User login
For MD-IQ use only
Cutaneous Sarcoidosis Presenting as a Cutaneous Horn
To the Editor:
A 53-year-old woman presented to our dermatology clinic with a painful growth on the right ear of 2 months’ duration. A complete review of systems was negative except for an isolated episode of shortness of breath prior to presentation that resolved without intervention. During this episode, her primary care physician made a diagnosis of chronic obstructive pulmonary disease based on a chest radiograph. The patient reported minimal tobacco use, specifically that she had smoked a few cigarettes daily for several years but had quit 6 months prior to the current presentation.

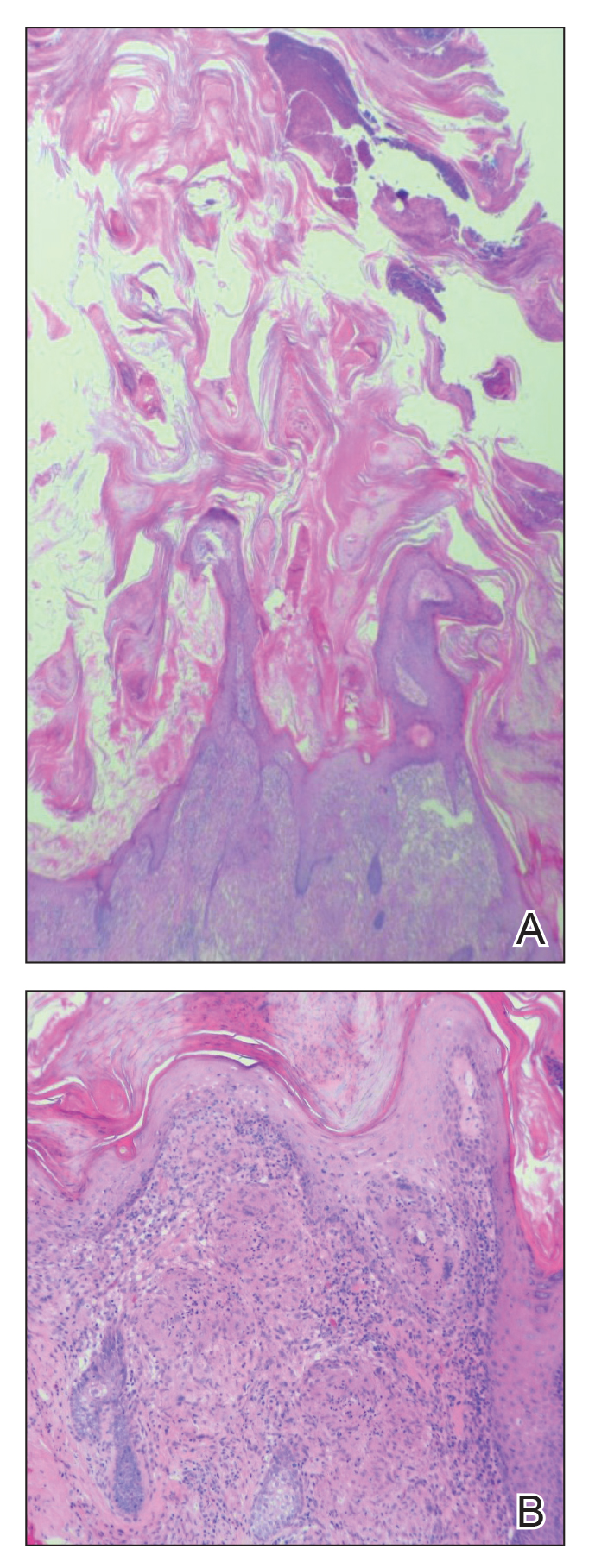
Cutaneous horn is a clinical term used to describe hyperkeratotic horn-shaped growths of highly variable shapes and sizes. Although the pathogenesis and incidence of cutaneous horns remain unknown, these lesions most often are the result of a neoplastic rather than an inflammatory process. The differential diagnosis typically includes entities characterized by marked hyperkeratosis, including hypertrophic actinic keratosis, squamous cell carcinoma (SCC), seborrheic keratosis, and verruca vulgaris. The base of the horn must be biopsied to determine the underlying etiology, paying careful attention to avoid a superficial biopsy, as it may be nondiagnostic.
Studies analyzing the underlying diagnoses and clinical features of cutaneous horns are limited. In a large retrospective study of 643 cutaneous horns, 61% were benign, 23% were premalignant, and 16% were malignant. In this study, 4 features were associated with premalignant or malignant pathology: (1) older age (mid- 60s to 70s); (2) male sex; (3) location on the nose, pinnae, dorsal hands, scalp, forearms, or face; and (4) a wide base (4.4 mm or larger) and a lower height-to-base ratio than benign lesions.1 Two additional studies of more than 200 horns each showed higher rates of premalignant horns (42% and 38%, respectively) with malignancy found in 7% and 20% of horns, respectively.2,3 One prospective study sought to identify clinical and dermatoscopic features of SCCs underlying cutaneous horns, concluding that SCC diagnosis was more likely if a horn had (1) a height less than the diameter of its base, (2) a lack of terrace morphology (a dermatoscopic feature defined as horizontal parallel layers of keratin), (3) erythema at the base, and (4) the presence of pain.4
Our patient had a cutaneous horn on the pinna that was painful, wider than it was tall, and erythematous at the base, suggesting a malignant process; however, a complete cutaneous physical examination revealed other skin lesions that were concerning for sarcoidosis and raised suspicion that the horn also was a manifestation of the same inflammatory process.
Although unusual, cutaneous sarcoidosis presenting as a cutaneous horn is not unexpected. In a histopathologic study of 62 cases of cutaneous sarcoidosis, 79% (49/62) showed epidermal changes and 13% (8/62) demonstrated hyperkeratosis. Other epidermal changes included parakeratosis (16% [10/62]), acanthosis (10% [6/62]), and epidermal atrophy (57% [35/62]).5 The spectrum of epidermal pathology in cutaneous sarcoidosis is evident in its well-documented verrucous, psoriasiform, and ichthyosiform presentations. For completeness, cutaneous horn is added to the list of clinical morphologies for this “great imitator” of cutaneous diseases.
- Yu RC, Pryce DW, Macfarlane AW, et al. A histopathological study of 643 cutaneous horns. Br J Dermatol. 1991;124:449-452.
- Schosser RH, Hodge SJ, Gaba CR, et al. Cutaneous horns: a histopathologic study. South Med J. 1979;72:1129-1131.
- Mantese SA, Diogo PM, Rocha A, et al. Cutaneous horn: a retrospective histopathological study of 222 cases. An Bras Dermatol. 2010;85:157-163.
- Pyne J, Sapkota D, Wong JC. Cutaneous horns: clues to invasive squamous cell carcinoma being present in the horn base. Dermatol Pract Concept. 2013;3:3-7.
- Hiroyuki O. Epidermal changes in cutaneous lesions of sarcoidosis. Am J Dermatopathol. 1999;21:229-233.
To the Editor:
A 53-year-old woman presented to our dermatology clinic with a painful growth on the right ear of 2 months’ duration. A complete review of systems was negative except for an isolated episode of shortness of breath prior to presentation that resolved without intervention. During this episode, her primary care physician made a diagnosis of chronic obstructive pulmonary disease based on a chest radiograph. The patient reported minimal tobacco use, specifically that she had smoked a few cigarettes daily for several years but had quit 6 months prior to the current presentation.
Cutaneous horn is a clinical term used to describe hyperkeratotic horn-shaped growths of highly variable shapes and sizes. Although the pathogenesis and incidence of cutaneous horns remain unknown, these lesions most often are the result of a neoplastic rather than an inflammatory process. The differential diagnosis typically includes entities characterized by marked hyperkeratosis, including hypertrophic actinic keratosis, squamous cell carcinoma (SCC), seborrheic keratosis, and verruca vulgaris. The base of the horn must be biopsied to determine the underlying etiology, paying careful attention to avoid a superficial biopsy, as it may be nondiagnostic.
Studies analyzing the underlying diagnoses and clinical features of cutaneous horns are limited. In a large retrospective study of 643 cutaneous horns, 61% were benign, 23% were premalignant, and 16% were malignant. In this study, 4 features were associated with premalignant or malignant pathology: (1) older age (mid- 60s to 70s); (2) male sex; (3) location on the nose, pinnae, dorsal hands, scalp, forearms, or face; and (4) a wide base (4.4 mm or larger) and a lower height-to-base ratio than benign lesions.1 Two additional studies of more than 200 horns each showed higher rates of premalignant horns (42% and 38%, respectively) with malignancy found in 7% and 20% of horns, respectively.2,3 One prospective study sought to identify clinical and dermatoscopic features of SCCs underlying cutaneous horns, concluding that SCC diagnosis was more likely if a horn had (1) a height less than the diameter of its base, (2) a lack of terrace morphology (a dermatoscopic feature defined as horizontal parallel layers of keratin), (3) erythema at the base, and (4) the presence of pain.4
Our patient had a cutaneous horn on the pinna that was painful, wider than it was tall, and erythematous at the base, suggesting a malignant process; however, a complete cutaneous physical examination revealed other skin lesions that were concerning for sarcoidosis and raised suspicion that the horn also was a manifestation of the same inflammatory process.
Although unusual, cutaneous sarcoidosis presenting as a cutaneous horn is not unexpected. In a histopathologic study of 62 cases of cutaneous sarcoidosis, 79% (49/62) showed epidermal changes and 13% (8/62) demonstrated hyperkeratosis. Other epidermal changes included parakeratosis (16% [10/62]), acanthosis (10% [6/62]), and epidermal atrophy (57% [35/62]).5 The spectrum of epidermal pathology in cutaneous sarcoidosis is evident in its well-documented verrucous, psoriasiform, and ichthyosiform presentations. For completeness, cutaneous horn is added to the list of clinical morphologies for this “great imitator” of cutaneous diseases.
To the Editor:
A 53-year-old woman presented to our dermatology clinic with a painful growth on the right ear of 2 months’ duration. A complete review of systems was negative except for an isolated episode of shortness of breath prior to presentation that resolved without intervention. During this episode, her primary care physician made a diagnosis of chronic obstructive pulmonary disease based on a chest radiograph. The patient reported minimal tobacco use, specifically that she had smoked a few cigarettes daily for several years but had quit 6 months prior to the current presentation.
Cutaneous horn is a clinical term used to describe hyperkeratotic horn-shaped growths of highly variable shapes and sizes. Although the pathogenesis and incidence of cutaneous horns remain unknown, these lesions most often are the result of a neoplastic rather than an inflammatory process. The differential diagnosis typically includes entities characterized by marked hyperkeratosis, including hypertrophic actinic keratosis, squamous cell carcinoma (SCC), seborrheic keratosis, and verruca vulgaris. The base of the horn must be biopsied to determine the underlying etiology, paying careful attention to avoid a superficial biopsy, as it may be nondiagnostic.
Studies analyzing the underlying diagnoses and clinical features of cutaneous horns are limited. In a large retrospective study of 643 cutaneous horns, 61% were benign, 23% were premalignant, and 16% were malignant. In this study, 4 features were associated with premalignant or malignant pathology: (1) older age (mid- 60s to 70s); (2) male sex; (3) location on the nose, pinnae, dorsal hands, scalp, forearms, or face; and (4) a wide base (4.4 mm or larger) and a lower height-to-base ratio than benign lesions.1 Two additional studies of more than 200 horns each showed higher rates of premalignant horns (42% and 38%, respectively) with malignancy found in 7% and 20% of horns, respectively.2,3 One prospective study sought to identify clinical and dermatoscopic features of SCCs underlying cutaneous horns, concluding that SCC diagnosis was more likely if a horn had (1) a height less than the diameter of its base, (2) a lack of terrace morphology (a dermatoscopic feature defined as horizontal parallel layers of keratin), (3) erythema at the base, and (4) the presence of pain.4
Our patient had a cutaneous horn on the pinna that was painful, wider than it was tall, and erythematous at the base, suggesting a malignant process; however, a complete cutaneous physical examination revealed other skin lesions that were concerning for sarcoidosis and raised suspicion that the horn also was a manifestation of the same inflammatory process.
Although unusual, cutaneous sarcoidosis presenting as a cutaneous horn is not unexpected. In a histopathologic study of 62 cases of cutaneous sarcoidosis, 79% (49/62) showed epidermal changes and 13% (8/62) demonstrated hyperkeratosis. Other epidermal changes included parakeratosis (16% [10/62]), acanthosis (10% [6/62]), and epidermal atrophy (57% [35/62]).5 The spectrum of epidermal pathology in cutaneous sarcoidosis is evident in its well-documented verrucous, psoriasiform, and ichthyosiform presentations. For completeness, cutaneous horn is added to the list of clinical morphologies for this “great imitator” of cutaneous diseases.
- Yu RC, Pryce DW, Macfarlane AW, et al. A histopathological study of 643 cutaneous horns. Br J Dermatol. 1991;124:449-452.
- Schosser RH, Hodge SJ, Gaba CR, et al. Cutaneous horns: a histopathologic study. South Med J. 1979;72:1129-1131.
- Mantese SA, Diogo PM, Rocha A, et al. Cutaneous horn: a retrospective histopathological study of 222 cases. An Bras Dermatol. 2010;85:157-163.
- Pyne J, Sapkota D, Wong JC. Cutaneous horns: clues to invasive squamous cell carcinoma being present in the horn base. Dermatol Pract Concept. 2013;3:3-7.
- Hiroyuki O. Epidermal changes in cutaneous lesions of sarcoidosis. Am J Dermatopathol. 1999;21:229-233.
- Yu RC, Pryce DW, Macfarlane AW, et al. A histopathological study of 643 cutaneous horns. Br J Dermatol. 1991;124:449-452.
- Schosser RH, Hodge SJ, Gaba CR, et al. Cutaneous horns: a histopathologic study. South Med J. 1979;72:1129-1131.
- Mantese SA, Diogo PM, Rocha A, et al. Cutaneous horn: a retrospective histopathological study of 222 cases. An Bras Dermatol. 2010;85:157-163.
- Pyne J, Sapkota D, Wong JC. Cutaneous horns: clues to invasive squamous cell carcinoma being present in the horn base. Dermatol Pract Concept. 2013;3:3-7.
- Hiroyuki O. Epidermal changes in cutaneous lesions of sarcoidosis. Am J Dermatopathol. 1999;21:229-233.
Practice Points
- Biopsy of a cutaneous horn should be deep enough to capture the neoplastic or inflammatory process at the base of the lesion.
- Cutaneous sarcoidosis can present with variable morphologies including the epidermal changes of a cutaneous horn.

New study confirms rise in U.S. suicide rates, particularly in rural areas
County-by-county analysis cites links to higher density of gun shops, other factors
Suicide rates in the United States climbed from 1999 to 2016, a new cross-sectional study found, and the increases were highest in rural areas.
“These findings are consistent with previous studies demonstrating higher and more rapidly increasing suicide rates in rural areas and are of considerable interest in light of the work by [Anne] Case and [Angus] Deaton,” wrote Danielle L. Steelesmith, PhD, and associates. “While increasing rates of suicide are well documented, little is known about contextual factors associated with county-level suicide rates.” The findings appear in JAMA Network Open.
To examine those contextual factors, Dr. Steelesmith, of the department of psychiatry and behavioral health at the Ohio State University, Columbus, and associates analyzed county-by-county suicide statistics from 1999 to 2016 for adults aged 25-64 years, noting that they “focused on this age range because most studies on mortality trends have focused on this age range.”
The researchers developed 3-year suicide averages for counties for rate “stabilization” purposes. They placed the counties into four categories (large metropolitan, small metropolitan, micropolitan, and rural), and used various data sources to gather various types of statistics about the communities.
Most of those who died by suicide were men (77%), and most (51%) were aged 45-64 years. The median suicide rate per county rose from 15 per 100,000 (1999-2001) to 21 per 100,000 (2014-2016), reported Dr. Steelesmith and associates.
Rural counties only made up 2% of the suicides, compared with 81% in large and small metropolitan counties, but suicide rates were “increasing most rapidly in rural areas, although all county types saw increases during the period studied,” Dr. Steelesmith and associates wrote.
They added that “counties with the highest excess risk of suicide tended to be in Western states (e.g., Colorado, New Mexico, Utah, and Wyoming), Appalachia (e.g., Kentucky, Virginia, and West Virginia), and the Ozarks (e.g., Arkansas and Missouri).”
In addition to the connections between increasing suicide rates, living in a rural area, and a higher density of gun shops, the researchers cited other contextual factors. Among those factors were higher median age and higher percentages of non-Hispanic whites, numbers of residents without health insurance, and veterans. They also found links between higher suicide rates and worse numbers on indexes designed to measure social capital; social fragmentation; and deprivation, a measure encompassing lower education, employment levels, and income.
“Long-term and persistent poverty appears to be more entrenched and economic opportunities more constrained in rural areas,” Dr. Steelesmith and associates wrote. “Greater social isolation, challenges related to transportation and interpersonal communication, and associated difficulties accessing health and mental health services likely contribute to the disproportionate association of deprivation with suicide in rural counties.”
Dr. Steelesmith and associates cited several limitations. One key limitation is that, because the study looked only at adults aged 25-64 years, the results might not be generalizable to youth or elderly adults.
No study funding was reported. One study author reported serving on the scientific advisory board of Clarigent Health and receiving grant support from the National Institute of Mental Health outside of the submitted work. No other disclosures were reported.
SOURCE: Steelesmith DL et al. JAMA Netw Open. 2019 Sep 6. doi: 10.1001/jamanetworkopen.2019.10936.
County-by-county analysis cites links to higher density of gun shops, other factors
County-by-county analysis cites links to higher density of gun shops, other factors
Suicide rates in the United States climbed from 1999 to 2016, a new cross-sectional study found, and the increases were highest in rural areas.
“These findings are consistent with previous studies demonstrating higher and more rapidly increasing suicide rates in rural areas and are of considerable interest in light of the work by [Anne] Case and [Angus] Deaton,” wrote Danielle L. Steelesmith, PhD, and associates. “While increasing rates of suicide are well documented, little is known about contextual factors associated with county-level suicide rates.” The findings appear in JAMA Network Open.
To examine those contextual factors, Dr. Steelesmith, of the department of psychiatry and behavioral health at the Ohio State University, Columbus, and associates analyzed county-by-county suicide statistics from 1999 to 2016 for adults aged 25-64 years, noting that they “focused on this age range because most studies on mortality trends have focused on this age range.”
The researchers developed 3-year suicide averages for counties for rate “stabilization” purposes. They placed the counties into four categories (large metropolitan, small metropolitan, micropolitan, and rural), and used various data sources to gather various types of statistics about the communities.
Most of those who died by suicide were men (77%), and most (51%) were aged 45-64 years. The median suicide rate per county rose from 15 per 100,000 (1999-2001) to 21 per 100,000 (2014-2016), reported Dr. Steelesmith and associates.
Rural counties only made up 2% of the suicides, compared with 81% in large and small metropolitan counties, but suicide rates were “increasing most rapidly in rural areas, although all county types saw increases during the period studied,” Dr. Steelesmith and associates wrote.
They added that “counties with the highest excess risk of suicide tended to be in Western states (e.g., Colorado, New Mexico, Utah, and Wyoming), Appalachia (e.g., Kentucky, Virginia, and West Virginia), and the Ozarks (e.g., Arkansas and Missouri).”
In addition to the connections between increasing suicide rates, living in a rural area, and a higher density of gun shops, the researchers cited other contextual factors. Among those factors were higher median age and higher percentages of non-Hispanic whites, numbers of residents without health insurance, and veterans. They also found links between higher suicide rates and worse numbers on indexes designed to measure social capital; social fragmentation; and deprivation, a measure encompassing lower education, employment levels, and income.
“Long-term and persistent poverty appears to be more entrenched and economic opportunities more constrained in rural areas,” Dr. Steelesmith and associates wrote. “Greater social isolation, challenges related to transportation and interpersonal communication, and associated difficulties accessing health and mental health services likely contribute to the disproportionate association of deprivation with suicide in rural counties.”
Dr. Steelesmith and associates cited several limitations. One key limitation is that, because the study looked only at adults aged 25-64 years, the results might not be generalizable to youth or elderly adults.
No study funding was reported. One study author reported serving on the scientific advisory board of Clarigent Health and receiving grant support from the National Institute of Mental Health outside of the submitted work. No other disclosures were reported.
SOURCE: Steelesmith DL et al. JAMA Netw Open. 2019 Sep 6. doi: 10.1001/jamanetworkopen.2019.10936.
Suicide rates in the United States climbed from 1999 to 2016, a new cross-sectional study found, and the increases were highest in rural areas.
“These findings are consistent with previous studies demonstrating higher and more rapidly increasing suicide rates in rural areas and are of considerable interest in light of the work by [Anne] Case and [Angus] Deaton,” wrote Danielle L. Steelesmith, PhD, and associates. “While increasing rates of suicide are well documented, little is known about contextual factors associated with county-level suicide rates.” The findings appear in JAMA Network Open.
To examine those contextual factors, Dr. Steelesmith, of the department of psychiatry and behavioral health at the Ohio State University, Columbus, and associates analyzed county-by-county suicide statistics from 1999 to 2016 for adults aged 25-64 years, noting that they “focused on this age range because most studies on mortality trends have focused on this age range.”
The researchers developed 3-year suicide averages for counties for rate “stabilization” purposes. They placed the counties into four categories (large metropolitan, small metropolitan, micropolitan, and rural), and used various data sources to gather various types of statistics about the communities.
Most of those who died by suicide were men (77%), and most (51%) were aged 45-64 years. The median suicide rate per county rose from 15 per 100,000 (1999-2001) to 21 per 100,000 (2014-2016), reported Dr. Steelesmith and associates.
Rural counties only made up 2% of the suicides, compared with 81% in large and small metropolitan counties, but suicide rates were “increasing most rapidly in rural areas, although all county types saw increases during the period studied,” Dr. Steelesmith and associates wrote.
They added that “counties with the highest excess risk of suicide tended to be in Western states (e.g., Colorado, New Mexico, Utah, and Wyoming), Appalachia (e.g., Kentucky, Virginia, and West Virginia), and the Ozarks (e.g., Arkansas and Missouri).”
In addition to the connections between increasing suicide rates, living in a rural area, and a higher density of gun shops, the researchers cited other contextual factors. Among those factors were higher median age and higher percentages of non-Hispanic whites, numbers of residents without health insurance, and veterans. They also found links between higher suicide rates and worse numbers on indexes designed to measure social capital; social fragmentation; and deprivation, a measure encompassing lower education, employment levels, and income.
“Long-term and persistent poverty appears to be more entrenched and economic opportunities more constrained in rural areas,” Dr. Steelesmith and associates wrote. “Greater social isolation, challenges related to transportation and interpersonal communication, and associated difficulties accessing health and mental health services likely contribute to the disproportionate association of deprivation with suicide in rural counties.”
Dr. Steelesmith and associates cited several limitations. One key limitation is that, because the study looked only at adults aged 25-64 years, the results might not be generalizable to youth or elderly adults.
No study funding was reported. One study author reported serving on the scientific advisory board of Clarigent Health and receiving grant support from the National Institute of Mental Health outside of the submitted work. No other disclosures were reported.
SOURCE: Steelesmith DL et al. JAMA Netw Open. 2019 Sep 6. doi: 10.1001/jamanetworkopen.2019.10936.
FROM JAMA NETWORK OPEN
Cancer Survivorship Clinic Utilizing an NP-led Model With Oncology Fellows
Background: Cancer survivors face unique posttreatment issues and require ongoing follow-up care. Per Commission on Cancer (CoC) and other cancer organizations, a survivorship care plan including a treatment summary and follow-up plan is standard of care. There are significant barriers to implementation of survivorship care plans due to the resources required. Our facility lacked a process to implement survivorship care plans. A need to expand clinical experiences for oncology fellows across the care continuum was also identified.
Methods: Researched existing private sector and VA models of providing cancer survivorship care. Analyzed literature regarding the unique care needs of veteran cancer survivors. NP led model was determined to support a holistic clinical care model including post treatment assessment, education, resources, and referrals.
Intervention: The Cancer Survivorship Clinic was implemented in August 2018, staffed by an oncology nurse practitioner and medical oncology fellows. Visits are face-to-face or by phone and one hour in length. Patients receive a survivorship care plan. The clinic provider addresses post-treatment health concerns and refers patients to other services when indicated. The clinic was created utilizing existing staffing and clinic space, no additional resources were needed.
Results: There were 30 Cancer Survivorship Clinic visits completed for veterans between 8/1/18 and 5/1/19. The clinic is part of an ongoing rotation for fellows and included in their annual orientation. Implementation of a Cancer Survivorship Clinic was effective in meeting the CoC Survivorship Care Plan standard. Oncology fellow rotation in the clinic has broadened their educational experience. Upon entering practice, fellows will be better equipped to address survivorship needs.
Discussion: The clinic was created utilizing existing medical oncology resources and staffing. Medical oncology is familiar with all cancer diagnoses and can therefore serve the entire cancer population. An NP-led model supports a holistic care approach, ensuring that physical and mental/emotional needs are addressed during the clinic visit. Oncology fellows receive an opportunity to care for patients following cancer treatment, expanding their understanding of cancer care. One drawback is the lack of fellow availability at certain times of the year.
Background: Cancer survivors face unique posttreatment issues and require ongoing follow-up care. Per Commission on Cancer (CoC) and other cancer organizations, a survivorship care plan including a treatment summary and follow-up plan is standard of care. There are significant barriers to implementation of survivorship care plans due to the resources required. Our facility lacked a process to implement survivorship care plans. A need to expand clinical experiences for oncology fellows across the care continuum was also identified.
Methods: Researched existing private sector and VA models of providing cancer survivorship care. Analyzed literature regarding the unique care needs of veteran cancer survivors. NP led model was determined to support a holistic clinical care model including post treatment assessment, education, resources, and referrals.
Intervention: The Cancer Survivorship Clinic was implemented in August 2018, staffed by an oncology nurse practitioner and medical oncology fellows. Visits are face-to-face or by phone and one hour in length. Patients receive a survivorship care plan. The clinic provider addresses post-treatment health concerns and refers patients to other services when indicated. The clinic was created utilizing existing staffing and clinic space, no additional resources were needed.
Results: There were 30 Cancer Survivorship Clinic visits completed for veterans between 8/1/18 and 5/1/19. The clinic is part of an ongoing rotation for fellows and included in their annual orientation. Implementation of a Cancer Survivorship Clinic was effective in meeting the CoC Survivorship Care Plan standard. Oncology fellow rotation in the clinic has broadened their educational experience. Upon entering practice, fellows will be better equipped to address survivorship needs.
Discussion: The clinic was created utilizing existing medical oncology resources and staffing. Medical oncology is familiar with all cancer diagnoses and can therefore serve the entire cancer population. An NP-led model supports a holistic care approach, ensuring that physical and mental/emotional needs are addressed during the clinic visit. Oncology fellows receive an opportunity to care for patients following cancer treatment, expanding their understanding of cancer care. One drawback is the lack of fellow availability at certain times of the year.
Background: Cancer survivors face unique posttreatment issues and require ongoing follow-up care. Per Commission on Cancer (CoC) and other cancer organizations, a survivorship care plan including a treatment summary and follow-up plan is standard of care. There are significant barriers to implementation of survivorship care plans due to the resources required. Our facility lacked a process to implement survivorship care plans. A need to expand clinical experiences for oncology fellows across the care continuum was also identified.
Methods: Researched existing private sector and VA models of providing cancer survivorship care. Analyzed literature regarding the unique care needs of veteran cancer survivors. NP led model was determined to support a holistic clinical care model including post treatment assessment, education, resources, and referrals.
Intervention: The Cancer Survivorship Clinic was implemented in August 2018, staffed by an oncology nurse practitioner and medical oncology fellows. Visits are face-to-face or by phone and one hour in length. Patients receive a survivorship care plan. The clinic provider addresses post-treatment health concerns and refers patients to other services when indicated. The clinic was created utilizing existing staffing and clinic space, no additional resources were needed.
Results: There were 30 Cancer Survivorship Clinic visits completed for veterans between 8/1/18 and 5/1/19. The clinic is part of an ongoing rotation for fellows and included in their annual orientation. Implementation of a Cancer Survivorship Clinic was effective in meeting the CoC Survivorship Care Plan standard. Oncology fellow rotation in the clinic has broadened their educational experience. Upon entering practice, fellows will be better equipped to address survivorship needs.
Discussion: The clinic was created utilizing existing medical oncology resources and staffing. Medical oncology is familiar with all cancer diagnoses and can therefore serve the entire cancer population. An NP-led model supports a holistic care approach, ensuring that physical and mental/emotional needs are addressed during the clinic visit. Oncology fellows receive an opportunity to care for patients following cancer treatment, expanding their understanding of cancer care. One drawback is the lack of fellow availability at certain times of the year.
Practical Application of Next Generation Sequencing (NGS) Results: A Single Center VA Experience
Introduction: Advancements in genomic profiling now allow for routine comprehensive somatic genomic alteration testing in all patients with advanced cancer. A subset of patients will have targetable genomic alterations, though the frequency of these alterations and the efficacy of the matched treatments have varied amongst published data. Several commercially available platforms exist, but the ideal method to appropriately interpret and apply this data across various clinical tumor types and disease stages is still unclear.
Methods: We obtained a list of all the next generation sequencing (NGS) panels submitted from our center to the National Precision Oncology Program (NPOP). A total of 53 patients were included in the analysis. We analyzed the most frequently altered genes, the tumor types most frequently profiled, the frequency of cases with targetable alterations, and the efficacy of the matched treatments in individual patients. We also compared the number and types of alterations reported as well as the length of reports generated by the three different commercial NGS platforms used in our cohort.
Results: A total of 19/53 (35.8%) patients had targetable alterations. Five out of 21 (23.8%) received a targeted therapy. Non-small cell lung cancer [NSCLC] (n = 14; 26%) and prostate cancer (n=9; 17%) were the most frequently profiled tumors. In the NSCLC cohort, 7/14 (50%) had targetable alterations, including two patients in whom a prior single gene test for the specific alteration [EGFR, BRAF] was negative. NGS panels produced on average 6.6-13.0 alterations per patient, and average report length ranged from 8.3-19.0 pages.
Conclusions: NGS testing has been implemented by providers across a variety of tumor types at our institution, though the number of patients receiving matched treatments is low. Reflexive serial single-gene testing in NSCLC for EGFR, ALK, ROS1, and BRAF is likely reducing the number of NGS panels sent in these patients. Two false-negative single gene tests in our small cohort suggests we are underdiagnosing driver alterations in these patients with this approach. We would suggest exploring decision support tools and provider education in order to encourage judicious and clinically meaningful use of this valuable resource.
Introduction: Advancements in genomic profiling now allow for routine comprehensive somatic genomic alteration testing in all patients with advanced cancer. A subset of patients will have targetable genomic alterations, though the frequency of these alterations and the efficacy of the matched treatments have varied amongst published data. Several commercially available platforms exist, but the ideal method to appropriately interpret and apply this data across various clinical tumor types and disease stages is still unclear.
Methods: We obtained a list of all the next generation sequencing (NGS) panels submitted from our center to the National Precision Oncology Program (NPOP). A total of 53 patients were included in the analysis. We analyzed the most frequently altered genes, the tumor types most frequently profiled, the frequency of cases with targetable alterations, and the efficacy of the matched treatments in individual patients. We also compared the number and types of alterations reported as well as the length of reports generated by the three different commercial NGS platforms used in our cohort.
Results: A total of 19/53 (35.8%) patients had targetable alterations. Five out of 21 (23.8%) received a targeted therapy. Non-small cell lung cancer [NSCLC] (n = 14; 26%) and prostate cancer (n=9; 17%) were the most frequently profiled tumors. In the NSCLC cohort, 7/14 (50%) had targetable alterations, including two patients in whom a prior single gene test for the specific alteration [EGFR, BRAF] was negative. NGS panels produced on average 6.6-13.0 alterations per patient, and average report length ranged from 8.3-19.0 pages.
Conclusions: NGS testing has been implemented by providers across a variety of tumor types at our institution, though the number of patients receiving matched treatments is low. Reflexive serial single-gene testing in NSCLC for EGFR, ALK, ROS1, and BRAF is likely reducing the number of NGS panels sent in these patients. Two false-negative single gene tests in our small cohort suggests we are underdiagnosing driver alterations in these patients with this approach. We would suggest exploring decision support tools and provider education in order to encourage judicious and clinically meaningful use of this valuable resource.
Introduction: Advancements in genomic profiling now allow for routine comprehensive somatic genomic alteration testing in all patients with advanced cancer. A subset of patients will have targetable genomic alterations, though the frequency of these alterations and the efficacy of the matched treatments have varied amongst published data. Several commercially available platforms exist, but the ideal method to appropriately interpret and apply this data across various clinical tumor types and disease stages is still unclear.
Methods: We obtained a list of all the next generation sequencing (NGS) panels submitted from our center to the National Precision Oncology Program (NPOP). A total of 53 patients were included in the analysis. We analyzed the most frequently altered genes, the tumor types most frequently profiled, the frequency of cases with targetable alterations, and the efficacy of the matched treatments in individual patients. We also compared the number and types of alterations reported as well as the length of reports generated by the three different commercial NGS platforms used in our cohort.
Results: A total of 19/53 (35.8%) patients had targetable alterations. Five out of 21 (23.8%) received a targeted therapy. Non-small cell lung cancer [NSCLC] (n = 14; 26%) and prostate cancer (n=9; 17%) were the most frequently profiled tumors. In the NSCLC cohort, 7/14 (50%) had targetable alterations, including two patients in whom a prior single gene test for the specific alteration [EGFR, BRAF] was negative. NGS panels produced on average 6.6-13.0 alterations per patient, and average report length ranged from 8.3-19.0 pages.
Conclusions: NGS testing has been implemented by providers across a variety of tumor types at our institution, though the number of patients receiving matched treatments is low. Reflexive serial single-gene testing in NSCLC for EGFR, ALK, ROS1, and BRAF is likely reducing the number of NGS panels sent in these patients. Two false-negative single gene tests in our small cohort suggests we are underdiagnosing driver alterations in these patients with this approach. We would suggest exploring decision support tools and provider education in order to encourage judicious and clinically meaningful use of this valuable resource.
Battling hospitalist burnout
Higher salaries are not sufficient
Hospitalist Rahul C. Borsadia, MD, had been working with Orlando Health Inpatient Medicine Group since the year of its founding in 2011.
The salaries of the practice’s physicians back then were based on relative value units (RVU) – the more patients that physicians saw, the higher their salaries. But a problem arose, Dr. Borsadia said. Physicians were trying to squeeze in two dozen or more patients a day “in a practice that is modeled for quality.”
“By the time the end of the day comes, it’s 9 or 10 p.m. and you are leaving but coming back at 6:30 the next morning. So, lack of sleep, more patients, striving to earn that higher salary,” he said. “The desire to perform quality work with that kind of patient load was not fulfilled and that lead to dissatisfaction and stress, which lead to irritation and exodus from the group.”
Three years ago, the practice transitioned to a throughput process with a census limit of 18 patients or less, without an RVU system, but with salary incentives based on patient satisfaction, billing, and documentation.
“We’ve not had anybody leave the hospital because of burnout or dissatisfaction” since the new system was put into place, Dr. Borsadia said. “Less burnout means more people are happy.”
Although symptoms of burnout still seem to be rampant across hospital medicine, hospitalists are putting potential solutions into place. And – sometimes – they are making progress, through tweaks in schedules and responsibilities, incentives suited to different goals, and better communication.
Scheduling problems
The need for continuing efforts to improve the work experience for hospitalists is apparent, said Henry Michtalik, MD, MPH, MHS, assistant professor of general internal medicine at Johns Hopkins, Baltimore, who led a workshop on the topic at the 2019 Annual Conference of the Society of Hospital Medicine (HM19).

A 2016 survey of academic general internal medicine clinicians – including about 600 hospitalists and outpatient physicians – found that 67% reported high stress, 38% said they were “burned out,” 50% said they felt they had “low control” over their work, and 60% said they felt high documentation pressures. Still, 68% said they were satisfied with the values of their departments.
Hospitalists surveyed were actually less likely to say they were burned out, compared with outpatient internists – 52%, compared with 55% – but they were more likely to score low on a scale measuring personal accomplishments, compared with the outpatient clinicians – 20% to 10%. The survey found no significant difference between the two groups in depression or suicidality. But with 40% reporting depression and 10% reporting thoughts of suicide, the numbers virtually cry out for solutions.
Hospitalists in the HM19 workshop, as in other sessions at the Annual Conference, questioned whether the standard 7-days-on, 7-days-off work schedule – seven 12-hour shifts followed by 7 days off – allows hospitalists to pair their works lives with their personal lives in a sustainable way. They described the way that the stress and fatigue of such an intense work period bleeds into the days off that follow after it.
“By the end of seven 12’s, they’re bleary eyed, they’re upset, they go home (for) 2 days of washout before they even start to enjoy whatever life they have left,” said Jonathan Martin, MD, director of medicine at Cumberland Medical Center in Crossville, Tenn. “It’s hard to get hospitalists to buy in, which increases their dissatisfaction.”
Dr. Michtalik had a similar perspective.
“You just shut the rest of your life down completely for those 7 days and then, on your 7 days off, you’ve scheduled your life,” he said. “But that last off day – day number 7 – you feel that pit in your stomach, that the streak is coming.” He joked that the feeling was similar to the dread inspired by the phrase “winter is coming” in the popular HBO series “Game of Thrones.”
Systematic reviews of the literature have found that it’s mostly changes at the organization level – rather than changes that an individual physician makes on his or her own – that tend to make significant differences. Changes to structure, communication, and scheduling tend to work better than working on mindfulness, education, or trying to improve resilience, Dr. Michtalik said.
In one study discussed at the HM19 workshop, researchers compared a schedule in which an intensivist works in-house for 7 days, with home call at night, to a schedule in which the intensivist is completely off at night, with an in-house intensivist covering the night shift. The schedule in which the intensivist was truly off for the night significantly reduced reports of burnout, while not affecting length of stay or patient-experience outcomes.
Dr. Michtalik said that another study compared 4-week rotations to 2-week rotations for attending physicians. Researchers found that the 2-week version resulted in lower reports of burnout, with readmissions and patient experience unaffected, although they noted that residents tended to prefer 4-week schedules because they felt it resulted in better relationships with the attending physician.
Perhaps the dominant factor in job satisfaction that’s been identified in surveys is how physicians, patients, and administrators relate to one another, Dr. Michtalik said.
“The important concept here is that relationships were really important in driving job satisfaction, whether that be with our colleagues, our patients, or with the staff that you’re working with,” he said. “It’s always easier to decline a consultation or have a bad interaction with someone over the phone than it is if you actually know them or you are communicating face to face. That’s why it’s important to develop these kinds of relationships, which also put a face to what’s going on.”
Beyond salary adjustments
Hospitalists attending the HM19 workshop said they thought that participating in administration committees at their own institutions helps keep hospitalists involved in hospital matters, limiting the effects of burnout and improving workplace satisfaction.
Kevin McAninch, DO, a hospitalist with Central Ohio Primary Care in Westerville, said a shift in work responsibilities has made an improvement at his hospital. There is now an “inpatient support center” – which has a physician and a nurse in an office taking calls from 6 p.m. to 7 a.m., so that rounders can stop taking floor calls during that time.
The system “takes the pressure off our admitters at night and our nurses because they’re not getting floor calls anymore, so they’re just taking care of the admissions from the ER,” he said.
A recurring theme of the discussion was that salary alone seems universally incapable of eradicating feelings of burnout. One hospitalist said that in surveys, higher-paid physicians insist that monetary compensation is their main driver, but still often complain of burnout because they must work extra shifts to earn that higher level of pay.
Instead, burnout and satisfaction indicators tend to have more do to with time, control, and support, Dr. Michtalik noted.
Mangla Gulati, MD, SFHM, chief quality officer at the University of Maryland Medical Center in Baltimore, said that there’s no big secret about what hospitalists want from their places of employment. They want things like getting patients to service faster so they can make diagnoses, making sure patients get the care they need, fixing the problems associated with electronic medical records, and having a work-life “integration.”
“The questions is – how do we get there?” Dr. Gulati wondered. She suggested that hospitalists have to be more assertive and explanatory in their interactions with members of the hospital C-suite.
“I think it’s really important for you to understand or ask your C-suite, ‘Where are you in this whole journey? What is your perception of wellness? Tell me some of the measures of staff wellness,’ ” she said.
If the C-suite says “we have no money” to make improvements, hospitalists must be willing to say, ‘Well, you’re going to have to invest a little bit.’ ” Dr. Gulati said. “What is the ROI (return on investment) on the turnover of a physician? Because when you turn a physician over, you have to recruit and hire new staff.”
Dr. Gulati said that hospitalists should provide C-suite leaders with a detailed walk-through of their actual workflows – what their workdays look like – because “it’s not something they’re familiar with.”
Aside from improving relations with hospital administration, Dr. Gulati suggested creating CME programs for wellness, offering time and funding for physician support meetings, supporting flexibility in work hours, and creating programs specifically to help clinicians with burnout symptoms.
She also touted the benefits of “Schwartz Rounds,” in which several medical disciplines gather to talk about a case that was particularly challenging, clinically complex, and emotionally draining for everyone involved.
At Cumberland Medical Center, Dr. Martin said he has two meetings a month with executives in the hospital’s C-suite. One is with his hospitalist group, TeamHealth, and one is more direct, between himself and hospital administrators. It’s just 2 hours a month, but these conversations have undoubtedly helped, he said, although he cautioned that “the meetings themselves don’t have as much meaning if you aren’t communicating effectively,” meaning hospitalists must understand how the C-suite thinks and learn to speak in terms they understand.
“When I go to the administration now and I say ‘Hey, this is a problem that we’re having. I need your help in solving it,’ the executives are much more likely to respond to me than if they’d never seen me, or only see me rarely,” Dr. Martin said.
As a result, a collaborative approach to such conversations tends to be more effective.
“If you go to the C-suite and say, ‘Here’s our issue, how can you help us?’ – as opposed to telling the administration, ‘This is what I need’ – they are more likely to work with you to generate a solution.”
Higher salaries are not sufficient
Higher salaries are not sufficient
Hospitalist Rahul C. Borsadia, MD, had been working with Orlando Health Inpatient Medicine Group since the year of its founding in 2011.
The salaries of the practice’s physicians back then were based on relative value units (RVU) – the more patients that physicians saw, the higher their salaries. But a problem arose, Dr. Borsadia said. Physicians were trying to squeeze in two dozen or more patients a day “in a practice that is modeled for quality.”
“By the time the end of the day comes, it’s 9 or 10 p.m. and you are leaving but coming back at 6:30 the next morning. So, lack of sleep, more patients, striving to earn that higher salary,” he said. “The desire to perform quality work with that kind of patient load was not fulfilled and that lead to dissatisfaction and stress, which lead to irritation and exodus from the group.”
Three years ago, the practice transitioned to a throughput process with a census limit of 18 patients or less, without an RVU system, but with salary incentives based on patient satisfaction, billing, and documentation.
“We’ve not had anybody leave the hospital because of burnout or dissatisfaction” since the new system was put into place, Dr. Borsadia said. “Less burnout means more people are happy.”
Although symptoms of burnout still seem to be rampant across hospital medicine, hospitalists are putting potential solutions into place. And – sometimes – they are making progress, through tweaks in schedules and responsibilities, incentives suited to different goals, and better communication.
Scheduling problems
The need for continuing efforts to improve the work experience for hospitalists is apparent, said Henry Michtalik, MD, MPH, MHS, assistant professor of general internal medicine at Johns Hopkins, Baltimore, who led a workshop on the topic at the 2019 Annual Conference of the Society of Hospital Medicine (HM19).
A 2016 survey of academic general internal medicine clinicians – including about 600 hospitalists and outpatient physicians – found that 67% reported high stress, 38% said they were “burned out,” 50% said they felt they had “low control” over their work, and 60% said they felt high documentation pressures. Still, 68% said they were satisfied with the values of their departments.
Hospitalists surveyed were actually less likely to say they were burned out, compared with outpatient internists – 52%, compared with 55% – but they were more likely to score low on a scale measuring personal accomplishments, compared with the outpatient clinicians – 20% to 10%. The survey found no significant difference between the two groups in depression or suicidality. But with 40% reporting depression and 10% reporting thoughts of suicide, the numbers virtually cry out for solutions.
Hospitalists in the HM19 workshop, as in other sessions at the Annual Conference, questioned whether the standard 7-days-on, 7-days-off work schedule – seven 12-hour shifts followed by 7 days off – allows hospitalists to pair their works lives with their personal lives in a sustainable way. They described the way that the stress and fatigue of such an intense work period bleeds into the days off that follow after it.
“By the end of seven 12’s, they’re bleary eyed, they’re upset, they go home (for) 2 days of washout before they even start to enjoy whatever life they have left,” said Jonathan Martin, MD, director of medicine at Cumberland Medical Center in Crossville, Tenn. “It’s hard to get hospitalists to buy in, which increases their dissatisfaction.”
Dr. Michtalik had a similar perspective.
“You just shut the rest of your life down completely for those 7 days and then, on your 7 days off, you’ve scheduled your life,” he said. “But that last off day – day number 7 – you feel that pit in your stomach, that the streak is coming.” He joked that the feeling was similar to the dread inspired by the phrase “winter is coming” in the popular HBO series “Game of Thrones.”
Systematic reviews of the literature have found that it’s mostly changes at the organization level – rather than changes that an individual physician makes on his or her own – that tend to make significant differences. Changes to structure, communication, and scheduling tend to work better than working on mindfulness, education, or trying to improve resilience, Dr. Michtalik said.
In one study discussed at the HM19 workshop, researchers compared a schedule in which an intensivist works in-house for 7 days, with home call at night, to a schedule in which the intensivist is completely off at night, with an in-house intensivist covering the night shift. The schedule in which the intensivist was truly off for the night significantly reduced reports of burnout, while not affecting length of stay or patient-experience outcomes.
Dr. Michtalik said that another study compared 4-week rotations to 2-week rotations for attending physicians. Researchers found that the 2-week version resulted in lower reports of burnout, with readmissions and patient experience unaffected, although they noted that residents tended to prefer 4-week schedules because they felt it resulted in better relationships with the attending physician.
Perhaps the dominant factor in job satisfaction that’s been identified in surveys is how physicians, patients, and administrators relate to one another, Dr. Michtalik said.
“The important concept here is that relationships were really important in driving job satisfaction, whether that be with our colleagues, our patients, or with the staff that you’re working with,” he said. “It’s always easier to decline a consultation or have a bad interaction with someone over the phone than it is if you actually know them or you are communicating face to face. That’s why it’s important to develop these kinds of relationships, which also put a face to what’s going on.”
Beyond salary adjustments
Hospitalists attending the HM19 workshop said they thought that participating in administration committees at their own institutions helps keep hospitalists involved in hospital matters, limiting the effects of burnout and improving workplace satisfaction.
Kevin McAninch, DO, a hospitalist with Central Ohio Primary Care in Westerville, said a shift in work responsibilities has made an improvement at his hospital. There is now an “inpatient support center” – which has a physician and a nurse in an office taking calls from 6 p.m. to 7 a.m., so that rounders can stop taking floor calls during that time.
The system “takes the pressure off our admitters at night and our nurses because they’re not getting floor calls anymore, so they’re just taking care of the admissions from the ER,” he said.
A recurring theme of the discussion was that salary alone seems universally incapable of eradicating feelings of burnout. One hospitalist said that in surveys, higher-paid physicians insist that monetary compensation is their main driver, but still often complain of burnout because they must work extra shifts to earn that higher level of pay.
Instead, burnout and satisfaction indicators tend to have more do to with time, control, and support, Dr. Michtalik noted.
Mangla Gulati, MD, SFHM, chief quality officer at the University of Maryland Medical Center in Baltimore, said that there’s no big secret about what hospitalists want from their places of employment. They want things like getting patients to service faster so they can make diagnoses, making sure patients get the care they need, fixing the problems associated with electronic medical records, and having a work-life “integration.”
“The questions is – how do we get there?” Dr. Gulati wondered. She suggested that hospitalists have to be more assertive and explanatory in their interactions with members of the hospital C-suite.
“I think it’s really important for you to understand or ask your C-suite, ‘Where are you in this whole journey? What is your perception of wellness? Tell me some of the measures of staff wellness,’ ” she said.
If the C-suite says “we have no money” to make improvements, hospitalists must be willing to say, ‘Well, you’re going to have to invest a little bit.’ ” Dr. Gulati said. “What is the ROI (return on investment) on the turnover of a physician? Because when you turn a physician over, you have to recruit and hire new staff.”
Dr. Gulati said that hospitalists should provide C-suite leaders with a detailed walk-through of their actual workflows – what their workdays look like – because “it’s not something they’re familiar with.”
Aside from improving relations with hospital administration, Dr. Gulati suggested creating CME programs for wellness, offering time and funding for physician support meetings, supporting flexibility in work hours, and creating programs specifically to help clinicians with burnout symptoms.
She also touted the benefits of “Schwartz Rounds,” in which several medical disciplines gather to talk about a case that was particularly challenging, clinically complex, and emotionally draining for everyone involved.
At Cumberland Medical Center, Dr. Martin said he has two meetings a month with executives in the hospital’s C-suite. One is with his hospitalist group, TeamHealth, and one is more direct, between himself and hospital administrators. It’s just 2 hours a month, but these conversations have undoubtedly helped, he said, although he cautioned that “the meetings themselves don’t have as much meaning if you aren’t communicating effectively,” meaning hospitalists must understand how the C-suite thinks and learn to speak in terms they understand.
“When I go to the administration now and I say ‘Hey, this is a problem that we’re having. I need your help in solving it,’ the executives are much more likely to respond to me than if they’d never seen me, or only see me rarely,” Dr. Martin said.
As a result, a collaborative approach to such conversations tends to be more effective.
“If you go to the C-suite and say, ‘Here’s our issue, how can you help us?’ – as opposed to telling the administration, ‘This is what I need’ – they are more likely to work with you to generate a solution.”
Hospitalist Rahul C. Borsadia, MD, had been working with Orlando Health Inpatient Medicine Group since the year of its founding in 2011.
The salaries of the practice’s physicians back then were based on relative value units (RVU) – the more patients that physicians saw, the higher their salaries. But a problem arose, Dr. Borsadia said. Physicians were trying to squeeze in two dozen or more patients a day “in a practice that is modeled for quality.”
“By the time the end of the day comes, it’s 9 or 10 p.m. and you are leaving but coming back at 6:30 the next morning. So, lack of sleep, more patients, striving to earn that higher salary,” he said. “The desire to perform quality work with that kind of patient load was not fulfilled and that lead to dissatisfaction and stress, which lead to irritation and exodus from the group.”
Three years ago, the practice transitioned to a throughput process with a census limit of 18 patients or less, without an RVU system, but with salary incentives based on patient satisfaction, billing, and documentation.
“We’ve not had anybody leave the hospital because of burnout or dissatisfaction” since the new system was put into place, Dr. Borsadia said. “Less burnout means more people are happy.”
Although symptoms of burnout still seem to be rampant across hospital medicine, hospitalists are putting potential solutions into place. And – sometimes – they are making progress, through tweaks in schedules and responsibilities, incentives suited to different goals, and better communication.
Scheduling problems
The need for continuing efforts to improve the work experience for hospitalists is apparent, said Henry Michtalik, MD, MPH, MHS, assistant professor of general internal medicine at Johns Hopkins, Baltimore, who led a workshop on the topic at the 2019 Annual Conference of the Society of Hospital Medicine (HM19).
A 2016 survey of academic general internal medicine clinicians – including about 600 hospitalists and outpatient physicians – found that 67% reported high stress, 38% said they were “burned out,” 50% said they felt they had “low control” over their work, and 60% said they felt high documentation pressures. Still, 68% said they were satisfied with the values of their departments.
Hospitalists surveyed were actually less likely to say they were burned out, compared with outpatient internists – 52%, compared with 55% – but they were more likely to score low on a scale measuring personal accomplishments, compared with the outpatient clinicians – 20% to 10%. The survey found no significant difference between the two groups in depression or suicidality. But with 40% reporting depression and 10% reporting thoughts of suicide, the numbers virtually cry out for solutions.
Hospitalists in the HM19 workshop, as in other sessions at the Annual Conference, questioned whether the standard 7-days-on, 7-days-off work schedule – seven 12-hour shifts followed by 7 days off – allows hospitalists to pair their works lives with their personal lives in a sustainable way. They described the way that the stress and fatigue of such an intense work period bleeds into the days off that follow after it.
“By the end of seven 12’s, they’re bleary eyed, they’re upset, they go home (for) 2 days of washout before they even start to enjoy whatever life they have left,” said Jonathan Martin, MD, director of medicine at Cumberland Medical Center in Crossville, Tenn. “It’s hard to get hospitalists to buy in, which increases their dissatisfaction.”
Dr. Michtalik had a similar perspective.
“You just shut the rest of your life down completely for those 7 days and then, on your 7 days off, you’ve scheduled your life,” he said. “But that last off day – day number 7 – you feel that pit in your stomach, that the streak is coming.” He joked that the feeling was similar to the dread inspired by the phrase “winter is coming” in the popular HBO series “Game of Thrones.”
Systematic reviews of the literature have found that it’s mostly changes at the organization level – rather than changes that an individual physician makes on his or her own – that tend to make significant differences. Changes to structure, communication, and scheduling tend to work better than working on mindfulness, education, or trying to improve resilience, Dr. Michtalik said.
In one study discussed at the HM19 workshop, researchers compared a schedule in which an intensivist works in-house for 7 days, with home call at night, to a schedule in which the intensivist is completely off at night, with an in-house intensivist covering the night shift. The schedule in which the intensivist was truly off for the night significantly reduced reports of burnout, while not affecting length of stay or patient-experience outcomes.
Dr. Michtalik said that another study compared 4-week rotations to 2-week rotations for attending physicians. Researchers found that the 2-week version resulted in lower reports of burnout, with readmissions and patient experience unaffected, although they noted that residents tended to prefer 4-week schedules because they felt it resulted in better relationships with the attending physician.
Perhaps the dominant factor in job satisfaction that’s been identified in surveys is how physicians, patients, and administrators relate to one another, Dr. Michtalik said.
“The important concept here is that relationships were really important in driving job satisfaction, whether that be with our colleagues, our patients, or with the staff that you’re working with,” he said. “It’s always easier to decline a consultation or have a bad interaction with someone over the phone than it is if you actually know them or you are communicating face to face. That’s why it’s important to develop these kinds of relationships, which also put a face to what’s going on.”
Beyond salary adjustments
Hospitalists attending the HM19 workshop said they thought that participating in administration committees at their own institutions helps keep hospitalists involved in hospital matters, limiting the effects of burnout and improving workplace satisfaction.
Kevin McAninch, DO, a hospitalist with Central Ohio Primary Care in Westerville, said a shift in work responsibilities has made an improvement at his hospital. There is now an “inpatient support center” – which has a physician and a nurse in an office taking calls from 6 p.m. to 7 a.m., so that rounders can stop taking floor calls during that time.
The system “takes the pressure off our admitters at night and our nurses because they’re not getting floor calls anymore, so they’re just taking care of the admissions from the ER,” he said.
A recurring theme of the discussion was that salary alone seems universally incapable of eradicating feelings of burnout. One hospitalist said that in surveys, higher-paid physicians insist that monetary compensation is their main driver, but still often complain of burnout because they must work extra shifts to earn that higher level of pay.
Instead, burnout and satisfaction indicators tend to have more do to with time, control, and support, Dr. Michtalik noted.
Mangla Gulati, MD, SFHM, chief quality officer at the University of Maryland Medical Center in Baltimore, said that there’s no big secret about what hospitalists want from their places of employment. They want things like getting patients to service faster so they can make diagnoses, making sure patients get the care they need, fixing the problems associated with electronic medical records, and having a work-life “integration.”
“The questions is – how do we get there?” Dr. Gulati wondered. She suggested that hospitalists have to be more assertive and explanatory in their interactions with members of the hospital C-suite.
“I think it’s really important for you to understand or ask your C-suite, ‘Where are you in this whole journey? What is your perception of wellness? Tell me some of the measures of staff wellness,’ ” she said.
If the C-suite says “we have no money” to make improvements, hospitalists must be willing to say, ‘Well, you’re going to have to invest a little bit.’ ” Dr. Gulati said. “What is the ROI (return on investment) on the turnover of a physician? Because when you turn a physician over, you have to recruit and hire new staff.”
Dr. Gulati said that hospitalists should provide C-suite leaders with a detailed walk-through of their actual workflows – what their workdays look like – because “it’s not something they’re familiar with.”
Aside from improving relations with hospital administration, Dr. Gulati suggested creating CME programs for wellness, offering time and funding for physician support meetings, supporting flexibility in work hours, and creating programs specifically to help clinicians with burnout symptoms.
She also touted the benefits of “Schwartz Rounds,” in which several medical disciplines gather to talk about a case that was particularly challenging, clinically complex, and emotionally draining for everyone involved.
At Cumberland Medical Center, Dr. Martin said he has two meetings a month with executives in the hospital’s C-suite. One is with his hospitalist group, TeamHealth, and one is more direct, between himself and hospital administrators. It’s just 2 hours a month, but these conversations have undoubtedly helped, he said, although he cautioned that “the meetings themselves don’t have as much meaning if you aren’t communicating effectively,” meaning hospitalists must understand how the C-suite thinks and learn to speak in terms they understand.
“When I go to the administration now and I say ‘Hey, this is a problem that we’re having. I need your help in solving it,’ the executives are much more likely to respond to me than if they’d never seen me, or only see me rarely,” Dr. Martin said.
As a result, a collaborative approach to such conversations tends to be more effective.
“If you go to the C-suite and say, ‘Here’s our issue, how can you help us?’ – as opposed to telling the administration, ‘This is what I need’ – they are more likely to work with you to generate a solution.”
Assessment of Barriers to Cancer Care
Purpose: The purpose of this quality improvement project was to determine barriers to cancer care in an urban, largely African-American veteran sample at the Washington DC Veterans Affairs Medical Center (DCVA). The DCVA veteran population has several characteristics associated with challenges in accessing cancer care, including a large African-American population and patients with mental health diagnoses.
Methods: Veterans completed an anonymous survey assess barriers to care as part of a larger survey examining veteran needs in cancer care. Descriptive statistics were conducted on the current responders (n = 128) with an ongoing recruitment goal of 150 survey completers.
Results indicated both logistical and psychosocial barriers, with trouble with transportation or parking (32%) and nancial dif culties (20%) most frequently reported. Nearly half of the sample (45%, n = 55) reported having a psychiatric or mental health diagnosis. A signi cant percentage of this subsample reported that their mental health symptoms caused them to avoid or delay cancer screening (18%), stop cancer treatment (13%), or delay follow-up visits after nishing cancer treatment (17%). Moreover, 62% of this sub-sample stated their mental health symptoms were worsened by their cancer care. The most common reported exacerbators were undergoing imaging (eg, MRI or PET scan) (35%), radiation therapy (33%), and attending follow-up visits (33%).
Conclusion: Logistical barriers are currently being addressed through expanding provider knowledge of transportation resources and opening of an expanded parking garage. Findings of transportation and parking barriers likely reflect specific construction projects at the DCVA and may not be generalizable to other settings. Further quality improvement work based on the results of this project include incorporating screening for mental health diagnoses and targeted interventions for patients identifying concerns related to mental health symptom stressors with the goal of increasing timeliness of care.
Purpose: The purpose of this quality improvement project was to determine barriers to cancer care in an urban, largely African-American veteran sample at the Washington DC Veterans Affairs Medical Center (DCVA). The DCVA veteran population has several characteristics associated with challenges in accessing cancer care, including a large African-American population and patients with mental health diagnoses.
Methods: Veterans completed an anonymous survey assess barriers to care as part of a larger survey examining veteran needs in cancer care. Descriptive statistics were conducted on the current responders (n = 128) with an ongoing recruitment goal of 150 survey completers.
Results indicated both logistical and psychosocial barriers, with trouble with transportation or parking (32%) and nancial dif culties (20%) most frequently reported. Nearly half of the sample (45%, n = 55) reported having a psychiatric or mental health diagnosis. A signi cant percentage of this subsample reported that their mental health symptoms caused them to avoid or delay cancer screening (18%), stop cancer treatment (13%), or delay follow-up visits after nishing cancer treatment (17%). Moreover, 62% of this sub-sample stated their mental health symptoms were worsened by their cancer care. The most common reported exacerbators were undergoing imaging (eg, MRI or PET scan) (35%), radiation therapy (33%), and attending follow-up visits (33%).
Conclusion: Logistical barriers are currently being addressed through expanding provider knowledge of transportation resources and opening of an expanded parking garage. Findings of transportation and parking barriers likely reflect specific construction projects at the DCVA and may not be generalizable to other settings. Further quality improvement work based on the results of this project include incorporating screening for mental health diagnoses and targeted interventions for patients identifying concerns related to mental health symptom stressors with the goal of increasing timeliness of care.
Purpose: The purpose of this quality improvement project was to determine barriers to cancer care in an urban, largely African-American veteran sample at the Washington DC Veterans Affairs Medical Center (DCVA). The DCVA veteran population has several characteristics associated with challenges in accessing cancer care, including a large African-American population and patients with mental health diagnoses.
Methods: Veterans completed an anonymous survey assess barriers to care as part of a larger survey examining veteran needs in cancer care. Descriptive statistics were conducted on the current responders (n = 128) with an ongoing recruitment goal of 150 survey completers.
Results indicated both logistical and psychosocial barriers, with trouble with transportation or parking (32%) and nancial dif culties (20%) most frequently reported. Nearly half of the sample (45%, n = 55) reported having a psychiatric or mental health diagnosis. A signi cant percentage of this subsample reported that their mental health symptoms caused them to avoid or delay cancer screening (18%), stop cancer treatment (13%), or delay follow-up visits after nishing cancer treatment (17%). Moreover, 62% of this sub-sample stated their mental health symptoms were worsened by their cancer care. The most common reported exacerbators were undergoing imaging (eg, MRI or PET scan) (35%), radiation therapy (33%), and attending follow-up visits (33%).
Conclusion: Logistical barriers are currently being addressed through expanding provider knowledge of transportation resources and opening of an expanded parking garage. Findings of transportation and parking barriers likely reflect specific construction projects at the DCVA and may not be generalizable to other settings. Further quality improvement work based on the results of this project include incorporating screening for mental health diagnoses and targeted interventions for patients identifying concerns related to mental health symptom stressors with the goal of increasing timeliness of care.
Primary Cardiac Sarcoma: An Analysis of the National Cancer Database (NCDB)
Introduction: Primary Cardiac Sarcomas (PCS) are exceptionally rare malignancies, representing approximately 25% of all malignant primary cardiac tumors. Due to the rarity of these neoplasms, literature on the characteristics, optimal management, and survival outcomes in these patients is limited.
Methods: The National Cancer Database (NCDB) for soft tissue tumors was utilized to identify 826 adult patients diagnosed with tumors localized to the heart or pericardium from 2004 to 2016. Demographic information was obtained and Kaplan-Meier analysis was used to analyze overall survival of PCS. Bivariate analysis was performed with Cox proportional hazards regression models to obtain hazard ratios and assess the association of patient characteristics and treatment methods with survival.
Results: The majority of PCS patients were male (51.5%) and white (79.4%), with a mean age at diagnosis of 53 years. 41.2% were blood vessel tumors and 27.7% were sarcomas. Leiomyosarcoma and epithelial neoplasms each represented 5.2% of tumors, followed by synovial sarcomas (4.2%) and rhabdomyosarcomas (2.8%). The majority of patients were diagnosed with metastatic disease (43.2%) and received treatment (85.2%), most often with surgical resection (58.1%) or chemotherapy (57.2%).
Median overall survival was 10.9 months (95% CI: 9.6 – 12.1 months), with a cumulative survival at 1-year, 5-years, and 10-years of 27%, 10%, and 4%, respectively. Factors associated with signi cantly increased mortality (P<0.05), include increased age (HR 1.017), increased Charleson-Deyo comorbidity score (HR 1.284), and elevated stage and grade at diagnosis. Compared to blood vessel tumors, leiomyosarcoma (HR 0.696), fibroblastic (HR 0.579), osseous (HR 0.537), and fibrohystocytic (HR 0.485) histologies were associated with improved survival (P<0.05). Factors associated with signi cantly improved survival (P<0.05) included treatment by surgical resection (HR 0.500), radiation (HR 0.808), and chemotherapy (HR 0.738).
Conclusion: This is the largest study of PCS to date, and the first to analyze the NCDB. The majority of these neoplasms are blood vessel tumors and are often diagnosed at advanced stage and grade. Prognosis is poor, and all treatment modalities are associated with improved survival. Understanding of patient characteristics and overall survival is important in enhancing patient outcomes for this rare diagnosis.
Introduction: Primary Cardiac Sarcomas (PCS) are exceptionally rare malignancies, representing approximately 25% of all malignant primary cardiac tumors. Due to the rarity of these neoplasms, literature on the characteristics, optimal management, and survival outcomes in these patients is limited.
Methods: The National Cancer Database (NCDB) for soft tissue tumors was utilized to identify 826 adult patients diagnosed with tumors localized to the heart or pericardium from 2004 to 2016. Demographic information was obtained and Kaplan-Meier analysis was used to analyze overall survival of PCS. Bivariate analysis was performed with Cox proportional hazards regression models to obtain hazard ratios and assess the association of patient characteristics and treatment methods with survival.
Results: The majority of PCS patients were male (51.5%) and white (79.4%), with a mean age at diagnosis of 53 years. 41.2% were blood vessel tumors and 27.7% were sarcomas. Leiomyosarcoma and epithelial neoplasms each represented 5.2% of tumors, followed by synovial sarcomas (4.2%) and rhabdomyosarcomas (2.8%). The majority of patients were diagnosed with metastatic disease (43.2%) and received treatment (85.2%), most often with surgical resection (58.1%) or chemotherapy (57.2%).
Median overall survival was 10.9 months (95% CI: 9.6 – 12.1 months), with a cumulative survival at 1-year, 5-years, and 10-years of 27%, 10%, and 4%, respectively. Factors associated with signi cantly increased mortality (P<0.05), include increased age (HR 1.017), increased Charleson-Deyo comorbidity score (HR 1.284), and elevated stage and grade at diagnosis. Compared to blood vessel tumors, leiomyosarcoma (HR 0.696), fibroblastic (HR 0.579), osseous (HR 0.537), and fibrohystocytic (HR 0.485) histologies were associated with improved survival (P<0.05). Factors associated with signi cantly improved survival (P<0.05) included treatment by surgical resection (HR 0.500), radiation (HR 0.808), and chemotherapy (HR 0.738).
Conclusion: This is the largest study of PCS to date, and the first to analyze the NCDB. The majority of these neoplasms are blood vessel tumors and are often diagnosed at advanced stage and grade. Prognosis is poor, and all treatment modalities are associated with improved survival. Understanding of patient characteristics and overall survival is important in enhancing patient outcomes for this rare diagnosis.
Introduction: Primary Cardiac Sarcomas (PCS) are exceptionally rare malignancies, representing approximately 25% of all malignant primary cardiac tumors. Due to the rarity of these neoplasms, literature on the characteristics, optimal management, and survival outcomes in these patients is limited.
Methods: The National Cancer Database (NCDB) for soft tissue tumors was utilized to identify 826 adult patients diagnosed with tumors localized to the heart or pericardium from 2004 to 2016. Demographic information was obtained and Kaplan-Meier analysis was used to analyze overall survival of PCS. Bivariate analysis was performed with Cox proportional hazards regression models to obtain hazard ratios and assess the association of patient characteristics and treatment methods with survival.
Results: The majority of PCS patients were male (51.5%) and white (79.4%), with a mean age at diagnosis of 53 years. 41.2% were blood vessel tumors and 27.7% were sarcomas. Leiomyosarcoma and epithelial neoplasms each represented 5.2% of tumors, followed by synovial sarcomas (4.2%) and rhabdomyosarcomas (2.8%). The majority of patients were diagnosed with metastatic disease (43.2%) and received treatment (85.2%), most often with surgical resection (58.1%) or chemotherapy (57.2%).
Median overall survival was 10.9 months (95% CI: 9.6 – 12.1 months), with a cumulative survival at 1-year, 5-years, and 10-years of 27%, 10%, and 4%, respectively. Factors associated with signi cantly increased mortality (P<0.05), include increased age (HR 1.017), increased Charleson-Deyo comorbidity score (HR 1.284), and elevated stage and grade at diagnosis. Compared to blood vessel tumors, leiomyosarcoma (HR 0.696), fibroblastic (HR 0.579), osseous (HR 0.537), and fibrohystocytic (HR 0.485) histologies were associated with improved survival (P<0.05). Factors associated with signi cantly improved survival (P<0.05) included treatment by surgical resection (HR 0.500), radiation (HR 0.808), and chemotherapy (HR 0.738).
Conclusion: This is the largest study of PCS to date, and the first to analyze the NCDB. The majority of these neoplasms are blood vessel tumors and are often diagnosed at advanced stage and grade. Prognosis is poor, and all treatment modalities are associated with improved survival. Understanding of patient characteristics and overall survival is important in enhancing patient outcomes for this rare diagnosis.
Veteran Symptom Assessment Scale (VSAS) in a Text Messaging Platform
Background: Oncologists are often not aware of the symptom burden their patients experience. Patient reported outcome (PRO) assessments are tools to measure symptoms. Higher symptom burden is associated with worse quality of life (QOL) and shorter survival, and implementation of PRO assessments is associated with improved QOL and longer survival. The Veteran Symptom Assessment Scale (VSAS) is a PRO template that is incorporated into the Veteran Administration’s (VA) computer patient record system. It is used by health care team members to record patient symptoms and is consistent and reproducible. However, as VSAS is administered at patient visits, it cannot measure between-visit symptoms. Thus, we sought to develop a platform by which veterans receiving hematology- oncology care can directly report their symptoms at any time.
Description: VA Office of Connected Care developed a text messaging platform called “Annie” which includes different disease-based assessment and automated management tools. Annie is named after Lieutenant Annie G. Fox, Chief Nurse in the Army Nurse Corps at Hickman Field, Pearl Harbor and the first woman to receive the Purple Heart for combat.
We developed an oncology symptom module in Annie that incorporates the VSAS symptoms, with a rating scale of 1 – 10 (1 = least severe, 10 = most severe). Veterans signed up for the oncology module receive weekday reminders to report symptoms, but may report symptoms on any day and time, even multiple times a day. After reporting a symptom and severity, a message with advice is texted to the veteran. This text is provided for self-help purposes, and does not replace individualized advice provided by an oncology nurse or provider. The Annie oncology module is available throughout the VA.
Implications: The Annie oncology module may improve implementation of VSAS at VA facilities, by removing the necessity for nurse administration. Using Annie will help VA facilities meet quality of care goals recommended by the American Society of Clinical Oncology and American College of Surgeon and will improve measurement of cancer related symptoms, a first step to developing symptom management tools for VA providers.
Background: Oncologists are often not aware of the symptom burden their patients experience. Patient reported outcome (PRO) assessments are tools to measure symptoms. Higher symptom burden is associated with worse quality of life (QOL) and shorter survival, and implementation of PRO assessments is associated with improved QOL and longer survival. The Veteran Symptom Assessment Scale (VSAS) is a PRO template that is incorporated into the Veteran Administration’s (VA) computer patient record system. It is used by health care team members to record patient symptoms and is consistent and reproducible. However, as VSAS is administered at patient visits, it cannot measure between-visit symptoms. Thus, we sought to develop a platform by which veterans receiving hematology- oncology care can directly report their symptoms at any time.
Description: VA Office of Connected Care developed a text messaging platform called “Annie” which includes different disease-based assessment and automated management tools. Annie is named after Lieutenant Annie G. Fox, Chief Nurse in the Army Nurse Corps at Hickman Field, Pearl Harbor and the first woman to receive the Purple Heart for combat.
We developed an oncology symptom module in Annie that incorporates the VSAS symptoms, with a rating scale of 1 – 10 (1 = least severe, 10 = most severe). Veterans signed up for the oncology module receive weekday reminders to report symptoms, but may report symptoms on any day and time, even multiple times a day. After reporting a symptom and severity, a message with advice is texted to the veteran. This text is provided for self-help purposes, and does not replace individualized advice provided by an oncology nurse or provider. The Annie oncology module is available throughout the VA.
Implications: The Annie oncology module may improve implementation of VSAS at VA facilities, by removing the necessity for nurse administration. Using Annie will help VA facilities meet quality of care goals recommended by the American Society of Clinical Oncology and American College of Surgeon and will improve measurement of cancer related symptoms, a first step to developing symptom management tools for VA providers.
Background: Oncologists are often not aware of the symptom burden their patients experience. Patient reported outcome (PRO) assessments are tools to measure symptoms. Higher symptom burden is associated with worse quality of life (QOL) and shorter survival, and implementation of PRO assessments is associated with improved QOL and longer survival. The Veteran Symptom Assessment Scale (VSAS) is a PRO template that is incorporated into the Veteran Administration’s (VA) computer patient record system. It is used by health care team members to record patient symptoms and is consistent and reproducible. However, as VSAS is administered at patient visits, it cannot measure between-visit symptoms. Thus, we sought to develop a platform by which veterans receiving hematology- oncology care can directly report their symptoms at any time.
Description: VA Office of Connected Care developed a text messaging platform called “Annie” which includes different disease-based assessment and automated management tools. Annie is named after Lieutenant Annie G. Fox, Chief Nurse in the Army Nurse Corps at Hickman Field, Pearl Harbor and the first woman to receive the Purple Heart for combat.
We developed an oncology symptom module in Annie that incorporates the VSAS symptoms, with a rating scale of 1 – 10 (1 = least severe, 10 = most severe). Veterans signed up for the oncology module receive weekday reminders to report symptoms, but may report symptoms on any day and time, even multiple times a day. After reporting a symptom and severity, a message with advice is texted to the veteran. This text is provided for self-help purposes, and does not replace individualized advice provided by an oncology nurse or provider. The Annie oncology module is available throughout the VA.
Implications: The Annie oncology module may improve implementation of VSAS at VA facilities, by removing the necessity for nurse administration. Using Annie will help VA facilities meet quality of care goals recommended by the American Society of Clinical Oncology and American College of Surgeon and will improve measurement of cancer related symptoms, a first step to developing symptom management tools for VA providers.
A Personable Infusion Room Experience
Background: A substantial percentage of veterans receiving chemotherapy in our infusion room reported some degree of feelings of distress. Distress can lead to patient dissatisfaction and an overall negative patient care experience.
Methods: We utilized the NCCN Distress Thermometer tool (scale 1-10) to gauge veterans self-reported level of distress after being seated in the infusion room. Of 88 veterans surveyed, 86% reported varying degrees of distress. Forty-two percent had scores of 4 or higher, and 18% with scores considered moderate to severe. Veterans reported that the fear of not knowing what to expect when starting treatment was a major contributor.
We created an informational video for veterans to view prior to their rst infusion room appointment. The video depicts a walk through the veterans shoes as they check into clinic, undergo a chemotherapy clearance appointment, access a peripheral vein or port, then ends with introducing the team of infusion nurses. Additionally, we have implemented chair-side service to veterans in the infusion room with physicians, volunteers and members of leadership rotating to offer coffee/tea, DVD players, electronic tablets, magazines, card games, and warm blankets.
Results: After implementation of this veteran centered initiative, there has been a reduction in overall distress levels. After implementation, 31% of scores were a 4 or higher, showing a decrease by 11%. Additionally, there were lower numbers of scores in the severe distress range, 4.4% compared to 6% before the intervention.
Conclusion: Helping veterans to understand what to expect with initiation of chemotherapy can help reduce distress and start their cancer journey on a positive note. Bringing members of the clinical team and leadership to the chair-side to serve our veterans creates a patient centric environment and supports the mission to enhance veterans’ experience.
Background: A substantial percentage of veterans receiving chemotherapy in our infusion room reported some degree of feelings of distress. Distress can lead to patient dissatisfaction and an overall negative patient care experience.
Methods: We utilized the NCCN Distress Thermometer tool (scale 1-10) to gauge veterans self-reported level of distress after being seated in the infusion room. Of 88 veterans surveyed, 86% reported varying degrees of distress. Forty-two percent had scores of 4 or higher, and 18% with scores considered moderate to severe. Veterans reported that the fear of not knowing what to expect when starting treatment was a major contributor.
We created an informational video for veterans to view prior to their rst infusion room appointment. The video depicts a walk through the veterans shoes as they check into clinic, undergo a chemotherapy clearance appointment, access a peripheral vein or port, then ends with introducing the team of infusion nurses. Additionally, we have implemented chair-side service to veterans in the infusion room with physicians, volunteers and members of leadership rotating to offer coffee/tea, DVD players, electronic tablets, magazines, card games, and warm blankets.
Results: After implementation of this veteran centered initiative, there has been a reduction in overall distress levels. After implementation, 31% of scores were a 4 or higher, showing a decrease by 11%. Additionally, there were lower numbers of scores in the severe distress range, 4.4% compared to 6% before the intervention.
Conclusion: Helping veterans to understand what to expect with initiation of chemotherapy can help reduce distress and start their cancer journey on a positive note. Bringing members of the clinical team and leadership to the chair-side to serve our veterans creates a patient centric environment and supports the mission to enhance veterans’ experience.
Background: A substantial percentage of veterans receiving chemotherapy in our infusion room reported some degree of feelings of distress. Distress can lead to patient dissatisfaction and an overall negative patient care experience.
Methods: We utilized the NCCN Distress Thermometer tool (scale 1-10) to gauge veterans self-reported level of distress after being seated in the infusion room. Of 88 veterans surveyed, 86% reported varying degrees of distress. Forty-two percent had scores of 4 or higher, and 18% with scores considered moderate to severe. Veterans reported that the fear of not knowing what to expect when starting treatment was a major contributor.
We created an informational video for veterans to view prior to their rst infusion room appointment. The video depicts a walk through the veterans shoes as they check into clinic, undergo a chemotherapy clearance appointment, access a peripheral vein or port, then ends with introducing the team of infusion nurses. Additionally, we have implemented chair-side service to veterans in the infusion room with physicians, volunteers and members of leadership rotating to offer coffee/tea, DVD players, electronic tablets, magazines, card games, and warm blankets.
Results: After implementation of this veteran centered initiative, there has been a reduction in overall distress levels. After implementation, 31% of scores were a 4 or higher, showing a decrease by 11%. Additionally, there were lower numbers of scores in the severe distress range, 4.4% compared to 6% before the intervention.
Conclusion: Helping veterans to understand what to expect with initiation of chemotherapy can help reduce distress and start their cancer journey on a positive note. Bringing members of the clinical team and leadership to the chair-side to serve our veterans creates a patient centric environment and supports the mission to enhance veterans’ experience.
Clinical Impact of Biweekly Liver Function Tests During the First Three Months of Abiraterone Therapy in a Veteran Population
Purpose: To evaluate the clinical impact of biweekly liver function tests (LFTs) during the first 3 months of abiraterone therapy in veterans with prostate cancer.
Background: Abiraterone monitoring recommendations include biweekly LFTs for 3 months, then monthly based on concerns of early hepatoxicity in a limited number of patients. Veterans at the Richard L. Roudebush Veterans Affairs Medical Center (RLRVAMC) appear to tolerate abiraterone without clinically significant hepatoxicity despite stringent monitoring. There appears to be an opportunity to improve patient satisfaction/ quality of life and decrease cost to the healthcare system.
Methods: Patients were included in this retrospective chart review if abiraterone was initiated through the RLRVAMC between May 2014 and July 2018. Exclusion criteria were discontinuation within three months due to rising prostate-specific antigen or adverse drug events unrelated to hepatotoxicity, prior abiraterone exposure, and management outside RLRVAMC. Primary outcome was incidence and severity of LFT changes. Secondary outcomes included incidence and cause of dose reduction and death. Descriptive statistics analyzed outcomes. Severity of toxicity was classified according to common terminology criteria for adverse events (CTCAE) version 5.
Results: Ninety patients were included. Across three months of treatment, 24 (26.7%), 2 (2.2%), 0, and 2 (2.2%) patients experienced maximum CTCAE grade 1, 2, 3, and 4 LFT changes, respectively. Two patients experienced grade 3 or 4 LFT changes, both with previous therapy modifications due to grade 1 or 2 LFT changes and acute illness. Therapy modifications for any reason occurred in 4.4% of patients, all due to acute illness, general tolerability concerns, or grade 1 or 2 LFT changes. Four patients experienced death. No deaths were considered directly related to abiraterone.
Implications: Need for week 10 laboratory monitoring may be determined based on patient specific criteria. Reduction in laboratory monitoring may increase patient satisfaction/quality of life and decrease unnecessary costs to the healthcare system. Patients initiated on abiraterone through the RLRVAMC will receive monthly monitoring starting at week eight in the absence of baseline risk factors for hepatoxicity, grade 2 or worsening grade 1 changes during the first two months of therapy, or new grade 1 changes identified at week eight of therapy
Purpose: To evaluate the clinical impact of biweekly liver function tests (LFTs) during the first 3 months of abiraterone therapy in veterans with prostate cancer.
Background: Abiraterone monitoring recommendations include biweekly LFTs for 3 months, then monthly based on concerns of early hepatoxicity in a limited number of patients. Veterans at the Richard L. Roudebush Veterans Affairs Medical Center (RLRVAMC) appear to tolerate abiraterone without clinically significant hepatoxicity despite stringent monitoring. There appears to be an opportunity to improve patient satisfaction/ quality of life and decrease cost to the healthcare system.
Methods: Patients were included in this retrospective chart review if abiraterone was initiated through the RLRVAMC between May 2014 and July 2018. Exclusion criteria were discontinuation within three months due to rising prostate-specific antigen or adverse drug events unrelated to hepatotoxicity, prior abiraterone exposure, and management outside RLRVAMC. Primary outcome was incidence and severity of LFT changes. Secondary outcomes included incidence and cause of dose reduction and death. Descriptive statistics analyzed outcomes. Severity of toxicity was classified according to common terminology criteria for adverse events (CTCAE) version 5.
Results: Ninety patients were included. Across three months of treatment, 24 (26.7%), 2 (2.2%), 0, and 2 (2.2%) patients experienced maximum CTCAE grade 1, 2, 3, and 4 LFT changes, respectively. Two patients experienced grade 3 or 4 LFT changes, both with previous therapy modifications due to grade 1 or 2 LFT changes and acute illness. Therapy modifications for any reason occurred in 4.4% of patients, all due to acute illness, general tolerability concerns, or grade 1 or 2 LFT changes. Four patients experienced death. No deaths were considered directly related to abiraterone.
Implications: Need for week 10 laboratory monitoring may be determined based on patient specific criteria. Reduction in laboratory monitoring may increase patient satisfaction/quality of life and decrease unnecessary costs to the healthcare system. Patients initiated on abiraterone through the RLRVAMC will receive monthly monitoring starting at week eight in the absence of baseline risk factors for hepatoxicity, grade 2 or worsening grade 1 changes during the first two months of therapy, or new grade 1 changes identified at week eight of therapy
Purpose: To evaluate the clinical impact of biweekly liver function tests (LFTs) during the first 3 months of abiraterone therapy in veterans with prostate cancer.
Background: Abiraterone monitoring recommendations include biweekly LFTs for 3 months, then monthly based on concerns of early hepatoxicity in a limited number of patients. Veterans at the Richard L. Roudebush Veterans Affairs Medical Center (RLRVAMC) appear to tolerate abiraterone without clinically significant hepatoxicity despite stringent monitoring. There appears to be an opportunity to improve patient satisfaction/ quality of life and decrease cost to the healthcare system.
Methods: Patients were included in this retrospective chart review if abiraterone was initiated through the RLRVAMC between May 2014 and July 2018. Exclusion criteria were discontinuation within three months due to rising prostate-specific antigen or adverse drug events unrelated to hepatotoxicity, prior abiraterone exposure, and management outside RLRVAMC. Primary outcome was incidence and severity of LFT changes. Secondary outcomes included incidence and cause of dose reduction and death. Descriptive statistics analyzed outcomes. Severity of toxicity was classified according to common terminology criteria for adverse events (CTCAE) version 5.
Results: Ninety patients were included. Across three months of treatment, 24 (26.7%), 2 (2.2%), 0, and 2 (2.2%) patients experienced maximum CTCAE grade 1, 2, 3, and 4 LFT changes, respectively. Two patients experienced grade 3 or 4 LFT changes, both with previous therapy modifications due to grade 1 or 2 LFT changes and acute illness. Therapy modifications for any reason occurred in 4.4% of patients, all due to acute illness, general tolerability concerns, or grade 1 or 2 LFT changes. Four patients experienced death. No deaths were considered directly related to abiraterone.
Implications: Need for week 10 laboratory monitoring may be determined based on patient specific criteria. Reduction in laboratory monitoring may increase patient satisfaction/quality of life and decrease unnecessary costs to the healthcare system. Patients initiated on abiraterone through the RLRVAMC will receive monthly monitoring starting at week eight in the absence of baseline risk factors for hepatoxicity, grade 2 or worsening grade 1 changes during the first two months of therapy, or new grade 1 changes identified at week eight of therapy