, 200735 | 8-week, double-blind, placebo-controlled; 20 subjects | 100 to 200 mg/d | Modafinil did not significantly improve neurocognitive or negative symptoms |
| Cocaine dependence | |||
| Dackis et al, 200538 | 8-week, double-blind, placebo-controlled; 62 cocaine-dependent subjects | 400 mg/d | Patients receiving modafinil provided significantly more cocaine-negative urine samples and were significantly more likely to achieve =3 weeks cocaine abstinence than those receiving placebo |
Related resource
- Ballon JS, Feifel D. A systematic review of modafinil: potential clinical uses and mechanisms of action. J Clin Psychiatry 2006;67(4):554-66.
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Carbamazepine • Carbatrol, Tegretol, others
- Citalopram • Celexa
- Dextroamphetamine • Dexedrine, DextroStat
- Diazepam • Valium
- Erythromycin • Ery-Tab, Eryc, others
- Fluoxetine • Prozac
- Lithium • Eskalith, Lithobid
- Methylphenidate • Ritalin, others
- Modafinil • Provigil
- Phenytoin • Dilantin
- Sertraline • Zoloft
- Venlafaxine • Effexor
- Zolpidem • Ambien
Dr. Ramaswamy receives research support from Bristol-Myers Squibb, Shire, and Forest Pharmaceuticals and is a consultant to Dainippon Sumitomo Pharma.
Dr. Mattai reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Wilson receives research support from, is a consultant to, or is a speaker for the National Institute of Mental Health, the Substance Abuse and Mental Health Services Administration, the Veterans Administration, the State of Nebraska, the State of Ohio, Health Futures Foundation, Inc., Abbott Laboratories, Astra-Zeneca, Bristol-Myers Squibb, Elan, Eli Lilly and Company, GlaxoSmithKline, Janssen, Ortho-McNeil, Pfizer, and Wyeth.
Ms. B, a middle-aged mother of 3, is being monitored for bipolar disorder. She has a history of stimulant abuse but has been in remission for 5 years. She complains of excessive daytime sleepiness. Most days she wakes at 7 AM, but sleeps on several occasions during the day. She also complains of fatigue and lack of motivation.
She is being treated with lithium, venlafaxine, and zolpidem and reports good adherence. Basic laboratory work and serum lithium levels are within acceptable ranges. Her symptoms do not improve when venlafaxine is titrated from 225 mg/d to 300 mg/d. She also reports previously failed trials with bupropion and fluoxetine.
We decide to try a psychostimulant as an augmenting agent. Because of her past stimulant abuse, we add modafinil, 100 mg/d and increase to 200 mg/d. Ms. B reports improvement in her daytime sleepiness and fatigue and—except for a mild headache—tolerates the medication well.
Modafinil is being investigated for potential roles in managing inattention, excess sleepiness, fatigue, and cognitive dysfunction associated with:
- mood disorders (major depression and bipolar depression)
- attention-deficit/hyperactivity disorder (ADHD)
- schizophrenia
- cocaine dependence.
This article discusses how the drug promotes wakefulness, how it might improve cognitive function, and what the evidence reveals about off-label indications.
How it works
Although modafinil’s precise mechanism of action is unknown, it is believed to promote wakefulness more selectively than conventional stimulants such as amphetamine and methylphenidate. Modafinil does not bind to norepinephrine, serotonin, dopamine, or benzodiazepine receptors.1,2 It might target specific hypothalamic regions such as the tuberomammillary nucleus and orexin neurons, which are peptide neurotransmitters that promote wakefulness.3,4
Clinical trials found that modafinil has beneficial effects on:
- working memory, recognition memory, and sustained attention in healthy humans
- prefrontal-dependent cognitive functions in schizophrenia, major depression, and adult ADHD.5
Evidence for approved indications
Modafinil is indicated to improve wakefulness in patients who have excessive sleepiness associated with narcolepsy, obstructive sleep apnea, or shift work sleep disorder. It was approved for reducing excessive sleepiness in narcoleptic patients after two 9-week placebo-controlled clinical trials. The drug significantly reduced sleepiness and improved overall disease status as measured by the Clinical Global Impression of Change (CGI-C) scale.6,7
In patients with shift work sleep disorder, a 12-week placebo-controlled clinical trial found that modafinil significantly improved sleep latency and CGI-C scores.10
Dosage and side effects. For patients with narcolepsy or obstructive sleep apnea, the recommended dose is 200 mg given in the morning.11 For patients prescribed modafinil for work-time wakefulness, the dose is 200 mg 1 hour before their work shift. Lower doses are recommended for patients who are elderly or have hepatic impairment. Those with severe hepatic impairment typically are prescribed 100 mg/d.11 Modafinil is rapidly absorbed and is metabolized primarily by the liver (Table 1). A summary of potential drug-drug interactions appears in Table 2.11
In pivotal trials, adverse events that occurred more frequently with modafinil than with placebo and in >5% of the study population included headache, nausea, nervousness, rhinitis, diarrhea, back pain, insomnia, dizziness, and dyspepsia. Headache was most commonly reported; in most patients, it resolved soon after they started taking modafinil. Post-marketing reports have included cases of psychosis, mania, and suspected serious skin reactions, including Stevens-Johnson syndrome.11 Modafinil lacks euphorigenic properties and has minimal potential for abuse.12
Table 1
Modafinil’s pharmacokinetics
| Absorbed rapidly, with peak plasma concentrations at 2 to 4 hours |
| Apparent steady states reached after 2 to 4 days of dosing |
| Half-life: 15 hours |
| Major route of elimination (~90%) is metabolism, primarily by the liver |
Selected drug-drug interactions with modafinil
| Action of modafinil | Potential drug interactions |
|---|---|
| Increases elimination of CYP 3A4 substrates | Carbamazepine, phenytoin may decrease modafinil levels Azole antifungals, protease inhibitors, and erythromycin may increase modafinil levels |
| Inhibits CYP 2C19 enzyme | Modafinil may increase levels of citalopram, diazepam, and sertraline |
| Decreases absorption of ethinyl estradiol | Modafinil can decrease effectiveness of oral contraceptives |
| CYP: cytochrome P-450 | |
| Source: Reference 11 | |
Evidence for off-label uses
Major depressive disorder (MDD). The fatigue and excessive sleepiness often seen with MDD often persist after other depressive symptoms have remitted with antidepressant treatment.13 Patients with these symptoms might benefit from modafinil’s stimulating properties. Conventional stimulants such as methylphenidate have been used to improve neurovegetative symptoms of depression, but modafinil offers several advantages:
- decreased adverse CNS effects
- fewer drug-drug interactions
- minimal risk for dependence or abuse.
A 6-week open-label study of 25 depressed patients with residual fatigue and sleepiness showed that adjunctive modafinil, 100 to 200 mg/d, significantly improved these symptoms, as well as Hamilton Rating Scale for Depression (HAM-D) score, as early as week 2. Seventy-six percent of patients responded to treatment, defined as a >50% reduction in HAM-D scores.16
Several open-label studies and case re-ports have evaluated adjunctive modafinil use in patients with:
- depression characterized by ongoing lethargy or apathy17
- depression with atypical features18
- seasonal affective disorder19
- partial response to antidepressants.20,21
Bipolar depression. A 6-week, double-blind, placebo-controlled trial randomly assigned 85 patients with bipolar depression to adjunctive modafinil, 100 to 200 mg/d, or placebo for 6 weeks (Table 3).22 The number of patients receiving an antidepressant or mood stabilizer was not significantly different between the modafinil and placebo groups.
The primary outcome measure was change in the Inventory for Depressive Symptoms (IDS) score from baseline to endpoint. Forty-four percent of patients receiving modafinil achieved a ≥50% reduction in IDS score, compared with 23% of the placebo group; this difference was statistically significant (P=0.03).
In this study, modafinil was well tolerated and did not induce mania or hypomania. Cases of modafinil-induced mania have been reported elsewhere.23,24
The mechanisms of modafinil’s antidepressant effects are unclear. The drug does not cause release of norepinephrine or dopamine. One study proposed that modafinil acts by releasing histamine and activating noradrenaline receptors.25 Activation of these receptors increases dopamine and norepinephrine in these areas, and excites histaminergic tuberomammillary neurons, increasing histamine levels. Another trial suggested that modafinil may improve mood by mechanisms similar to the antidepressant effects induced by sleep deprivation.26
Summary. Modafinil may have a role in managing residual fatigue and excessive sleepiness associated with MDD and bipolar depression. Evidence for a mood-elevating effect is minimal; additional studies are needed. Adjunctive modafinil and conventional stimulants have not been compared head-to-head in patients with mood disorders. Modafinil’s tolerability profile and lack of euphorigenic and reinforcing properties make it a potentially attractive alternative, however.
ADHD. Approximately 30% of ADHD patients do not respond to or are unable to tolerate conventional stimulant medications such as methylphenidate and dextroamphetamine.27 Several studies have evaluated modafinil as a potential treatment for ADHD based on the drug’s action on arousal and attention systems. Although modafinil’s precise mechanism of action in ADHD is unknown, proposed mechanisms include:
- hypothalamic and cerebral cortex neuronal activation
- action on histamine that results in internal vigilance.28
Can modafinil help patients with mood disorders?
| Author | Study design | Modafinil dose | Conclusion |
|---|---|---|---|
| Major depressive disorder | |||
| Fava et al, 200514 | 8-week, double-blind, placebo-controlled; 331 subjects with partial or no response to SSRI monotherapy | 200 mg/d | No significant difference between modafinil and placebo at final visit |
| DeBattista et al, 200315 | 6-week, double-blind, placebo-controlled; 136 subjects with partial response to antidepressant therapy | 100 to 400 mg/d | Significant improvement in sleepiness by week 1 and fatigue by week 2, but differences between modafinil and placebo were not statistically significant by end of study |
| Konuk et al, 200616 | 6-week, open-label; 25 subjects with residual sleepiness or fatigue after SSRI therapy | 100 to 200 mg/d | All patients showed significant improvement in sleepiness, fatigue, and HAM-D scores |
| Bipolar depression | |||
| Frye et al, 200722 | 6-week, double-blind, placebo-controlled trial; 85 subjects who did not respond to a mood stabilizer with or without concomitant antidepressant therapy | 100 to 200 mg/d (mean 177 mg/d) | 44% of modafinil patients achieved ≥50% reduction in IDS score compared with 23% in placebo group (P=0.03) |
| HAM-D: Hamilton Rating Scale for Depression; IDS: Inventory for Depressive Symptoms; SSRI: selective serotonin reuptake inhibitor | |||
CASE 2: Another Tx for ADHD
Matt, age 8, is referred to our outpatient child psychiatric clinic after his parents noted declining school performance associated with increased aggression and irritability. Our assessment strongly supports a diagnosis of ADHD without comorbid conditions. We start Matt on methylphenidate, 5 mg twice daily, which quickly improves his ADHD symptoms. However, the medication causes GI side effects and profound sleep and weight changes.
Matt’s parents request that their son be treated with a different type of agent. A trial of atomoxetine is not as effective as the initial methylphenidate dosage and produces similar side effects. We then consider modafinil because of its side effect profile. We start Matt on 100 mg once daily and titrate up to 200 mg/d 4 weeks later. Matt and his parents notice an immediate improvement in his ADHD symptoms with no side effects.
In children and adolescents. Wigal et al29 reviewed pooled data from 3 randomized, double-blind, placebo-controlled studies of modafinil in pediatric ADHD (Table 4). Modafinil was well tolerated and improved ADHD symptoms and behaviors regardless of patients’ stimulant use history.
In a recent open-label study, 220 children and young adolescents with ADHD who had completed 4 weeks of a double-blind, placebo-controlled trial were evaluated for an additional 8 weeks. Modafinil improved ADHD symptoms and overall clinical condition as determined by the parent- or clinician-completed ADHD Rating Scale-IV Home Version, the parent-completed Conners’ ADHD/DSM-IV Scale Parent Version, and the clinician-rated CGI scale.30 Insomnia, headache, and decreased appetite were the most commonly reported adverse events.
In adults. The results of 2 double-blind, placebo-controlled trials of modafinil in adults with ADHD have been positive:
- In 1 study, modafinil (mean 206.8 mg/d) was more effective than placebo and comparable to dextroamphetamine in improving ADHD symptoms.31
- In another, modafinil (a single 200-mg dose) increased cognitive performance during treatment.32
Schizophrenia. Double-blind, randomized placebo-controlled studies have evaluated modafinil for improving cognitive function and reducing negative symptoms in patients with schizophrenia. Results have been inconsistent.
One double-blind, randomized, placebo-controlled crossover study of 20 patients with chronic schizophrenia found that modafinil, 200 mg/d, significantly improved short-term verbal memory span and attentional set shifting—the ability to discriminate and selectively attend to various stimulus dimensions (Table 5).33 Two other controlled studies showed no differences between the effects of modafinil and placebo on schizophrenia’s fatigue, cognition, or positive or negative symptoms.34,35
Summary. Although open-label studies have shown modafinil has beneficial effects on cognitive symptoms, controlled data are scarce. Reports of modafinil-induced psychosis or mania11 may limit the drug’s usefulness in schizophrenia patients.
Cocaine dependence. No medications are FDA-approved for treating cocaine dependence. A placebo-controlled, double-blind trial found that modafinil blunts cocaine euphoria under controlled conditions.36 This effect is hypothesized to be secondary to modafinil’s glutamate-enhancing and gamma-aminobutyric acid inhibitory effects.37
Summary. A single study supports using modafinil to improve outcomes in cocaine-dependent patients receiving standardized psychosocial treatment. More research is needed.
Table 4
Modafinil and ADHD: What the evidence says
| Author | Study design | Modafinil dosage | Conclusion |
|---|---|---|---|
| Wigal et al, 200629 | Analysis of data from 3 double-blind, placebo-controlled trials; total 638 children/adolescents, some of whom had received prior stimulant therapy | 170 to 425 mg/d | Whether or not patients received prior stimulant treatment, modafinil significantly improved ADHD symptoms and was well tolerated |
| Boellner et al, 200630 | 8-week, open-label extension of a 4-week double-blind, placebo-controlled trial; 220 subjects ages 6-14 | 100 to 400 mg/d | Modafinil improved ADHD symptoms and overall clinical condition |
| Taylor et al, 200031 | 2-week, double-blind, placebo-controlled crossover comparing modafinil with dextroamphetamine; 22 adults | Mean 206.8 mg/d | Both modafinil and dextroamphetamine significantly improved ADHD symptoms compared with placebo |
| Turner et al, 200432 | Double-blind, placebo-controlled crossover; 20 adults | Single 200-mg dose | Modafinil improved results on cognitive tests, including short-term memory span, visual memory, spatial planning, and sustained attention |
| ADHD: attention-deficit/hyperactivity disorder | |||
Table 5
Modafinil for schizophrenia or cocaine dependence:
More research is needed
| Author | Study design | Modafinil dosage | Conclusion |
|---|---|---|---|
| Schizophrenia | |||
| Turner et al, 200433 | Double-blind, placebo-controlled crossover; 20 adults | 200 mg/d | Modafinil significantly improved attentional set shifting and short-term verbal memory span |
| Sevy et al, 200534 | 8-week, double-blind, placebo-controlled; 24 subjects | Up to 200 mg/d | No significant difference between modafinil and placebo in reducing fatigue or positive or negative symptoms or in improving cognition |
| Pierre et al, 200735 | 8-week, double-blind, placebo-controlled; 20 subjects | 100 to 200 mg/d | Modafinil did not significantly improve neurocognitive or negative symptoms |
| Cocaine dependence | |||
| Dackis et al, 200538 | 8-week, double-blind, placebo-controlled; 62 cocaine-dependent subjects | 400 mg/d | Patients receiving modafinil provided significantly more cocaine-negative urine samples and were significantly more likely to achieve =3 weeks cocaine abstinence than those receiving placebo |
Related resource
- Ballon JS, Feifel D. A systematic review of modafinil: potential clinical uses and mechanisms of action. J Clin Psychiatry 2006;67(4):554-66.
- Atomoxetine • Strattera
- Bupropion • Wellbutrin
- Carbamazepine • Carbatrol, Tegretol, others
- Citalopram • Celexa
- Dextroamphetamine • Dexedrine, DextroStat
- Diazepam • Valium
- Erythromycin • Ery-Tab, Eryc, others
- Fluoxetine • Prozac
- Lithium • Eskalith, Lithobid
- Methylphenidate • Ritalin, others
- Modafinil • Provigil
- Phenytoin • Dilantin
- Sertraline • Zoloft
- Venlafaxine • Effexor
- Zolpidem • Ambien
Dr. Ramaswamy receives research support from Bristol-Myers Squibb, Shire, and Forest Pharmaceuticals and is a consultant to Dainippon Sumitomo Pharma.
Dr. Mattai reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Wilson receives research support from, is a consultant to, or is a speaker for the National Institute of Mental Health, the Substance Abuse and Mental Health Services Administration, the Veterans Administration, the State of Nebraska, the State of Ohio, Health Futures Foundation, Inc., Abbott Laboratories, Astra-Zeneca, Bristol-Myers Squibb, Elan, Eli Lilly and Company, GlaxoSmithKline, Janssen, Ortho-McNeil, Pfizer, and Wyeth.
1. Mignot E, Nishino S, Guilleminault C, et al. Modafinil binds to dopamine uptake carrier site with low affinity. Sleep 1994;17:436-7.
2. Lin J-S, Hou Y, Jouvet M. Potential brain neuronal targets for amphetamine, methylphenidate, and modafinil induced wakefulness, evidenced by c-fos immunocytochemistry in the cat. Proc Natl Acad Sci USA 1996;93:14128-33.
3. Scammell TE, Estabrooke IV, McCarthy MT, et al. Hypothalamic arousal regions are activated during modafinil-induced wakefulness. J Neurosci 2000;20(22):8620-8.
4. Stenberg D. Neuroanatomy and neurochemistry of sleep. Cell Mol Life Sci 2007;64(10):1187-204.
5. Minzenberg MJ, Carter CS. Modafinil: a review of neurochemical actions and effects on cognition. Neuropsychopharmacology In press.
6. U.S. Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil for the treatment of pathological somnolence in narcolepsy. Ann Neurol 1998;43(1):88-97.
7. U.S. Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil as a treatment for the excessive daytime somnolence of narcolepsy. Neurology 2000;54:1166-75.
8. Black JE, Hirshkowitz M. Modafinil for treatment of residual excessive sleepiness in nasal continuous positive airway pressure-treated obstructive sleep apnea/hypopnea syndrome. Sleep 2005;28(4):464-71.
9. Pack AI, Black JE, Schwartz JR, Matheson JK. Modafinil as adjunct therapy for daytime sleepiness in obstructive sleep apnea. Am J Respir Crit Care Med 2001;164(9):1675-81.
10. Czeisler CA, Walsh JK, Roth T, et al. and the U.S. Modafinil in Shift Work Sleep Disorder Study Group. Modafinil for excessive sleepiness associated with shift-work sleep disorder. N Engl J Med. 2005;353(5):476-86. Published correction appears in: N Engl J Med 2005;353(10):1078.-
11. Provigil [package insert] West Chester, PA: Cephalon Inc; 2004.
12. Myrick H, Malcolm R, Taylor B, et al. Modafinil: preclinical, clinical, and post-marketing surveillance—a review of abuse liability issues. Ann Clin Psychiatry 2004;16(2):101-9.
13. Baldwin DS, Papakostas GI. Symptoms of fatigue and sleepiness in major depressive disorder. J Clin Psychiatry 2006;67(suppl 6):9-15.
14. Fava M, Thase ME, DeBattista C. A multicenter, placebo-controlled study of modafinil augmentation in partial responders to selective serotonin reuptake inhibitors with persistent fatigue and sleepiness. J Clin Psychiatry 2005;66(1):85-93.
15. DeBattista C, Doghramji K, Menza MA, et al. and the Modafinil in Depression Study Group. Adjunct modafinil for the short-term treatment of fatigue and sleepiness in patients with major depressive disorder: a preliminary double-blind, placebo-controlled study. J Clin Psychiatry 2003;64(9):1057-64.
16. Konuk N, Atasoy N, Atik L, Akay O. Open-label study of adjunct modafinil for the treatment of patients with fatigue, sleepiness, and major depression treated with selective serotonin reuptake inhibitors. Adv Ther 2006;23(4):646-54.
17. Markovitz PJ, Wagner S. An open-label trial of modafinil augmentation in patients with partial response to antidepressant therapy. J Clin Psychopharmacol 2003;23(2):207-9.
18. Vaishnavi S, Gadde K, Alamy S, et al. Modafinil for atypical depression: effects of open-label and double-blind discontinuation treatment. J Clin Psychopharmacol 2006; 26(4): 373-8. Published correction appears in: J Clin Psychopharmacol. 2006;26(5):523.
19. Lundt L. Modafinil treatment in patients with seasonal affective disorder/winter depression: an open-label pilot study. J Affect Disord 2004;81(2):173-8.
20. DeBattista C, Lembke A, Solvason HB, et al. A prospective trial of modafinil as an adjunctive treatment of major depression. J Clin Psychopharmacol 2004;24(1):87-90.
21. Rasmussen NA, Schroder P, Olsen LR, et al. Modafinil augmentation in depressed patients with partial response to antidepressants: a pilot study on self-reported symptoms covered by the Major Depression Inventory (MDI) and the Symptom Checklist (SCL-92). Nord J Psychiatry 2005;59(3):173-8.
22. Frye MA, Grunze H, Suppes T, et al. A placebo-controlled evaluation of adjunctive modafinil in the treatment of bipolar depression. Am J Psychiatry 2007;164:1242-9.
23. Wolf J, Fiedler U, Anghelescu I, Schwertfeger N. Manic switch in a patient with treatment-resistant bipolar depression treated with modafinil. J Clin Psychiatry 2006;67(11):1817.-
24. Vorspan F, Warot D, Consoli A, et al. Mania in a boy treated with modafinil for narcolepsy. Am J Psychiatry 2005;162(4):813-4.
25. McClellan KJ, Spencer CM. Modafinil: a review of its pharmacology and clinical efficacy in the management of narcolepsy. CNS Drugs 1998;9(4):311-24.
26. Ballon JS, Feifel D. A systematic review of modafinil: potential clinical uses and mechanisms of action. J Clin Psychiatry 2006;67(4):554-66.
27. Dulcan M. Practice parameters for the assessment and treatment of children, adolescents and adults with attentiondeficit hyperactivity disorder. American Academy of Child and Adolescent Psychiatry. J Am Acad Child Adolesc Psychiatry 1997;36(suppl 10):85S-121S.
28. Lindsay SE, Gudelsky GA, Heaton PC. Use of modafinil for the treatment of attention deficit/hyperactivity disorder. Ann Pharmacother 2006;40(10):1829-33.
29. Wigal SB, Biederman J, Swanson JM, et al. Efficacy and safety of modafinil film-coated tablets in children and adolescents with or without prior stimulant treatment for attention-deficit/hyperactivity disorder: pooled analysis of 3 randomized, double-blind, placebo-controlled studies. Prim Care Companion J Clin Psychiatry 2006;8(6):352-60.
30. Boellner SW, Earl CQ, Arora S. Modafinil in children and adolescents with attention-deficit/hyperactivity disorder: a preliminary 8-week, open-label study. Curr Med Res Opin 2006;22(12):2457-65.
31. Taylor FB, Russo J. Efficacy of modafinil compared to dextroamphetamine for the treatment of attention deficit hyperactivity disorder in adults. J Child Adolesc Psychopharmacol 2000;10(4):311-20.
32. Turner DC, Clark L, Dowson J, et al. Modafinil improves cognition and response inhibition in adult attention-deficit/ hyperactivity disorder. Biol Psychiatry 2004;55(10):1031-40.
33. Turner DC, Clark L, Pomarol-Clotet E, et al. Modafinil improves cognition and attentional set shifting in patients with chronic schizophrenia. Neuropsychopharmacology 2004;29(7):1363-73.
34. Sevy S, Rosenthal MH, Alvir J, et al. Double-blind, placebo-controlled study of modafinil for fatigue and cognition in schizophrenia patients treated with psychotropic medications. J Clin Psychiatry 2005;66(7):839-43.
35. Pierre JM, Peloian JH, Wirshing DA, et al. A randomized, double-blind, placebo-controlled trial of modafinil for negative symptoms in schizophrenia. J Clin Psychiatry 2007;68(5):705-10.
36. Dackis CA, Lynch KG, Yu E, et al. Modafinil and cocaine: a double-blind, placebo-controlled drug interaction study. Drug Alcohol Depend 2003;70(1):29-37.
37. Perez de la Mora M, Aguilar-Garcia A, Ramon-Frias T, et al. Effects of the vigilance promoting drug modafinil on the synthesis of GABA and glutamate in slices of rat hypothalamus. Neurosci Lett 1999;259:181-5.
38. Dackis CA, Kampman KM, Lynch KG, et al. A double-blind, placebo-controlled trial of modafinil for cocaine dependence. Neuropsychopharmacology 2005;30(1):205-11.
1. Mignot E, Nishino S, Guilleminault C, et al. Modafinil binds to dopamine uptake carrier site with low affinity. Sleep 1994;17:436-7.
2. Lin J-S, Hou Y, Jouvet M. Potential brain neuronal targets for amphetamine, methylphenidate, and modafinil induced wakefulness, evidenced by c-fos immunocytochemistry in the cat. Proc Natl Acad Sci USA 1996;93:14128-33.
3. Scammell TE, Estabrooke IV, McCarthy MT, et al. Hypothalamic arousal regions are activated during modafinil-induced wakefulness. J Neurosci 2000;20(22):8620-8.
4. Stenberg D. Neuroanatomy and neurochemistry of sleep. Cell Mol Life Sci 2007;64(10):1187-204.
5. Minzenberg MJ, Carter CS. Modafinil: a review of neurochemical actions and effects on cognition. Neuropsychopharmacology In press.
6. U.S. Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil for the treatment of pathological somnolence in narcolepsy. Ann Neurol 1998;43(1):88-97.
7. U.S. Modafinil in Narcolepsy Multicenter Study Group. Randomized trial of modafinil as a treatment for the excessive daytime somnolence of narcolepsy. Neurology 2000;54:1166-75.
8. Black JE, Hirshkowitz M. Modafinil for treatment of residual excessive sleepiness in nasal continuous positive airway pressure-treated obstructive sleep apnea/hypopnea syndrome. Sleep 2005;28(4):464-71.
9. Pack AI, Black JE, Schwartz JR, Matheson JK. Modafinil as adjunct therapy for daytime sleepiness in obstructive sleep apnea. Am J Respir Crit Care Med 2001;164(9):1675-81.
10. Czeisler CA, Walsh JK, Roth T, et al. and the U.S. Modafinil in Shift Work Sleep Disorder Study Group. Modafinil for excessive sleepiness associated with shift-work sleep disorder. N Engl J Med. 2005;353(5):476-86. Published correction appears in: N Engl J Med 2005;353(10):1078.-
11. Provigil [package insert] West Chester, PA: Cephalon Inc; 2004.
12. Myrick H, Malcolm R, Taylor B, et al. Modafinil: preclinical, clinical, and post-marketing surveillance—a review of abuse liability issues. Ann Clin Psychiatry 2004;16(2):101-9.
13. Baldwin DS, Papakostas GI. Symptoms of fatigue and sleepiness in major depressive disorder. J Clin Psychiatry 2006;67(suppl 6):9-15.
14. Fava M, Thase ME, DeBattista C. A multicenter, placebo-controlled study of modafinil augmentation in partial responders to selective serotonin reuptake inhibitors with persistent fatigue and sleepiness. J Clin Psychiatry 2005;66(1):85-93.
15. DeBattista C, Doghramji K, Menza MA, et al. and the Modafinil in Depression Study Group. Adjunct modafinil for the short-term treatment of fatigue and sleepiness in patients with major depressive disorder: a preliminary double-blind, placebo-controlled study. J Clin Psychiatry 2003;64(9):1057-64.
16. Konuk N, Atasoy N, Atik L, Akay O. Open-label study of adjunct modafinil for the treatment of patients with fatigue, sleepiness, and major depression treated with selective serotonin reuptake inhibitors. Adv Ther 2006;23(4):646-54.
17. Markovitz PJ, Wagner S. An open-label trial of modafinil augmentation in patients with partial response to antidepressant therapy. J Clin Psychopharmacol 2003;23(2):207-9.
18. Vaishnavi S, Gadde K, Alamy S, et al. Modafinil for atypical depression: effects of open-label and double-blind discontinuation treatment. J Clin Psychopharmacol 2006; 26(4): 373-8. Published correction appears in: J Clin Psychopharmacol. 2006;26(5):523.
19. Lundt L. Modafinil treatment in patients with seasonal affective disorder/winter depression: an open-label pilot study. J Affect Disord 2004;81(2):173-8.
20. DeBattista C, Lembke A, Solvason HB, et al. A prospective trial of modafinil as an adjunctive treatment of major depression. J Clin Psychopharmacol 2004;24(1):87-90.
21. Rasmussen NA, Schroder P, Olsen LR, et al. Modafinil augmentation in depressed patients with partial response to antidepressants: a pilot study on self-reported symptoms covered by the Major Depression Inventory (MDI) and the Symptom Checklist (SCL-92). Nord J Psychiatry 2005;59(3):173-8.
22. Frye MA, Grunze H, Suppes T, et al. A placebo-controlled evaluation of adjunctive modafinil in the treatment of bipolar depression. Am J Psychiatry 2007;164:1242-9.
23. Wolf J, Fiedler U, Anghelescu I, Schwertfeger N. Manic switch in a patient with treatment-resistant bipolar depression treated with modafinil. J Clin Psychiatry 2006;67(11):1817.-
24. Vorspan F, Warot D, Consoli A, et al. Mania in a boy treated with modafinil for narcolepsy. Am J Psychiatry 2005;162(4):813-4.
25. McClellan KJ, Spencer CM. Modafinil: a review of its pharmacology and clinical efficacy in the management of narcolepsy. CNS Drugs 1998;9(4):311-24.
26. Ballon JS, Feifel D. A systematic review of modafinil: potential clinical uses and mechanisms of action. J Clin Psychiatry 2006;67(4):554-66.
27. Dulcan M. Practice parameters for the assessment and treatment of children, adolescents and adults with attentiondeficit hyperactivity disorder. American Academy of Child and Adolescent Psychiatry. J Am Acad Child Adolesc Psychiatry 1997;36(suppl 10):85S-121S.
28. Lindsay SE, Gudelsky GA, Heaton PC. Use of modafinil for the treatment of attention deficit/hyperactivity disorder. Ann Pharmacother 2006;40(10):1829-33.
29. Wigal SB, Biederman J, Swanson JM, et al. Efficacy and safety of modafinil film-coated tablets in children and adolescents with or without prior stimulant treatment for attention-deficit/hyperactivity disorder: pooled analysis of 3 randomized, double-blind, placebo-controlled studies. Prim Care Companion J Clin Psychiatry 2006;8(6):352-60.
30. Boellner SW, Earl CQ, Arora S. Modafinil in children and adolescents with attention-deficit/hyperactivity disorder: a preliminary 8-week, open-label study. Curr Med Res Opin 2006;22(12):2457-65.
31. Taylor FB, Russo J. Efficacy of modafinil compared to dextroamphetamine for the treatment of attention deficit hyperactivity disorder in adults. J Child Adolesc Psychopharmacol 2000;10(4):311-20.
32. Turner DC, Clark L, Dowson J, et al. Modafinil improves cognition and response inhibition in adult attention-deficit/ hyperactivity disorder. Biol Psychiatry 2004;55(10):1031-40.
33. Turner DC, Clark L, Pomarol-Clotet E, et al. Modafinil improves cognition and attentional set shifting in patients with chronic schizophrenia. Neuropsychopharmacology 2004;29(7):1363-73.
34. Sevy S, Rosenthal MH, Alvir J, et al. Double-blind, placebo-controlled study of modafinil for fatigue and cognition in schizophrenia patients treated with psychotropic medications. J Clin Psychiatry 2005;66(7):839-43.
35. Pierre JM, Peloian JH, Wirshing DA, et al. A randomized, double-blind, placebo-controlled trial of modafinil for negative symptoms in schizophrenia. J Clin Psychiatry 2007;68(5):705-10.
36. Dackis CA, Lynch KG, Yu E, et al. Modafinil and cocaine: a double-blind, placebo-controlled drug interaction study. Drug Alcohol Depend 2003;70(1):29-37.
37. Perez de la Mora M, Aguilar-Garcia A, Ramon-Frias T, et al. Effects of the vigilance promoting drug modafinil on the synthesis of GABA and glutamate in slices of rat hypothalamus. Neurosci Lett 1999;259:181-5.
38. Dackis CA, Kampman KM, Lynch KG, et al. A double-blind, placebo-controlled trial of modafinil for cocaine dependence. Neuropsychopharmacology 2005;30(1):205-11.
Interoceptive cues: When ‘gut feelings’ point to anxiety
CASE: 'I don't know how I feel'
Ms. N, age 48, is seen in an outpatient clinic for episodic, impulsive aggression and evaluation of possible bipolar disorder. When you ask her to describe one of her episodes—which always involve a conflict with her partner or another loved one—Ms. N says, “I just lose control… I go blank.” You observe Ms. N’s deep, sighing respirations, trembling hands, and restless, fidgety leg movements. When you ask about her awareness of her physical state while she was recalling the incident, she immediately calms, looks at you quizzically, and states, “I don’t know how I feel.”
When assessing a patient who might have an anxiety disorder, don’t overlook the body. In addition to worry and avoidance, body-centered feelings are a vital component of anxiety and an important treatment target.1
This article:
- highlights clinically relevant neurobiology of anxious feelings
- discusses interoception—awareness of the physiologic state of one’s body—and its connection with anxiety
- explains the use of interoceptive cues as an aid to diagnosing and treating anxiety.
Affective neuroscience and fear
Interoceptive cues are questions directed toward the somatic manifestations of anxiety. Because these questions encourage patients to consciously experience the physical symptoms of anxiety, using interoceptive cues essentially is an exposure-based intervention that may feel counterintuitive to practitioners who are more accustomed to trying to relieve anxiety.
Emotions are thought to be grounded in brain areas that receive and regulate somatic signals, such as the amygdala and insula.2 A feeling-focused approach to anxiety weds affective neuroscience—the study of emotions—with clinical assessment and treatment of anxiety disorders, and conceptualizes that fear is a core component of many anxiety-related disorders.3,4
Although the DSM-IV-TR views anxiety disorders as clinically heterogeneous, affective neuroscience emphasizes what these disorders have in common.5 This unifying perspective allows clinicians to anchor anxiety disorders and anxiety-related disorders—such as hypochondriasis—in core emotional systems that have 3 clinically important aspects—actions (behavior and body), brain, and consciousness (mind) (Figure).4 Two emotional systems related to anxiety disorders are fear (anxious anticipation) and panic (evolutionarily related to separation anxiety and suffocation alarm signals). Viewing anxiety disorders as rooted in core emotion systems allows you to incorporate recent advances in emotional neuroscience, including interoception, into your clinical practice.
Figure: A,B,C model for understanding emotions
Affective neuroscience is a broad-based scientific discipline that explores emotions from 3 vantages: actions (behaviors and bodily responses), brain bases, and conscious manifestations. Two core emotional systems related to anxiety disorders are fear and panic.
Source: Adapted with permission from Panksepp J. Affective neuroscience. New York: Oxford University Press; 1998:31.
Detecting ‘hidden’ anxiety
Conscious symptoms. Activity in the brain’s fear system can generate conscious experiences, including worry, heightened arousal, attentional biases, and body-based feelings of fear. Anxious feelings—by definition, sensory experiences—are an important component of an anxiety assessment and relatively easy to identify.
Kroenke et al6 evaluated a 2-item screening tool, the Generalized Anxiety Disorder scale (GAD-2) that highlights both cognitive (worry) and somatic (feeling) sides of anxiety. Researchers asked 965 randomly sampled primary care patients, “Over the past 2 weeks, how often have you been bothered by the following problems:
- feeling nervous, anxious, or on edge
- not being able to stop or control worrying.
Possible responses ranged from 0 (not at all) to 3 (nearly every day). The GAD-2 was as specific for detecting anxiety disorders as a 7-item scale, the GAD-7, (88%), though less sensitive (65% vs 77%).
Nonconscious symptoms. A challenge arises, however, when patients demonstrate signs of anxiety (stress-related physical symptoms such as stomach pains or avoidance-related behaviors) without conscious awareness of anxious feelings. Though patients may intellectually understand the concept of body-based “gut feelings,” these sensations are often reflexively ignored, avoided, or mislabeled. Patients may use terms such as “stressed,” “distressed,” or “tense,” focus on the external source of the fear (rather than their response to it), or reflexively engage in behaviors (avoidance, impulsive behaviors) without being aware of their internal responses.
Anxiety symptoms that occur without corresponding awareness can be called occult, nonconscious, or unconscious anxiety. These symptoms, unique to each patient, can be used as:
- cues to the patient that he or she is anxious
- stimuli to be desensitized (via exposure-based interventions)
- markers of treatment progress.
Patients who experience occult anxiety often have a deficit in interoception (Box).2,7-11 Using interoceptive cues to foster awareness of these unrecognized body-based symptoms can provide insight into formerly unrecognized manifestations of anxiety.
Neurobiology of anxiety
The fear system. Dynamic changes in stimulus-specific physical sensations—anxious feelings—are linked to activity of the brain’s fear system. This system, which detects and rapidly learns to anticipate danger or distress, can exhibit low-level tonic activity (chronic, generalized anxiety), phasic high-amplitude reactivity (spikes of anxiety), and combinations of the 2.4,12
This precognitive, primary-process alarm system can generate:
- behaviors, often centered around avoidance—though other types (such as impulsive) can occur
- physiologic responses, which may or may not become conscious
- states of mind, including attention (hypervigilance, dissociation), cognitive contents (specific worries), and viscerosomatic awareness (“feelings”).
Through learning—and under the influence of temperamental/genetic predispositions—the fear system can be linked to internal and external stimuli, yielding a spectrum of clinical disorders that includes anxiety disorders.5
Consciously experiencing an emotion, attending to an emotionally arousing external stimulus, and remembering an emotionally arousing event all involve overlapping mental and neurobiologic processes in brain areas that process and regulate sensations from the body.2,7 Therefore, one does not need to remember “how one felt in the past” to elicit similar neurobiologic and physiologic responses in the present. These responses are recreated in the present when one consciously activates the memory. This understanding underlies the use of interoceptive cues.
Interoception is intentional, mindful awareness of the physiologic state of one’s body. Consciously directing attention to one’s internal state actively unifies the activity of the attending mind and brain with ongoing visceromotor sensations from the body.8,9 These body-based somatic markers often lie at the border of consciousness and can be brought into awareness via interoceptive cues.9 Awareness of and exposure to these often private, physiologic symptoms is an important part of many evidence-based therapies for anxiety disorders.10,11
Brain basis of fear. The amygdala and insula are 2 key components of the brain basis of fearful feelings.
The amygdala processes internal or external stimuli, alerts other brain areas that a threat is present, and triggers a fear or anxiety response (Table 1).13-16 Early, nonconscious threat detection by the amygdala may be a core component of the brain basis of many anxiety disorders.17
Amygdala activity has been associated with automatic fear perception, associative fear learning, trauma,18 and (on the treatment side) extinction of learned fears via active coping.19 The amygdala provides an extremely rapid response to fearful stimuli—within milliseconds—and can be active without conscious awareness of the stimuli (which may take several hundred milliseconds to develop).20,21
Inputs into the amygdala can come from:
- inside the brain (memories, images, emotions, predictions of the future)
- or outside (contemporary stimuli).
In treatment, the amygdala may be one site of activity of serotonergic medications.22 It is partially regulated by orbitofrontal and medial prefrontal areas that may be target sites of “top-down” psychotherapeutic interventions.23
The insula—a sector of cortex tucked beneath the fissure between the temporal and parietal lobes—is involved in interoception, modulation of emotional processing, and emotional learning, especially as related to aversive internal states.24,25
Paulus24 proposes that in anxiety-prone individuals the insula may create a negatively valenced, preattentive, body-centered warning of negative things to come—in a sense, a somatic semaphore that signals danger ahead. In a related study, Stein et al26 presented college students with emotion-provoking faces. Students prone to anxiety had elevated activity in the amygdala and insula compared with normal controls.
The insula also may respond to mindful mental exercise. Lazar et al27 found increased cortical thickness in prefrontal and anterior insula in 20 subjects with extensive experience in insight meditation, which involves focusing attention on internal states.
Table 1
Amygdala output pathways that result in anxiety symptoms
| Link to specific brain area | Clinically important responses |
|---|---|
| Hypothalamus | Sympathetic activation: increased heart rate, sweating, dilated pupils, striated muscle tension, strained breathing |
| Dorsal motor nucleus of vagus | Parasympathetic activation: slowed heart rate, bladder and bowel symptoms—frequent urination, diarrhea—via smooth muscle activity, gastric acid secretion |
| Parabrachial nucleus | Increased respiratory rate: sighing respirations |
| Ventral tegmental area/locus ceruleus | Generalized arousal, perceptual vigilance (excessive stimulation leads to disruption of attention/dissociation, via prefrontal cortical connections) |
| Nucleus reticularis pontis caudalis | Startle response, jumpiness |
| Periaqueductal gray matter | Automatic coping patterns, from passive (freeze, collapse) to active (confrontation, fight) |
| Trigeminal facial motor nuclei | Jaw tension, facial expressions of fear |
| Source: Adapted with permission from references 13 with additional information from references 14-16 | |
CASE CONTINUED: Using focused interoception
You help Ms. N become aware of her somatic symptoms of anxiety by using a series of questions to direct her attention to her physical responses in a “head-to-toe” approach: “Do you notice the tension in your jaw?” “Is your neck tense?” “How is your breathing now?” Though Ms. N had been unaware of these symptoms, she easily agrees: “Yes, now that you mention it, I am aware of that, but I never knew it was anxiety. I thought it was just stress.”
This exercise reveals marked generalized muscle tension, sweating, and a brief period of going “blank” in her mind when she recalled one of her impulsive, aggressive episodes. You explain that these physical reactions are part of the normal biologic fear response. Apart from these symptoms, Ms. N denies any prototypical manic symptoms and does not meet bipolar disorder criteria.
Using interoceptive cues
To frame an interoceptive inquiry, discuss with patients how the brain’s fear system is connected to the body, and explain that investigating these physical symptoms can assist diagnosis and treatment. For example, you might ask, “Could we look into your physical responses in these situations to help us better understand your difficulties?”
To actively explore somatic markers of anxiety (anxious feelings), encourage the patient to describe a specific stressful or avoided situation in detail. While he or she does this, direct the patient’s attention to objective physiologic markers of anxiety, such as strained breathing or increased heart rate. Use body-directed questions (interoceptive cues) to foreground these sensory experiences in the patient’s mind. For example:
- “As we are discussing this issue, I notice your breathing becomes more strained. Do you notice it?”
- “As you picture this incident in your mind, are you aware of what happens in your body?”
- “When you perceive her in that way, what do you notice about your physical response?”
You can further inquire into these somatic symptoms and their effect on the patient by asking, “How long have you been having these particular symptoms?” “How frequently do they occur?” or “How distressing are these symptoms?” These questions can separate transient physiologic arousal (normal) from pathologic (recurrent, disabling) responses that may respond to treatment. These cues and their responses can be used as person-specific biomarkers to assay a patient’s:
- ability to attend to his or her somatic state
- baseline level of autonomic arousal
- internal state before problematic behaviors (such as impulsive or self-harming behaviors, substance use)
- tendency toward anxiety-related perceptual disturbances (such as dissociation).
When the patient actively attends to and carefully describes his or her somatic sensations, the immediate outcome typically is anxiolytic. A shared awareness of the anxiolytic nature of this exercise—“It’s interesting that paying attention to these feelings actually reduces anxiety”—creates a positive first step toward further exploration. Patients can feel the power of the mind to regulate distress.
Overcoming barriers to interoception
Many patients—including those with dissociative disorders, impulse control disorders, or disorders with significant obsessive features—have difficulty using their attention to bring physical symptoms to mind. Some develop automatic, phobic patterns of disattention to contemporaneous somatic feelings of anxiety. This experiential avoidance is the fear of fear itself—fear of the conscious experience of fearful feelings. Their typical responses to interoceptive cues include:
- lack of awareness (“I don’t know,” “I wasn’t aware of anything”)
- perceptions, phrased as feelings (“I feel as if he doesn’t like me”)
- action tendencies or impulses, phrased as feelings (“I feel like I want to get out of there”)
- a verbal explanation of why they are anxious (“I’m worried about what might happen”).
Depending on the context of your inquiry, if the patient does not respond to an interoceptive cue with actual body-centered feelings, you can:
- reframe the question: “OK, but when you perceive him in that way, if you focus your mind on your physical reactions, what do you notice?”
- point out observable symptoms: “Did you notice as we were talking about this issue that your breathing got very shallow, and your hands got tense?”
Some patients may look transiently “spacey” or report “checking out” during the exercise. Inquire specifically about this because they may be demonstrating dissociative symptoms: “Does this sometimes happen when you are stressed, that you lose touch with your sense of your body, you go numb or your mind goes blank?” These symptoms warrant attention, as they may preclude effective retention of the exercise.
Explaining occult anxiety
Regardless of how far you choose to pursue an interoceptive inquiry, uncovering an interoceptive deficit—an inability to describe one’s somatic experience—may be diagnostically helpful. Doing so identifies a potentially modifiable component of self-awareness. So-called mindfulness-based and emotion-focused therapies assist patients in developing a more robust awareness and understanding of their emotions, including the somatic sensations of emotion (see Related Resources).
With appropriate psychoeducation, an interoceptive exploration makes anxiety a real, physical event anchored in brain-body function, and facilitates a nonshaming, organ-based explanation of anxiety. Psychoeducation about fear grounds physical symptoms of anxiety in a brain-based, evolutionarily selected neural system whose activity has a variety of inputs and outputs (Table 2).
An organ-based, body-centered discussion also may reduce defensiveness in patients who feel (or have been told) that anxiety is “not real” or signals personality weakness. This model may help trainees and medical colleagues avoid outdated distinctions between real/organic problems and functional/emotional problems and find a more conciliatory construct based in emotional neuroscience.
Serotonergic medications and psychotherapy—both of which work on the brain—have demonstrated broad efficacy for anxiety disorders.5 Several national organizations offer information about evidence-based psychotherapeutic treatments grounded in emotional awareness and neuroscience (see Related Resources).
Table 2
Activity of the fear system
| Inputs |
| Contemporary situations |
| Memories (visual and sensory) |
| Anticipated future situations |
| Other nonconscious body and brain processes (including the physiologic symptoms of emotions and anxiety—a ‘fear of fear’ or ‘fear of feelings’) |
| Outputs |
| Physical symptoms |
| Thoughts |
| Perceptions |
| Behaviors |
| States of attention |
CASE CONTINUED: Putting interoception to work
Your psychotherapeutic work with Ms. N focuses on attending to and consciously modulating her newly labeled anxiety For example, after an inquiry into a “stressful” situation, you help her use careful interoceptive attention—and when necessary, mindful relaxation and breathing—to regulate her fear symptoms.
She finds that these simple “exposure/regulation” exercises are enough to rapidly resolve her impulsive behaviors. In distressing situations, she can now be aware of her reactions and make a conscious choice of how to react. Your psychotherapeutic work now proceeds toward more effective interpersonal expression of other emotions.
- Barrett LF, Mesquita B, Ochsner K, Gross JJ. The experience of emotion. Annu Rev Psychol 2007;58:373-403.
- Damasio A. The feeling of what happens: body and emotion in the making of consciousness. New York: Harcourt; 1999.
- International Experiential Dynamic Therapy Association. www.iedta.net.
- International Center for Excellence in Emotionally Focused Therapy. www.eft.ca.
Disclosure
Dr. MacDonald reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Katon W, Lin EH, Kroenke K. The association of depression and anxiety with medical symptom burden in patients with chronic medical illness. Gen Hosp Psychiatry 2007;29(2):147-55.
2. Niedenthal PM. Embodying emotion. Science 2007;316(5827):1002-5.
3. McClure EB, Monk CS, Nelson EE, et al. Abnormal attention modulation of fear circuit function in pediatric generalized anxiety disorder. Arch Gen Psychiatry 2007;64(1):97-106.
4. Panksepp J. Affective neuroscience. New York: Oxford University Press; 1998:31.
5. Stein DJ. Advances in understanding the anxiety disorders: the cognitive-affective neuroscience of ‘false alarms’. Ann Clin Psychiatry 2006;18(3):173-82.
6. Kroenke K, Spitzer RL, Williams JBW, et al. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med 2007;146(5):317-25.
7. Damasio A. The feeling of what happens: body and emotion in the making of consciousness. New York: Harcourt; 1999.
8. Wiens S. Interoception in emotional experience. Curr Opin Neurol 2005;18(4):442-7.
9. Cameron OG. Interoception: the inside story—a model for psychosomatic processes. Psychosom Med 2001;63(5):697-710.
10. Wald J, Taylor S. Interoceptive exposure therapy combined with trauma-related exposure therapy for post-traumatic stress disorder: a case report. Cognit Behav Ther 2005;34(1):34-40.
11. Wells A, Papageorgiou C. Social phobic interoception: effects of bodily information on anxiety, beliefs and self-processing. Behav Res Ther 2001;39(1):1-11.
12. Davidson RJ. Anxiety and affective style: role of prefrontal cortex and amygdala. Biol Psychiatry 2002;51(1):68-80.
13. Kandel ER, Squire LR. Memory: from mind to molecules. New York: Henry Holt and Company, 1999.
14. Fokkema DS. The psychobiology of strained breathing and its cardiovascular implications: a functional system review. Psychophysiology 1999;36(2):164-75.
15. Arnsten AF. Fundamentals of attention-deficit/hyperactivity disorder: circuits and pathways. J Clin Psychiatry 2006;67 (suppl 8):7-12.
16. Keay KA, Bandler R. Parallel circuits mediating distinct emotional coping reactions to different types of stress. Neurosci Biobehav Rev 2001;25(7-8):669-78.
17. Garakani A, Mathew SJ, Charney DS. Neurobiology of anxiety disorders and implications for treatment. Mt Sinai J Med 2006;73(7):941-9.
18. Phelps EA. Emotion and cognition: insights from studies of the human amygdala. Annu Rev Psychol 2006;57:27-53.
19. LeDoux JE, Gorman JM. A call to action: overcoming anxiety through active coping. Am J Psychiatry 2001;158(12):1953-5.
20. LeDoux JE. The emotional brain. New York: Simon and Schuster, 1996.
21. Liddell BJ, Brown KJ, Kemp AH, et al. A direct brainstemamygdala-cortical ‘alarm’ system for subliminal signals of fear. Neuroimage 2005;24(1):235-43.
22. Harmer CJ, Mackay CE, Reid CB, et al. Antidepressant drug treatment modifies the neural processing of nonconscious threat cues. Biol Psychiatry 2006;59(9):816-20.
23. Hariri AR, Mattay VS, Tessitore A, et al. Neocortical modulation of the amygdala response to fearful stimuli. Biol Psychiatry 2003;53(6):494-501.
24. Paulus MP, Stein MB. An insular view of anxiety. Biol Psychiatry 2006;60(4):383-7.
25. Simmons A, Strigo I, Matthews SC, et al. Anticipation of aversive visual stimuli is associated with increased insula activation in anxiety-prone subjects. Biol Psychiatry 2006;60(4):402-9.
26. Stein MB, Simmons AN, Feinstein JS, et al. Increased amygdala and insula activation during emotion processing in anxiety-prone subjects. Am J Psychiatry 2007;164(2):318-27.
27. Lazar SW, Kerr CE, Wasserman RH, et al. Meditation experience is associated with increased cortical thickness. Neuroreport 2005;16(17):1893-7.
CASE: 'I don't know how I feel'
Ms. N, age 48, is seen in an outpatient clinic for episodic, impulsive aggression and evaluation of possible bipolar disorder. When you ask her to describe one of her episodes—which always involve a conflict with her partner or another loved one—Ms. N says, “I just lose control… I go blank.” You observe Ms. N’s deep, sighing respirations, trembling hands, and restless, fidgety leg movements. When you ask about her awareness of her physical state while she was recalling the incident, she immediately calms, looks at you quizzically, and states, “I don’t know how I feel.”
When assessing a patient who might have an anxiety disorder, don’t overlook the body. In addition to worry and avoidance, body-centered feelings are a vital component of anxiety and an important treatment target.1
This article:
- highlights clinically relevant neurobiology of anxious feelings
- discusses interoception—awareness of the physiologic state of one’s body—and its connection with anxiety
- explains the use of interoceptive cues as an aid to diagnosing and treating anxiety.
Affective neuroscience and fear
Interoceptive cues are questions directed toward the somatic manifestations of anxiety. Because these questions encourage patients to consciously experience the physical symptoms of anxiety, using interoceptive cues essentially is an exposure-based intervention that may feel counterintuitive to practitioners who are more accustomed to trying to relieve anxiety.
Emotions are thought to be grounded in brain areas that receive and regulate somatic signals, such as the amygdala and insula.2 A feeling-focused approach to anxiety weds affective neuroscience—the study of emotions—with clinical assessment and treatment of anxiety disorders, and conceptualizes that fear is a core component of many anxiety-related disorders.3,4
Although the DSM-IV-TR views anxiety disorders as clinically heterogeneous, affective neuroscience emphasizes what these disorders have in common.5 This unifying perspective allows clinicians to anchor anxiety disorders and anxiety-related disorders—such as hypochondriasis—in core emotional systems that have 3 clinically important aspects—actions (behavior and body), brain, and consciousness (mind) (Figure).4 Two emotional systems related to anxiety disorders are fear (anxious anticipation) and panic (evolutionarily related to separation anxiety and suffocation alarm signals). Viewing anxiety disorders as rooted in core emotion systems allows you to incorporate recent advances in emotional neuroscience, including interoception, into your clinical practice.
Figure: A,B,C model for understanding emotions
Affective neuroscience is a broad-based scientific discipline that explores emotions from 3 vantages: actions (behaviors and bodily responses), brain bases, and conscious manifestations. Two core emotional systems related to anxiety disorders are fear and panic.
Source: Adapted with permission from Panksepp J. Affective neuroscience. New York: Oxford University Press; 1998:31.
Detecting ‘hidden’ anxiety
Conscious symptoms. Activity in the brain’s fear system can generate conscious experiences, including worry, heightened arousal, attentional biases, and body-based feelings of fear. Anxious feelings—by definition, sensory experiences—are an important component of an anxiety assessment and relatively easy to identify.
Kroenke et al6 evaluated a 2-item screening tool, the Generalized Anxiety Disorder scale (GAD-2) that highlights both cognitive (worry) and somatic (feeling) sides of anxiety. Researchers asked 965 randomly sampled primary care patients, “Over the past 2 weeks, how often have you been bothered by the following problems:
- feeling nervous, anxious, or on edge
- not being able to stop or control worrying.
Possible responses ranged from 0 (not at all) to 3 (nearly every day). The GAD-2 was as specific for detecting anxiety disorders as a 7-item scale, the GAD-7, (88%), though less sensitive (65% vs 77%).
Nonconscious symptoms. A challenge arises, however, when patients demonstrate signs of anxiety (stress-related physical symptoms such as stomach pains or avoidance-related behaviors) without conscious awareness of anxious feelings. Though patients may intellectually understand the concept of body-based “gut feelings,” these sensations are often reflexively ignored, avoided, or mislabeled. Patients may use terms such as “stressed,” “distressed,” or “tense,” focus on the external source of the fear (rather than their response to it), or reflexively engage in behaviors (avoidance, impulsive behaviors) without being aware of their internal responses.
Anxiety symptoms that occur without corresponding awareness can be called occult, nonconscious, or unconscious anxiety. These symptoms, unique to each patient, can be used as:
- cues to the patient that he or she is anxious
- stimuli to be desensitized (via exposure-based interventions)
- markers of treatment progress.
Patients who experience occult anxiety often have a deficit in interoception (Box).2,7-11 Using interoceptive cues to foster awareness of these unrecognized body-based symptoms can provide insight into formerly unrecognized manifestations of anxiety.
Neurobiology of anxiety
The fear system. Dynamic changes in stimulus-specific physical sensations—anxious feelings—are linked to activity of the brain’s fear system. This system, which detects and rapidly learns to anticipate danger or distress, can exhibit low-level tonic activity (chronic, generalized anxiety), phasic high-amplitude reactivity (spikes of anxiety), and combinations of the 2.4,12
This precognitive, primary-process alarm system can generate:
- behaviors, often centered around avoidance—though other types (such as impulsive) can occur
- physiologic responses, which may or may not become conscious
- states of mind, including attention (hypervigilance, dissociation), cognitive contents (specific worries), and viscerosomatic awareness (“feelings”).
Through learning—and under the influence of temperamental/genetic predispositions—the fear system can be linked to internal and external stimuli, yielding a spectrum of clinical disorders that includes anxiety disorders.5
Consciously experiencing an emotion, attending to an emotionally arousing external stimulus, and remembering an emotionally arousing event all involve overlapping mental and neurobiologic processes in brain areas that process and regulate sensations from the body.2,7 Therefore, one does not need to remember “how one felt in the past” to elicit similar neurobiologic and physiologic responses in the present. These responses are recreated in the present when one consciously activates the memory. This understanding underlies the use of interoceptive cues.
Interoception is intentional, mindful awareness of the physiologic state of one’s body. Consciously directing attention to one’s internal state actively unifies the activity of the attending mind and brain with ongoing visceromotor sensations from the body.8,9 These body-based somatic markers often lie at the border of consciousness and can be brought into awareness via interoceptive cues.9 Awareness of and exposure to these often private, physiologic symptoms is an important part of many evidence-based therapies for anxiety disorders.10,11
Brain basis of fear. The amygdala and insula are 2 key components of the brain basis of fearful feelings.
The amygdala processes internal or external stimuli, alerts other brain areas that a threat is present, and triggers a fear or anxiety response (Table 1).13-16 Early, nonconscious threat detection by the amygdala may be a core component of the brain basis of many anxiety disorders.17
Amygdala activity has been associated with automatic fear perception, associative fear learning, trauma,18 and (on the treatment side) extinction of learned fears via active coping.19 The amygdala provides an extremely rapid response to fearful stimuli—within milliseconds—and can be active without conscious awareness of the stimuli (which may take several hundred milliseconds to develop).20,21
Inputs into the amygdala can come from:
- inside the brain (memories, images, emotions, predictions of the future)
- or outside (contemporary stimuli).
In treatment, the amygdala may be one site of activity of serotonergic medications.22 It is partially regulated by orbitofrontal and medial prefrontal areas that may be target sites of “top-down” psychotherapeutic interventions.23
The insula—a sector of cortex tucked beneath the fissure between the temporal and parietal lobes—is involved in interoception, modulation of emotional processing, and emotional learning, especially as related to aversive internal states.24,25
Paulus24 proposes that in anxiety-prone individuals the insula may create a negatively valenced, preattentive, body-centered warning of negative things to come—in a sense, a somatic semaphore that signals danger ahead. In a related study, Stein et al26 presented college students with emotion-provoking faces. Students prone to anxiety had elevated activity in the amygdala and insula compared with normal controls.
The insula also may respond to mindful mental exercise. Lazar et al27 found increased cortical thickness in prefrontal and anterior insula in 20 subjects with extensive experience in insight meditation, which involves focusing attention on internal states.
Table 1
Amygdala output pathways that result in anxiety symptoms
| Link to specific brain area | Clinically important responses |
|---|---|
| Hypothalamus | Sympathetic activation: increased heart rate, sweating, dilated pupils, striated muscle tension, strained breathing |
| Dorsal motor nucleus of vagus | Parasympathetic activation: slowed heart rate, bladder and bowel symptoms—frequent urination, diarrhea—via smooth muscle activity, gastric acid secretion |
| Parabrachial nucleus | Increased respiratory rate: sighing respirations |
| Ventral tegmental area/locus ceruleus | Generalized arousal, perceptual vigilance (excessive stimulation leads to disruption of attention/dissociation, via prefrontal cortical connections) |
| Nucleus reticularis pontis caudalis | Startle response, jumpiness |
| Periaqueductal gray matter | Automatic coping patterns, from passive (freeze, collapse) to active (confrontation, fight) |
| Trigeminal facial motor nuclei | Jaw tension, facial expressions of fear |
| Source: Adapted with permission from references 13 with additional information from references 14-16 | |
CASE CONTINUED: Using focused interoception
You help Ms. N become aware of her somatic symptoms of anxiety by using a series of questions to direct her attention to her physical responses in a “head-to-toe” approach: “Do you notice the tension in your jaw?” “Is your neck tense?” “How is your breathing now?” Though Ms. N had been unaware of these symptoms, she easily agrees: “Yes, now that you mention it, I am aware of that, but I never knew it was anxiety. I thought it was just stress.”
This exercise reveals marked generalized muscle tension, sweating, and a brief period of going “blank” in her mind when she recalled one of her impulsive, aggressive episodes. You explain that these physical reactions are part of the normal biologic fear response. Apart from these symptoms, Ms. N denies any prototypical manic symptoms and does not meet bipolar disorder criteria.
Using interoceptive cues
To frame an interoceptive inquiry, discuss with patients how the brain’s fear system is connected to the body, and explain that investigating these physical symptoms can assist diagnosis and treatment. For example, you might ask, “Could we look into your physical responses in these situations to help us better understand your difficulties?”
To actively explore somatic markers of anxiety (anxious feelings), encourage the patient to describe a specific stressful or avoided situation in detail. While he or she does this, direct the patient’s attention to objective physiologic markers of anxiety, such as strained breathing or increased heart rate. Use body-directed questions (interoceptive cues) to foreground these sensory experiences in the patient’s mind. For example:
- “As we are discussing this issue, I notice your breathing becomes more strained. Do you notice it?”
- “As you picture this incident in your mind, are you aware of what happens in your body?”
- “When you perceive her in that way, what do you notice about your physical response?”
You can further inquire into these somatic symptoms and their effect on the patient by asking, “How long have you been having these particular symptoms?” “How frequently do they occur?” or “How distressing are these symptoms?” These questions can separate transient physiologic arousal (normal) from pathologic (recurrent, disabling) responses that may respond to treatment. These cues and their responses can be used as person-specific biomarkers to assay a patient’s:
- ability to attend to his or her somatic state
- baseline level of autonomic arousal
- internal state before problematic behaviors (such as impulsive or self-harming behaviors, substance use)
- tendency toward anxiety-related perceptual disturbances (such as dissociation).
When the patient actively attends to and carefully describes his or her somatic sensations, the immediate outcome typically is anxiolytic. A shared awareness of the anxiolytic nature of this exercise—“It’s interesting that paying attention to these feelings actually reduces anxiety”—creates a positive first step toward further exploration. Patients can feel the power of the mind to regulate distress.
Overcoming barriers to interoception
Many patients—including those with dissociative disorders, impulse control disorders, or disorders with significant obsessive features—have difficulty using their attention to bring physical symptoms to mind. Some develop automatic, phobic patterns of disattention to contemporaneous somatic feelings of anxiety. This experiential avoidance is the fear of fear itself—fear of the conscious experience of fearful feelings. Their typical responses to interoceptive cues include:
- lack of awareness (“I don’t know,” “I wasn’t aware of anything”)
- perceptions, phrased as feelings (“I feel as if he doesn’t like me”)
- action tendencies or impulses, phrased as feelings (“I feel like I want to get out of there”)
- a verbal explanation of why they are anxious (“I’m worried about what might happen”).
Depending on the context of your inquiry, if the patient does not respond to an interoceptive cue with actual body-centered feelings, you can:
- reframe the question: “OK, but when you perceive him in that way, if you focus your mind on your physical reactions, what do you notice?”
- point out observable symptoms: “Did you notice as we were talking about this issue that your breathing got very shallow, and your hands got tense?”
Some patients may look transiently “spacey” or report “checking out” during the exercise. Inquire specifically about this because they may be demonstrating dissociative symptoms: “Does this sometimes happen when you are stressed, that you lose touch with your sense of your body, you go numb or your mind goes blank?” These symptoms warrant attention, as they may preclude effective retention of the exercise.
Explaining occult anxiety
Regardless of how far you choose to pursue an interoceptive inquiry, uncovering an interoceptive deficit—an inability to describe one’s somatic experience—may be diagnostically helpful. Doing so identifies a potentially modifiable component of self-awareness. So-called mindfulness-based and emotion-focused therapies assist patients in developing a more robust awareness and understanding of their emotions, including the somatic sensations of emotion (see Related Resources).
With appropriate psychoeducation, an interoceptive exploration makes anxiety a real, physical event anchored in brain-body function, and facilitates a nonshaming, organ-based explanation of anxiety. Psychoeducation about fear grounds physical symptoms of anxiety in a brain-based, evolutionarily selected neural system whose activity has a variety of inputs and outputs (Table 2).
An organ-based, body-centered discussion also may reduce defensiveness in patients who feel (or have been told) that anxiety is “not real” or signals personality weakness. This model may help trainees and medical colleagues avoid outdated distinctions between real/organic problems and functional/emotional problems and find a more conciliatory construct based in emotional neuroscience.
Serotonergic medications and psychotherapy—both of which work on the brain—have demonstrated broad efficacy for anxiety disorders.5 Several national organizations offer information about evidence-based psychotherapeutic treatments grounded in emotional awareness and neuroscience (see Related Resources).
Table 2
Activity of the fear system
| Inputs |
| Contemporary situations |
| Memories (visual and sensory) |
| Anticipated future situations |
| Other nonconscious body and brain processes (including the physiologic symptoms of emotions and anxiety—a ‘fear of fear’ or ‘fear of feelings’) |
| Outputs |
| Physical symptoms |
| Thoughts |
| Perceptions |
| Behaviors |
| States of attention |
CASE CONTINUED: Putting interoception to work
Your psychotherapeutic work with Ms. N focuses on attending to and consciously modulating her newly labeled anxiety For example, after an inquiry into a “stressful” situation, you help her use careful interoceptive attention—and when necessary, mindful relaxation and breathing—to regulate her fear symptoms.
She finds that these simple “exposure/regulation” exercises are enough to rapidly resolve her impulsive behaviors. In distressing situations, she can now be aware of her reactions and make a conscious choice of how to react. Your psychotherapeutic work now proceeds toward more effective interpersonal expression of other emotions.
- Barrett LF, Mesquita B, Ochsner K, Gross JJ. The experience of emotion. Annu Rev Psychol 2007;58:373-403.
- Damasio A. The feeling of what happens: body and emotion in the making of consciousness. New York: Harcourt; 1999.
- International Experiential Dynamic Therapy Association. www.iedta.net.
- International Center for Excellence in Emotionally Focused Therapy. www.eft.ca.
Disclosure
Dr. MacDonald reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: 'I don't know how I feel'
Ms. N, age 48, is seen in an outpatient clinic for episodic, impulsive aggression and evaluation of possible bipolar disorder. When you ask her to describe one of her episodes—which always involve a conflict with her partner or another loved one—Ms. N says, “I just lose control… I go blank.” You observe Ms. N’s deep, sighing respirations, trembling hands, and restless, fidgety leg movements. When you ask about her awareness of her physical state while she was recalling the incident, she immediately calms, looks at you quizzically, and states, “I don’t know how I feel.”
When assessing a patient who might have an anxiety disorder, don’t overlook the body. In addition to worry and avoidance, body-centered feelings are a vital component of anxiety and an important treatment target.1
This article:
- highlights clinically relevant neurobiology of anxious feelings
- discusses interoception—awareness of the physiologic state of one’s body—and its connection with anxiety
- explains the use of interoceptive cues as an aid to diagnosing and treating anxiety.
Affective neuroscience and fear
Interoceptive cues are questions directed toward the somatic manifestations of anxiety. Because these questions encourage patients to consciously experience the physical symptoms of anxiety, using interoceptive cues essentially is an exposure-based intervention that may feel counterintuitive to practitioners who are more accustomed to trying to relieve anxiety.
Emotions are thought to be grounded in brain areas that receive and regulate somatic signals, such as the amygdala and insula.2 A feeling-focused approach to anxiety weds affective neuroscience—the study of emotions—with clinical assessment and treatment of anxiety disorders, and conceptualizes that fear is a core component of many anxiety-related disorders.3,4
Although the DSM-IV-TR views anxiety disorders as clinically heterogeneous, affective neuroscience emphasizes what these disorders have in common.5 This unifying perspective allows clinicians to anchor anxiety disorders and anxiety-related disorders—such as hypochondriasis—in core emotional systems that have 3 clinically important aspects—actions (behavior and body), brain, and consciousness (mind) (Figure).4 Two emotional systems related to anxiety disorders are fear (anxious anticipation) and panic (evolutionarily related to separation anxiety and suffocation alarm signals). Viewing anxiety disorders as rooted in core emotion systems allows you to incorporate recent advances in emotional neuroscience, including interoception, into your clinical practice.
Figure: A,B,C model for understanding emotions
Affective neuroscience is a broad-based scientific discipline that explores emotions from 3 vantages: actions (behaviors and bodily responses), brain bases, and conscious manifestations. Two core emotional systems related to anxiety disorders are fear and panic.
Source: Adapted with permission from Panksepp J. Affective neuroscience. New York: Oxford University Press; 1998:31.
Detecting ‘hidden’ anxiety
Conscious symptoms. Activity in the brain’s fear system can generate conscious experiences, including worry, heightened arousal, attentional biases, and body-based feelings of fear. Anxious feelings—by definition, sensory experiences—are an important component of an anxiety assessment and relatively easy to identify.
Kroenke et al6 evaluated a 2-item screening tool, the Generalized Anxiety Disorder scale (GAD-2) that highlights both cognitive (worry) and somatic (feeling) sides of anxiety. Researchers asked 965 randomly sampled primary care patients, “Over the past 2 weeks, how often have you been bothered by the following problems:
- feeling nervous, anxious, or on edge
- not being able to stop or control worrying.
Possible responses ranged from 0 (not at all) to 3 (nearly every day). The GAD-2 was as specific for detecting anxiety disorders as a 7-item scale, the GAD-7, (88%), though less sensitive (65% vs 77%).
Nonconscious symptoms. A challenge arises, however, when patients demonstrate signs of anxiety (stress-related physical symptoms such as stomach pains or avoidance-related behaviors) without conscious awareness of anxious feelings. Though patients may intellectually understand the concept of body-based “gut feelings,” these sensations are often reflexively ignored, avoided, or mislabeled. Patients may use terms such as “stressed,” “distressed,” or “tense,” focus on the external source of the fear (rather than their response to it), or reflexively engage in behaviors (avoidance, impulsive behaviors) without being aware of their internal responses.
Anxiety symptoms that occur without corresponding awareness can be called occult, nonconscious, or unconscious anxiety. These symptoms, unique to each patient, can be used as:
- cues to the patient that he or she is anxious
- stimuli to be desensitized (via exposure-based interventions)
- markers of treatment progress.
Patients who experience occult anxiety often have a deficit in interoception (Box).2,7-11 Using interoceptive cues to foster awareness of these unrecognized body-based symptoms can provide insight into formerly unrecognized manifestations of anxiety.
Neurobiology of anxiety
The fear system. Dynamic changes in stimulus-specific physical sensations—anxious feelings—are linked to activity of the brain’s fear system. This system, which detects and rapidly learns to anticipate danger or distress, can exhibit low-level tonic activity (chronic, generalized anxiety), phasic high-amplitude reactivity (spikes of anxiety), and combinations of the 2.4,12
This precognitive, primary-process alarm system can generate:
- behaviors, often centered around avoidance—though other types (such as impulsive) can occur
- physiologic responses, which may or may not become conscious
- states of mind, including attention (hypervigilance, dissociation), cognitive contents (specific worries), and viscerosomatic awareness (“feelings”).
Through learning—and under the influence of temperamental/genetic predispositions—the fear system can be linked to internal and external stimuli, yielding a spectrum of clinical disorders that includes anxiety disorders.5
Consciously experiencing an emotion, attending to an emotionally arousing external stimulus, and remembering an emotionally arousing event all involve overlapping mental and neurobiologic processes in brain areas that process and regulate sensations from the body.2,7 Therefore, one does not need to remember “how one felt in the past” to elicit similar neurobiologic and physiologic responses in the present. These responses are recreated in the present when one consciously activates the memory. This understanding underlies the use of interoceptive cues.
Interoception is intentional, mindful awareness of the physiologic state of one’s body. Consciously directing attention to one’s internal state actively unifies the activity of the attending mind and brain with ongoing visceromotor sensations from the body.8,9 These body-based somatic markers often lie at the border of consciousness and can be brought into awareness via interoceptive cues.9 Awareness of and exposure to these often private, physiologic symptoms is an important part of many evidence-based therapies for anxiety disorders.10,11
Brain basis of fear. The amygdala and insula are 2 key components of the brain basis of fearful feelings.
The amygdala processes internal or external stimuli, alerts other brain areas that a threat is present, and triggers a fear or anxiety response (Table 1).13-16 Early, nonconscious threat detection by the amygdala may be a core component of the brain basis of many anxiety disorders.17
Amygdala activity has been associated with automatic fear perception, associative fear learning, trauma,18 and (on the treatment side) extinction of learned fears via active coping.19 The amygdala provides an extremely rapid response to fearful stimuli—within milliseconds—and can be active without conscious awareness of the stimuli (which may take several hundred milliseconds to develop).20,21
Inputs into the amygdala can come from:
- inside the brain (memories, images, emotions, predictions of the future)
- or outside (contemporary stimuli).
In treatment, the amygdala may be one site of activity of serotonergic medications.22 It is partially regulated by orbitofrontal and medial prefrontal areas that may be target sites of “top-down” psychotherapeutic interventions.23
The insula—a sector of cortex tucked beneath the fissure between the temporal and parietal lobes—is involved in interoception, modulation of emotional processing, and emotional learning, especially as related to aversive internal states.24,25
Paulus24 proposes that in anxiety-prone individuals the insula may create a negatively valenced, preattentive, body-centered warning of negative things to come—in a sense, a somatic semaphore that signals danger ahead. In a related study, Stein et al26 presented college students with emotion-provoking faces. Students prone to anxiety had elevated activity in the amygdala and insula compared with normal controls.
The insula also may respond to mindful mental exercise. Lazar et al27 found increased cortical thickness in prefrontal and anterior insula in 20 subjects with extensive experience in insight meditation, which involves focusing attention on internal states.
Table 1
Amygdala output pathways that result in anxiety symptoms
| Link to specific brain area | Clinically important responses |
|---|---|
| Hypothalamus | Sympathetic activation: increased heart rate, sweating, dilated pupils, striated muscle tension, strained breathing |
| Dorsal motor nucleus of vagus | Parasympathetic activation: slowed heart rate, bladder and bowel symptoms—frequent urination, diarrhea—via smooth muscle activity, gastric acid secretion |
| Parabrachial nucleus | Increased respiratory rate: sighing respirations |
| Ventral tegmental area/locus ceruleus | Generalized arousal, perceptual vigilance (excessive stimulation leads to disruption of attention/dissociation, via prefrontal cortical connections) |
| Nucleus reticularis pontis caudalis | Startle response, jumpiness |
| Periaqueductal gray matter | Automatic coping patterns, from passive (freeze, collapse) to active (confrontation, fight) |
| Trigeminal facial motor nuclei | Jaw tension, facial expressions of fear |
| Source: Adapted with permission from references 13 with additional information from references 14-16 | |
CASE CONTINUED: Using focused interoception
You help Ms. N become aware of her somatic symptoms of anxiety by using a series of questions to direct her attention to her physical responses in a “head-to-toe” approach: “Do you notice the tension in your jaw?” “Is your neck tense?” “How is your breathing now?” Though Ms. N had been unaware of these symptoms, she easily agrees: “Yes, now that you mention it, I am aware of that, but I never knew it was anxiety. I thought it was just stress.”
This exercise reveals marked generalized muscle tension, sweating, and a brief period of going “blank” in her mind when she recalled one of her impulsive, aggressive episodes. You explain that these physical reactions are part of the normal biologic fear response. Apart from these symptoms, Ms. N denies any prototypical manic symptoms and does not meet bipolar disorder criteria.
Using interoceptive cues
To frame an interoceptive inquiry, discuss with patients how the brain’s fear system is connected to the body, and explain that investigating these physical symptoms can assist diagnosis and treatment. For example, you might ask, “Could we look into your physical responses in these situations to help us better understand your difficulties?”
To actively explore somatic markers of anxiety (anxious feelings), encourage the patient to describe a specific stressful or avoided situation in detail. While he or she does this, direct the patient’s attention to objective physiologic markers of anxiety, such as strained breathing or increased heart rate. Use body-directed questions (interoceptive cues) to foreground these sensory experiences in the patient’s mind. For example:
- “As we are discussing this issue, I notice your breathing becomes more strained. Do you notice it?”
- “As you picture this incident in your mind, are you aware of what happens in your body?”
- “When you perceive her in that way, what do you notice about your physical response?”
You can further inquire into these somatic symptoms and their effect on the patient by asking, “How long have you been having these particular symptoms?” “How frequently do they occur?” or “How distressing are these symptoms?” These questions can separate transient physiologic arousal (normal) from pathologic (recurrent, disabling) responses that may respond to treatment. These cues and their responses can be used as person-specific biomarkers to assay a patient’s:
- ability to attend to his or her somatic state
- baseline level of autonomic arousal
- internal state before problematic behaviors (such as impulsive or self-harming behaviors, substance use)
- tendency toward anxiety-related perceptual disturbances (such as dissociation).
When the patient actively attends to and carefully describes his or her somatic sensations, the immediate outcome typically is anxiolytic. A shared awareness of the anxiolytic nature of this exercise—“It’s interesting that paying attention to these feelings actually reduces anxiety”—creates a positive first step toward further exploration. Patients can feel the power of the mind to regulate distress.
Overcoming barriers to interoception
Many patients—including those with dissociative disorders, impulse control disorders, or disorders with significant obsessive features—have difficulty using their attention to bring physical symptoms to mind. Some develop automatic, phobic patterns of disattention to contemporaneous somatic feelings of anxiety. This experiential avoidance is the fear of fear itself—fear of the conscious experience of fearful feelings. Their typical responses to interoceptive cues include:
- lack of awareness (“I don’t know,” “I wasn’t aware of anything”)
- perceptions, phrased as feelings (“I feel as if he doesn’t like me”)
- action tendencies or impulses, phrased as feelings (“I feel like I want to get out of there”)
- a verbal explanation of why they are anxious (“I’m worried about what might happen”).
Depending on the context of your inquiry, if the patient does not respond to an interoceptive cue with actual body-centered feelings, you can:
- reframe the question: “OK, but when you perceive him in that way, if you focus your mind on your physical reactions, what do you notice?”
- point out observable symptoms: “Did you notice as we were talking about this issue that your breathing got very shallow, and your hands got tense?”
Some patients may look transiently “spacey” or report “checking out” during the exercise. Inquire specifically about this because they may be demonstrating dissociative symptoms: “Does this sometimes happen when you are stressed, that you lose touch with your sense of your body, you go numb or your mind goes blank?” These symptoms warrant attention, as they may preclude effective retention of the exercise.
Explaining occult anxiety
Regardless of how far you choose to pursue an interoceptive inquiry, uncovering an interoceptive deficit—an inability to describe one’s somatic experience—may be diagnostically helpful. Doing so identifies a potentially modifiable component of self-awareness. So-called mindfulness-based and emotion-focused therapies assist patients in developing a more robust awareness and understanding of their emotions, including the somatic sensations of emotion (see Related Resources).
With appropriate psychoeducation, an interoceptive exploration makes anxiety a real, physical event anchored in brain-body function, and facilitates a nonshaming, organ-based explanation of anxiety. Psychoeducation about fear grounds physical symptoms of anxiety in a brain-based, evolutionarily selected neural system whose activity has a variety of inputs and outputs (Table 2).
An organ-based, body-centered discussion also may reduce defensiveness in patients who feel (or have been told) that anxiety is “not real” or signals personality weakness. This model may help trainees and medical colleagues avoid outdated distinctions between real/organic problems and functional/emotional problems and find a more conciliatory construct based in emotional neuroscience.
Serotonergic medications and psychotherapy—both of which work on the brain—have demonstrated broad efficacy for anxiety disorders.5 Several national organizations offer information about evidence-based psychotherapeutic treatments grounded in emotional awareness and neuroscience (see Related Resources).
Table 2
Activity of the fear system
| Inputs |
| Contemporary situations |
| Memories (visual and sensory) |
| Anticipated future situations |
| Other nonconscious body and brain processes (including the physiologic symptoms of emotions and anxiety—a ‘fear of fear’ or ‘fear of feelings’) |
| Outputs |
| Physical symptoms |
| Thoughts |
| Perceptions |
| Behaviors |
| States of attention |
CASE CONTINUED: Putting interoception to work
Your psychotherapeutic work with Ms. N focuses on attending to and consciously modulating her newly labeled anxiety For example, after an inquiry into a “stressful” situation, you help her use careful interoceptive attention—and when necessary, mindful relaxation and breathing—to regulate her fear symptoms.
She finds that these simple “exposure/regulation” exercises are enough to rapidly resolve her impulsive behaviors. In distressing situations, she can now be aware of her reactions and make a conscious choice of how to react. Your psychotherapeutic work now proceeds toward more effective interpersonal expression of other emotions.
- Barrett LF, Mesquita B, Ochsner K, Gross JJ. The experience of emotion. Annu Rev Psychol 2007;58:373-403.
- Damasio A. The feeling of what happens: body and emotion in the making of consciousness. New York: Harcourt; 1999.
- International Experiential Dynamic Therapy Association. www.iedta.net.
- International Center for Excellence in Emotionally Focused Therapy. www.eft.ca.
Disclosure
Dr. MacDonald reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Katon W, Lin EH, Kroenke K. The association of depression and anxiety with medical symptom burden in patients with chronic medical illness. Gen Hosp Psychiatry 2007;29(2):147-55.
2. Niedenthal PM. Embodying emotion. Science 2007;316(5827):1002-5.
3. McClure EB, Monk CS, Nelson EE, et al. Abnormal attention modulation of fear circuit function in pediatric generalized anxiety disorder. Arch Gen Psychiatry 2007;64(1):97-106.
4. Panksepp J. Affective neuroscience. New York: Oxford University Press; 1998:31.
5. Stein DJ. Advances in understanding the anxiety disorders: the cognitive-affective neuroscience of ‘false alarms’. Ann Clin Psychiatry 2006;18(3):173-82.
6. Kroenke K, Spitzer RL, Williams JBW, et al. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med 2007;146(5):317-25.
7. Damasio A. The feeling of what happens: body and emotion in the making of consciousness. New York: Harcourt; 1999.
8. Wiens S. Interoception in emotional experience. Curr Opin Neurol 2005;18(4):442-7.
9. Cameron OG. Interoception: the inside story—a model for psychosomatic processes. Psychosom Med 2001;63(5):697-710.
10. Wald J, Taylor S. Interoceptive exposure therapy combined with trauma-related exposure therapy for post-traumatic stress disorder: a case report. Cognit Behav Ther 2005;34(1):34-40.
11. Wells A, Papageorgiou C. Social phobic interoception: effects of bodily information on anxiety, beliefs and self-processing. Behav Res Ther 2001;39(1):1-11.
12. Davidson RJ. Anxiety and affective style: role of prefrontal cortex and amygdala. Biol Psychiatry 2002;51(1):68-80.
13. Kandel ER, Squire LR. Memory: from mind to molecules. New York: Henry Holt and Company, 1999.
14. Fokkema DS. The psychobiology of strained breathing and its cardiovascular implications: a functional system review. Psychophysiology 1999;36(2):164-75.
15. Arnsten AF. Fundamentals of attention-deficit/hyperactivity disorder: circuits and pathways. J Clin Psychiatry 2006;67 (suppl 8):7-12.
16. Keay KA, Bandler R. Parallel circuits mediating distinct emotional coping reactions to different types of stress. Neurosci Biobehav Rev 2001;25(7-8):669-78.
17. Garakani A, Mathew SJ, Charney DS. Neurobiology of anxiety disorders and implications for treatment. Mt Sinai J Med 2006;73(7):941-9.
18. Phelps EA. Emotion and cognition: insights from studies of the human amygdala. Annu Rev Psychol 2006;57:27-53.
19. LeDoux JE, Gorman JM. A call to action: overcoming anxiety through active coping. Am J Psychiatry 2001;158(12):1953-5.
20. LeDoux JE. The emotional brain. New York: Simon and Schuster, 1996.
21. Liddell BJ, Brown KJ, Kemp AH, et al. A direct brainstemamygdala-cortical ‘alarm’ system for subliminal signals of fear. Neuroimage 2005;24(1):235-43.
22. Harmer CJ, Mackay CE, Reid CB, et al. Antidepressant drug treatment modifies the neural processing of nonconscious threat cues. Biol Psychiatry 2006;59(9):816-20.
23. Hariri AR, Mattay VS, Tessitore A, et al. Neocortical modulation of the amygdala response to fearful stimuli. Biol Psychiatry 2003;53(6):494-501.
24. Paulus MP, Stein MB. An insular view of anxiety. Biol Psychiatry 2006;60(4):383-7.
25. Simmons A, Strigo I, Matthews SC, et al. Anticipation of aversive visual stimuli is associated with increased insula activation in anxiety-prone subjects. Biol Psychiatry 2006;60(4):402-9.
26. Stein MB, Simmons AN, Feinstein JS, et al. Increased amygdala and insula activation during emotion processing in anxiety-prone subjects. Am J Psychiatry 2007;164(2):318-27.
27. Lazar SW, Kerr CE, Wasserman RH, et al. Meditation experience is associated with increased cortical thickness. Neuroreport 2005;16(17):1893-7.
1. Katon W, Lin EH, Kroenke K. The association of depression and anxiety with medical symptom burden in patients with chronic medical illness. Gen Hosp Psychiatry 2007;29(2):147-55.
2. Niedenthal PM. Embodying emotion. Science 2007;316(5827):1002-5.
3. McClure EB, Monk CS, Nelson EE, et al. Abnormal attention modulation of fear circuit function in pediatric generalized anxiety disorder. Arch Gen Psychiatry 2007;64(1):97-106.
4. Panksepp J. Affective neuroscience. New York: Oxford University Press; 1998:31.
5. Stein DJ. Advances in understanding the anxiety disorders: the cognitive-affective neuroscience of ‘false alarms’. Ann Clin Psychiatry 2006;18(3):173-82.
6. Kroenke K, Spitzer RL, Williams JBW, et al. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med 2007;146(5):317-25.
7. Damasio A. The feeling of what happens: body and emotion in the making of consciousness. New York: Harcourt; 1999.
8. Wiens S. Interoception in emotional experience. Curr Opin Neurol 2005;18(4):442-7.
9. Cameron OG. Interoception: the inside story—a model for psychosomatic processes. Psychosom Med 2001;63(5):697-710.
10. Wald J, Taylor S. Interoceptive exposure therapy combined with trauma-related exposure therapy for post-traumatic stress disorder: a case report. Cognit Behav Ther 2005;34(1):34-40.
11. Wells A, Papageorgiou C. Social phobic interoception: effects of bodily information on anxiety, beliefs and self-processing. Behav Res Ther 2001;39(1):1-11.
12. Davidson RJ. Anxiety and affective style: role of prefrontal cortex and amygdala. Biol Psychiatry 2002;51(1):68-80.
13. Kandel ER, Squire LR. Memory: from mind to molecules. New York: Henry Holt and Company, 1999.
14. Fokkema DS. The psychobiology of strained breathing and its cardiovascular implications: a functional system review. Psychophysiology 1999;36(2):164-75.
15. Arnsten AF. Fundamentals of attention-deficit/hyperactivity disorder: circuits and pathways. J Clin Psychiatry 2006;67 (suppl 8):7-12.
16. Keay KA, Bandler R. Parallel circuits mediating distinct emotional coping reactions to different types of stress. Neurosci Biobehav Rev 2001;25(7-8):669-78.
17. Garakani A, Mathew SJ, Charney DS. Neurobiology of anxiety disorders and implications for treatment. Mt Sinai J Med 2006;73(7):941-9.
18. Phelps EA. Emotion and cognition: insights from studies of the human amygdala. Annu Rev Psychol 2006;57:27-53.
19. LeDoux JE, Gorman JM. A call to action: overcoming anxiety through active coping. Am J Psychiatry 2001;158(12):1953-5.
20. LeDoux JE. The emotional brain. New York: Simon and Schuster, 1996.
21. Liddell BJ, Brown KJ, Kemp AH, et al. A direct brainstemamygdala-cortical ‘alarm’ system for subliminal signals of fear. Neuroimage 2005;24(1):235-43.
22. Harmer CJ, Mackay CE, Reid CB, et al. Antidepressant drug treatment modifies the neural processing of nonconscious threat cues. Biol Psychiatry 2006;59(9):816-20.
23. Hariri AR, Mattay VS, Tessitore A, et al. Neocortical modulation of the amygdala response to fearful stimuli. Biol Psychiatry 2003;53(6):494-501.
24. Paulus MP, Stein MB. An insular view of anxiety. Biol Psychiatry 2006;60(4):383-7.
25. Simmons A, Strigo I, Matthews SC, et al. Anticipation of aversive visual stimuli is associated with increased insula activation in anxiety-prone subjects. Biol Psychiatry 2006;60(4):402-9.
26. Stein MB, Simmons AN, Feinstein JS, et al. Increased amygdala and insula activation during emotion processing in anxiety-prone subjects. Am J Psychiatry 2007;164(2):318-27.
27. Lazar SW, Kerr CE, Wasserman RH, et al. Meditation experience is associated with increased cortical thickness. Neuroreport 2005;16(17):1893-7.
Beating nicotine: Medication algorithm helps teens quit
CASE: Depressed, irritable — and smoking
Michael, age 16, is admitted to a psychiatric unit for severe depressive symptoms and suicidal ideation. The next day, he is irritable and refuses to cooperate with the interview. During group therapy he is distractible and unable to focus. The treating psychiatrist learns that before admission Michael had been smoking 10 to 15 cigarettes per day and now feels a strong craving for cigarettes.
Unrecognized nicotine dependence can be problematic on inpatient psychiatric units, where adolescents such as Michael are not permitted to smoke and rarely are offered nicotine replacement therapy (NRT). Unfortunately, psychiatrists seldom diagnose and treat nicotine dependence—particularly in adolescents—whether in outpatient or inpatient settings.1,2
Do adolescent smokers need help quitting? Do they experience withdrawal symptoms when they stop smoking? Are pharmacologic interventions appropriate? For each question, the answer is a resounding yes.
To help you treat young smokers, this article offers:
- tools for assessing adolescent tobacco use and dependence
- evidence-based treatment options
- an algorithm to guide treatment choice.
Not just a ‘phase’
Early smoking—especially among those younger than age 13—is associated with adolescent psychopathology, including depressive disorders and other substance use disorders.3 Compared with nonsmoking teens, those who smoke at least monthly are significantly more likely to smoke as adults.4 Among high school seniors:
- >20% report smoking cigarettes in the past 30 days
- 12% smoke daily
- 6% smoke ≥10 cigarettes per day.5
Nicotine dependence can develop very rapidly: nearly 25% of adolescents have ≥1 symptom within 2 weeks of starting to smoke at least once a month.6
Role of parents. Early intervention for teen nicotine addiction is particularly important because of the long-term health risks associated with tobacco use.7 In our experience, however, teen smokers’ parents’ attitudes can make addressing adolescent nicotine dependence a therapeutic challenge.
Modified Fagerstrom Tolerance Questionnaire8 (7 items)
Stanford Dependence Inventory (SDI)9 (5 items)
Hooked on Nicotine Checklist (HONC)10 (10 items)
Nicotine Dependence Scale for Adolescents11 (6 items)
Cigarette Dependence Scale (CDS-5 and CDS-12)12 (5 or 12 items)
Parents may be unaware of their teens’ smoking, and those who are aware may:
- not know what help is available
- dismiss teen smoking as “just a phase”
- feel that smoking cigarettes is preferable to smoking marijuana or using other illicit drugs.
Other parents have no objections because they themselves smoke. Some permit their teens to smoke and may even give them cigarettes.
Parents who want their teens to stop smoking often believe erroneously that the best method is to quit “cold turkey.”
Assessing use and dependence
Teen smokers’ nicotine withdrawal symptoms—such as irritability, anxiety, and impaired concentration—can imitate or exacerbate other psychiatric symptoms, thus complicating diagnosis and treatment. Ask all adolescent patients about the quantity, frequency, pattern, and duration of use of all forms of tobacco, including:
- cigarettes
- cigars
- cigarillos (short, narrow cigars)
- bidis (thin, flavored South Asian cigarettes wrapped in leaf)
- smokeless tobacco.
Dependence. Establishing nicotine dependence in young smokers is more complicated than in adults because of teen smokers’ variable smoking patterns. Several self-rating scales have been developed to assess nicotine dependence in adolescents (Box 1).8-12 Although some of these tools have been used primarily in research, outpatient psychiatrists may find these scales useful for evaluating adolescents’ smoking.
Some DSM-IV-TR criteria for substance dependence may not apply to nicotine dependence or correlate with other validated measures of nicotine dependence. For example, “significant time spent obtaining, using, or recovering from the effects of a substance” might not apply to all adolescent smokers.13 Based on our clinical experience, daily smoking for an extended period of time (several months) is a marker of dependence for almost all adolescents.
The Timeline Follow Back method can help you capture a more complete picture of adolescent tobacco use over time.14 This involves asking teens about tobacco use over the past 30 or 90 days, beginning with the assessment day and working backward. Record tobacco use on a calendar, using holidays, weekends, and events as anchor points to help teens recall their smoking.
Biomarker tests can be used to measure nicotine use. The 2 most common are:
- expired carbon monoxide (CO) level (essentially a “breathalyzer” for smoking)
- cotinine level—a metabolite of nicotine.
Expired CO testing is simple to conduct but requires specialized equipment that costs approximately $1,000. Marijuana use may affect CO results, but NRT will not. Measuring CO levels provides information about cigarette smoking over the past several hours, compared with the past several days with cotinine.15
Cotinine can be tested in serum, saliva, or urine. Serum testing can be expensive and may require shipping samples to a specialized laboratory for processing. Testing saliva or urine is less expensive and may be conducted in an office. Cotinine testing in teens who use NRT may be unreliable because the nicotine in these products will be metabolized to cotinine and yield a positive result.
CASE CONTINUED: Wanting to quit
Michael was placed on a 21-mg transdermal nicotine patch, which greatly reduced his craving and irritability. He expressed an interest in quitting smoking. Given Michael’s depressive symptoms, bupropion SR was initiated to treat his depression and assist with smoking cessation.
Treatment options
Optimal smoking cessation treatment includes a combination of medication and behavioral counseling.16
Pharmacologic treatments. FDA-approved medications for adult smoking cessation include NRT—available as a gum, inhaler, nasal spray, lozenge, or transdermal patch—bupropion SR, and varenicline. Although not FDA-approved for patients younger than age 18, NRT and bupropion SR have been evaluated for smoking in adolescents.
NRT helps smokers by reducing nicotine withdrawal symptoms during cessation. Only nicotine gum and transdermal nicotine patch have been studied in adolescents. Results are modest at best, although in some studies including behavioral treatments may have obscured any medication effect (Table 1).17-20
Bupropion SR. How bupropion SR helps patients stop smoking is not completely clear. Three studies have evaluated bupropion SR in adolescents; 2 had positive results, but all 3 had important limitations (Table 2).21-23
One of the 2 positive studies included only 16 patients and had an open-label design.22 The second—a larger randomized, placebo-controlled trial23—found that bupropion SR improved nicotine abstinence compared with placebo at 6 weeks, but this effect did not last after subjects stopped taking the drug.
The third bupropion SR study used 150 mg/d (the recommend adult dose is 300 mg/d) and had poor medication adherence.21 The difference in abstinence rate compared with placebo was not statistically significant.
Other medications. Varenicline—a partial nicotine receptor agonist recently approved for adult smoking cessation—has not been studied in adolescents. Nortriptyline, doxepin, selegiline, clonidine, and mecamylamine have shown promise in adult smokers but are not approved for smoking cessation and require further study, especially in young smokers.24-27
Pharmacotherapy risks. NRT can cause nicotine overdose symptoms, such as rapid heart rate or nausea, especially if used while smoking. Transdermal NRT can cause a local reaction at the application site and can cause burns if worn while undergoing magnetic resonance imaging.28
Adverse effects associated with bupropion SR include a small risk of seizure, weight loss, and insomnia. This drug is contraindicated for patients who:
- have a seizure disorder
- have ever been diagnosed with bulimia or anorexia nervosa
- are taking other bupropion formulations.
Patients should not take bupropion SR during abrupt discontinuation of alcohol or sedatives or within 14 days of taking a monoamine oxidase inhibitor.29
Table 1
Can the nicotine patch help teens quit smoking?
| Authors | Study population | Study design | Abstinence rate |
|---|---|---|---|
| Smith et al, 199617 | 13- to 17-year-olds (N=22) who smoked ≥20 cpd | 8 weeks of open-label treatment with transdermal NRT plus behavioral counseling and group support | 14% at 8 weeks, 4.5% at 3 and 6 months |
| Hurt et al, 200418 | 13- to 17-year-olds (N=101) who smoked ≥10 cpd | 6 weeks of open-label treatment with transdermal NRT plus self-help material and brief individual counseling if requested | 11% at 6 weeks, 5% at 6 months |
| Hanson et al, 200319 | 13- to 19-year-olds (N=100) who smoked ≥10 cpd | 10 weeks of double-blind treatment with transdermal NRT or placebo plus CBT and contingency management | 20% (active) vs 18% (placebo); not statistically significant |
| Moolchan et al, 200520 | 13- to 17-year-olds (N=120) who smoked ≥10 cpd | 12 weeks of double-blind treatment with:
| 17.7% (active transdermal NRT)* vs 6.5% (active gum) vs 2.5% (placebo only) |
| *P=0.04 for transdermal NRT vs placebo | |||
| CBT: cognitive-behavioral therapy; cpd: cigarettes per day; NRT: nicotine replacement therapy | |||
Table 2
Teen smoking cessation: Evidence for bupropion SR
| Authors | Study population | Study design | Abstinence rate |
|---|---|---|---|
| Upadhyaya et al, 200421 | 12- to 19-year-olds (N=16, 11 of whom had ADHD) who smoked ≥5 cpd | 7 weeks of open-label treatment with bupropion SR, 150 mg bid, with brief smoking cessation counseling | 31.3% after 4 weeks of medication |
| Killen et al, 200422 | 15- to 18-year-olds (N=211) who smoked ≥10 cpd | 9 weeks of double-blind treatment with bupropion SR, 150 mg/d, or placebo; subjects received 8 weeks of transdermal NRT and group skills training | 23% (active) vs 28% (placebo) at 10 weeks; 8% (active) vs 7% placebo) at 26 weeks; not statistically significant |
| Muramoto et al, 200523 | 14- to 17-year-olds (N=312) who smoked ≥6 cpd | 6 weeks of double-blind treatment with bupropion SR, 150 mg/d; 150 mg bid; or placebo, with CBT and motivational enhancement | 16.9% (150 mg bid) vs 10.3% (150 mg/d) vs 6.7% (placebo) at 6 weeks* No differences at 26 weeks |
| ADHD: attention-deficit/hyperactivity disorder; CBT: cognitive-behavioral therapy; cpd: cigarettes per day; NRT: nicotine replacement therapy | |||
| *P=0.019 for 150 mg bid vs placebo | |||
Behavioral therapy. Specialized treatments developed specifically for teen smoking cessation—such as Not On Tobacco (see Related Resources)—often are delivered in schools or other group settings. The most successful consist of ≥5 sessions and include motivational enhancement, cognitive-behavioral, and social influence-oriented approaches.30
Other behavioral treatments. Most psychiatrists are not equipped to deliver these specialized behavioral treatments. Instead, you can use simple yet effective behavioral treatments during routine office visits as adjuncts to pharmacotherapy. At the very least, we recommend the U.S. Public Health Service’s “5 As” strategy (Box 2).16
Educate patients about what to expect during withdrawal, how long withdrawal will last, and medication side effects. To help adolescents develop appropriate treatment expectations:
- discuss the difference between a “slip” (having 1 cigarette) and a “relapse” (returning to daily smoking)
- explain that many individuals need multiple attempts before they quit.
Encourage adolescent smokers to contact the National Network of Tobacco Cessation Quitlines (1-800-784-8669; www.smokefree.gov), which provides free access to telephone-based counseling services.
Ask every patient about tobacco use during every visit, and have a system for recording and tracking tobacco use in the chart
Advise patients clearly and unambiguously to stop smoking, and tailor that advice to each patient’s needs
Assess every patient’s readiness to quit
Assist patients who are ready to quit through self-help materials, referral, and/or smoking cessation treatment
Arrange follow-up visits for relapse prevention or to reassess readiness to quit
Source: Reference 16
Choosing treatment
Evidence guiding treatment choice for teen smoking cessation is limited but growing. Most studies examined daily cigarette smoking, with significantly less evidence to support treatment decisions for light (non-daily) smokers and teens who use other tobacco products.
Recommendations.We have developed a strategy to guide treatment of adolescent smokers (Algorithm). We recommend using pharmacologic interventions only for teens who smoke daily because:
- most studies have focused on daily smoking
- efficacy data are limited
- pharmacologic interventions carry potential risks.
Because of bupropion SR’s contraindications and potential side effect profile, we suggest NRT in combination with smoking cessation counseling as a first-line treatment for young smokers. We recommend beginning with transdermal NRT because of the low likelihood of underdosing with the patch’s once-daily application.20 With either NRT or bupropion SR, schedule follow-up appointments to target relapse prevention and solve any issues that arise.
Help your patient choose a “quit date,” preferably 1 to 2 weeks after your initial assessment. We recommend encouraging young smokers to reduce their smoking by 1 cigarette per day to help minimize withdrawal symptoms from “cold turkey” cessation.31
Some physicians have found it helpful to see the patient on the quit day—or 2 days after when withdrawal symptoms tend to be most robust—to provide support and encouragement. Ask the adolescent to bring and discard during the visit all smoking paraphernalia as a symbol of his or her new smoke-free status.
Step 1: NRT. Initiate smoking cessation counseling plus transdermal NRT using the dosing guidelines in Table 3,28,31 and adjust the dose depending on severity of withdrawal symptoms. Ideally, the patch delivery will be used for 12 weeks, with at least 3 and ideally 6 weeks on the initial dose, followed by a gradual taper.28 We strongly recommend using transdermal NRT on adolescent inpatient units, especially for daily smokers and those who exhibit nicotine withdrawal symptoms.
Step 2: Bupropion SR. If NRT fails, the next step is bupropion SR plus smoking cessation counseling, assuming the adolescent does not have contraindications to bupropion SR. Start the medication based on the dosing guidelines in Table 3,28,31 and set a quit date for 2 weeks after starting bupropion SR.
Again, encourage adolescents to reduce by 1 cigarette per day over the 2 weeks before the quit day to minimize withdrawal symptoms.31 Continue bupropion SR for at least 8 and optimally 12 weeks.31
Combination therapy? If teens are unable to successfully quit smoking with NRT or bupropion SR alone, experience with adults suggests combining the 2 therapies might be beneficial. However, no evidence supports combination therapy in adolescents. Instead, consider referring adolescents who can’t quit to a smoking cessation specialist.
AlgorithmA strategy to initiate smoking cessation in adolescents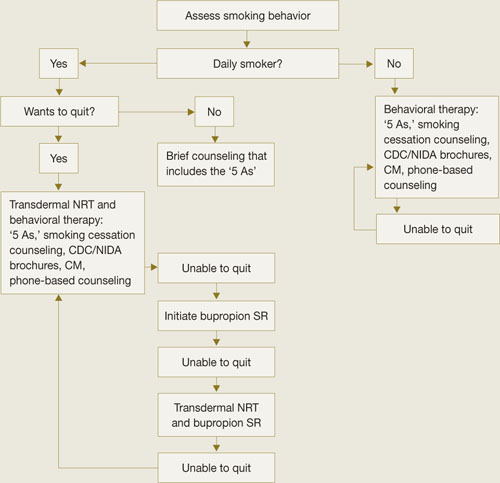
CDC: Centers for Disease Control and Prevention; CM: contingency management; NIDA: National Institute of Drug Abuse; NRT: nicotine replacement therapy
Source: Adapted from Upadhyaya H, Deas D, Brady K. A practical clinical approach to the treatment of nicotine dependence in adolescents. J Am Acad Child Adolesc Psychiatry 2005;44(9):942-6 with permission of Lippincott Williams & Wilkins.Table 3
Dosing guidelines for adolescent smoking cessation therapy
| Medication | Recommended regimen |
|---|---|
| Bupropion SR31 | Patient weight ≥90 lbs: 150 mg once in the morning for 3 to 6 days, then 150 mg bid for 12 weeks Patient weight <90 lbs: Maximum 150 mg once in the morning, if tolerated |
| Transdermal NRT28 | Patient smokes ≥10 cpd: 21 mg/d for 6 weeks, then 14 mg/d for 2 weeks, then 7 mg/d for 2 weeks, then discontinue Patient smokes <10 cpd: 14 mg/d for 6 weeks, then 7 mg/d for 2 weeks, then discontinue |
| cpd: cigarettes per day; NRT: nicotine replacement therapy | |
CASE CONTINUED: Staying smoke-free
Upon discharge, Michael discontinued NRT and followed up with his outpatient psychiatrist, who provided brief smoking cessation counseling in addition to bupropion SR, 150 mg bid. Michael’s depressive symptoms improved with the medication. He was able to stop smoking within 3 months with the combination of medication and behavioral therapy.
- Centers for Disease Control and Prevention, Youth Tobacco Prevention. www.cdc.gov/tobacco/youth/index.htm.
- Not On Tobacco model program. Substance Abuse and Mental Health Services Administration.www.modelprograms.samhsa.gov/pdfs/model/Not_On_Tobacco.pdf.
Drug brand names
- Bupropion SR • Zyban
- Clonidine • Catapres
- Doxepin • Sinequan
- Mecamylamine • Inversine
- Nicotine/inhalation system • Nicotrol Inhaler
- Nicotine/lozenge • Commit
- Nicotine/nasal spray • Nicotrol NS
- Nicotine/polacrilex • Nicorette
- Nicotine/transdermal • Nicotrol, Prostep
- Nortriptyline • Pamelor
- Selegiline • Eldepryl
- Varenicline • Chantix
Disclosures
Dr. Verduin has received research/grant support from the National Institute of Drug Abuse.
Dr. Upadhyaya is a consultant and speaker for Shire Pharmaceuticals and has received grant/research support from and is a consultant to Eli Lilly and Company.
1. Chassin L, Presson CC, Sherman SJ, Edwards DA. The natural history of cigarette smoking: predicting young-adult smoking outcomes from adolescent smoking patterns. Health Psychol 1990;9(6):701-16.
2. Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future national results on adolescent drug use: overview of key findings 2006. Bethesda, MD: National Institute on Drug Abuse; 2007. NIH publication no. 07-6202.
3. DiFranza JR, Rigotti NA, McNeill AD, et al. Initial symptoms of nicotine dependence in adolescence. Tob Control 2000;9(3):313-9.
4. Upadhyaya HP, Deas D, Brady KT, Kruesi M. Cigarette smoking and psychiatric comorbidity in children and adolescents. J Am Acad Child Adolesc Psychiatry 2002;41(11):1294-1305.
5. U.S. Department of Health and Human Services. The health consequences of smoking: a report of the surgeon general. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2004.
6. Himelhoch S, Daumit G. To whom do psychiatrists offer smoking-cessation counseling? Am J Psychiatry 2003;160(12):222-830.
7. Upadhyaya HP, Brady KT, Wharton M, Liao J. Psychiatric disorders and cigarette smoking among child and adolescent psychiatry inpatients. Am J Addict 2003;12(2):144-52.
8. Prokhorov AV, Pallonen UE, Fava JL, et al. Measuring nicotine dependence among high-risk adolescent smokers. Addict Behav 1996;21(1):117-27.
9. Rojas NL, Killen JD, Haydel KF, Robinson TN. Nicotine dependence among adolescent smokers. Arch Pediatr Adolesc Med 1998;152(2):151-6.
10. O’Loughlin J, DiFranza J, Tarasuk J, et al. Assessment of nicotine dependence symptoms in adolescents: a comparison of five indicators. Tob Control 2002;11(4):354-60.
11. Nonnemaker J, Mowery P, Hersey J, et al. Measurement properties of a nicotine dependence scale for adolescents. Nicotine Tob Res 2004;6(2):295-301.
12. Etter JF, LeHouezec J, Perneger TV. A self-administered questionnaire to measure addiction to cigarettes: the Cigarette Dependence Scale. Neuropsychopharmacology 2003;28(2):359-70.
13. Hughes JR, Oliveto AH, Riggs R, et al. Concordance of different measures of nicotine dependence: two pilot studies. Addict Behav 2004;29(8):1527-39.
14. Sobell LC, Sobell MB. Timeline Follow-Back: a technique for assessing self-reported alcohol consumption. In: Litten R, Allen J, eds. Measuring alcohol consumption: psychosocial and biochemical methods. Totowa, NJ: The Humana Press Inc.; 1992.
15. SRNT Subcommittee on Biochemical Verification. Biochemical verification of tobacco use and cessation. Nicotine Tob Res 2002;4(2):149-59.
16. Fiore MC, Bailey WC, Cohen SJ, et al. Treating tobacco use and dependence. Quick reference guide for clinicians. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service; 2000.
17. Smith TA, House RF, Croghan IT, et al. Nicotine patch therapy in adolescent smokers. Pediatrics 1996;98(4):659-67.
18. Hurt RD, Croghan GA, Beede SD, et al. Nicotine patch therapy in 101 adolescent smokers: efficacy, withdrawal symptom relief, and carbon monoxide and plasma cotinine levels. Arch Pediatr Adolesc Med 2000;154(1):31-7.
19. Hanson K, Allen S, Jensen S, Hatsukami D. Treatment of adolescent smokers with the nicotine patch. Nicotine Tob Res 2003;5(4):515-26.
20. Moolchan ET, Robinson ML, Ernst M, et al. Safety and efficacy of the nicotine patch and gum for the treatment of adolescent tobacco addiction. Pediatrics 2005;115(4):e407-14.
21. Upadhyaya HP, Brady KT, Wang W. Bupropion SR in adolescents with comorbid ADHD and nicotine dependence: a pilot study. J Am Acad Child Adolesc Psychiatry 2004;43(2):199-205.
22. Killen JD, Robinson TN, Ammerman S, et al. Randomized clinical trial of the efficacy of bupropion combined with nicotine patch in the treatment of adolescent smokers. J Consult Clin Psychol 2004;72(4):729-35.
23. Muramoto ML, Leischow SJ, Sherrill D. A randomized trial of the efficacy of bupropion for adolescent smoking cessation. Paper presented at: Annual Meeting of the Society for Research on Nicotine and Tobacco; March 20-23, 2005; Prague, Czech Republic.
24. Hall SM. Tricyclic antidepressants in the treatment of nicotine dependence. In: George TP, ed. Medication treatments for nicotine dependence. Boca Raton, FL: CRC Press; 2007:95-107.
25. Berlin I. Monoamine oxidase inhibitors for smoking cessation. In: George TP, ed. Medication treatments for nicotine dependence. Boca Raton, FL: CRC Press; 2007:109-21.
26. Weinberger AH, Reutenauer EL, George TP. Other nonapproved agents for smoking cessation. In: George TP, ed. Medication treatments for nicotine dependence. Boca Raton, FL: CRC Press; 2007:137-48.
27. Lancaster T, Stead LF. Mecamylamine (a nicotine antagonist) for smoking cessation. Cochrane Database Syst Rev 2005;2:CD001009.-
28. Nicoderm CQ [package insert]. Bridgewater, NJ: Sanofi Aventis; 2006.
29. Zyban [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2007.
30. Sussman S, Sun P, Dent CW. A meta-analysis of teen cigarette smoking cessation. Health Psychol 2006;25(5):549-57.
31. Upadhyaya H, Deas D, Brady K. A practical clinical approach to the treatment of nicotine dependence in adolescents. J Am Acad Child Adolesc Psychiatry 2005;44(9):942-6.
CASE: Depressed, irritable — and smoking
Michael, age 16, is admitted to a psychiatric unit for severe depressive symptoms and suicidal ideation. The next day, he is irritable and refuses to cooperate with the interview. During group therapy he is distractible and unable to focus. The treating psychiatrist learns that before admission Michael had been smoking 10 to 15 cigarettes per day and now feels a strong craving for cigarettes.
Unrecognized nicotine dependence can be problematic on inpatient psychiatric units, where adolescents such as Michael are not permitted to smoke and rarely are offered nicotine replacement therapy (NRT). Unfortunately, psychiatrists seldom diagnose and treat nicotine dependence—particularly in adolescents—whether in outpatient or inpatient settings.1,2
Do adolescent smokers need help quitting? Do they experience withdrawal symptoms when they stop smoking? Are pharmacologic interventions appropriate? For each question, the answer is a resounding yes.
To help you treat young smokers, this article offers:
- tools for assessing adolescent tobacco use and dependence
- evidence-based treatment options
- an algorithm to guide treatment choice.
Not just a ‘phase’
Early smoking—especially among those younger than age 13—is associated with adolescent psychopathology, including depressive disorders and other substance use disorders.3 Compared with nonsmoking teens, those who smoke at least monthly are significantly more likely to smoke as adults.4 Among high school seniors:
- >20% report smoking cigarettes in the past 30 days
- 12% smoke daily
- 6% smoke ≥10 cigarettes per day.5
Nicotine dependence can develop very rapidly: nearly 25% of adolescents have ≥1 symptom within 2 weeks of starting to smoke at least once a month.6
Role of parents. Early intervention for teen nicotine addiction is particularly important because of the long-term health risks associated with tobacco use.7 In our experience, however, teen smokers’ parents’ attitudes can make addressing adolescent nicotine dependence a therapeutic challenge.
Modified Fagerstrom Tolerance Questionnaire8 (7 items)
Stanford Dependence Inventory (SDI)9 (5 items)
Hooked on Nicotine Checklist (HONC)10 (10 items)
Nicotine Dependence Scale for Adolescents11 (6 items)
Cigarette Dependence Scale (CDS-5 and CDS-12)12 (5 or 12 items)
Parents may be unaware of their teens’ smoking, and those who are aware may:
- not know what help is available
- dismiss teen smoking as “just a phase”
- feel that smoking cigarettes is preferable to smoking marijuana or using other illicit drugs.
Other parents have no objections because they themselves smoke. Some permit their teens to smoke and may even give them cigarettes.
Parents who want their teens to stop smoking often believe erroneously that the best method is to quit “cold turkey.”
Assessing use and dependence
Teen smokers’ nicotine withdrawal symptoms—such as irritability, anxiety, and impaired concentration—can imitate or exacerbate other psychiatric symptoms, thus complicating diagnosis and treatment. Ask all adolescent patients about the quantity, frequency, pattern, and duration of use of all forms of tobacco, including:
- cigarettes
- cigars
- cigarillos (short, narrow cigars)
- bidis (thin, flavored South Asian cigarettes wrapped in leaf)
- smokeless tobacco.
Dependence. Establishing nicotine dependence in young smokers is more complicated than in adults because of teen smokers’ variable smoking patterns. Several self-rating scales have been developed to assess nicotine dependence in adolescents (Box 1).8-12 Although some of these tools have been used primarily in research, outpatient psychiatrists may find these scales useful for evaluating adolescents’ smoking.
Some DSM-IV-TR criteria for substance dependence may not apply to nicotine dependence or correlate with other validated measures of nicotine dependence. For example, “significant time spent obtaining, using, or recovering from the effects of a substance” might not apply to all adolescent smokers.13 Based on our clinical experience, daily smoking for an extended period of time (several months) is a marker of dependence for almost all adolescents.
The Timeline Follow Back method can help you capture a more complete picture of adolescent tobacco use over time.14 This involves asking teens about tobacco use over the past 30 or 90 days, beginning with the assessment day and working backward. Record tobacco use on a calendar, using holidays, weekends, and events as anchor points to help teens recall their smoking.
Biomarker tests can be used to measure nicotine use. The 2 most common are:
- expired carbon monoxide (CO) level (essentially a “breathalyzer” for smoking)
- cotinine level—a metabolite of nicotine.
Expired CO testing is simple to conduct but requires specialized equipment that costs approximately $1,000. Marijuana use may affect CO results, but NRT will not. Measuring CO levels provides information about cigarette smoking over the past several hours, compared with the past several days with cotinine.15
Cotinine can be tested in serum, saliva, or urine. Serum testing can be expensive and may require shipping samples to a specialized laboratory for processing. Testing saliva or urine is less expensive and may be conducted in an office. Cotinine testing in teens who use NRT may be unreliable because the nicotine in these products will be metabolized to cotinine and yield a positive result.
CASE CONTINUED: Wanting to quit
Michael was placed on a 21-mg transdermal nicotine patch, which greatly reduced his craving and irritability. He expressed an interest in quitting smoking. Given Michael’s depressive symptoms, bupropion SR was initiated to treat his depression and assist with smoking cessation.
Treatment options
Optimal smoking cessation treatment includes a combination of medication and behavioral counseling.16
Pharmacologic treatments. FDA-approved medications for adult smoking cessation include NRT—available as a gum, inhaler, nasal spray, lozenge, or transdermal patch—bupropion SR, and varenicline. Although not FDA-approved for patients younger than age 18, NRT and bupropion SR have been evaluated for smoking in adolescents.
NRT helps smokers by reducing nicotine withdrawal symptoms during cessation. Only nicotine gum and transdermal nicotine patch have been studied in adolescents. Results are modest at best, although in some studies including behavioral treatments may have obscured any medication effect (Table 1).17-20
Bupropion SR. How bupropion SR helps patients stop smoking is not completely clear. Three studies have evaluated bupropion SR in adolescents; 2 had positive results, but all 3 had important limitations (Table 2).21-23
One of the 2 positive studies included only 16 patients and had an open-label design.22 The second—a larger randomized, placebo-controlled trial23—found that bupropion SR improved nicotine abstinence compared with placebo at 6 weeks, but this effect did not last after subjects stopped taking the drug.
The third bupropion SR study used 150 mg/d (the recommend adult dose is 300 mg/d) and had poor medication adherence.21 The difference in abstinence rate compared with placebo was not statistically significant.
Other medications. Varenicline—a partial nicotine receptor agonist recently approved for adult smoking cessation—has not been studied in adolescents. Nortriptyline, doxepin, selegiline, clonidine, and mecamylamine have shown promise in adult smokers but are not approved for smoking cessation and require further study, especially in young smokers.24-27
Pharmacotherapy risks. NRT can cause nicotine overdose symptoms, such as rapid heart rate or nausea, especially if used while smoking. Transdermal NRT can cause a local reaction at the application site and can cause burns if worn while undergoing magnetic resonance imaging.28
Adverse effects associated with bupropion SR include a small risk of seizure, weight loss, and insomnia. This drug is contraindicated for patients who:
- have a seizure disorder
- have ever been diagnosed with bulimia or anorexia nervosa
- are taking other bupropion formulations.
Patients should not take bupropion SR during abrupt discontinuation of alcohol or sedatives or within 14 days of taking a monoamine oxidase inhibitor.29
Table 1
Can the nicotine patch help teens quit smoking?
| Authors | Study population | Study design | Abstinence rate |
|---|---|---|---|
| Smith et al, 199617 | 13- to 17-year-olds (N=22) who smoked ≥20 cpd | 8 weeks of open-label treatment with transdermal NRT plus behavioral counseling and group support | 14% at 8 weeks, 4.5% at 3 and 6 months |
| Hurt et al, 200418 | 13- to 17-year-olds (N=101) who smoked ≥10 cpd | 6 weeks of open-label treatment with transdermal NRT plus self-help material and brief individual counseling if requested | 11% at 6 weeks, 5% at 6 months |
| Hanson et al, 200319 | 13- to 19-year-olds (N=100) who smoked ≥10 cpd | 10 weeks of double-blind treatment with transdermal NRT or placebo plus CBT and contingency management | 20% (active) vs 18% (placebo); not statistically significant |
| Moolchan et al, 200520 | 13- to 17-year-olds (N=120) who smoked ≥10 cpd | 12 weeks of double-blind treatment with:
| 17.7% (active transdermal NRT)* vs 6.5% (active gum) vs 2.5% (placebo only) |
| *P=0.04 for transdermal NRT vs placebo | |||
| CBT: cognitive-behavioral therapy; cpd: cigarettes per day; NRT: nicotine replacement therapy | |||
Table 2
Teen smoking cessation: Evidence for bupropion SR
| Authors | Study population | Study design | Abstinence rate |
|---|---|---|---|
| Upadhyaya et al, 200421 | 12- to 19-year-olds (N=16, 11 of whom had ADHD) who smoked ≥5 cpd | 7 weeks of open-label treatment with bupropion SR, 150 mg bid, with brief smoking cessation counseling | 31.3% after 4 weeks of medication |
| Killen et al, 200422 | 15- to 18-year-olds (N=211) who smoked ≥10 cpd | 9 weeks of double-blind treatment with bupropion SR, 150 mg/d, or placebo; subjects received 8 weeks of transdermal NRT and group skills training | 23% (active) vs 28% (placebo) at 10 weeks; 8% (active) vs 7% placebo) at 26 weeks; not statistically significant |
| Muramoto et al, 200523 | 14- to 17-year-olds (N=312) who smoked ≥6 cpd | 6 weeks of double-blind treatment with bupropion SR, 150 mg/d; 150 mg bid; or placebo, with CBT and motivational enhancement | 16.9% (150 mg bid) vs 10.3% (150 mg/d) vs 6.7% (placebo) at 6 weeks* No differences at 26 weeks |
| ADHD: attention-deficit/hyperactivity disorder; CBT: cognitive-behavioral therapy; cpd: cigarettes per day; NRT: nicotine replacement therapy | |||
| *P=0.019 for 150 mg bid vs placebo | |||
Behavioral therapy. Specialized treatments developed specifically for teen smoking cessation—such as Not On Tobacco (see Related Resources)—often are delivered in schools or other group settings. The most successful consist of ≥5 sessions and include motivational enhancement, cognitive-behavioral, and social influence-oriented approaches.30
Other behavioral treatments. Most psychiatrists are not equipped to deliver these specialized behavioral treatments. Instead, you can use simple yet effective behavioral treatments during routine office visits as adjuncts to pharmacotherapy. At the very least, we recommend the U.S. Public Health Service’s “5 As” strategy (Box 2).16
Educate patients about what to expect during withdrawal, how long withdrawal will last, and medication side effects. To help adolescents develop appropriate treatment expectations:
- discuss the difference between a “slip” (having 1 cigarette) and a “relapse” (returning to daily smoking)
- explain that many individuals need multiple attempts before they quit.
Encourage adolescent smokers to contact the National Network of Tobacco Cessation Quitlines (1-800-784-8669; www.smokefree.gov), which provides free access to telephone-based counseling services.
Ask every patient about tobacco use during every visit, and have a system for recording and tracking tobacco use in the chart
Advise patients clearly and unambiguously to stop smoking, and tailor that advice to each patient’s needs
Assess every patient’s readiness to quit
Assist patients who are ready to quit through self-help materials, referral, and/or smoking cessation treatment
Arrange follow-up visits for relapse prevention or to reassess readiness to quit
Source: Reference 16
Choosing treatment
Evidence guiding treatment choice for teen smoking cessation is limited but growing. Most studies examined daily cigarette smoking, with significantly less evidence to support treatment decisions for light (non-daily) smokers and teens who use other tobacco products.
Recommendations.We have developed a strategy to guide treatment of adolescent smokers (Algorithm). We recommend using pharmacologic interventions only for teens who smoke daily because:
- most studies have focused on daily smoking
- efficacy data are limited
- pharmacologic interventions carry potential risks.
Because of bupropion SR’s contraindications and potential side effect profile, we suggest NRT in combination with smoking cessation counseling as a first-line treatment for young smokers. We recommend beginning with transdermal NRT because of the low likelihood of underdosing with the patch’s once-daily application.20 With either NRT or bupropion SR, schedule follow-up appointments to target relapse prevention and solve any issues that arise.
Help your patient choose a “quit date,” preferably 1 to 2 weeks after your initial assessment. We recommend encouraging young smokers to reduce their smoking by 1 cigarette per day to help minimize withdrawal symptoms from “cold turkey” cessation.31
Some physicians have found it helpful to see the patient on the quit day—or 2 days after when withdrawal symptoms tend to be most robust—to provide support and encouragement. Ask the adolescent to bring and discard during the visit all smoking paraphernalia as a symbol of his or her new smoke-free status.
Step 1: NRT. Initiate smoking cessation counseling plus transdermal NRT using the dosing guidelines in Table 3,28,31 and adjust the dose depending on severity of withdrawal symptoms. Ideally, the patch delivery will be used for 12 weeks, with at least 3 and ideally 6 weeks on the initial dose, followed by a gradual taper.28 We strongly recommend using transdermal NRT on adolescent inpatient units, especially for daily smokers and those who exhibit nicotine withdrawal symptoms.
Step 2: Bupropion SR. If NRT fails, the next step is bupropion SR plus smoking cessation counseling, assuming the adolescent does not have contraindications to bupropion SR. Start the medication based on the dosing guidelines in Table 3,28,31 and set a quit date for 2 weeks after starting bupropion SR.
Again, encourage adolescents to reduce by 1 cigarette per day over the 2 weeks before the quit day to minimize withdrawal symptoms.31 Continue bupropion SR for at least 8 and optimally 12 weeks.31
Combination therapy? If teens are unable to successfully quit smoking with NRT or bupropion SR alone, experience with adults suggests combining the 2 therapies might be beneficial. However, no evidence supports combination therapy in adolescents. Instead, consider referring adolescents who can’t quit to a smoking cessation specialist.
AlgorithmA strategy to initiate smoking cessation in adolescents
CDC: Centers for Disease Control and Prevention; CM: contingency management; NIDA: National Institute of Drug Abuse; NRT: nicotine replacement therapy
Source: Adapted from Upadhyaya H, Deas D, Brady K. A practical clinical approach to the treatment of nicotine dependence in adolescents. J Am Acad Child Adolesc Psychiatry 2005;44(9):942-6 with permission of Lippincott Williams & Wilkins.Table 3
Dosing guidelines for adolescent smoking cessation therapy
| Medication | Recommended regimen |
|---|---|
| Bupropion SR31 | Patient weight ≥90 lbs: 150 mg once in the morning for 3 to 6 days, then 150 mg bid for 12 weeks Patient weight <90 lbs: Maximum 150 mg once in the morning, if tolerated |
| Transdermal NRT28 | Patient smokes ≥10 cpd: 21 mg/d for 6 weeks, then 14 mg/d for 2 weeks, then 7 mg/d for 2 weeks, then discontinue Patient smokes <10 cpd: 14 mg/d for 6 weeks, then 7 mg/d for 2 weeks, then discontinue |
| cpd: cigarettes per day; NRT: nicotine replacement therapy | |
CASE CONTINUED: Staying smoke-free
Upon discharge, Michael discontinued NRT and followed up with his outpatient psychiatrist, who provided brief smoking cessation counseling in addition to bupropion SR, 150 mg bid. Michael’s depressive symptoms improved with the medication. He was able to stop smoking within 3 months with the combination of medication and behavioral therapy.
- Centers for Disease Control and Prevention, Youth Tobacco Prevention. www.cdc.gov/tobacco/youth/index.htm.
- Not On Tobacco model program. Substance Abuse and Mental Health Services Administration.www.modelprograms.samhsa.gov/pdfs/model/Not_On_Tobacco.pdf.
Drug brand names
- Bupropion SR • Zyban
- Clonidine • Catapres
- Doxepin • Sinequan
- Mecamylamine • Inversine
- Nicotine/inhalation system • Nicotrol Inhaler
- Nicotine/lozenge • Commit
- Nicotine/nasal spray • Nicotrol NS
- Nicotine/polacrilex • Nicorette
- Nicotine/transdermal • Nicotrol, Prostep
- Nortriptyline • Pamelor
- Selegiline • Eldepryl
- Varenicline • Chantix
Disclosures
Dr. Verduin has received research/grant support from the National Institute of Drug Abuse.
Dr. Upadhyaya is a consultant and speaker for Shire Pharmaceuticals and has received grant/research support from and is a consultant to Eli Lilly and Company.
CASE: Depressed, irritable — and smoking
Michael, age 16, is admitted to a psychiatric unit for severe depressive symptoms and suicidal ideation. The next day, he is irritable and refuses to cooperate with the interview. During group therapy he is distractible and unable to focus. The treating psychiatrist learns that before admission Michael had been smoking 10 to 15 cigarettes per day and now feels a strong craving for cigarettes.
Unrecognized nicotine dependence can be problematic on inpatient psychiatric units, where adolescents such as Michael are not permitted to smoke and rarely are offered nicotine replacement therapy (NRT). Unfortunately, psychiatrists seldom diagnose and treat nicotine dependence—particularly in adolescents—whether in outpatient or inpatient settings.1,2
Do adolescent smokers need help quitting? Do they experience withdrawal symptoms when they stop smoking? Are pharmacologic interventions appropriate? For each question, the answer is a resounding yes.
To help you treat young smokers, this article offers:
- tools for assessing adolescent tobacco use and dependence
- evidence-based treatment options
- an algorithm to guide treatment choice.
Not just a ‘phase’
Early smoking—especially among those younger than age 13—is associated with adolescent psychopathology, including depressive disorders and other substance use disorders.3 Compared with nonsmoking teens, those who smoke at least monthly are significantly more likely to smoke as adults.4 Among high school seniors:
- >20% report smoking cigarettes in the past 30 days
- 12% smoke daily
- 6% smoke ≥10 cigarettes per day.5
Nicotine dependence can develop very rapidly: nearly 25% of adolescents have ≥1 symptom within 2 weeks of starting to smoke at least once a month.6
Role of parents. Early intervention for teen nicotine addiction is particularly important because of the long-term health risks associated with tobacco use.7 In our experience, however, teen smokers’ parents’ attitudes can make addressing adolescent nicotine dependence a therapeutic challenge.
Modified Fagerstrom Tolerance Questionnaire8 (7 items)
Stanford Dependence Inventory (SDI)9 (5 items)
Hooked on Nicotine Checklist (HONC)10 (10 items)
Nicotine Dependence Scale for Adolescents11 (6 items)
Cigarette Dependence Scale (CDS-5 and CDS-12)12 (5 or 12 items)
Parents may be unaware of their teens’ smoking, and those who are aware may:
- not know what help is available
- dismiss teen smoking as “just a phase”
- feel that smoking cigarettes is preferable to smoking marijuana or using other illicit drugs.
Other parents have no objections because they themselves smoke. Some permit their teens to smoke and may even give them cigarettes.
Parents who want their teens to stop smoking often believe erroneously that the best method is to quit “cold turkey.”
Assessing use and dependence
Teen smokers’ nicotine withdrawal symptoms—such as irritability, anxiety, and impaired concentration—can imitate or exacerbate other psychiatric symptoms, thus complicating diagnosis and treatment. Ask all adolescent patients about the quantity, frequency, pattern, and duration of use of all forms of tobacco, including:
- cigarettes
- cigars
- cigarillos (short, narrow cigars)
- bidis (thin, flavored South Asian cigarettes wrapped in leaf)
- smokeless tobacco.
Dependence. Establishing nicotine dependence in young smokers is more complicated than in adults because of teen smokers’ variable smoking patterns. Several self-rating scales have been developed to assess nicotine dependence in adolescents (Box 1).8-12 Although some of these tools have been used primarily in research, outpatient psychiatrists may find these scales useful for evaluating adolescents’ smoking.
Some DSM-IV-TR criteria for substance dependence may not apply to nicotine dependence or correlate with other validated measures of nicotine dependence. For example, “significant time spent obtaining, using, or recovering from the effects of a substance” might not apply to all adolescent smokers.13 Based on our clinical experience, daily smoking for an extended period of time (several months) is a marker of dependence for almost all adolescents.
The Timeline Follow Back method can help you capture a more complete picture of adolescent tobacco use over time.14 This involves asking teens about tobacco use over the past 30 or 90 days, beginning with the assessment day and working backward. Record tobacco use on a calendar, using holidays, weekends, and events as anchor points to help teens recall their smoking.
Biomarker tests can be used to measure nicotine use. The 2 most common are:
- expired carbon monoxide (CO) level (essentially a “breathalyzer” for smoking)
- cotinine level—a metabolite of nicotine.
Expired CO testing is simple to conduct but requires specialized equipment that costs approximately $1,000. Marijuana use may affect CO results, but NRT will not. Measuring CO levels provides information about cigarette smoking over the past several hours, compared with the past several days with cotinine.15
Cotinine can be tested in serum, saliva, or urine. Serum testing can be expensive and may require shipping samples to a specialized laboratory for processing. Testing saliva or urine is less expensive and may be conducted in an office. Cotinine testing in teens who use NRT may be unreliable because the nicotine in these products will be metabolized to cotinine and yield a positive result.
CASE CONTINUED: Wanting to quit
Michael was placed on a 21-mg transdermal nicotine patch, which greatly reduced his craving and irritability. He expressed an interest in quitting smoking. Given Michael’s depressive symptoms, bupropion SR was initiated to treat his depression and assist with smoking cessation.
Treatment options
Optimal smoking cessation treatment includes a combination of medication and behavioral counseling.16
Pharmacologic treatments. FDA-approved medications for adult smoking cessation include NRT—available as a gum, inhaler, nasal spray, lozenge, or transdermal patch—bupropion SR, and varenicline. Although not FDA-approved for patients younger than age 18, NRT and bupropion SR have been evaluated for smoking in adolescents.
NRT helps smokers by reducing nicotine withdrawal symptoms during cessation. Only nicotine gum and transdermal nicotine patch have been studied in adolescents. Results are modest at best, although in some studies including behavioral treatments may have obscured any medication effect (Table 1).17-20
Bupropion SR. How bupropion SR helps patients stop smoking is not completely clear. Three studies have evaluated bupropion SR in adolescents; 2 had positive results, but all 3 had important limitations (Table 2).21-23
One of the 2 positive studies included only 16 patients and had an open-label design.22 The second—a larger randomized, placebo-controlled trial23—found that bupropion SR improved nicotine abstinence compared with placebo at 6 weeks, but this effect did not last after subjects stopped taking the drug.
The third bupropion SR study used 150 mg/d (the recommend adult dose is 300 mg/d) and had poor medication adherence.21 The difference in abstinence rate compared with placebo was not statistically significant.
Other medications. Varenicline—a partial nicotine receptor agonist recently approved for adult smoking cessation—has not been studied in adolescents. Nortriptyline, doxepin, selegiline, clonidine, and mecamylamine have shown promise in adult smokers but are not approved for smoking cessation and require further study, especially in young smokers.24-27
Pharmacotherapy risks. NRT can cause nicotine overdose symptoms, such as rapid heart rate or nausea, especially if used while smoking. Transdermal NRT can cause a local reaction at the application site and can cause burns if worn while undergoing magnetic resonance imaging.28
Adverse effects associated with bupropion SR include a small risk of seizure, weight loss, and insomnia. This drug is contraindicated for patients who:
- have a seizure disorder
- have ever been diagnosed with bulimia or anorexia nervosa
- are taking other bupropion formulations.
Patients should not take bupropion SR during abrupt discontinuation of alcohol or sedatives or within 14 days of taking a monoamine oxidase inhibitor.29
Table 1
Can the nicotine patch help teens quit smoking?
| Authors | Study population | Study design | Abstinence rate |
|---|---|---|---|
| Smith et al, 199617 | 13- to 17-year-olds (N=22) who smoked ≥20 cpd | 8 weeks of open-label treatment with transdermal NRT plus behavioral counseling and group support | 14% at 8 weeks, 4.5% at 3 and 6 months |
| Hurt et al, 200418 | 13- to 17-year-olds (N=101) who smoked ≥10 cpd | 6 weeks of open-label treatment with transdermal NRT plus self-help material and brief individual counseling if requested | 11% at 6 weeks, 5% at 6 months |
| Hanson et al, 200319 | 13- to 19-year-olds (N=100) who smoked ≥10 cpd | 10 weeks of double-blind treatment with transdermal NRT or placebo plus CBT and contingency management | 20% (active) vs 18% (placebo); not statistically significant |
| Moolchan et al, 200520 | 13- to 17-year-olds (N=120) who smoked ≥10 cpd | 12 weeks of double-blind treatment with:
| 17.7% (active transdermal NRT)* vs 6.5% (active gum) vs 2.5% (placebo only) |
| *P=0.04 for transdermal NRT vs placebo | |||
| CBT: cognitive-behavioral therapy; cpd: cigarettes per day; NRT: nicotine replacement therapy | |||
Table 2
Teen smoking cessation: Evidence for bupropion SR
| Authors | Study population | Study design | Abstinence rate |
|---|---|---|---|
| Upadhyaya et al, 200421 | 12- to 19-year-olds (N=16, 11 of whom had ADHD) who smoked ≥5 cpd | 7 weeks of open-label treatment with bupropion SR, 150 mg bid, with brief smoking cessation counseling | 31.3% after 4 weeks of medication |
| Killen et al, 200422 | 15- to 18-year-olds (N=211) who smoked ≥10 cpd | 9 weeks of double-blind treatment with bupropion SR, 150 mg/d, or placebo; subjects received 8 weeks of transdermal NRT and group skills training | 23% (active) vs 28% (placebo) at 10 weeks; 8% (active) vs 7% placebo) at 26 weeks; not statistically significant |
| Muramoto et al, 200523 | 14- to 17-year-olds (N=312) who smoked ≥6 cpd | 6 weeks of double-blind treatment with bupropion SR, 150 mg/d; 150 mg bid; or placebo, with CBT and motivational enhancement | 16.9% (150 mg bid) vs 10.3% (150 mg/d) vs 6.7% (placebo) at 6 weeks* No differences at 26 weeks |
| ADHD: attention-deficit/hyperactivity disorder; CBT: cognitive-behavioral therapy; cpd: cigarettes per day; NRT: nicotine replacement therapy | |||
| *P=0.019 for 150 mg bid vs placebo | |||
Behavioral therapy. Specialized treatments developed specifically for teen smoking cessation—such as Not On Tobacco (see Related Resources)—often are delivered in schools or other group settings. The most successful consist of ≥5 sessions and include motivational enhancement, cognitive-behavioral, and social influence-oriented approaches.30
Other behavioral treatments. Most psychiatrists are not equipped to deliver these specialized behavioral treatments. Instead, you can use simple yet effective behavioral treatments during routine office visits as adjuncts to pharmacotherapy. At the very least, we recommend the U.S. Public Health Service’s “5 As” strategy (Box 2).16
Educate patients about what to expect during withdrawal, how long withdrawal will last, and medication side effects. To help adolescents develop appropriate treatment expectations:
- discuss the difference between a “slip” (having 1 cigarette) and a “relapse” (returning to daily smoking)
- explain that many individuals need multiple attempts before they quit.
Encourage adolescent smokers to contact the National Network of Tobacco Cessation Quitlines (1-800-784-8669; www.smokefree.gov), which provides free access to telephone-based counseling services.
Ask every patient about tobacco use during every visit, and have a system for recording and tracking tobacco use in the chart
Advise patients clearly and unambiguously to stop smoking, and tailor that advice to each patient’s needs
Assess every patient’s readiness to quit
Assist patients who are ready to quit through self-help materials, referral, and/or smoking cessation treatment
Arrange follow-up visits for relapse prevention or to reassess readiness to quit
Source: Reference 16
Choosing treatment
Evidence guiding treatment choice for teen smoking cessation is limited but growing. Most studies examined daily cigarette smoking, with significantly less evidence to support treatment decisions for light (non-daily) smokers and teens who use other tobacco products.
Recommendations.We have developed a strategy to guide treatment of adolescent smokers (Algorithm). We recommend using pharmacologic interventions only for teens who smoke daily because:
- most studies have focused on daily smoking
- efficacy data are limited
- pharmacologic interventions carry potential risks.
Because of bupropion SR’s contraindications and potential side effect profile, we suggest NRT in combination with smoking cessation counseling as a first-line treatment for young smokers. We recommend beginning with transdermal NRT because of the low likelihood of underdosing with the patch’s once-daily application.20 With either NRT or bupropion SR, schedule follow-up appointments to target relapse prevention and solve any issues that arise.
Help your patient choose a “quit date,” preferably 1 to 2 weeks after your initial assessment. We recommend encouraging young smokers to reduce their smoking by 1 cigarette per day to help minimize withdrawal symptoms from “cold turkey” cessation.31
Some physicians have found it helpful to see the patient on the quit day—or 2 days after when withdrawal symptoms tend to be most robust—to provide support and encouragement. Ask the adolescent to bring and discard during the visit all smoking paraphernalia as a symbol of his or her new smoke-free status.
Step 1: NRT. Initiate smoking cessation counseling plus transdermal NRT using the dosing guidelines in Table 3,28,31 and adjust the dose depending on severity of withdrawal symptoms. Ideally, the patch delivery will be used for 12 weeks, with at least 3 and ideally 6 weeks on the initial dose, followed by a gradual taper.28 We strongly recommend using transdermal NRT on adolescent inpatient units, especially for daily smokers and those who exhibit nicotine withdrawal symptoms.
Step 2: Bupropion SR. If NRT fails, the next step is bupropion SR plus smoking cessation counseling, assuming the adolescent does not have contraindications to bupropion SR. Start the medication based on the dosing guidelines in Table 3,28,31 and set a quit date for 2 weeks after starting bupropion SR.
Again, encourage adolescents to reduce by 1 cigarette per day over the 2 weeks before the quit day to minimize withdrawal symptoms.31 Continue bupropion SR for at least 8 and optimally 12 weeks.31
Combination therapy? If teens are unable to successfully quit smoking with NRT or bupropion SR alone, experience with adults suggests combining the 2 therapies might be beneficial. However, no evidence supports combination therapy in adolescents. Instead, consider referring adolescents who can’t quit to a smoking cessation specialist.
AlgorithmA strategy to initiate smoking cessation in adolescents
CDC: Centers for Disease Control and Prevention; CM: contingency management; NIDA: National Institute of Drug Abuse; NRT: nicotine replacement therapy
Source: Adapted from Upadhyaya H, Deas D, Brady K. A practical clinical approach to the treatment of nicotine dependence in adolescents. J Am Acad Child Adolesc Psychiatry 2005;44(9):942-6 with permission of Lippincott Williams & Wilkins.Table 3
Dosing guidelines for adolescent smoking cessation therapy
| Medication | Recommended regimen |
|---|---|
| Bupropion SR31 | Patient weight ≥90 lbs: 150 mg once in the morning for 3 to 6 days, then 150 mg bid for 12 weeks Patient weight <90 lbs: Maximum 150 mg once in the morning, if tolerated |
| Transdermal NRT28 | Patient smokes ≥10 cpd: 21 mg/d for 6 weeks, then 14 mg/d for 2 weeks, then 7 mg/d for 2 weeks, then discontinue Patient smokes <10 cpd: 14 mg/d for 6 weeks, then 7 mg/d for 2 weeks, then discontinue |
| cpd: cigarettes per day; NRT: nicotine replacement therapy | |
CASE CONTINUED: Staying smoke-free
Upon discharge, Michael discontinued NRT and followed up with his outpatient psychiatrist, who provided brief smoking cessation counseling in addition to bupropion SR, 150 mg bid. Michael’s depressive symptoms improved with the medication. He was able to stop smoking within 3 months with the combination of medication and behavioral therapy.
- Centers for Disease Control and Prevention, Youth Tobacco Prevention. www.cdc.gov/tobacco/youth/index.htm.
- Not On Tobacco model program. Substance Abuse and Mental Health Services Administration.www.modelprograms.samhsa.gov/pdfs/model/Not_On_Tobacco.pdf.
Drug brand names
- Bupropion SR • Zyban
- Clonidine • Catapres
- Doxepin • Sinequan
- Mecamylamine • Inversine
- Nicotine/inhalation system • Nicotrol Inhaler
- Nicotine/lozenge • Commit
- Nicotine/nasal spray • Nicotrol NS
- Nicotine/polacrilex • Nicorette
- Nicotine/transdermal • Nicotrol, Prostep
- Nortriptyline • Pamelor
- Selegiline • Eldepryl
- Varenicline • Chantix
Disclosures
Dr. Verduin has received research/grant support from the National Institute of Drug Abuse.
Dr. Upadhyaya is a consultant and speaker for Shire Pharmaceuticals and has received grant/research support from and is a consultant to Eli Lilly and Company.
1. Chassin L, Presson CC, Sherman SJ, Edwards DA. The natural history of cigarette smoking: predicting young-adult smoking outcomes from adolescent smoking patterns. Health Psychol 1990;9(6):701-16.
2. Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future national results on adolescent drug use: overview of key findings 2006. Bethesda, MD: National Institute on Drug Abuse; 2007. NIH publication no. 07-6202.
3. DiFranza JR, Rigotti NA, McNeill AD, et al. Initial symptoms of nicotine dependence in adolescence. Tob Control 2000;9(3):313-9.
4. Upadhyaya HP, Deas D, Brady KT, Kruesi M. Cigarette smoking and psychiatric comorbidity in children and adolescents. J Am Acad Child Adolesc Psychiatry 2002;41(11):1294-1305.
5. U.S. Department of Health and Human Services. The health consequences of smoking: a report of the surgeon general. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2004.
6. Himelhoch S, Daumit G. To whom do psychiatrists offer smoking-cessation counseling? Am J Psychiatry 2003;160(12):222-830.
7. Upadhyaya HP, Brady KT, Wharton M, Liao J. Psychiatric disorders and cigarette smoking among child and adolescent psychiatry inpatients. Am J Addict 2003;12(2):144-52.
8. Prokhorov AV, Pallonen UE, Fava JL, et al. Measuring nicotine dependence among high-risk adolescent smokers. Addict Behav 1996;21(1):117-27.
9. Rojas NL, Killen JD, Haydel KF, Robinson TN. Nicotine dependence among adolescent smokers. Arch Pediatr Adolesc Med 1998;152(2):151-6.
10. O’Loughlin J, DiFranza J, Tarasuk J, et al. Assessment of nicotine dependence symptoms in adolescents: a comparison of five indicators. Tob Control 2002;11(4):354-60.
11. Nonnemaker J, Mowery P, Hersey J, et al. Measurement properties of a nicotine dependence scale for adolescents. Nicotine Tob Res 2004;6(2):295-301.
12. Etter JF, LeHouezec J, Perneger TV. A self-administered questionnaire to measure addiction to cigarettes: the Cigarette Dependence Scale. Neuropsychopharmacology 2003;28(2):359-70.
13. Hughes JR, Oliveto AH, Riggs R, et al. Concordance of different measures of nicotine dependence: two pilot studies. Addict Behav 2004;29(8):1527-39.
14. Sobell LC, Sobell MB. Timeline Follow-Back: a technique for assessing self-reported alcohol consumption. In: Litten R, Allen J, eds. Measuring alcohol consumption: psychosocial and biochemical methods. Totowa, NJ: The Humana Press Inc.; 1992.
15. SRNT Subcommittee on Biochemical Verification. Biochemical verification of tobacco use and cessation. Nicotine Tob Res 2002;4(2):149-59.
16. Fiore MC, Bailey WC, Cohen SJ, et al. Treating tobacco use and dependence. Quick reference guide for clinicians. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service; 2000.
17. Smith TA, House RF, Croghan IT, et al. Nicotine patch therapy in adolescent smokers. Pediatrics 1996;98(4):659-67.
18. Hurt RD, Croghan GA, Beede SD, et al. Nicotine patch therapy in 101 adolescent smokers: efficacy, withdrawal symptom relief, and carbon monoxide and plasma cotinine levels. Arch Pediatr Adolesc Med 2000;154(1):31-7.
19. Hanson K, Allen S, Jensen S, Hatsukami D. Treatment of adolescent smokers with the nicotine patch. Nicotine Tob Res 2003;5(4):515-26.
20. Moolchan ET, Robinson ML, Ernst M, et al. Safety and efficacy of the nicotine patch and gum for the treatment of adolescent tobacco addiction. Pediatrics 2005;115(4):e407-14.
21. Upadhyaya HP, Brady KT, Wang W. Bupropion SR in adolescents with comorbid ADHD and nicotine dependence: a pilot study. J Am Acad Child Adolesc Psychiatry 2004;43(2):199-205.
22. Killen JD, Robinson TN, Ammerman S, et al. Randomized clinical trial of the efficacy of bupropion combined with nicotine patch in the treatment of adolescent smokers. J Consult Clin Psychol 2004;72(4):729-35.
23. Muramoto ML, Leischow SJ, Sherrill D. A randomized trial of the efficacy of bupropion for adolescent smoking cessation. Paper presented at: Annual Meeting of the Society for Research on Nicotine and Tobacco; March 20-23, 2005; Prague, Czech Republic.
24. Hall SM. Tricyclic antidepressants in the treatment of nicotine dependence. In: George TP, ed. Medication treatments for nicotine dependence. Boca Raton, FL: CRC Press; 2007:95-107.
25. Berlin I. Monoamine oxidase inhibitors for smoking cessation. In: George TP, ed. Medication treatments for nicotine dependence. Boca Raton, FL: CRC Press; 2007:109-21.
26. Weinberger AH, Reutenauer EL, George TP. Other nonapproved agents for smoking cessation. In: George TP, ed. Medication treatments for nicotine dependence. Boca Raton, FL: CRC Press; 2007:137-48.
27. Lancaster T, Stead LF. Mecamylamine (a nicotine antagonist) for smoking cessation. Cochrane Database Syst Rev 2005;2:CD001009.-
28. Nicoderm CQ [package insert]. Bridgewater, NJ: Sanofi Aventis; 2006.
29. Zyban [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2007.
30. Sussman S, Sun P, Dent CW. A meta-analysis of teen cigarette smoking cessation. Health Psychol 2006;25(5):549-57.
31. Upadhyaya H, Deas D, Brady K. A practical clinical approach to the treatment of nicotine dependence in adolescents. J Am Acad Child Adolesc Psychiatry 2005;44(9):942-6.
1. Chassin L, Presson CC, Sherman SJ, Edwards DA. The natural history of cigarette smoking: predicting young-adult smoking outcomes from adolescent smoking patterns. Health Psychol 1990;9(6):701-16.
2. Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future national results on adolescent drug use: overview of key findings 2006. Bethesda, MD: National Institute on Drug Abuse; 2007. NIH publication no. 07-6202.
3. DiFranza JR, Rigotti NA, McNeill AD, et al. Initial symptoms of nicotine dependence in adolescence. Tob Control 2000;9(3):313-9.
4. Upadhyaya HP, Deas D, Brady KT, Kruesi M. Cigarette smoking and psychiatric comorbidity in children and adolescents. J Am Acad Child Adolesc Psychiatry 2002;41(11):1294-1305.
5. U.S. Department of Health and Human Services. The health consequences of smoking: a report of the surgeon general. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2004.
6. Himelhoch S, Daumit G. To whom do psychiatrists offer smoking-cessation counseling? Am J Psychiatry 2003;160(12):222-830.
7. Upadhyaya HP, Brady KT, Wharton M, Liao J. Psychiatric disorders and cigarette smoking among child and adolescent psychiatry inpatients. Am J Addict 2003;12(2):144-52.
8. Prokhorov AV, Pallonen UE, Fava JL, et al. Measuring nicotine dependence among high-risk adolescent smokers. Addict Behav 1996;21(1):117-27.
9. Rojas NL, Killen JD, Haydel KF, Robinson TN. Nicotine dependence among adolescent smokers. Arch Pediatr Adolesc Med 1998;152(2):151-6.
10. O’Loughlin J, DiFranza J, Tarasuk J, et al. Assessment of nicotine dependence symptoms in adolescents: a comparison of five indicators. Tob Control 2002;11(4):354-60.
11. Nonnemaker J, Mowery P, Hersey J, et al. Measurement properties of a nicotine dependence scale for adolescents. Nicotine Tob Res 2004;6(2):295-301.
12. Etter JF, LeHouezec J, Perneger TV. A self-administered questionnaire to measure addiction to cigarettes: the Cigarette Dependence Scale. Neuropsychopharmacology 2003;28(2):359-70.
13. Hughes JR, Oliveto AH, Riggs R, et al. Concordance of different measures of nicotine dependence: two pilot studies. Addict Behav 2004;29(8):1527-39.
14. Sobell LC, Sobell MB. Timeline Follow-Back: a technique for assessing self-reported alcohol consumption. In: Litten R, Allen J, eds. Measuring alcohol consumption: psychosocial and biochemical methods. Totowa, NJ: The Humana Press Inc.; 1992.
15. SRNT Subcommittee on Biochemical Verification. Biochemical verification of tobacco use and cessation. Nicotine Tob Res 2002;4(2):149-59.
16. Fiore MC, Bailey WC, Cohen SJ, et al. Treating tobacco use and dependence. Quick reference guide for clinicians. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service; 2000.
17. Smith TA, House RF, Croghan IT, et al. Nicotine patch therapy in adolescent smokers. Pediatrics 1996;98(4):659-67.
18. Hurt RD, Croghan GA, Beede SD, et al. Nicotine patch therapy in 101 adolescent smokers: efficacy, withdrawal symptom relief, and carbon monoxide and plasma cotinine levels. Arch Pediatr Adolesc Med 2000;154(1):31-7.
19. Hanson K, Allen S, Jensen S, Hatsukami D. Treatment of adolescent smokers with the nicotine patch. Nicotine Tob Res 2003;5(4):515-26.
20. Moolchan ET, Robinson ML, Ernst M, et al. Safety and efficacy of the nicotine patch and gum for the treatment of adolescent tobacco addiction. Pediatrics 2005;115(4):e407-14.
21. Upadhyaya HP, Brady KT, Wang W. Bupropion SR in adolescents with comorbid ADHD and nicotine dependence: a pilot study. J Am Acad Child Adolesc Psychiatry 2004;43(2):199-205.
22. Killen JD, Robinson TN, Ammerman S, et al. Randomized clinical trial of the efficacy of bupropion combined with nicotine patch in the treatment of adolescent smokers. J Consult Clin Psychol 2004;72(4):729-35.
23. Muramoto ML, Leischow SJ, Sherrill D. A randomized trial of the efficacy of bupropion for adolescent smoking cessation. Paper presented at: Annual Meeting of the Society for Research on Nicotine and Tobacco; March 20-23, 2005; Prague, Czech Republic.
24. Hall SM. Tricyclic antidepressants in the treatment of nicotine dependence. In: George TP, ed. Medication treatments for nicotine dependence. Boca Raton, FL: CRC Press; 2007:95-107.
25. Berlin I. Monoamine oxidase inhibitors for smoking cessation. In: George TP, ed. Medication treatments for nicotine dependence. Boca Raton, FL: CRC Press; 2007:109-21.
26. Weinberger AH, Reutenauer EL, George TP. Other nonapproved agents for smoking cessation. In: George TP, ed. Medication treatments for nicotine dependence. Boca Raton, FL: CRC Press; 2007:137-48.
27. Lancaster T, Stead LF. Mecamylamine (a nicotine antagonist) for smoking cessation. Cochrane Database Syst Rev 2005;2:CD001009.-
28. Nicoderm CQ [package insert]. Bridgewater, NJ: Sanofi Aventis; 2006.
29. Zyban [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2007.
30. Sussman S, Sun P, Dent CW. A meta-analysis of teen cigarette smoking cessation. Health Psychol 2006;25(5):549-57.
31. Upadhyaya H, Deas D, Brady K. A practical clinical approach to the treatment of nicotine dependence in adolescents. J Am Acad Child Adolesc Psychiatry 2005;44(9):942-6.
Why off-label antipsychotics remain first-choice drugs for delirium
Delirium is a medical emergency that needs to be identified and treated vigorously. Antipsychotics—including haloperidol and atypical agents—effectively manage a wide spectrum of delirium symptoms and are an essential component in the standard multimodal approach.1 Even so, antipsychotics are not FDA-approved for treating delirium, and evidence on their safety in medically ill patients is limited—particularly in the elderly, in whom delirium occurs most often.
The FDA has warned of increased risk of death when atypical antipsychotics are used to treat behavioral disturbances in elderly patients with dementia.2 Similarly, a retrospective study of elderly patients taking antipsychotics found higher mortality rates associated with typical antipsychotics than with atypicals.3
This article discusses the risks and benefits of using antipsychotics to manage delirium. Based on the literature and clinical experience, we offer recommendations on choosing among the available agents and avoiding side effects.
A challenging diagnosis
Delirium is a neuropsychiatric syndrome precipitated by an underlying medical condition or a medication effect on the brain. Its characteristic symptoms—abrupt onset of disturbed consciousness, attention, cognition, and perception—tend to fluctuate during the day. Delirium most often occurs in elderly patients (Box)1,4-7—particularly with dementia—but also occurs in younger patients with serious illnesses such as cancer or HIV-AIDS.
Delirium is underdiagnosed and under-treated in medical settings,4,8 most likely because of its protean symptoms (Table 1)9 and fluctuating clinical findings. Neurologic abnormalities—including cortical and motor symptoms—also can occur.1
Mortality risk. Delirium is an independent risk factor for mortality.1,4,5 It is a marker for serious and potentially life-threatening medical problems, such as organ failure or sepsis. When antipsychotics fail to control delirium, the 3 most common reasons are:
- delirium’s etiology has not been discovered or addressed
- delirium’s etiology is resistant to treatment or potentially irreversible
- antipsychotic dosage was inadequate.
3 subtypes. Delirium is classified as hyperactive, hypoactive, or mixed, depending on arousal disturbance and psychomotor behavior:
- the hyperactive subtype includes hallucinations, delusions, agitation, and disorientation.
- the hypoactive subtype includes confusion, sedation, and decreased alertness but rarely hallucinations or delusions.1
Up to 1 in 4 patients (14% to 24%) have delirium at hospital admission, and the annual incidence of delirium is 6% to 56% among hospital populations.4 Elderly inpatients who develop delirium have an estimated mortality rate of 22% to 76% during that hospitalization.1 At the end of life, the prevalence of delirium may be as high as 85%.5
Serotonergic, noradrenergic, opiatergic, glutamatergic, and histaminergic neurotransmitter systems may contribute to delirium as a syndrome. Evidence implicates underactivity of the cholinergic system as the final common pathway.6,7
The acetylcholine-dopamine hypothesis explains the efficacy of dopamine antagonists in treating delirium by regulating the imbalance between cholinergic and dopaminergic activity.5,6 Cytokines—including interleukin-1, interleukin-2, and interleukin-6—and chronic hypercortisolism may also contribute to delirium.4
Antipsychotics: Limited evidence
- identifying and eliminating contributing factors
- instituting nonpharmacologic interventions based on environmental strategies (Table 2)4
- providing pharmacologic interventions—primarily antipsychotics—as needed.
- delirium severity improved with haloperidol, chlorpromazine, olanzapine, risperidone, or quetiapine
- comparison trials did not identify any antipsychotic as more efficacious than another.
Michaud et al11 reviewed guidelines, systematic reviews, randomized controlled trials, and cohort studies on delirium management. They concluded that the experts agree on 3 points:
- prevention should be emphasized
- atypical antipsychotics are not first-choice drugs because of data on adverse events in the elderly
- pharmacologic treatment is recommended when the patient’s condition prevents adequate care or puts the patient or staff at risk.
Conventional antipsychotics
Haloperidol, the most-studied antipsychotic in delirium treatment, often is the drug of choice because of its high potency, low sedative effect, few anticholinergic side effects, minimal cardiovascular side effects, no active metabolites, and multiple administration routes.1
An IV route can facilitate rapid onset of medication effects. Compared with oral haloperidol, IV administration is associated with a lower risk of extrapyramidal symptoms (EPS), which allows use of higher doses.
Any IV use of injectable haloperidol is off-label, however. If you choose the IV route, monitor patients carefully for cardiac arrhythmias. Haloperidol’s prescribing information carries a new warning of sudden death, QT prolongation, and torsades de pointes in patients given IV haloperidol.
Chlorpromazine. In a double-blind, randomized comparison trial of 30 hospitalized AIDS patients, our group12 found oral and IM haloperidol (n=11) or chlorpromazine (n=13) highly effective in controlling delirium. Delirium symptoms improved significantly in both hypoactive and hyperactive subtypes with low doses of either antipsychotic (approximately 2 mg of haloperidol equivalent/day).
No patients developed dystonic or dyskinetic symptoms. Lorazepam, given to 6 patients, worsened delirium and cognitive impairment.
Table 1
Recognizing delirium: Diagnostic clinical features*
| Altered level of alertness and arousal |
| Rapidly fluctuating course |
| Attention disturbance |
| Increased or decreased psychomotor activity |
| Disturbance of sleep-wake cycle |
| Affective symptoms |
| Altered perceptions |
| Disorganized thinking and incoherent speech |
| Disorientation and memory impairment |
| * Not all symptoms are present in every case. |
| Source: Reference 9 |
Nonpharmacologic approaches to managing delirium
| Search for and correct all causes of delirium, including underlying disease or a medication effect |
| Create a calm, comfortable environment |
| Provide orienting objects such as calendars and clocks |
| Have family members present |
| Limit room and staff changes |
| Allow patients uninterrupted rest at night to improve the sleep-wake cycle |
| Consider 1-to-1 nursing observation, as necessary |
| Source: Reference 4 |
Atypicals in delirium: Trial data
Risperidone. Three open-label studies of risperidone in patients with delirium reported minimal risk of sedation and EPS.13-15
A 7-day, double-blind, flexible-dose trial of 24 patients with delirium16 found no significant difference between haloperidol (mean 1.71 mg/d) and risperidone (mean 1.02 mg/d) in clinical efficacy or response rate. The authors acknowledged, that they were unable to obtain identical-looking haloperidol and risperidone tablets for the trial.
Kim et al17 studied dopamine transporter gene polymorphism and use of haloperidol vs risperidone in 42 patients with delirium. Relatively low doses of both antipsychotics showed similar efficacy, and the authors concluded that dopamine transporter gene polymorphism did not influence delirium treatment.
Olanzapine. In an open trial of 79 inpatients with advanced cancer, olanzapine (mean 6.3 mg/d, range 2.5 to 20 mg/d) resolved delirium in 76% of patients, with no incidence of EPS.18 Age >70, history of dementia, hypoxia, cerebral metastasis, and hypoactive delirium were associated with poor response to olanzapine. This study is unique in assessing olanzapine’s efficacy in different delirium subtypes.
A prospective, randomized trial compared olanzapine (mean 4.5 mg/d, range 2.5 to 13.5 mg/d) with haloperidol (mean 6.5 mg/d, range 1 to 28 mg/d) in patients admitted with delirium to a critical care setting.19 Both treatment groups showed similar improvement over 5 days. No side effects were reported in the patients receiving olanzapine.
Ziprasidone. In the first case report in which ziprasidone was used to treat delirium,21 an HIV/AIDS patient was given 100 mg/d. Delirium symptoms improved, but treatment was discontinued because of side effects (hypokalemia, hypomagnesemia, premature ventricular contractions, and QT interval prolongation).
Aripiprazole. Straker et al22 reported 14 cases delirium treated with aripiprazole, which showed few side effects. Twelve patients had a ≥50% decrease in Delirium Rating Scale scores, and 13 showed improvement in Clinical Global Impression scale scores.
Clinical options
When choosing an antipsychotic to treat delirium, consider the individual patient’s risks of EPS, sedation, anticholinergic side effects, cardiac arrhythmias, and drug-drug interactions.
Haloperidol. When medication is necessary for delirium, American Psychiatric Association (APA) guidelines consider low-dose haloperidol as first-line treatment (see Related Resources). Recommended dosage is 1 to 2 mg (0.25 to 0.5 mg for the elderly) every 4 hours as needed.
Adding oral or IV lorazepam (0.5 to 1 mg every 1 to 2 hours) to haloperidol may help rapidly sedate the agitated delirious patient and minimize the risk of EPS associated with haloperidol.1 Avoid benzodiazepine monotherapy unless delirium is related to alcohol or benzodiazepine withdrawal.
Chlorpromazine. We have successfully used oral or IV chlorpromazine (12.5 to 50 mg every 4 to 12 hours) instead of haloperidol plus lorazepam when increased sedation was required, especially:
- in the ICU, where close blood pressure monitoring was feasible
- for severe agitation in terminally ill patients to decrease distress for the patient, family and staff.
Atypical antipsychotics also may be used to treat delirium, as supported by the literature. Recommended dosing, available routes administration routes, and clinical comments are summarized in Table 3.23
Table 3
Recommended antipsychotic dosing for delirium*
| Antipsychotic | Dosage | Route† | Comment | |
|---|---|---|---|---|
| Typical agents | ||||
| Haloperidol | Initial: 0.5 to 1 mg Range: 0.5 to 2 mg every 2 to 12 hours | Oral, IV, SC, IM | ‘First choice’ for delirium when antipsychotic treatment is needed (per APA guidelines) | |
| Chlorpromazine | Initial: 12.5 to 25 mg Range: 12.5 to 50 mg every 4 to 12 hours | Oral, IV, IM | Alternative to haloperidol plus lorazepam when increased sedation is needed | |
| Atypical agents | ||||
| Risperidone | Initial: 0.25 to 1 mg Range: 0.25 to 2 mg/d | Oral | Risk of sedation and orthostatic hypotension at higher doses | |
| Olanzapine | Initial: 2.5 to 5 mg nightly Range: 2.5 to 10 mg/d | Oral | Sedation (a potential limiting factor) may be beneficial for hyperactive delirium | |
| Quetiapine | Initial: 25 to 50 mg Range: 25 to 200 mg/d, usually divided into 2 daily doses | Oral | Sedation and orthostatic hypotension are dose-limiting factors | |
| Ziprasidone | Initial: 20 mg bid Range: 20 to 160 mg/d, usually divided into 2 daily doses | Oral | Limited data in delirium because of concerns about QT interval prolongation in medically ill patients | |
| Aripiprazole | Initial: 10 to 15 mg Range: 10 to 30 mg/d | Oral | ‘Dopamine stabilizing’ effect might be preferable in hypoactive delirium | |
| * For frail elderly patients, start with approximately one-half the suggested initial dose. | ||||
| † Risperidone and aripiprazole are available in liquid formulations. Risperidone, olanzapine, and aripiprazole are available in orally disintegrating tablets. | ||||
| APA: American Psychiatric Association; IM: intramuscular; IV: intravenous; SC: subcutaneous | ||||
| Source: Reference 23 | ||||
Managing adverse effects
Reassess patients frequently during a delirium episode to adjust the antipsychotic dose, search for underlying causes, and monitor for side effects (Table 4). In frail elderly patients, start with approximately one-half the recommended initial dose to reduce the side effect risk.
Antipsychotics may not be appropriate in certain populations with delirium, particularly in patients with:
- dementia of Lewy body type or Parkinson’s disease dementia
- stroke
- history of adverse reactions to antipsychotics.
Although the FDA advisory did not apply to typical antipsychotics, Wang et al3—in a retrospective cohort of nearly 23,000 patients age >65—found statistically significant higher mortality rates with typical vs atypical antipsychotics. The increased mortality risk with the typical agents was seen whether or not patients had dementia. The greatest increases in risk occurred early in therapy and with relatively high dosages.
The mortality risk associated with short-term antipsychotic treatment in medically ill elderly patients is unknown. Untreated delirium may impose a greater risk of morbidity and mortality than the risk associated with antipsychotics, however. Until more evidence becomes available, we recommend that you try to use low antipsychotic doses, especially for the elderly.
EPS are more common with conventional antipsychotics but also can be associated with the atypicals—particularly with risperidone at doses higher than 4 to 6 mg/d. To minimize EPS risk, monitor delirium patients daily during antipsychotic treatment and identify populations at risk.
QT interval prolongation. A prolonged QT interval increases the risk of ventricular arrhythmias—such as torsades de pointes and ventricular fibrillation—that can lead to syncope, cardiac arrest, or sudden cardiac death. Among the atypicals, ziprasidone has been associated with the highest rates of QT interval prolongation, followed by quetiapine, risperidone, and olanzapine.24 Thioridazine carries the greatest risk among the typical agents.25
When using antipsychotics for delirium, identify patients at risk for QT interval changes and monitor all patients during treatment. Risk factors include older age, female sex, preexisting heart disease, bradycardia, electrolyte abnormalities, and use of drugs that block potassium. APA guidelines recommend discontinuing antipsychotic therapy if QTc exceeds 450 msec or increases >25% from baseline.1 Consult with a cardiologist when antipsychotic treatment is necessary despite QT prolongation.
Metabolic syndrome. Long-term use of atypical antipsychotics—particularly olanzapine—has been associated with metabolic dysregulation and increased risk of obesity and diabetes. In the absence of data on the atypicals’ short-term effects on metabolism, we recommend careful monitoring for metabolic syndrome when using these agents, especially in patients with preexisting metabolic disturbances.26
Table 4
Monitoring for antipsychotic side effects during delirium treatment
| Side effects | How to monitor |
|---|---|
| EPS (parkinsonism, akathisia, dystonia) | Neurologic examination |
| Neuroleptic malignant syndrome | Neurologic examination, serum creatinine phosphokinase, serum prolactin |
| QT interval prolongation, torsades de pointes | ECG, serum potassium and magnesium, family history of QT prolongation |
| Metabolic syndrome (hyperglycemia, hyperlipidemia, weight gain) | Fasting blood glucose, lipid profile, weight, hemoglobin A1c |
| Anticholinergic symptoms (dry mouth, constipation) | History and physical examination |
| EPS: extrapyramidal symptoms | |
Discontinuing antipsychotics
No evidence-based or expert consensus guidelines have addressed when or how to discontinue antipsychotic treatment of delirium. Several studies—including a randomized, controlled trial by our group12—used protocols that reflect expert clinician practice.
Antipsychotic therapy is initiated to control delirium’s symptoms and is presumed to be needed until the causes have been identified or have resolved. Thus, antipsychotics are typically given in 3 phases:
Maintenance. Continue the antipsychotic 7 to 10 days—typically at two-thirds to one-half the initial-phase dosage—to allow delirium causes to be identified and resolve.
Tapering/discontinuation. If delirium symptoms resolve, taper and discontinue the antipsychotic relatively slowly over 3 to 5 days to allow for rapid control should delirium symptoms reemerge. Re-emergence suggests that new or unrecognized causes of delirium are present or identified causes have not resolved.
- American Psychiatric Association. Treating delirium: a quick reference guide. www.psych.org/psych_pract/treatg/quick_ref_guide/DeliriumQRG_4-15-05.pdf.
- American Psychiatric Association. Guideline watch: practice guideline for the treatment of patients with delirium. www.psych.org/psych_pract/treatg/pg/Delirium.watch.pdf.
- American Psychosocial Oncology Society. Multidisciplinary training in psycho-oncology: delirium. www.apos-society.org/professionals/meetings-ed/webcasts/webcasts-multidisciplinary.aspx.
- Aripiprazole • Abilify
- Chlorpromazine • various
- Haloperidol • various
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Dr. Breitbart is a consultant to Cephalon and a speaker for Cephalon, Janssen Pharmaceutica, Purdue Pharma, Eli Lilly and Company, and Bristol-Myers Squibb.
Dr. Alici-Evcimen reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. American Psychiatric Association. Practice guidelines for the treatment of patients with delirium. Am J Psychiatry 1999;156:S1-S20.
2. Schneider LS, Dagerman KS, Insel P. Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials. JAMA. 2005;294(15):1934-43.
3. Wang PS, Schneeweiss S, Avorn J, et al. Risk of death in elderly users of conventional vs. atypical antipsychotic medications. N Engl J Med 2005;353(22):2335-41.
4. Inouye SK. Delirium in older persons. N Engl J Med 2006;354(11):1157-65.
5. Casarett DJ, Inouye SK. Diagnosis and management of delirium near the end of life. Ann Intern Med 2001;135(1):32-40.
6. Trzepacz PT. Update on the neuropathogenesis of delirium. Dement Geriatr Cogn Disord 1999;10(5):330-4.
7. Trzepacz PT. Is there a final common neural pathway in delirium? Focus on acetylcholine and dopamine. Semin Clin Neuropsychiatry 2000;5(2):132-48.
8. Breitbart W, Gibson C, Tremblay A. The delirium experience: delirium recall and delirium-related distress in hospitalized patients with cancer, their spouses/caregivers, and their nurses. Psychosomatics 2002;43(3):183-94.
9. Diagnostic and statistical manual of mental disorders, 4th ed, text revision. Washington, DC: American Psychiatric Association; 2000.
10. Seitz DP, Gill SS, van Zyl LT. Antipsychotics in the treatment of delirium: a systematic review. J Clin Psychiatry 2007;68(1):11-21.
11. Michaud L, Bula C, Berney A, et al. Delirium: guidelines for general hospitals. J Psychosom Res 2007;62(3):371-83.
12. Breitbart W, Marotta R, Platt MM, et al. A double-blind trial of haloperidol, chlorpromazine, and lorazepam in the treatment of delirium in hospitalized AIDS patients. Am J Psychiatry 1996;153(2):231-7.
13. Horikawa N, Yamazaki T, Miyamoto K. Treatment for delirium with risperidone: results of a prospective open trial with 10 patients. Gen Hosp Psychiatry 2003;25:289-92.
14. Mittal D, Jimerson N, Neely E. Risperidone in the treatment of delirium: results from a prospective open-label trial. J Clin Psychiatry 2004;65:662-7.
15. Parellada E, Baeza I, de Pablo J. Risperidone in the treatment of patients with delirium. J Clin Psychiatry 2004;65:348-53.16.
16. Han C, Kim Y. A double-blind trial of risperidone and haloperidol for the treatment of delirium. Psychosomatics 2004;45(4):297-301.
17. Kim JY, Jung IK, Han C, et al. Antipsychotics and dopamine transporter gene polymorphisms in delirium patients. Psychiatry Clin Neurosci. 2005;59(2):183-8.
18. Breitbart W, Tremblay A, Gibson C. An open trial of olanzapine for the treatment of delirium in hospitalized cancer patients. Psychosomatics 2002;43(3):175-82.
19. Skrobik Y, Bergeron N, Dumont M. Olanzapine vs haloperidol: treating delirium in a critical care setting. Intensive Care Med 2004;30:444-9.
20. Pae C, Lee S, Lee C. A pilot trial of quetiapine for the treatment of patients with delirium. Hum Psychopharmacol 2004;19:125-7.
21. Leso L, Schwartz T. Ziprasidone treatment of delirium. Psychosomatics 2002;43:61-2.
22. Straker DA, Shapiro PA, Muskin PR. Aripiprazole in the treatment of delirium. Psychosomatics. 2006;47(5):385-91.
23. Boettger S, Breitbart W. Atypical antipsychotics in the management of delirium: a review of the empirical literature. Palliat Support Care 2005;3(3):227-37.
24. Al-Khatib SM, LaPointe NM, Kramer JM, Califf RM. What clinicians should know about the QT interval. JAMA 2003;289(16):2120-7.
25. Glassman AH, Bigger JT, Jr. Antipsychotic drugs: prolonged QTc interval, torsade de pointes, and sudden death. Am J Psychiatry. 2001;158(11):1774-82.
26. Nasrallah HA, Newcomer JW. Atypical antipsychotics and metabolic dysregulation: evaluating the risk/benefit equation and improving the standard of care. J Clin Psychopharmacol 2004;24(5 suppl 1):S7-S14.
Delirium is a medical emergency that needs to be identified and treated vigorously. Antipsychotics—including haloperidol and atypical agents—effectively manage a wide spectrum of delirium symptoms and are an essential component in the standard multimodal approach.1 Even so, antipsychotics are not FDA-approved for treating delirium, and evidence on their safety in medically ill patients is limited—particularly in the elderly, in whom delirium occurs most often.
The FDA has warned of increased risk of death when atypical antipsychotics are used to treat behavioral disturbances in elderly patients with dementia.2 Similarly, a retrospective study of elderly patients taking antipsychotics found higher mortality rates associated with typical antipsychotics than with atypicals.3
This article discusses the risks and benefits of using antipsychotics to manage delirium. Based on the literature and clinical experience, we offer recommendations on choosing among the available agents and avoiding side effects.
A challenging diagnosis
Delirium is a neuropsychiatric syndrome precipitated by an underlying medical condition or a medication effect on the brain. Its characteristic symptoms—abrupt onset of disturbed consciousness, attention, cognition, and perception—tend to fluctuate during the day. Delirium most often occurs in elderly patients (Box)1,4-7—particularly with dementia—but also occurs in younger patients with serious illnesses such as cancer or HIV-AIDS.
Delirium is underdiagnosed and under-treated in medical settings,4,8 most likely because of its protean symptoms (Table 1)9 and fluctuating clinical findings. Neurologic abnormalities—including cortical and motor symptoms—also can occur.1
Mortality risk. Delirium is an independent risk factor for mortality.1,4,5 It is a marker for serious and potentially life-threatening medical problems, such as organ failure or sepsis. When antipsychotics fail to control delirium, the 3 most common reasons are:
- delirium’s etiology has not been discovered or addressed
- delirium’s etiology is resistant to treatment or potentially irreversible
- antipsychotic dosage was inadequate.
3 subtypes. Delirium is classified as hyperactive, hypoactive, or mixed, depending on arousal disturbance and psychomotor behavior:
- the hyperactive subtype includes hallucinations, delusions, agitation, and disorientation.
- the hypoactive subtype includes confusion, sedation, and decreased alertness but rarely hallucinations or delusions.1
Up to 1 in 4 patients (14% to 24%) have delirium at hospital admission, and the annual incidence of delirium is 6% to 56% among hospital populations.4 Elderly inpatients who develop delirium have an estimated mortality rate of 22% to 76% during that hospitalization.1 At the end of life, the prevalence of delirium may be as high as 85%.5
Serotonergic, noradrenergic, opiatergic, glutamatergic, and histaminergic neurotransmitter systems may contribute to delirium as a syndrome. Evidence implicates underactivity of the cholinergic system as the final common pathway.6,7
The acetylcholine-dopamine hypothesis explains the efficacy of dopamine antagonists in treating delirium by regulating the imbalance between cholinergic and dopaminergic activity.5,6 Cytokines—including interleukin-1, interleukin-2, and interleukin-6—and chronic hypercortisolism may also contribute to delirium.4
Antipsychotics: Limited evidence
- identifying and eliminating contributing factors
- instituting nonpharmacologic interventions based on environmental strategies (Table 2)4
- providing pharmacologic interventions—primarily antipsychotics—as needed.
- delirium severity improved with haloperidol, chlorpromazine, olanzapine, risperidone, or quetiapine
- comparison trials did not identify any antipsychotic as more efficacious than another.
Michaud et al11 reviewed guidelines, systematic reviews, randomized controlled trials, and cohort studies on delirium management. They concluded that the experts agree on 3 points:
- prevention should be emphasized
- atypical antipsychotics are not first-choice drugs because of data on adverse events in the elderly
- pharmacologic treatment is recommended when the patient’s condition prevents adequate care or puts the patient or staff at risk.
Conventional antipsychotics
Haloperidol, the most-studied antipsychotic in delirium treatment, often is the drug of choice because of its high potency, low sedative effect, few anticholinergic side effects, minimal cardiovascular side effects, no active metabolites, and multiple administration routes.1
An IV route can facilitate rapid onset of medication effects. Compared with oral haloperidol, IV administration is associated with a lower risk of extrapyramidal symptoms (EPS), which allows use of higher doses.
Any IV use of injectable haloperidol is off-label, however. If you choose the IV route, monitor patients carefully for cardiac arrhythmias. Haloperidol’s prescribing information carries a new warning of sudden death, QT prolongation, and torsades de pointes in patients given IV haloperidol.
Chlorpromazine. In a double-blind, randomized comparison trial of 30 hospitalized AIDS patients, our group12 found oral and IM haloperidol (n=11) or chlorpromazine (n=13) highly effective in controlling delirium. Delirium symptoms improved significantly in both hypoactive and hyperactive subtypes with low doses of either antipsychotic (approximately 2 mg of haloperidol equivalent/day).
No patients developed dystonic or dyskinetic symptoms. Lorazepam, given to 6 patients, worsened delirium and cognitive impairment.
Table 1
Recognizing delirium: Diagnostic clinical features*
| Altered level of alertness and arousal |
| Rapidly fluctuating course |
| Attention disturbance |
| Increased or decreased psychomotor activity |
| Disturbance of sleep-wake cycle |
| Affective symptoms |
| Altered perceptions |
| Disorganized thinking and incoherent speech |
| Disorientation and memory impairment |
| * Not all symptoms are present in every case. |
| Source: Reference 9 |
Nonpharmacologic approaches to managing delirium
| Search for and correct all causes of delirium, including underlying disease or a medication effect |
| Create a calm, comfortable environment |
| Provide orienting objects such as calendars and clocks |
| Have family members present |
| Limit room and staff changes |
| Allow patients uninterrupted rest at night to improve the sleep-wake cycle |
| Consider 1-to-1 nursing observation, as necessary |
| Source: Reference 4 |
Atypicals in delirium: Trial data
Risperidone. Three open-label studies of risperidone in patients with delirium reported minimal risk of sedation and EPS.13-15
A 7-day, double-blind, flexible-dose trial of 24 patients with delirium16 found no significant difference between haloperidol (mean 1.71 mg/d) and risperidone (mean 1.02 mg/d) in clinical efficacy or response rate. The authors acknowledged, that they were unable to obtain identical-looking haloperidol and risperidone tablets for the trial.
Kim et al17 studied dopamine transporter gene polymorphism and use of haloperidol vs risperidone in 42 patients with delirium. Relatively low doses of both antipsychotics showed similar efficacy, and the authors concluded that dopamine transporter gene polymorphism did not influence delirium treatment.
Olanzapine. In an open trial of 79 inpatients with advanced cancer, olanzapine (mean 6.3 mg/d, range 2.5 to 20 mg/d) resolved delirium in 76% of patients, with no incidence of EPS.18 Age >70, history of dementia, hypoxia, cerebral metastasis, and hypoactive delirium were associated with poor response to olanzapine. This study is unique in assessing olanzapine’s efficacy in different delirium subtypes.
A prospective, randomized trial compared olanzapine (mean 4.5 mg/d, range 2.5 to 13.5 mg/d) with haloperidol (mean 6.5 mg/d, range 1 to 28 mg/d) in patients admitted with delirium to a critical care setting.19 Both treatment groups showed similar improvement over 5 days. No side effects were reported in the patients receiving olanzapine.
Ziprasidone. In the first case report in which ziprasidone was used to treat delirium,21 an HIV/AIDS patient was given 100 mg/d. Delirium symptoms improved, but treatment was discontinued because of side effects (hypokalemia, hypomagnesemia, premature ventricular contractions, and QT interval prolongation).
Aripiprazole. Straker et al22 reported 14 cases delirium treated with aripiprazole, which showed few side effects. Twelve patients had a ≥50% decrease in Delirium Rating Scale scores, and 13 showed improvement in Clinical Global Impression scale scores.
Clinical options
When choosing an antipsychotic to treat delirium, consider the individual patient’s risks of EPS, sedation, anticholinergic side effects, cardiac arrhythmias, and drug-drug interactions.
Haloperidol. When medication is necessary for delirium, American Psychiatric Association (APA) guidelines consider low-dose haloperidol as first-line treatment (see Related Resources). Recommended dosage is 1 to 2 mg (0.25 to 0.5 mg for the elderly) every 4 hours as needed.
Adding oral or IV lorazepam (0.5 to 1 mg every 1 to 2 hours) to haloperidol may help rapidly sedate the agitated delirious patient and minimize the risk of EPS associated with haloperidol.1 Avoid benzodiazepine monotherapy unless delirium is related to alcohol or benzodiazepine withdrawal.
Chlorpromazine. We have successfully used oral or IV chlorpromazine (12.5 to 50 mg every 4 to 12 hours) instead of haloperidol plus lorazepam when increased sedation was required, especially:
- in the ICU, where close blood pressure monitoring was feasible
- for severe agitation in terminally ill patients to decrease distress for the patient, family and staff.
Atypical antipsychotics also may be used to treat delirium, as supported by the literature. Recommended dosing, available routes administration routes, and clinical comments are summarized in Table 3.23
Table 3
Recommended antipsychotic dosing for delirium*
| Antipsychotic | Dosage | Route† | Comment | |
|---|---|---|---|---|
| Typical agents | ||||
| Haloperidol | Initial: 0.5 to 1 mg Range: 0.5 to 2 mg every 2 to 12 hours | Oral, IV, SC, IM | ‘First choice’ for delirium when antipsychotic treatment is needed (per APA guidelines) | |
| Chlorpromazine | Initial: 12.5 to 25 mg Range: 12.5 to 50 mg every 4 to 12 hours | Oral, IV, IM | Alternative to haloperidol plus lorazepam when increased sedation is needed | |
| Atypical agents | ||||
| Risperidone | Initial: 0.25 to 1 mg Range: 0.25 to 2 mg/d | Oral | Risk of sedation and orthostatic hypotension at higher doses | |
| Olanzapine | Initial: 2.5 to 5 mg nightly Range: 2.5 to 10 mg/d | Oral | Sedation (a potential limiting factor) may be beneficial for hyperactive delirium | |
| Quetiapine | Initial: 25 to 50 mg Range: 25 to 200 mg/d, usually divided into 2 daily doses | Oral | Sedation and orthostatic hypotension are dose-limiting factors | |
| Ziprasidone | Initial: 20 mg bid Range: 20 to 160 mg/d, usually divided into 2 daily doses | Oral | Limited data in delirium because of concerns about QT interval prolongation in medically ill patients | |
| Aripiprazole | Initial: 10 to 15 mg Range: 10 to 30 mg/d | Oral | ‘Dopamine stabilizing’ effect might be preferable in hypoactive delirium | |
| * For frail elderly patients, start with approximately one-half the suggested initial dose. | ||||
| † Risperidone and aripiprazole are available in liquid formulations. Risperidone, olanzapine, and aripiprazole are available in orally disintegrating tablets. | ||||
| APA: American Psychiatric Association; IM: intramuscular; IV: intravenous; SC: subcutaneous | ||||
| Source: Reference 23 | ||||
Managing adverse effects
Reassess patients frequently during a delirium episode to adjust the antipsychotic dose, search for underlying causes, and monitor for side effects (Table 4). In frail elderly patients, start with approximately one-half the recommended initial dose to reduce the side effect risk.
Antipsychotics may not be appropriate in certain populations with delirium, particularly in patients with:
- dementia of Lewy body type or Parkinson’s disease dementia
- stroke
- history of adverse reactions to antipsychotics.
Although the FDA advisory did not apply to typical antipsychotics, Wang et al3—in a retrospective cohort of nearly 23,000 patients age >65—found statistically significant higher mortality rates with typical vs atypical antipsychotics. The increased mortality risk with the typical agents was seen whether or not patients had dementia. The greatest increases in risk occurred early in therapy and with relatively high dosages.
The mortality risk associated with short-term antipsychotic treatment in medically ill elderly patients is unknown. Untreated delirium may impose a greater risk of morbidity and mortality than the risk associated with antipsychotics, however. Until more evidence becomes available, we recommend that you try to use low antipsychotic doses, especially for the elderly.
EPS are more common with conventional antipsychotics but also can be associated with the atypicals—particularly with risperidone at doses higher than 4 to 6 mg/d. To minimize EPS risk, monitor delirium patients daily during antipsychotic treatment and identify populations at risk.
QT interval prolongation. A prolonged QT interval increases the risk of ventricular arrhythmias—such as torsades de pointes and ventricular fibrillation—that can lead to syncope, cardiac arrest, or sudden cardiac death. Among the atypicals, ziprasidone has been associated with the highest rates of QT interval prolongation, followed by quetiapine, risperidone, and olanzapine.24 Thioridazine carries the greatest risk among the typical agents.25
When using antipsychotics for delirium, identify patients at risk for QT interval changes and monitor all patients during treatment. Risk factors include older age, female sex, preexisting heart disease, bradycardia, electrolyte abnormalities, and use of drugs that block potassium. APA guidelines recommend discontinuing antipsychotic therapy if QTc exceeds 450 msec or increases >25% from baseline.1 Consult with a cardiologist when antipsychotic treatment is necessary despite QT prolongation.
Metabolic syndrome. Long-term use of atypical antipsychotics—particularly olanzapine—has been associated with metabolic dysregulation and increased risk of obesity and diabetes. In the absence of data on the atypicals’ short-term effects on metabolism, we recommend careful monitoring for metabolic syndrome when using these agents, especially in patients with preexisting metabolic disturbances.26
Table 4
Monitoring for antipsychotic side effects during delirium treatment
| Side effects | How to monitor |
|---|---|
| EPS (parkinsonism, akathisia, dystonia) | Neurologic examination |
| Neuroleptic malignant syndrome | Neurologic examination, serum creatinine phosphokinase, serum prolactin |
| QT interval prolongation, torsades de pointes | ECG, serum potassium and magnesium, family history of QT prolongation |
| Metabolic syndrome (hyperglycemia, hyperlipidemia, weight gain) | Fasting blood glucose, lipid profile, weight, hemoglobin A1c |
| Anticholinergic symptoms (dry mouth, constipation) | History and physical examination |
| EPS: extrapyramidal symptoms | |
Discontinuing antipsychotics
No evidence-based or expert consensus guidelines have addressed when or how to discontinue antipsychotic treatment of delirium. Several studies—including a randomized, controlled trial by our group12—used protocols that reflect expert clinician practice.
Antipsychotic therapy is initiated to control delirium’s symptoms and is presumed to be needed until the causes have been identified or have resolved. Thus, antipsychotics are typically given in 3 phases:
Maintenance. Continue the antipsychotic 7 to 10 days—typically at two-thirds to one-half the initial-phase dosage—to allow delirium causes to be identified and resolve.
Tapering/discontinuation. If delirium symptoms resolve, taper and discontinue the antipsychotic relatively slowly over 3 to 5 days to allow for rapid control should delirium symptoms reemerge. Re-emergence suggests that new or unrecognized causes of delirium are present or identified causes have not resolved.
- American Psychiatric Association. Treating delirium: a quick reference guide. www.psych.org/psych_pract/treatg/quick_ref_guide/DeliriumQRG_4-15-05.pdf.
- American Psychiatric Association. Guideline watch: practice guideline for the treatment of patients with delirium. www.psych.org/psych_pract/treatg/pg/Delirium.watch.pdf.
- American Psychosocial Oncology Society. Multidisciplinary training in psycho-oncology: delirium. www.apos-society.org/professionals/meetings-ed/webcasts/webcasts-multidisciplinary.aspx.
- Aripiprazole • Abilify
- Chlorpromazine • various
- Haloperidol • various
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Dr. Breitbart is a consultant to Cephalon and a speaker for Cephalon, Janssen Pharmaceutica, Purdue Pharma, Eli Lilly and Company, and Bristol-Myers Squibb.
Dr. Alici-Evcimen reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Delirium is a medical emergency that needs to be identified and treated vigorously. Antipsychotics—including haloperidol and atypical agents—effectively manage a wide spectrum of delirium symptoms and are an essential component in the standard multimodal approach.1 Even so, antipsychotics are not FDA-approved for treating delirium, and evidence on their safety in medically ill patients is limited—particularly in the elderly, in whom delirium occurs most often.
The FDA has warned of increased risk of death when atypical antipsychotics are used to treat behavioral disturbances in elderly patients with dementia.2 Similarly, a retrospective study of elderly patients taking antipsychotics found higher mortality rates associated with typical antipsychotics than with atypicals.3
This article discusses the risks and benefits of using antipsychotics to manage delirium. Based on the literature and clinical experience, we offer recommendations on choosing among the available agents and avoiding side effects.
A challenging diagnosis
Delirium is a neuropsychiatric syndrome precipitated by an underlying medical condition or a medication effect on the brain. Its characteristic symptoms—abrupt onset of disturbed consciousness, attention, cognition, and perception—tend to fluctuate during the day. Delirium most often occurs in elderly patients (Box)1,4-7—particularly with dementia—but also occurs in younger patients with serious illnesses such as cancer or HIV-AIDS.
Delirium is underdiagnosed and under-treated in medical settings,4,8 most likely because of its protean symptoms (Table 1)9 and fluctuating clinical findings. Neurologic abnormalities—including cortical and motor symptoms—also can occur.1
Mortality risk. Delirium is an independent risk factor for mortality.1,4,5 It is a marker for serious and potentially life-threatening medical problems, such as organ failure or sepsis. When antipsychotics fail to control delirium, the 3 most common reasons are:
- delirium’s etiology has not been discovered or addressed
- delirium’s etiology is resistant to treatment or potentially irreversible
- antipsychotic dosage was inadequate.
3 subtypes. Delirium is classified as hyperactive, hypoactive, or mixed, depending on arousal disturbance and psychomotor behavior:
- the hyperactive subtype includes hallucinations, delusions, agitation, and disorientation.
- the hypoactive subtype includes confusion, sedation, and decreased alertness but rarely hallucinations or delusions.1
Up to 1 in 4 patients (14% to 24%) have delirium at hospital admission, and the annual incidence of delirium is 6% to 56% among hospital populations.4 Elderly inpatients who develop delirium have an estimated mortality rate of 22% to 76% during that hospitalization.1 At the end of life, the prevalence of delirium may be as high as 85%.5
Serotonergic, noradrenergic, opiatergic, glutamatergic, and histaminergic neurotransmitter systems may contribute to delirium as a syndrome. Evidence implicates underactivity of the cholinergic system as the final common pathway.6,7
The acetylcholine-dopamine hypothesis explains the efficacy of dopamine antagonists in treating delirium by regulating the imbalance between cholinergic and dopaminergic activity.5,6 Cytokines—including interleukin-1, interleukin-2, and interleukin-6—and chronic hypercortisolism may also contribute to delirium.4
Antipsychotics: Limited evidence
- identifying and eliminating contributing factors
- instituting nonpharmacologic interventions based on environmental strategies (Table 2)4
- providing pharmacologic interventions—primarily antipsychotics—as needed.
- delirium severity improved with haloperidol, chlorpromazine, olanzapine, risperidone, or quetiapine
- comparison trials did not identify any antipsychotic as more efficacious than another.
Michaud et al11 reviewed guidelines, systematic reviews, randomized controlled trials, and cohort studies on delirium management. They concluded that the experts agree on 3 points:
- prevention should be emphasized
- atypical antipsychotics are not first-choice drugs because of data on adverse events in the elderly
- pharmacologic treatment is recommended when the patient’s condition prevents adequate care or puts the patient or staff at risk.
Conventional antipsychotics
Haloperidol, the most-studied antipsychotic in delirium treatment, often is the drug of choice because of its high potency, low sedative effect, few anticholinergic side effects, minimal cardiovascular side effects, no active metabolites, and multiple administration routes.1
An IV route can facilitate rapid onset of medication effects. Compared with oral haloperidol, IV administration is associated with a lower risk of extrapyramidal symptoms (EPS), which allows use of higher doses.
Any IV use of injectable haloperidol is off-label, however. If you choose the IV route, monitor patients carefully for cardiac arrhythmias. Haloperidol’s prescribing information carries a new warning of sudden death, QT prolongation, and torsades de pointes in patients given IV haloperidol.
Chlorpromazine. In a double-blind, randomized comparison trial of 30 hospitalized AIDS patients, our group12 found oral and IM haloperidol (n=11) or chlorpromazine (n=13) highly effective in controlling delirium. Delirium symptoms improved significantly in both hypoactive and hyperactive subtypes with low doses of either antipsychotic (approximately 2 mg of haloperidol equivalent/day).
No patients developed dystonic or dyskinetic symptoms. Lorazepam, given to 6 patients, worsened delirium and cognitive impairment.
Table 1
Recognizing delirium: Diagnostic clinical features*
| Altered level of alertness and arousal |
| Rapidly fluctuating course |
| Attention disturbance |
| Increased or decreased psychomotor activity |
| Disturbance of sleep-wake cycle |
| Affective symptoms |
| Altered perceptions |
| Disorganized thinking and incoherent speech |
| Disorientation and memory impairment |
| * Not all symptoms are present in every case. |
| Source: Reference 9 |
Nonpharmacologic approaches to managing delirium
| Search for and correct all causes of delirium, including underlying disease or a medication effect |
| Create a calm, comfortable environment |
| Provide orienting objects such as calendars and clocks |
| Have family members present |
| Limit room and staff changes |
| Allow patients uninterrupted rest at night to improve the sleep-wake cycle |
| Consider 1-to-1 nursing observation, as necessary |
| Source: Reference 4 |
Atypicals in delirium: Trial data
Risperidone. Three open-label studies of risperidone in patients with delirium reported minimal risk of sedation and EPS.13-15
A 7-day, double-blind, flexible-dose trial of 24 patients with delirium16 found no significant difference between haloperidol (mean 1.71 mg/d) and risperidone (mean 1.02 mg/d) in clinical efficacy or response rate. The authors acknowledged, that they were unable to obtain identical-looking haloperidol and risperidone tablets for the trial.
Kim et al17 studied dopamine transporter gene polymorphism and use of haloperidol vs risperidone in 42 patients with delirium. Relatively low doses of both antipsychotics showed similar efficacy, and the authors concluded that dopamine transporter gene polymorphism did not influence delirium treatment.
Olanzapine. In an open trial of 79 inpatients with advanced cancer, olanzapine (mean 6.3 mg/d, range 2.5 to 20 mg/d) resolved delirium in 76% of patients, with no incidence of EPS.18 Age >70, history of dementia, hypoxia, cerebral metastasis, and hypoactive delirium were associated with poor response to olanzapine. This study is unique in assessing olanzapine’s efficacy in different delirium subtypes.
A prospective, randomized trial compared olanzapine (mean 4.5 mg/d, range 2.5 to 13.5 mg/d) with haloperidol (mean 6.5 mg/d, range 1 to 28 mg/d) in patients admitted with delirium to a critical care setting.19 Both treatment groups showed similar improvement over 5 days. No side effects were reported in the patients receiving olanzapine.
Ziprasidone. In the first case report in which ziprasidone was used to treat delirium,21 an HIV/AIDS patient was given 100 mg/d. Delirium symptoms improved, but treatment was discontinued because of side effects (hypokalemia, hypomagnesemia, premature ventricular contractions, and QT interval prolongation).
Aripiprazole. Straker et al22 reported 14 cases delirium treated with aripiprazole, which showed few side effects. Twelve patients had a ≥50% decrease in Delirium Rating Scale scores, and 13 showed improvement in Clinical Global Impression scale scores.
Clinical options
When choosing an antipsychotic to treat delirium, consider the individual patient’s risks of EPS, sedation, anticholinergic side effects, cardiac arrhythmias, and drug-drug interactions.
Haloperidol. When medication is necessary for delirium, American Psychiatric Association (APA) guidelines consider low-dose haloperidol as first-line treatment (see Related Resources). Recommended dosage is 1 to 2 mg (0.25 to 0.5 mg for the elderly) every 4 hours as needed.
Adding oral or IV lorazepam (0.5 to 1 mg every 1 to 2 hours) to haloperidol may help rapidly sedate the agitated delirious patient and minimize the risk of EPS associated with haloperidol.1 Avoid benzodiazepine monotherapy unless delirium is related to alcohol or benzodiazepine withdrawal.
Chlorpromazine. We have successfully used oral or IV chlorpromazine (12.5 to 50 mg every 4 to 12 hours) instead of haloperidol plus lorazepam when increased sedation was required, especially:
- in the ICU, where close blood pressure monitoring was feasible
- for severe agitation in terminally ill patients to decrease distress for the patient, family and staff.
Atypical antipsychotics also may be used to treat delirium, as supported by the literature. Recommended dosing, available routes administration routes, and clinical comments are summarized in Table 3.23
Table 3
Recommended antipsychotic dosing for delirium*
| Antipsychotic | Dosage | Route† | Comment | |
|---|---|---|---|---|
| Typical agents | ||||
| Haloperidol | Initial: 0.5 to 1 mg Range: 0.5 to 2 mg every 2 to 12 hours | Oral, IV, SC, IM | ‘First choice’ for delirium when antipsychotic treatment is needed (per APA guidelines) | |
| Chlorpromazine | Initial: 12.5 to 25 mg Range: 12.5 to 50 mg every 4 to 12 hours | Oral, IV, IM | Alternative to haloperidol plus lorazepam when increased sedation is needed | |
| Atypical agents | ||||
| Risperidone | Initial: 0.25 to 1 mg Range: 0.25 to 2 mg/d | Oral | Risk of sedation and orthostatic hypotension at higher doses | |
| Olanzapine | Initial: 2.5 to 5 mg nightly Range: 2.5 to 10 mg/d | Oral | Sedation (a potential limiting factor) may be beneficial for hyperactive delirium | |
| Quetiapine | Initial: 25 to 50 mg Range: 25 to 200 mg/d, usually divided into 2 daily doses | Oral | Sedation and orthostatic hypotension are dose-limiting factors | |
| Ziprasidone | Initial: 20 mg bid Range: 20 to 160 mg/d, usually divided into 2 daily doses | Oral | Limited data in delirium because of concerns about QT interval prolongation in medically ill patients | |
| Aripiprazole | Initial: 10 to 15 mg Range: 10 to 30 mg/d | Oral | ‘Dopamine stabilizing’ effect might be preferable in hypoactive delirium | |
| * For frail elderly patients, start with approximately one-half the suggested initial dose. | ||||
| † Risperidone and aripiprazole are available in liquid formulations. Risperidone, olanzapine, and aripiprazole are available in orally disintegrating tablets. | ||||
| APA: American Psychiatric Association; IM: intramuscular; IV: intravenous; SC: subcutaneous | ||||
| Source: Reference 23 | ||||
Managing adverse effects
Reassess patients frequently during a delirium episode to adjust the antipsychotic dose, search for underlying causes, and monitor for side effects (Table 4). In frail elderly patients, start with approximately one-half the recommended initial dose to reduce the side effect risk.
Antipsychotics may not be appropriate in certain populations with delirium, particularly in patients with:
- dementia of Lewy body type or Parkinson’s disease dementia
- stroke
- history of adverse reactions to antipsychotics.
Although the FDA advisory did not apply to typical antipsychotics, Wang et al3—in a retrospective cohort of nearly 23,000 patients age >65—found statistically significant higher mortality rates with typical vs atypical antipsychotics. The increased mortality risk with the typical agents was seen whether or not patients had dementia. The greatest increases in risk occurred early in therapy and with relatively high dosages.
The mortality risk associated with short-term antipsychotic treatment in medically ill elderly patients is unknown. Untreated delirium may impose a greater risk of morbidity and mortality than the risk associated with antipsychotics, however. Until more evidence becomes available, we recommend that you try to use low antipsychotic doses, especially for the elderly.
EPS are more common with conventional antipsychotics but also can be associated with the atypicals—particularly with risperidone at doses higher than 4 to 6 mg/d. To minimize EPS risk, monitor delirium patients daily during antipsychotic treatment and identify populations at risk.
QT interval prolongation. A prolonged QT interval increases the risk of ventricular arrhythmias—such as torsades de pointes and ventricular fibrillation—that can lead to syncope, cardiac arrest, or sudden cardiac death. Among the atypicals, ziprasidone has been associated with the highest rates of QT interval prolongation, followed by quetiapine, risperidone, and olanzapine.24 Thioridazine carries the greatest risk among the typical agents.25
When using antipsychotics for delirium, identify patients at risk for QT interval changes and monitor all patients during treatment. Risk factors include older age, female sex, preexisting heart disease, bradycardia, electrolyte abnormalities, and use of drugs that block potassium. APA guidelines recommend discontinuing antipsychotic therapy if QTc exceeds 450 msec or increases >25% from baseline.1 Consult with a cardiologist when antipsychotic treatment is necessary despite QT prolongation.
Metabolic syndrome. Long-term use of atypical antipsychotics—particularly olanzapine—has been associated with metabolic dysregulation and increased risk of obesity and diabetes. In the absence of data on the atypicals’ short-term effects on metabolism, we recommend careful monitoring for metabolic syndrome when using these agents, especially in patients with preexisting metabolic disturbances.26
Table 4
Monitoring for antipsychotic side effects during delirium treatment
| Side effects | How to monitor |
|---|---|
| EPS (parkinsonism, akathisia, dystonia) | Neurologic examination |
| Neuroleptic malignant syndrome | Neurologic examination, serum creatinine phosphokinase, serum prolactin |
| QT interval prolongation, torsades de pointes | ECG, serum potassium and magnesium, family history of QT prolongation |
| Metabolic syndrome (hyperglycemia, hyperlipidemia, weight gain) | Fasting blood glucose, lipid profile, weight, hemoglobin A1c |
| Anticholinergic symptoms (dry mouth, constipation) | History and physical examination |
| EPS: extrapyramidal symptoms | |
Discontinuing antipsychotics
No evidence-based or expert consensus guidelines have addressed when or how to discontinue antipsychotic treatment of delirium. Several studies—including a randomized, controlled trial by our group12—used protocols that reflect expert clinician practice.
Antipsychotic therapy is initiated to control delirium’s symptoms and is presumed to be needed until the causes have been identified or have resolved. Thus, antipsychotics are typically given in 3 phases:
Maintenance. Continue the antipsychotic 7 to 10 days—typically at two-thirds to one-half the initial-phase dosage—to allow delirium causes to be identified and resolve.
Tapering/discontinuation. If delirium symptoms resolve, taper and discontinue the antipsychotic relatively slowly over 3 to 5 days to allow for rapid control should delirium symptoms reemerge. Re-emergence suggests that new or unrecognized causes of delirium are present or identified causes have not resolved.
- American Psychiatric Association. Treating delirium: a quick reference guide. www.psych.org/psych_pract/treatg/quick_ref_guide/DeliriumQRG_4-15-05.pdf.
- American Psychiatric Association. Guideline watch: practice guideline for the treatment of patients with delirium. www.psych.org/psych_pract/treatg/pg/Delirium.watch.pdf.
- American Psychosocial Oncology Society. Multidisciplinary training in psycho-oncology: delirium. www.apos-society.org/professionals/meetings-ed/webcasts/webcasts-multidisciplinary.aspx.
- Aripiprazole • Abilify
- Chlorpromazine • various
- Haloperidol • various
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Dr. Breitbart is a consultant to Cephalon and a speaker for Cephalon, Janssen Pharmaceutica, Purdue Pharma, Eli Lilly and Company, and Bristol-Myers Squibb.
Dr. Alici-Evcimen reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. American Psychiatric Association. Practice guidelines for the treatment of patients with delirium. Am J Psychiatry 1999;156:S1-S20.
2. Schneider LS, Dagerman KS, Insel P. Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials. JAMA. 2005;294(15):1934-43.
3. Wang PS, Schneeweiss S, Avorn J, et al. Risk of death in elderly users of conventional vs. atypical antipsychotic medications. N Engl J Med 2005;353(22):2335-41.
4. Inouye SK. Delirium in older persons. N Engl J Med 2006;354(11):1157-65.
5. Casarett DJ, Inouye SK. Diagnosis and management of delirium near the end of life. Ann Intern Med 2001;135(1):32-40.
6. Trzepacz PT. Update on the neuropathogenesis of delirium. Dement Geriatr Cogn Disord 1999;10(5):330-4.
7. Trzepacz PT. Is there a final common neural pathway in delirium? Focus on acetylcholine and dopamine. Semin Clin Neuropsychiatry 2000;5(2):132-48.
8. Breitbart W, Gibson C, Tremblay A. The delirium experience: delirium recall and delirium-related distress in hospitalized patients with cancer, their spouses/caregivers, and their nurses. Psychosomatics 2002;43(3):183-94.
9. Diagnostic and statistical manual of mental disorders, 4th ed, text revision. Washington, DC: American Psychiatric Association; 2000.
10. Seitz DP, Gill SS, van Zyl LT. Antipsychotics in the treatment of delirium: a systematic review. J Clin Psychiatry 2007;68(1):11-21.
11. Michaud L, Bula C, Berney A, et al. Delirium: guidelines for general hospitals. J Psychosom Res 2007;62(3):371-83.
12. Breitbart W, Marotta R, Platt MM, et al. A double-blind trial of haloperidol, chlorpromazine, and lorazepam in the treatment of delirium in hospitalized AIDS patients. Am J Psychiatry 1996;153(2):231-7.
13. Horikawa N, Yamazaki T, Miyamoto K. Treatment for delirium with risperidone: results of a prospective open trial with 10 patients. Gen Hosp Psychiatry 2003;25:289-92.
14. Mittal D, Jimerson N, Neely E. Risperidone in the treatment of delirium: results from a prospective open-label trial. J Clin Psychiatry 2004;65:662-7.
15. Parellada E, Baeza I, de Pablo J. Risperidone in the treatment of patients with delirium. J Clin Psychiatry 2004;65:348-53.16.
16. Han C, Kim Y. A double-blind trial of risperidone and haloperidol for the treatment of delirium. Psychosomatics 2004;45(4):297-301.
17. Kim JY, Jung IK, Han C, et al. Antipsychotics and dopamine transporter gene polymorphisms in delirium patients. Psychiatry Clin Neurosci. 2005;59(2):183-8.
18. Breitbart W, Tremblay A, Gibson C. An open trial of olanzapine for the treatment of delirium in hospitalized cancer patients. Psychosomatics 2002;43(3):175-82.
19. Skrobik Y, Bergeron N, Dumont M. Olanzapine vs haloperidol: treating delirium in a critical care setting. Intensive Care Med 2004;30:444-9.
20. Pae C, Lee S, Lee C. A pilot trial of quetiapine for the treatment of patients with delirium. Hum Psychopharmacol 2004;19:125-7.
21. Leso L, Schwartz T. Ziprasidone treatment of delirium. Psychosomatics 2002;43:61-2.
22. Straker DA, Shapiro PA, Muskin PR. Aripiprazole in the treatment of delirium. Psychosomatics. 2006;47(5):385-91.
23. Boettger S, Breitbart W. Atypical antipsychotics in the management of delirium: a review of the empirical literature. Palliat Support Care 2005;3(3):227-37.
24. Al-Khatib SM, LaPointe NM, Kramer JM, Califf RM. What clinicians should know about the QT interval. JAMA 2003;289(16):2120-7.
25. Glassman AH, Bigger JT, Jr. Antipsychotic drugs: prolonged QTc interval, torsade de pointes, and sudden death. Am J Psychiatry. 2001;158(11):1774-82.
26. Nasrallah HA, Newcomer JW. Atypical antipsychotics and metabolic dysregulation: evaluating the risk/benefit equation and improving the standard of care. J Clin Psychopharmacol 2004;24(5 suppl 1):S7-S14.
1. American Psychiatric Association. Practice guidelines for the treatment of patients with delirium. Am J Psychiatry 1999;156:S1-S20.
2. Schneider LS, Dagerman KS, Insel P. Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials. JAMA. 2005;294(15):1934-43.
3. Wang PS, Schneeweiss S, Avorn J, et al. Risk of death in elderly users of conventional vs. atypical antipsychotic medications. N Engl J Med 2005;353(22):2335-41.
4. Inouye SK. Delirium in older persons. N Engl J Med 2006;354(11):1157-65.
5. Casarett DJ, Inouye SK. Diagnosis and management of delirium near the end of life. Ann Intern Med 2001;135(1):32-40.
6. Trzepacz PT. Update on the neuropathogenesis of delirium. Dement Geriatr Cogn Disord 1999;10(5):330-4.
7. Trzepacz PT. Is there a final common neural pathway in delirium? Focus on acetylcholine and dopamine. Semin Clin Neuropsychiatry 2000;5(2):132-48.
8. Breitbart W, Gibson C, Tremblay A. The delirium experience: delirium recall and delirium-related distress in hospitalized patients with cancer, their spouses/caregivers, and their nurses. Psychosomatics 2002;43(3):183-94.
9. Diagnostic and statistical manual of mental disorders, 4th ed, text revision. Washington, DC: American Psychiatric Association; 2000.
10. Seitz DP, Gill SS, van Zyl LT. Antipsychotics in the treatment of delirium: a systematic review. J Clin Psychiatry 2007;68(1):11-21.
11. Michaud L, Bula C, Berney A, et al. Delirium: guidelines for general hospitals. J Psychosom Res 2007;62(3):371-83.
12. Breitbart W, Marotta R, Platt MM, et al. A double-blind trial of haloperidol, chlorpromazine, and lorazepam in the treatment of delirium in hospitalized AIDS patients. Am J Psychiatry 1996;153(2):231-7.
13. Horikawa N, Yamazaki T, Miyamoto K. Treatment for delirium with risperidone: results of a prospective open trial with 10 patients. Gen Hosp Psychiatry 2003;25:289-92.
14. Mittal D, Jimerson N, Neely E. Risperidone in the treatment of delirium: results from a prospective open-label trial. J Clin Psychiatry 2004;65:662-7.
15. Parellada E, Baeza I, de Pablo J. Risperidone in the treatment of patients with delirium. J Clin Psychiatry 2004;65:348-53.16.
16. Han C, Kim Y. A double-blind trial of risperidone and haloperidol for the treatment of delirium. Psychosomatics 2004;45(4):297-301.
17. Kim JY, Jung IK, Han C, et al. Antipsychotics and dopamine transporter gene polymorphisms in delirium patients. Psychiatry Clin Neurosci. 2005;59(2):183-8.
18. Breitbart W, Tremblay A, Gibson C. An open trial of olanzapine for the treatment of delirium in hospitalized cancer patients. Psychosomatics 2002;43(3):175-82.
19. Skrobik Y, Bergeron N, Dumont M. Olanzapine vs haloperidol: treating delirium in a critical care setting. Intensive Care Med 2004;30:444-9.
20. Pae C, Lee S, Lee C. A pilot trial of quetiapine for the treatment of patients with delirium. Hum Psychopharmacol 2004;19:125-7.
21. Leso L, Schwartz T. Ziprasidone treatment of delirium. Psychosomatics 2002;43:61-2.
22. Straker DA, Shapiro PA, Muskin PR. Aripiprazole in the treatment of delirium. Psychosomatics. 2006;47(5):385-91.
23. Boettger S, Breitbart W. Atypical antipsychotics in the management of delirium: a review of the empirical literature. Palliat Support Care 2005;3(3):227-37.
24. Al-Khatib SM, LaPointe NM, Kramer JM, Califf RM. What clinicians should know about the QT interval. JAMA 2003;289(16):2120-7.
25. Glassman AH, Bigger JT, Jr. Antipsychotic drugs: prolonged QTc interval, torsade de pointes, and sudden death. Am J Psychiatry. 2001;158(11):1774-82.
26. Nasrallah HA, Newcomer JW. Atypical antipsychotics and metabolic dysregulation: evaluating the risk/benefit equation and improving the standard of care. J Clin Psychopharmacol 2004;24(5 suppl 1):S7-S14.
Antidepressants: The spectrum beyond depression
A molecule is a molecule is a molecule—until it becomes identified with a purpose. Consider, for example, (-)-trans-4R-(4’-fluorophenyl)-3S-[(3’,4’-methylenedioxyphenoxy) methyl] piperidine. You probably know this molecule as paroxetine—an antidepressant, of course, but it is more than that. If you examine paroxetine’s FDA-approved indications, it also has anti-panic, anti-social anxiety, anti-obsessive-compulsive disorder, anti-posttraumatic stress disorder, and anti-premenstrual dysphoric disorder effects.
“Antidepressants” have achieved fame as antidepressants; one could say these molecules’ search for meaning has been fulfilled. Yet even within psychiatry, their many other uses (Table) can create semantic misunderstandings. Beyond psychiatry, consider the nondepressed patient with neurocardiogenic syncope who wonders why he’s being treated with an antidepressant.
Rather than calling antidepressants “panaceas,” the better choice is to educate patients about the drugs’ wide spectrum of activity. Let’s look broadly across the so-called antidepressants and examine their varied uses in psychiatry and other medical specialties.
Table
FDA-approved psychiatric indications for serotonin uptake inhibitors*
| SSRIs | ||||||||
| Citalopram | X | |||||||
| Escitalopram | X | X | ||||||
| Fluoxetine | X | X | X | X | X | |||
| Fluvoxamine | X | |||||||
| Paroxetine | X | X | X | X | X | X | X | |
| Sertraline | X | X | X | X | X | X | ||
| SNRIs | ||||||||
| Duloxetine | X | X | ||||||
| Venlafaxine | X | X | X | X | ||||
| SSRIs: selective serotonin reuptake inhibitors; SNRIs: serotonin-norepinephrine reuptake inhibitors; MDD: major depressive disorder; PD: panic disorder; SAD: social anxiety disorder; PTSD: posttraumatic stress disorder; GAD: generalized anxiety disorder; OCD: obsessive-compulsive disorder; PMDD: premenstrual dysphoric disorder; BUL: bulimia | ||||||||
| * The absence of an X does not necessarily imply that a drug is ineffective for a given indication but, more likely, that definitive studies are lacking. | ||||||||
Pain syndromes
Peripheral neuropathy. The only antidepressant with an FDA-approved pain indication is duloxetine, a serotonin-norepinephrine reuptake inhibitor (SNRI). Its approval for diabetic peripheral neuropathic pain (DPNP) was based on two 12-week, randomized, double-blind, placebo-controlled studies using fixed doses of 60 mg once or twice daily.1,2 Another SNRI—venlafaxine XR, 150 to 225 mg/d, but not 75 mg/d—also was found to be more effective than placebo for this indication in a 6-week, double-blind study (Box 1).3
Using antidepressants to treat pain syndromes is neither new nor restricted to SNRIs, however. In combined double-blind, cross-over studies of patients with DPNP, Max et al4 found:
- moderate or greater pain relief in 74% and 61% of subjects, respectively, from the tricyclics amitriptyline, mean 105 mg/d, and desipramine, mean 111 mg/d—with pain reduced by equal amounts in depressed and nondepressed patients
- no statistically significant difference in pain relief between the selective serotonin reuptake inhibitor (SSRI) fluoxetine, 40 mg/d, and placebo.
- tricyclics: 1 in every 2 to 3 patients
- SNRIs: 1 in every 4 to 5 patients
- SSRIs: 1 in every 7 patients.
Chronic headache. A meta-analysis7 of randomized, placebo-controlled studies found antidepressants more effective than placebo for chronic migraine and tension headache prophylaxis. Although a subgroup meta-analysis found similar effects for tricyclics and SSRIs, the authors characterized the tricyclics’ results as well established and the SSRIs’ as “less certain.”
The results of this meta-analysis might not accurately reflect bona fide antidepressants, however. Some of the 38 studies (25 of migraine, 12 of tension headache, 1 of both) included treatment with serotonin antagonists—most commonly pizotifen, which is not available in the United States and does not appear to be an antidepressant.
Back pain. Patients with chronic low back pain (average 10 years) seem to benefit from antidepressants, according to a meta-analysis of 9 randomized, controlled trials by Salerno et al.8 The effect on pain in the total 504 patients was “small but significant,” and improvement in function was “small but nonsignificant.” Individual sample sizes also were small, however, and only 2 studies excluded depressed patients.
Fibromyalgia, with chronic generalized musculoskeletal pain and tenderness, has been a focus of antidepressant drug therapy. Goldenberg et al9 concluded from an ambitious literature review (505 articles) that evidence of efficacy was strong for amitripty-line and modest for SSRIs and SNRIs.
Overall, antidepressants are generally understood to have analgesic effects in the absence of depression. Benefits for patients with pain syndromes are well established for tricyclics (especially amitriptyline) and recently with SNRIs, whereas SSRIs are less effective.
Serotonin and norepinephrine are involved in pain modulation via descending inhibitory pathways in the brain and spinal cord. Serotonin-norepinephrine reuptake inhibitors (SNRIs) have been shown to reduce the severity of diabetic peripheral neuropathic pain (DPNP) in randomized controlled trials.
Duloxetine. In 2 double-blind studies,1,2 nondepressed patients with DPNP received duloxetine, 60 mg once daily; duloxetine, 60 mg bid; or placebo for 12 weeks. They rated the severity of neuropathic pain every 24 hours on an 11-point Likert scale, and weekly mean scores were the primary outcome measure. Average pain scores improved more in both duloxetine groups vs placebo. Duloxetine treatment did not interfere with diabetic control, and both dosages were well tolerated.
The FDA approved an added indication for duloxetine in the management of DPNP.
Venlafaxine. In a double-blind study,3 244 adult outpatients with moderately severe DPNP received venlafaxine ER, 75 or 150 to 225 mg/d, or placebo for 6 weeks. Daily scores on the Visual Analog Pain Intensity (VAS-PI) and Pain Relief (VAS-PR) scales were primary efficacy measures.
Patients receiving the higher venlafaxine dosage—but not 75 mg/d—showed statistically significant less-intensive pain vs placebo. VAS-PI scores were 27% lower than at enrollment with placebo, 32% lower with venlafaxine, 75 mg/d, and 50% lower with venlafaxine, 150 to 225 mg/d (P
Nausea and somnolence were the most common side effects; clinically important ECG changes occurred in 7 patients treated with venlafaxine, 150 to 225 mg/d.
Smoking cessation
Bupropion SR is FDA-approved to aid smoking cessation, and this effect is independent of the drug’s antidepressant activity. Bupropion may act as a nicotine receptor antagonist as well as a norepinephrine dopamine reuptake inhibitor.
Other antidepressants have been studied for smoking cessation, with nortriptyline showing benefit in 2 large placebo-controlled trials. Studies with doxepin, fluoxetine, and moclobemide found little or no benefit for this indication.
Cardiovascular uses
Angina. Monoamine oxidase inhibitor (MAOI) antidepressants were used to treat angina pectoris in the late 1950s and early 1960s. This practice stopped after evidence showed that whereas angina pain may have improved with MAOIs, stress-induced ischemia on ECG did not.
Antiarrhythmia. Tricyclics had a brief fling in cardiovascular therapeutics when their quinidine-like class I antiarrhythmic activity was recognized. Imipramine was one of several drugs included in the Cardiac Arrhythmia Pilot Study in the 1980s that involved 502 postmyocardial infarction patients with ventricular arrhythmias. Imipramine was the least effective of the 4 drugs studied and the least well tolerated.13
variety of medications. Options include the vasopressor midodrine, fludrocortisone, beta blockers, and SSRIs— none
FDA-approved for this indication. Paroxetine, 20 mg/d, was considerably more effective than placebo in preventing
recurrent syncope in 68 patients who had been unresponsive
to or intolerant of traditional medications. During a mean 25 months of treatment, 82% of patients remained syncope-free on paroxetine vs 47% on placebo.14
Selective serotonin reuptake inhibitors (SSRIs) often are used to treat irritable bowel syndrome (IBS), though evidence of their effectiveness is scarce. SSRIs can improve IBS patients’ quality of life, but effects on abdominal pain and bloating are less clear.
Paroxetine. In a randomized, double-blind trial,16 gastroenterologists tested a highfiber diet plus paroxetine in nondepressed patients with IBS. Ninety-eight patients ages 18 to 65 who experienced IBS symptoms on low- or average-fiber diets were first put on high-fiber diets and assessed for well-being and abdominal pain and bloating. Of these, 81 symptomatic patients continued highfiber diets with added paroxetine, 10 to 40 mg/d (n=38) or placebo (n=43).
With paroxetine, patients’ overall well-being improved more than with placebo, but abdominal pain and bloating and social functioning did not.
Fluoxetine. In a double-blind, randomized trial,17 44 patients with pain and constipation-predominant IBS received fluoxetine, 20 mg/d, or placebo for 12 weeks. These patients met Rome II criteria for IBS—abdominal discomfort/pain for ≥12 weeks in past year that met 2 of 3 criteria:
- relieved by defecation
- onset associated with change in stool frequency
- onset associated with change in stool appearance.
Patients receiving fluoxetine had less abdominal discomfort, less bloating, more frequent bowel movements, and decreased consistency of stool vs placebo 4 weeks after treatment stopped. Mean number of symptoms per patient decreased from 4.6 to 0.7 in the fluoxetine group vs 4.5 to 2.9 in controls (P
Citalopram. IBS symptom severity was the primary outcome in a crossover trial comparing citalopram (20 mg for 3 weeks and 40 mg for 3 weeks) with placebo in 23 nondepressed patients.18 Abdominal pain and bloating, impact of symptoms on daily life, and overall well-being improved significantly more with citalopram than with placebo after 3 and 6 weeks.
Symptom improvements were not related to changes in depression, anxiety, or colonic sensorimotor function.
Gastrointestinal
Peptic ulcer disease was shown in the 1980s to respond to tricyclic antidepressants. At the time, both anticholinergic and antihistaminic effects were thought to be responsible, but the later observation that trimipramine inhibited Campylobacter pylori in vitro suggested an additional explanation. Today, tricyclics are only of historic interest as treatments for peptic ulcer.
Irritable bowel syndrome (IBS) patients have responded favorably to antidepressants, although it is often difficult to know if the benefit is independent of improved coexisting anxiety or depression. A meta-analysis of 12 randomized, placebo-controlled trials—mostly with tricyclics—found an odds ratio for improvement of 4.2 and a number needed to treat of 3.2.15
More recently, a few placebo-controlled studies have shown SSRIs to be beneficial for IBS,16-18 although not all symptoms improved and some IBS subtypes might be more responsive than others (Box 2). In an editorial, Talley19 concluded that antidepressant therapy of IBS was “at best only a ‘band-aid’ approach to management.”
Genitourinary
Nocturnal enuresis. In the 1960s, imipramine was shown—in some but not all placebo-controlled studies—to be beneficial for nocturnal enuresis in children and adults. Although imipramine is not FDA-approved for this indication, it is thought to work by relaxing bladder muscle and contracting bladder neck smooth muscle. Imipramine appears to have a vasopressin-independent antidiuretic effect in enuretic patients with nocturnal polyuria.
Duloxetine is thought to improve stress urinary incontinence by increasing urethral sphincter tone and the force of sphincter contraction. This indication is not FDA- approved for duloxetine but is approved in the European Union.
Oncology
At one time antidepressants were suggested to promote tumors, based on observations that amitriptyline, fluoxetine, and several antihistamines promoted tumor growth in rodents.21 In 1995, a few case reports associated these 2 antidepressants with atypical cutaneous lymphoid infiltrates.22 A review by Sternback in 200323 concluded that a link between antidepressants and cancer was questionable but acknowledged the need for very long-term studies.
Recently, a nested case-control study found an association between high-dose SSRI use for ≤5 years and reduced risk of colorectal cancer, whereas no association was found with tricyclic use.24 A study of this design does not establish a causal relationship, how-ever, and one can only speculate whether SSRIs might have direct cytotoxic or anti-promoter effects.
At present, it seems reasonable to continue to treat depressed cancer patients with antidepressants without concern that cancer will worsen or hope that it will improve as a result.
Immunology
The pathogenesis of depression may be linked to pro-inflammatory cytokines—proteins such as tumor necrosis factor-alpha (TNF-α) and certain interleukins that mediate immune function. Bupropion markedly lowered pro-inflammatory cytokine levels in a mouse inflammation model, prompting the authors to suggest that this anti-inflammatory effect be explored in humans.25
Case reports have suggested benefit from bupropion in Crohn’s disease, recurrent aphthous ulcerations, psoriasis, atopic dermatitis, and Blau syndrome (a rare autosomal-dominant trait characterized by granulomatous arthritis, iritis, and skin rash). Whether this antidepressant has much anti-inflammatory potential remains to be determined, however.
Delayed ejaculation is among the sexual side effects commonly associated with antidepressant medication. In a 6-week trial,27 3 selective serotonin reuptake inhibitors (SSRIs)— paroxetine, fluoxetine, and sertraline— were shown to improve intravaginal ejaculatory latency time (IELT) in men with lifelong rapid ejaculation. Compared with baseline, the greatest delay in ejaculation was seen with paroxetine, 20 mg/d, followed by fluoxetine, 20 mg/d, and then sertraline, 50 mg/d, whereas delay with fluvoxamine, 100 mg/d, did not differ significantly from placebo.
Dapoxetine is a non-antidepressant SSRI under investigation for on-demand treatment of moderate-to-severe premature ejaculation.28 In two 12-week, randomized, double-blind, placebo-controlled trials, 870 men took placebo, 874 took 30-mg dapoxetine, and 870 took 60-mg dapoxetine 1 to 3 hours before sexual activity. Efficacy was determined by IELT measured at home by stopwatch.
Both dapoxetine doses improved IELT significantly more than placebo (P
Nausea, diarrhea, headache, and dizziness occurred in ≤20% of patients and were more common with the 60-mg than 30-mg dapoxetine dose.
Infectious disease
Pathogenic protozoa—such as Trypanosoma cruzi (Chagas disease), Leishmania donovani (Kala-azar), Leishmania major (Oriental sore), and Giardia lamblia (Giardiasis)—infect millions of humans worldwide. Clomipramine has been shown in vitro and in mice to inhibit or kill these protozoa, but these potential benefits have not been extended to humans.
Sertraline, on the other hand, might exert antifungal activity. Three patients with recurrent vulvovaginal candidiasis had no episodes while being treated with sertraline for premenstrual dysphoric disorder but relapsed when the drug was discontinued.26 Although sertraline demonstrated antifungal activity in vitro against several Candida species, this SSRI seems unlikely to gain prominence as an antifungal agent.
Sexual function
Premature ejaculation. SSRIs are well-known causes of delayed or absent orgasm, but a perceived liability can become an asset in treating premature ejaculation. By measuring intravaginal ejaculation latency time under double-blind, placebo-controlled conditions, Waldinger et al27 showed pronounced delay in ejaculation with sertraline, fluoxetine, and paroxetine in men with long-standing rapid ejaculation. Dapoxetine—a short-acting non-antidepressant SSRI—is being studied as a treatment for this condition (Box 3).28
Spermicidal effect. SSRIs—including fluoxetine— have demonstrated in vitro spermicidal and antitrichomonas activity29 but are unlikely to be developed as microbicidal contraceptives.
Related Resources
- Gorman JM, Kent JM. SSRIs and SMRIs: broad spectrum of efficacy beyond major depression. J Clin Psychiatry 1999;60(suppl 4):33-8.
- About.com: Mental Health. Antidepressants for more than depression. http://mentalhealth.about.com/cs/psychopharmacology/a/antimore.htm.
- Amitriptyline • Elavil, Endep
- Bupropion • Wellbutrin, Zyban
- Citalopram • Celexa
- Clomipramine • Anafranil
- Desipramine • Norpramin, Pertofrane
- Doxepin • Adapin, Sinequan
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fludrocortisone • Florinef
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranil
- Midodrine • ProAmitine
- Nortriptyline • Pamelor, Aventyl
- Paroxetine • Paxil
- Phenelzine • Nardil
- Sertraline • Zoloft
- Trimipramine • Surmontil
- Venlafaxine • Effexor
Dr. Jefferson receives research support from Bristol-Myers Squibb, Forest Pharmaceuticals, GlaxoSmithKline, Janssen Pharmaceutica, Eli Lilly and Company, Novartis, Pfizer, Roche, Solvay, UCB Pharma, and Wyeth. He is a consultant to GlaxoSmithKline, Schwarz Pharma, Shire, and Organon and a speaker for Abbott Laboratories, AstraZeneca, Bristol-Myers Squibb, Forest Pharmaceuticals, GlaxoSmithKline, Eli Lilly and Company, Pfizer, Schwarz Pharma, Shire, and Wyeth. He holds stock in Bristol-Myers Squibb, GlaxoSmithKline, and SciClone.
1. Wernicke JF, Pritchett YL, D’Souza DN, et al. A randomized controlled trial of duloxetine in diabetic peripheral neuropathic pain. Neurology 2006;67(8):1411-20.
2. Raskin J, Pritchett YL, Wang F, et al. A double-blind, randomized multicenter trial comparing duloxetine with placebo in the management of diabetic peripheral neuropathic pain. Pain Med 2005;6(5):346-56.
3. Rowbotham MC, Goli V, Kunz NR, Lei D. Venlafaxine extended release in the treatment of painful diabetic neuropathy: a double-blind, placebo-controlled study. Pain 2004;110:697-706.
4. Max MB, Lynch SA, Muir J, et al. Effects of desipramine, amitriptyline, and fluoxetine on pain in diabetic neuropathy. N Engl J Med 1992;326:1250-6.
5. Sindrup SH, Otto M, Finnerup NB, Jensen TS. Antidepressants in the treatment of neuropathic pain. Basic Clin Pharmacol Toxicol 2005;96:399-409.
6. Semenchuk MR, Sherman S, Davis B. Double-blind, randomized trial of bupropion SR for the treatment of neuropathic pain. Neurology 2001;57:1583-8.
7. Tomkins GE, Jackson JL, O’Malley PG, et al. Treatment of chronic headache with antidepressants: a meta-analysis. Am J Med 2001;111:54-63.
8. Salerno SM, Browning R, Jackson JL. The effect of antidepressant treatment on chronic back pain. Arch Intern Med 2002;162:19-24.
9. Goldenberg DL, Burckhardt C, Crofford L. Management of fibromyalgia syndrome. JAMA 2004;292:2388-95.
10. Littlejohn GO, Guymer EK. Fibromyalgia syndrome: which antidepressant drug should we choose. Curr Pharm Des 2006;12(1):3-9.
11. Arnold LM, Lu Y, Crofford LJ, et al. A double-blind, multicenter trial comparing duloxetine with placebo in the treatment of fibromyalgia patients with or without major depressive disorder. Arthritis Rheum 2004;50:2974-84.
12. Arnold LM, Rosen A, Pritchett YL, et al. A randomized, double-blind, placebo-controlled trial of duloxetine in the treatment of women with fibromyalgia with or without major depressive disorder. Pain 2005;119:5-15.
13. Effects of encainide, flecainide, imipramine and moricizine on ventricular arrhythmias during the year after acute myocardial infarction: The CAPS. The Cardiac Arrhythmia Pilot Study (CAPS) Investigators. Am J Cardiol 1988;61(8):501-9.
14. Di Girolamo E, Di Iorio C, Sabatini P, et al. Effects of paroxetine hydrochloride, a selective serotonin reuptake inhibitor, on refractory vasovagal syncope: a randomized, double-blind, placebo-controlled study. J Am Coll Cardiol 1999;33:1227-30.
15. Jackson JL, O’Malley PG, Tomkins G, et al. Treatment of functional gastrointestinal disorders with antidepressant medications: a meta-analysis. Am J Med 2000;108:65-72.
16. Tabas G, Beaves M, Wang J, et al. Paroxetine to treat irritable bowel syndrome not responding to high-fiber diet: a double-blind, placebo-controlled trial. Am J Gastroenterol 2004;99(5):914-20.
17. Vahedi H, Merat S, Rashidioon A, et al. The effect of fluoxetine in patients with pain and constipation-predominant irritable bowel syndrome: a double-blind randomized-controlled study. Aliment Pharmacol Ther 2005;22:381-5.
18. Tack J, Broekaert D, Fischler B, et al. A controlled crossover study of the selective serotonin reuptake inhibitor citalopram in irritable bowel syndrome. Gut 2006;55:1095-103.
19. Talley NJ. Antidepressants in IBS: are we deluding ourselves? [editorial]. Am J Gastroenterol 2004;99:921-3.
20. Mariappan P, Ballantyne Z, N’Dow JM, Alhasso AA. Serotonin and noradrenaline reuptake inhibitors (SNRI) for stress urinary incontinence in adults. Cochrane Database Syst Rev 2005;Jul 20;(3):CD004742.-
21. Brandes LJ, Arron RJ, Bogdanovic RP, et al. Stimulation of malignant growth in rodents by antidepressant drugs at clinically relevant doses. Cancer Res 1992;52:3796-800.
22. Crowson AN, Magro CM. Antidepressant therapy. Arch Dermatol 1995;131:925-9.
23. Sternbach H. Are antidepressants carcinogenic? A review of preclinical and clinical studies. J Clin Psychiatry 2003;64:1153-62.
24. Xu W, Tamim H, Shapiro S, et al. Use of antidepressants and risk of colorectal cancer: a nested case-control study. Lancet Oncol 2006;7:301-8.
25. Brustolim D, Ribeiro-dos-Santos R, Kast RE, et al. A new chapter opens in anti-inflammatory treatments: the antidepressant bupropion lowers production of tumor necrosis factor-alpha and interferon-gamma in mice. Int Immunopharmacol 2006;6:903-7.
26. Lass-Flörl C, Dierich MP, Fuchs D, et al. Antifungal activity against Candida species of the selective serotonin-reuptake inhibitor, sertraline. Clin Infect Dis 2001;33:e135-6.
27. Waldinger MD, Hengeveld MW, Zsinderman AH, Olivier B. Effect of SSRI antidepressants on ejaculation: a double-blind, randomized, placebo-controlled study with fluoxetine, fluvoxamine, paroxetine, and sertraline. J Clin Psychopharmacol 1998;18(4):274-81.
28. Pryor JL, Althof SE, Steidle C, et al. Efficacy and tolerability of dapoxetine in treatment of premature ejaculation: an integrated analysis of two double-blind, randomised controlled trials. Lancet 2006;368:929-37.
29. Kumar VS, Sharma VL, Tiwari P, et al. The spermicidal and antitrichomonas activities of SSRI antidepressants. Bioorg Med Chem Lett 2006;16:2509-12.
A molecule is a molecule is a molecule—until it becomes identified with a purpose. Consider, for example, (-)-trans-4R-(4’-fluorophenyl)-3S-[(3’,4’-methylenedioxyphenoxy) methyl] piperidine. You probably know this molecule as paroxetine—an antidepressant, of course, but it is more than that. If you examine paroxetine’s FDA-approved indications, it also has anti-panic, anti-social anxiety, anti-obsessive-compulsive disorder, anti-posttraumatic stress disorder, and anti-premenstrual dysphoric disorder effects.
“Antidepressants” have achieved fame as antidepressants; one could say these molecules’ search for meaning has been fulfilled. Yet even within psychiatry, their many other uses (Table) can create semantic misunderstandings. Beyond psychiatry, consider the nondepressed patient with neurocardiogenic syncope who wonders why he’s being treated with an antidepressant.
Rather than calling antidepressants “panaceas,” the better choice is to educate patients about the drugs’ wide spectrum of activity. Let’s look broadly across the so-called antidepressants and examine their varied uses in psychiatry and other medical specialties.
Table
FDA-approved psychiatric indications for serotonin uptake inhibitors*
| SSRIs | ||||||||
| Citalopram | X | |||||||
| Escitalopram | X | X | ||||||
| Fluoxetine | X | X | X | X | X | |||
| Fluvoxamine | X | |||||||
| Paroxetine | X | X | X | X | X | X | X | |
| Sertraline | X | X | X | X | X | X | ||
| SNRIs | ||||||||
| Duloxetine | X | X | ||||||
| Venlafaxine | X | X | X | X | ||||
| SSRIs: selective serotonin reuptake inhibitors; SNRIs: serotonin-norepinephrine reuptake inhibitors; MDD: major depressive disorder; PD: panic disorder; SAD: social anxiety disorder; PTSD: posttraumatic stress disorder; GAD: generalized anxiety disorder; OCD: obsessive-compulsive disorder; PMDD: premenstrual dysphoric disorder; BUL: bulimia | ||||||||
| * The absence of an X does not necessarily imply that a drug is ineffective for a given indication but, more likely, that definitive studies are lacking. | ||||||||
Pain syndromes
Peripheral neuropathy. The only antidepressant with an FDA-approved pain indication is duloxetine, a serotonin-norepinephrine reuptake inhibitor (SNRI). Its approval for diabetic peripheral neuropathic pain (DPNP) was based on two 12-week, randomized, double-blind, placebo-controlled studies using fixed doses of 60 mg once or twice daily.1,2 Another SNRI—venlafaxine XR, 150 to 225 mg/d, but not 75 mg/d—also was found to be more effective than placebo for this indication in a 6-week, double-blind study (Box 1).3
Using antidepressants to treat pain syndromes is neither new nor restricted to SNRIs, however. In combined double-blind, cross-over studies of patients with DPNP, Max et al4 found:
- moderate or greater pain relief in 74% and 61% of subjects, respectively, from the tricyclics amitriptyline, mean 105 mg/d, and desipramine, mean 111 mg/d—with pain reduced by equal amounts in depressed and nondepressed patients
- no statistically significant difference in pain relief between the selective serotonin reuptake inhibitor (SSRI) fluoxetine, 40 mg/d, and placebo.
- tricyclics: 1 in every 2 to 3 patients
- SNRIs: 1 in every 4 to 5 patients
- SSRIs: 1 in every 7 patients.
Chronic headache. A meta-analysis7 of randomized, placebo-controlled studies found antidepressants more effective than placebo for chronic migraine and tension headache prophylaxis. Although a subgroup meta-analysis found similar effects for tricyclics and SSRIs, the authors characterized the tricyclics’ results as well established and the SSRIs’ as “less certain.”
The results of this meta-analysis might not accurately reflect bona fide antidepressants, however. Some of the 38 studies (25 of migraine, 12 of tension headache, 1 of both) included treatment with serotonin antagonists—most commonly pizotifen, which is not available in the United States and does not appear to be an antidepressant.
Back pain. Patients with chronic low back pain (average 10 years) seem to benefit from antidepressants, according to a meta-analysis of 9 randomized, controlled trials by Salerno et al.8 The effect on pain in the total 504 patients was “small but significant,” and improvement in function was “small but nonsignificant.” Individual sample sizes also were small, however, and only 2 studies excluded depressed patients.
Fibromyalgia, with chronic generalized musculoskeletal pain and tenderness, has been a focus of antidepressant drug therapy. Goldenberg et al9 concluded from an ambitious literature review (505 articles) that evidence of efficacy was strong for amitripty-line and modest for SSRIs and SNRIs.
Overall, antidepressants are generally understood to have analgesic effects in the absence of depression. Benefits for patients with pain syndromes are well established for tricyclics (especially amitriptyline) and recently with SNRIs, whereas SSRIs are less effective.
Serotonin and norepinephrine are involved in pain modulation via descending inhibitory pathways in the brain and spinal cord. Serotonin-norepinephrine reuptake inhibitors (SNRIs) have been shown to reduce the severity of diabetic peripheral neuropathic pain (DPNP) in randomized controlled trials.
Duloxetine. In 2 double-blind studies,1,2 nondepressed patients with DPNP received duloxetine, 60 mg once daily; duloxetine, 60 mg bid; or placebo for 12 weeks. They rated the severity of neuropathic pain every 24 hours on an 11-point Likert scale, and weekly mean scores were the primary outcome measure. Average pain scores improved more in both duloxetine groups vs placebo. Duloxetine treatment did not interfere with diabetic control, and both dosages were well tolerated.
The FDA approved an added indication for duloxetine in the management of DPNP.
Venlafaxine. In a double-blind study,3 244 adult outpatients with moderately severe DPNP received venlafaxine ER, 75 or 150 to 225 mg/d, or placebo for 6 weeks. Daily scores on the Visual Analog Pain Intensity (VAS-PI) and Pain Relief (VAS-PR) scales were primary efficacy measures.
Patients receiving the higher venlafaxine dosage—but not 75 mg/d—showed statistically significant less-intensive pain vs placebo. VAS-PI scores were 27% lower than at enrollment with placebo, 32% lower with venlafaxine, 75 mg/d, and 50% lower with venlafaxine, 150 to 225 mg/d (P
Nausea and somnolence were the most common side effects; clinically important ECG changes occurred in 7 patients treated with venlafaxine, 150 to 225 mg/d.
Smoking cessation
Bupropion SR is FDA-approved to aid smoking cessation, and this effect is independent of the drug’s antidepressant activity. Bupropion may act as a nicotine receptor antagonist as well as a norepinephrine dopamine reuptake inhibitor.
Other antidepressants have been studied for smoking cessation, with nortriptyline showing benefit in 2 large placebo-controlled trials. Studies with doxepin, fluoxetine, and moclobemide found little or no benefit for this indication.
Cardiovascular uses
Angina. Monoamine oxidase inhibitor (MAOI) antidepressants were used to treat angina pectoris in the late 1950s and early 1960s. This practice stopped after evidence showed that whereas angina pain may have improved with MAOIs, stress-induced ischemia on ECG did not.
Antiarrhythmia. Tricyclics had a brief fling in cardiovascular therapeutics when their quinidine-like class I antiarrhythmic activity was recognized. Imipramine was one of several drugs included in the Cardiac Arrhythmia Pilot Study in the 1980s that involved 502 postmyocardial infarction patients with ventricular arrhythmias. Imipramine was the least effective of the 4 drugs studied and the least well tolerated.13
variety of medications. Options include the vasopressor midodrine, fludrocortisone, beta blockers, and SSRIs— none
FDA-approved for this indication. Paroxetine, 20 mg/d, was considerably more effective than placebo in preventing
recurrent syncope in 68 patients who had been unresponsive
to or intolerant of traditional medications. During a mean 25 months of treatment, 82% of patients remained syncope-free on paroxetine vs 47% on placebo.14
Selective serotonin reuptake inhibitors (SSRIs) often are used to treat irritable bowel syndrome (IBS), though evidence of their effectiveness is scarce. SSRIs can improve IBS patients’ quality of life, but effects on abdominal pain and bloating are less clear.
Paroxetine. In a randomized, double-blind trial,16 gastroenterologists tested a highfiber diet plus paroxetine in nondepressed patients with IBS. Ninety-eight patients ages 18 to 65 who experienced IBS symptoms on low- or average-fiber diets were first put on high-fiber diets and assessed for well-being and abdominal pain and bloating. Of these, 81 symptomatic patients continued highfiber diets with added paroxetine, 10 to 40 mg/d (n=38) or placebo (n=43).
With paroxetine, patients’ overall well-being improved more than with placebo, but abdominal pain and bloating and social functioning did not.
Fluoxetine. In a double-blind, randomized trial,17 44 patients with pain and constipation-predominant IBS received fluoxetine, 20 mg/d, or placebo for 12 weeks. These patients met Rome II criteria for IBS—abdominal discomfort/pain for ≥12 weeks in past year that met 2 of 3 criteria:
- relieved by defecation
- onset associated with change in stool frequency
- onset associated with change in stool appearance.
Patients receiving fluoxetine had less abdominal discomfort, less bloating, more frequent bowel movements, and decreased consistency of stool vs placebo 4 weeks after treatment stopped. Mean number of symptoms per patient decreased from 4.6 to 0.7 in the fluoxetine group vs 4.5 to 2.9 in controls (P
Citalopram. IBS symptom severity was the primary outcome in a crossover trial comparing citalopram (20 mg for 3 weeks and 40 mg for 3 weeks) with placebo in 23 nondepressed patients.18 Abdominal pain and bloating, impact of symptoms on daily life, and overall well-being improved significantly more with citalopram than with placebo after 3 and 6 weeks.
Symptom improvements were not related to changes in depression, anxiety, or colonic sensorimotor function.
Gastrointestinal
Peptic ulcer disease was shown in the 1980s to respond to tricyclic antidepressants. At the time, both anticholinergic and antihistaminic effects were thought to be responsible, but the later observation that trimipramine inhibited Campylobacter pylori in vitro suggested an additional explanation. Today, tricyclics are only of historic interest as treatments for peptic ulcer.
Irritable bowel syndrome (IBS) patients have responded favorably to antidepressants, although it is often difficult to know if the benefit is independent of improved coexisting anxiety or depression. A meta-analysis of 12 randomized, placebo-controlled trials—mostly with tricyclics—found an odds ratio for improvement of 4.2 and a number needed to treat of 3.2.15
More recently, a few placebo-controlled studies have shown SSRIs to be beneficial for IBS,16-18 although not all symptoms improved and some IBS subtypes might be more responsive than others (Box 2). In an editorial, Talley19 concluded that antidepressant therapy of IBS was “at best only a ‘band-aid’ approach to management.”
Genitourinary
Nocturnal enuresis. In the 1960s, imipramine was shown—in some but not all placebo-controlled studies—to be beneficial for nocturnal enuresis in children and adults. Although imipramine is not FDA-approved for this indication, it is thought to work by relaxing bladder muscle and contracting bladder neck smooth muscle. Imipramine appears to have a vasopressin-independent antidiuretic effect in enuretic patients with nocturnal polyuria.
Duloxetine is thought to improve stress urinary incontinence by increasing urethral sphincter tone and the force of sphincter contraction. This indication is not FDA- approved for duloxetine but is approved in the European Union.
Oncology
At one time antidepressants were suggested to promote tumors, based on observations that amitriptyline, fluoxetine, and several antihistamines promoted tumor growth in rodents.21 In 1995, a few case reports associated these 2 antidepressants with atypical cutaneous lymphoid infiltrates.22 A review by Sternback in 200323 concluded that a link between antidepressants and cancer was questionable but acknowledged the need for very long-term studies.
Recently, a nested case-control study found an association between high-dose SSRI use for ≤5 years and reduced risk of colorectal cancer, whereas no association was found with tricyclic use.24 A study of this design does not establish a causal relationship, how-ever, and one can only speculate whether SSRIs might have direct cytotoxic or anti-promoter effects.
At present, it seems reasonable to continue to treat depressed cancer patients with antidepressants without concern that cancer will worsen or hope that it will improve as a result.
Immunology
The pathogenesis of depression may be linked to pro-inflammatory cytokines—proteins such as tumor necrosis factor-alpha (TNF-α) and certain interleukins that mediate immune function. Bupropion markedly lowered pro-inflammatory cytokine levels in a mouse inflammation model, prompting the authors to suggest that this anti-inflammatory effect be explored in humans.25
Case reports have suggested benefit from bupropion in Crohn’s disease, recurrent aphthous ulcerations, psoriasis, atopic dermatitis, and Blau syndrome (a rare autosomal-dominant trait characterized by granulomatous arthritis, iritis, and skin rash). Whether this antidepressant has much anti-inflammatory potential remains to be determined, however.
Delayed ejaculation is among the sexual side effects commonly associated with antidepressant medication. In a 6-week trial,27 3 selective serotonin reuptake inhibitors (SSRIs)— paroxetine, fluoxetine, and sertraline— were shown to improve intravaginal ejaculatory latency time (IELT) in men with lifelong rapid ejaculation. Compared with baseline, the greatest delay in ejaculation was seen with paroxetine, 20 mg/d, followed by fluoxetine, 20 mg/d, and then sertraline, 50 mg/d, whereas delay with fluvoxamine, 100 mg/d, did not differ significantly from placebo.
Dapoxetine is a non-antidepressant SSRI under investigation for on-demand treatment of moderate-to-severe premature ejaculation.28 In two 12-week, randomized, double-blind, placebo-controlled trials, 870 men took placebo, 874 took 30-mg dapoxetine, and 870 took 60-mg dapoxetine 1 to 3 hours before sexual activity. Efficacy was determined by IELT measured at home by stopwatch.
Both dapoxetine doses improved IELT significantly more than placebo (P
Nausea, diarrhea, headache, and dizziness occurred in ≤20% of patients and were more common with the 60-mg than 30-mg dapoxetine dose.
Infectious disease
Pathogenic protozoa—such as Trypanosoma cruzi (Chagas disease), Leishmania donovani (Kala-azar), Leishmania major (Oriental sore), and Giardia lamblia (Giardiasis)—infect millions of humans worldwide. Clomipramine has been shown in vitro and in mice to inhibit or kill these protozoa, but these potential benefits have not been extended to humans.
Sertraline, on the other hand, might exert antifungal activity. Three patients with recurrent vulvovaginal candidiasis had no episodes while being treated with sertraline for premenstrual dysphoric disorder but relapsed when the drug was discontinued.26 Although sertraline demonstrated antifungal activity in vitro against several Candida species, this SSRI seems unlikely to gain prominence as an antifungal agent.
Sexual function
Premature ejaculation. SSRIs are well-known causes of delayed or absent orgasm, but a perceived liability can become an asset in treating premature ejaculation. By measuring intravaginal ejaculation latency time under double-blind, placebo-controlled conditions, Waldinger et al27 showed pronounced delay in ejaculation with sertraline, fluoxetine, and paroxetine in men with long-standing rapid ejaculation. Dapoxetine—a short-acting non-antidepressant SSRI—is being studied as a treatment for this condition (Box 3).28
Spermicidal effect. SSRIs—including fluoxetine— have demonstrated in vitro spermicidal and antitrichomonas activity29 but are unlikely to be developed as microbicidal contraceptives.
Related Resources
- Gorman JM, Kent JM. SSRIs and SMRIs: broad spectrum of efficacy beyond major depression. J Clin Psychiatry 1999;60(suppl 4):33-8.
- About.com: Mental Health. Antidepressants for more than depression. http://mentalhealth.about.com/cs/psychopharmacology/a/antimore.htm.
- Amitriptyline • Elavil, Endep
- Bupropion • Wellbutrin, Zyban
- Citalopram • Celexa
- Clomipramine • Anafranil
- Desipramine • Norpramin, Pertofrane
- Doxepin • Adapin, Sinequan
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fludrocortisone • Florinef
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranil
- Midodrine • ProAmitine
- Nortriptyline • Pamelor, Aventyl
- Paroxetine • Paxil
- Phenelzine • Nardil
- Sertraline • Zoloft
- Trimipramine • Surmontil
- Venlafaxine • Effexor
Dr. Jefferson receives research support from Bristol-Myers Squibb, Forest Pharmaceuticals, GlaxoSmithKline, Janssen Pharmaceutica, Eli Lilly and Company, Novartis, Pfizer, Roche, Solvay, UCB Pharma, and Wyeth. He is a consultant to GlaxoSmithKline, Schwarz Pharma, Shire, and Organon and a speaker for Abbott Laboratories, AstraZeneca, Bristol-Myers Squibb, Forest Pharmaceuticals, GlaxoSmithKline, Eli Lilly and Company, Pfizer, Schwarz Pharma, Shire, and Wyeth. He holds stock in Bristol-Myers Squibb, GlaxoSmithKline, and SciClone.
A molecule is a molecule is a molecule—until it becomes identified with a purpose. Consider, for example, (-)-trans-4R-(4’-fluorophenyl)-3S-[(3’,4’-methylenedioxyphenoxy) methyl] piperidine. You probably know this molecule as paroxetine—an antidepressant, of course, but it is more than that. If you examine paroxetine’s FDA-approved indications, it also has anti-panic, anti-social anxiety, anti-obsessive-compulsive disorder, anti-posttraumatic stress disorder, and anti-premenstrual dysphoric disorder effects.
“Antidepressants” have achieved fame as antidepressants; one could say these molecules’ search for meaning has been fulfilled. Yet even within psychiatry, their many other uses (Table) can create semantic misunderstandings. Beyond psychiatry, consider the nondepressed patient with neurocardiogenic syncope who wonders why he’s being treated with an antidepressant.
Rather than calling antidepressants “panaceas,” the better choice is to educate patients about the drugs’ wide spectrum of activity. Let’s look broadly across the so-called antidepressants and examine their varied uses in psychiatry and other medical specialties.
Table
FDA-approved psychiatric indications for serotonin uptake inhibitors*
| SSRIs | ||||||||
| Citalopram | X | |||||||
| Escitalopram | X | X | ||||||
| Fluoxetine | X | X | X | X | X | |||
| Fluvoxamine | X | |||||||
| Paroxetine | X | X | X | X | X | X | X | |
| Sertraline | X | X | X | X | X | X | ||
| SNRIs | ||||||||
| Duloxetine | X | X | ||||||
| Venlafaxine | X | X | X | X | ||||
| SSRIs: selective serotonin reuptake inhibitors; SNRIs: serotonin-norepinephrine reuptake inhibitors; MDD: major depressive disorder; PD: panic disorder; SAD: social anxiety disorder; PTSD: posttraumatic stress disorder; GAD: generalized anxiety disorder; OCD: obsessive-compulsive disorder; PMDD: premenstrual dysphoric disorder; BUL: bulimia | ||||||||
| * The absence of an X does not necessarily imply that a drug is ineffective for a given indication but, more likely, that definitive studies are lacking. | ||||||||
Pain syndromes
Peripheral neuropathy. The only antidepressant with an FDA-approved pain indication is duloxetine, a serotonin-norepinephrine reuptake inhibitor (SNRI). Its approval for diabetic peripheral neuropathic pain (DPNP) was based on two 12-week, randomized, double-blind, placebo-controlled studies using fixed doses of 60 mg once or twice daily.1,2 Another SNRI—venlafaxine XR, 150 to 225 mg/d, but not 75 mg/d—also was found to be more effective than placebo for this indication in a 6-week, double-blind study (Box 1).3
Using antidepressants to treat pain syndromes is neither new nor restricted to SNRIs, however. In combined double-blind, cross-over studies of patients with DPNP, Max et al4 found:
- moderate or greater pain relief in 74% and 61% of subjects, respectively, from the tricyclics amitriptyline, mean 105 mg/d, and desipramine, mean 111 mg/d—with pain reduced by equal amounts in depressed and nondepressed patients
- no statistically significant difference in pain relief between the selective serotonin reuptake inhibitor (SSRI) fluoxetine, 40 mg/d, and placebo.
- tricyclics: 1 in every 2 to 3 patients
- SNRIs: 1 in every 4 to 5 patients
- SSRIs: 1 in every 7 patients.
Chronic headache. A meta-analysis7 of randomized, placebo-controlled studies found antidepressants more effective than placebo for chronic migraine and tension headache prophylaxis. Although a subgroup meta-analysis found similar effects for tricyclics and SSRIs, the authors characterized the tricyclics’ results as well established and the SSRIs’ as “less certain.”
The results of this meta-analysis might not accurately reflect bona fide antidepressants, however. Some of the 38 studies (25 of migraine, 12 of tension headache, 1 of both) included treatment with serotonin antagonists—most commonly pizotifen, which is not available in the United States and does not appear to be an antidepressant.
Back pain. Patients with chronic low back pain (average 10 years) seem to benefit from antidepressants, according to a meta-analysis of 9 randomized, controlled trials by Salerno et al.8 The effect on pain in the total 504 patients was “small but significant,” and improvement in function was “small but nonsignificant.” Individual sample sizes also were small, however, and only 2 studies excluded depressed patients.
Fibromyalgia, with chronic generalized musculoskeletal pain and tenderness, has been a focus of antidepressant drug therapy. Goldenberg et al9 concluded from an ambitious literature review (505 articles) that evidence of efficacy was strong for amitripty-line and modest for SSRIs and SNRIs.
Overall, antidepressants are generally understood to have analgesic effects in the absence of depression. Benefits for patients with pain syndromes are well established for tricyclics (especially amitriptyline) and recently with SNRIs, whereas SSRIs are less effective.
Serotonin and norepinephrine are involved in pain modulation via descending inhibitory pathways in the brain and spinal cord. Serotonin-norepinephrine reuptake inhibitors (SNRIs) have been shown to reduce the severity of diabetic peripheral neuropathic pain (DPNP) in randomized controlled trials.
Duloxetine. In 2 double-blind studies,1,2 nondepressed patients with DPNP received duloxetine, 60 mg once daily; duloxetine, 60 mg bid; or placebo for 12 weeks. They rated the severity of neuropathic pain every 24 hours on an 11-point Likert scale, and weekly mean scores were the primary outcome measure. Average pain scores improved more in both duloxetine groups vs placebo. Duloxetine treatment did not interfere with diabetic control, and both dosages were well tolerated.
The FDA approved an added indication for duloxetine in the management of DPNP.
Venlafaxine. In a double-blind study,3 244 adult outpatients with moderately severe DPNP received venlafaxine ER, 75 or 150 to 225 mg/d, or placebo for 6 weeks. Daily scores on the Visual Analog Pain Intensity (VAS-PI) and Pain Relief (VAS-PR) scales were primary efficacy measures.
Patients receiving the higher venlafaxine dosage—but not 75 mg/d—showed statistically significant less-intensive pain vs placebo. VAS-PI scores were 27% lower than at enrollment with placebo, 32% lower with venlafaxine, 75 mg/d, and 50% lower with venlafaxine, 150 to 225 mg/d (P
Nausea and somnolence were the most common side effects; clinically important ECG changes occurred in 7 patients treated with venlafaxine, 150 to 225 mg/d.
Smoking cessation
Bupropion SR is FDA-approved to aid smoking cessation, and this effect is independent of the drug’s antidepressant activity. Bupropion may act as a nicotine receptor antagonist as well as a norepinephrine dopamine reuptake inhibitor.
Other antidepressants have been studied for smoking cessation, with nortriptyline showing benefit in 2 large placebo-controlled trials. Studies with doxepin, fluoxetine, and moclobemide found little or no benefit for this indication.
Cardiovascular uses
Angina. Monoamine oxidase inhibitor (MAOI) antidepressants were used to treat angina pectoris in the late 1950s and early 1960s. This practice stopped after evidence showed that whereas angina pain may have improved with MAOIs, stress-induced ischemia on ECG did not.
Antiarrhythmia. Tricyclics had a brief fling in cardiovascular therapeutics when their quinidine-like class I antiarrhythmic activity was recognized. Imipramine was one of several drugs included in the Cardiac Arrhythmia Pilot Study in the 1980s that involved 502 postmyocardial infarction patients with ventricular arrhythmias. Imipramine was the least effective of the 4 drugs studied and the least well tolerated.13
variety of medications. Options include the vasopressor midodrine, fludrocortisone, beta blockers, and SSRIs— none
FDA-approved for this indication. Paroxetine, 20 mg/d, was considerably more effective than placebo in preventing
recurrent syncope in 68 patients who had been unresponsive
to or intolerant of traditional medications. During a mean 25 months of treatment, 82% of patients remained syncope-free on paroxetine vs 47% on placebo.14
Selective serotonin reuptake inhibitors (SSRIs) often are used to treat irritable bowel syndrome (IBS), though evidence of their effectiveness is scarce. SSRIs can improve IBS patients’ quality of life, but effects on abdominal pain and bloating are less clear.
Paroxetine. In a randomized, double-blind trial,16 gastroenterologists tested a highfiber diet plus paroxetine in nondepressed patients with IBS. Ninety-eight patients ages 18 to 65 who experienced IBS symptoms on low- or average-fiber diets were first put on high-fiber diets and assessed for well-being and abdominal pain and bloating. Of these, 81 symptomatic patients continued highfiber diets with added paroxetine, 10 to 40 mg/d (n=38) or placebo (n=43).
With paroxetine, patients’ overall well-being improved more than with placebo, but abdominal pain and bloating and social functioning did not.
Fluoxetine. In a double-blind, randomized trial,17 44 patients with pain and constipation-predominant IBS received fluoxetine, 20 mg/d, or placebo for 12 weeks. These patients met Rome II criteria for IBS—abdominal discomfort/pain for ≥12 weeks in past year that met 2 of 3 criteria:
- relieved by defecation
- onset associated with change in stool frequency
- onset associated with change in stool appearance.
Patients receiving fluoxetine had less abdominal discomfort, less bloating, more frequent bowel movements, and decreased consistency of stool vs placebo 4 weeks after treatment stopped. Mean number of symptoms per patient decreased from 4.6 to 0.7 in the fluoxetine group vs 4.5 to 2.9 in controls (P
Citalopram. IBS symptom severity was the primary outcome in a crossover trial comparing citalopram (20 mg for 3 weeks and 40 mg for 3 weeks) with placebo in 23 nondepressed patients.18 Abdominal pain and bloating, impact of symptoms on daily life, and overall well-being improved significantly more with citalopram than with placebo after 3 and 6 weeks.
Symptom improvements were not related to changes in depression, anxiety, or colonic sensorimotor function.
Gastrointestinal
Peptic ulcer disease was shown in the 1980s to respond to tricyclic antidepressants. At the time, both anticholinergic and antihistaminic effects were thought to be responsible, but the later observation that trimipramine inhibited Campylobacter pylori in vitro suggested an additional explanation. Today, tricyclics are only of historic interest as treatments for peptic ulcer.
Irritable bowel syndrome (IBS) patients have responded favorably to antidepressants, although it is often difficult to know if the benefit is independent of improved coexisting anxiety or depression. A meta-analysis of 12 randomized, placebo-controlled trials—mostly with tricyclics—found an odds ratio for improvement of 4.2 and a number needed to treat of 3.2.15
More recently, a few placebo-controlled studies have shown SSRIs to be beneficial for IBS,16-18 although not all symptoms improved and some IBS subtypes might be more responsive than others (Box 2). In an editorial, Talley19 concluded that antidepressant therapy of IBS was “at best only a ‘band-aid’ approach to management.”
Genitourinary
Nocturnal enuresis. In the 1960s, imipramine was shown—in some but not all placebo-controlled studies—to be beneficial for nocturnal enuresis in children and adults. Although imipramine is not FDA-approved for this indication, it is thought to work by relaxing bladder muscle and contracting bladder neck smooth muscle. Imipramine appears to have a vasopressin-independent antidiuretic effect in enuretic patients with nocturnal polyuria.
Duloxetine is thought to improve stress urinary incontinence by increasing urethral sphincter tone and the force of sphincter contraction. This indication is not FDA- approved for duloxetine but is approved in the European Union.
Oncology
At one time antidepressants were suggested to promote tumors, based on observations that amitriptyline, fluoxetine, and several antihistamines promoted tumor growth in rodents.21 In 1995, a few case reports associated these 2 antidepressants with atypical cutaneous lymphoid infiltrates.22 A review by Sternback in 200323 concluded that a link between antidepressants and cancer was questionable but acknowledged the need for very long-term studies.
Recently, a nested case-control study found an association between high-dose SSRI use for ≤5 years and reduced risk of colorectal cancer, whereas no association was found with tricyclic use.24 A study of this design does not establish a causal relationship, how-ever, and one can only speculate whether SSRIs might have direct cytotoxic or anti-promoter effects.
At present, it seems reasonable to continue to treat depressed cancer patients with antidepressants without concern that cancer will worsen or hope that it will improve as a result.
Immunology
The pathogenesis of depression may be linked to pro-inflammatory cytokines—proteins such as tumor necrosis factor-alpha (TNF-α) and certain interleukins that mediate immune function. Bupropion markedly lowered pro-inflammatory cytokine levels in a mouse inflammation model, prompting the authors to suggest that this anti-inflammatory effect be explored in humans.25
Case reports have suggested benefit from bupropion in Crohn’s disease, recurrent aphthous ulcerations, psoriasis, atopic dermatitis, and Blau syndrome (a rare autosomal-dominant trait characterized by granulomatous arthritis, iritis, and skin rash). Whether this antidepressant has much anti-inflammatory potential remains to be determined, however.
Delayed ejaculation is among the sexual side effects commonly associated with antidepressant medication. In a 6-week trial,27 3 selective serotonin reuptake inhibitors (SSRIs)— paroxetine, fluoxetine, and sertraline— were shown to improve intravaginal ejaculatory latency time (IELT) in men with lifelong rapid ejaculation. Compared with baseline, the greatest delay in ejaculation was seen with paroxetine, 20 mg/d, followed by fluoxetine, 20 mg/d, and then sertraline, 50 mg/d, whereas delay with fluvoxamine, 100 mg/d, did not differ significantly from placebo.
Dapoxetine is a non-antidepressant SSRI under investigation for on-demand treatment of moderate-to-severe premature ejaculation.28 In two 12-week, randomized, double-blind, placebo-controlled trials, 870 men took placebo, 874 took 30-mg dapoxetine, and 870 took 60-mg dapoxetine 1 to 3 hours before sexual activity. Efficacy was determined by IELT measured at home by stopwatch.
Both dapoxetine doses improved IELT significantly more than placebo (P
Nausea, diarrhea, headache, and dizziness occurred in ≤20% of patients and were more common with the 60-mg than 30-mg dapoxetine dose.
Infectious disease
Pathogenic protozoa—such as Trypanosoma cruzi (Chagas disease), Leishmania donovani (Kala-azar), Leishmania major (Oriental sore), and Giardia lamblia (Giardiasis)—infect millions of humans worldwide. Clomipramine has been shown in vitro and in mice to inhibit or kill these protozoa, but these potential benefits have not been extended to humans.
Sertraline, on the other hand, might exert antifungal activity. Three patients with recurrent vulvovaginal candidiasis had no episodes while being treated with sertraline for premenstrual dysphoric disorder but relapsed when the drug was discontinued.26 Although sertraline demonstrated antifungal activity in vitro against several Candida species, this SSRI seems unlikely to gain prominence as an antifungal agent.
Sexual function
Premature ejaculation. SSRIs are well-known causes of delayed or absent orgasm, but a perceived liability can become an asset in treating premature ejaculation. By measuring intravaginal ejaculation latency time under double-blind, placebo-controlled conditions, Waldinger et al27 showed pronounced delay in ejaculation with sertraline, fluoxetine, and paroxetine in men with long-standing rapid ejaculation. Dapoxetine—a short-acting non-antidepressant SSRI—is being studied as a treatment for this condition (Box 3).28
Spermicidal effect. SSRIs—including fluoxetine— have demonstrated in vitro spermicidal and antitrichomonas activity29 but are unlikely to be developed as microbicidal contraceptives.
Related Resources
- Gorman JM, Kent JM. SSRIs and SMRIs: broad spectrum of efficacy beyond major depression. J Clin Psychiatry 1999;60(suppl 4):33-8.
- About.com: Mental Health. Antidepressants for more than depression. http://mentalhealth.about.com/cs/psychopharmacology/a/antimore.htm.
- Amitriptyline • Elavil, Endep
- Bupropion • Wellbutrin, Zyban
- Citalopram • Celexa
- Clomipramine • Anafranil
- Desipramine • Norpramin, Pertofrane
- Doxepin • Adapin, Sinequan
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fludrocortisone • Florinef
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranil
- Midodrine • ProAmitine
- Nortriptyline • Pamelor, Aventyl
- Paroxetine • Paxil
- Phenelzine • Nardil
- Sertraline • Zoloft
- Trimipramine • Surmontil
- Venlafaxine • Effexor
Dr. Jefferson receives research support from Bristol-Myers Squibb, Forest Pharmaceuticals, GlaxoSmithKline, Janssen Pharmaceutica, Eli Lilly and Company, Novartis, Pfizer, Roche, Solvay, UCB Pharma, and Wyeth. He is a consultant to GlaxoSmithKline, Schwarz Pharma, Shire, and Organon and a speaker for Abbott Laboratories, AstraZeneca, Bristol-Myers Squibb, Forest Pharmaceuticals, GlaxoSmithKline, Eli Lilly and Company, Pfizer, Schwarz Pharma, Shire, and Wyeth. He holds stock in Bristol-Myers Squibb, GlaxoSmithKline, and SciClone.
1. Wernicke JF, Pritchett YL, D’Souza DN, et al. A randomized controlled trial of duloxetine in diabetic peripheral neuropathic pain. Neurology 2006;67(8):1411-20.
2. Raskin J, Pritchett YL, Wang F, et al. A double-blind, randomized multicenter trial comparing duloxetine with placebo in the management of diabetic peripheral neuropathic pain. Pain Med 2005;6(5):346-56.
3. Rowbotham MC, Goli V, Kunz NR, Lei D. Venlafaxine extended release in the treatment of painful diabetic neuropathy: a double-blind, placebo-controlled study. Pain 2004;110:697-706.
4. Max MB, Lynch SA, Muir J, et al. Effects of desipramine, amitriptyline, and fluoxetine on pain in diabetic neuropathy. N Engl J Med 1992;326:1250-6.
5. Sindrup SH, Otto M, Finnerup NB, Jensen TS. Antidepressants in the treatment of neuropathic pain. Basic Clin Pharmacol Toxicol 2005;96:399-409.
6. Semenchuk MR, Sherman S, Davis B. Double-blind, randomized trial of bupropion SR for the treatment of neuropathic pain. Neurology 2001;57:1583-8.
7. Tomkins GE, Jackson JL, O’Malley PG, et al. Treatment of chronic headache with antidepressants: a meta-analysis. Am J Med 2001;111:54-63.
8. Salerno SM, Browning R, Jackson JL. The effect of antidepressant treatment on chronic back pain. Arch Intern Med 2002;162:19-24.
9. Goldenberg DL, Burckhardt C, Crofford L. Management of fibromyalgia syndrome. JAMA 2004;292:2388-95.
10. Littlejohn GO, Guymer EK. Fibromyalgia syndrome: which antidepressant drug should we choose. Curr Pharm Des 2006;12(1):3-9.
11. Arnold LM, Lu Y, Crofford LJ, et al. A double-blind, multicenter trial comparing duloxetine with placebo in the treatment of fibromyalgia patients with or without major depressive disorder. Arthritis Rheum 2004;50:2974-84.
12. Arnold LM, Rosen A, Pritchett YL, et al. A randomized, double-blind, placebo-controlled trial of duloxetine in the treatment of women with fibromyalgia with or without major depressive disorder. Pain 2005;119:5-15.
13. Effects of encainide, flecainide, imipramine and moricizine on ventricular arrhythmias during the year after acute myocardial infarction: The CAPS. The Cardiac Arrhythmia Pilot Study (CAPS) Investigators. Am J Cardiol 1988;61(8):501-9.
14. Di Girolamo E, Di Iorio C, Sabatini P, et al. Effects of paroxetine hydrochloride, a selective serotonin reuptake inhibitor, on refractory vasovagal syncope: a randomized, double-blind, placebo-controlled study. J Am Coll Cardiol 1999;33:1227-30.
15. Jackson JL, O’Malley PG, Tomkins G, et al. Treatment of functional gastrointestinal disorders with antidepressant medications: a meta-analysis. Am J Med 2000;108:65-72.
16. Tabas G, Beaves M, Wang J, et al. Paroxetine to treat irritable bowel syndrome not responding to high-fiber diet: a double-blind, placebo-controlled trial. Am J Gastroenterol 2004;99(5):914-20.
17. Vahedi H, Merat S, Rashidioon A, et al. The effect of fluoxetine in patients with pain and constipation-predominant irritable bowel syndrome: a double-blind randomized-controlled study. Aliment Pharmacol Ther 2005;22:381-5.
18. Tack J, Broekaert D, Fischler B, et al. A controlled crossover study of the selective serotonin reuptake inhibitor citalopram in irritable bowel syndrome. Gut 2006;55:1095-103.
19. Talley NJ. Antidepressants in IBS: are we deluding ourselves? [editorial]. Am J Gastroenterol 2004;99:921-3.
20. Mariappan P, Ballantyne Z, N’Dow JM, Alhasso AA. Serotonin and noradrenaline reuptake inhibitors (SNRI) for stress urinary incontinence in adults. Cochrane Database Syst Rev 2005;Jul 20;(3):CD004742.-
21. Brandes LJ, Arron RJ, Bogdanovic RP, et al. Stimulation of malignant growth in rodents by antidepressant drugs at clinically relevant doses. Cancer Res 1992;52:3796-800.
22. Crowson AN, Magro CM. Antidepressant therapy. Arch Dermatol 1995;131:925-9.
23. Sternbach H. Are antidepressants carcinogenic? A review of preclinical and clinical studies. J Clin Psychiatry 2003;64:1153-62.
24. Xu W, Tamim H, Shapiro S, et al. Use of antidepressants and risk of colorectal cancer: a nested case-control study. Lancet Oncol 2006;7:301-8.
25. Brustolim D, Ribeiro-dos-Santos R, Kast RE, et al. A new chapter opens in anti-inflammatory treatments: the antidepressant bupropion lowers production of tumor necrosis factor-alpha and interferon-gamma in mice. Int Immunopharmacol 2006;6:903-7.
26. Lass-Flörl C, Dierich MP, Fuchs D, et al. Antifungal activity against Candida species of the selective serotonin-reuptake inhibitor, sertraline. Clin Infect Dis 2001;33:e135-6.
27. Waldinger MD, Hengeveld MW, Zsinderman AH, Olivier B. Effect of SSRI antidepressants on ejaculation: a double-blind, randomized, placebo-controlled study with fluoxetine, fluvoxamine, paroxetine, and sertraline. J Clin Psychopharmacol 1998;18(4):274-81.
28. Pryor JL, Althof SE, Steidle C, et al. Efficacy and tolerability of dapoxetine in treatment of premature ejaculation: an integrated analysis of two double-blind, randomised controlled trials. Lancet 2006;368:929-37.
29. Kumar VS, Sharma VL, Tiwari P, et al. The spermicidal and antitrichomonas activities of SSRI antidepressants. Bioorg Med Chem Lett 2006;16:2509-12.
1. Wernicke JF, Pritchett YL, D’Souza DN, et al. A randomized controlled trial of duloxetine in diabetic peripheral neuropathic pain. Neurology 2006;67(8):1411-20.
2. Raskin J, Pritchett YL, Wang F, et al. A double-blind, randomized multicenter trial comparing duloxetine with placebo in the management of diabetic peripheral neuropathic pain. Pain Med 2005;6(5):346-56.
3. Rowbotham MC, Goli V, Kunz NR, Lei D. Venlafaxine extended release in the treatment of painful diabetic neuropathy: a double-blind, placebo-controlled study. Pain 2004;110:697-706.
4. Max MB, Lynch SA, Muir J, et al. Effects of desipramine, amitriptyline, and fluoxetine on pain in diabetic neuropathy. N Engl J Med 1992;326:1250-6.
5. Sindrup SH, Otto M, Finnerup NB, Jensen TS. Antidepressants in the treatment of neuropathic pain. Basic Clin Pharmacol Toxicol 2005;96:399-409.
6. Semenchuk MR, Sherman S, Davis B. Double-blind, randomized trial of bupropion SR for the treatment of neuropathic pain. Neurology 2001;57:1583-8.
7. Tomkins GE, Jackson JL, O’Malley PG, et al. Treatment of chronic headache with antidepressants: a meta-analysis. Am J Med 2001;111:54-63.
8. Salerno SM, Browning R, Jackson JL. The effect of antidepressant treatment on chronic back pain. Arch Intern Med 2002;162:19-24.
9. Goldenberg DL, Burckhardt C, Crofford L. Management of fibromyalgia syndrome. JAMA 2004;292:2388-95.
10. Littlejohn GO, Guymer EK. Fibromyalgia syndrome: which antidepressant drug should we choose. Curr Pharm Des 2006;12(1):3-9.
11. Arnold LM, Lu Y, Crofford LJ, et al. A double-blind, multicenter trial comparing duloxetine with placebo in the treatment of fibromyalgia patients with or without major depressive disorder. Arthritis Rheum 2004;50:2974-84.
12. Arnold LM, Rosen A, Pritchett YL, et al. A randomized, double-blind, placebo-controlled trial of duloxetine in the treatment of women with fibromyalgia with or without major depressive disorder. Pain 2005;119:5-15.
13. Effects of encainide, flecainide, imipramine and moricizine on ventricular arrhythmias during the year after acute myocardial infarction: The CAPS. The Cardiac Arrhythmia Pilot Study (CAPS) Investigators. Am J Cardiol 1988;61(8):501-9.
14. Di Girolamo E, Di Iorio C, Sabatini P, et al. Effects of paroxetine hydrochloride, a selective serotonin reuptake inhibitor, on refractory vasovagal syncope: a randomized, double-blind, placebo-controlled study. J Am Coll Cardiol 1999;33:1227-30.
15. Jackson JL, O’Malley PG, Tomkins G, et al. Treatment of functional gastrointestinal disorders with antidepressant medications: a meta-analysis. Am J Med 2000;108:65-72.
16. Tabas G, Beaves M, Wang J, et al. Paroxetine to treat irritable bowel syndrome not responding to high-fiber diet: a double-blind, placebo-controlled trial. Am J Gastroenterol 2004;99(5):914-20.
17. Vahedi H, Merat S, Rashidioon A, et al. The effect of fluoxetine in patients with pain and constipation-predominant irritable bowel syndrome: a double-blind randomized-controlled study. Aliment Pharmacol Ther 2005;22:381-5.
18. Tack J, Broekaert D, Fischler B, et al. A controlled crossover study of the selective serotonin reuptake inhibitor citalopram in irritable bowel syndrome. Gut 2006;55:1095-103.
19. Talley NJ. Antidepressants in IBS: are we deluding ourselves? [editorial]. Am J Gastroenterol 2004;99:921-3.
20. Mariappan P, Ballantyne Z, N’Dow JM, Alhasso AA. Serotonin and noradrenaline reuptake inhibitors (SNRI) for stress urinary incontinence in adults. Cochrane Database Syst Rev 2005;Jul 20;(3):CD004742.-
21. Brandes LJ, Arron RJ, Bogdanovic RP, et al. Stimulation of malignant growth in rodents by antidepressant drugs at clinically relevant doses. Cancer Res 1992;52:3796-800.
22. Crowson AN, Magro CM. Antidepressant therapy. Arch Dermatol 1995;131:925-9.
23. Sternbach H. Are antidepressants carcinogenic? A review of preclinical and clinical studies. J Clin Psychiatry 2003;64:1153-62.
24. Xu W, Tamim H, Shapiro S, et al. Use of antidepressants and risk of colorectal cancer: a nested case-control study. Lancet Oncol 2006;7:301-8.
25. Brustolim D, Ribeiro-dos-Santos R, Kast RE, et al. A new chapter opens in anti-inflammatory treatments: the antidepressant bupropion lowers production of tumor necrosis factor-alpha and interferon-gamma in mice. Int Immunopharmacol 2006;6:903-7.
26. Lass-Flörl C, Dierich MP, Fuchs D, et al. Antifungal activity against Candida species of the selective serotonin-reuptake inhibitor, sertraline. Clin Infect Dis 2001;33:e135-6.
27. Waldinger MD, Hengeveld MW, Zsinderman AH, Olivier B. Effect of SSRI antidepressants on ejaculation: a double-blind, randomized, placebo-controlled study with fluoxetine, fluvoxamine, paroxetine, and sertraline. J Clin Psychopharmacol 1998;18(4):274-81.
28. Pryor JL, Althof SE, Steidle C, et al. Efficacy and tolerability of dapoxetine in treatment of premature ejaculation: an integrated analysis of two double-blind, randomised controlled trials. Lancet 2006;368:929-37.
29. Kumar VS, Sharma VL, Tiwari P, et al. The spermicidal and antitrichomonas activities of SSRI antidepressants. Bioorg Med Chem Lett 2006;16:2509-12.
Is this child bipolar? What’s needed to improve diagnosis
When does bipolar disorder begin? That question confounds clinicians, worries parents, and is leading researchers such as Kiki D. Chang, MD, to look for answers in families with this highly heritable disorder.
“Parents with bipolar disorder know what’s happening if their children have early symptoms,” Dr. Chang says. “They tell me, ‘I don’t want my child to go through what I went through, and he’s having the same symptoms I did.’”
Dr. Chang believes early psychotherapy and medication might prevent prodromal bipolar disorder from fully developing. His team at Stanford University is among those seeking genetic and brain imaging biomarkers to make a pediatric bipolar diagnosis more reliable. Lack of age-specific criteria may be causing overdiagnosis, as suggested by a 40-fold increase in 10 years in the number of children and adolescents being treated for bipolar disorder.1
In this interview by Robert A. Kowatch, MD, PhD, Dr. Chang describes a child with probable early signs of bipolar disorder and discusses why early intervention is both complicated and promising.
Children at risk for bipolarity
DR. KOWATCH: You’re studying children considered at high risk for developing bipolar disorder; why are these studies important?
DR. CHANG: High-risk children represent a chance to understand risk factors for developing bipolar disorder and what the early symptoms are. By “high risk,” we mean children and adolescents who possess a genetic predisposition toward bipolar disorder.
Bipolar disorder develops over time; a boy such as “Brian” (Box 1) likely would have gone 3 to 5 years on the stimulant—not doing well—until he had a manic episode at age 14 or 15. The full mood episode usually does not develop until later, with the right—or you could say wrong— combination of environment and stressors acting on a genetic predisposition.
DR. KOWATCH: Do the parents of the children you’re studying have bipolar disorder?
DR. CHANG: Yes; we’re studying what we call “bipolar offspring”—children with biological parents with bipolar disorder (Box 2).2-4 One also could look at siblings; having a brother or sister with bipolar disorder increases risk as well. If you search back in these families, usually you’ll find many relatives with bipolar disorder who reflect the child’s genetic predisposition.
Mrs. M, age 35, had early-onset depression but was not diagnosed with bipolar disorder until age 22. She requests a consultation for her 10-year-old son, Brian, whom she suspects also may have bipolar disorder. “I know there’s something going on; he’s just like I was, but no one would listen to me,” she says.
The boy’s pediatrician prescribed methylphenidate for “a little inattention” but felt that Brian was doing okay in school and had some friends. The stimulant might be helping, says Mrs. M, but she is not sure.
You talk to Brian and learn he has some anxiety. He sometimes gets very excited and runs around, and sometimes he does not sleep well. If you consider all the symptoms, this child has anxiety, attention-deficit/hyperactivity disorder, short depressive periods that affect his functioning, and a parent with bipolar disorder.
You ask further, and Brian tells you about hearing conversations and voices of old friends, his parents, and unknown people in his head, usually neutral, and not commanding or commentating. No one has asked him about parapsychotic phenomena, and he’s never reported this to anyone.
In adults, the incidence of bipolar types I and II is approximately 4%.1 Because two-thirds of adults with bipolar disorder have onset during childhood or adolescence, the incidence of pediatric bipolar disorder may be 1% to 2%. It could be as high as 3% if you include children with prodromes or early forms of the disorder.
The risk of a child developing a bipolar disorder is probably 15% to 20% when 1 biological parent—or sibling—has a bipolar disorder.2 If both parents have bipolar disorder, some older studies suggest that the child’s risk of developing at least a mood disorder would be up to 75%,3 and depression in a child might develop into a bipolar disorder.
Therefore, the risk of bipolar disorder developing in a child whose parents both have bipolar disorder may be >50% and could approach 75%.
‘Kindling’ in bipolar disorder
DR. KOWATCH: What have you seen in children whose parents have bipolar disorder?
DR. CHANG: We’ve tracked more than 200 bipolar offspring for up to 10 years. In some families we’ve seen the natural progression toward full mania and bipolar disorder.
We’ve also seen children who start to show symptoms but don’t develop full bipolar disorder. These children have had clinical treatment, so we’re not sure if the intervention prevented full bipolar disorder or if they would not have developed it anyway. Some children have developed mood symptoms and other psychiatric problems that have resolved with early intervention.
DR. CHANG: Kindling, which originally referred to seizure disorders, also has been applied to affective disorders.5 Early stressors and triggers appear to add up over time and combine with genetic predisposition to create a full mood episode. After that break, it becomes easier and easier to have the next episode, and the disorder becomes chronic and more difficult to treat.
The goal of our work is to stop kindling in bipolar disorder—to prevent environmental or developmental “sparks” from interacting with genetic predisposition and igniting a chronic, spontaneous course of mood episodes.
Brain imaging biomarkers
DR. KOWATCH: Are researchers finding biomarkers for bipolar disorder?
DR. CHANG: The field is young but light-years ahead of where we were 10 years ago. Brain imaging has revealed consistently abnormal areas in children with bipolar disorder. These abnormalities are seen in adults with bipolar disorder as well, but chronic illness, substance abuse, and medication exposure affect the findings in adults. Children have had less exposure to these confounding variables.
We and other groups have identified areas of the prefrontal cortex, amygdala, cerebellum, and striatum that could represent biomarkers, although I wouldn’t say yet that there are any markers per se. A decrease in amygdala volume has been found consistently in children with bipolar disorder, for example, but it’s not specific to bipolar disorder. So we have a way to go before we find specific biomarkers.
In the future, clinicians will probably use a set of 10 to 20 biomarkers, and the more biomarkers a patient has, the greater the risk for bipolar disorder. Once a battery of biomarkers has been put together, the more certain a bipolar disorder diagnosis will become.
Genetic biomarkers
DR. KOWATCH: We’ve talked about high-risk families; are there genetic markers for bipolar disorder?
If you look at common polymorphisms in a set of genes, eventually you’ll be able to calculate the risk that a person will develop bipolar disorder. We’re also investigating whether genes control the age of onset.
DR. KOWATCH: How are you looking for genetic markers in the high-risk children you’re studying?
DR. CHANG: We start with the proband—the child of a bipolar parent—and then study as much of the family as we can. Approximately 50% of the probands’ first- or second-degree relatives have a mood disorder—so our samples are highly loaded.
We’re interested in the interaction between genes and brain function and structure: How do genetic predispositions lead to brain differences that create vulnerability for mood disorders—in this case, bipolar disorder?
To explore that question, we’re starting a 5-year study funded by the National Institutes of Health (NIH). We’re recruiting 50 sibling pairs in which 1 child has early bipolar symptoms and the other is healthy. We will compare these pairs’ genetic and brain imaging profiles with those of 30 healthy children with no genetic risk for bipolar disorder, as far as we can tell.
Something makes 1 child develop bipolar disorder and another child not. By matching siblings with shared environments, we’re trying to eliminate environmental factors and look at their genetic and brain function differences. We’ll use functional brain imaging to look at how children respond to mood-related tasks and standard tasks involving facial emotion exposure to activate brain areas bipolar disorder is thought to affect.
Preventing bipolar ‘kindling’
DR. KOWATCH: What interventions might interrupt kindling and help prevent bipolar I disorder from developing in high risk children?
DR. CHANG: Families affected by bipolar disorder are characterized by stress and high expressed emotion; they tend to fight a lot, and we’re trying to improve communication and their ability to work together. We think reduced stress could halt the progression of the disorder in at-risk children.
Our group is collaborating with Dr. David Miklowitz at the University of Colorado to develop a family psychotherapy program for children who have at least 1 parent or sibling with bipolar disorder and are showing early bipolar symptoms. In a 3-year, NIH-funded treatment development study, 40 children will be randomly assigned to receive 12 sessions of weekly family-focused therapy (FFT) or treatment as usual.
We also think some medications have potential for protecting the brain against the progression of bipolar disorder. In vitro evidence exists for lithium, valproate, and carbamazepine to some extent, other anticonvulsants such as lamotrigine, and atypical antipsychotics such as quetiapine and olanzapine. A few preliminary clinical trials have been conducted (Box 3)9-11 but no longitudinal studies.
A 12-week, open-label study of valproate8 showed symptom improvement in 18 of 23 (78%) children ages 6 to 18 with mood or behavioral symptoms and at least 1 parent with bipolar disorder. On the other hand, a double-blind, controlled trial found no difference in mood symptom changes in 56 children receiving valproate or placebo for up to 5 years. Children in this study were ages 5 to 17, met DSM-IV-TR criteria for cyclothymia or bipolar disorder not otherwise specified, and had at least 1 biological parent with bipolar disorder.9
A small, open-label, 12-week prospective study suggested that quetiapine may be useful for treating mood symptoms in adolescents with at least 1 first-degree relative with bipolar disorder. The 20 adolescents (ages 12 to 18) had mood disorder diagnoses but did not meet DSM-IV-TR criteria for bipolar I disorder.10
RECOMMENDATIONS
DR. KOWATCH: What do you recommend that psychiatrists do to help children at risk for bipolar disorder?
DR. CHANG: Ask your adult patients with bipolar disorder how their children are doing. If a child is not doing well, consider referral to a child and adolescent psychiatrist or take an interest yourself and assess the child for early signs of bipolar disorder.
DR. KOWATCH: What are the prodromal symptoms in children and adolescents?
DR. CHANG: In the past, the earliest reported symptoms were thought to include extreme hyperactivity, inappropriate sexuality, and severe depression at a very young age (preschool or school age children). Now data point to 2 major pathways toward bipolar disorder:
- early-onset depression, which elevates risk for later mania
- early attention-deficit/hyperactivity disorder (ADHD).
DR. KOWATCH: So you’ve got a group with depression and a group with severe ADHD that might develop into bipolar disorder?
DR. CHANG: The ADHD need not be severe. In these children, ADHD may reflect an underlying brain development trajectory toward mood dysregulation. We’ve also seen anxiety as an initial condition. A cross-sectional study found anxiety to be prevalent in bipolar offspring and a possible risk factor for later mania.12
Anxiety is very common in children, so it’s hard to tell if it’s a precursor for bipolar disorder in an individual child. But looking back, a lot of children who develop bipolar disorder had early anxiety, which may be a marker that they were not coping well with stress. What starts leaking out as anxiety eventually may leak out as a full mood episode.
DR. CHANG: Yes, although sometimes the risk comes not from the parents but from a second-degree or more distant relative. We have seen plenty of families in which (as far as we can tell) the parents don’t have any mood disorders, but a child has full bipolar disorder that began over time—as it usually does in bipolar offspring.
Children or adolescents who have first-break episodes after very little pre-morbid dysfunction comprise yet another subset. This group tends to present with episodic manic depression.
DR. KOWATCH: Do you think children with bipolar disorder have clear mood episodes?
DR. CHANG: Our research is trying to bypass that debate. We’re trying to understand whether biomarkers in the brain or blood can be used to distinguish different types of bipolar disorders, rather than relying on symptomatology.
Related resources
- Chang KD, Howe M, Gallelli, K, Miklowitz D. Prevention of pediatric bipolar disorder: integration of neurobiological and psychosocial processes. Ann NY Acad Sci 2006;1094:235–47.
- Chang KD, Gallelli KA. Bipolar disorders and genetics: clinical implications of high heritability. Medscape Psychiatry & Mental Health 2004;9(2). Available at: http://www.medscape.com/viewarticle/489331.
- Miklowitz D, Biuckians A, Richards JA. Early-onset bipolar disorder: a family treatment perspective. Dev Psychopathol 2006;18(4):1247–65.
- Carbamazepine • various
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Methylphenidate • Ritalin
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Valproate • Depakene, Depakote
Dr. Chang receives research support from AstraZeneca, Eli Lilly and Company, Otsuka, and the National Institute of Mental Health. He is a consultant to Abbott Laboratories, GlaxoSmithKline, and Shire, and a speaker for Abbott Laboratories and AstraZeneca.
Dr. Kowatch receives research support from Bristol-Myers Squibb, Stanley Research Foundation, National Institute of Mental Health, and National Institute of Child Health and Human Development. He is a speaker for Abbott Laboratories and AstraZeneca.
1. Moreno C, Laje G, Blanco C, et al. National trends in the outpatient diagnosis and treatment of bipolar disorder in youth. Arch Gen Psychiatry 2007;64(9):1032-9.
2. Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 2005;62(6):593-602.
3. Chang KD, Adleman N, Dienes K, et al. Bipolar offspring: a window into bipolar disorder evolution. Biol Psychiatry 2003;53:941-5.
4. Gershon ES, Hamovit J, Guroff JJ, et al. A family study of schizoaffective, bipolar I, bipolar II, unipolar, and normal control probands. Arch Gen Psychiatry 1982;39(10):1157-67.
5. Post RM. Do the epilepsies, pain syndromes, and affective disorders share common kindling-like mechanisms? Epilepsy Res 2002;50:203-19.
6. Caspi A, Sugden K, Moffitt TE, et al. Influence of life stress on depression: moderation by a polymorphism in the 5-HTT gene. Science 2003;18;301(5631):291-3.
7. Green EK, Raybould R, Macgregor S, et al. Genetic variation of brain-derived neurotrophic factor (BDNF) in bipolar disorder: case-control study of over 3000 individuals from the UK. Br J Psychiatry 2006;188:21-5.
8. Burdick KE, Funke B, Goldberg JF, et al. COMT genotype increases risk for bipolar I disorder and influences neurocognitive performance. Bipolar Disord 2007;9(4):370-6.
9. Chang KD, Dienes K, Blasey C, et al. Divalproex monotherapy in the treatment of bipolar offspring with mood and behavioral disorders and at least mild affective symptoms. J Clin Psychiatry 2003;64(8):936-42.
10. Findling RL, Frazier TW, Youngstrom EA, et al. Double-blind, placebo-controlled trial of divalproex monotherapy in the treatment of symptomatic youth at high risk for developing bipolar disorder. J Clin Psychiatry 2007;68(5):781-8.
11. DelBello MP, Adler CM, Whitsel RM, et al. A 12-week single-blind trial of quetiapine for the treatment of mood symptoms in adolescents at high risk for developing bipolar I disorder. J Clin Psychiatry 2007;68(5):789-95.
12. Henin A, Biederman J, Mick E, et al. Psychopathology in the offspring of parents with bipolar disorder: a controlled study. Biol Psychiatry 2005;58(7):554-61.
When does bipolar disorder begin? That question confounds clinicians, worries parents, and is leading researchers such as Kiki D. Chang, MD, to look for answers in families with this highly heritable disorder.
“Parents with bipolar disorder know what’s happening if their children have early symptoms,” Dr. Chang says. “They tell me, ‘I don’t want my child to go through what I went through, and he’s having the same symptoms I did.’”
Dr. Chang believes early psychotherapy and medication might prevent prodromal bipolar disorder from fully developing. His team at Stanford University is among those seeking genetic and brain imaging biomarkers to make a pediatric bipolar diagnosis more reliable. Lack of age-specific criteria may be causing overdiagnosis, as suggested by a 40-fold increase in 10 years in the number of children and adolescents being treated for bipolar disorder.1
In this interview by Robert A. Kowatch, MD, PhD, Dr. Chang describes a child with probable early signs of bipolar disorder and discusses why early intervention is both complicated and promising.
Children at risk for bipolarity
DR. KOWATCH: You’re studying children considered at high risk for developing bipolar disorder; why are these studies important?
DR. CHANG: High-risk children represent a chance to understand risk factors for developing bipolar disorder and what the early symptoms are. By “high risk,” we mean children and adolescents who possess a genetic predisposition toward bipolar disorder.
Bipolar disorder develops over time; a boy such as “Brian” (Box 1) likely would have gone 3 to 5 years on the stimulant—not doing well—until he had a manic episode at age 14 or 15. The full mood episode usually does not develop until later, with the right—or you could say wrong— combination of environment and stressors acting on a genetic predisposition.
DR. KOWATCH: Do the parents of the children you’re studying have bipolar disorder?
DR. CHANG: Yes; we’re studying what we call “bipolar offspring”—children with biological parents with bipolar disorder (Box 2).2-4 One also could look at siblings; having a brother or sister with bipolar disorder increases risk as well. If you search back in these families, usually you’ll find many relatives with bipolar disorder who reflect the child’s genetic predisposition.
Mrs. M, age 35, had early-onset depression but was not diagnosed with bipolar disorder until age 22. She requests a consultation for her 10-year-old son, Brian, whom she suspects also may have bipolar disorder. “I know there’s something going on; he’s just like I was, but no one would listen to me,” she says.
The boy’s pediatrician prescribed methylphenidate for “a little inattention” but felt that Brian was doing okay in school and had some friends. The stimulant might be helping, says Mrs. M, but she is not sure.
You talk to Brian and learn he has some anxiety. He sometimes gets very excited and runs around, and sometimes he does not sleep well. If you consider all the symptoms, this child has anxiety, attention-deficit/hyperactivity disorder, short depressive periods that affect his functioning, and a parent with bipolar disorder.
You ask further, and Brian tells you about hearing conversations and voices of old friends, his parents, and unknown people in his head, usually neutral, and not commanding or commentating. No one has asked him about parapsychotic phenomena, and he’s never reported this to anyone.
In adults, the incidence of bipolar types I and II is approximately 4%.1 Because two-thirds of adults with bipolar disorder have onset during childhood or adolescence, the incidence of pediatric bipolar disorder may be 1% to 2%. It could be as high as 3% if you include children with prodromes or early forms of the disorder.
The risk of a child developing a bipolar disorder is probably 15% to 20% when 1 biological parent—or sibling—has a bipolar disorder.2 If both parents have bipolar disorder, some older studies suggest that the child’s risk of developing at least a mood disorder would be up to 75%,3 and depression in a child might develop into a bipolar disorder.
Therefore, the risk of bipolar disorder developing in a child whose parents both have bipolar disorder may be >50% and could approach 75%.
‘Kindling’ in bipolar disorder
DR. KOWATCH: What have you seen in children whose parents have bipolar disorder?
DR. CHANG: We’ve tracked more than 200 bipolar offspring for up to 10 years. In some families we’ve seen the natural progression toward full mania and bipolar disorder.
We’ve also seen children who start to show symptoms but don’t develop full bipolar disorder. These children have had clinical treatment, so we’re not sure if the intervention prevented full bipolar disorder or if they would not have developed it anyway. Some children have developed mood symptoms and other psychiatric problems that have resolved with early intervention.
DR. CHANG: Kindling, which originally referred to seizure disorders, also has been applied to affective disorders.5 Early stressors and triggers appear to add up over time and combine with genetic predisposition to create a full mood episode. After that break, it becomes easier and easier to have the next episode, and the disorder becomes chronic and more difficult to treat.
The goal of our work is to stop kindling in bipolar disorder—to prevent environmental or developmental “sparks” from interacting with genetic predisposition and igniting a chronic, spontaneous course of mood episodes.
Brain imaging biomarkers
DR. KOWATCH: Are researchers finding biomarkers for bipolar disorder?
DR. CHANG: The field is young but light-years ahead of where we were 10 years ago. Brain imaging has revealed consistently abnormal areas in children with bipolar disorder. These abnormalities are seen in adults with bipolar disorder as well, but chronic illness, substance abuse, and medication exposure affect the findings in adults. Children have had less exposure to these confounding variables.
We and other groups have identified areas of the prefrontal cortex, amygdala, cerebellum, and striatum that could represent biomarkers, although I wouldn’t say yet that there are any markers per se. A decrease in amygdala volume has been found consistently in children with bipolar disorder, for example, but it’s not specific to bipolar disorder. So we have a way to go before we find specific biomarkers.
In the future, clinicians will probably use a set of 10 to 20 biomarkers, and the more biomarkers a patient has, the greater the risk for bipolar disorder. Once a battery of biomarkers has been put together, the more certain a bipolar disorder diagnosis will become.
Genetic biomarkers
DR. KOWATCH: We’ve talked about high-risk families; are there genetic markers for bipolar disorder?
If you look at common polymorphisms in a set of genes, eventually you’ll be able to calculate the risk that a person will develop bipolar disorder. We’re also investigating whether genes control the age of onset.
DR. KOWATCH: How are you looking for genetic markers in the high-risk children you’re studying?
DR. CHANG: We start with the proband—the child of a bipolar parent—and then study as much of the family as we can. Approximately 50% of the probands’ first- or second-degree relatives have a mood disorder—so our samples are highly loaded.
We’re interested in the interaction between genes and brain function and structure: How do genetic predispositions lead to brain differences that create vulnerability for mood disorders—in this case, bipolar disorder?
To explore that question, we’re starting a 5-year study funded by the National Institutes of Health (NIH). We’re recruiting 50 sibling pairs in which 1 child has early bipolar symptoms and the other is healthy. We will compare these pairs’ genetic and brain imaging profiles with those of 30 healthy children with no genetic risk for bipolar disorder, as far as we can tell.
Something makes 1 child develop bipolar disorder and another child not. By matching siblings with shared environments, we’re trying to eliminate environmental factors and look at their genetic and brain function differences. We’ll use functional brain imaging to look at how children respond to mood-related tasks and standard tasks involving facial emotion exposure to activate brain areas bipolar disorder is thought to affect.
Preventing bipolar ‘kindling’
DR. KOWATCH: What interventions might interrupt kindling and help prevent bipolar I disorder from developing in high risk children?
DR. CHANG: Families affected by bipolar disorder are characterized by stress and high expressed emotion; they tend to fight a lot, and we’re trying to improve communication and their ability to work together. We think reduced stress could halt the progression of the disorder in at-risk children.
Our group is collaborating with Dr. David Miklowitz at the University of Colorado to develop a family psychotherapy program for children who have at least 1 parent or sibling with bipolar disorder and are showing early bipolar symptoms. In a 3-year, NIH-funded treatment development study, 40 children will be randomly assigned to receive 12 sessions of weekly family-focused therapy (FFT) or treatment as usual.
We also think some medications have potential for protecting the brain against the progression of bipolar disorder. In vitro evidence exists for lithium, valproate, and carbamazepine to some extent, other anticonvulsants such as lamotrigine, and atypical antipsychotics such as quetiapine and olanzapine. A few preliminary clinical trials have been conducted (Box 3)9-11 but no longitudinal studies.
A 12-week, open-label study of valproate8 showed symptom improvement in 18 of 23 (78%) children ages 6 to 18 with mood or behavioral symptoms and at least 1 parent with bipolar disorder. On the other hand, a double-blind, controlled trial found no difference in mood symptom changes in 56 children receiving valproate or placebo for up to 5 years. Children in this study were ages 5 to 17, met DSM-IV-TR criteria for cyclothymia or bipolar disorder not otherwise specified, and had at least 1 biological parent with bipolar disorder.9
A small, open-label, 12-week prospective study suggested that quetiapine may be useful for treating mood symptoms in adolescents with at least 1 first-degree relative with bipolar disorder. The 20 adolescents (ages 12 to 18) had mood disorder diagnoses but did not meet DSM-IV-TR criteria for bipolar I disorder.10
RECOMMENDATIONS
DR. KOWATCH: What do you recommend that psychiatrists do to help children at risk for bipolar disorder?
DR. CHANG: Ask your adult patients with bipolar disorder how their children are doing. If a child is not doing well, consider referral to a child and adolescent psychiatrist or take an interest yourself and assess the child for early signs of bipolar disorder.
DR. KOWATCH: What are the prodromal symptoms in children and adolescents?
DR. CHANG: In the past, the earliest reported symptoms were thought to include extreme hyperactivity, inappropriate sexuality, and severe depression at a very young age (preschool or school age children). Now data point to 2 major pathways toward bipolar disorder:
- early-onset depression, which elevates risk for later mania
- early attention-deficit/hyperactivity disorder (ADHD).
DR. KOWATCH: So you’ve got a group with depression and a group with severe ADHD that might develop into bipolar disorder?
DR. CHANG: The ADHD need not be severe. In these children, ADHD may reflect an underlying brain development trajectory toward mood dysregulation. We’ve also seen anxiety as an initial condition. A cross-sectional study found anxiety to be prevalent in bipolar offspring and a possible risk factor for later mania.12
Anxiety is very common in children, so it’s hard to tell if it’s a precursor for bipolar disorder in an individual child. But looking back, a lot of children who develop bipolar disorder had early anxiety, which may be a marker that they were not coping well with stress. What starts leaking out as anxiety eventually may leak out as a full mood episode.
DR. CHANG: Yes, although sometimes the risk comes not from the parents but from a second-degree or more distant relative. We have seen plenty of families in which (as far as we can tell) the parents don’t have any mood disorders, but a child has full bipolar disorder that began over time—as it usually does in bipolar offspring.
Children or adolescents who have first-break episodes after very little pre-morbid dysfunction comprise yet another subset. This group tends to present with episodic manic depression.
DR. KOWATCH: Do you think children with bipolar disorder have clear mood episodes?
DR. CHANG: Our research is trying to bypass that debate. We’re trying to understand whether biomarkers in the brain or blood can be used to distinguish different types of bipolar disorders, rather than relying on symptomatology.
Related resources
- Chang KD, Howe M, Gallelli, K, Miklowitz D. Prevention of pediatric bipolar disorder: integration of neurobiological and psychosocial processes. Ann NY Acad Sci 2006;1094:235–47.
- Chang KD, Gallelli KA. Bipolar disorders and genetics: clinical implications of high heritability. Medscape Psychiatry & Mental Health 2004;9(2). Available at: http://www.medscape.com/viewarticle/489331.
- Miklowitz D, Biuckians A, Richards JA. Early-onset bipolar disorder: a family treatment perspective. Dev Psychopathol 2006;18(4):1247–65.
- Carbamazepine • various
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Methylphenidate • Ritalin
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Valproate • Depakene, Depakote
Dr. Chang receives research support from AstraZeneca, Eli Lilly and Company, Otsuka, and the National Institute of Mental Health. He is a consultant to Abbott Laboratories, GlaxoSmithKline, and Shire, and a speaker for Abbott Laboratories and AstraZeneca.
Dr. Kowatch receives research support from Bristol-Myers Squibb, Stanley Research Foundation, National Institute of Mental Health, and National Institute of Child Health and Human Development. He is a speaker for Abbott Laboratories and AstraZeneca.
When does bipolar disorder begin? That question confounds clinicians, worries parents, and is leading researchers such as Kiki D. Chang, MD, to look for answers in families with this highly heritable disorder.
“Parents with bipolar disorder know what’s happening if their children have early symptoms,” Dr. Chang says. “They tell me, ‘I don’t want my child to go through what I went through, and he’s having the same symptoms I did.’”
Dr. Chang believes early psychotherapy and medication might prevent prodromal bipolar disorder from fully developing. His team at Stanford University is among those seeking genetic and brain imaging biomarkers to make a pediatric bipolar diagnosis more reliable. Lack of age-specific criteria may be causing overdiagnosis, as suggested by a 40-fold increase in 10 years in the number of children and adolescents being treated for bipolar disorder.1
In this interview by Robert A. Kowatch, MD, PhD, Dr. Chang describes a child with probable early signs of bipolar disorder and discusses why early intervention is both complicated and promising.
Children at risk for bipolarity
DR. KOWATCH: You’re studying children considered at high risk for developing bipolar disorder; why are these studies important?
DR. CHANG: High-risk children represent a chance to understand risk factors for developing bipolar disorder and what the early symptoms are. By “high risk,” we mean children and adolescents who possess a genetic predisposition toward bipolar disorder.
Bipolar disorder develops over time; a boy such as “Brian” (Box 1) likely would have gone 3 to 5 years on the stimulant—not doing well—until he had a manic episode at age 14 or 15. The full mood episode usually does not develop until later, with the right—or you could say wrong— combination of environment and stressors acting on a genetic predisposition.
DR. KOWATCH: Do the parents of the children you’re studying have bipolar disorder?
DR. CHANG: Yes; we’re studying what we call “bipolar offspring”—children with biological parents with bipolar disorder (Box 2).2-4 One also could look at siblings; having a brother or sister with bipolar disorder increases risk as well. If you search back in these families, usually you’ll find many relatives with bipolar disorder who reflect the child’s genetic predisposition.
Mrs. M, age 35, had early-onset depression but was not diagnosed with bipolar disorder until age 22. She requests a consultation for her 10-year-old son, Brian, whom she suspects also may have bipolar disorder. “I know there’s something going on; he’s just like I was, but no one would listen to me,” she says.
The boy’s pediatrician prescribed methylphenidate for “a little inattention” but felt that Brian was doing okay in school and had some friends. The stimulant might be helping, says Mrs. M, but she is not sure.
You talk to Brian and learn he has some anxiety. He sometimes gets very excited and runs around, and sometimes he does not sleep well. If you consider all the symptoms, this child has anxiety, attention-deficit/hyperactivity disorder, short depressive periods that affect his functioning, and a parent with bipolar disorder.
You ask further, and Brian tells you about hearing conversations and voices of old friends, his parents, and unknown people in his head, usually neutral, and not commanding or commentating. No one has asked him about parapsychotic phenomena, and he’s never reported this to anyone.
In adults, the incidence of bipolar types I and II is approximately 4%.1 Because two-thirds of adults with bipolar disorder have onset during childhood or adolescence, the incidence of pediatric bipolar disorder may be 1% to 2%. It could be as high as 3% if you include children with prodromes or early forms of the disorder.
The risk of a child developing a bipolar disorder is probably 15% to 20% when 1 biological parent—or sibling—has a bipolar disorder.2 If both parents have bipolar disorder, some older studies suggest that the child’s risk of developing at least a mood disorder would be up to 75%,3 and depression in a child might develop into a bipolar disorder.
Therefore, the risk of bipolar disorder developing in a child whose parents both have bipolar disorder may be >50% and could approach 75%.
‘Kindling’ in bipolar disorder
DR. KOWATCH: What have you seen in children whose parents have bipolar disorder?
DR. CHANG: We’ve tracked more than 200 bipolar offspring for up to 10 years. In some families we’ve seen the natural progression toward full mania and bipolar disorder.
We’ve also seen children who start to show symptoms but don’t develop full bipolar disorder. These children have had clinical treatment, so we’re not sure if the intervention prevented full bipolar disorder or if they would not have developed it anyway. Some children have developed mood symptoms and other psychiatric problems that have resolved with early intervention.
DR. CHANG: Kindling, which originally referred to seizure disorders, also has been applied to affective disorders.5 Early stressors and triggers appear to add up over time and combine with genetic predisposition to create a full mood episode. After that break, it becomes easier and easier to have the next episode, and the disorder becomes chronic and more difficult to treat.
The goal of our work is to stop kindling in bipolar disorder—to prevent environmental or developmental “sparks” from interacting with genetic predisposition and igniting a chronic, spontaneous course of mood episodes.
Brain imaging biomarkers
DR. KOWATCH: Are researchers finding biomarkers for bipolar disorder?
DR. CHANG: The field is young but light-years ahead of where we were 10 years ago. Brain imaging has revealed consistently abnormal areas in children with bipolar disorder. These abnormalities are seen in adults with bipolar disorder as well, but chronic illness, substance abuse, and medication exposure affect the findings in adults. Children have had less exposure to these confounding variables.
We and other groups have identified areas of the prefrontal cortex, amygdala, cerebellum, and striatum that could represent biomarkers, although I wouldn’t say yet that there are any markers per se. A decrease in amygdala volume has been found consistently in children with bipolar disorder, for example, but it’s not specific to bipolar disorder. So we have a way to go before we find specific biomarkers.
In the future, clinicians will probably use a set of 10 to 20 biomarkers, and the more biomarkers a patient has, the greater the risk for bipolar disorder. Once a battery of biomarkers has been put together, the more certain a bipolar disorder diagnosis will become.
Genetic biomarkers
DR. KOWATCH: We’ve talked about high-risk families; are there genetic markers for bipolar disorder?
If you look at common polymorphisms in a set of genes, eventually you’ll be able to calculate the risk that a person will develop bipolar disorder. We’re also investigating whether genes control the age of onset.
DR. KOWATCH: How are you looking for genetic markers in the high-risk children you’re studying?
DR. CHANG: We start with the proband—the child of a bipolar parent—and then study as much of the family as we can. Approximately 50% of the probands’ first- or second-degree relatives have a mood disorder—so our samples are highly loaded.
We’re interested in the interaction between genes and brain function and structure: How do genetic predispositions lead to brain differences that create vulnerability for mood disorders—in this case, bipolar disorder?
To explore that question, we’re starting a 5-year study funded by the National Institutes of Health (NIH). We’re recruiting 50 sibling pairs in which 1 child has early bipolar symptoms and the other is healthy. We will compare these pairs’ genetic and brain imaging profiles with those of 30 healthy children with no genetic risk for bipolar disorder, as far as we can tell.
Something makes 1 child develop bipolar disorder and another child not. By matching siblings with shared environments, we’re trying to eliminate environmental factors and look at their genetic and brain function differences. We’ll use functional brain imaging to look at how children respond to mood-related tasks and standard tasks involving facial emotion exposure to activate brain areas bipolar disorder is thought to affect.
Preventing bipolar ‘kindling’
DR. KOWATCH: What interventions might interrupt kindling and help prevent bipolar I disorder from developing in high risk children?
DR. CHANG: Families affected by bipolar disorder are characterized by stress and high expressed emotion; they tend to fight a lot, and we’re trying to improve communication and their ability to work together. We think reduced stress could halt the progression of the disorder in at-risk children.
Our group is collaborating with Dr. David Miklowitz at the University of Colorado to develop a family psychotherapy program for children who have at least 1 parent or sibling with bipolar disorder and are showing early bipolar symptoms. In a 3-year, NIH-funded treatment development study, 40 children will be randomly assigned to receive 12 sessions of weekly family-focused therapy (FFT) or treatment as usual.
We also think some medications have potential for protecting the brain against the progression of bipolar disorder. In vitro evidence exists for lithium, valproate, and carbamazepine to some extent, other anticonvulsants such as lamotrigine, and atypical antipsychotics such as quetiapine and olanzapine. A few preliminary clinical trials have been conducted (Box 3)9-11 but no longitudinal studies.
A 12-week, open-label study of valproate8 showed symptom improvement in 18 of 23 (78%) children ages 6 to 18 with mood or behavioral symptoms and at least 1 parent with bipolar disorder. On the other hand, a double-blind, controlled trial found no difference in mood symptom changes in 56 children receiving valproate or placebo for up to 5 years. Children in this study were ages 5 to 17, met DSM-IV-TR criteria for cyclothymia or bipolar disorder not otherwise specified, and had at least 1 biological parent with bipolar disorder.9
A small, open-label, 12-week prospective study suggested that quetiapine may be useful for treating mood symptoms in adolescents with at least 1 first-degree relative with bipolar disorder. The 20 adolescents (ages 12 to 18) had mood disorder diagnoses but did not meet DSM-IV-TR criteria for bipolar I disorder.10
RECOMMENDATIONS
DR. KOWATCH: What do you recommend that psychiatrists do to help children at risk for bipolar disorder?
DR. CHANG: Ask your adult patients with bipolar disorder how their children are doing. If a child is not doing well, consider referral to a child and adolescent psychiatrist or take an interest yourself and assess the child for early signs of bipolar disorder.
DR. KOWATCH: What are the prodromal symptoms in children and adolescents?
DR. CHANG: In the past, the earliest reported symptoms were thought to include extreme hyperactivity, inappropriate sexuality, and severe depression at a very young age (preschool or school age children). Now data point to 2 major pathways toward bipolar disorder:
- early-onset depression, which elevates risk for later mania
- early attention-deficit/hyperactivity disorder (ADHD).
DR. KOWATCH: So you’ve got a group with depression and a group with severe ADHD that might develop into bipolar disorder?
DR. CHANG: The ADHD need not be severe. In these children, ADHD may reflect an underlying brain development trajectory toward mood dysregulation. We’ve also seen anxiety as an initial condition. A cross-sectional study found anxiety to be prevalent in bipolar offspring and a possible risk factor for later mania.12
Anxiety is very common in children, so it’s hard to tell if it’s a precursor for bipolar disorder in an individual child. But looking back, a lot of children who develop bipolar disorder had early anxiety, which may be a marker that they were not coping well with stress. What starts leaking out as anxiety eventually may leak out as a full mood episode.
DR. CHANG: Yes, although sometimes the risk comes not from the parents but from a second-degree or more distant relative. We have seen plenty of families in which (as far as we can tell) the parents don’t have any mood disorders, but a child has full bipolar disorder that began over time—as it usually does in bipolar offspring.
Children or adolescents who have first-break episodes after very little pre-morbid dysfunction comprise yet another subset. This group tends to present with episodic manic depression.
DR. KOWATCH: Do you think children with bipolar disorder have clear mood episodes?
DR. CHANG: Our research is trying to bypass that debate. We’re trying to understand whether biomarkers in the brain or blood can be used to distinguish different types of bipolar disorders, rather than relying on symptomatology.
Related resources
- Chang KD, Howe M, Gallelli, K, Miklowitz D. Prevention of pediatric bipolar disorder: integration of neurobiological and psychosocial processes. Ann NY Acad Sci 2006;1094:235–47.
- Chang KD, Gallelli KA. Bipolar disorders and genetics: clinical implications of high heritability. Medscape Psychiatry & Mental Health 2004;9(2). Available at: http://www.medscape.com/viewarticle/489331.
- Miklowitz D, Biuckians A, Richards JA. Early-onset bipolar disorder: a family treatment perspective. Dev Psychopathol 2006;18(4):1247–65.
- Carbamazepine • various
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Methylphenidate • Ritalin
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Valproate • Depakene, Depakote
Dr. Chang receives research support from AstraZeneca, Eli Lilly and Company, Otsuka, and the National Institute of Mental Health. He is a consultant to Abbott Laboratories, GlaxoSmithKline, and Shire, and a speaker for Abbott Laboratories and AstraZeneca.
Dr. Kowatch receives research support from Bristol-Myers Squibb, Stanley Research Foundation, National Institute of Mental Health, and National Institute of Child Health and Human Development. He is a speaker for Abbott Laboratories and AstraZeneca.
1. Moreno C, Laje G, Blanco C, et al. National trends in the outpatient diagnosis and treatment of bipolar disorder in youth. Arch Gen Psychiatry 2007;64(9):1032-9.
2. Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 2005;62(6):593-602.
3. Chang KD, Adleman N, Dienes K, et al. Bipolar offspring: a window into bipolar disorder evolution. Biol Psychiatry 2003;53:941-5.
4. Gershon ES, Hamovit J, Guroff JJ, et al. A family study of schizoaffective, bipolar I, bipolar II, unipolar, and normal control probands. Arch Gen Psychiatry 1982;39(10):1157-67.
5. Post RM. Do the epilepsies, pain syndromes, and affective disorders share common kindling-like mechanisms? Epilepsy Res 2002;50:203-19.
6. Caspi A, Sugden K, Moffitt TE, et al. Influence of life stress on depression: moderation by a polymorphism in the 5-HTT gene. Science 2003;18;301(5631):291-3.
7. Green EK, Raybould R, Macgregor S, et al. Genetic variation of brain-derived neurotrophic factor (BDNF) in bipolar disorder: case-control study of over 3000 individuals from the UK. Br J Psychiatry 2006;188:21-5.
8. Burdick KE, Funke B, Goldberg JF, et al. COMT genotype increases risk for bipolar I disorder and influences neurocognitive performance. Bipolar Disord 2007;9(4):370-6.
9. Chang KD, Dienes K, Blasey C, et al. Divalproex monotherapy in the treatment of bipolar offspring with mood and behavioral disorders and at least mild affective symptoms. J Clin Psychiatry 2003;64(8):936-42.
10. Findling RL, Frazier TW, Youngstrom EA, et al. Double-blind, placebo-controlled trial of divalproex monotherapy in the treatment of symptomatic youth at high risk for developing bipolar disorder. J Clin Psychiatry 2007;68(5):781-8.
11. DelBello MP, Adler CM, Whitsel RM, et al. A 12-week single-blind trial of quetiapine for the treatment of mood symptoms in adolescents at high risk for developing bipolar I disorder. J Clin Psychiatry 2007;68(5):789-95.
12. Henin A, Biederman J, Mick E, et al. Psychopathology in the offspring of parents with bipolar disorder: a controlled study. Biol Psychiatry 2005;58(7):554-61.
1. Moreno C, Laje G, Blanco C, et al. National trends in the outpatient diagnosis and treatment of bipolar disorder in youth. Arch Gen Psychiatry 2007;64(9):1032-9.
2. Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 2005;62(6):593-602.
3. Chang KD, Adleman N, Dienes K, et al. Bipolar offspring: a window into bipolar disorder evolution. Biol Psychiatry 2003;53:941-5.
4. Gershon ES, Hamovit J, Guroff JJ, et al. A family study of schizoaffective, bipolar I, bipolar II, unipolar, and normal control probands. Arch Gen Psychiatry 1982;39(10):1157-67.
5. Post RM. Do the epilepsies, pain syndromes, and affective disorders share common kindling-like mechanisms? Epilepsy Res 2002;50:203-19.
6. Caspi A, Sugden K, Moffitt TE, et al. Influence of life stress on depression: moderation by a polymorphism in the 5-HTT gene. Science 2003;18;301(5631):291-3.
7. Green EK, Raybould R, Macgregor S, et al. Genetic variation of brain-derived neurotrophic factor (BDNF) in bipolar disorder: case-control study of over 3000 individuals from the UK. Br J Psychiatry 2006;188:21-5.
8. Burdick KE, Funke B, Goldberg JF, et al. COMT genotype increases risk for bipolar I disorder and influences neurocognitive performance. Bipolar Disord 2007;9(4):370-6.
9. Chang KD, Dienes K, Blasey C, et al. Divalproex monotherapy in the treatment of bipolar offspring with mood and behavioral disorders and at least mild affective symptoms. J Clin Psychiatry 2003;64(8):936-42.
10. Findling RL, Frazier TW, Youngstrom EA, et al. Double-blind, placebo-controlled trial of divalproex monotherapy in the treatment of symptomatic youth at high risk for developing bipolar disorder. J Clin Psychiatry 2007;68(5):781-8.
11. DelBello MP, Adler CM, Whitsel RM, et al. A 12-week single-blind trial of quetiapine for the treatment of mood symptoms in adolescents at high risk for developing bipolar I disorder. J Clin Psychiatry 2007;68(5):789-95.
12. Henin A, Biederman J, Mick E, et al. Psychopathology in the offspring of parents with bipolar disorder: a controlled study. Biol Psychiatry 2005;58(7):554-61.
Paliperidone ER: Reformulated antipsychotic for schizophrenia Tx
In the 9 months since paliperidone extended-release was FDA-approved for schizophrenia, the 3 acute pivotal trials supporting its approval have been published.1-3 They join a handful of post hoc analyses of this second-generation antipsychotic (SGA) in schizophrenia subgroups, including patients over age 65, recently diagnosed patients, and those with predominant negative symptoms.
This article discusses the evidence and paliperidone ER’s probable clinical benefits and adverse effects, with focus on its:
- pharmacodynamics and pharmacokinetics
- potential efficacy in schizophrenia and for specific patients and symptoms
- safety and tolerability.
How does paliperidone ER work?
Paliperidone ER was approved for schizophrenia treatment in December 2006 based on three 6-week, randomized, placebo-controlled trials. Paliperidone ER is the active metabolite of risperidone (9-OH risperidone) delivered in a once-daily, time-released formulation (Table 1).
Pharmacodynamics. Similar to risperidone, paliperidone ER has high binding affinity for dopamine (D2) and serotonin (5-HT2A) receptors, with additional affinity for histaminic (H1) and adrenergic receptors (alpha1 and alpha2) but not for muscarinic-cholinergic receptors.
Pharmacokinetics. After oral administration, the medication is widely and rapidly distributed. The drug’s terminal half-life is about 23 hours, and steady-state concentration is reached in 4 to 5 days.4,5
Thus paliperidone ER—when compared with risperidone and other antipsychotics that are metabolized primarily in the liver—is less likely to be involved in hepatic drug-drug or drug-disease interactions. However, some drugs that can induce CYP-450 enzymes—such as carbamazepine—may affect paliperidone’s metabolism.7
Paliperidone has an osmotic controlled-release oral delivery system (OROS®) for steady medication delivery across 24 hours8 (Table 2).1-3 The tablet consists of an osmotically active tri-layer core surrounded by a semipermeable membrane. When the tablet is swallowed, the membrane controls the rate of water reaching the tablet core, which determines the rate of drug delivery.6 The result is less variation between peak and trough drug concentrations, compared with immediate-release formulations.
Table 1
How paliperidone ER compares with risperidone
| Characteristic | Paliperidone ER | Risperidone |
|---|---|---|
| Formulation | OROS extended-release | Immediate release |
| Active moiety | 9-OH risperidone | Risperidone plus 9-OH risperidone |
| Metabolism | Primarily renal | Primarily hepatic |
| Drug interactions | Minimal | Primarily through cytochrome P-450 enzyme 2D6 |
| Dosing | Start at target dose | Titrate to target dose |
| OROS: osmotic controlled-release oral delivery system | ||
Paliperidone ER’s clinical characteristics
| Second-generation antipsychotic approved for schizophrenia |
| 9-OH active metabolite of risperidone |
| Osmotic controlled-release system provides steady-state drug delivery over 24 hours |
| Terminal half-life (time for 50% of drug to be eliminated from the body) ~23 hours |
| Available in 3-mg, 6-mg, and 9-mg tablets; recommended starting dose is 6 mg/d, and labeled dose range is 3 to 12 mg/d |
| Excreted primarily by the kidney; maximum recommended dose for patients with oderate to severe renal impairment is 3 mg/d |
| Source: References 1-3 |
Clinical use
Paliperidone ER offers potential therapeutic benefits in treating schizophrenia patients, although not without the risk of adverse events such as extrapyramidal symptoms (EPS) (Table 3).1-3
Patient selection. Because of its slow-release formulation and relatively stable plasma concentrations, paliperidone ER might be useful for patients who are highly sensitive to antipsychotics’ side effects. In particular, paliperidone ER might be ideal for patients who respond to but may not tolerate risperidone.
Paliperidone ER appears to be safe in patients with liver disease. Its primary renal excretion should minimize the risk of hepatic-related drug interactions in patients taking multiple medications.
Dosage and titration. For treating schizophrenia, the suggested starting dose of paliperidone ER is 6 mg/d taken in the morning. In the 3 pivotal trials, 6 mg was the lowest dose to show broad efficacy with minimal adverse events.9
For many patients, the 6-mg starting dose will be the therapeutic dose. When needed, the dose may be increased in 3-mg increments every 1 to 2 weeks to a maximum 12 mg/d (a 15-mg dose was used in clinical trials, but the adverse effects out-weighed the benefits). Lower maximum doses are recommended for patients with renal impairment:
- 6 mg/d for those with creatinine clearance ≥50 to
- 3 mg/d for those with creatinine clearance 10 to 10
Safety and tolerability. Pooled data from the 3 trials indicate that adverse events (AEs) occurred during treatment in 66% to 77% of patients receiving paliperidone ER vs 66% in placebo groups. The most common AEs were headache (11% to 18%), insomnia (4% to 12%), and anxiety (6% to 9%).9
EPS. Risk of EPS-related AEs (such as akathisia and parkinsonian symptoms) with 3-mg and 6-mg paliperidone ER doses (13% and 10%, respectively) was similar to placebo (11%) but increased with the 9-mg, 12-mg, and 15-mg doses (25%, 26%, and 24%, respectively). Should EPS occur, reduce the paliperidone ER dose or consider adding antiparkinsonian medications.
Lab values. No clinically relevant changes were noted in blood glucose, insulin, or lipids.12 Similar to risperidone, paliperidone ER elevated prolactin levels.
Weight gain with paliperidone ER is dose-dependent; in the clinical trials, mean body weight change for all doses was ≤1.9 kg, which is similar to the weight gain seen with risperidone and in the moderate range compared with other SGAs. When using paliperidone ER, follow the American Diabetes Association/American Psychiatric Association guidelines13 for monitoring weight gain and metabolic parameters with antipsychotics. Also monitor patients for clinical symptoms of hyperprolactinemia, and—if intolerable—adjust the dose or switch to another SGA.
Tachycardia. Advise patients that they may experience a rapid heart rate while taking paliperidone ER. In clinical trials, tachycardia occurred in ≤14% of patients—twice the rate with placebo—but did not contribute to more serious cardiac rhythm disturbances or to discontinuation. Incidence of prolonged corrected QT interval (QTc) was 3% to 5% in the paliperidone ER group vs 3% in the placebo group.
Patient education. Because of paliperidone ER’s pharmacokinetic properties, counsel patients to:
- take 1 tablet each day in the morning
- not chew, split, or crush the tablets but swallow whole to preserve the controlled-release delivery.
Table 3
Paliperidone ER’s potential benefits and risks in clinical practice
| Potential benefits | Details |
|---|---|
| Efficacy | Data support acute (6 weeks) and chronic (up to 24 weeks) improvement in schizophrenia symptoms, patient function, and quality of life |
| Pharmacokinetics | Primarily renal excretion decreases risk of hepatic drug-drug or drug-disease interactions |
| Long-acting formulation | Once-daily dosing simplifies treatment and may improve adherence |
| EPS | Risk similar to placebo at 3-mg and 6-mg doses, but increased at higher doses |
| Weight gain | Similar to risperidone |
| Hyperprolactinemia | Similar to risperidone |
| Tachycardia | Occurred in up to 14% of patients in clinical trials (twice the rate of placebo [7%]) |
| QTc prolongation | Increase up to 12 msec on average, with no patients exceeding 500 msec and no clinically adverse events during trials; use paliperidone with caution in patients with arrhythmias or cardiovascular disease or who are taking other medication that can prolong the QT interval |
| EPS: extrapyramidal symptoms | |
| Source: References 1-3 | |
Efficacy trials in schizophrenia
Three 6-week trials1-3 examined paliperidone ER’s efficacy in a total of 1,692 patients with chronic schizophrenia who were hospitalized ≥14 days with acute exacerbations. The trials were double-blind, randomized, fixed-dose, parallel-group, and placebo- and active-controlled (compared with olanzapine, 10 mg/d). Patients showed no significant differences in demographic or baseline characteristics or in the use of rescue medications.
The primary outcome measure was mean change in Positive and Negative Syndrome Scale (PANSS) total score, which quantifies positive, negative, and global psychopathologic symptom severity. Secondary outcome measures included:
- PANSS Marder factor scores14 (derived from PANSS items that reflect positive and negative symptoms, anxiety and depression, hostility, and thought disorganization).
- Clinical Global Impressions-Severity (CGI-S) score, which measures overall illness severity.15
- Personal and Social Performance (PSP) scores, which rate socially useful activities, relationships, self-care, and disturbing and aggressive behaviors; improvement by 1 category (10 points) reflects a clinically meaningful change.16,17
A total of 43% of patients completed the study—34% taking placebo; 46% taking paliperidone ER, 6 mg; 48% taking paliperidone ER, 12 mg; and 45% taking olanzapine. Demographic and baseline characteristics of the 432 patients who received ≥1 dose were similar across all groups. Approximately 75% of patients in each group used rescue medications—primarily lorazepam—for agitation, restlessness, or insomnia for a mean of 8 days.
Patients taking either paliperidone ER dose showed statistically significant greater improvement in PANSS total score compared with those taking placebo (6 mg, P = 0.006; 12 mg, P
Clinical response rates were similar with the 6-mg and 12-mg paliperidone ER doses—50% and 51%, respectively—and greater than with placebo (34%). The higher response rates with paliperidone ER were statistically significant compared with placebo (6 mg, P
Discontinuation rates for lack of efficacy were lower with paliperidone ER (6 mg, 23%; 12 mg, 14%) than with placebo (35%). A substantially lower percentage of patients taking this agent remained classified as “marked/severe/extremely severe” on the CGI-S score from baseline to endpoint, compared with the placebo group;
- 6 mg paliperidone ER, 58% to 26%
- 12 mg paliperidone ER, 64% to 21%
- placebo, 60% to 45%.
The second study2 included U.S. and international sites and compared 3 fixed doses of paliperidone ER (6-, 9-, and 12-mg) with placebo. Among the 630 patients enrolled, 66% completed the study. Patients were randomly assigned to 6 mg, 9 mg, or 12 mg of paliperidone ER; 10 mg of olanzapine; or placebo. The number of patients who dropped out because of adverse events was comparable across the groups.
Patient groups assigned to paliperidone ER showed significant improvement when compared with placebo (P 30% reduction in PANSS total score from baseline to endpoint included:
- 6 mg paliperidone ER, 56%
- 9 mg paliperidone ER, 51%
- 12 mg paliperidone ER, 61%
- placebo, 30%.
- 6 mg paliperidone ER, 63% at baseline to 22% at endpoint
- 9 mg paliperidone ER, 58% to 23%
- 12 mg paliperidone ER, 64% to 16%
- placebo, 60% to 51%.
The third study3 was a multicenter international trial that compared 3 fixed doses of paliperidone ER (3, 9, and 15 mg) with placebo. Among the 618 randomized patients, 365 (59%) completed the study: 70 of 127 (55%) on 3-mg paliperidone ER, 78 of 125 (62%) on 9-mg paliperidone ER, 82 of 115 (71%) on 15-mg paliperidone ER, and 47 of 123 (38%) on placebo.
- 3 mg paliperidone ER, 40%
- 9 mg paliperidone ER, 46%
- 15 mg paliperidone ER, 53%
- placebo, 18% (P ≤0.005).
- 3 mg paliperidone ER, 54% to 32%
- 9 mg paliperidone ER, 52% to 23%
- 15 mg paliperidone ER, 57% to 17%
- placebo, 56% to 50%.
Additional trial evidence
Schizophrenia subpopulations. Post hoc analyses of data reported from the 3 pivotal trials suggest that paliperidone ER may be useful for specific groups of schizophrenia patients, including those who are recently diagnosed, age >65, or severely ill or have predominant negative symptoms or sleep problems (Table 4).18-23
Efficacy in delaying recurrence. Paliperidone ER’s efficacy in delaying symptom recurrence was examined in a randomized, double-blind, placebo-controlled study of 207 patients who had been stabilized on open-label, flexible-dosed paliperidone ER.24 Time to first recurrence of schizophrenia symptoms was the primary efficacy measure. Starting dose was 9 mg/d (flexible dose range 3 to 15 mg/d).
The study was halted at a planned interim analysis because time-to-recurrence was significantly longer for patients receiving paliperidone ER compared with placebo (P
Final analysis of the 179 patients who completed the study confirmed the interim findings. Ongoing treatment maintained improvement in patients’ acute symptoms, functioning, and quality-of-life measures.
Table 4
Studies of paliperidone ER in schizophrenia subpopulations
| Patient population | Study design | Findings |
|---|---|---|
| Recently diagnosed | 413 patients diagnosed within 5 years of study entry compared with 893 patients who had been ill ≥5 years*18,19 | Tolerability was similar, but recently diagnosed patients were more likely to experience movement disorders and somnolence |
| Age ≥65 years | 114 schizophrenia patients age ≥65 given paliperidone ER, 3 to 12 mg/d, or placebo in 6-week, double-blind, randomized, placebo-controlled trial20 | Rates of cardiovascular, cerebrovascular, neuromotor, and metabolic changes similar to placebo, except for tachycardia (16% with paliperidone vs 0% with placebo) |
| Severely ill | 217 patients with marked to severe symptoms (baseline total PANSS score ≥105)*21 | Patients treated with paliperidone showed significantly greater improvement vs placebo in mean total PANSS score (–26.7 vs –5.7) and other measures |
| Substantial negative symptoms | 299 patients with predominant negative symptoms from 3 acute efficacy trials*22 | Patients treated with paliperidone showed significant improvements vs placebo on primary and secondary measures of negative symptoms |
| Sleep problems | 36 patients age 18 to 45 diagnosed with schizophrenia and schizophrenia-related insomnia*23 | In stable patients, paliperidone improved sleep architecture, continuity, and patient-rated sleep quality without producing or worsening daytime sleepiness |
| * Studies marked with asterisks represent post hoc analyses of data from the 3 clinical trials on which the FDA based its approval of paliperidone ER. | ||
| PANSS: Positive and Negative Syndrome Scale | ||
- Paliperidone extended release. Prescribing information. www.invega.com.
- Johnson & Johnson. U.S. District Court upholds Risperdal® (risperidone) patent (press release). October 16, 2006. www.jnj.com/news/jnj_news/20061016_094453.htm.
- Carbamazepine • Tegretol
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Paliperidone ER • Invega
- Risperidone • Risperdal
Dr. Rado and Dr. Dowd receive research support from Neuronetics, sanofi-aventis, Janssen Pharmaceutica, and Solvay.
Dr. Janicak receives research support from Astra-Zeneca, Bristol-Myers Squibb, Janssen Pharmaceutica, Neuronetics, Solvay, and sanofi-aventis. He is a consultant to Astra-Zeneca, Bristol-Myers Squibb, Janssen Pharmaceutica, Neuronetics, and Solvay, and a speaker for Abbott Laboratories, Astra-Zeneca, Bristol-Myers Squibb, Janssen Pharmaceutica, and Pfizer.
1. Marder S, Kramer M, Ford L, et al. Efficacy and safety of paliperidone extended-release tablets: results of a 6-week, randomized, placebo-controlled study. Biol Psychiatry 2007; Jun 27; Epub ahead of print.
2. Kane J, Canas F, Kramer M, et al. Treatment of schizophrenia with paliperidone extended-release tablets: a 6-week placebo-controlled trial. Schizophr Res 2007;90(1-3):147-61.
3. Davidson M, Emsley R, Kramer M, et al. Efficacy, safety and early response of paliperidone extended-release tablets (paliperidone ER): results of a 6-week, randomized, placebo-controlled study. Schizophr Res 2007;93(1-3):117-30.
4. Rossenu SAC, Rusch S, Janssens L, et al. Extended release formulation of paliperidone shows dose proportional pharmacokinetics. Presented at: Annual Meeting of the American Association of Pharmaceutical Scientists; October 29, 2006; San Antonio, TX.
5. Vermeir M, Boom S, Naessens I, et al. Absorption, metabolism, and excretion of a single oral dose of 14C-paliperidone 1 mg in healthy subjects. Eur Neuropsychopharmacol 2005;15(suppl):S648-9.
6. Conley R, Gupta SK, Sathyan G. Clinical spectrum of the osmotic-controlled release oral delivery system (OROS), an advanced oral delivery form. Curr Med Res Opin 2006;22(10):1879-92.
7. Spina E, Avenoso A, Facciola G, et al. Plasma concentrations of risperidone and 9-hydroxyrisperidone: effect of comedication with carbamazepine or valproate. Ther Drug Monit 2000;22(4):481-5.
8. Paliperidone extended release. Prescribing information. Available at: http://www.invega.com. Accessed August 8, 2007.
9. Meltzer H, Kramer M, Gassmann-Mayer C, et al. Efficacy and tolerability of oral paliperidone extended-release tablets in the treatment of acute schizophrenia: pooled data from three 6-week placebo controlled studies. Int J Neuropsychopharmacol 2006;9(suppl 1):S225.-
10. Thyssen A, Cleton A, Osselae NV, et al. Effects of renal impairment on the pharmacokinetic profile of paliperidone extended-release tablets. Clin Pharmacol Ther 2007. In press.
11. Thyssen A, Crauwels H, Cleton A, et al. Effects of hepatic impairment on the pharmacokinetics of paliperidone immediate-release. Presented at: 46th Annual Meeting of the New Clinical Drug Evaluation Unit (NCDEU); June 12-15, 2006; Boca Raton, FL.
12. Meyer J, Kramer M, Lane R, et al. Metabolic outcomes in patients with schizophrenia treated with oral paliperidone extended release tablets: pooled analysis of three 6 week placebo-controlled studies. Int J Neuropsychopharmacol 2006;9(suppl 1):S282.-
13. American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, North American Association for the Study of Obesity. Consensus Development Conference on Antipsychotic Drugs and Obesity and Diabetes. J Clin Psychiatry 2004;65:267-72.
14. Marder SR, Davis JM, Chouinard G. The effects of risperidone on the five dimensions of schizophrenia derived by factor analysis: combined results of the North American trials. J Clin Psychiatry 1997;58:538-46.
15. Guy W. Clinical Global Impressions Scale. Early clinical drug evaluation unit (ECDEU) assessment manual for psychopharmacology. Rockville, MD: National Institute of Mental Health, Department of Health, Education, and Welfare; 1976:218-22. ADM publication 76-338.
16. Morosini PL, Magliano L, Brambilla L, et al. Development, reliability and acceptability of a new version of the DSMIV Social and Occupational Functioning Assessment Scale (SOFAS) to assess routine social functioning. Acta Psychiatr Scand 2000;101:323-9.
17. Patrick D, Adriaenssen I, Morosini P, Rothman M. Reliability, validity and sensitivity to change of the Personal and Social Performance scale in patients with acute schizophrenia. Int J Neuropsychopharmacol 2006;9(suppl 1):S287-8.
18. Kostic D, Bossie C, Turkoz I, et al. Paliperidone extended-release tablets in patients recently diagnosed with schizophrenia. Int J Neuropsychopharmacol 2006;9(suppl 1):S161.-
19. Kostic D, Bossie C, Turkoz I, et al. Paliperidone extended-release tablets in patients recently diagnosed with schizophrenia. Presented at: Congress of the Collegium Internationale Neruo-Psychopharmacologicum (CINP); July 9-13, 2006; Chicago, IL.
20. Tzimos A, Kramer M, Ford L, et al. A 6-week placebo-controlled study of the safety and tolerability of flexible doses of oral paliperidone extended release tablets in the treatment of schizophrenia in elderly patients. Int J Neuropsychopharmacol 2006;9(suppl 1):S155.-
21. Canuso C, Youssef E, Dirks B, et al. Paliperidone extended-release in severely-ill patients with schizophrenia. Presented at: 58th Annual Institute on Psychiatric Services; October 5-8, 2006; New York, NY.
22. Dirks B, Eerdekens M, Turkoz I, et al. Efficacy of paliperidone extended-release tablets in patients with schizophrenia and predominant negative symptoms. Int J Neuropsychopharmacol 2006;9(suppl 1):S162.-
23. Luthringer R, Staner L, Noel N, et al. Sleep assessments in patients with schizophrenia following treatment with paliperidone extended-release tablets. Eur Neuropsychopharmacol 2006;16(suppl 4):S224.-
24. Kramer M, Simpson G, Maciulis V, et al. Paliperidone extended-release tablets for prevention of symptom recurrence in patients with schizophrenia: a randomized double-blind, placebo-controlled study [published correction appears in J Clin Psychopharmacol. 2007;27(3):258]. J Clin Psychopharmacol 2007;27(1):6-14.
In the 9 months since paliperidone extended-release was FDA-approved for schizophrenia, the 3 acute pivotal trials supporting its approval have been published.1-3 They join a handful of post hoc analyses of this second-generation antipsychotic (SGA) in schizophrenia subgroups, including patients over age 65, recently diagnosed patients, and those with predominant negative symptoms.
This article discusses the evidence and paliperidone ER’s probable clinical benefits and adverse effects, with focus on its:
- pharmacodynamics and pharmacokinetics
- potential efficacy in schizophrenia and for specific patients and symptoms
- safety and tolerability.
How does paliperidone ER work?
Paliperidone ER was approved for schizophrenia treatment in December 2006 based on three 6-week, randomized, placebo-controlled trials. Paliperidone ER is the active metabolite of risperidone (9-OH risperidone) delivered in a once-daily, time-released formulation (Table 1).
Pharmacodynamics. Similar to risperidone, paliperidone ER has high binding affinity for dopamine (D2) and serotonin (5-HT2A) receptors, with additional affinity for histaminic (H1) and adrenergic receptors (alpha1 and alpha2) but not for muscarinic-cholinergic receptors.
Pharmacokinetics. After oral administration, the medication is widely and rapidly distributed. The drug’s terminal half-life is about 23 hours, and steady-state concentration is reached in 4 to 5 days.4,5
Thus paliperidone ER—when compared with risperidone and other antipsychotics that are metabolized primarily in the liver—is less likely to be involved in hepatic drug-drug or drug-disease interactions. However, some drugs that can induce CYP-450 enzymes—such as carbamazepine—may affect paliperidone’s metabolism.7
Paliperidone has an osmotic controlled-release oral delivery system (OROS®) for steady medication delivery across 24 hours8 (Table 2).1-3 The tablet consists of an osmotically active tri-layer core surrounded by a semipermeable membrane. When the tablet is swallowed, the membrane controls the rate of water reaching the tablet core, which determines the rate of drug delivery.6 The result is less variation between peak and trough drug concentrations, compared with immediate-release formulations.
Table 1
How paliperidone ER compares with risperidone
| Characteristic | Paliperidone ER | Risperidone |
|---|---|---|
| Formulation | OROS extended-release | Immediate release |
| Active moiety | 9-OH risperidone | Risperidone plus 9-OH risperidone |
| Metabolism | Primarily renal | Primarily hepatic |
| Drug interactions | Minimal | Primarily through cytochrome P-450 enzyme 2D6 |
| Dosing | Start at target dose | Titrate to target dose |
| OROS: osmotic controlled-release oral delivery system | ||
Paliperidone ER’s clinical characteristics
| Second-generation antipsychotic approved for schizophrenia |
| 9-OH active metabolite of risperidone |
| Osmotic controlled-release system provides steady-state drug delivery over 24 hours |
| Terminal half-life (time for 50% of drug to be eliminated from the body) ~23 hours |
| Available in 3-mg, 6-mg, and 9-mg tablets; recommended starting dose is 6 mg/d, and labeled dose range is 3 to 12 mg/d |
| Excreted primarily by the kidney; maximum recommended dose for patients with oderate to severe renal impairment is 3 mg/d |
| Source: References 1-3 |
Clinical use
Paliperidone ER offers potential therapeutic benefits in treating schizophrenia patients, although not without the risk of adverse events such as extrapyramidal symptoms (EPS) (Table 3).1-3
Patient selection. Because of its slow-release formulation and relatively stable plasma concentrations, paliperidone ER might be useful for patients who are highly sensitive to antipsychotics’ side effects. In particular, paliperidone ER might be ideal for patients who respond to but may not tolerate risperidone.
Paliperidone ER appears to be safe in patients with liver disease. Its primary renal excretion should minimize the risk of hepatic-related drug interactions in patients taking multiple medications.
Dosage and titration. For treating schizophrenia, the suggested starting dose of paliperidone ER is 6 mg/d taken in the morning. In the 3 pivotal trials, 6 mg was the lowest dose to show broad efficacy with minimal adverse events.9
For many patients, the 6-mg starting dose will be the therapeutic dose. When needed, the dose may be increased in 3-mg increments every 1 to 2 weeks to a maximum 12 mg/d (a 15-mg dose was used in clinical trials, but the adverse effects out-weighed the benefits). Lower maximum doses are recommended for patients with renal impairment:
- 6 mg/d for those with creatinine clearance ≥50 to
- 3 mg/d for those with creatinine clearance 10 to 10
Safety and tolerability. Pooled data from the 3 trials indicate that adverse events (AEs) occurred during treatment in 66% to 77% of patients receiving paliperidone ER vs 66% in placebo groups. The most common AEs were headache (11% to 18%), insomnia (4% to 12%), and anxiety (6% to 9%).9
EPS. Risk of EPS-related AEs (such as akathisia and parkinsonian symptoms) with 3-mg and 6-mg paliperidone ER doses (13% and 10%, respectively) was similar to placebo (11%) but increased with the 9-mg, 12-mg, and 15-mg doses (25%, 26%, and 24%, respectively). Should EPS occur, reduce the paliperidone ER dose or consider adding antiparkinsonian medications.
Lab values. No clinically relevant changes were noted in blood glucose, insulin, or lipids.12 Similar to risperidone, paliperidone ER elevated prolactin levels.
Weight gain with paliperidone ER is dose-dependent; in the clinical trials, mean body weight change for all doses was ≤1.9 kg, which is similar to the weight gain seen with risperidone and in the moderate range compared with other SGAs. When using paliperidone ER, follow the American Diabetes Association/American Psychiatric Association guidelines13 for monitoring weight gain and metabolic parameters with antipsychotics. Also monitor patients for clinical symptoms of hyperprolactinemia, and—if intolerable—adjust the dose or switch to another SGA.
Tachycardia. Advise patients that they may experience a rapid heart rate while taking paliperidone ER. In clinical trials, tachycardia occurred in ≤14% of patients—twice the rate with placebo—but did not contribute to more serious cardiac rhythm disturbances or to discontinuation. Incidence of prolonged corrected QT interval (QTc) was 3% to 5% in the paliperidone ER group vs 3% in the placebo group.
Patient education. Because of paliperidone ER’s pharmacokinetic properties, counsel patients to:
- take 1 tablet each day in the morning
- not chew, split, or crush the tablets but swallow whole to preserve the controlled-release delivery.
Table 3
Paliperidone ER’s potential benefits and risks in clinical practice
| Potential benefits | Details |
|---|---|
| Efficacy | Data support acute (6 weeks) and chronic (up to 24 weeks) improvement in schizophrenia symptoms, patient function, and quality of life |
| Pharmacokinetics | Primarily renal excretion decreases risk of hepatic drug-drug or drug-disease interactions |
| Long-acting formulation | Once-daily dosing simplifies treatment and may improve adherence |
| EPS | Risk similar to placebo at 3-mg and 6-mg doses, but increased at higher doses |
| Weight gain | Similar to risperidone |
| Hyperprolactinemia | Similar to risperidone |
| Tachycardia | Occurred in up to 14% of patients in clinical trials (twice the rate of placebo [7%]) |
| QTc prolongation | Increase up to 12 msec on average, with no patients exceeding 500 msec and no clinically adverse events during trials; use paliperidone with caution in patients with arrhythmias or cardiovascular disease or who are taking other medication that can prolong the QT interval |
| EPS: extrapyramidal symptoms | |
| Source: References 1-3 | |
Efficacy trials in schizophrenia
Three 6-week trials1-3 examined paliperidone ER’s efficacy in a total of 1,692 patients with chronic schizophrenia who were hospitalized ≥14 days with acute exacerbations. The trials were double-blind, randomized, fixed-dose, parallel-group, and placebo- and active-controlled (compared with olanzapine, 10 mg/d). Patients showed no significant differences in demographic or baseline characteristics or in the use of rescue medications.
The primary outcome measure was mean change in Positive and Negative Syndrome Scale (PANSS) total score, which quantifies positive, negative, and global psychopathologic symptom severity. Secondary outcome measures included:
- PANSS Marder factor scores14 (derived from PANSS items that reflect positive and negative symptoms, anxiety and depression, hostility, and thought disorganization).
- Clinical Global Impressions-Severity (CGI-S) score, which measures overall illness severity.15
- Personal and Social Performance (PSP) scores, which rate socially useful activities, relationships, self-care, and disturbing and aggressive behaviors; improvement by 1 category (10 points) reflects a clinically meaningful change.16,17
A total of 43% of patients completed the study—34% taking placebo; 46% taking paliperidone ER, 6 mg; 48% taking paliperidone ER, 12 mg; and 45% taking olanzapine. Demographic and baseline characteristics of the 432 patients who received ≥1 dose were similar across all groups. Approximately 75% of patients in each group used rescue medications—primarily lorazepam—for agitation, restlessness, or insomnia for a mean of 8 days.
Patients taking either paliperidone ER dose showed statistically significant greater improvement in PANSS total score compared with those taking placebo (6 mg, P = 0.006; 12 mg, P
Clinical response rates were similar with the 6-mg and 12-mg paliperidone ER doses—50% and 51%, respectively—and greater than with placebo (34%). The higher response rates with paliperidone ER were statistically significant compared with placebo (6 mg, P
Discontinuation rates for lack of efficacy were lower with paliperidone ER (6 mg, 23%; 12 mg, 14%) than with placebo (35%). A substantially lower percentage of patients taking this agent remained classified as “marked/severe/extremely severe” on the CGI-S score from baseline to endpoint, compared with the placebo group;
- 6 mg paliperidone ER, 58% to 26%
- 12 mg paliperidone ER, 64% to 21%
- placebo, 60% to 45%.
The second study2 included U.S. and international sites and compared 3 fixed doses of paliperidone ER (6-, 9-, and 12-mg) with placebo. Among the 630 patients enrolled, 66% completed the study. Patients were randomly assigned to 6 mg, 9 mg, or 12 mg of paliperidone ER; 10 mg of olanzapine; or placebo. The number of patients who dropped out because of adverse events was comparable across the groups.
Patient groups assigned to paliperidone ER showed significant improvement when compared with placebo (P 30% reduction in PANSS total score from baseline to endpoint included:
- 6 mg paliperidone ER, 56%
- 9 mg paliperidone ER, 51%
- 12 mg paliperidone ER, 61%
- placebo, 30%.
- 6 mg paliperidone ER, 63% at baseline to 22% at endpoint
- 9 mg paliperidone ER, 58% to 23%
- 12 mg paliperidone ER, 64% to 16%
- placebo, 60% to 51%.
The third study3 was a multicenter international trial that compared 3 fixed doses of paliperidone ER (3, 9, and 15 mg) with placebo. Among the 618 randomized patients, 365 (59%) completed the study: 70 of 127 (55%) on 3-mg paliperidone ER, 78 of 125 (62%) on 9-mg paliperidone ER, 82 of 115 (71%) on 15-mg paliperidone ER, and 47 of 123 (38%) on placebo.
- 3 mg paliperidone ER, 40%
- 9 mg paliperidone ER, 46%
- 15 mg paliperidone ER, 53%
- placebo, 18% (P ≤0.005).
- 3 mg paliperidone ER, 54% to 32%
- 9 mg paliperidone ER, 52% to 23%
- 15 mg paliperidone ER, 57% to 17%
- placebo, 56% to 50%.
Additional trial evidence
Schizophrenia subpopulations. Post hoc analyses of data reported from the 3 pivotal trials suggest that paliperidone ER may be useful for specific groups of schizophrenia patients, including those who are recently diagnosed, age >65, or severely ill or have predominant negative symptoms or sleep problems (Table 4).18-23
Efficacy in delaying recurrence. Paliperidone ER’s efficacy in delaying symptom recurrence was examined in a randomized, double-blind, placebo-controlled study of 207 patients who had been stabilized on open-label, flexible-dosed paliperidone ER.24 Time to first recurrence of schizophrenia symptoms was the primary efficacy measure. Starting dose was 9 mg/d (flexible dose range 3 to 15 mg/d).
The study was halted at a planned interim analysis because time-to-recurrence was significantly longer for patients receiving paliperidone ER compared with placebo (P
Final analysis of the 179 patients who completed the study confirmed the interim findings. Ongoing treatment maintained improvement in patients’ acute symptoms, functioning, and quality-of-life measures.
Table 4
Studies of paliperidone ER in schizophrenia subpopulations
| Patient population | Study design | Findings |
|---|---|---|
| Recently diagnosed | 413 patients diagnosed within 5 years of study entry compared with 893 patients who had been ill ≥5 years*18,19 | Tolerability was similar, but recently diagnosed patients were more likely to experience movement disorders and somnolence |
| Age ≥65 years | 114 schizophrenia patients age ≥65 given paliperidone ER, 3 to 12 mg/d, or placebo in 6-week, double-blind, randomized, placebo-controlled trial20 | Rates of cardiovascular, cerebrovascular, neuromotor, and metabolic changes similar to placebo, except for tachycardia (16% with paliperidone vs 0% with placebo) |
| Severely ill | 217 patients with marked to severe symptoms (baseline total PANSS score ≥105)*21 | Patients treated with paliperidone showed significantly greater improvement vs placebo in mean total PANSS score (–26.7 vs –5.7) and other measures |
| Substantial negative symptoms | 299 patients with predominant negative symptoms from 3 acute efficacy trials*22 | Patients treated with paliperidone showed significant improvements vs placebo on primary and secondary measures of negative symptoms |
| Sleep problems | 36 patients age 18 to 45 diagnosed with schizophrenia and schizophrenia-related insomnia*23 | In stable patients, paliperidone improved sleep architecture, continuity, and patient-rated sleep quality without producing or worsening daytime sleepiness |
| * Studies marked with asterisks represent post hoc analyses of data from the 3 clinical trials on which the FDA based its approval of paliperidone ER. | ||
| PANSS: Positive and Negative Syndrome Scale | ||
- Paliperidone extended release. Prescribing information. www.invega.com.
- Johnson & Johnson. U.S. District Court upholds Risperdal® (risperidone) patent (press release). October 16, 2006. www.jnj.com/news/jnj_news/20061016_094453.htm.
- Carbamazepine • Tegretol
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Paliperidone ER • Invega
- Risperidone • Risperdal
Dr. Rado and Dr. Dowd receive research support from Neuronetics, sanofi-aventis, Janssen Pharmaceutica, and Solvay.
Dr. Janicak receives research support from Astra-Zeneca, Bristol-Myers Squibb, Janssen Pharmaceutica, Neuronetics, Solvay, and sanofi-aventis. He is a consultant to Astra-Zeneca, Bristol-Myers Squibb, Janssen Pharmaceutica, Neuronetics, and Solvay, and a speaker for Abbott Laboratories, Astra-Zeneca, Bristol-Myers Squibb, Janssen Pharmaceutica, and Pfizer.
In the 9 months since paliperidone extended-release was FDA-approved for schizophrenia, the 3 acute pivotal trials supporting its approval have been published.1-3 They join a handful of post hoc analyses of this second-generation antipsychotic (SGA) in schizophrenia subgroups, including patients over age 65, recently diagnosed patients, and those with predominant negative symptoms.
This article discusses the evidence and paliperidone ER’s probable clinical benefits and adverse effects, with focus on its:
- pharmacodynamics and pharmacokinetics
- potential efficacy in schizophrenia and for specific patients and symptoms
- safety and tolerability.
How does paliperidone ER work?
Paliperidone ER was approved for schizophrenia treatment in December 2006 based on three 6-week, randomized, placebo-controlled trials. Paliperidone ER is the active metabolite of risperidone (9-OH risperidone) delivered in a once-daily, time-released formulation (Table 1).
Pharmacodynamics. Similar to risperidone, paliperidone ER has high binding affinity for dopamine (D2) and serotonin (5-HT2A) receptors, with additional affinity for histaminic (H1) and adrenergic receptors (alpha1 and alpha2) but not for muscarinic-cholinergic receptors.
Pharmacokinetics. After oral administration, the medication is widely and rapidly distributed. The drug’s terminal half-life is about 23 hours, and steady-state concentration is reached in 4 to 5 days.4,5
Thus paliperidone ER—when compared with risperidone and other antipsychotics that are metabolized primarily in the liver—is less likely to be involved in hepatic drug-drug or drug-disease interactions. However, some drugs that can induce CYP-450 enzymes—such as carbamazepine—may affect paliperidone’s metabolism.7
Paliperidone has an osmotic controlled-release oral delivery system (OROS®) for steady medication delivery across 24 hours8 (Table 2).1-3 The tablet consists of an osmotically active tri-layer core surrounded by a semipermeable membrane. When the tablet is swallowed, the membrane controls the rate of water reaching the tablet core, which determines the rate of drug delivery.6 The result is less variation between peak and trough drug concentrations, compared with immediate-release formulations.
Table 1
How paliperidone ER compares with risperidone
| Characteristic | Paliperidone ER | Risperidone |
|---|---|---|
| Formulation | OROS extended-release | Immediate release |
| Active moiety | 9-OH risperidone | Risperidone plus 9-OH risperidone |
| Metabolism | Primarily renal | Primarily hepatic |
| Drug interactions | Minimal | Primarily through cytochrome P-450 enzyme 2D6 |
| Dosing | Start at target dose | Titrate to target dose |
| OROS: osmotic controlled-release oral delivery system | ||
Paliperidone ER’s clinical characteristics
| Second-generation antipsychotic approved for schizophrenia |
| 9-OH active metabolite of risperidone |
| Osmotic controlled-release system provides steady-state drug delivery over 24 hours |
| Terminal half-life (time for 50% of drug to be eliminated from the body) ~23 hours |
| Available in 3-mg, 6-mg, and 9-mg tablets; recommended starting dose is 6 mg/d, and labeled dose range is 3 to 12 mg/d |
| Excreted primarily by the kidney; maximum recommended dose for patients with oderate to severe renal impairment is 3 mg/d |
| Source: References 1-3 |
Clinical use
Paliperidone ER offers potential therapeutic benefits in treating schizophrenia patients, although not without the risk of adverse events such as extrapyramidal symptoms (EPS) (Table 3).1-3
Patient selection. Because of its slow-release formulation and relatively stable plasma concentrations, paliperidone ER might be useful for patients who are highly sensitive to antipsychotics’ side effects. In particular, paliperidone ER might be ideal for patients who respond to but may not tolerate risperidone.
Paliperidone ER appears to be safe in patients with liver disease. Its primary renal excretion should minimize the risk of hepatic-related drug interactions in patients taking multiple medications.
Dosage and titration. For treating schizophrenia, the suggested starting dose of paliperidone ER is 6 mg/d taken in the morning. In the 3 pivotal trials, 6 mg was the lowest dose to show broad efficacy with minimal adverse events.9
For many patients, the 6-mg starting dose will be the therapeutic dose. When needed, the dose may be increased in 3-mg increments every 1 to 2 weeks to a maximum 12 mg/d (a 15-mg dose was used in clinical trials, but the adverse effects out-weighed the benefits). Lower maximum doses are recommended for patients with renal impairment:
- 6 mg/d for those with creatinine clearance ≥50 to
- 3 mg/d for those with creatinine clearance 10 to 10
Safety and tolerability. Pooled data from the 3 trials indicate that adverse events (AEs) occurred during treatment in 66% to 77% of patients receiving paliperidone ER vs 66% in placebo groups. The most common AEs were headache (11% to 18%), insomnia (4% to 12%), and anxiety (6% to 9%).9
EPS. Risk of EPS-related AEs (such as akathisia and parkinsonian symptoms) with 3-mg and 6-mg paliperidone ER doses (13% and 10%, respectively) was similar to placebo (11%) but increased with the 9-mg, 12-mg, and 15-mg doses (25%, 26%, and 24%, respectively). Should EPS occur, reduce the paliperidone ER dose or consider adding antiparkinsonian medications.
Lab values. No clinically relevant changes were noted in blood glucose, insulin, or lipids.12 Similar to risperidone, paliperidone ER elevated prolactin levels.
Weight gain with paliperidone ER is dose-dependent; in the clinical trials, mean body weight change for all doses was ≤1.9 kg, which is similar to the weight gain seen with risperidone and in the moderate range compared with other SGAs. When using paliperidone ER, follow the American Diabetes Association/American Psychiatric Association guidelines13 for monitoring weight gain and metabolic parameters with antipsychotics. Also monitor patients for clinical symptoms of hyperprolactinemia, and—if intolerable—adjust the dose or switch to another SGA.
Tachycardia. Advise patients that they may experience a rapid heart rate while taking paliperidone ER. In clinical trials, tachycardia occurred in ≤14% of patients—twice the rate with placebo—but did not contribute to more serious cardiac rhythm disturbances or to discontinuation. Incidence of prolonged corrected QT interval (QTc) was 3% to 5% in the paliperidone ER group vs 3% in the placebo group.
Patient education. Because of paliperidone ER’s pharmacokinetic properties, counsel patients to:
- take 1 tablet each day in the morning
- not chew, split, or crush the tablets but swallow whole to preserve the controlled-release delivery.
Table 3
Paliperidone ER’s potential benefits and risks in clinical practice
| Potential benefits | Details |
|---|---|
| Efficacy | Data support acute (6 weeks) and chronic (up to 24 weeks) improvement in schizophrenia symptoms, patient function, and quality of life |
| Pharmacokinetics | Primarily renal excretion decreases risk of hepatic drug-drug or drug-disease interactions |
| Long-acting formulation | Once-daily dosing simplifies treatment and may improve adherence |
| EPS | Risk similar to placebo at 3-mg and 6-mg doses, but increased at higher doses |
| Weight gain | Similar to risperidone |
| Hyperprolactinemia | Similar to risperidone |
| Tachycardia | Occurred in up to 14% of patients in clinical trials (twice the rate of placebo [7%]) |
| QTc prolongation | Increase up to 12 msec on average, with no patients exceeding 500 msec and no clinically adverse events during trials; use paliperidone with caution in patients with arrhythmias or cardiovascular disease or who are taking other medication that can prolong the QT interval |
| EPS: extrapyramidal symptoms | |
| Source: References 1-3 | |
Efficacy trials in schizophrenia
Three 6-week trials1-3 examined paliperidone ER’s efficacy in a total of 1,692 patients with chronic schizophrenia who were hospitalized ≥14 days with acute exacerbations. The trials were double-blind, randomized, fixed-dose, parallel-group, and placebo- and active-controlled (compared with olanzapine, 10 mg/d). Patients showed no significant differences in demographic or baseline characteristics or in the use of rescue medications.
The primary outcome measure was mean change in Positive and Negative Syndrome Scale (PANSS) total score, which quantifies positive, negative, and global psychopathologic symptom severity. Secondary outcome measures included:
- PANSS Marder factor scores14 (derived from PANSS items that reflect positive and negative symptoms, anxiety and depression, hostility, and thought disorganization).
- Clinical Global Impressions-Severity (CGI-S) score, which measures overall illness severity.15
- Personal and Social Performance (PSP) scores, which rate socially useful activities, relationships, self-care, and disturbing and aggressive behaviors; improvement by 1 category (10 points) reflects a clinically meaningful change.16,17
A total of 43% of patients completed the study—34% taking placebo; 46% taking paliperidone ER, 6 mg; 48% taking paliperidone ER, 12 mg; and 45% taking olanzapine. Demographic and baseline characteristics of the 432 patients who received ≥1 dose were similar across all groups. Approximately 75% of patients in each group used rescue medications—primarily lorazepam—for agitation, restlessness, or insomnia for a mean of 8 days.
Patients taking either paliperidone ER dose showed statistically significant greater improvement in PANSS total score compared with those taking placebo (6 mg, P = 0.006; 12 mg, P
Clinical response rates were similar with the 6-mg and 12-mg paliperidone ER doses—50% and 51%, respectively—and greater than with placebo (34%). The higher response rates with paliperidone ER were statistically significant compared with placebo (6 mg, P
Discontinuation rates for lack of efficacy were lower with paliperidone ER (6 mg, 23%; 12 mg, 14%) than with placebo (35%). A substantially lower percentage of patients taking this agent remained classified as “marked/severe/extremely severe” on the CGI-S score from baseline to endpoint, compared with the placebo group;
- 6 mg paliperidone ER, 58% to 26%
- 12 mg paliperidone ER, 64% to 21%
- placebo, 60% to 45%.
The second study2 included U.S. and international sites and compared 3 fixed doses of paliperidone ER (6-, 9-, and 12-mg) with placebo. Among the 630 patients enrolled, 66% completed the study. Patients were randomly assigned to 6 mg, 9 mg, or 12 mg of paliperidone ER; 10 mg of olanzapine; or placebo. The number of patients who dropped out because of adverse events was comparable across the groups.
Patient groups assigned to paliperidone ER showed significant improvement when compared with placebo (P 30% reduction in PANSS total score from baseline to endpoint included:
- 6 mg paliperidone ER, 56%
- 9 mg paliperidone ER, 51%
- 12 mg paliperidone ER, 61%
- placebo, 30%.
- 6 mg paliperidone ER, 63% at baseline to 22% at endpoint
- 9 mg paliperidone ER, 58% to 23%
- 12 mg paliperidone ER, 64% to 16%
- placebo, 60% to 51%.
The third study3 was a multicenter international trial that compared 3 fixed doses of paliperidone ER (3, 9, and 15 mg) with placebo. Among the 618 randomized patients, 365 (59%) completed the study: 70 of 127 (55%) on 3-mg paliperidone ER, 78 of 125 (62%) on 9-mg paliperidone ER, 82 of 115 (71%) on 15-mg paliperidone ER, and 47 of 123 (38%) on placebo.
- 3 mg paliperidone ER, 40%
- 9 mg paliperidone ER, 46%
- 15 mg paliperidone ER, 53%
- placebo, 18% (P ≤0.005).
- 3 mg paliperidone ER, 54% to 32%
- 9 mg paliperidone ER, 52% to 23%
- 15 mg paliperidone ER, 57% to 17%
- placebo, 56% to 50%.
Additional trial evidence
Schizophrenia subpopulations. Post hoc analyses of data reported from the 3 pivotal trials suggest that paliperidone ER may be useful for specific groups of schizophrenia patients, including those who are recently diagnosed, age >65, or severely ill or have predominant negative symptoms or sleep problems (Table 4).18-23
Efficacy in delaying recurrence. Paliperidone ER’s efficacy in delaying symptom recurrence was examined in a randomized, double-blind, placebo-controlled study of 207 patients who had been stabilized on open-label, flexible-dosed paliperidone ER.24 Time to first recurrence of schizophrenia symptoms was the primary efficacy measure. Starting dose was 9 mg/d (flexible dose range 3 to 15 mg/d).
The study was halted at a planned interim analysis because time-to-recurrence was significantly longer for patients receiving paliperidone ER compared with placebo (P
Final analysis of the 179 patients who completed the study confirmed the interim findings. Ongoing treatment maintained improvement in patients’ acute symptoms, functioning, and quality-of-life measures.
Table 4
Studies of paliperidone ER in schizophrenia subpopulations
| Patient population | Study design | Findings |
|---|---|---|
| Recently diagnosed | 413 patients diagnosed within 5 years of study entry compared with 893 patients who had been ill ≥5 years*18,19 | Tolerability was similar, but recently diagnosed patients were more likely to experience movement disorders and somnolence |
| Age ≥65 years | 114 schizophrenia patients age ≥65 given paliperidone ER, 3 to 12 mg/d, or placebo in 6-week, double-blind, randomized, placebo-controlled trial20 | Rates of cardiovascular, cerebrovascular, neuromotor, and metabolic changes similar to placebo, except for tachycardia (16% with paliperidone vs 0% with placebo) |
| Severely ill | 217 patients with marked to severe symptoms (baseline total PANSS score ≥105)*21 | Patients treated with paliperidone showed significantly greater improvement vs placebo in mean total PANSS score (–26.7 vs –5.7) and other measures |
| Substantial negative symptoms | 299 patients with predominant negative symptoms from 3 acute efficacy trials*22 | Patients treated with paliperidone showed significant improvements vs placebo on primary and secondary measures of negative symptoms |
| Sleep problems | 36 patients age 18 to 45 diagnosed with schizophrenia and schizophrenia-related insomnia*23 | In stable patients, paliperidone improved sleep architecture, continuity, and patient-rated sleep quality without producing or worsening daytime sleepiness |
| * Studies marked with asterisks represent post hoc analyses of data from the 3 clinical trials on which the FDA based its approval of paliperidone ER. | ||
| PANSS: Positive and Negative Syndrome Scale | ||
- Paliperidone extended release. Prescribing information. www.invega.com.
- Johnson & Johnson. U.S. District Court upholds Risperdal® (risperidone) patent (press release). October 16, 2006. www.jnj.com/news/jnj_news/20061016_094453.htm.
- Carbamazepine • Tegretol
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Paliperidone ER • Invega
- Risperidone • Risperdal
Dr. Rado and Dr. Dowd receive research support from Neuronetics, sanofi-aventis, Janssen Pharmaceutica, and Solvay.
Dr. Janicak receives research support from Astra-Zeneca, Bristol-Myers Squibb, Janssen Pharmaceutica, Neuronetics, Solvay, and sanofi-aventis. He is a consultant to Astra-Zeneca, Bristol-Myers Squibb, Janssen Pharmaceutica, Neuronetics, and Solvay, and a speaker for Abbott Laboratories, Astra-Zeneca, Bristol-Myers Squibb, Janssen Pharmaceutica, and Pfizer.
1. Marder S, Kramer M, Ford L, et al. Efficacy and safety of paliperidone extended-release tablets: results of a 6-week, randomized, placebo-controlled study. Biol Psychiatry 2007; Jun 27; Epub ahead of print.
2. Kane J, Canas F, Kramer M, et al. Treatment of schizophrenia with paliperidone extended-release tablets: a 6-week placebo-controlled trial. Schizophr Res 2007;90(1-3):147-61.
3. Davidson M, Emsley R, Kramer M, et al. Efficacy, safety and early response of paliperidone extended-release tablets (paliperidone ER): results of a 6-week, randomized, placebo-controlled study. Schizophr Res 2007;93(1-3):117-30.
4. Rossenu SAC, Rusch S, Janssens L, et al. Extended release formulation of paliperidone shows dose proportional pharmacokinetics. Presented at: Annual Meeting of the American Association of Pharmaceutical Scientists; October 29, 2006; San Antonio, TX.
5. Vermeir M, Boom S, Naessens I, et al. Absorption, metabolism, and excretion of a single oral dose of 14C-paliperidone 1 mg in healthy subjects. Eur Neuropsychopharmacol 2005;15(suppl):S648-9.
6. Conley R, Gupta SK, Sathyan G. Clinical spectrum of the osmotic-controlled release oral delivery system (OROS), an advanced oral delivery form. Curr Med Res Opin 2006;22(10):1879-92.
7. Spina E, Avenoso A, Facciola G, et al. Plasma concentrations of risperidone and 9-hydroxyrisperidone: effect of comedication with carbamazepine or valproate. Ther Drug Monit 2000;22(4):481-5.
8. Paliperidone extended release. Prescribing information. Available at: http://www.invega.com. Accessed August 8, 2007.
9. Meltzer H, Kramer M, Gassmann-Mayer C, et al. Efficacy and tolerability of oral paliperidone extended-release tablets in the treatment of acute schizophrenia: pooled data from three 6-week placebo controlled studies. Int J Neuropsychopharmacol 2006;9(suppl 1):S225.-
10. Thyssen A, Cleton A, Osselae NV, et al. Effects of renal impairment on the pharmacokinetic profile of paliperidone extended-release tablets. Clin Pharmacol Ther 2007. In press.
11. Thyssen A, Crauwels H, Cleton A, et al. Effects of hepatic impairment on the pharmacokinetics of paliperidone immediate-release. Presented at: 46th Annual Meeting of the New Clinical Drug Evaluation Unit (NCDEU); June 12-15, 2006; Boca Raton, FL.
12. Meyer J, Kramer M, Lane R, et al. Metabolic outcomes in patients with schizophrenia treated with oral paliperidone extended release tablets: pooled analysis of three 6 week placebo-controlled studies. Int J Neuropsychopharmacol 2006;9(suppl 1):S282.-
13. American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, North American Association for the Study of Obesity. Consensus Development Conference on Antipsychotic Drugs and Obesity and Diabetes. J Clin Psychiatry 2004;65:267-72.
14. Marder SR, Davis JM, Chouinard G. The effects of risperidone on the five dimensions of schizophrenia derived by factor analysis: combined results of the North American trials. J Clin Psychiatry 1997;58:538-46.
15. Guy W. Clinical Global Impressions Scale. Early clinical drug evaluation unit (ECDEU) assessment manual for psychopharmacology. Rockville, MD: National Institute of Mental Health, Department of Health, Education, and Welfare; 1976:218-22. ADM publication 76-338.
16. Morosini PL, Magliano L, Brambilla L, et al. Development, reliability and acceptability of a new version of the DSMIV Social and Occupational Functioning Assessment Scale (SOFAS) to assess routine social functioning. Acta Psychiatr Scand 2000;101:323-9.
17. Patrick D, Adriaenssen I, Morosini P, Rothman M. Reliability, validity and sensitivity to change of the Personal and Social Performance scale in patients with acute schizophrenia. Int J Neuropsychopharmacol 2006;9(suppl 1):S287-8.
18. Kostic D, Bossie C, Turkoz I, et al. Paliperidone extended-release tablets in patients recently diagnosed with schizophrenia. Int J Neuropsychopharmacol 2006;9(suppl 1):S161.-
19. Kostic D, Bossie C, Turkoz I, et al. Paliperidone extended-release tablets in patients recently diagnosed with schizophrenia. Presented at: Congress of the Collegium Internationale Neruo-Psychopharmacologicum (CINP); July 9-13, 2006; Chicago, IL.
20. Tzimos A, Kramer M, Ford L, et al. A 6-week placebo-controlled study of the safety and tolerability of flexible doses of oral paliperidone extended release tablets in the treatment of schizophrenia in elderly patients. Int J Neuropsychopharmacol 2006;9(suppl 1):S155.-
21. Canuso C, Youssef E, Dirks B, et al. Paliperidone extended-release in severely-ill patients with schizophrenia. Presented at: 58th Annual Institute on Psychiatric Services; October 5-8, 2006; New York, NY.
22. Dirks B, Eerdekens M, Turkoz I, et al. Efficacy of paliperidone extended-release tablets in patients with schizophrenia and predominant negative symptoms. Int J Neuropsychopharmacol 2006;9(suppl 1):S162.-
23. Luthringer R, Staner L, Noel N, et al. Sleep assessments in patients with schizophrenia following treatment with paliperidone extended-release tablets. Eur Neuropsychopharmacol 2006;16(suppl 4):S224.-
24. Kramer M, Simpson G, Maciulis V, et al. Paliperidone extended-release tablets for prevention of symptom recurrence in patients with schizophrenia: a randomized double-blind, placebo-controlled study [published correction appears in J Clin Psychopharmacol. 2007;27(3):258]. J Clin Psychopharmacol 2007;27(1):6-14.
1. Marder S, Kramer M, Ford L, et al. Efficacy and safety of paliperidone extended-release tablets: results of a 6-week, randomized, placebo-controlled study. Biol Psychiatry 2007; Jun 27; Epub ahead of print.
2. Kane J, Canas F, Kramer M, et al. Treatment of schizophrenia with paliperidone extended-release tablets: a 6-week placebo-controlled trial. Schizophr Res 2007;90(1-3):147-61.
3. Davidson M, Emsley R, Kramer M, et al. Efficacy, safety and early response of paliperidone extended-release tablets (paliperidone ER): results of a 6-week, randomized, placebo-controlled study. Schizophr Res 2007;93(1-3):117-30.
4. Rossenu SAC, Rusch S, Janssens L, et al. Extended release formulation of paliperidone shows dose proportional pharmacokinetics. Presented at: Annual Meeting of the American Association of Pharmaceutical Scientists; October 29, 2006; San Antonio, TX.
5. Vermeir M, Boom S, Naessens I, et al. Absorption, metabolism, and excretion of a single oral dose of 14C-paliperidone 1 mg in healthy subjects. Eur Neuropsychopharmacol 2005;15(suppl):S648-9.
6. Conley R, Gupta SK, Sathyan G. Clinical spectrum of the osmotic-controlled release oral delivery system (OROS), an advanced oral delivery form. Curr Med Res Opin 2006;22(10):1879-92.
7. Spina E, Avenoso A, Facciola G, et al. Plasma concentrations of risperidone and 9-hydroxyrisperidone: effect of comedication with carbamazepine or valproate. Ther Drug Monit 2000;22(4):481-5.
8. Paliperidone extended release. Prescribing information. Available at: http://www.invega.com. Accessed August 8, 2007.
9. Meltzer H, Kramer M, Gassmann-Mayer C, et al. Efficacy and tolerability of oral paliperidone extended-release tablets in the treatment of acute schizophrenia: pooled data from three 6-week placebo controlled studies. Int J Neuropsychopharmacol 2006;9(suppl 1):S225.-
10. Thyssen A, Cleton A, Osselae NV, et al. Effects of renal impairment on the pharmacokinetic profile of paliperidone extended-release tablets. Clin Pharmacol Ther 2007. In press.
11. Thyssen A, Crauwels H, Cleton A, et al. Effects of hepatic impairment on the pharmacokinetics of paliperidone immediate-release. Presented at: 46th Annual Meeting of the New Clinical Drug Evaluation Unit (NCDEU); June 12-15, 2006; Boca Raton, FL.
12. Meyer J, Kramer M, Lane R, et al. Metabolic outcomes in patients with schizophrenia treated with oral paliperidone extended release tablets: pooled analysis of three 6 week placebo-controlled studies. Int J Neuropsychopharmacol 2006;9(suppl 1):S282.-
13. American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, North American Association for the Study of Obesity. Consensus Development Conference on Antipsychotic Drugs and Obesity and Diabetes. J Clin Psychiatry 2004;65:267-72.
14. Marder SR, Davis JM, Chouinard G. The effects of risperidone on the five dimensions of schizophrenia derived by factor analysis: combined results of the North American trials. J Clin Psychiatry 1997;58:538-46.
15. Guy W. Clinical Global Impressions Scale. Early clinical drug evaluation unit (ECDEU) assessment manual for psychopharmacology. Rockville, MD: National Institute of Mental Health, Department of Health, Education, and Welfare; 1976:218-22. ADM publication 76-338.
16. Morosini PL, Magliano L, Brambilla L, et al. Development, reliability and acceptability of a new version of the DSMIV Social and Occupational Functioning Assessment Scale (SOFAS) to assess routine social functioning. Acta Psychiatr Scand 2000;101:323-9.
17. Patrick D, Adriaenssen I, Morosini P, Rothman M. Reliability, validity and sensitivity to change of the Personal and Social Performance scale in patients with acute schizophrenia. Int J Neuropsychopharmacol 2006;9(suppl 1):S287-8.
18. Kostic D, Bossie C, Turkoz I, et al. Paliperidone extended-release tablets in patients recently diagnosed with schizophrenia. Int J Neuropsychopharmacol 2006;9(suppl 1):S161.-
19. Kostic D, Bossie C, Turkoz I, et al. Paliperidone extended-release tablets in patients recently diagnosed with schizophrenia. Presented at: Congress of the Collegium Internationale Neruo-Psychopharmacologicum (CINP); July 9-13, 2006; Chicago, IL.
20. Tzimos A, Kramer M, Ford L, et al. A 6-week placebo-controlled study of the safety and tolerability of flexible doses of oral paliperidone extended release tablets in the treatment of schizophrenia in elderly patients. Int J Neuropsychopharmacol 2006;9(suppl 1):S155.-
21. Canuso C, Youssef E, Dirks B, et al. Paliperidone extended-release in severely-ill patients with schizophrenia. Presented at: 58th Annual Institute on Psychiatric Services; October 5-8, 2006; New York, NY.
22. Dirks B, Eerdekens M, Turkoz I, et al. Efficacy of paliperidone extended-release tablets in patients with schizophrenia and predominant negative symptoms. Int J Neuropsychopharmacol 2006;9(suppl 1):S162.-
23. Luthringer R, Staner L, Noel N, et al. Sleep assessments in patients with schizophrenia following treatment with paliperidone extended-release tablets. Eur Neuropsychopharmacol 2006;16(suppl 4):S224.-
24. Kramer M, Simpson G, Maciulis V, et al. Paliperidone extended-release tablets for prevention of symptom recurrence in patients with schizophrenia: a randomized double-blind, placebo-controlled study [published correction appears in J Clin Psychopharmacol. 2007;27(3):258]. J Clin Psychopharmacol 2007;27(1):6-14.
Can medications prevent PTSD in trauma victims?
Posttraumatic stress disorder (PTSD) is a preventable mental illness—without trauma, the illness does not occur. Primary prevention (such as eliminating war, rape, physical assaults, child abuse, or motor vehicle accidents) would be effective but is an unrealistic goal. Secondary prevention (such as preventing PTSD after individuals have been exposed to trauma) may be attainable.
No medication is FDA-approved to prevent PTSD, but patients recently exposed to trauma might benefit from drugs approved for other indications. Possibilities include noradrenergics such as propranolol, corticosteroids that affect the hypothalamic-pituitary-adrenal (HPA) axis, opioids, benzodiazepines, and antidepressants. Some investigational agents also might block the process that turns a traumatic experience into PTSD.
This article discusses these intriguing ideas and suggests which trauma victims might benefit now from acute pharmacologic PTSD prevention.
Who might be treated?
An estimated 8% to 10% of the U.S. population experiences PTSD at some point in life (Box 1).1,2 A person’s risk of developing PTSD after a traumatic event depends on the type of trauma. For example, 10% of motor vehicle accident survivors develop PTSD, compared with 60% of rape survivors.1
Targeting anyone who has experienced trauma for secondary PTSD prevention would expose large groups of people to medications they do not need. Targeting selected persons who are at the highest risk would be more efficient and cost-effective. In a group of acute trauma-exposed persons, 2 selection criteria could be considered simultaneously:
- Which patients may be most predisposed to PTSD?
- Which patients are showing early symptoms that may predict PTSD?
More than half of all American adults have been exposed to at least one traumatic event at some point in their lives.1 In most persons, the posttraumatic stress reaction causes short-term distress, with hyperarousal, agitation, intrusive memories, and exaggerated startle. Although these symptoms usually subside relatively quickly, they persist and evolve into posttraumatic stress disorder (PTSD) in a substantial number of trauma victims.
An estimated 8% to 10% of the U.S. population experiences PTSD at some point in life.2 Emotional distress, social and occupational disability, and persistent decrements in quality of life make PTSD a major public health problem.
Risk factors and resiliency. Certain factors have been shown to increase a person’s vulnerability for PTSD (Table 1).3 Other proposed risk factors include:
- personality types4
- psychophysiologic factors such as reactivity, conditionability, and resistance to extinction/habituation.5
Strong evidence also indicates that acute trauma-related symptoms—including excessive arousal and fear,6 peritraumatic dissociation, and depression—predict the later development of PTSD.
Once identified, individuals predisposed to developing PTSD could be given treatment to increase their resiliency after they have been exposed to trauma. Early evidence suggests that you also could consider giving these patients medications as secondary prevention (Table 2).
Table 1
Who develops PTSD? Risk and resiliency factors
Risk factors that may increase vulnerability for PTSD
|
Resiliency factors that may protect against PTSD
|
| Source: Reference 3 |
Table 2
Medications being studied for PTSD prevention
| Mechanism of action | Medication | FDA-approved indications | ||
|---|---|---|---|---|
| Psychiatric | Nonpsychiatric | |||
| Noradrenergic | Clonidine | No | Yes | |
| Guanfacine | No | Yes | ||
| Prazosin | No | Yes | ||
| Propranolol | No | Yes | ||
| Hypothalamic-pituitary-adrenal axis | Hydrocortisone | No | Yes | |
| Opioid | Morphine | No | Yes | |
| Antidepressant | Dual action | Duloxetine | Yes | Yes |
| Venlafaxine | Yes | No | ||
| SSRIs | Citalopram | Yes | No | |
| Fluoxetine | Yes | No | ||
| Paroxetine | Yes | No | ||
| Sertraline | Yes | No | ||
| TCAs | Amitriptyline | Yes | No | |
| Imipramine | Yes | No | ||
| GABA-benzodiazepine | Alprazolam | Yes | No | |
| Temazepam | Yes | No | ||
| Corticotropin-releasing hormone (CRH) | CRH antagonist | Investigational | ||
| Substance P | Substance P antagonist | Investigational | ||
| Neuropeptide Y | Neuropeptide Y agonist | Investigational | ||
| SSRIs: selective serotonin reuptake inhibitors | ||||
| TCAs: tricyclic antidepressants | ||||
Targeting noradrenergic activity
Increased noradrenergic activity has been associated with persistent memories and PTSD. Therefore, medications that reduce noradrenergic tone by blocking receptors or reduce norepinephrine release are being explored for PTSD prevention.
Propranolol. Three small studies have examined whether the beta-noradrenergic receptor blocker propranolol can prevent PTSD.
In a randomized, double-blind, placebo-controlled trial,7 41 emergency department patients who had a heart rate of ≥ 80 bpm within 6 hours of a traumatic accident received propranolol, 40 mg qid, or placebo for 10 days. After 1 month, the 11 patients who completed propranolol treatment showed a nonsignificant trend toward lower scores on the Clinician-Administered PTSD Scale (CAPS), compared with 20 patients taking placebo. At 3 months, the propranolol group had less physiologic reactivity (as measured by heart rate and skin conductance) to trauma-related cues than the placebo group.
In a nonrandomized study,8 PTSD developed within 2 months in 1 of 11 trauma victims who agreed to take propranolol, 40 mg tid, immediately after the trauma, compared with 3 of 8 victims who refused the medication.
In an unpublished randomized, double-blind trial,9 48 patients admitted to a level I trauma center received propranolol, 40 mg tid; gabapentin, 400 mg tid; or placebo for PTSD prevention. Gabapentin was chosen because it has few side effects or metabolic interactions and preliminary evidence of anxiolytic efficacy.
Neither propranolol nor gabapentin showed statistically significant benefit in preventing PTSD compared with placebo. Effect sizes with the 2 treatments were too small to suggest that larger samples would produce a statistically significant result.
Prazosin—an alpha-1 adrenergic receptor antagonist—has been evaluated in 3 controlled studies and found to reduce intrusive nightmares typical of chronic PTSD.
Ten combat veterans with chronic PTSD showed significantly improved sleep, fewer severe nightmares, and improved global clinical status after receiving prazosin (mean dose 9.5 mg at bedtime) in a 20-week, placebo-controlled, double-blind, crossover study.10
In a larger randomized, parallel group trial,11 the same authors compared prazosin with placebo in 40 combat veterans (mean age 56) with chronic PTSD. After 8 weeks, veterans taking prazosin (mean 13.3 ± 3 mg) had significantly fewer trauma nightmares, improved sleep (including return of normal dreams), and improved global clinical status vs placebo. Overall CAP scores did not decline significantly, however.
In a third placebo-controlled study,12 a midmorning dose of prazosin was added to the regimens of 11 civilian trauma patients already taking the drug at bedtime to suppress trauma-related nightmares. Their daytime PTSD symptoms improved, as shown by reduced psychological distress in response to verbal trauma cues.
Prazosin can reduce chronic PTSD manifestations of nightmares and disturbed sleep, but it has not been shown to ameliorate the full PTSD syndrome. Prazosin has not been studied as an early PTSD intervention.
Other antiadrenergics that reduce the release of norepinephrine—including clonidine and guanfacine—have been studied in open trials as treatment for PTSD. The only controlled study13 showed no benefit from guanfacine for PTSD prevention.
De-stressing the HPA axis
Hydrocortisone has been proposed to prevent PTSD by reducing HPA axis activation, acting as a countermeasure to elevated corticotropin-releasing factor found in patients with chronic PTSD.
IV hydrocortisone’s effect on the development of PTSD was compared with placebo in 20 septic shock survivors after discharge from intensive care.14 One of 9 patients (11%) in the hydrocortisone group was diagnosed with PTSD at follow-up (mean 31 months), compared with 7 of 11 (64%) in the placebo group.
In a similar study, the same researchers gave patients hydrocortisone before, during, and after cardiac surgery. Follow-up interviews revealed significantly lower PTSD and chronic stress symptom scores in the treatment group vs the placebo group.15
These studies—although provocative—are limited by the narrow range of trauma related to severe medical illness or extensive medical procedures.
Norepinephrine-blocking opioids
When the noradrenergic system is activated, one physiologic response is the activation of endogenous opioid systems, which may promote recovery by inhibiting the HPA axis. Opioid systems might be involved in PTSD, as suggested by:
- preclinical evidence that opioids modulate memory16
- studies showing low pain thresholds17 and abnormal beta-endorphin (an opioid peptide neurotransmitter)18 and methionine enkephalin (an opioid peptide)19 levels in PTSD patients.
In theory, opioid administration immediately after trauma may attenuate norepinephrine release, thus thwarting arousal-charged memory consolidation, hyperarousal, and re-experiencing.
One uncontrolled report of pediatric burn victims found a significant association between the morphine dose given for pain during hospitalization and reduced PTSD symptoms 6 months later.20 Decreased pain did not explain the reduction in PTSD, as no significant correlation was seen between pain symptoms and PTSD outcome measures. Similarly, a longitudinal study of substance use among Vietnam War veterans with PTSD found decreased hyperarousal symptoms in heroin users.21
Using opioids to prevent PTSD would be feasible and efficient in acute care settings because 80% to 90% of traumatically-injured patients are discharged on opioid analgesics (compared with <10% on beta blockers or corticosteroids).22 However, 20% to 40% of physically injured inpatients are diagnosed with a substance use disorder at some point in life, making the use of opioid analgesics a practical concern.23
GABA-benzodiazepine paradox
The GABA-benzodiazepine system plays an important role in mediating anxiety, which is consistent with the potent anxiolytic effects of benzodiazepines. Even so, trials of benzodiazepines have found these drugs surprisingly unhelpful—and perhaps harmful—in patients with acute trauma.
Alprazolam did not reduce PTSD symptoms in a small randomized, double-blind study.24 Another trial found that receiving benzodiazepines shortly after trauma exposure was associated with increased PTSD risk in trauma survivors. Nine of 13 patients (69%) who received alprazolam or clonazepam met PTSD diagnostic criteria 6 months after the trauma, compared with 3 of 13 controls (15%).25
Similarly, in a randomized controlled trial, 22 patients were given temazepam for 7 nights, starting approximately 14 days after exposure to a traumatic event. Six weeks later, 55% of those receiving temazepam and 27% of those receiving placebo met criteria for PTSD.26
In summary, benzodiazepines might be helpful when given for a few days after traumatization to control overwhelming anxiety but could be harmful over a longer term.
Other agents for PTSD
Antidepressants. Early trauma-related symptoms of depression predict later development of PTSD.27 Thus, antidepressants have been proposed for early intervention in addition to their well-established role as first-line treatment of PTSD.28
One study supports this idea: a 7-day randomized double-blind trial that compared the tricyclic antidepressant imipramine with chloral hydrate in pediatric burn patients with acute stress disorder (ASD). Imipramine was more effective (83% response) than chloral hydrate (38% response) in reducing ASD symptoms.29
Drugs in development. Three new medications being explored for treating anxiety and depression also might be useful for PTSD prevention. Neuropeptide Y (NPY) agonists,30 substance P antagonists,31 and CRH-antagonists32 are thought to hold promise because of their more proximate roles—compared with monoamine neurotransmitters such as dopamine, norepinephrine and serotonin—in mediating the stress response.
Manage the post-trauma environment:
- Move the victim to safety.
- Treat pain effectively.
- Avoid stress from interrogations, separation from loved ones, or unstable housing.
Avoid crisis incident stress debriefing (CISD), which could enhance physiologic hyperarousal and is not recommended as first-line treatment for most trauma victims. CISD was designed for and is best received by emergency personnel.
Consider prescribing antidepressants for patients thought to be particularly vulnerable to develop posttraumatic stress disorder (PTSD). Risk factors include:
- history of PTSD, depression, or anxiety disorder
- severe trauma (such as from sexual assault or torture)
- physical injury, when antidepressants with analgesic properties might be useful.
Analyzing the evidence
Insufficient evidence exists to determine which strategies might be most effective to prevent PTSD, what optimal dosing might be, and which traumatized individuals might be best targeted with these approaches.
- Beta-blockers and corticosteroids—the most theoretically compelling strategies—are the most difficult agents to use for PTSD prevention because they have the most medical contraindications. In addition, evidence supporting their ability to prevent PTSD is meager at best.
- Prazosin is intriguing but has contra-indications similar to those of beta blockers, no studies of secondary prevention, and no clear indication that it works for the overall PTSD syndrome.
- Opioids are restricted agents with substantial contraindications.
- Evidence is limited but points most strongly toward earlier use of antidepressants. Early trauma-related symptoms of depression predict later development of PTSD,27 and a number of selective serotonin reuptake inhibitors—such as citalopram, fluoxetine, paroxetine, and sertraline—are FDA-approved or used off-label for treating PTSD.33
Prescribing recommendations. Consider practicality, ease of use, and safety of the proposed medication when choosing a drug for PTSD prevention (Table 3).22 Based on the evidence, the most reasonable posttrauma approach (Box 2) might be to consider starting an approved antidepressant for individuals thought to be particularly vulnerable to PTSD because of:
- past history of PTSD, depression, or anxiety disorder
- severity of the trauma (such as in cases of sexual assault or torture)
- pain (antidepressants with analgesic properties—such as venlafaxine or duloxetine—might be useful in patients whose trauma is associated with physical injury, although neither is FDA-approved to treat PTSD).
Table 3
4 considerations when choosing a drug for PTSD prevention
| Potential benefits | Practicality, ease of use, and safety of the proposed medication |
| Potential drug-drug or drug-disease interactions | Asthma, diabetes, and trauma are relative contraindications to the use of antiadrenergics and corticosteroids |
| Psychiatric comorbidities | A patient’s history of substance use disorder makes opioid analgesics a concern |
| Clinical experience | Agents already prescribed safely and broadly in clinical practice are easiest to test and to use |
Related resources
- Mental health and mass violence: Evidence-based early psychological intervention for victims/survivors of mass violence. A workshop to reach consensus on best practices. Rockland, MD: National Institute of Mental Health; 2002. www.nimh.nih.gov.
- Post-traumatic stress disorder: the management of PTSD in adults and children in primary and secondary care (clinical guideline 26). London, UK: National Institute for Clinical Excellence; 2005. www.nice.org.uk.
- Ursano RJ, Bell C, Eth S, et al. Practice guideline for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Am J Psychiatry 2004;161(suppl 11):3-31.
Drug brand names
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Citalopram • Celexa
- Clonazepam • Klonopin
- Clonidine • Catapres
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Guanfacine • Tenex
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Paroxetine • Paxil
- Prazosin • Minipress
- Propranolol • Inderal
- Sertraline • Zoloft
- Temazepam • Restoril
- Venlafaxine • Effexor
Disclosure
Dr. Bennett and Dr. Zatzick report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Roy-Byrne is a consultant to Jazz Pharmaceuticals and Solvay and has received speaker honoraria from Wyeth and Forrest Pharmaceuticals.
1. Kessler RC, Sonnega A, Bromet E, et al. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1995;52(12):1048-60.
2. Zatzick D. Posttraumatic stress, functional impairment, and service utilization after injury: a public health approach. Semin Clin Neuropsychiatry 2003;8(3):149-57.
3. Yehuda R, Flory JD, Southwick S, Charney DS. Developing an agenda for translational studies of resilience and vulnerability following trauma exposure. Ann NY Acad Sci 2006;1071:379-96.
4. Schnurr P, Vielhauer M. Personality as a risk factor for PTSD. In: Yehuda R, ed. Risk factors for post-traumatic stress disorder. Washington, DC: American Psychiatric Publishing; 1999:191-222.
5. Shalev A. Psychophysiological expression of risk factors for PTSD. In: Yehuda R, ed. Risk factors for posttraumatic stress disorder. Washington, DC: American Psychiatric Publishing; 1995.
6. Bryant RA, Harvey AG, Guthrie RM, Moulds ML. A prospective study of psychophysiological arousal, acute stress disorder, and posttraumatic stress disorder. J Abnorm Psychol 2000;109(2):341-4.
7. Pitman RK, Sanders KM, Zusman RM, et al. Pilot study of secondary prevention of posttraumatic stress disorder with propranolol. Biol Psychiatry 2002;51(2):189-92.
8. Vaiva G, Ducrocq F, Jezequel K, et al. Immediate treatment with propranolol decreases posttraumatic stress disorder two months after trauma. Biol Psychiatry 2003;54(9):947-9.
9. Stein M. Pharmacoprevention of adverse psychiatric sequelae of physical injury. Paper presented at: 21st Annual Meeting of the International Society for Traumatic Stress Studies; November 2-5, 2005; Toronto, Ontario, Canada.
10. Raskind MA, Peskind ER, Kanter ED, et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo-controlled study. Am J Psychiatry 2003;160(2):371-3.
11. Raskind MA, Peskind ER, Hoff DJ, et al. A parallel group placebo controlled study of prazosin for trauma nightmares and sleep disturbance in combat veterans with post-traumatic stress disorder. Biol Psychiatry 2007;61(8):928-34.
12. Taylor FB, Lowe K, Thompson C, et al. Daytime prazosin reduces psychological distress to trauma specific cues in civilian trauma posttraumatic stress disorder. Biol Psychiatry 2006;59(7):577-81.
13. Neylan TC, Lenoci M, Samuelson KW, et al. No improvement of posttraumatic stress disorder symptoms with guanfacine treatment. Am J Psychiatry 2006;163(12):2186-8.
14. Schelling G, Briegel J, Roozendaal B, et al. The effect of stress doses of hydrocortisone during septic shock on posttraumatic stress disorder in survivors. Biol Psychiatry 2001;50(12):978-85.
15. Weis F, Kilger E, Roozendaal B, et al. Stress doses of hydrocortisone reduce chronic stress symptoms and improve health-related quality of life in high-risk patients after cardiac surgery: a randomized study. J Thorac Cardiovasc Surg 2006;131(2):277-82.
16. McGaugh JL, Introini-Collison IB, Nagahara AH, et al. Involvement of the amygdaloid complex in neuromodulatory influences on memory storage. Neurosci Biobehav Rev 1990;14(4):425-31.
17. Shalev AY, Peri T, Canetti L, Schreiber S. Predictors of PTSD in injured trauma survivors: a prospective study. Am J Psychiatry 1996;153(2):219-25.
18. Baker DG, West SA, Orth DN, et al. Cerebrospinal fluid and plasma beta-endorphin in combat veterans with post-traumatic stress disorder. Psychoneuroendocrinol 1997;22(7):517-29.
19. Wolf ME, Mosnaim AD, Puente J, Ignacio R. Plasma methionine-enkephalin in PTSD. Biol Psychiatry 1991;29(3):305-7.
20. Saxe G, Stoddard F, Courtney D, et al. Relationship between acute morphine and the course of PTSD in children with burns. J Am Acad Child Adolesc Psychiatry 2001;40(8):915-21.
21. Bremner JD, Southwick SM, Darnell A, Charney DS. Chronic PTSD in Vietnam combat veterans: course of illness and substance abuse. Am J Psychiatry 1996;153(3):369-75.
22. Zatzick D, Roy-Byrne PP. From bedside to bench: how the epidemiology of clinical practice can inform the secondary prevention of PTSD. Psychiatr Serv 2006;57(12):1726-30.
23. Zatzick D, Jurkovich G, Russo J, et al. Posttraumatic distress, alcohol disorders, and recurrent trauma across level 1 trauma centers. J Trauma 2004;57(2):360-6.
24. Braun P, Greenberg D, Dasberg H, Lerer B. Core symptoms of posttraumatic stress disorder unimproved by alprazolam treatment. J Clin Psychiatry 1990;51(6):236-8.
25. Gelpin E, Bonne O, Peri T, et al. Treatment of recent trauma survivors with benzodiazepines: a prospective study. J Clin Psychiatry 1996;57(9):390-4.
26. Mellman TA, Bustamante V, David D, et al. Hypnotic medication in the aftermath of trauma. J Clin Psychiatry 2002;63(12):1183-4.
27. Freedman SA, Brandes D, Peri T, Shalev A. Predictors of chronic post-traumatic stress disorder. A prospective study. Br J Psychiatry 1999;174:353-9.
28. Davidson JR. Pharmacologic treatment of acute and chronic stress following trauma. J Clin Psychiatry 2006;67(suppl 2):34-9.
29. Robert R, Blakeney PE, Villarreal C, et al. Imipramine treatment in pediatric burn patients with symptoms of acute stress disorder: a pilot study. J Am Acad Child Adolesc Psychiatry 1999;38(7):873-82.
30. Morgan CA, Wang S, Southwick SM, et al. Plasma neuropeptide-Y concentrations in humans exposed to military survival training. Biol Psychiatry 2000;47(10):902-9.
31. Geracioti TD, Carpenter LL, Owens MJ, et al. Elevated cerebrospinal fluid substance P concentrations in posttraumatic stress disorder and major depression. Am J Psychiatry 2006;163(4):637-43.
32. Zobel AW, Nickel T, Künzel HE, et al. Effects of the highaffinity corticotropin-releasing hormone receptor 1 antagonist R121919 in major depression: the first 20 patients treated. J Psychiatr Res 2000;34(3):171-81.
33. Davidson JR. Treatment of posttraumatic stress disorder: the impact of paroxetine. Psychopharmacol Bull 2003;37(suppl 1):76-88.
Posttraumatic stress disorder (PTSD) is a preventable mental illness—without trauma, the illness does not occur. Primary prevention (such as eliminating war, rape, physical assaults, child abuse, or motor vehicle accidents) would be effective but is an unrealistic goal. Secondary prevention (such as preventing PTSD after individuals have been exposed to trauma) may be attainable.
No medication is FDA-approved to prevent PTSD, but patients recently exposed to trauma might benefit from drugs approved for other indications. Possibilities include noradrenergics such as propranolol, corticosteroids that affect the hypothalamic-pituitary-adrenal (HPA) axis, opioids, benzodiazepines, and antidepressants. Some investigational agents also might block the process that turns a traumatic experience into PTSD.
This article discusses these intriguing ideas and suggests which trauma victims might benefit now from acute pharmacologic PTSD prevention.
Who might be treated?
An estimated 8% to 10% of the U.S. population experiences PTSD at some point in life (Box 1).1,2 A person’s risk of developing PTSD after a traumatic event depends on the type of trauma. For example, 10% of motor vehicle accident survivors develop PTSD, compared with 60% of rape survivors.1
Targeting anyone who has experienced trauma for secondary PTSD prevention would expose large groups of people to medications they do not need. Targeting selected persons who are at the highest risk would be more efficient and cost-effective. In a group of acute trauma-exposed persons, 2 selection criteria could be considered simultaneously:
- Which patients may be most predisposed to PTSD?
- Which patients are showing early symptoms that may predict PTSD?
More than half of all American adults have been exposed to at least one traumatic event at some point in their lives.1 In most persons, the posttraumatic stress reaction causes short-term distress, with hyperarousal, agitation, intrusive memories, and exaggerated startle. Although these symptoms usually subside relatively quickly, they persist and evolve into posttraumatic stress disorder (PTSD) in a substantial number of trauma victims.
An estimated 8% to 10% of the U.S. population experiences PTSD at some point in life.2 Emotional distress, social and occupational disability, and persistent decrements in quality of life make PTSD a major public health problem.
Risk factors and resiliency. Certain factors have been shown to increase a person’s vulnerability for PTSD (Table 1).3 Other proposed risk factors include:
- personality types4
- psychophysiologic factors such as reactivity, conditionability, and resistance to extinction/habituation.5
Strong evidence also indicates that acute trauma-related symptoms—including excessive arousal and fear,6 peritraumatic dissociation, and depression—predict the later development of PTSD.
Once identified, individuals predisposed to developing PTSD could be given treatment to increase their resiliency after they have been exposed to trauma. Early evidence suggests that you also could consider giving these patients medications as secondary prevention (Table 2).
Table 1
Who develops PTSD? Risk and resiliency factors
Risk factors that may increase vulnerability for PTSD
|
Resiliency factors that may protect against PTSD
|
| Source: Reference 3 |
Table 2
Medications being studied for PTSD prevention
| Mechanism of action | Medication | FDA-approved indications | ||
|---|---|---|---|---|
| Psychiatric | Nonpsychiatric | |||
| Noradrenergic | Clonidine | No | Yes | |
| Guanfacine | No | Yes | ||
| Prazosin | No | Yes | ||
| Propranolol | No | Yes | ||
| Hypothalamic-pituitary-adrenal axis | Hydrocortisone | No | Yes | |
| Opioid | Morphine | No | Yes | |
| Antidepressant | Dual action | Duloxetine | Yes | Yes |
| Venlafaxine | Yes | No | ||
| SSRIs | Citalopram | Yes | No | |
| Fluoxetine | Yes | No | ||
| Paroxetine | Yes | No | ||
| Sertraline | Yes | No | ||
| TCAs | Amitriptyline | Yes | No | |
| Imipramine | Yes | No | ||
| GABA-benzodiazepine | Alprazolam | Yes | No | |
| Temazepam | Yes | No | ||
| Corticotropin-releasing hormone (CRH) | CRH antagonist | Investigational | ||
| Substance P | Substance P antagonist | Investigational | ||
| Neuropeptide Y | Neuropeptide Y agonist | Investigational | ||
| SSRIs: selective serotonin reuptake inhibitors | ||||
| TCAs: tricyclic antidepressants | ||||
Targeting noradrenergic activity
Increased noradrenergic activity has been associated with persistent memories and PTSD. Therefore, medications that reduce noradrenergic tone by blocking receptors or reduce norepinephrine release are being explored for PTSD prevention.
Propranolol. Three small studies have examined whether the beta-noradrenergic receptor blocker propranolol can prevent PTSD.
In a randomized, double-blind, placebo-controlled trial,7 41 emergency department patients who had a heart rate of ≥ 80 bpm within 6 hours of a traumatic accident received propranolol, 40 mg qid, or placebo for 10 days. After 1 month, the 11 patients who completed propranolol treatment showed a nonsignificant trend toward lower scores on the Clinician-Administered PTSD Scale (CAPS), compared with 20 patients taking placebo. At 3 months, the propranolol group had less physiologic reactivity (as measured by heart rate and skin conductance) to trauma-related cues than the placebo group.
In a nonrandomized study,8 PTSD developed within 2 months in 1 of 11 trauma victims who agreed to take propranolol, 40 mg tid, immediately after the trauma, compared with 3 of 8 victims who refused the medication.
In an unpublished randomized, double-blind trial,9 48 patients admitted to a level I trauma center received propranolol, 40 mg tid; gabapentin, 400 mg tid; or placebo for PTSD prevention. Gabapentin was chosen because it has few side effects or metabolic interactions and preliminary evidence of anxiolytic efficacy.
Neither propranolol nor gabapentin showed statistically significant benefit in preventing PTSD compared with placebo. Effect sizes with the 2 treatments were too small to suggest that larger samples would produce a statistically significant result.
Prazosin—an alpha-1 adrenergic receptor antagonist—has been evaluated in 3 controlled studies and found to reduce intrusive nightmares typical of chronic PTSD.
Ten combat veterans with chronic PTSD showed significantly improved sleep, fewer severe nightmares, and improved global clinical status after receiving prazosin (mean dose 9.5 mg at bedtime) in a 20-week, placebo-controlled, double-blind, crossover study.10
In a larger randomized, parallel group trial,11 the same authors compared prazosin with placebo in 40 combat veterans (mean age 56) with chronic PTSD. After 8 weeks, veterans taking prazosin (mean 13.3 ± 3 mg) had significantly fewer trauma nightmares, improved sleep (including return of normal dreams), and improved global clinical status vs placebo. Overall CAP scores did not decline significantly, however.
In a third placebo-controlled study,12 a midmorning dose of prazosin was added to the regimens of 11 civilian trauma patients already taking the drug at bedtime to suppress trauma-related nightmares. Their daytime PTSD symptoms improved, as shown by reduced psychological distress in response to verbal trauma cues.
Prazosin can reduce chronic PTSD manifestations of nightmares and disturbed sleep, but it has not been shown to ameliorate the full PTSD syndrome. Prazosin has not been studied as an early PTSD intervention.
Other antiadrenergics that reduce the release of norepinephrine—including clonidine and guanfacine—have been studied in open trials as treatment for PTSD. The only controlled study13 showed no benefit from guanfacine for PTSD prevention.
De-stressing the HPA axis
Hydrocortisone has been proposed to prevent PTSD by reducing HPA axis activation, acting as a countermeasure to elevated corticotropin-releasing factor found in patients with chronic PTSD.
IV hydrocortisone’s effect on the development of PTSD was compared with placebo in 20 septic shock survivors after discharge from intensive care.14 One of 9 patients (11%) in the hydrocortisone group was diagnosed with PTSD at follow-up (mean 31 months), compared with 7 of 11 (64%) in the placebo group.
In a similar study, the same researchers gave patients hydrocortisone before, during, and after cardiac surgery. Follow-up interviews revealed significantly lower PTSD and chronic stress symptom scores in the treatment group vs the placebo group.15
These studies—although provocative—are limited by the narrow range of trauma related to severe medical illness or extensive medical procedures.
Norepinephrine-blocking opioids
When the noradrenergic system is activated, one physiologic response is the activation of endogenous opioid systems, which may promote recovery by inhibiting the HPA axis. Opioid systems might be involved in PTSD, as suggested by:
- preclinical evidence that opioids modulate memory16
- studies showing low pain thresholds17 and abnormal beta-endorphin (an opioid peptide neurotransmitter)18 and methionine enkephalin (an opioid peptide)19 levels in PTSD patients.
In theory, opioid administration immediately after trauma may attenuate norepinephrine release, thus thwarting arousal-charged memory consolidation, hyperarousal, and re-experiencing.
One uncontrolled report of pediatric burn victims found a significant association between the morphine dose given for pain during hospitalization and reduced PTSD symptoms 6 months later.20 Decreased pain did not explain the reduction in PTSD, as no significant correlation was seen between pain symptoms and PTSD outcome measures. Similarly, a longitudinal study of substance use among Vietnam War veterans with PTSD found decreased hyperarousal symptoms in heroin users.21
Using opioids to prevent PTSD would be feasible and efficient in acute care settings because 80% to 90% of traumatically-injured patients are discharged on opioid analgesics (compared with <10% on beta blockers or corticosteroids).22 However, 20% to 40% of physically injured inpatients are diagnosed with a substance use disorder at some point in life, making the use of opioid analgesics a practical concern.23
GABA-benzodiazepine paradox
The GABA-benzodiazepine system plays an important role in mediating anxiety, which is consistent with the potent anxiolytic effects of benzodiazepines. Even so, trials of benzodiazepines have found these drugs surprisingly unhelpful—and perhaps harmful—in patients with acute trauma.
Alprazolam did not reduce PTSD symptoms in a small randomized, double-blind study.24 Another trial found that receiving benzodiazepines shortly after trauma exposure was associated with increased PTSD risk in trauma survivors. Nine of 13 patients (69%) who received alprazolam or clonazepam met PTSD diagnostic criteria 6 months after the trauma, compared with 3 of 13 controls (15%).25
Similarly, in a randomized controlled trial, 22 patients were given temazepam for 7 nights, starting approximately 14 days after exposure to a traumatic event. Six weeks later, 55% of those receiving temazepam and 27% of those receiving placebo met criteria for PTSD.26
In summary, benzodiazepines might be helpful when given for a few days after traumatization to control overwhelming anxiety but could be harmful over a longer term.
Other agents for PTSD
Antidepressants. Early trauma-related symptoms of depression predict later development of PTSD.27 Thus, antidepressants have been proposed for early intervention in addition to their well-established role as first-line treatment of PTSD.28
One study supports this idea: a 7-day randomized double-blind trial that compared the tricyclic antidepressant imipramine with chloral hydrate in pediatric burn patients with acute stress disorder (ASD). Imipramine was more effective (83% response) than chloral hydrate (38% response) in reducing ASD symptoms.29
Drugs in development. Three new medications being explored for treating anxiety and depression also might be useful for PTSD prevention. Neuropeptide Y (NPY) agonists,30 substance P antagonists,31 and CRH-antagonists32 are thought to hold promise because of their more proximate roles—compared with monoamine neurotransmitters such as dopamine, norepinephrine and serotonin—in mediating the stress response.
Manage the post-trauma environment:
- Move the victim to safety.
- Treat pain effectively.
- Avoid stress from interrogations, separation from loved ones, or unstable housing.
Avoid crisis incident stress debriefing (CISD), which could enhance physiologic hyperarousal and is not recommended as first-line treatment for most trauma victims. CISD was designed for and is best received by emergency personnel.
Consider prescribing antidepressants for patients thought to be particularly vulnerable to develop posttraumatic stress disorder (PTSD). Risk factors include:
- history of PTSD, depression, or anxiety disorder
- severe trauma (such as from sexual assault or torture)
- physical injury, when antidepressants with analgesic properties might be useful.
Analyzing the evidence
Insufficient evidence exists to determine which strategies might be most effective to prevent PTSD, what optimal dosing might be, and which traumatized individuals might be best targeted with these approaches.
- Beta-blockers and corticosteroids—the most theoretically compelling strategies—are the most difficult agents to use for PTSD prevention because they have the most medical contraindications. In addition, evidence supporting their ability to prevent PTSD is meager at best.
- Prazosin is intriguing but has contra-indications similar to those of beta blockers, no studies of secondary prevention, and no clear indication that it works for the overall PTSD syndrome.
- Opioids are restricted agents with substantial contraindications.
- Evidence is limited but points most strongly toward earlier use of antidepressants. Early trauma-related symptoms of depression predict later development of PTSD,27 and a number of selective serotonin reuptake inhibitors—such as citalopram, fluoxetine, paroxetine, and sertraline—are FDA-approved or used off-label for treating PTSD.33
Prescribing recommendations. Consider practicality, ease of use, and safety of the proposed medication when choosing a drug for PTSD prevention (Table 3).22 Based on the evidence, the most reasonable posttrauma approach (Box 2) might be to consider starting an approved antidepressant for individuals thought to be particularly vulnerable to PTSD because of:
- past history of PTSD, depression, or anxiety disorder
- severity of the trauma (such as in cases of sexual assault or torture)
- pain (antidepressants with analgesic properties—such as venlafaxine or duloxetine—might be useful in patients whose trauma is associated with physical injury, although neither is FDA-approved to treat PTSD).
Table 3
4 considerations when choosing a drug for PTSD prevention
| Potential benefits | Practicality, ease of use, and safety of the proposed medication |
| Potential drug-drug or drug-disease interactions | Asthma, diabetes, and trauma are relative contraindications to the use of antiadrenergics and corticosteroids |
| Psychiatric comorbidities | A patient’s history of substance use disorder makes opioid analgesics a concern |
| Clinical experience | Agents already prescribed safely and broadly in clinical practice are easiest to test and to use |
Related resources
- Mental health and mass violence: Evidence-based early psychological intervention for victims/survivors of mass violence. A workshop to reach consensus on best practices. Rockland, MD: National Institute of Mental Health; 2002. www.nimh.nih.gov.
- Post-traumatic stress disorder: the management of PTSD in adults and children in primary and secondary care (clinical guideline 26). London, UK: National Institute for Clinical Excellence; 2005. www.nice.org.uk.
- Ursano RJ, Bell C, Eth S, et al. Practice guideline for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Am J Psychiatry 2004;161(suppl 11):3-31.
Drug brand names
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Citalopram • Celexa
- Clonazepam • Klonopin
- Clonidine • Catapres
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Guanfacine • Tenex
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Paroxetine • Paxil
- Prazosin • Minipress
- Propranolol • Inderal
- Sertraline • Zoloft
- Temazepam • Restoril
- Venlafaxine • Effexor
Disclosure
Dr. Bennett and Dr. Zatzick report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Roy-Byrne is a consultant to Jazz Pharmaceuticals and Solvay and has received speaker honoraria from Wyeth and Forrest Pharmaceuticals.
Posttraumatic stress disorder (PTSD) is a preventable mental illness—without trauma, the illness does not occur. Primary prevention (such as eliminating war, rape, physical assaults, child abuse, or motor vehicle accidents) would be effective but is an unrealistic goal. Secondary prevention (such as preventing PTSD after individuals have been exposed to trauma) may be attainable.
No medication is FDA-approved to prevent PTSD, but patients recently exposed to trauma might benefit from drugs approved for other indications. Possibilities include noradrenergics such as propranolol, corticosteroids that affect the hypothalamic-pituitary-adrenal (HPA) axis, opioids, benzodiazepines, and antidepressants. Some investigational agents also might block the process that turns a traumatic experience into PTSD.
This article discusses these intriguing ideas and suggests which trauma victims might benefit now from acute pharmacologic PTSD prevention.
Who might be treated?
An estimated 8% to 10% of the U.S. population experiences PTSD at some point in life (Box 1).1,2 A person’s risk of developing PTSD after a traumatic event depends on the type of trauma. For example, 10% of motor vehicle accident survivors develop PTSD, compared with 60% of rape survivors.1
Targeting anyone who has experienced trauma for secondary PTSD prevention would expose large groups of people to medications they do not need. Targeting selected persons who are at the highest risk would be more efficient and cost-effective. In a group of acute trauma-exposed persons, 2 selection criteria could be considered simultaneously:
- Which patients may be most predisposed to PTSD?
- Which patients are showing early symptoms that may predict PTSD?
More than half of all American adults have been exposed to at least one traumatic event at some point in their lives.1 In most persons, the posttraumatic stress reaction causes short-term distress, with hyperarousal, agitation, intrusive memories, and exaggerated startle. Although these symptoms usually subside relatively quickly, they persist and evolve into posttraumatic stress disorder (PTSD) in a substantial number of trauma victims.
An estimated 8% to 10% of the U.S. population experiences PTSD at some point in life.2 Emotional distress, social and occupational disability, and persistent decrements in quality of life make PTSD a major public health problem.
Risk factors and resiliency. Certain factors have been shown to increase a person’s vulnerability for PTSD (Table 1).3 Other proposed risk factors include:
- personality types4
- psychophysiologic factors such as reactivity, conditionability, and resistance to extinction/habituation.5
Strong evidence also indicates that acute trauma-related symptoms—including excessive arousal and fear,6 peritraumatic dissociation, and depression—predict the later development of PTSD.
Once identified, individuals predisposed to developing PTSD could be given treatment to increase their resiliency after they have been exposed to trauma. Early evidence suggests that you also could consider giving these patients medications as secondary prevention (Table 2).
Table 1
Who develops PTSD? Risk and resiliency factors
Risk factors that may increase vulnerability for PTSD
|
Resiliency factors that may protect against PTSD
|
| Source: Reference 3 |
Table 2
Medications being studied for PTSD prevention
| Mechanism of action | Medication | FDA-approved indications | ||
|---|---|---|---|---|
| Psychiatric | Nonpsychiatric | |||
| Noradrenergic | Clonidine | No | Yes | |
| Guanfacine | No | Yes | ||
| Prazosin | No | Yes | ||
| Propranolol | No | Yes | ||
| Hypothalamic-pituitary-adrenal axis | Hydrocortisone | No | Yes | |
| Opioid | Morphine | No | Yes | |
| Antidepressant | Dual action | Duloxetine | Yes | Yes |
| Venlafaxine | Yes | No | ||
| SSRIs | Citalopram | Yes | No | |
| Fluoxetine | Yes | No | ||
| Paroxetine | Yes | No | ||
| Sertraline | Yes | No | ||
| TCAs | Amitriptyline | Yes | No | |
| Imipramine | Yes | No | ||
| GABA-benzodiazepine | Alprazolam | Yes | No | |
| Temazepam | Yes | No | ||
| Corticotropin-releasing hormone (CRH) | CRH antagonist | Investigational | ||
| Substance P | Substance P antagonist | Investigational | ||
| Neuropeptide Y | Neuropeptide Y agonist | Investigational | ||
| SSRIs: selective serotonin reuptake inhibitors | ||||
| TCAs: tricyclic antidepressants | ||||
Targeting noradrenergic activity
Increased noradrenergic activity has been associated with persistent memories and PTSD. Therefore, medications that reduce noradrenergic tone by blocking receptors or reduce norepinephrine release are being explored for PTSD prevention.
Propranolol. Three small studies have examined whether the beta-noradrenergic receptor blocker propranolol can prevent PTSD.
In a randomized, double-blind, placebo-controlled trial,7 41 emergency department patients who had a heart rate of ≥ 80 bpm within 6 hours of a traumatic accident received propranolol, 40 mg qid, or placebo for 10 days. After 1 month, the 11 patients who completed propranolol treatment showed a nonsignificant trend toward lower scores on the Clinician-Administered PTSD Scale (CAPS), compared with 20 patients taking placebo. At 3 months, the propranolol group had less physiologic reactivity (as measured by heart rate and skin conductance) to trauma-related cues than the placebo group.
In a nonrandomized study,8 PTSD developed within 2 months in 1 of 11 trauma victims who agreed to take propranolol, 40 mg tid, immediately after the trauma, compared with 3 of 8 victims who refused the medication.
In an unpublished randomized, double-blind trial,9 48 patients admitted to a level I trauma center received propranolol, 40 mg tid; gabapentin, 400 mg tid; or placebo for PTSD prevention. Gabapentin was chosen because it has few side effects or metabolic interactions and preliminary evidence of anxiolytic efficacy.
Neither propranolol nor gabapentin showed statistically significant benefit in preventing PTSD compared with placebo. Effect sizes with the 2 treatments were too small to suggest that larger samples would produce a statistically significant result.
Prazosin—an alpha-1 adrenergic receptor antagonist—has been evaluated in 3 controlled studies and found to reduce intrusive nightmares typical of chronic PTSD.
Ten combat veterans with chronic PTSD showed significantly improved sleep, fewer severe nightmares, and improved global clinical status after receiving prazosin (mean dose 9.5 mg at bedtime) in a 20-week, placebo-controlled, double-blind, crossover study.10
In a larger randomized, parallel group trial,11 the same authors compared prazosin with placebo in 40 combat veterans (mean age 56) with chronic PTSD. After 8 weeks, veterans taking prazosin (mean 13.3 ± 3 mg) had significantly fewer trauma nightmares, improved sleep (including return of normal dreams), and improved global clinical status vs placebo. Overall CAP scores did not decline significantly, however.
In a third placebo-controlled study,12 a midmorning dose of prazosin was added to the regimens of 11 civilian trauma patients already taking the drug at bedtime to suppress trauma-related nightmares. Their daytime PTSD symptoms improved, as shown by reduced psychological distress in response to verbal trauma cues.
Prazosin can reduce chronic PTSD manifestations of nightmares and disturbed sleep, but it has not been shown to ameliorate the full PTSD syndrome. Prazosin has not been studied as an early PTSD intervention.
Other antiadrenergics that reduce the release of norepinephrine—including clonidine and guanfacine—have been studied in open trials as treatment for PTSD. The only controlled study13 showed no benefit from guanfacine for PTSD prevention.
De-stressing the HPA axis
Hydrocortisone has been proposed to prevent PTSD by reducing HPA axis activation, acting as a countermeasure to elevated corticotropin-releasing factor found in patients with chronic PTSD.
IV hydrocortisone’s effect on the development of PTSD was compared with placebo in 20 septic shock survivors after discharge from intensive care.14 One of 9 patients (11%) in the hydrocortisone group was diagnosed with PTSD at follow-up (mean 31 months), compared with 7 of 11 (64%) in the placebo group.
In a similar study, the same researchers gave patients hydrocortisone before, during, and after cardiac surgery. Follow-up interviews revealed significantly lower PTSD and chronic stress symptom scores in the treatment group vs the placebo group.15
These studies—although provocative—are limited by the narrow range of trauma related to severe medical illness or extensive medical procedures.
Norepinephrine-blocking opioids
When the noradrenergic system is activated, one physiologic response is the activation of endogenous opioid systems, which may promote recovery by inhibiting the HPA axis. Opioid systems might be involved in PTSD, as suggested by:
- preclinical evidence that opioids modulate memory16
- studies showing low pain thresholds17 and abnormal beta-endorphin (an opioid peptide neurotransmitter)18 and methionine enkephalin (an opioid peptide)19 levels in PTSD patients.
In theory, opioid administration immediately after trauma may attenuate norepinephrine release, thus thwarting arousal-charged memory consolidation, hyperarousal, and re-experiencing.
One uncontrolled report of pediatric burn victims found a significant association between the morphine dose given for pain during hospitalization and reduced PTSD symptoms 6 months later.20 Decreased pain did not explain the reduction in PTSD, as no significant correlation was seen between pain symptoms and PTSD outcome measures. Similarly, a longitudinal study of substance use among Vietnam War veterans with PTSD found decreased hyperarousal symptoms in heroin users.21
Using opioids to prevent PTSD would be feasible and efficient in acute care settings because 80% to 90% of traumatically-injured patients are discharged on opioid analgesics (compared with <10% on beta blockers or corticosteroids).22 However, 20% to 40% of physically injured inpatients are diagnosed with a substance use disorder at some point in life, making the use of opioid analgesics a practical concern.23
GABA-benzodiazepine paradox
The GABA-benzodiazepine system plays an important role in mediating anxiety, which is consistent with the potent anxiolytic effects of benzodiazepines. Even so, trials of benzodiazepines have found these drugs surprisingly unhelpful—and perhaps harmful—in patients with acute trauma.
Alprazolam did not reduce PTSD symptoms in a small randomized, double-blind study.24 Another trial found that receiving benzodiazepines shortly after trauma exposure was associated with increased PTSD risk in trauma survivors. Nine of 13 patients (69%) who received alprazolam or clonazepam met PTSD diagnostic criteria 6 months after the trauma, compared with 3 of 13 controls (15%).25
Similarly, in a randomized controlled trial, 22 patients were given temazepam for 7 nights, starting approximately 14 days after exposure to a traumatic event. Six weeks later, 55% of those receiving temazepam and 27% of those receiving placebo met criteria for PTSD.26
In summary, benzodiazepines might be helpful when given for a few days after traumatization to control overwhelming anxiety but could be harmful over a longer term.
Other agents for PTSD
Antidepressants. Early trauma-related symptoms of depression predict later development of PTSD.27 Thus, antidepressants have been proposed for early intervention in addition to their well-established role as first-line treatment of PTSD.28
One study supports this idea: a 7-day randomized double-blind trial that compared the tricyclic antidepressant imipramine with chloral hydrate in pediatric burn patients with acute stress disorder (ASD). Imipramine was more effective (83% response) than chloral hydrate (38% response) in reducing ASD symptoms.29
Drugs in development. Three new medications being explored for treating anxiety and depression also might be useful for PTSD prevention. Neuropeptide Y (NPY) agonists,30 substance P antagonists,31 and CRH-antagonists32 are thought to hold promise because of their more proximate roles—compared with monoamine neurotransmitters such as dopamine, norepinephrine and serotonin—in mediating the stress response.
Manage the post-trauma environment:
- Move the victim to safety.
- Treat pain effectively.
- Avoid stress from interrogations, separation from loved ones, or unstable housing.
Avoid crisis incident stress debriefing (CISD), which could enhance physiologic hyperarousal and is not recommended as first-line treatment for most trauma victims. CISD was designed for and is best received by emergency personnel.
Consider prescribing antidepressants for patients thought to be particularly vulnerable to develop posttraumatic stress disorder (PTSD). Risk factors include:
- history of PTSD, depression, or anxiety disorder
- severe trauma (such as from sexual assault or torture)
- physical injury, when antidepressants with analgesic properties might be useful.
Analyzing the evidence
Insufficient evidence exists to determine which strategies might be most effective to prevent PTSD, what optimal dosing might be, and which traumatized individuals might be best targeted with these approaches.
- Beta-blockers and corticosteroids—the most theoretically compelling strategies—are the most difficult agents to use for PTSD prevention because they have the most medical contraindications. In addition, evidence supporting their ability to prevent PTSD is meager at best.
- Prazosin is intriguing but has contra-indications similar to those of beta blockers, no studies of secondary prevention, and no clear indication that it works for the overall PTSD syndrome.
- Opioids are restricted agents with substantial contraindications.
- Evidence is limited but points most strongly toward earlier use of antidepressants. Early trauma-related symptoms of depression predict later development of PTSD,27 and a number of selective serotonin reuptake inhibitors—such as citalopram, fluoxetine, paroxetine, and sertraline—are FDA-approved or used off-label for treating PTSD.33
Prescribing recommendations. Consider practicality, ease of use, and safety of the proposed medication when choosing a drug for PTSD prevention (Table 3).22 Based on the evidence, the most reasonable posttrauma approach (Box 2) might be to consider starting an approved antidepressant for individuals thought to be particularly vulnerable to PTSD because of:
- past history of PTSD, depression, or anxiety disorder
- severity of the trauma (such as in cases of sexual assault or torture)
- pain (antidepressants with analgesic properties—such as venlafaxine or duloxetine—might be useful in patients whose trauma is associated with physical injury, although neither is FDA-approved to treat PTSD).
Table 3
4 considerations when choosing a drug for PTSD prevention
| Potential benefits | Practicality, ease of use, and safety of the proposed medication |
| Potential drug-drug or drug-disease interactions | Asthma, diabetes, and trauma are relative contraindications to the use of antiadrenergics and corticosteroids |
| Psychiatric comorbidities | A patient’s history of substance use disorder makes opioid analgesics a concern |
| Clinical experience | Agents already prescribed safely and broadly in clinical practice are easiest to test and to use |
Related resources
- Mental health and mass violence: Evidence-based early psychological intervention for victims/survivors of mass violence. A workshop to reach consensus on best practices. Rockland, MD: National Institute of Mental Health; 2002. www.nimh.nih.gov.
- Post-traumatic stress disorder: the management of PTSD in adults and children in primary and secondary care (clinical guideline 26). London, UK: National Institute for Clinical Excellence; 2005. www.nice.org.uk.
- Ursano RJ, Bell C, Eth S, et al. Practice guideline for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Am J Psychiatry 2004;161(suppl 11):3-31.
Drug brand names
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Citalopram • Celexa
- Clonazepam • Klonopin
- Clonidine • Catapres
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Guanfacine • Tenex
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Paroxetine • Paxil
- Prazosin • Minipress
- Propranolol • Inderal
- Sertraline • Zoloft
- Temazepam • Restoril
- Venlafaxine • Effexor
Disclosure
Dr. Bennett and Dr. Zatzick report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Roy-Byrne is a consultant to Jazz Pharmaceuticals and Solvay and has received speaker honoraria from Wyeth and Forrest Pharmaceuticals.
1. Kessler RC, Sonnega A, Bromet E, et al. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1995;52(12):1048-60.
2. Zatzick D. Posttraumatic stress, functional impairment, and service utilization after injury: a public health approach. Semin Clin Neuropsychiatry 2003;8(3):149-57.
3. Yehuda R, Flory JD, Southwick S, Charney DS. Developing an agenda for translational studies of resilience and vulnerability following trauma exposure. Ann NY Acad Sci 2006;1071:379-96.
4. Schnurr P, Vielhauer M. Personality as a risk factor for PTSD. In: Yehuda R, ed. Risk factors for post-traumatic stress disorder. Washington, DC: American Psychiatric Publishing; 1999:191-222.
5. Shalev A. Psychophysiological expression of risk factors for PTSD. In: Yehuda R, ed. Risk factors for posttraumatic stress disorder. Washington, DC: American Psychiatric Publishing; 1995.
6. Bryant RA, Harvey AG, Guthrie RM, Moulds ML. A prospective study of psychophysiological arousal, acute stress disorder, and posttraumatic stress disorder. J Abnorm Psychol 2000;109(2):341-4.
7. Pitman RK, Sanders KM, Zusman RM, et al. Pilot study of secondary prevention of posttraumatic stress disorder with propranolol. Biol Psychiatry 2002;51(2):189-92.
8. Vaiva G, Ducrocq F, Jezequel K, et al. Immediate treatment with propranolol decreases posttraumatic stress disorder two months after trauma. Biol Psychiatry 2003;54(9):947-9.
9. Stein M. Pharmacoprevention of adverse psychiatric sequelae of physical injury. Paper presented at: 21st Annual Meeting of the International Society for Traumatic Stress Studies; November 2-5, 2005; Toronto, Ontario, Canada.
10. Raskind MA, Peskind ER, Kanter ED, et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo-controlled study. Am J Psychiatry 2003;160(2):371-3.
11. Raskind MA, Peskind ER, Hoff DJ, et al. A parallel group placebo controlled study of prazosin for trauma nightmares and sleep disturbance in combat veterans with post-traumatic stress disorder. Biol Psychiatry 2007;61(8):928-34.
12. Taylor FB, Lowe K, Thompson C, et al. Daytime prazosin reduces psychological distress to trauma specific cues in civilian trauma posttraumatic stress disorder. Biol Psychiatry 2006;59(7):577-81.
13. Neylan TC, Lenoci M, Samuelson KW, et al. No improvement of posttraumatic stress disorder symptoms with guanfacine treatment. Am J Psychiatry 2006;163(12):2186-8.
14. Schelling G, Briegel J, Roozendaal B, et al. The effect of stress doses of hydrocortisone during septic shock on posttraumatic stress disorder in survivors. Biol Psychiatry 2001;50(12):978-85.
15. Weis F, Kilger E, Roozendaal B, et al. Stress doses of hydrocortisone reduce chronic stress symptoms and improve health-related quality of life in high-risk patients after cardiac surgery: a randomized study. J Thorac Cardiovasc Surg 2006;131(2):277-82.
16. McGaugh JL, Introini-Collison IB, Nagahara AH, et al. Involvement of the amygdaloid complex in neuromodulatory influences on memory storage. Neurosci Biobehav Rev 1990;14(4):425-31.
17. Shalev AY, Peri T, Canetti L, Schreiber S. Predictors of PTSD in injured trauma survivors: a prospective study. Am J Psychiatry 1996;153(2):219-25.
18. Baker DG, West SA, Orth DN, et al. Cerebrospinal fluid and plasma beta-endorphin in combat veterans with post-traumatic stress disorder. Psychoneuroendocrinol 1997;22(7):517-29.
19. Wolf ME, Mosnaim AD, Puente J, Ignacio R. Plasma methionine-enkephalin in PTSD. Biol Psychiatry 1991;29(3):305-7.
20. Saxe G, Stoddard F, Courtney D, et al. Relationship between acute morphine and the course of PTSD in children with burns. J Am Acad Child Adolesc Psychiatry 2001;40(8):915-21.
21. Bremner JD, Southwick SM, Darnell A, Charney DS. Chronic PTSD in Vietnam combat veterans: course of illness and substance abuse. Am J Psychiatry 1996;153(3):369-75.
22. Zatzick D, Roy-Byrne PP. From bedside to bench: how the epidemiology of clinical practice can inform the secondary prevention of PTSD. Psychiatr Serv 2006;57(12):1726-30.
23. Zatzick D, Jurkovich G, Russo J, et al. Posttraumatic distress, alcohol disorders, and recurrent trauma across level 1 trauma centers. J Trauma 2004;57(2):360-6.
24. Braun P, Greenberg D, Dasberg H, Lerer B. Core symptoms of posttraumatic stress disorder unimproved by alprazolam treatment. J Clin Psychiatry 1990;51(6):236-8.
25. Gelpin E, Bonne O, Peri T, et al. Treatment of recent trauma survivors with benzodiazepines: a prospective study. J Clin Psychiatry 1996;57(9):390-4.
26. Mellman TA, Bustamante V, David D, et al. Hypnotic medication in the aftermath of trauma. J Clin Psychiatry 2002;63(12):1183-4.
27. Freedman SA, Brandes D, Peri T, Shalev A. Predictors of chronic post-traumatic stress disorder. A prospective study. Br J Psychiatry 1999;174:353-9.
28. Davidson JR. Pharmacologic treatment of acute and chronic stress following trauma. J Clin Psychiatry 2006;67(suppl 2):34-9.
29. Robert R, Blakeney PE, Villarreal C, et al. Imipramine treatment in pediatric burn patients with symptoms of acute stress disorder: a pilot study. J Am Acad Child Adolesc Psychiatry 1999;38(7):873-82.
30. Morgan CA, Wang S, Southwick SM, et al. Plasma neuropeptide-Y concentrations in humans exposed to military survival training. Biol Psychiatry 2000;47(10):902-9.
31. Geracioti TD, Carpenter LL, Owens MJ, et al. Elevated cerebrospinal fluid substance P concentrations in posttraumatic stress disorder and major depression. Am J Psychiatry 2006;163(4):637-43.
32. Zobel AW, Nickel T, Künzel HE, et al. Effects of the highaffinity corticotropin-releasing hormone receptor 1 antagonist R121919 in major depression: the first 20 patients treated. J Psychiatr Res 2000;34(3):171-81.
33. Davidson JR. Treatment of posttraumatic stress disorder: the impact of paroxetine. Psychopharmacol Bull 2003;37(suppl 1):76-88.
1. Kessler RC, Sonnega A, Bromet E, et al. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1995;52(12):1048-60.
2. Zatzick D. Posttraumatic stress, functional impairment, and service utilization after injury: a public health approach. Semin Clin Neuropsychiatry 2003;8(3):149-57.
3. Yehuda R, Flory JD, Southwick S, Charney DS. Developing an agenda for translational studies of resilience and vulnerability following trauma exposure. Ann NY Acad Sci 2006;1071:379-96.
4. Schnurr P, Vielhauer M. Personality as a risk factor for PTSD. In: Yehuda R, ed. Risk factors for post-traumatic stress disorder. Washington, DC: American Psychiatric Publishing; 1999:191-222.
5. Shalev A. Psychophysiological expression of risk factors for PTSD. In: Yehuda R, ed. Risk factors for posttraumatic stress disorder. Washington, DC: American Psychiatric Publishing; 1995.
6. Bryant RA, Harvey AG, Guthrie RM, Moulds ML. A prospective study of psychophysiological arousal, acute stress disorder, and posttraumatic stress disorder. J Abnorm Psychol 2000;109(2):341-4.
7. Pitman RK, Sanders KM, Zusman RM, et al. Pilot study of secondary prevention of posttraumatic stress disorder with propranolol. Biol Psychiatry 2002;51(2):189-92.
8. Vaiva G, Ducrocq F, Jezequel K, et al. Immediate treatment with propranolol decreases posttraumatic stress disorder two months after trauma. Biol Psychiatry 2003;54(9):947-9.
9. Stein M. Pharmacoprevention of adverse psychiatric sequelae of physical injury. Paper presented at: 21st Annual Meeting of the International Society for Traumatic Stress Studies; November 2-5, 2005; Toronto, Ontario, Canada.
10. Raskind MA, Peskind ER, Kanter ED, et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo-controlled study. Am J Psychiatry 2003;160(2):371-3.
11. Raskind MA, Peskind ER, Hoff DJ, et al. A parallel group placebo controlled study of prazosin for trauma nightmares and sleep disturbance in combat veterans with post-traumatic stress disorder. Biol Psychiatry 2007;61(8):928-34.
12. Taylor FB, Lowe K, Thompson C, et al. Daytime prazosin reduces psychological distress to trauma specific cues in civilian trauma posttraumatic stress disorder. Biol Psychiatry 2006;59(7):577-81.
13. Neylan TC, Lenoci M, Samuelson KW, et al. No improvement of posttraumatic stress disorder symptoms with guanfacine treatment. Am J Psychiatry 2006;163(12):2186-8.
14. Schelling G, Briegel J, Roozendaal B, et al. The effect of stress doses of hydrocortisone during septic shock on posttraumatic stress disorder in survivors. Biol Psychiatry 2001;50(12):978-85.
15. Weis F, Kilger E, Roozendaal B, et al. Stress doses of hydrocortisone reduce chronic stress symptoms and improve health-related quality of life in high-risk patients after cardiac surgery: a randomized study. J Thorac Cardiovasc Surg 2006;131(2):277-82.
16. McGaugh JL, Introini-Collison IB, Nagahara AH, et al. Involvement of the amygdaloid complex in neuromodulatory influences on memory storage. Neurosci Biobehav Rev 1990;14(4):425-31.
17. Shalev AY, Peri T, Canetti L, Schreiber S. Predictors of PTSD in injured trauma survivors: a prospective study. Am J Psychiatry 1996;153(2):219-25.
18. Baker DG, West SA, Orth DN, et al. Cerebrospinal fluid and plasma beta-endorphin in combat veterans with post-traumatic stress disorder. Psychoneuroendocrinol 1997;22(7):517-29.
19. Wolf ME, Mosnaim AD, Puente J, Ignacio R. Plasma methionine-enkephalin in PTSD. Biol Psychiatry 1991;29(3):305-7.
20. Saxe G, Stoddard F, Courtney D, et al. Relationship between acute morphine and the course of PTSD in children with burns. J Am Acad Child Adolesc Psychiatry 2001;40(8):915-21.
21. Bremner JD, Southwick SM, Darnell A, Charney DS. Chronic PTSD in Vietnam combat veterans: course of illness and substance abuse. Am J Psychiatry 1996;153(3):369-75.
22. Zatzick D, Roy-Byrne PP. From bedside to bench: how the epidemiology of clinical practice can inform the secondary prevention of PTSD. Psychiatr Serv 2006;57(12):1726-30.
23. Zatzick D, Jurkovich G, Russo J, et al. Posttraumatic distress, alcohol disorders, and recurrent trauma across level 1 trauma centers. J Trauma 2004;57(2):360-6.
24. Braun P, Greenberg D, Dasberg H, Lerer B. Core symptoms of posttraumatic stress disorder unimproved by alprazolam treatment. J Clin Psychiatry 1990;51(6):236-8.
25. Gelpin E, Bonne O, Peri T, et al. Treatment of recent trauma survivors with benzodiazepines: a prospective study. J Clin Psychiatry 1996;57(9):390-4.
26. Mellman TA, Bustamante V, David D, et al. Hypnotic medication in the aftermath of trauma. J Clin Psychiatry 2002;63(12):1183-4.
27. Freedman SA, Brandes D, Peri T, Shalev A. Predictors of chronic post-traumatic stress disorder. A prospective study. Br J Psychiatry 1999;174:353-9.
28. Davidson JR. Pharmacologic treatment of acute and chronic stress following trauma. J Clin Psychiatry 2006;67(suppl 2):34-9.
29. Robert R, Blakeney PE, Villarreal C, et al. Imipramine treatment in pediatric burn patients with symptoms of acute stress disorder: a pilot study. J Am Acad Child Adolesc Psychiatry 1999;38(7):873-82.
30. Morgan CA, Wang S, Southwick SM, et al. Plasma neuropeptide-Y concentrations in humans exposed to military survival training. Biol Psychiatry 2000;47(10):902-9.
31. Geracioti TD, Carpenter LL, Owens MJ, et al. Elevated cerebrospinal fluid substance P concentrations in posttraumatic stress disorder and major depression. Am J Psychiatry 2006;163(4):637-43.
32. Zobel AW, Nickel T, Künzel HE, et al. Effects of the highaffinity corticotropin-releasing hormone receptor 1 antagonist R121919 in major depression: the first 20 patients treated. J Psychiatr Res 2000;34(3):171-81.
33. Davidson JR. Treatment of posttraumatic stress disorder: the impact of paroxetine. Psychopharmacol Bull 2003;37(suppl 1):76-88.
Suicide intervention: How to recognize risk, focus on patient safety
More than 50% of psychiatrists have experienced the death of a patient by suicide.1 For many of us, suicide represents the most feared outcome of a patient’s mental illness and makes managing suicide risk critical to everyday practice.
Unfortunately, we have little ability to predict suicide. Research into risk factors and the use of suicide rating scales have produced no consistently definitive methods to determine who will and who will not attempt or complete suicide.2 The purpose of suicide assessment, then, is not to predict suicide but to help us understand the sources of a patient’s suicidality and develop an informed intervention.
This article describes a practical, commonly accepted approach to suicide risk assessment and intervention, based on the B-SAFE model (Basic Suicide Assessment Five-step Evaluation) proposed by Jacobs et al (Figure).3 Using this method to assess suicide risk can help you answer questions such as:
- Which factors are most important to consider when evaluating suicide risk in my patient?
- What questions should I ask my patient to find out if he or she is suicidal?
- How do I know if a patient is at risk for suicide?
- What emergent interventions are called for when managing the acutely suicidal patient?
- How should I document a suicide risk assessment?
Figure Basic Suicide Assessment Five-step Evaluation (B-SAFE)
Source: Created from information in references 2,11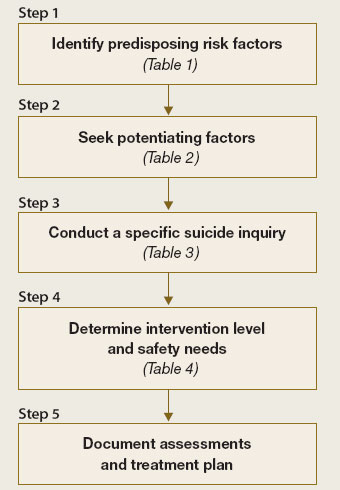
Why ask about suicide?
No single risk factor or combination of risk factors can predict or preclude suicide. Even so, attempting to evaluate an individual’s risk by asking about suicidal thinking, reviewing risk factors, or using clinical rating scales helps you determine the next appropriate action (discharge, medication, psychiatric referral, consultation, or hospitalization).
While talking to patients and evaluating their risk for suicide, you may begin to understand their suffering—described as the most common denominator in suicide2 and perhaps the most important clue to heightened suicide risk. Such an exploration allows you to identify potential:
- risk factors that can be modified
- preventative factors to promote.
Don’t be afraid to ask. Asking about suicidal thoughts is necessary—but not enough—to understand an individual’s potential for suicide. Never be afraid to ask patients about suicide, believing that doing so will “put ideas into their heads.” By the same token, a patient who denies thoughts or plans for suicide may still be at risk.
Identifying at-risk patients is much more difficult than just asking if they are considering suicide. Opening a concerned dialogue can provide a sense of relief to the patient while allowing you to explore:
- the extent and seriousness of the suicidal thoughts
- associated risk factors or conditions, such as depression.
Stepwise risk assessment
The first 3 steps of Jacobs’ B-SAFE model focus on identifying predisposing and protective factors for suicide.3 For an in-depth discussion, consult the American Psychiatric Association practice guideline for the assessment and treatment of patients with suicidal behaviors4 (available at http://www.psych.org/psych_pract/treatg/pg/suicidalbehavior_05-15-06.pdf).
STEP 1: Risk factors. Use the patient interview, medical records, and collateral information to uncover potential suicide risk factors (Table 1).2
Psychopathology. Focus on depression, bipolar disorder, schizophrenia, substance abuse, and personality disorders, which are strongly associated with suicide. These disorders are considered modifiable risk factors—diagnosis and appropriate treatment can diminish suicide risk.
Suicidality has been associated with early depression or bipolar disorder, often before patients receive a diagnosis or effective treatment. Recovery and immediate post-discharge periods also are thought to be times of heightened suicide risk.
Psychosocial variables. Demographic and psychosocial variables may influence suicide risk estimation. A retrospective study of 100 patients who attempted suicide suggests that the most predictive factors for suicide are:
- living alone
- being aged 17 to 35 (although in other studies, more advanced age also has been linked to increased suicide risk3)
- complaints of severe hopelessness, anhedonia, and insomnia.5
Physical illness may potentiate suicide risk. Medical illnesses that produce great pain, disfigurement, limited function, or fear of dependence may reduce a person’s will to live and increase suicide risk.6 Epilepsy has been associated with a 4- to 5-fold increase in suicide risk7 and is the only medical diagnosis to carry a documented increase in suicide among children and adolescents.8 Often these medical disorders coexist with psychiatric disorders, complicating the task of determining independent risk.
Severity of attempts or self-mutilation. When evaluating self-injurious or suicidal behavior in the emergency setting, consider the severity of the attempt as part of overall suicide assessment. Self-injurious behavior (cutting or burning) or impulsive suicide attempts (planned for <3 hours, committed in the presence others, or where discovery is very probable) appear to carry less severity or intent to die than do carefully planned and/or hidden suicide attempts.9 However, consider at high risk for suicide any patient with self-mutilating or suicidal behavior who expresses persistent intent to die; acute stabilization on an in-patient unit may be necessary.
STEP 2: ‘Protective’ factors. Discover and discuss internal and external factors that might help prevent the individual with suicidal thoughts from converting those thoughts into action (Table 2).2 When discussing these potentially protective effects, emphasize the patient’s:
- resilience during past personal crises
- family responsibilities
- religious or spiritual beliefs.
‘No-harm contracts.’ Suicide (or “no-harm”) contracts with patients might help open communication about factors that promote or mitigate suicide risk. Such contacts do not prevent suicide or lessen medicolegal risk in the event of a patient suicide, however.10
STEP 3: Suicide plans. Ask about suicide thoughts, plans, and behaviors (Table 3).11 Probe gently to allow the individual to discuss his or her feelings and to explore the next appropriate avenue of care.
In my experience, patients who reveal passive suicidal ideation (such as, “I sometimes wish I would just die in my sleep”) and strong deterrents to acting on thoughts of suicide (such as, “My children need me,” or “It’s against my religion”) should continue outpatient treatment. Those without deterrents or who discuss active and imminent thoughts and recent actions—writing suicide notes, buying a weapon, stockpiling pills—require emergent evaluation for psychiatric admission. Ask about thoughts of self-injury or mutilation (such as cutting or burning), as well as homicidal ideation.
Recognizing that patients with suicidal thoughts are almost always ambivalent about suicide to some extent—conflicted by simultaneous desires to live and to die—gives you the opportunity to intervene by allying with the part of the patient that wants to live. Creating a therapeutic connection also will help you determine the level of intervention required.
STEP 4: Intervention. Understanding why a patient feels suicidal—gathered in Steps 1 to 3—can help you choose the appropriate intervention. Among the 5 steps, Step 4 relies most heavily on clinical judgment:
- Is the suicidality acute or chronic?
- How great is the risk for suicide?
- To keep the patient safe, how urgent is the required intervention?
Acute risk. Suicidality related to Axis I psychiatric disorders tends to be acute, with prominent pain, anguish, and a desire to escape. Patients may describe a driven quality to the suicidality, which commands a treatment plan that maintains patient safety until suicidal feelings remit.
Hospitalization is often needed, plus focused treatments such as medication, psychotherapy, or electroconvulsive therapy. Intensive outpatient follow-up or partial hospitalization programs might be considered for patients:
- with whom you have a strong therapeutic alliance
- who have sturdy psychosocial support
- whose precipitating factors for suicidality have resolved.
Chronic risk. Suicide risk tends to be more chronic and has an impulsive quality for patients with suicidality related to personality disorders and environmental factors. Personality disordered patients may report feelings of anger, rage, or vengeance connected with their suicidal thoughts.
Hospitalization might become necessary, although multiple hospitalizations can be counter-therapeutic. Attempting in therapy to teach the patient to cope with suicidal thoughts and feelings might be a more effective intervention.
Malingering. Use your best judgment when patients make suicide threats that could represent malingering to achieve hospitalization.
Step 5: Documentation. Document your assessment of the suicidal patient and decision making to:
- clarify the treatment plan
- communicate to other caregivers
- manage medicolegal risk.
Include a brief summary (Box) that is timely, legible, and communicates the estimated degree of risk, known data, diagnosis, and planned interventions such as medications, tests, consultations, and follow-up reassessments.
This 46-year-old, recently divorced man is experiencing his second episode of major depression associated with clear-cut panic attacks and suspected psychotic features. Although he denies current suicidal ideation, the treatment team believes he is at moderate to high risk for suicide because of known past history of serious suicide attempt with first depression, the presence of panic/anxiety, and possibly psychotic features. Additional risk is posed by loss of marital support and his inability to verbalize meaningful protective factors.
The plan is to convert from observation status on the inpatient unit to full admission, as the suicide risk precludes discharge at present. Further medication management and consideration for electroconvulsive therapy will take place, with daily reassessments. Suicide precautions ordered.
Table 1
Factors associated with potential for increased suicide risk
| Variable | Risk Factors |
|---|---|
| Demographic | Male gender, Caucasian race, rural residence, possibly age (varies among studies) |
| Imprisoned; widowed, divorced, or separated; living alone; no children or no children living in the home | |
| Psychosocial | Lack or loss of social supports, recent loss of employment, decrease in socioeconomic status or poverty, hopelessness |
| History of victimization (physical or sexual abuse), psychological turmoil, severe relationship conflict, aggressive or impulsive traits | |
| Writing suicide notes; family history of suicide, previous attempts, ‘imitation’ suicide, gun ownership | |
| Occupational risk (physicians, dentists, nurses, pharmacists, veterinarians, farmers) | |
| Psychiatric | Psychiatric diagnosis of recent onset |
| Mood disorder, particularly major depression and bipolar disorder | |
| Schizophrenia; alcohol or other substance abuse or addiction; personality disorder; panic attacks or severe psychic anxiety | |
| Insomnia; poor concentration or confusion; anhedonia | |
| Medical | Huntington’s disease, stroke, multiple sclerosis, head injury, spinal cord injury, systemic lupus erythematosus, AIDS |
| Epilepsy, pain, malignant neoplasms, peptic ulcer disease, renal disease | |
| Source: Adapted with permission from reference 3 | |
Table 2
Potentially protective factors against suicide
| Internal |
| Successful past responses to stress |
| Positive coping skills |
| Spirituality |
| Capacity for reality testing |
| Frustration tolerance/optimism |
| Overall individual resiliency |
| External |
| Children or pets in the home |
| Religious prohibition or beliefs |
| Positive therapeutic relationships |
| Sense of responsibility to family |
| Social supports and connections |
| Financial incentives or deterrents |
| Source: Adapted from reference 11 |
Table 3
Evaluating suicide risk: Questions to ask patients
| Have you felt so sad or depressed that you thought life is not worth living? |
| Have you thought about hurting yourself or taking your own life? |
| Have you thought about a way or plan to kill yourself? |
| Do you have the means to complete the plan? (such as, do you have access to weapons or pills?) |
| Have you practiced or rehearsed this plan to end your own life? |
| Do you have a location picked out? |
| What has stopped you from following through with the plan? |
| Have you ever attempted suicide? |
| Has anyone in your family ever attempted or committed suicide? |
| Source: Adapted with permission from reference 3 |
Interventions for suicidal patients
Physical protection. Take decisive action when you determine that suicide risk is elevated and imminent. Pursue urgent psychiatric hospitalization, with or without patient consent, in accordance with local probate and involuntary commitment statutes.
The logistics of protective action can be challenging; transportation is often required, and the patient is not always cooperative with admission. Table 4 lists measures and precautions that can help keep the suicidal patient safe.
Disease-specific interventions. Because suicidal ideation is often symptomatic of a primary psychiatric disorder, rapidly identifying major depression, bipolar disorder, or a psychotic illness is crucial to reducing suicidal thoughts and behaviors. Prescribe appropriate antidepressants, mood stabilizers, and antipsychotics at adequate doses and for sufficient duration.
Be vigilant for distressing symptoms that may be elevating the patient’s suicide risk, such as anxiety, panic, agitation, insomnia, or pain. Pharmacotherapies—such as anxiolytics, sedative-hypnotics, antipsychotics, or analgesics—may rapidly reduce suffering.
Impulsivity associated with substance use disorders—particularly during intoxication and withdrawal syndromes—requires aggressive attempts by the treatment team to engage the patient in detoxification and rehabilitation.
Direct antisuicide therapy. Clozapine carries an FDA-approved indication for preventing suicide in patients with schizophrenia or schizoaffective disorder. The mechanism by which clozapine helps prevent suicide is not known, but its anti-suicidal effects appear to be independent of its antipsychotic effects.12
Lithium has been reported to reduce risk of suicide and suicide attempts in patients with bipolar disorder, perhaps by as much as 80%.13 Such benefit has not been observed with other mood stabilizers, suggesting that lithium confers protective effects against suicide beyond its mood-stabilizing effects. Suicide risk is known to increase after lithium is discontinued.14
Lithium’s antisuicidal effects may arise from its ability to enhance serotonin. This theory, although unproven, is consistent with observations associating central serotonergic deficiency with suicidal and aggressive behaviors.
Psychosocial measures. Address psychosocial variables that may increase suicide risk (Table 1). Recruit and involve the patient’s support system, augmented with a close follow-up plan. Case management to explore housing and job opportunities can help. Work with the patient’s family or others to remove guns from the patient’s access. Individual, marital, and family therapies can reduce conflicts and strengthen coping skills.
Table 4
Safety measures to protect the suicidal patient
| Hospitalize—voluntarily or involuntarily—on a locked psychiatric unit |
| Provide constant 1-to-1 observation by staff |
| Transport the patient, accompanied by adequate personnel |
| Use physical restraints or seclusion while maintaining continuous observation |
| Employ metal detector to remove dangerous, hidden objects |
| Remove and secure patient’s belongings (bags, coats, purses may contain pills or weapons) |
| Search visitors’ belongings before allowing access to unit |
| Ensure that inpatient unit meets all coded safety regulations |
Related resources
- National Suicide Prevention Lifeline, sponsored by the Substance Abuse & Mental Health Services Administration: 1-800-SUICIDE or 1-800-273-TALK (8255); www.suicidepreventionlifeline.org.
- American Foundation for Suicide Prevention (AFSP) 1-888-333-AFSP; www.afsp.org.
- Simon RI, Hales RE. Textbook of suicide assessment and management. Washington, DC: American Psychiatric Publishing; 2006.
Drug brand names
- Clozapine • Clozaril
- Lithium • Eskalith, Lithobid, others
Disclosure
Dr. Muzina has received grants from or served as a consultant to Abbott Laboratories, AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, Novartis Pharmaceuticals Corp., Pfizer, and Repligen.
1. Chemtob CM, Hamada RS, Bauer G, et al. Patients’ suicides: frequency and impact on psychiatrists. Am J Psychiatry 1988;145(2):224-8.
2. Muzina DJ. What physicians can do to prevent suicide. Cleve Clin J Med 2004;71(3):242-50.
3. Jacobs DG, Brewer ML, Klein-Benheim M. Suicide assessment: an overview and recommended protocol. In: Jacobs DG, ed. The Harvard Medical School guide to suicide assessment and intervention.. San Francisco, CA: Jossey-Bass Publishers; 1999:3-39.
4. Jacobs DG, Baldessarini RJ, Conwell Y, et al. American Psychiatric Association practice guideline for the assessment and treatment of patients with suicidal behaviors. Available at: http://www.psych.org/psych_pract/treatg/pg/suicidalbehavior_05-15-06.pdf. Accessed May 14, 2007.
5. Hall RC, Platt DE, Hall RC. Suicide risk assessment: a review of risk factors for suicide in 100 patients who made severe suicide attempts. Evaluation of suicide risk in a time of managed care. Psychosomatics 1999;40(1):18-27.
6. Mackenzie TB, Popkin MK. Suicide in the medical patient. Int J Psychiatry Med 1987;17(1):3-22.
7. Barraclough BM. The suicide rate of epilepsy. Acta Psychiatr Scand 1987;76(4):339-45
8. Brent DA, Kolko DJ, Allan MJ, Brown RV. Suicidality in affectively disordered adolescent inpatients. J Am Acad Child Adolesc Psychiatry 1990;29(4):586-93.
9. Polewka A, Mikolaszek-Boba M, Chrostek Maj J, Groszek B. The characteristics of suicide attempts based on the suicidal intent scale scores. Przegl Lek 2005;62(6):415-8.
10. Lewis LM. No-harm contracts: a review of what we know. Suicide Life Threat Behav 2007;37(1):50-7.
11. Jacobs DG. A resource guide for implementing the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) 2007 patient safety goals on suicide. Available at: http://www.sprc.org/library/jcahosafetygoals.pdf. Accessed May 14, 2007.
12. Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT). Arch Gen Psychiatry 2003;60(1):82-91.
13. Baldessarini RJ, Tondo L, Davis P, et al. Decreased risk of suicides and attempts during long-term lithium treatment: a meta-analytic review. Bipolar Disord 2006;8(5 Pt 2):625-39.
14. Baldessarini RJ, Tondo L, Viguera AC. Discontinuing lithium maintenance treatment in bipolar disorders: risks and implications. Bipolar Disord 1999;1(1):17-24.
More than 50% of psychiatrists have experienced the death of a patient by suicide.1 For many of us, suicide represents the most feared outcome of a patient’s mental illness and makes managing suicide risk critical to everyday practice.
Unfortunately, we have little ability to predict suicide. Research into risk factors and the use of suicide rating scales have produced no consistently definitive methods to determine who will and who will not attempt or complete suicide.2 The purpose of suicide assessment, then, is not to predict suicide but to help us understand the sources of a patient’s suicidality and develop an informed intervention.
This article describes a practical, commonly accepted approach to suicide risk assessment and intervention, based on the B-SAFE model (Basic Suicide Assessment Five-step Evaluation) proposed by Jacobs et al (Figure).3 Using this method to assess suicide risk can help you answer questions such as:
- Which factors are most important to consider when evaluating suicide risk in my patient?
- What questions should I ask my patient to find out if he or she is suicidal?
- How do I know if a patient is at risk for suicide?
- What emergent interventions are called for when managing the acutely suicidal patient?
- How should I document a suicide risk assessment?
Figure Basic Suicide Assessment Five-step Evaluation (B-SAFE)
Source: Created from information in references 2,11
Why ask about suicide?
No single risk factor or combination of risk factors can predict or preclude suicide. Even so, attempting to evaluate an individual’s risk by asking about suicidal thinking, reviewing risk factors, or using clinical rating scales helps you determine the next appropriate action (discharge, medication, psychiatric referral, consultation, or hospitalization).
While talking to patients and evaluating their risk for suicide, you may begin to understand their suffering—described as the most common denominator in suicide2 and perhaps the most important clue to heightened suicide risk. Such an exploration allows you to identify potential:
- risk factors that can be modified
- preventative factors to promote.
Don’t be afraid to ask. Asking about suicidal thoughts is necessary—but not enough—to understand an individual’s potential for suicide. Never be afraid to ask patients about suicide, believing that doing so will “put ideas into their heads.” By the same token, a patient who denies thoughts or plans for suicide may still be at risk.
Identifying at-risk patients is much more difficult than just asking if they are considering suicide. Opening a concerned dialogue can provide a sense of relief to the patient while allowing you to explore:
- the extent and seriousness of the suicidal thoughts
- associated risk factors or conditions, such as depression.
Stepwise risk assessment
The first 3 steps of Jacobs’ B-SAFE model focus on identifying predisposing and protective factors for suicide.3 For an in-depth discussion, consult the American Psychiatric Association practice guideline for the assessment and treatment of patients with suicidal behaviors4 (available at http://www.psych.org/psych_pract/treatg/pg/suicidalbehavior_05-15-06.pdf).
STEP 1: Risk factors. Use the patient interview, medical records, and collateral information to uncover potential suicide risk factors (Table 1).2
Psychopathology. Focus on depression, bipolar disorder, schizophrenia, substance abuse, and personality disorders, which are strongly associated with suicide. These disorders are considered modifiable risk factors—diagnosis and appropriate treatment can diminish suicide risk.
Suicidality has been associated with early depression or bipolar disorder, often before patients receive a diagnosis or effective treatment. Recovery and immediate post-discharge periods also are thought to be times of heightened suicide risk.
Psychosocial variables. Demographic and psychosocial variables may influence suicide risk estimation. A retrospective study of 100 patients who attempted suicide suggests that the most predictive factors for suicide are:
- living alone
- being aged 17 to 35 (although in other studies, more advanced age also has been linked to increased suicide risk3)
- complaints of severe hopelessness, anhedonia, and insomnia.5
Physical illness may potentiate suicide risk. Medical illnesses that produce great pain, disfigurement, limited function, or fear of dependence may reduce a person’s will to live and increase suicide risk.6 Epilepsy has been associated with a 4- to 5-fold increase in suicide risk7 and is the only medical diagnosis to carry a documented increase in suicide among children and adolescents.8 Often these medical disorders coexist with psychiatric disorders, complicating the task of determining independent risk.
Severity of attempts or self-mutilation. When evaluating self-injurious or suicidal behavior in the emergency setting, consider the severity of the attempt as part of overall suicide assessment. Self-injurious behavior (cutting or burning) or impulsive suicide attempts (planned for <3 hours, committed in the presence others, or where discovery is very probable) appear to carry less severity or intent to die than do carefully planned and/or hidden suicide attempts.9 However, consider at high risk for suicide any patient with self-mutilating or suicidal behavior who expresses persistent intent to die; acute stabilization on an in-patient unit may be necessary.
STEP 2: ‘Protective’ factors. Discover and discuss internal and external factors that might help prevent the individual with suicidal thoughts from converting those thoughts into action (Table 2).2 When discussing these potentially protective effects, emphasize the patient’s:
- resilience during past personal crises
- family responsibilities
- religious or spiritual beliefs.
‘No-harm contracts.’ Suicide (or “no-harm”) contracts with patients might help open communication about factors that promote or mitigate suicide risk. Such contacts do not prevent suicide or lessen medicolegal risk in the event of a patient suicide, however.10
STEP 3: Suicide plans. Ask about suicide thoughts, plans, and behaviors (Table 3).11 Probe gently to allow the individual to discuss his or her feelings and to explore the next appropriate avenue of care.
In my experience, patients who reveal passive suicidal ideation (such as, “I sometimes wish I would just die in my sleep”) and strong deterrents to acting on thoughts of suicide (such as, “My children need me,” or “It’s against my religion”) should continue outpatient treatment. Those without deterrents or who discuss active and imminent thoughts and recent actions—writing suicide notes, buying a weapon, stockpiling pills—require emergent evaluation for psychiatric admission. Ask about thoughts of self-injury or mutilation (such as cutting or burning), as well as homicidal ideation.
Recognizing that patients with suicidal thoughts are almost always ambivalent about suicide to some extent—conflicted by simultaneous desires to live and to die—gives you the opportunity to intervene by allying with the part of the patient that wants to live. Creating a therapeutic connection also will help you determine the level of intervention required.
STEP 4: Intervention. Understanding why a patient feels suicidal—gathered in Steps 1 to 3—can help you choose the appropriate intervention. Among the 5 steps, Step 4 relies most heavily on clinical judgment:
- Is the suicidality acute or chronic?
- How great is the risk for suicide?
- To keep the patient safe, how urgent is the required intervention?
Acute risk. Suicidality related to Axis I psychiatric disorders tends to be acute, with prominent pain, anguish, and a desire to escape. Patients may describe a driven quality to the suicidality, which commands a treatment plan that maintains patient safety until suicidal feelings remit.
Hospitalization is often needed, plus focused treatments such as medication, psychotherapy, or electroconvulsive therapy. Intensive outpatient follow-up or partial hospitalization programs might be considered for patients:
- with whom you have a strong therapeutic alliance
- who have sturdy psychosocial support
- whose precipitating factors for suicidality have resolved.
Chronic risk. Suicide risk tends to be more chronic and has an impulsive quality for patients with suicidality related to personality disorders and environmental factors. Personality disordered patients may report feelings of anger, rage, or vengeance connected with their suicidal thoughts.
Hospitalization might become necessary, although multiple hospitalizations can be counter-therapeutic. Attempting in therapy to teach the patient to cope with suicidal thoughts and feelings might be a more effective intervention.
Malingering. Use your best judgment when patients make suicide threats that could represent malingering to achieve hospitalization.
Step 5: Documentation. Document your assessment of the suicidal patient and decision making to:
- clarify the treatment plan
- communicate to other caregivers
- manage medicolegal risk.
Include a brief summary (Box) that is timely, legible, and communicates the estimated degree of risk, known data, diagnosis, and planned interventions such as medications, tests, consultations, and follow-up reassessments.
This 46-year-old, recently divorced man is experiencing his second episode of major depression associated with clear-cut panic attacks and suspected psychotic features. Although he denies current suicidal ideation, the treatment team believes he is at moderate to high risk for suicide because of known past history of serious suicide attempt with first depression, the presence of panic/anxiety, and possibly psychotic features. Additional risk is posed by loss of marital support and his inability to verbalize meaningful protective factors.
The plan is to convert from observation status on the inpatient unit to full admission, as the suicide risk precludes discharge at present. Further medication management and consideration for electroconvulsive therapy will take place, with daily reassessments. Suicide precautions ordered.
Table 1
Factors associated with potential for increased suicide risk
| Variable | Risk Factors |
|---|---|
| Demographic | Male gender, Caucasian race, rural residence, possibly age (varies among studies) |
| Imprisoned; widowed, divorced, or separated; living alone; no children or no children living in the home | |
| Psychosocial | Lack or loss of social supports, recent loss of employment, decrease in socioeconomic status or poverty, hopelessness |
| History of victimization (physical or sexual abuse), psychological turmoil, severe relationship conflict, aggressive or impulsive traits | |
| Writing suicide notes; family history of suicide, previous attempts, ‘imitation’ suicide, gun ownership | |
| Occupational risk (physicians, dentists, nurses, pharmacists, veterinarians, farmers) | |
| Psychiatric | Psychiatric diagnosis of recent onset |
| Mood disorder, particularly major depression and bipolar disorder | |
| Schizophrenia; alcohol or other substance abuse or addiction; personality disorder; panic attacks or severe psychic anxiety | |
| Insomnia; poor concentration or confusion; anhedonia | |
| Medical | Huntington’s disease, stroke, multiple sclerosis, head injury, spinal cord injury, systemic lupus erythematosus, AIDS |
| Epilepsy, pain, malignant neoplasms, peptic ulcer disease, renal disease | |
| Source: Adapted with permission from reference 3 | |
Table 2
Potentially protective factors against suicide
| Internal |
| Successful past responses to stress |
| Positive coping skills |
| Spirituality |
| Capacity for reality testing |
| Frustration tolerance/optimism |
| Overall individual resiliency |
| External |
| Children or pets in the home |
| Religious prohibition or beliefs |
| Positive therapeutic relationships |
| Sense of responsibility to family |
| Social supports and connections |
| Financial incentives or deterrents |
| Source: Adapted from reference 11 |
Table 3
Evaluating suicide risk: Questions to ask patients
| Have you felt so sad or depressed that you thought life is not worth living? |
| Have you thought about hurting yourself or taking your own life? |
| Have you thought about a way or plan to kill yourself? |
| Do you have the means to complete the plan? (such as, do you have access to weapons or pills?) |
| Have you practiced or rehearsed this plan to end your own life? |
| Do you have a location picked out? |
| What has stopped you from following through with the plan? |
| Have you ever attempted suicide? |
| Has anyone in your family ever attempted or committed suicide? |
| Source: Adapted with permission from reference 3 |
Interventions for suicidal patients
Physical protection. Take decisive action when you determine that suicide risk is elevated and imminent. Pursue urgent psychiatric hospitalization, with or without patient consent, in accordance with local probate and involuntary commitment statutes.
The logistics of protective action can be challenging; transportation is often required, and the patient is not always cooperative with admission. Table 4 lists measures and precautions that can help keep the suicidal patient safe.
Disease-specific interventions. Because suicidal ideation is often symptomatic of a primary psychiatric disorder, rapidly identifying major depression, bipolar disorder, or a psychotic illness is crucial to reducing suicidal thoughts and behaviors. Prescribe appropriate antidepressants, mood stabilizers, and antipsychotics at adequate doses and for sufficient duration.
Be vigilant for distressing symptoms that may be elevating the patient’s suicide risk, such as anxiety, panic, agitation, insomnia, or pain. Pharmacotherapies—such as anxiolytics, sedative-hypnotics, antipsychotics, or analgesics—may rapidly reduce suffering.
Impulsivity associated with substance use disorders—particularly during intoxication and withdrawal syndromes—requires aggressive attempts by the treatment team to engage the patient in detoxification and rehabilitation.
Direct antisuicide therapy. Clozapine carries an FDA-approved indication for preventing suicide in patients with schizophrenia or schizoaffective disorder. The mechanism by which clozapine helps prevent suicide is not known, but its anti-suicidal effects appear to be independent of its antipsychotic effects.12
Lithium has been reported to reduce risk of suicide and suicide attempts in patients with bipolar disorder, perhaps by as much as 80%.13 Such benefit has not been observed with other mood stabilizers, suggesting that lithium confers protective effects against suicide beyond its mood-stabilizing effects. Suicide risk is known to increase after lithium is discontinued.14
Lithium’s antisuicidal effects may arise from its ability to enhance serotonin. This theory, although unproven, is consistent with observations associating central serotonergic deficiency with suicidal and aggressive behaviors.
Psychosocial measures. Address psychosocial variables that may increase suicide risk (Table 1). Recruit and involve the patient’s support system, augmented with a close follow-up plan. Case management to explore housing and job opportunities can help. Work with the patient’s family or others to remove guns from the patient’s access. Individual, marital, and family therapies can reduce conflicts and strengthen coping skills.
Table 4
Safety measures to protect the suicidal patient
| Hospitalize—voluntarily or involuntarily—on a locked psychiatric unit |
| Provide constant 1-to-1 observation by staff |
| Transport the patient, accompanied by adequate personnel |
| Use physical restraints or seclusion while maintaining continuous observation |
| Employ metal detector to remove dangerous, hidden objects |
| Remove and secure patient’s belongings (bags, coats, purses may contain pills or weapons) |
| Search visitors’ belongings before allowing access to unit |
| Ensure that inpatient unit meets all coded safety regulations |
Related resources
- National Suicide Prevention Lifeline, sponsored by the Substance Abuse & Mental Health Services Administration: 1-800-SUICIDE or 1-800-273-TALK (8255); www.suicidepreventionlifeline.org.
- American Foundation for Suicide Prevention (AFSP) 1-888-333-AFSP; www.afsp.org.
- Simon RI, Hales RE. Textbook of suicide assessment and management. Washington, DC: American Psychiatric Publishing; 2006.
Drug brand names
- Clozapine • Clozaril
- Lithium • Eskalith, Lithobid, others
Disclosure
Dr. Muzina has received grants from or served as a consultant to Abbott Laboratories, AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, Novartis Pharmaceuticals Corp., Pfizer, and Repligen.
More than 50% of psychiatrists have experienced the death of a patient by suicide.1 For many of us, suicide represents the most feared outcome of a patient’s mental illness and makes managing suicide risk critical to everyday practice.
Unfortunately, we have little ability to predict suicide. Research into risk factors and the use of suicide rating scales have produced no consistently definitive methods to determine who will and who will not attempt or complete suicide.2 The purpose of suicide assessment, then, is not to predict suicide but to help us understand the sources of a patient’s suicidality and develop an informed intervention.
This article describes a practical, commonly accepted approach to suicide risk assessment and intervention, based on the B-SAFE model (Basic Suicide Assessment Five-step Evaluation) proposed by Jacobs et al (Figure).3 Using this method to assess suicide risk can help you answer questions such as:
- Which factors are most important to consider when evaluating suicide risk in my patient?
- What questions should I ask my patient to find out if he or she is suicidal?
- How do I know if a patient is at risk for suicide?
- What emergent interventions are called for when managing the acutely suicidal patient?
- How should I document a suicide risk assessment?
Figure Basic Suicide Assessment Five-step Evaluation (B-SAFE)
Source: Created from information in references 2,11
Why ask about suicide?
No single risk factor or combination of risk factors can predict or preclude suicide. Even so, attempting to evaluate an individual’s risk by asking about suicidal thinking, reviewing risk factors, or using clinical rating scales helps you determine the next appropriate action (discharge, medication, psychiatric referral, consultation, or hospitalization).
While talking to patients and evaluating their risk for suicide, you may begin to understand their suffering—described as the most common denominator in suicide2 and perhaps the most important clue to heightened suicide risk. Such an exploration allows you to identify potential:
- risk factors that can be modified
- preventative factors to promote.
Don’t be afraid to ask. Asking about suicidal thoughts is necessary—but not enough—to understand an individual’s potential for suicide. Never be afraid to ask patients about suicide, believing that doing so will “put ideas into their heads.” By the same token, a patient who denies thoughts or plans for suicide may still be at risk.
Identifying at-risk patients is much more difficult than just asking if they are considering suicide. Opening a concerned dialogue can provide a sense of relief to the patient while allowing you to explore:
- the extent and seriousness of the suicidal thoughts
- associated risk factors or conditions, such as depression.
Stepwise risk assessment
The first 3 steps of Jacobs’ B-SAFE model focus on identifying predisposing and protective factors for suicide.3 For an in-depth discussion, consult the American Psychiatric Association practice guideline for the assessment and treatment of patients with suicidal behaviors4 (available at http://www.psych.org/psych_pract/treatg/pg/suicidalbehavior_05-15-06.pdf).
STEP 1: Risk factors. Use the patient interview, medical records, and collateral information to uncover potential suicide risk factors (Table 1).2
Psychopathology. Focus on depression, bipolar disorder, schizophrenia, substance abuse, and personality disorders, which are strongly associated with suicide. These disorders are considered modifiable risk factors—diagnosis and appropriate treatment can diminish suicide risk.
Suicidality has been associated with early depression or bipolar disorder, often before patients receive a diagnosis or effective treatment. Recovery and immediate post-discharge periods also are thought to be times of heightened suicide risk.
Psychosocial variables. Demographic and psychosocial variables may influence suicide risk estimation. A retrospective study of 100 patients who attempted suicide suggests that the most predictive factors for suicide are:
- living alone
- being aged 17 to 35 (although in other studies, more advanced age also has been linked to increased suicide risk3)
- complaints of severe hopelessness, anhedonia, and insomnia.5
Physical illness may potentiate suicide risk. Medical illnesses that produce great pain, disfigurement, limited function, or fear of dependence may reduce a person’s will to live and increase suicide risk.6 Epilepsy has been associated with a 4- to 5-fold increase in suicide risk7 and is the only medical diagnosis to carry a documented increase in suicide among children and adolescents.8 Often these medical disorders coexist with psychiatric disorders, complicating the task of determining independent risk.
Severity of attempts or self-mutilation. When evaluating self-injurious or suicidal behavior in the emergency setting, consider the severity of the attempt as part of overall suicide assessment. Self-injurious behavior (cutting or burning) or impulsive suicide attempts (planned for <3 hours, committed in the presence others, or where discovery is very probable) appear to carry less severity or intent to die than do carefully planned and/or hidden suicide attempts.9 However, consider at high risk for suicide any patient with self-mutilating or suicidal behavior who expresses persistent intent to die; acute stabilization on an in-patient unit may be necessary.
STEP 2: ‘Protective’ factors. Discover and discuss internal and external factors that might help prevent the individual with suicidal thoughts from converting those thoughts into action (Table 2).2 When discussing these potentially protective effects, emphasize the patient’s:
- resilience during past personal crises
- family responsibilities
- religious or spiritual beliefs.
‘No-harm contracts.’ Suicide (or “no-harm”) contracts with patients might help open communication about factors that promote or mitigate suicide risk. Such contacts do not prevent suicide or lessen medicolegal risk in the event of a patient suicide, however.10
STEP 3: Suicide plans. Ask about suicide thoughts, plans, and behaviors (Table 3).11 Probe gently to allow the individual to discuss his or her feelings and to explore the next appropriate avenue of care.
In my experience, patients who reveal passive suicidal ideation (such as, “I sometimes wish I would just die in my sleep”) and strong deterrents to acting on thoughts of suicide (such as, “My children need me,” or “It’s against my religion”) should continue outpatient treatment. Those without deterrents or who discuss active and imminent thoughts and recent actions—writing suicide notes, buying a weapon, stockpiling pills—require emergent evaluation for psychiatric admission. Ask about thoughts of self-injury or mutilation (such as cutting or burning), as well as homicidal ideation.
Recognizing that patients with suicidal thoughts are almost always ambivalent about suicide to some extent—conflicted by simultaneous desires to live and to die—gives you the opportunity to intervene by allying with the part of the patient that wants to live. Creating a therapeutic connection also will help you determine the level of intervention required.
STEP 4: Intervention. Understanding why a patient feels suicidal—gathered in Steps 1 to 3—can help you choose the appropriate intervention. Among the 5 steps, Step 4 relies most heavily on clinical judgment:
- Is the suicidality acute or chronic?
- How great is the risk for suicide?
- To keep the patient safe, how urgent is the required intervention?
Acute risk. Suicidality related to Axis I psychiatric disorders tends to be acute, with prominent pain, anguish, and a desire to escape. Patients may describe a driven quality to the suicidality, which commands a treatment plan that maintains patient safety until suicidal feelings remit.
Hospitalization is often needed, plus focused treatments such as medication, psychotherapy, or electroconvulsive therapy. Intensive outpatient follow-up or partial hospitalization programs might be considered for patients:
- with whom you have a strong therapeutic alliance
- who have sturdy psychosocial support
- whose precipitating factors for suicidality have resolved.
Chronic risk. Suicide risk tends to be more chronic and has an impulsive quality for patients with suicidality related to personality disorders and environmental factors. Personality disordered patients may report feelings of anger, rage, or vengeance connected with their suicidal thoughts.
Hospitalization might become necessary, although multiple hospitalizations can be counter-therapeutic. Attempting in therapy to teach the patient to cope with suicidal thoughts and feelings might be a more effective intervention.
Malingering. Use your best judgment when patients make suicide threats that could represent malingering to achieve hospitalization.
Step 5: Documentation. Document your assessment of the suicidal patient and decision making to:
- clarify the treatment plan
- communicate to other caregivers
- manage medicolegal risk.
Include a brief summary (Box) that is timely, legible, and communicates the estimated degree of risk, known data, diagnosis, and planned interventions such as medications, tests, consultations, and follow-up reassessments.
This 46-year-old, recently divorced man is experiencing his second episode of major depression associated with clear-cut panic attacks and suspected psychotic features. Although he denies current suicidal ideation, the treatment team believes he is at moderate to high risk for suicide because of known past history of serious suicide attempt with first depression, the presence of panic/anxiety, and possibly psychotic features. Additional risk is posed by loss of marital support and his inability to verbalize meaningful protective factors.
The plan is to convert from observation status on the inpatient unit to full admission, as the suicide risk precludes discharge at present. Further medication management and consideration for electroconvulsive therapy will take place, with daily reassessments. Suicide precautions ordered.
Table 1
Factors associated with potential for increased suicide risk
| Variable | Risk Factors |
|---|---|
| Demographic | Male gender, Caucasian race, rural residence, possibly age (varies among studies) |
| Imprisoned; widowed, divorced, or separated; living alone; no children or no children living in the home | |
| Psychosocial | Lack or loss of social supports, recent loss of employment, decrease in socioeconomic status or poverty, hopelessness |
| History of victimization (physical or sexual abuse), psychological turmoil, severe relationship conflict, aggressive or impulsive traits | |
| Writing suicide notes; family history of suicide, previous attempts, ‘imitation’ suicide, gun ownership | |
| Occupational risk (physicians, dentists, nurses, pharmacists, veterinarians, farmers) | |
| Psychiatric | Psychiatric diagnosis of recent onset |
| Mood disorder, particularly major depression and bipolar disorder | |
| Schizophrenia; alcohol or other substance abuse or addiction; personality disorder; panic attacks or severe psychic anxiety | |
| Insomnia; poor concentration or confusion; anhedonia | |
| Medical | Huntington’s disease, stroke, multiple sclerosis, head injury, spinal cord injury, systemic lupus erythematosus, AIDS |
| Epilepsy, pain, malignant neoplasms, peptic ulcer disease, renal disease | |
| Source: Adapted with permission from reference 3 | |
Table 2
Potentially protective factors against suicide
| Internal |
| Successful past responses to stress |
| Positive coping skills |
| Spirituality |
| Capacity for reality testing |
| Frustration tolerance/optimism |
| Overall individual resiliency |
| External |
| Children or pets in the home |
| Religious prohibition or beliefs |
| Positive therapeutic relationships |
| Sense of responsibility to family |
| Social supports and connections |
| Financial incentives or deterrents |
| Source: Adapted from reference 11 |
Table 3
Evaluating suicide risk: Questions to ask patients
| Have you felt so sad or depressed that you thought life is not worth living? |
| Have you thought about hurting yourself or taking your own life? |
| Have you thought about a way or plan to kill yourself? |
| Do you have the means to complete the plan? (such as, do you have access to weapons or pills?) |
| Have you practiced or rehearsed this plan to end your own life? |
| Do you have a location picked out? |
| What has stopped you from following through with the plan? |
| Have you ever attempted suicide? |
| Has anyone in your family ever attempted or committed suicide? |
| Source: Adapted with permission from reference 3 |
Interventions for suicidal patients
Physical protection. Take decisive action when you determine that suicide risk is elevated and imminent. Pursue urgent psychiatric hospitalization, with or without patient consent, in accordance with local probate and involuntary commitment statutes.
The logistics of protective action can be challenging; transportation is often required, and the patient is not always cooperative with admission. Table 4 lists measures and precautions that can help keep the suicidal patient safe.
Disease-specific interventions. Because suicidal ideation is often symptomatic of a primary psychiatric disorder, rapidly identifying major depression, bipolar disorder, or a psychotic illness is crucial to reducing suicidal thoughts and behaviors. Prescribe appropriate antidepressants, mood stabilizers, and antipsychotics at adequate doses and for sufficient duration.
Be vigilant for distressing symptoms that may be elevating the patient’s suicide risk, such as anxiety, panic, agitation, insomnia, or pain. Pharmacotherapies—such as anxiolytics, sedative-hypnotics, antipsychotics, or analgesics—may rapidly reduce suffering.
Impulsivity associated with substance use disorders—particularly during intoxication and withdrawal syndromes—requires aggressive attempts by the treatment team to engage the patient in detoxification and rehabilitation.
Direct antisuicide therapy. Clozapine carries an FDA-approved indication for preventing suicide in patients with schizophrenia or schizoaffective disorder. The mechanism by which clozapine helps prevent suicide is not known, but its anti-suicidal effects appear to be independent of its antipsychotic effects.12
Lithium has been reported to reduce risk of suicide and suicide attempts in patients with bipolar disorder, perhaps by as much as 80%.13 Such benefit has not been observed with other mood stabilizers, suggesting that lithium confers protective effects against suicide beyond its mood-stabilizing effects. Suicide risk is known to increase after lithium is discontinued.14
Lithium’s antisuicidal effects may arise from its ability to enhance serotonin. This theory, although unproven, is consistent with observations associating central serotonergic deficiency with suicidal and aggressive behaviors.
Psychosocial measures. Address psychosocial variables that may increase suicide risk (Table 1). Recruit and involve the patient’s support system, augmented with a close follow-up plan. Case management to explore housing and job opportunities can help. Work with the patient’s family or others to remove guns from the patient’s access. Individual, marital, and family therapies can reduce conflicts and strengthen coping skills.
Table 4
Safety measures to protect the suicidal patient
| Hospitalize—voluntarily or involuntarily—on a locked psychiatric unit |
| Provide constant 1-to-1 observation by staff |
| Transport the patient, accompanied by adequate personnel |
| Use physical restraints or seclusion while maintaining continuous observation |
| Employ metal detector to remove dangerous, hidden objects |
| Remove and secure patient’s belongings (bags, coats, purses may contain pills or weapons) |
| Search visitors’ belongings before allowing access to unit |
| Ensure that inpatient unit meets all coded safety regulations |
Related resources
- National Suicide Prevention Lifeline, sponsored by the Substance Abuse & Mental Health Services Administration: 1-800-SUICIDE or 1-800-273-TALK (8255); www.suicidepreventionlifeline.org.
- American Foundation for Suicide Prevention (AFSP) 1-888-333-AFSP; www.afsp.org.
- Simon RI, Hales RE. Textbook of suicide assessment and management. Washington, DC: American Psychiatric Publishing; 2006.
Drug brand names
- Clozapine • Clozaril
- Lithium • Eskalith, Lithobid, others
Disclosure
Dr. Muzina has received grants from or served as a consultant to Abbott Laboratories, AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, Novartis Pharmaceuticals Corp., Pfizer, and Repligen.
1. Chemtob CM, Hamada RS, Bauer G, et al. Patients’ suicides: frequency and impact on psychiatrists. Am J Psychiatry 1988;145(2):224-8.
2. Muzina DJ. What physicians can do to prevent suicide. Cleve Clin J Med 2004;71(3):242-50.
3. Jacobs DG, Brewer ML, Klein-Benheim M. Suicide assessment: an overview and recommended protocol. In: Jacobs DG, ed. The Harvard Medical School guide to suicide assessment and intervention.. San Francisco, CA: Jossey-Bass Publishers; 1999:3-39.
4. Jacobs DG, Baldessarini RJ, Conwell Y, et al. American Psychiatric Association practice guideline for the assessment and treatment of patients with suicidal behaviors. Available at: http://www.psych.org/psych_pract/treatg/pg/suicidalbehavior_05-15-06.pdf. Accessed May 14, 2007.
5. Hall RC, Platt DE, Hall RC. Suicide risk assessment: a review of risk factors for suicide in 100 patients who made severe suicide attempts. Evaluation of suicide risk in a time of managed care. Psychosomatics 1999;40(1):18-27.
6. Mackenzie TB, Popkin MK. Suicide in the medical patient. Int J Psychiatry Med 1987;17(1):3-22.
7. Barraclough BM. The suicide rate of epilepsy. Acta Psychiatr Scand 1987;76(4):339-45
8. Brent DA, Kolko DJ, Allan MJ, Brown RV. Suicidality in affectively disordered adolescent inpatients. J Am Acad Child Adolesc Psychiatry 1990;29(4):586-93.
9. Polewka A, Mikolaszek-Boba M, Chrostek Maj J, Groszek B. The characteristics of suicide attempts based on the suicidal intent scale scores. Przegl Lek 2005;62(6):415-8.
10. Lewis LM. No-harm contracts: a review of what we know. Suicide Life Threat Behav 2007;37(1):50-7.
11. Jacobs DG. A resource guide for implementing the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) 2007 patient safety goals on suicide. Available at: http://www.sprc.org/library/jcahosafetygoals.pdf. Accessed May 14, 2007.
12. Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT). Arch Gen Psychiatry 2003;60(1):82-91.
13. Baldessarini RJ, Tondo L, Davis P, et al. Decreased risk of suicides and attempts during long-term lithium treatment: a meta-analytic review. Bipolar Disord 2006;8(5 Pt 2):625-39.
14. Baldessarini RJ, Tondo L, Viguera AC. Discontinuing lithium maintenance treatment in bipolar disorders: risks and implications. Bipolar Disord 1999;1(1):17-24.
1. Chemtob CM, Hamada RS, Bauer G, et al. Patients’ suicides: frequency and impact on psychiatrists. Am J Psychiatry 1988;145(2):224-8.
2. Muzina DJ. What physicians can do to prevent suicide. Cleve Clin J Med 2004;71(3):242-50.
3. Jacobs DG, Brewer ML, Klein-Benheim M. Suicide assessment: an overview and recommended protocol. In: Jacobs DG, ed. The Harvard Medical School guide to suicide assessment and intervention.. San Francisco, CA: Jossey-Bass Publishers; 1999:3-39.
4. Jacobs DG, Baldessarini RJ, Conwell Y, et al. American Psychiatric Association practice guideline for the assessment and treatment of patients with suicidal behaviors. Available at: http://www.psych.org/psych_pract/treatg/pg/suicidalbehavior_05-15-06.pdf. Accessed May 14, 2007.
5. Hall RC, Platt DE, Hall RC. Suicide risk assessment: a review of risk factors for suicide in 100 patients who made severe suicide attempts. Evaluation of suicide risk in a time of managed care. Psychosomatics 1999;40(1):18-27.
6. Mackenzie TB, Popkin MK. Suicide in the medical patient. Int J Psychiatry Med 1987;17(1):3-22.
7. Barraclough BM. The suicide rate of epilepsy. Acta Psychiatr Scand 1987;76(4):339-45
8. Brent DA, Kolko DJ, Allan MJ, Brown RV. Suicidality in affectively disordered adolescent inpatients. J Am Acad Child Adolesc Psychiatry 1990;29(4):586-93.
9. Polewka A, Mikolaszek-Boba M, Chrostek Maj J, Groszek B. The characteristics of suicide attempts based on the suicidal intent scale scores. Przegl Lek 2005;62(6):415-8.
10. Lewis LM. No-harm contracts: a review of what we know. Suicide Life Threat Behav 2007;37(1):50-7.
11. Jacobs DG. A resource guide for implementing the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) 2007 patient safety goals on suicide. Available at: http://www.sprc.org/library/jcahosafetygoals.pdf. Accessed May 14, 2007.
12. Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT). Arch Gen Psychiatry 2003;60(1):82-91.
13. Baldessarini RJ, Tondo L, Davis P, et al. Decreased risk of suicides and attempts during long-term lithium treatment: a meta-analytic review. Bipolar Disord 2006;8(5 Pt 2):625-39.
14. Baldessarini RJ, Tondo L, Viguera AC. Discontinuing lithium maintenance treatment in bipolar disorders: risks and implications. Bipolar Disord 1999;1(1):17-24.