User login
Pragmatic solutions to ‘catastrophic’ global stroke burden
Deaths and disability because of stroke are expected to rise alarmingly over the next 30 years, with almost 10 million stroke deaths forecast annually by 2050, according to a new report from the World Stroke Organization–Lancet Neurology Commission Stroke Collaboration Group.
“This highlights the need for urgent measures to reduce stroke burden worldwide, with an emphasis on low- and middle-income countries,” the report authors stated.
These measures include an increase in trained health care workers who can implement effective primary prevention strategies, including the early detection and adequate management of hypertension.
On the basis of a review of evidence-based guidelines, recent surveys, and in-depth interviews with stroke experts around the world, the WSO–Lancet Neurology Commission made evidence-based pragmatic recommendations to reduce the global burden of stroke, including measures to improve surveillance, prevention, acute care, and rehabilitation.
The report was announced on Oct. 10 by WSO President, Sheila Martins, MD, at the World Stroke Conference in Toronto. The report was also published online in The Lancet Neurology.
“Stroke care has changed a lot in the last few years,” said Dr. Martins, who is chief of neurology and neurosurgery at Hospital Moinhos de Vento, Porto Alegre, Brazil, and founder and president of the Brazilian Stroke Network. “We know what we need to do to reduce the global burden of stroke, and high-income countries are making progress in that regard. But the situation in low- and middle-income countries is catastrophic, with mortality rates of up to 80% in individuals who have had a stroke in some countries. There is a very large gap between knowledge and implementation.”
Dr. Martins said that the commission is offering potential innovative suggestions on how to change this reality.
“While we have the knowledge on the strategies needed to reduce stroke burden, the mechanisms needed to implement this knowledge will be different in different countries and cultures. Our commission includes several representatives from low- and middle-income countries, and we will be working with local stakeholders in these countries to try and implement our recommendations,” Dr. Martins explained.
Stroke mortality and disability is on the rise
In the report, the authors pointed out that the global burden of stroke is “huge.” In 2020, stroke was the second leading cause of death (6.6 million deaths) and the third leading cause of disability – responsible for 143 million disability-adjusted life-years – after neonatal disorders and ischemic heart disease. Stroke is also a leading cause of depression and dementia.
The absolute number of people affected by stroke, which includes those who die or remain disabled, has almost doubled in the past 30 years, the report authors noted. Most of the contemporary stroke burden is in low- and middle-income countries, and the burden of disability after a stroke is increasing at a faster pace in low- and middle-income countries than in high-income countries. Alarmingly, the incidence of stroke is increasing in young and middle-aged people globally.
The commission forecasts the burden of stroke from 2020 to 2050, with projections estimating that stroke mortality will increase by 50% to 9.7 million and disability-adjusted life-years growing to over 189.3 million by 2050.
“Stroke exerts an enormous toll on the world’s population, leading to the death and permanent disability of millions of people each year, and costing billions of dollars,” said Valery L. Feigin, MD, of Auckland (New Zealand) University of Technology, and commission cochair. “Precisely forecasting the health and economic impacts of stroke decades into the future is inherently challenging given the levels of uncertainty involved, but these estimates are indicative of the ever-increasing burden we will see in the years ahead unless urgent, effective action is taken.”
The report authors explained that multiple factors contribute to the high burden of stroke in low- and middle-income countries, including undetected and uncontrolled hypertension; lack of easily accessible, high-quality health services; insufficient attention to and investment in prevention, air pollution; population growth; unhealthy lifestyles (for example, poor diet, smoking, sedentary lifestyle, obesity); an earlier age of stroke onset and greater proportion of hemorrhagic strokes than in high-income countries; and the burden of infectious diseases resulting in competition for limited health care resources.
The enormous financial cost of stroke
The total cost of stroke (both direct treatment and rehabilitation costs and indirect costs due to loss of income) is estimated to rise from $891 billion per year in 2017 to as much as $2.31 trillion by 2050. “These substantial increases in the costs associated with stroke will cause distressing financial circumstances for many communities and national health systems,” the authors said.
However, this increase can be avoided because stroke is highly preventable and treatable, they stressed. “These unsustainable trends in burden and costs of stroke underline the importance of identifying interventions to prevent and manage stroke more effectively.”
The Commission pointed out that population-wide primary prevention across the lifespan is extremely cost effective. It has been estimated that for every $1 spent on the prevention of stroke and cardiovascular disease, there is a more than $10 return on investment.
Additionally, primary prevention efforts directed at stroke would probably yield large gains because of the secondary effects of reducing the risk for heart disease, type 2 diabetes, dementia, and some types of cancer that share common risk factors, the authors noted.
“One of the most common problems in implementing stroke prevention and care recommendations is the lack of funding. Our commission recommends introducing legislative regulations and taxations of unhealthy products (such as salt, alcohol, sugary drinks, trans fats) by each and every government in the world,” Dr. Feigin said.
“Such taxation would not only reduce consumption of these products – and therefore lead to the reduction of burden from stroke and major other noncommunicable diseases – but also generate a large revenue sufficient to fund not only prevention programs and services for stroke and other major disorders, but also reduce poverty, inequality in health service provision, and improve wellbeing of the population,” he added.
Recommendations
The commission authors made the following recommendations for key priorities to reduce the burden of stroke:
Surveillance and prevention
- Incorporate stroke events and risk factor surveillance into national stroke action plans.
- Establish a system for population-wide primary and secondary stroke prevention, with emphasis on lifestyle modification for people at any level of risk of stroke and cardiovascular disease.
- Primary and secondary stroke prevention services should be freely accessible and supported by universal health coverage, with access to affordable drugs for management of hypertension, dyslipidemia, diabetes, and clotting disorders.
- Governments must allocate a fixed proportion of their annual health care funding for prevention of stroke and related noncommunicable diseases. This funding could come from taxation of tobacco, salt, alcohol, and sugar.
- Raise public awareness and take action to encourage a healthy lifestyle and prevent stroke via population-wide deployment of digital technologies with simple, inexpensive screening for cardiovascular disease and modifiable risk factors.
- Establish protocol-based shifting of tasks from highly trained health care professionals to supervised paramedical health care workers, to facilitate population-wide primary stroke prevention interventions across rural and urban settings.
Acute care
- Prioritize effective planning of acute stroke care services; capacity building, training, and certification of a multidisciplinary workforce; provision of evidence-based equipment and affordable medicines; and adequate resource allocation at national and regional levels.
- Establish regional networks and protocol-driven services, including community-wide awareness campaigns for early recognition of a stroke, regionally coordinated prehospital services, telemedicine networks, and stroke centers that can triage and treat all cases of acute stroke, and facilitate timely access to reperfusion therapy.
- Integrate acute care networks into the four pillars of the stroke “quadrangle” of resources, including surveillance, prevention, and rehabilitation services, by involving all relevant stakeholders (that is, communities, policy makers, nongovernmental organizations, national and regional stroke organizations, and public and private health care providers) in the stroke care continuum.
Rehabilitation
- Establish multidisciplinary rehabilitation services and adapt evidence-based recommendations to the local context, including the training, support, and supervision of community health care workers and caregivers to assist in long-term care.
- Invest in research to generate innovative low-cost interventions, in public awareness to improve demand for rehabilitation services, and in advocacy to mobilize resources for multidisciplinary rehabilitation.
- Promote the training of stroke rehabilitation professionals. Use digital portals to improve training and to extend the use of assessment tools – such as the Modified Rankin Scale and the U.S. National Institutes of Health Stroke Scale – and quality of life measures to assess functional impairment and monitor recovery.
The commission concluded that, “overall, if the recommendations of this Commission are implemented, the burden of stroke will be reduced substantially ... which will improve brain health and overall wellbeing worldwide.”
Dr. Martins said that the WSO is committed to supporting and accelerating the implementation of these recommendations globally through the WSO Implementation Task Force, with stroke experts to advise the establishment of stroke prevention and care and to contribute with educational programs, and through Global Stroke Alliance meetings facilitating the discussions between stroke experts and policy makers, giving technical support to governments to elaborate national plans for stroke and to include stroke care in universal health coverage packages.
The Commission received funding from the WSO, Bill and Melinda Gates Foundation, Health Research Council of New Zealand, and National Health & Medical Research Council of Australia and was supported by the NIH.
A version of this article first appeared on Medscape.com.
Deaths and disability because of stroke are expected to rise alarmingly over the next 30 years, with almost 10 million stroke deaths forecast annually by 2050, according to a new report from the World Stroke Organization–Lancet Neurology Commission Stroke Collaboration Group.
“This highlights the need for urgent measures to reduce stroke burden worldwide, with an emphasis on low- and middle-income countries,” the report authors stated.
These measures include an increase in trained health care workers who can implement effective primary prevention strategies, including the early detection and adequate management of hypertension.
On the basis of a review of evidence-based guidelines, recent surveys, and in-depth interviews with stroke experts around the world, the WSO–Lancet Neurology Commission made evidence-based pragmatic recommendations to reduce the global burden of stroke, including measures to improve surveillance, prevention, acute care, and rehabilitation.
The report was announced on Oct. 10 by WSO President, Sheila Martins, MD, at the World Stroke Conference in Toronto. The report was also published online in The Lancet Neurology.
“Stroke care has changed a lot in the last few years,” said Dr. Martins, who is chief of neurology and neurosurgery at Hospital Moinhos de Vento, Porto Alegre, Brazil, and founder and president of the Brazilian Stroke Network. “We know what we need to do to reduce the global burden of stroke, and high-income countries are making progress in that regard. But the situation in low- and middle-income countries is catastrophic, with mortality rates of up to 80% in individuals who have had a stroke in some countries. There is a very large gap between knowledge and implementation.”
Dr. Martins said that the commission is offering potential innovative suggestions on how to change this reality.
“While we have the knowledge on the strategies needed to reduce stroke burden, the mechanisms needed to implement this knowledge will be different in different countries and cultures. Our commission includes several representatives from low- and middle-income countries, and we will be working with local stakeholders in these countries to try and implement our recommendations,” Dr. Martins explained.
Stroke mortality and disability is on the rise
In the report, the authors pointed out that the global burden of stroke is “huge.” In 2020, stroke was the second leading cause of death (6.6 million deaths) and the third leading cause of disability – responsible for 143 million disability-adjusted life-years – after neonatal disorders and ischemic heart disease. Stroke is also a leading cause of depression and dementia.
The absolute number of people affected by stroke, which includes those who die or remain disabled, has almost doubled in the past 30 years, the report authors noted. Most of the contemporary stroke burden is in low- and middle-income countries, and the burden of disability after a stroke is increasing at a faster pace in low- and middle-income countries than in high-income countries. Alarmingly, the incidence of stroke is increasing in young and middle-aged people globally.
The commission forecasts the burden of stroke from 2020 to 2050, with projections estimating that stroke mortality will increase by 50% to 9.7 million and disability-adjusted life-years growing to over 189.3 million by 2050.
“Stroke exerts an enormous toll on the world’s population, leading to the death and permanent disability of millions of people each year, and costing billions of dollars,” said Valery L. Feigin, MD, of Auckland (New Zealand) University of Technology, and commission cochair. “Precisely forecasting the health and economic impacts of stroke decades into the future is inherently challenging given the levels of uncertainty involved, but these estimates are indicative of the ever-increasing burden we will see in the years ahead unless urgent, effective action is taken.”
The report authors explained that multiple factors contribute to the high burden of stroke in low- and middle-income countries, including undetected and uncontrolled hypertension; lack of easily accessible, high-quality health services; insufficient attention to and investment in prevention, air pollution; population growth; unhealthy lifestyles (for example, poor diet, smoking, sedentary lifestyle, obesity); an earlier age of stroke onset and greater proportion of hemorrhagic strokes than in high-income countries; and the burden of infectious diseases resulting in competition for limited health care resources.
The enormous financial cost of stroke
The total cost of stroke (both direct treatment and rehabilitation costs and indirect costs due to loss of income) is estimated to rise from $891 billion per year in 2017 to as much as $2.31 trillion by 2050. “These substantial increases in the costs associated with stroke will cause distressing financial circumstances for many communities and national health systems,” the authors said.
However, this increase can be avoided because stroke is highly preventable and treatable, they stressed. “These unsustainable trends in burden and costs of stroke underline the importance of identifying interventions to prevent and manage stroke more effectively.”
The Commission pointed out that population-wide primary prevention across the lifespan is extremely cost effective. It has been estimated that for every $1 spent on the prevention of stroke and cardiovascular disease, there is a more than $10 return on investment.
Additionally, primary prevention efforts directed at stroke would probably yield large gains because of the secondary effects of reducing the risk for heart disease, type 2 diabetes, dementia, and some types of cancer that share common risk factors, the authors noted.
“One of the most common problems in implementing stroke prevention and care recommendations is the lack of funding. Our commission recommends introducing legislative regulations and taxations of unhealthy products (such as salt, alcohol, sugary drinks, trans fats) by each and every government in the world,” Dr. Feigin said.
“Such taxation would not only reduce consumption of these products – and therefore lead to the reduction of burden from stroke and major other noncommunicable diseases – but also generate a large revenue sufficient to fund not only prevention programs and services for stroke and other major disorders, but also reduce poverty, inequality in health service provision, and improve wellbeing of the population,” he added.
Recommendations
The commission authors made the following recommendations for key priorities to reduce the burden of stroke:
Surveillance and prevention
- Incorporate stroke events and risk factor surveillance into national stroke action plans.
- Establish a system for population-wide primary and secondary stroke prevention, with emphasis on lifestyle modification for people at any level of risk of stroke and cardiovascular disease.
- Primary and secondary stroke prevention services should be freely accessible and supported by universal health coverage, with access to affordable drugs for management of hypertension, dyslipidemia, diabetes, and clotting disorders.
- Governments must allocate a fixed proportion of their annual health care funding for prevention of stroke and related noncommunicable diseases. This funding could come from taxation of tobacco, salt, alcohol, and sugar.
- Raise public awareness and take action to encourage a healthy lifestyle and prevent stroke via population-wide deployment of digital technologies with simple, inexpensive screening for cardiovascular disease and modifiable risk factors.
- Establish protocol-based shifting of tasks from highly trained health care professionals to supervised paramedical health care workers, to facilitate population-wide primary stroke prevention interventions across rural and urban settings.
Acute care
- Prioritize effective planning of acute stroke care services; capacity building, training, and certification of a multidisciplinary workforce; provision of evidence-based equipment and affordable medicines; and adequate resource allocation at national and regional levels.
- Establish regional networks and protocol-driven services, including community-wide awareness campaigns for early recognition of a stroke, regionally coordinated prehospital services, telemedicine networks, and stroke centers that can triage and treat all cases of acute stroke, and facilitate timely access to reperfusion therapy.
- Integrate acute care networks into the four pillars of the stroke “quadrangle” of resources, including surveillance, prevention, and rehabilitation services, by involving all relevant stakeholders (that is, communities, policy makers, nongovernmental organizations, national and regional stroke organizations, and public and private health care providers) in the stroke care continuum.
Rehabilitation
- Establish multidisciplinary rehabilitation services and adapt evidence-based recommendations to the local context, including the training, support, and supervision of community health care workers and caregivers to assist in long-term care.
- Invest in research to generate innovative low-cost interventions, in public awareness to improve demand for rehabilitation services, and in advocacy to mobilize resources for multidisciplinary rehabilitation.
- Promote the training of stroke rehabilitation professionals. Use digital portals to improve training and to extend the use of assessment tools – such as the Modified Rankin Scale and the U.S. National Institutes of Health Stroke Scale – and quality of life measures to assess functional impairment and monitor recovery.
The commission concluded that, “overall, if the recommendations of this Commission are implemented, the burden of stroke will be reduced substantially ... which will improve brain health and overall wellbeing worldwide.”
Dr. Martins said that the WSO is committed to supporting and accelerating the implementation of these recommendations globally through the WSO Implementation Task Force, with stroke experts to advise the establishment of stroke prevention and care and to contribute with educational programs, and through Global Stroke Alliance meetings facilitating the discussions between stroke experts and policy makers, giving technical support to governments to elaborate national plans for stroke and to include stroke care in universal health coverage packages.
The Commission received funding from the WSO, Bill and Melinda Gates Foundation, Health Research Council of New Zealand, and National Health & Medical Research Council of Australia and was supported by the NIH.
A version of this article first appeared on Medscape.com.
Deaths and disability because of stroke are expected to rise alarmingly over the next 30 years, with almost 10 million stroke deaths forecast annually by 2050, according to a new report from the World Stroke Organization–Lancet Neurology Commission Stroke Collaboration Group.
“This highlights the need for urgent measures to reduce stroke burden worldwide, with an emphasis on low- and middle-income countries,” the report authors stated.
These measures include an increase in trained health care workers who can implement effective primary prevention strategies, including the early detection and adequate management of hypertension.
On the basis of a review of evidence-based guidelines, recent surveys, and in-depth interviews with stroke experts around the world, the WSO–Lancet Neurology Commission made evidence-based pragmatic recommendations to reduce the global burden of stroke, including measures to improve surveillance, prevention, acute care, and rehabilitation.
The report was announced on Oct. 10 by WSO President, Sheila Martins, MD, at the World Stroke Conference in Toronto. The report was also published online in The Lancet Neurology.
“Stroke care has changed a lot in the last few years,” said Dr. Martins, who is chief of neurology and neurosurgery at Hospital Moinhos de Vento, Porto Alegre, Brazil, and founder and president of the Brazilian Stroke Network. “We know what we need to do to reduce the global burden of stroke, and high-income countries are making progress in that regard. But the situation in low- and middle-income countries is catastrophic, with mortality rates of up to 80% in individuals who have had a stroke in some countries. There is a very large gap between knowledge and implementation.”
Dr. Martins said that the commission is offering potential innovative suggestions on how to change this reality.
“While we have the knowledge on the strategies needed to reduce stroke burden, the mechanisms needed to implement this knowledge will be different in different countries and cultures. Our commission includes several representatives from low- and middle-income countries, and we will be working with local stakeholders in these countries to try and implement our recommendations,” Dr. Martins explained.
Stroke mortality and disability is on the rise
In the report, the authors pointed out that the global burden of stroke is “huge.” In 2020, stroke was the second leading cause of death (6.6 million deaths) and the third leading cause of disability – responsible for 143 million disability-adjusted life-years – after neonatal disorders and ischemic heart disease. Stroke is also a leading cause of depression and dementia.
The absolute number of people affected by stroke, which includes those who die or remain disabled, has almost doubled in the past 30 years, the report authors noted. Most of the contemporary stroke burden is in low- and middle-income countries, and the burden of disability after a stroke is increasing at a faster pace in low- and middle-income countries than in high-income countries. Alarmingly, the incidence of stroke is increasing in young and middle-aged people globally.
The commission forecasts the burden of stroke from 2020 to 2050, with projections estimating that stroke mortality will increase by 50% to 9.7 million and disability-adjusted life-years growing to over 189.3 million by 2050.
“Stroke exerts an enormous toll on the world’s population, leading to the death and permanent disability of millions of people each year, and costing billions of dollars,” said Valery L. Feigin, MD, of Auckland (New Zealand) University of Technology, and commission cochair. “Precisely forecasting the health and economic impacts of stroke decades into the future is inherently challenging given the levels of uncertainty involved, but these estimates are indicative of the ever-increasing burden we will see in the years ahead unless urgent, effective action is taken.”
The report authors explained that multiple factors contribute to the high burden of stroke in low- and middle-income countries, including undetected and uncontrolled hypertension; lack of easily accessible, high-quality health services; insufficient attention to and investment in prevention, air pollution; population growth; unhealthy lifestyles (for example, poor diet, smoking, sedentary lifestyle, obesity); an earlier age of stroke onset and greater proportion of hemorrhagic strokes than in high-income countries; and the burden of infectious diseases resulting in competition for limited health care resources.
The enormous financial cost of stroke
The total cost of stroke (both direct treatment and rehabilitation costs and indirect costs due to loss of income) is estimated to rise from $891 billion per year in 2017 to as much as $2.31 trillion by 2050. “These substantial increases in the costs associated with stroke will cause distressing financial circumstances for many communities and national health systems,” the authors said.
However, this increase can be avoided because stroke is highly preventable and treatable, they stressed. “These unsustainable trends in burden and costs of stroke underline the importance of identifying interventions to prevent and manage stroke more effectively.”
The Commission pointed out that population-wide primary prevention across the lifespan is extremely cost effective. It has been estimated that for every $1 spent on the prevention of stroke and cardiovascular disease, there is a more than $10 return on investment.
Additionally, primary prevention efforts directed at stroke would probably yield large gains because of the secondary effects of reducing the risk for heart disease, type 2 diabetes, dementia, and some types of cancer that share common risk factors, the authors noted.
“One of the most common problems in implementing stroke prevention and care recommendations is the lack of funding. Our commission recommends introducing legislative regulations and taxations of unhealthy products (such as salt, alcohol, sugary drinks, trans fats) by each and every government in the world,” Dr. Feigin said.
“Such taxation would not only reduce consumption of these products – and therefore lead to the reduction of burden from stroke and major other noncommunicable diseases – but also generate a large revenue sufficient to fund not only prevention programs and services for stroke and other major disorders, but also reduce poverty, inequality in health service provision, and improve wellbeing of the population,” he added.
Recommendations
The commission authors made the following recommendations for key priorities to reduce the burden of stroke:
Surveillance and prevention
- Incorporate stroke events and risk factor surveillance into national stroke action plans.
- Establish a system for population-wide primary and secondary stroke prevention, with emphasis on lifestyle modification for people at any level of risk of stroke and cardiovascular disease.
- Primary and secondary stroke prevention services should be freely accessible and supported by universal health coverage, with access to affordable drugs for management of hypertension, dyslipidemia, diabetes, and clotting disorders.
- Governments must allocate a fixed proportion of their annual health care funding for prevention of stroke and related noncommunicable diseases. This funding could come from taxation of tobacco, salt, alcohol, and sugar.
- Raise public awareness and take action to encourage a healthy lifestyle and prevent stroke via population-wide deployment of digital technologies with simple, inexpensive screening for cardiovascular disease and modifiable risk factors.
- Establish protocol-based shifting of tasks from highly trained health care professionals to supervised paramedical health care workers, to facilitate population-wide primary stroke prevention interventions across rural and urban settings.
Acute care
- Prioritize effective planning of acute stroke care services; capacity building, training, and certification of a multidisciplinary workforce; provision of evidence-based equipment and affordable medicines; and adequate resource allocation at national and regional levels.
- Establish regional networks and protocol-driven services, including community-wide awareness campaigns for early recognition of a stroke, regionally coordinated prehospital services, telemedicine networks, and stroke centers that can triage and treat all cases of acute stroke, and facilitate timely access to reperfusion therapy.
- Integrate acute care networks into the four pillars of the stroke “quadrangle” of resources, including surveillance, prevention, and rehabilitation services, by involving all relevant stakeholders (that is, communities, policy makers, nongovernmental organizations, national and regional stroke organizations, and public and private health care providers) in the stroke care continuum.
Rehabilitation
- Establish multidisciplinary rehabilitation services and adapt evidence-based recommendations to the local context, including the training, support, and supervision of community health care workers and caregivers to assist in long-term care.
- Invest in research to generate innovative low-cost interventions, in public awareness to improve demand for rehabilitation services, and in advocacy to mobilize resources for multidisciplinary rehabilitation.
- Promote the training of stroke rehabilitation professionals. Use digital portals to improve training and to extend the use of assessment tools – such as the Modified Rankin Scale and the U.S. National Institutes of Health Stroke Scale – and quality of life measures to assess functional impairment and monitor recovery.
The commission concluded that, “overall, if the recommendations of this Commission are implemented, the burden of stroke will be reduced substantially ... which will improve brain health and overall wellbeing worldwide.”
Dr. Martins said that the WSO is committed to supporting and accelerating the implementation of these recommendations globally through the WSO Implementation Task Force, with stroke experts to advise the establishment of stroke prevention and care and to contribute with educational programs, and through Global Stroke Alliance meetings facilitating the discussions between stroke experts and policy makers, giving technical support to governments to elaborate national plans for stroke and to include stroke care in universal health coverage packages.
The Commission received funding from the WSO, Bill and Melinda Gates Foundation, Health Research Council of New Zealand, and National Health & Medical Research Council of Australia and was supported by the NIH.
A version of this article first appeared on Medscape.com.
FROM THE LANCET NEUROLOGY
New guidelines for determining brain death released
The consensus practice guideline on brain death, also known as death by neurologic criteria (BD/DNC), was developed by a panel of 20 experts from different specialties, institutions, and medical societies.
As with previous guidelines, the updated version stipulates that brain death should be declared when a patient with a known cause of catastrophic brain injury has permanent loss of function of the brain, including the brain stem, which results in coma, brain stem areflexia, and apnea in the setting of an adequate stimulus.
But the updated version also clarifies questions on neurological examinations and apnea testing and offers new guidance on pre-evaluation targets for blood pressure and body temperature and evaluating brain death in patients who are pregnant, are on extracorporeal membrane oxygenation, or have an injury to the base of the brain.
Also, for the first time, the guidance clarifies that clinicians don’t need to obtain consent before performing a brain death evaluation, unless institutional policy, state laws, or regulations stipulate otherwise.
“The 2023 guidelines will be considered the standard of care in the U.S.,” lead author David M. Greer, MD, chair and chief of neurology, Boston University, and chief of neurology, Boston Medical Center, said in an interview. “Each hospital in the U.S. is responsible for its own policy for BD/DNC determination, and our hope is that they will quickly revise their policies in accordance with this new national standard.”
The guidelines, which are accompanied by a three-page checklist and a free digital app, were published online in Neurology.
Four years in the making
Work on the 85 recommendations in the new report began more than 4 years ago as a collaborative effort by the American Academy of Neurology, the American Academy of Pediatrics, the Child Neurology Society, and the Society of Critical Care Medicine.
A lack of high-quality evidence on brain death determination led panelists to devise an evidence-informed formal consensus process to develop the guidelines, which involved three rounds of anonymous voting on each recommendation and the rationales behind them.
The strength of each recommendation was based on the level of consensus reached through voting, with Level A denoting a recommendation that “must” be followed, Level B one that “should” be followed, and Level C one that “may” be followed.
The majority of recommendations received an A or B rating. Only one recommendation, about whether a second clinical exam is needed in adults, garnered a C rating.
In children, the guidelines recommend that clinicians must perform two clinical examinations and two apnea tests 12 hours apart. In adults, only one exam is required. Both of those recommendations were rated Level A. A recommendation for a second exam in adults received the single Level C rating.
A uniform set of guidelines?
The new guidelines replace adult practice guidance published by AAN in 2010 and guideline for infants and children released in 2011 by AAP, CNS, and SCCM, and for the first time combine brain death guidelines for adult and pediatric patients into one document.
“It is important for clinicians to review the new guideline carefully and ensure their hospital brain death guidelines are updated to be consistent with the new guideline in order to prevent inaccurate determinations of death,” guidelines coauthor Ariane Lewis, MD, NYU Langone Health, New York, said in an interview.
The 1981 Uniform Determination of Death Act (UDDA) is the legal foundation for the declaration of BD/DNC in the United States, but it only stipulates that brain death determination must be made in accordance with accepted medical standards.
There is no single national standard, and states and hospitals are free to adopt their own, which many have done. One goal of the new guidelines was to create a uniform set of guidelines that all institutions follow.
“This is a step toward having a set of guidelines that are accepted by most of the societies and clinical specialties involved in this sort of diagnosis,” that could lead to a national-level policy, Fernando Goldenberg, MD, professor of neurology and director of neuroscience critical care, University of Chicago Medicine, said in an interview.
Dr. Goldenberg was not part of the panel that developed the updated guidelines, but was a coauthor of a consensus statement from the World Brain Death Project in 2020.
Developing a singular global guideline for brain death determination is unlikely, Dr. Goldenberg said. Policies vary widely across the world, and some countries don’t even recognize brain death.
“But this attempts to unify things at the U.S. level, which is very important,” he said.
Permanent vs. irreversible
Dr. Goldenberg said that combining adult and pediatric guidelines into one document will be very helpful for clinicians like him who treat patients from age 16 years and up.
The expanded guidance on apnea testing, recommendations on specific ancillary tests to use or avoid, and inclusion of language stipulating that prior consent is not needed to perform a brain death evaluation are also useful.
He also noted that the section on credentialing and training of clinicians who perform BD/DNC evaluations recognizes advanced practice providers, the first time he recalls seeing these professionals included in brain death guidelines.
However, the panel’s decision to use the term “permanent” to describe loss of brain function instead of “irreversible” gave Dr. Goldenberg pause.
The UDDA provides that an individual is declared legally dead when “circulatory and respiratory functions irreversibly stop; or all functions of the entire brain, including the brain stem, irreversibly stop.”
Earlier in October, the American College of Physicians released a position paper on cardiorespiratory death determination that called for a revision of the UDDA language.
The ACP suggested that “irreversibly” be replaced with “permanently” with regard to the cessation of circulatory and respiratory functions, but that “irreversible” be kept in the description of brain death.
“Permanent means that there is damage that is potentially reversible and irreversible means that the damage is so profound, it cannot be reversed even if an attempt to do so is performed,” Dr. Goldenberg said.
Even though the World Brain Death Project, on which he worked, also used “permanent” to describe brain function loss, Dr. Goldenberg said he aligns with ACP’s position.
“The understanding of brain death is that the damage is so profound, it is irreversible, even if you were to try,” he said. “Therefore, I think that the most appropriate term for brain death should be irreversible as opposed to permanent.”
The report was funded by the American Academy of Neurology. Dr. Greer has received travel funding from Boston University; serves as editor-in-chief for Seminars in Neurology; receives publishing royalties for 50 Studies Every Neurologist Should Know and Successful Leadership in Academic Medicine; has received honoraria from AAN; has received research funding from Becton, Dickinson, and Company; and has served as expert witness in legal proceedings. Dr. Lewis has received honoraria from AAN and Neurodiem, serves as Neurology deputy editor of disputes and debates, and serves as deputy editor of seminars in Neurology. Dr. Goldenberg reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The consensus practice guideline on brain death, also known as death by neurologic criteria (BD/DNC), was developed by a panel of 20 experts from different specialties, institutions, and medical societies.
As with previous guidelines, the updated version stipulates that brain death should be declared when a patient with a known cause of catastrophic brain injury has permanent loss of function of the brain, including the brain stem, which results in coma, brain stem areflexia, and apnea in the setting of an adequate stimulus.
But the updated version also clarifies questions on neurological examinations and apnea testing and offers new guidance on pre-evaluation targets for blood pressure and body temperature and evaluating brain death in patients who are pregnant, are on extracorporeal membrane oxygenation, or have an injury to the base of the brain.
Also, for the first time, the guidance clarifies that clinicians don’t need to obtain consent before performing a brain death evaluation, unless institutional policy, state laws, or regulations stipulate otherwise.
“The 2023 guidelines will be considered the standard of care in the U.S.,” lead author David M. Greer, MD, chair and chief of neurology, Boston University, and chief of neurology, Boston Medical Center, said in an interview. “Each hospital in the U.S. is responsible for its own policy for BD/DNC determination, and our hope is that they will quickly revise their policies in accordance with this new national standard.”
The guidelines, which are accompanied by a three-page checklist and a free digital app, were published online in Neurology.
Four years in the making
Work on the 85 recommendations in the new report began more than 4 years ago as a collaborative effort by the American Academy of Neurology, the American Academy of Pediatrics, the Child Neurology Society, and the Society of Critical Care Medicine.
A lack of high-quality evidence on brain death determination led panelists to devise an evidence-informed formal consensus process to develop the guidelines, which involved three rounds of anonymous voting on each recommendation and the rationales behind them.
The strength of each recommendation was based on the level of consensus reached through voting, with Level A denoting a recommendation that “must” be followed, Level B one that “should” be followed, and Level C one that “may” be followed.
The majority of recommendations received an A or B rating. Only one recommendation, about whether a second clinical exam is needed in adults, garnered a C rating.
In children, the guidelines recommend that clinicians must perform two clinical examinations and two apnea tests 12 hours apart. In adults, only one exam is required. Both of those recommendations were rated Level A. A recommendation for a second exam in adults received the single Level C rating.
A uniform set of guidelines?
The new guidelines replace adult practice guidance published by AAN in 2010 and guideline for infants and children released in 2011 by AAP, CNS, and SCCM, and for the first time combine brain death guidelines for adult and pediatric patients into one document.
“It is important for clinicians to review the new guideline carefully and ensure their hospital brain death guidelines are updated to be consistent with the new guideline in order to prevent inaccurate determinations of death,” guidelines coauthor Ariane Lewis, MD, NYU Langone Health, New York, said in an interview.
The 1981 Uniform Determination of Death Act (UDDA) is the legal foundation for the declaration of BD/DNC in the United States, but it only stipulates that brain death determination must be made in accordance with accepted medical standards.
There is no single national standard, and states and hospitals are free to adopt their own, which many have done. One goal of the new guidelines was to create a uniform set of guidelines that all institutions follow.
“This is a step toward having a set of guidelines that are accepted by most of the societies and clinical specialties involved in this sort of diagnosis,” that could lead to a national-level policy, Fernando Goldenberg, MD, professor of neurology and director of neuroscience critical care, University of Chicago Medicine, said in an interview.
Dr. Goldenberg was not part of the panel that developed the updated guidelines, but was a coauthor of a consensus statement from the World Brain Death Project in 2020.
Developing a singular global guideline for brain death determination is unlikely, Dr. Goldenberg said. Policies vary widely across the world, and some countries don’t even recognize brain death.
“But this attempts to unify things at the U.S. level, which is very important,” he said.
Permanent vs. irreversible
Dr. Goldenberg said that combining adult and pediatric guidelines into one document will be very helpful for clinicians like him who treat patients from age 16 years and up.
The expanded guidance on apnea testing, recommendations on specific ancillary tests to use or avoid, and inclusion of language stipulating that prior consent is not needed to perform a brain death evaluation are also useful.
He also noted that the section on credentialing and training of clinicians who perform BD/DNC evaluations recognizes advanced practice providers, the first time he recalls seeing these professionals included in brain death guidelines.
However, the panel’s decision to use the term “permanent” to describe loss of brain function instead of “irreversible” gave Dr. Goldenberg pause.
The UDDA provides that an individual is declared legally dead when “circulatory and respiratory functions irreversibly stop; or all functions of the entire brain, including the brain stem, irreversibly stop.”
Earlier in October, the American College of Physicians released a position paper on cardiorespiratory death determination that called for a revision of the UDDA language.
The ACP suggested that “irreversibly” be replaced with “permanently” with regard to the cessation of circulatory and respiratory functions, but that “irreversible” be kept in the description of brain death.
“Permanent means that there is damage that is potentially reversible and irreversible means that the damage is so profound, it cannot be reversed even if an attempt to do so is performed,” Dr. Goldenberg said.
Even though the World Brain Death Project, on which he worked, also used “permanent” to describe brain function loss, Dr. Goldenberg said he aligns with ACP’s position.
“The understanding of brain death is that the damage is so profound, it is irreversible, even if you were to try,” he said. “Therefore, I think that the most appropriate term for brain death should be irreversible as opposed to permanent.”
The report was funded by the American Academy of Neurology. Dr. Greer has received travel funding from Boston University; serves as editor-in-chief for Seminars in Neurology; receives publishing royalties for 50 Studies Every Neurologist Should Know and Successful Leadership in Academic Medicine; has received honoraria from AAN; has received research funding from Becton, Dickinson, and Company; and has served as expert witness in legal proceedings. Dr. Lewis has received honoraria from AAN and Neurodiem, serves as Neurology deputy editor of disputes and debates, and serves as deputy editor of seminars in Neurology. Dr. Goldenberg reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The consensus practice guideline on brain death, also known as death by neurologic criteria (BD/DNC), was developed by a panel of 20 experts from different specialties, institutions, and medical societies.
As with previous guidelines, the updated version stipulates that brain death should be declared when a patient with a known cause of catastrophic brain injury has permanent loss of function of the brain, including the brain stem, which results in coma, brain stem areflexia, and apnea in the setting of an adequate stimulus.
But the updated version also clarifies questions on neurological examinations and apnea testing and offers new guidance on pre-evaluation targets for blood pressure and body temperature and evaluating brain death in patients who are pregnant, are on extracorporeal membrane oxygenation, or have an injury to the base of the brain.
Also, for the first time, the guidance clarifies that clinicians don’t need to obtain consent before performing a brain death evaluation, unless institutional policy, state laws, or regulations stipulate otherwise.
“The 2023 guidelines will be considered the standard of care in the U.S.,” lead author David M. Greer, MD, chair and chief of neurology, Boston University, and chief of neurology, Boston Medical Center, said in an interview. “Each hospital in the U.S. is responsible for its own policy for BD/DNC determination, and our hope is that they will quickly revise their policies in accordance with this new national standard.”
The guidelines, which are accompanied by a three-page checklist and a free digital app, were published online in Neurology.
Four years in the making
Work on the 85 recommendations in the new report began more than 4 years ago as a collaborative effort by the American Academy of Neurology, the American Academy of Pediatrics, the Child Neurology Society, and the Society of Critical Care Medicine.
A lack of high-quality evidence on brain death determination led panelists to devise an evidence-informed formal consensus process to develop the guidelines, which involved three rounds of anonymous voting on each recommendation and the rationales behind them.
The strength of each recommendation was based on the level of consensus reached through voting, with Level A denoting a recommendation that “must” be followed, Level B one that “should” be followed, and Level C one that “may” be followed.
The majority of recommendations received an A or B rating. Only one recommendation, about whether a second clinical exam is needed in adults, garnered a C rating.
In children, the guidelines recommend that clinicians must perform two clinical examinations and two apnea tests 12 hours apart. In adults, only one exam is required. Both of those recommendations were rated Level A. A recommendation for a second exam in adults received the single Level C rating.
A uniform set of guidelines?
The new guidelines replace adult practice guidance published by AAN in 2010 and guideline for infants and children released in 2011 by AAP, CNS, and SCCM, and for the first time combine brain death guidelines for adult and pediatric patients into one document.
“It is important for clinicians to review the new guideline carefully and ensure their hospital brain death guidelines are updated to be consistent with the new guideline in order to prevent inaccurate determinations of death,” guidelines coauthor Ariane Lewis, MD, NYU Langone Health, New York, said in an interview.
The 1981 Uniform Determination of Death Act (UDDA) is the legal foundation for the declaration of BD/DNC in the United States, but it only stipulates that brain death determination must be made in accordance with accepted medical standards.
There is no single national standard, and states and hospitals are free to adopt their own, which many have done. One goal of the new guidelines was to create a uniform set of guidelines that all institutions follow.
“This is a step toward having a set of guidelines that are accepted by most of the societies and clinical specialties involved in this sort of diagnosis,” that could lead to a national-level policy, Fernando Goldenberg, MD, professor of neurology and director of neuroscience critical care, University of Chicago Medicine, said in an interview.
Dr. Goldenberg was not part of the panel that developed the updated guidelines, but was a coauthor of a consensus statement from the World Brain Death Project in 2020.
Developing a singular global guideline for brain death determination is unlikely, Dr. Goldenberg said. Policies vary widely across the world, and some countries don’t even recognize brain death.
“But this attempts to unify things at the U.S. level, which is very important,” he said.
Permanent vs. irreversible
Dr. Goldenberg said that combining adult and pediatric guidelines into one document will be very helpful for clinicians like him who treat patients from age 16 years and up.
The expanded guidance on apnea testing, recommendations on specific ancillary tests to use or avoid, and inclusion of language stipulating that prior consent is not needed to perform a brain death evaluation are also useful.
He also noted that the section on credentialing and training of clinicians who perform BD/DNC evaluations recognizes advanced practice providers, the first time he recalls seeing these professionals included in brain death guidelines.
However, the panel’s decision to use the term “permanent” to describe loss of brain function instead of “irreversible” gave Dr. Goldenberg pause.
The UDDA provides that an individual is declared legally dead when “circulatory and respiratory functions irreversibly stop; or all functions of the entire brain, including the brain stem, irreversibly stop.”
Earlier in October, the American College of Physicians released a position paper on cardiorespiratory death determination that called for a revision of the UDDA language.
The ACP suggested that “irreversibly” be replaced with “permanently” with regard to the cessation of circulatory and respiratory functions, but that “irreversible” be kept in the description of brain death.
“Permanent means that there is damage that is potentially reversible and irreversible means that the damage is so profound, it cannot be reversed even if an attempt to do so is performed,” Dr. Goldenberg said.
Even though the World Brain Death Project, on which he worked, also used “permanent” to describe brain function loss, Dr. Goldenberg said he aligns with ACP’s position.
“The understanding of brain death is that the damage is so profound, it is irreversible, even if you were to try,” he said. “Therefore, I think that the most appropriate term for brain death should be irreversible as opposed to permanent.”
The report was funded by the American Academy of Neurology. Dr. Greer has received travel funding from Boston University; serves as editor-in-chief for Seminars in Neurology; receives publishing royalties for 50 Studies Every Neurologist Should Know and Successful Leadership in Academic Medicine; has received honoraria from AAN; has received research funding from Becton, Dickinson, and Company; and has served as expert witness in legal proceedings. Dr. Lewis has received honoraria from AAN and Neurodiem, serves as Neurology deputy editor of disputes and debates, and serves as deputy editor of seminars in Neurology. Dr. Goldenberg reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NEUROLOGY
Proton pump inhibitors linked to increased dementia risk
TOPLINE:
and was highest among those diagnosed before age 70 years regardless of when PPI treatment was initiated.
METHODOLOGY:
- Researchers used four Danish registries to collect data on dementia diagnoses and prescription PPI use among 1,983,785 individuals aged 60-75 years between 2000 and 2018.
- The median follow-up time was 10.3 years.
TAKEAWAY:
- There were 99,384 (5.0%) cases of all-cause dementia during follow-up, with a median age of diagnosis of 79 years.
- Twenty-one-point-two percent of dementia cases and 18.9% of controls reported a history of PPI use.
- Risk for all-cause dementia before age 90 years was 36% higher with PPI use in people aged 60-69 years at baseline (adjusted incidence rate ratio, 1.36; 95% confidence interval, 1.29-1.43) and 6% higher in those who were age 80-89 years at baseline (aIRR, 1.06; 95% CI, 1.03-1.09).
- Investigators found significant increased dementia risk before age 90 years with PPI use regardless of when PPI treatment began and found no link between PPI use and dementia diagnoses after age 90 years.
IN PRACTICE:
“The association between PPI use and dementia was unambiguously largest among the youngest cases of dementia, potentially suggestive of a critical window of exposure where midlife PPI use affects dementia risk to a larger degree compared to late-life use,” the authors wrote. “Further, the finding could signify a declining impact of individual risk factors with advancing age owing to lengthy ongoing neuropathological processes.”
SOURCE:
Lead author of the study was Nelsan Pourhadi, MD, Danish Dementia Research Centre, department of neurology, Copenhagen University Hospital–Rigshospitalet. It was published online in Alzheimer’s and Dementia.
LIMITATIONS:
The study did not include data on PPI prescriptions before 1995, over-the-counter PPI use, and in-hospital intravenous use of PPI during the study period.
DISCLOSURES:
The study was funded by the Danish Ministry of Health. The authors reported no relevant conflicts.
A version of this article first appeared on Medscape.com.
TOPLINE:
and was highest among those diagnosed before age 70 years regardless of when PPI treatment was initiated.
METHODOLOGY:
- Researchers used four Danish registries to collect data on dementia diagnoses and prescription PPI use among 1,983,785 individuals aged 60-75 years between 2000 and 2018.
- The median follow-up time was 10.3 years.
TAKEAWAY:
- There were 99,384 (5.0%) cases of all-cause dementia during follow-up, with a median age of diagnosis of 79 years.
- Twenty-one-point-two percent of dementia cases and 18.9% of controls reported a history of PPI use.
- Risk for all-cause dementia before age 90 years was 36% higher with PPI use in people aged 60-69 years at baseline (adjusted incidence rate ratio, 1.36; 95% confidence interval, 1.29-1.43) and 6% higher in those who were age 80-89 years at baseline (aIRR, 1.06; 95% CI, 1.03-1.09).
- Investigators found significant increased dementia risk before age 90 years with PPI use regardless of when PPI treatment began and found no link between PPI use and dementia diagnoses after age 90 years.
IN PRACTICE:
“The association between PPI use and dementia was unambiguously largest among the youngest cases of dementia, potentially suggestive of a critical window of exposure where midlife PPI use affects dementia risk to a larger degree compared to late-life use,” the authors wrote. “Further, the finding could signify a declining impact of individual risk factors with advancing age owing to lengthy ongoing neuropathological processes.”
SOURCE:
Lead author of the study was Nelsan Pourhadi, MD, Danish Dementia Research Centre, department of neurology, Copenhagen University Hospital–Rigshospitalet. It was published online in Alzheimer’s and Dementia.
LIMITATIONS:
The study did not include data on PPI prescriptions before 1995, over-the-counter PPI use, and in-hospital intravenous use of PPI during the study period.
DISCLOSURES:
The study was funded by the Danish Ministry of Health. The authors reported no relevant conflicts.
A version of this article first appeared on Medscape.com.
TOPLINE:
and was highest among those diagnosed before age 70 years regardless of when PPI treatment was initiated.
METHODOLOGY:
- Researchers used four Danish registries to collect data on dementia diagnoses and prescription PPI use among 1,983,785 individuals aged 60-75 years between 2000 and 2018.
- The median follow-up time was 10.3 years.
TAKEAWAY:
- There were 99,384 (5.0%) cases of all-cause dementia during follow-up, with a median age of diagnosis of 79 years.
- Twenty-one-point-two percent of dementia cases and 18.9% of controls reported a history of PPI use.
- Risk for all-cause dementia before age 90 years was 36% higher with PPI use in people aged 60-69 years at baseline (adjusted incidence rate ratio, 1.36; 95% confidence interval, 1.29-1.43) and 6% higher in those who were age 80-89 years at baseline (aIRR, 1.06; 95% CI, 1.03-1.09).
- Investigators found significant increased dementia risk before age 90 years with PPI use regardless of when PPI treatment began and found no link between PPI use and dementia diagnoses after age 90 years.
IN PRACTICE:
“The association between PPI use and dementia was unambiguously largest among the youngest cases of dementia, potentially suggestive of a critical window of exposure where midlife PPI use affects dementia risk to a larger degree compared to late-life use,” the authors wrote. “Further, the finding could signify a declining impact of individual risk factors with advancing age owing to lengthy ongoing neuropathological processes.”
SOURCE:
Lead author of the study was Nelsan Pourhadi, MD, Danish Dementia Research Centre, department of neurology, Copenhagen University Hospital–Rigshospitalet. It was published online in Alzheimer’s and Dementia.
LIMITATIONS:
The study did not include data on PPI prescriptions before 1995, over-the-counter PPI use, and in-hospital intravenous use of PPI during the study period.
DISCLOSURES:
The study was funded by the Danish Ministry of Health. The authors reported no relevant conflicts.
A version of this article first appeared on Medscape.com.
A new clue into the cause, spread of Parkinson’s disease?
.
While defects in mitochondrial functions and in mitochondrial DNA have been implicated in PD in the past, the current study demonstrates “for the first time how damaged mitochondrial DNA can underlie the mechanisms of PD initiation and spread in brain,” lead investigator Shohreh Issazadeh-Navikas, PhD, with the University of Copenhagen, told this news organization.
“This has direct implication for clinical diagnosis” – if damaged mtDNA can be detected in blood, it could serve as an early biomarker for disease, she explained.
The study was published online in Molecular Psychiatry.
“Infectious-like” spread of PD pathology
In earlier work, the researchers identified dysregulated interferon-beta (IFN-beta) signaling as a “top candidate pathway” associated with sporadic PD and its progression to PD with dementia (PDD).
In mice PD models that were deficient in IFN-beta signaling, the investigators showed that neuronal IFN-beta is required to maintain mitochondrial homeostasis and metabolism.
Lack of neuronal IFN-beta or disruption of its downstream signaling causes the accumulation of damaged mitochondria with excessive oxidative stress and insufficient adenosine triphosphate production.
In the current study, using postmortem brain tissue samples from patients with sporadic PD, they confirmed that there were deletions of mtDNA in the medial frontal gyrus, a region implicated in cognitive impairments in PD, suggesting a potential role of damaged mtDNA in disease pathophysiology.
They also identified mtDNA deletions in a “hotspot” in complex I respiratory chain subunits that were associated with dysregulation of oxidative stress and DNA damage response pathways in cohorts with sporadic PD and PDD.
They confirmed the contribution of mtDNA damage to PD pathology in the PD mouse models. They showed that lack of neuronal IFN-beta signaling leads to oxidative damage and mutations in mtDNA in neurons, which are subsequently released outside the neurons.
Injecting damaged mtDNA into mouse brain induced PDD-like behavioral symptoms, including neuropsychiatric, motor, and cognitive impairments. It also caused neurodegeneration in brain regions distant from the injection site, suggesting that damaged mtDNA triggers spread of PDD characteristics in an “infectious-like” manner, the researchers report.
Further study revealed that the mechanism through which damaged mtDNA causes pathology in healthy neurons involves dual activation of Toll-like receptor (TLR) 9 and 4 pathways, leading to increased oxidative stress and neuronal cell death, respectively.
“Our proteomic analysis of extracellular vesicles containing damaged mtDNA identified the TLR4 activator, ribosomal protein S3, as a key protein involved in recognizing and extruding damaged mtDNA,” the investigators write.
In the future they plan to investigate how mtDNA damage can serve as a predictive marker for different disease stages and progression and to explore potential therapeutic strategies aimed at restoring normal mitochondrial function to rectify the mitochondrial dysfunctions implicated in PD.
Making a comeback?
Commenting on the research for this news organization, James Beck, PhD, chief scientific officer at the Parkinson’s Foundation, noted that the role of mitochondria in PD is “like a starlet that burst onto the scene in the 80s, faded into obscurity, and through diligence and continued research has moved beyond being a solid character actor and is reemerging as a force to reckon with.
“This paper only adds to the allure that mitochondria may have in contributing to PD by providing evidence of a novel process by which mitochondria may be not only contributing to PD and loss of dopamine neurons but may play a larger role in the subsequent effects that many people with PD experience – dementia,” Dr. Beck said.
He noted that the authors identified several proteins as facilitating the neurodegeneration that is wrought by damaged mitochondrial DNA.
“These could be potential targets for future drug development. In addition, this work implicates alterations in immune signaling and drugs in development to target inflammatory responses may also bring ancillary benefit,” Dr. Beck said.
However, he said, “while very interesting findings, this is really the first effort that demonstrates how damaged mitochondrial DNA may contribute to neurodegeneration in the context of PD and PD dementia. Further work needs to validate these findings as well as to elucidate mechanisms underlying the propagation of the mitochondrial DNA from cell to cell.”
Funding for this research was provided by the European Union’s Horizon 2020 Research and Innovation Program, the Lundbeck Foundation, and the Danish Council for Independent Research–Medicine. Dr. Issazadeh-Navikas and Dr. Beck have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
.
While defects in mitochondrial functions and in mitochondrial DNA have been implicated in PD in the past, the current study demonstrates “for the first time how damaged mitochondrial DNA can underlie the mechanisms of PD initiation and spread in brain,” lead investigator Shohreh Issazadeh-Navikas, PhD, with the University of Copenhagen, told this news organization.
“This has direct implication for clinical diagnosis” – if damaged mtDNA can be detected in blood, it could serve as an early biomarker for disease, she explained.
The study was published online in Molecular Psychiatry.
“Infectious-like” spread of PD pathology
In earlier work, the researchers identified dysregulated interferon-beta (IFN-beta) signaling as a “top candidate pathway” associated with sporadic PD and its progression to PD with dementia (PDD).
In mice PD models that were deficient in IFN-beta signaling, the investigators showed that neuronal IFN-beta is required to maintain mitochondrial homeostasis and metabolism.
Lack of neuronal IFN-beta or disruption of its downstream signaling causes the accumulation of damaged mitochondria with excessive oxidative stress and insufficient adenosine triphosphate production.
In the current study, using postmortem brain tissue samples from patients with sporadic PD, they confirmed that there were deletions of mtDNA in the medial frontal gyrus, a region implicated in cognitive impairments in PD, suggesting a potential role of damaged mtDNA in disease pathophysiology.
They also identified mtDNA deletions in a “hotspot” in complex I respiratory chain subunits that were associated with dysregulation of oxidative stress and DNA damage response pathways in cohorts with sporadic PD and PDD.
They confirmed the contribution of mtDNA damage to PD pathology in the PD mouse models. They showed that lack of neuronal IFN-beta signaling leads to oxidative damage and mutations in mtDNA in neurons, which are subsequently released outside the neurons.
Injecting damaged mtDNA into mouse brain induced PDD-like behavioral symptoms, including neuropsychiatric, motor, and cognitive impairments. It also caused neurodegeneration in brain regions distant from the injection site, suggesting that damaged mtDNA triggers spread of PDD characteristics in an “infectious-like” manner, the researchers report.
Further study revealed that the mechanism through which damaged mtDNA causes pathology in healthy neurons involves dual activation of Toll-like receptor (TLR) 9 and 4 pathways, leading to increased oxidative stress and neuronal cell death, respectively.
“Our proteomic analysis of extracellular vesicles containing damaged mtDNA identified the TLR4 activator, ribosomal protein S3, as a key protein involved in recognizing and extruding damaged mtDNA,” the investigators write.
In the future they plan to investigate how mtDNA damage can serve as a predictive marker for different disease stages and progression and to explore potential therapeutic strategies aimed at restoring normal mitochondrial function to rectify the mitochondrial dysfunctions implicated in PD.
Making a comeback?
Commenting on the research for this news organization, James Beck, PhD, chief scientific officer at the Parkinson’s Foundation, noted that the role of mitochondria in PD is “like a starlet that burst onto the scene in the 80s, faded into obscurity, and through diligence and continued research has moved beyond being a solid character actor and is reemerging as a force to reckon with.
“This paper only adds to the allure that mitochondria may have in contributing to PD by providing evidence of a novel process by which mitochondria may be not only contributing to PD and loss of dopamine neurons but may play a larger role in the subsequent effects that many people with PD experience – dementia,” Dr. Beck said.
He noted that the authors identified several proteins as facilitating the neurodegeneration that is wrought by damaged mitochondrial DNA.
“These could be potential targets for future drug development. In addition, this work implicates alterations in immune signaling and drugs in development to target inflammatory responses may also bring ancillary benefit,” Dr. Beck said.
However, he said, “while very interesting findings, this is really the first effort that demonstrates how damaged mitochondrial DNA may contribute to neurodegeneration in the context of PD and PD dementia. Further work needs to validate these findings as well as to elucidate mechanisms underlying the propagation of the mitochondrial DNA from cell to cell.”
Funding for this research was provided by the European Union’s Horizon 2020 Research and Innovation Program, the Lundbeck Foundation, and the Danish Council for Independent Research–Medicine. Dr. Issazadeh-Navikas and Dr. Beck have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
.
While defects in mitochondrial functions and in mitochondrial DNA have been implicated in PD in the past, the current study demonstrates “for the first time how damaged mitochondrial DNA can underlie the mechanisms of PD initiation and spread in brain,” lead investigator Shohreh Issazadeh-Navikas, PhD, with the University of Copenhagen, told this news organization.
“This has direct implication for clinical diagnosis” – if damaged mtDNA can be detected in blood, it could serve as an early biomarker for disease, she explained.
The study was published online in Molecular Psychiatry.
“Infectious-like” spread of PD pathology
In earlier work, the researchers identified dysregulated interferon-beta (IFN-beta) signaling as a “top candidate pathway” associated with sporadic PD and its progression to PD with dementia (PDD).
In mice PD models that were deficient in IFN-beta signaling, the investigators showed that neuronal IFN-beta is required to maintain mitochondrial homeostasis and metabolism.
Lack of neuronal IFN-beta or disruption of its downstream signaling causes the accumulation of damaged mitochondria with excessive oxidative stress and insufficient adenosine triphosphate production.
In the current study, using postmortem brain tissue samples from patients with sporadic PD, they confirmed that there were deletions of mtDNA in the medial frontal gyrus, a region implicated in cognitive impairments in PD, suggesting a potential role of damaged mtDNA in disease pathophysiology.
They also identified mtDNA deletions in a “hotspot” in complex I respiratory chain subunits that were associated with dysregulation of oxidative stress and DNA damage response pathways in cohorts with sporadic PD and PDD.
They confirmed the contribution of mtDNA damage to PD pathology in the PD mouse models. They showed that lack of neuronal IFN-beta signaling leads to oxidative damage and mutations in mtDNA in neurons, which are subsequently released outside the neurons.
Injecting damaged mtDNA into mouse brain induced PDD-like behavioral symptoms, including neuropsychiatric, motor, and cognitive impairments. It also caused neurodegeneration in brain regions distant from the injection site, suggesting that damaged mtDNA triggers spread of PDD characteristics in an “infectious-like” manner, the researchers report.
Further study revealed that the mechanism through which damaged mtDNA causes pathology in healthy neurons involves dual activation of Toll-like receptor (TLR) 9 and 4 pathways, leading to increased oxidative stress and neuronal cell death, respectively.
“Our proteomic analysis of extracellular vesicles containing damaged mtDNA identified the TLR4 activator, ribosomal protein S3, as a key protein involved in recognizing and extruding damaged mtDNA,” the investigators write.
In the future they plan to investigate how mtDNA damage can serve as a predictive marker for different disease stages and progression and to explore potential therapeutic strategies aimed at restoring normal mitochondrial function to rectify the mitochondrial dysfunctions implicated in PD.
Making a comeback?
Commenting on the research for this news organization, James Beck, PhD, chief scientific officer at the Parkinson’s Foundation, noted that the role of mitochondria in PD is “like a starlet that burst onto the scene in the 80s, faded into obscurity, and through diligence and continued research has moved beyond being a solid character actor and is reemerging as a force to reckon with.
“This paper only adds to the allure that mitochondria may have in contributing to PD by providing evidence of a novel process by which mitochondria may be not only contributing to PD and loss of dopamine neurons but may play a larger role in the subsequent effects that many people with PD experience – dementia,” Dr. Beck said.
He noted that the authors identified several proteins as facilitating the neurodegeneration that is wrought by damaged mitochondrial DNA.
“These could be potential targets for future drug development. In addition, this work implicates alterations in immune signaling and drugs in development to target inflammatory responses may also bring ancillary benefit,” Dr. Beck said.
However, he said, “while very interesting findings, this is really the first effort that demonstrates how damaged mitochondrial DNA may contribute to neurodegeneration in the context of PD and PD dementia. Further work needs to validate these findings as well as to elucidate mechanisms underlying the propagation of the mitochondrial DNA from cell to cell.”
Funding for this research was provided by the European Union’s Horizon 2020 Research and Innovation Program, the Lundbeck Foundation, and the Danish Council for Independent Research–Medicine. Dr. Issazadeh-Navikas and Dr. Beck have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM MOLECULAR PSYCHIATRY
Lead pollutants as harmful to health as particulate matter
in a presentation to the World Bank. Their work was published in The Lancet Planetary Health.
As Mr. Larsen and Mr. Sánchez-Triana report, the economic consequences of increased exposure to lead are already immense, especially in low- and middle-income countries (LMICs). The study was financed by the Korea Green Growth Trust Fund and the World Bank’s Pollution Management and Environmental Health Program.
Intellectual, cardiovascular effects
“It is a very important publication that affects all of us,” pediatrician Stephan Böse-O’Reilly, MD, of the Institute and Polyclinic for Occupational, Social, and Environmental Health at Ludwig Maximilian University Hospital in Munich, Germany, said in an interview. “The study, the results of which I think are very reliable, shows that elevated levels of lead in the blood have a much more drastic effect on children’s intelligence than we previously thought.”
It is well known that lead affects the antenatal and postnatal cognitive development of children, Dr. Böse-O’Reilly explained. But the extent of this effect has quite clearly been underestimated before now.
On the other hand, Mr. Larsen and Mr. Sánchez-Triana’s work could prove that lead may lead to more cardiovascular diseases in adulthood. “We already knew that increased exposure to lead increased the risk of high blood pressure and, as a result, mortality,” said Dr. Böse-O’Reilly. “This study now very clearly shows that the risk of arteriosclerosis, for example, also increases through lead exposure.”
Figures from 2019
“For the first time, to our knowledge, we aimed to estimate the global burden and cost of IQ loss and cardiovascular disease mortality from lead exposure,” wrote Mr. Larsen and Mr. Sánchez-Triana. For their calculations, the scientists used blood lead level estimates from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019.
They estimated IQ loss in children younger than 5 years using the internationally recognized blood lead level–IQ loss function. The researchers subsequently estimated the cost of this IQ loss based on the loss in lifetime income, presented as cost in U.S. dollars and percentage of gross domestic product (GDP).
Mr. Larsen and Mr. Sánchez-Triana estimated cardiovascular deaths caused by lead exposure in adults aged 25 years or older using a model that captures the effects of lead exposure on cardiovascular disease mortality that is mediated through mechanisms other than hypertension.
Finally, they used the statistical life expectancy to estimate the welfare cost of premature mortality, also presented as cost in U.S. dollars and percentage of GDP. All estimates were calculated according to the World Bank income classification for 2019.
Millions of deaths
As reported by Mr. Larsen and Mr. Sánchez-Triana, children younger than 5 years lost an estimated 765 million IQ points worldwide because of lead exposure in this period. In 2019, 5,545,000 adults died from cardiovascular diseases caused by lead exposure. The scientists recorded 729 million of the IQ points lost (95.3%) and 5,004,000 (90.2%) of the deaths as occurring in LMICs.
The IQ loss here was nearly 80% higher than a previous estimate, wrote Mr. Larsen and Mr. Sánchez-Triana. The number of cardiovascular disease deaths they determined was six times higher than the GBD 2019 estimate.
“These are results with which the expert societies, especially the German Society of Pediatrics and Adolescent Medicine and the German Cardiac Society, and the corresponding professional associations need to concern themselves,” said Dr. Böse-O’Reilly.
Although blood lead concentrations have declined substantially since the phase-out of leaded gasoline, especially in Western countries, lead still represents a major health issue because it stays in the bones for decades.
European situation moderate
“We need a broad discussion on questions such as whether lead levels should be included in prophylactic assessments in certain age groups, what blood level is even tolerable, and in what situation medicinal therapy with chelating agents would possibly be appropriate,” said Dr. Böse-O’Reilly.
“Of course, we cannot answer these questions on the basis of one individual study,” he added. “However, the work in question definitely illustrates how dangerous lead can be and that we need further research into the actual burden and the best preventive measures.”
In this respect, the situation in Europe is still comparatively moderate. “Globally, lead exposure has risen in recent years,” said Dr. Böse-O’Reilly. According to an investigation by the Planet Earth Foundation, outside of the European Union, lead can increasingly be found in toys, spices, and cooking utensils, for example.
“Especially in lower-income countries, there is a lack of consumer protection or a good monitoring program like we have here in the EU,” said Dr. Böse-O’Reilly. In these countries, lead is sometimes added to spices by unscrupulous retailers to make the color more intense or to simply add to its weight to gain more profit.
Recycling lead-acid batteries or other electrical waste, often transferred to poorer countries, constitutes a large problem. “In general, children in Germany have a blood lead level of less than 1 mcg/dL,” explained Dr. Böse-O’Reilly. “In some regions of Indonesia, where these recycling factories are located, more than 50% of children have levels of more than 20 mcg/dL.”
Particulate matter
According to Mr. Larsen and Mr. Sánchez-Triana, the global cost of increased lead exposure was around $6 trillion USD in 2019, which was equivalent to 6.9% of global GDP. About 77% of the cost ($4.62 trillion USD) comprised the welfare costs of cardiovascular disease mortality, and 23% ($1.38 trillion USD) comprised the present value of future income losses because of IQ loss in children.
“Our findings suggest that global lead exposure has health and economic costs on par with PM2.5 air pollution,” wrote the authors. This places lead as an environmental risk factor on par with particulate matter and above that of air pollution from solid fuels, ahead of unsafe drinking water, unhygienic sanitation, or insufficient handwashing.
“This finding is in contrast to that of GBD 2019, which ranked lead exposure as a distant fourth environmental risk factor, due to not accounting for IQ loss in children – other than idiopathic developmental intellectual disability in a small subset of children – and reporting a substantially lower estimate of adult cardiovascular disease mortality,” wrote Mr. Larsen and Mr. Sánchez-Triana.
“A central implication for future research and policy is that LMICs bear an extraordinarily large share of the health and cost burden of lead exposure,” wrote the authors. Consequently, improved quality of blood lead level measurements and identification of sources containing lead are urgently needed there.
Improved recycling methods
Dr. Böse-O’Reilly would like an increased focus on children. “If children’s cognitive skills are lost, this of course has a long-term effect on a country’s economic position,” he said. “Precisely that which LMICs actually need for their development is being stripped from them.
“We should think long and hard about whether we really need to send so much of our electrical waste and so many old cars to poorer countries, where they are incorrectly recycled,” he warned. “We should at least give the LMICs the support necessary for them to be able to process lead-containing products in the future so that less lead makes it into the environment.
“Through these global cycles, we all contribute a lot toward the worldwide lead burden,” Dr. Böse-O’Reilly said. “In my opinion, the German Supply Chain Act is therefore definitely sensible. Not only does it protect our own economy, but it also protects the health of people in other countries.”
This article was translated from Medscape’s German Edition. A version of this article appeared on Medscape.com.
in a presentation to the World Bank. Their work was published in The Lancet Planetary Health.
As Mr. Larsen and Mr. Sánchez-Triana report, the economic consequences of increased exposure to lead are already immense, especially in low- and middle-income countries (LMICs). The study was financed by the Korea Green Growth Trust Fund and the World Bank’s Pollution Management and Environmental Health Program.
Intellectual, cardiovascular effects
“It is a very important publication that affects all of us,” pediatrician Stephan Böse-O’Reilly, MD, of the Institute and Polyclinic for Occupational, Social, and Environmental Health at Ludwig Maximilian University Hospital in Munich, Germany, said in an interview. “The study, the results of which I think are very reliable, shows that elevated levels of lead in the blood have a much more drastic effect on children’s intelligence than we previously thought.”
It is well known that lead affects the antenatal and postnatal cognitive development of children, Dr. Böse-O’Reilly explained. But the extent of this effect has quite clearly been underestimated before now.
On the other hand, Mr. Larsen and Mr. Sánchez-Triana’s work could prove that lead may lead to more cardiovascular diseases in adulthood. “We already knew that increased exposure to lead increased the risk of high blood pressure and, as a result, mortality,” said Dr. Böse-O’Reilly. “This study now very clearly shows that the risk of arteriosclerosis, for example, also increases through lead exposure.”
Figures from 2019
“For the first time, to our knowledge, we aimed to estimate the global burden and cost of IQ loss and cardiovascular disease mortality from lead exposure,” wrote Mr. Larsen and Mr. Sánchez-Triana. For their calculations, the scientists used blood lead level estimates from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019.
They estimated IQ loss in children younger than 5 years using the internationally recognized blood lead level–IQ loss function. The researchers subsequently estimated the cost of this IQ loss based on the loss in lifetime income, presented as cost in U.S. dollars and percentage of gross domestic product (GDP).
Mr. Larsen and Mr. Sánchez-Triana estimated cardiovascular deaths caused by lead exposure in adults aged 25 years or older using a model that captures the effects of lead exposure on cardiovascular disease mortality that is mediated through mechanisms other than hypertension.
Finally, they used the statistical life expectancy to estimate the welfare cost of premature mortality, also presented as cost in U.S. dollars and percentage of GDP. All estimates were calculated according to the World Bank income classification for 2019.
Millions of deaths
As reported by Mr. Larsen and Mr. Sánchez-Triana, children younger than 5 years lost an estimated 765 million IQ points worldwide because of lead exposure in this period. In 2019, 5,545,000 adults died from cardiovascular diseases caused by lead exposure. The scientists recorded 729 million of the IQ points lost (95.3%) and 5,004,000 (90.2%) of the deaths as occurring in LMICs.
The IQ loss here was nearly 80% higher than a previous estimate, wrote Mr. Larsen and Mr. Sánchez-Triana. The number of cardiovascular disease deaths they determined was six times higher than the GBD 2019 estimate.
“These are results with which the expert societies, especially the German Society of Pediatrics and Adolescent Medicine and the German Cardiac Society, and the corresponding professional associations need to concern themselves,” said Dr. Böse-O’Reilly.
Although blood lead concentrations have declined substantially since the phase-out of leaded gasoline, especially in Western countries, lead still represents a major health issue because it stays in the bones for decades.
European situation moderate
“We need a broad discussion on questions such as whether lead levels should be included in prophylactic assessments in certain age groups, what blood level is even tolerable, and in what situation medicinal therapy with chelating agents would possibly be appropriate,” said Dr. Böse-O’Reilly.
“Of course, we cannot answer these questions on the basis of one individual study,” he added. “However, the work in question definitely illustrates how dangerous lead can be and that we need further research into the actual burden and the best preventive measures.”
In this respect, the situation in Europe is still comparatively moderate. “Globally, lead exposure has risen in recent years,” said Dr. Böse-O’Reilly. According to an investigation by the Planet Earth Foundation, outside of the European Union, lead can increasingly be found in toys, spices, and cooking utensils, for example.
“Especially in lower-income countries, there is a lack of consumer protection or a good monitoring program like we have here in the EU,” said Dr. Böse-O’Reilly. In these countries, lead is sometimes added to spices by unscrupulous retailers to make the color more intense or to simply add to its weight to gain more profit.
Recycling lead-acid batteries or other electrical waste, often transferred to poorer countries, constitutes a large problem. “In general, children in Germany have a blood lead level of less than 1 mcg/dL,” explained Dr. Böse-O’Reilly. “In some regions of Indonesia, where these recycling factories are located, more than 50% of children have levels of more than 20 mcg/dL.”
Particulate matter
According to Mr. Larsen and Mr. Sánchez-Triana, the global cost of increased lead exposure was around $6 trillion USD in 2019, which was equivalent to 6.9% of global GDP. About 77% of the cost ($4.62 trillion USD) comprised the welfare costs of cardiovascular disease mortality, and 23% ($1.38 trillion USD) comprised the present value of future income losses because of IQ loss in children.
“Our findings suggest that global lead exposure has health and economic costs on par with PM2.5 air pollution,” wrote the authors. This places lead as an environmental risk factor on par with particulate matter and above that of air pollution from solid fuels, ahead of unsafe drinking water, unhygienic sanitation, or insufficient handwashing.
“This finding is in contrast to that of GBD 2019, which ranked lead exposure as a distant fourth environmental risk factor, due to not accounting for IQ loss in children – other than idiopathic developmental intellectual disability in a small subset of children – and reporting a substantially lower estimate of adult cardiovascular disease mortality,” wrote Mr. Larsen and Mr. Sánchez-Triana.
“A central implication for future research and policy is that LMICs bear an extraordinarily large share of the health and cost burden of lead exposure,” wrote the authors. Consequently, improved quality of blood lead level measurements and identification of sources containing lead are urgently needed there.
Improved recycling methods
Dr. Böse-O’Reilly would like an increased focus on children. “If children’s cognitive skills are lost, this of course has a long-term effect on a country’s economic position,” he said. “Precisely that which LMICs actually need for their development is being stripped from them.
“We should think long and hard about whether we really need to send so much of our electrical waste and so many old cars to poorer countries, where they are incorrectly recycled,” he warned. “We should at least give the LMICs the support necessary for them to be able to process lead-containing products in the future so that less lead makes it into the environment.
“Through these global cycles, we all contribute a lot toward the worldwide lead burden,” Dr. Böse-O’Reilly said. “In my opinion, the German Supply Chain Act is therefore definitely sensible. Not only does it protect our own economy, but it also protects the health of people in other countries.”
This article was translated from Medscape’s German Edition. A version of this article appeared on Medscape.com.
in a presentation to the World Bank. Their work was published in The Lancet Planetary Health.
As Mr. Larsen and Mr. Sánchez-Triana report, the economic consequences of increased exposure to lead are already immense, especially in low- and middle-income countries (LMICs). The study was financed by the Korea Green Growth Trust Fund and the World Bank’s Pollution Management and Environmental Health Program.
Intellectual, cardiovascular effects
“It is a very important publication that affects all of us,” pediatrician Stephan Böse-O’Reilly, MD, of the Institute and Polyclinic for Occupational, Social, and Environmental Health at Ludwig Maximilian University Hospital in Munich, Germany, said in an interview. “The study, the results of which I think are very reliable, shows that elevated levels of lead in the blood have a much more drastic effect on children’s intelligence than we previously thought.”
It is well known that lead affects the antenatal and postnatal cognitive development of children, Dr. Böse-O’Reilly explained. But the extent of this effect has quite clearly been underestimated before now.
On the other hand, Mr. Larsen and Mr. Sánchez-Triana’s work could prove that lead may lead to more cardiovascular diseases in adulthood. “We already knew that increased exposure to lead increased the risk of high blood pressure and, as a result, mortality,” said Dr. Böse-O’Reilly. “This study now very clearly shows that the risk of arteriosclerosis, for example, also increases through lead exposure.”
Figures from 2019
“For the first time, to our knowledge, we aimed to estimate the global burden and cost of IQ loss and cardiovascular disease mortality from lead exposure,” wrote Mr. Larsen and Mr. Sánchez-Triana. For their calculations, the scientists used blood lead level estimates from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019.
They estimated IQ loss in children younger than 5 years using the internationally recognized blood lead level–IQ loss function. The researchers subsequently estimated the cost of this IQ loss based on the loss in lifetime income, presented as cost in U.S. dollars and percentage of gross domestic product (GDP).
Mr. Larsen and Mr. Sánchez-Triana estimated cardiovascular deaths caused by lead exposure in adults aged 25 years or older using a model that captures the effects of lead exposure on cardiovascular disease mortality that is mediated through mechanisms other than hypertension.
Finally, they used the statistical life expectancy to estimate the welfare cost of premature mortality, also presented as cost in U.S. dollars and percentage of GDP. All estimates were calculated according to the World Bank income classification for 2019.
Millions of deaths
As reported by Mr. Larsen and Mr. Sánchez-Triana, children younger than 5 years lost an estimated 765 million IQ points worldwide because of lead exposure in this period. In 2019, 5,545,000 adults died from cardiovascular diseases caused by lead exposure. The scientists recorded 729 million of the IQ points lost (95.3%) and 5,004,000 (90.2%) of the deaths as occurring in LMICs.
The IQ loss here was nearly 80% higher than a previous estimate, wrote Mr. Larsen and Mr. Sánchez-Triana. The number of cardiovascular disease deaths they determined was six times higher than the GBD 2019 estimate.
“These are results with which the expert societies, especially the German Society of Pediatrics and Adolescent Medicine and the German Cardiac Society, and the corresponding professional associations need to concern themselves,” said Dr. Böse-O’Reilly.
Although blood lead concentrations have declined substantially since the phase-out of leaded gasoline, especially in Western countries, lead still represents a major health issue because it stays in the bones for decades.
European situation moderate
“We need a broad discussion on questions such as whether lead levels should be included in prophylactic assessments in certain age groups, what blood level is even tolerable, and in what situation medicinal therapy with chelating agents would possibly be appropriate,” said Dr. Böse-O’Reilly.
“Of course, we cannot answer these questions on the basis of one individual study,” he added. “However, the work in question definitely illustrates how dangerous lead can be and that we need further research into the actual burden and the best preventive measures.”
In this respect, the situation in Europe is still comparatively moderate. “Globally, lead exposure has risen in recent years,” said Dr. Böse-O’Reilly. According to an investigation by the Planet Earth Foundation, outside of the European Union, lead can increasingly be found in toys, spices, and cooking utensils, for example.
“Especially in lower-income countries, there is a lack of consumer protection or a good monitoring program like we have here in the EU,” said Dr. Böse-O’Reilly. In these countries, lead is sometimes added to spices by unscrupulous retailers to make the color more intense or to simply add to its weight to gain more profit.
Recycling lead-acid batteries or other electrical waste, often transferred to poorer countries, constitutes a large problem. “In general, children in Germany have a blood lead level of less than 1 mcg/dL,” explained Dr. Böse-O’Reilly. “In some regions of Indonesia, where these recycling factories are located, more than 50% of children have levels of more than 20 mcg/dL.”
Particulate matter
According to Mr. Larsen and Mr. Sánchez-Triana, the global cost of increased lead exposure was around $6 trillion USD in 2019, which was equivalent to 6.9% of global GDP. About 77% of the cost ($4.62 trillion USD) comprised the welfare costs of cardiovascular disease mortality, and 23% ($1.38 trillion USD) comprised the present value of future income losses because of IQ loss in children.
“Our findings suggest that global lead exposure has health and economic costs on par with PM2.5 air pollution,” wrote the authors. This places lead as an environmental risk factor on par with particulate matter and above that of air pollution from solid fuels, ahead of unsafe drinking water, unhygienic sanitation, or insufficient handwashing.
“This finding is in contrast to that of GBD 2019, which ranked lead exposure as a distant fourth environmental risk factor, due to not accounting for IQ loss in children – other than idiopathic developmental intellectual disability in a small subset of children – and reporting a substantially lower estimate of adult cardiovascular disease mortality,” wrote Mr. Larsen and Mr. Sánchez-Triana.
“A central implication for future research and policy is that LMICs bear an extraordinarily large share of the health and cost burden of lead exposure,” wrote the authors. Consequently, improved quality of blood lead level measurements and identification of sources containing lead are urgently needed there.
Improved recycling methods
Dr. Böse-O’Reilly would like an increased focus on children. “If children’s cognitive skills are lost, this of course has a long-term effect on a country’s economic position,” he said. “Precisely that which LMICs actually need for their development is being stripped from them.
“We should think long and hard about whether we really need to send so much of our electrical waste and so many old cars to poorer countries, where they are incorrectly recycled,” he warned. “We should at least give the LMICs the support necessary for them to be able to process lead-containing products in the future so that less lead makes it into the environment.
“Through these global cycles, we all contribute a lot toward the worldwide lead burden,” Dr. Böse-O’Reilly said. “In my opinion, the German Supply Chain Act is therefore definitely sensible. Not only does it protect our own economy, but it also protects the health of people in other countries.”
This article was translated from Medscape’s German Edition. A version of this article appeared on Medscape.com.
FROM THE LANCET PLANETARY HEALTH
History of depression, stress tied to Alzheimer’s, MCI risk
TOPLINE:
compared with those without either condition, a new study found.
METHODOLOGY:
- Longitudinal cohort study of 1,362,548 people with records in the Region Stockholm administrative health care database with a diagnosis of stress-induced exhaustion disorder (SED), depression, or both between 2012 and 2013.
- Cohort followed for diagnosis of MCI or AD between 2014 and 2022.
TAKEAWAY:
- SED diagnosed in 0.3%, depression in 2.9% and both SED and depression in 0.1%
- Compared with people without SED or depression, AD risk was more than double in patients with SED (adjusted odds ratio [aOR], 2.45; 99% confidence interval [CI], 1.22-4.91) or depression (aOR, 2.32; 99% CI, 1.85-2.90) and four times higher in patients with both SED and depression (aOR, 4.00; 99% CI, 1.67-9.58)
- Risk for MCI was also higher in people with SED (aOR, 1.87; 99% CI,1.20-2.91), depression (aOR, 2.85; 99% CI, 2.53-3.22) or both SED and depression (aOR, 3.87; 99% CI, 2.39-6.27) vs patients with no history of SED or depression.
- Only patients with depression had a higher risk for another dementia type (aOR, 2.39; 99% CI, 1.92-2.96).
IN PRACTICE:
“Future studies should examine the possibility that symptoms of depression and/or chronic stress could be prodromal symptoms of dementia rather than risk factors,” study authors wrote.
SOURCE:
The study was conducted by Johanna Wallensten, doctoral student, department of clinical sciences, Danderyd Hospital, Stockholm, and colleagues and funded by the Karolinska Institute. It was published online in Alzheimer’s Research and Therapy.
LIMITATIONS:
Use of a health care registry could have led to over- or underestimation of depression, MCI and AD. The study probably captures most people with depression but not most people with depressive symptoms.
DISCLOSURES:
The authors reported no relevant conflicts.
A version of this article appeared on Medscape.com.
TOPLINE:
compared with those without either condition, a new study found.
METHODOLOGY:
- Longitudinal cohort study of 1,362,548 people with records in the Region Stockholm administrative health care database with a diagnosis of stress-induced exhaustion disorder (SED), depression, or both between 2012 and 2013.
- Cohort followed for diagnosis of MCI or AD between 2014 and 2022.
TAKEAWAY:
- SED diagnosed in 0.3%, depression in 2.9% and both SED and depression in 0.1%
- Compared with people without SED or depression, AD risk was more than double in patients with SED (adjusted odds ratio [aOR], 2.45; 99% confidence interval [CI], 1.22-4.91) or depression (aOR, 2.32; 99% CI, 1.85-2.90) and four times higher in patients with both SED and depression (aOR, 4.00; 99% CI, 1.67-9.58)
- Risk for MCI was also higher in people with SED (aOR, 1.87; 99% CI,1.20-2.91), depression (aOR, 2.85; 99% CI, 2.53-3.22) or both SED and depression (aOR, 3.87; 99% CI, 2.39-6.27) vs patients with no history of SED or depression.
- Only patients with depression had a higher risk for another dementia type (aOR, 2.39; 99% CI, 1.92-2.96).
IN PRACTICE:
“Future studies should examine the possibility that symptoms of depression and/or chronic stress could be prodromal symptoms of dementia rather than risk factors,” study authors wrote.
SOURCE:
The study was conducted by Johanna Wallensten, doctoral student, department of clinical sciences, Danderyd Hospital, Stockholm, and colleagues and funded by the Karolinska Institute. It was published online in Alzheimer’s Research and Therapy.
LIMITATIONS:
Use of a health care registry could have led to over- or underestimation of depression, MCI and AD. The study probably captures most people with depression but not most people with depressive symptoms.
DISCLOSURES:
The authors reported no relevant conflicts.
A version of this article appeared on Medscape.com.
TOPLINE:
compared with those without either condition, a new study found.
METHODOLOGY:
- Longitudinal cohort study of 1,362,548 people with records in the Region Stockholm administrative health care database with a diagnosis of stress-induced exhaustion disorder (SED), depression, or both between 2012 and 2013.
- Cohort followed for diagnosis of MCI or AD between 2014 and 2022.
TAKEAWAY:
- SED diagnosed in 0.3%, depression in 2.9% and both SED and depression in 0.1%
- Compared with people without SED or depression, AD risk was more than double in patients with SED (adjusted odds ratio [aOR], 2.45; 99% confidence interval [CI], 1.22-4.91) or depression (aOR, 2.32; 99% CI, 1.85-2.90) and four times higher in patients with both SED and depression (aOR, 4.00; 99% CI, 1.67-9.58)
- Risk for MCI was also higher in people with SED (aOR, 1.87; 99% CI,1.20-2.91), depression (aOR, 2.85; 99% CI, 2.53-3.22) or both SED and depression (aOR, 3.87; 99% CI, 2.39-6.27) vs patients with no history of SED or depression.
- Only patients with depression had a higher risk for another dementia type (aOR, 2.39; 99% CI, 1.92-2.96).
IN PRACTICE:
“Future studies should examine the possibility that symptoms of depression and/or chronic stress could be prodromal symptoms of dementia rather than risk factors,” study authors wrote.
SOURCE:
The study was conducted by Johanna Wallensten, doctoral student, department of clinical sciences, Danderyd Hospital, Stockholm, and colleagues and funded by the Karolinska Institute. It was published online in Alzheimer’s Research and Therapy.
LIMITATIONS:
Use of a health care registry could have led to over- or underestimation of depression, MCI and AD. The study probably captures most people with depression but not most people with depressive symptoms.
DISCLOSURES:
The authors reported no relevant conflicts.
A version of this article appeared on Medscape.com.
Hyperbaric oxygen therapy for traumatic brain injury: Promising or wishful thinking?
A recent review by Hadanny and colleagues recommends hyperbaric oxygen therapy (HBOT) for acute moderate to severe traumatic brain injury (TBI) and selected patients with prolonged postconcussive syndrome.
This article piqued my curiosity because I trained in HBOT more than 20 years ago. As a passionate scuba diver, my motivation was to master treatment for air embolism and decompression illness. Thankfully, these diving accidents are rare. However, I used HBOT for nonhealing wounds, and its efficacy was sometimes remarkable.
Paradoxical results with oxygen therapy
Although it may seem self-evident that “more oxygen is better” for medical illness, this is not necessarily true. I recently interviewed Ola Didrik Saugstad, MD, who demonstrated that the traditional practice of resuscitating newborns with 100% oxygen was more toxic than resuscitation with air (which contains 21% oxygen). His counterintuitive discovery led to a lifesaving change in the international newborn resuscitation guidelines.
The Food and Drug Administration has approved HBOT for a wide variety of conditions, but some practitioners enthusiastically promote it for off-label indications. These include antiaging, autism, multiple sclerosis, and the aforementioned TBI.
More than 50 years ago, HBOT was proposed for stroke, another disorder where the brain has been deprived of oxygen. Despite obvious logic, clinical trials have been unconvincing. The FDA has not approved HBOT for stroke.
HBOT in practice
During HBOT, the patient breathes 100% oxygen while the whole body is pressurized within a hyperbaric chamber. The chamber’s construction allows pressures above normal sea level of 1.0 atmosphere absolute (ATA). For example, The U.S. Navy Treatment Table for decompression sickness recommends 100% oxygen at 2.8 ATA. Chambers may hold one or more patients at a time.
The frequency of therapy varies but often consists of 20-60 sessions lasting 90-120 minutes. For off-label use like TBI, patients usually pay out of pocket. Given the multiple treatments, costs can add up.
Inconsistent evidence and sham controls
The unwieldy 33-page evidence review by Hadanny and colleagues cites multiple studies supporting HBOT for TBI. However, many, if not all, suffer from methodological flaws. These include vague inclusion criteria, lack of a control group, small patient numbers, treatment at different times since injury, poorly defined or varying HBOT protocols, varying outcome measures, and superficial results analysis.
A sham or control arm is essential for HBOT research trials, given the potential placebo effect of placing a human being inside a large, high-tech, sealed tube for an hour or more. In some sham-controlled studies, which consisted of low-pressure oxygen (that is, 1.3 ATA as sham vs. 2.4 ATA as treatment), all groups experienced symptom improvement. The review authors argue that the low-dose HBOT sham arms were biologically active and that the improvements seen mean that both high- and low-dose HBOT is therapeutic. The alternative explanation is that the placebo effect accounted for improvement in both groups.
The late Michael Bennett, a world authority on hyperbaric and underwater medicine, doubted that conventional HBOT sham controls could genuinely have a therapeutic effect, and I agree. The upcoming HOT-POCS trial (discussed below) should answer the question more definitively.
Mechanisms of action and safety
Mechanisms of benefit for HBOT include increased oxygen availability and angiogenesis. Animal research suggests that it may reduce secondary cell death from TBI, through stabilization of the blood-brain barrier and inflammation reduction.
HBOT is generally safe and well tolerated. A retrospective analysis of 1.5 million outpatient hyperbaric treatments revealed that less than 1% were associated with adverse events. The most common were ear and sinus barotrauma. Because HBOT uses increased air pressure, patients must equalize their ears and sinuses. Those who cannot because of altered consciousness, anatomical defects, or congestion must undergo myringotomy or terminate therapy. Claustrophobia was the second most common adverse effect. Convulsions and tension pneumocephalus were rare.
Perhaps the most concerning risk of HBOT for patients with TBI is the potential waste of human and financial resources.
Desperate physicians and patients
As a neurologist who regularly treats patients with TBI, I share the review authors’ frustration regarding the limited efficacy of available treatments. However, the suboptimal efficacy of currently available therapy is insufficient justification to recommend HBOT.
With respect to chronic TBI, it is difficult to imagine how HBOT could reverse brain injury that has been present for months or years. No other therapy exists that reliably encourages neuronal regeneration or prevents the development of posttraumatic epilepsy.
Frank Conidi, MD, a board-certified sports neurologist and headache specialist, shared his thoughts via email. He agrees that HBOT may have a role in TBI, but after reviewing Hadanny and colleagues’ paper, he concluded that there is insufficient evidence for the use of HBOT in all forms of TBI. He would like to see large multicenter, well-designed studies with standardized pressures and duration and a standard definition of the various types of head injury.
Ongoing research
There are at least five ongoing trials on HBOT for TBI or postconcussive syndrome, including the well-designed placebo-controlled HOT-POCS study. The latter has a novel placebo gas system that addresses Hadanny and colleagues’ contention that even low-dose HBOT might be effective.
The placebo arm in HOT-POCS mimics the HBO environment but provides only 0.21 ATA of oxygen, the same as room air. The active arm provides 100% oxygen at 2.0 ATA. If patients in both arms improve, the benefit will be caused by a placebo response, not HBOT.
Conflict of interest
Another concern with the review is that all three authors are affiliated with Aviv Scientific. This company has an exclusive partnership with the world’s largest hyperbaric medicine and research facility, the Sagol Center at Shamir Medical Center in Be’er Ya’akov, Israel.
This conflict of interest does not a priori invalidate their conclusions. However, official HBOT guidelines from a leading organization like the Undersea and Hyperbaric Medicine Society or the American Academy of Neurology would be preferable.
Conclusion
There is an urgent unmet need for more effective treatments for postconcussive syndrome and chronic TBI.
The review authors’ recommendations for HBOT seem premature. They are arguably a disservice to the many desperate patients and their families who will be tempted to expend valuable resources of time and money for an appealing but unproven therapy. Appropriately designed placebo-controlled studies such as HOT-POCS will help separate fact from wishful thinking.
Dr. Wilner is associate professor of neurology at University of Tennessee Health Science Center, Memphis. He reported a conflict of interest with Accordant Health Services.
A version of this article first appeared on Medscape.com.
A recent review by Hadanny and colleagues recommends hyperbaric oxygen therapy (HBOT) for acute moderate to severe traumatic brain injury (TBI) and selected patients with prolonged postconcussive syndrome.
This article piqued my curiosity because I trained in HBOT more than 20 years ago. As a passionate scuba diver, my motivation was to master treatment for air embolism and decompression illness. Thankfully, these diving accidents are rare. However, I used HBOT for nonhealing wounds, and its efficacy was sometimes remarkable.
Paradoxical results with oxygen therapy
Although it may seem self-evident that “more oxygen is better” for medical illness, this is not necessarily true. I recently interviewed Ola Didrik Saugstad, MD, who demonstrated that the traditional practice of resuscitating newborns with 100% oxygen was more toxic than resuscitation with air (which contains 21% oxygen). His counterintuitive discovery led to a lifesaving change in the international newborn resuscitation guidelines.
The Food and Drug Administration has approved HBOT for a wide variety of conditions, but some practitioners enthusiastically promote it for off-label indications. These include antiaging, autism, multiple sclerosis, and the aforementioned TBI.
More than 50 years ago, HBOT was proposed for stroke, another disorder where the brain has been deprived of oxygen. Despite obvious logic, clinical trials have been unconvincing. The FDA has not approved HBOT for stroke.
HBOT in practice
During HBOT, the patient breathes 100% oxygen while the whole body is pressurized within a hyperbaric chamber. The chamber’s construction allows pressures above normal sea level of 1.0 atmosphere absolute (ATA). For example, The U.S. Navy Treatment Table for decompression sickness recommends 100% oxygen at 2.8 ATA. Chambers may hold one or more patients at a time.
The frequency of therapy varies but often consists of 20-60 sessions lasting 90-120 minutes. For off-label use like TBI, patients usually pay out of pocket. Given the multiple treatments, costs can add up.
Inconsistent evidence and sham controls
The unwieldy 33-page evidence review by Hadanny and colleagues cites multiple studies supporting HBOT for TBI. However, many, if not all, suffer from methodological flaws. These include vague inclusion criteria, lack of a control group, small patient numbers, treatment at different times since injury, poorly defined or varying HBOT protocols, varying outcome measures, and superficial results analysis.
A sham or control arm is essential for HBOT research trials, given the potential placebo effect of placing a human being inside a large, high-tech, sealed tube for an hour or more. In some sham-controlled studies, which consisted of low-pressure oxygen (that is, 1.3 ATA as sham vs. 2.4 ATA as treatment), all groups experienced symptom improvement. The review authors argue that the low-dose HBOT sham arms were biologically active and that the improvements seen mean that both high- and low-dose HBOT is therapeutic. The alternative explanation is that the placebo effect accounted for improvement in both groups.
The late Michael Bennett, a world authority on hyperbaric and underwater medicine, doubted that conventional HBOT sham controls could genuinely have a therapeutic effect, and I agree. The upcoming HOT-POCS trial (discussed below) should answer the question more definitively.
Mechanisms of action and safety
Mechanisms of benefit for HBOT include increased oxygen availability and angiogenesis. Animal research suggests that it may reduce secondary cell death from TBI, through stabilization of the blood-brain barrier and inflammation reduction.
HBOT is generally safe and well tolerated. A retrospective analysis of 1.5 million outpatient hyperbaric treatments revealed that less than 1% were associated with adverse events. The most common were ear and sinus barotrauma. Because HBOT uses increased air pressure, patients must equalize their ears and sinuses. Those who cannot because of altered consciousness, anatomical defects, or congestion must undergo myringotomy or terminate therapy. Claustrophobia was the second most common adverse effect. Convulsions and tension pneumocephalus were rare.
Perhaps the most concerning risk of HBOT for patients with TBI is the potential waste of human and financial resources.
Desperate physicians and patients
As a neurologist who regularly treats patients with TBI, I share the review authors’ frustration regarding the limited efficacy of available treatments. However, the suboptimal efficacy of currently available therapy is insufficient justification to recommend HBOT.
With respect to chronic TBI, it is difficult to imagine how HBOT could reverse brain injury that has been present for months or years. No other therapy exists that reliably encourages neuronal regeneration or prevents the development of posttraumatic epilepsy.
Frank Conidi, MD, a board-certified sports neurologist and headache specialist, shared his thoughts via email. He agrees that HBOT may have a role in TBI, but after reviewing Hadanny and colleagues’ paper, he concluded that there is insufficient evidence for the use of HBOT in all forms of TBI. He would like to see large multicenter, well-designed studies with standardized pressures and duration and a standard definition of the various types of head injury.
Ongoing research
There are at least five ongoing trials on HBOT for TBI or postconcussive syndrome, including the well-designed placebo-controlled HOT-POCS study. The latter has a novel placebo gas system that addresses Hadanny and colleagues’ contention that even low-dose HBOT might be effective.
The placebo arm in HOT-POCS mimics the HBO environment but provides only 0.21 ATA of oxygen, the same as room air. The active arm provides 100% oxygen at 2.0 ATA. If patients in both arms improve, the benefit will be caused by a placebo response, not HBOT.
Conflict of interest
Another concern with the review is that all three authors are affiliated with Aviv Scientific. This company has an exclusive partnership with the world’s largest hyperbaric medicine and research facility, the Sagol Center at Shamir Medical Center in Be’er Ya’akov, Israel.
This conflict of interest does not a priori invalidate their conclusions. However, official HBOT guidelines from a leading organization like the Undersea and Hyperbaric Medicine Society or the American Academy of Neurology would be preferable.
Conclusion
There is an urgent unmet need for more effective treatments for postconcussive syndrome and chronic TBI.
The review authors’ recommendations for HBOT seem premature. They are arguably a disservice to the many desperate patients and their families who will be tempted to expend valuable resources of time and money for an appealing but unproven therapy. Appropriately designed placebo-controlled studies such as HOT-POCS will help separate fact from wishful thinking.
Dr. Wilner is associate professor of neurology at University of Tennessee Health Science Center, Memphis. He reported a conflict of interest with Accordant Health Services.
A version of this article first appeared on Medscape.com.
A recent review by Hadanny and colleagues recommends hyperbaric oxygen therapy (HBOT) for acute moderate to severe traumatic brain injury (TBI) and selected patients with prolonged postconcussive syndrome.
This article piqued my curiosity because I trained in HBOT more than 20 years ago. As a passionate scuba diver, my motivation was to master treatment for air embolism and decompression illness. Thankfully, these diving accidents are rare. However, I used HBOT for nonhealing wounds, and its efficacy was sometimes remarkable.
Paradoxical results with oxygen therapy
Although it may seem self-evident that “more oxygen is better” for medical illness, this is not necessarily true. I recently interviewed Ola Didrik Saugstad, MD, who demonstrated that the traditional practice of resuscitating newborns with 100% oxygen was more toxic than resuscitation with air (which contains 21% oxygen). His counterintuitive discovery led to a lifesaving change in the international newborn resuscitation guidelines.
The Food and Drug Administration has approved HBOT for a wide variety of conditions, but some practitioners enthusiastically promote it for off-label indications. These include antiaging, autism, multiple sclerosis, and the aforementioned TBI.
More than 50 years ago, HBOT was proposed for stroke, another disorder where the brain has been deprived of oxygen. Despite obvious logic, clinical trials have been unconvincing. The FDA has not approved HBOT for stroke.
HBOT in practice
During HBOT, the patient breathes 100% oxygen while the whole body is pressurized within a hyperbaric chamber. The chamber’s construction allows pressures above normal sea level of 1.0 atmosphere absolute (ATA). For example, The U.S. Navy Treatment Table for decompression sickness recommends 100% oxygen at 2.8 ATA. Chambers may hold one or more patients at a time.
The frequency of therapy varies but often consists of 20-60 sessions lasting 90-120 minutes. For off-label use like TBI, patients usually pay out of pocket. Given the multiple treatments, costs can add up.
Inconsistent evidence and sham controls
The unwieldy 33-page evidence review by Hadanny and colleagues cites multiple studies supporting HBOT for TBI. However, many, if not all, suffer from methodological flaws. These include vague inclusion criteria, lack of a control group, small patient numbers, treatment at different times since injury, poorly defined or varying HBOT protocols, varying outcome measures, and superficial results analysis.
A sham or control arm is essential for HBOT research trials, given the potential placebo effect of placing a human being inside a large, high-tech, sealed tube for an hour or more. In some sham-controlled studies, which consisted of low-pressure oxygen (that is, 1.3 ATA as sham vs. 2.4 ATA as treatment), all groups experienced symptom improvement. The review authors argue that the low-dose HBOT sham arms were biologically active and that the improvements seen mean that both high- and low-dose HBOT is therapeutic. The alternative explanation is that the placebo effect accounted for improvement in both groups.
The late Michael Bennett, a world authority on hyperbaric and underwater medicine, doubted that conventional HBOT sham controls could genuinely have a therapeutic effect, and I agree. The upcoming HOT-POCS trial (discussed below) should answer the question more definitively.
Mechanisms of action and safety
Mechanisms of benefit for HBOT include increased oxygen availability and angiogenesis. Animal research suggests that it may reduce secondary cell death from TBI, through stabilization of the blood-brain barrier and inflammation reduction.
HBOT is generally safe and well tolerated. A retrospective analysis of 1.5 million outpatient hyperbaric treatments revealed that less than 1% were associated with adverse events. The most common were ear and sinus barotrauma. Because HBOT uses increased air pressure, patients must equalize their ears and sinuses. Those who cannot because of altered consciousness, anatomical defects, or congestion must undergo myringotomy or terminate therapy. Claustrophobia was the second most common adverse effect. Convulsions and tension pneumocephalus were rare.
Perhaps the most concerning risk of HBOT for patients with TBI is the potential waste of human and financial resources.
Desperate physicians and patients
As a neurologist who regularly treats patients with TBI, I share the review authors’ frustration regarding the limited efficacy of available treatments. However, the suboptimal efficacy of currently available therapy is insufficient justification to recommend HBOT.
With respect to chronic TBI, it is difficult to imagine how HBOT could reverse brain injury that has been present for months or years. No other therapy exists that reliably encourages neuronal regeneration or prevents the development of posttraumatic epilepsy.
Frank Conidi, MD, a board-certified sports neurologist and headache specialist, shared his thoughts via email. He agrees that HBOT may have a role in TBI, but after reviewing Hadanny and colleagues’ paper, he concluded that there is insufficient evidence for the use of HBOT in all forms of TBI. He would like to see large multicenter, well-designed studies with standardized pressures and duration and a standard definition of the various types of head injury.
Ongoing research
There are at least five ongoing trials on HBOT for TBI or postconcussive syndrome, including the well-designed placebo-controlled HOT-POCS study. The latter has a novel placebo gas system that addresses Hadanny and colleagues’ contention that even low-dose HBOT might be effective.
The placebo arm in HOT-POCS mimics the HBO environment but provides only 0.21 ATA of oxygen, the same as room air. The active arm provides 100% oxygen at 2.0 ATA. If patients in both arms improve, the benefit will be caused by a placebo response, not HBOT.
Conflict of interest
Another concern with the review is that all three authors are affiliated with Aviv Scientific. This company has an exclusive partnership with the world’s largest hyperbaric medicine and research facility, the Sagol Center at Shamir Medical Center in Be’er Ya’akov, Israel.
This conflict of interest does not a priori invalidate their conclusions. However, official HBOT guidelines from a leading organization like the Undersea and Hyperbaric Medicine Society or the American Academy of Neurology would be preferable.
Conclusion
There is an urgent unmet need for more effective treatments for postconcussive syndrome and chronic TBI.
The review authors’ recommendations for HBOT seem premature. They are arguably a disservice to the many desperate patients and their families who will be tempted to expend valuable resources of time and money for an appealing but unproven therapy. Appropriately designed placebo-controlled studies such as HOT-POCS will help separate fact from wishful thinking.
Dr. Wilner is associate professor of neurology at University of Tennessee Health Science Center, Memphis. He reported a conflict of interest with Accordant Health Services.
A version of this article first appeared on Medscape.com.
Loneliness tied to increased risk for Parkinson’s disease
TOPLINE:
Loneliness is associated with a higher risk of developing Parkinson’s disease (PD) across demographic groups and independent of other risk factors, data from nearly 500,000 U.K. adults suggest.
METHODOLOGY:
- Loneliness is associated with illness and death, including higher risk of neurodegenerative diseases, but no study has examined whether the association between loneliness and detrimental outcomes extends to PD.
- The current analysis included 491,603 U.K. Biobank participants (mean age, 56; 54% women) without a diagnosis of PD at baseline.
- Loneliness was assessed by a single question at baseline and incident PD was ascertained via health records over 15 years.
- Researchers assessed whether the association between loneliness and PD was moderated by age, sex, or genetic risk and whether the association was accounted for by sociodemographic factors; behavioral, mental, physical, or social factors; or genetic risk.
TAKEAWAY:
- Roughly 19% of the cohort reported being lonely. Compared with those who were not lonely, those who did report being lonely were slightly younger and were more likely to be women. They also had fewer resources, more health risk behaviors (current smoker and physically inactive), and worse physical and mental health.
- Over 15+ years of follow-up, 2,822 participants developed PD (incidence rate: 47 per 100,000 person-years). Compared with those who did not develop PD, those who did were older and more likely to be male, former smokers, have higher BMI and PD polygenetic risk score, and to have diabetes, hypertension, myocardial infarction or stroke, anxiety, or depression.
- In the primary analysis, individuals who reported being lonely had a higher risk for PD (hazard ratio, 1.37) – an association that remained after accounting for demographic and socioeconomic status, social isolation, PD polygenetic risk score, smoking, physical activity, BMI, diabetes, hypertension, stroke, myocardial infarction, depression, and having ever seen a psychiatrist (fully adjusted HR, 1.25).
- The association between loneliness and incident PD was not moderated by sex, age, or polygenetic risk score.
- Contrary to expectations for a prodromal syndrome, loneliness was not associated with incident PD in the first 5 years after baseline but was associated with PD risk in the subsequent 10 years of follow-up (HR, 1.32).
IN PRACTICE:
“Our findings complement other evidence that loneliness is a psychosocial determinant of health associated with increased risk of morbidity and mortality [and] supports recent calls for the protective and healing effects of personally meaningful social connection,” the authors write.
SOURCE:
The study, with first author Antonio Terracciano, PhD, of Florida State University College of Medicine, Tallahassee, was published online in JAMA Neurology.
LIMITATIONS:
This observational study could not determine causality or whether reverse causality could explain the association. Loneliness was assessed by a single yes/no question. PD diagnosis relied on hospital admission and death records and may have missed early PD diagnoses.
DISCLOSURES:
Funding for the study was provided by the National Institutes of Health and National Institute on Aging. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
Loneliness is associated with a higher risk of developing Parkinson’s disease (PD) across demographic groups and independent of other risk factors, data from nearly 500,000 U.K. adults suggest.
METHODOLOGY:
- Loneliness is associated with illness and death, including higher risk of neurodegenerative diseases, but no study has examined whether the association between loneliness and detrimental outcomes extends to PD.
- The current analysis included 491,603 U.K. Biobank participants (mean age, 56; 54% women) without a diagnosis of PD at baseline.
- Loneliness was assessed by a single question at baseline and incident PD was ascertained via health records over 15 years.
- Researchers assessed whether the association between loneliness and PD was moderated by age, sex, or genetic risk and whether the association was accounted for by sociodemographic factors; behavioral, mental, physical, or social factors; or genetic risk.
TAKEAWAY:
- Roughly 19% of the cohort reported being lonely. Compared with those who were not lonely, those who did report being lonely were slightly younger and were more likely to be women. They also had fewer resources, more health risk behaviors (current smoker and physically inactive), and worse physical and mental health.
- Over 15+ years of follow-up, 2,822 participants developed PD (incidence rate: 47 per 100,000 person-years). Compared with those who did not develop PD, those who did were older and more likely to be male, former smokers, have higher BMI and PD polygenetic risk score, and to have diabetes, hypertension, myocardial infarction or stroke, anxiety, or depression.
- In the primary analysis, individuals who reported being lonely had a higher risk for PD (hazard ratio, 1.37) – an association that remained after accounting for demographic and socioeconomic status, social isolation, PD polygenetic risk score, smoking, physical activity, BMI, diabetes, hypertension, stroke, myocardial infarction, depression, and having ever seen a psychiatrist (fully adjusted HR, 1.25).
- The association between loneliness and incident PD was not moderated by sex, age, or polygenetic risk score.
- Contrary to expectations for a prodromal syndrome, loneliness was not associated with incident PD in the first 5 years after baseline but was associated with PD risk in the subsequent 10 years of follow-up (HR, 1.32).
IN PRACTICE:
“Our findings complement other evidence that loneliness is a psychosocial determinant of health associated with increased risk of morbidity and mortality [and] supports recent calls for the protective and healing effects of personally meaningful social connection,” the authors write.
SOURCE:
The study, with first author Antonio Terracciano, PhD, of Florida State University College of Medicine, Tallahassee, was published online in JAMA Neurology.
LIMITATIONS:
This observational study could not determine causality or whether reverse causality could explain the association. Loneliness was assessed by a single yes/no question. PD diagnosis relied on hospital admission and death records and may have missed early PD diagnoses.
DISCLOSURES:
Funding for the study was provided by the National Institutes of Health and National Institute on Aging. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
Loneliness is associated with a higher risk of developing Parkinson’s disease (PD) across demographic groups and independent of other risk factors, data from nearly 500,000 U.K. adults suggest.
METHODOLOGY:
- Loneliness is associated with illness and death, including higher risk of neurodegenerative diseases, but no study has examined whether the association between loneliness and detrimental outcomes extends to PD.
- The current analysis included 491,603 U.K. Biobank participants (mean age, 56; 54% women) without a diagnosis of PD at baseline.
- Loneliness was assessed by a single question at baseline and incident PD was ascertained via health records over 15 years.
- Researchers assessed whether the association between loneliness and PD was moderated by age, sex, or genetic risk and whether the association was accounted for by sociodemographic factors; behavioral, mental, physical, or social factors; or genetic risk.
TAKEAWAY:
- Roughly 19% of the cohort reported being lonely. Compared with those who were not lonely, those who did report being lonely were slightly younger and were more likely to be women. They also had fewer resources, more health risk behaviors (current smoker and physically inactive), and worse physical and mental health.
- Over 15+ years of follow-up, 2,822 participants developed PD (incidence rate: 47 per 100,000 person-years). Compared with those who did not develop PD, those who did were older and more likely to be male, former smokers, have higher BMI and PD polygenetic risk score, and to have diabetes, hypertension, myocardial infarction or stroke, anxiety, or depression.
- In the primary analysis, individuals who reported being lonely had a higher risk for PD (hazard ratio, 1.37) – an association that remained after accounting for demographic and socioeconomic status, social isolation, PD polygenetic risk score, smoking, physical activity, BMI, diabetes, hypertension, stroke, myocardial infarction, depression, and having ever seen a psychiatrist (fully adjusted HR, 1.25).
- The association between loneliness and incident PD was not moderated by sex, age, or polygenetic risk score.
- Contrary to expectations for a prodromal syndrome, loneliness was not associated with incident PD in the first 5 years after baseline but was associated with PD risk in the subsequent 10 years of follow-up (HR, 1.32).
IN PRACTICE:
“Our findings complement other evidence that loneliness is a psychosocial determinant of health associated with increased risk of morbidity and mortality [and] supports recent calls for the protective and healing effects of personally meaningful social connection,” the authors write.
SOURCE:
The study, with first author Antonio Terracciano, PhD, of Florida State University College of Medicine, Tallahassee, was published online in JAMA Neurology.
LIMITATIONS:
This observational study could not determine causality or whether reverse causality could explain the association. Loneliness was assessed by a single yes/no question. PD diagnosis relied on hospital admission and death records and may have missed early PD diagnoses.
DISCLOSURES:
Funding for the study was provided by the National Institutes of Health and National Institute on Aging. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The surprising link between loneliness and Parkinson’s disease
This transcript has been edited for clarity.
On May 3, 2023, Surgeon General Vivek Murthy issued an advisory raising an alarm about what he called an “epidemic of loneliness” in the United States.
Now, I am not saying that Vivek Murthy read my book, “How Medicine Works and When It Doesn’t” – released in January and available in bookstores now – where, in chapter 11, I call attention to the problem of loneliness and its relationship to the exponential rise in deaths of despair. But Vivek, if you did, let me know. I could use the publicity.
No, of course the idea that loneliness is a public health issue is not new, but I’m glad to see it finally getting attention. At this point, studies have linked loneliness to heart disease, stroke, dementia, and premature death.
The UK Biobank is really a treasure trove of data for epidemiologists. I must see three to four studies a week coming out of this mega-dataset. This one, appearing in JAMA Neurology, caught my eye for its focus specifically on loneliness as a risk factor – something I’m hoping to see more of in the future.
The study examines data from just under 500,000 individuals in the United Kingdom who answered a survey including the question “Do you often feel lonely?” between 2006 and 2010; 18.4% of people answered yes. Individuals’ electronic health record data were then monitored over time to see who would get a new diagnosis code consistent with Parkinson’s disease. Through 2021, 2822 people did – that’s just over half a percent.
So, now we do the statistics thing. Of the nonlonely folks, 2,273 went on to develop Parkinson’s disease. Of those who said they often feel lonely, 549 people did. The raw numbers here, to be honest, aren’t that compelling. Lonely people had an absolute risk for Parkinson’s disease about 0.03% higher than that of nonlonely people. Put another way, you’d need to take over 3,000 lonely souls and make them not lonely to prevent 1 case of Parkinson’s disease.
Still, the costs of loneliness are not measured exclusively in Parkinson’s disease, and I would argue that the real risks here come from other sources: alcohol abuse, drug abuse, and suicide. Nevertheless, the weak but significant association with Parkinson’s disease reminds us that loneliness is a neurologic phenomenon. There is something about social connection that affects our brain in a way that is not just spiritual; it is actually biological.
Of course, people who say they are often lonely are different in other ways from people who report not being lonely. Lonely people, in this dataset, were younger, more likely to be female, less likely to have a college degree, in worse physical health, and engaged in more high-risk health behaviors like smoking.
The authors adjusted for all of these factors and found that, on the relative scale, lonely people were still about 20%-30% more likely to develop Parkinson’s disease.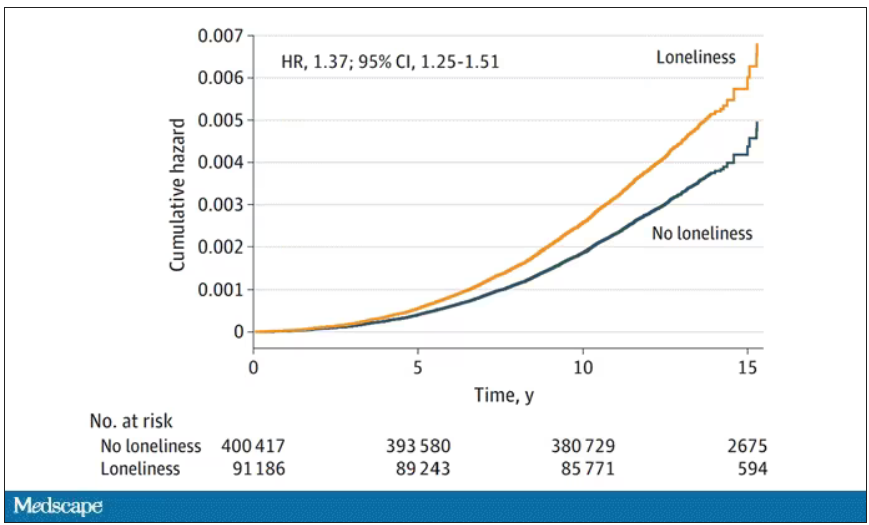
So, what do we do about this? There is no pill for loneliness, and God help us if there ever is. Recognizing the problem is a good start. But there are some policy things we can do to reduce loneliness. We can invest in public spaces that bring people together – parks, museums, libraries – and public transportation. We can deal with tech companies that are so optimized at capturing our attention that we cease to engage with other humans. And, individually, we can just reach out a bit more. We’ve spent the past few pandemic years with our attention focused sharply inward. It’s time to look out again.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
On May 3, 2023, Surgeon General Vivek Murthy issued an advisory raising an alarm about what he called an “epidemic of loneliness” in the United States.
Now, I am not saying that Vivek Murthy read my book, “How Medicine Works and When It Doesn’t” – released in January and available in bookstores now – where, in chapter 11, I call attention to the problem of loneliness and its relationship to the exponential rise in deaths of despair. But Vivek, if you did, let me know. I could use the publicity.
No, of course the idea that loneliness is a public health issue is not new, but I’m glad to see it finally getting attention. At this point, studies have linked loneliness to heart disease, stroke, dementia, and premature death.
The UK Biobank is really a treasure trove of data for epidemiologists. I must see three to four studies a week coming out of this mega-dataset. This one, appearing in JAMA Neurology, caught my eye for its focus specifically on loneliness as a risk factor – something I’m hoping to see more of in the future.
The study examines data from just under 500,000 individuals in the United Kingdom who answered a survey including the question “Do you often feel lonely?” between 2006 and 2010; 18.4% of people answered yes. Individuals’ electronic health record data were then monitored over time to see who would get a new diagnosis code consistent with Parkinson’s disease. Through 2021, 2822 people did – that’s just over half a percent.
So, now we do the statistics thing. Of the nonlonely folks, 2,273 went on to develop Parkinson’s disease. Of those who said they often feel lonely, 549 people did. The raw numbers here, to be honest, aren’t that compelling. Lonely people had an absolute risk for Parkinson’s disease about 0.03% higher than that of nonlonely people. Put another way, you’d need to take over 3,000 lonely souls and make them not lonely to prevent 1 case of Parkinson’s disease.
Still, the costs of loneliness are not measured exclusively in Parkinson’s disease, and I would argue that the real risks here come from other sources: alcohol abuse, drug abuse, and suicide. Nevertheless, the weak but significant association with Parkinson’s disease reminds us that loneliness is a neurologic phenomenon. There is something about social connection that affects our brain in a way that is not just spiritual; it is actually biological.
Of course, people who say they are often lonely are different in other ways from people who report not being lonely. Lonely people, in this dataset, were younger, more likely to be female, less likely to have a college degree, in worse physical health, and engaged in more high-risk health behaviors like smoking.
The authors adjusted for all of these factors and found that, on the relative scale, lonely people were still about 20%-30% more likely to develop Parkinson’s disease.
So, what do we do about this? There is no pill for loneliness, and God help us if there ever is. Recognizing the problem is a good start. But there are some policy things we can do to reduce loneliness. We can invest in public spaces that bring people together – parks, museums, libraries – and public transportation. We can deal with tech companies that are so optimized at capturing our attention that we cease to engage with other humans. And, individually, we can just reach out a bit more. We’ve spent the past few pandemic years with our attention focused sharply inward. It’s time to look out again.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
On May 3, 2023, Surgeon General Vivek Murthy issued an advisory raising an alarm about what he called an “epidemic of loneliness” in the United States.
Now, I am not saying that Vivek Murthy read my book, “How Medicine Works and When It Doesn’t” – released in January and available in bookstores now – where, in chapter 11, I call attention to the problem of loneliness and its relationship to the exponential rise in deaths of despair. But Vivek, if you did, let me know. I could use the publicity.
No, of course the idea that loneliness is a public health issue is not new, but I’m glad to see it finally getting attention. At this point, studies have linked loneliness to heart disease, stroke, dementia, and premature death.
The UK Biobank is really a treasure trove of data for epidemiologists. I must see three to four studies a week coming out of this mega-dataset. This one, appearing in JAMA Neurology, caught my eye for its focus specifically on loneliness as a risk factor – something I’m hoping to see more of in the future.
The study examines data from just under 500,000 individuals in the United Kingdom who answered a survey including the question “Do you often feel lonely?” between 2006 and 2010; 18.4% of people answered yes. Individuals’ electronic health record data were then monitored over time to see who would get a new diagnosis code consistent with Parkinson’s disease. Through 2021, 2822 people did – that’s just over half a percent.
So, now we do the statistics thing. Of the nonlonely folks, 2,273 went on to develop Parkinson’s disease. Of those who said they often feel lonely, 549 people did. The raw numbers here, to be honest, aren’t that compelling. Lonely people had an absolute risk for Parkinson’s disease about 0.03% higher than that of nonlonely people. Put another way, you’d need to take over 3,000 lonely souls and make them not lonely to prevent 1 case of Parkinson’s disease.
Still, the costs of loneliness are not measured exclusively in Parkinson’s disease, and I would argue that the real risks here come from other sources: alcohol abuse, drug abuse, and suicide. Nevertheless, the weak but significant association with Parkinson’s disease reminds us that loneliness is a neurologic phenomenon. There is something about social connection that affects our brain in a way that is not just spiritual; it is actually biological.
Of course, people who say they are often lonely are different in other ways from people who report not being lonely. Lonely people, in this dataset, were younger, more likely to be female, less likely to have a college degree, in worse physical health, and engaged in more high-risk health behaviors like smoking.
The authors adjusted for all of these factors and found that, on the relative scale, lonely people were still about 20%-30% more likely to develop Parkinson’s disease.
So, what do we do about this? There is no pill for loneliness, and God help us if there ever is. Recognizing the problem is a good start. But there are some policy things we can do to reduce loneliness. We can invest in public spaces that bring people together – parks, museums, libraries – and public transportation. We can deal with tech companies that are so optimized at capturing our attention that we cease to engage with other humans. And, individually, we can just reach out a bit more. We’ve spent the past few pandemic years with our attention focused sharply inward. It’s time to look out again.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Data Trends 2023: Migraine and Headache
22. Seng EK et al. Neurology. 2022;99(18):e1979-e1992. doi:10.1212/WNL.0000000000200888
23. Coffman C et al. Neurology. 2022;99(2):e187-e198. doi:10.1212/WNL.0000000000200518
24. Hesselbrock RR et al. Aerosp Med Hum Perform. 2022;93(1):26-31. doi:10.3357/amhp.5980.2022
25. Kuruvilla DE et al. BMC Complement Med Ther. 2022;22(1):22. doi:10.1186/s12906-022-03511-6
22. Seng EK et al. Neurology. 2022;99(18):e1979-e1992. doi:10.1212/WNL.0000000000200888
23. Coffman C et al. Neurology. 2022;99(2):e187-e198. doi:10.1212/WNL.0000000000200518
24. Hesselbrock RR et al. Aerosp Med Hum Perform. 2022;93(1):26-31. doi:10.3357/amhp.5980.2022
25. Kuruvilla DE et al. BMC Complement Med Ther. 2022;22(1):22. doi:10.1186/s12906-022-03511-6
22. Seng EK et al. Neurology. 2022;99(18):e1979-e1992. doi:10.1212/WNL.0000000000200888
23. Coffman C et al. Neurology. 2022;99(2):e187-e198. doi:10.1212/WNL.0000000000200518
24. Hesselbrock RR et al. Aerosp Med Hum Perform. 2022;93(1):26-31. doi:10.3357/amhp.5980.2022
25. Kuruvilla DE et al. BMC Complement Med Ther. 2022;22(1):22. doi:10.1186/s12906-022-03511-6