User login
The Official Newspaper of the American Association for Thoracic Surgery
Residents’ Forum: 2015 Cardiac training experience from the perspective of a trainee
At the 62nd annual Southern Thoracic Surgical Association meeting in Orlando, Fla., there were several pervasive themes, including measurement of quality metrics in pulmonary, esophageal, and cardiac surgery. Piggybacking on the topic of quality, Dr. Asad A. Shah of Duke University, Durham, N.C., and colleagues identified something inherent to improving a surgical product: the quality of resident training.
In the presentation titled Characterizing the Operative Experience of Cardiothoracic Surgery Residents in the United States: What are Residents Really Doing in the Operating Room?, Dr. Shah and his group utilized data from the 2015 Thoracic Surgery Directors Association Survey (to which 356 trainees responded) in order to analyze specific critical steps that are being performed by each PGY level in both traditional (2- and 3- year) and I-6 integrated programs.

In I-6 programs, trainees routinely performed sternotomy by PGY1; harvested LIMA, cannulated, and performed proximal anastomoses by PGY3; and performed all aspects of CABG by PGY4. Fully 100% of I-6 residents reported being the operative surgeon for both coronary artery bypass grafting (CABG) and aortic valve replacement (AVR) compared to 94% and 86% for CABG in 2-year and 3-year programs (respectively), and 89% and 83% for AVR in 2-year and 3-year programs (respectively).
Few trainees reported experience with other cardiac surgeries as an operative surgeon. Likely because of this lack of experience, 42% of trainees reported the need for further fellowship training to become facile with most standard cardiac procedures.
When we discuss quality metrics, qualifying an educational experience is critical. I commend Dr. Shah and colleagues for a well-analyzed, thoughtful study using the results of a survey that we all take at the end of our annual in-service training exam.
Graded operative responsibility is shown to work well in I-6 training programs where ALL residents reported experience as operative surgeon for CABG and AVR. Interestingly, traditional residents did not have the same experience: It is possible that a truncated training program makes graded learning more difficult in this population group, despite superior surgical skill at entry into cardiothoracic training. Or is this a matter of poor reporting? The definition of “operating surgeon” is not used or interpreted in a standard way and may be incorrectly used by I-6 trainees who have no basis of comparison to relative operative experience in a general surgery program.
Conversely, traditional cardiothoracic residents may have a different barometer of what it means to be an operating surgeon, potentially under-qualifying their experience. Either way, it is difficult to truly objectify a survey, as all individuals will interpret their experience based on their personal learning environment. Dr. Shah’s team is accurate in alluding to the heterogeneity of this experience.
If the operative experience is perceived to be so different amongst trainees across programs, how do we as a society standardize education in order to graduate more competent and capable cardiothoracic surgeons? Sending trainees to boot camps and increasing utilization of simulation labs is one step. Additionally, 360-degree Accreditation Council for Graduate Medical Education–mandated evaluations may open communication avenues that didn’t exist before between mentor and mentee in the operating room and encourage more stepwise teaching. And how do we augment operating surgeon experience across the other cardiac categories (i.e. mitral valve repair, aorta, TAVR, etc)?
In order for the composite body of new graduates to report better national outcomes, we must standardize quality teaching between programs. It is simply not acceptable that half of trainees feel that advanced fellowships are necessary to reach comfort in standard cardiac cases.
The aforementioned study is a great first start, and the analysis should be extended to thoracic experience. Specifically, it would be interesting to perform the same analysis for thoracoscopic cases, as these also include steps that can be learned and mastered prior to doing a case skin to skin on the operating-surgeon side of the table. Standardizing education is difficult in cardiothoracic surgery, but Dr. Shah and colleagues begin an excellent conversation about the heterogeneous training experience that prepares some but fails others.
Dr. Shersher is a cardiothoracic surgeon at Rush University Medical Center, Chicago, and a resident medical editor for Thoracic Surgery News.
At the 62nd annual Southern Thoracic Surgical Association meeting in Orlando, Fla., there were several pervasive themes, including measurement of quality metrics in pulmonary, esophageal, and cardiac surgery. Piggybacking on the topic of quality, Dr. Asad A. Shah of Duke University, Durham, N.C., and colleagues identified something inherent to improving a surgical product: the quality of resident training.
In the presentation titled Characterizing the Operative Experience of Cardiothoracic Surgery Residents in the United States: What are Residents Really Doing in the Operating Room?, Dr. Shah and his group utilized data from the 2015 Thoracic Surgery Directors Association Survey (to which 356 trainees responded) in order to analyze specific critical steps that are being performed by each PGY level in both traditional (2- and 3- year) and I-6 integrated programs.
In I-6 programs, trainees routinely performed sternotomy by PGY1; harvested LIMA, cannulated, and performed proximal anastomoses by PGY3; and performed all aspects of CABG by PGY4. Fully 100% of I-6 residents reported being the operative surgeon for both coronary artery bypass grafting (CABG) and aortic valve replacement (AVR) compared to 94% and 86% for CABG in 2-year and 3-year programs (respectively), and 89% and 83% for AVR in 2-year and 3-year programs (respectively).
Few trainees reported experience with other cardiac surgeries as an operative surgeon. Likely because of this lack of experience, 42% of trainees reported the need for further fellowship training to become facile with most standard cardiac procedures.
When we discuss quality metrics, qualifying an educational experience is critical. I commend Dr. Shah and colleagues for a well-analyzed, thoughtful study using the results of a survey that we all take at the end of our annual in-service training exam.
Graded operative responsibility is shown to work well in I-6 training programs where ALL residents reported experience as operative surgeon for CABG and AVR. Interestingly, traditional residents did not have the same experience: It is possible that a truncated training program makes graded learning more difficult in this population group, despite superior surgical skill at entry into cardiothoracic training. Or is this a matter of poor reporting? The definition of “operating surgeon” is not used or interpreted in a standard way and may be incorrectly used by I-6 trainees who have no basis of comparison to relative operative experience in a general surgery program.
Conversely, traditional cardiothoracic residents may have a different barometer of what it means to be an operating surgeon, potentially under-qualifying their experience. Either way, it is difficult to truly objectify a survey, as all individuals will interpret their experience based on their personal learning environment. Dr. Shah’s team is accurate in alluding to the heterogeneity of this experience.
If the operative experience is perceived to be so different amongst trainees across programs, how do we as a society standardize education in order to graduate more competent and capable cardiothoracic surgeons? Sending trainees to boot camps and increasing utilization of simulation labs is one step. Additionally, 360-degree Accreditation Council for Graduate Medical Education–mandated evaluations may open communication avenues that didn’t exist before between mentor and mentee in the operating room and encourage more stepwise teaching. And how do we augment operating surgeon experience across the other cardiac categories (i.e. mitral valve repair, aorta, TAVR, etc)?
In order for the composite body of new graduates to report better national outcomes, we must standardize quality teaching between programs. It is simply not acceptable that half of trainees feel that advanced fellowships are necessary to reach comfort in standard cardiac cases.
The aforementioned study is a great first start, and the analysis should be extended to thoracic experience. Specifically, it would be interesting to perform the same analysis for thoracoscopic cases, as these also include steps that can be learned and mastered prior to doing a case skin to skin on the operating-surgeon side of the table. Standardizing education is difficult in cardiothoracic surgery, but Dr. Shah and colleagues begin an excellent conversation about the heterogeneous training experience that prepares some but fails others.
Dr. Shersher is a cardiothoracic surgeon at Rush University Medical Center, Chicago, and a resident medical editor for Thoracic Surgery News.
At the 62nd annual Southern Thoracic Surgical Association meeting in Orlando, Fla., there were several pervasive themes, including measurement of quality metrics in pulmonary, esophageal, and cardiac surgery. Piggybacking on the topic of quality, Dr. Asad A. Shah of Duke University, Durham, N.C., and colleagues identified something inherent to improving a surgical product: the quality of resident training.
In the presentation titled Characterizing the Operative Experience of Cardiothoracic Surgery Residents in the United States: What are Residents Really Doing in the Operating Room?, Dr. Shah and his group utilized data from the 2015 Thoracic Surgery Directors Association Survey (to which 356 trainees responded) in order to analyze specific critical steps that are being performed by each PGY level in both traditional (2- and 3- year) and I-6 integrated programs.
In I-6 programs, trainees routinely performed sternotomy by PGY1; harvested LIMA, cannulated, and performed proximal anastomoses by PGY3; and performed all aspects of CABG by PGY4. Fully 100% of I-6 residents reported being the operative surgeon for both coronary artery bypass grafting (CABG) and aortic valve replacement (AVR) compared to 94% and 86% for CABG in 2-year and 3-year programs (respectively), and 89% and 83% for AVR in 2-year and 3-year programs (respectively).
Few trainees reported experience with other cardiac surgeries as an operative surgeon. Likely because of this lack of experience, 42% of trainees reported the need for further fellowship training to become facile with most standard cardiac procedures.
When we discuss quality metrics, qualifying an educational experience is critical. I commend Dr. Shah and colleagues for a well-analyzed, thoughtful study using the results of a survey that we all take at the end of our annual in-service training exam.
Graded operative responsibility is shown to work well in I-6 training programs where ALL residents reported experience as operative surgeon for CABG and AVR. Interestingly, traditional residents did not have the same experience: It is possible that a truncated training program makes graded learning more difficult in this population group, despite superior surgical skill at entry into cardiothoracic training. Or is this a matter of poor reporting? The definition of “operating surgeon” is not used or interpreted in a standard way and may be incorrectly used by I-6 trainees who have no basis of comparison to relative operative experience in a general surgery program.
Conversely, traditional cardiothoracic residents may have a different barometer of what it means to be an operating surgeon, potentially under-qualifying their experience. Either way, it is difficult to truly objectify a survey, as all individuals will interpret their experience based on their personal learning environment. Dr. Shah’s team is accurate in alluding to the heterogeneity of this experience.
If the operative experience is perceived to be so different amongst trainees across programs, how do we as a society standardize education in order to graduate more competent and capable cardiothoracic surgeons? Sending trainees to boot camps and increasing utilization of simulation labs is one step. Additionally, 360-degree Accreditation Council for Graduate Medical Education–mandated evaluations may open communication avenues that didn’t exist before between mentor and mentee in the operating room and encourage more stepwise teaching. And how do we augment operating surgeon experience across the other cardiac categories (i.e. mitral valve repair, aorta, TAVR, etc)?
In order for the composite body of new graduates to report better national outcomes, we must standardize quality teaching between programs. It is simply not acceptable that half of trainees feel that advanced fellowships are necessary to reach comfort in standard cardiac cases.
The aforementioned study is a great first start, and the analysis should be extended to thoracic experience. Specifically, it would be interesting to perform the same analysis for thoracoscopic cases, as these also include steps that can be learned and mastered prior to doing a case skin to skin on the operating-surgeon side of the table. Standardizing education is difficult in cardiothoracic surgery, but Dr. Shah and colleagues begin an excellent conversation about the heterogeneous training experience that prepares some but fails others.
Dr. Shersher is a cardiothoracic surgeon at Rush University Medical Center, Chicago, and a resident medical editor for Thoracic Surgery News.

AATS Week Registration & Housing Now Open
Register for AATS Week 2016 today and receive a $100 discount!
Aortic Symposium
May 12–13, 2016
New York, NY
Course Directors
Joseph S. Coselli
Steven L. Lansman
96th Annual Meeting
May 14-18, 2016
Baltimore, MD
President & Annual Meeting Chair
Joseph S. Coselli
Annual Meeting Co-Chairs
Charles D. Fraser
David R. Jones
Annual Meeting Registration Packages
Allied Health Package: Registration for the Saturday Courses, Sunday Symposium and the 96th Annual Meeting (Monday-Wednesday). Register before March 25, 2016 for only $400, after which the fee goes up to $500.
Resident/Fellow and Medical Student Package: Registration for the Saturday Courses, Sunday Symposium and the 96th Annual Meeting (Monday-Wednesday). Register before March 25, 2016 and attend for no charge. After that date, the fee is $300.
Saturday Courses and Sunday Symposium Registration: Register for a Saturday course and/or a Sunday symposium and have access to all other courses/symposia that same day. Note: Registration for the Saturday courses and/or Sunday symposium is separate from the Annual Meeting fee.
Register for AATS Week 2016 today and receive a $100 discount!
Aortic Symposium
May 12–13, 2016
New York, NY
Course Directors
Joseph S. Coselli
Steven L. Lansman
96th Annual Meeting
May 14-18, 2016
Baltimore, MD
President & Annual Meeting Chair
Joseph S. Coselli
Annual Meeting Co-Chairs
Charles D. Fraser
David R. Jones
Annual Meeting Registration Packages
Allied Health Package: Registration for the Saturday Courses, Sunday Symposium and the 96th Annual Meeting (Monday-Wednesday). Register before March 25, 2016 for only $400, after which the fee goes up to $500.
Resident/Fellow and Medical Student Package: Registration for the Saturday Courses, Sunday Symposium and the 96th Annual Meeting (Monday-Wednesday). Register before March 25, 2016 and attend for no charge. After that date, the fee is $300.
Saturday Courses and Sunday Symposium Registration: Register for a Saturday course and/or a Sunday symposium and have access to all other courses/symposia that same day. Note: Registration for the Saturday courses and/or Sunday symposium is separate from the Annual Meeting fee.
Register for AATS Week 2016 today and receive a $100 discount!
Aortic Symposium
May 12–13, 2016
New York, NY
Course Directors
Joseph S. Coselli
Steven L. Lansman
96th Annual Meeting
May 14-18, 2016
Baltimore, MD
President & Annual Meeting Chair
Joseph S. Coselli
Annual Meeting Co-Chairs
Charles D. Fraser
David R. Jones
Annual Meeting Registration Packages
Allied Health Package: Registration for the Saturday Courses, Sunday Symposium and the 96th Annual Meeting (Monday-Wednesday). Register before March 25, 2016 for only $400, after which the fee goes up to $500.
Resident/Fellow and Medical Student Package: Registration for the Saturday Courses, Sunday Symposium and the 96th Annual Meeting (Monday-Wednesday). Register before March 25, 2016 and attend for no charge. After that date, the fee is $300.
Saturday Courses and Sunday Symposium Registration: Register for a Saturday course and/or a Sunday symposium and have access to all other courses/symposia that same day. Note: Registration for the Saturday courses and/or Sunday symposium is separate from the Annual Meeting fee.

AHA: Coronary calcium personalizes ACC/AHA risk calculator
ORLANDO – Combining the coronary artery calcium score with the ACC/AHA cardiovascular risk calculator tool enables physicians to refine their decision making about who to recommend for statin therapy, Dr. Salman Waheed reported at the American Heart Association scientific sessions.
He presented an analysis of 1,225 asymptomatic adults followed for a median of 3.9 years in the observational arm of the St. Francis Health Study, an early landmark prospective study of the relationship between electron beam CT coronary artery calcium (CAC) score and cardiovascular event risk.
The 217 subjects who today would not be recommended for statin therapy on the basis of a 10-year atherosclerotic cardiovascular disease risk of 5%-7.4% as determined by the risk calculator included in the 2013 ACC/AHA cholesterol management guidelines (Circulation. 2014 Jun 24;129[25 Suppl 2]:S1-45) would be reclassified as warranting statin therapy if they had a CAC greater than 0, as was the case for 169 of the 217 (78%). Indeed, the presence of a CAC of 1 or more boosted their estimated 10-year risk to 10.8%.
On the other hand, there were 510 patients who would be classified as high risk by the ACC/AHA clinical risk calculator, with a 10-year risk of 7.5%-20%. Taking their CAC score into account would result in 73 being reclassified as low risk and becoming no longer statin candidates because their CAC of 0 was associated with a 10-year event risk of less than 1%. In contrast, for the 447 remaining subjects with a CAC greater than 0, the 10-year risk climbed to 21.9%, according to Dr. Waheed of the University of Kansas, Kansas City.
The composite outcome utilized in this analysis from the St. Francis Heart Study was comprised of nonfatal MI, coronary death, stroke, peripheral arterial revascularization, or coronary revascularization. Of note, heart failure wasn’t included.
Among the 545 subjects deemed at low cardiovascular risk because they weren’t eligible for statin therapy according to the 2013 ACC/AHA guidelines, 209 would be recategorized as high risk on the basis of a CAC score at or above the 80th percentile adjusted for age and gender. The adjusted risk of a cardiovascular event in the high CAC/low clinical risk group was 24.9-fold greater than in the low CAC/low clinical risk group.
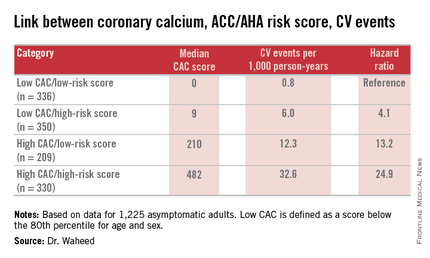
“Among those eligible for statin therapy based upon current guidelines, high CAC portends a sixfold higher outcome risk than low CAC,” Dr. Waheed added.
The magnitude of CAC progression over the course of 4 years was similar across the baseline risk categories; however, the absolute CAC progression was greater among those with a high CAC at baseline.
Audience member Dr. Daniel S. Berman observed that the results of Dr. Waheed’s study are highly concordant with an earlier report from the Multi-Ethnic Study of Atherosclerosis in which a CAC of 0 was quite common in patients for whom statins would be recommended under the current ACC/AHA guidelines.
“Your data support the idea that stratification based upon CAC could more personalize the statin recommendations,” said Dr. Berman, chief of cardiac imaging and nuclear cardiology at Cedars-Sinai Medical Center and professor of medicine at the University of California, Los Angeles.

Another audience member, Dr. Donald M. Lloyd-Jones, one of the architects of the current guidelines, commented that the analyses from the St. Francis Heart Study and the Multi-Ethnic Study of Atherosclerosis suggest CAC screening coupled with the ACC/AHA risk score provides added value in a select group of patients.
“Your analysis continues to reinforce the point that we probably shouldn’t be doing universal CAC screening because in the people with a 10-year risk of less than 5% the yield is low and the CAC didn’t change anything, while in the people with a 10-year risk of 20% or higher the yield is incredibly high and the CAC didn’t change anything,” observed Dr. Lloyd-Jones, professor and chair of the department of preventive medicine at Northwestern University, Chicago.
“So CAC really is for those intermediate-risk folks where we’re on the bubble, where we might consider withholding therapy. And I’d love to see a trial to show that’s safe, by the way, but maybe that day will come. But we certainly would be comfortable up-classifying somebody if more CAC is present than there should be,” he added.
Dr. Waheed reported having no financial conflicts regarding his study.
ORLANDO – Combining the coronary artery calcium score with the ACC/AHA cardiovascular risk calculator tool enables physicians to refine their decision making about who to recommend for statin therapy, Dr. Salman Waheed reported at the American Heart Association scientific sessions.
He presented an analysis of 1,225 asymptomatic adults followed for a median of 3.9 years in the observational arm of the St. Francis Health Study, an early landmark prospective study of the relationship between electron beam CT coronary artery calcium (CAC) score and cardiovascular event risk.
The 217 subjects who today would not be recommended for statin therapy on the basis of a 10-year atherosclerotic cardiovascular disease risk of 5%-7.4% as determined by the risk calculator included in the 2013 ACC/AHA cholesterol management guidelines (Circulation. 2014 Jun 24;129[25 Suppl 2]:S1-45) would be reclassified as warranting statin therapy if they had a CAC greater than 0, as was the case for 169 of the 217 (78%). Indeed, the presence of a CAC of 1 or more boosted their estimated 10-year risk to 10.8%.
On the other hand, there were 510 patients who would be classified as high risk by the ACC/AHA clinical risk calculator, with a 10-year risk of 7.5%-20%. Taking their CAC score into account would result in 73 being reclassified as low risk and becoming no longer statin candidates because their CAC of 0 was associated with a 10-year event risk of less than 1%. In contrast, for the 447 remaining subjects with a CAC greater than 0, the 10-year risk climbed to 21.9%, according to Dr. Waheed of the University of Kansas, Kansas City.
The composite outcome utilized in this analysis from the St. Francis Heart Study was comprised of nonfatal MI, coronary death, stroke, peripheral arterial revascularization, or coronary revascularization. Of note, heart failure wasn’t included.
Among the 545 subjects deemed at low cardiovascular risk because they weren’t eligible for statin therapy according to the 2013 ACC/AHA guidelines, 209 would be recategorized as high risk on the basis of a CAC score at or above the 80th percentile adjusted for age and gender. The adjusted risk of a cardiovascular event in the high CAC/low clinical risk group was 24.9-fold greater than in the low CAC/low clinical risk group.
“Among those eligible for statin therapy based upon current guidelines, high CAC portends a sixfold higher outcome risk than low CAC,” Dr. Waheed added.
The magnitude of CAC progression over the course of 4 years was similar across the baseline risk categories; however, the absolute CAC progression was greater among those with a high CAC at baseline.
Audience member Dr. Daniel S. Berman observed that the results of Dr. Waheed’s study are highly concordant with an earlier report from the Multi-Ethnic Study of Atherosclerosis in which a CAC of 0 was quite common in patients for whom statins would be recommended under the current ACC/AHA guidelines.
“Your data support the idea that stratification based upon CAC could more personalize the statin recommendations,” said Dr. Berman, chief of cardiac imaging and nuclear cardiology at Cedars-Sinai Medical Center and professor of medicine at the University of California, Los Angeles.
Another audience member, Dr. Donald M. Lloyd-Jones, one of the architects of the current guidelines, commented that the analyses from the St. Francis Heart Study and the Multi-Ethnic Study of Atherosclerosis suggest CAC screening coupled with the ACC/AHA risk score provides added value in a select group of patients.
“Your analysis continues to reinforce the point that we probably shouldn’t be doing universal CAC screening because in the people with a 10-year risk of less than 5% the yield is low and the CAC didn’t change anything, while in the people with a 10-year risk of 20% or higher the yield is incredibly high and the CAC didn’t change anything,” observed Dr. Lloyd-Jones, professor and chair of the department of preventive medicine at Northwestern University, Chicago.
“So CAC really is for those intermediate-risk folks where we’re on the bubble, where we might consider withholding therapy. And I’d love to see a trial to show that’s safe, by the way, but maybe that day will come. But we certainly would be comfortable up-classifying somebody if more CAC is present than there should be,” he added.
Dr. Waheed reported having no financial conflicts regarding his study.
ORLANDO – Combining the coronary artery calcium score with the ACC/AHA cardiovascular risk calculator tool enables physicians to refine their decision making about who to recommend for statin therapy, Dr. Salman Waheed reported at the American Heart Association scientific sessions.
He presented an analysis of 1,225 asymptomatic adults followed for a median of 3.9 years in the observational arm of the St. Francis Health Study, an early landmark prospective study of the relationship between electron beam CT coronary artery calcium (CAC) score and cardiovascular event risk.
The 217 subjects who today would not be recommended for statin therapy on the basis of a 10-year atherosclerotic cardiovascular disease risk of 5%-7.4% as determined by the risk calculator included in the 2013 ACC/AHA cholesterol management guidelines (Circulation. 2014 Jun 24;129[25 Suppl 2]:S1-45) would be reclassified as warranting statin therapy if they had a CAC greater than 0, as was the case for 169 of the 217 (78%). Indeed, the presence of a CAC of 1 or more boosted their estimated 10-year risk to 10.8%.
On the other hand, there were 510 patients who would be classified as high risk by the ACC/AHA clinical risk calculator, with a 10-year risk of 7.5%-20%. Taking their CAC score into account would result in 73 being reclassified as low risk and becoming no longer statin candidates because their CAC of 0 was associated with a 10-year event risk of less than 1%. In contrast, for the 447 remaining subjects with a CAC greater than 0, the 10-year risk climbed to 21.9%, according to Dr. Waheed of the University of Kansas, Kansas City.
The composite outcome utilized in this analysis from the St. Francis Heart Study was comprised of nonfatal MI, coronary death, stroke, peripheral arterial revascularization, or coronary revascularization. Of note, heart failure wasn’t included.
Among the 545 subjects deemed at low cardiovascular risk because they weren’t eligible for statin therapy according to the 2013 ACC/AHA guidelines, 209 would be recategorized as high risk on the basis of a CAC score at or above the 80th percentile adjusted for age and gender. The adjusted risk of a cardiovascular event in the high CAC/low clinical risk group was 24.9-fold greater than in the low CAC/low clinical risk group.
“Among those eligible for statin therapy based upon current guidelines, high CAC portends a sixfold higher outcome risk than low CAC,” Dr. Waheed added.
The magnitude of CAC progression over the course of 4 years was similar across the baseline risk categories; however, the absolute CAC progression was greater among those with a high CAC at baseline.
Audience member Dr. Daniel S. Berman observed that the results of Dr. Waheed’s study are highly concordant with an earlier report from the Multi-Ethnic Study of Atherosclerosis in which a CAC of 0 was quite common in patients for whom statins would be recommended under the current ACC/AHA guidelines.
“Your data support the idea that stratification based upon CAC could more personalize the statin recommendations,” said Dr. Berman, chief of cardiac imaging and nuclear cardiology at Cedars-Sinai Medical Center and professor of medicine at the University of California, Los Angeles.
Another audience member, Dr. Donald M. Lloyd-Jones, one of the architects of the current guidelines, commented that the analyses from the St. Francis Heart Study and the Multi-Ethnic Study of Atherosclerosis suggest CAC screening coupled with the ACC/AHA risk score provides added value in a select group of patients.
“Your analysis continues to reinforce the point that we probably shouldn’t be doing universal CAC screening because in the people with a 10-year risk of less than 5% the yield is low and the CAC didn’t change anything, while in the people with a 10-year risk of 20% or higher the yield is incredibly high and the CAC didn’t change anything,” observed Dr. Lloyd-Jones, professor and chair of the department of preventive medicine at Northwestern University, Chicago.
“So CAC really is for those intermediate-risk folks where we’re on the bubble, where we might consider withholding therapy. And I’d love to see a trial to show that’s safe, by the way, but maybe that day will come. But we certainly would be comfortable up-classifying somebody if more CAC is present than there should be,” he added.
Dr. Waheed reported having no financial conflicts regarding his study.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: Measuring coronary artery calcium provides added value in refining the 10-year atherosclerotic cardiovascular disease risk, especially in patients with an intermediate-risk score on the ACC/AHA risk calculator.
Major finding: Seventy-eight percent of a group of patients for whom statin therapy wouldn’t be recommended under the current ACC/AHA guidelines because their estimated 10-year event risk was 5%-7.5% would be reclassified as warranting statin therapy because their coronary artery calcium score was greater than 0, pushing their estimated risk to 10.8%.
Data source: A retrospective analysis of data on 1,225 asymptomatic adults followed prospectively with coronary artery calcium measurements in the St. Francis Health Study.
Disclosures: The study presenter reported having no financial conflicts of interest.
Cardiothoracic Surgery Resident Poster Competition
Represent your institution with a scientific poster of your clinical/investigative research at the 2016 AATS Annual Meeting in Baltimore, Maryland, May 14-18, 2016. The Competition is open to senior cardiothoracic surgery residents and/or congenital heart surgery fellows worldwide
North American residents must (1) Be in their last year of either an ACGME-accredited or RCPSC-accredited US or Canadian cardiothoracic surgery residency program or congenital heart surgery fellowship, and (2) Upload a support letter from their Program Director as part of their application.
International residents must (1) Be in their last year of a cardiothoracic training program at an AATS Member’s institution, and (2) Upload a sponsor letter from an AATS member at their institution as part of their application.
Application — Residents/fellows must provide a brief abstract of the research on their posters. Research may include information previously presented and/or published.
Benefits — Participant/institutions will (1) Receive a $500 stipend to offset travel and hotel accommodation to the Annual Meeting, (2) Receive a complimentary Annual Meeting registration, and (3) Have access to a Skills Course (Saturday, May 14) and Postgraduate Course (Sunday, May 15).
The participant’s training program will be responsible for the cost of any additional resident/fellow travel and accommodations.
Deadline: January 22, 2016
Represent your institution with a scientific poster of your clinical/investigative research at the 2016 AATS Annual Meeting in Baltimore, Maryland, May 14-18, 2016. The Competition is open to senior cardiothoracic surgery residents and/or congenital heart surgery fellows worldwide
North American residents must (1) Be in their last year of either an ACGME-accredited or RCPSC-accredited US or Canadian cardiothoracic surgery residency program or congenital heart surgery fellowship, and (2) Upload a support letter from their Program Director as part of their application.
International residents must (1) Be in their last year of a cardiothoracic training program at an AATS Member’s institution, and (2) Upload a sponsor letter from an AATS member at their institution as part of their application.
Application — Residents/fellows must provide a brief abstract of the research on their posters. Research may include information previously presented and/or published.
Benefits — Participant/institutions will (1) Receive a $500 stipend to offset travel and hotel accommodation to the Annual Meeting, (2) Receive a complimentary Annual Meeting registration, and (3) Have access to a Skills Course (Saturday, May 14) and Postgraduate Course (Sunday, May 15).
The participant’s training program will be responsible for the cost of any additional resident/fellow travel and accommodations.
Deadline: January 22, 2016
Represent your institution with a scientific poster of your clinical/investigative research at the 2016 AATS Annual Meeting in Baltimore, Maryland, May 14-18, 2016. The Competition is open to senior cardiothoracic surgery residents and/or congenital heart surgery fellows worldwide
North American residents must (1) Be in their last year of either an ACGME-accredited or RCPSC-accredited US or Canadian cardiothoracic surgery residency program or congenital heart surgery fellowship, and (2) Upload a support letter from their Program Director as part of their application.
International residents must (1) Be in their last year of a cardiothoracic training program at an AATS Member’s institution, and (2) Upload a sponsor letter from an AATS member at their institution as part of their application.
Application — Residents/fellows must provide a brief abstract of the research on their posters. Research may include information previously presented and/or published.
Benefits — Participant/institutions will (1) Receive a $500 stipend to offset travel and hotel accommodation to the Annual Meeting, (2) Receive a complimentary Annual Meeting registration, and (3) Have access to a Skills Course (Saturday, May 14) and Postgraduate Course (Sunday, May 15).
The participant’s training program will be responsible for the cost of any additional resident/fellow travel and accommodations.
Deadline: January 22, 2016

Apply to the AATS Summer Internship Scholarship
Medical students: Submissions are open for the AATS Summer Internship Scholarship giving up to 40 successful candidates the opportunity to spend eight weeks during the summer working in the cardiothoracic surgery department of a North American AATS member.
Program Goal — The program aims to broaden medical students’ educational experiences and to provide insight into cardiothoracic surgery.
Eligibility — (1) Candidates must be a North American first- or second-year medical student (as of January 2, 2016), (2) Host sponsor (an AATS member) must provide a letter of support/approval, and (3) Internships must take place at the institution of the host sponsor.
Application — The application must include no more than a one-page outline that includes what the candidate hopes to accomplish during his/her eight-week scholarship and specifies the proposed intern’s exposure to CT surgery, including both laboratory and clinical experience
Selection — (1) No more than two students from a single institution may receive a scholarship, (2) If two students from the same institution are selected, each must have a different host sponsor, and (3) Award recipients must agree to submit a summary report and evaluation of their experience to AATS within 60 days of internship completion.
Deadline: Friday, January 15, 2016
Medical students: Submissions are open for the AATS Summer Internship Scholarship giving up to 40 successful candidates the opportunity to spend eight weeks during the summer working in the cardiothoracic surgery department of a North American AATS member.
Program Goal — The program aims to broaden medical students’ educational experiences and to provide insight into cardiothoracic surgery.
Eligibility — (1) Candidates must be a North American first- or second-year medical student (as of January 2, 2016), (2) Host sponsor (an AATS member) must provide a letter of support/approval, and (3) Internships must take place at the institution of the host sponsor.
Application — The application must include no more than a one-page outline that includes what the candidate hopes to accomplish during his/her eight-week scholarship and specifies the proposed intern’s exposure to CT surgery, including both laboratory and clinical experience
Selection — (1) No more than two students from a single institution may receive a scholarship, (2) If two students from the same institution are selected, each must have a different host sponsor, and (3) Award recipients must agree to submit a summary report and evaluation of their experience to AATS within 60 days of internship completion.
Deadline: Friday, January 15, 2016
Medical students: Submissions are open for the AATS Summer Internship Scholarship giving up to 40 successful candidates the opportunity to spend eight weeks during the summer working in the cardiothoracic surgery department of a North American AATS member.
Program Goal — The program aims to broaden medical students’ educational experiences and to provide insight into cardiothoracic surgery.
Eligibility — (1) Candidates must be a North American first- or second-year medical student (as of January 2, 2016), (2) Host sponsor (an AATS member) must provide a letter of support/approval, and (3) Internships must take place at the institution of the host sponsor.
Application — The application must include no more than a one-page outline that includes what the candidate hopes to accomplish during his/her eight-week scholarship and specifies the proposed intern’s exposure to CT surgery, including both laboratory and clinical experience
Selection — (1) No more than two students from a single institution may receive a scholarship, (2) If two students from the same institution are selected, each must have a different host sponsor, and (3) Award recipients must agree to submit a summary report and evaluation of their experience to AATS within 60 days of internship completion.
Deadline: Friday, January 15, 2016

Be an AATS Member for a Day
Medical Students, General Surgery Residents and I-6 CT Surgical Residents — Submissions are open for the AATS Member for a Day program. Up to 30 successful candidates will have the opportunity to accompany an AATS Member Mentor for portions of the 2016 AATS Annual Meeting.
Dates/Location: May 14-18, 2016, Baltimore, MD
Eligibility — Applicants must be North American medical students, general surgery residents or I-6 cardiothoracic residents (within their first three years).
Program Goals — Are to (1) offer insight into cardiothoracic surgery, and (2) provide an opportunity to network and build relationships within the cardiothoracic surgical community.
Benefits — (1) Complimentary hotel accommodation for a minimum of three and maximum of four nights at an AATS Annual Meeting hotel, (2) a $500 stipend to help offset travel costs, and (3) an additional $250 stipend to offset the cost of meals.
Deadline: Friday, January 15, 2016
Medical Students, General Surgery Residents and I-6 CT Surgical Residents — Submissions are open for the AATS Member for a Day program. Up to 30 successful candidates will have the opportunity to accompany an AATS Member Mentor for portions of the 2016 AATS Annual Meeting.
Dates/Location: May 14-18, 2016, Baltimore, MD
Eligibility — Applicants must be North American medical students, general surgery residents or I-6 cardiothoracic residents (within their first three years).
Program Goals — Are to (1) offer insight into cardiothoracic surgery, and (2) provide an opportunity to network and build relationships within the cardiothoracic surgical community.
Benefits — (1) Complimentary hotel accommodation for a minimum of three and maximum of four nights at an AATS Annual Meeting hotel, (2) a $500 stipend to help offset travel costs, and (3) an additional $250 stipend to offset the cost of meals.
Deadline: Friday, January 15, 2016
Medical Students, General Surgery Residents and I-6 CT Surgical Residents — Submissions are open for the AATS Member for a Day program. Up to 30 successful candidates will have the opportunity to accompany an AATS Member Mentor for portions of the 2016 AATS Annual Meeting.
Dates/Location: May 14-18, 2016, Baltimore, MD
Eligibility — Applicants must be North American medical students, general surgery residents or I-6 cardiothoracic residents (within their first three years).
Program Goals — Are to (1) offer insight into cardiothoracic surgery, and (2) provide an opportunity to network and build relationships within the cardiothoracic surgical community.
Benefits — (1) Complimentary hotel accommodation for a minimum of three and maximum of four nights at an AATS Annual Meeting hotel, (2) a $500 stipend to help offset travel costs, and (3) an additional $250 stipend to offset the cost of meals.
Deadline: Friday, January 15, 2016

Apply for AATS Graham Foundation Programs
These AATS Graham Foundation programs are now open for submissions.
“Honoring Our Mentors” Fellowships acknowledge the leadership and dedication of surgeons in the field.
Marc de Leval Fellowship — This fellowship, for North American trainees and early career congenital heart surgeons, allows them to spend four to six weeks receiving an international surgical experience at a UK or European institution.
F. Griffith Pearson Fellowship — The fellowship, for surgeons who have finished their residences in general thoracic surgery, allows them to spend four to six weeks advancing their clinical techniques at a North American host institute.
North American Clinical Immersion in Advanced Minimally Invasive Thoracic Surgery
Sponsored by Medtronic
Young Chinese surgeons: Take advantage of this opportunity to spend up to three months at a North American institution. The program focuses on obtaining expertise in advanced minimally invasive thoracic surgery, comprehensive care screening and diagnosis.
Summer Intern Scholarship
The scholarship — for first- and second- year medical students — is an eight-week summer internships in the CT surgery department of an AATS member. Interns receive a $2,500 grant for living expenses.
Deadline: January 15, 2016
These AATS Graham Foundation programs are now open for submissions.
“Honoring Our Mentors” Fellowships acknowledge the leadership and dedication of surgeons in the field.
Marc de Leval Fellowship — This fellowship, for North American trainees and early career congenital heart surgeons, allows them to spend four to six weeks receiving an international surgical experience at a UK or European institution.
F. Griffith Pearson Fellowship — The fellowship, for surgeons who have finished their residences in general thoracic surgery, allows them to spend four to six weeks advancing their clinical techniques at a North American host institute.
North American Clinical Immersion in Advanced Minimally Invasive Thoracic Surgery
Sponsored by Medtronic
Young Chinese surgeons: Take advantage of this opportunity to spend up to three months at a North American institution. The program focuses on obtaining expertise in advanced minimally invasive thoracic surgery, comprehensive care screening and diagnosis.
Summer Intern Scholarship
The scholarship — for first- and second- year medical students — is an eight-week summer internships in the CT surgery department of an AATS member. Interns receive a $2,500 grant for living expenses.
Deadline: January 15, 2016
These AATS Graham Foundation programs are now open for submissions.
“Honoring Our Mentors” Fellowships acknowledge the leadership and dedication of surgeons in the field.
Marc de Leval Fellowship — This fellowship, for North American trainees and early career congenital heart surgeons, allows them to spend four to six weeks receiving an international surgical experience at a UK or European institution.
F. Griffith Pearson Fellowship — The fellowship, for surgeons who have finished their residences in general thoracic surgery, allows them to spend four to six weeks advancing their clinical techniques at a North American host institute.
North American Clinical Immersion in Advanced Minimally Invasive Thoracic Surgery
Sponsored by Medtronic
Young Chinese surgeons: Take advantage of this opportunity to spend up to three months at a North American institution. The program focuses on obtaining expertise in advanced minimally invasive thoracic surgery, comprehensive care screening and diagnosis.
Summer Intern Scholarship
The scholarship — for first- and second- year medical students — is an eight-week summer internships in the CT surgery department of an AATS member. Interns receive a $2,500 grant for living expenses.
Deadline: January 15, 2016
Submit to Perioperative/Team-based Care Poster Competition
Non-physician cardiothoracic surgical team professionals are invited to submit abstracts for the AATS Perioperative/Team-based Care Poster Competition at the AATS Annual Meeting in Baltimore, MD, May 14-16, 2016. The posters should reflect the participant’s research findings and/or new and innovative ideas for successful approaches in management of the cardiothoracic patient.
Eligibility — The competition is open to surgical team professionals: nurse practitioners, physician assistants, perfusionists and RNs.
Abstract Review — Abstracts will be reviewed and selected by the AATS Perioperative/Team-Based Care Review Committee. Successful applicants will be notified in mid-February 2016. Abstracts/posters may contain material that has been previously presented.
The Competition — All successful applicants will present their Competition poster during the AATS Welcome Reception on Sunday, May 15th from 5:00 pm - 7:00 pm. The winning presenter will receive a $1,000 stipend underwriting his/her travel to and accommodations at the Annual Meeting. The award winner will be announced during the Tuesday, May 17th Plenary Session and be published in Thoracic Surgery News and The Daily News.
Deadline: January 22, 2016
Non-physician cardiothoracic surgical team professionals are invited to submit abstracts for the AATS Perioperative/Team-based Care Poster Competition at the AATS Annual Meeting in Baltimore, MD, May 14-16, 2016. The posters should reflect the participant’s research findings and/or new and innovative ideas for successful approaches in management of the cardiothoracic patient.
Eligibility — The competition is open to surgical team professionals: nurse practitioners, physician assistants, perfusionists and RNs.
Abstract Review — Abstracts will be reviewed and selected by the AATS Perioperative/Team-Based Care Review Committee. Successful applicants will be notified in mid-February 2016. Abstracts/posters may contain material that has been previously presented.
The Competition — All successful applicants will present their Competition poster during the AATS Welcome Reception on Sunday, May 15th from 5:00 pm - 7:00 pm. The winning presenter will receive a $1,000 stipend underwriting his/her travel to and accommodations at the Annual Meeting. The award winner will be announced during the Tuesday, May 17th Plenary Session and be published in Thoracic Surgery News and The Daily News.
Deadline: January 22, 2016
Non-physician cardiothoracic surgical team professionals are invited to submit abstracts for the AATS Perioperative/Team-based Care Poster Competition at the AATS Annual Meeting in Baltimore, MD, May 14-16, 2016. The posters should reflect the participant’s research findings and/or new and innovative ideas for successful approaches in management of the cardiothoracic patient.
Eligibility — The competition is open to surgical team professionals: nurse practitioners, physician assistants, perfusionists and RNs.
Abstract Review — Abstracts will be reviewed and selected by the AATS Perioperative/Team-Based Care Review Committee. Successful applicants will be notified in mid-February 2016. Abstracts/posters may contain material that has been previously presented.
The Competition — All successful applicants will present their Competition poster during the AATS Welcome Reception on Sunday, May 15th from 5:00 pm - 7:00 pm. The winning presenter will receive a $1,000 stipend underwriting his/her travel to and accommodations at the Annual Meeting. The award winner will be announced during the Tuesday, May 17th Plenary Session and be published in Thoracic Surgery News and The Daily News.
Deadline: January 22, 2016

Alectinib shows promise in crizotinib-refractory ALK-rearranged NSCLC
Alectinib, an oral, small-molecule, ATP-competitive tyrosine kinase inhibitor of ALK, demonstrated good clinical activity in crizotinib-refractory patients with advanced non–small-cell lung cancer (NSCLC) harboring ALK rearrangements.
The overall response rate (ORR) for all 122 evaluable patients was 49%: 44% for the 96 patients who had received prior chemotherapy, and 69% for the 26 chemotherapy-naive patients. The median duration of response (DOR) for the 61 patients with a partial response was 11.2 months.
“The clinically meaningful ORR and DOR in patients with crizotinib-resistant disease and the sustained CNS response reported from this study, as well as the good tolerability profile, support the additional development of this promising new ALK inhibitor,” wrote Dr. Sai-Hong Ignatius Ou, clinical professor at the University of California, Irvine, and colleagues (J Clin Oncol. 2015 Nov. 23. doi:10.1200/JCO.2015.63.9443).
The observed clinical activity of alectinib in the CNS was consistent with preclinical data showing high CNS tissue penetration and earlier phase I/II results. Among 35 patients with baseline measurable CNS lesions, the ORR was 57%, including seven complete responses. CNS complete responses were observed in 10 of 23 patients (43%) who had no prior brain radiation.
The cumulative incidence rates of CNS progression were lower than were those of non-CNS progression, “which seems to suggest that alectinib can prevent or delay the emergence of CNS metastases,” the authors wrote. At 12 months, 33 patients had a CNS progression and 43 had a non-CNS progression.
Alectinib showed an acceptable safety profile. The most common adverse events were myalgia, fatigue, and gastrointestinal events, usually grade 1 or 2. Grade 3 or 4 adverse events occurred at a rate less than 5%. Most patients maintained therapeutic levels of alectinib throughout the study, indicated by a mean dose intensity of 97%.
The phase II study evaluated 122 patients who had locally advanced or metastatic NSCLC harboring an ALK rearrangement and who had progressed on crizotinib treatment.
Multiple oral doses at 600 mg twice daily produced an overall flat PK profile, supporting sustained alectinib exposure throughout the dosing interval. In contrast to results from the U.S. phase I/II study that reported differences in alectinib exposures between white and Asian patients, this study showed no marked differences between white (n = 6) and Asian (n = 20) patients evaluated.
F. Hoffmann-La Roche supported the study. Dr. Ou disclosed ties with Pfizer, F. Hoffmann-La Roche, Boehringer Ingelheim, ARIAD, AstraZeneca, Clovis Oncology, Astellas Pharma, Ignyta, and Daichi Sankyo. Several of his coauthors reported ties to industry.
Alectinib, an oral, small-molecule, ATP-competitive tyrosine kinase inhibitor of ALK, demonstrated good clinical activity in crizotinib-refractory patients with advanced non–small-cell lung cancer (NSCLC) harboring ALK rearrangements.
The overall response rate (ORR) for all 122 evaluable patients was 49%: 44% for the 96 patients who had received prior chemotherapy, and 69% for the 26 chemotherapy-naive patients. The median duration of response (DOR) for the 61 patients with a partial response was 11.2 months.
“The clinically meaningful ORR and DOR in patients with crizotinib-resistant disease and the sustained CNS response reported from this study, as well as the good tolerability profile, support the additional development of this promising new ALK inhibitor,” wrote Dr. Sai-Hong Ignatius Ou, clinical professor at the University of California, Irvine, and colleagues (J Clin Oncol. 2015 Nov. 23. doi:10.1200/JCO.2015.63.9443).
The observed clinical activity of alectinib in the CNS was consistent with preclinical data showing high CNS tissue penetration and earlier phase I/II results. Among 35 patients with baseline measurable CNS lesions, the ORR was 57%, including seven complete responses. CNS complete responses were observed in 10 of 23 patients (43%) who had no prior brain radiation.
The cumulative incidence rates of CNS progression were lower than were those of non-CNS progression, “which seems to suggest that alectinib can prevent or delay the emergence of CNS metastases,” the authors wrote. At 12 months, 33 patients had a CNS progression and 43 had a non-CNS progression.
Alectinib showed an acceptable safety profile. The most common adverse events were myalgia, fatigue, and gastrointestinal events, usually grade 1 or 2. Grade 3 or 4 adverse events occurred at a rate less than 5%. Most patients maintained therapeutic levels of alectinib throughout the study, indicated by a mean dose intensity of 97%.
The phase II study evaluated 122 patients who had locally advanced or metastatic NSCLC harboring an ALK rearrangement and who had progressed on crizotinib treatment.
Multiple oral doses at 600 mg twice daily produced an overall flat PK profile, supporting sustained alectinib exposure throughout the dosing interval. In contrast to results from the U.S. phase I/II study that reported differences in alectinib exposures between white and Asian patients, this study showed no marked differences between white (n = 6) and Asian (n = 20) patients evaluated.
F. Hoffmann-La Roche supported the study. Dr. Ou disclosed ties with Pfizer, F. Hoffmann-La Roche, Boehringer Ingelheim, ARIAD, AstraZeneca, Clovis Oncology, Astellas Pharma, Ignyta, and Daichi Sankyo. Several of his coauthors reported ties to industry.
Alectinib, an oral, small-molecule, ATP-competitive tyrosine kinase inhibitor of ALK, demonstrated good clinical activity in crizotinib-refractory patients with advanced non–small-cell lung cancer (NSCLC) harboring ALK rearrangements.
The overall response rate (ORR) for all 122 evaluable patients was 49%: 44% for the 96 patients who had received prior chemotherapy, and 69% for the 26 chemotherapy-naive patients. The median duration of response (DOR) for the 61 patients with a partial response was 11.2 months.
“The clinically meaningful ORR and DOR in patients with crizotinib-resistant disease and the sustained CNS response reported from this study, as well as the good tolerability profile, support the additional development of this promising new ALK inhibitor,” wrote Dr. Sai-Hong Ignatius Ou, clinical professor at the University of California, Irvine, and colleagues (J Clin Oncol. 2015 Nov. 23. doi:10.1200/JCO.2015.63.9443).
The observed clinical activity of alectinib in the CNS was consistent with preclinical data showing high CNS tissue penetration and earlier phase I/II results. Among 35 patients with baseline measurable CNS lesions, the ORR was 57%, including seven complete responses. CNS complete responses were observed in 10 of 23 patients (43%) who had no prior brain radiation.
The cumulative incidence rates of CNS progression were lower than were those of non-CNS progression, “which seems to suggest that alectinib can prevent or delay the emergence of CNS metastases,” the authors wrote. At 12 months, 33 patients had a CNS progression and 43 had a non-CNS progression.
Alectinib showed an acceptable safety profile. The most common adverse events were myalgia, fatigue, and gastrointestinal events, usually grade 1 or 2. Grade 3 or 4 adverse events occurred at a rate less than 5%. Most patients maintained therapeutic levels of alectinib throughout the study, indicated by a mean dose intensity of 97%.
The phase II study evaluated 122 patients who had locally advanced or metastatic NSCLC harboring an ALK rearrangement and who had progressed on crizotinib treatment.
Multiple oral doses at 600 mg twice daily produced an overall flat PK profile, supporting sustained alectinib exposure throughout the dosing interval. In contrast to results from the U.S. phase I/II study that reported differences in alectinib exposures between white and Asian patients, this study showed no marked differences between white (n = 6) and Asian (n = 20) patients evaluated.
F. Hoffmann-La Roche supported the study. Dr. Ou disclosed ties with Pfizer, F. Hoffmann-La Roche, Boehringer Ingelheim, ARIAD, AstraZeneca, Clovis Oncology, Astellas Pharma, Ignyta, and Daichi Sankyo. Several of his coauthors reported ties to industry.
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Alectinib, an oral, small molecule inhibitor of ALK, showed promising clinical activity in crizotinib-refractory patients with non–small-cell lung cancer (NSCLC).
Major finding: The overall response rate was 49% for all evaluable patients, 44% for those who had received prior chemotherapy, and 69% for chemotherapy-naive patients.
Data source: The phase II study evaluated 122 patients with locally advanced or metastatic NSCLC harboring an ALK rearrangement and who had progressed on crizotinib treatment.
Disclosures: F. Hoffmann-La Roche supported the study. Dr. Ou disclosed ties with Pfizer, F. Hoffmann-La Roche, Boehringer Ingelheim, ARIAD, AstraZeneca, Clovis Oncology, Astellas Pharma, Ignyta, and Daichi Sankyo. Several of his coauthors reported ties to industry.
Stroke risk boosted by adult congenital heart disease
Adult congenital heart disease significantly increases the risk of both hemorrhagic and ischemic stroke, particularly in individuals under 55 years of age, new data suggests.
A retrospective study of 29,638 adults aged 18-64 years with adult congenital heart disease (ACHD) showed that women aged 15-54 years with the disease were more than 12 times as likely to experience an ischemic stroke compared to the general population, while men had a nine-fold increase in risk.
Women aged over 55 years with ACHD had a four-fold higher risk of ischemic stroke, and men had a two-fold increase in risk, compared to the general population, according to a study published Nov. 23 in Circulation.
In the case of hemorrhagic stroke, women aged under 55 had a five-fold greater risk and men had a more than six-fold greater risk of ischemic stroke, while the risk for those older than 55 years was 2-3 times higher (Circulation 2015, November 23 [doi: 10.1161/CIRCULATIONAHA.115.011241]).
The risk of ischemic stroke increased significantly with heart failure, diabetes, or a recent myocardial infarction, and overall, 8.9% of men and 6.8% of women with ACHD who reached the age of 18 years had at least one stroke before age 65.
“Whether subgroups of patients with heart failure and sinus rhythm could benefit from an antithrombotic treatment is a matter of ongoing research in the general population and based on our findings may warrant further investigation in ACHD-patients,” wrote Dr. Jonas Lanz, from the McGill Adult Unit for Congenital Heart Disease Excellence, and co-authors.
The study was funded by the Heart and Stroke Foundation of Québec, the Fonds de Recherche en Santé Québec and the Canadian Institute of Health Research. There were no conflicts of interest declared.
Adult congenital heart disease significantly increases the risk of both hemorrhagic and ischemic stroke, particularly in individuals under 55 years of age, new data suggests.
A retrospective study of 29,638 adults aged 18-64 years with adult congenital heart disease (ACHD) showed that women aged 15-54 years with the disease were more than 12 times as likely to experience an ischemic stroke compared to the general population, while men had a nine-fold increase in risk.
Women aged over 55 years with ACHD had a four-fold higher risk of ischemic stroke, and men had a two-fold increase in risk, compared to the general population, according to a study published Nov. 23 in Circulation.
In the case of hemorrhagic stroke, women aged under 55 had a five-fold greater risk and men had a more than six-fold greater risk of ischemic stroke, while the risk for those older than 55 years was 2-3 times higher (Circulation 2015, November 23 [doi: 10.1161/CIRCULATIONAHA.115.011241]).
The risk of ischemic stroke increased significantly with heart failure, diabetes, or a recent myocardial infarction, and overall, 8.9% of men and 6.8% of women with ACHD who reached the age of 18 years had at least one stroke before age 65.
“Whether subgroups of patients with heart failure and sinus rhythm could benefit from an antithrombotic treatment is a matter of ongoing research in the general population and based on our findings may warrant further investigation in ACHD-patients,” wrote Dr. Jonas Lanz, from the McGill Adult Unit for Congenital Heart Disease Excellence, and co-authors.
The study was funded by the Heart and Stroke Foundation of Québec, the Fonds de Recherche en Santé Québec and the Canadian Institute of Health Research. There were no conflicts of interest declared.
Adult congenital heart disease significantly increases the risk of both hemorrhagic and ischemic stroke, particularly in individuals under 55 years of age, new data suggests.
A retrospective study of 29,638 adults aged 18-64 years with adult congenital heart disease (ACHD) showed that women aged 15-54 years with the disease were more than 12 times as likely to experience an ischemic stroke compared to the general population, while men had a nine-fold increase in risk.
Women aged over 55 years with ACHD had a four-fold higher risk of ischemic stroke, and men had a two-fold increase in risk, compared to the general population, according to a study published Nov. 23 in Circulation.
In the case of hemorrhagic stroke, women aged under 55 had a five-fold greater risk and men had a more than six-fold greater risk of ischemic stroke, while the risk for those older than 55 years was 2-3 times higher (Circulation 2015, November 23 [doi: 10.1161/CIRCULATIONAHA.115.011241]).
The risk of ischemic stroke increased significantly with heart failure, diabetes, or a recent myocardial infarction, and overall, 8.9% of men and 6.8% of women with ACHD who reached the age of 18 years had at least one stroke before age 65.
“Whether subgroups of patients with heart failure and sinus rhythm could benefit from an antithrombotic treatment is a matter of ongoing research in the general population and based on our findings may warrant further investigation in ACHD-patients,” wrote Dr. Jonas Lanz, from the McGill Adult Unit for Congenital Heart Disease Excellence, and co-authors.
The study was funded by the Heart and Stroke Foundation of Québec, the Fonds de Recherche en Santé Québec and the Canadian Institute of Health Research. There were no conflicts of interest declared.
FROM CIRCULATION
Key clinical point:Adult congenital heart disease significantly increases the risk of both hemorrhagic and ischemic stroke, particularly in younger patients.
Major finding: Younger women with adult congenital heart disease have a 12-fold higher risk of ischemic stroke than the general population.
Data source: A retrospective study of 29,638 adults aged 18-64 years with adult congenital heart disease.
Disclosures: Authors were funded by the Heart and Stroke Foundation of Québec, the Fonds de Recherche en Santé Québec and the Canadian Institute of Health Research. There were no conflicts of interest declared.