User login
For MD-IQ use only
Vesicles and Bullae on the Leg
The Diagnosis: Cutaneous B-cell Lymphoma
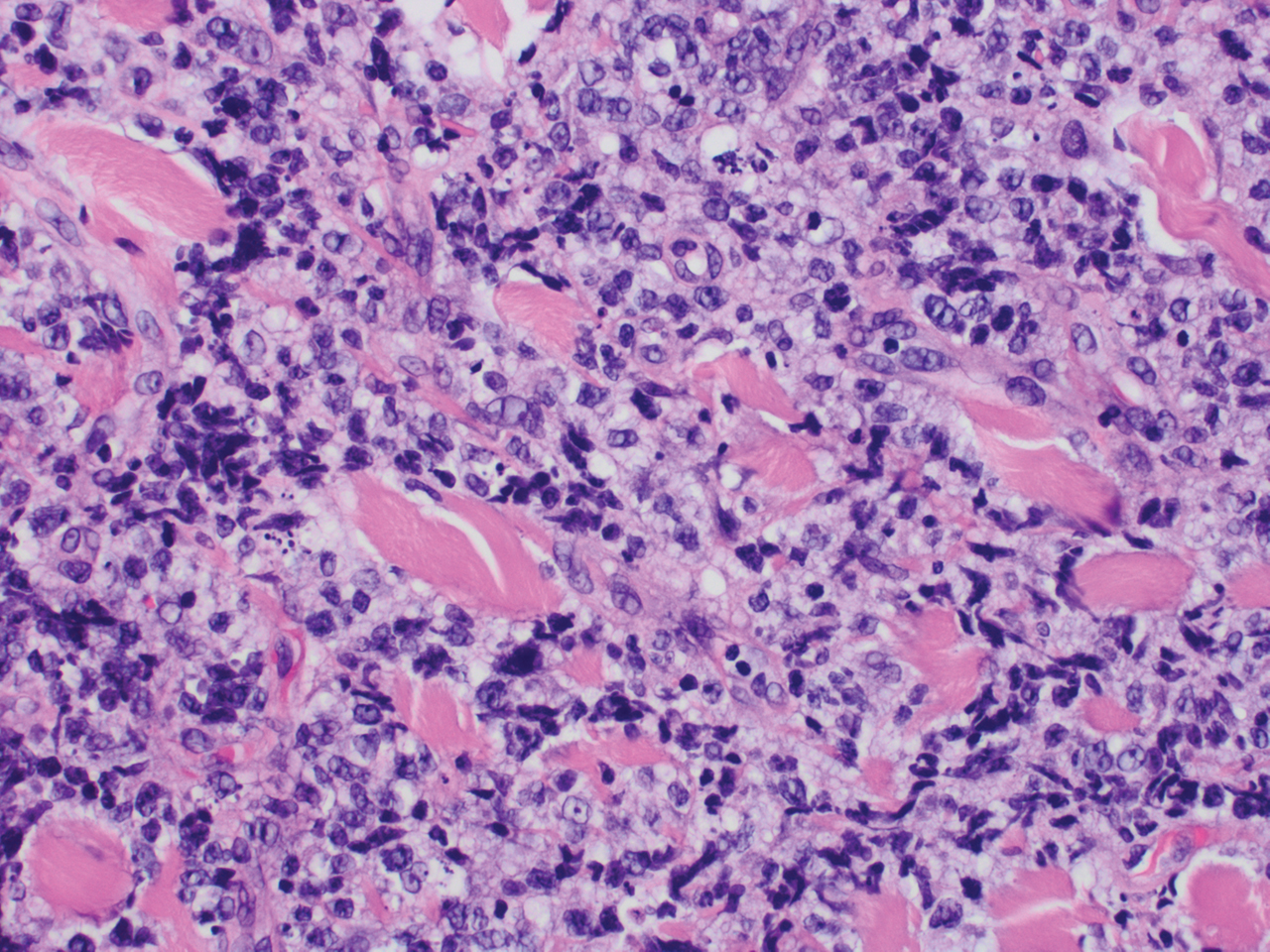
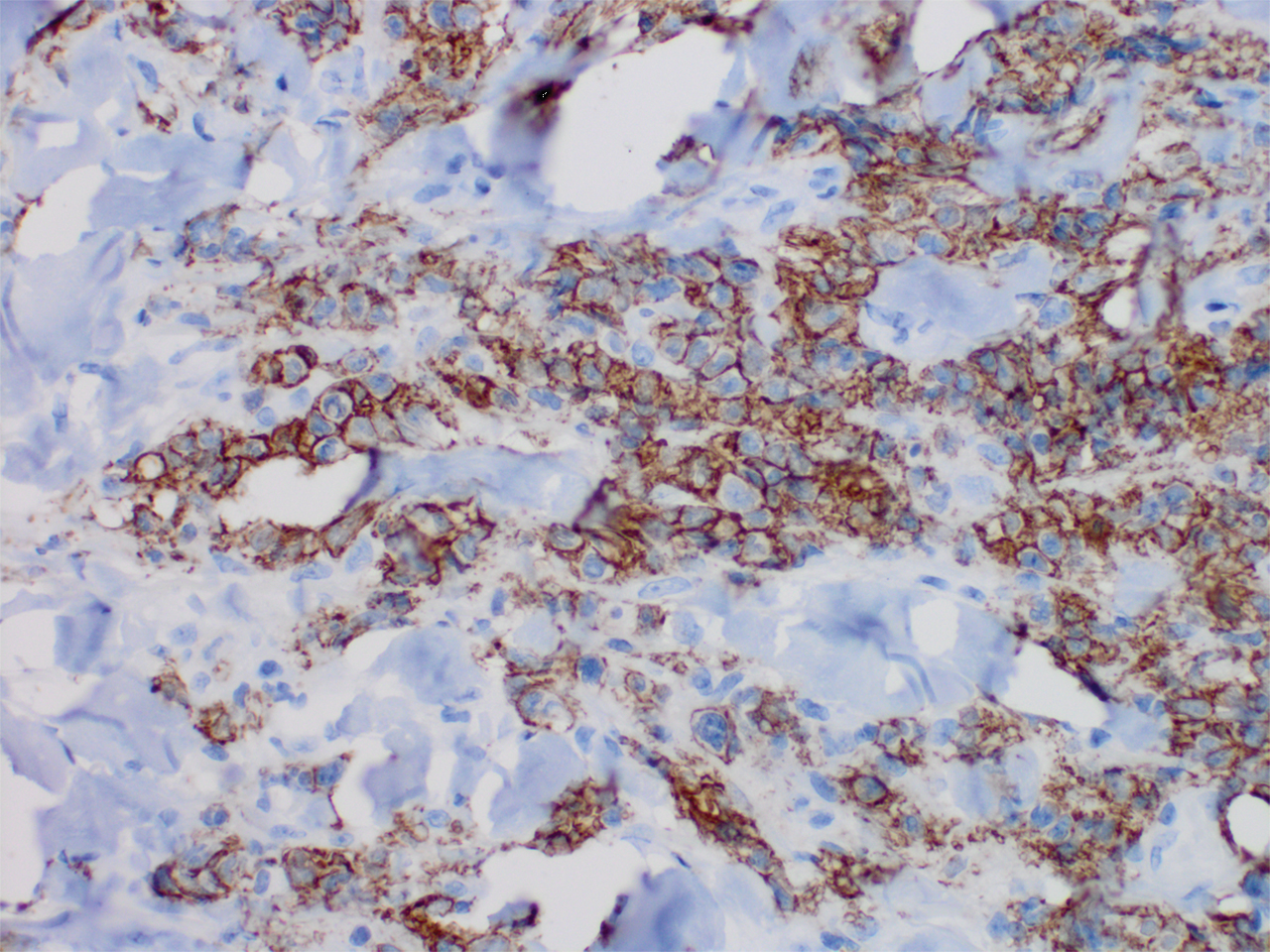
Histopathology revealed a dense and diffuse lymphocytic infiltrate throughout the dermis with occasional individual cell necrosis. On closer inspection, the infiltrate consisted of intermediate-sized lymphocytes, some with a vesiculated nucleus and ample amount of cytoplasm, while others contained hyperchromatic nuclei (Figure 1). These cells stained strongly positive for B-cell marker (CD20), while only a few mature lymphocytes demonstrated T-cell phenotype (CD3)(Figure 2).
Although the patient recounted a 3-month history of lower leg edema, he also reported that the rash began a few weeks after his diagnosis of systemic B-cell follicular lymphoma. Throughout this time, he was seen by various physicians who attributed the edema and skin changes to chronic stasis, peripheral venous insufficiency, and diabetic peripheral neuropathy. His primary care physician prescribed an antifungal lotion, which he discontinued on his own due to lack of improvement. Upon arrival to the emergency department, he was started on intravenous cefazolin and subcutaneous heparin. Doppler ultrasonography of the legs was ordered to rule out a deep venous thrombosis. Dermatology was consulted and proceeded with a punch biopsy to investigate for cutaneous B-cell lymphoma (BCL) with a plan to follow up as an outpatient for results upon discharge. He also was prescribed triamcinolone ointment 0.1% twice daily for symptomatic relief.
The patient's left axillary lymph node was biopsied for pathologic evaluation. Immunohistochemical staining revealed expression of B-cell markers CD20, CD79a, and PAX5, along with the antiapoptotic markers BCL-2 and BCL-6. Fluorescence in situ hybridization displayed gene rearrangements of BCL-2, BCL-6, and t(14;18)/IgH-BCL2 in the majority of cells. CD3 and CD5 immunostains were negative, indicating that T cells were not involved in this process. Flow cytometry identified a monoclonal κ B-cell population in 40% to 50% of the total cells, which co-expressed CD10, CD19, CD22, and CD38; the cells were negative for CD5, CD20, and CD23. Cell size was variably enlarged and CD71 positive, otherwise known as transferrin receptor 1, indicating the mediation of iron transport into cells of erythroid lineage that is necessary for proliferation.1 Bone marrow core biopsy did not identify features of bone marrow involvement by the lymphoma. Based on these results, the patient was diagnosed with systemic B-cell follicular lymphoma grade 3b stage IIIA. Oncology initiated a systemic chemotherapy regimen with obinutuzumab, cyclophosphamide, doxorubicin hydrochloride (hydroxydaunorubicin), vincristine sulfate, and prednisone.
Skin involvement in B-cell follicular lymphoma can be primary or secondary. Although all subtypes of BCL can have secondary cutaneous involvement, it is most common in advanced-stage disease (stages III or IV).2 Cutaneous manifestations of primary cutaneous follicle-center lymphoma (PCFCL) and systemic/nodal follicular lymphoma secondarily involving the skin can be difficult to distinguish clinically and histopathologically; both appear as solitary or grouped plaques and nodules most commonly on the head, neck, or trunk, and rarely on the legs.3 Although the pathologic features of these two diagnoses can seem almost identical, it is important to differentiate them due to their differing prognosis and management. Patients with follicular lymphoma involving the skin are more likely than those with PCFCL to develop lymphadenopathy and B symptoms.3 Primary cutaneous follicle-center lymphoma also generally runs an indolent course and requires local therapy, while secondary involvement of the skin due to systemic/nodal follicular lymphoma has a worse prognosis and requires systemic chemotherapy treatment.4
Immunohistochemical markers are the most helpful tool used to distinguish PCFCL from systemic/nodal follicular lymphoma involving the skin. Tumors of B-cell origin are expected to express associated B-cell markers such as CD20, CD79a, and PAX52; BCL-6, a marker of germinal center cells, also is expected to stain positive.2 CD10 is positive in a majority of cases with a follicular growth pattern, while those with a diffuse pattern of growth may have a negative stain.2 The most valuable histopathologic indicator differentiating primary and secondary skin involvement is the intensity of BCL-2 expression.5 The prognostic significance of the t(14;18)/IgH-BCL2 rearrangement is controversial, with rearrangement identified in more than 75% of systemic/nodal follicular lymphoma cases and less commonly found in PCFCL, with one report arguing an incidence ranging from 1% to 40%.5
A comprehensive history and physical examination are necessary to develop a differential diagnosis. Our patient's lower leg edema and extensive medical history made the diagnosis more complicated. Pitting edema was present on physical examination, making elephantiasis nostras verrucosa less likely, as it would instead present with nonpitting edema and a woody feel.6 Our patient did not have epidemiologic exposure to filariasis through foreign travel and did not present with any classic signs or symptoms of lymphatic filariasis, such as fever, eosinophilia, chyluria, or hydrocele.7 Although a negative history of HIV makes Kaposi sarcoma and bacillary angiomatosis less likely diagnoses, a biopsy would be useful to rule out these conditions. Positive inguinal lymphadenopathy present on physical examination may have contributed to lymphatic flow obstruction leading to the leg lymphedema in our patient.
- Marsee DK, Pinkus GS, Yu H. CD71 (transferrin receptor): an effective marker for erythroid precursors in bone marrow biopsy specimens. Am J Clin Pathol. 2010;134:429-435.
- Jaffe ES. Navigating the cutaneous B-cell lymphomas: avoiding the rocky shoals. Mod Pathol. 2020;33(suppl 1):96-106.
- Skala SL, Hristov B, Hristov AC. Primary cutaneous follicle center lymphoma. Arch Pathol Lab Med. 2018;142:1313-1321.
- Suárez AL, Pulitzer M, Horwitz S, et al. Primary cutaneous B-cell lymphomas: part I. clinical features, diagnosis, and classification. J Am Acad Dermatol. 2013;69:329.e1-13; quiz 341-342.
- Servitje O, Climent F, Colomo L, et al. Primary cutaneous vs secondary cutaneous follicular lymphomas: a comparative study focused on BCL2, CD10, and t(14;18) expression. J Cutan Pathol. 2018;46:182-189.
- Fredman R, Tenenhaus M. Elephantiasis nostras verrucose [published online October 12, 2012]. Eplasty. 2012;12:ic14.
- Lourens GB, Ferrell DK. Lymphatic filariasis. Nurs Clin of North Am. 2019;54:181-192.
The Diagnosis: Cutaneous B-cell Lymphoma
Histopathology revealed a dense and diffuse lymphocytic infiltrate throughout the dermis with occasional individual cell necrosis. On closer inspection, the infiltrate consisted of intermediate-sized lymphocytes, some with a vesiculated nucleus and ample amount of cytoplasm, while others contained hyperchromatic nuclei (Figure 1). These cells stained strongly positive for B-cell marker (CD20), while only a few mature lymphocytes demonstrated T-cell phenotype (CD3)(Figure 2).
Although the patient recounted a 3-month history of lower leg edema, he also reported that the rash began a few weeks after his diagnosis of systemic B-cell follicular lymphoma. Throughout this time, he was seen by various physicians who attributed the edema and skin changes to chronic stasis, peripheral venous insufficiency, and diabetic peripheral neuropathy. His primary care physician prescribed an antifungal lotion, which he discontinued on his own due to lack of improvement. Upon arrival to the emergency department, he was started on intravenous cefazolin and subcutaneous heparin. Doppler ultrasonography of the legs was ordered to rule out a deep venous thrombosis. Dermatology was consulted and proceeded with a punch biopsy to investigate for cutaneous B-cell lymphoma (BCL) with a plan to follow up as an outpatient for results upon discharge. He also was prescribed triamcinolone ointment 0.1% twice daily for symptomatic relief.
The patient's left axillary lymph node was biopsied for pathologic evaluation. Immunohistochemical staining revealed expression of B-cell markers CD20, CD79a, and PAX5, along with the antiapoptotic markers BCL-2 and BCL-6. Fluorescence in situ hybridization displayed gene rearrangements of BCL-2, BCL-6, and t(14;18)/IgH-BCL2 in the majority of cells. CD3 and CD5 immunostains were negative, indicating that T cells were not involved in this process. Flow cytometry identified a monoclonal κ B-cell population in 40% to 50% of the total cells, which co-expressed CD10, CD19, CD22, and CD38; the cells were negative for CD5, CD20, and CD23. Cell size was variably enlarged and CD71 positive, otherwise known as transferrin receptor 1, indicating the mediation of iron transport into cells of erythroid lineage that is necessary for proliferation.1 Bone marrow core biopsy did not identify features of bone marrow involvement by the lymphoma. Based on these results, the patient was diagnosed with systemic B-cell follicular lymphoma grade 3b stage IIIA. Oncology initiated a systemic chemotherapy regimen with obinutuzumab, cyclophosphamide, doxorubicin hydrochloride (hydroxydaunorubicin), vincristine sulfate, and prednisone.
Skin involvement in B-cell follicular lymphoma can be primary or secondary. Although all subtypes of BCL can have secondary cutaneous involvement, it is most common in advanced-stage disease (stages III or IV).2 Cutaneous manifestations of primary cutaneous follicle-center lymphoma (PCFCL) and systemic/nodal follicular lymphoma secondarily involving the skin can be difficult to distinguish clinically and histopathologically; both appear as solitary or grouped plaques and nodules most commonly on the head, neck, or trunk, and rarely on the legs.3 Although the pathologic features of these two diagnoses can seem almost identical, it is important to differentiate them due to their differing prognosis and management. Patients with follicular lymphoma involving the skin are more likely than those with PCFCL to develop lymphadenopathy and B symptoms.3 Primary cutaneous follicle-center lymphoma also generally runs an indolent course and requires local therapy, while secondary involvement of the skin due to systemic/nodal follicular lymphoma has a worse prognosis and requires systemic chemotherapy treatment.4
Immunohistochemical markers are the most helpful tool used to distinguish PCFCL from systemic/nodal follicular lymphoma involving the skin. Tumors of B-cell origin are expected to express associated B-cell markers such as CD20, CD79a, and PAX52; BCL-6, a marker of germinal center cells, also is expected to stain positive.2 CD10 is positive in a majority of cases with a follicular growth pattern, while those with a diffuse pattern of growth may have a negative stain.2 The most valuable histopathologic indicator differentiating primary and secondary skin involvement is the intensity of BCL-2 expression.5 The prognostic significance of the t(14;18)/IgH-BCL2 rearrangement is controversial, with rearrangement identified in more than 75% of systemic/nodal follicular lymphoma cases and less commonly found in PCFCL, with one report arguing an incidence ranging from 1% to 40%.5
A comprehensive history and physical examination are necessary to develop a differential diagnosis. Our patient's lower leg edema and extensive medical history made the diagnosis more complicated. Pitting edema was present on physical examination, making elephantiasis nostras verrucosa less likely, as it would instead present with nonpitting edema and a woody feel.6 Our patient did not have epidemiologic exposure to filariasis through foreign travel and did not present with any classic signs or symptoms of lymphatic filariasis, such as fever, eosinophilia, chyluria, or hydrocele.7 Although a negative history of HIV makes Kaposi sarcoma and bacillary angiomatosis less likely diagnoses, a biopsy would be useful to rule out these conditions. Positive inguinal lymphadenopathy present on physical examination may have contributed to lymphatic flow obstruction leading to the leg lymphedema in our patient.
The Diagnosis: Cutaneous B-cell Lymphoma
Histopathology revealed a dense and diffuse lymphocytic infiltrate throughout the dermis with occasional individual cell necrosis. On closer inspection, the infiltrate consisted of intermediate-sized lymphocytes, some with a vesiculated nucleus and ample amount of cytoplasm, while others contained hyperchromatic nuclei (Figure 1). These cells stained strongly positive for B-cell marker (CD20), while only a few mature lymphocytes demonstrated T-cell phenotype (CD3)(Figure 2).
Although the patient recounted a 3-month history of lower leg edema, he also reported that the rash began a few weeks after his diagnosis of systemic B-cell follicular lymphoma. Throughout this time, he was seen by various physicians who attributed the edema and skin changes to chronic stasis, peripheral venous insufficiency, and diabetic peripheral neuropathy. His primary care physician prescribed an antifungal lotion, which he discontinued on his own due to lack of improvement. Upon arrival to the emergency department, he was started on intravenous cefazolin and subcutaneous heparin. Doppler ultrasonography of the legs was ordered to rule out a deep venous thrombosis. Dermatology was consulted and proceeded with a punch biopsy to investigate for cutaneous B-cell lymphoma (BCL) with a plan to follow up as an outpatient for results upon discharge. He also was prescribed triamcinolone ointment 0.1% twice daily for symptomatic relief.
The patient's left axillary lymph node was biopsied for pathologic evaluation. Immunohistochemical staining revealed expression of B-cell markers CD20, CD79a, and PAX5, along with the antiapoptotic markers BCL-2 and BCL-6. Fluorescence in situ hybridization displayed gene rearrangements of BCL-2, BCL-6, and t(14;18)/IgH-BCL2 in the majority of cells. CD3 and CD5 immunostains were negative, indicating that T cells were not involved in this process. Flow cytometry identified a monoclonal κ B-cell population in 40% to 50% of the total cells, which co-expressed CD10, CD19, CD22, and CD38; the cells were negative for CD5, CD20, and CD23. Cell size was variably enlarged and CD71 positive, otherwise known as transferrin receptor 1, indicating the mediation of iron transport into cells of erythroid lineage that is necessary for proliferation.1 Bone marrow core biopsy did not identify features of bone marrow involvement by the lymphoma. Based on these results, the patient was diagnosed with systemic B-cell follicular lymphoma grade 3b stage IIIA. Oncology initiated a systemic chemotherapy regimen with obinutuzumab, cyclophosphamide, doxorubicin hydrochloride (hydroxydaunorubicin), vincristine sulfate, and prednisone.
Skin involvement in B-cell follicular lymphoma can be primary or secondary. Although all subtypes of BCL can have secondary cutaneous involvement, it is most common in advanced-stage disease (stages III or IV).2 Cutaneous manifestations of primary cutaneous follicle-center lymphoma (PCFCL) and systemic/nodal follicular lymphoma secondarily involving the skin can be difficult to distinguish clinically and histopathologically; both appear as solitary or grouped plaques and nodules most commonly on the head, neck, or trunk, and rarely on the legs.3 Although the pathologic features of these two diagnoses can seem almost identical, it is important to differentiate them due to their differing prognosis and management. Patients with follicular lymphoma involving the skin are more likely than those with PCFCL to develop lymphadenopathy and B symptoms.3 Primary cutaneous follicle-center lymphoma also generally runs an indolent course and requires local therapy, while secondary involvement of the skin due to systemic/nodal follicular lymphoma has a worse prognosis and requires systemic chemotherapy treatment.4
Immunohistochemical markers are the most helpful tool used to distinguish PCFCL from systemic/nodal follicular lymphoma involving the skin. Tumors of B-cell origin are expected to express associated B-cell markers such as CD20, CD79a, and PAX52; BCL-6, a marker of germinal center cells, also is expected to stain positive.2 CD10 is positive in a majority of cases with a follicular growth pattern, while those with a diffuse pattern of growth may have a negative stain.2 The most valuable histopathologic indicator differentiating primary and secondary skin involvement is the intensity of BCL-2 expression.5 The prognostic significance of the t(14;18)/IgH-BCL2 rearrangement is controversial, with rearrangement identified in more than 75% of systemic/nodal follicular lymphoma cases and less commonly found in PCFCL, with one report arguing an incidence ranging from 1% to 40%.5
A comprehensive history and physical examination are necessary to develop a differential diagnosis. Our patient's lower leg edema and extensive medical history made the diagnosis more complicated. Pitting edema was present on physical examination, making elephantiasis nostras verrucosa less likely, as it would instead present with nonpitting edema and a woody feel.6 Our patient did not have epidemiologic exposure to filariasis through foreign travel and did not present with any classic signs or symptoms of lymphatic filariasis, such as fever, eosinophilia, chyluria, or hydrocele.7 Although a negative history of HIV makes Kaposi sarcoma and bacillary angiomatosis less likely diagnoses, a biopsy would be useful to rule out these conditions. Positive inguinal lymphadenopathy present on physical examination may have contributed to lymphatic flow obstruction leading to the leg lymphedema in our patient.
- Marsee DK, Pinkus GS, Yu H. CD71 (transferrin receptor): an effective marker for erythroid precursors in bone marrow biopsy specimens. Am J Clin Pathol. 2010;134:429-435.
- Jaffe ES. Navigating the cutaneous B-cell lymphomas: avoiding the rocky shoals. Mod Pathol. 2020;33(suppl 1):96-106.
- Skala SL, Hristov B, Hristov AC. Primary cutaneous follicle center lymphoma. Arch Pathol Lab Med. 2018;142:1313-1321.
- Suárez AL, Pulitzer M, Horwitz S, et al. Primary cutaneous B-cell lymphomas: part I. clinical features, diagnosis, and classification. J Am Acad Dermatol. 2013;69:329.e1-13; quiz 341-342.
- Servitje O, Climent F, Colomo L, et al. Primary cutaneous vs secondary cutaneous follicular lymphomas: a comparative study focused on BCL2, CD10, and t(14;18) expression. J Cutan Pathol. 2018;46:182-189.
- Fredman R, Tenenhaus M. Elephantiasis nostras verrucose [published online October 12, 2012]. Eplasty. 2012;12:ic14.
- Lourens GB, Ferrell DK. Lymphatic filariasis. Nurs Clin of North Am. 2019;54:181-192.
- Marsee DK, Pinkus GS, Yu H. CD71 (transferrin receptor): an effective marker for erythroid precursors in bone marrow biopsy specimens. Am J Clin Pathol. 2010;134:429-435.
- Jaffe ES. Navigating the cutaneous B-cell lymphomas: avoiding the rocky shoals. Mod Pathol. 2020;33(suppl 1):96-106.
- Skala SL, Hristov B, Hristov AC. Primary cutaneous follicle center lymphoma. Arch Pathol Lab Med. 2018;142:1313-1321.
- Suárez AL, Pulitzer M, Horwitz S, et al. Primary cutaneous B-cell lymphomas: part I. clinical features, diagnosis, and classification. J Am Acad Dermatol. 2013;69:329.e1-13; quiz 341-342.
- Servitje O, Climent F, Colomo L, et al. Primary cutaneous vs secondary cutaneous follicular lymphomas: a comparative study focused on BCL2, CD10, and t(14;18) expression. J Cutan Pathol. 2018;46:182-189.
- Fredman R, Tenenhaus M. Elephantiasis nostras verrucose [published online October 12, 2012]. Eplasty. 2012;12:ic14.
- Lourens GB, Ferrell DK. Lymphatic filariasis. Nurs Clin of North Am. 2019;54:181-192.

A 60-year-old man presented to the emergency department with slowly progressing edema of the lower legs of 3 months’ duration. In the week prior to presentation to the emergency department, he noticed a sudden eruption of vesicles and bullae on the right leg that drained clear fluid and healed with brown crust. The lesions were associated with mild burning, pruritus, and pain. He denied fever, chills, recent travel, or injury. His medical history was notable for poorly controlled diabetes mellitus, congestive heart failure, hypertension, chronic kidney disease, hyperlipidemia, and chronic anemia. Physical examination revealed multiple scattered erythematous vesicles and bullae on the right leg on a background of hyperpigmentation. Bilateral 2+ pitting edema of the legs also was present. A punch biopsy of a lesion was performed.

Hospital medicine around the world
Similar needs, local adaptations
Hospital medicine has evolved rapidly and spread widely across the United States in the past 25 years in response to the health care system’s needs for patient safety, quality, efficiency, and effective coordination of care in the ever-more complex environment of the acute care hospital.
But hospital care can be just as complex in other countries, so it’s not surprising that there’s a lot of interest around the world in the U.S. model of hospital medicine. But adaptations of that model vary across – and within – countries, reflecting local culture, health care systems, payment models, and approaches to medical education.
Other countries have looked to U.S. experts for consultations, to U.S.-trained doctors who might be willing to relocate, and to the Society of Hospital Medicine as an internationally focused source of networking and other resources. Some U.S.-based institutions, led by the Cleveland Clinic, Johns Hopkins Medicine, and Weill-Cornell Medical School, have established teaching outposts in other countries, with opportunities for resident training that prepares future hospitalists on the ground.
SHM CEO Eric E. Howell, MD, MHM, said that he personally has interacted with developing hospital medicine programs in six countries, who called upon him in part because of his past research on managing length of hospital stays. Dr. Howell counts himself among a few dozen U.S. hospitalists who are regularly invited to come and consult or to give talks to established or developing hospitalist programs in other countries. Because of the COVID-19 epidemic, in-person visits to other countries have largely been curtailed, but that has introduced a more virtual world of online meetings.

“I think the interesting thing about the ‘international consultants’ for hospital medicine is that while they come from professionally diverse backgrounds, they are all working to solve remarkably similar problems: How to make health care more affordable and higher quality while staying abreast of up-to-date best practice for physicians,” he said.
“Hospital care is costly no matter where you go. Other countries are also trying to limit expense in ways that don’t compromise the quality of that care,” Dr. Howell said. Also, hospitalized patients are more complex than ever, with increasing severity of illness and comorbidities, which makes having a hospitalist available on site more important.
Dr. Howell hopes to encourage more dialogue with international colleagues. SHM has established collaborations with medical societies in other countries and makes time at its conferences for international hospitalist participants to meet and share their experiences. Hospitalists from 33 countries were represented at SHM’s 2017 conference, and the upcoming virtual SHM Converge, May 3-7, 2021, includes a dedicated international session. SHM chapters have formed in a number of other countries.
Flora Kisuule, MD, MPH, SFHM, director of the Division of Hospital Medicine at Johns Hopkins Bayview Medical Center in Baltimore, said her international hospital medicine work1 started 7 years ago when she was invited to the Middle East to help Aramco, the Saudi Arabian Oil Company, develop a hospital medicine program based on the U.S. model for its employees. This was a joint venture with Johns Hopkins Medicine. “We went there and looked at their processes and made recommendations such as duration of hospitalist shifts and how to expand the footprint of hospital medicine in the hospital,” she said.

Then Dr. Kisuule was asked to help develop a hospital medicine program in Panama, where the drivers for developing hospital medicine were improving quality of care and ensuring patient safety. The biggest barrier has been remuneration and how to pay salaries that will allow doctors to work at only one hospital. In Panama, doctors typically work at multiple hospitals or clinics so they can earn enough to make ends meet.
The need for professional identity
Arpana Vidyarthi, MD, “grew up” professionally in hospital medicine at the University of California, San Francisco, a pioneering institution for hospital medicine, and in SHM. “We used to say: If you’ve seen one hospital medicine group, you’ve seen one hospital medicine group,” she said.

Dr. Vidyarthi went to Singapore in 2011, taking a job as a hospitalist at Singapore General Hospital and the affiliated Duke–National University Medical School, eventually directing the Division of Advanced Internal Medicine (general and hospital medicine) at the National University Health System, before moving back to UCSF in 2020.
“Professional identity is one of the biggest benefits hospital medicine can bestow in Singapore and across Asia, where general medicine is underdeveloped. Just as it did 20 years ago in the U.S., that professional identity offers a road map to achieving competency in practicing medicine in the hospital setting,” Dr. Vidyarthi said.
At UCSF, the professional identity of a hospitalist is broad but defined. The research agenda, quality, safety, and educational competencies are specific, seen through a system lens, she added. “We take pride in that professional identify. This is an opportunity for countries where general medicine is underdeveloped and undervalued.”
But the term hospital medicine – or the American model – isn’t always welcomed by health care systems in other countries, Dr Vidyarthi said. “The label of 'hospital medicine' brings people together in professional identify, and that professional identity opens doors. But for it to have legs in other countries, those skills need to be of value to the local system. It needs to make sense, as it did in the United States, and to add value for the identified gaps that need to be filled.”
In Singapore, the health care system turned to the model of acute medical units (AMUs) and the acute medicine physician specialty developed in the United Kingdom, which created a new way of delivering care, a new geography of care, and new set of competencies around which to build training and certification.
AMUs manage the majority of acute medical patients who present to the emergency department and get admitted, with initial treatment for a maximum of 72 hours. Acute physicians, trained in the specialty of assessment, diagnosis, and treatment of adult patients with urgent medical needs, work in a unit situated between the emergency department entrance and the specialty care units. This specialty has been recognized since 2009.2
“Acute medicine is the standard care model in the UK and is now found in all government hospitals in Singapore. This model is being adapted across Europe, Asia, and the Pacific Islands,” Dr. Vidyarthi said. “Advantages include the specific geography of the unit, and outcomes that are value-added to these systems such as decreased use of hospital beds in areas with very high bed occupancy rates.”
In many locales, a variety of titles are used to describe doctors who are not hospitalists as we understand them but whose work is based in the hospital, including house officer, duty officer, junior officer, registrar, or general practitioner. Often these hospital-based doctors, who may in fact be residents or nongraduated trainees, lack the training and the scope of practice of a hospitalist. Because they typically need to consult the supervising physician before making inpatient management decisions, they aren’t able to provide the timely response to the patient’s changing medical condition that is needed to manage today’s acute patients.
Defining the fee schedule
In South Korea, a hospitalist model has emerged since 2015 in response to the insufficient number of hospital-based physicians needed to cover all admitted patients and to address related issues of patient safety, health care quality, and limitations on total hours per week medical residents are allowed to work.
South Korea in 1989 adopted a universal National Health Insurance System (NHIS), which took 12 years to implement. But inadequate coverage for medical work in the hospital has deterred physicians from choosing to work there. South Korea had longer lengths of hospital stay, fewer practicing physicians per 1,000 patients, and a much higher number of hospital patients per practicing physician than other countries in the Organization for Economic Cooperation and Development, according to a new study in the Journal of Hospital Medicine detailing hospitalist development in South Korea.3
A council representing leading medical associations was formed to develop a South Korean hospitalist system and charged by the Ministry of Health with designing an official proposal for implementing it. A pilot study focused on quality and on defining a fee schedule for hospital work was tested in four hospitals, and then a second phase in 31 of South Korea’s 344 general hospitals tested the proposed fee schedule, said Wonjeong Chae, MPH, the first named author on the study, based in the Department of Public Health in the College of Medicine at Yonsei University in Seoul. “But we’re still working on making the fee schedule better,” she said.
Ms. Chae estimates that there are about 250 working hospitalists in South Korea today, which leaves a lot of gaps in practice. “We did learn from America, but we have a different system, so the American concept had to be adapted. Hospital medicine is still growing in Korea despite the impact of the pandemic. We are at the beginning stages of development, but we expect it will grow more with government support.”
In Brazil, a handful of hospital medicine pioneers such as Guilherme Barcellos, MD, SFHM, in Porto Alegre have tried to grow the hospitalist model, networking with colleagues across Latin America through the Pan American Society of Hospitalists and the Brazilian chapter of SHM.
Individual hospitals have developed hospitalist programs, but there is no national model to lead the way. Frequent turnover for the Minister of Health position has made it harder to develop consistent national policy, and the country is largely still in the early stages of developing hospital medicine, depending on isolated initiatives, as Dr. Barcellos described it in a November 2015 article in The Hospitalist.4 Growth is slow but continuing, with new programs such as the one led by Reginaldo Filho, MD at Hospital São Vicente in Curitiba standing out in the confrontation against COVID-19, Dr. Barcellos said.
What can we learn from others?
India-born, U.S.-trained hospitalist Anand Kartha, MD, MS, SFHM, currently heads the Hospital Medicine Program at Hamad General Hospital in Doha, Qatar. He moved from Boston to this small nation on the Arabian Peninsula in 2014. Under the leadership of the hospital’s Department of Medicine, this program was developed to address difficulties such as scheduling, transitions of care, and networking with home care and other providers – the same issues seen in hospitals around the world.

These are not novel problems, Dr. Kartha said, but all of them have a common solution in evidence-based practice. “As hospitalists, our key is to collaborate with everyone in the hospital, using the multidisciplinary approach that is a unique feature of hospital medicine.”
The model has continued to spread across hospitals in Qatar, including academic and community programs. “We now have a full-fledged academic hospitalist system, which collaborates with community hospitals and community programs including a women’s hospital and an oncologic hospital,” he said. “Now the focus is on expanding resource capacity and the internal pipeline for hospitalists. I am getting graduates from Weill Cornell Medicine in Qatar.” Another key collaborator has been the Boston-based Institute for Healthcare Improvement, helping to develop best practices in Qatar and sponsoring the annual Middle East Forum on Quality and Safety in Health Care.
The residency training program at Hamad General is accredited by ACGME, with the same expected competencies as in the U.S. “We don’t use the term ‘hospitalist,’ ” Dr. Kartha said. “It’s better to focus on the model of care – which clearly was American. That model has encountered some resistance in some countries – on many of the same grounds U.S. hospitalists faced 20 years ago. You have to be sensitive to local culture. For hospitalists to succeed internationally, they have to possess a high degree of cultural intelligence.” There’s no shortage of issues such as language barriers, he said. “But that’s no different than at Boston Medical Center.”
SHM’s Middle East Chapter was off to a great start and then was slowed down by regional politics and COVID-19, but is looking forward to a great reboot in 2021, Dr. Kartha said. The pandemic also has been an opportunity to show how hospital medicine is the backbone of the hospital’s ability to respond, although of course many other professionals also pitched in.
Other countries around the world have learned a lot from the American model of hospital medicine. But sources for this article wonder if U.S. hospitalists, in turn, could learn from their adaptations and innovations.
“We can all learn better how to practice our field of medicine in the hospital with less resource utilization,” Dr. Vidyarthi concluded. “So many innovations are happening around us. If we open our eyes to our global colleagues and infuse some of their ideas, it could be wonderful for hospital professionals in the United States.”
References
1. Kisuule F, Howell E. Hospital medicine beyond the United States. Int J Gen Med. 2018;11:65-71. doi: 10.2147/IJGM.S151275.
2. Stosic J et al. The acute physician: The future of acute hospital care in the UK. Clin Med (Lond). 2010 Apr; 10(2):145-7. doi: 10.7861/clinmedicine.10-2-145.
3. Yan Y et al. Adoption of Hospitalist Care in Asia: Experiences From Singapore, Taiwan, Korea, and Japan. J Hosp Med. Published Online First 2021 June 11. doi: 10.12788/jhm.3621.
4. Beresford L. Hospital medicine flourishing around the world. The Hospitalist. Nov 2015.
Similar needs, local adaptations
Similar needs, local adaptations
Hospital medicine has evolved rapidly and spread widely across the United States in the past 25 years in response to the health care system’s needs for patient safety, quality, efficiency, and effective coordination of care in the ever-more complex environment of the acute care hospital.
But hospital care can be just as complex in other countries, so it’s not surprising that there’s a lot of interest around the world in the U.S. model of hospital medicine. But adaptations of that model vary across – and within – countries, reflecting local culture, health care systems, payment models, and approaches to medical education.
Other countries have looked to U.S. experts for consultations, to U.S.-trained doctors who might be willing to relocate, and to the Society of Hospital Medicine as an internationally focused source of networking and other resources. Some U.S.-based institutions, led by the Cleveland Clinic, Johns Hopkins Medicine, and Weill-Cornell Medical School, have established teaching outposts in other countries, with opportunities for resident training that prepares future hospitalists on the ground.
SHM CEO Eric E. Howell, MD, MHM, said that he personally has interacted with developing hospital medicine programs in six countries, who called upon him in part because of his past research on managing length of hospital stays. Dr. Howell counts himself among a few dozen U.S. hospitalists who are regularly invited to come and consult or to give talks to established or developing hospitalist programs in other countries. Because of the COVID-19 epidemic, in-person visits to other countries have largely been curtailed, but that has introduced a more virtual world of online meetings.
“I think the interesting thing about the ‘international consultants’ for hospital medicine is that while they come from professionally diverse backgrounds, they are all working to solve remarkably similar problems: How to make health care more affordable and higher quality while staying abreast of up-to-date best practice for physicians,” he said.
“Hospital care is costly no matter where you go. Other countries are also trying to limit expense in ways that don’t compromise the quality of that care,” Dr. Howell said. Also, hospitalized patients are more complex than ever, with increasing severity of illness and comorbidities, which makes having a hospitalist available on site more important.
Dr. Howell hopes to encourage more dialogue with international colleagues. SHM has established collaborations with medical societies in other countries and makes time at its conferences for international hospitalist participants to meet and share their experiences. Hospitalists from 33 countries were represented at SHM’s 2017 conference, and the upcoming virtual SHM Converge, May 3-7, 2021, includes a dedicated international session. SHM chapters have formed in a number of other countries.
Flora Kisuule, MD, MPH, SFHM, director of the Division of Hospital Medicine at Johns Hopkins Bayview Medical Center in Baltimore, said her international hospital medicine work1 started 7 years ago when she was invited to the Middle East to help Aramco, the Saudi Arabian Oil Company, develop a hospital medicine program based on the U.S. model for its employees. This was a joint venture with Johns Hopkins Medicine. “We went there and looked at their processes and made recommendations such as duration of hospitalist shifts and how to expand the footprint of hospital medicine in the hospital,” she said.
Then Dr. Kisuule was asked to help develop a hospital medicine program in Panama, where the drivers for developing hospital medicine were improving quality of care and ensuring patient safety. The biggest barrier has been remuneration and how to pay salaries that will allow doctors to work at only one hospital. In Panama, doctors typically work at multiple hospitals or clinics so they can earn enough to make ends meet.
The need for professional identity
Arpana Vidyarthi, MD, “grew up” professionally in hospital medicine at the University of California, San Francisco, a pioneering institution for hospital medicine, and in SHM. “We used to say: If you’ve seen one hospital medicine group, you’ve seen one hospital medicine group,” she said.
Dr. Vidyarthi went to Singapore in 2011, taking a job as a hospitalist at Singapore General Hospital and the affiliated Duke–National University Medical School, eventually directing the Division of Advanced Internal Medicine (general and hospital medicine) at the National University Health System, before moving back to UCSF in 2020.
“Professional identity is one of the biggest benefits hospital medicine can bestow in Singapore and across Asia, where general medicine is underdeveloped. Just as it did 20 years ago in the U.S., that professional identity offers a road map to achieving competency in practicing medicine in the hospital setting,” Dr. Vidyarthi said.
At UCSF, the professional identity of a hospitalist is broad but defined. The research agenda, quality, safety, and educational competencies are specific, seen through a system lens, she added. “We take pride in that professional identify. This is an opportunity for countries where general medicine is underdeveloped and undervalued.”
But the term hospital medicine – or the American model – isn’t always welcomed by health care systems in other countries, Dr Vidyarthi said. “The label of 'hospital medicine' brings people together in professional identify, and that professional identity opens doors. But for it to have legs in other countries, those skills need to be of value to the local system. It needs to make sense, as it did in the United States, and to add value for the identified gaps that need to be filled.”
In Singapore, the health care system turned to the model of acute medical units (AMUs) and the acute medicine physician specialty developed in the United Kingdom, which created a new way of delivering care, a new geography of care, and new set of competencies around which to build training and certification.
AMUs manage the majority of acute medical patients who present to the emergency department and get admitted, with initial treatment for a maximum of 72 hours. Acute physicians, trained in the specialty of assessment, diagnosis, and treatment of adult patients with urgent medical needs, work in a unit situated between the emergency department entrance and the specialty care units. This specialty has been recognized since 2009.2
“Acute medicine is the standard care model in the UK and is now found in all government hospitals in Singapore. This model is being adapted across Europe, Asia, and the Pacific Islands,” Dr. Vidyarthi said. “Advantages include the specific geography of the unit, and outcomes that are value-added to these systems such as decreased use of hospital beds in areas with very high bed occupancy rates.”
In many locales, a variety of titles are used to describe doctors who are not hospitalists as we understand them but whose work is based in the hospital, including house officer, duty officer, junior officer, registrar, or general practitioner. Often these hospital-based doctors, who may in fact be residents or nongraduated trainees, lack the training and the scope of practice of a hospitalist. Because they typically need to consult the supervising physician before making inpatient management decisions, they aren’t able to provide the timely response to the patient’s changing medical condition that is needed to manage today’s acute patients.
Defining the fee schedule
In South Korea, a hospitalist model has emerged since 2015 in response to the insufficient number of hospital-based physicians needed to cover all admitted patients and to address related issues of patient safety, health care quality, and limitations on total hours per week medical residents are allowed to work.
South Korea in 1989 adopted a universal National Health Insurance System (NHIS), which took 12 years to implement. But inadequate coverage for medical work in the hospital has deterred physicians from choosing to work there. South Korea had longer lengths of hospital stay, fewer practicing physicians per 1,000 patients, and a much higher number of hospital patients per practicing physician than other countries in the Organization for Economic Cooperation and Development, according to a new study in the Journal of Hospital Medicine detailing hospitalist development in South Korea.3
A council representing leading medical associations was formed to develop a South Korean hospitalist system and charged by the Ministry of Health with designing an official proposal for implementing it. A pilot study focused on quality and on defining a fee schedule for hospital work was tested in four hospitals, and then a second phase in 31 of South Korea’s 344 general hospitals tested the proposed fee schedule, said Wonjeong Chae, MPH, the first named author on the study, based in the Department of Public Health in the College of Medicine at Yonsei University in Seoul. “But we’re still working on making the fee schedule better,” she said.
Ms. Chae estimates that there are about 250 working hospitalists in South Korea today, which leaves a lot of gaps in practice. “We did learn from America, but we have a different system, so the American concept had to be adapted. Hospital medicine is still growing in Korea despite the impact of the pandemic. We are at the beginning stages of development, but we expect it will grow more with government support.”
In Brazil, a handful of hospital medicine pioneers such as Guilherme Barcellos, MD, SFHM, in Porto Alegre have tried to grow the hospitalist model, networking with colleagues across Latin America through the Pan American Society of Hospitalists and the Brazilian chapter of SHM.
Individual hospitals have developed hospitalist programs, but there is no national model to lead the way. Frequent turnover for the Minister of Health position has made it harder to develop consistent national policy, and the country is largely still in the early stages of developing hospital medicine, depending on isolated initiatives, as Dr. Barcellos described it in a November 2015 article in The Hospitalist.4 Growth is slow but continuing, with new programs such as the one led by Reginaldo Filho, MD at Hospital São Vicente in Curitiba standing out in the confrontation against COVID-19, Dr. Barcellos said.
What can we learn from others?
India-born, U.S.-trained hospitalist Anand Kartha, MD, MS, SFHM, currently heads the Hospital Medicine Program at Hamad General Hospital in Doha, Qatar. He moved from Boston to this small nation on the Arabian Peninsula in 2014. Under the leadership of the hospital’s Department of Medicine, this program was developed to address difficulties such as scheduling, transitions of care, and networking with home care and other providers – the same issues seen in hospitals around the world.
These are not novel problems, Dr. Kartha said, but all of them have a common solution in evidence-based practice. “As hospitalists, our key is to collaborate with everyone in the hospital, using the multidisciplinary approach that is a unique feature of hospital medicine.”
The model has continued to spread across hospitals in Qatar, including academic and community programs. “We now have a full-fledged academic hospitalist system, which collaborates with community hospitals and community programs including a women’s hospital and an oncologic hospital,” he said. “Now the focus is on expanding resource capacity and the internal pipeline for hospitalists. I am getting graduates from Weill Cornell Medicine in Qatar.” Another key collaborator has been the Boston-based Institute for Healthcare Improvement, helping to develop best practices in Qatar and sponsoring the annual Middle East Forum on Quality and Safety in Health Care.
The residency training program at Hamad General is accredited by ACGME, with the same expected competencies as in the U.S. “We don’t use the term ‘hospitalist,’ ” Dr. Kartha said. “It’s better to focus on the model of care – which clearly was American. That model has encountered some resistance in some countries – on many of the same grounds U.S. hospitalists faced 20 years ago. You have to be sensitive to local culture. For hospitalists to succeed internationally, they have to possess a high degree of cultural intelligence.” There’s no shortage of issues such as language barriers, he said. “But that’s no different than at Boston Medical Center.”
SHM’s Middle East Chapter was off to a great start and then was slowed down by regional politics and COVID-19, but is looking forward to a great reboot in 2021, Dr. Kartha said. The pandemic also has been an opportunity to show how hospital medicine is the backbone of the hospital’s ability to respond, although of course many other professionals also pitched in.
Other countries around the world have learned a lot from the American model of hospital medicine. But sources for this article wonder if U.S. hospitalists, in turn, could learn from their adaptations and innovations.
“We can all learn better how to practice our field of medicine in the hospital with less resource utilization,” Dr. Vidyarthi concluded. “So many innovations are happening around us. If we open our eyes to our global colleagues and infuse some of their ideas, it could be wonderful for hospital professionals in the United States.”
References
1. Kisuule F, Howell E. Hospital medicine beyond the United States. Int J Gen Med. 2018;11:65-71. doi: 10.2147/IJGM.S151275.
2. Stosic J et al. The acute physician: The future of acute hospital care in the UK. Clin Med (Lond). 2010 Apr; 10(2):145-7. doi: 10.7861/clinmedicine.10-2-145.
3. Yan Y et al. Adoption of Hospitalist Care in Asia: Experiences From Singapore, Taiwan, Korea, and Japan. J Hosp Med. Published Online First 2021 June 11. doi: 10.12788/jhm.3621.
4. Beresford L. Hospital medicine flourishing around the world. The Hospitalist. Nov 2015.
Hospital medicine has evolved rapidly and spread widely across the United States in the past 25 years in response to the health care system’s needs for patient safety, quality, efficiency, and effective coordination of care in the ever-more complex environment of the acute care hospital.
But hospital care can be just as complex in other countries, so it’s not surprising that there’s a lot of interest around the world in the U.S. model of hospital medicine. But adaptations of that model vary across – and within – countries, reflecting local culture, health care systems, payment models, and approaches to medical education.
Other countries have looked to U.S. experts for consultations, to U.S.-trained doctors who might be willing to relocate, and to the Society of Hospital Medicine as an internationally focused source of networking and other resources. Some U.S.-based institutions, led by the Cleveland Clinic, Johns Hopkins Medicine, and Weill-Cornell Medical School, have established teaching outposts in other countries, with opportunities for resident training that prepares future hospitalists on the ground.
SHM CEO Eric E. Howell, MD, MHM, said that he personally has interacted with developing hospital medicine programs in six countries, who called upon him in part because of his past research on managing length of hospital stays. Dr. Howell counts himself among a few dozen U.S. hospitalists who are regularly invited to come and consult or to give talks to established or developing hospitalist programs in other countries. Because of the COVID-19 epidemic, in-person visits to other countries have largely been curtailed, but that has introduced a more virtual world of online meetings.
“I think the interesting thing about the ‘international consultants’ for hospital medicine is that while they come from professionally diverse backgrounds, they are all working to solve remarkably similar problems: How to make health care more affordable and higher quality while staying abreast of up-to-date best practice for physicians,” he said.
“Hospital care is costly no matter where you go. Other countries are also trying to limit expense in ways that don’t compromise the quality of that care,” Dr. Howell said. Also, hospitalized patients are more complex than ever, with increasing severity of illness and comorbidities, which makes having a hospitalist available on site more important.
Dr. Howell hopes to encourage more dialogue with international colleagues. SHM has established collaborations with medical societies in other countries and makes time at its conferences for international hospitalist participants to meet and share their experiences. Hospitalists from 33 countries were represented at SHM’s 2017 conference, and the upcoming virtual SHM Converge, May 3-7, 2021, includes a dedicated international session. SHM chapters have formed in a number of other countries.
Flora Kisuule, MD, MPH, SFHM, director of the Division of Hospital Medicine at Johns Hopkins Bayview Medical Center in Baltimore, said her international hospital medicine work1 started 7 years ago when she was invited to the Middle East to help Aramco, the Saudi Arabian Oil Company, develop a hospital medicine program based on the U.S. model for its employees. This was a joint venture with Johns Hopkins Medicine. “We went there and looked at their processes and made recommendations such as duration of hospitalist shifts and how to expand the footprint of hospital medicine in the hospital,” she said.
Then Dr. Kisuule was asked to help develop a hospital medicine program in Panama, where the drivers for developing hospital medicine were improving quality of care and ensuring patient safety. The biggest barrier has been remuneration and how to pay salaries that will allow doctors to work at only one hospital. In Panama, doctors typically work at multiple hospitals or clinics so they can earn enough to make ends meet.
The need for professional identity
Arpana Vidyarthi, MD, “grew up” professionally in hospital medicine at the University of California, San Francisco, a pioneering institution for hospital medicine, and in SHM. “We used to say: If you’ve seen one hospital medicine group, you’ve seen one hospital medicine group,” she said.
Dr. Vidyarthi went to Singapore in 2011, taking a job as a hospitalist at Singapore General Hospital and the affiliated Duke–National University Medical School, eventually directing the Division of Advanced Internal Medicine (general and hospital medicine) at the National University Health System, before moving back to UCSF in 2020.
“Professional identity is one of the biggest benefits hospital medicine can bestow in Singapore and across Asia, where general medicine is underdeveloped. Just as it did 20 years ago in the U.S., that professional identity offers a road map to achieving competency in practicing medicine in the hospital setting,” Dr. Vidyarthi said.
At UCSF, the professional identity of a hospitalist is broad but defined. The research agenda, quality, safety, and educational competencies are specific, seen through a system lens, she added. “We take pride in that professional identify. This is an opportunity for countries where general medicine is underdeveloped and undervalued.”
But the term hospital medicine – or the American model – isn’t always welcomed by health care systems in other countries, Dr Vidyarthi said. “The label of 'hospital medicine' brings people together in professional identify, and that professional identity opens doors. But for it to have legs in other countries, those skills need to be of value to the local system. It needs to make sense, as it did in the United States, and to add value for the identified gaps that need to be filled.”
In Singapore, the health care system turned to the model of acute medical units (AMUs) and the acute medicine physician specialty developed in the United Kingdom, which created a new way of delivering care, a new geography of care, and new set of competencies around which to build training and certification.
AMUs manage the majority of acute medical patients who present to the emergency department and get admitted, with initial treatment for a maximum of 72 hours. Acute physicians, trained in the specialty of assessment, diagnosis, and treatment of adult patients with urgent medical needs, work in a unit situated between the emergency department entrance and the specialty care units. This specialty has been recognized since 2009.2
“Acute medicine is the standard care model in the UK and is now found in all government hospitals in Singapore. This model is being adapted across Europe, Asia, and the Pacific Islands,” Dr. Vidyarthi said. “Advantages include the specific geography of the unit, and outcomes that are value-added to these systems such as decreased use of hospital beds in areas with very high bed occupancy rates.”
In many locales, a variety of titles are used to describe doctors who are not hospitalists as we understand them but whose work is based in the hospital, including house officer, duty officer, junior officer, registrar, or general practitioner. Often these hospital-based doctors, who may in fact be residents or nongraduated trainees, lack the training and the scope of practice of a hospitalist. Because they typically need to consult the supervising physician before making inpatient management decisions, they aren’t able to provide the timely response to the patient’s changing medical condition that is needed to manage today’s acute patients.
Defining the fee schedule
In South Korea, a hospitalist model has emerged since 2015 in response to the insufficient number of hospital-based physicians needed to cover all admitted patients and to address related issues of patient safety, health care quality, and limitations on total hours per week medical residents are allowed to work.
South Korea in 1989 adopted a universal National Health Insurance System (NHIS), which took 12 years to implement. But inadequate coverage for medical work in the hospital has deterred physicians from choosing to work there. South Korea had longer lengths of hospital stay, fewer practicing physicians per 1,000 patients, and a much higher number of hospital patients per practicing physician than other countries in the Organization for Economic Cooperation and Development, according to a new study in the Journal of Hospital Medicine detailing hospitalist development in South Korea.3
A council representing leading medical associations was formed to develop a South Korean hospitalist system and charged by the Ministry of Health with designing an official proposal for implementing it. A pilot study focused on quality and on defining a fee schedule for hospital work was tested in four hospitals, and then a second phase in 31 of South Korea’s 344 general hospitals tested the proposed fee schedule, said Wonjeong Chae, MPH, the first named author on the study, based in the Department of Public Health in the College of Medicine at Yonsei University in Seoul. “But we’re still working on making the fee schedule better,” she said.
Ms. Chae estimates that there are about 250 working hospitalists in South Korea today, which leaves a lot of gaps in practice. “We did learn from America, but we have a different system, so the American concept had to be adapted. Hospital medicine is still growing in Korea despite the impact of the pandemic. We are at the beginning stages of development, but we expect it will grow more with government support.”
In Brazil, a handful of hospital medicine pioneers such as Guilherme Barcellos, MD, SFHM, in Porto Alegre have tried to grow the hospitalist model, networking with colleagues across Latin America through the Pan American Society of Hospitalists and the Brazilian chapter of SHM.
Individual hospitals have developed hospitalist programs, but there is no national model to lead the way. Frequent turnover for the Minister of Health position has made it harder to develop consistent national policy, and the country is largely still in the early stages of developing hospital medicine, depending on isolated initiatives, as Dr. Barcellos described it in a November 2015 article in The Hospitalist.4 Growth is slow but continuing, with new programs such as the one led by Reginaldo Filho, MD at Hospital São Vicente in Curitiba standing out in the confrontation against COVID-19, Dr. Barcellos said.
What can we learn from others?
India-born, U.S.-trained hospitalist Anand Kartha, MD, MS, SFHM, currently heads the Hospital Medicine Program at Hamad General Hospital in Doha, Qatar. He moved from Boston to this small nation on the Arabian Peninsula in 2014. Under the leadership of the hospital’s Department of Medicine, this program was developed to address difficulties such as scheduling, transitions of care, and networking with home care and other providers – the same issues seen in hospitals around the world.
These are not novel problems, Dr. Kartha said, but all of them have a common solution in evidence-based practice. “As hospitalists, our key is to collaborate with everyone in the hospital, using the multidisciplinary approach that is a unique feature of hospital medicine.”
The model has continued to spread across hospitals in Qatar, including academic and community programs. “We now have a full-fledged academic hospitalist system, which collaborates with community hospitals and community programs including a women’s hospital and an oncologic hospital,” he said. “Now the focus is on expanding resource capacity and the internal pipeline for hospitalists. I am getting graduates from Weill Cornell Medicine in Qatar.” Another key collaborator has been the Boston-based Institute for Healthcare Improvement, helping to develop best practices in Qatar and sponsoring the annual Middle East Forum on Quality and Safety in Health Care.
The residency training program at Hamad General is accredited by ACGME, with the same expected competencies as in the U.S. “We don’t use the term ‘hospitalist,’ ” Dr. Kartha said. “It’s better to focus on the model of care – which clearly was American. That model has encountered some resistance in some countries – on many of the same grounds U.S. hospitalists faced 20 years ago. You have to be sensitive to local culture. For hospitalists to succeed internationally, they have to possess a high degree of cultural intelligence.” There’s no shortage of issues such as language barriers, he said. “But that’s no different than at Boston Medical Center.”
SHM’s Middle East Chapter was off to a great start and then was slowed down by regional politics and COVID-19, but is looking forward to a great reboot in 2021, Dr. Kartha said. The pandemic also has been an opportunity to show how hospital medicine is the backbone of the hospital’s ability to respond, although of course many other professionals also pitched in.
Other countries around the world have learned a lot from the American model of hospital medicine. But sources for this article wonder if U.S. hospitalists, in turn, could learn from their adaptations and innovations.
“We can all learn better how to practice our field of medicine in the hospital with less resource utilization,” Dr. Vidyarthi concluded. “So many innovations are happening around us. If we open our eyes to our global colleagues and infuse some of their ideas, it could be wonderful for hospital professionals in the United States.”
References
1. Kisuule F, Howell E. Hospital medicine beyond the United States. Int J Gen Med. 2018;11:65-71. doi: 10.2147/IJGM.S151275.
2. Stosic J et al. The acute physician: The future of acute hospital care in the UK. Clin Med (Lond). 2010 Apr; 10(2):145-7. doi: 10.7861/clinmedicine.10-2-145.
3. Yan Y et al. Adoption of Hospitalist Care in Asia: Experiences From Singapore, Taiwan, Korea, and Japan. J Hosp Med. Published Online First 2021 June 11. doi: 10.12788/jhm.3621.
4. Beresford L. Hospital medicine flourishing around the world. The Hospitalist. Nov 2015.
FDA okays new indication for alirocumab in homozygous FH
The Food and Drug Administration has approved alirocumab (Praluent, Regeneron Pharmaceuticals) injection as add-on therapy for adults with homozygous familial hypercholesterolemia, the agency announced.
The proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor was originally approved in the United States in 2015 as an adjunct to diet, alone or in combination with other lipid-lowering therapies, to reduce LDL cholesterol in adults with primary hyperlipidemia, including heterozygous familial hypercholesterolemia (FH).
Heterozygous FH is one of the most common genetic disorders, affecting 1 in every 200-500 people worldwide, whereas homozygous FH is very rare, affecting about 1 in 1 million people worldwide.
Alirocumab is also approved to reduce the risk of myocardial infarction, stroke, and unstable angina requiring hospitalization in adults with cardiovascular disease.
The new indication is based on a 12-week randomized trial in 45 adults who received 150 mg alirocumab every 2 weeks and 24 patients who received placebo, both on top of other therapies to reduce LDL cholesterol. At week 12, patients receiving alirocumab had an average 27% decrease in LDL cholesterol, compared with an average 9% increase among patients on placebo.
Common side effects of alirocumab are nasopharyngitis, injection-site reactions, and influenza. Serious hypersensitivity reactions have occurred among people taking alirocumab.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved alirocumab (Praluent, Regeneron Pharmaceuticals) injection as add-on therapy for adults with homozygous familial hypercholesterolemia, the agency announced.
The proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor was originally approved in the United States in 2015 as an adjunct to diet, alone or in combination with other lipid-lowering therapies, to reduce LDL cholesterol in adults with primary hyperlipidemia, including heterozygous familial hypercholesterolemia (FH).
Heterozygous FH is one of the most common genetic disorders, affecting 1 in every 200-500 people worldwide, whereas homozygous FH is very rare, affecting about 1 in 1 million people worldwide.
Alirocumab is also approved to reduce the risk of myocardial infarction, stroke, and unstable angina requiring hospitalization in adults with cardiovascular disease.
The new indication is based on a 12-week randomized trial in 45 adults who received 150 mg alirocumab every 2 weeks and 24 patients who received placebo, both on top of other therapies to reduce LDL cholesterol. At week 12, patients receiving alirocumab had an average 27% decrease in LDL cholesterol, compared with an average 9% increase among patients on placebo.
Common side effects of alirocumab are nasopharyngitis, injection-site reactions, and influenza. Serious hypersensitivity reactions have occurred among people taking alirocumab.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved alirocumab (Praluent, Regeneron Pharmaceuticals) injection as add-on therapy for adults with homozygous familial hypercholesterolemia, the agency announced.
The proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor was originally approved in the United States in 2015 as an adjunct to diet, alone or in combination with other lipid-lowering therapies, to reduce LDL cholesterol in adults with primary hyperlipidemia, including heterozygous familial hypercholesterolemia (FH).
Heterozygous FH is one of the most common genetic disorders, affecting 1 in every 200-500 people worldwide, whereas homozygous FH is very rare, affecting about 1 in 1 million people worldwide.
Alirocumab is also approved to reduce the risk of myocardial infarction, stroke, and unstable angina requiring hospitalization in adults with cardiovascular disease.
The new indication is based on a 12-week randomized trial in 45 adults who received 150 mg alirocumab every 2 weeks and 24 patients who received placebo, both on top of other therapies to reduce LDL cholesterol. At week 12, patients receiving alirocumab had an average 27% decrease in LDL cholesterol, compared with an average 9% increase among patients on placebo.
Common side effects of alirocumab are nasopharyngitis, injection-site reactions, and influenza. Serious hypersensitivity reactions have occurred among people taking alirocumab.
A version of this article first appeared on Medscape.com.
Starting April 5, patients can read your notes: 5 things to consider
Change in writing style is not mandated
The mandate, called “open notes” by many, is part of the 21st Century Cures Act, a wide-ranging piece of federal health care legislation. The previous deadline of Nov. 2, 2020, for enacting open notes was extended last year because of the exigencies of the COVID-19 pandemic.
Organizations must provide access via patient portals to the following types of notes: consultations, discharge summaries, histories, physical examination findings, imaging narratives, laboratory and pathology report narratives, and procedure and progress notes. Noncompliant organizations will eventually be subject to fines from the Department of Health & Human Services for “information blocking.”
This news organization reported on the mandate in 2020, and some readers said it was an unwelcome intrusion into practice. Since then, this news organization has run additional open notes stories about physician concerns, a perspective essay addressing those fears, and a reader poll about the phenomenon.
Now, as the legislation turns into a practical clinical matter, there are five key points clinicians should consider.
Clinicians don’t have to change writing style.
The new law mandates timely patient access to notes and test results, but it doesn’t require that clinicians alter their writing, said Scott MacDonald, MD, an internist and electronic health record medical director at University of California Davis Health in Sacramento.
“You don’t have to change your notes,” he said. However, patients are now part of the note audience and some health care systems are directing clinicians to make patient-friendly style changes.
Everyday experience should guide clinicians when writing notes, said one expert.
“When you’re not sure [of how to write a note], just mirror the way you would speak in the office – that’s going to get you right, including for mental health issues,” advised Leonor Fernandez, MD, an internist at Beth Deaconess Israel Medical Center, Boston, in her “take-away” comments in the online video, How to Write an Open Note.
According to a 2020 Medscape poll of 1,050 physicians, a majority (56%) anticipate that they will write notes differently, knowing that patients can read them via open notes. Nearly two-thirds (64%) believe that this new wrinkle in medical records will increase their workload. However, actual practice suggests that this is true for a minority of practitioners, according to the results from a recent study of more than 1,000 physicians in Boston, Seattle, and rural Pennsylvania, who already work in open notes settings. Only about one-third (37%) reported “spending more time on documentation.”
Note writing is going to change because of the addition of the patient reader, and something will be lost, argued Steven Reidbord, MD, a psychiatrist in private practice in San Francisco. By watering down the language for patients, “you are trading away the technical precision and other advantages of having a professional language,” commented Dr. Reidbord, who blogs for Psychology Today and has criticized the open notes movement in the past.
However, years of investigation from OpenNotes, the Boston-based advocacy and research organization, indicates that there are many gains with patient-accessible notes, including improved medical record accuracy, greater medication adherence, and potentially improved health care disparities among a range of patient types. In a 2019 study, researchers said that worry and confusion among note-reading patients are uncommon (5% and 3%, respectively), which addresses two criticisms voiced by multiple people last year.
Some clinical notes can be withheld.
The new rules from the federal government permit information blocking if there is clear evidence that doing so “will substantially reduce the risk of harm” to patients or to other third parties, Tom Delbanco, MD, and Charlotte Blease, PhD, of OpenNotes in Boston wrote in a commentary in February 2021.
There are also state-level laws that can supersede the new U.S. law and block access to notes, points out MacDonald. For example, California law dictates that providers cannot post cancer test results without talking with the patient first.
The OpenNotes organization also points out that, with regard to sensitive psychotherapy notes that are separated from the rest of a medical record, those notes “can be kept from patients without their permission, and such rules vary state by state.”
Some patients are more likely readers.
Some patients are more likely to peer into their files than others, said Liz Salmi, senior strategist at OpenNotes, who is also a brain cancer patient.
“Those patients who have more serious or chronic conditions ... are more likely to read their notes,” she said in an interview.
A new study of nearly 6,000 medical oncology patients at the University of Wisconsin confirmed that opinion. Patients with incurable metastatic disease were much more likely than those with early-stage, curable disease to read notes. Notably, younger patients were more likely than older ones to access notes, likely the result of generational tech savvy.
Despite the unpredictability of serious disease such as cancer, oncology patients find satisfaction in reading their notes, say experts. “We’ve overwhelmingly heard that patients like it,” Thomas LeBlanc, MD, medical oncologist at Duke University, Durham, N.C., where all patients already have access to clinicians’ notes, told this news organization in 2018.
You are part of the avant garde.
The United States and Scandinavian countries are the world leaders in implementing open notes in clinical practice, Dr. Blease said in an interview.
“It’s a phenomenal achievement” to have enacted open notes nationally, she said. For example, there are no open notes in Northern Ireland, Dr. Blease’s home country, or most of Europe.
In the United States, there are more than 200 medical organizations, including at least one in every state, that were voluntarily providing open notes before April 5, including interstate giants such as Banner Health and big-name medical centers such as Cleveland Clinic.
It may be hard for the United States to top Sweden’s embrace of the practice. The national open notes program now has 7.2 million patient accounts in a country of 10 million people, noted Maria Häggland, PhD, of Uppsala (Sweden) MedTech Science Innovation Center during a webinar last year.
The start day will come, and you may not notice.
“When April 5 happens, something brand new is going to happen symbolically,” Ms. Salmi said. Its importance is hard to measure.
“Patients say they trust their doctor more because they understand their thinking with open notes. How do you value that? We don’t have metrics for that,” she said.
Dr. MacDonald suggested that open notes are both new and not new. In the fall of 2020, he predicted that the launch day would come, and few clinicians would notice, in part because many patients already access truncated information via patient portals.
However, there are “sensitive issues,” such as with adolescents and reproductive health, where “we know that some parents have sign-in information for their teen’s portal,” he commented. With clinical notes now on full display, potential problems “may be out of our control.”
Still, the Sacramento-based physician and IT officer acknowledged that concerns about open notes may be a bit inflated. “I’ve been more worried about reassuring physicians that everything will be okay than what’s actually going to happen [as the law takes effect],” Dr. MacDonald said.
The OpenNotes organization is grant funded, and staff disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Change in writing style is not mandated
Change in writing style is not mandated
The mandate, called “open notes” by many, is part of the 21st Century Cures Act, a wide-ranging piece of federal health care legislation. The previous deadline of Nov. 2, 2020, for enacting open notes was extended last year because of the exigencies of the COVID-19 pandemic.
Organizations must provide access via patient portals to the following types of notes: consultations, discharge summaries, histories, physical examination findings, imaging narratives, laboratory and pathology report narratives, and procedure and progress notes. Noncompliant organizations will eventually be subject to fines from the Department of Health & Human Services for “information blocking.”
This news organization reported on the mandate in 2020, and some readers said it was an unwelcome intrusion into practice. Since then, this news organization has run additional open notes stories about physician concerns, a perspective essay addressing those fears, and a reader poll about the phenomenon.
Now, as the legislation turns into a practical clinical matter, there are five key points clinicians should consider.
Clinicians don’t have to change writing style.
The new law mandates timely patient access to notes and test results, but it doesn’t require that clinicians alter their writing, said Scott MacDonald, MD, an internist and electronic health record medical director at University of California Davis Health in Sacramento.
“You don’t have to change your notes,” he said. However, patients are now part of the note audience and some health care systems are directing clinicians to make patient-friendly style changes.
Everyday experience should guide clinicians when writing notes, said one expert.
“When you’re not sure [of how to write a note], just mirror the way you would speak in the office – that’s going to get you right, including for mental health issues,” advised Leonor Fernandez, MD, an internist at Beth Deaconess Israel Medical Center, Boston, in her “take-away” comments in the online video, How to Write an Open Note.
According to a 2020 Medscape poll of 1,050 physicians, a majority (56%) anticipate that they will write notes differently, knowing that patients can read them via open notes. Nearly two-thirds (64%) believe that this new wrinkle in medical records will increase their workload. However, actual practice suggests that this is true for a minority of practitioners, according to the results from a recent study of more than 1,000 physicians in Boston, Seattle, and rural Pennsylvania, who already work in open notes settings. Only about one-third (37%) reported “spending more time on documentation.”
Note writing is going to change because of the addition of the patient reader, and something will be lost, argued Steven Reidbord, MD, a psychiatrist in private practice in San Francisco. By watering down the language for patients, “you are trading away the technical precision and other advantages of having a professional language,” commented Dr. Reidbord, who blogs for Psychology Today and has criticized the open notes movement in the past.
However, years of investigation from OpenNotes, the Boston-based advocacy and research organization, indicates that there are many gains with patient-accessible notes, including improved medical record accuracy, greater medication adherence, and potentially improved health care disparities among a range of patient types. In a 2019 study, researchers said that worry and confusion among note-reading patients are uncommon (5% and 3%, respectively), which addresses two criticisms voiced by multiple people last year.
Some clinical notes can be withheld.
The new rules from the federal government permit information blocking if there is clear evidence that doing so “will substantially reduce the risk of harm” to patients or to other third parties, Tom Delbanco, MD, and Charlotte Blease, PhD, of OpenNotes in Boston wrote in a commentary in February 2021.
There are also state-level laws that can supersede the new U.S. law and block access to notes, points out MacDonald. For example, California law dictates that providers cannot post cancer test results without talking with the patient first.
The OpenNotes organization also points out that, with regard to sensitive psychotherapy notes that are separated from the rest of a medical record, those notes “can be kept from patients without their permission, and such rules vary state by state.”
Some patients are more likely readers.
Some patients are more likely to peer into their files than others, said Liz Salmi, senior strategist at OpenNotes, who is also a brain cancer patient.
“Those patients who have more serious or chronic conditions ... are more likely to read their notes,” she said in an interview.
A new study of nearly 6,000 medical oncology patients at the University of Wisconsin confirmed that opinion. Patients with incurable metastatic disease were much more likely than those with early-stage, curable disease to read notes. Notably, younger patients were more likely than older ones to access notes, likely the result of generational tech savvy.
Despite the unpredictability of serious disease such as cancer, oncology patients find satisfaction in reading their notes, say experts. “We’ve overwhelmingly heard that patients like it,” Thomas LeBlanc, MD, medical oncologist at Duke University, Durham, N.C., where all patients already have access to clinicians’ notes, told this news organization in 2018.
You are part of the avant garde.
The United States and Scandinavian countries are the world leaders in implementing open notes in clinical practice, Dr. Blease said in an interview.
“It’s a phenomenal achievement” to have enacted open notes nationally, she said. For example, there are no open notes in Northern Ireland, Dr. Blease’s home country, or most of Europe.
In the United States, there are more than 200 medical organizations, including at least one in every state, that were voluntarily providing open notes before April 5, including interstate giants such as Banner Health and big-name medical centers such as Cleveland Clinic.
It may be hard for the United States to top Sweden’s embrace of the practice. The national open notes program now has 7.2 million patient accounts in a country of 10 million people, noted Maria Häggland, PhD, of Uppsala (Sweden) MedTech Science Innovation Center during a webinar last year.
The start day will come, and you may not notice.
“When April 5 happens, something brand new is going to happen symbolically,” Ms. Salmi said. Its importance is hard to measure.
“Patients say they trust their doctor more because they understand their thinking with open notes. How do you value that? We don’t have metrics for that,” she said.
Dr. MacDonald suggested that open notes are both new and not new. In the fall of 2020, he predicted that the launch day would come, and few clinicians would notice, in part because many patients already access truncated information via patient portals.
However, there are “sensitive issues,” such as with adolescents and reproductive health, where “we know that some parents have sign-in information for their teen’s portal,” he commented. With clinical notes now on full display, potential problems “may be out of our control.”
Still, the Sacramento-based physician and IT officer acknowledged that concerns about open notes may be a bit inflated. “I’ve been more worried about reassuring physicians that everything will be okay than what’s actually going to happen [as the law takes effect],” Dr. MacDonald said.
The OpenNotes organization is grant funded, and staff disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The mandate, called “open notes” by many, is part of the 21st Century Cures Act, a wide-ranging piece of federal health care legislation. The previous deadline of Nov. 2, 2020, for enacting open notes was extended last year because of the exigencies of the COVID-19 pandemic.
Organizations must provide access via patient portals to the following types of notes: consultations, discharge summaries, histories, physical examination findings, imaging narratives, laboratory and pathology report narratives, and procedure and progress notes. Noncompliant organizations will eventually be subject to fines from the Department of Health & Human Services for “information blocking.”
This news organization reported on the mandate in 2020, and some readers said it was an unwelcome intrusion into practice. Since then, this news organization has run additional open notes stories about physician concerns, a perspective essay addressing those fears, and a reader poll about the phenomenon.
Now, as the legislation turns into a practical clinical matter, there are five key points clinicians should consider.
Clinicians don’t have to change writing style.
The new law mandates timely patient access to notes and test results, but it doesn’t require that clinicians alter their writing, said Scott MacDonald, MD, an internist and electronic health record medical director at University of California Davis Health in Sacramento.
“You don’t have to change your notes,” he said. However, patients are now part of the note audience and some health care systems are directing clinicians to make patient-friendly style changes.
Everyday experience should guide clinicians when writing notes, said one expert.
“When you’re not sure [of how to write a note], just mirror the way you would speak in the office – that’s going to get you right, including for mental health issues,” advised Leonor Fernandez, MD, an internist at Beth Deaconess Israel Medical Center, Boston, in her “take-away” comments in the online video, How to Write an Open Note.
According to a 2020 Medscape poll of 1,050 physicians, a majority (56%) anticipate that they will write notes differently, knowing that patients can read them via open notes. Nearly two-thirds (64%) believe that this new wrinkle in medical records will increase their workload. However, actual practice suggests that this is true for a minority of practitioners, according to the results from a recent study of more than 1,000 physicians in Boston, Seattle, and rural Pennsylvania, who already work in open notes settings. Only about one-third (37%) reported “spending more time on documentation.”
Note writing is going to change because of the addition of the patient reader, and something will be lost, argued Steven Reidbord, MD, a psychiatrist in private practice in San Francisco. By watering down the language for patients, “you are trading away the technical precision and other advantages of having a professional language,” commented Dr. Reidbord, who blogs for Psychology Today and has criticized the open notes movement in the past.
However, years of investigation from OpenNotes, the Boston-based advocacy and research organization, indicates that there are many gains with patient-accessible notes, including improved medical record accuracy, greater medication adherence, and potentially improved health care disparities among a range of patient types. In a 2019 study, researchers said that worry and confusion among note-reading patients are uncommon (5% and 3%, respectively), which addresses two criticisms voiced by multiple people last year.
Some clinical notes can be withheld.
The new rules from the federal government permit information blocking if there is clear evidence that doing so “will substantially reduce the risk of harm” to patients or to other third parties, Tom Delbanco, MD, and Charlotte Blease, PhD, of OpenNotes in Boston wrote in a commentary in February 2021.
There are also state-level laws that can supersede the new U.S. law and block access to notes, points out MacDonald. For example, California law dictates that providers cannot post cancer test results without talking with the patient first.
The OpenNotes organization also points out that, with regard to sensitive psychotherapy notes that are separated from the rest of a medical record, those notes “can be kept from patients without their permission, and such rules vary state by state.”
Some patients are more likely readers.
Some patients are more likely to peer into their files than others, said Liz Salmi, senior strategist at OpenNotes, who is also a brain cancer patient.
“Those patients who have more serious or chronic conditions ... are more likely to read their notes,” she said in an interview.
A new study of nearly 6,000 medical oncology patients at the University of Wisconsin confirmed that opinion. Patients with incurable metastatic disease were much more likely than those with early-stage, curable disease to read notes. Notably, younger patients were more likely than older ones to access notes, likely the result of generational tech savvy.
Despite the unpredictability of serious disease such as cancer, oncology patients find satisfaction in reading their notes, say experts. “We’ve overwhelmingly heard that patients like it,” Thomas LeBlanc, MD, medical oncologist at Duke University, Durham, N.C., where all patients already have access to clinicians’ notes, told this news organization in 2018.
You are part of the avant garde.
The United States and Scandinavian countries are the world leaders in implementing open notes in clinical practice, Dr. Blease said in an interview.
“It’s a phenomenal achievement” to have enacted open notes nationally, she said. For example, there are no open notes in Northern Ireland, Dr. Blease’s home country, or most of Europe.
In the United States, there are more than 200 medical organizations, including at least one in every state, that were voluntarily providing open notes before April 5, including interstate giants such as Banner Health and big-name medical centers such as Cleveland Clinic.
It may be hard for the United States to top Sweden’s embrace of the practice. The national open notes program now has 7.2 million patient accounts in a country of 10 million people, noted Maria Häggland, PhD, of Uppsala (Sweden) MedTech Science Innovation Center during a webinar last year.
The start day will come, and you may not notice.
“When April 5 happens, something brand new is going to happen symbolically,” Ms. Salmi said. Its importance is hard to measure.
“Patients say they trust their doctor more because they understand their thinking with open notes. How do you value that? We don’t have metrics for that,” she said.
Dr. MacDonald suggested that open notes are both new and not new. In the fall of 2020, he predicted that the launch day would come, and few clinicians would notice, in part because many patients already access truncated information via patient portals.
However, there are “sensitive issues,” such as with adolescents and reproductive health, where “we know that some parents have sign-in information for their teen’s portal,” he commented. With clinical notes now on full display, potential problems “may be out of our control.”
Still, the Sacramento-based physician and IT officer acknowledged that concerns about open notes may be a bit inflated. “I’ve been more worried about reassuring physicians that everything will be okay than what’s actually going to happen [as the law takes effect],” Dr. MacDonald said.
The OpenNotes organization is grant funded, and staff disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
History made, history revisited
The Biden administration has passed and signed the $1.9 trillion American Rescue Plan, which contains a plethora of moneys targeted to people, businesses, and health systems impacted by the pandemic. According to the Economist, the bill would bring the amount of COVID-related spending since December 2020 to $3 trillion (14% of prepandemic GDP) and to $6 trillion since the start of the pandemic. This type of stimulus (regarded as income, not savings, by most people) will generate unprecedented consumer spending. The risk, of course, is inflation, rising interest rates, and long-term debt.

That said, there is substantial funding targeting scientific research, vaccine distribution, public health entities, global health initiatives, rural health care, and a variety of other health-related issues. By my rough estimation, the Centers for Disease Control and Prevention will see $12 billion in incremental funding, $10 billion for public health projects including $3 billion for community health centers and federally qualified health centers, and over $3 billion for mental and behavioral health. The Department of Health & Human Services will see substantial funding for a variety of projects. Teaching health centers will see $330 million additional funds (including a $10,000 per-resident increase and payments to establish new graduate residency training programs).
The impact on low-income families and childhood poverty will be substantial and reverses the philosophical underpinning of recent welfare reforms. U.S. welfare dates back to the early 1900s and the philosophical foundation has evolved over time. According to the Constitutional Rights Foundation (www.crf-usa.org), it began after food riots broke out during the Great Depression. The Great Depression affected children and the elderly most severely, so the nation’s willingness to implement federal welfare was high. Prior to the Depression, the only federal program providing money to low-income people was the “mothers pension” designed to support poor fatherless children, but it excluded divorced, deserted and minority mothers. President Roosevelt was able to pass the Social Security Act (1935), which supported the elderly and began Federal welfare. During the Clinton presidency, welfare “as we know it” changed to include work requirements. With the passage of the current Biden legislation, those requirements are rolled back and funds are targeted broadly to low income Americans and children.
John I. Allen, MD, MBA, AGAF
Editor in Chief
The Biden administration has passed and signed the $1.9 trillion American Rescue Plan, which contains a plethora of moneys targeted to people, businesses, and health systems impacted by the pandemic. According to the Economist, the bill would bring the amount of COVID-related spending since December 2020 to $3 trillion (14% of prepandemic GDP) and to $6 trillion since the start of the pandemic. This type of stimulus (regarded as income, not savings, by most people) will generate unprecedented consumer spending. The risk, of course, is inflation, rising interest rates, and long-term debt.
That said, there is substantial funding targeting scientific research, vaccine distribution, public health entities, global health initiatives, rural health care, and a variety of other health-related issues. By my rough estimation, the Centers for Disease Control and Prevention will see $12 billion in incremental funding, $10 billion for public health projects including $3 billion for community health centers and federally qualified health centers, and over $3 billion for mental and behavioral health. The Department of Health & Human Services will see substantial funding for a variety of projects. Teaching health centers will see $330 million additional funds (including a $10,000 per-resident increase and payments to establish new graduate residency training programs).
The impact on low-income families and childhood poverty will be substantial and reverses the philosophical underpinning of recent welfare reforms. U.S. welfare dates back to the early 1900s and the philosophical foundation has evolved over time. According to the Constitutional Rights Foundation (www.crf-usa.org), it began after food riots broke out during the Great Depression. The Great Depression affected children and the elderly most severely, so the nation’s willingness to implement federal welfare was high. Prior to the Depression, the only federal program providing money to low-income people was the “mothers pension” designed to support poor fatherless children, but it excluded divorced, deserted and minority mothers. President Roosevelt was able to pass the Social Security Act (1935), which supported the elderly and began Federal welfare. During the Clinton presidency, welfare “as we know it” changed to include work requirements. With the passage of the current Biden legislation, those requirements are rolled back and funds are targeted broadly to low income Americans and children.
John I. Allen, MD, MBA, AGAF
Editor in Chief
The Biden administration has passed and signed the $1.9 trillion American Rescue Plan, which contains a plethora of moneys targeted to people, businesses, and health systems impacted by the pandemic. According to the Economist, the bill would bring the amount of COVID-related spending since December 2020 to $3 trillion (14% of prepandemic GDP) and to $6 trillion since the start of the pandemic. This type of stimulus (regarded as income, not savings, by most people) will generate unprecedented consumer spending. The risk, of course, is inflation, rising interest rates, and long-term debt.
That said, there is substantial funding targeting scientific research, vaccine distribution, public health entities, global health initiatives, rural health care, and a variety of other health-related issues. By my rough estimation, the Centers for Disease Control and Prevention will see $12 billion in incremental funding, $10 billion for public health projects including $3 billion for community health centers and federally qualified health centers, and over $3 billion for mental and behavioral health. The Department of Health & Human Services will see substantial funding for a variety of projects. Teaching health centers will see $330 million additional funds (including a $10,000 per-resident increase and payments to establish new graduate residency training programs).
The impact on low-income families and childhood poverty will be substantial and reverses the philosophical underpinning of recent welfare reforms. U.S. welfare dates back to the early 1900s and the philosophical foundation has evolved over time. According to the Constitutional Rights Foundation (www.crf-usa.org), it began after food riots broke out during the Great Depression. The Great Depression affected children and the elderly most severely, so the nation’s willingness to implement federal welfare was high. Prior to the Depression, the only federal program providing money to low-income people was the “mothers pension” designed to support poor fatherless children, but it excluded divorced, deserted and minority mothers. President Roosevelt was able to pass the Social Security Act (1935), which supported the elderly and began Federal welfare. During the Clinton presidency, welfare “as we know it” changed to include work requirements. With the passage of the current Biden legislation, those requirements are rolled back and funds are targeted broadly to low income Americans and children.
John I. Allen, MD, MBA, AGAF
Editor in Chief
Question 2
Correct answer: B. Prednisone
Rationale
This is a case of Henoch-Schönlein purpura, which is a self-limited, systemic, nongranulomatous, autoimmune complex, small-vessel vasculitis with multiorgan involvement. It is characterized by a classic tetrad of nonthrombocytopenic palpable purpura, arthritis or arthralgias, gastrointestinal involvement, and renal involvement. GI involvement may mimic Crohn's disease, although the biopsies are usually diagnostic. Most cases are self-limiting, but oral steroids are indicated in patients with severe colicky abdominal pain; usually they're started as prednisone or methylprednisolone at 1-2 mg/kg per day for 1-2 weeks and then tapering to a stop in the next 1-2 weeks. Steroids may prevent major complications such as gastrointestinal bleeding or intussusception. Immunosuppressive drugs (cyclophosphamide, azathioprine, cyclosporine A, and mycophenolate mofetil) in combination with high-dose IV pulse steroids are recommended if there is no benefit from steroids alone.
Reference
Sohagia AB et al. Gastroenterol Res Pract. 2010. doi: 10.1155/2010/59764.
Correct answer: B. Prednisone
Rationale
This is a case of Henoch-Schönlein purpura, which is a self-limited, systemic, nongranulomatous, autoimmune complex, small-vessel vasculitis with multiorgan involvement. It is characterized by a classic tetrad of nonthrombocytopenic palpable purpura, arthritis or arthralgias, gastrointestinal involvement, and renal involvement. GI involvement may mimic Crohn's disease, although the biopsies are usually diagnostic. Most cases are self-limiting, but oral steroids are indicated in patients with severe colicky abdominal pain; usually they're started as prednisone or methylprednisolone at 1-2 mg/kg per day for 1-2 weeks and then tapering to a stop in the next 1-2 weeks. Steroids may prevent major complications such as gastrointestinal bleeding or intussusception. Immunosuppressive drugs (cyclophosphamide, azathioprine, cyclosporine A, and mycophenolate mofetil) in combination with high-dose IV pulse steroids are recommended if there is no benefit from steroids alone.
Reference
Sohagia AB et al. Gastroenterol Res Pract. 2010. doi: 10.1155/2010/59764.
Correct answer: B. Prednisone
Rationale
This is a case of Henoch-Schönlein purpura, which is a self-limited, systemic, nongranulomatous, autoimmune complex, small-vessel vasculitis with multiorgan involvement. It is characterized by a classic tetrad of nonthrombocytopenic palpable purpura, arthritis or arthralgias, gastrointestinal involvement, and renal involvement. GI involvement may mimic Crohn's disease, although the biopsies are usually diagnostic. Most cases are self-limiting, but oral steroids are indicated in patients with severe colicky abdominal pain; usually they're started as prednisone or methylprednisolone at 1-2 mg/kg per day for 1-2 weeks and then tapering to a stop in the next 1-2 weeks. Steroids may prevent major complications such as gastrointestinal bleeding or intussusception. Immunosuppressive drugs (cyclophosphamide, azathioprine, cyclosporine A, and mycophenolate mofetil) in combination with high-dose IV pulse steroids are recommended if there is no benefit from steroids alone.
Reference
Sohagia AB et al. Gastroenterol Res Pract. 2010. doi: 10.1155/2010/59764.
Q2. A 26-year-old White male presented with fever and sore throat for 5 days along with erythematous, nonpruritic rash involving the extremities and arthralgias. He subsequently developed right lower-quadrant pain, aggravated with meals, and associated with watery diarrhea. Labs show showed white blood cell count of 14,900/microL and a C-reactive protein level of 12.6 mg/dL. A magnetic resonance enterography showed 20 cm of thickened ileum. An upper endoscopy showed multiple erosions in the duodenum and antrum while a colonoscopy showed erythema and inflammation in the terminal ileum and cecum. Biopsies from both areas demonstrated evidence of leukocytoclastic vasculitis. Skin biopsy also showed leukocytoclastic vasculitis.
Question 1
Correct answer: D. Antienterocyte antibodies
Rationale
Autoimmune enteropathy (AIE) is characterized by a severe malabsorption and secretory diarrhea, and is differentiated from celiac disease on small-bowel biopsy by the decreased numbers or absence of surface intraepithelial lymphocytes, apoptotic bodies present in the intestinal crypts, and absent goblet and Paneth cells. Patients with AIE may also carry other autoimmune conditions such as rheumatoid arthritis and multiple sclerosis. A group at the Mayo Clinic has published a set of diagnostic criteria based on their case series of adult AIE that requires ruling out other causes of chronic diarrhea in adults, specific histology supportive of AIE, and presence of malabsorption and ruling out other causes of villous atrophy. The presence of antienterocyte or antigoblet cell antibodies are supportive of a diagnosis of AIE, but their absence does not exclude the diagnosis.
References
Akram S et al. Clin Gastroenterol Hepatol. 2007;5(11):1282-90.
Montalto M et al. Scan J Gastroenterol. 2009;44(9):1029-36.
Correct answer: D. Antienterocyte antibodies
Rationale
Autoimmune enteropathy (AIE) is characterized by a severe malabsorption and secretory diarrhea, and is differentiated from celiac disease on small-bowel biopsy by the decreased numbers or absence of surface intraepithelial lymphocytes, apoptotic bodies present in the intestinal crypts, and absent goblet and Paneth cells. Patients with AIE may also carry other autoimmune conditions such as rheumatoid arthritis and multiple sclerosis. A group at the Mayo Clinic has published a set of diagnostic criteria based on their case series of adult AIE that requires ruling out other causes of chronic diarrhea in adults, specific histology supportive of AIE, and presence of malabsorption and ruling out other causes of villous atrophy. The presence of antienterocyte or antigoblet cell antibodies are supportive of a diagnosis of AIE, but their absence does not exclude the diagnosis.
References
Akram S et al. Clin Gastroenterol Hepatol. 2007;5(11):1282-90.
Montalto M et al. Scan J Gastroenterol. 2009;44(9):1029-36.
Correct answer: D. Antienterocyte antibodies
Rationale
Autoimmune enteropathy (AIE) is characterized by a severe malabsorption and secretory diarrhea, and is differentiated from celiac disease on small-bowel biopsy by the decreased numbers or absence of surface intraepithelial lymphocytes, apoptotic bodies present in the intestinal crypts, and absent goblet and Paneth cells. Patients with AIE may also carry other autoimmune conditions such as rheumatoid arthritis and multiple sclerosis. A group at the Mayo Clinic has published a set of diagnostic criteria based on their case series of adult AIE that requires ruling out other causes of chronic diarrhea in adults, specific histology supportive of AIE, and presence of malabsorption and ruling out other causes of villous atrophy. The presence of antienterocyte or antigoblet cell antibodies are supportive of a diagnosis of AIE, but their absence does not exclude the diagnosis.
References
Akram S et al. Clin Gastroenterol Hepatol. 2007;5(11):1282-90.
Montalto M et al. Scan J Gastroenterol. 2009;44(9):1029-36.
Q1. A 55-year-old woman presents with a one-year history of large volume foul-smelling stools that float in water associated with 40-pound weight loss. Laboratory evaluation reveals low vitamin A and D levels. An upper endoscopy with duodenal biopsies reveals complete villous blunting with decreased goblet and Paneth cells, absence of surface intraepithelial lymphocytes, and increased crypt apoptosis. She denies nonsteroidal anti-inflammatory drug use, celiac serologies were not elevated, and a glucose hydrogen breath test was negative. She also has coexisting rheumatoid arthritis and multiple sclerosis.
The best exercises for BP control? European statement sorts it out
Recommendations for prescribing exercise to control high blood pressure have been put forward by various medical organizations and expert panels, but finding the bandwidth to craft personalized exercise training for their patients poses a challenge for clinicians.

Now, European cardiology societies have issued a consensus statement that offers an algorithm of sorts for developing personalized exercise programs as part of overall management approach for patients with or at risk of high BP.
The statement, published in the European Journal of Preventive Cardiology and issued by the European Association of Preventive Cardiology and the European Society of Cardiology Council on Hypertension, claims to be the first document to focus on personalized exercise for BP.
The statement draws on a systematic review, including meta-analyses, to produce guidance on how to lower BP in three specific types of patients: Those with hypertension (>140/90 mm Hg), high-normal blood pressure (130-139/85-89 mm Hg), and normal blood pressure (<130/84 mm Hg).
By making recommendations for these three specific groups, along with providing guidance for combined exercise – that is, blending aerobic exercise with resistance training (RT) – the consensus statement goes one step further than recommendations other organizations have issued, Matthew W. Martinez, MD, said in an interview.
“What it adds is an algorithmic approach, if you will,” said Dr. Martinez, a sports medicine cardiologist at Morristown (N.J.) Medical Center. “There are some recommendations to help the clinicians to decide what they’re going to offer individuals, but what’s a challenge for us when seeing patients is finding the time to deliver the message and explain how valuable nutrition and exercise are.”
Guidelines, updates, and statements that include the role of exercise in BP control have been issued by the European Society of Cardiology, American Heart Association, and American College of Sports Medicine (Med Sci Sports Exercise. 2019;51:1314-23).
The European consensus statement includes the expected range of BP lowering for each activity. For example, aerobic exercise for patients with hypertension should lead to a reduction from –4.9 to –12 mm Hg systolic and –3.4 to –5.8 mm Hg diastolic.
The consensus statement recommends the following exercise priorities based on a patient’s blood pressure:
- Hypertension: Aerobic training (AT) as a first-line exercise therapy; and low- to moderate-intensity RT – equally using dynamic and isometric RT – as second-line therapy. In non-White patients, dynamic RT should be considered as a first-line therapy. RT can be combined with aerobic exercise on an individual basis if the clinician determines either form of RT would provide a metabolic benefit.
- High-to-normal BP: Dynamic RT as a first-line exercise, which the systematic review determined led to greater BP reduction than that of aerobic training. “Isometric RT is likely to elicit similar if not superior BP-lowering effects as [dynamic RT], but the level of evidence is low and the available data are scarce,” wrote first author Henner Hanssen, MD, of the University of Basel, Switzerland, and coauthors. Combining dynamic resistance training with aerobic training “may be preferable” to dynamic RT alone in patients with a combination of cardiovascular risk factors.
- Normal BP: Isometric RT may be indicated as a first-line intervention in individuals with a family or gestational history or obese or overweight people currently with normal BP. This advice includes a caveat: “The number of studies is limited and the 95% confidence intervals are large,” Dr. Hanssen and coauthors noted. AT is also an option in these patients, with more high-quality meta-analyses than the recommendation for isometric RT. “Hence, the BP-lowering effects of [isometric RT] as compared to AT may be overestimated and both exercise modalities may have similar BP-lowering effects in individuals with normotension,” wrote the consensus statement authors.
They note that more research is needed to validate the BP-lowering effects of combined exercise.
The statement acknowledges the difficulty clinicians face in managing patients with high blood pressure. “From a socioeconomic health perspective, it is a major challenge to develop, promote, and implement individually tailored exercise programs for patients with hypertension under consideration of sustainable costs,” wrote Dr. Hanssen and coauthors.
Dr. Martinez noted that one strength of the consensus statement is that it addresses the impact exercise can have on vascular health and metabolic function. And, it points out existing knowledge gaps.
“Are we going to see greater applicability of this as we use IT health technology?” he asked. “Are wearables and telehealth going to help deliver this message more easily, more frequently? Is there work to be done in terms of differences in gender? Do men and women respond differently, and is there a different exercise prescription based on that as well as ethnicity? We well know there’s a different treatment for African Americans compared to other ethnic groups.”
The statement also raises the stakes for using exercise as part of a multifaceted, integrated approach to hypertension management, he said.
“It’s not enough to talk just about exercise or nutrition, or to just give an antihypertension medicine,” Dr. Martinez said. “Perhaps the sweet spot is in integrating an approach that includes all three.”
Consensus statement coauthor Antonio Coca, MD, reported financial relationships with Abbott, Berlin-Chemie, Biolab, Boehringer-Ingelheim, Ferrer, Menarini, Merck, Novartis and Sanofi-Aventis. Coauthor Maria Simonenko, MD, reported financial relationships with Novartis and Sanofi-Aventis. Linda Pescatello, PhD, is lead author of the American College of Sports Medicine 2019 statement. Dr. Hanssen and all other authors have no disclosures. Dr. Martinez has no relevant relationships to disclose.
Recommendations for prescribing exercise to control high blood pressure have been put forward by various medical organizations and expert panels, but finding the bandwidth to craft personalized exercise training for their patients poses a challenge for clinicians.
Now, European cardiology societies have issued a consensus statement that offers an algorithm of sorts for developing personalized exercise programs as part of overall management approach for patients with or at risk of high BP.
The statement, published in the European Journal of Preventive Cardiology and issued by the European Association of Preventive Cardiology and the European Society of Cardiology Council on Hypertension, claims to be the first document to focus on personalized exercise for BP.
The statement draws on a systematic review, including meta-analyses, to produce guidance on how to lower BP in three specific types of patients: Those with hypertension (>140/90 mm Hg), high-normal blood pressure (130-139/85-89 mm Hg), and normal blood pressure (<130/84 mm Hg).
By making recommendations for these three specific groups, along with providing guidance for combined exercise – that is, blending aerobic exercise with resistance training (RT) – the consensus statement goes one step further than recommendations other organizations have issued, Matthew W. Martinez, MD, said in an interview.
“What it adds is an algorithmic approach, if you will,” said Dr. Martinez, a sports medicine cardiologist at Morristown (N.J.) Medical Center. “There are some recommendations to help the clinicians to decide what they’re going to offer individuals, but what’s a challenge for us when seeing patients is finding the time to deliver the message and explain how valuable nutrition and exercise are.”
Guidelines, updates, and statements that include the role of exercise in BP control have been issued by the European Society of Cardiology, American Heart Association, and American College of Sports Medicine (Med Sci Sports Exercise. 2019;51:1314-23).
The European consensus statement includes the expected range of BP lowering for each activity. For example, aerobic exercise for patients with hypertension should lead to a reduction from –4.9 to –12 mm Hg systolic and –3.4 to –5.8 mm Hg diastolic.
The consensus statement recommends the following exercise priorities based on a patient’s blood pressure:
- Hypertension: Aerobic training (AT) as a first-line exercise therapy; and low- to moderate-intensity RT – equally using dynamic and isometric RT – as second-line therapy. In non-White patients, dynamic RT should be considered as a first-line therapy. RT can be combined with aerobic exercise on an individual basis if the clinician determines either form of RT would provide a metabolic benefit.
- High-to-normal BP: Dynamic RT as a first-line exercise, which the systematic review determined led to greater BP reduction than that of aerobic training. “Isometric RT is likely to elicit similar if not superior BP-lowering effects as [dynamic RT], but the level of evidence is low and the available data are scarce,” wrote first author Henner Hanssen, MD, of the University of Basel, Switzerland, and coauthors. Combining dynamic resistance training with aerobic training “may be preferable” to dynamic RT alone in patients with a combination of cardiovascular risk factors.
- Normal BP: Isometric RT may be indicated as a first-line intervention in individuals with a family or gestational history or obese or overweight people currently with normal BP. This advice includes a caveat: “The number of studies is limited and the 95% confidence intervals are large,” Dr. Hanssen and coauthors noted. AT is also an option in these patients, with more high-quality meta-analyses than the recommendation for isometric RT. “Hence, the BP-lowering effects of [isometric RT] as compared to AT may be overestimated and both exercise modalities may have similar BP-lowering effects in individuals with normotension,” wrote the consensus statement authors.
They note that more research is needed to validate the BP-lowering effects of combined exercise.
The statement acknowledges the difficulty clinicians face in managing patients with high blood pressure. “From a socioeconomic health perspective, it is a major challenge to develop, promote, and implement individually tailored exercise programs for patients with hypertension under consideration of sustainable costs,” wrote Dr. Hanssen and coauthors.
Dr. Martinez noted that one strength of the consensus statement is that it addresses the impact exercise can have on vascular health and metabolic function. And, it points out existing knowledge gaps.
“Are we going to see greater applicability of this as we use IT health technology?” he asked. “Are wearables and telehealth going to help deliver this message more easily, more frequently? Is there work to be done in terms of differences in gender? Do men and women respond differently, and is there a different exercise prescription based on that as well as ethnicity? We well know there’s a different treatment for African Americans compared to other ethnic groups.”
The statement also raises the stakes for using exercise as part of a multifaceted, integrated approach to hypertension management, he said.
“It’s not enough to talk just about exercise or nutrition, or to just give an antihypertension medicine,” Dr. Martinez said. “Perhaps the sweet spot is in integrating an approach that includes all three.”
Consensus statement coauthor Antonio Coca, MD, reported financial relationships with Abbott, Berlin-Chemie, Biolab, Boehringer-Ingelheim, Ferrer, Menarini, Merck, Novartis and Sanofi-Aventis. Coauthor Maria Simonenko, MD, reported financial relationships with Novartis and Sanofi-Aventis. Linda Pescatello, PhD, is lead author of the American College of Sports Medicine 2019 statement. Dr. Hanssen and all other authors have no disclosures. Dr. Martinez has no relevant relationships to disclose.
Recommendations for prescribing exercise to control high blood pressure have been put forward by various medical organizations and expert panels, but finding the bandwidth to craft personalized exercise training for their patients poses a challenge for clinicians.
Now, European cardiology societies have issued a consensus statement that offers an algorithm of sorts for developing personalized exercise programs as part of overall management approach for patients with or at risk of high BP.
The statement, published in the European Journal of Preventive Cardiology and issued by the European Association of Preventive Cardiology and the European Society of Cardiology Council on Hypertension, claims to be the first document to focus on personalized exercise for BP.
The statement draws on a systematic review, including meta-analyses, to produce guidance on how to lower BP in three specific types of patients: Those with hypertension (>140/90 mm Hg), high-normal blood pressure (130-139/85-89 mm Hg), and normal blood pressure (<130/84 mm Hg).
By making recommendations for these three specific groups, along with providing guidance for combined exercise – that is, blending aerobic exercise with resistance training (RT) – the consensus statement goes one step further than recommendations other organizations have issued, Matthew W. Martinez, MD, said in an interview.
“What it adds is an algorithmic approach, if you will,” said Dr. Martinez, a sports medicine cardiologist at Morristown (N.J.) Medical Center. “There are some recommendations to help the clinicians to decide what they’re going to offer individuals, but what’s a challenge for us when seeing patients is finding the time to deliver the message and explain how valuable nutrition and exercise are.”
Guidelines, updates, and statements that include the role of exercise in BP control have been issued by the European Society of Cardiology, American Heart Association, and American College of Sports Medicine (Med Sci Sports Exercise. 2019;51:1314-23).
The European consensus statement includes the expected range of BP lowering for each activity. For example, aerobic exercise for patients with hypertension should lead to a reduction from –4.9 to –12 mm Hg systolic and –3.4 to –5.8 mm Hg diastolic.
The consensus statement recommends the following exercise priorities based on a patient’s blood pressure:
- Hypertension: Aerobic training (AT) as a first-line exercise therapy; and low- to moderate-intensity RT – equally using dynamic and isometric RT – as second-line therapy. In non-White patients, dynamic RT should be considered as a first-line therapy. RT can be combined with aerobic exercise on an individual basis if the clinician determines either form of RT would provide a metabolic benefit.
- High-to-normal BP: Dynamic RT as a first-line exercise, which the systematic review determined led to greater BP reduction than that of aerobic training. “Isometric RT is likely to elicit similar if not superior BP-lowering effects as [dynamic RT], but the level of evidence is low and the available data are scarce,” wrote first author Henner Hanssen, MD, of the University of Basel, Switzerland, and coauthors. Combining dynamic resistance training with aerobic training “may be preferable” to dynamic RT alone in patients with a combination of cardiovascular risk factors.
- Normal BP: Isometric RT may be indicated as a first-line intervention in individuals with a family or gestational history or obese or overweight people currently with normal BP. This advice includes a caveat: “The number of studies is limited and the 95% confidence intervals are large,” Dr. Hanssen and coauthors noted. AT is also an option in these patients, with more high-quality meta-analyses than the recommendation for isometric RT. “Hence, the BP-lowering effects of [isometric RT] as compared to AT may be overestimated and both exercise modalities may have similar BP-lowering effects in individuals with normotension,” wrote the consensus statement authors.
They note that more research is needed to validate the BP-lowering effects of combined exercise.
The statement acknowledges the difficulty clinicians face in managing patients with high blood pressure. “From a socioeconomic health perspective, it is a major challenge to develop, promote, and implement individually tailored exercise programs for patients with hypertension under consideration of sustainable costs,” wrote Dr. Hanssen and coauthors.
Dr. Martinez noted that one strength of the consensus statement is that it addresses the impact exercise can have on vascular health and metabolic function. And, it points out existing knowledge gaps.
“Are we going to see greater applicability of this as we use IT health technology?” he asked. “Are wearables and telehealth going to help deliver this message more easily, more frequently? Is there work to be done in terms of differences in gender? Do men and women respond differently, and is there a different exercise prescription based on that as well as ethnicity? We well know there’s a different treatment for African Americans compared to other ethnic groups.”
The statement also raises the stakes for using exercise as part of a multifaceted, integrated approach to hypertension management, he said.
“It’s not enough to talk just about exercise or nutrition, or to just give an antihypertension medicine,” Dr. Martinez said. “Perhaps the sweet spot is in integrating an approach that includes all three.”
Consensus statement coauthor Antonio Coca, MD, reported financial relationships with Abbott, Berlin-Chemie, Biolab, Boehringer-Ingelheim, Ferrer, Menarini, Merck, Novartis and Sanofi-Aventis. Coauthor Maria Simonenko, MD, reported financial relationships with Novartis and Sanofi-Aventis. Linda Pescatello, PhD, is lead author of the American College of Sports Medicine 2019 statement. Dr. Hanssen and all other authors have no disclosures. Dr. Martinez has no relevant relationships to disclose.
FROM THE EUROPEAN JOURNAL OF PREVENTIVE CARDIOLOGY
Cardiologist forks out $2M to resolve unnecessary testing claims
Michigan cardiologist Dinesh M. Shah, MD, has paid the United States $2 million to resolve claims he violated the False Claims Act by knowingly billing federal health care programs for diagnostic tests that were unnecessary or not performed, the Department of Justice announced.
The settlement resolves allegations that, from 2006 to 2017, Dr. Shah and his practice, Michigan Physicians Group (MPG), of which he is sole owner, billed Medicare, Medicaid, and TRICARE for unnecessary diagnostic tests, including ankle brachial index and toe brachial index tests that were routinely performed on patients without first being ordered by a physician and without regard to medical necessity.
The prosecutors also alleged that Dr. Shah was routinely ordering, and MPG was providing, unnecessary nuclear stress tests to some patients.
“Subjecting patients to unnecessary testing in order to fill one’s pockets with taxpayer funds will not be tolerated. Such practices are particularly concerning because overuse of some tests can be harmful to patients,” acting U.S. Attorney Saima Mohsin said in the news release. “With these lawsuits and the accompanying resolution, Dr. Shah and Michigan Physicians Group are being held to account for these exploitative and improper past practices.”
In addition to the settlement, Dr. Shah and MPG entered into an Integrity Agreement with the Office of Inspector General for the Department of Health & Human Services, which will provide oversight of Dr. Shah and MPG’s billing practices for a 3-year period.
There was “no determination of liability” with the settlement, according to the Department of Justice. Dr. Shah’s case was sparked by two whistleblower lawsuits filed by Arlene Klinke and Khrystyna Malva, both former MPG employees.
The settlement comes after a years-long investigation by the HHS acting on behalf of TRICARE, a health care program for active and retired military members. Allegations that William Beaumont Hospital in Royal Oak, Mich., paid eight physicians excessive compensation to increase patient referrals led to an $84.5 million settlement in 2018.
Dr. Shah was one of three private practice cardiologists who denied involvement in the scheme but were named in the settlement, according to Crain’s Detroit Business.
A version of this article first appeared on Medscape.com.
Michigan cardiologist Dinesh M. Shah, MD, has paid the United States $2 million to resolve claims he violated the False Claims Act by knowingly billing federal health care programs for diagnostic tests that were unnecessary or not performed, the Department of Justice announced.
The settlement resolves allegations that, from 2006 to 2017, Dr. Shah and his practice, Michigan Physicians Group (MPG), of which he is sole owner, billed Medicare, Medicaid, and TRICARE for unnecessary diagnostic tests, including ankle brachial index and toe brachial index tests that were routinely performed on patients without first being ordered by a physician and without regard to medical necessity.
The prosecutors also alleged that Dr. Shah was routinely ordering, and MPG was providing, unnecessary nuclear stress tests to some patients.
“Subjecting patients to unnecessary testing in order to fill one’s pockets with taxpayer funds will not be tolerated. Such practices are particularly concerning because overuse of some tests can be harmful to patients,” acting U.S. Attorney Saima Mohsin said in the news release. “With these lawsuits and the accompanying resolution, Dr. Shah and Michigan Physicians Group are being held to account for these exploitative and improper past practices.”
In addition to the settlement, Dr. Shah and MPG entered into an Integrity Agreement with the Office of Inspector General for the Department of Health & Human Services, which will provide oversight of Dr. Shah and MPG’s billing practices for a 3-year period.
There was “no determination of liability” with the settlement, according to the Department of Justice. Dr. Shah’s case was sparked by two whistleblower lawsuits filed by Arlene Klinke and Khrystyna Malva, both former MPG employees.
The settlement comes after a years-long investigation by the HHS acting on behalf of TRICARE, a health care program for active and retired military members. Allegations that William Beaumont Hospital in Royal Oak, Mich., paid eight physicians excessive compensation to increase patient referrals led to an $84.5 million settlement in 2018.
Dr. Shah was one of three private practice cardiologists who denied involvement in the scheme but were named in the settlement, according to Crain’s Detroit Business.
A version of this article first appeared on Medscape.com.
Michigan cardiologist Dinesh M. Shah, MD, has paid the United States $2 million to resolve claims he violated the False Claims Act by knowingly billing federal health care programs for diagnostic tests that were unnecessary or not performed, the Department of Justice announced.
The settlement resolves allegations that, from 2006 to 2017, Dr. Shah and his practice, Michigan Physicians Group (MPG), of which he is sole owner, billed Medicare, Medicaid, and TRICARE for unnecessary diagnostic tests, including ankle brachial index and toe brachial index tests that were routinely performed on patients without first being ordered by a physician and without regard to medical necessity.
The prosecutors also alleged that Dr. Shah was routinely ordering, and MPG was providing, unnecessary nuclear stress tests to some patients.
“Subjecting patients to unnecessary testing in order to fill one’s pockets with taxpayer funds will not be tolerated. Such practices are particularly concerning because overuse of some tests can be harmful to patients,” acting U.S. Attorney Saima Mohsin said in the news release. “With these lawsuits and the accompanying resolution, Dr. Shah and Michigan Physicians Group are being held to account for these exploitative and improper past practices.”
In addition to the settlement, Dr. Shah and MPG entered into an Integrity Agreement with the Office of Inspector General for the Department of Health & Human Services, which will provide oversight of Dr. Shah and MPG’s billing practices for a 3-year period.
There was “no determination of liability” with the settlement, according to the Department of Justice. Dr. Shah’s case was sparked by two whistleblower lawsuits filed by Arlene Klinke and Khrystyna Malva, both former MPG employees.
The settlement comes after a years-long investigation by the HHS acting on behalf of TRICARE, a health care program for active and retired military members. Allegations that William Beaumont Hospital in Royal Oak, Mich., paid eight physicians excessive compensation to increase patient referrals led to an $84.5 million settlement in 2018.
Dr. Shah was one of three private practice cardiologists who denied involvement in the scheme but were named in the settlement, according to Crain’s Detroit Business.
A version of this article first appeared on Medscape.com.
Top cases
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. The following is a preview of a recent popular clinical discussion:
From John Fang, MD: Update on feeding tubes: Indications and troubleshooting complications.
Gastroenterologists are uniquely positioned to manage individuals with feeding tubes as their training underscores principles in digestion, nutrition support, and enteral tube placement. Adequate management of individuals with feeding tubes and, importantly, the complications that arise from feeding tube use and placement require both right education and experience. Therefore, gastroenterologists are well suited to both place and manage individuals with feeding tubes in the long term.
Questions:
1. Are gastroenterologist best suited for placement and management of feeding tubes (vs. interventional radiology or surgery)?
2. Are gastroenterologists adequately trained place and manage feeding tubes?
3. What are the most difficult complication(s) of feeding tubes to manage?
The conversation stems from the February In Focus article from The New Gastroenterologist, “Update on feeding tubes: Indications and troubleshooting complications.”
See how AGA members responded and join the discussion: https://community.gastro.org/posts/23639.
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. The following is a preview of a recent popular clinical discussion:
From John Fang, MD: Update on feeding tubes: Indications and troubleshooting complications.
Gastroenterologists are uniquely positioned to manage individuals with feeding tubes as their training underscores principles in digestion, nutrition support, and enteral tube placement. Adequate management of individuals with feeding tubes and, importantly, the complications that arise from feeding tube use and placement require both right education and experience. Therefore, gastroenterologists are well suited to both place and manage individuals with feeding tubes in the long term.
Questions:
1. Are gastroenterologist best suited for placement and management of feeding tubes (vs. interventional radiology or surgery)?
2. Are gastroenterologists adequately trained place and manage feeding tubes?
3. What are the most difficult complication(s) of feeding tubes to manage?
The conversation stems from the February In Focus article from The New Gastroenterologist, “Update on feeding tubes: Indications and troubleshooting complications.”
See how AGA members responded and join the discussion: https://community.gastro.org/posts/23639.
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. The following is a preview of a recent popular clinical discussion:
From John Fang, MD: Update on feeding tubes: Indications and troubleshooting complications.
Gastroenterologists are uniquely positioned to manage individuals with feeding tubes as their training underscores principles in digestion, nutrition support, and enteral tube placement. Adequate management of individuals with feeding tubes and, importantly, the complications that arise from feeding tube use and placement require both right education and experience. Therefore, gastroenterologists are well suited to both place and manage individuals with feeding tubes in the long term.
Questions:
1. Are gastroenterologist best suited for placement and management of feeding tubes (vs. interventional radiology or surgery)?
2. Are gastroenterologists adequately trained place and manage feeding tubes?
3. What are the most difficult complication(s) of feeding tubes to manage?
The conversation stems from the February In Focus article from The New Gastroenterologist, “Update on feeding tubes: Indications and troubleshooting complications.”
See how AGA members responded and join the discussion: https://community.gastro.org/posts/23639.