User login
Cell-Free DNA Blood Test Shows Strong Performance in Detecting Early-Stage CRC
Cell-Free DNA Blood Test Shows Strong Performance in Detecting Early-Stage CRC
TOPLINE:
A novel, blood-based test developed using fragmentomic features of cell-free DNA (cfDNA) detects colorectal cancer (CRC) with a 90.4% sensitivity and shows consistent performance across stages and tumor locations.
METHODOLOGY:
- Researchers conducted a prospective case-control study to develop and validate a noninvasive cfDNA-based screening test for CRC.
- Adults aged 40-89 years with CRC or advanced adenomas were enrolled at a tertiary center in South Korea between 2021 and 2024.
- Blood samples were drawn after colonoscopy, but prior to treatment, in patients with CRC, advanced adenomas, and asymptomatic controls with normal colonoscopy results.
- A model was trained on fragmentonic features derived from whole genome sequencing of cfDNA from 1250 participants and validated for its diagnostic performance in the remaining 427 participants, including all with advanced adenomas.
- The primary endpoint was the sensitivity of the cfDNA test for detecting CRC. The area under the receiver operating characteristic curve (AUROC) was also calculated.
TAKEAWAY:
- The cfDNA test detected CRC with 90.4% sensitivity and an AUROC of 0.978.
- Sensitivity by CRC stage was 84.2% for stage I, 85.0% for stage II, 94.4% for stage III, 100% for stage IV.
- Advanced adenomas were detected with 58.3% sensitivity and an AUROC of 0.862.
- Among individuals with normal colonoscopy findings, the test was correctly negative 94.7% of the time.
- Diagnostic sensitivities were consistent between left- and right-sided CRC tumors, among participants aged < 60 years and ≥ 60 years, and across left- and right-sided advanced adenomas.
IN PRACTICE:
"This highlights the potential clinical utility of the test in identifying candidates for minimally invasive therapeutic approaches tool for CRC," the authors wrote. "Notably, the high sensitivity observed for early-stage CRC and the favorable sensitivity for [advanced adenoma] suggest that this cfDNA test may offer benefits not only in diagnosis but also in prognosis and ultimately in CRC prevention."
SOURCE:
This study was led by Seung Wook Hong, MD, Asan Medical Center in Seoul, South Korea. It was published online on November 19, 2025, in the American Journal of Gastroenterology.
LIMITATIONS:
The case-control design introduced spectrum bias by comparing clearly defined CRC and advanced adenomas cases with individuals who had normal colonoscopy results. The CRC prevalence of 17% to 18% was higher than that observed in true screening populations, limiting generalizability. The exclusively Korean cohort limited extrapolation to non-Asian populations.
DISCLOSURES:
The study received support from GC Genome, Yongin, South Korea. The authors reported no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
A novel, blood-based test developed using fragmentomic features of cell-free DNA (cfDNA) detects colorectal cancer (CRC) with a 90.4% sensitivity and shows consistent performance across stages and tumor locations.
METHODOLOGY:
- Researchers conducted a prospective case-control study to develop and validate a noninvasive cfDNA-based screening test for CRC.
- Adults aged 40-89 years with CRC or advanced adenomas were enrolled at a tertiary center in South Korea between 2021 and 2024.
- Blood samples were drawn after colonoscopy, but prior to treatment, in patients with CRC, advanced adenomas, and asymptomatic controls with normal colonoscopy results.
- A model was trained on fragmentonic features derived from whole genome sequencing of cfDNA from 1250 participants and validated for its diagnostic performance in the remaining 427 participants, including all with advanced adenomas.
- The primary endpoint was the sensitivity of the cfDNA test for detecting CRC. The area under the receiver operating characteristic curve (AUROC) was also calculated.
TAKEAWAY:
- The cfDNA test detected CRC with 90.4% sensitivity and an AUROC of 0.978.
- Sensitivity by CRC stage was 84.2% for stage I, 85.0% for stage II, 94.4% for stage III, 100% for stage IV.
- Advanced adenomas were detected with 58.3% sensitivity and an AUROC of 0.862.
- Among individuals with normal colonoscopy findings, the test was correctly negative 94.7% of the time.
- Diagnostic sensitivities were consistent between left- and right-sided CRC tumors, among participants aged < 60 years and ≥ 60 years, and across left- and right-sided advanced adenomas.
IN PRACTICE:
"This highlights the potential clinical utility of the test in identifying candidates for minimally invasive therapeutic approaches tool for CRC," the authors wrote. "Notably, the high sensitivity observed for early-stage CRC and the favorable sensitivity for [advanced adenoma] suggest that this cfDNA test may offer benefits not only in diagnosis but also in prognosis and ultimately in CRC prevention."
SOURCE:
This study was led by Seung Wook Hong, MD, Asan Medical Center in Seoul, South Korea. It was published online on November 19, 2025, in the American Journal of Gastroenterology.
LIMITATIONS:
The case-control design introduced spectrum bias by comparing clearly defined CRC and advanced adenomas cases with individuals who had normal colonoscopy results. The CRC prevalence of 17% to 18% was higher than that observed in true screening populations, limiting generalizability. The exclusively Korean cohort limited extrapolation to non-Asian populations.
DISCLOSURES:
The study received support from GC Genome, Yongin, South Korea. The authors reported no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
A novel, blood-based test developed using fragmentomic features of cell-free DNA (cfDNA) detects colorectal cancer (CRC) with a 90.4% sensitivity and shows consistent performance across stages and tumor locations.
METHODOLOGY:
- Researchers conducted a prospective case-control study to develop and validate a noninvasive cfDNA-based screening test for CRC.
- Adults aged 40-89 years with CRC or advanced adenomas were enrolled at a tertiary center in South Korea between 2021 and 2024.
- Blood samples were drawn after colonoscopy, but prior to treatment, in patients with CRC, advanced adenomas, and asymptomatic controls with normal colonoscopy results.
- A model was trained on fragmentonic features derived from whole genome sequencing of cfDNA from 1250 participants and validated for its diagnostic performance in the remaining 427 participants, including all with advanced adenomas.
- The primary endpoint was the sensitivity of the cfDNA test for detecting CRC. The area under the receiver operating characteristic curve (AUROC) was also calculated.
TAKEAWAY:
- The cfDNA test detected CRC with 90.4% sensitivity and an AUROC of 0.978.
- Sensitivity by CRC stage was 84.2% for stage I, 85.0% for stage II, 94.4% for stage III, 100% for stage IV.
- Advanced adenomas were detected with 58.3% sensitivity and an AUROC of 0.862.
- Among individuals with normal colonoscopy findings, the test was correctly negative 94.7% of the time.
- Diagnostic sensitivities were consistent between left- and right-sided CRC tumors, among participants aged < 60 years and ≥ 60 years, and across left- and right-sided advanced adenomas.
IN PRACTICE:
"This highlights the potential clinical utility of the test in identifying candidates for minimally invasive therapeutic approaches tool for CRC," the authors wrote. "Notably, the high sensitivity observed for early-stage CRC and the favorable sensitivity for [advanced adenoma] suggest that this cfDNA test may offer benefits not only in diagnosis but also in prognosis and ultimately in CRC prevention."
SOURCE:
This study was led by Seung Wook Hong, MD, Asan Medical Center in Seoul, South Korea. It was published online on November 19, 2025, in the American Journal of Gastroenterology.
LIMITATIONS:
The case-control design introduced spectrum bias by comparing clearly defined CRC and advanced adenomas cases with individuals who had normal colonoscopy results. The CRC prevalence of 17% to 18% was higher than that observed in true screening populations, limiting generalizability. The exclusively Korean cohort limited extrapolation to non-Asian populations.
DISCLOSURES:
The study received support from GC Genome, Yongin, South Korea. The authors reported no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Cell-Free DNA Blood Test Shows Strong Performance in Detecting Early-Stage CRC
Cell-Free DNA Blood Test Shows Strong Performance in Detecting Early-Stage CRC

Geographic Clusters Show Uneven Cancer Screening in the US
Geographic Clusters Show Uneven Cancer Screening in the US
TOPLINE:
An analysis of 3142 US counties revealed that county-level screening for breast, cervical, and colorectal cancer increased overall between 1997 and 2019; however, despite the reduced geographic variation, persistently high-screening clusters remained in the Northeast, whereas persistently low-screening clusters remained in the Southwest.
METHODOLOGY:
- Cancer screening reduces mortality. Despite guideline recommendation, the uptake of breast, cervical, and colorectal cancer screening in the US falls short of national goals and varies across sociodemographic groups. To date, only a few studies have examined geographic and temporal patterns of screening.
- To address this gap, researchers conducted a cross-sectional study using an ecological panel design to analyze county-level screening prevalence across 3142 US mainland counties from 1997 to 2019, deriving prevalence estimates from Behavioral Risk Factor Surveillance System (BRFSS) and National Health Interview Survey (NHIS) data over 3- to 5-year periods.
- Spatial autocorrelation analyses, including Global Moran I and the bivariate local indicator of spatial autocorrelation, were performed to assess geographic clusters of cancer screening within each period. Four types of local geographic clusters of county-level cancer screening were identified: counties with persistently high screening rates, counties with persistently low screening rates, counties in which screening rates decreased from high to low, and counties in which screening rates increased from low to high.
- Screening prevalence was compared across multiple time windows for different modalities (mammography, a Papanicolaou test, colonoscopy, colorectal cancer test, endoscopy, and a fecal occult blood test [FOBT]). Overall, 3101 counties were analyzed for mammography and the Papanicolaou test, 3107 counties for colonoscopy, 3100 counties for colorectal cancer test, 3089 counties for endoscopy, and 3090 counties for the FOBT.
TAKEAWAY:
- Overall screening prevalence increased from 1997 to 2019, and global spatial autocorrelation declined over time. For instance, the distribution of mammography screening became 83% more uniform in more recent years (Moran I, 0.57 in 1997-1999 vs 0.10 in 2017-2019). Similarly, Papanicolaou test screening became more uniform in more recent years (Moran I, 0.44 vs. 0.07). These changes indicate reduced geographic heterogeneity.
- Colonoscopy and endoscopy use increased, surpassing a 50% prevalence in many counties for 2010; however, FOBT use declined. Spatial clustering also attenuated, with a 23.4% declined in Moran I for colonoscopy from 2011-2016 to 2017-2019, a 12.3% decline in the colorectal cancer test from 2004-2007 to 2008-2010, and a 14.0% decline for endoscopy from 2004-2007 to 2008-2010.
- Persistently high-/high-screening clusters were concentrated in the Northeast for mammography and colorectal cancer screening and in the East for Papanicolaou test screening, whereas persistently low-/low-screening clusters were concentrated in the Southwest for the same modalities.
- Clusters of low- and high-screening counties were more disadvantaged -- with lower socioeconomic status and a higher proportion of non-White residents -- than other cluster types, suggesting some improvement in screening uptake in more disadvantaged areas. Counties with persistently low screening exhibited greater socioeconomic disadvantages -- lower media household income, higher poverty, lower home values, and lower educational attainment -- than those with persistently high screening.
IN PRACTICE:
"This cross-sectional study found that despite secular increases that reduced geographic variation in screening, local clusters of high and low screening persisted in the Northeast and Southwest US, respectively. Future studies could incorporate health care access characteristics to explain why areas of low screening did not catch up to optimize cancer screening practice," the authors wrote.
SOURCE:
The study, led by Pranoti Pradhan, PhD, Harvard T.H. Chan School of Public Health, Boston, was published online in JAMA Network Open.
LIMITATIONS:
The county-level estimates were modeled using BRFSS, NHIS, and US Census data, which might be susceptible to sampling biases despite corrections for nonresponse and noncoverage. Researchers lacked data on specific health systems characteristics that may have directly driven changes in prevalence and were restricted to using screening time intervals available from the Small Area Estimates for Cancer-Relates Measures from the National Cancer Institute, rather than those according to US Preventive Services Task Force guidelines. Additionally, the spatial cluster method was sensitive to county size and arrangement, which may have influenced local cluster detection.
DISCLOSURES:
This research was supported by the T32 Cancer Prevention and Control Funding Fellowship and T32 Cancer Epidemiology Fellowship at the Harvard T.H. Chan School of Public Health. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
An analysis of 3142 US counties revealed that county-level screening for breast, cervical, and colorectal cancer increased overall between 1997 and 2019; however, despite the reduced geographic variation, persistently high-screening clusters remained in the Northeast, whereas persistently low-screening clusters remained in the Southwest.
METHODOLOGY:
- Cancer screening reduces mortality. Despite guideline recommendation, the uptake of breast, cervical, and colorectal cancer screening in the US falls short of national goals and varies across sociodemographic groups. To date, only a few studies have examined geographic and temporal patterns of screening.
- To address this gap, researchers conducted a cross-sectional study using an ecological panel design to analyze county-level screening prevalence across 3142 US mainland counties from 1997 to 2019, deriving prevalence estimates from Behavioral Risk Factor Surveillance System (BRFSS) and National Health Interview Survey (NHIS) data over 3- to 5-year periods.
- Spatial autocorrelation analyses, including Global Moran I and the bivariate local indicator of spatial autocorrelation, were performed to assess geographic clusters of cancer screening within each period. Four types of local geographic clusters of county-level cancer screening were identified: counties with persistently high screening rates, counties with persistently low screening rates, counties in which screening rates decreased from high to low, and counties in which screening rates increased from low to high.
- Screening prevalence was compared across multiple time windows for different modalities (mammography, a Papanicolaou test, colonoscopy, colorectal cancer test, endoscopy, and a fecal occult blood test [FOBT]). Overall, 3101 counties were analyzed for mammography and the Papanicolaou test, 3107 counties for colonoscopy, 3100 counties for colorectal cancer test, 3089 counties for endoscopy, and 3090 counties for the FOBT.
TAKEAWAY:
- Overall screening prevalence increased from 1997 to 2019, and global spatial autocorrelation declined over time. For instance, the distribution of mammography screening became 83% more uniform in more recent years (Moran I, 0.57 in 1997-1999 vs 0.10 in 2017-2019). Similarly, Papanicolaou test screening became more uniform in more recent years (Moran I, 0.44 vs. 0.07). These changes indicate reduced geographic heterogeneity.
- Colonoscopy and endoscopy use increased, surpassing a 50% prevalence in many counties for 2010; however, FOBT use declined. Spatial clustering also attenuated, with a 23.4% declined in Moran I for colonoscopy from 2011-2016 to 2017-2019, a 12.3% decline in the colorectal cancer test from 2004-2007 to 2008-2010, and a 14.0% decline for endoscopy from 2004-2007 to 2008-2010.
- Persistently high-/high-screening clusters were concentrated in the Northeast for mammography and colorectal cancer screening and in the East for Papanicolaou test screening, whereas persistently low-/low-screening clusters were concentrated in the Southwest for the same modalities.
- Clusters of low- and high-screening counties were more disadvantaged -- with lower socioeconomic status and a higher proportion of non-White residents -- than other cluster types, suggesting some improvement in screening uptake in more disadvantaged areas. Counties with persistently low screening exhibited greater socioeconomic disadvantages -- lower media household income, higher poverty, lower home values, and lower educational attainment -- than those with persistently high screening.
IN PRACTICE:
"This cross-sectional study found that despite secular increases that reduced geographic variation in screening, local clusters of high and low screening persisted in the Northeast and Southwest US, respectively. Future studies could incorporate health care access characteristics to explain why areas of low screening did not catch up to optimize cancer screening practice," the authors wrote.
SOURCE:
The study, led by Pranoti Pradhan, PhD, Harvard T.H. Chan School of Public Health, Boston, was published online in JAMA Network Open.
LIMITATIONS:
The county-level estimates were modeled using BRFSS, NHIS, and US Census data, which might be susceptible to sampling biases despite corrections for nonresponse and noncoverage. Researchers lacked data on specific health systems characteristics that may have directly driven changes in prevalence and were restricted to using screening time intervals available from the Small Area Estimates for Cancer-Relates Measures from the National Cancer Institute, rather than those according to US Preventive Services Task Force guidelines. Additionally, the spatial cluster method was sensitive to county size and arrangement, which may have influenced local cluster detection.
DISCLOSURES:
This research was supported by the T32 Cancer Prevention and Control Funding Fellowship and T32 Cancer Epidemiology Fellowship at the Harvard T.H. Chan School of Public Health. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
An analysis of 3142 US counties revealed that county-level screening for breast, cervical, and colorectal cancer increased overall between 1997 and 2019; however, despite the reduced geographic variation, persistently high-screening clusters remained in the Northeast, whereas persistently low-screening clusters remained in the Southwest.
METHODOLOGY:
- Cancer screening reduces mortality. Despite guideline recommendation, the uptake of breast, cervical, and colorectal cancer screening in the US falls short of national goals and varies across sociodemographic groups. To date, only a few studies have examined geographic and temporal patterns of screening.
- To address this gap, researchers conducted a cross-sectional study using an ecological panel design to analyze county-level screening prevalence across 3142 US mainland counties from 1997 to 2019, deriving prevalence estimates from Behavioral Risk Factor Surveillance System (BRFSS) and National Health Interview Survey (NHIS) data over 3- to 5-year periods.
- Spatial autocorrelation analyses, including Global Moran I and the bivariate local indicator of spatial autocorrelation, were performed to assess geographic clusters of cancer screening within each period. Four types of local geographic clusters of county-level cancer screening were identified: counties with persistently high screening rates, counties with persistently low screening rates, counties in which screening rates decreased from high to low, and counties in which screening rates increased from low to high.
- Screening prevalence was compared across multiple time windows for different modalities (mammography, a Papanicolaou test, colonoscopy, colorectal cancer test, endoscopy, and a fecal occult blood test [FOBT]). Overall, 3101 counties were analyzed for mammography and the Papanicolaou test, 3107 counties for colonoscopy, 3100 counties for colorectal cancer test, 3089 counties for endoscopy, and 3090 counties for the FOBT.
TAKEAWAY:
- Overall screening prevalence increased from 1997 to 2019, and global spatial autocorrelation declined over time. For instance, the distribution of mammography screening became 83% more uniform in more recent years (Moran I, 0.57 in 1997-1999 vs 0.10 in 2017-2019). Similarly, Papanicolaou test screening became more uniform in more recent years (Moran I, 0.44 vs. 0.07). These changes indicate reduced geographic heterogeneity.
- Colonoscopy and endoscopy use increased, surpassing a 50% prevalence in many counties for 2010; however, FOBT use declined. Spatial clustering also attenuated, with a 23.4% declined in Moran I for colonoscopy from 2011-2016 to 2017-2019, a 12.3% decline in the colorectal cancer test from 2004-2007 to 2008-2010, and a 14.0% decline for endoscopy from 2004-2007 to 2008-2010.
- Persistently high-/high-screening clusters were concentrated in the Northeast for mammography and colorectal cancer screening and in the East for Papanicolaou test screening, whereas persistently low-/low-screening clusters were concentrated in the Southwest for the same modalities.
- Clusters of low- and high-screening counties were more disadvantaged -- with lower socioeconomic status and a higher proportion of non-White residents -- than other cluster types, suggesting some improvement in screening uptake in more disadvantaged areas. Counties with persistently low screening exhibited greater socioeconomic disadvantages -- lower media household income, higher poverty, lower home values, and lower educational attainment -- than those with persistently high screening.
IN PRACTICE:
"This cross-sectional study found that despite secular increases that reduced geographic variation in screening, local clusters of high and low screening persisted in the Northeast and Southwest US, respectively. Future studies could incorporate health care access characteristics to explain why areas of low screening did not catch up to optimize cancer screening practice," the authors wrote.
SOURCE:
The study, led by Pranoti Pradhan, PhD, Harvard T.H. Chan School of Public Health, Boston, was published online in JAMA Network Open.
LIMITATIONS:
The county-level estimates were modeled using BRFSS, NHIS, and US Census data, which might be susceptible to sampling biases despite corrections for nonresponse and noncoverage. Researchers lacked data on specific health systems characteristics that may have directly driven changes in prevalence and were restricted to using screening time intervals available from the Small Area Estimates for Cancer-Relates Measures from the National Cancer Institute, rather than those according to US Preventive Services Task Force guidelines. Additionally, the spatial cluster method was sensitive to county size and arrangement, which may have influenced local cluster detection.
DISCLOSURES:
This research was supported by the T32 Cancer Prevention and Control Funding Fellowship and T32 Cancer Epidemiology Fellowship at the Harvard T.H. Chan School of Public Health. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Geographic Clusters Show Uneven Cancer Screening in the US
Geographic Clusters Show Uneven Cancer Screening in the US

Colorectal Cancer Characteristics and Mortality From Propensity Score-Matched Cohorts of Urban and Rural Veterans
Colorectal Cancer Characteristics and Mortality From Propensity Score-Matched Cohorts of Urban and Rural Veterans
Colorectal cancer (CRC) is the second-leading cause of cancer-related deaths in the United States, with an estimated 52,550 deaths in 2023.1 However, the disease burden varies among different segments of the population.2 While both CRC incidence and mortality have been decreasing due to screening and advances in treatment, there are disparities in incidence and mortality across the sociodemographic spectrum including race, ethnicity, education, and income.1-4 While CRC incidence is decreasing for older adults, it is increasing among those aged < 55 years.5 The incidence of CRC in adults aged 40 to 54 years has increased by 0.5% to 1.3% annually since the mid-1990s.6 The US Preventive Services Task Force now recommends starting CRC screening at age 45 years for asymptomatic adults with average risk.7
Disparities also exist across geographical boundaries and living environment. Rural Americans faces additional challenges in health and lifestyle that can affect CRC outcomes. Compared to their urban counterparts, rural residents are more likely to be older, have lower levels of education, higher levels of poverty, lack health insurance, and less access to health care practitioners (HCPs).8-10 Geographic proximity, defined as travel time or physical distance to a health facility, has been recognized as a predictor of inferior outcomes.11 These aspects of rural living may pose challenges for accessing care for CRC screening and treatment.11-13 National and local studies have shown disparities in CRC screening rates, incidence, and mortality between rural and urban populations.14-16
It is unclear whether rural/urban disparities persist under the Veterans Health Administration (VHA) health care delivery model. This study examined differences in baseline characteristics and mortality between rural and urban veterans newly diagnosed with CRC. We also focused on a subpopulation aged ≤ 45 years.
Methods
This study extracted national data from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW) hosted in the VA Informatics and Computing Infrastructure (VINCI) environment. VINCI is an initiative to improve access to VA data and facilitate the analysis of these data while ensuring veterans’ privacy and data security.17 CDW is the VHA business intelligence information repository, which extracts data from clinical and nonclinical sources following prescribed and validated protocols. Data extracted included demographics, diagnosis, and procedure codes for both inpatient and outpatient encounters, vital signs, and vital status. This study used data previously extracted from a national cohort of veterans that encompassed all patients who received a group of commonly prescribed medications, such as statins, proton pump inhibitors, histamine-2 blockers, acetaminophen-containing products, and hydrocortisone-containing skin applications. This cohort encompassed 8,648,754 veterans, from whom 2,460,727 had encounters during fiscal years (FY) 2016 to 2021 (study period). The cohort was used to ensure that subjects were VHA patients, allowing them to adequately capture their clinical profiles.
Patients were identified as rural or urban based on their residence address at the date of their first diagnosis of CRC. The Geospatial Service Support Center (GSSC) aggregates and updates veterans’ residence address records for all enrolled veterans from the National Change of Address database. The data contain 1 record per enrollee. GSSC Geocoded Enrollee File contains enrollee addresses and their rurality indicators, categorized as urban, rural, or highly rural.18 Rurality is defined by the Rural Urban Commuting Area (RUCA) categories developed by the Department of Agriculture and the Health Resources and Services Administration of the US Department of Health and Human Services.19 Urban areas had RUCA codes of 1.0 to 1.1, and highly rural areas had RUCA scores of 10.0. All other areas were classified as rural. Since the proportion of veterans from highly rural areas was small, we included residents from highly rural areas in the rural residents’ group.
Inclusion and Exclusion Criteria
All veterans newly diagnosed with CRC from FY 2016 to 2021 were included. We used the ninth and tenth clinical modification revisions of the International Classification of Diseases (ICD-9-CM and ICD-10-CM) to define CRC diagnosis (Supplemental materials).4,20 To ensure that patients were newly diagnosed with CRC, this study excluded patients with a previous ICD-9-CM code for CRC diagnosis since FY 2003.
Comorbidities were identified using diagnosis and procedure codes from inpatient and outpatient encounters, which were used to calculate the Charlson Comorbidity Index (CCI) at the time of CRC diagnosis using the weighted method described by Schneeweiss et al.21 We defined CRC high-risk conditions and CRC screening tests, including flexible sigmoidoscopy and stool tests, as described in previous studies (Supplemental materials).20
The main outcome was total mortality. The date of death was extracted from the VHA Death Ascertainment File, which contains mortality data from the Master Person Index file in CDW and the Social Security Administration Death Master File. We used the date of death from any cause, as cause of death was not available.
A propensity score (PS) was created to match rural (including highly rural) and urban residents at a ratio of 1:1. Using a standard procedure described in prior publications, multivariable logistic regression used all baseline characteristics to estimate the PS and perform nearest-number matching without replacement.22,23 A caliper of 0.01 maximized the matched cohort size and achieved balance (Supplemental materials). We then examined the balance of baseline characteristics between PS-matched groups.
Analyses
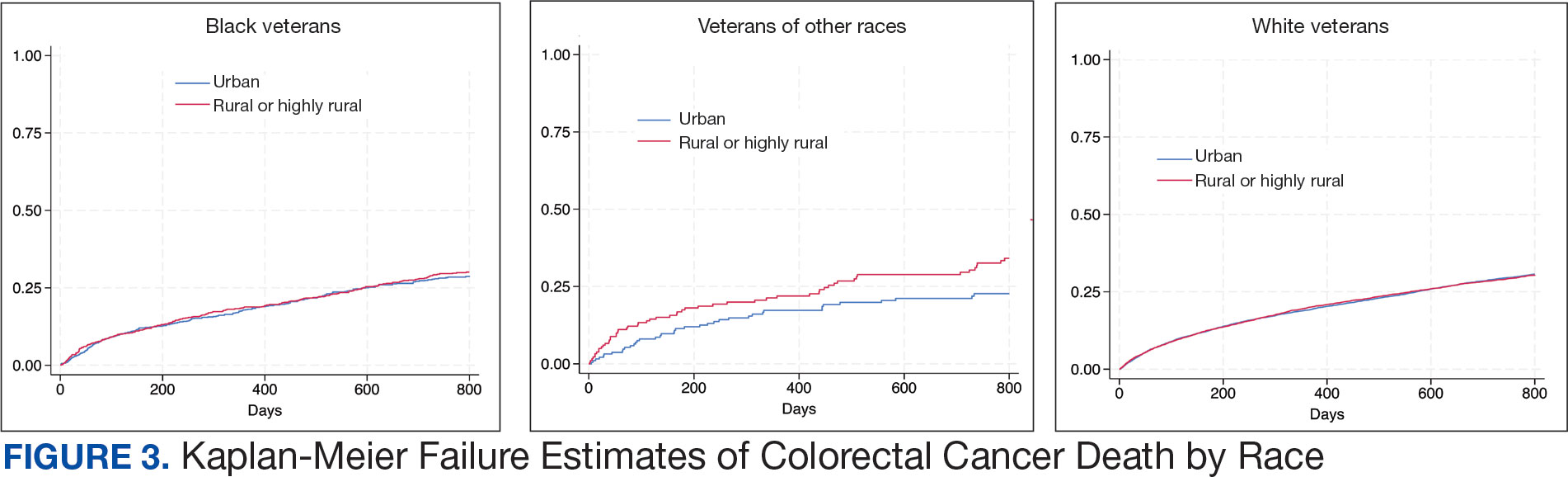
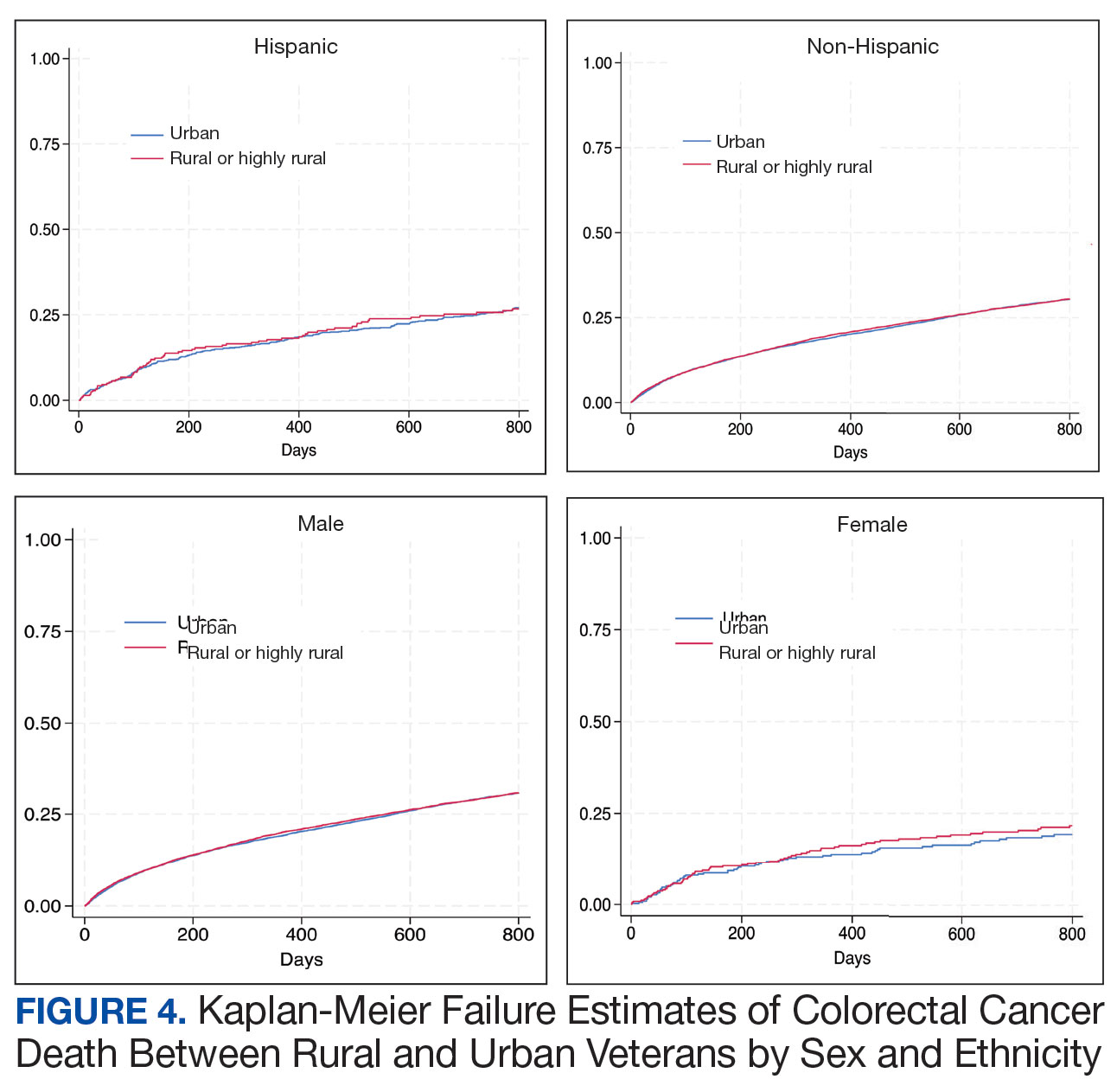
Cox proportional hazards regression analysis estimated the hazard ratio (HR) of death in rural residents compared to urban residents in the PS-matched cohort. The outcome event was the date of death during the study’s follow-up period (defined as period from first CRC diagnosis to death or study end), with censoring at the study’s end date (September 30, 2021). The proportional hazards assumption was assessed by inspecting the Kaplan-Meier curves. Multiple analyses examined the HR of total mortality in the PS-matched cohort, stratified by sex, race, and ethnicity. We also examined the HR of total mortality stratified by duration of follow-up.
Another PS-matching analysis among veterans aged ≤ 45 years was performed using the same techniques described earlier in this article. We performed a Cox proportional hazards regression analysis to compare mortality in PS-matched urban and rural veterans aged ≤ 45 years. The HR of death in all veterans aged ≤ 45 years (before PS-matching) was estimated using Cox proportional hazard regression analysis, adjusting for PS.
Dichotomous variables were compared using X2 tests and continuous variables were compared using t tests. Baseline characteristics with missing values were converted into categorical variables and the proportion of subjects with missing values was equalized between treatment groups after PS-matching. For subgroup analysis, we examined the HR of total mortality in each subgroup using separate Cox proportional hazards regression models similar to the primary analysis but adjusted for PS. Due to multiple comparisons in the subgroup analysis, the findings should be considered exploratory. Statistical tests were 2-tailed, and significance was defined as P < .05. Data management and statistical analyses were conducted from June 2022 to January 2023 using STATA, Version 17. The VA Orlando Healthcare System Institutional Review Board approved the study and waived requirements for informed consent because only deidentified data were used.
Results
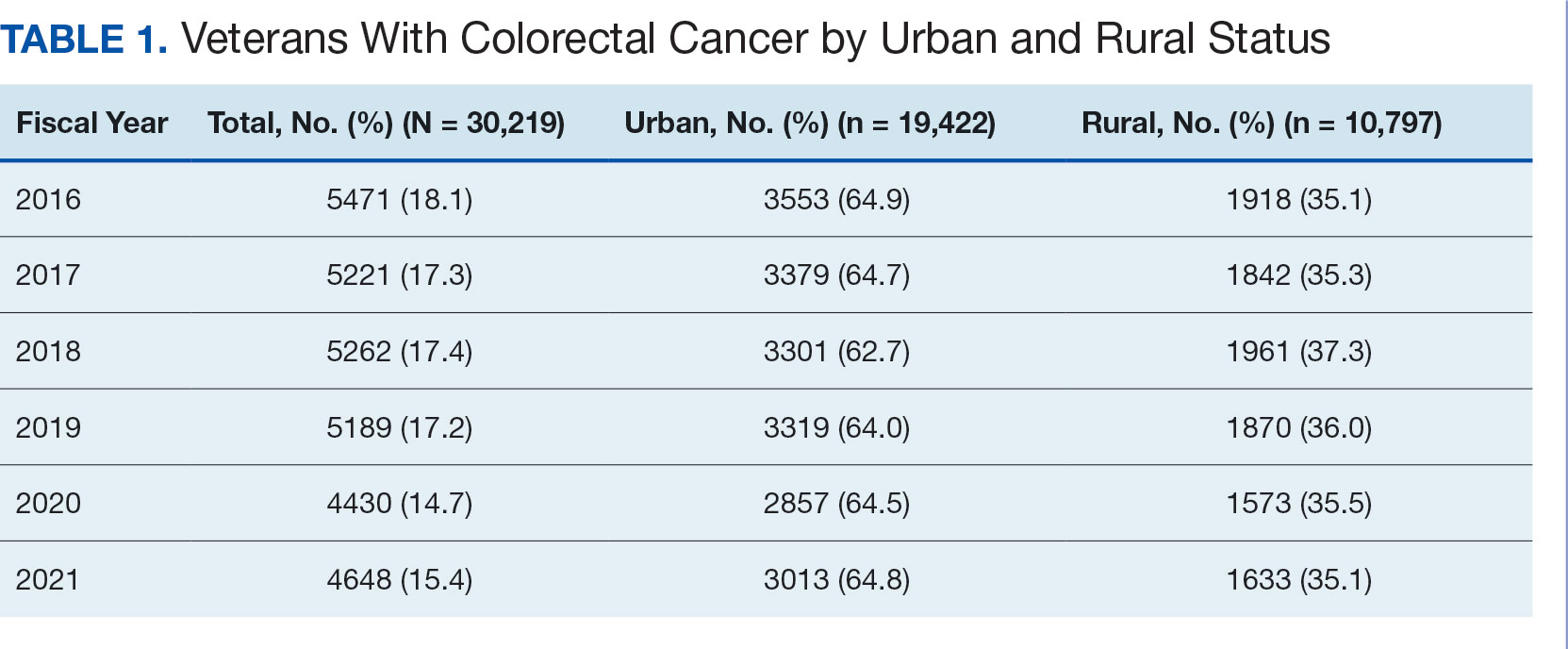
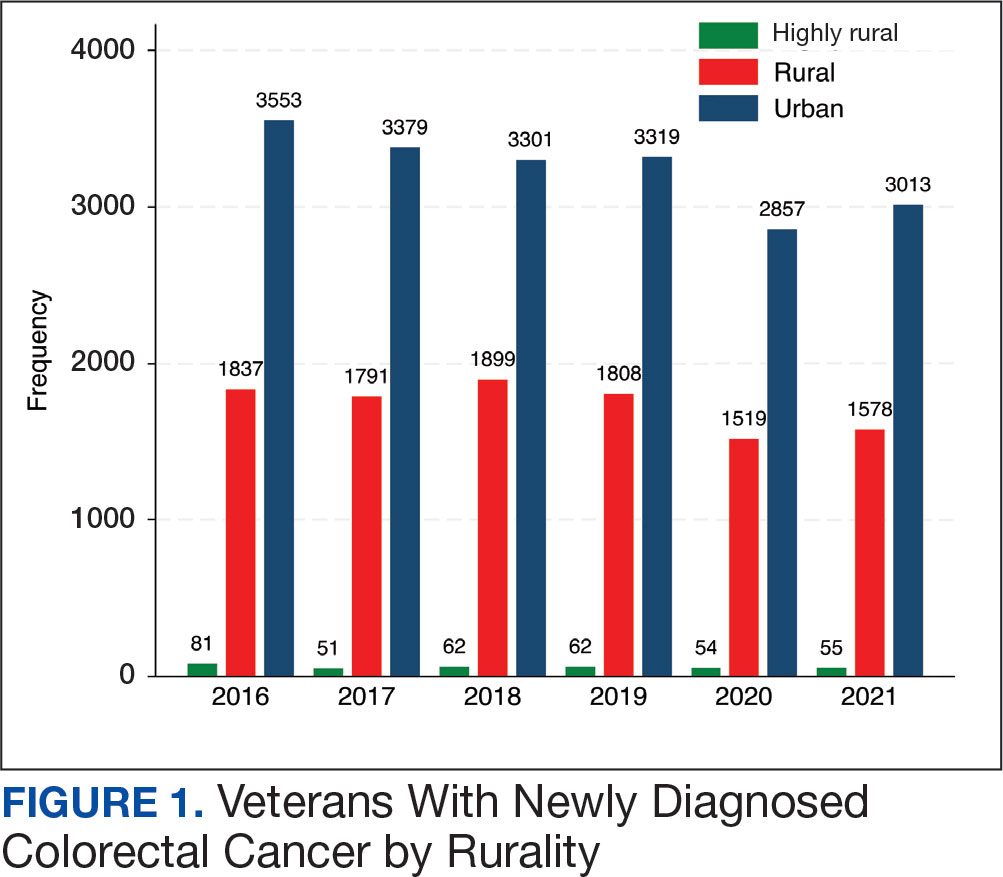
After excluding 49 patients (Supplemental materials, available at doi:10.12788/fp.0560), we identified 30,219 veterans with newly diagnosed CRC between FY 2016 to 2021 (Table 1). Of these, 19,422 (64.3%) resided in urban areas and 10,797 (35.7%) resided in rural areas (Table 2). The mean (SD) duration from the first CRC diagnosis to death or study end was 832 (640) days, and the median (IQR) was 723 (246–1330) days. Overall, incident CRC diagnoses were numerically highest in FY 2016 and lowest in FY 2020 (Figure 1). Patients with CRC in rural areas vs urban areas were significantly older (mean, 71.2 years vs 70.8 years, respectively; P < .001), more likely to be male (96.7% vs 95.7%, respectively; P < .001), more likely to be White (83.6% vs 67.8%, respectively; P < .001) and more likely to be non-Hispanic (92.2% vs 87.5%, respectively; P < .001). In terms of general health, rural veterans with CRC were more likely to be overweight or obese (81.5% rural vs 78.5% urban; P < .001) but had fewer mean comorbidities as measured by CCI (5.66 rural vs 5.90 urban; P < .001). A higher proportion of rural veterans with CRC had received stool-based (fecal occult blood test or fecal immunochemical test) CRC screening tests (61.6% rural vs 57.2% urban; P < .001). Fewer rural patients presented with systemic symptoms or signs within 1 year of CRC diagnosis (54.4% rural vs 57.5% urban, P < .001). Among urban patients with CRC, 6959 (35.8%) deaths were observed, compared with 3766 (34.9%) among rural patients (P = .10).
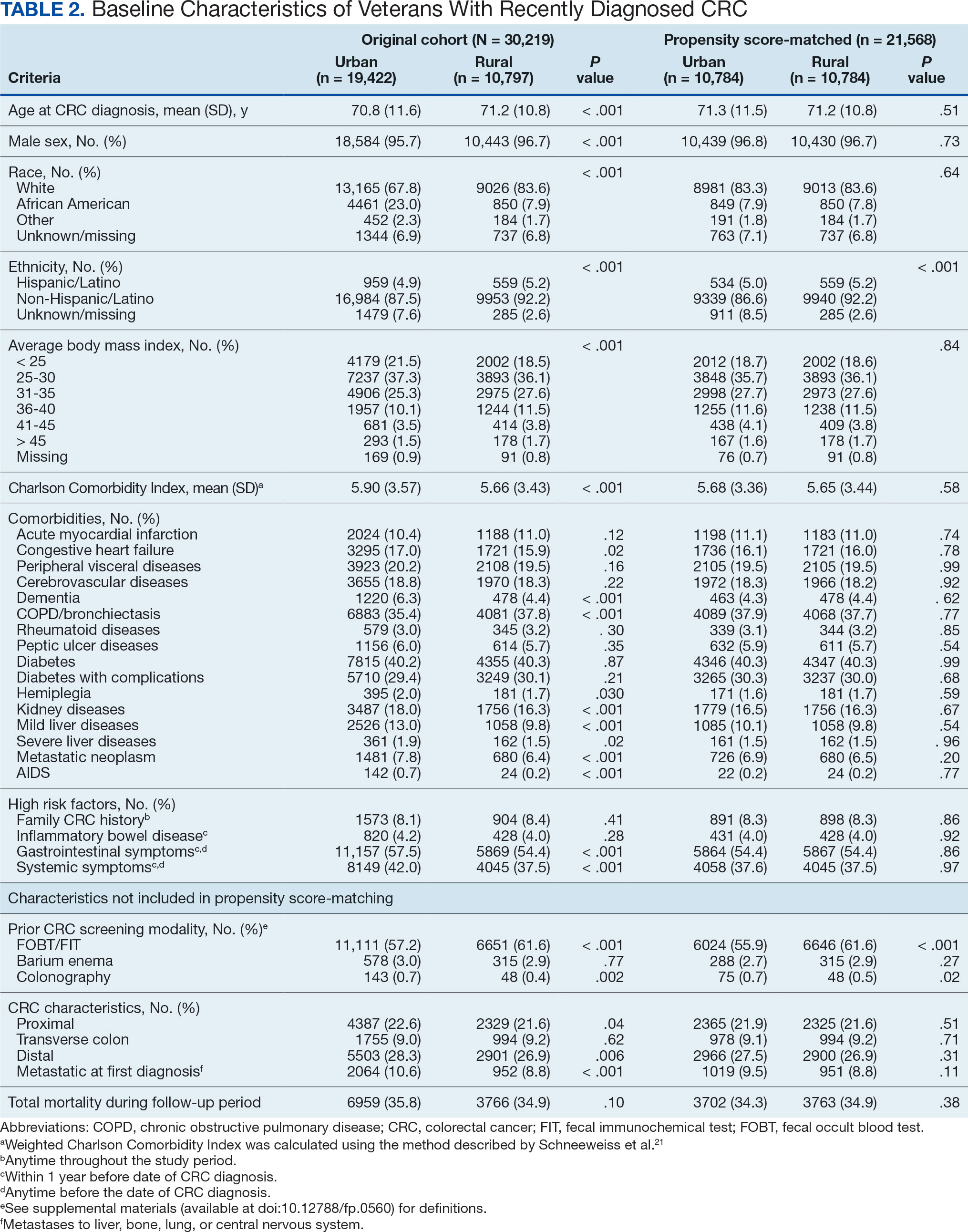
There were 21,568 PS-matched veterans: 10,784 in each group. In the PS-matched cohort, baseline characteristics were similar between veterans in urban and rural communities, including age, sex, race/ethnicity, body mass index, and comorbidities. Among rural patients with CRC, 3763 deaths (34.9%) were observed compared with 3702 (34.3%) among urban veterans. There was no significant difference in the HR of mortality between rural and urban CRC residents (HR, 1.01; 95% CI, 0.97-1.06; P = .53) (Figure 2).
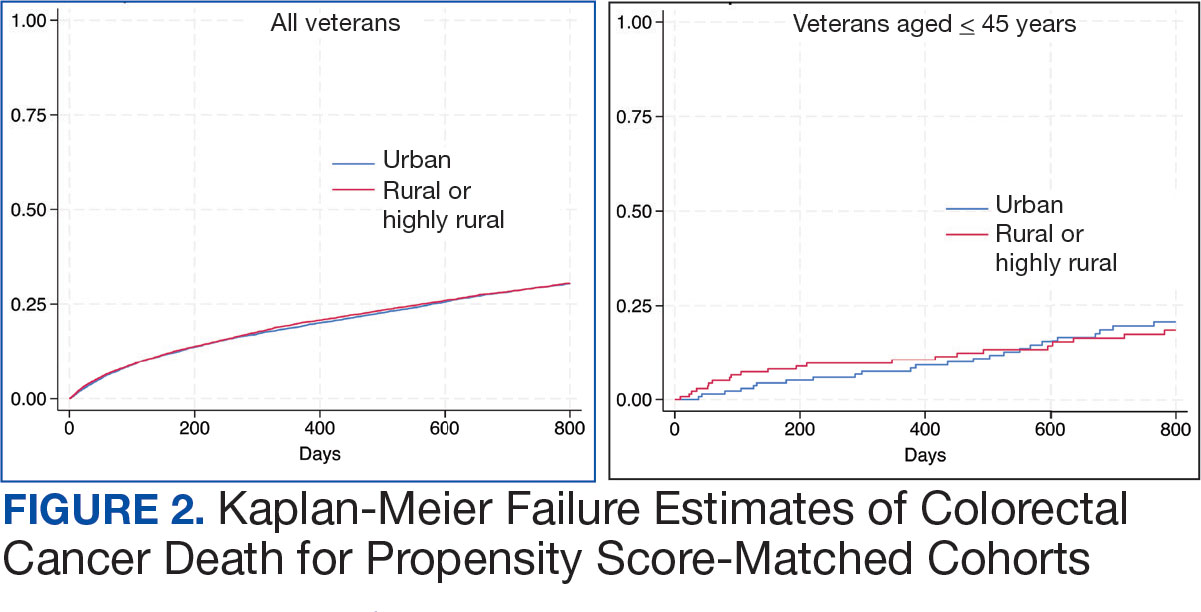
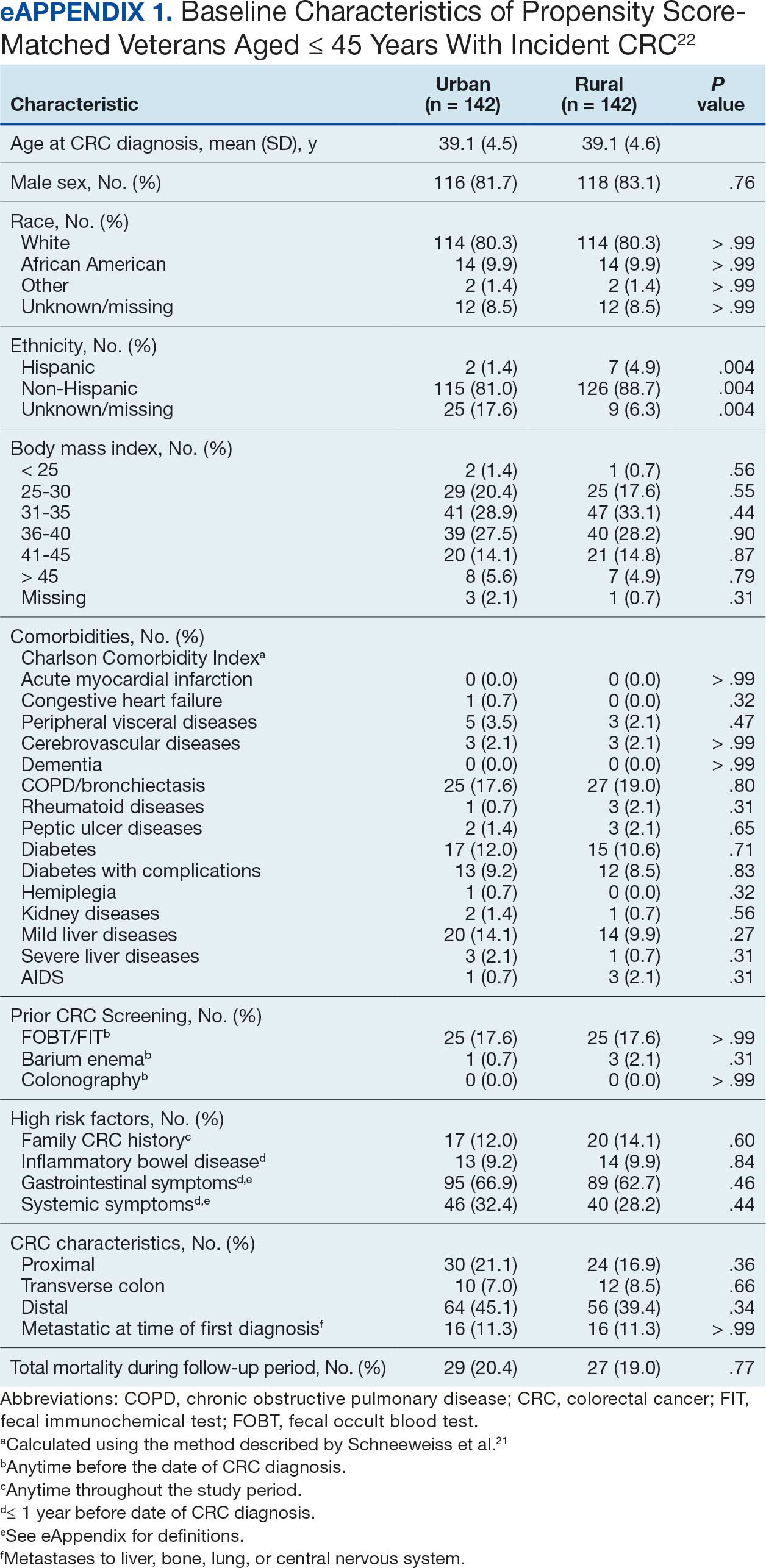
Among veterans aged ≤ 45 years, 551 were diagnosed with CRC (391 urban and 160 rural). We PS-matched 142 pairs of urban and rural veterans without residual differences in baseline characteristics (eAppendix 1). There was no significant difference in the HR of mortality between rural and urban veterans aged ≤ 45 years (HR, 0.97; 95% CI, 0.57-1.63; P = .90) (Figure 2). Similarly, no difference in mortality was observed adjusting for PS between all rural and urban veterans aged ≤ 45 years (HR, 1.03; 95% CI, 0.67-1.59; P = .88).
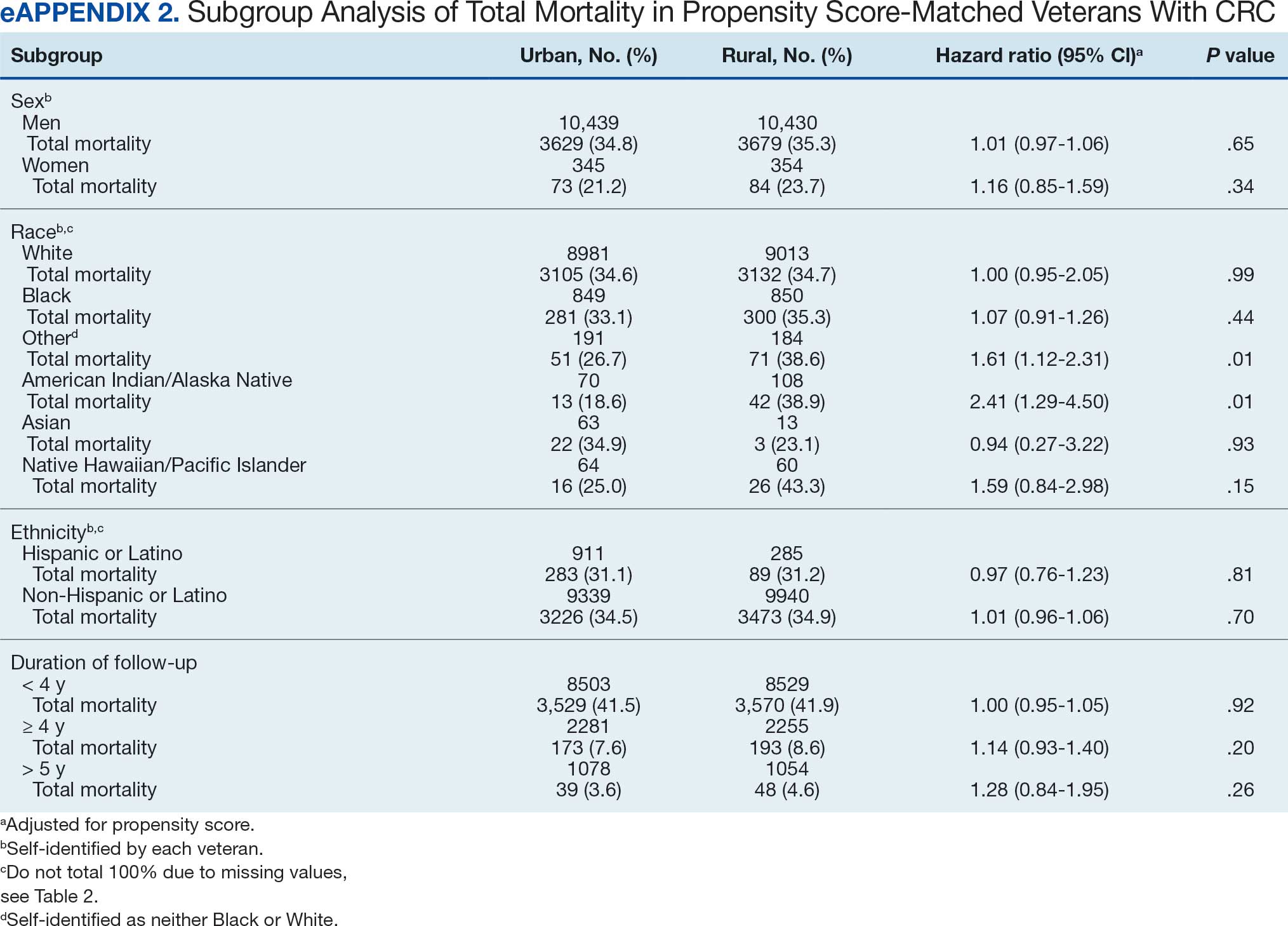
There was no difference in total mortality between rural and urban veterans in any subgroup except for American Indian or Alaska Native veterans (HR, 2.41; 95% CI, 1.29-4.50; P = .006) (eAppendix 2).
Discussion
This study examined characteristics of patients with CRC between urban and rural areas among veterans who were VHA patients. Similar to other studies, rural veterans with CRC were older, more likely to be White, and were obese, but exhibited fewer comorbidities (lower CCI and lower incidence of congestive heart failure, dementia, hemiplegia, kidney diseases, liver diseases and AIDS, but higher incidence of chronic obstructive lung disease).8,16 The incidence of CRC in this study population was lowest in FY 2020, which was reported by the Centers for Disease Control and Prevention and is attributed to COVID-19 pandemic disruption of health services.24 The overall mortality in this study was similar to rates reported in other studies from the VA Central Cancer Registry.4 In the PS-matched cohort, where baseline characteristics were similar between urban and rural patients with CRC, we found no disparities in CRC-specific mortality between veterans in rural and urban areas. Additionally, when analysis was restricted to veterans aged ≤ 45 years, the results remained consistent.
Subgroup analyses showed no significant difference in mortality between rural and urban areas by sex, race or ethnicity, except rural American Indian or Alaska Native veterans who had double the mortality of their urban counterparts (HR, 2.41; 95% CI, 1.29-4.50; P = .006). This finding is difficult to interpret due to the small number of events and the wide CI. While with a Bonferroni correction the adjusted P value was .08, which is not statistically significant, a previous study found that although CRC incidence was lower overall in American Indian or Alaska Native populations compared to non-Hispanic White populations, CRC incidence was higher among American Indian or Alaska Native individuals in some areas such as Alaska and the Northern Plains.25,26 Studies have noted that rural American Indian/Alaska Native populations experience greater poverty, less access to broadband internet, and limited access to care, contributing to poorer cancer outcomes and lower survival.27 Thus, the finding of disparity in mortality between rural and urban American Indian or Alaska Native veterans warrants further study.
Other studies have raised concerns that CRC disproportionately affects adults in rural areas with higher mortality rates.14-16 These disparities arise from sociodemographic factors and modifiable risk factors, including physical activity, dietary patterns, access to cancer screening, and gaps in quality treatment resources.16,28 These factors operate at multiple levels: from individual, local health system, to community and policy.2,27 For example, a South Carolina study (1996–2016) found that residents in rural areas were more likely to be diagnosed with advanced CRC, possibly indicating lower rates of CRC screening in rural areas. They also had higher likelihood of death from CRC.15 However, the study did not include any clinical parameters, such as comorbidities or obesity. A statewide, population-based study in Utah showed that rural men experienced a lower CRC survival in their unadjusted analysis.16 However, the study was small, with only 3948 urban and 712 rural residents. Additionally, there was no difference in total mortality in the whole cohort (HR, 0.96; 95% CI, 0.86-1.07) or in CRC-specific death (HR, 0.93; 95% CI, 0.81-1.08). A nationwide study also showed that CRC mortality rates were 8% higher in nonmetropolitan or rural areas than in the most urbanized areas containing large metropolitan counties.29 However, this study did not include descriptions of clinical confounders, such as comorbidities, making it difficult to ascertain whether the difference in CRC mortality was due to rurality or differences in baseline risk characteristics.
In this study, the lack of CRC-specific mortality disparities may be attributed to the structures and practices of VHA health care. Recent studies have noted that mortality of several chronic medical conditions treated at the VHA was lower than at non-VHA hospitals.30,31 One study that measured the quality of nonmetastatic CRC care based on National Comprehensive Cancer Network guidelines showed that > 72% of VHA patients received guideline-concordant care for each diagnostic and therapeutic measure, except for follow-up colonoscopy timing, which appear to be similar or superior to that of the private sector.30,32,33 Some of the VA initiative for CRC screening may bypass the urban-rurality divide such as the mailed fecal immunochemical test program for CRC. This program was implemented at the onset of the COVID-19 pandemic to avoid disruptions of medical care.34 Rural patients are more likely to undergo fecal immunochemical testing when compared to urban patients in this data. Beyond clinical care, the VHA uses processes to tackle social determinants of health such as housing, food security, and transportation, promoting equal access to health care, and promoting cultural competency among HCPs.35-37
The results suggest that solutions to CRC disparities between rural and urban areas need to consider known barriers to rural health care, including transportation, diminished rural health care workforce, and other social determinants of health.9,10,27,38 VHA makes considerable efforts to provide equitable care to all enrolled veterans, including specific programs for rural veterans, including ongoing outreach.39 This study demonstrated lack of disparity in CRC-specific mortality in veterans receiving VHA care, highlighting the importance of these efforts.
Strengths and Limitations
This study used the VHA cohort to compare patient characteristics and mortality between patients with CRC residing in rural and urban areas. The study provides nationwide perspectives on CRC across the geographical spectrum and used a longitudinal cohort with prolonged follow-up to account for comorbidities.
However, the study compared a cohort of rural and urban veterans enrolled in the VHA; hence, the results may not reflect CRC outcomes in veterans without access to VHA care. Rurality has been independently associated with decreased likelihood of meeting CRC screening guidelines among veterans and military service members.38 This study lacked sufficient information to compare CRC staging or treatment modalities among veterans. Although the data cannot identify CRC stage, the proportions of patients with metastatic CRC at diagnosis and CRC location were similar between groups. The study did not have information on their care outside of VHA setting.
This study could not ascertain whether disparities existed in CRC treatment modality since rural residence may result in referral to community-based CRC care, which did not appear in the data. To address these limitations, we used death from any cause as the primary outcome, since death is a hard outcome and is not subject to ascertainment bias. The relatively short follow-up time is another limitation, though subgroup analysis by follow-up did not show significant differences. Despite PS matching, residual unmeasured confounding may exist between urban and rural groups. The predominantly White, male VHA population with high CCI may limit the generalizability of the results.
Conclusions
Rural VHA enrollees had similar survival rates after CRC diagnosis compared to their urban counterparts in a PS-matched analysis. The VHA models of care—including mailed CRC screening tools, several socioeconomic determinants of health (housing, food security, and transportation), and promoting equal access to health care, as well as cultural competency among HCPs—HCPs—may help alleviate disparities across the rural-urban spectrum. The VHA should continue efforts to enroll veterans and provide comprehensive coordinated care in community partnerships.
- Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023;73(3):233-254. doi:10.3322/caac.21772
- Carethers JM, Doubeni CA. Causes of socioeconomic disparities in colorectal cancer and intervention framework and strategies. Gastroenterology. 2020;158(2):354-367. doi:10.1053/j.gastro.2019.10.029
- Murphy G, Devesa SS, Cross AJ, Inskip PD, McGlynn KA, Cook MB. Sex disparities in colorectal cancer incidence by anatomic subsite, race and age. Int J Cancer. 2011;128(7):1668-75. doi:10.1002/ijc.25481
- Zullig LL, Smith VA, Jackson GL, et al. Colorectal cancer statistics from the Veterans Affairs central cancer registry. Clin Colorectal Cancer. 2016;15(4):e199-e204. doi:10.1016/j.clcc.2016.04.005
- Lin JS, Perdue LA, Henrikson NB, Bean SI, Blasi PR. Screening for Colorectal Cancer: An Evidence Update for the US Preventive Services Task Force. 2021. U.S. Preventive Services Task Force Evidence Syntheses, formerly Systematic Evidence Reviews:Chapter 1. Agency for Healthcare Research and Quality (US); 2021. Accessed February 18, 2025. https://www.ncbi.nlm.nih.gov/books/NBK570917/
- Siegel RL, Fedewa SA, Anderson WF, et al. Colorectal cancer incidence patterns in the United States, 1974-2013. J Natl Cancer Inst. 2017;109(8). doi:10.1093/jnci/djw322
- Davidson KW, Barry MJ, Mangione CM, et al. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325(19):1965-1977. doi:10.1001/jama.2021.6238
- Hines R, Markossian T, Johnson A, Dong F, Bayakly R. Geographic residency status and census tract socioeconomic status as determinants of colorectal cancer outcomes. Am J Public Health. 2014;104(3):e63-e71. doi:10.2105/AJPH.2013.301572
- Cauwels J. The many barriers to high-quality rural health care. 2022;(9):1-32. NEJM Catal Innov Care Deliv. Accessed April 24, 2025. https://catalyst.nejm.org/doi/pdf/10.1056/CAT.22.0254
- Gong G, Phillips SG, Hudson C, Curti D, Philips BU. Higher US rural mortality rates linked to socioeconomic status, physician shortages, and lack of health insurance. Health Aff (Millwood);38(12):2003-2010. doi:10.1377/hlthaff.2019.00722
- Aboagye JK, Kaiser HE, Hayanga AJ. Rural-urban differences in access to specialist providers of colorectal cancer care in the United States: a physician workforce issue. JAMA Surg. 2014;149(6):537-543. doi:10.1001/jamasurg.2013.5062
- Lyckholm LJ, Hackney MH, Smith TJ. Ethics of rural health care. Crit Rev Oncol Hematol. 2001;40(2):131-138. doi:10.1016/s1040-8428(01)00139-1
- Krieger N, Williams DR, Moss NE. Measuring social class in US public health research: concepts, methodologies, and guidelines. Annu Rev Public Health. 1997;18:341-378. doi:10.1146/annurev.publhealth.18.1.341
- Singh GK, Jemal A. Socioeconomic and racial/ethnic disparities in cancer mortality, incidence, and survival in the United States, 1950-2014: over six decades of changing patterns and widening inequalities. J Environ Public Health. 2017;2017:2819372. doi:10.1155/2017/2819372
- Adams SA, Zahnd WE, Ranganathan R, et al. Rural and racial disparities in colorectal cancer incidence and mortality in South Carolina, 1996 - 2016. J Rural Health. 2022;38(1):34-39. doi:10.1111/jrh.12580
- Rogers CR, Blackburn BE, Huntington M, et al. Rural- urban disparities in colorectal cancer survival and risk among men in Utah: a statewide population-based study. Cancer Causes Control. 2020;31(3):241-253. doi:10.1007/s10552-020-01268-2
- US Department of Veterans Affairs. VA Informatics and Computing Infrastructure (VINCI), VA HSR RES 13-457. https://vincicentral.vinci.med.va.gov [Source not verified]
- US Department of Veterans Affairs Information Resource Center. VIReC Research User Guide: PSSG Geocoded Enrollee Files, 2015 Edition. US Department of Veterans Affairs, Health Services Research & Development Service, Information Resource Center; May. 2016. [source not verified]
- Goldsmith HF, Puskin DS, Stiles DJ. Improving the operational definition of “rural areas” for federal programs. US Department of Health and Human Services; 1993. Accessed February 27, 2025. https://www.ruralhealthinfo.org/pdf/improving-the-operational-definition-of-rural-areas.pdf
- Adams MA, Kerr EA, Dominitz JA, et al. Development and validation of a new ICD-10-based screening colonoscopy overuse measure in a large integrated healthcare system: a retrospective observational study. BMJ Qual Saf. 2023;32(7):414-424. doi:10.1136/bmjqs-2021-014236
- Schneeweiss S, Wang PS, Avorn J, Glynn RJ. Improved comorbidity adjustment for predicting mortality in Medicare populations. Health Serv Res. 2003;38(4):1103-1120. doi:10.1111/1475-6773.00165
- Becker S, Ichino A. Estimation of average treatment effects based on propensity scores. The Stata Journal. 2002;2(4):358-377.
- Leuven E, Sianesi B. PSMATCH2: Stata module to perform full Mahalanobis and propensity score matching, common support graphing, and covariate imbalance testing. Statistical software components. Revised February 1, 2018. Accessed February 27, 2025. https://ideas.repec.org/c/boc/bocode/s432001.html.
- US Cancer Statistics Working Group. US cancer statistics data visualizations tool. Centers for Disease Control and Prevention. June 2024. Accessed February 27, 2025. https://www.cdc.gov/cancer/dataviz
- Cao J, Zhang S. Multiple Comparison Procedures. JAMA. 2014;312(5):543-544. doi:10.1001/jama.2014.9440
- Gopalani SV, Janitz AE, Martinez SA, et al. Trends in cancer incidence among American Indians and Alaska Natives and Non-Hispanic Whites in the United States, 1999-2015. Epidemiology. 2020;31(2):205-213. doi:10.1097/EDE.0000000000001140
- Zahnd WE, Murphy C, Knoll M, et al. The intersection of rural residence and minority race/ethnicity in cancer disparities in the United States. Int J Environ Res Public Health. 2021;18(4). doi:10.3390/ijerph18041384
- Blake KD, Moss JL, Gaysynsky A, Srinivasan S, Croyle RT. Making the case for investment in rural cancer control: an analysis of rural cancer incidence, mortality, and funding trends. Cancer Epidemiol Biomarkers Prev. 2017;26(7):992-997. doi:10.1158/1055-9965.EPI-17-0092
- Singh GK, Williams SD, Siahpush M, Mulhollen A. Socioeconomic, rural-urban, and racial inequalities in US cancer mortality: part i-all cancers and lung cancer and part iicolorectal, prostate, breast, and cervical cancers. J Cancer Epidemiol. 2011;2011:107497. doi:10.1155/2011/107497
- Jackson GL, Melton LD, Abbott DH, et al. Quality of nonmetastatic colorectal cancer care in the Department of Veterans Affairs. J Clin Oncol. 2010;28(19):3176-3181. doi:10.1200/JCO.2009.26.7948
- Yoon J, Phibbs CS, Ong MK, et al. Outcomes of veterans treated in Veterans Affairs hospitals vs non-Veterans Affairs hospitals. JAMA Netw Open. 2023;6(12):e2345898. doi:10.1001/jamanetworkopen.2023.45898
- Malin JL, Schneider EC, Epstein AM, Adams J, Emanuel EJ, Kahn KL. Results of the National Initiative for Cancer Care Quality: how can we improve the quality of cancer care in the United States? J Clin Oncol. 2006;24(4):626-634. doi:10.1200/JCO.2005.03.3365
- Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology. 2008;134(5):1570-1595. doi:10.1053/j.gastro.2008.02.002
- Deeds SA, Moore CB, Gunnink EJ, et al. Implementation of a mailed faecal immunochemical test programme for colorectal cancer screening among Veterans. BMJ Open Qual. 2022;11(4). doi:10.1136/bmjoq-2022-001927
- Yehia BR, Greenstone CL, Hosenfeld CB, Matthews KL, Zephyrin LC. The role of VA community care in addressing health and health care disparities. Med Care. 2017;55(Suppl 9 suppl 2):S4-S5. doi:10.1097/MLR.0000000000000768
- Wright BN, MacDermid Wadsworth S, Wellnitz A, Eicher- Miller HA. Reaching rural veterans: a new mechanism to connect rural, low-income US Veterans with resources and improve food security. J Public Health (Oxf). 2019;41(4):714-723. doi:10.1093/pubmed/fdy203
- Nelson RE, Byrne TH, Suo Y, et al. Association of temporary financial assistance with housing stability among US veterans in the supportive services for veteran families program. JAMA Netw Open. 2021;4(2):e2037047. doi:10.1001/jamanetworkopen.2020.37047
- McDaniel JT, Albright D, Lee HY, et al. Rural–urban disparities in colorectal cancer screening among military service members and Veterans. J Mil Veteran Fam Health. 2019;5(1):40-48. doi:10.3138/jmvfh.2018-0013
- US Department of Veterans Affairs, Office of Rural Health. The rural veteran outreach toolkit. Updated February 12, 2025. Accessed February 18, 2025. https://www.ruralhealth.va.gov/partners/toolkit.asp
Colorectal cancer (CRC) is the second-leading cause of cancer-related deaths in the United States, with an estimated 52,550 deaths in 2023.1 However, the disease burden varies among different segments of the population.2 While both CRC incidence and mortality have been decreasing due to screening and advances in treatment, there are disparities in incidence and mortality across the sociodemographic spectrum including race, ethnicity, education, and income.1-4 While CRC incidence is decreasing for older adults, it is increasing among those aged < 55 years.5 The incidence of CRC in adults aged 40 to 54 years has increased by 0.5% to 1.3% annually since the mid-1990s.6 The US Preventive Services Task Force now recommends starting CRC screening at age 45 years for asymptomatic adults with average risk.7
Disparities also exist across geographical boundaries and living environment. Rural Americans faces additional challenges in health and lifestyle that can affect CRC outcomes. Compared to their urban counterparts, rural residents are more likely to be older, have lower levels of education, higher levels of poverty, lack health insurance, and less access to health care practitioners (HCPs).8-10 Geographic proximity, defined as travel time or physical distance to a health facility, has been recognized as a predictor of inferior outcomes.11 These aspects of rural living may pose challenges for accessing care for CRC screening and treatment.11-13 National and local studies have shown disparities in CRC screening rates, incidence, and mortality between rural and urban populations.14-16
It is unclear whether rural/urban disparities persist under the Veterans Health Administration (VHA) health care delivery model. This study examined differences in baseline characteristics and mortality between rural and urban veterans newly diagnosed with CRC. We also focused on a subpopulation aged ≤ 45 years.
Methods
This study extracted national data from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW) hosted in the VA Informatics and Computing Infrastructure (VINCI) environment. VINCI is an initiative to improve access to VA data and facilitate the analysis of these data while ensuring veterans’ privacy and data security.17 CDW is the VHA business intelligence information repository, which extracts data from clinical and nonclinical sources following prescribed and validated protocols. Data extracted included demographics, diagnosis, and procedure codes for both inpatient and outpatient encounters, vital signs, and vital status. This study used data previously extracted from a national cohort of veterans that encompassed all patients who received a group of commonly prescribed medications, such as statins, proton pump inhibitors, histamine-2 blockers, acetaminophen-containing products, and hydrocortisone-containing skin applications. This cohort encompassed 8,648,754 veterans, from whom 2,460,727 had encounters during fiscal years (FY) 2016 to 2021 (study period). The cohort was used to ensure that subjects were VHA patients, allowing them to adequately capture their clinical profiles.
Patients were identified as rural or urban based on their residence address at the date of their first diagnosis of CRC. The Geospatial Service Support Center (GSSC) aggregates and updates veterans’ residence address records for all enrolled veterans from the National Change of Address database. The data contain 1 record per enrollee. GSSC Geocoded Enrollee File contains enrollee addresses and their rurality indicators, categorized as urban, rural, or highly rural.18 Rurality is defined by the Rural Urban Commuting Area (RUCA) categories developed by the Department of Agriculture and the Health Resources and Services Administration of the US Department of Health and Human Services.19 Urban areas had RUCA codes of 1.0 to 1.1, and highly rural areas had RUCA scores of 10.0. All other areas were classified as rural. Since the proportion of veterans from highly rural areas was small, we included residents from highly rural areas in the rural residents’ group.
Inclusion and Exclusion Criteria
All veterans newly diagnosed with CRC from FY 2016 to 2021 were included. We used the ninth and tenth clinical modification revisions of the International Classification of Diseases (ICD-9-CM and ICD-10-CM) to define CRC diagnosis (Supplemental materials).4,20 To ensure that patients were newly diagnosed with CRC, this study excluded patients with a previous ICD-9-CM code for CRC diagnosis since FY 2003.
Comorbidities were identified using diagnosis and procedure codes from inpatient and outpatient encounters, which were used to calculate the Charlson Comorbidity Index (CCI) at the time of CRC diagnosis using the weighted method described by Schneeweiss et al.21 We defined CRC high-risk conditions and CRC screening tests, including flexible sigmoidoscopy and stool tests, as described in previous studies (Supplemental materials).20
The main outcome was total mortality. The date of death was extracted from the VHA Death Ascertainment File, which contains mortality data from the Master Person Index file in CDW and the Social Security Administration Death Master File. We used the date of death from any cause, as cause of death was not available.
A propensity score (PS) was created to match rural (including highly rural) and urban residents at a ratio of 1:1. Using a standard procedure described in prior publications, multivariable logistic regression used all baseline characteristics to estimate the PS and perform nearest-number matching without replacement.22,23 A caliper of 0.01 maximized the matched cohort size and achieved balance (Supplemental materials). We then examined the balance of baseline characteristics between PS-matched groups.
Analyses
Cox proportional hazards regression analysis estimated the hazard ratio (HR) of death in rural residents compared to urban residents in the PS-matched cohort. The outcome event was the date of death during the study’s follow-up period (defined as period from first CRC diagnosis to death or study end), with censoring at the study’s end date (September 30, 2021). The proportional hazards assumption was assessed by inspecting the Kaplan-Meier curves. Multiple analyses examined the HR of total mortality in the PS-matched cohort, stratified by sex, race, and ethnicity. We also examined the HR of total mortality stratified by duration of follow-up.
Another PS-matching analysis among veterans aged ≤ 45 years was performed using the same techniques described earlier in this article. We performed a Cox proportional hazards regression analysis to compare mortality in PS-matched urban and rural veterans aged ≤ 45 years. The HR of death in all veterans aged ≤ 45 years (before PS-matching) was estimated using Cox proportional hazard regression analysis, adjusting for PS.
Dichotomous variables were compared using X2 tests and continuous variables were compared using t tests. Baseline characteristics with missing values were converted into categorical variables and the proportion of subjects with missing values was equalized between treatment groups after PS-matching. For subgroup analysis, we examined the HR of total mortality in each subgroup using separate Cox proportional hazards regression models similar to the primary analysis but adjusted for PS. Due to multiple comparisons in the subgroup analysis, the findings should be considered exploratory. Statistical tests were 2-tailed, and significance was defined as P < .05. Data management and statistical analyses were conducted from June 2022 to January 2023 using STATA, Version 17. The VA Orlando Healthcare System Institutional Review Board approved the study and waived requirements for informed consent because only deidentified data were used.
Results
After excluding 49 patients (Supplemental materials, available at doi:10.12788/fp.0560), we identified 30,219 veterans with newly diagnosed CRC between FY 2016 to 2021 (Table 1). Of these, 19,422 (64.3%) resided in urban areas and 10,797 (35.7%) resided in rural areas (Table 2). The mean (SD) duration from the first CRC diagnosis to death or study end was 832 (640) days, and the median (IQR) was 723 (246–1330) days. Overall, incident CRC diagnoses were numerically highest in FY 2016 and lowest in FY 2020 (Figure 1). Patients with CRC in rural areas vs urban areas were significantly older (mean, 71.2 years vs 70.8 years, respectively; P < .001), more likely to be male (96.7% vs 95.7%, respectively; P < .001), more likely to be White (83.6% vs 67.8%, respectively; P < .001) and more likely to be non-Hispanic (92.2% vs 87.5%, respectively; P < .001). In terms of general health, rural veterans with CRC were more likely to be overweight or obese (81.5% rural vs 78.5% urban; P < .001) but had fewer mean comorbidities as measured by CCI (5.66 rural vs 5.90 urban; P < .001). A higher proportion of rural veterans with CRC had received stool-based (fecal occult blood test or fecal immunochemical test) CRC screening tests (61.6% rural vs 57.2% urban; P < .001). Fewer rural patients presented with systemic symptoms or signs within 1 year of CRC diagnosis (54.4% rural vs 57.5% urban, P < .001). Among urban patients with CRC, 6959 (35.8%) deaths were observed, compared with 3766 (34.9%) among rural patients (P = .10).
There were 21,568 PS-matched veterans: 10,784 in each group. In the PS-matched cohort, baseline characteristics were similar between veterans in urban and rural communities, including age, sex, race/ethnicity, body mass index, and comorbidities. Among rural patients with CRC, 3763 deaths (34.9%) were observed compared with 3702 (34.3%) among urban veterans. There was no significant difference in the HR of mortality between rural and urban CRC residents (HR, 1.01; 95% CI, 0.97-1.06; P = .53) (Figure 2).
Among veterans aged ≤ 45 years, 551 were diagnosed with CRC (391 urban and 160 rural). We PS-matched 142 pairs of urban and rural veterans without residual differences in baseline characteristics (eAppendix 1). There was no significant difference in the HR of mortality between rural and urban veterans aged ≤ 45 years (HR, 0.97; 95% CI, 0.57-1.63; P = .90) (Figure 2). Similarly, no difference in mortality was observed adjusting for PS between all rural and urban veterans aged ≤ 45 years (HR, 1.03; 95% CI, 0.67-1.59; P = .88).
There was no difference in total mortality between rural and urban veterans in any subgroup except for American Indian or Alaska Native veterans (HR, 2.41; 95% CI, 1.29-4.50; P = .006) (eAppendix 2).
Discussion
This study examined characteristics of patients with CRC between urban and rural areas among veterans who were VHA patients. Similar to other studies, rural veterans with CRC were older, more likely to be White, and were obese, but exhibited fewer comorbidities (lower CCI and lower incidence of congestive heart failure, dementia, hemiplegia, kidney diseases, liver diseases and AIDS, but higher incidence of chronic obstructive lung disease).8,16 The incidence of CRC in this study population was lowest in FY 2020, which was reported by the Centers for Disease Control and Prevention and is attributed to COVID-19 pandemic disruption of health services.24 The overall mortality in this study was similar to rates reported in other studies from the VA Central Cancer Registry.4 In the PS-matched cohort, where baseline characteristics were similar between urban and rural patients with CRC, we found no disparities in CRC-specific mortality between veterans in rural and urban areas. Additionally, when analysis was restricted to veterans aged ≤ 45 years, the results remained consistent.
Subgroup analyses showed no significant difference in mortality between rural and urban areas by sex, race or ethnicity, except rural American Indian or Alaska Native veterans who had double the mortality of their urban counterparts (HR, 2.41; 95% CI, 1.29-4.50; P = .006). This finding is difficult to interpret due to the small number of events and the wide CI. While with a Bonferroni correction the adjusted P value was .08, which is not statistically significant, a previous study found that although CRC incidence was lower overall in American Indian or Alaska Native populations compared to non-Hispanic White populations, CRC incidence was higher among American Indian or Alaska Native individuals in some areas such as Alaska and the Northern Plains.25,26 Studies have noted that rural American Indian/Alaska Native populations experience greater poverty, less access to broadband internet, and limited access to care, contributing to poorer cancer outcomes and lower survival.27 Thus, the finding of disparity in mortality between rural and urban American Indian or Alaska Native veterans warrants further study.
Other studies have raised concerns that CRC disproportionately affects adults in rural areas with higher mortality rates.14-16 These disparities arise from sociodemographic factors and modifiable risk factors, including physical activity, dietary patterns, access to cancer screening, and gaps in quality treatment resources.16,28 These factors operate at multiple levels: from individual, local health system, to community and policy.2,27 For example, a South Carolina study (1996–2016) found that residents in rural areas were more likely to be diagnosed with advanced CRC, possibly indicating lower rates of CRC screening in rural areas. They also had higher likelihood of death from CRC.15 However, the study did not include any clinical parameters, such as comorbidities or obesity. A statewide, population-based study in Utah showed that rural men experienced a lower CRC survival in their unadjusted analysis.16 However, the study was small, with only 3948 urban and 712 rural residents. Additionally, there was no difference in total mortality in the whole cohort (HR, 0.96; 95% CI, 0.86-1.07) or in CRC-specific death (HR, 0.93; 95% CI, 0.81-1.08). A nationwide study also showed that CRC mortality rates were 8% higher in nonmetropolitan or rural areas than in the most urbanized areas containing large metropolitan counties.29 However, this study did not include descriptions of clinical confounders, such as comorbidities, making it difficult to ascertain whether the difference in CRC mortality was due to rurality or differences in baseline risk characteristics.
In this study, the lack of CRC-specific mortality disparities may be attributed to the structures and practices of VHA health care. Recent studies have noted that mortality of several chronic medical conditions treated at the VHA was lower than at non-VHA hospitals.30,31 One study that measured the quality of nonmetastatic CRC care based on National Comprehensive Cancer Network guidelines showed that > 72% of VHA patients received guideline-concordant care for each diagnostic and therapeutic measure, except for follow-up colonoscopy timing, which appear to be similar or superior to that of the private sector.30,32,33 Some of the VA initiative for CRC screening may bypass the urban-rurality divide such as the mailed fecal immunochemical test program for CRC. This program was implemented at the onset of the COVID-19 pandemic to avoid disruptions of medical care.34 Rural patients are more likely to undergo fecal immunochemical testing when compared to urban patients in this data. Beyond clinical care, the VHA uses processes to tackle social determinants of health such as housing, food security, and transportation, promoting equal access to health care, and promoting cultural competency among HCPs.35-37
The results suggest that solutions to CRC disparities between rural and urban areas need to consider known barriers to rural health care, including transportation, diminished rural health care workforce, and other social determinants of health.9,10,27,38 VHA makes considerable efforts to provide equitable care to all enrolled veterans, including specific programs for rural veterans, including ongoing outreach.39 This study demonstrated lack of disparity in CRC-specific mortality in veterans receiving VHA care, highlighting the importance of these efforts.
Strengths and Limitations
This study used the VHA cohort to compare patient characteristics and mortality between patients with CRC residing in rural and urban areas. The study provides nationwide perspectives on CRC across the geographical spectrum and used a longitudinal cohort with prolonged follow-up to account for comorbidities.
However, the study compared a cohort of rural and urban veterans enrolled in the VHA; hence, the results may not reflect CRC outcomes in veterans without access to VHA care. Rurality has been independently associated with decreased likelihood of meeting CRC screening guidelines among veterans and military service members.38 This study lacked sufficient information to compare CRC staging or treatment modalities among veterans. Although the data cannot identify CRC stage, the proportions of patients with metastatic CRC at diagnosis and CRC location were similar between groups. The study did not have information on their care outside of VHA setting.
This study could not ascertain whether disparities existed in CRC treatment modality since rural residence may result in referral to community-based CRC care, which did not appear in the data. To address these limitations, we used death from any cause as the primary outcome, since death is a hard outcome and is not subject to ascertainment bias. The relatively short follow-up time is another limitation, though subgroup analysis by follow-up did not show significant differences. Despite PS matching, residual unmeasured confounding may exist between urban and rural groups. The predominantly White, male VHA population with high CCI may limit the generalizability of the results.
Conclusions
Rural VHA enrollees had similar survival rates after CRC diagnosis compared to their urban counterparts in a PS-matched analysis. The VHA models of care—including mailed CRC screening tools, several socioeconomic determinants of health (housing, food security, and transportation), and promoting equal access to health care, as well as cultural competency among HCPs—HCPs—may help alleviate disparities across the rural-urban spectrum. The VHA should continue efforts to enroll veterans and provide comprehensive coordinated care in community partnerships.
Colorectal cancer (CRC) is the second-leading cause of cancer-related deaths in the United States, with an estimated 52,550 deaths in 2023.1 However, the disease burden varies among different segments of the population.2 While both CRC incidence and mortality have been decreasing due to screening and advances in treatment, there are disparities in incidence and mortality across the sociodemographic spectrum including race, ethnicity, education, and income.1-4 While CRC incidence is decreasing for older adults, it is increasing among those aged < 55 years.5 The incidence of CRC in adults aged 40 to 54 years has increased by 0.5% to 1.3% annually since the mid-1990s.6 The US Preventive Services Task Force now recommends starting CRC screening at age 45 years for asymptomatic adults with average risk.7
Disparities also exist across geographical boundaries and living environment. Rural Americans faces additional challenges in health and lifestyle that can affect CRC outcomes. Compared to their urban counterparts, rural residents are more likely to be older, have lower levels of education, higher levels of poverty, lack health insurance, and less access to health care practitioners (HCPs).8-10 Geographic proximity, defined as travel time or physical distance to a health facility, has been recognized as a predictor of inferior outcomes.11 These aspects of rural living may pose challenges for accessing care for CRC screening and treatment.11-13 National and local studies have shown disparities in CRC screening rates, incidence, and mortality between rural and urban populations.14-16
It is unclear whether rural/urban disparities persist under the Veterans Health Administration (VHA) health care delivery model. This study examined differences in baseline characteristics and mortality between rural and urban veterans newly diagnosed with CRC. We also focused on a subpopulation aged ≤ 45 years.
Methods
This study extracted national data from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW) hosted in the VA Informatics and Computing Infrastructure (VINCI) environment. VINCI is an initiative to improve access to VA data and facilitate the analysis of these data while ensuring veterans’ privacy and data security.17 CDW is the VHA business intelligence information repository, which extracts data from clinical and nonclinical sources following prescribed and validated protocols. Data extracted included demographics, diagnosis, and procedure codes for both inpatient and outpatient encounters, vital signs, and vital status. This study used data previously extracted from a national cohort of veterans that encompassed all patients who received a group of commonly prescribed medications, such as statins, proton pump inhibitors, histamine-2 blockers, acetaminophen-containing products, and hydrocortisone-containing skin applications. This cohort encompassed 8,648,754 veterans, from whom 2,460,727 had encounters during fiscal years (FY) 2016 to 2021 (study period). The cohort was used to ensure that subjects were VHA patients, allowing them to adequately capture their clinical profiles.
Patients were identified as rural or urban based on their residence address at the date of their first diagnosis of CRC. The Geospatial Service Support Center (GSSC) aggregates and updates veterans’ residence address records for all enrolled veterans from the National Change of Address database. The data contain 1 record per enrollee. GSSC Geocoded Enrollee File contains enrollee addresses and their rurality indicators, categorized as urban, rural, or highly rural.18 Rurality is defined by the Rural Urban Commuting Area (RUCA) categories developed by the Department of Agriculture and the Health Resources and Services Administration of the US Department of Health and Human Services.19 Urban areas had RUCA codes of 1.0 to 1.1, and highly rural areas had RUCA scores of 10.0. All other areas were classified as rural. Since the proportion of veterans from highly rural areas was small, we included residents from highly rural areas in the rural residents’ group.
Inclusion and Exclusion Criteria
All veterans newly diagnosed with CRC from FY 2016 to 2021 were included. We used the ninth and tenth clinical modification revisions of the International Classification of Diseases (ICD-9-CM and ICD-10-CM) to define CRC diagnosis (Supplemental materials).4,20 To ensure that patients were newly diagnosed with CRC, this study excluded patients with a previous ICD-9-CM code for CRC diagnosis since FY 2003.
Comorbidities were identified using diagnosis and procedure codes from inpatient and outpatient encounters, which were used to calculate the Charlson Comorbidity Index (CCI) at the time of CRC diagnosis using the weighted method described by Schneeweiss et al.21 We defined CRC high-risk conditions and CRC screening tests, including flexible sigmoidoscopy and stool tests, as described in previous studies (Supplemental materials).20
The main outcome was total mortality. The date of death was extracted from the VHA Death Ascertainment File, which contains mortality data from the Master Person Index file in CDW and the Social Security Administration Death Master File. We used the date of death from any cause, as cause of death was not available.
A propensity score (PS) was created to match rural (including highly rural) and urban residents at a ratio of 1:1. Using a standard procedure described in prior publications, multivariable logistic regression used all baseline characteristics to estimate the PS and perform nearest-number matching without replacement.22,23 A caliper of 0.01 maximized the matched cohort size and achieved balance (Supplemental materials). We then examined the balance of baseline characteristics between PS-matched groups.
Analyses
Cox proportional hazards regression analysis estimated the hazard ratio (HR) of death in rural residents compared to urban residents in the PS-matched cohort. The outcome event was the date of death during the study’s follow-up period (defined as period from first CRC diagnosis to death or study end), with censoring at the study’s end date (September 30, 2021). The proportional hazards assumption was assessed by inspecting the Kaplan-Meier curves. Multiple analyses examined the HR of total mortality in the PS-matched cohort, stratified by sex, race, and ethnicity. We also examined the HR of total mortality stratified by duration of follow-up.
Another PS-matching analysis among veterans aged ≤ 45 years was performed using the same techniques described earlier in this article. We performed a Cox proportional hazards regression analysis to compare mortality in PS-matched urban and rural veterans aged ≤ 45 years. The HR of death in all veterans aged ≤ 45 years (before PS-matching) was estimated using Cox proportional hazard regression analysis, adjusting for PS.
Dichotomous variables were compared using X2 tests and continuous variables were compared using t tests. Baseline characteristics with missing values were converted into categorical variables and the proportion of subjects with missing values was equalized between treatment groups after PS-matching. For subgroup analysis, we examined the HR of total mortality in each subgroup using separate Cox proportional hazards regression models similar to the primary analysis but adjusted for PS. Due to multiple comparisons in the subgroup analysis, the findings should be considered exploratory. Statistical tests were 2-tailed, and significance was defined as P < .05. Data management and statistical analyses were conducted from June 2022 to January 2023 using STATA, Version 17. The VA Orlando Healthcare System Institutional Review Board approved the study and waived requirements for informed consent because only deidentified data were used.
Results
After excluding 49 patients (Supplemental materials, available at doi:10.12788/fp.0560), we identified 30,219 veterans with newly diagnosed CRC between FY 2016 to 2021 (Table 1). Of these, 19,422 (64.3%) resided in urban areas and 10,797 (35.7%) resided in rural areas (Table 2). The mean (SD) duration from the first CRC diagnosis to death or study end was 832 (640) days, and the median (IQR) was 723 (246–1330) days. Overall, incident CRC diagnoses were numerically highest in FY 2016 and lowest in FY 2020 (Figure 1). Patients with CRC in rural areas vs urban areas were significantly older (mean, 71.2 years vs 70.8 years, respectively; P < .001), more likely to be male (96.7% vs 95.7%, respectively; P < .001), more likely to be White (83.6% vs 67.8%, respectively; P < .001) and more likely to be non-Hispanic (92.2% vs 87.5%, respectively; P < .001). In terms of general health, rural veterans with CRC were more likely to be overweight or obese (81.5% rural vs 78.5% urban; P < .001) but had fewer mean comorbidities as measured by CCI (5.66 rural vs 5.90 urban; P < .001). A higher proportion of rural veterans with CRC had received stool-based (fecal occult blood test or fecal immunochemical test) CRC screening tests (61.6% rural vs 57.2% urban; P < .001). Fewer rural patients presented with systemic symptoms or signs within 1 year of CRC diagnosis (54.4% rural vs 57.5% urban, P < .001). Among urban patients with CRC, 6959 (35.8%) deaths were observed, compared with 3766 (34.9%) among rural patients (P = .10).
There were 21,568 PS-matched veterans: 10,784 in each group. In the PS-matched cohort, baseline characteristics were similar between veterans in urban and rural communities, including age, sex, race/ethnicity, body mass index, and comorbidities. Among rural patients with CRC, 3763 deaths (34.9%) were observed compared with 3702 (34.3%) among urban veterans. There was no significant difference in the HR of mortality between rural and urban CRC residents (HR, 1.01; 95% CI, 0.97-1.06; P = .53) (Figure 2).
Among veterans aged ≤ 45 years, 551 were diagnosed with CRC (391 urban and 160 rural). We PS-matched 142 pairs of urban and rural veterans without residual differences in baseline characteristics (eAppendix 1). There was no significant difference in the HR of mortality between rural and urban veterans aged ≤ 45 years (HR, 0.97; 95% CI, 0.57-1.63; P = .90) (Figure 2). Similarly, no difference in mortality was observed adjusting for PS between all rural and urban veterans aged ≤ 45 years (HR, 1.03; 95% CI, 0.67-1.59; P = .88).
There was no difference in total mortality between rural and urban veterans in any subgroup except for American Indian or Alaska Native veterans (HR, 2.41; 95% CI, 1.29-4.50; P = .006) (eAppendix 2).
Discussion
This study examined characteristics of patients with CRC between urban and rural areas among veterans who were VHA patients. Similar to other studies, rural veterans with CRC were older, more likely to be White, and were obese, but exhibited fewer comorbidities (lower CCI and lower incidence of congestive heart failure, dementia, hemiplegia, kidney diseases, liver diseases and AIDS, but higher incidence of chronic obstructive lung disease).8,16 The incidence of CRC in this study population was lowest in FY 2020, which was reported by the Centers for Disease Control and Prevention and is attributed to COVID-19 pandemic disruption of health services.24 The overall mortality in this study was similar to rates reported in other studies from the VA Central Cancer Registry.4 In the PS-matched cohort, where baseline characteristics were similar between urban and rural patients with CRC, we found no disparities in CRC-specific mortality between veterans in rural and urban areas. Additionally, when analysis was restricted to veterans aged ≤ 45 years, the results remained consistent.
Subgroup analyses showed no significant difference in mortality between rural and urban areas by sex, race or ethnicity, except rural American Indian or Alaska Native veterans who had double the mortality of their urban counterparts (HR, 2.41; 95% CI, 1.29-4.50; P = .006). This finding is difficult to interpret due to the small number of events and the wide CI. While with a Bonferroni correction the adjusted P value was .08, which is not statistically significant, a previous study found that although CRC incidence was lower overall in American Indian or Alaska Native populations compared to non-Hispanic White populations, CRC incidence was higher among American Indian or Alaska Native individuals in some areas such as Alaska and the Northern Plains.25,26 Studies have noted that rural American Indian/Alaska Native populations experience greater poverty, less access to broadband internet, and limited access to care, contributing to poorer cancer outcomes and lower survival.27 Thus, the finding of disparity in mortality between rural and urban American Indian or Alaska Native veterans warrants further study.
Other studies have raised concerns that CRC disproportionately affects adults in rural areas with higher mortality rates.14-16 These disparities arise from sociodemographic factors and modifiable risk factors, including physical activity, dietary patterns, access to cancer screening, and gaps in quality treatment resources.16,28 These factors operate at multiple levels: from individual, local health system, to community and policy.2,27 For example, a South Carolina study (1996–2016) found that residents in rural areas were more likely to be diagnosed with advanced CRC, possibly indicating lower rates of CRC screening in rural areas. They also had higher likelihood of death from CRC.15 However, the study did not include any clinical parameters, such as comorbidities or obesity. A statewide, population-based study in Utah showed that rural men experienced a lower CRC survival in their unadjusted analysis.16 However, the study was small, with only 3948 urban and 712 rural residents. Additionally, there was no difference in total mortality in the whole cohort (HR, 0.96; 95% CI, 0.86-1.07) or in CRC-specific death (HR, 0.93; 95% CI, 0.81-1.08). A nationwide study also showed that CRC mortality rates were 8% higher in nonmetropolitan or rural areas than in the most urbanized areas containing large metropolitan counties.29 However, this study did not include descriptions of clinical confounders, such as comorbidities, making it difficult to ascertain whether the difference in CRC mortality was due to rurality or differences in baseline risk characteristics.
In this study, the lack of CRC-specific mortality disparities may be attributed to the structures and practices of VHA health care. Recent studies have noted that mortality of several chronic medical conditions treated at the VHA was lower than at non-VHA hospitals.30,31 One study that measured the quality of nonmetastatic CRC care based on National Comprehensive Cancer Network guidelines showed that > 72% of VHA patients received guideline-concordant care for each diagnostic and therapeutic measure, except for follow-up colonoscopy timing, which appear to be similar or superior to that of the private sector.30,32,33 Some of the VA initiative for CRC screening may bypass the urban-rurality divide such as the mailed fecal immunochemical test program for CRC. This program was implemented at the onset of the COVID-19 pandemic to avoid disruptions of medical care.34 Rural patients are more likely to undergo fecal immunochemical testing when compared to urban patients in this data. Beyond clinical care, the VHA uses processes to tackle social determinants of health such as housing, food security, and transportation, promoting equal access to health care, and promoting cultural competency among HCPs.35-37
The results suggest that solutions to CRC disparities between rural and urban areas need to consider known barriers to rural health care, including transportation, diminished rural health care workforce, and other social determinants of health.9,10,27,38 VHA makes considerable efforts to provide equitable care to all enrolled veterans, including specific programs for rural veterans, including ongoing outreach.39 This study demonstrated lack of disparity in CRC-specific mortality in veterans receiving VHA care, highlighting the importance of these efforts.
Strengths and Limitations
This study used the VHA cohort to compare patient characteristics and mortality between patients with CRC residing in rural and urban areas. The study provides nationwide perspectives on CRC across the geographical spectrum and used a longitudinal cohort with prolonged follow-up to account for comorbidities.
However, the study compared a cohort of rural and urban veterans enrolled in the VHA; hence, the results may not reflect CRC outcomes in veterans without access to VHA care. Rurality has been independently associated with decreased likelihood of meeting CRC screening guidelines among veterans and military service members.38 This study lacked sufficient information to compare CRC staging or treatment modalities among veterans. Although the data cannot identify CRC stage, the proportions of patients with metastatic CRC at diagnosis and CRC location were similar between groups. The study did not have information on their care outside of VHA setting.
This study could not ascertain whether disparities existed in CRC treatment modality since rural residence may result in referral to community-based CRC care, which did not appear in the data. To address these limitations, we used death from any cause as the primary outcome, since death is a hard outcome and is not subject to ascertainment bias. The relatively short follow-up time is another limitation, though subgroup analysis by follow-up did not show significant differences. Despite PS matching, residual unmeasured confounding may exist between urban and rural groups. The predominantly White, male VHA population with high CCI may limit the generalizability of the results.
Conclusions
Rural VHA enrollees had similar survival rates after CRC diagnosis compared to their urban counterparts in a PS-matched analysis. The VHA models of care—including mailed CRC screening tools, several socioeconomic determinants of health (housing, food security, and transportation), and promoting equal access to health care, as well as cultural competency among HCPs—HCPs—may help alleviate disparities across the rural-urban spectrum. The VHA should continue efforts to enroll veterans and provide comprehensive coordinated care in community partnerships.
- Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023;73(3):233-254. doi:10.3322/caac.21772
- Carethers JM, Doubeni CA. Causes of socioeconomic disparities in colorectal cancer and intervention framework and strategies. Gastroenterology. 2020;158(2):354-367. doi:10.1053/j.gastro.2019.10.029
- Murphy G, Devesa SS, Cross AJ, Inskip PD, McGlynn KA, Cook MB. Sex disparities in colorectal cancer incidence by anatomic subsite, race and age. Int J Cancer. 2011;128(7):1668-75. doi:10.1002/ijc.25481
- Zullig LL, Smith VA, Jackson GL, et al. Colorectal cancer statistics from the Veterans Affairs central cancer registry. Clin Colorectal Cancer. 2016;15(4):e199-e204. doi:10.1016/j.clcc.2016.04.005
- Lin JS, Perdue LA, Henrikson NB, Bean SI, Blasi PR. Screening for Colorectal Cancer: An Evidence Update for the US Preventive Services Task Force. 2021. U.S. Preventive Services Task Force Evidence Syntheses, formerly Systematic Evidence Reviews:Chapter 1. Agency for Healthcare Research and Quality (US); 2021. Accessed February 18, 2025. https://www.ncbi.nlm.nih.gov/books/NBK570917/
- Siegel RL, Fedewa SA, Anderson WF, et al. Colorectal cancer incidence patterns in the United States, 1974-2013. J Natl Cancer Inst. 2017;109(8). doi:10.1093/jnci/djw322
- Davidson KW, Barry MJ, Mangione CM, et al. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325(19):1965-1977. doi:10.1001/jama.2021.6238
- Hines R, Markossian T, Johnson A, Dong F, Bayakly R. Geographic residency status and census tract socioeconomic status as determinants of colorectal cancer outcomes. Am J Public Health. 2014;104(3):e63-e71. doi:10.2105/AJPH.2013.301572
- Cauwels J. The many barriers to high-quality rural health care. 2022;(9):1-32. NEJM Catal Innov Care Deliv. Accessed April 24, 2025. https://catalyst.nejm.org/doi/pdf/10.1056/CAT.22.0254
- Gong G, Phillips SG, Hudson C, Curti D, Philips BU. Higher US rural mortality rates linked to socioeconomic status, physician shortages, and lack of health insurance. Health Aff (Millwood);38(12):2003-2010. doi:10.1377/hlthaff.2019.00722
- Aboagye JK, Kaiser HE, Hayanga AJ. Rural-urban differences in access to specialist providers of colorectal cancer care in the United States: a physician workforce issue. JAMA Surg. 2014;149(6):537-543. doi:10.1001/jamasurg.2013.5062
- Lyckholm LJ, Hackney MH, Smith TJ. Ethics of rural health care. Crit Rev Oncol Hematol. 2001;40(2):131-138. doi:10.1016/s1040-8428(01)00139-1
- Krieger N, Williams DR, Moss NE. Measuring social class in US public health research: concepts, methodologies, and guidelines. Annu Rev Public Health. 1997;18:341-378. doi:10.1146/annurev.publhealth.18.1.341
- Singh GK, Jemal A. Socioeconomic and racial/ethnic disparities in cancer mortality, incidence, and survival in the United States, 1950-2014: over six decades of changing patterns and widening inequalities. J Environ Public Health. 2017;2017:2819372. doi:10.1155/2017/2819372
- Adams SA, Zahnd WE, Ranganathan R, et al. Rural and racial disparities in colorectal cancer incidence and mortality in South Carolina, 1996 - 2016. J Rural Health. 2022;38(1):34-39. doi:10.1111/jrh.12580
- Rogers CR, Blackburn BE, Huntington M, et al. Rural- urban disparities in colorectal cancer survival and risk among men in Utah: a statewide population-based study. Cancer Causes Control. 2020;31(3):241-253. doi:10.1007/s10552-020-01268-2
- US Department of Veterans Affairs. VA Informatics and Computing Infrastructure (VINCI), VA HSR RES 13-457. https://vincicentral.vinci.med.va.gov [Source not verified]
- US Department of Veterans Affairs Information Resource Center. VIReC Research User Guide: PSSG Geocoded Enrollee Files, 2015 Edition. US Department of Veterans Affairs, Health Services Research & Development Service, Information Resource Center; May. 2016. [source not verified]
- Goldsmith HF, Puskin DS, Stiles DJ. Improving the operational definition of “rural areas” for federal programs. US Department of Health and Human Services; 1993. Accessed February 27, 2025. https://www.ruralhealthinfo.org/pdf/improving-the-operational-definition-of-rural-areas.pdf
- Adams MA, Kerr EA, Dominitz JA, et al. Development and validation of a new ICD-10-based screening colonoscopy overuse measure in a large integrated healthcare system: a retrospective observational study. BMJ Qual Saf. 2023;32(7):414-424. doi:10.1136/bmjqs-2021-014236
- Schneeweiss S, Wang PS, Avorn J, Glynn RJ. Improved comorbidity adjustment for predicting mortality in Medicare populations. Health Serv Res. 2003;38(4):1103-1120. doi:10.1111/1475-6773.00165
- Becker S, Ichino A. Estimation of average treatment effects based on propensity scores. The Stata Journal. 2002;2(4):358-377.
- Leuven E, Sianesi B. PSMATCH2: Stata module to perform full Mahalanobis and propensity score matching, common support graphing, and covariate imbalance testing. Statistical software components. Revised February 1, 2018. Accessed February 27, 2025. https://ideas.repec.org/c/boc/bocode/s432001.html.
- US Cancer Statistics Working Group. US cancer statistics data visualizations tool. Centers for Disease Control and Prevention. June 2024. Accessed February 27, 2025. https://www.cdc.gov/cancer/dataviz
- Cao J, Zhang S. Multiple Comparison Procedures. JAMA. 2014;312(5):543-544. doi:10.1001/jama.2014.9440
- Gopalani SV, Janitz AE, Martinez SA, et al. Trends in cancer incidence among American Indians and Alaska Natives and Non-Hispanic Whites in the United States, 1999-2015. Epidemiology. 2020;31(2):205-213. doi:10.1097/EDE.0000000000001140
- Zahnd WE, Murphy C, Knoll M, et al. The intersection of rural residence and minority race/ethnicity in cancer disparities in the United States. Int J Environ Res Public Health. 2021;18(4). doi:10.3390/ijerph18041384
- Blake KD, Moss JL, Gaysynsky A, Srinivasan S, Croyle RT. Making the case for investment in rural cancer control: an analysis of rural cancer incidence, mortality, and funding trends. Cancer Epidemiol Biomarkers Prev. 2017;26(7):992-997. doi:10.1158/1055-9965.EPI-17-0092
- Singh GK, Williams SD, Siahpush M, Mulhollen A. Socioeconomic, rural-urban, and racial inequalities in US cancer mortality: part i-all cancers and lung cancer and part iicolorectal, prostate, breast, and cervical cancers. J Cancer Epidemiol. 2011;2011:107497. doi:10.1155/2011/107497
- Jackson GL, Melton LD, Abbott DH, et al. Quality of nonmetastatic colorectal cancer care in the Department of Veterans Affairs. J Clin Oncol. 2010;28(19):3176-3181. doi:10.1200/JCO.2009.26.7948
- Yoon J, Phibbs CS, Ong MK, et al. Outcomes of veterans treated in Veterans Affairs hospitals vs non-Veterans Affairs hospitals. JAMA Netw Open. 2023;6(12):e2345898. doi:10.1001/jamanetworkopen.2023.45898
- Malin JL, Schneider EC, Epstein AM, Adams J, Emanuel EJ, Kahn KL. Results of the National Initiative for Cancer Care Quality: how can we improve the quality of cancer care in the United States? J Clin Oncol. 2006;24(4):626-634. doi:10.1200/JCO.2005.03.3365
- Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology. 2008;134(5):1570-1595. doi:10.1053/j.gastro.2008.02.002
- Deeds SA, Moore CB, Gunnink EJ, et al. Implementation of a mailed faecal immunochemical test programme for colorectal cancer screening among Veterans. BMJ Open Qual. 2022;11(4). doi:10.1136/bmjoq-2022-001927
- Yehia BR, Greenstone CL, Hosenfeld CB, Matthews KL, Zephyrin LC. The role of VA community care in addressing health and health care disparities. Med Care. 2017;55(Suppl 9 suppl 2):S4-S5. doi:10.1097/MLR.0000000000000768
- Wright BN, MacDermid Wadsworth S, Wellnitz A, Eicher- Miller HA. Reaching rural veterans: a new mechanism to connect rural, low-income US Veterans with resources and improve food security. J Public Health (Oxf). 2019;41(4):714-723. doi:10.1093/pubmed/fdy203
- Nelson RE, Byrne TH, Suo Y, et al. Association of temporary financial assistance with housing stability among US veterans in the supportive services for veteran families program. JAMA Netw Open. 2021;4(2):e2037047. doi:10.1001/jamanetworkopen.2020.37047
- McDaniel JT, Albright D, Lee HY, et al. Rural–urban disparities in colorectal cancer screening among military service members and Veterans. J Mil Veteran Fam Health. 2019;5(1):40-48. doi:10.3138/jmvfh.2018-0013
- US Department of Veterans Affairs, Office of Rural Health. The rural veteran outreach toolkit. Updated February 12, 2025. Accessed February 18, 2025. https://www.ruralhealth.va.gov/partners/toolkit.asp
- Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023;73(3):233-254. doi:10.3322/caac.21772
- Carethers JM, Doubeni CA. Causes of socioeconomic disparities in colorectal cancer and intervention framework and strategies. Gastroenterology. 2020;158(2):354-367. doi:10.1053/j.gastro.2019.10.029
- Murphy G, Devesa SS, Cross AJ, Inskip PD, McGlynn KA, Cook MB. Sex disparities in colorectal cancer incidence by anatomic subsite, race and age. Int J Cancer. 2011;128(7):1668-75. doi:10.1002/ijc.25481
- Zullig LL, Smith VA, Jackson GL, et al. Colorectal cancer statistics from the Veterans Affairs central cancer registry. Clin Colorectal Cancer. 2016;15(4):e199-e204. doi:10.1016/j.clcc.2016.04.005
- Lin JS, Perdue LA, Henrikson NB, Bean SI, Blasi PR. Screening for Colorectal Cancer: An Evidence Update for the US Preventive Services Task Force. 2021. U.S. Preventive Services Task Force Evidence Syntheses, formerly Systematic Evidence Reviews:Chapter 1. Agency for Healthcare Research and Quality (US); 2021. Accessed February 18, 2025. https://www.ncbi.nlm.nih.gov/books/NBK570917/
- Siegel RL, Fedewa SA, Anderson WF, et al. Colorectal cancer incidence patterns in the United States, 1974-2013. J Natl Cancer Inst. 2017;109(8). doi:10.1093/jnci/djw322
- Davidson KW, Barry MJ, Mangione CM, et al. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325(19):1965-1977. doi:10.1001/jama.2021.6238
- Hines R, Markossian T, Johnson A, Dong F, Bayakly R. Geographic residency status and census tract socioeconomic status as determinants of colorectal cancer outcomes. Am J Public Health. 2014;104(3):e63-e71. doi:10.2105/AJPH.2013.301572
- Cauwels J. The many barriers to high-quality rural health care. 2022;(9):1-32. NEJM Catal Innov Care Deliv. Accessed April 24, 2025. https://catalyst.nejm.org/doi/pdf/10.1056/CAT.22.0254
- Gong G, Phillips SG, Hudson C, Curti D, Philips BU. Higher US rural mortality rates linked to socioeconomic status, physician shortages, and lack of health insurance. Health Aff (Millwood);38(12):2003-2010. doi:10.1377/hlthaff.2019.00722
- Aboagye JK, Kaiser HE, Hayanga AJ. Rural-urban differences in access to specialist providers of colorectal cancer care in the United States: a physician workforce issue. JAMA Surg. 2014;149(6):537-543. doi:10.1001/jamasurg.2013.5062
- Lyckholm LJ, Hackney MH, Smith TJ. Ethics of rural health care. Crit Rev Oncol Hematol. 2001;40(2):131-138. doi:10.1016/s1040-8428(01)00139-1
- Krieger N, Williams DR, Moss NE. Measuring social class in US public health research: concepts, methodologies, and guidelines. Annu Rev Public Health. 1997;18:341-378. doi:10.1146/annurev.publhealth.18.1.341
- Singh GK, Jemal A. Socioeconomic and racial/ethnic disparities in cancer mortality, incidence, and survival in the United States, 1950-2014: over six decades of changing patterns and widening inequalities. J Environ Public Health. 2017;2017:2819372. doi:10.1155/2017/2819372
- Adams SA, Zahnd WE, Ranganathan R, et al. Rural and racial disparities in colorectal cancer incidence and mortality in South Carolina, 1996 - 2016. J Rural Health. 2022;38(1):34-39. doi:10.1111/jrh.12580
- Rogers CR, Blackburn BE, Huntington M, et al. Rural- urban disparities in colorectal cancer survival and risk among men in Utah: a statewide population-based study. Cancer Causes Control. 2020;31(3):241-253. doi:10.1007/s10552-020-01268-2
- US Department of Veterans Affairs. VA Informatics and Computing Infrastructure (VINCI), VA HSR RES 13-457. https://vincicentral.vinci.med.va.gov [Source not verified]
- US Department of Veterans Affairs Information Resource Center. VIReC Research User Guide: PSSG Geocoded Enrollee Files, 2015 Edition. US Department of Veterans Affairs, Health Services Research & Development Service, Information Resource Center; May. 2016. [source not verified]
- Goldsmith HF, Puskin DS, Stiles DJ. Improving the operational definition of “rural areas” for federal programs. US Department of Health and Human Services; 1993. Accessed February 27, 2025. https://www.ruralhealthinfo.org/pdf/improving-the-operational-definition-of-rural-areas.pdf
- Adams MA, Kerr EA, Dominitz JA, et al. Development and validation of a new ICD-10-based screening colonoscopy overuse measure in a large integrated healthcare system: a retrospective observational study. BMJ Qual Saf. 2023;32(7):414-424. doi:10.1136/bmjqs-2021-014236
- Schneeweiss S, Wang PS, Avorn J, Glynn RJ. Improved comorbidity adjustment for predicting mortality in Medicare populations. Health Serv Res. 2003;38(4):1103-1120. doi:10.1111/1475-6773.00165
- Becker S, Ichino A. Estimation of average treatment effects based on propensity scores. The Stata Journal. 2002;2(4):358-377.
- Leuven E, Sianesi B. PSMATCH2: Stata module to perform full Mahalanobis and propensity score matching, common support graphing, and covariate imbalance testing. Statistical software components. Revised February 1, 2018. Accessed February 27, 2025. https://ideas.repec.org/c/boc/bocode/s432001.html.
- US Cancer Statistics Working Group. US cancer statistics data visualizations tool. Centers for Disease Control and Prevention. June 2024. Accessed February 27, 2025. https://www.cdc.gov/cancer/dataviz
- Cao J, Zhang S. Multiple Comparison Procedures. JAMA. 2014;312(5):543-544. doi:10.1001/jama.2014.9440
- Gopalani SV, Janitz AE, Martinez SA, et al. Trends in cancer incidence among American Indians and Alaska Natives and Non-Hispanic Whites in the United States, 1999-2015. Epidemiology. 2020;31(2):205-213. doi:10.1097/EDE.0000000000001140
- Zahnd WE, Murphy C, Knoll M, et al. The intersection of rural residence and minority race/ethnicity in cancer disparities in the United States. Int J Environ Res Public Health. 2021;18(4). doi:10.3390/ijerph18041384
- Blake KD, Moss JL, Gaysynsky A, Srinivasan S, Croyle RT. Making the case for investment in rural cancer control: an analysis of rural cancer incidence, mortality, and funding trends. Cancer Epidemiol Biomarkers Prev. 2017;26(7):992-997. doi:10.1158/1055-9965.EPI-17-0092
- Singh GK, Williams SD, Siahpush M, Mulhollen A. Socioeconomic, rural-urban, and racial inequalities in US cancer mortality: part i-all cancers and lung cancer and part iicolorectal, prostate, breast, and cervical cancers. J Cancer Epidemiol. 2011;2011:107497. doi:10.1155/2011/107497
- Jackson GL, Melton LD, Abbott DH, et al. Quality of nonmetastatic colorectal cancer care in the Department of Veterans Affairs. J Clin Oncol. 2010;28(19):3176-3181. doi:10.1200/JCO.2009.26.7948
- Yoon J, Phibbs CS, Ong MK, et al. Outcomes of veterans treated in Veterans Affairs hospitals vs non-Veterans Affairs hospitals. JAMA Netw Open. 2023;6(12):e2345898. doi:10.1001/jamanetworkopen.2023.45898
- Malin JL, Schneider EC, Epstein AM, Adams J, Emanuel EJ, Kahn KL. Results of the National Initiative for Cancer Care Quality: how can we improve the quality of cancer care in the United States? J Clin Oncol. 2006;24(4):626-634. doi:10.1200/JCO.2005.03.3365
- Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology. 2008;134(5):1570-1595. doi:10.1053/j.gastro.2008.02.002
- Deeds SA, Moore CB, Gunnink EJ, et al. Implementation of a mailed faecal immunochemical test programme for colorectal cancer screening among Veterans. BMJ Open Qual. 2022;11(4). doi:10.1136/bmjoq-2022-001927
- Yehia BR, Greenstone CL, Hosenfeld CB, Matthews KL, Zephyrin LC. The role of VA community care in addressing health and health care disparities. Med Care. 2017;55(Suppl 9 suppl 2):S4-S5. doi:10.1097/MLR.0000000000000768
- Wright BN, MacDermid Wadsworth S, Wellnitz A, Eicher- Miller HA. Reaching rural veterans: a new mechanism to connect rural, low-income US Veterans with resources and improve food security. J Public Health (Oxf). 2019;41(4):714-723. doi:10.1093/pubmed/fdy203
- Nelson RE, Byrne TH, Suo Y, et al. Association of temporary financial assistance with housing stability among US veterans in the supportive services for veteran families program. JAMA Netw Open. 2021;4(2):e2037047. doi:10.1001/jamanetworkopen.2020.37047
- McDaniel JT, Albright D, Lee HY, et al. Rural–urban disparities in colorectal cancer screening among military service members and Veterans. J Mil Veteran Fam Health. 2019;5(1):40-48. doi:10.3138/jmvfh.2018-0013
- US Department of Veterans Affairs, Office of Rural Health. The rural veteran outreach toolkit. Updated February 12, 2025. Accessed February 18, 2025. https://www.ruralhealth.va.gov/partners/toolkit.asp
Colorectal Cancer Characteristics and Mortality From Propensity Score-Matched Cohorts of Urban and Rural Veterans
Colorectal Cancer Characteristics and Mortality From Propensity Score-Matched Cohorts of Urban and Rural Veterans

Cancer Data Trends 2025
The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.

In this issue:
- Access, Race, and "Colon Age": Improving CRC Screening
- Lung Cancer: Mortality Trends in Veterans and New Treatments
- Racial Disparities, Germline Testing, and Improved Overall Survival in Prostate Cancer
- Breast and Uterine Cancer: Screening Guidelines, Genetic Testing, and Mortality Trends
- HCC Updates: Quality Care Framework and Risk Stratification Data
- Rising Kidney Cancer Cases and Emerging Treatments for Veterans
- Advances in Blood Cancer Care for Veterans
- AI-Based Risk Stratification for Oropharyngeal Carcinomas: AIROC
- Brain Cancer: Epidemiology, TBI, and New Treatments
The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.
In this issue:
- Access, Race, and "Colon Age": Improving CRC Screening
- Lung Cancer: Mortality Trends in Veterans and New Treatments
- Racial Disparities, Germline Testing, and Improved Overall Survival in Prostate Cancer
- Breast and Uterine Cancer: Screening Guidelines, Genetic Testing, and Mortality Trends
- HCC Updates: Quality Care Framework and Risk Stratification Data
- Rising Kidney Cancer Cases and Emerging Treatments for Veterans
- Advances in Blood Cancer Care for Veterans
- AI-Based Risk Stratification for Oropharyngeal Carcinomas: AIROC
- Brain Cancer: Epidemiology, TBI, and New Treatments
The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.
In this issue:
- Access, Race, and "Colon Age": Improving CRC Screening
- Lung Cancer: Mortality Trends in Veterans and New Treatments
- Racial Disparities, Germline Testing, and Improved Overall Survival in Prostate Cancer
- Breast and Uterine Cancer: Screening Guidelines, Genetic Testing, and Mortality Trends
- HCC Updates: Quality Care Framework and Risk Stratification Data
- Rising Kidney Cancer Cases and Emerging Treatments for Veterans
- Advances in Blood Cancer Care for Veterans
- AI-Based Risk Stratification for Oropharyngeal Carcinomas: AIROC
- Brain Cancer: Epidemiology, TBI, and New Treatments

COVID-19 Pandemic Left Many Veteran Colon Cancers Undetected
Disruptions caused by the COVID-19 pandemic led to an estimated 619 missed cases of colorectal cancer (CRC) diagnoses among US veterans, and those whose cases were caught had larger tumors and more malignant bowel obstructions compared with a prepandemic period, a new longitudinal study finds.
The decline in diagnoses during the pandemic (March 2020-October 2023) represented a 5% decrease in anticipated cases compared with the prepandemic period (January 2017-February 2020) reported Veterans Health Administration (VHA) researchers in the Journal of Gastrointestinal Surgery.
Meanwhile, the percentage of cancers > 4 cm increased from 48.9% to 57.3% from the prepandemic to pandemic periods, and the percentage of patients with malignant bowel obstructions at presentation nearly doubled from 2.7% to 5.3%.
“The COVID-19 pandemic resulted in a significant initial decrease in rates of colon cancer diagnosis, with a slow return to baseline,” Louise Davies, MD, MS, a head-and-neck surgeon at the University of Wisconsin-Madison and senior author of the study told Federal Practitioner. “The length of time it took for things to return to normal surprised us. Patterns of detection did not return to more normal baselines until 2023.”
The Pandemic’s Toll on Colonoscopies
While mortality and diagnosis rates have fallen significantly over the past 3 decades, an estimated 158,850 colorectal cancer cases will be diagnosed in the US in 2026, and 55,230 patients will die. Within the VHA, an estimated 4000 new cases of colorectal cancer are diagnosed annually.
The pandemic disrupted medical care across the board, and colonoscopies were no exceptions. “There are various estimates that there were anywhere from 2 to 3 million missed exams,” said Timothy Pawlik, MD, PhD, MBA, MPH, a surgical oncologist and professor at The Ohio State University Wexner Medical Center, in an interview.
“At the height of the pandemic, all nonurgent procedures were put on hold,” explained Pawlik, who was not involved in the new study. “I suspect that a number of procedures were missed because different institutions and GI practices simply weren't providing that service at that time. In addition, I'm sure there was some reticence among patients to seek care even after the procedures were restarted and reoffered, especially at a hospital.”
Inside the VHA Data
The researchers found that 22,256 VHA patients were diagnosed with CRC during the study period (mean age, 71 years; 95.6% male; 72.1% White, 19.3% Black, and 6.4% Hispanic).
In a subset of 1087 patients, the percentage with an American Society of Anesthesiologists class ≥ 3 rose from 74.4% before the pandemic to 78.9% during it.
In light of the study findings, “clinicians should encourage their eligible patients to get screened for colon cancer, especially if they delayed screening as a result of the pandemic,” Davies said.
Why Colonoscopy Delays Matter
Pawlik, the Ohio State University Wexner Medical Center surgical oncologist, said even small delays in colonoscopies can be important.
“There are data suggesting that even a delay beyond 6 to 12 months can significantly increase the risk of advanced-stage cancer. Longer delays of a year, which were associated with the pandemic, definitely increase the risk of presenting with later stages of disease and potentially have a meaningful impact on your prognosis and survival.”
However, he noted that the study findings are limited because the results don’t clarify when patients were due for colonoscopies.
Still, in the big picture, the research “emphasizes the importance of timely colonoscopy compliance with national guidelines for screening of colon cancer,” he said.
Lessons About At-Home Tests
Pawlik added that the research also highlights that in times of limited access such as pandemics, there can be value to pivoting to home-based screening methods.
Study coauthor Douglas Robertson, MD, MPH, national deputy director of the Colorectal Cancer Screening Program with the US Department of Veterans Affairs National Gastroenterology and Hepatology Program, said the pandemic spurred a shift toward fecal immunochemical testing (FIT) via mail.
The VA is now mailing > 40,000 FIT tests per month to veterans. “This program was an outgrowth of and response to the pandemic and would enhance VA’s readiness to maintain CRC screening efforts should something similar occur in the future,” Robertson said in an interview.
The Department of Veterans Affairs funded the study. Davies, Robertson, and the other study authors have no disclosures. Pawlik is co-editor-in-chief of the Journal of Gastrointestinal Surgery and has no other disclosures.
Disruptions caused by the COVID-19 pandemic led to an estimated 619 missed cases of colorectal cancer (CRC) diagnoses among US veterans, and those whose cases were caught had larger tumors and more malignant bowel obstructions compared with a prepandemic period, a new longitudinal study finds.
The decline in diagnoses during the pandemic (March 2020-October 2023) represented a 5% decrease in anticipated cases compared with the prepandemic period (January 2017-February 2020) reported Veterans Health Administration (VHA) researchers in the Journal of Gastrointestinal Surgery.
Meanwhile, the percentage of cancers > 4 cm increased from 48.9% to 57.3% from the prepandemic to pandemic periods, and the percentage of patients with malignant bowel obstructions at presentation nearly doubled from 2.7% to 5.3%.
“The COVID-19 pandemic resulted in a significant initial decrease in rates of colon cancer diagnosis, with a slow return to baseline,” Louise Davies, MD, MS, a head-and-neck surgeon at the University of Wisconsin-Madison and senior author of the study told Federal Practitioner. “The length of time it took for things to return to normal surprised us. Patterns of detection did not return to more normal baselines until 2023.”
The Pandemic’s Toll on Colonoscopies
While mortality and diagnosis rates have fallen significantly over the past 3 decades, an estimated 158,850 colorectal cancer cases will be diagnosed in the US in 2026, and 55,230 patients will die. Within the VHA, an estimated 4000 new cases of colorectal cancer are diagnosed annually.
The pandemic disrupted medical care across the board, and colonoscopies were no exceptions. “There are various estimates that there were anywhere from 2 to 3 million missed exams,” said Timothy Pawlik, MD, PhD, MBA, MPH, a surgical oncologist and professor at The Ohio State University Wexner Medical Center, in an interview.
“At the height of the pandemic, all nonurgent procedures were put on hold,” explained Pawlik, who was not involved in the new study. “I suspect that a number of procedures were missed because different institutions and GI practices simply weren't providing that service at that time. In addition, I'm sure there was some reticence among patients to seek care even after the procedures were restarted and reoffered, especially at a hospital.”
Inside the VHA Data
The researchers found that 22,256 VHA patients were diagnosed with CRC during the study period (mean age, 71 years; 95.6% male; 72.1% White, 19.3% Black, and 6.4% Hispanic).
In a subset of 1087 patients, the percentage with an American Society of Anesthesiologists class ≥ 3 rose from 74.4% before the pandemic to 78.9% during it.
In light of the study findings, “clinicians should encourage their eligible patients to get screened for colon cancer, especially if they delayed screening as a result of the pandemic,” Davies said.
Why Colonoscopy Delays Matter
Pawlik, the Ohio State University Wexner Medical Center surgical oncologist, said even small delays in colonoscopies can be important.
“There are data suggesting that even a delay beyond 6 to 12 months can significantly increase the risk of advanced-stage cancer. Longer delays of a year, which were associated with the pandemic, definitely increase the risk of presenting with later stages of disease and potentially have a meaningful impact on your prognosis and survival.”
However, he noted that the study findings are limited because the results don’t clarify when patients were due for colonoscopies.
Still, in the big picture, the research “emphasizes the importance of timely colonoscopy compliance with national guidelines for screening of colon cancer,” he said.
Lessons About At-Home Tests
Pawlik added that the research also highlights that in times of limited access such as pandemics, there can be value to pivoting to home-based screening methods.
Study coauthor Douglas Robertson, MD, MPH, national deputy director of the Colorectal Cancer Screening Program with the US Department of Veterans Affairs National Gastroenterology and Hepatology Program, said the pandemic spurred a shift toward fecal immunochemical testing (FIT) via mail.
The VA is now mailing > 40,000 FIT tests per month to veterans. “This program was an outgrowth of and response to the pandemic and would enhance VA’s readiness to maintain CRC screening efforts should something similar occur in the future,” Robertson said in an interview.
The Department of Veterans Affairs funded the study. Davies, Robertson, and the other study authors have no disclosures. Pawlik is co-editor-in-chief of the Journal of Gastrointestinal Surgery and has no other disclosures.
Disruptions caused by the COVID-19 pandemic led to an estimated 619 missed cases of colorectal cancer (CRC) diagnoses among US veterans, and those whose cases were caught had larger tumors and more malignant bowel obstructions compared with a prepandemic period, a new longitudinal study finds.
The decline in diagnoses during the pandemic (March 2020-October 2023) represented a 5% decrease in anticipated cases compared with the prepandemic period (January 2017-February 2020) reported Veterans Health Administration (VHA) researchers in the Journal of Gastrointestinal Surgery.
Meanwhile, the percentage of cancers > 4 cm increased from 48.9% to 57.3% from the prepandemic to pandemic periods, and the percentage of patients with malignant bowel obstructions at presentation nearly doubled from 2.7% to 5.3%.
“The COVID-19 pandemic resulted in a significant initial decrease in rates of colon cancer diagnosis, with a slow return to baseline,” Louise Davies, MD, MS, a head-and-neck surgeon at the University of Wisconsin-Madison and senior author of the study told Federal Practitioner. “The length of time it took for things to return to normal surprised us. Patterns of detection did not return to more normal baselines until 2023.”
The Pandemic’s Toll on Colonoscopies
While mortality and diagnosis rates have fallen significantly over the past 3 decades, an estimated 158,850 colorectal cancer cases will be diagnosed in the US in 2026, and 55,230 patients will die. Within the VHA, an estimated 4000 new cases of colorectal cancer are diagnosed annually.
The pandemic disrupted medical care across the board, and colonoscopies were no exceptions. “There are various estimates that there were anywhere from 2 to 3 million missed exams,” said Timothy Pawlik, MD, PhD, MBA, MPH, a surgical oncologist and professor at The Ohio State University Wexner Medical Center, in an interview.
“At the height of the pandemic, all nonurgent procedures were put on hold,” explained Pawlik, who was not involved in the new study. “I suspect that a number of procedures were missed because different institutions and GI practices simply weren't providing that service at that time. In addition, I'm sure there was some reticence among patients to seek care even after the procedures were restarted and reoffered, especially at a hospital.”
Inside the VHA Data
The researchers found that 22,256 VHA patients were diagnosed with CRC during the study period (mean age, 71 years; 95.6% male; 72.1% White, 19.3% Black, and 6.4% Hispanic).
In a subset of 1087 patients, the percentage with an American Society of Anesthesiologists class ≥ 3 rose from 74.4% before the pandemic to 78.9% during it.
In light of the study findings, “clinicians should encourage their eligible patients to get screened for colon cancer, especially if they delayed screening as a result of the pandemic,” Davies said.
Why Colonoscopy Delays Matter
Pawlik, the Ohio State University Wexner Medical Center surgical oncologist, said even small delays in colonoscopies can be important.
“There are data suggesting that even a delay beyond 6 to 12 months can significantly increase the risk of advanced-stage cancer. Longer delays of a year, which were associated with the pandemic, definitely increase the risk of presenting with later stages of disease and potentially have a meaningful impact on your prognosis and survival.”
However, he noted that the study findings are limited because the results don’t clarify when patients were due for colonoscopies.
Still, in the big picture, the research “emphasizes the importance of timely colonoscopy compliance with national guidelines for screening of colon cancer,” he said.
Lessons About At-Home Tests
Pawlik added that the research also highlights that in times of limited access such as pandemics, there can be value to pivoting to home-based screening methods.
Study coauthor Douglas Robertson, MD, MPH, national deputy director of the Colorectal Cancer Screening Program with the US Department of Veterans Affairs National Gastroenterology and Hepatology Program, said the pandemic spurred a shift toward fecal immunochemical testing (FIT) via mail.
The VA is now mailing > 40,000 FIT tests per month to veterans. “This program was an outgrowth of and response to the pandemic and would enhance VA’s readiness to maintain CRC screening efforts should something similar occur in the future,” Robertson said in an interview.
The Department of Veterans Affairs funded the study. Davies, Robertson, and the other study authors have no disclosures. Pawlik is co-editor-in-chief of the Journal of Gastrointestinal Surgery and has no other disclosures.
Alcohol Intake Tied to Increased Colorectal Cancer Risk
Alcohol Intake Tied to Increased Colorectal Cancer Risk
Transcript generated from video captions.
Hello. I’m Dr Maurie Markman, from City of Hope. I’d like to discuss a very interesting paper that appeared in Cancer, entitled, “Association of alcohol intake over the lifetime with colorectal adenoma and colorectal cancer risk in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial.”
This is an important paper. It is very clear, certainly to those in the public health community and cancer doctors, that there is an association with alcohol intake and the risk of cancer. However, in population-based surveys, there is a very large percentage of individuals who do not appear to see the risk of alcohol intake, particularly excessive alcohol intake, related to cancer, or an even larger segment of population simply doesn’t know. This analysis is important to help address this question.
The investigators looked at adults in the United States who were enrolled in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial, which is a very important study that had been ongoing for many years. Individuals in this study reported at several timepoints during their participation what their current and past alcohol intake was.
What these investigators found is as follows. Among the 88,092 participants, there were a total of 1679 incident colorectal cancers that developed over 20 years of follow-up. Investigators demonstrated that current drinkers with an average lifetime alcohol intake of 14 or more drinks per week, or approximately 2 drinks per day, had a higher risk of colorectal cancer with a hazard ratio of 1.25, a 25% increase, compared to those individuals who had ≤ 1 drink per week.
Very importantly, individuals were characterized by their own information that they provided as consistent heavy drinking versus light drinking. This was associated with almost a doubling of the risk of the development of colorectal cancer over that 20-year period.
Clearly, heavy drinking and higher lifetime alcohol intake is associated with an increased risk of colorectal cancer. This is relevant information for public health officials, primary care doctors, and the public in general to understand that there is a risk if you drink often, particularly heavy drinking, with increased development of cancer in general — but in this case, we’re talking specifically about colorectal cancer.
I thank you for your attention.
A version of this article first appeared on Medscape.com.
Transcript generated from video captions.
Hello. I’m Dr Maurie Markman, from City of Hope. I’d like to discuss a very interesting paper that appeared in Cancer, entitled, “Association of alcohol intake over the lifetime with colorectal adenoma and colorectal cancer risk in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial.”
This is an important paper. It is very clear, certainly to those in the public health community and cancer doctors, that there is an association with alcohol intake and the risk of cancer. However, in population-based surveys, there is a very large percentage of individuals who do not appear to see the risk of alcohol intake, particularly excessive alcohol intake, related to cancer, or an even larger segment of population simply doesn’t know. This analysis is important to help address this question.
The investigators looked at adults in the United States who were enrolled in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial, which is a very important study that had been ongoing for many years. Individuals in this study reported at several timepoints during their participation what their current and past alcohol intake was.
What these investigators found is as follows. Among the 88,092 participants, there were a total of 1679 incident colorectal cancers that developed over 20 years of follow-up. Investigators demonstrated that current drinkers with an average lifetime alcohol intake of 14 or more drinks per week, or approximately 2 drinks per day, had a higher risk of colorectal cancer with a hazard ratio of 1.25, a 25% increase, compared to those individuals who had ≤ 1 drink per week.
Very importantly, individuals were characterized by their own information that they provided as consistent heavy drinking versus light drinking. This was associated with almost a doubling of the risk of the development of colorectal cancer over that 20-year period.
Clearly, heavy drinking and higher lifetime alcohol intake is associated with an increased risk of colorectal cancer. This is relevant information for public health officials, primary care doctors, and the public in general to understand that there is a risk if you drink often, particularly heavy drinking, with increased development of cancer in general — but in this case, we’re talking specifically about colorectal cancer.
I thank you for your attention.
A version of this article first appeared on Medscape.com.
Transcript generated from video captions.
Hello. I’m Dr Maurie Markman, from City of Hope. I’d like to discuss a very interesting paper that appeared in Cancer, entitled, “Association of alcohol intake over the lifetime with colorectal adenoma and colorectal cancer risk in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial.”
This is an important paper. It is very clear, certainly to those in the public health community and cancer doctors, that there is an association with alcohol intake and the risk of cancer. However, in population-based surveys, there is a very large percentage of individuals who do not appear to see the risk of alcohol intake, particularly excessive alcohol intake, related to cancer, or an even larger segment of population simply doesn’t know. This analysis is important to help address this question.
The investigators looked at adults in the United States who were enrolled in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial, which is a very important study that had been ongoing for many years. Individuals in this study reported at several timepoints during their participation what their current and past alcohol intake was.
What these investigators found is as follows. Among the 88,092 participants, there were a total of 1679 incident colorectal cancers that developed over 20 years of follow-up. Investigators demonstrated that current drinkers with an average lifetime alcohol intake of 14 or more drinks per week, or approximately 2 drinks per day, had a higher risk of colorectal cancer with a hazard ratio of 1.25, a 25% increase, compared to those individuals who had ≤ 1 drink per week.
Very importantly, individuals were characterized by their own information that they provided as consistent heavy drinking versus light drinking. This was associated with almost a doubling of the risk of the development of colorectal cancer over that 20-year period.
Clearly, heavy drinking and higher lifetime alcohol intake is associated with an increased risk of colorectal cancer. This is relevant information for public health officials, primary care doctors, and the public in general to understand that there is a risk if you drink often, particularly heavy drinking, with increased development of cancer in general — but in this case, we’re talking specifically about colorectal cancer.
I thank you for your attention.
A version of this article first appeared on Medscape.com.
Alcohol Intake Tied to Increased Colorectal Cancer Risk
Alcohol Intake Tied to Increased Colorectal Cancer Risk
VHA CRC Screening Has Blind Spots, Disparities
TOPLINE:
More than 1 in 8 colorectal cancer (CRC) cases among veterans occur outside the standard screening age of 50-75 years or those with high-risk personal or family history. High-risk patients face > 6 times the risk for CRC compared with average-risk patients aged 50-75 years who are up to date with screening, while Black patients have > 50% higher risk compared with White patients.
METHODOLOGY:
Researchers conducted a case-control analysis using Veterans Health Administration (VHA) Corporate Data Warehouse data from 2012-2018 at 2 sites: Veterans Affairs (VA) New York Harbor Health Care System and VA Puget Sound Health Care System.
Participants included 3714 cases among veterans with CRC matched to 14,856 controls (4:1), with matching on age (± 3 years), sex, and facility site; each control was used once.
Screening categories included 5 groups by age (50-75 years vs < 50 years or > 75 years), screening up-to-date status, and high-risk status (inflammatory bowel disease, hereditary cancer syndromes, or family history).
CRC screening was considered up to date if US Preventive Services Task Force-recommended tests were completed on time (colonoscopy ≤ 10 years; guaiac-based fecal occult blood test or fecal immunochemical test ≤ 1 year).
TAKEAWAY:
Compared with category 1 (age 50-75 years and up-to-date with screening), CRC was associated with category 4 (age < 50 years or > 75 years and not up to date) (odds ratio [OR], 1.40; 95% CI, 1.11-1.78), and category 5 (high risk) (OR, 6.23; 95% CI, 5.06-7.66).
Race and comorbidity associations included higher CRC risk for Black vs White patients (OR, 1.54; 95% CI, 1.37-1.73), and higher CRC risk with diabetes (OR, 1.65; 95% CI, 1.51-1.81) and alcohol use disorder (OR, 1.53; 95% CI, 1.35-1.73).
Among 3714 CRC cases, 71.1% occurred in individuals aged 50-75 years not up to date with screening.
A total of 12.5% of CRC cases occurred in people outside age 50-75 or with high-risk personal or family history, suggesting that conventional screening-adherence metrics may miss a clinically relevant minority.
IN PRACTICE:
“The conventional measure of CRC screening, focused on average-risk individuals aged 50 to 75, does not reflect screening status in an important minority of CRC patients," the authors wrote.
SOURCE:
The study was led by researchers at NYU Grossman School of Medicine and Veterans Affairs New York Harbor Health Care System, and published online July 9, 2026 in Medicine.
LIMITATIONS:
The study population consisted predominantly of male veterans (97.1%), who tend to be older and have more comorbidities compared with the US population, which may limit the generalizability of findings to other populations. Researchers defined screening status cross-sectionally relative to a single point in time rather than assessing longitudinal screening adherence, which may not fully capture the consistency of screening over time that is likely important for defining CRC risk. Veterans may receive screening at non-VA medical facilities, potentially leading to incomplete documentation of screening status and important covariates such as race, ethnicity, and comorbidities. The possibility of residual confounding cannot be excluded despite adjustment for multiple risk factors in the analysis.
DISCLOSURES:
This study received support from NIH grant K08 CA230162 and the AGA Caroline Craig Augustyn & Damian Augustyn Award in Digestive Cancer, both awarded to Peter S. Liang. Liang disclosed receiving research support from Freenome and serving on the advisory boards for Guardant Health and Natera. The remaining authors reported no funding or conflicts of interest to disclose.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE:
More than 1 in 8 colorectal cancer (CRC) cases among veterans occur outside the standard screening age of 50-75 years or those with high-risk personal or family history. High-risk patients face > 6 times the risk for CRC compared with average-risk patients aged 50-75 years who are up to date with screening, while Black patients have > 50% higher risk compared with White patients.
METHODOLOGY:
Researchers conducted a case-control analysis using Veterans Health Administration (VHA) Corporate Data Warehouse data from 2012-2018 at 2 sites: Veterans Affairs (VA) New York Harbor Health Care System and VA Puget Sound Health Care System.
Participants included 3714 cases among veterans with CRC matched to 14,856 controls (4:1), with matching on age (± 3 years), sex, and facility site; each control was used once.
Screening categories included 5 groups by age (50-75 years vs < 50 years or > 75 years), screening up-to-date status, and high-risk status (inflammatory bowel disease, hereditary cancer syndromes, or family history).
CRC screening was considered up to date if US Preventive Services Task Force-recommended tests were completed on time (colonoscopy ≤ 10 years; guaiac-based fecal occult blood test or fecal immunochemical test ≤ 1 year).
TAKEAWAY:
Compared with category 1 (age 50-75 years and up-to-date with screening), CRC was associated with category 4 (age < 50 years or > 75 years and not up to date) (odds ratio [OR], 1.40; 95% CI, 1.11-1.78), and category 5 (high risk) (OR, 6.23; 95% CI, 5.06-7.66).
Race and comorbidity associations included higher CRC risk for Black vs White patients (OR, 1.54; 95% CI, 1.37-1.73), and higher CRC risk with diabetes (OR, 1.65; 95% CI, 1.51-1.81) and alcohol use disorder (OR, 1.53; 95% CI, 1.35-1.73).
Among 3714 CRC cases, 71.1% occurred in individuals aged 50-75 years not up to date with screening.
A total of 12.5% of CRC cases occurred in people outside age 50-75 or with high-risk personal or family history, suggesting that conventional screening-adherence metrics may miss a clinically relevant minority.
IN PRACTICE:
“The conventional measure of CRC screening, focused on average-risk individuals aged 50 to 75, does not reflect screening status in an important minority of CRC patients," the authors wrote.
SOURCE:
The study was led by researchers at NYU Grossman School of Medicine and Veterans Affairs New York Harbor Health Care System, and published online July 9, 2026 in Medicine.
LIMITATIONS:
The study population consisted predominantly of male veterans (97.1%), who tend to be older and have more comorbidities compared with the US population, which may limit the generalizability of findings to other populations. Researchers defined screening status cross-sectionally relative to a single point in time rather than assessing longitudinal screening adherence, which may not fully capture the consistency of screening over time that is likely important for defining CRC risk. Veterans may receive screening at non-VA medical facilities, potentially leading to incomplete documentation of screening status and important covariates such as race, ethnicity, and comorbidities. The possibility of residual confounding cannot be excluded despite adjustment for multiple risk factors in the analysis.
DISCLOSURES:
This study received support from NIH grant K08 CA230162 and the AGA Caroline Craig Augustyn & Damian Augustyn Award in Digestive Cancer, both awarded to Peter S. Liang. Liang disclosed receiving research support from Freenome and serving on the advisory boards for Guardant Health and Natera. The remaining authors reported no funding or conflicts of interest to disclose.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE:
More than 1 in 8 colorectal cancer (CRC) cases among veterans occur outside the standard screening age of 50-75 years or those with high-risk personal or family history. High-risk patients face > 6 times the risk for CRC compared with average-risk patients aged 50-75 years who are up to date with screening, while Black patients have > 50% higher risk compared with White patients.
METHODOLOGY:
Researchers conducted a case-control analysis using Veterans Health Administration (VHA) Corporate Data Warehouse data from 2012-2018 at 2 sites: Veterans Affairs (VA) New York Harbor Health Care System and VA Puget Sound Health Care System.
Participants included 3714 cases among veterans with CRC matched to 14,856 controls (4:1), with matching on age (± 3 years), sex, and facility site; each control was used once.
Screening categories included 5 groups by age (50-75 years vs < 50 years or > 75 years), screening up-to-date status, and high-risk status (inflammatory bowel disease, hereditary cancer syndromes, or family history).
CRC screening was considered up to date if US Preventive Services Task Force-recommended tests were completed on time (colonoscopy ≤ 10 years; guaiac-based fecal occult blood test or fecal immunochemical test ≤ 1 year).
TAKEAWAY:
Compared with category 1 (age 50-75 years and up-to-date with screening), CRC was associated with category 4 (age < 50 years or > 75 years and not up to date) (odds ratio [OR], 1.40; 95% CI, 1.11-1.78), and category 5 (high risk) (OR, 6.23; 95% CI, 5.06-7.66).
Race and comorbidity associations included higher CRC risk for Black vs White patients (OR, 1.54; 95% CI, 1.37-1.73), and higher CRC risk with diabetes (OR, 1.65; 95% CI, 1.51-1.81) and alcohol use disorder (OR, 1.53; 95% CI, 1.35-1.73).
Among 3714 CRC cases, 71.1% occurred in individuals aged 50-75 years not up to date with screening.
A total of 12.5% of CRC cases occurred in people outside age 50-75 or with high-risk personal or family history, suggesting that conventional screening-adherence metrics may miss a clinically relevant minority.
IN PRACTICE:
“The conventional measure of CRC screening, focused on average-risk individuals aged 50 to 75, does not reflect screening status in an important minority of CRC patients," the authors wrote.
SOURCE:
The study was led by researchers at NYU Grossman School of Medicine and Veterans Affairs New York Harbor Health Care System, and published online July 9, 2026 in Medicine.
LIMITATIONS:
The study population consisted predominantly of male veterans (97.1%), who tend to be older and have more comorbidities compared with the US population, which may limit the generalizability of findings to other populations. Researchers defined screening status cross-sectionally relative to a single point in time rather than assessing longitudinal screening adherence, which may not fully capture the consistency of screening over time that is likely important for defining CRC risk. Veterans may receive screening at non-VA medical facilities, potentially leading to incomplete documentation of screening status and important covariates such as race, ethnicity, and comorbidities. The possibility of residual confounding cannot be excluded despite adjustment for multiple risk factors in the analysis.
DISCLOSURES:
This study received support from NIH grant K08 CA230162 and the AGA Caroline Craig Augustyn & Damian Augustyn Award in Digestive Cancer, both awarded to Peter S. Liang. Liang disclosed receiving research support from Freenome and serving on the advisory boards for Guardant Health and Natera. The remaining authors reported no funding or conflicts of interest to disclose.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
Tumor Debulking Fails to Boost Survival in Metastatic CRC
Tumor Debulking Fails to Boost Survival in Metastatic CRC
TOPLINE:
In a randomized phase 3 trial, adding tumor debulking to first-line chemotherapy did not significantly improve overall survival or progression-free survival (PFS) and was associated with an increased risk for serious adverse events in patients with multiorgan metastatic colorectal cancer (mCRC). The study found that patients receiving tumor debulking plus chemotherapy and those receiving chemotherapy alone had similar overall survival (median, 30.0 and 27.5 months, respectively) and PFS (median, 10.5 and 10.4 months, respectively).
METHODOLOGY:
- CRC frequently metastasizes, and when the spread is limited, local curative treatments (such as surgery and ablation) yield 5‑year survival rates of 35%-65%. With median overall survival from systemic therapy now exceeding 30 months, local ablative therapies are increasingly combined with systemic treatment for more extensive mCRC; however, randomized trial based-evidence of survival benefits of this approach is lacking.
- Researchers conducted an open-label, multicenter randomized clinical trial, involving 454 patients with multiorgan mCRC, to determine whether reducing the total amount of tumor (referred to as tumor debulking) could improve survival. Only those deemed amenable to at least 80% debulking prior to starting first-line palliative chemotherapy were included.
- A total of 382 patients were randomly assigned 1:1 to receive either chemotherapy alone (n = 192) or tumor debulking followed by chemotherapy (n = 190) after achieving an objective partial or complete response or stable disease following 3 cycles of capecitabine and oxaliplatin or 4 cycles of 5-fluorouracil or leucovorin and oxaliplatin with or without bevacizumab. The chemotherapy alone group continued standard oxaliplatin‑based chemotherapy; in the debulking group, patients with a response received one additional cycle without bevacizumab before local therapy.
- The primary outcome was overall survival, and secondary outcomes included PFS and serious adverse events. The median follow-up duration was 32.3 months.
TAKEAWAY:
- The median overall survival in the chemotherapy alone group vs chemotherapy plus tumor debulking group was 27.5 vs 30.0 months (adjusted hazard ratio [AHR], 0.88; 95% CI, 0.70-1.10; P = .26), indicating no overall survival benefit from adding tumor debulking to first-line palliative chemotherapy.
- The median PFS was also similar between the chemotherapy alone and chemotherapy plus tumor debulking groups (10.4 and 10.5 months, respectively; AHR, 0.83; 95% CI, 0.67-1.02; P = .08). More patients in the combination therapy group vs chemotherapy alone group experienced any serious adverse events of grade 1 or higher (53% vs 39%; P = .006).
- Among patients who achieved a state of stable disease at randomization, a significant overall survival benefit was observed in the intervention group (P for interaction = .04), although no differences in PFS were noted between subgroups (P for interaction = .13).
- Regarding exploratory outcomes, incomplete debulking was associated with much worse survival (median, 16.8 months), whereas maximal (80% or more) and radical debulking were associated with longer median survival (36.6 vs 35.3 months).
- Additionally, fewer patients in the debulking arm completed at least 6 months of chemotherapy (64% vs 77%), and prespecified analyses by BRAF V600E and RAS mutation status did not show a clear overall survival benefit from adding debulking for either mutant or wild‑type tumors.
IN PRACTICE:
“The results of this trial reveal no significant improvement in overall survival or PFS from additional tumor debulking compared with palliative systemic treatment alone in patients with multiorgan mCRC,” the authors of the study wrote, reiterating that “the addition of tumor debulking to palliative chemotherapy should therefore not be considered standard of care” and “use of local therapies for patients with more limited, oligometastatic CRC needs further consideration.”
SOURCE:
The study, led by Elske C. Gootjes, MD, PhD, and Lotte Bakkerus, MD, from the Radboud University Medical Center, Nijmegen, Netherlands, and Anviti A. Adhin, from Erasmus MC Cancer Institute, University Medical Center Rotterdam, Rotterdam, Netherlands, was published online in JAMA.
LIMITATIONS:
Prolonged enrollment could have led to outdated survival estimates and systemic therapy regimens. Additionally, modern systemic chemotherapy regimens such as triplet chemotherapy or chemotherapy plus anti-epidermal growth factor receptor antibodies for left-sided/RAS wild-type tumors were uniformly used.
DISCLOSURES:
The study received funding from the Dutch Cancer Society, the Blokker-Verwer Foundation, and Roche Nederland BV. Some authors reported receiving grants or personal fees or having other ties with various sources. Full disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
In a randomized phase 3 trial, adding tumor debulking to first-line chemotherapy did not significantly improve overall survival or progression-free survival (PFS) and was associated with an increased risk for serious adverse events in patients with multiorgan metastatic colorectal cancer (mCRC). The study found that patients receiving tumor debulking plus chemotherapy and those receiving chemotherapy alone had similar overall survival (median, 30.0 and 27.5 months, respectively) and PFS (median, 10.5 and 10.4 months, respectively).
METHODOLOGY:
- CRC frequently metastasizes, and when the spread is limited, local curative treatments (such as surgery and ablation) yield 5‑year survival rates of 35%-65%. With median overall survival from systemic therapy now exceeding 30 months, local ablative therapies are increasingly combined with systemic treatment for more extensive mCRC; however, randomized trial based-evidence of survival benefits of this approach is lacking.
- Researchers conducted an open-label, multicenter randomized clinical trial, involving 454 patients with multiorgan mCRC, to determine whether reducing the total amount of tumor (referred to as tumor debulking) could improve survival. Only those deemed amenable to at least 80% debulking prior to starting first-line palliative chemotherapy were included.
- A total of 382 patients were randomly assigned 1:1 to receive either chemotherapy alone (n = 192) or tumor debulking followed by chemotherapy (n = 190) after achieving an objective partial or complete response or stable disease following 3 cycles of capecitabine and oxaliplatin or 4 cycles of 5-fluorouracil or leucovorin and oxaliplatin with or without bevacizumab. The chemotherapy alone group continued standard oxaliplatin‑based chemotherapy; in the debulking group, patients with a response received one additional cycle without bevacizumab before local therapy.
- The primary outcome was overall survival, and secondary outcomes included PFS and serious adverse events. The median follow-up duration was 32.3 months.
TAKEAWAY:
- The median overall survival in the chemotherapy alone group vs chemotherapy plus tumor debulking group was 27.5 vs 30.0 months (adjusted hazard ratio [AHR], 0.88; 95% CI, 0.70-1.10; P = .26), indicating no overall survival benefit from adding tumor debulking to first-line palliative chemotherapy.
- The median PFS was also similar between the chemotherapy alone and chemotherapy plus tumor debulking groups (10.4 and 10.5 months, respectively; AHR, 0.83; 95% CI, 0.67-1.02; P = .08). More patients in the combination therapy group vs chemotherapy alone group experienced any serious adverse events of grade 1 or higher (53% vs 39%; P = .006).
- Among patients who achieved a state of stable disease at randomization, a significant overall survival benefit was observed in the intervention group (P for interaction = .04), although no differences in PFS were noted between subgroups (P for interaction = .13).
- Regarding exploratory outcomes, incomplete debulking was associated with much worse survival (median, 16.8 months), whereas maximal (80% or more) and radical debulking were associated with longer median survival (36.6 vs 35.3 months).
- Additionally, fewer patients in the debulking arm completed at least 6 months of chemotherapy (64% vs 77%), and prespecified analyses by BRAF V600E and RAS mutation status did not show a clear overall survival benefit from adding debulking for either mutant or wild‑type tumors.
IN PRACTICE:
“The results of this trial reveal no significant improvement in overall survival or PFS from additional tumor debulking compared with palliative systemic treatment alone in patients with multiorgan mCRC,” the authors of the study wrote, reiterating that “the addition of tumor debulking to palliative chemotherapy should therefore not be considered standard of care” and “use of local therapies for patients with more limited, oligometastatic CRC needs further consideration.”
SOURCE:
The study, led by Elske C. Gootjes, MD, PhD, and Lotte Bakkerus, MD, from the Radboud University Medical Center, Nijmegen, Netherlands, and Anviti A. Adhin, from Erasmus MC Cancer Institute, University Medical Center Rotterdam, Rotterdam, Netherlands, was published online in JAMA.
LIMITATIONS:
Prolonged enrollment could have led to outdated survival estimates and systemic therapy regimens. Additionally, modern systemic chemotherapy regimens such as triplet chemotherapy or chemotherapy plus anti-epidermal growth factor receptor antibodies for left-sided/RAS wild-type tumors were uniformly used.
DISCLOSURES:
The study received funding from the Dutch Cancer Society, the Blokker-Verwer Foundation, and Roche Nederland BV. Some authors reported receiving grants or personal fees or having other ties with various sources. Full disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
In a randomized phase 3 trial, adding tumor debulking to first-line chemotherapy did not significantly improve overall survival or progression-free survival (PFS) and was associated with an increased risk for serious adverse events in patients with multiorgan metastatic colorectal cancer (mCRC). The study found that patients receiving tumor debulking plus chemotherapy and those receiving chemotherapy alone had similar overall survival (median, 30.0 and 27.5 months, respectively) and PFS (median, 10.5 and 10.4 months, respectively).
METHODOLOGY:
- CRC frequently metastasizes, and when the spread is limited, local curative treatments (such as surgery and ablation) yield 5‑year survival rates of 35%-65%. With median overall survival from systemic therapy now exceeding 30 months, local ablative therapies are increasingly combined with systemic treatment for more extensive mCRC; however, randomized trial based-evidence of survival benefits of this approach is lacking.
- Researchers conducted an open-label, multicenter randomized clinical trial, involving 454 patients with multiorgan mCRC, to determine whether reducing the total amount of tumor (referred to as tumor debulking) could improve survival. Only those deemed amenable to at least 80% debulking prior to starting first-line palliative chemotherapy were included.
- A total of 382 patients were randomly assigned 1:1 to receive either chemotherapy alone (n = 192) or tumor debulking followed by chemotherapy (n = 190) after achieving an objective partial or complete response or stable disease following 3 cycles of capecitabine and oxaliplatin or 4 cycles of 5-fluorouracil or leucovorin and oxaliplatin with or without bevacizumab. The chemotherapy alone group continued standard oxaliplatin‑based chemotherapy; in the debulking group, patients with a response received one additional cycle without bevacizumab before local therapy.
- The primary outcome was overall survival, and secondary outcomes included PFS and serious adverse events. The median follow-up duration was 32.3 months.
TAKEAWAY:
- The median overall survival in the chemotherapy alone group vs chemotherapy plus tumor debulking group was 27.5 vs 30.0 months (adjusted hazard ratio [AHR], 0.88; 95% CI, 0.70-1.10; P = .26), indicating no overall survival benefit from adding tumor debulking to first-line palliative chemotherapy.
- The median PFS was also similar between the chemotherapy alone and chemotherapy plus tumor debulking groups (10.4 and 10.5 months, respectively; AHR, 0.83; 95% CI, 0.67-1.02; P = .08). More patients in the combination therapy group vs chemotherapy alone group experienced any serious adverse events of grade 1 or higher (53% vs 39%; P = .006).
- Among patients who achieved a state of stable disease at randomization, a significant overall survival benefit was observed in the intervention group (P for interaction = .04), although no differences in PFS were noted between subgroups (P for interaction = .13).
- Regarding exploratory outcomes, incomplete debulking was associated with much worse survival (median, 16.8 months), whereas maximal (80% or more) and radical debulking were associated with longer median survival (36.6 vs 35.3 months).
- Additionally, fewer patients in the debulking arm completed at least 6 months of chemotherapy (64% vs 77%), and prespecified analyses by BRAF V600E and RAS mutation status did not show a clear overall survival benefit from adding debulking for either mutant or wild‑type tumors.
IN PRACTICE:
“The results of this trial reveal no significant improvement in overall survival or PFS from additional tumor debulking compared with palliative systemic treatment alone in patients with multiorgan mCRC,” the authors of the study wrote, reiterating that “the addition of tumor debulking to palliative chemotherapy should therefore not be considered standard of care” and “use of local therapies for patients with more limited, oligometastatic CRC needs further consideration.”
SOURCE:
The study, led by Elske C. Gootjes, MD, PhD, and Lotte Bakkerus, MD, from the Radboud University Medical Center, Nijmegen, Netherlands, and Anviti A. Adhin, from Erasmus MC Cancer Institute, University Medical Center Rotterdam, Rotterdam, Netherlands, was published online in JAMA.
LIMITATIONS:
Prolonged enrollment could have led to outdated survival estimates and systemic therapy regimens. Additionally, modern systemic chemotherapy regimens such as triplet chemotherapy or chemotherapy plus anti-epidermal growth factor receptor antibodies for left-sided/RAS wild-type tumors were uniformly used.
DISCLOSURES:
The study received funding from the Dutch Cancer Society, the Blokker-Verwer Foundation, and Roche Nederland BV. Some authors reported receiving grants or personal fees or having other ties with various sources. Full disclosures are noted in the original article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Tumor Debulking Fails to Boost Survival in Metastatic CRC
Tumor Debulking Fails to Boost Survival in Metastatic CRC
Treatment Delays in Colorectal Cancer More Common in Urban Men, Racial Minorities
Treatment Delays in Colorectal Cancer More Common in Urban Men, Racial Minorities
TOPLINE:
Among patients with early-onset colorectal cancer (CRC), treatment delays exceeding 90 days were more common in all-urban populations and seemed to disproportionately affect men and Asian or Pacific Islander, Black, and Hispanic patients. Although several differences were statistically significant, the absolute differences in treatment timing were modest — for instance, the mean time to treatment was 20.7 days in all-urban areas vs 17.8 days in mostly rural areas.
METHODOLOGY:
- Adults with early-onset CRC frequently face diagnostic delays and present at an advanced stage, and this is particularly common among men and racially or ethnically minoritized groups in disadvantaged areas. However, studies evaluating how sex, race and ethnicity, and geography affect timely treatment are scarce.
- Researchers conducted a retrospective cross-sectional analysis using data from the Surveillance, Epidemiology, and End Results (SEER) Program, involving 79,090 patients with early-onset CRC between 2006 and 2020.
- Overall, 53.22% were men; 73.9% were aged 40-49 years; and 54.7% were White, 21.0% Hispanic, 13.8% Black, 9.0% Asian or Pacific Islander, and 0.6% American Indian or Alaska Native. More than half (66.5%) resided in all-urban areas, 20.6% in mostly urban areas, 7.0% in mostly rural areas, and 5.9% in all-rural areas.
- Researchers evaluated the time to treatment (defined as treatment initiation within 30, 60, or 90 days after diagnosis) and assessed its associations with sex, race, and rurality. False discovery rate (FDR) adjustment was applied to multivariable analyses to account for multiple comparisons, and FDR-adjusted two-sided P values were reported.
TAKEAWAY:
- The mean time to treatment in the overall cohort was 20.0 days; it was shortest in mostly rural areas (17.8 days) and longest in all-urban areas (20.7 days).
- Among patients in all-urban areas, men had 5% lower likelihood of initiating treatment within 90 days than women (hazard ratio [HR], 0.95; 95% CI, 0.93-0.97).
- Similarly, Asian or Pacific Islander (HR, 0.96; 95% CI, 0.93-0.99; P = .01), Black (HR, 0.95; 95% CI, 0.92-0.98; P = .001), and Hispanic (HR, 0.93; 95% CI, 0.91-0.95; P < .001) patients in all-urban areas were less likely than White patients to start treatment within 90 days. Comparable patterns were seen at the 30- and 60-day thresholds.
- In mostly rural areas, Black patients were more likely than White patients to start treatment earlier (30-day HR, 1.19; 95% CI, 1.06-1.34 and 90-day HR, 1.15; 95% CI, 1.02-1.28), whereas men were less likely than women to initiate treatment within 90 days (HR, 0.90; 95% CI, 0.85-0.96).
- Researchers found that several HRs were statistically significant but were numerically close to 1.00, indicating modest absolute differences in treatment timing.
IN PRACTICE:
“The consistency of these delays across sociodemographic groups challenges assumptions of uniformly timely access in urban settings. Overcrowded urban health care systems or inefficient public transportation may limit access to care,” the authors wrote, noting that “young adults face distinct challenges across life stages, including lack of health insurance among patients aged 18 to 29 years and financial strain among patients aged 30 to 39 years that hinder timely access to treatment.”
SOURCE:
The study, led by Meng-Han Tsai, PhD, Georgia Prevention Institute, Augusta University, Augusta, Georgia, was published online as a research letter in JAMA Network Open.
LIMITATIONS:
The study characterized time-to-treatment patterns rather than clinical outcomes and relied on SEER data without day-level treatment timing. Additionally, the observed HRs were small, but even modest delays may have led to population-level disparities.
DISCLOSURES:
This research was supported by the Augusta ROAR SCORE Career Enhancement Core through a grant awarded to Tsai. The authors declared having no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Among patients with early-onset colorectal cancer (CRC), treatment delays exceeding 90 days were more common in all-urban populations and seemed to disproportionately affect men and Asian or Pacific Islander, Black, and Hispanic patients. Although several differences were statistically significant, the absolute differences in treatment timing were modest — for instance, the mean time to treatment was 20.7 days in all-urban areas vs 17.8 days in mostly rural areas.
METHODOLOGY:
- Adults with early-onset CRC frequently face diagnostic delays and present at an advanced stage, and this is particularly common among men and racially or ethnically minoritized groups in disadvantaged areas. However, studies evaluating how sex, race and ethnicity, and geography affect timely treatment are scarce.
- Researchers conducted a retrospective cross-sectional analysis using data from the Surveillance, Epidemiology, and End Results (SEER) Program, involving 79,090 patients with early-onset CRC between 2006 and 2020.
- Overall, 53.22% were men; 73.9% were aged 40-49 years; and 54.7% were White, 21.0% Hispanic, 13.8% Black, 9.0% Asian or Pacific Islander, and 0.6% American Indian or Alaska Native. More than half (66.5%) resided in all-urban areas, 20.6% in mostly urban areas, 7.0% in mostly rural areas, and 5.9% in all-rural areas.
- Researchers evaluated the time to treatment (defined as treatment initiation within 30, 60, or 90 days after diagnosis) and assessed its associations with sex, race, and rurality. False discovery rate (FDR) adjustment was applied to multivariable analyses to account for multiple comparisons, and FDR-adjusted two-sided P values were reported.
TAKEAWAY:
- The mean time to treatment in the overall cohort was 20.0 days; it was shortest in mostly rural areas (17.8 days) and longest in all-urban areas (20.7 days).
- Among patients in all-urban areas, men had 5% lower likelihood of initiating treatment within 90 days than women (hazard ratio [HR], 0.95; 95% CI, 0.93-0.97).
- Similarly, Asian or Pacific Islander (HR, 0.96; 95% CI, 0.93-0.99; P = .01), Black (HR, 0.95; 95% CI, 0.92-0.98; P = .001), and Hispanic (HR, 0.93; 95% CI, 0.91-0.95; P < .001) patients in all-urban areas were less likely than White patients to start treatment within 90 days. Comparable patterns were seen at the 30- and 60-day thresholds.
- In mostly rural areas, Black patients were more likely than White patients to start treatment earlier (30-day HR, 1.19; 95% CI, 1.06-1.34 and 90-day HR, 1.15; 95% CI, 1.02-1.28), whereas men were less likely than women to initiate treatment within 90 days (HR, 0.90; 95% CI, 0.85-0.96).
- Researchers found that several HRs were statistically significant but were numerically close to 1.00, indicating modest absolute differences in treatment timing.
IN PRACTICE:
“The consistency of these delays across sociodemographic groups challenges assumptions of uniformly timely access in urban settings. Overcrowded urban health care systems or inefficient public transportation may limit access to care,” the authors wrote, noting that “young adults face distinct challenges across life stages, including lack of health insurance among patients aged 18 to 29 years and financial strain among patients aged 30 to 39 years that hinder timely access to treatment.”
SOURCE:
The study, led by Meng-Han Tsai, PhD, Georgia Prevention Institute, Augusta University, Augusta, Georgia, was published online as a research letter in JAMA Network Open.
LIMITATIONS:
The study characterized time-to-treatment patterns rather than clinical outcomes and relied on SEER data without day-level treatment timing. Additionally, the observed HRs were small, but even modest delays may have led to population-level disparities.
DISCLOSURES:
This research was supported by the Augusta ROAR SCORE Career Enhancement Core through a grant awarded to Tsai. The authors declared having no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Among patients with early-onset colorectal cancer (CRC), treatment delays exceeding 90 days were more common in all-urban populations and seemed to disproportionately affect men and Asian or Pacific Islander, Black, and Hispanic patients. Although several differences were statistically significant, the absolute differences in treatment timing were modest — for instance, the mean time to treatment was 20.7 days in all-urban areas vs 17.8 days in mostly rural areas.
METHODOLOGY:
- Adults with early-onset CRC frequently face diagnostic delays and present at an advanced stage, and this is particularly common among men and racially or ethnically minoritized groups in disadvantaged areas. However, studies evaluating how sex, race and ethnicity, and geography affect timely treatment are scarce.
- Researchers conducted a retrospective cross-sectional analysis using data from the Surveillance, Epidemiology, and End Results (SEER) Program, involving 79,090 patients with early-onset CRC between 2006 and 2020.
- Overall, 53.22% were men; 73.9% were aged 40-49 years; and 54.7% were White, 21.0% Hispanic, 13.8% Black, 9.0% Asian or Pacific Islander, and 0.6% American Indian or Alaska Native. More than half (66.5%) resided in all-urban areas, 20.6% in mostly urban areas, 7.0% in mostly rural areas, and 5.9% in all-rural areas.
- Researchers evaluated the time to treatment (defined as treatment initiation within 30, 60, or 90 days after diagnosis) and assessed its associations with sex, race, and rurality. False discovery rate (FDR) adjustment was applied to multivariable analyses to account for multiple comparisons, and FDR-adjusted two-sided P values were reported.
TAKEAWAY:
- The mean time to treatment in the overall cohort was 20.0 days; it was shortest in mostly rural areas (17.8 days) and longest in all-urban areas (20.7 days).
- Among patients in all-urban areas, men had 5% lower likelihood of initiating treatment within 90 days than women (hazard ratio [HR], 0.95; 95% CI, 0.93-0.97).
- Similarly, Asian or Pacific Islander (HR, 0.96; 95% CI, 0.93-0.99; P = .01), Black (HR, 0.95; 95% CI, 0.92-0.98; P = .001), and Hispanic (HR, 0.93; 95% CI, 0.91-0.95; P < .001) patients in all-urban areas were less likely than White patients to start treatment within 90 days. Comparable patterns were seen at the 30- and 60-day thresholds.
- In mostly rural areas, Black patients were more likely than White patients to start treatment earlier (30-day HR, 1.19; 95% CI, 1.06-1.34 and 90-day HR, 1.15; 95% CI, 1.02-1.28), whereas men were less likely than women to initiate treatment within 90 days (HR, 0.90; 95% CI, 0.85-0.96).
- Researchers found that several HRs were statistically significant but were numerically close to 1.00, indicating modest absolute differences in treatment timing.
IN PRACTICE:
“The consistency of these delays across sociodemographic groups challenges assumptions of uniformly timely access in urban settings. Overcrowded urban health care systems or inefficient public transportation may limit access to care,” the authors wrote, noting that “young adults face distinct challenges across life stages, including lack of health insurance among patients aged 18 to 29 years and financial strain among patients aged 30 to 39 years that hinder timely access to treatment.”
SOURCE:
The study, led by Meng-Han Tsai, PhD, Georgia Prevention Institute, Augusta University, Augusta, Georgia, was published online as a research letter in JAMA Network Open.
LIMITATIONS:
The study characterized time-to-treatment patterns rather than clinical outcomes and relied on SEER data without day-level treatment timing. Additionally, the observed HRs were small, but even modest delays may have led to population-level disparities.
DISCLOSURES:
This research was supported by the Augusta ROAR SCORE Career Enhancement Core through a grant awarded to Tsai. The authors declared having no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Treatment Delays in Colorectal Cancer More Common in Urban Men, Racial Minorities
Treatment Delays in Colorectal Cancer More Common in Urban Men, Racial Minorities
The GLP-1 Paradox in Colorectal Cancer
The GLP-1 Paradox in Colorectal Cancer
This transcript has been edited for clarity.
Hi. I'm David Kerr, professor of cancer medicine at University of Oxford. One of the harder lessons I've learned as a cancer doctor, not surprisingly, is that prevention's better than cure. This is something I've become increasingly interested in as I've become more senior in the profession. I say that rather than "becoming older."
I'd like to draw your attention to some interesting work that's been done looking at the risk of developing colorectal cancer. We talk about lifestyle factors, exercise, vitamin D, and sometimes aspirin. There is some plausible evidence, not from randomized trials, suggesting that these interventions can reduce the chance of developing colorectal cancer. With my friend Ian Tomlinson, colleague in Oxford, we have a huge interest in the genetics of predicting who will develop colorectal cancer.
Today I'd like to talk about these new agents, the so-called glucagon-like peptide 1 receptor agonists, or GLP-1 receptor agonists, which are being used widely now to treat type 2 diabetes and obesity. These are remarkably successful drugs with huge worldwide global uptake, but there is debate in the literature and in real-world evidence as to what they do about cancer risk.
You would think that if we reduce body weight and if we reduce adiposity, that truly would reduce the chance of developing cancer. We know that a number of cancers are related to body fat content and so on.
I'd like to focus particularly on my own field of interest, which is colorectal cancer, and an article I picked up recently by Professor Zhong and colleagues, where they did a meta-analysis. This is a statistical method for clumping together large datasets from different studies.
They did a meta-analysis using very conventional, widely accepted methods to look at a very large dataset of just over 5 million individuals from seven retrospective cohort studies, so a big database to study.
There was a pooled analysis, which revealed that there was a significant but slight increase in the risk for colorectal cancer in patients receiving the GLP-1 agonists. Overall, they felt that, given the small but significant increase in the risk of developing colorectal cancer, we need further evidence.
This was a retrospective review of a large dataset, but given debate in the literature, more forward-looking studies are required. It’s the sort of thing that, in real-world use, one might take into account when recommending these treatments, such as Mounjaro.
In patients who have a higher-than-expected risk of developing colorectal cancer, one might hesitate a little. Clearly, if they get diabetes or cardiac disease, those beneficial risks would, of course, weigh one in favor of using these effective new drugs.
For somebody who had borderline BMI, where there were some questions as to whether you would use the drugs or not, and if they had some other colorectal cancer risk factors, such as relatives affected, then one might pause for thought before using them.
This was a well-conducted study that adds to the rather confused literature on the effects of these widely used drugs on the risk for cancer. Again, just that thought that, although it would seem plausible to think the opposite, these drugs would reduce colorectal cancer risk, on review of a very large dataset, actually the opposite seems to be the case. Always go for evidence. The larger, the more convincing the dataset, the better.
I’d be interested in what you thought about this and whether information like this might tip your balance as to whether you would accept using these drugs to reduce your own body weight.
Thanks for listening. For the time being, Medscapers, over and out. Thank you.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I'm David Kerr, professor of cancer medicine at University of Oxford. One of the harder lessons I've learned as a cancer doctor, not surprisingly, is that prevention's better than cure. This is something I've become increasingly interested in as I've become more senior in the profession. I say that rather than "becoming older."
I'd like to draw your attention to some interesting work that's been done looking at the risk of developing colorectal cancer. We talk about lifestyle factors, exercise, vitamin D, and sometimes aspirin. There is some plausible evidence, not from randomized trials, suggesting that these interventions can reduce the chance of developing colorectal cancer. With my friend Ian Tomlinson, colleague in Oxford, we have a huge interest in the genetics of predicting who will develop colorectal cancer.
Today I'd like to talk about these new agents, the so-called glucagon-like peptide 1 receptor agonists, or GLP-1 receptor agonists, which are being used widely now to treat type 2 diabetes and obesity. These are remarkably successful drugs with huge worldwide global uptake, but there is debate in the literature and in real-world evidence as to what they do about cancer risk.
You would think that if we reduce body weight and if we reduce adiposity, that truly would reduce the chance of developing cancer. We know that a number of cancers are related to body fat content and so on.
I'd like to focus particularly on my own field of interest, which is colorectal cancer, and an article I picked up recently by Professor Zhong and colleagues, where they did a meta-analysis. This is a statistical method for clumping together large datasets from different studies.
They did a meta-analysis using very conventional, widely accepted methods to look at a very large dataset of just over 5 million individuals from seven retrospective cohort studies, so a big database to study.
There was a pooled analysis, which revealed that there was a significant but slight increase in the risk for colorectal cancer in patients receiving the GLP-1 agonists. Overall, they felt that, given the small but significant increase in the risk of developing colorectal cancer, we need further evidence.
This was a retrospective review of a large dataset, but given debate in the literature, more forward-looking studies are required. It’s the sort of thing that, in real-world use, one might take into account when recommending these treatments, such as Mounjaro.
In patients who have a higher-than-expected risk of developing colorectal cancer, one might hesitate a little. Clearly, if they get diabetes or cardiac disease, those beneficial risks would, of course, weigh one in favor of using these effective new drugs.
For somebody who had borderline BMI, where there were some questions as to whether you would use the drugs or not, and if they had some other colorectal cancer risk factors, such as relatives affected, then one might pause for thought before using them.
This was a well-conducted study that adds to the rather confused literature on the effects of these widely used drugs on the risk for cancer. Again, just that thought that, although it would seem plausible to think the opposite, these drugs would reduce colorectal cancer risk, on review of a very large dataset, actually the opposite seems to be the case. Always go for evidence. The larger, the more convincing the dataset, the better.
I’d be interested in what you thought about this and whether information like this might tip your balance as to whether you would accept using these drugs to reduce your own body weight.
Thanks for listening. For the time being, Medscapers, over and out. Thank you.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I'm David Kerr, professor of cancer medicine at University of Oxford. One of the harder lessons I've learned as a cancer doctor, not surprisingly, is that prevention's better than cure. This is something I've become increasingly interested in as I've become more senior in the profession. I say that rather than "becoming older."
I'd like to draw your attention to some interesting work that's been done looking at the risk of developing colorectal cancer. We talk about lifestyle factors, exercise, vitamin D, and sometimes aspirin. There is some plausible evidence, not from randomized trials, suggesting that these interventions can reduce the chance of developing colorectal cancer. With my friend Ian Tomlinson, colleague in Oxford, we have a huge interest in the genetics of predicting who will develop colorectal cancer.
Today I'd like to talk about these new agents, the so-called glucagon-like peptide 1 receptor agonists, or GLP-1 receptor agonists, which are being used widely now to treat type 2 diabetes and obesity. These are remarkably successful drugs with huge worldwide global uptake, but there is debate in the literature and in real-world evidence as to what they do about cancer risk.
You would think that if we reduce body weight and if we reduce adiposity, that truly would reduce the chance of developing cancer. We know that a number of cancers are related to body fat content and so on.
I'd like to focus particularly on my own field of interest, which is colorectal cancer, and an article I picked up recently by Professor Zhong and colleagues, where they did a meta-analysis. This is a statistical method for clumping together large datasets from different studies.
They did a meta-analysis using very conventional, widely accepted methods to look at a very large dataset of just over 5 million individuals from seven retrospective cohort studies, so a big database to study.
There was a pooled analysis, which revealed that there was a significant but slight increase in the risk for colorectal cancer in patients receiving the GLP-1 agonists. Overall, they felt that, given the small but significant increase in the risk of developing colorectal cancer, we need further evidence.
This was a retrospective review of a large dataset, but given debate in the literature, more forward-looking studies are required. It’s the sort of thing that, in real-world use, one might take into account when recommending these treatments, such as Mounjaro.
In patients who have a higher-than-expected risk of developing colorectal cancer, one might hesitate a little. Clearly, if they get diabetes or cardiac disease, those beneficial risks would, of course, weigh one in favor of using these effective new drugs.
For somebody who had borderline BMI, where there were some questions as to whether you would use the drugs or not, and if they had some other colorectal cancer risk factors, such as relatives affected, then one might pause for thought before using them.
This was a well-conducted study that adds to the rather confused literature on the effects of these widely used drugs on the risk for cancer. Again, just that thought that, although it would seem plausible to think the opposite, these drugs would reduce colorectal cancer risk, on review of a very large dataset, actually the opposite seems to be the case. Always go for evidence. The larger, the more convincing the dataset, the better.
I’d be interested in what you thought about this and whether information like this might tip your balance as to whether you would accept using these drugs to reduce your own body weight.
Thanks for listening. For the time being, Medscapers, over and out. Thank you.
A version of this article first appeared on Medscape.com.
The GLP-1 Paradox in Colorectal Cancer
The GLP-1 Paradox in Colorectal Cancer