User login
For MD-IQ use only
Conflicting psychiatric agendas in our polarized world
A series of case discussions recently engendered discord among colleagues of ours. The conflicts raised questions about systemic biases within our field and their possible ramifications.

The cases discussed, like many in psychiatry, involved patients with severely maladaptive coping skills who lived with punishing friends, had little rewarding purpose, and had dismissive or abusive families. The conflicts involved whether the treating psychiatrists should promote seemingly obvious life choices or whether those perspectives were based in socionormative stereotypes seeped in mistaken traditional values that do not account for the rich array of experiences our patients come from.
One such case involved a seemingly masochistic patient who repeatedly found herself in abusive relationships and whether the psychiatrist should consider criticizing her partner choices. Another case involved a severely suffering veteran who felt paralyzed at home and whether the psychiatrist should encourage employment to diminish isolation. Yet another case involved a suicidal transgender patient who was in despair when feeling little relief after receiving gender-conforming surgery and – whether the psychiatrist should or could discuss perspectives on gender.
Those cases have led to accusations of misunderstanding science on both sides – and questions about the political justifications and consequences of psychiatric recommendations.
The field of psychiatry is appropriately embarrassed by its former association to misogynistic, homophobic, and even racist schools of thought. However, we wonder whether our current attempts at penance are at times discouraging important discussions. In some cases, our lowest-functioning patients living on the fringe of society benefit the most from the stabilizing influences of family, employment, social institutions, or religious worship. This is especially true considering how much social isolation has become an increasing reality of modern life. As such, we worry when colleagues argue that the promotion of common values is inherently suspect.
This problem may be exemplified by the public attacks on Allan Josephson, MD. Dr. Josephson, a child psychiatrist at the University of Louisville (Ky.), contends that he was ostracized and later fired from his position for communicating at a Heritage Foundation forum on his concerns about current recommended treatments and approaches for gender dysphoria. It appears that, despite being a renowned and previously deeply respected expert in the field, his opinions on the subject now go beyond the acceptable discourse of psychiatry. It is not just that the establishment disagrees with him, he allegedly has gone beyond the acceptable bounds of professionalism.
This reaction is surprising from numerous perspectives. First, his opinions would have seemed mainstream to many only a few years ago. Second, there is no large body of scientific evidence that has been generated to confirm that he is promoting an unscientific perspective that should rightly get ostracized by the medical community – such as anti-vaccination. Actually, some evidence suggests that some medical approaches to gender dysphoria have not always ameliorated the distress found in some patients.

After reviewing the evidence on gender reassignment surgery a few years ago, the Centers for Medicare & Medicaid Services concluded: “Based on an extensive assessment of the clinical evidence as described above, there is not enough high-quality evidence to determine whether gender reassignment surgery improves health outcomes for Medicare beneficiaries with gender dysphoria and whether patients most likely to benefit from these types of surgical intervention can be identified prospectively.”
Whether such a diagnosis should exist at all in the DSM is a worthy topic of discussion with inclusive arguments on both sides. Pathologizing gender dysphoria is stigmatizing. At the same time, a diagnosis may permit one to receive assistance for a recognized condition. One may rightfully want to discuss the scientific merit of a diagnosis without the interference of arguments based on political or social ramifications of said diagnosis, despite their obvious existence and import.
One should be able to voice scientific opinions in a fair-minded, nonpolitically biased manner that is not designed to intimidate and harass dissenters. One should note that a debate about the appropriateness of having said diagnosis will bring up many philosophical and deeply uncomfortable questions. Those questions point out the apparent nosologic problems inherent in DSM methodology that are extraordinarily difficult to solve. If psychiatry chooses to produce or dismiss psychiatric diagnoses based on the inherent political inconvenience of said diagnoses, rather than their scientific and medical basis, the entire field will rightly be called into question.
One may deplore the static and at times oppressive nature of cultural biases. However, it should be noted that the ability to safely step outside the supportive structure of family, employment, and social and religious institution is itself a privilege, one in which some our patients do not have the luxury of engaging in.
It is not clear to us how we got to this juncture. Part of psychiatric and medical training does involve learning nonjudgmental approaches to human suffering and an identification with individual needs over societal demands. Our suspicion is that a nonjudgmental approach to the understanding of the human condition may be exaggerated into a desire to solve the human condition without challenging patients’ fundamental need for a well-rounded biologic, psychological, and social recovery. It is also possible that our desire to promote utopian hopes for society has blinded us from accepting the idea that, for many of our lowest-functioning patients, fitting in and participating in society can be their best path to recovery.
Psychiatry attempts to define and alleviate the suffering that accompanies some behaviors. As such, psychiatry has always and will always address and confront behaviors that society may condemn. At times, psychiatrists will be in sync or clash with societal trends. Sometimes science will contradict societal wishes. And ultimately, psychiatrists will hopefully make decisions informed in biopsychosocial constructs that best suit the patient in front of them no matter what society may want. In a polarized environment, psychiatry should remind itself that we cannot always or ever fix society, and that maintaining reasonable cultural norms and societal stability – while avoiding the traps of superficial culture wars and utopian visions – is often the wisest path.
Dr. Lehman is an associate professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He also is the course director for the UCSD third-year medical student psychiatry clerkship. Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at UCSD and the University of San Diego. Dr. Badre can be reached at his website, BadreMD.com.
A series of case discussions recently engendered discord among colleagues of ours. The conflicts raised questions about systemic biases within our field and their possible ramifications.
The cases discussed, like many in psychiatry, involved patients with severely maladaptive coping skills who lived with punishing friends, had little rewarding purpose, and had dismissive or abusive families. The conflicts involved whether the treating psychiatrists should promote seemingly obvious life choices or whether those perspectives were based in socionormative stereotypes seeped in mistaken traditional values that do not account for the rich array of experiences our patients come from.
One such case involved a seemingly masochistic patient who repeatedly found herself in abusive relationships and whether the psychiatrist should consider criticizing her partner choices. Another case involved a severely suffering veteran who felt paralyzed at home and whether the psychiatrist should encourage employment to diminish isolation. Yet another case involved a suicidal transgender patient who was in despair when feeling little relief after receiving gender-conforming surgery and – whether the psychiatrist should or could discuss perspectives on gender.
Those cases have led to accusations of misunderstanding science on both sides – and questions about the political justifications and consequences of psychiatric recommendations.
The field of psychiatry is appropriately embarrassed by its former association to misogynistic, homophobic, and even racist schools of thought. However, we wonder whether our current attempts at penance are at times discouraging important discussions. In some cases, our lowest-functioning patients living on the fringe of society benefit the most from the stabilizing influences of family, employment, social institutions, or religious worship. This is especially true considering how much social isolation has become an increasing reality of modern life. As such, we worry when colleagues argue that the promotion of common values is inherently suspect.
This problem may be exemplified by the public attacks on Allan Josephson, MD. Dr. Josephson, a child psychiatrist at the University of Louisville (Ky.), contends that he was ostracized and later fired from his position for communicating at a Heritage Foundation forum on his concerns about current recommended treatments and approaches for gender dysphoria. It appears that, despite being a renowned and previously deeply respected expert in the field, his opinions on the subject now go beyond the acceptable discourse of psychiatry. It is not just that the establishment disagrees with him, he allegedly has gone beyond the acceptable bounds of professionalism.
This reaction is surprising from numerous perspectives. First, his opinions would have seemed mainstream to many only a few years ago. Second, there is no large body of scientific evidence that has been generated to confirm that he is promoting an unscientific perspective that should rightly get ostracized by the medical community – such as anti-vaccination. Actually, some evidence suggests that some medical approaches to gender dysphoria have not always ameliorated the distress found in some patients.
After reviewing the evidence on gender reassignment surgery a few years ago, the Centers for Medicare & Medicaid Services concluded: “Based on an extensive assessment of the clinical evidence as described above, there is not enough high-quality evidence to determine whether gender reassignment surgery improves health outcomes for Medicare beneficiaries with gender dysphoria and whether patients most likely to benefit from these types of surgical intervention can be identified prospectively.”
Whether such a diagnosis should exist at all in the DSM is a worthy topic of discussion with inclusive arguments on both sides. Pathologizing gender dysphoria is stigmatizing. At the same time, a diagnosis may permit one to receive assistance for a recognized condition. One may rightfully want to discuss the scientific merit of a diagnosis without the interference of arguments based on political or social ramifications of said diagnosis, despite their obvious existence and import.
One should be able to voice scientific opinions in a fair-minded, nonpolitically biased manner that is not designed to intimidate and harass dissenters. One should note that a debate about the appropriateness of having said diagnosis will bring up many philosophical and deeply uncomfortable questions. Those questions point out the apparent nosologic problems inherent in DSM methodology that are extraordinarily difficult to solve. If psychiatry chooses to produce or dismiss psychiatric diagnoses based on the inherent political inconvenience of said diagnoses, rather than their scientific and medical basis, the entire field will rightly be called into question.
One may deplore the static and at times oppressive nature of cultural biases. However, it should be noted that the ability to safely step outside the supportive structure of family, employment, and social and religious institution is itself a privilege, one in which some our patients do not have the luxury of engaging in.
It is not clear to us how we got to this juncture. Part of psychiatric and medical training does involve learning nonjudgmental approaches to human suffering and an identification with individual needs over societal demands. Our suspicion is that a nonjudgmental approach to the understanding of the human condition may be exaggerated into a desire to solve the human condition without challenging patients’ fundamental need for a well-rounded biologic, psychological, and social recovery. It is also possible that our desire to promote utopian hopes for society has blinded us from accepting the idea that, for many of our lowest-functioning patients, fitting in and participating in society can be their best path to recovery.
Psychiatry attempts to define and alleviate the suffering that accompanies some behaviors. As such, psychiatry has always and will always address and confront behaviors that society may condemn. At times, psychiatrists will be in sync or clash with societal trends. Sometimes science will contradict societal wishes. And ultimately, psychiatrists will hopefully make decisions informed in biopsychosocial constructs that best suit the patient in front of them no matter what society may want. In a polarized environment, psychiatry should remind itself that we cannot always or ever fix society, and that maintaining reasonable cultural norms and societal stability – while avoiding the traps of superficial culture wars and utopian visions – is often the wisest path.
Dr. Lehman is an associate professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He also is the course director for the UCSD third-year medical student psychiatry clerkship. Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at UCSD and the University of San Diego. Dr. Badre can be reached at his website, BadreMD.com.
A series of case discussions recently engendered discord among colleagues of ours. The conflicts raised questions about systemic biases within our field and their possible ramifications.
The cases discussed, like many in psychiatry, involved patients with severely maladaptive coping skills who lived with punishing friends, had little rewarding purpose, and had dismissive or abusive families. The conflicts involved whether the treating psychiatrists should promote seemingly obvious life choices or whether those perspectives were based in socionormative stereotypes seeped in mistaken traditional values that do not account for the rich array of experiences our patients come from.
One such case involved a seemingly masochistic patient who repeatedly found herself in abusive relationships and whether the psychiatrist should consider criticizing her partner choices. Another case involved a severely suffering veteran who felt paralyzed at home and whether the psychiatrist should encourage employment to diminish isolation. Yet another case involved a suicidal transgender patient who was in despair when feeling little relief after receiving gender-conforming surgery and – whether the psychiatrist should or could discuss perspectives on gender.
Those cases have led to accusations of misunderstanding science on both sides – and questions about the political justifications and consequences of psychiatric recommendations.
The field of psychiatry is appropriately embarrassed by its former association to misogynistic, homophobic, and even racist schools of thought. However, we wonder whether our current attempts at penance are at times discouraging important discussions. In some cases, our lowest-functioning patients living on the fringe of society benefit the most from the stabilizing influences of family, employment, social institutions, or religious worship. This is especially true considering how much social isolation has become an increasing reality of modern life. As such, we worry when colleagues argue that the promotion of common values is inherently suspect.
This problem may be exemplified by the public attacks on Allan Josephson, MD. Dr. Josephson, a child psychiatrist at the University of Louisville (Ky.), contends that he was ostracized and later fired from his position for communicating at a Heritage Foundation forum on his concerns about current recommended treatments and approaches for gender dysphoria. It appears that, despite being a renowned and previously deeply respected expert in the field, his opinions on the subject now go beyond the acceptable discourse of psychiatry. It is not just that the establishment disagrees with him, he allegedly has gone beyond the acceptable bounds of professionalism.
This reaction is surprising from numerous perspectives. First, his opinions would have seemed mainstream to many only a few years ago. Second, there is no large body of scientific evidence that has been generated to confirm that he is promoting an unscientific perspective that should rightly get ostracized by the medical community – such as anti-vaccination. Actually, some evidence suggests that some medical approaches to gender dysphoria have not always ameliorated the distress found in some patients.
After reviewing the evidence on gender reassignment surgery a few years ago, the Centers for Medicare & Medicaid Services concluded: “Based on an extensive assessment of the clinical evidence as described above, there is not enough high-quality evidence to determine whether gender reassignment surgery improves health outcomes for Medicare beneficiaries with gender dysphoria and whether patients most likely to benefit from these types of surgical intervention can be identified prospectively.”
Whether such a diagnosis should exist at all in the DSM is a worthy topic of discussion with inclusive arguments on both sides. Pathologizing gender dysphoria is stigmatizing. At the same time, a diagnosis may permit one to receive assistance for a recognized condition. One may rightfully want to discuss the scientific merit of a diagnosis without the interference of arguments based on political or social ramifications of said diagnosis, despite their obvious existence and import.
One should be able to voice scientific opinions in a fair-minded, nonpolitically biased manner that is not designed to intimidate and harass dissenters. One should note that a debate about the appropriateness of having said diagnosis will bring up many philosophical and deeply uncomfortable questions. Those questions point out the apparent nosologic problems inherent in DSM methodology that are extraordinarily difficult to solve. If psychiatry chooses to produce or dismiss psychiatric diagnoses based on the inherent political inconvenience of said diagnoses, rather than their scientific and medical basis, the entire field will rightly be called into question.
One may deplore the static and at times oppressive nature of cultural biases. However, it should be noted that the ability to safely step outside the supportive structure of family, employment, and social and religious institution is itself a privilege, one in which some our patients do not have the luxury of engaging in.
It is not clear to us how we got to this juncture. Part of psychiatric and medical training does involve learning nonjudgmental approaches to human suffering and an identification with individual needs over societal demands. Our suspicion is that a nonjudgmental approach to the understanding of the human condition may be exaggerated into a desire to solve the human condition without challenging patients’ fundamental need for a well-rounded biologic, psychological, and social recovery. It is also possible that our desire to promote utopian hopes for society has blinded us from accepting the idea that, for many of our lowest-functioning patients, fitting in and participating in society can be their best path to recovery.
Psychiatry attempts to define and alleviate the suffering that accompanies some behaviors. As such, psychiatry has always and will always address and confront behaviors that society may condemn. At times, psychiatrists will be in sync or clash with societal trends. Sometimes science will contradict societal wishes. And ultimately, psychiatrists will hopefully make decisions informed in biopsychosocial constructs that best suit the patient in front of them no matter what society may want. In a polarized environment, psychiatry should remind itself that we cannot always or ever fix society, and that maintaining reasonable cultural norms and societal stability – while avoiding the traps of superficial culture wars and utopian visions – is often the wisest path.
Dr. Lehman is an associate professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He also is the course director for the UCSD third-year medical student psychiatry clerkship. Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at UCSD and the University of San Diego. Dr. Badre can be reached at his website, BadreMD.com.
Click for Credit: Long-term antibiotics & stroke, CHD; Postvaccination seizures; more
Here are 5 articles from the November issue of Clinician Reviews (individual articles are valid for one year from date of publication—expiration dates below):
1. Poor response to statins hikes risk of cardiovascular events
To take the posttest, go to: https://bit.ly/2MVHlDR
Expires April 17, 2020
2. Postvaccination febrile seizures are no more severe than other febrile seizures
To take the posttest, go to: https://bit.ly/2VUJzaE
Expires April 19, 2020
3. Hydroxychloroquine adherence in SLE: worse than you thought
To take the posttest, go to: https://bit.ly/2oT00Z9
Expires April 22, 2020
4. Long-term antibiotic use may heighten stroke, CHD risk
To take the posttest, go to: https://bit.ly/2OUUVu5
Expires April 28, 2020
5. Knowledge gaps about long-term osteoporosis drug therapy benefits, risks remain large
To take the posttest, go to: https://bit.ly/2Msgqkb
Expires May 1, 2020
Here are 5 articles from the November issue of Clinician Reviews (individual articles are valid for one year from date of publication—expiration dates below):
1. Poor response to statins hikes risk of cardiovascular events
To take the posttest, go to: https://bit.ly/2MVHlDR
Expires April 17, 2020
2. Postvaccination febrile seizures are no more severe than other febrile seizures
To take the posttest, go to: https://bit.ly/2VUJzaE
Expires April 19, 2020
3. Hydroxychloroquine adherence in SLE: worse than you thought
To take the posttest, go to: https://bit.ly/2oT00Z9
Expires April 22, 2020
4. Long-term antibiotic use may heighten stroke, CHD risk
To take the posttest, go to: https://bit.ly/2OUUVu5
Expires April 28, 2020
5. Knowledge gaps about long-term osteoporosis drug therapy benefits, risks remain large
To take the posttest, go to: https://bit.ly/2Msgqkb
Expires May 1, 2020
Here are 5 articles from the November issue of Clinician Reviews (individual articles are valid for one year from date of publication—expiration dates below):
1. Poor response to statins hikes risk of cardiovascular events
To take the posttest, go to: https://bit.ly/2MVHlDR
Expires April 17, 2020
2. Postvaccination febrile seizures are no more severe than other febrile seizures
To take the posttest, go to: https://bit.ly/2VUJzaE
Expires April 19, 2020
3. Hydroxychloroquine adherence in SLE: worse than you thought
To take the posttest, go to: https://bit.ly/2oT00Z9
Expires April 22, 2020
4. Long-term antibiotic use may heighten stroke, CHD risk
To take the posttest, go to: https://bit.ly/2OUUVu5
Expires April 28, 2020
5. Knowledge gaps about long-term osteoporosis drug therapy benefits, risks remain large
To take the posttest, go to: https://bit.ly/2Msgqkb
Expires May 1, 2020

Brain abscess with lung infection? Think Nocardia
ST. LOUIS – according to University of California, San Francisco, investigators.

Nocardia – an ubiquitous gram-positive rod normally found in standing water, decaying plants, and soil, that can cause problems when it is inhaled as dust or introduced through a nick in the skin – is an underappreciated cause of brain abscess that is not covered by standard empiric therapy targeting the more common causes: Staphylococcus and Streptococcus bacteria, said senior investigator Megan Richie, MD, an assistant neurology professor at UCSF.
“Patients that have a lung infection with a new brain abscess should be started on empiric therapy not just for pyogenic organisms, but also for Nocardia pending biopsy and operative culture data, especially given that empiric therapy of high-dose Bactrim for Nocardia is relatively benign,” she said at the annual meeting of the American Neurological Association.
The advice comes from a comparison of 14 Nocardia cases with 42 randomly selected Staph/Strep cases in a university radiologic database. Nine Nocardia cases were confirmed by operative specimen culture, the rest by lung, blood, or other tissue cultures.
Dr. Richie and colleagues suspected an association with lung infection, which has been reported anecdotally in the literature. The researchers wanted to take a quantitative look to see if it held up statistically after pushback on a brain abscess patient with a lung infection. “We were concerned this patient had Nocardia, but it took quite some time to convince other doctors that we really needed to start [Bactrim]. The patient was not immunocompromised and the infectious disease team said ‘Nocardia brain infections don’t happen in immunocompetent patients,’” Dr. Richie said,
The man did, however, turn out to have Nocardia, and of the 14 cases in the series, four patients (29%) were not immunosuppressed. “I think this would surprise [physicians] who have a little bit less experience with this organism,” Dr. Richie said.Patients with a Nocardia brain abscess were far more likely to have a concomitant lung infection (86% vs. 2%; odds ratio, 246; 95% confidence interval, 21-2953; P less than .0001). Staph/Strep brain abscess patients were more likely to have concomitant ear or sinus infections (40% versus 0%; P = .005). Immunosuppression did turn out to be more common in the Nocardia group, as well (71% vs. 19%; OR, 11; 95% CI, 3-43; P = .001), as did diabetes (36% vs. 10%; P = .03).
Nocardia patients were older (median age, 61 yrs vs. 46 yrs: P = .01) and more likely to be Hispanic (36% vs. 10%; P = .04). There were no differences in sex; neurosurgery history; intravenous drug use; or endocarditis.
On imaging, Nocardia brain abscesses were poorly circumscribed and tended to have multiple lobes, “often two in a figure-eight pattern,” Dr. Richie said. Nocardia diagnosis took longer (median, 7 vs. 4 days; P = .04), “which makes sense because it is a harder diagnosis to make,” she said.
Operative specimen culture was the most potent diagnostic tool. Blood cultures were positive in just one Nocardia patient and a few controls.
There was no external funding, and the investigators did not have any relevant disclosures.
ST. LOUIS – according to University of California, San Francisco, investigators.
Nocardia – an ubiquitous gram-positive rod normally found in standing water, decaying plants, and soil, that can cause problems when it is inhaled as dust or introduced through a nick in the skin – is an underappreciated cause of brain abscess that is not covered by standard empiric therapy targeting the more common causes: Staphylococcus and Streptococcus bacteria, said senior investigator Megan Richie, MD, an assistant neurology professor at UCSF.
“Patients that have a lung infection with a new brain abscess should be started on empiric therapy not just for pyogenic organisms, but also for Nocardia pending biopsy and operative culture data, especially given that empiric therapy of high-dose Bactrim for Nocardia is relatively benign,” she said at the annual meeting of the American Neurological Association.
The advice comes from a comparison of 14 Nocardia cases with 42 randomly selected Staph/Strep cases in a university radiologic database. Nine Nocardia cases were confirmed by operative specimen culture, the rest by lung, blood, or other tissue cultures.
Dr. Richie and colleagues suspected an association with lung infection, which has been reported anecdotally in the literature. The researchers wanted to take a quantitative look to see if it held up statistically after pushback on a brain abscess patient with a lung infection. “We were concerned this patient had Nocardia, but it took quite some time to convince other doctors that we really needed to start [Bactrim]. The patient was not immunocompromised and the infectious disease team said ‘Nocardia brain infections don’t happen in immunocompetent patients,’” Dr. Richie said,
The man did, however, turn out to have Nocardia, and of the 14 cases in the series, four patients (29%) were not immunosuppressed. “I think this would surprise [physicians] who have a little bit less experience with this organism,” Dr. Richie said.Patients with a Nocardia brain abscess were far more likely to have a concomitant lung infection (86% vs. 2%; odds ratio, 246; 95% confidence interval, 21-2953; P less than .0001). Staph/Strep brain abscess patients were more likely to have concomitant ear or sinus infections (40% versus 0%; P = .005). Immunosuppression did turn out to be more common in the Nocardia group, as well (71% vs. 19%; OR, 11; 95% CI, 3-43; P = .001), as did diabetes (36% vs. 10%; P = .03).
Nocardia patients were older (median age, 61 yrs vs. 46 yrs: P = .01) and more likely to be Hispanic (36% vs. 10%; P = .04). There were no differences in sex; neurosurgery history; intravenous drug use; or endocarditis.
On imaging, Nocardia brain abscesses were poorly circumscribed and tended to have multiple lobes, “often two in a figure-eight pattern,” Dr. Richie said. Nocardia diagnosis took longer (median, 7 vs. 4 days; P = .04), “which makes sense because it is a harder diagnosis to make,” she said.
Operative specimen culture was the most potent diagnostic tool. Blood cultures were positive in just one Nocardia patient and a few controls.
There was no external funding, and the investigators did not have any relevant disclosures.
ST. LOUIS – according to University of California, San Francisco, investigators.
Nocardia – an ubiquitous gram-positive rod normally found in standing water, decaying plants, and soil, that can cause problems when it is inhaled as dust or introduced through a nick in the skin – is an underappreciated cause of brain abscess that is not covered by standard empiric therapy targeting the more common causes: Staphylococcus and Streptococcus bacteria, said senior investigator Megan Richie, MD, an assistant neurology professor at UCSF.
“Patients that have a lung infection with a new brain abscess should be started on empiric therapy not just for pyogenic organisms, but also for Nocardia pending biopsy and operative culture data, especially given that empiric therapy of high-dose Bactrim for Nocardia is relatively benign,” she said at the annual meeting of the American Neurological Association.
The advice comes from a comparison of 14 Nocardia cases with 42 randomly selected Staph/Strep cases in a university radiologic database. Nine Nocardia cases were confirmed by operative specimen culture, the rest by lung, blood, or other tissue cultures.
Dr. Richie and colleagues suspected an association with lung infection, which has been reported anecdotally in the literature. The researchers wanted to take a quantitative look to see if it held up statistically after pushback on a brain abscess patient with a lung infection. “We were concerned this patient had Nocardia, but it took quite some time to convince other doctors that we really needed to start [Bactrim]. The patient was not immunocompromised and the infectious disease team said ‘Nocardia brain infections don’t happen in immunocompetent patients,’” Dr. Richie said,
The man did, however, turn out to have Nocardia, and of the 14 cases in the series, four patients (29%) were not immunosuppressed. “I think this would surprise [physicians] who have a little bit less experience with this organism,” Dr. Richie said.Patients with a Nocardia brain abscess were far more likely to have a concomitant lung infection (86% vs. 2%; odds ratio, 246; 95% confidence interval, 21-2953; P less than .0001). Staph/Strep brain abscess patients were more likely to have concomitant ear or sinus infections (40% versus 0%; P = .005). Immunosuppression did turn out to be more common in the Nocardia group, as well (71% vs. 19%; OR, 11; 95% CI, 3-43; P = .001), as did diabetes (36% vs. 10%; P = .03).
Nocardia patients were older (median age, 61 yrs vs. 46 yrs: P = .01) and more likely to be Hispanic (36% vs. 10%; P = .04). There were no differences in sex; neurosurgery history; intravenous drug use; or endocarditis.
On imaging, Nocardia brain abscesses were poorly circumscribed and tended to have multiple lobes, “often two in a figure-eight pattern,” Dr. Richie said. Nocardia diagnosis took longer (median, 7 vs. 4 days; P = .04), “which makes sense because it is a harder diagnosis to make,” she said.
Operative specimen culture was the most potent diagnostic tool. Blood cultures were positive in just one Nocardia patient and a few controls.
There was no external funding, and the investigators did not have any relevant disclosures.
REPORTING FROM ANA 2019
Taking the editorial torch
Dear colleagues,
I am excited to introduce the November issue of The New Gastroenterologist – which is also my first issue as the new Editor in Chief! First, I am incredibly grateful for this opportunity to be a part of the only existing publication tailored toward trainees and early-career gastroenterologists. Bryson Katona has done a remarkable job for the last 5 years as the publication’s inaugural EIC, as he has laid a great deal of groundwork and really set the standard going forward. Each issue has been a multifaceted compilation of salient clinical topics paired with brief but high-yield articles to help guide personal and professional growth; I hope to continue to do the same and maintain a high level of interest in our newsletter.

In this issue, the In Focus article, brought to you by Adeeti Chiplunker and Christina Ha (Cedars Sinai), discusses inpatient management of acute severe ulcerative colitis. It is an excellent review of the diagnostic workup and therapeutic options, and an important one, as therapies are quickly evolving in inflammatory bowel disease. We also have Manol Jovani (Johns Hopkins) help us navigate the daunting world of statistics, specifically focusing on the interpretation of the P value.
For those interested in or already pursuing careers in private practice but would not like to relinquish their research interests, Chris Fourment (Texas Digestive Disease Consultants) provides a series of helpful tips on how to be effective in conducting clinical research endeavors. In the realm of basic science, Melinda Engevik (Baylor College of Medicine) gives an informative breakdown on how to choose a lab that is the right fit for you.
Also in this issue, Sadeea Abbasi (Cedars Sinai) provides an array of tangible ways for gastroenterologists to become involved in health policy advocacy. Byron Cryer (UT Southwestern), Jesus Rivera-Nieves (UCSD), and Celena NuQuay (AGA) describe how the AGA has been promoting workforce diversity in academic gastroenterology via the FORWARD (Fostering Opportunities Resulting in Workforce and Research Diversity) program.
Finally, as the submission deadline for DDW® 2020 approaches, abstract reviewers for the fellow-directed quality improvement (QI) projects from this past year share helpful tips on crafting memorable QI abstracts (Mohammad Bilal, UT-Galveston; Chung Sang Tse, Brown University; Manol Jovani, Johns Hopkins; and Mer Mietzelfeld, AGA).
If you are interested in contributing or have ideas for future TNG topics, please contact me ([email protected]), or Ryan Farrell ([email protected]), managing editor of TNG.
Sincerely,
Vijaya L. Rao, MD
Editor in Chief
Dr. Rao is assistant professor of medicine, University of Chicago, section of gastroenterology, hepatology & nutrition.
Dear colleagues,
I am excited to introduce the November issue of The New Gastroenterologist – which is also my first issue as the new Editor in Chief! First, I am incredibly grateful for this opportunity to be a part of the only existing publication tailored toward trainees and early-career gastroenterologists. Bryson Katona has done a remarkable job for the last 5 years as the publication’s inaugural EIC, as he has laid a great deal of groundwork and really set the standard going forward. Each issue has been a multifaceted compilation of salient clinical topics paired with brief but high-yield articles to help guide personal and professional growth; I hope to continue to do the same and maintain a high level of interest in our newsletter.
In this issue, the In Focus article, brought to you by Adeeti Chiplunker and Christina Ha (Cedars Sinai), discusses inpatient management of acute severe ulcerative colitis. It is an excellent review of the diagnostic workup and therapeutic options, and an important one, as therapies are quickly evolving in inflammatory bowel disease. We also have Manol Jovani (Johns Hopkins) help us navigate the daunting world of statistics, specifically focusing on the interpretation of the P value.
For those interested in or already pursuing careers in private practice but would not like to relinquish their research interests, Chris Fourment (Texas Digestive Disease Consultants) provides a series of helpful tips on how to be effective in conducting clinical research endeavors. In the realm of basic science, Melinda Engevik (Baylor College of Medicine) gives an informative breakdown on how to choose a lab that is the right fit for you.
Also in this issue, Sadeea Abbasi (Cedars Sinai) provides an array of tangible ways for gastroenterologists to become involved in health policy advocacy. Byron Cryer (UT Southwestern), Jesus Rivera-Nieves (UCSD), and Celena NuQuay (AGA) describe how the AGA has been promoting workforce diversity in academic gastroenterology via the FORWARD (Fostering Opportunities Resulting in Workforce and Research Diversity) program.
Finally, as the submission deadline for DDW® 2020 approaches, abstract reviewers for the fellow-directed quality improvement (QI) projects from this past year share helpful tips on crafting memorable QI abstracts (Mohammad Bilal, UT-Galveston; Chung Sang Tse, Brown University; Manol Jovani, Johns Hopkins; and Mer Mietzelfeld, AGA).
If you are interested in contributing or have ideas for future TNG topics, please contact me ([email protected]), or Ryan Farrell ([email protected]), managing editor of TNG.
Sincerely,
Vijaya L. Rao, MD
Editor in Chief
Dr. Rao is assistant professor of medicine, University of Chicago, section of gastroenterology, hepatology & nutrition.
Dear colleagues,
I am excited to introduce the November issue of The New Gastroenterologist – which is also my first issue as the new Editor in Chief! First, I am incredibly grateful for this opportunity to be a part of the only existing publication tailored toward trainees and early-career gastroenterologists. Bryson Katona has done a remarkable job for the last 5 years as the publication’s inaugural EIC, as he has laid a great deal of groundwork and really set the standard going forward. Each issue has been a multifaceted compilation of salient clinical topics paired with brief but high-yield articles to help guide personal and professional growth; I hope to continue to do the same and maintain a high level of interest in our newsletter.
In this issue, the In Focus article, brought to you by Adeeti Chiplunker and Christina Ha (Cedars Sinai), discusses inpatient management of acute severe ulcerative colitis. It is an excellent review of the diagnostic workup and therapeutic options, and an important one, as therapies are quickly evolving in inflammatory bowel disease. We also have Manol Jovani (Johns Hopkins) help us navigate the daunting world of statistics, specifically focusing on the interpretation of the P value.
For those interested in or already pursuing careers in private practice but would not like to relinquish their research interests, Chris Fourment (Texas Digestive Disease Consultants) provides a series of helpful tips on how to be effective in conducting clinical research endeavors. In the realm of basic science, Melinda Engevik (Baylor College of Medicine) gives an informative breakdown on how to choose a lab that is the right fit for you.
Also in this issue, Sadeea Abbasi (Cedars Sinai) provides an array of tangible ways for gastroenterologists to become involved in health policy advocacy. Byron Cryer (UT Southwestern), Jesus Rivera-Nieves (UCSD), and Celena NuQuay (AGA) describe how the AGA has been promoting workforce diversity in academic gastroenterology via the FORWARD (Fostering Opportunities Resulting in Workforce and Research Diversity) program.
Finally, as the submission deadline for DDW® 2020 approaches, abstract reviewers for the fellow-directed quality improvement (QI) projects from this past year share helpful tips on crafting memorable QI abstracts (Mohammad Bilal, UT-Galveston; Chung Sang Tse, Brown University; Manol Jovani, Johns Hopkins; and Mer Mietzelfeld, AGA).
If you are interested in contributing or have ideas for future TNG topics, please contact me ([email protected]), or Ryan Farrell ([email protected]), managing editor of TNG.
Sincerely,
Vijaya L. Rao, MD
Editor in Chief
Dr. Rao is assistant professor of medicine, University of Chicago, section of gastroenterology, hepatology & nutrition.
Digital disruption
One of our lead articles stems from the annual Partners in Value meeting, which was developed by the AGA in partnership with the Digestive Health Physicians Association (Chicago, Oct. 4, 2019). This is an annual meeting about innovations and “what’s next” for GI practices. Anton Decker, MD, an expert in the business of GI and Chair of the Practice Management and Economics Committee, discussed “digital disruption.”

When we discuss digital innovations in health care, most think of telehealth, social media, self-care apps, and remote patient monitoring. As a health system executive, my viewpoint about digital technology has been expanded by other critical needs. At the University of Michigan, we are space constrained (land locked without sufficient parking) and are living with shrinking clinical margins. We see digital technology as a solution to both. As we consolidate our call centers from 27 sites to 1, we plan for 30% of our staff to work from home. Setting up a home work station costs $3,000, compared with office space costs (about $5,000/year). A new clinical site might cost $20 million to build, but that is a fraction of the true life-cycle cost of the building. We have a widely distributed patient base (imagine traveling from Michigan’s Upper Penisula to Ann Arbor for a 20-minute clinic visit).
Many people appreciate “seeing” their doctor from the comfort of their living room. We plan to convert at least 15% of patient visits to telehealth over the next few years although reimbursement rules are still limiting. This year, more than 80% of postsurgical visits (90-day bundled payment) were conducted virtually – mostly by NPs or PAs. Our GI psychologist converted 1,500 patient visit hours to virtual visits last year. In 2019, we completed over 4,000 evisits (management of simple conditions initiated by a patient – essential during flu season) and an increasing number of econsults (primary consultations to specialists). Project ECHO (N Engl J Med. 2011;364:2199) remains the star example of how digital health can improve access, especially for underserved communities.
Virtual care, telehealth, remote patient monitoring, telecommuting and other digital innovations are becoming standards for health systems. Now is the time to think of “face-to-face” visits as option B.
John I. Allen, MD, MBD, AGAF
Editor in Chief
One of our lead articles stems from the annual Partners in Value meeting, which was developed by the AGA in partnership with the Digestive Health Physicians Association (Chicago, Oct. 4, 2019). This is an annual meeting about innovations and “what’s next” for GI practices. Anton Decker, MD, an expert in the business of GI and Chair of the Practice Management and Economics Committee, discussed “digital disruption.”
When we discuss digital innovations in health care, most think of telehealth, social media, self-care apps, and remote patient monitoring. As a health system executive, my viewpoint about digital technology has been expanded by other critical needs. At the University of Michigan, we are space constrained (land locked without sufficient parking) and are living with shrinking clinical margins. We see digital technology as a solution to both. As we consolidate our call centers from 27 sites to 1, we plan for 30% of our staff to work from home. Setting up a home work station costs $3,000, compared with office space costs (about $5,000/year). A new clinical site might cost $20 million to build, but that is a fraction of the true life-cycle cost of the building. We have a widely distributed patient base (imagine traveling from Michigan’s Upper Penisula to Ann Arbor for a 20-minute clinic visit).
Many people appreciate “seeing” their doctor from the comfort of their living room. We plan to convert at least 15% of patient visits to telehealth over the next few years although reimbursement rules are still limiting. This year, more than 80% of postsurgical visits (90-day bundled payment) were conducted virtually – mostly by NPs or PAs. Our GI psychologist converted 1,500 patient visit hours to virtual visits last year. In 2019, we completed over 4,000 evisits (management of simple conditions initiated by a patient – essential during flu season) and an increasing number of econsults (primary consultations to specialists). Project ECHO (N Engl J Med. 2011;364:2199) remains the star example of how digital health can improve access, especially for underserved communities.
Virtual care, telehealth, remote patient monitoring, telecommuting and other digital innovations are becoming standards for health systems. Now is the time to think of “face-to-face” visits as option B.
John I. Allen, MD, MBD, AGAF
Editor in Chief
One of our lead articles stems from the annual Partners in Value meeting, which was developed by the AGA in partnership with the Digestive Health Physicians Association (Chicago, Oct. 4, 2019). This is an annual meeting about innovations and “what’s next” for GI practices. Anton Decker, MD, an expert in the business of GI and Chair of the Practice Management and Economics Committee, discussed “digital disruption.”
When we discuss digital innovations in health care, most think of telehealth, social media, self-care apps, and remote patient monitoring. As a health system executive, my viewpoint about digital technology has been expanded by other critical needs. At the University of Michigan, we are space constrained (land locked without sufficient parking) and are living with shrinking clinical margins. We see digital technology as a solution to both. As we consolidate our call centers from 27 sites to 1, we plan for 30% of our staff to work from home. Setting up a home work station costs $3,000, compared with office space costs (about $5,000/year). A new clinical site might cost $20 million to build, but that is a fraction of the true life-cycle cost of the building. We have a widely distributed patient base (imagine traveling from Michigan’s Upper Penisula to Ann Arbor for a 20-minute clinic visit).
Many people appreciate “seeing” their doctor from the comfort of their living room. We plan to convert at least 15% of patient visits to telehealth over the next few years although reimbursement rules are still limiting. This year, more than 80% of postsurgical visits (90-day bundled payment) were conducted virtually – mostly by NPs or PAs. Our GI psychologist converted 1,500 patient visit hours to virtual visits last year. In 2019, we completed over 4,000 evisits (management of simple conditions initiated by a patient – essential during flu season) and an increasing number of econsults (primary consultations to specialists). Project ECHO (N Engl J Med. 2011;364:2199) remains the star example of how digital health can improve access, especially for underserved communities.
Virtual care, telehealth, remote patient monitoring, telecommuting and other digital innovations are becoming standards for health systems. Now is the time to think of “face-to-face” visits as option B.
John I. Allen, MD, MBD, AGAF
Editor in Chief
2019 at a glance: Hem-onc U.S. drug approvals
The rapid development and identification of novel drugs has translated into innovative therapies in hematology and oncology. The aim of this piece is to present newly approved drugs and expanded indications to serve as a reference guide for practicing clinicians.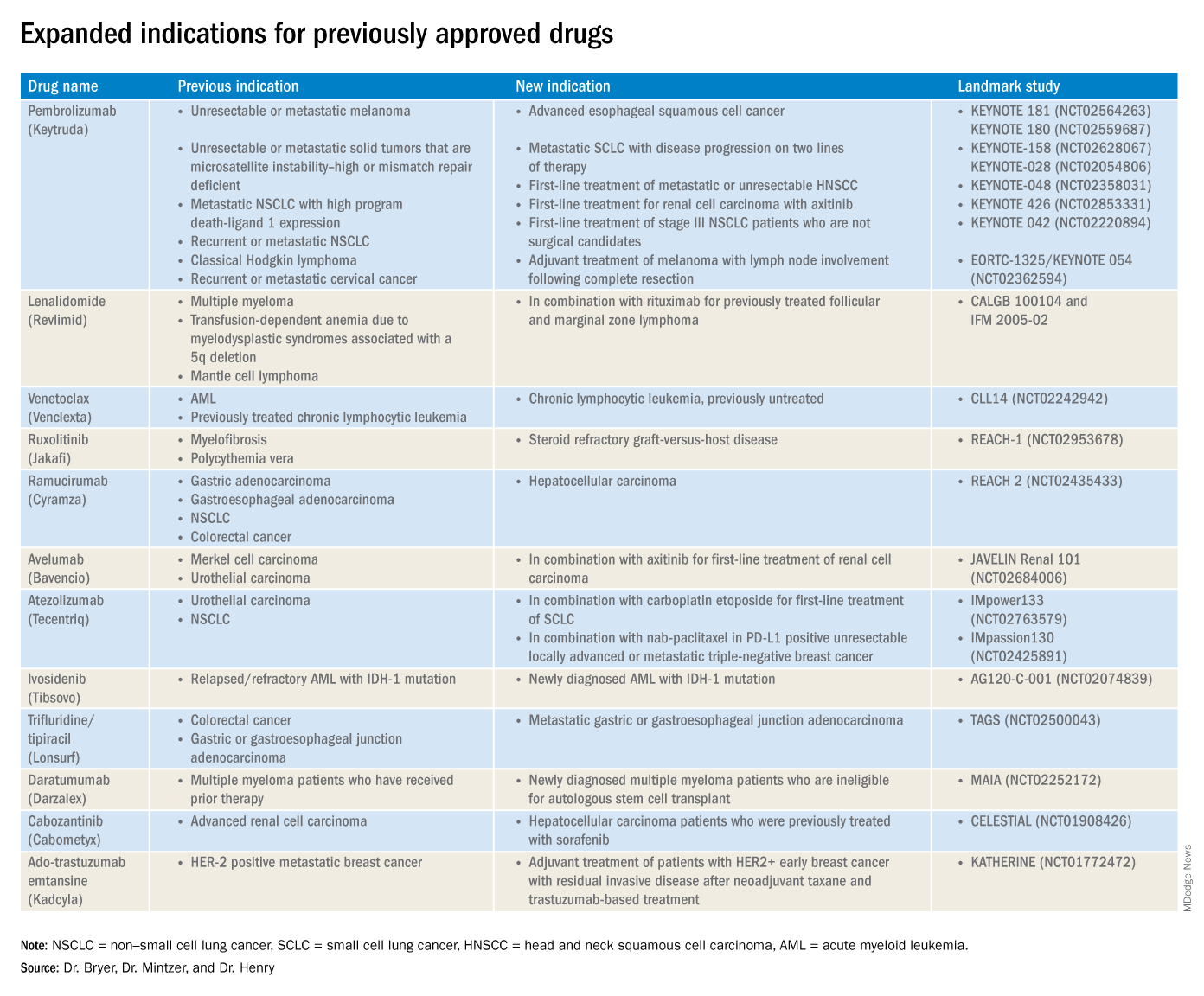
This article reviews therapies that were newly approved so far in 2019, as well as those previously approved whose indications were expanded this past year. The list highlights the most clinically important approvals, as well as adverse events that are unique or especially severe.
New approvals
Fedratinib (Inrebic)
Class: JAK2 and FLT3 selective kinase inhibitor.
Disease: Intermediate or high-risk primary or secondary (postpolycythemia vera or postessential thrombocythemia) myelofibrosis.
Dose: 400 mg orally once daily, with or without food.
Adverse events (AEs): Black box warning: Fatal encephalopathy, including Wernicke’s (thiamine level monitoring suggested).
Trials: In JAKARTA (NCT01437787), 37% of patients achieved a 35% or greater reduction in spleen volume and 40% received a 50% or greater reduction in myelofibrosis-related symptoms. In Jakarta-2, there was a 55% spleen response in patients resistant or intolerant to ruxolitinib.
Entrectinib (Rozlytrek)
Class: Tropomyosin receptor tyrosine kinase inhibitor.
Disease: Solid tumors that have a neurotrophic tyrosine receptor kinase (NTRK) gene fusion and for ROS-1 positive non–small cell lung cancer (NSCLC).
Dose: 600 mg orally once daily.
AEs: Heart failure, QT prolongation, skeletal fractures, hepatotoxicity, central nervous system effects, and hyperuricemia.
Trial: ALKA, STARTRK-1 (NCT02097810) and STARTRK-2 (NCT02568267): Overall response rate of 57% for NTRK positive patients; response rate of 77% in ROS-1 positive NSCLC.
Pexidartinib (Turalio)
Class: Small molecule tyrosine kinase inhibitor targeting CSF1R.
Disease: Symptomatic tenosynovial giant cell tumor.
Dose: 400 mg orally twice daily without food.
AEs: Black box warning on hepatotoxicity.
Trial: ENLIVEN (NCT02371369): Overall response rate of 38% at 25 weeks, with a 15% complete response rate and a 23% partial response rate.
Darolutamide (Nubeqa)
Class: Androgen receptor inhibitor.
Disease: Nonmetastatic castration-resistant prostate cancer.
Dose: 600 mg orally twice daily with food with concomitant androgen deprivation therapy.
AEs: Fatigue, extremity pain, and rash.
Trial: ARAMIS (NCT02200614): Median metastasis free survival was 40.4 months for patients with darolutamide, compared with 18.4 months for controls.
Selinexor (Xpovio)
Class: Reversible inhibitor of nuclear export of tumor suppressor proteins, growth regulators, and mRNAs of oncogenic proteins.
Disease: Relapsed or refractory multiple myeloma. Indicated for patients who have received at least four prior therapies, including at least two immunomodulatory agents and an anti-CD38 monoclonal antibody.
Dose: 80 mg orally in combination with oral dexamethasone on days 1 and 3 of each week.
AEs: Thrombocytopenia, fatigue, pancytopenia, and hyponatremia.
Trial: STORM (NCT02336815): Overall response rate 25.3% with a median time to first response of 4 weeks and 3.8-month median duration of response.
Polatuzumab vedotin-piiq (Polivy)
Class: CD79b-directed antibody-drug conjugate.
Disease: Relapsed or refractory diffuse large B-cell lymphoma. Indicated for patients who have had at least two prior therapies.
Dose: 1.8 mg/kg intravenous infusion every 21 days for six cycles in combination with bendamustine and a rituximab product.
AEs: Pancytopenia, peripheral neuropathy.
Trial: GO29365 (NCT02257567): Complete response rate was 40% for polatuzumab vedotin-piiq plus bendamustine/rituximab, compared with 18% with bendamustine/rituximab alone.*
Caplacizumab-yhdp (Cablivi)
Class: Monoclonal antibody fragment directed against von Willebrand factor.
Disease: Thrombotic thrombocytopenic purpura.
Dose: 11 mg IV initially, then daily subcutaneously; in combination with plasma exchange and immunosuppressive therapy.
AEs: Epistaxis, headache, and gingival bleeding.
Trial: Hercules trial (NCT02553317): More rapid normalization of platelets, lower incidence of composite TTP-related death, and lower rate of recurrence when added to plasma exchange and steroids.
Alpelisib (Piqray)
Class: Phosphatidylinositol-3-kinase (PI3K) inhibitor.
Disease: Hormone receptor positive HER2-negative PIK3CA-mutated, advanced or metastatic breast cancer.
Dose: 300 mg orally once daily with food with concomitant fulvestrant.
AEs: Hyperglycemia, pancytopenia.
Trial: SOLAR-1 (NCT02437318): 11-month progression-free survival among patients treated with alpelisib and fulvestrant, compared with 5.7 months in fulvestrant alone control arm; overall response rate of 36% versus 16%, respectively.
Erdafitinib (Balversa)
Class: Fibroblast growth factor receptor kinase inhibitor.
Disease: Locally advanced or metastatic urothelial carcinoma with FGFR3 or FGFR2 mutations.
Dose: 8 mg orally once daily, with or without food.
AEs: Ocular disorders including retinopathy or retinal detachment.
Trial: BLC2001 (NCT02365597): Objective response rate of 32.2%, with a complete response in 2.3% of patients and partial response in 29.9% of patients.
Biosimilar approvals
Trastuzumab and hyaluronidase-oysk (Herceptin Hylecta)
Biosimilar to: Trastuzumab.
Indication: HER2-overexpressing breast cancer.
Dr. Bryer is a resident in the department of internal medicine at the University of Pennsylvania, Philadelphia. Dr. Mintzer is chief of hematology-oncology at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania. Dr. Henry is a hematologist-oncologist at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania.
*Correction, 11/7/2019: An earlier version of this article misstated the drug combination in the GO29365 trial.
The rapid development and identification of novel drugs has translated into innovative therapies in hematology and oncology. The aim of this piece is to present newly approved drugs and expanded indications to serve as a reference guide for practicing clinicians.
This article reviews therapies that were newly approved so far in 2019, as well as those previously approved whose indications were expanded this past year. The list highlights the most clinically important approvals, as well as adverse events that are unique or especially severe.
New approvals
Fedratinib (Inrebic)
Class: JAK2 and FLT3 selective kinase inhibitor.
Disease: Intermediate or high-risk primary or secondary (postpolycythemia vera or postessential thrombocythemia) myelofibrosis.
Dose: 400 mg orally once daily, with or without food.
Adverse events (AEs): Black box warning: Fatal encephalopathy, including Wernicke’s (thiamine level monitoring suggested).
Trials: In JAKARTA (NCT01437787), 37% of patients achieved a 35% or greater reduction in spleen volume and 40% received a 50% or greater reduction in myelofibrosis-related symptoms. In Jakarta-2, there was a 55% spleen response in patients resistant or intolerant to ruxolitinib.
Entrectinib (Rozlytrek)
Class: Tropomyosin receptor tyrosine kinase inhibitor.
Disease: Solid tumors that have a neurotrophic tyrosine receptor kinase (NTRK) gene fusion and for ROS-1 positive non–small cell lung cancer (NSCLC).
Dose: 600 mg orally once daily.
AEs: Heart failure, QT prolongation, skeletal fractures, hepatotoxicity, central nervous system effects, and hyperuricemia.
Trial: ALKA, STARTRK-1 (NCT02097810) and STARTRK-2 (NCT02568267): Overall response rate of 57% for NTRK positive patients; response rate of 77% in ROS-1 positive NSCLC.
Pexidartinib (Turalio)
Class: Small molecule tyrosine kinase inhibitor targeting CSF1R.
Disease: Symptomatic tenosynovial giant cell tumor.
Dose: 400 mg orally twice daily without food.
AEs: Black box warning on hepatotoxicity.
Trial: ENLIVEN (NCT02371369): Overall response rate of 38% at 25 weeks, with a 15% complete response rate and a 23% partial response rate.
Darolutamide (Nubeqa)
Class: Androgen receptor inhibitor.
Disease: Nonmetastatic castration-resistant prostate cancer.
Dose: 600 mg orally twice daily with food with concomitant androgen deprivation therapy.
AEs: Fatigue, extremity pain, and rash.
Trial: ARAMIS (NCT02200614): Median metastasis free survival was 40.4 months for patients with darolutamide, compared with 18.4 months for controls.
Selinexor (Xpovio)
Class: Reversible inhibitor of nuclear export of tumor suppressor proteins, growth regulators, and mRNAs of oncogenic proteins.
Disease: Relapsed or refractory multiple myeloma. Indicated for patients who have received at least four prior therapies, including at least two immunomodulatory agents and an anti-CD38 monoclonal antibody.
Dose: 80 mg orally in combination with oral dexamethasone on days 1 and 3 of each week.
AEs: Thrombocytopenia, fatigue, pancytopenia, and hyponatremia.
Trial: STORM (NCT02336815): Overall response rate 25.3% with a median time to first response of 4 weeks and 3.8-month median duration of response.
Polatuzumab vedotin-piiq (Polivy)
Class: CD79b-directed antibody-drug conjugate.
Disease: Relapsed or refractory diffuse large B-cell lymphoma. Indicated for patients who have had at least two prior therapies.
Dose: 1.8 mg/kg intravenous infusion every 21 days for six cycles in combination with bendamustine and a rituximab product.
AEs: Pancytopenia, peripheral neuropathy.
Trial: GO29365 (NCT02257567): Complete response rate was 40% for polatuzumab vedotin-piiq plus bendamustine/rituximab, compared with 18% with bendamustine/rituximab alone.*
Caplacizumab-yhdp (Cablivi)
Class: Monoclonal antibody fragment directed against von Willebrand factor.
Disease: Thrombotic thrombocytopenic purpura.
Dose: 11 mg IV initially, then daily subcutaneously; in combination with plasma exchange and immunosuppressive therapy.
AEs: Epistaxis, headache, and gingival bleeding.
Trial: Hercules trial (NCT02553317): More rapid normalization of platelets, lower incidence of composite TTP-related death, and lower rate of recurrence when added to plasma exchange and steroids.
Alpelisib (Piqray)
Class: Phosphatidylinositol-3-kinase (PI3K) inhibitor.
Disease: Hormone receptor positive HER2-negative PIK3CA-mutated, advanced or metastatic breast cancer.
Dose: 300 mg orally once daily with food with concomitant fulvestrant.
AEs: Hyperglycemia, pancytopenia.
Trial: SOLAR-1 (NCT02437318): 11-month progression-free survival among patients treated with alpelisib and fulvestrant, compared with 5.7 months in fulvestrant alone control arm; overall response rate of 36% versus 16%, respectively.
Erdafitinib (Balversa)
Class: Fibroblast growth factor receptor kinase inhibitor.
Disease: Locally advanced or metastatic urothelial carcinoma with FGFR3 or FGFR2 mutations.
Dose: 8 mg orally once daily, with or without food.
AEs: Ocular disorders including retinopathy or retinal detachment.
Trial: BLC2001 (NCT02365597): Objective response rate of 32.2%, with a complete response in 2.3% of patients and partial response in 29.9% of patients.
Biosimilar approvals
Trastuzumab and hyaluronidase-oysk (Herceptin Hylecta)
Biosimilar to: Trastuzumab.
Indication: HER2-overexpressing breast cancer.
Dr. Bryer is a resident in the department of internal medicine at the University of Pennsylvania, Philadelphia. Dr. Mintzer is chief of hematology-oncology at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania. Dr. Henry is a hematologist-oncologist at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania.
*Correction, 11/7/2019: An earlier version of this article misstated the drug combination in the GO29365 trial.
The rapid development and identification of novel drugs has translated into innovative therapies in hematology and oncology. The aim of this piece is to present newly approved drugs and expanded indications to serve as a reference guide for practicing clinicians.
This article reviews therapies that were newly approved so far in 2019, as well as those previously approved whose indications were expanded this past year. The list highlights the most clinically important approvals, as well as adverse events that are unique or especially severe.
New approvals
Fedratinib (Inrebic)
Class: JAK2 and FLT3 selective kinase inhibitor.
Disease: Intermediate or high-risk primary or secondary (postpolycythemia vera or postessential thrombocythemia) myelofibrosis.
Dose: 400 mg orally once daily, with or without food.
Adverse events (AEs): Black box warning: Fatal encephalopathy, including Wernicke’s (thiamine level monitoring suggested).
Trials: In JAKARTA (NCT01437787), 37% of patients achieved a 35% or greater reduction in spleen volume and 40% received a 50% or greater reduction in myelofibrosis-related symptoms. In Jakarta-2, there was a 55% spleen response in patients resistant or intolerant to ruxolitinib.
Entrectinib (Rozlytrek)
Class: Tropomyosin receptor tyrosine kinase inhibitor.
Disease: Solid tumors that have a neurotrophic tyrosine receptor kinase (NTRK) gene fusion and for ROS-1 positive non–small cell lung cancer (NSCLC).
Dose: 600 mg orally once daily.
AEs: Heart failure, QT prolongation, skeletal fractures, hepatotoxicity, central nervous system effects, and hyperuricemia.
Trial: ALKA, STARTRK-1 (NCT02097810) and STARTRK-2 (NCT02568267): Overall response rate of 57% for NTRK positive patients; response rate of 77% in ROS-1 positive NSCLC.
Pexidartinib (Turalio)
Class: Small molecule tyrosine kinase inhibitor targeting CSF1R.
Disease: Symptomatic tenosynovial giant cell tumor.
Dose: 400 mg orally twice daily without food.
AEs: Black box warning on hepatotoxicity.
Trial: ENLIVEN (NCT02371369): Overall response rate of 38% at 25 weeks, with a 15% complete response rate and a 23% partial response rate.
Darolutamide (Nubeqa)
Class: Androgen receptor inhibitor.
Disease: Nonmetastatic castration-resistant prostate cancer.
Dose: 600 mg orally twice daily with food with concomitant androgen deprivation therapy.
AEs: Fatigue, extremity pain, and rash.
Trial: ARAMIS (NCT02200614): Median metastasis free survival was 40.4 months for patients with darolutamide, compared with 18.4 months for controls.
Selinexor (Xpovio)
Class: Reversible inhibitor of nuclear export of tumor suppressor proteins, growth regulators, and mRNAs of oncogenic proteins.
Disease: Relapsed or refractory multiple myeloma. Indicated for patients who have received at least four prior therapies, including at least two immunomodulatory agents and an anti-CD38 monoclonal antibody.
Dose: 80 mg orally in combination with oral dexamethasone on days 1 and 3 of each week.
AEs: Thrombocytopenia, fatigue, pancytopenia, and hyponatremia.
Trial: STORM (NCT02336815): Overall response rate 25.3% with a median time to first response of 4 weeks and 3.8-month median duration of response.
Polatuzumab vedotin-piiq (Polivy)
Class: CD79b-directed antibody-drug conjugate.
Disease: Relapsed or refractory diffuse large B-cell lymphoma. Indicated for patients who have had at least two prior therapies.
Dose: 1.8 mg/kg intravenous infusion every 21 days for six cycles in combination with bendamustine and a rituximab product.
AEs: Pancytopenia, peripheral neuropathy.
Trial: GO29365 (NCT02257567): Complete response rate was 40% for polatuzumab vedotin-piiq plus bendamustine/rituximab, compared with 18% with bendamustine/rituximab alone.*
Caplacizumab-yhdp (Cablivi)
Class: Monoclonal antibody fragment directed against von Willebrand factor.
Disease: Thrombotic thrombocytopenic purpura.
Dose: 11 mg IV initially, then daily subcutaneously; in combination with plasma exchange and immunosuppressive therapy.
AEs: Epistaxis, headache, and gingival bleeding.
Trial: Hercules trial (NCT02553317): More rapid normalization of platelets, lower incidence of composite TTP-related death, and lower rate of recurrence when added to plasma exchange and steroids.
Alpelisib (Piqray)
Class: Phosphatidylinositol-3-kinase (PI3K) inhibitor.
Disease: Hormone receptor positive HER2-negative PIK3CA-mutated, advanced or metastatic breast cancer.
Dose: 300 mg orally once daily with food with concomitant fulvestrant.
AEs: Hyperglycemia, pancytopenia.
Trial: SOLAR-1 (NCT02437318): 11-month progression-free survival among patients treated with alpelisib and fulvestrant, compared with 5.7 months in fulvestrant alone control arm; overall response rate of 36% versus 16%, respectively.
Erdafitinib (Balversa)
Class: Fibroblast growth factor receptor kinase inhibitor.
Disease: Locally advanced or metastatic urothelial carcinoma with FGFR3 or FGFR2 mutations.
Dose: 8 mg orally once daily, with or without food.
AEs: Ocular disorders including retinopathy or retinal detachment.
Trial: BLC2001 (NCT02365597): Objective response rate of 32.2%, with a complete response in 2.3% of patients and partial response in 29.9% of patients.
Biosimilar approvals
Trastuzumab and hyaluronidase-oysk (Herceptin Hylecta)
Biosimilar to: Trastuzumab.
Indication: HER2-overexpressing breast cancer.
Dr. Bryer is a resident in the department of internal medicine at the University of Pennsylvania, Philadelphia. Dr. Mintzer is chief of hematology-oncology at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania. Dr. Henry is a hematologist-oncologist at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania.
*Correction, 11/7/2019: An earlier version of this article misstated the drug combination in the GO29365 trial.
FDA advisory committee supports birth control patch approval

Most of the committee members based their decisions on the need for additional contraceptive options for patients. However, most also expressed concerns about its efficacy and offered suggestions for product labeling that called attention to high rates of unintended pregnancies and increased risk of venous thromboembolism (VTE) in obese women.
The agency’s Bone, Reproductive and Urologic Drugs Advisory Committee reviewed safety and efficacy data for AG200-15, a combined hormonal contraceptive patch developed by Agile Therapeutics. The treatment regimen involves application of a patch to the abdomen, buttock, or upper torso, and the patch is changed weekly for 3 weeks, followed by 1 week without a patch.
Elizabeth Garner, MD, consultant and former chief medical officer of Agile, presented study data on safety and effectiveness of the patch. The key study (known as Study 23) considered by the FDA included 1,736 women aged 35 years and younger. The primary efficacy endpoint was the pregnancy rate in the women who used the patch. Women reported sexual activity and back-up contraception use in e-diaries.
A total of 68 pregnancies occurred in the study population after 15,165 evaluable cycles, yielding an overall Pearl Index of 5.83 across all weight and body mass index groups. Historically, a Pearl Index of 5 has been the standard measure for effectiveness in contraceptive products, with lower being better. The index is defined as the number of pregnancies per 100 woman-years of product use. For example, a Pearl Index of 0.1 means that 1 in 1,000 women who use the same contraceptive method for 1 year becomes pregnant.
A subgroup analysis showed reduced efficacy in women with a higher BMI. The Pearl Index for women with a BMI of less than 30 kg/m2 (defined as nonobese) was 4.34, whereas in women with a BMI of 30 kg/m2 and higher (defined as obese), the index was 8.64, nearly double that of nonobese women. No significant differences in the index were noted based on race/ethnicity.
The company described the patch as filling a niche and providing an additional alternative for women seeking a noninvasive method of contraception. It proposed a limitation of use (LOU) as part of the product label that would provide detailed information on efficacy based on the Pearl Index for the different categories of BMI and would suggest that the patch may be less effective for women with obesity. Most of the committee members favored use of a LOU statement on the label, but some noted that it might limit prescriptions to nonobese women.
The committee expressed concern over the Pearl data in the study. The FDA has never approved a contraceptive product with a Pearl Index of greater than 5, said Yun Tang, PhD, a statistical reviewer for the agency’s Office of Translational Sciences, who presented the evaluation of the effectiveness of AG200-15.
Key safety concerns raised in discussion included the risk of venous thromboembolism and the risk of unscheduled bleeding. Both of those issues were significantly more common among obese women, said Nneka McNeal-Jackson, MD, clinical reviewer for the FDA, who presented details on the safety profile and risk-benefit considerations for the patch.
Overall, in Study 23, the incidence rate of VTE was 28/10,000 women-years, with cases in five participants. Four of those were deemed related to the patch, and all occurred in obese women.
Virginia C. “Jennie” Leslie, MD, of Oregon Health and Science University, Portland, voted no to recommending approval of the patch mainly because of efficacy concerns. “My goal is to do no harm, and I have concerns regarding efficacy and giving our patients a false sense of hope,” she said.
Even those members who voted yes expressed concerns about the efficacy data and VTE risk in obese women and recommended postmarketing studies and appropriate labeling to help clinicians in shared decision making with their patients.
Esther Eisenberg, MD, of the National Institutes of Health, noted that the patch fills a need, certainly for women with a BMI less than 30 kg/m2, and suggested that use be limited to women in that lower BMI category.
Other committee members suggested that the product not be restricted based on BMI, but rather that the LOU provide clear explanations of how effectiveness decreases as BMI increases.
David J. Margolis, MD, of the University of Pennsylvania, Philadelphia, opted to abstain from voting, in part based on concerns about the study design and a lack of additional data from the company.
Most of the committee members based their decisions on the need for additional contraceptive options for patients. However, most also expressed concerns about its efficacy and offered suggestions for product labeling that called attention to high rates of unintended pregnancies and increased risk of venous thromboembolism (VTE) in obese women.
The agency’s Bone, Reproductive and Urologic Drugs Advisory Committee reviewed safety and efficacy data for AG200-15, a combined hormonal contraceptive patch developed by Agile Therapeutics. The treatment regimen involves application of a patch to the abdomen, buttock, or upper torso, and the patch is changed weekly for 3 weeks, followed by 1 week without a patch.
Elizabeth Garner, MD, consultant and former chief medical officer of Agile, presented study data on safety and effectiveness of the patch. The key study (known as Study 23) considered by the FDA included 1,736 women aged 35 years and younger. The primary efficacy endpoint was the pregnancy rate in the women who used the patch. Women reported sexual activity and back-up contraception use in e-diaries.
A total of 68 pregnancies occurred in the study population after 15,165 evaluable cycles, yielding an overall Pearl Index of 5.83 across all weight and body mass index groups. Historically, a Pearl Index of 5 has been the standard measure for effectiveness in contraceptive products, with lower being better. The index is defined as the number of pregnancies per 100 woman-years of product use. For example, a Pearl Index of 0.1 means that 1 in 1,000 women who use the same contraceptive method for 1 year becomes pregnant.
A subgroup analysis showed reduced efficacy in women with a higher BMI. The Pearl Index for women with a BMI of less than 30 kg/m2 (defined as nonobese) was 4.34, whereas in women with a BMI of 30 kg/m2 and higher (defined as obese), the index was 8.64, nearly double that of nonobese women. No significant differences in the index were noted based on race/ethnicity.
The company described the patch as filling a niche and providing an additional alternative for women seeking a noninvasive method of contraception. It proposed a limitation of use (LOU) as part of the product label that would provide detailed information on efficacy based on the Pearl Index for the different categories of BMI and would suggest that the patch may be less effective for women with obesity. Most of the committee members favored use of a LOU statement on the label, but some noted that it might limit prescriptions to nonobese women.
The committee expressed concern over the Pearl data in the study. The FDA has never approved a contraceptive product with a Pearl Index of greater than 5, said Yun Tang, PhD, a statistical reviewer for the agency’s Office of Translational Sciences, who presented the evaluation of the effectiveness of AG200-15.
Key safety concerns raised in discussion included the risk of venous thromboembolism and the risk of unscheduled bleeding. Both of those issues were significantly more common among obese women, said Nneka McNeal-Jackson, MD, clinical reviewer for the FDA, who presented details on the safety profile and risk-benefit considerations for the patch.
Overall, in Study 23, the incidence rate of VTE was 28/10,000 women-years, with cases in five participants. Four of those were deemed related to the patch, and all occurred in obese women.
Virginia C. “Jennie” Leslie, MD, of Oregon Health and Science University, Portland, voted no to recommending approval of the patch mainly because of efficacy concerns. “My goal is to do no harm, and I have concerns regarding efficacy and giving our patients a false sense of hope,” she said.
Even those members who voted yes expressed concerns about the efficacy data and VTE risk in obese women and recommended postmarketing studies and appropriate labeling to help clinicians in shared decision making with their patients.
Esther Eisenberg, MD, of the National Institutes of Health, noted that the patch fills a need, certainly for women with a BMI less than 30 kg/m2, and suggested that use be limited to women in that lower BMI category.
Other committee members suggested that the product not be restricted based on BMI, but rather that the LOU provide clear explanations of how effectiveness decreases as BMI increases.
David J. Margolis, MD, of the University of Pennsylvania, Philadelphia, opted to abstain from voting, in part based on concerns about the study design and a lack of additional data from the company.
Most of the committee members based their decisions on the need for additional contraceptive options for patients. However, most also expressed concerns about its efficacy and offered suggestions for product labeling that called attention to high rates of unintended pregnancies and increased risk of venous thromboembolism (VTE) in obese women.
The agency’s Bone, Reproductive and Urologic Drugs Advisory Committee reviewed safety and efficacy data for AG200-15, a combined hormonal contraceptive patch developed by Agile Therapeutics. The treatment regimen involves application of a patch to the abdomen, buttock, or upper torso, and the patch is changed weekly for 3 weeks, followed by 1 week without a patch.
Elizabeth Garner, MD, consultant and former chief medical officer of Agile, presented study data on safety and effectiveness of the patch. The key study (known as Study 23) considered by the FDA included 1,736 women aged 35 years and younger. The primary efficacy endpoint was the pregnancy rate in the women who used the patch. Women reported sexual activity and back-up contraception use in e-diaries.
A total of 68 pregnancies occurred in the study population after 15,165 evaluable cycles, yielding an overall Pearl Index of 5.83 across all weight and body mass index groups. Historically, a Pearl Index of 5 has been the standard measure for effectiveness in contraceptive products, with lower being better. The index is defined as the number of pregnancies per 100 woman-years of product use. For example, a Pearl Index of 0.1 means that 1 in 1,000 women who use the same contraceptive method for 1 year becomes pregnant.
A subgroup analysis showed reduced efficacy in women with a higher BMI. The Pearl Index for women with a BMI of less than 30 kg/m2 (defined as nonobese) was 4.34, whereas in women with a BMI of 30 kg/m2 and higher (defined as obese), the index was 8.64, nearly double that of nonobese women. No significant differences in the index were noted based on race/ethnicity.
The company described the patch as filling a niche and providing an additional alternative for women seeking a noninvasive method of contraception. It proposed a limitation of use (LOU) as part of the product label that would provide detailed information on efficacy based on the Pearl Index for the different categories of BMI and would suggest that the patch may be less effective for women with obesity. Most of the committee members favored use of a LOU statement on the label, but some noted that it might limit prescriptions to nonobese women.
The committee expressed concern over the Pearl data in the study. The FDA has never approved a contraceptive product with a Pearl Index of greater than 5, said Yun Tang, PhD, a statistical reviewer for the agency’s Office of Translational Sciences, who presented the evaluation of the effectiveness of AG200-15.
Key safety concerns raised in discussion included the risk of venous thromboembolism and the risk of unscheduled bleeding. Both of those issues were significantly more common among obese women, said Nneka McNeal-Jackson, MD, clinical reviewer for the FDA, who presented details on the safety profile and risk-benefit considerations for the patch.
Overall, in Study 23, the incidence rate of VTE was 28/10,000 women-years, with cases in five participants. Four of those were deemed related to the patch, and all occurred in obese women.
Virginia C. “Jennie” Leslie, MD, of Oregon Health and Science University, Portland, voted no to recommending approval of the patch mainly because of efficacy concerns. “My goal is to do no harm, and I have concerns regarding efficacy and giving our patients a false sense of hope,” she said.
Even those members who voted yes expressed concerns about the efficacy data and VTE risk in obese women and recommended postmarketing studies and appropriate labeling to help clinicians in shared decision making with their patients.
Esther Eisenberg, MD, of the National Institutes of Health, noted that the patch fills a need, certainly for women with a BMI less than 30 kg/m2, and suggested that use be limited to women in that lower BMI category.
Other committee members suggested that the product not be restricted based on BMI, but rather that the LOU provide clear explanations of how effectiveness decreases as BMI increases.
David J. Margolis, MD, of the University of Pennsylvania, Philadelphia, opted to abstain from voting, in part based on concerns about the study design and a lack of additional data from the company.
FROM THE FDA
EHR prompt significantly reduced telemetry monitoring during inpatient stays
Background: Prior studies have shown multifaceted interventions that include EHR prompts can reduce the utilization of telemetry monitoring, but it is unclear if EHR prompts alone can reduce utilization.

Study design: Cluster-randomized, control trial.
Setting: November 2016 and May 2017 at a tertiary care medical center on the general medicine service.
Synopsis: The authors designed an EHR prompt for patients ordered for telemetry. The prompt would request the team to either discontinue or continue telemetry. Half of the general medicine teams (representing 499 hospitalizations) were randomized to receive the intervention, and the other half of the general medicine teams (representing 567 hospitalizations) did not receive the intervention. In the intervention group, 62% of prompts were followed by a discontinuation of telemetry. This led to a 17% reduction in the mean hours of telemetry monitoring (50 hours in the control group and 41.3 hours in the intervention group; P = .001). There was no significant difference in the rate of rapid responses or medical emergencies between the two groups.
Bottom line: A targeted EHR prompt alone may lead to a reduction in the utilization of telemetry monitoring.
Citation: Najafi N et al. Assessment of a targeted electronic health record intervention to reduce telemetry duration: A cluster-randomized clinical trial. JAMA Intern Med. 2019 Dec 10;179(1):11-5.
Dr. Biddick is a hospitalist at Beth Israel Deaconess Medical Center and instructor in medicine Harvard Medical School.
Background: Prior studies have shown multifaceted interventions that include EHR prompts can reduce the utilization of telemetry monitoring, but it is unclear if EHR prompts alone can reduce utilization.
Study design: Cluster-randomized, control trial.
Setting: November 2016 and May 2017 at a tertiary care medical center on the general medicine service.
Synopsis: The authors designed an EHR prompt for patients ordered for telemetry. The prompt would request the team to either discontinue or continue telemetry. Half of the general medicine teams (representing 499 hospitalizations) were randomized to receive the intervention, and the other half of the general medicine teams (representing 567 hospitalizations) did not receive the intervention. In the intervention group, 62% of prompts were followed by a discontinuation of telemetry. This led to a 17% reduction in the mean hours of telemetry monitoring (50 hours in the control group and 41.3 hours in the intervention group; P = .001). There was no significant difference in the rate of rapid responses or medical emergencies between the two groups.
Bottom line: A targeted EHR prompt alone may lead to a reduction in the utilization of telemetry monitoring.
Citation: Najafi N et al. Assessment of a targeted electronic health record intervention to reduce telemetry duration: A cluster-randomized clinical trial. JAMA Intern Med. 2019 Dec 10;179(1):11-5.
Dr. Biddick is a hospitalist at Beth Israel Deaconess Medical Center and instructor in medicine Harvard Medical School.
Background: Prior studies have shown multifaceted interventions that include EHR prompts can reduce the utilization of telemetry monitoring, but it is unclear if EHR prompts alone can reduce utilization.
Study design: Cluster-randomized, control trial.
Setting: November 2016 and May 2017 at a tertiary care medical center on the general medicine service.
Synopsis: The authors designed an EHR prompt for patients ordered for telemetry. The prompt would request the team to either discontinue or continue telemetry. Half of the general medicine teams (representing 499 hospitalizations) were randomized to receive the intervention, and the other half of the general medicine teams (representing 567 hospitalizations) did not receive the intervention. In the intervention group, 62% of prompts were followed by a discontinuation of telemetry. This led to a 17% reduction in the mean hours of telemetry monitoring (50 hours in the control group and 41.3 hours in the intervention group; P = .001). There was no significant difference in the rate of rapid responses or medical emergencies between the two groups.
Bottom line: A targeted EHR prompt alone may lead to a reduction in the utilization of telemetry monitoring.
Citation: Najafi N et al. Assessment of a targeted electronic health record intervention to reduce telemetry duration: A cluster-randomized clinical trial. JAMA Intern Med. 2019 Dec 10;179(1):11-5.
Dr. Biddick is a hospitalist at Beth Israel Deaconess Medical Center and instructor in medicine Harvard Medical School.
Quick Byte: DeepMind emerges
The science of prediction
Hundreds of scientists around the world enter a competition every 2 years called the Critical Assessment of Structure Prediction.
“Tackling a biological puzzle they call ‘the protein folding problem,’ they try to predict the three-dimensional shape of proteins in the human body. No one knows how to solve the problem. Even the winners only chip away at it. But a solution could streamline the way scientists create new medicines and fight disease,” according to a report in the New York Times.
In 2019, those scientists did not win the contest. “It was won by DeepMind, the artificial intelligence lab owned by Google’s parent company. DeepMind specializes in ‘deep learning,’ a type of artificial intelligence that is rapidly changing drug discovery science.”
Reference
1. Metz C. “Making New Drugs With a Dose of Artificial Intelligence,” New York Times. Feb. 5, 2019. https://www.nytimes.com/2019/02/05/technology/artificial-intelligence-drug-research-deepmind.html. Accessed Feb 7, 2019.
The science of prediction
The science of prediction
Hundreds of scientists around the world enter a competition every 2 years called the Critical Assessment of Structure Prediction.
“Tackling a biological puzzle they call ‘the protein folding problem,’ they try to predict the three-dimensional shape of proteins in the human body. No one knows how to solve the problem. Even the winners only chip away at it. But a solution could streamline the way scientists create new medicines and fight disease,” according to a report in the New York Times.
In 2019, those scientists did not win the contest. “It was won by DeepMind, the artificial intelligence lab owned by Google’s parent company. DeepMind specializes in ‘deep learning,’ a type of artificial intelligence that is rapidly changing drug discovery science.”
Reference
1. Metz C. “Making New Drugs With a Dose of Artificial Intelligence,” New York Times. Feb. 5, 2019. https://www.nytimes.com/2019/02/05/technology/artificial-intelligence-drug-research-deepmind.html. Accessed Feb 7, 2019.
Hundreds of scientists around the world enter a competition every 2 years called the Critical Assessment of Structure Prediction.
“Tackling a biological puzzle they call ‘the protein folding problem,’ they try to predict the three-dimensional shape of proteins in the human body. No one knows how to solve the problem. Even the winners only chip away at it. But a solution could streamline the way scientists create new medicines and fight disease,” according to a report in the New York Times.
In 2019, those scientists did not win the contest. “It was won by DeepMind, the artificial intelligence lab owned by Google’s parent company. DeepMind specializes in ‘deep learning,’ a type of artificial intelligence that is rapidly changing drug discovery science.”
Reference
1. Metz C. “Making New Drugs With a Dose of Artificial Intelligence,” New York Times. Feb. 5, 2019. https://www.nytimes.com/2019/02/05/technology/artificial-intelligence-drug-research-deepmind.html. Accessed Feb 7, 2019.
Thousands of Emergency-Care Claims Were Denied; Court Rules VA Must Reimburse
When veterans receive emergency care at non-VA facilities, they can file for reimbursement of non-VA emergency care costs. If the claims are denied or rejected, non-VA facilities and providers can bill the veterans for some or all of the costs.
A stunning VA Office of Inspector General (OIG) report issued in August revealed that the VA had wrongfully rejected thousands of those emergency-care claims between April 1, 2017 and September 30, 2017. The OIG report said VA supervisors had pressured staff to quickly decide claims and even deny claims to maximize productivity. That culture of “speed over accuracy” led to 31% of claims being “inappropriately processed.”
Under regulations, when a claim is denied it is because there is no basis for payment, but a claim may also be rejected, meaning it cannot be decided until the claimant provides additional or corrected information. When the Claims Adjudication and Reimbursement Directorate (CAR) in the VA Office of Community Care (OCC) denies a claim, the claimant may have to pay out of pocket for emergency care.
The billed amount of inappropriately processed claims in those 5 months that were denied or rejected was “large in the aggregate,” the report said: an estimated $716 million, presenting potential undue financial risk to an estimated 60,800 veterans. The OIG estimated that about 17,400 veterans, with bills of at least $53.3 million, were negatively affected during the audit period. If corrective actions are not taken, the OIG estimates that the errors could result in $533 million in improper underpayments over 5 years.
The OIG audit was initiated after then Representative Tim Walz (D-MN) raised the concern in September 2017 about claims processors denying non-VA claims not only to meet production goals, but also to receive incentives such as high-performance ratings, bonuses, and telework privileges. The OIG audit also found that examiners who did not consistently meet the production numbers were not considered for overtime and had their telework privileges removed.
Other processing errors were also significant, the report says. For example, claimants did not receive complete and accurate information regarding why their claims were denied or rejected. Those errors created a risk that claimants could not effectively respond with information to get their claims approved.
The pressure to approve or deny claims quickly stemmed from a backlog of claims > 30 days old, which OCC and CAR leaders tried to reduce, the report says.
The OIG notes that since FY 2017 the OCC “experienced several leadership changes,” including 3 CAR directors. While the audit’s findings cannot be tied directly to those changes, the instability “provided the context in which problems were allowed to continue without remediation.”
In May, VHA officials reported to the audit team that they had implemented process improvements and initiatives that affect claims processing nationwide, and “the environment in which claims are processed.” Richard Stone, executive in charge of the VHA, submitted plans to comply with the IG’s 11 recommendations, which included tying incentives to all performance standards rather than just production quantity.
The US Court of Appeals for Veterans Claims recently ruled that the VA must reimburse veterans for emergency medical care at non-VA facilities—potentially between $1.8 billion and $6.5 billion in reimbursements for veterans who have filed or will file claims between 2016 and 2025. The court also struck down an internal VA regulation that blocked such payments. In 2015, the court had struck down a previous version of the internal regulation that refused coverage for an emergency claim when another form of insurance covered even a small part of the bill. The court said that regulation violated a 2010 federal law. In last month’s ruling, the court found the department had violated the same federal law with its revision of the reimbursement regulation, issued in 2018. The new rule, the panel said, created a new obstacle for veterans.
When veterans receive emergency care at non-VA facilities, they can file for reimbursement of non-VA emergency care costs. If the claims are denied or rejected, non-VA facilities and providers can bill the veterans for some or all of the costs.
A stunning VA Office of Inspector General (OIG) report issued in August revealed that the VA had wrongfully rejected thousands of those emergency-care claims between April 1, 2017 and September 30, 2017. The OIG report said VA supervisors had pressured staff to quickly decide claims and even deny claims to maximize productivity. That culture of “speed over accuracy” led to 31% of claims being “inappropriately processed.”
Under regulations, when a claim is denied it is because there is no basis for payment, but a claim may also be rejected, meaning it cannot be decided until the claimant provides additional or corrected information. When the Claims Adjudication and Reimbursement Directorate (CAR) in the VA Office of Community Care (OCC) denies a claim, the claimant may have to pay out of pocket for emergency care.
The billed amount of inappropriately processed claims in those 5 months that were denied or rejected was “large in the aggregate,” the report said: an estimated $716 million, presenting potential undue financial risk to an estimated 60,800 veterans. The OIG estimated that about 17,400 veterans, with bills of at least $53.3 million, were negatively affected during the audit period. If corrective actions are not taken, the OIG estimates that the errors could result in $533 million in improper underpayments over 5 years.
The OIG audit was initiated after then Representative Tim Walz (D-MN) raised the concern in September 2017 about claims processors denying non-VA claims not only to meet production goals, but also to receive incentives such as high-performance ratings, bonuses, and telework privileges. The OIG audit also found that examiners who did not consistently meet the production numbers were not considered for overtime and had their telework privileges removed.
Other processing errors were also significant, the report says. For example, claimants did not receive complete and accurate information regarding why their claims were denied or rejected. Those errors created a risk that claimants could not effectively respond with information to get their claims approved.
The pressure to approve or deny claims quickly stemmed from a backlog of claims > 30 days old, which OCC and CAR leaders tried to reduce, the report says.
The OIG notes that since FY 2017 the OCC “experienced several leadership changes,” including 3 CAR directors. While the audit’s findings cannot be tied directly to those changes, the instability “provided the context in which problems were allowed to continue without remediation.”
In May, VHA officials reported to the audit team that they had implemented process improvements and initiatives that affect claims processing nationwide, and “the environment in which claims are processed.” Richard Stone, executive in charge of the VHA, submitted plans to comply with the IG’s 11 recommendations, which included tying incentives to all performance standards rather than just production quantity.
The US Court of Appeals for Veterans Claims recently ruled that the VA must reimburse veterans for emergency medical care at non-VA facilities—potentially between $1.8 billion and $6.5 billion in reimbursements for veterans who have filed or will file claims between 2016 and 2025. The court also struck down an internal VA regulation that blocked such payments. In 2015, the court had struck down a previous version of the internal regulation that refused coverage for an emergency claim when another form of insurance covered even a small part of the bill. The court said that regulation violated a 2010 federal law. In last month’s ruling, the court found the department had violated the same federal law with its revision of the reimbursement regulation, issued in 2018. The new rule, the panel said, created a new obstacle for veterans.
When veterans receive emergency care at non-VA facilities, they can file for reimbursement of non-VA emergency care costs. If the claims are denied or rejected, non-VA facilities and providers can bill the veterans for some or all of the costs.
A stunning VA Office of Inspector General (OIG) report issued in August revealed that the VA had wrongfully rejected thousands of those emergency-care claims between April 1, 2017 and September 30, 2017. The OIG report said VA supervisors had pressured staff to quickly decide claims and even deny claims to maximize productivity. That culture of “speed over accuracy” led to 31% of claims being “inappropriately processed.”
Under regulations, when a claim is denied it is because there is no basis for payment, but a claim may also be rejected, meaning it cannot be decided until the claimant provides additional or corrected information. When the Claims Adjudication and Reimbursement Directorate (CAR) in the VA Office of Community Care (OCC) denies a claim, the claimant may have to pay out of pocket for emergency care.
The billed amount of inappropriately processed claims in those 5 months that were denied or rejected was “large in the aggregate,” the report said: an estimated $716 million, presenting potential undue financial risk to an estimated 60,800 veterans. The OIG estimated that about 17,400 veterans, with bills of at least $53.3 million, were negatively affected during the audit period. If corrective actions are not taken, the OIG estimates that the errors could result in $533 million in improper underpayments over 5 years.
The OIG audit was initiated after then Representative Tim Walz (D-MN) raised the concern in September 2017 about claims processors denying non-VA claims not only to meet production goals, but also to receive incentives such as high-performance ratings, bonuses, and telework privileges. The OIG audit also found that examiners who did not consistently meet the production numbers were not considered for overtime and had their telework privileges removed.
Other processing errors were also significant, the report says. For example, claimants did not receive complete and accurate information regarding why their claims were denied or rejected. Those errors created a risk that claimants could not effectively respond with information to get their claims approved.
The pressure to approve or deny claims quickly stemmed from a backlog of claims > 30 days old, which OCC and CAR leaders tried to reduce, the report says.
The OIG notes that since FY 2017 the OCC “experienced several leadership changes,” including 3 CAR directors. While the audit’s findings cannot be tied directly to those changes, the instability “provided the context in which problems were allowed to continue without remediation.”
In May, VHA officials reported to the audit team that they had implemented process improvements and initiatives that affect claims processing nationwide, and “the environment in which claims are processed.” Richard Stone, executive in charge of the VHA, submitted plans to comply with the IG’s 11 recommendations, which included tying incentives to all performance standards rather than just production quantity.
The US Court of Appeals for Veterans Claims recently ruled that the VA must reimburse veterans for emergency medical care at non-VA facilities—potentially between $1.8 billion and $6.5 billion in reimbursements for veterans who have filed or will file claims between 2016 and 2025. The court also struck down an internal VA regulation that blocked such payments. In 2015, the court had struck down a previous version of the internal regulation that refused coverage for an emergency claim when another form of insurance covered even a small part of the bill. The court said that regulation violated a 2010 federal law. In last month’s ruling, the court found the department had violated the same federal law with its revision of the reimbursement regulation, issued in 2018. The new rule, the panel said, created a new obstacle for veterans.
