User login
Watch for nonpsychotropics causing psychiatric side effects
Mr. J, age 52, has a history of opioid dependence. Four weeks after starting interferon therapy for hepatitis C, he presents to the outpatient mental health clinic with depressed mood, irritability, decreased energy, poor concentration, insomnia, anhedonia, and suicidal ideation.
Because Mr. J has no history of depression, the psychiatrist diagnoses him with depressive disorder secondary to interferon. Interferon is stopped. Mr. J’s mood improves, but he wants to restart interferon.
The psychiatrist starts Mr. J on sertraline, 50 mg/d, then gradually increases the dose to 150 mg/d as Mr. J’s mood symptoms return. Subsequently, the patient continues interferon with a combination of sertraline and supportive psychotherapy.
Recognizing a medication as the possible cause of your patient’s psychiatric symptoms can avoid inaccurate diagnosis and nonindicated psychiatric treatment. Diligently evaluating patients for drug-related psychiatric side effects is critical because complications usually are reversed when the offending drug is discontinued. Unfortunately, a thin line separates available evidence from anecdotal myths about psychiatric complications of nonpsychotropics.
Almost two-thirds (65%) of drugs included in the Physicians’ Desk Reference list potential psychiatric side effects, according to a random sample review.1 In some patients, such as Mr. J, these effects can exacerbate mood symptoms and result in perceptual, cognitive, or behavioral disturbances.
A wide range of drugs can cause psychosis, agitation, anxiety, depression, delirium, or insomnia (Table). On the other hand, certain psychiatric side effects of nonpsychotropics can be beneficial (Box 1).
Improve your assessments by examining the evidence linking psychiatric side effects to commonly prescribed and over-the-counter (OTC) compounds, including:
- cardiovascular medications
- steroids (prescription and illegal)
- hormones
- interferons
- antimicrobials.
Table
New-onset psychiatric symptoms? Check patient’s drug list
| Symptom | Documented as a possible cause |
|---|---|
| Psychosis/agitation | Anabolic androgenic steroids, antihistamines, clonidine, corticosteroids, decongestants, didanosine, ethionamide, H2 blockers, isoniazid, nitrates, NSAIDs, opioids, proton pump inhibitors, quinolones, salbutamol, skeletal muscle relaxants, sulfonamides/trimethoprim |
| Anxiety | Acyclovir, anabolic androgenic steroids, clonidine, corticosteroids, cyclosporine, decongestants, didanosine, serotonin 5-HT1 agonists such as sumatriptan, foscarnet, ganciclovir, nitrates, ondansetron, penicillins, skeletal muscle relaxants |
| Depression | Anabolic androgenic steroids, beta blockers, chloramphenicol, clonidine, corticosteroids, didanosine, digoxin, efavirenz, foscarnet, GnRH agonists, H2 blockers, interferons, isoniazid, isotretinoin, NSAIDs, quinolones, statins, tetracyclines |
| Delirium | ACE inhibitors, anabolic androgenic steroids, antibiotics (most), anticholinergics, beta blockers, centrally acting antihypertensives such as methyldopa and reserpine, cimetidine, clonidine, corticosteroids, didanosine, digoxin, H2 blockers, lidocaine, naltrexone, nitrates, NSAIDs, opioids |
| Insomnia | Aminophylline, anabolic androgenic steroids, clonidine, corticosteroids, decongestants, didanosine, opioid antagonists, proton pump inhibitors, quinolone antibiotics, salbutamol, skeletal muscle relaxants, tetracyclines |
| NSAIDs: nonsteroidal anti-inflammatory drugs; ACE: angiotensin-converting enzyme; GnRH: gonadotropin-releasing hormone | |
| Source: Prepared for Current Psychiatry by Drs. Sidhu and Balon from references cited in this article | |
Cardiovascular medications
Beta blockers have CNS effects—some of which cause psychiatric syndromes—that might depend on an ancillary property such as lipophilicity.2 Unlike hydrophilic agents such as atenolol that are excreted unchanged by the kidneys, lipophilic drugs such as metoprolol and propranolol are metabolized by the liver and are believed to enter the brain. Metoprolol has a brain/plasma concentration ratio about 20 times higher than that of atenolol.3
Metoprolol and propranolol can induce delirium and psychosis.4,5 Psychiatric side effects with metoprolol are frequent,4 and propranolol has been associated with:
- sedation (affecting >10% of patients)
- nightmares
- visual impairment
- hallucinations
- delirium
- depression.5
The relationship between depressive symptoms and beta blockers has been increasingly questioned, however. One study did not find a higher prevalence of depression in patients receiving beta blockers vs those receiving other medications, although this trial had major methodologic limitations.7 One large study found no significant association between beta-blocker use and major depression, regardless of patient age, gender, or race.8
These studies stress the importance of carefully assessing the individual patient before assigning neurotoxicity to beta blockers, as these drugs have considerable benefits for cardiovascular disease.9
Angiotensin-converting enzyme (ACE) inhibitors also affect the CNS. About 4% to 8% of patients taking an ACE inhibitor experience altered mental status—typically increased arousal and psychomotor activity—although
- anxiety
- mania
- insomnia
- fatigue
- paresthesias
- hallucinations.5
Clonidine is a centrally acting alpha-agonist. The alpha-adrenergic system regulates arousal and has an important role in major depression, anxiety states, and other arousal disorders.
More than one-third (35%) of patients taking clonidine experience sedation or lethargy; less commonly, the drug causes anxiety (3%), agitation (3%), depression (1%), and insomnia (1%).5 Acute confusion, delirium, hypomania, and psychosis related to clonidine use have long been recognized, occurring in 5
In some instances, mood-elevating side effects of nonpsychotropic medications might be beneficial. This might be the case if your patient experiences a sudden, otherwise unexplainable improvement.
CASE Helped by corticosteroids
Ms. Q, age 44, has a history of asthma and major depressive disorder and is being treated by a resident psychiatrist with a combination of paroxetine, 60 mg/d, mirtazapine, 15 mg at night, and cognitive-behavioral therapy. Her treatment has been challenging, and the psychiatrist has tried multiple medications and psychotherapy modalities.
At a recent psychotherapy session, Ms. Q says she has been feeling much better, with improved mood and greater energy. Upon further questioning, she reports having an asthma exacerbation a week before that resulted in hospitalization. During her stay, Ms. Q was started on a tapering dose of prednisone, which elevated her mood. Depressive symptoms returned when the effects of the prednisone wore off.
Prednisone is not indicated for depression and has harmful effects when used long term. The psychiatrist adds bupropion, 300 mg/d, to Ms. Q’s regimen, and her symptoms improve.
Cholesterol-lowering statins might be linked to an increased risk of depression and suicide, but the evidence is inconclusive. Some studies have supported this link,10,11 whereas others have strongly refuted it12,13 or had mixed results.14 A recent review15 recommends being vigilant for psychiatric side effects in patients taking these drugs.
Steroids: prescription and illegal
Corticosteroids are prescribed for a variety of immune system-related diseases, including asthma, allergic rhinitis, rheumatoid arthritis, inflammatory bowel disease, and dermatologic disorders. Mood changes are the most common psychiatric symptoms caused by corticosteroid use; delirium is less common. Psychiatric side effects include:
- lethargy
- insomnia
- euphoria
- depression
- psychosis
- “personality changes”
- anxiety
- agitation.5
A prospective study of asthma patients found statistically significant changes in mood—primarily manic symptoms—during brief corticosteroid courses at modest dosages. Depressed persons did not become more depressed during prednisone therapy, however; in fact, some improved. Some patients with posttraumatic stress disorder reported increased depression and memories of the traumatic event during prednisone therapy.17
In a study of 50 ophthalmologic patients who did not have psychiatric illness receiving prednisolone (mean starting dose 119 mg/d) for 8 days, 26% developed mania and 10% depression.18 None reported psychotic symptoms.
The most common adverse effects of short-term corticosteroid therapy are euphoria and hypomania. Long-term therapy tends to induce depressive symptoms.19 A review of 79 cases of psychiatric syndromes induced by corticosteroids found that 41% reported depression, 28% mania, 6% mixed symptoms, and 14% psychosis.20
A group of 16 healthy volunteers receiving 80 mg/d of prednisone over 5 days exhibited depressed or elevated mood, irritability, lability, increased energy, anxiety, and depersonalization.21 Numerous case studies have reported anxiety, agitation, mania, and psychotic symptoms in children and adults taking inhaled corticosteroids.
In general, psychiatric side effects of corticosteroids occur within 2 weeks of starting therapy and resolve with dosage reduction or discontinuation. In severe cases or situations in which the dosage cannot be reduced, the patient may require antipsychotics or mood stabilizers.19
Female gender and past psychiatric history might be risk factors for developing psychiatric symptoms with corticosteroids,22 although not all studies have confirmed these findings.18
Anabolic androgenic steroids (AAS) have limited therapeutic benefits but are used illegally by some bodybuilders, wrestlers, and other amateur and professional athletes to increase muscle mass, enhance performance, and gain a competitive edge. AAS can cause acute paranoia, delirium, mania or hypomania, homicidal rage, aggression, and extreme mood swings, as well as a marked increase in libido, irritability, agitation, and anger.
In a large observational cohort study of 320 bodybuilding amateur and recreational athletes,23 AAS use induced many of these psychiatric side effects. The extent intensified as the abuse escalated. A study that used the Structured Clinical Interview for DSM-III-R to compare 88 athletes using steroids with 68 nonusers found that 23% of the AAS users reported major mood syndromes, including mania, hypomania, and major depression.24
In a 2-week, double-blind, fixed-order, placebo-controlled, crossover study of healthy male inpatient volunteers, AAS had both:
- mood-elevating effects—euphoria (“steroid rush”), increased energy, and increased sexual arousal and drive
- mood-dysphoric effects, such as irritability, mood swings, increasingly violent feelings, increased hostility, and cognitive impairments.25
Hormones
Gonadotropin-releasing hormone (GnRH) agonists such as leuprolide and nafarelin are approved for treating endometriosis, advanced prostate cancer, precocious puberty, and uterine leiomyomata. Some studies and case reports suggest that these agents cause depressive symptoms.26
Interferon
Various forms of interferon are used to treat hepatitis C, melanoma, multiple sclerosis, chronic myelogenous leukemia, and other illnesses. Psychiatric complications—particularly depression—are the most frequent side effect of interferon therapy and mainly occur within the first 12 weeks of therapy.28
In a prospective observational study of veterans undergoing interferon-alfa/ribavirin treatment for chronic hepatitis C:
- 48% of patients not receiving psychiatric care at baseline required treatment for neuropsychiatric side effects
- 23% developed symptoms of major depression.29
Because patients who receive interferon are far more likely to require psychiatric intervention if they have a family history of mood disorders, closely monitor them for depressive symptoms and treat such symptoms aggressively. Also closely monitor patients with multiple psychiatric diagnoses receiving interferon-alfa therapy.30
Jeungling et al31 speculated that hypometabolism in the prefrontal cortex may predispose patients to interferon-associated neuropsychological syndromes. Neuropsychiatric symptoms may be a characteristic of hepatitis C, interferon treatment, or both.32
Antimicrobial agents
Antibiotic and antiviral drugs can cause psychiatric side effects:
- directly by affecting neuronal functions
- indirectly by entering the brain rapidly, taking advantage of the compromised blood-brain barrier during sepsis or infection.
Antibiotics. Penicillin and its analogues are associated with sedation, anxiety, and hallucinations. Delirium has been reported as a side effect of most cephalosporins, especially in patients with compromised renal function. Quinolones such as ciprofloxacin and ofloxacin rarely cause restlessness, irritability, lethargy, tremors, insomnia, mania, depression, psychosis, delirium, seizures, or catatonia (incidence ≤1%).5 Though not commonly used, chloramphenicol may cause depression, confusion, and delirium. Many case reports have strongly associated clarithromycin with delirium.33
Isoniazid is one of the most commonly used antibiotics that can cause psychiatric side effects; it has been linked to delirium, mania, depression, and psychosis. Ethionamide is associated with sedation, irritability, depression, restlessness, and psychosis. Tetracyclines have been known to cause depression, insomnia, and irritability at high dosages.
Sulfonamides can cause delirium. Psychosis and confusion also have been reported, especially when sulfa drugs are combined with trimethoprim.5
Antivirals. When used intravenously and at high doses, acyclovir and ganciclovir can cause lethargy, anxiety, hallucinations, and frank delirium.5 Foscarnet—an antiviral used to treat herpes viruses—can cause depression, anxiety, hallucinations, and aggressive irritability.
Didanosine—an antiretroviral agent to treat HIV infections—can cause lethargy (5% to 7% of patients), depression (2%), anxiety (2%), emotional lability (25%), delirium (2%), insomnia (1%), and psychotic delusions (1%).5 Efavirenz treatment may be associated with major depression and severe suicidal ideation.34 Tenofovir, a nucleotide reverse transcriptase inhibitor, has not been associated with psychiatric side effects.27
Antifungals. Psychiatric side effects are rare.
OTC and other agents
Many common nonprescription agents can cause psychiatric symptoms. The most frequently used classes include cold and allergy preparations, reflux medications, and analgesics (Box 2).5,35
Cold preparations. Combined antihistamines and decongestants—such as phenylpropanolamine, azatadine, loratadine, ephedrine, phenylephrine, pseudoephedrine, and naphazoline—can cause an atropine-like psychosis that typically manifests as confusion, disorientation, agitation, hallucinations, and memory problems. Decongestants can cause dangerously high levels of norepinephrine when combined with monoamine oxidase inhibitors (MAOIs) and are contraindicated in patients taking MAOIs. Ephedrine can induce restlessness, dysphoria, irritability, anxiety, and insomnia.
Reflux medications. Two primary classes of reflux medications are proton pump inhibitors (omeprazole and lansoprazole) and H2 receptor antagonists (famotidine, nizatidine, ranitidine, and cimetidine). Although generally considered to have a benign side-effect profile, these medications have been reported to cause serious neuropsychiatric complications—including mental confusion, agitation, depression, and hallucinations—mainly in geriatric patients with impaired hepatic-renal function.36 These occur in only 37
Time to onset of psychiatric side effects from H2 antagonists varies. Ranitidine can cause depression 4 to 8 weeks after treatment begins. Cimetidine has been reported to cause adverse events within 2 to 3 weeks and delirium within 24 to 48 hours.38 These effects usually resolve within 3 days of discontinuing the drug. Cimetidine is also associated with sexual dysfunction.
Other medications. Ondansetron is a 5-hydroxytryptamine subclass 3 (5-HT3) antagonist used for antiemetic therapy. In case reports, it has been strongly associated with anxiety.40 This association is complex, however, and studies are evaluating 5-HT3 receptor antagonists for the treatment of anxiety, depression, phobia, and schizophrenia.
Isotretinoin—a retinoid used for severe acne—can cause severe depression and suicidal behavior.41
Aminophylline and salbutamol are associated with agitation, insomnia, euphoria, and delirium. Methotrexate is known to cause personality changes, irritability, and delirium.27
Up to 70% of persons in Western countries use analgesics regularly, primarily for headaches, other specific pains, and febrile illness. Nonsteroidal anti-inflammatory drugs (NSAIDs)—including aspirin, naproxen, ibuprofen, and indomethacin—are efficacious and have a wide safety margin, but potentially serious psychiatric side effects can occur even when these drugs are taken in recommended doses.
Salicylate intoxication, which can present as frank delirium, often goes unrecognized. Any NSAID can produce delirium in the elderly. Case reports have also implicated NSAIDs in mania, psychosis, and depressive disorders with suicidal ideation.35
Opioids may cause sedation, psychic slowing, dysphoria, mood changes, psychosis, and delirium. Epidural administration of morphine may induce hallucinations and catatonia. Opioid antagonists—such as naloxone and, particularly, naltrexone—can induce dysphoria, fatigue, sleep disturbances, suicidality, hallucinations, and delirium. The serotonin 5-HT1 agonist sumatriptan (an antimigraine medication) has been associated with fatigue, anxiety, and panic disorder.5
Skeletal muscle relaxants such as baclofen and dantrolene may induce sleep disturbances, anxiety, agitation, mood disturbances, hallucinations, and delirium.
Treating drug-related mood effects
If you suspect a nonpsychotropic medication is causing your patient’s psychiatric symptoms, discuss this with the patient and the prescribing physician. Switching to another similar agent may be an option. If this is not possible:
- work closely with the patient’s primary physician
- treat mood symptoms with appropriate psychotropics.
- Turjanski N, Lloyd GG. Psychiatric side-effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70.
- Brown TM, Stoudemire A. Psychiatric side effects of prescription and over-the-counter medications. Recognition and management. Washington, DC: American Psychiatric Publishing; 1998.
- Physicians’ Desk Reference. www.pdr.net.
- Acyclovir • Zovirax
- Aminophylline • Phyllocontin, Truphylline
- Atenolol • Tenormin
- Azatadine • Optimine
- Baclofen • Lioresal
- Chloramphenicol • Chloromycetin
- Cimetidine • Tagamet
- Ciprofloxacin • Cipro
- Clarithromycin • Biaxin
- Clonidine • Catapres
- Cyclosporine • Neoral, Sandimmune, others
- Dantrolene • Dantrium
- Didanosine • Videx
- Efavirenz • Sustiva
- Ethionamide • Trecator
- Famotidine • Pepcid
- Foscarnet • Foscavir
- Ganciclovir • Cytovene
- Indomethacin • Indocin
- Interferon alfa • Intron, Roferon
- Isoniazid • Nydrazid
- Isotretinoin • Accutane
- Lansoprazole • Prevacid
- Leuprolide • Lupron
- Lidocaine • Xylocaine, Xylocard
- Loratadine • Claritin
- Methotrexate • Rheumatrex, Trexall
- Methyldopa • Aldomet
- Metoprolol • Lopressor
- Mirtazapine • Remeron
- Nafarelin • Synarel
- Naloxone • Suboxone
- Naltrexone • Vivitrol
- Naphazoline • Naphcon-A, Clearine
- Naproxen • Aleve, others
- Nizatidine • Axid
- Ofloxacin • Floxin
- Omeprazole • Prilosec
- Ondansetron • Zofran
- Paroxetine • Paxil
- Peginterferon alfa • PEG-Intron, Pegasys
- Phenylephrine • Neo-Synephrine
- Prednisolone • Blephamide, Pred Forte, others
- Propranolol • Inderal
- Pseudoephedrine • Actifed, Sudafed
- Ranitidine • Zantac
- Reserpine • Serpasi
- Ribavirin • Copegus, Rebetol
- Salbutamol • Aerolin, Airomir, others
- Sertraline • Zoloft
- Sumatriptan • Imitrex
- Tenofovir • Viread
- Trimethoprim • Proloprim
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Smith DA. Psychiatric side effects of non-psychiatric drugs. S D J Med 1991;44(10):291-2.
2. Conant J, Engler R, Janowsky D, et al. Central nervous system side effects of beta-adrenergic blocking agents with high and low lipid solubility. J Cardiovasc Pharmacol 1989;13:656-61.
3. Cruickshank JM, Neil-Dwyer G. Beta-blocker brain concentrations in man. Eur J Clin Pharmacol 1985;28:21-3.
4. Sirois FJ. Visual hallucinations and metoprolol. Psychosomatics 2006;47(6):537-8.
5. Brown TM, Stoudemire A. Psychiatric side effects of prescription and over-the-counter medications. Recognition and management. Washington, DC: American Psychiatric Publishing; 1998.
6. Waal HF. Propranolol-induced depression (letter). Br Med J 1967;2:50.-
7. Carney RM, Rich MW, teVelde A, et al. Prevalence of major depressive disorder in patients receiving beta-blocker therapy versus other medications. Am J Med 1987;83(2):223-6.
8. Bright RA, Everitt DE. Beta-blockers and depression. Evidence against an association. JAMA 1992;267(13):1783-7.
9. Yudofsky SC. Beta-blockers and depression: the clinician’s dilemma. JAMA 1992;267:1826-7.
10. Law MR, Thompson SG, Wald NJ. Assessing possible hazards of reducing serum cholesterol. BMJ 1994;308:373-9.
11. Morales K, Wittink M, Datto C, et al. Simvastatin causes changes in affective processes in elderly volunteers. J Am Geriatr Soc 2006;54(1):70-6.
12. Yang CC, Jick SS, Jick H. Lipid-lowering drugs and the risk of depression and suicidal behavior. Arch Intern Med 2003;163(16):1926-32.
13. Callréus T, Agerskov Andersen U, Hallas J, et al. Cardiovascular drugs and the risk of suicide: a nested case-control study. Eur J Clin Pharmacol 2007;63(6):591-6.
14. Agostini JV, Tinetti ME, Han L, et al. Effects of statin use on muscle strength, cognition, and depressive symptoms in older adults. J Am Geriatr Soc 2007;55(3):420-5.
15. Tatley M, Savage R. Psychiatric adverse reactions with statins, fibrates and ezetimibe: implications for the use of lipid-lowering agents. Drug Saf 2007;30(3):195-201.
16. Boston Collaborative Drug Surveillance Program. Acute adverse reactions to prednisone in relation to dosage. Clin Pharm. Ther 1972;13:694-8.
17. Brown ES, Suppes T, Khan DA, Carmody TJ 3rd. Mood changes during prednisone bursts in outpatients with asthma. J Clin Psychopharmacol 2002;22:55-61.
18. Naber D, Sand P, Heigl B. Psychological and neuropsychological effects of 8 days’ corticosteroid treatment. A prospective study. Psychoneuroendocrinology 1996;21:25-31.
19. Warrington TP, Bostwick JM. Psychiatric adverse effects of corticosteroids. Mayo Clin Proc 2006;81(10):1361-7.
20. Lewis DA, Smith RE. Steroid-induced psychiatric syndromes: a report of 14 cases and a review of the literature. J Affect Disord 1983;5:319-32.
21. Wolkowitz OM, Rubinow D, Doran AR, et al. Prednisone effects on neurochemistry and behavior. Arch Gen Psych 1990;47:963-8.
22. Ling MHM, Perry PJ, Tsuang MT. Side effects of corticosteroid therapy. Arch Gen Psychiatry 1981;38:471-7.
23. Pagonis TA, Angelopoulos NV, Koukoulis GN, Hadjichristodoulou CS. Psychiatric side effects induced by supraphysiological doses of combinations of anabolic steroids correlate to the severity of abuse. Eur Psychiatry 2006;21(8):551-62.
24. Pope HG, Jr, Katz DL. Psychiatric and medical effects of anabolic-androgenic steroid use: a controlled study of 160 athletes. Arch Gen Psychiatry 1994;51:375-82.
25. Su T, Pagliaro M, Schmidt P, et al. Neuropsychiatric effects of anabolic steroids in male normal volunteers. JAMA 1993;269:2760-4.
26. Warnock JK, Bundren JC, Morris DW. Depressive symptoms associated with gonadotropin-releasing hormone agonists. Depress Anxiety 1998;7:171-7.
27. Turjanski N, Lloyd GG. Psychiatric side-effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70.
28. Lotrich FE, Rabinovitz M, Gironda P, Pollock BG. Depression following pegylated interferon-alpha: characteristics and vulnerability. J Psychosom Res 2007;63(2):131-5.
29. Dieperink E, Ho SB, Thuras P, Willenbring ML. A prospective study of neuropsychiatric symptoms associated with interferon-alpha-2b and ribavirin therapy for patients with chronic hepatitis C. Psychosomatics 2003;44(2):104-12.
30. Jakiche A, Paredez EC, Tannan PK, et al. Trend of depression and the use of psychiatric medications in U.S. Veterans with hepatitis C during interferon-based therapy. Am J Gastroenterol 2007;102(11):2426-33.
31. Juengling FD, Ebert D, Gut O, et al. Prefrontal cortical hypometabolism during low-dose interferon alpha treatment. Psychopharmacology.(Berl) 2000;152:383-9.
32. Matthews SC, Paulus MP, Dimsdale JE. Contribution of functional neuroimaging to understanding neuropsychiatric side effects of interferon in hepatitis C. Psychosomatics 2004;45(4):281-6.
33. Ozsoylar G, Sayin A, Bolay H. Clarithromycin monotherapy-induced delirium. J Antimicrob Chemother 2007;59(2):331.-
34. Puzantian T. Central nervous system adverse effects with efavirenz: case report and review. Pharmacotherapy 2002;22:930-3.
35. Browning CH. Nonsteroidal anti-inflammatory drugs and severe psychiatric side effects. Int J Psychiatry Med 1996;26(1):25-34.
36. Picotte-Prillmayer D, DiMaggio JR, Baile WF. H2 blocker delirium. Psychosomatics 1995;36(1):74-7.
37. Cantu TG, Korek JS. Central nervous system reactions to histamine-2 receptor blockers. Ann Intern Med 1991;114:1027-34.
38. Bernstein J. Handbook of drug therapy in psychiatry. St. Louis, MO: Mosby; 1995:380-1.
39. Rampello L, Nicoletti G. [The H2-antagonist therapy withdrawal syndrome: The possible role of hyperprolactinemia]. Medicina (Firenze) 1990;10:294-6.
40. Mitchell KE, Popkin MK, Trick W, Vercellotti G. Psychiatric complications associated with ondansetron. Psychosomatics 1994;35(2):161-3.
41. Brasic JR. Monitoring people treated with isotretinoin for depression. Psychol Rep 2007;100(3 Pt 2):1312-4.
Mr. J, age 52, has a history of opioid dependence. Four weeks after starting interferon therapy for hepatitis C, he presents to the outpatient mental health clinic with depressed mood, irritability, decreased energy, poor concentration, insomnia, anhedonia, and suicidal ideation.
Because Mr. J has no history of depression, the psychiatrist diagnoses him with depressive disorder secondary to interferon. Interferon is stopped. Mr. J’s mood improves, but he wants to restart interferon.
The psychiatrist starts Mr. J on sertraline, 50 mg/d, then gradually increases the dose to 150 mg/d as Mr. J’s mood symptoms return. Subsequently, the patient continues interferon with a combination of sertraline and supportive psychotherapy.
Recognizing a medication as the possible cause of your patient’s psychiatric symptoms can avoid inaccurate diagnosis and nonindicated psychiatric treatment. Diligently evaluating patients for drug-related psychiatric side effects is critical because complications usually are reversed when the offending drug is discontinued. Unfortunately, a thin line separates available evidence from anecdotal myths about psychiatric complications of nonpsychotropics.
Almost two-thirds (65%) of drugs included in the Physicians’ Desk Reference list potential psychiatric side effects, according to a random sample review.1 In some patients, such as Mr. J, these effects can exacerbate mood symptoms and result in perceptual, cognitive, or behavioral disturbances.
A wide range of drugs can cause psychosis, agitation, anxiety, depression, delirium, or insomnia (Table). On the other hand, certain psychiatric side effects of nonpsychotropics can be beneficial (Box 1).
Improve your assessments by examining the evidence linking psychiatric side effects to commonly prescribed and over-the-counter (OTC) compounds, including:
- cardiovascular medications
- steroids (prescription and illegal)
- hormones
- interferons
- antimicrobials.
Table
New-onset psychiatric symptoms? Check patient’s drug list
| Symptom | Documented as a possible cause |
|---|---|
| Psychosis/agitation | Anabolic androgenic steroids, antihistamines, clonidine, corticosteroids, decongestants, didanosine, ethionamide, H2 blockers, isoniazid, nitrates, NSAIDs, opioids, proton pump inhibitors, quinolones, salbutamol, skeletal muscle relaxants, sulfonamides/trimethoprim |
| Anxiety | Acyclovir, anabolic androgenic steroids, clonidine, corticosteroids, cyclosporine, decongestants, didanosine, serotonin 5-HT1 agonists such as sumatriptan, foscarnet, ganciclovir, nitrates, ondansetron, penicillins, skeletal muscle relaxants |
| Depression | Anabolic androgenic steroids, beta blockers, chloramphenicol, clonidine, corticosteroids, didanosine, digoxin, efavirenz, foscarnet, GnRH agonists, H2 blockers, interferons, isoniazid, isotretinoin, NSAIDs, quinolones, statins, tetracyclines |
| Delirium | ACE inhibitors, anabolic androgenic steroids, antibiotics (most), anticholinergics, beta blockers, centrally acting antihypertensives such as methyldopa and reserpine, cimetidine, clonidine, corticosteroids, didanosine, digoxin, H2 blockers, lidocaine, naltrexone, nitrates, NSAIDs, opioids |
| Insomnia | Aminophylline, anabolic androgenic steroids, clonidine, corticosteroids, decongestants, didanosine, opioid antagonists, proton pump inhibitors, quinolone antibiotics, salbutamol, skeletal muscle relaxants, tetracyclines |
| NSAIDs: nonsteroidal anti-inflammatory drugs; ACE: angiotensin-converting enzyme; GnRH: gonadotropin-releasing hormone | |
| Source: Prepared for Current Psychiatry by Drs. Sidhu and Balon from references cited in this article | |
Cardiovascular medications
Beta blockers have CNS effects—some of which cause psychiatric syndromes—that might depend on an ancillary property such as lipophilicity.2 Unlike hydrophilic agents such as atenolol that are excreted unchanged by the kidneys, lipophilic drugs such as metoprolol and propranolol are metabolized by the liver and are believed to enter the brain. Metoprolol has a brain/plasma concentration ratio about 20 times higher than that of atenolol.3
Metoprolol and propranolol can induce delirium and psychosis.4,5 Psychiatric side effects with metoprolol are frequent,4 and propranolol has been associated with:
- sedation (affecting >10% of patients)
- nightmares
- visual impairment
- hallucinations
- delirium
- depression.5
The relationship between depressive symptoms and beta blockers has been increasingly questioned, however. One study did not find a higher prevalence of depression in patients receiving beta blockers vs those receiving other medications, although this trial had major methodologic limitations.7 One large study found no significant association between beta-blocker use and major depression, regardless of patient age, gender, or race.8
These studies stress the importance of carefully assessing the individual patient before assigning neurotoxicity to beta blockers, as these drugs have considerable benefits for cardiovascular disease.9
Angiotensin-converting enzyme (ACE) inhibitors also affect the CNS. About 4% to 8% of patients taking an ACE inhibitor experience altered mental status—typically increased arousal and psychomotor activity—although
- anxiety
- mania
- insomnia
- fatigue
- paresthesias
- hallucinations.5
Clonidine is a centrally acting alpha-agonist. The alpha-adrenergic system regulates arousal and has an important role in major depression, anxiety states, and other arousal disorders.
More than one-third (35%) of patients taking clonidine experience sedation or lethargy; less commonly, the drug causes anxiety (3%), agitation (3%), depression (1%), and insomnia (1%).5 Acute confusion, delirium, hypomania, and psychosis related to clonidine use have long been recognized, occurring in 5
In some instances, mood-elevating side effects of nonpsychotropic medications might be beneficial. This might be the case if your patient experiences a sudden, otherwise unexplainable improvement.
CASE Helped by corticosteroids
Ms. Q, age 44, has a history of asthma and major depressive disorder and is being treated by a resident psychiatrist with a combination of paroxetine, 60 mg/d, mirtazapine, 15 mg at night, and cognitive-behavioral therapy. Her treatment has been challenging, and the psychiatrist has tried multiple medications and psychotherapy modalities.
At a recent psychotherapy session, Ms. Q says she has been feeling much better, with improved mood and greater energy. Upon further questioning, she reports having an asthma exacerbation a week before that resulted in hospitalization. During her stay, Ms. Q was started on a tapering dose of prednisone, which elevated her mood. Depressive symptoms returned when the effects of the prednisone wore off.
Prednisone is not indicated for depression and has harmful effects when used long term. The psychiatrist adds bupropion, 300 mg/d, to Ms. Q’s regimen, and her symptoms improve.
Cholesterol-lowering statins might be linked to an increased risk of depression and suicide, but the evidence is inconclusive. Some studies have supported this link,10,11 whereas others have strongly refuted it12,13 or had mixed results.14 A recent review15 recommends being vigilant for psychiatric side effects in patients taking these drugs.
Steroids: prescription and illegal
Corticosteroids are prescribed for a variety of immune system-related diseases, including asthma, allergic rhinitis, rheumatoid arthritis, inflammatory bowel disease, and dermatologic disorders. Mood changes are the most common psychiatric symptoms caused by corticosteroid use; delirium is less common. Psychiatric side effects include:
- lethargy
- insomnia
- euphoria
- depression
- psychosis
- “personality changes”
- anxiety
- agitation.5
A prospective study of asthma patients found statistically significant changes in mood—primarily manic symptoms—during brief corticosteroid courses at modest dosages. Depressed persons did not become more depressed during prednisone therapy, however; in fact, some improved. Some patients with posttraumatic stress disorder reported increased depression and memories of the traumatic event during prednisone therapy.17
In a study of 50 ophthalmologic patients who did not have psychiatric illness receiving prednisolone (mean starting dose 119 mg/d) for 8 days, 26% developed mania and 10% depression.18 None reported psychotic symptoms.
The most common adverse effects of short-term corticosteroid therapy are euphoria and hypomania. Long-term therapy tends to induce depressive symptoms.19 A review of 79 cases of psychiatric syndromes induced by corticosteroids found that 41% reported depression, 28% mania, 6% mixed symptoms, and 14% psychosis.20
A group of 16 healthy volunteers receiving 80 mg/d of prednisone over 5 days exhibited depressed or elevated mood, irritability, lability, increased energy, anxiety, and depersonalization.21 Numerous case studies have reported anxiety, agitation, mania, and psychotic symptoms in children and adults taking inhaled corticosteroids.
In general, psychiatric side effects of corticosteroids occur within 2 weeks of starting therapy and resolve with dosage reduction or discontinuation. In severe cases or situations in which the dosage cannot be reduced, the patient may require antipsychotics or mood stabilizers.19
Female gender and past psychiatric history might be risk factors for developing psychiatric symptoms with corticosteroids,22 although not all studies have confirmed these findings.18
Anabolic androgenic steroids (AAS) have limited therapeutic benefits but are used illegally by some bodybuilders, wrestlers, and other amateur and professional athletes to increase muscle mass, enhance performance, and gain a competitive edge. AAS can cause acute paranoia, delirium, mania or hypomania, homicidal rage, aggression, and extreme mood swings, as well as a marked increase in libido, irritability, agitation, and anger.
In a large observational cohort study of 320 bodybuilding amateur and recreational athletes,23 AAS use induced many of these psychiatric side effects. The extent intensified as the abuse escalated. A study that used the Structured Clinical Interview for DSM-III-R to compare 88 athletes using steroids with 68 nonusers found that 23% of the AAS users reported major mood syndromes, including mania, hypomania, and major depression.24
In a 2-week, double-blind, fixed-order, placebo-controlled, crossover study of healthy male inpatient volunteers, AAS had both:
- mood-elevating effects—euphoria (“steroid rush”), increased energy, and increased sexual arousal and drive
- mood-dysphoric effects, such as irritability, mood swings, increasingly violent feelings, increased hostility, and cognitive impairments.25
Hormones
Gonadotropin-releasing hormone (GnRH) agonists such as leuprolide and nafarelin are approved for treating endometriosis, advanced prostate cancer, precocious puberty, and uterine leiomyomata. Some studies and case reports suggest that these agents cause depressive symptoms.26
Interferon
Various forms of interferon are used to treat hepatitis C, melanoma, multiple sclerosis, chronic myelogenous leukemia, and other illnesses. Psychiatric complications—particularly depression—are the most frequent side effect of interferon therapy and mainly occur within the first 12 weeks of therapy.28
In a prospective observational study of veterans undergoing interferon-alfa/ribavirin treatment for chronic hepatitis C:
- 48% of patients not receiving psychiatric care at baseline required treatment for neuropsychiatric side effects
- 23% developed symptoms of major depression.29
Because patients who receive interferon are far more likely to require psychiatric intervention if they have a family history of mood disorders, closely monitor them for depressive symptoms and treat such symptoms aggressively. Also closely monitor patients with multiple psychiatric diagnoses receiving interferon-alfa therapy.30
Jeungling et al31 speculated that hypometabolism in the prefrontal cortex may predispose patients to interferon-associated neuropsychological syndromes. Neuropsychiatric symptoms may be a characteristic of hepatitis C, interferon treatment, or both.32
Antimicrobial agents
Antibiotic and antiviral drugs can cause psychiatric side effects:
- directly by affecting neuronal functions
- indirectly by entering the brain rapidly, taking advantage of the compromised blood-brain barrier during sepsis or infection.
Antibiotics. Penicillin and its analogues are associated with sedation, anxiety, and hallucinations. Delirium has been reported as a side effect of most cephalosporins, especially in patients with compromised renal function. Quinolones such as ciprofloxacin and ofloxacin rarely cause restlessness, irritability, lethargy, tremors, insomnia, mania, depression, psychosis, delirium, seizures, or catatonia (incidence ≤1%).5 Though not commonly used, chloramphenicol may cause depression, confusion, and delirium. Many case reports have strongly associated clarithromycin with delirium.33
Isoniazid is one of the most commonly used antibiotics that can cause psychiatric side effects; it has been linked to delirium, mania, depression, and psychosis. Ethionamide is associated with sedation, irritability, depression, restlessness, and psychosis. Tetracyclines have been known to cause depression, insomnia, and irritability at high dosages.
Sulfonamides can cause delirium. Psychosis and confusion also have been reported, especially when sulfa drugs are combined with trimethoprim.5
Antivirals. When used intravenously and at high doses, acyclovir and ganciclovir can cause lethargy, anxiety, hallucinations, and frank delirium.5 Foscarnet—an antiviral used to treat herpes viruses—can cause depression, anxiety, hallucinations, and aggressive irritability.
Didanosine—an antiretroviral agent to treat HIV infections—can cause lethargy (5% to 7% of patients), depression (2%), anxiety (2%), emotional lability (25%), delirium (2%), insomnia (1%), and psychotic delusions (1%).5 Efavirenz treatment may be associated with major depression and severe suicidal ideation.34 Tenofovir, a nucleotide reverse transcriptase inhibitor, has not been associated with psychiatric side effects.27
Antifungals. Psychiatric side effects are rare.
OTC and other agents
Many common nonprescription agents can cause psychiatric symptoms. The most frequently used classes include cold and allergy preparations, reflux medications, and analgesics (Box 2).5,35
Cold preparations. Combined antihistamines and decongestants—such as phenylpropanolamine, azatadine, loratadine, ephedrine, phenylephrine, pseudoephedrine, and naphazoline—can cause an atropine-like psychosis that typically manifests as confusion, disorientation, agitation, hallucinations, and memory problems. Decongestants can cause dangerously high levels of norepinephrine when combined with monoamine oxidase inhibitors (MAOIs) and are contraindicated in patients taking MAOIs. Ephedrine can induce restlessness, dysphoria, irritability, anxiety, and insomnia.
Reflux medications. Two primary classes of reflux medications are proton pump inhibitors (omeprazole and lansoprazole) and H2 receptor antagonists (famotidine, nizatidine, ranitidine, and cimetidine). Although generally considered to have a benign side-effect profile, these medications have been reported to cause serious neuropsychiatric complications—including mental confusion, agitation, depression, and hallucinations—mainly in geriatric patients with impaired hepatic-renal function.36 These occur in only 37
Time to onset of psychiatric side effects from H2 antagonists varies. Ranitidine can cause depression 4 to 8 weeks after treatment begins. Cimetidine has been reported to cause adverse events within 2 to 3 weeks and delirium within 24 to 48 hours.38 These effects usually resolve within 3 days of discontinuing the drug. Cimetidine is also associated with sexual dysfunction.
Other medications. Ondansetron is a 5-hydroxytryptamine subclass 3 (5-HT3) antagonist used for antiemetic therapy. In case reports, it has been strongly associated with anxiety.40 This association is complex, however, and studies are evaluating 5-HT3 receptor antagonists for the treatment of anxiety, depression, phobia, and schizophrenia.
Isotretinoin—a retinoid used for severe acne—can cause severe depression and suicidal behavior.41
Aminophylline and salbutamol are associated with agitation, insomnia, euphoria, and delirium. Methotrexate is known to cause personality changes, irritability, and delirium.27
Up to 70% of persons in Western countries use analgesics regularly, primarily for headaches, other specific pains, and febrile illness. Nonsteroidal anti-inflammatory drugs (NSAIDs)—including aspirin, naproxen, ibuprofen, and indomethacin—are efficacious and have a wide safety margin, but potentially serious psychiatric side effects can occur even when these drugs are taken in recommended doses.
Salicylate intoxication, which can present as frank delirium, often goes unrecognized. Any NSAID can produce delirium in the elderly. Case reports have also implicated NSAIDs in mania, psychosis, and depressive disorders with suicidal ideation.35
Opioids may cause sedation, psychic slowing, dysphoria, mood changes, psychosis, and delirium. Epidural administration of morphine may induce hallucinations and catatonia. Opioid antagonists—such as naloxone and, particularly, naltrexone—can induce dysphoria, fatigue, sleep disturbances, suicidality, hallucinations, and delirium. The serotonin 5-HT1 agonist sumatriptan (an antimigraine medication) has been associated with fatigue, anxiety, and panic disorder.5
Skeletal muscle relaxants such as baclofen and dantrolene may induce sleep disturbances, anxiety, agitation, mood disturbances, hallucinations, and delirium.
Treating drug-related mood effects
If you suspect a nonpsychotropic medication is causing your patient’s psychiatric symptoms, discuss this with the patient and the prescribing physician. Switching to another similar agent may be an option. If this is not possible:
- work closely with the patient’s primary physician
- treat mood symptoms with appropriate psychotropics.
- Turjanski N, Lloyd GG. Psychiatric side-effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70.
- Brown TM, Stoudemire A. Psychiatric side effects of prescription and over-the-counter medications. Recognition and management. Washington, DC: American Psychiatric Publishing; 1998.
- Physicians’ Desk Reference. www.pdr.net.
- Acyclovir • Zovirax
- Aminophylline • Phyllocontin, Truphylline
- Atenolol • Tenormin
- Azatadine • Optimine
- Baclofen • Lioresal
- Chloramphenicol • Chloromycetin
- Cimetidine • Tagamet
- Ciprofloxacin • Cipro
- Clarithromycin • Biaxin
- Clonidine • Catapres
- Cyclosporine • Neoral, Sandimmune, others
- Dantrolene • Dantrium
- Didanosine • Videx
- Efavirenz • Sustiva
- Ethionamide • Trecator
- Famotidine • Pepcid
- Foscarnet • Foscavir
- Ganciclovir • Cytovene
- Indomethacin • Indocin
- Interferon alfa • Intron, Roferon
- Isoniazid • Nydrazid
- Isotretinoin • Accutane
- Lansoprazole • Prevacid
- Leuprolide • Lupron
- Lidocaine • Xylocaine, Xylocard
- Loratadine • Claritin
- Methotrexate • Rheumatrex, Trexall
- Methyldopa • Aldomet
- Metoprolol • Lopressor
- Mirtazapine • Remeron
- Nafarelin • Synarel
- Naloxone • Suboxone
- Naltrexone • Vivitrol
- Naphazoline • Naphcon-A, Clearine
- Naproxen • Aleve, others
- Nizatidine • Axid
- Ofloxacin • Floxin
- Omeprazole • Prilosec
- Ondansetron • Zofran
- Paroxetine • Paxil
- Peginterferon alfa • PEG-Intron, Pegasys
- Phenylephrine • Neo-Synephrine
- Prednisolone • Blephamide, Pred Forte, others
- Propranolol • Inderal
- Pseudoephedrine • Actifed, Sudafed
- Ranitidine • Zantac
- Reserpine • Serpasi
- Ribavirin • Copegus, Rebetol
- Salbutamol • Aerolin, Airomir, others
- Sertraline • Zoloft
- Sumatriptan • Imitrex
- Tenofovir • Viread
- Trimethoprim • Proloprim
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Mr. J, age 52, has a history of opioid dependence. Four weeks after starting interferon therapy for hepatitis C, he presents to the outpatient mental health clinic with depressed mood, irritability, decreased energy, poor concentration, insomnia, anhedonia, and suicidal ideation.
Because Mr. J has no history of depression, the psychiatrist diagnoses him with depressive disorder secondary to interferon. Interferon is stopped. Mr. J’s mood improves, but he wants to restart interferon.
The psychiatrist starts Mr. J on sertraline, 50 mg/d, then gradually increases the dose to 150 mg/d as Mr. J’s mood symptoms return. Subsequently, the patient continues interferon with a combination of sertraline and supportive psychotherapy.
Recognizing a medication as the possible cause of your patient’s psychiatric symptoms can avoid inaccurate diagnosis and nonindicated psychiatric treatment. Diligently evaluating patients for drug-related psychiatric side effects is critical because complications usually are reversed when the offending drug is discontinued. Unfortunately, a thin line separates available evidence from anecdotal myths about psychiatric complications of nonpsychotropics.
Almost two-thirds (65%) of drugs included in the Physicians’ Desk Reference list potential psychiatric side effects, according to a random sample review.1 In some patients, such as Mr. J, these effects can exacerbate mood symptoms and result in perceptual, cognitive, or behavioral disturbances.
A wide range of drugs can cause psychosis, agitation, anxiety, depression, delirium, or insomnia (Table). On the other hand, certain psychiatric side effects of nonpsychotropics can be beneficial (Box 1).
Improve your assessments by examining the evidence linking psychiatric side effects to commonly prescribed and over-the-counter (OTC) compounds, including:
- cardiovascular medications
- steroids (prescription and illegal)
- hormones
- interferons
- antimicrobials.
Table
New-onset psychiatric symptoms? Check patient’s drug list
| Symptom | Documented as a possible cause |
|---|---|
| Psychosis/agitation | Anabolic androgenic steroids, antihistamines, clonidine, corticosteroids, decongestants, didanosine, ethionamide, H2 blockers, isoniazid, nitrates, NSAIDs, opioids, proton pump inhibitors, quinolones, salbutamol, skeletal muscle relaxants, sulfonamides/trimethoprim |
| Anxiety | Acyclovir, anabolic androgenic steroids, clonidine, corticosteroids, cyclosporine, decongestants, didanosine, serotonin 5-HT1 agonists such as sumatriptan, foscarnet, ganciclovir, nitrates, ondansetron, penicillins, skeletal muscle relaxants |
| Depression | Anabolic androgenic steroids, beta blockers, chloramphenicol, clonidine, corticosteroids, didanosine, digoxin, efavirenz, foscarnet, GnRH agonists, H2 blockers, interferons, isoniazid, isotretinoin, NSAIDs, quinolones, statins, tetracyclines |
| Delirium | ACE inhibitors, anabolic androgenic steroids, antibiotics (most), anticholinergics, beta blockers, centrally acting antihypertensives such as methyldopa and reserpine, cimetidine, clonidine, corticosteroids, didanosine, digoxin, H2 blockers, lidocaine, naltrexone, nitrates, NSAIDs, opioids |
| Insomnia | Aminophylline, anabolic androgenic steroids, clonidine, corticosteroids, decongestants, didanosine, opioid antagonists, proton pump inhibitors, quinolone antibiotics, salbutamol, skeletal muscle relaxants, tetracyclines |
| NSAIDs: nonsteroidal anti-inflammatory drugs; ACE: angiotensin-converting enzyme; GnRH: gonadotropin-releasing hormone | |
| Source: Prepared for Current Psychiatry by Drs. Sidhu and Balon from references cited in this article | |
Cardiovascular medications
Beta blockers have CNS effects—some of which cause psychiatric syndromes—that might depend on an ancillary property such as lipophilicity.2 Unlike hydrophilic agents such as atenolol that are excreted unchanged by the kidneys, lipophilic drugs such as metoprolol and propranolol are metabolized by the liver and are believed to enter the brain. Metoprolol has a brain/plasma concentration ratio about 20 times higher than that of atenolol.3
Metoprolol and propranolol can induce delirium and psychosis.4,5 Psychiatric side effects with metoprolol are frequent,4 and propranolol has been associated with:
- sedation (affecting >10% of patients)
- nightmares
- visual impairment
- hallucinations
- delirium
- depression.5
The relationship between depressive symptoms and beta blockers has been increasingly questioned, however. One study did not find a higher prevalence of depression in patients receiving beta blockers vs those receiving other medications, although this trial had major methodologic limitations.7 One large study found no significant association between beta-blocker use and major depression, regardless of patient age, gender, or race.8
These studies stress the importance of carefully assessing the individual patient before assigning neurotoxicity to beta blockers, as these drugs have considerable benefits for cardiovascular disease.9
Angiotensin-converting enzyme (ACE) inhibitors also affect the CNS. About 4% to 8% of patients taking an ACE inhibitor experience altered mental status—typically increased arousal and psychomotor activity—although
- anxiety
- mania
- insomnia
- fatigue
- paresthesias
- hallucinations.5
Clonidine is a centrally acting alpha-agonist. The alpha-adrenergic system regulates arousal and has an important role in major depression, anxiety states, and other arousal disorders.
More than one-third (35%) of patients taking clonidine experience sedation or lethargy; less commonly, the drug causes anxiety (3%), agitation (3%), depression (1%), and insomnia (1%).5 Acute confusion, delirium, hypomania, and psychosis related to clonidine use have long been recognized, occurring in 5
In some instances, mood-elevating side effects of nonpsychotropic medications might be beneficial. This might be the case if your patient experiences a sudden, otherwise unexplainable improvement.
CASE Helped by corticosteroids
Ms. Q, age 44, has a history of asthma and major depressive disorder and is being treated by a resident psychiatrist with a combination of paroxetine, 60 mg/d, mirtazapine, 15 mg at night, and cognitive-behavioral therapy. Her treatment has been challenging, and the psychiatrist has tried multiple medications and psychotherapy modalities.
At a recent psychotherapy session, Ms. Q says she has been feeling much better, with improved mood and greater energy. Upon further questioning, she reports having an asthma exacerbation a week before that resulted in hospitalization. During her stay, Ms. Q was started on a tapering dose of prednisone, which elevated her mood. Depressive symptoms returned when the effects of the prednisone wore off.
Prednisone is not indicated for depression and has harmful effects when used long term. The psychiatrist adds bupropion, 300 mg/d, to Ms. Q’s regimen, and her symptoms improve.
Cholesterol-lowering statins might be linked to an increased risk of depression and suicide, but the evidence is inconclusive. Some studies have supported this link,10,11 whereas others have strongly refuted it12,13 or had mixed results.14 A recent review15 recommends being vigilant for psychiatric side effects in patients taking these drugs.
Steroids: prescription and illegal
Corticosteroids are prescribed for a variety of immune system-related diseases, including asthma, allergic rhinitis, rheumatoid arthritis, inflammatory bowel disease, and dermatologic disorders. Mood changes are the most common psychiatric symptoms caused by corticosteroid use; delirium is less common. Psychiatric side effects include:
- lethargy
- insomnia
- euphoria
- depression
- psychosis
- “personality changes”
- anxiety
- agitation.5
A prospective study of asthma patients found statistically significant changes in mood—primarily manic symptoms—during brief corticosteroid courses at modest dosages. Depressed persons did not become more depressed during prednisone therapy, however; in fact, some improved. Some patients with posttraumatic stress disorder reported increased depression and memories of the traumatic event during prednisone therapy.17
In a study of 50 ophthalmologic patients who did not have psychiatric illness receiving prednisolone (mean starting dose 119 mg/d) for 8 days, 26% developed mania and 10% depression.18 None reported psychotic symptoms.
The most common adverse effects of short-term corticosteroid therapy are euphoria and hypomania. Long-term therapy tends to induce depressive symptoms.19 A review of 79 cases of psychiatric syndromes induced by corticosteroids found that 41% reported depression, 28% mania, 6% mixed symptoms, and 14% psychosis.20
A group of 16 healthy volunteers receiving 80 mg/d of prednisone over 5 days exhibited depressed or elevated mood, irritability, lability, increased energy, anxiety, and depersonalization.21 Numerous case studies have reported anxiety, agitation, mania, and psychotic symptoms in children and adults taking inhaled corticosteroids.
In general, psychiatric side effects of corticosteroids occur within 2 weeks of starting therapy and resolve with dosage reduction or discontinuation. In severe cases or situations in which the dosage cannot be reduced, the patient may require antipsychotics or mood stabilizers.19
Female gender and past psychiatric history might be risk factors for developing psychiatric symptoms with corticosteroids,22 although not all studies have confirmed these findings.18
Anabolic androgenic steroids (AAS) have limited therapeutic benefits but are used illegally by some bodybuilders, wrestlers, and other amateur and professional athletes to increase muscle mass, enhance performance, and gain a competitive edge. AAS can cause acute paranoia, delirium, mania or hypomania, homicidal rage, aggression, and extreme mood swings, as well as a marked increase in libido, irritability, agitation, and anger.
In a large observational cohort study of 320 bodybuilding amateur and recreational athletes,23 AAS use induced many of these psychiatric side effects. The extent intensified as the abuse escalated. A study that used the Structured Clinical Interview for DSM-III-R to compare 88 athletes using steroids with 68 nonusers found that 23% of the AAS users reported major mood syndromes, including mania, hypomania, and major depression.24
In a 2-week, double-blind, fixed-order, placebo-controlled, crossover study of healthy male inpatient volunteers, AAS had both:
- mood-elevating effects—euphoria (“steroid rush”), increased energy, and increased sexual arousal and drive
- mood-dysphoric effects, such as irritability, mood swings, increasingly violent feelings, increased hostility, and cognitive impairments.25
Hormones
Gonadotropin-releasing hormone (GnRH) agonists such as leuprolide and nafarelin are approved for treating endometriosis, advanced prostate cancer, precocious puberty, and uterine leiomyomata. Some studies and case reports suggest that these agents cause depressive symptoms.26
Interferon
Various forms of interferon are used to treat hepatitis C, melanoma, multiple sclerosis, chronic myelogenous leukemia, and other illnesses. Psychiatric complications—particularly depression—are the most frequent side effect of interferon therapy and mainly occur within the first 12 weeks of therapy.28
In a prospective observational study of veterans undergoing interferon-alfa/ribavirin treatment for chronic hepatitis C:
- 48% of patients not receiving psychiatric care at baseline required treatment for neuropsychiatric side effects
- 23% developed symptoms of major depression.29
Because patients who receive interferon are far more likely to require psychiatric intervention if they have a family history of mood disorders, closely monitor them for depressive symptoms and treat such symptoms aggressively. Also closely monitor patients with multiple psychiatric diagnoses receiving interferon-alfa therapy.30
Jeungling et al31 speculated that hypometabolism in the prefrontal cortex may predispose patients to interferon-associated neuropsychological syndromes. Neuropsychiatric symptoms may be a characteristic of hepatitis C, interferon treatment, or both.32
Antimicrobial agents
Antibiotic and antiviral drugs can cause psychiatric side effects:
- directly by affecting neuronal functions
- indirectly by entering the brain rapidly, taking advantage of the compromised blood-brain barrier during sepsis or infection.
Antibiotics. Penicillin and its analogues are associated with sedation, anxiety, and hallucinations. Delirium has been reported as a side effect of most cephalosporins, especially in patients with compromised renal function. Quinolones such as ciprofloxacin and ofloxacin rarely cause restlessness, irritability, lethargy, tremors, insomnia, mania, depression, psychosis, delirium, seizures, or catatonia (incidence ≤1%).5 Though not commonly used, chloramphenicol may cause depression, confusion, and delirium. Many case reports have strongly associated clarithromycin with delirium.33
Isoniazid is one of the most commonly used antibiotics that can cause psychiatric side effects; it has been linked to delirium, mania, depression, and psychosis. Ethionamide is associated with sedation, irritability, depression, restlessness, and psychosis. Tetracyclines have been known to cause depression, insomnia, and irritability at high dosages.
Sulfonamides can cause delirium. Psychosis and confusion also have been reported, especially when sulfa drugs are combined with trimethoprim.5
Antivirals. When used intravenously and at high doses, acyclovir and ganciclovir can cause lethargy, anxiety, hallucinations, and frank delirium.5 Foscarnet—an antiviral used to treat herpes viruses—can cause depression, anxiety, hallucinations, and aggressive irritability.
Didanosine—an antiretroviral agent to treat HIV infections—can cause lethargy (5% to 7% of patients), depression (2%), anxiety (2%), emotional lability (25%), delirium (2%), insomnia (1%), and psychotic delusions (1%).5 Efavirenz treatment may be associated with major depression and severe suicidal ideation.34 Tenofovir, a nucleotide reverse transcriptase inhibitor, has not been associated with psychiatric side effects.27
Antifungals. Psychiatric side effects are rare.
OTC and other agents
Many common nonprescription agents can cause psychiatric symptoms. The most frequently used classes include cold and allergy preparations, reflux medications, and analgesics (Box 2).5,35
Cold preparations. Combined antihistamines and decongestants—such as phenylpropanolamine, azatadine, loratadine, ephedrine, phenylephrine, pseudoephedrine, and naphazoline—can cause an atropine-like psychosis that typically manifests as confusion, disorientation, agitation, hallucinations, and memory problems. Decongestants can cause dangerously high levels of norepinephrine when combined with monoamine oxidase inhibitors (MAOIs) and are contraindicated in patients taking MAOIs. Ephedrine can induce restlessness, dysphoria, irritability, anxiety, and insomnia.
Reflux medications. Two primary classes of reflux medications are proton pump inhibitors (omeprazole and lansoprazole) and H2 receptor antagonists (famotidine, nizatidine, ranitidine, and cimetidine). Although generally considered to have a benign side-effect profile, these medications have been reported to cause serious neuropsychiatric complications—including mental confusion, agitation, depression, and hallucinations—mainly in geriatric patients with impaired hepatic-renal function.36 These occur in only 37
Time to onset of psychiatric side effects from H2 antagonists varies. Ranitidine can cause depression 4 to 8 weeks after treatment begins. Cimetidine has been reported to cause adverse events within 2 to 3 weeks and delirium within 24 to 48 hours.38 These effects usually resolve within 3 days of discontinuing the drug. Cimetidine is also associated with sexual dysfunction.
Other medications. Ondansetron is a 5-hydroxytryptamine subclass 3 (5-HT3) antagonist used for antiemetic therapy. In case reports, it has been strongly associated with anxiety.40 This association is complex, however, and studies are evaluating 5-HT3 receptor antagonists for the treatment of anxiety, depression, phobia, and schizophrenia.
Isotretinoin—a retinoid used for severe acne—can cause severe depression and suicidal behavior.41
Aminophylline and salbutamol are associated with agitation, insomnia, euphoria, and delirium. Methotrexate is known to cause personality changes, irritability, and delirium.27
Up to 70% of persons in Western countries use analgesics regularly, primarily for headaches, other specific pains, and febrile illness. Nonsteroidal anti-inflammatory drugs (NSAIDs)—including aspirin, naproxen, ibuprofen, and indomethacin—are efficacious and have a wide safety margin, but potentially serious psychiatric side effects can occur even when these drugs are taken in recommended doses.
Salicylate intoxication, which can present as frank delirium, often goes unrecognized. Any NSAID can produce delirium in the elderly. Case reports have also implicated NSAIDs in mania, psychosis, and depressive disorders with suicidal ideation.35
Opioids may cause sedation, psychic slowing, dysphoria, mood changes, psychosis, and delirium. Epidural administration of morphine may induce hallucinations and catatonia. Opioid antagonists—such as naloxone and, particularly, naltrexone—can induce dysphoria, fatigue, sleep disturbances, suicidality, hallucinations, and delirium. The serotonin 5-HT1 agonist sumatriptan (an antimigraine medication) has been associated with fatigue, anxiety, and panic disorder.5
Skeletal muscle relaxants such as baclofen and dantrolene may induce sleep disturbances, anxiety, agitation, mood disturbances, hallucinations, and delirium.
Treating drug-related mood effects
If you suspect a nonpsychotropic medication is causing your patient’s psychiatric symptoms, discuss this with the patient and the prescribing physician. Switching to another similar agent may be an option. If this is not possible:
- work closely with the patient’s primary physician
- treat mood symptoms with appropriate psychotropics.
- Turjanski N, Lloyd GG. Psychiatric side-effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70.
- Brown TM, Stoudemire A. Psychiatric side effects of prescription and over-the-counter medications. Recognition and management. Washington, DC: American Psychiatric Publishing; 1998.
- Physicians’ Desk Reference. www.pdr.net.
- Acyclovir • Zovirax
- Aminophylline • Phyllocontin, Truphylline
- Atenolol • Tenormin
- Azatadine • Optimine
- Baclofen • Lioresal
- Chloramphenicol • Chloromycetin
- Cimetidine • Tagamet
- Ciprofloxacin • Cipro
- Clarithromycin • Biaxin
- Clonidine • Catapres
- Cyclosporine • Neoral, Sandimmune, others
- Dantrolene • Dantrium
- Didanosine • Videx
- Efavirenz • Sustiva
- Ethionamide • Trecator
- Famotidine • Pepcid
- Foscarnet • Foscavir
- Ganciclovir • Cytovene
- Indomethacin • Indocin
- Interferon alfa • Intron, Roferon
- Isoniazid • Nydrazid
- Isotretinoin • Accutane
- Lansoprazole • Prevacid
- Leuprolide • Lupron
- Lidocaine • Xylocaine, Xylocard
- Loratadine • Claritin
- Methotrexate • Rheumatrex, Trexall
- Methyldopa • Aldomet
- Metoprolol • Lopressor
- Mirtazapine • Remeron
- Nafarelin • Synarel
- Naloxone • Suboxone
- Naltrexone • Vivitrol
- Naphazoline • Naphcon-A, Clearine
- Naproxen • Aleve, others
- Nizatidine • Axid
- Ofloxacin • Floxin
- Omeprazole • Prilosec
- Ondansetron • Zofran
- Paroxetine • Paxil
- Peginterferon alfa • PEG-Intron, Pegasys
- Phenylephrine • Neo-Synephrine
- Prednisolone • Blephamide, Pred Forte, others
- Propranolol • Inderal
- Pseudoephedrine • Actifed, Sudafed
- Ranitidine • Zantac
- Reserpine • Serpasi
- Ribavirin • Copegus, Rebetol
- Salbutamol • Aerolin, Airomir, others
- Sertraline • Zoloft
- Sumatriptan • Imitrex
- Tenofovir • Viread
- Trimethoprim • Proloprim
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Smith DA. Psychiatric side effects of non-psychiatric drugs. S D J Med 1991;44(10):291-2.
2. Conant J, Engler R, Janowsky D, et al. Central nervous system side effects of beta-adrenergic blocking agents with high and low lipid solubility. J Cardiovasc Pharmacol 1989;13:656-61.
3. Cruickshank JM, Neil-Dwyer G. Beta-blocker brain concentrations in man. Eur J Clin Pharmacol 1985;28:21-3.
4. Sirois FJ. Visual hallucinations and metoprolol. Psychosomatics 2006;47(6):537-8.
5. Brown TM, Stoudemire A. Psychiatric side effects of prescription and over-the-counter medications. Recognition and management. Washington, DC: American Psychiatric Publishing; 1998.
6. Waal HF. Propranolol-induced depression (letter). Br Med J 1967;2:50.-
7. Carney RM, Rich MW, teVelde A, et al. Prevalence of major depressive disorder in patients receiving beta-blocker therapy versus other medications. Am J Med 1987;83(2):223-6.
8. Bright RA, Everitt DE. Beta-blockers and depression. Evidence against an association. JAMA 1992;267(13):1783-7.
9. Yudofsky SC. Beta-blockers and depression: the clinician’s dilemma. JAMA 1992;267:1826-7.
10. Law MR, Thompson SG, Wald NJ. Assessing possible hazards of reducing serum cholesterol. BMJ 1994;308:373-9.
11. Morales K, Wittink M, Datto C, et al. Simvastatin causes changes in affective processes in elderly volunteers. J Am Geriatr Soc 2006;54(1):70-6.
12. Yang CC, Jick SS, Jick H. Lipid-lowering drugs and the risk of depression and suicidal behavior. Arch Intern Med 2003;163(16):1926-32.
13. Callréus T, Agerskov Andersen U, Hallas J, et al. Cardiovascular drugs and the risk of suicide: a nested case-control study. Eur J Clin Pharmacol 2007;63(6):591-6.
14. Agostini JV, Tinetti ME, Han L, et al. Effects of statin use on muscle strength, cognition, and depressive symptoms in older adults. J Am Geriatr Soc 2007;55(3):420-5.
15. Tatley M, Savage R. Psychiatric adverse reactions with statins, fibrates and ezetimibe: implications for the use of lipid-lowering agents. Drug Saf 2007;30(3):195-201.
16. Boston Collaborative Drug Surveillance Program. Acute adverse reactions to prednisone in relation to dosage. Clin Pharm. Ther 1972;13:694-8.
17. Brown ES, Suppes T, Khan DA, Carmody TJ 3rd. Mood changes during prednisone bursts in outpatients with asthma. J Clin Psychopharmacol 2002;22:55-61.
18. Naber D, Sand P, Heigl B. Psychological and neuropsychological effects of 8 days’ corticosteroid treatment. A prospective study. Psychoneuroendocrinology 1996;21:25-31.
19. Warrington TP, Bostwick JM. Psychiatric adverse effects of corticosteroids. Mayo Clin Proc 2006;81(10):1361-7.
20. Lewis DA, Smith RE. Steroid-induced psychiatric syndromes: a report of 14 cases and a review of the literature. J Affect Disord 1983;5:319-32.
21. Wolkowitz OM, Rubinow D, Doran AR, et al. Prednisone effects on neurochemistry and behavior. Arch Gen Psych 1990;47:963-8.
22. Ling MHM, Perry PJ, Tsuang MT. Side effects of corticosteroid therapy. Arch Gen Psychiatry 1981;38:471-7.
23. Pagonis TA, Angelopoulos NV, Koukoulis GN, Hadjichristodoulou CS. Psychiatric side effects induced by supraphysiological doses of combinations of anabolic steroids correlate to the severity of abuse. Eur Psychiatry 2006;21(8):551-62.
24. Pope HG, Jr, Katz DL. Psychiatric and medical effects of anabolic-androgenic steroid use: a controlled study of 160 athletes. Arch Gen Psychiatry 1994;51:375-82.
25. Su T, Pagliaro M, Schmidt P, et al. Neuropsychiatric effects of anabolic steroids in male normal volunteers. JAMA 1993;269:2760-4.
26. Warnock JK, Bundren JC, Morris DW. Depressive symptoms associated with gonadotropin-releasing hormone agonists. Depress Anxiety 1998;7:171-7.
27. Turjanski N, Lloyd GG. Psychiatric side-effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70.
28. Lotrich FE, Rabinovitz M, Gironda P, Pollock BG. Depression following pegylated interferon-alpha: characteristics and vulnerability. J Psychosom Res 2007;63(2):131-5.
29. Dieperink E, Ho SB, Thuras P, Willenbring ML. A prospective study of neuropsychiatric symptoms associated with interferon-alpha-2b and ribavirin therapy for patients with chronic hepatitis C. Psychosomatics 2003;44(2):104-12.
30. Jakiche A, Paredez EC, Tannan PK, et al. Trend of depression and the use of psychiatric medications in U.S. Veterans with hepatitis C during interferon-based therapy. Am J Gastroenterol 2007;102(11):2426-33.
31. Juengling FD, Ebert D, Gut O, et al. Prefrontal cortical hypometabolism during low-dose interferon alpha treatment. Psychopharmacology.(Berl) 2000;152:383-9.
32. Matthews SC, Paulus MP, Dimsdale JE. Contribution of functional neuroimaging to understanding neuropsychiatric side effects of interferon in hepatitis C. Psychosomatics 2004;45(4):281-6.
33. Ozsoylar G, Sayin A, Bolay H. Clarithromycin monotherapy-induced delirium. J Antimicrob Chemother 2007;59(2):331.-
34. Puzantian T. Central nervous system adverse effects with efavirenz: case report and review. Pharmacotherapy 2002;22:930-3.
35. Browning CH. Nonsteroidal anti-inflammatory drugs and severe psychiatric side effects. Int J Psychiatry Med 1996;26(1):25-34.
36. Picotte-Prillmayer D, DiMaggio JR, Baile WF. H2 blocker delirium. Psychosomatics 1995;36(1):74-7.
37. Cantu TG, Korek JS. Central nervous system reactions to histamine-2 receptor blockers. Ann Intern Med 1991;114:1027-34.
38. Bernstein J. Handbook of drug therapy in psychiatry. St. Louis, MO: Mosby; 1995:380-1.
39. Rampello L, Nicoletti G. [The H2-antagonist therapy withdrawal syndrome: The possible role of hyperprolactinemia]. Medicina (Firenze) 1990;10:294-6.
40. Mitchell KE, Popkin MK, Trick W, Vercellotti G. Psychiatric complications associated with ondansetron. Psychosomatics 1994;35(2):161-3.
41. Brasic JR. Monitoring people treated with isotretinoin for depression. Psychol Rep 2007;100(3 Pt 2):1312-4.
1. Smith DA. Psychiatric side effects of non-psychiatric drugs. S D J Med 1991;44(10):291-2.
2. Conant J, Engler R, Janowsky D, et al. Central nervous system side effects of beta-adrenergic blocking agents with high and low lipid solubility. J Cardiovasc Pharmacol 1989;13:656-61.
3. Cruickshank JM, Neil-Dwyer G. Beta-blocker brain concentrations in man. Eur J Clin Pharmacol 1985;28:21-3.
4. Sirois FJ. Visual hallucinations and metoprolol. Psychosomatics 2006;47(6):537-8.
5. Brown TM, Stoudemire A. Psychiatric side effects of prescription and over-the-counter medications. Recognition and management. Washington, DC: American Psychiatric Publishing; 1998.
6. Waal HF. Propranolol-induced depression (letter). Br Med J 1967;2:50.-
7. Carney RM, Rich MW, teVelde A, et al. Prevalence of major depressive disorder in patients receiving beta-blocker therapy versus other medications. Am J Med 1987;83(2):223-6.
8. Bright RA, Everitt DE. Beta-blockers and depression. Evidence against an association. JAMA 1992;267(13):1783-7.
9. Yudofsky SC. Beta-blockers and depression: the clinician’s dilemma. JAMA 1992;267:1826-7.
10. Law MR, Thompson SG, Wald NJ. Assessing possible hazards of reducing serum cholesterol. BMJ 1994;308:373-9.
11. Morales K, Wittink M, Datto C, et al. Simvastatin causes changes in affective processes in elderly volunteers. J Am Geriatr Soc 2006;54(1):70-6.
12. Yang CC, Jick SS, Jick H. Lipid-lowering drugs and the risk of depression and suicidal behavior. Arch Intern Med 2003;163(16):1926-32.
13. Callréus T, Agerskov Andersen U, Hallas J, et al. Cardiovascular drugs and the risk of suicide: a nested case-control study. Eur J Clin Pharmacol 2007;63(6):591-6.
14. Agostini JV, Tinetti ME, Han L, et al. Effects of statin use on muscle strength, cognition, and depressive symptoms in older adults. J Am Geriatr Soc 2007;55(3):420-5.
15. Tatley M, Savage R. Psychiatric adverse reactions with statins, fibrates and ezetimibe: implications for the use of lipid-lowering agents. Drug Saf 2007;30(3):195-201.
16. Boston Collaborative Drug Surveillance Program. Acute adverse reactions to prednisone in relation to dosage. Clin Pharm. Ther 1972;13:694-8.
17. Brown ES, Suppes T, Khan DA, Carmody TJ 3rd. Mood changes during prednisone bursts in outpatients with asthma. J Clin Psychopharmacol 2002;22:55-61.
18. Naber D, Sand P, Heigl B. Psychological and neuropsychological effects of 8 days’ corticosteroid treatment. A prospective study. Psychoneuroendocrinology 1996;21:25-31.
19. Warrington TP, Bostwick JM. Psychiatric adverse effects of corticosteroids. Mayo Clin Proc 2006;81(10):1361-7.
20. Lewis DA, Smith RE. Steroid-induced psychiatric syndromes: a report of 14 cases and a review of the literature. J Affect Disord 1983;5:319-32.
21. Wolkowitz OM, Rubinow D, Doran AR, et al. Prednisone effects on neurochemistry and behavior. Arch Gen Psych 1990;47:963-8.
22. Ling MHM, Perry PJ, Tsuang MT. Side effects of corticosteroid therapy. Arch Gen Psychiatry 1981;38:471-7.
23. Pagonis TA, Angelopoulos NV, Koukoulis GN, Hadjichristodoulou CS. Psychiatric side effects induced by supraphysiological doses of combinations of anabolic steroids correlate to the severity of abuse. Eur Psychiatry 2006;21(8):551-62.
24. Pope HG, Jr, Katz DL. Psychiatric and medical effects of anabolic-androgenic steroid use: a controlled study of 160 athletes. Arch Gen Psychiatry 1994;51:375-82.
25. Su T, Pagliaro M, Schmidt P, et al. Neuropsychiatric effects of anabolic steroids in male normal volunteers. JAMA 1993;269:2760-4.
26. Warnock JK, Bundren JC, Morris DW. Depressive symptoms associated with gonadotropin-releasing hormone agonists. Depress Anxiety 1998;7:171-7.
27. Turjanski N, Lloyd GG. Psychiatric side-effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70.
28. Lotrich FE, Rabinovitz M, Gironda P, Pollock BG. Depression following pegylated interferon-alpha: characteristics and vulnerability. J Psychosom Res 2007;63(2):131-5.
29. Dieperink E, Ho SB, Thuras P, Willenbring ML. A prospective study of neuropsychiatric symptoms associated with interferon-alpha-2b and ribavirin therapy for patients with chronic hepatitis C. Psychosomatics 2003;44(2):104-12.
30. Jakiche A, Paredez EC, Tannan PK, et al. Trend of depression and the use of psychiatric medications in U.S. Veterans with hepatitis C during interferon-based therapy. Am J Gastroenterol 2007;102(11):2426-33.
31. Juengling FD, Ebert D, Gut O, et al. Prefrontal cortical hypometabolism during low-dose interferon alpha treatment. Psychopharmacology.(Berl) 2000;152:383-9.
32. Matthews SC, Paulus MP, Dimsdale JE. Contribution of functional neuroimaging to understanding neuropsychiatric side effects of interferon in hepatitis C. Psychosomatics 2004;45(4):281-6.
33. Ozsoylar G, Sayin A, Bolay H. Clarithromycin monotherapy-induced delirium. J Antimicrob Chemother 2007;59(2):331.-
34. Puzantian T. Central nervous system adverse effects with efavirenz: case report and review. Pharmacotherapy 2002;22:930-3.
35. Browning CH. Nonsteroidal anti-inflammatory drugs and severe psychiatric side effects. Int J Psychiatry Med 1996;26(1):25-34.
36. Picotte-Prillmayer D, DiMaggio JR, Baile WF. H2 blocker delirium. Psychosomatics 1995;36(1):74-7.
37. Cantu TG, Korek JS. Central nervous system reactions to histamine-2 receptor blockers. Ann Intern Med 1991;114:1027-34.
38. Bernstein J. Handbook of drug therapy in psychiatry. St. Louis, MO: Mosby; 1995:380-1.
39. Rampello L, Nicoletti G. [The H2-antagonist therapy withdrawal syndrome: The possible role of hyperprolactinemia]. Medicina (Firenze) 1990;10:294-6.
40. Mitchell KE, Popkin MK, Trick W, Vercellotti G. Psychiatric complications associated with ondansetron. Psychosomatics 1994;35(2):161-3.
41. Brasic JR. Monitoring people treated with isotretinoin for depression. Psychol Rep 2007;100(3 Pt 2):1312-4.
Mild cognitive impairment: How can you be sure?
Mr. R, age 67, presents with what he describes as uncharacteristic “memory loss” that is affecting his ability to run his accounting business. He and his wife relate that he was doing well until approximately 9 months ago, when he started showing difficulties remembering clients’ names and addresses.
His wife became extremely concerned when he made serious accounting errors in a 1-month period that resulted in the loss of a longtime customer. Mr. R has become easily distracted and absentminded as well, and his wife reports he is misplacing things around the house.
Screening for mild cognitive impairment (MCI) is not recommended for asymptomatic, cognitively healthy older persons, but memory complaints in individuals age >50—especially when corroborated by a reliable informant—warrant further assessment. Your challenge is to determine whether subtle cognitive changes in patients such as Mr. R are part of normal aging, caused by medical or mental illnesses, or a harbinger of Alzheimer’s disease (AD) or another dementia.
Although no treatments can yet prevent dementia, substantial new research is defining the MCI diagnosis for clinicians. This article describes:
- the evolving understanding of MCI and its subtypes
- risk factors for converting from MCI to AD
- an evidence-based work-up (including functional, cognitive, and neuropsychological testing)
- neuroprotective strategies for patients with an MCI diagnosis, including evidence on cholinesterase inhibitors, vitamin E, and anti-inflammatory agents.
MCI’s evolving definition
MCI is characterized by subjective and objective cognitive decline greater than expected for an individual’s age and education but less than the functional deficit required for a dementia diagnosis. MCI is proposed to identify persons with early but pathologic cognitive impairment that has a high risk to progress to AD and possibly other dementias.
MCI subtypes. Some experts view MCI as a single entity, whereas others suggest amnestic (aMCI) and nonamnestic (nMCI) subtypes.1,3 Each subtype is further divided into single and multiple cognitive domains. So, for example, the diagnosis would be:
- aMCI-single cognitive domain for memory impairment only
- aMCI-multiple cognitive domains for memory impairment plus nonmemory deficits, such as in language, executive function, or visuospatial function
- nMCI-single or multiple cognitive domains for nonmemory deficits without memory impairment.
Determining a patient’s MCI subtype is still a research activity and calls for comprehensive neuropsychological testing. MCI patients perform at least 1.5 standard deviations below the average for age- and education-matched healthy individuals on objective measures of memory.1
Conversion to dementia
In longitudinal population studies patients with MCI have shown an 11% to 33% risk of developing dementia within 2 years, whereas 44% reverted to normal 1 year later. Reasons for reversibility may include variable definitions of MCI among the longitudinal studies and the possibility that patients who recovered or improved may have had reversible causes of dementia.1
Individuals with aMCI (Table 1)8 progress to AD at a rate of 10% to 15% per year, compared with 1% to 2% per year in normal elderly persons. The Mayo AD research center studies reported a conversion rate of up to 80% from aMCI to AD within 6 years.9
Research focuses on identifying preclinical AD states and potential targets for intervention using disease-modifying therapies. Some experts consider MCI to be the earliest clinical manifestation of AD, at least in a subgroup of patients.
Identifying markers to predict which patients are likely to convert from MCI to dementia also is a major research objective. In addition to ApoE status (Table 2),7,9-15 predictors of conversion may include:
- hippocampal atrophy13
- reduced metabolism in the temporoparietal cortex and posterior cingulum14
- elevated CSF tau and the 42 amino acid form of ß-amyloid (Aß 42).15
Neuropsychiatric symptoms. Individuals with MCI and neuropsychiatric symptoms may be at particular risk for progressing to dementia. Agitation or depression are more prevalent in persons with MCI than in normal elderly but less prevalent than in those with dementia (Table 3).10,16
- 16% of normal healthy elderly
- 43% of MCI patients
- 75% of dementia patients.16
Sleep disturbances and anxiety in persons with MCI may predict progression to AD.10 A baseline high frequency of apathy in aMCI patients has been associated with progression to AD within 1 year.11
Table 1
Amnestic MCI: Proposed diagnostic criteria
| Subjective memory impairment, preferably corroborated by a reliable informant |
| Reduced performance on objective memory tests, compared with persons of similar age and educational background |
| Typical general cognitive function |
| Intact basic activities of daily living and intact or minimally impaired instrumental activities of daily living |
| Absence of dementia |
| MCI: mild cognitive impairment |
| Source: Reference 8 |
Factors shown to predict conversion from MCI to dementia
| Category | Predictors of conversion |
|---|---|
| Clinical | Cognitive: Amnestic MCI Neuropsychiatric: Depression, apathy, and possibly nighttime behaviors and anxiety |
| Neuropsychological tests | Clock-drawing test, Trail-Making Test B, Symbol Digit Modalities Test, Delayed 10-Word List Recall, New York University Paragraph Recall Test (Delayed), ADAS-Cog total score |
| Neuroimaging | MRI: Entorhinal cortex and hippocampal atrophy PET: Medial temporal region, parietotemporal association cortex, and posterior cingulate hypometabolism fMRI: Abnormal hippocampal, posterior cingulate, and medial temporal region activation on memory tasks |
| CSF markers | Increase: t-tau, p-tau Decrease: Aß 42 |
| Genetic markers | ApoE e4 carriers |
| ADAS-Cog: Alzheimer’s Disease Assessment Scale-Cognitive subscale; ApoE e4: apolipoprotein E gene, e4 allele; CSF: cerebrospinal fluid; MCI: mild cognitive impairment; MRI: magnetic resonance imaging; fMRI: functional MRI; PET: positron-emission tomography | |
| Source: References 7,9-15 | |
Neuropsychiatric symptoms: Rising prevalence mirrors cognitive deterioration in elderly patients*
| Neuropsychiatric symptoms | Normal elderly | MCI | Mild AD |
|---|---|---|---|
| Depressed mood/dysphoria | + | ++ | +++ |
| Nighttime behaviors/sleep | + | ++ | +++ |
| Irritability | + | ++ | +++ |
| Anxiety | +/- | ++ | +++ |
| Apathy/indifference | +/- | ++ | +++ |
| Agitation/aggression | +/- | +/++ | +++ |
| Eating/appetite disturbance | +/- | + | ++ |
| Disinhibition | +/- | +/- | ++ |
| Aberrant motor behavior | 0 | + | ++ |
| Delusions | 0 | +/- | ++ |
| Euphoria | 0 | +/- | +/- |
| Hallucinations | 0 | 0 | + |
| * 0 = 0%; +/- = 1% to 5%; + = 6% to 10%; ++ = 11% to 20%; +++ = 21% to 40% | |||
| MCI: mild cognitive impairment; AD: Alzheimer’s disease | |||
| Source: References 10,16 | |||
Depression and MCI
Depression and cognitive complaints overlap considerably in older adults. Depressed patients without dementia show persistent cognitive deficits even after depression remits. In some patients, new-onset geriatric depression is considered a prodrome of MCI and AD. Given that AD neuropathologic changes precede clinical symptoms by many years, depression and AD have been proposed as different clinical manifestations of AD pathology.17
Depressed MCI patients are at higher risk of developing dementia than those without depression, especially if cognitive measures do not improve after depression is treated.12 Similarly, cognitively intact older persons who develop depression are at increased risk for MCI, particularly if they carry the ApoE e4 genotype.19
In the only study in which MCI patients’ neuropsychiatric symptoms have been treated, 39 elderly patients with depression and MCI received open-label sertraline, ≤200 mg/d, for 12 weeks. Among the 26 patients who completed the trial, 17 showed moderate improvement in depressive symptoms, attention, and executive function, and 9 showed no response.20
Recommendation. In clinical practice, antidepressant treatment—usually a selective serotonin reuptake inhibitor (SSRI), with or without psychotherapy—is recommended for the MCI patient with comorbid major depression.
CASE CONTINUED: No signs of depression
Mr. R’s medical, neurologic, and substance use history is unremarkable. Family history includes AD in a paternal aunt diagnosed at age 82. Mr. R reports no history of mood, sleep, or appetite changes and no psychotic symptoms. He shows no deficits in activities of daily living (ADL), although his wife recently took over paying household bills after he forgot to make a payment.
Evidence-based workup
Functional assessment. In the differential diagnosis of MCI, give special attention to functional impairment, which points toward dementia. ADL generally are preserved in MCI, and minimal deterioration is seen in instrumental activities of daily living (IADL). A relatively easy way to assess function is to use the Alzheimer’s Disease Functional Assessment and Change Scale (ADFACS), which is based on 16 ADL and IADL items (Table 4).21
A substantial functional decline precludes an MCI diagnosis, although the degree of functional decline can be difficult to assess in older adults with physical limitations caused by medical comorbidities.
Cognitive assessment. Because most individuals with MCI score in the normal range on the Folstein Mini-Mental State Examination (MMSE), the modified MMSE (3MS)22 may be more sensitive for detecting MCI. The 3MS retains the MMSE’s brevity (≤10 minutes to administer) but incorporates 4 additional items, has more graded scoring responses, and broadens the score range to 0 to 100. The clock-drawing test also is sensitive for MCI, especially in detecting early visuoconstructional dysfunction.
The Montreal Cognitive Assessment (MoCA) is a 10-minute, 30-point scale designed to help clinicians detect MCI (see Related Resources). The MoCA usually is given with the modified MMSE for a comprehensive cognitive assessment.
Nasreddine et al23 administered the MoCA and MMSE to 94 patients who met clinical criteria for MCI, 93 patients with mild AD, and 90 healthy cognitively normal elderly persons, using a cutoff score of 26. MoCA showed:
- 90% sensitivity for detecting MCI (compared with 18% for the MMSE)
- 87% specificity to exclude normal elderly persons.
Neuropsychological testing can be more sensitive than office-based screening tools in defining MCI subtypes. In the Alzheimer’s Disease Cooperative Study (ADCS), the neuropsychological measures that most accurately predicted progression of patients with aMCI to AD within 36 months were the:
- Symbol Digit Modalities Test
- New York University Paragraph Recall Test (Delayed)
- Delayed 10-Word List Recall
- Alzheimer’s Disease Assessment Scale-cognitive subscale (ADAS-Cog) total score.24
Table 4
Alzheimer’s Disease Functional Assessment and Change Scale (ADFACS)
| Basic ADL | Instrumental ADL (IADL) |
|---|---|
| Toileting | Use of telephone |
| Feeding | Household tasks |
| Dressing | Using household appliances |
| Personal hygiene and grooming | Managing money |
| Shopping | |
| Bathing | Food preparation |
| Walking | Ability to get around inside and outside home |
| Hobbies and leisure activities | |
| Handling personal mail | |
| Grasp of situations and explanations | |
The 16-item ADFACS total score ranges from 0 to 54 (best to worst):
| |
| Use total scores to assess for functional decline from baseline. A decline from 0 to 1 on individual ADL and IADL items is not considered clinically significant. | |
| ADL: activities of daily living | |
| Source: Reprinted with permission from reference 21 | |
Lab studies to rule out reversible causes of MCI
| Complete blood count with differential |
| Basic metabolic panel |
| Liver function tests |
| Serum calcium |
| Serum vitamin B12 and folate |
| Thyroid function tests |
| Rapid plasma reagin |
| HIV in high-risk individuals |
| CSF studies if CNS infection is suspected |
| CSF: cerebrospinal fluid; HIV: human immunodeficiency virus; MCI: mild cognitive impairment |
| Source: Reference 8 |
CASE CONTINUED: Subtle cognitive deficits
Mr. R scores 27/30 on the MMSE (losing 3 points on recall) and 25/30 on the MoCA (losing points on visuospatial/executive function, fluency, and delayed recall). Thyroid stimulating hormone, vitamin B12, folate, and rapid plasma reagin tests are unremarkable; brain MRI shows no significant abnormalities.
You refer Mr. R for neuropsychological testing, and most cognitive domains are normal. Exceptions include moderate impairment in immediate and delayed verbal and visual memory and mild executive dysfunction.
Based on your clinical evaluation and neuropsychological testing, you diagnose amnestic MCI. Mr. R shows abnormalities in memory and executive functioning without significant decline in basic and instrumental ADLs, is not taking medications, and has no other medical or psychiatric condition that could explain his cognitive deficits.
You discuss the diagnosis with him and his wife, including evidence on his risk for progression to dementia, neuroprotective strategies, and medications.
After an MCI diagnosis
Neuroprotection. Eliminate medications with anticholinergic effects, including:
- tricyclic antidepressants
- conventional antipsychotics
- antihistamines
- drugs used to treat urinary incontinence, such as oxybutynin
- muscle relaxants, such as cyclobenzaprine
- certain antiparkinsonian drugs, such as benztropine.
Monitoring. The American Academy of Neurology recommends monitoring patients diagnosed with MCI every 6 to 12 months for cognitive and functional decline.
In these visits, include:
- repeat office-based cognitive assessment, especially the modified MMSE, clock-drawing test, and MoCA
- careful history-taking from the patient and reliable informant
- repeat neuropsychological testing annually or when dementia is suspected
- assessment of the caregiver for distress.
- moderate exercise (at least 30 minutes per session, 3 times a week)
- cognitively stimulating activities that involve language and psychomotor coordination, such as dancing, crossword puzzles, and volunteer work.
Medications—yes or no? Cholinesterase inhibitors, rofecoxib, and vitamin E have not been shown to prevent MCI from progressing to AD. Thus, insufficient evidence exists to recommend medications for patients with MCI.
Donepezil has shown possible short-term benefits, however, and patients may choose to try this medication. Some find comfort in seeking this “extra time” to make decisions about advanced directives, attend to estate and will issues, and optimize relationships while they have only mild cognitive deficits and possess decision-making capacity.
Donepezil. The Alzheimer’s Disease Cooperative Study—supported by the National Institute on Aging—was designed to determine whether daily doses of donepezil or vitamin E can delay or prevent progression of aMCI to AD.25 In the double-blind, placebo-controlled, parallel group study, 769 patients with aMCI were randomly assigned to receive donepezil, 10 mg/d; vitamin E, 1,000 IU bid; or placebo for 3 years.
Overall progression to AD was 16% per year, and the 3-year risk of progression was the same in all 3 groups. Donepezil therapy was associated with a reduced rate of progression to AD compared with placebo during the first year of treatment. Donepezil’s benefit was evident among ApoE e4 carriers at 2-year follow-up, but none of the 3 groups showed statistically significant differences after 3 years. Vitamin E showed no effect on AD progression throughout the study.
Rivastigmine. A randomized, placebo-controlled trial in which 1,018 MCI patients received rivastigmine or placebo for 4 years found no statistically significant benefit of rivastigmine on AD progression.26
Galantamine. Two international randomized, double-blind, placebo-controlled trials failed to show a statistically significant benefit of galantamine in slowing progression from aMCI to AD. MRI data from one of these studies suggested that galantamine may have reduced the rate of brain atrophy over a 2-year period.27
Rofecoxib. Epidemiologic studies indicate that anti-inflammatory drugs may reduce the risk of developing AD, but the COX-2 inhibitor rofecoxib did not delay progression to AD among aMCI patients in a large, placebo-controlled trial.28
Educate patients and family members about supportive nonpharmacologic treatments and cholinesterase inhibitors. The Alzheimer’s Association, National Institute on Aging, and local department of aging agencies offer useful resources (see Related Resources).
CASE CONTINUED: Dealing with uncertainty
Mr. R and his wife are unsettled by his MCI diagnosis. They prefer to take a “wait and watch” approach, decline initiation of a cholinesterase inhibitor, and agree to adhere to nonpharmacologic interventions you discussed. You schedule a follow-up visit in 6 months and encourage them to call you with questions.
- Rosenberg PB, Johnston D, Lyketsos CG. A clinical approach to mild cognitive impairment. Am J Psychiatry 2006;163: 1884-90.
- Montreal Cognitive Assessment (MoCA). 10-minute screening test designed to help clinicians detect mild cognitive impairment. www.mocatest.org.
- Alzheimer’s Association. www.alz.org.
- National Institute on Aging. www.nia.nih.gov.
- Benztropine • Cogentin
- Cyclobenzaprine • Flexeril
- Donepezil • Aricept
- Galantamine • Razadyne
- Oxybutynin • Ditropan
- Rivastigmine • Exelon
- Rofecoxib • Vioxx
- Sertraline • Zoloft
Dr. Goveas and Dr. Dixon-Holbrook report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Kerwin is a consultant to Pfizer and a speaker for Pfizer and Novartis.
Dr. Antuono receives research support from Eisai, Pfizer, and Elan and is a speaker for Pfizer and Forest Pharmaceuticals.
1. Gauthier S, Reisberg B, Zaudig M, et al. Mild cognitive impairment. Lancet 2006;367:1262-70.
2. Lopez OL, Jagust WJ, DeKosky ST, et al. Prevalence and classification of mild cognitive impairment in the Cardiovascular Health Study Cognition Study: part 1. Arch Neurol 2003;60:1385-9.
3. Petersen RC. Conceptual review. In: Petersen RC, ed. Mild cognitive impairment: aging to Alzheimer’s disease. New York, NY: Oxford University Press; 2003:1-14.
4. Petersen RC, Morris JC. Mild cognitive impairment as a clinical entity and treatment target. Arch Neurol 2005;62:1160-3.
5. O’Brien JT. Vascular cognitive impairment. Am J Geriatr Psychiatry 2006;14:724-33.
6. Janvin CC, Larsen JP, Aarsland D, et al. Subtypes of mild cognitive impairment in Parkinson’s disease: progression to dementia. Mov Disord 2006;21:1343-9.
7. Farlow MR, He Y, Tekin S, et al. Impact of APOE in mild cognitive impairment. Neurology 2004;63:1898-1901.
8. Winblad B, Palmer K, Kivipelto M, et al. Mild cognitive impairment—beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment. J Intern Med 2004;256:240-6.
9. Petersen RC. Mild cognitive impairment as a diagnostic entity. J Intern Med 2004;256:183-94.
10. Geda YE, Smith GE, Knopman DS, et al. De novo genesis of neuropsychiatric symptoms in mild cognitive impairment (MCI). Int Psychogeriatr 2004;16:51-60.
11. Robert PH, Berr C, Volteau M, et al. Apathy in patients with mild cognitive impairment and the risk of developing dementia of Alzheimer’s disease: a one-year follow-up study. Clin Neurol Neurosurg 2006;108:733-6.
12. Modrego PJ, Ferrandez J. Depression in patients with mild cognitive impairment increases the risk of developing dementia of Alzheimer type. Arch Neurol 2004;61:1290-3.
13. Jack CR, Petersen RC, Xu YC, et al. Prediction of AD with MRI-based hippocampal volume in mild cognitive impairment. Neurology 1999;52:1397-1403.
14. Nestor PJ, Fryer TD, Smielewski P, et al. Limbic hypometabolism in Alzheimer’s disease and mild cognitive impairment. Ann Neurol 2003;54:343-51.
15. Sunderland T, Hampel H, Takeda M, et al. Biomarkers in the diagnosis of Alzheimer’s disease: are we ready? J Geriatr Psychiatry Neurol 2006;19:172-9.
16. Lyketsos CG, Lopez O, Jones B, et al. Prevalence of neuropsychiatric symptoms in dementia and mild cognitive impairment: results from the Cardiovascular Health Study. JAMA 2002;288:1475-83.
17. Steffens DC, Otey E, Alexoupolos GS, et al. Perspectives on depression, mild cognitive impairment, and cognitive decline. Arch Gen Psychiatry 2006;63:130-8.
18. Gabryelewicz T, Styczynska M, Pfeffer A, et al. Prevalence of major and minor depression in elderly persons with mild cognitive impairment: MADRS factor analysis. Int J Geriatr Psychiatry 2004;19:1168-72.
19. Geda YE, Knopman DS, Mrazek DA, et al. Depression, apolipoprotein E genotype, and the incidence of mild cognitive impairment: a prospective cohort study. Arch Neurol 2006;63:435-40.
20. Devanand DP, Pelton GH, Marston K, et al. Sertraline treatment of elderly patients with depression and cognitive impairment. Int J Geriatr Psychiatry 2003;18:123-30.
21. Mohs RC, Doody RS, Morris JC, et al. A 1-year, placebo-controlled preservation of function survival study of donepezil in AD patients. Neurology 2001;57:481-8.
22. Teng EL, Chui HC. The Modified Mini-Mental State (3MS) examination. J Clin Psychiatry 1987;48:314-8.
23. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment (MoCA): a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 2005;53:695-9.
24. Fleisher AS, Sowell BB, Taylor C, et al. Clinical predictors of progression to Alzheimer disease in amnestic mild cognitive impairment. Neurology 2007;68:1588-95.
25. Petersen RC, Thomas RG, Grundman M, et al. for the Alzheimer’s Disease Cooperative Study Group. Vitamin E and donepezil for the treatment of mild cognitive impairment. N Engl J Med 2005;352:2379-88.
26. Feldman HH, Ferris S, Winblad B, et al. Effect of rivastigmine on delay to diagnosis of Alzheimer’s disease from mild cognitive impairment: the InDDEx study. Lancet Neurol 2007;6:501-12.
27. Petersen RC. Mild cognitive impairment: current research and clinical implications. Semin Neurol 2007;27:22-31.
28. Thal LJ, Ferris SH, Kirby L, et al. A randomized, double-blind study of rofecoxib in patients with mild cognitive impairment. Neuropsychopharmacology 2005;30(6):1204-15.
Mr. R, age 67, presents with what he describes as uncharacteristic “memory loss” that is affecting his ability to run his accounting business. He and his wife relate that he was doing well until approximately 9 months ago, when he started showing difficulties remembering clients’ names and addresses.
His wife became extremely concerned when he made serious accounting errors in a 1-month period that resulted in the loss of a longtime customer. Mr. R has become easily distracted and absentminded as well, and his wife reports he is misplacing things around the house.
Screening for mild cognitive impairment (MCI) is not recommended for asymptomatic, cognitively healthy older persons, but memory complaints in individuals age >50—especially when corroborated by a reliable informant—warrant further assessment. Your challenge is to determine whether subtle cognitive changes in patients such as Mr. R are part of normal aging, caused by medical or mental illnesses, or a harbinger of Alzheimer’s disease (AD) or another dementia.
Although no treatments can yet prevent dementia, substantial new research is defining the MCI diagnosis for clinicians. This article describes:
- the evolving understanding of MCI and its subtypes
- risk factors for converting from MCI to AD
- an evidence-based work-up (including functional, cognitive, and neuropsychological testing)
- neuroprotective strategies for patients with an MCI diagnosis, including evidence on cholinesterase inhibitors, vitamin E, and anti-inflammatory agents.
MCI’s evolving definition
MCI is characterized by subjective and objective cognitive decline greater than expected for an individual’s age and education but less than the functional deficit required for a dementia diagnosis. MCI is proposed to identify persons with early but pathologic cognitive impairment that has a high risk to progress to AD and possibly other dementias.
MCI subtypes. Some experts view MCI as a single entity, whereas others suggest amnestic (aMCI) and nonamnestic (nMCI) subtypes.1,3 Each subtype is further divided into single and multiple cognitive domains. So, for example, the diagnosis would be:
- aMCI-single cognitive domain for memory impairment only
- aMCI-multiple cognitive domains for memory impairment plus nonmemory deficits, such as in language, executive function, or visuospatial function
- nMCI-single or multiple cognitive domains for nonmemory deficits without memory impairment.
Determining a patient’s MCI subtype is still a research activity and calls for comprehensive neuropsychological testing. MCI patients perform at least 1.5 standard deviations below the average for age- and education-matched healthy individuals on objective measures of memory.1
Conversion to dementia
In longitudinal population studies patients with MCI have shown an 11% to 33% risk of developing dementia within 2 years, whereas 44% reverted to normal 1 year later. Reasons for reversibility may include variable definitions of MCI among the longitudinal studies and the possibility that patients who recovered or improved may have had reversible causes of dementia.1
Individuals with aMCI (Table 1)8 progress to AD at a rate of 10% to 15% per year, compared with 1% to 2% per year in normal elderly persons. The Mayo AD research center studies reported a conversion rate of up to 80% from aMCI to AD within 6 years.9
Research focuses on identifying preclinical AD states and potential targets for intervention using disease-modifying therapies. Some experts consider MCI to be the earliest clinical manifestation of AD, at least in a subgroup of patients.
Identifying markers to predict which patients are likely to convert from MCI to dementia also is a major research objective. In addition to ApoE status (Table 2),7,9-15 predictors of conversion may include:
- hippocampal atrophy13
- reduced metabolism in the temporoparietal cortex and posterior cingulum14
- elevated CSF tau and the 42 amino acid form of ß-amyloid (Aß 42).15
Neuropsychiatric symptoms. Individuals with MCI and neuropsychiatric symptoms may be at particular risk for progressing to dementia. Agitation or depression are more prevalent in persons with MCI than in normal elderly but less prevalent than in those with dementia (Table 3).10,16
- 16% of normal healthy elderly
- 43% of MCI patients
- 75% of dementia patients.16
Sleep disturbances and anxiety in persons with MCI may predict progression to AD.10 A baseline high frequency of apathy in aMCI patients has been associated with progression to AD within 1 year.11
Table 1
Amnestic MCI: Proposed diagnostic criteria
| Subjective memory impairment, preferably corroborated by a reliable informant |
| Reduced performance on objective memory tests, compared with persons of similar age and educational background |
| Typical general cognitive function |
| Intact basic activities of daily living and intact or minimally impaired instrumental activities of daily living |
| Absence of dementia |
| MCI: mild cognitive impairment |
| Source: Reference 8 |
Factors shown to predict conversion from MCI to dementia
| Category | Predictors of conversion |
|---|---|
| Clinical | Cognitive: Amnestic MCI Neuropsychiatric: Depression, apathy, and possibly nighttime behaviors and anxiety |
| Neuropsychological tests | Clock-drawing test, Trail-Making Test B, Symbol Digit Modalities Test, Delayed 10-Word List Recall, New York University Paragraph Recall Test (Delayed), ADAS-Cog total score |
| Neuroimaging | MRI: Entorhinal cortex and hippocampal atrophy PET: Medial temporal region, parietotemporal association cortex, and posterior cingulate hypometabolism fMRI: Abnormal hippocampal, posterior cingulate, and medial temporal region activation on memory tasks |
| CSF markers | Increase: t-tau, p-tau Decrease: Aß 42 |
| Genetic markers | ApoE e4 carriers |
| ADAS-Cog: Alzheimer’s Disease Assessment Scale-Cognitive subscale; ApoE e4: apolipoprotein E gene, e4 allele; CSF: cerebrospinal fluid; MCI: mild cognitive impairment; MRI: magnetic resonance imaging; fMRI: functional MRI; PET: positron-emission tomography | |
| Source: References 7,9-15 | |
Neuropsychiatric symptoms: Rising prevalence mirrors cognitive deterioration in elderly patients*
| Neuropsychiatric symptoms | Normal elderly | MCI | Mild AD |
|---|---|---|---|
| Depressed mood/dysphoria | + | ++ | +++ |
| Nighttime behaviors/sleep | + | ++ | +++ |
| Irritability | + | ++ | +++ |
| Anxiety | +/- | ++ | +++ |
| Apathy/indifference | +/- | ++ | +++ |
| Agitation/aggression | +/- | +/++ | +++ |
| Eating/appetite disturbance | +/- | + | ++ |
| Disinhibition | +/- | +/- | ++ |
| Aberrant motor behavior | 0 | + | ++ |
| Delusions | 0 | +/- | ++ |
| Euphoria | 0 | +/- | +/- |
| Hallucinations | 0 | 0 | + |
| * 0 = 0%; +/- = 1% to 5%; + = 6% to 10%; ++ = 11% to 20%; +++ = 21% to 40% | |||
| MCI: mild cognitive impairment; AD: Alzheimer’s disease | |||
| Source: References 10,16 | |||
Depression and MCI
Depression and cognitive complaints overlap considerably in older adults. Depressed patients without dementia show persistent cognitive deficits even after depression remits. In some patients, new-onset geriatric depression is considered a prodrome of MCI and AD. Given that AD neuropathologic changes precede clinical symptoms by many years, depression and AD have been proposed as different clinical manifestations of AD pathology.17
Depressed MCI patients are at higher risk of developing dementia than those without depression, especially if cognitive measures do not improve after depression is treated.12 Similarly, cognitively intact older persons who develop depression are at increased risk for MCI, particularly if they carry the ApoE e4 genotype.19
In the only study in which MCI patients’ neuropsychiatric symptoms have been treated, 39 elderly patients with depression and MCI received open-label sertraline, ≤200 mg/d, for 12 weeks. Among the 26 patients who completed the trial, 17 showed moderate improvement in depressive symptoms, attention, and executive function, and 9 showed no response.20
Recommendation. In clinical practice, antidepressant treatment—usually a selective serotonin reuptake inhibitor (SSRI), with or without psychotherapy—is recommended for the MCI patient with comorbid major depression.
CASE CONTINUED: No signs of depression
Mr. R’s medical, neurologic, and substance use history is unremarkable. Family history includes AD in a paternal aunt diagnosed at age 82. Mr. R reports no history of mood, sleep, or appetite changes and no psychotic symptoms. He shows no deficits in activities of daily living (ADL), although his wife recently took over paying household bills after he forgot to make a payment.
Evidence-based workup
Functional assessment. In the differential diagnosis of MCI, give special attention to functional impairment, which points toward dementia. ADL generally are preserved in MCI, and minimal deterioration is seen in instrumental activities of daily living (IADL). A relatively easy way to assess function is to use the Alzheimer’s Disease Functional Assessment and Change Scale (ADFACS), which is based on 16 ADL and IADL items (Table 4).21
A substantial functional decline precludes an MCI diagnosis, although the degree of functional decline can be difficult to assess in older adults with physical limitations caused by medical comorbidities.
Cognitive assessment. Because most individuals with MCI score in the normal range on the Folstein Mini-Mental State Examination (MMSE), the modified MMSE (3MS)22 may be more sensitive for detecting MCI. The 3MS retains the MMSE’s brevity (≤10 minutes to administer) but incorporates 4 additional items, has more graded scoring responses, and broadens the score range to 0 to 100. The clock-drawing test also is sensitive for MCI, especially in detecting early visuoconstructional dysfunction.
The Montreal Cognitive Assessment (MoCA) is a 10-minute, 30-point scale designed to help clinicians detect MCI (see Related Resources). The MoCA usually is given with the modified MMSE for a comprehensive cognitive assessment.
Nasreddine et al23 administered the MoCA and MMSE to 94 patients who met clinical criteria for MCI, 93 patients with mild AD, and 90 healthy cognitively normal elderly persons, using a cutoff score of 26. MoCA showed:
- 90% sensitivity for detecting MCI (compared with 18% for the MMSE)
- 87% specificity to exclude normal elderly persons.
Neuropsychological testing can be more sensitive than office-based screening tools in defining MCI subtypes. In the Alzheimer’s Disease Cooperative Study (ADCS), the neuropsychological measures that most accurately predicted progression of patients with aMCI to AD within 36 months were the:
- Symbol Digit Modalities Test
- New York University Paragraph Recall Test (Delayed)
- Delayed 10-Word List Recall
- Alzheimer’s Disease Assessment Scale-cognitive subscale (ADAS-Cog) total score.24
Table 4
Alzheimer’s Disease Functional Assessment and Change Scale (ADFACS)
| Basic ADL | Instrumental ADL (IADL) |
|---|---|
| Toileting | Use of telephone |
| Feeding | Household tasks |
| Dressing | Using household appliances |
| Personal hygiene and grooming | Managing money |
| Shopping | |
| Bathing | Food preparation |
| Walking | Ability to get around inside and outside home |
| Hobbies and leisure activities | |
| Handling personal mail | |
| Grasp of situations and explanations | |
The 16-item ADFACS total score ranges from 0 to 54 (best to worst):
| |
| Use total scores to assess for functional decline from baseline. A decline from 0 to 1 on individual ADL and IADL items is not considered clinically significant. | |
| ADL: activities of daily living | |
| Source: Reprinted with permission from reference 21 | |
Lab studies to rule out reversible causes of MCI
| Complete blood count with differential |
| Basic metabolic panel |
| Liver function tests |
| Serum calcium |
| Serum vitamin B12 and folate |
| Thyroid function tests |
| Rapid plasma reagin |
| HIV in high-risk individuals |
| CSF studies if CNS infection is suspected |
| CSF: cerebrospinal fluid; HIV: human immunodeficiency virus; MCI: mild cognitive impairment |
| Source: Reference 8 |
CASE CONTINUED: Subtle cognitive deficits
Mr. R scores 27/30 on the MMSE (losing 3 points on recall) and 25/30 on the MoCA (losing points on visuospatial/executive function, fluency, and delayed recall). Thyroid stimulating hormone, vitamin B12, folate, and rapid plasma reagin tests are unremarkable; brain MRI shows no significant abnormalities.
You refer Mr. R for neuropsychological testing, and most cognitive domains are normal. Exceptions include moderate impairment in immediate and delayed verbal and visual memory and mild executive dysfunction.
Based on your clinical evaluation and neuropsychological testing, you diagnose amnestic MCI. Mr. R shows abnormalities in memory and executive functioning without significant decline in basic and instrumental ADLs, is not taking medications, and has no other medical or psychiatric condition that could explain his cognitive deficits.
You discuss the diagnosis with him and his wife, including evidence on his risk for progression to dementia, neuroprotective strategies, and medications.
After an MCI diagnosis
Neuroprotection. Eliminate medications with anticholinergic effects, including:
- tricyclic antidepressants
- conventional antipsychotics
- antihistamines
- drugs used to treat urinary incontinence, such as oxybutynin
- muscle relaxants, such as cyclobenzaprine
- certain antiparkinsonian drugs, such as benztropine.
Monitoring. The American Academy of Neurology recommends monitoring patients diagnosed with MCI every 6 to 12 months for cognitive and functional decline.
In these visits, include:
- repeat office-based cognitive assessment, especially the modified MMSE, clock-drawing test, and MoCA
- careful history-taking from the patient and reliable informant
- repeat neuropsychological testing annually or when dementia is suspected
- assessment of the caregiver for distress.
- moderate exercise (at least 30 minutes per session, 3 times a week)
- cognitively stimulating activities that involve language and psychomotor coordination, such as dancing, crossword puzzles, and volunteer work.
Medications—yes or no? Cholinesterase inhibitors, rofecoxib, and vitamin E have not been shown to prevent MCI from progressing to AD. Thus, insufficient evidence exists to recommend medications for patients with MCI.
Donepezil has shown possible short-term benefits, however, and patients may choose to try this medication. Some find comfort in seeking this “extra time” to make decisions about advanced directives, attend to estate and will issues, and optimize relationships while they have only mild cognitive deficits and possess decision-making capacity.
Donepezil. The Alzheimer’s Disease Cooperative Study—supported by the National Institute on Aging—was designed to determine whether daily doses of donepezil or vitamin E can delay or prevent progression of aMCI to AD.25 In the double-blind, placebo-controlled, parallel group study, 769 patients with aMCI were randomly assigned to receive donepezil, 10 mg/d; vitamin E, 1,000 IU bid; or placebo for 3 years.
Overall progression to AD was 16% per year, and the 3-year risk of progression was the same in all 3 groups. Donepezil therapy was associated with a reduced rate of progression to AD compared with placebo during the first year of treatment. Donepezil’s benefit was evident among ApoE e4 carriers at 2-year follow-up, but none of the 3 groups showed statistically significant differences after 3 years. Vitamin E showed no effect on AD progression throughout the study.
Rivastigmine. A randomized, placebo-controlled trial in which 1,018 MCI patients received rivastigmine or placebo for 4 years found no statistically significant benefit of rivastigmine on AD progression.26
Galantamine. Two international randomized, double-blind, placebo-controlled trials failed to show a statistically significant benefit of galantamine in slowing progression from aMCI to AD. MRI data from one of these studies suggested that galantamine may have reduced the rate of brain atrophy over a 2-year period.27
Rofecoxib. Epidemiologic studies indicate that anti-inflammatory drugs may reduce the risk of developing AD, but the COX-2 inhibitor rofecoxib did not delay progression to AD among aMCI patients in a large, placebo-controlled trial.28
Educate patients and family members about supportive nonpharmacologic treatments and cholinesterase inhibitors. The Alzheimer’s Association, National Institute on Aging, and local department of aging agencies offer useful resources (see Related Resources).
CASE CONTINUED: Dealing with uncertainty
Mr. R and his wife are unsettled by his MCI diagnosis. They prefer to take a “wait and watch” approach, decline initiation of a cholinesterase inhibitor, and agree to adhere to nonpharmacologic interventions you discussed. You schedule a follow-up visit in 6 months and encourage them to call you with questions.
- Rosenberg PB, Johnston D, Lyketsos CG. A clinical approach to mild cognitive impairment. Am J Psychiatry 2006;163: 1884-90.
- Montreal Cognitive Assessment (MoCA). 10-minute screening test designed to help clinicians detect mild cognitive impairment. www.mocatest.org.
- Alzheimer’s Association. www.alz.org.
- National Institute on Aging. www.nia.nih.gov.
- Benztropine • Cogentin
- Cyclobenzaprine • Flexeril
- Donepezil • Aricept
- Galantamine • Razadyne
- Oxybutynin • Ditropan
- Rivastigmine • Exelon
- Rofecoxib • Vioxx
- Sertraline • Zoloft
Dr. Goveas and Dr. Dixon-Holbrook report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Kerwin is a consultant to Pfizer and a speaker for Pfizer and Novartis.
Dr. Antuono receives research support from Eisai, Pfizer, and Elan and is a speaker for Pfizer and Forest Pharmaceuticals.
Mr. R, age 67, presents with what he describes as uncharacteristic “memory loss” that is affecting his ability to run his accounting business. He and his wife relate that he was doing well until approximately 9 months ago, when he started showing difficulties remembering clients’ names and addresses.
His wife became extremely concerned when he made serious accounting errors in a 1-month period that resulted in the loss of a longtime customer. Mr. R has become easily distracted and absentminded as well, and his wife reports he is misplacing things around the house.
Screening for mild cognitive impairment (MCI) is not recommended for asymptomatic, cognitively healthy older persons, but memory complaints in individuals age >50—especially when corroborated by a reliable informant—warrant further assessment. Your challenge is to determine whether subtle cognitive changes in patients such as Mr. R are part of normal aging, caused by medical or mental illnesses, or a harbinger of Alzheimer’s disease (AD) or another dementia.
Although no treatments can yet prevent dementia, substantial new research is defining the MCI diagnosis for clinicians. This article describes:
- the evolving understanding of MCI and its subtypes
- risk factors for converting from MCI to AD
- an evidence-based work-up (including functional, cognitive, and neuropsychological testing)
- neuroprotective strategies for patients with an MCI diagnosis, including evidence on cholinesterase inhibitors, vitamin E, and anti-inflammatory agents.
MCI’s evolving definition
MCI is characterized by subjective and objective cognitive decline greater than expected for an individual’s age and education but less than the functional deficit required for a dementia diagnosis. MCI is proposed to identify persons with early but pathologic cognitive impairment that has a high risk to progress to AD and possibly other dementias.
MCI subtypes. Some experts view MCI as a single entity, whereas others suggest amnestic (aMCI) and nonamnestic (nMCI) subtypes.1,3 Each subtype is further divided into single and multiple cognitive domains. So, for example, the diagnosis would be:
- aMCI-single cognitive domain for memory impairment only
- aMCI-multiple cognitive domains for memory impairment plus nonmemory deficits, such as in language, executive function, or visuospatial function
- nMCI-single or multiple cognitive domains for nonmemory deficits without memory impairment.
Determining a patient’s MCI subtype is still a research activity and calls for comprehensive neuropsychological testing. MCI patients perform at least 1.5 standard deviations below the average for age- and education-matched healthy individuals on objective measures of memory.1
Conversion to dementia
In longitudinal population studies patients with MCI have shown an 11% to 33% risk of developing dementia within 2 years, whereas 44% reverted to normal 1 year later. Reasons for reversibility may include variable definitions of MCI among the longitudinal studies and the possibility that patients who recovered or improved may have had reversible causes of dementia.1
Individuals with aMCI (Table 1)8 progress to AD at a rate of 10% to 15% per year, compared with 1% to 2% per year in normal elderly persons. The Mayo AD research center studies reported a conversion rate of up to 80% from aMCI to AD within 6 years.9
Research focuses on identifying preclinical AD states and potential targets for intervention using disease-modifying therapies. Some experts consider MCI to be the earliest clinical manifestation of AD, at least in a subgroup of patients.
Identifying markers to predict which patients are likely to convert from MCI to dementia also is a major research objective. In addition to ApoE status (Table 2),7,9-15 predictors of conversion may include:
- hippocampal atrophy13
- reduced metabolism in the temporoparietal cortex and posterior cingulum14
- elevated CSF tau and the 42 amino acid form of ß-amyloid (Aß 42).15
Neuropsychiatric symptoms. Individuals with MCI and neuropsychiatric symptoms may be at particular risk for progressing to dementia. Agitation or depression are more prevalent in persons with MCI than in normal elderly but less prevalent than in those with dementia (Table 3).10,16
- 16% of normal healthy elderly
- 43% of MCI patients
- 75% of dementia patients.16
Sleep disturbances and anxiety in persons with MCI may predict progression to AD.10 A baseline high frequency of apathy in aMCI patients has been associated with progression to AD within 1 year.11
Table 1
Amnestic MCI: Proposed diagnostic criteria
| Subjective memory impairment, preferably corroborated by a reliable informant |
| Reduced performance on objective memory tests, compared with persons of similar age and educational background |
| Typical general cognitive function |
| Intact basic activities of daily living and intact or minimally impaired instrumental activities of daily living |
| Absence of dementia |
| MCI: mild cognitive impairment |
| Source: Reference 8 |
Factors shown to predict conversion from MCI to dementia
| Category | Predictors of conversion |
|---|---|
| Clinical | Cognitive: Amnestic MCI Neuropsychiatric: Depression, apathy, and possibly nighttime behaviors and anxiety |
| Neuropsychological tests | Clock-drawing test, Trail-Making Test B, Symbol Digit Modalities Test, Delayed 10-Word List Recall, New York University Paragraph Recall Test (Delayed), ADAS-Cog total score |
| Neuroimaging | MRI: Entorhinal cortex and hippocampal atrophy PET: Medial temporal region, parietotemporal association cortex, and posterior cingulate hypometabolism fMRI: Abnormal hippocampal, posterior cingulate, and medial temporal region activation on memory tasks |
| CSF markers | Increase: t-tau, p-tau Decrease: Aß 42 |
| Genetic markers | ApoE e4 carriers |
| ADAS-Cog: Alzheimer’s Disease Assessment Scale-Cognitive subscale; ApoE e4: apolipoprotein E gene, e4 allele; CSF: cerebrospinal fluid; MCI: mild cognitive impairment; MRI: magnetic resonance imaging; fMRI: functional MRI; PET: positron-emission tomography | |
| Source: References 7,9-15 | |
Neuropsychiatric symptoms: Rising prevalence mirrors cognitive deterioration in elderly patients*
| Neuropsychiatric symptoms | Normal elderly | MCI | Mild AD |
|---|---|---|---|
| Depressed mood/dysphoria | + | ++ | +++ |
| Nighttime behaviors/sleep | + | ++ | +++ |
| Irritability | + | ++ | +++ |
| Anxiety | +/- | ++ | +++ |
| Apathy/indifference | +/- | ++ | +++ |
| Agitation/aggression | +/- | +/++ | +++ |
| Eating/appetite disturbance | +/- | + | ++ |
| Disinhibition | +/- | +/- | ++ |
| Aberrant motor behavior | 0 | + | ++ |
| Delusions | 0 | +/- | ++ |
| Euphoria | 0 | +/- | +/- |
| Hallucinations | 0 | 0 | + |
| * 0 = 0%; +/- = 1% to 5%; + = 6% to 10%; ++ = 11% to 20%; +++ = 21% to 40% | |||
| MCI: mild cognitive impairment; AD: Alzheimer’s disease | |||
| Source: References 10,16 | |||
Depression and MCI
Depression and cognitive complaints overlap considerably in older adults. Depressed patients without dementia show persistent cognitive deficits even after depression remits. In some patients, new-onset geriatric depression is considered a prodrome of MCI and AD. Given that AD neuropathologic changes precede clinical symptoms by many years, depression and AD have been proposed as different clinical manifestations of AD pathology.17
Depressed MCI patients are at higher risk of developing dementia than those without depression, especially if cognitive measures do not improve after depression is treated.12 Similarly, cognitively intact older persons who develop depression are at increased risk for MCI, particularly if they carry the ApoE e4 genotype.19
In the only study in which MCI patients’ neuropsychiatric symptoms have been treated, 39 elderly patients with depression and MCI received open-label sertraline, ≤200 mg/d, for 12 weeks. Among the 26 patients who completed the trial, 17 showed moderate improvement in depressive symptoms, attention, and executive function, and 9 showed no response.20
Recommendation. In clinical practice, antidepressant treatment—usually a selective serotonin reuptake inhibitor (SSRI), with or without psychotherapy—is recommended for the MCI patient with comorbid major depression.
CASE CONTINUED: No signs of depression
Mr. R’s medical, neurologic, and substance use history is unremarkable. Family history includes AD in a paternal aunt diagnosed at age 82. Mr. R reports no history of mood, sleep, or appetite changes and no psychotic symptoms. He shows no deficits in activities of daily living (ADL), although his wife recently took over paying household bills after he forgot to make a payment.
Evidence-based workup
Functional assessment. In the differential diagnosis of MCI, give special attention to functional impairment, which points toward dementia. ADL generally are preserved in MCI, and minimal deterioration is seen in instrumental activities of daily living (IADL). A relatively easy way to assess function is to use the Alzheimer’s Disease Functional Assessment and Change Scale (ADFACS), which is based on 16 ADL and IADL items (Table 4).21
A substantial functional decline precludes an MCI diagnosis, although the degree of functional decline can be difficult to assess in older adults with physical limitations caused by medical comorbidities.
Cognitive assessment. Because most individuals with MCI score in the normal range on the Folstein Mini-Mental State Examination (MMSE), the modified MMSE (3MS)22 may be more sensitive for detecting MCI. The 3MS retains the MMSE’s brevity (≤10 minutes to administer) but incorporates 4 additional items, has more graded scoring responses, and broadens the score range to 0 to 100. The clock-drawing test also is sensitive for MCI, especially in detecting early visuoconstructional dysfunction.
The Montreal Cognitive Assessment (MoCA) is a 10-minute, 30-point scale designed to help clinicians detect MCI (see Related Resources). The MoCA usually is given with the modified MMSE for a comprehensive cognitive assessment.
Nasreddine et al23 administered the MoCA and MMSE to 94 patients who met clinical criteria for MCI, 93 patients with mild AD, and 90 healthy cognitively normal elderly persons, using a cutoff score of 26. MoCA showed:
- 90% sensitivity for detecting MCI (compared with 18% for the MMSE)
- 87% specificity to exclude normal elderly persons.
Neuropsychological testing can be more sensitive than office-based screening tools in defining MCI subtypes. In the Alzheimer’s Disease Cooperative Study (ADCS), the neuropsychological measures that most accurately predicted progression of patients with aMCI to AD within 36 months were the:
- Symbol Digit Modalities Test
- New York University Paragraph Recall Test (Delayed)
- Delayed 10-Word List Recall
- Alzheimer’s Disease Assessment Scale-cognitive subscale (ADAS-Cog) total score.24
Table 4
Alzheimer’s Disease Functional Assessment and Change Scale (ADFACS)
| Basic ADL | Instrumental ADL (IADL) |
|---|---|
| Toileting | Use of telephone |
| Feeding | Household tasks |
| Dressing | Using household appliances |
| Personal hygiene and grooming | Managing money |
| Shopping | |
| Bathing | Food preparation |
| Walking | Ability to get around inside and outside home |
| Hobbies and leisure activities | |
| Handling personal mail | |
| Grasp of situations and explanations | |
The 16-item ADFACS total score ranges from 0 to 54 (best to worst):
| |
| Use total scores to assess for functional decline from baseline. A decline from 0 to 1 on individual ADL and IADL items is not considered clinically significant. | |
| ADL: activities of daily living | |
| Source: Reprinted with permission from reference 21 | |
Lab studies to rule out reversible causes of MCI
| Complete blood count with differential |
| Basic metabolic panel |
| Liver function tests |
| Serum calcium |
| Serum vitamin B12 and folate |
| Thyroid function tests |
| Rapid plasma reagin |
| HIV in high-risk individuals |
| CSF studies if CNS infection is suspected |
| CSF: cerebrospinal fluid; HIV: human immunodeficiency virus; MCI: mild cognitive impairment |
| Source: Reference 8 |
CASE CONTINUED: Subtle cognitive deficits
Mr. R scores 27/30 on the MMSE (losing 3 points on recall) and 25/30 on the MoCA (losing points on visuospatial/executive function, fluency, and delayed recall). Thyroid stimulating hormone, vitamin B12, folate, and rapid plasma reagin tests are unremarkable; brain MRI shows no significant abnormalities.
You refer Mr. R for neuropsychological testing, and most cognitive domains are normal. Exceptions include moderate impairment in immediate and delayed verbal and visual memory and mild executive dysfunction.
Based on your clinical evaluation and neuropsychological testing, you diagnose amnestic MCI. Mr. R shows abnormalities in memory and executive functioning without significant decline in basic and instrumental ADLs, is not taking medications, and has no other medical or psychiatric condition that could explain his cognitive deficits.
You discuss the diagnosis with him and his wife, including evidence on his risk for progression to dementia, neuroprotective strategies, and medications.
After an MCI diagnosis
Neuroprotection. Eliminate medications with anticholinergic effects, including:
- tricyclic antidepressants
- conventional antipsychotics
- antihistamines
- drugs used to treat urinary incontinence, such as oxybutynin
- muscle relaxants, such as cyclobenzaprine
- certain antiparkinsonian drugs, such as benztropine.
Monitoring. The American Academy of Neurology recommends monitoring patients diagnosed with MCI every 6 to 12 months for cognitive and functional decline.
In these visits, include:
- repeat office-based cognitive assessment, especially the modified MMSE, clock-drawing test, and MoCA
- careful history-taking from the patient and reliable informant
- repeat neuropsychological testing annually or when dementia is suspected
- assessment of the caregiver for distress.
- moderate exercise (at least 30 minutes per session, 3 times a week)
- cognitively stimulating activities that involve language and psychomotor coordination, such as dancing, crossword puzzles, and volunteer work.
Medications—yes or no? Cholinesterase inhibitors, rofecoxib, and vitamin E have not been shown to prevent MCI from progressing to AD. Thus, insufficient evidence exists to recommend medications for patients with MCI.
Donepezil has shown possible short-term benefits, however, and patients may choose to try this medication. Some find comfort in seeking this “extra time” to make decisions about advanced directives, attend to estate and will issues, and optimize relationships while they have only mild cognitive deficits and possess decision-making capacity.
Donepezil. The Alzheimer’s Disease Cooperative Study—supported by the National Institute on Aging—was designed to determine whether daily doses of donepezil or vitamin E can delay or prevent progression of aMCI to AD.25 In the double-blind, placebo-controlled, parallel group study, 769 patients with aMCI were randomly assigned to receive donepezil, 10 mg/d; vitamin E, 1,000 IU bid; or placebo for 3 years.
Overall progression to AD was 16% per year, and the 3-year risk of progression was the same in all 3 groups. Donepezil therapy was associated with a reduced rate of progression to AD compared with placebo during the first year of treatment. Donepezil’s benefit was evident among ApoE e4 carriers at 2-year follow-up, but none of the 3 groups showed statistically significant differences after 3 years. Vitamin E showed no effect on AD progression throughout the study.
Rivastigmine. A randomized, placebo-controlled trial in which 1,018 MCI patients received rivastigmine or placebo for 4 years found no statistically significant benefit of rivastigmine on AD progression.26
Galantamine. Two international randomized, double-blind, placebo-controlled trials failed to show a statistically significant benefit of galantamine in slowing progression from aMCI to AD. MRI data from one of these studies suggested that galantamine may have reduced the rate of brain atrophy over a 2-year period.27
Rofecoxib. Epidemiologic studies indicate that anti-inflammatory drugs may reduce the risk of developing AD, but the COX-2 inhibitor rofecoxib did not delay progression to AD among aMCI patients in a large, placebo-controlled trial.28
Educate patients and family members about supportive nonpharmacologic treatments and cholinesterase inhibitors. The Alzheimer’s Association, National Institute on Aging, and local department of aging agencies offer useful resources (see Related Resources).
CASE CONTINUED: Dealing with uncertainty
Mr. R and his wife are unsettled by his MCI diagnosis. They prefer to take a “wait and watch” approach, decline initiation of a cholinesterase inhibitor, and agree to adhere to nonpharmacologic interventions you discussed. You schedule a follow-up visit in 6 months and encourage them to call you with questions.
- Rosenberg PB, Johnston D, Lyketsos CG. A clinical approach to mild cognitive impairment. Am J Psychiatry 2006;163: 1884-90.
- Montreal Cognitive Assessment (MoCA). 10-minute screening test designed to help clinicians detect mild cognitive impairment. www.mocatest.org.
- Alzheimer’s Association. www.alz.org.
- National Institute on Aging. www.nia.nih.gov.
- Benztropine • Cogentin
- Cyclobenzaprine • Flexeril
- Donepezil • Aricept
- Galantamine • Razadyne
- Oxybutynin • Ditropan
- Rivastigmine • Exelon
- Rofecoxib • Vioxx
- Sertraline • Zoloft
Dr. Goveas and Dr. Dixon-Holbrook report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Kerwin is a consultant to Pfizer and a speaker for Pfizer and Novartis.
Dr. Antuono receives research support from Eisai, Pfizer, and Elan and is a speaker for Pfizer and Forest Pharmaceuticals.
1. Gauthier S, Reisberg B, Zaudig M, et al. Mild cognitive impairment. Lancet 2006;367:1262-70.
2. Lopez OL, Jagust WJ, DeKosky ST, et al. Prevalence and classification of mild cognitive impairment in the Cardiovascular Health Study Cognition Study: part 1. Arch Neurol 2003;60:1385-9.
3. Petersen RC. Conceptual review. In: Petersen RC, ed. Mild cognitive impairment: aging to Alzheimer’s disease. New York, NY: Oxford University Press; 2003:1-14.
4. Petersen RC, Morris JC. Mild cognitive impairment as a clinical entity and treatment target. Arch Neurol 2005;62:1160-3.
5. O’Brien JT. Vascular cognitive impairment. Am J Geriatr Psychiatry 2006;14:724-33.
6. Janvin CC, Larsen JP, Aarsland D, et al. Subtypes of mild cognitive impairment in Parkinson’s disease: progression to dementia. Mov Disord 2006;21:1343-9.
7. Farlow MR, He Y, Tekin S, et al. Impact of APOE in mild cognitive impairment. Neurology 2004;63:1898-1901.
8. Winblad B, Palmer K, Kivipelto M, et al. Mild cognitive impairment—beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment. J Intern Med 2004;256:240-6.
9. Petersen RC. Mild cognitive impairment as a diagnostic entity. J Intern Med 2004;256:183-94.
10. Geda YE, Smith GE, Knopman DS, et al. De novo genesis of neuropsychiatric symptoms in mild cognitive impairment (MCI). Int Psychogeriatr 2004;16:51-60.
11. Robert PH, Berr C, Volteau M, et al. Apathy in patients with mild cognitive impairment and the risk of developing dementia of Alzheimer’s disease: a one-year follow-up study. Clin Neurol Neurosurg 2006;108:733-6.
12. Modrego PJ, Ferrandez J. Depression in patients with mild cognitive impairment increases the risk of developing dementia of Alzheimer type. Arch Neurol 2004;61:1290-3.
13. Jack CR, Petersen RC, Xu YC, et al. Prediction of AD with MRI-based hippocampal volume in mild cognitive impairment. Neurology 1999;52:1397-1403.
14. Nestor PJ, Fryer TD, Smielewski P, et al. Limbic hypometabolism in Alzheimer’s disease and mild cognitive impairment. Ann Neurol 2003;54:343-51.
15. Sunderland T, Hampel H, Takeda M, et al. Biomarkers in the diagnosis of Alzheimer’s disease: are we ready? J Geriatr Psychiatry Neurol 2006;19:172-9.
16. Lyketsos CG, Lopez O, Jones B, et al. Prevalence of neuropsychiatric symptoms in dementia and mild cognitive impairment: results from the Cardiovascular Health Study. JAMA 2002;288:1475-83.
17. Steffens DC, Otey E, Alexoupolos GS, et al. Perspectives on depression, mild cognitive impairment, and cognitive decline. Arch Gen Psychiatry 2006;63:130-8.
18. Gabryelewicz T, Styczynska M, Pfeffer A, et al. Prevalence of major and minor depression in elderly persons with mild cognitive impairment: MADRS factor analysis. Int J Geriatr Psychiatry 2004;19:1168-72.
19. Geda YE, Knopman DS, Mrazek DA, et al. Depression, apolipoprotein E genotype, and the incidence of mild cognitive impairment: a prospective cohort study. Arch Neurol 2006;63:435-40.
20. Devanand DP, Pelton GH, Marston K, et al. Sertraline treatment of elderly patients with depression and cognitive impairment. Int J Geriatr Psychiatry 2003;18:123-30.
21. Mohs RC, Doody RS, Morris JC, et al. A 1-year, placebo-controlled preservation of function survival study of donepezil in AD patients. Neurology 2001;57:481-8.
22. Teng EL, Chui HC. The Modified Mini-Mental State (3MS) examination. J Clin Psychiatry 1987;48:314-8.
23. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment (MoCA): a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 2005;53:695-9.
24. Fleisher AS, Sowell BB, Taylor C, et al. Clinical predictors of progression to Alzheimer disease in amnestic mild cognitive impairment. Neurology 2007;68:1588-95.
25. Petersen RC, Thomas RG, Grundman M, et al. for the Alzheimer’s Disease Cooperative Study Group. Vitamin E and donepezil for the treatment of mild cognitive impairment. N Engl J Med 2005;352:2379-88.
26. Feldman HH, Ferris S, Winblad B, et al. Effect of rivastigmine on delay to diagnosis of Alzheimer’s disease from mild cognitive impairment: the InDDEx study. Lancet Neurol 2007;6:501-12.
27. Petersen RC. Mild cognitive impairment: current research and clinical implications. Semin Neurol 2007;27:22-31.
28. Thal LJ, Ferris SH, Kirby L, et al. A randomized, double-blind study of rofecoxib in patients with mild cognitive impairment. Neuropsychopharmacology 2005;30(6):1204-15.
1. Gauthier S, Reisberg B, Zaudig M, et al. Mild cognitive impairment. Lancet 2006;367:1262-70.
2. Lopez OL, Jagust WJ, DeKosky ST, et al. Prevalence and classification of mild cognitive impairment in the Cardiovascular Health Study Cognition Study: part 1. Arch Neurol 2003;60:1385-9.
3. Petersen RC. Conceptual review. In: Petersen RC, ed. Mild cognitive impairment: aging to Alzheimer’s disease. New York, NY: Oxford University Press; 2003:1-14.
4. Petersen RC, Morris JC. Mild cognitive impairment as a clinical entity and treatment target. Arch Neurol 2005;62:1160-3.
5. O’Brien JT. Vascular cognitive impairment. Am J Geriatr Psychiatry 2006;14:724-33.
6. Janvin CC, Larsen JP, Aarsland D, et al. Subtypes of mild cognitive impairment in Parkinson’s disease: progression to dementia. Mov Disord 2006;21:1343-9.
7. Farlow MR, He Y, Tekin S, et al. Impact of APOE in mild cognitive impairment. Neurology 2004;63:1898-1901.
8. Winblad B, Palmer K, Kivipelto M, et al. Mild cognitive impairment—beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment. J Intern Med 2004;256:240-6.
9. Petersen RC. Mild cognitive impairment as a diagnostic entity. J Intern Med 2004;256:183-94.
10. Geda YE, Smith GE, Knopman DS, et al. De novo genesis of neuropsychiatric symptoms in mild cognitive impairment (MCI). Int Psychogeriatr 2004;16:51-60.
11. Robert PH, Berr C, Volteau M, et al. Apathy in patients with mild cognitive impairment and the risk of developing dementia of Alzheimer’s disease: a one-year follow-up study. Clin Neurol Neurosurg 2006;108:733-6.
12. Modrego PJ, Ferrandez J. Depression in patients with mild cognitive impairment increases the risk of developing dementia of Alzheimer type. Arch Neurol 2004;61:1290-3.
13. Jack CR, Petersen RC, Xu YC, et al. Prediction of AD with MRI-based hippocampal volume in mild cognitive impairment. Neurology 1999;52:1397-1403.
14. Nestor PJ, Fryer TD, Smielewski P, et al. Limbic hypometabolism in Alzheimer’s disease and mild cognitive impairment. Ann Neurol 2003;54:343-51.
15. Sunderland T, Hampel H, Takeda M, et al. Biomarkers in the diagnosis of Alzheimer’s disease: are we ready? J Geriatr Psychiatry Neurol 2006;19:172-9.
16. Lyketsos CG, Lopez O, Jones B, et al. Prevalence of neuropsychiatric symptoms in dementia and mild cognitive impairment: results from the Cardiovascular Health Study. JAMA 2002;288:1475-83.
17. Steffens DC, Otey E, Alexoupolos GS, et al. Perspectives on depression, mild cognitive impairment, and cognitive decline. Arch Gen Psychiatry 2006;63:130-8.
18. Gabryelewicz T, Styczynska M, Pfeffer A, et al. Prevalence of major and minor depression in elderly persons with mild cognitive impairment: MADRS factor analysis. Int J Geriatr Psychiatry 2004;19:1168-72.
19. Geda YE, Knopman DS, Mrazek DA, et al. Depression, apolipoprotein E genotype, and the incidence of mild cognitive impairment: a prospective cohort study. Arch Neurol 2006;63:435-40.
20. Devanand DP, Pelton GH, Marston K, et al. Sertraline treatment of elderly patients with depression and cognitive impairment. Int J Geriatr Psychiatry 2003;18:123-30.
21. Mohs RC, Doody RS, Morris JC, et al. A 1-year, placebo-controlled preservation of function survival study of donepezil in AD patients. Neurology 2001;57:481-8.
22. Teng EL, Chui HC. The Modified Mini-Mental State (3MS) examination. J Clin Psychiatry 1987;48:314-8.
23. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment (MoCA): a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 2005;53:695-9.
24. Fleisher AS, Sowell BB, Taylor C, et al. Clinical predictors of progression to Alzheimer disease in amnestic mild cognitive impairment. Neurology 2007;68:1588-95.
25. Petersen RC, Thomas RG, Grundman M, et al. for the Alzheimer’s Disease Cooperative Study Group. Vitamin E and donepezil for the treatment of mild cognitive impairment. N Engl J Med 2005;352:2379-88.
26. Feldman HH, Ferris S, Winblad B, et al. Effect of rivastigmine on delay to diagnosis of Alzheimer’s disease from mild cognitive impairment: the InDDEx study. Lancet Neurol 2007;6:501-12.
27. Petersen RC. Mild cognitive impairment: current research and clinical implications. Semin Neurol 2007;27:22-31.
28. Thal LJ, Ferris SH, Kirby L, et al. A randomized, double-blind study of rofecoxib in patients with mild cognitive impairment. Neuropsychopharmacology 2005;30(6):1204-15.
Outpatient commitment: When it improves patient outcomes
On April 16, 2007, Seung Hui Cho shot and killed 32 students and faculty on the Virginia Tech campus and wounded 25 others before killing himself. A judge had declared Cho mentally ill in 2005 and placed him on involuntary outpatient commitment (OPC). Cho apparently never sought treatment, and no one made sure that he did (Box 1).1
Much second-guessing has occurred about whether enforcing Cho’s OPC could have prevented the Virginia Tech tragedy. Most states authorize OPC, but few make much use of OPC statues that require patients to adhere to prescribed treatment in the community. Virginia was typical; an OPC statute was on the books but rarely enforced.
This article discusses the evidence on OPC laws’ effectiveness and offers recommendations on how to use these tools in psychiatric practice.
Mandating needed treatment
OPC—also called “assisted outpatient treatment” or “mandated outpatient treatment”—is a civil court procedure whereby a judge can order a noncompliant mentally ill patient to adhere to needed treatment. OPC statutes exist in 42 states and the District of Columbia, although judges use these powers erratically.2,3
Most states have set identical thresholds for inpatient and outpatient commitment, such as when the patient is considered dangerous to self or others or (in some statutes) so gravely impaired that he is unable to safely care for himself in the community. These high thresholds have dramatically reduced inpatient commitment eligibility and yet may flag the patient as too dangerous for outpatient commitment.
Virginia’s commitment laws are in review because of the Virginia Tech shootings in April 2007. The state’s existing OPC provisions are embedded in involuntary commitment law, which is mainly directed toward inpatients. As a result, Virginia’s law:
- merely permits mandated outpatient treatment
- duplicates inpatient criteria for “imminent dangerousness” (although the state legislature is considering relaxing this criterion)
- provides no guidance on enforcement in the event of treatment nonadherence
- provides no administrative infrastructure to make the law work.
Virginia’s statute is typical. It lacks a separate threshold for outpatient commitment, using the same high threshold of imminent threat to self or others that is required for inpatient commitment.
Clinicians are uncomfortable using inpatient criteria for outpatient commitment. Labeling a patient as “ill enough” to be confined and then recommending that he or she be released to outpatient treatment feels like a liability risk.
Because the legislative intent in most state statutes was to set criteria and procedures for inpatient commitment, steps for implementing outpatient commitment are often ill-defined. An outpatient commitment process requires:
- notification to the responsible outpatient local mental health authority, clinicians, and local courts that the order is in place
- expectations regarding the order
- steps required to renew the order, if indicated.
States such as New York with fully operational outpatient commitment statutes have clear implementation processes.
- an alternative to hospitalization for patients who meet inpatient commitment criteria
- a form of conditional release for patients completing an involuntary inpatient commitment
- an alternative to hospitalization for noncompliant patients at risk for relapse and involuntary inpatient commitment.2
Enforcement. Courts typically can request that law officers transport patients who fail to comply with OPC to a treatment facility. There, patients will be encouraged to comply with treatment or evaluated for inpatient commitment.2 This relatively weak enforcement authority has led some to argue that OPC has no teeth.
Without clearly defined steps for implementation, an outpatient commitment order can be likened to a message in a bottle—a cry for help at risk for nondelivery. In the Virginia Tech case, the judge issued an outpatient commitment order for Cho, but how the local clinic understood its responsibilities and what resources and enforcement power it had were unclear.
Noncontrolled studies
Evidence from noncontrolled OPC studies is difficult to interpret because of:
- lack of comparable committed and noncommitted groups
- difficulty in comparing treatment across comparison groups
- selection effects, whereby clinicians and courts select patients for a predicted good outcome.2
Most noncontrolled studies have concluded that OPC improves treatment outcomes and decreases hospital readmission rates and lengths of stay under some circumstances.6-12 The largest study reported on New York’s initial 5 years’ experience with more than 3,000 patients under its OPC statute, known as “Kendra’s Law” (Box 2).12 Under this law—the most intensively implemented OPC statute in the United States—the court’s order specifies a detailed plan of medications and psychosocial treatment.
Most of New York’s OPC recipients stayed in assisted outpatient treatment longer than the court-mandated 6 months (average 16 months). The incidence of hospitalizations, homelessness, arrests, and incarcerations was far lower while patients participated in OPC, compared with the previous 3 years of their lives (Table). Medication adherence improved from 34% before OPC to 69% after commitment, and engagement with treatment improved from 41% to 62%, respectively.12
Table
Change in adverse events among OPC patients in New York
| Event | Incidence during 3 years prior to OPC* | Incidence during OPC treatment | Rate of decline |
|---|---|---|---|
| Incarceration | 23% | 3% | 87% |
| Arrest | 30% | 5% | 83% |
| Psychiatric hospitalization | 97% | 22% | 77% |
| Homelessness | 19% | 5% | 74% |
| * Adverse events reported as occurring at least once | |||
| OPC: outpatient commitment | |||
| Source: Reprinted from reference 12, table 10 | |||
Conflicting controlled trials
Duke Mental Health Study. In the first controlled study of OPC, the Duke Mental Health Study (DMHS) enrolled 331 seriously mentally ill inpatients being discharged from involuntarily hospitalization to court-ordered outpatient treatment between 1993 and 1996. Patients with a history of violent behavior in the previous year were placed in a nonrandomized comparison group and remained on OPC for at least 90 days. The remaining 264 patients were randomly assigned to:
- an experimental group that received OPC for ≤90 days (could be renewed for ≤180 days) plus consistent community mental health services
- a control group that was released from OPC but received the same community mental health services as the experimental group.13
Patients ordered to OPC had fewer hospital readmissions and spent fewer days in the hospital only if they received OPC plus consistent community services for ≥6 months.14 Patients who received this model of care were:
- less likely to be homeless,15 criminally victimized,16 arrested if they had past arrests,17 or violent18
- more likely than the control group to comply with recommended treatment.19
Outpatient service intensity was not controlled but varied according to clinical need and other unknown factors. As a result, selectively providing services could have influenced outcomes, although other analyses argue that this factor was not important.4
New York. In 1994, the state legislature established a 3-year pilot program to evaluate OPC in New York City’s Bellevue Hospital as a first step toward considering permanent OPC legislation.20 The randomized, controlled study compared a court-ordered group (N=78) and a control group (N=64) during 1 year after hospital discharge. Both groups received enhanced outpatient services, such as psychiatrist appointments, intensive case management, and treatment for co-occurring substance abuse as needed.
Andrew Goldstein and Kendra Webdale were strangers standing on a New York City subway platform as a train arrived on January 3, 1999. She was an aspiring journalist and he a troubled man with schizophrenia who had stopped taking his medication. Goldstein later admitted in court that he placed his hands on the back of her shoulders and pushed her into the train’s path.
“Kendra’s law”—first enacted in 1999 and renewed for 5 years in 2005—provides assisted outpatient treatment (AOT) for persons age ≥18 with mental illness who—in view of their treatment history—are unlikely to survive safely in the community without supervision. The patient also must:
- have a history of treatment noncompliance
- be unlikely to voluntarily participate in treatment
- need assisted outpatient treatment to prevent a deterioration that would likely result in a substantial risk of physical harm to himself or others
- be likely to benefit from assisted outpatient treatment.
Implementation starts with a petition to the court, asking that a person be evaluated for AOT suitability. Petitions can be filed by psychiatrists, psychologists, social workers, family members, adult roommates, hospital directors, mental health or social services directors, and parole or probation officers. The petition is followed by an investigation by local authorities and a court hearing.
If the patient is found to be eligible for AOT, the court orders a highly specific treatment plan. Initial orders for 6 months can be renewed at subsequent court hearings.
Control and experimental groups showed no statistically significant differences in hospitalizations, arrests, quality of life, symptoms, homelessness, or other outcomes. The authors interpreted these findings to suggest that in this study intensive services—and not OPC court orders—reduced hospital recidivism and other poor outcomes in seriously mentally ill patients.
Study limitations. Statute implementation and OPC enforcement were haphazard, and in most cases sanctions for noncompliance—such as orders to law enforcement to detain noncompliant patients—were not put into effect. Patients and providers often did not clearly distinguish between the control and experimental groups. And finally, the study likely was too small to demonstrate a positive effect for OPC. Nevertheless, the findings suggest that OPC might provide no added benefit if persons with serious mental illnesses have access to enhanced outpatient services.4
Do OPC laws prevent violence?
The North Carolina and New York controlled studies of OPC yielded contradictory findings and are difficult to compare. Even within North Carolina—where OPC has been shown most consistently to be effective—OPC orders’ duration (the “dose”) varies widely, as do the services patients receive.
No further randomized, controlled trials of OPC are underway. Our group is participating in a study supported by the MacArthur Foundation Research Network on Mandated Community Treatment and New York State Office of Mental Health to intensively review patient outcomes under New York’s OPC statute.
Given that most states permit OPC, attempts to standardize and implement OPC are needed. To make OPC effective, evidence indicates that states also must provide intensive community services to keep patients in treatment.
Strategies for using OPC
OPC is controversial in society and among clinicians. Some mental health organizations oppose outpatient commitment orders as coercive and intrusive, and some mental health professionals have concerns about legal or malpractice liability, increased paperwork, and administrative burden. Others may view OPC as:
- ineffective —providing weak sanctions that are impractical to enforce
- detrimental to the therapeutic alliance
- a less-desirable substitute for making high-quality voluntary treatment more widely available for the seriously mentally ill.
Select appropriate candidates. Our group’s experience suggests that patients with severe mental illness—especially schizophrenia spectrum disorders—are those most likely to benefit from OPC. There is no evidence that outpatient commitment helps patients with personality disorders or substance abuse without comorbid severe mental illness.
Maximize effectiveness. Evidence from the North Carolina studies suggests keeping OPC in place for ≥6 months and providing relatively intensive outpatient services. For schizophrenia-spectrum patients, combining OPC with depot antipsychotics may be more effective than oral agents for ensuring adherence and improving function.19
Decide when to terminate. OPC orders probably should last at least 6 months, but little evidence exists to guide discontinuing an order after 6 months. This dilemma is similar to deciding when a depot antipsychotic can or should be converted to an oral agent in previously nonadherent patients.
Our approach is to consider terminating the order in patients with restored insight who have ≥6 months of consistent treatment compliance without a need for or threat of OPC enforcement. In some cases, other leverage may preempt the need for continuing an order, such as:
- financial contingencies from family or others
- treatment required as a condition of probation or parole
- housing conditioned on treatment adherence.
- Treatment Advocacy Center. Nonprofit organization dedicated to eliminating barriers to timely, effective treatment of severe mental illnesses. www.psychlaws.org.
- MacArthur Foundation Research Network on Mandated Community Treatment. www.macarthur.virginia.edu/researchnetwork.html.
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
This work was supported by NIMH Grants MH 48103 and MH 51410 and the MacArthur Foundation Research Network on Mandated Community Treatment.
1. Swartz M. Taking issue: can mandated outpatient treatment prevent tragedies? Psychiatr Serv 2007;58(6):737.-
2. Swartz MS, Burns BJ, Hiday VA, et al. New directions in research on involuntary outpatient commitment. Psychiatr Serv 1995;46:381-5.
3. Torrey EF, Kaplan R. A national survey of the use of outpatient commitment. Psychiatr Serv 1995;46:778-84.
4. Swartz MS, Swanson JW. Involuntary outpatient commitment, community treatment orders, and assisted outpatient treatment: what’s in the data? Can J Psychiatry 2004;49(9):585-91.
5. Monahan J, Swartz M, Bonnie R. Mandated treatment in the community for people with mental disorders. Health Aff 2003;22:28-38.
6. Munetz MR, Grande T, Kleist J, Peterson GA. The effectiveness of outpatient civil commitment. Psychiatr Serv 1996;47:1251-3.
7. Rohland BM, Rohrer JE, Richard C. The long-term effects of outpatient commitment on service use. Adm Policy Ment Health 2000;27:383-94.
8. Keilitz I. Empirical studies of involuntary outpatient civil commitment: is it working? Ment Phys Disabil Law Rep 1990;14:368-79.
9. Hiday VA, Scheid-Cook TL. Outpatient commitment for revolving door patients: compliance and treatment. J Nerv Ment Dis 1991;179:83-8.
10. Moloy KA. Analysis: critiquing the empirical evidence. Does involuntary outpatient commitment work?. Washington, DC: Mental Health Policy Resource Center; 1992.
11. Ridgely MS, Borum J, Petrilla J. The effectiveness of outpatient commitment: empirical evidence and experience of eight states. Santa Monica, CA: RAND Corporation; 2001.
12. Kendra’s Law: final report on the status of assisted outpatient treatment. Albany, NY: New York State Office of Mental Health; 2005. Available at: http://www.omh.state.ny.us/omhweb/Kendra_web/finalreport. Accessed February 19, 2008.
13. Swartz MS, Swanson JW, Hiday VA, et al. A randomized controlled trial of outpatient commitment in North Carolina. Psychiatr Serv 2001;52:330-6.
14. Swartz MS, Swanson JW, Wagner RR, et al. Can involuntary outpatient commitment reduce hospital recidivism? Findings from a randomized trial in severely mentally ill individuals. Am J Psychiatry 1999;156:1968-75.
15. Compton SN, Swanson JW, Wagner HR, et al. Involuntary outpatient commitment and homelessness in persons with severe mental illness. J Ment Health Serv Res 2003;5:27-38.
16. Hiday VA, Swartz MS, Swanson JW, et al. Impact of outpatient commitment on victimization of people with severe mental illness. Am J Psychiatry 2002;159:1403-11.
17. Swanson JW, Borum R, Swartz MS, et al. Can involuntary outpatient commitment reduce arrests among persons with severe mental illness? Criminal Justice & Human Behavior 2001 28;156-89.
18. Swanson JW, Swartz MS, Borum R, et al. Involuntary outpatient commitment and reduction of violent behaviour in persons with severe mental illness. Br J Psychiatry 2000;176:324-31.
19. Swartz MS, Swanson JW, Wagner HR, et al. Effects of involuntary outpatient commitment and depot antipsychotics on treatment adherence in persons with severe mental illness. J Nerv Ment Dis 2001;189:583-92.
20. Steadman HJ, Gounis K, Dennis D, et al. Assessing the New York City outpatient commitment pilot program. Psychiatr Serv 2001;52:330-6.
On April 16, 2007, Seung Hui Cho shot and killed 32 students and faculty on the Virginia Tech campus and wounded 25 others before killing himself. A judge had declared Cho mentally ill in 2005 and placed him on involuntary outpatient commitment (OPC). Cho apparently never sought treatment, and no one made sure that he did (Box 1).1
Much second-guessing has occurred about whether enforcing Cho’s OPC could have prevented the Virginia Tech tragedy. Most states authorize OPC, but few make much use of OPC statues that require patients to adhere to prescribed treatment in the community. Virginia was typical; an OPC statute was on the books but rarely enforced.
This article discusses the evidence on OPC laws’ effectiveness and offers recommendations on how to use these tools in psychiatric practice.
Mandating needed treatment
OPC—also called “assisted outpatient treatment” or “mandated outpatient treatment”—is a civil court procedure whereby a judge can order a noncompliant mentally ill patient to adhere to needed treatment. OPC statutes exist in 42 states and the District of Columbia, although judges use these powers erratically.2,3
Most states have set identical thresholds for inpatient and outpatient commitment, such as when the patient is considered dangerous to self or others or (in some statutes) so gravely impaired that he is unable to safely care for himself in the community. These high thresholds have dramatically reduced inpatient commitment eligibility and yet may flag the patient as too dangerous for outpatient commitment.
Virginia’s commitment laws are in review because of the Virginia Tech shootings in April 2007. The state’s existing OPC provisions are embedded in involuntary commitment law, which is mainly directed toward inpatients. As a result, Virginia’s law:
- merely permits mandated outpatient treatment
- duplicates inpatient criteria for “imminent dangerousness” (although the state legislature is considering relaxing this criterion)
- provides no guidance on enforcement in the event of treatment nonadherence
- provides no administrative infrastructure to make the law work.
Virginia’s statute is typical. It lacks a separate threshold for outpatient commitment, using the same high threshold of imminent threat to self or others that is required for inpatient commitment.
Clinicians are uncomfortable using inpatient criteria for outpatient commitment. Labeling a patient as “ill enough” to be confined and then recommending that he or she be released to outpatient treatment feels like a liability risk.
Because the legislative intent in most state statutes was to set criteria and procedures for inpatient commitment, steps for implementing outpatient commitment are often ill-defined. An outpatient commitment process requires:
- notification to the responsible outpatient local mental health authority, clinicians, and local courts that the order is in place
- expectations regarding the order
- steps required to renew the order, if indicated.
States such as New York with fully operational outpatient commitment statutes have clear implementation processes.
- an alternative to hospitalization for patients who meet inpatient commitment criteria
- a form of conditional release for patients completing an involuntary inpatient commitment
- an alternative to hospitalization for noncompliant patients at risk for relapse and involuntary inpatient commitment.2
Enforcement. Courts typically can request that law officers transport patients who fail to comply with OPC to a treatment facility. There, patients will be encouraged to comply with treatment or evaluated for inpatient commitment.2 This relatively weak enforcement authority has led some to argue that OPC has no teeth.
Without clearly defined steps for implementation, an outpatient commitment order can be likened to a message in a bottle—a cry for help at risk for nondelivery. In the Virginia Tech case, the judge issued an outpatient commitment order for Cho, but how the local clinic understood its responsibilities and what resources and enforcement power it had were unclear.
Noncontrolled studies
Evidence from noncontrolled OPC studies is difficult to interpret because of:
- lack of comparable committed and noncommitted groups
- difficulty in comparing treatment across comparison groups
- selection effects, whereby clinicians and courts select patients for a predicted good outcome.2
Most noncontrolled studies have concluded that OPC improves treatment outcomes and decreases hospital readmission rates and lengths of stay under some circumstances.6-12 The largest study reported on New York’s initial 5 years’ experience with more than 3,000 patients under its OPC statute, known as “Kendra’s Law” (Box 2).12 Under this law—the most intensively implemented OPC statute in the United States—the court’s order specifies a detailed plan of medications and psychosocial treatment.
Most of New York’s OPC recipients stayed in assisted outpatient treatment longer than the court-mandated 6 months (average 16 months). The incidence of hospitalizations, homelessness, arrests, and incarcerations was far lower while patients participated in OPC, compared with the previous 3 years of their lives (Table). Medication adherence improved from 34% before OPC to 69% after commitment, and engagement with treatment improved from 41% to 62%, respectively.12
Table
Change in adverse events among OPC patients in New York
| Event | Incidence during 3 years prior to OPC* | Incidence during OPC treatment | Rate of decline |
|---|---|---|---|
| Incarceration | 23% | 3% | 87% |
| Arrest | 30% | 5% | 83% |
| Psychiatric hospitalization | 97% | 22% | 77% |
| Homelessness | 19% | 5% | 74% |
| * Adverse events reported as occurring at least once | |||
| OPC: outpatient commitment | |||
| Source: Reprinted from reference 12, table 10 | |||
Conflicting controlled trials
Duke Mental Health Study. In the first controlled study of OPC, the Duke Mental Health Study (DMHS) enrolled 331 seriously mentally ill inpatients being discharged from involuntarily hospitalization to court-ordered outpatient treatment between 1993 and 1996. Patients with a history of violent behavior in the previous year were placed in a nonrandomized comparison group and remained on OPC for at least 90 days. The remaining 264 patients were randomly assigned to:
- an experimental group that received OPC for ≤90 days (could be renewed for ≤180 days) plus consistent community mental health services
- a control group that was released from OPC but received the same community mental health services as the experimental group.13
Patients ordered to OPC had fewer hospital readmissions and spent fewer days in the hospital only if they received OPC plus consistent community services for ≥6 months.14 Patients who received this model of care were:
- less likely to be homeless,15 criminally victimized,16 arrested if they had past arrests,17 or violent18
- more likely than the control group to comply with recommended treatment.19
Outpatient service intensity was not controlled but varied according to clinical need and other unknown factors. As a result, selectively providing services could have influenced outcomes, although other analyses argue that this factor was not important.4
New York. In 1994, the state legislature established a 3-year pilot program to evaluate OPC in New York City’s Bellevue Hospital as a first step toward considering permanent OPC legislation.20 The randomized, controlled study compared a court-ordered group (N=78) and a control group (N=64) during 1 year after hospital discharge. Both groups received enhanced outpatient services, such as psychiatrist appointments, intensive case management, and treatment for co-occurring substance abuse as needed.
Andrew Goldstein and Kendra Webdale were strangers standing on a New York City subway platform as a train arrived on January 3, 1999. She was an aspiring journalist and he a troubled man with schizophrenia who had stopped taking his medication. Goldstein later admitted in court that he placed his hands on the back of her shoulders and pushed her into the train’s path.
“Kendra’s law”—first enacted in 1999 and renewed for 5 years in 2005—provides assisted outpatient treatment (AOT) for persons age ≥18 with mental illness who—in view of their treatment history—are unlikely to survive safely in the community without supervision. The patient also must:
- have a history of treatment noncompliance
- be unlikely to voluntarily participate in treatment
- need assisted outpatient treatment to prevent a deterioration that would likely result in a substantial risk of physical harm to himself or others
- be likely to benefit from assisted outpatient treatment.
Implementation starts with a petition to the court, asking that a person be evaluated for AOT suitability. Petitions can be filed by psychiatrists, psychologists, social workers, family members, adult roommates, hospital directors, mental health or social services directors, and parole or probation officers. The petition is followed by an investigation by local authorities and a court hearing.
If the patient is found to be eligible for AOT, the court orders a highly specific treatment plan. Initial orders for 6 months can be renewed at subsequent court hearings.
Control and experimental groups showed no statistically significant differences in hospitalizations, arrests, quality of life, symptoms, homelessness, or other outcomes. The authors interpreted these findings to suggest that in this study intensive services—and not OPC court orders—reduced hospital recidivism and other poor outcomes in seriously mentally ill patients.
Study limitations. Statute implementation and OPC enforcement were haphazard, and in most cases sanctions for noncompliance—such as orders to law enforcement to detain noncompliant patients—were not put into effect. Patients and providers often did not clearly distinguish between the control and experimental groups. And finally, the study likely was too small to demonstrate a positive effect for OPC. Nevertheless, the findings suggest that OPC might provide no added benefit if persons with serious mental illnesses have access to enhanced outpatient services.4
Do OPC laws prevent violence?
The North Carolina and New York controlled studies of OPC yielded contradictory findings and are difficult to compare. Even within North Carolina—where OPC has been shown most consistently to be effective—OPC orders’ duration (the “dose”) varies widely, as do the services patients receive.
No further randomized, controlled trials of OPC are underway. Our group is participating in a study supported by the MacArthur Foundation Research Network on Mandated Community Treatment and New York State Office of Mental Health to intensively review patient outcomes under New York’s OPC statute.
Given that most states permit OPC, attempts to standardize and implement OPC are needed. To make OPC effective, evidence indicates that states also must provide intensive community services to keep patients in treatment.
Strategies for using OPC
OPC is controversial in society and among clinicians. Some mental health organizations oppose outpatient commitment orders as coercive and intrusive, and some mental health professionals have concerns about legal or malpractice liability, increased paperwork, and administrative burden. Others may view OPC as:
- ineffective —providing weak sanctions that are impractical to enforce
- detrimental to the therapeutic alliance
- a less-desirable substitute for making high-quality voluntary treatment more widely available for the seriously mentally ill.
Select appropriate candidates. Our group’s experience suggests that patients with severe mental illness—especially schizophrenia spectrum disorders—are those most likely to benefit from OPC. There is no evidence that outpatient commitment helps patients with personality disorders or substance abuse without comorbid severe mental illness.
Maximize effectiveness. Evidence from the North Carolina studies suggests keeping OPC in place for ≥6 months and providing relatively intensive outpatient services. For schizophrenia-spectrum patients, combining OPC with depot antipsychotics may be more effective than oral agents for ensuring adherence and improving function.19
Decide when to terminate. OPC orders probably should last at least 6 months, but little evidence exists to guide discontinuing an order after 6 months. This dilemma is similar to deciding when a depot antipsychotic can or should be converted to an oral agent in previously nonadherent patients.
Our approach is to consider terminating the order in patients with restored insight who have ≥6 months of consistent treatment compliance without a need for or threat of OPC enforcement. In some cases, other leverage may preempt the need for continuing an order, such as:
- financial contingencies from family or others
- treatment required as a condition of probation or parole
- housing conditioned on treatment adherence.
- Treatment Advocacy Center. Nonprofit organization dedicated to eliminating barriers to timely, effective treatment of severe mental illnesses. www.psychlaws.org.
- MacArthur Foundation Research Network on Mandated Community Treatment. www.macarthur.virginia.edu/researchnetwork.html.
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
This work was supported by NIMH Grants MH 48103 and MH 51410 and the MacArthur Foundation Research Network on Mandated Community Treatment.
On April 16, 2007, Seung Hui Cho shot and killed 32 students and faculty on the Virginia Tech campus and wounded 25 others before killing himself. A judge had declared Cho mentally ill in 2005 and placed him on involuntary outpatient commitment (OPC). Cho apparently never sought treatment, and no one made sure that he did (Box 1).1
Much second-guessing has occurred about whether enforcing Cho’s OPC could have prevented the Virginia Tech tragedy. Most states authorize OPC, but few make much use of OPC statues that require patients to adhere to prescribed treatment in the community. Virginia was typical; an OPC statute was on the books but rarely enforced.
This article discusses the evidence on OPC laws’ effectiveness and offers recommendations on how to use these tools in psychiatric practice.
Mandating needed treatment
OPC—also called “assisted outpatient treatment” or “mandated outpatient treatment”—is a civil court procedure whereby a judge can order a noncompliant mentally ill patient to adhere to needed treatment. OPC statutes exist in 42 states and the District of Columbia, although judges use these powers erratically.2,3
Most states have set identical thresholds for inpatient and outpatient commitment, such as when the patient is considered dangerous to self or others or (in some statutes) so gravely impaired that he is unable to safely care for himself in the community. These high thresholds have dramatically reduced inpatient commitment eligibility and yet may flag the patient as too dangerous for outpatient commitment.
Virginia’s commitment laws are in review because of the Virginia Tech shootings in April 2007. The state’s existing OPC provisions are embedded in involuntary commitment law, which is mainly directed toward inpatients. As a result, Virginia’s law:
- merely permits mandated outpatient treatment
- duplicates inpatient criteria for “imminent dangerousness” (although the state legislature is considering relaxing this criterion)
- provides no guidance on enforcement in the event of treatment nonadherence
- provides no administrative infrastructure to make the law work.
Virginia’s statute is typical. It lacks a separate threshold for outpatient commitment, using the same high threshold of imminent threat to self or others that is required for inpatient commitment.
Clinicians are uncomfortable using inpatient criteria for outpatient commitment. Labeling a patient as “ill enough” to be confined and then recommending that he or she be released to outpatient treatment feels like a liability risk.
Because the legislative intent in most state statutes was to set criteria and procedures for inpatient commitment, steps for implementing outpatient commitment are often ill-defined. An outpatient commitment process requires:
- notification to the responsible outpatient local mental health authority, clinicians, and local courts that the order is in place
- expectations regarding the order
- steps required to renew the order, if indicated.
States such as New York with fully operational outpatient commitment statutes have clear implementation processes.
- an alternative to hospitalization for patients who meet inpatient commitment criteria
- a form of conditional release for patients completing an involuntary inpatient commitment
- an alternative to hospitalization for noncompliant patients at risk for relapse and involuntary inpatient commitment.2
Enforcement. Courts typically can request that law officers transport patients who fail to comply with OPC to a treatment facility. There, patients will be encouraged to comply with treatment or evaluated for inpatient commitment.2 This relatively weak enforcement authority has led some to argue that OPC has no teeth.
Without clearly defined steps for implementation, an outpatient commitment order can be likened to a message in a bottle—a cry for help at risk for nondelivery. In the Virginia Tech case, the judge issued an outpatient commitment order for Cho, but how the local clinic understood its responsibilities and what resources and enforcement power it had were unclear.
Noncontrolled studies
Evidence from noncontrolled OPC studies is difficult to interpret because of:
- lack of comparable committed and noncommitted groups
- difficulty in comparing treatment across comparison groups
- selection effects, whereby clinicians and courts select patients for a predicted good outcome.2
Most noncontrolled studies have concluded that OPC improves treatment outcomes and decreases hospital readmission rates and lengths of stay under some circumstances.6-12 The largest study reported on New York’s initial 5 years’ experience with more than 3,000 patients under its OPC statute, known as “Kendra’s Law” (Box 2).12 Under this law—the most intensively implemented OPC statute in the United States—the court’s order specifies a detailed plan of medications and psychosocial treatment.
Most of New York’s OPC recipients stayed in assisted outpatient treatment longer than the court-mandated 6 months (average 16 months). The incidence of hospitalizations, homelessness, arrests, and incarcerations was far lower while patients participated in OPC, compared with the previous 3 years of their lives (Table). Medication adherence improved from 34% before OPC to 69% after commitment, and engagement with treatment improved from 41% to 62%, respectively.12
Table
Change in adverse events among OPC patients in New York
| Event | Incidence during 3 years prior to OPC* | Incidence during OPC treatment | Rate of decline |
|---|---|---|---|
| Incarceration | 23% | 3% | 87% |
| Arrest | 30% | 5% | 83% |
| Psychiatric hospitalization | 97% | 22% | 77% |
| Homelessness | 19% | 5% | 74% |
| * Adverse events reported as occurring at least once | |||
| OPC: outpatient commitment | |||
| Source: Reprinted from reference 12, table 10 | |||
Conflicting controlled trials
Duke Mental Health Study. In the first controlled study of OPC, the Duke Mental Health Study (DMHS) enrolled 331 seriously mentally ill inpatients being discharged from involuntarily hospitalization to court-ordered outpatient treatment between 1993 and 1996. Patients with a history of violent behavior in the previous year were placed in a nonrandomized comparison group and remained on OPC for at least 90 days. The remaining 264 patients were randomly assigned to:
- an experimental group that received OPC for ≤90 days (could be renewed for ≤180 days) plus consistent community mental health services
- a control group that was released from OPC but received the same community mental health services as the experimental group.13
Patients ordered to OPC had fewer hospital readmissions and spent fewer days in the hospital only if they received OPC plus consistent community services for ≥6 months.14 Patients who received this model of care were:
- less likely to be homeless,15 criminally victimized,16 arrested if they had past arrests,17 or violent18
- more likely than the control group to comply with recommended treatment.19
Outpatient service intensity was not controlled but varied according to clinical need and other unknown factors. As a result, selectively providing services could have influenced outcomes, although other analyses argue that this factor was not important.4
New York. In 1994, the state legislature established a 3-year pilot program to evaluate OPC in New York City’s Bellevue Hospital as a first step toward considering permanent OPC legislation.20 The randomized, controlled study compared a court-ordered group (N=78) and a control group (N=64) during 1 year after hospital discharge. Both groups received enhanced outpatient services, such as psychiatrist appointments, intensive case management, and treatment for co-occurring substance abuse as needed.
Andrew Goldstein and Kendra Webdale were strangers standing on a New York City subway platform as a train arrived on January 3, 1999. She was an aspiring journalist and he a troubled man with schizophrenia who had stopped taking his medication. Goldstein later admitted in court that he placed his hands on the back of her shoulders and pushed her into the train’s path.
“Kendra’s law”—first enacted in 1999 and renewed for 5 years in 2005—provides assisted outpatient treatment (AOT) for persons age ≥18 with mental illness who—in view of their treatment history—are unlikely to survive safely in the community without supervision. The patient also must:
- have a history of treatment noncompliance
- be unlikely to voluntarily participate in treatment
- need assisted outpatient treatment to prevent a deterioration that would likely result in a substantial risk of physical harm to himself or others
- be likely to benefit from assisted outpatient treatment.
Implementation starts with a petition to the court, asking that a person be evaluated for AOT suitability. Petitions can be filed by psychiatrists, psychologists, social workers, family members, adult roommates, hospital directors, mental health or social services directors, and parole or probation officers. The petition is followed by an investigation by local authorities and a court hearing.
If the patient is found to be eligible for AOT, the court orders a highly specific treatment plan. Initial orders for 6 months can be renewed at subsequent court hearings.
Control and experimental groups showed no statistically significant differences in hospitalizations, arrests, quality of life, symptoms, homelessness, or other outcomes. The authors interpreted these findings to suggest that in this study intensive services—and not OPC court orders—reduced hospital recidivism and other poor outcomes in seriously mentally ill patients.
Study limitations. Statute implementation and OPC enforcement were haphazard, and in most cases sanctions for noncompliance—such as orders to law enforcement to detain noncompliant patients—were not put into effect. Patients and providers often did not clearly distinguish between the control and experimental groups. And finally, the study likely was too small to demonstrate a positive effect for OPC. Nevertheless, the findings suggest that OPC might provide no added benefit if persons with serious mental illnesses have access to enhanced outpatient services.4
Do OPC laws prevent violence?
The North Carolina and New York controlled studies of OPC yielded contradictory findings and are difficult to compare. Even within North Carolina—where OPC has been shown most consistently to be effective—OPC orders’ duration (the “dose”) varies widely, as do the services patients receive.
No further randomized, controlled trials of OPC are underway. Our group is participating in a study supported by the MacArthur Foundation Research Network on Mandated Community Treatment and New York State Office of Mental Health to intensively review patient outcomes under New York’s OPC statute.
Given that most states permit OPC, attempts to standardize and implement OPC are needed. To make OPC effective, evidence indicates that states also must provide intensive community services to keep patients in treatment.
Strategies for using OPC
OPC is controversial in society and among clinicians. Some mental health organizations oppose outpatient commitment orders as coercive and intrusive, and some mental health professionals have concerns about legal or malpractice liability, increased paperwork, and administrative burden. Others may view OPC as:
- ineffective —providing weak sanctions that are impractical to enforce
- detrimental to the therapeutic alliance
- a less-desirable substitute for making high-quality voluntary treatment more widely available for the seriously mentally ill.
Select appropriate candidates. Our group’s experience suggests that patients with severe mental illness—especially schizophrenia spectrum disorders—are those most likely to benefit from OPC. There is no evidence that outpatient commitment helps patients with personality disorders or substance abuse without comorbid severe mental illness.
Maximize effectiveness. Evidence from the North Carolina studies suggests keeping OPC in place for ≥6 months and providing relatively intensive outpatient services. For schizophrenia-spectrum patients, combining OPC with depot antipsychotics may be more effective than oral agents for ensuring adherence and improving function.19
Decide when to terminate. OPC orders probably should last at least 6 months, but little evidence exists to guide discontinuing an order after 6 months. This dilemma is similar to deciding when a depot antipsychotic can or should be converted to an oral agent in previously nonadherent patients.
Our approach is to consider terminating the order in patients with restored insight who have ≥6 months of consistent treatment compliance without a need for or threat of OPC enforcement. In some cases, other leverage may preempt the need for continuing an order, such as:
- financial contingencies from family or others
- treatment required as a condition of probation or parole
- housing conditioned on treatment adherence.
- Treatment Advocacy Center. Nonprofit organization dedicated to eliminating barriers to timely, effective treatment of severe mental illnesses. www.psychlaws.org.
- MacArthur Foundation Research Network on Mandated Community Treatment. www.macarthur.virginia.edu/researchnetwork.html.
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
This work was supported by NIMH Grants MH 48103 and MH 51410 and the MacArthur Foundation Research Network on Mandated Community Treatment.
1. Swartz M. Taking issue: can mandated outpatient treatment prevent tragedies? Psychiatr Serv 2007;58(6):737.-
2. Swartz MS, Burns BJ, Hiday VA, et al. New directions in research on involuntary outpatient commitment. Psychiatr Serv 1995;46:381-5.
3. Torrey EF, Kaplan R. A national survey of the use of outpatient commitment. Psychiatr Serv 1995;46:778-84.
4. Swartz MS, Swanson JW. Involuntary outpatient commitment, community treatment orders, and assisted outpatient treatment: what’s in the data? Can J Psychiatry 2004;49(9):585-91.
5. Monahan J, Swartz M, Bonnie R. Mandated treatment in the community for people with mental disorders. Health Aff 2003;22:28-38.
6. Munetz MR, Grande T, Kleist J, Peterson GA. The effectiveness of outpatient civil commitment. Psychiatr Serv 1996;47:1251-3.
7. Rohland BM, Rohrer JE, Richard C. The long-term effects of outpatient commitment on service use. Adm Policy Ment Health 2000;27:383-94.
8. Keilitz I. Empirical studies of involuntary outpatient civil commitment: is it working? Ment Phys Disabil Law Rep 1990;14:368-79.
9. Hiday VA, Scheid-Cook TL. Outpatient commitment for revolving door patients: compliance and treatment. J Nerv Ment Dis 1991;179:83-8.
10. Moloy KA. Analysis: critiquing the empirical evidence. Does involuntary outpatient commitment work?. Washington, DC: Mental Health Policy Resource Center; 1992.
11. Ridgely MS, Borum J, Petrilla J. The effectiveness of outpatient commitment: empirical evidence and experience of eight states. Santa Monica, CA: RAND Corporation; 2001.
12. Kendra’s Law: final report on the status of assisted outpatient treatment. Albany, NY: New York State Office of Mental Health; 2005. Available at: http://www.omh.state.ny.us/omhweb/Kendra_web/finalreport. Accessed February 19, 2008.
13. Swartz MS, Swanson JW, Hiday VA, et al. A randomized controlled trial of outpatient commitment in North Carolina. Psychiatr Serv 2001;52:330-6.
14. Swartz MS, Swanson JW, Wagner RR, et al. Can involuntary outpatient commitment reduce hospital recidivism? Findings from a randomized trial in severely mentally ill individuals. Am J Psychiatry 1999;156:1968-75.
15. Compton SN, Swanson JW, Wagner HR, et al. Involuntary outpatient commitment and homelessness in persons with severe mental illness. J Ment Health Serv Res 2003;5:27-38.
16. Hiday VA, Swartz MS, Swanson JW, et al. Impact of outpatient commitment on victimization of people with severe mental illness. Am J Psychiatry 2002;159:1403-11.
17. Swanson JW, Borum R, Swartz MS, et al. Can involuntary outpatient commitment reduce arrests among persons with severe mental illness? Criminal Justice & Human Behavior 2001 28;156-89.
18. Swanson JW, Swartz MS, Borum R, et al. Involuntary outpatient commitment and reduction of violent behaviour in persons with severe mental illness. Br J Psychiatry 2000;176:324-31.
19. Swartz MS, Swanson JW, Wagner HR, et al. Effects of involuntary outpatient commitment and depot antipsychotics on treatment adherence in persons with severe mental illness. J Nerv Ment Dis 2001;189:583-92.
20. Steadman HJ, Gounis K, Dennis D, et al. Assessing the New York City outpatient commitment pilot program. Psychiatr Serv 2001;52:330-6.
1. Swartz M. Taking issue: can mandated outpatient treatment prevent tragedies? Psychiatr Serv 2007;58(6):737.-
2. Swartz MS, Burns BJ, Hiday VA, et al. New directions in research on involuntary outpatient commitment. Psychiatr Serv 1995;46:381-5.
3. Torrey EF, Kaplan R. A national survey of the use of outpatient commitment. Psychiatr Serv 1995;46:778-84.
4. Swartz MS, Swanson JW. Involuntary outpatient commitment, community treatment orders, and assisted outpatient treatment: what’s in the data? Can J Psychiatry 2004;49(9):585-91.
5. Monahan J, Swartz M, Bonnie R. Mandated treatment in the community for people with mental disorders. Health Aff 2003;22:28-38.
6. Munetz MR, Grande T, Kleist J, Peterson GA. The effectiveness of outpatient civil commitment. Psychiatr Serv 1996;47:1251-3.
7. Rohland BM, Rohrer JE, Richard C. The long-term effects of outpatient commitment on service use. Adm Policy Ment Health 2000;27:383-94.
8. Keilitz I. Empirical studies of involuntary outpatient civil commitment: is it working? Ment Phys Disabil Law Rep 1990;14:368-79.
9. Hiday VA, Scheid-Cook TL. Outpatient commitment for revolving door patients: compliance and treatment. J Nerv Ment Dis 1991;179:83-8.
10. Moloy KA. Analysis: critiquing the empirical evidence. Does involuntary outpatient commitment work?. Washington, DC: Mental Health Policy Resource Center; 1992.
11. Ridgely MS, Borum J, Petrilla J. The effectiveness of outpatient commitment: empirical evidence and experience of eight states. Santa Monica, CA: RAND Corporation; 2001.
12. Kendra’s Law: final report on the status of assisted outpatient treatment. Albany, NY: New York State Office of Mental Health; 2005. Available at: http://www.omh.state.ny.us/omhweb/Kendra_web/finalreport. Accessed February 19, 2008.
13. Swartz MS, Swanson JW, Hiday VA, et al. A randomized controlled trial of outpatient commitment in North Carolina. Psychiatr Serv 2001;52:330-6.
14. Swartz MS, Swanson JW, Wagner RR, et al. Can involuntary outpatient commitment reduce hospital recidivism? Findings from a randomized trial in severely mentally ill individuals. Am J Psychiatry 1999;156:1968-75.
15. Compton SN, Swanson JW, Wagner HR, et al. Involuntary outpatient commitment and homelessness in persons with severe mental illness. J Ment Health Serv Res 2003;5:27-38.
16. Hiday VA, Swartz MS, Swanson JW, et al. Impact of outpatient commitment on victimization of people with severe mental illness. Am J Psychiatry 2002;159:1403-11.
17. Swanson JW, Borum R, Swartz MS, et al. Can involuntary outpatient commitment reduce arrests among persons with severe mental illness? Criminal Justice & Human Behavior 2001 28;156-89.
18. Swanson JW, Swartz MS, Borum R, et al. Involuntary outpatient commitment and reduction of violent behaviour in persons with severe mental illness. Br J Psychiatry 2000;176:324-31.
19. Swartz MS, Swanson JW, Wagner HR, et al. Effects of involuntary outpatient commitment and depot antipsychotics on treatment adherence in persons with severe mental illness. J Nerv Ment Dis 2001;189:583-92.
20. Steadman HJ, Gounis K, Dennis D, et al. Assessing the New York City outpatient commitment pilot program. Psychiatr Serv 2001;52:330-6.
A cry for help: Treating involuntary emotional expression disorder
Mrs. R, a 68-year-old retired teacher, is referred to you for suspected mania after a closed head injury from a car accident. The referring physician reports that Mrs. R experienced mild anterograde amnesia that has resolved, but she continues to suffer from “persistent mood swings as evidenced by substantial inappropriate laughter.”
Mrs. R is not manic. Her mood is normal, with a relatively euthymic affect. When asked about her accident or injury, however, she breaks into bouts of laughter that appear to be uncontrollable and last up to several minutes. These episodes include respiratory changes that make her laughter nearly indistinguishable from crying. Mrs. R explains that the episodes occur every time she discusses the accident—regardless of her efforts to prevent them—and complains they are extremely frustrating and embarrassing. She avoids situations that might trigger the episodes.
Patients with involuntary emotional expression disorder (IEED)—a neurologic disorder that manifests as brief bouts of uncontrollable crying, laughing, or both—may appear to have bipolar disorder, schizophrenia, depression, or another psychiatric disorder. Careful evaluation, however, can distinguish IEED from other conditions. Managing the disorder requires an understanding of IEED phenomenology, including:
- neurologic conditions that result in IEED
- underlying pathology
- diagnostic criteria
- effective treatments.
Brain dysfunction alters affect
IEED was introduced as an inclusive term, replacing previous nomenclature such as pathologic laughing and crying, pseudobulbar affect, affective lability, and emotional incontinence.1
IEED can present as episodes of laughter, as in Mrs. R’s case, but more commonly manifests as bouts of crying. Other presentations include a combination of laughing and crying, but episodic outbursts of other emotions that are out of the patient’s control—such as anger—can be included in this syndrome.2 IEED episodes can lead to embarrassment, frustration, and anger that eventually can affect mood and often cause patients to avoid social interaction.3
IEED can occur in any condition that damages and affects the brain areas critical to emotional motor output (Box 1).4-6 The broad pattern of lesions that can result in IEED stems from many disease states. IEED is often observed in amyotrophic lateral sclerosis (ALS), multiple sclerosis (MS), stroke, and traumatic brain injury. It also may occur in dementia, Parkinson’s disease, and other disorders (Table 1).7
Table 1
Neurologic conditions associated with IEED
| Amyotrophic lateral sclerosis |
| Multiple sclerosis |
| Traumatic brain injury |
| Stroke |
| Alzheimer’s disease |
| Frontotemporal dementia |
| Parkinson’s disease |
| Progressive supranuclear palsy |
| Multiple systems atrophy |
| Wilson’s disease |
| Normal pressure hydrocephalus |
| Olivopontine cerebellar atrophy |
| Source: Reference 7 |
Diagnosis can be elusive
Although IEED is not included in DSM-IV-TR, recently developed diagnostic criteria can help distinguish it from other disorders (Table 2).1 As with DSM-categorized disorders, IEED must result in clinically significant distress or impairment in social or occupational function and must not be better accounted for by another disorder or caused by a physiologic substance.
The patient must present with symptoms caused by brain dysfunction from brain injury or neurodegenerative disease. Underlying brain damage might not be apparent when the patient first presents, but to our knowledge no case of idiopathic IEED has been described. If a patient presents with symptoms thought to be IEED, first determine what underlying neurologic condition is causing the symptoms and optimally manage this disorder.
Symptoms must be incongruent with or in excess of the person’s underlying mood and independent or in excess of the provoking stimulus. Inappropriateness of the emotional response is the hallmark of IEED.
Some characteristics support—but are not essential for—an IEED diagnosis:
- autonomic symptoms, such as flushing of the face and increased salivary production during episodes
- pseudobulbar signs, such as increased jaw jerk, exaggerated gag reflex, dysarthria, and dysphagia
- other emotional outbursts.
Table 2
Is it IEED? Diagnostic criteria
| Presence of brain damage |
Episodes of involuntary emotional motor output that:
|
Disorder is not:
|
| Source: Reference 1 |
Characteristics of IEED episodes
| Paroxysmal, sudden onset with rapid offset |
| Brief (up to several minutes) |
| Stereotyped across patients (may manifest in similar fashion from patient to patient) |
| Stereotyped within patients (episodes often have similar type, severity, and eliciting stimuli) |
Damage to the descending inputs to the pontomedullary area once referred to as the faciorespiratory center is most likely to result in release of bulbar function and, subsequently, involuntary emotional expression disorder (IEED). Therefore, because of the progressive upper motor neuron degeneration associated with amyotrophic lateral sclerosis (ALS), nearly 50% of ALS patients will eventually demonstrate pathological affect.4
The lesions that can result in IEED are diffuse, however, and have been described in a review of IEED neuroanatomy as including a cortico-limbic-subcortico-thalamo-ponto-cerebellar network.5 Single lesions to white matter structures—such as the internal capsule—and gray matter structures—such as the thalamus, hypothalamus, basal ganglia, cerebellum, and several cortical locations—have been associated with IEED. Bilateral lesions are more likely to produce the disorder than single lesions.
With such varied neuroanatomic substrates, predicting the underlying neurochemical pathology of IEED is difficult. Among the neurotransmitters considered in IEED pathology and treatment are serotonin, glutamate, and dopamine. The sigma-1 receptor system may also play a role.6
CASE CONTINUED: Reaching a diagnosis
After thoroughly interviewing Mrs. R, you exclude mood disorders such as depression or bipolar disorder. The paroxysmal, episodic nature of her emotional outbursts and the consistency of the eliciting stimulus, suggest IEED.
Distinguishing IEED from depression. Physicians may be quick to diagnose a patient with consistent, recurrent crying as having a depressive disorder. In IEED, the patient’s family commonly (and inappropriately) will confirm this misperception, even if the patient claims otherwise. The hallmark distinctions between depression and IEED are:
- duration of crying
- associated mood state.
Patients who suffer from MDD, however, are not excluded from an IEED diagnosis. In 1 small study, almost one-half of patients with IEED also had major depression.12 Differentiating these syndromes—even in patients who suffer from both—is important to ensure proper management and patient and family understanding of the condition. Lastly, although IEED is not a mood disorder, the embarrassment and frustration it causes can change a patient’s mood over time.
Recommended treatment
Education. In our experience, education is critical to help patients and family members understand IEED and deal with embarrassment and other normal reactions they may experience. Explain that these emotional displays are not manic or psychotic episodes but periods of motor dyscontrol caused by a neurologic condition.
Teach them to cope with IEED by:
- identifying and avoiding stimuli that provoke IEED episodes
- ignoring the episodes and continuing with usual activities.
These agents have IEED-specific therapeutic effects through a mechanism independent of their antidepressant action. In patients with IEED and depression, antidepressants may resolve IEED while depression remains refractory.2,12 Potential drawbacks include anticholinergic effects with TCAs and sexual and gastrointestinal side effects with SSRIs. Nevertheless, these agents are the optimal first-line therapy for IEED among currently available options.
Other agents. Small studies have investigated other agents, but the data are insufficient to warrant recommendations for clinical practice. One study found that the novel antidepressant mirtazapine improved symptoms in 2 patients who did not respond to SSRIs.17 In another study, levodopa therapy resulted in improvement in 10 of 25 patients.18
Among scales that measure involuntary emotional expression disorder (IEED) severity, 2 have been used in studies of IEED therapeutic efficacy (see Related Resources):12,19,20
- Pathological Laughing and Crying Scale (PLACS) developed by Robinson et al12 is an interviewer-administered, 18-item tool that has been validated in IEED patients with stroke,12 dementia,22and traumatic brain injury.23
- 7-item Center for Neurologic Study-Lability Scale (CNS-LS) is a self-report measure that has been validated in IEED patients with amyotrophic lateral sclerosis24 and multiple sclerosis.25
Although these scales have been used primarily for research, you can use them clinically to establish a baseline of IEED severity and gauge treatment efficacy. Improved scores generally correlate with successful treatment; if a patient fails to show adequate response on 1 of these scales, consider changing treatment.
A combination dextromethorphan and quinidine (DM/Q) is being evaluated for IEED. This compound has demonstrated efficacy in IEED patients with ALS19 and MS20 and is in Phase III clinical development. DM/Q is thought to be a potent activator of the sigma-1 receptor system as well as an N-methyl-D-aspartate antagonist.21
Table 4
IEED: Evidence for antidepressants
| Drug | Study design/population | Dosage | Outcome |
|---|---|---|---|
| Tricyclics | |||
| Amitriptyline | Schiffer et al;13 double-blind crossover; 12 multiple sclerosis patients | Mean: 57.8 mg/d | 8 patients showed significant improvement compared with placebo |
| Nortriptyline | Robinson et al;12 double-blind, placebo-controlled; 28 stroke patients | ≤100 mg/d | Patients receiving nortriptyline reported significantly greater improvement on PLACS at 4 and 6 weeks compared with placebo |
| Selective serotonin reuptake inhibitors | |||
| Citalopram | Anderson et al;14 double-blind, placebo-controlled crossover; 16 stroke patients | 10 to 20 mg/d | Citalopram decreased the number of daily crying episodes by ≥50% compared with placebo |
| Fluoxetine | Choi-Kwon et al;2 double-blind placebo-controlled; 152 patients | 20 mg/d | Fluoxetine significantly improved measures of IEED and anger proneness but not depression |
| Paroxetine | Müller et al;15 consecutive case series, comparison with citalopram; 26 patients with traumatic brain injury or stroke | 10 to 40 mg/d | Both paroxetine and citalopram resulted in significant improvements in measures of emotionalism |
| Sertraline | Burns et al;16 double-blind, placebo-controlled; 28 stroke patients | 50 mg/d | Patients receiving sertraline had significant improvements in measures of emotionalism |
| IEED: involuntary emotional expression disorder; PLACS: Pathological Laughing and Crying Scale | |||
CASE CONTINUED: Effective pharmacotherapy
After diagnosing IEED, you start Mrs. R on sertraline, 50 mg/d. She experiences a nearly immediate reduction in the number of daily IEED episodes. As a result, she feels more comfortable engaging in social activities.
Effective pharmacologic intervention can greatly improve patients’ quality of life.19,20 Use scales that measure IEED severity to gauge treatment effectiveness (Box 2).12,19,20,22-25 Because treatment failure is a realistic possibility,17 you may need to try a variety of agents to determine which regimen provides the greatest efficacy and therapeutic effects.
- Involuntary emotional expressive disorder (for healthcare professionals). www.ieed.org/hp.
- Pathological laughing and crying scale (PLACS). Robinson RG, Parikh RM, Lipsey JR, et al. Pathological laughing and crying following stroke: validation of a measurement scale and a double-blind treatment study. Am J Psychiatry 1993;150:286-93.
- Center for neurologic study—lability scale (CNS-LS). Moore SR, Gresham LS, Bromberg MB, et al. A self report measure of affective lability. J Neurol Neurosurg Psychiatry 1997;63:89-93.
- Amitriptyline • Elavil, Endep
- Citalopram • Celexa
- Dextromethorphan/quinidine • Zenvia*
- Fluoxetine • Prozac
- Levodopa • Larodopa
- Mirtazapine • Remeron
- Nortriptyline • Aventyl
- Paroxetine • Paxil
- Sertraline • Zoloft
- * IN PHASE III DEVELOPMENT
Dr. Grill reports no financial relationship with any company whose products are mentioned in the article or with manufacturers of competing products.
Dr. Cummings is a consultant to Acadia Pharmaceuticals, Astellas Pharma, Avanir Pharmaceuticals, Cephalon, CoMentis, Eisai, Eli Lilly and Company, EnVivo Pharmaceuticals, Forest Pharmaceuticals, Janssen, L.P., Lundbeck, Merck, Merz Pharma, Myriad, Neurochem, Novartis, Ono Pharmaceutical Co., Pfizer Inc., and sanofi-aventis. He is a speaker for Eisai, Forest Pharmaceuticals, Janssen, L.P., Lundbeck, Merz Pharma, Novartis, and Pfizer Inc.
1. Cummings JL, Arciniegas DB, Brooks BR, et al. Defining and diagnosing involuntary emotional expression disorder. CNS Spectr 2006;11:1-7.
2. Choi-Kwon S, Han SW, Kwon SU, et al. Fluoxetine treatment in poststroke depression, emotional incontinence, and anger proneness: a double-blind, placebo-controlled study. Stroke 2006;37:156-61.
3. Lieberman A, Benson DF. Control of emotional expression in pseudobulbar palsy. A personal experience. Arch Neurol 1977;34:717-9.
4. Caroscio JT, Mulvihill MN, Sterling R, Abrams B. Amyotrophic lateral sclerosis. Its natural history. Neurol Clin 1987;5:1-8.
5. Arciniegas DB, Lauterbach EC, Anderson KE, et al. The differential diagnosis of pseudobulbar affect (PBA). Distinguishing PBA among disorders of mood and affect. Proceedings of a roundtable meeting. CNS Spectr 2005;10:1-14; quiz 15-16.-
6. Rabins PV, Arciniegas DB. Pathophysiology of involuntary emotional expression disorder. CNS Spectr 2007;12:17-22.
7. Arciniegas DB, Topkoff J. The neuropsychiatry of pathologic affect: an approach to evaluation and treatment. Semin Clin Neuropsychiatry 2000;5:290-306.
8. Green RL, McAllister TW, Bernat JL. A study of crying in medically and surgically hospitalized patients. Am J Psychiatry 1987;144:442-7.
9. Dark FL, McGrath JJ, Ron MA. Pathological laughing and crying. Aust N Z J Psychiatry 1996;30:472-9.
10. Wilson S. Some problems in neurology. II. Pathological laughing and crying. J Neurol Psychopathol 1924;16:299-333.
11. Diagnostic and statistical manual of mental disorders. 4th ed, text rev. Washington, D.C: American Psychiatric Association; 2000.
12. Robinson RG, Parikh RM, Lipsey JR, et al. Pathological laughing and crying following stroke: validation of a measurement scale and a double-blind treatment study. Am J Psychiatry 1993;150:286-93.
13. Schiffer RB, Herndon RM, Rudick RA. Treatment of pathologic laughing and weeping with amitriptyline. N Engl J Med 1985;312(23):1480-2.
14. Anderson G, Vestergaard K, Riis JO. Citalopram for post-stroke pathological crying. Lancet 1993;342(8875):837-9.
15. Müller U, Murai T, Bauer-Wittmund T, von Cramon DY. Paroxetine versus citalopram treatment of pathological crying after brain injury. Brain Inj 1999;13(10):805-11.
16. Burns A, Russell E, Stratton-Powell H, et al. Sertraline in stroke-associated lability of mood. Int J Geriatr Psychiatry 1999;14(8):681-5.
17. Kim SW, Shin IS, Kim JM, et al. Mirtazapine treatment for pathological laughing and crying after stroke. Clin Neuropharmacol 2005;28:249-51.
18. Udaka F, Yamao S, Nagata H, et al. Pathologic laughing and crying treated with levodopa. Arch Neurol 1984;41:1095-6.
19. Brooks BR, Thisted RA, Appel SH, et al. Treatment of pseudobulbar affect in ALS with dextromethorphan/quinidine: a randomized trial. Neurology 2004;63:1364-70.
20. Panitch HS, Thisted RA, Smith RA, et al. Randomized, controlled trial of dextromethorphan/quinidine for pseudobulbar affect in multiple sclerosis. Ann Neurol 2006;59:780-7.
21. Werling LL, Keller A, Frank JG, Nuwayhid SJ. A comparison of the binding profiles of dextromethorphan, memantine, fluoxetine and amitriptyline: treatment of involuntary emotional expression disorder. Exp Neurol 2007;207(2):248-57.
22. Starkstein SE, Migliorelli R, Teson A, et al. Prevalence and clinical correlates of pathological affective display in Alzheimer’s disease. J Neurol Neurosurg Psychiatry 1995;59:55-60.
23. Tateno A, Jorge RE, Robinson RG. Pathological laughing and crying following traumatic brain injury. J Neuropsychiatry Clin Neurosci 2004;16:426-34.
24. Moore SR, Gresham LS, Bromberg MB, et al. A self report measure of affective lability. J Neurol Neurosurg Psychiatry 1997;63:89-93.
25. Smith RA, Berg JE, Pope LE, et al. Validation of the CNS emotional lability scale for pseudobulbar affect (pathological laughing and crying) in multiple sclerosis patients. Mult Scler 2004;10:679-85.
Mrs. R, a 68-year-old retired teacher, is referred to you for suspected mania after a closed head injury from a car accident. The referring physician reports that Mrs. R experienced mild anterograde amnesia that has resolved, but she continues to suffer from “persistent mood swings as evidenced by substantial inappropriate laughter.”
Mrs. R is not manic. Her mood is normal, with a relatively euthymic affect. When asked about her accident or injury, however, she breaks into bouts of laughter that appear to be uncontrollable and last up to several minutes. These episodes include respiratory changes that make her laughter nearly indistinguishable from crying. Mrs. R explains that the episodes occur every time she discusses the accident—regardless of her efforts to prevent them—and complains they are extremely frustrating and embarrassing. She avoids situations that might trigger the episodes.
Patients with involuntary emotional expression disorder (IEED)—a neurologic disorder that manifests as brief bouts of uncontrollable crying, laughing, or both—may appear to have bipolar disorder, schizophrenia, depression, or another psychiatric disorder. Careful evaluation, however, can distinguish IEED from other conditions. Managing the disorder requires an understanding of IEED phenomenology, including:
- neurologic conditions that result in IEED
- underlying pathology
- diagnostic criteria
- effective treatments.
Brain dysfunction alters affect
IEED was introduced as an inclusive term, replacing previous nomenclature such as pathologic laughing and crying, pseudobulbar affect, affective lability, and emotional incontinence.1
IEED can present as episodes of laughter, as in Mrs. R’s case, but more commonly manifests as bouts of crying. Other presentations include a combination of laughing and crying, but episodic outbursts of other emotions that are out of the patient’s control—such as anger—can be included in this syndrome.2 IEED episodes can lead to embarrassment, frustration, and anger that eventually can affect mood and often cause patients to avoid social interaction.3
IEED can occur in any condition that damages and affects the brain areas critical to emotional motor output (Box 1).4-6 The broad pattern of lesions that can result in IEED stems from many disease states. IEED is often observed in amyotrophic lateral sclerosis (ALS), multiple sclerosis (MS), stroke, and traumatic brain injury. It also may occur in dementia, Parkinson’s disease, and other disorders (Table 1).7
Table 1
Neurologic conditions associated with IEED
| Amyotrophic lateral sclerosis |
| Multiple sclerosis |
| Traumatic brain injury |
| Stroke |
| Alzheimer’s disease |
| Frontotemporal dementia |
| Parkinson’s disease |
| Progressive supranuclear palsy |
| Multiple systems atrophy |
| Wilson’s disease |
| Normal pressure hydrocephalus |
| Olivopontine cerebellar atrophy |
| Source: Reference 7 |
Diagnosis can be elusive
Although IEED is not included in DSM-IV-TR, recently developed diagnostic criteria can help distinguish it from other disorders (Table 2).1 As with DSM-categorized disorders, IEED must result in clinically significant distress or impairment in social or occupational function and must not be better accounted for by another disorder or caused by a physiologic substance.
The patient must present with symptoms caused by brain dysfunction from brain injury or neurodegenerative disease. Underlying brain damage might not be apparent when the patient first presents, but to our knowledge no case of idiopathic IEED has been described. If a patient presents with symptoms thought to be IEED, first determine what underlying neurologic condition is causing the symptoms and optimally manage this disorder.
Symptoms must be incongruent with or in excess of the person’s underlying mood and independent or in excess of the provoking stimulus. Inappropriateness of the emotional response is the hallmark of IEED.
Some characteristics support—but are not essential for—an IEED diagnosis:
- autonomic symptoms, such as flushing of the face and increased salivary production during episodes
- pseudobulbar signs, such as increased jaw jerk, exaggerated gag reflex, dysarthria, and dysphagia
- other emotional outbursts.
Table 2
Is it IEED? Diagnostic criteria
| Presence of brain damage |
Episodes of involuntary emotional motor output that:
|
Disorder is not:
|
| Source: Reference 1 |
Characteristics of IEED episodes
| Paroxysmal, sudden onset with rapid offset |
| Brief (up to several minutes) |
| Stereotyped across patients (may manifest in similar fashion from patient to patient) |
| Stereotyped within patients (episodes often have similar type, severity, and eliciting stimuli) |
Damage to the descending inputs to the pontomedullary area once referred to as the faciorespiratory center is most likely to result in release of bulbar function and, subsequently, involuntary emotional expression disorder (IEED). Therefore, because of the progressive upper motor neuron degeneration associated with amyotrophic lateral sclerosis (ALS), nearly 50% of ALS patients will eventually demonstrate pathological affect.4
The lesions that can result in IEED are diffuse, however, and have been described in a review of IEED neuroanatomy as including a cortico-limbic-subcortico-thalamo-ponto-cerebellar network.5 Single lesions to white matter structures—such as the internal capsule—and gray matter structures—such as the thalamus, hypothalamus, basal ganglia, cerebellum, and several cortical locations—have been associated with IEED. Bilateral lesions are more likely to produce the disorder than single lesions.
With such varied neuroanatomic substrates, predicting the underlying neurochemical pathology of IEED is difficult. Among the neurotransmitters considered in IEED pathology and treatment are serotonin, glutamate, and dopamine. The sigma-1 receptor system may also play a role.6
CASE CONTINUED: Reaching a diagnosis
After thoroughly interviewing Mrs. R, you exclude mood disorders such as depression or bipolar disorder. The paroxysmal, episodic nature of her emotional outbursts and the consistency of the eliciting stimulus, suggest IEED.
Distinguishing IEED from depression. Physicians may be quick to diagnose a patient with consistent, recurrent crying as having a depressive disorder. In IEED, the patient’s family commonly (and inappropriately) will confirm this misperception, even if the patient claims otherwise. The hallmark distinctions between depression and IEED are:
- duration of crying
- associated mood state.
Patients who suffer from MDD, however, are not excluded from an IEED diagnosis. In 1 small study, almost one-half of patients with IEED also had major depression.12 Differentiating these syndromes—even in patients who suffer from both—is important to ensure proper management and patient and family understanding of the condition. Lastly, although IEED is not a mood disorder, the embarrassment and frustration it causes can change a patient’s mood over time.
Recommended treatment
Education. In our experience, education is critical to help patients and family members understand IEED and deal with embarrassment and other normal reactions they may experience. Explain that these emotional displays are not manic or psychotic episodes but periods of motor dyscontrol caused by a neurologic condition.
Teach them to cope with IEED by:
- identifying and avoiding stimuli that provoke IEED episodes
- ignoring the episodes and continuing with usual activities.
These agents have IEED-specific therapeutic effects through a mechanism independent of their antidepressant action. In patients with IEED and depression, antidepressants may resolve IEED while depression remains refractory.2,12 Potential drawbacks include anticholinergic effects with TCAs and sexual and gastrointestinal side effects with SSRIs. Nevertheless, these agents are the optimal first-line therapy for IEED among currently available options.
Other agents. Small studies have investigated other agents, but the data are insufficient to warrant recommendations for clinical practice. One study found that the novel antidepressant mirtazapine improved symptoms in 2 patients who did not respond to SSRIs.17 In another study, levodopa therapy resulted in improvement in 10 of 25 patients.18
Among scales that measure involuntary emotional expression disorder (IEED) severity, 2 have been used in studies of IEED therapeutic efficacy (see Related Resources):12,19,20
- Pathological Laughing and Crying Scale (PLACS) developed by Robinson et al12 is an interviewer-administered, 18-item tool that has been validated in IEED patients with stroke,12 dementia,22and traumatic brain injury.23
- 7-item Center for Neurologic Study-Lability Scale (CNS-LS) is a self-report measure that has been validated in IEED patients with amyotrophic lateral sclerosis24 and multiple sclerosis.25
Although these scales have been used primarily for research, you can use them clinically to establish a baseline of IEED severity and gauge treatment efficacy. Improved scores generally correlate with successful treatment; if a patient fails to show adequate response on 1 of these scales, consider changing treatment.
A combination dextromethorphan and quinidine (DM/Q) is being evaluated for IEED. This compound has demonstrated efficacy in IEED patients with ALS19 and MS20 and is in Phase III clinical development. DM/Q is thought to be a potent activator of the sigma-1 receptor system as well as an N-methyl-D-aspartate antagonist.21
Table 4
IEED: Evidence for antidepressants
| Drug | Study design/population | Dosage | Outcome |
|---|---|---|---|
| Tricyclics | |||
| Amitriptyline | Schiffer et al;13 double-blind crossover; 12 multiple sclerosis patients | Mean: 57.8 mg/d | 8 patients showed significant improvement compared with placebo |
| Nortriptyline | Robinson et al;12 double-blind, placebo-controlled; 28 stroke patients | ≤100 mg/d | Patients receiving nortriptyline reported significantly greater improvement on PLACS at 4 and 6 weeks compared with placebo |
| Selective serotonin reuptake inhibitors | |||
| Citalopram | Anderson et al;14 double-blind, placebo-controlled crossover; 16 stroke patients | 10 to 20 mg/d | Citalopram decreased the number of daily crying episodes by ≥50% compared with placebo |
| Fluoxetine | Choi-Kwon et al;2 double-blind placebo-controlled; 152 patients | 20 mg/d | Fluoxetine significantly improved measures of IEED and anger proneness but not depression |
| Paroxetine | Müller et al;15 consecutive case series, comparison with citalopram; 26 patients with traumatic brain injury or stroke | 10 to 40 mg/d | Both paroxetine and citalopram resulted in significant improvements in measures of emotionalism |
| Sertraline | Burns et al;16 double-blind, placebo-controlled; 28 stroke patients | 50 mg/d | Patients receiving sertraline had significant improvements in measures of emotionalism |
| IEED: involuntary emotional expression disorder; PLACS: Pathological Laughing and Crying Scale | |||
CASE CONTINUED: Effective pharmacotherapy
After diagnosing IEED, you start Mrs. R on sertraline, 50 mg/d. She experiences a nearly immediate reduction in the number of daily IEED episodes. As a result, she feels more comfortable engaging in social activities.
Effective pharmacologic intervention can greatly improve patients’ quality of life.19,20 Use scales that measure IEED severity to gauge treatment effectiveness (Box 2).12,19,20,22-25 Because treatment failure is a realistic possibility,17 you may need to try a variety of agents to determine which regimen provides the greatest efficacy and therapeutic effects.
- Involuntary emotional expressive disorder (for healthcare professionals). www.ieed.org/hp.
- Pathological laughing and crying scale (PLACS). Robinson RG, Parikh RM, Lipsey JR, et al. Pathological laughing and crying following stroke: validation of a measurement scale and a double-blind treatment study. Am J Psychiatry 1993;150:286-93.
- Center for neurologic study—lability scale (CNS-LS). Moore SR, Gresham LS, Bromberg MB, et al. A self report measure of affective lability. J Neurol Neurosurg Psychiatry 1997;63:89-93.
- Amitriptyline • Elavil, Endep
- Citalopram • Celexa
- Dextromethorphan/quinidine • Zenvia*
- Fluoxetine • Prozac
- Levodopa • Larodopa
- Mirtazapine • Remeron
- Nortriptyline • Aventyl
- Paroxetine • Paxil
- Sertraline • Zoloft
- * IN PHASE III DEVELOPMENT
Dr. Grill reports no financial relationship with any company whose products are mentioned in the article or with manufacturers of competing products.
Dr. Cummings is a consultant to Acadia Pharmaceuticals, Astellas Pharma, Avanir Pharmaceuticals, Cephalon, CoMentis, Eisai, Eli Lilly and Company, EnVivo Pharmaceuticals, Forest Pharmaceuticals, Janssen, L.P., Lundbeck, Merck, Merz Pharma, Myriad, Neurochem, Novartis, Ono Pharmaceutical Co., Pfizer Inc., and sanofi-aventis. He is a speaker for Eisai, Forest Pharmaceuticals, Janssen, L.P., Lundbeck, Merz Pharma, Novartis, and Pfizer Inc.
Mrs. R, a 68-year-old retired teacher, is referred to you for suspected mania after a closed head injury from a car accident. The referring physician reports that Mrs. R experienced mild anterograde amnesia that has resolved, but she continues to suffer from “persistent mood swings as evidenced by substantial inappropriate laughter.”
Mrs. R is not manic. Her mood is normal, with a relatively euthymic affect. When asked about her accident or injury, however, she breaks into bouts of laughter that appear to be uncontrollable and last up to several minutes. These episodes include respiratory changes that make her laughter nearly indistinguishable from crying. Mrs. R explains that the episodes occur every time she discusses the accident—regardless of her efforts to prevent them—and complains they are extremely frustrating and embarrassing. She avoids situations that might trigger the episodes.
Patients with involuntary emotional expression disorder (IEED)—a neurologic disorder that manifests as brief bouts of uncontrollable crying, laughing, or both—may appear to have bipolar disorder, schizophrenia, depression, or another psychiatric disorder. Careful evaluation, however, can distinguish IEED from other conditions. Managing the disorder requires an understanding of IEED phenomenology, including:
- neurologic conditions that result in IEED
- underlying pathology
- diagnostic criteria
- effective treatments.
Brain dysfunction alters affect
IEED was introduced as an inclusive term, replacing previous nomenclature such as pathologic laughing and crying, pseudobulbar affect, affective lability, and emotional incontinence.1
IEED can present as episodes of laughter, as in Mrs. R’s case, but more commonly manifests as bouts of crying. Other presentations include a combination of laughing and crying, but episodic outbursts of other emotions that are out of the patient’s control—such as anger—can be included in this syndrome.2 IEED episodes can lead to embarrassment, frustration, and anger that eventually can affect mood and often cause patients to avoid social interaction.3
IEED can occur in any condition that damages and affects the brain areas critical to emotional motor output (Box 1).4-6 The broad pattern of lesions that can result in IEED stems from many disease states. IEED is often observed in amyotrophic lateral sclerosis (ALS), multiple sclerosis (MS), stroke, and traumatic brain injury. It also may occur in dementia, Parkinson’s disease, and other disorders (Table 1).7
Table 1
Neurologic conditions associated with IEED
| Amyotrophic lateral sclerosis |
| Multiple sclerosis |
| Traumatic brain injury |
| Stroke |
| Alzheimer’s disease |
| Frontotemporal dementia |
| Parkinson’s disease |
| Progressive supranuclear palsy |
| Multiple systems atrophy |
| Wilson’s disease |
| Normal pressure hydrocephalus |
| Olivopontine cerebellar atrophy |
| Source: Reference 7 |
Diagnosis can be elusive
Although IEED is not included in DSM-IV-TR, recently developed diagnostic criteria can help distinguish it from other disorders (Table 2).1 As with DSM-categorized disorders, IEED must result in clinically significant distress or impairment in social or occupational function and must not be better accounted for by another disorder or caused by a physiologic substance.
The patient must present with symptoms caused by brain dysfunction from brain injury or neurodegenerative disease. Underlying brain damage might not be apparent when the patient first presents, but to our knowledge no case of idiopathic IEED has been described. If a patient presents with symptoms thought to be IEED, first determine what underlying neurologic condition is causing the symptoms and optimally manage this disorder.
Symptoms must be incongruent with or in excess of the person’s underlying mood and independent or in excess of the provoking stimulus. Inappropriateness of the emotional response is the hallmark of IEED.
Some characteristics support—but are not essential for—an IEED diagnosis:
- autonomic symptoms, such as flushing of the face and increased salivary production during episodes
- pseudobulbar signs, such as increased jaw jerk, exaggerated gag reflex, dysarthria, and dysphagia
- other emotional outbursts.
Table 2
Is it IEED? Diagnostic criteria
| Presence of brain damage |
Episodes of involuntary emotional motor output that:
|
Disorder is not:
|
| Source: Reference 1 |
Characteristics of IEED episodes
| Paroxysmal, sudden onset with rapid offset |
| Brief (up to several minutes) |
| Stereotyped across patients (may manifest in similar fashion from patient to patient) |
| Stereotyped within patients (episodes often have similar type, severity, and eliciting stimuli) |
Damage to the descending inputs to the pontomedullary area once referred to as the faciorespiratory center is most likely to result in release of bulbar function and, subsequently, involuntary emotional expression disorder (IEED). Therefore, because of the progressive upper motor neuron degeneration associated with amyotrophic lateral sclerosis (ALS), nearly 50% of ALS patients will eventually demonstrate pathological affect.4
The lesions that can result in IEED are diffuse, however, and have been described in a review of IEED neuroanatomy as including a cortico-limbic-subcortico-thalamo-ponto-cerebellar network.5 Single lesions to white matter structures—such as the internal capsule—and gray matter structures—such as the thalamus, hypothalamus, basal ganglia, cerebellum, and several cortical locations—have been associated with IEED. Bilateral lesions are more likely to produce the disorder than single lesions.
With such varied neuroanatomic substrates, predicting the underlying neurochemical pathology of IEED is difficult. Among the neurotransmitters considered in IEED pathology and treatment are serotonin, glutamate, and dopamine. The sigma-1 receptor system may also play a role.6
CASE CONTINUED: Reaching a diagnosis
After thoroughly interviewing Mrs. R, you exclude mood disorders such as depression or bipolar disorder. The paroxysmal, episodic nature of her emotional outbursts and the consistency of the eliciting stimulus, suggest IEED.
Distinguishing IEED from depression. Physicians may be quick to diagnose a patient with consistent, recurrent crying as having a depressive disorder. In IEED, the patient’s family commonly (and inappropriately) will confirm this misperception, even if the patient claims otherwise. The hallmark distinctions between depression and IEED are:
- duration of crying
- associated mood state.
Patients who suffer from MDD, however, are not excluded from an IEED diagnosis. In 1 small study, almost one-half of patients with IEED also had major depression.12 Differentiating these syndromes—even in patients who suffer from both—is important to ensure proper management and patient and family understanding of the condition. Lastly, although IEED is not a mood disorder, the embarrassment and frustration it causes can change a patient’s mood over time.
Recommended treatment
Education. In our experience, education is critical to help patients and family members understand IEED and deal with embarrassment and other normal reactions they may experience. Explain that these emotional displays are not manic or psychotic episodes but periods of motor dyscontrol caused by a neurologic condition.
Teach them to cope with IEED by:
- identifying and avoiding stimuli that provoke IEED episodes
- ignoring the episodes and continuing with usual activities.
These agents have IEED-specific therapeutic effects through a mechanism independent of their antidepressant action. In patients with IEED and depression, antidepressants may resolve IEED while depression remains refractory.2,12 Potential drawbacks include anticholinergic effects with TCAs and sexual and gastrointestinal side effects with SSRIs. Nevertheless, these agents are the optimal first-line therapy for IEED among currently available options.
Other agents. Small studies have investigated other agents, but the data are insufficient to warrant recommendations for clinical practice. One study found that the novel antidepressant mirtazapine improved symptoms in 2 patients who did not respond to SSRIs.17 In another study, levodopa therapy resulted in improvement in 10 of 25 patients.18
Among scales that measure involuntary emotional expression disorder (IEED) severity, 2 have been used in studies of IEED therapeutic efficacy (see Related Resources):12,19,20
- Pathological Laughing and Crying Scale (PLACS) developed by Robinson et al12 is an interviewer-administered, 18-item tool that has been validated in IEED patients with stroke,12 dementia,22and traumatic brain injury.23
- 7-item Center for Neurologic Study-Lability Scale (CNS-LS) is a self-report measure that has been validated in IEED patients with amyotrophic lateral sclerosis24 and multiple sclerosis.25
Although these scales have been used primarily for research, you can use them clinically to establish a baseline of IEED severity and gauge treatment efficacy. Improved scores generally correlate with successful treatment; if a patient fails to show adequate response on 1 of these scales, consider changing treatment.
A combination dextromethorphan and quinidine (DM/Q) is being evaluated for IEED. This compound has demonstrated efficacy in IEED patients with ALS19 and MS20 and is in Phase III clinical development. DM/Q is thought to be a potent activator of the sigma-1 receptor system as well as an N-methyl-D-aspartate antagonist.21
Table 4
IEED: Evidence for antidepressants
| Drug | Study design/population | Dosage | Outcome |
|---|---|---|---|
| Tricyclics | |||
| Amitriptyline | Schiffer et al;13 double-blind crossover; 12 multiple sclerosis patients | Mean: 57.8 mg/d | 8 patients showed significant improvement compared with placebo |
| Nortriptyline | Robinson et al;12 double-blind, placebo-controlled; 28 stroke patients | ≤100 mg/d | Patients receiving nortriptyline reported significantly greater improvement on PLACS at 4 and 6 weeks compared with placebo |
| Selective serotonin reuptake inhibitors | |||
| Citalopram | Anderson et al;14 double-blind, placebo-controlled crossover; 16 stroke patients | 10 to 20 mg/d | Citalopram decreased the number of daily crying episodes by ≥50% compared with placebo |
| Fluoxetine | Choi-Kwon et al;2 double-blind placebo-controlled; 152 patients | 20 mg/d | Fluoxetine significantly improved measures of IEED and anger proneness but not depression |
| Paroxetine | Müller et al;15 consecutive case series, comparison with citalopram; 26 patients with traumatic brain injury or stroke | 10 to 40 mg/d | Both paroxetine and citalopram resulted in significant improvements in measures of emotionalism |
| Sertraline | Burns et al;16 double-blind, placebo-controlled; 28 stroke patients | 50 mg/d | Patients receiving sertraline had significant improvements in measures of emotionalism |
| IEED: involuntary emotional expression disorder; PLACS: Pathological Laughing and Crying Scale | |||
CASE CONTINUED: Effective pharmacotherapy
After diagnosing IEED, you start Mrs. R on sertraline, 50 mg/d. She experiences a nearly immediate reduction in the number of daily IEED episodes. As a result, she feels more comfortable engaging in social activities.
Effective pharmacologic intervention can greatly improve patients’ quality of life.19,20 Use scales that measure IEED severity to gauge treatment effectiveness (Box 2).12,19,20,22-25 Because treatment failure is a realistic possibility,17 you may need to try a variety of agents to determine which regimen provides the greatest efficacy and therapeutic effects.
- Involuntary emotional expressive disorder (for healthcare professionals). www.ieed.org/hp.
- Pathological laughing and crying scale (PLACS). Robinson RG, Parikh RM, Lipsey JR, et al. Pathological laughing and crying following stroke: validation of a measurement scale and a double-blind treatment study. Am J Psychiatry 1993;150:286-93.
- Center for neurologic study—lability scale (CNS-LS). Moore SR, Gresham LS, Bromberg MB, et al. A self report measure of affective lability. J Neurol Neurosurg Psychiatry 1997;63:89-93.
- Amitriptyline • Elavil, Endep
- Citalopram • Celexa
- Dextromethorphan/quinidine • Zenvia*
- Fluoxetine • Prozac
- Levodopa • Larodopa
- Mirtazapine • Remeron
- Nortriptyline • Aventyl
- Paroxetine • Paxil
- Sertraline • Zoloft
- * IN PHASE III DEVELOPMENT
Dr. Grill reports no financial relationship with any company whose products are mentioned in the article or with manufacturers of competing products.
Dr. Cummings is a consultant to Acadia Pharmaceuticals, Astellas Pharma, Avanir Pharmaceuticals, Cephalon, CoMentis, Eisai, Eli Lilly and Company, EnVivo Pharmaceuticals, Forest Pharmaceuticals, Janssen, L.P., Lundbeck, Merck, Merz Pharma, Myriad, Neurochem, Novartis, Ono Pharmaceutical Co., Pfizer Inc., and sanofi-aventis. He is a speaker for Eisai, Forest Pharmaceuticals, Janssen, L.P., Lundbeck, Merz Pharma, Novartis, and Pfizer Inc.
1. Cummings JL, Arciniegas DB, Brooks BR, et al. Defining and diagnosing involuntary emotional expression disorder. CNS Spectr 2006;11:1-7.
2. Choi-Kwon S, Han SW, Kwon SU, et al. Fluoxetine treatment in poststroke depression, emotional incontinence, and anger proneness: a double-blind, placebo-controlled study. Stroke 2006;37:156-61.
3. Lieberman A, Benson DF. Control of emotional expression in pseudobulbar palsy. A personal experience. Arch Neurol 1977;34:717-9.
4. Caroscio JT, Mulvihill MN, Sterling R, Abrams B. Amyotrophic lateral sclerosis. Its natural history. Neurol Clin 1987;5:1-8.
5. Arciniegas DB, Lauterbach EC, Anderson KE, et al. The differential diagnosis of pseudobulbar affect (PBA). Distinguishing PBA among disorders of mood and affect. Proceedings of a roundtable meeting. CNS Spectr 2005;10:1-14; quiz 15-16.-
6. Rabins PV, Arciniegas DB. Pathophysiology of involuntary emotional expression disorder. CNS Spectr 2007;12:17-22.
7. Arciniegas DB, Topkoff J. The neuropsychiatry of pathologic affect: an approach to evaluation and treatment. Semin Clin Neuropsychiatry 2000;5:290-306.
8. Green RL, McAllister TW, Bernat JL. A study of crying in medically and surgically hospitalized patients. Am J Psychiatry 1987;144:442-7.
9. Dark FL, McGrath JJ, Ron MA. Pathological laughing and crying. Aust N Z J Psychiatry 1996;30:472-9.
10. Wilson S. Some problems in neurology. II. Pathological laughing and crying. J Neurol Psychopathol 1924;16:299-333.
11. Diagnostic and statistical manual of mental disorders. 4th ed, text rev. Washington, D.C: American Psychiatric Association; 2000.
12. Robinson RG, Parikh RM, Lipsey JR, et al. Pathological laughing and crying following stroke: validation of a measurement scale and a double-blind treatment study. Am J Psychiatry 1993;150:286-93.
13. Schiffer RB, Herndon RM, Rudick RA. Treatment of pathologic laughing and weeping with amitriptyline. N Engl J Med 1985;312(23):1480-2.
14. Anderson G, Vestergaard K, Riis JO. Citalopram for post-stroke pathological crying. Lancet 1993;342(8875):837-9.
15. Müller U, Murai T, Bauer-Wittmund T, von Cramon DY. Paroxetine versus citalopram treatment of pathological crying after brain injury. Brain Inj 1999;13(10):805-11.
16. Burns A, Russell E, Stratton-Powell H, et al. Sertraline in stroke-associated lability of mood. Int J Geriatr Psychiatry 1999;14(8):681-5.
17. Kim SW, Shin IS, Kim JM, et al. Mirtazapine treatment for pathological laughing and crying after stroke. Clin Neuropharmacol 2005;28:249-51.
18. Udaka F, Yamao S, Nagata H, et al. Pathologic laughing and crying treated with levodopa. Arch Neurol 1984;41:1095-6.
19. Brooks BR, Thisted RA, Appel SH, et al. Treatment of pseudobulbar affect in ALS with dextromethorphan/quinidine: a randomized trial. Neurology 2004;63:1364-70.
20. Panitch HS, Thisted RA, Smith RA, et al. Randomized, controlled trial of dextromethorphan/quinidine for pseudobulbar affect in multiple sclerosis. Ann Neurol 2006;59:780-7.
21. Werling LL, Keller A, Frank JG, Nuwayhid SJ. A comparison of the binding profiles of dextromethorphan, memantine, fluoxetine and amitriptyline: treatment of involuntary emotional expression disorder. Exp Neurol 2007;207(2):248-57.
22. Starkstein SE, Migliorelli R, Teson A, et al. Prevalence and clinical correlates of pathological affective display in Alzheimer’s disease. J Neurol Neurosurg Psychiatry 1995;59:55-60.
23. Tateno A, Jorge RE, Robinson RG. Pathological laughing and crying following traumatic brain injury. J Neuropsychiatry Clin Neurosci 2004;16:426-34.
24. Moore SR, Gresham LS, Bromberg MB, et al. A self report measure of affective lability. J Neurol Neurosurg Psychiatry 1997;63:89-93.
25. Smith RA, Berg JE, Pope LE, et al. Validation of the CNS emotional lability scale for pseudobulbar affect (pathological laughing and crying) in multiple sclerosis patients. Mult Scler 2004;10:679-85.
1. Cummings JL, Arciniegas DB, Brooks BR, et al. Defining and diagnosing involuntary emotional expression disorder. CNS Spectr 2006;11:1-7.
2. Choi-Kwon S, Han SW, Kwon SU, et al. Fluoxetine treatment in poststroke depression, emotional incontinence, and anger proneness: a double-blind, placebo-controlled study. Stroke 2006;37:156-61.
3. Lieberman A, Benson DF. Control of emotional expression in pseudobulbar palsy. A personal experience. Arch Neurol 1977;34:717-9.
4. Caroscio JT, Mulvihill MN, Sterling R, Abrams B. Amyotrophic lateral sclerosis. Its natural history. Neurol Clin 1987;5:1-8.
5. Arciniegas DB, Lauterbach EC, Anderson KE, et al. The differential diagnosis of pseudobulbar affect (PBA). Distinguishing PBA among disorders of mood and affect. Proceedings of a roundtable meeting. CNS Spectr 2005;10:1-14; quiz 15-16.-
6. Rabins PV, Arciniegas DB. Pathophysiology of involuntary emotional expression disorder. CNS Spectr 2007;12:17-22.
7. Arciniegas DB, Topkoff J. The neuropsychiatry of pathologic affect: an approach to evaluation and treatment. Semin Clin Neuropsychiatry 2000;5:290-306.
8. Green RL, McAllister TW, Bernat JL. A study of crying in medically and surgically hospitalized patients. Am J Psychiatry 1987;144:442-7.
9. Dark FL, McGrath JJ, Ron MA. Pathological laughing and crying. Aust N Z J Psychiatry 1996;30:472-9.
10. Wilson S. Some problems in neurology. II. Pathological laughing and crying. J Neurol Psychopathol 1924;16:299-333.
11. Diagnostic and statistical manual of mental disorders. 4th ed, text rev. Washington, D.C: American Psychiatric Association; 2000.
12. Robinson RG, Parikh RM, Lipsey JR, et al. Pathological laughing and crying following stroke: validation of a measurement scale and a double-blind treatment study. Am J Psychiatry 1993;150:286-93.
13. Schiffer RB, Herndon RM, Rudick RA. Treatment of pathologic laughing and weeping with amitriptyline. N Engl J Med 1985;312(23):1480-2.
14. Anderson G, Vestergaard K, Riis JO. Citalopram for post-stroke pathological crying. Lancet 1993;342(8875):837-9.
15. Müller U, Murai T, Bauer-Wittmund T, von Cramon DY. Paroxetine versus citalopram treatment of pathological crying after brain injury. Brain Inj 1999;13(10):805-11.
16. Burns A, Russell E, Stratton-Powell H, et al. Sertraline in stroke-associated lability of mood. Int J Geriatr Psychiatry 1999;14(8):681-5.
17. Kim SW, Shin IS, Kim JM, et al. Mirtazapine treatment for pathological laughing and crying after stroke. Clin Neuropharmacol 2005;28:249-51.
18. Udaka F, Yamao S, Nagata H, et al. Pathologic laughing and crying treated with levodopa. Arch Neurol 1984;41:1095-6.
19. Brooks BR, Thisted RA, Appel SH, et al. Treatment of pseudobulbar affect in ALS with dextromethorphan/quinidine: a randomized trial. Neurology 2004;63:1364-70.
20. Panitch HS, Thisted RA, Smith RA, et al. Randomized, controlled trial of dextromethorphan/quinidine for pseudobulbar affect in multiple sclerosis. Ann Neurol 2006;59:780-7.
21. Werling LL, Keller A, Frank JG, Nuwayhid SJ. A comparison of the binding profiles of dextromethorphan, memantine, fluoxetine and amitriptyline: treatment of involuntary emotional expression disorder. Exp Neurol 2007;207(2):248-57.
22. Starkstein SE, Migliorelli R, Teson A, et al. Prevalence and clinical correlates of pathological affective display in Alzheimer’s disease. J Neurol Neurosurg Psychiatry 1995;59:55-60.
23. Tateno A, Jorge RE, Robinson RG. Pathological laughing and crying following traumatic brain injury. J Neuropsychiatry Clin Neurosci 2004;16:426-34.
24. Moore SR, Gresham LS, Bromberg MB, et al. A self report measure of affective lability. J Neurol Neurosurg Psychiatry 1997;63:89-93.
25. Smith RA, Berg JE, Pope LE, et al. Validation of the CNS emotional lability scale for pseudobulbar affect (pathological laughing and crying) in multiple sclerosis patients. Mult Scler 2004;10:679-85.
Do cholinesterase inhibitors enhance cognition in schizophrenia?
Some schizophrenia patients have shown significant improvements in positive and negative symptoms when my colleagues and I added acetylcholinesterase inhibitors (AChEIs) to their anti-psychotic regimens. We cannot rule out these benefits as placebo effects, but nevertheless they have been sustained over time. When patients appear to have benefited from AChEIs but stopped them, the benefits rapidly disappeared. Then, when these patients restarted the medications, the benefits recurred.
Unfortunately, recent well-controlled clinical studies have not supported these anecdotal findings or the results of approximately 20 preliminary trials. Thus, this article explains:
- why we don’t recommend using off-label AChEIs as a “first choice” augmentation strategy in schizophrenia patients at this time
- under what circumstances the adjunctive use of these agents might be reasonable.
Why Alzheimer’s medications?
Schizophrenia and Alzheimer’s disease (AD) have dramatically different onset, symptoms, course, and pathophysiology. As reviewed below, schizophrenia patients are no more likely to develop AD than the general population, and AChEIs—even when effective—have a short-term, limited benefit in AD.
So why are psychiatrists trying AD medications in patients with schizophrenia? The answer has to do with the intriguing effects of cholinergic agents on cognition.
Toward cognitive enhancement
Schizophrenia’s cognitive impairments may occur at a very early age, often before other overt symptoms,1 then may worsen—sometimes to dementia levels—when obvious psychotic symptoms emerge.2
Positive symptoms (hallucinations, delusions, thought disorder, etc.) and—to a lesser extent—negative symptoms (anhedonia, asociality, blunted affect, etc.) often improve when patients are treated with antipsychotics. Antipsychotics do not significantly improve cognitive symptoms (attention, reaction time, working memory, verbal fluency, etc.), however, and cognitive symptoms are the strongest predictors of poor functional outcomes in our patients.
Heterogeneous disorder. In 2000, Cummings3 summarized evidence from case re-ports and small studies that AChEIs were useful in treating neuropsychiatric conditions other than AD (Table 1). Cholinergic agents, Cummings noted, “affect many aspects of cognition, which suggests that the primary effect may be on an attentional or executive system with a secondary, pan-intellectual modulating influence on memory, language, and visuospatial skills.”4
In schizophrenia, different patients have different types of cognitive impairment.5 Thus, broad-based cognitive enhancers such as AChEIs may be necessary for general use in this illness.
Acetyltransferase activity. Schizophrenia patients—even those meeting criteria for dementia—do not usually have typical AD neuropathology, and the incidence of AD is no different in elderly patients with or without comorbid schizophrenia.6 At autopsy, schizophrenia patients and normal controls have similar brain cortical choline acetyltransferase levels.
Nevertheless, persons with AD and those with schizophrenia show a similar, statistically significant negative correlation between premorbid Clinical Dementia Rating scale scores and brain cortical choline acetyltransferase activity (r=– 0.36, P 6 Furthermore, studies have found cholinergic neurotransmission alterations in schizophrenia patients, including:
- a deficit in regulation of the low-affinity alpha-7 nicotinic receptor in those with impaired sensory gating7
- altered high-affinity nicotinic receptor binding8
- decreased hippocampal muscarinic receptor binding compared with matched normal controls9
- reduced density of cholinergic inter-neurons in the ventral striatum.10
Table 1
Cholinesterase inhibitors have shown benefit in many neuropsychiatric conditions*
| Alcoholism with Wernicke’s encephalopathy |
| Attention-deficit/hyperactivity disorder |
| Autism |
| Bipolar disorder |
| Creutzfeldt-Jakob disease |
| Dementia pugilistica |
| Dementia with Lewy bodies |
| Olivopontocerebellar atrophy |
| Parkinson’s disease with dementia |
| Parkinsonism dementia complex of Guam |
| Pick’s disease |
| Progressive supranuclear palsy |
| Schizophrenia |
| Sleep disorders |
| Subacute sclerosing panencephalitis |
| Traumatic brain injury |
| Vascular dementia |
| * Data from case reports and small studies. Cholinesterase inhibitors are FDA-approved only for Alzheimer’s dementia. |
| Source: Reference 3 |
AChEI augmentation
Mixed results. A number of investigators—including myself—have published data indicating that adding AChEIs—most often donepezil, but also rivastigmine or galantamine—to antipsychotic regimens may improve some schizophrenia patients’ symptoms and general functioning. These benefits were modest, however, when they were seen in these relatively small case reports and studies (Box).
Approximately 20 published studies have reported clinically significant benefits (positive symptom, negative symptom, and/or cognitive improvement) when schizophrenia patients received cholinesterase inhibitors with their antipsychotic regimens. These include case reports, case series, and double-blind, placebo-controlled, crossover or parallel-design studies, most with relatively small numbers of subjects.a-o
Recent studies, however, have failed to show a clinically or statistically significant benefit from cholinesterase inhibitor augmentation in schizophrenia (Table 2). Some included larger sample sizes than earlier investigations and a placebo-active drug parallel design.
fMRI findings. A few crossover design studies of schizophrenia patients taking antipsychotics included functional magnetic resonance imaging (fMRI) at baseline and after cholinesterase inhibitor and placebo augmentation. Of interest, the basal “abnormal” pattern of the baseline fMR image became more “normal” when subjects were treated with donepezil.
Source: Click here to view references
Other studies of AChEI augmentation of typical or atypical antipsychotics have been:
- equivocal, reporting benefits in some but not all patients (with no clear statistical or clinical conclusions) or in schizophrenia patients with comorbid dementia11-14
- decisively negative, showing no benefits, particularly in comparatively larger, randomized, placebo-controlled trials (Table 2).15-19
The authors concluded that—based on preliminary data—adjunctive AChEIs seemed to have “some beneficial effects” on attention and memory for schizophrenia patients.
Both the treatment and placebo groups experienced statistically and clinically significant benefits from baseline in measures of cognition, positive symptoms, and negative symptoms. For all measures, placebo augmentation was equal to or superior to donepezil augmentation.
Table 2
Controlled trials: No benefit from AChEIs in schizophrenia
| Study design | Subjects | Drug (dosage) | Results |
|---|---|---|---|
| Friedman et al (2002),15 double-blind, placebo-controlled | 36 patients with schizophrenia | Donepezil, 5 or 10 mg/d for 12 weeks | Neither dose produced significant improvement in any cognitive measure |
| Tugal et al (2004),16 double-blind, placebo- controlled, crossover | 12 patients with stable schizophrenia | Donepezil, 5 mg/d for 6 weeks, with crossover to placebo for 6 weeks | Treatment effect was not significant in any cognitive measure |
| Freudenreich et al (2005),17 double-blind, placebo-controlled | 36 stable outpatients with schizophrenia | Donepezil, ≤10 mg/d for 8 weeks | No improvement in cognition or psychopathology measures |
| Sharma et al (2006),18 randomized, double-blind, placebo-controlled | 21 patients with stable schizophrenia | Rivastigmine, 12 mg/d for 24 weeks | No significant improvement in any cognitive measure |
| Fagerlund et al (2007),19 double-blind, placebo-controlled | 21 patients enrolled, 11 completed | Donepezil, 5 or 10 mg/d for 4 months added to ziprasidone | No differences in changes on PANSS scores or a global cognitive score |
| Keefe et al (2007),21 randomized, double-blind, placebo-controlled | 250 stable outpatients with schizophrenia or schizoaffective disorder | Donepezil, 5 mg for 6 weeks then 10 mg for 6 weeks | Donepezil was well-tolerated but did not improve cognition any more than placebo |
| PANSS: Positive and Negative Syndrome Scale | |||
Analyzing trial results
The large, well-designed clinical trial by Keefe et al21 suggests conclusively that donepezil augmentation is not more effective than placebo in most stable schizophrenia or schizoaffective disorder patients with mild to moderate cognitive impairment.
- Different dosages might have been more effective.
- Longer treatment (>3 months) might have been necessary for donepezil to “surpass” the large placebo effect.
- Other AChEIs—such as galantamine, which stimulates nicotinic receptors—might be more effective than donepezil, which is predominantly muscarinic.
If this hypothesis is true, clinicians would need to differentiate patients before giving them trials of AChEIs or other augmentation therapies. Genetic testing might identify different pathophysiologies among patients, but these technologies are not yet clinically available.
Recommendations
Clinical experience, case reports, and small case series indicate that occasional patients may benefit from AChEI augmentation. On the other hand, the only large, multi-center, placebo-controlled, parallel-design study found no difference between donepezil and placebo augmentation of atypical antipsychotics.21
Thus this review of available evidence does not support the routine use of AChEI augmentation of typical or atypical antipsychotics as a viable psychopharmacologic strategy. Until more supportive evidence has been reported, this reviewer cannot recommend AChEIs as a “first line” augmentation strategy. Furthermore, because these medications do not have an FDA-approved indication in schizophrenia and are expensive, a cost-benefit appraisal also would not support their routine use.
Nevertheless, AChEIs are relatively safe and occasionally have been dramatically effective in a small subgroup of schizophrenia patients when used as augmentation. They may represent a reasonable approach:
- when other adjuncts have failed
- as a supplement to other augmentation strategies, such as cognitive-behavioral therapy or family therapy.
- Mohamed S, Paulsen JS, O’Leary D, et al. Generalized cognitive deficits in schizophrenia. Arch Gen Psychiatry 1999;56:749-54.
- Risch SC, Horner MD, McGurk S, et al. Double-blind donepezil-placebo crossover augmentation study of atypical antipsychotics in chronic, stable schizophrenia: a pilot study. Schizophr Res 2007;93:131-5.
- Donepezil • Aricept
- Rivastigmine • Exelon
- Galantamine • Reminyl, Razadyne
- Ziprasidone • Geodon
Dr. Risch receives research support from the National Institute of Mental Health, Abbott Laboratories, GlaxoSmithKline, Bristol-Myers Squibb, and Forest Pharmaceuticals. He is a consultant to and speaker for AstraZeneca and Pfizer Inc.
1. Hans SL, Marcus J, Nuechterlein KH, et al. Neurobehavioral deficits at adolescence in children at risk for schizophrenia. The Jerusalem Infant Development Study. Arch Gen Psychiatry 1999;56:741-8.
2. Heaton R, Paulsen JS, McAdams LA, et al. Neuropsychological deficits in schizophrenia: relationship to age, chronicity and dementia. Arch Gen Psychiatry 1994;51(6):469-76.
3. Cummings JL. Cholinesterase inhibitors: a new class of psychotropic compounds. Am J Psychiatry 2000;157(1):4-15.
4. Lawrence AD, Sahakian BJ. Alzheimer disease, attention, and the cholinergic system. Alzheimer Dis Assoc Disord 1995;9(suppl 2):43-9.
5. Green MF, Kern RS, Broff DL, et al. Neurocognitive deficits and functional outcome in schizophrenia: are we measuring the “right stuff”? Schizophr Bull 2000;26:119-36.
6. Powchick P, Davidson M, Haroutunian V, et al. Postmortem studies in schizophrenia. Schizophr Bull 1998;24(3):325-41.
7. Breese CR, Lee MJ, Adams CE, et al. Abnormal regulation of high affinity nicotinic receptors in subjects with schizophrenia. Neuropsychopharmacol 2000;23(4):351-64.
8. Crook JM, Tomaskovic-Crook E, Copolov DL, Dean B. Decreased muscarinic receptor binding in subjects with schizophrenia: a study of the human hippocampal formation. Biol Psychiatry 2000;48(5):381-8.
9. Holt DJ, Bachus SE, Hyde TM, et al. Reduced density of cholinergic interneurons in the ventral striatum in schizophrenia: an in situ hybridization study. Biol Psychiatry 2005;58:408-16.
10. MacEwan GW, Ehmann TS, Khanbhai I, Wrixon C. Donepezil in schizophrenia—is it helpful? An experimental design case study. Acta Psychiatr Scand 2001;104(6):469-72.
11. Stryjer R, Strous RD, Bar F, et al. Beneficial effect of donepezil augmentation for the management of comorbid schizophrenia and dementia. Clin Neuropharmacol 2003;26:12-7.
12. Aasen I, Kumari V, Sharma T. Effects of rivastigmine on sustained attention in schizophrenia: an fMRI study. J Clin Psychopharmacol 2005;25:311-7.
13. Arnold DS, Rosse RB, Dickinson D, et al. Adjuvant therapeutic effects of galantamine on apathy in a schizophrenia patient. J Clin Psychiatry 2004;65:1723-4.
14. Friedman JI, Adler DN, Howanitz E, et al. A double blind placebo controlled trial of donepezil adjunctive treatment to risperidone for the cognitive impairment of schizophrenia. Biol Psychiatry 2002;51:349-57.
15. Tugal O, Yazici KM, Anil Y, Gögüs A. A double-blind placebo controlled, cross-over trial of adjunctive donepezil for cognitive impairment in schizophrenia. Int J Neuropsychopharmacol 2004;7:117-23.
16. Freudenreich O, Herz L, Deckersbach T, et al. Added donepezil for stable schizophrenia: a double-blind, placebo-controlled trial. Psychopharmacology. (Berl) 2005;181:358-63.
17. Sharma T, Reed C, Aasen I, Kumari V. Cognitive effects of adjunctive 24-weeks rivastigmine treatment to antipsychotics in schizophrenia: a randomized, placebo-controlled, double-blind investigation. Schizophr Res 2006;85:73-83.
18. Fagerlund B, Soholm B, Fink-Jensen A, et al. Effects of donepezil adjunctive treatment ziprasidone on cognitive deficits in schizophrenia: a double-blind, placebo-controlled study. Clin Neuropharmacol 2007;30:3-12.
19. Chouinard S, Sepehry A, Amir A, et al. Oral cholinesterase inhibitor add-on therapy for cognitive enhancement in schizophrenia: a quantitative systematic review, part I. Clin Neuropharmacol 2007;30:169-82.
20. Keefe RS, Malhotra AK, Meltzer HY, et al. Efficacy and safety of donepezil in patients with schizophrenia or schizoaffective disorder: significant placebo/practice effects in a 12-week, randomized, double-blind, placebo-controlled trial. Neuropharmacol 2007;July 11 [Epub ahead of print].
21. Maelicke A, Albuquerque EX. Allosteric modulation of nicotinic acetylcholine receptors as a treatment strategy for Alzheimer’s disease. Eur J Pharmacol 2000;393:165-70.
22. Miller AL. Combination treatments for schizophrenia. CNS. Spectr 2004;9(9):19-23.
Some schizophrenia patients have shown significant improvements in positive and negative symptoms when my colleagues and I added acetylcholinesterase inhibitors (AChEIs) to their anti-psychotic regimens. We cannot rule out these benefits as placebo effects, but nevertheless they have been sustained over time. When patients appear to have benefited from AChEIs but stopped them, the benefits rapidly disappeared. Then, when these patients restarted the medications, the benefits recurred.
Unfortunately, recent well-controlled clinical studies have not supported these anecdotal findings or the results of approximately 20 preliminary trials. Thus, this article explains:
- why we don’t recommend using off-label AChEIs as a “first choice” augmentation strategy in schizophrenia patients at this time
- under what circumstances the adjunctive use of these agents might be reasonable.
Why Alzheimer’s medications?
Schizophrenia and Alzheimer’s disease (AD) have dramatically different onset, symptoms, course, and pathophysiology. As reviewed below, schizophrenia patients are no more likely to develop AD than the general population, and AChEIs—even when effective—have a short-term, limited benefit in AD.
So why are psychiatrists trying AD medications in patients with schizophrenia? The answer has to do with the intriguing effects of cholinergic agents on cognition.
Toward cognitive enhancement
Schizophrenia’s cognitive impairments may occur at a very early age, often before other overt symptoms,1 then may worsen—sometimes to dementia levels—when obvious psychotic symptoms emerge.2
Positive symptoms (hallucinations, delusions, thought disorder, etc.) and—to a lesser extent—negative symptoms (anhedonia, asociality, blunted affect, etc.) often improve when patients are treated with antipsychotics. Antipsychotics do not significantly improve cognitive symptoms (attention, reaction time, working memory, verbal fluency, etc.), however, and cognitive symptoms are the strongest predictors of poor functional outcomes in our patients.
Heterogeneous disorder. In 2000, Cummings3 summarized evidence from case re-ports and small studies that AChEIs were useful in treating neuropsychiatric conditions other than AD (Table 1). Cholinergic agents, Cummings noted, “affect many aspects of cognition, which suggests that the primary effect may be on an attentional or executive system with a secondary, pan-intellectual modulating influence on memory, language, and visuospatial skills.”4
In schizophrenia, different patients have different types of cognitive impairment.5 Thus, broad-based cognitive enhancers such as AChEIs may be necessary for general use in this illness.
Acetyltransferase activity. Schizophrenia patients—even those meeting criteria for dementia—do not usually have typical AD neuropathology, and the incidence of AD is no different in elderly patients with or without comorbid schizophrenia.6 At autopsy, schizophrenia patients and normal controls have similar brain cortical choline acetyltransferase levels.
Nevertheless, persons with AD and those with schizophrenia show a similar, statistically significant negative correlation between premorbid Clinical Dementia Rating scale scores and brain cortical choline acetyltransferase activity (r=– 0.36, P 6 Furthermore, studies have found cholinergic neurotransmission alterations in schizophrenia patients, including:
- a deficit in regulation of the low-affinity alpha-7 nicotinic receptor in those with impaired sensory gating7
- altered high-affinity nicotinic receptor binding8
- decreased hippocampal muscarinic receptor binding compared with matched normal controls9
- reduced density of cholinergic inter-neurons in the ventral striatum.10
Table 1
Cholinesterase inhibitors have shown benefit in many neuropsychiatric conditions*
| Alcoholism with Wernicke’s encephalopathy |
| Attention-deficit/hyperactivity disorder |
| Autism |
| Bipolar disorder |
| Creutzfeldt-Jakob disease |
| Dementia pugilistica |
| Dementia with Lewy bodies |
| Olivopontocerebellar atrophy |
| Parkinson’s disease with dementia |
| Parkinsonism dementia complex of Guam |
| Pick’s disease |
| Progressive supranuclear palsy |
| Schizophrenia |
| Sleep disorders |
| Subacute sclerosing panencephalitis |
| Traumatic brain injury |
| Vascular dementia |
| * Data from case reports and small studies. Cholinesterase inhibitors are FDA-approved only for Alzheimer’s dementia. |
| Source: Reference 3 |
AChEI augmentation
Mixed results. A number of investigators—including myself—have published data indicating that adding AChEIs—most often donepezil, but also rivastigmine or galantamine—to antipsychotic regimens may improve some schizophrenia patients’ symptoms and general functioning. These benefits were modest, however, when they were seen in these relatively small case reports and studies (Box).
Approximately 20 published studies have reported clinically significant benefits (positive symptom, negative symptom, and/or cognitive improvement) when schizophrenia patients received cholinesterase inhibitors with their antipsychotic regimens. These include case reports, case series, and double-blind, placebo-controlled, crossover or parallel-design studies, most with relatively small numbers of subjects.a-o
Recent studies, however, have failed to show a clinically or statistically significant benefit from cholinesterase inhibitor augmentation in schizophrenia (Table 2). Some included larger sample sizes than earlier investigations and a placebo-active drug parallel design.
fMRI findings. A few crossover design studies of schizophrenia patients taking antipsychotics included functional magnetic resonance imaging (fMRI) at baseline and after cholinesterase inhibitor and placebo augmentation. Of interest, the basal “abnormal” pattern of the baseline fMR image became more “normal” when subjects were treated with donepezil.
Source: Click here to view references
Other studies of AChEI augmentation of typical or atypical antipsychotics have been:
- equivocal, reporting benefits in some but not all patients (with no clear statistical or clinical conclusions) or in schizophrenia patients with comorbid dementia11-14
- decisively negative, showing no benefits, particularly in comparatively larger, randomized, placebo-controlled trials (Table 2).15-19
The authors concluded that—based on preliminary data—adjunctive AChEIs seemed to have “some beneficial effects” on attention and memory for schizophrenia patients.
Both the treatment and placebo groups experienced statistically and clinically significant benefits from baseline in measures of cognition, positive symptoms, and negative symptoms. For all measures, placebo augmentation was equal to or superior to donepezil augmentation.
Table 2
Controlled trials: No benefit from AChEIs in schizophrenia
| Study design | Subjects | Drug (dosage) | Results |
|---|---|---|---|
| Friedman et al (2002),15 double-blind, placebo-controlled | 36 patients with schizophrenia | Donepezil, 5 or 10 mg/d for 12 weeks | Neither dose produced significant improvement in any cognitive measure |
| Tugal et al (2004),16 double-blind, placebo- controlled, crossover | 12 patients with stable schizophrenia | Donepezil, 5 mg/d for 6 weeks, with crossover to placebo for 6 weeks | Treatment effect was not significant in any cognitive measure |
| Freudenreich et al (2005),17 double-blind, placebo-controlled | 36 stable outpatients with schizophrenia | Donepezil, ≤10 mg/d for 8 weeks | No improvement in cognition or psychopathology measures |
| Sharma et al (2006),18 randomized, double-blind, placebo-controlled | 21 patients with stable schizophrenia | Rivastigmine, 12 mg/d for 24 weeks | No significant improvement in any cognitive measure |
| Fagerlund et al (2007),19 double-blind, placebo-controlled | 21 patients enrolled, 11 completed | Donepezil, 5 or 10 mg/d for 4 months added to ziprasidone | No differences in changes on PANSS scores or a global cognitive score |
| Keefe et al (2007),21 randomized, double-blind, placebo-controlled | 250 stable outpatients with schizophrenia or schizoaffective disorder | Donepezil, 5 mg for 6 weeks then 10 mg for 6 weeks | Donepezil was well-tolerated but did not improve cognition any more than placebo |
| PANSS: Positive and Negative Syndrome Scale | |||
Analyzing trial results
The large, well-designed clinical trial by Keefe et al21 suggests conclusively that donepezil augmentation is not more effective than placebo in most stable schizophrenia or schizoaffective disorder patients with mild to moderate cognitive impairment.
- Different dosages might have been more effective.
- Longer treatment (>3 months) might have been necessary for donepezil to “surpass” the large placebo effect.
- Other AChEIs—such as galantamine, which stimulates nicotinic receptors—might be more effective than donepezil, which is predominantly muscarinic.
If this hypothesis is true, clinicians would need to differentiate patients before giving them trials of AChEIs or other augmentation therapies. Genetic testing might identify different pathophysiologies among patients, but these technologies are not yet clinically available.
Recommendations
Clinical experience, case reports, and small case series indicate that occasional patients may benefit from AChEI augmentation. On the other hand, the only large, multi-center, placebo-controlled, parallel-design study found no difference between donepezil and placebo augmentation of atypical antipsychotics.21
Thus this review of available evidence does not support the routine use of AChEI augmentation of typical or atypical antipsychotics as a viable psychopharmacologic strategy. Until more supportive evidence has been reported, this reviewer cannot recommend AChEIs as a “first line” augmentation strategy. Furthermore, because these medications do not have an FDA-approved indication in schizophrenia and are expensive, a cost-benefit appraisal also would not support their routine use.
Nevertheless, AChEIs are relatively safe and occasionally have been dramatically effective in a small subgroup of schizophrenia patients when used as augmentation. They may represent a reasonable approach:
- when other adjuncts have failed
- as a supplement to other augmentation strategies, such as cognitive-behavioral therapy or family therapy.
- Mohamed S, Paulsen JS, O’Leary D, et al. Generalized cognitive deficits in schizophrenia. Arch Gen Psychiatry 1999;56:749-54.
- Risch SC, Horner MD, McGurk S, et al. Double-blind donepezil-placebo crossover augmentation study of atypical antipsychotics in chronic, stable schizophrenia: a pilot study. Schizophr Res 2007;93:131-5.
- Donepezil • Aricept
- Rivastigmine • Exelon
- Galantamine • Reminyl, Razadyne
- Ziprasidone • Geodon
Dr. Risch receives research support from the National Institute of Mental Health, Abbott Laboratories, GlaxoSmithKline, Bristol-Myers Squibb, and Forest Pharmaceuticals. He is a consultant to and speaker for AstraZeneca and Pfizer Inc.
Some schizophrenia patients have shown significant improvements in positive and negative symptoms when my colleagues and I added acetylcholinesterase inhibitors (AChEIs) to their anti-psychotic regimens. We cannot rule out these benefits as placebo effects, but nevertheless they have been sustained over time. When patients appear to have benefited from AChEIs but stopped them, the benefits rapidly disappeared. Then, when these patients restarted the medications, the benefits recurred.
Unfortunately, recent well-controlled clinical studies have not supported these anecdotal findings or the results of approximately 20 preliminary trials. Thus, this article explains:
- why we don’t recommend using off-label AChEIs as a “first choice” augmentation strategy in schizophrenia patients at this time
- under what circumstances the adjunctive use of these agents might be reasonable.
Why Alzheimer’s medications?
Schizophrenia and Alzheimer’s disease (AD) have dramatically different onset, symptoms, course, and pathophysiology. As reviewed below, schizophrenia patients are no more likely to develop AD than the general population, and AChEIs—even when effective—have a short-term, limited benefit in AD.
So why are psychiatrists trying AD medications in patients with schizophrenia? The answer has to do with the intriguing effects of cholinergic agents on cognition.
Toward cognitive enhancement
Schizophrenia’s cognitive impairments may occur at a very early age, often before other overt symptoms,1 then may worsen—sometimes to dementia levels—when obvious psychotic symptoms emerge.2
Positive symptoms (hallucinations, delusions, thought disorder, etc.) and—to a lesser extent—negative symptoms (anhedonia, asociality, blunted affect, etc.) often improve when patients are treated with antipsychotics. Antipsychotics do not significantly improve cognitive symptoms (attention, reaction time, working memory, verbal fluency, etc.), however, and cognitive symptoms are the strongest predictors of poor functional outcomes in our patients.
Heterogeneous disorder. In 2000, Cummings3 summarized evidence from case re-ports and small studies that AChEIs were useful in treating neuropsychiatric conditions other than AD (Table 1). Cholinergic agents, Cummings noted, “affect many aspects of cognition, which suggests that the primary effect may be on an attentional or executive system with a secondary, pan-intellectual modulating influence on memory, language, and visuospatial skills.”4
In schizophrenia, different patients have different types of cognitive impairment.5 Thus, broad-based cognitive enhancers such as AChEIs may be necessary for general use in this illness.
Acetyltransferase activity. Schizophrenia patients—even those meeting criteria for dementia—do not usually have typical AD neuropathology, and the incidence of AD is no different in elderly patients with or without comorbid schizophrenia.6 At autopsy, schizophrenia patients and normal controls have similar brain cortical choline acetyltransferase levels.
Nevertheless, persons with AD and those with schizophrenia show a similar, statistically significant negative correlation between premorbid Clinical Dementia Rating scale scores and brain cortical choline acetyltransferase activity (r=– 0.36, P 6 Furthermore, studies have found cholinergic neurotransmission alterations in schizophrenia patients, including:
- a deficit in regulation of the low-affinity alpha-7 nicotinic receptor in those with impaired sensory gating7
- altered high-affinity nicotinic receptor binding8
- decreased hippocampal muscarinic receptor binding compared with matched normal controls9
- reduced density of cholinergic inter-neurons in the ventral striatum.10
Table 1
Cholinesterase inhibitors have shown benefit in many neuropsychiatric conditions*
| Alcoholism with Wernicke’s encephalopathy |
| Attention-deficit/hyperactivity disorder |
| Autism |
| Bipolar disorder |
| Creutzfeldt-Jakob disease |
| Dementia pugilistica |
| Dementia with Lewy bodies |
| Olivopontocerebellar atrophy |
| Parkinson’s disease with dementia |
| Parkinsonism dementia complex of Guam |
| Pick’s disease |
| Progressive supranuclear palsy |
| Schizophrenia |
| Sleep disorders |
| Subacute sclerosing panencephalitis |
| Traumatic brain injury |
| Vascular dementia |
| * Data from case reports and small studies. Cholinesterase inhibitors are FDA-approved only for Alzheimer’s dementia. |
| Source: Reference 3 |
AChEI augmentation
Mixed results. A number of investigators—including myself—have published data indicating that adding AChEIs—most often donepezil, but also rivastigmine or galantamine—to antipsychotic regimens may improve some schizophrenia patients’ symptoms and general functioning. These benefits were modest, however, when they were seen in these relatively small case reports and studies (Box).
Approximately 20 published studies have reported clinically significant benefits (positive symptom, negative symptom, and/or cognitive improvement) when schizophrenia patients received cholinesterase inhibitors with their antipsychotic regimens. These include case reports, case series, and double-blind, placebo-controlled, crossover or parallel-design studies, most with relatively small numbers of subjects.a-o
Recent studies, however, have failed to show a clinically or statistically significant benefit from cholinesterase inhibitor augmentation in schizophrenia (Table 2). Some included larger sample sizes than earlier investigations and a placebo-active drug parallel design.
fMRI findings. A few crossover design studies of schizophrenia patients taking antipsychotics included functional magnetic resonance imaging (fMRI) at baseline and after cholinesterase inhibitor and placebo augmentation. Of interest, the basal “abnormal” pattern of the baseline fMR image became more “normal” when subjects were treated with donepezil.
Source: Click here to view references
Other studies of AChEI augmentation of typical or atypical antipsychotics have been:
- equivocal, reporting benefits in some but not all patients (with no clear statistical or clinical conclusions) or in schizophrenia patients with comorbid dementia11-14
- decisively negative, showing no benefits, particularly in comparatively larger, randomized, placebo-controlled trials (Table 2).15-19
The authors concluded that—based on preliminary data—adjunctive AChEIs seemed to have “some beneficial effects” on attention and memory for schizophrenia patients.
Both the treatment and placebo groups experienced statistically and clinically significant benefits from baseline in measures of cognition, positive symptoms, and negative symptoms. For all measures, placebo augmentation was equal to or superior to donepezil augmentation.
Table 2
Controlled trials: No benefit from AChEIs in schizophrenia
| Study design | Subjects | Drug (dosage) | Results |
|---|---|---|---|
| Friedman et al (2002),15 double-blind, placebo-controlled | 36 patients with schizophrenia | Donepezil, 5 or 10 mg/d for 12 weeks | Neither dose produced significant improvement in any cognitive measure |
| Tugal et al (2004),16 double-blind, placebo- controlled, crossover | 12 patients with stable schizophrenia | Donepezil, 5 mg/d for 6 weeks, with crossover to placebo for 6 weeks | Treatment effect was not significant in any cognitive measure |
| Freudenreich et al (2005),17 double-blind, placebo-controlled | 36 stable outpatients with schizophrenia | Donepezil, ≤10 mg/d for 8 weeks | No improvement in cognition or psychopathology measures |
| Sharma et al (2006),18 randomized, double-blind, placebo-controlled | 21 patients with stable schizophrenia | Rivastigmine, 12 mg/d for 24 weeks | No significant improvement in any cognitive measure |
| Fagerlund et al (2007),19 double-blind, placebo-controlled | 21 patients enrolled, 11 completed | Donepezil, 5 or 10 mg/d for 4 months added to ziprasidone | No differences in changes on PANSS scores or a global cognitive score |
| Keefe et al (2007),21 randomized, double-blind, placebo-controlled | 250 stable outpatients with schizophrenia or schizoaffective disorder | Donepezil, 5 mg for 6 weeks then 10 mg for 6 weeks | Donepezil was well-tolerated but did not improve cognition any more than placebo |
| PANSS: Positive and Negative Syndrome Scale | |||
Analyzing trial results
The large, well-designed clinical trial by Keefe et al21 suggests conclusively that donepezil augmentation is not more effective than placebo in most stable schizophrenia or schizoaffective disorder patients with mild to moderate cognitive impairment.
- Different dosages might have been more effective.
- Longer treatment (>3 months) might have been necessary for donepezil to “surpass” the large placebo effect.
- Other AChEIs—such as galantamine, which stimulates nicotinic receptors—might be more effective than donepezil, which is predominantly muscarinic.
If this hypothesis is true, clinicians would need to differentiate patients before giving them trials of AChEIs or other augmentation therapies. Genetic testing might identify different pathophysiologies among patients, but these technologies are not yet clinically available.
Recommendations
Clinical experience, case reports, and small case series indicate that occasional patients may benefit from AChEI augmentation. On the other hand, the only large, multi-center, placebo-controlled, parallel-design study found no difference between donepezil and placebo augmentation of atypical antipsychotics.21
Thus this review of available evidence does not support the routine use of AChEI augmentation of typical or atypical antipsychotics as a viable psychopharmacologic strategy. Until more supportive evidence has been reported, this reviewer cannot recommend AChEIs as a “first line” augmentation strategy. Furthermore, because these medications do not have an FDA-approved indication in schizophrenia and are expensive, a cost-benefit appraisal also would not support their routine use.
Nevertheless, AChEIs are relatively safe and occasionally have been dramatically effective in a small subgroup of schizophrenia patients when used as augmentation. They may represent a reasonable approach:
- when other adjuncts have failed
- as a supplement to other augmentation strategies, such as cognitive-behavioral therapy or family therapy.
- Mohamed S, Paulsen JS, O’Leary D, et al. Generalized cognitive deficits in schizophrenia. Arch Gen Psychiatry 1999;56:749-54.
- Risch SC, Horner MD, McGurk S, et al. Double-blind donepezil-placebo crossover augmentation study of atypical antipsychotics in chronic, stable schizophrenia: a pilot study. Schizophr Res 2007;93:131-5.
- Donepezil • Aricept
- Rivastigmine • Exelon
- Galantamine • Reminyl, Razadyne
- Ziprasidone • Geodon
Dr. Risch receives research support from the National Institute of Mental Health, Abbott Laboratories, GlaxoSmithKline, Bristol-Myers Squibb, and Forest Pharmaceuticals. He is a consultant to and speaker for AstraZeneca and Pfizer Inc.
1. Hans SL, Marcus J, Nuechterlein KH, et al. Neurobehavioral deficits at adolescence in children at risk for schizophrenia. The Jerusalem Infant Development Study. Arch Gen Psychiatry 1999;56:741-8.
2. Heaton R, Paulsen JS, McAdams LA, et al. Neuropsychological deficits in schizophrenia: relationship to age, chronicity and dementia. Arch Gen Psychiatry 1994;51(6):469-76.
3. Cummings JL. Cholinesterase inhibitors: a new class of psychotropic compounds. Am J Psychiatry 2000;157(1):4-15.
4. Lawrence AD, Sahakian BJ. Alzheimer disease, attention, and the cholinergic system. Alzheimer Dis Assoc Disord 1995;9(suppl 2):43-9.
5. Green MF, Kern RS, Broff DL, et al. Neurocognitive deficits and functional outcome in schizophrenia: are we measuring the “right stuff”? Schizophr Bull 2000;26:119-36.
6. Powchick P, Davidson M, Haroutunian V, et al. Postmortem studies in schizophrenia. Schizophr Bull 1998;24(3):325-41.
7. Breese CR, Lee MJ, Adams CE, et al. Abnormal regulation of high affinity nicotinic receptors in subjects with schizophrenia. Neuropsychopharmacol 2000;23(4):351-64.
8. Crook JM, Tomaskovic-Crook E, Copolov DL, Dean B. Decreased muscarinic receptor binding in subjects with schizophrenia: a study of the human hippocampal formation. Biol Psychiatry 2000;48(5):381-8.
9. Holt DJ, Bachus SE, Hyde TM, et al. Reduced density of cholinergic interneurons in the ventral striatum in schizophrenia: an in situ hybridization study. Biol Psychiatry 2005;58:408-16.
10. MacEwan GW, Ehmann TS, Khanbhai I, Wrixon C. Donepezil in schizophrenia—is it helpful? An experimental design case study. Acta Psychiatr Scand 2001;104(6):469-72.
11. Stryjer R, Strous RD, Bar F, et al. Beneficial effect of donepezil augmentation for the management of comorbid schizophrenia and dementia. Clin Neuropharmacol 2003;26:12-7.
12. Aasen I, Kumari V, Sharma T. Effects of rivastigmine on sustained attention in schizophrenia: an fMRI study. J Clin Psychopharmacol 2005;25:311-7.
13. Arnold DS, Rosse RB, Dickinson D, et al. Adjuvant therapeutic effects of galantamine on apathy in a schizophrenia patient. J Clin Psychiatry 2004;65:1723-4.
14. Friedman JI, Adler DN, Howanitz E, et al. A double blind placebo controlled trial of donepezil adjunctive treatment to risperidone for the cognitive impairment of schizophrenia. Biol Psychiatry 2002;51:349-57.
15. Tugal O, Yazici KM, Anil Y, Gögüs A. A double-blind placebo controlled, cross-over trial of adjunctive donepezil for cognitive impairment in schizophrenia. Int J Neuropsychopharmacol 2004;7:117-23.
16. Freudenreich O, Herz L, Deckersbach T, et al. Added donepezil for stable schizophrenia: a double-blind, placebo-controlled trial. Psychopharmacology. (Berl) 2005;181:358-63.
17. Sharma T, Reed C, Aasen I, Kumari V. Cognitive effects of adjunctive 24-weeks rivastigmine treatment to antipsychotics in schizophrenia: a randomized, placebo-controlled, double-blind investigation. Schizophr Res 2006;85:73-83.
18. Fagerlund B, Soholm B, Fink-Jensen A, et al. Effects of donepezil adjunctive treatment ziprasidone on cognitive deficits in schizophrenia: a double-blind, placebo-controlled study. Clin Neuropharmacol 2007;30:3-12.
19. Chouinard S, Sepehry A, Amir A, et al. Oral cholinesterase inhibitor add-on therapy for cognitive enhancement in schizophrenia: a quantitative systematic review, part I. Clin Neuropharmacol 2007;30:169-82.
20. Keefe RS, Malhotra AK, Meltzer HY, et al. Efficacy and safety of donepezil in patients with schizophrenia or schizoaffective disorder: significant placebo/practice effects in a 12-week, randomized, double-blind, placebo-controlled trial. Neuropharmacol 2007;July 11 [Epub ahead of print].
21. Maelicke A, Albuquerque EX. Allosteric modulation of nicotinic acetylcholine receptors as a treatment strategy for Alzheimer’s disease. Eur J Pharmacol 2000;393:165-70.
22. Miller AL. Combination treatments for schizophrenia. CNS. Spectr 2004;9(9):19-23.
1. Hans SL, Marcus J, Nuechterlein KH, et al. Neurobehavioral deficits at adolescence in children at risk for schizophrenia. The Jerusalem Infant Development Study. Arch Gen Psychiatry 1999;56:741-8.
2. Heaton R, Paulsen JS, McAdams LA, et al. Neuropsychological deficits in schizophrenia: relationship to age, chronicity and dementia. Arch Gen Psychiatry 1994;51(6):469-76.
3. Cummings JL. Cholinesterase inhibitors: a new class of psychotropic compounds. Am J Psychiatry 2000;157(1):4-15.
4. Lawrence AD, Sahakian BJ. Alzheimer disease, attention, and the cholinergic system. Alzheimer Dis Assoc Disord 1995;9(suppl 2):43-9.
5. Green MF, Kern RS, Broff DL, et al. Neurocognitive deficits and functional outcome in schizophrenia: are we measuring the “right stuff”? Schizophr Bull 2000;26:119-36.
6. Powchick P, Davidson M, Haroutunian V, et al. Postmortem studies in schizophrenia. Schizophr Bull 1998;24(3):325-41.
7. Breese CR, Lee MJ, Adams CE, et al. Abnormal regulation of high affinity nicotinic receptors in subjects with schizophrenia. Neuropsychopharmacol 2000;23(4):351-64.
8. Crook JM, Tomaskovic-Crook E, Copolov DL, Dean B. Decreased muscarinic receptor binding in subjects with schizophrenia: a study of the human hippocampal formation. Biol Psychiatry 2000;48(5):381-8.
9. Holt DJ, Bachus SE, Hyde TM, et al. Reduced density of cholinergic interneurons in the ventral striatum in schizophrenia: an in situ hybridization study. Biol Psychiatry 2005;58:408-16.
10. MacEwan GW, Ehmann TS, Khanbhai I, Wrixon C. Donepezil in schizophrenia—is it helpful? An experimental design case study. Acta Psychiatr Scand 2001;104(6):469-72.
11. Stryjer R, Strous RD, Bar F, et al. Beneficial effect of donepezil augmentation for the management of comorbid schizophrenia and dementia. Clin Neuropharmacol 2003;26:12-7.
12. Aasen I, Kumari V, Sharma T. Effects of rivastigmine on sustained attention in schizophrenia: an fMRI study. J Clin Psychopharmacol 2005;25:311-7.
13. Arnold DS, Rosse RB, Dickinson D, et al. Adjuvant therapeutic effects of galantamine on apathy in a schizophrenia patient. J Clin Psychiatry 2004;65:1723-4.
14. Friedman JI, Adler DN, Howanitz E, et al. A double blind placebo controlled trial of donepezil adjunctive treatment to risperidone for the cognitive impairment of schizophrenia. Biol Psychiatry 2002;51:349-57.
15. Tugal O, Yazici KM, Anil Y, Gögüs A. A double-blind placebo controlled, cross-over trial of adjunctive donepezil for cognitive impairment in schizophrenia. Int J Neuropsychopharmacol 2004;7:117-23.
16. Freudenreich O, Herz L, Deckersbach T, et al. Added donepezil for stable schizophrenia: a double-blind, placebo-controlled trial. Psychopharmacology. (Berl) 2005;181:358-63.
17. Sharma T, Reed C, Aasen I, Kumari V. Cognitive effects of adjunctive 24-weeks rivastigmine treatment to antipsychotics in schizophrenia: a randomized, placebo-controlled, double-blind investigation. Schizophr Res 2006;85:73-83.
18. Fagerlund B, Soholm B, Fink-Jensen A, et al. Effects of donepezil adjunctive treatment ziprasidone on cognitive deficits in schizophrenia: a double-blind, placebo-controlled study. Clin Neuropharmacol 2007;30:3-12.
19. Chouinard S, Sepehry A, Amir A, et al. Oral cholinesterase inhibitor add-on therapy for cognitive enhancement in schizophrenia: a quantitative systematic review, part I. Clin Neuropharmacol 2007;30:169-82.
20. Keefe RS, Malhotra AK, Meltzer HY, et al. Efficacy and safety of donepezil in patients with schizophrenia or schizoaffective disorder: significant placebo/practice effects in a 12-week, randomized, double-blind, placebo-controlled trial. Neuropharmacol 2007;July 11 [Epub ahead of print].
21. Maelicke A, Albuquerque EX. Allosteric modulation of nicotinic acetylcholine receptors as a treatment strategy for Alzheimer’s disease. Eur J Pharmacol 2000;393:165-70.
22. Miller AL. Combination treatments for schizophrenia. CNS. Spectr 2004;9(9):19-23.
Most effective, least worrisome therapies for late-life anxiety
Ms. W, a 73-year-old widow with no psychiatric history, visits her primary care physician because she is concerned about her memory. She denies impairment in other cognitive domains—such as executive function—or activities of daily living.
Ms. W relates prominent worries about her health and finances and those of her grandchildren. She describes daily restlessness, sleep-onset insomnia, difficulty concentrating, and mild episodic dysphoria. She says she’s always been a “worry wart” but her worry and other symptoms have become increasingly intrusive over the past 5 years with a series of deaths in her family. Ms. W’s medical history includes hypertension and type 2 diabetes. Unsure how to treat her, the physician refers Ms. W to a psychiatrist.
Older adults with anxiety symptoms often are dissatisfied with treatment because they believe they receive insufficient help. This complaint is probably valid because limited data support pharmacologic interventions for anxiety in older adults, and therapy is often based on inferences from studies in younger subjects. Moreover, many anxious older patients are treated with benzodiazepines, which increases their risk for cognitive impairment and injuries.1,2
Fortunately, growing evidence points to 2 treatment modalities for anxiety disorders in patients age ≥65:
- pharmacotherapy with antidepressants, benzodiazepines, and (perhaps) buspirone
- cognitive-behavioral therapy (CBT) for generalized anxiety disorder (GAD), panic disorder (PD), and mixed anxiety syndromes.
A common, debilitating problem
Anxious older adults report diminished perceived health, physical activities, and quality of life and increased loneliness compared with their nonanxious counterparts.1 The prevalence of anxiety disorders in older patients ranges from 0.4% for obsessive-compulsive disorder to 11.5% for GAD.3
Older adults with GAD present with a constellation of medical, psychiatric, psychological, and psychosocial features (Table 1).1,3-12 Anxiety disorders in older adults also may co-occur with major depressive disorder, other psychiatric conditions, or dementia, which can complicate diagnosis and treatment.
Table 1
Is it GAD? Common features in older adults
| Demographics |
| More prevalent at age |
| More common in women |
| Medical |
| Frequent visits to primary care |
| Low satisfaction with medical care |
| ≥2 chronic physical illnesses |
| ≥1 adaptive behavior limitations |
| Cognitive impairment, particularly verbal memory |
| Psychiatric |
| History of GAD symptoms (5 to ≥20 years) |
| Physiologic anxiety symptoms: restlessness, fatigue, muscle tension |
| Depressive symptoms |
| Prescribed a benzodiazepine |
| Presence of anxiety disorders |
| Suicidal ideation, particularly if depressed |
| Psychological |
| External locus of control |
| Neuroticism |
| Psychosocial |
| Limited social network |
| Perceived low instrumental support |
| Recent losses and traumatic life events |
| Loss of partner |
| GAD: generalized anxiety disorder |
| Source: References 1,3-12 |
CASE CONTINUED: Anxious, not depressed
You screen Ms. W with the Geriatric Depression Scale (short form; GDS) and Beck Anxiety Inventory (BAI). Her scores indicate no depression and moderate anxiousness. A neuropsychological screen finds no cognitive impairments. Based on the clinical interview and screening, Ms. W meets DSM-IV-TR criteria for GAD.
Psychopharmacologic interventions are first-line treatment for older adults with anxiety disorders, but you might consider other strategies because:
- Older patients may have increased vulnerability to medication side effects.
- Few randomized, placebo-controlled trials have examined psychopharmacologic interventions specifically for anxious older adults.
First-line pharmacotherapies
When selecting pharmacotherapy for an older adult with anxiety, take into account:
- physiologic changes in drug metabolism (older patients metabolize drugs more slowly than younger patients)
- comorbid medical problems
- polypharmacy (many older patients are taking multiple medications for multiple conditions, which increases the risk of drug-drug interactions).
Pharmacologic management of anxiety typically has included benzodiazepines, tricyclic antidepressants, barbiturates, and antihistamines. Newer antidepressants have emerged as first-line treatment for several anxiety disorders and mixed anxiety-depression syndromes, however, because of their more tolerable side-effect profiles, especially when used long-term.14 These antidepressants include:
- selective serotonin reuptake inhibitors (SSRIs)
- serotonin/norepinephrine reuptake inhibitors (SNRIs).
Citalopram—started at 10 mg/d and titrated to 30 mg/d as tolerated—was used in the only prospective, double-blind, randomized, controlled trial of an SSRI in older patients with anxiety disorders. In this 8-week trial, Clinical Global Impression scale scores and Hamilton Anxiety scale scores improved.15 In other investigations:
- Paroxetine, averaging approximately 28 mg/d, produced a similar response in older and younger adults with PD in terms of efficacy and tolerability in a naturalistic follow-up trial.16
- Sertraline, started at 25 mg/d and titrated to 100 mg/d (maximum 150 mg/d), when combined with CBT was effective for treating older adults with anxiety disorders in a randomized, placebo-controlled trial17 and specifically for those with PD in an open-label trial.18
- Fluvoxamine, median 200 mg/d, reduced anxiety symptoms in an open-label study of 12 older adults with various anxiety disorders. Most patients with GAD (57%) responded to fluvoxamine, but 3 patients with PD did not.19
- We found no studies of fluoxetine for anxiety symptoms in older adults.
SNRIs. In a retrospective, pooled analysis of 5 randomized, placebo-controlled trials24 venlafaxine ER, 37.5 to 225 mg/d, was significantly more effective than placebo in treating older adults with GAD. Several studies suggest duloxetine may be effective for treating GAD in adults, but none examined efficacy specifically for older adults.
Using benzodiazepines for more than a few weeks in older adults is not recommended, however.14 Potential complications of long-term benzodiazepine use in these patients include:
- excessive daytime drowsiness
- cognitive and psychomotor impairment
- confusion
- risk of falls
- depression
- paradoxical reactions
- amnesic syndromes
- respiratory problems
- potential for abuse/dependence
- breakthrough withdrawal reactions.2,25,26
Buspirone. Investigations of anxious older adults have suggested that buspirone is effective for addressing anxiety symptoms.28,29 Our experience, however, indicates that response to buspirone is inconsistent.
Recommendations. Based on this evidence and our clinical practice, we recommend using SSRIs or SNRIs as first-line treatment for most anxiety disorders in older adults (Table 3).
To minimize nonadherence associated with antidepressants’ delayed onset of action and initial transient “jitters”:
- provide patient education about medication onset and side effects
- add a short half-life benzodiazepine for the first few weeks of treatment only
- start with small doses and increase gradually.
Recommended dosages for treating anxiety in older adults
| Medication | Starting dosage | Maximum dosage |
|---|---|---|
| Selective serotonin reuptake inhibitors | ||
| Citalopram | 10 mg/d | 30 mg/d |
| Escitalopram | 5 mg/d | 10 mg/d |
| Fluvoxamine | 25 mg/d | 100 mg/d |
| Paroxetine | 10 mg/d | 20 mg/d |
| Sertraline | 12.5 mg/d | 50 mg/d |
| Serotonin/norepinephrine reuptake inhibitors | ||
| Duloxetine | 30 mg/d | 60 mg/d |
| Venlafaxine | 37.5 mg/d | 150 mg/d |
| Benzodiazepines | ||
| Lorazepam | 0.5 mg/d divided bid | 1 to 3 mg/d, divided bid or tid |
| Oxazepam | 30 mg/d divided tid | 45 to 60 mg/d divided tid or qid |
| Azapirone | ||
| Buspirone | 10 to 15 mg/d, divided bid or tid | 30 to 60 mg/d divided bid or tid |
Anxiety in older adults: Recommended interventions
| Disorder | First-line treatment(s) | Second-line treatment(s) |
|---|---|---|
| Generalized anxiety disorder | SSRIs, SNRIs, buspirone, and/or CBT | Other newer antidepressants* |
| Panic disorder, with or without agoraphobia | SSRIs, SNRIs, and/or CBT | Other newer antidepressants* |
| Mixed anxiety and depression | SSRIs or SNRIs | Buspirone, CBT |
| Anxiety and medical disorders | Identify and treat medical cause, use SSRIs or SNRIs for primary anxiety disorder | Benzodiazepines |
| * Novel agents such as mirtazapine | ||
| CBT: cognitive-behavioral therapy; SNRIs: serotonin/norepinephrine reuptake inhibitors; SSRIs: selective serotonin reuptake inhibitors | ||
Psychotherapy as an alternative or adjunct
Researchers have compared the efficacy of CBT—which is effective for depression in older adults30—with that of other psychotherapies for mixed and specific anxiety disorders, including GAD and PD.
For GAD. Multicomponent CBT for GAD typically includes:
- psychoeducation
- thought monitoring
- cognitive restructuring
- progressive muscle relaxation and similar techniques
- breathing retraining
- problem solving
- exposure (imaginal, in vivo, worry)
- time management
- problem solving.
Six months of group CBT or nondirective supportive psychotherapy have shown similar efficacy in reducing worry, anxiety, and depression scores in older adults with GAD.32 In a randomized trial,33 group CBT produced slightly greater improvements in anxiety, depression, and pathologic worry among 75 older adults with GAD, compared with a worry discussion group (DG). CBT’s only statistically significant advantage, however, was that patients spent less time worrying immediately after treatment, compared with DG patients. This difference disappeared at 6 months.
For PD. Evidence supports using CBT for older adults with PD. CBT for PD typically includes interventions used for GAD but also integrates interoceptive exposure and tailored psychoeducation regarding panic symptom onset and maintenance. Older adults with PD who received 10 sessions of CBT over 12 weeks improved significantly on all symptoms measured—cognitive, behavioral, physiologic, and depression—in a study by Swales et al.34 These improvements were seen immediately after treatment and at 3-month follow-up. In a separate study, a sample of 43 older adults—most of whom were diagnosed with PD—were randomly assigned to receive CBT or individual, in-home supportive therapy.35 The CBT group reported greater reductions in anxiety and depression.
For mixed anxiety disorders. Several investigations have assessed the efficacy of CBT for older adults with mixed anxiety diagnoses and symptoms.
In one randomized trial, 84 older adults with a principal anxiety disorder diagnosis—GAD, PD, agoraphobia, or social phobia—were assigned to CBT, sertraline (maximum dosage 150 mg/d), or a wait-list.17 Compared with patients assigned to the waitlist, those in the CBT and sertraline groups improved on measures of anxiety and worry immediately after treatment and at 3-month follow-up. Patients receiving sertraline worried slightly less than those who received CBT. The sertraline and CBT groups did not differ in percentage of subjects who responded to treatment or end-state functioning.
CASE CONTINUED: Combination pharmacotherapy CBT
You explain to Ms. W that depressed and anxious older adults frequently perceive memory difficulties. You further relate that it is possible that anxious older adults may experience memory changes because of medication side effects (particularly benzodiazepines) or interference of cognitive functioning by negative mood states. You prescribe sertraline, which is titrated to and maintained at 50 mg/d. Ms. W also participates in 10 psychotherapy sessions, which focus on psychoeducation about symptoms of GAD, relaxation strategies, sleep hygiene, grieving, and cognitive restructuring regarding her worries.
Modifying CBT for older adults. The quality of older adults’ cognitive functioning may affect their response to CBT,37 particularly if they exhibit impaired executive functioning.38 Modifying CBT to meet the needs of older adults has not been systematically investigated.
- weekly readings of psychoeducational materials that emphasized the relationship between cognitions, behaviors, physiological functioning, and emotions
- graphing symptom changes
- reminder/troubleshooting phone calls.
CASE CONTINUED: Follow-up evaluation
You refer Ms. W to her primary care physician for follow-up. After 12 weeks of treatment, she reports declining anxiety symptoms. A repeat BAI indicates mild anxiousness, which she describes as minimally affecting her day-to-day activities. She continues sertraline and participation in individual psychotherapy with a particular focus on recent losses in her life.
Delivering CBT in primary care. Integrating CBT into anxious older patients’ primary care may be desirable because:
- Older adults prefer to receive psychiatric care in this setting.40
- Collaborative-care models for depressed and anxious older adults have been successful.41
A small pilot study that provided CBT in a primary care setting for older adults who met DSM-IV-TR criteria for GAD found statistically and clinically significant declines in self-reported worry, depression, and GAD symptom severity compared with patients receiving care as usual.42
Related resources
- Anxiety Disorders Association of America. www.adaa.org.
- Lauderdale SA, Kelly K, Sheikh JI. Anxious older adults: prevalence, assessment, and treatment. In: Anthony ME, Maletta GJ, eds. Principles and practice of geriatric psychiatry. Philadelphia, PA: Lippincott Williams & Wilkins; 2006:429-48.
- Buspirone • BuSpar
- Citalopram • Celexa
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Lorazepam • Ativan
- Mirtazapine • Remeron
- Oxazepam • Serax
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. de Beurs E, Beekman AT, van Balkom AJ, et al. Consequences of anxiety in older persons: its effect on disability, well-being, and use of health services. Psychol Med 1999;29:583-93.
2. Wadsworth EJK, Moss SC, Simpson SA, Smith AP. Psychotropic medication use and accidents, injuries, and cognitive failures. Hum Psychopharmacol 2005;20:391-400.
3. Beekman AT, Bremmer MA, Deeg DJ, et al. Anxiety disorders in later life: a report from the Longitudinal Aging Study Amsterdam. Int J Geriatr Psychiatry 1998;13:717-26.
4. Lindesay J, Briggs K, Murphy E. The Guy’s/Age Concern survey: prevalence rates of cognitive impairment, depression, and anxiety in an urban elderly community. Br J Psychiatry 1989;155:317-29.
5. Manela M, Katona C, Livingston G. How common are the anxiety disorders in old age? Int J Geriatr Psychiatry 1996;11:65-70.
6. Beekman AT, de Beurs E, van Balkom AJ, et al. Anxiety and depression in later life: co-occurrence and communality of risk factors. Am J Psychiatry 2000;157:89-95.
7. DeLuca AK, Lenze EJ, Mulsant BH, et al. Comorbid anxiety disorder in late life depression: association with memory decline over four years. Int J Geriatr Psychiatry 2005;29:848-54.
8. Blazer D, George LK, Hughes D. The epidemiology of anxiety disorders: an age comparison. In: Salzman C, Lebowitz BD, eds. Anxiety in the elderly: treatment and research. New York, NY: Springer; 1991:17-30.
9. Wetherell JL, Le Roux H, Gatz M. DSM-IV criteria for generalized anxiety disorder in older adults: distinguishing the worried from the well. Psychol Aging 2003;18:622-7.
10. van Balkom AJ, Beekman AT, de Beurs E, et al. Comorbidity of the anxiety disorders in a community-based older population in the Netherlands. Acta Psychiatr Scand 2000;101:37-45.
11. Jeste ND, Hays JC, Steffens DC. Clinical correlates of anxious depression among elderly patients with depression. J Affect Disord 2006;90:37-41.
12. Schuurmans J, Comijs HC, Beekman AT, et al. The outcome of anxiety disorders in older people at 6-year follow-up: results from the Longitudinal Aging Study Amsterdam. Acta Psychiatr Scand 2005;111:420-8.
13. Nordhus IH, Pallesen S. Psychological treatment of late-life anxiety: an empirical review. J Consult Clin Psychol 2003;71:643-51.
14. Lenze E, Pollock BG, Shear MK, et al. Treatment considerations for anxiety in the elderly. CNS Spectr 2003;8 (suppl 3):6-13.
15. Lenze E, Mulsant BH, Shear MK, et al. Efficacy and tolerability of citalopram in the treatment of late-life anxiety disorders: results from an 8-week randomized, placebo-controlled trial. Am J Psychiatry 2005;162(1):146-50.
16. Dannon PN, Iancu I, Lowengrub K, et al. Pharmacotherapy of panic disorder in the elderly: a naturalistic 12-month follow-up outcome study. Therapy 2005;2:249-54.
17. Schuurmans J, Comijs H, Emmelkamp PM, et al. A randomized, controlled trial of the effectiveness of cognitive-behavioral therapy and sertraline versus a waitlist control group for anxiety disorders in older adults. Am J Geriatr Psychiatry 2006;14:255-63.
18. Sheikh JI, Lauderdale SA, Cassidy EL. Efficacy of sertraline for panic disorder in older adults: a preliminary open-label trial. Am J Geriatr Psychiatry 2004;12:230.-
19. Wylie ME, Miller MD, Shear MK, et al. Fluvoxamine pharmacotherapy of anxiety disorders in later life: preliminary open-trial data. J Geriatr Psychiatry Neurol 2000;13:43-8.
20. Andreescu C, Lenze EJ, Dew MA, et al. Effect of comorbid anxiety on treatment response and relapse risk in late-life depression: controlled study. Br J Psychiatry 2007;190:344-9.
21. Steffens DC, McQuoid DR. Impact of symptoms of generalized anxiety disorder on the course of late-life depression. Am J Geriatr Psychiatry 2005;13:40-7.
22. Lenze E, Mulsant BH, Dew MA, et al. Good treatment outcomes in late-life depression with comorbid anxiety. J Affect Disord 2003;77:247-54.
23. Mohamed S, Osatuke K, Aslam M, Kasckow J. Escitalopram for comorbid depression and anxiety in elderly patients: a 12-week, open-label, flexible-dose, pilot trial. Am J Geriatr Pharmacother 2006;4:201-9.
24. Katz IR, Reynolds CF, Alexopoulos GS, Hackett D. Venlafaxine ER as a treatment for generalized anxiety disorder in older adults: pooled analysis of five randomized placebo-controlled clinical trials. J Am Geriatr Soc 2002;50:18-25.
25. Hanlon JT, Schmader KE, Boult C, et al. Benzodiazepine use and cognitive function among community-dwelling elderly. Clin Pharmacol Ther 1998;64:684-92.
26. Leipzig RM, Cummings RG, Tinetti ME. Drugs and falls in older people: a systematic review and meta-analysis: I. psychotropic drugs. J Am Geriatr Soc 1999;47:30-9.
27. Sheikh JI. Anxiety in older adults. Assessment and management of three common presentations. Geriatrics 2003;58:44-5.
28. Böhm C, Robinson DS, Gammans RE. Buspirone therapy for elderly patients with anxiety or depressive neurosis. J Clin Psychiatry 1990;51:309.-
29. Napoliello MJ. An interim multicentre report on 677 anxious geriatric out-patients treated with buspirone. Br J Clin Pract 1986;40:71-3.
30. Scogin F, McElreath L. Efficacy of psychosocial treatments for geriatric depression: a quantitative review. J Consult Clin Psychol 1994;62:69-74.
31. Stanley MA, Beck JG, Novy DM, et al. Cognitive-behavioral treatment of late-life generalized anxiety disorder. J Consult Clin Psychol 2003;71:309-19.
32. Stanley MA, Beck JG, Glassco JD. Treatment of generalized anxiety in older adults: a preliminary comparison of cognitive-behavioral and supportive approaches. Behav Ther 1996;27:565-81.
33. Wetherell JL, Gatz M, Craske MG. Treatment of generalized anxiety disorder in older adults. J Consult Clin Psychol 2003;71:31-40.
34. Swales PJ, Solfvin JF, Sheikh JI. Cognitive-behavioral therapy in older panic disorder patients. Am J Geriatr Psychiatry 1996;4:46-60.
35. Barrowclough C, King P, Colville J, et al. A randomized trial of the effectiveness of cognitive-behavioral therapy and supportive counseling for anxiety symptoms in older adults. J Consult Clin Psychol 2001;69:756-62.
36. Gorenstein EE, Kleber MS, Mohlman J, et al. Cognitive-behavioral therapy for management of anxiety and medication taper in older adults. Am J Geriatr Psychiatry 2005;13:901-9.
37. Doubleday EK, King P, Papageorgiou C. Relationship between fluid intelligence and ability to benefit from cognitive-behavioural therapy in older adults: a preliminary investigation. Br J Clin Psychol 2002;41:423-8.
38. Mohlman J, Gorman JM. The role of executive functioning in CBT: a pilot study with anxious older adults. Behav Res Ther 2005;43:447-65.
39. Mohlman J, Gorenstein EE, Kleber M, et al. Standard and enhanced cognitive-behavioral therapy for late-life generalized anxiety disorder: two pilot investigations. Am J Geriatr Psychiatry 2003;11:24-32.
40. Chen H, Coakley EH, Cheal K, et al. Satisfaction with mental health services in older primary care patients. Am J Geriatr Psychiatry 2006;14:371-9.
41. Hegel MT, Unützer J, Tang L, et al. Impact of comorbid panic and posttraumatic stress disorder in outcomes of collaborative care for late-life depression in primary care. Am J Geriatr Psychiatry 2005;13:48-58.
42. Stanley MA, Hopko DR, Diefenbach GJ, et al. Cognitive-behavior therapy for late-life generalized anxiety disorder in primary care. Am J Geriatr Psychiatry 2003;11:92-6.
Ms. W, a 73-year-old widow with no psychiatric history, visits her primary care physician because she is concerned about her memory. She denies impairment in other cognitive domains—such as executive function—or activities of daily living.
Ms. W relates prominent worries about her health and finances and those of her grandchildren. She describes daily restlessness, sleep-onset insomnia, difficulty concentrating, and mild episodic dysphoria. She says she’s always been a “worry wart” but her worry and other symptoms have become increasingly intrusive over the past 5 years with a series of deaths in her family. Ms. W’s medical history includes hypertension and type 2 diabetes. Unsure how to treat her, the physician refers Ms. W to a psychiatrist.
Older adults with anxiety symptoms often are dissatisfied with treatment because they believe they receive insufficient help. This complaint is probably valid because limited data support pharmacologic interventions for anxiety in older adults, and therapy is often based on inferences from studies in younger subjects. Moreover, many anxious older patients are treated with benzodiazepines, which increases their risk for cognitive impairment and injuries.1,2
Fortunately, growing evidence points to 2 treatment modalities for anxiety disorders in patients age ≥65:
- pharmacotherapy with antidepressants, benzodiazepines, and (perhaps) buspirone
- cognitive-behavioral therapy (CBT) for generalized anxiety disorder (GAD), panic disorder (PD), and mixed anxiety syndromes.
A common, debilitating problem
Anxious older adults report diminished perceived health, physical activities, and quality of life and increased loneliness compared with their nonanxious counterparts.1 The prevalence of anxiety disorders in older patients ranges from 0.4% for obsessive-compulsive disorder to 11.5% for GAD.3
Older adults with GAD present with a constellation of medical, psychiatric, psychological, and psychosocial features (Table 1).1,3-12 Anxiety disorders in older adults also may co-occur with major depressive disorder, other psychiatric conditions, or dementia, which can complicate diagnosis and treatment.
Table 1
Is it GAD? Common features in older adults
| Demographics |
| More prevalent at age |
| More common in women |
| Medical |
| Frequent visits to primary care |
| Low satisfaction with medical care |
| ≥2 chronic physical illnesses |
| ≥1 adaptive behavior limitations |
| Cognitive impairment, particularly verbal memory |
| Psychiatric |
| History of GAD symptoms (5 to ≥20 years) |
| Physiologic anxiety symptoms: restlessness, fatigue, muscle tension |
| Depressive symptoms |
| Prescribed a benzodiazepine |
| Presence of anxiety disorders |
| Suicidal ideation, particularly if depressed |
| Psychological |
| External locus of control |
| Neuroticism |
| Psychosocial |
| Limited social network |
| Perceived low instrumental support |
| Recent losses and traumatic life events |
| Loss of partner |
| GAD: generalized anxiety disorder |
| Source: References 1,3-12 |
CASE CONTINUED: Anxious, not depressed
You screen Ms. W with the Geriatric Depression Scale (short form; GDS) and Beck Anxiety Inventory (BAI). Her scores indicate no depression and moderate anxiousness. A neuropsychological screen finds no cognitive impairments. Based on the clinical interview and screening, Ms. W meets DSM-IV-TR criteria for GAD.
Psychopharmacologic interventions are first-line treatment for older adults with anxiety disorders, but you might consider other strategies because:
- Older patients may have increased vulnerability to medication side effects.
- Few randomized, placebo-controlled trials have examined psychopharmacologic interventions specifically for anxious older adults.
First-line pharmacotherapies
When selecting pharmacotherapy for an older adult with anxiety, take into account:
- physiologic changes in drug metabolism (older patients metabolize drugs more slowly than younger patients)
- comorbid medical problems
- polypharmacy (many older patients are taking multiple medications for multiple conditions, which increases the risk of drug-drug interactions).
Pharmacologic management of anxiety typically has included benzodiazepines, tricyclic antidepressants, barbiturates, and antihistamines. Newer antidepressants have emerged as first-line treatment for several anxiety disorders and mixed anxiety-depression syndromes, however, because of their more tolerable side-effect profiles, especially when used long-term.14 These antidepressants include:
- selective serotonin reuptake inhibitors (SSRIs)
- serotonin/norepinephrine reuptake inhibitors (SNRIs).
Citalopram—started at 10 mg/d and titrated to 30 mg/d as tolerated—was used in the only prospective, double-blind, randomized, controlled trial of an SSRI in older patients with anxiety disorders. In this 8-week trial, Clinical Global Impression scale scores and Hamilton Anxiety scale scores improved.15 In other investigations:
- Paroxetine, averaging approximately 28 mg/d, produced a similar response in older and younger adults with PD in terms of efficacy and tolerability in a naturalistic follow-up trial.16
- Sertraline, started at 25 mg/d and titrated to 100 mg/d (maximum 150 mg/d), when combined with CBT was effective for treating older adults with anxiety disorders in a randomized, placebo-controlled trial17 and specifically for those with PD in an open-label trial.18
- Fluvoxamine, median 200 mg/d, reduced anxiety symptoms in an open-label study of 12 older adults with various anxiety disorders. Most patients with GAD (57%) responded to fluvoxamine, but 3 patients with PD did not.19
- We found no studies of fluoxetine for anxiety symptoms in older adults.
SNRIs. In a retrospective, pooled analysis of 5 randomized, placebo-controlled trials24 venlafaxine ER, 37.5 to 225 mg/d, was significantly more effective than placebo in treating older adults with GAD. Several studies suggest duloxetine may be effective for treating GAD in adults, but none examined efficacy specifically for older adults.
Using benzodiazepines for more than a few weeks in older adults is not recommended, however.14 Potential complications of long-term benzodiazepine use in these patients include:
- excessive daytime drowsiness
- cognitive and psychomotor impairment
- confusion
- risk of falls
- depression
- paradoxical reactions
- amnesic syndromes
- respiratory problems
- potential for abuse/dependence
- breakthrough withdrawal reactions.2,25,26
Buspirone. Investigations of anxious older adults have suggested that buspirone is effective for addressing anxiety symptoms.28,29 Our experience, however, indicates that response to buspirone is inconsistent.
Recommendations. Based on this evidence and our clinical practice, we recommend using SSRIs or SNRIs as first-line treatment for most anxiety disorders in older adults (Table 3).
To minimize nonadherence associated with antidepressants’ delayed onset of action and initial transient “jitters”:
- provide patient education about medication onset and side effects
- add a short half-life benzodiazepine for the first few weeks of treatment only
- start with small doses and increase gradually.
Recommended dosages for treating anxiety in older adults
| Medication | Starting dosage | Maximum dosage |
|---|---|---|
| Selective serotonin reuptake inhibitors | ||
| Citalopram | 10 mg/d | 30 mg/d |
| Escitalopram | 5 mg/d | 10 mg/d |
| Fluvoxamine | 25 mg/d | 100 mg/d |
| Paroxetine | 10 mg/d | 20 mg/d |
| Sertraline | 12.5 mg/d | 50 mg/d |
| Serotonin/norepinephrine reuptake inhibitors | ||
| Duloxetine | 30 mg/d | 60 mg/d |
| Venlafaxine | 37.5 mg/d | 150 mg/d |
| Benzodiazepines | ||
| Lorazepam | 0.5 mg/d divided bid | 1 to 3 mg/d, divided bid or tid |
| Oxazepam | 30 mg/d divided tid | 45 to 60 mg/d divided tid or qid |
| Azapirone | ||
| Buspirone | 10 to 15 mg/d, divided bid or tid | 30 to 60 mg/d divided bid or tid |
Anxiety in older adults: Recommended interventions
| Disorder | First-line treatment(s) | Second-line treatment(s) |
|---|---|---|
| Generalized anxiety disorder | SSRIs, SNRIs, buspirone, and/or CBT | Other newer antidepressants* |
| Panic disorder, with or without agoraphobia | SSRIs, SNRIs, and/or CBT | Other newer antidepressants* |
| Mixed anxiety and depression | SSRIs or SNRIs | Buspirone, CBT |
| Anxiety and medical disorders | Identify and treat medical cause, use SSRIs or SNRIs for primary anxiety disorder | Benzodiazepines |
| * Novel agents such as mirtazapine | ||
| CBT: cognitive-behavioral therapy; SNRIs: serotonin/norepinephrine reuptake inhibitors; SSRIs: selective serotonin reuptake inhibitors | ||
Psychotherapy as an alternative or adjunct
Researchers have compared the efficacy of CBT—which is effective for depression in older adults30—with that of other psychotherapies for mixed and specific anxiety disorders, including GAD and PD.
For GAD. Multicomponent CBT for GAD typically includes:
- psychoeducation
- thought monitoring
- cognitive restructuring
- progressive muscle relaxation and similar techniques
- breathing retraining
- problem solving
- exposure (imaginal, in vivo, worry)
- time management
- problem solving.
Six months of group CBT or nondirective supportive psychotherapy have shown similar efficacy in reducing worry, anxiety, and depression scores in older adults with GAD.32 In a randomized trial,33 group CBT produced slightly greater improvements in anxiety, depression, and pathologic worry among 75 older adults with GAD, compared with a worry discussion group (DG). CBT’s only statistically significant advantage, however, was that patients spent less time worrying immediately after treatment, compared with DG patients. This difference disappeared at 6 months.
For PD. Evidence supports using CBT for older adults with PD. CBT for PD typically includes interventions used for GAD but also integrates interoceptive exposure and tailored psychoeducation regarding panic symptom onset and maintenance. Older adults with PD who received 10 sessions of CBT over 12 weeks improved significantly on all symptoms measured—cognitive, behavioral, physiologic, and depression—in a study by Swales et al.34 These improvements were seen immediately after treatment and at 3-month follow-up. In a separate study, a sample of 43 older adults—most of whom were diagnosed with PD—were randomly assigned to receive CBT or individual, in-home supportive therapy.35 The CBT group reported greater reductions in anxiety and depression.
For mixed anxiety disorders. Several investigations have assessed the efficacy of CBT for older adults with mixed anxiety diagnoses and symptoms.
In one randomized trial, 84 older adults with a principal anxiety disorder diagnosis—GAD, PD, agoraphobia, or social phobia—were assigned to CBT, sertraline (maximum dosage 150 mg/d), or a wait-list.17 Compared with patients assigned to the waitlist, those in the CBT and sertraline groups improved on measures of anxiety and worry immediately after treatment and at 3-month follow-up. Patients receiving sertraline worried slightly less than those who received CBT. The sertraline and CBT groups did not differ in percentage of subjects who responded to treatment or end-state functioning.
CASE CONTINUED: Combination pharmacotherapy CBT
You explain to Ms. W that depressed and anxious older adults frequently perceive memory difficulties. You further relate that it is possible that anxious older adults may experience memory changes because of medication side effects (particularly benzodiazepines) or interference of cognitive functioning by negative mood states. You prescribe sertraline, which is titrated to and maintained at 50 mg/d. Ms. W also participates in 10 psychotherapy sessions, which focus on psychoeducation about symptoms of GAD, relaxation strategies, sleep hygiene, grieving, and cognitive restructuring regarding her worries.
Modifying CBT for older adults. The quality of older adults’ cognitive functioning may affect their response to CBT,37 particularly if they exhibit impaired executive functioning.38 Modifying CBT to meet the needs of older adults has not been systematically investigated.
- weekly readings of psychoeducational materials that emphasized the relationship between cognitions, behaviors, physiological functioning, and emotions
- graphing symptom changes
- reminder/troubleshooting phone calls.
CASE CONTINUED: Follow-up evaluation
You refer Ms. W to her primary care physician for follow-up. After 12 weeks of treatment, she reports declining anxiety symptoms. A repeat BAI indicates mild anxiousness, which she describes as minimally affecting her day-to-day activities. She continues sertraline and participation in individual psychotherapy with a particular focus on recent losses in her life.
Delivering CBT in primary care. Integrating CBT into anxious older patients’ primary care may be desirable because:
- Older adults prefer to receive psychiatric care in this setting.40
- Collaborative-care models for depressed and anxious older adults have been successful.41
A small pilot study that provided CBT in a primary care setting for older adults who met DSM-IV-TR criteria for GAD found statistically and clinically significant declines in self-reported worry, depression, and GAD symptom severity compared with patients receiving care as usual.42
Related resources
- Anxiety Disorders Association of America. www.adaa.org.
- Lauderdale SA, Kelly K, Sheikh JI. Anxious older adults: prevalence, assessment, and treatment. In: Anthony ME, Maletta GJ, eds. Principles and practice of geriatric psychiatry. Philadelphia, PA: Lippincott Williams & Wilkins; 2006:429-48.
- Buspirone • BuSpar
- Citalopram • Celexa
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Lorazepam • Ativan
- Mirtazapine • Remeron
- Oxazepam • Serax
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Ms. W, a 73-year-old widow with no psychiatric history, visits her primary care physician because she is concerned about her memory. She denies impairment in other cognitive domains—such as executive function—or activities of daily living.
Ms. W relates prominent worries about her health and finances and those of her grandchildren. She describes daily restlessness, sleep-onset insomnia, difficulty concentrating, and mild episodic dysphoria. She says she’s always been a “worry wart” but her worry and other symptoms have become increasingly intrusive over the past 5 years with a series of deaths in her family. Ms. W’s medical history includes hypertension and type 2 diabetes. Unsure how to treat her, the physician refers Ms. W to a psychiatrist.
Older adults with anxiety symptoms often are dissatisfied with treatment because they believe they receive insufficient help. This complaint is probably valid because limited data support pharmacologic interventions for anxiety in older adults, and therapy is often based on inferences from studies in younger subjects. Moreover, many anxious older patients are treated with benzodiazepines, which increases their risk for cognitive impairment and injuries.1,2
Fortunately, growing evidence points to 2 treatment modalities for anxiety disorders in patients age ≥65:
- pharmacotherapy with antidepressants, benzodiazepines, and (perhaps) buspirone
- cognitive-behavioral therapy (CBT) for generalized anxiety disorder (GAD), panic disorder (PD), and mixed anxiety syndromes.
A common, debilitating problem
Anxious older adults report diminished perceived health, physical activities, and quality of life and increased loneliness compared with their nonanxious counterparts.1 The prevalence of anxiety disorders in older patients ranges from 0.4% for obsessive-compulsive disorder to 11.5% for GAD.3
Older adults with GAD present with a constellation of medical, psychiatric, psychological, and psychosocial features (Table 1).1,3-12 Anxiety disorders in older adults also may co-occur with major depressive disorder, other psychiatric conditions, or dementia, which can complicate diagnosis and treatment.
Table 1
Is it GAD? Common features in older adults
| Demographics |
| More prevalent at age |
| More common in women |
| Medical |
| Frequent visits to primary care |
| Low satisfaction with medical care |
| ≥2 chronic physical illnesses |
| ≥1 adaptive behavior limitations |
| Cognitive impairment, particularly verbal memory |
| Psychiatric |
| History of GAD symptoms (5 to ≥20 years) |
| Physiologic anxiety symptoms: restlessness, fatigue, muscle tension |
| Depressive symptoms |
| Prescribed a benzodiazepine |
| Presence of anxiety disorders |
| Suicidal ideation, particularly if depressed |
| Psychological |
| External locus of control |
| Neuroticism |
| Psychosocial |
| Limited social network |
| Perceived low instrumental support |
| Recent losses and traumatic life events |
| Loss of partner |
| GAD: generalized anxiety disorder |
| Source: References 1,3-12 |
CASE CONTINUED: Anxious, not depressed
You screen Ms. W with the Geriatric Depression Scale (short form; GDS) and Beck Anxiety Inventory (BAI). Her scores indicate no depression and moderate anxiousness. A neuropsychological screen finds no cognitive impairments. Based on the clinical interview and screening, Ms. W meets DSM-IV-TR criteria for GAD.
Psychopharmacologic interventions are first-line treatment for older adults with anxiety disorders, but you might consider other strategies because:
- Older patients may have increased vulnerability to medication side effects.
- Few randomized, placebo-controlled trials have examined psychopharmacologic interventions specifically for anxious older adults.
First-line pharmacotherapies
When selecting pharmacotherapy for an older adult with anxiety, take into account:
- physiologic changes in drug metabolism (older patients metabolize drugs more slowly than younger patients)
- comorbid medical problems
- polypharmacy (many older patients are taking multiple medications for multiple conditions, which increases the risk of drug-drug interactions).
Pharmacologic management of anxiety typically has included benzodiazepines, tricyclic antidepressants, barbiturates, and antihistamines. Newer antidepressants have emerged as first-line treatment for several anxiety disorders and mixed anxiety-depression syndromes, however, because of their more tolerable side-effect profiles, especially when used long-term.14 These antidepressants include:
- selective serotonin reuptake inhibitors (SSRIs)
- serotonin/norepinephrine reuptake inhibitors (SNRIs).
Citalopram—started at 10 mg/d and titrated to 30 mg/d as tolerated—was used in the only prospective, double-blind, randomized, controlled trial of an SSRI in older patients with anxiety disorders. In this 8-week trial, Clinical Global Impression scale scores and Hamilton Anxiety scale scores improved.15 In other investigations:
- Paroxetine, averaging approximately 28 mg/d, produced a similar response in older and younger adults with PD in terms of efficacy and tolerability in a naturalistic follow-up trial.16
- Sertraline, started at 25 mg/d and titrated to 100 mg/d (maximum 150 mg/d), when combined with CBT was effective for treating older adults with anxiety disorders in a randomized, placebo-controlled trial17 and specifically for those with PD in an open-label trial.18
- Fluvoxamine, median 200 mg/d, reduced anxiety symptoms in an open-label study of 12 older adults with various anxiety disorders. Most patients with GAD (57%) responded to fluvoxamine, but 3 patients with PD did not.19
- We found no studies of fluoxetine for anxiety symptoms in older adults.
SNRIs. In a retrospective, pooled analysis of 5 randomized, placebo-controlled trials24 venlafaxine ER, 37.5 to 225 mg/d, was significantly more effective than placebo in treating older adults with GAD. Several studies suggest duloxetine may be effective for treating GAD in adults, but none examined efficacy specifically for older adults.
Using benzodiazepines for more than a few weeks in older adults is not recommended, however.14 Potential complications of long-term benzodiazepine use in these patients include:
- excessive daytime drowsiness
- cognitive and psychomotor impairment
- confusion
- risk of falls
- depression
- paradoxical reactions
- amnesic syndromes
- respiratory problems
- potential for abuse/dependence
- breakthrough withdrawal reactions.2,25,26
Buspirone. Investigations of anxious older adults have suggested that buspirone is effective for addressing anxiety symptoms.28,29 Our experience, however, indicates that response to buspirone is inconsistent.
Recommendations. Based on this evidence and our clinical practice, we recommend using SSRIs or SNRIs as first-line treatment for most anxiety disorders in older adults (Table 3).
To minimize nonadherence associated with antidepressants’ delayed onset of action and initial transient “jitters”:
- provide patient education about medication onset and side effects
- add a short half-life benzodiazepine for the first few weeks of treatment only
- start with small doses and increase gradually.
Recommended dosages for treating anxiety in older adults
| Medication | Starting dosage | Maximum dosage |
|---|---|---|
| Selective serotonin reuptake inhibitors | ||
| Citalopram | 10 mg/d | 30 mg/d |
| Escitalopram | 5 mg/d | 10 mg/d |
| Fluvoxamine | 25 mg/d | 100 mg/d |
| Paroxetine | 10 mg/d | 20 mg/d |
| Sertraline | 12.5 mg/d | 50 mg/d |
| Serotonin/norepinephrine reuptake inhibitors | ||
| Duloxetine | 30 mg/d | 60 mg/d |
| Venlafaxine | 37.5 mg/d | 150 mg/d |
| Benzodiazepines | ||
| Lorazepam | 0.5 mg/d divided bid | 1 to 3 mg/d, divided bid or tid |
| Oxazepam | 30 mg/d divided tid | 45 to 60 mg/d divided tid or qid |
| Azapirone | ||
| Buspirone | 10 to 15 mg/d, divided bid or tid | 30 to 60 mg/d divided bid or tid |
Anxiety in older adults: Recommended interventions
| Disorder | First-line treatment(s) | Second-line treatment(s) |
|---|---|---|
| Generalized anxiety disorder | SSRIs, SNRIs, buspirone, and/or CBT | Other newer antidepressants* |
| Panic disorder, with or without agoraphobia | SSRIs, SNRIs, and/or CBT | Other newer antidepressants* |
| Mixed anxiety and depression | SSRIs or SNRIs | Buspirone, CBT |
| Anxiety and medical disorders | Identify and treat medical cause, use SSRIs or SNRIs for primary anxiety disorder | Benzodiazepines |
| * Novel agents such as mirtazapine | ||
| CBT: cognitive-behavioral therapy; SNRIs: serotonin/norepinephrine reuptake inhibitors; SSRIs: selective serotonin reuptake inhibitors | ||
Psychotherapy as an alternative or adjunct
Researchers have compared the efficacy of CBT—which is effective for depression in older adults30—with that of other psychotherapies for mixed and specific anxiety disorders, including GAD and PD.
For GAD. Multicomponent CBT for GAD typically includes:
- psychoeducation
- thought monitoring
- cognitive restructuring
- progressive muscle relaxation and similar techniques
- breathing retraining
- problem solving
- exposure (imaginal, in vivo, worry)
- time management
- problem solving.
Six months of group CBT or nondirective supportive psychotherapy have shown similar efficacy in reducing worry, anxiety, and depression scores in older adults with GAD.32 In a randomized trial,33 group CBT produced slightly greater improvements in anxiety, depression, and pathologic worry among 75 older adults with GAD, compared with a worry discussion group (DG). CBT’s only statistically significant advantage, however, was that patients spent less time worrying immediately after treatment, compared with DG patients. This difference disappeared at 6 months.
For PD. Evidence supports using CBT for older adults with PD. CBT for PD typically includes interventions used for GAD but also integrates interoceptive exposure and tailored psychoeducation regarding panic symptom onset and maintenance. Older adults with PD who received 10 sessions of CBT over 12 weeks improved significantly on all symptoms measured—cognitive, behavioral, physiologic, and depression—in a study by Swales et al.34 These improvements were seen immediately after treatment and at 3-month follow-up. In a separate study, a sample of 43 older adults—most of whom were diagnosed with PD—were randomly assigned to receive CBT or individual, in-home supportive therapy.35 The CBT group reported greater reductions in anxiety and depression.
For mixed anxiety disorders. Several investigations have assessed the efficacy of CBT for older adults with mixed anxiety diagnoses and symptoms.
In one randomized trial, 84 older adults with a principal anxiety disorder diagnosis—GAD, PD, agoraphobia, or social phobia—were assigned to CBT, sertraline (maximum dosage 150 mg/d), or a wait-list.17 Compared with patients assigned to the waitlist, those in the CBT and sertraline groups improved on measures of anxiety and worry immediately after treatment and at 3-month follow-up. Patients receiving sertraline worried slightly less than those who received CBT. The sertraline and CBT groups did not differ in percentage of subjects who responded to treatment or end-state functioning.
CASE CONTINUED: Combination pharmacotherapy CBT
You explain to Ms. W that depressed and anxious older adults frequently perceive memory difficulties. You further relate that it is possible that anxious older adults may experience memory changes because of medication side effects (particularly benzodiazepines) or interference of cognitive functioning by negative mood states. You prescribe sertraline, which is titrated to and maintained at 50 mg/d. Ms. W also participates in 10 psychotherapy sessions, which focus on psychoeducation about symptoms of GAD, relaxation strategies, sleep hygiene, grieving, and cognitive restructuring regarding her worries.
Modifying CBT for older adults. The quality of older adults’ cognitive functioning may affect their response to CBT,37 particularly if they exhibit impaired executive functioning.38 Modifying CBT to meet the needs of older adults has not been systematically investigated.
- weekly readings of psychoeducational materials that emphasized the relationship between cognitions, behaviors, physiological functioning, and emotions
- graphing symptom changes
- reminder/troubleshooting phone calls.
CASE CONTINUED: Follow-up evaluation
You refer Ms. W to her primary care physician for follow-up. After 12 weeks of treatment, she reports declining anxiety symptoms. A repeat BAI indicates mild anxiousness, which she describes as minimally affecting her day-to-day activities. She continues sertraline and participation in individual psychotherapy with a particular focus on recent losses in her life.
Delivering CBT in primary care. Integrating CBT into anxious older patients’ primary care may be desirable because:
- Older adults prefer to receive psychiatric care in this setting.40
- Collaborative-care models for depressed and anxious older adults have been successful.41
A small pilot study that provided CBT in a primary care setting for older adults who met DSM-IV-TR criteria for GAD found statistically and clinically significant declines in self-reported worry, depression, and GAD symptom severity compared with patients receiving care as usual.42
Related resources
- Anxiety Disorders Association of America. www.adaa.org.
- Lauderdale SA, Kelly K, Sheikh JI. Anxious older adults: prevalence, assessment, and treatment. In: Anthony ME, Maletta GJ, eds. Principles and practice of geriatric psychiatry. Philadelphia, PA: Lippincott Williams & Wilkins; 2006:429-48.
- Buspirone • BuSpar
- Citalopram • Celexa
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Lorazepam • Ativan
- Mirtazapine • Remeron
- Oxazepam • Serax
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. de Beurs E, Beekman AT, van Balkom AJ, et al. Consequences of anxiety in older persons: its effect on disability, well-being, and use of health services. Psychol Med 1999;29:583-93.
2. Wadsworth EJK, Moss SC, Simpson SA, Smith AP. Psychotropic medication use and accidents, injuries, and cognitive failures. Hum Psychopharmacol 2005;20:391-400.
3. Beekman AT, Bremmer MA, Deeg DJ, et al. Anxiety disorders in later life: a report from the Longitudinal Aging Study Amsterdam. Int J Geriatr Psychiatry 1998;13:717-26.
4. Lindesay J, Briggs K, Murphy E. The Guy’s/Age Concern survey: prevalence rates of cognitive impairment, depression, and anxiety in an urban elderly community. Br J Psychiatry 1989;155:317-29.
5. Manela M, Katona C, Livingston G. How common are the anxiety disorders in old age? Int J Geriatr Psychiatry 1996;11:65-70.
6. Beekman AT, de Beurs E, van Balkom AJ, et al. Anxiety and depression in later life: co-occurrence and communality of risk factors. Am J Psychiatry 2000;157:89-95.
7. DeLuca AK, Lenze EJ, Mulsant BH, et al. Comorbid anxiety disorder in late life depression: association with memory decline over four years. Int J Geriatr Psychiatry 2005;29:848-54.
8. Blazer D, George LK, Hughes D. The epidemiology of anxiety disorders: an age comparison. In: Salzman C, Lebowitz BD, eds. Anxiety in the elderly: treatment and research. New York, NY: Springer; 1991:17-30.
9. Wetherell JL, Le Roux H, Gatz M. DSM-IV criteria for generalized anxiety disorder in older adults: distinguishing the worried from the well. Psychol Aging 2003;18:622-7.
10. van Balkom AJ, Beekman AT, de Beurs E, et al. Comorbidity of the anxiety disorders in a community-based older population in the Netherlands. Acta Psychiatr Scand 2000;101:37-45.
11. Jeste ND, Hays JC, Steffens DC. Clinical correlates of anxious depression among elderly patients with depression. J Affect Disord 2006;90:37-41.
12. Schuurmans J, Comijs HC, Beekman AT, et al. The outcome of anxiety disorders in older people at 6-year follow-up: results from the Longitudinal Aging Study Amsterdam. Acta Psychiatr Scand 2005;111:420-8.
13. Nordhus IH, Pallesen S. Psychological treatment of late-life anxiety: an empirical review. J Consult Clin Psychol 2003;71:643-51.
14. Lenze E, Pollock BG, Shear MK, et al. Treatment considerations for anxiety in the elderly. CNS Spectr 2003;8 (suppl 3):6-13.
15. Lenze E, Mulsant BH, Shear MK, et al. Efficacy and tolerability of citalopram in the treatment of late-life anxiety disorders: results from an 8-week randomized, placebo-controlled trial. Am J Psychiatry 2005;162(1):146-50.
16. Dannon PN, Iancu I, Lowengrub K, et al. Pharmacotherapy of panic disorder in the elderly: a naturalistic 12-month follow-up outcome study. Therapy 2005;2:249-54.
17. Schuurmans J, Comijs H, Emmelkamp PM, et al. A randomized, controlled trial of the effectiveness of cognitive-behavioral therapy and sertraline versus a waitlist control group for anxiety disorders in older adults. Am J Geriatr Psychiatry 2006;14:255-63.
18. Sheikh JI, Lauderdale SA, Cassidy EL. Efficacy of sertraline for panic disorder in older adults: a preliminary open-label trial. Am J Geriatr Psychiatry 2004;12:230.-
19. Wylie ME, Miller MD, Shear MK, et al. Fluvoxamine pharmacotherapy of anxiety disorders in later life: preliminary open-trial data. J Geriatr Psychiatry Neurol 2000;13:43-8.
20. Andreescu C, Lenze EJ, Dew MA, et al. Effect of comorbid anxiety on treatment response and relapse risk in late-life depression: controlled study. Br J Psychiatry 2007;190:344-9.
21. Steffens DC, McQuoid DR. Impact of symptoms of generalized anxiety disorder on the course of late-life depression. Am J Geriatr Psychiatry 2005;13:40-7.
22. Lenze E, Mulsant BH, Dew MA, et al. Good treatment outcomes in late-life depression with comorbid anxiety. J Affect Disord 2003;77:247-54.
23. Mohamed S, Osatuke K, Aslam M, Kasckow J. Escitalopram for comorbid depression and anxiety in elderly patients: a 12-week, open-label, flexible-dose, pilot trial. Am J Geriatr Pharmacother 2006;4:201-9.
24. Katz IR, Reynolds CF, Alexopoulos GS, Hackett D. Venlafaxine ER as a treatment for generalized anxiety disorder in older adults: pooled analysis of five randomized placebo-controlled clinical trials. J Am Geriatr Soc 2002;50:18-25.
25. Hanlon JT, Schmader KE, Boult C, et al. Benzodiazepine use and cognitive function among community-dwelling elderly. Clin Pharmacol Ther 1998;64:684-92.
26. Leipzig RM, Cummings RG, Tinetti ME. Drugs and falls in older people: a systematic review and meta-analysis: I. psychotropic drugs. J Am Geriatr Soc 1999;47:30-9.
27. Sheikh JI. Anxiety in older adults. Assessment and management of three common presentations. Geriatrics 2003;58:44-5.
28. Böhm C, Robinson DS, Gammans RE. Buspirone therapy for elderly patients with anxiety or depressive neurosis. J Clin Psychiatry 1990;51:309.-
29. Napoliello MJ. An interim multicentre report on 677 anxious geriatric out-patients treated with buspirone. Br J Clin Pract 1986;40:71-3.
30. Scogin F, McElreath L. Efficacy of psychosocial treatments for geriatric depression: a quantitative review. J Consult Clin Psychol 1994;62:69-74.
31. Stanley MA, Beck JG, Novy DM, et al. Cognitive-behavioral treatment of late-life generalized anxiety disorder. J Consult Clin Psychol 2003;71:309-19.
32. Stanley MA, Beck JG, Glassco JD. Treatment of generalized anxiety in older adults: a preliminary comparison of cognitive-behavioral and supportive approaches. Behav Ther 1996;27:565-81.
33. Wetherell JL, Gatz M, Craske MG. Treatment of generalized anxiety disorder in older adults. J Consult Clin Psychol 2003;71:31-40.
34. Swales PJ, Solfvin JF, Sheikh JI. Cognitive-behavioral therapy in older panic disorder patients. Am J Geriatr Psychiatry 1996;4:46-60.
35. Barrowclough C, King P, Colville J, et al. A randomized trial of the effectiveness of cognitive-behavioral therapy and supportive counseling for anxiety symptoms in older adults. J Consult Clin Psychol 2001;69:756-62.
36. Gorenstein EE, Kleber MS, Mohlman J, et al. Cognitive-behavioral therapy for management of anxiety and medication taper in older adults. Am J Geriatr Psychiatry 2005;13:901-9.
37. Doubleday EK, King P, Papageorgiou C. Relationship between fluid intelligence and ability to benefit from cognitive-behavioural therapy in older adults: a preliminary investigation. Br J Clin Psychol 2002;41:423-8.
38. Mohlman J, Gorman JM. The role of executive functioning in CBT: a pilot study with anxious older adults. Behav Res Ther 2005;43:447-65.
39. Mohlman J, Gorenstein EE, Kleber M, et al. Standard and enhanced cognitive-behavioral therapy for late-life generalized anxiety disorder: two pilot investigations. Am J Geriatr Psychiatry 2003;11:24-32.
40. Chen H, Coakley EH, Cheal K, et al. Satisfaction with mental health services in older primary care patients. Am J Geriatr Psychiatry 2006;14:371-9.
41. Hegel MT, Unützer J, Tang L, et al. Impact of comorbid panic and posttraumatic stress disorder in outcomes of collaborative care for late-life depression in primary care. Am J Geriatr Psychiatry 2005;13:48-58.
42. Stanley MA, Hopko DR, Diefenbach GJ, et al. Cognitive-behavior therapy for late-life generalized anxiety disorder in primary care. Am J Geriatr Psychiatry 2003;11:92-6.
1. de Beurs E, Beekman AT, van Balkom AJ, et al. Consequences of anxiety in older persons: its effect on disability, well-being, and use of health services. Psychol Med 1999;29:583-93.
2. Wadsworth EJK, Moss SC, Simpson SA, Smith AP. Psychotropic medication use and accidents, injuries, and cognitive failures. Hum Psychopharmacol 2005;20:391-400.
3. Beekman AT, Bremmer MA, Deeg DJ, et al. Anxiety disorders in later life: a report from the Longitudinal Aging Study Amsterdam. Int J Geriatr Psychiatry 1998;13:717-26.
4. Lindesay J, Briggs K, Murphy E. The Guy’s/Age Concern survey: prevalence rates of cognitive impairment, depression, and anxiety in an urban elderly community. Br J Psychiatry 1989;155:317-29.
5. Manela M, Katona C, Livingston G. How common are the anxiety disorders in old age? Int J Geriatr Psychiatry 1996;11:65-70.
6. Beekman AT, de Beurs E, van Balkom AJ, et al. Anxiety and depression in later life: co-occurrence and communality of risk factors. Am J Psychiatry 2000;157:89-95.
7. DeLuca AK, Lenze EJ, Mulsant BH, et al. Comorbid anxiety disorder in late life depression: association with memory decline over four years. Int J Geriatr Psychiatry 2005;29:848-54.
8. Blazer D, George LK, Hughes D. The epidemiology of anxiety disorders: an age comparison. In: Salzman C, Lebowitz BD, eds. Anxiety in the elderly: treatment and research. New York, NY: Springer; 1991:17-30.
9. Wetherell JL, Le Roux H, Gatz M. DSM-IV criteria for generalized anxiety disorder in older adults: distinguishing the worried from the well. Psychol Aging 2003;18:622-7.
10. van Balkom AJ, Beekman AT, de Beurs E, et al. Comorbidity of the anxiety disorders in a community-based older population in the Netherlands. Acta Psychiatr Scand 2000;101:37-45.
11. Jeste ND, Hays JC, Steffens DC. Clinical correlates of anxious depression among elderly patients with depression. J Affect Disord 2006;90:37-41.
12. Schuurmans J, Comijs HC, Beekman AT, et al. The outcome of anxiety disorders in older people at 6-year follow-up: results from the Longitudinal Aging Study Amsterdam. Acta Psychiatr Scand 2005;111:420-8.
13. Nordhus IH, Pallesen S. Psychological treatment of late-life anxiety: an empirical review. J Consult Clin Psychol 2003;71:643-51.
14. Lenze E, Pollock BG, Shear MK, et al. Treatment considerations for anxiety in the elderly. CNS Spectr 2003;8 (suppl 3):6-13.
15. Lenze E, Mulsant BH, Shear MK, et al. Efficacy and tolerability of citalopram in the treatment of late-life anxiety disorders: results from an 8-week randomized, placebo-controlled trial. Am J Psychiatry 2005;162(1):146-50.
16. Dannon PN, Iancu I, Lowengrub K, et al. Pharmacotherapy of panic disorder in the elderly: a naturalistic 12-month follow-up outcome study. Therapy 2005;2:249-54.
17. Schuurmans J, Comijs H, Emmelkamp PM, et al. A randomized, controlled trial of the effectiveness of cognitive-behavioral therapy and sertraline versus a waitlist control group for anxiety disorders in older adults. Am J Geriatr Psychiatry 2006;14:255-63.
18. Sheikh JI, Lauderdale SA, Cassidy EL. Efficacy of sertraline for panic disorder in older adults: a preliminary open-label trial. Am J Geriatr Psychiatry 2004;12:230.-
19. Wylie ME, Miller MD, Shear MK, et al. Fluvoxamine pharmacotherapy of anxiety disorders in later life: preliminary open-trial data. J Geriatr Psychiatry Neurol 2000;13:43-8.
20. Andreescu C, Lenze EJ, Dew MA, et al. Effect of comorbid anxiety on treatment response and relapse risk in late-life depression: controlled study. Br J Psychiatry 2007;190:344-9.
21. Steffens DC, McQuoid DR. Impact of symptoms of generalized anxiety disorder on the course of late-life depression. Am J Geriatr Psychiatry 2005;13:40-7.
22. Lenze E, Mulsant BH, Dew MA, et al. Good treatment outcomes in late-life depression with comorbid anxiety. J Affect Disord 2003;77:247-54.
23. Mohamed S, Osatuke K, Aslam M, Kasckow J. Escitalopram for comorbid depression and anxiety in elderly patients: a 12-week, open-label, flexible-dose, pilot trial. Am J Geriatr Pharmacother 2006;4:201-9.
24. Katz IR, Reynolds CF, Alexopoulos GS, Hackett D. Venlafaxine ER as a treatment for generalized anxiety disorder in older adults: pooled analysis of five randomized placebo-controlled clinical trials. J Am Geriatr Soc 2002;50:18-25.
25. Hanlon JT, Schmader KE, Boult C, et al. Benzodiazepine use and cognitive function among community-dwelling elderly. Clin Pharmacol Ther 1998;64:684-92.
26. Leipzig RM, Cummings RG, Tinetti ME. Drugs and falls in older people: a systematic review and meta-analysis: I. psychotropic drugs. J Am Geriatr Soc 1999;47:30-9.
27. Sheikh JI. Anxiety in older adults. Assessment and management of three common presentations. Geriatrics 2003;58:44-5.
28. Böhm C, Robinson DS, Gammans RE. Buspirone therapy for elderly patients with anxiety or depressive neurosis. J Clin Psychiatry 1990;51:309.-
29. Napoliello MJ. An interim multicentre report on 677 anxious geriatric out-patients treated with buspirone. Br J Clin Pract 1986;40:71-3.
30. Scogin F, McElreath L. Efficacy of psychosocial treatments for geriatric depression: a quantitative review. J Consult Clin Psychol 1994;62:69-74.
31. Stanley MA, Beck JG, Novy DM, et al. Cognitive-behavioral treatment of late-life generalized anxiety disorder. J Consult Clin Psychol 2003;71:309-19.
32. Stanley MA, Beck JG, Glassco JD. Treatment of generalized anxiety in older adults: a preliminary comparison of cognitive-behavioral and supportive approaches. Behav Ther 1996;27:565-81.
33. Wetherell JL, Gatz M, Craske MG. Treatment of generalized anxiety disorder in older adults. J Consult Clin Psychol 2003;71:31-40.
34. Swales PJ, Solfvin JF, Sheikh JI. Cognitive-behavioral therapy in older panic disorder patients. Am J Geriatr Psychiatry 1996;4:46-60.
35. Barrowclough C, King P, Colville J, et al. A randomized trial of the effectiveness of cognitive-behavioral therapy and supportive counseling for anxiety symptoms in older adults. J Consult Clin Psychol 2001;69:756-62.
36. Gorenstein EE, Kleber MS, Mohlman J, et al. Cognitive-behavioral therapy for management of anxiety and medication taper in older adults. Am J Geriatr Psychiatry 2005;13:901-9.
37. Doubleday EK, King P, Papageorgiou C. Relationship between fluid intelligence and ability to benefit from cognitive-behavioural therapy in older adults: a preliminary investigation. Br J Clin Psychol 2002;41:423-8.
38. Mohlman J, Gorman JM. The role of executive functioning in CBT: a pilot study with anxious older adults. Behav Res Ther 2005;43:447-65.
39. Mohlman J, Gorenstein EE, Kleber M, et al. Standard and enhanced cognitive-behavioral therapy for late-life generalized anxiety disorder: two pilot investigations. Am J Geriatr Psychiatry 2003;11:24-32.
40. Chen H, Coakley EH, Cheal K, et al. Satisfaction with mental health services in older primary care patients. Am J Geriatr Psychiatry 2006;14:371-9.
41. Hegel MT, Unützer J, Tang L, et al. Impact of comorbid panic and posttraumatic stress disorder in outcomes of collaborative care for late-life depression in primary care. Am J Geriatr Psychiatry 2005;13:48-58.
42. Stanley MA, Hopko DR, Diefenbach GJ, et al. Cognitive-behavior therapy for late-life generalized anxiety disorder in primary care. Am J Geriatr Psychiatry 2003;11:92-6.
Can genetics predict risk for alcohol dependence?
Children of alcoholics have a 40% to 60% increased risk of developing severe alcohol-related problems1—a harsh legacy recognized for >30 years. Now, as the result of rapidly growing evidence, we can explain in greater detail why alcoholism runs in families when discussing alcohol dependence with patients.
Individuals vary in response to medications and substances of abuse, and genetic research is revealing the heritable origins. Numerous genetic variations are known to influence response to alcohol, as well as alcoholism’s pathophysiology, clinical manifestations, and treatment. Pieces are still missing from this complex picture, but investigators are identifying possible risk factors for alcoholism and matching potential responders with treatments such as naltrexone and acamprosate.
This article provides a progress report on contemporary genetic research of alcoholism. Our goal is to inform your clinical practice by describing:
- new understandings of the genetics of alcoholism
- how researchers identify relationships between genetic variations and clinical/behavioral phenomena
- practical implications of this knowledge.
Genetic variations and risk of addiction
No single gene appears to cause alcoholism. Many genetic variations that accumulated during evolution likely contribute to individual differences in response to alcohol and susceptibility to developing alcohol-related problems. A growing number of genetic variations have been associated with increased alcohol tolerance, consumption, and other related phenotypes.
Like other addictive substances, alcohol triggers pharmacodynamic effects by interacting with a variety of molecular targets (Figure 1).2 These target proteins in turn interact with specific signaling proteins and trigger responses in complex functional pathways. Genetic variations may affect the structure of genes coding for proteins that constitute pathways involved in alcohol’s effects on target proteins (pharmacodynamics) or its metabolism (pharmacokinetics). If such variations alter the production, function, or stability of these proteins, the pathway’s function also may be altered and produce behavioral phenotypes—such as high or low sensitivity to alcohol’s effects.
Alcoholism-related phenotypes. DSM-IV-TR diagnostic criteria include some but not all of the multiple phenotypes within alcoholism’s clinical presentation. Researchers in the Collaborative Studies on Genetics of Alcoholism (COGA)3 identified chromosome regions linked to alcoholism-related phenotypes, including:
- alcohol dependence4
- later age of drinking onset and increased harm avoidance5
- alcoholism and depression6
- alcohol sensitivity7
- alcohol consumption.8
To identify genes of interest within these chromosome regions, researchers used transitional phenotypes (endophenotypes) that “lie on the pathway between genes and disease,”9,10 and allowed them to characterize the neural systems affected by gene risk variants.11 As a result, they found associations among variations in the GABRA2 gene, (encoding the alpha-2 subunit of the GABAA receptor), specific brain oscillations (electrophysiologic endophenotype), and predisposition to alcohol dependence.12,13 By this same strategy, researchers discovered an association between the endophenotype (low-level of response to alcohol) and some genotypes, including at least 1 short allele of the serotonin transporter gene SLC6A4.14
Figure 1
Known molecular targets for alcohol and other drugs of abuse
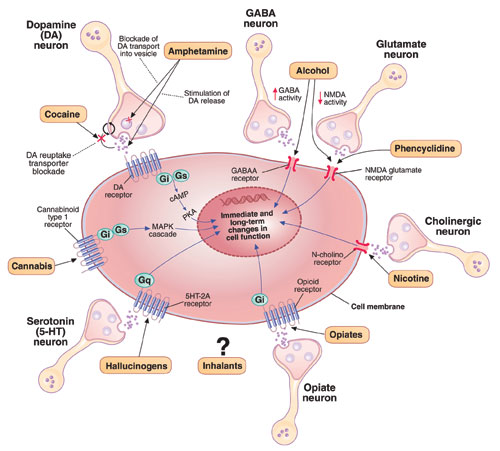
Effects of drugs of abuse (black arrows) influence intracellular signaling pathways (blue arrows) to produce immediate and long-term changes in cell function.
cAMP: cyclic adenosine monophosphate; GABAA: gamma-aminobutyric acid A receptor; Gi, Gs, Gq: G proteins (heterotrimeric guanine nucleotide-binding proteins) MAPK: mitogen-activated protein kinase; N-cholino receptor: nicotinic cholinoreceptor; NMDA: N-methyl-D-aspartate; PKA: protein kinase A
Source: Created for CURRENT PSYCHIATRY from information in reference 2
Alcohol metabolism
Alcohol is metabolized to acetic acid through primary and auxiliary pathways involving alcohol and acetaldehyde dehydrogenases (ADH/ALDH) and the microsomal ethanol oxidizing system (cytochrome P-450 [CYP] 2E1)15 (Figure 2). Auxiliary pathways become involved when the primary pathway is overwhelmed by the amount of alcohol needed to be metabolized. Catalase and fatty acid ethyl ester synthases play a minor role under normal conditions but may be implicated in alcohol-induced organ damage.16
ADH/ALDH pathway. From one individual to another, the ability to metabolize ethyl alcohol varies up to 3- to 4-fold.17 In European and Amerindian samples, a genetic link has been identified between alcoholism and the 4q21-23 region on chromosome 4.18 This region contains a cluster of 7 genes encoding for alcohol dehydrogenases (ADH), including 3 Class I genes—ADH1A, ADH1B, and ADH1C—coding for the corresponding proteins that play a major role in alcohol metabolism.19 In eastern Asian samples, alleles encoding high activity enzymes (ADH1B*47His and ADH1C*349Ile) are significantly less frequent in alcoholics compared with nonalcoholic controls.20
Mitochondrial ALDH2 protein plays the central role in acetaldehyde metabolism and is highly expressed in the liver, stomach, and other tissues—including the brain.21 The ALDH2*2 gene variant encodes for a catalytically inactive enzyme, thus inhibiting acetaldehyde metabolism and causing a facial flushing reaction.22 The ALDH2*2 allele has a relatively high frequency in Asians but also is found in other populations.23 Meta-analyses of published data indicate that possessing either of the variant alleles in the ADH1B and ALDH2 genes is protective against alcohol dependence in Asians.24
The ADH4 enzyme catalyzes oxidation or reduction of numerous substrates—including long-chain aliphatic alcohols and aromatic aldehydes—and becomes involved in alcohol metabolism at moderate to high concentrations. The -75A allele of the ADH4 gene has promoter activity more than twice that of the -75C allele and significantly affects its expression.25 This substitution in the promoter region, as well as A/G SNP (rs1042364)—a single nucleotide polymorphism (SNP)—at exon 9, has been associated with an increased risk for alcohol and drug dependence in European Americans.26
Finally, variations in the ADH7 gene may play a protective role against alcoholism through epistatic effects.27
The CYP 2E1 pathway has low initial catalytic efficiency compared with the ADH/ALDH pathway, but it may metabolize alcohol up to 10 times faster after chronic alcohol consumption or cigarette smoking and accounts for metabolic tolerance.28 CYP 2E1 is involved in metabolizing both alcohol and acetaldehyde.29 The CYP 2E1*1D polymorphism has been associated with greater inducibility as well as alcohol and nicotine dependence.30
Thus, linkage and association studies support the association of phenotypes related to alcohol response and dependence with variations in genes that code for proteins involved in alcohol’s pharmacodynamic and pharmacokinetic effects. Each of these findings is important, but conceptual models organizing them all and explaining their role in alcohol’s effects and predisposition to alcoholism have yet to be constructed.
Figure 2
Genetic variations that affect alcohol metabolism pathways
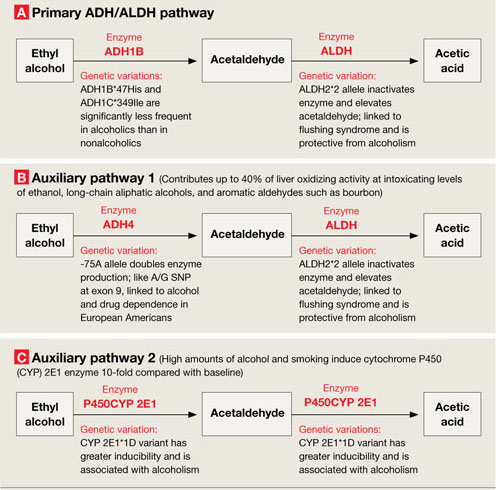
Genetic variations affect the efficiency of primary and auxiliary pathways by which ethyl alcohol is metabolized to acetaldehyde and acetic acid. Auxiliary pathways become involved when the primary pathway is overwhelmed by the amount of alcohol to be metabolized.
ADH: alcohol dehydrogenase; ALDH: acetaldehyde dehydrogenase; P450CYP 2E1: cytochrome P450, family 2, subfamily E, polypeptide 1; A/G SNP: adenine/guanine single nucleotide polymorphism
Phenotype-genotype relationships
Alcohol—unlike most other addictive substances—does not have a specific receptor and is believed to act by disturbing the balance between excitatory and inhibitory neurotransmission in the neural system. Consequently, researchers explore relationships between genetics and alcohol-related problems using 2 approaches:
- Forward genetics (discovering disease-related genes via genome-wide studies and then studying their function; examples include linkage and genome-wide association studies [GWAS]).
- Reverse genetics (testing whether candidate genes and polymorphisms identified in animal studies as relevant for biological effects also exist in humans and are relevant to the phenotype).31
When searching for relationships between genotypes and phenotypes, both approaches must take into account a framework of functional anatomic and physiologic connections (Figure 3).
Linkage studies. The goal of linkage studies is to find a link between a phenotypic variation (ideally a measurable trait, such as number of drinks necessary for intoxication) and the chromosomal marker expected to be in the vicinity of the disease-specific gene variation. An advantage of linkage studies is that they can be started without knowing specific DNA sequences. Their limitations include:
- limited power when applied to complex diseases such as alcoholism
- they do not yield gene-specific information
- their success is highly dependent on family members’ willingness to participate.
Association studies. Candidate gene-based association studies are designed to directly test a potential association between the phenotype of interest and a known genomic sequence variation. This approach provides adequate power to study variations with modest effects and allows use of DNA from unrelated individuals. The candidate gene approach has revealed associations between specific genomic variations and phenotypes related to alcohol misuse and alcoholism (Table).
Like linkage studies, association studies have their own challenges and limitations, such as:
- historically high false-positive rates
- confounding risks (allele frequencies may vary because of ethnic stratification rather than disease predisposition).
To address these challenges, researchers must carefully choose behavioral, physiologic, or intermediate phenotypes and genotype variations, as well as control subjects and sample sizes. Replication studies are necessary to rule out false-positive associations. In fact, only some of the findings depicted in the Table—those related to GABRA2 and GABRA6 and few other genes—have been replicated.
Genome-wide association studies are a powerful new method for studying relationships between genomic variability and behavior. With GWAS, thousands of DNA samples can be scanned for thousands of SNPs throughout the human genome, with the goal of identifying variations that modestly increase the risk of developing common diseases.
Unlike the candidate gene approach—which focuses on preselected genomic variations—GWAS scans the whole genome and may identify unexpected susceptibility factors. Unlike the family-based linkage approach, GWAS is not limited to specific families and can address all recombination events in a population.
Challenges are associated with GWAS, however, and include:
- need for substantial numbers (2,000 to 5,000) of rigorously described cases and matched controls
- need for accurate, high-throughput genotyping technologies and sophisticated algorithms for analyzing data
- risk of high false-positive rates related to multiple testing
- inability to scan 100% of the genome, which may lead to false-negative findings.
Table
Examples of gene variations related to alcohol misuse and alcoholism phenotypes
| Phenotype | Gene variation(s) |
|---|---|
| Related to alcohol misuse | |
| Low response/high tolerance to alcohol | L allele of serotonin transporter gene (SLC6A4) and Ser385 allele of alpha-6 subunit of GABAA receptor gene (GABRA6) in adolescents and healthy adult men;a,b 600G allele of alpha-2 subunit of GABAA receptor gene (GABRA2) in healthy social drinkersc |
| Cue-related craving for alcohol | 118G allele of opioid μ-receptor gene (OMPR) and L allele of dopamine receptor type 4 gene (DRD4) in young problem drinkersd,e |
| Binge drinking | S allele of serotonin transporter gene in college students; combination of SS genotype of serotonin transporter gene and HH genotype of MAOA gene in young womenf |
| Related to alcoholism | |
| Alcohol dependence | Two common haplotypes of GABRA2 geneg |
| Liver cirrhosis in alcoholics | -238A allele of tumor necrosis factor gene (TNFA)h |
| Protects against withdrawal symptoms in alcoholics | -141C Del variant of the dopamine receptor type 2 gene (DRD2)i |
| Associated with delirium tremens | 8 genetic polymorphisms in 3 candidate genes involved in the dopamine transmission (DRD2, DRD3, and SLC6A3), 1 gene involved in the glutamate pathway (GRIK3), 1 neuropeptide gene (BDNF), and 1 cannabinoid gene (CNR1)j |
| Associated with alcohol withdrawal seizures | 9 repeat allele of dopamine transporter (SLC6A3); 10 repeat allele of tyrosine hydroxylase gene (TH); Ser9 allele of dopamine receptor type 3 gene (DRD3); SS genotype of serotonin transporter gene; 2108A allele in NR1 subunit of NMDA receptor gene (GRIN1)k-m |
| GABAA: gamma-aminobutyric acid A; MAOA: monoamine oxidase A; NMDA: N-methyl-D-aspartate | |
| Source: Click here to view references | |
Figure 3
2 ways to seek relationships between genes and behavior
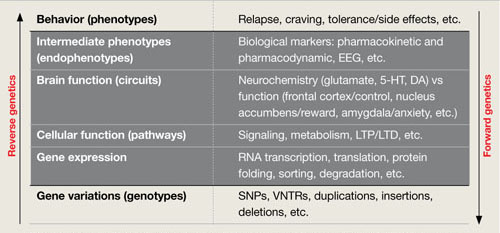
Researchers use ‘forward’ and ‘reverse’ genetics to connect behavioral phenotypes with predisposing genotypes. Each approach must consider intermediary functional anatomic and physiologic levels (black box), as shown in this conceptual framework.
DA: dopamine; EEG: electroencephalography; 5-HT: serotonin; LTD: long-term depression; LTP: long-term potentiation; RNA: ribonucleic acid; SNPs: single nucleotide polymorphisms; VNTRs: variable number tandem (triplet) repeats
Clinical implications
Genomic research is increasing our understanding of alcohol’s pharmacokinetic and pharmacodynamic interactions and of potential genetic associations with alcoholic phenotypes. These insights may lead to discovery of new therapies to compensate for specific physiologic and behavioral dysfunctions. For example, medications with pharmacologic profiles complimentary to addiction-related physiologic/behavioral deficits might be designed in the future.
Likewise, new understandings about genetic variability may allow us to predict an individual’s ability to tolerate and respond to existing medications used to treat alcohol dependence. For example, in studies of alcoholic and nonalcoholic subjects:
- Individuals with the 118G variant allele of the μ-opioid receptor may experience a stronger subjective response to alcohol and respond more robustly to naltrexone treatment than do carriers of the more common 118A allele.32
- Persons with a functional variation in the DRD4 gene (7 repeat allele–DRD4L) coding for type 4 dopamine receptor reported greater euphoria and reward while drinking alcohol and reduced alcohol consumption during 12-week treatment with olanzapine, a DRD2/DRD4 blocker.33
Applying this approach to the study of acamprosate has been difficult because of uncertainty about which protein molecules it targets. Variation in the Per2 gene (coding for protein involved in the circadian cycle) has been shown to be associated with brain glutamate levels, alcohol consumption, and the effects of acamprosate, although these interactions require further investigation.34
Pharmacogenomics of alcoholism treatment is in a very early stage of development. Findings require replication in different clinical samples and functional analysis. At the same time, if the reported association between the μ-opioid receptor genetic variation and naltrexone’s treatment efficacy is confirmed, this finding could help to guide clinical practice. Studies of genomic predictors of other medications’ efficacy and tolerability for alcoholism treatment would be expected to follow.
Related resources
- National Institute on Alcohol Abuse and Alcoholism. Collaborative Studies on Genetics of Alcoholism (COGA). www.niaaa.nih.gov (search NIAAA-funded collaborative research programs).
- Dick DM, Jones K, Saccone N, et al. Endophenotypes successfully lead to gene identification: results from the Collaborative Study on the Genetics of Alcoholism. Behav Genet 2006;36(1):112-26.
Drug brand names
- Acamprosate • Campral
- Naltrexone • ReVia, Vivitrol
- Olanzapine • Zyprexa
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgments
This work has been supported by the S.C. Johnson Genomic of Addictions Program. The authors thank Ms. Barbara Hall for expert technical assistance in preparing this manuscript.
1. Schuckit MA, Goodwin DA, Winokur G. A study of alcoholism in half siblings. Am J Psychiatry 1972;128(9):1132-6.
2. Nestler E. Molecular basis of long-term plasticity underlying addiction. Nat Rev Neurosci 2001;2(2):119-28.
3. National Institute of Alcohol Abuse and Alcoholism. Collaborative Studies on Genetics of Alcoholism (COGA). Available at: http://zork.wustl.edu/niaaa. Accessed January 28, 2008.
4. Foroud T, Edenberg HJ, Goate A, et al. Alcoholism susceptibility loci: confirmation studies in a replicate sample and further mapping. Alcohol Clin Exp Res 2000;24(7):933-45.
5. Dick DM, Nurnberger J, Jr, Edenberg HJ, et al. Suggestive linkage on chromosome 1 for a quantitative alcohol-related phenotype. Alcohol Clin Exp Res 2002;26(10):1453-60.
6. Nurnberger JI, Jr, Foroud T, Flury L, et al. Evidence for a locus on chromosome 1 that influences vulnerability to alcoholism and affective disorder. Am J Psychiatry 2001;158(5):718-24.
7. Schuckit MA, Edenberg HJ, Kalmijn J, et al. A genome-wide search for genes that relate to a low level of response to alcohol. Alcohol Clin Exp Res 2001;25(3):323-9.
8. Saccone NL, Kwon JM, Corbett J, et al. A genome screen of maximum number of drinks as an alcoholism phenotype. Am J Med Genet 2000;96(5):632-7.
9. Gottesman II, Shields J. Schizophrenia and genetics;a twin study vantage point. New York, NY: Academic Press;1972.
10. Rieder RO, Gershon ES. Genetic strategies in biological psychiatry. Arch Gen Psychiatry 1978;35(7):866-73.
11. Meyer-Lindenberg A, Weinberger DR. Intermediate phenotypes and genetic mechanisms of psychiatric disorders. Nat Rev Neurosci 2006;7(10):818-27.
12. Dick DM, Jones K, Saccone N, et al. Endophenotypes successfully lead to gene identification: results from the Collaborative Study on Genetics of Alcoholism. Behav Genet 2006;36(1):112-26.
13. Edenberg HJ, Dick DM, Xuei X, et al. Variations in GABRA2, encoding the alpha 2 subunit of the GABA(A) receptor, are associated with alcohol dependence and with brain oscillations. Am J Hum Genet 2004;74(4):705-14.
14. Hinckers AS, Laucht M, Schmidt MH, et al. Low level of response to alcohol as associated with serotonin transporter genotype and high alcohol intake in adolescents. Biol Psychiatry 2006;60(3):282-7.
15. Ramchandani VA, Bosron WF, Li TK. Research advances in ethanol metabolism. Pathol Biol (Paris) 2001;49(9):676-82.
16. Beckemeier ME, Bora PS. Fatty acid ethyl esters: potentially toxic products of myocardial ethanol metabolism. J Mol Cell Cardiol 1998;30(11):2487-94.
17. Li TK, Yin SJ, Crabb DW, et al. Genetic and environmental influences on alcohol metabolism in humans. Alcohol Clin Exp Res 2001;25(1):136-44.
18. Long JC, Knowler WC, Hanson RL, et al. Evidence for genetic linkage to alcohol dependence on chromosomes 4 and 11 from an autosome-wide scan in an American Indian population. Am J Med Genet 1998;81(3):216-21.
19. Edenberg HJ. Regulation of the mammalian alcohol dehydrogenase genes. Prog Nucleic Acid Res Mol Biol 2000;64:295-341.
20. Osier M, Pakstis A, Soodyall H, et al. A global perspective on genetic variation at the ADH genes reveals unusual patterns of linkage disequilibrium and diversity. Am J Hum Genet 2002;71(1):84-99.
21. Yoshida A, Rzhetsky A, Hsu LC, Chang C. Human aldehyde dehydrogenase gene family. Eur J Biochem 1998;251(3):549-57.
22. Harada S, Agarwal DP, Goedde HW. Aldehyde dehydrogenase deficiency as a cause of facial flashing reaction to alcohol in Japanese. Lancet 1981;2(8253):982.-
23. Goedde HW, Agarwal DP, Fritze G, et al. Distribution of ADH2 and ALDH2 genotypes in different populations. Hum Genet 1992;88(3):344-6.
24. Luczak SE, Glatt SJ, Wall TJ. Meta-analyses of ALDH2 and ADH1B with alcohol dependence in Asians. Psychol Bull 2006;132(4):607-21.
25. Edenberg HJ, Jerome RE, Li M. Polymorphism of the human alcohol dehydrogenase 4 (ADH4) promoter affects gene expression. Pharmacogenetics 1999;9(1):25-30.
26. Luo X, Kranzler HR, Zuo L, et al. ADH4 gene variation is associated with alcohol dependence and drug dependence in European Americans: results from HWD tests and case-control association studies. Neuropsychopharmacology 2006;31(5):1085-95.
27. Osier MV, Lu RB, Pakstis AJ, et al. Possible epistatic role of ADH7 in the protection against alcoholism. Am J Med Genet B Neuropsychiatr Genet 2004;126(1):19-22.
28. Lieber CS. Microsomal ethanol-oxidizing system (MEOS): the first 30 years (1968-1998)—a review. Alcohol Clin Exp Res 1999;23(6):991-1007.
29. Kunitoh S, Imaoka S, Hiroi T, et al. Acetaldehyde as well as ethanol is metabolized by human CYP2E1. J Pharmacol Exp Ther 1997;280(2):527-32.
30. Howard LA, Ahluwalia JS, Lin SK, et al. CYP2E1*1D regulatory polymorphism: association with alcohol and nicotine dependence [erratum in Pharmacogenetics. 2003;13(7):441-2]. Pharmacogenetics 2003;13(6):321-8.
31. Risch NJ. Searching for genetic determinants in the new millennium. Nature 2000;405(6788):847-56.
32. Oslin DW, Berrettini W, Kranzler HR, et al. A functional polymorphism of the mu-opioid receptor gene is associated with naltrexone response in alcohol-dependent patients. Neuropsychopharmacology 2003;28:1546-52.
33. Hutchison KE, Ray L, Sandman E, et al. The effect of olanzapine on craving and alcohol consumption. Neuropsychopharmacology 2006;31(6):1310-7.
34. Spanagel R, Pendyala G, Abarca C, et al. The clock gene Per2 influences the glutamatergic system and modulates alcohol consumption. Nat Med 2005;11(1):35-42.
Children of alcoholics have a 40% to 60% increased risk of developing severe alcohol-related problems1—a harsh legacy recognized for >30 years. Now, as the result of rapidly growing evidence, we can explain in greater detail why alcoholism runs in families when discussing alcohol dependence with patients.
Individuals vary in response to medications and substances of abuse, and genetic research is revealing the heritable origins. Numerous genetic variations are known to influence response to alcohol, as well as alcoholism’s pathophysiology, clinical manifestations, and treatment. Pieces are still missing from this complex picture, but investigators are identifying possible risk factors for alcoholism and matching potential responders with treatments such as naltrexone and acamprosate.
This article provides a progress report on contemporary genetic research of alcoholism. Our goal is to inform your clinical practice by describing:
- new understandings of the genetics of alcoholism
- how researchers identify relationships between genetic variations and clinical/behavioral phenomena
- practical implications of this knowledge.
Genetic variations and risk of addiction
No single gene appears to cause alcoholism. Many genetic variations that accumulated during evolution likely contribute to individual differences in response to alcohol and susceptibility to developing alcohol-related problems. A growing number of genetic variations have been associated with increased alcohol tolerance, consumption, and other related phenotypes.
Like other addictive substances, alcohol triggers pharmacodynamic effects by interacting with a variety of molecular targets (Figure 1).2 These target proteins in turn interact with specific signaling proteins and trigger responses in complex functional pathways. Genetic variations may affect the structure of genes coding for proteins that constitute pathways involved in alcohol’s effects on target proteins (pharmacodynamics) or its metabolism (pharmacokinetics). If such variations alter the production, function, or stability of these proteins, the pathway’s function also may be altered and produce behavioral phenotypes—such as high or low sensitivity to alcohol’s effects.
Alcoholism-related phenotypes. DSM-IV-TR diagnostic criteria include some but not all of the multiple phenotypes within alcoholism’s clinical presentation. Researchers in the Collaborative Studies on Genetics of Alcoholism (COGA)3 identified chromosome regions linked to alcoholism-related phenotypes, including:
- alcohol dependence4
- later age of drinking onset and increased harm avoidance5
- alcoholism and depression6
- alcohol sensitivity7
- alcohol consumption.8
To identify genes of interest within these chromosome regions, researchers used transitional phenotypes (endophenotypes) that “lie on the pathway between genes and disease,”9,10 and allowed them to characterize the neural systems affected by gene risk variants.11 As a result, they found associations among variations in the GABRA2 gene, (encoding the alpha-2 subunit of the GABAA receptor), specific brain oscillations (electrophysiologic endophenotype), and predisposition to alcohol dependence.12,13 By this same strategy, researchers discovered an association between the endophenotype (low-level of response to alcohol) and some genotypes, including at least 1 short allele of the serotonin transporter gene SLC6A4.14
Figure 1
Known molecular targets for alcohol and other drugs of abuse
Effects of drugs of abuse (black arrows) influence intracellular signaling pathways (blue arrows) to produce immediate and long-term changes in cell function.
cAMP: cyclic adenosine monophosphate; GABAA: gamma-aminobutyric acid A receptor; Gi, Gs, Gq: G proteins (heterotrimeric guanine nucleotide-binding proteins) MAPK: mitogen-activated protein kinase; N-cholino receptor: nicotinic cholinoreceptor; NMDA: N-methyl-D-aspartate; PKA: protein kinase A
Source: Created for CURRENT PSYCHIATRY from information in reference 2
Alcohol metabolism
Alcohol is metabolized to acetic acid through primary and auxiliary pathways involving alcohol and acetaldehyde dehydrogenases (ADH/ALDH) and the microsomal ethanol oxidizing system (cytochrome P-450 [CYP] 2E1)15 (Figure 2). Auxiliary pathways become involved when the primary pathway is overwhelmed by the amount of alcohol needed to be metabolized. Catalase and fatty acid ethyl ester synthases play a minor role under normal conditions but may be implicated in alcohol-induced organ damage.16
ADH/ALDH pathway. From one individual to another, the ability to metabolize ethyl alcohol varies up to 3- to 4-fold.17 In European and Amerindian samples, a genetic link has been identified between alcoholism and the 4q21-23 region on chromosome 4.18 This region contains a cluster of 7 genes encoding for alcohol dehydrogenases (ADH), including 3 Class I genes—ADH1A, ADH1B, and ADH1C—coding for the corresponding proteins that play a major role in alcohol metabolism.19 In eastern Asian samples, alleles encoding high activity enzymes (ADH1B*47His and ADH1C*349Ile) are significantly less frequent in alcoholics compared with nonalcoholic controls.20
Mitochondrial ALDH2 protein plays the central role in acetaldehyde metabolism and is highly expressed in the liver, stomach, and other tissues—including the brain.21 The ALDH2*2 gene variant encodes for a catalytically inactive enzyme, thus inhibiting acetaldehyde metabolism and causing a facial flushing reaction.22 The ALDH2*2 allele has a relatively high frequency in Asians but also is found in other populations.23 Meta-analyses of published data indicate that possessing either of the variant alleles in the ADH1B and ALDH2 genes is protective against alcohol dependence in Asians.24
The ADH4 enzyme catalyzes oxidation or reduction of numerous substrates—including long-chain aliphatic alcohols and aromatic aldehydes—and becomes involved in alcohol metabolism at moderate to high concentrations. The -75A allele of the ADH4 gene has promoter activity more than twice that of the -75C allele and significantly affects its expression.25 This substitution in the promoter region, as well as A/G SNP (rs1042364)—a single nucleotide polymorphism (SNP)—at exon 9, has been associated with an increased risk for alcohol and drug dependence in European Americans.26
Finally, variations in the ADH7 gene may play a protective role against alcoholism through epistatic effects.27
The CYP 2E1 pathway has low initial catalytic efficiency compared with the ADH/ALDH pathway, but it may metabolize alcohol up to 10 times faster after chronic alcohol consumption or cigarette smoking and accounts for metabolic tolerance.28 CYP 2E1 is involved in metabolizing both alcohol and acetaldehyde.29 The CYP 2E1*1D polymorphism has been associated with greater inducibility as well as alcohol and nicotine dependence.30
Thus, linkage and association studies support the association of phenotypes related to alcohol response and dependence with variations in genes that code for proteins involved in alcohol’s pharmacodynamic and pharmacokinetic effects. Each of these findings is important, but conceptual models organizing them all and explaining their role in alcohol’s effects and predisposition to alcoholism have yet to be constructed.
Figure 2
Genetic variations that affect alcohol metabolism pathways
Genetic variations affect the efficiency of primary and auxiliary pathways by which ethyl alcohol is metabolized to acetaldehyde and acetic acid. Auxiliary pathways become involved when the primary pathway is overwhelmed by the amount of alcohol to be metabolized.
ADH: alcohol dehydrogenase; ALDH: acetaldehyde dehydrogenase; P450CYP 2E1: cytochrome P450, family 2, subfamily E, polypeptide 1; A/G SNP: adenine/guanine single nucleotide polymorphism
Phenotype-genotype relationships
Alcohol—unlike most other addictive substances—does not have a specific receptor and is believed to act by disturbing the balance between excitatory and inhibitory neurotransmission in the neural system. Consequently, researchers explore relationships between genetics and alcohol-related problems using 2 approaches:
- Forward genetics (discovering disease-related genes via genome-wide studies and then studying their function; examples include linkage and genome-wide association studies [GWAS]).
- Reverse genetics (testing whether candidate genes and polymorphisms identified in animal studies as relevant for biological effects also exist in humans and are relevant to the phenotype).31
When searching for relationships between genotypes and phenotypes, both approaches must take into account a framework of functional anatomic and physiologic connections (Figure 3).
Linkage studies. The goal of linkage studies is to find a link between a phenotypic variation (ideally a measurable trait, such as number of drinks necessary for intoxication) and the chromosomal marker expected to be in the vicinity of the disease-specific gene variation. An advantage of linkage studies is that they can be started without knowing specific DNA sequences. Their limitations include:
- limited power when applied to complex diseases such as alcoholism
- they do not yield gene-specific information
- their success is highly dependent on family members’ willingness to participate.
Association studies. Candidate gene-based association studies are designed to directly test a potential association between the phenotype of interest and a known genomic sequence variation. This approach provides adequate power to study variations with modest effects and allows use of DNA from unrelated individuals. The candidate gene approach has revealed associations between specific genomic variations and phenotypes related to alcohol misuse and alcoholism (Table).
Like linkage studies, association studies have their own challenges and limitations, such as:
- historically high false-positive rates
- confounding risks (allele frequencies may vary because of ethnic stratification rather than disease predisposition).
To address these challenges, researchers must carefully choose behavioral, physiologic, or intermediate phenotypes and genotype variations, as well as control subjects and sample sizes. Replication studies are necessary to rule out false-positive associations. In fact, only some of the findings depicted in the Table—those related to GABRA2 and GABRA6 and few other genes—have been replicated.
Genome-wide association studies are a powerful new method for studying relationships between genomic variability and behavior. With GWAS, thousands of DNA samples can be scanned for thousands of SNPs throughout the human genome, with the goal of identifying variations that modestly increase the risk of developing common diseases.
Unlike the candidate gene approach—which focuses on preselected genomic variations—GWAS scans the whole genome and may identify unexpected susceptibility factors. Unlike the family-based linkage approach, GWAS is not limited to specific families and can address all recombination events in a population.
Challenges are associated with GWAS, however, and include:
- need for substantial numbers (2,000 to 5,000) of rigorously described cases and matched controls
- need for accurate, high-throughput genotyping technologies and sophisticated algorithms for analyzing data
- risk of high false-positive rates related to multiple testing
- inability to scan 100% of the genome, which may lead to false-negative findings.
Table
Examples of gene variations related to alcohol misuse and alcoholism phenotypes
| Phenotype | Gene variation(s) |
|---|---|
| Related to alcohol misuse | |
| Low response/high tolerance to alcohol | L allele of serotonin transporter gene (SLC6A4) and Ser385 allele of alpha-6 subunit of GABAA receptor gene (GABRA6) in adolescents and healthy adult men;a,b 600G allele of alpha-2 subunit of GABAA receptor gene (GABRA2) in healthy social drinkersc |
| Cue-related craving for alcohol | 118G allele of opioid μ-receptor gene (OMPR) and L allele of dopamine receptor type 4 gene (DRD4) in young problem drinkersd,e |
| Binge drinking | S allele of serotonin transporter gene in college students; combination of SS genotype of serotonin transporter gene and HH genotype of MAOA gene in young womenf |
| Related to alcoholism | |
| Alcohol dependence | Two common haplotypes of GABRA2 geneg |
| Liver cirrhosis in alcoholics | -238A allele of tumor necrosis factor gene (TNFA)h |
| Protects against withdrawal symptoms in alcoholics | -141C Del variant of the dopamine receptor type 2 gene (DRD2)i |
| Associated with delirium tremens | 8 genetic polymorphisms in 3 candidate genes involved in the dopamine transmission (DRD2, DRD3, and SLC6A3), 1 gene involved in the glutamate pathway (GRIK3), 1 neuropeptide gene (BDNF), and 1 cannabinoid gene (CNR1)j |
| Associated with alcohol withdrawal seizures | 9 repeat allele of dopamine transporter (SLC6A3); 10 repeat allele of tyrosine hydroxylase gene (TH); Ser9 allele of dopamine receptor type 3 gene (DRD3); SS genotype of serotonin transporter gene; 2108A allele in NR1 subunit of NMDA receptor gene (GRIN1)k-m |
| GABAA: gamma-aminobutyric acid A; MAOA: monoamine oxidase A; NMDA: N-methyl-D-aspartate | |
| Source: Click here to view references | |
Figure 3
2 ways to seek relationships between genes and behavior
Researchers use ‘forward’ and ‘reverse’ genetics to connect behavioral phenotypes with predisposing genotypes. Each approach must consider intermediary functional anatomic and physiologic levels (black box), as shown in this conceptual framework.
DA: dopamine; EEG: electroencephalography; 5-HT: serotonin; LTD: long-term depression; LTP: long-term potentiation; RNA: ribonucleic acid; SNPs: single nucleotide polymorphisms; VNTRs: variable number tandem (triplet) repeats
Clinical implications
Genomic research is increasing our understanding of alcohol’s pharmacokinetic and pharmacodynamic interactions and of potential genetic associations with alcoholic phenotypes. These insights may lead to discovery of new therapies to compensate for specific physiologic and behavioral dysfunctions. For example, medications with pharmacologic profiles complimentary to addiction-related physiologic/behavioral deficits might be designed in the future.
Likewise, new understandings about genetic variability may allow us to predict an individual’s ability to tolerate and respond to existing medications used to treat alcohol dependence. For example, in studies of alcoholic and nonalcoholic subjects:
- Individuals with the 118G variant allele of the μ-opioid receptor may experience a stronger subjective response to alcohol and respond more robustly to naltrexone treatment than do carriers of the more common 118A allele.32
- Persons with a functional variation in the DRD4 gene (7 repeat allele–DRD4L) coding for type 4 dopamine receptor reported greater euphoria and reward while drinking alcohol and reduced alcohol consumption during 12-week treatment with olanzapine, a DRD2/DRD4 blocker.33
Applying this approach to the study of acamprosate has been difficult because of uncertainty about which protein molecules it targets. Variation in the Per2 gene (coding for protein involved in the circadian cycle) has been shown to be associated with brain glutamate levels, alcohol consumption, and the effects of acamprosate, although these interactions require further investigation.34
Pharmacogenomics of alcoholism treatment is in a very early stage of development. Findings require replication in different clinical samples and functional analysis. At the same time, if the reported association between the μ-opioid receptor genetic variation and naltrexone’s treatment efficacy is confirmed, this finding could help to guide clinical practice. Studies of genomic predictors of other medications’ efficacy and tolerability for alcoholism treatment would be expected to follow.
Related resources
- National Institute on Alcohol Abuse and Alcoholism. Collaborative Studies on Genetics of Alcoholism (COGA). www.niaaa.nih.gov (search NIAAA-funded collaborative research programs).
- Dick DM, Jones K, Saccone N, et al. Endophenotypes successfully lead to gene identification: results from the Collaborative Study on the Genetics of Alcoholism. Behav Genet 2006;36(1):112-26.
Drug brand names
- Acamprosate • Campral
- Naltrexone • ReVia, Vivitrol
- Olanzapine • Zyprexa
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgments
This work has been supported by the S.C. Johnson Genomic of Addictions Program. The authors thank Ms. Barbara Hall for expert technical assistance in preparing this manuscript.
Children of alcoholics have a 40% to 60% increased risk of developing severe alcohol-related problems1—a harsh legacy recognized for >30 years. Now, as the result of rapidly growing evidence, we can explain in greater detail why alcoholism runs in families when discussing alcohol dependence with patients.
Individuals vary in response to medications and substances of abuse, and genetic research is revealing the heritable origins. Numerous genetic variations are known to influence response to alcohol, as well as alcoholism’s pathophysiology, clinical manifestations, and treatment. Pieces are still missing from this complex picture, but investigators are identifying possible risk factors for alcoholism and matching potential responders with treatments such as naltrexone and acamprosate.
This article provides a progress report on contemporary genetic research of alcoholism. Our goal is to inform your clinical practice by describing:
- new understandings of the genetics of alcoholism
- how researchers identify relationships between genetic variations and clinical/behavioral phenomena
- practical implications of this knowledge.
Genetic variations and risk of addiction
No single gene appears to cause alcoholism. Many genetic variations that accumulated during evolution likely contribute to individual differences in response to alcohol and susceptibility to developing alcohol-related problems. A growing number of genetic variations have been associated with increased alcohol tolerance, consumption, and other related phenotypes.
Like other addictive substances, alcohol triggers pharmacodynamic effects by interacting with a variety of molecular targets (Figure 1).2 These target proteins in turn interact with specific signaling proteins and trigger responses in complex functional pathways. Genetic variations may affect the structure of genes coding for proteins that constitute pathways involved in alcohol’s effects on target proteins (pharmacodynamics) or its metabolism (pharmacokinetics). If such variations alter the production, function, or stability of these proteins, the pathway’s function also may be altered and produce behavioral phenotypes—such as high or low sensitivity to alcohol’s effects.
Alcoholism-related phenotypes. DSM-IV-TR diagnostic criteria include some but not all of the multiple phenotypes within alcoholism’s clinical presentation. Researchers in the Collaborative Studies on Genetics of Alcoholism (COGA)3 identified chromosome regions linked to alcoholism-related phenotypes, including:
- alcohol dependence4
- later age of drinking onset and increased harm avoidance5
- alcoholism and depression6
- alcohol sensitivity7
- alcohol consumption.8
To identify genes of interest within these chromosome regions, researchers used transitional phenotypes (endophenotypes) that “lie on the pathway between genes and disease,”9,10 and allowed them to characterize the neural systems affected by gene risk variants.11 As a result, they found associations among variations in the GABRA2 gene, (encoding the alpha-2 subunit of the GABAA receptor), specific brain oscillations (electrophysiologic endophenotype), and predisposition to alcohol dependence.12,13 By this same strategy, researchers discovered an association between the endophenotype (low-level of response to alcohol) and some genotypes, including at least 1 short allele of the serotonin transporter gene SLC6A4.14
Figure 1
Known molecular targets for alcohol and other drugs of abuse
Effects of drugs of abuse (black arrows) influence intracellular signaling pathways (blue arrows) to produce immediate and long-term changes in cell function.
cAMP: cyclic adenosine monophosphate; GABAA: gamma-aminobutyric acid A receptor; Gi, Gs, Gq: G proteins (heterotrimeric guanine nucleotide-binding proteins) MAPK: mitogen-activated protein kinase; N-cholino receptor: nicotinic cholinoreceptor; NMDA: N-methyl-D-aspartate; PKA: protein kinase A
Source: Created for CURRENT PSYCHIATRY from information in reference 2
Alcohol metabolism
Alcohol is metabolized to acetic acid through primary and auxiliary pathways involving alcohol and acetaldehyde dehydrogenases (ADH/ALDH) and the microsomal ethanol oxidizing system (cytochrome P-450 [CYP] 2E1)15 (Figure 2). Auxiliary pathways become involved when the primary pathway is overwhelmed by the amount of alcohol needed to be metabolized. Catalase and fatty acid ethyl ester synthases play a minor role under normal conditions but may be implicated in alcohol-induced organ damage.16
ADH/ALDH pathway. From one individual to another, the ability to metabolize ethyl alcohol varies up to 3- to 4-fold.17 In European and Amerindian samples, a genetic link has been identified between alcoholism and the 4q21-23 region on chromosome 4.18 This region contains a cluster of 7 genes encoding for alcohol dehydrogenases (ADH), including 3 Class I genes—ADH1A, ADH1B, and ADH1C—coding for the corresponding proteins that play a major role in alcohol metabolism.19 In eastern Asian samples, alleles encoding high activity enzymes (ADH1B*47His and ADH1C*349Ile) are significantly less frequent in alcoholics compared with nonalcoholic controls.20
Mitochondrial ALDH2 protein plays the central role in acetaldehyde metabolism and is highly expressed in the liver, stomach, and other tissues—including the brain.21 The ALDH2*2 gene variant encodes for a catalytically inactive enzyme, thus inhibiting acetaldehyde metabolism and causing a facial flushing reaction.22 The ALDH2*2 allele has a relatively high frequency in Asians but also is found in other populations.23 Meta-analyses of published data indicate that possessing either of the variant alleles in the ADH1B and ALDH2 genes is protective against alcohol dependence in Asians.24
The ADH4 enzyme catalyzes oxidation or reduction of numerous substrates—including long-chain aliphatic alcohols and aromatic aldehydes—and becomes involved in alcohol metabolism at moderate to high concentrations. The -75A allele of the ADH4 gene has promoter activity more than twice that of the -75C allele and significantly affects its expression.25 This substitution in the promoter region, as well as A/G SNP (rs1042364)—a single nucleotide polymorphism (SNP)—at exon 9, has been associated with an increased risk for alcohol and drug dependence in European Americans.26
Finally, variations in the ADH7 gene may play a protective role against alcoholism through epistatic effects.27
The CYP 2E1 pathway has low initial catalytic efficiency compared with the ADH/ALDH pathway, but it may metabolize alcohol up to 10 times faster after chronic alcohol consumption or cigarette smoking and accounts for metabolic tolerance.28 CYP 2E1 is involved in metabolizing both alcohol and acetaldehyde.29 The CYP 2E1*1D polymorphism has been associated with greater inducibility as well as alcohol and nicotine dependence.30
Thus, linkage and association studies support the association of phenotypes related to alcohol response and dependence with variations in genes that code for proteins involved in alcohol’s pharmacodynamic and pharmacokinetic effects. Each of these findings is important, but conceptual models organizing them all and explaining their role in alcohol’s effects and predisposition to alcoholism have yet to be constructed.
Figure 2
Genetic variations that affect alcohol metabolism pathways
Genetic variations affect the efficiency of primary and auxiliary pathways by which ethyl alcohol is metabolized to acetaldehyde and acetic acid. Auxiliary pathways become involved when the primary pathway is overwhelmed by the amount of alcohol to be metabolized.
ADH: alcohol dehydrogenase; ALDH: acetaldehyde dehydrogenase; P450CYP 2E1: cytochrome P450, family 2, subfamily E, polypeptide 1; A/G SNP: adenine/guanine single nucleotide polymorphism
Phenotype-genotype relationships
Alcohol—unlike most other addictive substances—does not have a specific receptor and is believed to act by disturbing the balance between excitatory and inhibitory neurotransmission in the neural system. Consequently, researchers explore relationships between genetics and alcohol-related problems using 2 approaches:
- Forward genetics (discovering disease-related genes via genome-wide studies and then studying their function; examples include linkage and genome-wide association studies [GWAS]).
- Reverse genetics (testing whether candidate genes and polymorphisms identified in animal studies as relevant for biological effects also exist in humans and are relevant to the phenotype).31
When searching for relationships between genotypes and phenotypes, both approaches must take into account a framework of functional anatomic and physiologic connections (Figure 3).
Linkage studies. The goal of linkage studies is to find a link between a phenotypic variation (ideally a measurable trait, such as number of drinks necessary for intoxication) and the chromosomal marker expected to be in the vicinity of the disease-specific gene variation. An advantage of linkage studies is that they can be started without knowing specific DNA sequences. Their limitations include:
- limited power when applied to complex diseases such as alcoholism
- they do not yield gene-specific information
- their success is highly dependent on family members’ willingness to participate.
Association studies. Candidate gene-based association studies are designed to directly test a potential association between the phenotype of interest and a known genomic sequence variation. This approach provides adequate power to study variations with modest effects and allows use of DNA from unrelated individuals. The candidate gene approach has revealed associations between specific genomic variations and phenotypes related to alcohol misuse and alcoholism (Table).
Like linkage studies, association studies have their own challenges and limitations, such as:
- historically high false-positive rates
- confounding risks (allele frequencies may vary because of ethnic stratification rather than disease predisposition).
To address these challenges, researchers must carefully choose behavioral, physiologic, or intermediate phenotypes and genotype variations, as well as control subjects and sample sizes. Replication studies are necessary to rule out false-positive associations. In fact, only some of the findings depicted in the Table—those related to GABRA2 and GABRA6 and few other genes—have been replicated.
Genome-wide association studies are a powerful new method for studying relationships between genomic variability and behavior. With GWAS, thousands of DNA samples can be scanned for thousands of SNPs throughout the human genome, with the goal of identifying variations that modestly increase the risk of developing common diseases.
Unlike the candidate gene approach—which focuses on preselected genomic variations—GWAS scans the whole genome and may identify unexpected susceptibility factors. Unlike the family-based linkage approach, GWAS is not limited to specific families and can address all recombination events in a population.
Challenges are associated with GWAS, however, and include:
- need for substantial numbers (2,000 to 5,000) of rigorously described cases and matched controls
- need for accurate, high-throughput genotyping technologies and sophisticated algorithms for analyzing data
- risk of high false-positive rates related to multiple testing
- inability to scan 100% of the genome, which may lead to false-negative findings.
Table
Examples of gene variations related to alcohol misuse and alcoholism phenotypes
| Phenotype | Gene variation(s) |
|---|---|
| Related to alcohol misuse | |
| Low response/high tolerance to alcohol | L allele of serotonin transporter gene (SLC6A4) and Ser385 allele of alpha-6 subunit of GABAA receptor gene (GABRA6) in adolescents and healthy adult men;a,b 600G allele of alpha-2 subunit of GABAA receptor gene (GABRA2) in healthy social drinkersc |
| Cue-related craving for alcohol | 118G allele of opioid μ-receptor gene (OMPR) and L allele of dopamine receptor type 4 gene (DRD4) in young problem drinkersd,e |
| Binge drinking | S allele of serotonin transporter gene in college students; combination of SS genotype of serotonin transporter gene and HH genotype of MAOA gene in young womenf |
| Related to alcoholism | |
| Alcohol dependence | Two common haplotypes of GABRA2 geneg |
| Liver cirrhosis in alcoholics | -238A allele of tumor necrosis factor gene (TNFA)h |
| Protects against withdrawal symptoms in alcoholics | -141C Del variant of the dopamine receptor type 2 gene (DRD2)i |
| Associated with delirium tremens | 8 genetic polymorphisms in 3 candidate genes involved in the dopamine transmission (DRD2, DRD3, and SLC6A3), 1 gene involved in the glutamate pathway (GRIK3), 1 neuropeptide gene (BDNF), and 1 cannabinoid gene (CNR1)j |
| Associated with alcohol withdrawal seizures | 9 repeat allele of dopamine transporter (SLC6A3); 10 repeat allele of tyrosine hydroxylase gene (TH); Ser9 allele of dopamine receptor type 3 gene (DRD3); SS genotype of serotonin transporter gene; 2108A allele in NR1 subunit of NMDA receptor gene (GRIN1)k-m |
| GABAA: gamma-aminobutyric acid A; MAOA: monoamine oxidase A; NMDA: N-methyl-D-aspartate | |
| Source: Click here to view references | |
Figure 3
2 ways to seek relationships between genes and behavior
Researchers use ‘forward’ and ‘reverse’ genetics to connect behavioral phenotypes with predisposing genotypes. Each approach must consider intermediary functional anatomic and physiologic levels (black box), as shown in this conceptual framework.
DA: dopamine; EEG: electroencephalography; 5-HT: serotonin; LTD: long-term depression; LTP: long-term potentiation; RNA: ribonucleic acid; SNPs: single nucleotide polymorphisms; VNTRs: variable number tandem (triplet) repeats
Clinical implications
Genomic research is increasing our understanding of alcohol’s pharmacokinetic and pharmacodynamic interactions and of potential genetic associations with alcoholic phenotypes. These insights may lead to discovery of new therapies to compensate for specific physiologic and behavioral dysfunctions. For example, medications with pharmacologic profiles complimentary to addiction-related physiologic/behavioral deficits might be designed in the future.
Likewise, new understandings about genetic variability may allow us to predict an individual’s ability to tolerate and respond to existing medications used to treat alcohol dependence. For example, in studies of alcoholic and nonalcoholic subjects:
- Individuals with the 118G variant allele of the μ-opioid receptor may experience a stronger subjective response to alcohol and respond more robustly to naltrexone treatment than do carriers of the more common 118A allele.32
- Persons with a functional variation in the DRD4 gene (7 repeat allele–DRD4L) coding for type 4 dopamine receptor reported greater euphoria and reward while drinking alcohol and reduced alcohol consumption during 12-week treatment with olanzapine, a DRD2/DRD4 blocker.33
Applying this approach to the study of acamprosate has been difficult because of uncertainty about which protein molecules it targets. Variation in the Per2 gene (coding for protein involved in the circadian cycle) has been shown to be associated with brain glutamate levels, alcohol consumption, and the effects of acamprosate, although these interactions require further investigation.34
Pharmacogenomics of alcoholism treatment is in a very early stage of development. Findings require replication in different clinical samples and functional analysis. At the same time, if the reported association between the μ-opioid receptor genetic variation and naltrexone’s treatment efficacy is confirmed, this finding could help to guide clinical practice. Studies of genomic predictors of other medications’ efficacy and tolerability for alcoholism treatment would be expected to follow.
Related resources
- National Institute on Alcohol Abuse and Alcoholism. Collaborative Studies on Genetics of Alcoholism (COGA). www.niaaa.nih.gov (search NIAAA-funded collaborative research programs).
- Dick DM, Jones K, Saccone N, et al. Endophenotypes successfully lead to gene identification: results from the Collaborative Study on the Genetics of Alcoholism. Behav Genet 2006;36(1):112-26.
Drug brand names
- Acamprosate • Campral
- Naltrexone • ReVia, Vivitrol
- Olanzapine • Zyprexa
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgments
This work has been supported by the S.C. Johnson Genomic of Addictions Program. The authors thank Ms. Barbara Hall for expert technical assistance in preparing this manuscript.
1. Schuckit MA, Goodwin DA, Winokur G. A study of alcoholism in half siblings. Am J Psychiatry 1972;128(9):1132-6.
2. Nestler E. Molecular basis of long-term plasticity underlying addiction. Nat Rev Neurosci 2001;2(2):119-28.
3. National Institute of Alcohol Abuse and Alcoholism. Collaborative Studies on Genetics of Alcoholism (COGA). Available at: http://zork.wustl.edu/niaaa. Accessed January 28, 2008.
4. Foroud T, Edenberg HJ, Goate A, et al. Alcoholism susceptibility loci: confirmation studies in a replicate sample and further mapping. Alcohol Clin Exp Res 2000;24(7):933-45.
5. Dick DM, Nurnberger J, Jr, Edenberg HJ, et al. Suggestive linkage on chromosome 1 for a quantitative alcohol-related phenotype. Alcohol Clin Exp Res 2002;26(10):1453-60.
6. Nurnberger JI, Jr, Foroud T, Flury L, et al. Evidence for a locus on chromosome 1 that influences vulnerability to alcoholism and affective disorder. Am J Psychiatry 2001;158(5):718-24.
7. Schuckit MA, Edenberg HJ, Kalmijn J, et al. A genome-wide search for genes that relate to a low level of response to alcohol. Alcohol Clin Exp Res 2001;25(3):323-9.
8. Saccone NL, Kwon JM, Corbett J, et al. A genome screen of maximum number of drinks as an alcoholism phenotype. Am J Med Genet 2000;96(5):632-7.
9. Gottesman II, Shields J. Schizophrenia and genetics;a twin study vantage point. New York, NY: Academic Press;1972.
10. Rieder RO, Gershon ES. Genetic strategies in biological psychiatry. Arch Gen Psychiatry 1978;35(7):866-73.
11. Meyer-Lindenberg A, Weinberger DR. Intermediate phenotypes and genetic mechanisms of psychiatric disorders. Nat Rev Neurosci 2006;7(10):818-27.
12. Dick DM, Jones K, Saccone N, et al. Endophenotypes successfully lead to gene identification: results from the Collaborative Study on Genetics of Alcoholism. Behav Genet 2006;36(1):112-26.
13. Edenberg HJ, Dick DM, Xuei X, et al. Variations in GABRA2, encoding the alpha 2 subunit of the GABA(A) receptor, are associated with alcohol dependence and with brain oscillations. Am J Hum Genet 2004;74(4):705-14.
14. Hinckers AS, Laucht M, Schmidt MH, et al. Low level of response to alcohol as associated with serotonin transporter genotype and high alcohol intake in adolescents. Biol Psychiatry 2006;60(3):282-7.
15. Ramchandani VA, Bosron WF, Li TK. Research advances in ethanol metabolism. Pathol Biol (Paris) 2001;49(9):676-82.
16. Beckemeier ME, Bora PS. Fatty acid ethyl esters: potentially toxic products of myocardial ethanol metabolism. J Mol Cell Cardiol 1998;30(11):2487-94.
17. Li TK, Yin SJ, Crabb DW, et al. Genetic and environmental influences on alcohol metabolism in humans. Alcohol Clin Exp Res 2001;25(1):136-44.
18. Long JC, Knowler WC, Hanson RL, et al. Evidence for genetic linkage to alcohol dependence on chromosomes 4 and 11 from an autosome-wide scan in an American Indian population. Am J Med Genet 1998;81(3):216-21.
19. Edenberg HJ. Regulation of the mammalian alcohol dehydrogenase genes. Prog Nucleic Acid Res Mol Biol 2000;64:295-341.
20. Osier M, Pakstis A, Soodyall H, et al. A global perspective on genetic variation at the ADH genes reveals unusual patterns of linkage disequilibrium and diversity. Am J Hum Genet 2002;71(1):84-99.
21. Yoshida A, Rzhetsky A, Hsu LC, Chang C. Human aldehyde dehydrogenase gene family. Eur J Biochem 1998;251(3):549-57.
22. Harada S, Agarwal DP, Goedde HW. Aldehyde dehydrogenase deficiency as a cause of facial flashing reaction to alcohol in Japanese. Lancet 1981;2(8253):982.-
23. Goedde HW, Agarwal DP, Fritze G, et al. Distribution of ADH2 and ALDH2 genotypes in different populations. Hum Genet 1992;88(3):344-6.
24. Luczak SE, Glatt SJ, Wall TJ. Meta-analyses of ALDH2 and ADH1B with alcohol dependence in Asians. Psychol Bull 2006;132(4):607-21.
25. Edenberg HJ, Jerome RE, Li M. Polymorphism of the human alcohol dehydrogenase 4 (ADH4) promoter affects gene expression. Pharmacogenetics 1999;9(1):25-30.
26. Luo X, Kranzler HR, Zuo L, et al. ADH4 gene variation is associated with alcohol dependence and drug dependence in European Americans: results from HWD tests and case-control association studies. Neuropsychopharmacology 2006;31(5):1085-95.
27. Osier MV, Lu RB, Pakstis AJ, et al. Possible epistatic role of ADH7 in the protection against alcoholism. Am J Med Genet B Neuropsychiatr Genet 2004;126(1):19-22.
28. Lieber CS. Microsomal ethanol-oxidizing system (MEOS): the first 30 years (1968-1998)—a review. Alcohol Clin Exp Res 1999;23(6):991-1007.
29. Kunitoh S, Imaoka S, Hiroi T, et al. Acetaldehyde as well as ethanol is metabolized by human CYP2E1. J Pharmacol Exp Ther 1997;280(2):527-32.
30. Howard LA, Ahluwalia JS, Lin SK, et al. CYP2E1*1D regulatory polymorphism: association with alcohol and nicotine dependence [erratum in Pharmacogenetics. 2003;13(7):441-2]. Pharmacogenetics 2003;13(6):321-8.
31. Risch NJ. Searching for genetic determinants in the new millennium. Nature 2000;405(6788):847-56.
32. Oslin DW, Berrettini W, Kranzler HR, et al. A functional polymorphism of the mu-opioid receptor gene is associated with naltrexone response in alcohol-dependent patients. Neuropsychopharmacology 2003;28:1546-52.
33. Hutchison KE, Ray L, Sandman E, et al. The effect of olanzapine on craving and alcohol consumption. Neuropsychopharmacology 2006;31(6):1310-7.
34. Spanagel R, Pendyala G, Abarca C, et al. The clock gene Per2 influences the glutamatergic system and modulates alcohol consumption. Nat Med 2005;11(1):35-42.
1. Schuckit MA, Goodwin DA, Winokur G. A study of alcoholism in half siblings. Am J Psychiatry 1972;128(9):1132-6.
2. Nestler E. Molecular basis of long-term plasticity underlying addiction. Nat Rev Neurosci 2001;2(2):119-28.
3. National Institute of Alcohol Abuse and Alcoholism. Collaborative Studies on Genetics of Alcoholism (COGA). Available at: http://zork.wustl.edu/niaaa. Accessed January 28, 2008.
4. Foroud T, Edenberg HJ, Goate A, et al. Alcoholism susceptibility loci: confirmation studies in a replicate sample and further mapping. Alcohol Clin Exp Res 2000;24(7):933-45.
5. Dick DM, Nurnberger J, Jr, Edenberg HJ, et al. Suggestive linkage on chromosome 1 for a quantitative alcohol-related phenotype. Alcohol Clin Exp Res 2002;26(10):1453-60.
6. Nurnberger JI, Jr, Foroud T, Flury L, et al. Evidence for a locus on chromosome 1 that influences vulnerability to alcoholism and affective disorder. Am J Psychiatry 2001;158(5):718-24.
7. Schuckit MA, Edenberg HJ, Kalmijn J, et al. A genome-wide search for genes that relate to a low level of response to alcohol. Alcohol Clin Exp Res 2001;25(3):323-9.
8. Saccone NL, Kwon JM, Corbett J, et al. A genome screen of maximum number of drinks as an alcoholism phenotype. Am J Med Genet 2000;96(5):632-7.
9. Gottesman II, Shields J. Schizophrenia and genetics;a twin study vantage point. New York, NY: Academic Press;1972.
10. Rieder RO, Gershon ES. Genetic strategies in biological psychiatry. Arch Gen Psychiatry 1978;35(7):866-73.
11. Meyer-Lindenberg A, Weinberger DR. Intermediate phenotypes and genetic mechanisms of psychiatric disorders. Nat Rev Neurosci 2006;7(10):818-27.
12. Dick DM, Jones K, Saccone N, et al. Endophenotypes successfully lead to gene identification: results from the Collaborative Study on Genetics of Alcoholism. Behav Genet 2006;36(1):112-26.
13. Edenberg HJ, Dick DM, Xuei X, et al. Variations in GABRA2, encoding the alpha 2 subunit of the GABA(A) receptor, are associated with alcohol dependence and with brain oscillations. Am J Hum Genet 2004;74(4):705-14.
14. Hinckers AS, Laucht M, Schmidt MH, et al. Low level of response to alcohol as associated with serotonin transporter genotype and high alcohol intake in adolescents. Biol Psychiatry 2006;60(3):282-7.
15. Ramchandani VA, Bosron WF, Li TK. Research advances in ethanol metabolism. Pathol Biol (Paris) 2001;49(9):676-82.
16. Beckemeier ME, Bora PS. Fatty acid ethyl esters: potentially toxic products of myocardial ethanol metabolism. J Mol Cell Cardiol 1998;30(11):2487-94.
17. Li TK, Yin SJ, Crabb DW, et al. Genetic and environmental influences on alcohol metabolism in humans. Alcohol Clin Exp Res 2001;25(1):136-44.
18. Long JC, Knowler WC, Hanson RL, et al. Evidence for genetic linkage to alcohol dependence on chromosomes 4 and 11 from an autosome-wide scan in an American Indian population. Am J Med Genet 1998;81(3):216-21.
19. Edenberg HJ. Regulation of the mammalian alcohol dehydrogenase genes. Prog Nucleic Acid Res Mol Biol 2000;64:295-341.
20. Osier M, Pakstis A, Soodyall H, et al. A global perspective on genetic variation at the ADH genes reveals unusual patterns of linkage disequilibrium and diversity. Am J Hum Genet 2002;71(1):84-99.
21. Yoshida A, Rzhetsky A, Hsu LC, Chang C. Human aldehyde dehydrogenase gene family. Eur J Biochem 1998;251(3):549-57.
22. Harada S, Agarwal DP, Goedde HW. Aldehyde dehydrogenase deficiency as a cause of facial flashing reaction to alcohol in Japanese. Lancet 1981;2(8253):982.-
23. Goedde HW, Agarwal DP, Fritze G, et al. Distribution of ADH2 and ALDH2 genotypes in different populations. Hum Genet 1992;88(3):344-6.
24. Luczak SE, Glatt SJ, Wall TJ. Meta-analyses of ALDH2 and ADH1B with alcohol dependence in Asians. Psychol Bull 2006;132(4):607-21.
25. Edenberg HJ, Jerome RE, Li M. Polymorphism of the human alcohol dehydrogenase 4 (ADH4) promoter affects gene expression. Pharmacogenetics 1999;9(1):25-30.
26. Luo X, Kranzler HR, Zuo L, et al. ADH4 gene variation is associated with alcohol dependence and drug dependence in European Americans: results from HWD tests and case-control association studies. Neuropsychopharmacology 2006;31(5):1085-95.
27. Osier MV, Lu RB, Pakstis AJ, et al. Possible epistatic role of ADH7 in the protection against alcoholism. Am J Med Genet B Neuropsychiatr Genet 2004;126(1):19-22.
28. Lieber CS. Microsomal ethanol-oxidizing system (MEOS): the first 30 years (1968-1998)—a review. Alcohol Clin Exp Res 1999;23(6):991-1007.
29. Kunitoh S, Imaoka S, Hiroi T, et al. Acetaldehyde as well as ethanol is metabolized by human CYP2E1. J Pharmacol Exp Ther 1997;280(2):527-32.
30. Howard LA, Ahluwalia JS, Lin SK, et al. CYP2E1*1D regulatory polymorphism: association with alcohol and nicotine dependence [erratum in Pharmacogenetics. 2003;13(7):441-2]. Pharmacogenetics 2003;13(6):321-8.
31. Risch NJ. Searching for genetic determinants in the new millennium. Nature 2000;405(6788):847-56.
32. Oslin DW, Berrettini W, Kranzler HR, et al. A functional polymorphism of the mu-opioid receptor gene is associated with naltrexone response in alcohol-dependent patients. Neuropsychopharmacology 2003;28:1546-52.
33. Hutchison KE, Ray L, Sandman E, et al. The effect of olanzapine on craving and alcohol consumption. Neuropsychopharmacology 2006;31(6):1310-7.
34. Spanagel R, Pendyala G, Abarca C, et al. The clock gene Per2 influences the glutamatergic system and modulates alcohol consumption. Nat Med 2005;11(1):35-42.
Drug eruptions: Is your patient’s rash dangerous or benign?
Your patient who is taking psychotropics suddenly develops a rash. Rapidly identifying the cause is crucial to your decision to either stop the drug and risk decompensation or continue it and deal with the rash.
Adverse cutaneous drug reactions (ACDRs) develop in 2% to 5% of patients taking psychotropics1 and can occur with all drug classes.2 Most “drug eruptions” are benign and easily treated, but they can distress patients and lead to medication nonadherence. Other ACDRs can be disfiguring or life-threatening and require emergent medical treatment.
In this first installment of a 2-part article, we explain how to identify and manage benign ACDRs associated with psychotropics. In part 2, we’ll cover serious ACDRs—those that result in persistent or significant disability or are life-threatening3—as well as risk-reduction strategies.
Overall strategy
A psychiatric patient with a suspected drug eruption needs to be examined by you and, if necessary, another physician. Identify the lesion by taking a history and performing a physical examination (Box 1).4,5 If you are unable to perform this examination, promptly refer the patient to a primary care provider or dermatologist.
Once a rash is identified, determine its cause. Consider nonpharmacologic origins such as:
- infections
- insect bites
- collagen vascular disease
- neoplasms
- exposure to sun, toxins, etc.
Look for red flags that may indicate a serious reaction (Table 2).5,7 Treatment of a serious drug reaction may require care by physicians with training and clinical expertise likely to be beyond the scope of psychiatric practice. However, your responsibility is to ensure that the patient gets a timely—emergent, if indicated—referral so that treatment is not delayed. If an ACDR clearly is benign, follow the guidelines outlined below; otherwise, consult with a dermatologist, infectious diseases clinician, or other appropriate specialist.
Table 1
Benign rashes associated with psychotropics*
| Rash | Suspect drugs/classes |
|---|---|
| Exanthematous reactions | Any druga |
| Urticaria | Any druga |
| Fixed drug eruption | Any druga |
| Photosensitivity | Alprazolam,b antipsychotics,c bupropion,d carbamazepine,e citalopram,e eszopiclone,d fluoxetine,d oxcarbazepine,e paroxetine,e sertraline,e topiramate,e TCAs,d valproic acid,e zaleplon,d zolpideme |
| Acneiform eruptions | Antidepressants (most),d,e,f aripiprazole,e clonazepam,e eszopiclone,e lamotrigine,e lithium,g oxcarbazepine,e quetiapine,e risperidone,e topiramate,e zaleplon,e zolpideme |
| Pigmentation changes | Amitriptyline,h carbamazepine,e citalopram,e clomipramine,i desipramine,j,k eszopiclone,e fluoxetine,e lamotrigine,e paroxetine,e phenothiazines,a,c,d sertraline,e SGAs (most)e, thioridazine,l thiothixene,d topiramate,e venlafaxine,e zaleplone |
| Alopecia | Aripiprazole,e carbamazepine,e citalopram,e clonazepam,e dexmethylphenidate,e duloxetine,e escitalopram,e eszopiclone,e fluoxetine,a,e fluvoxamine,e haloperidol,d lamotrigine,e lithium,g,l methylphenidate,e mirtazapine,d olanzapine,e oxcarbazepine,e paroxetine,e risperidone,e sertraline,n trazodone,d TCAs,d valproic acid,e venlafaxine,e zaleplon,d ziprasidonee |
| Psoriaform eruptions | Carbamazepine,d fluoxetine,o lithium,b olanzapine,p oxcarbazepine,d paroxetine,q valproic acidd,r |
| * Suspect any drug with any reaction | |
| SGAs: second-generation antipsychotics; TCAs: tricyclic antidepressants | |
| Source: Click here to view references | |
Red flags: Warning signs of a serious drug rash
| Constitutional symptoms: fever, sore throat, malaise, arthralgia, lymphadenopathy, cough |
| Erythroderma |
| Facial or mucous membrane involvement |
| Skin tenderness or blistering, particularly if there is full-thickness epidermal detachment |
| Purpura |
| Source: References 5,7 |
When a patient presents with a suspected adverse cutaneous drug reaction, take a history to determine the rash onset, timing, relationship between symptoms and drug ingestion, associated symptoms, and history of previous drug reactions.
Ask your patient:
- What are your symptoms?
- How did the rash look initially?
- How has it changed?
- Have you used any new soaps, perfumes, cosmetics, medications, or supplements, or been exposed to insects, foliage, or someone with an illness?
Next, perform a physical examination. In addition to the photos and descriptions in this article (Table 3), review up-to-date textbooks, journal articles, and online resources to aid identification. Look for rashes that affect the mucosa and for lymphadenopathy or signs of internal organ involvement. Seek laboratory abnormalities, including elevated creatinine, positive fecal occult blood test, or hematuria. These and other red flags may indicate a serious rash that requires urgent treatment (Table 2). Consultation with a dermatologist may be indicated.
Dermatologic glossary
| Angioedema: a vascular reaction involving the deep dermis or subcutaneous or sub-mucosal tissue that results in localized swelling |
| Comedones: noninflammatory acne lesions; also called ‘blackheads’ |
| Effluvium, anagen: hair shedding during the growth phase of the hair cycle |
| Effluvium, telogen: hair shedding during the resting phase of the hair cycle |
| Erythema: skin redness |
| Macule: a discolored skin lesion that is not elevated above the surface |
| Papule: a small, circumscribed, superficial, solid elevation of the skin |
| Purpura: red or purple skin discolorations caused by bleeding underneath the skin |
| Pustule: a visible collection of pus within or beneath the epidermis |
| Wheal: a smooth, slightly elevated area that appears redder or paler than surrounding skin, is often accompanied by severe itching, and usually disappears within a few hours |
| Source: Dorland’s illustrated medical dictionary, 30th ed. Philadelphia, PA: Saunders; 2003 |
Benign rashes
© 2001-2008, DermAtlas Exanthematous reactions are the most common ACDR.1 Erythematous macules and papules may initially present on the trunk and spread peripherally within 1 to 2 weeks of a patient’s starting psychotropic therapy (Photo 1). Lesions may become confluent and involve the mucosa, hands, and feet. Differential diagnosis includes infections, collagen vascular diseases, and more serious drug rashes.1,5,6
Exanthems usually resolve within 2 weeks after the offending drug is discontinued.1,6 Because exanthems may resolve without drug discontinuation,1,8 you could continue treatment with the offending agent if other options are not feasible.9 Keep in mind, however, that exanthematous reactions may be the presenting symptom of a more serious condition, especially if associated with any of the red flags described in Table 2. If the suspect drug has been associated with a severe reaction, discontinue it permanently.4 Additional treatments for exanthems include corticosteroids, emollients, and oral antihistamines.6-8
© 2001-2008, DermAtlas Urticaria present as pruritic, blanching erythematous wheals of varying size (Photo 2). A single lesion will typically last 1,5-7,10
If a patient has unstable vital signs or a rash that affects the airway—or if you believe he or she is at risk for anaphylaxis—emergent treatment is indicated.1,6 This may include the use of epinephrine and corticosteroids.
© 2001-2008, DermAtlas Fixed drug eruptions can appear anywhere on the body as single or multiple sharply demarcated, pruritic erythematous macules (Photo 3). They may blister or cause a burning sensation; rarely, a patient may present with constitutional symptoms. Lesions might erupt hours to days after drug exposure. Although this condition usually is benign, consult a dermatologist if the patient exhibits constitutional symptoms or other red flags that may indicate a serious reaction.
© 2001-2008, DermAtlas Photosensitivity describes phototoxic and photoallergic reactions. A phototoxic response resembles sunburn and is distributed in areas exposed to the sun. This can present as erythema, edema, and skin tenderness (Photo 4).
Delayed hypersensitivity response is a photoallergic reaction. This reaction may be pruritic and appear after sunlight exposure as eczematous, bullous, vesicular, or urticarial lesions 1 to 2 weeks after the drug is started. Photoallergic lesions may extend beyond sun-exposed areas. Phototesting can confirm this diagnosis.1,5,13,14
Treat a phototoxic reaction as you would sunburn. Topical soothing agents should bring relief in 1 to 2 days.15 Instruct patients to use sunscreen and avoid the sun while taking the psychotropic.1,15 You may need to discontinue the medication if lesions persist.1
Managing a photoallergic response entails avoiding the sun or discontinuing the offending agent.14,16 For both phototoxic and photoallergic reactions, consider consulting a dermatologist if the above measures do not resolve the rash.1
© 2001-2008, DermAtlas Acne lesions present as papules or pustules, typically on the arms, legs, face, chest, or back (Photo 5).1 Comedones generally are not present.
Treatment options include benzoyl peroxide, antibiotics, and topical retinoids.1,12,17 If these measures are insufficient, or if your patient finds the eruption distressing, discontinuing the offending drug usually resolves the condition.12
© 2001-2008, DermAtlas Pigmentation changes. Blue, gray, or brown discoloration resulting from changes in melanin deposition can affect skin, hair, and nails, particularly in sun-exposed areas (Photo 6). Consider in the differential diagnosis other conditions that causes skin pigmentation changes such as:
1
Laser treatment has successfully improved pigmentation changes associated with imipramine without the patient discontinuing the offending drug.21 Pigmentation changes associated with chlorpromazine have resolved when the drug was replaced by haloperidol22 or phenothiazines, used individually or in combination.23
© 2001-2008, DermAtlas Alopecia is diffuse nonscarring hair loss (Photo 7). Anagen effluvium results in rapid hair loss, as seen with chemotherapeutic agents. Telogen effluvium may not occur until months after a drug is started. Frequently, patients experience only partial hair thinning.
Although alopecia is usually considered benign, patients may find it distressing. Improvement usually occurs within several months after the offending medication is discontinued.1,25 The benefits of continuing a medication associated with alopecia may outweigh the risks; discuss this with the patient.
© 2001-2008, DermAtlas Psoriasis presents as pruritic erythematous patches with scale (Photo 8). Psoriasis may appear at the beginning of drug therapy, or pharmacotherapy may worsen preexisting disease.2,26
Restarting a medication
By accurately identifying a rash and quickly determining its cause, you may avoid unnecessarily discontinuing a patient’s stabilizing medication (Box 2). If you need to discontinue a drug that is causing an ACDR, try to wait 2 weeks before initiating another drug. If this is not possible, cross-tapering a different medication from another class may diminish the risk of drug-rash relapse. To decrease the risk of drug-related rash, follow the manufacturer’s dosing recommendations28 and use the lowest effective dose.
Educate office and hospital staff about specifics pertaining to drug rashes to help ensure that:
- vital information gets to you immediately
- evaluation and treatment can start promptly.
While visiting the psychiatry clinic to complete paperwork, a patient receiving lamotrigine for bipolar disorder asks the office staff to tell her doctor she has a new rash on her face and in her mouth. Mrs. L, age 52, has been on the same lamotrigine dose (200 mg/d) for >1 year and was also taking lansoprazole (dosage unknown); loratadine, 10 mg/d; bupropion, 300 mg/d; quetiapine, 200 mg/d; clonazepam, 0.5 mg bid; atorvastatin, 10 mg/d; valsartan, 160 mg/d; and gabapentin, 300 mg/d. She has had no recent medication changes. Mrs. L leaves the office after finishing the paperwork.
Because lamotrigine carries an FDA “black-box” warning about serious, potentially life-threatening rashes, the psychiatrist attempts to contact Mrs. L immediately as soon as she learns of her symptoms. By phone, Mrs. L describes painful red lesions on her face and sores in her mouth that began the day before. She says she isn’t sure if these lesions have gotten worse. She denies having fever, chills, muscle aches, arthralgia, cough, neck stiffness, shortness of breath, or any other constitutional symptoms.
The psychiatrist tells Mrs. L she may be having a serious skin reaction to lamotrigine and instructs her to stop taking the drug and visit the ER immediately. She also explains that abruptly stopping lamotrigine might cause a relapse of Mrs. L’s bipolar disorder.
The ER physician examines Mrs. L, diagnoses herpes zoster, and prescribes the antiviral famciclovir, 500 mg tid for 7 days, and hydrocodone/acetaminophen, 7.5 mg/500 mg, as needed for pain. Three days later, Mrs. L sees the psychiatrist for a follow-up visit and resumes taking lamotrigine. She has no further complications.
- Dermatology Image Atlas. www.dermatlas.org.
- American Academy of Dermatology. www.aad.org.
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Atorvastatin • Lipitor
- Bupropion • Wellbutrin
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Cimetidine • Tagamet
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clonazepam • Klonopin
- Desipramine • Norpramin
- Dexmethylphenidate • Focalin
- Diphenhydramine • Benadryl
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Eszopiclone • Lunesta
- Famciclovir • Famvir
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Haloperidol • Haldol
- Hydrocodone/acetaminophen • Vicodin
- Hydroxyzine • Atarax
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lansoprazole • Prevacid
- Loratadine • Claritin
- Methylphenidate • Ritalin
- Mirtazapine • Remeron
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Ranitidine • Zantac
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Mellaril
- Thiothixene • Navane
- Topiramate • Topamax
- Trazodone • Desyrel
- Valproic acid • Depakote
- Valsartan • Diovan
- Venlafaxine • Effexor
- Zaleplon • Sonata
- Ziprasidone • Geodon
- Zolpidem • Ambien
Disclosure
Dr. Skonicki reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Warnock receives research/grant support from Boehringer Ingelheim, Forest Pharmaceuticals, and Wyeth Pharmaceuticals.
1. Kimyai-Asadi A, Harris JC, Nousari HC. Critical overview: adverse cutaneous reactions to psychotropic medications. J Clin Psychiatry 1999;60(10):714-25.
2. MacMorran WS, Krahn LE. Adverse cutaneous reactions to psychotropic drugs. Psychosomatics 1997;38(5):413-22.
3. Edwards IR, Aronson JK. Adverse drug reactions: definitions, diagnosis, and management. Lancet 2000;356(9237):1255-9.
4. Babu KS, Belgi G. Management of cutaneous drug reactions. Curr Allergy Asthma Rep 2002;2(1):26-33.
5. Shear NH, Knowles SR, Sullivan JR, Shapiro L. Cutaneous reactions to drugs. In: Freedburg IM, Eisen AZ, Wolff K, et al, eds. Fitzpatrick’s dermatology in general medicine. 6th ed. New York, NY: McGraw-Hill; 2003:1330-7.
6. Nigen S, Knowles SR, Shear NH. Drug eruptions: approaching the diagnosis of drug-induced skin diseases. J Drugs Dermatol 2003;3:278-99.
7. Chosidow OM, Stern RS, Wintroub BU. Cutaneous drug reactions. In: Kasper DL, Braunwald E, Fauci AS, et al, eds. Harrisons’s principles of internal medicine. 16th ed. New York, NY: McGraw-Hill; 2005:318-24.
8. Odom RB, James WD, Berger TG. Contact dermatitis and drug eruptions. In: Andrew’s diseases of the skin: clinical dermatology. 9th ed. Philadelphia, PA: W.B. Saunders Co.; 2000:95-145.
9. Rojeau JC, Stern RS. Medical progress: severe adverse cutaneous reactions to drugs. N Engl J Med 1994;331(19):1272-85.
10. Breathnach SM. Adverse cutaneous reactions to drugs. Clin Med 2002;2(1):15-9.
11. du Vivier A, McKee PH, Stoughton RB. Drug and toxic eruptions of the skin. In: du Vivier A, McKee PH, Stoughton RB. Atlas of clinical dermatology. Philadelphia, PA: W.B. Saunders Co.; 1986:14.1-14.18.
12. Warnock JK, Morris DW. Adverse cutaneous reactions to mood stabilizers. Am J Clin Dermatol 2003;4(1):21-30.
13. Mann SC, Walker MM. Leukocytoclastic vasculitis secondary to trazodone treatment. J Am Acad Dermatol 1984;10(4):669-70.
14. Hearn R. Recognition and management of cutaneous photosensitivity. Practitioner 2005;249(1671):418-32.
15. Moore DE. Drug-induced cutaneous photosensitivity: incidence, mechanism, prevention, and management. Drug Saf 2002;25(5):345-72.
16. Crowson AN, Brown TJ, Magro CM. Progress in the understanding of the pathology and pathogenesis of cutaneous drug eruptions. Am J Clin Dermatol 2003;4(6):407-28.
17. Remmer HI. Successful treatment of lithium-induced acne. J Clin Psychiatry 1986;47(1):48.-
18. Warnock JK, Morris DW. Adverse cutaneous reactions to antidepressants. Am J Clin Dermatol 2002;3(5):329-39.
19. Warnock JK, Morris DW. Adverse cutaneous reactions to antipsychotics. Am J Clin Dermatol 2002;3(9):629-36.
20. Physicians desk reference. 61st ed. Montvale, NJ: Thomson PDR; 2007.
21. Atkin DH, Fitzpatrick RE. Laser treatment of imipramine-induced hyperpigmentation. J Am Acad Dermatol 2000;43(1 Pt 1):77-80.
22. Thompson TR, Lal S, Yassa R, Gerstein W. Resolution of chlorpromazine-induced pigmentation with haloperidol substitution. Acta Psychiatr Scand 1988;78(6):763-5.
23. Bloom D, Krishnan B, Thavundayil JX, Lal S. Resolution of chlorpromazine-induced cutaneous pigmentation following substitution with levomepromazine or other neuroleptics. Acta Psychiatr Scand 1993;87(3):223-4.
24. Mercke Y, Sheng H, Khan T, Lippmann S. Hair loss in psychopharmacology. Ann Clin Psychiatry 2000;12(1):35-42.
25. Warnock JK. Psychotropic medication and drug-related alopecia. Psychosomatics 1999;32(2):149-52.
26. Gupta AK, Knowles SR, Gupta MA, et al. Lithium therapy associated with hidradenitis suppurativa: case report and review of the dermatologic side effects of lithium. J Am Acad Dermatol 1995;32(2 part 2):382-6.
27. Osborne SF, Stafford L, Orr KD. Paroxetine-associated psoriasis. Am J Psychiatry 2002;59(12):2113.-
28. Wong IC, Mawer GE, Sander JW. Factors influencing the incidence of lamotrigine-related skin rash. Ann Pharmacother 1999;33(10):1037-42.
Your patient who is taking psychotropics suddenly develops a rash. Rapidly identifying the cause is crucial to your decision to either stop the drug and risk decompensation or continue it and deal with the rash.
Adverse cutaneous drug reactions (ACDRs) develop in 2% to 5% of patients taking psychotropics1 and can occur with all drug classes.2 Most “drug eruptions” are benign and easily treated, but they can distress patients and lead to medication nonadherence. Other ACDRs can be disfiguring or life-threatening and require emergent medical treatment.
In this first installment of a 2-part article, we explain how to identify and manage benign ACDRs associated with psychotropics. In part 2, we’ll cover serious ACDRs—those that result in persistent or significant disability or are life-threatening3—as well as risk-reduction strategies.
Overall strategy
A psychiatric patient with a suspected drug eruption needs to be examined by you and, if necessary, another physician. Identify the lesion by taking a history and performing a physical examination (Box 1).4,5 If you are unable to perform this examination, promptly refer the patient to a primary care provider or dermatologist.
Once a rash is identified, determine its cause. Consider nonpharmacologic origins such as:
- infections
- insect bites
- collagen vascular disease
- neoplasms
- exposure to sun, toxins, etc.
Look for red flags that may indicate a serious reaction (Table 2).5,7 Treatment of a serious drug reaction may require care by physicians with training and clinical expertise likely to be beyond the scope of psychiatric practice. However, your responsibility is to ensure that the patient gets a timely—emergent, if indicated—referral so that treatment is not delayed. If an ACDR clearly is benign, follow the guidelines outlined below; otherwise, consult with a dermatologist, infectious diseases clinician, or other appropriate specialist.
Table 1
Benign rashes associated with psychotropics*
| Rash | Suspect drugs/classes |
|---|---|
| Exanthematous reactions | Any druga |
| Urticaria | Any druga |
| Fixed drug eruption | Any druga |
| Photosensitivity | Alprazolam,b antipsychotics,c bupropion,d carbamazepine,e citalopram,e eszopiclone,d fluoxetine,d oxcarbazepine,e paroxetine,e sertraline,e topiramate,e TCAs,d valproic acid,e zaleplon,d zolpideme |
| Acneiform eruptions | Antidepressants (most),d,e,f aripiprazole,e clonazepam,e eszopiclone,e lamotrigine,e lithium,g oxcarbazepine,e quetiapine,e risperidone,e topiramate,e zaleplon,e zolpideme |
| Pigmentation changes | Amitriptyline,h carbamazepine,e citalopram,e clomipramine,i desipramine,j,k eszopiclone,e fluoxetine,e lamotrigine,e paroxetine,e phenothiazines,a,c,d sertraline,e SGAs (most)e, thioridazine,l thiothixene,d topiramate,e venlafaxine,e zaleplone |
| Alopecia | Aripiprazole,e carbamazepine,e citalopram,e clonazepam,e dexmethylphenidate,e duloxetine,e escitalopram,e eszopiclone,e fluoxetine,a,e fluvoxamine,e haloperidol,d lamotrigine,e lithium,g,l methylphenidate,e mirtazapine,d olanzapine,e oxcarbazepine,e paroxetine,e risperidone,e sertraline,n trazodone,d TCAs,d valproic acid,e venlafaxine,e zaleplon,d ziprasidonee |
| Psoriaform eruptions | Carbamazepine,d fluoxetine,o lithium,b olanzapine,p oxcarbazepine,d paroxetine,q valproic acidd,r |
| * Suspect any drug with any reaction | |
| SGAs: second-generation antipsychotics; TCAs: tricyclic antidepressants | |
| Source: Click here to view references | |
Red flags: Warning signs of a serious drug rash
| Constitutional symptoms: fever, sore throat, malaise, arthralgia, lymphadenopathy, cough |
| Erythroderma |
| Facial or mucous membrane involvement |
| Skin tenderness or blistering, particularly if there is full-thickness epidermal detachment |
| Purpura |
| Source: References 5,7 |
When a patient presents with a suspected adverse cutaneous drug reaction, take a history to determine the rash onset, timing, relationship between symptoms and drug ingestion, associated symptoms, and history of previous drug reactions.
Ask your patient:
- What are your symptoms?
- How did the rash look initially?
- How has it changed?
- Have you used any new soaps, perfumes, cosmetics, medications, or supplements, or been exposed to insects, foliage, or someone with an illness?
Next, perform a physical examination. In addition to the photos and descriptions in this article (Table 3), review up-to-date textbooks, journal articles, and online resources to aid identification. Look for rashes that affect the mucosa and for lymphadenopathy or signs of internal organ involvement. Seek laboratory abnormalities, including elevated creatinine, positive fecal occult blood test, or hematuria. These and other red flags may indicate a serious rash that requires urgent treatment (Table 2). Consultation with a dermatologist may be indicated.
Dermatologic glossary
| Angioedema: a vascular reaction involving the deep dermis or subcutaneous or sub-mucosal tissue that results in localized swelling |
| Comedones: noninflammatory acne lesions; also called ‘blackheads’ |
| Effluvium, anagen: hair shedding during the growth phase of the hair cycle |
| Effluvium, telogen: hair shedding during the resting phase of the hair cycle |
| Erythema: skin redness |
| Macule: a discolored skin lesion that is not elevated above the surface |
| Papule: a small, circumscribed, superficial, solid elevation of the skin |
| Purpura: red or purple skin discolorations caused by bleeding underneath the skin |
| Pustule: a visible collection of pus within or beneath the epidermis |
| Wheal: a smooth, slightly elevated area that appears redder or paler than surrounding skin, is often accompanied by severe itching, and usually disappears within a few hours |
| Source: Dorland’s illustrated medical dictionary, 30th ed. Philadelphia, PA: Saunders; 2003 |
Benign rashes
© 2001-2008, DermAtlas Exanthematous reactions are the most common ACDR.1 Erythematous macules and papules may initially present on the trunk and spread peripherally within 1 to 2 weeks of a patient’s starting psychotropic therapy (Photo 1). Lesions may become confluent and involve the mucosa, hands, and feet. Differential diagnosis includes infections, collagen vascular diseases, and more serious drug rashes.1,5,6
Exanthems usually resolve within 2 weeks after the offending drug is discontinued.1,6 Because exanthems may resolve without drug discontinuation,1,8 you could continue treatment with the offending agent if other options are not feasible.9 Keep in mind, however, that exanthematous reactions may be the presenting symptom of a more serious condition, especially if associated with any of the red flags described in Table 2. If the suspect drug has been associated with a severe reaction, discontinue it permanently.4 Additional treatments for exanthems include corticosteroids, emollients, and oral antihistamines.6-8
© 2001-2008, DermAtlas Urticaria present as pruritic, blanching erythematous wheals of varying size (Photo 2). A single lesion will typically last 1,5-7,10
If a patient has unstable vital signs or a rash that affects the airway—or if you believe he or she is at risk for anaphylaxis—emergent treatment is indicated.1,6 This may include the use of epinephrine and corticosteroids.
© 2001-2008, DermAtlas Fixed drug eruptions can appear anywhere on the body as single or multiple sharply demarcated, pruritic erythematous macules (Photo 3). They may blister or cause a burning sensation; rarely, a patient may present with constitutional symptoms. Lesions might erupt hours to days after drug exposure. Although this condition usually is benign, consult a dermatologist if the patient exhibits constitutional symptoms or other red flags that may indicate a serious reaction.
© 2001-2008, DermAtlas Photosensitivity describes phototoxic and photoallergic reactions. A phototoxic response resembles sunburn and is distributed in areas exposed to the sun. This can present as erythema, edema, and skin tenderness (Photo 4).
Delayed hypersensitivity response is a photoallergic reaction. This reaction may be pruritic and appear after sunlight exposure as eczematous, bullous, vesicular, or urticarial lesions 1 to 2 weeks after the drug is started. Photoallergic lesions may extend beyond sun-exposed areas. Phototesting can confirm this diagnosis.1,5,13,14
Treat a phototoxic reaction as you would sunburn. Topical soothing agents should bring relief in 1 to 2 days.15 Instruct patients to use sunscreen and avoid the sun while taking the psychotropic.1,15 You may need to discontinue the medication if lesions persist.1
Managing a photoallergic response entails avoiding the sun or discontinuing the offending agent.14,16 For both phototoxic and photoallergic reactions, consider consulting a dermatologist if the above measures do not resolve the rash.1
© 2001-2008, DermAtlas Acne lesions present as papules or pustules, typically on the arms, legs, face, chest, or back (Photo 5).1 Comedones generally are not present.
Treatment options include benzoyl peroxide, antibiotics, and topical retinoids.1,12,17 If these measures are insufficient, or if your patient finds the eruption distressing, discontinuing the offending drug usually resolves the condition.12
© 2001-2008, DermAtlas Pigmentation changes. Blue, gray, or brown discoloration resulting from changes in melanin deposition can affect skin, hair, and nails, particularly in sun-exposed areas (Photo 6). Consider in the differential diagnosis other conditions that causes skin pigmentation changes such as:
1
Laser treatment has successfully improved pigmentation changes associated with imipramine without the patient discontinuing the offending drug.21 Pigmentation changes associated with chlorpromazine have resolved when the drug was replaced by haloperidol22 or phenothiazines, used individually or in combination.23
© 2001-2008, DermAtlas Alopecia is diffuse nonscarring hair loss (Photo 7). Anagen effluvium results in rapid hair loss, as seen with chemotherapeutic agents. Telogen effluvium may not occur until months after a drug is started. Frequently, patients experience only partial hair thinning.
Although alopecia is usually considered benign, patients may find it distressing. Improvement usually occurs within several months after the offending medication is discontinued.1,25 The benefits of continuing a medication associated with alopecia may outweigh the risks; discuss this with the patient.
© 2001-2008, DermAtlas Psoriasis presents as pruritic erythematous patches with scale (Photo 8). Psoriasis may appear at the beginning of drug therapy, or pharmacotherapy may worsen preexisting disease.2,26
Restarting a medication
By accurately identifying a rash and quickly determining its cause, you may avoid unnecessarily discontinuing a patient’s stabilizing medication (Box 2). If you need to discontinue a drug that is causing an ACDR, try to wait 2 weeks before initiating another drug. If this is not possible, cross-tapering a different medication from another class may diminish the risk of drug-rash relapse. To decrease the risk of drug-related rash, follow the manufacturer’s dosing recommendations28 and use the lowest effective dose.
Educate office and hospital staff about specifics pertaining to drug rashes to help ensure that:
- vital information gets to you immediately
- evaluation and treatment can start promptly.
While visiting the psychiatry clinic to complete paperwork, a patient receiving lamotrigine for bipolar disorder asks the office staff to tell her doctor she has a new rash on her face and in her mouth. Mrs. L, age 52, has been on the same lamotrigine dose (200 mg/d) for >1 year and was also taking lansoprazole (dosage unknown); loratadine, 10 mg/d; bupropion, 300 mg/d; quetiapine, 200 mg/d; clonazepam, 0.5 mg bid; atorvastatin, 10 mg/d; valsartan, 160 mg/d; and gabapentin, 300 mg/d. She has had no recent medication changes. Mrs. L leaves the office after finishing the paperwork.
Because lamotrigine carries an FDA “black-box” warning about serious, potentially life-threatening rashes, the psychiatrist attempts to contact Mrs. L immediately as soon as she learns of her symptoms. By phone, Mrs. L describes painful red lesions on her face and sores in her mouth that began the day before. She says she isn’t sure if these lesions have gotten worse. She denies having fever, chills, muscle aches, arthralgia, cough, neck stiffness, shortness of breath, or any other constitutional symptoms.
The psychiatrist tells Mrs. L she may be having a serious skin reaction to lamotrigine and instructs her to stop taking the drug and visit the ER immediately. She also explains that abruptly stopping lamotrigine might cause a relapse of Mrs. L’s bipolar disorder.
The ER physician examines Mrs. L, diagnoses herpes zoster, and prescribes the antiviral famciclovir, 500 mg tid for 7 days, and hydrocodone/acetaminophen, 7.5 mg/500 mg, as needed for pain. Three days later, Mrs. L sees the psychiatrist for a follow-up visit and resumes taking lamotrigine. She has no further complications.
- Dermatology Image Atlas. www.dermatlas.org.
- American Academy of Dermatology. www.aad.org.
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Atorvastatin • Lipitor
- Bupropion • Wellbutrin
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Cimetidine • Tagamet
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clonazepam • Klonopin
- Desipramine • Norpramin
- Dexmethylphenidate • Focalin
- Diphenhydramine • Benadryl
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Eszopiclone • Lunesta
- Famciclovir • Famvir
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Haloperidol • Haldol
- Hydrocodone/acetaminophen • Vicodin
- Hydroxyzine • Atarax
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lansoprazole • Prevacid
- Loratadine • Claritin
- Methylphenidate • Ritalin
- Mirtazapine • Remeron
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Ranitidine • Zantac
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Mellaril
- Thiothixene • Navane
- Topiramate • Topamax
- Trazodone • Desyrel
- Valproic acid • Depakote
- Valsartan • Diovan
- Venlafaxine • Effexor
- Zaleplon • Sonata
- Ziprasidone • Geodon
- Zolpidem • Ambien
Disclosure
Dr. Skonicki reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Warnock receives research/grant support from Boehringer Ingelheim, Forest Pharmaceuticals, and Wyeth Pharmaceuticals.
Your patient who is taking psychotropics suddenly develops a rash. Rapidly identifying the cause is crucial to your decision to either stop the drug and risk decompensation or continue it and deal with the rash.
Adverse cutaneous drug reactions (ACDRs) develop in 2% to 5% of patients taking psychotropics1 and can occur with all drug classes.2 Most “drug eruptions” are benign and easily treated, but they can distress patients and lead to medication nonadherence. Other ACDRs can be disfiguring or life-threatening and require emergent medical treatment.
In this first installment of a 2-part article, we explain how to identify and manage benign ACDRs associated with psychotropics. In part 2, we’ll cover serious ACDRs—those that result in persistent or significant disability or are life-threatening3—as well as risk-reduction strategies.
Overall strategy
A psychiatric patient with a suspected drug eruption needs to be examined by you and, if necessary, another physician. Identify the lesion by taking a history and performing a physical examination (Box 1).4,5 If you are unable to perform this examination, promptly refer the patient to a primary care provider or dermatologist.
Once a rash is identified, determine its cause. Consider nonpharmacologic origins such as:
- infections
- insect bites
- collagen vascular disease
- neoplasms
- exposure to sun, toxins, etc.
Look for red flags that may indicate a serious reaction (Table 2).5,7 Treatment of a serious drug reaction may require care by physicians with training and clinical expertise likely to be beyond the scope of psychiatric practice. However, your responsibility is to ensure that the patient gets a timely—emergent, if indicated—referral so that treatment is not delayed. If an ACDR clearly is benign, follow the guidelines outlined below; otherwise, consult with a dermatologist, infectious diseases clinician, or other appropriate specialist.
Table 1
Benign rashes associated with psychotropics*
| Rash | Suspect drugs/classes |
|---|---|
| Exanthematous reactions | Any druga |
| Urticaria | Any druga |
| Fixed drug eruption | Any druga |
| Photosensitivity | Alprazolam,b antipsychotics,c bupropion,d carbamazepine,e citalopram,e eszopiclone,d fluoxetine,d oxcarbazepine,e paroxetine,e sertraline,e topiramate,e TCAs,d valproic acid,e zaleplon,d zolpideme |
| Acneiform eruptions | Antidepressants (most),d,e,f aripiprazole,e clonazepam,e eszopiclone,e lamotrigine,e lithium,g oxcarbazepine,e quetiapine,e risperidone,e topiramate,e zaleplon,e zolpideme |
| Pigmentation changes | Amitriptyline,h carbamazepine,e citalopram,e clomipramine,i desipramine,j,k eszopiclone,e fluoxetine,e lamotrigine,e paroxetine,e phenothiazines,a,c,d sertraline,e SGAs (most)e, thioridazine,l thiothixene,d topiramate,e venlafaxine,e zaleplone |
| Alopecia | Aripiprazole,e carbamazepine,e citalopram,e clonazepam,e dexmethylphenidate,e duloxetine,e escitalopram,e eszopiclone,e fluoxetine,a,e fluvoxamine,e haloperidol,d lamotrigine,e lithium,g,l methylphenidate,e mirtazapine,d olanzapine,e oxcarbazepine,e paroxetine,e risperidone,e sertraline,n trazodone,d TCAs,d valproic acid,e venlafaxine,e zaleplon,d ziprasidonee |
| Psoriaform eruptions | Carbamazepine,d fluoxetine,o lithium,b olanzapine,p oxcarbazepine,d paroxetine,q valproic acidd,r |
| * Suspect any drug with any reaction | |
| SGAs: second-generation antipsychotics; TCAs: tricyclic antidepressants | |
| Source: Click here to view references | |
Red flags: Warning signs of a serious drug rash
| Constitutional symptoms: fever, sore throat, malaise, arthralgia, lymphadenopathy, cough |
| Erythroderma |
| Facial or mucous membrane involvement |
| Skin tenderness or blistering, particularly if there is full-thickness epidermal detachment |
| Purpura |
| Source: References 5,7 |
When a patient presents with a suspected adverse cutaneous drug reaction, take a history to determine the rash onset, timing, relationship between symptoms and drug ingestion, associated symptoms, and history of previous drug reactions.
Ask your patient:
- What are your symptoms?
- How did the rash look initially?
- How has it changed?
- Have you used any new soaps, perfumes, cosmetics, medications, or supplements, or been exposed to insects, foliage, or someone with an illness?
Next, perform a physical examination. In addition to the photos and descriptions in this article (Table 3), review up-to-date textbooks, journal articles, and online resources to aid identification. Look for rashes that affect the mucosa and for lymphadenopathy or signs of internal organ involvement. Seek laboratory abnormalities, including elevated creatinine, positive fecal occult blood test, or hematuria. These and other red flags may indicate a serious rash that requires urgent treatment (Table 2). Consultation with a dermatologist may be indicated.
Dermatologic glossary
| Angioedema: a vascular reaction involving the deep dermis or subcutaneous or sub-mucosal tissue that results in localized swelling |
| Comedones: noninflammatory acne lesions; also called ‘blackheads’ |
| Effluvium, anagen: hair shedding during the growth phase of the hair cycle |
| Effluvium, telogen: hair shedding during the resting phase of the hair cycle |
| Erythema: skin redness |
| Macule: a discolored skin lesion that is not elevated above the surface |
| Papule: a small, circumscribed, superficial, solid elevation of the skin |
| Purpura: red or purple skin discolorations caused by bleeding underneath the skin |
| Pustule: a visible collection of pus within or beneath the epidermis |
| Wheal: a smooth, slightly elevated area that appears redder or paler than surrounding skin, is often accompanied by severe itching, and usually disappears within a few hours |
| Source: Dorland’s illustrated medical dictionary, 30th ed. Philadelphia, PA: Saunders; 2003 |
Benign rashes
© 2001-2008, DermAtlas Exanthematous reactions are the most common ACDR.1 Erythematous macules and papules may initially present on the trunk and spread peripherally within 1 to 2 weeks of a patient’s starting psychotropic therapy (Photo 1). Lesions may become confluent and involve the mucosa, hands, and feet. Differential diagnosis includes infections, collagen vascular diseases, and more serious drug rashes.1,5,6
Exanthems usually resolve within 2 weeks after the offending drug is discontinued.1,6 Because exanthems may resolve without drug discontinuation,1,8 you could continue treatment with the offending agent if other options are not feasible.9 Keep in mind, however, that exanthematous reactions may be the presenting symptom of a more serious condition, especially if associated with any of the red flags described in Table 2. If the suspect drug has been associated with a severe reaction, discontinue it permanently.4 Additional treatments for exanthems include corticosteroids, emollients, and oral antihistamines.6-8
© 2001-2008, DermAtlas Urticaria present as pruritic, blanching erythematous wheals of varying size (Photo 2). A single lesion will typically last 1,5-7,10
If a patient has unstable vital signs or a rash that affects the airway—or if you believe he or she is at risk for anaphylaxis—emergent treatment is indicated.1,6 This may include the use of epinephrine and corticosteroids.
© 2001-2008, DermAtlas Fixed drug eruptions can appear anywhere on the body as single or multiple sharply demarcated, pruritic erythematous macules (Photo 3). They may blister or cause a burning sensation; rarely, a patient may present with constitutional symptoms. Lesions might erupt hours to days after drug exposure. Although this condition usually is benign, consult a dermatologist if the patient exhibits constitutional symptoms or other red flags that may indicate a serious reaction.
© 2001-2008, DermAtlas Photosensitivity describes phototoxic and photoallergic reactions. A phototoxic response resembles sunburn and is distributed in areas exposed to the sun. This can present as erythema, edema, and skin tenderness (Photo 4).
Delayed hypersensitivity response is a photoallergic reaction. This reaction may be pruritic and appear after sunlight exposure as eczematous, bullous, vesicular, or urticarial lesions 1 to 2 weeks after the drug is started. Photoallergic lesions may extend beyond sun-exposed areas. Phototesting can confirm this diagnosis.1,5,13,14
Treat a phototoxic reaction as you would sunburn. Topical soothing agents should bring relief in 1 to 2 days.15 Instruct patients to use sunscreen and avoid the sun while taking the psychotropic.1,15 You may need to discontinue the medication if lesions persist.1
Managing a photoallergic response entails avoiding the sun or discontinuing the offending agent.14,16 For both phototoxic and photoallergic reactions, consider consulting a dermatologist if the above measures do not resolve the rash.1
© 2001-2008, DermAtlas Acne lesions present as papules or pustules, typically on the arms, legs, face, chest, or back (Photo 5).1 Comedones generally are not present.
Treatment options include benzoyl peroxide, antibiotics, and topical retinoids.1,12,17 If these measures are insufficient, or if your patient finds the eruption distressing, discontinuing the offending drug usually resolves the condition.12
© 2001-2008, DermAtlas Pigmentation changes. Blue, gray, or brown discoloration resulting from changes in melanin deposition can affect skin, hair, and nails, particularly in sun-exposed areas (Photo 6). Consider in the differential diagnosis other conditions that causes skin pigmentation changes such as:
1
Laser treatment has successfully improved pigmentation changes associated with imipramine without the patient discontinuing the offending drug.21 Pigmentation changes associated with chlorpromazine have resolved when the drug was replaced by haloperidol22 or phenothiazines, used individually or in combination.23
© 2001-2008, DermAtlas Alopecia is diffuse nonscarring hair loss (Photo 7). Anagen effluvium results in rapid hair loss, as seen with chemotherapeutic agents. Telogen effluvium may not occur until months after a drug is started. Frequently, patients experience only partial hair thinning.
Although alopecia is usually considered benign, patients may find it distressing. Improvement usually occurs within several months after the offending medication is discontinued.1,25 The benefits of continuing a medication associated with alopecia may outweigh the risks; discuss this with the patient.
© 2001-2008, DermAtlas Psoriasis presents as pruritic erythematous patches with scale (Photo 8). Psoriasis may appear at the beginning of drug therapy, or pharmacotherapy may worsen preexisting disease.2,26
Restarting a medication
By accurately identifying a rash and quickly determining its cause, you may avoid unnecessarily discontinuing a patient’s stabilizing medication (Box 2). If you need to discontinue a drug that is causing an ACDR, try to wait 2 weeks before initiating another drug. If this is not possible, cross-tapering a different medication from another class may diminish the risk of drug-rash relapse. To decrease the risk of drug-related rash, follow the manufacturer’s dosing recommendations28 and use the lowest effective dose.
Educate office and hospital staff about specifics pertaining to drug rashes to help ensure that:
- vital information gets to you immediately
- evaluation and treatment can start promptly.
While visiting the psychiatry clinic to complete paperwork, a patient receiving lamotrigine for bipolar disorder asks the office staff to tell her doctor she has a new rash on her face and in her mouth. Mrs. L, age 52, has been on the same lamotrigine dose (200 mg/d) for >1 year and was also taking lansoprazole (dosage unknown); loratadine, 10 mg/d; bupropion, 300 mg/d; quetiapine, 200 mg/d; clonazepam, 0.5 mg bid; atorvastatin, 10 mg/d; valsartan, 160 mg/d; and gabapentin, 300 mg/d. She has had no recent medication changes. Mrs. L leaves the office after finishing the paperwork.
Because lamotrigine carries an FDA “black-box” warning about serious, potentially life-threatening rashes, the psychiatrist attempts to contact Mrs. L immediately as soon as she learns of her symptoms. By phone, Mrs. L describes painful red lesions on her face and sores in her mouth that began the day before. She says she isn’t sure if these lesions have gotten worse. She denies having fever, chills, muscle aches, arthralgia, cough, neck stiffness, shortness of breath, or any other constitutional symptoms.
The psychiatrist tells Mrs. L she may be having a serious skin reaction to lamotrigine and instructs her to stop taking the drug and visit the ER immediately. She also explains that abruptly stopping lamotrigine might cause a relapse of Mrs. L’s bipolar disorder.
The ER physician examines Mrs. L, diagnoses herpes zoster, and prescribes the antiviral famciclovir, 500 mg tid for 7 days, and hydrocodone/acetaminophen, 7.5 mg/500 mg, as needed for pain. Three days later, Mrs. L sees the psychiatrist for a follow-up visit and resumes taking lamotrigine. She has no further complications.
- Dermatology Image Atlas. www.dermatlas.org.
- American Academy of Dermatology. www.aad.org.
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Atorvastatin • Lipitor
- Bupropion • Wellbutrin
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Cimetidine • Tagamet
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clonazepam • Klonopin
- Desipramine • Norpramin
- Dexmethylphenidate • Focalin
- Diphenhydramine • Benadryl
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Eszopiclone • Lunesta
- Famciclovir • Famvir
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Haloperidol • Haldol
- Hydrocodone/acetaminophen • Vicodin
- Hydroxyzine • Atarax
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lansoprazole • Prevacid
- Loratadine • Claritin
- Methylphenidate • Ritalin
- Mirtazapine • Remeron
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Quetiapine • Seroquel
- Ranitidine • Zantac
- Risperidone • Risperdal
- Sertraline • Zoloft
- Thioridazine • Mellaril
- Thiothixene • Navane
- Topiramate • Topamax
- Trazodone • Desyrel
- Valproic acid • Depakote
- Valsartan • Diovan
- Venlafaxine • Effexor
- Zaleplon • Sonata
- Ziprasidone • Geodon
- Zolpidem • Ambien
Disclosure
Dr. Skonicki reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Warnock receives research/grant support from Boehringer Ingelheim, Forest Pharmaceuticals, and Wyeth Pharmaceuticals.
1. Kimyai-Asadi A, Harris JC, Nousari HC. Critical overview: adverse cutaneous reactions to psychotropic medications. J Clin Psychiatry 1999;60(10):714-25.
2. MacMorran WS, Krahn LE. Adverse cutaneous reactions to psychotropic drugs. Psychosomatics 1997;38(5):413-22.
3. Edwards IR, Aronson JK. Adverse drug reactions: definitions, diagnosis, and management. Lancet 2000;356(9237):1255-9.
4. Babu KS, Belgi G. Management of cutaneous drug reactions. Curr Allergy Asthma Rep 2002;2(1):26-33.
5. Shear NH, Knowles SR, Sullivan JR, Shapiro L. Cutaneous reactions to drugs. In: Freedburg IM, Eisen AZ, Wolff K, et al, eds. Fitzpatrick’s dermatology in general medicine. 6th ed. New York, NY: McGraw-Hill; 2003:1330-7.
6. Nigen S, Knowles SR, Shear NH. Drug eruptions: approaching the diagnosis of drug-induced skin diseases. J Drugs Dermatol 2003;3:278-99.
7. Chosidow OM, Stern RS, Wintroub BU. Cutaneous drug reactions. In: Kasper DL, Braunwald E, Fauci AS, et al, eds. Harrisons’s principles of internal medicine. 16th ed. New York, NY: McGraw-Hill; 2005:318-24.
8. Odom RB, James WD, Berger TG. Contact dermatitis and drug eruptions. In: Andrew’s diseases of the skin: clinical dermatology. 9th ed. Philadelphia, PA: W.B. Saunders Co.; 2000:95-145.
9. Rojeau JC, Stern RS. Medical progress: severe adverse cutaneous reactions to drugs. N Engl J Med 1994;331(19):1272-85.
10. Breathnach SM. Adverse cutaneous reactions to drugs. Clin Med 2002;2(1):15-9.
11. du Vivier A, McKee PH, Stoughton RB. Drug and toxic eruptions of the skin. In: du Vivier A, McKee PH, Stoughton RB. Atlas of clinical dermatology. Philadelphia, PA: W.B. Saunders Co.; 1986:14.1-14.18.
12. Warnock JK, Morris DW. Adverse cutaneous reactions to mood stabilizers. Am J Clin Dermatol 2003;4(1):21-30.
13. Mann SC, Walker MM. Leukocytoclastic vasculitis secondary to trazodone treatment. J Am Acad Dermatol 1984;10(4):669-70.
14. Hearn R. Recognition and management of cutaneous photosensitivity. Practitioner 2005;249(1671):418-32.
15. Moore DE. Drug-induced cutaneous photosensitivity: incidence, mechanism, prevention, and management. Drug Saf 2002;25(5):345-72.
16. Crowson AN, Brown TJ, Magro CM. Progress in the understanding of the pathology and pathogenesis of cutaneous drug eruptions. Am J Clin Dermatol 2003;4(6):407-28.
17. Remmer HI. Successful treatment of lithium-induced acne. J Clin Psychiatry 1986;47(1):48.-
18. Warnock JK, Morris DW. Adverse cutaneous reactions to antidepressants. Am J Clin Dermatol 2002;3(5):329-39.
19. Warnock JK, Morris DW. Adverse cutaneous reactions to antipsychotics. Am J Clin Dermatol 2002;3(9):629-36.
20. Physicians desk reference. 61st ed. Montvale, NJ: Thomson PDR; 2007.
21. Atkin DH, Fitzpatrick RE. Laser treatment of imipramine-induced hyperpigmentation. J Am Acad Dermatol 2000;43(1 Pt 1):77-80.
22. Thompson TR, Lal S, Yassa R, Gerstein W. Resolution of chlorpromazine-induced pigmentation with haloperidol substitution. Acta Psychiatr Scand 1988;78(6):763-5.
23. Bloom D, Krishnan B, Thavundayil JX, Lal S. Resolution of chlorpromazine-induced cutaneous pigmentation following substitution with levomepromazine or other neuroleptics. Acta Psychiatr Scand 1993;87(3):223-4.
24. Mercke Y, Sheng H, Khan T, Lippmann S. Hair loss in psychopharmacology. Ann Clin Psychiatry 2000;12(1):35-42.
25. Warnock JK. Psychotropic medication and drug-related alopecia. Psychosomatics 1999;32(2):149-52.
26. Gupta AK, Knowles SR, Gupta MA, et al. Lithium therapy associated with hidradenitis suppurativa: case report and review of the dermatologic side effects of lithium. J Am Acad Dermatol 1995;32(2 part 2):382-6.
27. Osborne SF, Stafford L, Orr KD. Paroxetine-associated psoriasis. Am J Psychiatry 2002;59(12):2113.-
28. Wong IC, Mawer GE, Sander JW. Factors influencing the incidence of lamotrigine-related skin rash. Ann Pharmacother 1999;33(10):1037-42.
1. Kimyai-Asadi A, Harris JC, Nousari HC. Critical overview: adverse cutaneous reactions to psychotropic medications. J Clin Psychiatry 1999;60(10):714-25.
2. MacMorran WS, Krahn LE. Adverse cutaneous reactions to psychotropic drugs. Psychosomatics 1997;38(5):413-22.
3. Edwards IR, Aronson JK. Adverse drug reactions: definitions, diagnosis, and management. Lancet 2000;356(9237):1255-9.
4. Babu KS, Belgi G. Management of cutaneous drug reactions. Curr Allergy Asthma Rep 2002;2(1):26-33.
5. Shear NH, Knowles SR, Sullivan JR, Shapiro L. Cutaneous reactions to drugs. In: Freedburg IM, Eisen AZ, Wolff K, et al, eds. Fitzpatrick’s dermatology in general medicine. 6th ed. New York, NY: McGraw-Hill; 2003:1330-7.
6. Nigen S, Knowles SR, Shear NH. Drug eruptions: approaching the diagnosis of drug-induced skin diseases. J Drugs Dermatol 2003;3:278-99.
7. Chosidow OM, Stern RS, Wintroub BU. Cutaneous drug reactions. In: Kasper DL, Braunwald E, Fauci AS, et al, eds. Harrisons’s principles of internal medicine. 16th ed. New York, NY: McGraw-Hill; 2005:318-24.
8. Odom RB, James WD, Berger TG. Contact dermatitis and drug eruptions. In: Andrew’s diseases of the skin: clinical dermatology. 9th ed. Philadelphia, PA: W.B. Saunders Co.; 2000:95-145.
9. Rojeau JC, Stern RS. Medical progress: severe adverse cutaneous reactions to drugs. N Engl J Med 1994;331(19):1272-85.
10. Breathnach SM. Adverse cutaneous reactions to drugs. Clin Med 2002;2(1):15-9.
11. du Vivier A, McKee PH, Stoughton RB. Drug and toxic eruptions of the skin. In: du Vivier A, McKee PH, Stoughton RB. Atlas of clinical dermatology. Philadelphia, PA: W.B. Saunders Co.; 1986:14.1-14.18.
12. Warnock JK, Morris DW. Adverse cutaneous reactions to mood stabilizers. Am J Clin Dermatol 2003;4(1):21-30.
13. Mann SC, Walker MM. Leukocytoclastic vasculitis secondary to trazodone treatment. J Am Acad Dermatol 1984;10(4):669-70.
14. Hearn R. Recognition and management of cutaneous photosensitivity. Practitioner 2005;249(1671):418-32.
15. Moore DE. Drug-induced cutaneous photosensitivity: incidence, mechanism, prevention, and management. Drug Saf 2002;25(5):345-72.
16. Crowson AN, Brown TJ, Magro CM. Progress in the understanding of the pathology and pathogenesis of cutaneous drug eruptions. Am J Clin Dermatol 2003;4(6):407-28.
17. Remmer HI. Successful treatment of lithium-induced acne. J Clin Psychiatry 1986;47(1):48.-
18. Warnock JK, Morris DW. Adverse cutaneous reactions to antidepressants. Am J Clin Dermatol 2002;3(5):329-39.
19. Warnock JK, Morris DW. Adverse cutaneous reactions to antipsychotics. Am J Clin Dermatol 2002;3(9):629-36.
20. Physicians desk reference. 61st ed. Montvale, NJ: Thomson PDR; 2007.
21. Atkin DH, Fitzpatrick RE. Laser treatment of imipramine-induced hyperpigmentation. J Am Acad Dermatol 2000;43(1 Pt 1):77-80.
22. Thompson TR, Lal S, Yassa R, Gerstein W. Resolution of chlorpromazine-induced pigmentation with haloperidol substitution. Acta Psychiatr Scand 1988;78(6):763-5.
23. Bloom D, Krishnan B, Thavundayil JX, Lal S. Resolution of chlorpromazine-induced cutaneous pigmentation following substitution with levomepromazine or other neuroleptics. Acta Psychiatr Scand 1993;87(3):223-4.
24. Mercke Y, Sheng H, Khan T, Lippmann S. Hair loss in psychopharmacology. Ann Clin Psychiatry 2000;12(1):35-42.
25. Warnock JK. Psychotropic medication and drug-related alopecia. Psychosomatics 1999;32(2):149-52.
26. Gupta AK, Knowles SR, Gupta MA, et al. Lithium therapy associated with hidradenitis suppurativa: case report and review of the dermatologic side effects of lithium. J Am Acad Dermatol 1995;32(2 part 2):382-6.
27. Osborne SF, Stafford L, Orr KD. Paroxetine-associated psoriasis. Am J Psychiatry 2002;59(12):2113.-
28. Wong IC, Mawer GE, Sander JW. Factors influencing the incidence of lamotrigine-related skin rash. Ann Pharmacother 1999;33(10):1037-42.
Deposition dos and don’ts: How to answer 8 tricky questions
During your deposition in a malpractice suit, would you know how to answer if the plaintiff’s counsel asked you: “Doctor, are you saying it was impossible to foresee Mr. Jones’ suicide?”
Ninety percent of malpractice cases are settled before trial, and the deposition often is the turning point.1-3 Your answer to tricky questions such as this could favorably affect a critical stage of litigation—or spur the plaintiff’s attorney to pursue the case more vigorously. Even if a case is settled in the plaintiff’s favor before trial, the deposition’s effectiveness may determine whether the settlement is $300,000 or $1 million.
Don’t go to a deposition unprepared. This article offers guidelines to help you anticipate many different scenarios and includes examples of honest, skillful answers to 8 difficult questions (Box 1).3-7
Digging for pay dirt
Discovery begins after a formal complaint alleges malpractice. The parties to a lawsuit gather information through written interrogatories, requests for documents, and witness depositions—out-of-court testimony to be used later in court or for discovery purposes.8 Discovery’s rationale is to reduce surprises at trial and encourage pretrial settlement. The witness being deposed is the “deponent,” and testimony is given under oath.9
A discovery deposition is designed to gather information, with almost all questions asked by opposing counsel. If you are sued for malpractice, this is the type of deposition you probably will encounter.
Rules of engagement. The plaintiff’s attorney initiates the discovery deposition. Ground rules vary by jurisdiction, but in general the Rules of Civil Procedure give deposing counsel substantial latitude in the questions that can be asked.10 The deponent and defending counsel, opposing counsel, and transcriptionist typically attend the deposition. To help you prepare appropriately, confirm with your defense counsel if other attorneys or the plaintiff will be present.
Not-so-hidden agendas. The plaintiff’s attorney’s primary goal is to gather as much information as possible about your side’s case4 (Table 1). No matter how accurate the medical records may be, they require interpretation and follow-up questioning of key players to get the full story. Opposing counsel also wants to:
- “lock down” your testimony for use at trial (testimony captured at a deposition can be used to impeach a witness who gives inconsistent testimony at trial)9
- “size up” your potential impact on a jury by assessing your strengths and weaknesses as a witness.11
The impression you make may influence the opposing attorney’s decision about how far to pursue the case. Plaintiffs’ attorney Bruce Fagel once told an interviewer that defense attorneys, too, may consider settling a case “if their client shows such arrogance in our deposition that they’re afraid to let him appear in front of a jury.”12
- The Impossible Dream
- The Hypothetical
- Invitation to Speculate
- Did I Say That?
- The Authoritative Treatise
- The Tyranny of Yes or No
- Convoluted Compounds
- Give Me More
Choosing a site. Most depositions take place in a conference room in one of the attorney’s law offices or at a neutral site. Avoid the temptation to schedule the de-position in your office, even though meeting there might seem more expedient and comfortable for you.9 Scheduling the deposition at your site:
- might make you feel it is “just another day at the office” and dissuade you from preparing sufficiently or taking the deposition seriously
- allows opposing counsel to scrutinize diplomas, books, journals, and other materials in your office.
Questioning you about these materials during the deposition is not off limits for the plaintiff’s attorney. You might find it difficult to explain why a book on your bookshelf is not “authoritative.”
Table 1
5 goals of the plaintiff’s attorney at a deposition
| Lock down testimony for trial |
| Scrutinize defendant’s qualifications |
| Size up defendant’s effectiveness as a witness |
| Probe defendant for bias, arrogance, or hostility |
| Learn as much as possible (‘fishing’) |
Prepare, prepare, prepare
Your emotional stress will probably wax and wane during the lengthy litigation process.13,14 Knowing what to expect and being well-prepared for the deposition may relieve some anxiety.
Review the case. At least twice, carefully review the entire database—including medical records and other fact witness discovery depositions. Perform 1 of these reviews just before the deposition.3 Having the details fresh in mind will help you if opposing counsel mischaracterizes information when questioning you.
Meet with your attorney. Insist on at least 2 predeposition conferences with defense counsel.
At the first conference, volunteer all pertinent information about the case as well as any noteworthy medical inconsistencies.2 Find out what documents to bring to the deposition, who will be present, and the expected duration. You might wish to prepare mentally by inquiring about the style and personality of opposing counsel.
Defense counsel does not control how long a deposition lasts but might be able to give a rough estimate. Plan accordingly, and allow for sufficient scheduling flexibility. Depositions typically last half a day, but they can last more than 1 day.
At a later predeposition conference, defense counsel might walk you through a mock deposition that involves difficult or anticipated questions. This is a good opportunity to master your anxiety and improve your effectiveness as a witness.
You also may wish to go over your curriculum vitae with defense counsel and check it for mistakes or other content that might raise problematic questions during the deposition (Table 2). Make sure your c.v. is up-to-date, and refresh your memory if it lists lectures given or articles written—no matter how long ago—on topics related to the litigation.
Table 2
Malpractice: How to prepare for your deposition
| Thoroughly review case records |
| Master the case (memorize key names, dates, facts) |
Meet with defense counsel at least twice to:
|
| Double-check your curriculum vitae for accuracy and updating |
| Come to the deposition well-rested |
On deposition day
Don’t open Pandora’s box. Keep your answers to deposition questions brief and clear. Opposing counsel may ask broad questions, hoping to encourage rambling answers that reveal new facts. Answering questions briefly provides the least information to opposing counsel and is best under most circumstances.
One exception may involve scenarios in which the defense attorney instructs you, for various reasons, to provide information beyond the question asked. For example, when a case is close to settling, your attorney might instruct you to lay out all evidence that supports your professional judgment and clinical decisions in the case. Do not use this approach, however, unless your attorney specifically instructs you to do so.
You are under no obligation to make op-posing counsel’s job easier. In a discovery deposition, volunteering information may:
- open up new areas for questioning
- equip the deposing attorney with more ammunition
- eliminate opportunities for your attorney to use surprise as a strategy, should the case go to trial.
Consider, for example, a scenario in which you and a hospital are sued in regard to an inpatient suicide case. At deposition, you might be asked whether you can identify written evidence anywhere in the patient’s chart that the decedent was checked every 15 minutes.
The correct answer would be “no,” even though you know 15-minute checks are documented in a log kept at the nursing station in this hospital. You might be tempted to reveal this information, but leave the timing of its disclosure to the defense attorney. Your attorney’s strategy may be to reveal this critical piece of information at trial, when the plaintiff’s attorney has less opportunity to strategize ways to discredit the evidence.
Keep your cool. Attorneys have different styles of questioning, depending on their personalities. Some may be excessively polite or friendly to get you to let down your guard—only to set you up for a devastating blow at the deposition’s end (or save this for trial). Other attorneys might employ a “bullying” style that seeks to intimidate. In responding to questions, always remain composed and resist the urge to counterattack.
In all circumstances, strive for humility and dignified confidence. Opposing counsel gains the advantage when defendants lose composure or become angry, defensive, or arrogant. Indeed, experienced plaintiff’s attorneys may be testing for precisely this reaction in the hope that a defendant will “demonstrate his arrogance” during the deposition or later on the witness stand.12
In working as expert witnesses in malpractice cases, we have observed many instances in which a defendant psychiatrist’s arrogant or hostile remarks at deposition played a key role in causing the case to be prematurely settled in the plaintiff’s favor.
Avoid making jokes or sarcastic comments. Even a well-timed, self-deprecating joke may backfire should opposing counsel take the opportunity to point out that the case is a “serious matter.”
Listen carefully to each question during the deposition. Pause for a moment to consider the question and allow time for other attorneys to object.5 Your attorney’s objection may suggest the best way for you to respond to the question. Refrain from answering any questions when defense counsel advises you to do so (Table 3).
Don’t answer questions you don’t understand. Rather, ask for clarification. Avoid using adjectives and superlatives such as “never” and “always,” which may be used to distort or mischaracterize your testimony at trial.
Don’t guess. No rule prevents opposing counsel from asking a witness to speculate, but generally avoid doing so. You are required to tell the truth—not to speculate or volunteer guesses. The best way to cause a jury to disbelieve your testimony is to make inaccurate or unfounded statements, which opposing counsel will surely point out at trial.
Don’t be tempted to “plumb the depths” of your memory for a forgotten piece of information, however. If asked, for example, if a patient displayed a specific symptom during an appointment 4 years ago, the true answer is likely to be “not that I recall,” rather than “no.” Qualify similar answers with statements such as “to the best of my recollection,” or “not that I recall at this time.”
If opposing counsel asks questions based on a particular document, request to see the document. Review it carefully for:
- who signed and/or authored it
- when it was prepared and dated
- whether it is a draft copy
- whether it contains confidential information relating to patients other than the plaintiff
- whether it is attorney-client privileged
- and—most importantly—whether opposing counsel has quoted portions of the document out of context.
Procedural pitfalls. Throughout the deposition, the attorneys may periodically tell the court reporter they wish to have a discussion “off the record.” Nothing is off the record for you, however. If you make a statement when the court reporter has been told to stop, opposing counsel can summarize on the record everything you said during that time.
At the beginning or end of the deposition, one of the attorneys may ask if you wish to retain or waive the right to read and sign the deposition transcript. Seek your counsel’s advice, but defendants usually choose to retain this right. Typically, you will have 30 days to read the transcript and correct any errors. Keep in mind, though, that substantive changes that go beyond typos are likely to be the subject of intense cross-examination should the case go to trial.9
Depositions are sometimes videotaped, usually because a witness will not be available at the time of trial. Because the jury will hear and see you, approach a videotaped deposition as if it were an actual trial. Dress appropriately, speak clearly, and look directly into the camera. Don’t feel embarrassed about making sure you are videotaped with the best possible lighting, camera angle, and background.
Table 3
Deposition dos and don’ts
| Always tell the truth |
| Actively listen to questions, and pause before answering |
| Keep your cool; never lose composure |
| Answer only the question asked |
| Stop speaking and listen carefully if your attorney makes an objection |
| Avoid long narratives, and don’t volunteer information |
| Don’t speculate or guess |
| Avoid absolutes such as ‘never’ or ‘always’ |
| Avoid jokes, sarcasm, and edgy comments |
| Ask for breaks if needed to keep from becoming inattentive |
| Carefully examine documents, reports, etc. before answering opposing counsel’s questions about them |
| Ask for clarification of confusing questions |
| Remember that nothing is ‘off the record’ |
| Don’t waive your right to read and sign the deposition transcript |
Keep your guard up
Don’t allow yourself to be distracted if op-posing counsel jumps from open-ended questions to clarification questions to “pinning down” questions. Using an erratic approach could be part of opposing counsel’s strategy. Answer only the question asked, and give the shortest correct answer to each question.
Opposing counsel may ask a question in a way that suggests substantial confusion or misunderstanding. If this confusion does not affect your testimony, you don’t need to clear up matters for opposing counsel. If, for example, opposing counsel asserts that one of your statements was contradictory, an appropriate response may be simply, “No, it wasn’t.” It is opposing counsel’s job to explicate further details.11
Opposing counsel may approach the deposition with a particular demeanor—such as friendly or eager to learn—in an attempt to get you to let down your guard and speak more freely (Box 2).
Particularly in a full-day deposition, the greatest likelihood of making mistakes begins around 4 pm. Indeed, some attorneys may reserve especially important questions for this time period, hoping that the witness will be less guarded. Be sure to start the day well rested, and ask for breaks if fatigue be-gins to affect your concentration.
Be alert to a pattern of questioning designed to elicit only “yes” answers. This technique—commonly used by salespersons—makes it difficult to say “no” in response to an ambiguous question.
Point out errors if opposing counsel misquotes earlier testimony or states facts incorrectly. These mistakes may be innocent or a deliberate attempt to distort your testimony.
‘Mr./Ms. Friendly.’ Some attorneys look for an opportunity before the deposition begins to show that they are ‘friendly’ and not to be feared. Remember that discussions with opposing counsel without defense counsel present are not appropriate.
‘Eager Student.’ Opposing counsel may play the ‘eager student’ to massage your ego and pave the way for long narratives and volunteered information.
‘Counselor Clueless.’ Opposing counsel may appear so ignorant of certain facts that you can scarcely resist jumping in to educate him or her.
Silent treatment. After you give a brief, honest answer, opposing counsel may sit silently as if expecting a more substantive response. Resist the temptation to fill the silence.
Related resources
- Professional Risk Management Services, Inc. The Psychiatrists’ Program. www.psychprogram.com.
- Simon R, Sadoff R. Psychiatric malpractice: cases and comments for clinicians. Washington DC: American Psychiatric Press, Inc; 1992.
Drug brand name
- Olanzapine • Zyprexa
1. Babitsky S, Mangraviti J. The discovery process. In: How to become a dangerous expert witness: advanced techniques and strategies. Falmouth, MA: Seak Inc;2005; 4-9:113-39.
2. Clark A, Fox P. The defendant physician’s deposition: fighting back—at last! Mo Med 2002;99(10):524-5.
3. Rice B. Malpractice: how to survive a deposition. Med Econ 2005;82:45-8.
4. Babitsky S, Mangraviti J. How to excel during depositions: techniques for experts that work. Falmouth, MA: Seak Inc; 1998.
5. Gutheil T. The psychiatrist as expert witness. Washington DC: American Psychiatric Publishing, Inc; 1998.
6. Babitsky S, Mangraviti J. How to excel during cross-examination: techniques for experts that work. Falmouth, MA: Seak Inc; 1997.
7. Hirsch C, Morris R, Moritz A. Handbook of legal medicine. 5th ed. St. Louis, MO: CV Mosby Co; 1979.
8. Black H. Black’s law dictionary. 8th ed. St. Paul, MN: West Publishing; 2004;440-
9. Babitsky S, Mangraviti J. Depositions: the comprehensive guide for expert witnesses. Falmouth, MA: Seak Inc; 2007.
10. Cornell Law School. Federal Rules of Civil Procedure. Depositions and discovery. Rule 26(5) B(1). Available at: http://www.law.cornell.edu/rules/frcp/Rule26.htm. Accessed January 18, 2008.
11. Culley C, Spisak L. So you’re being sued: do’s and don’ts for the defendant. Cleve Clin J Med 2002;69(10):752-60.
12. Rice B. How I pick the doctors I’ll sue. Med Econ 2004;81:54.-
13. Charles S. Coping with a medical malpractice suit. West J Med 2001;174:55-8.
14. Charles S. Malpractice distress: Help yourself and others survive. Current Psychiatry 2007;6(2):23-35.
During your deposition in a malpractice suit, would you know how to answer if the plaintiff’s counsel asked you: “Doctor, are you saying it was impossible to foresee Mr. Jones’ suicide?”
Ninety percent of malpractice cases are settled before trial, and the deposition often is the turning point.1-3 Your answer to tricky questions such as this could favorably affect a critical stage of litigation—or spur the plaintiff’s attorney to pursue the case more vigorously. Even if a case is settled in the plaintiff’s favor before trial, the deposition’s effectiveness may determine whether the settlement is $300,000 or $1 million.
Don’t go to a deposition unprepared. This article offers guidelines to help you anticipate many different scenarios and includes examples of honest, skillful answers to 8 difficult questions (Box 1).3-7
Digging for pay dirt
Discovery begins after a formal complaint alleges malpractice. The parties to a lawsuit gather information through written interrogatories, requests for documents, and witness depositions—out-of-court testimony to be used later in court or for discovery purposes.8 Discovery’s rationale is to reduce surprises at trial and encourage pretrial settlement. The witness being deposed is the “deponent,” and testimony is given under oath.9
A discovery deposition is designed to gather information, with almost all questions asked by opposing counsel. If you are sued for malpractice, this is the type of deposition you probably will encounter.
Rules of engagement. The plaintiff’s attorney initiates the discovery deposition. Ground rules vary by jurisdiction, but in general the Rules of Civil Procedure give deposing counsel substantial latitude in the questions that can be asked.10 The deponent and defending counsel, opposing counsel, and transcriptionist typically attend the deposition. To help you prepare appropriately, confirm with your defense counsel if other attorneys or the plaintiff will be present.
Not-so-hidden agendas. The plaintiff’s attorney’s primary goal is to gather as much information as possible about your side’s case4 (Table 1). No matter how accurate the medical records may be, they require interpretation and follow-up questioning of key players to get the full story. Opposing counsel also wants to:
- “lock down” your testimony for use at trial (testimony captured at a deposition can be used to impeach a witness who gives inconsistent testimony at trial)9
- “size up” your potential impact on a jury by assessing your strengths and weaknesses as a witness.11
The impression you make may influence the opposing attorney’s decision about how far to pursue the case. Plaintiffs’ attorney Bruce Fagel once told an interviewer that defense attorneys, too, may consider settling a case “if their client shows such arrogance in our deposition that they’re afraid to let him appear in front of a jury.”12
- The Impossible Dream
- The Hypothetical
- Invitation to Speculate
- Did I Say That?
- The Authoritative Treatise
- The Tyranny of Yes or No
- Convoluted Compounds
- Give Me More
Choosing a site. Most depositions take place in a conference room in one of the attorney’s law offices or at a neutral site. Avoid the temptation to schedule the de-position in your office, even though meeting there might seem more expedient and comfortable for you.9 Scheduling the deposition at your site:
- might make you feel it is “just another day at the office” and dissuade you from preparing sufficiently or taking the deposition seriously
- allows opposing counsel to scrutinize diplomas, books, journals, and other materials in your office.
Questioning you about these materials during the deposition is not off limits for the plaintiff’s attorney. You might find it difficult to explain why a book on your bookshelf is not “authoritative.”
Table 1
5 goals of the plaintiff’s attorney at a deposition
| Lock down testimony for trial |
| Scrutinize defendant’s qualifications |
| Size up defendant’s effectiveness as a witness |
| Probe defendant for bias, arrogance, or hostility |
| Learn as much as possible (‘fishing’) |
Prepare, prepare, prepare
Your emotional stress will probably wax and wane during the lengthy litigation process.13,14 Knowing what to expect and being well-prepared for the deposition may relieve some anxiety.
Review the case. At least twice, carefully review the entire database—including medical records and other fact witness discovery depositions. Perform 1 of these reviews just before the deposition.3 Having the details fresh in mind will help you if opposing counsel mischaracterizes information when questioning you.
Meet with your attorney. Insist on at least 2 predeposition conferences with defense counsel.
At the first conference, volunteer all pertinent information about the case as well as any noteworthy medical inconsistencies.2 Find out what documents to bring to the deposition, who will be present, and the expected duration. You might wish to prepare mentally by inquiring about the style and personality of opposing counsel.
Defense counsel does not control how long a deposition lasts but might be able to give a rough estimate. Plan accordingly, and allow for sufficient scheduling flexibility. Depositions typically last half a day, but they can last more than 1 day.
At a later predeposition conference, defense counsel might walk you through a mock deposition that involves difficult or anticipated questions. This is a good opportunity to master your anxiety and improve your effectiveness as a witness.
You also may wish to go over your curriculum vitae with defense counsel and check it for mistakes or other content that might raise problematic questions during the deposition (Table 2). Make sure your c.v. is up-to-date, and refresh your memory if it lists lectures given or articles written—no matter how long ago—on topics related to the litigation.
Table 2
Malpractice: How to prepare for your deposition
| Thoroughly review case records |
| Master the case (memorize key names, dates, facts) |
Meet with defense counsel at least twice to:
|
| Double-check your curriculum vitae for accuracy and updating |
| Come to the deposition well-rested |
On deposition day
Don’t open Pandora’s box. Keep your answers to deposition questions brief and clear. Opposing counsel may ask broad questions, hoping to encourage rambling answers that reveal new facts. Answering questions briefly provides the least information to opposing counsel and is best under most circumstances.
One exception may involve scenarios in which the defense attorney instructs you, for various reasons, to provide information beyond the question asked. For example, when a case is close to settling, your attorney might instruct you to lay out all evidence that supports your professional judgment and clinical decisions in the case. Do not use this approach, however, unless your attorney specifically instructs you to do so.
You are under no obligation to make op-posing counsel’s job easier. In a discovery deposition, volunteering information may:
- open up new areas for questioning
- equip the deposing attorney with more ammunition
- eliminate opportunities for your attorney to use surprise as a strategy, should the case go to trial.
Consider, for example, a scenario in which you and a hospital are sued in regard to an inpatient suicide case. At deposition, you might be asked whether you can identify written evidence anywhere in the patient’s chart that the decedent was checked every 15 minutes.
The correct answer would be “no,” even though you know 15-minute checks are documented in a log kept at the nursing station in this hospital. You might be tempted to reveal this information, but leave the timing of its disclosure to the defense attorney. Your attorney’s strategy may be to reveal this critical piece of information at trial, when the plaintiff’s attorney has less opportunity to strategize ways to discredit the evidence.
Keep your cool. Attorneys have different styles of questioning, depending on their personalities. Some may be excessively polite or friendly to get you to let down your guard—only to set you up for a devastating blow at the deposition’s end (or save this for trial). Other attorneys might employ a “bullying” style that seeks to intimidate. In responding to questions, always remain composed and resist the urge to counterattack.
In all circumstances, strive for humility and dignified confidence. Opposing counsel gains the advantage when defendants lose composure or become angry, defensive, or arrogant. Indeed, experienced plaintiff’s attorneys may be testing for precisely this reaction in the hope that a defendant will “demonstrate his arrogance” during the deposition or later on the witness stand.12
In working as expert witnesses in malpractice cases, we have observed many instances in which a defendant psychiatrist’s arrogant or hostile remarks at deposition played a key role in causing the case to be prematurely settled in the plaintiff’s favor.
Avoid making jokes or sarcastic comments. Even a well-timed, self-deprecating joke may backfire should opposing counsel take the opportunity to point out that the case is a “serious matter.”
Listen carefully to each question during the deposition. Pause for a moment to consider the question and allow time for other attorneys to object.5 Your attorney’s objection may suggest the best way for you to respond to the question. Refrain from answering any questions when defense counsel advises you to do so (Table 3).
Don’t answer questions you don’t understand. Rather, ask for clarification. Avoid using adjectives and superlatives such as “never” and “always,” which may be used to distort or mischaracterize your testimony at trial.
Don’t guess. No rule prevents opposing counsel from asking a witness to speculate, but generally avoid doing so. You are required to tell the truth—not to speculate or volunteer guesses. The best way to cause a jury to disbelieve your testimony is to make inaccurate or unfounded statements, which opposing counsel will surely point out at trial.
Don’t be tempted to “plumb the depths” of your memory for a forgotten piece of information, however. If asked, for example, if a patient displayed a specific symptom during an appointment 4 years ago, the true answer is likely to be “not that I recall,” rather than “no.” Qualify similar answers with statements such as “to the best of my recollection,” or “not that I recall at this time.”
If opposing counsel asks questions based on a particular document, request to see the document. Review it carefully for:
- who signed and/or authored it
- when it was prepared and dated
- whether it is a draft copy
- whether it contains confidential information relating to patients other than the plaintiff
- whether it is attorney-client privileged
- and—most importantly—whether opposing counsel has quoted portions of the document out of context.
Procedural pitfalls. Throughout the deposition, the attorneys may periodically tell the court reporter they wish to have a discussion “off the record.” Nothing is off the record for you, however. If you make a statement when the court reporter has been told to stop, opposing counsel can summarize on the record everything you said during that time.
At the beginning or end of the deposition, one of the attorneys may ask if you wish to retain or waive the right to read and sign the deposition transcript. Seek your counsel’s advice, but defendants usually choose to retain this right. Typically, you will have 30 days to read the transcript and correct any errors. Keep in mind, though, that substantive changes that go beyond typos are likely to be the subject of intense cross-examination should the case go to trial.9
Depositions are sometimes videotaped, usually because a witness will not be available at the time of trial. Because the jury will hear and see you, approach a videotaped deposition as if it were an actual trial. Dress appropriately, speak clearly, and look directly into the camera. Don’t feel embarrassed about making sure you are videotaped with the best possible lighting, camera angle, and background.
Table 3
Deposition dos and don’ts
| Always tell the truth |
| Actively listen to questions, and pause before answering |
| Keep your cool; never lose composure |
| Answer only the question asked |
| Stop speaking and listen carefully if your attorney makes an objection |
| Avoid long narratives, and don’t volunteer information |
| Don’t speculate or guess |
| Avoid absolutes such as ‘never’ or ‘always’ |
| Avoid jokes, sarcasm, and edgy comments |
| Ask for breaks if needed to keep from becoming inattentive |
| Carefully examine documents, reports, etc. before answering opposing counsel’s questions about them |
| Ask for clarification of confusing questions |
| Remember that nothing is ‘off the record’ |
| Don’t waive your right to read and sign the deposition transcript |
Keep your guard up
Don’t allow yourself to be distracted if op-posing counsel jumps from open-ended questions to clarification questions to “pinning down” questions. Using an erratic approach could be part of opposing counsel’s strategy. Answer only the question asked, and give the shortest correct answer to each question.
Opposing counsel may ask a question in a way that suggests substantial confusion or misunderstanding. If this confusion does not affect your testimony, you don’t need to clear up matters for opposing counsel. If, for example, opposing counsel asserts that one of your statements was contradictory, an appropriate response may be simply, “No, it wasn’t.” It is opposing counsel’s job to explicate further details.11
Opposing counsel may approach the deposition with a particular demeanor—such as friendly or eager to learn—in an attempt to get you to let down your guard and speak more freely (Box 2).
Particularly in a full-day deposition, the greatest likelihood of making mistakes begins around 4 pm. Indeed, some attorneys may reserve especially important questions for this time period, hoping that the witness will be less guarded. Be sure to start the day well rested, and ask for breaks if fatigue be-gins to affect your concentration.
Be alert to a pattern of questioning designed to elicit only “yes” answers. This technique—commonly used by salespersons—makes it difficult to say “no” in response to an ambiguous question.
Point out errors if opposing counsel misquotes earlier testimony or states facts incorrectly. These mistakes may be innocent or a deliberate attempt to distort your testimony.
‘Mr./Ms. Friendly.’ Some attorneys look for an opportunity before the deposition begins to show that they are ‘friendly’ and not to be feared. Remember that discussions with opposing counsel without defense counsel present are not appropriate.
‘Eager Student.’ Opposing counsel may play the ‘eager student’ to massage your ego and pave the way for long narratives and volunteered information.
‘Counselor Clueless.’ Opposing counsel may appear so ignorant of certain facts that you can scarcely resist jumping in to educate him or her.
Silent treatment. After you give a brief, honest answer, opposing counsel may sit silently as if expecting a more substantive response. Resist the temptation to fill the silence.
Related resources
- Professional Risk Management Services, Inc. The Psychiatrists’ Program. www.psychprogram.com.
- Simon R, Sadoff R. Psychiatric malpractice: cases and comments for clinicians. Washington DC: American Psychiatric Press, Inc; 1992.
Drug brand name
- Olanzapine • Zyprexa
During your deposition in a malpractice suit, would you know how to answer if the plaintiff’s counsel asked you: “Doctor, are you saying it was impossible to foresee Mr. Jones’ suicide?”
Ninety percent of malpractice cases are settled before trial, and the deposition often is the turning point.1-3 Your answer to tricky questions such as this could favorably affect a critical stage of litigation—or spur the plaintiff’s attorney to pursue the case more vigorously. Even if a case is settled in the plaintiff’s favor before trial, the deposition’s effectiveness may determine whether the settlement is $300,000 or $1 million.
Don’t go to a deposition unprepared. This article offers guidelines to help you anticipate many different scenarios and includes examples of honest, skillful answers to 8 difficult questions (Box 1).3-7
Digging for pay dirt
Discovery begins after a formal complaint alleges malpractice. The parties to a lawsuit gather information through written interrogatories, requests for documents, and witness depositions—out-of-court testimony to be used later in court or for discovery purposes.8 Discovery’s rationale is to reduce surprises at trial and encourage pretrial settlement. The witness being deposed is the “deponent,” and testimony is given under oath.9
A discovery deposition is designed to gather information, with almost all questions asked by opposing counsel. If you are sued for malpractice, this is the type of deposition you probably will encounter.
Rules of engagement. The plaintiff’s attorney initiates the discovery deposition. Ground rules vary by jurisdiction, but in general the Rules of Civil Procedure give deposing counsel substantial latitude in the questions that can be asked.10 The deponent and defending counsel, opposing counsel, and transcriptionist typically attend the deposition. To help you prepare appropriately, confirm with your defense counsel if other attorneys or the plaintiff will be present.
Not-so-hidden agendas. The plaintiff’s attorney’s primary goal is to gather as much information as possible about your side’s case4 (Table 1). No matter how accurate the medical records may be, they require interpretation and follow-up questioning of key players to get the full story. Opposing counsel also wants to:
- “lock down” your testimony for use at trial (testimony captured at a deposition can be used to impeach a witness who gives inconsistent testimony at trial)9
- “size up” your potential impact on a jury by assessing your strengths and weaknesses as a witness.11
The impression you make may influence the opposing attorney’s decision about how far to pursue the case. Plaintiffs’ attorney Bruce Fagel once told an interviewer that defense attorneys, too, may consider settling a case “if their client shows such arrogance in our deposition that they’re afraid to let him appear in front of a jury.”12
- The Impossible Dream
- The Hypothetical
- Invitation to Speculate
- Did I Say That?
- The Authoritative Treatise
- The Tyranny of Yes or No
- Convoluted Compounds
- Give Me More
Choosing a site. Most depositions take place in a conference room in one of the attorney’s law offices or at a neutral site. Avoid the temptation to schedule the de-position in your office, even though meeting there might seem more expedient and comfortable for you.9 Scheduling the deposition at your site:
- might make you feel it is “just another day at the office” and dissuade you from preparing sufficiently or taking the deposition seriously
- allows opposing counsel to scrutinize diplomas, books, journals, and other materials in your office.
Questioning you about these materials during the deposition is not off limits for the plaintiff’s attorney. You might find it difficult to explain why a book on your bookshelf is not “authoritative.”
Table 1
5 goals of the plaintiff’s attorney at a deposition
| Lock down testimony for trial |
| Scrutinize defendant’s qualifications |
| Size up defendant’s effectiveness as a witness |
| Probe defendant for bias, arrogance, or hostility |
| Learn as much as possible (‘fishing’) |
Prepare, prepare, prepare
Your emotional stress will probably wax and wane during the lengthy litigation process.13,14 Knowing what to expect and being well-prepared for the deposition may relieve some anxiety.
Review the case. At least twice, carefully review the entire database—including medical records and other fact witness discovery depositions. Perform 1 of these reviews just before the deposition.3 Having the details fresh in mind will help you if opposing counsel mischaracterizes information when questioning you.
Meet with your attorney. Insist on at least 2 predeposition conferences with defense counsel.
At the first conference, volunteer all pertinent information about the case as well as any noteworthy medical inconsistencies.2 Find out what documents to bring to the deposition, who will be present, and the expected duration. You might wish to prepare mentally by inquiring about the style and personality of opposing counsel.
Defense counsel does not control how long a deposition lasts but might be able to give a rough estimate. Plan accordingly, and allow for sufficient scheduling flexibility. Depositions typically last half a day, but they can last more than 1 day.
At a later predeposition conference, defense counsel might walk you through a mock deposition that involves difficult or anticipated questions. This is a good opportunity to master your anxiety and improve your effectiveness as a witness.
You also may wish to go over your curriculum vitae with defense counsel and check it for mistakes or other content that might raise problematic questions during the deposition (Table 2). Make sure your c.v. is up-to-date, and refresh your memory if it lists lectures given or articles written—no matter how long ago—on topics related to the litigation.
Table 2
Malpractice: How to prepare for your deposition
| Thoroughly review case records |
| Master the case (memorize key names, dates, facts) |
Meet with defense counsel at least twice to:
|
| Double-check your curriculum vitae for accuracy and updating |
| Come to the deposition well-rested |
On deposition day
Don’t open Pandora’s box. Keep your answers to deposition questions brief and clear. Opposing counsel may ask broad questions, hoping to encourage rambling answers that reveal new facts. Answering questions briefly provides the least information to opposing counsel and is best under most circumstances.
One exception may involve scenarios in which the defense attorney instructs you, for various reasons, to provide information beyond the question asked. For example, when a case is close to settling, your attorney might instruct you to lay out all evidence that supports your professional judgment and clinical decisions in the case. Do not use this approach, however, unless your attorney specifically instructs you to do so.
You are under no obligation to make op-posing counsel’s job easier. In a discovery deposition, volunteering information may:
- open up new areas for questioning
- equip the deposing attorney with more ammunition
- eliminate opportunities for your attorney to use surprise as a strategy, should the case go to trial.
Consider, for example, a scenario in which you and a hospital are sued in regard to an inpatient suicide case. At deposition, you might be asked whether you can identify written evidence anywhere in the patient’s chart that the decedent was checked every 15 minutes.
The correct answer would be “no,” even though you know 15-minute checks are documented in a log kept at the nursing station in this hospital. You might be tempted to reveal this information, but leave the timing of its disclosure to the defense attorney. Your attorney’s strategy may be to reveal this critical piece of information at trial, when the plaintiff’s attorney has less opportunity to strategize ways to discredit the evidence.
Keep your cool. Attorneys have different styles of questioning, depending on their personalities. Some may be excessively polite or friendly to get you to let down your guard—only to set you up for a devastating blow at the deposition’s end (or save this for trial). Other attorneys might employ a “bullying” style that seeks to intimidate. In responding to questions, always remain composed and resist the urge to counterattack.
In all circumstances, strive for humility and dignified confidence. Opposing counsel gains the advantage when defendants lose composure or become angry, defensive, or arrogant. Indeed, experienced plaintiff’s attorneys may be testing for precisely this reaction in the hope that a defendant will “demonstrate his arrogance” during the deposition or later on the witness stand.12
In working as expert witnesses in malpractice cases, we have observed many instances in which a defendant psychiatrist’s arrogant or hostile remarks at deposition played a key role in causing the case to be prematurely settled in the plaintiff’s favor.
Avoid making jokes or sarcastic comments. Even a well-timed, self-deprecating joke may backfire should opposing counsel take the opportunity to point out that the case is a “serious matter.”
Listen carefully to each question during the deposition. Pause for a moment to consider the question and allow time for other attorneys to object.5 Your attorney’s objection may suggest the best way for you to respond to the question. Refrain from answering any questions when defense counsel advises you to do so (Table 3).
Don’t answer questions you don’t understand. Rather, ask for clarification. Avoid using adjectives and superlatives such as “never” and “always,” which may be used to distort or mischaracterize your testimony at trial.
Don’t guess. No rule prevents opposing counsel from asking a witness to speculate, but generally avoid doing so. You are required to tell the truth—not to speculate or volunteer guesses. The best way to cause a jury to disbelieve your testimony is to make inaccurate or unfounded statements, which opposing counsel will surely point out at trial.
Don’t be tempted to “plumb the depths” of your memory for a forgotten piece of information, however. If asked, for example, if a patient displayed a specific symptom during an appointment 4 years ago, the true answer is likely to be “not that I recall,” rather than “no.” Qualify similar answers with statements such as “to the best of my recollection,” or “not that I recall at this time.”
If opposing counsel asks questions based on a particular document, request to see the document. Review it carefully for:
- who signed and/or authored it
- when it was prepared and dated
- whether it is a draft copy
- whether it contains confidential information relating to patients other than the plaintiff
- whether it is attorney-client privileged
- and—most importantly—whether opposing counsel has quoted portions of the document out of context.
Procedural pitfalls. Throughout the deposition, the attorneys may periodically tell the court reporter they wish to have a discussion “off the record.” Nothing is off the record for you, however. If you make a statement when the court reporter has been told to stop, opposing counsel can summarize on the record everything you said during that time.
At the beginning or end of the deposition, one of the attorneys may ask if you wish to retain or waive the right to read and sign the deposition transcript. Seek your counsel’s advice, but defendants usually choose to retain this right. Typically, you will have 30 days to read the transcript and correct any errors. Keep in mind, though, that substantive changes that go beyond typos are likely to be the subject of intense cross-examination should the case go to trial.9
Depositions are sometimes videotaped, usually because a witness will not be available at the time of trial. Because the jury will hear and see you, approach a videotaped deposition as if it were an actual trial. Dress appropriately, speak clearly, and look directly into the camera. Don’t feel embarrassed about making sure you are videotaped with the best possible lighting, camera angle, and background.
Table 3
Deposition dos and don’ts
| Always tell the truth |
| Actively listen to questions, and pause before answering |
| Keep your cool; never lose composure |
| Answer only the question asked |
| Stop speaking and listen carefully if your attorney makes an objection |
| Avoid long narratives, and don’t volunteer information |
| Don’t speculate or guess |
| Avoid absolutes such as ‘never’ or ‘always’ |
| Avoid jokes, sarcasm, and edgy comments |
| Ask for breaks if needed to keep from becoming inattentive |
| Carefully examine documents, reports, etc. before answering opposing counsel’s questions about them |
| Ask for clarification of confusing questions |
| Remember that nothing is ‘off the record’ |
| Don’t waive your right to read and sign the deposition transcript |
Keep your guard up
Don’t allow yourself to be distracted if op-posing counsel jumps from open-ended questions to clarification questions to “pinning down” questions. Using an erratic approach could be part of opposing counsel’s strategy. Answer only the question asked, and give the shortest correct answer to each question.
Opposing counsel may ask a question in a way that suggests substantial confusion or misunderstanding. If this confusion does not affect your testimony, you don’t need to clear up matters for opposing counsel. If, for example, opposing counsel asserts that one of your statements was contradictory, an appropriate response may be simply, “No, it wasn’t.” It is opposing counsel’s job to explicate further details.11
Opposing counsel may approach the deposition with a particular demeanor—such as friendly or eager to learn—in an attempt to get you to let down your guard and speak more freely (Box 2).
Particularly in a full-day deposition, the greatest likelihood of making mistakes begins around 4 pm. Indeed, some attorneys may reserve especially important questions for this time period, hoping that the witness will be less guarded. Be sure to start the day well rested, and ask for breaks if fatigue be-gins to affect your concentration.
Be alert to a pattern of questioning designed to elicit only “yes” answers. This technique—commonly used by salespersons—makes it difficult to say “no” in response to an ambiguous question.
Point out errors if opposing counsel misquotes earlier testimony or states facts incorrectly. These mistakes may be innocent or a deliberate attempt to distort your testimony.
‘Mr./Ms. Friendly.’ Some attorneys look for an opportunity before the deposition begins to show that they are ‘friendly’ and not to be feared. Remember that discussions with opposing counsel without defense counsel present are not appropriate.
‘Eager Student.’ Opposing counsel may play the ‘eager student’ to massage your ego and pave the way for long narratives and volunteered information.
‘Counselor Clueless.’ Opposing counsel may appear so ignorant of certain facts that you can scarcely resist jumping in to educate him or her.
Silent treatment. After you give a brief, honest answer, opposing counsel may sit silently as if expecting a more substantive response. Resist the temptation to fill the silence.
Related resources
- Professional Risk Management Services, Inc. The Psychiatrists’ Program. www.psychprogram.com.
- Simon R, Sadoff R. Psychiatric malpractice: cases and comments for clinicians. Washington DC: American Psychiatric Press, Inc; 1992.
Drug brand name
- Olanzapine • Zyprexa
1. Babitsky S, Mangraviti J. The discovery process. In: How to become a dangerous expert witness: advanced techniques and strategies. Falmouth, MA: Seak Inc;2005; 4-9:113-39.
2. Clark A, Fox P. The defendant physician’s deposition: fighting back—at last! Mo Med 2002;99(10):524-5.
3. Rice B. Malpractice: how to survive a deposition. Med Econ 2005;82:45-8.
4. Babitsky S, Mangraviti J. How to excel during depositions: techniques for experts that work. Falmouth, MA: Seak Inc; 1998.
5. Gutheil T. The psychiatrist as expert witness. Washington DC: American Psychiatric Publishing, Inc; 1998.
6. Babitsky S, Mangraviti J. How to excel during cross-examination: techniques for experts that work. Falmouth, MA: Seak Inc; 1997.
7. Hirsch C, Morris R, Moritz A. Handbook of legal medicine. 5th ed. St. Louis, MO: CV Mosby Co; 1979.
8. Black H. Black’s law dictionary. 8th ed. St. Paul, MN: West Publishing; 2004;440-
9. Babitsky S, Mangraviti J. Depositions: the comprehensive guide for expert witnesses. Falmouth, MA: Seak Inc; 2007.
10. Cornell Law School. Federal Rules of Civil Procedure. Depositions and discovery. Rule 26(5) B(1). Available at: http://www.law.cornell.edu/rules/frcp/Rule26.htm. Accessed January 18, 2008.
11. Culley C, Spisak L. So you’re being sued: do’s and don’ts for the defendant. Cleve Clin J Med 2002;69(10):752-60.
12. Rice B. How I pick the doctors I’ll sue. Med Econ 2004;81:54.-
13. Charles S. Coping with a medical malpractice suit. West J Med 2001;174:55-8.
14. Charles S. Malpractice distress: Help yourself and others survive. Current Psychiatry 2007;6(2):23-35.
1. Babitsky S, Mangraviti J. The discovery process. In: How to become a dangerous expert witness: advanced techniques and strategies. Falmouth, MA: Seak Inc;2005; 4-9:113-39.
2. Clark A, Fox P. The defendant physician’s deposition: fighting back—at last! Mo Med 2002;99(10):524-5.
3. Rice B. Malpractice: how to survive a deposition. Med Econ 2005;82:45-8.
4. Babitsky S, Mangraviti J. How to excel during depositions: techniques for experts that work. Falmouth, MA: Seak Inc; 1998.
5. Gutheil T. The psychiatrist as expert witness. Washington DC: American Psychiatric Publishing, Inc; 1998.
6. Babitsky S, Mangraviti J. How to excel during cross-examination: techniques for experts that work. Falmouth, MA: Seak Inc; 1997.
7. Hirsch C, Morris R, Moritz A. Handbook of legal medicine. 5th ed. St. Louis, MO: CV Mosby Co; 1979.
8. Black H. Black’s law dictionary. 8th ed. St. Paul, MN: West Publishing; 2004;440-
9. Babitsky S, Mangraviti J. Depositions: the comprehensive guide for expert witnesses. Falmouth, MA: Seak Inc; 2007.
10. Cornell Law School. Federal Rules of Civil Procedure. Depositions and discovery. Rule 26(5) B(1). Available at: http://www.law.cornell.edu/rules/frcp/Rule26.htm. Accessed January 18, 2008.
11. Culley C, Spisak L. So you’re being sued: do’s and don’ts for the defendant. Cleve Clin J Med 2002;69(10):752-60.
12. Rice B. How I pick the doctors I’ll sue. Med Econ 2004;81:54.-
13. Charles S. Coping with a medical malpractice suit. West J Med 2001;174:55-8.
14. Charles S. Malpractice distress: Help yourself and others survive. Current Psychiatry 2007;6(2):23-35.
Prevent drug-drug interactions with cholinesterase inhibitors
Mr. B, age 78, has a long history of well-controlled bipolar disorder and was diagnosed with Alzheimer’s dementia 6 months ago. He is living at home and has been taking donepezil, 10 mg/d, and lamotrigine, 100 mg bid.
This morning Mr. B’s wife calls and reports that he is experiencing sudden difficulty walking, dizziness, and “feeling drunk.” When you ask about Mr. B’s medications, his wife says that her husband’s internist had prescribed itraconazole, 200 mg/d, for onychomycosis, and Mr. B has taken 1 dose. You promptly discontinue the itraconazole, and Mr. B’s symptoms resolve.
Drug-drug interactions (DDIs) in Alzheimer’s disease (AD) patients such as Mr. B can be serious and even life-threatening. On average, persons age ≥65 use 4.5 prescription agents and 2 over-the-counter preparations per day,1 and the number of concurrently used medications is a significant predictor of adverse drug reactions.2
Cognitive enhancers, including acetylcholinesterase inhibitors (AChEIs) and memantine, are the most widely prescribed agents for AD patients. The FDA has approved galantamine and rivastigmine for mild to moderate dementia, memantine for moderate to severe dementia, and donepezil for mild to severe dementia (Table 1).3-5
To help you minimize adverse DDIs in AD patients, this article describes:
- pharmacokinetic and pharmacodynamic effects of cognitive enhancers used in AD management
- DDIs with medications commonly prescribed to AD patients
- how to avoid adverse events related to antipsychotics, antidepressants, and benzodiazepines.
Table 1
Pharmacokinetic features of cognitive enhancers
| Agent | Protein binding | CYP-450 activity | Other features |
|---|---|---|---|
| AChEIs | |||
| Donepezil | 96% | CYP 2D6, 3A4 substrate | Once-daily dosing |
| Rivastigmine | 40% | None | Metabolized by cholinesterases |
| Galantamine | 18% | CYP 2D6, 3A4 substrate | Nicotinic cholinergic receptor modulation |
| NMDA receptor antagonist | |||
| Memantine | 45% | None | No hepatic metabolism |
| CYP-450: cytochrome P-450; AChEIs: acetylcholinesterase inhibitors; NMDA: N-methyl-D-aspartate | |||
| Source: References 3-5 | |||
Pharmacologic changes with aging
Pharmacokinetics is the study of the time course of drugs and their metabolites through the body. Pharmacokinetic interactions involve alterations in the plasma concentration of a drug by a second agent.3
Absorption of medications is decreased in the elderly because of reduced intestinal blood flow and motility. Absorption further decreases if patients concomitantly take antacids, high-fiber supplements, or anticholinergic medications.
In plasma, drugs circulate freely or bound to proteins—mainly albumin and α1-acid glycoprotein. Aging can cause decreased plasma albumin and increased α1-acid glycoprotein.6 Additionally, malnutrition, diabetes mellitus, and hepatic and renal disease—all more common with advancing age—may cause hypoalbuminemia, which increases the free fraction of drugs bound to albumin.6Table 1 includes information about cognitive enhancers’ protein binding.
When 2 or more highly protein-bound drugs are coadministered, mutual displacement occurs and the free fraction of each drug increases. A recent case report described valproate toxicity with dizziness, ataxia, and falling in a 76-year-old man after aspirin was added to his regimen.7 The mechanism appeared to be mutual displacement from albumin combined with metabolism of valproate inhibited by aspirin.7
Metabolism. Liver size and hepatic blood flow decrease with aging.6 Cytochrome P-450 3A4 pathway activity slows, but the 2D6 pathway is not affected.4 Oxidative metabolism through CYP pathways is slower, but conjugation reactions are not.6Table 23,5,7,8 lists major substrates and inhibitors of CYP enzymes.
Azole antifungals are potent inhibitors of CYP 3A4,4 of which both donepezil and lamotrigine are substrates (Table 2). In Mr. B’s case, lamotrigine and donepezil levels increased because of this pharmacokinetic interaction. Because donepezil also is metabolized by the CYP 2D6 pathway, the increase in concentration is unlikely to modify the drug effect. Mr. B experienced symptoms consistent with lamotrigine toxicity.
Pharmacokinetics of AChEIs. AChEIs have relatively few pharmacokinetic interactions, although donepezil and galantamine are metabolized through the liver’s CYP 2D6 and 3A4 pathways.
Because rivastigmine does not undergo hepatic metabolism, it is least likely of the cognitive enhancers to have pharmacokinetic interactions with other medications. Rivastigmine did not lead to increased adverse events when administered concomitantly with 22 different classes of medications—including antidiabetics, cardiovascular drugs, gastrointestinal agents, and NSAIDs.9
Table 2
DDIs in AD patients: CYP-450 substrates and inhibitors*
| CYP 2D6 | CYP 3A4 | |
|---|---|---|
| Substrates (substances metabolized by enzyme) | Second-generation antipsychotics Citalopram Donepezil Duloxetine Galantamine Haloperidol Tricyclic antidepressants Trazodone Venlafaxine | Second-generation antipsychotics Benzodiazepines Buspirone Carbamazepine Donepezil Galantamine Haloperidol Lamotrigine Mirtazapine Nefazodone Sertraline Tricyclic antidepressants Trazodone Zolpidem |
| Inhibitors | Bupropion Cimetidine Duloxetine Fluoxetine Paroxetine Sertraline | Erythromycin Fluconazole Fluvoxamine Grapefruit juice Itraconazole Nefazodone |
| *All cytochrome P (CYP) 450 enzymes are induced by barbiturates, phenytoin, carbamazepine, and rifampicin. Smoking also induces CYP 1A2. | ||
| DDIs: drug-drug interactions; AD: Alzheimer’s disease | ||
| Source: References 3,5,7,8 | ||
Memantine, an amantadine derivative and N-methyl-D-aspartate (NMDA) receptor antagonist, is a weak dopaminergic agonist with atropinic effects.11 Because memantine is not metabolized by the CYP-450 pathway, it lacks pharmacokinetic DDIs.12 However, combining memantine with other NMDA antagonists—such as amantadine or dextromethorphan—could cause hallucinations, dizziness, headache, fatigue, and confusion.11 Concurrent use with drugs that lower seizure threshold, such as tricyclic antidepressants, may increase the risk of seizures.
Table 3
Potential drug-drug interactions in AD patients taking cognitive enhancers
| Interaction | Mechanism | Potential sequela(e) |
|---|---|---|
| AChEIs + anticholinergics | ↓ Acetylcholine in CNS | Cognitive worsening, delirium |
| AChEIs + beta blockers | Vagal stimulation and sympathetic blockade | Bradycardia, syncope |
| AChEIs + cholinergics | ↑ Acetylcholine in PNS | Cholinergic crisis: hypersalivation, abdominal pain, diarrhea |
| AChEIs + antipsychotics (rare) | ↑ Acetylcholine/↓ dopamine in striatum | Parkinsonian syndrome, rigidity |
| Ginkgo biloba + warfarin | Antiplatelet aggregation and anticoagulation | Gastrointestinal bleeding, hematuria, subcutaneous ecchymosis |
| AChEIs: acetylcholinesterase inhibitors; PNS: peripheral nervous system | ||
| Source: References 3,5,10 | ||
DDIs with cognitive enhancers
Anticholinergics. Because anticholinergic drugs can worsen cognitive impairment and cause delirium they are contraindicated in older patients—especially those with AD. Antihistamines, histamine H2 blockers, low-potency first-generation antipsychotics (FGAs), and tricyclic antidepressants are common medications with anticholinergic effects (Table 4).5,13,14
- 33% of those taking donepezil also were receiving anticholinergics, compared with 23% of controls
- 26% of all patients in the study used multiple anticholinergic medications.
Antiparkinsonian agents. Interaction of antiparkinsonian medications with AChEIs could limit the efficacy of either drug when treating comorbid AD and Parkinson’s disease (PD),5 although in practice, clinical deterioration of parkinsonism has not been reported.15 In one study, 25 PD patients stabilized on levodopa/carbidopa were given donepezil, 5 mg/d, or placebo for two 2-week courses separated by a washout of at least 2 weeks. At steady state, pharmacokinetic parameters were unchanged and no clinically significant DDIs were observed.16
Cardiovascular agents. Concurrent use of AChEIs and beta blockers, calcium channel inhibitors, or digoxin could worsen bradycardia and cause syncope. The risk is higher in patients:
- with sick sinus syndrome or other bradyarrhythmias
- taking antipsychotics that could induce torsades de pointes,11 such as ziprasidone or haloperidol.
Other agents. AChEIs inhibit the metabolism of succinylcholine and therefore augment and prolong this drug’s neuromuscular blockade. Discontinue AChEIs before administering succinylcholine for anesthesia, such as for electroconvulsive treatment.
AChEIs may lead to toxicity when added to cholinergic agents such as bethanechol.11 Similarly, AChEIs may precipitate a cholinergic crisis—with increasing weakness, hypersalivation, abdominal pains, and diarrhea—when used in conjunction with peripheral acetylcholinesterase inhibitors such as the myasthenia gravis agents pyridostigmine and neostigmine. The mechanism is increased acetylcholine available at the neuromuscular junction.
Table 4
Medications with moderate to strong anticholinergic activity
| Class | Examples | |||
|---|---|---|---|---|
| Antiarrhythmics | Disopyramide | |||
| Antiemetics | Meclizine | |||
| Antiparkinsonians | Benztropine, biperiden, trihexyphenidyl | |||
| Antipsychotics | Chlorpromazine, clozapine, olanzapine, pimozide, thioridazine | |||
| Antihistamines | Chlorpheniramine, cyproheptadine, diphenhydramine, hydroxyzine, Promethazine | |||
| Gastrointestinal/urinary antispasmodics | Atropine, belladonna alkaloids, dicyclomine, hyoscyamine, oxybutynin, scopolamine, tolterodine | |||
| H2 histamine | Cimetidine, ranitidine | |||
| Muscle relaxants | Cyclobenzaprine | |||
| Tricyclic antidepressants | Amitriptyline, amoxapine, clomipramine, doxepin, imipramine, protriptyline | |||
| Source: References 5,13,14 | ||||
DDIs with other psychotropics
Antipsychotics. Nearly one-half of AD patients experience delusions, often in the middle stage of the disease, and many are prescribed second-generation antipsychotics (SGAs) to control delusions, hallucinations, sundowning, agitation, or aggression. Concomitant use of AChEIs and antipsychotics may increase the risk of extrapyramidal symptoms by disrupting the acetylcholine/dopamine balance in the striatum.5
In AD patients taking donepezil and risperidone, case reports describe parkinsonian syndrome and rigidity with immobility, which resolved after the antipsychotic was discontinued.5,11 When rivastigmine and risperidone were coadministered, however, no clinically relevant adverse interactions were noted in a 20-week, open-label trial of 65 patients with AD, 10 with vascular dementia, and 10 with both.17
The FDA has warned of increased risk of death when SGAs are used to treat behavioral disturbances in dementia patients. In a recent meta-analysis of 15 placebo-controlled trials, cognitive tests scores worsened when AD patients took aripiprazole, olanzapine, quetiapine, or risperidone. A significant risk for cerebrovascular events was seen, especially with risperidone, although no clear causal relationship was established.18 Falls, injury, and syncope were not increased, and patients with less severe dementia, outpatients, and those selected for psychosis were less affected. Thus, provide careful follow-up and avoid long-term unwarranted antipsychotic use in AD patients.
Highly anticholinergic FGAs such as chlorpromazine are not recommended for AD patients (Table 4).
Antidepressants. Up to 30% of AD patients experience major depression.19 SSRIs are the antidepressants most often used to treat depression and anxiety in AD patients.
Citalopram, escitalopram, or venlafaxine are good choices for patients with AD because of minimal CYP inhibitory activity.4 Fluvoxamine, fluoxetine, and paroxetine inhibit CYP 2C9, through which warfarin and some other drugs with a narrow therapeutic index are metabolized.6
Herbal supplements. Ginkgo biloba and huperzine A (Chinese club moss) are the herbal supplements used most commonly by dementia patients. Ginkgo inhibits platelet aggregation and can cause bleeding complications, with or without concomitant antiplatelet or anticoagulant therapy such as aspirin, warfarin, and NSAIDs. Enzyme induction of CYP 2C19 by ginkgo, leading to subtherapeutic levels of anticonvulsants, has been implicated in a report of fatal seizures. Huperzine A is a natural cholinesterase inhibitor and should not be combined with AChEIs because of the risk of additive adverse effects.10
Related resources
- Jacobson SA, Pies RW, Greenblatt DJ. Handbook of geriatric psychopharmacology. Washington, DC: American Psychiatric Publishing; 2002.
- Sandson, NB. Drug-drug interaction primer. Washington, DC: American Psychiatric Publishing; 2007.
- Amantadine • Symmetrel
- Amitriptyline • Elavil
- Amoxapine • Asendin
- Aripiprazole • Abilify
- Atropine • Sal-Tropine
- Benztropine • Cogentin
- Bethanechol • Urecholine
- Biperiden • Akineton
- Bupropion • Wellbutrin
- Buspirone • BuSpar
- Carbamazepine • Tegretol
- Celecoxib • Celebrex
- Chlorpheniramine • Chlor-Trimeton
- Chlorpromazine • Thorazine
- Cimetidine • Tagamet
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clozapine • Clozaril
- Cyclobenzaprine • Flexeril
- Cyproheptadine • Periactin
- Dextromethorphan • Benylin, Delsym, others
- Dicyclomine • Bentyl
- Digoxin • Lanoxin
- Diphenhydramine • Benadryl
- Disopyramide • Norpace
- Donepezil • Aricept
- Doxepin • Adapin, Sinequan
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Erythromycin • E-Mycin
- Fluconazole • Diflucan
- Fluvoxamine • Luvox
- Fluoxetine • Prozac
- Galantamine • Reminyl, Razadyne
- Haloperidol • Haldol
- Hydroxyzine • Vistaril
- Hyoscyamine • Anaspaz, Levbid, Levsin
- Imipramine • Tofranil
- Itraconazole • Sporanox
- Lamotrigine • Lamictal
- Levodopa/carbidopa • Sinemet
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Meclizine • Antivert
- Memantine • Namenda
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Neostigmine • Prostigmin
- Olanzapine • Zyprexa
- Oxazepam • Serax
- Oxybutynin • Ditropan
- Paroxetine • Paxil
- Pimozide • Orap
- Promethazine • Phenergan
- Protriptyline • Vivactil
- Pyridostigmine • Mestinon
- Quetiapine • Seroquel
- Ranitidine • Zantac
- Risperidone • Risperdal
- Rivastigmine • Exelon
- Scopolamine • Scopace
- Sertraline • Zoloft
- Succinylcholine • Anectine
- Temazepam • Restoril
- Thioridazine • Mellaril
- Tolterodine • Detrol
- Trazodone • Desyrel
- Trihexyphenidyl • Artane
- Valproate • Depakote
- Venlafaxine • Effexor
- Warfarin • Coumadin
- Ziprasidone • Geodon
- Zolpidem • Ambien
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Prescription drugs and the elderly: many still receive potentially harmful drugs despite recent improvements. Washington, DC: United States General Accounting Office; 1996. Publication HEHS 95-152.
2. Atkin PA, Veitch PC, Veitch EM, Ogle SJ. The epidemiology of serious adverse drug reactions among the elderly. Drugs Aging 1999;14:141-52.
3. Marangell LB, Martinez JM, Silver JM, Yudofsky SC, eds. Concise guide to psychopharmacology. Washington, DC: American Psychiatric Publishing; 2002:4-7, 129,173, 171-80.
4. Roose SP, Pollock BG, Devanand DD. Treatment during late life. In: Schatzberg AF, Nemeroff CB, eds. Textbook of psychopharmacology. 3rd ed. Washington, DC: American Psychiatric Publishing; 2004:1083-5.
5. Bentue-Ferrer D, Tribut O, Polard E, Allain H. Clinically significant drug interactions with cholinesterase inhibitors: a guide for neurologists. CNS Drugs 2003;17:947-63.
6. Mulsant BH, Pollock BG. Psychopharmacology. In: Blazer DG, Steffens DC, Busse EW, eds. Textbook of geriatric psychiatry. 3rd ed. Washington, DC: American Psychiatric Publishing; 2004:387-411.
7. Sandson NB, Marcucci C, Bourke DL, Smith-Lamacchia R. An interaction between aspirin and valproate: the relevance of plasma protein displacement drug-drug interaction. Am J Psychiatry 2006;163:1891-6.
8. Spina E, Scordo MG, D’Arrigo C. Metabolic drug interactions with new psychotropic agents. Fundam Clin Pharmacol 2003;17:517-38.
9. Grossberg GT, Stahelin HB, Messina JC, et al. Lack of adverse pharmacodynamic drug interactions with rivastigmine and twenty-two classes of medications. Int J Geriatr Psychiatry 2000;15:242-7.
10. Beier MT. Harmless herbs? Think again: merits of a complete medication history. J Am Med Dir Assoc 2006;7:446-7.
11. [No authors listed]. Alzheimer’s disease: beware of interactions with cholinesterase inhibitors. Prescrire Int 2006;15:103-6.
12. Grossberg GT, Edwards KR, Zhao Q. Rationale for combining therapy with galantamine and memantine in Alzheimer’s disease. J Clin Pharmacol 2006;46(suppl 1):S17-S26.
13. Roe CM, Anderson MJ, Spivack B. Use of anticholinergic medications by older adults with dementia. J Am Geriatr Soc 2002;50:836-42.
14. Carnahan RM, Lund BC, Perry PJ, Chrischilles EA. The concurrent use of anticholinergics and cholinesterase inhibitors: rare event or common practice? J Am Geriatr Soc 2004;52:2082-7.
15. Schrag A. Psychiatric aspects of Parkinson’s disease. J Neurol 2004;251:795-804.
16. Okereke CS, Kirby L, Kumar D, et al. Concurrent administration of donepezil HCl and levodopa/carbidopa in patients with Parkinson’s disease: assessment of pharmacokinetic changes and safety following multiple oral doses. Br J Clin Pharmacol 2004;58(suppl 1):41-9.
17. Weiser M, Rotmensch HH, Korczyn AD, et al. A pilot, randomized, open-label trial assessing safety and pharmacokinetic parameters of co-administration of rivastigmine with risperidone in dementia patients with behavioral disturbances. Int J Geriatr Psychiatry 2002;17:343-6.
18. Schneider LS, Dagerman K, Insel PS. Efficacy and adverse events of atypical antipsychotics for dementia: meta-analysis of randomized, placebo-controlled trials. Am J Geriatr Psychiatry 2006;14(3):191-210.
19. Koenig HG, Blazer DG. Mood disorders. In: Blazer DG, Steffens DC, Busse EW, eds. Textbook of geriatric psychiatry 3rd ed. Washington, DC: American Psychiatric Publishing; 2004:254.
20. Jacobson SA, Pies RW, Greenblatt DJ. Anxiolytic and sedative-hypnotic medications. In: Handbook of geriatric psychopharmacology. Washington, DC: American Psychiatric Publishing; 2002:249-312.
Mr. B, age 78, has a long history of well-controlled bipolar disorder and was diagnosed with Alzheimer’s dementia 6 months ago. He is living at home and has been taking donepezil, 10 mg/d, and lamotrigine, 100 mg bid.
This morning Mr. B’s wife calls and reports that he is experiencing sudden difficulty walking, dizziness, and “feeling drunk.” When you ask about Mr. B’s medications, his wife says that her husband’s internist had prescribed itraconazole, 200 mg/d, for onychomycosis, and Mr. B has taken 1 dose. You promptly discontinue the itraconazole, and Mr. B’s symptoms resolve.
Drug-drug interactions (DDIs) in Alzheimer’s disease (AD) patients such as Mr. B can be serious and even life-threatening. On average, persons age ≥65 use 4.5 prescription agents and 2 over-the-counter preparations per day,1 and the number of concurrently used medications is a significant predictor of adverse drug reactions.2
Cognitive enhancers, including acetylcholinesterase inhibitors (AChEIs) and memantine, are the most widely prescribed agents for AD patients. The FDA has approved galantamine and rivastigmine for mild to moderate dementia, memantine for moderate to severe dementia, and donepezil for mild to severe dementia (Table 1).3-5
To help you minimize adverse DDIs in AD patients, this article describes:
- pharmacokinetic and pharmacodynamic effects of cognitive enhancers used in AD management
- DDIs with medications commonly prescribed to AD patients
- how to avoid adverse events related to antipsychotics, antidepressants, and benzodiazepines.
Table 1
Pharmacokinetic features of cognitive enhancers
| Agent | Protein binding | CYP-450 activity | Other features |
|---|---|---|---|
| AChEIs | |||
| Donepezil | 96% | CYP 2D6, 3A4 substrate | Once-daily dosing |
| Rivastigmine | 40% | None | Metabolized by cholinesterases |
| Galantamine | 18% | CYP 2D6, 3A4 substrate | Nicotinic cholinergic receptor modulation |
| NMDA receptor antagonist | |||
| Memantine | 45% | None | No hepatic metabolism |
| CYP-450: cytochrome P-450; AChEIs: acetylcholinesterase inhibitors; NMDA: N-methyl-D-aspartate | |||
| Source: References 3-5 | |||
Pharmacologic changes with aging
Pharmacokinetics is the study of the time course of drugs and their metabolites through the body. Pharmacokinetic interactions involve alterations in the plasma concentration of a drug by a second agent.3
Absorption of medications is decreased in the elderly because of reduced intestinal blood flow and motility. Absorption further decreases if patients concomitantly take antacids, high-fiber supplements, or anticholinergic medications.
In plasma, drugs circulate freely or bound to proteins—mainly albumin and α1-acid glycoprotein. Aging can cause decreased plasma albumin and increased α1-acid glycoprotein.6 Additionally, malnutrition, diabetes mellitus, and hepatic and renal disease—all more common with advancing age—may cause hypoalbuminemia, which increases the free fraction of drugs bound to albumin.6Table 1 includes information about cognitive enhancers’ protein binding.
When 2 or more highly protein-bound drugs are coadministered, mutual displacement occurs and the free fraction of each drug increases. A recent case report described valproate toxicity with dizziness, ataxia, and falling in a 76-year-old man after aspirin was added to his regimen.7 The mechanism appeared to be mutual displacement from albumin combined with metabolism of valproate inhibited by aspirin.7
Metabolism. Liver size and hepatic blood flow decrease with aging.6 Cytochrome P-450 3A4 pathway activity slows, but the 2D6 pathway is not affected.4 Oxidative metabolism through CYP pathways is slower, but conjugation reactions are not.6Table 23,5,7,8 lists major substrates and inhibitors of CYP enzymes.
Azole antifungals are potent inhibitors of CYP 3A4,4 of which both donepezil and lamotrigine are substrates (Table 2). In Mr. B’s case, lamotrigine and donepezil levels increased because of this pharmacokinetic interaction. Because donepezil also is metabolized by the CYP 2D6 pathway, the increase in concentration is unlikely to modify the drug effect. Mr. B experienced symptoms consistent with lamotrigine toxicity.
Pharmacokinetics of AChEIs. AChEIs have relatively few pharmacokinetic interactions, although donepezil and galantamine are metabolized through the liver’s CYP 2D6 and 3A4 pathways.
Because rivastigmine does not undergo hepatic metabolism, it is least likely of the cognitive enhancers to have pharmacokinetic interactions with other medications. Rivastigmine did not lead to increased adverse events when administered concomitantly with 22 different classes of medications—including antidiabetics, cardiovascular drugs, gastrointestinal agents, and NSAIDs.9
Table 2
DDIs in AD patients: CYP-450 substrates and inhibitors*
| CYP 2D6 | CYP 3A4 | |
|---|---|---|
| Substrates (substances metabolized by enzyme) | Second-generation antipsychotics Citalopram Donepezil Duloxetine Galantamine Haloperidol Tricyclic antidepressants Trazodone Venlafaxine | Second-generation antipsychotics Benzodiazepines Buspirone Carbamazepine Donepezil Galantamine Haloperidol Lamotrigine Mirtazapine Nefazodone Sertraline Tricyclic antidepressants Trazodone Zolpidem |
| Inhibitors | Bupropion Cimetidine Duloxetine Fluoxetine Paroxetine Sertraline | Erythromycin Fluconazole Fluvoxamine Grapefruit juice Itraconazole Nefazodone |
| *All cytochrome P (CYP) 450 enzymes are induced by barbiturates, phenytoin, carbamazepine, and rifampicin. Smoking also induces CYP 1A2. | ||
| DDIs: drug-drug interactions; AD: Alzheimer’s disease | ||
| Source: References 3,5,7,8 | ||
Memantine, an amantadine derivative and N-methyl-D-aspartate (NMDA) receptor antagonist, is a weak dopaminergic agonist with atropinic effects.11 Because memantine is not metabolized by the CYP-450 pathway, it lacks pharmacokinetic DDIs.12 However, combining memantine with other NMDA antagonists—such as amantadine or dextromethorphan—could cause hallucinations, dizziness, headache, fatigue, and confusion.11 Concurrent use with drugs that lower seizure threshold, such as tricyclic antidepressants, may increase the risk of seizures.
Table 3
Potential drug-drug interactions in AD patients taking cognitive enhancers
| Interaction | Mechanism | Potential sequela(e) |
|---|---|---|
| AChEIs + anticholinergics | ↓ Acetylcholine in CNS | Cognitive worsening, delirium |
| AChEIs + beta blockers | Vagal stimulation and sympathetic blockade | Bradycardia, syncope |
| AChEIs + cholinergics | ↑ Acetylcholine in PNS | Cholinergic crisis: hypersalivation, abdominal pain, diarrhea |
| AChEIs + antipsychotics (rare) | ↑ Acetylcholine/↓ dopamine in striatum | Parkinsonian syndrome, rigidity |
| Ginkgo biloba + warfarin | Antiplatelet aggregation and anticoagulation | Gastrointestinal bleeding, hematuria, subcutaneous ecchymosis |
| AChEIs: acetylcholinesterase inhibitors; PNS: peripheral nervous system | ||
| Source: References 3,5,10 | ||
DDIs with cognitive enhancers
Anticholinergics. Because anticholinergic drugs can worsen cognitive impairment and cause delirium they are contraindicated in older patients—especially those with AD. Antihistamines, histamine H2 blockers, low-potency first-generation antipsychotics (FGAs), and tricyclic antidepressants are common medications with anticholinergic effects (Table 4).5,13,14
- 33% of those taking donepezil also were receiving anticholinergics, compared with 23% of controls
- 26% of all patients in the study used multiple anticholinergic medications.
Antiparkinsonian agents. Interaction of antiparkinsonian medications with AChEIs could limit the efficacy of either drug when treating comorbid AD and Parkinson’s disease (PD),5 although in practice, clinical deterioration of parkinsonism has not been reported.15 In one study, 25 PD patients stabilized on levodopa/carbidopa were given donepezil, 5 mg/d, or placebo for two 2-week courses separated by a washout of at least 2 weeks. At steady state, pharmacokinetic parameters were unchanged and no clinically significant DDIs were observed.16
Cardiovascular agents. Concurrent use of AChEIs and beta blockers, calcium channel inhibitors, or digoxin could worsen bradycardia and cause syncope. The risk is higher in patients:
- with sick sinus syndrome or other bradyarrhythmias
- taking antipsychotics that could induce torsades de pointes,11 such as ziprasidone or haloperidol.
Other agents. AChEIs inhibit the metabolism of succinylcholine and therefore augment and prolong this drug’s neuromuscular blockade. Discontinue AChEIs before administering succinylcholine for anesthesia, such as for electroconvulsive treatment.
AChEIs may lead to toxicity when added to cholinergic agents such as bethanechol.11 Similarly, AChEIs may precipitate a cholinergic crisis—with increasing weakness, hypersalivation, abdominal pains, and diarrhea—when used in conjunction with peripheral acetylcholinesterase inhibitors such as the myasthenia gravis agents pyridostigmine and neostigmine. The mechanism is increased acetylcholine available at the neuromuscular junction.
Table 4
Medications with moderate to strong anticholinergic activity
| Class | Examples | |||
|---|---|---|---|---|
| Antiarrhythmics | Disopyramide | |||
| Antiemetics | Meclizine | |||
| Antiparkinsonians | Benztropine, biperiden, trihexyphenidyl | |||
| Antipsychotics | Chlorpromazine, clozapine, olanzapine, pimozide, thioridazine | |||
| Antihistamines | Chlorpheniramine, cyproheptadine, diphenhydramine, hydroxyzine, Promethazine | |||
| Gastrointestinal/urinary antispasmodics | Atropine, belladonna alkaloids, dicyclomine, hyoscyamine, oxybutynin, scopolamine, tolterodine | |||
| H2 histamine | Cimetidine, ranitidine | |||
| Muscle relaxants | Cyclobenzaprine | |||
| Tricyclic antidepressants | Amitriptyline, amoxapine, clomipramine, doxepin, imipramine, protriptyline | |||
| Source: References 5,13,14 | ||||
DDIs with other psychotropics
Antipsychotics. Nearly one-half of AD patients experience delusions, often in the middle stage of the disease, and many are prescribed second-generation antipsychotics (SGAs) to control delusions, hallucinations, sundowning, agitation, or aggression. Concomitant use of AChEIs and antipsychotics may increase the risk of extrapyramidal symptoms by disrupting the acetylcholine/dopamine balance in the striatum.5
In AD patients taking donepezil and risperidone, case reports describe parkinsonian syndrome and rigidity with immobility, which resolved after the antipsychotic was discontinued.5,11 When rivastigmine and risperidone were coadministered, however, no clinically relevant adverse interactions were noted in a 20-week, open-label trial of 65 patients with AD, 10 with vascular dementia, and 10 with both.17
The FDA has warned of increased risk of death when SGAs are used to treat behavioral disturbances in dementia patients. In a recent meta-analysis of 15 placebo-controlled trials, cognitive tests scores worsened when AD patients took aripiprazole, olanzapine, quetiapine, or risperidone. A significant risk for cerebrovascular events was seen, especially with risperidone, although no clear causal relationship was established.18 Falls, injury, and syncope were not increased, and patients with less severe dementia, outpatients, and those selected for psychosis were less affected. Thus, provide careful follow-up and avoid long-term unwarranted antipsychotic use in AD patients.
Highly anticholinergic FGAs such as chlorpromazine are not recommended for AD patients (Table 4).
Antidepressants. Up to 30% of AD patients experience major depression.19 SSRIs are the antidepressants most often used to treat depression and anxiety in AD patients.
Citalopram, escitalopram, or venlafaxine are good choices for patients with AD because of minimal CYP inhibitory activity.4 Fluvoxamine, fluoxetine, and paroxetine inhibit CYP 2C9, through which warfarin and some other drugs with a narrow therapeutic index are metabolized.6
Herbal supplements. Ginkgo biloba and huperzine A (Chinese club moss) are the herbal supplements used most commonly by dementia patients. Ginkgo inhibits platelet aggregation and can cause bleeding complications, with or without concomitant antiplatelet or anticoagulant therapy such as aspirin, warfarin, and NSAIDs. Enzyme induction of CYP 2C19 by ginkgo, leading to subtherapeutic levels of anticonvulsants, has been implicated in a report of fatal seizures. Huperzine A is a natural cholinesterase inhibitor and should not be combined with AChEIs because of the risk of additive adverse effects.10
Related resources
- Jacobson SA, Pies RW, Greenblatt DJ. Handbook of geriatric psychopharmacology. Washington, DC: American Psychiatric Publishing; 2002.
- Sandson, NB. Drug-drug interaction primer. Washington, DC: American Psychiatric Publishing; 2007.
- Amantadine • Symmetrel
- Amitriptyline • Elavil
- Amoxapine • Asendin
- Aripiprazole • Abilify
- Atropine • Sal-Tropine
- Benztropine • Cogentin
- Bethanechol • Urecholine
- Biperiden • Akineton
- Bupropion • Wellbutrin
- Buspirone • BuSpar
- Carbamazepine • Tegretol
- Celecoxib • Celebrex
- Chlorpheniramine • Chlor-Trimeton
- Chlorpromazine • Thorazine
- Cimetidine • Tagamet
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clozapine • Clozaril
- Cyclobenzaprine • Flexeril
- Cyproheptadine • Periactin
- Dextromethorphan • Benylin, Delsym, others
- Dicyclomine • Bentyl
- Digoxin • Lanoxin
- Diphenhydramine • Benadryl
- Disopyramide • Norpace
- Donepezil • Aricept
- Doxepin • Adapin, Sinequan
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Erythromycin • E-Mycin
- Fluconazole • Diflucan
- Fluvoxamine • Luvox
- Fluoxetine • Prozac
- Galantamine • Reminyl, Razadyne
- Haloperidol • Haldol
- Hydroxyzine • Vistaril
- Hyoscyamine • Anaspaz, Levbid, Levsin
- Imipramine • Tofranil
- Itraconazole • Sporanox
- Lamotrigine • Lamictal
- Levodopa/carbidopa • Sinemet
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Meclizine • Antivert
- Memantine • Namenda
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Neostigmine • Prostigmin
- Olanzapine • Zyprexa
- Oxazepam • Serax
- Oxybutynin • Ditropan
- Paroxetine • Paxil
- Pimozide • Orap
- Promethazine • Phenergan
- Protriptyline • Vivactil
- Pyridostigmine • Mestinon
- Quetiapine • Seroquel
- Ranitidine • Zantac
- Risperidone • Risperdal
- Rivastigmine • Exelon
- Scopolamine • Scopace
- Sertraline • Zoloft
- Succinylcholine • Anectine
- Temazepam • Restoril
- Thioridazine • Mellaril
- Tolterodine • Detrol
- Trazodone • Desyrel
- Trihexyphenidyl • Artane
- Valproate • Depakote
- Venlafaxine • Effexor
- Warfarin • Coumadin
- Ziprasidone • Geodon
- Zolpidem • Ambien
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Mr. B, age 78, has a long history of well-controlled bipolar disorder and was diagnosed with Alzheimer’s dementia 6 months ago. He is living at home and has been taking donepezil, 10 mg/d, and lamotrigine, 100 mg bid.
This morning Mr. B’s wife calls and reports that he is experiencing sudden difficulty walking, dizziness, and “feeling drunk.” When you ask about Mr. B’s medications, his wife says that her husband’s internist had prescribed itraconazole, 200 mg/d, for onychomycosis, and Mr. B has taken 1 dose. You promptly discontinue the itraconazole, and Mr. B’s symptoms resolve.
Drug-drug interactions (DDIs) in Alzheimer’s disease (AD) patients such as Mr. B can be serious and even life-threatening. On average, persons age ≥65 use 4.5 prescription agents and 2 over-the-counter preparations per day,1 and the number of concurrently used medications is a significant predictor of adverse drug reactions.2
Cognitive enhancers, including acetylcholinesterase inhibitors (AChEIs) and memantine, are the most widely prescribed agents for AD patients. The FDA has approved galantamine and rivastigmine for mild to moderate dementia, memantine for moderate to severe dementia, and donepezil for mild to severe dementia (Table 1).3-5
To help you minimize adverse DDIs in AD patients, this article describes:
- pharmacokinetic and pharmacodynamic effects of cognitive enhancers used in AD management
- DDIs with medications commonly prescribed to AD patients
- how to avoid adverse events related to antipsychotics, antidepressants, and benzodiazepines.
Table 1
Pharmacokinetic features of cognitive enhancers
| Agent | Protein binding | CYP-450 activity | Other features |
|---|---|---|---|
| AChEIs | |||
| Donepezil | 96% | CYP 2D6, 3A4 substrate | Once-daily dosing |
| Rivastigmine | 40% | None | Metabolized by cholinesterases |
| Galantamine | 18% | CYP 2D6, 3A4 substrate | Nicotinic cholinergic receptor modulation |
| NMDA receptor antagonist | |||
| Memantine | 45% | None | No hepatic metabolism |
| CYP-450: cytochrome P-450; AChEIs: acetylcholinesterase inhibitors; NMDA: N-methyl-D-aspartate | |||
| Source: References 3-5 | |||
Pharmacologic changes with aging
Pharmacokinetics is the study of the time course of drugs and their metabolites through the body. Pharmacokinetic interactions involve alterations in the plasma concentration of a drug by a second agent.3
Absorption of medications is decreased in the elderly because of reduced intestinal blood flow and motility. Absorption further decreases if patients concomitantly take antacids, high-fiber supplements, or anticholinergic medications.
In plasma, drugs circulate freely or bound to proteins—mainly albumin and α1-acid glycoprotein. Aging can cause decreased plasma albumin and increased α1-acid glycoprotein.6 Additionally, malnutrition, diabetes mellitus, and hepatic and renal disease—all more common with advancing age—may cause hypoalbuminemia, which increases the free fraction of drugs bound to albumin.6Table 1 includes information about cognitive enhancers’ protein binding.
When 2 or more highly protein-bound drugs are coadministered, mutual displacement occurs and the free fraction of each drug increases. A recent case report described valproate toxicity with dizziness, ataxia, and falling in a 76-year-old man after aspirin was added to his regimen.7 The mechanism appeared to be mutual displacement from albumin combined with metabolism of valproate inhibited by aspirin.7
Metabolism. Liver size and hepatic blood flow decrease with aging.6 Cytochrome P-450 3A4 pathway activity slows, but the 2D6 pathway is not affected.4 Oxidative metabolism through CYP pathways is slower, but conjugation reactions are not.6Table 23,5,7,8 lists major substrates and inhibitors of CYP enzymes.
Azole antifungals are potent inhibitors of CYP 3A4,4 of which both donepezil and lamotrigine are substrates (Table 2). In Mr. B’s case, lamotrigine and donepezil levels increased because of this pharmacokinetic interaction. Because donepezil also is metabolized by the CYP 2D6 pathway, the increase in concentration is unlikely to modify the drug effect. Mr. B experienced symptoms consistent with lamotrigine toxicity.
Pharmacokinetics of AChEIs. AChEIs have relatively few pharmacokinetic interactions, although donepezil and galantamine are metabolized through the liver’s CYP 2D6 and 3A4 pathways.
Because rivastigmine does not undergo hepatic metabolism, it is least likely of the cognitive enhancers to have pharmacokinetic interactions with other medications. Rivastigmine did not lead to increased adverse events when administered concomitantly with 22 different classes of medications—including antidiabetics, cardiovascular drugs, gastrointestinal agents, and NSAIDs.9
Table 2
DDIs in AD patients: CYP-450 substrates and inhibitors*
| CYP 2D6 | CYP 3A4 | |
|---|---|---|
| Substrates (substances metabolized by enzyme) | Second-generation antipsychotics Citalopram Donepezil Duloxetine Galantamine Haloperidol Tricyclic antidepressants Trazodone Venlafaxine | Second-generation antipsychotics Benzodiazepines Buspirone Carbamazepine Donepezil Galantamine Haloperidol Lamotrigine Mirtazapine Nefazodone Sertraline Tricyclic antidepressants Trazodone Zolpidem |
| Inhibitors | Bupropion Cimetidine Duloxetine Fluoxetine Paroxetine Sertraline | Erythromycin Fluconazole Fluvoxamine Grapefruit juice Itraconazole Nefazodone |
| *All cytochrome P (CYP) 450 enzymes are induced by barbiturates, phenytoin, carbamazepine, and rifampicin. Smoking also induces CYP 1A2. | ||
| DDIs: drug-drug interactions; AD: Alzheimer’s disease | ||
| Source: References 3,5,7,8 | ||
Memantine, an amantadine derivative and N-methyl-D-aspartate (NMDA) receptor antagonist, is a weak dopaminergic agonist with atropinic effects.11 Because memantine is not metabolized by the CYP-450 pathway, it lacks pharmacokinetic DDIs.12 However, combining memantine with other NMDA antagonists—such as amantadine or dextromethorphan—could cause hallucinations, dizziness, headache, fatigue, and confusion.11 Concurrent use with drugs that lower seizure threshold, such as tricyclic antidepressants, may increase the risk of seizures.
Table 3
Potential drug-drug interactions in AD patients taking cognitive enhancers
| Interaction | Mechanism | Potential sequela(e) |
|---|---|---|
| AChEIs + anticholinergics | ↓ Acetylcholine in CNS | Cognitive worsening, delirium |
| AChEIs + beta blockers | Vagal stimulation and sympathetic blockade | Bradycardia, syncope |
| AChEIs + cholinergics | ↑ Acetylcholine in PNS | Cholinergic crisis: hypersalivation, abdominal pain, diarrhea |
| AChEIs + antipsychotics (rare) | ↑ Acetylcholine/↓ dopamine in striatum | Parkinsonian syndrome, rigidity |
| Ginkgo biloba + warfarin | Antiplatelet aggregation and anticoagulation | Gastrointestinal bleeding, hematuria, subcutaneous ecchymosis |
| AChEIs: acetylcholinesterase inhibitors; PNS: peripheral nervous system | ||
| Source: References 3,5,10 | ||
DDIs with cognitive enhancers
Anticholinergics. Because anticholinergic drugs can worsen cognitive impairment and cause delirium they are contraindicated in older patients—especially those with AD. Antihistamines, histamine H2 blockers, low-potency first-generation antipsychotics (FGAs), and tricyclic antidepressants are common medications with anticholinergic effects (Table 4).5,13,14
- 33% of those taking donepezil also were receiving anticholinergics, compared with 23% of controls
- 26% of all patients in the study used multiple anticholinergic medications.
Antiparkinsonian agents. Interaction of antiparkinsonian medications with AChEIs could limit the efficacy of either drug when treating comorbid AD and Parkinson’s disease (PD),5 although in practice, clinical deterioration of parkinsonism has not been reported.15 In one study, 25 PD patients stabilized on levodopa/carbidopa were given donepezil, 5 mg/d, or placebo for two 2-week courses separated by a washout of at least 2 weeks. At steady state, pharmacokinetic parameters were unchanged and no clinically significant DDIs were observed.16
Cardiovascular agents. Concurrent use of AChEIs and beta blockers, calcium channel inhibitors, or digoxin could worsen bradycardia and cause syncope. The risk is higher in patients:
- with sick sinus syndrome or other bradyarrhythmias
- taking antipsychotics that could induce torsades de pointes,11 such as ziprasidone or haloperidol.
Other agents. AChEIs inhibit the metabolism of succinylcholine and therefore augment and prolong this drug’s neuromuscular blockade. Discontinue AChEIs before administering succinylcholine for anesthesia, such as for electroconvulsive treatment.
AChEIs may lead to toxicity when added to cholinergic agents such as bethanechol.11 Similarly, AChEIs may precipitate a cholinergic crisis—with increasing weakness, hypersalivation, abdominal pains, and diarrhea—when used in conjunction with peripheral acetylcholinesterase inhibitors such as the myasthenia gravis agents pyridostigmine and neostigmine. The mechanism is increased acetylcholine available at the neuromuscular junction.
Table 4
Medications with moderate to strong anticholinergic activity
| Class | Examples | |||
|---|---|---|---|---|
| Antiarrhythmics | Disopyramide | |||
| Antiemetics | Meclizine | |||
| Antiparkinsonians | Benztropine, biperiden, trihexyphenidyl | |||
| Antipsychotics | Chlorpromazine, clozapine, olanzapine, pimozide, thioridazine | |||
| Antihistamines | Chlorpheniramine, cyproheptadine, diphenhydramine, hydroxyzine, Promethazine | |||
| Gastrointestinal/urinary antispasmodics | Atropine, belladonna alkaloids, dicyclomine, hyoscyamine, oxybutynin, scopolamine, tolterodine | |||
| H2 histamine | Cimetidine, ranitidine | |||
| Muscle relaxants | Cyclobenzaprine | |||
| Tricyclic antidepressants | Amitriptyline, amoxapine, clomipramine, doxepin, imipramine, protriptyline | |||
| Source: References 5,13,14 | ||||
DDIs with other psychotropics
Antipsychotics. Nearly one-half of AD patients experience delusions, often in the middle stage of the disease, and many are prescribed second-generation antipsychotics (SGAs) to control delusions, hallucinations, sundowning, agitation, or aggression. Concomitant use of AChEIs and antipsychotics may increase the risk of extrapyramidal symptoms by disrupting the acetylcholine/dopamine balance in the striatum.5
In AD patients taking donepezil and risperidone, case reports describe parkinsonian syndrome and rigidity with immobility, which resolved after the antipsychotic was discontinued.5,11 When rivastigmine and risperidone were coadministered, however, no clinically relevant adverse interactions were noted in a 20-week, open-label trial of 65 patients with AD, 10 with vascular dementia, and 10 with both.17
The FDA has warned of increased risk of death when SGAs are used to treat behavioral disturbances in dementia patients. In a recent meta-analysis of 15 placebo-controlled trials, cognitive tests scores worsened when AD patients took aripiprazole, olanzapine, quetiapine, or risperidone. A significant risk for cerebrovascular events was seen, especially with risperidone, although no clear causal relationship was established.18 Falls, injury, and syncope were not increased, and patients with less severe dementia, outpatients, and those selected for psychosis were less affected. Thus, provide careful follow-up and avoid long-term unwarranted antipsychotic use in AD patients.
Highly anticholinergic FGAs such as chlorpromazine are not recommended for AD patients (Table 4).
Antidepressants. Up to 30% of AD patients experience major depression.19 SSRIs are the antidepressants most often used to treat depression and anxiety in AD patients.
Citalopram, escitalopram, or venlafaxine are good choices for patients with AD because of minimal CYP inhibitory activity.4 Fluvoxamine, fluoxetine, and paroxetine inhibit CYP 2C9, through which warfarin and some other drugs with a narrow therapeutic index are metabolized.6
Herbal supplements. Ginkgo biloba and huperzine A (Chinese club moss) are the herbal supplements used most commonly by dementia patients. Ginkgo inhibits platelet aggregation and can cause bleeding complications, with or without concomitant antiplatelet or anticoagulant therapy such as aspirin, warfarin, and NSAIDs. Enzyme induction of CYP 2C19 by ginkgo, leading to subtherapeutic levels of anticonvulsants, has been implicated in a report of fatal seizures. Huperzine A is a natural cholinesterase inhibitor and should not be combined with AChEIs because of the risk of additive adverse effects.10
Related resources
- Jacobson SA, Pies RW, Greenblatt DJ. Handbook of geriatric psychopharmacology. Washington, DC: American Psychiatric Publishing; 2002.
- Sandson, NB. Drug-drug interaction primer. Washington, DC: American Psychiatric Publishing; 2007.
- Amantadine • Symmetrel
- Amitriptyline • Elavil
- Amoxapine • Asendin
- Aripiprazole • Abilify
- Atropine • Sal-Tropine
- Benztropine • Cogentin
- Bethanechol • Urecholine
- Biperiden • Akineton
- Bupropion • Wellbutrin
- Buspirone • BuSpar
- Carbamazepine • Tegretol
- Celecoxib • Celebrex
- Chlorpheniramine • Chlor-Trimeton
- Chlorpromazine • Thorazine
- Cimetidine • Tagamet
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clozapine • Clozaril
- Cyclobenzaprine • Flexeril
- Cyproheptadine • Periactin
- Dextromethorphan • Benylin, Delsym, others
- Dicyclomine • Bentyl
- Digoxin • Lanoxin
- Diphenhydramine • Benadryl
- Disopyramide • Norpace
- Donepezil • Aricept
- Doxepin • Adapin, Sinequan
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Erythromycin • E-Mycin
- Fluconazole • Diflucan
- Fluvoxamine • Luvox
- Fluoxetine • Prozac
- Galantamine • Reminyl, Razadyne
- Haloperidol • Haldol
- Hydroxyzine • Vistaril
- Hyoscyamine • Anaspaz, Levbid, Levsin
- Imipramine • Tofranil
- Itraconazole • Sporanox
- Lamotrigine • Lamictal
- Levodopa/carbidopa • Sinemet
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Meclizine • Antivert
- Memantine • Namenda
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Neostigmine • Prostigmin
- Olanzapine • Zyprexa
- Oxazepam • Serax
- Oxybutynin • Ditropan
- Paroxetine • Paxil
- Pimozide • Orap
- Promethazine • Phenergan
- Protriptyline • Vivactil
- Pyridostigmine • Mestinon
- Quetiapine • Seroquel
- Ranitidine • Zantac
- Risperidone • Risperdal
- Rivastigmine • Exelon
- Scopolamine • Scopace
- Sertraline • Zoloft
- Succinylcholine • Anectine
- Temazepam • Restoril
- Thioridazine • Mellaril
- Tolterodine • Detrol
- Trazodone • Desyrel
- Trihexyphenidyl • Artane
- Valproate • Depakote
- Venlafaxine • Effexor
- Warfarin • Coumadin
- Ziprasidone • Geodon
- Zolpidem • Ambien
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Prescription drugs and the elderly: many still receive potentially harmful drugs despite recent improvements. Washington, DC: United States General Accounting Office; 1996. Publication HEHS 95-152.
2. Atkin PA, Veitch PC, Veitch EM, Ogle SJ. The epidemiology of serious adverse drug reactions among the elderly. Drugs Aging 1999;14:141-52.
3. Marangell LB, Martinez JM, Silver JM, Yudofsky SC, eds. Concise guide to psychopharmacology. Washington, DC: American Psychiatric Publishing; 2002:4-7, 129,173, 171-80.
4. Roose SP, Pollock BG, Devanand DD. Treatment during late life. In: Schatzberg AF, Nemeroff CB, eds. Textbook of psychopharmacology. 3rd ed. Washington, DC: American Psychiatric Publishing; 2004:1083-5.
5. Bentue-Ferrer D, Tribut O, Polard E, Allain H. Clinically significant drug interactions with cholinesterase inhibitors: a guide for neurologists. CNS Drugs 2003;17:947-63.
6. Mulsant BH, Pollock BG. Psychopharmacology. In: Blazer DG, Steffens DC, Busse EW, eds. Textbook of geriatric psychiatry. 3rd ed. Washington, DC: American Psychiatric Publishing; 2004:387-411.
7. Sandson NB, Marcucci C, Bourke DL, Smith-Lamacchia R. An interaction between aspirin and valproate: the relevance of plasma protein displacement drug-drug interaction. Am J Psychiatry 2006;163:1891-6.
8. Spina E, Scordo MG, D’Arrigo C. Metabolic drug interactions with new psychotropic agents. Fundam Clin Pharmacol 2003;17:517-38.
9. Grossberg GT, Stahelin HB, Messina JC, et al. Lack of adverse pharmacodynamic drug interactions with rivastigmine and twenty-two classes of medications. Int J Geriatr Psychiatry 2000;15:242-7.
10. Beier MT. Harmless herbs? Think again: merits of a complete medication history. J Am Med Dir Assoc 2006;7:446-7.
11. [No authors listed]. Alzheimer’s disease: beware of interactions with cholinesterase inhibitors. Prescrire Int 2006;15:103-6.
12. Grossberg GT, Edwards KR, Zhao Q. Rationale for combining therapy with galantamine and memantine in Alzheimer’s disease. J Clin Pharmacol 2006;46(suppl 1):S17-S26.
13. Roe CM, Anderson MJ, Spivack B. Use of anticholinergic medications by older adults with dementia. J Am Geriatr Soc 2002;50:836-42.
14. Carnahan RM, Lund BC, Perry PJ, Chrischilles EA. The concurrent use of anticholinergics and cholinesterase inhibitors: rare event or common practice? J Am Geriatr Soc 2004;52:2082-7.
15. Schrag A. Psychiatric aspects of Parkinson’s disease. J Neurol 2004;251:795-804.
16. Okereke CS, Kirby L, Kumar D, et al. Concurrent administration of donepezil HCl and levodopa/carbidopa in patients with Parkinson’s disease: assessment of pharmacokinetic changes and safety following multiple oral doses. Br J Clin Pharmacol 2004;58(suppl 1):41-9.
17. Weiser M, Rotmensch HH, Korczyn AD, et al. A pilot, randomized, open-label trial assessing safety and pharmacokinetic parameters of co-administration of rivastigmine with risperidone in dementia patients with behavioral disturbances. Int J Geriatr Psychiatry 2002;17:343-6.
18. Schneider LS, Dagerman K, Insel PS. Efficacy and adverse events of atypical antipsychotics for dementia: meta-analysis of randomized, placebo-controlled trials. Am J Geriatr Psychiatry 2006;14(3):191-210.
19. Koenig HG, Blazer DG. Mood disorders. In: Blazer DG, Steffens DC, Busse EW, eds. Textbook of geriatric psychiatry 3rd ed. Washington, DC: American Psychiatric Publishing; 2004:254.
20. Jacobson SA, Pies RW, Greenblatt DJ. Anxiolytic and sedative-hypnotic medications. In: Handbook of geriatric psychopharmacology. Washington, DC: American Psychiatric Publishing; 2002:249-312.
1. Prescription drugs and the elderly: many still receive potentially harmful drugs despite recent improvements. Washington, DC: United States General Accounting Office; 1996. Publication HEHS 95-152.
2. Atkin PA, Veitch PC, Veitch EM, Ogle SJ. The epidemiology of serious adverse drug reactions among the elderly. Drugs Aging 1999;14:141-52.
3. Marangell LB, Martinez JM, Silver JM, Yudofsky SC, eds. Concise guide to psychopharmacology. Washington, DC: American Psychiatric Publishing; 2002:4-7, 129,173, 171-80.
4. Roose SP, Pollock BG, Devanand DD. Treatment during late life. In: Schatzberg AF, Nemeroff CB, eds. Textbook of psychopharmacology. 3rd ed. Washington, DC: American Psychiatric Publishing; 2004:1083-5.
5. Bentue-Ferrer D, Tribut O, Polard E, Allain H. Clinically significant drug interactions with cholinesterase inhibitors: a guide for neurologists. CNS Drugs 2003;17:947-63.
6. Mulsant BH, Pollock BG. Psychopharmacology. In: Blazer DG, Steffens DC, Busse EW, eds. Textbook of geriatric psychiatry. 3rd ed. Washington, DC: American Psychiatric Publishing; 2004:387-411.
7. Sandson NB, Marcucci C, Bourke DL, Smith-Lamacchia R. An interaction between aspirin and valproate: the relevance of plasma protein displacement drug-drug interaction. Am J Psychiatry 2006;163:1891-6.
8. Spina E, Scordo MG, D’Arrigo C. Metabolic drug interactions with new psychotropic agents. Fundam Clin Pharmacol 2003;17:517-38.
9. Grossberg GT, Stahelin HB, Messina JC, et al. Lack of adverse pharmacodynamic drug interactions with rivastigmine and twenty-two classes of medications. Int J Geriatr Psychiatry 2000;15:242-7.
10. Beier MT. Harmless herbs? Think again: merits of a complete medication history. J Am Med Dir Assoc 2006;7:446-7.
11. [No authors listed]. Alzheimer’s disease: beware of interactions with cholinesterase inhibitors. Prescrire Int 2006;15:103-6.
12. Grossberg GT, Edwards KR, Zhao Q. Rationale for combining therapy with galantamine and memantine in Alzheimer’s disease. J Clin Pharmacol 2006;46(suppl 1):S17-S26.
13. Roe CM, Anderson MJ, Spivack B. Use of anticholinergic medications by older adults with dementia. J Am Geriatr Soc 2002;50:836-42.
14. Carnahan RM, Lund BC, Perry PJ, Chrischilles EA. The concurrent use of anticholinergics and cholinesterase inhibitors: rare event or common practice? J Am Geriatr Soc 2004;52:2082-7.
15. Schrag A. Psychiatric aspects of Parkinson’s disease. J Neurol 2004;251:795-804.
16. Okereke CS, Kirby L, Kumar D, et al. Concurrent administration of donepezil HCl and levodopa/carbidopa in patients with Parkinson’s disease: assessment of pharmacokinetic changes and safety following multiple oral doses. Br J Clin Pharmacol 2004;58(suppl 1):41-9.
17. Weiser M, Rotmensch HH, Korczyn AD, et al. A pilot, randomized, open-label trial assessing safety and pharmacokinetic parameters of co-administration of rivastigmine with risperidone in dementia patients with behavioral disturbances. Int J Geriatr Psychiatry 2002;17:343-6.
18. Schneider LS, Dagerman K, Insel PS. Efficacy and adverse events of atypical antipsychotics for dementia: meta-analysis of randomized, placebo-controlled trials. Am J Geriatr Psychiatry 2006;14(3):191-210.
19. Koenig HG, Blazer DG. Mood disorders. In: Blazer DG, Steffens DC, Busse EW, eds. Textbook of geriatric psychiatry 3rd ed. Washington, DC: American Psychiatric Publishing; 2004:254.
20. Jacobson SA, Pies RW, Greenblatt DJ. Anxiolytic and sedative-hypnotic medications. In: Handbook of geriatric psychopharmacology. Washington, DC: American Psychiatric Publishing; 2002:249-312.