User login
A focus on women with diabetes and their offspring
In 2021, diabetes and related complications was the 8th leading cause of death in the United States.1 As of 2022, more than 11% of the U.S. population had diabetes and 38% of the adult U.S. population had prediabetes.2 Diabetes is the most expensive chronic condition in the United States, where $1 of every $4 in health care costs is spent on care.3
Where this is most concerning is diabetes in pregnancy. While childbirth rates in the United States have decreased since the 2007 high of 4.32 million births4 to 3.66 million in 2021,5 the incidence of diabetes in pregnancy – both pregestational and gestational – has increased. The rate of pregestational diabetes in 2021 was 10.9 per 1,000 births, a 27% increase from 2016 (8.6 per 1,000).6 The percentage of those giving birth who also were diagnosed with gestational diabetes mellitus (GDM) was 8.3% in 2021, up from 6.0% in 2016.7
Adverse outcomes for an infant born to a mother with diabetes include a higher risk of obesity and diabetes as adults, potentially leading to a forward-feeding cycle.

We and our colleagues established the Diabetes in Pregnancy Study Group of North America in 1997 because we had witnessed too frequently the devastating diabetes-induced pregnancy complications in our patients. The mission we set forth was to provide a forum for dialogue among maternal-fetal medicine subspecialists. The three main goals we set forth to support this mission were to provide a catalyst for research, contribute to the creation and refinement of medical policies, and influence professional practices in diabetes in pregnancy.8
In the last quarter century, DPSG-NA, through its annual and biennial meetings, has brought together several hundred practitioners that include physicians, nurses, statisticians, researchers, nutritionists, and allied health professionals, among others. As a group, it has improved the detection and management of diabetes in pregnant women and their offspring through knowledge sharing and influencing policies on GDM screening, diagnosis, management, and treatment. Our members have shown that preconceptional counseling for women with diabetes can significantly reduce congenital malformation and perinatal mortality compared with those women with pregestational diabetes who receive no counseling.9,10
We have addressed a wide variety of topics including the paucity of data in determining the timing of delivery for women with diabetes and the Institute of Medicine/National Academy of Medicine recommendations of gestational weight gain and risks of not adhering to them. We have learned about new scientific discoveries that reveal underlying mechanisms to diabetes-related birth defects and potential therapeutic targets; and we have discussed the health literacy requirements, ethics, and opportunities for lifestyle intervention.11-16
But we need to do more.
Two risk factors are at play: Women continue to choose to have babies at later ages and their pregnancies continue to be complicated by the rising incidence of obesity (see Figure 1 and Figure 2). 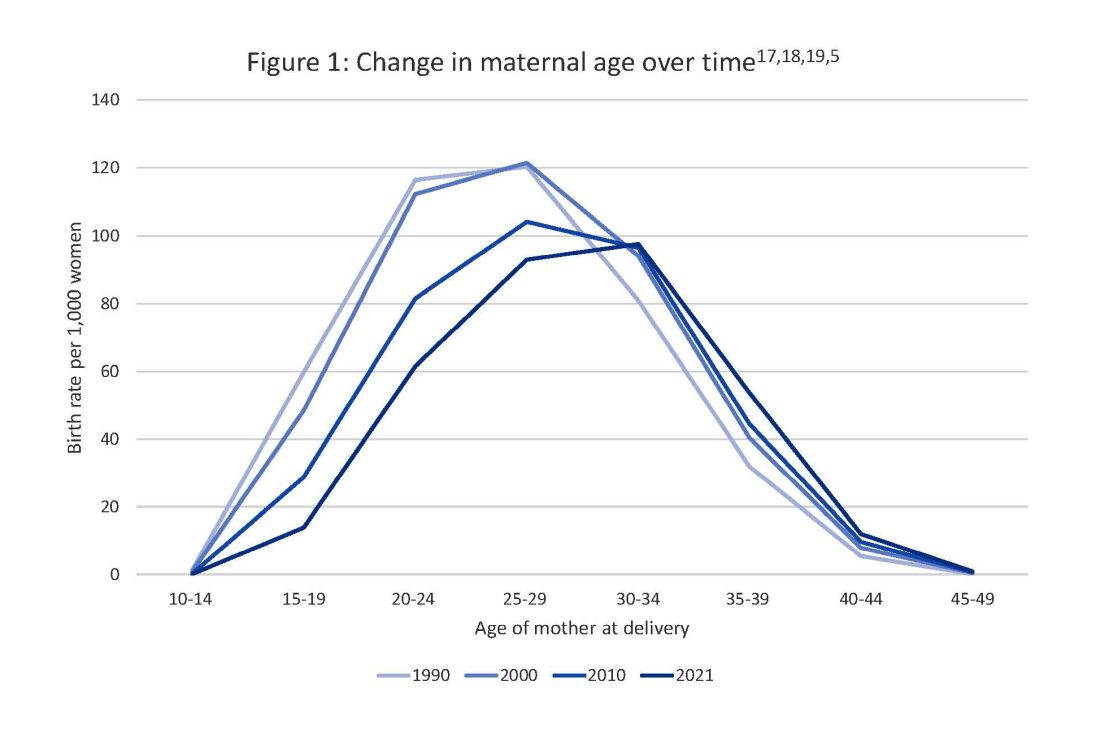
The global obesity epidemic has become a significant concern for all aspects of health and particularly for diabetes in pregnancy. 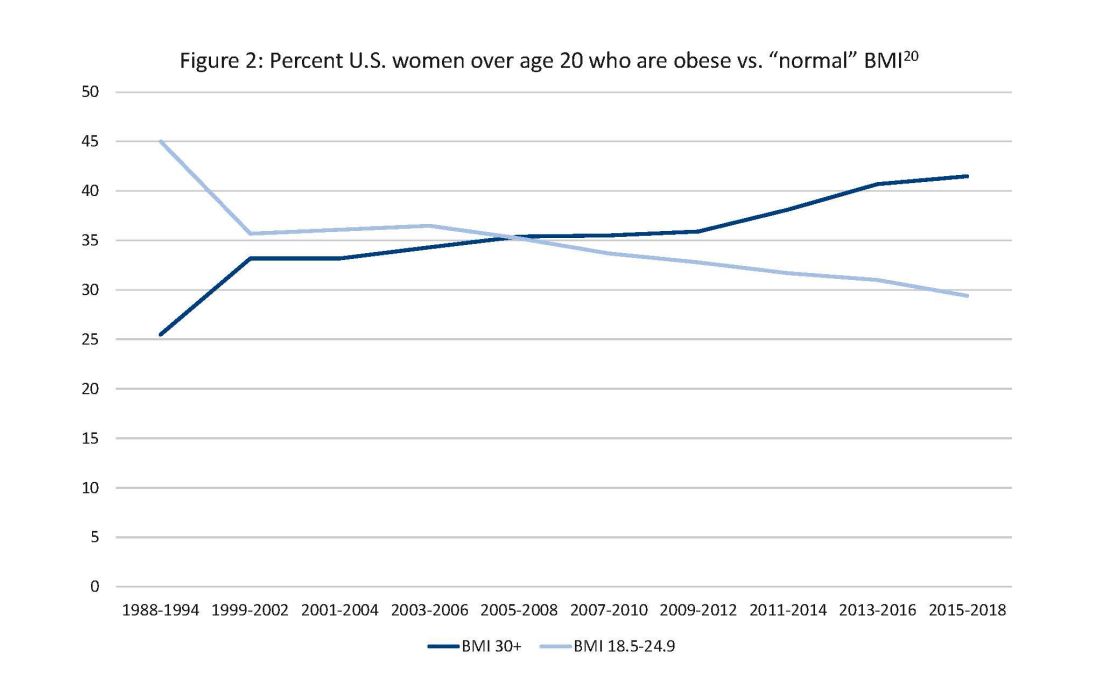
In 1990, 24.9% of women in the United States were obese; in 2010, 35.8%; and now more than 41%. Some experts project that by 2030 more than 80% of women in the United States will be overweight or obese.21
If we are to stop this cycle of diabetes begets more diabetes, now more than ever we need to come together and accelerate the research and education around the diabetes in pregnancy. Join us at this year’s DPSG-NA meeting Oct. 26-28 to take part in the knowledge sharing, discussions, and planning. More information can be found online at https://events.dpsg-na.com/home.
Dr. Miodovnik is adjunct professor of obstetrics, gynecology, and reproductive sciences at University of Maryland School of Medicine. Dr. Reece is professor of obstetrics, gynecology, and reproductive sciences and senior scientist at the Center for Birth Defects Research at University of Maryland School of Medicine.
References
1. Xu J et al. Mortality in the United States, 2021. NCHS Data Brief. 2022 Dec;(456):1-8. PMID: 36598387.
2. Centers for Disease Control and Prevention, diabetes data and statistics.
3. American Diabetes Association. The Cost of Diabetes.
4. Martin JA et al. Births: Final data for 2007. Natl Vital Stat Rep. 2010 Aug 9;58(24):1-85. PMID: 21254725.
5. Osterman MJK et al. Births: Final data for 2021. Natl Vital Stat Rep. 2023 Jan;72(1):1-53. PMID: 36723449.
6. Gregory ECW and Ely DM. Trends and characteristics in prepregnancy diabetes: United States, 2016-2021. Natl Vital Stat Rep. 2023 May;72(6):1-13. PMID: 37256333.
7. QuickStats: Percentage of mothers with gestational diabetes, by maternal age – National Vital Statistics System, United States, 2016 and 2021. MMWR Morb Mortal Wkly Rep. 2023 Jan 6;72(1):16. doi: 10.15585/mmwr.mm7201a4.
8. Langer O et al. The Diabetes in Pregnancy Study Group of North America – Introduction and summary statement. Prenat Neonat Med. 1998;3(6):514-6.
9. Willhoite MB et al. The impact of preconception counseling on pregnancy outcomes. The experience of the Maine Diabetes in Pregnancy Program. Diabetes Care. 1993 Feb;16(2):450-5. doi: 10.2337/diacare.16.2.450.
10. McElvy SS et al. A focused preconceptional and early pregnancy program in women with type 1 diabetes reduces perinatal mortality and malformation rates to general population levels. J Matern Fetal Med. 2000 Jan-Feb;9(1):14-20. doi: 10.1002/(SICI)1520-6661(200001/02)9:1<14::AID-MFM5>3.0.CO;2-K.
11. Rosen JA et al. The history and contributions of the Diabetes in Pregnancy Study Group of North America (1997-2015). Am J Perinatol. 2016 Nov;33(13):1223-6. doi: 10.1055/s-0036-1585082.
12. Driggers RW and Baschat A. The 12th meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA): Introduction and overview. J Matern Fetal Neonatal Med. 2012 Jan;25(1):3-4. doi: 10.3109/14767058.2012.626917.
13. Langer O et al. The proceedings of the Diabetes in Pregnancy Study Group of North America 2009 conference. J Matern Fetal Neonatal Med. 2010 Mar;23(3):196-8. doi: 10.3109/14767050903550634.
14. Reece EA et al. A consensus report of the Diabetes in Pregnancy Study Group of North America Conference, Little Rock, Ark., May 2002. J Matern Fetal Neonatal Med. 2002 Dec;12(6):362-4. doi: 10.1080/jmf.12.6.362.364.
15. Reece EA and Maulik D. A consensus conference of the Diabetes in Pregnancy Study Group of North America. J Matern Fetal Neonatal Med. 2002 Dec;12(6):361. doi: 10.1080/jmf.12.6.361.361.
16. Gabbe SG. Summation of the second meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA). J Matern Fetal Med. 2000 Jan-Feb;9(1):3-9.
17. Vital Statistics of the United States 1990: Volume I – Natality.
18. Martin JA et al. Births: final data for 2000. Natl Vital Stat Rep. 2002 Feb 12;50(5):1-101. PMID: 11876093.
19. Martin JA et al. Births: final data for 2010. Natl Vital Stat Rep. 2012 Aug 28;61(1):1-72. PMID: 24974589.
20. CDC Website. Normal weight, overweight, and obesity among adults aged 20 and over, by selected characteristics: United States.
21. Wang Y et al. Has the prevalence of overweight, obesity, and central obesity levelled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int J Epidemiol. 2020 Jun 1;49(3):810-23. doi: 10.1093/ije/dyz273.
In 2021, diabetes and related complications was the 8th leading cause of death in the United States.1 As of 2022, more than 11% of the U.S. population had diabetes and 38% of the adult U.S. population had prediabetes.2 Diabetes is the most expensive chronic condition in the United States, where $1 of every $4 in health care costs is spent on care.3
Where this is most concerning is diabetes in pregnancy. While childbirth rates in the United States have decreased since the 2007 high of 4.32 million births4 to 3.66 million in 2021,5 the incidence of diabetes in pregnancy – both pregestational and gestational – has increased. The rate of pregestational diabetes in 2021 was 10.9 per 1,000 births, a 27% increase from 2016 (8.6 per 1,000).6 The percentage of those giving birth who also were diagnosed with gestational diabetes mellitus (GDM) was 8.3% in 2021, up from 6.0% in 2016.7
Adverse outcomes for an infant born to a mother with diabetes include a higher risk of obesity and diabetes as adults, potentially leading to a forward-feeding cycle.
We and our colleagues established the Diabetes in Pregnancy Study Group of North America in 1997 because we had witnessed too frequently the devastating diabetes-induced pregnancy complications in our patients. The mission we set forth was to provide a forum for dialogue among maternal-fetal medicine subspecialists. The three main goals we set forth to support this mission were to provide a catalyst for research, contribute to the creation and refinement of medical policies, and influence professional practices in diabetes in pregnancy.8
In the last quarter century, DPSG-NA, through its annual and biennial meetings, has brought together several hundred practitioners that include physicians, nurses, statisticians, researchers, nutritionists, and allied health professionals, among others. As a group, it has improved the detection and management of diabetes in pregnant women and their offspring through knowledge sharing and influencing policies on GDM screening, diagnosis, management, and treatment. Our members have shown that preconceptional counseling for women with diabetes can significantly reduce congenital malformation and perinatal mortality compared with those women with pregestational diabetes who receive no counseling.9,10
We have addressed a wide variety of topics including the paucity of data in determining the timing of delivery for women with diabetes and the Institute of Medicine/National Academy of Medicine recommendations of gestational weight gain and risks of not adhering to them. We have learned about new scientific discoveries that reveal underlying mechanisms to diabetes-related birth defects and potential therapeutic targets; and we have discussed the health literacy requirements, ethics, and opportunities for lifestyle intervention.11-16
But we need to do more.
Two risk factors are at play: Women continue to choose to have babies at later ages and their pregnancies continue to be complicated by the rising incidence of obesity (see Figure 1 and Figure 2).
The global obesity epidemic has become a significant concern for all aspects of health and particularly for diabetes in pregnancy.
In 1990, 24.9% of women in the United States were obese; in 2010, 35.8%; and now more than 41%. Some experts project that by 2030 more than 80% of women in the United States will be overweight or obese.21
If we are to stop this cycle of diabetes begets more diabetes, now more than ever we need to come together and accelerate the research and education around the diabetes in pregnancy. Join us at this year’s DPSG-NA meeting Oct. 26-28 to take part in the knowledge sharing, discussions, and planning. More information can be found online at https://events.dpsg-na.com/home.
Dr. Miodovnik is adjunct professor of obstetrics, gynecology, and reproductive sciences at University of Maryland School of Medicine. Dr. Reece is professor of obstetrics, gynecology, and reproductive sciences and senior scientist at the Center for Birth Defects Research at University of Maryland School of Medicine.
References
1. Xu J et al. Mortality in the United States, 2021. NCHS Data Brief. 2022 Dec;(456):1-8. PMID: 36598387.
2. Centers for Disease Control and Prevention, diabetes data and statistics.
3. American Diabetes Association. The Cost of Diabetes.
4. Martin JA et al. Births: Final data for 2007. Natl Vital Stat Rep. 2010 Aug 9;58(24):1-85. PMID: 21254725.
5. Osterman MJK et al. Births: Final data for 2021. Natl Vital Stat Rep. 2023 Jan;72(1):1-53. PMID: 36723449.
6. Gregory ECW and Ely DM. Trends and characteristics in prepregnancy diabetes: United States, 2016-2021. Natl Vital Stat Rep. 2023 May;72(6):1-13. PMID: 37256333.
7. QuickStats: Percentage of mothers with gestational diabetes, by maternal age – National Vital Statistics System, United States, 2016 and 2021. MMWR Morb Mortal Wkly Rep. 2023 Jan 6;72(1):16. doi: 10.15585/mmwr.mm7201a4.
8. Langer O et al. The Diabetes in Pregnancy Study Group of North America – Introduction and summary statement. Prenat Neonat Med. 1998;3(6):514-6.
9. Willhoite MB et al. The impact of preconception counseling on pregnancy outcomes. The experience of the Maine Diabetes in Pregnancy Program. Diabetes Care. 1993 Feb;16(2):450-5. doi: 10.2337/diacare.16.2.450.
10. McElvy SS et al. A focused preconceptional and early pregnancy program in women with type 1 diabetes reduces perinatal mortality and malformation rates to general population levels. J Matern Fetal Med. 2000 Jan-Feb;9(1):14-20. doi: 10.1002/(SICI)1520-6661(200001/02)9:1<14::AID-MFM5>3.0.CO;2-K.
11. Rosen JA et al. The history and contributions of the Diabetes in Pregnancy Study Group of North America (1997-2015). Am J Perinatol. 2016 Nov;33(13):1223-6. doi: 10.1055/s-0036-1585082.
12. Driggers RW and Baschat A. The 12th meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA): Introduction and overview. J Matern Fetal Neonatal Med. 2012 Jan;25(1):3-4. doi: 10.3109/14767058.2012.626917.
13. Langer O et al. The proceedings of the Diabetes in Pregnancy Study Group of North America 2009 conference. J Matern Fetal Neonatal Med. 2010 Mar;23(3):196-8. doi: 10.3109/14767050903550634.
14. Reece EA et al. A consensus report of the Diabetes in Pregnancy Study Group of North America Conference, Little Rock, Ark., May 2002. J Matern Fetal Neonatal Med. 2002 Dec;12(6):362-4. doi: 10.1080/jmf.12.6.362.364.
15. Reece EA and Maulik D. A consensus conference of the Diabetes in Pregnancy Study Group of North America. J Matern Fetal Neonatal Med. 2002 Dec;12(6):361. doi: 10.1080/jmf.12.6.361.361.
16. Gabbe SG. Summation of the second meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA). J Matern Fetal Med. 2000 Jan-Feb;9(1):3-9.
17. Vital Statistics of the United States 1990: Volume I – Natality.
18. Martin JA et al. Births: final data for 2000. Natl Vital Stat Rep. 2002 Feb 12;50(5):1-101. PMID: 11876093.
19. Martin JA et al. Births: final data for 2010. Natl Vital Stat Rep. 2012 Aug 28;61(1):1-72. PMID: 24974589.
20. CDC Website. Normal weight, overweight, and obesity among adults aged 20 and over, by selected characteristics: United States.
21. Wang Y et al. Has the prevalence of overweight, obesity, and central obesity levelled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int J Epidemiol. 2020 Jun 1;49(3):810-23. doi: 10.1093/ije/dyz273.
In 2021, diabetes and related complications was the 8th leading cause of death in the United States.1 As of 2022, more than 11% of the U.S. population had diabetes and 38% of the adult U.S. population had prediabetes.2 Diabetes is the most expensive chronic condition in the United States, where $1 of every $4 in health care costs is spent on care.3
Where this is most concerning is diabetes in pregnancy. While childbirth rates in the United States have decreased since the 2007 high of 4.32 million births4 to 3.66 million in 2021,5 the incidence of diabetes in pregnancy – both pregestational and gestational – has increased. The rate of pregestational diabetes in 2021 was 10.9 per 1,000 births, a 27% increase from 2016 (8.6 per 1,000).6 The percentage of those giving birth who also were diagnosed with gestational diabetes mellitus (GDM) was 8.3% in 2021, up from 6.0% in 2016.7
Adverse outcomes for an infant born to a mother with diabetes include a higher risk of obesity and diabetes as adults, potentially leading to a forward-feeding cycle.
We and our colleagues established the Diabetes in Pregnancy Study Group of North America in 1997 because we had witnessed too frequently the devastating diabetes-induced pregnancy complications in our patients. The mission we set forth was to provide a forum for dialogue among maternal-fetal medicine subspecialists. The three main goals we set forth to support this mission were to provide a catalyst for research, contribute to the creation and refinement of medical policies, and influence professional practices in diabetes in pregnancy.8
In the last quarter century, DPSG-NA, through its annual and biennial meetings, has brought together several hundred practitioners that include physicians, nurses, statisticians, researchers, nutritionists, and allied health professionals, among others. As a group, it has improved the detection and management of diabetes in pregnant women and their offspring through knowledge sharing and influencing policies on GDM screening, diagnosis, management, and treatment. Our members have shown that preconceptional counseling for women with diabetes can significantly reduce congenital malformation and perinatal mortality compared with those women with pregestational diabetes who receive no counseling.9,10
We have addressed a wide variety of topics including the paucity of data in determining the timing of delivery for women with diabetes and the Institute of Medicine/National Academy of Medicine recommendations of gestational weight gain and risks of not adhering to them. We have learned about new scientific discoveries that reveal underlying mechanisms to diabetes-related birth defects and potential therapeutic targets; and we have discussed the health literacy requirements, ethics, and opportunities for lifestyle intervention.11-16
But we need to do more.
Two risk factors are at play: Women continue to choose to have babies at later ages and their pregnancies continue to be complicated by the rising incidence of obesity (see Figure 1 and Figure 2).
The global obesity epidemic has become a significant concern for all aspects of health and particularly for diabetes in pregnancy.
In 1990, 24.9% of women in the United States were obese; in 2010, 35.8%; and now more than 41%. Some experts project that by 2030 more than 80% of women in the United States will be overweight or obese.21
If we are to stop this cycle of diabetes begets more diabetes, now more than ever we need to come together and accelerate the research and education around the diabetes in pregnancy. Join us at this year’s DPSG-NA meeting Oct. 26-28 to take part in the knowledge sharing, discussions, and planning. More information can be found online at https://events.dpsg-na.com/home.
Dr. Miodovnik is adjunct professor of obstetrics, gynecology, and reproductive sciences at University of Maryland School of Medicine. Dr. Reece is professor of obstetrics, gynecology, and reproductive sciences and senior scientist at the Center for Birth Defects Research at University of Maryland School of Medicine.
References
1. Xu J et al. Mortality in the United States, 2021. NCHS Data Brief. 2022 Dec;(456):1-8. PMID: 36598387.
2. Centers for Disease Control and Prevention, diabetes data and statistics.
3. American Diabetes Association. The Cost of Diabetes.
4. Martin JA et al. Births: Final data for 2007. Natl Vital Stat Rep. 2010 Aug 9;58(24):1-85. PMID: 21254725.
5. Osterman MJK et al. Births: Final data for 2021. Natl Vital Stat Rep. 2023 Jan;72(1):1-53. PMID: 36723449.
6. Gregory ECW and Ely DM. Trends and characteristics in prepregnancy diabetes: United States, 2016-2021. Natl Vital Stat Rep. 2023 May;72(6):1-13. PMID: 37256333.
7. QuickStats: Percentage of mothers with gestational diabetes, by maternal age – National Vital Statistics System, United States, 2016 and 2021. MMWR Morb Mortal Wkly Rep. 2023 Jan 6;72(1):16. doi: 10.15585/mmwr.mm7201a4.
8. Langer O et al. The Diabetes in Pregnancy Study Group of North America – Introduction and summary statement. Prenat Neonat Med. 1998;3(6):514-6.
9. Willhoite MB et al. The impact of preconception counseling on pregnancy outcomes. The experience of the Maine Diabetes in Pregnancy Program. Diabetes Care. 1993 Feb;16(2):450-5. doi: 10.2337/diacare.16.2.450.
10. McElvy SS et al. A focused preconceptional and early pregnancy program in women with type 1 diabetes reduces perinatal mortality and malformation rates to general population levels. J Matern Fetal Med. 2000 Jan-Feb;9(1):14-20. doi: 10.1002/(SICI)1520-6661(200001/02)9:1<14::AID-MFM5>3.0.CO;2-K.
11. Rosen JA et al. The history and contributions of the Diabetes in Pregnancy Study Group of North America (1997-2015). Am J Perinatol. 2016 Nov;33(13):1223-6. doi: 10.1055/s-0036-1585082.
12. Driggers RW and Baschat A. The 12th meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA): Introduction and overview. J Matern Fetal Neonatal Med. 2012 Jan;25(1):3-4. doi: 10.3109/14767058.2012.626917.
13. Langer O et al. The proceedings of the Diabetes in Pregnancy Study Group of North America 2009 conference. J Matern Fetal Neonatal Med. 2010 Mar;23(3):196-8. doi: 10.3109/14767050903550634.
14. Reece EA et al. A consensus report of the Diabetes in Pregnancy Study Group of North America Conference, Little Rock, Ark., May 2002. J Matern Fetal Neonatal Med. 2002 Dec;12(6):362-4. doi: 10.1080/jmf.12.6.362.364.
15. Reece EA and Maulik D. A consensus conference of the Diabetes in Pregnancy Study Group of North America. J Matern Fetal Neonatal Med. 2002 Dec;12(6):361. doi: 10.1080/jmf.12.6.361.361.
16. Gabbe SG. Summation of the second meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA). J Matern Fetal Med. 2000 Jan-Feb;9(1):3-9.
17. Vital Statistics of the United States 1990: Volume I – Natality.
18. Martin JA et al. Births: final data for 2000. Natl Vital Stat Rep. 2002 Feb 12;50(5):1-101. PMID: 11876093.
19. Martin JA et al. Births: final data for 2010. Natl Vital Stat Rep. 2012 Aug 28;61(1):1-72. PMID: 24974589.
20. CDC Website. Normal weight, overweight, and obesity among adults aged 20 and over, by selected characteristics: United States.
21. Wang Y et al. Has the prevalence of overweight, obesity, and central obesity levelled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int J Epidemiol. 2020 Jun 1;49(3):810-23. doi: 10.1093/ije/dyz273.
Antidepressants ‘don’t blunt’ semaglutide and weight loss
in a post hoc analysis of the Semaglutide Treatment Effect in People with Obesity (STEP) program.
Adverse events, including psychiatric events, were slightly more usual in the patients on antidepressants, Robert Kushner, MD, noted, in an oral session at the annual meeting of the Obesity Society.
“It is very common that patients who present for weight management are taking antidepressants for various reasons, including depression, anxiety, insomnia, or chronic pain,”Dr. Kushner, from Northwestern University in Chicago, said in an email. “We wanted to see if these participants responded differently to semaglutide, compared to those not on antidepressants.”
“We found that antidepressants do not blunt the effect of semaglutide for weight loss,” he said. “However, there is a slight increase in reported adverse effects.”
“Semaglutide 2.4 mg provides an effective treatment option for weight management, regardless of antidepressant use at baseline,” Dr. Kushner summarized. “Clinicians should be assured that we can use semaglutide in this population of patients.”
Jack Yanovski, MD, PhD, said this was a “great presentation,” noting that “it’s really important that we understand what goes on in patients with depression.”
“Of course, all these trials still had rules that prevent the folks with the most severe depressive symptoms or past suicidality to participate,” added Dr. Yanovski, chief of the Growth and Obesity Section, Eunice Kennedy Shriver National Institute of Child Health and Human Development, Rockville, Md. “We need specific trials to know exactly how well we do.”
Dr. Kushner agreed, but also noted that, ever since some earlier antidepressants were associated with risk for suicidal ideation and death, strict guidelines were put in place that exclude certain patients from participating in clinical trials.
Dr. Yanovski suggested that now that the drugs are approved, it would be possible to study this, and the information would be important for clinicians.
Dr. Kushner said he hopes that such studies are forthcoming. In the meantime, “data like this will add some support and understanding,” he suggested.
36,000 Patients with obesity, 500 on antidepressants
Many people living with obesity report taking antidepressants for depression, anxiety, chronic pain, obsessive-compulsive disorder, sleep disturbance, neuropathy, panic disorder, or posttraumatic stress disorder, Dr. Kushner noted.
However, some of these medications can cause weight gain, and little is known about treatment outcomes for people with obesity who are on antidepressants, since most weight-loss studies exclude people with active major depressive disorder.
The researchers analyzed data from 1,961 patients in STEP 1 and 807 patients in STEP 2 as well as 611 patients in STEP 3 and 304 patients in STEP 5 – 3,683 participants in total, of which 539 were on antidepressants at baseline.
The patients were randomly assigned to 2.4 mg semaglutide vs. placebo plus a lifestyle intervention (STEP 1, 2, and 5) or intensive behavioral therapy (STEP 3 only), for 68 weeks, except STEP 5, which was 104 weeks.
Patients were included if they were aged 18 or older with a body mass index ≥30 kg/m2, or ≥27 kg/m2 with more than one weight-related complication (STEP 1, 3, and 5) or BMI ≥27 kg/m2 with type 2 diabetes (STEP 2 only), and at least one self-reported unsuccessful effort to lose weight by diet.
They were excluded if they had active major depressive disorder within 2 years prior to screening (or other severe psychiatric disorders such as schizophrenia or bipolar disorder) or a Patient Health Questionnaire-9 score of 15 or higher (indicating moderately severe or severe depression), or suicide ideation (type 4 or 5 on the Columbia Suicide Severity Rating Scale) or suicide behavior, within 30 days of screening.
From baseline to week 68, patients on semaglutide (with/without baseline antidepressant use) had a significantly greater change in weight vs. patients on placebo (with/without baseline antidepressant use), respectively:
- STEP 1: –15.7% / –14.7% vs. –0.2% / –2.8%
- STEP 2: –10.7% / –9.5% vs. –3.3% / –3.4%
- STEP 3: –16.2% / –15.9% vs. –5.0% / –5.9%
- STEP 5: –19.0% / –14.1% vs. +1.6% / – 4.0%.
The proportion of reported adverse events was generally slightly greater in patients receiving semaglutide (with/without baseline antidepressant use) than those on placebo (with/without baseline antidepressant use), respectively:
- STEP 1: 97.7% vs 88.6% and 92.9% vs. 86%
- STEP 2: 97.6% vs 86.5% and 88.6% vs. 77.2%
- STEP 3: 97.6% vs 95.3% and 100% vs. 95.8%
- STEP 5: 100% vs 94.8% and 95.5% vs. 89.2%.
Gastrointestinal adverse events were more frequently reported in the semaglutide group and in patients on antidepressants at baseline. The proportion of patients with psychiatric adverse events was greater in participants on antidepressants at baseline. There were no differences in suicidal ideation/behavior in patients with/without antidepressant use at baseline.
The STEP trials were funded by Novo Nordisk. Dr. Kushner discloses that he served as a consultant for Novo Nordisk, WeightWatchers, Eli Lilly, and Pfizer, and received a research grant from Epitomee.
A version of this article appeared on Medscape.com.
in a post hoc analysis of the Semaglutide Treatment Effect in People with Obesity (STEP) program.
Adverse events, including psychiatric events, were slightly more usual in the patients on antidepressants, Robert Kushner, MD, noted, in an oral session at the annual meeting of the Obesity Society.
“It is very common that patients who present for weight management are taking antidepressants for various reasons, including depression, anxiety, insomnia, or chronic pain,”Dr. Kushner, from Northwestern University in Chicago, said in an email. “We wanted to see if these participants responded differently to semaglutide, compared to those not on antidepressants.”
“We found that antidepressants do not blunt the effect of semaglutide for weight loss,” he said. “However, there is a slight increase in reported adverse effects.”
“Semaglutide 2.4 mg provides an effective treatment option for weight management, regardless of antidepressant use at baseline,” Dr. Kushner summarized. “Clinicians should be assured that we can use semaglutide in this population of patients.”
Jack Yanovski, MD, PhD, said this was a “great presentation,” noting that “it’s really important that we understand what goes on in patients with depression.”
“Of course, all these trials still had rules that prevent the folks with the most severe depressive symptoms or past suicidality to participate,” added Dr. Yanovski, chief of the Growth and Obesity Section, Eunice Kennedy Shriver National Institute of Child Health and Human Development, Rockville, Md. “We need specific trials to know exactly how well we do.”
Dr. Kushner agreed, but also noted that, ever since some earlier antidepressants were associated with risk for suicidal ideation and death, strict guidelines were put in place that exclude certain patients from participating in clinical trials.
Dr. Yanovski suggested that now that the drugs are approved, it would be possible to study this, and the information would be important for clinicians.
Dr. Kushner said he hopes that such studies are forthcoming. In the meantime, “data like this will add some support and understanding,” he suggested.
36,000 Patients with obesity, 500 on antidepressants
Many people living with obesity report taking antidepressants for depression, anxiety, chronic pain, obsessive-compulsive disorder, sleep disturbance, neuropathy, panic disorder, or posttraumatic stress disorder, Dr. Kushner noted.
However, some of these medications can cause weight gain, and little is known about treatment outcomes for people with obesity who are on antidepressants, since most weight-loss studies exclude people with active major depressive disorder.
The researchers analyzed data from 1,961 patients in STEP 1 and 807 patients in STEP 2 as well as 611 patients in STEP 3 and 304 patients in STEP 5 – 3,683 participants in total, of which 539 were on antidepressants at baseline.
The patients were randomly assigned to 2.4 mg semaglutide vs. placebo plus a lifestyle intervention (STEP 1, 2, and 5) or intensive behavioral therapy (STEP 3 only), for 68 weeks, except STEP 5, which was 104 weeks.
Patients were included if they were aged 18 or older with a body mass index ≥30 kg/m2, or ≥27 kg/m2 with more than one weight-related complication (STEP 1, 3, and 5) or BMI ≥27 kg/m2 with type 2 diabetes (STEP 2 only), and at least one self-reported unsuccessful effort to lose weight by diet.
They were excluded if they had active major depressive disorder within 2 years prior to screening (or other severe psychiatric disorders such as schizophrenia or bipolar disorder) or a Patient Health Questionnaire-9 score of 15 or higher (indicating moderately severe or severe depression), or suicide ideation (type 4 or 5 on the Columbia Suicide Severity Rating Scale) or suicide behavior, within 30 days of screening.
From baseline to week 68, patients on semaglutide (with/without baseline antidepressant use) had a significantly greater change in weight vs. patients on placebo (with/without baseline antidepressant use), respectively:
- STEP 1: –15.7% / –14.7% vs. –0.2% / –2.8%
- STEP 2: –10.7% / –9.5% vs. –3.3% / –3.4%
- STEP 3: –16.2% / –15.9% vs. –5.0% / –5.9%
- STEP 5: –19.0% / –14.1% vs. +1.6% / – 4.0%.
The proportion of reported adverse events was generally slightly greater in patients receiving semaglutide (with/without baseline antidepressant use) than those on placebo (with/without baseline antidepressant use), respectively:
- STEP 1: 97.7% vs 88.6% and 92.9% vs. 86%
- STEP 2: 97.6% vs 86.5% and 88.6% vs. 77.2%
- STEP 3: 97.6% vs 95.3% and 100% vs. 95.8%
- STEP 5: 100% vs 94.8% and 95.5% vs. 89.2%.
Gastrointestinal adverse events were more frequently reported in the semaglutide group and in patients on antidepressants at baseline. The proportion of patients with psychiatric adverse events was greater in participants on antidepressants at baseline. There were no differences in suicidal ideation/behavior in patients with/without antidepressant use at baseline.
The STEP trials were funded by Novo Nordisk. Dr. Kushner discloses that he served as a consultant for Novo Nordisk, WeightWatchers, Eli Lilly, and Pfizer, and received a research grant from Epitomee.
A version of this article appeared on Medscape.com.
in a post hoc analysis of the Semaglutide Treatment Effect in People with Obesity (STEP) program.
Adverse events, including psychiatric events, were slightly more usual in the patients on antidepressants, Robert Kushner, MD, noted, in an oral session at the annual meeting of the Obesity Society.
“It is very common that patients who present for weight management are taking antidepressants for various reasons, including depression, anxiety, insomnia, or chronic pain,”Dr. Kushner, from Northwestern University in Chicago, said in an email. “We wanted to see if these participants responded differently to semaglutide, compared to those not on antidepressants.”
“We found that antidepressants do not blunt the effect of semaglutide for weight loss,” he said. “However, there is a slight increase in reported adverse effects.”
“Semaglutide 2.4 mg provides an effective treatment option for weight management, regardless of antidepressant use at baseline,” Dr. Kushner summarized. “Clinicians should be assured that we can use semaglutide in this population of patients.”
Jack Yanovski, MD, PhD, said this was a “great presentation,” noting that “it’s really important that we understand what goes on in patients with depression.”
“Of course, all these trials still had rules that prevent the folks with the most severe depressive symptoms or past suicidality to participate,” added Dr. Yanovski, chief of the Growth and Obesity Section, Eunice Kennedy Shriver National Institute of Child Health and Human Development, Rockville, Md. “We need specific trials to know exactly how well we do.”
Dr. Kushner agreed, but also noted that, ever since some earlier antidepressants were associated with risk for suicidal ideation and death, strict guidelines were put in place that exclude certain patients from participating in clinical trials.
Dr. Yanovski suggested that now that the drugs are approved, it would be possible to study this, and the information would be important for clinicians.
Dr. Kushner said he hopes that such studies are forthcoming. In the meantime, “data like this will add some support and understanding,” he suggested.
36,000 Patients with obesity, 500 on antidepressants
Many people living with obesity report taking antidepressants for depression, anxiety, chronic pain, obsessive-compulsive disorder, sleep disturbance, neuropathy, panic disorder, or posttraumatic stress disorder, Dr. Kushner noted.
However, some of these medications can cause weight gain, and little is known about treatment outcomes for people with obesity who are on antidepressants, since most weight-loss studies exclude people with active major depressive disorder.
The researchers analyzed data from 1,961 patients in STEP 1 and 807 patients in STEP 2 as well as 611 patients in STEP 3 and 304 patients in STEP 5 – 3,683 participants in total, of which 539 were on antidepressants at baseline.
The patients were randomly assigned to 2.4 mg semaglutide vs. placebo plus a lifestyle intervention (STEP 1, 2, and 5) or intensive behavioral therapy (STEP 3 only), for 68 weeks, except STEP 5, which was 104 weeks.
Patients were included if they were aged 18 or older with a body mass index ≥30 kg/m2, or ≥27 kg/m2 with more than one weight-related complication (STEP 1, 3, and 5) or BMI ≥27 kg/m2 with type 2 diabetes (STEP 2 only), and at least one self-reported unsuccessful effort to lose weight by diet.
They were excluded if they had active major depressive disorder within 2 years prior to screening (or other severe psychiatric disorders such as schizophrenia or bipolar disorder) or a Patient Health Questionnaire-9 score of 15 or higher (indicating moderately severe or severe depression), or suicide ideation (type 4 or 5 on the Columbia Suicide Severity Rating Scale) or suicide behavior, within 30 days of screening.
From baseline to week 68, patients on semaglutide (with/without baseline antidepressant use) had a significantly greater change in weight vs. patients on placebo (with/without baseline antidepressant use), respectively:
- STEP 1: –15.7% / –14.7% vs. –0.2% / –2.8%
- STEP 2: –10.7% / –9.5% vs. –3.3% / –3.4%
- STEP 3: –16.2% / –15.9% vs. –5.0% / –5.9%
- STEP 5: –19.0% / –14.1% vs. +1.6% / – 4.0%.
The proportion of reported adverse events was generally slightly greater in patients receiving semaglutide (with/without baseline antidepressant use) than those on placebo (with/without baseline antidepressant use), respectively:
- STEP 1: 97.7% vs 88.6% and 92.9% vs. 86%
- STEP 2: 97.6% vs 86.5% and 88.6% vs. 77.2%
- STEP 3: 97.6% vs 95.3% and 100% vs. 95.8%
- STEP 5: 100% vs 94.8% and 95.5% vs. 89.2%.
Gastrointestinal adverse events were more frequently reported in the semaglutide group and in patients on antidepressants at baseline. The proportion of patients with psychiatric adverse events was greater in participants on antidepressants at baseline. There were no differences in suicidal ideation/behavior in patients with/without antidepressant use at baseline.
The STEP trials were funded by Novo Nordisk. Dr. Kushner discloses that he served as a consultant for Novo Nordisk, WeightWatchers, Eli Lilly, and Pfizer, and received a research grant from Epitomee.
A version of this article appeared on Medscape.com.
FROM OBESITYWEEK® 2023
Taking a new obesity drug and birth control pills? Be careful
For women who are obese, daily life is wrought with landmines. Whether it’s the challenges of air travel because plane seats are too small, the need to shield themselves from the world’s discriminating eyes, or the great lengths many will go to achieve better health and the promise of longevity, navigating life as an obese person requires a thick skin.
So, it’s no wonder so many are willing to pay more than $1,000 a month out of pocket to get their hands on drugs like semaglutide (Ozempic and Wegovy) or tirzepatide (Mounjaro). The benefits of these drugs, which are part of a new class called glucagonlike peptide–1 (GLP-1) receptor agonists, include significant and rapid weight loss, blood sugar control, and improved life quality; they are unprecedented in a setting where surgery has long been considered the most effective long-term option.
On the flip side, the desire for rapid weight loss and better blood sugar control also comes with an unexpected cost. , making an unintended pregnancy more likely.
Neel Shah, MD, an endocrinologist and associate professor at the University of Texas Health Science Center at Houston, said he has had several patients become pregnant without intending to.
“It was when Mounjaro came out on the market when we started using it,” he said of the drug the Food and Drug Administration approved for type 2 diabetes in 2022. “It [the warning] was in the product insert, but clinically speaking, I don’t know if it was at the top of providers’ minds when they were prescribing Mounjaro.”
When asked if he believed that we were going to be seeing a significant increase in so-called Mounjaro babies, Dr. Shah was sure in his response.
“Absolutely. We will because the sheer volume [of patients] will increase,” he said.
It’s all in the gut
One of the ways that drugs like Mounjaro work is by delaying the time that it takes for food to move from the stomach to the small intestine. Although data are still evolving, it is believed that this process – delayed gastric emptying – may affect the absorption of birth control pills.
Dr. Shah said another theory is that vomiting, which is a common side effect of these types of drugs, also affects the pills’ ability to prevent pregnancy.
And “there’s a prolonged period of ramping up the dose because of the GI side effects,” said Pinar Kodaman, MD, PhD, a reproductive endocrinologist and assistant professor of gynecology at Yale University in New Haven, Conn.
“Initially, at the lowest dose, there may not be a lot of potential effect on absorption and gastric emptying. But as the dose goes up, it becomes more common, and it can cause diarrhea, which is another condition that can affect the absorption of any medication,” she said.
Unanticipated outcomes, extra prevention
Roughly 42% of women in the United States are obese, 40% of whom are between the ages of 20 and 39. Although these new drugs can improve fertility outcomes for women who are obese (especially those with polycystic ovary syndrome, or PCOS), only one – Mounjaro – currently carries a warning about birth control pill effectiveness on its label. Unfortunately, it appears that some doctors are unaware or not counseling patients about this risk, and the data are unclear about whether other drugs in this class, like Ozempic and Wegovy, have the same risks.
“To date, it hasn’t been a typical thing that we counsel about,” said Dr. Kodaman. “It’s all fairly new, but when we have patients on birth control pills, we do review other medications that they are on because some can affect efficacy, and it’s something to keep in mind.”
It’s also unclear if other forms of birth control – for example, birth control patches that deliver through the skin – might carry similar pregnancy risks. Dr. Shah said some of his patients who became pregnant without intending to were using these patches. This raises even more questions, since they deliver drugs through the skin directly into the bloodstream and not through the GI system.
What can women do to help ensure that they don’t become pregnant while using these drugs?
“I really think that if patients want to protect themselves from an unplanned pregnancy, that as soon as they start the GLP receptor agonists, it wouldn’t be a bad idea to use condoms, because the onset of action is pretty quick,” said Dr. Kodaman, noting also that “at the lowest dose there may not be a lot of potential effect on gastric emptying. But as the dose goes up, it becomes much more common or can cause diarrhea.”
Dr. Shah said that in his practice he’s “been telling patients to add barrier contraception” 4 weeks before they start their first dose “and at any dose adjustment.”
Zoobia Chaudhry, an obesity medicine doctor and assistant professor of medicine at Johns Hopkins University in Baltimore, recommends that “patients just make sure that the injection and medication that they take are at least 1 hour apart.”
“Most of the time, patients do take birth control before bedtime, so if the two are spaced, it should be OK,” she said.
Another option is for women to speak to their doctors about other contraceptive options like IUDs or implantable rods, where gastric absorption is not going to be an issue.
“There’s very little research on this class of drugs,” said Emily Goodstein, a 40-year-old small-business owner in Washington, who recently switched from Ozempic to Mounjaro. “Being a person who lives in a larger body is such a horrifying experience because of the way that the world discriminates against you.”
She appreciates the feeling of being proactive that these new drugs grant. It has “opened up a bunch of opportunities for me to be seen as a full individual by the medical establishment,” she said. “I was willing to take the risk, knowing that I would be on these drugs for the rest of my life.”
In addition to being what Dr. Goodstein refers to as a guinea pig, she said she made sure that her primary care doctor was aware that she was not trying or planning to become pregnant again. (She has a 3-year-old child.) Still, her doctor mentioned only the most common side effects linked to these drugs, like nausea, vomiting, and diarrhea, and did not mention the risk of pregnancy.
“Folks are really not talking about the reproductive implications,” she said, referring to members of a Facebook group on these drugs that she belongs to.
Like patients themselves, many doctors are just beginning to get their arms around these agents. “Awareness, education, provider involvement, and having a multidisciplinary team could help patients achieve the goals that they set out for themselves,” said Dr. Shah.
Clear conversations are key.
A version of this article first appeared on WebMD.com.
For women who are obese, daily life is wrought with landmines. Whether it’s the challenges of air travel because plane seats are too small, the need to shield themselves from the world’s discriminating eyes, or the great lengths many will go to achieve better health and the promise of longevity, navigating life as an obese person requires a thick skin.
So, it’s no wonder so many are willing to pay more than $1,000 a month out of pocket to get their hands on drugs like semaglutide (Ozempic and Wegovy) or tirzepatide (Mounjaro). The benefits of these drugs, which are part of a new class called glucagonlike peptide–1 (GLP-1) receptor agonists, include significant and rapid weight loss, blood sugar control, and improved life quality; they are unprecedented in a setting where surgery has long been considered the most effective long-term option.
On the flip side, the desire for rapid weight loss and better blood sugar control also comes with an unexpected cost. , making an unintended pregnancy more likely.
Neel Shah, MD, an endocrinologist and associate professor at the University of Texas Health Science Center at Houston, said he has had several patients become pregnant without intending to.
“It was when Mounjaro came out on the market when we started using it,” he said of the drug the Food and Drug Administration approved for type 2 diabetes in 2022. “It [the warning] was in the product insert, but clinically speaking, I don’t know if it was at the top of providers’ minds when they were prescribing Mounjaro.”
When asked if he believed that we were going to be seeing a significant increase in so-called Mounjaro babies, Dr. Shah was sure in his response.
“Absolutely. We will because the sheer volume [of patients] will increase,” he said.
It’s all in the gut
One of the ways that drugs like Mounjaro work is by delaying the time that it takes for food to move from the stomach to the small intestine. Although data are still evolving, it is believed that this process – delayed gastric emptying – may affect the absorption of birth control pills.
Dr. Shah said another theory is that vomiting, which is a common side effect of these types of drugs, also affects the pills’ ability to prevent pregnancy.
And “there’s a prolonged period of ramping up the dose because of the GI side effects,” said Pinar Kodaman, MD, PhD, a reproductive endocrinologist and assistant professor of gynecology at Yale University in New Haven, Conn.
“Initially, at the lowest dose, there may not be a lot of potential effect on absorption and gastric emptying. But as the dose goes up, it becomes more common, and it can cause diarrhea, which is another condition that can affect the absorption of any medication,” she said.
Unanticipated outcomes, extra prevention
Roughly 42% of women in the United States are obese, 40% of whom are between the ages of 20 and 39. Although these new drugs can improve fertility outcomes for women who are obese (especially those with polycystic ovary syndrome, or PCOS), only one – Mounjaro – currently carries a warning about birth control pill effectiveness on its label. Unfortunately, it appears that some doctors are unaware or not counseling patients about this risk, and the data are unclear about whether other drugs in this class, like Ozempic and Wegovy, have the same risks.
“To date, it hasn’t been a typical thing that we counsel about,” said Dr. Kodaman. “It’s all fairly new, but when we have patients on birth control pills, we do review other medications that they are on because some can affect efficacy, and it’s something to keep in mind.”
It’s also unclear if other forms of birth control – for example, birth control patches that deliver through the skin – might carry similar pregnancy risks. Dr. Shah said some of his patients who became pregnant without intending to were using these patches. This raises even more questions, since they deliver drugs through the skin directly into the bloodstream and not through the GI system.
What can women do to help ensure that they don’t become pregnant while using these drugs?
“I really think that if patients want to protect themselves from an unplanned pregnancy, that as soon as they start the GLP receptor agonists, it wouldn’t be a bad idea to use condoms, because the onset of action is pretty quick,” said Dr. Kodaman, noting also that “at the lowest dose there may not be a lot of potential effect on gastric emptying. But as the dose goes up, it becomes much more common or can cause diarrhea.”
Dr. Shah said that in his practice he’s “been telling patients to add barrier contraception” 4 weeks before they start their first dose “and at any dose adjustment.”
Zoobia Chaudhry, an obesity medicine doctor and assistant professor of medicine at Johns Hopkins University in Baltimore, recommends that “patients just make sure that the injection and medication that they take are at least 1 hour apart.”
“Most of the time, patients do take birth control before bedtime, so if the two are spaced, it should be OK,” she said.
Another option is for women to speak to their doctors about other contraceptive options like IUDs or implantable rods, where gastric absorption is not going to be an issue.
“There’s very little research on this class of drugs,” said Emily Goodstein, a 40-year-old small-business owner in Washington, who recently switched from Ozempic to Mounjaro. “Being a person who lives in a larger body is such a horrifying experience because of the way that the world discriminates against you.”
She appreciates the feeling of being proactive that these new drugs grant. It has “opened up a bunch of opportunities for me to be seen as a full individual by the medical establishment,” she said. “I was willing to take the risk, knowing that I would be on these drugs for the rest of my life.”
In addition to being what Dr. Goodstein refers to as a guinea pig, she said she made sure that her primary care doctor was aware that she was not trying or planning to become pregnant again. (She has a 3-year-old child.) Still, her doctor mentioned only the most common side effects linked to these drugs, like nausea, vomiting, and diarrhea, and did not mention the risk of pregnancy.
“Folks are really not talking about the reproductive implications,” she said, referring to members of a Facebook group on these drugs that she belongs to.
Like patients themselves, many doctors are just beginning to get their arms around these agents. “Awareness, education, provider involvement, and having a multidisciplinary team could help patients achieve the goals that they set out for themselves,” said Dr. Shah.
Clear conversations are key.
A version of this article first appeared on WebMD.com.
For women who are obese, daily life is wrought with landmines. Whether it’s the challenges of air travel because plane seats are too small, the need to shield themselves from the world’s discriminating eyes, or the great lengths many will go to achieve better health and the promise of longevity, navigating life as an obese person requires a thick skin.
So, it’s no wonder so many are willing to pay more than $1,000 a month out of pocket to get their hands on drugs like semaglutide (Ozempic and Wegovy) or tirzepatide (Mounjaro). The benefits of these drugs, which are part of a new class called glucagonlike peptide–1 (GLP-1) receptor agonists, include significant and rapid weight loss, blood sugar control, and improved life quality; they are unprecedented in a setting where surgery has long been considered the most effective long-term option.
On the flip side, the desire for rapid weight loss and better blood sugar control also comes with an unexpected cost. , making an unintended pregnancy more likely.
Neel Shah, MD, an endocrinologist and associate professor at the University of Texas Health Science Center at Houston, said he has had several patients become pregnant without intending to.
“It was when Mounjaro came out on the market when we started using it,” he said of the drug the Food and Drug Administration approved for type 2 diabetes in 2022. “It [the warning] was in the product insert, but clinically speaking, I don’t know if it was at the top of providers’ minds when they were prescribing Mounjaro.”
When asked if he believed that we were going to be seeing a significant increase in so-called Mounjaro babies, Dr. Shah was sure in his response.
“Absolutely. We will because the sheer volume [of patients] will increase,” he said.
It’s all in the gut
One of the ways that drugs like Mounjaro work is by delaying the time that it takes for food to move from the stomach to the small intestine. Although data are still evolving, it is believed that this process – delayed gastric emptying – may affect the absorption of birth control pills.
Dr. Shah said another theory is that vomiting, which is a common side effect of these types of drugs, also affects the pills’ ability to prevent pregnancy.
And “there’s a prolonged period of ramping up the dose because of the GI side effects,” said Pinar Kodaman, MD, PhD, a reproductive endocrinologist and assistant professor of gynecology at Yale University in New Haven, Conn.
“Initially, at the lowest dose, there may not be a lot of potential effect on absorption and gastric emptying. But as the dose goes up, it becomes more common, and it can cause diarrhea, which is another condition that can affect the absorption of any medication,” she said.
Unanticipated outcomes, extra prevention
Roughly 42% of women in the United States are obese, 40% of whom are between the ages of 20 and 39. Although these new drugs can improve fertility outcomes for women who are obese (especially those with polycystic ovary syndrome, or PCOS), only one – Mounjaro – currently carries a warning about birth control pill effectiveness on its label. Unfortunately, it appears that some doctors are unaware or not counseling patients about this risk, and the data are unclear about whether other drugs in this class, like Ozempic and Wegovy, have the same risks.
“To date, it hasn’t been a typical thing that we counsel about,” said Dr. Kodaman. “It’s all fairly new, but when we have patients on birth control pills, we do review other medications that they are on because some can affect efficacy, and it’s something to keep in mind.”
It’s also unclear if other forms of birth control – for example, birth control patches that deliver through the skin – might carry similar pregnancy risks. Dr. Shah said some of his patients who became pregnant without intending to were using these patches. This raises even more questions, since they deliver drugs through the skin directly into the bloodstream and not through the GI system.
What can women do to help ensure that they don’t become pregnant while using these drugs?
“I really think that if patients want to protect themselves from an unplanned pregnancy, that as soon as they start the GLP receptor agonists, it wouldn’t be a bad idea to use condoms, because the onset of action is pretty quick,” said Dr. Kodaman, noting also that “at the lowest dose there may not be a lot of potential effect on gastric emptying. But as the dose goes up, it becomes much more common or can cause diarrhea.”
Dr. Shah said that in his practice he’s “been telling patients to add barrier contraception” 4 weeks before they start their first dose “and at any dose adjustment.”
Zoobia Chaudhry, an obesity medicine doctor and assistant professor of medicine at Johns Hopkins University in Baltimore, recommends that “patients just make sure that the injection and medication that they take are at least 1 hour apart.”
“Most of the time, patients do take birth control before bedtime, so if the two are spaced, it should be OK,” she said.
Another option is for women to speak to their doctors about other contraceptive options like IUDs or implantable rods, where gastric absorption is not going to be an issue.
“There’s very little research on this class of drugs,” said Emily Goodstein, a 40-year-old small-business owner in Washington, who recently switched from Ozempic to Mounjaro. “Being a person who lives in a larger body is such a horrifying experience because of the way that the world discriminates against you.”
She appreciates the feeling of being proactive that these new drugs grant. It has “opened up a bunch of opportunities for me to be seen as a full individual by the medical establishment,” she said. “I was willing to take the risk, knowing that I would be on these drugs for the rest of my life.”
In addition to being what Dr. Goodstein refers to as a guinea pig, she said she made sure that her primary care doctor was aware that she was not trying or planning to become pregnant again. (She has a 3-year-old child.) Still, her doctor mentioned only the most common side effects linked to these drugs, like nausea, vomiting, and diarrhea, and did not mention the risk of pregnancy.
“Folks are really not talking about the reproductive implications,” she said, referring to members of a Facebook group on these drugs that she belongs to.
Like patients themselves, many doctors are just beginning to get their arms around these agents. “Awareness, education, provider involvement, and having a multidisciplinary team could help patients achieve the goals that they set out for themselves,” said Dr. Shah.
Clear conversations are key.
A version of this article first appeared on WebMD.com.
Testosterone replacement benefits men with type 2 diabetes
HAMBURG, GERMANY – Testosterone replacement therapy was associated with significant reductions in hemoglobin A1c at 1 and 2 years among men with type 2 diabetes, a multinational audit shows.
“If you have a patient with type 2 diabetes, sexual dysfunction, or fatigue, please consider checking their testosterone level. And if they fulfill criteria for testosterone deficiency and have had their [prostate-specific antigen] checked, consider a trial of treatment and follow them,” study lead author T. Hugh Jones, MD, consultant physician and endocrinologist at Barnsley (England) Hospital NHS Foundation Trust advised, speaking with this news organization.
Dr. Jones also urges clinicians worldwide to enter their patients’ data into the ABCD Testosterone Audit, which aims to identify long-term outcomes and predictors of response to testosterone replacement therapy.
Dr. Jones, who is also professor of andrology at the University of Sheffield, presented the preliminary data analysis at the annual meeting of the European Association for the Study of Diabetes.
Thus far, a total of 428 men with type 2 diabetes and hypogonadism are entered into the audit, from 34 centers in eight countries: the United Kingdom, Germany, Canada, Brazil, South Africa, New Zealand, Malaysia, and Vietnam. Among 121 of the men at 12 months, there was a drop in A1c from a baseline level of 71.27 mmol/mol (8.7%) to 61.26 mmol/mol (7.8%). Among 104 men at 24 months, the drop was from 71.4 mmol/mol (8.7%) to 55.97 mmol/mol (7.3%). Both decreases were significant (P < .001).
Prior data from Dr. Jones’ group showed that about 40% of men with type 2 diabetes have symptomatic testosterone deficiency. Testosterone deficiency is also associated with adverse effects on cardiovascular risk factors, bone health, muscle strength, sexual function, and psychological well-being, yet it is often overlooked, Dr. Jones noted.
“It’s not typically measured in routine clinical practice. ... Deficiency is very common, but a lot of practitioners don’t treat it and don’t ask about it. But in fact, treatment has very significant benefits for patients. ... We know from sildenafil (Viagra) studies that 60%of people who didn’t respond were testosterone deficient. After being given testosterone, they converted to Viagra responders,” he noted.
Regarding safety concerns, the recent findings from the TRAVERSE study, in which about 70% of participants had type 2 diabetes, demonstrated no increased cardiovascular risk. There was also no association with prostate cancer, although it’s important to monitor prostate-specific antigen in patients for the first year on testosterone replacement, Dr. Jones said.
Asked to comment, endocrinologist Bradley D. Anawalt, MD, chief of medicine at the University of Washington Medical Center, Seattle, told this news organization, “This ‘worldwide survey’ confirms many studies from around the world over the past 20 years. ... [T]he association is due to ‘reverse causation,’ in that diabetes type 2 and obesity lower testosterone concentrations. Weight loss of 5%-10% may raise testosterone concentrations in men with high body mass indices, large waist circumferences, and low blood testosterone concentrations.”
At the same time, Dr. Anawalt pointed to data suggesting that “[t]reatment of androgen deficiency may facilitate lifestyle measures in men with high [body mass indexes] and high risk of type 2 diabetes to prevent, or more likely delay, the development of type 2 diabetes.”
However, both Dr. Jones and Dr. Anawalt emphasized that testosterone therapy would not be expected to affect blood glucose levels or any other cardiometabolic parameters in men who are not testosterone deficient, regardless of diabetes status.
“It’s important when you give testosterone to replace it to the normal level. Adequate treatment gives the greatest benefit,”Dr. Jones said.
As more centers contribute data to the ABCD audit, Jones anticipates collecting clinical practice data on a variety of clinical parameters, including complications, total insulin dose, kidney function, and eventually cardiovascular outcomes.
In the meantime, he said, giving testosterone replacement to men with deficiency can be very rewarding for many reasons. “People feel better. Individual patients come back and say ‘thank you doctor, you’ve given me my life back.’ It’s not often you get that. And the compliance is excellent.”
Dr. Jones is a speaker for, advisory board member for, and/or travel grant recipient of Besins Healthcare, Grantss, Grunenthal, and Simple Pharma. Dr. Anawalt has no disclosures.
A version of this article first appeared on Medscape.com.
HAMBURG, GERMANY – Testosterone replacement therapy was associated with significant reductions in hemoglobin A1c at 1 and 2 years among men with type 2 diabetes, a multinational audit shows.
“If you have a patient with type 2 diabetes, sexual dysfunction, or fatigue, please consider checking their testosterone level. And if they fulfill criteria for testosterone deficiency and have had their [prostate-specific antigen] checked, consider a trial of treatment and follow them,” study lead author T. Hugh Jones, MD, consultant physician and endocrinologist at Barnsley (England) Hospital NHS Foundation Trust advised, speaking with this news organization.
Dr. Jones also urges clinicians worldwide to enter their patients’ data into the ABCD Testosterone Audit, which aims to identify long-term outcomes and predictors of response to testosterone replacement therapy.
Dr. Jones, who is also professor of andrology at the University of Sheffield, presented the preliminary data analysis at the annual meeting of the European Association for the Study of Diabetes.
Thus far, a total of 428 men with type 2 diabetes and hypogonadism are entered into the audit, from 34 centers in eight countries: the United Kingdom, Germany, Canada, Brazil, South Africa, New Zealand, Malaysia, and Vietnam. Among 121 of the men at 12 months, there was a drop in A1c from a baseline level of 71.27 mmol/mol (8.7%) to 61.26 mmol/mol (7.8%). Among 104 men at 24 months, the drop was from 71.4 mmol/mol (8.7%) to 55.97 mmol/mol (7.3%). Both decreases were significant (P < .001).
Prior data from Dr. Jones’ group showed that about 40% of men with type 2 diabetes have symptomatic testosterone deficiency. Testosterone deficiency is also associated with adverse effects on cardiovascular risk factors, bone health, muscle strength, sexual function, and psychological well-being, yet it is often overlooked, Dr. Jones noted.
“It’s not typically measured in routine clinical practice. ... Deficiency is very common, but a lot of practitioners don’t treat it and don’t ask about it. But in fact, treatment has very significant benefits for patients. ... We know from sildenafil (Viagra) studies that 60%of people who didn’t respond were testosterone deficient. After being given testosterone, they converted to Viagra responders,” he noted.
Regarding safety concerns, the recent findings from the TRAVERSE study, in which about 70% of participants had type 2 diabetes, demonstrated no increased cardiovascular risk. There was also no association with prostate cancer, although it’s important to monitor prostate-specific antigen in patients for the first year on testosterone replacement, Dr. Jones said.
Asked to comment, endocrinologist Bradley D. Anawalt, MD, chief of medicine at the University of Washington Medical Center, Seattle, told this news organization, “This ‘worldwide survey’ confirms many studies from around the world over the past 20 years. ... [T]he association is due to ‘reverse causation,’ in that diabetes type 2 and obesity lower testosterone concentrations. Weight loss of 5%-10% may raise testosterone concentrations in men with high body mass indices, large waist circumferences, and low blood testosterone concentrations.”
At the same time, Dr. Anawalt pointed to data suggesting that “[t]reatment of androgen deficiency may facilitate lifestyle measures in men with high [body mass indexes] and high risk of type 2 diabetes to prevent, or more likely delay, the development of type 2 diabetes.”
However, both Dr. Jones and Dr. Anawalt emphasized that testosterone therapy would not be expected to affect blood glucose levels or any other cardiometabolic parameters in men who are not testosterone deficient, regardless of diabetes status.
“It’s important when you give testosterone to replace it to the normal level. Adequate treatment gives the greatest benefit,”Dr. Jones said.
As more centers contribute data to the ABCD audit, Jones anticipates collecting clinical practice data on a variety of clinical parameters, including complications, total insulin dose, kidney function, and eventually cardiovascular outcomes.
In the meantime, he said, giving testosterone replacement to men with deficiency can be very rewarding for many reasons. “People feel better. Individual patients come back and say ‘thank you doctor, you’ve given me my life back.’ It’s not often you get that. And the compliance is excellent.”
Dr. Jones is a speaker for, advisory board member for, and/or travel grant recipient of Besins Healthcare, Grantss, Grunenthal, and Simple Pharma. Dr. Anawalt has no disclosures.
A version of this article first appeared on Medscape.com.
HAMBURG, GERMANY – Testosterone replacement therapy was associated with significant reductions in hemoglobin A1c at 1 and 2 years among men with type 2 diabetes, a multinational audit shows.
“If you have a patient with type 2 diabetes, sexual dysfunction, or fatigue, please consider checking their testosterone level. And if they fulfill criteria for testosterone deficiency and have had their [prostate-specific antigen] checked, consider a trial of treatment and follow them,” study lead author T. Hugh Jones, MD, consultant physician and endocrinologist at Barnsley (England) Hospital NHS Foundation Trust advised, speaking with this news organization.
Dr. Jones also urges clinicians worldwide to enter their patients’ data into the ABCD Testosterone Audit, which aims to identify long-term outcomes and predictors of response to testosterone replacement therapy.
Dr. Jones, who is also professor of andrology at the University of Sheffield, presented the preliminary data analysis at the annual meeting of the European Association for the Study of Diabetes.
Thus far, a total of 428 men with type 2 diabetes and hypogonadism are entered into the audit, from 34 centers in eight countries: the United Kingdom, Germany, Canada, Brazil, South Africa, New Zealand, Malaysia, and Vietnam. Among 121 of the men at 12 months, there was a drop in A1c from a baseline level of 71.27 mmol/mol (8.7%) to 61.26 mmol/mol (7.8%). Among 104 men at 24 months, the drop was from 71.4 mmol/mol (8.7%) to 55.97 mmol/mol (7.3%). Both decreases were significant (P < .001).
Prior data from Dr. Jones’ group showed that about 40% of men with type 2 diabetes have symptomatic testosterone deficiency. Testosterone deficiency is also associated with adverse effects on cardiovascular risk factors, bone health, muscle strength, sexual function, and psychological well-being, yet it is often overlooked, Dr. Jones noted.
“It’s not typically measured in routine clinical practice. ... Deficiency is very common, but a lot of practitioners don’t treat it and don’t ask about it. But in fact, treatment has very significant benefits for patients. ... We know from sildenafil (Viagra) studies that 60%of people who didn’t respond were testosterone deficient. After being given testosterone, they converted to Viagra responders,” he noted.
Regarding safety concerns, the recent findings from the TRAVERSE study, in which about 70% of participants had type 2 diabetes, demonstrated no increased cardiovascular risk. There was also no association with prostate cancer, although it’s important to monitor prostate-specific antigen in patients for the first year on testosterone replacement, Dr. Jones said.
Asked to comment, endocrinologist Bradley D. Anawalt, MD, chief of medicine at the University of Washington Medical Center, Seattle, told this news organization, “This ‘worldwide survey’ confirms many studies from around the world over the past 20 years. ... [T]he association is due to ‘reverse causation,’ in that diabetes type 2 and obesity lower testosterone concentrations. Weight loss of 5%-10% may raise testosterone concentrations in men with high body mass indices, large waist circumferences, and low blood testosterone concentrations.”
At the same time, Dr. Anawalt pointed to data suggesting that “[t]reatment of androgen deficiency may facilitate lifestyle measures in men with high [body mass indexes] and high risk of type 2 diabetes to prevent, or more likely delay, the development of type 2 diabetes.”
However, both Dr. Jones and Dr. Anawalt emphasized that testosterone therapy would not be expected to affect blood glucose levels or any other cardiometabolic parameters in men who are not testosterone deficient, regardless of diabetes status.
“It’s important when you give testosterone to replace it to the normal level. Adequate treatment gives the greatest benefit,”Dr. Jones said.
As more centers contribute data to the ABCD audit, Jones anticipates collecting clinical practice data on a variety of clinical parameters, including complications, total insulin dose, kidney function, and eventually cardiovascular outcomes.
In the meantime, he said, giving testosterone replacement to men with deficiency can be very rewarding for many reasons. “People feel better. Individual patients come back and say ‘thank you doctor, you’ve given me my life back.’ It’s not often you get that. And the compliance is excellent.”
Dr. Jones is a speaker for, advisory board member for, and/or travel grant recipient of Besins Healthcare, Grantss, Grunenthal, and Simple Pharma. Dr. Anawalt has no disclosures.
A version of this article first appeared on Medscape.com.
AT EASD 2023
Debate: Is lasting remission of type 2 diabetes feasible in the real-world setting?
The prospect of remission of type 2 diabetes (T2D) has captured the hearts and minds of many patients with T2D and health care professionals, including myself.
I have changed my narrative when supporting my patients with T2D. I used to say that T2D is a progressive condition, but considering seminal recent evidence like the DiRECT trial, I now say that T2D can be a progressive condition. Through significant weight loss, patients can reverse it and achieve remission of T2D. This has given my patients hope that their T2D is no longer an inexorable condition. And hope, of course, is a powerful enabler of change.
However,
I therefore relished the opportunity to attend a debate on this topic at the annual meeting of the European Association for the Study of Diabetes in Hamburg, Germany, between Roy Taylor, MD, principal investigator for the DiRECT study and professor of medicine and metabolism at the University of Newcastle, England, and Kamlesh Khunti, MD, PhD, professor of primary care diabetes at the University of Leicester, England.
Remarkable weight loss
Dr. Taylor powerfully recapitulated the initial results of the DiRECT study. T2D remission was achieved in 46% of participants who underwent a low-energy formula diet (around 850 calories daily) for 3-5 months. After 2 years’ follow-up, an impressive 36% of participants were still in remission. Dr. Taylor then discussed unpublished 5-year extension follow-up data of the DiRECT study. Average weight loss in the remaining intervention group was 6.1 kg. I echo Taylor’s sentiment that this finding is remarkable in the context of a dietary study.
Overall, 13% of participants were still in remission, and this cohort maintained an average weight loss of 8.9 kg. Dr. Taylor concluded that lasting remission of T2D is indeed feasible in a primary care setting.
Yet he acknowledged that although remission appears feasible in the longer term, it was not necessarily easy, or indeed possible, for everyone. He used a wonderful analogy about climbing Mount Everest: It is feasible, but not everyone can or wants to climb it. And even if you try, you might not reach the top.
This analogy perfectly encapsulates the challenges I have observed when my patients have striven for T2D remission. In my opinion, intensive weight management with a low-energy formula diet is not a panacea for T2D but another tool in our toolbox to offer patients.
He also described some “jaw-dropping” results regarding incidence of cancer: There were no cases of cancer in the intervention group during the 5-year period, but there were eight cases of cancer in the control group. The latter figure is consistent with published data for cancer incidence in patients with T2D and the body mass index (BMI) inclusion criteria for the DiRECT study (a BMI of 27-45 kg/m2). Obesity is an established risk factor for 13 types of cancer, and excess body fat entails an approximately 17% increased risk for cancer-specific mortality. This indeed is a powerful motivator to facilitate meaningful lifestyle change.
In primary care, we also need to be aware that most weight regain usually occurs secondary to a life event (for example, financial, family, or illness). We should reiterate to our patients that weight regain is not a failure; it is just part of life. Once the life event has passed, rapid weight loss can be attempted again. In the “rescue plans” that were integral to the DiRECT study, participants were offered further periods of total diet replacement, depending on quantity of weight gain. In fact, 50% of participants in DiRECT required rescue therapy, and their outcomes, reassuringly, were the same as the other 50%.
Dr. Taylor also quoted data from the ReTUNE study suggesting that weight regain was less of an issue for those with initial BMI of 21-27, and there is “more bang for your buck” in approaching remission of T2D in patients with lower BMI. The fact that people with normal or near-normal BMI can also reverse their T2D was also a game changer for my clinical practice; the concept of an individual or personal fat threshold that results in T2D offers a pragmatic explanation to patients with T2D who are frustrated by the lack of improvements in cardiometabolic parameters despite significant weight loss.
Finally, Dr. Taylor acknowledged the breadth of the definition of T2D remission: A1c < 48 mmol/mol at least 2 months off all antidiabetic medication. This definition includes A1c values within the “prediabetes” range: 42-47 mmol/mol.
He cited 10-year cardiovascular risk data driven by hypertension and dyslipidemia before significant weight loss and compared it with 10-year cardiovascular risk data after significant weight loss. Cardiovascular risk profile was more favorable after weight loss, compared with controls with prediabetes without weight loss, even though some of the intervention group who lost significant weight still had an A1c of 42-47 mmol/mol. Dr. Taylor suggested that we not label these individuals who have lost significant weight as having prediabetes. Instead “postdiabetes” should be preferred, because these patients had more favorable cardiovascular profiles.
This is a very important take-home message for primary care: prediabetes is more than just dysglycemia.
New terminology proposed
Dr. Khunti outlined a recent large, systematic review that concluded that the definition of T2D remission encompassed substantial heterogeneity. This heterogeneity complicates the interpretation of previous research on T2D remission and complicates the implementation of remission pathways into routine clinical practice. Furthermore, Dr. Khunti highlighted a recent consensus report on the definition and interpretation of remission in T2D that explicitly stated that the underlying pathophysiology of T2D is rarely normalized completely by interventions, thus reducing the possibility of lasting remission.
Dr. Khunti also challenged the cardiovascular benefits seen after T2D remission. Recent Danish registry data were presented, demonstrating a twofold increased risk for major adverse cardiovascular events over 5 years in individuals who achieved remission of T2D, but not on glucose-lowering drug therapy.
Adherence to strict dietary interventions in the longer term was also addressed. Diet-induced weight loss causes changes in circulating hormones such as ghrelin, glucose-dependent insulinotropic polypeptide (GIP), and leptin, which mediate appetite and drive hunger and an increased preference for energy-dense foods (that is, high-fat or sugary foods), all of which encourage weight regain. Dr. Khunti suggested that other interventions, such as glucagon-like peptide 1 (GLP-1) receptor agonists or bariatric surgery, specifically target some of these hormonal responses.
The challenges in recruitment and retention for lifestyle studies were also discussed; they reflect the challenges of behavioral programs in primary care. The DiRECT study had 20% participation of screened candidates and an attrition rate approaching 30%. The seminal Diabetes Prevention Program study and Finnish Diabetes Prevention Study had similar results. At a population level, individuals do not appear to want to participate in behavioral programs.
Dr. Khunti also warned that the review of annual care processes for diabetes is declining for patients who had achieved remission, possibly because of a false sense of reassurance among health care professionals. It is essential that all those in remission remain under at least annual follow-up, because there is still a risk for future microvascular and macrovascular complications, especially in the event of weight regain.
Dr. Khunti concluded by proposing new terminology for remission: remission of hyperglycemia or euglycemia, aiming for A1c < 48 mmol/mol with or without glucose-lowering therapy. I do agree with this; it reflects the zeitgeist of cardiorenal protective diabetes therapies and is analogous to rheumatoid arthritis, where remission is defined as no disease activity while on therapy. But one size does not fit all.
Sir William Osler’s words provide a fitting conclusion: “If it were not for the great variability among individuals, medicine might as well be a science and not an art.”
Dr. Fernando has disclosed that he has received speakers’ fees from Eli Lilly and Novo Nordisk.
Dr. Fernando is a general practitioner near Edinburgh, with a specialist interest in diabetes; cardiovascular, renal, and metabolic diseases; and medical education.
A version of this article first appeared on Medscape.com.
The prospect of remission of type 2 diabetes (T2D) has captured the hearts and minds of many patients with T2D and health care professionals, including myself.
I have changed my narrative when supporting my patients with T2D. I used to say that T2D is a progressive condition, but considering seminal recent evidence like the DiRECT trial, I now say that T2D can be a progressive condition. Through significant weight loss, patients can reverse it and achieve remission of T2D. This has given my patients hope that their T2D is no longer an inexorable condition. And hope, of course, is a powerful enabler of change.
However,
I therefore relished the opportunity to attend a debate on this topic at the annual meeting of the European Association for the Study of Diabetes in Hamburg, Germany, between Roy Taylor, MD, principal investigator for the DiRECT study and professor of medicine and metabolism at the University of Newcastle, England, and Kamlesh Khunti, MD, PhD, professor of primary care diabetes at the University of Leicester, England.
Remarkable weight loss
Dr. Taylor powerfully recapitulated the initial results of the DiRECT study. T2D remission was achieved in 46% of participants who underwent a low-energy formula diet (around 850 calories daily) for 3-5 months. After 2 years’ follow-up, an impressive 36% of participants were still in remission. Dr. Taylor then discussed unpublished 5-year extension follow-up data of the DiRECT study. Average weight loss in the remaining intervention group was 6.1 kg. I echo Taylor’s sentiment that this finding is remarkable in the context of a dietary study.
Overall, 13% of participants were still in remission, and this cohort maintained an average weight loss of 8.9 kg. Dr. Taylor concluded that lasting remission of T2D is indeed feasible in a primary care setting.
Yet he acknowledged that although remission appears feasible in the longer term, it was not necessarily easy, or indeed possible, for everyone. He used a wonderful analogy about climbing Mount Everest: It is feasible, but not everyone can or wants to climb it. And even if you try, you might not reach the top.
This analogy perfectly encapsulates the challenges I have observed when my patients have striven for T2D remission. In my opinion, intensive weight management with a low-energy formula diet is not a panacea for T2D but another tool in our toolbox to offer patients.
He also described some “jaw-dropping” results regarding incidence of cancer: There were no cases of cancer in the intervention group during the 5-year period, but there were eight cases of cancer in the control group. The latter figure is consistent with published data for cancer incidence in patients with T2D and the body mass index (BMI) inclusion criteria for the DiRECT study (a BMI of 27-45 kg/m2). Obesity is an established risk factor for 13 types of cancer, and excess body fat entails an approximately 17% increased risk for cancer-specific mortality. This indeed is a powerful motivator to facilitate meaningful lifestyle change.
In primary care, we also need to be aware that most weight regain usually occurs secondary to a life event (for example, financial, family, or illness). We should reiterate to our patients that weight regain is not a failure; it is just part of life. Once the life event has passed, rapid weight loss can be attempted again. In the “rescue plans” that were integral to the DiRECT study, participants were offered further periods of total diet replacement, depending on quantity of weight gain. In fact, 50% of participants in DiRECT required rescue therapy, and their outcomes, reassuringly, were the same as the other 50%.
Dr. Taylor also quoted data from the ReTUNE study suggesting that weight regain was less of an issue for those with initial BMI of 21-27, and there is “more bang for your buck” in approaching remission of T2D in patients with lower BMI. The fact that people with normal or near-normal BMI can also reverse their T2D was also a game changer for my clinical practice; the concept of an individual or personal fat threshold that results in T2D offers a pragmatic explanation to patients with T2D who are frustrated by the lack of improvements in cardiometabolic parameters despite significant weight loss.
Finally, Dr. Taylor acknowledged the breadth of the definition of T2D remission: A1c < 48 mmol/mol at least 2 months off all antidiabetic medication. This definition includes A1c values within the “prediabetes” range: 42-47 mmol/mol.
He cited 10-year cardiovascular risk data driven by hypertension and dyslipidemia before significant weight loss and compared it with 10-year cardiovascular risk data after significant weight loss. Cardiovascular risk profile was more favorable after weight loss, compared with controls with prediabetes without weight loss, even though some of the intervention group who lost significant weight still had an A1c of 42-47 mmol/mol. Dr. Taylor suggested that we not label these individuals who have lost significant weight as having prediabetes. Instead “postdiabetes” should be preferred, because these patients had more favorable cardiovascular profiles.
This is a very important take-home message for primary care: prediabetes is more than just dysglycemia.
New terminology proposed
Dr. Khunti outlined a recent large, systematic review that concluded that the definition of T2D remission encompassed substantial heterogeneity. This heterogeneity complicates the interpretation of previous research on T2D remission and complicates the implementation of remission pathways into routine clinical practice. Furthermore, Dr. Khunti highlighted a recent consensus report on the definition and interpretation of remission in T2D that explicitly stated that the underlying pathophysiology of T2D is rarely normalized completely by interventions, thus reducing the possibility of lasting remission.
Dr. Khunti also challenged the cardiovascular benefits seen after T2D remission. Recent Danish registry data were presented, demonstrating a twofold increased risk for major adverse cardiovascular events over 5 years in individuals who achieved remission of T2D, but not on glucose-lowering drug therapy.
Adherence to strict dietary interventions in the longer term was also addressed. Diet-induced weight loss causes changes in circulating hormones such as ghrelin, glucose-dependent insulinotropic polypeptide (GIP), and leptin, which mediate appetite and drive hunger and an increased preference for energy-dense foods (that is, high-fat or sugary foods), all of which encourage weight regain. Dr. Khunti suggested that other interventions, such as glucagon-like peptide 1 (GLP-1) receptor agonists or bariatric surgery, specifically target some of these hormonal responses.
The challenges in recruitment and retention for lifestyle studies were also discussed; they reflect the challenges of behavioral programs in primary care. The DiRECT study had 20% participation of screened candidates and an attrition rate approaching 30%. The seminal Diabetes Prevention Program study and Finnish Diabetes Prevention Study had similar results. At a population level, individuals do not appear to want to participate in behavioral programs.
Dr. Khunti also warned that the review of annual care processes for diabetes is declining for patients who had achieved remission, possibly because of a false sense of reassurance among health care professionals. It is essential that all those in remission remain under at least annual follow-up, because there is still a risk for future microvascular and macrovascular complications, especially in the event of weight regain.
Dr. Khunti concluded by proposing new terminology for remission: remission of hyperglycemia or euglycemia, aiming for A1c < 48 mmol/mol with or without glucose-lowering therapy. I do agree with this; it reflects the zeitgeist of cardiorenal protective diabetes therapies and is analogous to rheumatoid arthritis, where remission is defined as no disease activity while on therapy. But one size does not fit all.
Sir William Osler’s words provide a fitting conclusion: “If it were not for the great variability among individuals, medicine might as well be a science and not an art.”
Dr. Fernando has disclosed that he has received speakers’ fees from Eli Lilly and Novo Nordisk.
Dr. Fernando is a general practitioner near Edinburgh, with a specialist interest in diabetes; cardiovascular, renal, and metabolic diseases; and medical education.
A version of this article first appeared on Medscape.com.
The prospect of remission of type 2 diabetes (T2D) has captured the hearts and minds of many patients with T2D and health care professionals, including myself.
I have changed my narrative when supporting my patients with T2D. I used to say that T2D is a progressive condition, but considering seminal recent evidence like the DiRECT trial, I now say that T2D can be a progressive condition. Through significant weight loss, patients can reverse it and achieve remission of T2D. This has given my patients hope that their T2D is no longer an inexorable condition. And hope, of course, is a powerful enabler of change.
However,
I therefore relished the opportunity to attend a debate on this topic at the annual meeting of the European Association for the Study of Diabetes in Hamburg, Germany, between Roy Taylor, MD, principal investigator for the DiRECT study and professor of medicine and metabolism at the University of Newcastle, England, and Kamlesh Khunti, MD, PhD, professor of primary care diabetes at the University of Leicester, England.
Remarkable weight loss
Dr. Taylor powerfully recapitulated the initial results of the DiRECT study. T2D remission was achieved in 46% of participants who underwent a low-energy formula diet (around 850 calories daily) for 3-5 months. After 2 years’ follow-up, an impressive 36% of participants were still in remission. Dr. Taylor then discussed unpublished 5-year extension follow-up data of the DiRECT study. Average weight loss in the remaining intervention group was 6.1 kg. I echo Taylor’s sentiment that this finding is remarkable in the context of a dietary study.
Overall, 13% of participants were still in remission, and this cohort maintained an average weight loss of 8.9 kg. Dr. Taylor concluded that lasting remission of T2D is indeed feasible in a primary care setting.
Yet he acknowledged that although remission appears feasible in the longer term, it was not necessarily easy, or indeed possible, for everyone. He used a wonderful analogy about climbing Mount Everest: It is feasible, but not everyone can or wants to climb it. And even if you try, you might not reach the top.
This analogy perfectly encapsulates the challenges I have observed when my patients have striven for T2D remission. In my opinion, intensive weight management with a low-energy formula diet is not a panacea for T2D but another tool in our toolbox to offer patients.
He also described some “jaw-dropping” results regarding incidence of cancer: There were no cases of cancer in the intervention group during the 5-year period, but there were eight cases of cancer in the control group. The latter figure is consistent with published data for cancer incidence in patients with T2D and the body mass index (BMI) inclusion criteria for the DiRECT study (a BMI of 27-45 kg/m2). Obesity is an established risk factor for 13 types of cancer, and excess body fat entails an approximately 17% increased risk for cancer-specific mortality. This indeed is a powerful motivator to facilitate meaningful lifestyle change.
In primary care, we also need to be aware that most weight regain usually occurs secondary to a life event (for example, financial, family, or illness). We should reiterate to our patients that weight regain is not a failure; it is just part of life. Once the life event has passed, rapid weight loss can be attempted again. In the “rescue plans” that were integral to the DiRECT study, participants were offered further periods of total diet replacement, depending on quantity of weight gain. In fact, 50% of participants in DiRECT required rescue therapy, and their outcomes, reassuringly, were the same as the other 50%.
Dr. Taylor also quoted data from the ReTUNE study suggesting that weight regain was less of an issue for those with initial BMI of 21-27, and there is “more bang for your buck” in approaching remission of T2D in patients with lower BMI. The fact that people with normal or near-normal BMI can also reverse their T2D was also a game changer for my clinical practice; the concept of an individual or personal fat threshold that results in T2D offers a pragmatic explanation to patients with T2D who are frustrated by the lack of improvements in cardiometabolic parameters despite significant weight loss.
Finally, Dr. Taylor acknowledged the breadth of the definition of T2D remission: A1c < 48 mmol/mol at least 2 months off all antidiabetic medication. This definition includes A1c values within the “prediabetes” range: 42-47 mmol/mol.
He cited 10-year cardiovascular risk data driven by hypertension and dyslipidemia before significant weight loss and compared it with 10-year cardiovascular risk data after significant weight loss. Cardiovascular risk profile was more favorable after weight loss, compared with controls with prediabetes without weight loss, even though some of the intervention group who lost significant weight still had an A1c of 42-47 mmol/mol. Dr. Taylor suggested that we not label these individuals who have lost significant weight as having prediabetes. Instead “postdiabetes” should be preferred, because these patients had more favorable cardiovascular profiles.
This is a very important take-home message for primary care: prediabetes is more than just dysglycemia.
New terminology proposed
Dr. Khunti outlined a recent large, systematic review that concluded that the definition of T2D remission encompassed substantial heterogeneity. This heterogeneity complicates the interpretation of previous research on T2D remission and complicates the implementation of remission pathways into routine clinical practice. Furthermore, Dr. Khunti highlighted a recent consensus report on the definition and interpretation of remission in T2D that explicitly stated that the underlying pathophysiology of T2D is rarely normalized completely by interventions, thus reducing the possibility of lasting remission.
Dr. Khunti also challenged the cardiovascular benefits seen after T2D remission. Recent Danish registry data were presented, demonstrating a twofold increased risk for major adverse cardiovascular events over 5 years in individuals who achieved remission of T2D, but not on glucose-lowering drug therapy.
Adherence to strict dietary interventions in the longer term was also addressed. Diet-induced weight loss causes changes in circulating hormones such as ghrelin, glucose-dependent insulinotropic polypeptide (GIP), and leptin, which mediate appetite and drive hunger and an increased preference for energy-dense foods (that is, high-fat or sugary foods), all of which encourage weight regain. Dr. Khunti suggested that other interventions, such as glucagon-like peptide 1 (GLP-1) receptor agonists or bariatric surgery, specifically target some of these hormonal responses.
The challenges in recruitment and retention for lifestyle studies were also discussed; they reflect the challenges of behavioral programs in primary care. The DiRECT study had 20% participation of screened candidates and an attrition rate approaching 30%. The seminal Diabetes Prevention Program study and Finnish Diabetes Prevention Study had similar results. At a population level, individuals do not appear to want to participate in behavioral programs.
Dr. Khunti also warned that the review of annual care processes for diabetes is declining for patients who had achieved remission, possibly because of a false sense of reassurance among health care professionals. It is essential that all those in remission remain under at least annual follow-up, because there is still a risk for future microvascular and macrovascular complications, especially in the event of weight regain.
Dr. Khunti concluded by proposing new terminology for remission: remission of hyperglycemia or euglycemia, aiming for A1c < 48 mmol/mol with or without glucose-lowering therapy. I do agree with this; it reflects the zeitgeist of cardiorenal protective diabetes therapies and is analogous to rheumatoid arthritis, where remission is defined as no disease activity while on therapy. But one size does not fit all.
Sir William Osler’s words provide a fitting conclusion: “If it were not for the great variability among individuals, medicine might as well be a science and not an art.”
Dr. Fernando has disclosed that he has received speakers’ fees from Eli Lilly and Novo Nordisk.
Dr. Fernando is a general practitioner near Edinburgh, with a specialist interest in diabetes; cardiovascular, renal, and metabolic diseases; and medical education.
A version of this article first appeared on Medscape.com.
Making time to care for patients with diabetes
Can busy primary care offices continue to care for patients with diabetes? No one would argue that it is involved and takes effort, and health care providers are bankrupt when it comes to sparing additional time for this chronic disease. With roughly 37 million people living with diabetes and 96 million with prediabetes or early type 2 diabetes, and just over 8,000 practicing endocrinologists in the United States, we all need to make time especially in primary care to provide insight and holistic care. With limited time and budget, how do we do this?
First, decide to be involved in caring for patients with diabetes. Diabetes is best managed by interprofessional care teams, so you’re not going it alone. These teams may include physicians; pharmacists; physician assistants; advanced practice nurses; registered nurses; certified diabetes care and education specialists (CDCES); dietitians; and other professionals such as social workers, behavioral health professionals, medical assistants, and community health workers. Know which professionals are available to serve on your team, either within your clinic or as a consultant, and reach out to them to share the care and ease the burden. Remember to refer to these professionals to reinforce the diabetes intervention message to the patient.
Second, incorporate “diabetes only” appointments into your schedule, allowing time to focus on current comprehensive diabetes treatment goals, barriers/inertia for care. Remember to have short-interval follow-up as needed to keep that patient engaged to achieve their targets. Instruct your office staff to create diabetes appointment templates and reminders to patients to bring diabetes-related technologies, medication lists, and diabetes questions to the appointment. When I implemented this change, my patients welcomed the focus on their diabetes health, and they knew we were prioritizing this disease that they have for a lifetime. These appointments did not take away from their other conditions; rather, they often reminded me to stay focused on their diabetes and associated coconditions.
Taking the time to establish efficient workflows before implementing diabetes care saves countless hours later and immediately maximizes health care provider–patient interactions. Assign specific staff duties and expectations related to diabetes appointments, such as downloading diabetes technology, medication reconciliation, laboratory data, point-of-care hemoglobin A1c, basic foot exam, and patient goals for diabetes care. This allows the prescriber to focus on the glycemic, cardiologic, renal, and metabolic goals and overcome the therapeutic inertia that plagues us all.
Incorporating diabetes-related technology into clinical practice can be a significant time-saver but requires initial onboarding. Set aside a few hours to create a technology clinic flow, and designate at least one team member to be responsible for obtaining patient data before, during, or after encounters. If possible, obtaining data ahead of the visit will enhance efficiency, allowing for meaningful discussion of blood glucose and lifestyle patterns. Diabetes technology reveals the gaps in care and enhances our ability to identify the areas where glycemic intervention is needed. In addition, it reveals the impact of food choices, activity level, stress, and medication adherence to the person living with diabetes.
Finally, be proactive about therapeutic inertia. This is defined as a prescribers’ failure to intensify or deintensify a patient’s treatment when appropriate to do so. Causes of therapeutic inertia can be placed at the primary care physician level, including time constraints or inexperience in treating diabetes; the patient level, such as concerns about side effects or new treatment regimens; or a systemic level, such as availability of medications or their costs. Be real with yourself: We all have inertia and can identify areas to overcome. Never let inertia be traced back to you.
Not all inertia lives with the health care provider. Patients bring apprehension and concerns, have questions, and just want to share the frustrations associated with living their best life with the disease. Don’t assume that you know what your patients’ treatment barriers are; ask them. If you don’t have an answer, then note it and come up with one by the next follow-up. Remember that this is a chronic disease – a marathon, not a sprint. You don’t have to solve everything at one appointment; rather, keep the momentum going.
Let’s put this into clinical practice. For the next patient with diabetes who comes into your office, discuss with them your intention to prioritize their diabetes by having an appointment set aside to specifically focus on their individual goals and targets for their disease. Have the patient list any barriers and treatment goals they would like to review; flag your schedule to indicate it is a diabetes-only visit; and orient your staff to reconcile diabetes medications and record the patient’s last eye exam, urine albumin-to-creatinine ratio, A1c result, and blood glucose data. During this encounter, identify the patient’s personal targets for control, examine their feet, and review or order necessary laboratory metrics. Explore the patient-reported barriers and make inroads to remove or alleviate these. Advance treatment intervention, and schedule follow-up: every 4-6 weeks if the A1c is > 9%, every 2 months if it’s 7% to < 9%, and every 3-6 months if it’s < 7%. Utilize team diabetes care, such as CDCES referrals, dietitians, online resources, and community members, to help reinforce care and enhance engagement.
We need to take steps in our clinical practice to make the necessary space to accommodate this pervasive disease affecting nearly one-third of our population. Take a moment to look up and determine what needs to be in place so that you can take care of the people in your practice with diabetes. Laying the groundwork for implementing diabetes-only appointments can be time-consuming, but establishing consistent procedures, developing efficient workflows, and clearly defining roles and responsibilities is well worth the effort. This solid foundation equips the office, health care providers, and staff to care for persons with diabetes and will be invaluable to ensure that time for this care is available in the day-to-day clinical practice.
A version of this article first appeared on Medscape.com.
Can busy primary care offices continue to care for patients with diabetes? No one would argue that it is involved and takes effort, and health care providers are bankrupt when it comes to sparing additional time for this chronic disease. With roughly 37 million people living with diabetes and 96 million with prediabetes or early type 2 diabetes, and just over 8,000 practicing endocrinologists in the United States, we all need to make time especially in primary care to provide insight and holistic care. With limited time and budget, how do we do this?
First, decide to be involved in caring for patients with diabetes. Diabetes is best managed by interprofessional care teams, so you’re not going it alone. These teams may include physicians; pharmacists; physician assistants; advanced practice nurses; registered nurses; certified diabetes care and education specialists (CDCES); dietitians; and other professionals such as social workers, behavioral health professionals, medical assistants, and community health workers. Know which professionals are available to serve on your team, either within your clinic or as a consultant, and reach out to them to share the care and ease the burden. Remember to refer to these professionals to reinforce the diabetes intervention message to the patient.
Second, incorporate “diabetes only” appointments into your schedule, allowing time to focus on current comprehensive diabetes treatment goals, barriers/inertia for care. Remember to have short-interval follow-up as needed to keep that patient engaged to achieve their targets. Instruct your office staff to create diabetes appointment templates and reminders to patients to bring diabetes-related technologies, medication lists, and diabetes questions to the appointment. When I implemented this change, my patients welcomed the focus on their diabetes health, and they knew we were prioritizing this disease that they have for a lifetime. These appointments did not take away from their other conditions; rather, they often reminded me to stay focused on their diabetes and associated coconditions.
Taking the time to establish efficient workflows before implementing diabetes care saves countless hours later and immediately maximizes health care provider–patient interactions. Assign specific staff duties and expectations related to diabetes appointments, such as downloading diabetes technology, medication reconciliation, laboratory data, point-of-care hemoglobin A1c, basic foot exam, and patient goals for diabetes care. This allows the prescriber to focus on the glycemic, cardiologic, renal, and metabolic goals and overcome the therapeutic inertia that plagues us all.
Incorporating diabetes-related technology into clinical practice can be a significant time-saver but requires initial onboarding. Set aside a few hours to create a technology clinic flow, and designate at least one team member to be responsible for obtaining patient data before, during, or after encounters. If possible, obtaining data ahead of the visit will enhance efficiency, allowing for meaningful discussion of blood glucose and lifestyle patterns. Diabetes technology reveals the gaps in care and enhances our ability to identify the areas where glycemic intervention is needed. In addition, it reveals the impact of food choices, activity level, stress, and medication adherence to the person living with diabetes.
Finally, be proactive about therapeutic inertia. This is defined as a prescribers’ failure to intensify or deintensify a patient’s treatment when appropriate to do so. Causes of therapeutic inertia can be placed at the primary care physician level, including time constraints or inexperience in treating diabetes; the patient level, such as concerns about side effects or new treatment regimens; or a systemic level, such as availability of medications or their costs. Be real with yourself: We all have inertia and can identify areas to overcome. Never let inertia be traced back to you.
Not all inertia lives with the health care provider. Patients bring apprehension and concerns, have questions, and just want to share the frustrations associated with living their best life with the disease. Don’t assume that you know what your patients’ treatment barriers are; ask them. If you don’t have an answer, then note it and come up with one by the next follow-up. Remember that this is a chronic disease – a marathon, not a sprint. You don’t have to solve everything at one appointment; rather, keep the momentum going.
Let’s put this into clinical practice. For the next patient with diabetes who comes into your office, discuss with them your intention to prioritize their diabetes by having an appointment set aside to specifically focus on their individual goals and targets for their disease. Have the patient list any barriers and treatment goals they would like to review; flag your schedule to indicate it is a diabetes-only visit; and orient your staff to reconcile diabetes medications and record the patient’s last eye exam, urine albumin-to-creatinine ratio, A1c result, and blood glucose data. During this encounter, identify the patient’s personal targets for control, examine their feet, and review or order necessary laboratory metrics. Explore the patient-reported barriers and make inroads to remove or alleviate these. Advance treatment intervention, and schedule follow-up: every 4-6 weeks if the A1c is > 9%, every 2 months if it’s 7% to < 9%, and every 3-6 months if it’s < 7%. Utilize team diabetes care, such as CDCES referrals, dietitians, online resources, and community members, to help reinforce care and enhance engagement.
We need to take steps in our clinical practice to make the necessary space to accommodate this pervasive disease affecting nearly one-third of our population. Take a moment to look up and determine what needs to be in place so that you can take care of the people in your practice with diabetes. Laying the groundwork for implementing diabetes-only appointments can be time-consuming, but establishing consistent procedures, developing efficient workflows, and clearly defining roles and responsibilities is well worth the effort. This solid foundation equips the office, health care providers, and staff to care for persons with diabetes and will be invaluable to ensure that time for this care is available in the day-to-day clinical practice.
A version of this article first appeared on Medscape.com.
Can busy primary care offices continue to care for patients with diabetes? No one would argue that it is involved and takes effort, and health care providers are bankrupt when it comes to sparing additional time for this chronic disease. With roughly 37 million people living with diabetes and 96 million with prediabetes or early type 2 diabetes, and just over 8,000 practicing endocrinologists in the United States, we all need to make time especially in primary care to provide insight and holistic care. With limited time and budget, how do we do this?
First, decide to be involved in caring for patients with diabetes. Diabetes is best managed by interprofessional care teams, so you’re not going it alone. These teams may include physicians; pharmacists; physician assistants; advanced practice nurses; registered nurses; certified diabetes care and education specialists (CDCES); dietitians; and other professionals such as social workers, behavioral health professionals, medical assistants, and community health workers. Know which professionals are available to serve on your team, either within your clinic or as a consultant, and reach out to them to share the care and ease the burden. Remember to refer to these professionals to reinforce the diabetes intervention message to the patient.
Second, incorporate “diabetes only” appointments into your schedule, allowing time to focus on current comprehensive diabetes treatment goals, barriers/inertia for care. Remember to have short-interval follow-up as needed to keep that patient engaged to achieve their targets. Instruct your office staff to create diabetes appointment templates and reminders to patients to bring diabetes-related technologies, medication lists, and diabetes questions to the appointment. When I implemented this change, my patients welcomed the focus on their diabetes health, and they knew we were prioritizing this disease that they have for a lifetime. These appointments did not take away from their other conditions; rather, they often reminded me to stay focused on their diabetes and associated coconditions.
Taking the time to establish efficient workflows before implementing diabetes care saves countless hours later and immediately maximizes health care provider–patient interactions. Assign specific staff duties and expectations related to diabetes appointments, such as downloading diabetes technology, medication reconciliation, laboratory data, point-of-care hemoglobin A1c, basic foot exam, and patient goals for diabetes care. This allows the prescriber to focus on the glycemic, cardiologic, renal, and metabolic goals and overcome the therapeutic inertia that plagues us all.
Incorporating diabetes-related technology into clinical practice can be a significant time-saver but requires initial onboarding. Set aside a few hours to create a technology clinic flow, and designate at least one team member to be responsible for obtaining patient data before, during, or after encounters. If possible, obtaining data ahead of the visit will enhance efficiency, allowing for meaningful discussion of blood glucose and lifestyle patterns. Diabetes technology reveals the gaps in care and enhances our ability to identify the areas where glycemic intervention is needed. In addition, it reveals the impact of food choices, activity level, stress, and medication adherence to the person living with diabetes.
Finally, be proactive about therapeutic inertia. This is defined as a prescribers’ failure to intensify or deintensify a patient’s treatment when appropriate to do so. Causes of therapeutic inertia can be placed at the primary care physician level, including time constraints or inexperience in treating diabetes; the patient level, such as concerns about side effects or new treatment regimens; or a systemic level, such as availability of medications or their costs. Be real with yourself: We all have inertia and can identify areas to overcome. Never let inertia be traced back to you.
Not all inertia lives with the health care provider. Patients bring apprehension and concerns, have questions, and just want to share the frustrations associated with living their best life with the disease. Don’t assume that you know what your patients’ treatment barriers are; ask them. If you don’t have an answer, then note it and come up with one by the next follow-up. Remember that this is a chronic disease – a marathon, not a sprint. You don’t have to solve everything at one appointment; rather, keep the momentum going.
Let’s put this into clinical practice. For the next patient with diabetes who comes into your office, discuss with them your intention to prioritize their diabetes by having an appointment set aside to specifically focus on their individual goals and targets for their disease. Have the patient list any barriers and treatment goals they would like to review; flag your schedule to indicate it is a diabetes-only visit; and orient your staff to reconcile diabetes medications and record the patient’s last eye exam, urine albumin-to-creatinine ratio, A1c result, and blood glucose data. During this encounter, identify the patient’s personal targets for control, examine their feet, and review or order necessary laboratory metrics. Explore the patient-reported barriers and make inroads to remove or alleviate these. Advance treatment intervention, and schedule follow-up: every 4-6 weeks if the A1c is > 9%, every 2 months if it’s 7% to < 9%, and every 3-6 months if it’s < 7%. Utilize team diabetes care, such as CDCES referrals, dietitians, online resources, and community members, to help reinforce care and enhance engagement.
We need to take steps in our clinical practice to make the necessary space to accommodate this pervasive disease affecting nearly one-third of our population. Take a moment to look up and determine what needs to be in place so that you can take care of the people in your practice with diabetes. Laying the groundwork for implementing diabetes-only appointments can be time-consuming, but establishing consistent procedures, developing efficient workflows, and clearly defining roles and responsibilities is well worth the effort. This solid foundation equips the office, health care providers, and staff to care for persons with diabetes and will be invaluable to ensure that time for this care is available in the day-to-day clinical practice.
A version of this article first appeared on Medscape.com.
Metformin, weight management to stop type 2 diabetes in kids
TOPLINE:
Nearly one in five adolescents are living with prediabetes, a condition where blood glucose levels are elevated, but are not high enough for a type 2 diabetes (T2D) diagnosis. According to a new study, higher levels of nonfasting glucose and hemoglobin A1c, and worsening obesity are important predictors of progression to T2D. In addition, metformin and weight stabilization may prove to be important interventions for preventing T2D in kids.
METHODOLOGY:
- Researchers did a retrospective chart review of patient data from Vanderbilt University Medical Center Pediatric Prediabetes Clinic, Nashville, Tenn., from May 2015 to August 2022.
- The study included 552 children with prediabetes, defined as abnormal blood glucose (fasting plasma glucose [FPG] ≥ 100 mg/dL, random glucose ≥ 150 mg/dL), or hemoglobin A1c equal to or greater than 5.9%.
- Based on follow-up visits, patients were classified as having progressed to T2D, or nonprogression.
- Researchers analyzed the patients’ initial visit A1c, fasting C-peptide, 2-hour glucose, fasting glucose, and body mass index (BMI), among other baseline characteristics.
TAKEAWAY:
- Thirty-six children (6.5%) progressed to T2D during the duration of the study period.
- The average time to T2D diagnosis was much longer in patients taking metformin (43 months), compared with those not taking the prescribed medication (28 months).
- Worsening obesity was strongly associated with T2D progression – patients who progressed to T2D had a higher BMI at baseline and had continued weight gain.
- A higher baseline A1c, fasting C-peptide, and 2-hour glucose were also associated with progression to T2D.
- In the multivariable analysis, both A1c and 2-hour glucose were strong independent predictors of progression.
- Fasting plasma glucose was not associated with progression to T2D.
IN PRACTICE:
“Weight stabilization and metformin therapy could be important interventions for diabetes prevention in children,” study author Ashley H. Shoemaker, MD, MSci, a pediatric endocrinologist at Vanderbilt University Medical Center in Nashville, Tenn., said in a press release.
In addition, A1c plus a nonfasting glucose may be a feasible way to identify high-risk pediatric patients in a clinical setting.
SOURCE:
This study was performed by Natasha Belsky, Jaclyn Tamaroff, and Ashley H. Shoemaker of the Vanderbilt University Medical Center and the Vanderbilt University School of Medicine in Nashville, Tenn. It was published October 12, 2023, in the Journal of the Endocrine Society
LIMITATIONS:
Additional patients who developed T2D may have been lost to follow-up, since the authors did not contact patients to confirm their disease status. The authors were also unable to establish racial differences in the progression to T2D because of missing data.
DISCLOSURES:
Funding for this study was provided by the National Center for Advancing Translational Sciences. One author has research contracts with Novo Nordisk and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
TOPLINE:
Nearly one in five adolescents are living with prediabetes, a condition where blood glucose levels are elevated, but are not high enough for a type 2 diabetes (T2D) diagnosis. According to a new study, higher levels of nonfasting glucose and hemoglobin A1c, and worsening obesity are important predictors of progression to T2D. In addition, metformin and weight stabilization may prove to be important interventions for preventing T2D in kids.
METHODOLOGY:
- Researchers did a retrospective chart review of patient data from Vanderbilt University Medical Center Pediatric Prediabetes Clinic, Nashville, Tenn., from May 2015 to August 2022.
- The study included 552 children with prediabetes, defined as abnormal blood glucose (fasting plasma glucose [FPG] ≥ 100 mg/dL, random glucose ≥ 150 mg/dL), or hemoglobin A1c equal to or greater than 5.9%.
- Based on follow-up visits, patients were classified as having progressed to T2D, or nonprogression.
- Researchers analyzed the patients’ initial visit A1c, fasting C-peptide, 2-hour glucose, fasting glucose, and body mass index (BMI), among other baseline characteristics.
TAKEAWAY:
- Thirty-six children (6.5%) progressed to T2D during the duration of the study period.
- The average time to T2D diagnosis was much longer in patients taking metformin (43 months), compared with those not taking the prescribed medication (28 months).
- Worsening obesity was strongly associated with T2D progression – patients who progressed to T2D had a higher BMI at baseline and had continued weight gain.
- A higher baseline A1c, fasting C-peptide, and 2-hour glucose were also associated with progression to T2D.
- In the multivariable analysis, both A1c and 2-hour glucose were strong independent predictors of progression.
- Fasting plasma glucose was not associated with progression to T2D.
IN PRACTICE:
“Weight stabilization and metformin therapy could be important interventions for diabetes prevention in children,” study author Ashley H. Shoemaker, MD, MSci, a pediatric endocrinologist at Vanderbilt University Medical Center in Nashville, Tenn., said in a press release.
In addition, A1c plus a nonfasting glucose may be a feasible way to identify high-risk pediatric patients in a clinical setting.
SOURCE:
This study was performed by Natasha Belsky, Jaclyn Tamaroff, and Ashley H. Shoemaker of the Vanderbilt University Medical Center and the Vanderbilt University School of Medicine in Nashville, Tenn. It was published October 12, 2023, in the Journal of the Endocrine Society
LIMITATIONS:
Additional patients who developed T2D may have been lost to follow-up, since the authors did not contact patients to confirm their disease status. The authors were also unable to establish racial differences in the progression to T2D because of missing data.
DISCLOSURES:
Funding for this study was provided by the National Center for Advancing Translational Sciences. One author has research contracts with Novo Nordisk and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
TOPLINE:
Nearly one in five adolescents are living with prediabetes, a condition where blood glucose levels are elevated, but are not high enough for a type 2 diabetes (T2D) diagnosis. According to a new study, higher levels of nonfasting glucose and hemoglobin A1c, and worsening obesity are important predictors of progression to T2D. In addition, metformin and weight stabilization may prove to be important interventions for preventing T2D in kids.
METHODOLOGY:
- Researchers did a retrospective chart review of patient data from Vanderbilt University Medical Center Pediatric Prediabetes Clinic, Nashville, Tenn., from May 2015 to August 2022.
- The study included 552 children with prediabetes, defined as abnormal blood glucose (fasting plasma glucose [FPG] ≥ 100 mg/dL, random glucose ≥ 150 mg/dL), or hemoglobin A1c equal to or greater than 5.9%.
- Based on follow-up visits, patients were classified as having progressed to T2D, or nonprogression.
- Researchers analyzed the patients’ initial visit A1c, fasting C-peptide, 2-hour glucose, fasting glucose, and body mass index (BMI), among other baseline characteristics.
TAKEAWAY:
- Thirty-six children (6.5%) progressed to T2D during the duration of the study period.
- The average time to T2D diagnosis was much longer in patients taking metformin (43 months), compared with those not taking the prescribed medication (28 months).
- Worsening obesity was strongly associated with T2D progression – patients who progressed to T2D had a higher BMI at baseline and had continued weight gain.
- A higher baseline A1c, fasting C-peptide, and 2-hour glucose were also associated with progression to T2D.
- In the multivariable analysis, both A1c and 2-hour glucose were strong independent predictors of progression.
- Fasting plasma glucose was not associated with progression to T2D.
IN PRACTICE:
“Weight stabilization and metformin therapy could be important interventions for diabetes prevention in children,” study author Ashley H. Shoemaker, MD, MSci, a pediatric endocrinologist at Vanderbilt University Medical Center in Nashville, Tenn., said in a press release.
In addition, A1c plus a nonfasting glucose may be a feasible way to identify high-risk pediatric patients in a clinical setting.
SOURCE:
This study was performed by Natasha Belsky, Jaclyn Tamaroff, and Ashley H. Shoemaker of the Vanderbilt University Medical Center and the Vanderbilt University School of Medicine in Nashville, Tenn. It was published October 12, 2023, in the Journal of the Endocrine Society
LIMITATIONS:
Additional patients who developed T2D may have been lost to follow-up, since the authors did not contact patients to confirm their disease status. The authors were also unable to establish racial differences in the progression to T2D because of missing data.
DISCLOSURES:
Funding for this study was provided by the National Center for Advancing Translational Sciences. One author has research contracts with Novo Nordisk and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
Alert! A decade of type 2 diabetes shortens life by 3.5 years
researchers estimate on the basis of data from studies conducted in 19 high-income countries.
They estimated that, among 50-year-olds, life expectancy of those diagnosed with type 2 diabetes at age 30 is 14 years shorter than that of their peers without diabetes. Among those diagnosed at age 50, life expectancy is 6 years shorter.
The study was recently published in The Lancet – Diabetes and Endocrinology.
The team analyzed data from the Emerging Risk Factors Collaboration and the UK Biobank. The data were from 97 long-term, prospective cohorts and involved 1.5 million participants who were followed for 23.1 million person-years.
“The strongest associations with earlier age at diagnosis of diabetes were for vascular (for example, myocardial infarction and stroke) and other causes of death – mainly respiratory, neurological, and infectious diseases and external causes,” they reported.
Their findings are consistent with previous studies that suggested that younger individuals who develop type 2 diabetes might have higher body mass index (BMI), blood pressure, and lipid levels and that they might experience faster deterioration in glycemic control than individuals who develop diabetes later, potentially leading to premature mortality.

Asked to comment, Anne Peters, MD, director of clinical diabetes programs at the University of Southern California, Los Angeles, who was not involved with this study, said: “We’ve long known that diabetes reduces life expectancy, and the younger you get it the more years you lose. However, this study was from a broader and larger population base than prior studies.
“In this study, the major reason for death was vascular disease, and undertreatment of cardiovascular risk factors may have occurred in the younger individuals. We also don’t know about glucose control.
“I personally think the findings show that we should treat cardiovascular risk factors more aggressively in people diagnosed with [type 2] diabetes in their 30s and 40s,” urged Dr. Peters.
High priority should be given to prevention globally
“Type 2 diabetes used to be seen as a disease that affected older adults, but we’re increasingly seeing people diagnosed earlier in life,” senior author Emanuele Di Angelantonio, MD, PhD, from the University of Cambridge (England), explained in a press release. “As we’ve shown, this means they are at risk of a much shorter life expectancy than they would otherwise have.”
The findings suggest that “high priority should be given to developing and implementing interventions that prevent or delay the onset of [type 2 diabetes], especially as its prevalence among younger age groups is increasing globally,” the study authors wrote.
The results “support the idea that the younger an individual is when they develop type 2 diabetes, the more damage their body accumulates from its impaired metabolism,” added co–senior author Naveed Sattar, MD, PhD, of the University of Glasgow,
Dr. Peters agreed: “People who develop type 2 diabetes at a younger age might have a different, potentially more aggressive type of type 2 diabetes and perhaps need treatment targets that are lower than people who develop type 2 diabetes when they are older.”
“The findings ... suggest that early detection of diabetes by screening followed by intensive glucose management could help prevent long-term complications from the condition,” Dr. Sattar said.
Dr. Peters added: “An issue for some is pregnancy. ... Many of the medications taken for management of CVD [cardiovascular disease] risk factors are contraindicated in pregnancy (as are many of the medications [for treating type 2 diabetes]).
“We need to be careful to risk reduce but take care of the ‘whole person,’ and if of childbearing age, consider the safest approaches to healthy management,” she emphasized.
Study results: Type 2 diabetes diagnosed at age 30, 40, and 50
Previous studies estimated that adults with type 2 diabetes die 6 years earlier on average in comparison with their counterparts who do not have diabetes, but it was not known how diabetes duration affects life span.
To investigate this, the team analyzed individual records from the Emerging Risk Factors Collaboration and the UK Biobank. The primary outcome was all-cause mortality. Other outcomes were deaths from CVD, cancer, and other causes.
Over a median follow-up of 12.5 years, there were 246,670 deaths: 84,443 from cardiovascular causes, 150, 972 from noncardiovascular causes, and 11,255 from unknown/ill-defined causes.
Compared with participants who did not have a history of type 2 diabetes, the hazard ratios for all-cause mortality, adjusted for age and sex, were 2.69 for participants diagnosed at age 30-39, 2.26 for those diagnosed aged 40-49, 1.84 aged 50-59, 1.57 for those aged 60-69, and 1.39 for those diagnosed 70 and older.
These hazard ratios were similar after adjusting for BMI, systolic blood pressure, and total cholesterol, but they were substantially attenuated after further adjusting for fasting glucose or hemoglobin A1c level.
Similar patterns were observed for cause-specific mortality.
“Every decade of earlier diagnosis of diabetes was associated with about 3-4 years of lower life expectancy, highlighting the need to develop and implement interventions that prevent or delay the onset of diabetes and to intensify the treatment of risk factors among young adults diagnosed with diabetes,” the researchers wrote.
The study was funded the British Heart Foundation, the Medical Research Council, the National Institute for Health and Care Research, and Health Data Research UK. Dr. Peters is on advisory boards for Vertex, Eli Lilly, and Medscape, receives research funding from Abbott Diabetes Care and Insulet, and has stock options for Omada Health.
A version of this article first appeared on Medscape.com.
researchers estimate on the basis of data from studies conducted in 19 high-income countries.
They estimated that, among 50-year-olds, life expectancy of those diagnosed with type 2 diabetes at age 30 is 14 years shorter than that of their peers without diabetes. Among those diagnosed at age 50, life expectancy is 6 years shorter.
The study was recently published in The Lancet – Diabetes and Endocrinology.
The team analyzed data from the Emerging Risk Factors Collaboration and the UK Biobank. The data were from 97 long-term, prospective cohorts and involved 1.5 million participants who were followed for 23.1 million person-years.
“The strongest associations with earlier age at diagnosis of diabetes were for vascular (for example, myocardial infarction and stroke) and other causes of death – mainly respiratory, neurological, and infectious diseases and external causes,” they reported.
Their findings are consistent with previous studies that suggested that younger individuals who develop type 2 diabetes might have higher body mass index (BMI), blood pressure, and lipid levels and that they might experience faster deterioration in glycemic control than individuals who develop diabetes later, potentially leading to premature mortality.
Asked to comment, Anne Peters, MD, director of clinical diabetes programs at the University of Southern California, Los Angeles, who was not involved with this study, said: “We’ve long known that diabetes reduces life expectancy, and the younger you get it the more years you lose. However, this study was from a broader and larger population base than prior studies.
“In this study, the major reason for death was vascular disease, and undertreatment of cardiovascular risk factors may have occurred in the younger individuals. We also don’t know about glucose control.
“I personally think the findings show that we should treat cardiovascular risk factors more aggressively in people diagnosed with [type 2] diabetes in their 30s and 40s,” urged Dr. Peters.
High priority should be given to prevention globally
“Type 2 diabetes used to be seen as a disease that affected older adults, but we’re increasingly seeing people diagnosed earlier in life,” senior author Emanuele Di Angelantonio, MD, PhD, from the University of Cambridge (England), explained in a press release. “As we’ve shown, this means they are at risk of a much shorter life expectancy than they would otherwise have.”
The findings suggest that “high priority should be given to developing and implementing interventions that prevent or delay the onset of [type 2 diabetes], especially as its prevalence among younger age groups is increasing globally,” the study authors wrote.
The results “support the idea that the younger an individual is when they develop type 2 diabetes, the more damage their body accumulates from its impaired metabolism,” added co–senior author Naveed Sattar, MD, PhD, of the University of Glasgow,
Dr. Peters agreed: “People who develop type 2 diabetes at a younger age might have a different, potentially more aggressive type of type 2 diabetes and perhaps need treatment targets that are lower than people who develop type 2 diabetes when they are older.”
“The findings ... suggest that early detection of diabetes by screening followed by intensive glucose management could help prevent long-term complications from the condition,” Dr. Sattar said.
Dr. Peters added: “An issue for some is pregnancy. ... Many of the medications taken for management of CVD [cardiovascular disease] risk factors are contraindicated in pregnancy (as are many of the medications [for treating type 2 diabetes]).
“We need to be careful to risk reduce but take care of the ‘whole person,’ and if of childbearing age, consider the safest approaches to healthy management,” she emphasized.
Study results: Type 2 diabetes diagnosed at age 30, 40, and 50
Previous studies estimated that adults with type 2 diabetes die 6 years earlier on average in comparison with their counterparts who do not have diabetes, but it was not known how diabetes duration affects life span.
To investigate this, the team analyzed individual records from the Emerging Risk Factors Collaboration and the UK Biobank. The primary outcome was all-cause mortality. Other outcomes were deaths from CVD, cancer, and other causes.
Over a median follow-up of 12.5 years, there were 246,670 deaths: 84,443 from cardiovascular causes, 150, 972 from noncardiovascular causes, and 11,255 from unknown/ill-defined causes.
Compared with participants who did not have a history of type 2 diabetes, the hazard ratios for all-cause mortality, adjusted for age and sex, were 2.69 for participants diagnosed at age 30-39, 2.26 for those diagnosed aged 40-49, 1.84 aged 50-59, 1.57 for those aged 60-69, and 1.39 for those diagnosed 70 and older.
These hazard ratios were similar after adjusting for BMI, systolic blood pressure, and total cholesterol, but they were substantially attenuated after further adjusting for fasting glucose or hemoglobin A1c level.
Similar patterns were observed for cause-specific mortality.
“Every decade of earlier diagnosis of diabetes was associated with about 3-4 years of lower life expectancy, highlighting the need to develop and implement interventions that prevent or delay the onset of diabetes and to intensify the treatment of risk factors among young adults diagnosed with diabetes,” the researchers wrote.
The study was funded the British Heart Foundation, the Medical Research Council, the National Institute for Health and Care Research, and Health Data Research UK. Dr. Peters is on advisory boards for Vertex, Eli Lilly, and Medscape, receives research funding from Abbott Diabetes Care and Insulet, and has stock options for Omada Health.
A version of this article first appeared on Medscape.com.
researchers estimate on the basis of data from studies conducted in 19 high-income countries.
They estimated that, among 50-year-olds, life expectancy of those diagnosed with type 2 diabetes at age 30 is 14 years shorter than that of their peers without diabetes. Among those diagnosed at age 50, life expectancy is 6 years shorter.
The study was recently published in The Lancet – Diabetes and Endocrinology.
The team analyzed data from the Emerging Risk Factors Collaboration and the UK Biobank. The data were from 97 long-term, prospective cohorts and involved 1.5 million participants who were followed for 23.1 million person-years.
“The strongest associations with earlier age at diagnosis of diabetes were for vascular (for example, myocardial infarction and stroke) and other causes of death – mainly respiratory, neurological, and infectious diseases and external causes,” they reported.
Their findings are consistent with previous studies that suggested that younger individuals who develop type 2 diabetes might have higher body mass index (BMI), blood pressure, and lipid levels and that they might experience faster deterioration in glycemic control than individuals who develop diabetes later, potentially leading to premature mortality.
Asked to comment, Anne Peters, MD, director of clinical diabetes programs at the University of Southern California, Los Angeles, who was not involved with this study, said: “We’ve long known that diabetes reduces life expectancy, and the younger you get it the more years you lose. However, this study was from a broader and larger population base than prior studies.
“In this study, the major reason for death was vascular disease, and undertreatment of cardiovascular risk factors may have occurred in the younger individuals. We also don’t know about glucose control.
“I personally think the findings show that we should treat cardiovascular risk factors more aggressively in people diagnosed with [type 2] diabetes in their 30s and 40s,” urged Dr. Peters.
High priority should be given to prevention globally
“Type 2 diabetes used to be seen as a disease that affected older adults, but we’re increasingly seeing people diagnosed earlier in life,” senior author Emanuele Di Angelantonio, MD, PhD, from the University of Cambridge (England), explained in a press release. “As we’ve shown, this means they are at risk of a much shorter life expectancy than they would otherwise have.”
The findings suggest that “high priority should be given to developing and implementing interventions that prevent or delay the onset of [type 2 diabetes], especially as its prevalence among younger age groups is increasing globally,” the study authors wrote.
The results “support the idea that the younger an individual is when they develop type 2 diabetes, the more damage their body accumulates from its impaired metabolism,” added co–senior author Naveed Sattar, MD, PhD, of the University of Glasgow,
Dr. Peters agreed: “People who develop type 2 diabetes at a younger age might have a different, potentially more aggressive type of type 2 diabetes and perhaps need treatment targets that are lower than people who develop type 2 diabetes when they are older.”
“The findings ... suggest that early detection of diabetes by screening followed by intensive glucose management could help prevent long-term complications from the condition,” Dr. Sattar said.
Dr. Peters added: “An issue for some is pregnancy. ... Many of the medications taken for management of CVD [cardiovascular disease] risk factors are contraindicated in pregnancy (as are many of the medications [for treating type 2 diabetes]).
“We need to be careful to risk reduce but take care of the ‘whole person,’ and if of childbearing age, consider the safest approaches to healthy management,” she emphasized.
Study results: Type 2 diabetes diagnosed at age 30, 40, and 50
Previous studies estimated that adults with type 2 diabetes die 6 years earlier on average in comparison with their counterparts who do not have diabetes, but it was not known how diabetes duration affects life span.
To investigate this, the team analyzed individual records from the Emerging Risk Factors Collaboration and the UK Biobank. The primary outcome was all-cause mortality. Other outcomes were deaths from CVD, cancer, and other causes.
Over a median follow-up of 12.5 years, there were 246,670 deaths: 84,443 from cardiovascular causes, 150, 972 from noncardiovascular causes, and 11,255 from unknown/ill-defined causes.
Compared with participants who did not have a history of type 2 diabetes, the hazard ratios for all-cause mortality, adjusted for age and sex, were 2.69 for participants diagnosed at age 30-39, 2.26 for those diagnosed aged 40-49, 1.84 aged 50-59, 1.57 for those aged 60-69, and 1.39 for those diagnosed 70 and older.
These hazard ratios were similar after adjusting for BMI, systolic blood pressure, and total cholesterol, but they were substantially attenuated after further adjusting for fasting glucose or hemoglobin A1c level.
Similar patterns were observed for cause-specific mortality.
“Every decade of earlier diagnosis of diabetes was associated with about 3-4 years of lower life expectancy, highlighting the need to develop and implement interventions that prevent or delay the onset of diabetes and to intensify the treatment of risk factors among young adults diagnosed with diabetes,” the researchers wrote.
The study was funded the British Heart Foundation, the Medical Research Council, the National Institute for Health and Care Research, and Health Data Research UK. Dr. Peters is on advisory boards for Vertex, Eli Lilly, and Medscape, receives research funding from Abbott Diabetes Care and Insulet, and has stock options for Omada Health.
A version of this article first appeared on Medscape.com.
FROM THE LANCET – DIABETES AND ENDOCRINOLOGY
Many young adults with type 2 diabetes skip medications
Young adults who developed type 2 diabetes as children often do not take medications to control blood pressure or cholesterol, according to a new study in JAMA Network Open. Researchers expressed alarm that young people who forgo these medications increase their chances of developing kidney disease or having a stroke.
“We’re learning more and more that those with youth onset [type 2 diabetes] really differ from those with adult onset: It looks like a more virulent form of the disease because kids are getting complications and comorbidities at much earlier ages and more severe levels,” said study author Paula Trief, PhD, a professor of psychiatry and behavioral science at State University of New York, Syracuse.
Participants in the new study were on average aged 26 years. They also had previously been part of the Treating Options for Type 2 Diabetes in Adolescents and Youth study, known as TODAY, which took place from 2004 to 2011. TODAY enrolled children between ages 10 and 17 years with type 2 diabetes who received either metformin, metformin plus rosiglitazone, or metformin plus a lifestyle intervention.
The study included extensive education and contact from medical professionals to the participants about managing diabetes.
“This cohort was followed a long time and they had a lot of support. It may be better than the real world where people haven’t had the history of this much attention,” said Lorraine Katz, MD, who specializes in endocrinology and diabetes at the Children’s Hospital of Philadelphia. Dr. Katz has enrolled participants in TODAY and published about medication adherence rates but was not part of the recent analysis.
Unannounced pill counts, addressing concerns about medication
The analysis, known as iCount, included 243 participants from the original TODAY study (159 girls) who had hypertension, neuropathy, or dyslipidemia that required ongoing medication. As the TODAY study was concluding between 2017 and 2019, researchers made unannounced phone calls to participants to request the numbers of pills they had prescribed, number of refills, and the refill date. Participants also counted aloud every pill in their possession twice.
Those phone calls continued for 3 consecutive months after iCount began and again at the same intervals 1 year later.
If the number of pills counted at a later time was at least 80% of the starting total, researchers considered this rate as low adherence. Anything less than 80% was considered high adherence.
“That’s kind of an arbitrary cutoff, but it’s one that’s used consistently in the literature” to measure medication adherence for many conditions including cancer and heart disease, Dr. Trief said. Unannounced calls to initiate pill counts were first used to understand how often people took medications for HIV, and this method was found to be a more reliable method than are self-reports.
Of 196 participants with hypertension or neuropathy, 157 (80.1%) had low adherence. And of the 146 people with high cholesterol, 137 (93.8%) had low adherence. Ninety-nine people with high cholesterol also had neuropathy or diabetes.
“This is new to the literature: We don’t really know as much about this age group,” because medication adherence studies of people who have had diabetes for more than a decade and are still in their 20s are rare, Dr. Katz said.
During the core TODAY study period, all medications were provided for free. In contrast, in the current study, participants had to obtain their prescriptions on their own. The researchers found that many participants who showed low adherence to blood pressure medications reported sometimes having trouble obtaining food (n = 62), struggling with securing stable housing (n = 47), or lacking reliable health care insurance (n = 28), all factors linked to medication adherence success, according to the analysis authors.
Researchers also assessed the impact of concerns that taking blood pressure medications may be harmful and found that people with these concerns were 37% less likely to maintain high adherence than others were by the 1-year follow-up point (odds ratio, 0.63; 95% confidence interval, 0.40-0.96; P = .01).
To some extent, the reasons people avoid medications are understandable, according to pediatric endocrinologist Tamara Hannon, MD, of Indiana University, Indianapolis.
“Rather than taking a medicine to feel better, you’re taking one not to have a problem in the future: You might not feel blood pressure, you certainly don’t feel cholesterol,” Dr. Hannon, who was not involved in the analysis, said. “Scolding them or telling them you’re going to be sorry one day doesn’t generally work.”
Dr. Hannon added that education alone about the benefits of medications does not generally drive people to adherence but that adding reminders to their phone calendar when refills are due could help. Or, the clinician could reach out to a trusted person in the patient’s life and enlist their support in taking medications consistently.
Dr. Trief advised that clinicians should carve out time for people to express their concerns about medications rather than simply writing a prescription and sending them on their way and to ask patients open-ended questions.
“If you just say to people do you have any questions, they usually say, ‘no.’ ”
No disclosures were reported.
A version of this article first appeared on Medscape.com.
Young adults who developed type 2 diabetes as children often do not take medications to control blood pressure or cholesterol, according to a new study in JAMA Network Open. Researchers expressed alarm that young people who forgo these medications increase their chances of developing kidney disease or having a stroke.
“We’re learning more and more that those with youth onset [type 2 diabetes] really differ from those with adult onset: It looks like a more virulent form of the disease because kids are getting complications and comorbidities at much earlier ages and more severe levels,” said study author Paula Trief, PhD, a professor of psychiatry and behavioral science at State University of New York, Syracuse.
Participants in the new study were on average aged 26 years. They also had previously been part of the Treating Options for Type 2 Diabetes in Adolescents and Youth study, known as TODAY, which took place from 2004 to 2011. TODAY enrolled children between ages 10 and 17 years with type 2 diabetes who received either metformin, metformin plus rosiglitazone, or metformin plus a lifestyle intervention.
The study included extensive education and contact from medical professionals to the participants about managing diabetes.
“This cohort was followed a long time and they had a lot of support. It may be better than the real world where people haven’t had the history of this much attention,” said Lorraine Katz, MD, who specializes in endocrinology and diabetes at the Children’s Hospital of Philadelphia. Dr. Katz has enrolled participants in TODAY and published about medication adherence rates but was not part of the recent analysis.
Unannounced pill counts, addressing concerns about medication
The analysis, known as iCount, included 243 participants from the original TODAY study (159 girls) who had hypertension, neuropathy, or dyslipidemia that required ongoing medication. As the TODAY study was concluding between 2017 and 2019, researchers made unannounced phone calls to participants to request the numbers of pills they had prescribed, number of refills, and the refill date. Participants also counted aloud every pill in their possession twice.
Those phone calls continued for 3 consecutive months after iCount began and again at the same intervals 1 year later.
If the number of pills counted at a later time was at least 80% of the starting total, researchers considered this rate as low adherence. Anything less than 80% was considered high adherence.
“That’s kind of an arbitrary cutoff, but it’s one that’s used consistently in the literature” to measure medication adherence for many conditions including cancer and heart disease, Dr. Trief said. Unannounced calls to initiate pill counts were first used to understand how often people took medications for HIV, and this method was found to be a more reliable method than are self-reports.
Of 196 participants with hypertension or neuropathy, 157 (80.1%) had low adherence. And of the 146 people with high cholesterol, 137 (93.8%) had low adherence. Ninety-nine people with high cholesterol also had neuropathy or diabetes.
“This is new to the literature: We don’t really know as much about this age group,” because medication adherence studies of people who have had diabetes for more than a decade and are still in their 20s are rare, Dr. Katz said.
During the core TODAY study period, all medications were provided for free. In contrast, in the current study, participants had to obtain their prescriptions on their own. The researchers found that many participants who showed low adherence to blood pressure medications reported sometimes having trouble obtaining food (n = 62), struggling with securing stable housing (n = 47), or lacking reliable health care insurance (n = 28), all factors linked to medication adherence success, according to the analysis authors.
Researchers also assessed the impact of concerns that taking blood pressure medications may be harmful and found that people with these concerns were 37% less likely to maintain high adherence than others were by the 1-year follow-up point (odds ratio, 0.63; 95% confidence interval, 0.40-0.96; P = .01).
To some extent, the reasons people avoid medications are understandable, according to pediatric endocrinologist Tamara Hannon, MD, of Indiana University, Indianapolis.
“Rather than taking a medicine to feel better, you’re taking one not to have a problem in the future: You might not feel blood pressure, you certainly don’t feel cholesterol,” Dr. Hannon, who was not involved in the analysis, said. “Scolding them or telling them you’re going to be sorry one day doesn’t generally work.”
Dr. Hannon added that education alone about the benefits of medications does not generally drive people to adherence but that adding reminders to their phone calendar when refills are due could help. Or, the clinician could reach out to a trusted person in the patient’s life and enlist their support in taking medications consistently.
Dr. Trief advised that clinicians should carve out time for people to express their concerns about medications rather than simply writing a prescription and sending them on their way and to ask patients open-ended questions.
“If you just say to people do you have any questions, they usually say, ‘no.’ ”
No disclosures were reported.
A version of this article first appeared on Medscape.com.
Young adults who developed type 2 diabetes as children often do not take medications to control blood pressure or cholesterol, according to a new study in JAMA Network Open. Researchers expressed alarm that young people who forgo these medications increase their chances of developing kidney disease or having a stroke.
“We’re learning more and more that those with youth onset [type 2 diabetes] really differ from those with adult onset: It looks like a more virulent form of the disease because kids are getting complications and comorbidities at much earlier ages and more severe levels,” said study author Paula Trief, PhD, a professor of psychiatry and behavioral science at State University of New York, Syracuse.
Participants in the new study were on average aged 26 years. They also had previously been part of the Treating Options for Type 2 Diabetes in Adolescents and Youth study, known as TODAY, which took place from 2004 to 2011. TODAY enrolled children between ages 10 and 17 years with type 2 diabetes who received either metformin, metformin plus rosiglitazone, or metformin plus a lifestyle intervention.
The study included extensive education and contact from medical professionals to the participants about managing diabetes.
“This cohort was followed a long time and they had a lot of support. It may be better than the real world where people haven’t had the history of this much attention,” said Lorraine Katz, MD, who specializes in endocrinology and diabetes at the Children’s Hospital of Philadelphia. Dr. Katz has enrolled participants in TODAY and published about medication adherence rates but was not part of the recent analysis.
Unannounced pill counts, addressing concerns about medication
The analysis, known as iCount, included 243 participants from the original TODAY study (159 girls) who had hypertension, neuropathy, or dyslipidemia that required ongoing medication. As the TODAY study was concluding between 2017 and 2019, researchers made unannounced phone calls to participants to request the numbers of pills they had prescribed, number of refills, and the refill date. Participants also counted aloud every pill in their possession twice.
Those phone calls continued for 3 consecutive months after iCount began and again at the same intervals 1 year later.
If the number of pills counted at a later time was at least 80% of the starting total, researchers considered this rate as low adherence. Anything less than 80% was considered high adherence.
“That’s kind of an arbitrary cutoff, but it’s one that’s used consistently in the literature” to measure medication adherence for many conditions including cancer and heart disease, Dr. Trief said. Unannounced calls to initiate pill counts were first used to understand how often people took medications for HIV, and this method was found to be a more reliable method than are self-reports.
Of 196 participants with hypertension or neuropathy, 157 (80.1%) had low adherence. And of the 146 people with high cholesterol, 137 (93.8%) had low adherence. Ninety-nine people with high cholesterol also had neuropathy or diabetes.
“This is new to the literature: We don’t really know as much about this age group,” because medication adherence studies of people who have had diabetes for more than a decade and are still in their 20s are rare, Dr. Katz said.
During the core TODAY study period, all medications were provided for free. In contrast, in the current study, participants had to obtain their prescriptions on their own. The researchers found that many participants who showed low adherence to blood pressure medications reported sometimes having trouble obtaining food (n = 62), struggling with securing stable housing (n = 47), or lacking reliable health care insurance (n = 28), all factors linked to medication adherence success, according to the analysis authors.
Researchers also assessed the impact of concerns that taking blood pressure medications may be harmful and found that people with these concerns were 37% less likely to maintain high adherence than others were by the 1-year follow-up point (odds ratio, 0.63; 95% confidence interval, 0.40-0.96; P = .01).
To some extent, the reasons people avoid medications are understandable, according to pediatric endocrinologist Tamara Hannon, MD, of Indiana University, Indianapolis.
“Rather than taking a medicine to feel better, you’re taking one not to have a problem in the future: You might not feel blood pressure, you certainly don’t feel cholesterol,” Dr. Hannon, who was not involved in the analysis, said. “Scolding them or telling them you’re going to be sorry one day doesn’t generally work.”
Dr. Hannon added that education alone about the benefits of medications does not generally drive people to adherence but that adding reminders to their phone calendar when refills are due could help. Or, the clinician could reach out to a trusted person in the patient’s life and enlist their support in taking medications consistently.
Dr. Trief advised that clinicians should carve out time for people to express their concerns about medications rather than simply writing a prescription and sending them on their way and to ask patients open-ended questions.
“If you just say to people do you have any questions, they usually say, ‘no.’ ”
No disclosures were reported.
A version of this article first appeared on Medscape.com.
Redefining CVD risk: Cardiovascular-kidney-metabolic (CKM) syndrome
“This work was prompted by the fact that CKM syndrome leads to premature morbidity and mortality, primarily because of a higher burden of CVD,” writing committee chair Chiadi Ndumele, MD, PhD, said in an interview.
“While CKM syndrome is a public health emergency, there is also great potential for improving CKM health in the population, with an increasing number of therapies that favorably impact metabolic risk factors, risk for adverse kidney events, or both, which also protect against CVD,” added Dr. Ndumele, director of obesity and cardiometabolic research in the division of cardiology at Johns Hopkins University, Baltimore.
The AHA presidential advisory and accompanying scientific statement, which provides a synopsis of evidence for the science and clinical management of CKM, were published online in the journal Circulation.
CKM syndrome staging
According to the AHA, one in three U.S. adults have three or more risk factors that contribute to CVD, metabolic disorders, and/or kidney disease.
In addition to defining CKM syndrome, the advisory provides a “staging construct, to be used in both adults and youth, that reflects the progressive pathophysiology and risk within CKM syndrome, with therapeutic guidance tied to CKM stages,” Dr. Ndumele told this news organization.
The AHA outlines four stages of CKM syndrome:
Stage 0: At this stage, no CKM risk factors are present, and the goal is to prevent CKM syndrome (particularly unhealthy weight gain) by achieving and maintaining ideal health based on the AHA’s Life’s Essential 8 recommendations. Adults in this stage should be screened every 3-5 years to assess lipids, blood pressure, and blood sugar.
Stage 1: At this stage, excess weight, abdominal obesity, or dysfunctional adipose tissue (clinically manifest as impaired glucose tolerance or prediabetes) is present without other metabolic risk factors or CVD. Management includes providing support for healthy lifestyle changes (healthy eating and regular physical activity), with a goal of at least 5% weight loss and addressing glucose intolerance if needed. Screening adults with stage 1 CKM every 2-3 years is advised to assess blood pressure, triglycerides, cholesterol, and blood sugar.
Stage 2: At this stage, metabolic risk factors (hypertriglyceridemia, hypertension, metabolic syndrome, diabetes) and kidney disease are present. The goal is to address risk factors to prevent progression to CVD and kidney failure. Screening for stage 2 CKM syndrome aligns with AHA/ACC guidelines, which include yearly assessment of blood pressure, triglycerides, cholesterol, blood sugar, and kidney function. More frequent kidney screening is recommended for individuals with increased risk of kidney failure based on kidney function assessments.
Stage 3: This stage describes individuals with subclinical CVD with metabolic risk factors or kidney disease or those at high predicted risk for CVD. The goal is to intensify efforts to prevent progression to symptomatic CVD and kidney failure. This may involve increasing or changing medications, and additional focus on lifestyle changes. Coronary artery calcium (CAC) measurement in some adults is recommended to assess narrowing of the arteries when treatment decisions are unclear.
Stage 4: Individuals with stage 4 CKM syndrome have symptomatic CVD, excess body fat, metabolic risk factors, or kidney disease. Stage 4 CKM syndrome is divided into two subcategories: (4a) no kidney failure and (4b) kidney failure. In this stage, patients may have already had a myocardial infarction (MI) or stroke or may already have heart failure. They also may have additional CV conditions such as peripheral artery disease or atrial fibrillation. The goal of care is individualized treatment for CVD with consideration for CKM syndrome conditions.
The advisory also describes CKM syndrome regression, “an important concept and public health message in which people making healthy lifestyle changes and achieving weight loss may regress to lower CKM syndrome stages and a better state of health,” the AHA says in a news release.
They note that a “critical” next step is to update the pooled cohort equation (PCE) risk prediction algorithm to include measures of kidney function, type 2 diabetes control, and social determinants of health for a more comprehensive risk estimate.
The advisory also recommends risk calculator updates be expanded to assess risk in people as young as age 30 and to calculate both 10- and 30-year CVD risk.
“Clearly defining the patient with CKM syndrome, and providing new approaches for CKM syndrome staging and risk prediction, will help health care professionals to identify these individuals earlier and to provide timely, holistic, and patient-centered care,” Dr. Ndumele said.
This presidential advisory was prepared by the volunteer writing group on behalf of the AHA . The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“This work was prompted by the fact that CKM syndrome leads to premature morbidity and mortality, primarily because of a higher burden of CVD,” writing committee chair Chiadi Ndumele, MD, PhD, said in an interview.
“While CKM syndrome is a public health emergency, there is also great potential for improving CKM health in the population, with an increasing number of therapies that favorably impact metabolic risk factors, risk for adverse kidney events, or both, which also protect against CVD,” added Dr. Ndumele, director of obesity and cardiometabolic research in the division of cardiology at Johns Hopkins University, Baltimore.
The AHA presidential advisory and accompanying scientific statement, which provides a synopsis of evidence for the science and clinical management of CKM, were published online in the journal Circulation.
CKM syndrome staging
According to the AHA, one in three U.S. adults have three or more risk factors that contribute to CVD, metabolic disorders, and/or kidney disease.
In addition to defining CKM syndrome, the advisory provides a “staging construct, to be used in both adults and youth, that reflects the progressive pathophysiology and risk within CKM syndrome, with therapeutic guidance tied to CKM stages,” Dr. Ndumele told this news organization.
The AHA outlines four stages of CKM syndrome:
Stage 0: At this stage, no CKM risk factors are present, and the goal is to prevent CKM syndrome (particularly unhealthy weight gain) by achieving and maintaining ideal health based on the AHA’s Life’s Essential 8 recommendations. Adults in this stage should be screened every 3-5 years to assess lipids, blood pressure, and blood sugar.
Stage 1: At this stage, excess weight, abdominal obesity, or dysfunctional adipose tissue (clinically manifest as impaired glucose tolerance or prediabetes) is present without other metabolic risk factors or CVD. Management includes providing support for healthy lifestyle changes (healthy eating and regular physical activity), with a goal of at least 5% weight loss and addressing glucose intolerance if needed. Screening adults with stage 1 CKM every 2-3 years is advised to assess blood pressure, triglycerides, cholesterol, and blood sugar.
Stage 2: At this stage, metabolic risk factors (hypertriglyceridemia, hypertension, metabolic syndrome, diabetes) and kidney disease are present. The goal is to address risk factors to prevent progression to CVD and kidney failure. Screening for stage 2 CKM syndrome aligns with AHA/ACC guidelines, which include yearly assessment of blood pressure, triglycerides, cholesterol, blood sugar, and kidney function. More frequent kidney screening is recommended for individuals with increased risk of kidney failure based on kidney function assessments.
Stage 3: This stage describes individuals with subclinical CVD with metabolic risk factors or kidney disease or those at high predicted risk for CVD. The goal is to intensify efforts to prevent progression to symptomatic CVD and kidney failure. This may involve increasing or changing medications, and additional focus on lifestyle changes. Coronary artery calcium (CAC) measurement in some adults is recommended to assess narrowing of the arteries when treatment decisions are unclear.
Stage 4: Individuals with stage 4 CKM syndrome have symptomatic CVD, excess body fat, metabolic risk factors, or kidney disease. Stage 4 CKM syndrome is divided into two subcategories: (4a) no kidney failure and (4b) kidney failure. In this stage, patients may have already had a myocardial infarction (MI) or stroke or may already have heart failure. They also may have additional CV conditions such as peripheral artery disease or atrial fibrillation. The goal of care is individualized treatment for CVD with consideration for CKM syndrome conditions.
The advisory also describes CKM syndrome regression, “an important concept and public health message in which people making healthy lifestyle changes and achieving weight loss may regress to lower CKM syndrome stages and a better state of health,” the AHA says in a news release.
They note that a “critical” next step is to update the pooled cohort equation (PCE) risk prediction algorithm to include measures of kidney function, type 2 diabetes control, and social determinants of health for a more comprehensive risk estimate.
The advisory also recommends risk calculator updates be expanded to assess risk in people as young as age 30 and to calculate both 10- and 30-year CVD risk.
“Clearly defining the patient with CKM syndrome, and providing new approaches for CKM syndrome staging and risk prediction, will help health care professionals to identify these individuals earlier and to provide timely, holistic, and patient-centered care,” Dr. Ndumele said.
This presidential advisory was prepared by the volunteer writing group on behalf of the AHA . The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“This work was prompted by the fact that CKM syndrome leads to premature morbidity and mortality, primarily because of a higher burden of CVD,” writing committee chair Chiadi Ndumele, MD, PhD, said in an interview.
“While CKM syndrome is a public health emergency, there is also great potential for improving CKM health in the population, with an increasing number of therapies that favorably impact metabolic risk factors, risk for adverse kidney events, or both, which also protect against CVD,” added Dr. Ndumele, director of obesity and cardiometabolic research in the division of cardiology at Johns Hopkins University, Baltimore.
The AHA presidential advisory and accompanying scientific statement, which provides a synopsis of evidence for the science and clinical management of CKM, were published online in the journal Circulation.
CKM syndrome staging
According to the AHA, one in three U.S. adults have three or more risk factors that contribute to CVD, metabolic disorders, and/or kidney disease.
In addition to defining CKM syndrome, the advisory provides a “staging construct, to be used in both adults and youth, that reflects the progressive pathophysiology and risk within CKM syndrome, with therapeutic guidance tied to CKM stages,” Dr. Ndumele told this news organization.
The AHA outlines four stages of CKM syndrome:
Stage 0: At this stage, no CKM risk factors are present, and the goal is to prevent CKM syndrome (particularly unhealthy weight gain) by achieving and maintaining ideal health based on the AHA’s Life’s Essential 8 recommendations. Adults in this stage should be screened every 3-5 years to assess lipids, blood pressure, and blood sugar.
Stage 1: At this stage, excess weight, abdominal obesity, or dysfunctional adipose tissue (clinically manifest as impaired glucose tolerance or prediabetes) is present without other metabolic risk factors or CVD. Management includes providing support for healthy lifestyle changes (healthy eating and regular physical activity), with a goal of at least 5% weight loss and addressing glucose intolerance if needed. Screening adults with stage 1 CKM every 2-3 years is advised to assess blood pressure, triglycerides, cholesterol, and blood sugar.
Stage 2: At this stage, metabolic risk factors (hypertriglyceridemia, hypertension, metabolic syndrome, diabetes) and kidney disease are present. The goal is to address risk factors to prevent progression to CVD and kidney failure. Screening for stage 2 CKM syndrome aligns with AHA/ACC guidelines, which include yearly assessment of blood pressure, triglycerides, cholesterol, blood sugar, and kidney function. More frequent kidney screening is recommended for individuals with increased risk of kidney failure based on kidney function assessments.
Stage 3: This stage describes individuals with subclinical CVD with metabolic risk factors or kidney disease or those at high predicted risk for CVD. The goal is to intensify efforts to prevent progression to symptomatic CVD and kidney failure. This may involve increasing or changing medications, and additional focus on lifestyle changes. Coronary artery calcium (CAC) measurement in some adults is recommended to assess narrowing of the arteries when treatment decisions are unclear.
Stage 4: Individuals with stage 4 CKM syndrome have symptomatic CVD, excess body fat, metabolic risk factors, or kidney disease. Stage 4 CKM syndrome is divided into two subcategories: (4a) no kidney failure and (4b) kidney failure. In this stage, patients may have already had a myocardial infarction (MI) or stroke or may already have heart failure. They also may have additional CV conditions such as peripheral artery disease or atrial fibrillation. The goal of care is individualized treatment for CVD with consideration for CKM syndrome conditions.
The advisory also describes CKM syndrome regression, “an important concept and public health message in which people making healthy lifestyle changes and achieving weight loss may regress to lower CKM syndrome stages and a better state of health,” the AHA says in a news release.
They note that a “critical” next step is to update the pooled cohort equation (PCE) risk prediction algorithm to include measures of kidney function, type 2 diabetes control, and social determinants of health for a more comprehensive risk estimate.
The advisory also recommends risk calculator updates be expanded to assess risk in people as young as age 30 and to calculate both 10- and 30-year CVD risk.
“Clearly defining the patient with CKM syndrome, and providing new approaches for CKM syndrome staging and risk prediction, will help health care professionals to identify these individuals earlier and to provide timely, holistic, and patient-centered care,” Dr. Ndumele said.
This presidential advisory was prepared by the volunteer writing group on behalf of the AHA . The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CIRCULATION