User login
For MD-IQ use only
HM19: Interprofessional rounds
Better process, outcomes
Session presenters
Surekha Bhamidipati, MD, FACP; Preetham Talari, MD, FACP, SFHM; Mark V. Williams, MD, FACP, MHM
Session title
Interprofessional rounds: What’s the right way?
Session summary
Interprofessional or multidisciplinary rounds involve all members of the care delivery team, including physicians, nurses, case managers, social workers, pharmacists, nurse facilitators, and of course, patients. The primary goal for these rounds is patient-centered care, and to improve communication among the health care team members, as well as with patients and their families.
At HM19, Dr. Preetham Talari and Dr. Mark Williams of the University of Kentucky, and Dr. Surekha Bhamidipati of Christiana Care Health System in Newark, Del., discussed their system-based efforts to try to implement interprofessional rounds, and the role of these rounds in improving patient outcome measures.
The presenters noted that the purpose of these rounds is effective communication and efficient patient care. As shown by multiple studies, there is significant impact in team member satisfaction, decrease in length of stay,1 reduction in adverse events2 and improvement in patient experience.3 They emphasized the importance of implementing these rounds at the bedside, so that patients and families can be engaged in the patient’s care, thereby improving closed communication among the team and the patient. These rounds always offer an opportunity for the patient to ask questions of multiple health care team members as they are gathered together at the same time.

The University of Kentucky named these rounds the “Interprofessional Teamwork Innovation Model (ITIM),” to promote communication and patient-centered coordinated care. Their model showed a significant reduction in readmission rates, and no increase in costs despite adding pharmacy and case managers to the rounds.
Dr. Bhamidipati described how Christiana Care Health System designed multidisciplinary rounds based on the application of Team STEPPS 2.0, a teamwork system developed by the Department of Defense and the Agency for Healthcare Research and Quality to improve the institutional collaboration and communication relating to patient safety.

The Christiana Care model is based on a few principles of team structure, communication, leadership, situation monitoring, and mutual support. The interprofessional team was trained and observed, and a short video recording was made. This video was used as an educational tool in coaching the rest of the team. Dr. Bhamidipati described the importance of interprofessional leaders as coaches to train other team members, and highlighted the engagement of unit leaders in successfully implementing these rounds. The Christiana Care team used its informational technology system to collect real-time data, which was then used for team review.
In summary, the presenters from both the University of Kentucky and Christiana Care highlighted the importance of interprofessional rounds, as well as the need for continued measurement of process and outcome metrics.
Dr. Jonnalagadda is a physician advisor, and Dr. Medarametla is medical director, Hospital Medicine, at Baystate Medical Center, Springfield, Mass.
References
1. Yoo JW et al. Effects of an internal medicine floor interdisciplinary team on hospital and clinical outcomes of seniors with acute medical illness. Geriatr Gerontol Int. 2013 Oct;13(4):942-8. doi: 10.1111/ggi.12035. Epub 2013 Feb 26.
2. O’Leary KJ et al. Structured interdisciplinary rounds in a medical teaching unit: improving patient safety. Arch Intern Med. 2011 Apr 11;171(7):678-84. doi: 10.1001/archinternmed.2011.128.
3. Ratelle JT et al. Implementing bedside rounds to improve patient-centred outcomes: a systematic review. BMJ Qual Saf. 2019;28:317-326.
Better process, outcomes
Better process, outcomes
Session presenters
Surekha Bhamidipati, MD, FACP; Preetham Talari, MD, FACP, SFHM; Mark V. Williams, MD, FACP, MHM
Session title
Interprofessional rounds: What’s the right way?
Session summary
Interprofessional or multidisciplinary rounds involve all members of the care delivery team, including physicians, nurses, case managers, social workers, pharmacists, nurse facilitators, and of course, patients. The primary goal for these rounds is patient-centered care, and to improve communication among the health care team members, as well as with patients and their families.
At HM19, Dr. Preetham Talari and Dr. Mark Williams of the University of Kentucky, and Dr. Surekha Bhamidipati of Christiana Care Health System in Newark, Del., discussed their system-based efforts to try to implement interprofessional rounds, and the role of these rounds in improving patient outcome measures.
The presenters noted that the purpose of these rounds is effective communication and efficient patient care. As shown by multiple studies, there is significant impact in team member satisfaction, decrease in length of stay,1 reduction in adverse events2 and improvement in patient experience.3 They emphasized the importance of implementing these rounds at the bedside, so that patients and families can be engaged in the patient’s care, thereby improving closed communication among the team and the patient. These rounds always offer an opportunity for the patient to ask questions of multiple health care team members as they are gathered together at the same time.
The University of Kentucky named these rounds the “Interprofessional Teamwork Innovation Model (ITIM),” to promote communication and patient-centered coordinated care. Their model showed a significant reduction in readmission rates, and no increase in costs despite adding pharmacy and case managers to the rounds.
Dr. Bhamidipati described how Christiana Care Health System designed multidisciplinary rounds based on the application of Team STEPPS 2.0, a teamwork system developed by the Department of Defense and the Agency for Healthcare Research and Quality to improve the institutional collaboration and communication relating to patient safety.
The Christiana Care model is based on a few principles of team structure, communication, leadership, situation monitoring, and mutual support. The interprofessional team was trained and observed, and a short video recording was made. This video was used as an educational tool in coaching the rest of the team. Dr. Bhamidipati described the importance of interprofessional leaders as coaches to train other team members, and highlighted the engagement of unit leaders in successfully implementing these rounds. The Christiana Care team used its informational technology system to collect real-time data, which was then used for team review.
In summary, the presenters from both the University of Kentucky and Christiana Care highlighted the importance of interprofessional rounds, as well as the need for continued measurement of process and outcome metrics.
Dr. Jonnalagadda is a physician advisor, and Dr. Medarametla is medical director, Hospital Medicine, at Baystate Medical Center, Springfield, Mass.
References
1. Yoo JW et al. Effects of an internal medicine floor interdisciplinary team on hospital and clinical outcomes of seniors with acute medical illness. Geriatr Gerontol Int. 2013 Oct;13(4):942-8. doi: 10.1111/ggi.12035. Epub 2013 Feb 26.
2. O’Leary KJ et al. Structured interdisciplinary rounds in a medical teaching unit: improving patient safety. Arch Intern Med. 2011 Apr 11;171(7):678-84. doi: 10.1001/archinternmed.2011.128.
3. Ratelle JT et al. Implementing bedside rounds to improve patient-centred outcomes: a systematic review. BMJ Qual Saf. 2019;28:317-326.
Session presenters
Surekha Bhamidipati, MD, FACP; Preetham Talari, MD, FACP, SFHM; Mark V. Williams, MD, FACP, MHM
Session title
Interprofessional rounds: What’s the right way?
Session summary
Interprofessional or multidisciplinary rounds involve all members of the care delivery team, including physicians, nurses, case managers, social workers, pharmacists, nurse facilitators, and of course, patients. The primary goal for these rounds is patient-centered care, and to improve communication among the health care team members, as well as with patients and their families.
At HM19, Dr. Preetham Talari and Dr. Mark Williams of the University of Kentucky, and Dr. Surekha Bhamidipati of Christiana Care Health System in Newark, Del., discussed their system-based efforts to try to implement interprofessional rounds, and the role of these rounds in improving patient outcome measures.
The presenters noted that the purpose of these rounds is effective communication and efficient patient care. As shown by multiple studies, there is significant impact in team member satisfaction, decrease in length of stay,1 reduction in adverse events2 and improvement in patient experience.3 They emphasized the importance of implementing these rounds at the bedside, so that patients and families can be engaged in the patient’s care, thereby improving closed communication among the team and the patient. These rounds always offer an opportunity for the patient to ask questions of multiple health care team members as they are gathered together at the same time.
The University of Kentucky named these rounds the “Interprofessional Teamwork Innovation Model (ITIM),” to promote communication and patient-centered coordinated care. Their model showed a significant reduction in readmission rates, and no increase in costs despite adding pharmacy and case managers to the rounds.
Dr. Bhamidipati described how Christiana Care Health System designed multidisciplinary rounds based on the application of Team STEPPS 2.0, a teamwork system developed by the Department of Defense and the Agency for Healthcare Research and Quality to improve the institutional collaboration and communication relating to patient safety.
The Christiana Care model is based on a few principles of team structure, communication, leadership, situation monitoring, and mutual support. The interprofessional team was trained and observed, and a short video recording was made. This video was used as an educational tool in coaching the rest of the team. Dr. Bhamidipati described the importance of interprofessional leaders as coaches to train other team members, and highlighted the engagement of unit leaders in successfully implementing these rounds. The Christiana Care team used its informational technology system to collect real-time data, which was then used for team review.
In summary, the presenters from both the University of Kentucky and Christiana Care highlighted the importance of interprofessional rounds, as well as the need for continued measurement of process and outcome metrics.
Dr. Jonnalagadda is a physician advisor, and Dr. Medarametla is medical director, Hospital Medicine, at Baystate Medical Center, Springfield, Mass.
References
1. Yoo JW et al. Effects of an internal medicine floor interdisciplinary team on hospital and clinical outcomes of seniors with acute medical illness. Geriatr Gerontol Int. 2013 Oct;13(4):942-8. doi: 10.1111/ggi.12035. Epub 2013 Feb 26.
2. O’Leary KJ et al. Structured interdisciplinary rounds in a medical teaching unit: improving patient safety. Arch Intern Med. 2011 Apr 11;171(7):678-84. doi: 10.1001/archinternmed.2011.128.
3. Ratelle JT et al. Implementing bedside rounds to improve patient-centred outcomes: a systematic review. BMJ Qual Saf. 2019;28:317-326.
What We Don’t Know About Osteoporosis Treatment
A 5-member panel of experts in primary care, geriatrics, and behavioral sciences, among others, convened by the National Institutes of Health (NIH), sought to answer that question. In the Pathways to Prevention (P2P) Workshop: Appropriate Use of Drug Therapies for Osteoporotic Fracture Prevention, the panel discussed the available evidence on long-term drug therapies, in hopes of identifying research gaps and ways to “advance the field.” Then they published a report that summarizes their findings, along with recommendations for “new strengthened research.”
Trials have found 3 to 5 years of ODT is safe and effective, the panel notes, and that some ODTs reduce the incidence of nonvertebral fractures. But those studies have been done mainly in white postmenopausal women. Men, people of other race and ethnicity, residents in facilities, people with advanced and multiple comorbid conditions, and other populations are absent or underrepresented. Thus, estimates on benefits and harms may differ in practice. Moreover, the trial results presented no data on nonfracture patient outcomes or sequelae, such as mobility, hospitalizations, and nursing home placement. The studies also offered limited or no evidence on whether patient characteristics would result in different fracture outcomes.
The panel also noted that few trials extended beyond 5 years, although some observational studies provided “limited evidence” on potential benefits and harms from longer term use. Gaps exist in how to use information on bone biomarkers and other patient characteristics, such as concurrent medication use, that might modify the effects of ODT, the panel concluded.
One of the main issues the panel investigated was how to make sure that the people at highest risk of fracture get the medicine they need. Only about one-third of women at high risk have reported treatment with osteoporosis medication. And among older adults with a hip fracture, only 11% to 13% filled any prescription for osteoporosis medication within 3 months of the fracture.
Information about ODT use and adherence was not included in the systematic evidence review, so the report relies on material provided by the workshop speakers, who say low rates of diagnosis and treatment probably stem from multiple clinician and patient factors. For instance, they said, with regard to clinicians, the problems may be lack of time, knowledge gaps, and lack of appropriate systems in primary care.
The panelists also cited another gap: in communication between clinicians about treatment as patients transition from one setting to another. One solution could be a hospital-based fracture liaison service to coordinate care, they suggest.
Patient factors include perceptions that osteoporosis is a normal part of aging, or that drugs do not work or that they are harmful and risky. Studies about decision making have found that people often overestimate their risk for rare adverse effects (AEs) and underestimate the likelihood of having a fracture.
In their assessment of studies, the workshop panelists found education-based interventions sometimes increase rates of filled prescriptions but not adherence 6 or 10 months down the road. They also found coaching and counseling have been “largely ineffective.”
“We need to identify the reasons why,” the panelists concluded, and made a number of recommendations about how to do the research. For instance, they suggest using a broader array of trial designs, such as innovative platform trials as used in cancer research, where the target of the investigation is the disease and not the drug. Studies also should focus on fracture sequelae, and include diverse populations that “more closely match” the characteristics of people who actually have fractures.
Gaps in knowledge about the uncommon AEs reported with bisphosphonates and other questions mean questions to be answered include which class of drugs should be used first, when treatment should start and how long it should last, and which doses are preferable.
Knowing how to treat can help clinicians and their patients decide whom to treat, the report suggests. Addressing the research gaps will improve the shared decision making needed for answering those questions.
The report was published in Annals of Internal Medicine on April 23, 2019.
A 5-member panel of experts in primary care, geriatrics, and behavioral sciences, among others, convened by the National Institutes of Health (NIH), sought to answer that question. In the Pathways to Prevention (P2P) Workshop: Appropriate Use of Drug Therapies for Osteoporotic Fracture Prevention, the panel discussed the available evidence on long-term drug therapies, in hopes of identifying research gaps and ways to “advance the field.” Then they published a report that summarizes their findings, along with recommendations for “new strengthened research.”
Trials have found 3 to 5 years of ODT is safe and effective, the panel notes, and that some ODTs reduce the incidence of nonvertebral fractures. But those studies have been done mainly in white postmenopausal women. Men, people of other race and ethnicity, residents in facilities, people with advanced and multiple comorbid conditions, and other populations are absent or underrepresented. Thus, estimates on benefits and harms may differ in practice. Moreover, the trial results presented no data on nonfracture patient outcomes or sequelae, such as mobility, hospitalizations, and nursing home placement. The studies also offered limited or no evidence on whether patient characteristics would result in different fracture outcomes.
The panel also noted that few trials extended beyond 5 years, although some observational studies provided “limited evidence” on potential benefits and harms from longer term use. Gaps exist in how to use information on bone biomarkers and other patient characteristics, such as concurrent medication use, that might modify the effects of ODT, the panel concluded.
One of the main issues the panel investigated was how to make sure that the people at highest risk of fracture get the medicine they need. Only about one-third of women at high risk have reported treatment with osteoporosis medication. And among older adults with a hip fracture, only 11% to 13% filled any prescription for osteoporosis medication within 3 months of the fracture.
Information about ODT use and adherence was not included in the systematic evidence review, so the report relies on material provided by the workshop speakers, who say low rates of diagnosis and treatment probably stem from multiple clinician and patient factors. For instance, they said, with regard to clinicians, the problems may be lack of time, knowledge gaps, and lack of appropriate systems in primary care.
The panelists also cited another gap: in communication between clinicians about treatment as patients transition from one setting to another. One solution could be a hospital-based fracture liaison service to coordinate care, they suggest.
Patient factors include perceptions that osteoporosis is a normal part of aging, or that drugs do not work or that they are harmful and risky. Studies about decision making have found that people often overestimate their risk for rare adverse effects (AEs) and underestimate the likelihood of having a fracture.
In their assessment of studies, the workshop panelists found education-based interventions sometimes increase rates of filled prescriptions but not adherence 6 or 10 months down the road. They also found coaching and counseling have been “largely ineffective.”
“We need to identify the reasons why,” the panelists concluded, and made a number of recommendations about how to do the research. For instance, they suggest using a broader array of trial designs, such as innovative platform trials as used in cancer research, where the target of the investigation is the disease and not the drug. Studies also should focus on fracture sequelae, and include diverse populations that “more closely match” the characteristics of people who actually have fractures.
Gaps in knowledge about the uncommon AEs reported with bisphosphonates and other questions mean questions to be answered include which class of drugs should be used first, when treatment should start and how long it should last, and which doses are preferable.
Knowing how to treat can help clinicians and their patients decide whom to treat, the report suggests. Addressing the research gaps will improve the shared decision making needed for answering those questions.
The report was published in Annals of Internal Medicine on April 23, 2019.
A 5-member panel of experts in primary care, geriatrics, and behavioral sciences, among others, convened by the National Institutes of Health (NIH), sought to answer that question. In the Pathways to Prevention (P2P) Workshop: Appropriate Use of Drug Therapies for Osteoporotic Fracture Prevention, the panel discussed the available evidence on long-term drug therapies, in hopes of identifying research gaps and ways to “advance the field.” Then they published a report that summarizes their findings, along with recommendations for “new strengthened research.”
Trials have found 3 to 5 years of ODT is safe and effective, the panel notes, and that some ODTs reduce the incidence of nonvertebral fractures. But those studies have been done mainly in white postmenopausal women. Men, people of other race and ethnicity, residents in facilities, people with advanced and multiple comorbid conditions, and other populations are absent or underrepresented. Thus, estimates on benefits and harms may differ in practice. Moreover, the trial results presented no data on nonfracture patient outcomes or sequelae, such as mobility, hospitalizations, and nursing home placement. The studies also offered limited or no evidence on whether patient characteristics would result in different fracture outcomes.
The panel also noted that few trials extended beyond 5 years, although some observational studies provided “limited evidence” on potential benefits and harms from longer term use. Gaps exist in how to use information on bone biomarkers and other patient characteristics, such as concurrent medication use, that might modify the effects of ODT, the panel concluded.
One of the main issues the panel investigated was how to make sure that the people at highest risk of fracture get the medicine they need. Only about one-third of women at high risk have reported treatment with osteoporosis medication. And among older adults with a hip fracture, only 11% to 13% filled any prescription for osteoporosis medication within 3 months of the fracture.
Information about ODT use and adherence was not included in the systematic evidence review, so the report relies on material provided by the workshop speakers, who say low rates of diagnosis and treatment probably stem from multiple clinician and patient factors. For instance, they said, with regard to clinicians, the problems may be lack of time, knowledge gaps, and lack of appropriate systems in primary care.
The panelists also cited another gap: in communication between clinicians about treatment as patients transition from one setting to another. One solution could be a hospital-based fracture liaison service to coordinate care, they suggest.
Patient factors include perceptions that osteoporosis is a normal part of aging, or that drugs do not work or that they are harmful and risky. Studies about decision making have found that people often overestimate their risk for rare adverse effects (AEs) and underestimate the likelihood of having a fracture.
In their assessment of studies, the workshop panelists found education-based interventions sometimes increase rates of filled prescriptions but not adherence 6 or 10 months down the road. They also found coaching and counseling have been “largely ineffective.”
“We need to identify the reasons why,” the panelists concluded, and made a number of recommendations about how to do the research. For instance, they suggest using a broader array of trial designs, such as innovative platform trials as used in cancer research, where the target of the investigation is the disease and not the drug. Studies also should focus on fracture sequelae, and include diverse populations that “more closely match” the characteristics of people who actually have fractures.
Gaps in knowledge about the uncommon AEs reported with bisphosphonates and other questions mean questions to be answered include which class of drugs should be used first, when treatment should start and how long it should last, and which doses are preferable.
Knowing how to treat can help clinicians and their patients decide whom to treat, the report suggests. Addressing the research gaps will improve the shared decision making needed for answering those questions.
The report was published in Annals of Internal Medicine on April 23, 2019.
Unit-based models of care
A tool for ensuring patient safety
“To me, teamwork is the beauty of our sport, where you have five acting as one. You become selfless.” – Mike Krzyzewski
High-performing teams plan, communicate, reflect, and take action together. Teamwork can transform seemingly impossible tasks into opportunities for people to come together and create value.

The increasing complexity of health care makes team-based care necessary to achieve successful health outcomes for patients. At the Brooklyn (N.Y.) Hospital Center, a 464-bed care center, we transformed the model of care on the medical wards into a geographic, unit-based team model. Here we describe our journey – the successes, the challenges, and the opportunities for growth.
Previous model
In the previous care model on our medical wards, no set structures were in place. Teams would travel to multiple wards throughout the hospital to see the patients they were rounding on. Each floor had its own set of social workers and case managers, therefore a hospital medicine team routinely dealt with more than eight social workers and case managers to address their patients’ needs in a single day.
Multidisciplinary rounds for all medical patients were held at 11 a.m. in a room located a significant distance away from the medical wards. All case managers and social workers would sit in this room from 11 a.m. until noon, and teams would travel to that room to discuss their patients.
Many challenges were identified in this model, including a lack of communication, a de-emphasis on teamwork, and a design that did not take physician workflows into account resulting in low efficiency. Thus, these challenges sparked a desire to create a more effective and team-based methodology of accomplishing excellence in delivery of clinical care. Dr. Pendharkar, having worked primarily in centers with unit-based care, determined that a geographic, unit-based model of care could transform care delivery at the Brooklyn Hospital Center.
Looking ahead
The efforts for transforming the vision of geographic, unit-based teams into a reality started by gathering all stakeholders together to unite for a common mission. Initial meetings were held with all parties including social workers, case managers, residents, nursing staff, bed board and attending physicians in internal medicine, and the emergency department.
The vision of a geographic, unit-based team was shared and explained to all team members. Exercises in LEAN methodology were conducted, including one-piece flow exercises, to highlight the possibilities of what could be accomplished through teamwork. Once support for the vision was in place from all parties, the logistics were addressed.
The biggest challenge to overcome was how to place all of one team’s patients on a singular medical ward. In our hospital, a medical ward holds anywhere from 30 to 33 patients. Each hospital medicine team, of which there are many, typically carries 20-23 patients. We created a blueprint to map out the floor to which each team and attending would be assigned. Next, we partnered with both IT and bed board to design an admission order set that specified the particular geographic location that a team and attending were associated with so that patients could be placed accordingly from the ED.
It was important for the ED doctors, bed board, and the internal medicine residents to understand these changes because all of these parties were involved in the initial admitting process. Dr. Pendharkar and Dr. Malieckal provided all groups with in-person training on how the logistics of the system would unfold. Noon conference lectures were also held to explain the vision to residents.
Over 3 weeks, the first ward we chose to implement our model on slowly accumulated the patients of one team – this was the gradual trickle phase. We then selected a “re-set” date. On the re-set date, it was determined that all patients would go to the team that was assigned to that floor, with the exception of any private attendings’ patients.
On the day before the re-set date, time was spent ensuring that all hand-offs were safe. Dr. Pendharkar and Dr. Malieckal spoke with every intern and team that would be handing off and/or receiving patients as a result of the re-set policy. The goal was to ensure that on that date a ward had close to 100% of its patients belonging to the team/attending that was assigned to that area.
The good
Once we began our geographic, unit-based model, our rounding process was transformed.
Now, our morning rounds were joined by the bedside nurse, case manager, social worker, clinical pharmacy, and nutrition in addition to the core team. The entire team went from room to room on one ward rounding on all 20 to 25 patients back to back, which created an unparalleled level of efficiency and a forum for effective communication lasting throughout the day.

We also added workstations on wheels (WOWS) to the rounding process so that labs, radiology, and more could be reviewed on rounds with the entire team. A standard script was developed so that each patient was introduced to all members of the team, and the care plan was disclosed and highlighted. One patient noted, “I feel so cared for, knowing I have this entire team taking care of me.” We also rounded in the afternoon with the case managers and social workers to follow up tasks that were to be completed that day.
Our first few weeks utilizing the geographic, unit-based model of rounding was largely successful. The residents, now able to round on all of their patients in one location with one case manager and one social worker, noted, “This model of rounding makes my life so much easier, I feel like I can focus on the patient rather than running around. … and I know the social worker and case manager will help me.”
Provider satisfaction had improved, from residents to physicians to nurses, case managers, social workers, and more. Our case manager also noted her satisfaction with the new model, stating that her communication with the medical team was much easier. As the attending, I witnessed firsthand how working together with the team moved care forward much more quickly, compared with the previous model, because of the simple factor of increased ease of communication.
Now all team members were together in the patient room and discussion was much easier. There was less confusion, fewer delays, and better communication – I think unit-based teams can even be described as a lifesaving measure that reduces harm to patients. An additional benefit is the relationship that now developed between doctors, social workers, and case managers – they spent more time together and really got to know one another, creating a feeling of shared success and a deeper drive to help one another succeed.
In our model, 87% of surveyed residents said they felt less burned out in the new geographic, unit-based model of care, and 91% of physicians surveyed said it was easier to talk with team members to coordinate care. Additionally, our HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) scores saw a drastic increase in many domains. Nursing communication improved by more than 42% on domain 7B; doctor communication improved by more than 31%. Additionally, all other domains saw at least 10% improvement. We are now 5 months out from our initial rollout of the model and continue to see sustained improvements in quality measures.
The bad
The biggest challenges that we are working through with this model are hand-offs and transfer of patients from one team to another. Sometimes, it happens that one team’s patient will wind up on a floor that is the designated floor of another team because of bed availability. We continue to work with bed board to address this issue. We want to minimize transfers and hand-offs to promote continuity and have to balance that with the need for geographic location. With clear communication, hospital collaboration from bed board and safe hand-off methods, this problem can be safely addressed.
Conclusions
The experience of implementing the unit-based team model has been an eye-opening journey. One thing that stands out is that, in an increasingly complex health care system, design thinking is critical.
Design thinking takes into consideration the needs of those who are using a system. In this case, patients and health care workers including doctors, nurses, case managers, and social workers are the end users of the health care system. All parties are utilizing the health care system to optimize patient health. Therefore, we must create systems that are easy to navigate and use by patients and health care workers so that they can ensure the success of patients.
Unit-based teams offer a basic framework to optimize the inpatient system to facilitate better workflow. In our system, it allowed us to optimize communications between health care workers and also between health care workers and patients. It allowed team members to work in close proximity to better share ideas with each other.
We spent a significant amount of time upfront earning the support of all of the disciplines for this effort. We had support from all leaders within the organization and continue to make our case for this model by sharing metrics and holding forums to discuss the process.
Initial data show a marked improvement in many domains of HCAHPS scores. Our frontline staff, including attendings, residents, nursing, case managers, and social workers, also continue to support this effort since it has a positive impact on their workflow and improves their workday quality. One nurse mentioned specifically, “in my 30 years at this hospital I have never seen people work together so well.”
To sustain this effort, we continue to have regular meetings, and there are new features that we would like to add to the program. For example, we are working with our IT group to ensure that each unit-based team will have dashboards available to incorporate real time, actionable data into daily workflows.
We are excited by the potential of our high-performing teams to highlight the patient experience, placing the patient at the center for care, decision making, and rounding. Health care is a team sport, and anytime you build something where all teams are playing together and approaching the finish line as a unit, you will never go wrong!
Dr. Pendharkar is division chief of hospital medicine at the Brooklyn (N.Y.) Hospital Center, medical director of inpatient services and director of quality for the department of medicine at the Brooklyn Hospital Center and assistant professor of medicine, Icahn School of Medicine at Mount Sinai, New York. Dr. Malieckal is chief resident, internal medicine, at the Brooklyn Hospital Center. Dr. Gasperino is chair, department of medicine; vice president for critical care, perioperative, and hospital medicine; and associate chief medical officer at the Brooklyn Hospital Center.
A tool for ensuring patient safety
A tool for ensuring patient safety
“To me, teamwork is the beauty of our sport, where you have five acting as one. You become selfless.” – Mike Krzyzewski
High-performing teams plan, communicate, reflect, and take action together. Teamwork can transform seemingly impossible tasks into opportunities for people to come together and create value.
The increasing complexity of health care makes team-based care necessary to achieve successful health outcomes for patients. At the Brooklyn (N.Y.) Hospital Center, a 464-bed care center, we transformed the model of care on the medical wards into a geographic, unit-based team model. Here we describe our journey – the successes, the challenges, and the opportunities for growth.
Previous model
In the previous care model on our medical wards, no set structures were in place. Teams would travel to multiple wards throughout the hospital to see the patients they were rounding on. Each floor had its own set of social workers and case managers, therefore a hospital medicine team routinely dealt with more than eight social workers and case managers to address their patients’ needs in a single day.
Multidisciplinary rounds for all medical patients were held at 11 a.m. in a room located a significant distance away from the medical wards. All case managers and social workers would sit in this room from 11 a.m. until noon, and teams would travel to that room to discuss their patients.
Many challenges were identified in this model, including a lack of communication, a de-emphasis on teamwork, and a design that did not take physician workflows into account resulting in low efficiency. Thus, these challenges sparked a desire to create a more effective and team-based methodology of accomplishing excellence in delivery of clinical care. Dr. Pendharkar, having worked primarily in centers with unit-based care, determined that a geographic, unit-based model of care could transform care delivery at the Brooklyn Hospital Center.
Looking ahead
The efforts for transforming the vision of geographic, unit-based teams into a reality started by gathering all stakeholders together to unite for a common mission. Initial meetings were held with all parties including social workers, case managers, residents, nursing staff, bed board and attending physicians in internal medicine, and the emergency department.
The vision of a geographic, unit-based team was shared and explained to all team members. Exercises in LEAN methodology were conducted, including one-piece flow exercises, to highlight the possibilities of what could be accomplished through teamwork. Once support for the vision was in place from all parties, the logistics were addressed.
The biggest challenge to overcome was how to place all of one team’s patients on a singular medical ward. In our hospital, a medical ward holds anywhere from 30 to 33 patients. Each hospital medicine team, of which there are many, typically carries 20-23 patients. We created a blueprint to map out the floor to which each team and attending would be assigned. Next, we partnered with both IT and bed board to design an admission order set that specified the particular geographic location that a team and attending were associated with so that patients could be placed accordingly from the ED.
It was important for the ED doctors, bed board, and the internal medicine residents to understand these changes because all of these parties were involved in the initial admitting process. Dr. Pendharkar and Dr. Malieckal provided all groups with in-person training on how the logistics of the system would unfold. Noon conference lectures were also held to explain the vision to residents.
Over 3 weeks, the first ward we chose to implement our model on slowly accumulated the patients of one team – this was the gradual trickle phase. We then selected a “re-set” date. On the re-set date, it was determined that all patients would go to the team that was assigned to that floor, with the exception of any private attendings’ patients.
On the day before the re-set date, time was spent ensuring that all hand-offs were safe. Dr. Pendharkar and Dr. Malieckal spoke with every intern and team that would be handing off and/or receiving patients as a result of the re-set policy. The goal was to ensure that on that date a ward had close to 100% of its patients belonging to the team/attending that was assigned to that area.
The good
Once we began our geographic, unit-based model, our rounding process was transformed.
Now, our morning rounds were joined by the bedside nurse, case manager, social worker, clinical pharmacy, and nutrition in addition to the core team. The entire team went from room to room on one ward rounding on all 20 to 25 patients back to back, which created an unparalleled level of efficiency and a forum for effective communication lasting throughout the day.
We also added workstations on wheels (WOWS) to the rounding process so that labs, radiology, and more could be reviewed on rounds with the entire team. A standard script was developed so that each patient was introduced to all members of the team, and the care plan was disclosed and highlighted. One patient noted, “I feel so cared for, knowing I have this entire team taking care of me.” We also rounded in the afternoon with the case managers and social workers to follow up tasks that were to be completed that day.
Our first few weeks utilizing the geographic, unit-based model of rounding was largely successful. The residents, now able to round on all of their patients in one location with one case manager and one social worker, noted, “This model of rounding makes my life so much easier, I feel like I can focus on the patient rather than running around. … and I know the social worker and case manager will help me.”
Provider satisfaction had improved, from residents to physicians to nurses, case managers, social workers, and more. Our case manager also noted her satisfaction with the new model, stating that her communication with the medical team was much easier. As the attending, I witnessed firsthand how working together with the team moved care forward much more quickly, compared with the previous model, because of the simple factor of increased ease of communication.
Now all team members were together in the patient room and discussion was much easier. There was less confusion, fewer delays, and better communication – I think unit-based teams can even be described as a lifesaving measure that reduces harm to patients. An additional benefit is the relationship that now developed between doctors, social workers, and case managers – they spent more time together and really got to know one another, creating a feeling of shared success and a deeper drive to help one another succeed.
In our model, 87% of surveyed residents said they felt less burned out in the new geographic, unit-based model of care, and 91% of physicians surveyed said it was easier to talk with team members to coordinate care. Additionally, our HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) scores saw a drastic increase in many domains. Nursing communication improved by more than 42% on domain 7B; doctor communication improved by more than 31%. Additionally, all other domains saw at least 10% improvement. We are now 5 months out from our initial rollout of the model and continue to see sustained improvements in quality measures.
The bad
The biggest challenges that we are working through with this model are hand-offs and transfer of patients from one team to another. Sometimes, it happens that one team’s patient will wind up on a floor that is the designated floor of another team because of bed availability. We continue to work with bed board to address this issue. We want to minimize transfers and hand-offs to promote continuity and have to balance that with the need for geographic location. With clear communication, hospital collaboration from bed board and safe hand-off methods, this problem can be safely addressed.
Conclusions
The experience of implementing the unit-based team model has been an eye-opening journey. One thing that stands out is that, in an increasingly complex health care system, design thinking is critical.
Design thinking takes into consideration the needs of those who are using a system. In this case, patients and health care workers including doctors, nurses, case managers, and social workers are the end users of the health care system. All parties are utilizing the health care system to optimize patient health. Therefore, we must create systems that are easy to navigate and use by patients and health care workers so that they can ensure the success of patients.
Unit-based teams offer a basic framework to optimize the inpatient system to facilitate better workflow. In our system, it allowed us to optimize communications between health care workers and also between health care workers and patients. It allowed team members to work in close proximity to better share ideas with each other.
We spent a significant amount of time upfront earning the support of all of the disciplines for this effort. We had support from all leaders within the organization and continue to make our case for this model by sharing metrics and holding forums to discuss the process.
Initial data show a marked improvement in many domains of HCAHPS scores. Our frontline staff, including attendings, residents, nursing, case managers, and social workers, also continue to support this effort since it has a positive impact on their workflow and improves their workday quality. One nurse mentioned specifically, “in my 30 years at this hospital I have never seen people work together so well.”
To sustain this effort, we continue to have regular meetings, and there are new features that we would like to add to the program. For example, we are working with our IT group to ensure that each unit-based team will have dashboards available to incorporate real time, actionable data into daily workflows.
We are excited by the potential of our high-performing teams to highlight the patient experience, placing the patient at the center for care, decision making, and rounding. Health care is a team sport, and anytime you build something where all teams are playing together and approaching the finish line as a unit, you will never go wrong!
Dr. Pendharkar is division chief of hospital medicine at the Brooklyn (N.Y.) Hospital Center, medical director of inpatient services and director of quality for the department of medicine at the Brooklyn Hospital Center and assistant professor of medicine, Icahn School of Medicine at Mount Sinai, New York. Dr. Malieckal is chief resident, internal medicine, at the Brooklyn Hospital Center. Dr. Gasperino is chair, department of medicine; vice president for critical care, perioperative, and hospital medicine; and associate chief medical officer at the Brooklyn Hospital Center.
“To me, teamwork is the beauty of our sport, where you have five acting as one. You become selfless.” – Mike Krzyzewski
High-performing teams plan, communicate, reflect, and take action together. Teamwork can transform seemingly impossible tasks into opportunities for people to come together and create value.
The increasing complexity of health care makes team-based care necessary to achieve successful health outcomes for patients. At the Brooklyn (N.Y.) Hospital Center, a 464-bed care center, we transformed the model of care on the medical wards into a geographic, unit-based team model. Here we describe our journey – the successes, the challenges, and the opportunities for growth.
Previous model
In the previous care model on our medical wards, no set structures were in place. Teams would travel to multiple wards throughout the hospital to see the patients they were rounding on. Each floor had its own set of social workers and case managers, therefore a hospital medicine team routinely dealt with more than eight social workers and case managers to address their patients’ needs in a single day.
Multidisciplinary rounds for all medical patients were held at 11 a.m. in a room located a significant distance away from the medical wards. All case managers and social workers would sit in this room from 11 a.m. until noon, and teams would travel to that room to discuss their patients.
Many challenges were identified in this model, including a lack of communication, a de-emphasis on teamwork, and a design that did not take physician workflows into account resulting in low efficiency. Thus, these challenges sparked a desire to create a more effective and team-based methodology of accomplishing excellence in delivery of clinical care. Dr. Pendharkar, having worked primarily in centers with unit-based care, determined that a geographic, unit-based model of care could transform care delivery at the Brooklyn Hospital Center.
Looking ahead
The efforts for transforming the vision of geographic, unit-based teams into a reality started by gathering all stakeholders together to unite for a common mission. Initial meetings were held with all parties including social workers, case managers, residents, nursing staff, bed board and attending physicians in internal medicine, and the emergency department.
The vision of a geographic, unit-based team was shared and explained to all team members. Exercises in LEAN methodology were conducted, including one-piece flow exercises, to highlight the possibilities of what could be accomplished through teamwork. Once support for the vision was in place from all parties, the logistics were addressed.
The biggest challenge to overcome was how to place all of one team’s patients on a singular medical ward. In our hospital, a medical ward holds anywhere from 30 to 33 patients. Each hospital medicine team, of which there are many, typically carries 20-23 patients. We created a blueprint to map out the floor to which each team and attending would be assigned. Next, we partnered with both IT and bed board to design an admission order set that specified the particular geographic location that a team and attending were associated with so that patients could be placed accordingly from the ED.
It was important for the ED doctors, bed board, and the internal medicine residents to understand these changes because all of these parties were involved in the initial admitting process. Dr. Pendharkar and Dr. Malieckal provided all groups with in-person training on how the logistics of the system would unfold. Noon conference lectures were also held to explain the vision to residents.
Over 3 weeks, the first ward we chose to implement our model on slowly accumulated the patients of one team – this was the gradual trickle phase. We then selected a “re-set” date. On the re-set date, it was determined that all patients would go to the team that was assigned to that floor, with the exception of any private attendings’ patients.
On the day before the re-set date, time was spent ensuring that all hand-offs were safe. Dr. Pendharkar and Dr. Malieckal spoke with every intern and team that would be handing off and/or receiving patients as a result of the re-set policy. The goal was to ensure that on that date a ward had close to 100% of its patients belonging to the team/attending that was assigned to that area.
The good
Once we began our geographic, unit-based model, our rounding process was transformed.
Now, our morning rounds were joined by the bedside nurse, case manager, social worker, clinical pharmacy, and nutrition in addition to the core team. The entire team went from room to room on one ward rounding on all 20 to 25 patients back to back, which created an unparalleled level of efficiency and a forum for effective communication lasting throughout the day.
We also added workstations on wheels (WOWS) to the rounding process so that labs, radiology, and more could be reviewed on rounds with the entire team. A standard script was developed so that each patient was introduced to all members of the team, and the care plan was disclosed and highlighted. One patient noted, “I feel so cared for, knowing I have this entire team taking care of me.” We also rounded in the afternoon with the case managers and social workers to follow up tasks that were to be completed that day.
Our first few weeks utilizing the geographic, unit-based model of rounding was largely successful. The residents, now able to round on all of their patients in one location with one case manager and one social worker, noted, “This model of rounding makes my life so much easier, I feel like I can focus on the patient rather than running around. … and I know the social worker and case manager will help me.”
Provider satisfaction had improved, from residents to physicians to nurses, case managers, social workers, and more. Our case manager also noted her satisfaction with the new model, stating that her communication with the medical team was much easier. As the attending, I witnessed firsthand how working together with the team moved care forward much more quickly, compared with the previous model, because of the simple factor of increased ease of communication.
Now all team members were together in the patient room and discussion was much easier. There was less confusion, fewer delays, and better communication – I think unit-based teams can even be described as a lifesaving measure that reduces harm to patients. An additional benefit is the relationship that now developed between doctors, social workers, and case managers – they spent more time together and really got to know one another, creating a feeling of shared success and a deeper drive to help one another succeed.
In our model, 87% of surveyed residents said they felt less burned out in the new geographic, unit-based model of care, and 91% of physicians surveyed said it was easier to talk with team members to coordinate care. Additionally, our HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) scores saw a drastic increase in many domains. Nursing communication improved by more than 42% on domain 7B; doctor communication improved by more than 31%. Additionally, all other domains saw at least 10% improvement. We are now 5 months out from our initial rollout of the model and continue to see sustained improvements in quality measures.
The bad
The biggest challenges that we are working through with this model are hand-offs and transfer of patients from one team to another. Sometimes, it happens that one team’s patient will wind up on a floor that is the designated floor of another team because of bed availability. We continue to work with bed board to address this issue. We want to minimize transfers and hand-offs to promote continuity and have to balance that with the need for geographic location. With clear communication, hospital collaboration from bed board and safe hand-off methods, this problem can be safely addressed.
Conclusions
The experience of implementing the unit-based team model has been an eye-opening journey. One thing that stands out is that, in an increasingly complex health care system, design thinking is critical.
Design thinking takes into consideration the needs of those who are using a system. In this case, patients and health care workers including doctors, nurses, case managers, and social workers are the end users of the health care system. All parties are utilizing the health care system to optimize patient health. Therefore, we must create systems that are easy to navigate and use by patients and health care workers so that they can ensure the success of patients.
Unit-based teams offer a basic framework to optimize the inpatient system to facilitate better workflow. In our system, it allowed us to optimize communications between health care workers and also between health care workers and patients. It allowed team members to work in close proximity to better share ideas with each other.
We spent a significant amount of time upfront earning the support of all of the disciplines for this effort. We had support from all leaders within the organization and continue to make our case for this model by sharing metrics and holding forums to discuss the process.
Initial data show a marked improvement in many domains of HCAHPS scores. Our frontline staff, including attendings, residents, nursing, case managers, and social workers, also continue to support this effort since it has a positive impact on their workflow and improves their workday quality. One nurse mentioned specifically, “in my 30 years at this hospital I have never seen people work together so well.”
To sustain this effort, we continue to have regular meetings, and there are new features that we would like to add to the program. For example, we are working with our IT group to ensure that each unit-based team will have dashboards available to incorporate real time, actionable data into daily workflows.
We are excited by the potential of our high-performing teams to highlight the patient experience, placing the patient at the center for care, decision making, and rounding. Health care is a team sport, and anytime you build something where all teams are playing together and approaching the finish line as a unit, you will never go wrong!
Dr. Pendharkar is division chief of hospital medicine at the Brooklyn (N.Y.) Hospital Center, medical director of inpatient services and director of quality for the department of medicine at the Brooklyn Hospital Center and assistant professor of medicine, Icahn School of Medicine at Mount Sinai, New York. Dr. Malieckal is chief resident, internal medicine, at the Brooklyn Hospital Center. Dr. Gasperino is chair, department of medicine; vice president for critical care, perioperative, and hospital medicine; and associate chief medical officer at the Brooklyn Hospital Center.
Sunscreen ingredients found in bloodstream, but health impact unknown
for sunscreens, in a phase 1 randomized controlled study of 24 healthy volunteers.

In the open-label study, 24 people (mean age 35.5 years) were randomized to one of four commercially available sunscreens (two sprays, one lotion, or one cream formulation); 2 mg of sunscreen per 1 cm2 was applied to 75% of their body surface four times a day for 4 days (described as “maximal use conditions consistent with current sunscreen labeling”), and 30 blood samples were collected over 7 days.
The primary outcome was the maximum plasma concentration of avobenzone, from days 1-7; secondary outcomes were maximum plasma concentrations of sunscreen ingredients oxybenzone, octocrylene, and ecamsule over the same period of time.
All but one participant completed the study. “All four sunscreen active ingredients tested resulted in exposures exceeding 0.5 ng/mL,” reported Murali Matta, PhD, of the FDA’s Center for Drug Evaluation and Research, and coauthors. “The clinical effect of plasma concentrations exceeding 0.5 ng/mL is unknown, necessitating further research,” they added.
According to the study, FDA sunscreen guidance and the proposed rule for over-the-counter sunscreen monograph, nonclinical toxicology studies, such as carcinogenicity and reproductive studies, “may be waived if results of an adequately conducted human pharmacokinetic maximal usage trial show a steady state blood level less than 0.5 ng/mL and an adequately conducted toxicology assessment does not reveal any potential safety concerns.”
The results of this study “do not indicate that individuals should refrain from the use of sunscreen,” the authors concluded, adding that the “systemic absorption of sunscreen ingredients supports the need for further studies to determine the clinical significance of these findings.” The study was published in JAMA.
In an accompanying editorial, former FDA commissioner Robert Califf, MD, professor of cardiology, Duke University, Durham, N.C., and JAMA Dermatology Editor Kanade Shinkai, MD, PhD, of the department of dermatology, University of California, San Francisco, noted that “the demonstration of systemic absorption well above the FDA guideline does not mean these ingredients are unsafe” (JAMA. 2019 May 6. doi: 10.1001/jama.2019.5528). But, they added, the results “raise many important questions about sunscreen and the process by which the sunscreen industry, clinicians, specialty organizations, and regulatory agencies evaluate the benefits and risks of this topical OTC medication. First and foremost, it is essential to determine whether systemic absorption of sunscreen poses risks to human health. Second, the effects of different sunscreen formulations, clinical characteristics (that is, skin type, age, presence of skin diseases that disrupt the skin barrier), physical activity level, and exposure to sun and water on systemic sunscreen levels require further study.”
In a statement, former American Academy of Dermatology President Darrel Rigel, MD, of the department of dermatology, New York University, said that he was concerned that the results were misleading. “We have always known that there is a very small amount of absorption of sunscreens in the bloodstream,” and there are no data that this is a problem, he said, adding: “Tens of millions of people use sunscreens in the U.S. every summer weekend for many years with no incidence. Daily use of a broad-spectrum SPF of at least 30 is the best way to protect yourself from skin cancer. For many people, the chemical formulations cited in the study are the only ones that feel cosmetically elegant enough to wear. Consumers should continue to use their preferred formulation if it means they will actually wear it.”
SOURCE: JAMA. 2019 May 6. doi: 10.1001/jama.2019.5586
It comes as no real surprise that in the wake of the recent FDA proposed rule on sunscreen, which is currently in the “open season” phase for public input, a pilot study supporting said proposal emerges from this very group. We certainly need a watchdog – one that protects us from potentially harmful things in this world. The study presented validates this role. However, let’s not misconstrue what is presented here. In fact, I credit the authors with highlighting a key point in the last sentence of their abstract: These data do not suggest that individuals should refrain from using sunscreen. This paper serves a purpose, which is to support the recommendation to evaluate the potential of these ingredients to penetrate, permeate, and absorb into the systemic circulation. And yes, these data certainly suggest specific filters and formulations can enable systemic absorption, but these findings cannot be correlated to toxicity or pathology.

Let’s critically evaluate what was investigated. The experimental protocol was not exactly realistic, rather, representative of optimal use (2mg/cm2, covering 75% body surface area, four times a day – let’s be real, who actually does that?). The number of those evaluated was low (six per group) and did not account for all skin type and external environments that do play a role in barrier integrity.
While the clinical relevance is unclear, let’s turn to what is not unclear: Ultraviolet radiation causes skin cancer, plain and simple. Therefore, a comprehensive sun protective regimen that includes sunscreen, sun avoidance, and protective clothing is central to prevention. If one is still concerned, there are always mineral sunscreens, zinc and titanium, which the FDA has deemed safe (“generally recognized as safe and effective” or GRASE).
Adam Friedman, MD, is professor and interim chief of dermatology, and director of the supportive oncodermatology clinic, at George Washington University, Washington. He is an advisor and consultant to Aveeno and LaRoche Posay.
It comes as no real surprise that in the wake of the recent FDA proposed rule on sunscreen, which is currently in the “open season” phase for public input, a pilot study supporting said proposal emerges from this very group. We certainly need a watchdog – one that protects us from potentially harmful things in this world. The study presented validates this role. However, let’s not misconstrue what is presented here. In fact, I credit the authors with highlighting a key point in the last sentence of their abstract: These data do not suggest that individuals should refrain from using sunscreen. This paper serves a purpose, which is to support the recommendation to evaluate the potential of these ingredients to penetrate, permeate, and absorb into the systemic circulation. And yes, these data certainly suggest specific filters and formulations can enable systemic absorption, but these findings cannot be correlated to toxicity or pathology.
Let’s critically evaluate what was investigated. The experimental protocol was not exactly realistic, rather, representative of optimal use (2mg/cm2, covering 75% body surface area, four times a day – let’s be real, who actually does that?). The number of those evaluated was low (six per group) and did not account for all skin type and external environments that do play a role in barrier integrity.
While the clinical relevance is unclear, let’s turn to what is not unclear: Ultraviolet radiation causes skin cancer, plain and simple. Therefore, a comprehensive sun protective regimen that includes sunscreen, sun avoidance, and protective clothing is central to prevention. If one is still concerned, there are always mineral sunscreens, zinc and titanium, which the FDA has deemed safe (“generally recognized as safe and effective” or GRASE).
Adam Friedman, MD, is professor and interim chief of dermatology, and director of the supportive oncodermatology clinic, at George Washington University, Washington. He is an advisor and consultant to Aveeno and LaRoche Posay.
It comes as no real surprise that in the wake of the recent FDA proposed rule on sunscreen, which is currently in the “open season” phase for public input, a pilot study supporting said proposal emerges from this very group. We certainly need a watchdog – one that protects us from potentially harmful things in this world. The study presented validates this role. However, let’s not misconstrue what is presented here. In fact, I credit the authors with highlighting a key point in the last sentence of their abstract: These data do not suggest that individuals should refrain from using sunscreen. This paper serves a purpose, which is to support the recommendation to evaluate the potential of these ingredients to penetrate, permeate, and absorb into the systemic circulation. And yes, these data certainly suggest specific filters and formulations can enable systemic absorption, but these findings cannot be correlated to toxicity or pathology.
Let’s critically evaluate what was investigated. The experimental protocol was not exactly realistic, rather, representative of optimal use (2mg/cm2, covering 75% body surface area, four times a day – let’s be real, who actually does that?). The number of those evaluated was low (six per group) and did not account for all skin type and external environments that do play a role in barrier integrity.
While the clinical relevance is unclear, let’s turn to what is not unclear: Ultraviolet radiation causes skin cancer, plain and simple. Therefore, a comprehensive sun protective regimen that includes sunscreen, sun avoidance, and protective clothing is central to prevention. If one is still concerned, there are always mineral sunscreens, zinc and titanium, which the FDA has deemed safe (“generally recognized as safe and effective” or GRASE).
Adam Friedman, MD, is professor and interim chief of dermatology, and director of the supportive oncodermatology clinic, at George Washington University, Washington. He is an advisor and consultant to Aveeno and LaRoche Posay.
for sunscreens, in a phase 1 randomized controlled study of 24 healthy volunteers.
In the open-label study, 24 people (mean age 35.5 years) were randomized to one of four commercially available sunscreens (two sprays, one lotion, or one cream formulation); 2 mg of sunscreen per 1 cm2 was applied to 75% of their body surface four times a day for 4 days (described as “maximal use conditions consistent with current sunscreen labeling”), and 30 blood samples were collected over 7 days.
The primary outcome was the maximum plasma concentration of avobenzone, from days 1-7; secondary outcomes were maximum plasma concentrations of sunscreen ingredients oxybenzone, octocrylene, and ecamsule over the same period of time.
All but one participant completed the study. “All four sunscreen active ingredients tested resulted in exposures exceeding 0.5 ng/mL,” reported Murali Matta, PhD, of the FDA’s Center for Drug Evaluation and Research, and coauthors. “The clinical effect of plasma concentrations exceeding 0.5 ng/mL is unknown, necessitating further research,” they added.
According to the study, FDA sunscreen guidance and the proposed rule for over-the-counter sunscreen monograph, nonclinical toxicology studies, such as carcinogenicity and reproductive studies, “may be waived if results of an adequately conducted human pharmacokinetic maximal usage trial show a steady state blood level less than 0.5 ng/mL and an adequately conducted toxicology assessment does not reveal any potential safety concerns.”
The results of this study “do not indicate that individuals should refrain from the use of sunscreen,” the authors concluded, adding that the “systemic absorption of sunscreen ingredients supports the need for further studies to determine the clinical significance of these findings.” The study was published in JAMA.
In an accompanying editorial, former FDA commissioner Robert Califf, MD, professor of cardiology, Duke University, Durham, N.C., and JAMA Dermatology Editor Kanade Shinkai, MD, PhD, of the department of dermatology, University of California, San Francisco, noted that “the demonstration of systemic absorption well above the FDA guideline does not mean these ingredients are unsafe” (JAMA. 2019 May 6. doi: 10.1001/jama.2019.5528). But, they added, the results “raise many important questions about sunscreen and the process by which the sunscreen industry, clinicians, specialty organizations, and regulatory agencies evaluate the benefits and risks of this topical OTC medication. First and foremost, it is essential to determine whether systemic absorption of sunscreen poses risks to human health. Second, the effects of different sunscreen formulations, clinical characteristics (that is, skin type, age, presence of skin diseases that disrupt the skin barrier), physical activity level, and exposure to sun and water on systemic sunscreen levels require further study.”
In a statement, former American Academy of Dermatology President Darrel Rigel, MD, of the department of dermatology, New York University, said that he was concerned that the results were misleading. “We have always known that there is a very small amount of absorption of sunscreens in the bloodstream,” and there are no data that this is a problem, he said, adding: “Tens of millions of people use sunscreens in the U.S. every summer weekend for many years with no incidence. Daily use of a broad-spectrum SPF of at least 30 is the best way to protect yourself from skin cancer. For many people, the chemical formulations cited in the study are the only ones that feel cosmetically elegant enough to wear. Consumers should continue to use their preferred formulation if it means they will actually wear it.”
SOURCE: JAMA. 2019 May 6. doi: 10.1001/jama.2019.5586
for sunscreens, in a phase 1 randomized controlled study of 24 healthy volunteers.
In the open-label study, 24 people (mean age 35.5 years) were randomized to one of four commercially available sunscreens (two sprays, one lotion, or one cream formulation); 2 mg of sunscreen per 1 cm2 was applied to 75% of their body surface four times a day for 4 days (described as “maximal use conditions consistent with current sunscreen labeling”), and 30 blood samples were collected over 7 days.
The primary outcome was the maximum plasma concentration of avobenzone, from days 1-7; secondary outcomes were maximum plasma concentrations of sunscreen ingredients oxybenzone, octocrylene, and ecamsule over the same period of time.
All but one participant completed the study. “All four sunscreen active ingredients tested resulted in exposures exceeding 0.5 ng/mL,” reported Murali Matta, PhD, of the FDA’s Center for Drug Evaluation and Research, and coauthors. “The clinical effect of plasma concentrations exceeding 0.5 ng/mL is unknown, necessitating further research,” they added.
According to the study, FDA sunscreen guidance and the proposed rule for over-the-counter sunscreen monograph, nonclinical toxicology studies, such as carcinogenicity and reproductive studies, “may be waived if results of an adequately conducted human pharmacokinetic maximal usage trial show a steady state blood level less than 0.5 ng/mL and an adequately conducted toxicology assessment does not reveal any potential safety concerns.”
The results of this study “do not indicate that individuals should refrain from the use of sunscreen,” the authors concluded, adding that the “systemic absorption of sunscreen ingredients supports the need for further studies to determine the clinical significance of these findings.” The study was published in JAMA.
In an accompanying editorial, former FDA commissioner Robert Califf, MD, professor of cardiology, Duke University, Durham, N.C., and JAMA Dermatology Editor Kanade Shinkai, MD, PhD, of the department of dermatology, University of California, San Francisco, noted that “the demonstration of systemic absorption well above the FDA guideline does not mean these ingredients are unsafe” (JAMA. 2019 May 6. doi: 10.1001/jama.2019.5528). But, they added, the results “raise many important questions about sunscreen and the process by which the sunscreen industry, clinicians, specialty organizations, and regulatory agencies evaluate the benefits and risks of this topical OTC medication. First and foremost, it is essential to determine whether systemic absorption of sunscreen poses risks to human health. Second, the effects of different sunscreen formulations, clinical characteristics (that is, skin type, age, presence of skin diseases that disrupt the skin barrier), physical activity level, and exposure to sun and water on systemic sunscreen levels require further study.”
In a statement, former American Academy of Dermatology President Darrel Rigel, MD, of the department of dermatology, New York University, said that he was concerned that the results were misleading. “We have always known that there is a very small amount of absorption of sunscreens in the bloodstream,” and there are no data that this is a problem, he said, adding: “Tens of millions of people use sunscreens in the U.S. every summer weekend for many years with no incidence. Daily use of a broad-spectrum SPF of at least 30 is the best way to protect yourself from skin cancer. For many people, the chemical formulations cited in the study are the only ones that feel cosmetically elegant enough to wear. Consumers should continue to use their preferred formulation if it means they will actually wear it.”
SOURCE: JAMA. 2019 May 6. doi: 10.1001/jama.2019.5586
FROM JAMA
Adult-Onset Asymmetrical Lipomatosis
To the Editor:
An 85-year-old woman presented with extra growth of subcutaneous fat at the left anterior infradiaphragm that expanded circumferentially to the left back over the last 4 years. Two years prior to the current presentation, the left thigh became visibly thicker than the right. Diffuse subtle lipomatosis affecting the ipsilateral face, neck, arms, calf, and foot was noted at that time. Additionally, the patient had hyperlipidemia, gastroesophageal reflux disease, osteoporosis, and scoliosis, all beginning in her late 60s. She reported no alcohol or tobacco use and was taking rosuvastatin, esomeprazole, calcium, vitamin D, and glucosamine. There was no reported family history of asymmetric growth or bony deformities, and her children were healthy.
On physical examination, the lipomatosis affected the entire left side, most prominently around the abdomen, back, and thighs. The affected side was nontender and nonpruritic; there was no atrophy of the unaffected side (Figure). Maximum thigh circumference was 55.1 cm on the affected side and 52.6 cm on the unaffected side. There were no differences in power, reflex, or sensation between the 2 sides, and no hyperhidrosis or vascular malformations were present. Laboratory investigations, including complete blood cell count, complete metabolic panel, lipids, and thyroid-stimulating and sex hormone panels all were within reference range.

Enzi et al1 reported 2 women who developed asymmetrical lipomatosis between the ages of 13 and 20 years. Acquired asymmetrical lipomatosis should be differentiated from the asymmetrical overgrowth diagnosed in neonates and infants.
Proteus syndrome (PS) is a progressive disease involving a combination of overgrowth in a mosaic distribution, connective tissue and epidermal nevi, ovarian cysts, parotid gland tumor, dysregulated adipose tissue, lymphovascular malformation, and certain facial phenotypes.2,3 The average age of onset is 6 to 18 months, and half of cases present at birth.3,4 Hemihyperplasia-multiple lipomatosis syndrome (HHML) describes a mild and nonprogressive variant that does not satisfy the diagnostic criteria of PS; it typically is diagnosed at birth.5 One case of mild and delayed-onset PS was described in a woman who started developing signs at 15 years of age.6 In comparison, asymmetrical lipomatosis and scoliosis were the only abnormal clinical signs present in our patient, and the lipomatosis developed diffusely, as opposed to the typical mosaic distribution found in PS and HHML. Scoliosis can be found in PS and HHML secondary to hemihypertrophy of vertebra or infiltrative intraspinal lipomatosis.7,8 Our patient’s scoliosis was diagnosed more than 10 years prior to the onset of lipomatosis, likely representing degenerative joint disease.9
Prior reported cases of asymmetrical lipomatosis did not describe treatment.1 Ultrasound-guided or conventional liposuction and lipectomy are mainstream therapies for multiple symmetrical lipomatosis, an acquired lipomatosis typically affecting alcoholics in the fourth decade of life. However, recurrence rates are high for surgical treatment of unencapsulated lipomatosis, likely due to incomplete removal of the adipose tissue.10 Alternative treatments found in case reports, including oral salbutamol, mesotherapy using phosphatidylcholine, and fenofibrate (200 mg/d), require further study.11-13 Our patient was not aesthetically bothered by her lipomatosis; therefore, imaging and treatment options were not pursued. In conclusion, we report a patient with acquired asymmetrical lipomatosis with onset in late adulthood, unique from the existing syndromes of asymmetrical hemihyperplasia.1,14
- Enzi G, Digito M, Enzi GB, et al. Asymmetrical lipomatosis: report of two cases. Postgrad Med J. 1985;61:797-800.
- Biesecker LG, Happle R, Mulliken JB, et al. Proteus syndrome: diagnostic criteria, differential diagnosis, and patient evaluation. Am J Med Genet. 1999;84:389-395.
- Biesecker L. The challenges of Proteus syndrome: diagnosis and management. Eur J Hum Genet. 2006;14:1151-1157.
- Cohen MM Jr. Proteus syndrome: an update. Am J Med Genet C Semin Med Genet. 2005;137C:38-52.
- Biesecker LG, Peters KF, Darling TN, et al. Clinical differentiation between Proteus syndrome and hemihyperplasia: description of a distinct form of hemihyperplasia. Am J Med Genet. 1998;79:311-318.
- Luo S, Feng Y, Zheng Y, et al. Mild and delayed-onset Proteus syndrome. Eur J Dermatol. 2007;17:172-173.
- Takebayashi T, Yamashita T, Yokogushi K, et al. Scoliosis in Proteus syndrome: case report. Spine. 2001;26:E395-E398.
- Schulte TL, Liljenqvist U, Görgens H, et al. Hemihyperplasia-multiple lipomatosis syndrome (HHML): a challenge in spinal care. Acta Orthop Belg. 2008;74:714-719.
- Robin GC, Span Y, Steinberg R, et al. Scoliosis in the elderly: a follow-up study. Spine. 1982;7:355-359.
- Brea-García B, Cameselle-Teijeiro J, Couto-González I, et al. Madelung’s disease: comorbidities, fatty mass distribution, and response to treatment of 22 patients. Aesthet Plast Surg. 2013;37:409-416.
- Hasegawa T, Matsukura T, Ikeda S. Mesotherapy for benign symmetric lipomatosis. Aesthet Plast Surg. 2010;34:153-156.
- Zeitler H, Ulrich-Merzenich G, Richter DF, et al. Multiple benign symmetric lipomatosis—a differential diagnosis of obesity. is there a rationale for fibrate treatment? Obes Surg. 2008;18:1354-1356.
- Leung N, Gaer J, Beggs D, et al. Multiple symmetric lipomatosis (Launois‐Bensaude syndrome): effect of oral salbutamol. Clin Endocrinol. 1987;27:601-606.
- Craiglow BG, Ko CJ, Antaya RJ. Two cases of hemihyperplasia-multiple lipomatosis syndrome and review of asymmetric hemihyperplasia syndromes. Pediatr Dermatol. 2014;31:507-510.
To the Editor:
An 85-year-old woman presented with extra growth of subcutaneous fat at the left anterior infradiaphragm that expanded circumferentially to the left back over the last 4 years. Two years prior to the current presentation, the left thigh became visibly thicker than the right. Diffuse subtle lipomatosis affecting the ipsilateral face, neck, arms, calf, and foot was noted at that time. Additionally, the patient had hyperlipidemia, gastroesophageal reflux disease, osteoporosis, and scoliosis, all beginning in her late 60s. She reported no alcohol or tobacco use and was taking rosuvastatin, esomeprazole, calcium, vitamin D, and glucosamine. There was no reported family history of asymmetric growth or bony deformities, and her children were healthy.
On physical examination, the lipomatosis affected the entire left side, most prominently around the abdomen, back, and thighs. The affected side was nontender and nonpruritic; there was no atrophy of the unaffected side (Figure). Maximum thigh circumference was 55.1 cm on the affected side and 52.6 cm on the unaffected side. There were no differences in power, reflex, or sensation between the 2 sides, and no hyperhidrosis or vascular malformations were present. Laboratory investigations, including complete blood cell count, complete metabolic panel, lipids, and thyroid-stimulating and sex hormone panels all were within reference range.
Enzi et al1 reported 2 women who developed asymmetrical lipomatosis between the ages of 13 and 20 years. Acquired asymmetrical lipomatosis should be differentiated from the asymmetrical overgrowth diagnosed in neonates and infants.
Proteus syndrome (PS) is a progressive disease involving a combination of overgrowth in a mosaic distribution, connective tissue and epidermal nevi, ovarian cysts, parotid gland tumor, dysregulated adipose tissue, lymphovascular malformation, and certain facial phenotypes.2,3 The average age of onset is 6 to 18 months, and half of cases present at birth.3,4 Hemihyperplasia-multiple lipomatosis syndrome (HHML) describes a mild and nonprogressive variant that does not satisfy the diagnostic criteria of PS; it typically is diagnosed at birth.5 One case of mild and delayed-onset PS was described in a woman who started developing signs at 15 years of age.6 In comparison, asymmetrical lipomatosis and scoliosis were the only abnormal clinical signs present in our patient, and the lipomatosis developed diffusely, as opposed to the typical mosaic distribution found in PS and HHML. Scoliosis can be found in PS and HHML secondary to hemihypertrophy of vertebra or infiltrative intraspinal lipomatosis.7,8 Our patient’s scoliosis was diagnosed more than 10 years prior to the onset of lipomatosis, likely representing degenerative joint disease.9
Prior reported cases of asymmetrical lipomatosis did not describe treatment.1 Ultrasound-guided or conventional liposuction and lipectomy are mainstream therapies for multiple symmetrical lipomatosis, an acquired lipomatosis typically affecting alcoholics in the fourth decade of life. However, recurrence rates are high for surgical treatment of unencapsulated lipomatosis, likely due to incomplete removal of the adipose tissue.10 Alternative treatments found in case reports, including oral salbutamol, mesotherapy using phosphatidylcholine, and fenofibrate (200 mg/d), require further study.11-13 Our patient was not aesthetically bothered by her lipomatosis; therefore, imaging and treatment options were not pursued. In conclusion, we report a patient with acquired asymmetrical lipomatosis with onset in late adulthood, unique from the existing syndromes of asymmetrical hemihyperplasia.1,14
To the Editor:
An 85-year-old woman presented with extra growth of subcutaneous fat at the left anterior infradiaphragm that expanded circumferentially to the left back over the last 4 years. Two years prior to the current presentation, the left thigh became visibly thicker than the right. Diffuse subtle lipomatosis affecting the ipsilateral face, neck, arms, calf, and foot was noted at that time. Additionally, the patient had hyperlipidemia, gastroesophageal reflux disease, osteoporosis, and scoliosis, all beginning in her late 60s. She reported no alcohol or tobacco use and was taking rosuvastatin, esomeprazole, calcium, vitamin D, and glucosamine. There was no reported family history of asymmetric growth or bony deformities, and her children were healthy.
On physical examination, the lipomatosis affected the entire left side, most prominently around the abdomen, back, and thighs. The affected side was nontender and nonpruritic; there was no atrophy of the unaffected side (Figure). Maximum thigh circumference was 55.1 cm on the affected side and 52.6 cm on the unaffected side. There were no differences in power, reflex, or sensation between the 2 sides, and no hyperhidrosis or vascular malformations were present. Laboratory investigations, including complete blood cell count, complete metabolic panel, lipids, and thyroid-stimulating and sex hormone panels all were within reference range.
Enzi et al1 reported 2 women who developed asymmetrical lipomatosis between the ages of 13 and 20 years. Acquired asymmetrical lipomatosis should be differentiated from the asymmetrical overgrowth diagnosed in neonates and infants.
Proteus syndrome (PS) is a progressive disease involving a combination of overgrowth in a mosaic distribution, connective tissue and epidermal nevi, ovarian cysts, parotid gland tumor, dysregulated adipose tissue, lymphovascular malformation, and certain facial phenotypes.2,3 The average age of onset is 6 to 18 months, and half of cases present at birth.3,4 Hemihyperplasia-multiple lipomatosis syndrome (HHML) describes a mild and nonprogressive variant that does not satisfy the diagnostic criteria of PS; it typically is diagnosed at birth.5 One case of mild and delayed-onset PS was described in a woman who started developing signs at 15 years of age.6 In comparison, asymmetrical lipomatosis and scoliosis were the only abnormal clinical signs present in our patient, and the lipomatosis developed diffusely, as opposed to the typical mosaic distribution found in PS and HHML. Scoliosis can be found in PS and HHML secondary to hemihypertrophy of vertebra or infiltrative intraspinal lipomatosis.7,8 Our patient’s scoliosis was diagnosed more than 10 years prior to the onset of lipomatosis, likely representing degenerative joint disease.9
Prior reported cases of asymmetrical lipomatosis did not describe treatment.1 Ultrasound-guided or conventional liposuction and lipectomy are mainstream therapies for multiple symmetrical lipomatosis, an acquired lipomatosis typically affecting alcoholics in the fourth decade of life. However, recurrence rates are high for surgical treatment of unencapsulated lipomatosis, likely due to incomplete removal of the adipose tissue.10 Alternative treatments found in case reports, including oral salbutamol, mesotherapy using phosphatidylcholine, and fenofibrate (200 mg/d), require further study.11-13 Our patient was not aesthetically bothered by her lipomatosis; therefore, imaging and treatment options were not pursued. In conclusion, we report a patient with acquired asymmetrical lipomatosis with onset in late adulthood, unique from the existing syndromes of asymmetrical hemihyperplasia.1,14
- Enzi G, Digito M, Enzi GB, et al. Asymmetrical lipomatosis: report of two cases. Postgrad Med J. 1985;61:797-800.
- Biesecker LG, Happle R, Mulliken JB, et al. Proteus syndrome: diagnostic criteria, differential diagnosis, and patient evaluation. Am J Med Genet. 1999;84:389-395.
- Biesecker L. The challenges of Proteus syndrome: diagnosis and management. Eur J Hum Genet. 2006;14:1151-1157.
- Cohen MM Jr. Proteus syndrome: an update. Am J Med Genet C Semin Med Genet. 2005;137C:38-52.
- Biesecker LG, Peters KF, Darling TN, et al. Clinical differentiation between Proteus syndrome and hemihyperplasia: description of a distinct form of hemihyperplasia. Am J Med Genet. 1998;79:311-318.
- Luo S, Feng Y, Zheng Y, et al. Mild and delayed-onset Proteus syndrome. Eur J Dermatol. 2007;17:172-173.
- Takebayashi T, Yamashita T, Yokogushi K, et al. Scoliosis in Proteus syndrome: case report. Spine. 2001;26:E395-E398.
- Schulte TL, Liljenqvist U, Görgens H, et al. Hemihyperplasia-multiple lipomatosis syndrome (HHML): a challenge in spinal care. Acta Orthop Belg. 2008;74:714-719.
- Robin GC, Span Y, Steinberg R, et al. Scoliosis in the elderly: a follow-up study. Spine. 1982;7:355-359.
- Brea-García B, Cameselle-Teijeiro J, Couto-González I, et al. Madelung’s disease: comorbidities, fatty mass distribution, and response to treatment of 22 patients. Aesthet Plast Surg. 2013;37:409-416.
- Hasegawa T, Matsukura T, Ikeda S. Mesotherapy for benign symmetric lipomatosis. Aesthet Plast Surg. 2010;34:153-156.
- Zeitler H, Ulrich-Merzenich G, Richter DF, et al. Multiple benign symmetric lipomatosis—a differential diagnosis of obesity. is there a rationale for fibrate treatment? Obes Surg. 2008;18:1354-1356.
- Leung N, Gaer J, Beggs D, et al. Multiple symmetric lipomatosis (Launois‐Bensaude syndrome): effect of oral salbutamol. Clin Endocrinol. 1987;27:601-606.
- Craiglow BG, Ko CJ, Antaya RJ. Two cases of hemihyperplasia-multiple lipomatosis syndrome and review of asymmetric hemihyperplasia syndromes. Pediatr Dermatol. 2014;31:507-510.
- Enzi G, Digito M, Enzi GB, et al. Asymmetrical lipomatosis: report of two cases. Postgrad Med J. 1985;61:797-800.
- Biesecker LG, Happle R, Mulliken JB, et al. Proteus syndrome: diagnostic criteria, differential diagnosis, and patient evaluation. Am J Med Genet. 1999;84:389-395.
- Biesecker L. The challenges of Proteus syndrome: diagnosis and management. Eur J Hum Genet. 2006;14:1151-1157.
- Cohen MM Jr. Proteus syndrome: an update. Am J Med Genet C Semin Med Genet. 2005;137C:38-52.
- Biesecker LG, Peters KF, Darling TN, et al. Clinical differentiation between Proteus syndrome and hemihyperplasia: description of a distinct form of hemihyperplasia. Am J Med Genet. 1998;79:311-318.
- Luo S, Feng Y, Zheng Y, et al. Mild and delayed-onset Proteus syndrome. Eur J Dermatol. 2007;17:172-173.
- Takebayashi T, Yamashita T, Yokogushi K, et al. Scoliosis in Proteus syndrome: case report. Spine. 2001;26:E395-E398.
- Schulte TL, Liljenqvist U, Görgens H, et al. Hemihyperplasia-multiple lipomatosis syndrome (HHML): a challenge in spinal care. Acta Orthop Belg. 2008;74:714-719.
- Robin GC, Span Y, Steinberg R, et al. Scoliosis in the elderly: a follow-up study. Spine. 1982;7:355-359.
- Brea-García B, Cameselle-Teijeiro J, Couto-González I, et al. Madelung’s disease: comorbidities, fatty mass distribution, and response to treatment of 22 patients. Aesthet Plast Surg. 2013;37:409-416.
- Hasegawa T, Matsukura T, Ikeda S. Mesotherapy for benign symmetric lipomatosis. Aesthet Plast Surg. 2010;34:153-156.
- Zeitler H, Ulrich-Merzenich G, Richter DF, et al. Multiple benign symmetric lipomatosis—a differential diagnosis of obesity. is there a rationale for fibrate treatment? Obes Surg. 2008;18:1354-1356.
- Leung N, Gaer J, Beggs D, et al. Multiple symmetric lipomatosis (Launois‐Bensaude syndrome): effect of oral salbutamol. Clin Endocrinol. 1987;27:601-606.
- Craiglow BG, Ko CJ, Antaya RJ. Two cases of hemihyperplasia-multiple lipomatosis syndrome and review of asymmetric hemihyperplasia syndromes. Pediatr Dermatol. 2014;31:507-510.
Practice Points
- Acquired asymmetrical lipomatosis is a rare condition that can develop at any age; it should be differentiated from existing syndromes of asymmetrical hemihyperplasia.
- Acquired asymmetrical lipomatosis is a clinical diagnosis with no laboratory changes. If the patient is clinically stable and asymptomatic, no further investigation or management is required.

Coalescing Papules on Bilateral Mastectomy Scars
The Diagnosis: Scar Sarcoidosis
Although scars on both breasts were involved, the decision was made to biopsy the right breast because the patient reported more pain on the left breast. Biopsy showed noncaseating granulomas consistent with scar sarcoidosis (Figure). Additional screening tests were performed to evaluate for any systemic involvement of sarcoidosis, including a complete blood cell count, comprehensive metabolic panel, angiotensin-converting enzyme level, tuberculosis serology screening, electrocardiogram, chest radiograph, and pulmonary function tests. She also was referred to rheumatology and ophthalmology for consultation. The results of all screenings were within reference range, and no sign of systemic sarcoidosis was found. She was treated with hydrocortisone ointment 2.5% for several weeks without notable improvement. She elected not to pursue any additional treatment and to monitor the symptoms with close follow-up only. One year after the initial visit, the skin lesions spontaneously and notably improved.
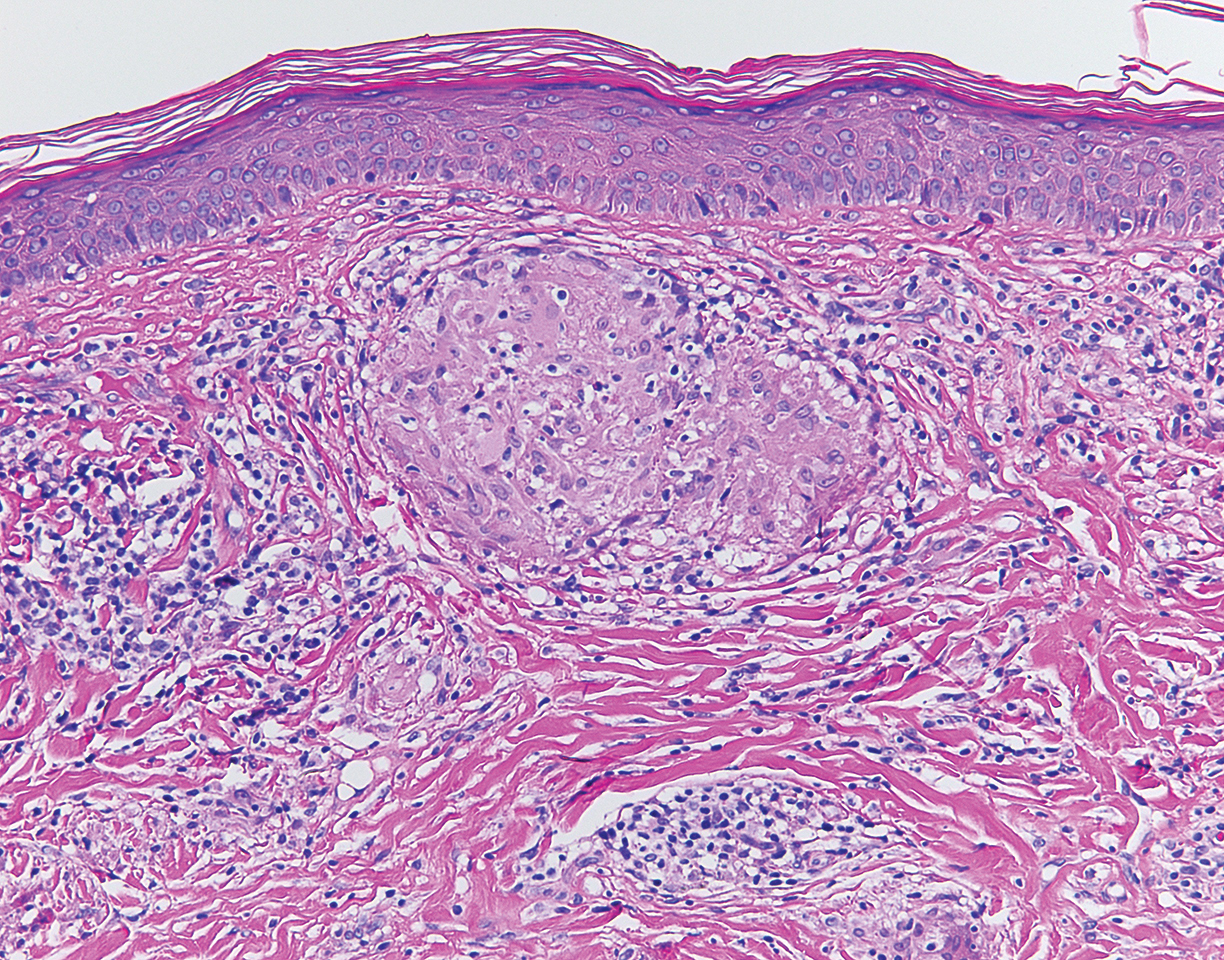
Sarcoidosis is a systemic granulomatous disorder of unknown etiology that most commonly affects the lungs. It also can involve the lymph nodes, liver, spleen, bones, gastrointestinal tract, eyes, and skin. Cutaneous sarcoidosis has been documented in the literature since the late 1800s and occurs in up to one-third of sarcoid patients.1 Cutaneous lesions developing within a preexisting scar is a well-known variant, occurring in 29% of patients with cutaneous sarcoidosis in one clinical study (N=818).2 There have been many reports describing scar sarcoidosis, with its development at prior sites of surgery, trauma, acne, or venipuncture.3 Other case reports have described variants of scar sarcoidosis developing at sites of hyaluronic acid injection, laser surgery, ritual scarification, tattoos, and desensitization injections, as well as prior herpes zoster infections.4-9
Cutaneous sarcoidosis has a wide range of clinical presentations. Lesions can be described as specific or nonspecific. Specific lesions demonstrate the typical sarcoid granuloma on histology and more often are seen in chronic disease, while nonspecific lesions more often are seen in acute disease.3,10 Scar sarcoidosis is an example of a specific lesion in which old scars become infiltrated with noncaseating granulomas. The granulomas typically are in the superficial dermis but may involve the full thickness of the dermis, extending into the subcutaneous tissue.11 The cause of granulomas developing in scars is unknown. Prior contamination of the scar with foreign material, possibly at the time of the trauma, is a possible underlying cause.12
Typical scar sarcoidosis presents as swollen, erythematous, indurated lesions with a purple-red hue that may become brown.3,12 Tenderness or pruritus also may be present.13 Interestingly, our patient's scar sarcoidosis presented with a yellow hue at both mastectomy sites.
Diagnosing scar sarcoidosis can be challenging. Patients are diagnosed with sarcoidosis when a compatible clinical or radiologic picture is present along with histologic evidence of a noncaseating granuloma and other potential causes are excluded.11 The differential includes an infectious etiology, other types of granulomatous dermatitis, hypertrophic scar, keloid, or foreign body granuloma.
Scar sarcoidosis can be isolated in occurrence. It also can precede or occur concomitantly or during a relapse of systemic sarcoidosis.10 Most commonly, patients with scar sarcoidosis also have systemic manifestations of sarcoidosis, and changing scars may be an indicator of disease exacerbation or relapse.10 For patients who only demonstrate specific skin lesions of cutaneous sarcoidosis, approximately 30% develop systemic involvement later in life.3 For this reason, close monitoring and regular follow-up are necessary.
Treatment of scar sarcoidosis is dependent on the extent of the disease and presence of systemic sarcoidosis. Topical and systemic corticosteroids, hydroxychloroquine, chloroquine phosphate, and methotrexate all have been shown to be helpful in treating cutaneous sarcoidosis.3 For scar sarcoidosis that is limited to only the scar site, as seen in our case, monitoring and close follow-up is acceptable. Topical steroids can be prescribed for symptomatic relief. Scar sarcoidosis can resolve slowly and spontaneously over time.10 Our patient notably improved 1 year after the initial presentation without treatment.
Scar sarcoidosis is a well-documented variant of cutaneous sarcoidosis that can have important implications for diagnosing systemic sarcoidosis. Although there are typical lesions that represent scar sarcoidosis, it is important to have a high degree of suspicion with any changing scar. Once diagnosed through biopsy, a thorough investigation for systemic signs of sarcoidosis needs to be performed to guide treatment.
- Bolognia JL, Jorizzo JL, Shaffer JV, eds. Dermatology. 3rd ed. Vol 2. Philadelphia, PA: Elsevier/Saunders; 2012.
- Neville E, Walker AN, James DG. Prognostic factors predicting the outcome of sarcoidosis: an analysis of 818 patients. Q J Med. 1983;52:525-533.
- Mañá J, Marcoval J, Graells J, et al. Cutaneous involvement in sarcoidosis: relationship to systemic disease. Arch Dermatol. 1997;133:882-888.
- Dal Sacco D, Cozzani E, Parodi A, et al. Scar sarcoidosis after hyaluronic acid injection. Int J Dermatol. 2005;44:411-412.
- Kormeili T, Neel V, Moy RL. Cutaneous sarcoidosis at sites of previous laser surgery. Cutis. 2004;73:53-55.
- Nayar M. Sarcoidosis on ritual scarification. Int J Dermatol. 1993;32:116-118.
- James WD, Elston DM, Berger TG, et al. Andrews' Diseases of the Skin: Clinical Dermatology. 11th ed. Philadelphia, PA: Elsevier/Saunders; 2011.
- Healsmith MF, Hutchinson PE. The development of scar sarcoidosis at the site of desensitization injections. Clin Exp Dermatol. 1992;17:369-370.
- Singal A, Vij A, Pandhi D. Post herpes-zoster scar sarcoidosis with pulmonary involvement. Indian Dermatol Online J. 2014;5:77-79.
- Chudomirova K, Velichkova L, Anavi B, et al. Recurrent sarcoidosis in skin scars accompanying systemic sarcoidosis. J Eur Acad Dermatol Venereol. 2003;17:360-361.
- Selim A, Ehrsam E, Atassi MB, et al. Scar sarcoidosis: a case report and brief review. Cutis. 2006;78:418-422.
- Singal A, Thami GP, Goraya JS. Scar sarcoidosis in childhood: case report and review of the literature. Clin Exp Dermatol. 2005;30:244-246.
- Marchell RM, Judson MA. Chronic cutaneous lesions of sarcoidosis. Clin Dermatol. 2007;25:295-302.
The Diagnosis: Scar Sarcoidosis
Although scars on both breasts were involved, the decision was made to biopsy the right breast because the patient reported more pain on the left breast. Biopsy showed noncaseating granulomas consistent with scar sarcoidosis (Figure). Additional screening tests were performed to evaluate for any systemic involvement of sarcoidosis, including a complete blood cell count, comprehensive metabolic panel, angiotensin-converting enzyme level, tuberculosis serology screening, electrocardiogram, chest radiograph, and pulmonary function tests. She also was referred to rheumatology and ophthalmology for consultation. The results of all screenings were within reference range, and no sign of systemic sarcoidosis was found. She was treated with hydrocortisone ointment 2.5% for several weeks without notable improvement. She elected not to pursue any additional treatment and to monitor the symptoms with close follow-up only. One year after the initial visit, the skin lesions spontaneously and notably improved.
Sarcoidosis is a systemic granulomatous disorder of unknown etiology that most commonly affects the lungs. It also can involve the lymph nodes, liver, spleen, bones, gastrointestinal tract, eyes, and skin. Cutaneous sarcoidosis has been documented in the literature since the late 1800s and occurs in up to one-third of sarcoid patients.1 Cutaneous lesions developing within a preexisting scar is a well-known variant, occurring in 29% of patients with cutaneous sarcoidosis in one clinical study (N=818).2 There have been many reports describing scar sarcoidosis, with its development at prior sites of surgery, trauma, acne, or venipuncture.3 Other case reports have described variants of scar sarcoidosis developing at sites of hyaluronic acid injection, laser surgery, ritual scarification, tattoos, and desensitization injections, as well as prior herpes zoster infections.4-9
Cutaneous sarcoidosis has a wide range of clinical presentations. Lesions can be described as specific or nonspecific. Specific lesions demonstrate the typical sarcoid granuloma on histology and more often are seen in chronic disease, while nonspecific lesions more often are seen in acute disease.3,10 Scar sarcoidosis is an example of a specific lesion in which old scars become infiltrated with noncaseating granulomas. The granulomas typically are in the superficial dermis but may involve the full thickness of the dermis, extending into the subcutaneous tissue.11 The cause of granulomas developing in scars is unknown. Prior contamination of the scar with foreign material, possibly at the time of the trauma, is a possible underlying cause.12
Typical scar sarcoidosis presents as swollen, erythematous, indurated lesions with a purple-red hue that may become brown.3,12 Tenderness or pruritus also may be present.13 Interestingly, our patient's scar sarcoidosis presented with a yellow hue at both mastectomy sites.
Diagnosing scar sarcoidosis can be challenging. Patients are diagnosed with sarcoidosis when a compatible clinical or radiologic picture is present along with histologic evidence of a noncaseating granuloma and other potential causes are excluded.11 The differential includes an infectious etiology, other types of granulomatous dermatitis, hypertrophic scar, keloid, or foreign body granuloma.
Scar sarcoidosis can be isolated in occurrence. It also can precede or occur concomitantly or during a relapse of systemic sarcoidosis.10 Most commonly, patients with scar sarcoidosis also have systemic manifestations of sarcoidosis, and changing scars may be an indicator of disease exacerbation or relapse.10 For patients who only demonstrate specific skin lesions of cutaneous sarcoidosis, approximately 30% develop systemic involvement later in life.3 For this reason, close monitoring and regular follow-up are necessary.
Treatment of scar sarcoidosis is dependent on the extent of the disease and presence of systemic sarcoidosis. Topical and systemic corticosteroids, hydroxychloroquine, chloroquine phosphate, and methotrexate all have been shown to be helpful in treating cutaneous sarcoidosis.3 For scar sarcoidosis that is limited to only the scar site, as seen in our case, monitoring and close follow-up is acceptable. Topical steroids can be prescribed for symptomatic relief. Scar sarcoidosis can resolve slowly and spontaneously over time.10 Our patient notably improved 1 year after the initial presentation without treatment.
Scar sarcoidosis is a well-documented variant of cutaneous sarcoidosis that can have important implications for diagnosing systemic sarcoidosis. Although there are typical lesions that represent scar sarcoidosis, it is important to have a high degree of suspicion with any changing scar. Once diagnosed through biopsy, a thorough investigation for systemic signs of sarcoidosis needs to be performed to guide treatment.
The Diagnosis: Scar Sarcoidosis
Although scars on both breasts were involved, the decision was made to biopsy the right breast because the patient reported more pain on the left breast. Biopsy showed noncaseating granulomas consistent with scar sarcoidosis (Figure). Additional screening tests were performed to evaluate for any systemic involvement of sarcoidosis, including a complete blood cell count, comprehensive metabolic panel, angiotensin-converting enzyme level, tuberculosis serology screening, electrocardiogram, chest radiograph, and pulmonary function tests. She also was referred to rheumatology and ophthalmology for consultation. The results of all screenings were within reference range, and no sign of systemic sarcoidosis was found. She was treated with hydrocortisone ointment 2.5% for several weeks without notable improvement. She elected not to pursue any additional treatment and to monitor the symptoms with close follow-up only. One year after the initial visit, the skin lesions spontaneously and notably improved.
Sarcoidosis is a systemic granulomatous disorder of unknown etiology that most commonly affects the lungs. It also can involve the lymph nodes, liver, spleen, bones, gastrointestinal tract, eyes, and skin. Cutaneous sarcoidosis has been documented in the literature since the late 1800s and occurs in up to one-third of sarcoid patients.1 Cutaneous lesions developing within a preexisting scar is a well-known variant, occurring in 29% of patients with cutaneous sarcoidosis in one clinical study (N=818).2 There have been many reports describing scar sarcoidosis, with its development at prior sites of surgery, trauma, acne, or venipuncture.3 Other case reports have described variants of scar sarcoidosis developing at sites of hyaluronic acid injection, laser surgery, ritual scarification, tattoos, and desensitization injections, as well as prior herpes zoster infections.4-9
Cutaneous sarcoidosis has a wide range of clinical presentations. Lesions can be described as specific or nonspecific. Specific lesions demonstrate the typical sarcoid granuloma on histology and more often are seen in chronic disease, while nonspecific lesions more often are seen in acute disease.3,10 Scar sarcoidosis is an example of a specific lesion in which old scars become infiltrated with noncaseating granulomas. The granulomas typically are in the superficial dermis but may involve the full thickness of the dermis, extending into the subcutaneous tissue.11 The cause of granulomas developing in scars is unknown. Prior contamination of the scar with foreign material, possibly at the time of the trauma, is a possible underlying cause.12
Typical scar sarcoidosis presents as swollen, erythematous, indurated lesions with a purple-red hue that may become brown.3,12 Tenderness or pruritus also may be present.13 Interestingly, our patient's scar sarcoidosis presented with a yellow hue at both mastectomy sites.
Diagnosing scar sarcoidosis can be challenging. Patients are diagnosed with sarcoidosis when a compatible clinical or radiologic picture is present along with histologic evidence of a noncaseating granuloma and other potential causes are excluded.11 The differential includes an infectious etiology, other types of granulomatous dermatitis, hypertrophic scar, keloid, or foreign body granuloma.
Scar sarcoidosis can be isolated in occurrence. It also can precede or occur concomitantly or during a relapse of systemic sarcoidosis.10 Most commonly, patients with scar sarcoidosis also have systemic manifestations of sarcoidosis, and changing scars may be an indicator of disease exacerbation or relapse.10 For patients who only demonstrate specific skin lesions of cutaneous sarcoidosis, approximately 30% develop systemic involvement later in life.3 For this reason, close monitoring and regular follow-up are necessary.
Treatment of scar sarcoidosis is dependent on the extent of the disease and presence of systemic sarcoidosis. Topical and systemic corticosteroids, hydroxychloroquine, chloroquine phosphate, and methotrexate all have been shown to be helpful in treating cutaneous sarcoidosis.3 For scar sarcoidosis that is limited to only the scar site, as seen in our case, monitoring and close follow-up is acceptable. Topical steroids can be prescribed for symptomatic relief. Scar sarcoidosis can resolve slowly and spontaneously over time.10 Our patient notably improved 1 year after the initial presentation without treatment.
Scar sarcoidosis is a well-documented variant of cutaneous sarcoidosis that can have important implications for diagnosing systemic sarcoidosis. Although there are typical lesions that represent scar sarcoidosis, it is important to have a high degree of suspicion with any changing scar. Once diagnosed through biopsy, a thorough investigation for systemic signs of sarcoidosis needs to be performed to guide treatment.
- Bolognia JL, Jorizzo JL, Shaffer JV, eds. Dermatology. 3rd ed. Vol 2. Philadelphia, PA: Elsevier/Saunders; 2012.
- Neville E, Walker AN, James DG. Prognostic factors predicting the outcome of sarcoidosis: an analysis of 818 patients. Q J Med. 1983;52:525-533.
- Mañá J, Marcoval J, Graells J, et al. Cutaneous involvement in sarcoidosis: relationship to systemic disease. Arch Dermatol. 1997;133:882-888.
- Dal Sacco D, Cozzani E, Parodi A, et al. Scar sarcoidosis after hyaluronic acid injection. Int J Dermatol. 2005;44:411-412.
- Kormeili T, Neel V, Moy RL. Cutaneous sarcoidosis at sites of previous laser surgery. Cutis. 2004;73:53-55.
- Nayar M. Sarcoidosis on ritual scarification. Int J Dermatol. 1993;32:116-118.
- James WD, Elston DM, Berger TG, et al. Andrews' Diseases of the Skin: Clinical Dermatology. 11th ed. Philadelphia, PA: Elsevier/Saunders; 2011.
- Healsmith MF, Hutchinson PE. The development of scar sarcoidosis at the site of desensitization injections. Clin Exp Dermatol. 1992;17:369-370.
- Singal A, Vij A, Pandhi D. Post herpes-zoster scar sarcoidosis with pulmonary involvement. Indian Dermatol Online J. 2014;5:77-79.
- Chudomirova K, Velichkova L, Anavi B, et al. Recurrent sarcoidosis in skin scars accompanying systemic sarcoidosis. J Eur Acad Dermatol Venereol. 2003;17:360-361.
- Selim A, Ehrsam E, Atassi MB, et al. Scar sarcoidosis: a case report and brief review. Cutis. 2006;78:418-422.
- Singal A, Thami GP, Goraya JS. Scar sarcoidosis in childhood: case report and review of the literature. Clin Exp Dermatol. 2005;30:244-246.
- Marchell RM, Judson MA. Chronic cutaneous lesions of sarcoidosis. Clin Dermatol. 2007;25:295-302.
- Bolognia JL, Jorizzo JL, Shaffer JV, eds. Dermatology. 3rd ed. Vol 2. Philadelphia, PA: Elsevier/Saunders; 2012.
- Neville E, Walker AN, James DG. Prognostic factors predicting the outcome of sarcoidosis: an analysis of 818 patients. Q J Med. 1983;52:525-533.
- Mañá J, Marcoval J, Graells J, et al. Cutaneous involvement in sarcoidosis: relationship to systemic disease. Arch Dermatol. 1997;133:882-888.
- Dal Sacco D, Cozzani E, Parodi A, et al. Scar sarcoidosis after hyaluronic acid injection. Int J Dermatol. 2005;44:411-412.
- Kormeili T, Neel V, Moy RL. Cutaneous sarcoidosis at sites of previous laser surgery. Cutis. 2004;73:53-55.
- Nayar M. Sarcoidosis on ritual scarification. Int J Dermatol. 1993;32:116-118.
- James WD, Elston DM, Berger TG, et al. Andrews' Diseases of the Skin: Clinical Dermatology. 11th ed. Philadelphia, PA: Elsevier/Saunders; 2011.
- Healsmith MF, Hutchinson PE. The development of scar sarcoidosis at the site of desensitization injections. Clin Exp Dermatol. 1992;17:369-370.
- Singal A, Vij A, Pandhi D. Post herpes-zoster scar sarcoidosis with pulmonary involvement. Indian Dermatol Online J. 2014;5:77-79.
- Chudomirova K, Velichkova L, Anavi B, et al. Recurrent sarcoidosis in skin scars accompanying systemic sarcoidosis. J Eur Acad Dermatol Venereol. 2003;17:360-361.
- Selim A, Ehrsam E, Atassi MB, et al. Scar sarcoidosis: a case report and brief review. Cutis. 2006;78:418-422.
- Singal A, Thami GP, Goraya JS. Scar sarcoidosis in childhood: case report and review of the literature. Clin Exp Dermatol. 2005;30:244-246.
- Marchell RM, Judson MA. Chronic cutaneous lesions of sarcoidosis. Clin Dermatol. 2007;25:295-302.

A 57-year-old woman with triple-negative ductal breast cancer presented with a mildly pruritic rash on bilateral mastectomy scars of 3 to 4 months' duration. More than a year prior to presentation, she was diagnosed with breast cancer and treated with a bilateral mastectomy and chemotherapy. On physical examination, faintly yellow, slightly indurated, coalescing papules with red rims were present on the bilateral mastectomy scars, with the scar on the left side appearing worse than the right. She previously had not sought treatment.

Management of Rodenticide Poisoning Associated with Synthetic Cannabinoids
Between March 7, 2018, and May 9, 2018, at least 164 people in Illinois were sickened by synthetic cannabinoids laced with rodenticides. The Illinois Department of Public Health has reported 4 deaths connected with the use of synthetic cannabinoids (sold under names such as Spice, K2, Legal Weed, etc).1 Synthetic cannabinoids are mind-altering chemicals that are sprayed on dried plant material and often sold at convenience stores. Some users have reported smoking these substances because they are generally not detected by standard urine toxicology tests.
Recreational use of synthetic cannabinoids can lead to serious and, at times, deadly complications. Chemicals found in rat poison have contaminated batches of synthetic cannabinoids, leading to coagulopathy and severe bleeding. Affected patients have reported hemoptysis, hematuria, severe epistaxis, bleeding gums, conjunctival hemorrhages, and gastrointestinal bleeding. The following case is of a patient who presented to an emergency department (ED) with severe coagulopathy and cardiotoxicity after using an adulterated synthetic cannabinoid product.
Case Presentation
A 65-year-old man presented to the ED reporting hematochezia, hematuria, and hemoptysis. He reported that these symptoms began about 1 day after he had smoked a synthetic cannabinoid called K2. The patient stated that some of his friends who used the same product were experiencing similar symptoms. He reported mild generalized abdominal pain but reported no chest pain, dyspnea, headache, fevers, chills, or dysuria.
The patient’s past medical history included hypertension, dyslipidemia, chronic lower back pain, and vitamin D deficiency. His past surgical history was notable for an exploratory laparotomy after a stab wound to the abdomen. The patient reported taking the following medications: morphine SA 30 mg bid, meloxicam 15 mg daily, amitriptyline 100 mg qhs, amlodipine 5 mg daily, hydrocodone/acetaminophen 5/325 mg q12h prn, atorvastatin 20 mg qhs, omeprazole 20 mg qam, senna 187 mg daily prn, psyllium 1 packet dissolved in water daily prn, and cholecalciferol 1,000 IU daily.
The patient’s temperature was 98o F, blood pressure, 144/80 mm Hg; pulse, 131 beats per minute; respiratory rate, 18 breaths per minute; and O2 saturation, 98% (ambient air). A physical examination revealed no acute distress; he was coughing up blood; clear lungs; heart sounds were tachycardic and irregularly irregular; soft, nondistended, mild generalized tenderness in the abdomen with no guarding and no rebound. The pertinent laboratory tests were international normalized ratio (INR), > 20; prothrombin time, > 150 seconds; prothrombin thromboplastin time, 157 seconds; hemoglobin, 13.3 g/dL; platelet count, 195 k/uL; white blood count, 11.3 k/uL; creatinine, 0.57mg/dL; potassium, 3.8 mmol/L, D-dimertest, 0.87 ug/mL fibrinogen equivalent units; fibrinogen level, 624 mg/dL; troponin, < 0.04 ng/mL; lactic acid, 1.3 mmol/L; total bilirubin, 0.8 mg/dL; alanine aminotransferase, 22 U/L, aspartate aminotransferase, 22 U/L; alkaline phosphatase, 89 U/L; urinalysis with > 50 red blood cells/high power field; large blood, negative leukocyte esterase, negative nitrite. The patient’s urine toxicology was negative for cannabinoids, methadone, amphetamines, cocaine, and benzodiazepines; but was positive for opiates. An anticoagulant poisoning panel also was ordered.
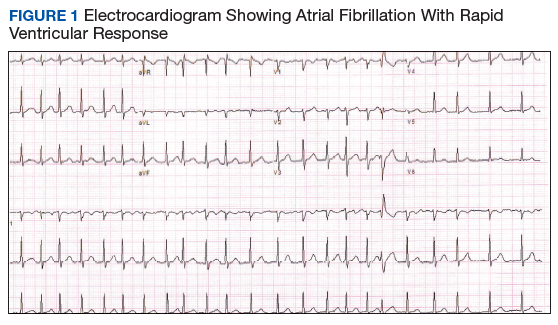
An electrocardiogram (ECG) and imaging studies were ordered. The ECG showed atrial fibrillation (AF) with rapid ventricular response (Figure 1). A chest X-ray indicated bibasilar consolidations that were worse on the right side. A noncontrast computed tomography (CT) of the head did not show intracranial bleeding. An abdomen/pelvis CT showed bilateral diffuse patchy peribronchovascular ground-glass opacities in the lung bases that could represent pulmonary hemorrhage, but no peritoneal or retroperitoneal bleeding.
Treatment
In the ED, the case was discussed with the Illinois Poison Control Center. The patient was diagnosed with coagulopathy likely due to anticoagulant poisoning. He was immediately treated with 10 mg of IV vitamin K, a fixed dose of 2,000 units of 4-factor prothrombin complex concentrate, and 4 units of fresh frozen plasma. His INR improved to 1.42 within several hours. He received 5 mg of IV metoprolol for uncontrolled AF and was admitted to the intensive care unit (ICU) for further care.
In the ICU the patient was started on oral vitamin K 50 mg tid for ongoing treatment of coagulopathy due to concern for possible rodenticide poisoning associated with very long half-life. This dose was then decreased to 50 mg bid. He was given IV fluid resuscitation with normal saline and started on rate control for AF with oral metoprolol. His heart rate improved. An echocardiogram showed new cardiomyopathy with an ejection fraction of 25% to 30%. Given basilar infiltrates and 1 episode of low-grade fever, he was started on ceftriaxone for possible community-acquired pneumonia. The patient was started on cholestyramine to help with washout of the possible rodenticide. No endoscopic interventions were performed.
The patient was transferred to an inpatient telemetry floor 24 hours after admission to the ICU once his tachycardia and bleeding improved. He did not require transfusion of packed red blood cells. In the ICU his INR had ranged between 1.62 and 2.46 (down from > 20 in the ED). His hemoglobin dropped from 13.3 g/dL on admission to 12 g/dL on transfer from the ICU, before stabilizing around 11 g/dL on the floor. The patient’s heart rate required better control, so metoprolol was increased to a total daily dose of 200 mg on the telemetry floor. Oral digoxin was then added after a digoxin load for additional rate control, as the patient remained tachycardic. Twice a day the patient continued to take 50 mg vitamin K. Cholestyramine and ceftriaxone were initially continued, but when the INR started increasing again, the cholestyramine was stopped to allow for an increase to more frequent 3-times daily vitamin 50 mg K administration (cholestyramine can interfere with vitamin K absorption). According to the toxicology service, there was only weak evidence to support use of cholestyramine in this setting.
Given his ongoing mild hemoptysis, the patient received first 1 unit, and then another 4 units of FFP when the INR increased to 3.96 despite oral vitamin K. After FFP, the INR decreased to 1.93 and subsequently to 1.52. A CT of the chest showed patchy ground-glass densities throughout the lungs, predominantly at the lung bases and to a lesser extent in the upper lobes. The findings were felt to represent pulmonary hemorrhage given the patient’s history of hemoptysis (Figure 2). 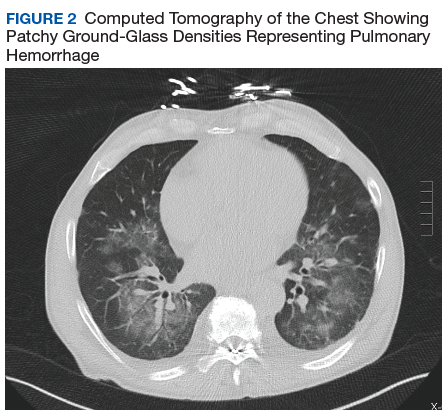
The patient’s heart rate control improved, and he remained hemodynamically stable. A thyroid function test was within normal limits. Lisinopril was added to metoprolol and digoxin given his newly diagnosed cardiomyopathy. The patient was observed for a total of 4 days on the inpatient floor and discharged after his INR stabilized around 1.5 on twice daily 50 mg vitamin K. The patient’s hematuria and hematochezia completely resolved, and hemoptysis was much improved at the time of discharge. His hemoglobin remained stable. The anticoagulant poisoning panel came back positive for
The patient has remained in AF at all follow-up visits. The INR normalized by 6 weeks after hospital discharge, and the dose of vitamin K slowly was tapered with close monitoring of the INR. Vitamin K was tapered for about 6 months after his initial presentation, and the patient was started on a direct oral anticoagulant (DOAC) for anticoagulation when the INR remained stable off vitamin K. He subsequently underwent a transesophageal echocardiogram followed by an attempt at direct current (DC) cardioversion; however, he did not remain in sinus rhythm, and is being continued on anticoagulation and rate control for his AF.
Discussion
Users generally smoke synthetic cannabinoids, which produce cannabis-like effects. However, atypical intoxication effects with worse complications often occur.2 These products typically contain dried shredded plant material that is soaked in or sprayed with several synthetic cannabinoids, varying in dosage and combination.3 Synthetic cannabinoids have been associated with serious adverse effects (AEs), including drowsiness, light-headedness, and fast or irregular heartbeat.4 More severe clinical features such as psychosis, delirium, cardiotoxicity, seizures, rhabdomyolysis, acute kidney injury, hyperthermia, myocardial ischemia, ischemic strokes, and death have also been noted.4
It is not known how some batches of synthetic cannabinoids came to be contaminated with rat poison or how commonly such an adulteration is found across the country. Several different guidelines provide pathways for the treatment of acute bleeding in the setting of coagulopathy due to vitamin K antagonists.5,6 Each guideline divides the indications for reversal into either severity of bleeding or the criticality of the bleeding based on location.5,6 All guidelines recommend the use of vitamin K (either oral or IV) followed by FFP or 4-factor prothrombin complex concentrate (PCC) for more severe bleeding.5,6 However, recommendations regarding the use of PCC vary in dosing for vitamin K antagonists (in contrast to treatment of coagulopathy due to DOACs). Recent studies and guidelines suggest that fixed-dose (rather than weight-based dose) PCC is effective for the reversal of coagulopathy due to vitamin K antagonists.6,7 Using fixed rather than weight-based dosing decreases cost and may decrease the possibility of thrombotic AEs.7 In this patient, a fixed-dose of 2,000 units of PCC was given based on data that were extrapolated from warfarin reversal using PCC.7
The vitamin K antagonists that adulterated this patient’s synthetic cannabinoid were difenacoum and brodifacoum, which are 4-hydroxycoumarin derivatives. These are second-generation long-acting anticoagulant rodenticides (LAARs) that are about 100 times more potent than warfarin.8 As the name implies, LAARs have a longer duration of action in the body of any organism that ingests the poison, which is due to the highly lipophilic groups that have been added to the warfarin molecule to combat resistance in rodents.9
As a result of the deposition in the tissues, there have been reports of the duration of action of brodifacoum ranging from 51 days to 9 months after ingestion, with the latter caused by an intentional overdose in a human.9-12 Reports suggest that coagulopathy is not likely to occur when the serum brodifacoum concentration is < 10 ng/mL.13,14 Animal models show difenacoum has a tissue half-life of about 62 days.15 Reports of difenacoum poisoning in humans have shown variable lengths of treatment, ranging from 30 to 47 days.16-18 The length of treatment for either brodifacoum or difenacoum will depend on the amount of poison exposure.
The long duration of action and treatment duration may lead to problems with drug procurement, especially in the early phase of treatment in which IV vitamin K is used. The supply of IV vitamin K recently has been limited for at least some manufacturers. According to the American Society of Health System Pharmacists Current Drug Shortage List, the increased demand is thought to be due to increased use of synthetic inhaled cannabinoids laced with anticoagulant.19 IV vitamin K products are available from suppliers such as Amphastar (Rancho Cucamonga, CA) and Hospira (Lake Forest, IL).
The American College of Chest Physicians recommends IV vitamin K administration in patients with major bleeding secondary to vitamin K antagonists.20 The oral route is thought to be more effective than a subcutaneous route in the treatment of nonbleeding patients with rodenticide-associated coagulopathy. Due to erratic and unpredictable absorption, the subcutaneous route of administration has fallen out of favor. Oral vitamin K products were not affected by the recent shortage. However, large doses of oral vitamin K can be costly. Due to the long half-life of LAAR, many patients are discharged with a prescription for oral vitamin K. Although vitamin K is found in most over-the-counter (OTC) multivitamins, the strength is insufficient. Most OTC formulations are ≤ 100 μg, whereas the prescription strength is 5 mg, but patients being treated for rodenticide poisoning require much larger doses.
Commercial insurance carriers and Medicare Part D usually do not cover vitamins and minerals unless it is for a medically accepted indication or is an indication supported by citation in either the American Hospital Formulary System, United States Pharmacopeia drug information book, or an electronic information resource that is supported by evidence such as Micromedex.21 For a patient without insurance coverage being treated with high-dose vitamin K therapy for rodenticide poisoning outside of a federal health care system, the cost could be as high as $500 to $1,000 per day, depending on the dose of vitamin K needed to maintain an acceptable INR.
Conclusion
In addition to bleeding as a result of coagulopathy, this patient presented with new onset of AF with rapid ventricular response and a newly diagnosed cardiomyopathy. Although the patient had other cardiovascular risk factors, such as hypertension, dyslipidemia, and a remote history of cocaine use, it is likely that the use of the synthetic cannabinoids contributed to the development and/or worsening of this arrhythmia and cardiomyopathy. The patient remained in AF 6 weeks after hospital discharge with a controlled ventricular rate on metoprolol and digoxin. An interval echocardiogram 6 weeks after hospital discharge showed a recovered ejection fraction. In cases of tachycardia-induced cardiomyopathy, the ejection fraction often recovers with control of the tachycardia. The patient was weaned off vitamin K about 6 months after his initial presentation and started on a DOAC for anticoagulation. He subsequently underwent a transesophageal echocardiogram followed by an attempt at DC cardioversion; however, he did not remain in sinus rhythm and is being continued on anticoagulation and rate control for his AF.
Although unclear how synthetic cannabinoids became adulterated with a potent vitamin K antagonist, health care practitioners should consider this if a patient presents with unexplained coagulopathy and widespread bleeding. Fixed-dose PCC should be considered as an alternative to weight-based dosing in these cases. Physicians and pharmacy personnel should anticipate a need for long-term high doses of vitamin K in order to begin work early to obtain sufficient supplies to treat presenting patients.
1. Illinois Department of Public Health. Synthetic cannabinoids. http://dph.illinois.gov/topics-services/prevention-wellness/medical-cannabis/synthetic-cannabinoids. Updated May 30, 2018. Accessed April 8, 2019.
2. Tournebize J, Gibaja V, Kahn JP. Acute effects of synthetic cannabinoids: update 2015. Subst Abus. 2017;38(3):344-366.
3. United Nations Office on Drugs and Crime. Global SMART update. https://www.unodc.org/documents/scientific/Global_SMART_Update_13_web.pdf. Published March 2015. Accessed April 8, 2019.
4. Adams AJ, Banister SD, Irizarry L, Trecki J, Schwartz M, Gerona R, “Zombie” outbreak caused by the synthetic cannabinoid AMB-FUBINACA in New York. N Engl J Med. 2017;376(3):235-242.
5. Tomaselli GF, Mahaffey KW, Cuker A, et al. 2017 ACC expert consensus decision pathway on management of bleeding in patients on oral anticoagulants: a report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J Am Coll Cardiol. 2017;70(24):3042-3067.
6. Cushman M, Lim W, Zakai NA. 2011 Clinical Practice guide on anticoagulant dosing and management of anticoagulant-associated bleeding complications in adults. http://www.hematology.org/Clinicians/Guidelines-Quality/Quick-Ref/525.aspx. Published 2011. Accessed April 8, 2019.
7. Klein L, Peters J, Miner J, Gorlin J. Evaluation of fixed dose 4-factor prothrombin complex concentrate for emergent warfarin reversal. Am J Emerg Med. 2015;33(9):1213-1218.
8. Bachmann KA, Sullivan TJ. Dispositional and pharmacodynamic characteristics of brodifacoum in warfarin-sensitive rats. Pharmacology. 1983;27(5):281-288.
9. Lipton RA, Klass EM. Human ingestion of ‘superwarfarin’ rodenticide resulting in a prolonged anticoagulant effect. JAMA. 1984;252(21):3004-3005.
10. Chong LL, Chau WK, Ho CH. A case of ‘superwarfarin’ poisoning. Scand J Haematol. 1986;36(3):314-331.
11. Jones EC, Growe GH, Naiman SC. Prolonged anticoagulation in rat poisoning. JAMA. 1984;252(21):3005-3007.
12. Babcock J, Hartman K, Pedersen A, Murphy M, Alving B. Rodenticide-induced coagulopathy in a young child. A case of Munchausen syndrome by proxy. Am J Pediatr Hematol Oncol. 1993;15(1):126-130.
13. Hollinger BR, Pastoor TP. Case management and plasma half-life in a case of brodifacoum poisoning. Arch Intern Med. 1993;153(16):1925-1928.
14. Bruno GR, Howland MA, McMeeking A, Hoffman RS. Long-acting anticoagulant overdose: brodifacoum kinetics and optimal vitamin K dosing. Ann Emerg Med. 2000;36(3):262-267.
15. Vandenbrouke V, Bousquet-Meloua A, De Backer P, Croubels S. Pharmacokinetics of eight anticoagulant rodenticides in mice after single oral administration. J Vet Pharmacol Ther. 2008;31(5):437-445.
16. Barlow AM, Gay AL, Park BK. Difenacoum (Neosorexa) poisoning. Br Med J (Clin Res Ed). 1982;285(6341):541.
17. Katona B, Wason S. Superwarfarin poisoning. J Emerg Med. 1989;7(6):627-631.
18. Butcher GP, Shearer MJ, MacNicoll AD, Kelly MJ, Ind PW. Difenacoum poisoning as a cause of haematuria. Hum Exp Toxicol. 1992;11(6):553-554.
19. American Society of Health System Pharmacists. Current drug shortages. Vitamin K (phytonadione) injection. https://www.ashp.org/drug-shortages/current-shortages/Drug-Shortage-Detail.aspx?id=100. Updated July 5, 2018. Accessed April 8, 2019.
20. Holbrook A, Schulman S, Witt DM, et al. Evidence-based management of anticoagulant therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(suppl 2):e152S-e184S.
21. Centers for Medicare and Medicaid Services. Part D Excluded Drugs. https://www.medicareadvocacy.org/old-site/News/Archives/PartD_ExcludedDrugsByState.htm. Accessed on August 23, 2018.
Between March 7, 2018, and May 9, 2018, at least 164 people in Illinois were sickened by synthetic cannabinoids laced with rodenticides. The Illinois Department of Public Health has reported 4 deaths connected with the use of synthetic cannabinoids (sold under names such as Spice, K2, Legal Weed, etc).1 Synthetic cannabinoids are mind-altering chemicals that are sprayed on dried plant material and often sold at convenience stores. Some users have reported smoking these substances because they are generally not detected by standard urine toxicology tests.
Recreational use of synthetic cannabinoids can lead to serious and, at times, deadly complications. Chemicals found in rat poison have contaminated batches of synthetic cannabinoids, leading to coagulopathy and severe bleeding. Affected patients have reported hemoptysis, hematuria, severe epistaxis, bleeding gums, conjunctival hemorrhages, and gastrointestinal bleeding. The following case is of a patient who presented to an emergency department (ED) with severe coagulopathy and cardiotoxicity after using an adulterated synthetic cannabinoid product.
Case Presentation
A 65-year-old man presented to the ED reporting hematochezia, hematuria, and hemoptysis. He reported that these symptoms began about 1 day after he had smoked a synthetic cannabinoid called K2. The patient stated that some of his friends who used the same product were experiencing similar symptoms. He reported mild generalized abdominal pain but reported no chest pain, dyspnea, headache, fevers, chills, or dysuria.
The patient’s past medical history included hypertension, dyslipidemia, chronic lower back pain, and vitamin D deficiency. His past surgical history was notable for an exploratory laparotomy after a stab wound to the abdomen. The patient reported taking the following medications: morphine SA 30 mg bid, meloxicam 15 mg daily, amitriptyline 100 mg qhs, amlodipine 5 mg daily, hydrocodone/acetaminophen 5/325 mg q12h prn, atorvastatin 20 mg qhs, omeprazole 20 mg qam, senna 187 mg daily prn, psyllium 1 packet dissolved in water daily prn, and cholecalciferol 1,000 IU daily.
The patient’s temperature was 98o F, blood pressure, 144/80 mm Hg; pulse, 131 beats per minute; respiratory rate, 18 breaths per minute; and O2 saturation, 98% (ambient air). A physical examination revealed no acute distress; he was coughing up blood; clear lungs; heart sounds were tachycardic and irregularly irregular; soft, nondistended, mild generalized tenderness in the abdomen with no guarding and no rebound. The pertinent laboratory tests were international normalized ratio (INR), > 20; prothrombin time, > 150 seconds; prothrombin thromboplastin time, 157 seconds; hemoglobin, 13.3 g/dL; platelet count, 195 k/uL; white blood count, 11.3 k/uL; creatinine, 0.57mg/dL; potassium, 3.8 mmol/L, D-dimertest, 0.87 ug/mL fibrinogen equivalent units; fibrinogen level, 624 mg/dL; troponin, < 0.04 ng/mL; lactic acid, 1.3 mmol/L; total bilirubin, 0.8 mg/dL; alanine aminotransferase, 22 U/L, aspartate aminotransferase, 22 U/L; alkaline phosphatase, 89 U/L; urinalysis with > 50 red blood cells/high power field; large blood, negative leukocyte esterase, negative nitrite. The patient’s urine toxicology was negative for cannabinoids, methadone, amphetamines, cocaine, and benzodiazepines; but was positive for opiates. An anticoagulant poisoning panel also was ordered.
An electrocardiogram (ECG) and imaging studies were ordered. The ECG showed atrial fibrillation (AF) with rapid ventricular response (Figure 1). A chest X-ray indicated bibasilar consolidations that were worse on the right side. A noncontrast computed tomography (CT) of the head did not show intracranial bleeding. An abdomen/pelvis CT showed bilateral diffuse patchy peribronchovascular ground-glass opacities in the lung bases that could represent pulmonary hemorrhage, but no peritoneal or retroperitoneal bleeding.
Treatment
In the ED, the case was discussed with the Illinois Poison Control Center. The patient was diagnosed with coagulopathy likely due to anticoagulant poisoning. He was immediately treated with 10 mg of IV vitamin K, a fixed dose of 2,000 units of 4-factor prothrombin complex concentrate, and 4 units of fresh frozen plasma. His INR improved to 1.42 within several hours. He received 5 mg of IV metoprolol for uncontrolled AF and was admitted to the intensive care unit (ICU) for further care.
In the ICU the patient was started on oral vitamin K 50 mg tid for ongoing treatment of coagulopathy due to concern for possible rodenticide poisoning associated with very long half-life. This dose was then decreased to 50 mg bid. He was given IV fluid resuscitation with normal saline and started on rate control for AF with oral metoprolol. His heart rate improved. An echocardiogram showed new cardiomyopathy with an ejection fraction of 25% to 30%. Given basilar infiltrates and 1 episode of low-grade fever, he was started on ceftriaxone for possible community-acquired pneumonia. The patient was started on cholestyramine to help with washout of the possible rodenticide. No endoscopic interventions were performed.
The patient was transferred to an inpatient telemetry floor 24 hours after admission to the ICU once his tachycardia and bleeding improved. He did not require transfusion of packed red blood cells. In the ICU his INR had ranged between 1.62 and 2.46 (down from > 20 in the ED). His hemoglobin dropped from 13.3 g/dL on admission to 12 g/dL on transfer from the ICU, before stabilizing around 11 g/dL on the floor. The patient’s heart rate required better control, so metoprolol was increased to a total daily dose of 200 mg on the telemetry floor. Oral digoxin was then added after a digoxin load for additional rate control, as the patient remained tachycardic. Twice a day the patient continued to take 50 mg vitamin K. Cholestyramine and ceftriaxone were initially continued, but when the INR started increasing again, the cholestyramine was stopped to allow for an increase to more frequent 3-times daily vitamin 50 mg K administration (cholestyramine can interfere with vitamin K absorption). According to the toxicology service, there was only weak evidence to support use of cholestyramine in this setting.
Given his ongoing mild hemoptysis, the patient received first 1 unit, and then another 4 units of FFP when the INR increased to 3.96 despite oral vitamin K. After FFP, the INR decreased to 1.93 and subsequently to 1.52. A CT of the chest showed patchy ground-glass densities throughout the lungs, predominantly at the lung bases and to a lesser extent in the upper lobes. The findings were felt to represent pulmonary hemorrhage given the patient’s history of hemoptysis (Figure 2).
The patient’s heart rate control improved, and he remained hemodynamically stable. A thyroid function test was within normal limits. Lisinopril was added to metoprolol and digoxin given his newly diagnosed cardiomyopathy. The patient was observed for a total of 4 days on the inpatient floor and discharged after his INR stabilized around 1.5 on twice daily 50 mg vitamin K. The patient’s hematuria and hematochezia completely resolved, and hemoptysis was much improved at the time of discharge. His hemoglobin remained stable. The anticoagulant poisoning panel came back positive for
The patient has remained in AF at all follow-up visits. The INR normalized by 6 weeks after hospital discharge, and the dose of vitamin K slowly was tapered with close monitoring of the INR. Vitamin K was tapered for about 6 months after his initial presentation, and the patient was started on a direct oral anticoagulant (DOAC) for anticoagulation when the INR remained stable off vitamin K. He subsequently underwent a transesophageal echocardiogram followed by an attempt at direct current (DC) cardioversion; however, he did not remain in sinus rhythm, and is being continued on anticoagulation and rate control for his AF.
Discussion
Users generally smoke synthetic cannabinoids, which produce cannabis-like effects. However, atypical intoxication effects with worse complications often occur.2 These products typically contain dried shredded plant material that is soaked in or sprayed with several synthetic cannabinoids, varying in dosage and combination.3 Synthetic cannabinoids have been associated with serious adverse effects (AEs), including drowsiness, light-headedness, and fast or irregular heartbeat.4 More severe clinical features such as psychosis, delirium, cardiotoxicity, seizures, rhabdomyolysis, acute kidney injury, hyperthermia, myocardial ischemia, ischemic strokes, and death have also been noted.4
It is not known how some batches of synthetic cannabinoids came to be contaminated with rat poison or how commonly such an adulteration is found across the country. Several different guidelines provide pathways for the treatment of acute bleeding in the setting of coagulopathy due to vitamin K antagonists.5,6 Each guideline divides the indications for reversal into either severity of bleeding or the criticality of the bleeding based on location.5,6 All guidelines recommend the use of vitamin K (either oral or IV) followed by FFP or 4-factor prothrombin complex concentrate (PCC) for more severe bleeding.5,6 However, recommendations regarding the use of PCC vary in dosing for vitamin K antagonists (in contrast to treatment of coagulopathy due to DOACs). Recent studies and guidelines suggest that fixed-dose (rather than weight-based dose) PCC is effective for the reversal of coagulopathy due to vitamin K antagonists.6,7 Using fixed rather than weight-based dosing decreases cost and may decrease the possibility of thrombotic AEs.7 In this patient, a fixed-dose of 2,000 units of PCC was given based on data that were extrapolated from warfarin reversal using PCC.7
The vitamin K antagonists that adulterated this patient’s synthetic cannabinoid were difenacoum and brodifacoum, which are 4-hydroxycoumarin derivatives. These are second-generation long-acting anticoagulant rodenticides (LAARs) that are about 100 times more potent than warfarin.8 As the name implies, LAARs have a longer duration of action in the body of any organism that ingests the poison, which is due to the highly lipophilic groups that have been added to the warfarin molecule to combat resistance in rodents.9
As a result of the deposition in the tissues, there have been reports of the duration of action of brodifacoum ranging from 51 days to 9 months after ingestion, with the latter caused by an intentional overdose in a human.9-12 Reports suggest that coagulopathy is not likely to occur when the serum brodifacoum concentration is < 10 ng/mL.13,14 Animal models show difenacoum has a tissue half-life of about 62 days.15 Reports of difenacoum poisoning in humans have shown variable lengths of treatment, ranging from 30 to 47 days.16-18 The length of treatment for either brodifacoum or difenacoum will depend on the amount of poison exposure.
The long duration of action and treatment duration may lead to problems with drug procurement, especially in the early phase of treatment in which IV vitamin K is used. The supply of IV vitamin K recently has been limited for at least some manufacturers. According to the American Society of Health System Pharmacists Current Drug Shortage List, the increased demand is thought to be due to increased use of synthetic inhaled cannabinoids laced with anticoagulant.19 IV vitamin K products are available from suppliers such as Amphastar (Rancho Cucamonga, CA) and Hospira (Lake Forest, IL).
The American College of Chest Physicians recommends IV vitamin K administration in patients with major bleeding secondary to vitamin K antagonists.20 The oral route is thought to be more effective than a subcutaneous route in the treatment of nonbleeding patients with rodenticide-associated coagulopathy. Due to erratic and unpredictable absorption, the subcutaneous route of administration has fallen out of favor. Oral vitamin K products were not affected by the recent shortage. However, large doses of oral vitamin K can be costly. Due to the long half-life of LAAR, many patients are discharged with a prescription for oral vitamin K. Although vitamin K is found in most over-the-counter (OTC) multivitamins, the strength is insufficient. Most OTC formulations are ≤ 100 μg, whereas the prescription strength is 5 mg, but patients being treated for rodenticide poisoning require much larger doses.
Commercial insurance carriers and Medicare Part D usually do not cover vitamins and minerals unless it is for a medically accepted indication or is an indication supported by citation in either the American Hospital Formulary System, United States Pharmacopeia drug information book, or an electronic information resource that is supported by evidence such as Micromedex.21 For a patient without insurance coverage being treated with high-dose vitamin K therapy for rodenticide poisoning outside of a federal health care system, the cost could be as high as $500 to $1,000 per day, depending on the dose of vitamin K needed to maintain an acceptable INR.
Conclusion
In addition to bleeding as a result of coagulopathy, this patient presented with new onset of AF with rapid ventricular response and a newly diagnosed cardiomyopathy. Although the patient had other cardiovascular risk factors, such as hypertension, dyslipidemia, and a remote history of cocaine use, it is likely that the use of the synthetic cannabinoids contributed to the development and/or worsening of this arrhythmia and cardiomyopathy. The patient remained in AF 6 weeks after hospital discharge with a controlled ventricular rate on metoprolol and digoxin. An interval echocardiogram 6 weeks after hospital discharge showed a recovered ejection fraction. In cases of tachycardia-induced cardiomyopathy, the ejection fraction often recovers with control of the tachycardia. The patient was weaned off vitamin K about 6 months after his initial presentation and started on a DOAC for anticoagulation. He subsequently underwent a transesophageal echocardiogram followed by an attempt at DC cardioversion; however, he did not remain in sinus rhythm and is being continued on anticoagulation and rate control for his AF.
Although unclear how synthetic cannabinoids became adulterated with a potent vitamin K antagonist, health care practitioners should consider this if a patient presents with unexplained coagulopathy and widespread bleeding. Fixed-dose PCC should be considered as an alternative to weight-based dosing in these cases. Physicians and pharmacy personnel should anticipate a need for long-term high doses of vitamin K in order to begin work early to obtain sufficient supplies to treat presenting patients.
Between March 7, 2018, and May 9, 2018, at least 164 people in Illinois were sickened by synthetic cannabinoids laced with rodenticides. The Illinois Department of Public Health has reported 4 deaths connected with the use of synthetic cannabinoids (sold under names such as Spice, K2, Legal Weed, etc).1 Synthetic cannabinoids are mind-altering chemicals that are sprayed on dried plant material and often sold at convenience stores. Some users have reported smoking these substances because they are generally not detected by standard urine toxicology tests.
Recreational use of synthetic cannabinoids can lead to serious and, at times, deadly complications. Chemicals found in rat poison have contaminated batches of synthetic cannabinoids, leading to coagulopathy and severe bleeding. Affected patients have reported hemoptysis, hematuria, severe epistaxis, bleeding gums, conjunctival hemorrhages, and gastrointestinal bleeding. The following case is of a patient who presented to an emergency department (ED) with severe coagulopathy and cardiotoxicity after using an adulterated synthetic cannabinoid product.
Case Presentation
A 65-year-old man presented to the ED reporting hematochezia, hematuria, and hemoptysis. He reported that these symptoms began about 1 day after he had smoked a synthetic cannabinoid called K2. The patient stated that some of his friends who used the same product were experiencing similar symptoms. He reported mild generalized abdominal pain but reported no chest pain, dyspnea, headache, fevers, chills, or dysuria.
The patient’s past medical history included hypertension, dyslipidemia, chronic lower back pain, and vitamin D deficiency. His past surgical history was notable for an exploratory laparotomy after a stab wound to the abdomen. The patient reported taking the following medications: morphine SA 30 mg bid, meloxicam 15 mg daily, amitriptyline 100 mg qhs, amlodipine 5 mg daily, hydrocodone/acetaminophen 5/325 mg q12h prn, atorvastatin 20 mg qhs, omeprazole 20 mg qam, senna 187 mg daily prn, psyllium 1 packet dissolved in water daily prn, and cholecalciferol 1,000 IU daily.
The patient’s temperature was 98o F, blood pressure, 144/80 mm Hg; pulse, 131 beats per minute; respiratory rate, 18 breaths per minute; and O2 saturation, 98% (ambient air). A physical examination revealed no acute distress; he was coughing up blood; clear lungs; heart sounds were tachycardic and irregularly irregular; soft, nondistended, mild generalized tenderness in the abdomen with no guarding and no rebound. The pertinent laboratory tests were international normalized ratio (INR), > 20; prothrombin time, > 150 seconds; prothrombin thromboplastin time, 157 seconds; hemoglobin, 13.3 g/dL; platelet count, 195 k/uL; white blood count, 11.3 k/uL; creatinine, 0.57mg/dL; potassium, 3.8 mmol/L, D-dimertest, 0.87 ug/mL fibrinogen equivalent units; fibrinogen level, 624 mg/dL; troponin, < 0.04 ng/mL; lactic acid, 1.3 mmol/L; total bilirubin, 0.8 mg/dL; alanine aminotransferase, 22 U/L, aspartate aminotransferase, 22 U/L; alkaline phosphatase, 89 U/L; urinalysis with > 50 red blood cells/high power field; large blood, negative leukocyte esterase, negative nitrite. The patient’s urine toxicology was negative for cannabinoids, methadone, amphetamines, cocaine, and benzodiazepines; but was positive for opiates. An anticoagulant poisoning panel also was ordered.
An electrocardiogram (ECG) and imaging studies were ordered. The ECG showed atrial fibrillation (AF) with rapid ventricular response (Figure 1). A chest X-ray indicated bibasilar consolidations that were worse on the right side. A noncontrast computed tomography (CT) of the head did not show intracranial bleeding. An abdomen/pelvis CT showed bilateral diffuse patchy peribronchovascular ground-glass opacities in the lung bases that could represent pulmonary hemorrhage, but no peritoneal or retroperitoneal bleeding.
Treatment
In the ED, the case was discussed with the Illinois Poison Control Center. The patient was diagnosed with coagulopathy likely due to anticoagulant poisoning. He was immediately treated with 10 mg of IV vitamin K, a fixed dose of 2,000 units of 4-factor prothrombin complex concentrate, and 4 units of fresh frozen plasma. His INR improved to 1.42 within several hours. He received 5 mg of IV metoprolol for uncontrolled AF and was admitted to the intensive care unit (ICU) for further care.
In the ICU the patient was started on oral vitamin K 50 mg tid for ongoing treatment of coagulopathy due to concern for possible rodenticide poisoning associated with very long half-life. This dose was then decreased to 50 mg bid. He was given IV fluid resuscitation with normal saline and started on rate control for AF with oral metoprolol. His heart rate improved. An echocardiogram showed new cardiomyopathy with an ejection fraction of 25% to 30%. Given basilar infiltrates and 1 episode of low-grade fever, he was started on ceftriaxone for possible community-acquired pneumonia. The patient was started on cholestyramine to help with washout of the possible rodenticide. No endoscopic interventions were performed.
The patient was transferred to an inpatient telemetry floor 24 hours after admission to the ICU once his tachycardia and bleeding improved. He did not require transfusion of packed red blood cells. In the ICU his INR had ranged between 1.62 and 2.46 (down from > 20 in the ED). His hemoglobin dropped from 13.3 g/dL on admission to 12 g/dL on transfer from the ICU, before stabilizing around 11 g/dL on the floor. The patient’s heart rate required better control, so metoprolol was increased to a total daily dose of 200 mg on the telemetry floor. Oral digoxin was then added after a digoxin load for additional rate control, as the patient remained tachycardic. Twice a day the patient continued to take 50 mg vitamin K. Cholestyramine and ceftriaxone were initially continued, but when the INR started increasing again, the cholestyramine was stopped to allow for an increase to more frequent 3-times daily vitamin 50 mg K administration (cholestyramine can interfere with vitamin K absorption). According to the toxicology service, there was only weak evidence to support use of cholestyramine in this setting.
Given his ongoing mild hemoptysis, the patient received first 1 unit, and then another 4 units of FFP when the INR increased to 3.96 despite oral vitamin K. After FFP, the INR decreased to 1.93 and subsequently to 1.52. A CT of the chest showed patchy ground-glass densities throughout the lungs, predominantly at the lung bases and to a lesser extent in the upper lobes. The findings were felt to represent pulmonary hemorrhage given the patient’s history of hemoptysis (Figure 2).
The patient’s heart rate control improved, and he remained hemodynamically stable. A thyroid function test was within normal limits. Lisinopril was added to metoprolol and digoxin given his newly diagnosed cardiomyopathy. The patient was observed for a total of 4 days on the inpatient floor and discharged after his INR stabilized around 1.5 on twice daily 50 mg vitamin K. The patient’s hematuria and hematochezia completely resolved, and hemoptysis was much improved at the time of discharge. His hemoglobin remained stable. The anticoagulant poisoning panel came back positive for
The patient has remained in AF at all follow-up visits. The INR normalized by 6 weeks after hospital discharge, and the dose of vitamin K slowly was tapered with close monitoring of the INR. Vitamin K was tapered for about 6 months after his initial presentation, and the patient was started on a direct oral anticoagulant (DOAC) for anticoagulation when the INR remained stable off vitamin K. He subsequently underwent a transesophageal echocardiogram followed by an attempt at direct current (DC) cardioversion; however, he did not remain in sinus rhythm, and is being continued on anticoagulation and rate control for his AF.
Discussion
Users generally smoke synthetic cannabinoids, which produce cannabis-like effects. However, atypical intoxication effects with worse complications often occur.2 These products typically contain dried shredded plant material that is soaked in or sprayed with several synthetic cannabinoids, varying in dosage and combination.3 Synthetic cannabinoids have been associated with serious adverse effects (AEs), including drowsiness, light-headedness, and fast or irregular heartbeat.4 More severe clinical features such as psychosis, delirium, cardiotoxicity, seizures, rhabdomyolysis, acute kidney injury, hyperthermia, myocardial ischemia, ischemic strokes, and death have also been noted.4
It is not known how some batches of synthetic cannabinoids came to be contaminated with rat poison or how commonly such an adulteration is found across the country. Several different guidelines provide pathways for the treatment of acute bleeding in the setting of coagulopathy due to vitamin K antagonists.5,6 Each guideline divides the indications for reversal into either severity of bleeding or the criticality of the bleeding based on location.5,6 All guidelines recommend the use of vitamin K (either oral or IV) followed by FFP or 4-factor prothrombin complex concentrate (PCC) for more severe bleeding.5,6 However, recommendations regarding the use of PCC vary in dosing for vitamin K antagonists (in contrast to treatment of coagulopathy due to DOACs). Recent studies and guidelines suggest that fixed-dose (rather than weight-based dose) PCC is effective for the reversal of coagulopathy due to vitamin K antagonists.6,7 Using fixed rather than weight-based dosing decreases cost and may decrease the possibility of thrombotic AEs.7 In this patient, a fixed-dose of 2,000 units of PCC was given based on data that were extrapolated from warfarin reversal using PCC.7
The vitamin K antagonists that adulterated this patient’s synthetic cannabinoid were difenacoum and brodifacoum, which are 4-hydroxycoumarin derivatives. These are second-generation long-acting anticoagulant rodenticides (LAARs) that are about 100 times more potent than warfarin.8 As the name implies, LAARs have a longer duration of action in the body of any organism that ingests the poison, which is due to the highly lipophilic groups that have been added to the warfarin molecule to combat resistance in rodents.9
As a result of the deposition in the tissues, there have been reports of the duration of action of brodifacoum ranging from 51 days to 9 months after ingestion, with the latter caused by an intentional overdose in a human.9-12 Reports suggest that coagulopathy is not likely to occur when the serum brodifacoum concentration is < 10 ng/mL.13,14 Animal models show difenacoum has a tissue half-life of about 62 days.15 Reports of difenacoum poisoning in humans have shown variable lengths of treatment, ranging from 30 to 47 days.16-18 The length of treatment for either brodifacoum or difenacoum will depend on the amount of poison exposure.
The long duration of action and treatment duration may lead to problems with drug procurement, especially in the early phase of treatment in which IV vitamin K is used. The supply of IV vitamin K recently has been limited for at least some manufacturers. According to the American Society of Health System Pharmacists Current Drug Shortage List, the increased demand is thought to be due to increased use of synthetic inhaled cannabinoids laced with anticoagulant.19 IV vitamin K products are available from suppliers such as Amphastar (Rancho Cucamonga, CA) and Hospira (Lake Forest, IL).
The American College of Chest Physicians recommends IV vitamin K administration in patients with major bleeding secondary to vitamin K antagonists.20 The oral route is thought to be more effective than a subcutaneous route in the treatment of nonbleeding patients with rodenticide-associated coagulopathy. Due to erratic and unpredictable absorption, the subcutaneous route of administration has fallen out of favor. Oral vitamin K products were not affected by the recent shortage. However, large doses of oral vitamin K can be costly. Due to the long half-life of LAAR, many patients are discharged with a prescription for oral vitamin K. Although vitamin K is found in most over-the-counter (OTC) multivitamins, the strength is insufficient. Most OTC formulations are ≤ 100 μg, whereas the prescription strength is 5 mg, but patients being treated for rodenticide poisoning require much larger doses.
Commercial insurance carriers and Medicare Part D usually do not cover vitamins and minerals unless it is for a medically accepted indication or is an indication supported by citation in either the American Hospital Formulary System, United States Pharmacopeia drug information book, or an electronic information resource that is supported by evidence such as Micromedex.21 For a patient without insurance coverage being treated with high-dose vitamin K therapy for rodenticide poisoning outside of a federal health care system, the cost could be as high as $500 to $1,000 per day, depending on the dose of vitamin K needed to maintain an acceptable INR.
Conclusion
In addition to bleeding as a result of coagulopathy, this patient presented with new onset of AF with rapid ventricular response and a newly diagnosed cardiomyopathy. Although the patient had other cardiovascular risk factors, such as hypertension, dyslipidemia, and a remote history of cocaine use, it is likely that the use of the synthetic cannabinoids contributed to the development and/or worsening of this arrhythmia and cardiomyopathy. The patient remained in AF 6 weeks after hospital discharge with a controlled ventricular rate on metoprolol and digoxin. An interval echocardiogram 6 weeks after hospital discharge showed a recovered ejection fraction. In cases of tachycardia-induced cardiomyopathy, the ejection fraction often recovers with control of the tachycardia. The patient was weaned off vitamin K about 6 months after his initial presentation and started on a DOAC for anticoagulation. He subsequently underwent a transesophageal echocardiogram followed by an attempt at DC cardioversion; however, he did not remain in sinus rhythm and is being continued on anticoagulation and rate control for his AF.
Although unclear how synthetic cannabinoids became adulterated with a potent vitamin K antagonist, health care practitioners should consider this if a patient presents with unexplained coagulopathy and widespread bleeding. Fixed-dose PCC should be considered as an alternative to weight-based dosing in these cases. Physicians and pharmacy personnel should anticipate a need for long-term high doses of vitamin K in order to begin work early to obtain sufficient supplies to treat presenting patients.
1. Illinois Department of Public Health. Synthetic cannabinoids. http://dph.illinois.gov/topics-services/prevention-wellness/medical-cannabis/synthetic-cannabinoids. Updated May 30, 2018. Accessed April 8, 2019.
2. Tournebize J, Gibaja V, Kahn JP. Acute effects of synthetic cannabinoids: update 2015. Subst Abus. 2017;38(3):344-366.
3. United Nations Office on Drugs and Crime. Global SMART update. https://www.unodc.org/documents/scientific/Global_SMART_Update_13_web.pdf. Published March 2015. Accessed April 8, 2019.
4. Adams AJ, Banister SD, Irizarry L, Trecki J, Schwartz M, Gerona R, “Zombie” outbreak caused by the synthetic cannabinoid AMB-FUBINACA in New York. N Engl J Med. 2017;376(3):235-242.
5. Tomaselli GF, Mahaffey KW, Cuker A, et al. 2017 ACC expert consensus decision pathway on management of bleeding in patients on oral anticoagulants: a report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J Am Coll Cardiol. 2017;70(24):3042-3067.
6. Cushman M, Lim W, Zakai NA. 2011 Clinical Practice guide on anticoagulant dosing and management of anticoagulant-associated bleeding complications in adults. http://www.hematology.org/Clinicians/Guidelines-Quality/Quick-Ref/525.aspx. Published 2011. Accessed April 8, 2019.
7. Klein L, Peters J, Miner J, Gorlin J. Evaluation of fixed dose 4-factor prothrombin complex concentrate for emergent warfarin reversal. Am J Emerg Med. 2015;33(9):1213-1218.
8. Bachmann KA, Sullivan TJ. Dispositional and pharmacodynamic characteristics of brodifacoum in warfarin-sensitive rats. Pharmacology. 1983;27(5):281-288.
9. Lipton RA, Klass EM. Human ingestion of ‘superwarfarin’ rodenticide resulting in a prolonged anticoagulant effect. JAMA. 1984;252(21):3004-3005.
10. Chong LL, Chau WK, Ho CH. A case of ‘superwarfarin’ poisoning. Scand J Haematol. 1986;36(3):314-331.
11. Jones EC, Growe GH, Naiman SC. Prolonged anticoagulation in rat poisoning. JAMA. 1984;252(21):3005-3007.
12. Babcock J, Hartman K, Pedersen A, Murphy M, Alving B. Rodenticide-induced coagulopathy in a young child. A case of Munchausen syndrome by proxy. Am J Pediatr Hematol Oncol. 1993;15(1):126-130.
13. Hollinger BR, Pastoor TP. Case management and plasma half-life in a case of brodifacoum poisoning. Arch Intern Med. 1993;153(16):1925-1928.
14. Bruno GR, Howland MA, McMeeking A, Hoffman RS. Long-acting anticoagulant overdose: brodifacoum kinetics and optimal vitamin K dosing. Ann Emerg Med. 2000;36(3):262-267.
15. Vandenbrouke V, Bousquet-Meloua A, De Backer P, Croubels S. Pharmacokinetics of eight anticoagulant rodenticides in mice after single oral administration. J Vet Pharmacol Ther. 2008;31(5):437-445.
16. Barlow AM, Gay AL, Park BK. Difenacoum (Neosorexa) poisoning. Br Med J (Clin Res Ed). 1982;285(6341):541.
17. Katona B, Wason S. Superwarfarin poisoning. J Emerg Med. 1989;7(6):627-631.
18. Butcher GP, Shearer MJ, MacNicoll AD, Kelly MJ, Ind PW. Difenacoum poisoning as a cause of haematuria. Hum Exp Toxicol. 1992;11(6):553-554.
19. American Society of Health System Pharmacists. Current drug shortages. Vitamin K (phytonadione) injection. https://www.ashp.org/drug-shortages/current-shortages/Drug-Shortage-Detail.aspx?id=100. Updated July 5, 2018. Accessed April 8, 2019.
20. Holbrook A, Schulman S, Witt DM, et al. Evidence-based management of anticoagulant therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(suppl 2):e152S-e184S.
21. Centers for Medicare and Medicaid Services. Part D Excluded Drugs. https://www.medicareadvocacy.org/old-site/News/Archives/PartD_ExcludedDrugsByState.htm. Accessed on August 23, 2018.
1. Illinois Department of Public Health. Synthetic cannabinoids. http://dph.illinois.gov/topics-services/prevention-wellness/medical-cannabis/synthetic-cannabinoids. Updated May 30, 2018. Accessed April 8, 2019.
2. Tournebize J, Gibaja V, Kahn JP. Acute effects of synthetic cannabinoids: update 2015. Subst Abus. 2017;38(3):344-366.
3. United Nations Office on Drugs and Crime. Global SMART update. https://www.unodc.org/documents/scientific/Global_SMART_Update_13_web.pdf. Published March 2015. Accessed April 8, 2019.
4. Adams AJ, Banister SD, Irizarry L, Trecki J, Schwartz M, Gerona R, “Zombie” outbreak caused by the synthetic cannabinoid AMB-FUBINACA in New York. N Engl J Med. 2017;376(3):235-242.
5. Tomaselli GF, Mahaffey KW, Cuker A, et al. 2017 ACC expert consensus decision pathway on management of bleeding in patients on oral anticoagulants: a report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J Am Coll Cardiol. 2017;70(24):3042-3067.
6. Cushman M, Lim W, Zakai NA. 2011 Clinical Practice guide on anticoagulant dosing and management of anticoagulant-associated bleeding complications in adults. http://www.hematology.org/Clinicians/Guidelines-Quality/Quick-Ref/525.aspx. Published 2011. Accessed April 8, 2019.
7. Klein L, Peters J, Miner J, Gorlin J. Evaluation of fixed dose 4-factor prothrombin complex concentrate for emergent warfarin reversal. Am J Emerg Med. 2015;33(9):1213-1218.
8. Bachmann KA, Sullivan TJ. Dispositional and pharmacodynamic characteristics of brodifacoum in warfarin-sensitive rats. Pharmacology. 1983;27(5):281-288.
9. Lipton RA, Klass EM. Human ingestion of ‘superwarfarin’ rodenticide resulting in a prolonged anticoagulant effect. JAMA. 1984;252(21):3004-3005.
10. Chong LL, Chau WK, Ho CH. A case of ‘superwarfarin’ poisoning. Scand J Haematol. 1986;36(3):314-331.
11. Jones EC, Growe GH, Naiman SC. Prolonged anticoagulation in rat poisoning. JAMA. 1984;252(21):3005-3007.
12. Babcock J, Hartman K, Pedersen A, Murphy M, Alving B. Rodenticide-induced coagulopathy in a young child. A case of Munchausen syndrome by proxy. Am J Pediatr Hematol Oncol. 1993;15(1):126-130.
13. Hollinger BR, Pastoor TP. Case management and plasma half-life in a case of brodifacoum poisoning. Arch Intern Med. 1993;153(16):1925-1928.
14. Bruno GR, Howland MA, McMeeking A, Hoffman RS. Long-acting anticoagulant overdose: brodifacoum kinetics and optimal vitamin K dosing. Ann Emerg Med. 2000;36(3):262-267.
15. Vandenbrouke V, Bousquet-Meloua A, De Backer P, Croubels S. Pharmacokinetics of eight anticoagulant rodenticides in mice after single oral administration. J Vet Pharmacol Ther. 2008;31(5):437-445.
16. Barlow AM, Gay AL, Park BK. Difenacoum (Neosorexa) poisoning. Br Med J (Clin Res Ed). 1982;285(6341):541.
17. Katona B, Wason S. Superwarfarin poisoning. J Emerg Med. 1989;7(6):627-631.
18. Butcher GP, Shearer MJ, MacNicoll AD, Kelly MJ, Ind PW. Difenacoum poisoning as a cause of haematuria. Hum Exp Toxicol. 1992;11(6):553-554.
19. American Society of Health System Pharmacists. Current drug shortages. Vitamin K (phytonadione) injection. https://www.ashp.org/drug-shortages/current-shortages/Drug-Shortage-Detail.aspx?id=100. Updated July 5, 2018. Accessed April 8, 2019.
20. Holbrook A, Schulman S, Witt DM, et al. Evidence-based management of anticoagulant therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(suppl 2):e152S-e184S.
21. Centers for Medicare and Medicaid Services. Part D Excluded Drugs. https://www.medicareadvocacy.org/old-site/News/Archives/PartD_ExcludedDrugsByState.htm. Accessed on August 23, 2018.
Evaluation of the Mantram Repetition Program for Health Care Providers
According to the National Institute for Occupational Safety and Health (NIOSH), stress is a major problem for more than 18 million US health care workers (HCWs).1 Increases in technology, high patient acuity, and new demands for meeting institutional benchmarks create stressful clinical work environments. HCWs at the US Department of Veterans Affairs (VA) are perhaps at particular risk of experiencing burnout due to the unique needs of VA patients and bureaucratic demands.2 Stress may lead to depression, decreased job satisfaction, and other psychological distress among HCWs.3 This, in turn, affects the delivery of care. High levels of burnout have been associated with increased medication errors, lower quality of care, and lower patient satisfaction scores.4-10
A Cochrane Review found that mental and physical relaxation reduce stress in HCWs.11 Among these, meditative interventions (eg, mindfulness, meditation, yoga) have demonstrated promise.12-14 Results from a systematic meta-analysis of meditative interventions for HCWs indicated small-to-moderate improvements in emotional exhaustion, sense of personal accomplishment, and life satisfaction. Additional research is needed to determine effects of meditative interventions on burnout and caregiver burden.15
Unfortunately, many meditative intervention programs are lengthy and require a significant investment of time. They also require some form of sitting meditation every day, placing additional demands on busy HCWs. There remains a need for practical strategies to reduce HCW stress that are easier to master and practice.
Background
We developed, implemented, evaluated, and modified an evidence-based meditative intervention called the Mantram Repetition Program (MRP) to address workplace stress and burnout. The MRP is a mind-body, spiritually enhanced intervention that offers benefits similar to other types of meditative interventions.16 MRP is composed of 3 primary components: (1) silently repeating a self-selected, meaningful word or phrase (here called a mantram); (2) intentionally slowing down thoughts and behaviors; and (3) developing the ability to focus on a single task at a time (ie, one-pointed attention). The MRP does not require participants to set aside a specific place to practice, and mantram repetition can be initiated intermittently and privately throughout the day (eg, between tasks, while walking or waiting). Examples of 4 sessions (eg, Mantram 1, 2, 3, and 4) can be found on the PsychArmor Institute website (www.psycharmor.org; San Diego, CA).
Initially, the MRP was offered in a group format, in 6 or 8 weekly, 90-minute face-to-face sessions to both patient and nonpatient populations. Studies in veterans with chronic diseases demonstrated improvements in perceived stress, anxiety, and anger, and increased levels of spiritual well-being and quality of life (QOL).17-19 Veterans with posttraumatic stress disorder (PTSD) reported improvements in PTSD symptoms, QOL, and spiritual well-being.20-23 Family caregivers of veterans with dementia reported significant reductions in caregiver burden, depression, and anxiety after participating in the MRP.24
Similar results have substantiated the effects of the MRP among HCWs, including reductions in perceived stress, stress of conscience (ie, the conflict that results from competing values and behaviors in the workplace), and burnout.25-27 HCWs also reported improvements in mindfulness and spiritual well-being.28 In a randomized controlled trial, South Korean nurse managers who completed the MRP demonstrated significant improvements in psychosocial and spiritual well-being and leadership practice and experienced reductions in burnout compared with that of the control group.27 In a qualitative study, the most frequently reported benefits of the MRP were improvements in managing symptoms of stress, anxiety, and feeling out of control.18
HCWs reported they found it difficult to attend the 8-week MRP face-to-face group classes. Therefore, we developed a shorter online version of the MRP consisting of six 1-hour educational sessions: 4 online self-learning modules, and 2 live meeting webinars with the course facilitator.28 VA employees were invited to enroll in the program from June 2013 through 2016 through group e-mails and announcements in the VA Employee Education Service newsletters. Those eligible to participate could earn up to 6 hours of continuing education.
Although the program was generally well accepted, feedback from HCWs indicated that providers still lacked enough time to participate fully. We therefore condensed the MRP into one 90-minute, videotaped webinar entitled “Mind-Body-Spiritual Strategies for a Healthy Workforce: The Mantram Repetition Program.” The webinar was delivered in real time in June 2013 and archived for viewing later. This condensed course provided an overview of the development, theory, and practice of MRP core components. Specific instructions included how to choose and use a mantram; the importance of acting slowly with intention to avoid mistakes; and ways of developing single-pointed attention. Participants were invited to complete a standard course evaluation using an online survey.
This article presents results from qualitative analyses of participant feedback for the condensed MRP in a nationwide sample of more than 1,700 HCWs within the VA. We used template summary analysis to identify themes in participants’ responses to 2 open-ended questions: “What about this learning activity was most useful to you?” and “What about this learning activity was least useful to you?” These results have implications for reducing HCW stress and developing training programs for HCWs.
Analysis
Responses to the what was most useful question were downloaded to a spreadsheet file for analyses. Investigators chose summary template analysis, a rapid qualitative analytic technique, as the best strategy for analyzing these textual data. This technique is often used in health services research when it is unrealistic to use more time-consuming qualitative methods, such as coding.29
To begin, the analyst, a PhD-level anthropologist, read through the feedback to identify similar words, phrases, and/or concepts (ie, themes). Once the analyst gained a sense of general themes, she developed category labels using verbatim words and/or phrases in the feedback (similar to developing in vivo codes.30 She listed these categories at the top of a summary template document, providing a definition for each to ensure analytic rigor.
Next, each category was listed down the left side of the template. Participant feedback was copied and pasted from the spreadsheet form into the appropriate category for each of 200 responses. The investigator identified subthemes within each category. After analysis was completed for the first 200 course participants, the analyst grouped similar categories together into broader domains to further organize the data. She then read through the feedback from the remaining 917 course participants to identify negative cases (ie, dissimilarities in feedback). An additional researcher familiar with the condensed MRP training then examined the categories and domains. Together, they discussed and resolved any inconsistencies in interpretation of the data.
To get a better sense of the full range of perspectives about the training, the analyst then read through the written feedback for the what was least useful question. She scanned the feedback for negative cases that contradicted template findings and noted these in a document. A more balanced evaluation of the course emerged through this secondary analysis.
Results
Online surveys were completed by 1,117 participants, of which three-quarters (841) were female. Two hundred eleven (19%) viewed the condensed MRP in real time. The remaining participants viewed an online video of the course. Anonymous course evaluations captured only gender and professional classification of participants. Participants represented a wide range of professional roles. The majority (63%) held clinical positions with direct patient care. The next largest category included administrative or health information personnel (21%). There were also students and trainees among these categories.
Qualitative Findings
Feedback about the course was organized into categories during analysis: (1) instructional format; (2) mode of delivery; (3) course content; (4) professional and personal empowerment; (5) religion and spirituality; and (6) ease of mantram practice. These categories represented 2 broad domains: feedback about the course and feedback about the intervention.
Instructional Format
HCWs often reported that the most useful aspect of the course was the instructional format. Most cited the ease with which they could understand the materials and helpfulness of the examples of mantram practice. The option to download course materials for later reference was also useful. Some HCWs indicated that the course could have been improved by incorporating an experiential component in which participants paused to practice a mantram.
Mode of Delivery
Delivery mode including the convenience of the training and the flexibility of having the course available at both work and home was mentioned in the feedback. Some HCWs reported that the most useful aspect of the training was the on-demand feature, which allowed them to stop and restart the program as needed. A few, however, referenced technical difficulties with the webinar.
Content
HCWs also indicated that general information about mantram repetition and information regarding the benefits of the intervention (eg, stress reduction) were useful. The scientific basis of mantram was described as useful by some, though others reported it as least useful. Practical guidance regarding the appropriate time and place to practice a mantram as well as concrete information regarding how to select a mantram was mentioned as the most useful by other participants.
Professional and Personal Empowerment
Professional and personal empowerment was referenced in evaluations. Professional development, such as learning a strategy for enhancing work performance, was reported as positive. HCWs also reported that learning a new strategy for self-care and coping with stress was useful. Some described having experienced a sense of validation by participating in the course that was empowering. Finally, some HCWs indicated the personal growth experienced as the most useful.
Religion and Spirituality
General statements regarding the utility of having learned a spiritually-based practice that crossed religious boundaries as well as general references to the power of prayer were listed in the feedback. Other HCWs indicated the usefulness of having learned that a mantram could be secular.
Ease of Mantram
HCWs referenced the ease with which a mantram can be learned and/or practiced. Course participants described the simplicity of mantram repetition and referenced its portability (ie, it can be practiced in many different settings). Finally, the overall flexibility of mantram practice of where and when it can be performed was also described as useful.
Discussion
Qualitative feedback from participant evaluations of a 90-minute, virtual online MRP course suggests that HCWs representing all areas of care are interested in learning practical strategies for managing workplace stress. Participants overwhelmingly perceived mantram practice as feasible to implement, with the portability of mantram repetition described as particularly useful. This aspect of mantram repetition represents a distinct advantage over meditative interventions that require a dedicated space and time in which to practice (eg, yoga postures, sitting meditation).
These preliminary findings also suggest that mantram practice is acceptable to HCWs representing a variety of roles. Participants indicated that they valued learning a meditative practice that can be interpreted as spiritual or secular, depending on the word or phrase chosen. Only 1 participant reported that the practice of mantram conflicted with his/her personal beliefs. A small minority of participants who found the discussion of spirituality disconcerting nevertheless indicated that the intervention was acceptable to them.
The finding that even a 90-minute course was challenging for some HCWs to accommodate speaks to the importance of developing short-duration stress-reduction programs. The standardized Mindfulness Based Stress Reduction (MBSR) program consists of 8 weekly 2.5-hour sessions and a full-day retreat for an overall commitment of 29 to 33 hours.31 Additionally, a systematic review of meditative interventions for informal and professional caregivers found that programs ranged from 4 to 8 weeks.15 These lengthier programs are likely more challenging than the condensed MRP.
These results also suggest the importance of general guidelines for meditative intervention courses for reducing HCW stress. The mode of delivery should be as flexible as possible, allowing course participants to start, stop, and restart the program as needed and to participate from a location most convenient to them. Although presenting evidence for clinical effectiveness is critical for establishing credibility, statistical data should be briefly summarized. An experiential component in which participants are encouraged to practice the intervention will enhance learning and ensure the translation of knowledge into practice. Finally, framing meditative practices as compatible with many different faiths and/or secular will enhance their acceptability.
Three recommended components of an overall strategy for reducing occupational burnout in health care settings include modifying the organizational structure and work processes, improving the fit between the organization and HCWs, and promoting and allowing time for individuals to learn strategies for coping with work-related stress.32 This 90-minute online MRP course represents an aspect of an overall strategy to reduce HCW stress and burnout. Providing opportunities for HCWs to learn strategies for managing stress could enhance the quality of care and improve patient outcomes. Future pragmatic trials could determine whether mantram practice impacts clinical care at the VA and elsewhere.
Limitations
All participants were self-selected; therefore, the findings may be biased favorably toward the intervention. These qualitative analyses are not generalizable. HCWs in other, non-VA settings might have different needs and/or stressors that should be considered in future program development. If this intervention is offered to a wider audience, then other formats ought to be offered, such as print, at-home recordings, live meeting, and face-to-face.
Conclusion
Course participants reported that the condensed 90-minute virtual MRP was convenient to complete. They described the intervention as flexible and easy to learn. Participants indicated that they intended to implement what they learned in the course to reduce work-related stress. This feedback can be used to recommend guidelines for developing meditative interventions aimed at reducing stress in HCWs.
Acknowledgments
This material is based on work supported by the US Department of Veterans Affairs (VA), VA Employee Education Service and with resources from the VA San Diego Healthcare System and the VA Center for Mental Healthcare & Outcomes Research, South Central Mental Illness Research, Education, and Clinical Center at the Central Arkansas Veterans Healthcare System.
1. Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health (NIOSH). Workplace safety and health topic: health care workers. http://www.cdc.gov/niosh/topics/healthcare. Updated May 9, 2018. Accessed April 8, 2019.
2. Voss Horrell SC, Holohan DR, Didion LM, Vance GT. Treating traumatized OEF/OIF veterans: how does trauma treatment affect the clinician? Prof Psychol Res Pract. 2011;42(1):79-86.
3. Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health. Exposure to stress: occupational hazards in hospitals. http://www.cdc.gov/niosh/docs/2008-136/default.html. Published July 2008. Accessed April 9, 2019.
4. Fahrenkopf AM, Sectish TC, Barger LK. Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ. 2008;336(7642):488-491.
5. Melnyk BM, Orsolini L, Tan A, et al. A national study links nurses’ physical and mental health to medical errors and perceived worksite wellness. J Occup Environ Med. 2018;60(2):126-131.
6. Shanafelt TD, Balch CM, Bechamps G, et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251(6):995-1000.
7. Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA. 2002;288(16):1987-1993.
8. Poghosyan L, Clarke SP, Finlayson M, Aiken LH. Nurse burnout and quality of care: cross-national investigation in six countries. Res Nurs Health. 2010;33(4):288-298.
9. Rios-Risquez MI, García-Izquierdo M. Patient satisfaction, stress and burnout in nursing personnel in emergency departments: a cross-sectional study. Int J Nurs Stud. 2016;59:60-67.
10. Vahey DC, Aiken LH, Sloane DM, Clarke SP, Delfino V. Nurse burnout and patient satisfaction. Med Care. 2004;42(2 suppl):II57-II66.
11. Ruotsalainen JH, Verbeek JH, Mariné A, Serra C. Preventing occupational stress in health care workers. Cochrane Database Syst Rev. 2015;7(4):CD002892.
12. Elder C, Nidich S, Moriarty F, Nidich R. Effect of transcendental meditation on employee stress, depression, and burnout: a randomized controlled study. Perm J. 2014;18(1):19-23.
13. Prasad K, Wahner-Roedler DL, Cha SS, Sood A. Effect of a single-session meditation training to reduce stress and improve quality of life among health care professionals: a “dose-ranging” feasibility study. Altern Ther Health Med. 2011;17(3):46-49.
14. Jamieson SD, Tuckey MR. Mindfulness interventions in the workplace: a critique of the current state of the literature. J Occup Health Psychol. 2017;22(2):180-193.
15. Dharmawardene M, Givens J, Wachholtz A, Makowski S, Tjia J. A systematic review and meta-analysis of meditative interventions for informal caregivers and health professionals. BMJ Support Palliat Care. 2016;6(2):160-169.
16. Goyal M, Singh S, Sibinga EM, et al. Meditation programs for psychological stress and well-being: a systematic review and meta-analysis. JAMA Intern Med. 2014;174(3):357-368.
17. Bormann JE, Smith TL, Becker S, et al. Efficacy of frequent mantram repetition on stress, quality of life, and spiritual well-being in veterans: a pilot study. J Holist Nurs. 2005;23(4):395-414.
18. Bormann JE, Oman D, Kemppainen JK, Becker S, Gershwin M, Kelly A. Mantram repetition for stress management in veterans and employees: a critical incident study. J Adv Nurs. 2006;53(5):502-512.
19. Buttner MM, Bormann JE, Weingart K, Andrews T, Ferguson M, Afari N. Multi-site evaluation of a complementary, spiritually-based intervention for veterans: the mantram repetition program. Complement Ther Clin Pract. 2016;22:74-79.
20. Bormann JE, Hurst S, Kelly A. Responses to mantram repetition program from veterans with posttraumatic stress disorder: a qualitative analysis. J Rehabil Res Dev. 2013;50(6):769-784.
21. Bormann JE, Thorp S, Wetherell JL, Golshan S. A spiritually based group intervention for combat veterans with posttraumatic stress disorder: feasibility study. J Holist Nurs. 2008;26(2):109-116.
22. Bormann JE, Thorp SR, Wetherell JL, Golshan S, Lang AJ. Meditation-based mantram intervention for veterans with posttraumatic stress disorder: a randomized trial. Psychol Trauma: Theory Res Pract Policy. 2013;5(3):259-267.
23. Bormann JE, Thorp SR, Smith E, et al. Individual treatment of posttraumatic stress disorder using mantram repetition: a randomized clinical trial. Am J Psych. 2018;175(10):979-988.
24. Bormann JE, Warren KA, Regalbuto L, et al. A spiritually-based caregiver intervention with telephone delivery for family caregivers of veterans with dementia. Fam Community Health. 2009;32(4):345-353.
25. Bormann JE, Becker S, Gershwin M, et al. Relationship of frequent mantram repetition to emotional and spiritual well-being in healthcare workers. J Contin Educ Nurs. 2006;37(5):218-224.
26. Leary F, Weingart K, Topp R, Bormann JE. The effect of mantram repetition on burnout and stress among VA staff. Workplace Health Saf. 2018;66(3):120-128.
27. Yong J, Kim J, Park J, Seo I, Swinton BD. Effects of a spirituality training program on the spiritual and psychosocial well-being of hospital middle manager nurses in Korea. J Contin Educ Nurs. 2011;42(6):280-288.
28. Bormann JE, Walter KH, Leary S, Glaser D. An internet-delivered mantram repetition program for spiritual well-being and mindfulness for health care workers. Spirit Clin Pract. 2017;4(1):64-73.
29. Hamilton S, Pinfold V, Cotney J. Qualitative analysis of mental health service users’ reported experiences of discrimination. Acta Psychiatr Scand. 2016;134(suppl 446):14-22.
30. Ryan GW, Bernard HR. Techniques to identify themes. Field Meth. 2003;15(1):85-109.
31. Hoge EA, Bui E, Marques L, et al. Randomized controlled trial of mindfulness meditation for generalized anxiety disorder: effects on anxiety and stress reactivity. J Clin Psychiatry. 2013;74(8):786-792.
32. Lee RT, Seo B, Hladkyj S, Lovell BL, Schwartzmann L. Correlates of physician burnout across regions and specialties: a meta-analysis. Hum Resour Health. 2013;11(1):48.
According to the National Institute for Occupational Safety and Health (NIOSH), stress is a major problem for more than 18 million US health care workers (HCWs).1 Increases in technology, high patient acuity, and new demands for meeting institutional benchmarks create stressful clinical work environments. HCWs at the US Department of Veterans Affairs (VA) are perhaps at particular risk of experiencing burnout due to the unique needs of VA patients and bureaucratic demands.2 Stress may lead to depression, decreased job satisfaction, and other psychological distress among HCWs.3 This, in turn, affects the delivery of care. High levels of burnout have been associated with increased medication errors, lower quality of care, and lower patient satisfaction scores.4-10
A Cochrane Review found that mental and physical relaxation reduce stress in HCWs.11 Among these, meditative interventions (eg, mindfulness, meditation, yoga) have demonstrated promise.12-14 Results from a systematic meta-analysis of meditative interventions for HCWs indicated small-to-moderate improvements in emotional exhaustion, sense of personal accomplishment, and life satisfaction. Additional research is needed to determine effects of meditative interventions on burnout and caregiver burden.15
Unfortunately, many meditative intervention programs are lengthy and require a significant investment of time. They also require some form of sitting meditation every day, placing additional demands on busy HCWs. There remains a need for practical strategies to reduce HCW stress that are easier to master and practice.
Background
We developed, implemented, evaluated, and modified an evidence-based meditative intervention called the Mantram Repetition Program (MRP) to address workplace stress and burnout. The MRP is a mind-body, spiritually enhanced intervention that offers benefits similar to other types of meditative interventions.16 MRP is composed of 3 primary components: (1) silently repeating a self-selected, meaningful word or phrase (here called a mantram); (2) intentionally slowing down thoughts and behaviors; and (3) developing the ability to focus on a single task at a time (ie, one-pointed attention). The MRP does not require participants to set aside a specific place to practice, and mantram repetition can be initiated intermittently and privately throughout the day (eg, between tasks, while walking or waiting). Examples of 4 sessions (eg, Mantram 1, 2, 3, and 4) can be found on the PsychArmor Institute website (www.psycharmor.org; San Diego, CA).
Initially, the MRP was offered in a group format, in 6 or 8 weekly, 90-minute face-to-face sessions to both patient and nonpatient populations. Studies in veterans with chronic diseases demonstrated improvements in perceived stress, anxiety, and anger, and increased levels of spiritual well-being and quality of life (QOL).17-19 Veterans with posttraumatic stress disorder (PTSD) reported improvements in PTSD symptoms, QOL, and spiritual well-being.20-23 Family caregivers of veterans with dementia reported significant reductions in caregiver burden, depression, and anxiety after participating in the MRP.24
Similar results have substantiated the effects of the MRP among HCWs, including reductions in perceived stress, stress of conscience (ie, the conflict that results from competing values and behaviors in the workplace), and burnout.25-27 HCWs also reported improvements in mindfulness and spiritual well-being.28 In a randomized controlled trial, South Korean nurse managers who completed the MRP demonstrated significant improvements in psychosocial and spiritual well-being and leadership practice and experienced reductions in burnout compared with that of the control group.27 In a qualitative study, the most frequently reported benefits of the MRP were improvements in managing symptoms of stress, anxiety, and feeling out of control.18
HCWs reported they found it difficult to attend the 8-week MRP face-to-face group classes. Therefore, we developed a shorter online version of the MRP consisting of six 1-hour educational sessions: 4 online self-learning modules, and 2 live meeting webinars with the course facilitator.28 VA employees were invited to enroll in the program from June 2013 through 2016 through group e-mails and announcements in the VA Employee Education Service newsletters. Those eligible to participate could earn up to 6 hours of continuing education.
Although the program was generally well accepted, feedback from HCWs indicated that providers still lacked enough time to participate fully. We therefore condensed the MRP into one 90-minute, videotaped webinar entitled “Mind-Body-Spiritual Strategies for a Healthy Workforce: The Mantram Repetition Program.” The webinar was delivered in real time in June 2013 and archived for viewing later. This condensed course provided an overview of the development, theory, and practice of MRP core components. Specific instructions included how to choose and use a mantram; the importance of acting slowly with intention to avoid mistakes; and ways of developing single-pointed attention. Participants were invited to complete a standard course evaluation using an online survey.
This article presents results from qualitative analyses of participant feedback for the condensed MRP in a nationwide sample of more than 1,700 HCWs within the VA. We used template summary analysis to identify themes in participants’ responses to 2 open-ended questions: “What about this learning activity was most useful to you?” and “What about this learning activity was least useful to you?” These results have implications for reducing HCW stress and developing training programs for HCWs.
Analysis
Responses to the what was most useful question were downloaded to a spreadsheet file for analyses. Investigators chose summary template analysis, a rapid qualitative analytic technique, as the best strategy for analyzing these textual data. This technique is often used in health services research when it is unrealistic to use more time-consuming qualitative methods, such as coding.29
To begin, the analyst, a PhD-level anthropologist, read through the feedback to identify similar words, phrases, and/or concepts (ie, themes). Once the analyst gained a sense of general themes, she developed category labels using verbatim words and/or phrases in the feedback (similar to developing in vivo codes.30 She listed these categories at the top of a summary template document, providing a definition for each to ensure analytic rigor.
Next, each category was listed down the left side of the template. Participant feedback was copied and pasted from the spreadsheet form into the appropriate category for each of 200 responses. The investigator identified subthemes within each category. After analysis was completed for the first 200 course participants, the analyst grouped similar categories together into broader domains to further organize the data. She then read through the feedback from the remaining 917 course participants to identify negative cases (ie, dissimilarities in feedback). An additional researcher familiar with the condensed MRP training then examined the categories and domains. Together, they discussed and resolved any inconsistencies in interpretation of the data.
To get a better sense of the full range of perspectives about the training, the analyst then read through the written feedback for the what was least useful question. She scanned the feedback for negative cases that contradicted template findings and noted these in a document. A more balanced evaluation of the course emerged through this secondary analysis.
Results
Online surveys were completed by 1,117 participants, of which three-quarters (841) were female. Two hundred eleven (19%) viewed the condensed MRP in real time. The remaining participants viewed an online video of the course. Anonymous course evaluations captured only gender and professional classification of participants. Participants represented a wide range of professional roles. The majority (63%) held clinical positions with direct patient care. The next largest category included administrative or health information personnel (21%). There were also students and trainees among these categories.
Qualitative Findings
Feedback about the course was organized into categories during analysis: (1) instructional format; (2) mode of delivery; (3) course content; (4) professional and personal empowerment; (5) religion and spirituality; and (6) ease of mantram practice. These categories represented 2 broad domains: feedback about the course and feedback about the intervention.
Instructional Format
HCWs often reported that the most useful aspect of the course was the instructional format. Most cited the ease with which they could understand the materials and helpfulness of the examples of mantram practice. The option to download course materials for later reference was also useful. Some HCWs indicated that the course could have been improved by incorporating an experiential component in which participants paused to practice a mantram.
Mode of Delivery
Delivery mode including the convenience of the training and the flexibility of having the course available at both work and home was mentioned in the feedback. Some HCWs reported that the most useful aspect of the training was the on-demand feature, which allowed them to stop and restart the program as needed. A few, however, referenced technical difficulties with the webinar.
Content
HCWs also indicated that general information about mantram repetition and information regarding the benefits of the intervention (eg, stress reduction) were useful. The scientific basis of mantram was described as useful by some, though others reported it as least useful. Practical guidance regarding the appropriate time and place to practice a mantram as well as concrete information regarding how to select a mantram was mentioned as the most useful by other participants.
Professional and Personal Empowerment
Professional and personal empowerment was referenced in evaluations. Professional development, such as learning a strategy for enhancing work performance, was reported as positive. HCWs also reported that learning a new strategy for self-care and coping with stress was useful. Some described having experienced a sense of validation by participating in the course that was empowering. Finally, some HCWs indicated the personal growth experienced as the most useful.
Religion and Spirituality
General statements regarding the utility of having learned a spiritually-based practice that crossed religious boundaries as well as general references to the power of prayer were listed in the feedback. Other HCWs indicated the usefulness of having learned that a mantram could be secular.
Ease of Mantram
HCWs referenced the ease with which a mantram can be learned and/or practiced. Course participants described the simplicity of mantram repetition and referenced its portability (ie, it can be practiced in many different settings). Finally, the overall flexibility of mantram practice of where and when it can be performed was also described as useful.
Discussion
Qualitative feedback from participant evaluations of a 90-minute, virtual online MRP course suggests that HCWs representing all areas of care are interested in learning practical strategies for managing workplace stress. Participants overwhelmingly perceived mantram practice as feasible to implement, with the portability of mantram repetition described as particularly useful. This aspect of mantram repetition represents a distinct advantage over meditative interventions that require a dedicated space and time in which to practice (eg, yoga postures, sitting meditation).
These preliminary findings also suggest that mantram practice is acceptable to HCWs representing a variety of roles. Participants indicated that they valued learning a meditative practice that can be interpreted as spiritual or secular, depending on the word or phrase chosen. Only 1 participant reported that the practice of mantram conflicted with his/her personal beliefs. A small minority of participants who found the discussion of spirituality disconcerting nevertheless indicated that the intervention was acceptable to them.
The finding that even a 90-minute course was challenging for some HCWs to accommodate speaks to the importance of developing short-duration stress-reduction programs. The standardized Mindfulness Based Stress Reduction (MBSR) program consists of 8 weekly 2.5-hour sessions and a full-day retreat for an overall commitment of 29 to 33 hours.31 Additionally, a systematic review of meditative interventions for informal and professional caregivers found that programs ranged from 4 to 8 weeks.15 These lengthier programs are likely more challenging than the condensed MRP.
These results also suggest the importance of general guidelines for meditative intervention courses for reducing HCW stress. The mode of delivery should be as flexible as possible, allowing course participants to start, stop, and restart the program as needed and to participate from a location most convenient to them. Although presenting evidence for clinical effectiveness is critical for establishing credibility, statistical data should be briefly summarized. An experiential component in which participants are encouraged to practice the intervention will enhance learning and ensure the translation of knowledge into practice. Finally, framing meditative practices as compatible with many different faiths and/or secular will enhance their acceptability.
Three recommended components of an overall strategy for reducing occupational burnout in health care settings include modifying the organizational structure and work processes, improving the fit between the organization and HCWs, and promoting and allowing time for individuals to learn strategies for coping with work-related stress.32 This 90-minute online MRP course represents an aspect of an overall strategy to reduce HCW stress and burnout. Providing opportunities for HCWs to learn strategies for managing stress could enhance the quality of care and improve patient outcomes. Future pragmatic trials could determine whether mantram practice impacts clinical care at the VA and elsewhere.
Limitations
All participants were self-selected; therefore, the findings may be biased favorably toward the intervention. These qualitative analyses are not generalizable. HCWs in other, non-VA settings might have different needs and/or stressors that should be considered in future program development. If this intervention is offered to a wider audience, then other formats ought to be offered, such as print, at-home recordings, live meeting, and face-to-face.
Conclusion
Course participants reported that the condensed 90-minute virtual MRP was convenient to complete. They described the intervention as flexible and easy to learn. Participants indicated that they intended to implement what they learned in the course to reduce work-related stress. This feedback can be used to recommend guidelines for developing meditative interventions aimed at reducing stress in HCWs.
Acknowledgments
This material is based on work supported by the US Department of Veterans Affairs (VA), VA Employee Education Service and with resources from the VA San Diego Healthcare System and the VA Center for Mental Healthcare & Outcomes Research, South Central Mental Illness Research, Education, and Clinical Center at the Central Arkansas Veterans Healthcare System.
According to the National Institute for Occupational Safety and Health (NIOSH), stress is a major problem for more than 18 million US health care workers (HCWs).1 Increases in technology, high patient acuity, and new demands for meeting institutional benchmarks create stressful clinical work environments. HCWs at the US Department of Veterans Affairs (VA) are perhaps at particular risk of experiencing burnout due to the unique needs of VA patients and bureaucratic demands.2 Stress may lead to depression, decreased job satisfaction, and other psychological distress among HCWs.3 This, in turn, affects the delivery of care. High levels of burnout have been associated with increased medication errors, lower quality of care, and lower patient satisfaction scores.4-10
A Cochrane Review found that mental and physical relaxation reduce stress in HCWs.11 Among these, meditative interventions (eg, mindfulness, meditation, yoga) have demonstrated promise.12-14 Results from a systematic meta-analysis of meditative interventions for HCWs indicated small-to-moderate improvements in emotional exhaustion, sense of personal accomplishment, and life satisfaction. Additional research is needed to determine effects of meditative interventions on burnout and caregiver burden.15
Unfortunately, many meditative intervention programs are lengthy and require a significant investment of time. They also require some form of sitting meditation every day, placing additional demands on busy HCWs. There remains a need for practical strategies to reduce HCW stress that are easier to master and practice.
Background
We developed, implemented, evaluated, and modified an evidence-based meditative intervention called the Mantram Repetition Program (MRP) to address workplace stress and burnout. The MRP is a mind-body, spiritually enhanced intervention that offers benefits similar to other types of meditative interventions.16 MRP is composed of 3 primary components: (1) silently repeating a self-selected, meaningful word or phrase (here called a mantram); (2) intentionally slowing down thoughts and behaviors; and (3) developing the ability to focus on a single task at a time (ie, one-pointed attention). The MRP does not require participants to set aside a specific place to practice, and mantram repetition can be initiated intermittently and privately throughout the day (eg, between tasks, while walking or waiting). Examples of 4 sessions (eg, Mantram 1, 2, 3, and 4) can be found on the PsychArmor Institute website (www.psycharmor.org; San Diego, CA).
Initially, the MRP was offered in a group format, in 6 or 8 weekly, 90-minute face-to-face sessions to both patient and nonpatient populations. Studies in veterans with chronic diseases demonstrated improvements in perceived stress, anxiety, and anger, and increased levels of spiritual well-being and quality of life (QOL).17-19 Veterans with posttraumatic stress disorder (PTSD) reported improvements in PTSD symptoms, QOL, and spiritual well-being.20-23 Family caregivers of veterans with dementia reported significant reductions in caregiver burden, depression, and anxiety after participating in the MRP.24
Similar results have substantiated the effects of the MRP among HCWs, including reductions in perceived stress, stress of conscience (ie, the conflict that results from competing values and behaviors in the workplace), and burnout.25-27 HCWs also reported improvements in mindfulness and spiritual well-being.28 In a randomized controlled trial, South Korean nurse managers who completed the MRP demonstrated significant improvements in psychosocial and spiritual well-being and leadership practice and experienced reductions in burnout compared with that of the control group.27 In a qualitative study, the most frequently reported benefits of the MRP were improvements in managing symptoms of stress, anxiety, and feeling out of control.18
HCWs reported they found it difficult to attend the 8-week MRP face-to-face group classes. Therefore, we developed a shorter online version of the MRP consisting of six 1-hour educational sessions: 4 online self-learning modules, and 2 live meeting webinars with the course facilitator.28 VA employees were invited to enroll in the program from June 2013 through 2016 through group e-mails and announcements in the VA Employee Education Service newsletters. Those eligible to participate could earn up to 6 hours of continuing education.
Although the program was generally well accepted, feedback from HCWs indicated that providers still lacked enough time to participate fully. We therefore condensed the MRP into one 90-minute, videotaped webinar entitled “Mind-Body-Spiritual Strategies for a Healthy Workforce: The Mantram Repetition Program.” The webinar was delivered in real time in June 2013 and archived for viewing later. This condensed course provided an overview of the development, theory, and practice of MRP core components. Specific instructions included how to choose and use a mantram; the importance of acting slowly with intention to avoid mistakes; and ways of developing single-pointed attention. Participants were invited to complete a standard course evaluation using an online survey.
This article presents results from qualitative analyses of participant feedback for the condensed MRP in a nationwide sample of more than 1,700 HCWs within the VA. We used template summary analysis to identify themes in participants’ responses to 2 open-ended questions: “What about this learning activity was most useful to you?” and “What about this learning activity was least useful to you?” These results have implications for reducing HCW stress and developing training programs for HCWs.
Analysis
Responses to the what was most useful question were downloaded to a spreadsheet file for analyses. Investigators chose summary template analysis, a rapid qualitative analytic technique, as the best strategy for analyzing these textual data. This technique is often used in health services research when it is unrealistic to use more time-consuming qualitative methods, such as coding.29
To begin, the analyst, a PhD-level anthropologist, read through the feedback to identify similar words, phrases, and/or concepts (ie, themes). Once the analyst gained a sense of general themes, she developed category labels using verbatim words and/or phrases in the feedback (similar to developing in vivo codes.30 She listed these categories at the top of a summary template document, providing a definition for each to ensure analytic rigor.
Next, each category was listed down the left side of the template. Participant feedback was copied and pasted from the spreadsheet form into the appropriate category for each of 200 responses. The investigator identified subthemes within each category. After analysis was completed for the first 200 course participants, the analyst grouped similar categories together into broader domains to further organize the data. She then read through the feedback from the remaining 917 course participants to identify negative cases (ie, dissimilarities in feedback). An additional researcher familiar with the condensed MRP training then examined the categories and domains. Together, they discussed and resolved any inconsistencies in interpretation of the data.
To get a better sense of the full range of perspectives about the training, the analyst then read through the written feedback for the what was least useful question. She scanned the feedback for negative cases that contradicted template findings and noted these in a document. A more balanced evaluation of the course emerged through this secondary analysis.
Results
Online surveys were completed by 1,117 participants, of which three-quarters (841) were female. Two hundred eleven (19%) viewed the condensed MRP in real time. The remaining participants viewed an online video of the course. Anonymous course evaluations captured only gender and professional classification of participants. Participants represented a wide range of professional roles. The majority (63%) held clinical positions with direct patient care. The next largest category included administrative or health information personnel (21%). There were also students and trainees among these categories.
Qualitative Findings
Feedback about the course was organized into categories during analysis: (1) instructional format; (2) mode of delivery; (3) course content; (4) professional and personal empowerment; (5) religion and spirituality; and (6) ease of mantram practice. These categories represented 2 broad domains: feedback about the course and feedback about the intervention.
Instructional Format
HCWs often reported that the most useful aspect of the course was the instructional format. Most cited the ease with which they could understand the materials and helpfulness of the examples of mantram practice. The option to download course materials for later reference was also useful. Some HCWs indicated that the course could have been improved by incorporating an experiential component in which participants paused to practice a mantram.
Mode of Delivery
Delivery mode including the convenience of the training and the flexibility of having the course available at both work and home was mentioned in the feedback. Some HCWs reported that the most useful aspect of the training was the on-demand feature, which allowed them to stop and restart the program as needed. A few, however, referenced technical difficulties with the webinar.
Content
HCWs also indicated that general information about mantram repetition and information regarding the benefits of the intervention (eg, stress reduction) were useful. The scientific basis of mantram was described as useful by some, though others reported it as least useful. Practical guidance regarding the appropriate time and place to practice a mantram as well as concrete information regarding how to select a mantram was mentioned as the most useful by other participants.
Professional and Personal Empowerment
Professional and personal empowerment was referenced in evaluations. Professional development, such as learning a strategy for enhancing work performance, was reported as positive. HCWs also reported that learning a new strategy for self-care and coping with stress was useful. Some described having experienced a sense of validation by participating in the course that was empowering. Finally, some HCWs indicated the personal growth experienced as the most useful.
Religion and Spirituality
General statements regarding the utility of having learned a spiritually-based practice that crossed religious boundaries as well as general references to the power of prayer were listed in the feedback. Other HCWs indicated the usefulness of having learned that a mantram could be secular.
Ease of Mantram
HCWs referenced the ease with which a mantram can be learned and/or practiced. Course participants described the simplicity of mantram repetition and referenced its portability (ie, it can be practiced in many different settings). Finally, the overall flexibility of mantram practice of where and when it can be performed was also described as useful.
Discussion
Qualitative feedback from participant evaluations of a 90-minute, virtual online MRP course suggests that HCWs representing all areas of care are interested in learning practical strategies for managing workplace stress. Participants overwhelmingly perceived mantram practice as feasible to implement, with the portability of mantram repetition described as particularly useful. This aspect of mantram repetition represents a distinct advantage over meditative interventions that require a dedicated space and time in which to practice (eg, yoga postures, sitting meditation).
These preliminary findings also suggest that mantram practice is acceptable to HCWs representing a variety of roles. Participants indicated that they valued learning a meditative practice that can be interpreted as spiritual or secular, depending on the word or phrase chosen. Only 1 participant reported that the practice of mantram conflicted with his/her personal beliefs. A small minority of participants who found the discussion of spirituality disconcerting nevertheless indicated that the intervention was acceptable to them.
The finding that even a 90-minute course was challenging for some HCWs to accommodate speaks to the importance of developing short-duration stress-reduction programs. The standardized Mindfulness Based Stress Reduction (MBSR) program consists of 8 weekly 2.5-hour sessions and a full-day retreat for an overall commitment of 29 to 33 hours.31 Additionally, a systematic review of meditative interventions for informal and professional caregivers found that programs ranged from 4 to 8 weeks.15 These lengthier programs are likely more challenging than the condensed MRP.
These results also suggest the importance of general guidelines for meditative intervention courses for reducing HCW stress. The mode of delivery should be as flexible as possible, allowing course participants to start, stop, and restart the program as needed and to participate from a location most convenient to them. Although presenting evidence for clinical effectiveness is critical for establishing credibility, statistical data should be briefly summarized. An experiential component in which participants are encouraged to practice the intervention will enhance learning and ensure the translation of knowledge into practice. Finally, framing meditative practices as compatible with many different faiths and/or secular will enhance their acceptability.
Three recommended components of an overall strategy for reducing occupational burnout in health care settings include modifying the organizational structure and work processes, improving the fit between the organization and HCWs, and promoting and allowing time for individuals to learn strategies for coping with work-related stress.32 This 90-minute online MRP course represents an aspect of an overall strategy to reduce HCW stress and burnout. Providing opportunities for HCWs to learn strategies for managing stress could enhance the quality of care and improve patient outcomes. Future pragmatic trials could determine whether mantram practice impacts clinical care at the VA and elsewhere.
Limitations
All participants were self-selected; therefore, the findings may be biased favorably toward the intervention. These qualitative analyses are not generalizable. HCWs in other, non-VA settings might have different needs and/or stressors that should be considered in future program development. If this intervention is offered to a wider audience, then other formats ought to be offered, such as print, at-home recordings, live meeting, and face-to-face.
Conclusion
Course participants reported that the condensed 90-minute virtual MRP was convenient to complete. They described the intervention as flexible and easy to learn. Participants indicated that they intended to implement what they learned in the course to reduce work-related stress. This feedback can be used to recommend guidelines for developing meditative interventions aimed at reducing stress in HCWs.
Acknowledgments
This material is based on work supported by the US Department of Veterans Affairs (VA), VA Employee Education Service and with resources from the VA San Diego Healthcare System and the VA Center for Mental Healthcare & Outcomes Research, South Central Mental Illness Research, Education, and Clinical Center at the Central Arkansas Veterans Healthcare System.
1. Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health (NIOSH). Workplace safety and health topic: health care workers. http://www.cdc.gov/niosh/topics/healthcare. Updated May 9, 2018. Accessed April 8, 2019.
2. Voss Horrell SC, Holohan DR, Didion LM, Vance GT. Treating traumatized OEF/OIF veterans: how does trauma treatment affect the clinician? Prof Psychol Res Pract. 2011;42(1):79-86.
3. Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health. Exposure to stress: occupational hazards in hospitals. http://www.cdc.gov/niosh/docs/2008-136/default.html. Published July 2008. Accessed April 9, 2019.
4. Fahrenkopf AM, Sectish TC, Barger LK. Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ. 2008;336(7642):488-491.
5. Melnyk BM, Orsolini L, Tan A, et al. A national study links nurses’ physical and mental health to medical errors and perceived worksite wellness. J Occup Environ Med. 2018;60(2):126-131.
6. Shanafelt TD, Balch CM, Bechamps G, et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251(6):995-1000.
7. Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA. 2002;288(16):1987-1993.
8. Poghosyan L, Clarke SP, Finlayson M, Aiken LH. Nurse burnout and quality of care: cross-national investigation in six countries. Res Nurs Health. 2010;33(4):288-298.
9. Rios-Risquez MI, García-Izquierdo M. Patient satisfaction, stress and burnout in nursing personnel in emergency departments: a cross-sectional study. Int J Nurs Stud. 2016;59:60-67.
10. Vahey DC, Aiken LH, Sloane DM, Clarke SP, Delfino V. Nurse burnout and patient satisfaction. Med Care. 2004;42(2 suppl):II57-II66.
11. Ruotsalainen JH, Verbeek JH, Mariné A, Serra C. Preventing occupational stress in health care workers. Cochrane Database Syst Rev. 2015;7(4):CD002892.
12. Elder C, Nidich S, Moriarty F, Nidich R. Effect of transcendental meditation on employee stress, depression, and burnout: a randomized controlled study. Perm J. 2014;18(1):19-23.
13. Prasad K, Wahner-Roedler DL, Cha SS, Sood A. Effect of a single-session meditation training to reduce stress and improve quality of life among health care professionals: a “dose-ranging” feasibility study. Altern Ther Health Med. 2011;17(3):46-49.
14. Jamieson SD, Tuckey MR. Mindfulness interventions in the workplace: a critique of the current state of the literature. J Occup Health Psychol. 2017;22(2):180-193.
15. Dharmawardene M, Givens J, Wachholtz A, Makowski S, Tjia J. A systematic review and meta-analysis of meditative interventions for informal caregivers and health professionals. BMJ Support Palliat Care. 2016;6(2):160-169.
16. Goyal M, Singh S, Sibinga EM, et al. Meditation programs for psychological stress and well-being: a systematic review and meta-analysis. JAMA Intern Med. 2014;174(3):357-368.
17. Bormann JE, Smith TL, Becker S, et al. Efficacy of frequent mantram repetition on stress, quality of life, and spiritual well-being in veterans: a pilot study. J Holist Nurs. 2005;23(4):395-414.
18. Bormann JE, Oman D, Kemppainen JK, Becker S, Gershwin M, Kelly A. Mantram repetition for stress management in veterans and employees: a critical incident study. J Adv Nurs. 2006;53(5):502-512.
19. Buttner MM, Bormann JE, Weingart K, Andrews T, Ferguson M, Afari N. Multi-site evaluation of a complementary, spiritually-based intervention for veterans: the mantram repetition program. Complement Ther Clin Pract. 2016;22:74-79.
20. Bormann JE, Hurst S, Kelly A. Responses to mantram repetition program from veterans with posttraumatic stress disorder: a qualitative analysis. J Rehabil Res Dev. 2013;50(6):769-784.
21. Bormann JE, Thorp S, Wetherell JL, Golshan S. A spiritually based group intervention for combat veterans with posttraumatic stress disorder: feasibility study. J Holist Nurs. 2008;26(2):109-116.
22. Bormann JE, Thorp SR, Wetherell JL, Golshan S, Lang AJ. Meditation-based mantram intervention for veterans with posttraumatic stress disorder: a randomized trial. Psychol Trauma: Theory Res Pract Policy. 2013;5(3):259-267.
23. Bormann JE, Thorp SR, Smith E, et al. Individual treatment of posttraumatic stress disorder using mantram repetition: a randomized clinical trial. Am J Psych. 2018;175(10):979-988.
24. Bormann JE, Warren KA, Regalbuto L, et al. A spiritually-based caregiver intervention with telephone delivery for family caregivers of veterans with dementia. Fam Community Health. 2009;32(4):345-353.
25. Bormann JE, Becker S, Gershwin M, et al. Relationship of frequent mantram repetition to emotional and spiritual well-being in healthcare workers. J Contin Educ Nurs. 2006;37(5):218-224.
26. Leary F, Weingart K, Topp R, Bormann JE. The effect of mantram repetition on burnout and stress among VA staff. Workplace Health Saf. 2018;66(3):120-128.
27. Yong J, Kim J, Park J, Seo I, Swinton BD. Effects of a spirituality training program on the spiritual and psychosocial well-being of hospital middle manager nurses in Korea. J Contin Educ Nurs. 2011;42(6):280-288.
28. Bormann JE, Walter KH, Leary S, Glaser D. An internet-delivered mantram repetition program for spiritual well-being and mindfulness for health care workers. Spirit Clin Pract. 2017;4(1):64-73.
29. Hamilton S, Pinfold V, Cotney J. Qualitative analysis of mental health service users’ reported experiences of discrimination. Acta Psychiatr Scand. 2016;134(suppl 446):14-22.
30. Ryan GW, Bernard HR. Techniques to identify themes. Field Meth. 2003;15(1):85-109.
31. Hoge EA, Bui E, Marques L, et al. Randomized controlled trial of mindfulness meditation for generalized anxiety disorder: effects on anxiety and stress reactivity. J Clin Psychiatry. 2013;74(8):786-792.
32. Lee RT, Seo B, Hladkyj S, Lovell BL, Schwartzmann L. Correlates of physician burnout across regions and specialties: a meta-analysis. Hum Resour Health. 2013;11(1):48.
1. Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health (NIOSH). Workplace safety and health topic: health care workers. http://www.cdc.gov/niosh/topics/healthcare. Updated May 9, 2018. Accessed April 8, 2019.
2. Voss Horrell SC, Holohan DR, Didion LM, Vance GT. Treating traumatized OEF/OIF veterans: how does trauma treatment affect the clinician? Prof Psychol Res Pract. 2011;42(1):79-86.
3. Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health. Exposure to stress: occupational hazards in hospitals. http://www.cdc.gov/niosh/docs/2008-136/default.html. Published July 2008. Accessed April 9, 2019.
4. Fahrenkopf AM, Sectish TC, Barger LK. Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ. 2008;336(7642):488-491.
5. Melnyk BM, Orsolini L, Tan A, et al. A national study links nurses’ physical and mental health to medical errors and perceived worksite wellness. J Occup Environ Med. 2018;60(2):126-131.
6. Shanafelt TD, Balch CM, Bechamps G, et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251(6):995-1000.
7. Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA. 2002;288(16):1987-1993.
8. Poghosyan L, Clarke SP, Finlayson M, Aiken LH. Nurse burnout and quality of care: cross-national investigation in six countries. Res Nurs Health. 2010;33(4):288-298.
9. Rios-Risquez MI, García-Izquierdo M. Patient satisfaction, stress and burnout in nursing personnel in emergency departments: a cross-sectional study. Int J Nurs Stud. 2016;59:60-67.
10. Vahey DC, Aiken LH, Sloane DM, Clarke SP, Delfino V. Nurse burnout and patient satisfaction. Med Care. 2004;42(2 suppl):II57-II66.
11. Ruotsalainen JH, Verbeek JH, Mariné A, Serra C. Preventing occupational stress in health care workers. Cochrane Database Syst Rev. 2015;7(4):CD002892.
12. Elder C, Nidich S, Moriarty F, Nidich R. Effect of transcendental meditation on employee stress, depression, and burnout: a randomized controlled study. Perm J. 2014;18(1):19-23.
13. Prasad K, Wahner-Roedler DL, Cha SS, Sood A. Effect of a single-session meditation training to reduce stress and improve quality of life among health care professionals: a “dose-ranging” feasibility study. Altern Ther Health Med. 2011;17(3):46-49.
14. Jamieson SD, Tuckey MR. Mindfulness interventions in the workplace: a critique of the current state of the literature. J Occup Health Psychol. 2017;22(2):180-193.
15. Dharmawardene M, Givens J, Wachholtz A, Makowski S, Tjia J. A systematic review and meta-analysis of meditative interventions for informal caregivers and health professionals. BMJ Support Palliat Care. 2016;6(2):160-169.
16. Goyal M, Singh S, Sibinga EM, et al. Meditation programs for psychological stress and well-being: a systematic review and meta-analysis. JAMA Intern Med. 2014;174(3):357-368.
17. Bormann JE, Smith TL, Becker S, et al. Efficacy of frequent mantram repetition on stress, quality of life, and spiritual well-being in veterans: a pilot study. J Holist Nurs. 2005;23(4):395-414.
18. Bormann JE, Oman D, Kemppainen JK, Becker S, Gershwin M, Kelly A. Mantram repetition for stress management in veterans and employees: a critical incident study. J Adv Nurs. 2006;53(5):502-512.
19. Buttner MM, Bormann JE, Weingart K, Andrews T, Ferguson M, Afari N. Multi-site evaluation of a complementary, spiritually-based intervention for veterans: the mantram repetition program. Complement Ther Clin Pract. 2016;22:74-79.
20. Bormann JE, Hurst S, Kelly A. Responses to mantram repetition program from veterans with posttraumatic stress disorder: a qualitative analysis. J Rehabil Res Dev. 2013;50(6):769-784.
21. Bormann JE, Thorp S, Wetherell JL, Golshan S. A spiritually based group intervention for combat veterans with posttraumatic stress disorder: feasibility study. J Holist Nurs. 2008;26(2):109-116.
22. Bormann JE, Thorp SR, Wetherell JL, Golshan S, Lang AJ. Meditation-based mantram intervention for veterans with posttraumatic stress disorder: a randomized trial. Psychol Trauma: Theory Res Pract Policy. 2013;5(3):259-267.
23. Bormann JE, Thorp SR, Smith E, et al. Individual treatment of posttraumatic stress disorder using mantram repetition: a randomized clinical trial. Am J Psych. 2018;175(10):979-988.
24. Bormann JE, Warren KA, Regalbuto L, et al. A spiritually-based caregiver intervention with telephone delivery for family caregivers of veterans with dementia. Fam Community Health. 2009;32(4):345-353.
25. Bormann JE, Becker S, Gershwin M, et al. Relationship of frequent mantram repetition to emotional and spiritual well-being in healthcare workers. J Contin Educ Nurs. 2006;37(5):218-224.
26. Leary F, Weingart K, Topp R, Bormann JE. The effect of mantram repetition on burnout and stress among VA staff. Workplace Health Saf. 2018;66(3):120-128.
27. Yong J, Kim J, Park J, Seo I, Swinton BD. Effects of a spirituality training program on the spiritual and psychosocial well-being of hospital middle manager nurses in Korea. J Contin Educ Nurs. 2011;42(6):280-288.
28. Bormann JE, Walter KH, Leary S, Glaser D. An internet-delivered mantram repetition program for spiritual well-being and mindfulness for health care workers. Spirit Clin Pract. 2017;4(1):64-73.
29. Hamilton S, Pinfold V, Cotney J. Qualitative analysis of mental health service users’ reported experiences of discrimination. Acta Psychiatr Scand. 2016;134(suppl 446):14-22.
30. Ryan GW, Bernard HR. Techniques to identify themes. Field Meth. 2003;15(1):85-109.
31. Hoge EA, Bui E, Marques L, et al. Randomized controlled trial of mindfulness meditation for generalized anxiety disorder: effects on anxiety and stress reactivity. J Clin Psychiatry. 2013;74(8):786-792.
32. Lee RT, Seo B, Hladkyj S, Lovell BL, Schwartzmann L. Correlates of physician burnout across regions and specialties: a meta-analysis. Hum Resour Health. 2013;11(1):48.
Top 10 tips community hospitalists need to know for implementing a QI project
Consider low-cost, high-impact projects
Quality improvement (QI) is essential to the advancement of medicine. QI differs from research as it focuses on already proven knowledge and aims to make quick, sustainable change in local health care systems. Community hospitals may not have organized quality improvement initiatives and often rely on individual hospitalists to be their champions.

Although there are resources for quality improvement projects, initiating a project can seem daunting to a hospitalist. Our aim is to equip the community hospitalist with basic skills to initiate their own successful project. We present our “Top 10” tips to review.
1. Start small: Many quality improvement ideas include grandiose changes that require a large buy-in or worse, more money. When starting a QI project, you need to consider low-cost, high-impact projects. Even the smallest projects can make considerable change. Focus on ideas that require only one or two improvement cycles to implement. Understand your hospital culture, flow, and processes, and then pick a project that is reasonable.
Projects can be as simple as decreasing the number of daily labs ordered by your hospitalist group. Projects that are small could still improve patient satisfaction and decrease costs. Listen to your colleagues, if they are discussing an issue, turn this into an idea! As you learn the culture of your hospital you will be able to tackle larger projects. Plus, it gets your name out there!
2. Establish buy-in: Surround yourself with champions of your cause. Properly identifying and engaging key players is paramount to a successful QI project. First, start with your hospital administration, and garner their support by aligning your project with the goals and objectives that the administration leaders have identified to be important for your institution. Next, select a motivated multidisciplinary team. When choosing your team, be sure to include a representative from the various stakeholders, that is, the individuals who have a variety of hospital roles likely to be affected by the outcome of the project. Stakeholders ensure the success of the project because they have a fundamental understanding of how the project will influence workflow, can predict issues before they arise, and often become empowered to make changes that directly influence their work.
Lastly, include at least one well-respected and highly influential member on your team. Change is always hard, and this person’s support and endorsement of the project, can often move mountains when challenges arise.
3. Know the data collector: It is important to understand what data can be collected because, without data, you cannot measure your success. Arrange a meeting and develop a partnership with the data collector. Obtain a general understanding of how and what specific data is collected. Be sure the data collector has a clear understanding of the project design and the specific details of the project. Include the overall project mission, specific aims of the project, the time frame in which data should be collected, and specific inclusion and exclusion criteria.
Often, data collectors prefer to collect extra data points upfront, even if you end up not using some of them, rather than having to find missing data after the fact. Communication is key, so be available for questions and open to the suggestions of the data collector.
4. Don’t reinvent the wheel: Prior to starting any QI projects, evaluate available resources for project ideas and implementation. The Society of Hospital Medicine and the American College of Physicians outline multiple projects on their websites. Reach out to colleagues at other institutions and obtain their input as they are likely struggling with similar issues and/or have worked on similar project ideas. Use these resources as scaffolding and edit them to fit your institution’s processes and culture, and use their metrics as your measures of success.

5. Remove waste: When determining QI projects, consider focusing on health care waste. Many of the current processes at our institutions have redundancies that add unhealthy time, effort, and inefficiency to our days that can not only impede patient care but also can lead to burnout. When outlining a project idea, consider mapping the process in your interested area to identify those redundancies and inefficiencies. Consider focusing on these instead of building an entirely new process. Improving inefficiencies also can help with provider buy-in with process changes, especially if this helps in improving their everyday frustrations.
6. Express your values: Create a sense of urgency around the problem you are trying to solve. Educate your colleagues to understand the depth of the QI initiative and its impact on their ability to care for patients and patient safety. Express genuine interest in improving your colleagues’ ability to care for patients and improve their days.
Sharing your passion about your project allows people to understand your vested interest in improving the system. This will inspire team members to lead the way to change and encourage colleagues to adopt the recommended changes.
7. Recognize and reward your team: Involve “champions” in every process change. Identify people who are part of your team and ensure they feel valued. Recognition and acknowledgment will allow people to feel more involved and to gain their buy-in. When it comes to results or progress, consider your group’s dynamics. If they are competitive, consider posting progress results on a publicly displayed run chart. If your group is less likely to be motivated by competition, hold individual meetings to help show progress. This is a crucial dynamic to understand, because creating a competitive environment may alienate some members of your group. Remember, the final result is not to blame those lagging behind but to encourage everyone to find the best pathway to success.

8. Be okay with failure: Celebrate your failures because failure is a chance to learn. Every failure is an educational opportunity to understand what not to do, or a chance to gain insight into a process that did not work.
Be a divergent thinker. Start considering problems as part of the path to solution, rather than a barrier in the way. Be open to change and learn from your mistakes. Don’t just be okay with your failures, own them. This will lead to trust with your team members and show your commitment.
9. Finish: This is key. You must finish your project. Even if you anticipate that the project will fail, you should see the project through to its completion. This proves both you and the process of QI are valid and worthwhile; you have to see results and share them with others.
Completing your project also shows your colleagues that you are resilient, committed, and dedicated. Completing a QI project, even with disappointing results, is a success in and of itself. In the end, it is most important to remember to show progress, not perfection.
10. Create sustainability: When your QI project is finished, you need to decide if the changes are sustainable. Some projects show small change and do not need permanent implementation, rather reminders over time. Other projects may be sustainable with EHR or organizational changes. Once you have successful results, your goal should be to find a way to ensure that the process stays in place over time. This is where all your hard work establishing buy-in comes in handy. Your team is more likely to create sustainable change with the hard work you forged through following these key tips.
These Top 10 tips are a hospitalist’s starting point to begin making changes at their own community hospital. Your motivation and effort in making quality change will not go unnoticed. Small ideas will open doors for larger, more sustainable QI projects. Remember, a failure just means a new idea for the next cycle! Enjoy the process of working collaboratively with your hospital on improving quality. Good luck!
Dr. Astik is a hospitalist and instructor of medicine at Northwestern Memorial Hospital, Chicago. Dr. Corbett is a hospitalist and assistant professor at the University of Oklahoma, Tulsa. Dr. Patel is a hospitalist and assistant professor at the University of Colorado, Denver. Dr. Ronan is a hospitalist and associate professor at Christus St. Vincent Regional Medical Center, Santa Fe, NM.
Consider low-cost, high-impact projects
Consider low-cost, high-impact projects
Quality improvement (QI) is essential to the advancement of medicine. QI differs from research as it focuses on already proven knowledge and aims to make quick, sustainable change in local health care systems. Community hospitals may not have organized quality improvement initiatives and often rely on individual hospitalists to be their champions.
Although there are resources for quality improvement projects, initiating a project can seem daunting to a hospitalist. Our aim is to equip the community hospitalist with basic skills to initiate their own successful project. We present our “Top 10” tips to review.
1. Start small: Many quality improvement ideas include grandiose changes that require a large buy-in or worse, more money. When starting a QI project, you need to consider low-cost, high-impact projects. Even the smallest projects can make considerable change. Focus on ideas that require only one or two improvement cycles to implement. Understand your hospital culture, flow, and processes, and then pick a project that is reasonable.
Projects can be as simple as decreasing the number of daily labs ordered by your hospitalist group. Projects that are small could still improve patient satisfaction and decrease costs. Listen to your colleagues, if they are discussing an issue, turn this into an idea! As you learn the culture of your hospital you will be able to tackle larger projects. Plus, it gets your name out there!
2. Establish buy-in: Surround yourself with champions of your cause. Properly identifying and engaging key players is paramount to a successful QI project. First, start with your hospital administration, and garner their support by aligning your project with the goals and objectives that the administration leaders have identified to be important for your institution. Next, select a motivated multidisciplinary team. When choosing your team, be sure to include a representative from the various stakeholders, that is, the individuals who have a variety of hospital roles likely to be affected by the outcome of the project. Stakeholders ensure the success of the project because they have a fundamental understanding of how the project will influence workflow, can predict issues before they arise, and often become empowered to make changes that directly influence their work.
Lastly, include at least one well-respected and highly influential member on your team. Change is always hard, and this person’s support and endorsement of the project, can often move mountains when challenges arise.
3. Know the data collector: It is important to understand what data can be collected because, without data, you cannot measure your success. Arrange a meeting and develop a partnership with the data collector. Obtain a general understanding of how and what specific data is collected. Be sure the data collector has a clear understanding of the project design and the specific details of the project. Include the overall project mission, specific aims of the project, the time frame in which data should be collected, and specific inclusion and exclusion criteria.
Often, data collectors prefer to collect extra data points upfront, even if you end up not using some of them, rather than having to find missing data after the fact. Communication is key, so be available for questions and open to the suggestions of the data collector.
4. Don’t reinvent the wheel: Prior to starting any QI projects, evaluate available resources for project ideas and implementation. The Society of Hospital Medicine and the American College of Physicians outline multiple projects on their websites. Reach out to colleagues at other institutions and obtain their input as they are likely struggling with similar issues and/or have worked on similar project ideas. Use these resources as scaffolding and edit them to fit your institution’s processes and culture, and use their metrics as your measures of success.
5. Remove waste: When determining QI projects, consider focusing on health care waste. Many of the current processes at our institutions have redundancies that add unhealthy time, effort, and inefficiency to our days that can not only impede patient care but also can lead to burnout. When outlining a project idea, consider mapping the process in your interested area to identify those redundancies and inefficiencies. Consider focusing on these instead of building an entirely new process. Improving inefficiencies also can help with provider buy-in with process changes, especially if this helps in improving their everyday frustrations.
6. Express your values: Create a sense of urgency around the problem you are trying to solve. Educate your colleagues to understand the depth of the QI initiative and its impact on their ability to care for patients and patient safety. Express genuine interest in improving your colleagues’ ability to care for patients and improve their days.
Sharing your passion about your project allows people to understand your vested interest in improving the system. This will inspire team members to lead the way to change and encourage colleagues to adopt the recommended changes.
7. Recognize and reward your team: Involve “champions” in every process change. Identify people who are part of your team and ensure they feel valued. Recognition and acknowledgment will allow people to feel more involved and to gain their buy-in. When it comes to results or progress, consider your group’s dynamics. If they are competitive, consider posting progress results on a publicly displayed run chart. If your group is less likely to be motivated by competition, hold individual meetings to help show progress. This is a crucial dynamic to understand, because creating a competitive environment may alienate some members of your group. Remember, the final result is not to blame those lagging behind but to encourage everyone to find the best pathway to success.
8. Be okay with failure: Celebrate your failures because failure is a chance to learn. Every failure is an educational opportunity to understand what not to do, or a chance to gain insight into a process that did not work.
Be a divergent thinker. Start considering problems as part of the path to solution, rather than a barrier in the way. Be open to change and learn from your mistakes. Don’t just be okay with your failures, own them. This will lead to trust with your team members and show your commitment.
9. Finish: This is key. You must finish your project. Even if you anticipate that the project will fail, you should see the project through to its completion. This proves both you and the process of QI are valid and worthwhile; you have to see results and share them with others.
Completing your project also shows your colleagues that you are resilient, committed, and dedicated. Completing a QI project, even with disappointing results, is a success in and of itself. In the end, it is most important to remember to show progress, not perfection.
10. Create sustainability: When your QI project is finished, you need to decide if the changes are sustainable. Some projects show small change and do not need permanent implementation, rather reminders over time. Other projects may be sustainable with EHR or organizational changes. Once you have successful results, your goal should be to find a way to ensure that the process stays in place over time. This is where all your hard work establishing buy-in comes in handy. Your team is more likely to create sustainable change with the hard work you forged through following these key tips.
These Top 10 tips are a hospitalist’s starting point to begin making changes at their own community hospital. Your motivation and effort in making quality change will not go unnoticed. Small ideas will open doors for larger, more sustainable QI projects. Remember, a failure just means a new idea for the next cycle! Enjoy the process of working collaboratively with your hospital on improving quality. Good luck!
Dr. Astik is a hospitalist and instructor of medicine at Northwestern Memorial Hospital, Chicago. Dr. Corbett is a hospitalist and assistant professor at the University of Oklahoma, Tulsa. Dr. Patel is a hospitalist and assistant professor at the University of Colorado, Denver. Dr. Ronan is a hospitalist and associate professor at Christus St. Vincent Regional Medical Center, Santa Fe, NM.
Quality improvement (QI) is essential to the advancement of medicine. QI differs from research as it focuses on already proven knowledge and aims to make quick, sustainable change in local health care systems. Community hospitals may not have organized quality improvement initiatives and often rely on individual hospitalists to be their champions.
Although there are resources for quality improvement projects, initiating a project can seem daunting to a hospitalist. Our aim is to equip the community hospitalist with basic skills to initiate their own successful project. We present our “Top 10” tips to review.
1. Start small: Many quality improvement ideas include grandiose changes that require a large buy-in or worse, more money. When starting a QI project, you need to consider low-cost, high-impact projects. Even the smallest projects can make considerable change. Focus on ideas that require only one or two improvement cycles to implement. Understand your hospital culture, flow, and processes, and then pick a project that is reasonable.
Projects can be as simple as decreasing the number of daily labs ordered by your hospitalist group. Projects that are small could still improve patient satisfaction and decrease costs. Listen to your colleagues, if they are discussing an issue, turn this into an idea! As you learn the culture of your hospital you will be able to tackle larger projects. Plus, it gets your name out there!
2. Establish buy-in: Surround yourself with champions of your cause. Properly identifying and engaging key players is paramount to a successful QI project. First, start with your hospital administration, and garner their support by aligning your project with the goals and objectives that the administration leaders have identified to be important for your institution. Next, select a motivated multidisciplinary team. When choosing your team, be sure to include a representative from the various stakeholders, that is, the individuals who have a variety of hospital roles likely to be affected by the outcome of the project. Stakeholders ensure the success of the project because they have a fundamental understanding of how the project will influence workflow, can predict issues before they arise, and often become empowered to make changes that directly influence their work.
Lastly, include at least one well-respected and highly influential member on your team. Change is always hard, and this person’s support and endorsement of the project, can often move mountains when challenges arise.
3. Know the data collector: It is important to understand what data can be collected because, without data, you cannot measure your success. Arrange a meeting and develop a partnership with the data collector. Obtain a general understanding of how and what specific data is collected. Be sure the data collector has a clear understanding of the project design and the specific details of the project. Include the overall project mission, specific aims of the project, the time frame in which data should be collected, and specific inclusion and exclusion criteria.
Often, data collectors prefer to collect extra data points upfront, even if you end up not using some of them, rather than having to find missing data after the fact. Communication is key, so be available for questions and open to the suggestions of the data collector.
4. Don’t reinvent the wheel: Prior to starting any QI projects, evaluate available resources for project ideas and implementation. The Society of Hospital Medicine and the American College of Physicians outline multiple projects on their websites. Reach out to colleagues at other institutions and obtain their input as they are likely struggling with similar issues and/or have worked on similar project ideas. Use these resources as scaffolding and edit them to fit your institution’s processes and culture, and use their metrics as your measures of success.
5. Remove waste: When determining QI projects, consider focusing on health care waste. Many of the current processes at our institutions have redundancies that add unhealthy time, effort, and inefficiency to our days that can not only impede patient care but also can lead to burnout. When outlining a project idea, consider mapping the process in your interested area to identify those redundancies and inefficiencies. Consider focusing on these instead of building an entirely new process. Improving inefficiencies also can help with provider buy-in with process changes, especially if this helps in improving their everyday frustrations.
6. Express your values: Create a sense of urgency around the problem you are trying to solve. Educate your colleagues to understand the depth of the QI initiative and its impact on their ability to care for patients and patient safety. Express genuine interest in improving your colleagues’ ability to care for patients and improve their days.
Sharing your passion about your project allows people to understand your vested interest in improving the system. This will inspire team members to lead the way to change and encourage colleagues to adopt the recommended changes.
7. Recognize and reward your team: Involve “champions” in every process change. Identify people who are part of your team and ensure they feel valued. Recognition and acknowledgment will allow people to feel more involved and to gain their buy-in. When it comes to results or progress, consider your group’s dynamics. If they are competitive, consider posting progress results on a publicly displayed run chart. If your group is less likely to be motivated by competition, hold individual meetings to help show progress. This is a crucial dynamic to understand, because creating a competitive environment may alienate some members of your group. Remember, the final result is not to blame those lagging behind but to encourage everyone to find the best pathway to success.
8. Be okay with failure: Celebrate your failures because failure is a chance to learn. Every failure is an educational opportunity to understand what not to do, or a chance to gain insight into a process that did not work.
Be a divergent thinker. Start considering problems as part of the path to solution, rather than a barrier in the way. Be open to change and learn from your mistakes. Don’t just be okay with your failures, own them. This will lead to trust with your team members and show your commitment.
9. Finish: This is key. You must finish your project. Even if you anticipate that the project will fail, you should see the project through to its completion. This proves both you and the process of QI are valid and worthwhile; you have to see results and share them with others.
Completing your project also shows your colleagues that you are resilient, committed, and dedicated. Completing a QI project, even with disappointing results, is a success in and of itself. In the end, it is most important to remember to show progress, not perfection.
10. Create sustainability: When your QI project is finished, you need to decide if the changes are sustainable. Some projects show small change and do not need permanent implementation, rather reminders over time. Other projects may be sustainable with EHR or organizational changes. Once you have successful results, your goal should be to find a way to ensure that the process stays in place over time. This is where all your hard work establishing buy-in comes in handy. Your team is more likely to create sustainable change with the hard work you forged through following these key tips.
These Top 10 tips are a hospitalist’s starting point to begin making changes at their own community hospital. Your motivation and effort in making quality change will not go unnoticed. Small ideas will open doors for larger, more sustainable QI projects. Remember, a failure just means a new idea for the next cycle! Enjoy the process of working collaboratively with your hospital on improving quality. Good luck!
Dr. Astik is a hospitalist and instructor of medicine at Northwestern Memorial Hospital, Chicago. Dr. Corbett is a hospitalist and assistant professor at the University of Oklahoma, Tulsa. Dr. Patel is a hospitalist and assistant professor at the University of Colorado, Denver. Dr. Ronan is a hospitalist and associate professor at Christus St. Vincent Regional Medical Center, Santa Fe, NM.
Outpatient Management and Follow-up Recommendations for Adverse Drug Reactions: Guidelines for Posthospitalization Care
It has been estimated that 2 million serious adverse drug reactions (ADRs) occur annually in the United States, resulting in 100,000 deaths.1 Although the acute morbidity and mortality of these ADRs are readily apparent, postdischarge sequalae are critical aspects of a patient’s care. Herein, we present an approach to outpatient dermatologic follow-up of 3 ADRs: acute generalized exanthematous pustulosis (AGEP), drug rash with eosinophilia and systemic symptoms (DRESS) syndrome, and Stevens-Johnson syndrome (SJS)/toxic epidermal necrolysis (TEN). For these ADRs, the first step is prompt diagnosis and discontinuation of any potentially causative medications.
ACUTE GENERALIZED EXANTHEMATOUS PUSTULOSIS
Ninety percent of the time, AGEP is caused by medications, most commonly antibiotics, and less often it is caused by viruses.2-4 It presents as a cutaneous eruption with nonfollicular sterile pustules, fever, and leukocytosis, usually within 5 days after starting a causative medication.5 After stopping the medication, cutaneous findings generally improve within 1 week, and leukocytosis often resolves within 1 week.3
Notable Sequelae
Although AGEP typically is considered benign,2 there have been reports of severe sequelae including death from a systemic inflammatory response and complications such as bacterial superinfection and sepsis.6,7 Visceral involvement can be seen in up to 20% of AGEP patients, with systemic symptoms similar to those seen in DRESS syndrome. Mortality has been reported in up to 5% of cases, mainly in patients with comorbidities and notable mucosal involvement.8 More severe disease can be seen in patients with known dermatologic disease, as AGEP can provoke an isomorphic phenomenon.9 Laboratory alterations typically seen in AGEP include neutrophilia, eosinophilia, and elevated liver enzymes.2
Follow-up Recommendations
Patients should be informed of the expected timeline for resolution and should be counseled on the possibility of rare systemic symptoms. Laboratory abnormalities should be monitored every 2 to 4 weeks until normalized.
DRESS SYNDROME
DRESS syndrome is characterized by a morbilliform eruption that can be accompanied by fever; eosinophilia; purpura; facial edema; lymphadenopathy; and liver, renal, or other organ dysfunction. DRESS syndrome most often presents within 8 weeks of exposure to a causative drug.10,11 The most common causative agents are anticonvulsants, antimicrobials, and allopurinol.12 Treatment includes topical corticosteroids and systemic corticosteroids for internal organ involvement.10
Short-term Sequelae
Several potential sequelae may occur within 6 months of resolution of DRESS syndrome, resulting from both the ADR itself and/or systemic corticosteroids that often are required for treatment.13 Complications secondary to herpesviruses have been reported.14 Cases of cytomegalovirus-induced gastric ulcers can lead to gastrointestinal tract bleeds.15
Infections including Cryptococcus species and herpes zoster also have been reported.16 Patients, particularly those treated with systemic corticosteroids, should be monitored with close follow-up for infectious complications and treatment-related adverse effects.13
Long-term Sequelae
Endocrine
Thyroid gland abnormalities secondary to DRESS syndrome include Graves disease and Hashimoto disease as well as variations in biomarkers including elevated free thyroxine and low and elevated thyroid-stimulating hormone levels.16,17 Type 1 diabetes mellitus also has been seen after DRESS syndrome, developing within the first 10 months after onset with unknown pathogenesis.18
Autoimmune
Other reported sequelae of DRESS syndrome include elevated antinuclear antibodies with possible development into systemic lupus erythematosus, autoimmune hemolytic anemia, vitiligo, and rheumatoid arthritis.11,16 Symptoms may be exacerbated in patients with preexisting autoimmune diseases such as systemic lupus erythematosus and rheumatoid arthritis, and patients with preexisting renal disease are at an increased risk for requiring lifelong hemodialysis after DRESS syndrome.16
Other
Studies have demonstrated that pneumonia, thrombosis, and alopecia can be complications of DRESS syndrome.11,16 Psychiatric disturbances including fear of taking new medications, anxiety, and depression also have been reported.19 Children with DRESS syndrome may develop vitiligo, alopecia, sclerodermatous lesions, photophobia, uveitis, and Vogt-Koyanagi-Harada disease.17
Follow-up Recommendations
It is important to inform patients of both the potential short-term and long-term sequelae of DRESS syndrome, including those associated with treatment. A thorough review of systems should be performed at each visit, along with laboratory evaluation including a complete blood cell count with differential and liver function testing every 1 to 2 weeks after discharge until normalized, with monthly monitoring of glucose, thyroid-stimulating hormone, and free thyroxine levels for 3 months after discharge.
STEVENS-JOHNSON SYNDROME/TOXIC EPIDERMAL NECROLYSIS
Stevens-Johnson syndrome/toxic epidermal necrolysis are severe ADRs that present with dusky violaceous macules. Inciting medications include nonsteroidal anti-inflammatory drugs, allopurinol, antibiotics, and anticonvulsants, and symptoms begin 1 to 3 weeks after medication exposure.12 Initially, the lesions often begin on the trunk and can progress to full-body erythema and exfoliation with a necrotic epidermis and mucosal involvement.12,20
Notable Sequelae
Cutaneous
Chronic eczema can present at any time and can vary in severity in SJS/TEN patients.21 Xerosis and pruritus can be treated with emollients.11 Dyschromia is common. Hypertrophic and keloidal scarring can result from surgical debridement and are best prevented with the use of nonadherent dressings.22 Nail changes such as anonychia, dystrophy, longitudinal ridges, and pterygium also are seen, and topical steroids can be helpful. Other reported dermatologic sequelae include dyschromia and eruption of ectopic sebaceous glands.21,22
Ocular
Ocular sequelae include dry eyes, photophobia, symblepharon, corneal scarring, corneal neovascularization, corneal xerosis, trichiasis, reduced visual acuity, blindness, and subconjunctival fibrosis. The most common sequelae are bilateral conjunctivitis and corneal ulcerations.22,23 Early and regular ophthalmologic follow-up is recommended, as SJS/TEN-induced blindness can result from delayed therapy, destroying corneal stem cells.21 Amniotic membrane transplantation replaces the damaged corneal membrane, which may reduce corneal inflammation.24
Chronic dry eye syndrome can recur for years after SJS/TEN resolves and progresses over time.22 Frequent use of nonpreserved artificial tears and salivary gland transplantation can be helpful.24 Unfortunately, ocular disease may develop months after discharge; therefore, it is recommended that dermatologists ask all SJS/TEN patients about ocular symptoms in follow-up visits. If ocular involvement was present initially, patients should be followed by ophthalmology for at least 1 year after discharge.23
Genitourinary
Genitourinary sequelae in SJS/TEN include adhesions, particularly in the female urethra and vaginal opening; vaginal adenosis; vulvovaginal endometriosis; and persistent genital ulcerations most commonly reported in females.22 Prompt inpatient gynecologic or urologic consultation is critical to reduce these potentially permanent outcomes. Topical corticosteroid therapy is recommended in the acute phase.22
Psychologic
Posttraumatic stress disorder may occur in patients with SJS/TEN. One study showed that 23% (7/30) of patients had posttraumatic stress disorder 6 months after hospitalization for SJS/TEN. The investigators recommended routine psychiatric assessment in the acute disease period and for at least 1 year after discharge.25
Pulmonary, Gastrointestinal, and Renal
Interstitial pneumonia and obliterative bronchitis/bronchiolitis can be caused by SJS/TEN. Interstitial pneumonia tends to occur during the acute course, while obliterative airway disease manifests after resolution of SJS/TEN.21,22 Abnormal pulmonary function testing can be seen in more than half of SJS/TEN patients 2 months after the ADR.22 Gastrointestinal sequelae include esophageal strictures, intestinal ulceration, and cholestasis.22 Renal sequelae include acute kidney injury and glomerulonephritis, which may be secondary to the volume loss seen in SJS/TEN but may be irreversible.21
Special Populations
A correlation with infertility in women has been documented in patients with SJS/TEN; thus, follow-up with obstetrics and gynecology is recommended in women of child-bearing potential. The most considerable risk in pregnant women with SJS/TEN is premature birth, and mucosal necrosis of SJS/TEN can impair vaginal delivery.26 Antiretrovirals can be a cause of SJS/TEN in the human immunodeficiency virus–positive population.27 In those cases, it is best to discontinue the medication and find an alternative.
Risk factors for children can be different and can include viral and febrile illnesses as well as mycoplasma infection.28 Children also can be at an increased risk for poor ocular outcomes, such as permanent deficiency in visual acuity and blindness.29
Follow-up Recommendations
Patients should be counseled regarding sequelae and the multisystem nature of SJS/TEN. Inpatient referrals should be given as needed. It is important to watch for ocular symptoms for 1 year after SJS/TEN resolution. When ocular involvement is present, follow-up with ophthalmology is recommended within 1 month of discharge and then at the discretion of the ophthalmologist. Pulmonary function should be monitored for 1 year after SJS/TEN, starting 1 month after discharge and then at the discretion of the pulmonologist. Patients also should be screened for psychologic sequelae for at least 1 year after discharge.
FINAL THOUGHTS
Adverse drug reactions are notable causes of inpatient hospitalization and may lead to considerable sequelae. These ADRs range in severity from more common and benign maculopapular exanthems to severe multiorgan ADRs such as DRESS syndrome and SJS/TEN.
In AGEP, it is important to monitor patients with preexisting dermatologic diseases and to screen for visceral involvement. DRESS syndrome has the potential to cause immune dysregulation and variable long-term adverse sequelae, both from the disease itself and from corticosteroid therapy. Mucocutaneous sequelae of SJS/TEN can potentially affect a patient’s cutaneous, ocular, genitourinary, mental, pulmonary, gastrointestinal, and renal health.
The baseline recommendations provided here warrant more frequent monitoring if the findings and symptoms are severe. In all of these cases, if a causative medication is identified, it should be added to the patient’s allergy list and the patient should be counseled extensively to avoid this medication and other medications in the same class. If a single agent cannot be identified, referrals for patch testing may be of some utility, particularly in AGEP and DRESS syndrome.30,31
- Preventable adverse drug reactions: a focus on drug interactions. US Food and Drug Administration website. https://www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/DrugInteractionsLabeling/ucm110632.htm. Updated March 6, 2018. Accessed April 12, 2019.
- Thienvibul C, Vachiramon V, Chanprapaph K. Five-year retrospective review of acute generalized exanthematous pustulosis. Dermatol Res Pract. 2015;3:1-8.
- Lee HY, Chou D, Pang SM, et al. Acute generalized exanthematous pustulosis: analysis of cases managed in a tertiary hospital in Singapore. Int J Dermatol. 2010
;49:507-512. - Ropars N, Darrieux L, Tisseau L, et al. Acute generalized exanthematous pustulosis associated with primary Epstein-Barr virus infection. JAAD Case Rep. 2014;1:9-11.
- Hattem S, Beerthuizen G, Kardaun S. Severe flucloxacillin‐induced acute generalized exanthematous pustulosis (AGEP), with toxic epidermal necrolysis (TEN)‐like features: does overlap between AGEP and TEN exist? clinical report and review of the literature. Br J Dermatol. 2014;171:1539-1545.
- Tajmir-Riahi A, Wörl P, Harrer T, et al. Life-threatening atypical case of acute generalized exanthematous pustulosis. Int Arch Allergy Immunol. 2017;174:108-111.
- Feldmeyer L, Heidemeyer K, Yawalkar N. Acute generalized exanthematous pustulosis: pathogenesis, genetic background, clinical variants and therapy. Int J Mol Sci. 2016;17:E1214.
- Szatkowski J, Schwartz RA. Acute generalized exanthematous pustulosis (AGEP). a review and update. J Am Acad Dermatol. 2015;73:843-848.
- Totonchy MB, McNiff JM, Bunick CG. Koebnerization of Hailey-Hailey disease into a cutaneous drug eruption of acute generalized exanthematous pustulosis associated with systemic symptoms. J Cutan Pathol. 2016;43:1031-1035.
- Husain Z, Reddy BY, Schwartz RA. DRESS syndrome: part II. management and therapeutics. J Am Acad Dermatol. 2013;68:709.e1-e9; quiz 718-720.
- Kano Y, Shiohara T. Long-term outcome of patients with severe cutaneous adverse reactions. Dermatologica Sinica. 2013;31:211-216.
- Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. Vol 1. Philadelphia, PA: Elsevier Saunders; 2012.
- Ushigome Y, Kano Y, Ishida T, et al. Short- and long-term outcomes of 34 patients with drug-induced hypersensitivity syndrome in a single institution. J Am Acad Dermatol. 2013;68:721-728.
- Ljungman P, Wang FZ, Clark DA, et al. High levels of human herpesvirus 6 DNA in peripheral blood leucocytes are correlated to platelet engraftment and disease in allogeneic stem cell transplant patients. Br J Haematol. 2000;111:774-781.
- Asano Y, Kagawa H, Kano Y, et al. Cytomegalovirus disease during severe drug eruptions: report of 2 cases and retrospective study of 18 patients with drug-induced hypersensitivity syndrome. Arch Dermatol. 2009;145:1030-1036.
- Kano Y , Tohyama M, Aihara M, et al. Sequelae in 145 patients with drug‐induced hypersensitivity syndrome/drug reaction with eosinophilia and systemic symptoms: survey conducted by the Asian Research Committee on Severe Cutaneous Adverse Reactions (ASCAR). J Dermatol. 2015;42:276-282.
- Morita C, Yanase T, Shiohara T, et al. Aggressive treatment in paediatric or young patients with drug-induced hypersensitivity syndrome (DiHS)/ drug reaction with eosinophilia and systemic symptoms (DRESS) is associated with future development of type III polyglandular autoimmune syndrome [published online October 27, 2018]. BMJ Case Rep. doi:10.1136/bcr-2018-225528.
- Chiang A, Shiu J, Elsensohn AN, et al. Classic autoimmune type 1 diabetes mellitus after a case of drug reaction with eosinophilia and systemic symptoms (DRESS). JAAD Case Rep. 2018;4:295-297.
- Lew TT, Creamer D, Mackenzie J, et al. Post-traumatic stress disorder following drug reaction with eosinophilia and systemic symptoms. Br J Dermatol. 2015;172:836-837.
- Kumar R, Das A, Das S. Management of Stevens-Johnson syndrome-toxic epidermal necrolysis: looking beyond guidelines! Indian J Dermatol. 2018;63:117-124.
- Yang CW, Cho YT, Chen KL, et al. Long-term sequelae of Stevens-Johnson syndrome/toxic epidermal necrolysis. Acta Derm Venereol. 2016;96:525-529.
- Lee HY, Walsh SA, Creamer D. Long‐term complications of Stevens-Johnson syndrome/toxic epidermal necrolysis (SJS/TEN): the spectrum of chronic problems in patients who survive an episode of SJS/TEN necessitates multidisciplinary follow‐up. Br J Dermatol. 2017;177:924-935.
- Hsu M, Jayaram A, Verner R, et al. Indications and outcomes of amniotic membrane transplantation in the management of acute Stevens-Johnson syndrome and toxic epidermal necrolysis: a case-control study. Cornea. 2012;31:1394-1402.
- Sant’ Anna AE, Hazarbassanov RM, de Freitas D, et al. Minor salivary glands and labial mucous membrane graft in the treatment of severe symblepharon and dry eye in patients with Stevens-Johnson syndrome. Br J Ophthalmol. 2012;96:234-239.
- Hefez L, Zaghbib K, Sbidian E, et al. Post-traumatic stress disorder in Stevens-Johnson syndrome and toxic epidermal necrolysis: prevalence and risk factors. a prospective study of 31 patients [published online October 3, 2018]. Br J Dermatol. doi:10.1111/bjd.17267.
- Knight L, Todd G, Muloiwa R, et al. Stevens Johnson syndrome and toxic epidermal necrolysis: maternal and foetal outcomes intwenty-two consecutive pregnant HIV infected women [published online August 12, 2015]. PLoS One. doi:10.1371/journal.pone.0135501.
- Tchetnya X, Ngwasiri CA, Munge T, et al. Severe eye complications from toxic epidermal necrolysis following initiation of nevirapine based HAART regimen in a child with HIV infection: a case from Cameroon. BMC Pediatr. 2018;18:108.
- Antoon JW, Goldman JL, Lee B, et al. Incidence, outcomes, and resource use in children with Stevens-Johnson syndrome and toxic epidermal necrolysis. Pediatr Dermatol. 2018;35:182-187.
- Basu S, Shanbhag SS, Gokani A, et al. Chronic ocular sequelae of Stevens-Johnson syndrome in children: long-term impact of appropriate therapy on natural history of disease. Am J Ophthalmol. 2018;189:17-28.
- Pinho A, Marta A, Coutinho I, et al. Long‐term reproducibility of positive patch test reactions in patients with non‐immediate cutaneous adverse drug reactions to antibiotics. Contact Dermatitis. 2017;76:204-209.
- Barbaud A, Collet E, Milpied B, et al. A multicentre study to determine the value and safety of drug patch tests for the three main classes of severe cutaneous adverse drug reactions. Br J Dermatol. 2013;168:555-562.
It has been estimated that 2 million serious adverse drug reactions (ADRs) occur annually in the United States, resulting in 100,000 deaths.1 Although the acute morbidity and mortality of these ADRs are readily apparent, postdischarge sequalae are critical aspects of a patient’s care. Herein, we present an approach to outpatient dermatologic follow-up of 3 ADRs: acute generalized exanthematous pustulosis (AGEP), drug rash with eosinophilia and systemic symptoms (DRESS) syndrome, and Stevens-Johnson syndrome (SJS)/toxic epidermal necrolysis (TEN). For these ADRs, the first step is prompt diagnosis and discontinuation of any potentially causative medications.
ACUTE GENERALIZED EXANTHEMATOUS PUSTULOSIS
Ninety percent of the time, AGEP is caused by medications, most commonly antibiotics, and less often it is caused by viruses.2-4 It presents as a cutaneous eruption with nonfollicular sterile pustules, fever, and leukocytosis, usually within 5 days after starting a causative medication.5 After stopping the medication, cutaneous findings generally improve within 1 week, and leukocytosis often resolves within 1 week.3
Notable Sequelae
Although AGEP typically is considered benign,2 there have been reports of severe sequelae including death from a systemic inflammatory response and complications such as bacterial superinfection and sepsis.6,7 Visceral involvement can be seen in up to 20% of AGEP patients, with systemic symptoms similar to those seen in DRESS syndrome. Mortality has been reported in up to 5% of cases, mainly in patients with comorbidities and notable mucosal involvement.8 More severe disease can be seen in patients with known dermatologic disease, as AGEP can provoke an isomorphic phenomenon.9 Laboratory alterations typically seen in AGEP include neutrophilia, eosinophilia, and elevated liver enzymes.2
Follow-up Recommendations
Patients should be informed of the expected timeline for resolution and should be counseled on the possibility of rare systemic symptoms. Laboratory abnormalities should be monitored every 2 to 4 weeks until normalized.
DRESS SYNDROME
DRESS syndrome is characterized by a morbilliform eruption that can be accompanied by fever; eosinophilia; purpura; facial edema; lymphadenopathy; and liver, renal, or other organ dysfunction. DRESS syndrome most often presents within 8 weeks of exposure to a causative drug.10,11 The most common causative agents are anticonvulsants, antimicrobials, and allopurinol.12 Treatment includes topical corticosteroids and systemic corticosteroids for internal organ involvement.10
Short-term Sequelae
Several potential sequelae may occur within 6 months of resolution of DRESS syndrome, resulting from both the ADR itself and/or systemic corticosteroids that often are required for treatment.13 Complications secondary to herpesviruses have been reported.14 Cases of cytomegalovirus-induced gastric ulcers can lead to gastrointestinal tract bleeds.15
Infections including Cryptococcus species and herpes zoster also have been reported.16 Patients, particularly those treated with systemic corticosteroids, should be monitored with close follow-up for infectious complications and treatment-related adverse effects.13
Long-term Sequelae
Endocrine
Thyroid gland abnormalities secondary to DRESS syndrome include Graves disease and Hashimoto disease as well as variations in biomarkers including elevated free thyroxine and low and elevated thyroid-stimulating hormone levels.16,17 Type 1 diabetes mellitus also has been seen after DRESS syndrome, developing within the first 10 months after onset with unknown pathogenesis.18
Autoimmune
Other reported sequelae of DRESS syndrome include elevated antinuclear antibodies with possible development into systemic lupus erythematosus, autoimmune hemolytic anemia, vitiligo, and rheumatoid arthritis.11,16 Symptoms may be exacerbated in patients with preexisting autoimmune diseases such as systemic lupus erythematosus and rheumatoid arthritis, and patients with preexisting renal disease are at an increased risk for requiring lifelong hemodialysis after DRESS syndrome.16
Other
Studies have demonstrated that pneumonia, thrombosis, and alopecia can be complications of DRESS syndrome.11,16 Psychiatric disturbances including fear of taking new medications, anxiety, and depression also have been reported.19 Children with DRESS syndrome may develop vitiligo, alopecia, sclerodermatous lesions, photophobia, uveitis, and Vogt-Koyanagi-Harada disease.17
Follow-up Recommendations
It is important to inform patients of both the potential short-term and long-term sequelae of DRESS syndrome, including those associated with treatment. A thorough review of systems should be performed at each visit, along with laboratory evaluation including a complete blood cell count with differential and liver function testing every 1 to 2 weeks after discharge until normalized, with monthly monitoring of glucose, thyroid-stimulating hormone, and free thyroxine levels for 3 months after discharge.
STEVENS-JOHNSON SYNDROME/TOXIC EPIDERMAL NECROLYSIS
Stevens-Johnson syndrome/toxic epidermal necrolysis are severe ADRs that present with dusky violaceous macules. Inciting medications include nonsteroidal anti-inflammatory drugs, allopurinol, antibiotics, and anticonvulsants, and symptoms begin 1 to 3 weeks after medication exposure.12 Initially, the lesions often begin on the trunk and can progress to full-body erythema and exfoliation with a necrotic epidermis and mucosal involvement.12,20
Notable Sequelae
Cutaneous
Chronic eczema can present at any time and can vary in severity in SJS/TEN patients.21 Xerosis and pruritus can be treated with emollients.11 Dyschromia is common. Hypertrophic and keloidal scarring can result from surgical debridement and are best prevented with the use of nonadherent dressings.22 Nail changes such as anonychia, dystrophy, longitudinal ridges, and pterygium also are seen, and topical steroids can be helpful. Other reported dermatologic sequelae include dyschromia and eruption of ectopic sebaceous glands.21,22
Ocular
Ocular sequelae include dry eyes, photophobia, symblepharon, corneal scarring, corneal neovascularization, corneal xerosis, trichiasis, reduced visual acuity, blindness, and subconjunctival fibrosis. The most common sequelae are bilateral conjunctivitis and corneal ulcerations.22,23 Early and regular ophthalmologic follow-up is recommended, as SJS/TEN-induced blindness can result from delayed therapy, destroying corneal stem cells.21 Amniotic membrane transplantation replaces the damaged corneal membrane, which may reduce corneal inflammation.24
Chronic dry eye syndrome can recur for years after SJS/TEN resolves and progresses over time.22 Frequent use of nonpreserved artificial tears and salivary gland transplantation can be helpful.24 Unfortunately, ocular disease may develop months after discharge; therefore, it is recommended that dermatologists ask all SJS/TEN patients about ocular symptoms in follow-up visits. If ocular involvement was present initially, patients should be followed by ophthalmology for at least 1 year after discharge.23
Genitourinary
Genitourinary sequelae in SJS/TEN include adhesions, particularly in the female urethra and vaginal opening; vaginal adenosis; vulvovaginal endometriosis; and persistent genital ulcerations most commonly reported in females.22 Prompt inpatient gynecologic or urologic consultation is critical to reduce these potentially permanent outcomes. Topical corticosteroid therapy is recommended in the acute phase.22
Psychologic
Posttraumatic stress disorder may occur in patients with SJS/TEN. One study showed that 23% (7/30) of patients had posttraumatic stress disorder 6 months after hospitalization for SJS/TEN. The investigators recommended routine psychiatric assessment in the acute disease period and for at least 1 year after discharge.25
Pulmonary, Gastrointestinal, and Renal
Interstitial pneumonia and obliterative bronchitis/bronchiolitis can be caused by SJS/TEN. Interstitial pneumonia tends to occur during the acute course, while obliterative airway disease manifests after resolution of SJS/TEN.21,22 Abnormal pulmonary function testing can be seen in more than half of SJS/TEN patients 2 months after the ADR.22 Gastrointestinal sequelae include esophageal strictures, intestinal ulceration, and cholestasis.22 Renal sequelae include acute kidney injury and glomerulonephritis, which may be secondary to the volume loss seen in SJS/TEN but may be irreversible.21
Special Populations
A correlation with infertility in women has been documented in patients with SJS/TEN; thus, follow-up with obstetrics and gynecology is recommended in women of child-bearing potential. The most considerable risk in pregnant women with SJS/TEN is premature birth, and mucosal necrosis of SJS/TEN can impair vaginal delivery.26 Antiretrovirals can be a cause of SJS/TEN in the human immunodeficiency virus–positive population.27 In those cases, it is best to discontinue the medication and find an alternative.
Risk factors for children can be different and can include viral and febrile illnesses as well as mycoplasma infection.28 Children also can be at an increased risk for poor ocular outcomes, such as permanent deficiency in visual acuity and blindness.29
Follow-up Recommendations
Patients should be counseled regarding sequelae and the multisystem nature of SJS/TEN. Inpatient referrals should be given as needed. It is important to watch for ocular symptoms for 1 year after SJS/TEN resolution. When ocular involvement is present, follow-up with ophthalmology is recommended within 1 month of discharge and then at the discretion of the ophthalmologist. Pulmonary function should be monitored for 1 year after SJS/TEN, starting 1 month after discharge and then at the discretion of the pulmonologist. Patients also should be screened for psychologic sequelae for at least 1 year after discharge.
FINAL THOUGHTS
Adverse drug reactions are notable causes of inpatient hospitalization and may lead to considerable sequelae. These ADRs range in severity from more common and benign maculopapular exanthems to severe multiorgan ADRs such as DRESS syndrome and SJS/TEN.
In AGEP, it is important to monitor patients with preexisting dermatologic diseases and to screen for visceral involvement. DRESS syndrome has the potential to cause immune dysregulation and variable long-term adverse sequelae, both from the disease itself and from corticosteroid therapy. Mucocutaneous sequelae of SJS/TEN can potentially affect a patient’s cutaneous, ocular, genitourinary, mental, pulmonary, gastrointestinal, and renal health.
The baseline recommendations provided here warrant more frequent monitoring if the findings and symptoms are severe. In all of these cases, if a causative medication is identified, it should be added to the patient’s allergy list and the patient should be counseled extensively to avoid this medication and other medications in the same class. If a single agent cannot be identified, referrals for patch testing may be of some utility, particularly in AGEP and DRESS syndrome.30,31
It has been estimated that 2 million serious adverse drug reactions (ADRs) occur annually in the United States, resulting in 100,000 deaths.1 Although the acute morbidity and mortality of these ADRs are readily apparent, postdischarge sequalae are critical aspects of a patient’s care. Herein, we present an approach to outpatient dermatologic follow-up of 3 ADRs: acute generalized exanthematous pustulosis (AGEP), drug rash with eosinophilia and systemic symptoms (DRESS) syndrome, and Stevens-Johnson syndrome (SJS)/toxic epidermal necrolysis (TEN). For these ADRs, the first step is prompt diagnosis and discontinuation of any potentially causative medications.
ACUTE GENERALIZED EXANTHEMATOUS PUSTULOSIS
Ninety percent of the time, AGEP is caused by medications, most commonly antibiotics, and less often it is caused by viruses.2-4 It presents as a cutaneous eruption with nonfollicular sterile pustules, fever, and leukocytosis, usually within 5 days after starting a causative medication.5 After stopping the medication, cutaneous findings generally improve within 1 week, and leukocytosis often resolves within 1 week.3
Notable Sequelae
Although AGEP typically is considered benign,2 there have been reports of severe sequelae including death from a systemic inflammatory response and complications such as bacterial superinfection and sepsis.6,7 Visceral involvement can be seen in up to 20% of AGEP patients, with systemic symptoms similar to those seen in DRESS syndrome. Mortality has been reported in up to 5% of cases, mainly in patients with comorbidities and notable mucosal involvement.8 More severe disease can be seen in patients with known dermatologic disease, as AGEP can provoke an isomorphic phenomenon.9 Laboratory alterations typically seen in AGEP include neutrophilia, eosinophilia, and elevated liver enzymes.2
Follow-up Recommendations
Patients should be informed of the expected timeline for resolution and should be counseled on the possibility of rare systemic symptoms. Laboratory abnormalities should be monitored every 2 to 4 weeks until normalized.
DRESS SYNDROME
DRESS syndrome is characterized by a morbilliform eruption that can be accompanied by fever; eosinophilia; purpura; facial edema; lymphadenopathy; and liver, renal, or other organ dysfunction. DRESS syndrome most often presents within 8 weeks of exposure to a causative drug.10,11 The most common causative agents are anticonvulsants, antimicrobials, and allopurinol.12 Treatment includes topical corticosteroids and systemic corticosteroids for internal organ involvement.10
Short-term Sequelae
Several potential sequelae may occur within 6 months of resolution of DRESS syndrome, resulting from both the ADR itself and/or systemic corticosteroids that often are required for treatment.13 Complications secondary to herpesviruses have been reported.14 Cases of cytomegalovirus-induced gastric ulcers can lead to gastrointestinal tract bleeds.15
Infections including Cryptococcus species and herpes zoster also have been reported.16 Patients, particularly those treated with systemic corticosteroids, should be monitored with close follow-up for infectious complications and treatment-related adverse effects.13
Long-term Sequelae
Endocrine
Thyroid gland abnormalities secondary to DRESS syndrome include Graves disease and Hashimoto disease as well as variations in biomarkers including elevated free thyroxine and low and elevated thyroid-stimulating hormone levels.16,17 Type 1 diabetes mellitus also has been seen after DRESS syndrome, developing within the first 10 months after onset with unknown pathogenesis.18
Autoimmune
Other reported sequelae of DRESS syndrome include elevated antinuclear antibodies with possible development into systemic lupus erythematosus, autoimmune hemolytic anemia, vitiligo, and rheumatoid arthritis.11,16 Symptoms may be exacerbated in patients with preexisting autoimmune diseases such as systemic lupus erythematosus and rheumatoid arthritis, and patients with preexisting renal disease are at an increased risk for requiring lifelong hemodialysis after DRESS syndrome.16
Other
Studies have demonstrated that pneumonia, thrombosis, and alopecia can be complications of DRESS syndrome.11,16 Psychiatric disturbances including fear of taking new medications, anxiety, and depression also have been reported.19 Children with DRESS syndrome may develop vitiligo, alopecia, sclerodermatous lesions, photophobia, uveitis, and Vogt-Koyanagi-Harada disease.17
Follow-up Recommendations
It is important to inform patients of both the potential short-term and long-term sequelae of DRESS syndrome, including those associated with treatment. A thorough review of systems should be performed at each visit, along with laboratory evaluation including a complete blood cell count with differential and liver function testing every 1 to 2 weeks after discharge until normalized, with monthly monitoring of glucose, thyroid-stimulating hormone, and free thyroxine levels for 3 months after discharge.
STEVENS-JOHNSON SYNDROME/TOXIC EPIDERMAL NECROLYSIS
Stevens-Johnson syndrome/toxic epidermal necrolysis are severe ADRs that present with dusky violaceous macules. Inciting medications include nonsteroidal anti-inflammatory drugs, allopurinol, antibiotics, and anticonvulsants, and symptoms begin 1 to 3 weeks after medication exposure.12 Initially, the lesions often begin on the trunk and can progress to full-body erythema and exfoliation with a necrotic epidermis and mucosal involvement.12,20
Notable Sequelae
Cutaneous
Chronic eczema can present at any time and can vary in severity in SJS/TEN patients.21 Xerosis and pruritus can be treated with emollients.11 Dyschromia is common. Hypertrophic and keloidal scarring can result from surgical debridement and are best prevented with the use of nonadherent dressings.22 Nail changes such as anonychia, dystrophy, longitudinal ridges, and pterygium also are seen, and topical steroids can be helpful. Other reported dermatologic sequelae include dyschromia and eruption of ectopic sebaceous glands.21,22
Ocular
Ocular sequelae include dry eyes, photophobia, symblepharon, corneal scarring, corneal neovascularization, corneal xerosis, trichiasis, reduced visual acuity, blindness, and subconjunctival fibrosis. The most common sequelae are bilateral conjunctivitis and corneal ulcerations.22,23 Early and regular ophthalmologic follow-up is recommended, as SJS/TEN-induced blindness can result from delayed therapy, destroying corneal stem cells.21 Amniotic membrane transplantation replaces the damaged corneal membrane, which may reduce corneal inflammation.24
Chronic dry eye syndrome can recur for years after SJS/TEN resolves and progresses over time.22 Frequent use of nonpreserved artificial tears and salivary gland transplantation can be helpful.24 Unfortunately, ocular disease may develop months after discharge; therefore, it is recommended that dermatologists ask all SJS/TEN patients about ocular symptoms in follow-up visits. If ocular involvement was present initially, patients should be followed by ophthalmology for at least 1 year after discharge.23
Genitourinary
Genitourinary sequelae in SJS/TEN include adhesions, particularly in the female urethra and vaginal opening; vaginal adenosis; vulvovaginal endometriosis; and persistent genital ulcerations most commonly reported in females.22 Prompt inpatient gynecologic or urologic consultation is critical to reduce these potentially permanent outcomes. Topical corticosteroid therapy is recommended in the acute phase.22
Psychologic
Posttraumatic stress disorder may occur in patients with SJS/TEN. One study showed that 23% (7/30) of patients had posttraumatic stress disorder 6 months after hospitalization for SJS/TEN. The investigators recommended routine psychiatric assessment in the acute disease period and for at least 1 year after discharge.25
Pulmonary, Gastrointestinal, and Renal
Interstitial pneumonia and obliterative bronchitis/bronchiolitis can be caused by SJS/TEN. Interstitial pneumonia tends to occur during the acute course, while obliterative airway disease manifests after resolution of SJS/TEN.21,22 Abnormal pulmonary function testing can be seen in more than half of SJS/TEN patients 2 months after the ADR.22 Gastrointestinal sequelae include esophageal strictures, intestinal ulceration, and cholestasis.22 Renal sequelae include acute kidney injury and glomerulonephritis, which may be secondary to the volume loss seen in SJS/TEN but may be irreversible.21
Special Populations
A correlation with infertility in women has been documented in patients with SJS/TEN; thus, follow-up with obstetrics and gynecology is recommended in women of child-bearing potential. The most considerable risk in pregnant women with SJS/TEN is premature birth, and mucosal necrosis of SJS/TEN can impair vaginal delivery.26 Antiretrovirals can be a cause of SJS/TEN in the human immunodeficiency virus–positive population.27 In those cases, it is best to discontinue the medication and find an alternative.
Risk factors for children can be different and can include viral and febrile illnesses as well as mycoplasma infection.28 Children also can be at an increased risk for poor ocular outcomes, such as permanent deficiency in visual acuity and blindness.29
Follow-up Recommendations
Patients should be counseled regarding sequelae and the multisystem nature of SJS/TEN. Inpatient referrals should be given as needed. It is important to watch for ocular symptoms for 1 year after SJS/TEN resolution. When ocular involvement is present, follow-up with ophthalmology is recommended within 1 month of discharge and then at the discretion of the ophthalmologist. Pulmonary function should be monitored for 1 year after SJS/TEN, starting 1 month after discharge and then at the discretion of the pulmonologist. Patients also should be screened for psychologic sequelae for at least 1 year after discharge.
FINAL THOUGHTS
Adverse drug reactions are notable causes of inpatient hospitalization and may lead to considerable sequelae. These ADRs range in severity from more common and benign maculopapular exanthems to severe multiorgan ADRs such as DRESS syndrome and SJS/TEN.
In AGEP, it is important to monitor patients with preexisting dermatologic diseases and to screen for visceral involvement. DRESS syndrome has the potential to cause immune dysregulation and variable long-term adverse sequelae, both from the disease itself and from corticosteroid therapy. Mucocutaneous sequelae of SJS/TEN can potentially affect a patient’s cutaneous, ocular, genitourinary, mental, pulmonary, gastrointestinal, and renal health.
The baseline recommendations provided here warrant more frequent monitoring if the findings and symptoms are severe. In all of these cases, if a causative medication is identified, it should be added to the patient’s allergy list and the patient should be counseled extensively to avoid this medication and other medications in the same class. If a single agent cannot be identified, referrals for patch testing may be of some utility, particularly in AGEP and DRESS syndrome.30,31
- Preventable adverse drug reactions: a focus on drug interactions. US Food and Drug Administration website. https://www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/DrugInteractionsLabeling/ucm110632.htm. Updated March 6, 2018. Accessed April 12, 2019.
- Thienvibul C, Vachiramon V, Chanprapaph K. Five-year retrospective review of acute generalized exanthematous pustulosis. Dermatol Res Pract. 2015;3:1-8.
- Lee HY, Chou D, Pang SM, et al. Acute generalized exanthematous pustulosis: analysis of cases managed in a tertiary hospital in Singapore. Int J Dermatol. 2010
;49:507-512. - Ropars N, Darrieux L, Tisseau L, et al. Acute generalized exanthematous pustulosis associated with primary Epstein-Barr virus infection. JAAD Case Rep. 2014;1:9-11.
- Hattem S, Beerthuizen G, Kardaun S. Severe flucloxacillin‐induced acute generalized exanthematous pustulosis (AGEP), with toxic epidermal necrolysis (TEN)‐like features: does overlap between AGEP and TEN exist? clinical report and review of the literature. Br J Dermatol. 2014;171:1539-1545.
- Tajmir-Riahi A, Wörl P, Harrer T, et al. Life-threatening atypical case of acute generalized exanthematous pustulosis. Int Arch Allergy Immunol. 2017;174:108-111.
- Feldmeyer L, Heidemeyer K, Yawalkar N. Acute generalized exanthematous pustulosis: pathogenesis, genetic background, clinical variants and therapy. Int J Mol Sci. 2016;17:E1214.
- Szatkowski J, Schwartz RA. Acute generalized exanthematous pustulosis (AGEP). a review and update. J Am Acad Dermatol. 2015;73:843-848.
- Totonchy MB, McNiff JM, Bunick CG. Koebnerization of Hailey-Hailey disease into a cutaneous drug eruption of acute generalized exanthematous pustulosis associated with systemic symptoms. J Cutan Pathol. 2016;43:1031-1035.
- Husain Z, Reddy BY, Schwartz RA. DRESS syndrome: part II. management and therapeutics. J Am Acad Dermatol. 2013;68:709.e1-e9; quiz 718-720.
- Kano Y, Shiohara T. Long-term outcome of patients with severe cutaneous adverse reactions. Dermatologica Sinica. 2013;31:211-216.
- Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. Vol 1. Philadelphia, PA: Elsevier Saunders; 2012.
- Ushigome Y, Kano Y, Ishida T, et al. Short- and long-term outcomes of 34 patients with drug-induced hypersensitivity syndrome in a single institution. J Am Acad Dermatol. 2013;68:721-728.
- Ljungman P, Wang FZ, Clark DA, et al. High levels of human herpesvirus 6 DNA in peripheral blood leucocytes are correlated to platelet engraftment and disease in allogeneic stem cell transplant patients. Br J Haematol. 2000;111:774-781.
- Asano Y, Kagawa H, Kano Y, et al. Cytomegalovirus disease during severe drug eruptions: report of 2 cases and retrospective study of 18 patients with drug-induced hypersensitivity syndrome. Arch Dermatol. 2009;145:1030-1036.
- Kano Y , Tohyama M, Aihara M, et al. Sequelae in 145 patients with drug‐induced hypersensitivity syndrome/drug reaction with eosinophilia and systemic symptoms: survey conducted by the Asian Research Committee on Severe Cutaneous Adverse Reactions (ASCAR). J Dermatol. 2015;42:276-282.
- Morita C, Yanase T, Shiohara T, et al. Aggressive treatment in paediatric or young patients with drug-induced hypersensitivity syndrome (DiHS)/ drug reaction with eosinophilia and systemic symptoms (DRESS) is associated with future development of type III polyglandular autoimmune syndrome [published online October 27, 2018]. BMJ Case Rep. doi:10.1136/bcr-2018-225528.
- Chiang A, Shiu J, Elsensohn AN, et al. Classic autoimmune type 1 diabetes mellitus after a case of drug reaction with eosinophilia and systemic symptoms (DRESS). JAAD Case Rep. 2018;4:295-297.
- Lew TT, Creamer D, Mackenzie J, et al. Post-traumatic stress disorder following drug reaction with eosinophilia and systemic symptoms. Br J Dermatol. 2015;172:836-837.
- Kumar R, Das A, Das S. Management of Stevens-Johnson syndrome-toxic epidermal necrolysis: looking beyond guidelines! Indian J Dermatol. 2018;63:117-124.
- Yang CW, Cho YT, Chen KL, et al. Long-term sequelae of Stevens-Johnson syndrome/toxic epidermal necrolysis. Acta Derm Venereol. 2016;96:525-529.
- Lee HY, Walsh SA, Creamer D. Long‐term complications of Stevens-Johnson syndrome/toxic epidermal necrolysis (SJS/TEN): the spectrum of chronic problems in patients who survive an episode of SJS/TEN necessitates multidisciplinary follow‐up. Br J Dermatol. 2017;177:924-935.
- Hsu M, Jayaram A, Verner R, et al. Indications and outcomes of amniotic membrane transplantation in the management of acute Stevens-Johnson syndrome and toxic epidermal necrolysis: a case-control study. Cornea. 2012;31:1394-1402.
- Sant’ Anna AE, Hazarbassanov RM, de Freitas D, et al. Minor salivary glands and labial mucous membrane graft in the treatment of severe symblepharon and dry eye in patients with Stevens-Johnson syndrome. Br J Ophthalmol. 2012;96:234-239.
- Hefez L, Zaghbib K, Sbidian E, et al. Post-traumatic stress disorder in Stevens-Johnson syndrome and toxic epidermal necrolysis: prevalence and risk factors. a prospective study of 31 patients [published online October 3, 2018]. Br J Dermatol. doi:10.1111/bjd.17267.
- Knight L, Todd G, Muloiwa R, et al. Stevens Johnson syndrome and toxic epidermal necrolysis: maternal and foetal outcomes intwenty-two consecutive pregnant HIV infected women [published online August 12, 2015]. PLoS One. doi:10.1371/journal.pone.0135501.
- Tchetnya X, Ngwasiri CA, Munge T, et al. Severe eye complications from toxic epidermal necrolysis following initiation of nevirapine based HAART regimen in a child with HIV infection: a case from Cameroon. BMC Pediatr. 2018;18:108.
- Antoon JW, Goldman JL, Lee B, et al. Incidence, outcomes, and resource use in children with Stevens-Johnson syndrome and toxic epidermal necrolysis. Pediatr Dermatol. 2018;35:182-187.
- Basu S, Shanbhag SS, Gokani A, et al. Chronic ocular sequelae of Stevens-Johnson syndrome in children: long-term impact of appropriate therapy on natural history of disease. Am J Ophthalmol. 2018;189:17-28.
- Pinho A, Marta A, Coutinho I, et al. Long‐term reproducibility of positive patch test reactions in patients with non‐immediate cutaneous adverse drug reactions to antibiotics. Contact Dermatitis. 2017;76:204-209.
- Barbaud A, Collet E, Milpied B, et al. A multicentre study to determine the value and safety of drug patch tests for the three main classes of severe cutaneous adverse drug reactions. Br J Dermatol. 2013;168:555-562.
- Preventable adverse drug reactions: a focus on drug interactions. US Food and Drug Administration website. https://www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/DrugInteractionsLabeling/ucm110632.htm. Updated March 6, 2018. Accessed April 12, 2019.
- Thienvibul C, Vachiramon V, Chanprapaph K. Five-year retrospective review of acute generalized exanthematous pustulosis. Dermatol Res Pract. 2015;3:1-8.
- Lee HY, Chou D, Pang SM, et al. Acute generalized exanthematous pustulosis: analysis of cases managed in a tertiary hospital in Singapore. Int J Dermatol. 2010
;49:507-512. - Ropars N, Darrieux L, Tisseau L, et al. Acute generalized exanthematous pustulosis associated with primary Epstein-Barr virus infection. JAAD Case Rep. 2014;1:9-11.
- Hattem S, Beerthuizen G, Kardaun S. Severe flucloxacillin‐induced acute generalized exanthematous pustulosis (AGEP), with toxic epidermal necrolysis (TEN)‐like features: does overlap between AGEP and TEN exist? clinical report and review of the literature. Br J Dermatol. 2014;171:1539-1545.
- Tajmir-Riahi A, Wörl P, Harrer T, et al. Life-threatening atypical case of acute generalized exanthematous pustulosis. Int Arch Allergy Immunol. 2017;174:108-111.
- Feldmeyer L, Heidemeyer K, Yawalkar N. Acute generalized exanthematous pustulosis: pathogenesis, genetic background, clinical variants and therapy. Int J Mol Sci. 2016;17:E1214.
- Szatkowski J, Schwartz RA. Acute generalized exanthematous pustulosis (AGEP). a review and update. J Am Acad Dermatol. 2015;73:843-848.
- Totonchy MB, McNiff JM, Bunick CG. Koebnerization of Hailey-Hailey disease into a cutaneous drug eruption of acute generalized exanthematous pustulosis associated with systemic symptoms. J Cutan Pathol. 2016;43:1031-1035.
- Husain Z, Reddy BY, Schwartz RA. DRESS syndrome: part II. management and therapeutics. J Am Acad Dermatol. 2013;68:709.e1-e9; quiz 718-720.
- Kano Y, Shiohara T. Long-term outcome of patients with severe cutaneous adverse reactions. Dermatologica Sinica. 2013;31:211-216.
- Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. Vol 1. Philadelphia, PA: Elsevier Saunders; 2012.
- Ushigome Y, Kano Y, Ishida T, et al. Short- and long-term outcomes of 34 patients with drug-induced hypersensitivity syndrome in a single institution. J Am Acad Dermatol. 2013;68:721-728.
- Ljungman P, Wang FZ, Clark DA, et al. High levels of human herpesvirus 6 DNA in peripheral blood leucocytes are correlated to platelet engraftment and disease in allogeneic stem cell transplant patients. Br J Haematol. 2000;111:774-781.
- Asano Y, Kagawa H, Kano Y, et al. Cytomegalovirus disease during severe drug eruptions: report of 2 cases and retrospective study of 18 patients with drug-induced hypersensitivity syndrome. Arch Dermatol. 2009;145:1030-1036.
- Kano Y , Tohyama M, Aihara M, et al. Sequelae in 145 patients with drug‐induced hypersensitivity syndrome/drug reaction with eosinophilia and systemic symptoms: survey conducted by the Asian Research Committee on Severe Cutaneous Adverse Reactions (ASCAR). J Dermatol. 2015;42:276-282.
- Morita C, Yanase T, Shiohara T, et al. Aggressive treatment in paediatric or young patients with drug-induced hypersensitivity syndrome (DiHS)/ drug reaction with eosinophilia and systemic symptoms (DRESS) is associated with future development of type III polyglandular autoimmune syndrome [published online October 27, 2018]. BMJ Case Rep. doi:10.1136/bcr-2018-225528.
- Chiang A, Shiu J, Elsensohn AN, et al. Classic autoimmune type 1 diabetes mellitus after a case of drug reaction with eosinophilia and systemic symptoms (DRESS). JAAD Case Rep. 2018;4:295-297.
- Lew TT, Creamer D, Mackenzie J, et al. Post-traumatic stress disorder following drug reaction with eosinophilia and systemic symptoms. Br J Dermatol. 2015;172:836-837.
- Kumar R, Das A, Das S. Management of Stevens-Johnson syndrome-toxic epidermal necrolysis: looking beyond guidelines! Indian J Dermatol. 2018;63:117-124.
- Yang CW, Cho YT, Chen KL, et al. Long-term sequelae of Stevens-Johnson syndrome/toxic epidermal necrolysis. Acta Derm Venereol. 2016;96:525-529.
- Lee HY, Walsh SA, Creamer D. Long‐term complications of Stevens-Johnson syndrome/toxic epidermal necrolysis (SJS/TEN): the spectrum of chronic problems in patients who survive an episode of SJS/TEN necessitates multidisciplinary follow‐up. Br J Dermatol. 2017;177:924-935.
- Hsu M, Jayaram A, Verner R, et al. Indications and outcomes of amniotic membrane transplantation in the management of acute Stevens-Johnson syndrome and toxic epidermal necrolysis: a case-control study. Cornea. 2012;31:1394-1402.
- Sant’ Anna AE, Hazarbassanov RM, de Freitas D, et al. Minor salivary glands and labial mucous membrane graft in the treatment of severe symblepharon and dry eye in patients with Stevens-Johnson syndrome. Br J Ophthalmol. 2012;96:234-239.
- Hefez L, Zaghbib K, Sbidian E, et al. Post-traumatic stress disorder in Stevens-Johnson syndrome and toxic epidermal necrolysis: prevalence and risk factors. a prospective study of 31 patients [published online October 3, 2018]. Br J Dermatol. doi:10.1111/bjd.17267.
- Knight L, Todd G, Muloiwa R, et al. Stevens Johnson syndrome and toxic epidermal necrolysis: maternal and foetal outcomes intwenty-two consecutive pregnant HIV infected women [published online August 12, 2015]. PLoS One. doi:10.1371/journal.pone.0135501.
- Tchetnya X, Ngwasiri CA, Munge T, et al. Severe eye complications from toxic epidermal necrolysis following initiation of nevirapine based HAART regimen in a child with HIV infection: a case from Cameroon. BMC Pediatr. 2018;18:108.
- Antoon JW, Goldman JL, Lee B, et al. Incidence, outcomes, and resource use in children with Stevens-Johnson syndrome and toxic epidermal necrolysis. Pediatr Dermatol. 2018;35:182-187.
- Basu S, Shanbhag SS, Gokani A, et al. Chronic ocular sequelae of Stevens-Johnson syndrome in children: long-term impact of appropriate therapy on natural history of disease. Am J Ophthalmol. 2018;189:17-28.
- Pinho A, Marta A, Coutinho I, et al. Long‐term reproducibility of positive patch test reactions in patients with non‐immediate cutaneous adverse drug reactions to antibiotics. Contact Dermatitis. 2017;76:204-209.
- Barbaud A, Collet E, Milpied B, et al. A multicentre study to determine the value and safety of drug patch tests for the three main classes of severe cutaneous adverse drug reactions. Br J Dermatol. 2013;168:555-562.
Practice Points
- In the setting of an adverse drug reaction (ADR), discontinuing the concerning medication is the first and most important step.
- Acute generalized exanthematous pustulosis, drug rash with eosinophilia and systemic symptoms (DRESS) syndrome, and Stevens-Johnson syndrome/toxic epidermal necrolysis all require specific outpatient follow-up after discharge.