User login
For MD-IQ use only
ACGME deepening its commitment to physician well-being, leader says
NEW ORLEANS – When Timothy P. Brigham, MDiv, PhD, thinks about the impact of burnout and stress on the ability of physicians to practice medicine, Lewin’s equation comes to mind.

Developed by psychologist Kurt Lewin in 1936, the equation holds that behavior stems from a person’s personality and the environment that person inhabits.
Dr. Brigham, chief of staff and chief education and organizational development officer at the Chicago-based Accreditation Council for Graduate Medical Education (ACGME), said at the annual meeting of the American Academy of Pediatrics.
“It’s a toxic mine, in some ways. What we tend to do is when we detect that physicians in general are, or a particular residency program is, too stressed out or burned out, we give them resilience training. Not that that’s unimportant, but it’s like putting a canary in a toxic mine full of poison and saying, ‘We’re going to teach you to hold your breath a little bit longer.’ Our job is to detoxify the mine.”
Troubled by the rise of suicides among physicians in recent years as well as mounting evidence about the adverse impact of burnout and stress on the practice of medicine, Dr. Brigham said that the ACGME is deepening its commitment to the well-being of faculty, residents, patients, and all members of the health care team. Since launching a “call to arms” on the topic at its annual educational conference in 2015, the ACGME has added courses on well-being to its annual meeting and remolded its Clinical Learning Environmental Review program to include all clinicians, “because everybody is affected by this: nurses, coordinators, et cetera,” he said. The ACGME also has revised Common Program Requirements, disseminated tools and resources to promote well-being and new knowledge on the topic, and partnered with the National Academy of Medicine Action Collaborative on Clinician Well-Being and Resilience – all in an effort to bring about culture change.
“But we’re well aware that the ACGME can’t do this alone,” Dr. Brigham said. “We can’t ‘requirement’ our way out of this problem. It’s going to take a culture shift. Only you physicians, in collaboration with everyone in your community of learning, can create the systemic change required to improve our culture. We have a good handle on the problem at this point, but the solutions are a little bit more difficult to get a hold of. As Martin Luther King Jr. once said, ‘You don’t have to see the whole staircase, just take the first step.’ ”
The ACGME wants to work with physicians “to collect data and do joint research, to share insights, and to share tools and resources to create a better world for practicing physicians, for other members of the health care team, and for patients. After all, clinicians who care for themselves provide better care for others. They’re less likely to make errors or leave the profession,” Dr. Brigham told attendees.
He added that clinicians can gauge their risk for burnout by asking themselves three simple questions about their work environment: Does it support self-care? Does it increase and support connection with colleagues? Does it connect people to purpose and meaningful work?
“One of the problems with our resident clinical work hours is not terrible program directors saying, ‘work longer.’ It’s residents who want to take care of families for 1 more hour,” Dr. Brigham continued. “It’s residents who want to take care of patients who are going through a difficult time. You represent the top 2% in the world in terms of your intelligence and achievement, yet that’s not what makes you special. What makes you special is that the level of self-doubt in this room exceeds that of the general population by about 10 times. You also tend to run toward what everyone else runs away from: disease, despair, people who are injured and suffering. That takes a toll.”

He emphasized that positive social relationships with others are crucial to joy and well-being in the practice of medicine. “Burnout isn’t just about exhaustion; it’s about loneliness,” Dr. Brigham said. “There’s a surprising power in just asking people how they’re doing, and really wanting to know the answer.”
Negative social connections are highly correlated with burnout and depression, such as harassment, bullying, mistreatment, discrimination, “and using the power gradient to squash somebody who’s trying their best to be a physician,” he said.
Dr. Brigham acknowledged the tall task of bringing a spotlight to well-being as physicians continue to engage in tasks such as the burden and lack of standardization of prior authorization requirements, the burden of clinical documentation requirements, electronic health records and related work flow, and quality payment programs. “This is what we need to shift; this is what we need to take away so you can get back in touch with why you became a physician in the first place.”
Dr. Brigham reported having no financial disclosures.
NEW ORLEANS – When Timothy P. Brigham, MDiv, PhD, thinks about the impact of burnout and stress on the ability of physicians to practice medicine, Lewin’s equation comes to mind.
Developed by psychologist Kurt Lewin in 1936, the equation holds that behavior stems from a person’s personality and the environment that person inhabits.
Dr. Brigham, chief of staff and chief education and organizational development officer at the Chicago-based Accreditation Council for Graduate Medical Education (ACGME), said at the annual meeting of the American Academy of Pediatrics.
“It’s a toxic mine, in some ways. What we tend to do is when we detect that physicians in general are, or a particular residency program is, too stressed out or burned out, we give them resilience training. Not that that’s unimportant, but it’s like putting a canary in a toxic mine full of poison and saying, ‘We’re going to teach you to hold your breath a little bit longer.’ Our job is to detoxify the mine.”
Troubled by the rise of suicides among physicians in recent years as well as mounting evidence about the adverse impact of burnout and stress on the practice of medicine, Dr. Brigham said that the ACGME is deepening its commitment to the well-being of faculty, residents, patients, and all members of the health care team. Since launching a “call to arms” on the topic at its annual educational conference in 2015, the ACGME has added courses on well-being to its annual meeting and remolded its Clinical Learning Environmental Review program to include all clinicians, “because everybody is affected by this: nurses, coordinators, et cetera,” he said. The ACGME also has revised Common Program Requirements, disseminated tools and resources to promote well-being and new knowledge on the topic, and partnered with the National Academy of Medicine Action Collaborative on Clinician Well-Being and Resilience – all in an effort to bring about culture change.
“But we’re well aware that the ACGME can’t do this alone,” Dr. Brigham said. “We can’t ‘requirement’ our way out of this problem. It’s going to take a culture shift. Only you physicians, in collaboration with everyone in your community of learning, can create the systemic change required to improve our culture. We have a good handle on the problem at this point, but the solutions are a little bit more difficult to get a hold of. As Martin Luther King Jr. once said, ‘You don’t have to see the whole staircase, just take the first step.’ ”
The ACGME wants to work with physicians “to collect data and do joint research, to share insights, and to share tools and resources to create a better world for practicing physicians, for other members of the health care team, and for patients. After all, clinicians who care for themselves provide better care for others. They’re less likely to make errors or leave the profession,” Dr. Brigham told attendees.
He added that clinicians can gauge their risk for burnout by asking themselves three simple questions about their work environment: Does it support self-care? Does it increase and support connection with colleagues? Does it connect people to purpose and meaningful work?
“One of the problems with our resident clinical work hours is not terrible program directors saying, ‘work longer.’ It’s residents who want to take care of families for 1 more hour,” Dr. Brigham continued. “It’s residents who want to take care of patients who are going through a difficult time. You represent the top 2% in the world in terms of your intelligence and achievement, yet that’s not what makes you special. What makes you special is that the level of self-doubt in this room exceeds that of the general population by about 10 times. You also tend to run toward what everyone else runs away from: disease, despair, people who are injured and suffering. That takes a toll.”
He emphasized that positive social relationships with others are crucial to joy and well-being in the practice of medicine. “Burnout isn’t just about exhaustion; it’s about loneliness,” Dr. Brigham said. “There’s a surprising power in just asking people how they’re doing, and really wanting to know the answer.”
Negative social connections are highly correlated with burnout and depression, such as harassment, bullying, mistreatment, discrimination, “and using the power gradient to squash somebody who’s trying their best to be a physician,” he said.
Dr. Brigham acknowledged the tall task of bringing a spotlight to well-being as physicians continue to engage in tasks such as the burden and lack of standardization of prior authorization requirements, the burden of clinical documentation requirements, electronic health records and related work flow, and quality payment programs. “This is what we need to shift; this is what we need to take away so you can get back in touch with why you became a physician in the first place.”
Dr. Brigham reported having no financial disclosures.
NEW ORLEANS – When Timothy P. Brigham, MDiv, PhD, thinks about the impact of burnout and stress on the ability of physicians to practice medicine, Lewin’s equation comes to mind.
Developed by psychologist Kurt Lewin in 1936, the equation holds that behavior stems from a person’s personality and the environment that person inhabits.
Dr. Brigham, chief of staff and chief education and organizational development officer at the Chicago-based Accreditation Council for Graduate Medical Education (ACGME), said at the annual meeting of the American Academy of Pediatrics.
“It’s a toxic mine, in some ways. What we tend to do is when we detect that physicians in general are, or a particular residency program is, too stressed out or burned out, we give them resilience training. Not that that’s unimportant, but it’s like putting a canary in a toxic mine full of poison and saying, ‘We’re going to teach you to hold your breath a little bit longer.’ Our job is to detoxify the mine.”
Troubled by the rise of suicides among physicians in recent years as well as mounting evidence about the adverse impact of burnout and stress on the practice of medicine, Dr. Brigham said that the ACGME is deepening its commitment to the well-being of faculty, residents, patients, and all members of the health care team. Since launching a “call to arms” on the topic at its annual educational conference in 2015, the ACGME has added courses on well-being to its annual meeting and remolded its Clinical Learning Environmental Review program to include all clinicians, “because everybody is affected by this: nurses, coordinators, et cetera,” he said. The ACGME also has revised Common Program Requirements, disseminated tools and resources to promote well-being and new knowledge on the topic, and partnered with the National Academy of Medicine Action Collaborative on Clinician Well-Being and Resilience – all in an effort to bring about culture change.
“But we’re well aware that the ACGME can’t do this alone,” Dr. Brigham said. “We can’t ‘requirement’ our way out of this problem. It’s going to take a culture shift. Only you physicians, in collaboration with everyone in your community of learning, can create the systemic change required to improve our culture. We have a good handle on the problem at this point, but the solutions are a little bit more difficult to get a hold of. As Martin Luther King Jr. once said, ‘You don’t have to see the whole staircase, just take the first step.’ ”
The ACGME wants to work with physicians “to collect data and do joint research, to share insights, and to share tools and resources to create a better world for practicing physicians, for other members of the health care team, and for patients. After all, clinicians who care for themselves provide better care for others. They’re less likely to make errors or leave the profession,” Dr. Brigham told attendees.
He added that clinicians can gauge their risk for burnout by asking themselves three simple questions about their work environment: Does it support self-care? Does it increase and support connection with colleagues? Does it connect people to purpose and meaningful work?
“One of the problems with our resident clinical work hours is not terrible program directors saying, ‘work longer.’ It’s residents who want to take care of families for 1 more hour,” Dr. Brigham continued. “It’s residents who want to take care of patients who are going through a difficult time. You represent the top 2% in the world in terms of your intelligence and achievement, yet that’s not what makes you special. What makes you special is that the level of self-doubt in this room exceeds that of the general population by about 10 times. You also tend to run toward what everyone else runs away from: disease, despair, people who are injured and suffering. That takes a toll.”
He emphasized that positive social relationships with others are crucial to joy and well-being in the practice of medicine. “Burnout isn’t just about exhaustion; it’s about loneliness,” Dr. Brigham said. “There’s a surprising power in just asking people how they’re doing, and really wanting to know the answer.”
Negative social connections are highly correlated with burnout and depression, such as harassment, bullying, mistreatment, discrimination, “and using the power gradient to squash somebody who’s trying their best to be a physician,” he said.
Dr. Brigham acknowledged the tall task of bringing a spotlight to well-being as physicians continue to engage in tasks such as the burden and lack of standardization of prior authorization requirements, the burden of clinical documentation requirements, electronic health records and related work flow, and quality payment programs. “This is what we need to shift; this is what we need to take away so you can get back in touch with why you became a physician in the first place.”
Dr. Brigham reported having no financial disclosures.
EXPERT ANALYSIS AT AAP 2019
Anticipating the A.I. revolution
Goal is to augment human performance
Artificial intelligence (A.I.) is likely to change almost everything in medical practice, according to a new book called “Deep Medicine: How Artificial Intelligence Can Make Healthcare Human Again,” by Eric Topol, MD.
Dr. Topol told The Hospitalist that his book’s subtitle “is the paradox: the unexpected, far-reaching goal of A.I. that can, if used properly, restore the most important part of medicine – a deep patient-doctor relationship.”
That’s because A.I. can do more than enhance diagnoses; it can also help with tasks such as note-taking and reading scans, making it possible for hospitalists to spend more time connecting with their patients. “Hospitalists could have a much better handle on a patient’s dataset via algorithmic processing, providing alerts and augmented performance of hospitalists (when validated),” Dr. Topol said. “They can also expect far less keyboard use with the help of speech recognition, natural language processing, and deep learning.”In an interview with the New York Times, Dr. Topol said that by augmenting human performance, A.I. has the potential to markedly improve productivity, efficiency, work flow, accuracy and speed, both for doctors and for patients, giving more charge and control to consumers through algorithmic support of their data.
“We can’t, and will never, rely on only algorithms for interpretation of life and death matters,” he said. “That requires human expert contextualization, something machines can’t do.”Of course, there could be pitfalls. “The liabilities include breaches of privacy and security, hacking, the lack of explainability of most A.I. algorithms, the potential to worsen inequities, the embedded bias, and ethical quandaries,” he said.
Reference
1. O’Connor A. How Artificial Intelligence Could Transform Medicine. New York Times. March 11, 2019. https://www.nytimes.com/2019/03/11/well/live/how-artificial-intelligence-could-transform-medicine.html.
Goal is to augment human performance
Goal is to augment human performance
Artificial intelligence (A.I.) is likely to change almost everything in medical practice, according to a new book called “Deep Medicine: How Artificial Intelligence Can Make Healthcare Human Again,” by Eric Topol, MD.
Dr. Topol told The Hospitalist that his book’s subtitle “is the paradox: the unexpected, far-reaching goal of A.I. that can, if used properly, restore the most important part of medicine – a deep patient-doctor relationship.”
That’s because A.I. can do more than enhance diagnoses; it can also help with tasks such as note-taking and reading scans, making it possible for hospitalists to spend more time connecting with their patients. “Hospitalists could have a much better handle on a patient’s dataset via algorithmic processing, providing alerts and augmented performance of hospitalists (when validated),” Dr. Topol said. “They can also expect far less keyboard use with the help of speech recognition, natural language processing, and deep learning.”In an interview with the New York Times, Dr. Topol said that by augmenting human performance, A.I. has the potential to markedly improve productivity, efficiency, work flow, accuracy and speed, both for doctors and for patients, giving more charge and control to consumers through algorithmic support of their data.
“We can’t, and will never, rely on only algorithms for interpretation of life and death matters,” he said. “That requires human expert contextualization, something machines can’t do.”Of course, there could be pitfalls. “The liabilities include breaches of privacy and security, hacking, the lack of explainability of most A.I. algorithms, the potential to worsen inequities, the embedded bias, and ethical quandaries,” he said.
Reference
1. O’Connor A. How Artificial Intelligence Could Transform Medicine. New York Times. March 11, 2019. https://www.nytimes.com/2019/03/11/well/live/how-artificial-intelligence-could-transform-medicine.html.
Artificial intelligence (A.I.) is likely to change almost everything in medical practice, according to a new book called “Deep Medicine: How Artificial Intelligence Can Make Healthcare Human Again,” by Eric Topol, MD.
Dr. Topol told The Hospitalist that his book’s subtitle “is the paradox: the unexpected, far-reaching goal of A.I. that can, if used properly, restore the most important part of medicine – a deep patient-doctor relationship.”
That’s because A.I. can do more than enhance diagnoses; it can also help with tasks such as note-taking and reading scans, making it possible for hospitalists to spend more time connecting with their patients. “Hospitalists could have a much better handle on a patient’s dataset via algorithmic processing, providing alerts and augmented performance of hospitalists (when validated),” Dr. Topol said. “They can also expect far less keyboard use with the help of speech recognition, natural language processing, and deep learning.”In an interview with the New York Times, Dr. Topol said that by augmenting human performance, A.I. has the potential to markedly improve productivity, efficiency, work flow, accuracy and speed, both for doctors and for patients, giving more charge and control to consumers through algorithmic support of their data.
“We can’t, and will never, rely on only algorithms for interpretation of life and death matters,” he said. “That requires human expert contextualization, something machines can’t do.”Of course, there could be pitfalls. “The liabilities include breaches of privacy and security, hacking, the lack of explainability of most A.I. algorithms, the potential to worsen inequities, the embedded bias, and ethical quandaries,” he said.
Reference
1. O’Connor A. How Artificial Intelligence Could Transform Medicine. New York Times. March 11, 2019. https://www.nytimes.com/2019/03/11/well/live/how-artificial-intelligence-could-transform-medicine.html.
Poor OR posture a key cause of vascular burnout
NEW YORK – Career burnout is common is common among physicians and surgeons, but vascular surgeons might be able to lower their risk simply by taking steps to improve their posture in the operating room, according to data presented at a symposium on vascular and endovascular issues on an evolution that is already underway.

“We looked at physical pain and we were able to demonstrate a correlation with burnout. More pain, more burnout,” said Samuel R. Money, MD, division of vascular surgery, Mayo Clinic, Phoenix, Arizona.
Pain was a reasonable focus for efforts to identify causes of burnout because it is so common among vascular surgeons. In data recently published by Dr. Money and his coinvestigators, 78.3% reported moderate to severe physical pain at the end of a day of surgery (J Vasc Surg 2018;70:913-920).
“Forty percent of vascular surgeons have chronic pain,” Dr. Money said at the symposium sponsored by the Cleveland Clinic Foundation.
Physical pain is not the only cause of burnout, which affects 30% of vascular surgeons, according to data recently presented at the annual meeting of the Society of Vascular Surgery (J Vasc Surg 2019;69[6]:e97.). In that survey, physical pain was joined by work hours, documentation tasks, on-call frequency, and conflicts between work and personal life as significant factors.
“The average vascular surgeon in North America works 63 hours per week,” noted Dr. Money, adding that his survey found nearly 90% of surgeons operate on 3 or more days of every week. This amount of time in the operating room is relevant because almost all surgeons report some degree of pain after a procedure. In the survey, the proportion was greater than 95%.
Yet, risk of pain is modifiable.
“Body position matters,” said Dr. Money, citing studies showing that open procedures are most closely associated with neck pain whereas endovascular procedures are more likely to produce back pain. Although there is a high risk of either type of pain with these procedures, the types of predominant pain are consistent with the demands on body positioning.
“The more you lean forward, the more stress is placed on your neck and back. When standing straight, your head weighs 10-12 pounds, but leaning forward, it can put 60 pounds of pressure on your neck,” he said.
The relative stress can be measured objectively. Dr. Money cited work with a device that measures the body force in inertial measurement units (IMU). According to Dr. Money, the neck is in a high stress position about 75% of the time spent performing typical vascular surgery.
“The trunk is placed in a high stress position approximately 40% of the time, while the other parts of the body that were measured were not generally that bad,” Dr. Money said.
To avoid postural pain, which is not often stressed in surgical training, Dr. Money had specific recommendations. Some are obvious, such as positioning the operating table to minimize the amount of time the head is inclined. He also recommended positioning display monitors no more than 10-20 degrees below and no higher than eye level.
“If you sit down to perform tasks during the procedure, use an adjustable chair so that you can optimize the height,” he said.
He identified loupes as a risk factor for bad posture, and he stressed the importance of wearing lead garments only when necessary and adjusted properly.
“Padded floor mats? They really help,” Dr. Money said. He also recommended appropriate footwear and support stocking.
“Microbreaks are being used in a lot of professions. This means stopping for a moment to stretch every 15-30 minutes,” Dr. Money said.
As a first step, Dr. Money recommended simply developing posture awareness. Many surgeons are simply ignoring the risk and failing to optimize the ways they can increase their comfort during surgery.
Even before entering the surgical suite, regular exercise, yoga, and stretching are all strategies that have the potential to make a difference, according to Dr. Money.
The immediate goal is to reduce the physical pain that is an important occupational hazard for vascular surgeons, but the ultimate goal is to improve job satisfaction, an important defense against professional burnout.
NEW YORK – Career burnout is common is common among physicians and surgeons, but vascular surgeons might be able to lower their risk simply by taking steps to improve their posture in the operating room, according to data presented at a symposium on vascular and endovascular issues on an evolution that is already underway.
“We looked at physical pain and we were able to demonstrate a correlation with burnout. More pain, more burnout,” said Samuel R. Money, MD, division of vascular surgery, Mayo Clinic, Phoenix, Arizona.
Pain was a reasonable focus for efforts to identify causes of burnout because it is so common among vascular surgeons. In data recently published by Dr. Money and his coinvestigators, 78.3% reported moderate to severe physical pain at the end of a day of surgery (J Vasc Surg 2018;70:913-920).
“Forty percent of vascular surgeons have chronic pain,” Dr. Money said at the symposium sponsored by the Cleveland Clinic Foundation.
Physical pain is not the only cause of burnout, which affects 30% of vascular surgeons, according to data recently presented at the annual meeting of the Society of Vascular Surgery (J Vasc Surg 2019;69[6]:e97.). In that survey, physical pain was joined by work hours, documentation tasks, on-call frequency, and conflicts between work and personal life as significant factors.
“The average vascular surgeon in North America works 63 hours per week,” noted Dr. Money, adding that his survey found nearly 90% of surgeons operate on 3 or more days of every week. This amount of time in the operating room is relevant because almost all surgeons report some degree of pain after a procedure. In the survey, the proportion was greater than 95%.
Yet, risk of pain is modifiable.
“Body position matters,” said Dr. Money, citing studies showing that open procedures are most closely associated with neck pain whereas endovascular procedures are more likely to produce back pain. Although there is a high risk of either type of pain with these procedures, the types of predominant pain are consistent with the demands on body positioning.
“The more you lean forward, the more stress is placed on your neck and back. When standing straight, your head weighs 10-12 pounds, but leaning forward, it can put 60 pounds of pressure on your neck,” he said.
The relative stress can be measured objectively. Dr. Money cited work with a device that measures the body force in inertial measurement units (IMU). According to Dr. Money, the neck is in a high stress position about 75% of the time spent performing typical vascular surgery.
“The trunk is placed in a high stress position approximately 40% of the time, while the other parts of the body that were measured were not generally that bad,” Dr. Money said.
To avoid postural pain, which is not often stressed in surgical training, Dr. Money had specific recommendations. Some are obvious, such as positioning the operating table to minimize the amount of time the head is inclined. He also recommended positioning display monitors no more than 10-20 degrees below and no higher than eye level.
“If you sit down to perform tasks during the procedure, use an adjustable chair so that you can optimize the height,” he said.
He identified loupes as a risk factor for bad posture, and he stressed the importance of wearing lead garments only when necessary and adjusted properly.
“Padded floor mats? They really help,” Dr. Money said. He also recommended appropriate footwear and support stocking.
“Microbreaks are being used in a lot of professions. This means stopping for a moment to stretch every 15-30 minutes,” Dr. Money said.
As a first step, Dr. Money recommended simply developing posture awareness. Many surgeons are simply ignoring the risk and failing to optimize the ways they can increase their comfort during surgery.
Even before entering the surgical suite, regular exercise, yoga, and stretching are all strategies that have the potential to make a difference, according to Dr. Money.
The immediate goal is to reduce the physical pain that is an important occupational hazard for vascular surgeons, but the ultimate goal is to improve job satisfaction, an important defense against professional burnout.
NEW YORK – Career burnout is common is common among physicians and surgeons, but vascular surgeons might be able to lower their risk simply by taking steps to improve their posture in the operating room, according to data presented at a symposium on vascular and endovascular issues on an evolution that is already underway.
“We looked at physical pain and we were able to demonstrate a correlation with burnout. More pain, more burnout,” said Samuel R. Money, MD, division of vascular surgery, Mayo Clinic, Phoenix, Arizona.
Pain was a reasonable focus for efforts to identify causes of burnout because it is so common among vascular surgeons. In data recently published by Dr. Money and his coinvestigators, 78.3% reported moderate to severe physical pain at the end of a day of surgery (J Vasc Surg 2018;70:913-920).
“Forty percent of vascular surgeons have chronic pain,” Dr. Money said at the symposium sponsored by the Cleveland Clinic Foundation.
Physical pain is not the only cause of burnout, which affects 30% of vascular surgeons, according to data recently presented at the annual meeting of the Society of Vascular Surgery (J Vasc Surg 2019;69[6]:e97.). In that survey, physical pain was joined by work hours, documentation tasks, on-call frequency, and conflicts between work and personal life as significant factors.
“The average vascular surgeon in North America works 63 hours per week,” noted Dr. Money, adding that his survey found nearly 90% of surgeons operate on 3 or more days of every week. This amount of time in the operating room is relevant because almost all surgeons report some degree of pain after a procedure. In the survey, the proportion was greater than 95%.
Yet, risk of pain is modifiable.
“Body position matters,” said Dr. Money, citing studies showing that open procedures are most closely associated with neck pain whereas endovascular procedures are more likely to produce back pain. Although there is a high risk of either type of pain with these procedures, the types of predominant pain are consistent with the demands on body positioning.
“The more you lean forward, the more stress is placed on your neck and back. When standing straight, your head weighs 10-12 pounds, but leaning forward, it can put 60 pounds of pressure on your neck,” he said.
The relative stress can be measured objectively. Dr. Money cited work with a device that measures the body force in inertial measurement units (IMU). According to Dr. Money, the neck is in a high stress position about 75% of the time spent performing typical vascular surgery.
“The trunk is placed in a high stress position approximately 40% of the time, while the other parts of the body that were measured were not generally that bad,” Dr. Money said.
To avoid postural pain, which is not often stressed in surgical training, Dr. Money had specific recommendations. Some are obvious, such as positioning the operating table to minimize the amount of time the head is inclined. He also recommended positioning display monitors no more than 10-20 degrees below and no higher than eye level.
“If you sit down to perform tasks during the procedure, use an adjustable chair so that you can optimize the height,” he said.
He identified loupes as a risk factor for bad posture, and he stressed the importance of wearing lead garments only when necessary and adjusted properly.
“Padded floor mats? They really help,” Dr. Money said. He also recommended appropriate footwear and support stocking.
“Microbreaks are being used in a lot of professions. This means stopping for a moment to stretch every 15-30 minutes,” Dr. Money said.
As a first step, Dr. Money recommended simply developing posture awareness. Many surgeons are simply ignoring the risk and failing to optimize the ways they can increase their comfort during surgery.
Even before entering the surgical suite, regular exercise, yoga, and stretching are all strategies that have the potential to make a difference, according to Dr. Money.
The immediate goal is to reduce the physical pain that is an important occupational hazard for vascular surgeons, but the ultimate goal is to improve job satisfaction, an important defense against professional burnout.
REPORTING FROM VEITHsymposium
ID Blog: The waters of death
Diseases of the American Civil War, Part I
If cleanliness is next to godliness, then the average soldier in the American Civil War lived just down the street from hell. In a land at war, before the formal tenets of germ theory had spread beyond the confines of Louis Pasteur’s laboratory in France, the lack of basic hygiene, both cultural and situational, coupled to an almost complete lack of curative therapies created an appalling death toll. Waterborne diseases in particular spared neither general nor private, and neither doctor nor nurse.
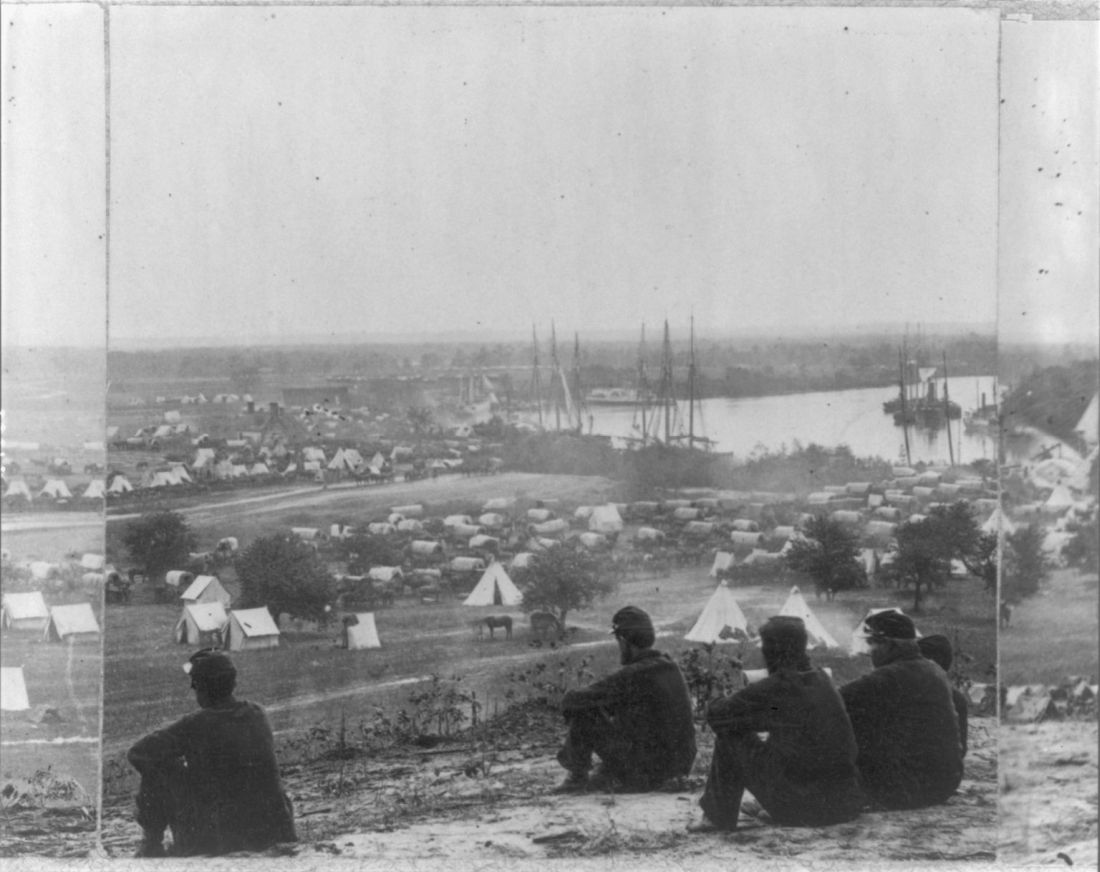
“Of all the adversities that Union and Confederate soldiers confronted, none was more deadly or more prevalent than contaminated water,” according to Jeffrey S. Sartin, MD, in his survey of Civil War diseases.1
The Union Army records list 1,765,000 cases of diarrhea or dysentery with 45,000 deaths and 149,000 cases of typhoid fever with 35,000 deaths. Add to these the 1,316,000 cases of malaria (borne by mosquitoes breeding in the waters) with its 10,000 deaths, and it is easy to see how the battlefield itself took second place in service to the grim reaper. (Overall, there were roughly two deaths from disease for every one from wounds.)
The chief waterborne plague, infectious diarrhea – including bacterial, amoebic, and other parasites – as well as cholera and typhoid, was an all-year-long problem, and, with the typical wry humor of soldiers, these maladies were given popular names, including the “Tennessee trots” and the “Virginia quick-step.”
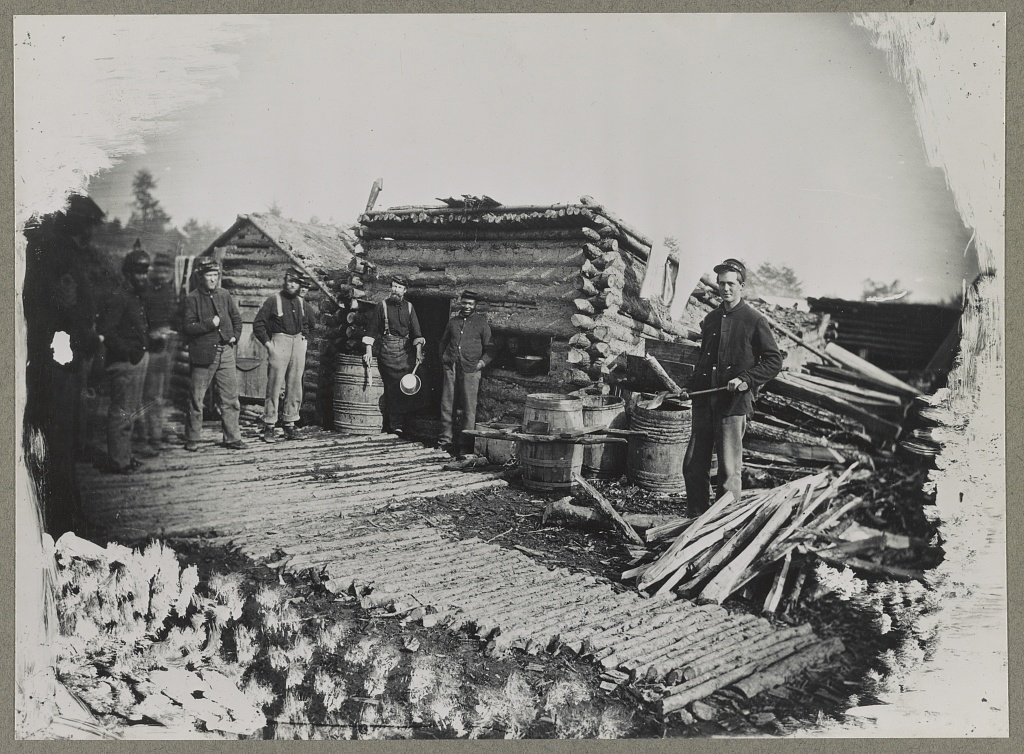
Unsanitary conditions in the camps were primarily to blame, and this problem of sanitation was obvious to many observers at the time.
Despite a lack of knowledge of germ theory, doctors were fully aware of the relationship of unsanitary conditions to disease, even if they ascribed the link to miasmas or particles of filth.
Hospitals, which were under more strict control than the regular army camps, were meticulous about the placement of latrines and about keeping high standards of cleanliness among the patients, including routine washing. However, this was insufficient for complete protection, because what passed for clean in the absence of the knowledge of bacterial contamination was often totally ineffective. As one Civil War surgeon stated: “We operated in old bloodstained and often pus-stained coats, we used undisinfected instruments from undisinfected plush-lined cases. If a sponge (if they had sponges) or instrument fell on the floor it was washed and squeezed in a basin of water and used as if it was clean.”2
Overall, efforts at what passed for sanitation remained a constant goal and constant struggle in the field.
After the First Battle of Bull Run, Women’s Central Association of Relief President Henry W. Bellows met with Secretary of War Simon Cameron to discuss the abysmal sanitary conditions witnessed by WCAR volunteers. This meeting led to the creation of what would become the U.S. Sanitary Commission, which was approved by President Abraham Lincoln on June 13, 1861.
The U.S. Sanitary Commission served as a means for funneling civilian assistance to the military, with volunteers providing assistance in the organization of military hospitals and camps and aiding in the transportation of the wounded. However, despite these efforts, the setup of army camps and the behavior of the soldiers were not often directed toward proper sanitation. “The principal causes of disease, however, in our camps were the same that we have always to deplore and find it so difficult to remedy, simply because citizens suddenly called to the field cannot comprehend that men in masses require the attention of their officers to enforce certain hygienic conditions without which health cannot be preserved.”3
Breaches of sanitation were common in the confines of the camps, despite regulations designed to protect the soldiers. According to one U.S. Army surgeon of the time: “Especially [needed] was policing of the latrines. The trench is generally too shallow, the daily covering ... with dirt is entirely neglected. Large numbers of the men will not use the sinks [latrines], ... but instead every clump of bushes, every fence border in the vicinity.” Another pointed out that, after the Battle of Seven Pines, “the only water was infiltrated with the decaying animal matter of the battlefield.” Commenting on the placement of latrines in one encampment, another surgeon described how “the sink [latrine] is the ground in the vicinity, which slopes down to the stream, from which all water from the camp is obtained.”4
Treatment for diarrhea and dysentery was varied. Opiates were one of the most common treatments for diarrhea, whether in an alcohol solution as laudanum or in pill form, with belladonna being used to treat intestinal cramps, according to Glenna R. Schroeder-Lein in her book “The Encyclopedia of Civil War Medicine.” However, useless or damaging treatments were also prescribed, including the use of calomel (a mercury compound), turpentine, castor oil, and quinine.5
Acute diarrhea and dysentery illnesses occurred in at least 641/1,000 troops per year in the Union army. And even though the death rate was comparatively low (20/1,000 cases), it frequently led to chronic diarrhea, which was responsible for 288 deaths per 1,000 cases, and was the third highest cause of medical discharge after gunshot wounds and tuberculosis, according to Ms. Schroeder-Lein.
Although the American Civil War was the last major conflict before the spread of the knowledge of germ theory, the struggle to prevent the spread of waterborne diseases under wartime conditions remains ongoing. Hygiene is difficult under conditions of abject poverty and especially under conditions of armed conflict, and until the era of curative antibiotics there was no recourse.
Antibiotics are not the final solution for antibiotic resistance in intestinal disease pathogens, as outlined in a recent CDC report, is an increasing problem.6 For example, nontyphoidal Salmonella causes an estimated 1.35 million infections, 26,500 hospitalizations, and 420 deaths each year in the United States, with 16% of strains being resistant to at least one essential antibiotic. On a global scale, according to the World Health Organization, poor sanitation causes up to 432,000 diarrheal deaths annually and is linked to the transmission of other diseases like cholera, dysentery, typhoid, hepatitis A, and polio.7
With regard to actual epidemics, the world is only a hygienic crisis away from a major outbreak of dysentery (the last occurring between 1969 and 1972, when 20,000 people in Central America died), according to researchers who have detected antibiotic resistance in all but 1% of circulating Shigella dysenteriae strains surveyed since the 1990s. “This bacterium is still in circulation, and could be responsible for future epidemics if conditions should prove favorable – such as a large gathering of people without access to drinking water or treatment of human waste,” wrote François-Xavier Weill of the Pasteur Institute’s Enteric Bacterial Pathogens Unit.8
References
1. Sartin JS. Clin Infec Dis. 1993;16:580-4. (Correction published in 2002).
2. Civil War Battlefield Surgery. eHistory. The Ohio State University.
3. “Myths About Antiseptics and Camp Life – George Wunderlich,” published online Oct. 11, 2011. http://civilwarscholars.com/2011/10/myths-about-antiseptics-and-camp-life-george-wunderlich/
4. Dorwart BB. “Death is in the Breeze: Disease during the American Civil War” (The National Museum of the American Civil War Press, 2009).
5. Glenna R, Schroeder-Lein GR. “The Encyclopedia of Civil War Medicine” (New York: M. E. Sharpe, 2008).
6. “Antibiotic resistance threats in the United States 2019” Centers for Disease Control and Prevention.
7. “New report exposes horror of working conditions for millions of sanitation workers in the developing world,” World Health Organization. 2019 Nov 14.
8. Grant B. Origins of Dysentery. The Scientist. Published online March 22, 2016.
Mark Lesney is the managing editor of MDedge.com/IDPractioner. He has a PhD in plant virology and a PhD in the history of science, with a focus on the history of biotechnology and medicine. He has served as an adjunct assistant professor of the department of biochemistry and molecular & cellular biology at Georgetown University, Washington.
Diseases of the American Civil War, Part I
Diseases of the American Civil War, Part I
If cleanliness is next to godliness, then the average soldier in the American Civil War lived just down the street from hell. In a land at war, before the formal tenets of germ theory had spread beyond the confines of Louis Pasteur’s laboratory in France, the lack of basic hygiene, both cultural and situational, coupled to an almost complete lack of curative therapies created an appalling death toll. Waterborne diseases in particular spared neither general nor private, and neither doctor nor nurse.
“Of all the adversities that Union and Confederate soldiers confronted, none was more deadly or more prevalent than contaminated water,” according to Jeffrey S. Sartin, MD, in his survey of Civil War diseases.1
The Union Army records list 1,765,000 cases of diarrhea or dysentery with 45,000 deaths and 149,000 cases of typhoid fever with 35,000 deaths. Add to these the 1,316,000 cases of malaria (borne by mosquitoes breeding in the waters) with its 10,000 deaths, and it is easy to see how the battlefield itself took second place in service to the grim reaper. (Overall, there were roughly two deaths from disease for every one from wounds.)
The chief waterborne plague, infectious diarrhea – including bacterial, amoebic, and other parasites – as well as cholera and typhoid, was an all-year-long problem, and, with the typical wry humor of soldiers, these maladies were given popular names, including the “Tennessee trots” and the “Virginia quick-step.”
Unsanitary conditions in the camps were primarily to blame, and this problem of sanitation was obvious to many observers at the time.
Despite a lack of knowledge of germ theory, doctors were fully aware of the relationship of unsanitary conditions to disease, even if they ascribed the link to miasmas or particles of filth.
Hospitals, which were under more strict control than the regular army camps, were meticulous about the placement of latrines and about keeping high standards of cleanliness among the patients, including routine washing. However, this was insufficient for complete protection, because what passed for clean in the absence of the knowledge of bacterial contamination was often totally ineffective. As one Civil War surgeon stated: “We operated in old bloodstained and often pus-stained coats, we used undisinfected instruments from undisinfected plush-lined cases. If a sponge (if they had sponges) or instrument fell on the floor it was washed and squeezed in a basin of water and used as if it was clean.”2
Overall, efforts at what passed for sanitation remained a constant goal and constant struggle in the field.
After the First Battle of Bull Run, Women’s Central Association of Relief President Henry W. Bellows met with Secretary of War Simon Cameron to discuss the abysmal sanitary conditions witnessed by WCAR volunteers. This meeting led to the creation of what would become the U.S. Sanitary Commission, which was approved by President Abraham Lincoln on June 13, 1861.
The U.S. Sanitary Commission served as a means for funneling civilian assistance to the military, with volunteers providing assistance in the organization of military hospitals and camps and aiding in the transportation of the wounded. However, despite these efforts, the setup of army camps and the behavior of the soldiers were not often directed toward proper sanitation. “The principal causes of disease, however, in our camps were the same that we have always to deplore and find it so difficult to remedy, simply because citizens suddenly called to the field cannot comprehend that men in masses require the attention of their officers to enforce certain hygienic conditions without which health cannot be preserved.”3
Breaches of sanitation were common in the confines of the camps, despite regulations designed to protect the soldiers. According to one U.S. Army surgeon of the time: “Especially [needed] was policing of the latrines. The trench is generally too shallow, the daily covering ... with dirt is entirely neglected. Large numbers of the men will not use the sinks [latrines], ... but instead every clump of bushes, every fence border in the vicinity.” Another pointed out that, after the Battle of Seven Pines, “the only water was infiltrated with the decaying animal matter of the battlefield.” Commenting on the placement of latrines in one encampment, another surgeon described how “the sink [latrine] is the ground in the vicinity, which slopes down to the stream, from which all water from the camp is obtained.”4
Treatment for diarrhea and dysentery was varied. Opiates were one of the most common treatments for diarrhea, whether in an alcohol solution as laudanum or in pill form, with belladonna being used to treat intestinal cramps, according to Glenna R. Schroeder-Lein in her book “The Encyclopedia of Civil War Medicine.” However, useless or damaging treatments were also prescribed, including the use of calomel (a mercury compound), turpentine, castor oil, and quinine.5
Acute diarrhea and dysentery illnesses occurred in at least 641/1,000 troops per year in the Union army. And even though the death rate was comparatively low (20/1,000 cases), it frequently led to chronic diarrhea, which was responsible for 288 deaths per 1,000 cases, and was the third highest cause of medical discharge after gunshot wounds and tuberculosis, according to Ms. Schroeder-Lein.
Although the American Civil War was the last major conflict before the spread of the knowledge of germ theory, the struggle to prevent the spread of waterborne diseases under wartime conditions remains ongoing. Hygiene is difficult under conditions of abject poverty and especially under conditions of armed conflict, and until the era of curative antibiotics there was no recourse.
Antibiotics are not the final solution for antibiotic resistance in intestinal disease pathogens, as outlined in a recent CDC report, is an increasing problem.6 For example, nontyphoidal Salmonella causes an estimated 1.35 million infections, 26,500 hospitalizations, and 420 deaths each year in the United States, with 16% of strains being resistant to at least one essential antibiotic. On a global scale, according to the World Health Organization, poor sanitation causes up to 432,000 diarrheal deaths annually and is linked to the transmission of other diseases like cholera, dysentery, typhoid, hepatitis A, and polio.7
With regard to actual epidemics, the world is only a hygienic crisis away from a major outbreak of dysentery (the last occurring between 1969 and 1972, when 20,000 people in Central America died), according to researchers who have detected antibiotic resistance in all but 1% of circulating Shigella dysenteriae strains surveyed since the 1990s. “This bacterium is still in circulation, and could be responsible for future epidemics if conditions should prove favorable – such as a large gathering of people without access to drinking water or treatment of human waste,” wrote François-Xavier Weill of the Pasteur Institute’s Enteric Bacterial Pathogens Unit.8
References
1. Sartin JS. Clin Infec Dis. 1993;16:580-4. (Correction published in 2002).
2. Civil War Battlefield Surgery. eHistory. The Ohio State University.
3. “Myths About Antiseptics and Camp Life – George Wunderlich,” published online Oct. 11, 2011. http://civilwarscholars.com/2011/10/myths-about-antiseptics-and-camp-life-george-wunderlich/
4. Dorwart BB. “Death is in the Breeze: Disease during the American Civil War” (The National Museum of the American Civil War Press, 2009).
5. Glenna R, Schroeder-Lein GR. “The Encyclopedia of Civil War Medicine” (New York: M. E. Sharpe, 2008).
6. “Antibiotic resistance threats in the United States 2019” Centers for Disease Control and Prevention.
7. “New report exposes horror of working conditions for millions of sanitation workers in the developing world,” World Health Organization. 2019 Nov 14.
8. Grant B. Origins of Dysentery. The Scientist. Published online March 22, 2016.
Mark Lesney is the managing editor of MDedge.com/IDPractioner. He has a PhD in plant virology and a PhD in the history of science, with a focus on the history of biotechnology and medicine. He has served as an adjunct assistant professor of the department of biochemistry and molecular & cellular biology at Georgetown University, Washington.
If cleanliness is next to godliness, then the average soldier in the American Civil War lived just down the street from hell. In a land at war, before the formal tenets of germ theory had spread beyond the confines of Louis Pasteur’s laboratory in France, the lack of basic hygiene, both cultural and situational, coupled to an almost complete lack of curative therapies created an appalling death toll. Waterborne diseases in particular spared neither general nor private, and neither doctor nor nurse.
“Of all the adversities that Union and Confederate soldiers confronted, none was more deadly or more prevalent than contaminated water,” according to Jeffrey S. Sartin, MD, in his survey of Civil War diseases.1
The Union Army records list 1,765,000 cases of diarrhea or dysentery with 45,000 deaths and 149,000 cases of typhoid fever with 35,000 deaths. Add to these the 1,316,000 cases of malaria (borne by mosquitoes breeding in the waters) with its 10,000 deaths, and it is easy to see how the battlefield itself took second place in service to the grim reaper. (Overall, there were roughly two deaths from disease for every one from wounds.)
The chief waterborne plague, infectious diarrhea – including bacterial, amoebic, and other parasites – as well as cholera and typhoid, was an all-year-long problem, and, with the typical wry humor of soldiers, these maladies were given popular names, including the “Tennessee trots” and the “Virginia quick-step.”
Unsanitary conditions in the camps were primarily to blame, and this problem of sanitation was obvious to many observers at the time.
Despite a lack of knowledge of germ theory, doctors were fully aware of the relationship of unsanitary conditions to disease, even if they ascribed the link to miasmas or particles of filth.
Hospitals, which were under more strict control than the regular army camps, were meticulous about the placement of latrines and about keeping high standards of cleanliness among the patients, including routine washing. However, this was insufficient for complete protection, because what passed for clean in the absence of the knowledge of bacterial contamination was often totally ineffective. As one Civil War surgeon stated: “We operated in old bloodstained and often pus-stained coats, we used undisinfected instruments from undisinfected plush-lined cases. If a sponge (if they had sponges) or instrument fell on the floor it was washed and squeezed in a basin of water and used as if it was clean.”2
Overall, efforts at what passed for sanitation remained a constant goal and constant struggle in the field.
After the First Battle of Bull Run, Women’s Central Association of Relief President Henry W. Bellows met with Secretary of War Simon Cameron to discuss the abysmal sanitary conditions witnessed by WCAR volunteers. This meeting led to the creation of what would become the U.S. Sanitary Commission, which was approved by President Abraham Lincoln on June 13, 1861.
The U.S. Sanitary Commission served as a means for funneling civilian assistance to the military, with volunteers providing assistance in the organization of military hospitals and camps and aiding in the transportation of the wounded. However, despite these efforts, the setup of army camps and the behavior of the soldiers were not often directed toward proper sanitation. “The principal causes of disease, however, in our camps were the same that we have always to deplore and find it so difficult to remedy, simply because citizens suddenly called to the field cannot comprehend that men in masses require the attention of their officers to enforce certain hygienic conditions without which health cannot be preserved.”3
Breaches of sanitation were common in the confines of the camps, despite regulations designed to protect the soldiers. According to one U.S. Army surgeon of the time: “Especially [needed] was policing of the latrines. The trench is generally too shallow, the daily covering ... with dirt is entirely neglected. Large numbers of the men will not use the sinks [latrines], ... but instead every clump of bushes, every fence border in the vicinity.” Another pointed out that, after the Battle of Seven Pines, “the only water was infiltrated with the decaying animal matter of the battlefield.” Commenting on the placement of latrines in one encampment, another surgeon described how “the sink [latrine] is the ground in the vicinity, which slopes down to the stream, from which all water from the camp is obtained.”4
Treatment for diarrhea and dysentery was varied. Opiates were one of the most common treatments for diarrhea, whether in an alcohol solution as laudanum or in pill form, with belladonna being used to treat intestinal cramps, according to Glenna R. Schroeder-Lein in her book “The Encyclopedia of Civil War Medicine.” However, useless or damaging treatments were also prescribed, including the use of calomel (a mercury compound), turpentine, castor oil, and quinine.5
Acute diarrhea and dysentery illnesses occurred in at least 641/1,000 troops per year in the Union army. And even though the death rate was comparatively low (20/1,000 cases), it frequently led to chronic diarrhea, which was responsible for 288 deaths per 1,000 cases, and was the third highest cause of medical discharge after gunshot wounds and tuberculosis, according to Ms. Schroeder-Lein.
Although the American Civil War was the last major conflict before the spread of the knowledge of germ theory, the struggle to prevent the spread of waterborne diseases under wartime conditions remains ongoing. Hygiene is difficult under conditions of abject poverty and especially under conditions of armed conflict, and until the era of curative antibiotics there was no recourse.
Antibiotics are not the final solution for antibiotic resistance in intestinal disease pathogens, as outlined in a recent CDC report, is an increasing problem.6 For example, nontyphoidal Salmonella causes an estimated 1.35 million infections, 26,500 hospitalizations, and 420 deaths each year in the United States, with 16% of strains being resistant to at least one essential antibiotic. On a global scale, according to the World Health Organization, poor sanitation causes up to 432,000 diarrheal deaths annually and is linked to the transmission of other diseases like cholera, dysentery, typhoid, hepatitis A, and polio.7
With regard to actual epidemics, the world is only a hygienic crisis away from a major outbreak of dysentery (the last occurring between 1969 and 1972, when 20,000 people in Central America died), according to researchers who have detected antibiotic resistance in all but 1% of circulating Shigella dysenteriae strains surveyed since the 1990s. “This bacterium is still in circulation, and could be responsible for future epidemics if conditions should prove favorable – such as a large gathering of people without access to drinking water or treatment of human waste,” wrote François-Xavier Weill of the Pasteur Institute’s Enteric Bacterial Pathogens Unit.8
References
1. Sartin JS. Clin Infec Dis. 1993;16:580-4. (Correction published in 2002).
2. Civil War Battlefield Surgery. eHistory. The Ohio State University.
3. “Myths About Antiseptics and Camp Life – George Wunderlich,” published online Oct. 11, 2011. http://civilwarscholars.com/2011/10/myths-about-antiseptics-and-camp-life-george-wunderlich/
4. Dorwart BB. “Death is in the Breeze: Disease during the American Civil War” (The National Museum of the American Civil War Press, 2009).
5. Glenna R, Schroeder-Lein GR. “The Encyclopedia of Civil War Medicine” (New York: M. E. Sharpe, 2008).
6. “Antibiotic resistance threats in the United States 2019” Centers for Disease Control and Prevention.
7. “New report exposes horror of working conditions for millions of sanitation workers in the developing world,” World Health Organization. 2019 Nov 14.
8. Grant B. Origins of Dysentery. The Scientist. Published online March 22, 2016.
Mark Lesney is the managing editor of MDedge.com/IDPractioner. He has a PhD in plant virology and a PhD in the history of science, with a focus on the history of biotechnology and medicine. He has served as an adjunct assistant professor of the department of biochemistry and molecular & cellular biology at Georgetown University, Washington.
Proposed RESPONSE Act targets potential shooters
As I’m writing, my Twitter feed announces yet another public shooting, this one at a Walmart in Oklahoma. It’s a problem that gets worse as it gets more attention and the argument over how to approach the issue of mass shootings still continues down two separate and distinct pathways: Is this the result of too-easy access to firearms or is it one of untreated mental illness?

Sen. John Cornyn (R-Tex.) spoke on the Senate floor on Oct. 23, 2019, about new legislation he is cosponsoring in the aftermath of two mass shootings in Texas this past August. The Restoring, Enhancing, Strengthening, and Promoting Our Nation’s Safety Efforts Act of 2019 (S. 2690), or the RESPONSE Act, is designed to “reduce mass violence, strengthen mental health collaboration in communities, improve school safety, and for other purposes.” Sen. Cornyn notes that in the aftermath of those shootings he met with his constituents and he heard a common refrain: Please do something.
“Unfortunately, there is no quick fix, no simple answer, instead we are left to look at the factors that led to these attacks and to try to do something to prevent the sequence of events from playing out again in the future,” Sen. Cornyn said.
“While mental illness is not the prevailing cause of mass violence, enhanced mental health resources are critical to saving lives,” he said, adding that most gun deaths are from suicide. In his speech, he outlined the issues it would address – and despite his statement that mental illness is not the cause of mass violence – he went on to elaborate on the issues that the bill would address.
“First, this legislation takes aim at unlicensed firearms dealers who are breaking the law,” he said. This legislation would create a task force to prosecute those who buy and sell firearms through unlicensed dealers, and he notes that one of the Texas shooters was denied a gun by a licensed firearms dealer before purchasing one from an unlicensed dealer. That Sen. Cornyn’s proposed legislation would not create any new gun legislation is not a surprise: he has an A+ rating from the National Rifle Association and his website’s fun facts include the statement: “Sen. Cornyn owns several firearms and hunts as often as he can.”
The rest of the RESPONSE Act takes aim at those who have or might have psychiatric disorders or a tendency toward violence. Sen. Cornyn noted that the act would expand assisted outpatient treatment (AOT, or outpatient civil commitment). He referenced this as a way for families to get care for their loved ones in the community rather than in a hospital and did not allude to the involuntary nature of the treatment.
Marvin Swartz, MD, is professor of psychiatry at Duke University, Durham, N.C., and lead investigator on outcome studies following the implementation of outpatient civil commitment legislation.
“AOT may be justified in improving treatment adherence and service provision,” Dr. Swartz noted, “but there is no direct line to serious violence. The violence we documented as reduced were mainly minor acts of interpersonal violence – pushing and shoving – what we call minor acts of violence. There is no evidence that AOT is a remedy to serious acts of violence – mass shootings included.”
In addition, Sen. Cornyn noted there would be expanded crisis intervention teams and increased coordination between mental health providers and law enforcement. Furthermore, the bill would make schools safer by identifying students whose behavior indicated a threat of violence and providing those students with the services they need. This would be done “by promoting best practices within our schools and promoting Internet safety.”
Finally, Sen. Cornyn talked about using social media as a means to identify those who might be a danger. “Because so often these shooters advertise on social media ... this legislation includes provisions to [ensure] that law enforcement can receive timely information about threats made online.”
The bill already has garnered both support and opposition. It has been supported by the National Council for Behavioral Health, the National Alliance on Mental Illness (NAMI), and the Treatment Advocacy Center. Those opposed to the legislation include the National Disability Rights Network, the American Association of People with Disabilities, the National Council on Independent Living, the Disability Rights Education & Defense Fund, the Bazelon Center for Mental Health Law, and the Autistic Self Advocacy Network. The American Psychiatric Association has not made a statement on the proposed legislation as of this writing.
The National Council for Behavioral Health posted an endorsement on its website. It notes: “The RESPONSE Act authorizes up to $10 million of existing funds in the Department of Justice for partnership between law enforcement and mental health providers to increase access to long-acting medically assisted treatment. Additionally, it requires the Department of Health and Human Services (HHS) to develop and disseminate guidance for states to fund mental health programs and crisis intervention teams through Medicaid as well as to issue a report to Congress on best practices to expand the mental health workforce. These provisions aim to divert more individuals from incarceration and will create more opportunities for community-based treatment and recovery.”
There is no question that psychiatric treatment for those with mental illness is underfunded and often inaccessible. But while it is true that some individuals become violent when they are ill, most do not, and targeting those one in five Americans who suffer from a psychiatric disorder each year in an effort to identify, then thwart, the rare mass murderer among us makes no sense.
Acts of mass violence remain rare. In 2018, the year we had a record-breaking number of mass shootings, there were 12 mass murders in the United States, according to the criteria used by Mother Jones, and 27 active shooter incidents using the FBI’s criteria. Approximately half of all mass shooters showed signs of mental illness prior to the shooting and of those, some had never come to the attention of mental health professionals in a way that would have predicted violence. While linking mass violence to mental illness may seem reasonable, the numbers just don’t make sense and targeting this presumed link between mental illness and mass violence is stigmatizing.
The text of the RESPONSE Act reveals proposed legislation that is perhaps more thoughtful than Sen. Cornyn’s speech suggested; the bill starts with funding services for those with psychiatric disorders who are being released from the correctional system, a population that may be at higher risk for acts of violence. The funding for outpatient civil commitment is worded in such a way that it is hard to know exactly what is required. The bill starts by mandating that each state must use 10% of the funding it gets from this bill for court-ordered treatment (AOT), but then lists alternative ways states may use that 10%, including “otherwise support evidence-based programs that address the needs of eligible patients.” In all, the proposed legislation is long and complex and attempts to address issues related to terrorism, the Internet, mental health, and the educational system. It’s an ambitious use of $10 million a year for our entire country.

At a time when mental health care is desperately underfunded and many are unable to access treatment, it is tempting to endorse any legislation that improves funding. But does it serve society to endorse legislation that suggests psychiatrists can prevent mass shootings? Does that ultimately serve our patients?
Dr. Miller is coauthor with Annette Hanson, MD, of “Committed: The Battle of Inpatient Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016), and has a private practice in Baltimore.
As I’m writing, my Twitter feed announces yet another public shooting, this one at a Walmart in Oklahoma. It’s a problem that gets worse as it gets more attention and the argument over how to approach the issue of mass shootings still continues down two separate and distinct pathways: Is this the result of too-easy access to firearms or is it one of untreated mental illness?
Sen. John Cornyn (R-Tex.) spoke on the Senate floor on Oct. 23, 2019, about new legislation he is cosponsoring in the aftermath of two mass shootings in Texas this past August. The Restoring, Enhancing, Strengthening, and Promoting Our Nation’s Safety Efforts Act of 2019 (S. 2690), or the RESPONSE Act, is designed to “reduce mass violence, strengthen mental health collaboration in communities, improve school safety, and for other purposes.” Sen. Cornyn notes that in the aftermath of those shootings he met with his constituents and he heard a common refrain: Please do something.
“Unfortunately, there is no quick fix, no simple answer, instead we are left to look at the factors that led to these attacks and to try to do something to prevent the sequence of events from playing out again in the future,” Sen. Cornyn said.
“While mental illness is not the prevailing cause of mass violence, enhanced mental health resources are critical to saving lives,” he said, adding that most gun deaths are from suicide. In his speech, he outlined the issues it would address – and despite his statement that mental illness is not the cause of mass violence – he went on to elaborate on the issues that the bill would address.
“First, this legislation takes aim at unlicensed firearms dealers who are breaking the law,” he said. This legislation would create a task force to prosecute those who buy and sell firearms through unlicensed dealers, and he notes that one of the Texas shooters was denied a gun by a licensed firearms dealer before purchasing one from an unlicensed dealer. That Sen. Cornyn’s proposed legislation would not create any new gun legislation is not a surprise: he has an A+ rating from the National Rifle Association and his website’s fun facts include the statement: “Sen. Cornyn owns several firearms and hunts as often as he can.”
The rest of the RESPONSE Act takes aim at those who have or might have psychiatric disorders or a tendency toward violence. Sen. Cornyn noted that the act would expand assisted outpatient treatment (AOT, or outpatient civil commitment). He referenced this as a way for families to get care for their loved ones in the community rather than in a hospital and did not allude to the involuntary nature of the treatment.
Marvin Swartz, MD, is professor of psychiatry at Duke University, Durham, N.C., and lead investigator on outcome studies following the implementation of outpatient civil commitment legislation.
“AOT may be justified in improving treatment adherence and service provision,” Dr. Swartz noted, “but there is no direct line to serious violence. The violence we documented as reduced were mainly minor acts of interpersonal violence – pushing and shoving – what we call minor acts of violence. There is no evidence that AOT is a remedy to serious acts of violence – mass shootings included.”
In addition, Sen. Cornyn noted there would be expanded crisis intervention teams and increased coordination between mental health providers and law enforcement. Furthermore, the bill would make schools safer by identifying students whose behavior indicated a threat of violence and providing those students with the services they need. This would be done “by promoting best practices within our schools and promoting Internet safety.”
Finally, Sen. Cornyn talked about using social media as a means to identify those who might be a danger. “Because so often these shooters advertise on social media ... this legislation includes provisions to [ensure] that law enforcement can receive timely information about threats made online.”
The bill already has garnered both support and opposition. It has been supported by the National Council for Behavioral Health, the National Alliance on Mental Illness (NAMI), and the Treatment Advocacy Center. Those opposed to the legislation include the National Disability Rights Network, the American Association of People with Disabilities, the National Council on Independent Living, the Disability Rights Education & Defense Fund, the Bazelon Center for Mental Health Law, and the Autistic Self Advocacy Network. The American Psychiatric Association has not made a statement on the proposed legislation as of this writing.
The National Council for Behavioral Health posted an endorsement on its website. It notes: “The RESPONSE Act authorizes up to $10 million of existing funds in the Department of Justice for partnership between law enforcement and mental health providers to increase access to long-acting medically assisted treatment. Additionally, it requires the Department of Health and Human Services (HHS) to develop and disseminate guidance for states to fund mental health programs and crisis intervention teams through Medicaid as well as to issue a report to Congress on best practices to expand the mental health workforce. These provisions aim to divert more individuals from incarceration and will create more opportunities for community-based treatment and recovery.”
There is no question that psychiatric treatment for those with mental illness is underfunded and often inaccessible. But while it is true that some individuals become violent when they are ill, most do not, and targeting those one in five Americans who suffer from a psychiatric disorder each year in an effort to identify, then thwart, the rare mass murderer among us makes no sense.
Acts of mass violence remain rare. In 2018, the year we had a record-breaking number of mass shootings, there were 12 mass murders in the United States, according to the criteria used by Mother Jones, and 27 active shooter incidents using the FBI’s criteria. Approximately half of all mass shooters showed signs of mental illness prior to the shooting and of those, some had never come to the attention of mental health professionals in a way that would have predicted violence. While linking mass violence to mental illness may seem reasonable, the numbers just don’t make sense and targeting this presumed link between mental illness and mass violence is stigmatizing.
The text of the RESPONSE Act reveals proposed legislation that is perhaps more thoughtful than Sen. Cornyn’s speech suggested; the bill starts with funding services for those with psychiatric disorders who are being released from the correctional system, a population that may be at higher risk for acts of violence. The funding for outpatient civil commitment is worded in such a way that it is hard to know exactly what is required. The bill starts by mandating that each state must use 10% of the funding it gets from this bill for court-ordered treatment (AOT), but then lists alternative ways states may use that 10%, including “otherwise support evidence-based programs that address the needs of eligible patients.” In all, the proposed legislation is long and complex and attempts to address issues related to terrorism, the Internet, mental health, and the educational system. It’s an ambitious use of $10 million a year for our entire country.
At a time when mental health care is desperately underfunded and many are unable to access treatment, it is tempting to endorse any legislation that improves funding. But does it serve society to endorse legislation that suggests psychiatrists can prevent mass shootings? Does that ultimately serve our patients?
Dr. Miller is coauthor with Annette Hanson, MD, of “Committed: The Battle of Inpatient Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016), and has a private practice in Baltimore.
As I’m writing, my Twitter feed announces yet another public shooting, this one at a Walmart in Oklahoma. It’s a problem that gets worse as it gets more attention and the argument over how to approach the issue of mass shootings still continues down two separate and distinct pathways: Is this the result of too-easy access to firearms or is it one of untreated mental illness?
Sen. John Cornyn (R-Tex.) spoke on the Senate floor on Oct. 23, 2019, about new legislation he is cosponsoring in the aftermath of two mass shootings in Texas this past August. The Restoring, Enhancing, Strengthening, and Promoting Our Nation’s Safety Efforts Act of 2019 (S. 2690), or the RESPONSE Act, is designed to “reduce mass violence, strengthen mental health collaboration in communities, improve school safety, and for other purposes.” Sen. Cornyn notes that in the aftermath of those shootings he met with his constituents and he heard a common refrain: Please do something.
“Unfortunately, there is no quick fix, no simple answer, instead we are left to look at the factors that led to these attacks and to try to do something to prevent the sequence of events from playing out again in the future,” Sen. Cornyn said.
“While mental illness is not the prevailing cause of mass violence, enhanced mental health resources are critical to saving lives,” he said, adding that most gun deaths are from suicide. In his speech, he outlined the issues it would address – and despite his statement that mental illness is not the cause of mass violence – he went on to elaborate on the issues that the bill would address.
“First, this legislation takes aim at unlicensed firearms dealers who are breaking the law,” he said. This legislation would create a task force to prosecute those who buy and sell firearms through unlicensed dealers, and he notes that one of the Texas shooters was denied a gun by a licensed firearms dealer before purchasing one from an unlicensed dealer. That Sen. Cornyn’s proposed legislation would not create any new gun legislation is not a surprise: he has an A+ rating from the National Rifle Association and his website’s fun facts include the statement: “Sen. Cornyn owns several firearms and hunts as often as he can.”
The rest of the RESPONSE Act takes aim at those who have or might have psychiatric disorders or a tendency toward violence. Sen. Cornyn noted that the act would expand assisted outpatient treatment (AOT, or outpatient civil commitment). He referenced this as a way for families to get care for their loved ones in the community rather than in a hospital and did not allude to the involuntary nature of the treatment.
Marvin Swartz, MD, is professor of psychiatry at Duke University, Durham, N.C., and lead investigator on outcome studies following the implementation of outpatient civil commitment legislation.
“AOT may be justified in improving treatment adherence and service provision,” Dr. Swartz noted, “but there is no direct line to serious violence. The violence we documented as reduced were mainly minor acts of interpersonal violence – pushing and shoving – what we call minor acts of violence. There is no evidence that AOT is a remedy to serious acts of violence – mass shootings included.”
In addition, Sen. Cornyn noted there would be expanded crisis intervention teams and increased coordination between mental health providers and law enforcement. Furthermore, the bill would make schools safer by identifying students whose behavior indicated a threat of violence and providing those students with the services they need. This would be done “by promoting best practices within our schools and promoting Internet safety.”
Finally, Sen. Cornyn talked about using social media as a means to identify those who might be a danger. “Because so often these shooters advertise on social media ... this legislation includes provisions to [ensure] that law enforcement can receive timely information about threats made online.”
The bill already has garnered both support and opposition. It has been supported by the National Council for Behavioral Health, the National Alliance on Mental Illness (NAMI), and the Treatment Advocacy Center. Those opposed to the legislation include the National Disability Rights Network, the American Association of People with Disabilities, the National Council on Independent Living, the Disability Rights Education & Defense Fund, the Bazelon Center for Mental Health Law, and the Autistic Self Advocacy Network. The American Psychiatric Association has not made a statement on the proposed legislation as of this writing.
The National Council for Behavioral Health posted an endorsement on its website. It notes: “The RESPONSE Act authorizes up to $10 million of existing funds in the Department of Justice for partnership between law enforcement and mental health providers to increase access to long-acting medically assisted treatment. Additionally, it requires the Department of Health and Human Services (HHS) to develop and disseminate guidance for states to fund mental health programs and crisis intervention teams through Medicaid as well as to issue a report to Congress on best practices to expand the mental health workforce. These provisions aim to divert more individuals from incarceration and will create more opportunities for community-based treatment and recovery.”
There is no question that psychiatric treatment for those with mental illness is underfunded and often inaccessible. But while it is true that some individuals become violent when they are ill, most do not, and targeting those one in five Americans who suffer from a psychiatric disorder each year in an effort to identify, then thwart, the rare mass murderer among us makes no sense.
Acts of mass violence remain rare. In 2018, the year we had a record-breaking number of mass shootings, there were 12 mass murders in the United States, according to the criteria used by Mother Jones, and 27 active shooter incidents using the FBI’s criteria. Approximately half of all mass shooters showed signs of mental illness prior to the shooting and of those, some had never come to the attention of mental health professionals in a way that would have predicted violence. While linking mass violence to mental illness may seem reasonable, the numbers just don’t make sense and targeting this presumed link between mental illness and mass violence is stigmatizing.
The text of the RESPONSE Act reveals proposed legislation that is perhaps more thoughtful than Sen. Cornyn’s speech suggested; the bill starts with funding services for those with psychiatric disorders who are being released from the correctional system, a population that may be at higher risk for acts of violence. The funding for outpatient civil commitment is worded in such a way that it is hard to know exactly what is required. The bill starts by mandating that each state must use 10% of the funding it gets from this bill for court-ordered treatment (AOT), but then lists alternative ways states may use that 10%, including “otherwise support evidence-based programs that address the needs of eligible patients.” In all, the proposed legislation is long and complex and attempts to address issues related to terrorism, the Internet, mental health, and the educational system. It’s an ambitious use of $10 million a year for our entire country.
At a time when mental health care is desperately underfunded and many are unable to access treatment, it is tempting to endorse any legislation that improves funding. But does it serve society to endorse legislation that suggests psychiatrists can prevent mass shootings? Does that ultimately serve our patients?
Dr. Miller is coauthor with Annette Hanson, MD, of “Committed: The Battle of Inpatient Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016), and has a private practice in Baltimore.

Going beyond the QI project
Role modeling for residents
Quality improvement (QI) education has become increasingly seen as core content in graduate medical education, said Brian Wong, MD, FRCPC, of the University of Toronto. One of the most common strategies for teaching QI is to have residents participate in a QI project, in which hospitalists often take a leading role.

“Given the investment made and time spent carrying out these projects, it is important to know whether or not the training has led to the desired outcome from both a learning and a project standpoint,” Dr. Wong said, which is why he coauthored a recent editorial on the subject in BMJ Quality and Safety. QI educators have long recognized that it’s difficult to know whether the education was successful.
“For example, if the project was not successful, does it matter if the residents learned key QI principles that they were able to apply to their project work?” Dr. Wong noted. “Our perspective extends this discussion by asking, ‘What does success look like in QI education?’ We argue that rather than focusing on whether the project was successful or not, our real goal should be to create QI educational experiences that will ensure that residents change their behaviors in future practice to embrace QI as an activity that is core to their everyday work.”
Hospitalists have an important role in that. “They can set the stage for learners to recognize just how important it is to incorporate QI into daily work. Through this role modeling, residents who carry out QI projects can see that the lessons learned contribute to lifelong engagement in QI.”
Dr. Wong’s hope is to focus on the type of QI experience that fosters long-term behavior changes.
“We want residents, when they graduate, to embrace QI, to volunteer to participate in organizational initiatives, to welcome practice data and reflect on it for the purposes of continuous improvement, to collaborate interprofessionally to make small iterative changes to the care delivery system to ensure that patients receive the highest quality of care possible,” he said. “My hope is that we can start to think differently about how we measure success in QI education.”
Reference
1. Myers JS, Wong BM. Measuring outcomes in quality improvement education: Success is in the eye of the beholder. BMJ Qual Saf. 2019 Mar 18. doi: 10.1136/bmjqs-2018-008305.
Role modeling for residents
Role modeling for residents
Quality improvement (QI) education has become increasingly seen as core content in graduate medical education, said Brian Wong, MD, FRCPC, of the University of Toronto. One of the most common strategies for teaching QI is to have residents participate in a QI project, in which hospitalists often take a leading role.
“Given the investment made and time spent carrying out these projects, it is important to know whether or not the training has led to the desired outcome from both a learning and a project standpoint,” Dr. Wong said, which is why he coauthored a recent editorial on the subject in BMJ Quality and Safety. QI educators have long recognized that it’s difficult to know whether the education was successful.
“For example, if the project was not successful, does it matter if the residents learned key QI principles that they were able to apply to their project work?” Dr. Wong noted. “Our perspective extends this discussion by asking, ‘What does success look like in QI education?’ We argue that rather than focusing on whether the project was successful or not, our real goal should be to create QI educational experiences that will ensure that residents change their behaviors in future practice to embrace QI as an activity that is core to their everyday work.”
Hospitalists have an important role in that. “They can set the stage for learners to recognize just how important it is to incorporate QI into daily work. Through this role modeling, residents who carry out QI projects can see that the lessons learned contribute to lifelong engagement in QI.”
Dr. Wong’s hope is to focus on the type of QI experience that fosters long-term behavior changes.
“We want residents, when they graduate, to embrace QI, to volunteer to participate in organizational initiatives, to welcome practice data and reflect on it for the purposes of continuous improvement, to collaborate interprofessionally to make small iterative changes to the care delivery system to ensure that patients receive the highest quality of care possible,” he said. “My hope is that we can start to think differently about how we measure success in QI education.”
Reference
1. Myers JS, Wong BM. Measuring outcomes in quality improvement education: Success is in the eye of the beholder. BMJ Qual Saf. 2019 Mar 18. doi: 10.1136/bmjqs-2018-008305.
Quality improvement (QI) education has become increasingly seen as core content in graduate medical education, said Brian Wong, MD, FRCPC, of the University of Toronto. One of the most common strategies for teaching QI is to have residents participate in a QI project, in which hospitalists often take a leading role.
“Given the investment made and time spent carrying out these projects, it is important to know whether or not the training has led to the desired outcome from both a learning and a project standpoint,” Dr. Wong said, which is why he coauthored a recent editorial on the subject in BMJ Quality and Safety. QI educators have long recognized that it’s difficult to know whether the education was successful.
“For example, if the project was not successful, does it matter if the residents learned key QI principles that they were able to apply to their project work?” Dr. Wong noted. “Our perspective extends this discussion by asking, ‘What does success look like in QI education?’ We argue that rather than focusing on whether the project was successful or not, our real goal should be to create QI educational experiences that will ensure that residents change their behaviors in future practice to embrace QI as an activity that is core to their everyday work.”
Hospitalists have an important role in that. “They can set the stage for learners to recognize just how important it is to incorporate QI into daily work. Through this role modeling, residents who carry out QI projects can see that the lessons learned contribute to lifelong engagement in QI.”
Dr. Wong’s hope is to focus on the type of QI experience that fosters long-term behavior changes.
“We want residents, when they graduate, to embrace QI, to volunteer to participate in organizational initiatives, to welcome practice data and reflect on it for the purposes of continuous improvement, to collaborate interprofessionally to make small iterative changes to the care delivery system to ensure that patients receive the highest quality of care possible,” he said. “My hope is that we can start to think differently about how we measure success in QI education.”
Reference
1. Myers JS, Wong BM. Measuring outcomes in quality improvement education: Success is in the eye of the beholder. BMJ Qual Saf. 2019 Mar 18. doi: 10.1136/bmjqs-2018-008305.
Short Takes
E-cigarettes with behavioral support more effective than nicotine replacement for smoking cessation
A study of 886 randomized United Kingdom National Health Service stop-smoking service attendees showed better 1-year abstinence rates in the e-cigarette (18%) vs. nicotine replacement product (9%) group (risk ratio,1.83; 95% confidence interval, 1.30-2.58) when both groups received behavioral support.
Citation: Hajek P et al. A randomized trial of e-cigarettes versus nicotine-replacement therapy. N Eng J Med. 2019 Feb 14;380:629-37.
New scoring system more accurate in diagnosing sepsis than qSOFA
Using retrospective data from 2,759,529 ED patients in 49 urban hospitals, and a supervised machine-learning process, the authors developed a Risk of Sepsis score, which demonstrated significantly higher sensitivity for detecting sepsis than the qSOFA (Quick Sequential Organ Failure Assessment) score.
Citation: Delahanty R et al. Development and evaluation of a machine learning model for the early identification of patients at risk for sepsis. Ann Emerg Med. 2019 Apr;73(4):334-44.
Shared decision making may decrease risk of legal action
A randomized, controlled simulation experiment using a clinical vignette with an adverse outcome showed that when engaged in shared decision making, participants were less likely to consider taking legal action.
Citation: Schoenfeld EM et al. The effect of shared decision making on patients’ likelihood of filing a complaint or lawsuit: A simulation study. Ann Emerg Med. 2019 Jan 3. doi: 10.1016/j.annemergmed.2018.11.017.
ADA issues new inpatient diabetes care recommendations
The American Diabetes Association recommends that insulin therapy be initiated for a majority of inpatients who have persistent hyperglycemia greater than 180 mg/dL to target a blood glucose range of 140-180 mg/dL. They recommend the use of basal insulin or basal plus bolus insulin and discourage the sole use of sliding scale insulin.
Citation: American Diabetes Association. 15. Diabetes care in the hospital: Standards of Medical Care in Diabetes-2019. Diabetes Care. 2019;42(Suppl. 1):S173-81.
Beta-blocker use may reduce risk of COPD hospitalization

In a retrospective longitudinal study of 301,542 patients newly prescribed beta-blockers and 1,000,633 patients newly prescribed any other antihypertensive drug, patients who were treated with beta-blockers continuously for more than 6 months had a significantly lower risk of chronic obstructive pulmonary disease (COPD) hospitalization, all-cause mortality, and COPD death than did patients who received alternative antihypertensives. Patients with a history of COPD hospitalization were excluded from this study.
Citation: Nielsen AO et al. Beta-blocker therapy and risk of chronic obstructive pulmonary disease: A Danish nationwide study of 1.3 million individuals. EClinicalMedicine. 2019;7:21-6. doi: 10.1016/j.eclinm.2019.01.004.
E-cigarettes with behavioral support more effective than nicotine replacement for smoking cessation
A study of 886 randomized United Kingdom National Health Service stop-smoking service attendees showed better 1-year abstinence rates in the e-cigarette (18%) vs. nicotine replacement product (9%) group (risk ratio,1.83; 95% confidence interval, 1.30-2.58) when both groups received behavioral support.
Citation: Hajek P et al. A randomized trial of e-cigarettes versus nicotine-replacement therapy. N Eng J Med. 2019 Feb 14;380:629-37.
New scoring system more accurate in diagnosing sepsis than qSOFA
Using retrospective data from 2,759,529 ED patients in 49 urban hospitals, and a supervised machine-learning process, the authors developed a Risk of Sepsis score, which demonstrated significantly higher sensitivity for detecting sepsis than the qSOFA (Quick Sequential Organ Failure Assessment) score.
Citation: Delahanty R et al. Development and evaluation of a machine learning model for the early identification of patients at risk for sepsis. Ann Emerg Med. 2019 Apr;73(4):334-44.
Shared decision making may decrease risk of legal action
A randomized, controlled simulation experiment using a clinical vignette with an adverse outcome showed that when engaged in shared decision making, participants were less likely to consider taking legal action.
Citation: Schoenfeld EM et al. The effect of shared decision making on patients’ likelihood of filing a complaint or lawsuit: A simulation study. Ann Emerg Med. 2019 Jan 3. doi: 10.1016/j.annemergmed.2018.11.017.
ADA issues new inpatient diabetes care recommendations
The American Diabetes Association recommends that insulin therapy be initiated for a majority of inpatients who have persistent hyperglycemia greater than 180 mg/dL to target a blood glucose range of 140-180 mg/dL. They recommend the use of basal insulin or basal plus bolus insulin and discourage the sole use of sliding scale insulin.
Citation: American Diabetes Association. 15. Diabetes care in the hospital: Standards of Medical Care in Diabetes-2019. Diabetes Care. 2019;42(Suppl. 1):S173-81.
Beta-blocker use may reduce risk of COPD hospitalization
In a retrospective longitudinal study of 301,542 patients newly prescribed beta-blockers and 1,000,633 patients newly prescribed any other antihypertensive drug, patients who were treated with beta-blockers continuously for more than 6 months had a significantly lower risk of chronic obstructive pulmonary disease (COPD) hospitalization, all-cause mortality, and COPD death than did patients who received alternative antihypertensives. Patients with a history of COPD hospitalization were excluded from this study.
Citation: Nielsen AO et al. Beta-blocker therapy and risk of chronic obstructive pulmonary disease: A Danish nationwide study of 1.3 million individuals. EClinicalMedicine. 2019;7:21-6. doi: 10.1016/j.eclinm.2019.01.004.
E-cigarettes with behavioral support more effective than nicotine replacement for smoking cessation
A study of 886 randomized United Kingdom National Health Service stop-smoking service attendees showed better 1-year abstinence rates in the e-cigarette (18%) vs. nicotine replacement product (9%) group (risk ratio,1.83; 95% confidence interval, 1.30-2.58) when both groups received behavioral support.
Citation: Hajek P et al. A randomized trial of e-cigarettes versus nicotine-replacement therapy. N Eng J Med. 2019 Feb 14;380:629-37.
New scoring system more accurate in diagnosing sepsis than qSOFA
Using retrospective data from 2,759,529 ED patients in 49 urban hospitals, and a supervised machine-learning process, the authors developed a Risk of Sepsis score, which demonstrated significantly higher sensitivity for detecting sepsis than the qSOFA (Quick Sequential Organ Failure Assessment) score.
Citation: Delahanty R et al. Development and evaluation of a machine learning model for the early identification of patients at risk for sepsis. Ann Emerg Med. 2019 Apr;73(4):334-44.
Shared decision making may decrease risk of legal action
A randomized, controlled simulation experiment using a clinical vignette with an adverse outcome showed that when engaged in shared decision making, participants were less likely to consider taking legal action.
Citation: Schoenfeld EM et al. The effect of shared decision making on patients’ likelihood of filing a complaint or lawsuit: A simulation study. Ann Emerg Med. 2019 Jan 3. doi: 10.1016/j.annemergmed.2018.11.017.
ADA issues new inpatient diabetes care recommendations
The American Diabetes Association recommends that insulin therapy be initiated for a majority of inpatients who have persistent hyperglycemia greater than 180 mg/dL to target a blood glucose range of 140-180 mg/dL. They recommend the use of basal insulin or basal plus bolus insulin and discourage the sole use of sliding scale insulin.
Citation: American Diabetes Association. 15. Diabetes care in the hospital: Standards of Medical Care in Diabetes-2019. Diabetes Care. 2019;42(Suppl. 1):S173-81.
Beta-blocker use may reduce risk of COPD hospitalization
In a retrospective longitudinal study of 301,542 patients newly prescribed beta-blockers and 1,000,633 patients newly prescribed any other antihypertensive drug, patients who were treated with beta-blockers continuously for more than 6 months had a significantly lower risk of chronic obstructive pulmonary disease (COPD) hospitalization, all-cause mortality, and COPD death than did patients who received alternative antihypertensives. Patients with a history of COPD hospitalization were excluded from this study.
Citation: Nielsen AO et al. Beta-blocker therapy and risk of chronic obstructive pulmonary disease: A Danish nationwide study of 1.3 million individuals. EClinicalMedicine. 2019;7:21-6. doi: 10.1016/j.eclinm.2019.01.004.
What psychiatrists need to know about the Green New Deal
My final appointment for the day was very late, with only 10 minutes left in the session. I was closing my office door when my patient, a middle-aged woman, rushed up and said: “I am sorry to be so late, but traffic was terrible. I am out of my meds. Will you still see me?” I agreed. She was touched and thanked me.
As she sat down, still breathless, she said: “I have had a lot on my mind. After we work out the meds, could we please talk about them? One thing is the climate problem, but there is really no point in worrying about something you cannot do anything about.”
I refilled her meds, then I responded to her offhand comment about climate by saying, “I, too, have been concerned about climate change. Tell me your concerns.” She opened up and, to my surprise, burst into tears, saying, “how terrible it is, what we’re doing to the earth, and how bad it will be for those to come. How could we leave the earth in such a mess?” She was clearly grieving. I agreed and said: “There is a lot to be done, and we can do many things to help. Have you heard about the Green New Deal?” We talked about this for a few minutes, and she was very interested.
At first, she disavowed the problem, saying that, while it bothered her, nothing could be done about it, so why talk about it? Disavowal is a common defense that shields us from our real feelings about disturbing problems. Once I invited her to talk about it, she opened up with grief and near paralyzing sadness. This was my opportunity to let her know that there is a realistic plan for dealing with climate change. If she were to get politically active or involved with like-minded groups, hope could be possible. (As young Greta Thunberg, the Swedish youth climate action leader, teaches us, “Where there is no action, there is no hope, but where there is action, hope is everywhere.”)
So, what does a psychiatrist need to know about the Green New Deal?
It is essentially a broad legislative conceptual agenda with wide-ranging implications. The resolution has growing support in Congress. Its scope has been compared to the 1960s moon landing or the New Deal that helped this nation come out of the Great Depression. The primary goal is to bring the United States to 100% sustainable clean energy by 2030. It also proposes to help those most vulnerable to the stresses of climate change, such as “indigenous communities, communities of color, migrant communities, deinstitutionalized communities, depopulated communities, the poor, lower income workers, women, the elderly, the unhoused, people with disabilities, and youth.” Our patient population reflects many of those cohorts and will likely be helped directly by this ambitious agenda.
Specifically, the Green New Deal would transition the United States from fossil fuel dependence to clean energy sources, such as solar and wind power, upgrade the power grid, refurbish and retrofit buildings to become sustainable and energy efficient, overhaul transportation systems, and promote the transition to electric vehicles and high-speed rail. This transition of the infrastructure and economy will, in turn, create millions of good jobs, including meaningful and rewarding work for workers and communities transitioning away from fossil fuel industry–related activities.
The Green New Deal is intended to address the reality and risks of climate change. The World Health Organization has deemed climate change the greatest public health threat of the 21st century. Consider the following ominous developments:
The current atmospheric CO2 level is 415 parts per million and rising, an increase from preindustrial levels of 278 ppm. Earthworms have now expanded their territory to include boreal forests near the Arctic, munching the foot-thick organic forest floor, potentially releasing much more CO2. Permafrost is melting near the Arctic, as is sea ice, reducing the amount of solar radiation reflected back to space. Perversely and ironically, the loss of sea ice is touted by some climate deniers as an opportunity for expanded oil and gas exploration in the Arctic.
Extreme weather events are increasing in frequency and duration. Record-setting hurricanes, floods, tornadoes, heat waves, and wildfires are becoming the “new normal,” except for the fact that they are expected to continue worsening.
If the United States continues business as usual without addressing our climate trajectory, there will be dire consequences for all future generations. Without serious efforts to combat global warming, a 4- to 5-degree Celsius increase by the end of the century is likely. This would be catastrophic, leading to the collapse of the ice sheets, massive coastal inundation, unrelenting heat waves, wildfires beyond imagination, severe droughts, starvation, immense storms, and vast areas of the earth becoming uninhabitable.
It is time for the United States to join the rest of the world in dealing with global warming. The nations of the earth need to unite for the common good and to save our planet. The Green New Deal would represent a major step in that direction and would certainly help our patients to have more meaningful, hopeful, and healthier lives.
Dr. Peterson is assistant clinical professor in the department of psychiatry at Georgetown University in Washington. He is an active member of the Climate Psychiatry Alliance and the Caucus on Climate Change and Mental Health at the American Psychiatric Association. Dr. Peterson changed key facts about the patient’s story to protect her confidentiality.
My final appointment for the day was very late, with only 10 minutes left in the session. I was closing my office door when my patient, a middle-aged woman, rushed up and said: “I am sorry to be so late, but traffic was terrible. I am out of my meds. Will you still see me?” I agreed. She was touched and thanked me.
As she sat down, still breathless, she said: “I have had a lot on my mind. After we work out the meds, could we please talk about them? One thing is the climate problem, but there is really no point in worrying about something you cannot do anything about.”
I refilled her meds, then I responded to her offhand comment about climate by saying, “I, too, have been concerned about climate change. Tell me your concerns.” She opened up and, to my surprise, burst into tears, saying, “how terrible it is, what we’re doing to the earth, and how bad it will be for those to come. How could we leave the earth in such a mess?” She was clearly grieving. I agreed and said: “There is a lot to be done, and we can do many things to help. Have you heard about the Green New Deal?” We talked about this for a few minutes, and she was very interested.
At first, she disavowed the problem, saying that, while it bothered her, nothing could be done about it, so why talk about it? Disavowal is a common defense that shields us from our real feelings about disturbing problems. Once I invited her to talk about it, she opened up with grief and near paralyzing sadness. This was my opportunity to let her know that there is a realistic plan for dealing with climate change. If she were to get politically active or involved with like-minded groups, hope could be possible. (As young Greta Thunberg, the Swedish youth climate action leader, teaches us, “Where there is no action, there is no hope, but where there is action, hope is everywhere.”)
So, what does a psychiatrist need to know about the Green New Deal?
It is essentially a broad legislative conceptual agenda with wide-ranging implications. The resolution has growing support in Congress. Its scope has been compared to the 1960s moon landing or the New Deal that helped this nation come out of the Great Depression. The primary goal is to bring the United States to 100% sustainable clean energy by 2030. It also proposes to help those most vulnerable to the stresses of climate change, such as “indigenous communities, communities of color, migrant communities, deinstitutionalized communities, depopulated communities, the poor, lower income workers, women, the elderly, the unhoused, people with disabilities, and youth.” Our patient population reflects many of those cohorts and will likely be helped directly by this ambitious agenda.
Specifically, the Green New Deal would transition the United States from fossil fuel dependence to clean energy sources, such as solar and wind power, upgrade the power grid, refurbish and retrofit buildings to become sustainable and energy efficient, overhaul transportation systems, and promote the transition to electric vehicles and high-speed rail. This transition of the infrastructure and economy will, in turn, create millions of good jobs, including meaningful and rewarding work for workers and communities transitioning away from fossil fuel industry–related activities.
The Green New Deal is intended to address the reality and risks of climate change. The World Health Organization has deemed climate change the greatest public health threat of the 21st century. Consider the following ominous developments:
The current atmospheric CO2 level is 415 parts per million and rising, an increase from preindustrial levels of 278 ppm. Earthworms have now expanded their territory to include boreal forests near the Arctic, munching the foot-thick organic forest floor, potentially releasing much more CO2. Permafrost is melting near the Arctic, as is sea ice, reducing the amount of solar radiation reflected back to space. Perversely and ironically, the loss of sea ice is touted by some climate deniers as an opportunity for expanded oil and gas exploration in the Arctic.
Extreme weather events are increasing in frequency and duration. Record-setting hurricanes, floods, tornadoes, heat waves, and wildfires are becoming the “new normal,” except for the fact that they are expected to continue worsening.
If the United States continues business as usual without addressing our climate trajectory, there will be dire consequences for all future generations. Without serious efforts to combat global warming, a 4- to 5-degree Celsius increase by the end of the century is likely. This would be catastrophic, leading to the collapse of the ice sheets, massive coastal inundation, unrelenting heat waves, wildfires beyond imagination, severe droughts, starvation, immense storms, and vast areas of the earth becoming uninhabitable.
It is time for the United States to join the rest of the world in dealing with global warming. The nations of the earth need to unite for the common good and to save our planet. The Green New Deal would represent a major step in that direction and would certainly help our patients to have more meaningful, hopeful, and healthier lives.
Dr. Peterson is assistant clinical professor in the department of psychiatry at Georgetown University in Washington. He is an active member of the Climate Psychiatry Alliance and the Caucus on Climate Change and Mental Health at the American Psychiatric Association. Dr. Peterson changed key facts about the patient’s story to protect her confidentiality.
My final appointment for the day was very late, with only 10 minutes left in the session. I was closing my office door when my patient, a middle-aged woman, rushed up and said: “I am sorry to be so late, but traffic was terrible. I am out of my meds. Will you still see me?” I agreed. She was touched and thanked me.
As she sat down, still breathless, she said: “I have had a lot on my mind. After we work out the meds, could we please talk about them? One thing is the climate problem, but there is really no point in worrying about something you cannot do anything about.”
I refilled her meds, then I responded to her offhand comment about climate by saying, “I, too, have been concerned about climate change. Tell me your concerns.” She opened up and, to my surprise, burst into tears, saying, “how terrible it is, what we’re doing to the earth, and how bad it will be for those to come. How could we leave the earth in such a mess?” She was clearly grieving. I agreed and said: “There is a lot to be done, and we can do many things to help. Have you heard about the Green New Deal?” We talked about this for a few minutes, and she was very interested.
At first, she disavowed the problem, saying that, while it bothered her, nothing could be done about it, so why talk about it? Disavowal is a common defense that shields us from our real feelings about disturbing problems. Once I invited her to talk about it, she opened up with grief and near paralyzing sadness. This was my opportunity to let her know that there is a realistic plan for dealing with climate change. If she were to get politically active or involved with like-minded groups, hope could be possible. (As young Greta Thunberg, the Swedish youth climate action leader, teaches us, “Where there is no action, there is no hope, but where there is action, hope is everywhere.”)
So, what does a psychiatrist need to know about the Green New Deal?
It is essentially a broad legislative conceptual agenda with wide-ranging implications. The resolution has growing support in Congress. Its scope has been compared to the 1960s moon landing or the New Deal that helped this nation come out of the Great Depression. The primary goal is to bring the United States to 100% sustainable clean energy by 2030. It also proposes to help those most vulnerable to the stresses of climate change, such as “indigenous communities, communities of color, migrant communities, deinstitutionalized communities, depopulated communities, the poor, lower income workers, women, the elderly, the unhoused, people with disabilities, and youth.” Our patient population reflects many of those cohorts and will likely be helped directly by this ambitious agenda.
Specifically, the Green New Deal would transition the United States from fossil fuel dependence to clean energy sources, such as solar and wind power, upgrade the power grid, refurbish and retrofit buildings to become sustainable and energy efficient, overhaul transportation systems, and promote the transition to electric vehicles and high-speed rail. This transition of the infrastructure and economy will, in turn, create millions of good jobs, including meaningful and rewarding work for workers and communities transitioning away from fossil fuel industry–related activities.
The Green New Deal is intended to address the reality and risks of climate change. The World Health Organization has deemed climate change the greatest public health threat of the 21st century. Consider the following ominous developments:
The current atmospheric CO2 level is 415 parts per million and rising, an increase from preindustrial levels of 278 ppm. Earthworms have now expanded their territory to include boreal forests near the Arctic, munching the foot-thick organic forest floor, potentially releasing much more CO2. Permafrost is melting near the Arctic, as is sea ice, reducing the amount of solar radiation reflected back to space. Perversely and ironically, the loss of sea ice is touted by some climate deniers as an opportunity for expanded oil and gas exploration in the Arctic.
Extreme weather events are increasing in frequency and duration. Record-setting hurricanes, floods, tornadoes, heat waves, and wildfires are becoming the “new normal,” except for the fact that they are expected to continue worsening.
If the United States continues business as usual without addressing our climate trajectory, there will be dire consequences for all future generations. Without serious efforts to combat global warming, a 4- to 5-degree Celsius increase by the end of the century is likely. This would be catastrophic, leading to the collapse of the ice sheets, massive coastal inundation, unrelenting heat waves, wildfires beyond imagination, severe droughts, starvation, immense storms, and vast areas of the earth becoming uninhabitable.
It is time for the United States to join the rest of the world in dealing with global warming. The nations of the earth need to unite for the common good and to save our planet. The Green New Deal would represent a major step in that direction and would certainly help our patients to have more meaningful, hopeful, and healthier lives.
Dr. Peterson is assistant clinical professor in the department of psychiatry at Georgetown University in Washington. He is an active member of the Climate Psychiatry Alliance and the Caucus on Climate Change and Mental Health at the American Psychiatric Association. Dr. Peterson changed key facts about the patient’s story to protect her confidentiality.
FDA still concerned about biotin affecting troponin tests
The

However, not all troponin tests are affected, according to the update. “Since the FDA’s safety communication on this topic in 2017, some lab test developers have been successful at mitigating the biotin interference of their assays, but others have not yet addressed it,” according to the new communication, issued in early November.
Also known as vitamin B7 and appearing in many dietary supplements, including prenatal multivitamins and supplements for hair, skin, and nail growth, biotin can lead to falsely low results on some troponin tests, especially at high levels. The worry is that biotin interference could therefore lead to missed diagnoses. The FDA has provided a list of those tests that have not taken biotin’s effects into account, titled “Biotin Interference with Troponin Lab Tests – Assays Subject to Biotin Interference.”
The daily recommended allowance for biotin, according to the communication, is about 0.3 mg, but it isn’t always clear how much is actually included in supplements – some can contain 20 mg or even as much as 100 mg per pill of biotin. The communication includes recommendations for patients, health care professionals, laboratory personnel, and lab test manufacturers and developers.
The full safety communication can be found on the FDA website, and problems with tests can be reported via the FDA’s MedWatch Voluntary Reporting Form.
The
However, not all troponin tests are affected, according to the update. “Since the FDA’s safety communication on this topic in 2017, some lab test developers have been successful at mitigating the biotin interference of their assays, but others have not yet addressed it,” according to the new communication, issued in early November.
Also known as vitamin B7 and appearing in many dietary supplements, including prenatal multivitamins and supplements for hair, skin, and nail growth, biotin can lead to falsely low results on some troponin tests, especially at high levels. The worry is that biotin interference could therefore lead to missed diagnoses. The FDA has provided a list of those tests that have not taken biotin’s effects into account, titled “Biotin Interference with Troponin Lab Tests – Assays Subject to Biotin Interference.”
The daily recommended allowance for biotin, according to the communication, is about 0.3 mg, but it isn’t always clear how much is actually included in supplements – some can contain 20 mg or even as much as 100 mg per pill of biotin. The communication includes recommendations for patients, health care professionals, laboratory personnel, and lab test manufacturers and developers.
The full safety communication can be found on the FDA website, and problems with tests can be reported via the FDA’s MedWatch Voluntary Reporting Form.
The
However, not all troponin tests are affected, according to the update. “Since the FDA’s safety communication on this topic in 2017, some lab test developers have been successful at mitigating the biotin interference of their assays, but others have not yet addressed it,” according to the new communication, issued in early November.
Also known as vitamin B7 and appearing in many dietary supplements, including prenatal multivitamins and supplements for hair, skin, and nail growth, biotin can lead to falsely low results on some troponin tests, especially at high levels. The worry is that biotin interference could therefore lead to missed diagnoses. The FDA has provided a list of those tests that have not taken biotin’s effects into account, titled “Biotin Interference with Troponin Lab Tests – Assays Subject to Biotin Interference.”
The daily recommended allowance for biotin, according to the communication, is about 0.3 mg, but it isn’t always clear how much is actually included in supplements – some can contain 20 mg or even as much as 100 mg per pill of biotin. The communication includes recommendations for patients, health care professionals, laboratory personnel, and lab test manufacturers and developers.
The full safety communication can be found on the FDA website, and problems with tests can be reported via the FDA’s MedWatch Voluntary Reporting Form.
How I became a better doctor
I became a better doctor on the day I became a cardiac patient. On that day, I experienced the helpless, vulnerable, and needy feelings of a patient’s dependency and blind trust of a physician whom I did not know. I suddenly realized how it feels to be a patient.

My entire life, I had always been an athlete in excellent shape. My 7-day-a-week daily schedule included seeing patients, being an expert psychiatric witness for disability cases, playing 2 hours of tennis, walking/running for 1 hour, and ending the night with 1 hour on a stationary bike.
I get to see my children all the time. I am so fortunate to get to travel with them and play national father-son and father-daughter tennis tournaments. We have been ranked No. 1 in the country many times. I have won 16 gold balls in these tournaments, each symbolic of a U.S. championship.
As a busy board-certified psychiatrist, I had been featured in an article, “Well being: Tennis is doctor’s favorite medicine,” by Art Carey, in the Philadelphia Inquirer, posted May 2, 2011. The author discussed my diet and exercise regime, and how I used exercise to stay healthy and to deal with the stress of being a physician.
‘Take me to the hospital’
At the end of 2018, I had a complete blood count performed, and the results indicated that I had a lipid panel of a healthy 30-year-old; however, my delusional bubble burst in March 2019. I was the No. 1 seed in a National Father-Daughter Tennis Tournament in Chicago. We were in the semifinal match, we had won the first set, and we were up 3-0. I fell, hit my head on the net post, and was feeling nauseated. I checked for bleeding and continued playing, though I was not feeling well. Five minutes later, I experienced symptoms of very extreme gastrointestinal pain and nausea. I ran off the tennis court wanting to vomit and get rid of the symptom so I could go back and finish the match. I wanted to play in the finals the following day and try to win the tournament.
The kind, competent, compassionate, and warm tournament director said I looked gray – and he promptly called 911. The paramedics came and said they thought I may be having a heart attack. I was in denial since I had no chest pain and I thought I was super healthy; therefore, I could not be experiencing an acute myocardial infarction. I finally agreed to let technicians perform an EKG, and they told me that I had ST elevation. Reality finally set in and I realized I was having a heart attack. “Take me to the hospital,” I said.
At the Chicago hospital where I was taken, I told doctors and staff I was a physician. To my surprise, they did not care. I was not going to get any prioritized treatment. Despite all of my devotion to medicine, I was not even getting their top physician to treat me. I was being evaluated by a resident. I felt even more deflated.
They performed a cardiac catheterization and put in one stent in one vessel in the right cardiac vessel. I had many questions to ask, but everyone seemed very impatient and abrupt with me, acting like this was just a very routine procedure. No one ever adequately answered my questions. I was very disillusioned, and I felt very insignificant, scared, and invisible.
I was discharged a few days later and was told my heart problem was fixed. I was instructed to follow up with a cardiologist in Philadelphia when I got home.
The first night home, I experienced chest pain. I was alarmed and thought my stent may have collapsed, so I went to the emergency room of the Philadelphia area hospital I knew had the best cardiac staff. After another blood test, indicating raised troponin levels, I was informed they needed to perform another cardiac catheterization. I learned I had two more coronary artery blockages, each 95%-99%, in the left ventricle.
I was shocked. How could the doctor in Chicago have made such a significant mistake? What happened? I would never know.
The interventional cardiologist in Philadelphia was able to repair one coronary artery, but the other blockage in the LED vessel (yes, the widow maker) had calcified too much for a stent. I would need cardiac bypass surgery. This was very unbelievable to me, and furthermore, I would have to wait 2 long weeks for the anticoagulant effect of the Brilinta to wear off before I could undergo bypass surgery.
While I anxiously waited for the big day, I was calling either my cardiologist, surgeon, or his nurse practitioner almost daily with questions and concerns; after all, this was a life-threatening and momentous event. Thankfully, I was met with great patience, understanding, and promptness of detailed answers and explanations by all involved with my cardiac care. The reactions of the staff made me mindful of the importance of really hearing my patients’ concerns and addressing their issues in a prompt, nonjudgmental, patient, and genuine manner. I am grateful that my robotic cardiac bypass surgery on March 26, 2019, went very well, and I am now back to work, playing tennis, jogging slowly, and riding my stationery bike.
Changed perspective on practice
I had always thought of myself as a warm, caring, and empathic psychiatrist, but my experience as a cardiac patient made me realize that there is always room for improvement in treating my patients.
Remember, every doctor will become a patient one day, and the reality of illness, injury, and mortality may really hit you hard, as it did me. You may not receive any prioritized treatment and you will know what it feels like to be helpless, vulnerable, and at the mercy of a physician while you regress in the service of the ego and become a patient.
You can be a better doctor now if you are mindful that whatever the physical, emotional, or mental issue facing your patients, the problem may be catastrophic to them. They need your undivided attention. Any problem is a significant event to your presenting patient. Really listen to his or her concerns or questions, and address every one with patience, understanding, and accurate information. If you follow these lessons, which I learned the hard way, you can become a better doctor.
I followed my doctor’s instructions and I started hitting tennis balls gradually. I worked myself back into shape and with my daughter Julia Cohen, and we won the USTA National Father Daughter Clay Court Championship in Florida 6 months after I had the heart attack during a national tennis tournament. This is the comeback of the year in tennis!
Dr. Cohen has had a private practice in psychiatry for more than 35 years. He is a former professor of psychiatry, family medicine, and otolaryngology at Thomas Jefferson University in Philadelphia. Dr. Cohen has been a nationally ranked tennis player from age 12 to the present, served as captain of the University of Pennsylvania tennis team, and ranked No. 1 in tennis in the middle states section and in the country in various categories and times. He was inducted into the Philadelphia Jewish Sports Hall of Fame in 2012.
I became a better doctor on the day I became a cardiac patient. On that day, I experienced the helpless, vulnerable, and needy feelings of a patient’s dependency and blind trust of a physician whom I did not know. I suddenly realized how it feels to be a patient.
My entire life, I had always been an athlete in excellent shape. My 7-day-a-week daily schedule included seeing patients, being an expert psychiatric witness for disability cases, playing 2 hours of tennis, walking/running for 1 hour, and ending the night with 1 hour on a stationary bike.
I get to see my children all the time. I am so fortunate to get to travel with them and play national father-son and father-daughter tennis tournaments. We have been ranked No. 1 in the country many times. I have won 16 gold balls in these tournaments, each symbolic of a U.S. championship.
As a busy board-certified psychiatrist, I had been featured in an article, “Well being: Tennis is doctor’s favorite medicine,” by Art Carey, in the Philadelphia Inquirer, posted May 2, 2011. The author discussed my diet and exercise regime, and how I used exercise to stay healthy and to deal with the stress of being a physician.
‘Take me to the hospital’
At the end of 2018, I had a complete blood count performed, and the results indicated that I had a lipid panel of a healthy 30-year-old; however, my delusional bubble burst in March 2019. I was the No. 1 seed in a National Father-Daughter Tennis Tournament in Chicago. We were in the semifinal match, we had won the first set, and we were up 3-0. I fell, hit my head on the net post, and was feeling nauseated. I checked for bleeding and continued playing, though I was not feeling well. Five minutes later, I experienced symptoms of very extreme gastrointestinal pain and nausea. I ran off the tennis court wanting to vomit and get rid of the symptom so I could go back and finish the match. I wanted to play in the finals the following day and try to win the tournament.
The kind, competent, compassionate, and warm tournament director said I looked gray – and he promptly called 911. The paramedics came and said they thought I may be having a heart attack. I was in denial since I had no chest pain and I thought I was super healthy; therefore, I could not be experiencing an acute myocardial infarction. I finally agreed to let technicians perform an EKG, and they told me that I had ST elevation. Reality finally set in and I realized I was having a heart attack. “Take me to the hospital,” I said.
At the Chicago hospital where I was taken, I told doctors and staff I was a physician. To my surprise, they did not care. I was not going to get any prioritized treatment. Despite all of my devotion to medicine, I was not even getting their top physician to treat me. I was being evaluated by a resident. I felt even more deflated.
They performed a cardiac catheterization and put in one stent in one vessel in the right cardiac vessel. I had many questions to ask, but everyone seemed very impatient and abrupt with me, acting like this was just a very routine procedure. No one ever adequately answered my questions. I was very disillusioned, and I felt very insignificant, scared, and invisible.
I was discharged a few days later and was told my heart problem was fixed. I was instructed to follow up with a cardiologist in Philadelphia when I got home.
The first night home, I experienced chest pain. I was alarmed and thought my stent may have collapsed, so I went to the emergency room of the Philadelphia area hospital I knew had the best cardiac staff. After another blood test, indicating raised troponin levels, I was informed they needed to perform another cardiac catheterization. I learned I had two more coronary artery blockages, each 95%-99%, in the left ventricle.
I was shocked. How could the doctor in Chicago have made such a significant mistake? What happened? I would never know.
The interventional cardiologist in Philadelphia was able to repair one coronary artery, but the other blockage in the LED vessel (yes, the widow maker) had calcified too much for a stent. I would need cardiac bypass surgery. This was very unbelievable to me, and furthermore, I would have to wait 2 long weeks for the anticoagulant effect of the Brilinta to wear off before I could undergo bypass surgery.
While I anxiously waited for the big day, I was calling either my cardiologist, surgeon, or his nurse practitioner almost daily with questions and concerns; after all, this was a life-threatening and momentous event. Thankfully, I was met with great patience, understanding, and promptness of detailed answers and explanations by all involved with my cardiac care. The reactions of the staff made me mindful of the importance of really hearing my patients’ concerns and addressing their issues in a prompt, nonjudgmental, patient, and genuine manner. I am grateful that my robotic cardiac bypass surgery on March 26, 2019, went very well, and I am now back to work, playing tennis, jogging slowly, and riding my stationery bike.
Changed perspective on practice
I had always thought of myself as a warm, caring, and empathic psychiatrist, but my experience as a cardiac patient made me realize that there is always room for improvement in treating my patients.
Remember, every doctor will become a patient one day, and the reality of illness, injury, and mortality may really hit you hard, as it did me. You may not receive any prioritized treatment and you will know what it feels like to be helpless, vulnerable, and at the mercy of a physician while you regress in the service of the ego and become a patient.
You can be a better doctor now if you are mindful that whatever the physical, emotional, or mental issue facing your patients, the problem may be catastrophic to them. They need your undivided attention. Any problem is a significant event to your presenting patient. Really listen to his or her concerns or questions, and address every one with patience, understanding, and accurate information. If you follow these lessons, which I learned the hard way, you can become a better doctor.
I followed my doctor’s instructions and I started hitting tennis balls gradually. I worked myself back into shape and with my daughter Julia Cohen, and we won the USTA National Father Daughter Clay Court Championship in Florida 6 months after I had the heart attack during a national tennis tournament. This is the comeback of the year in tennis!
Dr. Cohen has had a private practice in psychiatry for more than 35 years. He is a former professor of psychiatry, family medicine, and otolaryngology at Thomas Jefferson University in Philadelphia. Dr. Cohen has been a nationally ranked tennis player from age 12 to the present, served as captain of the University of Pennsylvania tennis team, and ranked No. 1 in tennis in the middle states section and in the country in various categories and times. He was inducted into the Philadelphia Jewish Sports Hall of Fame in 2012.
I became a better doctor on the day I became a cardiac patient. On that day, I experienced the helpless, vulnerable, and needy feelings of a patient’s dependency and blind trust of a physician whom I did not know. I suddenly realized how it feels to be a patient.
My entire life, I had always been an athlete in excellent shape. My 7-day-a-week daily schedule included seeing patients, being an expert psychiatric witness for disability cases, playing 2 hours of tennis, walking/running for 1 hour, and ending the night with 1 hour on a stationary bike.
I get to see my children all the time. I am so fortunate to get to travel with them and play national father-son and father-daughter tennis tournaments. We have been ranked No. 1 in the country many times. I have won 16 gold balls in these tournaments, each symbolic of a U.S. championship.
As a busy board-certified psychiatrist, I had been featured in an article, “Well being: Tennis is doctor’s favorite medicine,” by Art Carey, in the Philadelphia Inquirer, posted May 2, 2011. The author discussed my diet and exercise regime, and how I used exercise to stay healthy and to deal with the stress of being a physician.
‘Take me to the hospital’
At the end of 2018, I had a complete blood count performed, and the results indicated that I had a lipid panel of a healthy 30-year-old; however, my delusional bubble burst in March 2019. I was the No. 1 seed in a National Father-Daughter Tennis Tournament in Chicago. We were in the semifinal match, we had won the first set, and we were up 3-0. I fell, hit my head on the net post, and was feeling nauseated. I checked for bleeding and continued playing, though I was not feeling well. Five minutes later, I experienced symptoms of very extreme gastrointestinal pain and nausea. I ran off the tennis court wanting to vomit and get rid of the symptom so I could go back and finish the match. I wanted to play in the finals the following day and try to win the tournament.
The kind, competent, compassionate, and warm tournament director said I looked gray – and he promptly called 911. The paramedics came and said they thought I may be having a heart attack. I was in denial since I had no chest pain and I thought I was super healthy; therefore, I could not be experiencing an acute myocardial infarction. I finally agreed to let technicians perform an EKG, and they told me that I had ST elevation. Reality finally set in and I realized I was having a heart attack. “Take me to the hospital,” I said.
At the Chicago hospital where I was taken, I told doctors and staff I was a physician. To my surprise, they did not care. I was not going to get any prioritized treatment. Despite all of my devotion to medicine, I was not even getting their top physician to treat me. I was being evaluated by a resident. I felt even more deflated.
They performed a cardiac catheterization and put in one stent in one vessel in the right cardiac vessel. I had many questions to ask, but everyone seemed very impatient and abrupt with me, acting like this was just a very routine procedure. No one ever adequately answered my questions. I was very disillusioned, and I felt very insignificant, scared, and invisible.
I was discharged a few days later and was told my heart problem was fixed. I was instructed to follow up with a cardiologist in Philadelphia when I got home.
The first night home, I experienced chest pain. I was alarmed and thought my stent may have collapsed, so I went to the emergency room of the Philadelphia area hospital I knew had the best cardiac staff. After another blood test, indicating raised troponin levels, I was informed they needed to perform another cardiac catheterization. I learned I had two more coronary artery blockages, each 95%-99%, in the left ventricle.
I was shocked. How could the doctor in Chicago have made such a significant mistake? What happened? I would never know.
The interventional cardiologist in Philadelphia was able to repair one coronary artery, but the other blockage in the LED vessel (yes, the widow maker) had calcified too much for a stent. I would need cardiac bypass surgery. This was very unbelievable to me, and furthermore, I would have to wait 2 long weeks for the anticoagulant effect of the Brilinta to wear off before I could undergo bypass surgery.
While I anxiously waited for the big day, I was calling either my cardiologist, surgeon, or his nurse practitioner almost daily with questions and concerns; after all, this was a life-threatening and momentous event. Thankfully, I was met with great patience, understanding, and promptness of detailed answers and explanations by all involved with my cardiac care. The reactions of the staff made me mindful of the importance of really hearing my patients’ concerns and addressing their issues in a prompt, nonjudgmental, patient, and genuine manner. I am grateful that my robotic cardiac bypass surgery on March 26, 2019, went very well, and I am now back to work, playing tennis, jogging slowly, and riding my stationery bike.
Changed perspective on practice
I had always thought of myself as a warm, caring, and empathic psychiatrist, but my experience as a cardiac patient made me realize that there is always room for improvement in treating my patients.
Remember, every doctor will become a patient one day, and the reality of illness, injury, and mortality may really hit you hard, as it did me. You may not receive any prioritized treatment and you will know what it feels like to be helpless, vulnerable, and at the mercy of a physician while you regress in the service of the ego and become a patient.
You can be a better doctor now if you are mindful that whatever the physical, emotional, or mental issue facing your patients, the problem may be catastrophic to them. They need your undivided attention. Any problem is a significant event to your presenting patient. Really listen to his or her concerns or questions, and address every one with patience, understanding, and accurate information. If you follow these lessons, which I learned the hard way, you can become a better doctor.
I followed my doctor’s instructions and I started hitting tennis balls gradually. I worked myself back into shape and with my daughter Julia Cohen, and we won the USTA National Father Daughter Clay Court Championship in Florida 6 months after I had the heart attack during a national tennis tournament. This is the comeback of the year in tennis!
Dr. Cohen has had a private practice in psychiatry for more than 35 years. He is a former professor of psychiatry, family medicine, and otolaryngology at Thomas Jefferson University in Philadelphia. Dr. Cohen has been a nationally ranked tennis player from age 12 to the present, served as captain of the University of Pennsylvania tennis team, and ranked No. 1 in tennis in the middle states section and in the country in various categories and times. He was inducted into the Philadelphia Jewish Sports Hall of Fame in 2012.