User login
For MD-IQ use only
Progress still needed for pregnant and postpartum gastroenterologists
Despite increasing numbers joining the field, women remain a minority group in gastroenterology, where they constitute only 18% of these physicians.1 Additionally, women continue to be underrepresented among senior faculty and in leadership roles in both academic and private practice settings.2 While women now make up a majority of medical school matriculants3,4 women trainees are frequently dissuaded from pursuing specialty fellowships following residency, particularly in procedurally based fields like gastroenterology, because of perceived incompatibility with childbearing and child-rearing.5-8 For many who choose to enter the field despite these challenges, gastroenterology training and early practice often coincide with childbearing years.910 These structural impediments may contribute to the “leaky pipeline” and female physician attrition during the first decade of independent practice after fellowship.11-13 Urgent changes are needed in order to retain and support clinicians and physician-scientists through this period so that they, their offspring, their patients, and the field are able to thrive.

Fertility and pregnancy
The decision to have a child is a major milestone for many physicians and often occurs during gastroenterology training or early practice.10 Medical-training and early-career environments are not yet optimized to support women who become pregnant. At baseline, the formative years of a career are challenging ones, punctuated by long hours and both intellectually and emotionally demanding work. They are also often physically grueling, particularly while one is learning and becoming efficient in endoscopy. The ergonomics in the endoscopy suite (as in other areas of medicine) are not optimized for physicians of shorter stature, smaller hand sizes, and those who may have difficulty pushing a several-hundred-pound endoscopy cart bedside, all of which contribute to increased injury risk for female proceduralists.7,14-16 Methods to reduce endoscopic injuries in pregnant endoscopists have not yet been studied. Additionally, the existence of maternity and gender bias has been well-documented, in our field and beyond.17-20 Not surprisingly, women in gastroenterology commonly report delayed childbearing, with expected consequences, including increased infertility rates, compared with nonphysician peers.21 After 5 and 10 years as attendings, female gastroenterologists continue to report fewer children than male colleagues.22,23 Once pregnant, there are a number of field-specific challenges to navigate. These include decisions about the safety of performing procedures involving fluoroscopy or high infectious risk, particularly early in pregnancy when organogenesis occurs.7,24 Additionally, engaging in appropriate obstetric care can be challenging given the need for regular physician and ultrasound appointments.

Simple, cost-efficient interventions may be effective in decreasing infertility rates, pregnancy loss, and poor physician experiences during pregnancy. For one, all gastroenterology divisions could craft written policies that include a no-tolerance approach to expressions of maternity bias against pregnant or postpartum trainees and faculty.12,25 Additionally, ergonomic improvements, such as standing pads, dial extenders, and adjusted screen heights may decrease injury rates and increase comfort for female endoscopists.26,27 There should also be a no-penalty, no-questions-asked approach for any female endoscopist who defers performance of an obstetrically high-risk procedure to a nonpregnant colleague. Additionally, pregnant gastroenterologists should be supported in obtaining high-quality obstetric care. At an individual level, nonpregnant gastroenterologists, and particularly male allies, can support pregnant colleagues by agreeing to perform higher-risk procedures, stepping in if a fellow is unable to perform endoscopy because of pregnancy, and by offering to push the endoscopy cart on behalf of a pregnant colleague to bedside, if necessary.10,28
Parental leave
Following delivery, parental leave presents an additional challenge for the physician parent. Paid maternal leave has been associated with improved child and maternal outcomes and is widely available to physicians outside the United States.29,30 At present, duration of leave varies significantly by career stage (fellows versus attending), practice setting (academic center versus private practice), and geographic location. The American Academy of Pediatrics recommends a minimum of 12 weeks of leave.31 This length has been associated with lower rates of postpartum depression and higher rates of sustained breastfeeding, with subsequent improved health outcomes for mother and child.32-34 An increasing number of states have passed laws mandating minimum paid and unpaid parental leave time (for example, in Massachusetts, gastroenterology trainees and faculty are afforded 12 weeks of leave, in accordance with state law).35 Recent changes to board eligibility and training requirements via the American Board of Medical Specialties and the American Council for Graduate Medical Education now provide 6 weeks for parental leave. This is an improvement over prior policies which rendered many physician-parents board-ineligible if they took more than 4 weeks of leave, although it must be noted that even the revised policies allow for less time than either that of Obstetricians and Gynecologists or than the American Academy of Pediatrics recommends.
Our data, presented at the 2021 ACG conference, suggest that many trainees report receiving 4 weeks or less of parental leave, despite the ACGME and ABMS policies described above. We also found that physicians were frequently not aware of their institution or division leave policies.10 Ideally, all gastroenterology divisions in the United States would follow the recommended leave duration set forth by the medical societies of specialties that care for pregnant and postpartum mothers and their infants. Additionally, the impact of leave time on graduation and board eligibility, as well as academic and practice promotion, should be made clear at the time of leave and should minimize adverse consequences for the careers of pregnant and postpartum gastroenterologists. Gastroenterology trainees and faculty should be educated in the existence and details of their institution or practice policies, and these policies should be made readily available to all physicians and administrators.
Postpartum period
The transition back to work is a challenging one for mothers in all fields of medicine, particularly for those returning to procedurally based subspecialties such as gastroenterology. This is especially true for trainees and faculty who have returned to work sooner than the recommended 12 weeks and for those who are post cesarean section, for whom physical healing may not be complete. Long days performing endoscopy may be physically challenging or impossible for some women during the postpartum period. Additionally, expressing breast milk, a metabolically intensive activity, also necessitates time, space, and privacy to perform and is frequently made more difficult by insufficient lactation accommodations. The COVID-19 pandemic has increased logistic challenges for lactating mothers, because of the need for well-ventilated lactation spaces to minimize infectious risk.19 Our colleagues have reported pumping in their vehicles, in supply closets, and in spaces that require so much travel time (in addition to time required to express milk, store milk, and clean pump equipment) that the practice was unsustainable, and the physician stopped breastfeeding prematurely.36
The benefits of breastfeeding for mother and infant are well-established, and exclusive breastfeeding for the first 6 months of life is supported by the American College of Obstetricians and Gynecologists, whose position statement reads as follows: “Policies that protect the right of a woman and her child to breastfeed ... and that accommodate milk expression, such as ... paid maternity leave, on-site childcare, break time for expressing milk, and a clean, private location for expressing milk, are essential to sustaining breastfeeding.”37 We would add to these recommendations provision of dedicated milk storage space and establishment of clear, supportive policies that allow lactating physicians to breastfeed and express breast milk if they choose without career penalty. Several institutions offer scheduled protected clinical time and modified work relative value units (RVU) for lactating physicians, such that returning parents can have protected time for expressing breast milk and still meet RVU targets.38 Additionally, many academic institutions offer productivity adjustments for tenure-track faculty who have recently had children.
Creating a more supportive environment for women gastroenterologists who desire children allows the field to be more representative of our patient population and has been shown to positively impact outcomes from improved colorectal cancer screening rates to more guideline-directed informed consent conversations.39-41 Gastroenterology should comprise a physician workforce predicated on clinical and research excellence alone and should not require its practitioners to delay or abstain from pregnancy and child rearing. Robust, clear, and generous parental leave and postpartum accommodations will allow the field to retain and promote talented physicians, who will then contribute to the betterment of patients and the field over decades.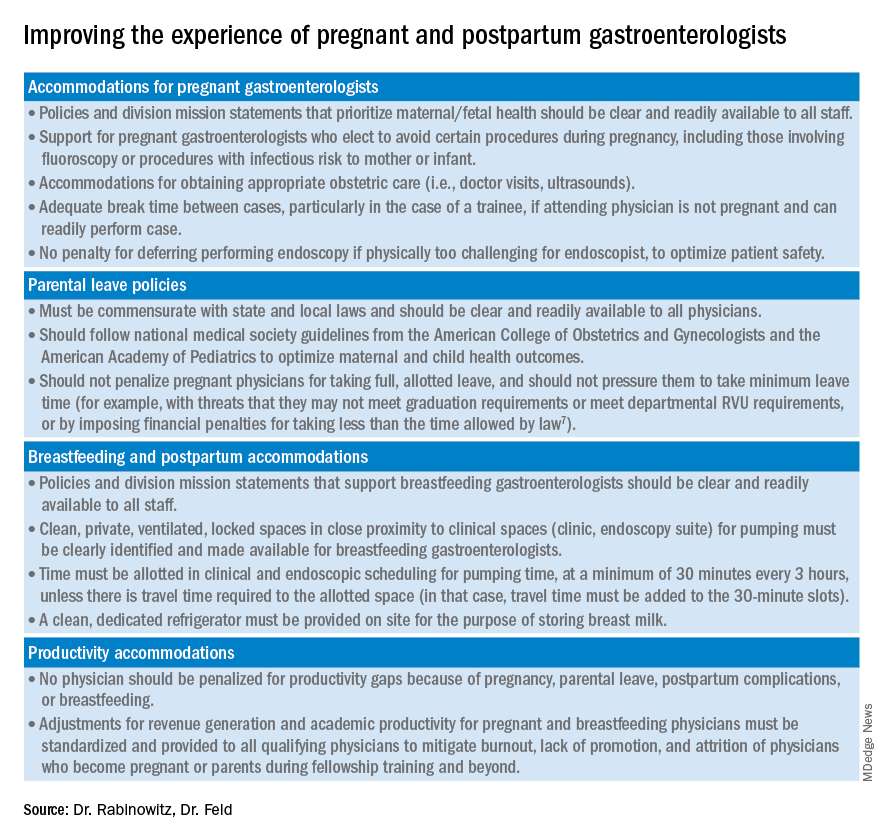
Dr. Rabinowitz is a faculty member in the department of medicine and division of gastroenterology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston. Dr. Feld is a transplant hepatology fellow, division of gastroenterology, department of medicine, University of Washington, Seattle. Dr. Rabinowitz and Dr. Feld have no conflicts of interest to disclose.
References
1. AAMC. Diversity in Medicine: Facts and Figures 2019. 2018.
2. Colleges AoAM. The State of Women in Academic Medicine: The Pipeline and Pathways to Leadership, 2015-2016. 2016. www.aamc.org/download/481206/data/2015table11.pdf.
3. AAMC. Table B-3: Total U.S. Medical School Enrollment by Race/Ethnicity and Sex, 2014-2015 through 2018-2019, 2019.
4. Rabinowitz LG. Recognizing blind spots – a remedy for gender bias in medicine? (N Engl. J Med. 2018; 378[24]: 2253-5).
5. Douglas PS et al. Career preferences and perceptions of cardiology among US internal medicine trainees: Factors influencing cardiology career choice. JAMA Cardiol 2018; 3(8):682-91.
6. Stack SW et al. Childbearing decisions in residency: A multicenter survey of female residents. Acad Med 2020;95(10):1550-7.
7. David YN et al. Pregnancy and the working gastroenterologist: Perceptions, realities, and systemic challenges. Gastroenterology 2021;161(3):756-60.
8. Rembacken BJ et al. Barriers and bias standing in the way of female trainees wanting to learn advanced endoscopy. United European Gastroenterol J. 2019;7(8):1141-5.
9. Arlow FL et al. Gastroenterology training and career choices: A prospective longitudinal study of the impact of gender and of managed care. Am J Gastroenterol. 2002;97(2):459-69.
10. Feld L et al. Parental leave for gastroenterology fellows: A national survey of current fellows. Am J Gastroenterol. 2021;116:S611-2.
11. Rabinowitz LG et al. Addressing gender in gastroenterology: opportunities for change. Gastrointest Endosc. 2020;91(1):155-61.
12. Feld LD. Baby steps in the right direction: Toward a parental leave policy for gastroenterology fellows. Am J Gastroenterol. 2021;116(3):505-8.
13. Feld LD. Interviewing for two. Am J Gastroenterol. 2020;116(3):445-6
14. Rabinowitz LG et al. Gender dynamics in education and practice of gastroenterology. Gastrointest Endosc. 2021;93(5):1047-56.e5.
15. Harvin G. Review of musculoskeletal injuries and prevention in the endoscopy practitioner. J Clin Gastroenterol. 2014;48(7):590-4.
16. LabX Oecs. www.labx.com/product/endoscopy-cart (accessed 2021 Nov 19.
17. Heilman ME and Okimoto TG. Motherhood: A potential source of bias in employment decisions. J Appl Psychol. 2008;93(1):189-98.
18. Robinson K et al. Racism, bias, and discrimination as modifiable barriers to breastfeeding for African American women: A scoping review of the literature. J Midwifery Womens Health. 2019;64(6):734-42.
19. Rabinowitz LG and Rabinowitz DG. Women on the Frontline: A Changed Workforce and the Fight Against COVID-19. Acad Med. 2021 Jun 1;96(6):808-12.
20. Rabinowitz LG et al. Gender in the endoscopy suite. Lancet Gastroenterol Hepatol. 2020 Dec;5(12):1032-4.
21. Stentz NC et al. Fertility and childbearing among American female physicians. J Womens Health. 2016; 25(10):1059-65.
22. Burke CA et al. Gender disparity in the practice of gastroenterology: The first 5 years of a career. Am J Gastroenterol. 2005;100(2):259-64.
23. Singh A et al. Women in gastroenterology committee of American College of G. Do gender disparities persist in gastroenterology after 10 years of practice? Am J Gastroenterol. 2008;103(7):1589-95.
24. Krueger KJ and Hoffman BJ. Radiation exposure during gastroenterologic fluoroscopy: Risk assessment for pregnant workers. Am J Gastroenterol. 1992;87(4):429-31.
25. Krause ML et al. Impact of pregnancy and gender on internal medicine resident evaluations: A retrospective cohort study. J Gen Intern Med. 2017;32(6):648-53.
26. Pawa S et al. Are all endoscopy-related musculoskeletal injuries created equal? Results of a national gender-based survey. Am J Gastroenterol. 2021;116(3):530-8.
27. David YN et al. Gender-specific factors influencing gastroenterologists to pursue careers in advanced endoscopy: perceptions vs reality. Am J Gastroenterol. 2021;116(3):539-50.
28. Bilal M et al. The need for allyship in achieving gender equity in gastroenterology. Am J Gastroenterol. 2021 Oct 19. doi: 10.14309/ajg.0000000000001508. Online ahead of print.
29. Jou J et al. Paid maternity leave in the United States: Associations with maternal and infant health. Matern Child Health J. 2018;22(2):216-25.
30. Aitken Z et al. The maternal health outcomes of paid maternity leave: A systematic review. Soc Sci Med. 2015;130:32-41.
31. Dodson NA and Talib HJ. Paid parental leave for mothers and fathers can improve physician wellness. AAP News. 2020 Jul 1. https://publications.aap.org/aapnews/news/12432.
32. Kornfeind KR and Sipsma HL. Exploring the link between maternity leave and postpartum depression. Womens Health Issues 2018;28(4):321-6.
33. Navarro-Rosenblatt D and Garmendia ML. Maternity leave and its impact on breastfeeding: A review of the literature. Breastfeed Med 2018;13(9):589-97.
34. Stack SW et al. Maternity leave in residency: A multicenter study of determinants and wellness outcomes. Acad Med. 2019;94(11):1738-45.
35. Mass.gov. Paid Family and Medical Leave Information for Massachusetts Employers. 2020.
36. Ares Segura S et al. en representacion del Comite de Lactancia Materna de la Asociacion Espanola de P. [The importance of maternal nutrition during breastfeeding: Do breastfeeding mothers need nutritional supplements?]. An Pediatr. (Barc) 2016;84(6):347 e1-7.
37. American College of Obstetricians and Gynecologists, Committee on Obstetric Practice. Committee Opinion No. 658: Optimizing Support for Breastfeeding as Part of Obstetric Practice. Obstet Gynecol. 2016;127(2):e86-92.
38. Porter KK et al. A lactation credit model to support breastfeeding in radiology: The new gold standard to support “liquid gold.” Clin Imaging 2021;80:16-8.
39. Davis J et al. Clinical practice patterns suggest female patients prefer female endoscopists. Dig Dis Sci. 2015;60(10):3149-50.
40. Menees SB et al. Women patients’ preference for women physicians is a barrier to colon cancer screening. Gastrointest Endosc. 2005;62(2):219-23.
41. Feld LD et al. Management of code status in the periendoscopic period: A national survey of current practices and beliefs of U.S. gastroenterologists. Gastrointest Endosc. 2021;94(1):172-7.e2.
Despite increasing numbers joining the field, women remain a minority group in gastroenterology, where they constitute only 18% of these physicians.1 Additionally, women continue to be underrepresented among senior faculty and in leadership roles in both academic and private practice settings.2 While women now make up a majority of medical school matriculants3,4 women trainees are frequently dissuaded from pursuing specialty fellowships following residency, particularly in procedurally based fields like gastroenterology, because of perceived incompatibility with childbearing and child-rearing.5-8 For many who choose to enter the field despite these challenges, gastroenterology training and early practice often coincide with childbearing years.910 These structural impediments may contribute to the “leaky pipeline” and female physician attrition during the first decade of independent practice after fellowship.11-13 Urgent changes are needed in order to retain and support clinicians and physician-scientists through this period so that they, their offspring, their patients, and the field are able to thrive.
Fertility and pregnancy
The decision to have a child is a major milestone for many physicians and often occurs during gastroenterology training or early practice.10 Medical-training and early-career environments are not yet optimized to support women who become pregnant. At baseline, the formative years of a career are challenging ones, punctuated by long hours and both intellectually and emotionally demanding work. They are also often physically grueling, particularly while one is learning and becoming efficient in endoscopy. The ergonomics in the endoscopy suite (as in other areas of medicine) are not optimized for physicians of shorter stature, smaller hand sizes, and those who may have difficulty pushing a several-hundred-pound endoscopy cart bedside, all of which contribute to increased injury risk for female proceduralists.7,14-16 Methods to reduce endoscopic injuries in pregnant endoscopists have not yet been studied. Additionally, the existence of maternity and gender bias has been well-documented, in our field and beyond.17-20 Not surprisingly, women in gastroenterology commonly report delayed childbearing, with expected consequences, including increased infertility rates, compared with nonphysician peers.21 After 5 and 10 years as attendings, female gastroenterologists continue to report fewer children than male colleagues.22,23 Once pregnant, there are a number of field-specific challenges to navigate. These include decisions about the safety of performing procedures involving fluoroscopy or high infectious risk, particularly early in pregnancy when organogenesis occurs.7,24 Additionally, engaging in appropriate obstetric care can be challenging given the need for regular physician and ultrasound appointments.
Simple, cost-efficient interventions may be effective in decreasing infertility rates, pregnancy loss, and poor physician experiences during pregnancy. For one, all gastroenterology divisions could craft written policies that include a no-tolerance approach to expressions of maternity bias against pregnant or postpartum trainees and faculty.12,25 Additionally, ergonomic improvements, such as standing pads, dial extenders, and adjusted screen heights may decrease injury rates and increase comfort for female endoscopists.26,27 There should also be a no-penalty, no-questions-asked approach for any female endoscopist who defers performance of an obstetrically high-risk procedure to a nonpregnant colleague. Additionally, pregnant gastroenterologists should be supported in obtaining high-quality obstetric care. At an individual level, nonpregnant gastroenterologists, and particularly male allies, can support pregnant colleagues by agreeing to perform higher-risk procedures, stepping in if a fellow is unable to perform endoscopy because of pregnancy, and by offering to push the endoscopy cart on behalf of a pregnant colleague to bedside, if necessary.10,28
Parental leave
Following delivery, parental leave presents an additional challenge for the physician parent. Paid maternal leave has been associated with improved child and maternal outcomes and is widely available to physicians outside the United States.29,30 At present, duration of leave varies significantly by career stage (fellows versus attending), practice setting (academic center versus private practice), and geographic location. The American Academy of Pediatrics recommends a minimum of 12 weeks of leave.31 This length has been associated with lower rates of postpartum depression and higher rates of sustained breastfeeding, with subsequent improved health outcomes for mother and child.32-34 An increasing number of states have passed laws mandating minimum paid and unpaid parental leave time (for example, in Massachusetts, gastroenterology trainees and faculty are afforded 12 weeks of leave, in accordance with state law).35 Recent changes to board eligibility and training requirements via the American Board of Medical Specialties and the American Council for Graduate Medical Education now provide 6 weeks for parental leave. This is an improvement over prior policies which rendered many physician-parents board-ineligible if they took more than 4 weeks of leave, although it must be noted that even the revised policies allow for less time than either that of Obstetricians and Gynecologists or than the American Academy of Pediatrics recommends.
Our data, presented at the 2021 ACG conference, suggest that many trainees report receiving 4 weeks or less of parental leave, despite the ACGME and ABMS policies described above. We also found that physicians were frequently not aware of their institution or division leave policies.10 Ideally, all gastroenterology divisions in the United States would follow the recommended leave duration set forth by the medical societies of specialties that care for pregnant and postpartum mothers and their infants. Additionally, the impact of leave time on graduation and board eligibility, as well as academic and practice promotion, should be made clear at the time of leave and should minimize adverse consequences for the careers of pregnant and postpartum gastroenterologists. Gastroenterology trainees and faculty should be educated in the existence and details of their institution or practice policies, and these policies should be made readily available to all physicians and administrators.
Postpartum period
The transition back to work is a challenging one for mothers in all fields of medicine, particularly for those returning to procedurally based subspecialties such as gastroenterology. This is especially true for trainees and faculty who have returned to work sooner than the recommended 12 weeks and for those who are post cesarean section, for whom physical healing may not be complete. Long days performing endoscopy may be physically challenging or impossible for some women during the postpartum period. Additionally, expressing breast milk, a metabolically intensive activity, also necessitates time, space, and privacy to perform and is frequently made more difficult by insufficient lactation accommodations. The COVID-19 pandemic has increased logistic challenges for lactating mothers, because of the need for well-ventilated lactation spaces to minimize infectious risk.19 Our colleagues have reported pumping in their vehicles, in supply closets, and in spaces that require so much travel time (in addition to time required to express milk, store milk, and clean pump equipment) that the practice was unsustainable, and the physician stopped breastfeeding prematurely.36
The benefits of breastfeeding for mother and infant are well-established, and exclusive breastfeeding for the first 6 months of life is supported by the American College of Obstetricians and Gynecologists, whose position statement reads as follows: “Policies that protect the right of a woman and her child to breastfeed ... and that accommodate milk expression, such as ... paid maternity leave, on-site childcare, break time for expressing milk, and a clean, private location for expressing milk, are essential to sustaining breastfeeding.”37 We would add to these recommendations provision of dedicated milk storage space and establishment of clear, supportive policies that allow lactating physicians to breastfeed and express breast milk if they choose without career penalty. Several institutions offer scheduled protected clinical time and modified work relative value units (RVU) for lactating physicians, such that returning parents can have protected time for expressing breast milk and still meet RVU targets.38 Additionally, many academic institutions offer productivity adjustments for tenure-track faculty who have recently had children.
Creating a more supportive environment for women gastroenterologists who desire children allows the field to be more representative of our patient population and has been shown to positively impact outcomes from improved colorectal cancer screening rates to more guideline-directed informed consent conversations.39-41 Gastroenterology should comprise a physician workforce predicated on clinical and research excellence alone and should not require its practitioners to delay or abstain from pregnancy and child rearing. Robust, clear, and generous parental leave and postpartum accommodations will allow the field to retain and promote talented physicians, who will then contribute to the betterment of patients and the field over decades.
Dr. Rabinowitz is a faculty member in the department of medicine and division of gastroenterology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston. Dr. Feld is a transplant hepatology fellow, division of gastroenterology, department of medicine, University of Washington, Seattle. Dr. Rabinowitz and Dr. Feld have no conflicts of interest to disclose.
References
1. AAMC. Diversity in Medicine: Facts and Figures 2019. 2018.
2. Colleges AoAM. The State of Women in Academic Medicine: The Pipeline and Pathways to Leadership, 2015-2016. 2016. www.aamc.org/download/481206/data/2015table11.pdf.
3. AAMC. Table B-3: Total U.S. Medical School Enrollment by Race/Ethnicity and Sex, 2014-2015 through 2018-2019, 2019.
4. Rabinowitz LG. Recognizing blind spots – a remedy for gender bias in medicine? (N Engl. J Med. 2018; 378[24]: 2253-5).
5. Douglas PS et al. Career preferences and perceptions of cardiology among US internal medicine trainees: Factors influencing cardiology career choice. JAMA Cardiol 2018; 3(8):682-91.
6. Stack SW et al. Childbearing decisions in residency: A multicenter survey of female residents. Acad Med 2020;95(10):1550-7.
7. David YN et al. Pregnancy and the working gastroenterologist: Perceptions, realities, and systemic challenges. Gastroenterology 2021;161(3):756-60.
8. Rembacken BJ et al. Barriers and bias standing in the way of female trainees wanting to learn advanced endoscopy. United European Gastroenterol J. 2019;7(8):1141-5.
9. Arlow FL et al. Gastroenterology training and career choices: A prospective longitudinal study of the impact of gender and of managed care. Am J Gastroenterol. 2002;97(2):459-69.
10. Feld L et al. Parental leave for gastroenterology fellows: A national survey of current fellows. Am J Gastroenterol. 2021;116:S611-2.
11. Rabinowitz LG et al. Addressing gender in gastroenterology: opportunities for change. Gastrointest Endosc. 2020;91(1):155-61.
12. Feld LD. Baby steps in the right direction: Toward a parental leave policy for gastroenterology fellows. Am J Gastroenterol. 2021;116(3):505-8.
13. Feld LD. Interviewing for two. Am J Gastroenterol. 2020;116(3):445-6
14. Rabinowitz LG et al. Gender dynamics in education and practice of gastroenterology. Gastrointest Endosc. 2021;93(5):1047-56.e5.
15. Harvin G. Review of musculoskeletal injuries and prevention in the endoscopy practitioner. J Clin Gastroenterol. 2014;48(7):590-4.
16. LabX Oecs. www.labx.com/product/endoscopy-cart (accessed 2021 Nov 19.
17. Heilman ME and Okimoto TG. Motherhood: A potential source of bias in employment decisions. J Appl Psychol. 2008;93(1):189-98.
18. Robinson K et al. Racism, bias, and discrimination as modifiable barriers to breastfeeding for African American women: A scoping review of the literature. J Midwifery Womens Health. 2019;64(6):734-42.
19. Rabinowitz LG and Rabinowitz DG. Women on the Frontline: A Changed Workforce and the Fight Against COVID-19. Acad Med. 2021 Jun 1;96(6):808-12.
20. Rabinowitz LG et al. Gender in the endoscopy suite. Lancet Gastroenterol Hepatol. 2020 Dec;5(12):1032-4.
21. Stentz NC et al. Fertility and childbearing among American female physicians. J Womens Health. 2016; 25(10):1059-65.
22. Burke CA et al. Gender disparity in the practice of gastroenterology: The first 5 years of a career. Am J Gastroenterol. 2005;100(2):259-64.
23. Singh A et al. Women in gastroenterology committee of American College of G. Do gender disparities persist in gastroenterology after 10 years of practice? Am J Gastroenterol. 2008;103(7):1589-95.
24. Krueger KJ and Hoffman BJ. Radiation exposure during gastroenterologic fluoroscopy: Risk assessment for pregnant workers. Am J Gastroenterol. 1992;87(4):429-31.
25. Krause ML et al. Impact of pregnancy and gender on internal medicine resident evaluations: A retrospective cohort study. J Gen Intern Med. 2017;32(6):648-53.
26. Pawa S et al. Are all endoscopy-related musculoskeletal injuries created equal? Results of a national gender-based survey. Am J Gastroenterol. 2021;116(3):530-8.
27. David YN et al. Gender-specific factors influencing gastroenterologists to pursue careers in advanced endoscopy: perceptions vs reality. Am J Gastroenterol. 2021;116(3):539-50.
28. Bilal M et al. The need for allyship in achieving gender equity in gastroenterology. Am J Gastroenterol. 2021 Oct 19. doi: 10.14309/ajg.0000000000001508. Online ahead of print.
29. Jou J et al. Paid maternity leave in the United States: Associations with maternal and infant health. Matern Child Health J. 2018;22(2):216-25.
30. Aitken Z et al. The maternal health outcomes of paid maternity leave: A systematic review. Soc Sci Med. 2015;130:32-41.
31. Dodson NA and Talib HJ. Paid parental leave for mothers and fathers can improve physician wellness. AAP News. 2020 Jul 1. https://publications.aap.org/aapnews/news/12432.
32. Kornfeind KR and Sipsma HL. Exploring the link between maternity leave and postpartum depression. Womens Health Issues 2018;28(4):321-6.
33. Navarro-Rosenblatt D and Garmendia ML. Maternity leave and its impact on breastfeeding: A review of the literature. Breastfeed Med 2018;13(9):589-97.
34. Stack SW et al. Maternity leave in residency: A multicenter study of determinants and wellness outcomes. Acad Med. 2019;94(11):1738-45.
35. Mass.gov. Paid Family and Medical Leave Information for Massachusetts Employers. 2020.
36. Ares Segura S et al. en representacion del Comite de Lactancia Materna de la Asociacion Espanola de P. [The importance of maternal nutrition during breastfeeding: Do breastfeeding mothers need nutritional supplements?]. An Pediatr. (Barc) 2016;84(6):347 e1-7.
37. American College of Obstetricians and Gynecologists, Committee on Obstetric Practice. Committee Opinion No. 658: Optimizing Support for Breastfeeding as Part of Obstetric Practice. Obstet Gynecol. 2016;127(2):e86-92.
38. Porter KK et al. A lactation credit model to support breastfeeding in radiology: The new gold standard to support “liquid gold.” Clin Imaging 2021;80:16-8.
39. Davis J et al. Clinical practice patterns suggest female patients prefer female endoscopists. Dig Dis Sci. 2015;60(10):3149-50.
40. Menees SB et al. Women patients’ preference for women physicians is a barrier to colon cancer screening. Gastrointest Endosc. 2005;62(2):219-23.
41. Feld LD et al. Management of code status in the periendoscopic period: A national survey of current practices and beliefs of U.S. gastroenterologists. Gastrointest Endosc. 2021;94(1):172-7.e2.
Despite increasing numbers joining the field, women remain a minority group in gastroenterology, where they constitute only 18% of these physicians.1 Additionally, women continue to be underrepresented among senior faculty and in leadership roles in both academic and private practice settings.2 While women now make up a majority of medical school matriculants3,4 women trainees are frequently dissuaded from pursuing specialty fellowships following residency, particularly in procedurally based fields like gastroenterology, because of perceived incompatibility with childbearing and child-rearing.5-8 For many who choose to enter the field despite these challenges, gastroenterology training and early practice often coincide with childbearing years.910 These structural impediments may contribute to the “leaky pipeline” and female physician attrition during the first decade of independent practice after fellowship.11-13 Urgent changes are needed in order to retain and support clinicians and physician-scientists through this period so that they, their offspring, their patients, and the field are able to thrive.
Fertility and pregnancy
The decision to have a child is a major milestone for many physicians and often occurs during gastroenterology training or early practice.10 Medical-training and early-career environments are not yet optimized to support women who become pregnant. At baseline, the formative years of a career are challenging ones, punctuated by long hours and both intellectually and emotionally demanding work. They are also often physically grueling, particularly while one is learning and becoming efficient in endoscopy. The ergonomics in the endoscopy suite (as in other areas of medicine) are not optimized for physicians of shorter stature, smaller hand sizes, and those who may have difficulty pushing a several-hundred-pound endoscopy cart bedside, all of which contribute to increased injury risk for female proceduralists.7,14-16 Methods to reduce endoscopic injuries in pregnant endoscopists have not yet been studied. Additionally, the existence of maternity and gender bias has been well-documented, in our field and beyond.17-20 Not surprisingly, women in gastroenterology commonly report delayed childbearing, with expected consequences, including increased infertility rates, compared with nonphysician peers.21 After 5 and 10 years as attendings, female gastroenterologists continue to report fewer children than male colleagues.22,23 Once pregnant, there are a number of field-specific challenges to navigate. These include decisions about the safety of performing procedures involving fluoroscopy or high infectious risk, particularly early in pregnancy when organogenesis occurs.7,24 Additionally, engaging in appropriate obstetric care can be challenging given the need for regular physician and ultrasound appointments.
Simple, cost-efficient interventions may be effective in decreasing infertility rates, pregnancy loss, and poor physician experiences during pregnancy. For one, all gastroenterology divisions could craft written policies that include a no-tolerance approach to expressions of maternity bias against pregnant or postpartum trainees and faculty.12,25 Additionally, ergonomic improvements, such as standing pads, dial extenders, and adjusted screen heights may decrease injury rates and increase comfort for female endoscopists.26,27 There should also be a no-penalty, no-questions-asked approach for any female endoscopist who defers performance of an obstetrically high-risk procedure to a nonpregnant colleague. Additionally, pregnant gastroenterologists should be supported in obtaining high-quality obstetric care. At an individual level, nonpregnant gastroenterologists, and particularly male allies, can support pregnant colleagues by agreeing to perform higher-risk procedures, stepping in if a fellow is unable to perform endoscopy because of pregnancy, and by offering to push the endoscopy cart on behalf of a pregnant colleague to bedside, if necessary.10,28
Parental leave
Following delivery, parental leave presents an additional challenge for the physician parent. Paid maternal leave has been associated with improved child and maternal outcomes and is widely available to physicians outside the United States.29,30 At present, duration of leave varies significantly by career stage (fellows versus attending), practice setting (academic center versus private practice), and geographic location. The American Academy of Pediatrics recommends a minimum of 12 weeks of leave.31 This length has been associated with lower rates of postpartum depression and higher rates of sustained breastfeeding, with subsequent improved health outcomes for mother and child.32-34 An increasing number of states have passed laws mandating minimum paid and unpaid parental leave time (for example, in Massachusetts, gastroenterology trainees and faculty are afforded 12 weeks of leave, in accordance with state law).35 Recent changes to board eligibility and training requirements via the American Board of Medical Specialties and the American Council for Graduate Medical Education now provide 6 weeks for parental leave. This is an improvement over prior policies which rendered many physician-parents board-ineligible if they took more than 4 weeks of leave, although it must be noted that even the revised policies allow for less time than either that of Obstetricians and Gynecologists or than the American Academy of Pediatrics recommends.
Our data, presented at the 2021 ACG conference, suggest that many trainees report receiving 4 weeks or less of parental leave, despite the ACGME and ABMS policies described above. We also found that physicians were frequently not aware of their institution or division leave policies.10 Ideally, all gastroenterology divisions in the United States would follow the recommended leave duration set forth by the medical societies of specialties that care for pregnant and postpartum mothers and their infants. Additionally, the impact of leave time on graduation and board eligibility, as well as academic and practice promotion, should be made clear at the time of leave and should minimize adverse consequences for the careers of pregnant and postpartum gastroenterologists. Gastroenterology trainees and faculty should be educated in the existence and details of their institution or practice policies, and these policies should be made readily available to all physicians and administrators.
Postpartum period
The transition back to work is a challenging one for mothers in all fields of medicine, particularly for those returning to procedurally based subspecialties such as gastroenterology. This is especially true for trainees and faculty who have returned to work sooner than the recommended 12 weeks and for those who are post cesarean section, for whom physical healing may not be complete. Long days performing endoscopy may be physically challenging or impossible for some women during the postpartum period. Additionally, expressing breast milk, a metabolically intensive activity, also necessitates time, space, and privacy to perform and is frequently made more difficult by insufficient lactation accommodations. The COVID-19 pandemic has increased logistic challenges for lactating mothers, because of the need for well-ventilated lactation spaces to minimize infectious risk.19 Our colleagues have reported pumping in their vehicles, in supply closets, and in spaces that require so much travel time (in addition to time required to express milk, store milk, and clean pump equipment) that the practice was unsustainable, and the physician stopped breastfeeding prematurely.36
The benefits of breastfeeding for mother and infant are well-established, and exclusive breastfeeding for the first 6 months of life is supported by the American College of Obstetricians and Gynecologists, whose position statement reads as follows: “Policies that protect the right of a woman and her child to breastfeed ... and that accommodate milk expression, such as ... paid maternity leave, on-site childcare, break time for expressing milk, and a clean, private location for expressing milk, are essential to sustaining breastfeeding.”37 We would add to these recommendations provision of dedicated milk storage space and establishment of clear, supportive policies that allow lactating physicians to breastfeed and express breast milk if they choose without career penalty. Several institutions offer scheduled protected clinical time and modified work relative value units (RVU) for lactating physicians, such that returning parents can have protected time for expressing breast milk and still meet RVU targets.38 Additionally, many academic institutions offer productivity adjustments for tenure-track faculty who have recently had children.
Creating a more supportive environment for women gastroenterologists who desire children allows the field to be more representative of our patient population and has been shown to positively impact outcomes from improved colorectal cancer screening rates to more guideline-directed informed consent conversations.39-41 Gastroenterology should comprise a physician workforce predicated on clinical and research excellence alone and should not require its practitioners to delay or abstain from pregnancy and child rearing. Robust, clear, and generous parental leave and postpartum accommodations will allow the field to retain and promote talented physicians, who will then contribute to the betterment of patients and the field over decades.
Dr. Rabinowitz is a faculty member in the department of medicine and division of gastroenterology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston. Dr. Feld is a transplant hepatology fellow, division of gastroenterology, department of medicine, University of Washington, Seattle. Dr. Rabinowitz and Dr. Feld have no conflicts of interest to disclose.
References
1. AAMC. Diversity in Medicine: Facts and Figures 2019. 2018.
2. Colleges AoAM. The State of Women in Academic Medicine: The Pipeline and Pathways to Leadership, 2015-2016. 2016. www.aamc.org/download/481206/data/2015table11.pdf.
3. AAMC. Table B-3: Total U.S. Medical School Enrollment by Race/Ethnicity and Sex, 2014-2015 through 2018-2019, 2019.
4. Rabinowitz LG. Recognizing blind spots – a remedy for gender bias in medicine? (N Engl. J Med. 2018; 378[24]: 2253-5).
5. Douglas PS et al. Career preferences and perceptions of cardiology among US internal medicine trainees: Factors influencing cardiology career choice. JAMA Cardiol 2018; 3(8):682-91.
6. Stack SW et al. Childbearing decisions in residency: A multicenter survey of female residents. Acad Med 2020;95(10):1550-7.
7. David YN et al. Pregnancy and the working gastroenterologist: Perceptions, realities, and systemic challenges. Gastroenterology 2021;161(3):756-60.
8. Rembacken BJ et al. Barriers and bias standing in the way of female trainees wanting to learn advanced endoscopy. United European Gastroenterol J. 2019;7(8):1141-5.
9. Arlow FL et al. Gastroenterology training and career choices: A prospective longitudinal study of the impact of gender and of managed care. Am J Gastroenterol. 2002;97(2):459-69.
10. Feld L et al. Parental leave for gastroenterology fellows: A national survey of current fellows. Am J Gastroenterol. 2021;116:S611-2.
11. Rabinowitz LG et al. Addressing gender in gastroenterology: opportunities for change. Gastrointest Endosc. 2020;91(1):155-61.
12. Feld LD. Baby steps in the right direction: Toward a parental leave policy for gastroenterology fellows. Am J Gastroenterol. 2021;116(3):505-8.
13. Feld LD. Interviewing for two. Am J Gastroenterol. 2020;116(3):445-6
14. Rabinowitz LG et al. Gender dynamics in education and practice of gastroenterology. Gastrointest Endosc. 2021;93(5):1047-56.e5.
15. Harvin G. Review of musculoskeletal injuries and prevention in the endoscopy practitioner. J Clin Gastroenterol. 2014;48(7):590-4.
16. LabX Oecs. www.labx.com/product/endoscopy-cart (accessed 2021 Nov 19.
17. Heilman ME and Okimoto TG. Motherhood: A potential source of bias in employment decisions. J Appl Psychol. 2008;93(1):189-98.
18. Robinson K et al. Racism, bias, and discrimination as modifiable barriers to breastfeeding for African American women: A scoping review of the literature. J Midwifery Womens Health. 2019;64(6):734-42.
19. Rabinowitz LG and Rabinowitz DG. Women on the Frontline: A Changed Workforce and the Fight Against COVID-19. Acad Med. 2021 Jun 1;96(6):808-12.
20. Rabinowitz LG et al. Gender in the endoscopy suite. Lancet Gastroenterol Hepatol. 2020 Dec;5(12):1032-4.
21. Stentz NC et al. Fertility and childbearing among American female physicians. J Womens Health. 2016; 25(10):1059-65.
22. Burke CA et al. Gender disparity in the practice of gastroenterology: The first 5 years of a career. Am J Gastroenterol. 2005;100(2):259-64.
23. Singh A et al. Women in gastroenterology committee of American College of G. Do gender disparities persist in gastroenterology after 10 years of practice? Am J Gastroenterol. 2008;103(7):1589-95.
24. Krueger KJ and Hoffman BJ. Radiation exposure during gastroenterologic fluoroscopy: Risk assessment for pregnant workers. Am J Gastroenterol. 1992;87(4):429-31.
25. Krause ML et al. Impact of pregnancy and gender on internal medicine resident evaluations: A retrospective cohort study. J Gen Intern Med. 2017;32(6):648-53.
26. Pawa S et al. Are all endoscopy-related musculoskeletal injuries created equal? Results of a national gender-based survey. Am J Gastroenterol. 2021;116(3):530-8.
27. David YN et al. Gender-specific factors influencing gastroenterologists to pursue careers in advanced endoscopy: perceptions vs reality. Am J Gastroenterol. 2021;116(3):539-50.
28. Bilal M et al. The need for allyship in achieving gender equity in gastroenterology. Am J Gastroenterol. 2021 Oct 19. doi: 10.14309/ajg.0000000000001508. Online ahead of print.
29. Jou J et al. Paid maternity leave in the United States: Associations with maternal and infant health. Matern Child Health J. 2018;22(2):216-25.
30. Aitken Z et al. The maternal health outcomes of paid maternity leave: A systematic review. Soc Sci Med. 2015;130:32-41.
31. Dodson NA and Talib HJ. Paid parental leave for mothers and fathers can improve physician wellness. AAP News. 2020 Jul 1. https://publications.aap.org/aapnews/news/12432.
32. Kornfeind KR and Sipsma HL. Exploring the link between maternity leave and postpartum depression. Womens Health Issues 2018;28(4):321-6.
33. Navarro-Rosenblatt D and Garmendia ML. Maternity leave and its impact on breastfeeding: A review of the literature. Breastfeed Med 2018;13(9):589-97.
34. Stack SW et al. Maternity leave in residency: A multicenter study of determinants and wellness outcomes. Acad Med. 2019;94(11):1738-45.
35. Mass.gov. Paid Family and Medical Leave Information for Massachusetts Employers. 2020.
36. Ares Segura S et al. en representacion del Comite de Lactancia Materna de la Asociacion Espanola de P. [The importance of maternal nutrition during breastfeeding: Do breastfeeding mothers need nutritional supplements?]. An Pediatr. (Barc) 2016;84(6):347 e1-7.
37. American College of Obstetricians and Gynecologists, Committee on Obstetric Practice. Committee Opinion No. 658: Optimizing Support for Breastfeeding as Part of Obstetric Practice. Obstet Gynecol. 2016;127(2):e86-92.
38. Porter KK et al. A lactation credit model to support breastfeeding in radiology: The new gold standard to support “liquid gold.” Clin Imaging 2021;80:16-8.
39. Davis J et al. Clinical practice patterns suggest female patients prefer female endoscopists. Dig Dis Sci. 2015;60(10):3149-50.
40. Menees SB et al. Women patients’ preference for women physicians is a barrier to colon cancer screening. Gastrointest Endosc. 2005;62(2):219-23.
41. Feld LD et al. Management of code status in the periendoscopic period: A national survey of current practices and beliefs of U.S. gastroenterologists. Gastrointest Endosc. 2021;94(1):172-7.e2.
Olive oil intake tied to reduced mortality
Compared with men and women who rarely or never consumed olive oil (the lowest intake), those who consumed greater than 0.5 tablespoon/day or more than 7 g/day (the highest intake) had a 19% lower mortality risk over a 28-year follow-up, starting from an average age of 56 years.
Moreover, compared with those with the lowest olive oil intake, those with the highest intake had a 19% lower cardiovascular disease (CVD) mortality, a 17% lower risk of dying from cancer, a 29% lower risk of dying from neurodegenerative disease, and an 18% lower risk of dying from respiratory disease during follow-up.
The researchers estimate that replacing 10 g/day of margarine, butter, mayonnaise, or dairy fat with the same amount of olive oil is associated with an 8%-34% lower risk of death from various causes.
The study by Marta Guasch-Ferré, PhD, and colleagues was published online Jan. 10 in the Journal of the American College of Cardiology.
Results support plant-based dietary fat recommendations
“Our results support current dietary recommendations to increase the intake of olive oil and other unsaturated vegetable oils in place of other fats to improve overall health and longevity,” the researchers summarize.
However, “I wouldn’t say that olive oil is the only way to help you live longer,” Dr. Guasch-Ferré, a senior research scientist in the department of nutrition, Harvard T.H. Chan School of Public Health, Boston, cautioned in an interview with this news organization.
“Other things are very important, such as not smoking, doing physical activity, etc., but one recommendation could be to try to eat more plant-based food including olive oil and healthy fat,” she added, and to use it for cooking, salad dressing, and baking, and substitute it for saturated fat or animal fat, especially for cooking.
The study suggests that people should “consume a more plant-based diet and prioritize fatty acids such as olive oil because they have a better nutritional composition (high in phenols and antioxidants), instead of using butter or margarines or other animal fats that have been shown to have detrimental effects for health,” she added, which is consistent with recommendations in the Dietary Guidelines for Americans.
“That said,” Dr. Guasch-Ferré summarized, “replication is needed in other cohorts and populations to see if the results are similar.”
In an accompanying editorial, Susanna C. Larsson, PhD, writes that “this was a well-designed study, with long-term follow-up and repeated measurements of dietary intake and other risk factors for diseases.”
“However, the difference in olive oil consumption between those with the highest and those with the lowest/no olive oil consumption was very low (0.5 tablespoon) and a [12%] reduced mortality risk was observed already at a much lower intake (0.5 teaspoon, about 1.5 g/day) of olive oil,” she noted in an email to this news organization.
“It’s a bit hard to believe that such a small amount could have an independent effect on mortality risk,” Dr. Larsson, associate professor of epidemiology at the Karolinska Institutet, Stockholm, cautioned.
Like Dr. Guasch-Ferré, she noted that “just adding one or two teaspoons of olive oil to the diet each day will likely not change the risk of mortality.”
Rather, “people may need to make larger changes in the whole diet, not focus on fat only. An overall healthier diet, rich in nonrefined plant-based foods (vegetables, whole grains, nuts), low/no intake of processed foods, and a switch to healthier fat (eg, olive oil) is needed.”
Importantly, “this study cannot say anything about causality, that is, whether it’s olive oil specifically that reduces mortality risk or if there are many other beneficial factors that act together to reduce mortality rate among those with high olive oil consumption.”
The researchers acknowledge this observational study limitation and that the findings may not be generalizable to other populations.
Novel findings regarding Alzheimer’s and respiratory disease
Dr. Larsson highlights two novel findings of this study.
First, it showed a 27% reduction in risk of dementia-related mortality for those in the highest versus lowest category of olive oil consumption. “Considering the lack of preventive strategies for Alzheimer’s disease and the high morbidity and mortality related to this disease, this finding, if confirmed, is of great public health importance,” she said.
Second, the study reported an inverse association of olive oil consumption with risk of respiratory disease mortality. “Because residual confounding from smoking cannot be ruled out,” Dr. Larsson said, “this finding is tentative and requires confirmation in a study that is less susceptible to confounding, such as a randomized trial.”
And although the current study and previous studies have found that consumption of olive oil may have health benefits, she identified several remaining questions.
“Are the associations causal or spurious?” she noted. Is olive oil consumption protective for certain cardiovascular diseases like stroke or atrial fibrillation only, as has been shown in other studies, or also for other major diseases and causes of death, she added. What is the amount of olive oil required for a protective effect?
Further, is the potential effect related to monounsaturated fatty acids (MUFAs) or phenolic compounds; that is, “is the protective effect confined to polyphenol-rich extra-virgin olive oil or are refined olive oil and other vegetable oils as beneficial? More research is needed to address these questions,” she concludes.
“Further studies are needed,” the researchers agree, “to confirm the association of olive oil consumption with reduced mortality, clarify the mechanisms responsible, and quantify the dose/volume boundaries around this effect.”
Virgin olive oil has more polyphenols
Olive oil, a key component of the Mediterranean diet, is high in MUFAs, especially oleic acid, as well as vitamin E and polyphenols, which contribute to its anti-inflammatory and antioxidant properties, the researchers explain.
Virgin olive oil, produced by mechanically pressing ripe olives, contains multiple bioactive and antioxidant components and has an acidity of less than 1.5%. And extra-virgin olive oil is produced the same way but has a higher quality, more intense taste, and lower acidity (less than 1%).
Refined or processed olive oil contains less phytochemicals, as some are lost during processing; it usually contains more than 80% refined oil, plus virgin oil added back to enhance flavor, and may also be labeled “pure” or “light.” However, refined olive oil “still has a good amount of healthy fatty acids but less bioactive compounds,” Dr. Guasch-Ferré noted.
Until now, no large prospective study has examined the link between olive oil intake and all-cause and cause-specific mortality in a U.S. population, where olive oil consumption is limited, compared with Mediterranean countries.
The researchers identified 60,582 women in the Nurses’ Health Study and 31,801 men in the Health Professionals Follow-up Study who were free of CVD or cancer in 1990, the first year that food frequency questionnaires in these studies asked about olive oil.
Participants replied to questionnaires every 4 years that asked about use of olive oil (for salad dressing, baking, frying, sautéing, and spreading on bread), other vegetable oils (for example, corn, safflower, soybean, canola oil), margarine, butter, and dairy fat. The researchers averaged the consumption of these fats during the follow-up years.
From 1990 to 2019, the average consumption of olive oil increased from 1.6 g/day to 4 g/day. Margarine in the 1990s contained saturated fat and trans fats, whereas more recently margarine contains beneficial olive oil or vegetable fat, Dr. Guasch-Ferré noted.
Baseline olive oil consumption in this U.S. population “differed remarkably” from that in the Spanish population in the PREDIMED (Prevención con Dieta Mediterránea) trial, which was, on average, 20-22 g/day of extra-virgin olive oil and 16-18 g/day of refined/mixed olive oil, Larsson pointed out.
Because olive oil consumption was so low in this U.S. study, the researchers did not distinguish between virgin/extra-virgin olive oil and refined/processed olive oil.
The participants were almost all White (99%) and were generally healthier than the average U.S. population; on average, they had a body mass index of 25.3-25.8 kg/m2 and ate 4.8-7.2 fruits and vegetables/day.
Those with the highest olive oil consumption were more physically active, had a healthier diet, were more likely to have Southern European or Mediterranean ancestry, and were less likely to smoke.
During 28 years of follow-up, 36,856 participants died. The researchers classified the deaths into five categories: CVD, cancer, neurodegenerative disease (including Alzheimer’s disease, Parkinson’s disease, multiple sclerosis), respiratory disease (such as chronic obstructive pulmonary disease), and all other causes (including suicide, injury, infections, diabetes, and kidney disease).
After adjusting for multiple confounders, compared with participants who rarely or never consumed olive oil, those in the highest quartile for olive oil consumption had a decreased risk of death from all causes (hazard ratio, 0.81; 95% confidence interval, 0.78 - 0.84) and from CVD (HR, 0.81; 95% CI, 0.75-0.87), cancer (HR, 0.83; 95% CI, 0.78-0.89), neurodegenerative disease (HR, 0.71; 95% CI, 0.64-0.78), and respiratory disease (HR, 0.82; 95% CI, 0.72-0.93).
There was no decrease in mortality in models where the researchers substituted olive oil for vegetable oil, suggesting that vegetable oils may provide similar health benefits as olive oil.
The research was supported by grants from the National Institutes of Health. Dr. Guasch-Ferré was supported by the American Diabetes Association. Coauthor Salas-Salvadó is partially supported by the Catalan Institution for Research and Advanced Studies and received the virgin olive oil that was used in the PREDIMED and PREDIMED-Plus studies from the Patrimonio Communal Olivalero and Hojiblanca (Málaga, Spain). The other study authors and Dr. Larsson have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Compared with men and women who rarely or never consumed olive oil (the lowest intake), those who consumed greater than 0.5 tablespoon/day or more than 7 g/day (the highest intake) had a 19% lower mortality risk over a 28-year follow-up, starting from an average age of 56 years.
Moreover, compared with those with the lowest olive oil intake, those with the highest intake had a 19% lower cardiovascular disease (CVD) mortality, a 17% lower risk of dying from cancer, a 29% lower risk of dying from neurodegenerative disease, and an 18% lower risk of dying from respiratory disease during follow-up.
The researchers estimate that replacing 10 g/day of margarine, butter, mayonnaise, or dairy fat with the same amount of olive oil is associated with an 8%-34% lower risk of death from various causes.
The study by Marta Guasch-Ferré, PhD, and colleagues was published online Jan. 10 in the Journal of the American College of Cardiology.
Results support plant-based dietary fat recommendations
“Our results support current dietary recommendations to increase the intake of olive oil and other unsaturated vegetable oils in place of other fats to improve overall health and longevity,” the researchers summarize.
However, “I wouldn’t say that olive oil is the only way to help you live longer,” Dr. Guasch-Ferré, a senior research scientist in the department of nutrition, Harvard T.H. Chan School of Public Health, Boston, cautioned in an interview with this news organization.
“Other things are very important, such as not smoking, doing physical activity, etc., but one recommendation could be to try to eat more plant-based food including olive oil and healthy fat,” she added, and to use it for cooking, salad dressing, and baking, and substitute it for saturated fat or animal fat, especially for cooking.
The study suggests that people should “consume a more plant-based diet and prioritize fatty acids such as olive oil because they have a better nutritional composition (high in phenols and antioxidants), instead of using butter or margarines or other animal fats that have been shown to have detrimental effects for health,” she added, which is consistent with recommendations in the Dietary Guidelines for Americans.
“That said,” Dr. Guasch-Ferré summarized, “replication is needed in other cohorts and populations to see if the results are similar.”
In an accompanying editorial, Susanna C. Larsson, PhD, writes that “this was a well-designed study, with long-term follow-up and repeated measurements of dietary intake and other risk factors for diseases.”
“However, the difference in olive oil consumption between those with the highest and those with the lowest/no olive oil consumption was very low (0.5 tablespoon) and a [12%] reduced mortality risk was observed already at a much lower intake (0.5 teaspoon, about 1.5 g/day) of olive oil,” she noted in an email to this news organization.
“It’s a bit hard to believe that such a small amount could have an independent effect on mortality risk,” Dr. Larsson, associate professor of epidemiology at the Karolinska Institutet, Stockholm, cautioned.
Like Dr. Guasch-Ferré, she noted that “just adding one or two teaspoons of olive oil to the diet each day will likely not change the risk of mortality.”
Rather, “people may need to make larger changes in the whole diet, not focus on fat only. An overall healthier diet, rich in nonrefined plant-based foods (vegetables, whole grains, nuts), low/no intake of processed foods, and a switch to healthier fat (eg, olive oil) is needed.”
Importantly, “this study cannot say anything about causality, that is, whether it’s olive oil specifically that reduces mortality risk or if there are many other beneficial factors that act together to reduce mortality rate among those with high olive oil consumption.”
The researchers acknowledge this observational study limitation and that the findings may not be generalizable to other populations.
Novel findings regarding Alzheimer’s and respiratory disease
Dr. Larsson highlights two novel findings of this study.
First, it showed a 27% reduction in risk of dementia-related mortality for those in the highest versus lowest category of olive oil consumption. “Considering the lack of preventive strategies for Alzheimer’s disease and the high morbidity and mortality related to this disease, this finding, if confirmed, is of great public health importance,” she said.
Second, the study reported an inverse association of olive oil consumption with risk of respiratory disease mortality. “Because residual confounding from smoking cannot be ruled out,” Dr. Larsson said, “this finding is tentative and requires confirmation in a study that is less susceptible to confounding, such as a randomized trial.”
And although the current study and previous studies have found that consumption of olive oil may have health benefits, she identified several remaining questions.
“Are the associations causal or spurious?” she noted. Is olive oil consumption protective for certain cardiovascular diseases like stroke or atrial fibrillation only, as has been shown in other studies, or also for other major diseases and causes of death, she added. What is the amount of olive oil required for a protective effect?
Further, is the potential effect related to monounsaturated fatty acids (MUFAs) or phenolic compounds; that is, “is the protective effect confined to polyphenol-rich extra-virgin olive oil or are refined olive oil and other vegetable oils as beneficial? More research is needed to address these questions,” she concludes.
“Further studies are needed,” the researchers agree, “to confirm the association of olive oil consumption with reduced mortality, clarify the mechanisms responsible, and quantify the dose/volume boundaries around this effect.”
Virgin olive oil has more polyphenols
Olive oil, a key component of the Mediterranean diet, is high in MUFAs, especially oleic acid, as well as vitamin E and polyphenols, which contribute to its anti-inflammatory and antioxidant properties, the researchers explain.
Virgin olive oil, produced by mechanically pressing ripe olives, contains multiple bioactive and antioxidant components and has an acidity of less than 1.5%. And extra-virgin olive oil is produced the same way but has a higher quality, more intense taste, and lower acidity (less than 1%).
Refined or processed olive oil contains less phytochemicals, as some are lost during processing; it usually contains more than 80% refined oil, plus virgin oil added back to enhance flavor, and may also be labeled “pure” or “light.” However, refined olive oil “still has a good amount of healthy fatty acids but less bioactive compounds,” Dr. Guasch-Ferré noted.
Until now, no large prospective study has examined the link between olive oil intake and all-cause and cause-specific mortality in a U.S. population, where olive oil consumption is limited, compared with Mediterranean countries.
The researchers identified 60,582 women in the Nurses’ Health Study and 31,801 men in the Health Professionals Follow-up Study who were free of CVD or cancer in 1990, the first year that food frequency questionnaires in these studies asked about olive oil.
Participants replied to questionnaires every 4 years that asked about use of olive oil (for salad dressing, baking, frying, sautéing, and spreading on bread), other vegetable oils (for example, corn, safflower, soybean, canola oil), margarine, butter, and dairy fat. The researchers averaged the consumption of these fats during the follow-up years.
From 1990 to 2019, the average consumption of olive oil increased from 1.6 g/day to 4 g/day. Margarine in the 1990s contained saturated fat and trans fats, whereas more recently margarine contains beneficial olive oil or vegetable fat, Dr. Guasch-Ferré noted.
Baseline olive oil consumption in this U.S. population “differed remarkably” from that in the Spanish population in the PREDIMED (Prevención con Dieta Mediterránea) trial, which was, on average, 20-22 g/day of extra-virgin olive oil and 16-18 g/day of refined/mixed olive oil, Larsson pointed out.
Because olive oil consumption was so low in this U.S. study, the researchers did not distinguish between virgin/extra-virgin olive oil and refined/processed olive oil.
The participants were almost all White (99%) and were generally healthier than the average U.S. population; on average, they had a body mass index of 25.3-25.8 kg/m2 and ate 4.8-7.2 fruits and vegetables/day.
Those with the highest olive oil consumption were more physically active, had a healthier diet, were more likely to have Southern European or Mediterranean ancestry, and were less likely to smoke.
During 28 years of follow-up, 36,856 participants died. The researchers classified the deaths into five categories: CVD, cancer, neurodegenerative disease (including Alzheimer’s disease, Parkinson’s disease, multiple sclerosis), respiratory disease (such as chronic obstructive pulmonary disease), and all other causes (including suicide, injury, infections, diabetes, and kidney disease).
After adjusting for multiple confounders, compared with participants who rarely or never consumed olive oil, those in the highest quartile for olive oil consumption had a decreased risk of death from all causes (hazard ratio, 0.81; 95% confidence interval, 0.78 - 0.84) and from CVD (HR, 0.81; 95% CI, 0.75-0.87), cancer (HR, 0.83; 95% CI, 0.78-0.89), neurodegenerative disease (HR, 0.71; 95% CI, 0.64-0.78), and respiratory disease (HR, 0.82; 95% CI, 0.72-0.93).
There was no decrease in mortality in models where the researchers substituted olive oil for vegetable oil, suggesting that vegetable oils may provide similar health benefits as olive oil.
The research was supported by grants from the National Institutes of Health. Dr. Guasch-Ferré was supported by the American Diabetes Association. Coauthor Salas-Salvadó is partially supported by the Catalan Institution for Research and Advanced Studies and received the virgin olive oil that was used in the PREDIMED and PREDIMED-Plus studies from the Patrimonio Communal Olivalero and Hojiblanca (Málaga, Spain). The other study authors and Dr. Larsson have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Compared with men and women who rarely or never consumed olive oil (the lowest intake), those who consumed greater than 0.5 tablespoon/day or more than 7 g/day (the highest intake) had a 19% lower mortality risk over a 28-year follow-up, starting from an average age of 56 years.
Moreover, compared with those with the lowest olive oil intake, those with the highest intake had a 19% lower cardiovascular disease (CVD) mortality, a 17% lower risk of dying from cancer, a 29% lower risk of dying from neurodegenerative disease, and an 18% lower risk of dying from respiratory disease during follow-up.
The researchers estimate that replacing 10 g/day of margarine, butter, mayonnaise, or dairy fat with the same amount of olive oil is associated with an 8%-34% lower risk of death from various causes.
The study by Marta Guasch-Ferré, PhD, and colleagues was published online Jan. 10 in the Journal of the American College of Cardiology.
Results support plant-based dietary fat recommendations
“Our results support current dietary recommendations to increase the intake of olive oil and other unsaturated vegetable oils in place of other fats to improve overall health and longevity,” the researchers summarize.
However, “I wouldn’t say that olive oil is the only way to help you live longer,” Dr. Guasch-Ferré, a senior research scientist in the department of nutrition, Harvard T.H. Chan School of Public Health, Boston, cautioned in an interview with this news organization.
“Other things are very important, such as not smoking, doing physical activity, etc., but one recommendation could be to try to eat more plant-based food including olive oil and healthy fat,” she added, and to use it for cooking, salad dressing, and baking, and substitute it for saturated fat or animal fat, especially for cooking.
The study suggests that people should “consume a more plant-based diet and prioritize fatty acids such as olive oil because they have a better nutritional composition (high in phenols and antioxidants), instead of using butter or margarines or other animal fats that have been shown to have detrimental effects for health,” she added, which is consistent with recommendations in the Dietary Guidelines for Americans.
“That said,” Dr. Guasch-Ferré summarized, “replication is needed in other cohorts and populations to see if the results are similar.”
In an accompanying editorial, Susanna C. Larsson, PhD, writes that “this was a well-designed study, with long-term follow-up and repeated measurements of dietary intake and other risk factors for diseases.”
“However, the difference in olive oil consumption between those with the highest and those with the lowest/no olive oil consumption was very low (0.5 tablespoon) and a [12%] reduced mortality risk was observed already at a much lower intake (0.5 teaspoon, about 1.5 g/day) of olive oil,” she noted in an email to this news organization.
“It’s a bit hard to believe that such a small amount could have an independent effect on mortality risk,” Dr. Larsson, associate professor of epidemiology at the Karolinska Institutet, Stockholm, cautioned.
Like Dr. Guasch-Ferré, she noted that “just adding one or two teaspoons of olive oil to the diet each day will likely not change the risk of mortality.”
Rather, “people may need to make larger changes in the whole diet, not focus on fat only. An overall healthier diet, rich in nonrefined plant-based foods (vegetables, whole grains, nuts), low/no intake of processed foods, and a switch to healthier fat (eg, olive oil) is needed.”
Importantly, “this study cannot say anything about causality, that is, whether it’s olive oil specifically that reduces mortality risk or if there are many other beneficial factors that act together to reduce mortality rate among those with high olive oil consumption.”
The researchers acknowledge this observational study limitation and that the findings may not be generalizable to other populations.
Novel findings regarding Alzheimer’s and respiratory disease
Dr. Larsson highlights two novel findings of this study.
First, it showed a 27% reduction in risk of dementia-related mortality for those in the highest versus lowest category of olive oil consumption. “Considering the lack of preventive strategies for Alzheimer’s disease and the high morbidity and mortality related to this disease, this finding, if confirmed, is of great public health importance,” she said.
Second, the study reported an inverse association of olive oil consumption with risk of respiratory disease mortality. “Because residual confounding from smoking cannot be ruled out,” Dr. Larsson said, “this finding is tentative and requires confirmation in a study that is less susceptible to confounding, such as a randomized trial.”
And although the current study and previous studies have found that consumption of olive oil may have health benefits, she identified several remaining questions.
“Are the associations causal or spurious?” she noted. Is olive oil consumption protective for certain cardiovascular diseases like stroke or atrial fibrillation only, as has been shown in other studies, or also for other major diseases and causes of death, she added. What is the amount of olive oil required for a protective effect?
Further, is the potential effect related to monounsaturated fatty acids (MUFAs) or phenolic compounds; that is, “is the protective effect confined to polyphenol-rich extra-virgin olive oil or are refined olive oil and other vegetable oils as beneficial? More research is needed to address these questions,” she concludes.
“Further studies are needed,” the researchers agree, “to confirm the association of olive oil consumption with reduced mortality, clarify the mechanisms responsible, and quantify the dose/volume boundaries around this effect.”
Virgin olive oil has more polyphenols
Olive oil, a key component of the Mediterranean diet, is high in MUFAs, especially oleic acid, as well as vitamin E and polyphenols, which contribute to its anti-inflammatory and antioxidant properties, the researchers explain.
Virgin olive oil, produced by mechanically pressing ripe olives, contains multiple bioactive and antioxidant components and has an acidity of less than 1.5%. And extra-virgin olive oil is produced the same way but has a higher quality, more intense taste, and lower acidity (less than 1%).
Refined or processed olive oil contains less phytochemicals, as some are lost during processing; it usually contains more than 80% refined oil, plus virgin oil added back to enhance flavor, and may also be labeled “pure” or “light.” However, refined olive oil “still has a good amount of healthy fatty acids but less bioactive compounds,” Dr. Guasch-Ferré noted.
Until now, no large prospective study has examined the link between olive oil intake and all-cause and cause-specific mortality in a U.S. population, where olive oil consumption is limited, compared with Mediterranean countries.
The researchers identified 60,582 women in the Nurses’ Health Study and 31,801 men in the Health Professionals Follow-up Study who were free of CVD or cancer in 1990, the first year that food frequency questionnaires in these studies asked about olive oil.
Participants replied to questionnaires every 4 years that asked about use of olive oil (for salad dressing, baking, frying, sautéing, and spreading on bread), other vegetable oils (for example, corn, safflower, soybean, canola oil), margarine, butter, and dairy fat. The researchers averaged the consumption of these fats during the follow-up years.
From 1990 to 2019, the average consumption of olive oil increased from 1.6 g/day to 4 g/day. Margarine in the 1990s contained saturated fat and trans fats, whereas more recently margarine contains beneficial olive oil or vegetable fat, Dr. Guasch-Ferré noted.
Baseline olive oil consumption in this U.S. population “differed remarkably” from that in the Spanish population in the PREDIMED (Prevención con Dieta Mediterránea) trial, which was, on average, 20-22 g/day of extra-virgin olive oil and 16-18 g/day of refined/mixed olive oil, Larsson pointed out.
Because olive oil consumption was so low in this U.S. study, the researchers did not distinguish between virgin/extra-virgin olive oil and refined/processed olive oil.
The participants were almost all White (99%) and were generally healthier than the average U.S. population; on average, they had a body mass index of 25.3-25.8 kg/m2 and ate 4.8-7.2 fruits and vegetables/day.
Those with the highest olive oil consumption were more physically active, had a healthier diet, were more likely to have Southern European or Mediterranean ancestry, and were less likely to smoke.
During 28 years of follow-up, 36,856 participants died. The researchers classified the deaths into five categories: CVD, cancer, neurodegenerative disease (including Alzheimer’s disease, Parkinson’s disease, multiple sclerosis), respiratory disease (such as chronic obstructive pulmonary disease), and all other causes (including suicide, injury, infections, diabetes, and kidney disease).
After adjusting for multiple confounders, compared with participants who rarely or never consumed olive oil, those in the highest quartile for olive oil consumption had a decreased risk of death from all causes (hazard ratio, 0.81; 95% confidence interval, 0.78 - 0.84) and from CVD (HR, 0.81; 95% CI, 0.75-0.87), cancer (HR, 0.83; 95% CI, 0.78-0.89), neurodegenerative disease (HR, 0.71; 95% CI, 0.64-0.78), and respiratory disease (HR, 0.82; 95% CI, 0.72-0.93).
There was no decrease in mortality in models where the researchers substituted olive oil for vegetable oil, suggesting that vegetable oils may provide similar health benefits as olive oil.
The research was supported by grants from the National Institutes of Health. Dr. Guasch-Ferré was supported by the American Diabetes Association. Coauthor Salas-Salvadó is partially supported by the Catalan Institution for Research and Advanced Studies and received the virgin olive oil that was used in the PREDIMED and PREDIMED-Plus studies from the Patrimonio Communal Olivalero and Hojiblanca (Málaga, Spain). The other study authors and Dr. Larsson have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AGA News - February 2022
Registration now open: Gut Microbiota for Health World Summit 2022
Registration is now open for the Gut Microbiota for Health (GMFH) World Summit 2022, taking place March 12-13 in Washington, D.C., and virtually.
Organized by AGA and the European Society of Neurogastroenterology and Motility (ESNM), the GMFH World Summit is the preeminent international meeting on the gut microbiome for clinicians, dietitians, and researchers.
Now in its tenth year, this year’s program will focus on “The Gut Microbiome in Precision Nutrition and Medicine.” Join us to gain a deeper understanding of the role of the gut microbiome in precision medicine and discover personalized approaches to modulating the gut microbiome that may promote health and improve patient outcomes for a variety of disorders and diseases.
https://www.gutmicrobiotaforhealth.com/summit
See Gastroenterology’s curated Equity in GI journal collection
Gastroenterology is proud to announce the release of a special collection of articles focused on the intersection of diversity, equity, and inclusion (DEI) and gastroenterology and hepatology. This curated collection, under the guidance of the journal’s new DEI section editor Dr. Chyke Doubeni, includes original research, reviews, commentaries and editorials on matters of health disparities, socioeconomic determinants of health outcomes, and population-based studies on disease incidence among races and ethnicities, among other topics. New articles are added to the collection as they are published.
View the special collection on Gastroenterology’s website, which is designed to help you quickly and easily look over the latest DEI articles and content of interest. Recent articles include:
- How to incorporate health equity training into GI/hepatology fellowships by Jannel Lee-Allen and Brijen J. Shah
- Disparities in preventable mortality from colorectal cancer: are they the result of structural racism? By Chyke A. Doubeni, Kevin Selby and Theodore R. Levin
- COVID-19 pediatric patients: GI symptoms, presentations and disparities by race/ethnicity in a large, multicenter U.S. study by Yusuf Ashktorab, Anas Brim, Antonio Pizuorno, Vijay Gayam, Sahar Nikdel and Hassan Brim
View all of Gastroenterology’s curated article collections.
Registration now open: Gut Microbiota for Health World Summit 2022
Registration is now open for the Gut Microbiota for Health (GMFH) World Summit 2022, taking place March 12-13 in Washington, D.C., and virtually.
Organized by AGA and the European Society of Neurogastroenterology and Motility (ESNM), the GMFH World Summit is the preeminent international meeting on the gut microbiome for clinicians, dietitians, and researchers.
Now in its tenth year, this year’s program will focus on “The Gut Microbiome in Precision Nutrition and Medicine.” Join us to gain a deeper understanding of the role of the gut microbiome in precision medicine and discover personalized approaches to modulating the gut microbiome that may promote health and improve patient outcomes for a variety of disorders and diseases.
https://www.gutmicrobiotaforhealth.com/summit
See Gastroenterology’s curated Equity in GI journal collection
Gastroenterology is proud to announce the release of a special collection of articles focused on the intersection of diversity, equity, and inclusion (DEI) and gastroenterology and hepatology. This curated collection, under the guidance of the journal’s new DEI section editor Dr. Chyke Doubeni, includes original research, reviews, commentaries and editorials on matters of health disparities, socioeconomic determinants of health outcomes, and population-based studies on disease incidence among races and ethnicities, among other topics. New articles are added to the collection as they are published.
View the special collection on Gastroenterology’s website, which is designed to help you quickly and easily look over the latest DEI articles and content of interest. Recent articles include:
- How to incorporate health equity training into GI/hepatology fellowships by Jannel Lee-Allen and Brijen J. Shah
- Disparities in preventable mortality from colorectal cancer: are they the result of structural racism? By Chyke A. Doubeni, Kevin Selby and Theodore R. Levin
- COVID-19 pediatric patients: GI symptoms, presentations and disparities by race/ethnicity in a large, multicenter U.S. study by Yusuf Ashktorab, Anas Brim, Antonio Pizuorno, Vijay Gayam, Sahar Nikdel and Hassan Brim
View all of Gastroenterology’s curated article collections.
Registration now open: Gut Microbiota for Health World Summit 2022
Registration is now open for the Gut Microbiota for Health (GMFH) World Summit 2022, taking place March 12-13 in Washington, D.C., and virtually.
Organized by AGA and the European Society of Neurogastroenterology and Motility (ESNM), the GMFH World Summit is the preeminent international meeting on the gut microbiome for clinicians, dietitians, and researchers.
Now in its tenth year, this year’s program will focus on “The Gut Microbiome in Precision Nutrition and Medicine.” Join us to gain a deeper understanding of the role of the gut microbiome in precision medicine and discover personalized approaches to modulating the gut microbiome that may promote health and improve patient outcomes for a variety of disorders and diseases.
https://www.gutmicrobiotaforhealth.com/summit
See Gastroenterology’s curated Equity in GI journal collection
Gastroenterology is proud to announce the release of a special collection of articles focused on the intersection of diversity, equity, and inclusion (DEI) and gastroenterology and hepatology. This curated collection, under the guidance of the journal’s new DEI section editor Dr. Chyke Doubeni, includes original research, reviews, commentaries and editorials on matters of health disparities, socioeconomic determinants of health outcomes, and population-based studies on disease incidence among races and ethnicities, among other topics. New articles are added to the collection as they are published.
View the special collection on Gastroenterology’s website, which is designed to help you quickly and easily look over the latest DEI articles and content of interest. Recent articles include:
- How to incorporate health equity training into GI/hepatology fellowships by Jannel Lee-Allen and Brijen J. Shah
- Disparities in preventable mortality from colorectal cancer: are they the result of structural racism? By Chyke A. Doubeni, Kevin Selby and Theodore R. Levin
- COVID-19 pediatric patients: GI symptoms, presentations and disparities by race/ethnicity in a large, multicenter U.S. study by Yusuf Ashktorab, Anas Brim, Antonio Pizuorno, Vijay Gayam, Sahar Nikdel and Hassan Brim
View all of Gastroenterology’s curated article collections.
February 2022 – ICYMI
Gastroenterology
November 2021
How to navigate national societal organizations for leadership development and academic promotion: A guide for trainees and young faculty
Aby ES et al. Gastroenterology. 2021 Nov;161(5):1361-1365. doi: 10.1053/j.gastro.2021.08.044.
Value of pH impedance monitoring while on twice-daily proton pump inhibitor therapy to identify need for escalation of reflux management
Gyawali CG et al. Gastroenterology. 2021 Nov;161(5):1412-1422. doi: 10.1053/j.gastro.2021.07.004.
The sulfur microbial diet is associated with increased risk of early-onset colorectal cancer precursors
Nguyen LH et al. Gastroenterology. 2021 Nov;161(5):1423-1432.e4. doi: 10.1053/j.gastro.2021.07.008.
Underwater vs conventional endoscopic mucosal resection of large sessile or flat colorectal polyps: A prospective randomized controlled trial
Nagl S et al. Gastroenterology. 2021 Nov;161(5):1460-1474.e1. doi: 10.1053/j.gastro.2021.07.044.
December 2021
How to approach long-term enteral and parenteral nutrition
Hadefi A, Arvanitakis M. Gastroenterology. 2021 Dec;161(6):1780-1786. doi: 10.1053/j.gastro.2021.09.030.
Regular use of proton pump inhibitor and the risk of inflammatory bowel disease: Pooled analysis of 3 prospective cohorts
Xia B et al. Gastroenterology. 2021 Dec;161(6):1842-1852.e10. doi: 10.1053/j.gastro.2021.08.005.
January 2022
Serologic response to Coronavirus Disease 2019 (COVID-19) vaccination in patients with immune-mediated inflammatory diseases: A systematic review and meta-analysis
Sakuraba A et al. Gastroenterology. 2022 Jan;162(1):88-108.e9. doi: 10.1053/j.gastro.2021.09.055.
Advancing diversity, equity, and inclusion in scientific publishing
Doubeni CA et al. Gastroenterology. 2022 Jan;162(1):59-62.e1. doi: 10.1053/j.gastro.2021.10.043.
How we approach difficult to eradicate Helicobacter pylori
Argueta EA, Moss SF. Gastroenterology. 2022 Jan;162(1):32-37. doi: 10.1053/j.gastro.2021.10.048.
Global incidence of acute pancreatitis is increasing over time: A systematic review and meta-analysis
Iannuzzi JP et al. Gastroenterology. 2022 Jan;162(1):122-134. doi: 10.1053/j.gastro.2021.09.043.
Epidemiology, etiology, and treatment of gastroparesis: Real-world evidence from a large US national claims database
Ye Y et al. Gastroenterology. 2022 Jan;162(1):109-121.e5. doi: 10.1053/j.gastro.2021.09.064.
Clinical Gastroenterology and Hepatology
November 2021
AGA Clinical Practice Update on endoscopic management of perforations in gastrointestinal tract: Expert Review
Lee JH et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2252-2261.e2. doi: 10.1016/j.cgh.2021.06.045.
Food allergies and intolerances: A clinical approach to the diagnosis and management of adverse reactions to food
Onyimba F et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2230-2240.e1. doi: 10.1016/j.cgh.2021.01.025.
Management of gastrointestinal side effects of immune checkpoint inhibitors
Lui RN et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2262-2265. doi: 10.1016/j.cgh.2021.06.038.
December 2021
Optimizing the endoscopic examination in eosinophilic esophagitis
Dellon ES. Clin Gastroenterol Hepatol. 2021 Dec;19(12):2489-2492.e1. doi: 10.1016/j.cgh.2021.07.011.
Diagnostic accuracy of fecal calprotectin concentration in evaluating therapeutic outcomes of patients with ulcerative colitis
Stevens TW et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2333-2342. doi: 10.1016/j.cgh.2020.08.019.
Factors associated with inpatient endoscopy delay and its impact on hospital length-of-stay and 30-day readmission
Jacobs CC et al. Clin Gastroenterol Hepatol. 2021 Dec;19(12):2648-2655. doi: 10.1016/j.cgh.2021.06.009.
January 2022
Comparing costs and outcomes of treatments for irritable bowel syndrome with diarrhea: Cost-benefit analysis
Shah ED et al. Clin Gastroenterol Hepatol. 2022 Jan;20(1):136-144.e31. doi: 10.1016/j.cgh.2020.09.043.
Next generation academic gastroenterology
Allen JI, Berry S. Clin Gastroenterol Hepatol. 2022 Jan;20(1):5-8. doi: 10.1016/j.cgh.2021.09.038.
Beyond metoclopramide for gastroparesis
Camilleri M. Clin Gastroenterol Hepatol. 2022 Jan;20(1):19-24. doi: 10.1016/j.cgh.2021.08.052.
Comparative safety and effectiveness of vedolizumab to tumor necrosis factor antagonist therapy for ulcerative colitis
Lukin D et al. Clin Gastroenterol Hepatol. 2022 Jan;20(1):126-135. doi: 10.1016/j.cgh.2020.10.003.
Techniques and Innovations in Gastrointestinal Endoscopy
Impact of the COVID-19 pandemic on utilization of EGD and colonoscopy in the United States: An analysis of the GIQuIC registry
Calderwood AH et al. Tech Innov Gastrointest Endosc. 2021;23(4):313-321. doi: 10.1016/j.tige.2021.07.003.
How to approach small polyps in colon: Tips and tricks
Mahmood S et al. Tech Inov Gastroinest Endosc. 2021;23(4):238-335. doi: 10.1016/j.tige.2021.06.007
Gastroenterology
November 2021
How to navigate national societal organizations for leadership development and academic promotion: A guide for trainees and young faculty
Aby ES et al. Gastroenterology. 2021 Nov;161(5):1361-1365. doi: 10.1053/j.gastro.2021.08.044.
Value of pH impedance monitoring while on twice-daily proton pump inhibitor therapy to identify need for escalation of reflux management
Gyawali CG et al. Gastroenterology. 2021 Nov;161(5):1412-1422. doi: 10.1053/j.gastro.2021.07.004.
The sulfur microbial diet is associated with increased risk of early-onset colorectal cancer precursors
Nguyen LH et al. Gastroenterology. 2021 Nov;161(5):1423-1432.e4. doi: 10.1053/j.gastro.2021.07.008.
Underwater vs conventional endoscopic mucosal resection of large sessile or flat colorectal polyps: A prospective randomized controlled trial
Nagl S et al. Gastroenterology. 2021 Nov;161(5):1460-1474.e1. doi: 10.1053/j.gastro.2021.07.044.
December 2021
How to approach long-term enteral and parenteral nutrition
Hadefi A, Arvanitakis M. Gastroenterology. 2021 Dec;161(6):1780-1786. doi: 10.1053/j.gastro.2021.09.030.
Regular use of proton pump inhibitor and the risk of inflammatory bowel disease: Pooled analysis of 3 prospective cohorts
Xia B et al. Gastroenterology. 2021 Dec;161(6):1842-1852.e10. doi: 10.1053/j.gastro.2021.08.005.
January 2022
Serologic response to Coronavirus Disease 2019 (COVID-19) vaccination in patients with immune-mediated inflammatory diseases: A systematic review and meta-analysis
Sakuraba A et al. Gastroenterology. 2022 Jan;162(1):88-108.e9. doi: 10.1053/j.gastro.2021.09.055.
Advancing diversity, equity, and inclusion in scientific publishing
Doubeni CA et al. Gastroenterology. 2022 Jan;162(1):59-62.e1. doi: 10.1053/j.gastro.2021.10.043.
How we approach difficult to eradicate Helicobacter pylori
Argueta EA, Moss SF. Gastroenterology. 2022 Jan;162(1):32-37. doi: 10.1053/j.gastro.2021.10.048.
Global incidence of acute pancreatitis is increasing over time: A systematic review and meta-analysis
Iannuzzi JP et al. Gastroenterology. 2022 Jan;162(1):122-134. doi: 10.1053/j.gastro.2021.09.043.
Epidemiology, etiology, and treatment of gastroparesis: Real-world evidence from a large US national claims database
Ye Y et al. Gastroenterology. 2022 Jan;162(1):109-121.e5. doi: 10.1053/j.gastro.2021.09.064.
Clinical Gastroenterology and Hepatology
November 2021
AGA Clinical Practice Update on endoscopic management of perforations in gastrointestinal tract: Expert Review
Lee JH et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2252-2261.e2. doi: 10.1016/j.cgh.2021.06.045.
Food allergies and intolerances: A clinical approach to the diagnosis and management of adverse reactions to food
Onyimba F et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2230-2240.e1. doi: 10.1016/j.cgh.2021.01.025.
Management of gastrointestinal side effects of immune checkpoint inhibitors
Lui RN et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2262-2265. doi: 10.1016/j.cgh.2021.06.038.
December 2021
Optimizing the endoscopic examination in eosinophilic esophagitis
Dellon ES. Clin Gastroenterol Hepatol. 2021 Dec;19(12):2489-2492.e1. doi: 10.1016/j.cgh.2021.07.011.
Diagnostic accuracy of fecal calprotectin concentration in evaluating therapeutic outcomes of patients with ulcerative colitis
Stevens TW et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2333-2342. doi: 10.1016/j.cgh.2020.08.019.
Factors associated with inpatient endoscopy delay and its impact on hospital length-of-stay and 30-day readmission
Jacobs CC et al. Clin Gastroenterol Hepatol. 2021 Dec;19(12):2648-2655. doi: 10.1016/j.cgh.2021.06.009.
January 2022
Comparing costs and outcomes of treatments for irritable bowel syndrome with diarrhea: Cost-benefit analysis
Shah ED et al. Clin Gastroenterol Hepatol. 2022 Jan;20(1):136-144.e31. doi: 10.1016/j.cgh.2020.09.043.
Next generation academic gastroenterology
Allen JI, Berry S. Clin Gastroenterol Hepatol. 2022 Jan;20(1):5-8. doi: 10.1016/j.cgh.2021.09.038.
Beyond metoclopramide for gastroparesis
Camilleri M. Clin Gastroenterol Hepatol. 2022 Jan;20(1):19-24. doi: 10.1016/j.cgh.2021.08.052.
Comparative safety and effectiveness of vedolizumab to tumor necrosis factor antagonist therapy for ulcerative colitis
Lukin D et al. Clin Gastroenterol Hepatol. 2022 Jan;20(1):126-135. doi: 10.1016/j.cgh.2020.10.003.
Techniques and Innovations in Gastrointestinal Endoscopy
Impact of the COVID-19 pandemic on utilization of EGD and colonoscopy in the United States: An analysis of the GIQuIC registry
Calderwood AH et al. Tech Innov Gastrointest Endosc. 2021;23(4):313-321. doi: 10.1016/j.tige.2021.07.003.
How to approach small polyps in colon: Tips and tricks
Mahmood S et al. Tech Inov Gastroinest Endosc. 2021;23(4):238-335. doi: 10.1016/j.tige.2021.06.007
Gastroenterology
November 2021
How to navigate national societal organizations for leadership development and academic promotion: A guide for trainees and young faculty
Aby ES et al. Gastroenterology. 2021 Nov;161(5):1361-1365. doi: 10.1053/j.gastro.2021.08.044.
Value of pH impedance monitoring while on twice-daily proton pump inhibitor therapy to identify need for escalation of reflux management
Gyawali CG et al. Gastroenterology. 2021 Nov;161(5):1412-1422. doi: 10.1053/j.gastro.2021.07.004.
The sulfur microbial diet is associated with increased risk of early-onset colorectal cancer precursors
Nguyen LH et al. Gastroenterology. 2021 Nov;161(5):1423-1432.e4. doi: 10.1053/j.gastro.2021.07.008.
Underwater vs conventional endoscopic mucosal resection of large sessile or flat colorectal polyps: A prospective randomized controlled trial
Nagl S et al. Gastroenterology. 2021 Nov;161(5):1460-1474.e1. doi: 10.1053/j.gastro.2021.07.044.
December 2021
How to approach long-term enteral and parenteral nutrition
Hadefi A, Arvanitakis M. Gastroenterology. 2021 Dec;161(6):1780-1786. doi: 10.1053/j.gastro.2021.09.030.
Regular use of proton pump inhibitor and the risk of inflammatory bowel disease: Pooled analysis of 3 prospective cohorts
Xia B et al. Gastroenterology. 2021 Dec;161(6):1842-1852.e10. doi: 10.1053/j.gastro.2021.08.005.
January 2022
Serologic response to Coronavirus Disease 2019 (COVID-19) vaccination in patients with immune-mediated inflammatory diseases: A systematic review and meta-analysis
Sakuraba A et al. Gastroenterology. 2022 Jan;162(1):88-108.e9. doi: 10.1053/j.gastro.2021.09.055.
Advancing diversity, equity, and inclusion in scientific publishing
Doubeni CA et al. Gastroenterology. 2022 Jan;162(1):59-62.e1. doi: 10.1053/j.gastro.2021.10.043.
How we approach difficult to eradicate Helicobacter pylori
Argueta EA, Moss SF. Gastroenterology. 2022 Jan;162(1):32-37. doi: 10.1053/j.gastro.2021.10.048.
Global incidence of acute pancreatitis is increasing over time: A systematic review and meta-analysis
Iannuzzi JP et al. Gastroenterology. 2022 Jan;162(1):122-134. doi: 10.1053/j.gastro.2021.09.043.
Epidemiology, etiology, and treatment of gastroparesis: Real-world evidence from a large US national claims database
Ye Y et al. Gastroenterology. 2022 Jan;162(1):109-121.e5. doi: 10.1053/j.gastro.2021.09.064.
Clinical Gastroenterology and Hepatology
November 2021
AGA Clinical Practice Update on endoscopic management of perforations in gastrointestinal tract: Expert Review
Lee JH et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2252-2261.e2. doi: 10.1016/j.cgh.2021.06.045.
Food allergies and intolerances: A clinical approach to the diagnosis and management of adverse reactions to food
Onyimba F et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2230-2240.e1. doi: 10.1016/j.cgh.2021.01.025.
Management of gastrointestinal side effects of immune checkpoint inhibitors
Lui RN et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2262-2265. doi: 10.1016/j.cgh.2021.06.038.
December 2021
Optimizing the endoscopic examination in eosinophilic esophagitis
Dellon ES. Clin Gastroenterol Hepatol. 2021 Dec;19(12):2489-2492.e1. doi: 10.1016/j.cgh.2021.07.011.
Diagnostic accuracy of fecal calprotectin concentration in evaluating therapeutic outcomes of patients with ulcerative colitis
Stevens TW et al. Clin Gastroenterol Hepatol. 2021 Nov;19(11):2333-2342. doi: 10.1016/j.cgh.2020.08.019.
Factors associated with inpatient endoscopy delay and its impact on hospital length-of-stay and 30-day readmission
Jacobs CC et al. Clin Gastroenterol Hepatol. 2021 Dec;19(12):2648-2655. doi: 10.1016/j.cgh.2021.06.009.
January 2022
Comparing costs and outcomes of treatments for irritable bowel syndrome with diarrhea: Cost-benefit analysis
Shah ED et al. Clin Gastroenterol Hepatol. 2022 Jan;20(1):136-144.e31. doi: 10.1016/j.cgh.2020.09.043.
Next generation academic gastroenterology
Allen JI, Berry S. Clin Gastroenterol Hepatol. 2022 Jan;20(1):5-8. doi: 10.1016/j.cgh.2021.09.038.
Beyond metoclopramide for gastroparesis
Camilleri M. Clin Gastroenterol Hepatol. 2022 Jan;20(1):19-24. doi: 10.1016/j.cgh.2021.08.052.
Comparative safety and effectiveness of vedolizumab to tumor necrosis factor antagonist therapy for ulcerative colitis
Lukin D et al. Clin Gastroenterol Hepatol. 2022 Jan;20(1):126-135. doi: 10.1016/j.cgh.2020.10.003.
Techniques and Innovations in Gastrointestinal Endoscopy
Impact of the COVID-19 pandemic on utilization of EGD and colonoscopy in the United States: An analysis of the GIQuIC registry
Calderwood AH et al. Tech Innov Gastrointest Endosc. 2021;23(4):313-321. doi: 10.1016/j.tige.2021.07.003.
How to approach small polyps in colon: Tips and tricks
Mahmood S et al. Tech Inov Gastroinest Endosc. 2021;23(4):238-335. doi: 10.1016/j.tige.2021.06.007
Pig heart successfully transplanted to man
A genetically modified pig heart has been successfully transplanted into a 57-year-old man who had no other treatment options but is “doing well” 3 days after the procedure, officials at the University of Maryland Medical Center (UMMC), Baltimore, announced Jan. 10.
“This organ transplant demonstrated for the first time that a genetically modified animal heart can function like a human heart without immediate rejection by the body,” they said.
Three genes associated with antibody-mediated rejection had been knocked out in the pig supplying the transplanted heart, and six human genes associated with immune acceptance of the organ had been inserted into the pig’s genome, notes a UMMC press release.

“Lastly, one additional gene in the pig was knocked out to prevent excessive growth of the pig heart tissue, which totaled 10 unique gene edits made in the donor pig,” the release states.
The patient, Maryland resident David Bennett, had required mechanical circulatory support to stay alive but was rejected for standard heart transplantation at UMMC and other centers. He was ineligible for an implanted ventricular assist device due to ventricular arrhythmias.
Mr. Bennett “is being carefully monitored over the next days and weeks to determine whether the transplant provides lifesaving benefits,” the announcement says.
“We are proceeding cautiously, but we are also optimistic that this first-in-the-world surgery will provide an important new option for patients in the future,” notes a quote from Bartley P. Griffith, MD, the UMMC surgeon who performed the procedure.
The pig supplying the heart was provided to the center by Revivicor (Blacksburg, Virginia), a regenerative medicine company. An experimental antirejection medication (Kiniksa Pharmaceuticals; Lexington, Massachusetts) was also used, in addition to standard immunosuppressants.
A version of this article first appeared on Medscape.com.
A genetically modified pig heart has been successfully transplanted into a 57-year-old man who had no other treatment options but is “doing well” 3 days after the procedure, officials at the University of Maryland Medical Center (UMMC), Baltimore, announced Jan. 10.
“This organ transplant demonstrated for the first time that a genetically modified animal heart can function like a human heart without immediate rejection by the body,” they said.
Three genes associated with antibody-mediated rejection had been knocked out in the pig supplying the transplanted heart, and six human genes associated with immune acceptance of the organ had been inserted into the pig’s genome, notes a UMMC press release.
“Lastly, one additional gene in the pig was knocked out to prevent excessive growth of the pig heart tissue, which totaled 10 unique gene edits made in the donor pig,” the release states.
The patient, Maryland resident David Bennett, had required mechanical circulatory support to stay alive but was rejected for standard heart transplantation at UMMC and other centers. He was ineligible for an implanted ventricular assist device due to ventricular arrhythmias.
Mr. Bennett “is being carefully monitored over the next days and weeks to determine whether the transplant provides lifesaving benefits,” the announcement says.
“We are proceeding cautiously, but we are also optimistic that this first-in-the-world surgery will provide an important new option for patients in the future,” notes a quote from Bartley P. Griffith, MD, the UMMC surgeon who performed the procedure.
The pig supplying the heart was provided to the center by Revivicor (Blacksburg, Virginia), a regenerative medicine company. An experimental antirejection medication (Kiniksa Pharmaceuticals; Lexington, Massachusetts) was also used, in addition to standard immunosuppressants.
A version of this article first appeared on Medscape.com.
A genetically modified pig heart has been successfully transplanted into a 57-year-old man who had no other treatment options but is “doing well” 3 days after the procedure, officials at the University of Maryland Medical Center (UMMC), Baltimore, announced Jan. 10.
“This organ transplant demonstrated for the first time that a genetically modified animal heart can function like a human heart without immediate rejection by the body,” they said.
Three genes associated with antibody-mediated rejection had been knocked out in the pig supplying the transplanted heart, and six human genes associated with immune acceptance of the organ had been inserted into the pig’s genome, notes a UMMC press release.
“Lastly, one additional gene in the pig was knocked out to prevent excessive growth of the pig heart tissue, which totaled 10 unique gene edits made in the donor pig,” the release states.
The patient, Maryland resident David Bennett, had required mechanical circulatory support to stay alive but was rejected for standard heart transplantation at UMMC and other centers. He was ineligible for an implanted ventricular assist device due to ventricular arrhythmias.
Mr. Bennett “is being carefully monitored over the next days and weeks to determine whether the transplant provides lifesaving benefits,” the announcement says.
“We are proceeding cautiously, but we are also optimistic that this first-in-the-world surgery will provide an important new option for patients in the future,” notes a quote from Bartley P. Griffith, MD, the UMMC surgeon who performed the procedure.
The pig supplying the heart was provided to the center by Revivicor (Blacksburg, Virginia), a regenerative medicine company. An experimental antirejection medication (Kiniksa Pharmaceuticals; Lexington, Massachusetts) was also used, in addition to standard immunosuppressants.
A version of this article first appeared on Medscape.com.
COVID-vaccine myocarditis: Rare, mild, and usually in young men
The risk of myocarditis after immunization with mRNA-based vaccines against SARS-CoV-2 raised concerns when it came to light in early 2021. But as report after report showed such cases to be rare and usually mild and self-limited, focus has turned to the “how and why.”
The mechanism linking the BNT162b2 (Pfizer-BioNTech) and especially mRNA-1273 (Moderna) vaccines to the occurrence of myocarditis is unclear for now, but one potential driver may be tied to a peculiarity that became apparent early: It occurs overwhelmingly in younger males, from 16 to perhaps 40 or 50 years of age. Excess risk has not been consistently seen among women, girls, and older men.
That observation has led to speculation that higher testosterone levels in adolescent boys and young men may somehow promote the adverse vaccine effect, whereas greater levels of estrogen among girls and women in the same age range may be cardioprotective.
Unlikely, brief, and ‘benign’
“Most of the myocarditis is benign, by which I mean that maybe the patients are admitted due to chest pain, but without reduction in ventricular function,” Enrico Ammirati, MD, PhD, a myocarditis expert at De Gasperis Cardio Center and Transplant Center, Niguarda Hospital, Milan, said in an interview.
In a Nov. 14 address on this topic at the annual scientific sessions of the American Heart Association, Dror Mevorach, MD, described the typical case presentation as “mild” and one that clears in fairly short order based on resolution of “clinical symptoms, inflammatory markers and troponin decline, EKG normalization, echo normalization, and a relatively short length of hospital stay.”
Dr. Mevorach, of Hadassah Hebrew University Medical Center, Jerusalem, subsequently published the findings in a report in the New England Journal of Medicine that described 136 confirmed myocarditis cases among more than 5 million people in Israel immunized with the Pfizer-BioNTech vaccine. Myocarditis was considered “mild” in 129 cases, or 95%.
And the risk is tiny, compared with myocarditis from infection by SARS-CoV-2, not to mention the possibility of nasty clinical COVID-19 complications such as pneumonia and pulmonary embolism, Dr. Mevorach observed.
Many other reports agree that the incidence is minimal, especially given the rewards of vaccination. In a separate NEJM publication in September 2021 – from Noam Barda, MD, Clalit (Israel) Research Institute, and colleagues on 1.7 million people in that country, about half unvaccinated and half given the Pfizer-BioNTech vaccine – there were an estimated 2.7 cases of myocarditis per 100,000 vaccinated persons. There were also 11 cases of myocarditis per 100,000 persons who were positive for SARS-CoV-2 infection.
And in a recent case series of vaccinated people aged 16 or older, the myocarditis rate after a first or second Pfizer-BioNTech or Moderna injection was estimated at 1 or fewer per 100,000. The corresponding estimate was 4 such cases per 100,000 after a positive SARS-CoV-2 test among the same population, notes a report published Dec.14, 2021, in Nature Medicine.
In general, “the risk of any kind of cardiac injury is vastly lower with a vaccine than it is with the actual viral infection,” Leslie T. Cooper Jr., MD, a myocarditis expert and clinical trialist at the Mayo Clinic, Jacksonville, Fla., said in an interview. With the mRNA-based vaccines, “we do not have any conceivable danger signal that would outweigh the benefit of vaccination.”
Males of a certain age
Evidence that such myocarditis predominates in young adult men and adolescent boys, especially following a second vaccine dose, is remarkably consistent.
The risk was elevated only among mRNA-based vaccine recipients who were younger than 40 in the recent Nature Medicine analysis. Among that group, estimates after a second dose numbered fewer than 1 case per 100,000 for Pfizer-BioNTech and 1.5 per 100,000 for Moderna.
In a third analysis from Israel – also in NEJM, from Guy Witberg, MD, Rabin Medical Center, Petah Tikva, and colleagues, based on 2.5 million people aged 16 and older with at least one Pfizer-BioNTech injection – 2.1 cases per 100,000 were estimated overall, but the number rose to 10.7 per 100,000 among those aged 16-29 years.
In Dr. Mevorach’s NEJM report, estimates after a second Pfizer-BioNTech vaccine dose were 1 per 26,000 males versus 1 in 218,000 females, compared with 1 myocarditis case in 10,857 persons among “the general unvaccinated population.”
Most recipients of a first vaccine dose were younger than 50, and 16- to 29-year-olds accounted for most who completed two doses, noted Dr. Mevorach. Younger males bore the brunt of any myocarditis: the estimated prevalence after a second dose among males aged 16-19 was 1 per 6,637, compared with 1 per 99,853 females in the same age range, the group reported.
In the BMJ report, based on about 5 million people 12 years of age or older in Denmark, the estimated rates of myocarditis or pericarditis associated with Moderna immunization were 2 per 100,000 among women but 6.3 per 100,000 for men. The incidence and sex difference was much lower among those getting the Pfizer-BioNTech vaccine: 1.3 per 100,000 and 1.5 per 100,000 in women and men, respectively.
Sex hormones may be key
The predominance of vaccine-associated myocarditis among adolescent and young adult males is probably more about the myocarditis itself than the vaccines, observed Biykem Bozkurt, MD, PhD, who has been studying COVID-related myocarditis at Baylor College of Medicine, Houston.
Male sex historically is associated in both epidemiologic studies and experimental models with a greater propensity for most any form of myocarditis, Dr. Bozkurt said in an interview. Given that males aged 16-19 or so appear to be at highest risk of myocarditis as a complication of SARS-CoV-2 vaccination, the mechanism may well be related to sex hormones.
“Therefore, testosterone is implicated as a player in their higher risk of inflammation and injury and lack of adaptive response in terms of healing, and in terms of prevention of injury,” Dr. Bozkurt said. For its part, estrogen inhibits proinflammatory processes and, in particular, “blunts cell-mediated immune responses.”
“We don’t know the mechanism, but a theory that attributes a protective role to estrogen, or a risk associated with testosterone, is reasonable. It makes sense, at least based on epidemiological data,” Dr. Ammirati agreed. Still, “we do not have any direct evidence in human beings.”
Sex-associated differences in experimental myocarditis have been reported in the journals for at least 70 years, but “the testosterone literature and the estrogen literature have not been evaluated in detail in vaccine-associated myocarditis,” Dr. Cooper said.
Most myocarditis in the laboratory is viral, Dr. Cooper observed, and “the links between testosterone, viruses, and inflammation have been pretty well worked out, I would say, if you’re a mouse. If you’re a human, I think it’s still a bit uncertain.”
Were it to apply in humans, greater testosterone levels might independently promote myocarditis, “and if estrogen is cardioprotective, it would be another mechanism,” Dr. Cooper said. “That would translate to slight male predominance in most kinds of myocarditis.”
In males, compared with females, “the heart can be more vulnerable to events such as arrhythmias or to immune-mediated phenomena. So, probably there is also higher vulnerability to myocarditis in men,” Dr. Ammirati noted.
Male predominance in vaccine-related myocarditis is provocative, so it’s worth considering whether testosterone is part of the mechanism as well as the possibility of estrogen cardioprotection, Dr. Ammirati said. But given limitations of the animal models, “we don’t really have robust data to support any part of that.”
Although myocarditis is in some way immune mediated, “and hormones can modulate the response,” the mechanism has to be more than just sex hormones, he said. “They probably cannot explain the specificity for the heart. It’s not a systemic response, it’s an organ-specific response.”
Modulation of immune responses
Details about the immune processes underlying mRNA-vaccine myocarditis, hormone modulated or not, have been elusive. The complication doesn’t resemble serum sickness, nor does it seem to be a reaction to infection by other cardiotropic viruses, such as coxsackie virus B, a cause of viral myocarditis, Dr. Bozkurt said. The latter had been a compelling possibility because such hypersensitivity to smallpox vaccination is well recognized.
“We don’t know the mechanism, that’s the short answer. But there are many hypotheses,” she said. One candidate widely proposed in the literature: autoantibodies driven by molecular mimicry between the SARS-CoV-2 spike protein targeted by the mRNA vaccines and a structurally similar myocardial protein, possibly alpha-myosin, noted Dr. Bozkurt and colleagues in a recent publication.
But elevations in specific “antiheart antibodies” have not been documented in recipients of the two mRNA-based vaccines, said Dr. Cooper. “So, I would say that – although molecular mimicry is a well-established mechanism of, for example, rheumatic carditis after a streptococcal A infection – that has not been demonstrated yet for COVID-19 mRNA vaccination–related myocarditis.”
“We probably won’t know, ever, with a huge level of certainty, the exact mechanisms,” Dr. Cooper added. There is no animal model for vaccine-induced myocarditis, and “We’re still talking very, very small numbers of patients. The vast majority of them recover,” and so don’t generally provide mechanistic clues.
Prospects for younger children
Vaccination against SARS-CoV-2 has now been authorized by the Centers for Disease Control and Prevention for kids as young as 5-11 years, using the Pfizer-BioNTech vaccine. Experience so far suggests the immunization is safe in that age group with negligible risk of myocarditis or other complications. But with prospects of possible authorization in children younger than 5, should myocarditis be a concern for them?
Probably not, if the complication is driven primarily by sex hormones, Dr. Cooper proposed. “One would predict that before puberty you would have a lower – much, much lower – rate of myocarditis in males than you would in the 16- to 19-year-old range, and that it would be roughly equal to females.” Dr. Ammirati and Dr. Bozkurt largely agreed.
It remains to be seen whether the vaccine-related myocarditis risk applies to children younger than 12, “but I doubt it. I think it’s going to be puberty-related,” Dr. Bozkurt said. Still, “I don’t want to hypothesize without data.”
A version of this article first appeared on Medscape.com.
The risk of myocarditis after immunization with mRNA-based vaccines against SARS-CoV-2 raised concerns when it came to light in early 2021. But as report after report showed such cases to be rare and usually mild and self-limited, focus has turned to the “how and why.”
The mechanism linking the BNT162b2 (Pfizer-BioNTech) and especially mRNA-1273 (Moderna) vaccines to the occurrence of myocarditis is unclear for now, but one potential driver may be tied to a peculiarity that became apparent early: It occurs overwhelmingly in younger males, from 16 to perhaps 40 or 50 years of age. Excess risk has not been consistently seen among women, girls, and older men.
That observation has led to speculation that higher testosterone levels in adolescent boys and young men may somehow promote the adverse vaccine effect, whereas greater levels of estrogen among girls and women in the same age range may be cardioprotective.
Unlikely, brief, and ‘benign’
“Most of the myocarditis is benign, by which I mean that maybe the patients are admitted due to chest pain, but without reduction in ventricular function,” Enrico Ammirati, MD, PhD, a myocarditis expert at De Gasperis Cardio Center and Transplant Center, Niguarda Hospital, Milan, said in an interview.
In a Nov. 14 address on this topic at the annual scientific sessions of the American Heart Association, Dror Mevorach, MD, described the typical case presentation as “mild” and one that clears in fairly short order based on resolution of “clinical symptoms, inflammatory markers and troponin decline, EKG normalization, echo normalization, and a relatively short length of hospital stay.”
Dr. Mevorach, of Hadassah Hebrew University Medical Center, Jerusalem, subsequently published the findings in a report in the New England Journal of Medicine that described 136 confirmed myocarditis cases among more than 5 million people in Israel immunized with the Pfizer-BioNTech vaccine. Myocarditis was considered “mild” in 129 cases, or 95%.
And the risk is tiny, compared with myocarditis from infection by SARS-CoV-2, not to mention the possibility of nasty clinical COVID-19 complications such as pneumonia and pulmonary embolism, Dr. Mevorach observed.
Many other reports agree that the incidence is minimal, especially given the rewards of vaccination. In a separate NEJM publication in September 2021 – from Noam Barda, MD, Clalit (Israel) Research Institute, and colleagues on 1.7 million people in that country, about half unvaccinated and half given the Pfizer-BioNTech vaccine – there were an estimated 2.7 cases of myocarditis per 100,000 vaccinated persons. There were also 11 cases of myocarditis per 100,000 persons who were positive for SARS-CoV-2 infection.
And in a recent case series of vaccinated people aged 16 or older, the myocarditis rate after a first or second Pfizer-BioNTech or Moderna injection was estimated at 1 or fewer per 100,000. The corresponding estimate was 4 such cases per 100,000 after a positive SARS-CoV-2 test among the same population, notes a report published Dec.14, 2021, in Nature Medicine.
In general, “the risk of any kind of cardiac injury is vastly lower with a vaccine than it is with the actual viral infection,” Leslie T. Cooper Jr., MD, a myocarditis expert and clinical trialist at the Mayo Clinic, Jacksonville, Fla., said in an interview. With the mRNA-based vaccines, “we do not have any conceivable danger signal that would outweigh the benefit of vaccination.”
Males of a certain age
Evidence that such myocarditis predominates in young adult men and adolescent boys, especially following a second vaccine dose, is remarkably consistent.
The risk was elevated only among mRNA-based vaccine recipients who were younger than 40 in the recent Nature Medicine analysis. Among that group, estimates after a second dose numbered fewer than 1 case per 100,000 for Pfizer-BioNTech and 1.5 per 100,000 for Moderna.
In a third analysis from Israel – also in NEJM, from Guy Witberg, MD, Rabin Medical Center, Petah Tikva, and colleagues, based on 2.5 million people aged 16 and older with at least one Pfizer-BioNTech injection – 2.1 cases per 100,000 were estimated overall, but the number rose to 10.7 per 100,000 among those aged 16-29 years.
In Dr. Mevorach’s NEJM report, estimates after a second Pfizer-BioNTech vaccine dose were 1 per 26,000 males versus 1 in 218,000 females, compared with 1 myocarditis case in 10,857 persons among “the general unvaccinated population.”
Most recipients of a first vaccine dose were younger than 50, and 16- to 29-year-olds accounted for most who completed two doses, noted Dr. Mevorach. Younger males bore the brunt of any myocarditis: the estimated prevalence after a second dose among males aged 16-19 was 1 per 6,637, compared with 1 per 99,853 females in the same age range, the group reported.
In the BMJ report, based on about 5 million people 12 years of age or older in Denmark, the estimated rates of myocarditis or pericarditis associated with Moderna immunization were 2 per 100,000 among women but 6.3 per 100,000 for men. The incidence and sex difference was much lower among those getting the Pfizer-BioNTech vaccine: 1.3 per 100,000 and 1.5 per 100,000 in women and men, respectively.
Sex hormones may be key
The predominance of vaccine-associated myocarditis among adolescent and young adult males is probably more about the myocarditis itself than the vaccines, observed Biykem Bozkurt, MD, PhD, who has been studying COVID-related myocarditis at Baylor College of Medicine, Houston.
Male sex historically is associated in both epidemiologic studies and experimental models with a greater propensity for most any form of myocarditis, Dr. Bozkurt said in an interview. Given that males aged 16-19 or so appear to be at highest risk of myocarditis as a complication of SARS-CoV-2 vaccination, the mechanism may well be related to sex hormones.
“Therefore, testosterone is implicated as a player in their higher risk of inflammation and injury and lack of adaptive response in terms of healing, and in terms of prevention of injury,” Dr. Bozkurt said. For its part, estrogen inhibits proinflammatory processes and, in particular, “blunts cell-mediated immune responses.”
“We don’t know the mechanism, but a theory that attributes a protective role to estrogen, or a risk associated with testosterone, is reasonable. It makes sense, at least based on epidemiological data,” Dr. Ammirati agreed. Still, “we do not have any direct evidence in human beings.”
Sex-associated differences in experimental myocarditis have been reported in the journals for at least 70 years, but “the testosterone literature and the estrogen literature have not been evaluated in detail in vaccine-associated myocarditis,” Dr. Cooper said.
Most myocarditis in the laboratory is viral, Dr. Cooper observed, and “the links between testosterone, viruses, and inflammation have been pretty well worked out, I would say, if you’re a mouse. If you’re a human, I think it’s still a bit uncertain.”
Were it to apply in humans, greater testosterone levels might independently promote myocarditis, “and if estrogen is cardioprotective, it would be another mechanism,” Dr. Cooper said. “That would translate to slight male predominance in most kinds of myocarditis.”
In males, compared with females, “the heart can be more vulnerable to events such as arrhythmias or to immune-mediated phenomena. So, probably there is also higher vulnerability to myocarditis in men,” Dr. Ammirati noted.
Male predominance in vaccine-related myocarditis is provocative, so it’s worth considering whether testosterone is part of the mechanism as well as the possibility of estrogen cardioprotection, Dr. Ammirati said. But given limitations of the animal models, “we don’t really have robust data to support any part of that.”
Although myocarditis is in some way immune mediated, “and hormones can modulate the response,” the mechanism has to be more than just sex hormones, he said. “They probably cannot explain the specificity for the heart. It’s not a systemic response, it’s an organ-specific response.”
Modulation of immune responses
Details about the immune processes underlying mRNA-vaccine myocarditis, hormone modulated or not, have been elusive. The complication doesn’t resemble serum sickness, nor does it seem to be a reaction to infection by other cardiotropic viruses, such as coxsackie virus B, a cause of viral myocarditis, Dr. Bozkurt said. The latter had been a compelling possibility because such hypersensitivity to smallpox vaccination is well recognized.
“We don’t know the mechanism, that’s the short answer. But there are many hypotheses,” she said. One candidate widely proposed in the literature: autoantibodies driven by molecular mimicry between the SARS-CoV-2 spike protein targeted by the mRNA vaccines and a structurally similar myocardial protein, possibly alpha-myosin, noted Dr. Bozkurt and colleagues in a recent publication.
But elevations in specific “antiheart antibodies” have not been documented in recipients of the two mRNA-based vaccines, said Dr. Cooper. “So, I would say that – although molecular mimicry is a well-established mechanism of, for example, rheumatic carditis after a streptococcal A infection – that has not been demonstrated yet for COVID-19 mRNA vaccination–related myocarditis.”
“We probably won’t know, ever, with a huge level of certainty, the exact mechanisms,” Dr. Cooper added. There is no animal model for vaccine-induced myocarditis, and “We’re still talking very, very small numbers of patients. The vast majority of them recover,” and so don’t generally provide mechanistic clues.
Prospects for younger children
Vaccination against SARS-CoV-2 has now been authorized by the Centers for Disease Control and Prevention for kids as young as 5-11 years, using the Pfizer-BioNTech vaccine. Experience so far suggests the immunization is safe in that age group with negligible risk of myocarditis or other complications. But with prospects of possible authorization in children younger than 5, should myocarditis be a concern for them?
Probably not, if the complication is driven primarily by sex hormones, Dr. Cooper proposed. “One would predict that before puberty you would have a lower – much, much lower – rate of myocarditis in males than you would in the 16- to 19-year-old range, and that it would be roughly equal to females.” Dr. Ammirati and Dr. Bozkurt largely agreed.
It remains to be seen whether the vaccine-related myocarditis risk applies to children younger than 12, “but I doubt it. I think it’s going to be puberty-related,” Dr. Bozkurt said. Still, “I don’t want to hypothesize without data.”
A version of this article first appeared on Medscape.com.
The risk of myocarditis after immunization with mRNA-based vaccines against SARS-CoV-2 raised concerns when it came to light in early 2021. But as report after report showed such cases to be rare and usually mild and self-limited, focus has turned to the “how and why.”
The mechanism linking the BNT162b2 (Pfizer-BioNTech) and especially mRNA-1273 (Moderna) vaccines to the occurrence of myocarditis is unclear for now, but one potential driver may be tied to a peculiarity that became apparent early: It occurs overwhelmingly in younger males, from 16 to perhaps 40 or 50 years of age. Excess risk has not been consistently seen among women, girls, and older men.
That observation has led to speculation that higher testosterone levels in adolescent boys and young men may somehow promote the adverse vaccine effect, whereas greater levels of estrogen among girls and women in the same age range may be cardioprotective.
Unlikely, brief, and ‘benign’
“Most of the myocarditis is benign, by which I mean that maybe the patients are admitted due to chest pain, but without reduction in ventricular function,” Enrico Ammirati, MD, PhD, a myocarditis expert at De Gasperis Cardio Center and Transplant Center, Niguarda Hospital, Milan, said in an interview.
In a Nov. 14 address on this topic at the annual scientific sessions of the American Heart Association, Dror Mevorach, MD, described the typical case presentation as “mild” and one that clears in fairly short order based on resolution of “clinical symptoms, inflammatory markers and troponin decline, EKG normalization, echo normalization, and a relatively short length of hospital stay.”
Dr. Mevorach, of Hadassah Hebrew University Medical Center, Jerusalem, subsequently published the findings in a report in the New England Journal of Medicine that described 136 confirmed myocarditis cases among more than 5 million people in Israel immunized with the Pfizer-BioNTech vaccine. Myocarditis was considered “mild” in 129 cases, or 95%.
And the risk is tiny, compared with myocarditis from infection by SARS-CoV-2, not to mention the possibility of nasty clinical COVID-19 complications such as pneumonia and pulmonary embolism, Dr. Mevorach observed.
Many other reports agree that the incidence is minimal, especially given the rewards of vaccination. In a separate NEJM publication in September 2021 – from Noam Barda, MD, Clalit (Israel) Research Institute, and colleagues on 1.7 million people in that country, about half unvaccinated and half given the Pfizer-BioNTech vaccine – there were an estimated 2.7 cases of myocarditis per 100,000 vaccinated persons. There were also 11 cases of myocarditis per 100,000 persons who were positive for SARS-CoV-2 infection.
And in a recent case series of vaccinated people aged 16 or older, the myocarditis rate after a first or second Pfizer-BioNTech or Moderna injection was estimated at 1 or fewer per 100,000. The corresponding estimate was 4 such cases per 100,000 after a positive SARS-CoV-2 test among the same population, notes a report published Dec.14, 2021, in Nature Medicine.
In general, “the risk of any kind of cardiac injury is vastly lower with a vaccine than it is with the actual viral infection,” Leslie T. Cooper Jr., MD, a myocarditis expert and clinical trialist at the Mayo Clinic, Jacksonville, Fla., said in an interview. With the mRNA-based vaccines, “we do not have any conceivable danger signal that would outweigh the benefit of vaccination.”
Males of a certain age
Evidence that such myocarditis predominates in young adult men and adolescent boys, especially following a second vaccine dose, is remarkably consistent.
The risk was elevated only among mRNA-based vaccine recipients who were younger than 40 in the recent Nature Medicine analysis. Among that group, estimates after a second dose numbered fewer than 1 case per 100,000 for Pfizer-BioNTech and 1.5 per 100,000 for Moderna.
In a third analysis from Israel – also in NEJM, from Guy Witberg, MD, Rabin Medical Center, Petah Tikva, and colleagues, based on 2.5 million people aged 16 and older with at least one Pfizer-BioNTech injection – 2.1 cases per 100,000 were estimated overall, but the number rose to 10.7 per 100,000 among those aged 16-29 years.
In Dr. Mevorach’s NEJM report, estimates after a second Pfizer-BioNTech vaccine dose were 1 per 26,000 males versus 1 in 218,000 females, compared with 1 myocarditis case in 10,857 persons among “the general unvaccinated population.”
Most recipients of a first vaccine dose were younger than 50, and 16- to 29-year-olds accounted for most who completed two doses, noted Dr. Mevorach. Younger males bore the brunt of any myocarditis: the estimated prevalence after a second dose among males aged 16-19 was 1 per 6,637, compared with 1 per 99,853 females in the same age range, the group reported.
In the BMJ report, based on about 5 million people 12 years of age or older in Denmark, the estimated rates of myocarditis or pericarditis associated with Moderna immunization were 2 per 100,000 among women but 6.3 per 100,000 for men. The incidence and sex difference was much lower among those getting the Pfizer-BioNTech vaccine: 1.3 per 100,000 and 1.5 per 100,000 in women and men, respectively.
Sex hormones may be key
The predominance of vaccine-associated myocarditis among adolescent and young adult males is probably more about the myocarditis itself than the vaccines, observed Biykem Bozkurt, MD, PhD, who has been studying COVID-related myocarditis at Baylor College of Medicine, Houston.
Male sex historically is associated in both epidemiologic studies and experimental models with a greater propensity for most any form of myocarditis, Dr. Bozkurt said in an interview. Given that males aged 16-19 or so appear to be at highest risk of myocarditis as a complication of SARS-CoV-2 vaccination, the mechanism may well be related to sex hormones.
“Therefore, testosterone is implicated as a player in their higher risk of inflammation and injury and lack of adaptive response in terms of healing, and in terms of prevention of injury,” Dr. Bozkurt said. For its part, estrogen inhibits proinflammatory processes and, in particular, “blunts cell-mediated immune responses.”
“We don’t know the mechanism, but a theory that attributes a protective role to estrogen, or a risk associated with testosterone, is reasonable. It makes sense, at least based on epidemiological data,” Dr. Ammirati agreed. Still, “we do not have any direct evidence in human beings.”
Sex-associated differences in experimental myocarditis have been reported in the journals for at least 70 years, but “the testosterone literature and the estrogen literature have not been evaluated in detail in vaccine-associated myocarditis,” Dr. Cooper said.
Most myocarditis in the laboratory is viral, Dr. Cooper observed, and “the links between testosterone, viruses, and inflammation have been pretty well worked out, I would say, if you’re a mouse. If you’re a human, I think it’s still a bit uncertain.”
Were it to apply in humans, greater testosterone levels might independently promote myocarditis, “and if estrogen is cardioprotective, it would be another mechanism,” Dr. Cooper said. “That would translate to slight male predominance in most kinds of myocarditis.”
In males, compared with females, “the heart can be more vulnerable to events such as arrhythmias or to immune-mediated phenomena. So, probably there is also higher vulnerability to myocarditis in men,” Dr. Ammirati noted.
Male predominance in vaccine-related myocarditis is provocative, so it’s worth considering whether testosterone is part of the mechanism as well as the possibility of estrogen cardioprotection, Dr. Ammirati said. But given limitations of the animal models, “we don’t really have robust data to support any part of that.”
Although myocarditis is in some way immune mediated, “and hormones can modulate the response,” the mechanism has to be more than just sex hormones, he said. “They probably cannot explain the specificity for the heart. It’s not a systemic response, it’s an organ-specific response.”
Modulation of immune responses
Details about the immune processes underlying mRNA-vaccine myocarditis, hormone modulated or not, have been elusive. The complication doesn’t resemble serum sickness, nor does it seem to be a reaction to infection by other cardiotropic viruses, such as coxsackie virus B, a cause of viral myocarditis, Dr. Bozkurt said. The latter had been a compelling possibility because such hypersensitivity to smallpox vaccination is well recognized.
“We don’t know the mechanism, that’s the short answer. But there are many hypotheses,” she said. One candidate widely proposed in the literature: autoantibodies driven by molecular mimicry between the SARS-CoV-2 spike protein targeted by the mRNA vaccines and a structurally similar myocardial protein, possibly alpha-myosin, noted Dr. Bozkurt and colleagues in a recent publication.
But elevations in specific “antiheart antibodies” have not been documented in recipients of the two mRNA-based vaccines, said Dr. Cooper. “So, I would say that – although molecular mimicry is a well-established mechanism of, for example, rheumatic carditis after a streptococcal A infection – that has not been demonstrated yet for COVID-19 mRNA vaccination–related myocarditis.”
“We probably won’t know, ever, with a huge level of certainty, the exact mechanisms,” Dr. Cooper added. There is no animal model for vaccine-induced myocarditis, and “We’re still talking very, very small numbers of patients. The vast majority of them recover,” and so don’t generally provide mechanistic clues.
Prospects for younger children
Vaccination against SARS-CoV-2 has now been authorized by the Centers for Disease Control and Prevention for kids as young as 5-11 years, using the Pfizer-BioNTech vaccine. Experience so far suggests the immunization is safe in that age group with negligible risk of myocarditis or other complications. But with prospects of possible authorization in children younger than 5, should myocarditis be a concern for them?
Probably not, if the complication is driven primarily by sex hormones, Dr. Cooper proposed. “One would predict that before puberty you would have a lower – much, much lower – rate of myocarditis in males than you would in the 16- to 19-year-old range, and that it would be roughly equal to females.” Dr. Ammirati and Dr. Bozkurt largely agreed.
It remains to be seen whether the vaccine-related myocarditis risk applies to children younger than 12, “but I doubt it. I think it’s going to be puberty-related,” Dr. Bozkurt said. Still, “I don’t want to hypothesize without data.”
A version of this article first appeared on Medscape.com.
One doctor’s psychedelic journey to confront his cancer
Pradeep Bansal considered the five capsules he was about to swallow. Together they made up a 25-mg dose of a substance that, in another setting, could have landed him in federal prison.
The substance was psilocybin, the active ingredient in magic mushrooms. To be more exact, it was a synthetic form of psilocybin called COMP360, made to pharmaceutical standards by a company called COMPASS Pathways. He was taking it as part of an Food and Drug Administration–approved clinical study on mental health therapy for people with cancer.
Dr. Bansal, a New York gastroenterologist, was far more comfortable giving medical treatment than receiving it. But he was getting used to it.
He had already been through surgery and a number of other treatments to address the physical aspects of his cancer. The psilocybin was to address the mental aspects – the crushing anxiety and depression that had stuck with him after his diagnosis.
Dr. Bansal did not arrive at this moment lightly.
“I was extremely skeptical going into this process,” said Dr. Bansal, who during a long medical career had looked with distrust and even disdain at alternative therapies.
“I don’t have much patience for holistic medicine, homeopathy, acupuncture, or alternative medicines with claims of spiritual upliftment or altered states of mind.”
But Bansal had done his homework on psilocybin and was impressed.
according to studies published in 2011, 2014, and 2016.
One study from Johns Hopkins University tracked the effects of a single guided dose of psilocybin in terminal cancer patients with anxiety and depression. More than 80% had a “significant decrease” in symptoms – even 6 months after treatment – with more than 60% of the group remaining in the normal mood range.
For the study Dr. Bansal joined, there had been weeks of screening and consultation and preparation in a strictly controlled scientific trial.
And yet, even with all that he had learned, even with his psychiatrist-guide by his side, he was afraid. Afraid of what he might experience under the powerful effects of psilocybin. And afraid that this was all a misguided waste of time – that his mental angst would still be there when it was all over.
He knew that psilocybin, like other psychedelic substances, could take you on a “trip” – could remove you, at least for a time, from normal conscious experience.
Maybe he would feel “funny,” he thought. Maybe he would have some hallucinations. But how would that change the reality of his cancer? How would it lift the black dread and anxiety he felt about his future?
Stuck in a dark place
Dr. Bansal had first noticed blood in his urine – a lot of it – in September 2019.
Two months later, doctors diagnosed cancer in his right kidney. He would need surgery to remove the kidney and surrounding lymph nodes (an operation called radical nephrectomy).
It was a shock, said Dr. Bansal. But the diagnosis and the surgery happened so quickly that he hardly had time to think. And treatment results seemed good. The cancer was only in stage I and the CT scans showed no signs of cancer after surgery.
“We were so relieved. Everyone was so happy,” Dr. Bansal said. “They didn’t even give me chemotherapy after surgery because it seemed so early.”
But a routine scan in June 2020 revealed more cancer in his lung. Within a couple of months, it was in his bladder too.
“It was devastating,” Dr. Bansal said. “I went from thinking I was healthy again to stage IV cancer.”
As doctors scheduled surgery to remove part of his lung, Dr. Bansal started on painful immunotherapy (BCG therapy) for his bladder.
At this point, from a psychological standpoint, Dr. Bansal was reeling. As a doctor, he knew all too well the meaning of stage IV cancer.
With two adult children and a grandchild on the way, Dr. Bansal had been looking forward to retirement with his wife of almost 40 years. “Suddenly, I wasn’t sure I was going to last that long,” Bansal recalled. “I was in a very dark place. I was very anxious, very depressed from lack of sleep.”
He saw a therapist about his cancer diagnosis and maintained his regular meditation practice at home. He hired a personal trainer and tried to focus on any good news that he got about his treatment.
Those things helped, but not enough.
The basic facts were inescapable. His cancer might end everything. He couldn’t stop thinking about it. And then he couldn’t stop thinking about how he couldn’t stop thinking about it.
If the worst happened, he didn’t want to spend his last days in a state of such relentless existential angst. And it wasn’t just for himself. He wanted to be strong and mentally present for his family and his loved ones and his patients.
As he searched for something to ease his mental anguish, Dr. Bansal recalled some psychedelic research on end-of-life anxiety and depression that he’d read about in Michael Pollan’s book on psychedelics, “How to Change Your Mind” (New York, Penguin Press, 2018).
The studies were small and the research was new, but Dr. Bansal was impressed enough with the results to take a chance. He called a lead researcher of one of the studies, a fellow New York doctor, and eventually found himself accepted into a new study.
Starting the journey
By the time Dr. Bansal arrived at the Bill Richards Center for Healing at the Aquilino Cancer Center in Rockville, Md., he had already been through weeks of screening.
The main requirements for the study were a cancer diagnosis and a measurable level of depression. But study participants also had to be physically fit enough to handle the medication, and psychologically free from a personal or family history of psychosis or schizophrenia. (The study also required participants to slowly wean themselves from medications like SSRIs for depression or antianxiety medications under the strict supervision of a qualified doctor.)
Dr. Bansal’s week of treatment began almost immediately on arrival at Aquilino. Everything was carefully choreographed but not rushed. From Monday to Wednesday, doctors followed his physical health with exams, ECGs, and blood work. And most importantly, they began to prepare him for the “dosing session” on Thursday when he would take the psilocybin.
This is the careful crafting of “set and setting” stressed in so many psychedelic therapies. “Set” refers to your mindset going into the drug experience. “Setting” is the space and people around you when the drug sends you into an altered state of consciousness.
Dr. Bansal met several times with at least three therapists in the days leading up to his dosing. He attended 4-plus hours of therapist-led group sessions with other people who would get a dosing on the same day. Together, they talked about what to expect during the experience and what to do in the face of fear or panic.
He connected with a therapist who would be his personal guide. Dr. Bansal’s therapist was a military psychiatrist with over 30 years’ experience.
“He was there with me from day 1, and so we established a relationship,” Dr. Bansal said.
“He asked me a lot of personal background history – you know, my religious convictions, aspirations, all those things.”
“Trust and let go,” was a kind of mantra for the treatment repeated by his guide and other doctors.
For Dr. Bansal, a doctor and scientist accustomed to using hard facts rather than touchy-feely slogans to navigate the care of patients, it was an adjustment, to say the least.
But he did his best to set aside his doubts and embrace the journey he was about to take.
The day of the trip
Thursday morning finally arrived. The setting of the dosing room was warm and welcoming, more like a cozy home study than a hospital room.
This matters more than you might think. First, because it’s important that you feel safe, open, and comfortable enough to let go and enter into a therapeutic process. But also because though rare, it’s possible – especially with psilocybin – for people to lose track of where they are and what they’re doing and put themselves or others in danger.
The dose, 25 mg, had been carefully calibrated to induce a psychedelic experience sufficient for therapy. Much less than that, say 10 mg, isn’t enough for most people to enter this state. A double dose, 50 mg, though not physically unsafe, may leave you too incoherent to have the useful insights key to therapeutic value.
A doctor, the lead investigator of the study, brought the five capsules into the room in an intricately carved crucible with a small ceremonial cup that held the water with which to take it.
“It was very solemn,” Dr. Bansal said. “He sat down with me in a very calming way.”
The doctor said: “Don’t worry about it. Just trust and let go.”
And that’s just what he did.
Dr. Bansal swallowed the capsules and lay down. The doctor quietly left the room so that Dr. Bansal and his psychiatrist guide could begin their session together.
Special eye shades kept him in the pitch dark whether his eyes were open or closed. Headphones streamed a curated musical playlist – much of it Western classical like Strauss, Bach, Mozart, and Beethoven – but also modern electronica and other music from cultures around the globe.
Dr. Bansal would remain here, with his therapist-guide by his side, in largely this same position, for the next 7-and-a-half hours.
It took about 45 minutes for the medication to kick in.
The investigator
The doctor who brought the capsules into the dosing room was Manish Agrawal, MD, codirector of clinical research at the Aquilino Cancer Center and lead investigator of the study.
Dr. Agrawal trained at the National Cancer Institute and practiced for many years as an oncologist before developing an interest in psychedelic therapies. It was his work with cancer patients that drew him to psychedelics in the first place.
He had seen too many of his patients mentally wrecked by a cancer diagnosis, and he often felt helpless to comfort them.
“You take care of the physical aspects of the cancer, right? You talk about side effects and recommend another scan to look for recurrence.”
“But what about the psychological effects?”
They can be very serious and too often go ignored, said Dr. Agrawal. Your plans for the future suddenly become moot. You may be concerned about your ability to work or worried about the pain and suffering and financial strain that might be ahead for both you and your family. And to top it all off, you’re staring into the face of your own mortality.
So it’s no wonder, said Dr. Agrawal, that many people develop clinical levels of anxiety and depression after a cancer diagnosis.
Like Dr. Bansal, Dr. Agrawal had been impressed by early studies on psilocybin-assisted therapies for end-of-life anxiety and depression. He had tried other approaches – support groups, one-on-one therapy, religious counselors, psychiatrist-prescribed medication – but he was never really happy with the results.
To Dr. Agrawal, psilocybin-assisted therapy was the first thing that looked like it could really make a difference.
And so after his psychedelic certification at the California Institute of Integral Studies, Dr. Agrawal was determined to change his approach.
The result was the Bill Richards Center for Healing at Aquilino Cancer Center, built specifically to study psychedelic-assisted therapies for psychological distress in people with cancer. The mission of the center is to help develop safe, FDA-approved psychedelic therapies for the mental health of cancer patients, and, once approved, provide a state-of-the-art facility and staff to administer those treatments.
A trip into the unknown
Back in the dosing room, Dr. Bansal was starting to feel the effects of the medication. As the psilocybin kicked in, spectacular images swirled.
“It was as if a million stained glass windows had suddenly come to life and were dancing in front of my vision,” Dr. Bansal said.
There were moving landscapes and intricate swirling patterns and massive stages in the sky where he saw orchestras playing the music he was hearing.
Dr. Bansal saw himself being crushed by a huge machine and buried, dead, in the Earth. He died and returned to life several times, glided over the top of New York City with the skyscrapers just below him, and took in the vision of the entire universe.
“I saw this expanse of the sky that was limitless. And there was this prehistoric reptile creature that spanned galaxies in the sky ahead of me who was dying. I said: ‘My God, the universe is dying,’ but then after a few moments, the universe came to life again in a burst of stars exploding.”
All the while, Dr. Bansal said, he was well aware that it was simply his mind creating these images, thoughts, and ideas. He knew he was in a safe room wearing eyeshades and headphones.
And yet, he says, it felt true. “The images and feelings are so powerful that you cannot help but believe they are in some way a part of reality.”
“At one point, I saw this giant Ferris wheel coming towards me and it was full of giant crabs, clicking and clacking their pincers. And my brain told me: ‘That’s my cancer!’ ”
Dr. Bansal was terrified. But he and his therapist had arranged a system of signals before the session. “If I was feeling afraid, I would hold his hand and if I had other issues, I would raise my hand. If I was feeling good, I would give him a thumbs up.”
Dr. Bansal reached out to his therapist and grasped his hand. “I said, ‘My cancer is coming at me!’ ”
His therapist was clear about what to do: Stand firm and walk toward it.
“That’s what they tell you: If you see anything frightening, you face it. And that’s the whole point of this exercise. And so, I stood and walked forward, and it just blew off in a puff of smoke.”
A state of peace
Around 3 hours into the experience, Dr. Bansal started to feel an immense sense of peace, happiness, and even comfort.
“I felt like I was watching a movie or a multidimensional slideshow. I was also a part of the movie. I felt like I could tell my mind what I wanted to see, and it would show it to me. It’s almost like you can mold your own visions. It was mystical.”
After about 8 hours, as the effects of the drug wore off, Dr. Bansal removed his eyeshades and headphones. He was completely drained.
“Even though I was lying down on my back for 7 hours, I felt like I had been run over by a truck. I was exhausted beyond belief physically and mentally.”
This was partly because of the fact that he hadn’t eaten much during the session. But mostly, said Dr. Bansal, it was because of the searing emotional intensity of the experience.
After the journey
It’s hard to put into words, said Dr. Bansal, what this treatment has done for his life. He feels as if he has stumbled onto something very precious that had been right in front of him all along. He wrote of his change in perspective almost obsessively in his journal in the days and weeks after treatment. One passage reads:
“It seems that, as time is passing on, I’m becoming more relaxed and hopeful, more calm, and at peace. Family has become even more important to me now. Money, politics, material gains, alcohol, seem less important.”
And yet there was nothing “easy” about the experience. In fact, in some ways the experience demanded more from him. “I feel I need to be more compassionate and considerate – less irritable and angry, more understanding of others’ needs. I feel I need to be a better human being, a better patient, a better father, and a better doctor for my patients.”
The experience, he said, gave him something far more important than mere ease. It gave him a sense of meaning.
From his journal:
“I died, and I was reborn. If I survived this, then I can face anything and anybody in the cosmic scheme. I can become part of it.
“How many sorrows in the universe? My cancer is nothing. Life does not end with the end of life. What was will be again. Eternally.”
That’s not an unusual response, according to the namesake of the Bill Richards Center for Healing. Bill Richards, PhD, has worked in the world of psychedelic-assisted psychotherapy since 1963.
A psychologist with decades of experience, Dr. Richards and colleagues figure that, with few possible exceptions, he has helped treat more people with psychedelic therapies than anyone alive in Western medicine today. At Aquilino, he works directly with patients and oversees the therapy protocol that goes along with the psilocybin dosing sessions.
“It’s inspiring,” Dr. Richards said.
“You meet someone who’s very depressed and scared and isolating from family and having all kinds of physical complaints. And a few days later, you talk to the same person and they have a whole new lease on life.”
And the positive effects can extend deep into the family system, he said.
After psilocybin treatment, said Dr. Richards, the person with cancer can become a kind of social worker for the family. They’re often far better able to talk about death and loss and even money and family issues than their loved ones. It’s not uncommon after treatment to see the resolution of years-old resentments or grievances that have dogged a family for many years.
Plus, said Dr. Richards, the cancer patient often ends up as a kind model to other family members for how to approach death. “They can demonstrate how to live fully – right to the last breath – which is a real gift because those relatives and loved ones have to die someday too, you know.”
At 80 years old, Dr. Richards is still in active practice and hopes to spend the rest of his days working with people in end-of-life care.
After the experience
Psychedelic-assisted therapy does not end with the dosing session. Integration sessions, where you discuss what happened during the dosing session, are a key part of most treatments.
The goal is to help participants absorb and “integrate” their experience. It typically happens over two or more sessions of 60-90 minutes with a therapist. In some cases, the therapist may invite a significant other to join in the integration process.
Dr. Agrawal’s trial at the Bill Richards center added something new: group therapy. Not only did Dr. Bansal meet with his therapist, he also met with a group of three other people in the trial who had their dosing the same day.
The point, said Dr. Agrawal, is to try and determine the effect of the group on the therapy. After their private dosing sessions, they come back together to discuss their experiences.
“After the psilocybin, they feel like they’ve been to war together,” Dr. Agrawal said. “There is this profound openness and connection. They feel able to share things with each other that they wouldn’t with other people.”
It will take some time to figure out how the group affects the overall outcome, but Dr. Bansal thinks it was integral to the success of his treatment.
In fact, he continues to meet regularly with his therapy group, even though it’s long since past the requirements of the study.
Pradeep 2.0
Dr. Bansal still has tough days with his cancer. Recently, immunotherapy treatment for his bladder caused side effects – pain, bleeding, fever, and chills – for most of the night. He felt like he was “passing razor blades” when he peed.
“And yet it was somehow okay,” he said. “It was only pain.”
“It’s as if there is a part of me that is watching myself objectively, going through the painful process of treatments saying: ‘It’s all right. I will be with you through this journey, through this experience. Don’t worry.’”
Months after taking that one dose, Dr. Bansal still calls it as “the single most powerful experience of my life.”
The change in his mental outlook, Dr. Bansal said, was profound, particularly in regard to his cancer.
“I understood that I still had cancer and that it could kill me in a few weeks, or months, or years. But my perspective had shifted.”
Dr. Bansal was as surprised as anyone. “Had somebody told me going into this that I would come out a transformed being or a person with a completely different perspective on life, I would never have believed it.”
He even named his new outlook. “I call it Pradeep 2.0.”
A version of this article first appeared on WebMD.com.
Pradeep Bansal considered the five capsules he was about to swallow. Together they made up a 25-mg dose of a substance that, in another setting, could have landed him in federal prison.
The substance was psilocybin, the active ingredient in magic mushrooms. To be more exact, it was a synthetic form of psilocybin called COMP360, made to pharmaceutical standards by a company called COMPASS Pathways. He was taking it as part of an Food and Drug Administration–approved clinical study on mental health therapy for people with cancer.
Dr. Bansal, a New York gastroenterologist, was far more comfortable giving medical treatment than receiving it. But he was getting used to it.
He had already been through surgery and a number of other treatments to address the physical aspects of his cancer. The psilocybin was to address the mental aspects – the crushing anxiety and depression that had stuck with him after his diagnosis.
Dr. Bansal did not arrive at this moment lightly.
“I was extremely skeptical going into this process,” said Dr. Bansal, who during a long medical career had looked with distrust and even disdain at alternative therapies.
“I don’t have much patience for holistic medicine, homeopathy, acupuncture, or alternative medicines with claims of spiritual upliftment or altered states of mind.”
But Bansal had done his homework on psilocybin and was impressed.
according to studies published in 2011, 2014, and 2016.
One study from Johns Hopkins University tracked the effects of a single guided dose of psilocybin in terminal cancer patients with anxiety and depression. More than 80% had a “significant decrease” in symptoms – even 6 months after treatment – with more than 60% of the group remaining in the normal mood range.
For the study Dr. Bansal joined, there had been weeks of screening and consultation and preparation in a strictly controlled scientific trial.
And yet, even with all that he had learned, even with his psychiatrist-guide by his side, he was afraid. Afraid of what he might experience under the powerful effects of psilocybin. And afraid that this was all a misguided waste of time – that his mental angst would still be there when it was all over.
He knew that psilocybin, like other psychedelic substances, could take you on a “trip” – could remove you, at least for a time, from normal conscious experience.
Maybe he would feel “funny,” he thought. Maybe he would have some hallucinations. But how would that change the reality of his cancer? How would it lift the black dread and anxiety he felt about his future?
Stuck in a dark place
Dr. Bansal had first noticed blood in his urine – a lot of it – in September 2019.
Two months later, doctors diagnosed cancer in his right kidney. He would need surgery to remove the kidney and surrounding lymph nodes (an operation called radical nephrectomy).
It was a shock, said Dr. Bansal. But the diagnosis and the surgery happened so quickly that he hardly had time to think. And treatment results seemed good. The cancer was only in stage I and the CT scans showed no signs of cancer after surgery.
“We were so relieved. Everyone was so happy,” Dr. Bansal said. “They didn’t even give me chemotherapy after surgery because it seemed so early.”
But a routine scan in June 2020 revealed more cancer in his lung. Within a couple of months, it was in his bladder too.
“It was devastating,” Dr. Bansal said. “I went from thinking I was healthy again to stage IV cancer.”
As doctors scheduled surgery to remove part of his lung, Dr. Bansal started on painful immunotherapy (BCG therapy) for his bladder.
At this point, from a psychological standpoint, Dr. Bansal was reeling. As a doctor, he knew all too well the meaning of stage IV cancer.
With two adult children and a grandchild on the way, Dr. Bansal had been looking forward to retirement with his wife of almost 40 years. “Suddenly, I wasn’t sure I was going to last that long,” Bansal recalled. “I was in a very dark place. I was very anxious, very depressed from lack of sleep.”
He saw a therapist about his cancer diagnosis and maintained his regular meditation practice at home. He hired a personal trainer and tried to focus on any good news that he got about his treatment.
Those things helped, but not enough.
The basic facts were inescapable. His cancer might end everything. He couldn’t stop thinking about it. And then he couldn’t stop thinking about how he couldn’t stop thinking about it.
If the worst happened, he didn’t want to spend his last days in a state of such relentless existential angst. And it wasn’t just for himself. He wanted to be strong and mentally present for his family and his loved ones and his patients.
As he searched for something to ease his mental anguish, Dr. Bansal recalled some psychedelic research on end-of-life anxiety and depression that he’d read about in Michael Pollan’s book on psychedelics, “How to Change Your Mind” (New York, Penguin Press, 2018).
The studies were small and the research was new, but Dr. Bansal was impressed enough with the results to take a chance. He called a lead researcher of one of the studies, a fellow New York doctor, and eventually found himself accepted into a new study.
Starting the journey
By the time Dr. Bansal arrived at the Bill Richards Center for Healing at the Aquilino Cancer Center in Rockville, Md., he had already been through weeks of screening.
The main requirements for the study were a cancer diagnosis and a measurable level of depression. But study participants also had to be physically fit enough to handle the medication, and psychologically free from a personal or family history of psychosis or schizophrenia. (The study also required participants to slowly wean themselves from medications like SSRIs for depression or antianxiety medications under the strict supervision of a qualified doctor.)
Dr. Bansal’s week of treatment began almost immediately on arrival at Aquilino. Everything was carefully choreographed but not rushed. From Monday to Wednesday, doctors followed his physical health with exams, ECGs, and blood work. And most importantly, they began to prepare him for the “dosing session” on Thursday when he would take the psilocybin.
This is the careful crafting of “set and setting” stressed in so many psychedelic therapies. “Set” refers to your mindset going into the drug experience. “Setting” is the space and people around you when the drug sends you into an altered state of consciousness.
Dr. Bansal met several times with at least three therapists in the days leading up to his dosing. He attended 4-plus hours of therapist-led group sessions with other people who would get a dosing on the same day. Together, they talked about what to expect during the experience and what to do in the face of fear or panic.
He connected with a therapist who would be his personal guide. Dr. Bansal’s therapist was a military psychiatrist with over 30 years’ experience.
“He was there with me from day 1, and so we established a relationship,” Dr. Bansal said.
“He asked me a lot of personal background history – you know, my religious convictions, aspirations, all those things.”
“Trust and let go,” was a kind of mantra for the treatment repeated by his guide and other doctors.
For Dr. Bansal, a doctor and scientist accustomed to using hard facts rather than touchy-feely slogans to navigate the care of patients, it was an adjustment, to say the least.
But he did his best to set aside his doubts and embrace the journey he was about to take.
The day of the trip
Thursday morning finally arrived. The setting of the dosing room was warm and welcoming, more like a cozy home study than a hospital room.
This matters more than you might think. First, because it’s important that you feel safe, open, and comfortable enough to let go and enter into a therapeutic process. But also because though rare, it’s possible – especially with psilocybin – for people to lose track of where they are and what they’re doing and put themselves or others in danger.
The dose, 25 mg, had been carefully calibrated to induce a psychedelic experience sufficient for therapy. Much less than that, say 10 mg, isn’t enough for most people to enter this state. A double dose, 50 mg, though not physically unsafe, may leave you too incoherent to have the useful insights key to therapeutic value.
A doctor, the lead investigator of the study, brought the five capsules into the room in an intricately carved crucible with a small ceremonial cup that held the water with which to take it.
“It was very solemn,” Dr. Bansal said. “He sat down with me in a very calming way.”
The doctor said: “Don’t worry about it. Just trust and let go.”
And that’s just what he did.
Dr. Bansal swallowed the capsules and lay down. The doctor quietly left the room so that Dr. Bansal and his psychiatrist guide could begin their session together.
Special eye shades kept him in the pitch dark whether his eyes were open or closed. Headphones streamed a curated musical playlist – much of it Western classical like Strauss, Bach, Mozart, and Beethoven – but also modern electronica and other music from cultures around the globe.
Dr. Bansal would remain here, with his therapist-guide by his side, in largely this same position, for the next 7-and-a-half hours.
It took about 45 minutes for the medication to kick in.
The investigator
The doctor who brought the capsules into the dosing room was Manish Agrawal, MD, codirector of clinical research at the Aquilino Cancer Center and lead investigator of the study.
Dr. Agrawal trained at the National Cancer Institute and practiced for many years as an oncologist before developing an interest in psychedelic therapies. It was his work with cancer patients that drew him to psychedelics in the first place.
He had seen too many of his patients mentally wrecked by a cancer diagnosis, and he often felt helpless to comfort them.
“You take care of the physical aspects of the cancer, right? You talk about side effects and recommend another scan to look for recurrence.”
“But what about the psychological effects?”
They can be very serious and too often go ignored, said Dr. Agrawal. Your plans for the future suddenly become moot. You may be concerned about your ability to work or worried about the pain and suffering and financial strain that might be ahead for both you and your family. And to top it all off, you’re staring into the face of your own mortality.
So it’s no wonder, said Dr. Agrawal, that many people develop clinical levels of anxiety and depression after a cancer diagnosis.
Like Dr. Bansal, Dr. Agrawal had been impressed by early studies on psilocybin-assisted therapies for end-of-life anxiety and depression. He had tried other approaches – support groups, one-on-one therapy, religious counselors, psychiatrist-prescribed medication – but he was never really happy with the results.
To Dr. Agrawal, psilocybin-assisted therapy was the first thing that looked like it could really make a difference.
And so after his psychedelic certification at the California Institute of Integral Studies, Dr. Agrawal was determined to change his approach.
The result was the Bill Richards Center for Healing at Aquilino Cancer Center, built specifically to study psychedelic-assisted therapies for psychological distress in people with cancer. The mission of the center is to help develop safe, FDA-approved psychedelic therapies for the mental health of cancer patients, and, once approved, provide a state-of-the-art facility and staff to administer those treatments.
A trip into the unknown
Back in the dosing room, Dr. Bansal was starting to feel the effects of the medication. As the psilocybin kicked in, spectacular images swirled.
“It was as if a million stained glass windows had suddenly come to life and were dancing in front of my vision,” Dr. Bansal said.
There were moving landscapes and intricate swirling patterns and massive stages in the sky where he saw orchestras playing the music he was hearing.
Dr. Bansal saw himself being crushed by a huge machine and buried, dead, in the Earth. He died and returned to life several times, glided over the top of New York City with the skyscrapers just below him, and took in the vision of the entire universe.
“I saw this expanse of the sky that was limitless. And there was this prehistoric reptile creature that spanned galaxies in the sky ahead of me who was dying. I said: ‘My God, the universe is dying,’ but then after a few moments, the universe came to life again in a burst of stars exploding.”
All the while, Dr. Bansal said, he was well aware that it was simply his mind creating these images, thoughts, and ideas. He knew he was in a safe room wearing eyeshades and headphones.
And yet, he says, it felt true. “The images and feelings are so powerful that you cannot help but believe they are in some way a part of reality.”
“At one point, I saw this giant Ferris wheel coming towards me and it was full of giant crabs, clicking and clacking their pincers. And my brain told me: ‘That’s my cancer!’ ”
Dr. Bansal was terrified. But he and his therapist had arranged a system of signals before the session. “If I was feeling afraid, I would hold his hand and if I had other issues, I would raise my hand. If I was feeling good, I would give him a thumbs up.”
Dr. Bansal reached out to his therapist and grasped his hand. “I said, ‘My cancer is coming at me!’ ”
His therapist was clear about what to do: Stand firm and walk toward it.
“That’s what they tell you: If you see anything frightening, you face it. And that’s the whole point of this exercise. And so, I stood and walked forward, and it just blew off in a puff of smoke.”
A state of peace
Around 3 hours into the experience, Dr. Bansal started to feel an immense sense of peace, happiness, and even comfort.
“I felt like I was watching a movie or a multidimensional slideshow. I was also a part of the movie. I felt like I could tell my mind what I wanted to see, and it would show it to me. It’s almost like you can mold your own visions. It was mystical.”
After about 8 hours, as the effects of the drug wore off, Dr. Bansal removed his eyeshades and headphones. He was completely drained.
“Even though I was lying down on my back for 7 hours, I felt like I had been run over by a truck. I was exhausted beyond belief physically and mentally.”
This was partly because of the fact that he hadn’t eaten much during the session. But mostly, said Dr. Bansal, it was because of the searing emotional intensity of the experience.
After the journey
It’s hard to put into words, said Dr. Bansal, what this treatment has done for his life. He feels as if he has stumbled onto something very precious that had been right in front of him all along. He wrote of his change in perspective almost obsessively in his journal in the days and weeks after treatment. One passage reads:
“It seems that, as time is passing on, I’m becoming more relaxed and hopeful, more calm, and at peace. Family has become even more important to me now. Money, politics, material gains, alcohol, seem less important.”
And yet there was nothing “easy” about the experience. In fact, in some ways the experience demanded more from him. “I feel I need to be more compassionate and considerate – less irritable and angry, more understanding of others’ needs. I feel I need to be a better human being, a better patient, a better father, and a better doctor for my patients.”
The experience, he said, gave him something far more important than mere ease. It gave him a sense of meaning.
From his journal:
“I died, and I was reborn. If I survived this, then I can face anything and anybody in the cosmic scheme. I can become part of it.
“How many sorrows in the universe? My cancer is nothing. Life does not end with the end of life. What was will be again. Eternally.”
That’s not an unusual response, according to the namesake of the Bill Richards Center for Healing. Bill Richards, PhD, has worked in the world of psychedelic-assisted psychotherapy since 1963.
A psychologist with decades of experience, Dr. Richards and colleagues figure that, with few possible exceptions, he has helped treat more people with psychedelic therapies than anyone alive in Western medicine today. At Aquilino, he works directly with patients and oversees the therapy protocol that goes along with the psilocybin dosing sessions.
“It’s inspiring,” Dr. Richards said.
“You meet someone who’s very depressed and scared and isolating from family and having all kinds of physical complaints. And a few days later, you talk to the same person and they have a whole new lease on life.”
And the positive effects can extend deep into the family system, he said.
After psilocybin treatment, said Dr. Richards, the person with cancer can become a kind of social worker for the family. They’re often far better able to talk about death and loss and even money and family issues than their loved ones. It’s not uncommon after treatment to see the resolution of years-old resentments or grievances that have dogged a family for many years.
Plus, said Dr. Richards, the cancer patient often ends up as a kind model to other family members for how to approach death. “They can demonstrate how to live fully – right to the last breath – which is a real gift because those relatives and loved ones have to die someday too, you know.”
At 80 years old, Dr. Richards is still in active practice and hopes to spend the rest of his days working with people in end-of-life care.
After the experience
Psychedelic-assisted therapy does not end with the dosing session. Integration sessions, where you discuss what happened during the dosing session, are a key part of most treatments.
The goal is to help participants absorb and “integrate” their experience. It typically happens over two or more sessions of 60-90 minutes with a therapist. In some cases, the therapist may invite a significant other to join in the integration process.
Dr. Agrawal’s trial at the Bill Richards center added something new: group therapy. Not only did Dr. Bansal meet with his therapist, he also met with a group of three other people in the trial who had their dosing the same day.
The point, said Dr. Agrawal, is to try and determine the effect of the group on the therapy. After their private dosing sessions, they come back together to discuss their experiences.
“After the psilocybin, they feel like they’ve been to war together,” Dr. Agrawal said. “There is this profound openness and connection. They feel able to share things with each other that they wouldn’t with other people.”
It will take some time to figure out how the group affects the overall outcome, but Dr. Bansal thinks it was integral to the success of his treatment.
In fact, he continues to meet regularly with his therapy group, even though it’s long since past the requirements of the study.
Pradeep 2.0
Dr. Bansal still has tough days with his cancer. Recently, immunotherapy treatment for his bladder caused side effects – pain, bleeding, fever, and chills – for most of the night. He felt like he was “passing razor blades” when he peed.
“And yet it was somehow okay,” he said. “It was only pain.”
“It’s as if there is a part of me that is watching myself objectively, going through the painful process of treatments saying: ‘It’s all right. I will be with you through this journey, through this experience. Don’t worry.’”
Months after taking that one dose, Dr. Bansal still calls it as “the single most powerful experience of my life.”
The change in his mental outlook, Dr. Bansal said, was profound, particularly in regard to his cancer.
“I understood that I still had cancer and that it could kill me in a few weeks, or months, or years. But my perspective had shifted.”
Dr. Bansal was as surprised as anyone. “Had somebody told me going into this that I would come out a transformed being or a person with a completely different perspective on life, I would never have believed it.”
He even named his new outlook. “I call it Pradeep 2.0.”
A version of this article first appeared on WebMD.com.
Pradeep Bansal considered the five capsules he was about to swallow. Together they made up a 25-mg dose of a substance that, in another setting, could have landed him in federal prison.
The substance was psilocybin, the active ingredient in magic mushrooms. To be more exact, it was a synthetic form of psilocybin called COMP360, made to pharmaceutical standards by a company called COMPASS Pathways. He was taking it as part of an Food and Drug Administration–approved clinical study on mental health therapy for people with cancer.
Dr. Bansal, a New York gastroenterologist, was far more comfortable giving medical treatment than receiving it. But he was getting used to it.
He had already been through surgery and a number of other treatments to address the physical aspects of his cancer. The psilocybin was to address the mental aspects – the crushing anxiety and depression that had stuck with him after his diagnosis.
Dr. Bansal did not arrive at this moment lightly.
“I was extremely skeptical going into this process,” said Dr. Bansal, who during a long medical career had looked with distrust and even disdain at alternative therapies.
“I don’t have much patience for holistic medicine, homeopathy, acupuncture, or alternative medicines with claims of spiritual upliftment or altered states of mind.”
But Bansal had done his homework on psilocybin and was impressed.
according to studies published in 2011, 2014, and 2016.
One study from Johns Hopkins University tracked the effects of a single guided dose of psilocybin in terminal cancer patients with anxiety and depression. More than 80% had a “significant decrease” in symptoms – even 6 months after treatment – with more than 60% of the group remaining in the normal mood range.
For the study Dr. Bansal joined, there had been weeks of screening and consultation and preparation in a strictly controlled scientific trial.
And yet, even with all that he had learned, even with his psychiatrist-guide by his side, he was afraid. Afraid of what he might experience under the powerful effects of psilocybin. And afraid that this was all a misguided waste of time – that his mental angst would still be there when it was all over.
He knew that psilocybin, like other psychedelic substances, could take you on a “trip” – could remove you, at least for a time, from normal conscious experience.
Maybe he would feel “funny,” he thought. Maybe he would have some hallucinations. But how would that change the reality of his cancer? How would it lift the black dread and anxiety he felt about his future?
Stuck in a dark place
Dr. Bansal had first noticed blood in his urine – a lot of it – in September 2019.
Two months later, doctors diagnosed cancer in his right kidney. He would need surgery to remove the kidney and surrounding lymph nodes (an operation called radical nephrectomy).
It was a shock, said Dr. Bansal. But the diagnosis and the surgery happened so quickly that he hardly had time to think. And treatment results seemed good. The cancer was only in stage I and the CT scans showed no signs of cancer after surgery.
“We were so relieved. Everyone was so happy,” Dr. Bansal said. “They didn’t even give me chemotherapy after surgery because it seemed so early.”
But a routine scan in June 2020 revealed more cancer in his lung. Within a couple of months, it was in his bladder too.
“It was devastating,” Dr. Bansal said. “I went from thinking I was healthy again to stage IV cancer.”
As doctors scheduled surgery to remove part of his lung, Dr. Bansal started on painful immunotherapy (BCG therapy) for his bladder.
At this point, from a psychological standpoint, Dr. Bansal was reeling. As a doctor, he knew all too well the meaning of stage IV cancer.
With two adult children and a grandchild on the way, Dr. Bansal had been looking forward to retirement with his wife of almost 40 years. “Suddenly, I wasn’t sure I was going to last that long,” Bansal recalled. “I was in a very dark place. I was very anxious, very depressed from lack of sleep.”
He saw a therapist about his cancer diagnosis and maintained his regular meditation practice at home. He hired a personal trainer and tried to focus on any good news that he got about his treatment.
Those things helped, but not enough.
The basic facts were inescapable. His cancer might end everything. He couldn’t stop thinking about it. And then he couldn’t stop thinking about how he couldn’t stop thinking about it.
If the worst happened, he didn’t want to spend his last days in a state of such relentless existential angst. And it wasn’t just for himself. He wanted to be strong and mentally present for his family and his loved ones and his patients.
As he searched for something to ease his mental anguish, Dr. Bansal recalled some psychedelic research on end-of-life anxiety and depression that he’d read about in Michael Pollan’s book on psychedelics, “How to Change Your Mind” (New York, Penguin Press, 2018).
The studies were small and the research was new, but Dr. Bansal was impressed enough with the results to take a chance. He called a lead researcher of one of the studies, a fellow New York doctor, and eventually found himself accepted into a new study.
Starting the journey
By the time Dr. Bansal arrived at the Bill Richards Center for Healing at the Aquilino Cancer Center in Rockville, Md., he had already been through weeks of screening.
The main requirements for the study were a cancer diagnosis and a measurable level of depression. But study participants also had to be physically fit enough to handle the medication, and psychologically free from a personal or family history of psychosis or schizophrenia. (The study also required participants to slowly wean themselves from medications like SSRIs for depression or antianxiety medications under the strict supervision of a qualified doctor.)
Dr. Bansal’s week of treatment began almost immediately on arrival at Aquilino. Everything was carefully choreographed but not rushed. From Monday to Wednesday, doctors followed his physical health with exams, ECGs, and blood work. And most importantly, they began to prepare him for the “dosing session” on Thursday when he would take the psilocybin.
This is the careful crafting of “set and setting” stressed in so many psychedelic therapies. “Set” refers to your mindset going into the drug experience. “Setting” is the space and people around you when the drug sends you into an altered state of consciousness.
Dr. Bansal met several times with at least three therapists in the days leading up to his dosing. He attended 4-plus hours of therapist-led group sessions with other people who would get a dosing on the same day. Together, they talked about what to expect during the experience and what to do in the face of fear or panic.
He connected with a therapist who would be his personal guide. Dr. Bansal’s therapist was a military psychiatrist with over 30 years’ experience.
“He was there with me from day 1, and so we established a relationship,” Dr. Bansal said.
“He asked me a lot of personal background history – you know, my religious convictions, aspirations, all those things.”
“Trust and let go,” was a kind of mantra for the treatment repeated by his guide and other doctors.
For Dr. Bansal, a doctor and scientist accustomed to using hard facts rather than touchy-feely slogans to navigate the care of patients, it was an adjustment, to say the least.
But he did his best to set aside his doubts and embrace the journey he was about to take.
The day of the trip
Thursday morning finally arrived. The setting of the dosing room was warm and welcoming, more like a cozy home study than a hospital room.
This matters more than you might think. First, because it’s important that you feel safe, open, and comfortable enough to let go and enter into a therapeutic process. But also because though rare, it’s possible – especially with psilocybin – for people to lose track of where they are and what they’re doing and put themselves or others in danger.
The dose, 25 mg, had been carefully calibrated to induce a psychedelic experience sufficient for therapy. Much less than that, say 10 mg, isn’t enough for most people to enter this state. A double dose, 50 mg, though not physically unsafe, may leave you too incoherent to have the useful insights key to therapeutic value.
A doctor, the lead investigator of the study, brought the five capsules into the room in an intricately carved crucible with a small ceremonial cup that held the water with which to take it.
“It was very solemn,” Dr. Bansal said. “He sat down with me in a very calming way.”
The doctor said: “Don’t worry about it. Just trust and let go.”
And that’s just what he did.
Dr. Bansal swallowed the capsules and lay down. The doctor quietly left the room so that Dr. Bansal and his psychiatrist guide could begin their session together.
Special eye shades kept him in the pitch dark whether his eyes were open or closed. Headphones streamed a curated musical playlist – much of it Western classical like Strauss, Bach, Mozart, and Beethoven – but also modern electronica and other music from cultures around the globe.
Dr. Bansal would remain here, with his therapist-guide by his side, in largely this same position, for the next 7-and-a-half hours.
It took about 45 minutes for the medication to kick in.
The investigator
The doctor who brought the capsules into the dosing room was Manish Agrawal, MD, codirector of clinical research at the Aquilino Cancer Center and lead investigator of the study.
Dr. Agrawal trained at the National Cancer Institute and practiced for many years as an oncologist before developing an interest in psychedelic therapies. It was his work with cancer patients that drew him to psychedelics in the first place.
He had seen too many of his patients mentally wrecked by a cancer diagnosis, and he often felt helpless to comfort them.
“You take care of the physical aspects of the cancer, right? You talk about side effects and recommend another scan to look for recurrence.”
“But what about the psychological effects?”
They can be very serious and too often go ignored, said Dr. Agrawal. Your plans for the future suddenly become moot. You may be concerned about your ability to work or worried about the pain and suffering and financial strain that might be ahead for both you and your family. And to top it all off, you’re staring into the face of your own mortality.
So it’s no wonder, said Dr. Agrawal, that many people develop clinical levels of anxiety and depression after a cancer diagnosis.
Like Dr. Bansal, Dr. Agrawal had been impressed by early studies on psilocybin-assisted therapies for end-of-life anxiety and depression. He had tried other approaches – support groups, one-on-one therapy, religious counselors, psychiatrist-prescribed medication – but he was never really happy with the results.
To Dr. Agrawal, psilocybin-assisted therapy was the first thing that looked like it could really make a difference.
And so after his psychedelic certification at the California Institute of Integral Studies, Dr. Agrawal was determined to change his approach.
The result was the Bill Richards Center for Healing at Aquilino Cancer Center, built specifically to study psychedelic-assisted therapies for psychological distress in people with cancer. The mission of the center is to help develop safe, FDA-approved psychedelic therapies for the mental health of cancer patients, and, once approved, provide a state-of-the-art facility and staff to administer those treatments.
A trip into the unknown
Back in the dosing room, Dr. Bansal was starting to feel the effects of the medication. As the psilocybin kicked in, spectacular images swirled.
“It was as if a million stained glass windows had suddenly come to life and were dancing in front of my vision,” Dr. Bansal said.
There were moving landscapes and intricate swirling patterns and massive stages in the sky where he saw orchestras playing the music he was hearing.
Dr. Bansal saw himself being crushed by a huge machine and buried, dead, in the Earth. He died and returned to life several times, glided over the top of New York City with the skyscrapers just below him, and took in the vision of the entire universe.
“I saw this expanse of the sky that was limitless. And there was this prehistoric reptile creature that spanned galaxies in the sky ahead of me who was dying. I said: ‘My God, the universe is dying,’ but then after a few moments, the universe came to life again in a burst of stars exploding.”
All the while, Dr. Bansal said, he was well aware that it was simply his mind creating these images, thoughts, and ideas. He knew he was in a safe room wearing eyeshades and headphones.
And yet, he says, it felt true. “The images and feelings are so powerful that you cannot help but believe they are in some way a part of reality.”
“At one point, I saw this giant Ferris wheel coming towards me and it was full of giant crabs, clicking and clacking their pincers. And my brain told me: ‘That’s my cancer!’ ”
Dr. Bansal was terrified. But he and his therapist had arranged a system of signals before the session. “If I was feeling afraid, I would hold his hand and if I had other issues, I would raise my hand. If I was feeling good, I would give him a thumbs up.”
Dr. Bansal reached out to his therapist and grasped his hand. “I said, ‘My cancer is coming at me!’ ”
His therapist was clear about what to do: Stand firm and walk toward it.
“That’s what they tell you: If you see anything frightening, you face it. And that’s the whole point of this exercise. And so, I stood and walked forward, and it just blew off in a puff of smoke.”
A state of peace
Around 3 hours into the experience, Dr. Bansal started to feel an immense sense of peace, happiness, and even comfort.
“I felt like I was watching a movie or a multidimensional slideshow. I was also a part of the movie. I felt like I could tell my mind what I wanted to see, and it would show it to me. It’s almost like you can mold your own visions. It was mystical.”
After about 8 hours, as the effects of the drug wore off, Dr. Bansal removed his eyeshades and headphones. He was completely drained.
“Even though I was lying down on my back for 7 hours, I felt like I had been run over by a truck. I was exhausted beyond belief physically and mentally.”
This was partly because of the fact that he hadn’t eaten much during the session. But mostly, said Dr. Bansal, it was because of the searing emotional intensity of the experience.
After the journey
It’s hard to put into words, said Dr. Bansal, what this treatment has done for his life. He feels as if he has stumbled onto something very precious that had been right in front of him all along. He wrote of his change in perspective almost obsessively in his journal in the days and weeks after treatment. One passage reads:
“It seems that, as time is passing on, I’m becoming more relaxed and hopeful, more calm, and at peace. Family has become even more important to me now. Money, politics, material gains, alcohol, seem less important.”
And yet there was nothing “easy” about the experience. In fact, in some ways the experience demanded more from him. “I feel I need to be more compassionate and considerate – less irritable and angry, more understanding of others’ needs. I feel I need to be a better human being, a better patient, a better father, and a better doctor for my patients.”
The experience, he said, gave him something far more important than mere ease. It gave him a sense of meaning.
From his journal:
“I died, and I was reborn. If I survived this, then I can face anything and anybody in the cosmic scheme. I can become part of it.
“How many sorrows in the universe? My cancer is nothing. Life does not end with the end of life. What was will be again. Eternally.”
That’s not an unusual response, according to the namesake of the Bill Richards Center for Healing. Bill Richards, PhD, has worked in the world of psychedelic-assisted psychotherapy since 1963.
A psychologist with decades of experience, Dr. Richards and colleagues figure that, with few possible exceptions, he has helped treat more people with psychedelic therapies than anyone alive in Western medicine today. At Aquilino, he works directly with patients and oversees the therapy protocol that goes along with the psilocybin dosing sessions.
“It’s inspiring,” Dr. Richards said.
“You meet someone who’s very depressed and scared and isolating from family and having all kinds of physical complaints. And a few days later, you talk to the same person and they have a whole new lease on life.”
And the positive effects can extend deep into the family system, he said.
After psilocybin treatment, said Dr. Richards, the person with cancer can become a kind of social worker for the family. They’re often far better able to talk about death and loss and even money and family issues than their loved ones. It’s not uncommon after treatment to see the resolution of years-old resentments or grievances that have dogged a family for many years.
Plus, said Dr. Richards, the cancer patient often ends up as a kind model to other family members for how to approach death. “They can demonstrate how to live fully – right to the last breath – which is a real gift because those relatives and loved ones have to die someday too, you know.”
At 80 years old, Dr. Richards is still in active practice and hopes to spend the rest of his days working with people in end-of-life care.
After the experience
Psychedelic-assisted therapy does not end with the dosing session. Integration sessions, where you discuss what happened during the dosing session, are a key part of most treatments.
The goal is to help participants absorb and “integrate” their experience. It typically happens over two or more sessions of 60-90 minutes with a therapist. In some cases, the therapist may invite a significant other to join in the integration process.
Dr. Agrawal’s trial at the Bill Richards center added something new: group therapy. Not only did Dr. Bansal meet with his therapist, he also met with a group of three other people in the trial who had their dosing the same day.
The point, said Dr. Agrawal, is to try and determine the effect of the group on the therapy. After their private dosing sessions, they come back together to discuss their experiences.
“After the psilocybin, they feel like they’ve been to war together,” Dr. Agrawal said. “There is this profound openness and connection. They feel able to share things with each other that they wouldn’t with other people.”
It will take some time to figure out how the group affects the overall outcome, but Dr. Bansal thinks it was integral to the success of his treatment.
In fact, he continues to meet regularly with his therapy group, even though it’s long since past the requirements of the study.
Pradeep 2.0
Dr. Bansal still has tough days with his cancer. Recently, immunotherapy treatment for his bladder caused side effects – pain, bleeding, fever, and chills – for most of the night. He felt like he was “passing razor blades” when he peed.
“And yet it was somehow okay,” he said. “It was only pain.”
“It’s as if there is a part of me that is watching myself objectively, going through the painful process of treatments saying: ‘It’s all right. I will be with you through this journey, through this experience. Don’t worry.’”
Months after taking that one dose, Dr. Bansal still calls it as “the single most powerful experience of my life.”
The change in his mental outlook, Dr. Bansal said, was profound, particularly in regard to his cancer.
“I understood that I still had cancer and that it could kill me in a few weeks, or months, or years. But my perspective had shifted.”
Dr. Bansal was as surprised as anyone. “Had somebody told me going into this that I would come out a transformed being or a person with a completely different perspective on life, I would never have believed it.”
He even named his new outlook. “I call it Pradeep 2.0.”
A version of this article first appeared on WebMD.com.
My favorite physical exam pearls
I would like to start the new year off by returning to the past – when the physical exam was emphasized and utilized in decision making. I think a big reason that its use has diminished in recent years is due to the physical exam not having been emphasized in training.
For those seeking to increase their comfort with conducting the physical exam, below are several methods I have found helpful to use in practice.
Examining the pharynx
We were usually taught to ask the patient to say ahhh, with or without a nasty tongue depressor.

When I was on my pediatrics rotation, I was taught to ask the patients to roar like a lion, which always gave a nice look at their posterior pharynx. The kids also really liked doing this, but it might seem a little strange to ask adults to do this.
A technique I have found that works well with adults is to ask them to yawn. I have found that this get me a great look at the pharynx for about half of my patients.
Auscultatory percussion for pleural effusions
Guarino and colleagues described a technique that is easily mastered and very effective for determining the presence of pleural effusions.1 It involves placing the stethoscope 3 cm below the last rib in the mid clavicular line and tapping from the apex down to the last rib.
For patients without effusion, a sharp change to a loud percussion note will occur at the last rib.
If the patient has an effusion, the loud percussion note will start at the top of the effusion.
This method was remarkably successful at finding pleural effusions. In the study, Dr. Guarino found a sensitivity of 96% and a specificity of 100%.
Physical exam for anemia
Look at the nails and see if they look pale. How can we do this?
The first step is to know what your own hematocrit is. You can then compare the color of your nail to that of the patient.
If you have a normal hematocrit and the patient’s nail bed color is lighter than yours, the patient likely has anemia. If you do this frequently, you will get good at estimating hematocrit. This is especially important if you do not have labs readily available.
Another way to assess for anemia is to look at the color tint of the lower conjunctiva. The best way to look for this is to look at whether there is a generous amount of visible capillaries in the lower conjunctiva. Patients without anemia have a darker red color because of these vessels, whereas patients with anemia are a lighter pink.
Strobach and colleagues2 looked at both nail bed rubor and color tint of the lower conjunctiva and found that both reliably predicted presence and degree of anemia.
Determining if clubbing is present
Most physicians are aware of Shamroth sign, and use it to evaluate for clubbing. Shamroth sign is the loss of the diamond that is created by placing the back surfaces of opposite terminal phalanges together.
I have found that it’s easier to diagnose mild clubbing by looking at the finger in profile. If the ratio of the distal phalangeal depth compared to the depth across the distal interphalangeal joint is greater than 1:1, then clubbing is present.3
Pearls
1. Have the patient try yawning to better see the pharynx without using a tongue blade.
2. Try the technique of auscultatory percussion to be more accurate at picking up pleural effusions.
3. Know your hematocrit, so you can better use color shade to assess for anemia.
4. Try looking at fingers in profile to pick up clubbing.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as 3rd-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. Guarino JR and Guarino JC. Auscultatory percussion: A simple method to detect pleural effusion. J Gen Intern Med. 1994 Feb;9(2):71-4.
2. Strobach RS et al. The value of the physical examination in the diagnosis of anemia. Correlation of the physical findings and the hemoglobin concentration. Arch Intern Med. 1988 Apr;148(4):831-2.
3. Spicknall KE et al. Clubbing: an update on diagnosis, differential diagnosis, pathophysiology, and clinical relevance. J Am Acad Dermatol. 2005 Jun;52(6):1020-8.
I would like to start the new year off by returning to the past – when the physical exam was emphasized and utilized in decision making. I think a big reason that its use has diminished in recent years is due to the physical exam not having been emphasized in training.
For those seeking to increase their comfort with conducting the physical exam, below are several methods I have found helpful to use in practice.
Examining the pharynx
We were usually taught to ask the patient to say ahhh, with or without a nasty tongue depressor.
When I was on my pediatrics rotation, I was taught to ask the patients to roar like a lion, which always gave a nice look at their posterior pharynx. The kids also really liked doing this, but it might seem a little strange to ask adults to do this.
A technique I have found that works well with adults is to ask them to yawn. I have found that this get me a great look at the pharynx for about half of my patients.
Auscultatory percussion for pleural effusions
Guarino and colleagues described a technique that is easily mastered and very effective for determining the presence of pleural effusions.1 It involves placing the stethoscope 3 cm below the last rib in the mid clavicular line and tapping from the apex down to the last rib.
For patients without effusion, a sharp change to a loud percussion note will occur at the last rib.
If the patient has an effusion, the loud percussion note will start at the top of the effusion.
This method was remarkably successful at finding pleural effusions. In the study, Dr. Guarino found a sensitivity of 96% and a specificity of 100%.
Physical exam for anemia
Look at the nails and see if they look pale. How can we do this?
The first step is to know what your own hematocrit is. You can then compare the color of your nail to that of the patient.
If you have a normal hematocrit and the patient’s nail bed color is lighter than yours, the patient likely has anemia. If you do this frequently, you will get good at estimating hematocrit. This is especially important if you do not have labs readily available.
Another way to assess for anemia is to look at the color tint of the lower conjunctiva. The best way to look for this is to look at whether there is a generous amount of visible capillaries in the lower conjunctiva. Patients without anemia have a darker red color because of these vessels, whereas patients with anemia are a lighter pink.
Strobach and colleagues2 looked at both nail bed rubor and color tint of the lower conjunctiva and found that both reliably predicted presence and degree of anemia.
Determining if clubbing is present
Most physicians are aware of Shamroth sign, and use it to evaluate for clubbing. Shamroth sign is the loss of the diamond that is created by placing the back surfaces of opposite terminal phalanges together.
I have found that it’s easier to diagnose mild clubbing by looking at the finger in profile. If the ratio of the distal phalangeal depth compared to the depth across the distal interphalangeal joint is greater than 1:1, then clubbing is present.3
Pearls
1. Have the patient try yawning to better see the pharynx without using a tongue blade.
2. Try the technique of auscultatory percussion to be more accurate at picking up pleural effusions.
3. Know your hematocrit, so you can better use color shade to assess for anemia.
4. Try looking at fingers in profile to pick up clubbing.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as 3rd-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. Guarino JR and Guarino JC. Auscultatory percussion: A simple method to detect pleural effusion. J Gen Intern Med. 1994 Feb;9(2):71-4.
2. Strobach RS et al. The value of the physical examination in the diagnosis of anemia. Correlation of the physical findings and the hemoglobin concentration. Arch Intern Med. 1988 Apr;148(4):831-2.
3. Spicknall KE et al. Clubbing: an update on diagnosis, differential diagnosis, pathophysiology, and clinical relevance. J Am Acad Dermatol. 2005 Jun;52(6):1020-8.
I would like to start the new year off by returning to the past – when the physical exam was emphasized and utilized in decision making. I think a big reason that its use has diminished in recent years is due to the physical exam not having been emphasized in training.
For those seeking to increase their comfort with conducting the physical exam, below are several methods I have found helpful to use in practice.
Examining the pharynx
We were usually taught to ask the patient to say ahhh, with or without a nasty tongue depressor.
When I was on my pediatrics rotation, I was taught to ask the patients to roar like a lion, which always gave a nice look at their posterior pharynx. The kids also really liked doing this, but it might seem a little strange to ask adults to do this.
A technique I have found that works well with adults is to ask them to yawn. I have found that this get me a great look at the pharynx for about half of my patients.
Auscultatory percussion for pleural effusions
Guarino and colleagues described a technique that is easily mastered and very effective for determining the presence of pleural effusions.1 It involves placing the stethoscope 3 cm below the last rib in the mid clavicular line and tapping from the apex down to the last rib.
For patients without effusion, a sharp change to a loud percussion note will occur at the last rib.
If the patient has an effusion, the loud percussion note will start at the top of the effusion.
This method was remarkably successful at finding pleural effusions. In the study, Dr. Guarino found a sensitivity of 96% and a specificity of 100%.
Physical exam for anemia
Look at the nails and see if they look pale. How can we do this?
The first step is to know what your own hematocrit is. You can then compare the color of your nail to that of the patient.
If you have a normal hematocrit and the patient’s nail bed color is lighter than yours, the patient likely has anemia. If you do this frequently, you will get good at estimating hematocrit. This is especially important if you do not have labs readily available.
Another way to assess for anemia is to look at the color tint of the lower conjunctiva. The best way to look for this is to look at whether there is a generous amount of visible capillaries in the lower conjunctiva. Patients without anemia have a darker red color because of these vessels, whereas patients with anemia are a lighter pink.
Strobach and colleagues2 looked at both nail bed rubor and color tint of the lower conjunctiva and found that both reliably predicted presence and degree of anemia.
Determining if clubbing is present
Most physicians are aware of Shamroth sign, and use it to evaluate for clubbing. Shamroth sign is the loss of the diamond that is created by placing the back surfaces of opposite terminal phalanges together.
I have found that it’s easier to diagnose mild clubbing by looking at the finger in profile. If the ratio of the distal phalangeal depth compared to the depth across the distal interphalangeal joint is greater than 1:1, then clubbing is present.3
Pearls
1. Have the patient try yawning to better see the pharynx without using a tongue blade.
2. Try the technique of auscultatory percussion to be more accurate at picking up pleural effusions.
3. Know your hematocrit, so you can better use color shade to assess for anemia.
4. Try looking at fingers in profile to pick up clubbing.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as 3rd-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. Guarino JR and Guarino JC. Auscultatory percussion: A simple method to detect pleural effusion. J Gen Intern Med. 1994 Feb;9(2):71-4.
2. Strobach RS et al. The value of the physical examination in the diagnosis of anemia. Correlation of the physical findings and the hemoglobin concentration. Arch Intern Med. 1988 Apr;148(4):831-2.
3. Spicknall KE et al. Clubbing: an update on diagnosis, differential diagnosis, pathophysiology, and clinical relevance. J Am Acad Dermatol. 2005 Jun;52(6):1020-8.
‘No one’s talking about it’: Infertility and one specialty’s onerous board exams
It would be impossible for her to fly the 2,500 miles from New York to the test site in Tucson, Ariz., when she could go into labor at any moment. She asked the American Board of Radiology – which oversees the process – if she could take the oral exam on Zoom or shift the timing a few weeks earlier or later.
The response: If she decided not to sit for the exam in person on the date specified, she would have to wait an entire year for the next test.
“I felt: Angry. Sad. Helpless. Inconsequential,” Dr. Dover tweeted. “But I will not be silent.”
The experience motivated Dr. Dover and six colleagues to conduct a study about how radiation oncology’s onerous four-exam board certification process has disproportionately burdened women.
The study, published online in Practical Radiation Oncology on Nov. 3, 2021, revealed that almost 60% of the early-career female radiation oncologists surveyed had delayed or were timing their pregnancies to accommodate their board exams. Women who chose to delay pregnancy were 2.5 times more likely to experience infertility.
“When we started doing the study, we didn’t realize just how common it was for people to wrap so much of their [family planning decisions] around taking these board exams,” said study coauthor Adrianna Henson Masters, MD, a radiation oncologist at Springfield (Ill.) Clinic. “How crazy is that? And no one’s talking about it.”
However, once the study appeared online, physicians took to Twitter to comment on the challenges of the board certification process, while others demanded change. One radiation oncologist even shared her decision not to have a child until she passed her board exams.
The study also got the attention of the American Board of Radiology, which governs certification for the specialty. In a response, leaders of the organization agreed that “the issues raised are significant and worthy of thoughtful consideration” and highlighted how, in light of the COVID-19 pandemic, the board has provided greater flexibility to the exam process – transitioning to remote testing and offering two dates for each exam in 2021.
But will the changes last? And will they help reduce the burden these exams place on families and family planning?
Inside board certification before the pandemic
While other specialties require one or two exams for board certification, radiation oncology is the only medical field that requires candidates pass four exams – three qualifying written tests, followed by a certifying oral exam. Since 2004, these exams, which cover physics, radiation biology, and clinical radiation oncology, have taken place over 3 years at specific locations across the country.
Radiation oncology residents have reported spending hundreds of hours preparing for each of these high-stakes evaluations. Fail or miss one and an already time-consuming process draws out, with major repercussions for career advancement and earnings.
“Passing and achieving board certification is the capstone of medical specialty training and, for many, is a prerequisite for attaining partnership or a promotion,” said study coauthor Chelain Goodman, MD, PhD, a radiation oncologist at the University of Texas MD Anderson Cancer Center, Houston.
To top it off, this process may be contributing to the gender disparity in radiation oncology, the study suggests. Only 25%-30% of practicing radiation oncologists are women, making it one of the lowest-ranking specialties when it comes to female representation.
“I think [this exam process] creates some disincentive when female medical students see that these are issues that early-career radiation oncologists are facing,” said Dr. Dover, who practices at Memorial Sloan Kettering Cancer Center, New York. “[Students may instead] choose a specialty that they believe will be more supportive of them and their family planning goals. That’s definitely a big concern for a field that wants to attract the top candidates.”
For those who do pick radiation oncology, the system of board exams often requires prospective parents to choose among three options: Try to time delivery before or between exams, put off pregnancy or adoption until exams are done, or delay board certification.
A balancing act: Board exams and family planning
Like Dr. Dover, Dr. Masters opted for door No. 1. She tried to time the birth of her daughter to fall several months before her first board exam.
She hoped her careful planning would reduce the stress of both major life events. But that was not the case. At 35 weeks, Dr. Masters found herself in the hospital with preeclampsia and symptomatic hypertension.
While receiving a magnesium sulfate drip to prevent a seizure, she frantically typed her patient list before her vision got too blurry to see the screen.
“That is ridiculous,” Dr. Masters said. “But so is a system that makes this the expectation [for pregnant physicians].”
During her hospital stay, Dr. Masters was induced. She suspects the stress of prepping for the board exam coupled with being pregnant and continuing to work long hours as a resident contributed to her pregnancy complications.
This juggling act can bleed into exam day as well. When interviewing women for their study, Dr. Masters and colleagues uncovered personal accounts of the challenges pregnant women and new mothers faced during their exams.
One woman described being granted lactation accommodation ahead of time, but when she arrived for her first two written exams, the testing center had no record of her request. She ended up breast-pumping in a coat closet next to the cleaning supplies while her male coresidents ate lunch and reviewed their notes.
“I started my physics exam in tears, completely anxious,” she reported. “I didn’t get to eat lunch. I was physically uncomfortable and emotionally wiped during both exams.”
Another woman had contractions during her written clinical boards, but “thankfully” passed her exam and gave birth 2 days later.
“It might sound crazy that we would put ourselves through things like that just to take an exam,” Dr. Dover said. “But because it does have the potential to sharply shape our early professional trajectory, we push through it. Otherwise, we’re going to be left behind by our male peers.”
This pressure to push through can be intense.
Still recovering from a difficult pregnancy, Dr. Masters returned to work when her daughter was just 5 weeks old. Although not ready to return to work, she felt too scared to ask for more time off after seeing other new mothers receive negative comments about not working hard enough.
Enter door No. 2: The pregnancy and postpregnancy experiences were so traumatizing that she decided to put off trying for a second child until after her exams.
Now board certified and 38 years old, Dr. Masters is worried she won’t be able to conceive as easily as before.
“So, we’re stuck in limbo, starting the process again and being nervous about it because what if it’s not so easy at this age?” she said. “And what if it could have been easy, in different circumstances, with a different specialty?”
Dr. Masters’ concerns are justified. Of the 126 women interviewed for the study, those who delayed pregnancy because of the board exams were significantly more likely to have fertility problems (46% vs. 18%), and 20% reported experiencing infertility.
This finding dovetails with previous research showing that almost 25% of female physicians who attempt to become pregnant are diagnosed with infertility – nearly twice the rate of the general population. This high rate of infertility has been attributed to professional pressures and stress, long hours on the job, and delaying pregnancy during medical training.
But choosing door No. 3 – focusing on family over exams – has downsides as well. Board certification is a prerequisite for almost every partnership position or promotion track within academic medicine and delaying certification can significantly hinder a physician’s career and finances.
Radiation oncologists who aren’t certified often remain in salaried positions until they can make partnership and earn a portion of the practice’s profits, “which could easily change your annual compensation by six digits,” Dr. Dover said.
According to the team’s study, annual compensation typically increases by $30,000-$50,000 after board certification, with some reporting an increase of over $100,000. That salary hike also impacts physicians’ ability to pay off medical school loans, make financial investments, and afford the cost of childcare.
In other words, when it comes to family planning, there’s often no good option.
Change on the horizon
When the pandemic struck, the American Board of Radiology quickly went into triage mode, postponing in-person board certification exams scheduled in 2020 and brainstorming solutions.
By June, the organization announced that the exams would switch to a virtual format in 2021. Each test would be offered twice – once early in the year for candidates like Dover whose postponed 2020 exams had ultimately been canceled, and then again for those already planning to take their tests in 2021.
The shift to remote testing was a boon. Taking the tests from home not only allowed candidates to forgo the cost, stress, and time of travel, it also mitigated the burden of juggling pregnancy and parenting needs.
For example, Courtney Hentz, MD, a pediatric radiation oncologist at Loyola University Chicago, Maywood, Ill., and a study coauthor, was given the choice to take a virtual exam in one day with two breastfeeding breaks or to spread the exam over 2 days with one breastfeeding break each day.
“Transitioning exams to a virtual format has been a really big achievement that the American Board of Radiology should be applauded for,” Dr. Dover said.
Not only that, offering the exams multiple times a year has “significantly increased flexibility for candidates as they juggle completing residency, starting at their first practice, and balancing time with their family,” Dr. Goodman added.
Brent Wagner, MD, MBA, executive director of the American Board of Radiology, Tucson, Ariz., said in an interviewthat remote exams are here to stay. “I don’t foresee us ever going back to in-person board exams,” said Dr. Wagner, a diagnostic radiologist. “Administering exams remotely last year worked better than I could have expected.”
Dr. Wagner said the American Board of Radiology also plans to keep two dates for the oral certifying exam for the foreseeable future, though will revert to one date for the written qualifying exams.
“In a perfect world, we’d offer an exam every quarter,” he said. However, providing multiple dates for the written exams “is not practical with a cohort of a few hundred people,” given the staff resources needed to create and score twice the number of items each year. The board did not rule out reassessing this decision in the future, “as examination development software improves and more resources become available.”
Another big change, proposed by Dr. Dover, Dr. Goodman, and others, would be to combine the four exams into fewer tests, such as consolidating the three written exams into one. Such a shift would allow physicians to launch their careers sooner and begin focusing on other career-advancing endeavors such as research and publishing. It would also significantly improve radiation oncologists’ quality of life.
“The amount of time that you spend studying for these very high-level, high-stakes exams really puts a toll on your mental health,” Dr. Dover said. “The longer it’s dragged out, the longer you’re dealing with that, and it contributes tremendously to poor job satisfaction and work-life balance.”
The American Board of Radiology said it is discussing options for consolidating the exams, but the challenge with combining the three written exams into one comes down to scoring. “We need to get a statistically valid result in all three categories,” Dr. Wagner said.
Another recent change: The American Board of Radiology is now allowing residents flexibility on the sequence of the written exams.
“In the past, we said you had to pass the physics exam before moving on to clinical radiology, but now we’re letting residents decide the order for themselves,” Dr. Wagner said. “This change may introduce more flexibility for someone who missed their first opportunity to take the physics exam but is ready to take the clinical exam.”
Dr. Wagner added: “We’re learning as we go, and I tell our staff that there’s no reason we should think we’re done making improvements. It’s going to keep getting better.”
The recent changes have already made a difference to radiation oncologists. And many hope to build on this new foundation to move the specialty toward a more family-friendly, equitable culture.
“I think as people in a caregiver profession, it’s hard to prioritize doing things for yourself or your own family sometimes; it’s hard to speak up and say: ‘We need something different,’ ” Dr. Masters said. “I think we have [an opportunity] to capitalize on the momentum we have now.”
A version of this article first appeared on Medscape.com.
It would be impossible for her to fly the 2,500 miles from New York to the test site in Tucson, Ariz., when she could go into labor at any moment. She asked the American Board of Radiology – which oversees the process – if she could take the oral exam on Zoom or shift the timing a few weeks earlier or later.
The response: If she decided not to sit for the exam in person on the date specified, she would have to wait an entire year for the next test.
“I felt: Angry. Sad. Helpless. Inconsequential,” Dr. Dover tweeted. “But I will not be silent.”
The experience motivated Dr. Dover and six colleagues to conduct a study about how radiation oncology’s onerous four-exam board certification process has disproportionately burdened women.
The study, published online in Practical Radiation Oncology on Nov. 3, 2021, revealed that almost 60% of the early-career female radiation oncologists surveyed had delayed or were timing their pregnancies to accommodate their board exams. Women who chose to delay pregnancy were 2.5 times more likely to experience infertility.
“When we started doing the study, we didn’t realize just how common it was for people to wrap so much of their [family planning decisions] around taking these board exams,” said study coauthor Adrianna Henson Masters, MD, a radiation oncologist at Springfield (Ill.) Clinic. “How crazy is that? And no one’s talking about it.”
However, once the study appeared online, physicians took to Twitter to comment on the challenges of the board certification process, while others demanded change. One radiation oncologist even shared her decision not to have a child until she passed her board exams.
The study also got the attention of the American Board of Radiology, which governs certification for the specialty. In a response, leaders of the organization agreed that “the issues raised are significant and worthy of thoughtful consideration” and highlighted how, in light of the COVID-19 pandemic, the board has provided greater flexibility to the exam process – transitioning to remote testing and offering two dates for each exam in 2021.
But will the changes last? And will they help reduce the burden these exams place on families and family planning?
Inside board certification before the pandemic
While other specialties require one or two exams for board certification, radiation oncology is the only medical field that requires candidates pass four exams – three qualifying written tests, followed by a certifying oral exam. Since 2004, these exams, which cover physics, radiation biology, and clinical radiation oncology, have taken place over 3 years at specific locations across the country.
Radiation oncology residents have reported spending hundreds of hours preparing for each of these high-stakes evaluations. Fail or miss one and an already time-consuming process draws out, with major repercussions for career advancement and earnings.
“Passing and achieving board certification is the capstone of medical specialty training and, for many, is a prerequisite for attaining partnership or a promotion,” said study coauthor Chelain Goodman, MD, PhD, a radiation oncologist at the University of Texas MD Anderson Cancer Center, Houston.
To top it off, this process may be contributing to the gender disparity in radiation oncology, the study suggests. Only 25%-30% of practicing radiation oncologists are women, making it one of the lowest-ranking specialties when it comes to female representation.
“I think [this exam process] creates some disincentive when female medical students see that these are issues that early-career radiation oncologists are facing,” said Dr. Dover, who practices at Memorial Sloan Kettering Cancer Center, New York. “[Students may instead] choose a specialty that they believe will be more supportive of them and their family planning goals. That’s definitely a big concern for a field that wants to attract the top candidates.”
For those who do pick radiation oncology, the system of board exams often requires prospective parents to choose among three options: Try to time delivery before or between exams, put off pregnancy or adoption until exams are done, or delay board certification.
A balancing act: Board exams and family planning
Like Dr. Dover, Dr. Masters opted for door No. 1. She tried to time the birth of her daughter to fall several months before her first board exam.
She hoped her careful planning would reduce the stress of both major life events. But that was not the case. At 35 weeks, Dr. Masters found herself in the hospital with preeclampsia and symptomatic hypertension.
While receiving a magnesium sulfate drip to prevent a seizure, she frantically typed her patient list before her vision got too blurry to see the screen.
“That is ridiculous,” Dr. Masters said. “But so is a system that makes this the expectation [for pregnant physicians].”
During her hospital stay, Dr. Masters was induced. She suspects the stress of prepping for the board exam coupled with being pregnant and continuing to work long hours as a resident contributed to her pregnancy complications.
This juggling act can bleed into exam day as well. When interviewing women for their study, Dr. Masters and colleagues uncovered personal accounts of the challenges pregnant women and new mothers faced during their exams.
One woman described being granted lactation accommodation ahead of time, but when she arrived for her first two written exams, the testing center had no record of her request. She ended up breast-pumping in a coat closet next to the cleaning supplies while her male coresidents ate lunch and reviewed their notes.
“I started my physics exam in tears, completely anxious,” she reported. “I didn’t get to eat lunch. I was physically uncomfortable and emotionally wiped during both exams.”
Another woman had contractions during her written clinical boards, but “thankfully” passed her exam and gave birth 2 days later.
“It might sound crazy that we would put ourselves through things like that just to take an exam,” Dr. Dover said. “But because it does have the potential to sharply shape our early professional trajectory, we push through it. Otherwise, we’re going to be left behind by our male peers.”
This pressure to push through can be intense.
Still recovering from a difficult pregnancy, Dr. Masters returned to work when her daughter was just 5 weeks old. Although not ready to return to work, she felt too scared to ask for more time off after seeing other new mothers receive negative comments about not working hard enough.
Enter door No. 2: The pregnancy and postpregnancy experiences were so traumatizing that she decided to put off trying for a second child until after her exams.
Now board certified and 38 years old, Dr. Masters is worried she won’t be able to conceive as easily as before.
“So, we’re stuck in limbo, starting the process again and being nervous about it because what if it’s not so easy at this age?” she said. “And what if it could have been easy, in different circumstances, with a different specialty?”
Dr. Masters’ concerns are justified. Of the 126 women interviewed for the study, those who delayed pregnancy because of the board exams were significantly more likely to have fertility problems (46% vs. 18%), and 20% reported experiencing infertility.
This finding dovetails with previous research showing that almost 25% of female physicians who attempt to become pregnant are diagnosed with infertility – nearly twice the rate of the general population. This high rate of infertility has been attributed to professional pressures and stress, long hours on the job, and delaying pregnancy during medical training.
But choosing door No. 3 – focusing on family over exams – has downsides as well. Board certification is a prerequisite for almost every partnership position or promotion track within academic medicine and delaying certification can significantly hinder a physician’s career and finances.
Radiation oncologists who aren’t certified often remain in salaried positions until they can make partnership and earn a portion of the practice’s profits, “which could easily change your annual compensation by six digits,” Dr. Dover said.
According to the team’s study, annual compensation typically increases by $30,000-$50,000 after board certification, with some reporting an increase of over $100,000. That salary hike also impacts physicians’ ability to pay off medical school loans, make financial investments, and afford the cost of childcare.
In other words, when it comes to family planning, there’s often no good option.
Change on the horizon
When the pandemic struck, the American Board of Radiology quickly went into triage mode, postponing in-person board certification exams scheduled in 2020 and brainstorming solutions.
By June, the organization announced that the exams would switch to a virtual format in 2021. Each test would be offered twice – once early in the year for candidates like Dover whose postponed 2020 exams had ultimately been canceled, and then again for those already planning to take their tests in 2021.
The shift to remote testing was a boon. Taking the tests from home not only allowed candidates to forgo the cost, stress, and time of travel, it also mitigated the burden of juggling pregnancy and parenting needs.
For example, Courtney Hentz, MD, a pediatric radiation oncologist at Loyola University Chicago, Maywood, Ill., and a study coauthor, was given the choice to take a virtual exam in one day with two breastfeeding breaks or to spread the exam over 2 days with one breastfeeding break each day.
“Transitioning exams to a virtual format has been a really big achievement that the American Board of Radiology should be applauded for,” Dr. Dover said.
Not only that, offering the exams multiple times a year has “significantly increased flexibility for candidates as they juggle completing residency, starting at their first practice, and balancing time with their family,” Dr. Goodman added.
Brent Wagner, MD, MBA, executive director of the American Board of Radiology, Tucson, Ariz., said in an interviewthat remote exams are here to stay. “I don’t foresee us ever going back to in-person board exams,” said Dr. Wagner, a diagnostic radiologist. “Administering exams remotely last year worked better than I could have expected.”
Dr. Wagner said the American Board of Radiology also plans to keep two dates for the oral certifying exam for the foreseeable future, though will revert to one date for the written qualifying exams.
“In a perfect world, we’d offer an exam every quarter,” he said. However, providing multiple dates for the written exams “is not practical with a cohort of a few hundred people,” given the staff resources needed to create and score twice the number of items each year. The board did not rule out reassessing this decision in the future, “as examination development software improves and more resources become available.”
Another big change, proposed by Dr. Dover, Dr. Goodman, and others, would be to combine the four exams into fewer tests, such as consolidating the three written exams into one. Such a shift would allow physicians to launch their careers sooner and begin focusing on other career-advancing endeavors such as research and publishing. It would also significantly improve radiation oncologists’ quality of life.
“The amount of time that you spend studying for these very high-level, high-stakes exams really puts a toll on your mental health,” Dr. Dover said. “The longer it’s dragged out, the longer you’re dealing with that, and it contributes tremendously to poor job satisfaction and work-life balance.”
The American Board of Radiology said it is discussing options for consolidating the exams, but the challenge with combining the three written exams into one comes down to scoring. “We need to get a statistically valid result in all three categories,” Dr. Wagner said.
Another recent change: The American Board of Radiology is now allowing residents flexibility on the sequence of the written exams.
“In the past, we said you had to pass the physics exam before moving on to clinical radiology, but now we’re letting residents decide the order for themselves,” Dr. Wagner said. “This change may introduce more flexibility for someone who missed their first opportunity to take the physics exam but is ready to take the clinical exam.”
Dr. Wagner added: “We’re learning as we go, and I tell our staff that there’s no reason we should think we’re done making improvements. It’s going to keep getting better.”
The recent changes have already made a difference to radiation oncologists. And many hope to build on this new foundation to move the specialty toward a more family-friendly, equitable culture.
“I think as people in a caregiver profession, it’s hard to prioritize doing things for yourself or your own family sometimes; it’s hard to speak up and say: ‘We need something different,’ ” Dr. Masters said. “I think we have [an opportunity] to capitalize on the momentum we have now.”
A version of this article first appeared on Medscape.com.
It would be impossible for her to fly the 2,500 miles from New York to the test site in Tucson, Ariz., when she could go into labor at any moment. She asked the American Board of Radiology – which oversees the process – if she could take the oral exam on Zoom or shift the timing a few weeks earlier or later.
The response: If she decided not to sit for the exam in person on the date specified, she would have to wait an entire year for the next test.
“I felt: Angry. Sad. Helpless. Inconsequential,” Dr. Dover tweeted. “But I will not be silent.”
The experience motivated Dr. Dover and six colleagues to conduct a study about how radiation oncology’s onerous four-exam board certification process has disproportionately burdened women.
The study, published online in Practical Radiation Oncology on Nov. 3, 2021, revealed that almost 60% of the early-career female radiation oncologists surveyed had delayed or were timing their pregnancies to accommodate their board exams. Women who chose to delay pregnancy were 2.5 times more likely to experience infertility.
“When we started doing the study, we didn’t realize just how common it was for people to wrap so much of their [family planning decisions] around taking these board exams,” said study coauthor Adrianna Henson Masters, MD, a radiation oncologist at Springfield (Ill.) Clinic. “How crazy is that? And no one’s talking about it.”
However, once the study appeared online, physicians took to Twitter to comment on the challenges of the board certification process, while others demanded change. One radiation oncologist even shared her decision not to have a child until she passed her board exams.
The study also got the attention of the American Board of Radiology, which governs certification for the specialty. In a response, leaders of the organization agreed that “the issues raised are significant and worthy of thoughtful consideration” and highlighted how, in light of the COVID-19 pandemic, the board has provided greater flexibility to the exam process – transitioning to remote testing and offering two dates for each exam in 2021.
But will the changes last? And will they help reduce the burden these exams place on families and family planning?
Inside board certification before the pandemic
While other specialties require one or two exams for board certification, radiation oncology is the only medical field that requires candidates pass four exams – three qualifying written tests, followed by a certifying oral exam. Since 2004, these exams, which cover physics, radiation biology, and clinical radiation oncology, have taken place over 3 years at specific locations across the country.
Radiation oncology residents have reported spending hundreds of hours preparing for each of these high-stakes evaluations. Fail or miss one and an already time-consuming process draws out, with major repercussions for career advancement and earnings.
“Passing and achieving board certification is the capstone of medical specialty training and, for many, is a prerequisite for attaining partnership or a promotion,” said study coauthor Chelain Goodman, MD, PhD, a radiation oncologist at the University of Texas MD Anderson Cancer Center, Houston.
To top it off, this process may be contributing to the gender disparity in radiation oncology, the study suggests. Only 25%-30% of practicing radiation oncologists are women, making it one of the lowest-ranking specialties when it comes to female representation.
“I think [this exam process] creates some disincentive when female medical students see that these are issues that early-career radiation oncologists are facing,” said Dr. Dover, who practices at Memorial Sloan Kettering Cancer Center, New York. “[Students may instead] choose a specialty that they believe will be more supportive of them and their family planning goals. That’s definitely a big concern for a field that wants to attract the top candidates.”
For those who do pick radiation oncology, the system of board exams often requires prospective parents to choose among three options: Try to time delivery before or between exams, put off pregnancy or adoption until exams are done, or delay board certification.
A balancing act: Board exams and family planning
Like Dr. Dover, Dr. Masters opted for door No. 1. She tried to time the birth of her daughter to fall several months before her first board exam.
She hoped her careful planning would reduce the stress of both major life events. But that was not the case. At 35 weeks, Dr. Masters found herself in the hospital with preeclampsia and symptomatic hypertension.
While receiving a magnesium sulfate drip to prevent a seizure, she frantically typed her patient list before her vision got too blurry to see the screen.
“That is ridiculous,” Dr. Masters said. “But so is a system that makes this the expectation [for pregnant physicians].”
During her hospital stay, Dr. Masters was induced. She suspects the stress of prepping for the board exam coupled with being pregnant and continuing to work long hours as a resident contributed to her pregnancy complications.
This juggling act can bleed into exam day as well. When interviewing women for their study, Dr. Masters and colleagues uncovered personal accounts of the challenges pregnant women and new mothers faced during their exams.
One woman described being granted lactation accommodation ahead of time, but when she arrived for her first two written exams, the testing center had no record of her request. She ended up breast-pumping in a coat closet next to the cleaning supplies while her male coresidents ate lunch and reviewed their notes.
“I started my physics exam in tears, completely anxious,” she reported. “I didn’t get to eat lunch. I was physically uncomfortable and emotionally wiped during both exams.”
Another woman had contractions during her written clinical boards, but “thankfully” passed her exam and gave birth 2 days later.
“It might sound crazy that we would put ourselves through things like that just to take an exam,” Dr. Dover said. “But because it does have the potential to sharply shape our early professional trajectory, we push through it. Otherwise, we’re going to be left behind by our male peers.”
This pressure to push through can be intense.
Still recovering from a difficult pregnancy, Dr. Masters returned to work when her daughter was just 5 weeks old. Although not ready to return to work, she felt too scared to ask for more time off after seeing other new mothers receive negative comments about not working hard enough.
Enter door No. 2: The pregnancy and postpregnancy experiences were so traumatizing that she decided to put off trying for a second child until after her exams.
Now board certified and 38 years old, Dr. Masters is worried she won’t be able to conceive as easily as before.
“So, we’re stuck in limbo, starting the process again and being nervous about it because what if it’s not so easy at this age?” she said. “And what if it could have been easy, in different circumstances, with a different specialty?”
Dr. Masters’ concerns are justified. Of the 126 women interviewed for the study, those who delayed pregnancy because of the board exams were significantly more likely to have fertility problems (46% vs. 18%), and 20% reported experiencing infertility.
This finding dovetails with previous research showing that almost 25% of female physicians who attempt to become pregnant are diagnosed with infertility – nearly twice the rate of the general population. This high rate of infertility has been attributed to professional pressures and stress, long hours on the job, and delaying pregnancy during medical training.
But choosing door No. 3 – focusing on family over exams – has downsides as well. Board certification is a prerequisite for almost every partnership position or promotion track within academic medicine and delaying certification can significantly hinder a physician’s career and finances.
Radiation oncologists who aren’t certified often remain in salaried positions until they can make partnership and earn a portion of the practice’s profits, “which could easily change your annual compensation by six digits,” Dr. Dover said.
According to the team’s study, annual compensation typically increases by $30,000-$50,000 after board certification, with some reporting an increase of over $100,000. That salary hike also impacts physicians’ ability to pay off medical school loans, make financial investments, and afford the cost of childcare.
In other words, when it comes to family planning, there’s often no good option.
Change on the horizon
When the pandemic struck, the American Board of Radiology quickly went into triage mode, postponing in-person board certification exams scheduled in 2020 and brainstorming solutions.
By June, the organization announced that the exams would switch to a virtual format in 2021. Each test would be offered twice – once early in the year for candidates like Dover whose postponed 2020 exams had ultimately been canceled, and then again for those already planning to take their tests in 2021.
The shift to remote testing was a boon. Taking the tests from home not only allowed candidates to forgo the cost, stress, and time of travel, it also mitigated the burden of juggling pregnancy and parenting needs.
For example, Courtney Hentz, MD, a pediatric radiation oncologist at Loyola University Chicago, Maywood, Ill., and a study coauthor, was given the choice to take a virtual exam in one day with two breastfeeding breaks or to spread the exam over 2 days with one breastfeeding break each day.
“Transitioning exams to a virtual format has been a really big achievement that the American Board of Radiology should be applauded for,” Dr. Dover said.
Not only that, offering the exams multiple times a year has “significantly increased flexibility for candidates as they juggle completing residency, starting at their first practice, and balancing time with their family,” Dr. Goodman added.
Brent Wagner, MD, MBA, executive director of the American Board of Radiology, Tucson, Ariz., said in an interviewthat remote exams are here to stay. “I don’t foresee us ever going back to in-person board exams,” said Dr. Wagner, a diagnostic radiologist. “Administering exams remotely last year worked better than I could have expected.”
Dr. Wagner said the American Board of Radiology also plans to keep two dates for the oral certifying exam for the foreseeable future, though will revert to one date for the written qualifying exams.
“In a perfect world, we’d offer an exam every quarter,” he said. However, providing multiple dates for the written exams “is not practical with a cohort of a few hundred people,” given the staff resources needed to create and score twice the number of items each year. The board did not rule out reassessing this decision in the future, “as examination development software improves and more resources become available.”
Another big change, proposed by Dr. Dover, Dr. Goodman, and others, would be to combine the four exams into fewer tests, such as consolidating the three written exams into one. Such a shift would allow physicians to launch their careers sooner and begin focusing on other career-advancing endeavors such as research and publishing. It would also significantly improve radiation oncologists’ quality of life.
“The amount of time that you spend studying for these very high-level, high-stakes exams really puts a toll on your mental health,” Dr. Dover said. “The longer it’s dragged out, the longer you’re dealing with that, and it contributes tremendously to poor job satisfaction and work-life balance.”
The American Board of Radiology said it is discussing options for consolidating the exams, but the challenge with combining the three written exams into one comes down to scoring. “We need to get a statistically valid result in all three categories,” Dr. Wagner said.
Another recent change: The American Board of Radiology is now allowing residents flexibility on the sequence of the written exams.
“In the past, we said you had to pass the physics exam before moving on to clinical radiology, but now we’re letting residents decide the order for themselves,” Dr. Wagner said. “This change may introduce more flexibility for someone who missed their first opportunity to take the physics exam but is ready to take the clinical exam.”
Dr. Wagner added: “We’re learning as we go, and I tell our staff that there’s no reason we should think we’re done making improvements. It’s going to keep getting better.”
The recent changes have already made a difference to radiation oncologists. And many hope to build on this new foundation to move the specialty toward a more family-friendly, equitable culture.
“I think as people in a caregiver profession, it’s hard to prioritize doing things for yourself or your own family sometimes; it’s hard to speak up and say: ‘We need something different,’ ” Dr. Masters said. “I think we have [an opportunity] to capitalize on the momentum we have now.”
A version of this article first appeared on Medscape.com.
Study finds sharp drop in opioid scripts among most specialties
The volume of prescription opioids dispensed at retail pharmacies in the United States dropped by 21% in recent years amid efforts to reduce unnecessary use of the painkillers, but the rate of decline varied greatly among types of patients and by type of clinician, a study found.
In a brief report published by Annals of Internal Medicine, researchers from the nonprofit RAND Corp reported an analysis of opioid prescriptions from two periods, 2008-2009 and 2017-2018.
The researchers sought to assess total opioid use rather than simply track the number of pills dispensed. So they used days’ supply and total daily dose to calculate per capita morphine milligram equivalents (MME) for opioid prescriptions, write Bradley D. Stein, MD, PhD, MPH, the study’s lead author and a senior physician researcher at RAND Corp, and his coauthors in their paper.
For the study, the researchers used data from the consulting firm IQVIA, which they say covers about 90% of U.S. prescriptions. Total opioid volume per capita by prescriptions filled in retail pharmacies decreased from 951.4 MME in 2008-2009 to 749.3 MME in 2017-2018, Dr. Stein’s group found.
(In 2020, IQVIA separately said that prescription opioid use per adult in this country rose from an average of 16 pills, or 134 MMEs, in 1992 to a peak of about 55 pills a person, or 790 MMEs, in 2011. By 2019, opioid use per adult had declined to 29 pills and 366 MMEs per capita.)
The RAND report found substantial variation in opioid volume by type of insurance, including a 41.5% decline (636.5 MME to 372.6 MME) among people covered by commercial health plans. That exceeded the 27.7% drop seen for people enrolled in Medicaid (646.8 MME to 467.7 MME). The decline was smaller (17.5%; 2,780.2 MME to 2,294.2 MME) for those on Medicare, who as a group used the most opioids.
‘Almost functions as a Rorschach test’
The causes of the decline are easy to guess, although definitive conclusions are impossible, Dr. Stein told this news organization.
Significant work has been done in recent years to change attitudes about opioid prescriptions by physicians, researchers, and lawmakers. Aggressive promotion of prescription painkillers, particularly Purdue Pharma’s OxyContin, in the 1990s, is widely cited as the triggering event for the national opioid crisis.
In response, states created databases known as prescription drug monitoring programs. The Centers for Disease Control and Prevention in 2016 issued guidelines intended to curb unnecessary use of opioids. The guidelines noted that other medicines could treat chronic pain without raising the risk of addiction. The Choosing Wisely campaign, run by a foundation of the American Board of Internal Medicine, also offered recommendations about limiting use of opioids. And insurers have restricted access to opioids through the prior authorization process. As a result, researchers will make their own guesses at the causes of the decline in opioid prescriptions, based on their own experiences and research interests, Dr. Stein said.
“It almost functions as a Rorschach test,” he said.
Dr. Stein’s group also looked at trends among medical specialties. They found the largest reduction between 2008-2009 and 2017-2018 among emergency physicians (70.5% drop from 99,254.5 MME to 29,234.3 MME), psychiatrists (67.2% drop from 50,464.3 MME to 16,533.0 MME) and oncologists (59.5% drop from 51,731.2 MME to 20,941.4).
Among surgeons, the RAND researchers found a drop of 49.3% from 220,764.6 to 111,904.4. Among dentists, they found a drop of 41.3% from 22,345.3 to 13,126.1.
Among pain specialists, they found a drop of 15.4% from 1,020,808.4 MME to 863,140.7 MME.
Among adult primary care clinicians, Dr. Stein and his colleagues found a drop of 40% from 651,489.4 MME in 2008-2009 to 390,841.0 MME in 2017-2018.
However, one of the groups tracked in the study increased the volume of opioid prescriptions written: advanced practice providers, among whom scripts for the drugs rose 22.7%, from 112,873.9 MME to 138,459.3 MME.
Dr. Stein said he suspects that this gain reflects a change in the nature of the practice of primary care, with nurse practitioners and physician assistants taking more active roles in treatment of patients. Some of the reduction seen among primary care clinicians who treat adults may reflect a shift in which medical personnel in a practice write the opioid prescriptions.
Still, the trends in general seen by Dr. Stein and coauthors are encouraging, even if further study of these patterns is needed, he said.
“This is one of those papers that I think potentially raises as many questions as it provides answers for,” he said.
What’s missing
Maya Hambright, MD, a family medicine physician in New York’s Hudson Valley, who has been working mainly in addiction in response to the opioid overdose crisis, observed that the drop in total prescribed volume of prescription painkillers does not necessarily translate into a reduction in use of opioids
“No one is taking fewer opioids,” Dr. Hambright told this news organization. “I can say that comfortably. They are just getting them from other sources.”
CDC data support Dr. Hambright’s view.
An estimated 100,306 people in the United States died of a drug overdose in the 12 months that ended in April 2021, an increase of 28.5% from the 78,056 deaths during the same period the year before, according to the CDC.
Dr. Hambright said more physicians need to be involved in prescribing medication-assisted treatment (MAT).
The federal government has in the past year loosened restrictions on a requirement, known as an X waiver. Certain clinicians have been exempted from training requirements, as explained in the frequently asked questions page on the Substance Abuse and Mental Health Services Administration website.
SAMHSA says legislation is required to eliminate the waiver. As of Dec. 30, 2021, more than half of the members of the U.S. House of Representatives were listed as sponsors of the Mainstreaming Addiction Treatment (MAT) Act (HR 1384), which would end the need for X waivers. The bill has the backing of 187 Democrats and 43 Republicans.
At this time, too many physicians shy away from offering MAT, Dr. Hambright said.
“People are still scared of it,” she said. “People don’t want to deal with addicts.”
But Dr. Hambright said it’s well worth the initial time invested in having the needed conversations with patients about MAT.
“Afterwards, it’s so straightforward. People feel better. They’re healthier. It’s amazing,” she said. “You’re changing lives.”
The research was supported by grants from the National Institutes of Health. Dr. Stein and coauthors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The volume of prescription opioids dispensed at retail pharmacies in the United States dropped by 21% in recent years amid efforts to reduce unnecessary use of the painkillers, but the rate of decline varied greatly among types of patients and by type of clinician, a study found.
In a brief report published by Annals of Internal Medicine, researchers from the nonprofit RAND Corp reported an analysis of opioid prescriptions from two periods, 2008-2009 and 2017-2018.
The researchers sought to assess total opioid use rather than simply track the number of pills dispensed. So they used days’ supply and total daily dose to calculate per capita morphine milligram equivalents (MME) for opioid prescriptions, write Bradley D. Stein, MD, PhD, MPH, the study’s lead author and a senior physician researcher at RAND Corp, and his coauthors in their paper.
For the study, the researchers used data from the consulting firm IQVIA, which they say covers about 90% of U.S. prescriptions. Total opioid volume per capita by prescriptions filled in retail pharmacies decreased from 951.4 MME in 2008-2009 to 749.3 MME in 2017-2018, Dr. Stein’s group found.
(In 2020, IQVIA separately said that prescription opioid use per adult in this country rose from an average of 16 pills, or 134 MMEs, in 1992 to a peak of about 55 pills a person, or 790 MMEs, in 2011. By 2019, opioid use per adult had declined to 29 pills and 366 MMEs per capita.)
The RAND report found substantial variation in opioid volume by type of insurance, including a 41.5% decline (636.5 MME to 372.6 MME) among people covered by commercial health plans. That exceeded the 27.7% drop seen for people enrolled in Medicaid (646.8 MME to 467.7 MME). The decline was smaller (17.5%; 2,780.2 MME to 2,294.2 MME) for those on Medicare, who as a group used the most opioids.
‘Almost functions as a Rorschach test’
The causes of the decline are easy to guess, although definitive conclusions are impossible, Dr. Stein told this news organization.
Significant work has been done in recent years to change attitudes about opioid prescriptions by physicians, researchers, and lawmakers. Aggressive promotion of prescription painkillers, particularly Purdue Pharma’s OxyContin, in the 1990s, is widely cited as the triggering event for the national opioid crisis.
In response, states created databases known as prescription drug monitoring programs. The Centers for Disease Control and Prevention in 2016 issued guidelines intended to curb unnecessary use of opioids. The guidelines noted that other medicines could treat chronic pain without raising the risk of addiction. The Choosing Wisely campaign, run by a foundation of the American Board of Internal Medicine, also offered recommendations about limiting use of opioids. And insurers have restricted access to opioids through the prior authorization process. As a result, researchers will make their own guesses at the causes of the decline in opioid prescriptions, based on their own experiences and research interests, Dr. Stein said.
“It almost functions as a Rorschach test,” he said.
Dr. Stein’s group also looked at trends among medical specialties. They found the largest reduction between 2008-2009 and 2017-2018 among emergency physicians (70.5% drop from 99,254.5 MME to 29,234.3 MME), psychiatrists (67.2% drop from 50,464.3 MME to 16,533.0 MME) and oncologists (59.5% drop from 51,731.2 MME to 20,941.4).
Among surgeons, the RAND researchers found a drop of 49.3% from 220,764.6 to 111,904.4. Among dentists, they found a drop of 41.3% from 22,345.3 to 13,126.1.
Among pain specialists, they found a drop of 15.4% from 1,020,808.4 MME to 863,140.7 MME.
Among adult primary care clinicians, Dr. Stein and his colleagues found a drop of 40% from 651,489.4 MME in 2008-2009 to 390,841.0 MME in 2017-2018.
However, one of the groups tracked in the study increased the volume of opioid prescriptions written: advanced practice providers, among whom scripts for the drugs rose 22.7%, from 112,873.9 MME to 138,459.3 MME.
Dr. Stein said he suspects that this gain reflects a change in the nature of the practice of primary care, with nurse practitioners and physician assistants taking more active roles in treatment of patients. Some of the reduction seen among primary care clinicians who treat adults may reflect a shift in which medical personnel in a practice write the opioid prescriptions.
Still, the trends in general seen by Dr. Stein and coauthors are encouraging, even if further study of these patterns is needed, he said.
“This is one of those papers that I think potentially raises as many questions as it provides answers for,” he said.
What’s missing
Maya Hambright, MD, a family medicine physician in New York’s Hudson Valley, who has been working mainly in addiction in response to the opioid overdose crisis, observed that the drop in total prescribed volume of prescription painkillers does not necessarily translate into a reduction in use of opioids
“No one is taking fewer opioids,” Dr. Hambright told this news organization. “I can say that comfortably. They are just getting them from other sources.”
CDC data support Dr. Hambright’s view.
An estimated 100,306 people in the United States died of a drug overdose in the 12 months that ended in April 2021, an increase of 28.5% from the 78,056 deaths during the same period the year before, according to the CDC.
Dr. Hambright said more physicians need to be involved in prescribing medication-assisted treatment (MAT).
The federal government has in the past year loosened restrictions on a requirement, known as an X waiver. Certain clinicians have been exempted from training requirements, as explained in the frequently asked questions page on the Substance Abuse and Mental Health Services Administration website.
SAMHSA says legislation is required to eliminate the waiver. As of Dec. 30, 2021, more than half of the members of the U.S. House of Representatives were listed as sponsors of the Mainstreaming Addiction Treatment (MAT) Act (HR 1384), which would end the need for X waivers. The bill has the backing of 187 Democrats and 43 Republicans.
At this time, too many physicians shy away from offering MAT, Dr. Hambright said.
“People are still scared of it,” she said. “People don’t want to deal with addicts.”
But Dr. Hambright said it’s well worth the initial time invested in having the needed conversations with patients about MAT.
“Afterwards, it’s so straightforward. People feel better. They’re healthier. It’s amazing,” she said. “You’re changing lives.”
The research was supported by grants from the National Institutes of Health. Dr. Stein and coauthors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The volume of prescription opioids dispensed at retail pharmacies in the United States dropped by 21% in recent years amid efforts to reduce unnecessary use of the painkillers, but the rate of decline varied greatly among types of patients and by type of clinician, a study found.
In a brief report published by Annals of Internal Medicine, researchers from the nonprofit RAND Corp reported an analysis of opioid prescriptions from two periods, 2008-2009 and 2017-2018.
The researchers sought to assess total opioid use rather than simply track the number of pills dispensed. So they used days’ supply and total daily dose to calculate per capita morphine milligram equivalents (MME) for opioid prescriptions, write Bradley D. Stein, MD, PhD, MPH, the study’s lead author and a senior physician researcher at RAND Corp, and his coauthors in their paper.
For the study, the researchers used data from the consulting firm IQVIA, which they say covers about 90% of U.S. prescriptions. Total opioid volume per capita by prescriptions filled in retail pharmacies decreased from 951.4 MME in 2008-2009 to 749.3 MME in 2017-2018, Dr. Stein’s group found.
(In 2020, IQVIA separately said that prescription opioid use per adult in this country rose from an average of 16 pills, or 134 MMEs, in 1992 to a peak of about 55 pills a person, or 790 MMEs, in 2011. By 2019, opioid use per adult had declined to 29 pills and 366 MMEs per capita.)
The RAND report found substantial variation in opioid volume by type of insurance, including a 41.5% decline (636.5 MME to 372.6 MME) among people covered by commercial health plans. That exceeded the 27.7% drop seen for people enrolled in Medicaid (646.8 MME to 467.7 MME). The decline was smaller (17.5%; 2,780.2 MME to 2,294.2 MME) for those on Medicare, who as a group used the most opioids.
‘Almost functions as a Rorschach test’
The causes of the decline are easy to guess, although definitive conclusions are impossible, Dr. Stein told this news organization.
Significant work has been done in recent years to change attitudes about opioid prescriptions by physicians, researchers, and lawmakers. Aggressive promotion of prescription painkillers, particularly Purdue Pharma’s OxyContin, in the 1990s, is widely cited as the triggering event for the national opioid crisis.
In response, states created databases known as prescription drug monitoring programs. The Centers for Disease Control and Prevention in 2016 issued guidelines intended to curb unnecessary use of opioids. The guidelines noted that other medicines could treat chronic pain without raising the risk of addiction. The Choosing Wisely campaign, run by a foundation of the American Board of Internal Medicine, also offered recommendations about limiting use of opioids. And insurers have restricted access to opioids through the prior authorization process. As a result, researchers will make their own guesses at the causes of the decline in opioid prescriptions, based on their own experiences and research interests, Dr. Stein said.
“It almost functions as a Rorschach test,” he said.
Dr. Stein’s group also looked at trends among medical specialties. They found the largest reduction between 2008-2009 and 2017-2018 among emergency physicians (70.5% drop from 99,254.5 MME to 29,234.3 MME), psychiatrists (67.2% drop from 50,464.3 MME to 16,533.0 MME) and oncologists (59.5% drop from 51,731.2 MME to 20,941.4).
Among surgeons, the RAND researchers found a drop of 49.3% from 220,764.6 to 111,904.4. Among dentists, they found a drop of 41.3% from 22,345.3 to 13,126.1.
Among pain specialists, they found a drop of 15.4% from 1,020,808.4 MME to 863,140.7 MME.
Among adult primary care clinicians, Dr. Stein and his colleagues found a drop of 40% from 651,489.4 MME in 2008-2009 to 390,841.0 MME in 2017-2018.
However, one of the groups tracked in the study increased the volume of opioid prescriptions written: advanced practice providers, among whom scripts for the drugs rose 22.7%, from 112,873.9 MME to 138,459.3 MME.
Dr. Stein said he suspects that this gain reflects a change in the nature of the practice of primary care, with nurse practitioners and physician assistants taking more active roles in treatment of patients. Some of the reduction seen among primary care clinicians who treat adults may reflect a shift in which medical personnel in a practice write the opioid prescriptions.
Still, the trends in general seen by Dr. Stein and coauthors are encouraging, even if further study of these patterns is needed, he said.
“This is one of those papers that I think potentially raises as many questions as it provides answers for,” he said.
What’s missing
Maya Hambright, MD, a family medicine physician in New York’s Hudson Valley, who has been working mainly in addiction in response to the opioid overdose crisis, observed that the drop in total prescribed volume of prescription painkillers does not necessarily translate into a reduction in use of opioids
“No one is taking fewer opioids,” Dr. Hambright told this news organization. “I can say that comfortably. They are just getting them from other sources.”
CDC data support Dr. Hambright’s view.
An estimated 100,306 people in the United States died of a drug overdose in the 12 months that ended in April 2021, an increase of 28.5% from the 78,056 deaths during the same period the year before, according to the CDC.
Dr. Hambright said more physicians need to be involved in prescribing medication-assisted treatment (MAT).
The federal government has in the past year loosened restrictions on a requirement, known as an X waiver. Certain clinicians have been exempted from training requirements, as explained in the frequently asked questions page on the Substance Abuse and Mental Health Services Administration website.
SAMHSA says legislation is required to eliminate the waiver. As of Dec. 30, 2021, more than half of the members of the U.S. House of Representatives were listed as sponsors of the Mainstreaming Addiction Treatment (MAT) Act (HR 1384), which would end the need for X waivers. The bill has the backing of 187 Democrats and 43 Republicans.
At this time, too many physicians shy away from offering MAT, Dr. Hambright said.
“People are still scared of it,” she said. “People don’t want to deal with addicts.”
But Dr. Hambright said it’s well worth the initial time invested in having the needed conversations with patients about MAT.
“Afterwards, it’s so straightforward. People feel better. They’re healthier. It’s amazing,” she said. “You’re changing lives.”
The research was supported by grants from the National Institutes of Health. Dr. Stein and coauthors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.