User login
For MD-IQ use only
A new world awaits us all
July is typically the month when new students/physicians arrive at academic medical centers, schools, and hospitals to begin the next phase of training. July also marks the beginning of practice for graduating fellows. In the post-COVID world, these settings will have changed dramatically from the past.

Community practices are consolidating rapidly, with many being acquired by private equity firms, hospitals, and health systems. Private equity made its first investment in GI in 2016, when Audax acquired Miami-based Gastro Health. It was announced this past May that Audax sold Gastro Health to Omers (a larger, Canadian PE firm), marking the first PE sale of a practice (second bite) (Newitt P. “Gastro Health sold to private equity company.” Becker’s GI & Endoscopy. 2021 May 19). The financial success of this model has not been lost on any community practice, so expect more such transactions.
Health systems are bouncing back from 2020, with balance sheets that are recovering quickly. But operating margins are still narrow so physician productivity is being pushed and burnout is a hot-button issue. Older workers are retiring at increasing rates, and low-wage workers are often reluctant to return to the workforce. Both trends increase Medicare and Medicaid rolls. As more patients enter government insurance programs, provider reimbursement falls. “Manage to Medicare” (bringing costs down to levels that are sustainable on Medicare rates) has again become a common goal. The historic reaction to these financial pressures has been to push commercial rates higher thru market consolidation and emphasize margin-producing services.
COVID has changed medicine. We will deliver care differently, and health inequities inherent in the current system will not be tolerable. We now can analyze population-level health outcomes by mining data from enormous databases containing both administrative and health records. Imagine the information we could derive by analyzing IBD populations scattered across multiple states, all cared for by 1,000 gastroenterologists working in a mega practice that uses a single electronic medical record. That might break down the town-gown barrier quickly.
John I. Allen, MD, MBA, AGAF
Editor in Chief
July is typically the month when new students/physicians arrive at academic medical centers, schools, and hospitals to begin the next phase of training. July also marks the beginning of practice for graduating fellows. In the post-COVID world, these settings will have changed dramatically from the past.
Community practices are consolidating rapidly, with many being acquired by private equity firms, hospitals, and health systems. Private equity made its first investment in GI in 2016, when Audax acquired Miami-based Gastro Health. It was announced this past May that Audax sold Gastro Health to Omers (a larger, Canadian PE firm), marking the first PE sale of a practice (second bite) (Newitt P. “Gastro Health sold to private equity company.” Becker’s GI & Endoscopy. 2021 May 19). The financial success of this model has not been lost on any community practice, so expect more such transactions.
Health systems are bouncing back from 2020, with balance sheets that are recovering quickly. But operating margins are still narrow so physician productivity is being pushed and burnout is a hot-button issue. Older workers are retiring at increasing rates, and low-wage workers are often reluctant to return to the workforce. Both trends increase Medicare and Medicaid rolls. As more patients enter government insurance programs, provider reimbursement falls. “Manage to Medicare” (bringing costs down to levels that are sustainable on Medicare rates) has again become a common goal. The historic reaction to these financial pressures has been to push commercial rates higher thru market consolidation and emphasize margin-producing services.
COVID has changed medicine. We will deliver care differently, and health inequities inherent in the current system will not be tolerable. We now can analyze population-level health outcomes by mining data from enormous databases containing both administrative and health records. Imagine the information we could derive by analyzing IBD populations scattered across multiple states, all cared for by 1,000 gastroenterologists working in a mega practice that uses a single electronic medical record. That might break down the town-gown barrier quickly.
John I. Allen, MD, MBA, AGAF
Editor in Chief
July is typically the month when new students/physicians arrive at academic medical centers, schools, and hospitals to begin the next phase of training. July also marks the beginning of practice for graduating fellows. In the post-COVID world, these settings will have changed dramatically from the past.
Community practices are consolidating rapidly, with many being acquired by private equity firms, hospitals, and health systems. Private equity made its first investment in GI in 2016, when Audax acquired Miami-based Gastro Health. It was announced this past May that Audax sold Gastro Health to Omers (a larger, Canadian PE firm), marking the first PE sale of a practice (second bite) (Newitt P. “Gastro Health sold to private equity company.” Becker’s GI & Endoscopy. 2021 May 19). The financial success of this model has not been lost on any community practice, so expect more such transactions.
Health systems are bouncing back from 2020, with balance sheets that are recovering quickly. But operating margins are still narrow so physician productivity is being pushed and burnout is a hot-button issue. Older workers are retiring at increasing rates, and low-wage workers are often reluctant to return to the workforce. Both trends increase Medicare and Medicaid rolls. As more patients enter government insurance programs, provider reimbursement falls. “Manage to Medicare” (bringing costs down to levels that are sustainable on Medicare rates) has again become a common goal. The historic reaction to these financial pressures has been to push commercial rates higher thru market consolidation and emphasize margin-producing services.
COVID has changed medicine. We will deliver care differently, and health inequities inherent in the current system will not be tolerable. We now can analyze population-level health outcomes by mining data from enormous databases containing both administrative and health records. Imagine the information we could derive by analyzing IBD populations scattered across multiple states, all cared for by 1,000 gastroenterologists working in a mega practice that uses a single electronic medical record. That might break down the town-gown barrier quickly.
John I. Allen, MD, MBA, AGAF
Editor in Chief

July 2021 - What's the diagnosis?
Answer: Erythropoietic protoporphyria.Figure B demonstrated massive cholestasis with brown deposits that represented protoporphyrin precipitates, which plugged the bile ducts and led to a cholestatic pattern of liver injury. Under polarized light, protoporhyrin precipitates produced Maltese crosses (Figure C), which are pathognomonic of erythropoietic protoporphyria (EPP). Porphyria is a rare group of inherited heme biosynthesis disorders. EPP is an uncommon type of porphyria and is secondary to a ferrochelatase (FECH) gene mutation, which results in deficient activity of the mitochondrial enzyme FECH.1
FECH catalyzes chelation of iron into proptoporphyrin IX to form heme. The inability of protoporphyrins to be transformed into heme inhibits hepatic elimination and results in hepatocyte accumulation of protoporphyrins, leading to protoporphyrin precipitation in bile canaliculi. Painful photosensitivity (Figure A) is the most common manifestation of EPP, beginning in childhood.2 Only a small proportion of patients with EPP develop liver dysfunction but the consequences can be severe.2 Therefore, therapeutic decisions are based on limited published experience without randomized, controlled data.2 One treatment method is to attempt to remove protoporphyrins from the blood via therapeutic plasma exchange.2Our patient underwent one session of therapeutic plasma exchange; however, after this initial course of treatment, the patient’s goals of care changed and she elected to enroll in hospice. Patients with severe liver dysfunction as a result of EPP require consideration of liver transplantation in the setting of fulminant hepatic failure. Liver transplantation does not cure EPP; the graft is at risk for similar EPP-related changes.1 Only bone marrow transplantation can correct the underlying enzymatic defect in FECH.1 Although physicians are often taught “common things are common,” this case highlights a rare complication of a rare disease such as porphyria is an often forgotten or missed condition. Vigilance should be kept for other rare conditions, especially ones with curative treatments or fatal consequences. In an era where the role of liver biopsy is often questioned in favor of prediction models or noninvasive testing, we must have a low threshold to safely perform a liver biopsy when the diagnosis is unclear or a patient is deteriorating.
The quiz authors disclosed no conflicts of interest.
References
1. Windon AL et al. Am J Transplant. 2018 Mar;18(3):745-9.
2. Pagano MB et al. J Clin Apher. 2012;27(6):336-41.
Answer: Erythropoietic protoporphyria.Figure B demonstrated massive cholestasis with brown deposits that represented protoporphyrin precipitates, which plugged the bile ducts and led to a cholestatic pattern of liver injury. Under polarized light, protoporhyrin precipitates produced Maltese crosses (Figure C), which are pathognomonic of erythropoietic protoporphyria (EPP). Porphyria is a rare group of inherited heme biosynthesis disorders. EPP is an uncommon type of porphyria and is secondary to a ferrochelatase (FECH) gene mutation, which results in deficient activity of the mitochondrial enzyme FECH.1
FECH catalyzes chelation of iron into proptoporphyrin IX to form heme. The inability of protoporphyrins to be transformed into heme inhibits hepatic elimination and results in hepatocyte accumulation of protoporphyrins, leading to protoporphyrin precipitation in bile canaliculi. Painful photosensitivity (Figure A) is the most common manifestation of EPP, beginning in childhood.2 Only a small proportion of patients with EPP develop liver dysfunction but the consequences can be severe.2 Therefore, therapeutic decisions are based on limited published experience without randomized, controlled data.2 One treatment method is to attempt to remove protoporphyrins from the blood via therapeutic plasma exchange.2Our patient underwent one session of therapeutic plasma exchange; however, after this initial course of treatment, the patient’s goals of care changed and she elected to enroll in hospice. Patients with severe liver dysfunction as a result of EPP require consideration of liver transplantation in the setting of fulminant hepatic failure. Liver transplantation does not cure EPP; the graft is at risk for similar EPP-related changes.1 Only bone marrow transplantation can correct the underlying enzymatic defect in FECH.1 Although physicians are often taught “common things are common,” this case highlights a rare complication of a rare disease such as porphyria is an often forgotten or missed condition. Vigilance should be kept for other rare conditions, especially ones with curative treatments or fatal consequences. In an era where the role of liver biopsy is often questioned in favor of prediction models or noninvasive testing, we must have a low threshold to safely perform a liver biopsy when the diagnosis is unclear or a patient is deteriorating.
The quiz authors disclosed no conflicts of interest.
References
1. Windon AL et al. Am J Transplant. 2018 Mar;18(3):745-9.
2. Pagano MB et al. J Clin Apher. 2012;27(6):336-41.
Answer: Erythropoietic protoporphyria.Figure B demonstrated massive cholestasis with brown deposits that represented protoporphyrin precipitates, which plugged the bile ducts and led to a cholestatic pattern of liver injury. Under polarized light, protoporhyrin precipitates produced Maltese crosses (Figure C), which are pathognomonic of erythropoietic protoporphyria (EPP). Porphyria is a rare group of inherited heme biosynthesis disorders. EPP is an uncommon type of porphyria and is secondary to a ferrochelatase (FECH) gene mutation, which results in deficient activity of the mitochondrial enzyme FECH.1
FECH catalyzes chelation of iron into proptoporphyrin IX to form heme. The inability of protoporphyrins to be transformed into heme inhibits hepatic elimination and results in hepatocyte accumulation of protoporphyrins, leading to protoporphyrin precipitation in bile canaliculi. Painful photosensitivity (Figure A) is the most common manifestation of EPP, beginning in childhood.2 Only a small proportion of patients with EPP develop liver dysfunction but the consequences can be severe.2 Therefore, therapeutic decisions are based on limited published experience without randomized, controlled data.2 One treatment method is to attempt to remove protoporphyrins from the blood via therapeutic plasma exchange.2Our patient underwent one session of therapeutic plasma exchange; however, after this initial course of treatment, the patient’s goals of care changed and she elected to enroll in hospice. Patients with severe liver dysfunction as a result of EPP require consideration of liver transplantation in the setting of fulminant hepatic failure. Liver transplantation does not cure EPP; the graft is at risk for similar EPP-related changes.1 Only bone marrow transplantation can correct the underlying enzymatic defect in FECH.1 Although physicians are often taught “common things are common,” this case highlights a rare complication of a rare disease such as porphyria is an often forgotten or missed condition. Vigilance should be kept for other rare conditions, especially ones with curative treatments or fatal consequences. In an era where the role of liver biopsy is often questioned in favor of prediction models or noninvasive testing, we must have a low threshold to safely perform a liver biopsy when the diagnosis is unclear or a patient is deteriorating.
The quiz authors disclosed no conflicts of interest.
References
1. Windon AL et al. Am J Transplant. 2018 Mar;18(3):745-9.
2. Pagano MB et al. J Clin Apher. 2012;27(6):336-41.
A 66-year-old White woman with tetralogy of Fallot status after remote pulmonic valve surgery, hypothyroidism, and previous cholecystectomy presented to her primary care provider with 2 days of constant, dull, right upper quadrant pain with nausea but without fever, association with meals, or association with defecation. Her home medications included low-dose aspirin and levothyroxine. Her physical examination revealed normal vital signs, a body mass index of 29 kg/m2, right upper quadrant tenderness to palpation without peritoneal signs, and normal bowel sounds. The remainder of her examination was normal.
The patient underwent an exhaustive evaluation beginning with laboratory tests, which revealed a normal complete blood count, basic metabolic panel, lipase, international normalized ratio, and urinalysis. Her liver function tests results showed aspartate aminotransferase 118 international IU/L, alanine aminotransferase 117 IU/L, alkaline phosphatase 147 IU/L, and total bilirubin 17.6 mg/dL, with a direct bilirubin of 11.9 mg/dL.
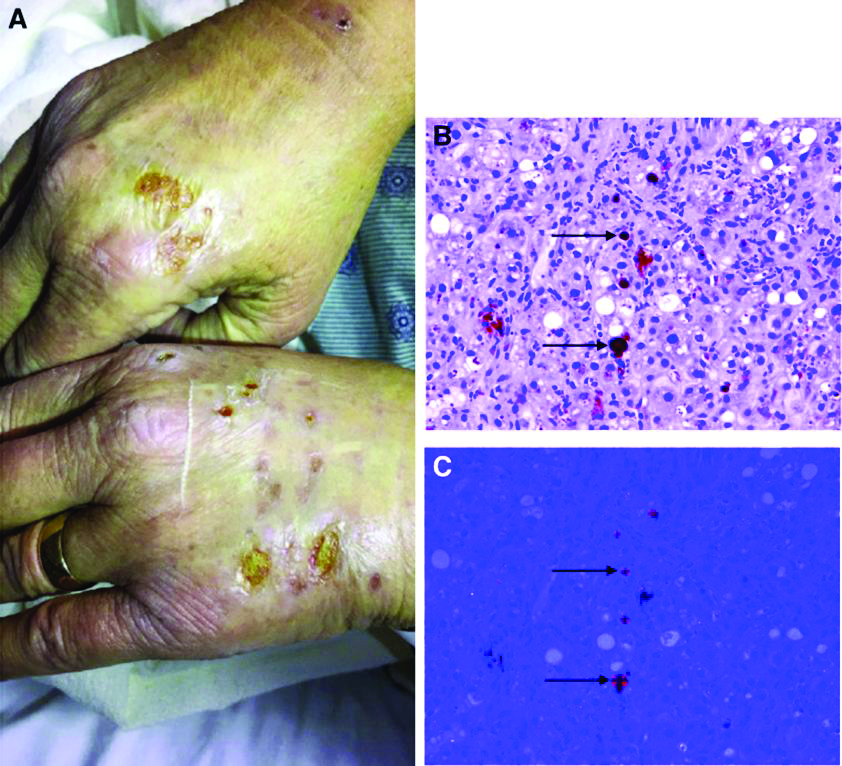
Her liver function tests were last checked 18 months prior and were normal. A liver ultrasound examination revealed cirrhotic morphology without ascites or hepatic or portal vein thrombosis. A magnetic resonance imaging study of the liver revealed morphologic changes of hepatic cirrhosis without portal hypertension, biliary dilation, or stricturing. Additionally, hepatitis A IgM, hepatitis B surface antigen, hepatitis B core IgM and IgG, hepatitis C antibody, ceruloplasmin, antinuclear antibody, anti-smooth muscle antibody, anti-liver-kidney-microsomal antibody, quantitative immunoglobulins, antimitochondrial antibody, alpha-1 antitrypsin phenotype, phosphatidylethanolamine, serum protein electrophoresis, and alpha fetoprotein were reassuring. Later, the patient reported sensitivity to the sun, described as a "sun allergy" with irritation on her hands (Figure A). Mentation remained normal; however, given progressive worsening hepatic function evidenced by international normalized ratio of 1.7 and bilirubin of 27.6 mg/dL, the patient was urgently admitted for expedited portal manometry with transjugular liver biopsy. The hepatic venous pressure gradient was 23 mm Hg. The liver biopsy images are shown in Figure B, C.
What's the diagnosis?
Britney Spears battles conservatorship for mental health protection
In a 24-minute statement, Ms. Spears told the judge overseeing the conservatorship that she wants it to end “without having to be evaluated.” She called the arrangement “abusive” and said she’s been “traumatized” and “in denial” despite the upbeat messages that she’s posted on Instagram during the past year, according to Reuters.
“I just want my life back,” she said. “I’m not here to be anyone’s slave.”
After the statement, the court recessed, and the audio transmission was stopped, Reuters reported. Full transcripts have been published by several news outlets, including this lightly edited version by Variety.
Ms. Spears’ statement came as a shock after years of silence about the conservatorship. Public speculation about the arrangement has resurfaced during the past year because of the #FreeBritney movement on social media, news reports of leaked court documents, and a 2021 documentary that showed she may feel trapped.
During the hearing, Ms. Spears spoke by phone to Los Angeles Superior Court Judge Brenda Penny about the court-approved arrangement that began in 2008 after she had a mental health breakdown. Judge Penny said Ms. Spears would need to submit a petition to the court to ask for the conservatorship to be terminated.
Under the terms of the conservatorship, Ms. Spears would have to demonstrate that she can take responsibility for her personal and financial affairs, Reuters reported. During the hearing, Judge Penny supported Ms. Spears for speaking out.
“I know it took a lot of courage for you to say everything you have to say today,” she said. “I want to let you know that the court does appreciate your coming on the line and sharing how you’re feeling.”
Ms. Spears, 39, said she wanted to get married again and have a baby but that she’s not allowed to go to the doctor to get a contraceptive device removed. She spoke up about her mental health and said doctors had put her on the drug lithium, which made her less able to function. Ms. Spears also said she was forced to perform in the past and is now required to attend numerous therapy sessions each week against her will.
“I’m not happy. I can’t sleep. I’m so angry, it’s insane,” she said. “And I’m depressed. I cry every day.”
Ms. Spears last spoke with the court in May 2019, but the hearing was closed to the public and her testimony was sealed. Ms. Spears recently said she wanted people to hear her thoughts.
“I feel ganged-up on and I feel bullied and I feel left out and alone,” she said. “I deserve to have the same rights as anybody does, by having a child, a family, any of those things, and more so.”
A version of this article first appeared on WebMD.com.
In a 24-minute statement, Ms. Spears told the judge overseeing the conservatorship that she wants it to end “without having to be evaluated.” She called the arrangement “abusive” and said she’s been “traumatized” and “in denial” despite the upbeat messages that she’s posted on Instagram during the past year, according to Reuters.
“I just want my life back,” she said. “I’m not here to be anyone’s slave.”
After the statement, the court recessed, and the audio transmission was stopped, Reuters reported. Full transcripts have been published by several news outlets, including this lightly edited version by Variety.
Ms. Spears’ statement came as a shock after years of silence about the conservatorship. Public speculation about the arrangement has resurfaced during the past year because of the #FreeBritney movement on social media, news reports of leaked court documents, and a 2021 documentary that showed she may feel trapped.
During the hearing, Ms. Spears spoke by phone to Los Angeles Superior Court Judge Brenda Penny about the court-approved arrangement that began in 2008 after she had a mental health breakdown. Judge Penny said Ms. Spears would need to submit a petition to the court to ask for the conservatorship to be terminated.
Under the terms of the conservatorship, Ms. Spears would have to demonstrate that she can take responsibility for her personal and financial affairs, Reuters reported. During the hearing, Judge Penny supported Ms. Spears for speaking out.
“I know it took a lot of courage for you to say everything you have to say today,” she said. “I want to let you know that the court does appreciate your coming on the line and sharing how you’re feeling.”
Ms. Spears, 39, said she wanted to get married again and have a baby but that she’s not allowed to go to the doctor to get a contraceptive device removed. She spoke up about her mental health and said doctors had put her on the drug lithium, which made her less able to function. Ms. Spears also said she was forced to perform in the past and is now required to attend numerous therapy sessions each week against her will.
“I’m not happy. I can’t sleep. I’m so angry, it’s insane,” she said. “And I’m depressed. I cry every day.”
Ms. Spears last spoke with the court in May 2019, but the hearing was closed to the public and her testimony was sealed. Ms. Spears recently said she wanted people to hear her thoughts.
“I feel ganged-up on and I feel bullied and I feel left out and alone,” she said. “I deserve to have the same rights as anybody does, by having a child, a family, any of those things, and more so.”
A version of this article first appeared on WebMD.com.
In a 24-minute statement, Ms. Spears told the judge overseeing the conservatorship that she wants it to end “without having to be evaluated.” She called the arrangement “abusive” and said she’s been “traumatized” and “in denial” despite the upbeat messages that she’s posted on Instagram during the past year, according to Reuters.
“I just want my life back,” she said. “I’m not here to be anyone’s slave.”
After the statement, the court recessed, and the audio transmission was stopped, Reuters reported. Full transcripts have been published by several news outlets, including this lightly edited version by Variety.
Ms. Spears’ statement came as a shock after years of silence about the conservatorship. Public speculation about the arrangement has resurfaced during the past year because of the #FreeBritney movement on social media, news reports of leaked court documents, and a 2021 documentary that showed she may feel trapped.
During the hearing, Ms. Spears spoke by phone to Los Angeles Superior Court Judge Brenda Penny about the court-approved arrangement that began in 2008 after she had a mental health breakdown. Judge Penny said Ms. Spears would need to submit a petition to the court to ask for the conservatorship to be terminated.
Under the terms of the conservatorship, Ms. Spears would have to demonstrate that she can take responsibility for her personal and financial affairs, Reuters reported. During the hearing, Judge Penny supported Ms. Spears for speaking out.
“I know it took a lot of courage for you to say everything you have to say today,” she said. “I want to let you know that the court does appreciate your coming on the line and sharing how you’re feeling.”
Ms. Spears, 39, said she wanted to get married again and have a baby but that she’s not allowed to go to the doctor to get a contraceptive device removed. She spoke up about her mental health and said doctors had put her on the drug lithium, which made her less able to function. Ms. Spears also said she was forced to perform in the past and is now required to attend numerous therapy sessions each week against her will.
“I’m not happy. I can’t sleep. I’m so angry, it’s insane,” she said. “And I’m depressed. I cry every day.”
Ms. Spears last spoke with the court in May 2019, but the hearing was closed to the public and her testimony was sealed. Ms. Spears recently said she wanted people to hear her thoughts.
“I feel ganged-up on and I feel bullied and I feel left out and alone,” she said. “I deserve to have the same rights as anybody does, by having a child, a family, any of those things, and more so.”
A version of this article first appeared on WebMD.com.
New! Spotlight on medical power couples: Their extraordinary lives
When people started dying from lethal anthrax spores sent through the mail in 2001, infectious disease expert Jeannette Guarner, MD, was called to Florida and Connecticut to analyze the bodies. She and her pathology team investigated how the bacteria had entered the victims and examined tissue samples from across the country to discern the scale of the attacks.

After conducting autopsies and identifying that inhalation anthrax had caused the deaths, Dr. Guarner rushed home to Atlanta just in time for Thanksgiving. Exhausted, the beloved family chef still managed to cook the big turkey that holiday, but she enlisted help with dessert.
“She returned home on Thanksgiving at like three in the morning,” recalls Carlos del Rio, MD. “She said to me, ‘In order for us to have Thanksgiving, you have to be in charge of the pies.’ When I told my daughter, she said, ‘This is going to be a disaster! If mom’s not cooking, this is not going to be good.’”
“It didn’t turn out that bad,” Dr. Guarner laughs. “There was dessert.”
As two of the top infectious disease experts in the country, Dr. Guarner and Dr. del Rio are no strangers to juggling their personal lives around disease outbreaks, last-minute travel, and pressing research.
Former director of the clinical laboratory at Mexico’s National Cancer Institute, Dr. Guarner worked for the Centers for Disease Control and Prevention for 10 years, where she played an integral part in the discovery of SARS. She and her team identified that a coronavirus was in cultures taken from a health care worker who died after working in Asia and determined through molecular testing that the virus was different from any other coronaviruses at the time.
Dr. Guarner went on to search for the novel virus in tissue samples and determine that it was SARS that had caused the damage. She is now a professor in the department of pathology and laboratory medicine at Emory University, Atlanta, medical director of the clinical laboratory at Emory University Hospital Midtown, and vice chair for faculty affairs.
Dr. Del Rio, who served as director of the National AIDS Council of Mexico, is a distinguished professor of medicine in Emory University’s division of infectious diseases and a professor of global health and epidemiology in the Rollins School of Public Health at Emory University. He is also co-director of the Emory Center for AIDS Research and co-principal investigator of the Emory-CDC HIV Clinical Trials Unit and the Emory Vaccine and Treatment Evaluation Unit.
Dr. Del Rio’s work in HIV prevention and care has made great strides, including developing the concept for the HIV Care Continuum, a public health model that outlines the stages that HIV patients go through, from diagnosis to achieving viral suppression. Dr. Del Rio, who is foreign secretary of the National Academy of Medicine, has also worked on emerging infections such as pandemic influenza and was a member of the WHO Influenza A (H1N1) Clinical Advisory Group and of the CDC Influenza A Task Force during the 2009 pandemic.
Dr. Del Rio and Dr. Guarner met during medical school in Mexico City. At first, the two carpooled to classes, but when Dr. Guarner fell ill with hepatitis A, Dr. del Rio brought Dr. Guarner the class notes so she wouldn’t fall behind. The study buddies later became a couple and married just before coming to the United States for residency.
With their expertise in infectious disease, Dr. del Rio and Dr. Guarner have worked collaboratively in the past, but the couple says they’ve always maintained separate professional identities.
“We try to create our own spaces,” Dr. del Rio said. “You try to keep your personal and professional identity independent as much as possible. You don’t want people to say, ‘Oh, you got this or you’re doing this because you are married to this other person.’ You want, to a certain degree, intellectual independence.”
This has been easier in some ways because Dr. del Rio and Dr. Guarner have different last names. Over the years they have frequently encountered people who had no idea that they are married.
“One time, we were both down in the lab and Jeanette was discussing a case, and she started teasing me or poking me, making fun,” recalls Dr. del Rio. “Some of the ID fellows were like, ‘Oh my God, who the hell is this woman?’ They didn’t realize she was my wife.”
Since the COVID-19 outbreak, both Dr. Guarner and Dr. del Rio have been involved in different ways with the pandemic. Dr. Del Rio has seen patients, conducted clinical trials, and given hundreds of local and national interviews about the virus. As a laboratory director, Dr. Guarner has validated tests for the diagnosis of COVID-19 and counseled staff on exposure concerns.
“An important aspect has also been to make sure that our laboratory technologists understand the disease and the need for the different protection elements we have had to use in the hospital,” she said. “In many ways I have had to scale down fears the techs have had when handling specimens from these patients.”
In their own words
What was one of your most surprising discoveries?
Jeannette: During the anthrax attacks, we received lots of tissues on live patients, particularly skin biopsies from different parts of the country where pathologists had concerns that there was anthrax. From New York, we received more than 50 skin biopsies and discovered that the necrotic lesions suspected of anthrax had Rickettsia in them. In other words, we discovered that rickettsialpox – a mite-borne infectious disease – was circulating in the city, which was unknown at the time.
Describe a challenge that you overcame:
Carlos: When I was appointed as director of the National AIDS Council of Mexico (CONASIDA), I was quite young, only 32 years old. I had to learn to listen to others who had expertise and institutional memory, to respect their opinions, and at the same time to push for change. A huge challenge was the role of the Catholic Church and conservative groups that were adamantly against condom promotion. Thus, I learned how to advance policies based in science without being confrontational.
Have you ever been famous for anything other than your work?
Jeannette: In 2017, a tree fell on our house during Hurricane Irma. It fell right on my husband’s office a few minutes after he left the room. Fortunately, I have always been small and flexible, and I crawled through the rubble to save our valuables before they were ruined by the rain. Later, a local Atlanta TV news crew was in the neighborhood reporting on the damage, and I told them to come to our house if they wanted to see real damage. That night, we were on the local news.
Power couple Paul and Mary Klotman
When Mary Klotman, MD, was offered an opportunity with the National Institutes of Health in 1991, Paul Klotman, MD, didn’t hesitate to resign his post at Duke University, Durham, N.C., and join his wife in Washington. Paul says he wanted to support Mary’s aspirations, even though it meant an uncertain track for his own career.

Fortunately for the Klotmans, the move proved instrumental for both of their careers and spurred one of their proudest scientific breakthroughs.
At NIH, Mary was a member of the Public Health Service and worked in the laboratory of tumor cell biology, and Paul became chief of the institute’s molecular medicine section in the laboratory of developmental biology. Together, their work led to the first animal model of HIV-associated nephropathy using transgenic techniques. The Klotmans and their team demonstrated that HIV resides in and evolves separately in kidney cells, a critical step in HIV-associated kidney disease.
“That’s where our longstanding collaboration around HIV-associated nephropathy started,” Mary says. “Paul and I have a passion for research, and we’ve had the same grant together for 25 years.”
After their successful stint at NIH, the Klotmans next climbed the ranks at the Icahn School of Medicine at Mount Sinai, where Paul started as chief of the nephrology division and became chair of medicine, and Mary became chief of infectious diseases and co-director of Mount Sinai’s Global Health and Emerging Pathogens Institute.
Today, Mary and Paul are the first – and only – married couple in the United States to lead separate medical schools. Mary is dean and vice chancellor for health affairs at Duke, and Paul is president and executive dean of Baylor College of Medicine, Houston.
Despite their 1,100-mile separation, the Klotmans manage their relationship in an unconventional way that some might balk at: Every Friday, one spouse hops on a plane and travels to the other for a date night and weekend.
“When we started this crazy lifestyle, we committed to being together every weekend,” says Mary. “And in 10 years – before COVID – we missed only one weekend together.”
The Klotmans say the scheduled time together places a hard end to each work week and enables them to truly enjoy their quality time.
“Friday at noon, I’m on the plane going to Durham, and I know that in 2 hours I’m going to have a date with my wife,” Paul said. “There are institutions that we’ve run into that think you have to be 7 days a week on site. But Duke and Baylor have been very supportive [of our situation].”
No doubt, the arrangement means a lot of time in the air for the couple. Paul says he travels about 150,000 miles every year by plane.
Having dual leadership positions in academic medicine has kept the Klotmans tightly connected, and the couple says their strong partnership has contributed to their success.
“It’s really been helpful having a deep understanding of our career paths, because we’ve been able to understand when one of us needed to be really focused on work and the other one would step back a bit with the kids and vice versa,” Mary said.
“There’s no question that we wouldn’t be in the positions we are in now if it weren’t for the fact that we’ve had each other,” Paul said.
In their own words
What is a little-known title that you have?
Paul: Purse-carrier for my wife. When she is honored at a national meeting or event, she often stands up and hands me her purse. I now make sure I have on an appropriate outfit that matches the purse.
Tell us about your children.
Mary: We had a very traumatic first pregnancy that we lost. Six years later, we adopted our first child, which was an amazing blessing. Our second son was Duke’s first successful frozen embryo transfer.
Describe a memorable moment in your relationship.
Paul: As we were leaving for our honeymoon, Mary’s dad handed me this booklet. It was the receipts for Mary’s medical school loans for the next 10 years. He said, “Congratulations, she’s all yours!”
A version of this article first appeared on Medscape.com.
When people started dying from lethal anthrax spores sent through the mail in 2001, infectious disease expert Jeannette Guarner, MD, was called to Florida and Connecticut to analyze the bodies. She and her pathology team investigated how the bacteria had entered the victims and examined tissue samples from across the country to discern the scale of the attacks.
After conducting autopsies and identifying that inhalation anthrax had caused the deaths, Dr. Guarner rushed home to Atlanta just in time for Thanksgiving. Exhausted, the beloved family chef still managed to cook the big turkey that holiday, but she enlisted help with dessert.
“She returned home on Thanksgiving at like three in the morning,” recalls Carlos del Rio, MD. “She said to me, ‘In order for us to have Thanksgiving, you have to be in charge of the pies.’ When I told my daughter, she said, ‘This is going to be a disaster! If mom’s not cooking, this is not going to be good.’”
“It didn’t turn out that bad,” Dr. Guarner laughs. “There was dessert.”
As two of the top infectious disease experts in the country, Dr. Guarner and Dr. del Rio are no strangers to juggling their personal lives around disease outbreaks, last-minute travel, and pressing research.
Former director of the clinical laboratory at Mexico’s National Cancer Institute, Dr. Guarner worked for the Centers for Disease Control and Prevention for 10 years, where she played an integral part in the discovery of SARS. She and her team identified that a coronavirus was in cultures taken from a health care worker who died after working in Asia and determined through molecular testing that the virus was different from any other coronaviruses at the time.
Dr. Guarner went on to search for the novel virus in tissue samples and determine that it was SARS that had caused the damage. She is now a professor in the department of pathology and laboratory medicine at Emory University, Atlanta, medical director of the clinical laboratory at Emory University Hospital Midtown, and vice chair for faculty affairs.
Dr. Del Rio, who served as director of the National AIDS Council of Mexico, is a distinguished professor of medicine in Emory University’s division of infectious diseases and a professor of global health and epidemiology in the Rollins School of Public Health at Emory University. He is also co-director of the Emory Center for AIDS Research and co-principal investigator of the Emory-CDC HIV Clinical Trials Unit and the Emory Vaccine and Treatment Evaluation Unit.
Dr. Del Rio’s work in HIV prevention and care has made great strides, including developing the concept for the HIV Care Continuum, a public health model that outlines the stages that HIV patients go through, from diagnosis to achieving viral suppression. Dr. Del Rio, who is foreign secretary of the National Academy of Medicine, has also worked on emerging infections such as pandemic influenza and was a member of the WHO Influenza A (H1N1) Clinical Advisory Group and of the CDC Influenza A Task Force during the 2009 pandemic.
Dr. Del Rio and Dr. Guarner met during medical school in Mexico City. At first, the two carpooled to classes, but when Dr. Guarner fell ill with hepatitis A, Dr. del Rio brought Dr. Guarner the class notes so she wouldn’t fall behind. The study buddies later became a couple and married just before coming to the United States for residency.
With their expertise in infectious disease, Dr. del Rio and Dr. Guarner have worked collaboratively in the past, but the couple says they’ve always maintained separate professional identities.
“We try to create our own spaces,” Dr. del Rio said. “You try to keep your personal and professional identity independent as much as possible. You don’t want people to say, ‘Oh, you got this or you’re doing this because you are married to this other person.’ You want, to a certain degree, intellectual independence.”
This has been easier in some ways because Dr. del Rio and Dr. Guarner have different last names. Over the years they have frequently encountered people who had no idea that they are married.
“One time, we were both down in the lab and Jeanette was discussing a case, and she started teasing me or poking me, making fun,” recalls Dr. del Rio. “Some of the ID fellows were like, ‘Oh my God, who the hell is this woman?’ They didn’t realize she was my wife.”
Since the COVID-19 outbreak, both Dr. Guarner and Dr. del Rio have been involved in different ways with the pandemic. Dr. Del Rio has seen patients, conducted clinical trials, and given hundreds of local and national interviews about the virus. As a laboratory director, Dr. Guarner has validated tests for the diagnosis of COVID-19 and counseled staff on exposure concerns.
“An important aspect has also been to make sure that our laboratory technologists understand the disease and the need for the different protection elements we have had to use in the hospital,” she said. “In many ways I have had to scale down fears the techs have had when handling specimens from these patients.”
In their own words
What was one of your most surprising discoveries?
Jeannette: During the anthrax attacks, we received lots of tissues on live patients, particularly skin biopsies from different parts of the country where pathologists had concerns that there was anthrax. From New York, we received more than 50 skin biopsies and discovered that the necrotic lesions suspected of anthrax had Rickettsia in them. In other words, we discovered that rickettsialpox – a mite-borne infectious disease – was circulating in the city, which was unknown at the time.
Describe a challenge that you overcame:
Carlos: When I was appointed as director of the National AIDS Council of Mexico (CONASIDA), I was quite young, only 32 years old. I had to learn to listen to others who had expertise and institutional memory, to respect their opinions, and at the same time to push for change. A huge challenge was the role of the Catholic Church and conservative groups that were adamantly against condom promotion. Thus, I learned how to advance policies based in science without being confrontational.
Have you ever been famous for anything other than your work?
Jeannette: In 2017, a tree fell on our house during Hurricane Irma. It fell right on my husband’s office a few minutes after he left the room. Fortunately, I have always been small and flexible, and I crawled through the rubble to save our valuables before they were ruined by the rain. Later, a local Atlanta TV news crew was in the neighborhood reporting on the damage, and I told them to come to our house if they wanted to see real damage. That night, we were on the local news.
Power couple Paul and Mary Klotman
When Mary Klotman, MD, was offered an opportunity with the National Institutes of Health in 1991, Paul Klotman, MD, didn’t hesitate to resign his post at Duke University, Durham, N.C., and join his wife in Washington. Paul says he wanted to support Mary’s aspirations, even though it meant an uncertain track for his own career.
Fortunately for the Klotmans, the move proved instrumental for both of their careers and spurred one of their proudest scientific breakthroughs.
At NIH, Mary was a member of the Public Health Service and worked in the laboratory of tumor cell biology, and Paul became chief of the institute’s molecular medicine section in the laboratory of developmental biology. Together, their work led to the first animal model of HIV-associated nephropathy using transgenic techniques. The Klotmans and their team demonstrated that HIV resides in and evolves separately in kidney cells, a critical step in HIV-associated kidney disease.
“That’s where our longstanding collaboration around HIV-associated nephropathy started,” Mary says. “Paul and I have a passion for research, and we’ve had the same grant together for 25 years.”
After their successful stint at NIH, the Klotmans next climbed the ranks at the Icahn School of Medicine at Mount Sinai, where Paul started as chief of the nephrology division and became chair of medicine, and Mary became chief of infectious diseases and co-director of Mount Sinai’s Global Health and Emerging Pathogens Institute.
Today, Mary and Paul are the first – and only – married couple in the United States to lead separate medical schools. Mary is dean and vice chancellor for health affairs at Duke, and Paul is president and executive dean of Baylor College of Medicine, Houston.
Despite their 1,100-mile separation, the Klotmans manage their relationship in an unconventional way that some might balk at: Every Friday, one spouse hops on a plane and travels to the other for a date night and weekend.
“When we started this crazy lifestyle, we committed to being together every weekend,” says Mary. “And in 10 years – before COVID – we missed only one weekend together.”
The Klotmans say the scheduled time together places a hard end to each work week and enables them to truly enjoy their quality time.
“Friday at noon, I’m on the plane going to Durham, and I know that in 2 hours I’m going to have a date with my wife,” Paul said. “There are institutions that we’ve run into that think you have to be 7 days a week on site. But Duke and Baylor have been very supportive [of our situation].”
No doubt, the arrangement means a lot of time in the air for the couple. Paul says he travels about 150,000 miles every year by plane.
Having dual leadership positions in academic medicine has kept the Klotmans tightly connected, and the couple says their strong partnership has contributed to their success.
“It’s really been helpful having a deep understanding of our career paths, because we’ve been able to understand when one of us needed to be really focused on work and the other one would step back a bit with the kids and vice versa,” Mary said.
“There’s no question that we wouldn’t be in the positions we are in now if it weren’t for the fact that we’ve had each other,” Paul said.
In their own words
What is a little-known title that you have?
Paul: Purse-carrier for my wife. When she is honored at a national meeting or event, she often stands up and hands me her purse. I now make sure I have on an appropriate outfit that matches the purse.
Tell us about your children.
Mary: We had a very traumatic first pregnancy that we lost. Six years later, we adopted our first child, which was an amazing blessing. Our second son was Duke’s first successful frozen embryo transfer.
Describe a memorable moment in your relationship.
Paul: As we were leaving for our honeymoon, Mary’s dad handed me this booklet. It was the receipts for Mary’s medical school loans for the next 10 years. He said, “Congratulations, she’s all yours!”
A version of this article first appeared on Medscape.com.
When people started dying from lethal anthrax spores sent through the mail in 2001, infectious disease expert Jeannette Guarner, MD, was called to Florida and Connecticut to analyze the bodies. She and her pathology team investigated how the bacteria had entered the victims and examined tissue samples from across the country to discern the scale of the attacks.
After conducting autopsies and identifying that inhalation anthrax had caused the deaths, Dr. Guarner rushed home to Atlanta just in time for Thanksgiving. Exhausted, the beloved family chef still managed to cook the big turkey that holiday, but she enlisted help with dessert.
“She returned home on Thanksgiving at like three in the morning,” recalls Carlos del Rio, MD. “She said to me, ‘In order for us to have Thanksgiving, you have to be in charge of the pies.’ When I told my daughter, she said, ‘This is going to be a disaster! If mom’s not cooking, this is not going to be good.’”
“It didn’t turn out that bad,” Dr. Guarner laughs. “There was dessert.”
As two of the top infectious disease experts in the country, Dr. Guarner and Dr. del Rio are no strangers to juggling their personal lives around disease outbreaks, last-minute travel, and pressing research.
Former director of the clinical laboratory at Mexico’s National Cancer Institute, Dr. Guarner worked for the Centers for Disease Control and Prevention for 10 years, where she played an integral part in the discovery of SARS. She and her team identified that a coronavirus was in cultures taken from a health care worker who died after working in Asia and determined through molecular testing that the virus was different from any other coronaviruses at the time.
Dr. Guarner went on to search for the novel virus in tissue samples and determine that it was SARS that had caused the damage. She is now a professor in the department of pathology and laboratory medicine at Emory University, Atlanta, medical director of the clinical laboratory at Emory University Hospital Midtown, and vice chair for faculty affairs.
Dr. Del Rio, who served as director of the National AIDS Council of Mexico, is a distinguished professor of medicine in Emory University’s division of infectious diseases and a professor of global health and epidemiology in the Rollins School of Public Health at Emory University. He is also co-director of the Emory Center for AIDS Research and co-principal investigator of the Emory-CDC HIV Clinical Trials Unit and the Emory Vaccine and Treatment Evaluation Unit.
Dr. Del Rio’s work in HIV prevention and care has made great strides, including developing the concept for the HIV Care Continuum, a public health model that outlines the stages that HIV patients go through, from diagnosis to achieving viral suppression. Dr. Del Rio, who is foreign secretary of the National Academy of Medicine, has also worked on emerging infections such as pandemic influenza and was a member of the WHO Influenza A (H1N1) Clinical Advisory Group and of the CDC Influenza A Task Force during the 2009 pandemic.
Dr. Del Rio and Dr. Guarner met during medical school in Mexico City. At first, the two carpooled to classes, but when Dr. Guarner fell ill with hepatitis A, Dr. del Rio brought Dr. Guarner the class notes so she wouldn’t fall behind. The study buddies later became a couple and married just before coming to the United States for residency.
With their expertise in infectious disease, Dr. del Rio and Dr. Guarner have worked collaboratively in the past, but the couple says they’ve always maintained separate professional identities.
“We try to create our own spaces,” Dr. del Rio said. “You try to keep your personal and professional identity independent as much as possible. You don’t want people to say, ‘Oh, you got this or you’re doing this because you are married to this other person.’ You want, to a certain degree, intellectual independence.”
This has been easier in some ways because Dr. del Rio and Dr. Guarner have different last names. Over the years they have frequently encountered people who had no idea that they are married.
“One time, we were both down in the lab and Jeanette was discussing a case, and she started teasing me or poking me, making fun,” recalls Dr. del Rio. “Some of the ID fellows were like, ‘Oh my God, who the hell is this woman?’ They didn’t realize she was my wife.”
Since the COVID-19 outbreak, both Dr. Guarner and Dr. del Rio have been involved in different ways with the pandemic. Dr. Del Rio has seen patients, conducted clinical trials, and given hundreds of local and national interviews about the virus. As a laboratory director, Dr. Guarner has validated tests for the diagnosis of COVID-19 and counseled staff on exposure concerns.
“An important aspect has also been to make sure that our laboratory technologists understand the disease and the need for the different protection elements we have had to use in the hospital,” she said. “In many ways I have had to scale down fears the techs have had when handling specimens from these patients.”
In their own words
What was one of your most surprising discoveries?
Jeannette: During the anthrax attacks, we received lots of tissues on live patients, particularly skin biopsies from different parts of the country where pathologists had concerns that there was anthrax. From New York, we received more than 50 skin biopsies and discovered that the necrotic lesions suspected of anthrax had Rickettsia in them. In other words, we discovered that rickettsialpox – a mite-borne infectious disease – was circulating in the city, which was unknown at the time.
Describe a challenge that you overcame:
Carlos: When I was appointed as director of the National AIDS Council of Mexico (CONASIDA), I was quite young, only 32 years old. I had to learn to listen to others who had expertise and institutional memory, to respect their opinions, and at the same time to push for change. A huge challenge was the role of the Catholic Church and conservative groups that were adamantly against condom promotion. Thus, I learned how to advance policies based in science without being confrontational.
Have you ever been famous for anything other than your work?
Jeannette: In 2017, a tree fell on our house during Hurricane Irma. It fell right on my husband’s office a few minutes after he left the room. Fortunately, I have always been small and flexible, and I crawled through the rubble to save our valuables before they were ruined by the rain. Later, a local Atlanta TV news crew was in the neighborhood reporting on the damage, and I told them to come to our house if they wanted to see real damage. That night, we were on the local news.
Power couple Paul and Mary Klotman
When Mary Klotman, MD, was offered an opportunity with the National Institutes of Health in 1991, Paul Klotman, MD, didn’t hesitate to resign his post at Duke University, Durham, N.C., and join his wife in Washington. Paul says he wanted to support Mary’s aspirations, even though it meant an uncertain track for his own career.
Fortunately for the Klotmans, the move proved instrumental for both of their careers and spurred one of their proudest scientific breakthroughs.
At NIH, Mary was a member of the Public Health Service and worked in the laboratory of tumor cell biology, and Paul became chief of the institute’s molecular medicine section in the laboratory of developmental biology. Together, their work led to the first animal model of HIV-associated nephropathy using transgenic techniques. The Klotmans and their team demonstrated that HIV resides in and evolves separately in kidney cells, a critical step in HIV-associated kidney disease.
“That’s where our longstanding collaboration around HIV-associated nephropathy started,” Mary says. “Paul and I have a passion for research, and we’ve had the same grant together for 25 years.”
After their successful stint at NIH, the Klotmans next climbed the ranks at the Icahn School of Medicine at Mount Sinai, where Paul started as chief of the nephrology division and became chair of medicine, and Mary became chief of infectious diseases and co-director of Mount Sinai’s Global Health and Emerging Pathogens Institute.
Today, Mary and Paul are the first – and only – married couple in the United States to lead separate medical schools. Mary is dean and vice chancellor for health affairs at Duke, and Paul is president and executive dean of Baylor College of Medicine, Houston.
Despite their 1,100-mile separation, the Klotmans manage their relationship in an unconventional way that some might balk at: Every Friday, one spouse hops on a plane and travels to the other for a date night and weekend.
“When we started this crazy lifestyle, we committed to being together every weekend,” says Mary. “And in 10 years – before COVID – we missed only one weekend together.”
The Klotmans say the scheduled time together places a hard end to each work week and enables them to truly enjoy their quality time.
“Friday at noon, I’m on the plane going to Durham, and I know that in 2 hours I’m going to have a date with my wife,” Paul said. “There are institutions that we’ve run into that think you have to be 7 days a week on site. But Duke and Baylor have been very supportive [of our situation].”
No doubt, the arrangement means a lot of time in the air for the couple. Paul says he travels about 150,000 miles every year by plane.
Having dual leadership positions in academic medicine has kept the Klotmans tightly connected, and the couple says their strong partnership has contributed to their success.
“It’s really been helpful having a deep understanding of our career paths, because we’ve been able to understand when one of us needed to be really focused on work and the other one would step back a bit with the kids and vice versa,” Mary said.
“There’s no question that we wouldn’t be in the positions we are in now if it weren’t for the fact that we’ve had each other,” Paul said.
In their own words
What is a little-known title that you have?
Paul: Purse-carrier for my wife. When she is honored at a national meeting or event, she often stands up and hands me her purse. I now make sure I have on an appropriate outfit that matches the purse.
Tell us about your children.
Mary: We had a very traumatic first pregnancy that we lost. Six years later, we adopted our first child, which was an amazing blessing. Our second son was Duke’s first successful frozen embryo transfer.
Describe a memorable moment in your relationship.
Paul: As we were leaving for our honeymoon, Mary’s dad handed me this booklet. It was the receipts for Mary’s medical school loans for the next 10 years. He said, “Congratulations, she’s all yours!”
A version of this article first appeared on Medscape.com.
Pfizer halts distribution of stop-smoking pill Chantix
The pharmaceutical company is also recalling some lots of Chantix that may have high levels of NDMA, Reuters reported.
Pfizer told Reuters the distribution pause was ordered out of abundance of caution while further testing is conducted. The FDA approved varenicline, which is marketed as Chantix, in 2006.
“The benefits of Chantix outweigh the very low potential risks, if any, posed by nitrosamine exposure from varenicline on top of other common sources over a lifetime,” Pfizer spokesperson Steven Danehy said in an email, according to Reuters.
The FDA has not issued a recall on Chantix. In Canada, however, health authorities on June 8 instituted a recall for Champix, the name under which the drug is sold in that nation.
The Chantix website says it’s a 3- to 6-month treatment that helps people overcome the need to smoke tobacco. The website says more than 13 million people have been prescribed Chantix.
Other health concerns have been raised about Chantix, such as mental health side effects.
In 2016, however, researchers concluded Chantix did not appear to raise the risk of serious health disorders such as depression, anxiety, and suicidal thoughts.
A version of this article first appeared on WebMD.com.
The pharmaceutical company is also recalling some lots of Chantix that may have high levels of NDMA, Reuters reported.
Pfizer told Reuters the distribution pause was ordered out of abundance of caution while further testing is conducted. The FDA approved varenicline, which is marketed as Chantix, in 2006.
“The benefits of Chantix outweigh the very low potential risks, if any, posed by nitrosamine exposure from varenicline on top of other common sources over a lifetime,” Pfizer spokesperson Steven Danehy said in an email, according to Reuters.
The FDA has not issued a recall on Chantix. In Canada, however, health authorities on June 8 instituted a recall for Champix, the name under which the drug is sold in that nation.
The Chantix website says it’s a 3- to 6-month treatment that helps people overcome the need to smoke tobacco. The website says more than 13 million people have been prescribed Chantix.
Other health concerns have been raised about Chantix, such as mental health side effects.
In 2016, however, researchers concluded Chantix did not appear to raise the risk of serious health disorders such as depression, anxiety, and suicidal thoughts.
A version of this article first appeared on WebMD.com.
The pharmaceutical company is also recalling some lots of Chantix that may have high levels of NDMA, Reuters reported.
Pfizer told Reuters the distribution pause was ordered out of abundance of caution while further testing is conducted. The FDA approved varenicline, which is marketed as Chantix, in 2006.
“The benefits of Chantix outweigh the very low potential risks, if any, posed by nitrosamine exposure from varenicline on top of other common sources over a lifetime,” Pfizer spokesperson Steven Danehy said in an email, according to Reuters.
The FDA has not issued a recall on Chantix. In Canada, however, health authorities on June 8 instituted a recall for Champix, the name under which the drug is sold in that nation.
The Chantix website says it’s a 3- to 6-month treatment that helps people overcome the need to smoke tobacco. The website says more than 13 million people have been prescribed Chantix.
Other health concerns have been raised about Chantix, such as mental health side effects.
In 2016, however, researchers concluded Chantix did not appear to raise the risk of serious health disorders such as depression, anxiety, and suicidal thoughts.
A version of this article first appeared on WebMD.com.
Few clinical guidelines exist for treating post-COVID symptoms
As doctors struggled through several surges of COVID-19 infections, most of what we learned was acquired through real-life experience. While many treatment options were promoted, most flat-out failed to be real therapeutics at all. Now that we have a safe and effective vaccine, we can prevent many infections from this virus. However, we are still left to manage the many post-COVID symptoms our patients continue to suffer with.

Symptoms following infection can last for months and range widely from “brain fog,” fatigue, dyspnea, chest pain, generalized weakness, depression, and a host of others. Patients may experience one or all of these symptoms, and there is currently no good way to predict who will go on to become a COVID “long hauler”.
Following the example of being educated by COVID as it happened, the same is true for managing post-COVID symptoms. The medical community still has a poor understanding of why some people develop it and there are few evidence-based studies to support any treatment modalities.
which they define as “new, recurring, or ongoing symptoms more than 4 weeks after infection, sometimes after initial symptom recovery.” It is important to note that these symptoms can occur in any degree of sickness during the acute infection, including in those who were asymptomatic. Even the actual name of this post-COVID syndrome is still being developed, with several other names being used for it as well.
While the guidelines are quite extensive, the actual clinical recommendations are still vague. For example, it is advised to let the patient know that post-COVID symptoms are still not well understood. While it is important to be transparent with patients, this does little to reassure them. Patients look to doctors, especially their primary care physicians, to guide them on the best treatment paths. Yet, we currently have none for post-COVID syndrome.
It is also advised to treat the patients’ symptoms and help improve functioning. For many diseases, doctors like to get to the root cause of the problem. Treating a symptom often masks an underlying condition. It may make the patient feel better and improve what they are capable of doing, which is important, but it also fails to unmask the real problem. It is also important to note that symptoms can be out of proportion to clinical findings and should not be dismissed: we just don’t have the answers yet.
One helpful recommendation is having a patient keep a diary of their symptoms. This will help both the patient and doctor learn what may be triggering factors. If it is, for example, exertion that induces breathlessness, perhaps the patient can gradually increase their level of activity to minimize symptoms. Additionally, a “comprehensive rehabilitation program” is also advised and this can greatly assist addressing all the issues a patient is experiencing, physically and medically.
It is also advised that management of underlying medical conditions be optimized. While this is very important, it is not something specific to post-COVID syndrome: All patients should have their underlying medical conditions well controlled. It might be that the patient is paying more attention to their overall health, which is a good thing. However, this does not necessarily reduce the current symptoms a patient is experiencing.
The CDC makes a good attempt to offer guidance in the frustrating management of post-COVID syndrome. However, their clinical guidelines fail to offer specific management tools specific to treating post-COVID patients. The recommendations offered are more helpful to health in general. The fact that more specific recommendations are lacking is simply caused by the lack of knowledge of this condition at present. As more research is conducted and more knowledge obtained, new guidelines should become more detailed.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
As doctors struggled through several surges of COVID-19 infections, most of what we learned was acquired through real-life experience. While many treatment options were promoted, most flat-out failed to be real therapeutics at all. Now that we have a safe and effective vaccine, we can prevent many infections from this virus. However, we are still left to manage the many post-COVID symptoms our patients continue to suffer with.
Symptoms following infection can last for months and range widely from “brain fog,” fatigue, dyspnea, chest pain, generalized weakness, depression, and a host of others. Patients may experience one or all of these symptoms, and there is currently no good way to predict who will go on to become a COVID “long hauler”.
Following the example of being educated by COVID as it happened, the same is true for managing post-COVID symptoms. The medical community still has a poor understanding of why some people develop it and there are few evidence-based studies to support any treatment modalities.
which they define as “new, recurring, or ongoing symptoms more than 4 weeks after infection, sometimes after initial symptom recovery.” It is important to note that these symptoms can occur in any degree of sickness during the acute infection, including in those who were asymptomatic. Even the actual name of this post-COVID syndrome is still being developed, with several other names being used for it as well.
While the guidelines are quite extensive, the actual clinical recommendations are still vague. For example, it is advised to let the patient know that post-COVID symptoms are still not well understood. While it is important to be transparent with patients, this does little to reassure them. Patients look to doctors, especially their primary care physicians, to guide them on the best treatment paths. Yet, we currently have none for post-COVID syndrome.
It is also advised to treat the patients’ symptoms and help improve functioning. For many diseases, doctors like to get to the root cause of the problem. Treating a symptom often masks an underlying condition. It may make the patient feel better and improve what they are capable of doing, which is important, but it also fails to unmask the real problem. It is also important to note that symptoms can be out of proportion to clinical findings and should not be dismissed: we just don’t have the answers yet.
One helpful recommendation is having a patient keep a diary of their symptoms. This will help both the patient and doctor learn what may be triggering factors. If it is, for example, exertion that induces breathlessness, perhaps the patient can gradually increase their level of activity to minimize symptoms. Additionally, a “comprehensive rehabilitation program” is also advised and this can greatly assist addressing all the issues a patient is experiencing, physically and medically.
It is also advised that management of underlying medical conditions be optimized. While this is very important, it is not something specific to post-COVID syndrome: All patients should have their underlying medical conditions well controlled. It might be that the patient is paying more attention to their overall health, which is a good thing. However, this does not necessarily reduce the current symptoms a patient is experiencing.
The CDC makes a good attempt to offer guidance in the frustrating management of post-COVID syndrome. However, their clinical guidelines fail to offer specific management tools specific to treating post-COVID patients. The recommendations offered are more helpful to health in general. The fact that more specific recommendations are lacking is simply caused by the lack of knowledge of this condition at present. As more research is conducted and more knowledge obtained, new guidelines should become more detailed.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
As doctors struggled through several surges of COVID-19 infections, most of what we learned was acquired through real-life experience. While many treatment options were promoted, most flat-out failed to be real therapeutics at all. Now that we have a safe and effective vaccine, we can prevent many infections from this virus. However, we are still left to manage the many post-COVID symptoms our patients continue to suffer with.
Symptoms following infection can last for months and range widely from “brain fog,” fatigue, dyspnea, chest pain, generalized weakness, depression, and a host of others. Patients may experience one or all of these symptoms, and there is currently no good way to predict who will go on to become a COVID “long hauler”.
Following the example of being educated by COVID as it happened, the same is true for managing post-COVID symptoms. The medical community still has a poor understanding of why some people develop it and there are few evidence-based studies to support any treatment modalities.
which they define as “new, recurring, or ongoing symptoms more than 4 weeks after infection, sometimes after initial symptom recovery.” It is important to note that these symptoms can occur in any degree of sickness during the acute infection, including in those who were asymptomatic. Even the actual name of this post-COVID syndrome is still being developed, with several other names being used for it as well.
While the guidelines are quite extensive, the actual clinical recommendations are still vague. For example, it is advised to let the patient know that post-COVID symptoms are still not well understood. While it is important to be transparent with patients, this does little to reassure them. Patients look to doctors, especially their primary care physicians, to guide them on the best treatment paths. Yet, we currently have none for post-COVID syndrome.
It is also advised to treat the patients’ symptoms and help improve functioning. For many diseases, doctors like to get to the root cause of the problem. Treating a symptom often masks an underlying condition. It may make the patient feel better and improve what they are capable of doing, which is important, but it also fails to unmask the real problem. It is also important to note that symptoms can be out of proportion to clinical findings and should not be dismissed: we just don’t have the answers yet.
One helpful recommendation is having a patient keep a diary of their symptoms. This will help both the patient and doctor learn what may be triggering factors. If it is, for example, exertion that induces breathlessness, perhaps the patient can gradually increase their level of activity to minimize symptoms. Additionally, a “comprehensive rehabilitation program” is also advised and this can greatly assist addressing all the issues a patient is experiencing, physically and medically.
It is also advised that management of underlying medical conditions be optimized. While this is very important, it is not something specific to post-COVID syndrome: All patients should have their underlying medical conditions well controlled. It might be that the patient is paying more attention to their overall health, which is a good thing. However, this does not necessarily reduce the current symptoms a patient is experiencing.
The CDC makes a good attempt to offer guidance in the frustrating management of post-COVID syndrome. However, their clinical guidelines fail to offer specific management tools specific to treating post-COVID patients. The recommendations offered are more helpful to health in general. The fact that more specific recommendations are lacking is simply caused by the lack of knowledge of this condition at present. As more research is conducted and more knowledge obtained, new guidelines should become more detailed.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
FIND: A framework for success as a first-year hospitalist
Congratulations! You’re about to start your first year as a hospitalist, and in many cases your first real job. Hospital medicine is an incredibly rewarding subspecialty, but the progression from resident to attending physician can be daunting. To facilitate this transition, we present FIND (Familiarity, Identity, Network, and Direction) – a novel, sequential framework for success as a first-year hospitalist. For each component, we provide a narrative overview and a summary bullet point for quick reference.
Familiarity
- Lay the foundation: Learn the ins and outs of your job, EMR, and team.
Familiarize yourself with your surroundings. Know where your patients are located, where you can document, where to find equipment for procedures, and how to reach information technology. Proactively set up the electronic medical record on your home computer and phone. Make sure to review your responsibilities, including your call schedule, your shifts, your assigned patient panel, when you can leave campus, and how people should contact you. Also, others should know your expectations of them, especially if you are working with trainees.
Maintain a file with all of your orientation materials, including phone numbers and emails of key personnel. Know who your people are – who can access your calendar, who you can call with a clinical question or to escalate care, who can assist you with billing, and who helps with the throughput of your patients in the hospital. Take time to review your benefits, including parental leave, insurance coverage, retirement planning, vacation time, and ancillary services like laundry for your white coat. Familiarizing yourself with these basics will provide comfort and lay the foundation for your first year.
Identity
- Perform self-reflection: Overcome imposter syndrome and invest in hobbies.

One of the fundamental realizations that will occur with your first hospitalist job is that you are the attending. You walk in with a vision of your first job; be prepared to be surprised. You have earned the privilege of deciding on patient plans, and you are no longer obligated to staff with a senior physician. This is both empowering and terrifying. In a way, it may oddly remind you of intern year. A new hospital, new EMR, new colleagues, and imposter syndrome will trick you into doubting your decisions.
How to battle it? Positive thinking. You do know the basics of inpatient medicine and you do have a support system to cheer you on. As part of imposter syndrome, you may feel pressured to focus solely on work. Yet, your first job as a hospitalist is finally an amazing opportunity to focus on you. What hobbies have you been neglecting: cooking, photography, reading, more time with family, a new pet? You have the power to schedule your off-weeks. Are you interested in academics? Reserve a portion of your time off to explore scholarship opportunities at your institution. Your first job as a hospitalist is a chance to develop your identity, both as a physician and as an individual.
Network
- Engage your support system: Communicate with nursing, administration, colleagues.

Networking, or building a web of mutually beneficial professional relationships, is imperative for long-term career success. Hospitalists should focus on developing their network across multiple departments, such as nursing, subspecialties, medical education, and hospital administration. Curating a broad network will increase your visibility within your organization, showcase your unique services, and demonstrate your value.
To make networking encounters impactful, express interest, actively listen, ask relevant questions, and seek areas of mutual benefit. It’s equally important to cultivate these new relationships after the initial encounter and to demonstrate how your skill set will aid colleagues in achieving their professional goals. Over time, as you establish your niche, deliberate networking with those who share similar interests can lead to a wealth of new experiences and opportunities. Intentionally mastering networking early in your career provides insight into different aspects of the hospital system, new perspectives on ideas, and access to valuable guidance from other professionals. Engaging in networking to establish your support system is an essential step towards success as a first-year hospitalist.
Direction
- Visualize your path: Find a mentor and develop a mission statement and career plan.
Once you’re familiar with your work environment, confident in your identity, and acquainted with your support network, you’re ready for the final step – direction. Hospital medicine offers many professional avenues and clarifying your career path is challenging when attempted alone. A mentor is the necessary catalyst to find direction and purpose.
Selecting and engaging with a mentor will bolster your professional advancement, academic productivity, and most importantly, career satisfaction.1 At its best, mentorship is a symbiotic relationship. Your mentor should inspire you, challenge you, and support your growth and emotional well-being. In turn, as the mentee, you should be proactive, establish expectations, and take responsibility for maintaining communication to ensure a successful relationship. As your career takes shape over time, you may require a mentorship team to fulfill your unique needs.
When you’ve established a relationship with your mentor, take time to develop 1-year and 5-year plans. Your 1-year plan should focus on a few “quick wins,” often projects or opportunities at your home institution. Small victories in your first year will boost your confidence, motivation, and sense of control. Your 5-year plan should delineate the steps necessary to make your first major career transition, such as from instructor to assistant professor. Working with your mentor to draft a career mission statement is a useful first step in this process. Beginning with the end in mind, will help you visualize your direction.2
We hope that the FIND framework will help you find your path to success as a first-year hospitalist.
Dr. Nelson is a hospitalist and instructor of medicine at Harvard Medical School and Beth Israel Deaconess Medical Center, both in Boston. Dr. Ashford is assistant professor and program director, department of internal medicine/pediatrics, at the University of Nebraska Medical Center, Omaha. Dr. Rawal is clinical assistant professor of medicine at the University of Pittsburgh Medical Center. Dr. Crecelius is assistant professor of clinical medicine at Indiana University, Indianapolis. This article is sponsored by the SHM Physicians in Training committee, which submits quarterly content to the Hospitalist on topics relevant to trainees and early -career hospitalists.
References
1. Zerzan JT et al. Making the most of mentors: a guide for mentees. Acad Med. 2009;84:140-4. doi: 10.1097/ACM.0b013e3181906e8f.
2. Covey F. The seven habits of highly effective people. 25th anniversary edition. New York: Simon and Schuster, 2013.
Congratulations! You’re about to start your first year as a hospitalist, and in many cases your first real job. Hospital medicine is an incredibly rewarding subspecialty, but the progression from resident to attending physician can be daunting. To facilitate this transition, we present FIND (Familiarity, Identity, Network, and Direction) – a novel, sequential framework for success as a first-year hospitalist. For each component, we provide a narrative overview and a summary bullet point for quick reference.
Familiarity
- Lay the foundation: Learn the ins and outs of your job, EMR, and team.
Familiarize yourself with your surroundings. Know where your patients are located, where you can document, where to find equipment for procedures, and how to reach information technology. Proactively set up the electronic medical record on your home computer and phone. Make sure to review your responsibilities, including your call schedule, your shifts, your assigned patient panel, when you can leave campus, and how people should contact you. Also, others should know your expectations of them, especially if you are working with trainees.
Maintain a file with all of your orientation materials, including phone numbers and emails of key personnel. Know who your people are – who can access your calendar, who you can call with a clinical question or to escalate care, who can assist you with billing, and who helps with the throughput of your patients in the hospital. Take time to review your benefits, including parental leave, insurance coverage, retirement planning, vacation time, and ancillary services like laundry for your white coat. Familiarizing yourself with these basics will provide comfort and lay the foundation for your first year.
Identity
- Perform self-reflection: Overcome imposter syndrome and invest in hobbies.
One of the fundamental realizations that will occur with your first hospitalist job is that you are the attending. You walk in with a vision of your first job; be prepared to be surprised. You have earned the privilege of deciding on patient plans, and you are no longer obligated to staff with a senior physician. This is both empowering and terrifying. In a way, it may oddly remind you of intern year. A new hospital, new EMR, new colleagues, and imposter syndrome will trick you into doubting your decisions.
How to battle it? Positive thinking. You do know the basics of inpatient medicine and you do have a support system to cheer you on. As part of imposter syndrome, you may feel pressured to focus solely on work. Yet, your first job as a hospitalist is finally an amazing opportunity to focus on you. What hobbies have you been neglecting: cooking, photography, reading, more time with family, a new pet? You have the power to schedule your off-weeks. Are you interested in academics? Reserve a portion of your time off to explore scholarship opportunities at your institution. Your first job as a hospitalist is a chance to develop your identity, both as a physician and as an individual.
Network
- Engage your support system: Communicate with nursing, administration, colleagues.
Networking, or building a web of mutually beneficial professional relationships, is imperative for long-term career success. Hospitalists should focus on developing their network across multiple departments, such as nursing, subspecialties, medical education, and hospital administration. Curating a broad network will increase your visibility within your organization, showcase your unique services, and demonstrate your value.
To make networking encounters impactful, express interest, actively listen, ask relevant questions, and seek areas of mutual benefit. It’s equally important to cultivate these new relationships after the initial encounter and to demonstrate how your skill set will aid colleagues in achieving their professional goals. Over time, as you establish your niche, deliberate networking with those who share similar interests can lead to a wealth of new experiences and opportunities. Intentionally mastering networking early in your career provides insight into different aspects of the hospital system, new perspectives on ideas, and access to valuable guidance from other professionals. Engaging in networking to establish your support system is an essential step towards success as a first-year hospitalist.
Direction
- Visualize your path: Find a mentor and develop a mission statement and career plan.
Once you’re familiar with your work environment, confident in your identity, and acquainted with your support network, you’re ready for the final step – direction. Hospital medicine offers many professional avenues and clarifying your career path is challenging when attempted alone. A mentor is the necessary catalyst to find direction and purpose.
Selecting and engaging with a mentor will bolster your professional advancement, academic productivity, and most importantly, career satisfaction.1 At its best, mentorship is a symbiotic relationship. Your mentor should inspire you, challenge you, and support your growth and emotional well-being. In turn, as the mentee, you should be proactive, establish expectations, and take responsibility for maintaining communication to ensure a successful relationship. As your career takes shape over time, you may require a mentorship team to fulfill your unique needs.
When you’ve established a relationship with your mentor, take time to develop 1-year and 5-year plans. Your 1-year plan should focus on a few “quick wins,” often projects or opportunities at your home institution. Small victories in your first year will boost your confidence, motivation, and sense of control. Your 5-year plan should delineate the steps necessary to make your first major career transition, such as from instructor to assistant professor. Working with your mentor to draft a career mission statement is a useful first step in this process. Beginning with the end in mind, will help you visualize your direction.2
We hope that the FIND framework will help you find your path to success as a first-year hospitalist.
Dr. Nelson is a hospitalist and instructor of medicine at Harvard Medical School and Beth Israel Deaconess Medical Center, both in Boston. Dr. Ashford is assistant professor and program director, department of internal medicine/pediatrics, at the University of Nebraska Medical Center, Omaha. Dr. Rawal is clinical assistant professor of medicine at the University of Pittsburgh Medical Center. Dr. Crecelius is assistant professor of clinical medicine at Indiana University, Indianapolis. This article is sponsored by the SHM Physicians in Training committee, which submits quarterly content to the Hospitalist on topics relevant to trainees and early -career hospitalists.
References
1. Zerzan JT et al. Making the most of mentors: a guide for mentees. Acad Med. 2009;84:140-4. doi: 10.1097/ACM.0b013e3181906e8f.
2. Covey F. The seven habits of highly effective people. 25th anniversary edition. New York: Simon and Schuster, 2013.
Congratulations! You’re about to start your first year as a hospitalist, and in many cases your first real job. Hospital medicine is an incredibly rewarding subspecialty, but the progression from resident to attending physician can be daunting. To facilitate this transition, we present FIND (Familiarity, Identity, Network, and Direction) – a novel, sequential framework for success as a first-year hospitalist. For each component, we provide a narrative overview and a summary bullet point for quick reference.
Familiarity
- Lay the foundation: Learn the ins and outs of your job, EMR, and team.
Familiarize yourself with your surroundings. Know where your patients are located, where you can document, where to find equipment for procedures, and how to reach information technology. Proactively set up the electronic medical record on your home computer and phone. Make sure to review your responsibilities, including your call schedule, your shifts, your assigned patient panel, when you can leave campus, and how people should contact you. Also, others should know your expectations of them, especially if you are working with trainees.
Maintain a file with all of your orientation materials, including phone numbers and emails of key personnel. Know who your people are – who can access your calendar, who you can call with a clinical question or to escalate care, who can assist you with billing, and who helps with the throughput of your patients in the hospital. Take time to review your benefits, including parental leave, insurance coverage, retirement planning, vacation time, and ancillary services like laundry for your white coat. Familiarizing yourself with these basics will provide comfort and lay the foundation for your first year.
Identity
- Perform self-reflection: Overcome imposter syndrome and invest in hobbies.
One of the fundamental realizations that will occur with your first hospitalist job is that you are the attending. You walk in with a vision of your first job; be prepared to be surprised. You have earned the privilege of deciding on patient plans, and you are no longer obligated to staff with a senior physician. This is both empowering and terrifying. In a way, it may oddly remind you of intern year. A new hospital, new EMR, new colleagues, and imposter syndrome will trick you into doubting your decisions.
How to battle it? Positive thinking. You do know the basics of inpatient medicine and you do have a support system to cheer you on. As part of imposter syndrome, you may feel pressured to focus solely on work. Yet, your first job as a hospitalist is finally an amazing opportunity to focus on you. What hobbies have you been neglecting: cooking, photography, reading, more time with family, a new pet? You have the power to schedule your off-weeks. Are you interested in academics? Reserve a portion of your time off to explore scholarship opportunities at your institution. Your first job as a hospitalist is a chance to develop your identity, both as a physician and as an individual.
Network
- Engage your support system: Communicate with nursing, administration, colleagues.
Networking, or building a web of mutually beneficial professional relationships, is imperative for long-term career success. Hospitalists should focus on developing their network across multiple departments, such as nursing, subspecialties, medical education, and hospital administration. Curating a broad network will increase your visibility within your organization, showcase your unique services, and demonstrate your value.
To make networking encounters impactful, express interest, actively listen, ask relevant questions, and seek areas of mutual benefit. It’s equally important to cultivate these new relationships after the initial encounter and to demonstrate how your skill set will aid colleagues in achieving their professional goals. Over time, as you establish your niche, deliberate networking with those who share similar interests can lead to a wealth of new experiences and opportunities. Intentionally mastering networking early in your career provides insight into different aspects of the hospital system, new perspectives on ideas, and access to valuable guidance from other professionals. Engaging in networking to establish your support system is an essential step towards success as a first-year hospitalist.
Direction
- Visualize your path: Find a mentor and develop a mission statement and career plan.
Once you’re familiar with your work environment, confident in your identity, and acquainted with your support network, you’re ready for the final step – direction. Hospital medicine offers many professional avenues and clarifying your career path is challenging when attempted alone. A mentor is the necessary catalyst to find direction and purpose.
Selecting and engaging with a mentor will bolster your professional advancement, academic productivity, and most importantly, career satisfaction.1 At its best, mentorship is a symbiotic relationship. Your mentor should inspire you, challenge you, and support your growth and emotional well-being. In turn, as the mentee, you should be proactive, establish expectations, and take responsibility for maintaining communication to ensure a successful relationship. As your career takes shape over time, you may require a mentorship team to fulfill your unique needs.
When you’ve established a relationship with your mentor, take time to develop 1-year and 5-year plans. Your 1-year plan should focus on a few “quick wins,” often projects or opportunities at your home institution. Small victories in your first year will boost your confidence, motivation, and sense of control. Your 5-year plan should delineate the steps necessary to make your first major career transition, such as from instructor to assistant professor. Working with your mentor to draft a career mission statement is a useful first step in this process. Beginning with the end in mind, will help you visualize your direction.2
We hope that the FIND framework will help you find your path to success as a first-year hospitalist.
Dr. Nelson is a hospitalist and instructor of medicine at Harvard Medical School and Beth Israel Deaconess Medical Center, both in Boston. Dr. Ashford is assistant professor and program director, department of internal medicine/pediatrics, at the University of Nebraska Medical Center, Omaha. Dr. Rawal is clinical assistant professor of medicine at the University of Pittsburgh Medical Center. Dr. Crecelius is assistant professor of clinical medicine at Indiana University, Indianapolis. This article is sponsored by the SHM Physicians in Training committee, which submits quarterly content to the Hospitalist on topics relevant to trainees and early -career hospitalists.
References
1. Zerzan JT et al. Making the most of mentors: a guide for mentees. Acad Med. 2009;84:140-4. doi: 10.1097/ACM.0b013e3181906e8f.
2. Covey F. The seven habits of highly effective people. 25th anniversary edition. New York: Simon and Schuster, 2013.
Sotagliflozin use in T2D patients linked with posthospitalization benefits in analysis

The outcome measure –days alive and out of the hospital – may be a meaningful, patient-centered way of capturing disease burden, the researchers wrote in their paper, published in Annals of Internal Medicine.
“The question was: Can we keep patients alive and out of the hospital for any reason, accounting for the duration of each hospitalization?” author Michael Szarek, PhD, a visiting professor in the division of cardiology at the University of Colorado at Denver, Aurora, said in an interview.
“For every 100 days of follow-up, patients in the sotagliflozin group were alive and out of the hospital 3% more days in relative terms or 2.9 days in absolute terms than those in the placebo group (91.8 vs. 88.9 days),” the researchers reported in their analysis of data from the SOLOIST-WHF trial.
“If you translate that to over the course of a year, that’s more than 10 days,” said Dr. Szarek, who is also a faculty member of CPC Clinical Research, an academic research organization affiliated with the University of Colorado.
Most patients in both groups survived to the end of the study without hospitalization, according to the paper.
Sotagliflozin, a sodium-glucose cotransporter 1 and SGLT2 inhibitor, is not approved in the United States. In 2019, the Food and Drug Administration rejected sotagliflozin as an adjunct to insulin for the treatment of type 1 diabetes after members of an advisory committee expressed concerns about an increased risk for diabetic ketoacidosis with the drug.
Methods and results
To examine whether sotagliflozin increased days alive and out of the hospital in the SOLOIST-WHF trial, Dr. Szarek and colleagues analyzed data from this randomized, double-blind, placebo-controlled study. The trial’s primary results were published in the New England Journal of Medicine in January 2021. Researchers conducted SOLOIST-WHF at more than 300 sites in 32 countries. The trial included 1,222 patients with type 2 diabetes and reduced or preserved ejection fraction who were recently hospitalized for worsening heart failure.
In the new analysis the researchers looked at hospitalizations for any reason and the duration of hospital admissions after randomization. They analyzed days alive and out of the hospital using prespecified models.
Similar proportions of patients who received sotagliflozin and placebo were hospitalized at least once (38.5% vs. 41.4%) during a median follow-up of 9 months. Fewer patients who received sotagliflozin were hospitalized more than once (16.3% vs. 22.1%). In all, 64 patients in the sotagliflozin group and 76 patients in the placebo group died.
The reason for each hospitalization was unspecified, except for cases of heart failure, the authors noted. About 62% of hospitalizations during the trial were for reasons other than heart failure.
Outside expert cites similarities to initial trial
The results for days alive and out of the hospital are “not particularly surprising given the previous publication” of the trial’s primary results, but the new analysis provides a “different view of outcomes that might be clinically meaningful for patients,” commented Frank Brosius, MD, a professor of medicine at the University of Arizona, Tucson.
The SOLOIST-WHF trial indicated that doctors may be able to effectively treat patients with relatively new heart failure with sotagliflozin as long as patients are relatively stable, said Dr. Brosius, who coauthored an editorial in the New England Journal of Medicine that accompanied the initial results from the SOLOIST-WHF trial. It appears that previously reported benefits with regard to heart failure outcomes “showed up in these other indicators” in the secondary analysis.
Still, the effect sizes in the new analysis were relatively small and “probably more studies will be necessary” to examine these end points, he added.
SOLOIST-WHF was funded by Sanofi at initiation and by Lexicon Pharmaceuticals at completion. Dr. Szarek disclosed grants from Lexicon and grants and personal fees from Sanofi, as well as personal fees from other companies. His coauthors included employees of Lexicon and other researchers with financial ties to Lexicon and other pharmaceutical companies. Dr. Brosius disclosed personal fees from the American Diabetes Association and is a member of the Diabetic Kidney Disease Collaborative task force for the American Society of Nephrology that is broadly advocating the use of SGLT2 inhibitors by patients with diabetic kidney diseases. He also has participated in an advisory group for treatment of diabetic kidney disease for Gilead.
The outcome measure –days alive and out of the hospital – may be a meaningful, patient-centered way of capturing disease burden, the researchers wrote in their paper, published in Annals of Internal Medicine.
“The question was: Can we keep patients alive and out of the hospital for any reason, accounting for the duration of each hospitalization?” author Michael Szarek, PhD, a visiting professor in the division of cardiology at the University of Colorado at Denver, Aurora, said in an interview.
“For every 100 days of follow-up, patients in the sotagliflozin group were alive and out of the hospital 3% more days in relative terms or 2.9 days in absolute terms than those in the placebo group (91.8 vs. 88.9 days),” the researchers reported in their analysis of data from the SOLOIST-WHF trial.
“If you translate that to over the course of a year, that’s more than 10 days,” said Dr. Szarek, who is also a faculty member of CPC Clinical Research, an academic research organization affiliated with the University of Colorado.
Most patients in both groups survived to the end of the study without hospitalization, according to the paper.
Sotagliflozin, a sodium-glucose cotransporter 1 and SGLT2 inhibitor, is not approved in the United States. In 2019, the Food and Drug Administration rejected sotagliflozin as an adjunct to insulin for the treatment of type 1 diabetes after members of an advisory committee expressed concerns about an increased risk for diabetic ketoacidosis with the drug.
Methods and results
To examine whether sotagliflozin increased days alive and out of the hospital in the SOLOIST-WHF trial, Dr. Szarek and colleagues analyzed data from this randomized, double-blind, placebo-controlled study. The trial’s primary results were published in the New England Journal of Medicine in January 2021. Researchers conducted SOLOIST-WHF at more than 300 sites in 32 countries. The trial included 1,222 patients with type 2 diabetes and reduced or preserved ejection fraction who were recently hospitalized for worsening heart failure.
In the new analysis the researchers looked at hospitalizations for any reason and the duration of hospital admissions after randomization. They analyzed days alive and out of the hospital using prespecified models.
Similar proportions of patients who received sotagliflozin and placebo were hospitalized at least once (38.5% vs. 41.4%) during a median follow-up of 9 months. Fewer patients who received sotagliflozin were hospitalized more than once (16.3% vs. 22.1%). In all, 64 patients in the sotagliflozin group and 76 patients in the placebo group died.
The reason for each hospitalization was unspecified, except for cases of heart failure, the authors noted. About 62% of hospitalizations during the trial were for reasons other than heart failure.
Outside expert cites similarities to initial trial
The results for days alive and out of the hospital are “not particularly surprising given the previous publication” of the trial’s primary results, but the new analysis provides a “different view of outcomes that might be clinically meaningful for patients,” commented Frank Brosius, MD, a professor of medicine at the University of Arizona, Tucson.
The SOLOIST-WHF trial indicated that doctors may be able to effectively treat patients with relatively new heart failure with sotagliflozin as long as patients are relatively stable, said Dr. Brosius, who coauthored an editorial in the New England Journal of Medicine that accompanied the initial results from the SOLOIST-WHF trial. It appears that previously reported benefits with regard to heart failure outcomes “showed up in these other indicators” in the secondary analysis.
Still, the effect sizes in the new analysis were relatively small and “probably more studies will be necessary” to examine these end points, he added.
SOLOIST-WHF was funded by Sanofi at initiation and by Lexicon Pharmaceuticals at completion. Dr. Szarek disclosed grants from Lexicon and grants and personal fees from Sanofi, as well as personal fees from other companies. His coauthors included employees of Lexicon and other researchers with financial ties to Lexicon and other pharmaceutical companies. Dr. Brosius disclosed personal fees from the American Diabetes Association and is a member of the Diabetic Kidney Disease Collaborative task force for the American Society of Nephrology that is broadly advocating the use of SGLT2 inhibitors by patients with diabetic kidney diseases. He also has participated in an advisory group for treatment of diabetic kidney disease for Gilead.
The outcome measure –days alive and out of the hospital – may be a meaningful, patient-centered way of capturing disease burden, the researchers wrote in their paper, published in Annals of Internal Medicine.
“The question was: Can we keep patients alive and out of the hospital for any reason, accounting for the duration of each hospitalization?” author Michael Szarek, PhD, a visiting professor in the division of cardiology at the University of Colorado at Denver, Aurora, said in an interview.
“For every 100 days of follow-up, patients in the sotagliflozin group were alive and out of the hospital 3% more days in relative terms or 2.9 days in absolute terms than those in the placebo group (91.8 vs. 88.9 days),” the researchers reported in their analysis of data from the SOLOIST-WHF trial.
“If you translate that to over the course of a year, that’s more than 10 days,” said Dr. Szarek, who is also a faculty member of CPC Clinical Research, an academic research organization affiliated with the University of Colorado.
Most patients in both groups survived to the end of the study without hospitalization, according to the paper.
Sotagliflozin, a sodium-glucose cotransporter 1 and SGLT2 inhibitor, is not approved in the United States. In 2019, the Food and Drug Administration rejected sotagliflozin as an adjunct to insulin for the treatment of type 1 diabetes after members of an advisory committee expressed concerns about an increased risk for diabetic ketoacidosis with the drug.
Methods and results
To examine whether sotagliflozin increased days alive and out of the hospital in the SOLOIST-WHF trial, Dr. Szarek and colleagues analyzed data from this randomized, double-blind, placebo-controlled study. The trial’s primary results were published in the New England Journal of Medicine in January 2021. Researchers conducted SOLOIST-WHF at more than 300 sites in 32 countries. The trial included 1,222 patients with type 2 diabetes and reduced or preserved ejection fraction who were recently hospitalized for worsening heart failure.
In the new analysis the researchers looked at hospitalizations for any reason and the duration of hospital admissions after randomization. They analyzed days alive and out of the hospital using prespecified models.
Similar proportions of patients who received sotagliflozin and placebo were hospitalized at least once (38.5% vs. 41.4%) during a median follow-up of 9 months. Fewer patients who received sotagliflozin were hospitalized more than once (16.3% vs. 22.1%). In all, 64 patients in the sotagliflozin group and 76 patients in the placebo group died.
The reason for each hospitalization was unspecified, except for cases of heart failure, the authors noted. About 62% of hospitalizations during the trial were for reasons other than heart failure.
Outside expert cites similarities to initial trial
The results for days alive and out of the hospital are “not particularly surprising given the previous publication” of the trial’s primary results, but the new analysis provides a “different view of outcomes that might be clinically meaningful for patients,” commented Frank Brosius, MD, a professor of medicine at the University of Arizona, Tucson.
The SOLOIST-WHF trial indicated that doctors may be able to effectively treat patients with relatively new heart failure with sotagliflozin as long as patients are relatively stable, said Dr. Brosius, who coauthored an editorial in the New England Journal of Medicine that accompanied the initial results from the SOLOIST-WHF trial. It appears that previously reported benefits with regard to heart failure outcomes “showed up in these other indicators” in the secondary analysis.
Still, the effect sizes in the new analysis were relatively small and “probably more studies will be necessary” to examine these end points, he added.
SOLOIST-WHF was funded by Sanofi at initiation and by Lexicon Pharmaceuticals at completion. Dr. Szarek disclosed grants from Lexicon and grants and personal fees from Sanofi, as well as personal fees from other companies. His coauthors included employees of Lexicon and other researchers with financial ties to Lexicon and other pharmaceutical companies. Dr. Brosius disclosed personal fees from the American Diabetes Association and is a member of the Diabetic Kidney Disease Collaborative task force for the American Society of Nephrology that is broadly advocating the use of SGLT2 inhibitors by patients with diabetic kidney diseases. He also has participated in an advisory group for treatment of diabetic kidney disease for Gilead.
FROM ANNALS OF INTERNAL MEDICINE
Hard Nodular Plaque on the Scalp
The Diagnosis: Platelike Osteoma Cutis
Histopathologic examination revealed extensive cutaneous ossification in the dermis and subcutis with dermal fibrosis and minimal surrounding inflammation (Figure 1). There was no evidence of infection or neoplasm. Further evaluation did not demonstrate any additional physical dysmorphia, and there were no imbalances of calcium-phosphate metabolism or abnormalities in parathyroid hormone or thyroid hormone function. A diagnosis of platelike osteoma cutis (PLOC) was favored. Computed tomography of the head showed material at the posterior skull of similar density to the adjacent calvarial skull and centered within the dermis, consistent with osteoma cutis (Figure 2).
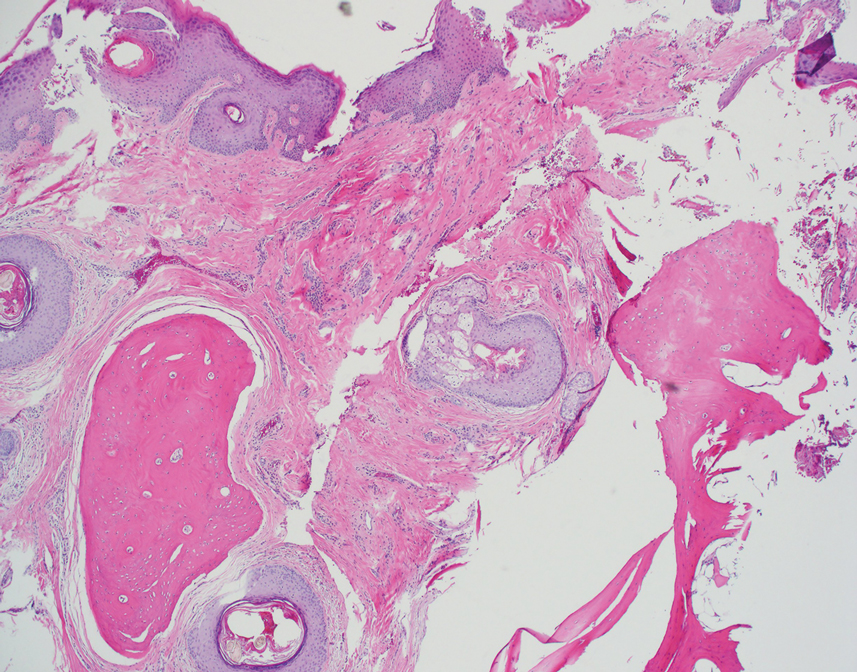

Osteoma cutis describes the formation of bone within the skin. It occurs when hydroxyapatite crystals in a proteinaceous matrix are deposited within the skin, ultimately leading to the formation of bone ultrastructure. Ossification of the skin most often occurs secondary to trauma, inflammation, or neoplasm; however, it rarely may be a primary event.1,2
Platelike osteoma cutis is a rare form of primary cutaneous ossification in which bone forms within the skin in a platelike manner. It most frequently affects the scalp but also has been observed on the trunk and extremities.1 A driving metabolic or endocrine abnormality typically is not identified.2
Platelike osteoma cutis can occur as an isolated finding or as a feature of Albright hereditary osteodystrophy (AHO) or progressive osseous heteroplasia (POH). In addition to cutaneous ossification, AHO involves short stature, endocrinopathy, obesity, shortened fourth and fifth metacarpals, and mental retardation. Progressive osseous heteroplasia is characterized by progressive ossification of the skin and deeper tissues such as muscle and fascia, leading to severe movement restriction; it is believed to be a localized nonprogressive variant of POH.3,4 Mutations in the guanine nucleotide binding protein, alpha stimulating activity polypeptide 1 gene, GNAS1, a key regulatory gene involved in AHO and POH, have been found in several cases of PLOC.3 Our patient lacked any dysmorphic features or laboratory abnormalities suggestive of AHO or POH. Moreover, testing of the tissue and blood for the GNAS1 mutation was negative. Treatment of PLOC often is difficult. Our patient underwent a trial of ablative fractional laser resurfacing, which failed to lead to perceivable improvement.
The differential diagnoses include a kerion, dissecting cellulitis of the scalp, folliculitis decalvans, and acne keloidalis nuchae. A kerion is a manifestation of tinea capitis characterized by an inflammatory plaque, often with pain or tenderness. Kerions most frequently occur in children aged 5 to 10 years.5 Failure to treat a kerion may result in scarring alopecia. Treatment consists of oral antifungals.
Dissecting cellulitis of the scalp is thought to occur secondary to follicular occlusion. It is characterized by boggy suppurative nodules primarily on the posterior and vertex scalp. Patchy hair loss is present and typically progresses to cicatricial alopecia. Histology characteristically shows areas of dense, predominantly neutrophilic, perifollicular dermal infiltrates.6
Folliculitis decalvans is a primary neutrophilic cicatricial alopecia that primarily occurs in adults. Patients with folliculitis decalvans tend to have multiple pustules on the periphery of confluent areas of scarring alopecia. It is theorized that an immune response to staphylococcal superantigens contributes to this disease process.7
The clinical findings of acne keloidalis nuchae include inflammatory pustules and papules with keloidlike plaques on the posterior neck and scalp. It occurs predominantly in teenaged and adult males of African ancestry.8 Treatment is aimed at reducing inflammation and preventing exacerbating factors. Severe disease courses may lead to scarring alopecia.
- Sanmartín O, Alegre V, Martinez-Aparicio A, et al. Congenital platelike osteoma cutis: case report and review of the literature. Pediatr Dermatol. 1993;10:182-186.
- Talsania N, Jolliffe V, O’Toole EA, et al. Platelike osteoma cutis. J Am Acad Dermatol. 2009;64:613-615.
- Yeh GL, Mathur S, Wivel A, et al. GNAS1 mutation and Cbfa1 misexpression in a child with severe congenital platelike osteoma cutis. J Bone Miner Res. 2000;15:2063-2073.
- Hernandez-Martin A, Perez-Mies B, Torrelo A. Congenital plate-like osteoma cutis in an infant. Pediatr Dermatol. 2009;26:479-481.
- Zaraa I, Hawilo A, Aounallah A, et al. Inflammatory tinea capitis: a 12-year study and a review of the literature. Mycoses. 2013;56:110-116.
- Scheinfeld N. Dissecting cellulitis (perifolliculitis capitis abscedens et suffodiens): a comprehensive review focusing on new treatments and findings of the last decade with commentary comparing the therapies and causes of dissecting cellulitis to hidradenitis suppurativa. Dermatol Online J. 2014;20:22692.
- Ross EK, Tan E, Shapiro J. Update on primary cicatricial alopecias. J Am Acad Dermatol. 2005;53:1-37.
- Knable AL Jr, Hanke CW, Gonin R. Prevalence of acne keloidalis nuchae in football players. J Am Acad Dermatol. 1997;37:570-574.
The Diagnosis: Platelike Osteoma Cutis
Histopathologic examination revealed extensive cutaneous ossification in the dermis and subcutis with dermal fibrosis and minimal surrounding inflammation (Figure 1). There was no evidence of infection or neoplasm. Further evaluation did not demonstrate any additional physical dysmorphia, and there were no imbalances of calcium-phosphate metabolism or abnormalities in parathyroid hormone or thyroid hormone function. A diagnosis of platelike osteoma cutis (PLOC) was favored. Computed tomography of the head showed material at the posterior skull of similar density to the adjacent calvarial skull and centered within the dermis, consistent with osteoma cutis (Figure 2).
Osteoma cutis describes the formation of bone within the skin. It occurs when hydroxyapatite crystals in a proteinaceous matrix are deposited within the skin, ultimately leading to the formation of bone ultrastructure. Ossification of the skin most often occurs secondary to trauma, inflammation, or neoplasm; however, it rarely may be a primary event.1,2
Platelike osteoma cutis is a rare form of primary cutaneous ossification in which bone forms within the skin in a platelike manner. It most frequently affects the scalp but also has been observed on the trunk and extremities.1 A driving metabolic or endocrine abnormality typically is not identified.2
Platelike osteoma cutis can occur as an isolated finding or as a feature of Albright hereditary osteodystrophy (AHO) or progressive osseous heteroplasia (POH). In addition to cutaneous ossification, AHO involves short stature, endocrinopathy, obesity, shortened fourth and fifth metacarpals, and mental retardation. Progressive osseous heteroplasia is characterized by progressive ossification of the skin and deeper tissues such as muscle and fascia, leading to severe movement restriction; it is believed to be a localized nonprogressive variant of POH.3,4 Mutations in the guanine nucleotide binding protein, alpha stimulating activity polypeptide 1 gene, GNAS1, a key regulatory gene involved in AHO and POH, have been found in several cases of PLOC.3 Our patient lacked any dysmorphic features or laboratory abnormalities suggestive of AHO or POH. Moreover, testing of the tissue and blood for the GNAS1 mutation was negative. Treatment of PLOC often is difficult. Our patient underwent a trial of ablative fractional laser resurfacing, which failed to lead to perceivable improvement.
The differential diagnoses include a kerion, dissecting cellulitis of the scalp, folliculitis decalvans, and acne keloidalis nuchae. A kerion is a manifestation of tinea capitis characterized by an inflammatory plaque, often with pain or tenderness. Kerions most frequently occur in children aged 5 to 10 years.5 Failure to treat a kerion may result in scarring alopecia. Treatment consists of oral antifungals.
Dissecting cellulitis of the scalp is thought to occur secondary to follicular occlusion. It is characterized by boggy suppurative nodules primarily on the posterior and vertex scalp. Patchy hair loss is present and typically progresses to cicatricial alopecia. Histology characteristically shows areas of dense, predominantly neutrophilic, perifollicular dermal infiltrates.6
Folliculitis decalvans is a primary neutrophilic cicatricial alopecia that primarily occurs in adults. Patients with folliculitis decalvans tend to have multiple pustules on the periphery of confluent areas of scarring alopecia. It is theorized that an immune response to staphylococcal superantigens contributes to this disease process.7
The clinical findings of acne keloidalis nuchae include inflammatory pustules and papules with keloidlike plaques on the posterior neck and scalp. It occurs predominantly in teenaged and adult males of African ancestry.8 Treatment is aimed at reducing inflammation and preventing exacerbating factors. Severe disease courses may lead to scarring alopecia.
The Diagnosis: Platelike Osteoma Cutis
Histopathologic examination revealed extensive cutaneous ossification in the dermis and subcutis with dermal fibrosis and minimal surrounding inflammation (Figure 1). There was no evidence of infection or neoplasm. Further evaluation did not demonstrate any additional physical dysmorphia, and there were no imbalances of calcium-phosphate metabolism or abnormalities in parathyroid hormone or thyroid hormone function. A diagnosis of platelike osteoma cutis (PLOC) was favored. Computed tomography of the head showed material at the posterior skull of similar density to the adjacent calvarial skull and centered within the dermis, consistent with osteoma cutis (Figure 2).
Osteoma cutis describes the formation of bone within the skin. It occurs when hydroxyapatite crystals in a proteinaceous matrix are deposited within the skin, ultimately leading to the formation of bone ultrastructure. Ossification of the skin most often occurs secondary to trauma, inflammation, or neoplasm; however, it rarely may be a primary event.1,2
Platelike osteoma cutis is a rare form of primary cutaneous ossification in which bone forms within the skin in a platelike manner. It most frequently affects the scalp but also has been observed on the trunk and extremities.1 A driving metabolic or endocrine abnormality typically is not identified.2
Platelike osteoma cutis can occur as an isolated finding or as a feature of Albright hereditary osteodystrophy (AHO) or progressive osseous heteroplasia (POH). In addition to cutaneous ossification, AHO involves short stature, endocrinopathy, obesity, shortened fourth and fifth metacarpals, and mental retardation. Progressive osseous heteroplasia is characterized by progressive ossification of the skin and deeper tissues such as muscle and fascia, leading to severe movement restriction; it is believed to be a localized nonprogressive variant of POH.3,4 Mutations in the guanine nucleotide binding protein, alpha stimulating activity polypeptide 1 gene, GNAS1, a key regulatory gene involved in AHO and POH, have been found in several cases of PLOC.3 Our patient lacked any dysmorphic features or laboratory abnormalities suggestive of AHO or POH. Moreover, testing of the tissue and blood for the GNAS1 mutation was negative. Treatment of PLOC often is difficult. Our patient underwent a trial of ablative fractional laser resurfacing, which failed to lead to perceivable improvement.
The differential diagnoses include a kerion, dissecting cellulitis of the scalp, folliculitis decalvans, and acne keloidalis nuchae. A kerion is a manifestation of tinea capitis characterized by an inflammatory plaque, often with pain or tenderness. Kerions most frequently occur in children aged 5 to 10 years.5 Failure to treat a kerion may result in scarring alopecia. Treatment consists of oral antifungals.
Dissecting cellulitis of the scalp is thought to occur secondary to follicular occlusion. It is characterized by boggy suppurative nodules primarily on the posterior and vertex scalp. Patchy hair loss is present and typically progresses to cicatricial alopecia. Histology characteristically shows areas of dense, predominantly neutrophilic, perifollicular dermal infiltrates.6
Folliculitis decalvans is a primary neutrophilic cicatricial alopecia that primarily occurs in adults. Patients with folliculitis decalvans tend to have multiple pustules on the periphery of confluent areas of scarring alopecia. It is theorized that an immune response to staphylococcal superantigens contributes to this disease process.7
The clinical findings of acne keloidalis nuchae include inflammatory pustules and papules with keloidlike plaques on the posterior neck and scalp. It occurs predominantly in teenaged and adult males of African ancestry.8 Treatment is aimed at reducing inflammation and preventing exacerbating factors. Severe disease courses may lead to scarring alopecia.
- Sanmartín O, Alegre V, Martinez-Aparicio A, et al. Congenital platelike osteoma cutis: case report and review of the literature. Pediatr Dermatol. 1993;10:182-186.
- Talsania N, Jolliffe V, O’Toole EA, et al. Platelike osteoma cutis. J Am Acad Dermatol. 2009;64:613-615.
- Yeh GL, Mathur S, Wivel A, et al. GNAS1 mutation and Cbfa1 misexpression in a child with severe congenital platelike osteoma cutis. J Bone Miner Res. 2000;15:2063-2073.
- Hernandez-Martin A, Perez-Mies B, Torrelo A. Congenital plate-like osteoma cutis in an infant. Pediatr Dermatol. 2009;26:479-481.
- Zaraa I, Hawilo A, Aounallah A, et al. Inflammatory tinea capitis: a 12-year study and a review of the literature. Mycoses. 2013;56:110-116.
- Scheinfeld N. Dissecting cellulitis (perifolliculitis capitis abscedens et suffodiens): a comprehensive review focusing on new treatments and findings of the last decade with commentary comparing the therapies and causes of dissecting cellulitis to hidradenitis suppurativa. Dermatol Online J. 2014;20:22692.
- Ross EK, Tan E, Shapiro J. Update on primary cicatricial alopecias. J Am Acad Dermatol. 2005;53:1-37.
- Knable AL Jr, Hanke CW, Gonin R. Prevalence of acne keloidalis nuchae in football players. J Am Acad Dermatol. 1997;37:570-574.
- Sanmartín O, Alegre V, Martinez-Aparicio A, et al. Congenital platelike osteoma cutis: case report and review of the literature. Pediatr Dermatol. 1993;10:182-186.
- Talsania N, Jolliffe V, O’Toole EA, et al. Platelike osteoma cutis. J Am Acad Dermatol. 2009;64:613-615.
- Yeh GL, Mathur S, Wivel A, et al. GNAS1 mutation and Cbfa1 misexpression in a child with severe congenital platelike osteoma cutis. J Bone Miner Res. 2000;15:2063-2073.
- Hernandez-Martin A, Perez-Mies B, Torrelo A. Congenital plate-like osteoma cutis in an infant. Pediatr Dermatol. 2009;26:479-481.
- Zaraa I, Hawilo A, Aounallah A, et al. Inflammatory tinea capitis: a 12-year study and a review of the literature. Mycoses. 2013;56:110-116.
- Scheinfeld N. Dissecting cellulitis (perifolliculitis capitis abscedens et suffodiens): a comprehensive review focusing on new treatments and findings of the last decade with commentary comparing the therapies and causes of dissecting cellulitis to hidradenitis suppurativa. Dermatol Online J. 2014;20:22692.
- Ross EK, Tan E, Shapiro J. Update on primary cicatricial alopecias. J Am Acad Dermatol. 2005;53:1-37.
- Knable AL Jr, Hanke CW, Gonin R. Prevalence of acne keloidalis nuchae in football players. J Am Acad Dermatol. 1997;37:570-574.

A 35-year-old man presented to the dermatology clinic with a slow-growing plaque on the scalp of 10 years’ duration. The lesion was mildly pruritic and was never associated with any pain or discharge. He denied antecedent trauma or infection. A hard, erythematous, nodular, alopecic plaque with punctate hyperkeratosis on the left posterior temporal and parietal scalp was noted on physical examination. The lesion was slightly tender to palpation.

Memory benefit seen with antihypertensives crossing blood-brain barrier
Over a 3-year period, cognitively normal older adults taking BBB-crossing antihypertensives demonstrated superior verbal memory, compared with similar individuals receiving non–BBB-crossing antihypertensives, reported lead author Jean K. Ho, PhD, of the Institute for Memory Impairments and Neurological Disorders at the University of California, Irvine, and colleagues.
According to the investigators, the findings add color to a known link between hypertension and neurologic degeneration, and may aid the search for new therapeutic targets.
“Hypertension is a well-established risk factor for cognitive decline and dementia, possibly through its effects on both cerebrovascular disease and Alzheimer’s disease,” Dr. Ho and colleagues wrote in Hypertension. “Studies of antihypertensive treatments have reported possible salutary effects on cognition and cerebrovascular disease, as well as Alzheimer’s disease neuropathology.”
In a previous study, individuals younger than 75 years exposed to antihypertensives had an 8% decreased risk of dementia per year of use, while another trial showed that intensive blood pressure–lowering therapy reduced mild cognitive impairment by 19%.
“Despite these encouraging findings ... larger meta-analytic studies have been hampered by the fact that pharmacokinetic properties are typically not considered in existing studies or routine clinical practice,” wrote Dr. Ho and colleagues. “The present study sought to fill this gap [in that it was] a large and longitudinal meta-analytic study of existing data recoded to assess the effects of BBB-crossing potential in renin-angiotensin system [RAS] treatments among hypertensive adults.”
Methods and results
The meta-analysis included randomized clinical trials, prospective cohort studies, and retrospective observational studies. The researchers assessed data on 12,849 individuals from 14 cohorts that received either BBB-crossing or non–BBB-crossing antihypertensives.
The BBB-crossing properties of RAS treatments were identified by a literature review. Of ACE inhibitors, captopril, fosinopril, lisinopril, perindopril, ramipril, and trandolapril were classified as BBB crossing, and benazepril, enalapril, moexipril, and quinapril were classified as non–BBB-crossing. Of ARBs, telmisartan and candesartan were considered BBB-crossing, and olmesartan, eprosartan, irbesartan, and losartan were tagged as non–BBB-crossing.
Cognition was assessed via the following seven domains: executive function, attention, verbal memory learning, language, mental status, recall, and processing speed.
Compared with individuals taking non–BBB-crossing antihypertensives, those taking BBB-crossing agents had significantly superior verbal memory (recall), with a maximum effect size of 0.07 (P = .03).
According to the investigators, this finding was particularly noteworthy, as the BBB-crossing group had relatively higher vascular risk burden and lower mean education level.
“These differences make it all the more remarkable that the BBB-crossing group displayed better memory ability over time despite these cognitive disadvantages,” the investigators wrote.
Still, not all the findings favored BBB-crossing agents. Individuals in the BBB-crossing group had relatively inferior attention ability, with a minimum effect size of –0.17 (P = .02).
The other cognitive measures were not significantly different between groups.
Clinicians may consider findings after accounting for other factors
Principal investigator Daniel A. Nation, PhD, associate professor of psychological science and a faculty member of the Institute for Memory Impairments and Neurological Disorders at the University of California, Irvine, suggested that the small difference in verbal memory between groups could be clinically significant over a longer period of time.
“Although the overall effect size was pretty small, if you look at how long it would take for someone [with dementia] to progress over many years of decline, it would actually end up being a pretty big effect,” Dr. Nation said in an interview. “Small effect sizes could actually end up preventing a lot of cases of dementia,” he added.
The conflicting results in the BBB-crossing group – better verbal memory but worse attention ability – were “surprising,” he noted.
“I sort of didn’t believe it at first,” Dr. Nation said, “because the memory finding is sort of replication – we’d observed the same exact effect on memory in a smaller sample in another study. ... The attention [finding], going another way, was a new thing.”
Dr. Nation suggested that the intergroup differences in attention ability may stem from idiosyncrasies of the tests used to measure that domain, which can be impacted by cardiovascular or brain vascular disease. Or it could be caused by something else entirely, he said, noting that further investigation is needed.
He added that the improvements in verbal memory within the BBB-crossing group could be caused by direct effects on the brain. He pointed out that certain ACE polymorphisms have been linked with Alzheimer’s disease risk, and those same polymorphisms, in animal models, lead to neurodegeneration, with reversal possible through administration of ACE inhibitors.
“It could be that what we’re observing has nothing really to do with blood pressure,” Dr. Nation explained. “This could be a neuronal effect on learning memory systems.”
He went on to suggest that clinicians may consider these findings when selecting antihypertensive agents for their patients, with the caveat that all other prescribing factors have already been taking to account.
“In the event that you’re going to give an ACE inhibitor or an angiotensin receptor blocker anyway, and it ends up being a somewhat arbitrary decision in terms of which specific drug you’re going to give, then perhaps this is a piece of information you would take into account – that one gets in the brain and one doesn’t – in somebody at risk for cognitive decline,” Dr. Nation said.
Exact mechanisms of action unknown
Hélène Girouard, PhD, assistant professor of pharmacology and physiology at the University of Montreal, said in an interview that the findings are “of considerable importance, knowing that brain alterations could begin as much as 30 years before manifestation of dementia.”

Since 2003, Dr. Girouard has been studying the cognitive effects of antihypertensive medications. She noted that previous studies involving rodents “have shown beneficial effects [of BBB-crossing antihypertensive drugs] on cognition independent of their effects on blood pressure.”
The drugs’ exact mechanisms of action, however, remain elusive, according to Dr. Girouard, who offered several possible explanations, including amelioration of BBB disruption, brain inflammation, cerebral blood flow dysregulation, cholinergic dysfunction, and neurologic deficits. “Whether these mechanisms may explain Ho and colleagues’ observations remains to be established,” she added.
Andrea L. Schneider, MD, PhD, assistant professor of neurology at the University of Pennsylvania, Philadelphia, applauded the study, but ultimately suggested that more research is needed to impact clinical decision-making.
“The results of this important and well-done study suggest that further investigation into targeted mechanism-based approaches to selecting hypertension treatment agents, with a specific focus on cognitive outcomes, is warranted,” Dr. Schneider said in an interview. “Before changing clinical practice, further work is necessary to disentangle contributions of medication mechanism, comorbid vascular risk factors, and achieved blood pressure reduction, among others.”
The investigators disclosed support from the National Institutes of Health, the Alzheimer’s Association, the Waksman Foundation of Japan, and others. The interviewees reported no relevant conflicts of interest.
Over a 3-year period, cognitively normal older adults taking BBB-crossing antihypertensives demonstrated superior verbal memory, compared with similar individuals receiving non–BBB-crossing antihypertensives, reported lead author Jean K. Ho, PhD, of the Institute for Memory Impairments and Neurological Disorders at the University of California, Irvine, and colleagues.
According to the investigators, the findings add color to a known link between hypertension and neurologic degeneration, and may aid the search for new therapeutic targets.
“Hypertension is a well-established risk factor for cognitive decline and dementia, possibly through its effects on both cerebrovascular disease and Alzheimer’s disease,” Dr. Ho and colleagues wrote in Hypertension. “Studies of antihypertensive treatments have reported possible salutary effects on cognition and cerebrovascular disease, as well as Alzheimer’s disease neuropathology.”
In a previous study, individuals younger than 75 years exposed to antihypertensives had an 8% decreased risk of dementia per year of use, while another trial showed that intensive blood pressure–lowering therapy reduced mild cognitive impairment by 19%.
“Despite these encouraging findings ... larger meta-analytic studies have been hampered by the fact that pharmacokinetic properties are typically not considered in existing studies or routine clinical practice,” wrote Dr. Ho and colleagues. “The present study sought to fill this gap [in that it was] a large and longitudinal meta-analytic study of existing data recoded to assess the effects of BBB-crossing potential in renin-angiotensin system [RAS] treatments among hypertensive adults.”
Methods and results
The meta-analysis included randomized clinical trials, prospective cohort studies, and retrospective observational studies. The researchers assessed data on 12,849 individuals from 14 cohorts that received either BBB-crossing or non–BBB-crossing antihypertensives.
The BBB-crossing properties of RAS treatments were identified by a literature review. Of ACE inhibitors, captopril, fosinopril, lisinopril, perindopril, ramipril, and trandolapril were classified as BBB crossing, and benazepril, enalapril, moexipril, and quinapril were classified as non–BBB-crossing. Of ARBs, telmisartan and candesartan were considered BBB-crossing, and olmesartan, eprosartan, irbesartan, and losartan were tagged as non–BBB-crossing.
Cognition was assessed via the following seven domains: executive function, attention, verbal memory learning, language, mental status, recall, and processing speed.
Compared with individuals taking non–BBB-crossing antihypertensives, those taking BBB-crossing agents had significantly superior verbal memory (recall), with a maximum effect size of 0.07 (P = .03).
According to the investigators, this finding was particularly noteworthy, as the BBB-crossing group had relatively higher vascular risk burden and lower mean education level.
“These differences make it all the more remarkable that the BBB-crossing group displayed better memory ability over time despite these cognitive disadvantages,” the investigators wrote.
Still, not all the findings favored BBB-crossing agents. Individuals in the BBB-crossing group had relatively inferior attention ability, with a minimum effect size of –0.17 (P = .02).
The other cognitive measures were not significantly different between groups.
Clinicians may consider findings after accounting for other factors
Principal investigator Daniel A. Nation, PhD, associate professor of psychological science and a faculty member of the Institute for Memory Impairments and Neurological Disorders at the University of California, Irvine, suggested that the small difference in verbal memory between groups could be clinically significant over a longer period of time.
“Although the overall effect size was pretty small, if you look at how long it would take for someone [with dementia] to progress over many years of decline, it would actually end up being a pretty big effect,” Dr. Nation said in an interview. “Small effect sizes could actually end up preventing a lot of cases of dementia,” he added.
The conflicting results in the BBB-crossing group – better verbal memory but worse attention ability – were “surprising,” he noted.
“I sort of didn’t believe it at first,” Dr. Nation said, “because the memory finding is sort of replication – we’d observed the same exact effect on memory in a smaller sample in another study. ... The attention [finding], going another way, was a new thing.”
Dr. Nation suggested that the intergroup differences in attention ability may stem from idiosyncrasies of the tests used to measure that domain, which can be impacted by cardiovascular or brain vascular disease. Or it could be caused by something else entirely, he said, noting that further investigation is needed.
He added that the improvements in verbal memory within the BBB-crossing group could be caused by direct effects on the brain. He pointed out that certain ACE polymorphisms have been linked with Alzheimer’s disease risk, and those same polymorphisms, in animal models, lead to neurodegeneration, with reversal possible through administration of ACE inhibitors.
“It could be that what we’re observing has nothing really to do with blood pressure,” Dr. Nation explained. “This could be a neuronal effect on learning memory systems.”
He went on to suggest that clinicians may consider these findings when selecting antihypertensive agents for their patients, with the caveat that all other prescribing factors have already been taking to account.
“In the event that you’re going to give an ACE inhibitor or an angiotensin receptor blocker anyway, and it ends up being a somewhat arbitrary decision in terms of which specific drug you’re going to give, then perhaps this is a piece of information you would take into account – that one gets in the brain and one doesn’t – in somebody at risk for cognitive decline,” Dr. Nation said.
Exact mechanisms of action unknown
Hélène Girouard, PhD, assistant professor of pharmacology and physiology at the University of Montreal, said in an interview that the findings are “of considerable importance, knowing that brain alterations could begin as much as 30 years before manifestation of dementia.”
Since 2003, Dr. Girouard has been studying the cognitive effects of antihypertensive medications. She noted that previous studies involving rodents “have shown beneficial effects [of BBB-crossing antihypertensive drugs] on cognition independent of their effects on blood pressure.”
The drugs’ exact mechanisms of action, however, remain elusive, according to Dr. Girouard, who offered several possible explanations, including amelioration of BBB disruption, brain inflammation, cerebral blood flow dysregulation, cholinergic dysfunction, and neurologic deficits. “Whether these mechanisms may explain Ho and colleagues’ observations remains to be established,” she added.
Andrea L. Schneider, MD, PhD, assistant professor of neurology at the University of Pennsylvania, Philadelphia, applauded the study, but ultimately suggested that more research is needed to impact clinical decision-making.
“The results of this important and well-done study suggest that further investigation into targeted mechanism-based approaches to selecting hypertension treatment agents, with a specific focus on cognitive outcomes, is warranted,” Dr. Schneider said in an interview. “Before changing clinical practice, further work is necessary to disentangle contributions of medication mechanism, comorbid vascular risk factors, and achieved blood pressure reduction, among others.”
The investigators disclosed support from the National Institutes of Health, the Alzheimer’s Association, the Waksman Foundation of Japan, and others. The interviewees reported no relevant conflicts of interest.
Over a 3-year period, cognitively normal older adults taking BBB-crossing antihypertensives demonstrated superior verbal memory, compared with similar individuals receiving non–BBB-crossing antihypertensives, reported lead author Jean K. Ho, PhD, of the Institute for Memory Impairments and Neurological Disorders at the University of California, Irvine, and colleagues.
According to the investigators, the findings add color to a known link between hypertension and neurologic degeneration, and may aid the search for new therapeutic targets.
“Hypertension is a well-established risk factor for cognitive decline and dementia, possibly through its effects on both cerebrovascular disease and Alzheimer’s disease,” Dr. Ho and colleagues wrote in Hypertension. “Studies of antihypertensive treatments have reported possible salutary effects on cognition and cerebrovascular disease, as well as Alzheimer’s disease neuropathology.”
In a previous study, individuals younger than 75 years exposed to antihypertensives had an 8% decreased risk of dementia per year of use, while another trial showed that intensive blood pressure–lowering therapy reduced mild cognitive impairment by 19%.
“Despite these encouraging findings ... larger meta-analytic studies have been hampered by the fact that pharmacokinetic properties are typically not considered in existing studies or routine clinical practice,” wrote Dr. Ho and colleagues. “The present study sought to fill this gap [in that it was] a large and longitudinal meta-analytic study of existing data recoded to assess the effects of BBB-crossing potential in renin-angiotensin system [RAS] treatments among hypertensive adults.”
Methods and results
The meta-analysis included randomized clinical trials, prospective cohort studies, and retrospective observational studies. The researchers assessed data on 12,849 individuals from 14 cohorts that received either BBB-crossing or non–BBB-crossing antihypertensives.
The BBB-crossing properties of RAS treatments were identified by a literature review. Of ACE inhibitors, captopril, fosinopril, lisinopril, perindopril, ramipril, and trandolapril were classified as BBB crossing, and benazepril, enalapril, moexipril, and quinapril were classified as non–BBB-crossing. Of ARBs, telmisartan and candesartan were considered BBB-crossing, and olmesartan, eprosartan, irbesartan, and losartan were tagged as non–BBB-crossing.
Cognition was assessed via the following seven domains: executive function, attention, verbal memory learning, language, mental status, recall, and processing speed.
Compared with individuals taking non–BBB-crossing antihypertensives, those taking BBB-crossing agents had significantly superior verbal memory (recall), with a maximum effect size of 0.07 (P = .03).
According to the investigators, this finding was particularly noteworthy, as the BBB-crossing group had relatively higher vascular risk burden and lower mean education level.
“These differences make it all the more remarkable that the BBB-crossing group displayed better memory ability over time despite these cognitive disadvantages,” the investigators wrote.
Still, not all the findings favored BBB-crossing agents. Individuals in the BBB-crossing group had relatively inferior attention ability, with a minimum effect size of –0.17 (P = .02).
The other cognitive measures were not significantly different between groups.
Clinicians may consider findings after accounting for other factors
Principal investigator Daniel A. Nation, PhD, associate professor of psychological science and a faculty member of the Institute for Memory Impairments and Neurological Disorders at the University of California, Irvine, suggested that the small difference in verbal memory between groups could be clinically significant over a longer period of time.
“Although the overall effect size was pretty small, if you look at how long it would take for someone [with dementia] to progress over many years of decline, it would actually end up being a pretty big effect,” Dr. Nation said in an interview. “Small effect sizes could actually end up preventing a lot of cases of dementia,” he added.
The conflicting results in the BBB-crossing group – better verbal memory but worse attention ability – were “surprising,” he noted.
“I sort of didn’t believe it at first,” Dr. Nation said, “because the memory finding is sort of replication – we’d observed the same exact effect on memory in a smaller sample in another study. ... The attention [finding], going another way, was a new thing.”
Dr. Nation suggested that the intergroup differences in attention ability may stem from idiosyncrasies of the tests used to measure that domain, which can be impacted by cardiovascular or brain vascular disease. Or it could be caused by something else entirely, he said, noting that further investigation is needed.
He added that the improvements in verbal memory within the BBB-crossing group could be caused by direct effects on the brain. He pointed out that certain ACE polymorphisms have been linked with Alzheimer’s disease risk, and those same polymorphisms, in animal models, lead to neurodegeneration, with reversal possible through administration of ACE inhibitors.
“It could be that what we’re observing has nothing really to do with blood pressure,” Dr. Nation explained. “This could be a neuronal effect on learning memory systems.”
He went on to suggest that clinicians may consider these findings when selecting antihypertensive agents for their patients, with the caveat that all other prescribing factors have already been taking to account.
“In the event that you’re going to give an ACE inhibitor or an angiotensin receptor blocker anyway, and it ends up being a somewhat arbitrary decision in terms of which specific drug you’re going to give, then perhaps this is a piece of information you would take into account – that one gets in the brain and one doesn’t – in somebody at risk for cognitive decline,” Dr. Nation said.
Exact mechanisms of action unknown
Hélène Girouard, PhD, assistant professor of pharmacology and physiology at the University of Montreal, said in an interview that the findings are “of considerable importance, knowing that brain alterations could begin as much as 30 years before manifestation of dementia.”
Since 2003, Dr. Girouard has been studying the cognitive effects of antihypertensive medications. She noted that previous studies involving rodents “have shown beneficial effects [of BBB-crossing antihypertensive drugs] on cognition independent of their effects on blood pressure.”
The drugs’ exact mechanisms of action, however, remain elusive, according to Dr. Girouard, who offered several possible explanations, including amelioration of BBB disruption, brain inflammation, cerebral blood flow dysregulation, cholinergic dysfunction, and neurologic deficits. “Whether these mechanisms may explain Ho and colleagues’ observations remains to be established,” she added.
Andrea L. Schneider, MD, PhD, assistant professor of neurology at the University of Pennsylvania, Philadelphia, applauded the study, but ultimately suggested that more research is needed to impact clinical decision-making.
“The results of this important and well-done study suggest that further investigation into targeted mechanism-based approaches to selecting hypertension treatment agents, with a specific focus on cognitive outcomes, is warranted,” Dr. Schneider said in an interview. “Before changing clinical practice, further work is necessary to disentangle contributions of medication mechanism, comorbid vascular risk factors, and achieved blood pressure reduction, among others.”
The investigators disclosed support from the National Institutes of Health, the Alzheimer’s Association, the Waksman Foundation of Japan, and others. The interviewees reported no relevant conflicts of interest.
FROM HYPERTENSION
