User login
For MD-IQ use only
Appendectomy or antibiotics? Large trial helps decision-making
The presence of mineralized stool, known as appendicolith, was associated with a nearly twofold increased risk of undergoing appendectomy within 30 days of initiating antibiotics, write David Flum, MD, of the University of Washington, Seattle, and coauthors in a paper published in JAMA Surgery on Jan. 12, 2021.
But the surprise was the lack of an association between appendectomy and factors often presumed to be consistent with more severe appendicitis.
Physicians have had their own ideas about what factors make a patient more likely to need an appendectomy after an initial round of treatment with antibiotics, such as a high white blood cell count or a perforation seen on CT scan, Dr. Flum said in an interview. But the research didn’t support some of these theories.
“This is why we do the studies,” Dr. Flum said. “Sometimes we find out that our hunches were wrong.”
Dr. Flum and coauthors measured the association between different patient factors and disease severity and the need for appendectomy following a course of antibiotics. They used adjusted odds ratios to describe these relationships while accounting for other differences.
An OR of 1.0 – or when the confidence interval around an OR crosses 1 – signals that there is no association between that factor and appendectomy. Positive ORs with confidence intervals that exclude 1.0 suggest the factor was associated with appendectomy.
The OR was 1.99 for the presence of appendicolith, a finding with a 95% confidence interval of 1.28-3.10. The OR was 1.53 (95% CI, 1.01-2.31) for female sex.
But the OR was 1.14 (95% CI, 0.66-1.98) for perforation, abscess, or fat stranding.
The OR was 1.09 (95% CI, 1.00-1.18) for radiographic finding of a larger appendix, as measured by diameter.
And the OR was 1.03 (95% CI, 0.98-1.09) for having a higher white blood cell count, as measured by a 1,000-cells/mcL increase.
Appy or not?
This paper draws from the Comparison of Outcomes of Antibiotic Drugs and Appendectomy (CODA) trial (NCT02800785), for which top-line results were published in 2020 in the New England Journal of Medicine. In that paper, Dr. Flum and colleagues reported on results for 1,552 adults (414 with an appendicolith) who were evenly randomized to either antibiotics treatment or appendectomy. After 30 days, antibiotics were found to be noninferior to appendectomy, as reported by this news organization.
The federal Patient-Centered Outcomes Research Institute funded the CODA research. Dr. Flum said the National Institutes of Health had not appeared interested in funding a look at the different options available to patients experiencing appendicitis. Congress created PCORI as part of the Affordable Care Act of 2010, seeking to encourage researchers to study which treatments best serve patients through direct comparisons. Its support was critical for Dr. Flum and colleagues in seeking to help people weigh their options for treating appendicitis.
The CODA study “models what the patient’s experience is like, and this has not been the focus of NIH as much,” Dr. Flum said.
The CODA team has sought to make it easy for patients to consider what its findings and other research on appendicitis mean for them. They created an online decision-making tool, available at the aptly named http://www.appyornot.org/ website, which has videos in English and Spanish explaining patients’ options in simple terms. The website also asks questions about personal preferences, priorities, and resources to help them choose a treatment based on their individual situation.
Shift away from ‘paternalistic framing’
In the past, surgeons focused on the risk for patients from procedures, making the decisions for them about whether or not to proceed. There’s now a drive to shift away from this “paternalistic framing” toward shared decision-making, Dr. Flum said.
Surgeons need to have conversations with their patients about what’s happening in their lives as well as to assess their fears and concerns about treatment options, he said. These are aspects of patient care that were not covered in medical school or surgical training, but they lead to “less paternalistic” treatment. A patient’s decision about whether to choose surgery or antibiotics for appendicitis may hinge on factors such as insurance coverage, access to childcare, and the ability to miss days of work.
Dr. Flum said his fellow surgeons by and large have reacted well to the CODA team’s work.
“To their credit, the surgical community has embraced a healthy skepticism about the role of surgery,” Dr. Flum said.
The guidelines of the American College of Surgeons state that there is “high-quality evidence” that most patients with appendicitis can be managed with antibiotics instead of appendectomy (69% overall avoid appendectomy by 90 days, 75% of those without appendicolith, and 59% of those with appendicolith).
“Based on the surgeon’s judgment, patient preferences, and local resources (e.g., hospital staff, bed, and PPE supply availability) antibiotics are an acceptable first-line treatment, with appendectomy offered for those with worsening or recurrent symptoms,” the ACS guidelines say.
In an interview, Samir M. Fakhry, MD, vice president of HCA Center for Trauma and Acute Care Surgery Research in Nashville, Tenn., agreed with Dr. Flum about the shift taking place in medicine.
The CODA research, including the new paper in JAMA Surgery, makes it easier for physicians to work with patients and their families to reach decisions about how to treat appendicitis, Dr. Fakhry said.
These important discussions take time, he said, and patients must be allowed that time. Patients might feel misled, for example, if a surgeon pressed for appendectomy without explaining that a course of antibiotics may have served them well. Other patients may opt for surgery right away, especially in cases with appendicoliths, to avoid the potential for repeat episodes of medical care.
“You’ve got people who just want to get it done and over with. You’ve got people who want to avoid surgery no matter what,” Dr. Fakhry said. “It’s not just about the science and the data.”
This study was supported by a grant from PCORI. The authors reported having served as consultants or reviewers or have received fees for work outside of this paper from Stryker, Kerecis, Acera, Medline, Shriner’s Research Fund, UpToDate, and Tetraphase Pharmaceuticals Stryker.
A version of this article first appeared on Medscape.com.
The presence of mineralized stool, known as appendicolith, was associated with a nearly twofold increased risk of undergoing appendectomy within 30 days of initiating antibiotics, write David Flum, MD, of the University of Washington, Seattle, and coauthors in a paper published in JAMA Surgery on Jan. 12, 2021.
But the surprise was the lack of an association between appendectomy and factors often presumed to be consistent with more severe appendicitis.
Physicians have had their own ideas about what factors make a patient more likely to need an appendectomy after an initial round of treatment with antibiotics, such as a high white blood cell count or a perforation seen on CT scan, Dr. Flum said in an interview. But the research didn’t support some of these theories.
“This is why we do the studies,” Dr. Flum said. “Sometimes we find out that our hunches were wrong.”
Dr. Flum and coauthors measured the association between different patient factors and disease severity and the need for appendectomy following a course of antibiotics. They used adjusted odds ratios to describe these relationships while accounting for other differences.
An OR of 1.0 – or when the confidence interval around an OR crosses 1 – signals that there is no association between that factor and appendectomy. Positive ORs with confidence intervals that exclude 1.0 suggest the factor was associated with appendectomy.
The OR was 1.99 for the presence of appendicolith, a finding with a 95% confidence interval of 1.28-3.10. The OR was 1.53 (95% CI, 1.01-2.31) for female sex.
But the OR was 1.14 (95% CI, 0.66-1.98) for perforation, abscess, or fat stranding.
The OR was 1.09 (95% CI, 1.00-1.18) for radiographic finding of a larger appendix, as measured by diameter.
And the OR was 1.03 (95% CI, 0.98-1.09) for having a higher white blood cell count, as measured by a 1,000-cells/mcL increase.
Appy or not?
This paper draws from the Comparison of Outcomes of Antibiotic Drugs and Appendectomy (CODA) trial (NCT02800785), for which top-line results were published in 2020 in the New England Journal of Medicine. In that paper, Dr. Flum and colleagues reported on results for 1,552 adults (414 with an appendicolith) who were evenly randomized to either antibiotics treatment or appendectomy. After 30 days, antibiotics were found to be noninferior to appendectomy, as reported by this news organization.
The federal Patient-Centered Outcomes Research Institute funded the CODA research. Dr. Flum said the National Institutes of Health had not appeared interested in funding a look at the different options available to patients experiencing appendicitis. Congress created PCORI as part of the Affordable Care Act of 2010, seeking to encourage researchers to study which treatments best serve patients through direct comparisons. Its support was critical for Dr. Flum and colleagues in seeking to help people weigh their options for treating appendicitis.
The CODA study “models what the patient’s experience is like, and this has not been the focus of NIH as much,” Dr. Flum said.
The CODA team has sought to make it easy for patients to consider what its findings and other research on appendicitis mean for them. They created an online decision-making tool, available at the aptly named http://www.appyornot.org/ website, which has videos in English and Spanish explaining patients’ options in simple terms. The website also asks questions about personal preferences, priorities, and resources to help them choose a treatment based on their individual situation.
Shift away from ‘paternalistic framing’
In the past, surgeons focused on the risk for patients from procedures, making the decisions for them about whether or not to proceed. There’s now a drive to shift away from this “paternalistic framing” toward shared decision-making, Dr. Flum said.
Surgeons need to have conversations with their patients about what’s happening in their lives as well as to assess their fears and concerns about treatment options, he said. These are aspects of patient care that were not covered in medical school or surgical training, but they lead to “less paternalistic” treatment. A patient’s decision about whether to choose surgery or antibiotics for appendicitis may hinge on factors such as insurance coverage, access to childcare, and the ability to miss days of work.
Dr. Flum said his fellow surgeons by and large have reacted well to the CODA team’s work.
“To their credit, the surgical community has embraced a healthy skepticism about the role of surgery,” Dr. Flum said.
The guidelines of the American College of Surgeons state that there is “high-quality evidence” that most patients with appendicitis can be managed with antibiotics instead of appendectomy (69% overall avoid appendectomy by 90 days, 75% of those without appendicolith, and 59% of those with appendicolith).
“Based on the surgeon’s judgment, patient preferences, and local resources (e.g., hospital staff, bed, and PPE supply availability) antibiotics are an acceptable first-line treatment, with appendectomy offered for those with worsening or recurrent symptoms,” the ACS guidelines say.
In an interview, Samir M. Fakhry, MD, vice president of HCA Center for Trauma and Acute Care Surgery Research in Nashville, Tenn., agreed with Dr. Flum about the shift taking place in medicine.
The CODA research, including the new paper in JAMA Surgery, makes it easier for physicians to work with patients and their families to reach decisions about how to treat appendicitis, Dr. Fakhry said.
These important discussions take time, he said, and patients must be allowed that time. Patients might feel misled, for example, if a surgeon pressed for appendectomy without explaining that a course of antibiotics may have served them well. Other patients may opt for surgery right away, especially in cases with appendicoliths, to avoid the potential for repeat episodes of medical care.
“You’ve got people who just want to get it done and over with. You’ve got people who want to avoid surgery no matter what,” Dr. Fakhry said. “It’s not just about the science and the data.”
This study was supported by a grant from PCORI. The authors reported having served as consultants or reviewers or have received fees for work outside of this paper from Stryker, Kerecis, Acera, Medline, Shriner’s Research Fund, UpToDate, and Tetraphase Pharmaceuticals Stryker.
A version of this article first appeared on Medscape.com.
The presence of mineralized stool, known as appendicolith, was associated with a nearly twofold increased risk of undergoing appendectomy within 30 days of initiating antibiotics, write David Flum, MD, of the University of Washington, Seattle, and coauthors in a paper published in JAMA Surgery on Jan. 12, 2021.
But the surprise was the lack of an association between appendectomy and factors often presumed to be consistent with more severe appendicitis.
Physicians have had their own ideas about what factors make a patient more likely to need an appendectomy after an initial round of treatment with antibiotics, such as a high white blood cell count or a perforation seen on CT scan, Dr. Flum said in an interview. But the research didn’t support some of these theories.
“This is why we do the studies,” Dr. Flum said. “Sometimes we find out that our hunches were wrong.”
Dr. Flum and coauthors measured the association between different patient factors and disease severity and the need for appendectomy following a course of antibiotics. They used adjusted odds ratios to describe these relationships while accounting for other differences.
An OR of 1.0 – or when the confidence interval around an OR crosses 1 – signals that there is no association between that factor and appendectomy. Positive ORs with confidence intervals that exclude 1.0 suggest the factor was associated with appendectomy.
The OR was 1.99 for the presence of appendicolith, a finding with a 95% confidence interval of 1.28-3.10. The OR was 1.53 (95% CI, 1.01-2.31) for female sex.
But the OR was 1.14 (95% CI, 0.66-1.98) for perforation, abscess, or fat stranding.
The OR was 1.09 (95% CI, 1.00-1.18) for radiographic finding of a larger appendix, as measured by diameter.
And the OR was 1.03 (95% CI, 0.98-1.09) for having a higher white blood cell count, as measured by a 1,000-cells/mcL increase.
Appy or not?
This paper draws from the Comparison of Outcomes of Antibiotic Drugs and Appendectomy (CODA) trial (NCT02800785), for which top-line results were published in 2020 in the New England Journal of Medicine. In that paper, Dr. Flum and colleagues reported on results for 1,552 adults (414 with an appendicolith) who were evenly randomized to either antibiotics treatment or appendectomy. After 30 days, antibiotics were found to be noninferior to appendectomy, as reported by this news organization.
The federal Patient-Centered Outcomes Research Institute funded the CODA research. Dr. Flum said the National Institutes of Health had not appeared interested in funding a look at the different options available to patients experiencing appendicitis. Congress created PCORI as part of the Affordable Care Act of 2010, seeking to encourage researchers to study which treatments best serve patients through direct comparisons. Its support was critical for Dr. Flum and colleagues in seeking to help people weigh their options for treating appendicitis.
The CODA study “models what the patient’s experience is like, and this has not been the focus of NIH as much,” Dr. Flum said.
The CODA team has sought to make it easy for patients to consider what its findings and other research on appendicitis mean for them. They created an online decision-making tool, available at the aptly named http://www.appyornot.org/ website, which has videos in English and Spanish explaining patients’ options in simple terms. The website also asks questions about personal preferences, priorities, and resources to help them choose a treatment based on their individual situation.
Shift away from ‘paternalistic framing’
In the past, surgeons focused on the risk for patients from procedures, making the decisions for them about whether or not to proceed. There’s now a drive to shift away from this “paternalistic framing” toward shared decision-making, Dr. Flum said.
Surgeons need to have conversations with their patients about what’s happening in their lives as well as to assess their fears and concerns about treatment options, he said. These are aspects of patient care that were not covered in medical school or surgical training, but they lead to “less paternalistic” treatment. A patient’s decision about whether to choose surgery or antibiotics for appendicitis may hinge on factors such as insurance coverage, access to childcare, and the ability to miss days of work.
Dr. Flum said his fellow surgeons by and large have reacted well to the CODA team’s work.
“To their credit, the surgical community has embraced a healthy skepticism about the role of surgery,” Dr. Flum said.
The guidelines of the American College of Surgeons state that there is “high-quality evidence” that most patients with appendicitis can be managed with antibiotics instead of appendectomy (69% overall avoid appendectomy by 90 days, 75% of those without appendicolith, and 59% of those with appendicolith).
“Based on the surgeon’s judgment, patient preferences, and local resources (e.g., hospital staff, bed, and PPE supply availability) antibiotics are an acceptable first-line treatment, with appendectomy offered for those with worsening or recurrent symptoms,” the ACS guidelines say.
In an interview, Samir M. Fakhry, MD, vice president of HCA Center for Trauma and Acute Care Surgery Research in Nashville, Tenn., agreed with Dr. Flum about the shift taking place in medicine.
The CODA research, including the new paper in JAMA Surgery, makes it easier for physicians to work with patients and their families to reach decisions about how to treat appendicitis, Dr. Fakhry said.
These important discussions take time, he said, and patients must be allowed that time. Patients might feel misled, for example, if a surgeon pressed for appendectomy without explaining that a course of antibiotics may have served them well. Other patients may opt for surgery right away, especially in cases with appendicoliths, to avoid the potential for repeat episodes of medical care.
“You’ve got people who just want to get it done and over with. You’ve got people who want to avoid surgery no matter what,” Dr. Fakhry said. “It’s not just about the science and the data.”
This study was supported by a grant from PCORI. The authors reported having served as consultants or reviewers or have received fees for work outside of this paper from Stryker, Kerecis, Acera, Medline, Shriner’s Research Fund, UpToDate, and Tetraphase Pharmaceuticals Stryker.
A version of this article first appeared on Medscape.com.
FROM JAMA SURGERY
Survey: Medical cannabis use for skin conditions lags behind interest, acceptance
A , according to the results of a recent survey.
Almost 89% of respondents were in favor of medical cannabis use for dermatologic diseases, and 73% said that they would be comfortable seeing a dermatologist who recommended such products to them, Samuel Yeroushalmi, a 4th-year medical student at George Washington University, Washington, and associates reported.
“Consumers and patients are already using MCPs [medical cannabis products] to treat inflammatory skin conditions, such as acne, rosacea, atopic dermatitis, and psoriasis, even without guidance from a dermatologist. While acceptance was high, there were clear barriers reported limiting use and uptake, such as patient skepticism and a lack of understanding,” Adam Friedman, MD, senior author and chair of the department of dermatology at the university, said in a separate statement.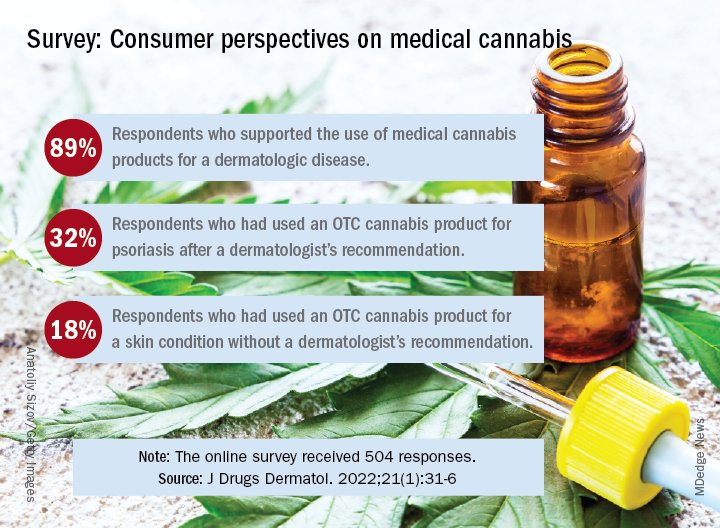
Dermatologic use of OTC cannabis products without the recommendation of a dermatologist was reported by 18% of the 504 of 700 adults who responded in the SurveyMonkey online panel. Of the two-thirds who had seen a dermatologist, 20% received a recommendation for an OTC product and 11% were recommended a product that required a department of health medical card, the investigators said.
Uptake among the patients who did receive a recommendation, however, was high: 76% for OTC products and 72% for those that required a medical card. Among those who had received an OTC recommendation, 32% used the cannabis product for psoriasis and 30% each for acne and rosacea, Mr. Yeroushalmi and his coauthors said.
The most common indication among the respondents with dermatologist recommendations for products requiring a medical card was for acne (68%), followed by psoriasis and rosacea (28% each). Cost was the main deterrent (60%) for those who declined to use the recommended cannabis product, with skepticism, limited understanding, and product illegality in their state each at 50%, the researchers said.
“Though cost and legality concerns are nonmodifiable barriers, dermatologists have an opportunity to educate those who know little in the way of medical cannabis or are skeptic[s],” they wrote. The survey results show that many patients are interested, and “the future should be bright for MCPs; we just need to show and disseminate the science,” Dr. Friedman commented in the statement.
One of the authors was from the University of Maryland, College Park. The authors had no disclosures to report.
A , according to the results of a recent survey.
Almost 89% of respondents were in favor of medical cannabis use for dermatologic diseases, and 73% said that they would be comfortable seeing a dermatologist who recommended such products to them, Samuel Yeroushalmi, a 4th-year medical student at George Washington University, Washington, and associates reported.
“Consumers and patients are already using MCPs [medical cannabis products] to treat inflammatory skin conditions, such as acne, rosacea, atopic dermatitis, and psoriasis, even without guidance from a dermatologist. While acceptance was high, there were clear barriers reported limiting use and uptake, such as patient skepticism and a lack of understanding,” Adam Friedman, MD, senior author and chair of the department of dermatology at the university, said in a separate statement.
Dermatologic use of OTC cannabis products without the recommendation of a dermatologist was reported by 18% of the 504 of 700 adults who responded in the SurveyMonkey online panel. Of the two-thirds who had seen a dermatologist, 20% received a recommendation for an OTC product and 11% were recommended a product that required a department of health medical card, the investigators said.
Uptake among the patients who did receive a recommendation, however, was high: 76% for OTC products and 72% for those that required a medical card. Among those who had received an OTC recommendation, 32% used the cannabis product for psoriasis and 30% each for acne and rosacea, Mr. Yeroushalmi and his coauthors said.
The most common indication among the respondents with dermatologist recommendations for products requiring a medical card was for acne (68%), followed by psoriasis and rosacea (28% each). Cost was the main deterrent (60%) for those who declined to use the recommended cannabis product, with skepticism, limited understanding, and product illegality in their state each at 50%, the researchers said.
“Though cost and legality concerns are nonmodifiable barriers, dermatologists have an opportunity to educate those who know little in the way of medical cannabis or are skeptic[s],” they wrote. The survey results show that many patients are interested, and “the future should be bright for MCPs; we just need to show and disseminate the science,” Dr. Friedman commented in the statement.
One of the authors was from the University of Maryland, College Park. The authors had no disclosures to report.
A , according to the results of a recent survey.
Almost 89% of respondents were in favor of medical cannabis use for dermatologic diseases, and 73% said that they would be comfortable seeing a dermatologist who recommended such products to them, Samuel Yeroushalmi, a 4th-year medical student at George Washington University, Washington, and associates reported.
“Consumers and patients are already using MCPs [medical cannabis products] to treat inflammatory skin conditions, such as acne, rosacea, atopic dermatitis, and psoriasis, even without guidance from a dermatologist. While acceptance was high, there were clear barriers reported limiting use and uptake, such as patient skepticism and a lack of understanding,” Adam Friedman, MD, senior author and chair of the department of dermatology at the university, said in a separate statement.
Dermatologic use of OTC cannabis products without the recommendation of a dermatologist was reported by 18% of the 504 of 700 adults who responded in the SurveyMonkey online panel. Of the two-thirds who had seen a dermatologist, 20% received a recommendation for an OTC product and 11% were recommended a product that required a department of health medical card, the investigators said.
Uptake among the patients who did receive a recommendation, however, was high: 76% for OTC products and 72% for those that required a medical card. Among those who had received an OTC recommendation, 32% used the cannabis product for psoriasis and 30% each for acne and rosacea, Mr. Yeroushalmi and his coauthors said.
The most common indication among the respondents with dermatologist recommendations for products requiring a medical card was for acne (68%), followed by psoriasis and rosacea (28% each). Cost was the main deterrent (60%) for those who declined to use the recommended cannabis product, with skepticism, limited understanding, and product illegality in their state each at 50%, the researchers said.
“Though cost and legality concerns are nonmodifiable barriers, dermatologists have an opportunity to educate those who know little in the way of medical cannabis or are skeptic[s],” they wrote. The survey results show that many patients are interested, and “the future should be bright for MCPs; we just need to show and disseminate the science,” Dr. Friedman commented in the statement.
One of the authors was from the University of Maryland, College Park. The authors had no disclosures to report.
FROM JOURNAL OF DRUGS IN DERMATOLOGY
Can supercomputers really keep up with the human brain?
An adult brain contains about 86 billion neurons and even more supercomputing power to closely monitor the entire human brain.
All those neurons have trillions of synapses – or connection points – that make up the circuitry the brain uses to control everything we do from reasoning to breathing to walking. And scientists with the Human Brain Project are trying to build new computing tools that can zoom in on every one of these synapses, peer inside cells, and zoom out to focus on entire regions of the brain at once.
, researchers from the Human Brain Project report in Science. If you have an old smartphone or tablet with 32GB of storage, you’d need more than 31,000 of them to get a single petabyte of storage.
Using an electron microscope to image the entire brain would require more than one exabyte of data, the scientists point out. That’s more than a million petabytes.
Giacomo Indiveri, PhD, professor of neuroinformatics at the University of Zurich, Switzerland, says we need to fundamentally change the way we build computers. Delivering the keynote address at the Human Brain Project Summit in October, he warned we will use 20% of all the world’s electricity on computing by the year 2025.
To meet the computing challenges posed by the quest to map every bit of the human brain, researchers are working to produce the first two exascale supercomputers within the next 5 years. When they’re done, these machines will provide brain scientists with supercomputers powerful enough to explore the human brain in all its complexities.
A version of this article first appeared on Medscape.com.
An adult brain contains about 86 billion neurons and even more supercomputing power to closely monitor the entire human brain.
All those neurons have trillions of synapses – or connection points – that make up the circuitry the brain uses to control everything we do from reasoning to breathing to walking. And scientists with the Human Brain Project are trying to build new computing tools that can zoom in on every one of these synapses, peer inside cells, and zoom out to focus on entire regions of the brain at once.
, researchers from the Human Brain Project report in Science. If you have an old smartphone or tablet with 32GB of storage, you’d need more than 31,000 of them to get a single petabyte of storage.
Using an electron microscope to image the entire brain would require more than one exabyte of data, the scientists point out. That’s more than a million petabytes.
Giacomo Indiveri, PhD, professor of neuroinformatics at the University of Zurich, Switzerland, says we need to fundamentally change the way we build computers. Delivering the keynote address at the Human Brain Project Summit in October, he warned we will use 20% of all the world’s electricity on computing by the year 2025.
To meet the computing challenges posed by the quest to map every bit of the human brain, researchers are working to produce the first two exascale supercomputers within the next 5 years. When they’re done, these machines will provide brain scientists with supercomputers powerful enough to explore the human brain in all its complexities.
A version of this article first appeared on Medscape.com.
An adult brain contains about 86 billion neurons and even more supercomputing power to closely monitor the entire human brain.
All those neurons have trillions of synapses – or connection points – that make up the circuitry the brain uses to control everything we do from reasoning to breathing to walking. And scientists with the Human Brain Project are trying to build new computing tools that can zoom in on every one of these synapses, peer inside cells, and zoom out to focus on entire regions of the brain at once.
, researchers from the Human Brain Project report in Science. If you have an old smartphone or tablet with 32GB of storage, you’d need more than 31,000 of them to get a single petabyte of storage.
Using an electron microscope to image the entire brain would require more than one exabyte of data, the scientists point out. That’s more than a million petabytes.
Giacomo Indiveri, PhD, professor of neuroinformatics at the University of Zurich, Switzerland, says we need to fundamentally change the way we build computers. Delivering the keynote address at the Human Brain Project Summit in October, he warned we will use 20% of all the world’s electricity on computing by the year 2025.
To meet the computing challenges posed by the quest to map every bit of the human brain, researchers are working to produce the first two exascale supercomputers within the next 5 years. When they’re done, these machines will provide brain scientists with supercomputers powerful enough to explore the human brain in all its complexities.
A version of this article first appeared on Medscape.com.
FROM SCIENCE
FDA updates status of iPLEDGE access problems
The, one month after a modified program was launched, the Food and Drug Administration announced on Jan. 14.
The IPMG has “created a new tool within the system to help resolve account access for some user groups without using the call center. This tool is intended to allow prescribers and designees to send login links directly to their patients’ desired email address through the Manage Patients page of the iPLEDGE REMS portal,” the FDA statement said.

“Prescribers can also send login links to their designees still having difficulty accessing their iPLEDGE account,” and users should check their emails for messages from iPLEDGE, including spam folders, the FDA advises. The iPLEDGE strategy is designed to prevent fetal exposure to isotretinoin, which is highly teratogenic.
Days after the new, gender-neutral approach to the isotretinoin risk mitigation program was launched on Dec. 13, the FDA convened an emergency meeting with representatives from the American Academy of Dermatology Association (AADA) to discuss the problematic rollout of the program, which was described as disastrous, chaotic, and a failure, with dermatologists on Twitter and elsewhere expressing anger and frustration over not being able to access the program or reach the call center.
A statement by the FDA on Dec. 23 followed, urging manufacturers to develop solutions for the website and to work with the AADA and pharmacy organizations to find solutions that would minimize treatment interruptions during the transition.
The modified REMS, launched on Dec. 13, is designed to make it more inclusive for transgender patients prescribed isotretinoin. Instead of three risk categories (females of reproductive potential, females not of reproductive potential, and males), patients who are prescribed isotretinoin for acne are assigned to one of two risk categories: those who can get pregnant and those who cannot get pregnant.
In the Jan. 14 statement, the FDA notes that the agency is continuing to work with the IPMG regarding the problems clinicians, pharmacists, and patients have had with accessing iPLEDGE over the last month.
“Although there has been progress, there is a significant amount of work still to be done,” the FDA acknowledged. “While we consider potential steps within the scope of FDA’s authorities, we will continue to meet with the IPMG for updates on the status of the problems with the iPLEDGE REMS and their progress towards having the system work as intended for all users.”
The, one month after a modified program was launched, the Food and Drug Administration announced on Jan. 14.
The IPMG has “created a new tool within the system to help resolve account access for some user groups without using the call center. This tool is intended to allow prescribers and designees to send login links directly to their patients’ desired email address through the Manage Patients page of the iPLEDGE REMS portal,” the FDA statement said.
“Prescribers can also send login links to their designees still having difficulty accessing their iPLEDGE account,” and users should check their emails for messages from iPLEDGE, including spam folders, the FDA advises. The iPLEDGE strategy is designed to prevent fetal exposure to isotretinoin, which is highly teratogenic.
Days after the new, gender-neutral approach to the isotretinoin risk mitigation program was launched on Dec. 13, the FDA convened an emergency meeting with representatives from the American Academy of Dermatology Association (AADA) to discuss the problematic rollout of the program, which was described as disastrous, chaotic, and a failure, with dermatologists on Twitter and elsewhere expressing anger and frustration over not being able to access the program or reach the call center.
A statement by the FDA on Dec. 23 followed, urging manufacturers to develop solutions for the website and to work with the AADA and pharmacy organizations to find solutions that would minimize treatment interruptions during the transition.
The modified REMS, launched on Dec. 13, is designed to make it more inclusive for transgender patients prescribed isotretinoin. Instead of three risk categories (females of reproductive potential, females not of reproductive potential, and males), patients who are prescribed isotretinoin for acne are assigned to one of two risk categories: those who can get pregnant and those who cannot get pregnant.
In the Jan. 14 statement, the FDA notes that the agency is continuing to work with the IPMG regarding the problems clinicians, pharmacists, and patients have had with accessing iPLEDGE over the last month.
“Although there has been progress, there is a significant amount of work still to be done,” the FDA acknowledged. “While we consider potential steps within the scope of FDA’s authorities, we will continue to meet with the IPMG for updates on the status of the problems with the iPLEDGE REMS and their progress towards having the system work as intended for all users.”
The, one month after a modified program was launched, the Food and Drug Administration announced on Jan. 14.
The IPMG has “created a new tool within the system to help resolve account access for some user groups without using the call center. This tool is intended to allow prescribers and designees to send login links directly to their patients’ desired email address through the Manage Patients page of the iPLEDGE REMS portal,” the FDA statement said.
“Prescribers can also send login links to their designees still having difficulty accessing their iPLEDGE account,” and users should check their emails for messages from iPLEDGE, including spam folders, the FDA advises. The iPLEDGE strategy is designed to prevent fetal exposure to isotretinoin, which is highly teratogenic.
Days after the new, gender-neutral approach to the isotretinoin risk mitigation program was launched on Dec. 13, the FDA convened an emergency meeting with representatives from the American Academy of Dermatology Association (AADA) to discuss the problematic rollout of the program, which was described as disastrous, chaotic, and a failure, with dermatologists on Twitter and elsewhere expressing anger and frustration over not being able to access the program or reach the call center.
A statement by the FDA on Dec. 23 followed, urging manufacturers to develop solutions for the website and to work with the AADA and pharmacy organizations to find solutions that would minimize treatment interruptions during the transition.
The modified REMS, launched on Dec. 13, is designed to make it more inclusive for transgender patients prescribed isotretinoin. Instead of three risk categories (females of reproductive potential, females not of reproductive potential, and males), patients who are prescribed isotretinoin for acne are assigned to one of two risk categories: those who can get pregnant and those who cannot get pregnant.
In the Jan. 14 statement, the FDA notes that the agency is continuing to work with the IPMG regarding the problems clinicians, pharmacists, and patients have had with accessing iPLEDGE over the last month.
“Although there has been progress, there is a significant amount of work still to be done,” the FDA acknowledged. “While we consider potential steps within the scope of FDA’s authorities, we will continue to meet with the IPMG for updates on the status of the problems with the iPLEDGE REMS and their progress towards having the system work as intended for all users.”
Reducing night-time checks is safe and helps patients sleep
Routine checks of vital signs during the night often prevent hospitalized patients from getting sufficient recuperative sleep. But patients who are judged to be clinically stable by an algorithm that uses real-time data can be safely spared these checks, according to a recent study published in JAMA Internal Medicine.
In their study,
“Sleep is crucial to health,” writes Hyung J. Cho, MD, from the New York University Grossman School of Medicine, in an accompanying editorial. “Ironically, hospitals, where people go to recover from illness, are among the most difficult places to sleep.”
Noise from the surrounding area, night-time examinations, multibed rooms, an unfamiliar environment, early morning blood sample collections, and frequent vital sign checks often prevent patients from sleeping through the night.
The goal of the study was to see if the elimination of one of these disrupting factors – the frequent checks of vital signs – would improve sleep and lead to a reduction in delirium, the primary endpoint.
To do this, the researchers incorporated a predictive algorithm they developed “to identify patients who are at low risk for abnormal night-time vital signs” into the hospitals electronic health records system. Attending physicians received a notification, based on real-time patient data, if it was predicted with a high degree of probability that a patient’s night-time vital signs would be within the normal range. Each physician was free to decide whether they would forgo night-time checks of the vital signs or whether they would turn off the notifications for a specific period.
The randomized clinical trial was conducted at a tertiary care academic teaching hospital from March to November 2019. Half the 1,930 patients were randomized to the algorithm group and half to standard care. None of the patients were receiving intensive care.
Number of night-time checks successfully reduced
The mean number of night-time checks was significantly lower in the algorithm group than in the standard-care group (0.97 vs. 1.41; P < .001).
The reduction in night-time checks had no effect on patient safety. There was no increase in transfers to the intensive care unit in the algorithm or standard-care groups (5% vs 5%; P = .92), and no difference between the number of heart alarms (0.2% vs. 0.9%; P = .07).
However, the reduction also had no effect on the incidence of episodes of delirium in the algorithm or standard-care groups (11% vs. 13%; P = .32).
“The reduction in vital signs checking, although statistically significant, was relatively small,” Dr. Cho explains. But the primary endpoint might have been different had the adherence to intervention been better, he notes.
In fact, the analysis confirmed that changes to routine daily practice in a hospital are not always easy to implement. In 35% of cases, the patients’ vital signs were checked at night, despite the physician’s order to the contrary.
“Busy patient-care assistants and nurses may check vital signs out of habit without noticing that the order has changed for some of the patients,” Dr. Najafi and his coauthors write. Many hospitals are used to thinking that regular measurements of the vital signs are part of good practice.
Include nursing staff
Future projects should use an interdisciplinary approach that includes nursing staff, Dr. Cho recommends. More user-friendly displays and optimized alerts in the electronic patient records could also encourage better implementation of the orders.
Less frequent checks of the vital signs would be welcomed by frontline staff because it would lighten their already heavy workload, he adds.
Although the study didn’t meet its primary endpoint, patients subjected to fewer night-time checks because of the algorithm were able to get a good night’s sleep. Other aspects of hospital care that are based on the patient’s stability, such as cardiac monitoring, could also potentially benefit from this type of intervention, Dr. Najafi and his colleagues suggest.
A version of this article first appeared on Medscape.com.
Routine checks of vital signs during the night often prevent hospitalized patients from getting sufficient recuperative sleep. But patients who are judged to be clinically stable by an algorithm that uses real-time data can be safely spared these checks, according to a recent study published in JAMA Internal Medicine.
In their study,
“Sleep is crucial to health,” writes Hyung J. Cho, MD, from the New York University Grossman School of Medicine, in an accompanying editorial. “Ironically, hospitals, where people go to recover from illness, are among the most difficult places to sleep.”
Noise from the surrounding area, night-time examinations, multibed rooms, an unfamiliar environment, early morning blood sample collections, and frequent vital sign checks often prevent patients from sleeping through the night.
The goal of the study was to see if the elimination of one of these disrupting factors – the frequent checks of vital signs – would improve sleep and lead to a reduction in delirium, the primary endpoint.
To do this, the researchers incorporated a predictive algorithm they developed “to identify patients who are at low risk for abnormal night-time vital signs” into the hospitals electronic health records system. Attending physicians received a notification, based on real-time patient data, if it was predicted with a high degree of probability that a patient’s night-time vital signs would be within the normal range. Each physician was free to decide whether they would forgo night-time checks of the vital signs or whether they would turn off the notifications for a specific period.
The randomized clinical trial was conducted at a tertiary care academic teaching hospital from March to November 2019. Half the 1,930 patients were randomized to the algorithm group and half to standard care. None of the patients were receiving intensive care.
Number of night-time checks successfully reduced
The mean number of night-time checks was significantly lower in the algorithm group than in the standard-care group (0.97 vs. 1.41; P < .001).
The reduction in night-time checks had no effect on patient safety. There was no increase in transfers to the intensive care unit in the algorithm or standard-care groups (5% vs 5%; P = .92), and no difference between the number of heart alarms (0.2% vs. 0.9%; P = .07).
However, the reduction also had no effect on the incidence of episodes of delirium in the algorithm or standard-care groups (11% vs. 13%; P = .32).
“The reduction in vital signs checking, although statistically significant, was relatively small,” Dr. Cho explains. But the primary endpoint might have been different had the adherence to intervention been better, he notes.
In fact, the analysis confirmed that changes to routine daily practice in a hospital are not always easy to implement. In 35% of cases, the patients’ vital signs were checked at night, despite the physician’s order to the contrary.
“Busy patient-care assistants and nurses may check vital signs out of habit without noticing that the order has changed for some of the patients,” Dr. Najafi and his coauthors write. Many hospitals are used to thinking that regular measurements of the vital signs are part of good practice.
Include nursing staff
Future projects should use an interdisciplinary approach that includes nursing staff, Dr. Cho recommends. More user-friendly displays and optimized alerts in the electronic patient records could also encourage better implementation of the orders.
Less frequent checks of the vital signs would be welcomed by frontline staff because it would lighten their already heavy workload, he adds.
Although the study didn’t meet its primary endpoint, patients subjected to fewer night-time checks because of the algorithm were able to get a good night’s sleep. Other aspects of hospital care that are based on the patient’s stability, such as cardiac monitoring, could also potentially benefit from this type of intervention, Dr. Najafi and his colleagues suggest.
A version of this article first appeared on Medscape.com.
Routine checks of vital signs during the night often prevent hospitalized patients from getting sufficient recuperative sleep. But patients who are judged to be clinically stable by an algorithm that uses real-time data can be safely spared these checks, according to a recent study published in JAMA Internal Medicine.
In their study,
“Sleep is crucial to health,” writes Hyung J. Cho, MD, from the New York University Grossman School of Medicine, in an accompanying editorial. “Ironically, hospitals, where people go to recover from illness, are among the most difficult places to sleep.”
Noise from the surrounding area, night-time examinations, multibed rooms, an unfamiliar environment, early morning blood sample collections, and frequent vital sign checks often prevent patients from sleeping through the night.
The goal of the study was to see if the elimination of one of these disrupting factors – the frequent checks of vital signs – would improve sleep and lead to a reduction in delirium, the primary endpoint.
To do this, the researchers incorporated a predictive algorithm they developed “to identify patients who are at low risk for abnormal night-time vital signs” into the hospitals electronic health records system. Attending physicians received a notification, based on real-time patient data, if it was predicted with a high degree of probability that a patient’s night-time vital signs would be within the normal range. Each physician was free to decide whether they would forgo night-time checks of the vital signs or whether they would turn off the notifications for a specific period.
The randomized clinical trial was conducted at a tertiary care academic teaching hospital from March to November 2019. Half the 1,930 patients were randomized to the algorithm group and half to standard care. None of the patients were receiving intensive care.
Number of night-time checks successfully reduced
The mean number of night-time checks was significantly lower in the algorithm group than in the standard-care group (0.97 vs. 1.41; P < .001).
The reduction in night-time checks had no effect on patient safety. There was no increase in transfers to the intensive care unit in the algorithm or standard-care groups (5% vs 5%; P = .92), and no difference between the number of heart alarms (0.2% vs. 0.9%; P = .07).
However, the reduction also had no effect on the incidence of episodes of delirium in the algorithm or standard-care groups (11% vs. 13%; P = .32).
“The reduction in vital signs checking, although statistically significant, was relatively small,” Dr. Cho explains. But the primary endpoint might have been different had the adherence to intervention been better, he notes.
In fact, the analysis confirmed that changes to routine daily practice in a hospital are not always easy to implement. In 35% of cases, the patients’ vital signs were checked at night, despite the physician’s order to the contrary.
“Busy patient-care assistants and nurses may check vital signs out of habit without noticing that the order has changed for some of the patients,” Dr. Najafi and his coauthors write. Many hospitals are used to thinking that regular measurements of the vital signs are part of good practice.
Include nursing staff
Future projects should use an interdisciplinary approach that includes nursing staff, Dr. Cho recommends. More user-friendly displays and optimized alerts in the electronic patient records could also encourage better implementation of the orders.
Less frequent checks of the vital signs would be welcomed by frontline staff because it would lighten their already heavy workload, he adds.
Although the study didn’t meet its primary endpoint, patients subjected to fewer night-time checks because of the algorithm were able to get a good night’s sleep. Other aspects of hospital care that are based on the patient’s stability, such as cardiac monitoring, could also potentially benefit from this type of intervention, Dr. Najafi and his colleagues suggest.
A version of this article first appeared on Medscape.com.
Infectious disease pop quiz: Clinical challenge #10 for the ObGyn
What are the characteristic mucocutaneous lesions of primary, secondary, and tertiary syphilis?
Continue to answer...
The characteristic mucosal lesion of primary syphilis is the painless chancre. The usual mucocutaneous manifestations of secondary syphilis are maculopapular lesions (red or violet in color) on the palms and soles, mucous patches on the oral membranes, and condyloma lata on the genitalia. The classic mucocutaneous lesion of tertiary syphilis is the gumma.
Other serious manifestations of advanced syphilis include central nervous system abnormalities, such as tabes dorsalis, the Argyll Robertson pupil, and dementia, and cardiac abnormalities, such as aortitis, which can lead to a dissecting aneurysm of the aortic root. (Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Morbid Mortal Wkly Rep. 2015;64[RR3]:1-137.)
- Duff P. Maternal and perinatal infections: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al. Gabbe’s Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021:1124-1146.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TJ, et al. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862-919.

Dr. Edwards is a Resident in the Department of Medicine, University of Florida College of Medicine, Gainesville.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The authors report no financial relationships relevant to this article.
Dr. Edwards is a Resident in the Department of Medicine, University of Florida College of Medicine, Gainesville.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The authors report no financial relationships relevant to this article.
Dr. Edwards is a Resident in the Department of Medicine, University of Florida College of Medicine, Gainesville.
Dr. Duff is Professor of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville.
The authors report no financial relationships relevant to this article.
What are the characteristic mucocutaneous lesions of primary, secondary, and tertiary syphilis?
Continue to answer...
The characteristic mucosal lesion of primary syphilis is the painless chancre. The usual mucocutaneous manifestations of secondary syphilis are maculopapular lesions (red or violet in color) on the palms and soles, mucous patches on the oral membranes, and condyloma lata on the genitalia. The classic mucocutaneous lesion of tertiary syphilis is the gumma.
Other serious manifestations of advanced syphilis include central nervous system abnormalities, such as tabes dorsalis, the Argyll Robertson pupil, and dementia, and cardiac abnormalities, such as aortitis, which can lead to a dissecting aneurysm of the aortic root. (Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Morbid Mortal Wkly Rep. 2015;64[RR3]:1-137.)
What are the characteristic mucocutaneous lesions of primary, secondary, and tertiary syphilis?
Continue to answer...
The characteristic mucosal lesion of primary syphilis is the painless chancre. The usual mucocutaneous manifestations of secondary syphilis are maculopapular lesions (red or violet in color) on the palms and soles, mucous patches on the oral membranes, and condyloma lata on the genitalia. The classic mucocutaneous lesion of tertiary syphilis is the gumma.
Other serious manifestations of advanced syphilis include central nervous system abnormalities, such as tabes dorsalis, the Argyll Robertson pupil, and dementia, and cardiac abnormalities, such as aortitis, which can lead to a dissecting aneurysm of the aortic root. (Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Morbid Mortal Wkly Rep. 2015;64[RR3]:1-137.)
- Duff P. Maternal and perinatal infections: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al. Gabbe’s Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021:1124-1146.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TJ, et al. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862-919.
- Duff P. Maternal and perinatal infections: bacterial. In: Landon MB, Galan HL, Jauniaux ERM, et al. Gabbe’s Obstetrics: Normal and Problem Pregnancies. 8th ed. Elsevier; 2021:1124-1146.
- Duff P. Maternal and fetal infections. In: Resnik R, Lockwood CJ, Moore TJ, et al. Creasy & Resnik’s Maternal-Fetal Medicine: Principles and Practice. 8th ed. Elsevier; 2019:862-919.
Wilderness Medical Society issues clinical guidelines for tick-borne illness
The recently published “Clinical Practice Guidelines for the Prevention and Management of Tick-Borne Illness,” from the Wilderness Medical Society, are a good compilation of treatment suggestions but are not, in fact, new recommendations, lead author Benjamin Ho, MD, of Southern Wisconsin Emergency Associates in Janesville, acknowledged in an interview.
Dr. Ho emphasized that the focus of the report was on “practitioners who practice in resource-limited settings” and are “the group’s way of solidifying a ... standard of practice” for such physicians. Dr. Ho also said that, while “a lot of the recommendations aren’t well supported, the risk-benefit ratio, we believe, supports the recommendations.”
The article first reviewed the different types of ticks and their distribution in the United States, the specific pathogen associated with each, the disease it causes, and comments about seasonal variations in biting behavior. Another table outlines the most common clinical syndromes, typical lab findings, recommended diagnostic testing, and antibiotic treatments. A third section contains images of different types of ticks and photos of ticks in various life-cycle stages and different levels of engorgement.
The authors were careful to note: “Several tick species are able to carry multiple pathogens. In one study, nearly 25% of Ixodes were coinfected with some combination of the bacteria or parasites causing Lyme disease, anaplasmosis, or babesiosis. Although TBI [tick-borne illness] diagnosis is not the focus of this [clinical practice guideline], providers should be aware of high rates of coinfection; the presence of one TBI should in many instances prompt testing for others.”
In terms of recommendations for preventing TBIs, the authors challenge the suggestion of wearing light-colored clothing. For repellents, they recommend DEET, picaridin, and permethrin. And they also give instructions for laundering clothing and removing ticks.
One recommendation is controversial: that of providing single-dose doxycycline as prophylaxis against Lyme disease. Dr. Ho stresses that this was only for “high-risk” tick bites, defined as a tick bite from an identified Ixodes vector species in which the tick was attached for at least 36 hours and that occurred in an endemic area.
The recommendation for prophylactic doxycycline originated with an article by Robert Nadelman and colleagues in the New England Journal of Medicine and has been strongly challenged by ILADS (International Lyme and Associated Diseases Society) physicians, including Daniel Cameron, MD, and others.
Sam Donta, MD, a recent member of the Department of Health & Human Services Tick-borne Working Group and a member of the Infectious Disease Society of America, said in an interview: “The problem with the one-dose doxycycline is you may not begin to develop symptoms until 2 months later.” It might mask the early symptoms of Lyme. “My impression is that the doxycycline – even the single dose – might have abrogated the ability to see an immune response. The idea, though, if you’ve had a tick bite, is to do nothing and to wait for symptoms to develop. That becomes a little bit more complex. But even then, you could choose to follow the patient and see the patient in 2 weeks and then get blood testing.”
Dr. Donta added: “I think the screening test is inadequate. So you have to go directly to the Western blot. And you have to do both the IgM and IgG” and look for specific bands.
Dr. Donta emphasized that patients should be encouraged to save any ticks that were attached and that, if at all possible, ticks should be sent to a reference lab for testing before committing a patient to a course of antibiotics. There is no harm in that brief delay, he said, and most labs can identify an array of pathogens.
The Wilderness Society guidelines on TBIs provide a good overview for clinicians practicing in limited resource settings and mirror those from the IDSA.
Dr. Ho and Dr. Donta reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The recently published “Clinical Practice Guidelines for the Prevention and Management of Tick-Borne Illness,” from the Wilderness Medical Society, are a good compilation of treatment suggestions but are not, in fact, new recommendations, lead author Benjamin Ho, MD, of Southern Wisconsin Emergency Associates in Janesville, acknowledged in an interview.
Dr. Ho emphasized that the focus of the report was on “practitioners who practice in resource-limited settings” and are “the group’s way of solidifying a ... standard of practice” for such physicians. Dr. Ho also said that, while “a lot of the recommendations aren’t well supported, the risk-benefit ratio, we believe, supports the recommendations.”
The article first reviewed the different types of ticks and their distribution in the United States, the specific pathogen associated with each, the disease it causes, and comments about seasonal variations in biting behavior. Another table outlines the most common clinical syndromes, typical lab findings, recommended diagnostic testing, and antibiotic treatments. A third section contains images of different types of ticks and photos of ticks in various life-cycle stages and different levels of engorgement.
The authors were careful to note: “Several tick species are able to carry multiple pathogens. In one study, nearly 25% of Ixodes were coinfected with some combination of the bacteria or parasites causing Lyme disease, anaplasmosis, or babesiosis. Although TBI [tick-borne illness] diagnosis is not the focus of this [clinical practice guideline], providers should be aware of high rates of coinfection; the presence of one TBI should in many instances prompt testing for others.”
In terms of recommendations for preventing TBIs, the authors challenge the suggestion of wearing light-colored clothing. For repellents, they recommend DEET, picaridin, and permethrin. And they also give instructions for laundering clothing and removing ticks.
One recommendation is controversial: that of providing single-dose doxycycline as prophylaxis against Lyme disease. Dr. Ho stresses that this was only for “high-risk” tick bites, defined as a tick bite from an identified Ixodes vector species in which the tick was attached for at least 36 hours and that occurred in an endemic area.
The recommendation for prophylactic doxycycline originated with an article by Robert Nadelman and colleagues in the New England Journal of Medicine and has been strongly challenged by ILADS (International Lyme and Associated Diseases Society) physicians, including Daniel Cameron, MD, and others.
Sam Donta, MD, a recent member of the Department of Health & Human Services Tick-borne Working Group and a member of the Infectious Disease Society of America, said in an interview: “The problem with the one-dose doxycycline is you may not begin to develop symptoms until 2 months later.” It might mask the early symptoms of Lyme. “My impression is that the doxycycline – even the single dose – might have abrogated the ability to see an immune response. The idea, though, if you’ve had a tick bite, is to do nothing and to wait for symptoms to develop. That becomes a little bit more complex. But even then, you could choose to follow the patient and see the patient in 2 weeks and then get blood testing.”
Dr. Donta added: “I think the screening test is inadequate. So you have to go directly to the Western blot. And you have to do both the IgM and IgG” and look for specific bands.
Dr. Donta emphasized that patients should be encouraged to save any ticks that were attached and that, if at all possible, ticks should be sent to a reference lab for testing before committing a patient to a course of antibiotics. There is no harm in that brief delay, he said, and most labs can identify an array of pathogens.
The Wilderness Society guidelines on TBIs provide a good overview for clinicians practicing in limited resource settings and mirror those from the IDSA.
Dr. Ho and Dr. Donta reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The recently published “Clinical Practice Guidelines for the Prevention and Management of Tick-Borne Illness,” from the Wilderness Medical Society, are a good compilation of treatment suggestions but are not, in fact, new recommendations, lead author Benjamin Ho, MD, of Southern Wisconsin Emergency Associates in Janesville, acknowledged in an interview.
Dr. Ho emphasized that the focus of the report was on “practitioners who practice in resource-limited settings” and are “the group’s way of solidifying a ... standard of practice” for such physicians. Dr. Ho also said that, while “a lot of the recommendations aren’t well supported, the risk-benefit ratio, we believe, supports the recommendations.”
The article first reviewed the different types of ticks and their distribution in the United States, the specific pathogen associated with each, the disease it causes, and comments about seasonal variations in biting behavior. Another table outlines the most common clinical syndromes, typical lab findings, recommended diagnostic testing, and antibiotic treatments. A third section contains images of different types of ticks and photos of ticks in various life-cycle stages and different levels of engorgement.
The authors were careful to note: “Several tick species are able to carry multiple pathogens. In one study, nearly 25% of Ixodes were coinfected with some combination of the bacteria or parasites causing Lyme disease, anaplasmosis, or babesiosis. Although TBI [tick-borne illness] diagnosis is not the focus of this [clinical practice guideline], providers should be aware of high rates of coinfection; the presence of one TBI should in many instances prompt testing for others.”
In terms of recommendations for preventing TBIs, the authors challenge the suggestion of wearing light-colored clothing. For repellents, they recommend DEET, picaridin, and permethrin. And they also give instructions for laundering clothing and removing ticks.
One recommendation is controversial: that of providing single-dose doxycycline as prophylaxis against Lyme disease. Dr. Ho stresses that this was only for “high-risk” tick bites, defined as a tick bite from an identified Ixodes vector species in which the tick was attached for at least 36 hours and that occurred in an endemic area.
The recommendation for prophylactic doxycycline originated with an article by Robert Nadelman and colleagues in the New England Journal of Medicine and has been strongly challenged by ILADS (International Lyme and Associated Diseases Society) physicians, including Daniel Cameron, MD, and others.
Sam Donta, MD, a recent member of the Department of Health & Human Services Tick-borne Working Group and a member of the Infectious Disease Society of America, said in an interview: “The problem with the one-dose doxycycline is you may not begin to develop symptoms until 2 months later.” It might mask the early symptoms of Lyme. “My impression is that the doxycycline – even the single dose – might have abrogated the ability to see an immune response. The idea, though, if you’ve had a tick bite, is to do nothing and to wait for symptoms to develop. That becomes a little bit more complex. But even then, you could choose to follow the patient and see the patient in 2 weeks and then get blood testing.”
Dr. Donta added: “I think the screening test is inadequate. So you have to go directly to the Western blot. And you have to do both the IgM and IgG” and look for specific bands.
Dr. Donta emphasized that patients should be encouraged to save any ticks that were attached and that, if at all possible, ticks should be sent to a reference lab for testing before committing a patient to a course of antibiotics. There is no harm in that brief delay, he said, and most labs can identify an array of pathogens.
The Wilderness Society guidelines on TBIs provide a good overview for clinicians practicing in limited resource settings and mirror those from the IDSA.
Dr. Ho and Dr. Donta reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM WILDERNESS ENVIRONMENTAL MEDICINE
More vitamin D not better for reducing cancer or CVD incidence
according to a new randomized controlled study.
In the cohort of nearly 2,500 healthy individuals, the researchers found no differences in cancer or CVD incidence over 5 years between the groups randomly assigned to vitamin D supplementation and to placebo.
The findings, published online Jan. 4, 2022, in the American Journal of Clinical Nutrition, may be influenced by the fact that most participants had sufficient vitamin D levels at baseline, and thus received higher than recommended doses of vitamin D during the study.
“Vitamin D3 supplementation with 1600 or 3200 IU/day for 5 years did not reduce the incidence of major CVD events, any invasive cancer, or mortality among generally healthy and mostly vitamin D sufficient older adults in Finland,” write the authors, led by Jyrki Virtanen, RD, PhD, associate professor of nutrition and public health at University of Eastern Finland, Kuopio.
“The low number of subjects with low vitamin D concentrations was a bit of a surprise for us also, but it likely reflects the quite successful food fortification policy in Finland,” Dr. Virtanen told this news organization.
Prior research has found that vitamin D insufficiency is associated with a higher risk of nearly all diseases. Although the evidence on the benefits of vitamin D supplementation remains more limited, a meta-analysis reported a consistent and significant 13% reduction in cancer mortality in those who received vitamin D supplements.
In this study, Dr. Virtanen and colleagues investigated the effects of vitamin D3 supplementation on cancer and CVD incidence in a cohort of 2,495 healthy participants.
Men 60 years or older and women 65 years or older were randomly assigned to one of three groups: placebo, 40 mcg (1,600 IU) of daily vitamin D3, or 80 mcg (3,200 IU) of daily vitamin D3.
Data collected at baseline and throughout the trial included serum 25(OH)D concentrations, nutrition, sun exposure, medication use, mental health, and other factors that could affect the risk of disease.
The study’s primary endpoints were incident of major CVD and invasive cancer. Secondary endpoints included incidence of myocardial infarction, stroke, and CVD mortality as well as site-specific cancers and cancer death.
Follow-up occurred via annual study questionnaires and national registry data. A representative subcohort of 551 participants had more detailed in-person evaluations. In the sub-cohort, mean serum 25(OH)D concentration was 75 nmol/L (30 ng/mL) at baseline; 9.1% had concentrations less than 50 nmol/L (20 ng/mL) and 50.0% had concentrations of at least 75 nmol/L (30 ng/mL).
The authors identified no major differences between the three arms at baseline, but noted that, compared with the overall study population, those in the subcohort were younger, more likely to use their own vitamin D supplements, and more likely to rate their health as good or excellent.
Among 503 participants that had complete data from baseline, the mean increase in serum 25(OH)D in participants receiving 1,600 IU/day vitamin D3 was 23.4 nmol/L (9.4 ng/mL) and 43.6 nmol/L (17.4 ng/mL) in the arm receiving 3,200 IU/day between baseline and 6 months. The authors observed a small additional increase in levels between the 6-month and 12-month visits, but few changes in vitamin D3 levels in the placebo arm.
At the 5-year follow-up, major CVD events occurred in 4.9% of participants in the placebo arm, 5% in those in the 1,600 IU/d arm (hazard ratio, 0.97), and 4.3% of those in the 3,200 IU/d arm (HR, 0.84; P = .44). Invasive cancer at follow-up was diagnosed in 4.9% of placebo recipients, 5.8% of those on 1,600 IU/d supplementation (HR, 1.14; P = .55), and 4.8% in the 3,200 IU/d group (HR, 0.95; P = .81). No significant differences were observed in the secondary endpoints or in total mortality.
The authors did not conduct a subanalysis in participants who had low 25(OH)D concentrations levels at baseline because “there were too few participants to do any meaningful analyses,” said Dr. Virtanen, who noted that blood samples were available for a representative subgroup of 550 subjects, and only 9% of them had low 25(OH)D concentrations at baseline.
Dr. Virtanen noted that future vitamin D supplementation trials should focus on recruiting participants with low vitamin D status.
The study was supported by funding from the Academy of Finland, University of Eastern Finland, Juho Vainio Foundation, Medicinska Understödsföreningen Liv och Hälsa, Finnish Foundation for Cardiovascular Research, Finnish Diabetes Research Foundation, and Finnish Cultural Foundation. Dr. Virtanen disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new randomized controlled study.
In the cohort of nearly 2,500 healthy individuals, the researchers found no differences in cancer or CVD incidence over 5 years between the groups randomly assigned to vitamin D supplementation and to placebo.
The findings, published online Jan. 4, 2022, in the American Journal of Clinical Nutrition, may be influenced by the fact that most participants had sufficient vitamin D levels at baseline, and thus received higher than recommended doses of vitamin D during the study.
“Vitamin D3 supplementation with 1600 or 3200 IU/day for 5 years did not reduce the incidence of major CVD events, any invasive cancer, or mortality among generally healthy and mostly vitamin D sufficient older adults in Finland,” write the authors, led by Jyrki Virtanen, RD, PhD, associate professor of nutrition and public health at University of Eastern Finland, Kuopio.
“The low number of subjects with low vitamin D concentrations was a bit of a surprise for us also, but it likely reflects the quite successful food fortification policy in Finland,” Dr. Virtanen told this news organization.
Prior research has found that vitamin D insufficiency is associated with a higher risk of nearly all diseases. Although the evidence on the benefits of vitamin D supplementation remains more limited, a meta-analysis reported a consistent and significant 13% reduction in cancer mortality in those who received vitamin D supplements.
In this study, Dr. Virtanen and colleagues investigated the effects of vitamin D3 supplementation on cancer and CVD incidence in a cohort of 2,495 healthy participants.
Men 60 years or older and women 65 years or older were randomly assigned to one of three groups: placebo, 40 mcg (1,600 IU) of daily vitamin D3, or 80 mcg (3,200 IU) of daily vitamin D3.
Data collected at baseline and throughout the trial included serum 25(OH)D concentrations, nutrition, sun exposure, medication use, mental health, and other factors that could affect the risk of disease.
The study’s primary endpoints were incident of major CVD and invasive cancer. Secondary endpoints included incidence of myocardial infarction, stroke, and CVD mortality as well as site-specific cancers and cancer death.
Follow-up occurred via annual study questionnaires and national registry data. A representative subcohort of 551 participants had more detailed in-person evaluations. In the sub-cohort, mean serum 25(OH)D concentration was 75 nmol/L (30 ng/mL) at baseline; 9.1% had concentrations less than 50 nmol/L (20 ng/mL) and 50.0% had concentrations of at least 75 nmol/L (30 ng/mL).
The authors identified no major differences between the three arms at baseline, but noted that, compared with the overall study population, those in the subcohort were younger, more likely to use their own vitamin D supplements, and more likely to rate their health as good or excellent.
Among 503 participants that had complete data from baseline, the mean increase in serum 25(OH)D in participants receiving 1,600 IU/day vitamin D3 was 23.4 nmol/L (9.4 ng/mL) and 43.6 nmol/L (17.4 ng/mL) in the arm receiving 3,200 IU/day between baseline and 6 months. The authors observed a small additional increase in levels between the 6-month and 12-month visits, but few changes in vitamin D3 levels in the placebo arm.
At the 5-year follow-up, major CVD events occurred in 4.9% of participants in the placebo arm, 5% in those in the 1,600 IU/d arm (hazard ratio, 0.97), and 4.3% of those in the 3,200 IU/d arm (HR, 0.84; P = .44). Invasive cancer at follow-up was diagnosed in 4.9% of placebo recipients, 5.8% of those on 1,600 IU/d supplementation (HR, 1.14; P = .55), and 4.8% in the 3,200 IU/d group (HR, 0.95; P = .81). No significant differences were observed in the secondary endpoints or in total mortality.
The authors did not conduct a subanalysis in participants who had low 25(OH)D concentrations levels at baseline because “there were too few participants to do any meaningful analyses,” said Dr. Virtanen, who noted that blood samples were available for a representative subgroup of 550 subjects, and only 9% of them had low 25(OH)D concentrations at baseline.
Dr. Virtanen noted that future vitamin D supplementation trials should focus on recruiting participants with low vitamin D status.
The study was supported by funding from the Academy of Finland, University of Eastern Finland, Juho Vainio Foundation, Medicinska Understödsföreningen Liv och Hälsa, Finnish Foundation for Cardiovascular Research, Finnish Diabetes Research Foundation, and Finnish Cultural Foundation. Dr. Virtanen disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new randomized controlled study.
In the cohort of nearly 2,500 healthy individuals, the researchers found no differences in cancer or CVD incidence over 5 years between the groups randomly assigned to vitamin D supplementation and to placebo.
The findings, published online Jan. 4, 2022, in the American Journal of Clinical Nutrition, may be influenced by the fact that most participants had sufficient vitamin D levels at baseline, and thus received higher than recommended doses of vitamin D during the study.
“Vitamin D3 supplementation with 1600 or 3200 IU/day for 5 years did not reduce the incidence of major CVD events, any invasive cancer, or mortality among generally healthy and mostly vitamin D sufficient older adults in Finland,” write the authors, led by Jyrki Virtanen, RD, PhD, associate professor of nutrition and public health at University of Eastern Finland, Kuopio.
“The low number of subjects with low vitamin D concentrations was a bit of a surprise for us also, but it likely reflects the quite successful food fortification policy in Finland,” Dr. Virtanen told this news organization.
Prior research has found that vitamin D insufficiency is associated with a higher risk of nearly all diseases. Although the evidence on the benefits of vitamin D supplementation remains more limited, a meta-analysis reported a consistent and significant 13% reduction in cancer mortality in those who received vitamin D supplements.
In this study, Dr. Virtanen and colleagues investigated the effects of vitamin D3 supplementation on cancer and CVD incidence in a cohort of 2,495 healthy participants.
Men 60 years or older and women 65 years or older were randomly assigned to one of three groups: placebo, 40 mcg (1,600 IU) of daily vitamin D3, or 80 mcg (3,200 IU) of daily vitamin D3.
Data collected at baseline and throughout the trial included serum 25(OH)D concentrations, nutrition, sun exposure, medication use, mental health, and other factors that could affect the risk of disease.
The study’s primary endpoints were incident of major CVD and invasive cancer. Secondary endpoints included incidence of myocardial infarction, stroke, and CVD mortality as well as site-specific cancers and cancer death.
Follow-up occurred via annual study questionnaires and national registry data. A representative subcohort of 551 participants had more detailed in-person evaluations. In the sub-cohort, mean serum 25(OH)D concentration was 75 nmol/L (30 ng/mL) at baseline; 9.1% had concentrations less than 50 nmol/L (20 ng/mL) and 50.0% had concentrations of at least 75 nmol/L (30 ng/mL).
The authors identified no major differences between the three arms at baseline, but noted that, compared with the overall study population, those in the subcohort were younger, more likely to use their own vitamin D supplements, and more likely to rate their health as good or excellent.
Among 503 participants that had complete data from baseline, the mean increase in serum 25(OH)D in participants receiving 1,600 IU/day vitamin D3 was 23.4 nmol/L (9.4 ng/mL) and 43.6 nmol/L (17.4 ng/mL) in the arm receiving 3,200 IU/day between baseline and 6 months. The authors observed a small additional increase in levels between the 6-month and 12-month visits, but few changes in vitamin D3 levels in the placebo arm.
At the 5-year follow-up, major CVD events occurred in 4.9% of participants in the placebo arm, 5% in those in the 1,600 IU/d arm (hazard ratio, 0.97), and 4.3% of those in the 3,200 IU/d arm (HR, 0.84; P = .44). Invasive cancer at follow-up was diagnosed in 4.9% of placebo recipients, 5.8% of those on 1,600 IU/d supplementation (HR, 1.14; P = .55), and 4.8% in the 3,200 IU/d group (HR, 0.95; P = .81). No significant differences were observed in the secondary endpoints or in total mortality.
The authors did not conduct a subanalysis in participants who had low 25(OH)D concentrations levels at baseline because “there were too few participants to do any meaningful analyses,” said Dr. Virtanen, who noted that blood samples were available for a representative subgroup of 550 subjects, and only 9% of them had low 25(OH)D concentrations at baseline.
Dr. Virtanen noted that future vitamin D supplementation trials should focus on recruiting participants with low vitamin D status.
The study was supported by funding from the Academy of Finland, University of Eastern Finland, Juho Vainio Foundation, Medicinska Understödsföreningen Liv och Hälsa, Finnish Foundation for Cardiovascular Research, Finnish Diabetes Research Foundation, and Finnish Cultural Foundation. Dr. Virtanen disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE AMERICAN JOURNAL OF CLINICAL NUTRITION
Docs react: Crowd crush survival guide, more dewormer, sizzling earwax
New year, same old TikTok.
You would think after 2021’s often perilous online health trends that the people of the internet would learn a thing or two. Just kidding, who actually thought that? Luckily,
Here’s to another year of “wow,” “ugh,” and “omg” moments. But let’s start with great advice from a doctor using TikTok to help save lives.
The good: Doctor explains how to survive crowd crush
J. Mack Slaughter, MD, (@drjmackslaughter_md) is an emergency physician who’s built his platform by engaging with and educating people on TikTok and Instagram. He recently reacted to the tragedy at the Travis Scott Astroworld music festival in Houston, where 10 people died due to a crowd surge. “This isn’t the first time this has happened, and it won’t be the last,” Dr. Slaughter captioned his post.
He used a video to spread awareness of how to best react to a crowd surge to his audience of over 368,000 followers, laying out four tips that people can use in case this ever happens to them.
Dr. Slaughter’s four tips are to (1) keep your arms up in front of you to give your chest as much room between someone in front of you as possible; (2) stay upright in order to avoid collapsing; (3) go with the flow of the crowd’s movement to conserve energy; (4) stay away from hard surfaces like walls or barriers “that can’t ebb and flow with the crowd.”
“When you get a densely packed area of people, not only can you lose control over your own movements, but you can have your chest compressed to the point where you can’t inhale,” Dr. Slaughter says. Hopefully, this crowd crush phenomenon is something that no one ever has to experience, but it’s better to have the knowledge on how to get through it.
The bad: Papaya seeds and parasites
TikTok user Jacqueline Rae posted about using papaya seeds as a detox method and dewormer in a video that has more than 32.5K likes and over a thousand comments – and she is just one of many TikTok users to promote this. “Papaya seeds on an empty stomach first thing in the morning is an antiparasitic,” Ms. Rae claims.
The papaya seed trend doesn’t come out of thin air, though. There was a study in 2007 where 60 Nigerian children who showed evidence of having intestinal parasites received papaya seeds as a treatment. For 71% of them, the treatment worked to clear their stool of the parasites. However, this is just one study with a pretty small sample size.
Unfortunately, TikTok’s algorithm can cater to hypochondriacs, and after scrolling through dewormer video after dewormer video, where people tout various products and cleanses, patients may really be convinced they have something they don’t.
Terry Simpson, MD, is a California-based physician and weight loss surgeon whose TikTok (@drterrysimpson) bio says: “Know your guts inside and out.” Dr. Simpson made his own video responding to the papaya seed craze, assuaging any anxiety or fears about contracting parasites.
In his video, Dr. Simpson says that most first-world countries like the United States have very few parasites, so patients shouldn’t be worried about them if they haven’t traveled to other countries recently. Additionally, he explains that what many people are seeing expelled after papaya seed cleanses is just fiber, and parasites aren’t visible to the naked eye.
“Papaya seeds are not a cure for parasites,” Dr. Simpson explains. “If you think you have parasites, see a doctor. One pill will get rid of all of the parasites that you can have, but the chances are you don’t have them.”
Symptoms that make people point toward parasites, such as low energy, frequent diarrhea, or other gut issues, can be symptoms of other issues unrelated to parasites, like irritable bowel syndrome or celiac disease. Because of this, it’s important to get a proper diagnosis amid signs of gut trouble.
The ugly: Hydrogen peroxide ear wax cleanse
TikTok user Ayisha Friedman-Negrin (@ayishafrita) got a whopping 2.7 million likes on her video where she puts hydrogen peroxide in her ear (yes, 2.7 million likes). This home remedy, she says, dissolves earwax that is stuck together. She lays her head on one side and waits for the hydrogen peroxide to “sizzle.” It bubbles like a hot spring before yellow-tinged liquid drips out. Yuck.
She isn’t totally wrong – hydrogen peroxide has been used for years to irrigate ears and help soften earwax. But there’s a lot of important information that people replicating this trend on TikTok tend to leave out of their videos. Thankfully, Sina Joorabchi, MD, is here to make sure TikTokers (and the rest of us) aren’t damaging their ears.
Dr. Joorabchi is a board-certified ear, nose, and throat doctor with his own TikTok account (@doctor.sina). He recommends in his video that if hydrogen peroxide is a patient’s go-to ear cleaner, it’s best to stick with one that’s of a 3% hydrogen peroxide concentration, as anything more can damage ears. Additionally, in the original video, Ms. Friedman-Negrin uses too much liquid, and 5 drops a day should work just fine for helping soften earwax.
“Definitely do not attempt [this] if you have an ear infection or history of ear perforation,” Dr. Joorabchi says. “And you don’t want to be using peroxide for an extended period of time. That can cause a lot of ear itching.”
A version of this article first appeared on Medscape.com.
New year, same old TikTok.
You would think after 2021’s often perilous online health trends that the people of the internet would learn a thing or two. Just kidding, who actually thought that? Luckily,
Here’s to another year of “wow,” “ugh,” and “omg” moments. But let’s start with great advice from a doctor using TikTok to help save lives.
The good: Doctor explains how to survive crowd crush
J. Mack Slaughter, MD, (@drjmackslaughter_md) is an emergency physician who’s built his platform by engaging with and educating people on TikTok and Instagram. He recently reacted to the tragedy at the Travis Scott Astroworld music festival in Houston, where 10 people died due to a crowd surge. “This isn’t the first time this has happened, and it won’t be the last,” Dr. Slaughter captioned his post.
He used a video to spread awareness of how to best react to a crowd surge to his audience of over 368,000 followers, laying out four tips that people can use in case this ever happens to them.
Dr. Slaughter’s four tips are to (1) keep your arms up in front of you to give your chest as much room between someone in front of you as possible; (2) stay upright in order to avoid collapsing; (3) go with the flow of the crowd’s movement to conserve energy; (4) stay away from hard surfaces like walls or barriers “that can’t ebb and flow with the crowd.”
“When you get a densely packed area of people, not only can you lose control over your own movements, but you can have your chest compressed to the point where you can’t inhale,” Dr. Slaughter says. Hopefully, this crowd crush phenomenon is something that no one ever has to experience, but it’s better to have the knowledge on how to get through it.
The bad: Papaya seeds and parasites
TikTok user Jacqueline Rae posted about using papaya seeds as a detox method and dewormer in a video that has more than 32.5K likes and over a thousand comments – and she is just one of many TikTok users to promote this. “Papaya seeds on an empty stomach first thing in the morning is an antiparasitic,” Ms. Rae claims.
The papaya seed trend doesn’t come out of thin air, though. There was a study in 2007 where 60 Nigerian children who showed evidence of having intestinal parasites received papaya seeds as a treatment. For 71% of them, the treatment worked to clear their stool of the parasites. However, this is just one study with a pretty small sample size.
Unfortunately, TikTok’s algorithm can cater to hypochondriacs, and after scrolling through dewormer video after dewormer video, where people tout various products and cleanses, patients may really be convinced they have something they don’t.
Terry Simpson, MD, is a California-based physician and weight loss surgeon whose TikTok (@drterrysimpson) bio says: “Know your guts inside and out.” Dr. Simpson made his own video responding to the papaya seed craze, assuaging any anxiety or fears about contracting parasites.
In his video, Dr. Simpson says that most first-world countries like the United States have very few parasites, so patients shouldn’t be worried about them if they haven’t traveled to other countries recently. Additionally, he explains that what many people are seeing expelled after papaya seed cleanses is just fiber, and parasites aren’t visible to the naked eye.
“Papaya seeds are not a cure for parasites,” Dr. Simpson explains. “If you think you have parasites, see a doctor. One pill will get rid of all of the parasites that you can have, but the chances are you don’t have them.”
Symptoms that make people point toward parasites, such as low energy, frequent diarrhea, or other gut issues, can be symptoms of other issues unrelated to parasites, like irritable bowel syndrome or celiac disease. Because of this, it’s important to get a proper diagnosis amid signs of gut trouble.
The ugly: Hydrogen peroxide ear wax cleanse
TikTok user Ayisha Friedman-Negrin (@ayishafrita) got a whopping 2.7 million likes on her video where she puts hydrogen peroxide in her ear (yes, 2.7 million likes). This home remedy, she says, dissolves earwax that is stuck together. She lays her head on one side and waits for the hydrogen peroxide to “sizzle.” It bubbles like a hot spring before yellow-tinged liquid drips out. Yuck.
She isn’t totally wrong – hydrogen peroxide has been used for years to irrigate ears and help soften earwax. But there’s a lot of important information that people replicating this trend on TikTok tend to leave out of their videos. Thankfully, Sina Joorabchi, MD, is here to make sure TikTokers (and the rest of us) aren’t damaging their ears.
Dr. Joorabchi is a board-certified ear, nose, and throat doctor with his own TikTok account (@doctor.sina). He recommends in his video that if hydrogen peroxide is a patient’s go-to ear cleaner, it’s best to stick with one that’s of a 3% hydrogen peroxide concentration, as anything more can damage ears. Additionally, in the original video, Ms. Friedman-Negrin uses too much liquid, and 5 drops a day should work just fine for helping soften earwax.
“Definitely do not attempt [this] if you have an ear infection or history of ear perforation,” Dr. Joorabchi says. “And you don’t want to be using peroxide for an extended period of time. That can cause a lot of ear itching.”
A version of this article first appeared on Medscape.com.
New year, same old TikTok.
You would think after 2021’s often perilous online health trends that the people of the internet would learn a thing or two. Just kidding, who actually thought that? Luckily,
Here’s to another year of “wow,” “ugh,” and “omg” moments. But let’s start with great advice from a doctor using TikTok to help save lives.
The good: Doctor explains how to survive crowd crush
J. Mack Slaughter, MD, (@drjmackslaughter_md) is an emergency physician who’s built his platform by engaging with and educating people on TikTok and Instagram. He recently reacted to the tragedy at the Travis Scott Astroworld music festival in Houston, where 10 people died due to a crowd surge. “This isn’t the first time this has happened, and it won’t be the last,” Dr. Slaughter captioned his post.
He used a video to spread awareness of how to best react to a crowd surge to his audience of over 368,000 followers, laying out four tips that people can use in case this ever happens to them.
Dr. Slaughter’s four tips are to (1) keep your arms up in front of you to give your chest as much room between someone in front of you as possible; (2) stay upright in order to avoid collapsing; (3) go with the flow of the crowd’s movement to conserve energy; (4) stay away from hard surfaces like walls or barriers “that can’t ebb and flow with the crowd.”
“When you get a densely packed area of people, not only can you lose control over your own movements, but you can have your chest compressed to the point where you can’t inhale,” Dr. Slaughter says. Hopefully, this crowd crush phenomenon is something that no one ever has to experience, but it’s better to have the knowledge on how to get through it.
The bad: Papaya seeds and parasites
TikTok user Jacqueline Rae posted about using papaya seeds as a detox method and dewormer in a video that has more than 32.5K likes and over a thousand comments – and she is just one of many TikTok users to promote this. “Papaya seeds on an empty stomach first thing in the morning is an antiparasitic,” Ms. Rae claims.
The papaya seed trend doesn’t come out of thin air, though. There was a study in 2007 where 60 Nigerian children who showed evidence of having intestinal parasites received papaya seeds as a treatment. For 71% of them, the treatment worked to clear their stool of the parasites. However, this is just one study with a pretty small sample size.
Unfortunately, TikTok’s algorithm can cater to hypochondriacs, and after scrolling through dewormer video after dewormer video, where people tout various products and cleanses, patients may really be convinced they have something they don’t.
Terry Simpson, MD, is a California-based physician and weight loss surgeon whose TikTok (@drterrysimpson) bio says: “Know your guts inside and out.” Dr. Simpson made his own video responding to the papaya seed craze, assuaging any anxiety or fears about contracting parasites.
In his video, Dr. Simpson says that most first-world countries like the United States have very few parasites, so patients shouldn’t be worried about them if they haven’t traveled to other countries recently. Additionally, he explains that what many people are seeing expelled after papaya seed cleanses is just fiber, and parasites aren’t visible to the naked eye.
“Papaya seeds are not a cure for parasites,” Dr. Simpson explains. “If you think you have parasites, see a doctor. One pill will get rid of all of the parasites that you can have, but the chances are you don’t have them.”
Symptoms that make people point toward parasites, such as low energy, frequent diarrhea, or other gut issues, can be symptoms of other issues unrelated to parasites, like irritable bowel syndrome or celiac disease. Because of this, it’s important to get a proper diagnosis amid signs of gut trouble.
The ugly: Hydrogen peroxide ear wax cleanse
TikTok user Ayisha Friedman-Negrin (@ayishafrita) got a whopping 2.7 million likes on her video where she puts hydrogen peroxide in her ear (yes, 2.7 million likes). This home remedy, she says, dissolves earwax that is stuck together. She lays her head on one side and waits for the hydrogen peroxide to “sizzle.” It bubbles like a hot spring before yellow-tinged liquid drips out. Yuck.
She isn’t totally wrong – hydrogen peroxide has been used for years to irrigate ears and help soften earwax. But there’s a lot of important information that people replicating this trend on TikTok tend to leave out of their videos. Thankfully, Sina Joorabchi, MD, is here to make sure TikTokers (and the rest of us) aren’t damaging their ears.
Dr. Joorabchi is a board-certified ear, nose, and throat doctor with his own TikTok account (@doctor.sina). He recommends in his video that if hydrogen peroxide is a patient’s go-to ear cleaner, it’s best to stick with one that’s of a 3% hydrogen peroxide concentration, as anything more can damage ears. Additionally, in the original video, Ms. Friedman-Negrin uses too much liquid, and 5 drops a day should work just fine for helping soften earwax.
“Definitely do not attempt [this] if you have an ear infection or history of ear perforation,” Dr. Joorabchi says. “And you don’t want to be using peroxide for an extended period of time. That can cause a lot of ear itching.”
A version of this article first appeared on Medscape.com.
What does a pig-to-human heart transplant mean for medicine?
Scientific achievements usually raise big new questions, and the remarkable surgery that took place on Jan. 7, when Maryland resident David Bennett was transplanted with a genetically modified heart from a pig, has been no different.
The 57-year-old with end-stage heart failure had been repeatedly turned down for a standard transplant and was judged a poor candidate for a ventricular assist device. Now his new heart is beating soundly and apparently accepted by his immune system as Mr. Bennett, his physicians at the University of Maryland where the procedure took place, and indeed the world set out on a journey with far more unknowns than knowns.

“I think even just a couple of years ago, people felt that xenotransplantation for the heart and other organs was still a long way off. And it seems like it’s started to move very quickly,” Larry A. Allen, MD, University of Colorado, Aurora, said in an interview.
Demand for donor hearts far outstrips supply, and despite advances in the development of ventricular assist pumps and artificial hearts, “there are still significant limitations to them in terms of clotting, stroke, and infection. We’ve seen the use of those devices plateau,” Dr. Allen said. “So, the concept of a nonhuman source of organs is exciting and very much in need, if people can get it to work.”
“I really credit the surgeons at the University of Maryland for courageous clinical work and a brilliant scientific innovation,” Clyde W. Yancy, MD, MSc, Northwestern University, Chicago, said in an interview. “But it’s always in the implementation that we have to hold our breath.” Heart xenotransplantation is an old idea that “has never before been successful,” he said. And standard heart transplantation has set a high bar, with a 1-year survival of about 90% and low 1-year risk for rejection. Whether the new procedure can meet that standard is unknown, as is its potential for complications, such as chronic rejection or cancers due to long-term immunosuppression. Those are “major questions requiring more time and careful follow-up.”

‘Still a nascent technology’
“This is an exciting and courageous step forward in heart transplantation, and kudos to the team at the University of Maryland,” said Mandeep R. Mehra, MD, Brigham and Woman’s Hospital, Boston. But “there are many challenges here.”
The procedure’s 10 gene modifications were reportedly aimed at preventing hyperacute rejection of the heart and its excessive growth after transplantation, and making the organ less immunogenic, Dr. Mehra said in an interview. But even if those goals are met, could the same changes potentially impede the heart’s adaptation to human physiology, such as during ambulation or stress?
That kind of adaptation may become important. For example, Dr. Mehra observed, normally a pig heart “provides flow in a four-footed configuration, and pig temperature is inherently higher than humans by several degrees, so it will be functioning in a relatively hypothermic environment.”
Transplantation remains the gold standard for patients with advanced heart failure despite modern medical and device therapy, Dr. Allen agreed. But “if we can raise pig hearts that provide the organ, and it can be implanted with a surgery that’s been done for 50 years, and rejection can be managed with gene editing and tailored immunosuppression, then it’s not hard to think about this very rapidly replacing a lot of what we do in the advanced heart failure and transplantation world.”
Certainly, it would be a major advance if the gene editing technique successfully improves the heart’s immunologic compatibility, Dr. Yancy noted. But do we have enough genomic knowledge to select gene deletions and insertions in the safest way for a successful outcome? “We have to appreciate that this is still a nascent technology, and we should be careful that there might be consequences that we haven’t anticipated.”
For example, he said, the xenotransplantation and gene-modifying techniques should be explored in a range of patients, including older and younger people, women and men, and people of different ethnicities and races.
“There may be some differences based on ancestry, based on gender, based on aging, that will influence the way in which these engineered donor hearts are experienced clinically,” Dr. Yancy said.
The xenotransplantation technique’s potential impact on health equity should also be considered, as it “almost assuredly will be a very expensive technology that will be utilized in a very select population,” he noted. “We need to have a really wide lens to think about all of the potential ramifications.”
‘This field needs to evolve’
Dr. Mehra also flagged the procedure’s potential cost should it become mainstream. Perhaps that would promote dialogue on how to primarily use it “after legitimately exhausting all available options, such as total artificial heart support.”
It might also teach the field to take greater advantage of the many donated hearts discarded as suboptimal. “The general usage rate for offered organs is around a third,” despite opportunities to expand use of those that are “less than perfect,” Dr. Mehra said. “I think that the field will grow with the community focusing on reduced discards of current available heart organs, and not necessarily grow because of the availability of ‘xeno-organs.’ ”
“This field needs to evolve because we’re actively transplanting patients today. But in my mind, the real future is to have such a sufficient understanding of the biology of left ventricular dysfunction that transplantation is a rare event,” Dr. Yancy proposed.
“I’m not certain that heart transplantation per se is the endgame. I think the avoidance of transplantation is the real endgame,” he said. “This may be controversial, but my vision of the future is not one where we have a supply of animals that we can use for transplantation. My vision of the future is that heart transplantation becomes obsolete.”
A version of this article first appeared on Medscape.com.
Scientific achievements usually raise big new questions, and the remarkable surgery that took place on Jan. 7, when Maryland resident David Bennett was transplanted with a genetically modified heart from a pig, has been no different.
The 57-year-old with end-stage heart failure had been repeatedly turned down for a standard transplant and was judged a poor candidate for a ventricular assist device. Now his new heart is beating soundly and apparently accepted by his immune system as Mr. Bennett, his physicians at the University of Maryland where the procedure took place, and indeed the world set out on a journey with far more unknowns than knowns.
“I think even just a couple of years ago, people felt that xenotransplantation for the heart and other organs was still a long way off. And it seems like it’s started to move very quickly,” Larry A. Allen, MD, University of Colorado, Aurora, said in an interview.
Demand for donor hearts far outstrips supply, and despite advances in the development of ventricular assist pumps and artificial hearts, “there are still significant limitations to them in terms of clotting, stroke, and infection. We’ve seen the use of those devices plateau,” Dr. Allen said. “So, the concept of a nonhuman source of organs is exciting and very much in need, if people can get it to work.”
“I really credit the surgeons at the University of Maryland for courageous clinical work and a brilliant scientific innovation,” Clyde W. Yancy, MD, MSc, Northwestern University, Chicago, said in an interview. “But it’s always in the implementation that we have to hold our breath.” Heart xenotransplantation is an old idea that “has never before been successful,” he said. And standard heart transplantation has set a high bar, with a 1-year survival of about 90% and low 1-year risk for rejection. Whether the new procedure can meet that standard is unknown, as is its potential for complications, such as chronic rejection or cancers due to long-term immunosuppression. Those are “major questions requiring more time and careful follow-up.”
‘Still a nascent technology’
“This is an exciting and courageous step forward in heart transplantation, and kudos to the team at the University of Maryland,” said Mandeep R. Mehra, MD, Brigham and Woman’s Hospital, Boston. But “there are many challenges here.”
The procedure’s 10 gene modifications were reportedly aimed at preventing hyperacute rejection of the heart and its excessive growth after transplantation, and making the organ less immunogenic, Dr. Mehra said in an interview. But even if those goals are met, could the same changes potentially impede the heart’s adaptation to human physiology, such as during ambulation or stress?
That kind of adaptation may become important. For example, Dr. Mehra observed, normally a pig heart “provides flow in a four-footed configuration, and pig temperature is inherently higher than humans by several degrees, so it will be functioning in a relatively hypothermic environment.”
Transplantation remains the gold standard for patients with advanced heart failure despite modern medical and device therapy, Dr. Allen agreed. But “if we can raise pig hearts that provide the organ, and it can be implanted with a surgery that’s been done for 50 years, and rejection can be managed with gene editing and tailored immunosuppression, then it’s not hard to think about this very rapidly replacing a lot of what we do in the advanced heart failure and transplantation world.”
Certainly, it would be a major advance if the gene editing technique successfully improves the heart’s immunologic compatibility, Dr. Yancy noted. But do we have enough genomic knowledge to select gene deletions and insertions in the safest way for a successful outcome? “We have to appreciate that this is still a nascent technology, and we should be careful that there might be consequences that we haven’t anticipated.”
For example, he said, the xenotransplantation and gene-modifying techniques should be explored in a range of patients, including older and younger people, women and men, and people of different ethnicities and races.
“There may be some differences based on ancestry, based on gender, based on aging, that will influence the way in which these engineered donor hearts are experienced clinically,” Dr. Yancy said.
The xenotransplantation technique’s potential impact on health equity should also be considered, as it “almost assuredly will be a very expensive technology that will be utilized in a very select population,” he noted. “We need to have a really wide lens to think about all of the potential ramifications.”
‘This field needs to evolve’
Dr. Mehra also flagged the procedure’s potential cost should it become mainstream. Perhaps that would promote dialogue on how to primarily use it “after legitimately exhausting all available options, such as total artificial heart support.”
It might also teach the field to take greater advantage of the many donated hearts discarded as suboptimal. “The general usage rate for offered organs is around a third,” despite opportunities to expand use of those that are “less than perfect,” Dr. Mehra said. “I think that the field will grow with the community focusing on reduced discards of current available heart organs, and not necessarily grow because of the availability of ‘xeno-organs.’ ”
“This field needs to evolve because we’re actively transplanting patients today. But in my mind, the real future is to have such a sufficient understanding of the biology of left ventricular dysfunction that transplantation is a rare event,” Dr. Yancy proposed.
“I’m not certain that heart transplantation per se is the endgame. I think the avoidance of transplantation is the real endgame,” he said. “This may be controversial, but my vision of the future is not one where we have a supply of animals that we can use for transplantation. My vision of the future is that heart transplantation becomes obsolete.”
A version of this article first appeared on Medscape.com.
Scientific achievements usually raise big new questions, and the remarkable surgery that took place on Jan. 7, when Maryland resident David Bennett was transplanted with a genetically modified heart from a pig, has been no different.
The 57-year-old with end-stage heart failure had been repeatedly turned down for a standard transplant and was judged a poor candidate for a ventricular assist device. Now his new heart is beating soundly and apparently accepted by his immune system as Mr. Bennett, his physicians at the University of Maryland where the procedure took place, and indeed the world set out on a journey with far more unknowns than knowns.
“I think even just a couple of years ago, people felt that xenotransplantation for the heart and other organs was still a long way off. And it seems like it’s started to move very quickly,” Larry A. Allen, MD, University of Colorado, Aurora, said in an interview.
Demand for donor hearts far outstrips supply, and despite advances in the development of ventricular assist pumps and artificial hearts, “there are still significant limitations to them in terms of clotting, stroke, and infection. We’ve seen the use of those devices plateau,” Dr. Allen said. “So, the concept of a nonhuman source of organs is exciting and very much in need, if people can get it to work.”
“I really credit the surgeons at the University of Maryland for courageous clinical work and a brilliant scientific innovation,” Clyde W. Yancy, MD, MSc, Northwestern University, Chicago, said in an interview. “But it’s always in the implementation that we have to hold our breath.” Heart xenotransplantation is an old idea that “has never before been successful,” he said. And standard heart transplantation has set a high bar, with a 1-year survival of about 90% and low 1-year risk for rejection. Whether the new procedure can meet that standard is unknown, as is its potential for complications, such as chronic rejection or cancers due to long-term immunosuppression. Those are “major questions requiring more time and careful follow-up.”
‘Still a nascent technology’
“This is an exciting and courageous step forward in heart transplantation, and kudos to the team at the University of Maryland,” said Mandeep R. Mehra, MD, Brigham and Woman’s Hospital, Boston. But “there are many challenges here.”
The procedure’s 10 gene modifications were reportedly aimed at preventing hyperacute rejection of the heart and its excessive growth after transplantation, and making the organ less immunogenic, Dr. Mehra said in an interview. But even if those goals are met, could the same changes potentially impede the heart’s adaptation to human physiology, such as during ambulation or stress?
That kind of adaptation may become important. For example, Dr. Mehra observed, normally a pig heart “provides flow in a four-footed configuration, and pig temperature is inherently higher than humans by several degrees, so it will be functioning in a relatively hypothermic environment.”
Transplantation remains the gold standard for patients with advanced heart failure despite modern medical and device therapy, Dr. Allen agreed. But “if we can raise pig hearts that provide the organ, and it can be implanted with a surgery that’s been done for 50 years, and rejection can be managed with gene editing and tailored immunosuppression, then it’s not hard to think about this very rapidly replacing a lot of what we do in the advanced heart failure and transplantation world.”
Certainly, it would be a major advance if the gene editing technique successfully improves the heart’s immunologic compatibility, Dr. Yancy noted. But do we have enough genomic knowledge to select gene deletions and insertions in the safest way for a successful outcome? “We have to appreciate that this is still a nascent technology, and we should be careful that there might be consequences that we haven’t anticipated.”
For example, he said, the xenotransplantation and gene-modifying techniques should be explored in a range of patients, including older and younger people, women and men, and people of different ethnicities and races.
“There may be some differences based on ancestry, based on gender, based on aging, that will influence the way in which these engineered donor hearts are experienced clinically,” Dr. Yancy said.
The xenotransplantation technique’s potential impact on health equity should also be considered, as it “almost assuredly will be a very expensive technology that will be utilized in a very select population,” he noted. “We need to have a really wide lens to think about all of the potential ramifications.”
‘This field needs to evolve’
Dr. Mehra also flagged the procedure’s potential cost should it become mainstream. Perhaps that would promote dialogue on how to primarily use it “after legitimately exhausting all available options, such as total artificial heart support.”
It might also teach the field to take greater advantage of the many donated hearts discarded as suboptimal. “The general usage rate for offered organs is around a third,” despite opportunities to expand use of those that are “less than perfect,” Dr. Mehra said. “I think that the field will grow with the community focusing on reduced discards of current available heart organs, and not necessarily grow because of the availability of ‘xeno-organs.’ ”
“This field needs to evolve because we’re actively transplanting patients today. But in my mind, the real future is to have such a sufficient understanding of the biology of left ventricular dysfunction that transplantation is a rare event,” Dr. Yancy proposed.
“I’m not certain that heart transplantation per se is the endgame. I think the avoidance of transplantation is the real endgame,” he said. “This may be controversial, but my vision of the future is not one where we have a supply of animals that we can use for transplantation. My vision of the future is that heart transplantation becomes obsolete.”
A version of this article first appeared on Medscape.com.