User login
For MD-IQ use only
Infectious disease pop quiz: Clinical challenge #8 for the ObGyn
For uncomplicated gonorrhea in a pregnant woman, what is the most appropriate treatment?
Continue to the answer...
The current recommendation from the Centers for Disease Control and Prevention for treatment of uncomplicated gonorrhea is a single 500-mg intramuscular dose of ceftriaxone. For the patient who is opposed to an intramuscular injection, an alternative treatment is cefixime 800 mg orally. With either of these regimens, if chlamydia infection cannot be excluded, the pregnant patient also should receive azithromycin 1,000 mg orally in a single dose. In a nonpregnant patient, doxycycline 100 mg orally twice daily for 7 days should be used to cover for concurrent chlamydia infection.
In a patient with an allergy to β-lactam antibiotics, an alternative regimen for treatment of uncomplicated gonorrhea is intramuscular gentamicin 240 mg plus a single 2,000-mg dose of oral azithromycin. (St Cyr S, Barbee L, Workowski KA, et al. Update to CDC’s treatment guidelines for gonococcal infection, 2020. MMWR Morbid Mortal Wkly Rep. 2020;69:1911-1916.)
- Duff P. Maternal and perinatal infections: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al. Gabbe’s Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021:1124-1146.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TJ, et al. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862-919.

Dr. Edwards is a Resident in the Department of Medicine, University of Florida College of Medicine, Gainesville.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The authors report no financial relationships relevant to this article.
Dr. Edwards is a Resident in the Department of Medicine, University of Florida College of Medicine, Gainesville.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The authors report no financial relationships relevant to this article.
Dr. Edwards is a Resident in the Department of Medicine, University of Florida College of Medicine, Gainesville.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The authors report no financial relationships relevant to this article.
For uncomplicated gonorrhea in a pregnant woman, what is the most appropriate treatment?
Continue to the answer...
The current recommendation from the Centers for Disease Control and Prevention for treatment of uncomplicated gonorrhea is a single 500-mg intramuscular dose of ceftriaxone. For the patient who is opposed to an intramuscular injection, an alternative treatment is cefixime 800 mg orally. With either of these regimens, if chlamydia infection cannot be excluded, the pregnant patient also should receive azithromycin 1,000 mg orally in a single dose. In a nonpregnant patient, doxycycline 100 mg orally twice daily for 7 days should be used to cover for concurrent chlamydia infection.
In a patient with an allergy to β-lactam antibiotics, an alternative regimen for treatment of uncomplicated gonorrhea is intramuscular gentamicin 240 mg plus a single 2,000-mg dose of oral azithromycin. (St Cyr S, Barbee L, Workowski KA, et al. Update to CDC’s treatment guidelines for gonococcal infection, 2020. MMWR Morbid Mortal Wkly Rep. 2020;69:1911-1916.)
For uncomplicated gonorrhea in a pregnant woman, what is the most appropriate treatment?
Continue to the answer...
The current recommendation from the Centers for Disease Control and Prevention for treatment of uncomplicated gonorrhea is a single 500-mg intramuscular dose of ceftriaxone. For the patient who is opposed to an intramuscular injection, an alternative treatment is cefixime 800 mg orally. With either of these regimens, if chlamydia infection cannot be excluded, the pregnant patient also should receive azithromycin 1,000 mg orally in a single dose. In a nonpregnant patient, doxycycline 100 mg orally twice daily for 7 days should be used to cover for concurrent chlamydia infection.
In a patient with an allergy to β-lactam antibiotics, an alternative regimen for treatment of uncomplicated gonorrhea is intramuscular gentamicin 240 mg plus a single 2,000-mg dose of oral azithromycin. (St Cyr S, Barbee L, Workowski KA, et al. Update to CDC’s treatment guidelines for gonococcal infection, 2020. MMWR Morbid Mortal Wkly Rep. 2020;69:1911-1916.)
- Duff P. Maternal and perinatal infections: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al. Gabbe’s Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021:1124-1146.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TJ, et al. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862-919.
- Duff P. Maternal and perinatal infections: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al. Gabbe’s Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021:1124-1146.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TJ, et al. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862-919.
Severe GI distress: Is clozapine to blame?
CASE GI distress while taking clozapine
Mr. F, age 29, has a history of psychiatric hospitalizations for psychotic episodes. It took a herculean effort to get him to agree to try clozapine, to which he has experienced a modest to good response. Unfortunately, recently he has been experiencing significant upper gastrointestinal (GI) distress. He attributes this to clozapine, and asks if he can discontinue this medication.
HISTORY Nausea becomes severe
Mr. F, age 29, resides in a long-term residential setting for patients with serious mental illness who need additional support following acute hospitalization. He has treatment-refractory schizophrenia. He first developed symptoms at age 18, and experienced multiple psychotic episodes requiring psychiatric hospitalizations that lasted for months. He has had numerous antipsychotic trials and a course of electroconvulsive therapy, with limited benefit.
More recently, Mr. F’s symptoms began to stabilize on a medication regimen that includes clozapine, 350 mg/d at bedtime, and haloperidol, 2 mg/d. He has not required psychiatric hospitalization for the past year.
Within months of initiating clozapine, Mr. F starts to complain daily about symptoms of worsening abdominal pain, abdominal bloating, nausea, intermittent episodes of emesis, and heartburn. The symptoms begin when he wakes up, are worse in the morning, and persist throughout the morning. He has experienced occasional mild constipation, but no diarrhea or weight loss. There have been no major changes in his diet, addition of new medications, or significant use of nonsteroidal anti-inflammatory drugs.
Mr. F’s nausea worsens over the next several weeks, to the point he begins to significantly limit how much he eats to cope with it. His GI symptoms are also impacting his mood and daily functioning.
This is not Mr. F’s first experience with significant GI distress. A few months before his first psychotic episode, Mr. F began developing vision problems, joint and abdominal pain, and a general decline in social and academic functioning. At that time, he underwent a significant workup by both GI and integrative medicine, including stool testing, upper endoscopy, and a Cyrex panel (a complementary medicine approach to exploring for specific autoimmune conditions). Results were largely within expected parameters, though a hydrogen breath test was suggestive of possible small intestine bowel overgrowth. More recently, he has been adhering to a gluten-free diet, which his family felt may help prevent some of his physical symptoms as well as mitigate some of his psychotic symptoms. He now asks if he can stop taking clozapine.
[polldaddy:11008393]
EVALUATION Establishing the correct diagnosis
Initially, Mr. F is diagnosed with gastroesophageal reflux disease (GERD) and attempts to manage his symptoms with pharmacologic and diet-based interventions. He significantly cuts down on soda consumption, and undergoes trials of calcium carbonate, antiemetics, and a PPI. Unfortunately, no material improvements are noted, and he continued to experience significant upper GI distress, especially after meals.
The psychiatric treatment team, Mr. F, and his family seek consultation with a GI specialist, who recommends that Mr. F. undergo a nuclear medicine solid gastric emptying scintigraphy study to evaluate for gastroparesis (delayed gastric emptying).1 Results demonstrate grade 3 gastroparesis, with 56% radiotracer retainment at 4 hours. Mr. F is relieved to finally have an explanation for his persistent GI symptoms, and discusses his treatment options with the GI consultant and psychiatry team.
Continue to: The authors’ observations...
The authors’ observations
Mr. F and his family are opposed to starting a dopamine antagonist such as metoclopramide or domperidone (the latter is not FDA-approved but is available by special application to the FDA). These are first-line treatments for gastroparesis, but Mr. F and his family do not want them because of the risk of tardive dyskinesia. This is consistent with their previously expressed concerns regarding first-generation antipsychotics, and is why Mr. F has only been treated with a very low dose of haloperidol while the clozapine was titrated. Instead, Mr. F, his family, the psychiatry treatment team, and the GI specialist agree to pursue a combination of a GI hypomotility diet—which includes frequent small meals (4 to 6 per day), ideally with low fiber, low fat, and increased fluid intake—and a trial of the second line agent for gastroparesis, erythromycin, a medication with known hepatic cytochrome P450 (CYP) drug-drug interactions that impacts the clearance of clozapine.
Shared decision making is an evidence-based approach to engaging patients in medical decision making. It allows clinicians to provide education on potential treatment options and includes a discussion of risks and benefits. It also includes an assessment of the patient’s understanding of their condition, explores attitudes towards treatment, and elicits patient values specific to the desired outcome. Even in very ill patients with schizophrenia, shared decision making has been demonstrated to increase patient perception of involvement in their own care and knowledge about their condition.2 Using this framework, Mr. F and his family, as well as the GI and psychiatric teams, felt confident that the agreed-upon approach was the best one for Mr. F.
TREATMENT Erythromycin and continued clozapine
Mr. F. is started on erythromycin, 100 mg 3 times a day. Erythromycin is a prokinetic agent that acts as a motilin agonist and increases the rate of gastric emptying. The liquid formulation of the medication is a suspension typically taken in 3- to 4-week courses, with 1 week “off” to prevent tachyphylaxis.3 Compared to the tablet, the liquid suspension has higher bioavailability, allows for easier dose adjustment, and takes less time to reach peak serum concentrations, which make it the preferred formulation for gastroparesis treatment.
Per the GI consultant’s recommendation, Mr. F receives a total of 3 courses of erythromycin, with some improvement in the frequency of his nausea noted only during the third erythromycin course. His clozapine levels are closely monitored during this time, as well as symptoms of clozapine toxicity (ie, sedation, confusion, hypersalivation, seizures, myoclonic jerks), because erythromycin can directly affect clozapine levels.4,5 Case reports suggest that when these 2 medications are taken concomitantly, erythromycin inhibits the metabolism of hepatic enzyme CYP3A4, causing increased plasma concentrations of clozapine. Before starting erythromycin, Mr. F’s clozapine levels were 809 ng/mL at 350 mg/d. During the erythromycin courses, his levels are 1,043 to 1,074 ng/mL, despite reducing clozapine to 300 mg/d. However, he does not experience any adverse effects of clozapine (including seizures), which were being monitored closely.
The authors’ observations
Clozapine is the most effective medication for treatment-refractory schizophrenia.6 Compared to the other second-generation antipsychotics, it is associated with a lower risk of rehospitalization and treatment discontinuation, a significant decrease of positive symptom burden, and a reduction in suicidality.7,8 Unfortunately, clozapine use is not without significant risk. FDA black box warnings highlight severe neutropenia, myocarditis, seizures, and hypotension as potentially life-threatening adverse effects that require close monitoring.9
Recently, clinicians have increasingly focused on the underrecognized but well-established finding that clozapine can cause significant GI adverse effects. While constipation is a known adverse effect of other antipsychotics, a 2016 meta-analysis of 32 studies estimated that the pooled prevalence of clozapine-associated constipation was 31.2%, and showed that patients receiving clozapine were 3 times more likely to be constipated than patients receiving other antipsychotics (odds ratio 3.02, CI 1.91-4.77, P < .001, n = 11 studies).10 A 2012 review of 16 studies involving potentially lethal adverse effects of clozapine demonstrated that rates of agranulocytosis and GI hypomotility were nearly identical, but that mortality from constipation was 3.6 to 12.5 times higher than mortality from agranulocytosis.11
In 2020, the FDA issued an increased warning regarding severe bowel-related complications in patients receiving clozapine, ranging in severity from mild discomfort to ileus, bowel obstruction, toxic megacolon, and death.9
As exemplified by Mr. F’s case, upper GI symptoms associated with clozapine also are distressing and can have a significant impact on quality of life. Dyspepsia is a common complaint in patients with chronic psychiatric illness. A study of 79 psychiatric inpatients hospitalized long-term found that 80% reported at least 1 symptom of dyspepsia.12 There are few older studies describing the effect of clozapine on the upper GI system. We and others previously reported on significantly increased use of—not only antacids—but also H2 blockers and prokinetic agents after initiating clozapine, but sample sizes are small.13-15 These older data and newer studies suggest that GERD is a common upper GI disorder diagnosis following clozapine initiation, perhaps reflecting a knowledge gap and infrequent use of the more complex testing required to confirm a diagnosis of GI motility disorders such as gastroparesis.
In a study of 17 patients receiving clozapine, wireless motility capsules were used to measure whole gut motility, including gastric emptying time, small bowel transit time, and colonic transit time. In 82% of patients, there was demonstrated GI hypomotility in at least 1 region, and 41% of participants exhibited delayed gastric emptying, with a cut-off time of >5 hours required for a gastroparesis diagnosis.16 This is significantly higher than the prevalence of gastroparesis observed in studies of the general community.17 The Table18,19 summarizes the differences between GERD and gastroparesis.

OUTCOME Some improvement
Mr. F experiences limited improvement of some of his nausea symptoms during the third erythromycin cycle and returns to the gastroenterologist for a follow-up appointment. The GI specialist decides to discontinue erythromycin in view of potential drug-drug interactions and Mr. F’s elevated clozapine levels and the associated risks that might entail. Mr. F is again offered the D2 dopamine antagonist metoclopramide, but again refuses due to the risk for tardive dyskinesia. He is asked to continue the GI dysmotility diet. Mr. F finds some relief of nausea symptoms from an over-the-counter product for nausea (a nasal inhalant containing essential oils) and is advised to follow up with the GI specialist in 3 months. Shortly thereafter, he is discharged to live in a less restrictive supportive housing environment, and his follow-up psychiatric care is provided by an assertive community treatment team. Over the next several months, the dosage of clozapine is decreased to 250 mg/d. Mr. F initially experiences worsening psychiatric symptoms, but stabilizes thereafter. He then moves out of state to be closer to his family.
Bottom Line
In patients receiving clozapine, frequent nausea along with clustering of heartburn, abdominal pain, bloating, early satiety, and vomiting (especially after meals) may signal gastroparesis rather than gastroesophageal reflux disease. Such patients may require consultation with a gastroenterologist, a scintigraphy-based gastric emptying test, and treatment if gastroparesis is confirmed.
1. Camilleri M, Chedid V, Ford AC, et al. Gastroparesis. Nat Rev Dis Primers. 2018;4(1):41. doi:10.1038/s41572-018-0038-z
2. Hamann J, Langer B, Winkler V, et al. Shared decision making for in-patients with schizophrenia. Acta Psychiatr Scand. 2006;114(4):265-273. doi: 10.1111/j.1600-0447.2006.00798.x
3. Maganti K, Onyemere K, Jones MP. Oral erythromycin and symptomatic relief of gastroparesis: a systematic review. Am J Gastroenterol. 2003;98(2):259-263. doi:10.1111/j.1572-0241.2003.07167.x
4. Taylor D. Pharmacokinetic interactions involving clozapine. Br J Psychiatry. 1997;171:109-112. doi:10.1192/bjp.171.2.109
5. Edge SC, Markowitz JS, Devane CL. Clozapine drug-drug interactions: a review of the literature. Human Psychopharmacology: Clinical and Experimental. 1997;12(1):5-20.
6. Vanasse A, Blais L, Courteau J, et al. Comparative effectiveness and safety of antipsychotic drugs in schizophrenia treatment: a real-world observational study. Acta Psychiatr Scand. 2016;134(5):374-384. doi:10.1111/acps.12621
7. Siskind D, McCartney L, Goldschlager R, et al. Clozapine v. first- and second-generation antipsychotics in treatment-refractory schizophrenia: systematic review and meta-analysis. Br J Psychiatry. 2016;209(5):385-392. doi:10.1192/bjp.bp.115.177261
8. Azorin JM, Spiegel R, Remington G, et al. A double-blind comparative study of clozapine and risperidone in the management of severe chronic schizophrenia. Am J Psychiatry. 2001;158(8):1305-1313. doi:10.1176/appi.ajp.158.8.1305
9. National Alliance on Mental Illness. Clozapine. Accessed June 13, 2021. https://www.nami.org/About-Mental-Illness/Treatments/Mental-Health-Medications/Types-of-Medication/Clozapine-(Clozaril-and-FazaClo)
10. Shirazi A, Stubbs B, Gomez L, et al. Prevalence and predictors of clozapine-associated constipation: a systematic review and meta-analysis. Int J Mol Sci. 2016;17(6):863. doi:10.3390/ijms17060863
11. Cohen D, Bogers JP, van Dijk D, et al. Beyond white blood cell monitoring: screening in the initial phase of clozapine therapy. J Clin Psychiatry. 2012;73(10):1307-1312. doi:10.4088/JCP.11r06977
12. Mookhoek EJ, Meijs VM, Loonen AJ, et al. Dyspepsia in chronic psychiatric patients. Pharmacopsychiatry. 2005;38(3):125-127. doi:10.1055/s-2005-864123
13. John JP, Chengappa KN, Baker RW, et al. Assessment of changes in both weight and frequency of use of medications for the treatment of gastrointestinal symptoms among clozapine-treated patients. Ann Clin Psychiatry. 1995;7(3):119-125. doi: 10.3109/10401239509149038
14. Schwartz BJ, Frisolone JA. A case report of clozapine-induced gastric outlet obstruction. Am J Psychiatry. 1993;150(10):1563. doi:10.1176/ajp.150.10.1563a
15. Taylor D, Olofinjana O, Rahimi T. Use of antacid medication in patients receiving clozapine: a comparison with other second-generation antipsychotics. J Clin Psychopharmacol. 2010;30(4):460-461. doi:10.1097/JCP.0b013e3181e5c0f7
16. Every-Palmer S, Inns SJ, Grant E, et al. Effects of clozapine on the gut: cross-sectional study of delayed gastric emptying and small and large intestinal dysmotility. CNS Drugs. 2019;33(1):81-91. doi:10.1007/s40263-018-0587-4
17. Jung HK, Choung RS, Locke GR 3rd, et al. The incidence, prevalence, and outcomes of patients with gastroparesis in Olmsted County, Minnesota, from 1996 to 2006. Gastroenterology. 2009;136(4):1225-1233. doi: 10.1053/j.gastro.2008.12.047
18. Antunes C, Aleem A, Curtis SA. Gastroesophageal reflux disease. StatPearls Publishing. Updated July 7, 2021. Accessed December 8, 2021. https://www.ncbi.nlm.nih.gov/books/NBK441938/
19. Reddivari AKR, Mehta P. Gastroparesis. StatPearls Publishing. Updated June 30, 2021. Accessed December 8, 2021. https://www.ncbi.nlm.nih.gov/books/NBK551528/
CASE GI distress while taking clozapine
Mr. F, age 29, has a history of psychiatric hospitalizations for psychotic episodes. It took a herculean effort to get him to agree to try clozapine, to which he has experienced a modest to good response. Unfortunately, recently he has been experiencing significant upper gastrointestinal (GI) distress. He attributes this to clozapine, and asks if he can discontinue this medication.
HISTORY Nausea becomes severe
Mr. F, age 29, resides in a long-term residential setting for patients with serious mental illness who need additional support following acute hospitalization. He has treatment-refractory schizophrenia. He first developed symptoms at age 18, and experienced multiple psychotic episodes requiring psychiatric hospitalizations that lasted for months. He has had numerous antipsychotic trials and a course of electroconvulsive therapy, with limited benefit.
More recently, Mr. F’s symptoms began to stabilize on a medication regimen that includes clozapine, 350 mg/d at bedtime, and haloperidol, 2 mg/d. He has not required psychiatric hospitalization for the past year.
Within months of initiating clozapine, Mr. F starts to complain daily about symptoms of worsening abdominal pain, abdominal bloating, nausea, intermittent episodes of emesis, and heartburn. The symptoms begin when he wakes up, are worse in the morning, and persist throughout the morning. He has experienced occasional mild constipation, but no diarrhea or weight loss. There have been no major changes in his diet, addition of new medications, or significant use of nonsteroidal anti-inflammatory drugs.
Mr. F’s nausea worsens over the next several weeks, to the point he begins to significantly limit how much he eats to cope with it. His GI symptoms are also impacting his mood and daily functioning.
This is not Mr. F’s first experience with significant GI distress. A few months before his first psychotic episode, Mr. F began developing vision problems, joint and abdominal pain, and a general decline in social and academic functioning. At that time, he underwent a significant workup by both GI and integrative medicine, including stool testing, upper endoscopy, and a Cyrex panel (a complementary medicine approach to exploring for specific autoimmune conditions). Results were largely within expected parameters, though a hydrogen breath test was suggestive of possible small intestine bowel overgrowth. More recently, he has been adhering to a gluten-free diet, which his family felt may help prevent some of his physical symptoms as well as mitigate some of his psychotic symptoms. He now asks if he can stop taking clozapine.
[polldaddy:11008393]
EVALUATION Establishing the correct diagnosis
Initially, Mr. F is diagnosed with gastroesophageal reflux disease (GERD) and attempts to manage his symptoms with pharmacologic and diet-based interventions. He significantly cuts down on soda consumption, and undergoes trials of calcium carbonate, antiemetics, and a PPI. Unfortunately, no material improvements are noted, and he continued to experience significant upper GI distress, especially after meals.
The psychiatric treatment team, Mr. F, and his family seek consultation with a GI specialist, who recommends that Mr. F. undergo a nuclear medicine solid gastric emptying scintigraphy study to evaluate for gastroparesis (delayed gastric emptying).1 Results demonstrate grade 3 gastroparesis, with 56% radiotracer retainment at 4 hours. Mr. F is relieved to finally have an explanation for his persistent GI symptoms, and discusses his treatment options with the GI consultant and psychiatry team.
Continue to: The authors’ observations...
The authors’ observations
Mr. F and his family are opposed to starting a dopamine antagonist such as metoclopramide or domperidone (the latter is not FDA-approved but is available by special application to the FDA). These are first-line treatments for gastroparesis, but Mr. F and his family do not want them because of the risk of tardive dyskinesia. This is consistent with their previously expressed concerns regarding first-generation antipsychotics, and is why Mr. F has only been treated with a very low dose of haloperidol while the clozapine was titrated. Instead, Mr. F, his family, the psychiatry treatment team, and the GI specialist agree to pursue a combination of a GI hypomotility diet—which includes frequent small meals (4 to 6 per day), ideally with low fiber, low fat, and increased fluid intake—and a trial of the second line agent for gastroparesis, erythromycin, a medication with known hepatic cytochrome P450 (CYP) drug-drug interactions that impacts the clearance of clozapine.
Shared decision making is an evidence-based approach to engaging patients in medical decision making. It allows clinicians to provide education on potential treatment options and includes a discussion of risks and benefits. It also includes an assessment of the patient’s understanding of their condition, explores attitudes towards treatment, and elicits patient values specific to the desired outcome. Even in very ill patients with schizophrenia, shared decision making has been demonstrated to increase patient perception of involvement in their own care and knowledge about their condition.2 Using this framework, Mr. F and his family, as well as the GI and psychiatric teams, felt confident that the agreed-upon approach was the best one for Mr. F.
TREATMENT Erythromycin and continued clozapine
Mr. F. is started on erythromycin, 100 mg 3 times a day. Erythromycin is a prokinetic agent that acts as a motilin agonist and increases the rate of gastric emptying. The liquid formulation of the medication is a suspension typically taken in 3- to 4-week courses, with 1 week “off” to prevent tachyphylaxis.3 Compared to the tablet, the liquid suspension has higher bioavailability, allows for easier dose adjustment, and takes less time to reach peak serum concentrations, which make it the preferred formulation for gastroparesis treatment.
Per the GI consultant’s recommendation, Mr. F receives a total of 3 courses of erythromycin, with some improvement in the frequency of his nausea noted only during the third erythromycin course. His clozapine levels are closely monitored during this time, as well as symptoms of clozapine toxicity (ie, sedation, confusion, hypersalivation, seizures, myoclonic jerks), because erythromycin can directly affect clozapine levels.4,5 Case reports suggest that when these 2 medications are taken concomitantly, erythromycin inhibits the metabolism of hepatic enzyme CYP3A4, causing increased plasma concentrations of clozapine. Before starting erythromycin, Mr. F’s clozapine levels were 809 ng/mL at 350 mg/d. During the erythromycin courses, his levels are 1,043 to 1,074 ng/mL, despite reducing clozapine to 300 mg/d. However, he does not experience any adverse effects of clozapine (including seizures), which were being monitored closely.
The authors’ observations
Clozapine is the most effective medication for treatment-refractory schizophrenia.6 Compared to the other second-generation antipsychotics, it is associated with a lower risk of rehospitalization and treatment discontinuation, a significant decrease of positive symptom burden, and a reduction in suicidality.7,8 Unfortunately, clozapine use is not without significant risk. FDA black box warnings highlight severe neutropenia, myocarditis, seizures, and hypotension as potentially life-threatening adverse effects that require close monitoring.9
Recently, clinicians have increasingly focused on the underrecognized but well-established finding that clozapine can cause significant GI adverse effects. While constipation is a known adverse effect of other antipsychotics, a 2016 meta-analysis of 32 studies estimated that the pooled prevalence of clozapine-associated constipation was 31.2%, and showed that patients receiving clozapine were 3 times more likely to be constipated than patients receiving other antipsychotics (odds ratio 3.02, CI 1.91-4.77, P < .001, n = 11 studies).10 A 2012 review of 16 studies involving potentially lethal adverse effects of clozapine demonstrated that rates of agranulocytosis and GI hypomotility were nearly identical, but that mortality from constipation was 3.6 to 12.5 times higher than mortality from agranulocytosis.11
In 2020, the FDA issued an increased warning regarding severe bowel-related complications in patients receiving clozapine, ranging in severity from mild discomfort to ileus, bowel obstruction, toxic megacolon, and death.9
As exemplified by Mr. F’s case, upper GI symptoms associated with clozapine also are distressing and can have a significant impact on quality of life. Dyspepsia is a common complaint in patients with chronic psychiatric illness. A study of 79 psychiatric inpatients hospitalized long-term found that 80% reported at least 1 symptom of dyspepsia.12 There are few older studies describing the effect of clozapine on the upper GI system. We and others previously reported on significantly increased use of—not only antacids—but also H2 blockers and prokinetic agents after initiating clozapine, but sample sizes are small.13-15 These older data and newer studies suggest that GERD is a common upper GI disorder diagnosis following clozapine initiation, perhaps reflecting a knowledge gap and infrequent use of the more complex testing required to confirm a diagnosis of GI motility disorders such as gastroparesis.
In a study of 17 patients receiving clozapine, wireless motility capsules were used to measure whole gut motility, including gastric emptying time, small bowel transit time, and colonic transit time. In 82% of patients, there was demonstrated GI hypomotility in at least 1 region, and 41% of participants exhibited delayed gastric emptying, with a cut-off time of >5 hours required for a gastroparesis diagnosis.16 This is significantly higher than the prevalence of gastroparesis observed in studies of the general community.17 The Table18,19 summarizes the differences between GERD and gastroparesis.
OUTCOME Some improvement
Mr. F experiences limited improvement of some of his nausea symptoms during the third erythromycin cycle and returns to the gastroenterologist for a follow-up appointment. The GI specialist decides to discontinue erythromycin in view of potential drug-drug interactions and Mr. F’s elevated clozapine levels and the associated risks that might entail. Mr. F is again offered the D2 dopamine antagonist metoclopramide, but again refuses due to the risk for tardive dyskinesia. He is asked to continue the GI dysmotility diet. Mr. F finds some relief of nausea symptoms from an over-the-counter product for nausea (a nasal inhalant containing essential oils) and is advised to follow up with the GI specialist in 3 months. Shortly thereafter, he is discharged to live in a less restrictive supportive housing environment, and his follow-up psychiatric care is provided by an assertive community treatment team. Over the next several months, the dosage of clozapine is decreased to 250 mg/d. Mr. F initially experiences worsening psychiatric symptoms, but stabilizes thereafter. He then moves out of state to be closer to his family.
Bottom Line
In patients receiving clozapine, frequent nausea along with clustering of heartburn, abdominal pain, bloating, early satiety, and vomiting (especially after meals) may signal gastroparesis rather than gastroesophageal reflux disease. Such patients may require consultation with a gastroenterologist, a scintigraphy-based gastric emptying test, and treatment if gastroparesis is confirmed.
CASE GI distress while taking clozapine
Mr. F, age 29, has a history of psychiatric hospitalizations for psychotic episodes. It took a herculean effort to get him to agree to try clozapine, to which he has experienced a modest to good response. Unfortunately, recently he has been experiencing significant upper gastrointestinal (GI) distress. He attributes this to clozapine, and asks if he can discontinue this medication.
HISTORY Nausea becomes severe
Mr. F, age 29, resides in a long-term residential setting for patients with serious mental illness who need additional support following acute hospitalization. He has treatment-refractory schizophrenia. He first developed symptoms at age 18, and experienced multiple psychotic episodes requiring psychiatric hospitalizations that lasted for months. He has had numerous antipsychotic trials and a course of electroconvulsive therapy, with limited benefit.
More recently, Mr. F’s symptoms began to stabilize on a medication regimen that includes clozapine, 350 mg/d at bedtime, and haloperidol, 2 mg/d. He has not required psychiatric hospitalization for the past year.
Within months of initiating clozapine, Mr. F starts to complain daily about symptoms of worsening abdominal pain, abdominal bloating, nausea, intermittent episodes of emesis, and heartburn. The symptoms begin when he wakes up, are worse in the morning, and persist throughout the morning. He has experienced occasional mild constipation, but no diarrhea or weight loss. There have been no major changes in his diet, addition of new medications, or significant use of nonsteroidal anti-inflammatory drugs.
Mr. F’s nausea worsens over the next several weeks, to the point he begins to significantly limit how much he eats to cope with it. His GI symptoms are also impacting his mood and daily functioning.
This is not Mr. F’s first experience with significant GI distress. A few months before his first psychotic episode, Mr. F began developing vision problems, joint and abdominal pain, and a general decline in social and academic functioning. At that time, he underwent a significant workup by both GI and integrative medicine, including stool testing, upper endoscopy, and a Cyrex panel (a complementary medicine approach to exploring for specific autoimmune conditions). Results were largely within expected parameters, though a hydrogen breath test was suggestive of possible small intestine bowel overgrowth. More recently, he has been adhering to a gluten-free diet, which his family felt may help prevent some of his physical symptoms as well as mitigate some of his psychotic symptoms. He now asks if he can stop taking clozapine.
[polldaddy:11008393]
EVALUATION Establishing the correct diagnosis
Initially, Mr. F is diagnosed with gastroesophageal reflux disease (GERD) and attempts to manage his symptoms with pharmacologic and diet-based interventions. He significantly cuts down on soda consumption, and undergoes trials of calcium carbonate, antiemetics, and a PPI. Unfortunately, no material improvements are noted, and he continued to experience significant upper GI distress, especially after meals.
The psychiatric treatment team, Mr. F, and his family seek consultation with a GI specialist, who recommends that Mr. F. undergo a nuclear medicine solid gastric emptying scintigraphy study to evaluate for gastroparesis (delayed gastric emptying).1 Results demonstrate grade 3 gastroparesis, with 56% radiotracer retainment at 4 hours. Mr. F is relieved to finally have an explanation for his persistent GI symptoms, and discusses his treatment options with the GI consultant and psychiatry team.
Continue to: The authors’ observations...
The authors’ observations
Mr. F and his family are opposed to starting a dopamine antagonist such as metoclopramide or domperidone (the latter is not FDA-approved but is available by special application to the FDA). These are first-line treatments for gastroparesis, but Mr. F and his family do not want them because of the risk of tardive dyskinesia. This is consistent with their previously expressed concerns regarding first-generation antipsychotics, and is why Mr. F has only been treated with a very low dose of haloperidol while the clozapine was titrated. Instead, Mr. F, his family, the psychiatry treatment team, and the GI specialist agree to pursue a combination of a GI hypomotility diet—which includes frequent small meals (4 to 6 per day), ideally with low fiber, low fat, and increased fluid intake—and a trial of the second line agent for gastroparesis, erythromycin, a medication with known hepatic cytochrome P450 (CYP) drug-drug interactions that impacts the clearance of clozapine.
Shared decision making is an evidence-based approach to engaging patients in medical decision making. It allows clinicians to provide education on potential treatment options and includes a discussion of risks and benefits. It also includes an assessment of the patient’s understanding of their condition, explores attitudes towards treatment, and elicits patient values specific to the desired outcome. Even in very ill patients with schizophrenia, shared decision making has been demonstrated to increase patient perception of involvement in their own care and knowledge about their condition.2 Using this framework, Mr. F and his family, as well as the GI and psychiatric teams, felt confident that the agreed-upon approach was the best one for Mr. F.
TREATMENT Erythromycin and continued clozapine
Mr. F. is started on erythromycin, 100 mg 3 times a day. Erythromycin is a prokinetic agent that acts as a motilin agonist and increases the rate of gastric emptying. The liquid formulation of the medication is a suspension typically taken in 3- to 4-week courses, with 1 week “off” to prevent tachyphylaxis.3 Compared to the tablet, the liquid suspension has higher bioavailability, allows for easier dose adjustment, and takes less time to reach peak serum concentrations, which make it the preferred formulation for gastroparesis treatment.
Per the GI consultant’s recommendation, Mr. F receives a total of 3 courses of erythromycin, with some improvement in the frequency of his nausea noted only during the third erythromycin course. His clozapine levels are closely monitored during this time, as well as symptoms of clozapine toxicity (ie, sedation, confusion, hypersalivation, seizures, myoclonic jerks), because erythromycin can directly affect clozapine levels.4,5 Case reports suggest that when these 2 medications are taken concomitantly, erythromycin inhibits the metabolism of hepatic enzyme CYP3A4, causing increased plasma concentrations of clozapine. Before starting erythromycin, Mr. F’s clozapine levels were 809 ng/mL at 350 mg/d. During the erythromycin courses, his levels are 1,043 to 1,074 ng/mL, despite reducing clozapine to 300 mg/d. However, he does not experience any adverse effects of clozapine (including seizures), which were being monitored closely.
The authors’ observations
Clozapine is the most effective medication for treatment-refractory schizophrenia.6 Compared to the other second-generation antipsychotics, it is associated with a lower risk of rehospitalization and treatment discontinuation, a significant decrease of positive symptom burden, and a reduction in suicidality.7,8 Unfortunately, clozapine use is not without significant risk. FDA black box warnings highlight severe neutropenia, myocarditis, seizures, and hypotension as potentially life-threatening adverse effects that require close monitoring.9
Recently, clinicians have increasingly focused on the underrecognized but well-established finding that clozapine can cause significant GI adverse effects. While constipation is a known adverse effect of other antipsychotics, a 2016 meta-analysis of 32 studies estimated that the pooled prevalence of clozapine-associated constipation was 31.2%, and showed that patients receiving clozapine were 3 times more likely to be constipated than patients receiving other antipsychotics (odds ratio 3.02, CI 1.91-4.77, P < .001, n = 11 studies).10 A 2012 review of 16 studies involving potentially lethal adverse effects of clozapine demonstrated that rates of agranulocytosis and GI hypomotility were nearly identical, but that mortality from constipation was 3.6 to 12.5 times higher than mortality from agranulocytosis.11
In 2020, the FDA issued an increased warning regarding severe bowel-related complications in patients receiving clozapine, ranging in severity from mild discomfort to ileus, bowel obstruction, toxic megacolon, and death.9
As exemplified by Mr. F’s case, upper GI symptoms associated with clozapine also are distressing and can have a significant impact on quality of life. Dyspepsia is a common complaint in patients with chronic psychiatric illness. A study of 79 psychiatric inpatients hospitalized long-term found that 80% reported at least 1 symptom of dyspepsia.12 There are few older studies describing the effect of clozapine on the upper GI system. We and others previously reported on significantly increased use of—not only antacids—but also H2 blockers and prokinetic agents after initiating clozapine, but sample sizes are small.13-15 These older data and newer studies suggest that GERD is a common upper GI disorder diagnosis following clozapine initiation, perhaps reflecting a knowledge gap and infrequent use of the more complex testing required to confirm a diagnosis of GI motility disorders such as gastroparesis.
In a study of 17 patients receiving clozapine, wireless motility capsules were used to measure whole gut motility, including gastric emptying time, small bowel transit time, and colonic transit time. In 82% of patients, there was demonstrated GI hypomotility in at least 1 region, and 41% of participants exhibited delayed gastric emptying, with a cut-off time of >5 hours required for a gastroparesis diagnosis.16 This is significantly higher than the prevalence of gastroparesis observed in studies of the general community.17 The Table18,19 summarizes the differences between GERD and gastroparesis.
OUTCOME Some improvement
Mr. F experiences limited improvement of some of his nausea symptoms during the third erythromycin cycle and returns to the gastroenterologist for a follow-up appointment. The GI specialist decides to discontinue erythromycin in view of potential drug-drug interactions and Mr. F’s elevated clozapine levels and the associated risks that might entail. Mr. F is again offered the D2 dopamine antagonist metoclopramide, but again refuses due to the risk for tardive dyskinesia. He is asked to continue the GI dysmotility diet. Mr. F finds some relief of nausea symptoms from an over-the-counter product for nausea (a nasal inhalant containing essential oils) and is advised to follow up with the GI specialist in 3 months. Shortly thereafter, he is discharged to live in a less restrictive supportive housing environment, and his follow-up psychiatric care is provided by an assertive community treatment team. Over the next several months, the dosage of clozapine is decreased to 250 mg/d. Mr. F initially experiences worsening psychiatric symptoms, but stabilizes thereafter. He then moves out of state to be closer to his family.
Bottom Line
In patients receiving clozapine, frequent nausea along with clustering of heartburn, abdominal pain, bloating, early satiety, and vomiting (especially after meals) may signal gastroparesis rather than gastroesophageal reflux disease. Such patients may require consultation with a gastroenterologist, a scintigraphy-based gastric emptying test, and treatment if gastroparesis is confirmed.
1. Camilleri M, Chedid V, Ford AC, et al. Gastroparesis. Nat Rev Dis Primers. 2018;4(1):41. doi:10.1038/s41572-018-0038-z
2. Hamann J, Langer B, Winkler V, et al. Shared decision making for in-patients with schizophrenia. Acta Psychiatr Scand. 2006;114(4):265-273. doi: 10.1111/j.1600-0447.2006.00798.x
3. Maganti K, Onyemere K, Jones MP. Oral erythromycin and symptomatic relief of gastroparesis: a systematic review. Am J Gastroenterol. 2003;98(2):259-263. doi:10.1111/j.1572-0241.2003.07167.x
4. Taylor D. Pharmacokinetic interactions involving clozapine. Br J Psychiatry. 1997;171:109-112. doi:10.1192/bjp.171.2.109
5. Edge SC, Markowitz JS, Devane CL. Clozapine drug-drug interactions: a review of the literature. Human Psychopharmacology: Clinical and Experimental. 1997;12(1):5-20.
6. Vanasse A, Blais L, Courteau J, et al. Comparative effectiveness and safety of antipsychotic drugs in schizophrenia treatment: a real-world observational study. Acta Psychiatr Scand. 2016;134(5):374-384. doi:10.1111/acps.12621
7. Siskind D, McCartney L, Goldschlager R, et al. Clozapine v. first- and second-generation antipsychotics in treatment-refractory schizophrenia: systematic review and meta-analysis. Br J Psychiatry. 2016;209(5):385-392. doi:10.1192/bjp.bp.115.177261
8. Azorin JM, Spiegel R, Remington G, et al. A double-blind comparative study of clozapine and risperidone in the management of severe chronic schizophrenia. Am J Psychiatry. 2001;158(8):1305-1313. doi:10.1176/appi.ajp.158.8.1305
9. National Alliance on Mental Illness. Clozapine. Accessed June 13, 2021. https://www.nami.org/About-Mental-Illness/Treatments/Mental-Health-Medications/Types-of-Medication/Clozapine-(Clozaril-and-FazaClo)
10. Shirazi A, Stubbs B, Gomez L, et al. Prevalence and predictors of clozapine-associated constipation: a systematic review and meta-analysis. Int J Mol Sci. 2016;17(6):863. doi:10.3390/ijms17060863
11. Cohen D, Bogers JP, van Dijk D, et al. Beyond white blood cell monitoring: screening in the initial phase of clozapine therapy. J Clin Psychiatry. 2012;73(10):1307-1312. doi:10.4088/JCP.11r06977
12. Mookhoek EJ, Meijs VM, Loonen AJ, et al. Dyspepsia in chronic psychiatric patients. Pharmacopsychiatry. 2005;38(3):125-127. doi:10.1055/s-2005-864123
13. John JP, Chengappa KN, Baker RW, et al. Assessment of changes in both weight and frequency of use of medications for the treatment of gastrointestinal symptoms among clozapine-treated patients. Ann Clin Psychiatry. 1995;7(3):119-125. doi: 10.3109/10401239509149038
14. Schwartz BJ, Frisolone JA. A case report of clozapine-induced gastric outlet obstruction. Am J Psychiatry. 1993;150(10):1563. doi:10.1176/ajp.150.10.1563a
15. Taylor D, Olofinjana O, Rahimi T. Use of antacid medication in patients receiving clozapine: a comparison with other second-generation antipsychotics. J Clin Psychopharmacol. 2010;30(4):460-461. doi:10.1097/JCP.0b013e3181e5c0f7
16. Every-Palmer S, Inns SJ, Grant E, et al. Effects of clozapine on the gut: cross-sectional study of delayed gastric emptying and small and large intestinal dysmotility. CNS Drugs. 2019;33(1):81-91. doi:10.1007/s40263-018-0587-4
17. Jung HK, Choung RS, Locke GR 3rd, et al. The incidence, prevalence, and outcomes of patients with gastroparesis in Olmsted County, Minnesota, from 1996 to 2006. Gastroenterology. 2009;136(4):1225-1233. doi: 10.1053/j.gastro.2008.12.047
18. Antunes C, Aleem A, Curtis SA. Gastroesophageal reflux disease. StatPearls Publishing. Updated July 7, 2021. Accessed December 8, 2021. https://www.ncbi.nlm.nih.gov/books/NBK441938/
19. Reddivari AKR, Mehta P. Gastroparesis. StatPearls Publishing. Updated June 30, 2021. Accessed December 8, 2021. https://www.ncbi.nlm.nih.gov/books/NBK551528/
1. Camilleri M, Chedid V, Ford AC, et al. Gastroparesis. Nat Rev Dis Primers. 2018;4(1):41. doi:10.1038/s41572-018-0038-z
2. Hamann J, Langer B, Winkler V, et al. Shared decision making for in-patients with schizophrenia. Acta Psychiatr Scand. 2006;114(4):265-273. doi: 10.1111/j.1600-0447.2006.00798.x
3. Maganti K, Onyemere K, Jones MP. Oral erythromycin and symptomatic relief of gastroparesis: a systematic review. Am J Gastroenterol. 2003;98(2):259-263. doi:10.1111/j.1572-0241.2003.07167.x
4. Taylor D. Pharmacokinetic interactions involving clozapine. Br J Psychiatry. 1997;171:109-112. doi:10.1192/bjp.171.2.109
5. Edge SC, Markowitz JS, Devane CL. Clozapine drug-drug interactions: a review of the literature. Human Psychopharmacology: Clinical and Experimental. 1997;12(1):5-20.
6. Vanasse A, Blais L, Courteau J, et al. Comparative effectiveness and safety of antipsychotic drugs in schizophrenia treatment: a real-world observational study. Acta Psychiatr Scand. 2016;134(5):374-384. doi:10.1111/acps.12621
7. Siskind D, McCartney L, Goldschlager R, et al. Clozapine v. first- and second-generation antipsychotics in treatment-refractory schizophrenia: systematic review and meta-analysis. Br J Psychiatry. 2016;209(5):385-392. doi:10.1192/bjp.bp.115.177261
8. Azorin JM, Spiegel R, Remington G, et al. A double-blind comparative study of clozapine and risperidone in the management of severe chronic schizophrenia. Am J Psychiatry. 2001;158(8):1305-1313. doi:10.1176/appi.ajp.158.8.1305
9. National Alliance on Mental Illness. Clozapine. Accessed June 13, 2021. https://www.nami.org/About-Mental-Illness/Treatments/Mental-Health-Medications/Types-of-Medication/Clozapine-(Clozaril-and-FazaClo)
10. Shirazi A, Stubbs B, Gomez L, et al. Prevalence and predictors of clozapine-associated constipation: a systematic review and meta-analysis. Int J Mol Sci. 2016;17(6):863. doi:10.3390/ijms17060863
11. Cohen D, Bogers JP, van Dijk D, et al. Beyond white blood cell monitoring: screening in the initial phase of clozapine therapy. J Clin Psychiatry. 2012;73(10):1307-1312. doi:10.4088/JCP.11r06977
12. Mookhoek EJ, Meijs VM, Loonen AJ, et al. Dyspepsia in chronic psychiatric patients. Pharmacopsychiatry. 2005;38(3):125-127. doi:10.1055/s-2005-864123
13. John JP, Chengappa KN, Baker RW, et al. Assessment of changes in both weight and frequency of use of medications for the treatment of gastrointestinal symptoms among clozapine-treated patients. Ann Clin Psychiatry. 1995;7(3):119-125. doi: 10.3109/10401239509149038
14. Schwartz BJ, Frisolone JA. A case report of clozapine-induced gastric outlet obstruction. Am J Psychiatry. 1993;150(10):1563. doi:10.1176/ajp.150.10.1563a
15. Taylor D, Olofinjana O, Rahimi T. Use of antacid medication in patients receiving clozapine: a comparison with other second-generation antipsychotics. J Clin Psychopharmacol. 2010;30(4):460-461. doi:10.1097/JCP.0b013e3181e5c0f7
16. Every-Palmer S, Inns SJ, Grant E, et al. Effects of clozapine on the gut: cross-sectional study of delayed gastric emptying and small and large intestinal dysmotility. CNS Drugs. 2019;33(1):81-91. doi:10.1007/s40263-018-0587-4
17. Jung HK, Choung RS, Locke GR 3rd, et al. The incidence, prevalence, and outcomes of patients with gastroparesis in Olmsted County, Minnesota, from 1996 to 2006. Gastroenterology. 2009;136(4):1225-1233. doi: 10.1053/j.gastro.2008.12.047
18. Antunes C, Aleem A, Curtis SA. Gastroesophageal reflux disease. StatPearls Publishing. Updated July 7, 2021. Accessed December 8, 2021. https://www.ncbi.nlm.nih.gov/books/NBK441938/
19. Reddivari AKR, Mehta P. Gastroparesis. StatPearls Publishing. Updated June 30, 2021. Accessed December 8, 2021. https://www.ncbi.nlm.nih.gov/books/NBK551528/

Most Americans approve of the death penalty. Do you?
As a health care provider, I have always been interested in topics that concern incarcerated citizens, whether the discussion is related to the pursuit of aggressive care or jurisprudence in general. Additionally, I have followed the issue of capital punishment for most of my career, wondering if our democracy would continue this form of punishment for violent crimes.
In the early 2000s, public opinion moved away from capital punishment. The days of executing violent criminals such as Ted Bundy (who was killed in the electric chair in 1989) seemed to be in the rearview mirror. The ability of prison systems to obtain drugs for execution had become arduous, and Americans appeared disinterested in continuing with the process. Slowly, states began opting out of executions. Currently, 27 U.S. states offer the death penalty as an option at prosecution.
Botched executions
So far in 2021, 11 prisoners have been put to death by the federal government as well as five states, using either a one-drug or three-drug intravenous protocol. Of those prisoners, one was female.
The length of time from sentencing to date of execution varied from a low of 9 years to a high of 29 years, according to the Death Penalty Information Center. Of the executions performed this year, one was considered “botched.” The victim convulsed and vomited for several minutes before his ultimate demise. In fact, in the history of using the death penalty, from 1890 to 2010, approximately 3% of total executions (276 prisoners) were botched. They involved failed electric shocks, convulsions, labored breathing, and in one particularly horrific incident, a victim who was shot in the hip and abdomen by a firing squad and took several minutes to die.
One of the more difficult tasks for conducting an execution is intravenous access, with acquisition of an intravenous site proving to be a common issue. Another concern involves intravenous efficacy, or failure of the site to remain patent until death is achieved. That is why a few states that still practice capital punishment have returned to an electric chair option for execution (the method is chosen by the prisoner).
Majority favor capital punishment
But why do most Americans believe we need the death penalty? According to a 2021 poll by the Pew Research Center, 60% of U.S. citizens favor the use of capital punishment for those convicted of murder, including 27% who strongly favor its use. About 4 in 10 oppose the punishment, but only 15% are strongly opposed. The belief of those who favor retaining execution is that use of the death penalty deters violent crime.
Surprisingly, the American South has both the highest murder rate in the country and the highest percentage of executions. This geographic area encompasses 81% of the nation’s executions. A 2012 National Research Council poll determined that studies claiming the death penalty deters violent crime are “fundamentally flawed.” States that have abolished the death penalty do not show an increase in murder rates; in fact, the opposite is true, the organization concluded.
Since 1990, states without death penalty punishment have had consistently lower murder rates than those that retain capital punishment.
Where does that leave us?
Place my attitude in the column labeled “undecided.” I would love to believe capital punishment is a deterrent to violent crime, yet statistics do not prove the hypothesis to be true. We live in one of the more violent times in history, with mass shootings becoming commonplace. Large-scale retail theft has also been on the rise, especially in recent weeks.
The idea of severe punishment for heinous crime appeals to me, yet in 2001 Timothy McVeigh was executed after eating ice cream and gazing at the moon. His treatment before execution and the length of time he served were in opposition to other inmates sentenced to death. This, despite being punished for killing 168 people (including 19 children) in the Oklahoma City bombings.
I know we cannot be complacent. Violent crime needs to be reduced, and Americans need to feel safe. The process for achieving that goal? You tell me.
Nurses in prisons
About 1% of employed nurses (i.e., close to 21,000) in the United States work in prisons. This figure does not include the many LPNs and unlicensed assistive personnel who are also working in the field and may underrepresent actual numbers.
Correctional nurses have their own scope and standards of practice. They demonstrate superb assessment skills and organization.
If you can hire a correctional nurse, or even aspire to be one, do not hesitate. Patients will thank you.
A version of this article first appeared on Medscape.com.
As a health care provider, I have always been interested in topics that concern incarcerated citizens, whether the discussion is related to the pursuit of aggressive care or jurisprudence in general. Additionally, I have followed the issue of capital punishment for most of my career, wondering if our democracy would continue this form of punishment for violent crimes.
In the early 2000s, public opinion moved away from capital punishment. The days of executing violent criminals such as Ted Bundy (who was killed in the electric chair in 1989) seemed to be in the rearview mirror. The ability of prison systems to obtain drugs for execution had become arduous, and Americans appeared disinterested in continuing with the process. Slowly, states began opting out of executions. Currently, 27 U.S. states offer the death penalty as an option at prosecution.
Botched executions
So far in 2021, 11 prisoners have been put to death by the federal government as well as five states, using either a one-drug or three-drug intravenous protocol. Of those prisoners, one was female.
The length of time from sentencing to date of execution varied from a low of 9 years to a high of 29 years, according to the Death Penalty Information Center. Of the executions performed this year, one was considered “botched.” The victim convulsed and vomited for several minutes before his ultimate demise. In fact, in the history of using the death penalty, from 1890 to 2010, approximately 3% of total executions (276 prisoners) were botched. They involved failed electric shocks, convulsions, labored breathing, and in one particularly horrific incident, a victim who was shot in the hip and abdomen by a firing squad and took several minutes to die.
One of the more difficult tasks for conducting an execution is intravenous access, with acquisition of an intravenous site proving to be a common issue. Another concern involves intravenous efficacy, or failure of the site to remain patent until death is achieved. That is why a few states that still practice capital punishment have returned to an electric chair option for execution (the method is chosen by the prisoner).
Majority favor capital punishment
But why do most Americans believe we need the death penalty? According to a 2021 poll by the Pew Research Center, 60% of U.S. citizens favor the use of capital punishment for those convicted of murder, including 27% who strongly favor its use. About 4 in 10 oppose the punishment, but only 15% are strongly opposed. The belief of those who favor retaining execution is that use of the death penalty deters violent crime.
Surprisingly, the American South has both the highest murder rate in the country and the highest percentage of executions. This geographic area encompasses 81% of the nation’s executions. A 2012 National Research Council poll determined that studies claiming the death penalty deters violent crime are “fundamentally flawed.” States that have abolished the death penalty do not show an increase in murder rates; in fact, the opposite is true, the organization concluded.
Since 1990, states without death penalty punishment have had consistently lower murder rates than those that retain capital punishment.
Where does that leave us?
Place my attitude in the column labeled “undecided.” I would love to believe capital punishment is a deterrent to violent crime, yet statistics do not prove the hypothesis to be true. We live in one of the more violent times in history, with mass shootings becoming commonplace. Large-scale retail theft has also been on the rise, especially in recent weeks.
The idea of severe punishment for heinous crime appeals to me, yet in 2001 Timothy McVeigh was executed after eating ice cream and gazing at the moon. His treatment before execution and the length of time he served were in opposition to other inmates sentenced to death. This, despite being punished for killing 168 people (including 19 children) in the Oklahoma City bombings.
I know we cannot be complacent. Violent crime needs to be reduced, and Americans need to feel safe. The process for achieving that goal? You tell me.
Nurses in prisons
About 1% of employed nurses (i.e., close to 21,000) in the United States work in prisons. This figure does not include the many LPNs and unlicensed assistive personnel who are also working in the field and may underrepresent actual numbers.
Correctional nurses have their own scope and standards of practice. They demonstrate superb assessment skills and organization.
If you can hire a correctional nurse, or even aspire to be one, do not hesitate. Patients will thank you.
A version of this article first appeared on Medscape.com.
As a health care provider, I have always been interested in topics that concern incarcerated citizens, whether the discussion is related to the pursuit of aggressive care or jurisprudence in general. Additionally, I have followed the issue of capital punishment for most of my career, wondering if our democracy would continue this form of punishment for violent crimes.
In the early 2000s, public opinion moved away from capital punishment. The days of executing violent criminals such as Ted Bundy (who was killed in the electric chair in 1989) seemed to be in the rearview mirror. The ability of prison systems to obtain drugs for execution had become arduous, and Americans appeared disinterested in continuing with the process. Slowly, states began opting out of executions. Currently, 27 U.S. states offer the death penalty as an option at prosecution.
Botched executions
So far in 2021, 11 prisoners have been put to death by the federal government as well as five states, using either a one-drug or three-drug intravenous protocol. Of those prisoners, one was female.
The length of time from sentencing to date of execution varied from a low of 9 years to a high of 29 years, according to the Death Penalty Information Center. Of the executions performed this year, one was considered “botched.” The victim convulsed and vomited for several minutes before his ultimate demise. In fact, in the history of using the death penalty, from 1890 to 2010, approximately 3% of total executions (276 prisoners) were botched. They involved failed electric shocks, convulsions, labored breathing, and in one particularly horrific incident, a victim who was shot in the hip and abdomen by a firing squad and took several minutes to die.
One of the more difficult tasks for conducting an execution is intravenous access, with acquisition of an intravenous site proving to be a common issue. Another concern involves intravenous efficacy, or failure of the site to remain patent until death is achieved. That is why a few states that still practice capital punishment have returned to an electric chair option for execution (the method is chosen by the prisoner).
Majority favor capital punishment
But why do most Americans believe we need the death penalty? According to a 2021 poll by the Pew Research Center, 60% of U.S. citizens favor the use of capital punishment for those convicted of murder, including 27% who strongly favor its use. About 4 in 10 oppose the punishment, but only 15% are strongly opposed. The belief of those who favor retaining execution is that use of the death penalty deters violent crime.
Surprisingly, the American South has both the highest murder rate in the country and the highest percentage of executions. This geographic area encompasses 81% of the nation’s executions. A 2012 National Research Council poll determined that studies claiming the death penalty deters violent crime are “fundamentally flawed.” States that have abolished the death penalty do not show an increase in murder rates; in fact, the opposite is true, the organization concluded.
Since 1990, states without death penalty punishment have had consistently lower murder rates than those that retain capital punishment.
Where does that leave us?
Place my attitude in the column labeled “undecided.” I would love to believe capital punishment is a deterrent to violent crime, yet statistics do not prove the hypothesis to be true. We live in one of the more violent times in history, with mass shootings becoming commonplace. Large-scale retail theft has also been on the rise, especially in recent weeks.
The idea of severe punishment for heinous crime appeals to me, yet in 2001 Timothy McVeigh was executed after eating ice cream and gazing at the moon. His treatment before execution and the length of time he served were in opposition to other inmates sentenced to death. This, despite being punished for killing 168 people (including 19 children) in the Oklahoma City bombings.
I know we cannot be complacent. Violent crime needs to be reduced, and Americans need to feel safe. The process for achieving that goal? You tell me.
Nurses in prisons
About 1% of employed nurses (i.e., close to 21,000) in the United States work in prisons. This figure does not include the many LPNs and unlicensed assistive personnel who are also working in the field and may underrepresent actual numbers.
Correctional nurses have their own scope and standards of practice. They demonstrate superb assessment skills and organization.
If you can hire a correctional nurse, or even aspire to be one, do not hesitate. Patients will thank you.
A version of this article first appeared on Medscape.com.
Gender-based pay inequity in gastroenterology
In 2017, the number of women students entering medical school surpassed that of men.1 However, the future generation of women doctors is unlikely to be paid the same as their male colleagues for equal work unless something changes in health care. About 34% of gastroenterology fellows are women,2 and there are increasing proportions of women in all academic and community practices, as well as in leadership positions.

Despite this progress, equity in pay between male and female physicians has been unequal in many areas of the country, despite the same level of training.3 Doximity, a social network for physicians, surveyed 65,000 doctors in the United States and found a difference in pay between male and female physicians who worked full time.4 This is an issue that the medical field has been aware of for many years, and articles have been published on this topic in several medical journals.5-11 Doximity found that women physicians are paid less than men, although the extent of the difference varies among regions.

In 2017, per the Doximity report, the field of gastroenterology was one of the top five specialties with the biggest pay gap: Women gastroenterologists earn 19% less (or $86,447) than men gastroenterologists. This study did not differentiate among practice types (academic, private practice, hospital, or multispecialty), but it did break down the data for all physicians into general groups of owner/partner, independent contractor, and employee – it found a gender-based gap in pay among all three of these groups. For owner/partners, the gap was a $114,590 (27.2%) difference.4 According to Doximity survey data from 2018, gastroenterology is no longer in the top five specialties with the largest gender pay gap, indicating the gap is shrinking but still exists.12
A questionnaire sent to gastroenterologists 3, 5, or 10 years after they completed their fellowships (in 1993 or 1995) revealed that after 3 years women earned 23% less per hour than men, and at 5 years, the gap had decreased to 19% less per hour.6-7 The statistical data showed that the mean annual gross income of males was significantly higher at 3 years and 5 years.7 Unfortunately, at 10 years the income gap increased up to 22%.6 The researchers found that female gastroenterologists at academic centers earned 39% less than male gastroenterologists at academic centers, whereas women at nonacademic centers earned 24% less than men, despite similar work hours and call schedules.6-7
Desai and colleauges analyzed health care provider reimbursement data for various medical specialties using the 2014 Medicare Fee-for-Service Provider Utilization and Payment Data Physician and Other Supplier Public Use File, and they found a disparity in reimbursements of female versus male physicians.11 Female physicians received significantly lower Medicare reimbursements in 11 of 13 medical specialties,4 despite adjustments for productivity, work hours, and years of experience. Factors that might affect Medicare reimbursement include variations in payment among different locations, types of service provided, location of procedures performed (hospital vs. clinic), and missing data because of privacy concerns.
Among medical specialties, the gender-based payment gap is highest among vascular surgeons, followed by occupational medicine physicians, gastroenterologists, pediatric endocrinologists, and rheumatologists. In these specialties, men earn approximately 20% more than women (approximately $89,000 more for a male vascular surgeon or about $45,000 more for a male pediatric rheumatologist).4
Gender-based gaps in pay, leadership opportunities, and other opportunities exist in the health care field regardless of whether physicians are employed at academic institutions, community-based private practices, or large health care systems. Women physicians occupy fewer leadership positions, and female physician leaders have greater disparities in pay, compared with men than women who are not in leadership positions.6,10 A 2016 survey of the 50 medical schools with the largest amounts of funding from the National Institutes of Health revealed that only 13% of the department leaders were women.
The Fair Pay Act of 2013 and the Paycheck Fairness Act of 2014 aimed to close the salary gap between men and women.13 So why are women paid less than men for the same work? Some researchers have proposed “gender differences in negotiation skills, lack of opportunities to join networks of influence within organizations, and implicit or explicit bias and discrimination.”8,10
The fee for service model based on relative value units can result in lower pay for female physicians, who spend more time with patients, compared with male physicians, because of fewer billable RVUs per hour and per day.15
What should be done?
The American Medical Women’s Association leadership stated that the key to pay equity is transparency, which has been a struggle. Some states, such as New York, require state contractors, including providers that work with the state health department, to disclose salary information. Because of the persistent gender gap in pay in all medical specialties (even after adjustments for age, experience, faculty rank, and measures of research productivity and clinical revenue), the American Medical Association House of Delegates announced a plan to balance salaries within the AMA, and in medicine overall, by promoting research, action, and advocacy.14 In the American College of Physicians, 37% of the members are women. This organization published a position paper in 2018 on gender disparity in pay, and proposed solutions included reviewing and addressing recruitment and advancement of women and other underrepresented groups.15
The executive director of Indiana University’s National Center of Excellence in Women’s Health in Indianapolis, Theresa Rohr-Kirchgraber, MD, who is a professor of clinical care and pediatrics, said that women physicians should bill and code in ways that better reflect the services they provide. Women should also demand more transparency in salaries and push to remove patient satisfaction scores from being a factor in salary determination.16
It is also important to note that there are medical groups and hospitals at which disparities in gender pay might not be an issue, because of physician compensation models. These include but are not limited to Kaiser Permanente and large private practice groups (such as MNGI Digestive Health). For example, with MNGI Digestive Health, shareholder track, ambulatory surgical center distributions are based on full-time equivalent status and not on production. Shareholder compensation is transparent and communicated to all. For Kaiser Permanente, salary is based on specialty and years of service. We will have the opportunity to evaluate the effects of different compensation models as health care delivery moves toward value-based care.
There is a limitation in data presented, as we were unable to obtain specialty salary data from the Association of American Medical Colleges or Medical Group Management Association to confirm findings from the Doximity survey, etc.
Conclusions
It is important to acknowledge that we have made great strides in ensuring gender diversity in the field of gastroenterology. All professional medical and gastroenterological societies are working to address gender disparities in compensation and leadership opportunities. Medical schools and fellowship programs have incorporated training on negotiation skills into their curriculums. The medical profession and overall society will benefit from providing thriving workplaces to female physicians, allowing them to achieve their full potential by ensuring gender equity in compensation and opportunities.
Dr. Perera is a gastroenterologist at Advocate Aurora Health, Grafton, Wisc. Dr. Toriz is a gastroenterologist, treasurer, and board member, MNGI Digestive Health, Bloomington, Minn. They disclosed having no relevant conflicts of interest.
References
1. The American Association of Medical Colleges. “More Women Than Men Enrolled in U.S. Medical schools in 2017.” 2017 Dec 17. http://news.aamc.org/press-releases/article/applicants-enrollment
2. The American Association of Medical Colleges data. https://aamc.org/downlaod/280338/data/tablel3.pdf
3. CBS Business. “The gender pay gap for women doctors is big – and getting worse.” 2018 Mar 14. https://money.CNN.com/2018/03/14/news/economy/gender-pay-gap-doctors/index.html4. Doximity. “Doxmity 2018 Physician Compensation Report.” 2018 Mar 27. https://blog.doximity.com/articles/doximity-2018-physician-compensation-report
5. Tomer G et al. Gastroenterology. 2015;60: 481-5.
6. Singh A et al. Am J Gastroenterol. 2008 Jul;103(7):1589-95.
7. Burke CA et al. Am J Gastroenterol. 2005 Feb;100(2):259-64.
8. Achkar E. Am J Gastroenterol. 2008 Jul;103(7):1587-8.
9. Hoff TJ. Inquiry. 2004;41(3):301-15.
10. Weaver AC et al. J Hosp Med. 2015 Aug;10(8):486-90.
11. Desai T et al. Postgrad Med J. 2016 Oct;92(1092):571-5.
12. Doximity. “Women in Medicine: The Gender Pay Gap” 2018 Oct 2. https://blog.finder.doximity.info/women-in-medicine-the-gender-pay-gap
13. H.R.438. Fair Pay Act of 2013. 113th Congress (2013-2014)
14. O’Reilly KB. American Medical Association. “Physicians adopt plan to combat pay gap in medicine.” 2018 Jun 13. https://www.ama-assn.org/delivering-care/health-equity/physicians-adopt-plan-combat-pay-gap-medicine
15. Butkus R et al. Ann Intern Med. 2018 May 15;168(10):721-3.
16. Commins J. “5 Reasons Women Doctors Earn Less Than Men.” Health Leaders. 2018 Aug 6. https://www.healthleadersmedia.com/clinical-care /5-reasons-women-doctors-earn-less-men
In 2017, the number of women students entering medical school surpassed that of men.1 However, the future generation of women doctors is unlikely to be paid the same as their male colleagues for equal work unless something changes in health care. About 34% of gastroenterology fellows are women,2 and there are increasing proportions of women in all academic and community practices, as well as in leadership positions.
Despite this progress, equity in pay between male and female physicians has been unequal in many areas of the country, despite the same level of training.3 Doximity, a social network for physicians, surveyed 65,000 doctors in the United States and found a difference in pay between male and female physicians who worked full time.4 This is an issue that the medical field has been aware of for many years, and articles have been published on this topic in several medical journals.5-11 Doximity found that women physicians are paid less than men, although the extent of the difference varies among regions.
In 2017, per the Doximity report, the field of gastroenterology was one of the top five specialties with the biggest pay gap: Women gastroenterologists earn 19% less (or $86,447) than men gastroenterologists. This study did not differentiate among practice types (academic, private practice, hospital, or multispecialty), but it did break down the data for all physicians into general groups of owner/partner, independent contractor, and employee – it found a gender-based gap in pay among all three of these groups. For owner/partners, the gap was a $114,590 (27.2%) difference.4 According to Doximity survey data from 2018, gastroenterology is no longer in the top five specialties with the largest gender pay gap, indicating the gap is shrinking but still exists.12
A questionnaire sent to gastroenterologists 3, 5, or 10 years after they completed their fellowships (in 1993 or 1995) revealed that after 3 years women earned 23% less per hour than men, and at 5 years, the gap had decreased to 19% less per hour.6-7 The statistical data showed that the mean annual gross income of males was significantly higher at 3 years and 5 years.7 Unfortunately, at 10 years the income gap increased up to 22%.6 The researchers found that female gastroenterologists at academic centers earned 39% less than male gastroenterologists at academic centers, whereas women at nonacademic centers earned 24% less than men, despite similar work hours and call schedules.6-7
Desai and colleauges analyzed health care provider reimbursement data for various medical specialties using the 2014 Medicare Fee-for-Service Provider Utilization and Payment Data Physician and Other Supplier Public Use File, and they found a disparity in reimbursements of female versus male physicians.11 Female physicians received significantly lower Medicare reimbursements in 11 of 13 medical specialties,4 despite adjustments for productivity, work hours, and years of experience. Factors that might affect Medicare reimbursement include variations in payment among different locations, types of service provided, location of procedures performed (hospital vs. clinic), and missing data because of privacy concerns.
Among medical specialties, the gender-based payment gap is highest among vascular surgeons, followed by occupational medicine physicians, gastroenterologists, pediatric endocrinologists, and rheumatologists. In these specialties, men earn approximately 20% more than women (approximately $89,000 more for a male vascular surgeon or about $45,000 more for a male pediatric rheumatologist).4
Gender-based gaps in pay, leadership opportunities, and other opportunities exist in the health care field regardless of whether physicians are employed at academic institutions, community-based private practices, or large health care systems. Women physicians occupy fewer leadership positions, and female physician leaders have greater disparities in pay, compared with men than women who are not in leadership positions.6,10 A 2016 survey of the 50 medical schools with the largest amounts of funding from the National Institutes of Health revealed that only 13% of the department leaders were women.
The Fair Pay Act of 2013 and the Paycheck Fairness Act of 2014 aimed to close the salary gap between men and women.13 So why are women paid less than men for the same work? Some researchers have proposed “gender differences in negotiation skills, lack of opportunities to join networks of influence within organizations, and implicit or explicit bias and discrimination.”8,10
The fee for service model based on relative value units can result in lower pay for female physicians, who spend more time with patients, compared with male physicians, because of fewer billable RVUs per hour and per day.15
What should be done?
The American Medical Women’s Association leadership stated that the key to pay equity is transparency, which has been a struggle. Some states, such as New York, require state contractors, including providers that work with the state health department, to disclose salary information. Because of the persistent gender gap in pay in all medical specialties (even after adjustments for age, experience, faculty rank, and measures of research productivity and clinical revenue), the American Medical Association House of Delegates announced a plan to balance salaries within the AMA, and in medicine overall, by promoting research, action, and advocacy.14 In the American College of Physicians, 37% of the members are women. This organization published a position paper in 2018 on gender disparity in pay, and proposed solutions included reviewing and addressing recruitment and advancement of women and other underrepresented groups.15
The executive director of Indiana University’s National Center of Excellence in Women’s Health in Indianapolis, Theresa Rohr-Kirchgraber, MD, who is a professor of clinical care and pediatrics, said that women physicians should bill and code in ways that better reflect the services they provide. Women should also demand more transparency in salaries and push to remove patient satisfaction scores from being a factor in salary determination.16
It is also important to note that there are medical groups and hospitals at which disparities in gender pay might not be an issue, because of physician compensation models. These include but are not limited to Kaiser Permanente and large private practice groups (such as MNGI Digestive Health). For example, with MNGI Digestive Health, shareholder track, ambulatory surgical center distributions are based on full-time equivalent status and not on production. Shareholder compensation is transparent and communicated to all. For Kaiser Permanente, salary is based on specialty and years of service. We will have the opportunity to evaluate the effects of different compensation models as health care delivery moves toward value-based care.
There is a limitation in data presented, as we were unable to obtain specialty salary data from the Association of American Medical Colleges or Medical Group Management Association to confirm findings from the Doximity survey, etc.
Conclusions
It is important to acknowledge that we have made great strides in ensuring gender diversity in the field of gastroenterology. All professional medical and gastroenterological societies are working to address gender disparities in compensation and leadership opportunities. Medical schools and fellowship programs have incorporated training on negotiation skills into their curriculums. The medical profession and overall society will benefit from providing thriving workplaces to female physicians, allowing them to achieve their full potential by ensuring gender equity in compensation and opportunities.
Dr. Perera is a gastroenterologist at Advocate Aurora Health, Grafton, Wisc. Dr. Toriz is a gastroenterologist, treasurer, and board member, MNGI Digestive Health, Bloomington, Minn. They disclosed having no relevant conflicts of interest.
References
1. The American Association of Medical Colleges. “More Women Than Men Enrolled in U.S. Medical schools in 2017.” 2017 Dec 17. http://news.aamc.org/press-releases/article/applicants-enrollment
2. The American Association of Medical Colleges data. https://aamc.org/downlaod/280338/data/tablel3.pdf
3. CBS Business. “The gender pay gap for women doctors is big – and getting worse.” 2018 Mar 14. https://money.CNN.com/2018/03/14/news/economy/gender-pay-gap-doctors/index.html4. Doximity. “Doxmity 2018 Physician Compensation Report.” 2018 Mar 27. https://blog.doximity.com/articles/doximity-2018-physician-compensation-report
5. Tomer G et al. Gastroenterology. 2015;60: 481-5.
6. Singh A et al. Am J Gastroenterol. 2008 Jul;103(7):1589-95.
7. Burke CA et al. Am J Gastroenterol. 2005 Feb;100(2):259-64.
8. Achkar E. Am J Gastroenterol. 2008 Jul;103(7):1587-8.
9. Hoff TJ. Inquiry. 2004;41(3):301-15.
10. Weaver AC et al. J Hosp Med. 2015 Aug;10(8):486-90.
11. Desai T et al. Postgrad Med J. 2016 Oct;92(1092):571-5.
12. Doximity. “Women in Medicine: The Gender Pay Gap” 2018 Oct 2. https://blog.finder.doximity.info/women-in-medicine-the-gender-pay-gap
13. H.R.438. Fair Pay Act of 2013. 113th Congress (2013-2014)
14. O’Reilly KB. American Medical Association. “Physicians adopt plan to combat pay gap in medicine.” 2018 Jun 13. https://www.ama-assn.org/delivering-care/health-equity/physicians-adopt-plan-combat-pay-gap-medicine
15. Butkus R et al. Ann Intern Med. 2018 May 15;168(10):721-3.
16. Commins J. “5 Reasons Women Doctors Earn Less Than Men.” Health Leaders. 2018 Aug 6. https://www.healthleadersmedia.com/clinical-care /5-reasons-women-doctors-earn-less-men
In 2017, the number of women students entering medical school surpassed that of men.1 However, the future generation of women doctors is unlikely to be paid the same as their male colleagues for equal work unless something changes in health care. About 34% of gastroenterology fellows are women,2 and there are increasing proportions of women in all academic and community practices, as well as in leadership positions.
Despite this progress, equity in pay between male and female physicians has been unequal in many areas of the country, despite the same level of training.3 Doximity, a social network for physicians, surveyed 65,000 doctors in the United States and found a difference in pay between male and female physicians who worked full time.4 This is an issue that the medical field has been aware of for many years, and articles have been published on this topic in several medical journals.5-11 Doximity found that women physicians are paid less than men, although the extent of the difference varies among regions.
In 2017, per the Doximity report, the field of gastroenterology was one of the top five specialties with the biggest pay gap: Women gastroenterologists earn 19% less (or $86,447) than men gastroenterologists. This study did not differentiate among practice types (academic, private practice, hospital, or multispecialty), but it did break down the data for all physicians into general groups of owner/partner, independent contractor, and employee – it found a gender-based gap in pay among all three of these groups. For owner/partners, the gap was a $114,590 (27.2%) difference.4 According to Doximity survey data from 2018, gastroenterology is no longer in the top five specialties with the largest gender pay gap, indicating the gap is shrinking but still exists.12
A questionnaire sent to gastroenterologists 3, 5, or 10 years after they completed their fellowships (in 1993 or 1995) revealed that after 3 years women earned 23% less per hour than men, and at 5 years, the gap had decreased to 19% less per hour.6-7 The statistical data showed that the mean annual gross income of males was significantly higher at 3 years and 5 years.7 Unfortunately, at 10 years the income gap increased up to 22%.6 The researchers found that female gastroenterologists at academic centers earned 39% less than male gastroenterologists at academic centers, whereas women at nonacademic centers earned 24% less than men, despite similar work hours and call schedules.6-7
Desai and colleauges analyzed health care provider reimbursement data for various medical specialties using the 2014 Medicare Fee-for-Service Provider Utilization and Payment Data Physician and Other Supplier Public Use File, and they found a disparity in reimbursements of female versus male physicians.11 Female physicians received significantly lower Medicare reimbursements in 11 of 13 medical specialties,4 despite adjustments for productivity, work hours, and years of experience. Factors that might affect Medicare reimbursement include variations in payment among different locations, types of service provided, location of procedures performed (hospital vs. clinic), and missing data because of privacy concerns.
Among medical specialties, the gender-based payment gap is highest among vascular surgeons, followed by occupational medicine physicians, gastroenterologists, pediatric endocrinologists, and rheumatologists. In these specialties, men earn approximately 20% more than women (approximately $89,000 more for a male vascular surgeon or about $45,000 more for a male pediatric rheumatologist).4
Gender-based gaps in pay, leadership opportunities, and other opportunities exist in the health care field regardless of whether physicians are employed at academic institutions, community-based private practices, or large health care systems. Women physicians occupy fewer leadership positions, and female physician leaders have greater disparities in pay, compared with men than women who are not in leadership positions.6,10 A 2016 survey of the 50 medical schools with the largest amounts of funding from the National Institutes of Health revealed that only 13% of the department leaders were women.
The Fair Pay Act of 2013 and the Paycheck Fairness Act of 2014 aimed to close the salary gap between men and women.13 So why are women paid less than men for the same work? Some researchers have proposed “gender differences in negotiation skills, lack of opportunities to join networks of influence within organizations, and implicit or explicit bias and discrimination.”8,10
The fee for service model based on relative value units can result in lower pay for female physicians, who spend more time with patients, compared with male physicians, because of fewer billable RVUs per hour and per day.15
What should be done?
The American Medical Women’s Association leadership stated that the key to pay equity is transparency, which has been a struggle. Some states, such as New York, require state contractors, including providers that work with the state health department, to disclose salary information. Because of the persistent gender gap in pay in all medical specialties (even after adjustments for age, experience, faculty rank, and measures of research productivity and clinical revenue), the American Medical Association House of Delegates announced a plan to balance salaries within the AMA, and in medicine overall, by promoting research, action, and advocacy.14 In the American College of Physicians, 37% of the members are women. This organization published a position paper in 2018 on gender disparity in pay, and proposed solutions included reviewing and addressing recruitment and advancement of women and other underrepresented groups.15
The executive director of Indiana University’s National Center of Excellence in Women’s Health in Indianapolis, Theresa Rohr-Kirchgraber, MD, who is a professor of clinical care and pediatrics, said that women physicians should bill and code in ways that better reflect the services they provide. Women should also demand more transparency in salaries and push to remove patient satisfaction scores from being a factor in salary determination.16
It is also important to note that there are medical groups and hospitals at which disparities in gender pay might not be an issue, because of physician compensation models. These include but are not limited to Kaiser Permanente and large private practice groups (such as MNGI Digestive Health). For example, with MNGI Digestive Health, shareholder track, ambulatory surgical center distributions are based on full-time equivalent status and not on production. Shareholder compensation is transparent and communicated to all. For Kaiser Permanente, salary is based on specialty and years of service. We will have the opportunity to evaluate the effects of different compensation models as health care delivery moves toward value-based care.
There is a limitation in data presented, as we were unable to obtain specialty salary data from the Association of American Medical Colleges or Medical Group Management Association to confirm findings from the Doximity survey, etc.
Conclusions
It is important to acknowledge that we have made great strides in ensuring gender diversity in the field of gastroenterology. All professional medical and gastroenterological societies are working to address gender disparities in compensation and leadership opportunities. Medical schools and fellowship programs have incorporated training on negotiation skills into their curriculums. The medical profession and overall society will benefit from providing thriving workplaces to female physicians, allowing them to achieve their full potential by ensuring gender equity in compensation and opportunities.
Dr. Perera is a gastroenterologist at Advocate Aurora Health, Grafton, Wisc. Dr. Toriz is a gastroenterologist, treasurer, and board member, MNGI Digestive Health, Bloomington, Minn. They disclosed having no relevant conflicts of interest.
References
1. The American Association of Medical Colleges. “More Women Than Men Enrolled in U.S. Medical schools in 2017.” 2017 Dec 17. http://news.aamc.org/press-releases/article/applicants-enrollment
2. The American Association of Medical Colleges data. https://aamc.org/downlaod/280338/data/tablel3.pdf
3. CBS Business. “The gender pay gap for women doctors is big – and getting worse.” 2018 Mar 14. https://money.CNN.com/2018/03/14/news/economy/gender-pay-gap-doctors/index.html4. Doximity. “Doxmity 2018 Physician Compensation Report.” 2018 Mar 27. https://blog.doximity.com/articles/doximity-2018-physician-compensation-report
5. Tomer G et al. Gastroenterology. 2015;60: 481-5.
6. Singh A et al. Am J Gastroenterol. 2008 Jul;103(7):1589-95.
7. Burke CA et al. Am J Gastroenterol. 2005 Feb;100(2):259-64.
8. Achkar E. Am J Gastroenterol. 2008 Jul;103(7):1587-8.
9. Hoff TJ. Inquiry. 2004;41(3):301-15.
10. Weaver AC et al. J Hosp Med. 2015 Aug;10(8):486-90.
11. Desai T et al. Postgrad Med J. 2016 Oct;92(1092):571-5.
12. Doximity. “Women in Medicine: The Gender Pay Gap” 2018 Oct 2. https://blog.finder.doximity.info/women-in-medicine-the-gender-pay-gap
13. H.R.438. Fair Pay Act of 2013. 113th Congress (2013-2014)
14. O’Reilly KB. American Medical Association. “Physicians adopt plan to combat pay gap in medicine.” 2018 Jun 13. https://www.ama-assn.org/delivering-care/health-equity/physicians-adopt-plan-combat-pay-gap-medicine
15. Butkus R et al. Ann Intern Med. 2018 May 15;168(10):721-3.
16. Commins J. “5 Reasons Women Doctors Earn Less Than Men.” Health Leaders. 2018 Aug 6. https://www.healthleadersmedia.com/clinical-care /5-reasons-women-doctors-earn-less-men
Your money. Your voice. Your wellness.
I was a third-year gastroenterology fellow when I realized that something had to change. I was on a one-way trip to burnout.

I went through medical school with the sole goal of becoming an excellent physician. Like many physicians, I was six figures deep in student loan debt by the end of training. I remember clearly being told, “You are going to be physicians. Money won’t be a problem.” In fact, in 2021, money remains a taboo topic in medicine, and most of medical education remains void of the fundamentals of money management.
Although I was surrounded by some of the most brilliant minds in medicine, burnout was spreading like a wave. Physicians are becoming increasingly broken, burned out by a system through which we have vowed to care for our patients: For better or for worse. We are required to attend lectures about burnout, yet nothing about money or finances. We can all agree that talking about resilience and burnout during odd hours of the morning are ironic measures that by themselves have done nothing to help us through the crisis that exists.
I noticed that there seemed to be a difference between physicians who had their finances in order and those who didn’t. This eventually made sense as I became more aware of the data that now exists. Healthy financial practices can lead to financial independence, which may in turn decrease burnout-associated stressors.1 This is what we need.
My observation about the difference in satisfaction between physicians led me to decide to explore that path for myself. My hypothesis? Empowering myself financially is an anti-burnout tool that will improve my satisfaction, longevity in medicine, and my well-being. I traded my financial illiteracy for empowerment and I am now on a mission to help physicians become financially empowered. This is an important step toward preventing and recovering from burnout. The surprising part is that it is not difficult. You need to be committed. Our math literacy is already higher than needed. When we physicians are financially independent, we will have the ability to practice medicine in a way that is healthy. In a world where physician suicide, burnout, and dissatisfaction continue to rise, there is an urgent call to financial action. This is a critical key that will help us change the future of medicine.
In this article, I am going to share four myths that are preventing physicians from truly managing their finances.
1. I love medicine. I have no plans of leaving: I love gastroenterology. The ability to use our critical internal medicine skills as well as intervene procedurally is truly a privilege. As a gastroenterologist with a focus on inflammatory bowel diseases, I have the honor of walking patients through seasons of life and making decisions that truly impact their lives. It is an honor. I also believe that good money management allows physicians to become even better physicians. The platforms of medicine continue to change. According to Physician Advocacy Institute, about 70% of physicians report being employed.2 As physicians graduate from training, joining large hospitals, physician autonomy in the practice of medicine is affected. To ensure that we continue to practice medicine at the fullest extent of our oath, it is essential that our finances allow us the ability and capacity to fulfill that oath. Furthermore, the pandemic has shown that physician income is not pandemic-proof. Having a healthy emergency fund and diversifying our income sources is critical as we move forward.
2. I have a financial adviser or planner. They will figure it out for me: Financial advisers and planners are hired professionals with varied levels of training and expertise. A great financial adviser can be an important part of your team. A team that is led by you, the CEO, because no one will care about your finances as much as you do. Investing the time to learn the basics can pay dividends. When I started my financial education journey, I was completely illiterate. I knew I wanted to have money but didn’t know how. One of the first things in my financial competency journey was to hire a financial adviser. Unfortunately, as I learned more about money, I realized that my investments favored him more than they did me. Coincidentally, we had similar starting balances in a different self-management investment account. At the end of our time together, our self-managed funds fared better than his actively picked funds. As humans, we assume that actively picking investments and stocks would be better than passive investments. Based on experience and data, investing in boring, diverse funds such as index funds averagely do better than actively managed funds. Is it wrong then to hire an adviser? No, but you are still the CEO of you-incorporated. Choosing to completely delegate to someone else, avoiding the basic education that would allow you to better screen for effectiveness and competence, may in fact be negligence. After empowering themselves financially, some physicians who have gone through my money curriculum have chosen to keep their advisers; others chose to self-manage. The key is giving yourself the gift of choice: Choosing to have an adviser because you want to rather than because you thought you had no choice.
3. Money management looks complicated. This is one of the most common statements I get for why physicians avoid their own money management. I remember the complex biochemical pathways we learned in medical school. Those were hard and complicated. We chose to stay the course because we believed that, with repetition and simplifying, it would eventually become less difficult. Why then is it any different with money? A physician shared a discussion she once had with a banker. She was told, “Doctors are bad with money.” When did we become the stereotype for being bad with money? If we can learn channelopathies and memorize mechanisms and save lives, we can do money. We have to start somewhere. We may not get it the first time. However, as physicians, we are the more persistent people and are excellent examples of what happens when you commit to learning something new. After coaching hundreds of physicians regarding money management, I have concluded that physicians are not bad with money. We simply may not be committed to learning it. Once we commit, the rest becomes history.
4. I don’t have time. For practicing gastroenterologists dealing with post-lockdown influx of patients, the days can be long. As a gastroenterologist who is also a parent, I know firsthand how time can be tight. When we had two children, we were busy. We thought we were at our capacity on time with two children. Then we had a third. Suddenly, life with two children looked easier than with three. As humans, we have the capacity to create. Things take exactly how much time we commit to them. If I give myself a month to write an article, I will write it in a month. If I give myself 2 weeks, I will be done in 2 weeks. The key is to remember that we all have 24 hours. David Frankel is the author of “The Freedom Formula: How to Succeed in Business Without Sacrificing Your Family, Health, or Life.”3 He analyzed a poll of business owners. He showed that they were wasting an average of 21.8 hours per week. Many times, we talk about our to-do list. We don’t talk enough about our “to don’t list.” This refers to the list of things we need to stop doing so that we can spend time on things that give or add value to our lives. Starting with as little as 30 minutes per day or per week dedicated to learning and/or managing our finances, the result will compound.
As the platform of medicine continues to evolve, it is important for astute gastroenterologists to be part of these conversations. When we are confident in our finances, they become a vehicle that gives strength to the power of our voice. We are less likely to overwork and more likely to find joy and meaning within and outside medicine.
If we want to care for our patients at a high level and keep our oath to do no harm, we have to remember that includes doing no harm to self as well.
Money management tools and empowering ourselves financially should be an essential component of our training; until then, the onus is on you to learn, so that you can be well.
Your voice matters. Your wellness matters. Your time matters. Your money matters.
Dr. Alli-Akintade is a gastroenterologist with Kaiser Permanente South Sacramento (Calif.) Medical Center. She is the CEO of MoneyFitMD, a financial empowerment coaching platform for female physicians. She is also the host of The MoneyFitMD podcast.
References
1. Royce TJ et al. Pract Radiat Oncol. Jul-Aug 2019;9(4):231-8.
2. Physician Advocacy Institute. “COVID-19’s Impact on Acquisitions of Physician Practices and Physician Employment 2019-2020.” 2021 Jun.
3. Finkel D. “New Study Shows You’re Wasting 21.8 hours a Week.” Inc.com. 2018 Mar 1.
I was a third-year gastroenterology fellow when I realized that something had to change. I was on a one-way trip to burnout.
I went through medical school with the sole goal of becoming an excellent physician. Like many physicians, I was six figures deep in student loan debt by the end of training. I remember clearly being told, “You are going to be physicians. Money won’t be a problem.” In fact, in 2021, money remains a taboo topic in medicine, and most of medical education remains void of the fundamentals of money management.
Although I was surrounded by some of the most brilliant minds in medicine, burnout was spreading like a wave. Physicians are becoming increasingly broken, burned out by a system through which we have vowed to care for our patients: For better or for worse. We are required to attend lectures about burnout, yet nothing about money or finances. We can all agree that talking about resilience and burnout during odd hours of the morning are ironic measures that by themselves have done nothing to help us through the crisis that exists.
I noticed that there seemed to be a difference between physicians who had their finances in order and those who didn’t. This eventually made sense as I became more aware of the data that now exists. Healthy financial practices can lead to financial independence, which may in turn decrease burnout-associated stressors.1 This is what we need.
My observation about the difference in satisfaction between physicians led me to decide to explore that path for myself. My hypothesis? Empowering myself financially is an anti-burnout tool that will improve my satisfaction, longevity in medicine, and my well-being. I traded my financial illiteracy for empowerment and I am now on a mission to help physicians become financially empowered. This is an important step toward preventing and recovering from burnout. The surprising part is that it is not difficult. You need to be committed. Our math literacy is already higher than needed. When we physicians are financially independent, we will have the ability to practice medicine in a way that is healthy. In a world where physician suicide, burnout, and dissatisfaction continue to rise, there is an urgent call to financial action. This is a critical key that will help us change the future of medicine.
In this article, I am going to share four myths that are preventing physicians from truly managing their finances.
1. I love medicine. I have no plans of leaving: I love gastroenterology. The ability to use our critical internal medicine skills as well as intervene procedurally is truly a privilege. As a gastroenterologist with a focus on inflammatory bowel diseases, I have the honor of walking patients through seasons of life and making decisions that truly impact their lives. It is an honor. I also believe that good money management allows physicians to become even better physicians. The platforms of medicine continue to change. According to Physician Advocacy Institute, about 70% of physicians report being employed.2 As physicians graduate from training, joining large hospitals, physician autonomy in the practice of medicine is affected. To ensure that we continue to practice medicine at the fullest extent of our oath, it is essential that our finances allow us the ability and capacity to fulfill that oath. Furthermore, the pandemic has shown that physician income is not pandemic-proof. Having a healthy emergency fund and diversifying our income sources is critical as we move forward.
2. I have a financial adviser or planner. They will figure it out for me: Financial advisers and planners are hired professionals with varied levels of training and expertise. A great financial adviser can be an important part of your team. A team that is led by you, the CEO, because no one will care about your finances as much as you do. Investing the time to learn the basics can pay dividends. When I started my financial education journey, I was completely illiterate. I knew I wanted to have money but didn’t know how. One of the first things in my financial competency journey was to hire a financial adviser. Unfortunately, as I learned more about money, I realized that my investments favored him more than they did me. Coincidentally, we had similar starting balances in a different self-management investment account. At the end of our time together, our self-managed funds fared better than his actively picked funds. As humans, we assume that actively picking investments and stocks would be better than passive investments. Based on experience and data, investing in boring, diverse funds such as index funds averagely do better than actively managed funds. Is it wrong then to hire an adviser? No, but you are still the CEO of you-incorporated. Choosing to completely delegate to someone else, avoiding the basic education that would allow you to better screen for effectiveness and competence, may in fact be negligence. After empowering themselves financially, some physicians who have gone through my money curriculum have chosen to keep their advisers; others chose to self-manage. The key is giving yourself the gift of choice: Choosing to have an adviser because you want to rather than because you thought you had no choice.
3. Money management looks complicated. This is one of the most common statements I get for why physicians avoid their own money management. I remember the complex biochemical pathways we learned in medical school. Those were hard and complicated. We chose to stay the course because we believed that, with repetition and simplifying, it would eventually become less difficult. Why then is it any different with money? A physician shared a discussion she once had with a banker. She was told, “Doctors are bad with money.” When did we become the stereotype for being bad with money? If we can learn channelopathies and memorize mechanisms and save lives, we can do money. We have to start somewhere. We may not get it the first time. However, as physicians, we are the more persistent people and are excellent examples of what happens when you commit to learning something new. After coaching hundreds of physicians regarding money management, I have concluded that physicians are not bad with money. We simply may not be committed to learning it. Once we commit, the rest becomes history.
4. I don’t have time. For practicing gastroenterologists dealing with post-lockdown influx of patients, the days can be long. As a gastroenterologist who is also a parent, I know firsthand how time can be tight. When we had two children, we were busy. We thought we were at our capacity on time with two children. Then we had a third. Suddenly, life with two children looked easier than with three. As humans, we have the capacity to create. Things take exactly how much time we commit to them. If I give myself a month to write an article, I will write it in a month. If I give myself 2 weeks, I will be done in 2 weeks. The key is to remember that we all have 24 hours. David Frankel is the author of “The Freedom Formula: How to Succeed in Business Without Sacrificing Your Family, Health, or Life.”3 He analyzed a poll of business owners. He showed that they were wasting an average of 21.8 hours per week. Many times, we talk about our to-do list. We don’t talk enough about our “to don’t list.” This refers to the list of things we need to stop doing so that we can spend time on things that give or add value to our lives. Starting with as little as 30 minutes per day or per week dedicated to learning and/or managing our finances, the result will compound.
As the platform of medicine continues to evolve, it is important for astute gastroenterologists to be part of these conversations. When we are confident in our finances, they become a vehicle that gives strength to the power of our voice. We are less likely to overwork and more likely to find joy and meaning within and outside medicine.
If we want to care for our patients at a high level and keep our oath to do no harm, we have to remember that includes doing no harm to self as well.
Money management tools and empowering ourselves financially should be an essential component of our training; until then, the onus is on you to learn, so that you can be well.
Your voice matters. Your wellness matters. Your time matters. Your money matters.
Dr. Alli-Akintade is a gastroenterologist with Kaiser Permanente South Sacramento (Calif.) Medical Center. She is the CEO of MoneyFitMD, a financial empowerment coaching platform for female physicians. She is also the host of The MoneyFitMD podcast.
References
1. Royce TJ et al. Pract Radiat Oncol. Jul-Aug 2019;9(4):231-8.
2. Physician Advocacy Institute. “COVID-19’s Impact on Acquisitions of Physician Practices and Physician Employment 2019-2020.” 2021 Jun.
3. Finkel D. “New Study Shows You’re Wasting 21.8 hours a Week.” Inc.com. 2018 Mar 1.
I was a third-year gastroenterology fellow when I realized that something had to change. I was on a one-way trip to burnout.
I went through medical school with the sole goal of becoming an excellent physician. Like many physicians, I was six figures deep in student loan debt by the end of training. I remember clearly being told, “You are going to be physicians. Money won’t be a problem.” In fact, in 2021, money remains a taboo topic in medicine, and most of medical education remains void of the fundamentals of money management.
Although I was surrounded by some of the most brilliant minds in medicine, burnout was spreading like a wave. Physicians are becoming increasingly broken, burned out by a system through which we have vowed to care for our patients: For better or for worse. We are required to attend lectures about burnout, yet nothing about money or finances. We can all agree that talking about resilience and burnout during odd hours of the morning are ironic measures that by themselves have done nothing to help us through the crisis that exists.
I noticed that there seemed to be a difference between physicians who had their finances in order and those who didn’t. This eventually made sense as I became more aware of the data that now exists. Healthy financial practices can lead to financial independence, which may in turn decrease burnout-associated stressors.1 This is what we need.
My observation about the difference in satisfaction between physicians led me to decide to explore that path for myself. My hypothesis? Empowering myself financially is an anti-burnout tool that will improve my satisfaction, longevity in medicine, and my well-being. I traded my financial illiteracy for empowerment and I am now on a mission to help physicians become financially empowered. This is an important step toward preventing and recovering from burnout. The surprising part is that it is not difficult. You need to be committed. Our math literacy is already higher than needed. When we physicians are financially independent, we will have the ability to practice medicine in a way that is healthy. In a world where physician suicide, burnout, and dissatisfaction continue to rise, there is an urgent call to financial action. This is a critical key that will help us change the future of medicine.
In this article, I am going to share four myths that are preventing physicians from truly managing their finances.
1. I love medicine. I have no plans of leaving: I love gastroenterology. The ability to use our critical internal medicine skills as well as intervene procedurally is truly a privilege. As a gastroenterologist with a focus on inflammatory bowel diseases, I have the honor of walking patients through seasons of life and making decisions that truly impact their lives. It is an honor. I also believe that good money management allows physicians to become even better physicians. The platforms of medicine continue to change. According to Physician Advocacy Institute, about 70% of physicians report being employed.2 As physicians graduate from training, joining large hospitals, physician autonomy in the practice of medicine is affected. To ensure that we continue to practice medicine at the fullest extent of our oath, it is essential that our finances allow us the ability and capacity to fulfill that oath. Furthermore, the pandemic has shown that physician income is not pandemic-proof. Having a healthy emergency fund and diversifying our income sources is critical as we move forward.
2. I have a financial adviser or planner. They will figure it out for me: Financial advisers and planners are hired professionals with varied levels of training and expertise. A great financial adviser can be an important part of your team. A team that is led by you, the CEO, because no one will care about your finances as much as you do. Investing the time to learn the basics can pay dividends. When I started my financial education journey, I was completely illiterate. I knew I wanted to have money but didn’t know how. One of the first things in my financial competency journey was to hire a financial adviser. Unfortunately, as I learned more about money, I realized that my investments favored him more than they did me. Coincidentally, we had similar starting balances in a different self-management investment account. At the end of our time together, our self-managed funds fared better than his actively picked funds. As humans, we assume that actively picking investments and stocks would be better than passive investments. Based on experience and data, investing in boring, diverse funds such as index funds averagely do better than actively managed funds. Is it wrong then to hire an adviser? No, but you are still the CEO of you-incorporated. Choosing to completely delegate to someone else, avoiding the basic education that would allow you to better screen for effectiveness and competence, may in fact be negligence. After empowering themselves financially, some physicians who have gone through my money curriculum have chosen to keep their advisers; others chose to self-manage. The key is giving yourself the gift of choice: Choosing to have an adviser because you want to rather than because you thought you had no choice.
3. Money management looks complicated. This is one of the most common statements I get for why physicians avoid their own money management. I remember the complex biochemical pathways we learned in medical school. Those were hard and complicated. We chose to stay the course because we believed that, with repetition and simplifying, it would eventually become less difficult. Why then is it any different with money? A physician shared a discussion she once had with a banker. She was told, “Doctors are bad with money.” When did we become the stereotype for being bad with money? If we can learn channelopathies and memorize mechanisms and save lives, we can do money. We have to start somewhere. We may not get it the first time. However, as physicians, we are the more persistent people and are excellent examples of what happens when you commit to learning something new. After coaching hundreds of physicians regarding money management, I have concluded that physicians are not bad with money. We simply may not be committed to learning it. Once we commit, the rest becomes history.
4. I don’t have time. For practicing gastroenterologists dealing with post-lockdown influx of patients, the days can be long. As a gastroenterologist who is also a parent, I know firsthand how time can be tight. When we had two children, we were busy. We thought we were at our capacity on time with two children. Then we had a third. Suddenly, life with two children looked easier than with three. As humans, we have the capacity to create. Things take exactly how much time we commit to them. If I give myself a month to write an article, I will write it in a month. If I give myself 2 weeks, I will be done in 2 weeks. The key is to remember that we all have 24 hours. David Frankel is the author of “The Freedom Formula: How to Succeed in Business Without Sacrificing Your Family, Health, or Life.”3 He analyzed a poll of business owners. He showed that they were wasting an average of 21.8 hours per week. Many times, we talk about our to-do list. We don’t talk enough about our “to don’t list.” This refers to the list of things we need to stop doing so that we can spend time on things that give or add value to our lives. Starting with as little as 30 minutes per day or per week dedicated to learning and/or managing our finances, the result will compound.
As the platform of medicine continues to evolve, it is important for astute gastroenterologists to be part of these conversations. When we are confident in our finances, they become a vehicle that gives strength to the power of our voice. We are less likely to overwork and more likely to find joy and meaning within and outside medicine.
If we want to care for our patients at a high level and keep our oath to do no harm, we have to remember that includes doing no harm to self as well.
Money management tools and empowering ourselves financially should be an essential component of our training; until then, the onus is on you to learn, so that you can be well.
Your voice matters. Your wellness matters. Your time matters. Your money matters.
Dr. Alli-Akintade is a gastroenterologist with Kaiser Permanente South Sacramento (Calif.) Medical Center. She is the CEO of MoneyFitMD, a financial empowerment coaching platform for female physicians. She is also the host of The MoneyFitMD podcast.
References
1. Royce TJ et al. Pract Radiat Oncol. Jul-Aug 2019;9(4):231-8.
2. Physician Advocacy Institute. “COVID-19’s Impact on Acquisitions of Physician Practices and Physician Employment 2019-2020.” 2021 Jun.
3. Finkel D. “New Study Shows You’re Wasting 21.8 hours a Week.” Inc.com. 2018 Mar 1.
What causes cancer? There’s a lot we don’t know
People with cancer are often desperate to know what caused their disease. Was it something they did? Something they could have prevented?

In a recent analysis, experts estimated that about 40% of cancers can be explained by known, often modifiable risk factors. Smoking and obesity represent the primary drivers, though a host of other factors – germline mutations, alcohol, infections, or environmental pollutants like asbestos – contribute to cancer risk as well.
But what about the remaining 60% of cancers?
The study suggests that, And a small but significant number may simply be caused by chance.
Here’s what experts suspect those missing causes might be, and why they can be so difficult to confirm.
Possibility 1: Known risk factors contribute more than we realize
For certain factors, a straight line can be drawn to cancer.
Take smoking, for instance. Decades of research have helped scientists clearly delineate tobacco’s carcinogenic effects. Researchers have pinpointed a unique set of mutations in the tumors of smokers that can be seen when cells grown in a dish are exposed to the carcinogens present in tobacco.
In addition, experts have been able to collect robust data from epidemiologic studies on smoking prevalence as well as associated cancer risks and deaths, in large part because an individual’s lifetime tobacco exposure is fairly easy to measure.
“The evidence for smoking is incredibly consistent,” Paul Brennan, PhD, a cancer epidemiologist at the World Health Organization’s International Agency for Research on Cancer, said in an interview.
For other known risk factors, such as obesity and air pollution, many more questions than answers remain.
Because of the limitations in how such factors are measured, we are likely downplaying their effects, said Richard Martin, PhD, a professor of clinical epidemiology at the University of Bristol (England).
Take obesity. Excess body weight is associated with an increased risk of at least 13 cancers. Although risk estimates vary by study and cancer type, according to a global snapshot from 2012, being overweight or obese accounted for about 4% of all cancers worldwide – 1% in low-income countries and as high as 8% in high-income countries.
However, Dr. Brennan believes “we have underestimated the effect of obesity [on cancer].”
A key reason, he said, is most studies use body mass index to determine whether someone is overweight or obese, but BMI is a poor measure of body fat. BMI does not differentiate between fat and muscle, which means two people with the same height and weight can have the same BMI, even if one is an athlete who eats lean meats and vegetables while the other lives a sedentary life and consumes large quantities of processed foods and alcohol.
On top of that, studies often only calculate a person’s BMI once, and a single measurement can’t tell you how a person’s weight has fluctuated in recent years or across different stages of their life. However, recent analyses suggest that obesity status over time may be more relevant to cancer risk than one-off measures.
In addition, many studies now suggest that alterations to our gut microbes and high blood insulin level – often seen in people who are overweight or obese – may increase the risk of cancer and speed the growth of tumors.
When these additional factors are considered, the impact of excess body fat may ultimately play a much more significant role in cancer risk. In fact, according to Dr. Brennan, “if we estimate [the effects of obesity] properly, it might at some point become the main cause of cancer.”
Possibility 2: Environmental or lifestyle factors remain under the radar
Researchers have linked many substances we consume or are exposed to in our daily lives – air pollution, toxins from industrial waste, and highly processed foods – to cancer. But the extent or contribution of potential carcinogens in our surroundings, particularly those found almost everywhere at low levels, is still largely unknown.
One simple reason is the effects of many of these substances remain difficult to assess. For instance, it is much harder to study the impact of pollutants found in food or water, in which a given population will share similar exposure levels versus tobacco, where it is possible to compare a person who smokes a pack of cigarettes a day with a person who does not smoke.
“If you’ve got exposures that are ubiquitous, it can be difficult to discern their [individual] roles,” Dr. Martin said. “There are many causes that we [likely] don’t really know because everyone has been exposed.”
On the flip side, some carcinogenic substances that people encounter for limited periods might be missed if studies are not performed at the time of exposure.
“What’s in the body at age 40 may not reflect what you were exposed at age 5-10 on the playground or soccer field,” said Graham Colditz, MD, PhD, an epidemiologist and public health expert at Washington University, St. Louis. “The technology keeps changing so we can get better measures of what you’ve got exposure to today, but how that relates to 5, 10, 15 years ago is probably very variable.”
In addition, researchers have found that many carcinogens do not cause specific mutations in a cell’s DNA; rather, studies suggest that most carcinogens lead to cancer-promoting changes in cells, such as inflammation.
“We need to think of how potential carcinogens are causing cancer,” Dr. Brennan said. Instead of provoking mutations, potential carcinogens may use a “whole other kind of pathway.” When, for instance, inflammation becomes chronic, it may spur a cascade of events that ultimately leads to cancer.
Finally, not much is known about what causes cancers in low- and middle-income countries. Most of the research to date has been in high-income countries, such the United States, Australia, and parts of Europe.
“There’s a real lack of robust epidemiological studies in other parts of the world, Latin America, Africa, parts of Asia,” Marc Gunter, PhD, a molecular epidemiologist at the IARC, told this news organization.
Possibility 3: Some cancers occur by chance
When it comes to cancer risk, an element of chance may be at play. Cancer can occur in individuals who have very little exposure to known carcinogens or have no family history of cancer.
“We all know there are people who get cancer who eat very healthy diets, are never overweight, and never smoke,” Dr. Gunter said. “Then there are people on the other end of the extreme who don’t get cancer.”
But what fraction of cancers are attributable to chance?
A controversial 2017 study published in Science suggested that, based on the rate of cell turnover in healthy tissues in the lung, pancreas, and other parts of the body, only about one-third of cancers could be linked to environmental or genetic factors. The rest, the authors claimed, occurred because of random mutations that accumulated in a person’s DNA – in other words, bad luck.
That study brought on a flood of criticism from scientists who pointed to serious flaws in the work that led the researchers to significantly overestimate the share of chance-related cancers.
The actual proportion of cancers that occur by chance is much lower, according to Dr. Brennan. “If you look at international comparisons [of cancer rates] and take a conservative estimate, you see that maybe 10% or 15% of cancers are really chance.”
Whether some cancers are caused by bad luck or undiscovered risk factors remains an open question.
But the bottom line is many unknown causes of cancer are likely environmental or lifestyle related, which means that, in theory, they can be altered, even prevented.
“There is always going to be some element of chance, but you can modify your chance, depending on your lifestyle and maybe other factors, which we don’t fully understand yet,” Dr. Gunter said.
The good news is that, when it comes to prevention, there are many ways to modify our behaviors – such as consuming fewer processed meats, going for a daily walk, or getting vaccinated against cancer-causing viruses – to improve our chances of living cancer free. And as scientists better understand more about what causes cancer, possibilities for prevention will only grow.
“There is a constant, slow growth [in knowledge] that is lowering the overall risk of cancer,” Dr. Brennan said. “We’re never going to eliminate cancer, but we will be able to control it as a disease.”
A version of this article first appeared on Medscape.com.
People with cancer are often desperate to know what caused their disease. Was it something they did? Something they could have prevented?
In a recent analysis, experts estimated that about 40% of cancers can be explained by known, often modifiable risk factors. Smoking and obesity represent the primary drivers, though a host of other factors – germline mutations, alcohol, infections, or environmental pollutants like asbestos – contribute to cancer risk as well.
But what about the remaining 60% of cancers?
The study suggests that, And a small but significant number may simply be caused by chance.
Here’s what experts suspect those missing causes might be, and why they can be so difficult to confirm.
Possibility 1: Known risk factors contribute more than we realize
For certain factors, a straight line can be drawn to cancer.
Take smoking, for instance. Decades of research have helped scientists clearly delineate tobacco’s carcinogenic effects. Researchers have pinpointed a unique set of mutations in the tumors of smokers that can be seen when cells grown in a dish are exposed to the carcinogens present in tobacco.
In addition, experts have been able to collect robust data from epidemiologic studies on smoking prevalence as well as associated cancer risks and deaths, in large part because an individual’s lifetime tobacco exposure is fairly easy to measure.
“The evidence for smoking is incredibly consistent,” Paul Brennan, PhD, a cancer epidemiologist at the World Health Organization’s International Agency for Research on Cancer, said in an interview.
For other known risk factors, such as obesity and air pollution, many more questions than answers remain.
Because of the limitations in how such factors are measured, we are likely downplaying their effects, said Richard Martin, PhD, a professor of clinical epidemiology at the University of Bristol (England).
Take obesity. Excess body weight is associated with an increased risk of at least 13 cancers. Although risk estimates vary by study and cancer type, according to a global snapshot from 2012, being overweight or obese accounted for about 4% of all cancers worldwide – 1% in low-income countries and as high as 8% in high-income countries.
However, Dr. Brennan believes “we have underestimated the effect of obesity [on cancer].”
A key reason, he said, is most studies use body mass index to determine whether someone is overweight or obese, but BMI is a poor measure of body fat. BMI does not differentiate between fat and muscle, which means two people with the same height and weight can have the same BMI, even if one is an athlete who eats lean meats and vegetables while the other lives a sedentary life and consumes large quantities of processed foods and alcohol.
On top of that, studies often only calculate a person’s BMI once, and a single measurement can’t tell you how a person’s weight has fluctuated in recent years or across different stages of their life. However, recent analyses suggest that obesity status over time may be more relevant to cancer risk than one-off measures.
In addition, many studies now suggest that alterations to our gut microbes and high blood insulin level – often seen in people who are overweight or obese – may increase the risk of cancer and speed the growth of tumors.
When these additional factors are considered, the impact of excess body fat may ultimately play a much more significant role in cancer risk. In fact, according to Dr. Brennan, “if we estimate [the effects of obesity] properly, it might at some point become the main cause of cancer.”
Possibility 2: Environmental or lifestyle factors remain under the radar
Researchers have linked many substances we consume or are exposed to in our daily lives – air pollution, toxins from industrial waste, and highly processed foods – to cancer. But the extent or contribution of potential carcinogens in our surroundings, particularly those found almost everywhere at low levels, is still largely unknown.
One simple reason is the effects of many of these substances remain difficult to assess. For instance, it is much harder to study the impact of pollutants found in food or water, in which a given population will share similar exposure levels versus tobacco, where it is possible to compare a person who smokes a pack of cigarettes a day with a person who does not smoke.
“If you’ve got exposures that are ubiquitous, it can be difficult to discern their [individual] roles,” Dr. Martin said. “There are many causes that we [likely] don’t really know because everyone has been exposed.”
On the flip side, some carcinogenic substances that people encounter for limited periods might be missed if studies are not performed at the time of exposure.
“What’s in the body at age 40 may not reflect what you were exposed at age 5-10 on the playground or soccer field,” said Graham Colditz, MD, PhD, an epidemiologist and public health expert at Washington University, St. Louis. “The technology keeps changing so we can get better measures of what you’ve got exposure to today, but how that relates to 5, 10, 15 years ago is probably very variable.”
In addition, researchers have found that many carcinogens do not cause specific mutations in a cell’s DNA; rather, studies suggest that most carcinogens lead to cancer-promoting changes in cells, such as inflammation.
“We need to think of how potential carcinogens are causing cancer,” Dr. Brennan said. Instead of provoking mutations, potential carcinogens may use a “whole other kind of pathway.” When, for instance, inflammation becomes chronic, it may spur a cascade of events that ultimately leads to cancer.
Finally, not much is known about what causes cancers in low- and middle-income countries. Most of the research to date has been in high-income countries, such the United States, Australia, and parts of Europe.
“There’s a real lack of robust epidemiological studies in other parts of the world, Latin America, Africa, parts of Asia,” Marc Gunter, PhD, a molecular epidemiologist at the IARC, told this news organization.
Possibility 3: Some cancers occur by chance
When it comes to cancer risk, an element of chance may be at play. Cancer can occur in individuals who have very little exposure to known carcinogens or have no family history of cancer.
“We all know there are people who get cancer who eat very healthy diets, are never overweight, and never smoke,” Dr. Gunter said. “Then there are people on the other end of the extreme who don’t get cancer.”
But what fraction of cancers are attributable to chance?
A controversial 2017 study published in Science suggested that, based on the rate of cell turnover in healthy tissues in the lung, pancreas, and other parts of the body, only about one-third of cancers could be linked to environmental or genetic factors. The rest, the authors claimed, occurred because of random mutations that accumulated in a person’s DNA – in other words, bad luck.
That study brought on a flood of criticism from scientists who pointed to serious flaws in the work that led the researchers to significantly overestimate the share of chance-related cancers.
The actual proportion of cancers that occur by chance is much lower, according to Dr. Brennan. “If you look at international comparisons [of cancer rates] and take a conservative estimate, you see that maybe 10% or 15% of cancers are really chance.”
Whether some cancers are caused by bad luck or undiscovered risk factors remains an open question.
But the bottom line is many unknown causes of cancer are likely environmental or lifestyle related, which means that, in theory, they can be altered, even prevented.
“There is always going to be some element of chance, but you can modify your chance, depending on your lifestyle and maybe other factors, which we don’t fully understand yet,” Dr. Gunter said.
The good news is that, when it comes to prevention, there are many ways to modify our behaviors – such as consuming fewer processed meats, going for a daily walk, or getting vaccinated against cancer-causing viruses – to improve our chances of living cancer free. And as scientists better understand more about what causes cancer, possibilities for prevention will only grow.
“There is a constant, slow growth [in knowledge] that is lowering the overall risk of cancer,” Dr. Brennan said. “We’re never going to eliminate cancer, but we will be able to control it as a disease.”
A version of this article first appeared on Medscape.com.
People with cancer are often desperate to know what caused their disease. Was it something they did? Something they could have prevented?
In a recent analysis, experts estimated that about 40% of cancers can be explained by known, often modifiable risk factors. Smoking and obesity represent the primary drivers, though a host of other factors – germline mutations, alcohol, infections, or environmental pollutants like asbestos – contribute to cancer risk as well.
But what about the remaining 60% of cancers?
The study suggests that, And a small but significant number may simply be caused by chance.
Here’s what experts suspect those missing causes might be, and why they can be so difficult to confirm.
Possibility 1: Known risk factors contribute more than we realize
For certain factors, a straight line can be drawn to cancer.
Take smoking, for instance. Decades of research have helped scientists clearly delineate tobacco’s carcinogenic effects. Researchers have pinpointed a unique set of mutations in the tumors of smokers that can be seen when cells grown in a dish are exposed to the carcinogens present in tobacco.
In addition, experts have been able to collect robust data from epidemiologic studies on smoking prevalence as well as associated cancer risks and deaths, in large part because an individual’s lifetime tobacco exposure is fairly easy to measure.
“The evidence for smoking is incredibly consistent,” Paul Brennan, PhD, a cancer epidemiologist at the World Health Organization’s International Agency for Research on Cancer, said in an interview.
For other known risk factors, such as obesity and air pollution, many more questions than answers remain.
Because of the limitations in how such factors are measured, we are likely downplaying their effects, said Richard Martin, PhD, a professor of clinical epidemiology at the University of Bristol (England).
Take obesity. Excess body weight is associated with an increased risk of at least 13 cancers. Although risk estimates vary by study and cancer type, according to a global snapshot from 2012, being overweight or obese accounted for about 4% of all cancers worldwide – 1% in low-income countries and as high as 8% in high-income countries.
However, Dr. Brennan believes “we have underestimated the effect of obesity [on cancer].”
A key reason, he said, is most studies use body mass index to determine whether someone is overweight or obese, but BMI is a poor measure of body fat. BMI does not differentiate between fat and muscle, which means two people with the same height and weight can have the same BMI, even if one is an athlete who eats lean meats and vegetables while the other lives a sedentary life and consumes large quantities of processed foods and alcohol.
On top of that, studies often only calculate a person’s BMI once, and a single measurement can’t tell you how a person’s weight has fluctuated in recent years or across different stages of their life. However, recent analyses suggest that obesity status over time may be more relevant to cancer risk than one-off measures.
In addition, many studies now suggest that alterations to our gut microbes and high blood insulin level – often seen in people who are overweight or obese – may increase the risk of cancer and speed the growth of tumors.
When these additional factors are considered, the impact of excess body fat may ultimately play a much more significant role in cancer risk. In fact, according to Dr. Brennan, “if we estimate [the effects of obesity] properly, it might at some point become the main cause of cancer.”
Possibility 2: Environmental or lifestyle factors remain under the radar
Researchers have linked many substances we consume or are exposed to in our daily lives – air pollution, toxins from industrial waste, and highly processed foods – to cancer. But the extent or contribution of potential carcinogens in our surroundings, particularly those found almost everywhere at low levels, is still largely unknown.
One simple reason is the effects of many of these substances remain difficult to assess. For instance, it is much harder to study the impact of pollutants found in food or water, in which a given population will share similar exposure levels versus tobacco, where it is possible to compare a person who smokes a pack of cigarettes a day with a person who does not smoke.
“If you’ve got exposures that are ubiquitous, it can be difficult to discern their [individual] roles,” Dr. Martin said. “There are many causes that we [likely] don’t really know because everyone has been exposed.”
On the flip side, some carcinogenic substances that people encounter for limited periods might be missed if studies are not performed at the time of exposure.
“What’s in the body at age 40 may not reflect what you were exposed at age 5-10 on the playground or soccer field,” said Graham Colditz, MD, PhD, an epidemiologist and public health expert at Washington University, St. Louis. “The technology keeps changing so we can get better measures of what you’ve got exposure to today, but how that relates to 5, 10, 15 years ago is probably very variable.”
In addition, researchers have found that many carcinogens do not cause specific mutations in a cell’s DNA; rather, studies suggest that most carcinogens lead to cancer-promoting changes in cells, such as inflammation.
“We need to think of how potential carcinogens are causing cancer,” Dr. Brennan said. Instead of provoking mutations, potential carcinogens may use a “whole other kind of pathway.” When, for instance, inflammation becomes chronic, it may spur a cascade of events that ultimately leads to cancer.
Finally, not much is known about what causes cancers in low- and middle-income countries. Most of the research to date has been in high-income countries, such the United States, Australia, and parts of Europe.
“There’s a real lack of robust epidemiological studies in other parts of the world, Latin America, Africa, parts of Asia,” Marc Gunter, PhD, a molecular epidemiologist at the IARC, told this news organization.
Possibility 3: Some cancers occur by chance
When it comes to cancer risk, an element of chance may be at play. Cancer can occur in individuals who have very little exposure to known carcinogens or have no family history of cancer.
“We all know there are people who get cancer who eat very healthy diets, are never overweight, and never smoke,” Dr. Gunter said. “Then there are people on the other end of the extreme who don’t get cancer.”
But what fraction of cancers are attributable to chance?
A controversial 2017 study published in Science suggested that, based on the rate of cell turnover in healthy tissues in the lung, pancreas, and other parts of the body, only about one-third of cancers could be linked to environmental or genetic factors. The rest, the authors claimed, occurred because of random mutations that accumulated in a person’s DNA – in other words, bad luck.
That study brought on a flood of criticism from scientists who pointed to serious flaws in the work that led the researchers to significantly overestimate the share of chance-related cancers.
The actual proportion of cancers that occur by chance is much lower, according to Dr. Brennan. “If you look at international comparisons [of cancer rates] and take a conservative estimate, you see that maybe 10% or 15% of cancers are really chance.”
Whether some cancers are caused by bad luck or undiscovered risk factors remains an open question.
But the bottom line is many unknown causes of cancer are likely environmental or lifestyle related, which means that, in theory, they can be altered, even prevented.
“There is always going to be some element of chance, but you can modify your chance, depending on your lifestyle and maybe other factors, which we don’t fully understand yet,” Dr. Gunter said.
The good news is that, when it comes to prevention, there are many ways to modify our behaviors – such as consuming fewer processed meats, going for a daily walk, or getting vaccinated against cancer-causing viruses – to improve our chances of living cancer free. And as scientists better understand more about what causes cancer, possibilities for prevention will only grow.
“There is a constant, slow growth [in knowledge] that is lowering the overall risk of cancer,” Dr. Brennan said. “We’re never going to eliminate cancer, but we will be able to control it as a disease.”
A version of this article first appeared on Medscape.com.
Are we failing to diagnose and treat the many faces of catatonia?
I had seen many new and exciting presentations of psychopathology during my intern year, yet one patient was uniquely memorable. When stable, he worked as a counselor, though for any number of reasons (eg, missing a dose of medication, smoking marijuana) his manic symptoms would emerge quickly, the disease rearing its ugly head within hours. He would become extremely hyperactive, elated, disinhibited (running naked in the streets), and grandiose (believing he was working for the president). He would be escorted to our psychiatric emergency department (ED) by police, who would have to resort to handcuffing him. His symptoms were described by ED and inpatient nursing staff and residents as “disorganized,” “psychotic,” “agitated,”’ or “combative.” He would receive large doses of intramuscular (IM) haloperidol, chlorpromazine, and diphenhydramine in desperate attempts to rein in his mania. Frustratingly—and paradoxically— this would make him more confused, disoriented, restless, and hyperactive, and often led to the need for restraints.
This behavior persisted for days until an attending I was working with assessed him. The attending observed that the patient did not know his current location, day of the week or month, or how he ended up in the hospital. He observed this patient intermittently staring, making abnormal repetitive movements with his arms and hands, occasionally freezing, making impulsive movements, and becoming combative without provocation. His heart rate and temperature were elevated; he was diaphoretic, especially after receiving parenteral antipsychotics. The attending, a pupil of Max Fink, made the diagnosis: delirious mania, a form of catatonia.1,2 Resolution was quick and complete after 6 bilateral electroconvulsive therapy (ECT) sessions.
Catatonia, a neuropsychiatric phenomenon characterized by abnormal speech, movement, and affect, has undergone numerous paradigm shifts since it was recognized by Karl Ludwig Kahlbaum in 1874.3 Shortly after Kahlbaum, Emil Kraepelin held the belief that catatonia was a subtype of dementia praecox, or what is now known as schizophrenia.4 Due to this, patients were likely receiving less-than-optimal treatments, because their catatonia was being diagnosed as acute psychosis. Finally, in DSM-5, catatonia was unshackled from the constraints of schizophrenia and is now an entity of its own.5 However, catatonia is often met with incertitude (despite being present in up to 15% of inpatients),1 with its treatment typically delayed or not even pursued. This is amplified because many forms of catatonia are often misdiagnosed as disorders that are more common or better understood.
Potential catatonia presentations
Delirious mania. Patients with delirious mania typically present with acute delirium, severe paranoia, hyperactivity, and visual/auditory hallucinations.2,6,7 They usually have excited catatonic signs, such as excessive movement, combativeness, impulsivity, stereotypy, and echophenomena. Unfortunately, the catatonia is overshadowed by extreme psychotic and manic symptoms, or delirium (for which an underlying medical cause is usually not found). As was the case for the patient I described earlier, large doses of IM antipsychotics usually are administered, which can cause neuroleptic malignant syndrome (NMS) or precipitate seizures.8
Neuroleptic malignant syndrome. NMS is marked by fever, elevated blood pressure and heart rate, lead-pipe rigidity, parkinsonian features, altered mental status, and lab abnormalities (elevated liver enzymes or creatinine phosphokinase). This syndrome is preceded by the administration of an antipsychotic. It has features of catatonia that include mutism, negativism, and posturing.9 NMS is commonly interpreted as a subtype of malignant catatonia. Some argue that the diagnosis of malignant catatonia yields a more favorable outcome because it leads to more effective treatments (ie, benzodiazepines and ECT as opposed to dopamine agonists and dantrolene).10 Because NMS has much overlap with serotonin syndrome and drug-induced parkinsonism, initiation of benzodiazepines and ECT often is delayed.11
Retarded catatonia. This version of catatonia usually is well recognized. The typical presentation is a patient who does not speak (mutism) or move (stupor), stares, becomes withdrawn (does not eat or drink), or maintains abnormal posturing. Retarded catatonia can be confused with a major depressive episode or hypoactive delirium.
Catatonia in autism spectrum disorder. Historically, co-occurring catatonia and autism spectrum disorder (ASD) was believed to be extremely rare. However, recent retrospective studies have found that up to 17% of patients with ASD older than age 15 have catatonia.12 Many pediatric psychiatrists fail to recognize catatonia; in 1 study, only 2 patients (of 18) were correctly identified as having catatonia.13 The catatonic signs may vary, but the core features include withdrawal (children may need a feeding tube), decreased communication and/or worsening psychomotor slowing, agitation, or stereotypical movements, which can manifest as worsening self-injurious behavior.14,15
An approach to treatment
Regardless of the etiology or presentation, first-line treatment for catatonia is benzodiazepines and/or ECT. A lorazepam challenge is used for diagnostic clarification; if effective, lorazepam can be titrated until symptoms fully resolve.16,17 Doses >20 mg have been reported as effective and well-tolerated, without the feared sedation and respiratory depression.6 An unsuccessful lorazepam challenge does not rule out catatonia. If benzodiazepine therapy fails or the patient requires immediate symptom relief, ECT is the most effective treatment. Many clinicians use a bilateral electrode placement with high-energy dosing and frequent sessions until the catatonia resolves.1,18
In my experience, catatonia in all its forms remains poorly recognized, with its treatment questioned. Residents—especially those in psychiatry—must understand that catatonia can result in systemic illness or death.
1. Fink M. Expanding the catatonia tent: recognizing electroconvulsive therapy responsive syndromes. J ECT. 2021;37(2):77-79.
2. Fink M. Delirious mania. Bipolar Disord. 1999;1(1):54-60.
3. Starkstein SE, Goldar JC, Hodgkiss A. Karl Ludwig Kahlbaum’s concept of catatonia. Hist Psychiatry. 1995;6(22 Pt 2):201-207.
4. Jain A, Mitra P. Catatonic schizophrenia. StatPearls Publishing. Last updated July 31, 2021. Accessed December 9, 2021. https://www.ncbi.nlm.nih.gov/books/NBK563222/
5. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013.
6. Karmacharya R, England ML, Ongür D. Delirious mania: clinical features and treatment response. J Affect Disord. 2008;109(3):312-316.
7. Jacobowski NL, Heckers S, Bobo WV. Delirious mania: detection, diagnosis, and clinical management in the acute setting. J Psychiatr Pract. 2013;19(1):15-28.
8. Fink M. Electroconvulsive Therapy: A Guide for Professionals and Their Patients. Oxford University Press; 2009.
9. Francis A, Yacoub A. Catatonia and neuroleptic malignant syndrome. Ann Clin Psychiatry. 2008:231; author reply 232-233.
10. Fink M. Hidden in plain sight: catatonia in pediatrics: “An editorial comment to Shorter E. “Making childhood catatonia visible (Separate from competing diagnoses”, (1) Dhossche D, Ross CA, Stoppelbein L. ‘The role of deprivation, abuse, and trauma in pediatric catatonia without a clear medical cause’, (2) Ghaziuddin N, Dhossche D, Marcotte K. ‘Retrospective chart review of catatonia in child and adolescent psychiatric patients’ (3)”. Acta Psychiatr Scand. 2012;125(1):11-12.
11. Perry PJ, Wilborn CA. Serotonin syndrome vs neuroleptic malignant syndrome: a contrast of causes, diagnoses, and management. Ann Clin Psychiatry. 2012;24(2):155-162.
12. Wing L, Shah A. Catatonia in autistic spectrum disorders. Br J Psychiatry. 2000;176:357-362.
13. Ghaziuddin N, Dhossche D, Marcotte K. Retrospective chart review of catatonia in child and adolescent psychiatric patients. Acta Psychiatr Scand. 2012;125(1):33-38.
14. Wachtel LE, Hermida A, Dhossche DM. Maintenance electroconvulsive therapy in autistic catatonia: a case series review. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(4):581-587.
15. Wachtel LE. The multiple faces of catatonia in autism spectrum disorders: descriptive clinical experience of 22 patients over 12 years. Eur Child Adolesc Psychiatry. 2019;28(4):471-480.
16. Bush G, Fink M, Petrides G, et al. Catatonia. I. Rating scale and standardized examination. Acta Psychiatr Scand. 1996;93(2):129-136.
17. Bush G, Fink M, Petrides G, et al. Catatonia. II. Treatment with lorazepam and electroconvulsive therapy. Acta Psychiatr Scand. 1996;93(2):137-143.
18. Fink M, Kellner CH, McCall WV. Optimizing ECT technique in treating catatonia. J ECT. 2016;32(3):149-150.
I had seen many new and exciting presentations of psychopathology during my intern year, yet one patient was uniquely memorable. When stable, he worked as a counselor, though for any number of reasons (eg, missing a dose of medication, smoking marijuana) his manic symptoms would emerge quickly, the disease rearing its ugly head within hours. He would become extremely hyperactive, elated, disinhibited (running naked in the streets), and grandiose (believing he was working for the president). He would be escorted to our psychiatric emergency department (ED) by police, who would have to resort to handcuffing him. His symptoms were described by ED and inpatient nursing staff and residents as “disorganized,” “psychotic,” “agitated,”’ or “combative.” He would receive large doses of intramuscular (IM) haloperidol, chlorpromazine, and diphenhydramine in desperate attempts to rein in his mania. Frustratingly—and paradoxically— this would make him more confused, disoriented, restless, and hyperactive, and often led to the need for restraints.
This behavior persisted for days until an attending I was working with assessed him. The attending observed that the patient did not know his current location, day of the week or month, or how he ended up in the hospital. He observed this patient intermittently staring, making abnormal repetitive movements with his arms and hands, occasionally freezing, making impulsive movements, and becoming combative without provocation. His heart rate and temperature were elevated; he was diaphoretic, especially after receiving parenteral antipsychotics. The attending, a pupil of Max Fink, made the diagnosis: delirious mania, a form of catatonia.1,2 Resolution was quick and complete after 6 bilateral electroconvulsive therapy (ECT) sessions.
Catatonia, a neuropsychiatric phenomenon characterized by abnormal speech, movement, and affect, has undergone numerous paradigm shifts since it was recognized by Karl Ludwig Kahlbaum in 1874.3 Shortly after Kahlbaum, Emil Kraepelin held the belief that catatonia was a subtype of dementia praecox, or what is now known as schizophrenia.4 Due to this, patients were likely receiving less-than-optimal treatments, because their catatonia was being diagnosed as acute psychosis. Finally, in DSM-5, catatonia was unshackled from the constraints of schizophrenia and is now an entity of its own.5 However, catatonia is often met with incertitude (despite being present in up to 15% of inpatients),1 with its treatment typically delayed or not even pursued. This is amplified because many forms of catatonia are often misdiagnosed as disorders that are more common or better understood.
Potential catatonia presentations
Delirious mania. Patients with delirious mania typically present with acute delirium, severe paranoia, hyperactivity, and visual/auditory hallucinations.2,6,7 They usually have excited catatonic signs, such as excessive movement, combativeness, impulsivity, stereotypy, and echophenomena. Unfortunately, the catatonia is overshadowed by extreme psychotic and manic symptoms, or delirium (for which an underlying medical cause is usually not found). As was the case for the patient I described earlier, large doses of IM antipsychotics usually are administered, which can cause neuroleptic malignant syndrome (NMS) or precipitate seizures.8
Neuroleptic malignant syndrome. NMS is marked by fever, elevated blood pressure and heart rate, lead-pipe rigidity, parkinsonian features, altered mental status, and lab abnormalities (elevated liver enzymes or creatinine phosphokinase). This syndrome is preceded by the administration of an antipsychotic. It has features of catatonia that include mutism, negativism, and posturing.9 NMS is commonly interpreted as a subtype of malignant catatonia. Some argue that the diagnosis of malignant catatonia yields a more favorable outcome because it leads to more effective treatments (ie, benzodiazepines and ECT as opposed to dopamine agonists and dantrolene).10 Because NMS has much overlap with serotonin syndrome and drug-induced parkinsonism, initiation of benzodiazepines and ECT often is delayed.11
Retarded catatonia. This version of catatonia usually is well recognized. The typical presentation is a patient who does not speak (mutism) or move (stupor), stares, becomes withdrawn (does not eat or drink), or maintains abnormal posturing. Retarded catatonia can be confused with a major depressive episode or hypoactive delirium.
Catatonia in autism spectrum disorder. Historically, co-occurring catatonia and autism spectrum disorder (ASD) was believed to be extremely rare. However, recent retrospective studies have found that up to 17% of patients with ASD older than age 15 have catatonia.12 Many pediatric psychiatrists fail to recognize catatonia; in 1 study, only 2 patients (of 18) were correctly identified as having catatonia.13 The catatonic signs may vary, but the core features include withdrawal (children may need a feeding tube), decreased communication and/or worsening psychomotor slowing, agitation, or stereotypical movements, which can manifest as worsening self-injurious behavior.14,15
An approach to treatment
Regardless of the etiology or presentation, first-line treatment for catatonia is benzodiazepines and/or ECT. A lorazepam challenge is used for diagnostic clarification; if effective, lorazepam can be titrated until symptoms fully resolve.16,17 Doses >20 mg have been reported as effective and well-tolerated, without the feared sedation and respiratory depression.6 An unsuccessful lorazepam challenge does not rule out catatonia. If benzodiazepine therapy fails or the patient requires immediate symptom relief, ECT is the most effective treatment. Many clinicians use a bilateral electrode placement with high-energy dosing and frequent sessions until the catatonia resolves.1,18
In my experience, catatonia in all its forms remains poorly recognized, with its treatment questioned. Residents—especially those in psychiatry—must understand that catatonia can result in systemic illness or death.
I had seen many new and exciting presentations of psychopathology during my intern year, yet one patient was uniquely memorable. When stable, he worked as a counselor, though for any number of reasons (eg, missing a dose of medication, smoking marijuana) his manic symptoms would emerge quickly, the disease rearing its ugly head within hours. He would become extremely hyperactive, elated, disinhibited (running naked in the streets), and grandiose (believing he was working for the president). He would be escorted to our psychiatric emergency department (ED) by police, who would have to resort to handcuffing him. His symptoms were described by ED and inpatient nursing staff and residents as “disorganized,” “psychotic,” “agitated,”’ or “combative.” He would receive large doses of intramuscular (IM) haloperidol, chlorpromazine, and diphenhydramine in desperate attempts to rein in his mania. Frustratingly—and paradoxically— this would make him more confused, disoriented, restless, and hyperactive, and often led to the need for restraints.
This behavior persisted for days until an attending I was working with assessed him. The attending observed that the patient did not know his current location, day of the week or month, or how he ended up in the hospital. He observed this patient intermittently staring, making abnormal repetitive movements with his arms and hands, occasionally freezing, making impulsive movements, and becoming combative without provocation. His heart rate and temperature were elevated; he was diaphoretic, especially after receiving parenteral antipsychotics. The attending, a pupil of Max Fink, made the diagnosis: delirious mania, a form of catatonia.1,2 Resolution was quick and complete after 6 bilateral electroconvulsive therapy (ECT) sessions.
Catatonia, a neuropsychiatric phenomenon characterized by abnormal speech, movement, and affect, has undergone numerous paradigm shifts since it was recognized by Karl Ludwig Kahlbaum in 1874.3 Shortly after Kahlbaum, Emil Kraepelin held the belief that catatonia was a subtype of dementia praecox, or what is now known as schizophrenia.4 Due to this, patients were likely receiving less-than-optimal treatments, because their catatonia was being diagnosed as acute psychosis. Finally, in DSM-5, catatonia was unshackled from the constraints of schizophrenia and is now an entity of its own.5 However, catatonia is often met with incertitude (despite being present in up to 15% of inpatients),1 with its treatment typically delayed or not even pursued. This is amplified because many forms of catatonia are often misdiagnosed as disorders that are more common or better understood.
Potential catatonia presentations
Delirious mania. Patients with delirious mania typically present with acute delirium, severe paranoia, hyperactivity, and visual/auditory hallucinations.2,6,7 They usually have excited catatonic signs, such as excessive movement, combativeness, impulsivity, stereotypy, and echophenomena. Unfortunately, the catatonia is overshadowed by extreme psychotic and manic symptoms, or delirium (for which an underlying medical cause is usually not found). As was the case for the patient I described earlier, large doses of IM antipsychotics usually are administered, which can cause neuroleptic malignant syndrome (NMS) or precipitate seizures.8
Neuroleptic malignant syndrome. NMS is marked by fever, elevated blood pressure and heart rate, lead-pipe rigidity, parkinsonian features, altered mental status, and lab abnormalities (elevated liver enzymes or creatinine phosphokinase). This syndrome is preceded by the administration of an antipsychotic. It has features of catatonia that include mutism, negativism, and posturing.9 NMS is commonly interpreted as a subtype of malignant catatonia. Some argue that the diagnosis of malignant catatonia yields a more favorable outcome because it leads to more effective treatments (ie, benzodiazepines and ECT as opposed to dopamine agonists and dantrolene).10 Because NMS has much overlap with serotonin syndrome and drug-induced parkinsonism, initiation of benzodiazepines and ECT often is delayed.11
Retarded catatonia. This version of catatonia usually is well recognized. The typical presentation is a patient who does not speak (mutism) or move (stupor), stares, becomes withdrawn (does not eat or drink), or maintains abnormal posturing. Retarded catatonia can be confused with a major depressive episode or hypoactive delirium.
Catatonia in autism spectrum disorder. Historically, co-occurring catatonia and autism spectrum disorder (ASD) was believed to be extremely rare. However, recent retrospective studies have found that up to 17% of patients with ASD older than age 15 have catatonia.12 Many pediatric psychiatrists fail to recognize catatonia; in 1 study, only 2 patients (of 18) were correctly identified as having catatonia.13 The catatonic signs may vary, but the core features include withdrawal (children may need a feeding tube), decreased communication and/or worsening psychomotor slowing, agitation, or stereotypical movements, which can manifest as worsening self-injurious behavior.14,15
An approach to treatment
Regardless of the etiology or presentation, first-line treatment for catatonia is benzodiazepines and/or ECT. A lorazepam challenge is used for diagnostic clarification; if effective, lorazepam can be titrated until symptoms fully resolve.16,17 Doses >20 mg have been reported as effective and well-tolerated, without the feared sedation and respiratory depression.6 An unsuccessful lorazepam challenge does not rule out catatonia. If benzodiazepine therapy fails or the patient requires immediate symptom relief, ECT is the most effective treatment. Many clinicians use a bilateral electrode placement with high-energy dosing and frequent sessions until the catatonia resolves.1,18
In my experience, catatonia in all its forms remains poorly recognized, with its treatment questioned. Residents—especially those in psychiatry—must understand that catatonia can result in systemic illness or death.
1. Fink M. Expanding the catatonia tent: recognizing electroconvulsive therapy responsive syndromes. J ECT. 2021;37(2):77-79.
2. Fink M. Delirious mania. Bipolar Disord. 1999;1(1):54-60.
3. Starkstein SE, Goldar JC, Hodgkiss A. Karl Ludwig Kahlbaum’s concept of catatonia. Hist Psychiatry. 1995;6(22 Pt 2):201-207.
4. Jain A, Mitra P. Catatonic schizophrenia. StatPearls Publishing. Last updated July 31, 2021. Accessed December 9, 2021. https://www.ncbi.nlm.nih.gov/books/NBK563222/
5. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013.
6. Karmacharya R, England ML, Ongür D. Delirious mania: clinical features and treatment response. J Affect Disord. 2008;109(3):312-316.
7. Jacobowski NL, Heckers S, Bobo WV. Delirious mania: detection, diagnosis, and clinical management in the acute setting. J Psychiatr Pract. 2013;19(1):15-28.
8. Fink M. Electroconvulsive Therapy: A Guide for Professionals and Their Patients. Oxford University Press; 2009.
9. Francis A, Yacoub A. Catatonia and neuroleptic malignant syndrome. Ann Clin Psychiatry. 2008:231; author reply 232-233.
10. Fink M. Hidden in plain sight: catatonia in pediatrics: “An editorial comment to Shorter E. “Making childhood catatonia visible (Separate from competing diagnoses”, (1) Dhossche D, Ross CA, Stoppelbein L. ‘The role of deprivation, abuse, and trauma in pediatric catatonia without a clear medical cause’, (2) Ghaziuddin N, Dhossche D, Marcotte K. ‘Retrospective chart review of catatonia in child and adolescent psychiatric patients’ (3)”. Acta Psychiatr Scand. 2012;125(1):11-12.
11. Perry PJ, Wilborn CA. Serotonin syndrome vs neuroleptic malignant syndrome: a contrast of causes, diagnoses, and management. Ann Clin Psychiatry. 2012;24(2):155-162.
12. Wing L, Shah A. Catatonia in autistic spectrum disorders. Br J Psychiatry. 2000;176:357-362.
13. Ghaziuddin N, Dhossche D, Marcotte K. Retrospective chart review of catatonia in child and adolescent psychiatric patients. Acta Psychiatr Scand. 2012;125(1):33-38.
14. Wachtel LE, Hermida A, Dhossche DM. Maintenance electroconvulsive therapy in autistic catatonia: a case series review. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(4):581-587.
15. Wachtel LE. The multiple faces of catatonia in autism spectrum disorders: descriptive clinical experience of 22 patients over 12 years. Eur Child Adolesc Psychiatry. 2019;28(4):471-480.
16. Bush G, Fink M, Petrides G, et al. Catatonia. I. Rating scale and standardized examination. Acta Psychiatr Scand. 1996;93(2):129-136.
17. Bush G, Fink M, Petrides G, et al. Catatonia. II. Treatment with lorazepam and electroconvulsive therapy. Acta Psychiatr Scand. 1996;93(2):137-143.
18. Fink M, Kellner CH, McCall WV. Optimizing ECT technique in treating catatonia. J ECT. 2016;32(3):149-150.
1. Fink M. Expanding the catatonia tent: recognizing electroconvulsive therapy responsive syndromes. J ECT. 2021;37(2):77-79.
2. Fink M. Delirious mania. Bipolar Disord. 1999;1(1):54-60.
3. Starkstein SE, Goldar JC, Hodgkiss A. Karl Ludwig Kahlbaum’s concept of catatonia. Hist Psychiatry. 1995;6(22 Pt 2):201-207.
4. Jain A, Mitra P. Catatonic schizophrenia. StatPearls Publishing. Last updated July 31, 2021. Accessed December 9, 2021. https://www.ncbi.nlm.nih.gov/books/NBK563222/
5. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013.
6. Karmacharya R, England ML, Ongür D. Delirious mania: clinical features and treatment response. J Affect Disord. 2008;109(3):312-316.
7. Jacobowski NL, Heckers S, Bobo WV. Delirious mania: detection, diagnosis, and clinical management in the acute setting. J Psychiatr Pract. 2013;19(1):15-28.
8. Fink M. Electroconvulsive Therapy: A Guide for Professionals and Their Patients. Oxford University Press; 2009.
9. Francis A, Yacoub A. Catatonia and neuroleptic malignant syndrome. Ann Clin Psychiatry. 2008:231; author reply 232-233.
10. Fink M. Hidden in plain sight: catatonia in pediatrics: “An editorial comment to Shorter E. “Making childhood catatonia visible (Separate from competing diagnoses”, (1) Dhossche D, Ross CA, Stoppelbein L. ‘The role of deprivation, abuse, and trauma in pediatric catatonia without a clear medical cause’, (2) Ghaziuddin N, Dhossche D, Marcotte K. ‘Retrospective chart review of catatonia in child and adolescent psychiatric patients’ (3)”. Acta Psychiatr Scand. 2012;125(1):11-12.
11. Perry PJ, Wilborn CA. Serotonin syndrome vs neuroleptic malignant syndrome: a contrast of causes, diagnoses, and management. Ann Clin Psychiatry. 2012;24(2):155-162.
12. Wing L, Shah A. Catatonia in autistic spectrum disorders. Br J Psychiatry. 2000;176:357-362.
13. Ghaziuddin N, Dhossche D, Marcotte K. Retrospective chart review of catatonia in child and adolescent psychiatric patients. Acta Psychiatr Scand. 2012;125(1):33-38.
14. Wachtel LE, Hermida A, Dhossche DM. Maintenance electroconvulsive therapy in autistic catatonia: a case series review. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(4):581-587.
15. Wachtel LE. The multiple faces of catatonia in autism spectrum disorders: descriptive clinical experience of 22 patients over 12 years. Eur Child Adolesc Psychiatry. 2019;28(4):471-480.
16. Bush G, Fink M, Petrides G, et al. Catatonia. I. Rating scale and standardized examination. Acta Psychiatr Scand. 1996;93(2):129-136.
17. Bush G, Fink M, Petrides G, et al. Catatonia. II. Treatment with lorazepam and electroconvulsive therapy. Acta Psychiatr Scand. 1996;93(2):137-143.
18. Fink M, Kellner CH, McCall WV. Optimizing ECT technique in treating catatonia. J ECT. 2016;32(3):149-150.
High GI spending reveals research, public health need
GI, liver, and pancreatic diseases cost the U.S. health care system about $120B per year and account for approximately 250,000 annual deaths, according to a “conservative” estimate from a recent analysis.
These figures emphasize the need for more research funding in the area, along with additional clinical and public health initiatives, reported lead author Anne F. Peery, MD, of the University of North Carolina School of Medicine, Chapel Hill, and colleagues.
“Reports detailing the burden of GI diseases are necessary for clinical research, decision making, and priority setting,” the investigators wrote in Gastroenterology. “Our aim was to describe health care use, expenditures, and research funding across GI, liver, and pancreatic diseases in the United States.”
Dr. Peery and colleagues analyzed data from 14 sources, including the National Institutes of Health; the Centers for Disease Control and Prevention; the National Ambulatory Medical Care Survey; and others. GI-specific outcomes included mortality, readmissions, hospitalizations, office-based visits, and emergency department visits. The investigators also characterized trends in cancers, organ transplants, and GI endoscopy, as well as GI-specific health care costs and NIH research funding. Annual findings were presented for various periods.
Total GI health care spending was $119.6 billion in 2018, down from $135.9 billion in 2015. The top five most costly conditions were biliary tract diseases ($16.9 billion), esophageal disorders ($12.1 billion), abdominal pain ($9.5 billion), abdominal hernias ($9.0 billion), and diverticular disease ($9.0 billion). The investigators noted that medication costs were particularly high for two categories: inflammatory bowel diseases and esophageal disorders, which had prescription drug costs relative to total expenditures of 71% and 53%, respectively.
“This conservative estimate [of $119.6 billion] did not include most GI cancers and likely underestimated the costs associated with some GI conditions,” the investigators noted. “For example, the Medical Expenditure Panel Survey estimate associated with GI bleeding was $300 million. In comparison, the aggregate cost of GI bleeding was more realistically $3.7 billion, as estimated using inpatient data from the National Inpatient Sample.”
In 2016, the most common GI-related diagnosis in the U.S. was abdominal pain (15.7 million annual visits), followed by nausea and vomiting (5.0 million visits), gastroesophageal reflux disorder and reflux esophagitis (4.7 million visits), constipation (3.1 million visits), and abdominal wall/inguinal hernia (2.8 million visits).
The top three most common GI-related hospital admissions in 2018 were GI bleeding (1.3 million admissions), followed by cholelithiasis and cholecystitis (741,060 admissions), then pancreatitis (685,880 admissions). GI bleeding was also the leading cause of 30-day readmission in 2018 (84,533 readmissions).
“We found substantial numbers of GI conditions and symptoms listed in secondary positions on the discharge record,” the investigators wrote. “For example, liver disease accounted for 280,645 discharges with a primary diagnosis; however, there were 13-fold as many discharges (3.6 million in 2018) with liver disease as a secondary diagnosis. Including all diagnoses captures a burden of GI disease not previously reported.”
In 2018 and 2019, GI diseases and cancers caused 255,407 annual deaths. The most common noncancer deaths were caused by alcohol-associated liver disease (24,110 deaths), hepatic fibrosis/cirrhosis (20,184 deaths), and GI bleeding (9,548 deaths). Among GI-cancer related deaths, colorectal cancer (CRC) caused the most mortalities (52,163 deaths), followed by pancreatic cancer (44,914 deaths), and hepatic/biliary cancer (44,914 deaths). The investigators noted that CRC was disproportionately common among non-Hispanic Black individuals, whereas gastric cancer was relatively high among Hispanic individuals.
“GI cancers account for a large number of diagnoses and deaths annually, with persistent disparities in incidence and mortality rates by race/ethnicity,” the investigators wrote. “Racial, ethnic, and regional disparities in access to most GI endoscopy procedures exist, which suggests an unmet need for GI procedures across the United States.”
A total of 22.2 million endoscopies were performed in 2019, most commonly colonoscopy (13.8 million procedures), followed by upper endoscopy (7.5 million procedures), and flexible sigmoidoscopy (379,883 procedures).
In 2020, the NIH spent $3.1 billion, or approximately 7.5% of its budget, on GI disease research. Digestive diseases captured the bulk of this spending, with $2.3 billion. In the same year, the NIH spent 10.5% of its cancer research budget on GI cancers, with the greatest proportion ($325 million) awarded to CRC research.
“Carefully examining the data in this report can help generate areas for future investigation, prioritize research funding, identify areas of unmet need or disparities, and provide an important overview of the impact of digestive and liver conditions,” the investigators concluded. “We hope that others will use this report as motivation to take a deeper dive into individual diseases. There is much to learn from carefully studying existing data sources.”
The study was supported by the National Center for Advancing Translational Sciences, National Institutes of Health. The investigators disclosed no conflicts of interest.
GI, liver, and pancreatic diseases cost the U.S. health care system about $120B per year and account for approximately 250,000 annual deaths, according to a “conservative” estimate from a recent analysis.
These figures emphasize the need for more research funding in the area, along with additional clinical and public health initiatives, reported lead author Anne F. Peery, MD, of the University of North Carolina School of Medicine, Chapel Hill, and colleagues.
“Reports detailing the burden of GI diseases are necessary for clinical research, decision making, and priority setting,” the investigators wrote in Gastroenterology. “Our aim was to describe health care use, expenditures, and research funding across GI, liver, and pancreatic diseases in the United States.”
Dr. Peery and colleagues analyzed data from 14 sources, including the National Institutes of Health; the Centers for Disease Control and Prevention; the National Ambulatory Medical Care Survey; and others. GI-specific outcomes included mortality, readmissions, hospitalizations, office-based visits, and emergency department visits. The investigators also characterized trends in cancers, organ transplants, and GI endoscopy, as well as GI-specific health care costs and NIH research funding. Annual findings were presented for various periods.
Total GI health care spending was $119.6 billion in 2018, down from $135.9 billion in 2015. The top five most costly conditions were biliary tract diseases ($16.9 billion), esophageal disorders ($12.1 billion), abdominal pain ($9.5 billion), abdominal hernias ($9.0 billion), and diverticular disease ($9.0 billion). The investigators noted that medication costs were particularly high for two categories: inflammatory bowel diseases and esophageal disorders, which had prescription drug costs relative to total expenditures of 71% and 53%, respectively.
“This conservative estimate [of $119.6 billion] did not include most GI cancers and likely underestimated the costs associated with some GI conditions,” the investigators noted. “For example, the Medical Expenditure Panel Survey estimate associated with GI bleeding was $300 million. In comparison, the aggregate cost of GI bleeding was more realistically $3.7 billion, as estimated using inpatient data from the National Inpatient Sample.”
In 2016, the most common GI-related diagnosis in the U.S. was abdominal pain (15.7 million annual visits), followed by nausea and vomiting (5.0 million visits), gastroesophageal reflux disorder and reflux esophagitis (4.7 million visits), constipation (3.1 million visits), and abdominal wall/inguinal hernia (2.8 million visits).
The top three most common GI-related hospital admissions in 2018 were GI bleeding (1.3 million admissions), followed by cholelithiasis and cholecystitis (741,060 admissions), then pancreatitis (685,880 admissions). GI bleeding was also the leading cause of 30-day readmission in 2018 (84,533 readmissions).
“We found substantial numbers of GI conditions and symptoms listed in secondary positions on the discharge record,” the investigators wrote. “For example, liver disease accounted for 280,645 discharges with a primary diagnosis; however, there were 13-fold as many discharges (3.6 million in 2018) with liver disease as a secondary diagnosis. Including all diagnoses captures a burden of GI disease not previously reported.”
In 2018 and 2019, GI diseases and cancers caused 255,407 annual deaths. The most common noncancer deaths were caused by alcohol-associated liver disease (24,110 deaths), hepatic fibrosis/cirrhosis (20,184 deaths), and GI bleeding (9,548 deaths). Among GI-cancer related deaths, colorectal cancer (CRC) caused the most mortalities (52,163 deaths), followed by pancreatic cancer (44,914 deaths), and hepatic/biliary cancer (44,914 deaths). The investigators noted that CRC was disproportionately common among non-Hispanic Black individuals, whereas gastric cancer was relatively high among Hispanic individuals.
“GI cancers account for a large number of diagnoses and deaths annually, with persistent disparities in incidence and mortality rates by race/ethnicity,” the investigators wrote. “Racial, ethnic, and regional disparities in access to most GI endoscopy procedures exist, which suggests an unmet need for GI procedures across the United States.”
A total of 22.2 million endoscopies were performed in 2019, most commonly colonoscopy (13.8 million procedures), followed by upper endoscopy (7.5 million procedures), and flexible sigmoidoscopy (379,883 procedures).
In 2020, the NIH spent $3.1 billion, or approximately 7.5% of its budget, on GI disease research. Digestive diseases captured the bulk of this spending, with $2.3 billion. In the same year, the NIH spent 10.5% of its cancer research budget on GI cancers, with the greatest proportion ($325 million) awarded to CRC research.
“Carefully examining the data in this report can help generate areas for future investigation, prioritize research funding, identify areas of unmet need or disparities, and provide an important overview of the impact of digestive and liver conditions,” the investigators concluded. “We hope that others will use this report as motivation to take a deeper dive into individual diseases. There is much to learn from carefully studying existing data sources.”
The study was supported by the National Center for Advancing Translational Sciences, National Institutes of Health. The investigators disclosed no conflicts of interest.
GI, liver, and pancreatic diseases cost the U.S. health care system about $120B per year and account for approximately 250,000 annual deaths, according to a “conservative” estimate from a recent analysis.
These figures emphasize the need for more research funding in the area, along with additional clinical and public health initiatives, reported lead author Anne F. Peery, MD, of the University of North Carolina School of Medicine, Chapel Hill, and colleagues.
“Reports detailing the burden of GI diseases are necessary for clinical research, decision making, and priority setting,” the investigators wrote in Gastroenterology. “Our aim was to describe health care use, expenditures, and research funding across GI, liver, and pancreatic diseases in the United States.”
Dr. Peery and colleagues analyzed data from 14 sources, including the National Institutes of Health; the Centers for Disease Control and Prevention; the National Ambulatory Medical Care Survey; and others. GI-specific outcomes included mortality, readmissions, hospitalizations, office-based visits, and emergency department visits. The investigators also characterized trends in cancers, organ transplants, and GI endoscopy, as well as GI-specific health care costs and NIH research funding. Annual findings were presented for various periods.
Total GI health care spending was $119.6 billion in 2018, down from $135.9 billion in 2015. The top five most costly conditions were biliary tract diseases ($16.9 billion), esophageal disorders ($12.1 billion), abdominal pain ($9.5 billion), abdominal hernias ($9.0 billion), and diverticular disease ($9.0 billion). The investigators noted that medication costs were particularly high for two categories: inflammatory bowel diseases and esophageal disorders, which had prescription drug costs relative to total expenditures of 71% and 53%, respectively.
“This conservative estimate [of $119.6 billion] did not include most GI cancers and likely underestimated the costs associated with some GI conditions,” the investigators noted. “For example, the Medical Expenditure Panel Survey estimate associated with GI bleeding was $300 million. In comparison, the aggregate cost of GI bleeding was more realistically $3.7 billion, as estimated using inpatient data from the National Inpatient Sample.”
In 2016, the most common GI-related diagnosis in the U.S. was abdominal pain (15.7 million annual visits), followed by nausea and vomiting (5.0 million visits), gastroesophageal reflux disorder and reflux esophagitis (4.7 million visits), constipation (3.1 million visits), and abdominal wall/inguinal hernia (2.8 million visits).
The top three most common GI-related hospital admissions in 2018 were GI bleeding (1.3 million admissions), followed by cholelithiasis and cholecystitis (741,060 admissions), then pancreatitis (685,880 admissions). GI bleeding was also the leading cause of 30-day readmission in 2018 (84,533 readmissions).
“We found substantial numbers of GI conditions and symptoms listed in secondary positions on the discharge record,” the investigators wrote. “For example, liver disease accounted for 280,645 discharges with a primary diagnosis; however, there were 13-fold as many discharges (3.6 million in 2018) with liver disease as a secondary diagnosis. Including all diagnoses captures a burden of GI disease not previously reported.”
In 2018 and 2019, GI diseases and cancers caused 255,407 annual deaths. The most common noncancer deaths were caused by alcohol-associated liver disease (24,110 deaths), hepatic fibrosis/cirrhosis (20,184 deaths), and GI bleeding (9,548 deaths). Among GI-cancer related deaths, colorectal cancer (CRC) caused the most mortalities (52,163 deaths), followed by pancreatic cancer (44,914 deaths), and hepatic/biliary cancer (44,914 deaths). The investigators noted that CRC was disproportionately common among non-Hispanic Black individuals, whereas gastric cancer was relatively high among Hispanic individuals.
“GI cancers account for a large number of diagnoses and deaths annually, with persistent disparities in incidence and mortality rates by race/ethnicity,” the investigators wrote. “Racial, ethnic, and regional disparities in access to most GI endoscopy procedures exist, which suggests an unmet need for GI procedures across the United States.”
A total of 22.2 million endoscopies were performed in 2019, most commonly colonoscopy (13.8 million procedures), followed by upper endoscopy (7.5 million procedures), and flexible sigmoidoscopy (379,883 procedures).
In 2020, the NIH spent $3.1 billion, or approximately 7.5% of its budget, on GI disease research. Digestive diseases captured the bulk of this spending, with $2.3 billion. In the same year, the NIH spent 10.5% of its cancer research budget on GI cancers, with the greatest proportion ($325 million) awarded to CRC research.
“Carefully examining the data in this report can help generate areas for future investigation, prioritize research funding, identify areas of unmet need or disparities, and provide an important overview of the impact of digestive and liver conditions,” the investigators concluded. “We hope that others will use this report as motivation to take a deeper dive into individual diseases. There is much to learn from carefully studying existing data sources.”
The study was supported by the National Center for Advancing Translational Sciences, National Institutes of Health. The investigators disclosed no conflicts of interest.
FROM GASTROENTEROLOGY
Infectious disease pop quiz: Clinical challenge #7 for the ObGyn
What is the most appropriate treatment for trichomonas infection in pregnancy?
Continue to the answer...
Trichomonas infection should be treated with oral metronidazole 500 mg twice daily for 7 days. Metronidazole also can be given as a single oral 2-g dose. This treatment is not quite as effective as the multidose regimen, but it may be appropriate for patients who are not likely to be adherent with the longer course of treatment.
Resistance to metronidazole is rare; in such instances, oral tinidazole 2 g in a single dose may be effective.
- Duff P. Maternal and perinatal infections: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al. Gabbe’s Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021:1124-1146.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TJ, et al. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862-919.

Dr. Edwards is a Resident in the Department of Medicine, University of Florida College of Medicine, Gainesville.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The authors report no financial relationships relevant to this article.
Dr. Edwards is a Resident in the Department of Medicine, University of Florida College of Medicine, Gainesville.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The authors report no financial relationships relevant to this article.
Dr. Edwards is a Resident in the Department of Medicine, University of Florida College of Medicine, Gainesville.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The authors report no financial relationships relevant to this article.
What is the most appropriate treatment for trichomonas infection in pregnancy?
Continue to the answer...
Trichomonas infection should be treated with oral metronidazole 500 mg twice daily for 7 days. Metronidazole also can be given as a single oral 2-g dose. This treatment is not quite as effective as the multidose regimen, but it may be appropriate for patients who are not likely to be adherent with the longer course of treatment.
Resistance to metronidazole is rare; in such instances, oral tinidazole 2 g in a single dose may be effective.
What is the most appropriate treatment for trichomonas infection in pregnancy?
Continue to the answer...
Trichomonas infection should be treated with oral metronidazole 500 mg twice daily for 7 days. Metronidazole also can be given as a single oral 2-g dose. This treatment is not quite as effective as the multidose regimen, but it may be appropriate for patients who are not likely to be adherent with the longer course of treatment.
Resistance to metronidazole is rare; in such instances, oral tinidazole 2 g in a single dose may be effective.
- Duff P. Maternal and perinatal infections: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al. Gabbe’s Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021:1124-1146.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TJ, et al. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862-919.
- Duff P. Maternal and perinatal infections: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al. Gabbe’s Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021:1124-1146.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TJ, et al. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862-919.
Even light physical activity linked to lower dementia risk
Older adults who participate in even light physical activity (LPA) may have a lower risk of developing dementia, new research suggests.
In a retrospective analysis of more than 62,000 individuals aged 65 or older without preexisting dementia, 6% developed dementia.
Compared with inactive individuals, “insufficiently active,” “active,” and “highly active” individuals all had a 10%, 20%, and 28% lower risk for dementia, respectively. And this association was consistent regardless of age, sex, other comorbidities, or after the researchers censored for stroke.
Even the lowest amount of LPA was associated with reduced dementia risk, investigators noted.
“In older adults, an increased physical activity level, including a low amount of LPA, was associated with a reduced risk of dementia,” Minjae Yoon, MD, division of cardiology, Severance Cardiovascular Hospital, Yonsei University, Seoul, South Korea, and colleagues wrote.
“Promotion of LPA might reduce the risk of dementia in older adults,” they added.
The findings were published online in JAMA Network Open.
Reverse causation?
Physical activity has been shown previously to be associated with reduced dementia risk. Current World Health Organization guidelines recommend that adults with normal cognition should engage in PA to reduce their risk for cognitive decline.
However, some studies have not yielded this result, “suggesting that previous findings showing a lower risk of dementia in physically active people could be attributed to reverse causation,” the investigators noted. Additionally, previous research regarding exercise intensity has been “inconsistent” concerning the role of LPA in reducing dementia risk.
Many older adults with frailty and comorbidity cannot perform intense or even moderate PA, therefore “these adults would have to gain the benefits of physical activity from LPA,” the researchers noted.
To clarify the potential association between PA and new-onset dementia, they focused specifically on the “dose-response association” between PA and dementia – especially LPA.
Between 2009 and 2012, the investigators enrolled 62,286 older individuals (60.4% women; mean age, 73.2 years) with available health checkup data from the National Health Insurance Service–Senior Database of Korea. All had no history of dementia.
Leisure-time PA was assessed with self-report questionnaires that used a 7-day recall method and included three questions regarding usual frequency (in days per week):
- Vigorous PA (VPA) for at least 20 minutes
- Moderate-intensity PA (MPA) for at least 30 minutes
- LPA for at least 30 minutes
VPA was defined as “intense exercise that caused severe shortness of breath, MPA was defined as activity causing mild shortness of breath, and LPA was defined as “walking at a slow or leisurely pace.”
PA-related energy expenditure was also calculated in metabolic equivalent (MET) minutes per week by “summing the product of frequency, intensity, and duration,” the investigators noted.
Participants were stratified on the basis of their weekly total PA levels into the following groups:
- Inactive (no LPA beyond basic movements)
- Insufficiently active (less than the recommended target range of 1-499 MET-min/wk)
- Active (meeting the recommended target range of 500-999 MET-min/wk)
- Highly active (exceeding the recommended target range of at least 1,000 MET-min/wk)
Of all participants, 35% were categorized as inactive, 25% were insufficiently active, 24.4% were active, and 15.2% were highly active.
Controversy remains
During the total median follow-up of 42 months, 6% of participants had all-cause dementia. After the researchers excluded the first 2 years, incidence of dementia was 21.6 per 1000 person-years during follow-up.
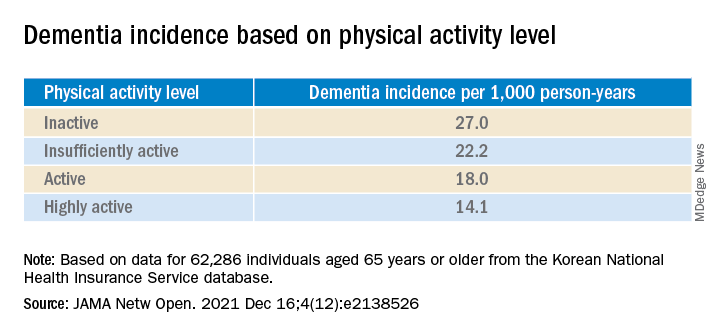
“The cumulative incidence of dementia was associated with a progressively decreasing trend with increasing physical activity” (P = .001 for trend), the investigators reported.
When using a competing-risk multivariable regression model, they found that higher levels of PA were associated with lower risk for dementia, compared with the inactive group.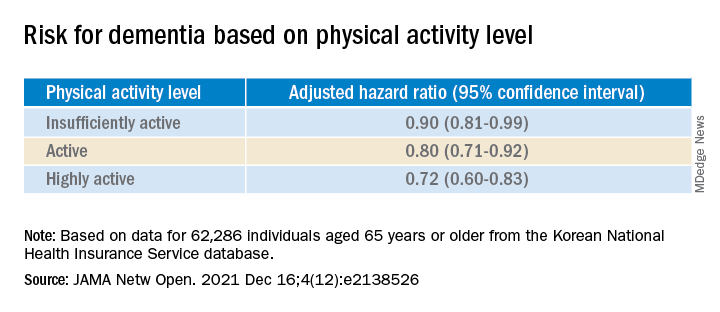
Similar findings were obtained after censoring for stroke, and were consistent for all follow-up periods. In subgroup analysis, the association between PA level and dementia risk remained consistent, regardless of age, sex, and comorbidities.
Even a low amount of LPA (1-299 MET-min/wk) was linked to reduced risk for dementia versus total sedentary behavior (adjusted HR, 0.86; 95% CI, 0.74-0.99).
The investigators noted that some “controversy” remains regarding the possibility of reverse causation and, because their study was observational in nature, “it cannot be used to establish causal relationship.”
Nevertheless, the study had important strengths, including the large number of older adults with available data, the assessment of dose-response association between PA and dementia, and the sensitivity analyses they performed, the researchers added.
Piece of important evidence
Commenting on the findings, Takashi Tarumi, PhD, senior research investigator, National Institute of Advanced Industrial Science and Technology, Ibaraki, Japan, said previous studies have suggested “an inverse association between physical activity and dementia risk, such that older adults performing a higher dose of exercise may have a greater benefit for reducing the dementia risk.”
Dr. Tarumi, an associate editor at the Journal of Alzheimer’s Disease, added the current study “significantly extends our knowledge by showing that dementia risk can also be reduced by light physical activities when they are performed for longer hours.”
This provides “another piece of important evidence” to support clinicians recommending regular physical activity for the prevention of dementia in later life, said Dr. Tarumi, who was not involved with the research.
Also commenting, Martin Underwood, MD, Warwick Medical School, Coventry, England, described the association between reduced physical inactivity and dementia as well established – and noted the current study “appears to confirm earlier observational data showing this relationship.”
The current results have “still not been able to fully exclude the possibility of reverse causation,” said Dr. Underwood, who was also not associated with the study.
However, the finding that more physically active individuals are less likely to develop dementia “only becomes of real interest if we can show that increased physical activity prevents the onset, or slows the progression, of dementia,” he noted.
“To my knowledge this has not yet been established” in randomized clinical trials, Dr. Underwood added.
The study was supported by grants from the Patient-Centered Clinical Research Coordinating Center, funded by the Ministry of Health & Welfare, Republic of Korea; and by a research grant from Yonsei University. One coauthor reported serving as a speaker for Bayer, Bristol-Myers Squibb/Pfizer, Medtronic, and Daiichi-Sankyo, and receiving research funds from Medtronic and Abbott. No other author disclosures were reported. Dr. Tarumi and Dr. Underwood have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Older adults who participate in even light physical activity (LPA) may have a lower risk of developing dementia, new research suggests.
In a retrospective analysis of more than 62,000 individuals aged 65 or older without preexisting dementia, 6% developed dementia.
Compared with inactive individuals, “insufficiently active,” “active,” and “highly active” individuals all had a 10%, 20%, and 28% lower risk for dementia, respectively. And this association was consistent regardless of age, sex, other comorbidities, or after the researchers censored for stroke.
Even the lowest amount of LPA was associated with reduced dementia risk, investigators noted.
“In older adults, an increased physical activity level, including a low amount of LPA, was associated with a reduced risk of dementia,” Minjae Yoon, MD, division of cardiology, Severance Cardiovascular Hospital, Yonsei University, Seoul, South Korea, and colleagues wrote.
“Promotion of LPA might reduce the risk of dementia in older adults,” they added.
The findings were published online in JAMA Network Open.
Reverse causation?
Physical activity has been shown previously to be associated with reduced dementia risk. Current World Health Organization guidelines recommend that adults with normal cognition should engage in PA to reduce their risk for cognitive decline.
However, some studies have not yielded this result, “suggesting that previous findings showing a lower risk of dementia in physically active people could be attributed to reverse causation,” the investigators noted. Additionally, previous research regarding exercise intensity has been “inconsistent” concerning the role of LPA in reducing dementia risk.
Many older adults with frailty and comorbidity cannot perform intense or even moderate PA, therefore “these adults would have to gain the benefits of physical activity from LPA,” the researchers noted.
To clarify the potential association between PA and new-onset dementia, they focused specifically on the “dose-response association” between PA and dementia – especially LPA.
Between 2009 and 2012, the investigators enrolled 62,286 older individuals (60.4% women; mean age, 73.2 years) with available health checkup data from the National Health Insurance Service–Senior Database of Korea. All had no history of dementia.
Leisure-time PA was assessed with self-report questionnaires that used a 7-day recall method and included three questions regarding usual frequency (in days per week):
- Vigorous PA (VPA) for at least 20 minutes
- Moderate-intensity PA (MPA) for at least 30 minutes
- LPA for at least 30 minutes
VPA was defined as “intense exercise that caused severe shortness of breath, MPA was defined as activity causing mild shortness of breath, and LPA was defined as “walking at a slow or leisurely pace.”
PA-related energy expenditure was also calculated in metabolic equivalent (MET) minutes per week by “summing the product of frequency, intensity, and duration,” the investigators noted.
Participants were stratified on the basis of their weekly total PA levels into the following groups:
- Inactive (no LPA beyond basic movements)
- Insufficiently active (less than the recommended target range of 1-499 MET-min/wk)
- Active (meeting the recommended target range of 500-999 MET-min/wk)
- Highly active (exceeding the recommended target range of at least 1,000 MET-min/wk)
Of all participants, 35% were categorized as inactive, 25% were insufficiently active, 24.4% were active, and 15.2% were highly active.
Controversy remains
During the total median follow-up of 42 months, 6% of participants had all-cause dementia. After the researchers excluded the first 2 years, incidence of dementia was 21.6 per 1000 person-years during follow-up.
“The cumulative incidence of dementia was associated with a progressively decreasing trend with increasing physical activity” (P = .001 for trend), the investigators reported.
When using a competing-risk multivariable regression model, they found that higher levels of PA were associated with lower risk for dementia, compared with the inactive group.
Similar findings were obtained after censoring for stroke, and were consistent for all follow-up periods. In subgroup analysis, the association between PA level and dementia risk remained consistent, regardless of age, sex, and comorbidities.
Even a low amount of LPA (1-299 MET-min/wk) was linked to reduced risk for dementia versus total sedentary behavior (adjusted HR, 0.86; 95% CI, 0.74-0.99).
The investigators noted that some “controversy” remains regarding the possibility of reverse causation and, because their study was observational in nature, “it cannot be used to establish causal relationship.”
Nevertheless, the study had important strengths, including the large number of older adults with available data, the assessment of dose-response association between PA and dementia, and the sensitivity analyses they performed, the researchers added.
Piece of important evidence
Commenting on the findings, Takashi Tarumi, PhD, senior research investigator, National Institute of Advanced Industrial Science and Technology, Ibaraki, Japan, said previous studies have suggested “an inverse association between physical activity and dementia risk, such that older adults performing a higher dose of exercise may have a greater benefit for reducing the dementia risk.”
Dr. Tarumi, an associate editor at the Journal of Alzheimer’s Disease, added the current study “significantly extends our knowledge by showing that dementia risk can also be reduced by light physical activities when they are performed for longer hours.”
This provides “another piece of important evidence” to support clinicians recommending regular physical activity for the prevention of dementia in later life, said Dr. Tarumi, who was not involved with the research.
Also commenting, Martin Underwood, MD, Warwick Medical School, Coventry, England, described the association between reduced physical inactivity and dementia as well established – and noted the current study “appears to confirm earlier observational data showing this relationship.”
The current results have “still not been able to fully exclude the possibility of reverse causation,” said Dr. Underwood, who was also not associated with the study.
However, the finding that more physically active individuals are less likely to develop dementia “only becomes of real interest if we can show that increased physical activity prevents the onset, or slows the progression, of dementia,” he noted.
“To my knowledge this has not yet been established” in randomized clinical trials, Dr. Underwood added.
The study was supported by grants from the Patient-Centered Clinical Research Coordinating Center, funded by the Ministry of Health & Welfare, Republic of Korea; and by a research grant from Yonsei University. One coauthor reported serving as a speaker for Bayer, Bristol-Myers Squibb/Pfizer, Medtronic, and Daiichi-Sankyo, and receiving research funds from Medtronic and Abbott. No other author disclosures were reported. Dr. Tarumi and Dr. Underwood have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Older adults who participate in even light physical activity (LPA) may have a lower risk of developing dementia, new research suggests.
In a retrospective analysis of more than 62,000 individuals aged 65 or older without preexisting dementia, 6% developed dementia.
Compared with inactive individuals, “insufficiently active,” “active,” and “highly active” individuals all had a 10%, 20%, and 28% lower risk for dementia, respectively. And this association was consistent regardless of age, sex, other comorbidities, or after the researchers censored for stroke.
Even the lowest amount of LPA was associated with reduced dementia risk, investigators noted.
“In older adults, an increased physical activity level, including a low amount of LPA, was associated with a reduced risk of dementia,” Minjae Yoon, MD, division of cardiology, Severance Cardiovascular Hospital, Yonsei University, Seoul, South Korea, and colleagues wrote.
“Promotion of LPA might reduce the risk of dementia in older adults,” they added.
The findings were published online in JAMA Network Open.
Reverse causation?
Physical activity has been shown previously to be associated with reduced dementia risk. Current World Health Organization guidelines recommend that adults with normal cognition should engage in PA to reduce their risk for cognitive decline.
However, some studies have not yielded this result, “suggesting that previous findings showing a lower risk of dementia in physically active people could be attributed to reverse causation,” the investigators noted. Additionally, previous research regarding exercise intensity has been “inconsistent” concerning the role of LPA in reducing dementia risk.
Many older adults with frailty and comorbidity cannot perform intense or even moderate PA, therefore “these adults would have to gain the benefits of physical activity from LPA,” the researchers noted.
To clarify the potential association between PA and new-onset dementia, they focused specifically on the “dose-response association” between PA and dementia – especially LPA.
Between 2009 and 2012, the investigators enrolled 62,286 older individuals (60.4% women; mean age, 73.2 years) with available health checkup data from the National Health Insurance Service–Senior Database of Korea. All had no history of dementia.
Leisure-time PA was assessed with self-report questionnaires that used a 7-day recall method and included three questions regarding usual frequency (in days per week):
- Vigorous PA (VPA) for at least 20 minutes
- Moderate-intensity PA (MPA) for at least 30 minutes
- LPA for at least 30 minutes
VPA was defined as “intense exercise that caused severe shortness of breath, MPA was defined as activity causing mild shortness of breath, and LPA was defined as “walking at a slow or leisurely pace.”
PA-related energy expenditure was also calculated in metabolic equivalent (MET) minutes per week by “summing the product of frequency, intensity, and duration,” the investigators noted.
Participants were stratified on the basis of their weekly total PA levels into the following groups:
- Inactive (no LPA beyond basic movements)
- Insufficiently active (less than the recommended target range of 1-499 MET-min/wk)
- Active (meeting the recommended target range of 500-999 MET-min/wk)
- Highly active (exceeding the recommended target range of at least 1,000 MET-min/wk)
Of all participants, 35% were categorized as inactive, 25% were insufficiently active, 24.4% were active, and 15.2% were highly active.
Controversy remains
During the total median follow-up of 42 months, 6% of participants had all-cause dementia. After the researchers excluded the first 2 years, incidence of dementia was 21.6 per 1000 person-years during follow-up.
“The cumulative incidence of dementia was associated with a progressively decreasing trend with increasing physical activity” (P = .001 for trend), the investigators reported.
When using a competing-risk multivariable regression model, they found that higher levels of PA were associated with lower risk for dementia, compared with the inactive group.
Similar findings were obtained after censoring for stroke, and were consistent for all follow-up periods. In subgroup analysis, the association between PA level and dementia risk remained consistent, regardless of age, sex, and comorbidities.
Even a low amount of LPA (1-299 MET-min/wk) was linked to reduced risk for dementia versus total sedentary behavior (adjusted HR, 0.86; 95% CI, 0.74-0.99).
The investigators noted that some “controversy” remains regarding the possibility of reverse causation and, because their study was observational in nature, “it cannot be used to establish causal relationship.”
Nevertheless, the study had important strengths, including the large number of older adults with available data, the assessment of dose-response association between PA and dementia, and the sensitivity analyses they performed, the researchers added.
Piece of important evidence
Commenting on the findings, Takashi Tarumi, PhD, senior research investigator, National Institute of Advanced Industrial Science and Technology, Ibaraki, Japan, said previous studies have suggested “an inverse association between physical activity and dementia risk, such that older adults performing a higher dose of exercise may have a greater benefit for reducing the dementia risk.”
Dr. Tarumi, an associate editor at the Journal of Alzheimer’s Disease, added the current study “significantly extends our knowledge by showing that dementia risk can also be reduced by light physical activities when they are performed for longer hours.”
This provides “another piece of important evidence” to support clinicians recommending regular physical activity for the prevention of dementia in later life, said Dr. Tarumi, who was not involved with the research.
Also commenting, Martin Underwood, MD, Warwick Medical School, Coventry, England, described the association between reduced physical inactivity and dementia as well established – and noted the current study “appears to confirm earlier observational data showing this relationship.”
The current results have “still not been able to fully exclude the possibility of reverse causation,” said Dr. Underwood, who was also not associated with the study.
However, the finding that more physically active individuals are less likely to develop dementia “only becomes of real interest if we can show that increased physical activity prevents the onset, or slows the progression, of dementia,” he noted.
“To my knowledge this has not yet been established” in randomized clinical trials, Dr. Underwood added.
The study was supported by grants from the Patient-Centered Clinical Research Coordinating Center, funded by the Ministry of Health & Welfare, Republic of Korea; and by a research grant from Yonsei University. One coauthor reported serving as a speaker for Bayer, Bristol-Myers Squibb/Pfizer, Medtronic, and Daiichi-Sankyo, and receiving research funds from Medtronic and Abbott. No other author disclosures were reported. Dr. Tarumi and Dr. Underwood have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.