User login
For MD-IQ use only
Quick Byte: Conversations about cost
Patients want to talk
Seventy percent of Americans would like to have conversations about the costs of care with their health care providers, but only 28% do so, according to polling conducted for the Robert Wood Johnson Foundation (RWJF) by Avalere Health.

With those polling results in hand, 2 years ago RWJF and Avalere Health launched the Cost Conversation projects to help. Practice briefs for these kinds of conversations are now available on America’s Essential Hospitals’ website (https://essentialhospitals.org/cost-care/practice-briefs/).
Reference
1. Ganos E, Steinberg K, Seidman J, Masi D, Gomez-Rexode A, Fraser A. Talking About Costs: Innovation In Clinician-Patient Conversations. Health Affairs. Published online Nov. 27, 2018. doi: 10.1377/hblog20181126.366161. Accessed Dec. 11, 2018.
Patients want to talk
Patients want to talk
Seventy percent of Americans would like to have conversations about the costs of care with their health care providers, but only 28% do so, according to polling conducted for the Robert Wood Johnson Foundation (RWJF) by Avalere Health.
With those polling results in hand, 2 years ago RWJF and Avalere Health launched the Cost Conversation projects to help. Practice briefs for these kinds of conversations are now available on America’s Essential Hospitals’ website (https://essentialhospitals.org/cost-care/practice-briefs/).
Reference
1. Ganos E, Steinberg K, Seidman J, Masi D, Gomez-Rexode A, Fraser A. Talking About Costs: Innovation In Clinician-Patient Conversations. Health Affairs. Published online Nov. 27, 2018. doi: 10.1377/hblog20181126.366161. Accessed Dec. 11, 2018.
Seventy percent of Americans would like to have conversations about the costs of care with their health care providers, but only 28% do so, according to polling conducted for the Robert Wood Johnson Foundation (RWJF) by Avalere Health.
With those polling results in hand, 2 years ago RWJF and Avalere Health launched the Cost Conversation projects to help. Practice briefs for these kinds of conversations are now available on America’s Essential Hospitals’ website (https://essentialhospitals.org/cost-care/practice-briefs/).
Reference
1. Ganos E, Steinberg K, Seidman J, Masi D, Gomez-Rexode A, Fraser A. Talking About Costs: Innovation In Clinician-Patient Conversations. Health Affairs. Published online Nov. 27, 2018. doi: 10.1377/hblog20181126.366161. Accessed Dec. 11, 2018.
View, Review VAM at Home with VAM on Demand Library
The inability to be in two places at one time makes VAM On Demand an essential component of the Vascular Annual Meeting.

VAM on Demand lets people review — in depth and on their own timeline —sessions they attended and “attend” electronically the ones they couldn’t in person. VAM on Demand will include hundreds of individual presentations, with accompanying PowerPoint slides and audio. Select video sessions will be available.
The fee is $199 for attendees after the meeting ends. (Non-attendees may purchase VAM on Demand for $499.) All purchasers receive unlimited access, plus downloads to the library, for up to one year. Access begins several weeks after VAM ends and will be available on the SVS website vascular.org.
Contact [email protected] with questions.
The inability to be in two places at one time makes VAM On Demand an essential component of the Vascular Annual Meeting.
VAM on Demand lets people review — in depth and on their own timeline —sessions they attended and “attend” electronically the ones they couldn’t in person. VAM on Demand will include hundreds of individual presentations, with accompanying PowerPoint slides and audio. Select video sessions will be available.
The fee is $199 for attendees after the meeting ends. (Non-attendees may purchase VAM on Demand for $499.) All purchasers receive unlimited access, plus downloads to the library, for up to one year. Access begins several weeks after VAM ends and will be available on the SVS website vascular.org.
Contact [email protected] with questions.
The inability to be in two places at one time makes VAM On Demand an essential component of the Vascular Annual Meeting.
VAM on Demand lets people review — in depth and on their own timeline —sessions they attended and “attend” electronically the ones they couldn’t in person. VAM on Demand will include hundreds of individual presentations, with accompanying PowerPoint slides and audio. Select video sessions will be available.
The fee is $199 for attendees after the meeting ends. (Non-attendees may purchase VAM on Demand for $499.) All purchasers receive unlimited access, plus downloads to the library, for up to one year. Access begins several weeks after VAM ends and will be available on the SVS website vascular.org.
Contact [email protected] with questions.
How to Earn Your CME, MOC Credits from VAM
Physician registrants can get a big boost in collecting required Continuing Medical Education (CME) and Maintenance of Certification (MOC) self-assessment credits at the Vascular Annual Meeting.
The Society for Vascular Surgery is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. SVS has designated the 2019 Vascular Annual Meeting for a maximum of 30 AMA PRA Category 1 Credits™.
Physicians should claim only the credits commensurate with the extent of their participation in the activity.
Full credit is not available for attendance at two sessions occurring simultaneously.
A number of sessions also permit earning of MOC credits.
Participants may claim credits beginning Wednesday, June 12. Credits must be claimed by Dec. 31, 2019.
Physician registrants can get a big boost in collecting required Continuing Medical Education (CME) and Maintenance of Certification (MOC) self-assessment credits at the Vascular Annual Meeting.
The Society for Vascular Surgery is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. SVS has designated the 2019 Vascular Annual Meeting for a maximum of 30 AMA PRA Category 1 Credits™.
Physicians should claim only the credits commensurate with the extent of their participation in the activity.
Full credit is not available for attendance at two sessions occurring simultaneously.
A number of sessions also permit earning of MOC credits.
Participants may claim credits beginning Wednesday, June 12. Credits must be claimed by Dec. 31, 2019.
Physician registrants can get a big boost in collecting required Continuing Medical Education (CME) and Maintenance of Certification (MOC) self-assessment credits at the Vascular Annual Meeting.
The Society for Vascular Surgery is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. SVS has designated the 2019 Vascular Annual Meeting for a maximum of 30 AMA PRA Category 1 Credits™.
Physicians should claim only the credits commensurate with the extent of their participation in the activity.
Full credit is not available for attendance at two sessions occurring simultaneously.
A number of sessions also permit earning of MOC credits.
Participants may claim credits beginning Wednesday, June 12. Credits must be claimed by Dec. 31, 2019.
‘Good Outcomes Not Good Enough’
A tradition at the Vascular Annual Meeting, the E. Stanley Crawford Critical Issues Forum is organized by the incoming SVS President and devotes itself to assessing and discussing particular challenges currently facing the society. This year’s Forum focused on how vascular surgeons could use evidence-based medicine to develop tools to improve outcomes, reduce costs, and ensure appropriate utilization of resources.

Session moderator and organizer Kim J. Hodgson, MD, SVS president-elect and chair of the division of vascular surgery at Southern Illinois University School of Medicine, outlined the problem in his introductory presentation “Why Good Outcomes Are No Longer Good Enough.”
He pointed out how there are several driving forces influencing the inappropriate use of medical procedures, resulting in diminished quality of outcomes and increased costs of health care: These comprise incorrect evaluation, incorrect treatment and planning, and improper motivation. The first two factors can be improved through education and development and promulgation of evidence-based medical practices, but the last is correctable only through enforced regulation and peer-review. This has become increasingly more difficult as procedures move from the hospital to outpatient centers, where the profit motive for performing inappropriate procedures, and the means to satisfy it, are increasingly more tempting.
He emphasized how SVS has tools such as the Vascular Quality Initiative and its registries to provide evidence-based input on the appropriateness of procedures and whether an institution is matching up to its peers in providing appropriate patient care. The importance of the VQI was also stressed by the majority of the Crawford Forum speakers.
“Unfortunately, like it or not, the reality is that some degree of regulation is inevitable, and if we don’t step up and regulate ourselves, there are plenty of other people willing to do it for us. I would say that we let the bureaucrats develop our EHRs, and you know how that worked out. So, I think it is incumbent upon us to be able to regulate ourselves.”
Dr. Hodgson turned over the discussion to Arlene Seid, MD, MPH, medical director of the quality assurance office within the Pennsylvania Department of Health. Her presentation, “The Government’s Perspective on When & Where Endovascular Interventions Should Be Performed,” detailed how her department recently became concerned about an increase in the volume of endovascular procedures, and complications thereof, mainly in outpatient settings. The department also raised questions about the procedures and discussed whether reimbursement via programs such as Medicaid should be ceased.
She pointed out how federal regulations from the Centers for Medicare & Medicaid Services (CMS) only regulate through payments and their choice of procedures to be reimbursed, the vast majority of other regulations are established at the state level and vary widely from state to state. And at the state level, such as hers, there was great difficulty finding trustworthy expert opinion, and she added how organizations like the SVS could be of tremendous use in providing guidance in developing regulations.

As an example she used Ambulatory Surgical Centers, which are defined differently from state to state and vary widely in their requirements for licensing. The state’s job is made much simpler, and more effective, when expert organizations like the SVS can provide certification programs as a firm foundation for basing such licensing efforts.
She also suggested that if individuals have problems with or disagree with state regulations, they must become knowledgeable as to what level of state organization is involved, and ideally enlist the help of groups such as SVS to provide the expert justification for change.
Anton Sidawy, MD, MPH, FACS, professor and chair of the Department of Surgery at the George Washington University Medical Center, discussed how SVS is working with the American College of Surgeons to develop certification for vascular surgery centers. He addressed the need for organizations such as SVS to take the initiative in defining quality and value for the field, in no small part because payment models are shifting from the rewarding of volume to the rewarding of value.
Defining value may come from many sources: government, private insurers, and the public. Unless SVS has a strong voice in defining value, it may find itself not pleased with the results, according to Dr. Sidawy.
Then Fred A. Weaver, MD, chair of the SVS Patient Safety Organization and professor of surgery and chief of the vascular surgery division at Keck School of Medicine of University of Southern California, described the current state of the Vascular Quality Initiative. This is an SVS database whose 12 registries have gathered demographic, clinical, procedural and outcomes data from more than 500,000 vascular procedures performed in North America in 18 regional quality groups.
Currently, the VQI is comprised of 571 centers in the United States and Canada, with one in Singapore. Of particular importance, the makeup of the practitioners involved in the VQI is very diverse in specialty training, with only 41% of the membership being vascular surgeons.
In the near future, three more VQI registries are coming, according to Dr. Weaver: An ultrasound registry (in concert with the Society of Vascular Ultrasound); Venous Stenting; and Vascular Medicine (in concert with the American Heart Association).
Dr. Weaver emphasized how tracking outcomes is crucial for both vascular surgeons and certified vascular surgery centers to assess and improve their performance and how the VQI is critical to these endeavors.
Finally, Larry Kraiss, MD, chair of the SVS Quality Council and professor and chief of the vascular surgery division at the University of Utah, presented the goals of the new SVS council and described how the council is expanding the quality mission to include appropriate use criteria in addition to the long-standing clinical practice guidelines the SVS produces.
Dr. Kraiss elaborated how Appropriate Use Criteria (AUC) perform a substantially different role than that of Clinical Practice Guidelines (CPG).
Since 2006, SVS has developed 13 active guidelines, with more on the way. Guidelines provide positive yes/no statements with regard to treatment decision-making. However, many patients fall outside the guidelines, often due to comorbidities or other confounding factors, and appropriate use criteria are vital in these cases to evaluate where on a spectrum the patient fits for making a decision with regard to performing an operation or the use of a device.
Appropriate use criteria can be developed through the use of risk assessment to determine where on the spectrum of safety and effectiveness a particular patient falls with regard to a particular procedure or device. A major role of the new SVS Quality Council is to develop appropriate use criteria using outcome tools such as VQI and to provide recommendations as to how individuals and institutions could improve their performance by taking into account risk factors and assess infrastructural needs.
“The SVS board has authorized development of AUC in particular areas,” said Dr. Kraiss. “This process with be closely tied with updating the CPG. The first commissioned AUC will be to address intermittent claudication. But I invite the membership to participate in this process, especially on the panels, which can have up to 17 members, and we envision AUC coming out in carotid intervention, AAA management, and venous disease,” he added.
A tradition at the Vascular Annual Meeting, the E. Stanley Crawford Critical Issues Forum is organized by the incoming SVS President and devotes itself to assessing and discussing particular challenges currently facing the society. This year’s Forum focused on how vascular surgeons could use evidence-based medicine to develop tools to improve outcomes, reduce costs, and ensure appropriate utilization of resources.
Session moderator and organizer Kim J. Hodgson, MD, SVS president-elect and chair of the division of vascular surgery at Southern Illinois University School of Medicine, outlined the problem in his introductory presentation “Why Good Outcomes Are No Longer Good Enough.”
He pointed out how there are several driving forces influencing the inappropriate use of medical procedures, resulting in diminished quality of outcomes and increased costs of health care: These comprise incorrect evaluation, incorrect treatment and planning, and improper motivation. The first two factors can be improved through education and development and promulgation of evidence-based medical practices, but the last is correctable only through enforced regulation and peer-review. This has become increasingly more difficult as procedures move from the hospital to outpatient centers, where the profit motive for performing inappropriate procedures, and the means to satisfy it, are increasingly more tempting.
He emphasized how SVS has tools such as the Vascular Quality Initiative and its registries to provide evidence-based input on the appropriateness of procedures and whether an institution is matching up to its peers in providing appropriate patient care. The importance of the VQI was also stressed by the majority of the Crawford Forum speakers.
“Unfortunately, like it or not, the reality is that some degree of regulation is inevitable, and if we don’t step up and regulate ourselves, there are plenty of other people willing to do it for us. I would say that we let the bureaucrats develop our EHRs, and you know how that worked out. So, I think it is incumbent upon us to be able to regulate ourselves.”
Dr. Hodgson turned over the discussion to Arlene Seid, MD, MPH, medical director of the quality assurance office within the Pennsylvania Department of Health. Her presentation, “The Government’s Perspective on When & Where Endovascular Interventions Should Be Performed,” detailed how her department recently became concerned about an increase in the volume of endovascular procedures, and complications thereof, mainly in outpatient settings. The department also raised questions about the procedures and discussed whether reimbursement via programs such as Medicaid should be ceased.
She pointed out how federal regulations from the Centers for Medicare & Medicaid Services (CMS) only regulate through payments and their choice of procedures to be reimbursed, the vast majority of other regulations are established at the state level and vary widely from state to state. And at the state level, such as hers, there was great difficulty finding trustworthy expert opinion, and she added how organizations like the SVS could be of tremendous use in providing guidance in developing regulations.
As an example she used Ambulatory Surgical Centers, which are defined differently from state to state and vary widely in their requirements for licensing. The state’s job is made much simpler, and more effective, when expert organizations like the SVS can provide certification programs as a firm foundation for basing such licensing efforts.
She also suggested that if individuals have problems with or disagree with state regulations, they must become knowledgeable as to what level of state organization is involved, and ideally enlist the help of groups such as SVS to provide the expert justification for change.
Anton Sidawy, MD, MPH, FACS, professor and chair of the Department of Surgery at the George Washington University Medical Center, discussed how SVS is working with the American College of Surgeons to develop certification for vascular surgery centers. He addressed the need for organizations such as SVS to take the initiative in defining quality and value for the field, in no small part because payment models are shifting from the rewarding of volume to the rewarding of value.
Defining value may come from many sources: government, private insurers, and the public. Unless SVS has a strong voice in defining value, it may find itself not pleased with the results, according to Dr. Sidawy.
Then Fred A. Weaver, MD, chair of the SVS Patient Safety Organization and professor of surgery and chief of the vascular surgery division at Keck School of Medicine of University of Southern California, described the current state of the Vascular Quality Initiative. This is an SVS database whose 12 registries have gathered demographic, clinical, procedural and outcomes data from more than 500,000 vascular procedures performed in North America in 18 regional quality groups.
Currently, the VQI is comprised of 571 centers in the United States and Canada, with one in Singapore. Of particular importance, the makeup of the practitioners involved in the VQI is very diverse in specialty training, with only 41% of the membership being vascular surgeons.
In the near future, three more VQI registries are coming, according to Dr. Weaver: An ultrasound registry (in concert with the Society of Vascular Ultrasound); Venous Stenting; and Vascular Medicine (in concert with the American Heart Association).
Dr. Weaver emphasized how tracking outcomes is crucial for both vascular surgeons and certified vascular surgery centers to assess and improve their performance and how the VQI is critical to these endeavors.
Finally, Larry Kraiss, MD, chair of the SVS Quality Council and professor and chief of the vascular surgery division at the University of Utah, presented the goals of the new SVS council and described how the council is expanding the quality mission to include appropriate use criteria in addition to the long-standing clinical practice guidelines the SVS produces.
Dr. Kraiss elaborated how Appropriate Use Criteria (AUC) perform a substantially different role than that of Clinical Practice Guidelines (CPG).
Since 2006, SVS has developed 13 active guidelines, with more on the way. Guidelines provide positive yes/no statements with regard to treatment decision-making. However, many patients fall outside the guidelines, often due to comorbidities or other confounding factors, and appropriate use criteria are vital in these cases to evaluate where on a spectrum the patient fits for making a decision with regard to performing an operation or the use of a device.
Appropriate use criteria can be developed through the use of risk assessment to determine where on the spectrum of safety and effectiveness a particular patient falls with regard to a particular procedure or device. A major role of the new SVS Quality Council is to develop appropriate use criteria using outcome tools such as VQI and to provide recommendations as to how individuals and institutions could improve their performance by taking into account risk factors and assess infrastructural needs.
“The SVS board has authorized development of AUC in particular areas,” said Dr. Kraiss. “This process with be closely tied with updating the CPG. The first commissioned AUC will be to address intermittent claudication. But I invite the membership to participate in this process, especially on the panels, which can have up to 17 members, and we envision AUC coming out in carotid intervention, AAA management, and venous disease,” he added.
A tradition at the Vascular Annual Meeting, the E. Stanley Crawford Critical Issues Forum is organized by the incoming SVS President and devotes itself to assessing and discussing particular challenges currently facing the society. This year’s Forum focused on how vascular surgeons could use evidence-based medicine to develop tools to improve outcomes, reduce costs, and ensure appropriate utilization of resources.
Session moderator and organizer Kim J. Hodgson, MD, SVS president-elect and chair of the division of vascular surgery at Southern Illinois University School of Medicine, outlined the problem in his introductory presentation “Why Good Outcomes Are No Longer Good Enough.”
He pointed out how there are several driving forces influencing the inappropriate use of medical procedures, resulting in diminished quality of outcomes and increased costs of health care: These comprise incorrect evaluation, incorrect treatment and planning, and improper motivation. The first two factors can be improved through education and development and promulgation of evidence-based medical practices, but the last is correctable only through enforced regulation and peer-review. This has become increasingly more difficult as procedures move from the hospital to outpatient centers, where the profit motive for performing inappropriate procedures, and the means to satisfy it, are increasingly more tempting.
He emphasized how SVS has tools such as the Vascular Quality Initiative and its registries to provide evidence-based input on the appropriateness of procedures and whether an institution is matching up to its peers in providing appropriate patient care. The importance of the VQI was also stressed by the majority of the Crawford Forum speakers.
“Unfortunately, like it or not, the reality is that some degree of regulation is inevitable, and if we don’t step up and regulate ourselves, there are plenty of other people willing to do it for us. I would say that we let the bureaucrats develop our EHRs, and you know how that worked out. So, I think it is incumbent upon us to be able to regulate ourselves.”
Dr. Hodgson turned over the discussion to Arlene Seid, MD, MPH, medical director of the quality assurance office within the Pennsylvania Department of Health. Her presentation, “The Government’s Perspective on When & Where Endovascular Interventions Should Be Performed,” detailed how her department recently became concerned about an increase in the volume of endovascular procedures, and complications thereof, mainly in outpatient settings. The department also raised questions about the procedures and discussed whether reimbursement via programs such as Medicaid should be ceased.
She pointed out how federal regulations from the Centers for Medicare & Medicaid Services (CMS) only regulate through payments and their choice of procedures to be reimbursed, the vast majority of other regulations are established at the state level and vary widely from state to state. And at the state level, such as hers, there was great difficulty finding trustworthy expert opinion, and she added how organizations like the SVS could be of tremendous use in providing guidance in developing regulations.
As an example she used Ambulatory Surgical Centers, which are defined differently from state to state and vary widely in their requirements for licensing. The state’s job is made much simpler, and more effective, when expert organizations like the SVS can provide certification programs as a firm foundation for basing such licensing efforts.
She also suggested that if individuals have problems with or disagree with state regulations, they must become knowledgeable as to what level of state organization is involved, and ideally enlist the help of groups such as SVS to provide the expert justification for change.
Anton Sidawy, MD, MPH, FACS, professor and chair of the Department of Surgery at the George Washington University Medical Center, discussed how SVS is working with the American College of Surgeons to develop certification for vascular surgery centers. He addressed the need for organizations such as SVS to take the initiative in defining quality and value for the field, in no small part because payment models are shifting from the rewarding of volume to the rewarding of value.
Defining value may come from many sources: government, private insurers, and the public. Unless SVS has a strong voice in defining value, it may find itself not pleased with the results, according to Dr. Sidawy.
Then Fred A. Weaver, MD, chair of the SVS Patient Safety Organization and professor of surgery and chief of the vascular surgery division at Keck School of Medicine of University of Southern California, described the current state of the Vascular Quality Initiative. This is an SVS database whose 12 registries have gathered demographic, clinical, procedural and outcomes data from more than 500,000 vascular procedures performed in North America in 18 regional quality groups.
Currently, the VQI is comprised of 571 centers in the United States and Canada, with one in Singapore. Of particular importance, the makeup of the practitioners involved in the VQI is very diverse in specialty training, with only 41% of the membership being vascular surgeons.
In the near future, three more VQI registries are coming, according to Dr. Weaver: An ultrasound registry (in concert with the Society of Vascular Ultrasound); Venous Stenting; and Vascular Medicine (in concert with the American Heart Association).
Dr. Weaver emphasized how tracking outcomes is crucial for both vascular surgeons and certified vascular surgery centers to assess and improve their performance and how the VQI is critical to these endeavors.
Finally, Larry Kraiss, MD, chair of the SVS Quality Council and professor and chief of the vascular surgery division at the University of Utah, presented the goals of the new SVS council and described how the council is expanding the quality mission to include appropriate use criteria in addition to the long-standing clinical practice guidelines the SVS produces.
Dr. Kraiss elaborated how Appropriate Use Criteria (AUC) perform a substantially different role than that of Clinical Practice Guidelines (CPG).
Since 2006, SVS has developed 13 active guidelines, with more on the way. Guidelines provide positive yes/no statements with regard to treatment decision-making. However, many patients fall outside the guidelines, often due to comorbidities or other confounding factors, and appropriate use criteria are vital in these cases to evaluate where on a spectrum the patient fits for making a decision with regard to performing an operation or the use of a device.
Appropriate use criteria can be developed through the use of risk assessment to determine where on the spectrum of safety and effectiveness a particular patient falls with regard to a particular procedure or device. A major role of the new SVS Quality Council is to develop appropriate use criteria using outcome tools such as VQI and to provide recommendations as to how individuals and institutions could improve their performance by taking into account risk factors and assess infrastructural needs.
“The SVS board has authorized development of AUC in particular areas,” said Dr. Kraiss. “This process with be closely tied with updating the CPG. The first commissioned AUC will be to address intermittent claudication. But I invite the membership to participate in this process, especially on the panels, which can have up to 17 members, and we envision AUC coming out in carotid intervention, AAA management, and venous disease,” he added.
Change Doesn’t Come Easy! But Is Needed
In selecting the subject of his presidential address, SVS President Michel Makaroun, MD, decided to focus on the inadequacy of vascular manpower to meet the demands and needs of the public.

In introducing the subject, he quoted a favorite saying from Mark Twain that gave him the topic of his address, “I am in favor of progress; it’s change I don’t like.” He then proceeded to outline why changes are necessary and what the Society for Vascular Surgery is doing to help implement them.
“You are all familiar with the highlights of the problem: It is in our numbers! A problem with multiple facets, including unfilled jobs, increasing demand, maldistribution and a demographic cliff of our membership,” Dr. Makaroun said.
The manifestations of this shortage are multiple. The number of advertised jobs far exceeds the number of graduates. There is also a significant maldistribution of the workforce. “We are concentrated in the northeast, and many populous states including Texas, Florida and California are well below average,” he said.
Additionally, many community hospitals, in both suburban areas or small towns completely lack any access to vascular surgical care, even in states with seemingly adequate numbers.
The shortage problem in vascular surgery will get worse before it gets better, he added, saying “Our pipeline is simply not large enough to overcome an older retiring generation of vascular surgeons, with nearly half retiring before 65.”
“Change does not come easy!” Dr. Makaroun warned.
“We cannot ignore in the discussion of workforce issues, the major shifts, change and uncertainty we are experiencing in health care delivery, education and the generational change of our newest members,” he said.
More than 10% of vascular surgeons now practice primarily if not exclusively in ambulatory facilities. This direction is gathering steam and reduces the pool of vascular surgeons available to accept hospital practices and cover emergencies, particularly in underserved communities.
Despite this movement, nearly two-thirds of SVS members are currently employed by hospital systems that are getting larger and larger, making it essential to navigate an ever more complex decision-making process in employment, compensation and spectrum of activities. Practice environments are becoming more corporate and bureaucratic.
Dr. Makaroun pointed out that the current landscape of our manpower has a clear two tiers divided by hospital size and location. “The most pressing concern is the inability of our specialty to provide vascular surgery services to the multitude of hospitals located in smaller communities.
“The SVS established a task force to study our manpower issues last fall. The taskforce was divided into three workgroups to focus on different areas of the problem.
The first workgroup, under the leadership of Malachi Sheehan III, MD, and Jeffrey Jim, MD, focused on the obvious solution: a campaign to increase training programs and available positions. Unfortunately, this is only aspirational, since reality fails the SVS in this effort. The pool of general surgery graduates is finite, with competition from several specialties that are more analogous to modern general surgery than vascular surgery.
Increasing the number of integrated programs is less efficient because of a 5- to 6-year lag between initiation of a new program and graduation, but it can tap into an almost unlimited pool of applicants from medical school, and more recently some very qualified international medical graduates. This makes it potentially a far more effective solution for the long term, Dr. Makaroun said.
The workgroup attempted to contact all hospitals with a general surgery program and no associated vascular fellowship. Help in navigating the process of securing financing and applying for a new program was offered. A session was conducted at VAM for interested potential sites to start discussing the process, and representatives from 27 hospitals were there expressing interest.
The second workgroup, under the leadership of Rick Powell, MD, and Andy Schanzer, MD, was tasked with analyzing and understanding the entire spectrum of surgeons’ clinical activities and producing a valuation study that illustrates the economic and vital impact of vascular surgery for hospitals and patients. “The work of this group is essential to promote a healthier relationship between our specialty and our institutions, making vascular surgery more attractive for future recruits,” according to Dr. Makaroun.
The third workgroup under the leadership of Will Jordan, MD, and Tim Sarac, MD, had the toughest job, said Dr. Makaroun. It was tasked with thinking outside the box and suggesting methods to address the most glaring need: the community hospitals, where most of the advertised jobs are, jobs that are being shunned by graduates of current training programs.
Dr. Makaroun cited the difficulties of recruitment of vascular surgeons to community hospital systems in small towns and rural areas, and he reminded people that recent general surgery graduates continue to offer vascular surgery services in such communities. Unfortunately, this is without any additional vascular training and most hospitals grant privileges without a VSB certificate when the need is demonstrated. “You all appreciate that recent graduates of general surgery programs do not have the breadth or depth of exposure to modern vascular surgery that an older generation did,” he added.
The workgroup explored many options to provide relief to community hospitals. But probably the most efficient, according to Dr. Makaroun, is to consider strategies that tap into new constituencies. One consideration to be explored is to offer a 3-year vascular surgery training opportunity to the dozens of qualified candidates in preliminary surgical positions unable to locate a categorical spot to finish their training. This process will lead to VSB certification, but will take some time to establish through the ACGME structure.
The workgroup developed an outline of a proposal for a community vascular surgery training program, as a first step. It has been sketched and will be part of the task force report submitted for review by the Executive Board of the Society.
The goals of the new pathway would be to improve local vascular care in underserved communities, while increasing the referral of appropriate cases to vascular centers. It would provide stress relief to isolated vascular surgeons, and where none exist, plant the seeds of a better work environment for vascular surgery graduates to reconsider this currently undesirable career choice.
The program is designed to offer an additional year of vascular surgery training to general surgery graduates already committed to a community practice, many of whom are already planning to offer vascular services anyway. The program will individualize training but focus only on low-complexity procedures, both open and endovascular, and more importantly the clinical situations that dictate referral, said Dr. Makaroun.
To maintain quality, the program will mandate the availability of mentorship, support and real-time advice after completion of the program, through a regional “sponsoring vascular surgery service.” This service will also be responsible for retrospective peer review and root cause analysis of complications. In addition, the association with a sponsoring institution will facilitate and increase referrals of appropriate patients to higher level of care at a vascular surgery center.
“The suggested program graduates will not be board-certified and will be performing mostly general surgery and low-complexity vascular cases part- time in smaller communities. They will also require supervision by the board-certified graduates of the current training pathways, working in a regional vascular center, typically in a larger urban center. Instead of competing they will actually complement our current trainees and provide an extension of their reach.” Dr. Makaroun stated.
“We must find a way to fill the vacuum now before the reality on the ground permanently excludes our specialty from this primary level of vascular care,” Dr. Makaroun said. “It is time for another bold step to preserve the legacy of our specialty in meeting the needs of our patients and the public.
“Progress is made through change even if we don’t like it!” Dr. Makaroun concluded.
In selecting the subject of his presidential address, SVS President Michel Makaroun, MD, decided to focus on the inadequacy of vascular manpower to meet the demands and needs of the public.
In introducing the subject, he quoted a favorite saying from Mark Twain that gave him the topic of his address, “I am in favor of progress; it’s change I don’t like.” He then proceeded to outline why changes are necessary and what the Society for Vascular Surgery is doing to help implement them.
“You are all familiar with the highlights of the problem: It is in our numbers! A problem with multiple facets, including unfilled jobs, increasing demand, maldistribution and a demographic cliff of our membership,” Dr. Makaroun said.
The manifestations of this shortage are multiple. The number of advertised jobs far exceeds the number of graduates. There is also a significant maldistribution of the workforce. “We are concentrated in the northeast, and many populous states including Texas, Florida and California are well below average,” he said.
Additionally, many community hospitals, in both suburban areas or small towns completely lack any access to vascular surgical care, even in states with seemingly adequate numbers.
The shortage problem in vascular surgery will get worse before it gets better, he added, saying “Our pipeline is simply not large enough to overcome an older retiring generation of vascular surgeons, with nearly half retiring before 65.”
“Change does not come easy!” Dr. Makaroun warned.
“We cannot ignore in the discussion of workforce issues, the major shifts, change and uncertainty we are experiencing in health care delivery, education and the generational change of our newest members,” he said.
More than 10% of vascular surgeons now practice primarily if not exclusively in ambulatory facilities. This direction is gathering steam and reduces the pool of vascular surgeons available to accept hospital practices and cover emergencies, particularly in underserved communities.
Despite this movement, nearly two-thirds of SVS members are currently employed by hospital systems that are getting larger and larger, making it essential to navigate an ever more complex decision-making process in employment, compensation and spectrum of activities. Practice environments are becoming more corporate and bureaucratic.
Dr. Makaroun pointed out that the current landscape of our manpower has a clear two tiers divided by hospital size and location. “The most pressing concern is the inability of our specialty to provide vascular surgery services to the multitude of hospitals located in smaller communities.
“The SVS established a task force to study our manpower issues last fall. The taskforce was divided into three workgroups to focus on different areas of the problem.
The first workgroup, under the leadership of Malachi Sheehan III, MD, and Jeffrey Jim, MD, focused on the obvious solution: a campaign to increase training programs and available positions. Unfortunately, this is only aspirational, since reality fails the SVS in this effort. The pool of general surgery graduates is finite, with competition from several specialties that are more analogous to modern general surgery than vascular surgery.
Increasing the number of integrated programs is less efficient because of a 5- to 6-year lag between initiation of a new program and graduation, but it can tap into an almost unlimited pool of applicants from medical school, and more recently some very qualified international medical graduates. This makes it potentially a far more effective solution for the long term, Dr. Makaroun said.
The workgroup attempted to contact all hospitals with a general surgery program and no associated vascular fellowship. Help in navigating the process of securing financing and applying for a new program was offered. A session was conducted at VAM for interested potential sites to start discussing the process, and representatives from 27 hospitals were there expressing interest.
The second workgroup, under the leadership of Rick Powell, MD, and Andy Schanzer, MD, was tasked with analyzing and understanding the entire spectrum of surgeons’ clinical activities and producing a valuation study that illustrates the economic and vital impact of vascular surgery for hospitals and patients. “The work of this group is essential to promote a healthier relationship between our specialty and our institutions, making vascular surgery more attractive for future recruits,” according to Dr. Makaroun.
The third workgroup under the leadership of Will Jordan, MD, and Tim Sarac, MD, had the toughest job, said Dr. Makaroun. It was tasked with thinking outside the box and suggesting methods to address the most glaring need: the community hospitals, where most of the advertised jobs are, jobs that are being shunned by graduates of current training programs.
Dr. Makaroun cited the difficulties of recruitment of vascular surgeons to community hospital systems in small towns and rural areas, and he reminded people that recent general surgery graduates continue to offer vascular surgery services in such communities. Unfortunately, this is without any additional vascular training and most hospitals grant privileges without a VSB certificate when the need is demonstrated. “You all appreciate that recent graduates of general surgery programs do not have the breadth or depth of exposure to modern vascular surgery that an older generation did,” he added.
The workgroup explored many options to provide relief to community hospitals. But probably the most efficient, according to Dr. Makaroun, is to consider strategies that tap into new constituencies. One consideration to be explored is to offer a 3-year vascular surgery training opportunity to the dozens of qualified candidates in preliminary surgical positions unable to locate a categorical spot to finish their training. This process will lead to VSB certification, but will take some time to establish through the ACGME structure.
The workgroup developed an outline of a proposal for a community vascular surgery training program, as a first step. It has been sketched and will be part of the task force report submitted for review by the Executive Board of the Society.
The goals of the new pathway would be to improve local vascular care in underserved communities, while increasing the referral of appropriate cases to vascular centers. It would provide stress relief to isolated vascular surgeons, and where none exist, plant the seeds of a better work environment for vascular surgery graduates to reconsider this currently undesirable career choice.
The program is designed to offer an additional year of vascular surgery training to general surgery graduates already committed to a community practice, many of whom are already planning to offer vascular services anyway. The program will individualize training but focus only on low-complexity procedures, both open and endovascular, and more importantly the clinical situations that dictate referral, said Dr. Makaroun.
To maintain quality, the program will mandate the availability of mentorship, support and real-time advice after completion of the program, through a regional “sponsoring vascular surgery service.” This service will also be responsible for retrospective peer review and root cause analysis of complications. In addition, the association with a sponsoring institution will facilitate and increase referrals of appropriate patients to higher level of care at a vascular surgery center.
“The suggested program graduates will not be board-certified and will be performing mostly general surgery and low-complexity vascular cases part- time in smaller communities. They will also require supervision by the board-certified graduates of the current training pathways, working in a regional vascular center, typically in a larger urban center. Instead of competing they will actually complement our current trainees and provide an extension of their reach.” Dr. Makaroun stated.
“We must find a way to fill the vacuum now before the reality on the ground permanently excludes our specialty from this primary level of vascular care,” Dr. Makaroun said. “It is time for another bold step to preserve the legacy of our specialty in meeting the needs of our patients and the public.
“Progress is made through change even if we don’t like it!” Dr. Makaroun concluded.
In selecting the subject of his presidential address, SVS President Michel Makaroun, MD, decided to focus on the inadequacy of vascular manpower to meet the demands and needs of the public.
In introducing the subject, he quoted a favorite saying from Mark Twain that gave him the topic of his address, “I am in favor of progress; it’s change I don’t like.” He then proceeded to outline why changes are necessary and what the Society for Vascular Surgery is doing to help implement them.
“You are all familiar with the highlights of the problem: It is in our numbers! A problem with multiple facets, including unfilled jobs, increasing demand, maldistribution and a demographic cliff of our membership,” Dr. Makaroun said.
The manifestations of this shortage are multiple. The number of advertised jobs far exceeds the number of graduates. There is also a significant maldistribution of the workforce. “We are concentrated in the northeast, and many populous states including Texas, Florida and California are well below average,” he said.
Additionally, many community hospitals, in both suburban areas or small towns completely lack any access to vascular surgical care, even in states with seemingly adequate numbers.
The shortage problem in vascular surgery will get worse before it gets better, he added, saying “Our pipeline is simply not large enough to overcome an older retiring generation of vascular surgeons, with nearly half retiring before 65.”
“Change does not come easy!” Dr. Makaroun warned.
“We cannot ignore in the discussion of workforce issues, the major shifts, change and uncertainty we are experiencing in health care delivery, education and the generational change of our newest members,” he said.
More than 10% of vascular surgeons now practice primarily if not exclusively in ambulatory facilities. This direction is gathering steam and reduces the pool of vascular surgeons available to accept hospital practices and cover emergencies, particularly in underserved communities.
Despite this movement, nearly two-thirds of SVS members are currently employed by hospital systems that are getting larger and larger, making it essential to navigate an ever more complex decision-making process in employment, compensation and spectrum of activities. Practice environments are becoming more corporate and bureaucratic.
Dr. Makaroun pointed out that the current landscape of our manpower has a clear two tiers divided by hospital size and location. “The most pressing concern is the inability of our specialty to provide vascular surgery services to the multitude of hospitals located in smaller communities.
“The SVS established a task force to study our manpower issues last fall. The taskforce was divided into three workgroups to focus on different areas of the problem.
The first workgroup, under the leadership of Malachi Sheehan III, MD, and Jeffrey Jim, MD, focused on the obvious solution: a campaign to increase training programs and available positions. Unfortunately, this is only aspirational, since reality fails the SVS in this effort. The pool of general surgery graduates is finite, with competition from several specialties that are more analogous to modern general surgery than vascular surgery.
Increasing the number of integrated programs is less efficient because of a 5- to 6-year lag between initiation of a new program and graduation, but it can tap into an almost unlimited pool of applicants from medical school, and more recently some very qualified international medical graduates. This makes it potentially a far more effective solution for the long term, Dr. Makaroun said.
The workgroup attempted to contact all hospitals with a general surgery program and no associated vascular fellowship. Help in navigating the process of securing financing and applying for a new program was offered. A session was conducted at VAM for interested potential sites to start discussing the process, and representatives from 27 hospitals were there expressing interest.
The second workgroup, under the leadership of Rick Powell, MD, and Andy Schanzer, MD, was tasked with analyzing and understanding the entire spectrum of surgeons’ clinical activities and producing a valuation study that illustrates the economic and vital impact of vascular surgery for hospitals and patients. “The work of this group is essential to promote a healthier relationship between our specialty and our institutions, making vascular surgery more attractive for future recruits,” according to Dr. Makaroun.
The third workgroup under the leadership of Will Jordan, MD, and Tim Sarac, MD, had the toughest job, said Dr. Makaroun. It was tasked with thinking outside the box and suggesting methods to address the most glaring need: the community hospitals, where most of the advertised jobs are, jobs that are being shunned by graduates of current training programs.
Dr. Makaroun cited the difficulties of recruitment of vascular surgeons to community hospital systems in small towns and rural areas, and he reminded people that recent general surgery graduates continue to offer vascular surgery services in such communities. Unfortunately, this is without any additional vascular training and most hospitals grant privileges without a VSB certificate when the need is demonstrated. “You all appreciate that recent graduates of general surgery programs do not have the breadth or depth of exposure to modern vascular surgery that an older generation did,” he added.
The workgroup explored many options to provide relief to community hospitals. But probably the most efficient, according to Dr. Makaroun, is to consider strategies that tap into new constituencies. One consideration to be explored is to offer a 3-year vascular surgery training opportunity to the dozens of qualified candidates in preliminary surgical positions unable to locate a categorical spot to finish their training. This process will lead to VSB certification, but will take some time to establish through the ACGME structure.
The workgroup developed an outline of a proposal for a community vascular surgery training program, as a first step. It has been sketched and will be part of the task force report submitted for review by the Executive Board of the Society.
The goals of the new pathway would be to improve local vascular care in underserved communities, while increasing the referral of appropriate cases to vascular centers. It would provide stress relief to isolated vascular surgeons, and where none exist, plant the seeds of a better work environment for vascular surgery graduates to reconsider this currently undesirable career choice.
The program is designed to offer an additional year of vascular surgery training to general surgery graduates already committed to a community practice, many of whom are already planning to offer vascular services anyway. The program will individualize training but focus only on low-complexity procedures, both open and endovascular, and more importantly the clinical situations that dictate referral, said Dr. Makaroun.
To maintain quality, the program will mandate the availability of mentorship, support and real-time advice after completion of the program, through a regional “sponsoring vascular surgery service.” This service will also be responsible for retrospective peer review and root cause analysis of complications. In addition, the association with a sponsoring institution will facilitate and increase referrals of appropriate patients to higher level of care at a vascular surgery center.
“The suggested program graduates will not be board-certified and will be performing mostly general surgery and low-complexity vascular cases part- time in smaller communities. They will also require supervision by the board-certified graduates of the current training pathways, working in a regional vascular center, typically in a larger urban center. Instead of competing they will actually complement our current trainees and provide an extension of their reach.” Dr. Makaroun stated.
“We must find a way to fill the vacuum now before the reality on the ground permanently excludes our specialty from this primary level of vascular care,” Dr. Makaroun said. “It is time for another bold step to preserve the legacy of our specialty in meeting the needs of our patients and the public.
“Progress is made through change even if we don’t like it!” Dr. Makaroun concluded.
Creating better performance incentives
P4P programs suffer from several flaws
Many performance improvement programs try to create a higher value health system by incentivizing physicians and health systems to behave in particular ways. These have often been pay-for-performance programs that offer bonuses or impose penalties depending on how providers perform on various metrics.

“In theory, this makes sense,” said Dhruv Khullar, MD, MPP, lead author of a JAMA article about the future of incentives, and assistant professor at Weill Cornell Medicine in New York. “But in practice, these programs have not been successful in consistently improving quality, and sometimes they have been counterproductive. In our article, we argued that focusing too narrowly on financial rewards is not the right strategy to improve health system performance – and is sometimes at odds with the physician professionalism and what really motivates most clinicians.”
Pay-for-performance programs suffer from several fundamental flaws: they focus too narrowly on financial incentives and use centralized accountability instead of local culture, for example, Dr. Khullar said.
“A better future state would involve capitalizing on physician professionalism through nonfinancial rewards, resources for quality improvement, team-based assessments, and emphasizing continuous learning and organizational culture,” he noted. Performance programs would take a more global view of clinical care by emphasizing culture, teams, trust, and learning. Such a system would allow hospitalists and other physicians to worry less about meeting specific metrics and focus more on providing high-quality care to their patients.
“I would hope physicians, payers, and administrators would reconsider some previously held beliefs about quality improvement, especially the idea that better quality requires giving people bonus payments or imposing financial penalties,” Dr. Khullar said. “We believe the next wave of performance improvement programs should entertain other paths to better quality, which are more in line with human motivation and physician professionalism.”
Reference
1. Khullar D, Wolfson D, Casalino LP. Professionalism, Performance, and the Future of Physician Incentives. JAMA. 2018 Nov 26 (Epub ahead of print). doi: 10.1001/jama.2018.17719. Accessed Dec. 11, 2018.
P4P programs suffer from several flaws
P4P programs suffer from several flaws
Many performance improvement programs try to create a higher value health system by incentivizing physicians and health systems to behave in particular ways. These have often been pay-for-performance programs that offer bonuses or impose penalties depending on how providers perform on various metrics.
“In theory, this makes sense,” said Dhruv Khullar, MD, MPP, lead author of a JAMA article about the future of incentives, and assistant professor at Weill Cornell Medicine in New York. “But in practice, these programs have not been successful in consistently improving quality, and sometimes they have been counterproductive. In our article, we argued that focusing too narrowly on financial rewards is not the right strategy to improve health system performance – and is sometimes at odds with the physician professionalism and what really motivates most clinicians.”
Pay-for-performance programs suffer from several fundamental flaws: they focus too narrowly on financial incentives and use centralized accountability instead of local culture, for example, Dr. Khullar said.
“A better future state would involve capitalizing on physician professionalism through nonfinancial rewards, resources for quality improvement, team-based assessments, and emphasizing continuous learning and organizational culture,” he noted. Performance programs would take a more global view of clinical care by emphasizing culture, teams, trust, and learning. Such a system would allow hospitalists and other physicians to worry less about meeting specific metrics and focus more on providing high-quality care to their patients.
“I would hope physicians, payers, and administrators would reconsider some previously held beliefs about quality improvement, especially the idea that better quality requires giving people bonus payments or imposing financial penalties,” Dr. Khullar said. “We believe the next wave of performance improvement programs should entertain other paths to better quality, which are more in line with human motivation and physician professionalism.”
Reference
1. Khullar D, Wolfson D, Casalino LP. Professionalism, Performance, and the Future of Physician Incentives. JAMA. 2018 Nov 26 (Epub ahead of print). doi: 10.1001/jama.2018.17719. Accessed Dec. 11, 2018.
Many performance improvement programs try to create a higher value health system by incentivizing physicians and health systems to behave in particular ways. These have often been pay-for-performance programs that offer bonuses or impose penalties depending on how providers perform on various metrics.
“In theory, this makes sense,” said Dhruv Khullar, MD, MPP, lead author of a JAMA article about the future of incentives, and assistant professor at Weill Cornell Medicine in New York. “But in practice, these programs have not been successful in consistently improving quality, and sometimes they have been counterproductive. In our article, we argued that focusing too narrowly on financial rewards is not the right strategy to improve health system performance – and is sometimes at odds with the physician professionalism and what really motivates most clinicians.”
Pay-for-performance programs suffer from several fundamental flaws: they focus too narrowly on financial incentives and use centralized accountability instead of local culture, for example, Dr. Khullar said.
“A better future state would involve capitalizing on physician professionalism through nonfinancial rewards, resources for quality improvement, team-based assessments, and emphasizing continuous learning and organizational culture,” he noted. Performance programs would take a more global view of clinical care by emphasizing culture, teams, trust, and learning. Such a system would allow hospitalists and other physicians to worry less about meeting specific metrics and focus more on providing high-quality care to their patients.
“I would hope physicians, payers, and administrators would reconsider some previously held beliefs about quality improvement, especially the idea that better quality requires giving people bonus payments or imposing financial penalties,” Dr. Khullar said. “We believe the next wave of performance improvement programs should entertain other paths to better quality, which are more in line with human motivation and physician professionalism.”
Reference
1. Khullar D, Wolfson D, Casalino LP. Professionalism, Performance, and the Future of Physician Incentives. JAMA. 2018 Nov 26 (Epub ahead of print). doi: 10.1001/jama.2018.17719. Accessed Dec. 11, 2018.
A “Ray of light”
Finding inspiration in our patients
I rush into the room at 4:30 p.m., hoping for a quick visit and maybe an early exit from the hospital; I had been asked to see Mr. Bryant in room 6765 with sigmoid volvulus.

“Hey, Dr. Hass, my brother!” he says with a huge smile. Somehow, he must have gotten a glimpse of me before I could see him. I peek over the nurse’s shoulder, and then I see that unforgettable smile with only a few teeth and big bright eyes. Immediately I recognize him and think, “How could I have forgotten his name? Ray – like a beam of light.” He certainly had not forgotten me.
“It’s been more than a year since I was last here,” he says proudly.
When we met during his last hospitalization, I was struck by a thought that implanted itself deep in my brain: This guy is the happiest person I have ever met. And after what must have been 18 hard months for him, he is still smiling – and more than that, he is radiating love.
The fact that he is the “happiest person” is made more remarkable by all the hardship he has endured. Ray was born with cerebral palsy and didn’t walk until he was 10. The continuous spasms in his muscles led to severe cervical disc disease. His worsening pain and weakness were missed by his health care providers until he had lost significant strength in his hands and legs. When he finally got an MRI and then emergency surgery, it was too late. He never regained the dexterity of his hands or the ability to walk. He can climb onto his scooter chair only with the help of a lift.
“Wow! How you been, Ray?”
He replies with a phrase that jumped back out from my memory as he was saying it: “I just wake up every day and think about what I can do to make people happy.”
The goosebumps rise on my arms; I remember feeling this same sense of awe the last time we met – a feeling of real spiritual love for this guy.
“Today I feel so much better, too. I want to thank y’all who helped my stomach go down. Man, it got so huge, I thought I might blow up.” One of the consequences of the nerve damage he sustained is a very slow gut that has led to a stretched-out colon. The other day, his big, floppy colon got twisted, and neither our gastroenterologist nor radiologist was able to untwist it. He still has a tube in his rectum to help decompress his bowel.
Ray fills me in on the details in the slightly strained and slurred speech that sometimes comes with cerebral palsy. As he relays his story, my mind goes to work trying to diagnosis this mysterious case of happiness. How can I not try to get to the origins of this wellspring of love? I can’t help but thinking: Was it Ray’s joy and his speech impediment that made him seem childlike, or was it some brain injury that blessedly knocked out his self-pity? I would be wallowing in self-pity if I were as gravely disabled as him.
After a moment’s reflection, I recall the research on the amazing stability of our happiness set point: Good things and bad only move our happiness for a while before we return to our innate level of happiness. I see I had likely fallen prey to a stereotype of the disabled as heroic for just being themselves. Ray’s happiness is largely because of his lack of self-absorption and his focus on service and love.
Finishing our conversation and leaving the room feeling enlivened, I realize that Ray‘s generous spirit is a gift.
That night, my heart aches. I think about the inadequate care that led to Ray’s profound loss of function, leading to a surge of anger toward our flawed health care system – one that routinely lets down the most vulnerable among us.
The next day, two sisters and an aunt join Ray in his room. They ask for hugs, and I happily supply them. “Ray told us about you,” says Sheila, one of his sisters.
“Well, we have been talking about him here at the hospital, because he brightens everyone’s day. He is truly amazing. Has Ray always been so full of love?” I say, hoping to get some insight into his remarkable spirit.
Tonya, his aunt, responds first. “We were raised that way – to look for the good and keep love in our hearts. But Ray has always been the best. He never, ever complains. He brings joy to so many people. You should see him every day out on his scooter. That’s how he got that big sore on his butt.”
Ray indeed had developed a pressure sore, one that was going to need some thoughtful, ongoing care.
“But I finally got the right kind of cushion, before it was real hard,” he says.
I move from hospitalist mode to primary care mode and ask about his home equipment and his dental care. But they all want to keep talking about love.
“If doctors showed more love and their human side, they could bring more healing,” his sister says.
After 20 minutes of chatting, I pause. It is my last day on service, I had run out of medical reason to stay and I have others to see. So, I reluctantly give my goodbye hugs and leave. At the door, I turn back around. “Hey, Ray, can I get a picture with you?”
“Yeah, I want one with you, too!”
So, not surprisingly, Ray never complains. Maybe his spinal cord injury wasn’t from negligent care. Maybe he was so accustomed to looking past discomfort and too busy with his ministry of love, it didn’t occur to him to seek care.
Still, such a tragedy that he lost so much of the little mobility he did have. But maybe not so bad. His injury brought him back in contact with me and our staff. He is still waking up trying to make people happy and I can see his efforts are working. “He made my day!” I hear from a nurse. There is a healthy buzz at the nurses’ station after visits to his room.
Before walking out the door, he gives me an awkward fist bump from the bed and says, “I want to thank y’all again for everything. And I want you to know I love you.”
I find myself tearing up. “I love you too, my brother. And I am the one who should be grateful, Ray.” Saying it, I feel myself playing a part in the cycle of gratitude. Even small gifts put us under an obligation to give back. With great gifts, the desire to give is inescapable.
There is only one Ray, but he has given me something to aspire toward and what feels like urgency to do it. I want to “wake up each day thinking about ways to make other people happy.”
And understanding the potency of the gift from him has alerted me to the value of looking for other gifts and other inspirations from those I care for – something those of us who tend to be in the “doing” part of the provider-patient relationship can easy miss.
I will never be the beacon of light and love that Ray is, but being compelled to be my most authentic caring self with him, I see that for years I have held back – in the name of professionalism – the positive emotions that naturally arise from the work I do. I will try to shine and try to connect with that “Ray of light” residing in all my patients. I hope, too, that the cycle of giving Ray started will continue spreading to all those I care for.
Dr. Hass is a hospitalist at Sutter Health in Oakland, Calif. This article appeared originally in SHM's official blog The Hospital Leader. Read more recent posts here.
Finding inspiration in our patients
Finding inspiration in our patients
I rush into the room at 4:30 p.m., hoping for a quick visit and maybe an early exit from the hospital; I had been asked to see Mr. Bryant in room 6765 with sigmoid volvulus.
“Hey, Dr. Hass, my brother!” he says with a huge smile. Somehow, he must have gotten a glimpse of me before I could see him. I peek over the nurse’s shoulder, and then I see that unforgettable smile with only a few teeth and big bright eyes. Immediately I recognize him and think, “How could I have forgotten his name? Ray – like a beam of light.” He certainly had not forgotten me.
“It’s been more than a year since I was last here,” he says proudly.
When we met during his last hospitalization, I was struck by a thought that implanted itself deep in my brain: This guy is the happiest person I have ever met. And after what must have been 18 hard months for him, he is still smiling – and more than that, he is radiating love.
The fact that he is the “happiest person” is made more remarkable by all the hardship he has endured. Ray was born with cerebral palsy and didn’t walk until he was 10. The continuous spasms in his muscles led to severe cervical disc disease. His worsening pain and weakness were missed by his health care providers until he had lost significant strength in his hands and legs. When he finally got an MRI and then emergency surgery, it was too late. He never regained the dexterity of his hands or the ability to walk. He can climb onto his scooter chair only with the help of a lift.
“Wow! How you been, Ray?”
He replies with a phrase that jumped back out from my memory as he was saying it: “I just wake up every day and think about what I can do to make people happy.”
The goosebumps rise on my arms; I remember feeling this same sense of awe the last time we met – a feeling of real spiritual love for this guy.
“Today I feel so much better, too. I want to thank y’all who helped my stomach go down. Man, it got so huge, I thought I might blow up.” One of the consequences of the nerve damage he sustained is a very slow gut that has led to a stretched-out colon. The other day, his big, floppy colon got twisted, and neither our gastroenterologist nor radiologist was able to untwist it. He still has a tube in his rectum to help decompress his bowel.
Ray fills me in on the details in the slightly strained and slurred speech that sometimes comes with cerebral palsy. As he relays his story, my mind goes to work trying to diagnosis this mysterious case of happiness. How can I not try to get to the origins of this wellspring of love? I can’t help but thinking: Was it Ray’s joy and his speech impediment that made him seem childlike, or was it some brain injury that blessedly knocked out his self-pity? I would be wallowing in self-pity if I were as gravely disabled as him.
After a moment’s reflection, I recall the research on the amazing stability of our happiness set point: Good things and bad only move our happiness for a while before we return to our innate level of happiness. I see I had likely fallen prey to a stereotype of the disabled as heroic for just being themselves. Ray’s happiness is largely because of his lack of self-absorption and his focus on service and love.
Finishing our conversation and leaving the room feeling enlivened, I realize that Ray‘s generous spirit is a gift.
That night, my heart aches. I think about the inadequate care that led to Ray’s profound loss of function, leading to a surge of anger toward our flawed health care system – one that routinely lets down the most vulnerable among us.
The next day, two sisters and an aunt join Ray in his room. They ask for hugs, and I happily supply them. “Ray told us about you,” says Sheila, one of his sisters.
“Well, we have been talking about him here at the hospital, because he brightens everyone’s day. He is truly amazing. Has Ray always been so full of love?” I say, hoping to get some insight into his remarkable spirit.
Tonya, his aunt, responds first. “We were raised that way – to look for the good and keep love in our hearts. But Ray has always been the best. He never, ever complains. He brings joy to so many people. You should see him every day out on his scooter. That’s how he got that big sore on his butt.”
Ray indeed had developed a pressure sore, one that was going to need some thoughtful, ongoing care.
“But I finally got the right kind of cushion, before it was real hard,” he says.
I move from hospitalist mode to primary care mode and ask about his home equipment and his dental care. But they all want to keep talking about love.
“If doctors showed more love and their human side, they could bring more healing,” his sister says.
After 20 minutes of chatting, I pause. It is my last day on service, I had run out of medical reason to stay and I have others to see. So, I reluctantly give my goodbye hugs and leave. At the door, I turn back around. “Hey, Ray, can I get a picture with you?”
“Yeah, I want one with you, too!”
So, not surprisingly, Ray never complains. Maybe his spinal cord injury wasn’t from negligent care. Maybe he was so accustomed to looking past discomfort and too busy with his ministry of love, it didn’t occur to him to seek care.
Still, such a tragedy that he lost so much of the little mobility he did have. But maybe not so bad. His injury brought him back in contact with me and our staff. He is still waking up trying to make people happy and I can see his efforts are working. “He made my day!” I hear from a nurse. There is a healthy buzz at the nurses’ station after visits to his room.
Before walking out the door, he gives me an awkward fist bump from the bed and says, “I want to thank y’all again for everything. And I want you to know I love you.”
I find myself tearing up. “I love you too, my brother. And I am the one who should be grateful, Ray.” Saying it, I feel myself playing a part in the cycle of gratitude. Even small gifts put us under an obligation to give back. With great gifts, the desire to give is inescapable.
There is only one Ray, but he has given me something to aspire toward and what feels like urgency to do it. I want to “wake up each day thinking about ways to make other people happy.”
And understanding the potency of the gift from him has alerted me to the value of looking for other gifts and other inspirations from those I care for – something those of us who tend to be in the “doing” part of the provider-patient relationship can easy miss.
I will never be the beacon of light and love that Ray is, but being compelled to be my most authentic caring self with him, I see that for years I have held back – in the name of professionalism – the positive emotions that naturally arise from the work I do. I will try to shine and try to connect with that “Ray of light” residing in all my patients. I hope, too, that the cycle of giving Ray started will continue spreading to all those I care for.
Dr. Hass is a hospitalist at Sutter Health in Oakland, Calif. This article appeared originally in SHM's official blog The Hospital Leader. Read more recent posts here.
I rush into the room at 4:30 p.m., hoping for a quick visit and maybe an early exit from the hospital; I had been asked to see Mr. Bryant in room 6765 with sigmoid volvulus.
“Hey, Dr. Hass, my brother!” he says with a huge smile. Somehow, he must have gotten a glimpse of me before I could see him. I peek over the nurse’s shoulder, and then I see that unforgettable smile with only a few teeth and big bright eyes. Immediately I recognize him and think, “How could I have forgotten his name? Ray – like a beam of light.” He certainly had not forgotten me.
“It’s been more than a year since I was last here,” he says proudly.
When we met during his last hospitalization, I was struck by a thought that implanted itself deep in my brain: This guy is the happiest person I have ever met. And after what must have been 18 hard months for him, he is still smiling – and more than that, he is radiating love.
The fact that he is the “happiest person” is made more remarkable by all the hardship he has endured. Ray was born with cerebral palsy and didn’t walk until he was 10. The continuous spasms in his muscles led to severe cervical disc disease. His worsening pain and weakness were missed by his health care providers until he had lost significant strength in his hands and legs. When he finally got an MRI and then emergency surgery, it was too late. He never regained the dexterity of his hands or the ability to walk. He can climb onto his scooter chair only with the help of a lift.
“Wow! How you been, Ray?”
He replies with a phrase that jumped back out from my memory as he was saying it: “I just wake up every day and think about what I can do to make people happy.”
The goosebumps rise on my arms; I remember feeling this same sense of awe the last time we met – a feeling of real spiritual love for this guy.
“Today I feel so much better, too. I want to thank y’all who helped my stomach go down. Man, it got so huge, I thought I might blow up.” One of the consequences of the nerve damage he sustained is a very slow gut that has led to a stretched-out colon. The other day, his big, floppy colon got twisted, and neither our gastroenterologist nor radiologist was able to untwist it. He still has a tube in his rectum to help decompress his bowel.
Ray fills me in on the details in the slightly strained and slurred speech that sometimes comes with cerebral palsy. As he relays his story, my mind goes to work trying to diagnosis this mysterious case of happiness. How can I not try to get to the origins of this wellspring of love? I can’t help but thinking: Was it Ray’s joy and his speech impediment that made him seem childlike, or was it some brain injury that blessedly knocked out his self-pity? I would be wallowing in self-pity if I were as gravely disabled as him.
After a moment’s reflection, I recall the research on the amazing stability of our happiness set point: Good things and bad only move our happiness for a while before we return to our innate level of happiness. I see I had likely fallen prey to a stereotype of the disabled as heroic for just being themselves. Ray’s happiness is largely because of his lack of self-absorption and his focus on service and love.
Finishing our conversation and leaving the room feeling enlivened, I realize that Ray‘s generous spirit is a gift.
That night, my heart aches. I think about the inadequate care that led to Ray’s profound loss of function, leading to a surge of anger toward our flawed health care system – one that routinely lets down the most vulnerable among us.
The next day, two sisters and an aunt join Ray in his room. They ask for hugs, and I happily supply them. “Ray told us about you,” says Sheila, one of his sisters.
“Well, we have been talking about him here at the hospital, because he brightens everyone’s day. He is truly amazing. Has Ray always been so full of love?” I say, hoping to get some insight into his remarkable spirit.
Tonya, his aunt, responds first. “We were raised that way – to look for the good and keep love in our hearts. But Ray has always been the best. He never, ever complains. He brings joy to so many people. You should see him every day out on his scooter. That’s how he got that big sore on his butt.”
Ray indeed had developed a pressure sore, one that was going to need some thoughtful, ongoing care.
“But I finally got the right kind of cushion, before it was real hard,” he says.
I move from hospitalist mode to primary care mode and ask about his home equipment and his dental care. But they all want to keep talking about love.
“If doctors showed more love and their human side, they could bring more healing,” his sister says.
After 20 minutes of chatting, I pause. It is my last day on service, I had run out of medical reason to stay and I have others to see. So, I reluctantly give my goodbye hugs and leave. At the door, I turn back around. “Hey, Ray, can I get a picture with you?”
“Yeah, I want one with you, too!”
So, not surprisingly, Ray never complains. Maybe his spinal cord injury wasn’t from negligent care. Maybe he was so accustomed to looking past discomfort and too busy with his ministry of love, it didn’t occur to him to seek care.
Still, such a tragedy that he lost so much of the little mobility he did have. But maybe not so bad. His injury brought him back in contact with me and our staff. He is still waking up trying to make people happy and I can see his efforts are working. “He made my day!” I hear from a nurse. There is a healthy buzz at the nurses’ station after visits to his room.
Before walking out the door, he gives me an awkward fist bump from the bed and says, “I want to thank y’all again for everything. And I want you to know I love you.”
I find myself tearing up. “I love you too, my brother. And I am the one who should be grateful, Ray.” Saying it, I feel myself playing a part in the cycle of gratitude. Even small gifts put us under an obligation to give back. With great gifts, the desire to give is inescapable.
There is only one Ray, but he has given me something to aspire toward and what feels like urgency to do it. I want to “wake up each day thinking about ways to make other people happy.”
And understanding the potency of the gift from him has alerted me to the value of looking for other gifts and other inspirations from those I care for – something those of us who tend to be in the “doing” part of the provider-patient relationship can easy miss.
I will never be the beacon of light and love that Ray is, but being compelled to be my most authentic caring self with him, I see that for years I have held back – in the name of professionalism – the positive emotions that naturally arise from the work I do. I will try to shine and try to connect with that “Ray of light” residing in all my patients. I hope, too, that the cycle of giving Ray started will continue spreading to all those I care for.
Dr. Hass is a hospitalist at Sutter Health in Oakland, Calif. This article appeared originally in SHM's official blog The Hospital Leader. Read more recent posts here.
Are hospitalists being more highly valued?
An uptrend in financial support
Since the inception of hospital medicine more than 2 decades ago, the total number of hospitalists has rapidly increased to more than 60,000. The Society of Hospital Medicine’s State of Hospital Medicine Report (SoHM), published biennially, captures new changes in our growing field and sheds light on current practice trends.

Among its findings, the 2018 SoHM Report reassuringly reveals that financial support from hospitals to hospital medicine groups (HMGs) continues to climb, even in the setting of rising health care costs and ongoing budget pressure.
The median amount of financial support per full-time equivalent (FTE) physician for HMGs serving adults was $176,658, according to the 2018 SoHM Report, which is up 12% from the 2016 median of $157,535. While there is no correlation between group sizes and the amount of financial support per FTE physician, there are significant differences across regions, with HMGs in the Midwest garnering the highest median support, at $193,121 per FTE physician.
The report also reveals big differences by employment model. For example, private multispecialty and primary care medical groups receive much less financial support ($58,396 per FTE physician) than HMGs employed by hospitals. This likely signifies that their main source of revenue is from professional service fees. Regardless of the types of employment models, past surveys have reported more than 95% of HMGs receive support from their hospitals to help cover expenses.
The median amount of financial support per FTE provider (including nurse practitioners, physician assistants, and locum tenens) was $134,300, which represents a 3.3% decrease, compared with the 2016 SoHM Report. For the first time, the 2018 SoHM also collected data on financial support per “work relative value unit” (wRVU) in addition to support per FTE physician and support per FTE provider. HMGs and their hospitals can use support per wRVU data to evaluate the support per unit of work, regardless of who (whether it is a physician, an advanced practice provider, and/or others) performed that work.
The median amount of financial support per wRVU for HMGs serving adults in 2018 was $41.92, with academic HMGs reporting a higher amount ($45.81) than nonacademic HMGs ($41.28). It will be interesting to track these numbers over time.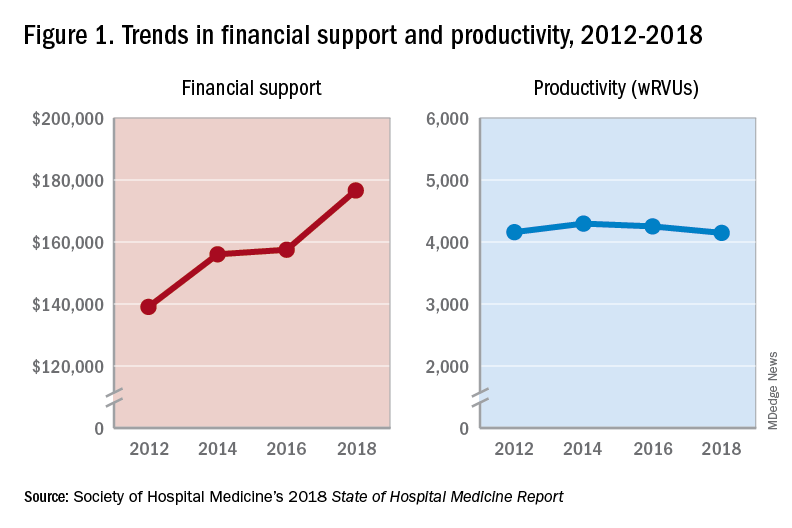
One of the most intriguing findings from the SHM’s 2018 SoHM Report is that financial support has risen despite relatively flat professional fee productivity (see Figure 1). Productivity, calculated as work relative value units (wRVUs) per physician declined slightly from 4,252 in 2016 to 4,147 in 2018.
There may be a few reasons why wRVUs per physician has remained relatively unchanged over the years. Many hospitals emphasize quality of care above provider productivity. The volume-to-value shift in theory serves as a means to reduce hospital-associated complications, length of stay, and readmission rates, thereby avoiding penalties and saving the overall costs for the hospitals in the long run.
Hospitalists involved in quality improvement projects and other essential nonclinical work perform tasks that are rarely captured in the wRVU metric. Improving patient experience, one of the Triple Aim components, necessitates extra time and effort, which also are nonbillable. In addition, increasing productivity can be challenging, a double-edged sword that may further escalate burnout and turnover rates. The static productivity may portend that it has leveled off or hit the ceiling in spite of ongoing efforts to improve efficacy.
In my view, the decision to invest in hospitalists for their contributions and dedications should not be determined based on a single metric such as wRVUs per physician. Hospitalist work on quality improvements; patient safety; efficiency, from direct bedside patient care to nonclinical efforts; teaching; research; involvements in various committees; administrative tasks; and leadership roles in improving health care systems are immeasurable. These are the reasons that most hospitals chose to adopt the hospitalist model and continue to support it. In fact, demand for hospitalists still outstrips supply, as evidenced by more than half of the hospital medicine groups with unfilled positions and an overall high turnover rate per 2018 SoHM data.
Although hospitalists are needed for the value that they provide, they should not take the status quo for granted. Instead, in return for the favorable financial support and in appreciation of being valued, hospitalists have a responsibility to prove that they are the right group chosen to do the work and help achieve their hospital’s mission and goals.
Dr. Vuong is a hospitalist at HealthPartners Medical Group in St Paul, Minn., and an assistant professor of medicine at the University of Minnesota. He is a member of SHM’s Practice Analysis Committee.
References
Afsar N. Looking into the Future and Making History. Hospitalist. 2019;23(1):31.
Beresford L. The State of Hospital Medicine in 2018. Hospitalist. 2019;23(1):1-11.
FitzGerald S. Not a Time for Modesty. Oct. 2009. Retrieved from https://acphospitalist.org/archives/2009/10/value.htm.
Watcher RM et al. Zero to 50,000 – The 20th Anniversary of the Hospitalist. N Eng J Med. 2016. 375(11):1009-11.
An uptrend in financial support
An uptrend in financial support
Since the inception of hospital medicine more than 2 decades ago, the total number of hospitalists has rapidly increased to more than 60,000. The Society of Hospital Medicine’s State of Hospital Medicine Report (SoHM), published biennially, captures new changes in our growing field and sheds light on current practice trends.
Among its findings, the 2018 SoHM Report reassuringly reveals that financial support from hospitals to hospital medicine groups (HMGs) continues to climb, even in the setting of rising health care costs and ongoing budget pressure.
The median amount of financial support per full-time equivalent (FTE) physician for HMGs serving adults was $176,658, according to the 2018 SoHM Report, which is up 12% from the 2016 median of $157,535. While there is no correlation between group sizes and the amount of financial support per FTE physician, there are significant differences across regions, with HMGs in the Midwest garnering the highest median support, at $193,121 per FTE physician.
The report also reveals big differences by employment model. For example, private multispecialty and primary care medical groups receive much less financial support ($58,396 per FTE physician) than HMGs employed by hospitals. This likely signifies that their main source of revenue is from professional service fees. Regardless of the types of employment models, past surveys have reported more than 95% of HMGs receive support from their hospitals to help cover expenses.
The median amount of financial support per FTE provider (including nurse practitioners, physician assistants, and locum tenens) was $134,300, which represents a 3.3% decrease, compared with the 2016 SoHM Report. For the first time, the 2018 SoHM also collected data on financial support per “work relative value unit” (wRVU) in addition to support per FTE physician and support per FTE provider. HMGs and their hospitals can use support per wRVU data to evaluate the support per unit of work, regardless of who (whether it is a physician, an advanced practice provider, and/or others) performed that work.
The median amount of financial support per wRVU for HMGs serving adults in 2018 was $41.92, with academic HMGs reporting a higher amount ($45.81) than nonacademic HMGs ($41.28). It will be interesting to track these numbers over time.
One of the most intriguing findings from the SHM’s 2018 SoHM Report is that financial support has risen despite relatively flat professional fee productivity (see Figure 1). Productivity, calculated as work relative value units (wRVUs) per physician declined slightly from 4,252 in 2016 to 4,147 in 2018.
There may be a few reasons why wRVUs per physician has remained relatively unchanged over the years. Many hospitals emphasize quality of care above provider productivity. The volume-to-value shift in theory serves as a means to reduce hospital-associated complications, length of stay, and readmission rates, thereby avoiding penalties and saving the overall costs for the hospitals in the long run.
Hospitalists involved in quality improvement projects and other essential nonclinical work perform tasks that are rarely captured in the wRVU metric. Improving patient experience, one of the Triple Aim components, necessitates extra time and effort, which also are nonbillable. In addition, increasing productivity can be challenging, a double-edged sword that may further escalate burnout and turnover rates. The static productivity may portend that it has leveled off or hit the ceiling in spite of ongoing efforts to improve efficacy.
In my view, the decision to invest in hospitalists for their contributions and dedications should not be determined based on a single metric such as wRVUs per physician. Hospitalist work on quality improvements; patient safety; efficiency, from direct bedside patient care to nonclinical efforts; teaching; research; involvements in various committees; administrative tasks; and leadership roles in improving health care systems are immeasurable. These are the reasons that most hospitals chose to adopt the hospitalist model and continue to support it. In fact, demand for hospitalists still outstrips supply, as evidenced by more than half of the hospital medicine groups with unfilled positions and an overall high turnover rate per 2018 SoHM data.
Although hospitalists are needed for the value that they provide, they should not take the status quo for granted. Instead, in return for the favorable financial support and in appreciation of being valued, hospitalists have a responsibility to prove that they are the right group chosen to do the work and help achieve their hospital’s mission and goals.
Dr. Vuong is a hospitalist at HealthPartners Medical Group in St Paul, Minn., and an assistant professor of medicine at the University of Minnesota. He is a member of SHM’s Practice Analysis Committee.
References
Afsar N. Looking into the Future and Making History. Hospitalist. 2019;23(1):31.
Beresford L. The State of Hospital Medicine in 2018. Hospitalist. 2019;23(1):1-11.
FitzGerald S. Not a Time for Modesty. Oct. 2009. Retrieved from https://acphospitalist.org/archives/2009/10/value.htm.
Watcher RM et al. Zero to 50,000 – The 20th Anniversary of the Hospitalist. N Eng J Med. 2016. 375(11):1009-11.
Since the inception of hospital medicine more than 2 decades ago, the total number of hospitalists has rapidly increased to more than 60,000. The Society of Hospital Medicine’s State of Hospital Medicine Report (SoHM), published biennially, captures new changes in our growing field and sheds light on current practice trends.
Among its findings, the 2018 SoHM Report reassuringly reveals that financial support from hospitals to hospital medicine groups (HMGs) continues to climb, even in the setting of rising health care costs and ongoing budget pressure.
The median amount of financial support per full-time equivalent (FTE) physician for HMGs serving adults was $176,658, according to the 2018 SoHM Report, which is up 12% from the 2016 median of $157,535. While there is no correlation between group sizes and the amount of financial support per FTE physician, there are significant differences across regions, with HMGs in the Midwest garnering the highest median support, at $193,121 per FTE physician.
The report also reveals big differences by employment model. For example, private multispecialty and primary care medical groups receive much less financial support ($58,396 per FTE physician) than HMGs employed by hospitals. This likely signifies that their main source of revenue is from professional service fees. Regardless of the types of employment models, past surveys have reported more than 95% of HMGs receive support from their hospitals to help cover expenses.
The median amount of financial support per FTE provider (including nurse practitioners, physician assistants, and locum tenens) was $134,300, which represents a 3.3% decrease, compared with the 2016 SoHM Report. For the first time, the 2018 SoHM also collected data on financial support per “work relative value unit” (wRVU) in addition to support per FTE physician and support per FTE provider. HMGs and their hospitals can use support per wRVU data to evaluate the support per unit of work, regardless of who (whether it is a physician, an advanced practice provider, and/or others) performed that work.
The median amount of financial support per wRVU for HMGs serving adults in 2018 was $41.92, with academic HMGs reporting a higher amount ($45.81) than nonacademic HMGs ($41.28). It will be interesting to track these numbers over time.
One of the most intriguing findings from the SHM’s 2018 SoHM Report is that financial support has risen despite relatively flat professional fee productivity (see Figure 1). Productivity, calculated as work relative value units (wRVUs) per physician declined slightly from 4,252 in 2016 to 4,147 in 2018.
There may be a few reasons why wRVUs per physician has remained relatively unchanged over the years. Many hospitals emphasize quality of care above provider productivity. The volume-to-value shift in theory serves as a means to reduce hospital-associated complications, length of stay, and readmission rates, thereby avoiding penalties and saving the overall costs for the hospitals in the long run.
Hospitalists involved in quality improvement projects and other essential nonclinical work perform tasks that are rarely captured in the wRVU metric. Improving patient experience, one of the Triple Aim components, necessitates extra time and effort, which also are nonbillable. In addition, increasing productivity can be challenging, a double-edged sword that may further escalate burnout and turnover rates. The static productivity may portend that it has leveled off or hit the ceiling in spite of ongoing efforts to improve efficacy.
In my view, the decision to invest in hospitalists for their contributions and dedications should not be determined based on a single metric such as wRVUs per physician. Hospitalist work on quality improvements; patient safety; efficiency, from direct bedside patient care to nonclinical efforts; teaching; research; involvements in various committees; administrative tasks; and leadership roles in improving health care systems are immeasurable. These are the reasons that most hospitals chose to adopt the hospitalist model and continue to support it. In fact, demand for hospitalists still outstrips supply, as evidenced by more than half of the hospital medicine groups with unfilled positions and an overall high turnover rate per 2018 SoHM data.
Although hospitalists are needed for the value that they provide, they should not take the status quo for granted. Instead, in return for the favorable financial support and in appreciation of being valued, hospitalists have a responsibility to prove that they are the right group chosen to do the work and help achieve their hospital’s mission and goals.
Dr. Vuong is a hospitalist at HealthPartners Medical Group in St Paul, Minn., and an assistant professor of medicine at the University of Minnesota. He is a member of SHM’s Practice Analysis Committee.
References
Afsar N. Looking into the Future and Making History. Hospitalist. 2019;23(1):31.
Beresford L. The State of Hospital Medicine in 2018. Hospitalist. 2019;23(1):1-11.
FitzGerald S. Not a Time for Modesty. Oct. 2009. Retrieved from https://acphospitalist.org/archives/2009/10/value.htm.
Watcher RM et al. Zero to 50,000 – The 20th Anniversary of the Hospitalist. N Eng J Med. 2016. 375(11):1009-11.
Early Outcomes To Be Presented From ROADSTER 2
Vikram S. Kashyap, MD, of the University Hospitals Cleveland Medical Center, will present results from ROADSTER 2, a prospective, multicenter, postapproval registry for patients undergoing transcarotid artery revascularization (TCAR). This technique involves carotid artery stenting with cerebral protection via reversal of carotid arterial flow. The aim of the study was to evaluate the real- world safety and efficacy of TCAR.
Dr. Kashyap and his colleagues enrolled 623 patients who were considered at high risk for complications from carotid endarterectomy (CEA) and who had symptomatic stenosis equal to or greater than 50% or asymptomatic stenosis equal to or greater than 80%. The primary endpoint was procedural success, which encompassed technical success plus the absence of stroke, myocardial infarction, or death within the 30-day postoperative period. Secondary endpoints were acute device success (delivery of device, establishment of flow reversal, and retrieval), technical success (acute device success plus introduction of interventional tools), stroke, death, and the composite of stroke, death, or myocardial infarction (S/D/MI), according to Dr. Kashyap.
A total of 599 of the patients completed 30-day follow-up. The cohort included 67.0% men, 42% older than 75 years, and 26.8% with symptoms Overall, 68.2% of the patients had anatomic-related high-risk factors, 56.5% had physiologic high-risk factors, and 24.7% had both. The majority (81.2%) of the operators in this study were new to TCAR and did not participate in the ROADSTER 1 trial.
The early postoperative outcomes included five patients (0.8%) suffering a stroke, one patient (0.2%) dying from a ruptured AAA two weeks post-procedure, and six (1.0%) having an MI. The composite stroke/death/MI rate was 1.9%.
“TCAR results in excellent early outcomes with a combined stroke/death rate of 1.0%. Broader, longer- term, comparative studies are needed in this area. But if these results can be confirmed, I believe TCAR may become a favorable alternative to transfemoral carotid artery stenting, and even rival carotid endarterectomy,” Dr. Kashyap concluded.
Saturday, June 15
1:30-2:30 p.m.
Gaylord National, Potomac 4-6
S10: Scientific Session 10/Late-Breaking: LB2
Vikram S. Kashyap, MD, of the University Hospitals Cleveland Medical Center, will present results from ROADSTER 2, a prospective, multicenter, postapproval registry for patients undergoing transcarotid artery revascularization (TCAR). This technique involves carotid artery stenting with cerebral protection via reversal of carotid arterial flow. The aim of the study was to evaluate the real- world safety and efficacy of TCAR.
Dr. Kashyap and his colleagues enrolled 623 patients who were considered at high risk for complications from carotid endarterectomy (CEA) and who had symptomatic stenosis equal to or greater than 50% or asymptomatic stenosis equal to or greater than 80%. The primary endpoint was procedural success, which encompassed technical success plus the absence of stroke, myocardial infarction, or death within the 30-day postoperative period. Secondary endpoints were acute device success (delivery of device, establishment of flow reversal, and retrieval), technical success (acute device success plus introduction of interventional tools), stroke, death, and the composite of stroke, death, or myocardial infarction (S/D/MI), according to Dr. Kashyap.
A total of 599 of the patients completed 30-day follow-up. The cohort included 67.0% men, 42% older than 75 years, and 26.8% with symptoms Overall, 68.2% of the patients had anatomic-related high-risk factors, 56.5% had physiologic high-risk factors, and 24.7% had both. The majority (81.2%) of the operators in this study were new to TCAR and did not participate in the ROADSTER 1 trial.
The early postoperative outcomes included five patients (0.8%) suffering a stroke, one patient (0.2%) dying from a ruptured AAA two weeks post-procedure, and six (1.0%) having an MI. The composite stroke/death/MI rate was 1.9%.
“TCAR results in excellent early outcomes with a combined stroke/death rate of 1.0%. Broader, longer- term, comparative studies are needed in this area. But if these results can be confirmed, I believe TCAR may become a favorable alternative to transfemoral carotid artery stenting, and even rival carotid endarterectomy,” Dr. Kashyap concluded.
Saturday, June 15
1:30-2:30 p.m.
Gaylord National, Potomac 4-6
S10: Scientific Session 10/Late-Breaking: LB2
Vikram S. Kashyap, MD, of the University Hospitals Cleveland Medical Center, will present results from ROADSTER 2, a prospective, multicenter, postapproval registry for patients undergoing transcarotid artery revascularization (TCAR). This technique involves carotid artery stenting with cerebral protection via reversal of carotid arterial flow. The aim of the study was to evaluate the real- world safety and efficacy of TCAR.
Dr. Kashyap and his colleagues enrolled 623 patients who were considered at high risk for complications from carotid endarterectomy (CEA) and who had symptomatic stenosis equal to or greater than 50% or asymptomatic stenosis equal to or greater than 80%. The primary endpoint was procedural success, which encompassed technical success plus the absence of stroke, myocardial infarction, or death within the 30-day postoperative period. Secondary endpoints were acute device success (delivery of device, establishment of flow reversal, and retrieval), technical success (acute device success plus introduction of interventional tools), stroke, death, and the composite of stroke, death, or myocardial infarction (S/D/MI), according to Dr. Kashyap.
A total of 599 of the patients completed 30-day follow-up. The cohort included 67.0% men, 42% older than 75 years, and 26.8% with symptoms Overall, 68.2% of the patients had anatomic-related high-risk factors, 56.5% had physiologic high-risk factors, and 24.7% had both. The majority (81.2%) of the operators in this study were new to TCAR and did not participate in the ROADSTER 1 trial.
The early postoperative outcomes included five patients (0.8%) suffering a stroke, one patient (0.2%) dying from a ruptured AAA two weeks post-procedure, and six (1.0%) having an MI. The composite stroke/death/MI rate was 1.9%.
“TCAR results in excellent early outcomes with a combined stroke/death rate of 1.0%. Broader, longer- term, comparative studies are needed in this area. But if these results can be confirmed, I believe TCAR may become a favorable alternative to transfemoral carotid artery stenting, and even rival carotid endarterectomy,” Dr. Kashyap concluded.
Saturday, June 15
1:30-2:30 p.m.
Gaylord National, Potomac 4-6
S10: Scientific Session 10/Late-Breaking: LB2

Lifetime Achievement, Innovation Award On Tap
Three of the Vascular Annual Meeting’s signature events – celebrations along with distinguished lectures – occur on Saturday, VAM’s closing day. All conveniently occur in the morning, shortly before the start of the SVS Annual Business Meeting and luncheon and take place in Potomac A/B.
The John Homans Lecture, 9:30 to 10 a.m.: Jack Cronenwett, MD, Dartmouth-Hitchcock Medical Center, Lebanon, N.H., will present the lecture, “Why Should I Join the Vascular Quality Initiative?” Dr. Cronenwett spearheaded a regional quality outcomes registry, the eventual model for VQI. He later helped launch the SVS-Patient Safety Organization, which operates VQI and served as medical director until 2016. Dr. Cronenwett will discuss the VQI’s benefits for vascular practitioners and examine the VQI’s research and quality improvement opportunities.
The Roy Greenberg Distinguished Lecture, 10:15 to 10:45 a.m.: Michael Dake, MD, professor at Stanford (Calif.) University, will present “The Vision Beyond the Vision: Same as it Ever Was, but Different.” Dr. Dake is an internationally recognized pioneer of image-guided therapies whose contributions have changed the treatment of both common and complex vascular disease issues. His groundbreaking research with CT angiography, endovascular stents and stent-grafts has forever altered the interventional landscape and his publications have dramatically influenced several fields, including vascular imaging.
Awards Ceremony, 10 to 10:15 a.m.: Who will win two of the SVS’s top honors? Attendees will find out at the Awards Ceremony, during which the Lifetime Achievement Award AND the Medal for Innovation in Vascular Surgery will be presented.
The Lifetime Achievement Award recognizes an individual’s outstanding and sustained contributions to the profession and SVS, and his or her exemplary professional practice and leadership. The 2018 recipient was Gregorio Sicard, MD.
The Medal for Innovation is not an annual award; it recognizes individual whose contributions have had a transforming impact on the practice or science of vascular surgery. Past recipients include Juan Parodi, MD (2006); Timothy Chuter, MD (2008); Thomas Fogarty, MD (2010); Roy Greenberg, MD (2012); and, most recently, Edward Diethrich, MD (2013).
The identities of these two recipients are a closely guarded secret until the presentation. Be part of the unveiling and celebration.
Three of the Vascular Annual Meeting’s signature events – celebrations along with distinguished lectures – occur on Saturday, VAM’s closing day. All conveniently occur in the morning, shortly before the start of the SVS Annual Business Meeting and luncheon and take place in Potomac A/B.
The John Homans Lecture, 9:30 to 10 a.m.: Jack Cronenwett, MD, Dartmouth-Hitchcock Medical Center, Lebanon, N.H., will present the lecture, “Why Should I Join the Vascular Quality Initiative?” Dr. Cronenwett spearheaded a regional quality outcomes registry, the eventual model for VQI. He later helped launch the SVS-Patient Safety Organization, which operates VQI and served as medical director until 2016. Dr. Cronenwett will discuss the VQI’s benefits for vascular practitioners and examine the VQI’s research and quality improvement opportunities.
The Roy Greenberg Distinguished Lecture, 10:15 to 10:45 a.m.: Michael Dake, MD, professor at Stanford (Calif.) University, will present “The Vision Beyond the Vision: Same as it Ever Was, but Different.” Dr. Dake is an internationally recognized pioneer of image-guided therapies whose contributions have changed the treatment of both common and complex vascular disease issues. His groundbreaking research with CT angiography, endovascular stents and stent-grafts has forever altered the interventional landscape and his publications have dramatically influenced several fields, including vascular imaging.
Awards Ceremony, 10 to 10:15 a.m.: Who will win two of the SVS’s top honors? Attendees will find out at the Awards Ceremony, during which the Lifetime Achievement Award AND the Medal for Innovation in Vascular Surgery will be presented.
The Lifetime Achievement Award recognizes an individual’s outstanding and sustained contributions to the profession and SVS, and his or her exemplary professional practice and leadership. The 2018 recipient was Gregorio Sicard, MD.
The Medal for Innovation is not an annual award; it recognizes individual whose contributions have had a transforming impact on the practice or science of vascular surgery. Past recipients include Juan Parodi, MD (2006); Timothy Chuter, MD (2008); Thomas Fogarty, MD (2010); Roy Greenberg, MD (2012); and, most recently, Edward Diethrich, MD (2013).
The identities of these two recipients are a closely guarded secret until the presentation. Be part of the unveiling and celebration.
Three of the Vascular Annual Meeting’s signature events – celebrations along with distinguished lectures – occur on Saturday, VAM’s closing day. All conveniently occur in the morning, shortly before the start of the SVS Annual Business Meeting and luncheon and take place in Potomac A/B.
The John Homans Lecture, 9:30 to 10 a.m.: Jack Cronenwett, MD, Dartmouth-Hitchcock Medical Center, Lebanon, N.H., will present the lecture, “Why Should I Join the Vascular Quality Initiative?” Dr. Cronenwett spearheaded a regional quality outcomes registry, the eventual model for VQI. He later helped launch the SVS-Patient Safety Organization, which operates VQI and served as medical director until 2016. Dr. Cronenwett will discuss the VQI’s benefits for vascular practitioners and examine the VQI’s research and quality improvement opportunities.
The Roy Greenberg Distinguished Lecture, 10:15 to 10:45 a.m.: Michael Dake, MD, professor at Stanford (Calif.) University, will present “The Vision Beyond the Vision: Same as it Ever Was, but Different.” Dr. Dake is an internationally recognized pioneer of image-guided therapies whose contributions have changed the treatment of both common and complex vascular disease issues. His groundbreaking research with CT angiography, endovascular stents and stent-grafts has forever altered the interventional landscape and his publications have dramatically influenced several fields, including vascular imaging.
Awards Ceremony, 10 to 10:15 a.m.: Who will win two of the SVS’s top honors? Attendees will find out at the Awards Ceremony, during which the Lifetime Achievement Award AND the Medal for Innovation in Vascular Surgery will be presented.
The Lifetime Achievement Award recognizes an individual’s outstanding and sustained contributions to the profession and SVS, and his or her exemplary professional practice and leadership. The 2018 recipient was Gregorio Sicard, MD.
The Medal for Innovation is not an annual award; it recognizes individual whose contributions have had a transforming impact on the practice or science of vascular surgery. Past recipients include Juan Parodi, MD (2006); Timothy Chuter, MD (2008); Thomas Fogarty, MD (2010); Roy Greenberg, MD (2012); and, most recently, Edward Diethrich, MD (2013).
The identities of these two recipients are a closely guarded secret until the presentation. Be part of the unveiling and celebration.
